User login
CMS’ proposal to pay for care coordination: the ACO bridge?
Betting that it will more than pay for itself in savings, on July 5 the Centers for Medicare and Medicaid Services issued a proposed rule to pay physicians for non–face-to-face chronic care management. This would cover such things as development of care plans, reports on a patient’s status, coordination along the care continuum, and integration of health information across settings.
The proposal requires the patient to have had an annual Medicare wellness visit in the last 12 months. In addition, the physician must meet electronic health record (EHR) meaningful use standards and must have care coordinators who assist in care for patients with complex chronic conditions. CMS believes that these efforts, heretofore largely not reimbursed under the fee-for-service system, will actually end up reducing spending while simultaneously improving quality. How? By reducing downstream costs through reduced hospitalizations, the use of post–acute care services, and reduced emergency department visits. The public may comment until Sept. 6, 2013. The final policies will be issued in November and go into effect in 2015.
An ACO bridge? Readers of this column know that this pretty much describes the success strategy for a primary care physician–led accountable care organization (ACO) (less the webbing of joint financial accountability, a common technology platform, access to a full patient population, and the expense of setting one up).
What is great is that this is a relatively painless way for primary care physicians to get compensation to change behavior patterns in ways Dr. Jeffrey Cain, president of the American Academy of Family Physicians, declares necessary for primary care’s "survival." It will further prove the value proposition of the medical home model. The benefits then can be leveraged through common pursuit with colleagues of care coordination for a patient population empowered by data, best practices, and resources of a primary care–led ACO.
While the final details of the CMS proposal will not be known until the fall, presumably primary care physicians could obtain both up-front payment for non–face-to-face chronic care management and qualify for ACO shared savings distributions on the back end.
Worst case, the final rules will be unworkably burdensome. Better case, recognition of the "value" of the medical home model is being recognized. Best case, this is a nice bridge for physicians to develop the habits to thrive in the accountable-care era while getting paid to do it.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612).
Betting that it will more than pay for itself in savings, on July 5 the Centers for Medicare and Medicaid Services issued a proposed rule to pay physicians for non–face-to-face chronic care management. This would cover such things as development of care plans, reports on a patient’s status, coordination along the care continuum, and integration of health information across settings.
The proposal requires the patient to have had an annual Medicare wellness visit in the last 12 months. In addition, the physician must meet electronic health record (EHR) meaningful use standards and must have care coordinators who assist in care for patients with complex chronic conditions. CMS believes that these efforts, heretofore largely not reimbursed under the fee-for-service system, will actually end up reducing spending while simultaneously improving quality. How? By reducing downstream costs through reduced hospitalizations, the use of post–acute care services, and reduced emergency department visits. The public may comment until Sept. 6, 2013. The final policies will be issued in November and go into effect in 2015.
An ACO bridge? Readers of this column know that this pretty much describes the success strategy for a primary care physician–led accountable care organization (ACO) (less the webbing of joint financial accountability, a common technology platform, access to a full patient population, and the expense of setting one up).
What is great is that this is a relatively painless way for primary care physicians to get compensation to change behavior patterns in ways Dr. Jeffrey Cain, president of the American Academy of Family Physicians, declares necessary for primary care’s "survival." It will further prove the value proposition of the medical home model. The benefits then can be leveraged through common pursuit with colleagues of care coordination for a patient population empowered by data, best practices, and resources of a primary care–led ACO.
While the final details of the CMS proposal will not be known until the fall, presumably primary care physicians could obtain both up-front payment for non–face-to-face chronic care management and qualify for ACO shared savings distributions on the back end.
Worst case, the final rules will be unworkably burdensome. Better case, recognition of the "value" of the medical home model is being recognized. Best case, this is a nice bridge for physicians to develop the habits to thrive in the accountable-care era while getting paid to do it.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612).
Betting that it will more than pay for itself in savings, on July 5 the Centers for Medicare and Medicaid Services issued a proposed rule to pay physicians for non–face-to-face chronic care management. This would cover such things as development of care plans, reports on a patient’s status, coordination along the care continuum, and integration of health information across settings.
The proposal requires the patient to have had an annual Medicare wellness visit in the last 12 months. In addition, the physician must meet electronic health record (EHR) meaningful use standards and must have care coordinators who assist in care for patients with complex chronic conditions. CMS believes that these efforts, heretofore largely not reimbursed under the fee-for-service system, will actually end up reducing spending while simultaneously improving quality. How? By reducing downstream costs through reduced hospitalizations, the use of post–acute care services, and reduced emergency department visits. The public may comment until Sept. 6, 2013. The final policies will be issued in November and go into effect in 2015.
An ACO bridge? Readers of this column know that this pretty much describes the success strategy for a primary care physician–led accountable care organization (ACO) (less the webbing of joint financial accountability, a common technology platform, access to a full patient population, and the expense of setting one up).
What is great is that this is a relatively painless way for primary care physicians to get compensation to change behavior patterns in ways Dr. Jeffrey Cain, president of the American Academy of Family Physicians, declares necessary for primary care’s "survival." It will further prove the value proposition of the medical home model. The benefits then can be leveraged through common pursuit with colleagues of care coordination for a patient population empowered by data, best practices, and resources of a primary care–led ACO.
While the final details of the CMS proposal will not be known until the fall, presumably primary care physicians could obtain both up-front payment for non–face-to-face chronic care management and qualify for ACO shared savings distributions on the back end.
Worst case, the final rules will be unworkably burdensome. Better case, recognition of the "value" of the medical home model is being recognized. Best case, this is a nice bridge for physicians to develop the habits to thrive in the accountable-care era while getting paid to do it.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612).

Empathy: Getting Past the Fluff
There has been a lot of recent news about empathy in the medical and lay press; likely because it translates into better patient satisfaction ratings (think Press-Ganey’s mission) and improved institutional finances (think patient compliance and reduced medical malpractice claims). However, isn’t empathy just a bunch of touchy-feely vegans (no-offense) talking about stuff that really doesn’t matter in the long run? Let’s see!
A working definition would be a good place to start. Empathy is actually a “cognitive” event whereby the clinician (us) “understands” what patients are feeling, but does not actually “feel” what they are feeling. Feeling a patient’s pain is considered sympathy, and too much of this leads one down the road to extra testing and/or procedures. So, how can understanding a patient’s feelings improve your patient satisfaction ratings (and maybe your pay or bonus) and keep a subpoena out of your future?
1. Recent studies reveal that physicians (insert PAs or NPs) with higher empathy scores have better clinical outcomes in improving their patients’ compliance with chronic disease management such as diabetes mellitus as well as improved advice or instruction retention in mothers with sick children. This means better A1Cs and less re-admits for sick kids.
2. Studies further reveal that empathetic residents and physicians have far fewer conversations with risk managers and are rarely sued. Lower lawsuit risks are less dependent upon severity of the medical/surgical outcome and more closely tied to empathetic behaviors; listening, eye-contact, a simple human touch, and returning phone calls. You got it, showing genuine concern and warmth (even after a long surgery) promotes a strong and trusting relationship, allowing you to do your job without adverse outcomes.
3. But does empathy actually affect you as a physician assistant or nurse practitioner? Well, yes it does. Simply being empathetic in your daily practice reduces your stress level. You say, ‘come on!’ Studies of medical residents support statistically lower medical errors, improved personal life, less depression, and greater career satisfaction in those scoring higher on a highly validated and reliable empathy survey.
4. Well, we all know that listening to your patient eats into lunch time and gets you home even later than usual. Not so. Allowing patients to present their narrative results in a better history and permits the PA/NP to actively listen and digest the information. Patients feel the difference and the time it takes, and you may find yourself ahead on the clock as well as feel better about your own performance.
Being the empathetic PA that I am (harrumph) let me and others know your feelings about empathy in your practice. Feel free to nicely and anonymously lambast, (oops I mean describe) empathy stories in your clinical world. The good and the bad are welcome! Really.
There has been a lot of recent news about empathy in the medical and lay press; likely because it translates into better patient satisfaction ratings (think Press-Ganey’s mission) and improved institutional finances (think patient compliance and reduced medical malpractice claims). However, isn’t empathy just a bunch of touchy-feely vegans (no-offense) talking about stuff that really doesn’t matter in the long run? Let’s see!
A working definition would be a good place to start. Empathy is actually a “cognitive” event whereby the clinician (us) “understands” what patients are feeling, but does not actually “feel” what they are feeling. Feeling a patient’s pain is considered sympathy, and too much of this leads one down the road to extra testing and/or procedures. So, how can understanding a patient’s feelings improve your patient satisfaction ratings (and maybe your pay or bonus) and keep a subpoena out of your future?
1. Recent studies reveal that physicians (insert PAs or NPs) with higher empathy scores have better clinical outcomes in improving their patients’ compliance with chronic disease management such as diabetes mellitus as well as improved advice or instruction retention in mothers with sick children. This means better A1Cs and less re-admits for sick kids.
2. Studies further reveal that empathetic residents and physicians have far fewer conversations with risk managers and are rarely sued. Lower lawsuit risks are less dependent upon severity of the medical/surgical outcome and more closely tied to empathetic behaviors; listening, eye-contact, a simple human touch, and returning phone calls. You got it, showing genuine concern and warmth (even after a long surgery) promotes a strong and trusting relationship, allowing you to do your job without adverse outcomes.
3. But does empathy actually affect you as a physician assistant or nurse practitioner? Well, yes it does. Simply being empathetic in your daily practice reduces your stress level. You say, ‘come on!’ Studies of medical residents support statistically lower medical errors, improved personal life, less depression, and greater career satisfaction in those scoring higher on a highly validated and reliable empathy survey.
4. Well, we all know that listening to your patient eats into lunch time and gets you home even later than usual. Not so. Allowing patients to present their narrative results in a better history and permits the PA/NP to actively listen and digest the information. Patients feel the difference and the time it takes, and you may find yourself ahead on the clock as well as feel better about your own performance.
Being the empathetic PA that I am (harrumph) let me and others know your feelings about empathy in your practice. Feel free to nicely and anonymously lambast, (oops I mean describe) empathy stories in your clinical world. The good and the bad are welcome! Really.
There has been a lot of recent news about empathy in the medical and lay press; likely because it translates into better patient satisfaction ratings (think Press-Ganey’s mission) and improved institutional finances (think patient compliance and reduced medical malpractice claims). However, isn’t empathy just a bunch of touchy-feely vegans (no-offense) talking about stuff that really doesn’t matter in the long run? Let’s see!
A working definition would be a good place to start. Empathy is actually a “cognitive” event whereby the clinician (us) “understands” what patients are feeling, but does not actually “feel” what they are feeling. Feeling a patient’s pain is considered sympathy, and too much of this leads one down the road to extra testing and/or procedures. So, how can understanding a patient’s feelings improve your patient satisfaction ratings (and maybe your pay or bonus) and keep a subpoena out of your future?
1. Recent studies reveal that physicians (insert PAs or NPs) with higher empathy scores have better clinical outcomes in improving their patients’ compliance with chronic disease management such as diabetes mellitus as well as improved advice or instruction retention in mothers with sick children. This means better A1Cs and less re-admits for sick kids.
2. Studies further reveal that empathetic residents and physicians have far fewer conversations with risk managers and are rarely sued. Lower lawsuit risks are less dependent upon severity of the medical/surgical outcome and more closely tied to empathetic behaviors; listening, eye-contact, a simple human touch, and returning phone calls. You got it, showing genuine concern and warmth (even after a long surgery) promotes a strong and trusting relationship, allowing you to do your job without adverse outcomes.
3. But does empathy actually affect you as a physician assistant or nurse practitioner? Well, yes it does. Simply being empathetic in your daily practice reduces your stress level. You say, ‘come on!’ Studies of medical residents support statistically lower medical errors, improved personal life, less depression, and greater career satisfaction in those scoring higher on a highly validated and reliable empathy survey.
4. Well, we all know that listening to your patient eats into lunch time and gets you home even later than usual. Not so. Allowing patients to present their narrative results in a better history and permits the PA/NP to actively listen and digest the information. Patients feel the difference and the time it takes, and you may find yourself ahead on the clock as well as feel better about your own performance.
Being the empathetic PA that I am (harrumph) let me and others know your feelings about empathy in your practice. Feel free to nicely and anonymously lambast, (oops I mean describe) empathy stories in your clinical world. The good and the bad are welcome! Really.
Primary care-centric ACOs are working
Guess what? Physician-driven accountable care organizations with a strong primary care core are working – and, in a historic change, primary care physicians are the most highly compensated group.
The even better news? This trend is predictable and inevitable.
ACOs are working
As earlier posts to this column show, there are eight fairly straightforward elements required to create a successful and sustainable ACO:
• A change in financial incentives from those that reward volume, such as fee-for-service, to those that reward value, such as shared savings, if quality benchmarks are met.
• A primary care core.
• Physician cultural change.
• Patient engagement.
• Robust data collection.
• Clinical best practices.
• Administrative infrastructure.
• Enough scale.
A number of ACOs that do not have these elements will fail; but fortunately, more and more are being set up properly.
Recently, the Boston Consulting Group reported that ACO-like Medicare Advantage plans are reporting positive results. They are all distinguished by having "a selective network of providers, financial incentives that are aligned with clinical best practices, and active care management that emphasizes prevention in an effort to minimize expensive acute care."
Not only are emergency department and ambulatory surgery procedures down 20%-30% at these plans, but analysis of their data on 3 million Medicare patients showed that quality went up. These patients had lower single-year mortality rates, shorter average hospital stays, fewer readmissions, and better sustainability of health over time.1
Physician-led ACOs are better
If ACOs are good, physician-sponsored ones are better.
At a recent national meeting of health insurance companies, Paul Ginsburg, Ph.D., president of the Center for Studying Health System Change, told the insurers, "I think physician-led ACOs inherently make markets more competitive, because they have an opportunity to shift patients toward high-value hospitals."
Similarly, Charlie Baker, former secretary of health and human services for Massachusetts, told the group that nearly all of the Medicare Advantage risk contracts are with physician groups and not hospitals. Medicare Advantage participants are chosen by insurers, and he indicated that they know that contracting with physician ACOs is the best way to save money.2
As reported in an earlier column, this truth is becoming more evident, and there are now more physician-led ACOs than any other.
Primary care reaping rewards
Primary care is the only discipline mandated to be in ACOs participating in the Medicare Shared Savings Program. This is because ACO success stems from keeping people out of the hospital, avoiding expensive procedures, and reducing unnecessary tests and imaging. The "target-rich fields" for ACOs to accomplish this are primarily prevention and wellness, coordination of high-cost complex patients, reduced hospitalizations, and transition management across our fragmented system. These are all in primary care’s wheelhouse. It is no wonder that you are the darlings of the accountable care movement.
Successful and sustainable ACOs will tie shared savings distributions to relative contribution. A merit system thus likely will be primary care weighted.
For example, one ACO posted this planned distribution of shared savings: 12% to infrastructure; of the remainder, 60% to primary care, 40% to specialists, and 0% to hospitals.
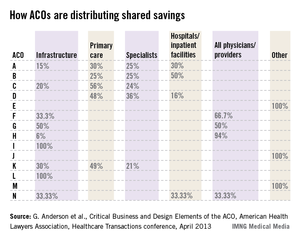
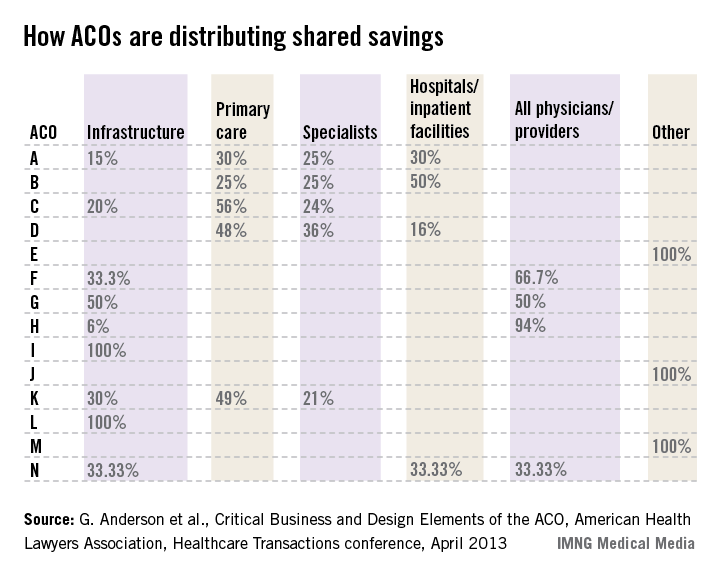
The following small sample survey shows widely varying models; but in all cases where distribution is broken out, primary care receives as much or more than specialists and, with one exception, hospitals.
There are some primary-care-only ACOs that are distributing 100% of savings to their primary care physicians under Medicare Advantage risk or Medicare Shared Savings Program contracts. One interviewed primary care physician ACO member stated that for his full-risk Medicare Advantage patient population, he was seeing half as many patients and making three times the income.
While income recognition for what you do is way overdue, keeping all the savings might be going too far. A fully evolved ACO should incentivize all providers and facilities along the entire continuum of care, but always in proportion to their value-adding contribution.
Primary care physicians tell me that while this economic reward is gratifying and validating, their surprise biggest reward has been empowerment to do health care right and regain control of the physician/patient relationship. They say that seeing happier, healthier patients, and being able to spend more time with them, has returned the fun to the practice of medicine.
References
1. Kaplan, J., et al., Alternative Payer Models Show Improved Health-Care Value, BCG Perspective, May 14, 2013.
2. Pittman, D., Doc-Led ACOs Better Model for Saving $$$, MedPage Today, May 15, 2013.
3. Anderson, G., et al., Critical Business and Design Elements of the ACO, American Health Lawyers Association, Healthcare Transactions conference (April 2013).
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
Guess what? Physician-driven accountable care organizations with a strong primary care core are working – and, in a historic change, primary care physicians are the most highly compensated group.
The even better news? This trend is predictable and inevitable.
ACOs are working
As earlier posts to this column show, there are eight fairly straightforward elements required to create a successful and sustainable ACO:
• A change in financial incentives from those that reward volume, such as fee-for-service, to those that reward value, such as shared savings, if quality benchmarks are met.
• A primary care core.
• Physician cultural change.
• Patient engagement.
• Robust data collection.
• Clinical best practices.
• Administrative infrastructure.
• Enough scale.
A number of ACOs that do not have these elements will fail; but fortunately, more and more are being set up properly.
Recently, the Boston Consulting Group reported that ACO-like Medicare Advantage plans are reporting positive results. They are all distinguished by having "a selective network of providers, financial incentives that are aligned with clinical best practices, and active care management that emphasizes prevention in an effort to minimize expensive acute care."
Not only are emergency department and ambulatory surgery procedures down 20%-30% at these plans, but analysis of their data on 3 million Medicare patients showed that quality went up. These patients had lower single-year mortality rates, shorter average hospital stays, fewer readmissions, and better sustainability of health over time.1
Physician-led ACOs are better
If ACOs are good, physician-sponsored ones are better.
At a recent national meeting of health insurance companies, Paul Ginsburg, Ph.D., president of the Center for Studying Health System Change, told the insurers, "I think physician-led ACOs inherently make markets more competitive, because they have an opportunity to shift patients toward high-value hospitals."
Similarly, Charlie Baker, former secretary of health and human services for Massachusetts, told the group that nearly all of the Medicare Advantage risk contracts are with physician groups and not hospitals. Medicare Advantage participants are chosen by insurers, and he indicated that they know that contracting with physician ACOs is the best way to save money.2
As reported in an earlier column, this truth is becoming more evident, and there are now more physician-led ACOs than any other.
Primary care reaping rewards
Primary care is the only discipline mandated to be in ACOs participating in the Medicare Shared Savings Program. This is because ACO success stems from keeping people out of the hospital, avoiding expensive procedures, and reducing unnecessary tests and imaging. The "target-rich fields" for ACOs to accomplish this are primarily prevention and wellness, coordination of high-cost complex patients, reduced hospitalizations, and transition management across our fragmented system. These are all in primary care’s wheelhouse. It is no wonder that you are the darlings of the accountable care movement.
Successful and sustainable ACOs will tie shared savings distributions to relative contribution. A merit system thus likely will be primary care weighted.
For example, one ACO posted this planned distribution of shared savings: 12% to infrastructure; of the remainder, 60% to primary care, 40% to specialists, and 0% to hospitals.
The following small sample survey shows widely varying models; but in all cases where distribution is broken out, primary care receives as much or more than specialists and, with one exception, hospitals.
There are some primary-care-only ACOs that are distributing 100% of savings to their primary care physicians under Medicare Advantage risk or Medicare Shared Savings Program contracts. One interviewed primary care physician ACO member stated that for his full-risk Medicare Advantage patient population, he was seeing half as many patients and making three times the income.
While income recognition for what you do is way overdue, keeping all the savings might be going too far. A fully evolved ACO should incentivize all providers and facilities along the entire continuum of care, but always in proportion to their value-adding contribution.
Primary care physicians tell me that while this economic reward is gratifying and validating, their surprise biggest reward has been empowerment to do health care right and regain control of the physician/patient relationship. They say that seeing happier, healthier patients, and being able to spend more time with them, has returned the fun to the practice of medicine.
References
1. Kaplan, J., et al., Alternative Payer Models Show Improved Health-Care Value, BCG Perspective, May 14, 2013.
2. Pittman, D., Doc-Led ACOs Better Model for Saving $$$, MedPage Today, May 15, 2013.
3. Anderson, G., et al., Critical Business and Design Elements of the ACO, American Health Lawyers Association, Healthcare Transactions conference (April 2013).
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
Guess what? Physician-driven accountable care organizations with a strong primary care core are working – and, in a historic change, primary care physicians are the most highly compensated group.
The even better news? This trend is predictable and inevitable.
ACOs are working
As earlier posts to this column show, there are eight fairly straightforward elements required to create a successful and sustainable ACO:
• A change in financial incentives from those that reward volume, such as fee-for-service, to those that reward value, such as shared savings, if quality benchmarks are met.
• A primary care core.
• Physician cultural change.
• Patient engagement.
• Robust data collection.
• Clinical best practices.
• Administrative infrastructure.
• Enough scale.
A number of ACOs that do not have these elements will fail; but fortunately, more and more are being set up properly.
Recently, the Boston Consulting Group reported that ACO-like Medicare Advantage plans are reporting positive results. They are all distinguished by having "a selective network of providers, financial incentives that are aligned with clinical best practices, and active care management that emphasizes prevention in an effort to minimize expensive acute care."
Not only are emergency department and ambulatory surgery procedures down 20%-30% at these plans, but analysis of their data on 3 million Medicare patients showed that quality went up. These patients had lower single-year mortality rates, shorter average hospital stays, fewer readmissions, and better sustainability of health over time.1
Physician-led ACOs are better
If ACOs are good, physician-sponsored ones are better.
At a recent national meeting of health insurance companies, Paul Ginsburg, Ph.D., president of the Center for Studying Health System Change, told the insurers, "I think physician-led ACOs inherently make markets more competitive, because they have an opportunity to shift patients toward high-value hospitals."
Similarly, Charlie Baker, former secretary of health and human services for Massachusetts, told the group that nearly all of the Medicare Advantage risk contracts are with physician groups and not hospitals. Medicare Advantage participants are chosen by insurers, and he indicated that they know that contracting with physician ACOs is the best way to save money.2
As reported in an earlier column, this truth is becoming more evident, and there are now more physician-led ACOs than any other.
Primary care reaping rewards
Primary care is the only discipline mandated to be in ACOs participating in the Medicare Shared Savings Program. This is because ACO success stems from keeping people out of the hospital, avoiding expensive procedures, and reducing unnecessary tests and imaging. The "target-rich fields" for ACOs to accomplish this are primarily prevention and wellness, coordination of high-cost complex patients, reduced hospitalizations, and transition management across our fragmented system. These are all in primary care’s wheelhouse. It is no wonder that you are the darlings of the accountable care movement.
Successful and sustainable ACOs will tie shared savings distributions to relative contribution. A merit system thus likely will be primary care weighted.
For example, one ACO posted this planned distribution of shared savings: 12% to infrastructure; of the remainder, 60% to primary care, 40% to specialists, and 0% to hospitals.
The following small sample survey shows widely varying models; but in all cases where distribution is broken out, primary care receives as much or more than specialists and, with one exception, hospitals.
There are some primary-care-only ACOs that are distributing 100% of savings to their primary care physicians under Medicare Advantage risk or Medicare Shared Savings Program contracts. One interviewed primary care physician ACO member stated that for his full-risk Medicare Advantage patient population, he was seeing half as many patients and making three times the income.
While income recognition for what you do is way overdue, keeping all the savings might be going too far. A fully evolved ACO should incentivize all providers and facilities along the entire continuum of care, but always in proportion to their value-adding contribution.
Primary care physicians tell me that while this economic reward is gratifying and validating, their surprise biggest reward has been empowerment to do health care right and regain control of the physician/patient relationship. They say that seeing happier, healthier patients, and being able to spend more time with them, has returned the fun to the practice of medicine.
References
1. Kaplan, J., et al., Alternative Payer Models Show Improved Health-Care Value, BCG Perspective, May 14, 2013.
2. Pittman, D., Doc-Led ACOs Better Model for Saving $$$, MedPage Today, May 15, 2013.
3. Anderson, G., et al., Critical Business and Design Elements of the ACO, American Health Lawyers Association, Healthcare Transactions conference (April 2013).
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
PDL Versus PDT for Port-wine Stains

In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?
In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?
In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?

MelaFind: Invaluable or Inane?
JAMA Dermatology (formerly Archives of Dermatology) reported a study (Arch Dermatol. 2012;148:1083-1084) on the diagnosis of pigmented lesions by dermatologists compared with the MelaFind device (Mela Sciences), a handheld light unit that produces a 3-dimensional computer image of a pigmented lesion with subsequent recommendation of “high disorganization” versus “low disorganization.” Of 47 pigmented lesions (23 melanoma; 24 nonmelanoma), MelaFind recommended biopsy in 44 cases and no biopsy in 3 cases, with 1 lesion that was truly melanoma (96% sensitivity; 8% specificity), compared with a range of 48% to 100% (mean, 80%) sensitivity and 4% to 71% (mean, 43%) specificity among the study dermatologists. The authors quote in their conclusion paragraph that MelaFind is a “very sensitive tool to guide dermatologists.”
What’s the issue?
A recent patient forcefully suggested to me that our department should “keep up with the times” and invest in MelaFind. MelaFind’s Web site states that it is “not a screening device.” The physician fact sheet says that it is “the world’s first and only multi-spectral, non-invasive, painless, and 100% objective and automated computer vision technology that evaluates clinically atypical pigmented skin lesions and classifies them unambiguously and clearly based upon their level of 3-dimensional morphological disorganization.” Given these claims and its US Food and Drug Administration approval, how can we not own one? The word unambiguous has never been used to describe the clinical decision making and diagnosis of pigmented lesions, but we all hope for it. Quite well-known leaders in our field have spoken highly of this technology, though I await better-powered studies and more poignant data, or perhaps just a better grasp of how it works. Can someone aid us in understanding its true niche in clinical practice?
JAMA Dermatology (formerly Archives of Dermatology) reported a study (Arch Dermatol. 2012;148:1083-1084) on the diagnosis of pigmented lesions by dermatologists compared with the MelaFind device (Mela Sciences), a handheld light unit that produces a 3-dimensional computer image of a pigmented lesion with subsequent recommendation of “high disorganization” versus “low disorganization.” Of 47 pigmented lesions (23 melanoma; 24 nonmelanoma), MelaFind recommended biopsy in 44 cases and no biopsy in 3 cases, with 1 lesion that was truly melanoma (96% sensitivity; 8% specificity), compared with a range of 48% to 100% (mean, 80%) sensitivity and 4% to 71% (mean, 43%) specificity among the study dermatologists. The authors quote in their conclusion paragraph that MelaFind is a “very sensitive tool to guide dermatologists.”
What’s the issue?
A recent patient forcefully suggested to me that our department should “keep up with the times” and invest in MelaFind. MelaFind’s Web site states that it is “not a screening device.” The physician fact sheet says that it is “the world’s first and only multi-spectral, non-invasive, painless, and 100% objective and automated computer vision technology that evaluates clinically atypical pigmented skin lesions and classifies them unambiguously and clearly based upon their level of 3-dimensional morphological disorganization.” Given these claims and its US Food and Drug Administration approval, how can we not own one? The word unambiguous has never been used to describe the clinical decision making and diagnosis of pigmented lesions, but we all hope for it. Quite well-known leaders in our field have spoken highly of this technology, though I await better-powered studies and more poignant data, or perhaps just a better grasp of how it works. Can someone aid us in understanding its true niche in clinical practice?
JAMA Dermatology (formerly Archives of Dermatology) reported a study (Arch Dermatol. 2012;148:1083-1084) on the diagnosis of pigmented lesions by dermatologists compared with the MelaFind device (Mela Sciences), a handheld light unit that produces a 3-dimensional computer image of a pigmented lesion with subsequent recommendation of “high disorganization” versus “low disorganization.” Of 47 pigmented lesions (23 melanoma; 24 nonmelanoma), MelaFind recommended biopsy in 44 cases and no biopsy in 3 cases, with 1 lesion that was truly melanoma (96% sensitivity; 8% specificity), compared with a range of 48% to 100% (mean, 80%) sensitivity and 4% to 71% (mean, 43%) specificity among the study dermatologists. The authors quote in their conclusion paragraph that MelaFind is a “very sensitive tool to guide dermatologists.”
What’s the issue?
A recent patient forcefully suggested to me that our department should “keep up with the times” and invest in MelaFind. MelaFind’s Web site states that it is “not a screening device.” The physician fact sheet says that it is “the world’s first and only multi-spectral, non-invasive, painless, and 100% objective and automated computer vision technology that evaluates clinically atypical pigmented skin lesions and classifies them unambiguously and clearly based upon their level of 3-dimensional morphological disorganization.” Given these claims and its US Food and Drug Administration approval, how can we not own one? The word unambiguous has never been used to describe the clinical decision making and diagnosis of pigmented lesions, but we all hope for it. Quite well-known leaders in our field have spoken highly of this technology, though I await better-powered studies and more poignant data, or perhaps just a better grasp of how it works. Can someone aid us in understanding its true niche in clinical practice?

The Deplorable Imprisonment of a Doctor: A Warning Signal for Physicians

Professor Cyril Karabus is a 78-year-old pediatric oncologist who has dedicated his life to treating children with malignancy and is widely respected for his expertise and compassion. He was arrested in the United Arab Emirates (UAE) on August 18, 2012, while returning to his home in South Africa with his wife and daughter following his son’s wedding in Canada. The flight had stopped at Abu Dhabi International Airport overnight and he was detained by passport control. He was unaware that more than 10 years earlier he had been tried and convicted in absentia for manslaughter and falsifying documents (medical records) after the death of a 3-year-old girl with acute myeloblastic leukemia in 2002 while he was temporarily working in the UAE (Br Med J. 2012;345:e6815)(The Cancer Letter. 2012;38[46]:11).
The injustice of Professor Karabus’ arrest and detention by the UAE’s judicial system is deplorable. A South African activist organization called the Treatment Action Campaign stated that by no modern principle of jurisprudence is it acceptable to try a foreign citizen in absentia without informing him/her. The South African Medical Association has cautioned members about working in the UAE and the British Medical Association has protested the conditions in which he had been held (Br Med J. 2012;345:e6815). More recently, the World Medical Association (WMA) stated that an advisory notice will be published in the World Medical Journal and on the WMA Web site about the working conditions and legal risks for physicians working in the UAE (http://www.wma.net/en/30publications/10policies/30council/cr_16/).
Professor Karabus recently was released after being held for 9 months (since August 2012) even though the prosecution could not find the disputed medical records. On March 21, 2013, a judge acquitted Professor Karabus of all charges. However, the prosecution elected to appeal the judge’s decision, keeping Professor Karabus in the UAE. He was finally released and was back home in South Africa on May 18, 2013. The WMA continues to emphasize the risks for physicians working in the UAE (http://www.wma.net/en/40news/20archives/2013/2013_15/index.html).
What’s the issue?
First, is it still safe for doctors to accept locum tenens abroad? Perhaps yes, but it may be prudent to carefully assess the judicial system of the country in which one is considering to work before accepting the employment opportunity.
Second, should academic centers and particularly medical institutions be receiving large sums of money from foreign dictatorships, such as the UAE? Currently, there are several major medical institutions—Johns Hopkins University in Baltimore, Maryland; the Children’s National Medical Center in Washington, DC; and The University of Texas MD Anderson Cancer Center in Houston—that accept substantial financial contributions from the Zayed family who govern the UAE (Clin Dermatol. 2013;31:325-326).
Professor Cyril Karabus is a 78-year-old pediatric oncologist who has dedicated his life to treating children with malignancy and is widely respected for his expertise and compassion. He was arrested in the United Arab Emirates (UAE) on August 18, 2012, while returning to his home in South Africa with his wife and daughter following his son’s wedding in Canada. The flight had stopped at Abu Dhabi International Airport overnight and he was detained by passport control. He was unaware that more than 10 years earlier he had been tried and convicted in absentia for manslaughter and falsifying documents (medical records) after the death of a 3-year-old girl with acute myeloblastic leukemia in 2002 while he was temporarily working in the UAE (Br Med J. 2012;345:e6815)(The Cancer Letter. 2012;38[46]:11).
The injustice of Professor Karabus’ arrest and detention by the UAE’s judicial system is deplorable. A South African activist organization called the Treatment Action Campaign stated that by no modern principle of jurisprudence is it acceptable to try a foreign citizen in absentia without informing him/her. The South African Medical Association has cautioned members about working in the UAE and the British Medical Association has protested the conditions in which he had been held (Br Med J. 2012;345:e6815). More recently, the World Medical Association (WMA) stated that an advisory notice will be published in the World Medical Journal and on the WMA Web site about the working conditions and legal risks for physicians working in the UAE (http://www.wma.net/en/30publications/10policies/30council/cr_16/).
Professor Karabus recently was released after being held for 9 months (since August 2012) even though the prosecution could not find the disputed medical records. On March 21, 2013, a judge acquitted Professor Karabus of all charges. However, the prosecution elected to appeal the judge’s decision, keeping Professor Karabus in the UAE. He was finally released and was back home in South Africa on May 18, 2013. The WMA continues to emphasize the risks for physicians working in the UAE (http://www.wma.net/en/40news/20archives/2013/2013_15/index.html).
What’s the issue?
First, is it still safe for doctors to accept locum tenens abroad? Perhaps yes, but it may be prudent to carefully assess the judicial system of the country in which one is considering to work before accepting the employment opportunity.
Second, should academic centers and particularly medical institutions be receiving large sums of money from foreign dictatorships, such as the UAE? Currently, there are several major medical institutions—Johns Hopkins University in Baltimore, Maryland; the Children’s National Medical Center in Washington, DC; and The University of Texas MD Anderson Cancer Center in Houston—that accept substantial financial contributions from the Zayed family who govern the UAE (Clin Dermatol. 2013;31:325-326).
Professor Cyril Karabus is a 78-year-old pediatric oncologist who has dedicated his life to treating children with malignancy and is widely respected for his expertise and compassion. He was arrested in the United Arab Emirates (UAE) on August 18, 2012, while returning to his home in South Africa with his wife and daughter following his son’s wedding in Canada. The flight had stopped at Abu Dhabi International Airport overnight and he was detained by passport control. He was unaware that more than 10 years earlier he had been tried and convicted in absentia for manslaughter and falsifying documents (medical records) after the death of a 3-year-old girl with acute myeloblastic leukemia in 2002 while he was temporarily working in the UAE (Br Med J. 2012;345:e6815)(The Cancer Letter. 2012;38[46]:11).
The injustice of Professor Karabus’ arrest and detention by the UAE’s judicial system is deplorable. A South African activist organization called the Treatment Action Campaign stated that by no modern principle of jurisprudence is it acceptable to try a foreign citizen in absentia without informing him/her. The South African Medical Association has cautioned members about working in the UAE and the British Medical Association has protested the conditions in which he had been held (Br Med J. 2012;345:e6815). More recently, the World Medical Association (WMA) stated that an advisory notice will be published in the World Medical Journal and on the WMA Web site about the working conditions and legal risks for physicians working in the UAE (http://www.wma.net/en/30publications/10policies/30council/cr_16/).
Professor Karabus recently was released after being held for 9 months (since August 2012) even though the prosecution could not find the disputed medical records. On March 21, 2013, a judge acquitted Professor Karabus of all charges. However, the prosecution elected to appeal the judge’s decision, keeping Professor Karabus in the UAE. He was finally released and was back home in South Africa on May 18, 2013. The WMA continues to emphasize the risks for physicians working in the UAE (http://www.wma.net/en/40news/20archives/2013/2013_15/index.html).
What’s the issue?
First, is it still safe for doctors to accept locum tenens abroad? Perhaps yes, but it may be prudent to carefully assess the judicial system of the country in which one is considering to work before accepting the employment opportunity.
Second, should academic centers and particularly medical institutions be receiving large sums of money from foreign dictatorships, such as the UAE? Currently, there are several major medical institutions—Johns Hopkins University in Baltimore, Maryland; the Children’s National Medical Center in Washington, DC; and The University of Texas MD Anderson Cancer Center in Houston—that accept substantial financial contributions from the Zayed family who govern the UAE (Clin Dermatol. 2013;31:325-326).

Safety First: Fractional Nonablative Laser Resurfacing in Fitzpatrick Skin Types IV to VI

In the April 2013 issue of the Journal of Drugs in Dermatology (2013;12:428-431), Clark et al retrospectively reviewed 115 laser sessions with the 1550-nm erbium-doped fractional nonablative laser (Fraxel Re:Store SR 1550, Solta Medical) in 45 patients with Fitzpatrick skin types IV to VI to assess the rate of postinflammatory hyperpigmentation and the associated laser parameters. The fluence, treatment level, and number of passes were all reviewed, as well as any posttreatment complications (ie, erythema, blistering, edema, bruising, pain) and long-term (1 month) complications (ie, hypopigmentation, hyperpigmentation). All patients were pretreated with hydroquinone cream 4% 2 weeks before, stopping 7 days before treatment and then continuing 4 weeks thereafter. Also, continuous forced-air cooling was used during treatment as well as posttreatment ice packs. Fifty-eight percent (26/45) of treatments were performed in patients with Fitzpatrick skin type IV, 24% (11/45) with type V, and 18% (8/45) with type VI. Laser parameters ranged from 4 to 70 mJ, treatment level 2 to 9, and 4 to 8 passes. Of 115 sessions, 5 (4%) were associated with postinflammatory hyperpigmentation; 2 of these instances occurred in 1 patient. The occurrence of postinflammatory hyperpigmentation was found to be statistically significant (P=.05), correlating with higher mean energy levels compared to those without hyperpigmentation (60.8 vs 44.7 mJ). Only 1 episode of postinflammatory hyperpigmentation lasted longer than 1 month, and 2 of 5 cases had only transient (<7 days) hyperpigmentation. All 5 cases resolved.
What’s the issue?
The 1550-nm erbium-doped fractional nonablative laser is being used for many skin conditions and has a low incidence of adverse effects when appropriate laser parameters are chosen. When treating darker skin phototypes with this technology, the concern for postinflammatory pigmentary alteration is more concerning. Higher treatment densities used in darker phototypes have been associated with a greater risk for postinflammatory hyperpigmentation. In their review, the authors showed that higher energy levels were associated with their cases of postinflammatory hyperpigmentation, with the caveat that they were careful not to use higher density or treatment levels than they would have used in lighter phototypes. Importantly, all 5 cases of hyperpigmentation did resolve and only 1 lasted longer than 1 month (2 months in total). This analysis reinforces that the 1550-nm erbium-doped fractional nonablative laser is quite safe in Fitzpatrick skin types IV to VI when appropriate parameters are utilized, as well as methodical pretreatment and posttreatment with hydroquinone, concomitant cooling, and strict posttreatment sun protection. With the right parameters, the treatment is quite safe; however, what are the optimal treatment parameters to provide efficacious and lasting results?
In the April 2013 issue of the Journal of Drugs in Dermatology (2013;12:428-431), Clark et al retrospectively reviewed 115 laser sessions with the 1550-nm erbium-doped fractional nonablative laser (Fraxel Re:Store SR 1550, Solta Medical) in 45 patients with Fitzpatrick skin types IV to VI to assess the rate of postinflammatory hyperpigmentation and the associated laser parameters. The fluence, treatment level, and number of passes were all reviewed, as well as any posttreatment complications (ie, erythema, blistering, edema, bruising, pain) and long-term (1 month) complications (ie, hypopigmentation, hyperpigmentation). All patients were pretreated with hydroquinone cream 4% 2 weeks before, stopping 7 days before treatment and then continuing 4 weeks thereafter. Also, continuous forced-air cooling was used during treatment as well as posttreatment ice packs. Fifty-eight percent (26/45) of treatments were performed in patients with Fitzpatrick skin type IV, 24% (11/45) with type V, and 18% (8/45) with type VI. Laser parameters ranged from 4 to 70 mJ, treatment level 2 to 9, and 4 to 8 passes. Of 115 sessions, 5 (4%) were associated with postinflammatory hyperpigmentation; 2 of these instances occurred in 1 patient. The occurrence of postinflammatory hyperpigmentation was found to be statistically significant (P=.05), correlating with higher mean energy levels compared to those without hyperpigmentation (60.8 vs 44.7 mJ). Only 1 episode of postinflammatory hyperpigmentation lasted longer than 1 month, and 2 of 5 cases had only transient (<7 days) hyperpigmentation. All 5 cases resolved.
What’s the issue?
The 1550-nm erbium-doped fractional nonablative laser is being used for many skin conditions and has a low incidence of adverse effects when appropriate laser parameters are chosen. When treating darker skin phototypes with this technology, the concern for postinflammatory pigmentary alteration is more concerning. Higher treatment densities used in darker phototypes have been associated with a greater risk for postinflammatory hyperpigmentation. In their review, the authors showed that higher energy levels were associated with their cases of postinflammatory hyperpigmentation, with the caveat that they were careful not to use higher density or treatment levels than they would have used in lighter phototypes. Importantly, all 5 cases of hyperpigmentation did resolve and only 1 lasted longer than 1 month (2 months in total). This analysis reinforces that the 1550-nm erbium-doped fractional nonablative laser is quite safe in Fitzpatrick skin types IV to VI when appropriate parameters are utilized, as well as methodical pretreatment and posttreatment with hydroquinone, concomitant cooling, and strict posttreatment sun protection. With the right parameters, the treatment is quite safe; however, what are the optimal treatment parameters to provide efficacious and lasting results?
In the April 2013 issue of the Journal of Drugs in Dermatology (2013;12:428-431), Clark et al retrospectively reviewed 115 laser sessions with the 1550-nm erbium-doped fractional nonablative laser (Fraxel Re:Store SR 1550, Solta Medical) in 45 patients with Fitzpatrick skin types IV to VI to assess the rate of postinflammatory hyperpigmentation and the associated laser parameters. The fluence, treatment level, and number of passes were all reviewed, as well as any posttreatment complications (ie, erythema, blistering, edema, bruising, pain) and long-term (1 month) complications (ie, hypopigmentation, hyperpigmentation). All patients were pretreated with hydroquinone cream 4% 2 weeks before, stopping 7 days before treatment and then continuing 4 weeks thereafter. Also, continuous forced-air cooling was used during treatment as well as posttreatment ice packs. Fifty-eight percent (26/45) of treatments were performed in patients with Fitzpatrick skin type IV, 24% (11/45) with type V, and 18% (8/45) with type VI. Laser parameters ranged from 4 to 70 mJ, treatment level 2 to 9, and 4 to 8 passes. Of 115 sessions, 5 (4%) were associated with postinflammatory hyperpigmentation; 2 of these instances occurred in 1 patient. The occurrence of postinflammatory hyperpigmentation was found to be statistically significant (P=.05), correlating with higher mean energy levels compared to those without hyperpigmentation (60.8 vs 44.7 mJ). Only 1 episode of postinflammatory hyperpigmentation lasted longer than 1 month, and 2 of 5 cases had only transient (<7 days) hyperpigmentation. All 5 cases resolved.
What’s the issue?
The 1550-nm erbium-doped fractional nonablative laser is being used for many skin conditions and has a low incidence of adverse effects when appropriate laser parameters are chosen. When treating darker skin phototypes with this technology, the concern for postinflammatory pigmentary alteration is more concerning. Higher treatment densities used in darker phototypes have been associated with a greater risk for postinflammatory hyperpigmentation. In their review, the authors showed that higher energy levels were associated with their cases of postinflammatory hyperpigmentation, with the caveat that they were careful not to use higher density or treatment levels than they would have used in lighter phototypes. Importantly, all 5 cases of hyperpigmentation did resolve and only 1 lasted longer than 1 month (2 months in total). This analysis reinforces that the 1550-nm erbium-doped fractional nonablative laser is quite safe in Fitzpatrick skin types IV to VI when appropriate parameters are utilized, as well as methodical pretreatment and posttreatment with hydroquinone, concomitant cooling, and strict posttreatment sun protection. With the right parameters, the treatment is quite safe; however, what are the optimal treatment parameters to provide efficacious and lasting results?
Get ready now for 2014 Medicare ACO program
The Centers for Medicare and Medicaid Services has just announced key dates for the 2014 Medicare Shared Savings Program application cycle – and although the upcoming Jan. 1, 2014, start date for the MSSP seems far off, physicians should start organizing now.
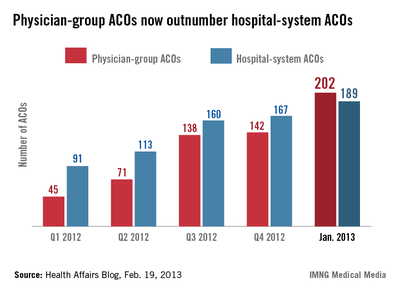
Physician interest in participating is mounting, as physician-led accountable care organizations are emerging as leaders in improving quality while eradicating waste. In fact, there are now more physician-run ACOs than any other model (see chart below).
Physicians see opportunity
The MSSP has embraced the accountable care concept to improve the quality of care for Medicare fee-for-service beneficiaries. Eligible providers and suppliers may participate in the MSSP by creating or participating in an ACO. The MSSP rewards ACOs that lower their rate of growth in health care costs while meeting quality performance standards.
On Jan. 10, 2013, the Centers for Medicare and Medicaid Services (CMS) announced that 106 new organizations were selected to participate in the program. That’s in addition to the 87 ACOs approved in July 2012 and the 27 selected in April 2012 – bringing the total to 220 ACOs selected to participate in the MSSP. Early evidence indicates that these ACOs are decreasing costs while improving clinical outcomes.
For many of those ACOs, Medicare will be just the beginning. Private insurers such as Aetna, UnitedHealth Group, Humana, Cigna, and most Blue Cross plans are contracting with ACOs to care for more patients. Many state Medicaid programs have moved or are considering moving to accountable care.
These multiple streams of shared savings will be generated through the same ACO infrastructure needed for the MSSP, encouraging more physician-owned ACOs to form.
With the rise of ACOs, "providers are doing things in a positive way rather than a reactive way. We are seeing the beginnings of a tsunami," noted Dr. Michael Cryer, national medical director at employee benefits consultancy Aon Hewitt, in a New York Times article ("Small-picture approach flips medical economics," March 12, 2012).
According to a recent study by consulting firm Oliver Wyman entitled "The ACO Surprise," roughly 10% of the U.S. population, or from 25 million to 31 million patients, are being served by ACOs. "Successful ACOs won’t just siphon patients away from traditional providers. They will change the rules of the game," the report’s authors conclude.
Don’t miss these 2013 deadlines
CMS has just released its 2013 application cycle for 2014 (see table). The time to act is now. It will take time to understand ACOs and enlist a critical mass of informed and committed primary care providers. Though the notice of intent ("NOI") is not binding, failure to file in May is binding – you are barred from applying. Likewise, you must obtain your user ID by May 31.
The application is not hard, but it basically reflects your ACO game plan. You must be organized, have a focused care plan, and complete the application by the end of July – much earlier than last year’s deadline.
Bottom line: Do not let the start date lull you into procrastination.
Let’s have a closer look at some of the things that must be covered in the application. In addition to a culture of teamwork, patient engagement, and alignment of financial incentives, which are chief among the eight essential elements necessary for a successful ACO ("The essential elements of an ACO," Internal Medicine News, Oct. 1, 2012, p. 38), the MSSP application requires:
• Compliance with the required definitions of "ACO applicant" and "participant."
• A certification that the ACO, its ACO-provider participants, and its ACO providers/suppliers have agreed to become accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the ACO.
• Establishment of a governing body.
• Implementation of a comprehensive compliance plan.
• Execution of an ACO Participation Agreement.
In addition, certain organizational milestones should be reached in advance of the application. In particular, planning for a successful ACO requires identification of a physician-champion, completion of a feasibility analysis, implementation of sufficient information technology, and internal reporting on quality and cost metrics. As in any entrepreneurial pursuit, timing is critical, and delay equates to lost potential.
Given that primary care providers are the only providers mandated for inclusion in the MSSP, it is apparent that CMS expects primary care to drive ACO value via prevention and wellness; chronic disease management; care transitions and navigation; reduced hospitalizations; and multispecialty care coordination of complex patients.
ACOs, in one form or another, are sure to be permanent fixtures in American health care, as the nation’s economy and its residents eagerly await the benefits stemming from primary care–driven innovation.
Opportunity knocks – get going!
For more information about the Medicare Shared Savings Program, click here.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612). Mr. McNeill is a practicing attorney pursuing his LLM at Duke University, currently focusing on accountable care.
Medicare Shared Savings Program deadlines
Key dates for Jan. 1, 2014, start:
| Notice of intent (NOI) accepted | May 1-31, 2013 |
| CMS user ID forms accepted | May 1-31, 2013 |
| Applications accepted | July 1-31, 2013 |
| Application approval or denial decision | Fall 2013 |
| Start date for MSSP ACO | Jan. 1, 2014 |
Source: Centers for Medicare and Medicaid Services
The Centers for Medicare and Medicaid Services has just announced key dates for the 2014 Medicare Shared Savings Program application cycle – and although the upcoming Jan. 1, 2014, start date for the MSSP seems far off, physicians should start organizing now.
Physician interest in participating is mounting, as physician-led accountable care organizations are emerging as leaders in improving quality while eradicating waste. In fact, there are now more physician-run ACOs than any other model (see chart below).
Physicians see opportunity
The MSSP has embraced the accountable care concept to improve the quality of care for Medicare fee-for-service beneficiaries. Eligible providers and suppliers may participate in the MSSP by creating or participating in an ACO. The MSSP rewards ACOs that lower their rate of growth in health care costs while meeting quality performance standards.
On Jan. 10, 2013, the Centers for Medicare and Medicaid Services (CMS) announced that 106 new organizations were selected to participate in the program. That’s in addition to the 87 ACOs approved in July 2012 and the 27 selected in April 2012 – bringing the total to 220 ACOs selected to participate in the MSSP. Early evidence indicates that these ACOs are decreasing costs while improving clinical outcomes.
For many of those ACOs, Medicare will be just the beginning. Private insurers such as Aetna, UnitedHealth Group, Humana, Cigna, and most Blue Cross plans are contracting with ACOs to care for more patients. Many state Medicaid programs have moved or are considering moving to accountable care.
These multiple streams of shared savings will be generated through the same ACO infrastructure needed for the MSSP, encouraging more physician-owned ACOs to form.
With the rise of ACOs, "providers are doing things in a positive way rather than a reactive way. We are seeing the beginnings of a tsunami," noted Dr. Michael Cryer, national medical director at employee benefits consultancy Aon Hewitt, in a New York Times article ("Small-picture approach flips medical economics," March 12, 2012).
According to a recent study by consulting firm Oliver Wyman entitled "The ACO Surprise," roughly 10% of the U.S. population, or from 25 million to 31 million patients, are being served by ACOs. "Successful ACOs won’t just siphon patients away from traditional providers. They will change the rules of the game," the report’s authors conclude.
Don’t miss these 2013 deadlines
CMS has just released its 2013 application cycle for 2014 (see table). The time to act is now. It will take time to understand ACOs and enlist a critical mass of informed and committed primary care providers. Though the notice of intent ("NOI") is not binding, failure to file in May is binding – you are barred from applying. Likewise, you must obtain your user ID by May 31.
The application is not hard, but it basically reflects your ACO game plan. You must be organized, have a focused care plan, and complete the application by the end of July – much earlier than last year’s deadline.
Bottom line: Do not let the start date lull you into procrastination.
Let’s have a closer look at some of the things that must be covered in the application. In addition to a culture of teamwork, patient engagement, and alignment of financial incentives, which are chief among the eight essential elements necessary for a successful ACO ("The essential elements of an ACO," Internal Medicine News, Oct. 1, 2012, p. 38), the MSSP application requires:
• Compliance with the required definitions of "ACO applicant" and "participant."
• A certification that the ACO, its ACO-provider participants, and its ACO providers/suppliers have agreed to become accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the ACO.
• Establishment of a governing body.
• Implementation of a comprehensive compliance plan.
• Execution of an ACO Participation Agreement.
In addition, certain organizational milestones should be reached in advance of the application. In particular, planning for a successful ACO requires identification of a physician-champion, completion of a feasibility analysis, implementation of sufficient information technology, and internal reporting on quality and cost metrics. As in any entrepreneurial pursuit, timing is critical, and delay equates to lost potential.
Given that primary care providers are the only providers mandated for inclusion in the MSSP, it is apparent that CMS expects primary care to drive ACO value via prevention and wellness; chronic disease management; care transitions and navigation; reduced hospitalizations; and multispecialty care coordination of complex patients.
ACOs, in one form or another, are sure to be permanent fixtures in American health care, as the nation’s economy and its residents eagerly await the benefits stemming from primary care–driven innovation.
Opportunity knocks – get going!
For more information about the Medicare Shared Savings Program, click here.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612). Mr. McNeill is a practicing attorney pursuing his LLM at Duke University, currently focusing on accountable care.
Medicare Shared Savings Program deadlines
Key dates for Jan. 1, 2014, start:
| Notice of intent (NOI) accepted | May 1-31, 2013 |
| CMS user ID forms accepted | May 1-31, 2013 |
| Applications accepted | July 1-31, 2013 |
| Application approval or denial decision | Fall 2013 |
| Start date for MSSP ACO | Jan. 1, 2014 |
Source: Centers for Medicare and Medicaid Services
The Centers for Medicare and Medicaid Services has just announced key dates for the 2014 Medicare Shared Savings Program application cycle – and although the upcoming Jan. 1, 2014, start date for the MSSP seems far off, physicians should start organizing now.
Physician interest in participating is mounting, as physician-led accountable care organizations are emerging as leaders in improving quality while eradicating waste. In fact, there are now more physician-run ACOs than any other model (see chart below).
Physicians see opportunity
The MSSP has embraced the accountable care concept to improve the quality of care for Medicare fee-for-service beneficiaries. Eligible providers and suppliers may participate in the MSSP by creating or participating in an ACO. The MSSP rewards ACOs that lower their rate of growth in health care costs while meeting quality performance standards.
On Jan. 10, 2013, the Centers for Medicare and Medicaid Services (CMS) announced that 106 new organizations were selected to participate in the program. That’s in addition to the 87 ACOs approved in July 2012 and the 27 selected in April 2012 – bringing the total to 220 ACOs selected to participate in the MSSP. Early evidence indicates that these ACOs are decreasing costs while improving clinical outcomes.
For many of those ACOs, Medicare will be just the beginning. Private insurers such as Aetna, UnitedHealth Group, Humana, Cigna, and most Blue Cross plans are contracting with ACOs to care for more patients. Many state Medicaid programs have moved or are considering moving to accountable care.
These multiple streams of shared savings will be generated through the same ACO infrastructure needed for the MSSP, encouraging more physician-owned ACOs to form.
With the rise of ACOs, "providers are doing things in a positive way rather than a reactive way. We are seeing the beginnings of a tsunami," noted Dr. Michael Cryer, national medical director at employee benefits consultancy Aon Hewitt, in a New York Times article ("Small-picture approach flips medical economics," March 12, 2012).
According to a recent study by consulting firm Oliver Wyman entitled "The ACO Surprise," roughly 10% of the U.S. population, or from 25 million to 31 million patients, are being served by ACOs. "Successful ACOs won’t just siphon patients away from traditional providers. They will change the rules of the game," the report’s authors conclude.
Don’t miss these 2013 deadlines
CMS has just released its 2013 application cycle for 2014 (see table). The time to act is now. It will take time to understand ACOs and enlist a critical mass of informed and committed primary care providers. Though the notice of intent ("NOI") is not binding, failure to file in May is binding – you are barred from applying. Likewise, you must obtain your user ID by May 31.
The application is not hard, but it basically reflects your ACO game plan. You must be organized, have a focused care plan, and complete the application by the end of July – much earlier than last year’s deadline.
Bottom line: Do not let the start date lull you into procrastination.
Let’s have a closer look at some of the things that must be covered in the application. In addition to a culture of teamwork, patient engagement, and alignment of financial incentives, which are chief among the eight essential elements necessary for a successful ACO ("The essential elements of an ACO," Internal Medicine News, Oct. 1, 2012, p. 38), the MSSP application requires:
• Compliance with the required definitions of "ACO applicant" and "participant."
• A certification that the ACO, its ACO-provider participants, and its ACO providers/suppliers have agreed to become accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the ACO.
• Establishment of a governing body.
• Implementation of a comprehensive compliance plan.
• Execution of an ACO Participation Agreement.
In addition, certain organizational milestones should be reached in advance of the application. In particular, planning for a successful ACO requires identification of a physician-champion, completion of a feasibility analysis, implementation of sufficient information technology, and internal reporting on quality and cost metrics. As in any entrepreneurial pursuit, timing is critical, and delay equates to lost potential.
Given that primary care providers are the only providers mandated for inclusion in the MSSP, it is apparent that CMS expects primary care to drive ACO value via prevention and wellness; chronic disease management; care transitions and navigation; reduced hospitalizations; and multispecialty care coordination of complex patients.
ACOs, in one form or another, are sure to be permanent fixtures in American health care, as the nation’s economy and its residents eagerly await the benefits stemming from primary care–driven innovation.
Opportunity knocks – get going!
For more information about the Medicare Shared Savings Program, click here.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, North Carolina. He has many years’ experience assisting physicians in forming integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author (bbobbitt@smithlaw.com or 919-821-6612). Mr. McNeill is a practicing attorney pursuing his LLM at Duke University, currently focusing on accountable care.
Medicare Shared Savings Program deadlines
Key dates for Jan. 1, 2014, start:
| Notice of intent (NOI) accepted | May 1-31, 2013 |
| CMS user ID forms accepted | May 1-31, 2013 |
| Applications accepted | July 1-31, 2013 |
| Application approval or denial decision | Fall 2013 |
| Start date for MSSP ACO | Jan. 1, 2014 |
Source: Centers for Medicare and Medicaid Services
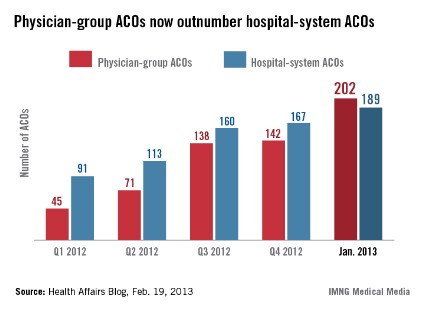
AAD 2013 Miami Highlights: A Resident’s Perspective
One of the challenges of the American Academy of Dermatology (AAD) annual meeting is attending all the lectures that spark your interest while trying to attend lectures that offer a variety of topics. Many of the lectures that you want to attend are offered at the same time and there is just no way to attend every lecture that is appealing. The dermatology review 2-day course (C009) is the answer to this problem. This course was one of the highlights of my AAD experience this year. It brought together some of the top presenters and clinical investigators to highlight emerging discoveries in their respective areas of expertise. It was an honor to sit among these dermatologists and quite a compliment to the course design that they actually stayed the full 2 days to learn as well. Topics covered a wide range of dermatologic areas including advanced treatment of melanoma, actinic keratoses, photoprotection, contact dermatitis, flap design, and cosmeceuticals. I would highly recommend this course to second- or third-year dermatology residents who are preparing for the boards examination, as much of the presented material recently had been published in the literature and will likely end up on our boards. Not to mention the lectures were captivating.
Another must for residents was Dr. Christine Ko’s forum entitled “Dermatopathology Made Simple” (F131). Dr. Ko discussed basic pattern analysis that dermatology residents must know for the boards and the most important differential diagnoses to be included in each pattern. She made dermatopathology seem easy and she was an engaging speaker. As a forum-style lecture, personal computers were set up throughout the room for the audience to follow along. She covered 33 patterns and 174 entities in this 2-hour course. She also provided a session handout that is available on the official AAD 2013 CD-ROM. I would encourage all residents to attend this lecture next year.
One final suggestion is to attend the Skin Cancer Foundation annual meeting and reception. It is truly an amazing group of dermatologists who have given back so much to the community and are dedicated to raising awareness of and preventing skin cancer. Residents and medical students could attend for free and had the opportunity to meet some of the great names in our field, such as Dr. Perry Robins, president of the Skin Cancer Foundation. It was an excellent networking opportunity. At the end of the evening, Skin Cancer Foundation members received complimentary copies of a patient education DVD for office use. The DVD included interviews with 2 young women who have battled melanoma after using tanning beds as teenagers and aimed to help physicians communicate the dangers of indoor tanning to patients.
I hope some of these suggestions help you navigate through next year’s program book, and I look forward to attending next year’s event in my hometown of Denver, Colorado. What were your favorite sessions at this year’s annual meeting?
One of the challenges of the American Academy of Dermatology (AAD) annual meeting is attending all the lectures that spark your interest while trying to attend lectures that offer a variety of topics. Many of the lectures that you want to attend are offered at the same time and there is just no way to attend every lecture that is appealing. The dermatology review 2-day course (C009) is the answer to this problem. This course was one of the highlights of my AAD experience this year. It brought together some of the top presenters and clinical investigators to highlight emerging discoveries in their respective areas of expertise. It was an honor to sit among these dermatologists and quite a compliment to the course design that they actually stayed the full 2 days to learn as well. Topics covered a wide range of dermatologic areas including advanced treatment of melanoma, actinic keratoses, photoprotection, contact dermatitis, flap design, and cosmeceuticals. I would highly recommend this course to second- or third-year dermatology residents who are preparing for the boards examination, as much of the presented material recently had been published in the literature and will likely end up on our boards. Not to mention the lectures were captivating.
Another must for residents was Dr. Christine Ko’s forum entitled “Dermatopathology Made Simple” (F131). Dr. Ko discussed basic pattern analysis that dermatology residents must know for the boards and the most important differential diagnoses to be included in each pattern. She made dermatopathology seem easy and she was an engaging speaker. As a forum-style lecture, personal computers were set up throughout the room for the audience to follow along. She covered 33 patterns and 174 entities in this 2-hour course. She also provided a session handout that is available on the official AAD 2013 CD-ROM. I would encourage all residents to attend this lecture next year.
One final suggestion is to attend the Skin Cancer Foundation annual meeting and reception. It is truly an amazing group of dermatologists who have given back so much to the community and are dedicated to raising awareness of and preventing skin cancer. Residents and medical students could attend for free and had the opportunity to meet some of the great names in our field, such as Dr. Perry Robins, president of the Skin Cancer Foundation. It was an excellent networking opportunity. At the end of the evening, Skin Cancer Foundation members received complimentary copies of a patient education DVD for office use. The DVD included interviews with 2 young women who have battled melanoma after using tanning beds as teenagers and aimed to help physicians communicate the dangers of indoor tanning to patients.
I hope some of these suggestions help you navigate through next year’s program book, and I look forward to attending next year’s event in my hometown of Denver, Colorado. What were your favorite sessions at this year’s annual meeting?
One of the challenges of the American Academy of Dermatology (AAD) annual meeting is attending all the lectures that spark your interest while trying to attend lectures that offer a variety of topics. Many of the lectures that you want to attend are offered at the same time and there is just no way to attend every lecture that is appealing. The dermatology review 2-day course (C009) is the answer to this problem. This course was one of the highlights of my AAD experience this year. It brought together some of the top presenters and clinical investigators to highlight emerging discoveries in their respective areas of expertise. It was an honor to sit among these dermatologists and quite a compliment to the course design that they actually stayed the full 2 days to learn as well. Topics covered a wide range of dermatologic areas including advanced treatment of melanoma, actinic keratoses, photoprotection, contact dermatitis, flap design, and cosmeceuticals. I would highly recommend this course to second- or third-year dermatology residents who are preparing for the boards examination, as much of the presented material recently had been published in the literature and will likely end up on our boards. Not to mention the lectures were captivating.
Another must for residents was Dr. Christine Ko’s forum entitled “Dermatopathology Made Simple” (F131). Dr. Ko discussed basic pattern analysis that dermatology residents must know for the boards and the most important differential diagnoses to be included in each pattern. She made dermatopathology seem easy and she was an engaging speaker. As a forum-style lecture, personal computers were set up throughout the room for the audience to follow along. She covered 33 patterns and 174 entities in this 2-hour course. She also provided a session handout that is available on the official AAD 2013 CD-ROM. I would encourage all residents to attend this lecture next year.
One final suggestion is to attend the Skin Cancer Foundation annual meeting and reception. It is truly an amazing group of dermatologists who have given back so much to the community and are dedicated to raising awareness of and preventing skin cancer. Residents and medical students could attend for free and had the opportunity to meet some of the great names in our field, such as Dr. Perry Robins, president of the Skin Cancer Foundation. It was an excellent networking opportunity. At the end of the evening, Skin Cancer Foundation members received complimentary copies of a patient education DVD for office use. The DVD included interviews with 2 young women who have battled melanoma after using tanning beds as teenagers and aimed to help physicians communicate the dangers of indoor tanning to patients.
I hope some of these suggestions help you navigate through next year’s program book, and I look forward to attending next year’s event in my hometown of Denver, Colorado. What were your favorite sessions at this year’s annual meeting?

ACO Insider: An Rx for rising health spending
With the looming federal "sequestration" threatening drastic spending cuts, our nation’s leaders are finally confronting the main drivers of our deficit dilemma: government "entitlement" programs such as Social Security, Medicare, and Medicaid.
Meanwhile, there is broad consensus that many of our runaway health care costs are avoidable. Our current fee-for-service health care payment system rewards higher-intensity care in greater volume, with no consequence for lack of coordination. It is a significant reason that our health care system is fragmented, inefficient, and too costly.
Federal government receipts total approximately 19% of our nation’s gross domestic product. Yet if our health care spending trends remain unchecked, by 2035 Medicare and Medicaid alone are predicted to consume 13% of GDP. By 2080, Medicare and Medicaid will consume all federal taxes, while total public and private health spending will claim almost 50% of GDP. We will have to borrow to pay for the rest of the federal government’s obligations: defense, education, transportation, etc.
As of 2012, our nation is already $16 trillion in the hole and counting. Sticking with the status quo would be a disastrous choice.
However, if medical providers work together and accept new payment incentives that reward value instead of volume, we can help fix America’s broken health care system.
That cannot be done remotely in Washington. It requires health care providers in each community cooperating to increase health care quality and cut cumulative costs.
Quality, savings, and patient satisfaction all must be achieved for providers to receive incentive payments under the new health care payment model, called "value-based reimbursement."
There is plenty of waste to be found and eliminated. Last summer, the Institute of Medicine concluded that America wastes about 30% of its health care spending – some $750 billion a year – on unneeded care, excessive paperwork, fraud, and other inefficiencies.
With basic health care becoming unaffordable for many ordinary working families and individuals, that amount of waste is unacceptable.
Although no one can hope to eradicate it overnight, it’s time somebody did something about it. America is asking physicians to step up and form teams, teams such as accountable care organizations.
By doing so, you can help ensure access, improve patient care, promote efficiency, stretch health care dollars, and make patients more of a partner in their treatment. ACOs typically receive 50% of the savings they create, which should be considered compensation to you for professional services.
As healers with a calling to serve, you have an opportunity to do your part to enhance patient care while helping to improve our nation’s fiscal health. Besides empowering, and paying, physicians to regain control of the physician/patient relationship, your patients, your profession, and your nation need you.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com, or at 919-821-6612.
With the looming federal "sequestration" threatening drastic spending cuts, our nation’s leaders are finally confronting the main drivers of our deficit dilemma: government "entitlement" programs such as Social Security, Medicare, and Medicaid.
Meanwhile, there is broad consensus that many of our runaway health care costs are avoidable. Our current fee-for-service health care payment system rewards higher-intensity care in greater volume, with no consequence for lack of coordination. It is a significant reason that our health care system is fragmented, inefficient, and too costly.
Federal government receipts total approximately 19% of our nation’s gross domestic product. Yet if our health care spending trends remain unchecked, by 2035 Medicare and Medicaid alone are predicted to consume 13% of GDP. By 2080, Medicare and Medicaid will consume all federal taxes, while total public and private health spending will claim almost 50% of GDP. We will have to borrow to pay for the rest of the federal government’s obligations: defense, education, transportation, etc.
As of 2012, our nation is already $16 trillion in the hole and counting. Sticking with the status quo would be a disastrous choice.
However, if medical providers work together and accept new payment incentives that reward value instead of volume, we can help fix America’s broken health care system.
That cannot be done remotely in Washington. It requires health care providers in each community cooperating to increase health care quality and cut cumulative costs.
Quality, savings, and patient satisfaction all must be achieved for providers to receive incentive payments under the new health care payment model, called "value-based reimbursement."
There is plenty of waste to be found and eliminated. Last summer, the Institute of Medicine concluded that America wastes about 30% of its health care spending – some $750 billion a year – on unneeded care, excessive paperwork, fraud, and other inefficiencies.
With basic health care becoming unaffordable for many ordinary working families and individuals, that amount of waste is unacceptable.
Although no one can hope to eradicate it overnight, it’s time somebody did something about it. America is asking physicians to step up and form teams, teams such as accountable care organizations.
By doing so, you can help ensure access, improve patient care, promote efficiency, stretch health care dollars, and make patients more of a partner in their treatment. ACOs typically receive 50% of the savings they create, which should be considered compensation to you for professional services.
As healers with a calling to serve, you have an opportunity to do your part to enhance patient care while helping to improve our nation’s fiscal health. Besides empowering, and paying, physicians to regain control of the physician/patient relationship, your patients, your profession, and your nation need you.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com, or at 919-821-6612.
With the looming federal "sequestration" threatening drastic spending cuts, our nation’s leaders are finally confronting the main drivers of our deficit dilemma: government "entitlement" programs such as Social Security, Medicare, and Medicaid.
Meanwhile, there is broad consensus that many of our runaway health care costs are avoidable. Our current fee-for-service health care payment system rewards higher-intensity care in greater volume, with no consequence for lack of coordination. It is a significant reason that our health care system is fragmented, inefficient, and too costly.
Federal government receipts total approximately 19% of our nation’s gross domestic product. Yet if our health care spending trends remain unchecked, by 2035 Medicare and Medicaid alone are predicted to consume 13% of GDP. By 2080, Medicare and Medicaid will consume all federal taxes, while total public and private health spending will claim almost 50% of GDP. We will have to borrow to pay for the rest of the federal government’s obligations: defense, education, transportation, etc.
As of 2012, our nation is already $16 trillion in the hole and counting. Sticking with the status quo would be a disastrous choice.
However, if medical providers work together and accept new payment incentives that reward value instead of volume, we can help fix America’s broken health care system.
That cannot be done remotely in Washington. It requires health care providers in each community cooperating to increase health care quality and cut cumulative costs.
Quality, savings, and patient satisfaction all must be achieved for providers to receive incentive payments under the new health care payment model, called "value-based reimbursement."
There is plenty of waste to be found and eliminated. Last summer, the Institute of Medicine concluded that America wastes about 30% of its health care spending – some $750 billion a year – on unneeded care, excessive paperwork, fraud, and other inefficiencies.
With basic health care becoming unaffordable for many ordinary working families and individuals, that amount of waste is unacceptable.
Although no one can hope to eradicate it overnight, it’s time somebody did something about it. America is asking physicians to step up and form teams, teams such as accountable care organizations.
By doing so, you can help ensure access, improve patient care, promote efficiency, stretch health care dollars, and make patients more of a partner in their treatment. ACOs typically receive 50% of the savings they create, which should be considered compensation to you for professional services.
As healers with a calling to serve, you have an opportunity to do your part to enhance patient care while helping to improve our nation’s fiscal health. Besides empowering, and paying, physicians to regain control of the physician/patient relationship, your patients, your profession, and your nation need you.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com, or at 919-821-6612.
