User login
What Makes Squamous Cell Cancers Different? Genomics May Explain
Squamous cell carcinomas (SCCs) associated with smoking and human papillomavirus (HPV) have distinct genomic signatures, say researchers from a National Institutes of Health-supported study. That is one of the findings that may help distinguish SCCs from other cancers and point the way to new research and treatment.
The researchers used new analytic tools and data from the recently completed PanCancer Atlas to investigate similarities and differences among SCCs in the head and neck, lung, esophagus, cervix, and bladder. The PanCancer Atlas is a detailed analysis from a dataset containing molecular and clinical information on more than 10,000 tumors from 33 forms of cancer.
The researchers combined multiple platforms of genomic data from 1,400 SCC samples into integrated analyses, creating visual clusters of tumors based on genomic characteristics.
Squamous cell carcinomas had genomic features that set them apart from other cancers, the researchers found. The most common were gains or losses of the sections of certain chromosomes, making it likely that those regions harbor genes important to the development of SCCs.
The current study expands on research reported in 2014 and 2015, which compared genomic features of SCCs in head and neck cancer associated with smoking (a risk factor for head and neck cancer [HNC]) and HPV (a risk factor for cervical and some HNCs). Certain features were present in tumors associated with both, whereas others were exclusive to only 1 of the 2. The researchers also found similarities in the genomic characteristics of HNCs with lung cancers, some bladder cancers, and cervical cancer.
Squamous cell carcinomas (SCCs) associated with smoking and human papillomavirus (HPV) have distinct genomic signatures, say researchers from a National Institutes of Health-supported study. That is one of the findings that may help distinguish SCCs from other cancers and point the way to new research and treatment.
The researchers used new analytic tools and data from the recently completed PanCancer Atlas to investigate similarities and differences among SCCs in the head and neck, lung, esophagus, cervix, and bladder. The PanCancer Atlas is a detailed analysis from a dataset containing molecular and clinical information on more than 10,000 tumors from 33 forms of cancer.
The researchers combined multiple platforms of genomic data from 1,400 SCC samples into integrated analyses, creating visual clusters of tumors based on genomic characteristics.
Squamous cell carcinomas had genomic features that set them apart from other cancers, the researchers found. The most common were gains or losses of the sections of certain chromosomes, making it likely that those regions harbor genes important to the development of SCCs.
The current study expands on research reported in 2014 and 2015, which compared genomic features of SCCs in head and neck cancer associated with smoking (a risk factor for head and neck cancer [HNC]) and HPV (a risk factor for cervical and some HNCs). Certain features were present in tumors associated with both, whereas others were exclusive to only 1 of the 2. The researchers also found similarities in the genomic characteristics of HNCs with lung cancers, some bladder cancers, and cervical cancer.
Squamous cell carcinomas (SCCs) associated with smoking and human papillomavirus (HPV) have distinct genomic signatures, say researchers from a National Institutes of Health-supported study. That is one of the findings that may help distinguish SCCs from other cancers and point the way to new research and treatment.
The researchers used new analytic tools and data from the recently completed PanCancer Atlas to investigate similarities and differences among SCCs in the head and neck, lung, esophagus, cervix, and bladder. The PanCancer Atlas is a detailed analysis from a dataset containing molecular and clinical information on more than 10,000 tumors from 33 forms of cancer.
The researchers combined multiple platforms of genomic data from 1,400 SCC samples into integrated analyses, creating visual clusters of tumors based on genomic characteristics.
Squamous cell carcinomas had genomic features that set them apart from other cancers, the researchers found. The most common were gains or losses of the sections of certain chromosomes, making it likely that those regions harbor genes important to the development of SCCs.
The current study expands on research reported in 2014 and 2015, which compared genomic features of SCCs in head and neck cancer associated with smoking (a risk factor for head and neck cancer [HNC]) and HPV (a risk factor for cervical and some HNCs). Certain features were present in tumors associated with both, whereas others were exclusive to only 1 of the 2. The researchers also found similarities in the genomic characteristics of HNCs with lung cancers, some bladder cancers, and cervical cancer.
Five-year survival for non-Hodgkin lymphoma tops 71%
The overall 5-year survival rate for non-Hodgkin lymphoma (NHL) is 71.4%, according to the National Cancer Institute.
That number falls neatly into the middle of the range for survival by stage at diagnosis, with stage I (81.8%) and stage II (75.3%) disease on the high side and stage III (69.1%) and stage IV (61.7%) on the low side, the most recent data from the Surveillance, Epidemiology, and End Results (SEER) Program show. Five-year survival for NHL of unknown stage at diagnosis is 76.4%.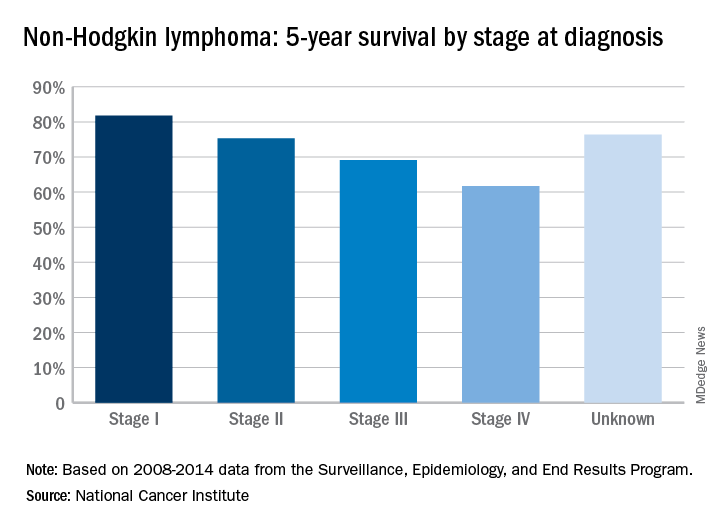
The overall 5-year survival rate for non-Hodgkin lymphoma (NHL) is 71.4%, according to the National Cancer Institute.
That number falls neatly into the middle of the range for survival by stage at diagnosis, with stage I (81.8%) and stage II (75.3%) disease on the high side and stage III (69.1%) and stage IV (61.7%) on the low side, the most recent data from the Surveillance, Epidemiology, and End Results (SEER) Program show. Five-year survival for NHL of unknown stage at diagnosis is 76.4%.
The overall 5-year survival rate for non-Hodgkin lymphoma (NHL) is 71.4%, according to the National Cancer Institute.
That number falls neatly into the middle of the range for survival by stage at diagnosis, with stage I (81.8%) and stage II (75.3%) disease on the high side and stage III (69.1%) and stage IV (61.7%) on the low side, the most recent data from the Surveillance, Epidemiology, and End Results (SEER) Program show. Five-year survival for NHL of unknown stage at diagnosis is 76.4%.
Islet Transplantation Improves Diabetes-Related Quality of Life
Participants reported the greatest improvements in diabetes-related quality of life (QOL) and better overall health status even though they would need lifelong immune-suppressing drugs to prevent transplant rejection.
The study, conducted by the Clinical Islet Transplantation Consortium, involved 48 people with hypoglycemia unawareness who experienced frequent episodes of severe hypoglycemia despite receiving expert care. Each participant received at least 1 islet transplant.
One year after the first transplant, 42 participants (88%) were free of severe hypoglycemic events, had near-normal blood glucose control, and had restored awareness of hypoglycemia. About half of the recipients needed to continue on insulin to control blood glucose, but the reported improvements in QOL were similar between those who did and those who did not. The researchers say the elimination of severe hypoglycemia and the associated fears outweighed concerns about the need for continued insulin treatment.
Islet transplantation is investigational in the US. Although the results are promising, the National Institutes of Health cautions that the process is not appropriate for all patients with type 1 diabetes mellitus due to risks and adverse effects.
Participants reported the greatest improvements in diabetes-related quality of life (QOL) and better overall health status even though they would need lifelong immune-suppressing drugs to prevent transplant rejection.
The study, conducted by the Clinical Islet Transplantation Consortium, involved 48 people with hypoglycemia unawareness who experienced frequent episodes of severe hypoglycemia despite receiving expert care. Each participant received at least 1 islet transplant.
One year after the first transplant, 42 participants (88%) were free of severe hypoglycemic events, had near-normal blood glucose control, and had restored awareness of hypoglycemia. About half of the recipients needed to continue on insulin to control blood glucose, but the reported improvements in QOL were similar between those who did and those who did not. The researchers say the elimination of severe hypoglycemia and the associated fears outweighed concerns about the need for continued insulin treatment.
Islet transplantation is investigational in the US. Although the results are promising, the National Institutes of Health cautions that the process is not appropriate for all patients with type 1 diabetes mellitus due to risks and adverse effects.
Participants reported the greatest improvements in diabetes-related quality of life (QOL) and better overall health status even though they would need lifelong immune-suppressing drugs to prevent transplant rejection.
The study, conducted by the Clinical Islet Transplantation Consortium, involved 48 people with hypoglycemia unawareness who experienced frequent episodes of severe hypoglycemia despite receiving expert care. Each participant received at least 1 islet transplant.
One year after the first transplant, 42 participants (88%) were free of severe hypoglycemic events, had near-normal blood glucose control, and had restored awareness of hypoglycemia. About half of the recipients needed to continue on insulin to control blood glucose, but the reported improvements in QOL were similar between those who did and those who did not. The researchers say the elimination of severe hypoglycemia and the associated fears outweighed concerns about the need for continued insulin treatment.
Islet transplantation is investigational in the US. Although the results are promising, the National Institutes of Health cautions that the process is not appropriate for all patients with type 1 diabetes mellitus due to risks and adverse effects.
FDA: More COPD patients can use triple therapy
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.

“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.
“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.
“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
Getting At-Risk Kids to Change Sexual Behavior
In 2015, young people aged 13- 24 years accounted for > 1 in 5 new HIV diagnoses in the US. Young people aged 15-24 years also account for half of all new sexually transmitted disease infections. Many of those high-risk youth are caught in the juvenile justice system, where they experience more mental illness, substance abuse, and STDs than their peers in the general population.
It is a challenge to identify and implement effective prevention strategies for these young people, but a study at the University of Illinois shows potential. PHAT Life: Preventing HIV/AIDS Among Teens uses role-playing, videos, games, and skill-building exercises to promote knowledge about HIV/AIDS, positive coping, and problem-solving skills.
The study was conducted with 310 urban teens, mostly African American boys, on probation in Chicago’s Cook County, the second-largest county justice system in the US. The participants were assigned to PHAT Life or an equally intensive health information program. Both 2-week programs consisted of 8 90- to 120-minute sessions, delivered at detention-alternative after-school programs.
The study measured the degree of condom use and number of sexual partners in the 6 months before and after the intervention. Among participants who reported the highest-risk sexual behavior at baseline, those assigned to PHAT Life were over 4 times more likely than those in the control group to report a reduction in number of sexual partners and more consistent condom use. Of those who reported having had sex before age 12, the PHAT Life participants reported significantly fewer sexual partners after the intervention.
“Uniquely tailored interventions like PHAT Life … are essential to mitigate young offenders’ poor long-term trajectories,” says Geri Donenberg, PhD, study leader.
The next step, the researchers say, is to identify how best to disseminate PHAT Life resources to ensure it’s self-sustaining in the juvenile justice system.
In 2015, young people aged 13- 24 years accounted for > 1 in 5 new HIV diagnoses in the US. Young people aged 15-24 years also account for half of all new sexually transmitted disease infections. Many of those high-risk youth are caught in the juvenile justice system, where they experience more mental illness, substance abuse, and STDs than their peers in the general population.
It is a challenge to identify and implement effective prevention strategies for these young people, but a study at the University of Illinois shows potential. PHAT Life: Preventing HIV/AIDS Among Teens uses role-playing, videos, games, and skill-building exercises to promote knowledge about HIV/AIDS, positive coping, and problem-solving skills.
The study was conducted with 310 urban teens, mostly African American boys, on probation in Chicago’s Cook County, the second-largest county justice system in the US. The participants were assigned to PHAT Life or an equally intensive health information program. Both 2-week programs consisted of 8 90- to 120-minute sessions, delivered at detention-alternative after-school programs.
The study measured the degree of condom use and number of sexual partners in the 6 months before and after the intervention. Among participants who reported the highest-risk sexual behavior at baseline, those assigned to PHAT Life were over 4 times more likely than those in the control group to report a reduction in number of sexual partners and more consistent condom use. Of those who reported having had sex before age 12, the PHAT Life participants reported significantly fewer sexual partners after the intervention.
“Uniquely tailored interventions like PHAT Life … are essential to mitigate young offenders’ poor long-term trajectories,” says Geri Donenberg, PhD, study leader.
The next step, the researchers say, is to identify how best to disseminate PHAT Life resources to ensure it’s self-sustaining in the juvenile justice system.
In 2015, young people aged 13- 24 years accounted for > 1 in 5 new HIV diagnoses in the US. Young people aged 15-24 years also account for half of all new sexually transmitted disease infections. Many of those high-risk youth are caught in the juvenile justice system, where they experience more mental illness, substance abuse, and STDs than their peers in the general population.
It is a challenge to identify and implement effective prevention strategies for these young people, but a study at the University of Illinois shows potential. PHAT Life: Preventing HIV/AIDS Among Teens uses role-playing, videos, games, and skill-building exercises to promote knowledge about HIV/AIDS, positive coping, and problem-solving skills.
The study was conducted with 310 urban teens, mostly African American boys, on probation in Chicago’s Cook County, the second-largest county justice system in the US. The participants were assigned to PHAT Life or an equally intensive health information program. Both 2-week programs consisted of 8 90- to 120-minute sessions, delivered at detention-alternative after-school programs.
The study measured the degree of condom use and number of sexual partners in the 6 months before and after the intervention. Among participants who reported the highest-risk sexual behavior at baseline, those assigned to PHAT Life were over 4 times more likely than those in the control group to report a reduction in number of sexual partners and more consistent condom use. Of those who reported having had sex before age 12, the PHAT Life participants reported significantly fewer sexual partners after the intervention.
“Uniquely tailored interventions like PHAT Life … are essential to mitigate young offenders’ poor long-term trajectories,” says Geri Donenberg, PhD, study leader.
The next step, the researchers say, is to identify how best to disseminate PHAT Life resources to ensure it’s self-sustaining in the juvenile justice system.
FDA approves epinephrine autoinjector for infants and toddlers
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
An Easier Way to Track Genetic Influences
The research paradigm had been: examine a person’s traits or symptomsthen, then search for genes or gene variants that cause or contribute to them. But it was difficult for researchers to recontact people with genotypes of interest for “downstream” follow-up.
Now, the National Institute of Health (NIH) and Inova Health System are launching The Genomic Ascertainment Cohort (TGAC), a 2-year pilot project that will allow researchers to recall genotyped people and examine the influence of genes and gene variants on phenotypes. “This is essentially match-making between genes and gene variants and the researchers who study them,” says Richard Siegel, MD, PhD, TGAC co-organizer, and clinical director and chief of the Autoimmunity Branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases. For instance, a researcher might locate a genotype of interest in the database and ask participants with the genotype to come to the NIH Clinical Center in Bethesda.
Participating NIH institutes will contribute genome and exome sequences from existing research programs to the database. Another 1,000 patients will be recruited to have genome sequencing performed. Half of the new recruits will be from Hispanic backgrounds.
The researchers are aiming for 10,000 genomes and exomes to allow recruitment of people with both common and rarer gene variants.
“We’re trying to advance science in a new, creative, and slightly radical way,” says Leslie Biesecker, MD, TGAC co-organizer and chief of the Medical Genomics and Metabolic Genetics Branch at the National Human Genome Research Institute. “We’re especially interested in using this as a platform to test our ability to predict phenotype from genotype—one of the key underpinnings of predictive genomic medicine.”
The research paradigm had been: examine a person’s traits or symptomsthen, then search for genes or gene variants that cause or contribute to them. But it was difficult for researchers to recontact people with genotypes of interest for “downstream” follow-up.
Now, the National Institute of Health (NIH) and Inova Health System are launching The Genomic Ascertainment Cohort (TGAC), a 2-year pilot project that will allow researchers to recall genotyped people and examine the influence of genes and gene variants on phenotypes. “This is essentially match-making between genes and gene variants and the researchers who study them,” says Richard Siegel, MD, PhD, TGAC co-organizer, and clinical director and chief of the Autoimmunity Branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases. For instance, a researcher might locate a genotype of interest in the database and ask participants with the genotype to come to the NIH Clinical Center in Bethesda.
Participating NIH institutes will contribute genome and exome sequences from existing research programs to the database. Another 1,000 patients will be recruited to have genome sequencing performed. Half of the new recruits will be from Hispanic backgrounds.
The researchers are aiming for 10,000 genomes and exomes to allow recruitment of people with both common and rarer gene variants.
“We’re trying to advance science in a new, creative, and slightly radical way,” says Leslie Biesecker, MD, TGAC co-organizer and chief of the Medical Genomics and Metabolic Genetics Branch at the National Human Genome Research Institute. “We’re especially interested in using this as a platform to test our ability to predict phenotype from genotype—one of the key underpinnings of predictive genomic medicine.”
The research paradigm had been: examine a person’s traits or symptomsthen, then search for genes or gene variants that cause or contribute to them. But it was difficult for researchers to recontact people with genotypes of interest for “downstream” follow-up.
Now, the National Institute of Health (NIH) and Inova Health System are launching The Genomic Ascertainment Cohort (TGAC), a 2-year pilot project that will allow researchers to recall genotyped people and examine the influence of genes and gene variants on phenotypes. “This is essentially match-making between genes and gene variants and the researchers who study them,” says Richard Siegel, MD, PhD, TGAC co-organizer, and clinical director and chief of the Autoimmunity Branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases. For instance, a researcher might locate a genotype of interest in the database and ask participants with the genotype to come to the NIH Clinical Center in Bethesda.
Participating NIH institutes will contribute genome and exome sequences from existing research programs to the database. Another 1,000 patients will be recruited to have genome sequencing performed. Half of the new recruits will be from Hispanic backgrounds.
The researchers are aiming for 10,000 genomes and exomes to allow recruitment of people with both common and rarer gene variants.
“We’re trying to advance science in a new, creative, and slightly radical way,” says Leslie Biesecker, MD, TGAC co-organizer and chief of the Medical Genomics and Metabolic Genetics Branch at the National Human Genome Research Institute. “We’re especially interested in using this as a platform to test our ability to predict phenotype from genotype—one of the key underpinnings of predictive genomic medicine.”
Giving Dexamethasone a New Lease on Life
Dexamethasone (Dex), a synthetic glucocorticoid, for years has been widely used both to treat adverse effects of antitumor agents and in direct chemotherapy regimens for hematologic malignancies, such as leukemia and lymphoma. But might it be modified to work against solid cancers as well? Researchers from Advanced Radiation Technology Institute, Medical Device Development Center, and University of Science and Technology in South Korea, suggest that ionizing radiation could produce new anticancer options from an old drug.
The researchers irradiated Dex with γ- rays to produce ionizing-radiation-irradiated.
Dex (Dex-IR), then investigated its effects on human lung cancer cells (cell lines H1650, A549, and H1299). The researchers used ionizing radiation because introducing energy into materials can produce favorable changes; irradiated materials with sufficiently high energy can decompose to yield very reactive intermediate molecules and form new ones. In this study, γ -irradiation produced “remarkable changes” in the chemical properties of dexamethasone; changes included degradation products, such as methanol vapor and carbon monoxide.
Original Dex inhibits the proliferation of non-small cell lung cancer (NSCLC) cells but has minimal cytotoxic effects, the researchers say. However, Dex-IR not only significantly inhibited the proliferation of NSCLC cells, but also induced apoptosis, arrested cell cycles of H1650 lung cancer cells, and significantly reduced cells’ invasiveness.
The researchers say their results “strongly suggest” a direct link between the chemical derivatives of Dex and inhibition of NSCLC cell growth. Their findings are the first evidence that γ -irradiated Dex represents a novel class of anticancer agents for lung cancer.
Lee EH, Park CH, Choi HJ, Kawala RA, Bai HW, Chung BY. PLoS One. 2018;13(4):e0194341.
doi: 10.1371/journal.pone.0194341.
Dexamethasone (Dex), a synthetic glucocorticoid, for years has been widely used both to treat adverse effects of antitumor agents and in direct chemotherapy regimens for hematologic malignancies, such as leukemia and lymphoma. But might it be modified to work against solid cancers as well? Researchers from Advanced Radiation Technology Institute, Medical Device Development Center, and University of Science and Technology in South Korea, suggest that ionizing radiation could produce new anticancer options from an old drug.
The researchers irradiated Dex with γ- rays to produce ionizing-radiation-irradiated.
Dex (Dex-IR), then investigated its effects on human lung cancer cells (cell lines H1650, A549, and H1299). The researchers used ionizing radiation because introducing energy into materials can produce favorable changes; irradiated materials with sufficiently high energy can decompose to yield very reactive intermediate molecules and form new ones. In this study, γ -irradiation produced “remarkable changes” in the chemical properties of dexamethasone; changes included degradation products, such as methanol vapor and carbon monoxide.
Original Dex inhibits the proliferation of non-small cell lung cancer (NSCLC) cells but has minimal cytotoxic effects, the researchers say. However, Dex-IR not only significantly inhibited the proliferation of NSCLC cells, but also induced apoptosis, arrested cell cycles of H1650 lung cancer cells, and significantly reduced cells’ invasiveness.
The researchers say their results “strongly suggest” a direct link between the chemical derivatives of Dex and inhibition of NSCLC cell growth. Their findings are the first evidence that γ -irradiated Dex represents a novel class of anticancer agents for lung cancer.
Lee EH, Park CH, Choi HJ, Kawala RA, Bai HW, Chung BY. PLoS One. 2018;13(4):e0194341.
doi: 10.1371/journal.pone.0194341.
Dexamethasone (Dex), a synthetic glucocorticoid, for years has been widely used both to treat adverse effects of antitumor agents and in direct chemotherapy regimens for hematologic malignancies, such as leukemia and lymphoma. But might it be modified to work against solid cancers as well? Researchers from Advanced Radiation Technology Institute, Medical Device Development Center, and University of Science and Technology in South Korea, suggest that ionizing radiation could produce new anticancer options from an old drug.
The researchers irradiated Dex with γ- rays to produce ionizing-radiation-irradiated.
Dex (Dex-IR), then investigated its effects on human lung cancer cells (cell lines H1650, A549, and H1299). The researchers used ionizing radiation because introducing energy into materials can produce favorable changes; irradiated materials with sufficiently high energy can decompose to yield very reactive intermediate molecules and form new ones. In this study, γ -irradiation produced “remarkable changes” in the chemical properties of dexamethasone; changes included degradation products, such as methanol vapor and carbon monoxide.
Original Dex inhibits the proliferation of non-small cell lung cancer (NSCLC) cells but has minimal cytotoxic effects, the researchers say. However, Dex-IR not only significantly inhibited the proliferation of NSCLC cells, but also induced apoptosis, arrested cell cycles of H1650 lung cancer cells, and significantly reduced cells’ invasiveness.
The researchers say their results “strongly suggest” a direct link between the chemical derivatives of Dex and inhibition of NSCLC cell growth. Their findings are the first evidence that γ -irradiated Dex represents a novel class of anticancer agents for lung cancer.
Lee EH, Park CH, Choi HJ, Kawala RA, Bai HW, Chung BY. PLoS One. 2018;13(4):e0194341.
doi: 10.1371/journal.pone.0194341.
FDA places partial hold on trials after secondary lymphoma
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
Stroke patients benefited from CPAP
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
FROM THE JOURNAL OF CLINICAL SLEEP MEDICINE
Key clinical point: Continuous positive airway pressure (CPAP) treatment may prevent vascular events in patients with stroke who have OSA.
Major finding: There was one vascular event (3.33%) at 12 months for CPAP-treated patients, versus six events (15%) in non-CPAP patients, though the difference was not significant (P = .23).
Study details: A single-blind, randomized, controlled trial including 70 patients with imaging-confirmed first arterial stroke and OSA.
Disclosures: The authors reported no conflicts of interest related to the study.
Source: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.