User login
VA is First Hospital System to Release Opioid-Prescribing Rates
The VA has begun publicly posting information on opioids dispensed from VA pharmacies, becoming the only health care system in the country to do so.
An interactive map is available, showing data from 2012-2017, with opioid-dispensing rates for each facility and how much those rates have changed over time. The prescribing-rate information will be updated twice a year. According to the data, opioid prescribing rates dropped 41% between 2012-2017.
Nearly all (99%) facilities reduced their prescribing rates. El Paso, Texas, and Fayetteville, North Carolina are “most improved,” cutting prescribing rates by > 60% since 2012. San Juan, Puerto Rico, and Cleveland, Ohio, have the lowest prescribing rates, at 3%.
The map is available at https://www.data.va.gov/story/department-veterans-affairs-opioid-prescribing-data.
The VA has begun publicly posting information on opioids dispensed from VA pharmacies, becoming the only health care system in the country to do so.
An interactive map is available, showing data from 2012-2017, with opioid-dispensing rates for each facility and how much those rates have changed over time. The prescribing-rate information will be updated twice a year. According to the data, opioid prescribing rates dropped 41% between 2012-2017.
Nearly all (99%) facilities reduced their prescribing rates. El Paso, Texas, and Fayetteville, North Carolina are “most improved,” cutting prescribing rates by > 60% since 2012. San Juan, Puerto Rico, and Cleveland, Ohio, have the lowest prescribing rates, at 3%.
The map is available at https://www.data.va.gov/story/department-veterans-affairs-opioid-prescribing-data.
The VA has begun publicly posting information on opioids dispensed from VA pharmacies, becoming the only health care system in the country to do so.
An interactive map is available, showing data from 2012-2017, with opioid-dispensing rates for each facility and how much those rates have changed over time. The prescribing-rate information will be updated twice a year. According to the data, opioid prescribing rates dropped 41% between 2012-2017.
Nearly all (99%) facilities reduced their prescribing rates. El Paso, Texas, and Fayetteville, North Carolina are “most improved,” cutting prescribing rates by > 60% since 2012. San Juan, Puerto Rico, and Cleveland, Ohio, have the lowest prescribing rates, at 3%.
The map is available at https://www.data.va.gov/story/department-veterans-affairs-opioid-prescribing-data.
Ibrutinib plus venetoclax is active in mantle cell lymphoma
In mantle cell lymphoma (MCL), ibrutinib plus venetoclax significantly improved the complete response rate, compared with what has been previously reported for ibrutinib alone, according to results of a phase 2 study.
Clinical outcomes with the combination seem superior to previously reported results for either treatment alone, said lead investigator Constantine S. Tam, MBBS, MD, of the Peter MacCallum Cancer Centre, Melbourne, and his coinvestigators.
“The results of our study, which used a historical cohort as a control, are consistent with the notion that the combination of ibrutinib and venetoclax is highly effective in mantle-cell lymphoma,” the investigators wrote in the New England Journal of Medicine.
The BTK inhibitor ibrutinib and the BCL2 inhibitor venetoclax are two of the most active agents for this B-cell cancer, investigators reported. The rationale for combining the agents is “compelling” because they affect different critical pathways in the malignant B cell.
Both agents have demonstrated complete response rates of 21% in previous studies of relapsed or refractory MCL, and preclinical studies suggest the combination of ibrutinib and venetoclax would be synergistic.
In the present single-group, phase 2 study, 24 patients with MCL (23 relapsed or refractory, 1 previously untreated) started ibrutinib 560 mg daily; at 4 weeks, venetoclax was started at a low dose and increased to 400 mg daily.
The study primary end point – complete response rate at week 16 assessed by CT – was 42%, compared with 9% for ibrutinib monotherapy in the phase 2 PCYC-1104-CA study (P less than .001).
Computed tomography assessment was used for the primary end point to allow comparison to the ibrutinib monotherapy study, which did not use positron emission tomography for restaging. “Our study was designed to have 80% power to reject a complete response rate of 9% (at a one-sided alpha level of 0.05) if the rate of complete response was at least 30%,” the investigators noted.
Complete response rate assessed by positron emission tomography at week 16 was 62%, and was 71% overall.
In all, 67% of patients had absence of minimal residual disease by flow cytometry. At 15 months, 78% of the responses were ongoing, and at 18 months, 57% of patients were alive and progression free.
“Such outcomes appear to be substantially better than those that have been reported for ibrutinib or venetoclax monotherapy,” the investigators wrote.
The combination had side effects that are “acceptable to both patients and physicians,” investigators wrote. Side effects, usually low grade, included diarrhea in 83% of patients, fatigue in 75%, and nausea or vomiting in 71%. Tumor lysis syndrome was seen in two patients.
Whether ibrutinib plus venetoclax is superior to ibrutinib alone is being formally evaluated in an ongoing phase 3 study.
Janssen and AbbVie partially funded the current phase 2 study. Dr. Tam reported financial ties to Janssen, AbbVie, and Pharmacyclics. Other study authors reported financial ties to various pharmaceutical companies.
SOURCE: Tam C et al. N Engl J Med. 2018;378:1211-23.
In mantle cell lymphoma (MCL), ibrutinib plus venetoclax significantly improved the complete response rate, compared with what has been previously reported for ibrutinib alone, according to results of a phase 2 study.
Clinical outcomes with the combination seem superior to previously reported results for either treatment alone, said lead investigator Constantine S. Tam, MBBS, MD, of the Peter MacCallum Cancer Centre, Melbourne, and his coinvestigators.
“The results of our study, which used a historical cohort as a control, are consistent with the notion that the combination of ibrutinib and venetoclax is highly effective in mantle-cell lymphoma,” the investigators wrote in the New England Journal of Medicine.
The BTK inhibitor ibrutinib and the BCL2 inhibitor venetoclax are two of the most active agents for this B-cell cancer, investigators reported. The rationale for combining the agents is “compelling” because they affect different critical pathways in the malignant B cell.
Both agents have demonstrated complete response rates of 21% in previous studies of relapsed or refractory MCL, and preclinical studies suggest the combination of ibrutinib and venetoclax would be synergistic.
In the present single-group, phase 2 study, 24 patients with MCL (23 relapsed or refractory, 1 previously untreated) started ibrutinib 560 mg daily; at 4 weeks, venetoclax was started at a low dose and increased to 400 mg daily.
The study primary end point – complete response rate at week 16 assessed by CT – was 42%, compared with 9% for ibrutinib monotherapy in the phase 2 PCYC-1104-CA study (P less than .001).
Computed tomography assessment was used for the primary end point to allow comparison to the ibrutinib monotherapy study, which did not use positron emission tomography for restaging. “Our study was designed to have 80% power to reject a complete response rate of 9% (at a one-sided alpha level of 0.05) if the rate of complete response was at least 30%,” the investigators noted.
Complete response rate assessed by positron emission tomography at week 16 was 62%, and was 71% overall.
In all, 67% of patients had absence of minimal residual disease by flow cytometry. At 15 months, 78% of the responses were ongoing, and at 18 months, 57% of patients were alive and progression free.
“Such outcomes appear to be substantially better than those that have been reported for ibrutinib or venetoclax monotherapy,” the investigators wrote.
The combination had side effects that are “acceptable to both patients and physicians,” investigators wrote. Side effects, usually low grade, included diarrhea in 83% of patients, fatigue in 75%, and nausea or vomiting in 71%. Tumor lysis syndrome was seen in two patients.
Whether ibrutinib plus venetoclax is superior to ibrutinib alone is being formally evaluated in an ongoing phase 3 study.
Janssen and AbbVie partially funded the current phase 2 study. Dr. Tam reported financial ties to Janssen, AbbVie, and Pharmacyclics. Other study authors reported financial ties to various pharmaceutical companies.
SOURCE: Tam C et al. N Engl J Med. 2018;378:1211-23.
In mantle cell lymphoma (MCL), ibrutinib plus venetoclax significantly improved the complete response rate, compared with what has been previously reported for ibrutinib alone, according to results of a phase 2 study.
Clinical outcomes with the combination seem superior to previously reported results for either treatment alone, said lead investigator Constantine S. Tam, MBBS, MD, of the Peter MacCallum Cancer Centre, Melbourne, and his coinvestigators.
“The results of our study, which used a historical cohort as a control, are consistent with the notion that the combination of ibrutinib and venetoclax is highly effective in mantle-cell lymphoma,” the investigators wrote in the New England Journal of Medicine.
The BTK inhibitor ibrutinib and the BCL2 inhibitor venetoclax are two of the most active agents for this B-cell cancer, investigators reported. The rationale for combining the agents is “compelling” because they affect different critical pathways in the malignant B cell.
Both agents have demonstrated complete response rates of 21% in previous studies of relapsed or refractory MCL, and preclinical studies suggest the combination of ibrutinib and venetoclax would be synergistic.
In the present single-group, phase 2 study, 24 patients with MCL (23 relapsed or refractory, 1 previously untreated) started ibrutinib 560 mg daily; at 4 weeks, venetoclax was started at a low dose and increased to 400 mg daily.
The study primary end point – complete response rate at week 16 assessed by CT – was 42%, compared with 9% for ibrutinib monotherapy in the phase 2 PCYC-1104-CA study (P less than .001).
Computed tomography assessment was used for the primary end point to allow comparison to the ibrutinib monotherapy study, which did not use positron emission tomography for restaging. “Our study was designed to have 80% power to reject a complete response rate of 9% (at a one-sided alpha level of 0.05) if the rate of complete response was at least 30%,” the investigators noted.
Complete response rate assessed by positron emission tomography at week 16 was 62%, and was 71% overall.
In all, 67% of patients had absence of minimal residual disease by flow cytometry. At 15 months, 78% of the responses were ongoing, and at 18 months, 57% of patients were alive and progression free.
“Such outcomes appear to be substantially better than those that have been reported for ibrutinib or venetoclax monotherapy,” the investigators wrote.
The combination had side effects that are “acceptable to both patients and physicians,” investigators wrote. Side effects, usually low grade, included diarrhea in 83% of patients, fatigue in 75%, and nausea or vomiting in 71%. Tumor lysis syndrome was seen in two patients.
Whether ibrutinib plus venetoclax is superior to ibrutinib alone is being formally evaluated in an ongoing phase 3 study.
Janssen and AbbVie partially funded the current phase 2 study. Dr. Tam reported financial ties to Janssen, AbbVie, and Pharmacyclics. Other study authors reported financial ties to various pharmaceutical companies.
SOURCE: Tam C et al. N Engl J Med. 2018;378:1211-23.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Dual targeting of BTK and BCL2 with ibrutinib and venetoclax may improve complete response rate versus ibrutinib alone in patients with mantle cell lymphoma.
Major finding: Complete response rate at week 16 as assessed by CT was 42%, compared with 9% with ibrutinib monotherapy in a previous study (P less than .001).
Study details: A single-group phase 2 study of daily oral ibrutinib and venetoclax in 24 patients with mantle cell lymphoma (23 relapsed or refractory, 1 previously untreated), as compared with historical controls.
Disclosures: Janssen and AbbVie partially funded the study. Dr. Tam reported financial ties to Janssen, Abbvie, and Pharmacyclics. Other study authors reported financial ties to various pharmaceutical companies.
Source: Tam C et al. N Engl J Med. 2018;378:1211-23.
Waning vaccine immunity linked to pertussis resurgence
researchers said.
In the March 28, 2018, edition of Science Translational Medicine, researchers reported on a study that used different models of transmission to explore what might be the cause of the steady increase in pertussis infections since the mid-1970s.
Using 16 years’ worth of detailed, age-stratified incidence data from Massachusetts, researchers found that the model which assumed a gradual waning in protection was the best fit for the observed patterns of pertussis incidence across the population.
This model suggested significant variability in how the level of protection changes over time, with a 10% risk of vaccine protection waning to zero within 10 years of completing routine vaccination and a 55% chance that the vaccine would confer lifelong protection.
“Crucially, we find that the vaccine is effective at reducing pathogen circulation but not so effective that eradication of this highly contagious bacterium should be possible without targeted booster campaigns,” wrote Dr. Matthieu Domenech de Cellès, PhD, of the Institut Pasteur at the University of Versailles (France) and his coauthors.
The model also considered the possibility that the whole-cell and acellular pertussis vaccines might show differences in immunity, which had been suggested as one explanation for the resurgence of the disease. However, the authors found little evidence of a marked epidemiological switch from the whole-cell to acellular vaccines, although their results did suggest the acellular vaccine has a moderately reduced efficacy.
“Our results suggest that the train of events leading to the resurgence of pertussis was set in motion well before the shift to the DTaP vaccine,” Dr. Domenech de Cellès and his associates said.
The model also pointed to big shifts in the age-specific immunological profile caused by introduction of vaccination, which led to a reduction in transmission and also a reduction in natural infections both in vaccinated and unvaccinated individuals.
This meant individuals who either did not get vaccinated as children or who did not gain immunity from vaccination were growing to adulthood without ever being exposed to natural infection.
“Concurrently, older cohorts, with their long-lived immunity derived from natural infections experienced during the prevaccine period, were gradually dying out,” the authors said. “The resulting rise in the number of susceptible adults sets the stage for the pertussis resurgence, especially among adults.”
Two authors were supported by the National Institutes of Health and by Models of Infectious Disease Agent Study–National Institute of General Medical Sciences. No conflicts of interest were declared.
SOURCE: Domenech de Cellès M et al. Sci Transl Med. 2018 Mar 28;10:eaaj1748.
researchers said.
In the March 28, 2018, edition of Science Translational Medicine, researchers reported on a study that used different models of transmission to explore what might be the cause of the steady increase in pertussis infections since the mid-1970s.
Using 16 years’ worth of detailed, age-stratified incidence data from Massachusetts, researchers found that the model which assumed a gradual waning in protection was the best fit for the observed patterns of pertussis incidence across the population.
This model suggested significant variability in how the level of protection changes over time, with a 10% risk of vaccine protection waning to zero within 10 years of completing routine vaccination and a 55% chance that the vaccine would confer lifelong protection.
“Crucially, we find that the vaccine is effective at reducing pathogen circulation but not so effective that eradication of this highly contagious bacterium should be possible without targeted booster campaigns,” wrote Dr. Matthieu Domenech de Cellès, PhD, of the Institut Pasteur at the University of Versailles (France) and his coauthors.
The model also considered the possibility that the whole-cell and acellular pertussis vaccines might show differences in immunity, which had been suggested as one explanation for the resurgence of the disease. However, the authors found little evidence of a marked epidemiological switch from the whole-cell to acellular vaccines, although their results did suggest the acellular vaccine has a moderately reduced efficacy.
“Our results suggest that the train of events leading to the resurgence of pertussis was set in motion well before the shift to the DTaP vaccine,” Dr. Domenech de Cellès and his associates said.
The model also pointed to big shifts in the age-specific immunological profile caused by introduction of vaccination, which led to a reduction in transmission and also a reduction in natural infections both in vaccinated and unvaccinated individuals.
This meant individuals who either did not get vaccinated as children or who did not gain immunity from vaccination were growing to adulthood without ever being exposed to natural infection.
“Concurrently, older cohorts, with their long-lived immunity derived from natural infections experienced during the prevaccine period, were gradually dying out,” the authors said. “The resulting rise in the number of susceptible adults sets the stage for the pertussis resurgence, especially among adults.”
Two authors were supported by the National Institutes of Health and by Models of Infectious Disease Agent Study–National Institute of General Medical Sciences. No conflicts of interest were declared.
SOURCE: Domenech de Cellès M et al. Sci Transl Med. 2018 Mar 28;10:eaaj1748.
researchers said.
In the March 28, 2018, edition of Science Translational Medicine, researchers reported on a study that used different models of transmission to explore what might be the cause of the steady increase in pertussis infections since the mid-1970s.
Using 16 years’ worth of detailed, age-stratified incidence data from Massachusetts, researchers found that the model which assumed a gradual waning in protection was the best fit for the observed patterns of pertussis incidence across the population.
This model suggested significant variability in how the level of protection changes over time, with a 10% risk of vaccine protection waning to zero within 10 years of completing routine vaccination and a 55% chance that the vaccine would confer lifelong protection.
“Crucially, we find that the vaccine is effective at reducing pathogen circulation but not so effective that eradication of this highly contagious bacterium should be possible without targeted booster campaigns,” wrote Dr. Matthieu Domenech de Cellès, PhD, of the Institut Pasteur at the University of Versailles (France) and his coauthors.
The model also considered the possibility that the whole-cell and acellular pertussis vaccines might show differences in immunity, which had been suggested as one explanation for the resurgence of the disease. However, the authors found little evidence of a marked epidemiological switch from the whole-cell to acellular vaccines, although their results did suggest the acellular vaccine has a moderately reduced efficacy.
“Our results suggest that the train of events leading to the resurgence of pertussis was set in motion well before the shift to the DTaP vaccine,” Dr. Domenech de Cellès and his associates said.
The model also pointed to big shifts in the age-specific immunological profile caused by introduction of vaccination, which led to a reduction in transmission and also a reduction in natural infections both in vaccinated and unvaccinated individuals.
This meant individuals who either did not get vaccinated as children or who did not gain immunity from vaccination were growing to adulthood without ever being exposed to natural infection.
“Concurrently, older cohorts, with their long-lived immunity derived from natural infections experienced during the prevaccine period, were gradually dying out,” the authors said. “The resulting rise in the number of susceptible adults sets the stage for the pertussis resurgence, especially among adults.”
Two authors were supported by the National Institutes of Health and by Models of Infectious Disease Agent Study–National Institute of General Medical Sciences. No conflicts of interest were declared.
SOURCE: Domenech de Cellès M et al. Sci Transl Med. 2018 Mar 28;10:eaaj1748.
FROM SCIENCE TRANSLATIONAL MEDICINE
TB in 2017: Good news and bad news
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.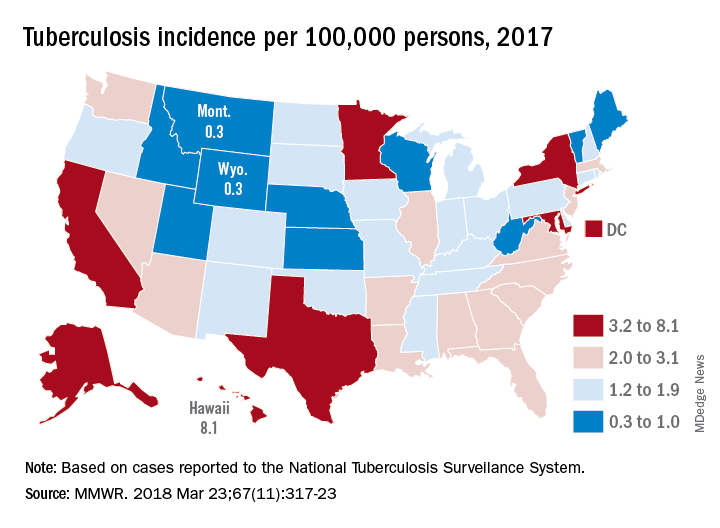
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
according to the Centers for Disease Control and Prevention.
Those new lows – TB incidence of 2.8 per 100,000 persons and 9,093 new cases – continue a downward trend that started in 1993, but the current rate of decline is much lower than the threshold needed to eliminate TB by the year 2100, Rebekah J. Stewart and her associates at the CDC’s Division of Tuberculosis Elimination, Atlanta, wrote in the Morbidity and Mortality Weekly Report.
Geographically, at least, the states with populations at the highest risk are Hawaii, which had a TB incidence of 8.1 per 100,000 persons in 2017, and Alaska, with an incidence of 7.0 per 100,000. California and the District of Columbia were next, each with an incidence of 5.2. The states with the lowest rates were Montana and Wyoming at 0.3 per 100,000, the investigators reported, based on data from the National Tuberculosis Surveillance System as of Feb. 12, 2018.
Groups most affected by TB include persons housed in congregate settings – homeless shelters, long-term care facilities, and correctional facilities – and those from countries that have high TB prevalence. Overall incidence for non–U.S. born residents was 14.6 per 100,000 in 2017, compared with 1.0 for the native born, with large discrepancies seen between U.S. and non–U.S. born blacks (2.8 vs. 22.0), native Hawaiian/Pacific Islanders (6.5 vs. 21.0), and Asians (2.0 vs. 27.0), Ms. Stewart and her associates said.
“Increased support of global TB elimination efforts would help to reduce global … prevalence, thereby indirectly reducing the incidence of reactivation TB in the United States among non–U.S. born persons from higher-prevalence countries,” they wrote.
The issue of global action on TB was addressed by the Forum of International Respiratory Societies in a statement recognizing World TB Day (March 24). “TB is the world’s most common infectious disease killer, yet is identifiable, treatable and preventable; what is missing is the political will to dedicate the resources necessary to eradicate it, once and for all,” said Dean E. Schraufnagel, MD, the organization’s executive director.
SOURCE: Stewart RJ et al. MMWR 2018 Mar 23;67(11):317-23.
FROM MMWR
Filling a Gender Gap in Research
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
Women, the VA wants your brains. It sounds a little disconcerting at first, but the National Center for PTSD and the nonprofit PINK Concussions are encouraging women to donate their brains for research.
In the past, says Dr. Carolyn Clancy, executive in charge of Veterans Health Administration, “the focus on TBI and PTSD brain research has primarily been based on male brains, without any active recruitment for women.” There has been almost no postmortem brain tissue available for study of injury in women. The VA also notes a lack of research on chronic traumatic encephalopathy in women. Only 2 peer-reviewed journal articles, both published in the early 1990s, have focused on women.
Women who are interested can take the “PINK Brain Pledge,” a nonbinding promise to leave their brains to science. They do not have to have a history of TBI or PTSD; brains also are needed for controls.
All VA Facilities Now Offer Same-Day Service
Calling it “a major milestone,” the VA announced same-day services for urgent primary and mental health care are now available at 100% of its > 1,000 medical facilities.
Now a veteran can more conveniently have a face-to-face visit with a clinician, call a nurse, have a telehealth or video care visit, get an appointment with a specialist, or have a prescription filled in the same day, “depending upon what best meets the needs of the veteran.”
The VA also has reduced patient wait time, and implemented a new process to ensure timely follow-up appointments for time-sensitive medical needs.
Calling it “a major milestone,” the VA announced same-day services for urgent primary and mental health care are now available at 100% of its > 1,000 medical facilities.
Now a veteran can more conveniently have a face-to-face visit with a clinician, call a nurse, have a telehealth or video care visit, get an appointment with a specialist, or have a prescription filled in the same day, “depending upon what best meets the needs of the veteran.”
The VA also has reduced patient wait time, and implemented a new process to ensure timely follow-up appointments for time-sensitive medical needs.
Calling it “a major milestone,” the VA announced same-day services for urgent primary and mental health care are now available at 100% of its > 1,000 medical facilities.
Now a veteran can more conveniently have a face-to-face visit with a clinician, call a nurse, have a telehealth or video care visit, get an appointment with a specialist, or have a prescription filled in the same day, “depending upon what best meets the needs of the veteran.”
The VA also has reduced patient wait time, and implemented a new process to ensure timely follow-up appointments for time-sensitive medical needs.
RSV immunoprophylaxis in premature infants doesn’t prevent later asthma
reported Nienke M. Scheltema, MD, of Wilhelmina Children’s Hospital, Utrecht, the Netherlands, and associates.
In a study of 395 otherwise healthy premature infants who were randomized to receive palivizumab for respiratory syncytial virus (RSV) immunoprophylaxis or placebo and followed for 6 years, 14% of the 199 infants in the RSV prevention group had parent-reported asthma, compared with 24% of the 196 in the placebo group (absolute risk reduction, 9.9%). This was explained mostly by differences in infrequent wheeze, the researchers said. However, physician-diagnosed asthma in the past 12 months was not significantly different between the two groups at 6 years: 10.3% in the RSV prevention group and 9.9% in the placebo group.

SOURCE: Scheltema NM et al. Lancet. 2018 Feb 27. doi: 10.1016/S2213-2600(18)30055-9.
reported Nienke M. Scheltema, MD, of Wilhelmina Children’s Hospital, Utrecht, the Netherlands, and associates.
In a study of 395 otherwise healthy premature infants who were randomized to receive palivizumab for respiratory syncytial virus (RSV) immunoprophylaxis or placebo and followed for 6 years, 14% of the 199 infants in the RSV prevention group had parent-reported asthma, compared with 24% of the 196 in the placebo group (absolute risk reduction, 9.9%). This was explained mostly by differences in infrequent wheeze, the researchers said. However, physician-diagnosed asthma in the past 12 months was not significantly different between the two groups at 6 years: 10.3% in the RSV prevention group and 9.9% in the placebo group.
SOURCE: Scheltema NM et al. Lancet. 2018 Feb 27. doi: 10.1016/S2213-2600(18)30055-9.
reported Nienke M. Scheltema, MD, of Wilhelmina Children’s Hospital, Utrecht, the Netherlands, and associates.
In a study of 395 otherwise healthy premature infants who were randomized to receive palivizumab for respiratory syncytial virus (RSV) immunoprophylaxis or placebo and followed for 6 years, 14% of the 199 infants in the RSV prevention group had parent-reported asthma, compared with 24% of the 196 in the placebo group (absolute risk reduction, 9.9%). This was explained mostly by differences in infrequent wheeze, the researchers said. However, physician-diagnosed asthma in the past 12 months was not significantly different between the two groups at 6 years: 10.3% in the RSV prevention group and 9.9% in the placebo group.
SOURCE: Scheltema NM et al. Lancet. 2018 Feb 27. doi: 10.1016/S2213-2600(18)30055-9.
FROM THE LANCET
Different OSA subtypes respond differently to therapy
Patients with obstructive sleep apnea can be grouped into distinct clinical subtypes that differ in response to positive airway pressure treatment, according to two studies published in the March issue of the journal Sleep.
In the first study, investigators evaluated whether patients in different clinical clusters responded differently to positive airway pressure (PAP) treatment. Authors identified 706 patients with moderate to severe obstructive sleep apnea (OSA) from the Icelandic Sleep Apnea Cohort. All patients completed a sleep study prior to starting PAP treatment, and completed questionnaires to assess symptoms. Patients were grouped into one of three clusters based on symptomatology: disturbed sleep, minimally symptomatic, or sleepy, wrote Grace W. Pien, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and her coauthors.
Patients in the minimally symptomatic cluster reported symptoms at lower rates than patients in the other clusters at baseline, and they remained relatively asymptomatic at follow-up, the authors noted. By comparison, patients in the sleepy group reported the highest Epworth Sleepiness Scale scores at baseline (16.0 plus or minus 3.4), which fell by five points at follow-up (mean change, −5.3; 95% confidence interval, −5.8 to −4.8). Also, patients in the sleepy group reported higher rates of drowsy driving (37.8%) at baseline, which dropped to 8.1% at follow-up (odds ratio, 0.06; 95% CI, 0.03-0.14).
At baseline, the disturbed-sleep group reported mainly insomnia-related symptoms, including difficulty falling asleep (43.2%), waking often at night (90.8%), restless sleep (74.2%), and waking up early (62.3%). At follow-up, improvements in the frequency of insomnia-related symptoms ranged from 0.28 to 1.25 points, and Epworth Sleepiness Scale scores fell significantly (−2.06; 95% CI, −2.64 to −1.48). Reductions in the proportion of patients with insomnia symptoms ranged from 13.1% (OR, 0.35; 95% CI, 0.20-0.59) for difficulty falling asleep to 39.0% (OR, 0.08; 95% CI, 0.04-0.14) for restless sleep, Dr. Pien and her colleagues reported.
The results “demonstrate that although symptoms improved overall among each of the three clinical phenotypes of moderate to severe OSA, patterns of treatment response … varied based on initial clinical presentation,” the authors wrote. “Our findings underscore the need to consider initial OSA phenotype when designing future trials.”
In the second study, also published in Sleep, investigators confirmed the three clinical OSA subtypes previously identified in the Icelandic Sleep Apnea Cohort. In analysis of an international sample, they also expanded these clusters to include two additional disease subtypes. One of these subtypes consisted of patients with symptoms dominated by indications of upper airway obstruction. The other new subtype, sleepiness dominant OSA, included patients who had excessive sleepiness but no symptoms of upper airway obstruction.
The study authors performed a cluster analysis using data from 972 patients from the Sleep Apnea Global Interdisciplinary Consortium with moderate to severe OSA, with 215 of these patients being from Iceland.
In total, 688 (70.8%) patients were diagnosed using laboratory-based polysomnography and 284 (29.2%) with home-based sleep studies. Patients completed questionnaires related to symptoms including sleepiness, insomnia, sleep disturbance, abnormal behaviors during sleep, upper airway symptoms, and other symptoms such as headaches and excessive sweating, wrote Brendan T. Keenan, of the University of Pennsylvania, Philadelphia, and his coauthors.
In the Icelandic group, results identified 72 (33.5%) patients in the disturbed-sleep cluster, 62 (28.8%) in the minimally symptomatic cluster, and 81 (37.7%) in the excessively sleepy cluster, similar to prior research. The three subtypes were found in the international sample of patients as well, with 150 (19.8%) in the disturbed-sleep cluster, 306 (40.4%) in the minimally symptomatic cluster, and 301 (39.8%) in the excessively sleepy cluster.
“Overall, this study provides a novel approach to better characterize patients with OSA presenting at sleep clinics worldwide,” wrote the authors of the second study. “This information can help inform personalized medicine approaches to OSA treatment by allowing clinicians to focus interventions on the most relevant OSA symptoms and consequences within an individual patient.”
Both studies were funded by the National Institutes of Health.
SOURCES: Pien GW et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx201; Keenan BT et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx214.
The results of these studies “advance the personalization of sleep apnea care by validating distinct symptom-based groups that generalize across nations and assessing how members of these clinical phenotypes respond to therapy,” wrote Vishesh K. Kapur, MD, of the division of pulmonary, critical care and sleep medicine at the University of Washington, Seattle, in an editorial published in the March issue of Sleep (2018 Mar. doi: 10.1093/sleep/zsy042).
“Patients with OSA differ in their presenting symptoms,” he said, and future studies should aim to “elucidate whether the proposed phenotypes will enable a more personalized paradigm of sleep apnea care that results in better tailored and more effective care.”
Dr. Kapur did not report any relevant disclosures.
The results of these studies “advance the personalization of sleep apnea care by validating distinct symptom-based groups that generalize across nations and assessing how members of these clinical phenotypes respond to therapy,” wrote Vishesh K. Kapur, MD, of the division of pulmonary, critical care and sleep medicine at the University of Washington, Seattle, in an editorial published in the March issue of Sleep (2018 Mar. doi: 10.1093/sleep/zsy042).
“Patients with OSA differ in their presenting symptoms,” he said, and future studies should aim to “elucidate whether the proposed phenotypes will enable a more personalized paradigm of sleep apnea care that results in better tailored and more effective care.”
Dr. Kapur did not report any relevant disclosures.
The results of these studies “advance the personalization of sleep apnea care by validating distinct symptom-based groups that generalize across nations and assessing how members of these clinical phenotypes respond to therapy,” wrote Vishesh K. Kapur, MD, of the division of pulmonary, critical care and sleep medicine at the University of Washington, Seattle, in an editorial published in the March issue of Sleep (2018 Mar. doi: 10.1093/sleep/zsy042).
“Patients with OSA differ in their presenting symptoms,” he said, and future studies should aim to “elucidate whether the proposed phenotypes will enable a more personalized paradigm of sleep apnea care that results in better tailored and more effective care.”
Dr. Kapur did not report any relevant disclosures.
Patients with obstructive sleep apnea can be grouped into distinct clinical subtypes that differ in response to positive airway pressure treatment, according to two studies published in the March issue of the journal Sleep.
In the first study, investigators evaluated whether patients in different clinical clusters responded differently to positive airway pressure (PAP) treatment. Authors identified 706 patients with moderate to severe obstructive sleep apnea (OSA) from the Icelandic Sleep Apnea Cohort. All patients completed a sleep study prior to starting PAP treatment, and completed questionnaires to assess symptoms. Patients were grouped into one of three clusters based on symptomatology: disturbed sleep, minimally symptomatic, or sleepy, wrote Grace W. Pien, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and her coauthors.
Patients in the minimally symptomatic cluster reported symptoms at lower rates than patients in the other clusters at baseline, and they remained relatively asymptomatic at follow-up, the authors noted. By comparison, patients in the sleepy group reported the highest Epworth Sleepiness Scale scores at baseline (16.0 plus or minus 3.4), which fell by five points at follow-up (mean change, −5.3; 95% confidence interval, −5.8 to −4.8). Also, patients in the sleepy group reported higher rates of drowsy driving (37.8%) at baseline, which dropped to 8.1% at follow-up (odds ratio, 0.06; 95% CI, 0.03-0.14).
At baseline, the disturbed-sleep group reported mainly insomnia-related symptoms, including difficulty falling asleep (43.2%), waking often at night (90.8%), restless sleep (74.2%), and waking up early (62.3%). At follow-up, improvements in the frequency of insomnia-related symptoms ranged from 0.28 to 1.25 points, and Epworth Sleepiness Scale scores fell significantly (−2.06; 95% CI, −2.64 to −1.48). Reductions in the proportion of patients with insomnia symptoms ranged from 13.1% (OR, 0.35; 95% CI, 0.20-0.59) for difficulty falling asleep to 39.0% (OR, 0.08; 95% CI, 0.04-0.14) for restless sleep, Dr. Pien and her colleagues reported.
The results “demonstrate that although symptoms improved overall among each of the three clinical phenotypes of moderate to severe OSA, patterns of treatment response … varied based on initial clinical presentation,” the authors wrote. “Our findings underscore the need to consider initial OSA phenotype when designing future trials.”
In the second study, also published in Sleep, investigators confirmed the three clinical OSA subtypes previously identified in the Icelandic Sleep Apnea Cohort. In analysis of an international sample, they also expanded these clusters to include two additional disease subtypes. One of these subtypes consisted of patients with symptoms dominated by indications of upper airway obstruction. The other new subtype, sleepiness dominant OSA, included patients who had excessive sleepiness but no symptoms of upper airway obstruction.
The study authors performed a cluster analysis using data from 972 patients from the Sleep Apnea Global Interdisciplinary Consortium with moderate to severe OSA, with 215 of these patients being from Iceland.
In total, 688 (70.8%) patients were diagnosed using laboratory-based polysomnography and 284 (29.2%) with home-based sleep studies. Patients completed questionnaires related to symptoms including sleepiness, insomnia, sleep disturbance, abnormal behaviors during sleep, upper airway symptoms, and other symptoms such as headaches and excessive sweating, wrote Brendan T. Keenan, of the University of Pennsylvania, Philadelphia, and his coauthors.
In the Icelandic group, results identified 72 (33.5%) patients in the disturbed-sleep cluster, 62 (28.8%) in the minimally symptomatic cluster, and 81 (37.7%) in the excessively sleepy cluster, similar to prior research. The three subtypes were found in the international sample of patients as well, with 150 (19.8%) in the disturbed-sleep cluster, 306 (40.4%) in the minimally symptomatic cluster, and 301 (39.8%) in the excessively sleepy cluster.
“Overall, this study provides a novel approach to better characterize patients with OSA presenting at sleep clinics worldwide,” wrote the authors of the second study. “This information can help inform personalized medicine approaches to OSA treatment by allowing clinicians to focus interventions on the most relevant OSA symptoms and consequences within an individual patient.”
Both studies were funded by the National Institutes of Health.
SOURCES: Pien GW et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx201; Keenan BT et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx214.
Patients with obstructive sleep apnea can be grouped into distinct clinical subtypes that differ in response to positive airway pressure treatment, according to two studies published in the March issue of the journal Sleep.
In the first study, investigators evaluated whether patients in different clinical clusters responded differently to positive airway pressure (PAP) treatment. Authors identified 706 patients with moderate to severe obstructive sleep apnea (OSA) from the Icelandic Sleep Apnea Cohort. All patients completed a sleep study prior to starting PAP treatment, and completed questionnaires to assess symptoms. Patients were grouped into one of three clusters based on symptomatology: disturbed sleep, minimally symptomatic, or sleepy, wrote Grace W. Pien, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and her coauthors.
Patients in the minimally symptomatic cluster reported symptoms at lower rates than patients in the other clusters at baseline, and they remained relatively asymptomatic at follow-up, the authors noted. By comparison, patients in the sleepy group reported the highest Epworth Sleepiness Scale scores at baseline (16.0 plus or minus 3.4), which fell by five points at follow-up (mean change, −5.3; 95% confidence interval, −5.8 to −4.8). Also, patients in the sleepy group reported higher rates of drowsy driving (37.8%) at baseline, which dropped to 8.1% at follow-up (odds ratio, 0.06; 95% CI, 0.03-0.14).
At baseline, the disturbed-sleep group reported mainly insomnia-related symptoms, including difficulty falling asleep (43.2%), waking often at night (90.8%), restless sleep (74.2%), and waking up early (62.3%). At follow-up, improvements in the frequency of insomnia-related symptoms ranged from 0.28 to 1.25 points, and Epworth Sleepiness Scale scores fell significantly (−2.06; 95% CI, −2.64 to −1.48). Reductions in the proportion of patients with insomnia symptoms ranged from 13.1% (OR, 0.35; 95% CI, 0.20-0.59) for difficulty falling asleep to 39.0% (OR, 0.08; 95% CI, 0.04-0.14) for restless sleep, Dr. Pien and her colleagues reported.
The results “demonstrate that although symptoms improved overall among each of the three clinical phenotypes of moderate to severe OSA, patterns of treatment response … varied based on initial clinical presentation,” the authors wrote. “Our findings underscore the need to consider initial OSA phenotype when designing future trials.”
In the second study, also published in Sleep, investigators confirmed the three clinical OSA subtypes previously identified in the Icelandic Sleep Apnea Cohort. In analysis of an international sample, they also expanded these clusters to include two additional disease subtypes. One of these subtypes consisted of patients with symptoms dominated by indications of upper airway obstruction. The other new subtype, sleepiness dominant OSA, included patients who had excessive sleepiness but no symptoms of upper airway obstruction.
The study authors performed a cluster analysis using data from 972 patients from the Sleep Apnea Global Interdisciplinary Consortium with moderate to severe OSA, with 215 of these patients being from Iceland.
In total, 688 (70.8%) patients were diagnosed using laboratory-based polysomnography and 284 (29.2%) with home-based sleep studies. Patients completed questionnaires related to symptoms including sleepiness, insomnia, sleep disturbance, abnormal behaviors during sleep, upper airway symptoms, and other symptoms such as headaches and excessive sweating, wrote Brendan T. Keenan, of the University of Pennsylvania, Philadelphia, and his coauthors.
In the Icelandic group, results identified 72 (33.5%) patients in the disturbed-sleep cluster, 62 (28.8%) in the minimally symptomatic cluster, and 81 (37.7%) in the excessively sleepy cluster, similar to prior research. The three subtypes were found in the international sample of patients as well, with 150 (19.8%) in the disturbed-sleep cluster, 306 (40.4%) in the minimally symptomatic cluster, and 301 (39.8%) in the excessively sleepy cluster.
“Overall, this study provides a novel approach to better characterize patients with OSA presenting at sleep clinics worldwide,” wrote the authors of the second study. “This information can help inform personalized medicine approaches to OSA treatment by allowing clinicians to focus interventions on the most relevant OSA symptoms and consequences within an individual patient.”
Both studies were funded by the National Institutes of Health.
SOURCES: Pien GW et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx201; Keenan BT et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx214.
FROM SLEEP
Key clinical point: Obstructive sleep apnea patients can be grouped into distinct subtypes depending on disease presentation, and these clusters differ in their responses to positive air pressure treatment.
Major finding: Though improvements were seen in all groups, presentation and changes in symptoms varied widely across clusters; for instance, patients in the sleepy group reported the highest Epworth Sleepiness Scale scores at baseline (16.0 plus or minus 3.4), which fell by five points at follow-up (mean change, −5.3; 95% CI, −5.8 to −4.8); whereas the disturbed-sleep group reported mainly insomnia-related symptoms including difficulty falling asleep (43.2%), waking often at night (90.8%), restless sleep (74.2%), and waking up early (62.3%).
Study details: A study of 706 patients with moderate to severe OSA from the Icelandic Sleep Apnea Cohort, and a study of 972 patients from the Sleep Apnea Global Interdisciplinary Consortium with moderate to severe OSA.
Disclosures: Both studies were funded by the National Institutes of Health.
Sources: Pien GW et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx201; Keenan B et al. Sleep. 2018 Mar. doi: 10.1093/sleep/zsx214.
Experimental voxtalisib shows mixed results in phase 2 study
Voxtalisib, an investigational agent that targets both mTOR and multiple isoforms of PI3K, showed “promising” efficacy with acceptable safety in patients with relapsed or refractory follicular lymphoma (FL), results of a phase 2 trial indicate.
Among 46 patients with FL, the overall response rate was 41.3%, including five (10.9%) complete responses. The median progression-free survival in this group was 58 weeks, reported Jennifer R. Brown, MD, PhD, of the Dana-Farber Cancer Institute in Boston, and her colleagues.
“The observed activity of voxtalisib in relapsed or refractory follicular lymphoma, notable for inducing complete responses in 10.9% of patients, warrants further study,” the investigators wrote in a study published in the Lancet Haematology.
Efficacy of the drug was limited, however, against aggressive malignancies, including mantle cell lymphoma (MCL), diffuse large B-cell lymphoma (DLBCL), or chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Voxtalisib (XL765) is a potent inhibitor of all four class I PI3Ks, as well as a less robust inhibitor of the mammalian target of rapamycin (mTOR). In contrast, idelalisib (Zydelig) – which is approved by the Food and Drug Administration for treatment of relapsed/refractory FL or for CLL, in combination with rituximab – inhibits only the delta isoform of PI3K, and does not have marked anti–mTOR properties.
The investigators conducted an open-label, nonrandomized trial of voxtalisib in 30 centers in the United States, Belgium, France, Germany, the Netherlands, and Australia.
Adults 18 years or older with relapsed or refractory MCL, FL, DLBCL or CLL/SLL with Eastern Cooperative Oncology Group performance status of 2 or less were enrolled. All patients received voxtalisib 50 mg orally twice daily in 28-day continuous dosing cycles until progression or unacceptable toxicity.
All patients who received more the 4 weeks of treatment and had both a baseline and one or more on-treatment tumor assessments were included in the efficacy analysis. Patients with lymphoma had received a median of three prior lines of therapy, and those with CLL had received a median of four prior lines.
The overall response rate in the entire study population was 18.3% (30 patients), including 22 partial and 8 complete responses. ORR rates were as follows:
- FL: 41.3% (19 of 46 patients).
- MCL: 11.9% (5 of 42 patients).
- DLBCL: 4.9% (2 of 41 patients).
- CLL/SLL: 11.4% (4 of 35 patients).
The safety analysis, which included all 167 patients enrolled, was consistent with that of previous studies of voxtalisib, the investigators said. The most frequently reported adverse events of any grade or type were diarrhea in 35% of patients, fatigue in 32%, nausea in 27%, pyrexia in 26%, cough 24%, and decreased appetite in 21%.
Grade 3 or greater adverse events include anemia in 12%, and pneumonia and thrombocytopenia in 8% each. Slightly more than half of all patients (58.1%) had a serious adverse event.
The investigators noted that voxtalisib’s short plasma half-life may explain the drug’s lack of efficacy against the aggressive lymphomas and CLL/SLL. Longer-acting formulations of the drug or more frequent dosing might address this problem, although the latter solution could be challenging for patients to follow, the investigators acknowledged.
In light of the results, no further studies of voxtalisib in CLL are planned, thought investigation of the drug alone or in combination with chemoimmunotherapy is warranted for patients with follicular lymphoma, the investigators wrote.
The study was funded by Sanofi. Dr. Brown reported consulting for Janssen, Gilead, Celgene, Sun BioPharma, Novartis, AbbVie, Pfizer, AstraZeneca, Astellas, RedX, Pharmacyclics, Genentech/Roche, Verastem, and TG Therapeutics, and grants from Gilead and Sun BioPharma.
SOURCE: Brown J et al. Lancet Haematol. 2018 Mar 14. doi: 10.1016/S2352-3026(18)30030-9.
Voxtalisib, an investigational agent that targets both mTOR and multiple isoforms of PI3K, showed “promising” efficacy with acceptable safety in patients with relapsed or refractory follicular lymphoma (FL), results of a phase 2 trial indicate.
Among 46 patients with FL, the overall response rate was 41.3%, including five (10.9%) complete responses. The median progression-free survival in this group was 58 weeks, reported Jennifer R. Brown, MD, PhD, of the Dana-Farber Cancer Institute in Boston, and her colleagues.
“The observed activity of voxtalisib in relapsed or refractory follicular lymphoma, notable for inducing complete responses in 10.9% of patients, warrants further study,” the investigators wrote in a study published in the Lancet Haematology.
Efficacy of the drug was limited, however, against aggressive malignancies, including mantle cell lymphoma (MCL), diffuse large B-cell lymphoma (DLBCL), or chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Voxtalisib (XL765) is a potent inhibitor of all four class I PI3Ks, as well as a less robust inhibitor of the mammalian target of rapamycin (mTOR). In contrast, idelalisib (Zydelig) – which is approved by the Food and Drug Administration for treatment of relapsed/refractory FL or for CLL, in combination with rituximab – inhibits only the delta isoform of PI3K, and does not have marked anti–mTOR properties.
The investigators conducted an open-label, nonrandomized trial of voxtalisib in 30 centers in the United States, Belgium, France, Germany, the Netherlands, and Australia.
Adults 18 years or older with relapsed or refractory MCL, FL, DLBCL or CLL/SLL with Eastern Cooperative Oncology Group performance status of 2 or less were enrolled. All patients received voxtalisib 50 mg orally twice daily in 28-day continuous dosing cycles until progression or unacceptable toxicity.
All patients who received more the 4 weeks of treatment and had both a baseline and one or more on-treatment tumor assessments were included in the efficacy analysis. Patients with lymphoma had received a median of three prior lines of therapy, and those with CLL had received a median of four prior lines.
The overall response rate in the entire study population was 18.3% (30 patients), including 22 partial and 8 complete responses. ORR rates were as follows:
- FL: 41.3% (19 of 46 patients).
- MCL: 11.9% (5 of 42 patients).
- DLBCL: 4.9% (2 of 41 patients).
- CLL/SLL: 11.4% (4 of 35 patients).
The safety analysis, which included all 167 patients enrolled, was consistent with that of previous studies of voxtalisib, the investigators said. The most frequently reported adverse events of any grade or type were diarrhea in 35% of patients, fatigue in 32%, nausea in 27%, pyrexia in 26%, cough 24%, and decreased appetite in 21%.
Grade 3 or greater adverse events include anemia in 12%, and pneumonia and thrombocytopenia in 8% each. Slightly more than half of all patients (58.1%) had a serious adverse event.
The investigators noted that voxtalisib’s short plasma half-life may explain the drug’s lack of efficacy against the aggressive lymphomas and CLL/SLL. Longer-acting formulations of the drug or more frequent dosing might address this problem, although the latter solution could be challenging for patients to follow, the investigators acknowledged.
In light of the results, no further studies of voxtalisib in CLL are planned, thought investigation of the drug alone or in combination with chemoimmunotherapy is warranted for patients with follicular lymphoma, the investigators wrote.
The study was funded by Sanofi. Dr. Brown reported consulting for Janssen, Gilead, Celgene, Sun BioPharma, Novartis, AbbVie, Pfizer, AstraZeneca, Astellas, RedX, Pharmacyclics, Genentech/Roche, Verastem, and TG Therapeutics, and grants from Gilead and Sun BioPharma.
SOURCE: Brown J et al. Lancet Haematol. 2018 Mar 14. doi: 10.1016/S2352-3026(18)30030-9.
Voxtalisib, an investigational agent that targets both mTOR and multiple isoforms of PI3K, showed “promising” efficacy with acceptable safety in patients with relapsed or refractory follicular lymphoma (FL), results of a phase 2 trial indicate.
Among 46 patients with FL, the overall response rate was 41.3%, including five (10.9%) complete responses. The median progression-free survival in this group was 58 weeks, reported Jennifer R. Brown, MD, PhD, of the Dana-Farber Cancer Institute in Boston, and her colleagues.
“The observed activity of voxtalisib in relapsed or refractory follicular lymphoma, notable for inducing complete responses in 10.9% of patients, warrants further study,” the investigators wrote in a study published in the Lancet Haematology.
Efficacy of the drug was limited, however, against aggressive malignancies, including mantle cell lymphoma (MCL), diffuse large B-cell lymphoma (DLBCL), or chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Voxtalisib (XL765) is a potent inhibitor of all four class I PI3Ks, as well as a less robust inhibitor of the mammalian target of rapamycin (mTOR). In contrast, idelalisib (Zydelig) – which is approved by the Food and Drug Administration for treatment of relapsed/refractory FL or for CLL, in combination with rituximab – inhibits only the delta isoform of PI3K, and does not have marked anti–mTOR properties.
The investigators conducted an open-label, nonrandomized trial of voxtalisib in 30 centers in the United States, Belgium, France, Germany, the Netherlands, and Australia.
Adults 18 years or older with relapsed or refractory MCL, FL, DLBCL or CLL/SLL with Eastern Cooperative Oncology Group performance status of 2 or less were enrolled. All patients received voxtalisib 50 mg orally twice daily in 28-day continuous dosing cycles until progression or unacceptable toxicity.
All patients who received more the 4 weeks of treatment and had both a baseline and one or more on-treatment tumor assessments were included in the efficacy analysis. Patients with lymphoma had received a median of three prior lines of therapy, and those with CLL had received a median of four prior lines.
The overall response rate in the entire study population was 18.3% (30 patients), including 22 partial and 8 complete responses. ORR rates were as follows:
- FL: 41.3% (19 of 46 patients).
- MCL: 11.9% (5 of 42 patients).
- DLBCL: 4.9% (2 of 41 patients).
- CLL/SLL: 11.4% (4 of 35 patients).
The safety analysis, which included all 167 patients enrolled, was consistent with that of previous studies of voxtalisib, the investigators said. The most frequently reported adverse events of any grade or type were diarrhea in 35% of patients, fatigue in 32%, nausea in 27%, pyrexia in 26%, cough 24%, and decreased appetite in 21%.
Grade 3 or greater adverse events include anemia in 12%, and pneumonia and thrombocytopenia in 8% each. Slightly more than half of all patients (58.1%) had a serious adverse event.
The investigators noted that voxtalisib’s short plasma half-life may explain the drug’s lack of efficacy against the aggressive lymphomas and CLL/SLL. Longer-acting formulations of the drug or more frequent dosing might address this problem, although the latter solution could be challenging for patients to follow, the investigators acknowledged.
In light of the results, no further studies of voxtalisib in CLL are planned, thought investigation of the drug alone or in combination with chemoimmunotherapy is warranted for patients with follicular lymphoma, the investigators wrote.
The study was funded by Sanofi. Dr. Brown reported consulting for Janssen, Gilead, Celgene, Sun BioPharma, Novartis, AbbVie, Pfizer, AstraZeneca, Astellas, RedX, Pharmacyclics, Genentech/Roche, Verastem, and TG Therapeutics, and grants from Gilead and Sun BioPharma.
SOURCE: Brown J et al. Lancet Haematol. 2018 Mar 14. doi: 10.1016/S2352-3026(18)30030-9.
FROM THE LANCET HAEMATOLOGY
Key clinical point:
Major finding: The overall response rate in patients with relapsed/refractory FL was 41.3%.
Study details: Open-label, nonrandomized trial in 167 patients from 30 centers in six countries.
Disclosures: The study was funded by Sanofi. Dr. Brown disclosed consulting for Janssen, Gilead, Celgene, Sun BioPharma, Novartis, AbbVie, Pfizer, AstraZeneca, Astellas, RedX, Pharmacyclics, Genentech/Roche, Verastem, and TG Therapeutics, and grants from Gilead and Sun BioPharma.
Source: Brown J et al. Lancet Haematol. 2018 Mar 14. doi: 10.1016/S2352-3026(18)30030-9.
FDA updates breast implant–associated lymphoma cases, risk
(BIA-ALCL), including nine deaths.
This figure includes all medical device reports received by the agency between 2011 and September 2017. The FDA recently provided an update on ALCL linked to breast implants and an estimate of lifetime risk of developing ALCL.
Based on available medical literature, the lifetime risk of developing BIA-ALCL for patients with textured breast implants ranges from 1 in 3,817 to 1 in 30,000, according to the update.
Of the 272 reports with data on surface type, 242 were textured implants and 30 were smooth implants. In addition, 413 reports include information on the implant fill type: 234 used silicone gel and 179 were saline filled.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association. We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health. “As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
The possible association between breast implants and the development of anaplastic large cell lymphoma (ALCL) was first identified in 2011. At that time, there were not enough cases of to determine what factors increased a patient’s risk of developing the disease. As more information became available, the World Health Organization designated BIA-ALCL as a T-cell lymphoma that can develop following breast implants.
(BIA-ALCL), including nine deaths.
This figure includes all medical device reports received by the agency between 2011 and September 2017. The FDA recently provided an update on ALCL linked to breast implants and an estimate of lifetime risk of developing ALCL.
Based on available medical literature, the lifetime risk of developing BIA-ALCL for patients with textured breast implants ranges from 1 in 3,817 to 1 in 30,000, according to the update.
Of the 272 reports with data on surface type, 242 were textured implants and 30 were smooth implants. In addition, 413 reports include information on the implant fill type: 234 used silicone gel and 179 were saline filled.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association. We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health. “As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
The possible association between breast implants and the development of anaplastic large cell lymphoma (ALCL) was first identified in 2011. At that time, there were not enough cases of to determine what factors increased a patient’s risk of developing the disease. As more information became available, the World Health Organization designated BIA-ALCL as a T-cell lymphoma that can develop following breast implants.
(BIA-ALCL), including nine deaths.
This figure includes all medical device reports received by the agency between 2011 and September 2017. The FDA recently provided an update on ALCL linked to breast implants and an estimate of lifetime risk of developing ALCL.
Based on available medical literature, the lifetime risk of developing BIA-ALCL for patients with textured breast implants ranges from 1 in 3,817 to 1 in 30,000, according to the update.
Of the 272 reports with data on surface type, 242 were textured implants and 30 were smooth implants. In addition, 413 reports include information on the implant fill type: 234 used silicone gel and 179 were saline filled.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association. We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health. “As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
The possible association between breast implants and the development of anaplastic large cell lymphoma (ALCL) was first identified in 2011. At that time, there were not enough cases of to determine what factors increased a patient’s risk of developing the disease. As more information became available, the World Health Organization designated BIA-ALCL as a T-cell lymphoma that can develop following breast implants.