User login
FDA approves epinephrine autoinjector for infants, small children
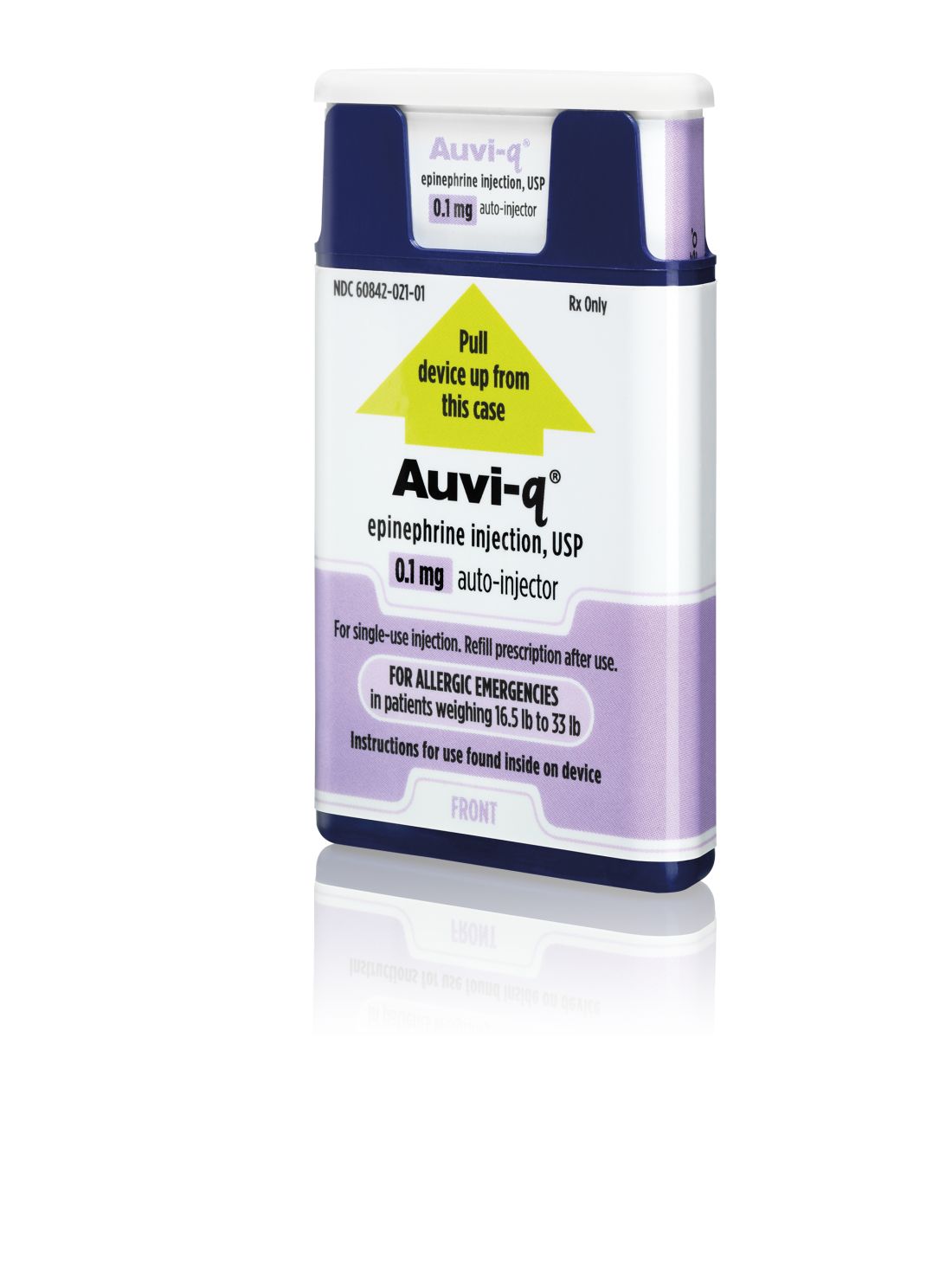
The Food and Drug Administration approved an epinephrine autoinjector constructed specifically to treat life-threatening allergic reactions in infants and small children weighing 16.5-33 pounds.
The Auvi-Q 0.1 mg autoinjector by kaléo was approved after a priority review by the FDA, with features such as “a voice prompt system that guides a user with step-by-step instructions through the delivery process,” according to a written statement from the company. This auto-injector has a shorter needle length and lower dose of epinephrine than other FDA-approved 0.15-mg and 0.3-mg epinephrine autoinjectors.
In a previous study of 51 infants with a mean weight of 24 pounds who were treated with a 0.15-mg epinephrine auto-injector with a standard 12.7-mm needle length, 43% were at risk of having the needle strike the bone. Unintentional injection of epinephrine into the intraosseous space can cause systemic absorption of the epinephrine and possible cardiac complications (Ann Allergy Asthma Immunol. 2017 Jun;118[6]:719-25.e1).
This new autoinjector with a shorter needle length was designed to obviate this problem, according to kaléo’s statement.
The Auvi-Q 0.1 mg autoinjector should be available to patients in the first half of 2018, the company said.
The Food and Drug Administration approved an epinephrine autoinjector constructed specifically to treat life-threatening allergic reactions in infants and small children weighing 16.5-33 pounds.
The Auvi-Q 0.1 mg autoinjector by kaléo was approved after a priority review by the FDA, with features such as “a voice prompt system that guides a user with step-by-step instructions through the delivery process,” according to a written statement from the company. This auto-injector has a shorter needle length and lower dose of epinephrine than other FDA-approved 0.15-mg and 0.3-mg epinephrine autoinjectors.
In a previous study of 51 infants with a mean weight of 24 pounds who were treated with a 0.15-mg epinephrine auto-injector with a standard 12.7-mm needle length, 43% were at risk of having the needle strike the bone. Unintentional injection of epinephrine into the intraosseous space can cause systemic absorption of the epinephrine and possible cardiac complications (Ann Allergy Asthma Immunol. 2017 Jun;118[6]:719-25.e1).
This new autoinjector with a shorter needle length was designed to obviate this problem, according to kaléo’s statement.
The Auvi-Q 0.1 mg autoinjector should be available to patients in the first half of 2018, the company said.
The Food and Drug Administration approved an epinephrine autoinjector constructed specifically to treat life-threatening allergic reactions in infants and small children weighing 16.5-33 pounds.
The Auvi-Q 0.1 mg autoinjector by kaléo was approved after a priority review by the FDA, with features such as “a voice prompt system that guides a user with step-by-step instructions through the delivery process,” according to a written statement from the company. This auto-injector has a shorter needle length and lower dose of epinephrine than other FDA-approved 0.15-mg and 0.3-mg epinephrine autoinjectors.
In a previous study of 51 infants with a mean weight of 24 pounds who were treated with a 0.15-mg epinephrine auto-injector with a standard 12.7-mm needle length, 43% were at risk of having the needle strike the bone. Unintentional injection of epinephrine into the intraosseous space can cause systemic absorption of the epinephrine and possible cardiac complications (Ann Allergy Asthma Immunol. 2017 Jun;118[6]:719-25.e1).
This new autoinjector with a shorter needle length was designed to obviate this problem, according to kaléo’s statement.
The Auvi-Q 0.1 mg autoinjector should be available to patients in the first half of 2018, the company said.
Monitoring HIV and Kidney Disease in Aging Asians
More people who are HIV-1 positive are living longer and better managing comorbidities—especially those associated with kidney disease. This becomes critical since the medications patients with HIV must take can be nephrotoxic with long-term use. Researchers from the AIDS Clinical Center, National Center for Global Health and Medicine, in Tokyo, Japan note that Asian patients may be at higher risk because of their generally smaller body weight and metabolism differences, compared with whites and blacks.
Few studies in Asia had assessed the prevalence and factors associated with chronic kidney disease (CKD) and end-stage renal disease (ERSD) in patients with HIV-1, the researchers say, so they conducted the first, to their knowledge, with a cross-sectional study of 1,990 patients.
One third of the patients were aged ≥ 50 years. Nearly all (94%) had HIV-load < 50 copies/mL. The median time from diagnosis to study enrollment was 9.1 years; the median duration of antiretroviral therapy (ART) was 7.35 years. Of the study patients, 256 (13%) had chronic kidney disease and 9 (0.5%) had ESRD. It is noteworthy, the researchers say, that 5 of those 9 developed ESRD long after the diagnosis of HIV infection and that the age of the ESRD patients varied from 30s to 60s.
The incidence of CKD rose from 18.6% among those aged 50-59 years to 47% for those aged > 70 years. Heavier body weight, diabetes, hypertension, and longer duration of ART also were associated with CKD. Duration of exposure to tenofovir disoproxil fumarate (TDF), however, was not associated with CKD. Of all the patients, 61% had a history of TDF use. At the time of the study, 774 patients were taking TDF; 69 in the group with CKD and 705 in the group without CKD.
Tenofovir disoproxil fumarate nephrotoxicity had been well publicized by 2016, when the data were collected for this study, the researchers note, which is why they used “duration of TDF exposure” in their logistic regression model. Tenofovir disoproxil fumarate may have been discontinued early on for the patients at risk for CKD in their study cohort. However, they note that while TDF will be replaced with its prodrug tenofovir alafenamide, other antiretroviral drugs that inhibit excretion of creatinine in the renal proximal tubules and increase serum creatinine value, such as dolutegravir, cobicistat, rilpivirine, raltegravir, and ritonavir, will still be widely used.
Source:
Nishijima T, Kawasaki Y, Mutoh Y, et al. Sci Rep. 2017;7(14565) doi:10.1038/s41598-017-15214-x
More people who are HIV-1 positive are living longer and better managing comorbidities—especially those associated with kidney disease. This becomes critical since the medications patients with HIV must take can be nephrotoxic with long-term use. Researchers from the AIDS Clinical Center, National Center for Global Health and Medicine, in Tokyo, Japan note that Asian patients may be at higher risk because of their generally smaller body weight and metabolism differences, compared with whites and blacks.
Few studies in Asia had assessed the prevalence and factors associated with chronic kidney disease (CKD) and end-stage renal disease (ERSD) in patients with HIV-1, the researchers say, so they conducted the first, to their knowledge, with a cross-sectional study of 1,990 patients.
One third of the patients were aged ≥ 50 years. Nearly all (94%) had HIV-load < 50 copies/mL. The median time from diagnosis to study enrollment was 9.1 years; the median duration of antiretroviral therapy (ART) was 7.35 years. Of the study patients, 256 (13%) had chronic kidney disease and 9 (0.5%) had ESRD. It is noteworthy, the researchers say, that 5 of those 9 developed ESRD long after the diagnosis of HIV infection and that the age of the ESRD patients varied from 30s to 60s.
The incidence of CKD rose from 18.6% among those aged 50-59 years to 47% for those aged > 70 years. Heavier body weight, diabetes, hypertension, and longer duration of ART also were associated with CKD. Duration of exposure to tenofovir disoproxil fumarate (TDF), however, was not associated with CKD. Of all the patients, 61% had a history of TDF use. At the time of the study, 774 patients were taking TDF; 69 in the group with CKD and 705 in the group without CKD.
Tenofovir disoproxil fumarate nephrotoxicity had been well publicized by 2016, when the data were collected for this study, the researchers note, which is why they used “duration of TDF exposure” in their logistic regression model. Tenofovir disoproxil fumarate may have been discontinued early on for the patients at risk for CKD in their study cohort. However, they note that while TDF will be replaced with its prodrug tenofovir alafenamide, other antiretroviral drugs that inhibit excretion of creatinine in the renal proximal tubules and increase serum creatinine value, such as dolutegravir, cobicistat, rilpivirine, raltegravir, and ritonavir, will still be widely used.
Source:
Nishijima T, Kawasaki Y, Mutoh Y, et al. Sci Rep. 2017;7(14565) doi:10.1038/s41598-017-15214-x
More people who are HIV-1 positive are living longer and better managing comorbidities—especially those associated with kidney disease. This becomes critical since the medications patients with HIV must take can be nephrotoxic with long-term use. Researchers from the AIDS Clinical Center, National Center for Global Health and Medicine, in Tokyo, Japan note that Asian patients may be at higher risk because of their generally smaller body weight and metabolism differences, compared with whites and blacks.
Few studies in Asia had assessed the prevalence and factors associated with chronic kidney disease (CKD) and end-stage renal disease (ERSD) in patients with HIV-1, the researchers say, so they conducted the first, to their knowledge, with a cross-sectional study of 1,990 patients.
One third of the patients were aged ≥ 50 years. Nearly all (94%) had HIV-load < 50 copies/mL. The median time from diagnosis to study enrollment was 9.1 years; the median duration of antiretroviral therapy (ART) was 7.35 years. Of the study patients, 256 (13%) had chronic kidney disease and 9 (0.5%) had ESRD. It is noteworthy, the researchers say, that 5 of those 9 developed ESRD long after the diagnosis of HIV infection and that the age of the ESRD patients varied from 30s to 60s.
The incidence of CKD rose from 18.6% among those aged 50-59 years to 47% for those aged > 70 years. Heavier body weight, diabetes, hypertension, and longer duration of ART also were associated with CKD. Duration of exposure to tenofovir disoproxil fumarate (TDF), however, was not associated with CKD. Of all the patients, 61% had a history of TDF use. At the time of the study, 774 patients were taking TDF; 69 in the group with CKD and 705 in the group without CKD.
Tenofovir disoproxil fumarate nephrotoxicity had been well publicized by 2016, when the data were collected for this study, the researchers note, which is why they used “duration of TDF exposure” in their logistic regression model. Tenofovir disoproxil fumarate may have been discontinued early on for the patients at risk for CKD in their study cohort. However, they note that while TDF will be replaced with its prodrug tenofovir alafenamide, other antiretroviral drugs that inhibit excretion of creatinine in the renal proximal tubules and increase serum creatinine value, such as dolutegravir, cobicistat, rilpivirine, raltegravir, and ritonavir, will still be widely used.
Source:
Nishijima T, Kawasaki Y, Mutoh Y, et al. Sci Rep. 2017;7(14565) doi:10.1038/s41598-017-15214-x
FDA approves obinutuzumab for follicular lymphoma
The Food and Drug Administration has approved obinutuzumab in combination with chemotherapy, followed by obinutuzumab alone in those who responded, for people with previously untreated advanced follicular lymphoma (stage II bulky, III or IV).

The most common adverse events associated with obinutuzumab were infusion reactions, low white blood cell count, upper respiratory tract infection, cough, constipation, and diarrhea. The most common significant adverse events are low white blood cell count, low white blood cell count with fever, and low platelet count.
Obinutuzumab is marketed as Gazyva by Genentech.
“Today’s Gazyva approval is an important advance for the thousands of people diagnosed each year with follicular lymphoma who hope to delay disease progression for as long as possible,” said Sarah Horning, MD, chief medical officer and head of global product development at Genentech, in the company press release.
The Food and Drug Administration has approved obinutuzumab in combination with chemotherapy, followed by obinutuzumab alone in those who responded, for people with previously untreated advanced follicular lymphoma (stage II bulky, III or IV).
The most common adverse events associated with obinutuzumab were infusion reactions, low white blood cell count, upper respiratory tract infection, cough, constipation, and diarrhea. The most common significant adverse events are low white blood cell count, low white blood cell count with fever, and low platelet count.
Obinutuzumab is marketed as Gazyva by Genentech.
“Today’s Gazyva approval is an important advance for the thousands of people diagnosed each year with follicular lymphoma who hope to delay disease progression for as long as possible,” said Sarah Horning, MD, chief medical officer and head of global product development at Genentech, in the company press release.
The Food and Drug Administration has approved obinutuzumab in combination with chemotherapy, followed by obinutuzumab alone in those who responded, for people with previously untreated advanced follicular lymphoma (stage II bulky, III or IV).
The most common adverse events associated with obinutuzumab were infusion reactions, low white blood cell count, upper respiratory tract infection, cough, constipation, and diarrhea. The most common significant adverse events are low white blood cell count, low white blood cell count with fever, and low platelet count.
Obinutuzumab is marketed as Gazyva by Genentech.
“Today’s Gazyva approval is an important advance for the thousands of people diagnosed each year with follicular lymphoma who hope to delay disease progression for as long as possible,” said Sarah Horning, MD, chief medical officer and head of global product development at Genentech, in the company press release.
Chinese school-based flu vaccination program reduced outbreaks
, said Yang Pan, PhD, of the Institute for Infectious Disease and Endemic Disease Control, Beijing Center for Disease Prevention and Control, and associates.
School-based trivalent inactivated influenza vaccination programs generally occurred Oct. 15-Nov. 30 each year since 2007, with greater than 50% vaccination coverage. In an 11-year retrospective study of school outbreaks of influenza in elementary, middle, and high schools in the Beijing area during Sept. 1, 2006-March 31, 2017, there were 286 febrile outbreaks in schools, involving 6,863 children.
During the 11 years, a mismatch between circulating strains and vaccine strains was identified in two influenza seasons, such as “the A(H3N2) 3C.1 (vaccine strain)-A(H3N2) 3C.3a (circulating strains) mismatch in 2014-2015, the B(Yamagata) Clade 2 (vaccine strain)-B(Yamagata) Clade 3 (circulating strain) mismatch in the 2014-2015 influenza season, and B(Yamagata) (vaccine strain)-B(Victoria) (circulating strains) mismatch in 2015-2016,” they reported.
A combination of high flu vaccine coverage because of school-based vaccinations and a good vaccine match reduced influenza outbreaks in schools by 89% (odds ratio, 0.111), Dr. Pan and associates concluded.
“The school-based influenza vaccination program has been in operation for nearly 10 years in the Beijing area, is unique in China, and is one of the few school-based influenza programs in the world,” the researchers explained. “These data can inform and improve vaccination policy locally and nationally.”
Read more in Vaccine (2017 Nov 8. doi: 10.1016/j.vaccine.2017.10.096).
, said Yang Pan, PhD, of the Institute for Infectious Disease and Endemic Disease Control, Beijing Center for Disease Prevention and Control, and associates.
School-based trivalent inactivated influenza vaccination programs generally occurred Oct. 15-Nov. 30 each year since 2007, with greater than 50% vaccination coverage. In an 11-year retrospective study of school outbreaks of influenza in elementary, middle, and high schools in the Beijing area during Sept. 1, 2006-March 31, 2017, there were 286 febrile outbreaks in schools, involving 6,863 children.
During the 11 years, a mismatch between circulating strains and vaccine strains was identified in two influenza seasons, such as “the A(H3N2) 3C.1 (vaccine strain)-A(H3N2) 3C.3a (circulating strains) mismatch in 2014-2015, the B(Yamagata) Clade 2 (vaccine strain)-B(Yamagata) Clade 3 (circulating strain) mismatch in the 2014-2015 influenza season, and B(Yamagata) (vaccine strain)-B(Victoria) (circulating strains) mismatch in 2015-2016,” they reported.
A combination of high flu vaccine coverage because of school-based vaccinations and a good vaccine match reduced influenza outbreaks in schools by 89% (odds ratio, 0.111), Dr. Pan and associates concluded.
“The school-based influenza vaccination program has been in operation for nearly 10 years in the Beijing area, is unique in China, and is one of the few school-based influenza programs in the world,” the researchers explained. “These data can inform and improve vaccination policy locally and nationally.”
Read more in Vaccine (2017 Nov 8. doi: 10.1016/j.vaccine.2017.10.096).
, said Yang Pan, PhD, of the Institute for Infectious Disease and Endemic Disease Control, Beijing Center for Disease Prevention and Control, and associates.
School-based trivalent inactivated influenza vaccination programs generally occurred Oct. 15-Nov. 30 each year since 2007, with greater than 50% vaccination coverage. In an 11-year retrospective study of school outbreaks of influenza in elementary, middle, and high schools in the Beijing area during Sept. 1, 2006-March 31, 2017, there were 286 febrile outbreaks in schools, involving 6,863 children.
During the 11 years, a mismatch between circulating strains and vaccine strains was identified in two influenza seasons, such as “the A(H3N2) 3C.1 (vaccine strain)-A(H3N2) 3C.3a (circulating strains) mismatch in 2014-2015, the B(Yamagata) Clade 2 (vaccine strain)-B(Yamagata) Clade 3 (circulating strain) mismatch in the 2014-2015 influenza season, and B(Yamagata) (vaccine strain)-B(Victoria) (circulating strains) mismatch in 2015-2016,” they reported.
A combination of high flu vaccine coverage because of school-based vaccinations and a good vaccine match reduced influenza outbreaks in schools by 89% (odds ratio, 0.111), Dr. Pan and associates concluded.
“The school-based influenza vaccination program has been in operation for nearly 10 years in the Beijing area, is unique in China, and is one of the few school-based influenza programs in the world,” the researchers explained. “These data can inform and improve vaccination policy locally and nationally.”
Read more in Vaccine (2017 Nov 8. doi: 10.1016/j.vaccine.2017.10.096).
FROM VACCINE
Benralizumab approved for eosinophilic asthma
This is the only respiratory biologic to provide fast and “near-complete depletion of eosinophils within 24 hours,” according to the statement from AstraZeneca.![]()
Similar adverse events were seen in patients who took benralizumab and the placebo. AstraZeneca will market benralizumab under the trade name Fasenra.
“This is an important day for severe, eosinophilic asthma patients who have had limited treatment options for far too long,” said Eugene Bleecker, MD, professor and codirector of genetics, genomics, and precision medicine at the University of Arizona in Tucson, in the statement.
This is the only respiratory biologic to provide fast and “near-complete depletion of eosinophils within 24 hours,” according to the statement from AstraZeneca.![]()
Similar adverse events were seen in patients who took benralizumab and the placebo. AstraZeneca will market benralizumab under the trade name Fasenra.
“This is an important day for severe, eosinophilic asthma patients who have had limited treatment options for far too long,” said Eugene Bleecker, MD, professor and codirector of genetics, genomics, and precision medicine at the University of Arizona in Tucson, in the statement.
This is the only respiratory biologic to provide fast and “near-complete depletion of eosinophils within 24 hours,” according to the statement from AstraZeneca.![]()
Similar adverse events were seen in patients who took benralizumab and the placebo. AstraZeneca will market benralizumab under the trade name Fasenra.
“This is an important day for severe, eosinophilic asthma patients who have had limited treatment options for far too long,” said Eugene Bleecker, MD, professor and codirector of genetics, genomics, and precision medicine at the University of Arizona in Tucson, in the statement.
Rituximab key to survival after transplant for mantle cell lymphoma
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
This study confirms the value of maintenance rituximab for a large cohort of patients with mantle cell lymphoma who have undergone high-dose chemotherapy and autologous stem cell transplantation outside of clinical trials.
The findings also affirm results of a recent phase 3 randomized trial (LyMa) suggesting that in previously untreated MCL patients who have undergone ASCT, rituximab maintenance is superior to observation in improving overall survival and progression-free survival.
However, the most interesting aspect of this study is the positron emission tomography data. Namely, the benefit of rituximab maintenance was apparent in patients regardless of whether they were in a PET-positive or PET-negative first complete remission at ASCT. “This important finding implies that the benefit of rituximab maintenance after ASCT is present for low- and high-risk MCL patients.”
Despite these confirmatory findings, the treatment landscape for MCL has changed significantly in recent years, particularly with the introduction of treatments such as ibrutinib.
In a clinical trial currently underway, the European Mantle Cell Lymphoma Network is evaluating ibrutinib as an upfront treatment for young and fit patients. Specifically, the study compares first-line ASCT and rituximab maintenance, ASCT with ibrutinib maintenance, or a transplant-free approach with ibrutinib and chemotherapy.
Unless and until the data from this study “redefine the value of ASCT in the ibrutinib era, ASCT and rituximab maintenance should be recommended as the standard treatment after ASCT for transplant-eligible patients with MCL.”
Tobias Roider, MD, and Sascha Dietrich, MD, are with the Department of Medicine V, University of Heidelberg, Germany. Their comments are in an editorial (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.09.008). The authors reported no financial disclosures or conflicts of interest.
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
The study, which outlines the experience across a variety of different treatment patterns at City of Hope National Medical Center, Duarte, Calif., between January 1997 and November 2013, suggests a “large benefit” of adding rituximab, wrote Matthew G. Mei, MD, of the center’s department of hematology and hematopoietic cell transplantation, and his colleagues. Further, maintenance rituximab was associated with improved survival outcomes in patients with positron emission tomography (PET)-negative status at first complete remission.
The benefit of rituximab “stands out, and adds to the increasing body of evidence supporting this practice for all MCL patients after ASCT, regardless of age and frontline induction regimens,” wrote Dr. Mei and his colleagues (Biol Blood Marrow Transplant 2017 November. doi: 10.1016/j.bbmt.2017.07.006). This was the case even with improvements in early diagnosis and supportive care, and the incorporation of novel agents such as bortezomib, lenalidomide, and ibrutinib, they wrote, noting significantly better outcomes for patients who underwent ASCT after 2007.
In multivariate analysis, maintenance rituximab therapy after ASCT was the single most important factor associated with improvement in progression-free survival (relative risk [RR], .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Positron emission tomography scans were done prior to ASCT for 133 patients; after ASCT, 105 (79%) were found to be in a PET-negative complete remission. All but one of the patients with PET-negative disease received rituximab before ASCT. For that PET-negative subset, maintenance rituximab was significantly associated with improvements in progression-free survival (RR, .20; 95% CI, .09-.43) and overall survival (RR, .17; 95% CI, .05-.59).
This study represents one of the largest single-center reports to date on MCL patients who have undergone ASCT, according to the authors. “This study also sets the stage for prospective investigation aiming at optimization of maintenance therapy following ASCT.”
Dr. Mei reported no disclosures, and senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium. The study was supported by research funding from the National Cancer Institute.
FROM BIOLOGY OF BLOOD AND MARROW TRANSPLANTATION
Key clinical point: Over time and in many different patterns, rituximab maintenance therapy stood out as the prominent factor influencing survival in patients with mantle cell lymphoma who undergo autologous stem cell transplant.
Major finding: Maintenance rituximab was significantly associated with superior progression-free survival (relative risk, .25; 95% confidence interval, .14-.44) and overall survival (RR, .17; 95% CI, .07-.38).
Data source: Retrospective analysis of data for 191 patients with MCL who underwent ASCT at a medical center in California between January 1997 and November 2013.
Disclosures: The study was supported by research funding from the National Cancer Institute. Senior author Lihua E. Budde, MD, PhD, reported being a member of the Lymphoma Research Foundation MCL consortium.
DTaP vaccination rate highest in Maryland
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).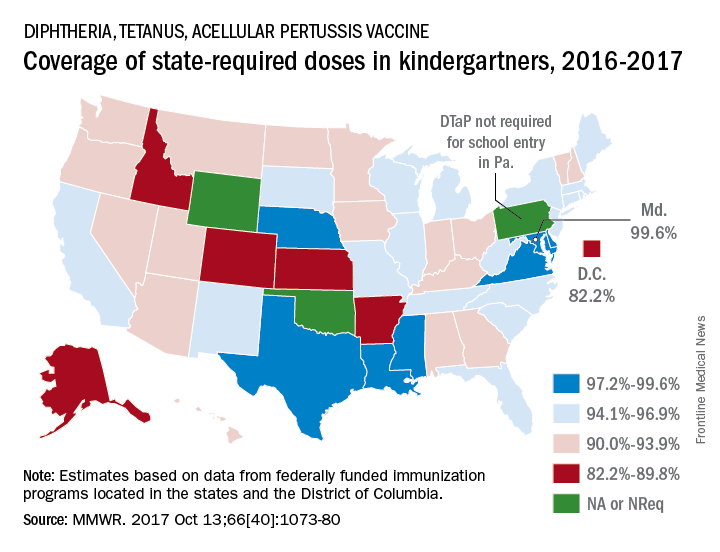
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
FROM MMWR
NCI-MATCH: Nivolumab shows promising activity in noncolorectal cancers
NATIONAL HARBOR, MD. – The immune checkpoint inhibitor nivolumab has promising activity in mismatch repair–deficient noncolorectal cancers, according to preliminary findings from the first sub-arm of the National Cancer Institute’s landmark Molecular Analysis for Therapy Choice (NCI-MATCH) trial.
NCI-MATCH is a 1,173-site precision medicine trial launched in 2015 to study targeted therapies for patients with relapsed/refractory solid tumors, lymphomas, and myelomas. In the first substudy (arm Z1D), the investigators identified 4,900 subjects with samples that could be tested for “actionable molecular abnormalities,” and from among those, they identified 77 with loss of mismatch repair proteins MLH1 or MSH2. Ultimately 47 patients were treated with nivolumab in the substudy.

The confirmed overall response rate was 24%, and an additional 27% of patients had stable disease, said Dr. Azad of Johns Hopkins University, Baltimore.
The patients had a median age of 60 years and were heavily pretreated with a median of three prior therapies. The most common histologies among them were endometrioid endometrial cancer (10 patients), prostate cancer (6 patients), and breast cancer (3 patients).
The safety and tolerability of treatment was as expected for single-agent nivolumab treatment. Toxicity was predominantly low-grade fatigue. Anemia was the most common grade 3 toxicity.
“DNA repair defects due to mismatch repair–deficiency are most commonly caused by silencing of mismatch repair proteins MLH1 or MSH2 and, a little less commonly, MSH6 or PMS2. This can happen through DNA mutation, as well as promoter methylation,” Dr. Azad explained. “In fact, nivolumab has already been tested in patients with mismatch repair–deficient colorectal cancer, both alone and in combination with anti-CTLA-4 ipilimumab ... in addition, pembrolizumab was approved earlier this year for pretreated mismatch repair–deficient cancer.”
“So this formed the nidus for our interest and hypothesis that nivolumab would also have activity in mismatch repair–deficient noncolorectal cancer,” she said.
Study subjects had relapsed/refractory cancers, good end-organ function, and good performance status. They were screened for molecular alterations by centralized testing on fresh biopsy tissue, and mismatch repair deficiency was defined through immunohistochemistry as loss of nuclear expression of MLH1 or MSH2. Patients with mismatch repair–deficient colorectal cancer were excluded.
Those in the nivolumab arm received 3 mg/kg every 2 weeks, and after cycle 4, they could be switched to receive treatment every 4 weeks. Imaging was performed every 2 weeks, and patients were allowed to remain in the study as long as their disease had not progressed. A caveat was that patients with progression within the first 24 weeks, but with no more than four new lesions or 40% increase in tumor index lesions, could remain in the study as long as they were clinically stable.
The overall response rate was compared against a null value of 5%.
“We enrolled 35 patients so that we could have 31 evaluable patients, looking for a signal of 5 or greater responses in that patient group to conclude that the arm was promising and worth further testing,” Dr. Azad said. “This gave us 91.8% power to conclude that an agent was promising if the overall response was truly 25%.”
The study met its primary endpoint, with 8 responses out of 34 evaluable patients, she reported.
“Of note, we had five more patients that had unconfirmed responses. Two of those remained on study at the time of data cutoff, so these response numbers may change as the study matures,” she said.
The disease control rate was 56%, and benefit was seen across tumor histologies, she noted.
“The duration of benefit was compelling for these patients,” she said. “The median time to response was 2.1 cycles, and the 6-month progression-free survival was 49%.”
The median duration of response has not been reached.
Follow-up is ongoing, and 12 patients are enrolled in an expansion cohort; results should be reported within the next year.
“Future work includes interrogating tumor tissue and blood to identify possible predictive markers of response and resistance,” Dr. Azad concluded.
Dr. Azad reported having no disclosures.
NATIONAL HARBOR, MD. – The immune checkpoint inhibitor nivolumab has promising activity in mismatch repair–deficient noncolorectal cancers, according to preliminary findings from the first sub-arm of the National Cancer Institute’s landmark Molecular Analysis for Therapy Choice (NCI-MATCH) trial.
NCI-MATCH is a 1,173-site precision medicine trial launched in 2015 to study targeted therapies for patients with relapsed/refractory solid tumors, lymphomas, and myelomas. In the first substudy (arm Z1D), the investigators identified 4,900 subjects with samples that could be tested for “actionable molecular abnormalities,” and from among those, they identified 77 with loss of mismatch repair proteins MLH1 or MSH2. Ultimately 47 patients were treated with nivolumab in the substudy.
The confirmed overall response rate was 24%, and an additional 27% of patients had stable disease, said Dr. Azad of Johns Hopkins University, Baltimore.
The patients had a median age of 60 years and were heavily pretreated with a median of three prior therapies. The most common histologies among them were endometrioid endometrial cancer (10 patients), prostate cancer (6 patients), and breast cancer (3 patients).
The safety and tolerability of treatment was as expected for single-agent nivolumab treatment. Toxicity was predominantly low-grade fatigue. Anemia was the most common grade 3 toxicity.
“DNA repair defects due to mismatch repair–deficiency are most commonly caused by silencing of mismatch repair proteins MLH1 or MSH2 and, a little less commonly, MSH6 or PMS2. This can happen through DNA mutation, as well as promoter methylation,” Dr. Azad explained. “In fact, nivolumab has already been tested in patients with mismatch repair–deficient colorectal cancer, both alone and in combination with anti-CTLA-4 ipilimumab ... in addition, pembrolizumab was approved earlier this year for pretreated mismatch repair–deficient cancer.”
“So this formed the nidus for our interest and hypothesis that nivolumab would also have activity in mismatch repair–deficient noncolorectal cancer,” she said.
Study subjects had relapsed/refractory cancers, good end-organ function, and good performance status. They were screened for molecular alterations by centralized testing on fresh biopsy tissue, and mismatch repair deficiency was defined through immunohistochemistry as loss of nuclear expression of MLH1 or MSH2. Patients with mismatch repair–deficient colorectal cancer were excluded.
Those in the nivolumab arm received 3 mg/kg every 2 weeks, and after cycle 4, they could be switched to receive treatment every 4 weeks. Imaging was performed every 2 weeks, and patients were allowed to remain in the study as long as their disease had not progressed. A caveat was that patients with progression within the first 24 weeks, but with no more than four new lesions or 40% increase in tumor index lesions, could remain in the study as long as they were clinically stable.
The overall response rate was compared against a null value of 5%.
“We enrolled 35 patients so that we could have 31 evaluable patients, looking for a signal of 5 or greater responses in that patient group to conclude that the arm was promising and worth further testing,” Dr. Azad said. “This gave us 91.8% power to conclude that an agent was promising if the overall response was truly 25%.”
The study met its primary endpoint, with 8 responses out of 34 evaluable patients, she reported.
“Of note, we had five more patients that had unconfirmed responses. Two of those remained on study at the time of data cutoff, so these response numbers may change as the study matures,” she said.
The disease control rate was 56%, and benefit was seen across tumor histologies, she noted.
“The duration of benefit was compelling for these patients,” she said. “The median time to response was 2.1 cycles, and the 6-month progression-free survival was 49%.”
The median duration of response has not been reached.
Follow-up is ongoing, and 12 patients are enrolled in an expansion cohort; results should be reported within the next year.
“Future work includes interrogating tumor tissue and blood to identify possible predictive markers of response and resistance,” Dr. Azad concluded.
Dr. Azad reported having no disclosures.
NATIONAL HARBOR, MD. – The immune checkpoint inhibitor nivolumab has promising activity in mismatch repair–deficient noncolorectal cancers, according to preliminary findings from the first sub-arm of the National Cancer Institute’s landmark Molecular Analysis for Therapy Choice (NCI-MATCH) trial.
NCI-MATCH is a 1,173-site precision medicine trial launched in 2015 to study targeted therapies for patients with relapsed/refractory solid tumors, lymphomas, and myelomas. In the first substudy (arm Z1D), the investigators identified 4,900 subjects with samples that could be tested for “actionable molecular abnormalities,” and from among those, they identified 77 with loss of mismatch repair proteins MLH1 or MSH2. Ultimately 47 patients were treated with nivolumab in the substudy.
The confirmed overall response rate was 24%, and an additional 27% of patients had stable disease, said Dr. Azad of Johns Hopkins University, Baltimore.
The patients had a median age of 60 years and were heavily pretreated with a median of three prior therapies. The most common histologies among them were endometrioid endometrial cancer (10 patients), prostate cancer (6 patients), and breast cancer (3 patients).
The safety and tolerability of treatment was as expected for single-agent nivolumab treatment. Toxicity was predominantly low-grade fatigue. Anemia was the most common grade 3 toxicity.
“DNA repair defects due to mismatch repair–deficiency are most commonly caused by silencing of mismatch repair proteins MLH1 or MSH2 and, a little less commonly, MSH6 or PMS2. This can happen through DNA mutation, as well as promoter methylation,” Dr. Azad explained. “In fact, nivolumab has already been tested in patients with mismatch repair–deficient colorectal cancer, both alone and in combination with anti-CTLA-4 ipilimumab ... in addition, pembrolizumab was approved earlier this year for pretreated mismatch repair–deficient cancer.”
“So this formed the nidus for our interest and hypothesis that nivolumab would also have activity in mismatch repair–deficient noncolorectal cancer,” she said.
Study subjects had relapsed/refractory cancers, good end-organ function, and good performance status. They were screened for molecular alterations by centralized testing on fresh biopsy tissue, and mismatch repair deficiency was defined through immunohistochemistry as loss of nuclear expression of MLH1 or MSH2. Patients with mismatch repair–deficient colorectal cancer were excluded.
Those in the nivolumab arm received 3 mg/kg every 2 weeks, and after cycle 4, they could be switched to receive treatment every 4 weeks. Imaging was performed every 2 weeks, and patients were allowed to remain in the study as long as their disease had not progressed. A caveat was that patients with progression within the first 24 weeks, but with no more than four new lesions or 40% increase in tumor index lesions, could remain in the study as long as they were clinically stable.
The overall response rate was compared against a null value of 5%.
“We enrolled 35 patients so that we could have 31 evaluable patients, looking for a signal of 5 or greater responses in that patient group to conclude that the arm was promising and worth further testing,” Dr. Azad said. “This gave us 91.8% power to conclude that an agent was promising if the overall response was truly 25%.”
The study met its primary endpoint, with 8 responses out of 34 evaluable patients, she reported.
“Of note, we had five more patients that had unconfirmed responses. Two of those remained on study at the time of data cutoff, so these response numbers may change as the study matures,” she said.
The disease control rate was 56%, and benefit was seen across tumor histologies, she noted.
“The duration of benefit was compelling for these patients,” she said. “The median time to response was 2.1 cycles, and the 6-month progression-free survival was 49%.”
The median duration of response has not been reached.
Follow-up is ongoing, and 12 patients are enrolled in an expansion cohort; results should be reported within the next year.
“Future work includes interrogating tumor tissue and blood to identify possible predictive markers of response and resistance,” Dr. Azad concluded.
Dr. Azad reported having no disclosures.
AT SITC 2017
Key clinical point:
Major finding: The confirmed overall response rate was 24%, and an additional 27% of patients had stable disease.
Data source: Arm Z1D (35 patients) of the NCI-MATCH trial.
Disclosures: Dr. Azad reported having no disclosures.
Study Will Compare Mammography Screening Methods
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
The Return of Scarlet Fever?
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”