User login
Patients With Concussions Aren’t Getting Enough Follow-Up
Many patients with traumatic brain injury (TBI) may not be receiving follow-up care, according to findings from Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI), a long-term NIH-funded study.
Of 831 patients who completed questionnaires 2 weeks and 3 months after sustaining TBI, 44% reported seeing a health care provider within 3 months. Of those, 15% visited a clinic that specialized in head injury. Approximately half saw a general practitioner; close to a third reported seeing ≥ 1 type of doctor.
Among the 279 patients with ≥ 3 symptoms of moderate to severe postconcussion, 41% had not had a follow-up visit at 3 months. Moreover, half of the patients were discharged without TBI educational materials.
Rates and components of follow-up care varied widely from institution to institution even among patients with the same initial degree of injury.
Many patients with traumatic brain injury (TBI) may not be receiving follow-up care, according to findings from Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI), a long-term NIH-funded study.
Of 831 patients who completed questionnaires 2 weeks and 3 months after sustaining TBI, 44% reported seeing a health care provider within 3 months. Of those, 15% visited a clinic that specialized in head injury. Approximately half saw a general practitioner; close to a third reported seeing ≥ 1 type of doctor.
Among the 279 patients with ≥ 3 symptoms of moderate to severe postconcussion, 41% had not had a follow-up visit at 3 months. Moreover, half of the patients were discharged without TBI educational materials.
Rates and components of follow-up care varied widely from institution to institution even among patients with the same initial degree of injury.
Many patients with traumatic brain injury (TBI) may not be receiving follow-up care, according to findings from Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI), a long-term NIH-funded study.
Of 831 patients who completed questionnaires 2 weeks and 3 months after sustaining TBI, 44% reported seeing a health care provider within 3 months. Of those, 15% visited a clinic that specialized in head injury. Approximately half saw a general practitioner; close to a third reported seeing ≥ 1 type of doctor.
Among the 279 patients with ≥ 3 symptoms of moderate to severe postconcussion, 41% had not had a follow-up visit at 3 months. Moreover, half of the patients were discharged without TBI educational materials.
Rates and components of follow-up care varied widely from institution to institution even among patients with the same initial degree of injury.
Talk Therapy—Without Words
Many forms of therapy rely on the patient being able to verbally communicate thoughts and feelings. Arts-based therapies, however, can help people explore sensitive and controversial topics that might be hard to talk about.
Body mapping, which has been in use for more than 30 years, is an interesting, revealing, and productive way of using art to help patients “talk” about their thoughts and feelings. Several studies have used body maps as therapy for patients with HIV/AIDS, but researchers from University of New South Wales, Sydney, theorized that it could be particularly helpful for patients with cognitive disability who have complex support needs as well as those who are socially marginalized.
In body-mapping sessions, participants trace outlines of their bodies and then “populate” the outlines with drawings, magazine photos, symbols, words, and other visual representations of the experience they are investigating. It is a form of storytelling that allows the participant to engage physically, visually, verbally, and relationally (through dialogue and interaction with the researcher).
The researchers used body mapping in 2 studies, first with 29 adults with cognitive disability and complex support needs, such as mental illness and sensory impairment, to explore experiences of support planning. In the second study, one of the researchers used body mapping with 13 teens and young adults with complex support needs (eg, drug and alcohol misuse) to explore support they received during a life transition.
The body-mapping technique, the researchers say, shifts the power balance between researcher and participant, because the patient is in control of the images used and where they are placed on the map. Patients could decide not only how they spoke about the topic, but also which topic they spoke about. The researchers say, “we were often taken to surprising places” that might not have come up in an interview, as when participants used images to reveal aspects of cultural heritage and sexual orientation that had not come up in conversation. For example, a transsexual woman in the second study was uncomfortable with the process until she covered her incorrectly gendered body with another piece of paper on which she could redraw her body as she wished.
Body mapping does not suit everyone, the researchers acknowledge. Participants need to be able to engage in a level of abstraction and reflection about personal experiences. It is important to have other methods available for those who do not want to take part. The researchers say one way they protected patients was by recruiting through service providers so support could be “embedded in existing relationships.” The potential vulnerabilities of the patients mean researchers need to be flexible, they add, and allow the method to evolve, much like the patients’ personal stories.
Source:
Dew A, Smith L, Collings S, Savage ID. FQS. 2018;19(2).
doi: http://dx.doi.org/10.17169/fqs-19.2.2929.
Many forms of therapy rely on the patient being able to verbally communicate thoughts and feelings. Arts-based therapies, however, can help people explore sensitive and controversial topics that might be hard to talk about.
Body mapping, which has been in use for more than 30 years, is an interesting, revealing, and productive way of using art to help patients “talk” about their thoughts and feelings. Several studies have used body maps as therapy for patients with HIV/AIDS, but researchers from University of New South Wales, Sydney, theorized that it could be particularly helpful for patients with cognitive disability who have complex support needs as well as those who are socially marginalized.
In body-mapping sessions, participants trace outlines of their bodies and then “populate” the outlines with drawings, magazine photos, symbols, words, and other visual representations of the experience they are investigating. It is a form of storytelling that allows the participant to engage physically, visually, verbally, and relationally (through dialogue and interaction with the researcher).
The researchers used body mapping in 2 studies, first with 29 adults with cognitive disability and complex support needs, such as mental illness and sensory impairment, to explore experiences of support planning. In the second study, one of the researchers used body mapping with 13 teens and young adults with complex support needs (eg, drug and alcohol misuse) to explore support they received during a life transition.
The body-mapping technique, the researchers say, shifts the power balance between researcher and participant, because the patient is in control of the images used and where they are placed on the map. Patients could decide not only how they spoke about the topic, but also which topic they spoke about. The researchers say, “we were often taken to surprising places” that might not have come up in an interview, as when participants used images to reveal aspects of cultural heritage and sexual orientation that had not come up in conversation. For example, a transsexual woman in the second study was uncomfortable with the process until she covered her incorrectly gendered body with another piece of paper on which she could redraw her body as she wished.
Body mapping does not suit everyone, the researchers acknowledge. Participants need to be able to engage in a level of abstraction and reflection about personal experiences. It is important to have other methods available for those who do not want to take part. The researchers say one way they protected patients was by recruiting through service providers so support could be “embedded in existing relationships.” The potential vulnerabilities of the patients mean researchers need to be flexible, they add, and allow the method to evolve, much like the patients’ personal stories.
Source:
Dew A, Smith L, Collings S, Savage ID. FQS. 2018;19(2).
doi: http://dx.doi.org/10.17169/fqs-19.2.2929.
Many forms of therapy rely on the patient being able to verbally communicate thoughts and feelings. Arts-based therapies, however, can help people explore sensitive and controversial topics that might be hard to talk about.
Body mapping, which has been in use for more than 30 years, is an interesting, revealing, and productive way of using art to help patients “talk” about their thoughts and feelings. Several studies have used body maps as therapy for patients with HIV/AIDS, but researchers from University of New South Wales, Sydney, theorized that it could be particularly helpful for patients with cognitive disability who have complex support needs as well as those who are socially marginalized.
In body-mapping sessions, participants trace outlines of their bodies and then “populate” the outlines with drawings, magazine photos, symbols, words, and other visual representations of the experience they are investigating. It is a form of storytelling that allows the participant to engage physically, visually, verbally, and relationally (through dialogue and interaction with the researcher).
The researchers used body mapping in 2 studies, first with 29 adults with cognitive disability and complex support needs, such as mental illness and sensory impairment, to explore experiences of support planning. In the second study, one of the researchers used body mapping with 13 teens and young adults with complex support needs (eg, drug and alcohol misuse) to explore support they received during a life transition.
The body-mapping technique, the researchers say, shifts the power balance between researcher and participant, because the patient is in control of the images used and where they are placed on the map. Patients could decide not only how they spoke about the topic, but also which topic they spoke about. The researchers say, “we were often taken to surprising places” that might not have come up in an interview, as when participants used images to reveal aspects of cultural heritage and sexual orientation that had not come up in conversation. For example, a transsexual woman in the second study was uncomfortable with the process until she covered her incorrectly gendered body with another piece of paper on which she could redraw her body as she wished.
Body mapping does not suit everyone, the researchers acknowledge. Participants need to be able to engage in a level of abstraction and reflection about personal experiences. It is important to have other methods available for those who do not want to take part. The researchers say one way they protected patients was by recruiting through service providers so support could be “embedded in existing relationships.” The potential vulnerabilities of the patients mean researchers need to be flexible, they add, and allow the method to evolve, much like the patients’ personal stories.
Source:
Dew A, Smith L, Collings S, Savage ID. FQS. 2018;19(2).
doi: http://dx.doi.org/10.17169/fqs-19.2.2929.
Study profiles sleep disruption in depression
Waking theta reduced in depression
BALTIMORE – Disruption of slow-wave activity may potentially explain the positive influence that sleep deprivation may have on major depressive disorder, according to results of a study presented at the annual meeting of the Associated Professional Sleep Societies.
Jennifer Goldschmied, PhD, of the University of Pennsylvania, Philadelphia, reported preliminary results of a study of slow-wave activity (SWA) disruption in 26 subjects – 12 healthy controls and 14 people diagnosed with major depressive disorder – that found a significant decrease of about 20% in waking theta activity, as measured with EEG, in the MDD group. In the 3-night sleep study, conducted at the University of Michigan, Ann Arbor, an adaptation night was followed by baseline and SWA disruption nights with EEGs performed each night. After the baseline night, patients also had a morning and afternoon EEG.
Across the baseline day, patients with depression showed “no modulation of theta activity whatsoever,” Dr. Goldschmied said. “And then we see, following slow-wave disruption, a significant decrease in theta activity,” whereas, healthy controls showed no change in waking theta following slow-wave disruption. “So what this means is that the presence of SWA may actually be facilitating the reduction of theta or sleep propensity during typical sleep in healthy individuals,” she added. In MDD patients, the decline in theta power following slow-wave disruption was from around 5.4 to 4.3.
Dr. Goldschmied noted that this finding somewhat supports what is known as the synaptic homeostasis hypothesis that University of Wisconsin researchers Giulio Tononi, MD, PhD, and Chiara Cirelli, MD, PhD, reported (Brain Res Bull. 2003;62:143-50). This hypothesis holds that SWA is a marker of synaptic strength and promotes the downscaling of synaptic strength during sleep. No method for measuring synaptic strength in humans exists, Dr. Goldschmied added, but waking theta can be considered a proxy for net synaptic strength across the cortex.
Dr. Goldschmied noted other research that has found SWA disruption improves mood (Psychiatry Res. 2015;228:715-8; J Psychiatr Res. 2011;45:1019-26), but the study she reported on found no role of decreased theta activity in that change. “To go even further,” she said, “we looked at the entire data set and found no relationship between the decrease in theta and any of the measures of sleep architecture – so there’s really no way to predict this decrease in our sample of people with depression.”
SWA plays a significant role in depression and merits more study, Dr. Goldschmied said. She noted that future research should examine the effects of SWA disruption in a larger sample, investigate theta findings with other proxy measures of synaptic strength such as brain-derived neurotrophic factor and transcranial magnetic stimulation, explore differences in SWA between sexes, and explore how SWA enhancement influences mood and theta activity.
Dr. Goldschmied reported having no financial relationships.
SOURCE: Goldschmied J et al. Sleep 2018, Abstract 0245.
Waking theta reduced in depression
Waking theta reduced in depression
BALTIMORE – Disruption of slow-wave activity may potentially explain the positive influence that sleep deprivation may have on major depressive disorder, according to results of a study presented at the annual meeting of the Associated Professional Sleep Societies.
Jennifer Goldschmied, PhD, of the University of Pennsylvania, Philadelphia, reported preliminary results of a study of slow-wave activity (SWA) disruption in 26 subjects – 12 healthy controls and 14 people diagnosed with major depressive disorder – that found a significant decrease of about 20% in waking theta activity, as measured with EEG, in the MDD group. In the 3-night sleep study, conducted at the University of Michigan, Ann Arbor, an adaptation night was followed by baseline and SWA disruption nights with EEGs performed each night. After the baseline night, patients also had a morning and afternoon EEG.
Across the baseline day, patients with depression showed “no modulation of theta activity whatsoever,” Dr. Goldschmied said. “And then we see, following slow-wave disruption, a significant decrease in theta activity,” whereas, healthy controls showed no change in waking theta following slow-wave disruption. “So what this means is that the presence of SWA may actually be facilitating the reduction of theta or sleep propensity during typical sleep in healthy individuals,” she added. In MDD patients, the decline in theta power following slow-wave disruption was from around 5.4 to 4.3.
Dr. Goldschmied noted that this finding somewhat supports what is known as the synaptic homeostasis hypothesis that University of Wisconsin researchers Giulio Tononi, MD, PhD, and Chiara Cirelli, MD, PhD, reported (Brain Res Bull. 2003;62:143-50). This hypothesis holds that SWA is a marker of synaptic strength and promotes the downscaling of synaptic strength during sleep. No method for measuring synaptic strength in humans exists, Dr. Goldschmied added, but waking theta can be considered a proxy for net synaptic strength across the cortex.
Dr. Goldschmied noted other research that has found SWA disruption improves mood (Psychiatry Res. 2015;228:715-8; J Psychiatr Res. 2011;45:1019-26), but the study she reported on found no role of decreased theta activity in that change. “To go even further,” she said, “we looked at the entire data set and found no relationship between the decrease in theta and any of the measures of sleep architecture – so there’s really no way to predict this decrease in our sample of people with depression.”
SWA plays a significant role in depression and merits more study, Dr. Goldschmied said. She noted that future research should examine the effects of SWA disruption in a larger sample, investigate theta findings with other proxy measures of synaptic strength such as brain-derived neurotrophic factor and transcranial magnetic stimulation, explore differences in SWA between sexes, and explore how SWA enhancement influences mood and theta activity.
Dr. Goldschmied reported having no financial relationships.
SOURCE: Goldschmied J et al. Sleep 2018, Abstract 0245.
BALTIMORE – Disruption of slow-wave activity may potentially explain the positive influence that sleep deprivation may have on major depressive disorder, according to results of a study presented at the annual meeting of the Associated Professional Sleep Societies.
Jennifer Goldschmied, PhD, of the University of Pennsylvania, Philadelphia, reported preliminary results of a study of slow-wave activity (SWA) disruption in 26 subjects – 12 healthy controls and 14 people diagnosed with major depressive disorder – that found a significant decrease of about 20% in waking theta activity, as measured with EEG, in the MDD group. In the 3-night sleep study, conducted at the University of Michigan, Ann Arbor, an adaptation night was followed by baseline and SWA disruption nights with EEGs performed each night. After the baseline night, patients also had a morning and afternoon EEG.
Across the baseline day, patients with depression showed “no modulation of theta activity whatsoever,” Dr. Goldschmied said. “And then we see, following slow-wave disruption, a significant decrease in theta activity,” whereas, healthy controls showed no change in waking theta following slow-wave disruption. “So what this means is that the presence of SWA may actually be facilitating the reduction of theta or sleep propensity during typical sleep in healthy individuals,” she added. In MDD patients, the decline in theta power following slow-wave disruption was from around 5.4 to 4.3.
Dr. Goldschmied noted that this finding somewhat supports what is known as the synaptic homeostasis hypothesis that University of Wisconsin researchers Giulio Tononi, MD, PhD, and Chiara Cirelli, MD, PhD, reported (Brain Res Bull. 2003;62:143-50). This hypothesis holds that SWA is a marker of synaptic strength and promotes the downscaling of synaptic strength during sleep. No method for measuring synaptic strength in humans exists, Dr. Goldschmied added, but waking theta can be considered a proxy for net synaptic strength across the cortex.
Dr. Goldschmied noted other research that has found SWA disruption improves mood (Psychiatry Res. 2015;228:715-8; J Psychiatr Res. 2011;45:1019-26), but the study she reported on found no role of decreased theta activity in that change. “To go even further,” she said, “we looked at the entire data set and found no relationship between the decrease in theta and any of the measures of sleep architecture – so there’s really no way to predict this decrease in our sample of people with depression.”
SWA plays a significant role in depression and merits more study, Dr. Goldschmied said. She noted that future research should examine the effects of SWA disruption in a larger sample, investigate theta findings with other proxy measures of synaptic strength such as brain-derived neurotrophic factor and transcranial magnetic stimulation, explore differences in SWA between sexes, and explore how SWA enhancement influences mood and theta activity.
Dr. Goldschmied reported having no financial relationships.
SOURCE: Goldschmied J et al. Sleep 2018, Abstract 0245.
REPORTING FROM SLEEP 2018
Key clinical point: Patients with major depression have reduced brain activity after sleep disruption.
Major finding: Morning theta activity was 20% lower following slow-wave disruption in patients with major depressive disorder than in healthy controls.
Data source: EEG measures of 14 individuals with major depressive disorder and 12 healthy controls in the evening before sleep and the morning following sleep after 1 night of baseline and 1 night of selective slow-wave disrupted sleep.
Disclosure: Dr. Goldschmied had no financial relationships to disclose.
Source: Goldschmied J et al. Sleep 2018, Abstract 0245.
Youth Suicide Rates Steady Climb
Black children aged 5 to 12 years are roughly twice as likely as white children to commit suicide, according to a study funded by the National Institute of Mental Health. But that trend reverses in adolescence: From ages 13 to 17 years, the suicide rates for white children are double those of black children.
The researchers used the CDC’s web-based Injury Statistics Query and Reporting System, analyzing data from 2001-2015 separately for each age group. The data were limited, the researchers say, and did not include information on contributing factors. They add that their findings highlight the need for a greater understanding of age-related racial disparities in youth suicide.
The disturbing findings are part of an overall rise in suicide nationwide. Suicide is the tenth leading cause of death in the US, according to the latest figures from the CDC. In 2016, nearly 45,000 Americans aged ≥ 10 years died by suicide.
In 2017, the CDC released Preventing Suicide: A Technical Package of Policy, Programs, and Practices, with evidence-based strategies (https://www.cdc.gov/media/releases/2018/p0607-suicide-prevention.html). The strategies include creating protective environments by reducing access to lethal means among at-risk individuals and intervening at “suicide hotspots” by, for example, putting barriers on tall structures. “Like most public health problems,” the guide says, “suicide is preventable.”
Black children aged 5 to 12 years are roughly twice as likely as white children to commit suicide, according to a study funded by the National Institute of Mental Health. But that trend reverses in adolescence: From ages 13 to 17 years, the suicide rates for white children are double those of black children.
The researchers used the CDC’s web-based Injury Statistics Query and Reporting System, analyzing data from 2001-2015 separately for each age group. The data were limited, the researchers say, and did not include information on contributing factors. They add that their findings highlight the need for a greater understanding of age-related racial disparities in youth suicide.
The disturbing findings are part of an overall rise in suicide nationwide. Suicide is the tenth leading cause of death in the US, according to the latest figures from the CDC. In 2016, nearly 45,000 Americans aged ≥ 10 years died by suicide.
In 2017, the CDC released Preventing Suicide: A Technical Package of Policy, Programs, and Practices, with evidence-based strategies (https://www.cdc.gov/media/releases/2018/p0607-suicide-prevention.html). The strategies include creating protective environments by reducing access to lethal means among at-risk individuals and intervening at “suicide hotspots” by, for example, putting barriers on tall structures. “Like most public health problems,” the guide says, “suicide is preventable.”
Black children aged 5 to 12 years are roughly twice as likely as white children to commit suicide, according to a study funded by the National Institute of Mental Health. But that trend reverses in adolescence: From ages 13 to 17 years, the suicide rates for white children are double those of black children.
The researchers used the CDC’s web-based Injury Statistics Query and Reporting System, analyzing data from 2001-2015 separately for each age group. The data were limited, the researchers say, and did not include information on contributing factors. They add that their findings highlight the need for a greater understanding of age-related racial disparities in youth suicide.
The disturbing findings are part of an overall rise in suicide nationwide. Suicide is the tenth leading cause of death in the US, according to the latest figures from the CDC. In 2016, nearly 45,000 Americans aged ≥ 10 years died by suicide.
In 2017, the CDC released Preventing Suicide: A Technical Package of Policy, Programs, and Practices, with evidence-based strategies (https://www.cdc.gov/media/releases/2018/p0607-suicide-prevention.html). The strategies include creating protective environments by reducing access to lethal means among at-risk individuals and intervening at “suicide hotspots” by, for example, putting barriers on tall structures. “Like most public health problems,” the guide says, “suicide is preventable.”
Swim at Your Own Risk
Hotel pools and hot tubs are breeding grounds for waterborne bacteria—and they can be deadly. Between 2000 and 2014, germs spread through treated recreational water caused at least 27,219 illnesses and 8 deaths.
According to a CDC study, efforts to prevent outbreaks have had mixed results. The number of Legionella-related respiratory disease outbreaks increased over time, while Pseudomonas-related skin infection outbreaks declined and Cryptosporidium-related diarrheal disease outbreaks leveled off.
Legionella, which can cause severe pneumonia and flulike symptoms, was responsible for 16% of outbreaks. Another 13% was due to Pseudomonas, which can cause “hot tub rash” and swimmer’s ear. When a pool, hot tub, or water playground isn’t cleaned properly, bacteria grow and form “biofilm” on wet surfaces, ideal growing grounds for bacteria like Legionella and Pseudomonas. It’s harder for disinfectants to kill these bacteria when they are protected by biofilm, the CDC says.
The worst offender was Cryptosporidium, which caused 58% of the outbreaks and 89% of the illnesses. “Swallowing just a mouthful of water with Crypto in it can make otherwise healthy kids and adults sick for weeks,” said Michele Hlavsa, RN, MPH, chief of the CDC’s Healthy Swimming Program. Chlorine can’t kill Cryptosporidium quickly, she cautions. The best way to avoid it is to keep it out of the water in the first place. That means keeping anyone (usually young children) with stomach problems or diarrhea out of the pool.
Other CDC tips:
- Check the inspection scores for pools, hot tubs, and water playgrounds.
- Use a test strip from a pool supply store to check the pH and bromine or free chlorine levels.
- Don’t swallow pool water.
- Take kids on regular bathroom breaks; change diapers in the diaper-changing area, away from the water.
Hotel pools and hot tubs are breeding grounds for waterborne bacteria—and they can be deadly. Between 2000 and 2014, germs spread through treated recreational water caused at least 27,219 illnesses and 8 deaths.
According to a CDC study, efforts to prevent outbreaks have had mixed results. The number of Legionella-related respiratory disease outbreaks increased over time, while Pseudomonas-related skin infection outbreaks declined and Cryptosporidium-related diarrheal disease outbreaks leveled off.
Legionella, which can cause severe pneumonia and flulike symptoms, was responsible for 16% of outbreaks. Another 13% was due to Pseudomonas, which can cause “hot tub rash” and swimmer’s ear. When a pool, hot tub, or water playground isn’t cleaned properly, bacteria grow and form “biofilm” on wet surfaces, ideal growing grounds for bacteria like Legionella and Pseudomonas. It’s harder for disinfectants to kill these bacteria when they are protected by biofilm, the CDC says.
The worst offender was Cryptosporidium, which caused 58% of the outbreaks and 89% of the illnesses. “Swallowing just a mouthful of water with Crypto in it can make otherwise healthy kids and adults sick for weeks,” said Michele Hlavsa, RN, MPH, chief of the CDC’s Healthy Swimming Program. Chlorine can’t kill Cryptosporidium quickly, she cautions. The best way to avoid it is to keep it out of the water in the first place. That means keeping anyone (usually young children) with stomach problems or diarrhea out of the pool.
Other CDC tips:
- Check the inspection scores for pools, hot tubs, and water playgrounds.
- Use a test strip from a pool supply store to check the pH and bromine or free chlorine levels.
- Don’t swallow pool water.
- Take kids on regular bathroom breaks; change diapers in the diaper-changing area, away from the water.
Hotel pools and hot tubs are breeding grounds for waterborne bacteria—and they can be deadly. Between 2000 and 2014, germs spread through treated recreational water caused at least 27,219 illnesses and 8 deaths.
According to a CDC study, efforts to prevent outbreaks have had mixed results. The number of Legionella-related respiratory disease outbreaks increased over time, while Pseudomonas-related skin infection outbreaks declined and Cryptosporidium-related diarrheal disease outbreaks leveled off.
Legionella, which can cause severe pneumonia and flulike symptoms, was responsible for 16% of outbreaks. Another 13% was due to Pseudomonas, which can cause “hot tub rash” and swimmer’s ear. When a pool, hot tub, or water playground isn’t cleaned properly, bacteria grow and form “biofilm” on wet surfaces, ideal growing grounds for bacteria like Legionella and Pseudomonas. It’s harder for disinfectants to kill these bacteria when they are protected by biofilm, the CDC says.
The worst offender was Cryptosporidium, which caused 58% of the outbreaks and 89% of the illnesses. “Swallowing just a mouthful of water with Crypto in it can make otherwise healthy kids and adults sick for weeks,” said Michele Hlavsa, RN, MPH, chief of the CDC’s Healthy Swimming Program. Chlorine can’t kill Cryptosporidium quickly, she cautions. The best way to avoid it is to keep it out of the water in the first place. That means keeping anyone (usually young children) with stomach problems or diarrhea out of the pool.
Other CDC tips:
- Check the inspection scores for pools, hot tubs, and water playgrounds.
- Use a test strip from a pool supply store to check the pH and bromine or free chlorine levels.
- Don’t swallow pool water.
- Take kids on regular bathroom breaks; change diapers in the diaper-changing area, away from the water.
Infectious Diseases Federal Health Data Trends (FULL)
The VA and DoD health care systems have long recognized the dangers posed by infectious diseases and the importance of vaccines. After the Spanish-American War, Walter Reed, MD, led U.S. Army boards that investigated typhoid fever and yellow fever, which had killed more soldiers than had died on the battlefield during the war. That tradition of infectious disease epidemiology continues today. Recently, scientists at Walter Reed Army Institute of Research have developed 2 possible Ebola vaccines (currently in phase 2 trials), a possible Zika vaccine (phase 1 trials), and vaccine candidates for Middle East Respiratory Syndrome (MERS), HIV, and simian immunodeficiency virus.
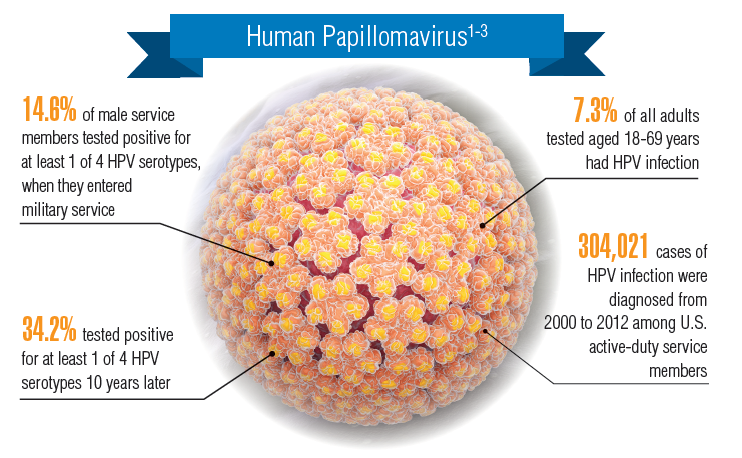
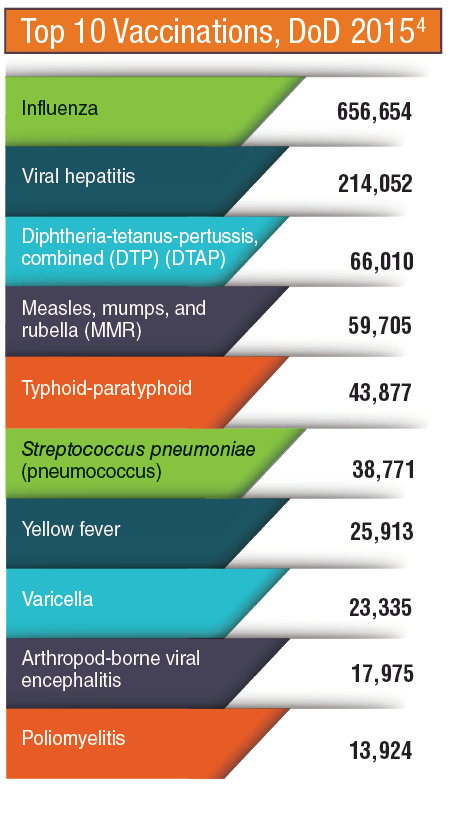
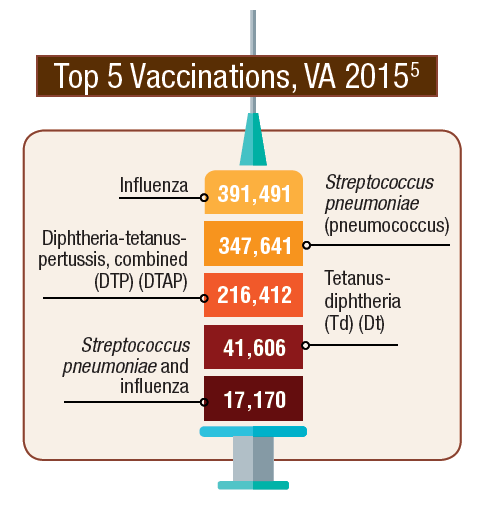
Vaccines are among the safest medical products available and are considered the most effective. It’s not surprising, therefore, that the VA and DoD actively promote the use of vaccines. In 2015, the VA and DoD each dispensed more than 1 million vaccines to prevent the spread of infectious diseases, ranging from influenza and viral hepatitis to Streptococcus pneumoniae and yellow fever. Increasingly, researchers are exploring the use of vaccines to prevent cancers. The human papillomavirus (HPV) vaccine not only prevents cervical cancer, but also anal, vulvar, and vaginal cancers.
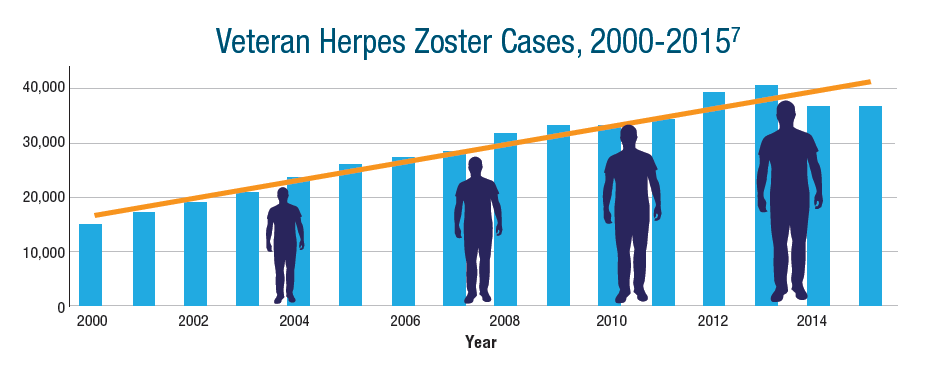
Despite the successful development of vaccines, controlling infectious diseases remains a challenge in both the VA and DoD health care systems. Cases of many infectious diseases continue to grow. The number of veterans with herpes zoster/shingles more than doubled between 2000 and 2015.
Click here to read the digital edition.
The VA and DoD health care systems have long recognized the dangers posed by infectious diseases and the importance of vaccines. After the Spanish-American War, Walter Reed, MD, led U.S. Army boards that investigated typhoid fever and yellow fever, which had killed more soldiers than had died on the battlefield during the war. That tradition of infectious disease epidemiology continues today. Recently, scientists at Walter Reed Army Institute of Research have developed 2 possible Ebola vaccines (currently in phase 2 trials), a possible Zika vaccine (phase 1 trials), and vaccine candidates for Middle East Respiratory Syndrome (MERS), HIV, and simian immunodeficiency virus.
Vaccines are among the safest medical products available and are considered the most effective. It’s not surprising, therefore, that the VA and DoD actively promote the use of vaccines. In 2015, the VA and DoD each dispensed more than 1 million vaccines to prevent the spread of infectious diseases, ranging from influenza and viral hepatitis to Streptococcus pneumoniae and yellow fever. Increasingly, researchers are exploring the use of vaccines to prevent cancers. The human papillomavirus (HPV) vaccine not only prevents cervical cancer, but also anal, vulvar, and vaginal cancers.
Despite the successful development of vaccines, controlling infectious diseases remains a challenge in both the VA and DoD health care systems. Cases of many infectious diseases continue to grow. The number of veterans with herpes zoster/shingles more than doubled between 2000 and 2015.
Click here to read the digital edition.
The VA and DoD health care systems have long recognized the dangers posed by infectious diseases and the importance of vaccines. After the Spanish-American War, Walter Reed, MD, led U.S. Army boards that investigated typhoid fever and yellow fever, which had killed more soldiers than had died on the battlefield during the war. That tradition of infectious disease epidemiology continues today. Recently, scientists at Walter Reed Army Institute of Research have developed 2 possible Ebola vaccines (currently in phase 2 trials), a possible Zika vaccine (phase 1 trials), and vaccine candidates for Middle East Respiratory Syndrome (MERS), HIV, and simian immunodeficiency virus.
Vaccines are among the safest medical products available and are considered the most effective. It’s not surprising, therefore, that the VA and DoD actively promote the use of vaccines. In 2015, the VA and DoD each dispensed more than 1 million vaccines to prevent the spread of infectious diseases, ranging from influenza and viral hepatitis to Streptococcus pneumoniae and yellow fever. Increasingly, researchers are exploring the use of vaccines to prevent cancers. The human papillomavirus (HPV) vaccine not only prevents cervical cancer, but also anal, vulvar, and vaginal cancers.
Despite the successful development of vaccines, controlling infectious diseases remains a challenge in both the VA and DoD health care systems. Cases of many infectious diseases continue to grow. The number of veterans with herpes zoster/shingles more than doubled between 2000 and 2015.
Click here to read the digital edition.
Falls: Still a Deadly Danger for Elderly
Falls have long been a major hazard for older adults—accounting for the largest percentage of deaths from unintentional injuries. Each year, about 1 in 4 older adults in the US reports falling, and an estimated 3 million emergency department visits every year are related to falls.
According to the CDC, things are getting worse. Overall, deaths due to falls among older adults increased 31% from 2007- 2016, a rate of 3% per year. The rate increased in every demographic category except among American Indians/Alaska Natives, with the largest increase (4%) among people aged ≥ 85 years. Nationwide, nearly 30,000 older adults died from fall-related causes in 2016.
But falls are not an inevitable part of aging, the CDC reminds. Advanced age is a well-known independent risk factor; other risk factors include reduced activity, chronic conditions (including incontinence), prescription medications (which may act synergistically on the central nervous system), and changes in gait and balance. The CDC says health care providers can address the problem by asking patients about falls, assessing gait and balance, reviewing medications, and prescribing interventions such as strength and balance exercises or physical therapy.
Initiatives such as CDC’s STEADI (Stopping Elderly Accidents, Deaths, and Injuries) can help with risk assessment, patient education, and interventions (https://www.cdc.gov/steadi).
Falls have long been a major hazard for older adults—accounting for the largest percentage of deaths from unintentional injuries. Each year, about 1 in 4 older adults in the US reports falling, and an estimated 3 million emergency department visits every year are related to falls.
According to the CDC, things are getting worse. Overall, deaths due to falls among older adults increased 31% from 2007- 2016, a rate of 3% per year. The rate increased in every demographic category except among American Indians/Alaska Natives, with the largest increase (4%) among people aged ≥ 85 years. Nationwide, nearly 30,000 older adults died from fall-related causes in 2016.
But falls are not an inevitable part of aging, the CDC reminds. Advanced age is a well-known independent risk factor; other risk factors include reduced activity, chronic conditions (including incontinence), prescription medications (which may act synergistically on the central nervous system), and changes in gait and balance. The CDC says health care providers can address the problem by asking patients about falls, assessing gait and balance, reviewing medications, and prescribing interventions such as strength and balance exercises or physical therapy.
Initiatives such as CDC’s STEADI (Stopping Elderly Accidents, Deaths, and Injuries) can help with risk assessment, patient education, and interventions (https://www.cdc.gov/steadi).
Falls have long been a major hazard for older adults—accounting for the largest percentage of deaths from unintentional injuries. Each year, about 1 in 4 older adults in the US reports falling, and an estimated 3 million emergency department visits every year are related to falls.
According to the CDC, things are getting worse. Overall, deaths due to falls among older adults increased 31% from 2007- 2016, a rate of 3% per year. The rate increased in every demographic category except among American Indians/Alaska Natives, with the largest increase (4%) among people aged ≥ 85 years. Nationwide, nearly 30,000 older adults died from fall-related causes in 2016.
But falls are not an inevitable part of aging, the CDC reminds. Advanced age is a well-known independent risk factor; other risk factors include reduced activity, chronic conditions (including incontinence), prescription medications (which may act synergistically on the central nervous system), and changes in gait and balance. The CDC says health care providers can address the problem by asking patients about falls, assessing gait and balance, reviewing medications, and prescribing interventions such as strength and balance exercises or physical therapy.
Initiatives such as CDC’s STEADI (Stopping Elderly Accidents, Deaths, and Injuries) can help with risk assessment, patient education, and interventions (https://www.cdc.gov/steadi).
FDA approves Zephyr endobronchial valve to treat severe emphysema
The valve is the first minimally invasive device approved in the United States for treating such patients, according to Pulmonx, the device manufacturer.
The FDA previously granted the novel device expedited review, as patients who did not respond to drug treatment had only limited alternative options, including lung volume reduction and lung transplant, Tina Kiang, PhD, of the FDA’s Center for Devices and Radiological Health, said in a press release. “This novel device is a less invasive treatment that expands the options available to patients,” said Dr. Kiang, acting director of the center’s Division of Anesthesiology, General Hospital, Respiratory, Infection Control, and Dental Devices.![]()
The approval is based on a multicenter study of 190 patients with severe emphysema. A total of 128 received Zephyr valves and medical management, while 62 received medical management only. The primary measure was the number of patients who achieved at least a 15% improvement in their pulmonary function score: At 1 year, 47.7% of the Zephyr valve patients had achieved such improvement versus 16.8% of the control group, according to the FDA.
Adverse events included death, pneumothorax, pneumonia, worsening of emphysema, coughing up blood, shortness of breath, and chest pain. The valve is contraindicated in patients with active lung infections; those allergic to nitinol, nickel, titanium, or silicone; and active smokers.
Read more about this approval in the full FDA press announcement.
The valve is the first minimally invasive device approved in the United States for treating such patients, according to Pulmonx, the device manufacturer.
The FDA previously granted the novel device expedited review, as patients who did not respond to drug treatment had only limited alternative options, including lung volume reduction and lung transplant, Tina Kiang, PhD, of the FDA’s Center for Devices and Radiological Health, said in a press release. “This novel device is a less invasive treatment that expands the options available to patients,” said Dr. Kiang, acting director of the center’s Division of Anesthesiology, General Hospital, Respiratory, Infection Control, and Dental Devices.![]()
The approval is based on a multicenter study of 190 patients with severe emphysema. A total of 128 received Zephyr valves and medical management, while 62 received medical management only. The primary measure was the number of patients who achieved at least a 15% improvement in their pulmonary function score: At 1 year, 47.7% of the Zephyr valve patients had achieved such improvement versus 16.8% of the control group, according to the FDA.
Adverse events included death, pneumothorax, pneumonia, worsening of emphysema, coughing up blood, shortness of breath, and chest pain. The valve is contraindicated in patients with active lung infections; those allergic to nitinol, nickel, titanium, or silicone; and active smokers.
Read more about this approval in the full FDA press announcement.
The valve is the first minimally invasive device approved in the United States for treating such patients, according to Pulmonx, the device manufacturer.
The FDA previously granted the novel device expedited review, as patients who did not respond to drug treatment had only limited alternative options, including lung volume reduction and lung transplant, Tina Kiang, PhD, of the FDA’s Center for Devices and Radiological Health, said in a press release. “This novel device is a less invasive treatment that expands the options available to patients,” said Dr. Kiang, acting director of the center’s Division of Anesthesiology, General Hospital, Respiratory, Infection Control, and Dental Devices.![]()
The approval is based on a multicenter study of 190 patients with severe emphysema. A total of 128 received Zephyr valves and medical management, while 62 received medical management only. The primary measure was the number of patients who achieved at least a 15% improvement in their pulmonary function score: At 1 year, 47.7% of the Zephyr valve patients had achieved such improvement versus 16.8% of the control group, according to the FDA.
Adverse events included death, pneumothorax, pneumonia, worsening of emphysema, coughing up blood, shortness of breath, and chest pain. The valve is contraindicated in patients with active lung infections; those allergic to nitinol, nickel, titanium, or silicone; and active smokers.
Read more about this approval in the full FDA press announcement.
European Medicines Agency recommends CAR T-cell approvals
The European Medicines Agency (EMA) has recommended a handful of hematology medications for approval, including two chimeric antigen receptor (CAR) T-cell therapies.
All of the drugs must next be approved by the European Commission in order to be marketed to patients throughout Europe.
At the end of June, the EMA’s Committee for Medicinal Products for Human Use tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta).

The EMA approval recommendations come with risk management measures to address the potential for cytokine release syndrome with both of these treatments. Drug makers must use a patient registry to monitor the long-term safety and efficacy of the therapies.
The EMA is also recommending approval of caplacizumab for acquired thrombotic thrombocytopenic purpura, vonicog alfa for the treatment of von Willebrand disease, and daunorubicin/cytarabine for the treatment of acute myeloid leukemia.
The European Medicines Agency (EMA) has recommended a handful of hematology medications for approval, including two chimeric antigen receptor (CAR) T-cell therapies.
All of the drugs must next be approved by the European Commission in order to be marketed to patients throughout Europe.
At the end of June, the EMA’s Committee for Medicinal Products for Human Use tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta).
The EMA approval recommendations come with risk management measures to address the potential for cytokine release syndrome with both of these treatments. Drug makers must use a patient registry to monitor the long-term safety and efficacy of the therapies.
The EMA is also recommending approval of caplacizumab for acquired thrombotic thrombocytopenic purpura, vonicog alfa for the treatment of von Willebrand disease, and daunorubicin/cytarabine for the treatment of acute myeloid leukemia.
The European Medicines Agency (EMA) has recommended a handful of hematology medications for approval, including two chimeric antigen receptor (CAR) T-cell therapies.
All of the drugs must next be approved by the European Commission in order to be marketed to patients throughout Europe.
At the end of June, the EMA’s Committee for Medicinal Products for Human Use tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta).
The EMA approval recommendations come with risk management measures to address the potential for cytokine release syndrome with both of these treatments. Drug makers must use a patient registry to monitor the long-term safety and efficacy of the therapies.
The EMA is also recommending approval of caplacizumab for acquired thrombotic thrombocytopenic purpura, vonicog alfa for the treatment of von Willebrand disease, and daunorubicin/cytarabine for the treatment of acute myeloid leukemia.
Bortezomib plus vorinostat shows modest response in MCL
but was less impressive among patients with diffuse large B-cell lymphoma (DLBCL).
Victor Yazbeck, MD, of the Massey Cancer Center at Virginia Commonwealth University in Richmond, and his colleagues reported the findings from the multicenter, nonrandomized, phase 2 trial with 65 treated patients. The trial included three cohorts: 22 patients with MCL and no prior treatment with bortezomib; 4 patients with MCL and prior treatment with bortezomib; and 39 patients with relapsed or refractory DLBCL and no prior bortezomib.
The best results were seen among MCL patients with no prior bortezomib treatment, with an overall response rate of 31.8% and a median progression-free survival (PFS) of 7.6 months. Responses were limited among the DLBCL cohort, which had an overall response rate of 7.7% and a median PFS of just 1.8 months. Among MCL patients who had received prior bortezomib treatment, there were no responses.
From a safety perspective, the combination treatment was well tolerated. The most common grade 3 and 4 hematologic toxicities were thrombocytopenia, lymphopenia, and neutropenia. There was one death among the DLBCL patients and it was unclear if it was related to treatment or progression of disease.
“Patients with MCL had a higher [overall response rate] compared to those with DLBCL, most likely due to the single-agent activity of bortezomib in MCL,” the researchers wrote. “Overall, the synergism previously demonstrated in preclinical models could not be confirmed.”
The study was supported by the Southeast Phase 2 Consortium and by a grant from the National Cancer Institute. Dr. Yazbeck reported having no financial disclosures. One of his coauthors is an employee of Amgen and owns Amgen stock. Another coauthor receives research support from Takeda, Celgene, Karyopharm Therapeutics, Bristol-Myers Squibb, Merck, and Signal Genetics.
SOURCE: Yazbeck V et al. Clin Lymphoma Myeloma Leuk. 2018 Jun 6. doi: 10.1016/j.clml.2018.05.023.
but was less impressive among patients with diffuse large B-cell lymphoma (DLBCL).
Victor Yazbeck, MD, of the Massey Cancer Center at Virginia Commonwealth University in Richmond, and his colleagues reported the findings from the multicenter, nonrandomized, phase 2 trial with 65 treated patients. The trial included three cohorts: 22 patients with MCL and no prior treatment with bortezomib; 4 patients with MCL and prior treatment with bortezomib; and 39 patients with relapsed or refractory DLBCL and no prior bortezomib.
The best results were seen among MCL patients with no prior bortezomib treatment, with an overall response rate of 31.8% and a median progression-free survival (PFS) of 7.6 months. Responses were limited among the DLBCL cohort, which had an overall response rate of 7.7% and a median PFS of just 1.8 months. Among MCL patients who had received prior bortezomib treatment, there were no responses.
From a safety perspective, the combination treatment was well tolerated. The most common grade 3 and 4 hematologic toxicities were thrombocytopenia, lymphopenia, and neutropenia. There was one death among the DLBCL patients and it was unclear if it was related to treatment or progression of disease.
“Patients with MCL had a higher [overall response rate] compared to those with DLBCL, most likely due to the single-agent activity of bortezomib in MCL,” the researchers wrote. “Overall, the synergism previously demonstrated in preclinical models could not be confirmed.”
The study was supported by the Southeast Phase 2 Consortium and by a grant from the National Cancer Institute. Dr. Yazbeck reported having no financial disclosures. One of his coauthors is an employee of Amgen and owns Amgen stock. Another coauthor receives research support from Takeda, Celgene, Karyopharm Therapeutics, Bristol-Myers Squibb, Merck, and Signal Genetics.
SOURCE: Yazbeck V et al. Clin Lymphoma Myeloma Leuk. 2018 Jun 6. doi: 10.1016/j.clml.2018.05.023.
but was less impressive among patients with diffuse large B-cell lymphoma (DLBCL).
Victor Yazbeck, MD, of the Massey Cancer Center at Virginia Commonwealth University in Richmond, and his colleagues reported the findings from the multicenter, nonrandomized, phase 2 trial with 65 treated patients. The trial included three cohorts: 22 patients with MCL and no prior treatment with bortezomib; 4 patients with MCL and prior treatment with bortezomib; and 39 patients with relapsed or refractory DLBCL and no prior bortezomib.
The best results were seen among MCL patients with no prior bortezomib treatment, with an overall response rate of 31.8% and a median progression-free survival (PFS) of 7.6 months. Responses were limited among the DLBCL cohort, which had an overall response rate of 7.7% and a median PFS of just 1.8 months. Among MCL patients who had received prior bortezomib treatment, there were no responses.
From a safety perspective, the combination treatment was well tolerated. The most common grade 3 and 4 hematologic toxicities were thrombocytopenia, lymphopenia, and neutropenia. There was one death among the DLBCL patients and it was unclear if it was related to treatment or progression of disease.
“Patients with MCL had a higher [overall response rate] compared to those with DLBCL, most likely due to the single-agent activity of bortezomib in MCL,” the researchers wrote. “Overall, the synergism previously demonstrated in preclinical models could not be confirmed.”
The study was supported by the Southeast Phase 2 Consortium and by a grant from the National Cancer Institute. Dr. Yazbeck reported having no financial disclosures. One of his coauthors is an employee of Amgen and owns Amgen stock. Another coauthor receives research support from Takeda, Celgene, Karyopharm Therapeutics, Bristol-Myers Squibb, Merck, and Signal Genetics.
SOURCE: Yazbeck V et al. Clin Lymphoma Myeloma Leuk. 2018 Jun 6. doi: 10.1016/j.clml.2018.05.023.
FROM CLINICAL LYMPHOMA, MYELOMA AND LEUKEMIA