User login
Ventricular Arrhythmia Due to MS Treatment
Fingolimod, a sphingosine-1-phosphate receptor modulator, has been used to treat > 55,000 patients in the US, according to the manufacturer (Gilenya/Novartis). It is believed to work by keeping lymphocytes from migrating into the CNS, sequestering them in the lymph nodes.
Although it has been found effective in randomized controlled trials, fingolimod is also known to have a wide range of adverse effects (AEs), including some that are serious and even life-threatening, such as bradycardia and atrioventricular block. The drug is contraindicated for patients who have had myocardial infarction, unstable angina, or heart failure, among other conditions. Ventricular tachycardia has been reported only once, but clinicians from Hurley Medical Center in Flint, Michigan, suggest that it may actually be an underrecognized cause of sudden death.
They describe the case of their patient, a 63-year-old woman with relapsing-remitting multiple sclerosis and hypertension who was about to start fingolomod. She underwent a basal ECG to be cleared before starting treatment. She received her first dose of fingolimod at the cardiology office, was monitored for 6 hours, and went home with a surface-mounted Holter monitor.
Two weeks later, she was in the emergency department because the monitor had captured ventricular tachycardia, and she was reporting palpitations.
Lab work was normal; the echocardiogram was normal. Cardiac monitoring showed no other evidence of cardiac arrhythmias. Her only other medication was amlodipine. The fingolimod was held back. She was observed for4 days then discharged in a stable condition. Her clinicians followed her for 2 months but the arrhythmia did not return.
Although this patient had no further arrhythmias, the authors warn that serious outcomes are possible. They urge health care practitioners to let patients know of this potential AE and advise them to report symptoms such as palpitations immediately.
Fingolimod, a sphingosine-1-phosphate receptor modulator, has been used to treat > 55,000 patients in the US, according to the manufacturer (Gilenya/Novartis). It is believed to work by keeping lymphocytes from migrating into the CNS, sequestering them in the lymph nodes.
Although it has been found effective in randomized controlled trials, fingolimod is also known to have a wide range of adverse effects (AEs), including some that are serious and even life-threatening, such as bradycardia and atrioventricular block. The drug is contraindicated for patients who have had myocardial infarction, unstable angina, or heart failure, among other conditions. Ventricular tachycardia has been reported only once, but clinicians from Hurley Medical Center in Flint, Michigan, suggest that it may actually be an underrecognized cause of sudden death.
They describe the case of their patient, a 63-year-old woman with relapsing-remitting multiple sclerosis and hypertension who was about to start fingolomod. She underwent a basal ECG to be cleared before starting treatment. She received her first dose of fingolimod at the cardiology office, was monitored for 6 hours, and went home with a surface-mounted Holter monitor.
Two weeks later, she was in the emergency department because the monitor had captured ventricular tachycardia, and she was reporting palpitations.
Lab work was normal; the echocardiogram was normal. Cardiac monitoring showed no other evidence of cardiac arrhythmias. Her only other medication was amlodipine. The fingolimod was held back. She was observed for4 days then discharged in a stable condition. Her clinicians followed her for 2 months but the arrhythmia did not return.
Although this patient had no further arrhythmias, the authors warn that serious outcomes are possible. They urge health care practitioners to let patients know of this potential AE and advise them to report symptoms such as palpitations immediately.
Fingolimod, a sphingosine-1-phosphate receptor modulator, has been used to treat > 55,000 patients in the US, according to the manufacturer (Gilenya/Novartis). It is believed to work by keeping lymphocytes from migrating into the CNS, sequestering them in the lymph nodes.
Although it has been found effective in randomized controlled trials, fingolimod is also known to have a wide range of adverse effects (AEs), including some that are serious and even life-threatening, such as bradycardia and atrioventricular block. The drug is contraindicated for patients who have had myocardial infarction, unstable angina, or heart failure, among other conditions. Ventricular tachycardia has been reported only once, but clinicians from Hurley Medical Center in Flint, Michigan, suggest that it may actually be an underrecognized cause of sudden death.
They describe the case of their patient, a 63-year-old woman with relapsing-remitting multiple sclerosis and hypertension who was about to start fingolomod. She underwent a basal ECG to be cleared before starting treatment. She received her first dose of fingolimod at the cardiology office, was monitored for 6 hours, and went home with a surface-mounted Holter monitor.
Two weeks later, she was in the emergency department because the monitor had captured ventricular tachycardia, and she was reporting palpitations.
Lab work was normal; the echocardiogram was normal. Cardiac monitoring showed no other evidence of cardiac arrhythmias. Her only other medication was amlodipine. The fingolimod was held back. She was observed for4 days then discharged in a stable condition. Her clinicians followed her for 2 months but the arrhythmia did not return.
Although this patient had no further arrhythmias, the authors warn that serious outcomes are possible. They urge health care practitioners to let patients know of this potential AE and advise them to report symptoms such as palpitations immediately.
Ibrexafungerp effective against C. auris in two early case reports
A novel antifungal successfully eradicated Candida auris in two critically ill patients with fungemia, according to data presented in a poster session at the European Congress of Clinical Microbiology & Infectious Diseases.

The case reports, drawn from the phase 3 CARES study of the oral formulation of ibrexafungerp, demonstrated complete response to the glucan synthase inhibitor, according to Deven Juneja, MD, and his coauthors of the Max Super Specialty Hospital, New Delhi.
The first patient was an Asian male, aged 58 years, who had a previous history of diabetes and experienced a protracted ICU stay after acute ischemic stroke. He developed septic shock after aspiration pneumonia, and also experienced a popliteal thrombosis and liver, spleen, and kidney infarcts.
The patient had received empiric antibiotics with the addition of fluconazole; the antifungal was later switched to micafungin after C. auris was identified from blood cultures. Despite clinical improvement on micafungin, blood cultures remained positive for C. auris, so ibrexafungerp was started and continued for 17 days. Blood cultures became negative by day 3 of ibrexafungerp and remained negative for the follow-up period. The patient later developed Klebsiella pneumonia and died.
The second patient, an Asian female, aged 64 years, presented with a lower respiratory tract infection accompanied by fever and hypotension. She had a previous history of diabetes, hypertension, and chronic kidney disease with maintenance hemodialysis. Her fever also persisted despite antibiotics, and C. auris was isolated from her blood cultures with the subsequent initiation of ibrexafungerp. Her blood cultures were still positive at day 3 of ibrexafungerp, but negative at day 9 and 21. She completed 22 days of ibrexafungerp therapy and was asymptomatic with no evidence of C. auris recurrence at a 6-week follow-up visit.
The male patient experienced 2 days of loose stools soon after initiating ibrexafungerp; the female patient had no adverse events.
“These cases provide initial evidence of efficacy and safety of ibrexafungerp in the treatment of candidemia caused by C. auris, including in patients who failed previous therapies,” wrote Dr. Juneja and his coauthors in the late-breaking poster.
Ibrexafungerp belongs to a novel class of glucan synthase inhibitors called triterpenoids. Scynexis funded the CARES study and also is evaluating it alone or in combination with other antifungals for treatment of vulvovaginal candidiasis, invasive pulmonary aspergillosis, and refractory invasive and/or severe fungal disease.
SOURCE: Juneja D et al. ECCMID 2019, Poster L0028.
A novel antifungal successfully eradicated Candida auris in two critically ill patients with fungemia, according to data presented in a poster session at the European Congress of Clinical Microbiology & Infectious Diseases.
The case reports, drawn from the phase 3 CARES study of the oral formulation of ibrexafungerp, demonstrated complete response to the glucan synthase inhibitor, according to Deven Juneja, MD, and his coauthors of the Max Super Specialty Hospital, New Delhi.
The first patient was an Asian male, aged 58 years, who had a previous history of diabetes and experienced a protracted ICU stay after acute ischemic stroke. He developed septic shock after aspiration pneumonia, and also experienced a popliteal thrombosis and liver, spleen, and kidney infarcts.
The patient had received empiric antibiotics with the addition of fluconazole; the antifungal was later switched to micafungin after C. auris was identified from blood cultures. Despite clinical improvement on micafungin, blood cultures remained positive for C. auris, so ibrexafungerp was started and continued for 17 days. Blood cultures became negative by day 3 of ibrexafungerp and remained negative for the follow-up period. The patient later developed Klebsiella pneumonia and died.
The second patient, an Asian female, aged 64 years, presented with a lower respiratory tract infection accompanied by fever and hypotension. She had a previous history of diabetes, hypertension, and chronic kidney disease with maintenance hemodialysis. Her fever also persisted despite antibiotics, and C. auris was isolated from her blood cultures with the subsequent initiation of ibrexafungerp. Her blood cultures were still positive at day 3 of ibrexafungerp, but negative at day 9 and 21. She completed 22 days of ibrexafungerp therapy and was asymptomatic with no evidence of C. auris recurrence at a 6-week follow-up visit.
The male patient experienced 2 days of loose stools soon after initiating ibrexafungerp; the female patient had no adverse events.
“These cases provide initial evidence of efficacy and safety of ibrexafungerp in the treatment of candidemia caused by C. auris, including in patients who failed previous therapies,” wrote Dr. Juneja and his coauthors in the late-breaking poster.
Ibrexafungerp belongs to a novel class of glucan synthase inhibitors called triterpenoids. Scynexis funded the CARES study and also is evaluating it alone or in combination with other antifungals for treatment of vulvovaginal candidiasis, invasive pulmonary aspergillosis, and refractory invasive and/or severe fungal disease.
SOURCE: Juneja D et al. ECCMID 2019, Poster L0028.
A novel antifungal successfully eradicated Candida auris in two critically ill patients with fungemia, according to data presented in a poster session at the European Congress of Clinical Microbiology & Infectious Diseases.
The case reports, drawn from the phase 3 CARES study of the oral formulation of ibrexafungerp, demonstrated complete response to the glucan synthase inhibitor, according to Deven Juneja, MD, and his coauthors of the Max Super Specialty Hospital, New Delhi.
The first patient was an Asian male, aged 58 years, who had a previous history of diabetes and experienced a protracted ICU stay after acute ischemic stroke. He developed septic shock after aspiration pneumonia, and also experienced a popliteal thrombosis and liver, spleen, and kidney infarcts.
The patient had received empiric antibiotics with the addition of fluconazole; the antifungal was later switched to micafungin after C. auris was identified from blood cultures. Despite clinical improvement on micafungin, blood cultures remained positive for C. auris, so ibrexafungerp was started and continued for 17 days. Blood cultures became negative by day 3 of ibrexafungerp and remained negative for the follow-up period. The patient later developed Klebsiella pneumonia and died.
The second patient, an Asian female, aged 64 years, presented with a lower respiratory tract infection accompanied by fever and hypotension. She had a previous history of diabetes, hypertension, and chronic kidney disease with maintenance hemodialysis. Her fever also persisted despite antibiotics, and C. auris was isolated from her blood cultures with the subsequent initiation of ibrexafungerp. Her blood cultures were still positive at day 3 of ibrexafungerp, but negative at day 9 and 21. She completed 22 days of ibrexafungerp therapy and was asymptomatic with no evidence of C. auris recurrence at a 6-week follow-up visit.
The male patient experienced 2 days of loose stools soon after initiating ibrexafungerp; the female patient had no adverse events.
“These cases provide initial evidence of efficacy and safety of ibrexafungerp in the treatment of candidemia caused by C. auris, including in patients who failed previous therapies,” wrote Dr. Juneja and his coauthors in the late-breaking poster.
Ibrexafungerp belongs to a novel class of glucan synthase inhibitors called triterpenoids. Scynexis funded the CARES study and also is evaluating it alone or in combination with other antifungals for treatment of vulvovaginal candidiasis, invasive pulmonary aspergillosis, and refractory invasive and/or severe fungal disease.
SOURCE: Juneja D et al. ECCMID 2019, Poster L0028.
FROM ECCMID 2019

During Flu Season Risk of Heart Failure Rises
A study of > 450,000 adults has “confirmed the long-held notion” that flu and heart failure are connected. The Atherosclerosis Risk in Communities study (ARIC), led by a VA researcher, found influenza significantly increased the risk of hospitalization for heart failure.
Every flu season about 36,000 people die, and > 200,000 are hospitalized due to flu, which is known to be associated with a higher risk of cardiovascular events. Several mechanisms likely contribute: Some form of immunocompromise is thought to be a key link. But few studies, the researchers note, have explored the temporal association between influenza activity and hospitalizations, particularly those caused by heart failure.
In ARIC, the researchers analyzed hospitalization data for adults aged 35 to 84 years between 2010 and 2014 in geographically diverse communities in Mississippi, Minnesota, North Carolina, and Maryland. They correlated those data with reports of influenza activity from the CDC Surveillance Network.
A 5% monthly increase in influenza activity was associated with a 24% relative increase in heart failure hospitalization rates. Myocardial infarction hospitalizations did not rise significantly. The most pneumonia and influenza-associated deaths were during the 2012-2013 season, when influenza-like illness (ILI) activity was highest, and the fewest deaths occurred during 2011-2012, when ILI activity was lowest. The model suggests that in a month with high influenza activity, about 19% of hospitalizations could be attributable to influenza, the researchers say.
“The study’s findings support VA’s aggressive effort every year to provide veterans with influenza vaccine,” said VA Secretary Robert Wilkie. Although the flu season is winding down, he added, it is not too late for veterans—and others—to get vaccinated.
A study of > 450,000 adults has “confirmed the long-held notion” that flu and heart failure are connected. The Atherosclerosis Risk in Communities study (ARIC), led by a VA researcher, found influenza significantly increased the risk of hospitalization for heart failure.
Every flu season about 36,000 people die, and > 200,000 are hospitalized due to flu, which is known to be associated with a higher risk of cardiovascular events. Several mechanisms likely contribute: Some form of immunocompromise is thought to be a key link. But few studies, the researchers note, have explored the temporal association between influenza activity and hospitalizations, particularly those caused by heart failure.
In ARIC, the researchers analyzed hospitalization data for adults aged 35 to 84 years between 2010 and 2014 in geographically diverse communities in Mississippi, Minnesota, North Carolina, and Maryland. They correlated those data with reports of influenza activity from the CDC Surveillance Network.
A 5% monthly increase in influenza activity was associated with a 24% relative increase in heart failure hospitalization rates. Myocardial infarction hospitalizations did not rise significantly. The most pneumonia and influenza-associated deaths were during the 2012-2013 season, when influenza-like illness (ILI) activity was highest, and the fewest deaths occurred during 2011-2012, when ILI activity was lowest. The model suggests that in a month with high influenza activity, about 19% of hospitalizations could be attributable to influenza, the researchers say.
“The study’s findings support VA’s aggressive effort every year to provide veterans with influenza vaccine,” said VA Secretary Robert Wilkie. Although the flu season is winding down, he added, it is not too late for veterans—and others—to get vaccinated.
A study of > 450,000 adults has “confirmed the long-held notion” that flu and heart failure are connected. The Atherosclerosis Risk in Communities study (ARIC), led by a VA researcher, found influenza significantly increased the risk of hospitalization for heart failure.
Every flu season about 36,000 people die, and > 200,000 are hospitalized due to flu, which is known to be associated with a higher risk of cardiovascular events. Several mechanisms likely contribute: Some form of immunocompromise is thought to be a key link. But few studies, the researchers note, have explored the temporal association between influenza activity and hospitalizations, particularly those caused by heart failure.
In ARIC, the researchers analyzed hospitalization data for adults aged 35 to 84 years between 2010 and 2014 in geographically diverse communities in Mississippi, Minnesota, North Carolina, and Maryland. They correlated those data with reports of influenza activity from the CDC Surveillance Network.
A 5% monthly increase in influenza activity was associated with a 24% relative increase in heart failure hospitalization rates. Myocardial infarction hospitalizations did not rise significantly. The most pneumonia and influenza-associated deaths were during the 2012-2013 season, when influenza-like illness (ILI) activity was highest, and the fewest deaths occurred during 2011-2012, when ILI activity was lowest. The model suggests that in a month with high influenza activity, about 19% of hospitalizations could be attributable to influenza, the researchers say.
“The study’s findings support VA’s aggressive effort every year to provide veterans with influenza vaccine,” said VA Secretary Robert Wilkie. Although the flu season is winding down, he added, it is not too late for veterans—and others—to get vaccinated.
Gout Drug May Help in Metabolic Syndrome
Colchicine inhibits the formation of the Nod-like Receptor Family Pyrin Domain Containing 3 (NLRP3) inflammasome, a key component in the obesity-associated inflammatory cascade. In a retrospective study, long-term colchicine treatment had glycemic benefit in patients with gout. Other research has suggested that suppressing NLRP3 could improve peripheral insulin resistance as well as β-cell insulin production. However, no randomized controlled trial had yet investigated colchicine’s long-term effects on glucose metabolism in adults with obesity and metabolic syndrome (MetS).
The NIH researchers enrolled 40 adults to receive either colchicine or placebo; 37 completed the 3-month study. Adherence was high in both groups.
Colchicine significantly reduced multiple markers of obesity-associated inflammation, including high sensitivity C-reactive protein and erythrocyte sedimentation rate. The colchicine group also had moderate but statistically significant reductions in white blood cell count, monocytes, neutrophils, and platelets, without significant effects on lymphocyte count.
Although colchicine’s effects on the primary outcome of insulin sensitivity were not significant, some of the secondary outcomes related to glucose homeostasis—eg, insulin resistance and fasting insulin—suggest colchicine treatment may improve hepatic insulin sensitivity. Moreover, the researchers say, a trend toward improvement in disposition index suggests that the drug might potentially delay the onset of diabetes in people at risk.
While some small, short-term studies had suggested that colchicine might worsen metabolic variables by inhibiting insulin secretion, other recent retrospective studies found long-term colchicine use did not negatively affect insulin secretion or glycemic control. In this study, similarly, the researchers say, chronic colchicine use did not impair first-phase insulin response or insulin sensitivity, and other markers of metabolic health, such as hemoglobin A1c and cholesterol, were not significantly changed. However, the researchers acknowledge that their study may have been too small to confirm those differences, and say larger studies are warranted.
Colchicine inhibits the formation of the Nod-like Receptor Family Pyrin Domain Containing 3 (NLRP3) inflammasome, a key component in the obesity-associated inflammatory cascade. In a retrospective study, long-term colchicine treatment had glycemic benefit in patients with gout. Other research has suggested that suppressing NLRP3 could improve peripheral insulin resistance as well as β-cell insulin production. However, no randomized controlled trial had yet investigated colchicine’s long-term effects on glucose metabolism in adults with obesity and metabolic syndrome (MetS).
The NIH researchers enrolled 40 adults to receive either colchicine or placebo; 37 completed the 3-month study. Adherence was high in both groups.
Colchicine significantly reduced multiple markers of obesity-associated inflammation, including high sensitivity C-reactive protein and erythrocyte sedimentation rate. The colchicine group also had moderate but statistically significant reductions in white blood cell count, monocytes, neutrophils, and platelets, without significant effects on lymphocyte count.
Although colchicine’s effects on the primary outcome of insulin sensitivity were not significant, some of the secondary outcomes related to glucose homeostasis—eg, insulin resistance and fasting insulin—suggest colchicine treatment may improve hepatic insulin sensitivity. Moreover, the researchers say, a trend toward improvement in disposition index suggests that the drug might potentially delay the onset of diabetes in people at risk.
While some small, short-term studies had suggested that colchicine might worsen metabolic variables by inhibiting insulin secretion, other recent retrospective studies found long-term colchicine use did not negatively affect insulin secretion or glycemic control. In this study, similarly, the researchers say, chronic colchicine use did not impair first-phase insulin response or insulin sensitivity, and other markers of metabolic health, such as hemoglobin A1c and cholesterol, were not significantly changed. However, the researchers acknowledge that their study may have been too small to confirm those differences, and say larger studies are warranted.
Colchicine inhibits the formation of the Nod-like Receptor Family Pyrin Domain Containing 3 (NLRP3) inflammasome, a key component in the obesity-associated inflammatory cascade. In a retrospective study, long-term colchicine treatment had glycemic benefit in patients with gout. Other research has suggested that suppressing NLRP3 could improve peripheral insulin resistance as well as β-cell insulin production. However, no randomized controlled trial had yet investigated colchicine’s long-term effects on glucose metabolism in adults with obesity and metabolic syndrome (MetS).
The NIH researchers enrolled 40 adults to receive either colchicine or placebo; 37 completed the 3-month study. Adherence was high in both groups.
Colchicine significantly reduced multiple markers of obesity-associated inflammation, including high sensitivity C-reactive protein and erythrocyte sedimentation rate. The colchicine group also had moderate but statistically significant reductions in white blood cell count, monocytes, neutrophils, and platelets, without significant effects on lymphocyte count.
Although colchicine’s effects on the primary outcome of insulin sensitivity were not significant, some of the secondary outcomes related to glucose homeostasis—eg, insulin resistance and fasting insulin—suggest colchicine treatment may improve hepatic insulin sensitivity. Moreover, the researchers say, a trend toward improvement in disposition index suggests that the drug might potentially delay the onset of diabetes in people at risk.
While some small, short-term studies had suggested that colchicine might worsen metabolic variables by inhibiting insulin secretion, other recent retrospective studies found long-term colchicine use did not negatively affect insulin secretion or glycemic control. In this study, similarly, the researchers say, chronic colchicine use did not impair first-phase insulin response or insulin sensitivity, and other markers of metabolic health, such as hemoglobin A1c and cholesterol, were not significantly changed. However, the researchers acknowledge that their study may have been too small to confirm those differences, and say larger studies are warranted.
Busiest week yet brings 2019 measles total to 555 cases
according to the Centers for Disease Control and Prevention.
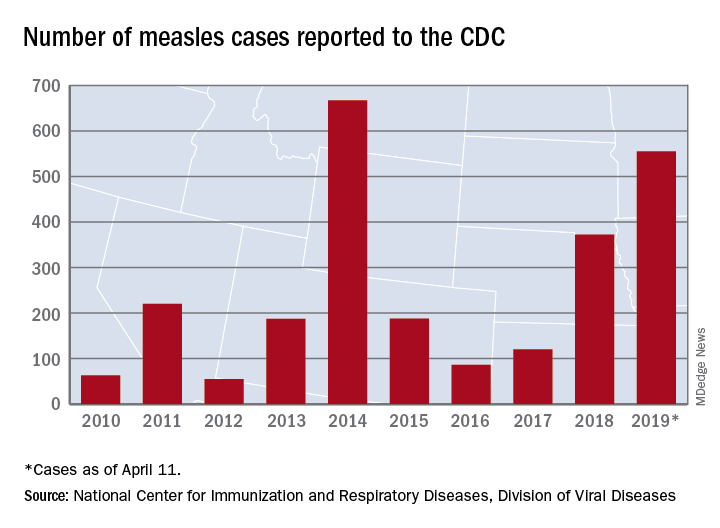
The 90 measles cases reported during the week ending April 11 mark the third consecutive weekly high for 2019, topping the 78 recorded during the week of April 4 and the 73 reported during the week of March 28. Meanwhile, this year’s total trails only the 667 cases reported in 2014 for the highest in the postelimination era, the CDC said April 15.
New York reported 26 new cases in Brooklyn’s Williamsburg neighborhood last week, which puts the borough at 227 for the year, with another two occurring in the Flushing section of Queens. A public health emergency declared on April 9 covers several zip codes in Williamsburg and requires unvaccinated individuals who may have been exposed to measles to receive “the measles-mumps-rubella vaccine in order to protect others in the community and help curtail the ongoing outbreak,” the city’s health department said in a written statement.
Maryland became the 20th state to report a measles case this year, and the state’s department of health said it was notifying those in the vicinity of a medical office building in Pikesville about possible exposure on April 2.
The recent outbreak in Michigan’s Oakland County did not result in any new patients over the last week and remains at 38 cases, with the state reporting one additional case in Wayne County. More recent reports of a case in Washtenaw County and another in Oakland County were reversed after additional testing, the state health department reported.
according to the Centers for Disease Control and Prevention.
The 90 measles cases reported during the week ending April 11 mark the third consecutive weekly high for 2019, topping the 78 recorded during the week of April 4 and the 73 reported during the week of March 28. Meanwhile, this year’s total trails only the 667 cases reported in 2014 for the highest in the postelimination era, the CDC said April 15.
New York reported 26 new cases in Brooklyn’s Williamsburg neighborhood last week, which puts the borough at 227 for the year, with another two occurring in the Flushing section of Queens. A public health emergency declared on April 9 covers several zip codes in Williamsburg and requires unvaccinated individuals who may have been exposed to measles to receive “the measles-mumps-rubella vaccine in order to protect others in the community and help curtail the ongoing outbreak,” the city’s health department said in a written statement.
Maryland became the 20th state to report a measles case this year, and the state’s department of health said it was notifying those in the vicinity of a medical office building in Pikesville about possible exposure on April 2.
The recent outbreak in Michigan’s Oakland County did not result in any new patients over the last week and remains at 38 cases, with the state reporting one additional case in Wayne County. More recent reports of a case in Washtenaw County and another in Oakland County were reversed after additional testing, the state health department reported.
according to the Centers for Disease Control and Prevention.
The 90 measles cases reported during the week ending April 11 mark the third consecutive weekly high for 2019, topping the 78 recorded during the week of April 4 and the 73 reported during the week of March 28. Meanwhile, this year’s total trails only the 667 cases reported in 2014 for the highest in the postelimination era, the CDC said April 15.
New York reported 26 new cases in Brooklyn’s Williamsburg neighborhood last week, which puts the borough at 227 for the year, with another two occurring in the Flushing section of Queens. A public health emergency declared on April 9 covers several zip codes in Williamsburg and requires unvaccinated individuals who may have been exposed to measles to receive “the measles-mumps-rubella vaccine in order to protect others in the community and help curtail the ongoing outbreak,” the city’s health department said in a written statement.
Maryland became the 20th state to report a measles case this year, and the state’s department of health said it was notifying those in the vicinity of a medical office building in Pikesville about possible exposure on April 2.
The recent outbreak in Michigan’s Oakland County did not result in any new patients over the last week and remains at 38 cases, with the state reporting one additional case in Wayne County. More recent reports of a case in Washtenaw County and another in Oakland County were reversed after additional testing, the state health department reported.
The VA vs HCV: Making a Deadly Disease a Memory
“This is terrific news,” said US Department of Veterans Affairs (VA) Secretary Robert Wilkie, noting that the VA is the largest single provider of hepatitis C virus (HCV) care in the US. “Diagnosing, treating, and curing hepatitis C virus infection among veterans has been a significant priority for VA.” According to the Review of Hepatitis C Virus Care within the Veterans Health Administration, published last month by the VA Office of Inspector General (OIG), the VA cares for more than 180,000 confirmed patients who are disproportionately affected by HCV infection, at rates about 3 times that of the national average.
As of March, nearly 116,000 veterans had started all-oral HCV medications. Almost 100,000 have completed treatment and are now cured. As an article in Forbes magazine pointed out, that is a story very different from the one reported just a few years earlier, when HCV treatment was out of reach for the tens of thousands of service members seriously ill with HCV, most of whom contracted it during blood transfusions in the Vietnam War.
The good news is due largely to the use of highly effective direct-acting antivirals (DAAs), which have revolutionized HCV treatment. Before 2014, HCV treatment required weekly interferon injections for up to a year, with low cure rates (35%-55%) and significant physical and psychiatric adverse effects (AEs), leading to frequent early discontinuation. Of the approximately 180,000 veterans in VA care at that time who had been diagnosed with chronic HCV infection, only 12,000 had been treated and cured. More than 30,000 had advanced liver disease.
In 2014, the VA launched an “aggressive program” to identify all undiagnosed veterans with HCV, link them to care, and offer them treatment with the new medications: sofosbuvir (Sovaldi) and simeprevir (Olysio). They have few AEs and can be administered once daily for as few as 8 weeks.
However, those drugs were incredibly expensive, prohibitively so for many people. Sovaldi cost $1,000 a pill. But the VA, allowed by law to negotiate prices, brought down the price. The VA estimated that the drugs would cost roughly $750 million and provide about 60,000 treatments over 2017 and 2018, at about $25,300 per service member .
The VA then began treating close to 2,000 veterans with HCV every week—nearly 1 treatment started every minute of every workday. As a result, by the next year the overall death rate had dropped dramatically. Veterans cured of HCV were also 84% less likely to develop liver cancer.
Still, some patients have been left out. The OIG conducted a study to, among other things, assess why some patients with chronic HCV infection were not treated with DAAs. Acceptable reasons included pregnancy, being in hospice or palliative care, the possibility of drug interactions with current medications, a diagnosis of liver cancer, and adherence challenges (eg, being homeless). Unacceptable reasons included HIV co-infection and prior treatment failure with DAAs.
The decision to disqualify a patient from receiving HCV treatment must be made on a case-by-case basis by individual providers in consultation with their patients, the OIG says. If a patient is deferred for treatment based on “problematic levels of alcohol or substance use,” the report adds, he/she should be referred for substance use treatment and must have a plan for re-evaluation for HCV treatment within 3 to 6 months. However, the VHA notes that patients with drug or alcohol addiction “should not be automatically excluded from hepatitis C treatment.”
The VA says it is on track to treat more than 125,000 veterans with HCV by October. As of March, fewer than 27,000 remained to be treated.
“This is terrific news,” said US Department of Veterans Affairs (VA) Secretary Robert Wilkie, noting that the VA is the largest single provider of hepatitis C virus (HCV) care in the US. “Diagnosing, treating, and curing hepatitis C virus infection among veterans has been a significant priority for VA.” According to the Review of Hepatitis C Virus Care within the Veterans Health Administration, published last month by the VA Office of Inspector General (OIG), the VA cares for more than 180,000 confirmed patients who are disproportionately affected by HCV infection, at rates about 3 times that of the national average.
As of March, nearly 116,000 veterans had started all-oral HCV medications. Almost 100,000 have completed treatment and are now cured. As an article in Forbes magazine pointed out, that is a story very different from the one reported just a few years earlier, when HCV treatment was out of reach for the tens of thousands of service members seriously ill with HCV, most of whom contracted it during blood transfusions in the Vietnam War.
The good news is due largely to the use of highly effective direct-acting antivirals (DAAs), which have revolutionized HCV treatment. Before 2014, HCV treatment required weekly interferon injections for up to a year, with low cure rates (35%-55%) and significant physical and psychiatric adverse effects (AEs), leading to frequent early discontinuation. Of the approximately 180,000 veterans in VA care at that time who had been diagnosed with chronic HCV infection, only 12,000 had been treated and cured. More than 30,000 had advanced liver disease.
In 2014, the VA launched an “aggressive program” to identify all undiagnosed veterans with HCV, link them to care, and offer them treatment with the new medications: sofosbuvir (Sovaldi) and simeprevir (Olysio). They have few AEs and can be administered once daily for as few as 8 weeks.
However, those drugs were incredibly expensive, prohibitively so for many people. Sovaldi cost $1,000 a pill. But the VA, allowed by law to negotiate prices, brought down the price. The VA estimated that the drugs would cost roughly $750 million and provide about 60,000 treatments over 2017 and 2018, at about $25,300 per service member .
The VA then began treating close to 2,000 veterans with HCV every week—nearly 1 treatment started every minute of every workday. As a result, by the next year the overall death rate had dropped dramatically. Veterans cured of HCV were also 84% less likely to develop liver cancer.
Still, some patients have been left out. The OIG conducted a study to, among other things, assess why some patients with chronic HCV infection were not treated with DAAs. Acceptable reasons included pregnancy, being in hospice or palliative care, the possibility of drug interactions with current medications, a diagnosis of liver cancer, and adherence challenges (eg, being homeless). Unacceptable reasons included HIV co-infection and prior treatment failure with DAAs.
The decision to disqualify a patient from receiving HCV treatment must be made on a case-by-case basis by individual providers in consultation with their patients, the OIG says. If a patient is deferred for treatment based on “problematic levels of alcohol or substance use,” the report adds, he/she should be referred for substance use treatment and must have a plan for re-evaluation for HCV treatment within 3 to 6 months. However, the VHA notes that patients with drug or alcohol addiction “should not be automatically excluded from hepatitis C treatment.”
The VA says it is on track to treat more than 125,000 veterans with HCV by October. As of March, fewer than 27,000 remained to be treated.
“This is terrific news,” said US Department of Veterans Affairs (VA) Secretary Robert Wilkie, noting that the VA is the largest single provider of hepatitis C virus (HCV) care in the US. “Diagnosing, treating, and curing hepatitis C virus infection among veterans has been a significant priority for VA.” According to the Review of Hepatitis C Virus Care within the Veterans Health Administration, published last month by the VA Office of Inspector General (OIG), the VA cares for more than 180,000 confirmed patients who are disproportionately affected by HCV infection, at rates about 3 times that of the national average.
As of March, nearly 116,000 veterans had started all-oral HCV medications. Almost 100,000 have completed treatment and are now cured. As an article in Forbes magazine pointed out, that is a story very different from the one reported just a few years earlier, when HCV treatment was out of reach for the tens of thousands of service members seriously ill with HCV, most of whom contracted it during blood transfusions in the Vietnam War.
The good news is due largely to the use of highly effective direct-acting antivirals (DAAs), which have revolutionized HCV treatment. Before 2014, HCV treatment required weekly interferon injections for up to a year, with low cure rates (35%-55%) and significant physical and psychiatric adverse effects (AEs), leading to frequent early discontinuation. Of the approximately 180,000 veterans in VA care at that time who had been diagnosed with chronic HCV infection, only 12,000 had been treated and cured. More than 30,000 had advanced liver disease.
In 2014, the VA launched an “aggressive program” to identify all undiagnosed veterans with HCV, link them to care, and offer them treatment with the new medications: sofosbuvir (Sovaldi) and simeprevir (Olysio). They have few AEs and can be administered once daily for as few as 8 weeks.
However, those drugs were incredibly expensive, prohibitively so for many people. Sovaldi cost $1,000 a pill. But the VA, allowed by law to negotiate prices, brought down the price. The VA estimated that the drugs would cost roughly $750 million and provide about 60,000 treatments over 2017 and 2018, at about $25,300 per service member .
The VA then began treating close to 2,000 veterans with HCV every week—nearly 1 treatment started every minute of every workday. As a result, by the next year the overall death rate had dropped dramatically. Veterans cured of HCV were also 84% less likely to develop liver cancer.
Still, some patients have been left out. The OIG conducted a study to, among other things, assess why some patients with chronic HCV infection were not treated with DAAs. Acceptable reasons included pregnancy, being in hospice or palliative care, the possibility of drug interactions with current medications, a diagnosis of liver cancer, and adherence challenges (eg, being homeless). Unacceptable reasons included HIV co-infection and prior treatment failure with DAAs.
The decision to disqualify a patient from receiving HCV treatment must be made on a case-by-case basis by individual providers in consultation with their patients, the OIG says. If a patient is deferred for treatment based on “problematic levels of alcohol or substance use,” the report adds, he/she should be referred for substance use treatment and must have a plan for re-evaluation for HCV treatment within 3 to 6 months. However, the VHA notes that patients with drug or alcohol addiction “should not be automatically excluded from hepatitis C treatment.”
The VA says it is on track to treat more than 125,000 veterans with HCV by October. As of March, fewer than 27,000 remained to be treated.
FDA warns of possible temporary shortage of trach tube
manufactured by Smiths Medical caused by the closure of a large ethylene oxide sterilization facilities in Willowbrook, Ill., and the future planned closure of a similar facility.

The shortage may affect pediatric use because, although tubes are used for both adults and children, there are fewer alternative products on the market for pediatric patients. Parents and caregivers of children who use the Bivona tube are encouraged to check with Smiths Medical about available inventory and with their health care providers about alternative products.
Jeff Shuren, MD, director of the Center for Devices and Radiological Health, wrote in a press release, “I want to assure you that the FDA is working closely with the company to quickly resolve their sterilization challenges and bring these critical devices to the patients who need them as quickly as possible, which we anticipate will be made available again beginning the week of April 22.”
For patients currently using the Bivona tubes, Dr. Shuren noted, “The closure of the Willowbrook facility does not impact tubes already in use by patients at home or in health care settings. The company is communicating with patients about the tubes and how patients and caregivers can mitigate any potential impact, including reusing and cleaning tubes in accordance with the manufacturer’s instructions for use.”
Read the entire announcement at the FDA website.
manufactured by Smiths Medical caused by the closure of a large ethylene oxide sterilization facilities in Willowbrook, Ill., and the future planned closure of a similar facility.
The shortage may affect pediatric use because, although tubes are used for both adults and children, there are fewer alternative products on the market for pediatric patients. Parents and caregivers of children who use the Bivona tube are encouraged to check with Smiths Medical about available inventory and with their health care providers about alternative products.
Jeff Shuren, MD, director of the Center for Devices and Radiological Health, wrote in a press release, “I want to assure you that the FDA is working closely with the company to quickly resolve their sterilization challenges and bring these critical devices to the patients who need them as quickly as possible, which we anticipate will be made available again beginning the week of April 22.”
For patients currently using the Bivona tubes, Dr. Shuren noted, “The closure of the Willowbrook facility does not impact tubes already in use by patients at home or in health care settings. The company is communicating with patients about the tubes and how patients and caregivers can mitigate any potential impact, including reusing and cleaning tubes in accordance with the manufacturer’s instructions for use.”
Read the entire announcement at the FDA website.
manufactured by Smiths Medical caused by the closure of a large ethylene oxide sterilization facilities in Willowbrook, Ill., and the future planned closure of a similar facility.
The shortage may affect pediatric use because, although tubes are used for both adults and children, there are fewer alternative products on the market for pediatric patients. Parents and caregivers of children who use the Bivona tube are encouraged to check with Smiths Medical about available inventory and with their health care providers about alternative products.
Jeff Shuren, MD, director of the Center for Devices and Radiological Health, wrote in a press release, “I want to assure you that the FDA is working closely with the company to quickly resolve their sterilization challenges and bring these critical devices to the patients who need them as quickly as possible, which we anticipate will be made available again beginning the week of April 22.”
For patients currently using the Bivona tubes, Dr. Shuren noted, “The closure of the Willowbrook facility does not impact tubes already in use by patients at home or in health care settings. The company is communicating with patients about the tubes and how patients and caregivers can mitigate any potential impact, including reusing and cleaning tubes in accordance with the manufacturer’s instructions for use.”
Read the entire announcement at the FDA website.
Help for Guard and Reserve Members at Risk for Suicide
Every day in 2005, 18.5 service members and veterans committed suicide; of those, 2.7 were active-duty and non-activated Guard or Reserve. In 2015, those numbers had risen to 20.6 deaths per day, of which 3.8 were among active-duty or non-activated Guard and Reserve members. According to the VA’s most recent analysis, 7,298 current and former service members committed suicide in 2016. Of those, 902 were former Guard and Reserve members.
National Guard and Reserve members may not have veteran legal status due to their type of service, which can limit their access to VA benefits and services under current laws and regulations. In partnership with the DoD, VA now operates a mobile Vet Center to increase Guard and Reserve members’ access to mental health care.
To further help them, their families, and their health care providers, the VA also has developed a tool kit with links to mental health and suicide prevention resources that are available through the VA and their communities. “Extending support to former Guard and Reserve members at the community level is an important aspect of VA’s public health approach to preventing suicide,” said Dr. Keita Franklin, executive director for suicide prevention in the VA Office of Mental Health and Suicide Prevention.
The resources include online suicide prevention training, mobile apps that help with managing daily stressors, and supportive services for family members who are seeking care for former service members.
InTransition, for instance, is a free confidential program that offers coaching and specialized assistance over the phone for service members who need access to mental health care. Military OneSource provides military personnel and their families with round-the-clock support for a wide range of civilian necessities, such as tax preparation and spouse employment. PsychArmor Institute provides free online education to anyone who works with, lives with, or cares for service members, veterans, and their families. The MY3-Support Network app allows users to add the contact information of 3 people they would like to talk to when they are having thoughts of suicide.
The tool kit also offers links to programs for community members who want to learn how to help prevent suicides and support families who have gone through the trauma. The #BeThere Campaign teaches how simple acts can help save the life of a veteran in crisis. The S.A.V.E. Training video, designed in collaboration with PsychArmor Institute, teaches how to demonstrate support and compassion when talking with a veteran who may be at risk. Other links lead users to ways to help those whose loved one has committed suicide, such as the Tragedy Assistance Program for Survivors (TAPS).
Further expansion of suicide prevention activities for the former Guard and Reserve population is planned for fiscal year 2019.
The Veterans Crisis Line is available with free confidential support and crisis intervention 24 hours a day, 7 days a week, 365 days a year: Call 800.273.8255 (press 1), text to 838255, or chat online at VeteransCrisisLine.net/Chat. The tool kit is available at https://www.mentalhealth.va.gov/suicide_prevention/docs/toolkit_National_Guard_and_Reserve_members_cleared_2-21-19.pdf.
Every day in 2005, 18.5 service members and veterans committed suicide; of those, 2.7 were active-duty and non-activated Guard or Reserve. In 2015, those numbers had risen to 20.6 deaths per day, of which 3.8 were among active-duty or non-activated Guard and Reserve members. According to the VA’s most recent analysis, 7,298 current and former service members committed suicide in 2016. Of those, 902 were former Guard and Reserve members.
National Guard and Reserve members may not have veteran legal status due to their type of service, which can limit their access to VA benefits and services under current laws and regulations. In partnership with the DoD, VA now operates a mobile Vet Center to increase Guard and Reserve members’ access to mental health care.
To further help them, their families, and their health care providers, the VA also has developed a tool kit with links to mental health and suicide prevention resources that are available through the VA and their communities. “Extending support to former Guard and Reserve members at the community level is an important aspect of VA’s public health approach to preventing suicide,” said Dr. Keita Franklin, executive director for suicide prevention in the VA Office of Mental Health and Suicide Prevention.
The resources include online suicide prevention training, mobile apps that help with managing daily stressors, and supportive services for family members who are seeking care for former service members.
InTransition, for instance, is a free confidential program that offers coaching and specialized assistance over the phone for service members who need access to mental health care. Military OneSource provides military personnel and their families with round-the-clock support for a wide range of civilian necessities, such as tax preparation and spouse employment. PsychArmor Institute provides free online education to anyone who works with, lives with, or cares for service members, veterans, and their families. The MY3-Support Network app allows users to add the contact information of 3 people they would like to talk to when they are having thoughts of suicide.
The tool kit also offers links to programs for community members who want to learn how to help prevent suicides and support families who have gone through the trauma. The #BeThere Campaign teaches how simple acts can help save the life of a veteran in crisis. The S.A.V.E. Training video, designed in collaboration with PsychArmor Institute, teaches how to demonstrate support and compassion when talking with a veteran who may be at risk. Other links lead users to ways to help those whose loved one has committed suicide, such as the Tragedy Assistance Program for Survivors (TAPS).
Further expansion of suicide prevention activities for the former Guard and Reserve population is planned for fiscal year 2019.
The Veterans Crisis Line is available with free confidential support and crisis intervention 24 hours a day, 7 days a week, 365 days a year: Call 800.273.8255 (press 1), text to 838255, or chat online at VeteransCrisisLine.net/Chat. The tool kit is available at https://www.mentalhealth.va.gov/suicide_prevention/docs/toolkit_National_Guard_and_Reserve_members_cleared_2-21-19.pdf.
Every day in 2005, 18.5 service members and veterans committed suicide; of those, 2.7 were active-duty and non-activated Guard or Reserve. In 2015, those numbers had risen to 20.6 deaths per day, of which 3.8 were among active-duty or non-activated Guard and Reserve members. According to the VA’s most recent analysis, 7,298 current and former service members committed suicide in 2016. Of those, 902 were former Guard and Reserve members.
National Guard and Reserve members may not have veteran legal status due to their type of service, which can limit their access to VA benefits and services under current laws and regulations. In partnership with the DoD, VA now operates a mobile Vet Center to increase Guard and Reserve members’ access to mental health care.
To further help them, their families, and their health care providers, the VA also has developed a tool kit with links to mental health and suicide prevention resources that are available through the VA and their communities. “Extending support to former Guard and Reserve members at the community level is an important aspect of VA’s public health approach to preventing suicide,” said Dr. Keita Franklin, executive director for suicide prevention in the VA Office of Mental Health and Suicide Prevention.
The resources include online suicide prevention training, mobile apps that help with managing daily stressors, and supportive services for family members who are seeking care for former service members.
InTransition, for instance, is a free confidential program that offers coaching and specialized assistance over the phone for service members who need access to mental health care. Military OneSource provides military personnel and their families with round-the-clock support for a wide range of civilian necessities, such as tax preparation and spouse employment. PsychArmor Institute provides free online education to anyone who works with, lives with, or cares for service members, veterans, and their families. The MY3-Support Network app allows users to add the contact information of 3 people they would like to talk to when they are having thoughts of suicide.
The tool kit also offers links to programs for community members who want to learn how to help prevent suicides and support families who have gone through the trauma. The #BeThere Campaign teaches how simple acts can help save the life of a veteran in crisis. The S.A.V.E. Training video, designed in collaboration with PsychArmor Institute, teaches how to demonstrate support and compassion when talking with a veteran who may be at risk. Other links lead users to ways to help those whose loved one has committed suicide, such as the Tragedy Assistance Program for Survivors (TAPS).
Further expansion of suicide prevention activities for the former Guard and Reserve population is planned for fiscal year 2019.
The Veterans Crisis Line is available with free confidential support and crisis intervention 24 hours a day, 7 days a week, 365 days a year: Call 800.273.8255 (press 1), text to 838255, or chat online at VeteransCrisisLine.net/Chat. The tool kit is available at https://www.mentalhealth.va.gov/suicide_prevention/docs/toolkit_National_Guard_and_Reserve_members_cleared_2-21-19.pdf.
Mucus buildup precedes lung damage in children with CF
according to a cross-sectional cohort study.
It has been difficult for researchers to pinpoint the mechanisms that initiate lung disease in people with CF, because it is challenging to study young people with the disease and “CF animal models often fail to recapitulate aspects of human CF disease and yield disparate findings,” wrote Charles R. Esther Jr., MD, of the division of pediatric pulmonology at the University of North Carolina at Chapel Hill and his colleagues in Science Translational Medicine.
The researchers studied 46 clinically stable young children (aged 3.3 years, plus or minus 1.7 years) with CF and 16 age-matched controls who did not have CF, but had respiratory symptoms (aged 3.2 years, plus or minus 2.0 years) using chest CT imaging and bronchoalveolar lavage fluid. BALF samples in CF patients were collected over 62 study visits and subsequently cultured for detection and quantification of pathogens. The children with CF were enrolled in the Australian Respiratory Early Surveillance Team for Cystic Fibrosis (AREST CF) program.
“We analyzed the relationships between airway mucus, inflammation, and bacterial culture/microbiome,” the researchers wrote.
BALF total mucin levels were higher in CF samples versus non-CF controls. In addition, Dr. Esther and his colleagues found that these results were the same regardless of infection status and that increased densities of mucus flakes were also seen in samples from the CF patients. “Elevated total mucin concentrations and inflammatory markers were observed in children with CF despite a low incidence of pathogens identified by culture or molecular microbiology. This muco-inflammatory state also characterized our CF population with the earliest lung disease [without substantial CT-defined structural changes] in the setting of little or no pathogen infection,” they wrote.
Based on the findings, the investigators postulated that the airways of children with CF may show distinct defects in the clearance of recently created mucins, which could contribute to early CF lung disease.
A key limitation of the study was the prophylactic use of intermittent antibiotics. As a result, bacterial infection could have contributed to the development of early CF lung disease.
“Agents designed to remove permanent mucus covering airway surfaces of young children with CF appear to be rational strategies to prevent bacterial infection and disease progression,” they concluded.
The study was supported by the National Heart, Lung, and Blood Institute; the North Carolina Translational and Clinical Sciences Institute; the National Health and Medical Research Council; and the Cystic Fibrosis Foundation. Two coauthors reported financial affiliations with Parion Sciences.
SOURCE: Esther CR et al. Sci Transl Med. 2019 Apr 3. doi: 10.1126/scitranslmed.aav3488.
according to a cross-sectional cohort study.
It has been difficult for researchers to pinpoint the mechanisms that initiate lung disease in people with CF, because it is challenging to study young people with the disease and “CF animal models often fail to recapitulate aspects of human CF disease and yield disparate findings,” wrote Charles R. Esther Jr., MD, of the division of pediatric pulmonology at the University of North Carolina at Chapel Hill and his colleagues in Science Translational Medicine.
The researchers studied 46 clinically stable young children (aged 3.3 years, plus or minus 1.7 years) with CF and 16 age-matched controls who did not have CF, but had respiratory symptoms (aged 3.2 years, plus or minus 2.0 years) using chest CT imaging and bronchoalveolar lavage fluid. BALF samples in CF patients were collected over 62 study visits and subsequently cultured for detection and quantification of pathogens. The children with CF were enrolled in the Australian Respiratory Early Surveillance Team for Cystic Fibrosis (AREST CF) program.
“We analyzed the relationships between airway mucus, inflammation, and bacterial culture/microbiome,” the researchers wrote.
BALF total mucin levels were higher in CF samples versus non-CF controls. In addition, Dr. Esther and his colleagues found that these results were the same regardless of infection status and that increased densities of mucus flakes were also seen in samples from the CF patients. “Elevated total mucin concentrations and inflammatory markers were observed in children with CF despite a low incidence of pathogens identified by culture or molecular microbiology. This muco-inflammatory state also characterized our CF population with the earliest lung disease [without substantial CT-defined structural changes] in the setting of little or no pathogen infection,” they wrote.
Based on the findings, the investigators postulated that the airways of children with CF may show distinct defects in the clearance of recently created mucins, which could contribute to early CF lung disease.
A key limitation of the study was the prophylactic use of intermittent antibiotics. As a result, bacterial infection could have contributed to the development of early CF lung disease.
“Agents designed to remove permanent mucus covering airway surfaces of young children with CF appear to be rational strategies to prevent bacterial infection and disease progression,” they concluded.
The study was supported by the National Heart, Lung, and Blood Institute; the North Carolina Translational and Clinical Sciences Institute; the National Health and Medical Research Council; and the Cystic Fibrosis Foundation. Two coauthors reported financial affiliations with Parion Sciences.
SOURCE: Esther CR et al. Sci Transl Med. 2019 Apr 3. doi: 10.1126/scitranslmed.aav3488.
according to a cross-sectional cohort study.
It has been difficult for researchers to pinpoint the mechanisms that initiate lung disease in people with CF, because it is challenging to study young people with the disease and “CF animal models often fail to recapitulate aspects of human CF disease and yield disparate findings,” wrote Charles R. Esther Jr., MD, of the division of pediatric pulmonology at the University of North Carolina at Chapel Hill and his colleagues in Science Translational Medicine.
The researchers studied 46 clinically stable young children (aged 3.3 years, plus or minus 1.7 years) with CF and 16 age-matched controls who did not have CF, but had respiratory symptoms (aged 3.2 years, plus or minus 2.0 years) using chest CT imaging and bronchoalveolar lavage fluid. BALF samples in CF patients were collected over 62 study visits and subsequently cultured for detection and quantification of pathogens. The children with CF were enrolled in the Australian Respiratory Early Surveillance Team for Cystic Fibrosis (AREST CF) program.
“We analyzed the relationships between airway mucus, inflammation, and bacterial culture/microbiome,” the researchers wrote.
BALF total mucin levels were higher in CF samples versus non-CF controls. In addition, Dr. Esther and his colleagues found that these results were the same regardless of infection status and that increased densities of mucus flakes were also seen in samples from the CF patients. “Elevated total mucin concentrations and inflammatory markers were observed in children with CF despite a low incidence of pathogens identified by culture or molecular microbiology. This muco-inflammatory state also characterized our CF population with the earliest lung disease [without substantial CT-defined structural changes] in the setting of little or no pathogen infection,” they wrote.
Based on the findings, the investigators postulated that the airways of children with CF may show distinct defects in the clearance of recently created mucins, which could contribute to early CF lung disease.
A key limitation of the study was the prophylactic use of intermittent antibiotics. As a result, bacterial infection could have contributed to the development of early CF lung disease.
“Agents designed to remove permanent mucus covering airway surfaces of young children with CF appear to be rational strategies to prevent bacterial infection and disease progression,” they concluded.
The study was supported by the National Heart, Lung, and Blood Institute; the North Carolina Translational and Clinical Sciences Institute; the National Health and Medical Research Council; and the Cystic Fibrosis Foundation. Two coauthors reported financial affiliations with Parion Sciences.
SOURCE: Esther CR et al. Sci Transl Med. 2019 Apr 3. doi: 10.1126/scitranslmed.aav3488.
FROM SCIENCE TRANSLATIONAL MEDICINE
CT scan honeycombing key to hypersensitivity pneumonitis prognosis
In patients with hypersensitivity pneumonitis, presence of radiologic honeycombing suggests a poor prognosis in line with what might be expected with idiopathic pulmonary fibrosis, results of a recent study suggest.
When radiologic honeycombing was present, event-free survival was uniformly poor, regardless of whether the patient had hypersensitivity pneumonitis (HP) or idiopathic pulmonary fibrosis (IPF). By contrast, HP patients with nonhoneycomb fibrosis had longer event-free survival than IPF patients with honeycomb features on CT, wrote researchers led by Margaret L. Salisbury, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
“Given the uniformly poor outcome among subjects with radiologic honeycombing, pursuit of invasive diagnostic tests directed at differentiating IPF from HP may be of limited value,” Dr. Salisbury and her coinvestigators wrote in Chest.
In the study, 117 patients with HP and 161 with IPF underwent high-resolution CT, results of which were evaluated by three thoracic radiologists. Patients with HP who had no fibrosis on CT had the best event-free median survival, or time to transplant or death, at greater than 14.73 years. For HP patients with nonhoneycomb fibrosis, that median survival was greater than 7.95 years, compared with just 5.20 years in IPF patients without honeycomb features.
Looking specifically at patients with honeycomb features, median event-free survival was poor for both HP and IPF patients, at 2.76 and 2.81 years, respectively.
The HP patients with no fibrosis had a significant improvement in percent predicted forced vital capacity over time, while fibrotic patients experienced significant declines, the investigators wrote. Thus, HP patients with nonhoneycomb fibrosis had forced vital capacity declines despite longer transplant-free survival.
“These results highlight the importance of making a correct diagnosis of HP versus IPF in patients with nonhoneycomb fibrosis, as well as the limited utility in differentiating HP from IPF among patients with radiologic honeycombing,” Dr. Salisbury and her coinvestigators concluded.
Dr. Salisbury reported grants from the National Institutes of Health during the study. Her coauthors reported disclosures related to the NIH, Bayer, Centocor, Gilead, Promedior, Ikaria, Genentech, Nycomed/Takeda, Pfizer, and others.
SOURCE: Salisbury ML et al. Chest. 2019 Apr;155(4):699-711.
This study provides “clearly defined” phenotypes that are practical and potentially important for stratification and prognosis in patients with hypersensitivity pneumonitis (HP), according to David A. Lynch, MB.
“They should be widely adopted,” Dr. Lynch wrote of the three HP CT phenotypes in an editorial.
The study adds further evidence on the significance of honeycombing in the clinical course of fibrotic HP versus that of idiopathic pulmonary fibrosis, he added. Symptom duration in the HP patients was similar regardless of nonfibrotic, fibrotic, or honeycomb patterns, and was not linked to survival time. With that in mind, classifying HP based on fibrosis and its pattern may be more useful in determining prognosis than traditional acute, subacute, or chronic classification
That said, the present study does not provide much information on what demographic or exposure factors were associated with three phenotypes.
“Further study of this question will be important,” Dr. Lynch wrote. “Additionally, it will be important to understand the histologic correlates of the CT phenotypes.”
Dr. Lynch is with the department of radiology at National Jewish Health in Denver. His remarks are taken from his editorial that appeared in Chest (2019;155[4]:655-6). Dr. Lynch reported disclosures related to Genentech, Boehringer Ingelheim, Veracyte, Boehringer Ingelheim, and the France Foundation.
This study provides “clearly defined” phenotypes that are practical and potentially important for stratification and prognosis in patients with hypersensitivity pneumonitis (HP), according to David A. Lynch, MB.
“They should be widely adopted,” Dr. Lynch wrote of the three HP CT phenotypes in an editorial.
The study adds further evidence on the significance of honeycombing in the clinical course of fibrotic HP versus that of idiopathic pulmonary fibrosis, he added. Symptom duration in the HP patients was similar regardless of nonfibrotic, fibrotic, or honeycomb patterns, and was not linked to survival time. With that in mind, classifying HP based on fibrosis and its pattern may be more useful in determining prognosis than traditional acute, subacute, or chronic classification
That said, the present study does not provide much information on what demographic or exposure factors were associated with three phenotypes.
“Further study of this question will be important,” Dr. Lynch wrote. “Additionally, it will be important to understand the histologic correlates of the CT phenotypes.”
Dr. Lynch is with the department of radiology at National Jewish Health in Denver. His remarks are taken from his editorial that appeared in Chest (2019;155[4]:655-6). Dr. Lynch reported disclosures related to Genentech, Boehringer Ingelheim, Veracyte, Boehringer Ingelheim, and the France Foundation.
This study provides “clearly defined” phenotypes that are practical and potentially important for stratification and prognosis in patients with hypersensitivity pneumonitis (HP), according to David A. Lynch, MB.
“They should be widely adopted,” Dr. Lynch wrote of the three HP CT phenotypes in an editorial.
The study adds further evidence on the significance of honeycombing in the clinical course of fibrotic HP versus that of idiopathic pulmonary fibrosis, he added. Symptom duration in the HP patients was similar regardless of nonfibrotic, fibrotic, or honeycomb patterns, and was not linked to survival time. With that in mind, classifying HP based on fibrosis and its pattern may be more useful in determining prognosis than traditional acute, subacute, or chronic classification
That said, the present study does not provide much information on what demographic or exposure factors were associated with three phenotypes.
“Further study of this question will be important,” Dr. Lynch wrote. “Additionally, it will be important to understand the histologic correlates of the CT phenotypes.”
Dr. Lynch is with the department of radiology at National Jewish Health in Denver. His remarks are taken from his editorial that appeared in Chest (2019;155[4]:655-6). Dr. Lynch reported disclosures related to Genentech, Boehringer Ingelheim, Veracyte, Boehringer Ingelheim, and the France Foundation.
In patients with hypersensitivity pneumonitis, presence of radiologic honeycombing suggests a poor prognosis in line with what might be expected with idiopathic pulmonary fibrosis, results of a recent study suggest.
When radiologic honeycombing was present, event-free survival was uniformly poor, regardless of whether the patient had hypersensitivity pneumonitis (HP) or idiopathic pulmonary fibrosis (IPF). By contrast, HP patients with nonhoneycomb fibrosis had longer event-free survival than IPF patients with honeycomb features on CT, wrote researchers led by Margaret L. Salisbury, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
“Given the uniformly poor outcome among subjects with radiologic honeycombing, pursuit of invasive diagnostic tests directed at differentiating IPF from HP may be of limited value,” Dr. Salisbury and her coinvestigators wrote in Chest.
In the study, 117 patients with HP and 161 with IPF underwent high-resolution CT, results of which were evaluated by three thoracic radiologists. Patients with HP who had no fibrosis on CT had the best event-free median survival, or time to transplant or death, at greater than 14.73 years. For HP patients with nonhoneycomb fibrosis, that median survival was greater than 7.95 years, compared with just 5.20 years in IPF patients without honeycomb features.
Looking specifically at patients with honeycomb features, median event-free survival was poor for both HP and IPF patients, at 2.76 and 2.81 years, respectively.
The HP patients with no fibrosis had a significant improvement in percent predicted forced vital capacity over time, while fibrotic patients experienced significant declines, the investigators wrote. Thus, HP patients with nonhoneycomb fibrosis had forced vital capacity declines despite longer transplant-free survival.
“These results highlight the importance of making a correct diagnosis of HP versus IPF in patients with nonhoneycomb fibrosis, as well as the limited utility in differentiating HP from IPF among patients with radiologic honeycombing,” Dr. Salisbury and her coinvestigators concluded.
Dr. Salisbury reported grants from the National Institutes of Health during the study. Her coauthors reported disclosures related to the NIH, Bayer, Centocor, Gilead, Promedior, Ikaria, Genentech, Nycomed/Takeda, Pfizer, and others.
SOURCE: Salisbury ML et al. Chest. 2019 Apr;155(4):699-711.
In patients with hypersensitivity pneumonitis, presence of radiologic honeycombing suggests a poor prognosis in line with what might be expected with idiopathic pulmonary fibrosis, results of a recent study suggest.
When radiologic honeycombing was present, event-free survival was uniformly poor, regardless of whether the patient had hypersensitivity pneumonitis (HP) or idiopathic pulmonary fibrosis (IPF). By contrast, HP patients with nonhoneycomb fibrosis had longer event-free survival than IPF patients with honeycomb features on CT, wrote researchers led by Margaret L. Salisbury, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
“Given the uniformly poor outcome among subjects with radiologic honeycombing, pursuit of invasive diagnostic tests directed at differentiating IPF from HP may be of limited value,” Dr. Salisbury and her coinvestigators wrote in Chest.
In the study, 117 patients with HP and 161 with IPF underwent high-resolution CT, results of which were evaluated by three thoracic radiologists. Patients with HP who had no fibrosis on CT had the best event-free median survival, or time to transplant or death, at greater than 14.73 years. For HP patients with nonhoneycomb fibrosis, that median survival was greater than 7.95 years, compared with just 5.20 years in IPF patients without honeycomb features.
Looking specifically at patients with honeycomb features, median event-free survival was poor for both HP and IPF patients, at 2.76 and 2.81 years, respectively.
The HP patients with no fibrosis had a significant improvement in percent predicted forced vital capacity over time, while fibrotic patients experienced significant declines, the investigators wrote. Thus, HP patients with nonhoneycomb fibrosis had forced vital capacity declines despite longer transplant-free survival.
“These results highlight the importance of making a correct diagnosis of HP versus IPF in patients with nonhoneycomb fibrosis, as well as the limited utility in differentiating HP from IPF among patients with radiologic honeycombing,” Dr. Salisbury and her coinvestigators concluded.
Dr. Salisbury reported grants from the National Institutes of Health during the study. Her coauthors reported disclosures related to the NIH, Bayer, Centocor, Gilead, Promedior, Ikaria, Genentech, Nycomed/Takeda, Pfizer, and others.
SOURCE: Salisbury ML et al. Chest. 2019 Apr;155(4):699-711.
FROM CHEST®