User login
FDA lifts partial hold on tazemetostat trials
The U.S. Food and Drug Administration has lifted the partial clinical hold on trials of tazemetostat, an EZH2 inhibitor being developed to treat solid tumors and lymphomas, according to a press release from the drug’s developer Epizyme.

The patient had been on study for approximately 15 months and had achieved a confirmed partial response. The patient has since discontinued tazemetostat and responded to treatment for T-LBL.
“This remains the only case of T-LBL we’ve seen in more than 750 patients treated with tazemetostat,” Robert Bazemore, president and chief executive officer of Epizyme, said in a webcast on Sept. 24.
Epizyme assessed the risk of secondary malignancies, including T-LBL, as well as the overall risks and benefits of tazemetostat treatment, conducting a review of the published literature and an examination of efficacy and safety data across all of its tazemetostat trials. A panel of external scientific and medical experts who reviewed the findings concluded that T-LBL risks appear to be confined to pediatric patients who received higher doses of the drug. The phase 1 pediatric study in which the patient developed T-LBL included higher doses of tazemetostat than those used in the phase 2 adult studies.
“The team at Epizyme has worked diligently in collaboration with external experts and the FDA over the past several months,” Mr. Bazemore said.
The company is not making any substantial changes to trial designs or the patient populations involved in tazemetostat trials. However, Epizyme is modifying dosing in the pediatric studies, improving patient monitoring, and making changes to exclusion criteria to reduce the potential risk of T-LBL and other secondary malignancies. Mr. Bazemore said Epizyme hopes to submit a New Drug Application for tazemetostat in the treatment of epithelioid sarcoma.
Tazemetostat is under investigation as monotherapy in phase 2 trials of follicular lymphoma and solid-tumor malignancies. The drug is also being studied as part of combination therapy for non–small cell lung cancer and diffuse large B-cell lymphoma (DLBCL).
In August, Epizyme announced its decision to stop developing tazemetostat for use as monotherapy or in combination with prednisolone for patients with DLBCL. However, tazemetostat is still under investigation as a potential treatment for DLBCL as part of other combination regimens.
Epizyme is now working to resolve partial clinical holds placed on tazemetostat in France and Germany in order to resume trial enrollment in those countries.
The U.S. Food and Drug Administration has lifted the partial clinical hold on trials of tazemetostat, an EZH2 inhibitor being developed to treat solid tumors and lymphomas, according to a press release from the drug’s developer Epizyme.
The patient had been on study for approximately 15 months and had achieved a confirmed partial response. The patient has since discontinued tazemetostat and responded to treatment for T-LBL.
“This remains the only case of T-LBL we’ve seen in more than 750 patients treated with tazemetostat,” Robert Bazemore, president and chief executive officer of Epizyme, said in a webcast on Sept. 24.
Epizyme assessed the risk of secondary malignancies, including T-LBL, as well as the overall risks and benefits of tazemetostat treatment, conducting a review of the published literature and an examination of efficacy and safety data across all of its tazemetostat trials. A panel of external scientific and medical experts who reviewed the findings concluded that T-LBL risks appear to be confined to pediatric patients who received higher doses of the drug. The phase 1 pediatric study in which the patient developed T-LBL included higher doses of tazemetostat than those used in the phase 2 adult studies.
“The team at Epizyme has worked diligently in collaboration with external experts and the FDA over the past several months,” Mr. Bazemore said.
The company is not making any substantial changes to trial designs or the patient populations involved in tazemetostat trials. However, Epizyme is modifying dosing in the pediatric studies, improving patient monitoring, and making changes to exclusion criteria to reduce the potential risk of T-LBL and other secondary malignancies. Mr. Bazemore said Epizyme hopes to submit a New Drug Application for tazemetostat in the treatment of epithelioid sarcoma.
Tazemetostat is under investigation as monotherapy in phase 2 trials of follicular lymphoma and solid-tumor malignancies. The drug is also being studied as part of combination therapy for non–small cell lung cancer and diffuse large B-cell lymphoma (DLBCL).
In August, Epizyme announced its decision to stop developing tazemetostat for use as monotherapy or in combination with prednisolone for patients with DLBCL. However, tazemetostat is still under investigation as a potential treatment for DLBCL as part of other combination regimens.
Epizyme is now working to resolve partial clinical holds placed on tazemetostat in France and Germany in order to resume trial enrollment in those countries.
The U.S. Food and Drug Administration has lifted the partial clinical hold on trials of tazemetostat, an EZH2 inhibitor being developed to treat solid tumors and lymphomas, according to a press release from the drug’s developer Epizyme.
The patient had been on study for approximately 15 months and had achieved a confirmed partial response. The patient has since discontinued tazemetostat and responded to treatment for T-LBL.
“This remains the only case of T-LBL we’ve seen in more than 750 patients treated with tazemetostat,” Robert Bazemore, president and chief executive officer of Epizyme, said in a webcast on Sept. 24.
Epizyme assessed the risk of secondary malignancies, including T-LBL, as well as the overall risks and benefits of tazemetostat treatment, conducting a review of the published literature and an examination of efficacy and safety data across all of its tazemetostat trials. A panel of external scientific and medical experts who reviewed the findings concluded that T-LBL risks appear to be confined to pediatric patients who received higher doses of the drug. The phase 1 pediatric study in which the patient developed T-LBL included higher doses of tazemetostat than those used in the phase 2 adult studies.
“The team at Epizyme has worked diligently in collaboration with external experts and the FDA over the past several months,” Mr. Bazemore said.
The company is not making any substantial changes to trial designs or the patient populations involved in tazemetostat trials. However, Epizyme is modifying dosing in the pediatric studies, improving patient monitoring, and making changes to exclusion criteria to reduce the potential risk of T-LBL and other secondary malignancies. Mr. Bazemore said Epizyme hopes to submit a New Drug Application for tazemetostat in the treatment of epithelioid sarcoma.
Tazemetostat is under investigation as monotherapy in phase 2 trials of follicular lymphoma and solid-tumor malignancies. The drug is also being studied as part of combination therapy for non–small cell lung cancer and diffuse large B-cell lymphoma (DLBCL).
In August, Epizyme announced its decision to stop developing tazemetostat for use as monotherapy or in combination with prednisolone for patients with DLBCL. However, tazemetostat is still under investigation as a potential treatment for DLBCL as part of other combination regimens.
Epizyme is now working to resolve partial clinical holds placed on tazemetostat in France and Germany in order to resume trial enrollment in those countries.
Pulmonary artery denervation boosts walking capacity in left heart failure
SAN DIEGO – Pulmonary artery denervation is efficacious for treating combined pre- and postcapillary pulmonary hypertension attributable to left heart failure, based on results of the Chinese PADN-5 trial reported at the Transcatheter Cardiovascular Therapeutics annual meeting.

This ablative treatment has been studied among patients with pulmonary hypertension attributable to other etiologies, but not in randomized fashion among this population, noted lead investigator Shao-Liang Chen, MD, of Nanjing (China) First Hospital, Nanjing Medical University. The treatment is an attractive one, as medications recommended for pulmonary arterial hypertension are not recommended for joint pre- and postcapillary pulmonary hypertension (group II pulmonary hypertension).
In PADN-5, 98 patients were randomized to pulmonary artery denervation or to sham denervation plus open-label sildenafil (Viagra), which at the time of trial initiation was thought to be safe and potentially beneficial.
The trial’s main outcome, 6-minute walk distance at 6 months, improved in both groups, according to data reported at the meeting and simultaneously published in JACC Cardiovascular Interventions. But the improvement was about four times greater in the pulmonary artery denervation group. Secondary efficacy outcomes also favored that group, and the rate of fatal pulmonary embolism did not differ for the two groups.
“The PADN-5 trial demonstrates the benefits of pulmonary artery denervation for patients with combined pre- and postcapillary pulmonary hypertension. Patients with preserved and with reduced ejection fraction equally benefited,” summarized Dr. Chen, who pioneered this procedure about 7 years ago. “There was no sign of any harm of sildenafil in patients with combined pre- and postcapillary pulmonary hypertension.”
Trial critique
“This is a very difficult study to conduct, being able to recruit patients and actually have these procedures done,” commented press conference moderator Ori Ben-Yehuda, MD, professor of clinical medicine and director, coronary care unit, UC San Diego Medical Center.
At the same time, he expressed some reservations about the trial. “Sildenafil in the control group might actually be expected to ... decrease your effect size. Also, particularly in men, perhaps even in women, it might unblind them to which group they are in and undermine your sham design,” he noted. In addition, some hemodynamic changes after pulmonary artery denervation – a decrease in wedge pressure and an increase in ejection fraction – were puzzling.
“We need a lot more data here. There are some issues with this trial in terms of design, and we haven’t even gotten into the issue of whether there were core labs, whether the echoes, the hemodynamics, were read blindly,” Dr. Ben-Yehuda maintained. “This issue of secondary or group II pulmonary hypertension due to left heart failure is one that has been very frustrating in terms of actual PA-specific therapies. So this is an important step further, but it needs confirmation in truly sham-controlled trials that have no potential for unblinding.”
The catheter used in PADN-5 is available in China but has not received clearance in the United States, he pointed out. “There are alternative or competing technologies, one using ultrasound, for example, that has a very similar approach. … We’ll have to see how it ends up [performing].”
Trial details
Patients in the PADN-5 pulmonary artery denervation group underwent ablation only in the periconjunctional area between the distal main trunk and the left ostial branch with a multifunction catheter having premounted electrodes. Those in the control group underwent a sham procedure, with catheter positioning at the target sites and connection to a generator but no ablation, and were given open-label sildenafil. All additionally received standard heart failure medical therapy. (No sildenafil placebo was used in the denervation group.)
Trial results reported at the meeting, which is sponsored by the Cardiovascular Research Foundation, showed that most echocardiographic and hemodynamic measures improved more in the pulmonary artery denervation group.
The greater improvement in 6-minute walk test with denervation versus sham sildenafil at 6 months was evident in a variety of measures: absolute median distance walked (432.5 m vs. 358 m) and mean distance walked (434.6 m vs. 359.4 m), and absolute increase (80 m vs. 17.5 m) and relative increase (21.4% vs. 4.9%) The difference was significant for all measures at P less than .001.
The denervation group had a comparatively greater reduction of pulmonary vascular resistance (29.8% vs. 3.4%; P less than .001) and were less likely to experience clinical worsening (16.7% vs. 40.0%; P = .014).
There was a single fatal pulmonary embolism in each treatment group. Of the seven total deaths, two occurred in the denervation group (one attributable to pump failure, one a sudden death) and five occurred in the sham sildenafil group (all but one attributable to pump failure).
Dr. Chen disclosed that he had no relevant conflicts of interest. The trial was sponsored by Nanjing First Hospital, Nanjing Medical University.
SOURCE: Chen S-J et al. TCT 2018. JACC Cardiovasc Interv. 2018 Sep 23.
SAN DIEGO – Pulmonary artery denervation is efficacious for treating combined pre- and postcapillary pulmonary hypertension attributable to left heart failure, based on results of the Chinese PADN-5 trial reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
This ablative treatment has been studied among patients with pulmonary hypertension attributable to other etiologies, but not in randomized fashion among this population, noted lead investigator Shao-Liang Chen, MD, of Nanjing (China) First Hospital, Nanjing Medical University. The treatment is an attractive one, as medications recommended for pulmonary arterial hypertension are not recommended for joint pre- and postcapillary pulmonary hypertension (group II pulmonary hypertension).
In PADN-5, 98 patients were randomized to pulmonary artery denervation or to sham denervation plus open-label sildenafil (Viagra), which at the time of trial initiation was thought to be safe and potentially beneficial.
The trial’s main outcome, 6-minute walk distance at 6 months, improved in both groups, according to data reported at the meeting and simultaneously published in JACC Cardiovascular Interventions. But the improvement was about four times greater in the pulmonary artery denervation group. Secondary efficacy outcomes also favored that group, and the rate of fatal pulmonary embolism did not differ for the two groups.
“The PADN-5 trial demonstrates the benefits of pulmonary artery denervation for patients with combined pre- and postcapillary pulmonary hypertension. Patients with preserved and with reduced ejection fraction equally benefited,” summarized Dr. Chen, who pioneered this procedure about 7 years ago. “There was no sign of any harm of sildenafil in patients with combined pre- and postcapillary pulmonary hypertension.”
Trial critique
“This is a very difficult study to conduct, being able to recruit patients and actually have these procedures done,” commented press conference moderator Ori Ben-Yehuda, MD, professor of clinical medicine and director, coronary care unit, UC San Diego Medical Center.
At the same time, he expressed some reservations about the trial. “Sildenafil in the control group might actually be expected to ... decrease your effect size. Also, particularly in men, perhaps even in women, it might unblind them to which group they are in and undermine your sham design,” he noted. In addition, some hemodynamic changes after pulmonary artery denervation – a decrease in wedge pressure and an increase in ejection fraction – were puzzling.
“We need a lot more data here. There are some issues with this trial in terms of design, and we haven’t even gotten into the issue of whether there were core labs, whether the echoes, the hemodynamics, were read blindly,” Dr. Ben-Yehuda maintained. “This issue of secondary or group II pulmonary hypertension due to left heart failure is one that has been very frustrating in terms of actual PA-specific therapies. So this is an important step further, but it needs confirmation in truly sham-controlled trials that have no potential for unblinding.”
The catheter used in PADN-5 is available in China but has not received clearance in the United States, he pointed out. “There are alternative or competing technologies, one using ultrasound, for example, that has a very similar approach. … We’ll have to see how it ends up [performing].”
Trial details
Patients in the PADN-5 pulmonary artery denervation group underwent ablation only in the periconjunctional area between the distal main trunk and the left ostial branch with a multifunction catheter having premounted electrodes. Those in the control group underwent a sham procedure, with catheter positioning at the target sites and connection to a generator but no ablation, and were given open-label sildenafil. All additionally received standard heart failure medical therapy. (No sildenafil placebo was used in the denervation group.)
Trial results reported at the meeting, which is sponsored by the Cardiovascular Research Foundation, showed that most echocardiographic and hemodynamic measures improved more in the pulmonary artery denervation group.
The greater improvement in 6-minute walk test with denervation versus sham sildenafil at 6 months was evident in a variety of measures: absolute median distance walked (432.5 m vs. 358 m) and mean distance walked (434.6 m vs. 359.4 m), and absolute increase (80 m vs. 17.5 m) and relative increase (21.4% vs. 4.9%) The difference was significant for all measures at P less than .001.
The denervation group had a comparatively greater reduction of pulmonary vascular resistance (29.8% vs. 3.4%; P less than .001) and were less likely to experience clinical worsening (16.7% vs. 40.0%; P = .014).
There was a single fatal pulmonary embolism in each treatment group. Of the seven total deaths, two occurred in the denervation group (one attributable to pump failure, one a sudden death) and five occurred in the sham sildenafil group (all but one attributable to pump failure).
Dr. Chen disclosed that he had no relevant conflicts of interest. The trial was sponsored by Nanjing First Hospital, Nanjing Medical University.
SOURCE: Chen S-J et al. TCT 2018. JACC Cardiovasc Interv. 2018 Sep 23.
SAN DIEGO – Pulmonary artery denervation is efficacious for treating combined pre- and postcapillary pulmonary hypertension attributable to left heart failure, based on results of the Chinese PADN-5 trial reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
This ablative treatment has been studied among patients with pulmonary hypertension attributable to other etiologies, but not in randomized fashion among this population, noted lead investigator Shao-Liang Chen, MD, of Nanjing (China) First Hospital, Nanjing Medical University. The treatment is an attractive one, as medications recommended for pulmonary arterial hypertension are not recommended for joint pre- and postcapillary pulmonary hypertension (group II pulmonary hypertension).
In PADN-5, 98 patients were randomized to pulmonary artery denervation or to sham denervation plus open-label sildenafil (Viagra), which at the time of trial initiation was thought to be safe and potentially beneficial.
The trial’s main outcome, 6-minute walk distance at 6 months, improved in both groups, according to data reported at the meeting and simultaneously published in JACC Cardiovascular Interventions. But the improvement was about four times greater in the pulmonary artery denervation group. Secondary efficacy outcomes also favored that group, and the rate of fatal pulmonary embolism did not differ for the two groups.
“The PADN-5 trial demonstrates the benefits of pulmonary artery denervation for patients with combined pre- and postcapillary pulmonary hypertension. Patients with preserved and with reduced ejection fraction equally benefited,” summarized Dr. Chen, who pioneered this procedure about 7 years ago. “There was no sign of any harm of sildenafil in patients with combined pre- and postcapillary pulmonary hypertension.”
Trial critique
“This is a very difficult study to conduct, being able to recruit patients and actually have these procedures done,” commented press conference moderator Ori Ben-Yehuda, MD, professor of clinical medicine and director, coronary care unit, UC San Diego Medical Center.
At the same time, he expressed some reservations about the trial. “Sildenafil in the control group might actually be expected to ... decrease your effect size. Also, particularly in men, perhaps even in women, it might unblind them to which group they are in and undermine your sham design,” he noted. In addition, some hemodynamic changes after pulmonary artery denervation – a decrease in wedge pressure and an increase in ejection fraction – were puzzling.
“We need a lot more data here. There are some issues with this trial in terms of design, and we haven’t even gotten into the issue of whether there were core labs, whether the echoes, the hemodynamics, were read blindly,” Dr. Ben-Yehuda maintained. “This issue of secondary or group II pulmonary hypertension due to left heart failure is one that has been very frustrating in terms of actual PA-specific therapies. So this is an important step further, but it needs confirmation in truly sham-controlled trials that have no potential for unblinding.”
The catheter used in PADN-5 is available in China but has not received clearance in the United States, he pointed out. “There are alternative or competing technologies, one using ultrasound, for example, that has a very similar approach. … We’ll have to see how it ends up [performing].”
Trial details
Patients in the PADN-5 pulmonary artery denervation group underwent ablation only in the periconjunctional area between the distal main trunk and the left ostial branch with a multifunction catheter having premounted electrodes. Those in the control group underwent a sham procedure, with catheter positioning at the target sites and connection to a generator but no ablation, and were given open-label sildenafil. All additionally received standard heart failure medical therapy. (No sildenafil placebo was used in the denervation group.)
Trial results reported at the meeting, which is sponsored by the Cardiovascular Research Foundation, showed that most echocardiographic and hemodynamic measures improved more in the pulmonary artery denervation group.
The greater improvement in 6-minute walk test with denervation versus sham sildenafil at 6 months was evident in a variety of measures: absolute median distance walked (432.5 m vs. 358 m) and mean distance walked (434.6 m vs. 359.4 m), and absolute increase (80 m vs. 17.5 m) and relative increase (21.4% vs. 4.9%) The difference was significant for all measures at P less than .001.
The denervation group had a comparatively greater reduction of pulmonary vascular resistance (29.8% vs. 3.4%; P less than .001) and were less likely to experience clinical worsening (16.7% vs. 40.0%; P = .014).
There was a single fatal pulmonary embolism in each treatment group. Of the seven total deaths, two occurred in the denervation group (one attributable to pump failure, one a sudden death) and five occurred in the sham sildenafil group (all but one attributable to pump failure).
Dr. Chen disclosed that he had no relevant conflicts of interest. The trial was sponsored by Nanjing First Hospital, Nanjing Medical University.
SOURCE: Chen S-J et al. TCT 2018. JACC Cardiovasc Interv. 2018 Sep 23.
REPORTING FROM TCT 2018
Key clinical point: Pulmonary artery denervation is efficacious for treating pulmonary hypertension related to heart failure.
Major finding: Improvement in 6-minute walk distance was greater with pulmonary artery denervation than with sham denervation plus sildenafil (21.4% vs. 4.9%; P less than .001).
Study details: PADN-5 is a randomized controlled trial among 98 patients with combined pre- and postcapillary pulmonary hypertension secondary to left heart failure (group II pulmonary hypertension).
Disclosures: Dr. Chen disclosed that he had no relevant conflicts of interest. The trial was sponsored by Nanjing First Hospital, Nanjing Medical University.
Source: Chen S-L et al. TCT 2018. JACC Cardiovasc Interv. 2018 Sep 23.
Teaching Kids About Flu Variants—Graphically
A group of teenage 4-H members take part in a state agricultural fair, after which one of the boys comes sick. But luckily they have also attended the CDC’s Disease Detective Camp in Atlanta and use their newly acquired detective skills to find out why their friend got sick.
That is the story in “The Junior Disease Detectives: Operation Outbreak,” the new graphic novel the CDC has developed with the Department of Agriculture and 4-H.
Spoiler alert: it was the flu. The novel is designed to help young people understand the potential health risks of human influenza viruses that normally circulate in swine, known as variant flu infections.
Four new variant virus infections have been associated with attendance at agricultural fairs in 2 US states, the CDC reports. Most are connected to infected pigs or their environments in fair settings. While variant flu infections in people are rare, the CDC says, they can lead to hospitalization and death. In 2017, 67 variant virus infections were reported in the US; 6 resulted in hospitalization, including 2 ICU admissions.
The novel is intended for use in middle and high school science, technology, engineering, and mathematics (STEM) classrooms. It is the first of a planned series of educational activities being rolled out throughout the 2018-2019 school year.
The novel is available as a free mobile app, and can be downloaded at https://www.cdc.gov/flu/resource-center/freeresources/graphic-novel/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fflu%2Fgraphicnovel%2Findex.html.
A group of teenage 4-H members take part in a state agricultural fair, after which one of the boys comes sick. But luckily they have also attended the CDC’s Disease Detective Camp in Atlanta and use their newly acquired detective skills to find out why their friend got sick.
That is the story in “The Junior Disease Detectives: Operation Outbreak,” the new graphic novel the CDC has developed with the Department of Agriculture and 4-H.
Spoiler alert: it was the flu. The novel is designed to help young people understand the potential health risks of human influenza viruses that normally circulate in swine, known as variant flu infections.
Four new variant virus infections have been associated with attendance at agricultural fairs in 2 US states, the CDC reports. Most are connected to infected pigs or their environments in fair settings. While variant flu infections in people are rare, the CDC says, they can lead to hospitalization and death. In 2017, 67 variant virus infections were reported in the US; 6 resulted in hospitalization, including 2 ICU admissions.
The novel is intended for use in middle and high school science, technology, engineering, and mathematics (STEM) classrooms. It is the first of a planned series of educational activities being rolled out throughout the 2018-2019 school year.
The novel is available as a free mobile app, and can be downloaded at https://www.cdc.gov/flu/resource-center/freeresources/graphic-novel/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fflu%2Fgraphicnovel%2Findex.html.
A group of teenage 4-H members take part in a state agricultural fair, after which one of the boys comes sick. But luckily they have also attended the CDC’s Disease Detective Camp in Atlanta and use their newly acquired detective skills to find out why their friend got sick.
That is the story in “The Junior Disease Detectives: Operation Outbreak,” the new graphic novel the CDC has developed with the Department of Agriculture and 4-H.
Spoiler alert: it was the flu. The novel is designed to help young people understand the potential health risks of human influenza viruses that normally circulate in swine, known as variant flu infections.
Four new variant virus infections have been associated with attendance at agricultural fairs in 2 US states, the CDC reports. Most are connected to infected pigs or their environments in fair settings. While variant flu infections in people are rare, the CDC says, they can lead to hospitalization and death. In 2017, 67 variant virus infections were reported in the US; 6 resulted in hospitalization, including 2 ICU admissions.
The novel is intended for use in middle and high school science, technology, engineering, and mathematics (STEM) classrooms. It is the first of a planned series of educational activities being rolled out throughout the 2018-2019 school year.
The novel is available as a free mobile app, and can be downloaded at https://www.cdc.gov/flu/resource-center/freeresources/graphic-novel/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fflu%2Fgraphicnovel%2Findex.html.
FDA Grants Fund Rare Disease Research
Twelve FDA grants fund new clinical trials to advance the development of medical products for the treatment of rare diseases.
On September 24, 2018, the FDA announced that it awarded 12 new clinical trial research grants totaling more than $18 million over the next four years to enhance the development of medical products for patients with rare diseases. These new grants were awarded to principal investigators from academia and industry across the country.
“Developing a treatment for a rare disease can be especially challenging. Given the often small number of patients affected by certain very rare diseases, there can be limited markets for new treatments, and as a result fewer resources devoted to researching these opportunities,” said FDA Commissioner Scott Gottlieb, MD. “The FDA is committed to doing its part to facilitate continued progress toward more treatments, and even potential cures, for patients with rare diseases. New scientific advances offer more opportunities to develop these potential cures. With efficient regulation, proper incentives for product development, and the continued support of patients, providers, and researchers, we have more opportunities to pursue these advances than ever before. For 35 years, the FDA has provided much-needed financial support for clinical trials of potentially life-changing treatments for patients with rare diseases. This funding helps support early-stage development activities targeting rare diseases that do not have effective treatments. By providing seed capital, these FDA-administered grants enable researchers to prove out important concepts. The FDA grants also provide some important recognition to promising development programs that ultimately can help researchers attract additional funding.”

The FDA awarded the grants through the Orphan Products Clinical Trials Grants Program. This program is funded by Congressional appropriations and encourages clinical development of drugs, biologics, medical devices, or medical foods for use in rare diseases. The grants are intended for clinical studies evaluating the safety and effectiveness of products that could either result in, or substantially contribute to, the FDA approval of products targeted to the treatment of rare diseases. Grant applications were reviewed and evaluated for scientific and technical merit by more than 100 rare disease experts, which included representatives from academia, the NIH, and the FDA.
The grant recipients, principal investigators, and approximate funding amounts, listed alphabetically, are:
Alkeus Pharmaceuticals, Inc (Cambridge, Massachusetts), Leonide Saad, phase 2 study of ALK-001 for the treatment of Stargardt disease—$1.75 million over four years
Arizona State University–Tempe Campus (Tempe, Arizona), Keith Lindor, phase 2 study of oral vancomycin for the treatment of primary sclerosing cholangitis—$2 million over four years
Cedars-Sinai Medical Center (Los Angeles), Shlomo Melmed, phase 2 study of seliciclib for the treatment of Cushing disease—$2 million over four years
Columbia University (New York), Yvonne Saenger, phase 1 study of talimogene laherparepvec for the treatment for advanced pancreatic cancer—$750,000 over three years
Emory University (Atlanta), Eric Sorscher, phase 1/ 2 study of Ad/PNP fludarabine for the treatment of head and neck squamous cell carcinoma—$1.5 million over three years
Fibrocell Technologies, Inc (Exton, Pennsylvania), John Maslowski, phase 1/2 study of gene-modified ex-vivo autologous fibroblasts for the treatment of dystrophic epidermolysis bullosa—$1.5 million over four years
Johns Hopkins University (Baltimore), Amy Dezern, phase 1/2 study of CD8-reduced T cells for the treatment of myelodysplastic syndrome or acute myeloid leukemia—$750,000 over three years
Oncolmmune, Inc (Rockville, Maryland) Yang Liu, phase 2b study of CD24Fc for the prevention of graft versus host disease—$2 million over four years
Patagonia Pharmaceuticals, LLC (Woodcliff Lake, New Jersey), Zachary Rome, phase 2 study of PAT-001 (isotretinoin) for the treatment of congenital ichthyosis—$1.5 million over three years
The General Hospital Corporation (Boston), Stephanie Seminara, phase 2 study of kisspeptin for the treatment of dopamine agonist intolerant hyperprolactinemia—$1.4 million over four years
University of Minnesota (Minneapolis), Kyriakie Sarafoglou, phase 2a study of subcutaneous hydrocortisone infusion pump for the treatment of congenital adrenal hyperplasia—$1.4 million over three years
University of North Carolina at Chapel Hill (Chapel Hill, North Carolina), Matthew Laughon, phase 2 study of sildenafil for the prevention of bronchopulmonary dysplasia—$2 million over four years.
“Since its creation in 1983, the Orphan Products Grants Program has provided more than $400 million to fund more than 600 new clinical studies,” said Debra Lewis, OD, Acting Director of the FDA’s Office of Orphan Products Development. “We are encouraged to see so much interest in our grants program and are pleased to support research for a variety of rare diseases that have little, or no, treatment options for patients.”
One-third of the new awards aim to accelerate cancer research by enrolling patients with rare forms of cancer, including advanced pancreatic cancer, head and neck squamous cell carcinoma, myelodysplastic syndrome, and acute myeloid leukemia. Another 25% of the new awards fund studies evaluating drug products for rare endocrine disorders, including Cushing disease, dopamine agonist intolerant hyperprolactinemia, and congenital adrenal hyperplasia. Another study addresses an unmet need in primary sclerosing cholangitis, a rare, chronic, and potentially serious bile duct disease.
About 42% of the grants fund studies that enroll children and adolescents, targeting a variety of rare diseases in children such as Stargardt disease, a juvenile genetic eye disorder that causes progressive vision loss; dystrophic epidermolysis bullosa, a genetic condition that causes the skin to be fragile resulting in painful blisters; and bronchopulmonary dysplasia, a serious lung condition that affects infants.
To date, the program’s grants have supported research that led to the marketing approval of more than 60 orphan products. Among the recent product approvals which were supported by studies funded by this grants program are a marketing approval for a much-needed treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults with multidrug resistant HIV-1 infection and another approval to reduce the acute complications of sickle cell disease in adult and pediatric patients.
The FDA is also currently supporting six natural history studies for rare diseases to further advance the mission of bringing new therapies to market.
Twelve FDA grants fund new clinical trials to advance the development of medical products for the treatment of rare diseases.
Twelve FDA grants fund new clinical trials to advance the development of medical products for the treatment of rare diseases.
On September 24, 2018, the FDA announced that it awarded 12 new clinical trial research grants totaling more than $18 million over the next four years to enhance the development of medical products for patients with rare diseases. These new grants were awarded to principal investigators from academia and industry across the country.
“Developing a treatment for a rare disease can be especially challenging. Given the often small number of patients affected by certain very rare diseases, there can be limited markets for new treatments, and as a result fewer resources devoted to researching these opportunities,” said FDA Commissioner Scott Gottlieb, MD. “The FDA is committed to doing its part to facilitate continued progress toward more treatments, and even potential cures, for patients with rare diseases. New scientific advances offer more opportunities to develop these potential cures. With efficient regulation, proper incentives for product development, and the continued support of patients, providers, and researchers, we have more opportunities to pursue these advances than ever before. For 35 years, the FDA has provided much-needed financial support for clinical trials of potentially life-changing treatments for patients with rare diseases. This funding helps support early-stage development activities targeting rare diseases that do not have effective treatments. By providing seed capital, these FDA-administered grants enable researchers to prove out important concepts. The FDA grants also provide some important recognition to promising development programs that ultimately can help researchers attract additional funding.”
The FDA awarded the grants through the Orphan Products Clinical Trials Grants Program. This program is funded by Congressional appropriations and encourages clinical development of drugs, biologics, medical devices, or medical foods for use in rare diseases. The grants are intended for clinical studies evaluating the safety and effectiveness of products that could either result in, or substantially contribute to, the FDA approval of products targeted to the treatment of rare diseases. Grant applications were reviewed and evaluated for scientific and technical merit by more than 100 rare disease experts, which included representatives from academia, the NIH, and the FDA.
The grant recipients, principal investigators, and approximate funding amounts, listed alphabetically, are:
Alkeus Pharmaceuticals, Inc (Cambridge, Massachusetts), Leonide Saad, phase 2 study of ALK-001 for the treatment of Stargardt disease—$1.75 million over four years
Arizona State University–Tempe Campus (Tempe, Arizona), Keith Lindor, phase 2 study of oral vancomycin for the treatment of primary sclerosing cholangitis—$2 million over four years
Cedars-Sinai Medical Center (Los Angeles), Shlomo Melmed, phase 2 study of seliciclib for the treatment of Cushing disease—$2 million over four years
Columbia University (New York), Yvonne Saenger, phase 1 study of talimogene laherparepvec for the treatment for advanced pancreatic cancer—$750,000 over three years
Emory University (Atlanta), Eric Sorscher, phase 1/ 2 study of Ad/PNP fludarabine for the treatment of head and neck squamous cell carcinoma—$1.5 million over three years
Fibrocell Technologies, Inc (Exton, Pennsylvania), John Maslowski, phase 1/2 study of gene-modified ex-vivo autologous fibroblasts for the treatment of dystrophic epidermolysis bullosa—$1.5 million over four years
Johns Hopkins University (Baltimore), Amy Dezern, phase 1/2 study of CD8-reduced T cells for the treatment of myelodysplastic syndrome or acute myeloid leukemia—$750,000 over three years
Oncolmmune, Inc (Rockville, Maryland) Yang Liu, phase 2b study of CD24Fc for the prevention of graft versus host disease—$2 million over four years
Patagonia Pharmaceuticals, LLC (Woodcliff Lake, New Jersey), Zachary Rome, phase 2 study of PAT-001 (isotretinoin) for the treatment of congenital ichthyosis—$1.5 million over three years
The General Hospital Corporation (Boston), Stephanie Seminara, phase 2 study of kisspeptin for the treatment of dopamine agonist intolerant hyperprolactinemia—$1.4 million over four years
University of Minnesota (Minneapolis), Kyriakie Sarafoglou, phase 2a study of subcutaneous hydrocortisone infusion pump for the treatment of congenital adrenal hyperplasia—$1.4 million over three years
University of North Carolina at Chapel Hill (Chapel Hill, North Carolina), Matthew Laughon, phase 2 study of sildenafil for the prevention of bronchopulmonary dysplasia—$2 million over four years.
“Since its creation in 1983, the Orphan Products Grants Program has provided more than $400 million to fund more than 600 new clinical studies,” said Debra Lewis, OD, Acting Director of the FDA’s Office of Orphan Products Development. “We are encouraged to see so much interest in our grants program and are pleased to support research for a variety of rare diseases that have little, or no, treatment options for patients.”
One-third of the new awards aim to accelerate cancer research by enrolling patients with rare forms of cancer, including advanced pancreatic cancer, head and neck squamous cell carcinoma, myelodysplastic syndrome, and acute myeloid leukemia. Another 25% of the new awards fund studies evaluating drug products for rare endocrine disorders, including Cushing disease, dopamine agonist intolerant hyperprolactinemia, and congenital adrenal hyperplasia. Another study addresses an unmet need in primary sclerosing cholangitis, a rare, chronic, and potentially serious bile duct disease.
About 42% of the grants fund studies that enroll children and adolescents, targeting a variety of rare diseases in children such as Stargardt disease, a juvenile genetic eye disorder that causes progressive vision loss; dystrophic epidermolysis bullosa, a genetic condition that causes the skin to be fragile resulting in painful blisters; and bronchopulmonary dysplasia, a serious lung condition that affects infants.
To date, the program’s grants have supported research that led to the marketing approval of more than 60 orphan products. Among the recent product approvals which were supported by studies funded by this grants program are a marketing approval for a much-needed treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults with multidrug resistant HIV-1 infection and another approval to reduce the acute complications of sickle cell disease in adult and pediatric patients.
The FDA is also currently supporting six natural history studies for rare diseases to further advance the mission of bringing new therapies to market.
On September 24, 2018, the FDA announced that it awarded 12 new clinical trial research grants totaling more than $18 million over the next four years to enhance the development of medical products for patients with rare diseases. These new grants were awarded to principal investigators from academia and industry across the country.
“Developing a treatment for a rare disease can be especially challenging. Given the often small number of patients affected by certain very rare diseases, there can be limited markets for new treatments, and as a result fewer resources devoted to researching these opportunities,” said FDA Commissioner Scott Gottlieb, MD. “The FDA is committed to doing its part to facilitate continued progress toward more treatments, and even potential cures, for patients with rare diseases. New scientific advances offer more opportunities to develop these potential cures. With efficient regulation, proper incentives for product development, and the continued support of patients, providers, and researchers, we have more opportunities to pursue these advances than ever before. For 35 years, the FDA has provided much-needed financial support for clinical trials of potentially life-changing treatments for patients with rare diseases. This funding helps support early-stage development activities targeting rare diseases that do not have effective treatments. By providing seed capital, these FDA-administered grants enable researchers to prove out important concepts. The FDA grants also provide some important recognition to promising development programs that ultimately can help researchers attract additional funding.”
The FDA awarded the grants through the Orphan Products Clinical Trials Grants Program. This program is funded by Congressional appropriations and encourages clinical development of drugs, biologics, medical devices, or medical foods for use in rare diseases. The grants are intended for clinical studies evaluating the safety and effectiveness of products that could either result in, or substantially contribute to, the FDA approval of products targeted to the treatment of rare diseases. Grant applications were reviewed and evaluated for scientific and technical merit by more than 100 rare disease experts, which included representatives from academia, the NIH, and the FDA.
The grant recipients, principal investigators, and approximate funding amounts, listed alphabetically, are:
Alkeus Pharmaceuticals, Inc (Cambridge, Massachusetts), Leonide Saad, phase 2 study of ALK-001 for the treatment of Stargardt disease—$1.75 million over four years
Arizona State University–Tempe Campus (Tempe, Arizona), Keith Lindor, phase 2 study of oral vancomycin for the treatment of primary sclerosing cholangitis—$2 million over four years
Cedars-Sinai Medical Center (Los Angeles), Shlomo Melmed, phase 2 study of seliciclib for the treatment of Cushing disease—$2 million over four years
Columbia University (New York), Yvonne Saenger, phase 1 study of talimogene laherparepvec for the treatment for advanced pancreatic cancer—$750,000 over three years
Emory University (Atlanta), Eric Sorscher, phase 1/ 2 study of Ad/PNP fludarabine for the treatment of head and neck squamous cell carcinoma—$1.5 million over three years
Fibrocell Technologies, Inc (Exton, Pennsylvania), John Maslowski, phase 1/2 study of gene-modified ex-vivo autologous fibroblasts for the treatment of dystrophic epidermolysis bullosa—$1.5 million over four years
Johns Hopkins University (Baltimore), Amy Dezern, phase 1/2 study of CD8-reduced T cells for the treatment of myelodysplastic syndrome or acute myeloid leukemia—$750,000 over three years
Oncolmmune, Inc (Rockville, Maryland) Yang Liu, phase 2b study of CD24Fc for the prevention of graft versus host disease—$2 million over four years
Patagonia Pharmaceuticals, LLC (Woodcliff Lake, New Jersey), Zachary Rome, phase 2 study of PAT-001 (isotretinoin) for the treatment of congenital ichthyosis—$1.5 million over three years
The General Hospital Corporation (Boston), Stephanie Seminara, phase 2 study of kisspeptin for the treatment of dopamine agonist intolerant hyperprolactinemia—$1.4 million over four years
University of Minnesota (Minneapolis), Kyriakie Sarafoglou, phase 2a study of subcutaneous hydrocortisone infusion pump for the treatment of congenital adrenal hyperplasia—$1.4 million over three years
University of North Carolina at Chapel Hill (Chapel Hill, North Carolina), Matthew Laughon, phase 2 study of sildenafil for the prevention of bronchopulmonary dysplasia—$2 million over four years.
“Since its creation in 1983, the Orphan Products Grants Program has provided more than $400 million to fund more than 600 new clinical studies,” said Debra Lewis, OD, Acting Director of the FDA’s Office of Orphan Products Development. “We are encouraged to see so much interest in our grants program and are pleased to support research for a variety of rare diseases that have little, or no, treatment options for patients.”
One-third of the new awards aim to accelerate cancer research by enrolling patients with rare forms of cancer, including advanced pancreatic cancer, head and neck squamous cell carcinoma, myelodysplastic syndrome, and acute myeloid leukemia. Another 25% of the new awards fund studies evaluating drug products for rare endocrine disorders, including Cushing disease, dopamine agonist intolerant hyperprolactinemia, and congenital adrenal hyperplasia. Another study addresses an unmet need in primary sclerosing cholangitis, a rare, chronic, and potentially serious bile duct disease.
About 42% of the grants fund studies that enroll children and adolescents, targeting a variety of rare diseases in children such as Stargardt disease, a juvenile genetic eye disorder that causes progressive vision loss; dystrophic epidermolysis bullosa, a genetic condition that causes the skin to be fragile resulting in painful blisters; and bronchopulmonary dysplasia, a serious lung condition that affects infants.
To date, the program’s grants have supported research that led to the marketing approval of more than 60 orphan products. Among the recent product approvals which were supported by studies funded by this grants program are a marketing approval for a much-needed treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults with multidrug resistant HIV-1 infection and another approval to reduce the acute complications of sickle cell disease in adult and pediatric patients.
The FDA is also currently supporting six natural history studies for rare diseases to further advance the mission of bringing new therapies to market.
ID experts urge widespread flu vaccination for 2018-2019 season
WASHINGTON – The flu vaccine may not be perfect, but it can reduce the severity of illness and curb the risk of spreading the disease to others, William Schaffner, MD, emphasized at a press conference held by the National Foundation for Infectious Diseases.
“Give the vaccine credit for softening the blow,” said Dr. Schaffner, medical director of NFID and a professor at Vanderbilt University in Nashville.
Dr. Schaffner and a panel of experts including U.S. Surgeon General Jerome M. Adams, MD, encouraged the public and the health care community to follow recommendation from the Centers for Disease Control & Prevention that everyone aged 6 months and older receive an influenza vaccine.
Dr. Schaffner shared recent data showing that complications from the flu don’t stop when the acute illness resolves. Acute influenza causes a whole-body inflammatory reaction, and consequently “there is an increased risk of heart attack and stroke during the 2-4 weeks of recovery from acute influenza,” he said. In addition, older adults who experience acute flu and are already frail may never regain their pre-flu level of function, as the flu can start a “domino effect of decline and disability.”
Despite last year’s severe flu season that included 180 deaths in children, vaccination remains the most effective protection against the flu, Dr. Adams said.
This year, between 163 million and 168 million doses of vaccine will be available in the United States. The vaccine is available in a range of settings including doctors’ offices, pharmacies, grocery stores, and workplaces, said Dr. Adams.
Flu vaccine choices this year include a return of the live-attenuated influenza vaccine (LAIV) given via nasal spray, along with the standard influenza vaccine that includes either three influenza viruses (trivalent, with two influenza A and one influenza B) or four influenza viruses (quadrivalent, with two influenza A and two influenza B). Other options are adjuvanted vaccine and high-dose vaccine for adults aged 65 years and older, and a cell-based and recombinant vaccine as alternatives to egg-based vaccines.
Dr. Adams emphasized the importance of healthy people getting vaccinated to protect the community. “All the people who died from the flu caught it from someone else,” he said.

The message to health care providers remains the same: Recommend the flu vaccine to patients at every opportunity, and lead by example and get vaccinated yourself, Dr. Adams said. He noted this year’s strategies to promote flu vaccination on social media, and encouraged clinicians to recommend the flu shot to their patients and to showcase their own shots via the #FightFlu hashtag.
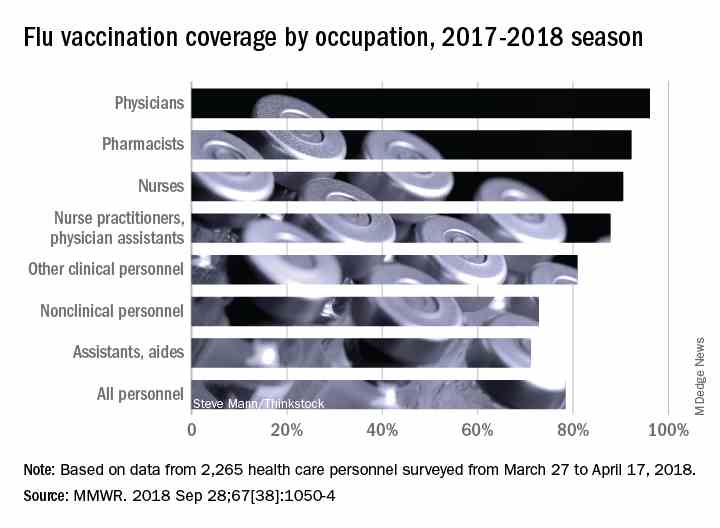
Vaccination among health care personnel last year was approximately 78%, which is a plateau over the past several years (MMWR 2018; 67:1050-54).
Be prepared to offer antivirals to patients as appropriate, and to promote the pneumococcal vaccine to eligible older adults as well, to protect not only themselves, but their contacts and the community, Dr. Adams emphasized. Currently approved antiviral drugs recommended for the 2018-2019 flu season: oseltamivir, zanamivir, and peramivir.
Wendy Sue Swanson, MD, of Seattle Children’s Hospital, stressed the importance of flu vaccination for all children, given their ability to spread viral infections. She noted a concerning 2% drop in vaccinations for children aged 6 months to 4 years, although vaccination coverage in this group was highest among children overall, at approximately 68% last season.
Last year, approximately 80% of the child deaths from flu occurred in unvaccinated children, but the vaccine has been shown to reduce the likelihood of hospitalization or death even if a child does become ill, Dr. Swanson said.
Laura E. Riley, MD, of Weill Cornell Medical Center, noted that vaccination of pregnant women has plateaued in recent years, and was 49% last year. “Our goal is 80% plus,” she said. Data show that pregnant women who received flu vaccination were 40% less likely to be hospitalized for the flu, she noted. The American College of Obstetricians and Gynecologists recommends flu vaccination as safe during any trimester, and valuable to both mothers and newborns because it provides protective antibodies during the first 6 months of life before babies can receive their own vaccinations, Dr. Riley said.
More information about this year’s flu season is available from the CDC and NFID.
WASHINGTON – The flu vaccine may not be perfect, but it can reduce the severity of illness and curb the risk of spreading the disease to others, William Schaffner, MD, emphasized at a press conference held by the National Foundation for Infectious Diseases.
“Give the vaccine credit for softening the blow,” said Dr. Schaffner, medical director of NFID and a professor at Vanderbilt University in Nashville.
Dr. Schaffner and a panel of experts including U.S. Surgeon General Jerome M. Adams, MD, encouraged the public and the health care community to follow recommendation from the Centers for Disease Control & Prevention that everyone aged 6 months and older receive an influenza vaccine.
Dr. Schaffner shared recent data showing that complications from the flu don’t stop when the acute illness resolves. Acute influenza causes a whole-body inflammatory reaction, and consequently “there is an increased risk of heart attack and stroke during the 2-4 weeks of recovery from acute influenza,” he said. In addition, older adults who experience acute flu and are already frail may never regain their pre-flu level of function, as the flu can start a “domino effect of decline and disability.”
Despite last year’s severe flu season that included 180 deaths in children, vaccination remains the most effective protection against the flu, Dr. Adams said.
This year, between 163 million and 168 million doses of vaccine will be available in the United States. The vaccine is available in a range of settings including doctors’ offices, pharmacies, grocery stores, and workplaces, said Dr. Adams.
Flu vaccine choices this year include a return of the live-attenuated influenza vaccine (LAIV) given via nasal spray, along with the standard influenza vaccine that includes either three influenza viruses (trivalent, with two influenza A and one influenza B) or four influenza viruses (quadrivalent, with two influenza A and two influenza B). Other options are adjuvanted vaccine and high-dose vaccine for adults aged 65 years and older, and a cell-based and recombinant vaccine as alternatives to egg-based vaccines.
Dr. Adams emphasized the importance of healthy people getting vaccinated to protect the community. “All the people who died from the flu caught it from someone else,” he said.
The message to health care providers remains the same: Recommend the flu vaccine to patients at every opportunity, and lead by example and get vaccinated yourself, Dr. Adams said. He noted this year’s strategies to promote flu vaccination on social media, and encouraged clinicians to recommend the flu shot to their patients and to showcase their own shots via the #FightFlu hashtag.
Vaccination among health care personnel last year was approximately 78%, which is a plateau over the past several years (MMWR 2018; 67:1050-54).
Be prepared to offer antivirals to patients as appropriate, and to promote the pneumococcal vaccine to eligible older adults as well, to protect not only themselves, but their contacts and the community, Dr. Adams emphasized. Currently approved antiviral drugs recommended for the 2018-2019 flu season: oseltamivir, zanamivir, and peramivir.
Wendy Sue Swanson, MD, of Seattle Children’s Hospital, stressed the importance of flu vaccination for all children, given their ability to spread viral infections. She noted a concerning 2% drop in vaccinations for children aged 6 months to 4 years, although vaccination coverage in this group was highest among children overall, at approximately 68% last season.
Last year, approximately 80% of the child deaths from flu occurred in unvaccinated children, but the vaccine has been shown to reduce the likelihood of hospitalization or death even if a child does become ill, Dr. Swanson said.
Laura E. Riley, MD, of Weill Cornell Medical Center, noted that vaccination of pregnant women has plateaued in recent years, and was 49% last year. “Our goal is 80% plus,” she said. Data show that pregnant women who received flu vaccination were 40% less likely to be hospitalized for the flu, she noted. The American College of Obstetricians and Gynecologists recommends flu vaccination as safe during any trimester, and valuable to both mothers and newborns because it provides protective antibodies during the first 6 months of life before babies can receive their own vaccinations, Dr. Riley said.
More information about this year’s flu season is available from the CDC and NFID.
WASHINGTON – The flu vaccine may not be perfect, but it can reduce the severity of illness and curb the risk of spreading the disease to others, William Schaffner, MD, emphasized at a press conference held by the National Foundation for Infectious Diseases.
“Give the vaccine credit for softening the blow,” said Dr. Schaffner, medical director of NFID and a professor at Vanderbilt University in Nashville.
Dr. Schaffner and a panel of experts including U.S. Surgeon General Jerome M. Adams, MD, encouraged the public and the health care community to follow recommendation from the Centers for Disease Control & Prevention that everyone aged 6 months and older receive an influenza vaccine.
Dr. Schaffner shared recent data showing that complications from the flu don’t stop when the acute illness resolves. Acute influenza causes a whole-body inflammatory reaction, and consequently “there is an increased risk of heart attack and stroke during the 2-4 weeks of recovery from acute influenza,” he said. In addition, older adults who experience acute flu and are already frail may never regain their pre-flu level of function, as the flu can start a “domino effect of decline and disability.”
Despite last year’s severe flu season that included 180 deaths in children, vaccination remains the most effective protection against the flu, Dr. Adams said.
This year, between 163 million and 168 million doses of vaccine will be available in the United States. The vaccine is available in a range of settings including doctors’ offices, pharmacies, grocery stores, and workplaces, said Dr. Adams.
Flu vaccine choices this year include a return of the live-attenuated influenza vaccine (LAIV) given via nasal spray, along with the standard influenza vaccine that includes either three influenza viruses (trivalent, with two influenza A and one influenza B) or four influenza viruses (quadrivalent, with two influenza A and two influenza B). Other options are adjuvanted vaccine and high-dose vaccine for adults aged 65 years and older, and a cell-based and recombinant vaccine as alternatives to egg-based vaccines.
Dr. Adams emphasized the importance of healthy people getting vaccinated to protect the community. “All the people who died from the flu caught it from someone else,” he said.
The message to health care providers remains the same: Recommend the flu vaccine to patients at every opportunity, and lead by example and get vaccinated yourself, Dr. Adams said. He noted this year’s strategies to promote flu vaccination on social media, and encouraged clinicians to recommend the flu shot to their patients and to showcase their own shots via the #FightFlu hashtag.
Vaccination among health care personnel last year was approximately 78%, which is a plateau over the past several years (MMWR 2018; 67:1050-54).
Be prepared to offer antivirals to patients as appropriate, and to promote the pneumococcal vaccine to eligible older adults as well, to protect not only themselves, but their contacts and the community, Dr. Adams emphasized. Currently approved antiviral drugs recommended for the 2018-2019 flu season: oseltamivir, zanamivir, and peramivir.
Wendy Sue Swanson, MD, of Seattle Children’s Hospital, stressed the importance of flu vaccination for all children, given their ability to spread viral infections. She noted a concerning 2% drop in vaccinations for children aged 6 months to 4 years, although vaccination coverage in this group was highest among children overall, at approximately 68% last season.
Last year, approximately 80% of the child deaths from flu occurred in unvaccinated children, but the vaccine has been shown to reduce the likelihood of hospitalization or death even if a child does become ill, Dr. Swanson said.
Laura E. Riley, MD, of Weill Cornell Medical Center, noted that vaccination of pregnant women has plateaued in recent years, and was 49% last year. “Our goal is 80% plus,” she said. Data show that pregnant women who received flu vaccination were 40% less likely to be hospitalized for the flu, she noted. The American College of Obstetricians and Gynecologists recommends flu vaccination as safe during any trimester, and valuable to both mothers and newborns because it provides protective antibodies during the first 6 months of life before babies can receive their own vaccinations, Dr. Riley said.
More information about this year’s flu season is available from the CDC and NFID.
FROM AN NFID PRESS CONFERENCE
Point-of-care test for respiratory viruses lowers antibiotic use
Routine testing in the ED is advocated
PARIS – Using a point-of-care test for viral pathogens, hospital admissions were avoided in about a third of emergency department patients with suspected respiratory infection when other clinical signs also suggested a low risk of a bacterial pathogen, according to a single-center experience presented at the annual congress of the European Respiratory Society.
“We found that when patients had point-of-care respiratory viral testing soon after they were admitted to the emergency department, we were able to reduce unnecessary admission and improve bed flow in our center,” reported Kay Roy, MBBS, consultant physician in respiratory medicine, West Hertfordshire (England) Hospital NHS Trust.
In a protocol that was launched at Dr. Kay’s institution in January 2018, the point-of-care viral test was combined with other clinical factors, particularly chest x-rays and elevated C-reactive protein (CRP), to determine whether patients had a viral pathogen and whether they could be discharged without antibiotics.
“Clinical judgment will always be required in individual patient decisions regarding antibiotic avoidance and early discharge,” Dr. Roy maintained. “But the point-of-care viral assay can be integrated into a strategy that permits more informed and rapid decision-making.”
This assertion is supported by the experience using a protocol anchored with the point-of-care viral test over a 4-month period. During this time, 901 patients with respiratory symptoms suspected of having a viral etiology were evaluated with the proprietary point-of-care device called FilmArray (bioMérieux).
From a sample taken with a nasopharyngeal swab, the test can identify a broad array of viruses using polymerase chain reaction technology in less than 45 minutes. However, the ED protocol for considering discharge without antibiotics requires additional evidence that the pathogen is viral, including a normal chest x-ray and a CRP less than 50 mg/L.
Of the 901 patients tested, a substantial proportion of whom had chronic obstructive pulmonary disease (COPD) or asthma, 507 (56%) tested positive for at least one virus, including influenza, rhinoviruses, coronaviruses, and adenovirus. Of these, 239 had normal chest x-rays and CRPs less than 50 mg/L. Because of the severity of symptoms or other clinical considerations, 154 patients were admitted, but 85 (36% of those meeting protocol criteria) were discharged without an antibiotic prescription.
“Antibiotics were continued in 90% of the patients who had an abnormal chest x-ray and abnormal CRP,” Dr. Roy reported. However, an objective strategy that permits clinicians to discharge patients at very low risk of a bacterial infection has many advantages even if it applies to a relatively modest proportion of those tested, according to Dr. Roy.
“Each respiratory admission can cost around [2,000 pounds] at our center,” reported Dr. Kay, referring to a figure equivalent to more than $2,600. In addition, she said that avoiding hospitalization frees up hospital beds and facilitates improved antimicrobial stewardship, which is vital to stem resistance.
Avoiding antibiotic use in patients with viral respiratory infections also is relevant to improved antibiotic stewardship in the community. For this reason, a randomized trial with a similar protocol involving the point-of-care viral test is planned in the outpatient setting. According to Dr. Roy, this will involve a community hub to which patients can be referred for testing and clinical evaluation.
“We hope that the quality of care can be improved with the point-of-care test for respiratory viruses as well as helping to reduce antibiotic resistance,” Dr. Roy said.
This approach is promising, according to Tobias Welte, MD, of the department of respiratory medicine at Hannover (Germany) Medical School, but he cautioned that it is not a standard approach.
“The protocol described by Dr. Roy will have to be compared to guidelines and recommended best clinical practice to confirm its usefulness,” he said, while conceding that any strategy that reduces unnecessary hospitalizations deserves further evaluation.
Routine testing in the ED is advocated
Routine testing in the ED is advocated
PARIS – Using a point-of-care test for viral pathogens, hospital admissions were avoided in about a third of emergency department patients with suspected respiratory infection when other clinical signs also suggested a low risk of a bacterial pathogen, according to a single-center experience presented at the annual congress of the European Respiratory Society.
“We found that when patients had point-of-care respiratory viral testing soon after they were admitted to the emergency department, we were able to reduce unnecessary admission and improve bed flow in our center,” reported Kay Roy, MBBS, consultant physician in respiratory medicine, West Hertfordshire (England) Hospital NHS Trust.
In a protocol that was launched at Dr. Kay’s institution in January 2018, the point-of-care viral test was combined with other clinical factors, particularly chest x-rays and elevated C-reactive protein (CRP), to determine whether patients had a viral pathogen and whether they could be discharged without antibiotics.
“Clinical judgment will always be required in individual patient decisions regarding antibiotic avoidance and early discharge,” Dr. Roy maintained. “But the point-of-care viral assay can be integrated into a strategy that permits more informed and rapid decision-making.”
This assertion is supported by the experience using a protocol anchored with the point-of-care viral test over a 4-month period. During this time, 901 patients with respiratory symptoms suspected of having a viral etiology were evaluated with the proprietary point-of-care device called FilmArray (bioMérieux).
From a sample taken with a nasopharyngeal swab, the test can identify a broad array of viruses using polymerase chain reaction technology in less than 45 minutes. However, the ED protocol for considering discharge without antibiotics requires additional evidence that the pathogen is viral, including a normal chest x-ray and a CRP less than 50 mg/L.
Of the 901 patients tested, a substantial proportion of whom had chronic obstructive pulmonary disease (COPD) or asthma, 507 (56%) tested positive for at least one virus, including influenza, rhinoviruses, coronaviruses, and adenovirus. Of these, 239 had normal chest x-rays and CRPs less than 50 mg/L. Because of the severity of symptoms or other clinical considerations, 154 patients were admitted, but 85 (36% of those meeting protocol criteria) were discharged without an antibiotic prescription.
“Antibiotics were continued in 90% of the patients who had an abnormal chest x-ray and abnormal CRP,” Dr. Roy reported. However, an objective strategy that permits clinicians to discharge patients at very low risk of a bacterial infection has many advantages even if it applies to a relatively modest proportion of those tested, according to Dr. Roy.
“Each respiratory admission can cost around [2,000 pounds] at our center,” reported Dr. Kay, referring to a figure equivalent to more than $2,600. In addition, she said that avoiding hospitalization frees up hospital beds and facilitates improved antimicrobial stewardship, which is vital to stem resistance.
Avoiding antibiotic use in patients with viral respiratory infections also is relevant to improved antibiotic stewardship in the community. For this reason, a randomized trial with a similar protocol involving the point-of-care viral test is planned in the outpatient setting. According to Dr. Roy, this will involve a community hub to which patients can be referred for testing and clinical evaluation.
“We hope that the quality of care can be improved with the point-of-care test for respiratory viruses as well as helping to reduce antibiotic resistance,” Dr. Roy said.
This approach is promising, according to Tobias Welte, MD, of the department of respiratory medicine at Hannover (Germany) Medical School, but he cautioned that it is not a standard approach.
“The protocol described by Dr. Roy will have to be compared to guidelines and recommended best clinical practice to confirm its usefulness,” he said, while conceding that any strategy that reduces unnecessary hospitalizations deserves further evaluation.
PARIS – Using a point-of-care test for viral pathogens, hospital admissions were avoided in about a third of emergency department patients with suspected respiratory infection when other clinical signs also suggested a low risk of a bacterial pathogen, according to a single-center experience presented at the annual congress of the European Respiratory Society.
“We found that when patients had point-of-care respiratory viral testing soon after they were admitted to the emergency department, we were able to reduce unnecessary admission and improve bed flow in our center,” reported Kay Roy, MBBS, consultant physician in respiratory medicine, West Hertfordshire (England) Hospital NHS Trust.
In a protocol that was launched at Dr. Kay’s institution in January 2018, the point-of-care viral test was combined with other clinical factors, particularly chest x-rays and elevated C-reactive protein (CRP), to determine whether patients had a viral pathogen and whether they could be discharged without antibiotics.
“Clinical judgment will always be required in individual patient decisions regarding antibiotic avoidance and early discharge,” Dr. Roy maintained. “But the point-of-care viral assay can be integrated into a strategy that permits more informed and rapid decision-making.”
This assertion is supported by the experience using a protocol anchored with the point-of-care viral test over a 4-month period. During this time, 901 patients with respiratory symptoms suspected of having a viral etiology were evaluated with the proprietary point-of-care device called FilmArray (bioMérieux).
From a sample taken with a nasopharyngeal swab, the test can identify a broad array of viruses using polymerase chain reaction technology in less than 45 minutes. However, the ED protocol for considering discharge without antibiotics requires additional evidence that the pathogen is viral, including a normal chest x-ray and a CRP less than 50 mg/L.
Of the 901 patients tested, a substantial proportion of whom had chronic obstructive pulmonary disease (COPD) or asthma, 507 (56%) tested positive for at least one virus, including influenza, rhinoviruses, coronaviruses, and adenovirus. Of these, 239 had normal chest x-rays and CRPs less than 50 mg/L. Because of the severity of symptoms or other clinical considerations, 154 patients were admitted, but 85 (36% of those meeting protocol criteria) were discharged without an antibiotic prescription.
“Antibiotics were continued in 90% of the patients who had an abnormal chest x-ray and abnormal CRP,” Dr. Roy reported. However, an objective strategy that permits clinicians to discharge patients at very low risk of a bacterial infection has many advantages even if it applies to a relatively modest proportion of those tested, according to Dr. Roy.
“Each respiratory admission can cost around [2,000 pounds] at our center,” reported Dr. Kay, referring to a figure equivalent to more than $2,600. In addition, she said that avoiding hospitalization frees up hospital beds and facilitates improved antimicrobial stewardship, which is vital to stem resistance.
Avoiding antibiotic use in patients with viral respiratory infections also is relevant to improved antibiotic stewardship in the community. For this reason, a randomized trial with a similar protocol involving the point-of-care viral test is planned in the outpatient setting. According to Dr. Roy, this will involve a community hub to which patients can be referred for testing and clinical evaluation.
“We hope that the quality of care can be improved with the point-of-care test for respiratory viruses as well as helping to reduce antibiotic resistance,” Dr. Roy said.
This approach is promising, according to Tobias Welte, MD, of the department of respiratory medicine at Hannover (Germany) Medical School, but he cautioned that it is not a standard approach.
“The protocol described by Dr. Roy will have to be compared to guidelines and recommended best clinical practice to confirm its usefulness,” he said, while conceding that any strategy that reduces unnecessary hospitalizations deserves further evaluation.
REPORTING FROM THE ERS CONGRESS 2018
Key clinical point:
Major finding: Of patients with a negative chest x-ray and low CRP level, 36% avoided hospital admission due to a positive test for a virus.
Study details: A case series.
Disclosures: Dr. Roy reports no financial relationships relevant to this study.
Viruses Form Gangs
In 2015, researchers showed that polioviruses could travel in groups—or “packets”—that is, membrane-bound vesicles containing multiple virus particles. The researchers used the Trojan horse analogy to describe it. But they could not say whether the system applied to animals and humans, or how effective the “horses” were in infecting host cells.
To find out, the researchers focused on rotaviruses and noroviruses, which are mainly spread through stool-contaminated food or liquids. And they found that the viruses were indeed shed as packet-enclosed clusters in the stool. Moreover, the virus clusters were significantly more infectious than the free, unbound viruses in the fecal samples tested.
The researchers say the high level of infectiousness is likely due to the vesicles delivering many viruses at once to the target tissue. The vesicles also protect their “viral cargo” from being destroyed by prolonged exposure to enzymes and may even make it invisible to the antibodies in the stool or gut.
The virus packets are not only extremely potent, but aggressive. More studies are needed, and more antivirals, the researchers say, but in the meantime, soap and water can help keep them down.
In 2015, researchers showed that polioviruses could travel in groups—or “packets”—that is, membrane-bound vesicles containing multiple virus particles. The researchers used the Trojan horse analogy to describe it. But they could not say whether the system applied to animals and humans, or how effective the “horses” were in infecting host cells.
To find out, the researchers focused on rotaviruses and noroviruses, which are mainly spread through stool-contaminated food or liquids. And they found that the viruses were indeed shed as packet-enclosed clusters in the stool. Moreover, the virus clusters were significantly more infectious than the free, unbound viruses in the fecal samples tested.
The researchers say the high level of infectiousness is likely due to the vesicles delivering many viruses at once to the target tissue. The vesicles also protect their “viral cargo” from being destroyed by prolonged exposure to enzymes and may even make it invisible to the antibodies in the stool or gut.
The virus packets are not only extremely potent, but aggressive. More studies are needed, and more antivirals, the researchers say, but in the meantime, soap and water can help keep them down.
In 2015, researchers showed that polioviruses could travel in groups—or “packets”—that is, membrane-bound vesicles containing multiple virus particles. The researchers used the Trojan horse analogy to describe it. But they could not say whether the system applied to animals and humans, or how effective the “horses” were in infecting host cells.
To find out, the researchers focused on rotaviruses and noroviruses, which are mainly spread through stool-contaminated food or liquids. And they found that the viruses were indeed shed as packet-enclosed clusters in the stool. Moreover, the virus clusters were significantly more infectious than the free, unbound viruses in the fecal samples tested.
The researchers say the high level of infectiousness is likely due to the vesicles delivering many viruses at once to the target tissue. The vesicles also protect their “viral cargo” from being destroyed by prolonged exposure to enzymes and may even make it invisible to the antibodies in the stool or gut.
The virus packets are not only extremely potent, but aggressive. More studies are needed, and more antivirals, the researchers say, but in the meantime, soap and water can help keep them down.
Teva Announces FDA Approval of Ajovy (fremanezumab-vfrm)
Teva Pharmaceutical Industries Ltd. announced that the FDA approved Ajovy (fremanezumab-vfrm) injection for the preventive treatment of migraine in adults. Ajovy, a humanized monoclonal antibody that binds to the calcitonin gene-related peptide (CGRP) ligand and blocks its binding to the receptor, is the first and only anti-CGRP treatment for the prevention of migraine with quarterly (675 mg) and monthly (225 mg) dosing options.
“Migraine is a disabling neurological disease that affects more than 36 million people in the United States,” said Stephen Silberstein
Ajovy was evaluated in two Phase III, placebo-controlled clinical trials that enrolled patients with disabling migraine and was studied as both a stand-alone preventive treatment and in combination with oral preventive treatments. In these trials, patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions (≥ 5% and greater than placebo) were injection site reactions.
Teva Pharmaceutical Industries Ltd. announced that the FDA approved Ajovy (fremanezumab-vfrm) injection for the preventive treatment of migraine in adults. Ajovy, a humanized monoclonal antibody that binds to the calcitonin gene-related peptide (CGRP) ligand and blocks its binding to the receptor, is the first and only anti-CGRP treatment for the prevention of migraine with quarterly (675 mg) and monthly (225 mg) dosing options.
“Migraine is a disabling neurological disease that affects more than 36 million people in the United States,” said Stephen Silberstein
Ajovy was evaluated in two Phase III, placebo-controlled clinical trials that enrolled patients with disabling migraine and was studied as both a stand-alone preventive treatment and in combination with oral preventive treatments. In these trials, patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions (≥ 5% and greater than placebo) were injection site reactions.
Teva Pharmaceutical Industries Ltd. announced that the FDA approved Ajovy (fremanezumab-vfrm) injection for the preventive treatment of migraine in adults. Ajovy, a humanized monoclonal antibody that binds to the calcitonin gene-related peptide (CGRP) ligand and blocks its binding to the receptor, is the first and only anti-CGRP treatment for the prevention of migraine with quarterly (675 mg) and monthly (225 mg) dosing options.
“Migraine is a disabling neurological disease that affects more than 36 million people in the United States,” said Stephen Silberstein
Ajovy was evaluated in two Phase III, placebo-controlled clinical trials that enrolled patients with disabling migraine and was studied as both a stand-alone preventive treatment and in combination with oral preventive treatments. In these trials, patients experienced a reduction in monthly migraine days during a 12-week period. The most common adverse reactions (≥ 5% and greater than placebo) were injection site reactions.
NELSON trial: CT Screening reduces lung cancer deaths
TORONTO – Computed tomography screening among asymptomatic men at high risk for lung cancer reduced lung cancer deaths by a highly statistically significant 26% at 10 years and appeared to reduce lung cancer mortality risk even more in women in the population-based, NELSON trial.

The findings from this large controlled trial encompassing more than 27,000 CT scans in 15,792 individuals support those from the National Lung Screening Trials (NLST), published in 2011, and should “inform and direct future CT screening programs worldwide,” according to Harry de Koning, MD, who presented the findings at the World Conference on Lung Cancer.
Participants were randomized to CT screening at baseline, 1, 3, and 5.5 years after randomization, or to a control group that received usual care. Overall 157 lung cancer deaths occurred in the screening arm vs. 250 in the control arm. Detection rates varied between 0.8% and 1.1% across screenings (0.9% overall), and the positive predictive value of screening was 41%, Dr. de Koning of Erasmus Medical Center, Rotterdam, the Netherlands, said at the meeting sponsored by the International Association for the Study of Lung Cancer.
Notably, 69% of the 243 lung cancers detected by screening were detected at stage 1A or 1B, compared with 10%-12% being detected at stage 4 in about 50% of control patients and based on registry data in the Netherlands.
“There’s huge importance of this early detection in the screening arm,” Dr. de Koning said.
Additionally, an analysis of a subset of those with lung cancer showed a significant threefold increase in surgical treatment among the screened patients vs. those in the control arm who developed lung cancer (67.7% vs. 24.5%), he said.
CT screening reduced the risk of death from lung cancer by 9% to 41% in men over the course of the study, with an overall reduction of 26% at 10 years, and in a smaller subset of women, the rate-ratio of dying from lung cancer varied from 0.39 to 0.61 at different years of follow-up, he said, noting that this suggests a “significant and even larger reduction” in women.
Study participants were individuals aged 50-74 years in the Netherlands and Leuven, Belgium, who were considered at high risk for lung cancer based on responses to a general questionnaire. Participants’ records were linked with national registries with 100% coverage regarding cancer diagnosis and date and cause of death, and medical records for deceased lung cancer patients were reviewed by a blinded expert panel through 2013, and for the remaining study years cause of death as reported by Statistics Netherlands was used. Compliance among those randomized to the screening group was 86%, Dr. de Koning said.
“These findings show that CT screenings are an effective way to assess lung nodules in people at high risk for lung cancer, often leading to detection of suspicious nodules and subsequent surgical intervention at relatively low rates and with few false positives, and can positively increase the chances of cure in this devastating disease,” Dr. de Koning said in a press statement. “It is the second-largest trial in the world, with an even more favorable outcome than the first trial, the NLST, showed. These results should be used to inform and direct future CT screening in the world.”
During a press briefing, in response to a question about whether lung cancer screening should be offered more widely, he said that yes, countries – including the United States – should take note that “now two large-scale trials show large benefit.”
Dr. de Koning reported having no disclosures.
TORONTO – Computed tomography screening among asymptomatic men at high risk for lung cancer reduced lung cancer deaths by a highly statistically significant 26% at 10 years and appeared to reduce lung cancer mortality risk even more in women in the population-based, NELSON trial.
The findings from this large controlled trial encompassing more than 27,000 CT scans in 15,792 individuals support those from the National Lung Screening Trials (NLST), published in 2011, and should “inform and direct future CT screening programs worldwide,” according to Harry de Koning, MD, who presented the findings at the World Conference on Lung Cancer.
Participants were randomized to CT screening at baseline, 1, 3, and 5.5 years after randomization, or to a control group that received usual care. Overall 157 lung cancer deaths occurred in the screening arm vs. 250 in the control arm. Detection rates varied between 0.8% and 1.1% across screenings (0.9% overall), and the positive predictive value of screening was 41%, Dr. de Koning of Erasmus Medical Center, Rotterdam, the Netherlands, said at the meeting sponsored by the International Association for the Study of Lung Cancer.
Notably, 69% of the 243 lung cancers detected by screening were detected at stage 1A or 1B, compared with 10%-12% being detected at stage 4 in about 50% of control patients and based on registry data in the Netherlands.
“There’s huge importance of this early detection in the screening arm,” Dr. de Koning said.
Additionally, an analysis of a subset of those with lung cancer showed a significant threefold increase in surgical treatment among the screened patients vs. those in the control arm who developed lung cancer (67.7% vs. 24.5%), he said.
CT screening reduced the risk of death from lung cancer by 9% to 41% in men over the course of the study, with an overall reduction of 26% at 10 years, and in a smaller subset of women, the rate-ratio of dying from lung cancer varied from 0.39 to 0.61 at different years of follow-up, he said, noting that this suggests a “significant and even larger reduction” in women.
Study participants were individuals aged 50-74 years in the Netherlands and Leuven, Belgium, who were considered at high risk for lung cancer based on responses to a general questionnaire. Participants’ records were linked with national registries with 100% coverage regarding cancer diagnosis and date and cause of death, and medical records for deceased lung cancer patients were reviewed by a blinded expert panel through 2013, and for the remaining study years cause of death as reported by Statistics Netherlands was used. Compliance among those randomized to the screening group was 86%, Dr. de Koning said.
“These findings show that CT screenings are an effective way to assess lung nodules in people at high risk for lung cancer, often leading to detection of suspicious nodules and subsequent surgical intervention at relatively low rates and with few false positives, and can positively increase the chances of cure in this devastating disease,” Dr. de Koning said in a press statement. “It is the second-largest trial in the world, with an even more favorable outcome than the first trial, the NLST, showed. These results should be used to inform and direct future CT screening in the world.”
During a press briefing, in response to a question about whether lung cancer screening should be offered more widely, he said that yes, countries – including the United States – should take note that “now two large-scale trials show large benefit.”
Dr. de Koning reported having no disclosures.
TORONTO – Computed tomography screening among asymptomatic men at high risk for lung cancer reduced lung cancer deaths by a highly statistically significant 26% at 10 years and appeared to reduce lung cancer mortality risk even more in women in the population-based, NELSON trial.
The findings from this large controlled trial encompassing more than 27,000 CT scans in 15,792 individuals support those from the National Lung Screening Trials (NLST), published in 2011, and should “inform and direct future CT screening programs worldwide,” according to Harry de Koning, MD, who presented the findings at the World Conference on Lung Cancer.
Participants were randomized to CT screening at baseline, 1, 3, and 5.5 years after randomization, or to a control group that received usual care. Overall 157 lung cancer deaths occurred in the screening arm vs. 250 in the control arm. Detection rates varied between 0.8% and 1.1% across screenings (0.9% overall), and the positive predictive value of screening was 41%, Dr. de Koning of Erasmus Medical Center, Rotterdam, the Netherlands, said at the meeting sponsored by the International Association for the Study of Lung Cancer.
Notably, 69% of the 243 lung cancers detected by screening were detected at stage 1A or 1B, compared with 10%-12% being detected at stage 4 in about 50% of control patients and based on registry data in the Netherlands.
“There’s huge importance of this early detection in the screening arm,” Dr. de Koning said.
Additionally, an analysis of a subset of those with lung cancer showed a significant threefold increase in surgical treatment among the screened patients vs. those in the control arm who developed lung cancer (67.7% vs. 24.5%), he said.
CT screening reduced the risk of death from lung cancer by 9% to 41% in men over the course of the study, with an overall reduction of 26% at 10 years, and in a smaller subset of women, the rate-ratio of dying from lung cancer varied from 0.39 to 0.61 at different years of follow-up, he said, noting that this suggests a “significant and even larger reduction” in women.
Study participants were individuals aged 50-74 years in the Netherlands and Leuven, Belgium, who were considered at high risk for lung cancer based on responses to a general questionnaire. Participants’ records were linked with national registries with 100% coverage regarding cancer diagnosis and date and cause of death, and medical records for deceased lung cancer patients were reviewed by a blinded expert panel through 2013, and for the remaining study years cause of death as reported by Statistics Netherlands was used. Compliance among those randomized to the screening group was 86%, Dr. de Koning said.
“These findings show that CT screenings are an effective way to assess lung nodules in people at high risk for lung cancer, often leading to detection of suspicious nodules and subsequent surgical intervention at relatively low rates and with few false positives, and can positively increase the chances of cure in this devastating disease,” Dr. de Koning said in a press statement. “It is the second-largest trial in the world, with an even more favorable outcome than the first trial, the NLST, showed. These results should be used to inform and direct future CT screening in the world.”
During a press briefing, in response to a question about whether lung cancer screening should be offered more widely, he said that yes, countries – including the United States – should take note that “now two large-scale trials show large benefit.”
Dr. de Koning reported having no disclosures.
REPORTING FROM WCLC 2018
Key clinical point: CT screening among high-risk patients significantly reduces lung cancer mortality.
Major finding: CT screening in high-risk patients reduced lung cancer deaths by 26% in men, 39%-61% in women.
Study details: A population-based controlled trial of 15,792 individuals.
Disclosures: Dr. de Koning reported having no disclosures.
Outpatient lenalidomide/rituximab yields long-term MCL remission
After 5 years, the combination of lenalidomide and rituximab as first-line therapy for mantle cell lymphoma (MCL) continues to show durable responses with manageable toxicities, long-term results from a phase 2 clinical trial show.
After a median follow-up of 64 months, 21 of 33 patients with initial responses remained in durable, minimal residual disease (MRD)-negative remission following induction with lenalidomide and rituximab and maintenance with those same two agents for at least 3 years.
The patients with durable responses included five who opted to discontinue maintenance after 3 years, reported Jia Ruan, MD, PhD, of Cornell University, New York, and her colleagues.
“Our long-term data provide proof of concept that an outpatient-based induction and maintenance strategy free of conventional chemotherapy is effective, safe, and feasible as first-line therapy for MCL,” they wrote. Their report was published in Blood.
In the multicenter, phase 2 single-arm study, 38 patients with untreated MCL were enrolled and treated with lenalidomide 20 mg daily on days 1-21 of each 28-day cycle for 12 cycles during induction, followed by dose reduction to 15 mg during the maintenance phase. Patients also received standard dose rituximab 375 mg/m2 weekly for 4 weeks during cycle 1, then once every other cycle.
Patients remained on treatment until disease progression, unacceptable toxicities, or study withdrawal. Patients who remained in remission after 3 years, based on routine surveillance CT scans, had the option to discontinue maintenance.
Of the original 38 patients enrolled, 36 were evaluable for response, including 23 with a complete response (CR) and 10 with a partial response.
At the 64-month median follow-up, neither the median progression-free survival (PFS) nor duration of response had been reached.
Overall, 21 of the 33 patients with responses (64%) had ongoing responses, including six patients with responses beyond 6 years.
Estimated 3-year and 5-year PFS rates were 80.3% and 63.9%, respectively. Respective estimated 3- and 5-year overall survival rates were 89.5% and 77.4%.
Mantle cell lymphoma international prognostic index (MIPI) scores were not associated with either response or PFS rates, but patients with high-risk MIPI scores were significantly more likely to have worse overall survival (P = .04).
Grade 3 or greater hematologic toxicities included neutropenia in 42% of patients in both induction and maintenance, anemia in 8% and 3%, thrombocytopenia in 11% and 5%, and febrile neutropenia in 3% and 5%.
Secondary primary malignancies occurred in six patients. These included five noninvasive skin cancers requiring only local therapy without the need for study interruption. Two patients, including one with a skin cancer, died from the secondary malignancies, including one from Merkel cell carcinoma and one from pancreatic cancer.
“The efficacy and survival outcome observed in our study compared favorably to those reported with lenalidomide either as single agent, or in combination with rituximab in relapsed and refractory setting, lending support for prioritizing novel agents such as lenalidomide early in the treatment sequence, to compare to conventional chemotherapy-based approach,” the investigators wrote.
The study was supported in part by Celgene Corporation, a Clinical Translational Science Center grant, and the Lymphoma Foundation. Dr. Ruan has received research support and been a consultant for Celgene, and other coauthors reported research support and consultant relationships with the company.
SOURCE: Ruan J et al. Blood. 2018 Sep 4. doi: 10.1182/blood-2018-07-859769.
After 5 years, the combination of lenalidomide and rituximab as first-line therapy for mantle cell lymphoma (MCL) continues to show durable responses with manageable toxicities, long-term results from a phase 2 clinical trial show.
After a median follow-up of 64 months, 21 of 33 patients with initial responses remained in durable, minimal residual disease (MRD)-negative remission following induction with lenalidomide and rituximab and maintenance with those same two agents for at least 3 years.
The patients with durable responses included five who opted to discontinue maintenance after 3 years, reported Jia Ruan, MD, PhD, of Cornell University, New York, and her colleagues.
“Our long-term data provide proof of concept that an outpatient-based induction and maintenance strategy free of conventional chemotherapy is effective, safe, and feasible as first-line therapy for MCL,” they wrote. Their report was published in Blood.
In the multicenter, phase 2 single-arm study, 38 patients with untreated MCL were enrolled and treated with lenalidomide 20 mg daily on days 1-21 of each 28-day cycle for 12 cycles during induction, followed by dose reduction to 15 mg during the maintenance phase. Patients also received standard dose rituximab 375 mg/m2 weekly for 4 weeks during cycle 1, then once every other cycle.
Patients remained on treatment until disease progression, unacceptable toxicities, or study withdrawal. Patients who remained in remission after 3 years, based on routine surveillance CT scans, had the option to discontinue maintenance.
Of the original 38 patients enrolled, 36 were evaluable for response, including 23 with a complete response (CR) and 10 with a partial response.
At the 64-month median follow-up, neither the median progression-free survival (PFS) nor duration of response had been reached.
Overall, 21 of the 33 patients with responses (64%) had ongoing responses, including six patients with responses beyond 6 years.
Estimated 3-year and 5-year PFS rates were 80.3% and 63.9%, respectively. Respective estimated 3- and 5-year overall survival rates were 89.5% and 77.4%.
Mantle cell lymphoma international prognostic index (MIPI) scores were not associated with either response or PFS rates, but patients with high-risk MIPI scores were significantly more likely to have worse overall survival (P = .04).
Grade 3 or greater hematologic toxicities included neutropenia in 42% of patients in both induction and maintenance, anemia in 8% and 3%, thrombocytopenia in 11% and 5%, and febrile neutropenia in 3% and 5%.
Secondary primary malignancies occurred in six patients. These included five noninvasive skin cancers requiring only local therapy without the need for study interruption. Two patients, including one with a skin cancer, died from the secondary malignancies, including one from Merkel cell carcinoma and one from pancreatic cancer.
“The efficacy and survival outcome observed in our study compared favorably to those reported with lenalidomide either as single agent, or in combination with rituximab in relapsed and refractory setting, lending support for prioritizing novel agents such as lenalidomide early in the treatment sequence, to compare to conventional chemotherapy-based approach,” the investigators wrote.
The study was supported in part by Celgene Corporation, a Clinical Translational Science Center grant, and the Lymphoma Foundation. Dr. Ruan has received research support and been a consultant for Celgene, and other coauthors reported research support and consultant relationships with the company.
SOURCE: Ruan J et al. Blood. 2018 Sep 4. doi: 10.1182/blood-2018-07-859769.
After 5 years, the combination of lenalidomide and rituximab as first-line therapy for mantle cell lymphoma (MCL) continues to show durable responses with manageable toxicities, long-term results from a phase 2 clinical trial show.
After a median follow-up of 64 months, 21 of 33 patients with initial responses remained in durable, minimal residual disease (MRD)-negative remission following induction with lenalidomide and rituximab and maintenance with those same two agents for at least 3 years.
The patients with durable responses included five who opted to discontinue maintenance after 3 years, reported Jia Ruan, MD, PhD, of Cornell University, New York, and her colleagues.
“Our long-term data provide proof of concept that an outpatient-based induction and maintenance strategy free of conventional chemotherapy is effective, safe, and feasible as first-line therapy for MCL,” they wrote. Their report was published in Blood.
In the multicenter, phase 2 single-arm study, 38 patients with untreated MCL were enrolled and treated with lenalidomide 20 mg daily on days 1-21 of each 28-day cycle for 12 cycles during induction, followed by dose reduction to 15 mg during the maintenance phase. Patients also received standard dose rituximab 375 mg/m2 weekly for 4 weeks during cycle 1, then once every other cycle.
Patients remained on treatment until disease progression, unacceptable toxicities, or study withdrawal. Patients who remained in remission after 3 years, based on routine surveillance CT scans, had the option to discontinue maintenance.
Of the original 38 patients enrolled, 36 were evaluable for response, including 23 with a complete response (CR) and 10 with a partial response.
At the 64-month median follow-up, neither the median progression-free survival (PFS) nor duration of response had been reached.
Overall, 21 of the 33 patients with responses (64%) had ongoing responses, including six patients with responses beyond 6 years.
Estimated 3-year and 5-year PFS rates were 80.3% and 63.9%, respectively. Respective estimated 3- and 5-year overall survival rates were 89.5% and 77.4%.
Mantle cell lymphoma international prognostic index (MIPI) scores were not associated with either response or PFS rates, but patients with high-risk MIPI scores were significantly more likely to have worse overall survival (P = .04).
Grade 3 or greater hematologic toxicities included neutropenia in 42% of patients in both induction and maintenance, anemia in 8% and 3%, thrombocytopenia in 11% and 5%, and febrile neutropenia in 3% and 5%.
Secondary primary malignancies occurred in six patients. These included five noninvasive skin cancers requiring only local therapy without the need for study interruption. Two patients, including one with a skin cancer, died from the secondary malignancies, including one from Merkel cell carcinoma and one from pancreatic cancer.
“The efficacy and survival outcome observed in our study compared favorably to those reported with lenalidomide either as single agent, or in combination with rituximab in relapsed and refractory setting, lending support for prioritizing novel agents such as lenalidomide early in the treatment sequence, to compare to conventional chemotherapy-based approach,” the investigators wrote.
The study was supported in part by Celgene Corporation, a Clinical Translational Science Center grant, and the Lymphoma Foundation. Dr. Ruan has received research support and been a consultant for Celgene, and other coauthors reported research support and consultant relationships with the company.
SOURCE: Ruan J et al. Blood. 2018 Sep 4. doi: 10.1182/blood-2018-07-859769.
FROM BLOOD
Key clinical point:
Major finding: After 64-months of median follow-up, 21 of 33 patients with initial responses remained in remission.
Study details: Five-year follow-up of a phase 2 single arm trial of lenalidomide/rituximab induction and maintenance in 38 patients with mantle cell lymphoma.
Disclosures: The study was supported in part by Celgene Corporation, a Clinical Translational Science Center grant, and the Lymphoma Foundation. Dr. Ruan has received research support and been a consultant for Celgene, and other coauthors reported research support and consultant relationships with the company.
Source: Ruan J et al. Blood. 2018 Sep 4. doi: 10.1182/blood-2018-07-859769.