User login
Lines Blur Between Dysplasia, Carcinoma in Situ
SAN DIEGO – It’s not getting any easier to make the histological distinction between carcinoma in situ and simple dysplasia in a sun-damaged epidermis, but it may be getting less critical to get it right, noted Dr. John B. Campbell.
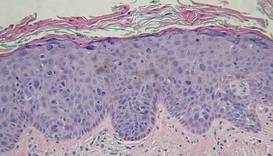
During his presentation at a meeting sponsored by the American Society for Mohs Surgery, Dr. Campbell, a Mohs pathologist in private practice in San Diego, showed slides depicting disorderly cells that typify dysplasia extending high up into the epidermis along the edges of specimens containing in situ carcinoma. "There are a lot of things that go along with dysplastic changes," he said. "The nuclei become larger; they stain darker; they have less cytoplasm so that the N/C [nuclear to cytoplasmic] ratio increases."
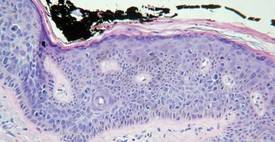
"At some place along the edges of the specimen you’re going to have to draw a line between in situ carcinoma and simple dysplasia. There are gradations that are somewhat subjective."
Pathologists commonly envision a line midway through the epidermis. If the dark and disorganized cells reach that point, they call it "moderate dysplasia." If they’re clumped in the lower third of the epidermis, it merits a call of "mild dysplasia," and if they extend to near the surface, it’s "severe."
"Dysplastic changes that are wall-to-wall, top-to-bottom are carcinoma in situ," he said. "You’ll need to develop criteria on your own."
In the meantime, the pressure to make the right call may be easing.
"What I’ve seen happening in the last few years is that we’re becoming less and less sensitive about dysplasia at the edges of in situ carcinomas because we can treat them so easily topically," said Dr. Campbell. Beyond watchful waiting or freezing, such regions can now be well managed with topical therapies such as Aldara (imiquimod) or Efudex (fluorouracil).
"Once we’ve cleared the unequivocal carcinoma in situ, people are letting a significant amount of dysplasia remain and then treating it in follow-up.
"There’s really no downside to [conservative or topical management] as long as the patient is reliable," he said.
Taking a careful look at the site during follow-up visits will easily reveal any cell changes that might prompt a fresh biopsy. One finding of note in such cases is the proclivity of dysplastic cells to take a downward course along appendage structures such as eccrine ducts and follicles in the epithelium. "They can go down quite deep ... maybe 2 mm deep to the surface," he said.
In his practice, Dr. Campbell and his colleagues characterize such findings as "advanced actinic keratoses," and note the presence of dysplastic cells along appendage structures.
Dr. Campbell reported no relevant disclosures.
SAN DIEGO – It’s not getting any easier to make the histological distinction between carcinoma in situ and simple dysplasia in a sun-damaged epidermis, but it may be getting less critical to get it right, noted Dr. John B. Campbell.
During his presentation at a meeting sponsored by the American Society for Mohs Surgery, Dr. Campbell, a Mohs pathologist in private practice in San Diego, showed slides depicting disorderly cells that typify dysplasia extending high up into the epidermis along the edges of specimens containing in situ carcinoma. "There are a lot of things that go along with dysplastic changes," he said. "The nuclei become larger; they stain darker; they have less cytoplasm so that the N/C [nuclear to cytoplasmic] ratio increases."
"At some place along the edges of the specimen you’re going to have to draw a line between in situ carcinoma and simple dysplasia. There are gradations that are somewhat subjective."
Pathologists commonly envision a line midway through the epidermis. If the dark and disorganized cells reach that point, they call it "moderate dysplasia." If they’re clumped in the lower third of the epidermis, it merits a call of "mild dysplasia," and if they extend to near the surface, it’s "severe."
"Dysplastic changes that are wall-to-wall, top-to-bottom are carcinoma in situ," he said. "You’ll need to develop criteria on your own."
In the meantime, the pressure to make the right call may be easing.
"What I’ve seen happening in the last few years is that we’re becoming less and less sensitive about dysplasia at the edges of in situ carcinomas because we can treat them so easily topically," said Dr. Campbell. Beyond watchful waiting or freezing, such regions can now be well managed with topical therapies such as Aldara (imiquimod) or Efudex (fluorouracil).
"Once we’ve cleared the unequivocal carcinoma in situ, people are letting a significant amount of dysplasia remain and then treating it in follow-up.
"There’s really no downside to [conservative or topical management] as long as the patient is reliable," he said.
Taking a careful look at the site during follow-up visits will easily reveal any cell changes that might prompt a fresh biopsy. One finding of note in such cases is the proclivity of dysplastic cells to take a downward course along appendage structures such as eccrine ducts and follicles in the epithelium. "They can go down quite deep ... maybe 2 mm deep to the surface," he said.
In his practice, Dr. Campbell and his colleagues characterize such findings as "advanced actinic keratoses," and note the presence of dysplastic cells along appendage structures.
Dr. Campbell reported no relevant disclosures.
SAN DIEGO – It’s not getting any easier to make the histological distinction between carcinoma in situ and simple dysplasia in a sun-damaged epidermis, but it may be getting less critical to get it right, noted Dr. John B. Campbell.
During his presentation at a meeting sponsored by the American Society for Mohs Surgery, Dr. Campbell, a Mohs pathologist in private practice in San Diego, showed slides depicting disorderly cells that typify dysplasia extending high up into the epidermis along the edges of specimens containing in situ carcinoma. "There are a lot of things that go along with dysplastic changes," he said. "The nuclei become larger; they stain darker; they have less cytoplasm so that the N/C [nuclear to cytoplasmic] ratio increases."
"At some place along the edges of the specimen you’re going to have to draw a line between in situ carcinoma and simple dysplasia. There are gradations that are somewhat subjective."
Pathologists commonly envision a line midway through the epidermis. If the dark and disorganized cells reach that point, they call it "moderate dysplasia." If they’re clumped in the lower third of the epidermis, it merits a call of "mild dysplasia," and if they extend to near the surface, it’s "severe."
"Dysplastic changes that are wall-to-wall, top-to-bottom are carcinoma in situ," he said. "You’ll need to develop criteria on your own."
In the meantime, the pressure to make the right call may be easing.
"What I’ve seen happening in the last few years is that we’re becoming less and less sensitive about dysplasia at the edges of in situ carcinomas because we can treat them so easily topically," said Dr. Campbell. Beyond watchful waiting or freezing, such regions can now be well managed with topical therapies such as Aldara (imiquimod) or Efudex (fluorouracil).
"Once we’ve cleared the unequivocal carcinoma in situ, people are letting a significant amount of dysplasia remain and then treating it in follow-up.
"There’s really no downside to [conservative or topical management] as long as the patient is reliable," he said.
Taking a careful look at the site during follow-up visits will easily reveal any cell changes that might prompt a fresh biopsy. One finding of note in such cases is the proclivity of dysplastic cells to take a downward course along appendage structures such as eccrine ducts and follicles in the epithelium. "They can go down quite deep ... maybe 2 mm deep to the surface," he said.
In his practice, Dr. Campbell and his colleagues characterize such findings as "advanced actinic keratoses," and note the presence of dysplastic cells along appendage structures.
Dr. Campbell reported no relevant disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN SOCIETY FOR MOHS SURGERY
Blog: The Vampire Lift
What the heck is the vampire lift, and how does it work? No biting is involved, but you will have to draw some blood.

Dr. Julie Woodward discussed the research, or lack thereof, behind this autologous blood plasma injection at the Cosmetic Surgery Forum in Las Vegas.
What the heck is the vampire lift, and how does it work? No biting is involved, but you will have to draw some blood.
Dr. Julie Woodward discussed the research, or lack thereof, behind this autologous blood plasma injection at the Cosmetic Surgery Forum in Las Vegas.
What the heck is the vampire lift, and how does it work? No biting is involved, but you will have to draw some blood.
Dr. Julie Woodward discussed the research, or lack thereof, behind this autologous blood plasma injection at the Cosmetic Surgery Forum in Las Vegas.
Mohs Microscope Shopping? Expert Describes Must Haves
SAN DIEGO – Like choosing a cell phone, stereo system, or new car, shopping for a microscope suitable for a Mohs surgery practice can be a delicate balance between what is needed, what is wanted, and how much money there is to spend.
Consumer Reports doesn’t have a special Mohs edition to help out on the microscope hunt, but Dr. Kenneth G. Gross offered his perspective on must-haves, don’t-wants, and "highly desirable features" to look for in a microscope designated for the special needs inherent in Mohs.
For starters, he emphasized that an appropriate microscope is a necessity, not a luxury.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice. You don’t bring a knife to a gun fight," he said at a meeting sponsored by the American Society for Mohs Surgery.
Dr. Gross, a dermatologic surgeon practicing in San Diego, explained that several competitive companies market technical microscopes that work well for Mohs and that all make quality products. He stated no personal preference but recommended shopping for a microscope that contains certain specifications, no matter the manufacturer.
Binocular or Trinocular?
Mohs surgeons really need a microscope with a teaching head – a binocular design – and ideally, the addition of a trinocular scope for photography.
A dual head is valuable not only for teaching or consultation with a resident, colleague, or pathologist, but it also allows for demonstrating to a technician the errors that can thwart a complete and accurate view of a specimen.
A third head for a camera is not 100% necessary, but is very nice to have, according to Dr. Gross.
"Photography is so easy nowadays, it is really stone simple. Everything is through the viewfinder and through the lens," automatically optimizing the F-stop, speed, and color balance.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice."
"Really, there’s no trick to it," said Dr. Gross. "You just attach a digital camera on top and shoot."
Point it Out
An adjustable, lighted pointer further assists communication and identification of focal regions on a slide.
"If there’s something I don’t see, [the pathologist] can flip on the pointer and say, "There you are, man. There it is."
Focusing on Lenses
Objective lenses, those closest to the specimen, come in three quality levels, and the middle level is acceptable for Mohs, according to Dr. Gross.
The lowest power objective lens should be no bigger than a 2.5x; a 2x is preferable. A 1x or 1.5x is fine as well, but not necessary, he said. With a 2.5x objective lens, "You can orient yourself to a pretty big specimen ... without getting lost."
He compared the view of a large specimen with a 10x objective lens to looking at ink dots and then trying to figure out how they combine to form letters on a book page.
Nose pieces hold five objective lenses, with a 2x, 4x, 10x, 20x, and 40x of middle-quality a good selection.
"You do not need an oil immersion lens on your microscope," he said.
Proper lighting with different lenses is achieved by using swing-out condensers, the best of which "clunk" into place like a solid car door.
The ones that freely slide from side to side are "kind of a piece of junk in my opinion," he said, "because they get out of focus easily."
When it comes to ocular lenses, pony up for the focusable, highest-quality, wide-angle options available, Dr. Gross said.
Each person viewing the specimen should be able to separately focus the image to accommodate individual differences in visual acuity.
Angle for Tilt Heads
Opting for a system with tilt heads isn’t imperative, but is wise if more than one doctor is sharing the microscope, according to Dr. Gross.
"Unless you’re identical twins, you’re going to [have one doctor who is] taller or shorter, sits up straight or slumped, use[s] different style chairs. If you have tilt heads, they’re really easy to adjust."
You can economize, though, by foregoing an option that allows the microscope heads to push in or out. "That’s a waste of money," he said.
Dr. Gross said he had no financial disclosures with regard to any company that manufactures or maintains microscopes used in Mohs surgery.
SAN DIEGO – Like choosing a cell phone, stereo system, or new car, shopping for a microscope suitable for a Mohs surgery practice can be a delicate balance between what is needed, what is wanted, and how much money there is to spend.
Consumer Reports doesn’t have a special Mohs edition to help out on the microscope hunt, but Dr. Kenneth G. Gross offered his perspective on must-haves, don’t-wants, and "highly desirable features" to look for in a microscope designated for the special needs inherent in Mohs.
For starters, he emphasized that an appropriate microscope is a necessity, not a luxury.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice. You don’t bring a knife to a gun fight," he said at a meeting sponsored by the American Society for Mohs Surgery.
Dr. Gross, a dermatologic surgeon practicing in San Diego, explained that several competitive companies market technical microscopes that work well for Mohs and that all make quality products. He stated no personal preference but recommended shopping for a microscope that contains certain specifications, no matter the manufacturer.
Binocular or Trinocular?
Mohs surgeons really need a microscope with a teaching head – a binocular design – and ideally, the addition of a trinocular scope for photography.
A dual head is valuable not only for teaching or consultation with a resident, colleague, or pathologist, but it also allows for demonstrating to a technician the errors that can thwart a complete and accurate view of a specimen.
A third head for a camera is not 100% necessary, but is very nice to have, according to Dr. Gross.
"Photography is so easy nowadays, it is really stone simple. Everything is through the viewfinder and through the lens," automatically optimizing the F-stop, speed, and color balance.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice."
"Really, there’s no trick to it," said Dr. Gross. "You just attach a digital camera on top and shoot."
Point it Out
An adjustable, lighted pointer further assists communication and identification of focal regions on a slide.
"If there’s something I don’t see, [the pathologist] can flip on the pointer and say, "There you are, man. There it is."
Focusing on Lenses
Objective lenses, those closest to the specimen, come in three quality levels, and the middle level is acceptable for Mohs, according to Dr. Gross.
The lowest power objective lens should be no bigger than a 2.5x; a 2x is preferable. A 1x or 1.5x is fine as well, but not necessary, he said. With a 2.5x objective lens, "You can orient yourself to a pretty big specimen ... without getting lost."
He compared the view of a large specimen with a 10x objective lens to looking at ink dots and then trying to figure out how they combine to form letters on a book page.
Nose pieces hold five objective lenses, with a 2x, 4x, 10x, 20x, and 40x of middle-quality a good selection.
"You do not need an oil immersion lens on your microscope," he said.
Proper lighting with different lenses is achieved by using swing-out condensers, the best of which "clunk" into place like a solid car door.
The ones that freely slide from side to side are "kind of a piece of junk in my opinion," he said, "because they get out of focus easily."
When it comes to ocular lenses, pony up for the focusable, highest-quality, wide-angle options available, Dr. Gross said.
Each person viewing the specimen should be able to separately focus the image to accommodate individual differences in visual acuity.
Angle for Tilt Heads
Opting for a system with tilt heads isn’t imperative, but is wise if more than one doctor is sharing the microscope, according to Dr. Gross.
"Unless you’re identical twins, you’re going to [have one doctor who is] taller or shorter, sits up straight or slumped, use[s] different style chairs. If you have tilt heads, they’re really easy to adjust."
You can economize, though, by foregoing an option that allows the microscope heads to push in or out. "That’s a waste of money," he said.
Dr. Gross said he had no financial disclosures with regard to any company that manufactures or maintains microscopes used in Mohs surgery.
SAN DIEGO – Like choosing a cell phone, stereo system, or new car, shopping for a microscope suitable for a Mohs surgery practice can be a delicate balance between what is needed, what is wanted, and how much money there is to spend.
Consumer Reports doesn’t have a special Mohs edition to help out on the microscope hunt, but Dr. Kenneth G. Gross offered his perspective on must-haves, don’t-wants, and "highly desirable features" to look for in a microscope designated for the special needs inherent in Mohs.
For starters, he emphasized that an appropriate microscope is a necessity, not a luxury.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice. You don’t bring a knife to a gun fight," he said at a meeting sponsored by the American Society for Mohs Surgery.
Dr. Gross, a dermatologic surgeon practicing in San Diego, explained that several competitive companies market technical microscopes that work well for Mohs and that all make quality products. He stated no personal preference but recommended shopping for a microscope that contains certain specifications, no matter the manufacturer.
Binocular or Trinocular?
Mohs surgeons really need a microscope with a teaching head – a binocular design – and ideally, the addition of a trinocular scope for photography.
A dual head is valuable not only for teaching or consultation with a resident, colleague, or pathologist, but it also allows for demonstrating to a technician the errors that can thwart a complete and accurate view of a specimen.
A third head for a camera is not 100% necessary, but is very nice to have, according to Dr. Gross.
"Photography is so easy nowadays, it is really stone simple. Everything is through the viewfinder and through the lens," automatically optimizing the F-stop, speed, and color balance.
"That little student microscope you used in medical school is really not the kind of microscope you want to use in a Mohs practice."
"Really, there’s no trick to it," said Dr. Gross. "You just attach a digital camera on top and shoot."
Point it Out
An adjustable, lighted pointer further assists communication and identification of focal regions on a slide.
"If there’s something I don’t see, [the pathologist] can flip on the pointer and say, "There you are, man. There it is."
Focusing on Lenses
Objective lenses, those closest to the specimen, come in three quality levels, and the middle level is acceptable for Mohs, according to Dr. Gross.
The lowest power objective lens should be no bigger than a 2.5x; a 2x is preferable. A 1x or 1.5x is fine as well, but not necessary, he said. With a 2.5x objective lens, "You can orient yourself to a pretty big specimen ... without getting lost."
He compared the view of a large specimen with a 10x objective lens to looking at ink dots and then trying to figure out how they combine to form letters on a book page.
Nose pieces hold five objective lenses, with a 2x, 4x, 10x, 20x, and 40x of middle-quality a good selection.
"You do not need an oil immersion lens on your microscope," he said.
Proper lighting with different lenses is achieved by using swing-out condensers, the best of which "clunk" into place like a solid car door.
The ones that freely slide from side to side are "kind of a piece of junk in my opinion," he said, "because they get out of focus easily."
When it comes to ocular lenses, pony up for the focusable, highest-quality, wide-angle options available, Dr. Gross said.
Each person viewing the specimen should be able to separately focus the image to accommodate individual differences in visual acuity.
Angle for Tilt Heads
Opting for a system with tilt heads isn’t imperative, but is wise if more than one doctor is sharing the microscope, according to Dr. Gross.
"Unless you’re identical twins, you’re going to [have one doctor who is] taller or shorter, sits up straight or slumped, use[s] different style chairs. If you have tilt heads, they’re really easy to adjust."
You can economize, though, by foregoing an option that allows the microscope heads to push in or out. "That’s a waste of money," he said.
Dr. Gross said he had no financial disclosures with regard to any company that manufactures or maintains microscopes used in Mohs surgery.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN SOCIETY FOR MOHS SURGERY
Blog: Goggle Removal, IPL Treatment Never Mix
Dr. Tzu, an ophthalmology resident at the University of Miami's Bascom Palmer Eye Institute, presented two cases highlighting the danger of removing eye goggles during IPL treatment for any reason.

In the first case, a 36-year-old female presented with burning, decreased vision, and photophobia in the right eye. She had undergone IPL treatment 1 hour before her symptoms began. She reported that her eye protection was removed during treatment of the eyelid area.
On eye examination, she was 20/20 in both eyes. However, her right pupil was 3 mm with decreased reactivity, compared with her left pupil, which was 5 mm and reactive. On slit lamp examination, inflammatory reaction was seen in the anterior chamber. She was treated with the steroid dexamethasone.
At 2-week follow-up, the patient's inflammation of the eye had improved; however, posterior synechiae was noted, as was iris transillumination defects. Topical steroids were increased.
At 2 years, the patient still has photophobia, iris defects, and abnormal pupils. She was given colored contact lenses to mitigate the photophobia.
In the second case presented by Dr. Tzu, a 27-year-old female presented 2 days after undergoing IPL treatment for freckles over the left upper eyelid. She reported that her goggles were removed for some applications of IPL to the eyelid. She reported pain, photophobia, and redness in her left eye.
On eye exam, she was 20/30 in the left eye. Her right pupil was 5 mm and reactive, while her left pupil was 3 mm with minimal reactivity. On slit lamp exam, inflammatory reaction in the anterior chamber of her eye could be seen. She was treated with topical prednisone.
At 3-week follow-up her vision had returned to 20/20 in the left eye and inflammation was improved. Posterior synechiae was noted, as was iris transillumination defects and atrophy.
The patient continues to have photophobia and glare, and is unhappy with the cosmetic asymmetry between her two pupils, Dr. Tzu noted.
Shutter goggles need to be worn by the clinician, and patient's need to wear nontransparent goggles. For treatment around the eye area, corneal shields can be placed directly on the globe area of the eye.
Dr. Tzu, an ophthalmology resident at the University of Miami's Bascom Palmer Eye Institute, presented two cases highlighting the danger of removing eye goggles during IPL treatment for any reason.
In the first case, a 36-year-old female presented with burning, decreased vision, and photophobia in the right eye. She had undergone IPL treatment 1 hour before her symptoms began. She reported that her eye protection was removed during treatment of the eyelid area.
On eye examination, she was 20/20 in both eyes. However, her right pupil was 3 mm with decreased reactivity, compared with her left pupil, which was 5 mm and reactive. On slit lamp examination, inflammatory reaction was seen in the anterior chamber. She was treated with the steroid dexamethasone.
At 2-week follow-up, the patient's inflammation of the eye had improved; however, posterior synechiae was noted, as was iris transillumination defects. Topical steroids were increased.
At 2 years, the patient still has photophobia, iris defects, and abnormal pupils. She was given colored contact lenses to mitigate the photophobia.
In the second case presented by Dr. Tzu, a 27-year-old female presented 2 days after undergoing IPL treatment for freckles over the left upper eyelid. She reported that her goggles were removed for some applications of IPL to the eyelid. She reported pain, photophobia, and redness in her left eye.
On eye exam, she was 20/30 in the left eye. Her right pupil was 5 mm and reactive, while her left pupil was 3 mm with minimal reactivity. On slit lamp exam, inflammatory reaction in the anterior chamber of her eye could be seen. She was treated with topical prednisone.
At 3-week follow-up her vision had returned to 20/20 in the left eye and inflammation was improved. Posterior synechiae was noted, as was iris transillumination defects and atrophy.
The patient continues to have photophobia and glare, and is unhappy with the cosmetic asymmetry between her two pupils, Dr. Tzu noted.
Shutter goggles need to be worn by the clinician, and patient's need to wear nontransparent goggles. For treatment around the eye area, corneal shields can be placed directly on the globe area of the eye.
Dr. Tzu, an ophthalmology resident at the University of Miami's Bascom Palmer Eye Institute, presented two cases highlighting the danger of removing eye goggles during IPL treatment for any reason.
In the first case, a 36-year-old female presented with burning, decreased vision, and photophobia in the right eye. She had undergone IPL treatment 1 hour before her symptoms began. She reported that her eye protection was removed during treatment of the eyelid area.
On eye examination, she was 20/20 in both eyes. However, her right pupil was 3 mm with decreased reactivity, compared with her left pupil, which was 5 mm and reactive. On slit lamp examination, inflammatory reaction was seen in the anterior chamber. She was treated with the steroid dexamethasone.
At 2-week follow-up, the patient's inflammation of the eye had improved; however, posterior synechiae was noted, as was iris transillumination defects. Topical steroids were increased.
At 2 years, the patient still has photophobia, iris defects, and abnormal pupils. She was given colored contact lenses to mitigate the photophobia.
In the second case presented by Dr. Tzu, a 27-year-old female presented 2 days after undergoing IPL treatment for freckles over the left upper eyelid. She reported that her goggles were removed for some applications of IPL to the eyelid. She reported pain, photophobia, and redness in her left eye.
On eye exam, she was 20/30 in the left eye. Her right pupil was 5 mm and reactive, while her left pupil was 3 mm with minimal reactivity. On slit lamp exam, inflammatory reaction in the anterior chamber of her eye could be seen. She was treated with topical prednisone.
At 3-week follow-up her vision had returned to 20/20 in the left eye and inflammation was improved. Posterior synechiae was noted, as was iris transillumination defects and atrophy.
The patient continues to have photophobia and glare, and is unhappy with the cosmetic asymmetry between her two pupils, Dr. Tzu noted.
Shutter goggles need to be worn by the clinician, and patient's need to wear nontransparent goggles. For treatment around the eye area, corneal shields can be placed directly on the globe area of the eye.
‘Keep it Simple,’ for a Satisfactory ASMS Grade
SAN DIEGO – If you want to receive a coveted "satisfactory" grade from peer reviewers of the American Society for Mohs Surgery, "keep it simple," advised Dr. Sharon F. Tiefenbrunn, a member of the ASMS peer review committee..
"The goal of this is to show us that you can recognize a perfect case and can produce a perfect case," she said at a meeting sponsored by the ASMS.
Highly complex or controversial cases are frequently "unreviewable," she noted.

"We don’t want your greatest case, where you worked until almost midnight, and it took 10 stages to clear, and the patient had to have a free flap to repair the defect, and you were ready to tear out your hair and swear off Mohs forever," stressed Dr. Tiefenbrunn, a procedural dermatologist in private practice in St. Louis.
Instead, peer reviewers want to see a stage II to III Mohs case, with tumor evident on stage I and a tumor-free final stage, she said.
Dr. Tiefenbrunn explained that the peer review program was launched in 2000, reviewing cases from the previous year. Its purpose is to improve the quality of Mohs surgery, track the organization’s success in teaching Mohs techniques, and provide practitioners with one of the two episodes of peer review required by the Clinical Laboratory Improvement Act (CLIA).
Cases are submitted to the ASMS administrative office and cycled to reviewers, who classify them as satisfactory, unreviewable, or "comments only."
A typical comment might be: "not enough overlap to determine clear margin." Such cases are sent to the peer review chairman, who forwards the case, along with a critique, back to the presenter.
In essence, a "comments" case fails to meet peer review standards, while an "unreviewable" case potentially might be corrected according to reviewers’ comments and resubmitted, said Dr. Tiefenbrunn.
Satisfactory cases demonstrate use of standard Mohs technique, have a minimal number of slides, and represent noncontroversial histology.
Some common reasons that cases are judged "unreviewable" include problems with the tumor map and ink legend, failure to mark the tumor on the map, unlabeled sections, confusing slide labeling, use of a nonstandard Mohs technique, bubbles, or a failure to identify tumor on stage I.
Dr. Tiefenbrunn reminded attendees of several cardinal rules, among them the need to include a complete skin edge (at least 90%), a complete deep margin, visible structural details, an adequate stain, visible ink for orientation, and a stage II showing a 2.5-mm margin in every direction.
Reviewers appreciate a legible presenter form; an orderly, precisely drawn map; well-packaged and well-organized slides; and simple explanations for anything on histology, such as actinic keratoses or nevi that might be mistaken for a tumor, said Dr. Tiefenbrunn.
"Presentation matters," she said. "Reviewers are your colleagues who are just as busy as you. We want to whip through these cases and just circle ‘satisfactory’ and go home."
Dr. Tiefenbrunn reported no relevant financial disclosures.
SAN DIEGO – If you want to receive a coveted "satisfactory" grade from peer reviewers of the American Society for Mohs Surgery, "keep it simple," advised Dr. Sharon F. Tiefenbrunn, a member of the ASMS peer review committee..
"The goal of this is to show us that you can recognize a perfect case and can produce a perfect case," she said at a meeting sponsored by the ASMS.
Highly complex or controversial cases are frequently "unreviewable," she noted.
"We don’t want your greatest case, where you worked until almost midnight, and it took 10 stages to clear, and the patient had to have a free flap to repair the defect, and you were ready to tear out your hair and swear off Mohs forever," stressed Dr. Tiefenbrunn, a procedural dermatologist in private practice in St. Louis.
Instead, peer reviewers want to see a stage II to III Mohs case, with tumor evident on stage I and a tumor-free final stage, she said.
Dr. Tiefenbrunn explained that the peer review program was launched in 2000, reviewing cases from the previous year. Its purpose is to improve the quality of Mohs surgery, track the organization’s success in teaching Mohs techniques, and provide practitioners with one of the two episodes of peer review required by the Clinical Laboratory Improvement Act (CLIA).
Cases are submitted to the ASMS administrative office and cycled to reviewers, who classify them as satisfactory, unreviewable, or "comments only."
A typical comment might be: "not enough overlap to determine clear margin." Such cases are sent to the peer review chairman, who forwards the case, along with a critique, back to the presenter.
In essence, a "comments" case fails to meet peer review standards, while an "unreviewable" case potentially might be corrected according to reviewers’ comments and resubmitted, said Dr. Tiefenbrunn.
Satisfactory cases demonstrate use of standard Mohs technique, have a minimal number of slides, and represent noncontroversial histology.
Some common reasons that cases are judged "unreviewable" include problems with the tumor map and ink legend, failure to mark the tumor on the map, unlabeled sections, confusing slide labeling, use of a nonstandard Mohs technique, bubbles, or a failure to identify tumor on stage I.
Dr. Tiefenbrunn reminded attendees of several cardinal rules, among them the need to include a complete skin edge (at least 90%), a complete deep margin, visible structural details, an adequate stain, visible ink for orientation, and a stage II showing a 2.5-mm margin in every direction.
Reviewers appreciate a legible presenter form; an orderly, precisely drawn map; well-packaged and well-organized slides; and simple explanations for anything on histology, such as actinic keratoses or nevi that might be mistaken for a tumor, said Dr. Tiefenbrunn.
"Presentation matters," she said. "Reviewers are your colleagues who are just as busy as you. We want to whip through these cases and just circle ‘satisfactory’ and go home."
Dr. Tiefenbrunn reported no relevant financial disclosures.
SAN DIEGO – If you want to receive a coveted "satisfactory" grade from peer reviewers of the American Society for Mohs Surgery, "keep it simple," advised Dr. Sharon F. Tiefenbrunn, a member of the ASMS peer review committee..
"The goal of this is to show us that you can recognize a perfect case and can produce a perfect case," she said at a meeting sponsored by the ASMS.
Highly complex or controversial cases are frequently "unreviewable," she noted.
"We don’t want your greatest case, where you worked until almost midnight, and it took 10 stages to clear, and the patient had to have a free flap to repair the defect, and you were ready to tear out your hair and swear off Mohs forever," stressed Dr. Tiefenbrunn, a procedural dermatologist in private practice in St. Louis.
Instead, peer reviewers want to see a stage II to III Mohs case, with tumor evident on stage I and a tumor-free final stage, she said.
Dr. Tiefenbrunn explained that the peer review program was launched in 2000, reviewing cases from the previous year. Its purpose is to improve the quality of Mohs surgery, track the organization’s success in teaching Mohs techniques, and provide practitioners with one of the two episodes of peer review required by the Clinical Laboratory Improvement Act (CLIA).
Cases are submitted to the ASMS administrative office and cycled to reviewers, who classify them as satisfactory, unreviewable, or "comments only."
A typical comment might be: "not enough overlap to determine clear margin." Such cases are sent to the peer review chairman, who forwards the case, along with a critique, back to the presenter.
In essence, a "comments" case fails to meet peer review standards, while an "unreviewable" case potentially might be corrected according to reviewers’ comments and resubmitted, said Dr. Tiefenbrunn.
Satisfactory cases demonstrate use of standard Mohs technique, have a minimal number of slides, and represent noncontroversial histology.
Some common reasons that cases are judged "unreviewable" include problems with the tumor map and ink legend, failure to mark the tumor on the map, unlabeled sections, confusing slide labeling, use of a nonstandard Mohs technique, bubbles, or a failure to identify tumor on stage I.
Dr. Tiefenbrunn reminded attendees of several cardinal rules, among them the need to include a complete skin edge (at least 90%), a complete deep margin, visible structural details, an adequate stain, visible ink for orientation, and a stage II showing a 2.5-mm margin in every direction.
Reviewers appreciate a legible presenter form; an orderly, precisely drawn map; well-packaged and well-organized slides; and simple explanations for anything on histology, such as actinic keratoses or nevi that might be mistaken for a tumor, said Dr. Tiefenbrunn.
"Presentation matters," she said. "Reviewers are your colleagues who are just as busy as you. We want to whip through these cases and just circle ‘satisfactory’ and go home."
Dr. Tiefenbrunn reported no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING SPONSORED BY THE AMERICAN SOCIETY FOR MOHS SURGERY
Neck Liposuction: A 'Home Run' Dermatologic Surgery Procedure
LISBON – Neck liposuction using tumescent local anesthesia is the cosmetic dermatology procedure having the optimal combination of high patient satisfaction, minimal complications, and a short learning curve.
"What I consider to be the No. 1, home-run procedure in all of dermatosurgery is liposuction of the neck," Dr. C. William Hanke, a dermatologic surgeon, said during a plenary lecture at the annual congress of the European Academy of Dermatology and Venereology.
"A long, youthful neck is felt to be a sign of beauty. When patients lose that – when their neck fills in with fat, and when the face and the neck become one – it’s not felt to be a sign of beauty. And that’s when liposuction of the neck comes in," explained Dr. Hanke of the Laser and Skin Surgery Center of Indiana, Carmel.
It is important to understand, however, that liposuction is no substitute for weight loss. The ideal candidate for neck liposuction is a young patient with good skin elasticity who has excess submandibular fat resulting in lost definition of the mandibular border.
Using liposuction to remove adipose tissue lying superficial to the platysmal muscle in such a patient, and redraping the skin to reduce the cervicomental angle to a well-defined 105-120 degrees with sharp mandibular demarcation, brings stellar cosmetic results.
In contrast, an elderly patient who is overweight or obese and has poor skin quality and redundant neck skin may need additional procedures, such as platysmal plication and laser resurfacing, he said.
Basically, neck liposuction entails filling the neck with tumescent anesthesia. "Any dermatologist can learn this," Dr. Hanke said. The fat is then suctioned using a combination of 1- to 3-mm cannulas with spatula tips placed through a primary entry point located in the mental crease. Additional holes can be placed for suctioning the lateral neck. The patient is entirely awake for the procedure, which can be performed in an office surgical suite, an ambulatory surgery center, or a hospital operating room.
"We sweep across the neck, suctioning the fat and transecting the septae that run through the fat. We can march into the jowls as well," he said.
Neuropraxia of the marginal mandibular nerve occurs in roughly 5% of cases of neck liposuction. The interruption of motor function typically lasts 4-6 weeks and is never permanent. The marginal mandibular nerve lies deep to the platysma, and the muscle would actually have to be punctured by the cannula to cause permanent nerve injury, Dr. Hanke said.
Immediately after the procedure he has patients wear a compression garment 24 hours a day for the first 1-2 days except while showering, then for 2-4 hours daily for 1-2 weeks. The compression garment helps in redraping the skin, prevents hematomas, speeds absorption of tumescent fluid, and prevents skin wrinkling.
Serious complications are exceedingly rare. In fact, in an early national survey of more than 15,000 patients treated with liposuction using tumescent local anesthesia, Dr. Hanke and coworkers reported no deaths or complications requiring hospital transfer (Dermatol. Surg. 1995;21:459-62).
The finding was confirmed in another national survey, this one involving nearly 67,000 liposuction procedures performed by dermatologic surgeons from 1994 to 2000 (Dermatol. Surg. 2002;28:971-8).
Occasionally, the platysmal bands are unmasked by neck liposuction. This is an unwelcome event, but marked improvement can be achieved through injection of small doses of botulinum toxin.
Dr. Hanke noted that he and Dr. William G. Stebbins recently performed an in-depth review of neck rejuvenation via liposuction, including proper patient selection, technical aspects of the procedure, postop care, and ancillary techniques (Dermatol. Ther. 2011;24:28-40).
Dr. Hanke reported having no financial conflicts of interest.
LISBON – Neck liposuction using tumescent local anesthesia is the cosmetic dermatology procedure having the optimal combination of high patient satisfaction, minimal complications, and a short learning curve.
"What I consider to be the No. 1, home-run procedure in all of dermatosurgery is liposuction of the neck," Dr. C. William Hanke, a dermatologic surgeon, said during a plenary lecture at the annual congress of the European Academy of Dermatology and Venereology.
"A long, youthful neck is felt to be a sign of beauty. When patients lose that – when their neck fills in with fat, and when the face and the neck become one – it’s not felt to be a sign of beauty. And that’s when liposuction of the neck comes in," explained Dr. Hanke of the Laser and Skin Surgery Center of Indiana, Carmel.
It is important to understand, however, that liposuction is no substitute for weight loss. The ideal candidate for neck liposuction is a young patient with good skin elasticity who has excess submandibular fat resulting in lost definition of the mandibular border.
Using liposuction to remove adipose tissue lying superficial to the platysmal muscle in such a patient, and redraping the skin to reduce the cervicomental angle to a well-defined 105-120 degrees with sharp mandibular demarcation, brings stellar cosmetic results.
In contrast, an elderly patient who is overweight or obese and has poor skin quality and redundant neck skin may need additional procedures, such as platysmal plication and laser resurfacing, he said.
Basically, neck liposuction entails filling the neck with tumescent anesthesia. "Any dermatologist can learn this," Dr. Hanke said. The fat is then suctioned using a combination of 1- to 3-mm cannulas with spatula tips placed through a primary entry point located in the mental crease. Additional holes can be placed for suctioning the lateral neck. The patient is entirely awake for the procedure, which can be performed in an office surgical suite, an ambulatory surgery center, or a hospital operating room.
"We sweep across the neck, suctioning the fat and transecting the septae that run through the fat. We can march into the jowls as well," he said.
Neuropraxia of the marginal mandibular nerve occurs in roughly 5% of cases of neck liposuction. The interruption of motor function typically lasts 4-6 weeks and is never permanent. The marginal mandibular nerve lies deep to the platysma, and the muscle would actually have to be punctured by the cannula to cause permanent nerve injury, Dr. Hanke said.
Immediately after the procedure he has patients wear a compression garment 24 hours a day for the first 1-2 days except while showering, then for 2-4 hours daily for 1-2 weeks. The compression garment helps in redraping the skin, prevents hematomas, speeds absorption of tumescent fluid, and prevents skin wrinkling.
Serious complications are exceedingly rare. In fact, in an early national survey of more than 15,000 patients treated with liposuction using tumescent local anesthesia, Dr. Hanke and coworkers reported no deaths or complications requiring hospital transfer (Dermatol. Surg. 1995;21:459-62).
The finding was confirmed in another national survey, this one involving nearly 67,000 liposuction procedures performed by dermatologic surgeons from 1994 to 2000 (Dermatol. Surg. 2002;28:971-8).
Occasionally, the platysmal bands are unmasked by neck liposuction. This is an unwelcome event, but marked improvement can be achieved through injection of small doses of botulinum toxin.
Dr. Hanke noted that he and Dr. William G. Stebbins recently performed an in-depth review of neck rejuvenation via liposuction, including proper patient selection, technical aspects of the procedure, postop care, and ancillary techniques (Dermatol. Ther. 2011;24:28-40).
Dr. Hanke reported having no financial conflicts of interest.
LISBON – Neck liposuction using tumescent local anesthesia is the cosmetic dermatology procedure having the optimal combination of high patient satisfaction, minimal complications, and a short learning curve.
"What I consider to be the No. 1, home-run procedure in all of dermatosurgery is liposuction of the neck," Dr. C. William Hanke, a dermatologic surgeon, said during a plenary lecture at the annual congress of the European Academy of Dermatology and Venereology.
"A long, youthful neck is felt to be a sign of beauty. When patients lose that – when their neck fills in with fat, and when the face and the neck become one – it’s not felt to be a sign of beauty. And that’s when liposuction of the neck comes in," explained Dr. Hanke of the Laser and Skin Surgery Center of Indiana, Carmel.
It is important to understand, however, that liposuction is no substitute for weight loss. The ideal candidate for neck liposuction is a young patient with good skin elasticity who has excess submandibular fat resulting in lost definition of the mandibular border.
Using liposuction to remove adipose tissue lying superficial to the platysmal muscle in such a patient, and redraping the skin to reduce the cervicomental angle to a well-defined 105-120 degrees with sharp mandibular demarcation, brings stellar cosmetic results.
In contrast, an elderly patient who is overweight or obese and has poor skin quality and redundant neck skin may need additional procedures, such as platysmal plication and laser resurfacing, he said.
Basically, neck liposuction entails filling the neck with tumescent anesthesia. "Any dermatologist can learn this," Dr. Hanke said. The fat is then suctioned using a combination of 1- to 3-mm cannulas with spatula tips placed through a primary entry point located in the mental crease. Additional holes can be placed for suctioning the lateral neck. The patient is entirely awake for the procedure, which can be performed in an office surgical suite, an ambulatory surgery center, or a hospital operating room.
"We sweep across the neck, suctioning the fat and transecting the septae that run through the fat. We can march into the jowls as well," he said.
Neuropraxia of the marginal mandibular nerve occurs in roughly 5% of cases of neck liposuction. The interruption of motor function typically lasts 4-6 weeks and is never permanent. The marginal mandibular nerve lies deep to the platysma, and the muscle would actually have to be punctured by the cannula to cause permanent nerve injury, Dr. Hanke said.
Immediately after the procedure he has patients wear a compression garment 24 hours a day for the first 1-2 days except while showering, then for 2-4 hours daily for 1-2 weeks. The compression garment helps in redraping the skin, prevents hematomas, speeds absorption of tumescent fluid, and prevents skin wrinkling.
Serious complications are exceedingly rare. In fact, in an early national survey of more than 15,000 patients treated with liposuction using tumescent local anesthesia, Dr. Hanke and coworkers reported no deaths or complications requiring hospital transfer (Dermatol. Surg. 1995;21:459-62).
The finding was confirmed in another national survey, this one involving nearly 67,000 liposuction procedures performed by dermatologic surgeons from 1994 to 2000 (Dermatol. Surg. 2002;28:971-8).
Occasionally, the platysmal bands are unmasked by neck liposuction. This is an unwelcome event, but marked improvement can be achieved through injection of small doses of botulinum toxin.
Dr. Hanke noted that he and Dr. William G. Stebbins recently performed an in-depth review of neck rejuvenation via liposuction, including proper patient selection, technical aspects of the procedure, postop care, and ancillary techniques (Dermatol. Ther. 2011;24:28-40).
Dr. Hanke reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL CONGRESS OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Role of Phototherapy in Patients with Skin of Color
Zain U. Syed, MD, and Iltefat H. Hamzavi, MD
Phototherapy has proven to be one of the most versatile and effective treatment options for a variety of inflammatory and pigmentary skin diseases. However, the use of these treatment modalities in patients of color requires some special considerations. The modality chosen, the dosing of the treatment and duration of treatment are all issues to be considered for patients of color treated with ultraviolet phototherapy. In addition, there are some diseases which are more commonly seen in patients of color. These diseases may have better treatment outcomes using newer phototherapeutic options such as the long pulsed Nd:YAG laser or UVA1. As our population in the United States becomes more diverse it would behoove all dermatologists to acquaint themselves with the special circumstances of treating ethnic patients with phototherapy.
*For a PDF of the full article, click on the link to the left of this introduction.
Zain U. Syed, MD, and Iltefat H. Hamzavi, MD
Phototherapy has proven to be one of the most versatile and effective treatment options for a variety of inflammatory and pigmentary skin diseases. However, the use of these treatment modalities in patients of color requires some special considerations. The modality chosen, the dosing of the treatment and duration of treatment are all issues to be considered for patients of color treated with ultraviolet phototherapy. In addition, there are some diseases which are more commonly seen in patients of color. These diseases may have better treatment outcomes using newer phototherapeutic options such as the long pulsed Nd:YAG laser or UVA1. As our population in the United States becomes more diverse it would behoove all dermatologists to acquaint themselves with the special circumstances of treating ethnic patients with phototherapy.
*For a PDF of the full article, click on the link to the left of this introduction.
Zain U. Syed, MD, and Iltefat H. Hamzavi, MD
Phototherapy has proven to be one of the most versatile and effective treatment options for a variety of inflammatory and pigmentary skin diseases. However, the use of these treatment modalities in patients of color requires some special considerations. The modality chosen, the dosing of the treatment and duration of treatment are all issues to be considered for patients of color treated with ultraviolet phototherapy. In addition, there are some diseases which are more commonly seen in patients of color. These diseases may have better treatment outcomes using newer phototherapeutic options such as the long pulsed Nd:YAG laser or UVA1. As our population in the United States becomes more diverse it would behoove all dermatologists to acquaint themselves with the special circumstances of treating ethnic patients with phototherapy.
*For a PDF of the full article, click on the link to the left of this introduction.
Update on Photodermatoses
Frank A. Santoro, MD, and Henry W. Lim, MD
Interactions with ultraviolet radiation (UVR) and chromophores in the skin happen on a daily basis. Photodermatoses, which are abnormal responses to UV exposure, can be classified into subgroups based on pathogenesis. This review will discuss the clinical features, pathogenesis, photobiologic evaluation, prognosis and therapies of the most common photodermatoses.
*For a PDF of the full article, click on the link to the left of this introduction.
Frank A. Santoro, MD, and Henry W. Lim, MD
Interactions with ultraviolet radiation (UVR) and chromophores in the skin happen on a daily basis. Photodermatoses, which are abnormal responses to UV exposure, can be classified into subgroups based on pathogenesis. This review will discuss the clinical features, pathogenesis, photobiologic evaluation, prognosis and therapies of the most common photodermatoses.
*For a PDF of the full article, click on the link to the left of this introduction.
Frank A. Santoro, MD, and Henry W. Lim, MD
Interactions with ultraviolet radiation (UVR) and chromophores in the skin happen on a daily basis. Photodermatoses, which are abnormal responses to UV exposure, can be classified into subgroups based on pathogenesis. This review will discuss the clinical features, pathogenesis, photobiologic evaluation, prognosis and therapies of the most common photodermatoses.
*For a PDF of the full article, click on the link to the left of this introduction.
In this review we will discuss the clinical features, pathogenesis, photobiologic evaluation, prognosis, and therapies of the more commonly encountered photodermatoses: polymorphous light eruption, chronic actinic dermatitis, solar urticarial, phototoxicity, photoallergy, porphyria cutanea tarda, and erythropoietic protoporphyria.