User login
Good Advice, Bad Advice?

Do you view your medical school and residency training the same way I see mine? I think I received really good training and education in the clinical knowledge base (e.g. which tests and drugs are useful in pneumonia) but really poor training and guidance into how to get the job done efficiently and organize my career. My problem was an inability to separate the good and bad advice about organizing my work; I essentially tried to follow all advice.
An energetic ENT attending who really seemed to care about students and trainees told me during my third year of medical school that failure to palpate the floor of the mouth on every new patient was a failure to do an adequate exam, not just on the ENT service but also on every patient in the hospital. While less dogmatic about it, he also encouraged documenting the presence or absence of a Darwinian tubercle. So I was determined to do these things—on all patients. No shortcuts for me!
But on my next rotation a few weeks later, I noticed that none of the neurosurgery attendings palpated the floor of the mouth on their patients. I stopped doing it routinely not long after.
By the time I was a resident, I was catching on to the fact that, like the ENT attending, my superiors were sometimes providing misguided, or even bad, advice. Meanwhile, I got a little better at knowing the difference. If I didn’t hear the same advice from multiple people, I gave it much less credibility. But if enough different people gave me advice, I typically accepted it as well-founded and tried to follow it.
Bad Advice: Keeping Up with the Literature
There must have been dozens of people who told me that the best strategy to keep up with the medical literature was to pick one, maybe two, medical journals with original scientific research and read all the articles in every issue. So that is exactly what I tried to do.
But after a few years, I decided that “pick one journal and read every issue” was bad advice. I think it is a poor way for most doctors in community practice to keep up with the latest and most important information. How many of us can really understand the strengths and weaknesses of study design and statistics? For example, outside of those who spend their career writing and analyzing original research (and are proficient in the complex and counterintuitive statistics they contain), how many of us have been able to make sense of all the conflicting studies of perioperative beta-blocker use? Outcomes of these studies vary a lot. So what should we do in clinical practice?
Better Advice: Keep Up with Literature
I finally concluded that in the pre-Internet era, the best way to keep up was to let academicians and researchers study the original research articles and write review articles, editorials, and letters to the editor. These seemed to pay much greater dividends in improving my clinical practice.
The traditional literature sources I’ve relied on for these kinds of articles are the New England Journal of Medicine, Annals of Internal Medicine, and the Cleveland Clinic Journal of Medicine. The latter is my favorite; it provides concise articles written to address very focused questions that come up all the time in my practice.
Since the arrival of the Internet, there are so many more ways to keep up with literature other than just deciding which journals and articles you’ll read. I’ll leave it to others to provide thoughts about that.
Get a Gimmick: Good Advice?
It was a tradition in my residency that at the end of a month “on the wards,” the attending (who rounded with us seven days a week for the whole month) took the whole team out to lunch or dinner. I think this once-common tradition has largely disappeared as a result of both the residency work-hour restrictions and attendings usually staying “on service” for only a couple of weeks, rather than the whole month. Right? (I’d love to hear from someone at a place where the attending-led, end-of-the-month team social event is still a common practice.)
On every such occasion, I would ask the attending, “What do you know now about ensuring a good career as a doctor that you wish you knew when you were a resident?” A number of the attendings didn’t seem willing to give it much thought: “I dunno,” most would say. “Maybe just make sure to leave time for nonprofessional activities like regular exercise.” Others gave generic advice: “Be sure to keep up with the literature.”
But one successful GI attending surprised me. When asked to provide career advice, he said, “Get a gimmick.” This is not what a young and idealistic trainee wanted to hear. A gimmick sounds like cheating or taking a shortcut.
He went on to explain that he meant that focusing only on being a good doctor for the next patient on your list, although it might be the most important thing you can do, might not be enough to keep your career interesting and energizing. So he advocated for finding an additional special interest, such as becoming a super-expert in a particular disease (e.g. you’re the snakebite expert at your hospital) or becoming a quality-improvement (QI) expert for your institution.
I’ve since fully embraced this idea and consider it among the best pearls of wisdom I’ve collected in my career. But “gimmick” is probably the wrong word choice; maybe it’s better to just say that you should get a special interest.
It would be best if you are the only one, or one of only a few, who pursues an area of interest at your institution. It can be rewarding to be the “go-to guy” for certain issues. And it might even lead to invitations to speak on the topic elsewhere, additional compensation, etc.
For nonacademic hospitalists, most of us will see our direct-patient-care activities as the core of what defines our career. I do many things other than patient care, but when I’m asked by a stranger about my occupation, I almost always end up talking about being a doctor who takes care of hospitalized patients. But my non-patient-care activities, my “gimmicks,” have been vitally important and satisfying components of my career.
If I were an attending at an end-of-the-month dinner with my team, I would talk with them about the value of developing these additional interests as part of a healthy and balanced career. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Do you view your medical school and residency training the same way I see mine? I think I received really good training and education in the clinical knowledge base (e.g. which tests and drugs are useful in pneumonia) but really poor training and guidance into how to get the job done efficiently and organize my career. My problem was an inability to separate the good and bad advice about organizing my work; I essentially tried to follow all advice.
An energetic ENT attending who really seemed to care about students and trainees told me during my third year of medical school that failure to palpate the floor of the mouth on every new patient was a failure to do an adequate exam, not just on the ENT service but also on every patient in the hospital. While less dogmatic about it, he also encouraged documenting the presence or absence of a Darwinian tubercle. So I was determined to do these things—on all patients. No shortcuts for me!
But on my next rotation a few weeks later, I noticed that none of the neurosurgery attendings palpated the floor of the mouth on their patients. I stopped doing it routinely not long after.
By the time I was a resident, I was catching on to the fact that, like the ENT attending, my superiors were sometimes providing misguided, or even bad, advice. Meanwhile, I got a little better at knowing the difference. If I didn’t hear the same advice from multiple people, I gave it much less credibility. But if enough different people gave me advice, I typically accepted it as well-founded and tried to follow it.
Bad Advice: Keeping Up with the Literature
There must have been dozens of people who told me that the best strategy to keep up with the medical literature was to pick one, maybe two, medical journals with original scientific research and read all the articles in every issue. So that is exactly what I tried to do.
But after a few years, I decided that “pick one journal and read every issue” was bad advice. I think it is a poor way for most doctors in community practice to keep up with the latest and most important information. How many of us can really understand the strengths and weaknesses of study design and statistics? For example, outside of those who spend their career writing and analyzing original research (and are proficient in the complex and counterintuitive statistics they contain), how many of us have been able to make sense of all the conflicting studies of perioperative beta-blocker use? Outcomes of these studies vary a lot. So what should we do in clinical practice?
Better Advice: Keep Up with Literature
I finally concluded that in the pre-Internet era, the best way to keep up was to let academicians and researchers study the original research articles and write review articles, editorials, and letters to the editor. These seemed to pay much greater dividends in improving my clinical practice.
The traditional literature sources I’ve relied on for these kinds of articles are the New England Journal of Medicine, Annals of Internal Medicine, and the Cleveland Clinic Journal of Medicine. The latter is my favorite; it provides concise articles written to address very focused questions that come up all the time in my practice.
Since the arrival of the Internet, there are so many more ways to keep up with literature other than just deciding which journals and articles you’ll read. I’ll leave it to others to provide thoughts about that.
Get a Gimmick: Good Advice?
It was a tradition in my residency that at the end of a month “on the wards,” the attending (who rounded with us seven days a week for the whole month) took the whole team out to lunch or dinner. I think this once-common tradition has largely disappeared as a result of both the residency work-hour restrictions and attendings usually staying “on service” for only a couple of weeks, rather than the whole month. Right? (I’d love to hear from someone at a place where the attending-led, end-of-the-month team social event is still a common practice.)
On every such occasion, I would ask the attending, “What do you know now about ensuring a good career as a doctor that you wish you knew when you were a resident?” A number of the attendings didn’t seem willing to give it much thought: “I dunno,” most would say. “Maybe just make sure to leave time for nonprofessional activities like regular exercise.” Others gave generic advice: “Be sure to keep up with the literature.”
But one successful GI attending surprised me. When asked to provide career advice, he said, “Get a gimmick.” This is not what a young and idealistic trainee wanted to hear. A gimmick sounds like cheating or taking a shortcut.
He went on to explain that he meant that focusing only on being a good doctor for the next patient on your list, although it might be the most important thing you can do, might not be enough to keep your career interesting and energizing. So he advocated for finding an additional special interest, such as becoming a super-expert in a particular disease (e.g. you’re the snakebite expert at your hospital) or becoming a quality-improvement (QI) expert for your institution.
I’ve since fully embraced this idea and consider it among the best pearls of wisdom I’ve collected in my career. But “gimmick” is probably the wrong word choice; maybe it’s better to just say that you should get a special interest.
It would be best if you are the only one, or one of only a few, who pursues an area of interest at your institution. It can be rewarding to be the “go-to guy” for certain issues. And it might even lead to invitations to speak on the topic elsewhere, additional compensation, etc.
For nonacademic hospitalists, most of us will see our direct-patient-care activities as the core of what defines our career. I do many things other than patient care, but when I’m asked by a stranger about my occupation, I almost always end up talking about being a doctor who takes care of hospitalized patients. But my non-patient-care activities, my “gimmicks,” have been vitally important and satisfying components of my career.
If I were an attending at an end-of-the-month dinner with my team, I would talk with them about the value of developing these additional interests as part of a healthy and balanced career. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Do you view your medical school and residency training the same way I see mine? I think I received really good training and education in the clinical knowledge base (e.g. which tests and drugs are useful in pneumonia) but really poor training and guidance into how to get the job done efficiently and organize my career. My problem was an inability to separate the good and bad advice about organizing my work; I essentially tried to follow all advice.
An energetic ENT attending who really seemed to care about students and trainees told me during my third year of medical school that failure to palpate the floor of the mouth on every new patient was a failure to do an adequate exam, not just on the ENT service but also on every patient in the hospital. While less dogmatic about it, he also encouraged documenting the presence or absence of a Darwinian tubercle. So I was determined to do these things—on all patients. No shortcuts for me!
But on my next rotation a few weeks later, I noticed that none of the neurosurgery attendings palpated the floor of the mouth on their patients. I stopped doing it routinely not long after.
By the time I was a resident, I was catching on to the fact that, like the ENT attending, my superiors were sometimes providing misguided, or even bad, advice. Meanwhile, I got a little better at knowing the difference. If I didn’t hear the same advice from multiple people, I gave it much less credibility. But if enough different people gave me advice, I typically accepted it as well-founded and tried to follow it.
Bad Advice: Keeping Up with the Literature
There must have been dozens of people who told me that the best strategy to keep up with the medical literature was to pick one, maybe two, medical journals with original scientific research and read all the articles in every issue. So that is exactly what I tried to do.
But after a few years, I decided that “pick one journal and read every issue” was bad advice. I think it is a poor way for most doctors in community practice to keep up with the latest and most important information. How many of us can really understand the strengths and weaknesses of study design and statistics? For example, outside of those who spend their career writing and analyzing original research (and are proficient in the complex and counterintuitive statistics they contain), how many of us have been able to make sense of all the conflicting studies of perioperative beta-blocker use? Outcomes of these studies vary a lot. So what should we do in clinical practice?
Better Advice: Keep Up with Literature
I finally concluded that in the pre-Internet era, the best way to keep up was to let academicians and researchers study the original research articles and write review articles, editorials, and letters to the editor. These seemed to pay much greater dividends in improving my clinical practice.
The traditional literature sources I’ve relied on for these kinds of articles are the New England Journal of Medicine, Annals of Internal Medicine, and the Cleveland Clinic Journal of Medicine. The latter is my favorite; it provides concise articles written to address very focused questions that come up all the time in my practice.
Since the arrival of the Internet, there are so many more ways to keep up with literature other than just deciding which journals and articles you’ll read. I’ll leave it to others to provide thoughts about that.
Get a Gimmick: Good Advice?
It was a tradition in my residency that at the end of a month “on the wards,” the attending (who rounded with us seven days a week for the whole month) took the whole team out to lunch or dinner. I think this once-common tradition has largely disappeared as a result of both the residency work-hour restrictions and attendings usually staying “on service” for only a couple of weeks, rather than the whole month. Right? (I’d love to hear from someone at a place where the attending-led, end-of-the-month team social event is still a common practice.)
On every such occasion, I would ask the attending, “What do you know now about ensuring a good career as a doctor that you wish you knew when you were a resident?” A number of the attendings didn’t seem willing to give it much thought: “I dunno,” most would say. “Maybe just make sure to leave time for nonprofessional activities like regular exercise.” Others gave generic advice: “Be sure to keep up with the literature.”
But one successful GI attending surprised me. When asked to provide career advice, he said, “Get a gimmick.” This is not what a young and idealistic trainee wanted to hear. A gimmick sounds like cheating or taking a shortcut.
He went on to explain that he meant that focusing only on being a good doctor for the next patient on your list, although it might be the most important thing you can do, might not be enough to keep your career interesting and energizing. So he advocated for finding an additional special interest, such as becoming a super-expert in a particular disease (e.g. you’re the snakebite expert at your hospital) or becoming a quality-improvement (QI) expert for your institution.
I’ve since fully embraced this idea and consider it among the best pearls of wisdom I’ve collected in my career. But “gimmick” is probably the wrong word choice; maybe it’s better to just say that you should get a special interest.
It would be best if you are the only one, or one of only a few, who pursues an area of interest at your institution. It can be rewarding to be the “go-to guy” for certain issues. And it might even lead to invitations to speak on the topic elsewhere, additional compensation, etc.
For nonacademic hospitalists, most of us will see our direct-patient-care activities as the core of what defines our career. I do many things other than patient care, but when I’m asked by a stranger about my occupation, I almost always end up talking about being a doctor who takes care of hospitalized patients. But my non-patient-care activities, my “gimmicks,” have been vitally important and satisfying components of my career.
If I were an attending at an end-of-the-month dinner with my team, I would talk with them about the value of developing these additional interests as part of a healthy and balanced career. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Establish Clear Goals Before Changing Improvement Projects

I recently was appointed the director of my hospitalist group at a 53-bed hospital in rural Wisconsin. Including myself, we have three hospitalist FTEs, one part-time hospitalist, and one nurse practitioner; we are all seasoned internists, but we are relatively new to HM and the 24/7 nature of the business. The hospital administration has charged me with making the program more efficient. What do you suggest I do to improve our efficiency and standard of patient care?
Andrew Neubauer, DO, MPH
Dr. Hospitalist responds: Congratulations aside, one of the first items at hand is to understand the question being asked. Your hospital administration potentially has many moving parts: a CEO for vision, a chief operating officer (COO) for execution, a chief medical officer (CMO) for medical staff initiatives, and a chief financial officer (CFO) for the hard truth of hospital finances.
Before you take any steps to improve efficiency, you need to ask what “efficiency” means.
- Is it the CFO asking for better financial returns?
- Is the CEO trying to woo a large surgical group and needs to tout his high-functioning hospitalist group to make it more attractive?
- Does the CMO want to improve staff relations and primary-care referrals?
- Does the COO want higher patient satisfaction?
Whatever the answer is, the first thing to do is define the question. So, in a non-confrontational, inquisitive way, ask your administrators what they mean by “efficiency.”
The immediate corollary to this is that you must then get baseline data. You have to know where you are starting from in order to show demonstrable progress toward a goal. Whether it’s the case-mix index, the readmission rate, or adherence to protocols, defining the baseline and the goal is paramount.
Why is this so important? You need to be able to prove you met the goals, because as soon as you meet this one, a new one will be placed in front of you.
Let’s assume, by way of example, that “efficiency” in this case means an earlier time of discharge. For starters, ask what the average time of discharge is now, how it is measured, what the desired result is, and why. Once you have that information, look for ways that your group can improve, and make sure that the hospital is measuring you only on things you can control. Your physicians can determine the time the discharge order is written, but they have no say in when the patient physically leaves the building. It might seem like a subtle distinction, but it can make all the difference depending on how “time of discharge” is defined. Don’t promise what you can’t deliver—you’ll disappoint both the hospital and your practice partners.
Going forward, you should keep a playbook of past goals asked of you, and your group’s actions. This is incredibly important if (when) your contract comes up for renewal, since you will need to gently (and sometimes forcefully) remind the hospital of your group’s value. In addition, the other main constant in any hospital administration is change; last I checked, the average tenure for a hospital CEO is four years. You want to always be able to communicate your group’s achievements to serve as a visible reminder of your central role in the hospital.
As the newly appointed medical director, everyone is looking to you for answers. Just make sure to focus on the question first. TH
I recently was appointed the director of my hospitalist group at a 53-bed hospital in rural Wisconsin. Including myself, we have three hospitalist FTEs, one part-time hospitalist, and one nurse practitioner; we are all seasoned internists, but we are relatively new to HM and the 24/7 nature of the business. The hospital administration has charged me with making the program more efficient. What do you suggest I do to improve our efficiency and standard of patient care?
Andrew Neubauer, DO, MPH
Dr. Hospitalist responds: Congratulations aside, one of the first items at hand is to understand the question being asked. Your hospital administration potentially has many moving parts: a CEO for vision, a chief operating officer (COO) for execution, a chief medical officer (CMO) for medical staff initiatives, and a chief financial officer (CFO) for the hard truth of hospital finances.
Before you take any steps to improve efficiency, you need to ask what “efficiency” means.
- Is it the CFO asking for better financial returns?
- Is the CEO trying to woo a large surgical group and needs to tout his high-functioning hospitalist group to make it more attractive?
- Does the CMO want to improve staff relations and primary-care referrals?
- Does the COO want higher patient satisfaction?
Whatever the answer is, the first thing to do is define the question. So, in a non-confrontational, inquisitive way, ask your administrators what they mean by “efficiency.”
The immediate corollary to this is that you must then get baseline data. You have to know where you are starting from in order to show demonstrable progress toward a goal. Whether it’s the case-mix index, the readmission rate, or adherence to protocols, defining the baseline and the goal is paramount.
Why is this so important? You need to be able to prove you met the goals, because as soon as you meet this one, a new one will be placed in front of you.
Let’s assume, by way of example, that “efficiency” in this case means an earlier time of discharge. For starters, ask what the average time of discharge is now, how it is measured, what the desired result is, and why. Once you have that information, look for ways that your group can improve, and make sure that the hospital is measuring you only on things you can control. Your physicians can determine the time the discharge order is written, but they have no say in when the patient physically leaves the building. It might seem like a subtle distinction, but it can make all the difference depending on how “time of discharge” is defined. Don’t promise what you can’t deliver—you’ll disappoint both the hospital and your practice partners.
Going forward, you should keep a playbook of past goals asked of you, and your group’s actions. This is incredibly important if (when) your contract comes up for renewal, since you will need to gently (and sometimes forcefully) remind the hospital of your group’s value. In addition, the other main constant in any hospital administration is change; last I checked, the average tenure for a hospital CEO is four years. You want to always be able to communicate your group’s achievements to serve as a visible reminder of your central role in the hospital.
As the newly appointed medical director, everyone is looking to you for answers. Just make sure to focus on the question first. TH
I recently was appointed the director of my hospitalist group at a 53-bed hospital in rural Wisconsin. Including myself, we have three hospitalist FTEs, one part-time hospitalist, and one nurse practitioner; we are all seasoned internists, but we are relatively new to HM and the 24/7 nature of the business. The hospital administration has charged me with making the program more efficient. What do you suggest I do to improve our efficiency and standard of patient care?
Andrew Neubauer, DO, MPH
Dr. Hospitalist responds: Congratulations aside, one of the first items at hand is to understand the question being asked. Your hospital administration potentially has many moving parts: a CEO for vision, a chief operating officer (COO) for execution, a chief medical officer (CMO) for medical staff initiatives, and a chief financial officer (CFO) for the hard truth of hospital finances.
Before you take any steps to improve efficiency, you need to ask what “efficiency” means.
- Is it the CFO asking for better financial returns?
- Is the CEO trying to woo a large surgical group and needs to tout his high-functioning hospitalist group to make it more attractive?
- Does the CMO want to improve staff relations and primary-care referrals?
- Does the COO want higher patient satisfaction?
Whatever the answer is, the first thing to do is define the question. So, in a non-confrontational, inquisitive way, ask your administrators what they mean by “efficiency.”
The immediate corollary to this is that you must then get baseline data. You have to know where you are starting from in order to show demonstrable progress toward a goal. Whether it’s the case-mix index, the readmission rate, or adherence to protocols, defining the baseline and the goal is paramount.
Why is this so important? You need to be able to prove you met the goals, because as soon as you meet this one, a new one will be placed in front of you.
Let’s assume, by way of example, that “efficiency” in this case means an earlier time of discharge. For starters, ask what the average time of discharge is now, how it is measured, what the desired result is, and why. Once you have that information, look for ways that your group can improve, and make sure that the hospital is measuring you only on things you can control. Your physicians can determine the time the discharge order is written, but they have no say in when the patient physically leaves the building. It might seem like a subtle distinction, but it can make all the difference depending on how “time of discharge” is defined. Don’t promise what you can’t deliver—you’ll disappoint both the hospital and your practice partners.
Going forward, you should keep a playbook of past goals asked of you, and your group’s actions. This is incredibly important if (when) your contract comes up for renewal, since you will need to gently (and sometimes forcefully) remind the hospital of your group’s value. In addition, the other main constant in any hospital administration is change; last I checked, the average tenure for a hospital CEO is four years. You want to always be able to communicate your group’s achievements to serve as a visible reminder of your central role in the hospital.
As the newly appointed medical director, everyone is looking to you for answers. Just make sure to focus on the question first. TH
Compartment Syndrome...
The Billing & Coding Bandwagon

It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?

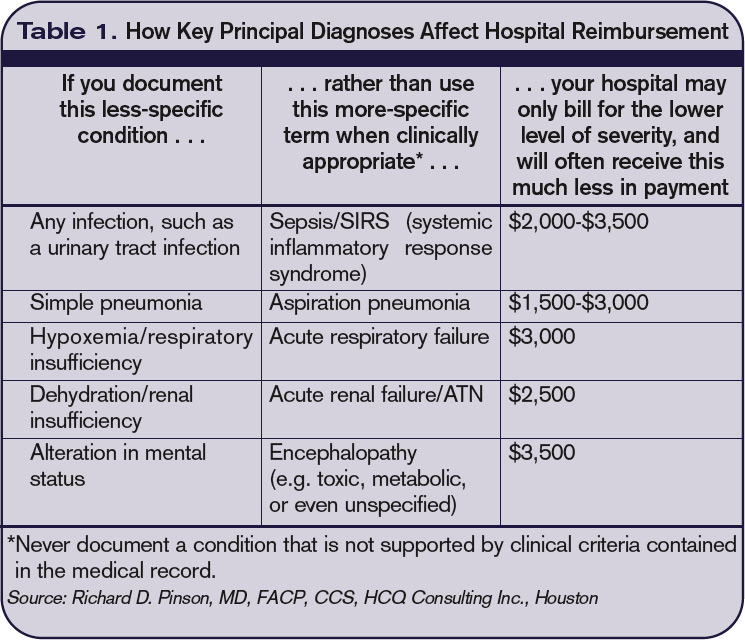
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset

Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.

Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
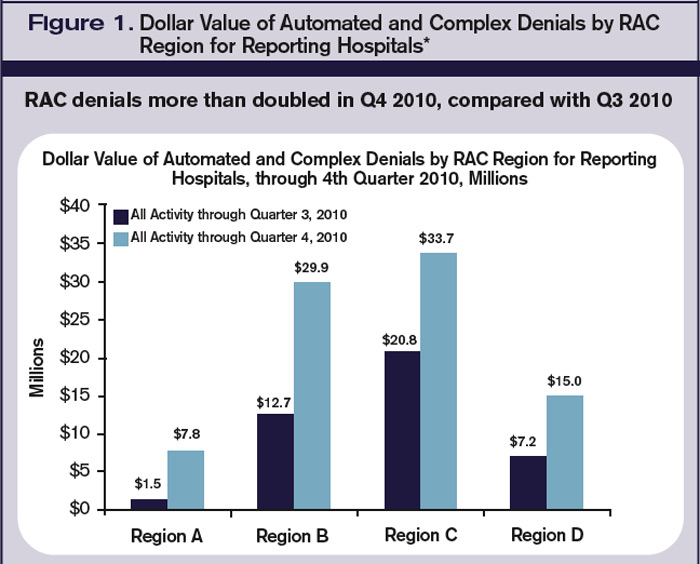
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
POLICY CORNER: new documentation requirement could burden hospitalists
As of April 1, physicians who order home care services for their Medicare patients are required to document that they had a face-to-face encounter with the patient prior to certifying the patient’s eligibility for home care services. The face-to-face encounter is a mandated provision of the Affordable Care Act (ACA) of 2010, which is intended to reduce fraud and abuse among home health providers.
Despite this goal, the new documentation requirement poses the threat of a significant paperwork burden on practitioners, including hospitalists.
Many providers have remained unaware of this new requirement, but those who are aware have been experiencing confusion as to what, if any, additional paperwork is required of physicians. SHM, along with the American Medical Association (AMA) and other physician groups, have requested clarification from the Centers for Medicare & Medicaid Services (CMS) regarding the documentation requirement. SHM also is advocating that CMS keep the additional paperwork burden to a minimum.
CMS denied a request to extend the implementation deadline to allow for more provider education. Despite denying the extension, CMS has committed to continue monitoring for problems and unintended consequences caused by the new requirement.
CMS also has clarified the face-to-face documentation requirements: “Physicians may attach existing documentation as long as it includes necessary information and evidences the need for home health services.”
An example would be for a physician to attach the patient’s discharge summary or relevant portion of the patient’s medical record that evidences the need for home health services. Instead of creating an entirely new document or filling out an additional form to evidence the face-to-face encounter, physicians will have some flexibility in determining the existing documentation they will use. This is an option that hopefully will reduce some of the burden.
CMS could produce further guidelines in the future. SHM intends to continue following the issue and advocating on behalf of hospitalists. For the most up-to-date information, visit http://questions.cms.hhs.gov and enter the search term “home health face-to-face.” TH
As of April 1, physicians who order home care services for their Medicare patients are required to document that they had a face-to-face encounter with the patient prior to certifying the patient’s eligibility for home care services. The face-to-face encounter is a mandated provision of the Affordable Care Act (ACA) of 2010, which is intended to reduce fraud and abuse among home health providers.
Despite this goal, the new documentation requirement poses the threat of a significant paperwork burden on practitioners, including hospitalists.
Many providers have remained unaware of this new requirement, but those who are aware have been experiencing confusion as to what, if any, additional paperwork is required of physicians. SHM, along with the American Medical Association (AMA) and other physician groups, have requested clarification from the Centers for Medicare & Medicaid Services (CMS) regarding the documentation requirement. SHM also is advocating that CMS keep the additional paperwork burden to a minimum.
CMS denied a request to extend the implementation deadline to allow for more provider education. Despite denying the extension, CMS has committed to continue monitoring for problems and unintended consequences caused by the new requirement.
CMS also has clarified the face-to-face documentation requirements: “Physicians may attach existing documentation as long as it includes necessary information and evidences the need for home health services.”
An example would be for a physician to attach the patient’s discharge summary or relevant portion of the patient’s medical record that evidences the need for home health services. Instead of creating an entirely new document or filling out an additional form to evidence the face-to-face encounter, physicians will have some flexibility in determining the existing documentation they will use. This is an option that hopefully will reduce some of the burden.
CMS could produce further guidelines in the future. SHM intends to continue following the issue and advocating on behalf of hospitalists. For the most up-to-date information, visit http://questions.cms.hhs.gov and enter the search term “home health face-to-face.” TH
As of April 1, physicians who order home care services for their Medicare patients are required to document that they had a face-to-face encounter with the patient prior to certifying the patient’s eligibility for home care services. The face-to-face encounter is a mandated provision of the Affordable Care Act (ACA) of 2010, which is intended to reduce fraud and abuse among home health providers.
Despite this goal, the new documentation requirement poses the threat of a significant paperwork burden on practitioners, including hospitalists.
Many providers have remained unaware of this new requirement, but those who are aware have been experiencing confusion as to what, if any, additional paperwork is required of physicians. SHM, along with the American Medical Association (AMA) and other physician groups, have requested clarification from the Centers for Medicare & Medicaid Services (CMS) regarding the documentation requirement. SHM also is advocating that CMS keep the additional paperwork burden to a minimum.
CMS denied a request to extend the implementation deadline to allow for more provider education. Despite denying the extension, CMS has committed to continue monitoring for problems and unintended consequences caused by the new requirement.
CMS also has clarified the face-to-face documentation requirements: “Physicians may attach existing documentation as long as it includes necessary information and evidences the need for home health services.”
An example would be for a physician to attach the patient’s discharge summary or relevant portion of the patient’s medical record that evidences the need for home health services. Instead of creating an entirely new document or filling out an additional form to evidence the face-to-face encounter, physicians will have some flexibility in determining the existing documentation they will use. This is an option that hopefully will reduce some of the burden.
CMS could produce further guidelines in the future. SHM intends to continue following the issue and advocating on behalf of hospitalists. For the most up-to-date information, visit http://questions.cms.hhs.gov and enter the search term “home health face-to-face.” TH
Due Diligence: Denials
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
The To-Don’t List, Part 2


A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
CMS Requires “In-Person Encounter” to Initiate Home Health Services

I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
I’ve been told by home health agencies that I have to fill out some additional paperwork to get my patients outpatient services. Can you explain to me what these new rules are all about?
Alicia Farrouk, MD
Evansville, Ind.
Dr. Hospitalist responds: In June 2010, the Affordable Care Act changed the rules regarding physician orders for durable medical equipment and for certifying or recertifying the need for home health services. Last November, the Center for Medicare & Medicaid Services (CMS) published the final rules in the Federal Register.
The new law went into effect Jan. 1, and I suspect that is why you have been asked to adjust the way you fill out your paperwork. The upshot of the change in the law is that providers can no longer use the discharge plan or transfer form as evidence of “certification” of need for home health services. The ordering provider, as a condition for payment for services, must document an in-person encounter within the 90 days prior or 30 days after the initiation of home health services. The documentation must detail the clinical findings supporting the need for home health services.
If you are a hospitalist and discharging the patient from the hospital but will not be following the patient as an outpatient, you must document the name of the primary-care physician (PCP) who will follow the patient’s need for home health services and initiate the order and plan of care. The PCP will then sign the home health certification and document that they reviewed your note and plan for home health services and agree with the plan.
If you are a hospitalist working in a teaching hospital, the resident can fill out the form, but it must list your name (as attending physician) and your NPI number. This new rule applies only to home health services and durable medical equipment (things that can be used over and over again for medical purposes, such as crutches, walkers, wheelchairs, etc.) but does not include drugs or supplemental oxygen.
HM Model Spreads to Surgical Specialists
I have a friend who told me there is a neurologist in the hospital where he works who I understand is calling himself a hospitalist. What gives? I thought hospitalists were all internists or family physicians.
Bill Mulley, MD
Flagstaff, Ariz.
Dr. Hospitalist responds: The vast majority of hospitalists in the U.S. are general internists. There are smaller numbers of family physicians, pediatricians, and medical subspecialists who also work as hospitalists. Although this is the face of HM in America, we are seeing other fields of medicine adopting this model of care.
I know of surgical hospitalists, OB-GYN hospitalists, and yes, even neurohospitalists (see “Generation Next,” October 2010, p. 1). It is hard for some people to get their heads around the notion of a surgeon as a hospitalist because when one thinks of a surgeon, you are thinking of a physician who works in the operating room. But the traditional surgeon also has a clinic where they provide pre- and post-operative care.
Herein lies the difference between traditional surgeons and surgical hospitalists: The surgical hospitalist is, for the most part, only doing work in the hospital—sound familiar? (Think traditional internist vs. internist working as hospitalist.) The traditional general surgeon performs scheduled elective surgeries and typically only does emergency surgeries when they are on call for the hospital. As I understand it, the life of a surgical hospitalist is spending a shift in the hospital waiting for a patient to show up needing emergency surgery.
The hospital CEO today has increasing challenges convincing physicians to take hospital call. Some find themselves paying sizable sums of money for surgeons to take call from home. Some have decided their money is better spent paying for surgical hospitalists to spend nights in the hospital waiting for their pager to go off.
From a patient’s perspective, this seems to be a no-brainer. Having a surgeon in the hospital increases their chances of more timely care. You have to believe the providers in the ED and the medical hospitalist also love having a surgeon in-house, available to provide consults when requested.
I am a bit surprised that we don’t already have a large number of surgical hospitalists in the country. Then again, I have no idea of how many surgeons are working as surgical hospitalists. I am not sure anybody knows that answer.
There is a belief that we are going to see the continued growth of “specialty hospitalists” in the U.S. I believe we are going to see neurohospitalists managing inpatients with stroke and other neurosurgical issues, working side by side with medical hospitalists. I share in the excitement that was pervasive in the early days of the hospitalist movement, even though I’m not sure what we are going to see next.
I never imagined that we would have more than 30,000 hospitalists, as we do today. But while the HM model can help improve care, I will always feel strongly that no system will improve care without the dedication of motivated and compassionate healthcare providers driving the system. TH
Alleged violation of EMTALA...
The Comanagement Conundrum

As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.

Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”

Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying

Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.

Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”

For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB
As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.
Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”
Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying
Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.
Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”
For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB
As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.
Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”
Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying
Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.
Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”
For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB