User login
Brain abscess with lung infection? Think Nocardia
ST. LOUIS – according to University of California, San Francisco, investigators.

Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
ST. LOUIS – according to University of California, San Francisco, investigators.
Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
ST. LOUIS – according to University of California, San Francisco, investigators.
Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
REPORTING FROM ANA 2019
Open Clinical Trials for Diabetes Mellitus Harm Reduction (FULL)
Providing access to clinical trials for native American, veteran, and active-duty military patients can be a challenge, but a significant number of trials are now recruiting from those populations. Many trials explicitly recruit patients from the US Department of Veterans
Affairs (VA), the military, and Indian Health Service. The VA Office of Research and Development alone sponsors more than 480 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of October 24, 2018; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on preventing diabetes mellitus or improving patient care. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials. gov.
Diabetes Prevention Program Outcomes Study (DPPOS)
The Diabetes Prevention Program (DPP) was a multicenter trial examining the ability of an intensive lifestyle or metformin to prevent or delay the development of diabetes in a high risk population due to the presence of impaired glucose tolerance (IGT). The DPP has ended early demonstrating that lifestyle reduced diabetes onset by 58% and metformin reduced diabetes onset by 31%.
ID: NCT00038727
Sponsor: National Institute of Diabetes and Digestive and Kidney Diseases
Location: George Washington University, Rockville, Maryland
Efforts to Improve Diabetes Control
The primary objectives of this study are: (1) test the longterm effectiveness of a peer mentor model on improving glucose control, blood pressure, LDL levels, diabetes mellitus quality of life, and depression scores in a mixed race population of poorly controlled diabetic veterans; (2) test the effectiveness of using former peer mentees as peer mentors as a means of creating a self-sustaining program; and (3) test the effects of becoming a mentor on those who were originally mentees given a growing literature that being a mentor is good for your health. Secondary objectives include: (1) in those randomized to being a mentee, explore mentor characteristics associated with improved HbA1c.
ID: NCT01651117
Sponsor: VA Office of Research and Development
Location: Corporal Michael J. Crescenz VA Medical Center, Philadelphia, Pennsylvania
A Patient-Centered Strategy for Improving Diabetes Prevention in Urban American Indians
The goal of the proposed research is to identify effective patient-centered strategies to prevent diabetes in high-risk populations in real world settings. The investigators will accomplish this by conducting a randomized controlled trial comparing an enhanced Diabetes Prevention Program addressing psychosocial stressors to a standard version in a high-risk population of urban American Indian
and Alaskan Native peoples within a primary care setting.
ID: NCT02266576
Sponsor: Stanford University
Locations: Timpany Center of San Jose State University, California; Stanford University School of Medicine, California
Physical Activity and Participation
Physical activity is the cornerstone of good diabetes management, and yet effective physical activity intervention is not available. The investigators developed a lifestyle intervention based on individual’s home activity patterns. The goal of the study is to test the efficacy of this intervention among veterans with diabetes in a randomized-controlled trial. In addition to physical activity, the investigators will also assess if the intervention will improve social participation among veterans.
ID: NCT02268916
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Caring Others Increasing EngageMent in PACT (CO-IMPACT)
This trial will compare two methods of increasing engagement in care and success in diabetes management, among patients with diabetes with high-risk features, who also have family members involved in their care.
ID: NCT02328326
Sponsor: VA Office of Research and Development
Locations: VA Ann Arbor Healthcare System, Michigan;VA Pittsburgh Healthcare System, Pennsylvania
STEP UP to Avert Amputation in Diabetes (STEP UP)
This study will evaluate a comprehensive tailored behavioral intervention aimed to improve foot self-care and self-monitoring (combined with dermal thermometry) to prevent recurrent ulcers in Veterans at highest risk of amputation. This intervention may be a novel strategy for improving self-care and early detection of foot abnormalities in this at-risk population using psychological theories to target multiple health behaviors simultaneously. This could be an efficient and cost-effective approach to improve diabetes-related foot health behavior, and other risk factors in patients who are vulnerable to devastating consequences related to amputation.
ID: NCT02356848
Sponsor: VA Office of Research and Development
Location: Manhattan Campus of the VA NY Harbor Healthcare System
Physical Activity Behavior Change for Older Adults After Dysvascular Amputation (PABC)
This pilot study will use mobile-health technology to deliver an intervention designed for lasting physical activity behavior change. The study will assess the feasibility of using the Physical Activity Behavior Change (PABC) intervention for Veterans with lower limb amputation. This intervention will be delivered using wrist-worn wearable activity sensors and a home-based tablet computer to allow real-time physical activity feedback and video interface between the participants and the therapist.
ID: NCT02738086
Sponsor: VA Office of Research and Development
Location: Rocky Mountain Regional VA Medical Center, Aurora, Colorado
ForgIng New Paths to Prevent DIabeTes (FINDIT)
This study will evaluate the effects of screening for type 2 diabetes mellitus (T2DM) and brief counseling about screening test results on weight and key health behaviors among veterans with risk factors for T2DM. Study participants will be randomly assigned to 1 of 2 study groups: (1) Blood Test Group; or (2) Brochure Group. Participants in the Blood Test Group will complete a blood test called hemoglobin A1c (HbA1c) which measures average blood sugar levels. Participants will receive brief counseling about the results from their primary care provider or someone authorized to speak on their behalf. Participants randomly selected for the Brochure Group will review a handout from the VA National Center for Health Promotion and Disease Prevention (NCP) on recommended screening tests and immunizations. All participants will be asked to complete a survey prior to study group assignment, immediately after a Primary Care appointment, 3 months after enrollment, and 12 months after enrollment.
ID: NCT02747108
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Using Technology to Share Fitness Goals and Results to Improve Diabetes Outcomes
The investigators will recruit DoD beneficiaries, aged 18 years or older and diagnosed with type 2 diabetes. Patients will be randomized into one of two groups. Group 1 will use a fitness tracker but will not be able to see other participants data and group 2 will use a fitness tracker and will be able to see other members daily and weekly results. Outcome measures will be assessed at baseline, 3 months and 6 months to include hemoglobin A1c, weight, body mass index, blood pressure, and number of hours and days fitness tracker is used. The goal is to see if the group randomized into an online community will have improved activity and outcome measurements compared with those who use the pedometer alone.
ID: NCT02761018
Sponsor: Mike O’Callaghan Military Hospital
Location: Mike O’Callaghan Federal Medical Center, Nellis Air Force Base, Nevada
Healthy Living Partnerships to Prevent Diabetes in Veterans Pilot Study (HELP Vets)
Diabetes and obesity are both major public health concerns and the prevalence of diabetes is even higher in the patient population of the VA. This planning project is designed to adapt a successful weight-loss program for delivery through an existing outpatient clinic to reach local veterans at risk for developing diabetes. The information gathered as a part of this project will be used to plan a larger trial designed to improve the health of veterans by offering them a diabetes prevention program through their usual source of healthcare.
ID: NCT02835495
Sponsor: Wake Forest University Health Sciences
Location: Wake Forest School of Medicine
Mindful Stress Reduction in Diabetes Self-Management Education for Veterans (MindSTRIDE)
The purpose of this study is to see if adding Mindfulness training to diabetes education reduces feelings of stress and makes it easier to adhere to healthy behaviors that improve diabetes outcomes (such as hemoglobin A1c).
ID: NCT02928952
Sponsor: VA Office of Research and Development
Location: VA Pittsburgh Healthcare System University Drive Division, Pittsburgh, Pennsylvania
Improving Diabetes Care Through Effective Personalized Patient Portal Interactions
Patient-facing eHealth technologies are those that connect patients and the healthcare system, and include online patient portals. Although many organizations are adopting patient portals, there is limited understanding of how the different portal features help improve health outcomes. This study is designed to develop and test an intervention to improve adoption and use of patient portal features for diabetes management.
ID: NCT02953262
Sponsor: VA Office of Research and Development
Locations: Edith Nourse Rogers Memorial Veterans Hospital, Bedford, Massachusetts; VA Boston Healthcare System Jamaica Plain Campus, Massachusetts.
Home-Based Kidney Care in Native American’s of New Mexico (HBKC)
People reach end stage renal disease (ESRD) due to progressive chronic kidney disease (CKD), which is associated with increased risk for heart disease and death. The burden of chronic kidney disease is increased among minority populations compared to Caucasians. New Mexico American Indians are experiencing an epidemic of chronic kidney disease due primarily to the high rates of obesity and diabetes. The present study entitled Home-Based Kidney Care is designed to delay / reduce rates of ESRD by early interventions in CKD. Investigators propose to assess the safety and efficacy of conducting a full-scale study to determine if home based care delivered
by a collaborative team composed of community health workers, the Albuquerque Area Indian Health Board and University of New Mexico faculty will decrease the risk for the development and the progression of CKD.
ID: NCT03179085
Sponsor: University of New Mexico
Location: University of New Mexico, Albuquerque
INcreasing Veteran EngagemeNT to Prevent Diabetes (INVENT)
This study will evaluate a VA MyHealtheVet Secure Messaging intervention that uses different intervention messaging strategies designed to increase engagement in behaviors to prevent type 2 diabetes (T2DM). After completing a baseline survey, participants will be randomly assigned to receive different novel presentations of information about ways to prevent T2DM through both secure messaging and US mail. The investigators will test the 5 presentations that each: (1) represent an innovative approach from behavioral economics or health psychology with great promise to increase engagement in behaviors to prevent T2DM among patients with prediabetes; and (2) have not been tested in this setting.
ID: NCT03403231
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Self-efficacy, Beliefs and Adherence—Pilot and Feasibility Trial of a Pharmacist-led Intervention
This study uses an intervention mixed methods design. The overall purpose is to improve medication adherence and assess the clinical impact on diabetes outcomes among patients with uncontrolled diabetes. We will examine if usual care combined with a clinic-based health literacy/psychosocial support intervention improves medication adherence compared to usual care alone. A randomized controlled trial will be conducted at William S. Middleton Memorial Veterans Hospital in Madison, targeting individuals with
uncontrolled diabetes. The patient-centered health literacy intervention will focus on enhancing patients’ self-efficacy and addressing patients’ negative beliefs in medicine and illness.
ID: NCT03406923
Sponsor: University of Wisconsin, Madison
Location: William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin
Practical Telemedicine to Improve Control and Engagement for Veterans With Clinic-Refractory Diabetes Mellitus (PRACTICE-DM)
Diabetes generates significant morbidity, mortality, and costs within the Veterans Health Administration (VHA). Veterans with persistently poor diabetes control despite clinic-based care are among the highest-risk diabetes patients in VHA, and contribute disproportionately to VHA’s massive burden of diabetes complications and costs. VHA critically needs effective, practical management alternatives for veterans whose diabetes does not respond to clinic-based management. The proposed study will address this need by leveraging VHA’s unique Home Telehealth capacity to deliver comprehensive telemedicine-based management for veterans with persistently poor diabetes control despite clinic-based care. Because this intensive intervention is delivered using only existing Home Telehealth workforce, infrastructure, and technical resources—which are ubiquitous at VHA centers nationwide—it could represent an effective, practical approach to improving outcomes in veterans with PPDM, potentially translating to a substantial reduction in VHA’s diabetes burden.
ID: NCT03520413
Sponsor: VA Office of Research and Development
Locations: Durham VA Medical Center, North Carolina; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Cooking for Health
Type 2 diabetes is a leading cause of morbidity and mortality among American Indians in the US. Although healthy diet is a key component of diabetes management programs, many American Indians face contextual barriers to adopting a healthy diet including: difficulty budgeting for food on low-incomes, low literacy and numeracy when purchasing food, and limited cooking skills. The proposed project will develop, implement, and evaluate a culturally-targeted healthy foods budgeting, purchasing, and cooking skills intervention aimed at improving the cardio-metabolic health of American Indians with type 2 diabetes who live in rural areas.
ID: NCT03699709
Sponsor: University of Washington
Location: Missouri Breaks Industries Research, Eagle Butte, South Dakota
Providing access to clinical trials for native American, veteran, and active-duty military patients can be a challenge, but a significant number of trials are now recruiting from those populations. Many trials explicitly recruit patients from the US Department of Veterans
Affairs (VA), the military, and Indian Health Service. The VA Office of Research and Development alone sponsors more than 480 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of October 24, 2018; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on preventing diabetes mellitus or improving patient care. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials. gov.
Diabetes Prevention Program Outcomes Study (DPPOS)
The Diabetes Prevention Program (DPP) was a multicenter trial examining the ability of an intensive lifestyle or metformin to prevent or delay the development of diabetes in a high risk population due to the presence of impaired glucose tolerance (IGT). The DPP has ended early demonstrating that lifestyle reduced diabetes onset by 58% and metformin reduced diabetes onset by 31%.
ID: NCT00038727
Sponsor: National Institute of Diabetes and Digestive and Kidney Diseases
Location: George Washington University, Rockville, Maryland
Efforts to Improve Diabetes Control
The primary objectives of this study are: (1) test the longterm effectiveness of a peer mentor model on improving glucose control, blood pressure, LDL levels, diabetes mellitus quality of life, and depression scores in a mixed race population of poorly controlled diabetic veterans; (2) test the effectiveness of using former peer mentees as peer mentors as a means of creating a self-sustaining program; and (3) test the effects of becoming a mentor on those who were originally mentees given a growing literature that being a mentor is good for your health. Secondary objectives include: (1) in those randomized to being a mentee, explore mentor characteristics associated with improved HbA1c.
ID: NCT01651117
Sponsor: VA Office of Research and Development
Location: Corporal Michael J. Crescenz VA Medical Center, Philadelphia, Pennsylvania
A Patient-Centered Strategy for Improving Diabetes Prevention in Urban American Indians
The goal of the proposed research is to identify effective patient-centered strategies to prevent diabetes in high-risk populations in real world settings. The investigators will accomplish this by conducting a randomized controlled trial comparing an enhanced Diabetes Prevention Program addressing psychosocial stressors to a standard version in a high-risk population of urban American Indian
and Alaskan Native peoples within a primary care setting.
ID: NCT02266576
Sponsor: Stanford University
Locations: Timpany Center of San Jose State University, California; Stanford University School of Medicine, California
Physical Activity and Participation
Physical activity is the cornerstone of good diabetes management, and yet effective physical activity intervention is not available. The investigators developed a lifestyle intervention based on individual’s home activity patterns. The goal of the study is to test the efficacy of this intervention among veterans with diabetes in a randomized-controlled trial. In addition to physical activity, the investigators will also assess if the intervention will improve social participation among veterans.
ID: NCT02268916
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Caring Others Increasing EngageMent in PACT (CO-IMPACT)
This trial will compare two methods of increasing engagement in care and success in diabetes management, among patients with diabetes with high-risk features, who also have family members involved in their care.
ID: NCT02328326
Sponsor: VA Office of Research and Development
Locations: VA Ann Arbor Healthcare System, Michigan;VA Pittsburgh Healthcare System, Pennsylvania
STEP UP to Avert Amputation in Diabetes (STEP UP)
This study will evaluate a comprehensive tailored behavioral intervention aimed to improve foot self-care and self-monitoring (combined with dermal thermometry) to prevent recurrent ulcers in Veterans at highest risk of amputation. This intervention may be a novel strategy for improving self-care and early detection of foot abnormalities in this at-risk population using psychological theories to target multiple health behaviors simultaneously. This could be an efficient and cost-effective approach to improve diabetes-related foot health behavior, and other risk factors in patients who are vulnerable to devastating consequences related to amputation.
ID: NCT02356848
Sponsor: VA Office of Research and Development
Location: Manhattan Campus of the VA NY Harbor Healthcare System
Physical Activity Behavior Change for Older Adults After Dysvascular Amputation (PABC)
This pilot study will use mobile-health technology to deliver an intervention designed for lasting physical activity behavior change. The study will assess the feasibility of using the Physical Activity Behavior Change (PABC) intervention for Veterans with lower limb amputation. This intervention will be delivered using wrist-worn wearable activity sensors and a home-based tablet computer to allow real-time physical activity feedback and video interface between the participants and the therapist.
ID: NCT02738086
Sponsor: VA Office of Research and Development
Location: Rocky Mountain Regional VA Medical Center, Aurora, Colorado
ForgIng New Paths to Prevent DIabeTes (FINDIT)
This study will evaluate the effects of screening for type 2 diabetes mellitus (T2DM) and brief counseling about screening test results on weight and key health behaviors among veterans with risk factors for T2DM. Study participants will be randomly assigned to 1 of 2 study groups: (1) Blood Test Group; or (2) Brochure Group. Participants in the Blood Test Group will complete a blood test called hemoglobin A1c (HbA1c) which measures average blood sugar levels. Participants will receive brief counseling about the results from their primary care provider or someone authorized to speak on their behalf. Participants randomly selected for the Brochure Group will review a handout from the VA National Center for Health Promotion and Disease Prevention (NCP) on recommended screening tests and immunizations. All participants will be asked to complete a survey prior to study group assignment, immediately after a Primary Care appointment, 3 months after enrollment, and 12 months after enrollment.
ID: NCT02747108
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Using Technology to Share Fitness Goals and Results to Improve Diabetes Outcomes
The investigators will recruit DoD beneficiaries, aged 18 years or older and diagnosed with type 2 diabetes. Patients will be randomized into one of two groups. Group 1 will use a fitness tracker but will not be able to see other participants data and group 2 will use a fitness tracker and will be able to see other members daily and weekly results. Outcome measures will be assessed at baseline, 3 months and 6 months to include hemoglobin A1c, weight, body mass index, blood pressure, and number of hours and days fitness tracker is used. The goal is to see if the group randomized into an online community will have improved activity and outcome measurements compared with those who use the pedometer alone.
ID: NCT02761018
Sponsor: Mike O’Callaghan Military Hospital
Location: Mike O’Callaghan Federal Medical Center, Nellis Air Force Base, Nevada
Healthy Living Partnerships to Prevent Diabetes in Veterans Pilot Study (HELP Vets)
Diabetes and obesity are both major public health concerns and the prevalence of diabetes is even higher in the patient population of the VA. This planning project is designed to adapt a successful weight-loss program for delivery through an existing outpatient clinic to reach local veterans at risk for developing diabetes. The information gathered as a part of this project will be used to plan a larger trial designed to improve the health of veterans by offering them a diabetes prevention program through their usual source of healthcare.
ID: NCT02835495
Sponsor: Wake Forest University Health Sciences
Location: Wake Forest School of Medicine
Mindful Stress Reduction in Diabetes Self-Management Education for Veterans (MindSTRIDE)
The purpose of this study is to see if adding Mindfulness training to diabetes education reduces feelings of stress and makes it easier to adhere to healthy behaviors that improve diabetes outcomes (such as hemoglobin A1c).
ID: NCT02928952
Sponsor: VA Office of Research and Development
Location: VA Pittsburgh Healthcare System University Drive Division, Pittsburgh, Pennsylvania
Improving Diabetes Care Through Effective Personalized Patient Portal Interactions
Patient-facing eHealth technologies are those that connect patients and the healthcare system, and include online patient portals. Although many organizations are adopting patient portals, there is limited understanding of how the different portal features help improve health outcomes. This study is designed to develop and test an intervention to improve adoption and use of patient portal features for diabetes management.
ID: NCT02953262
Sponsor: VA Office of Research and Development
Locations: Edith Nourse Rogers Memorial Veterans Hospital, Bedford, Massachusetts; VA Boston Healthcare System Jamaica Plain Campus, Massachusetts.
Home-Based Kidney Care in Native American’s of New Mexico (HBKC)
People reach end stage renal disease (ESRD) due to progressive chronic kidney disease (CKD), which is associated with increased risk for heart disease and death. The burden of chronic kidney disease is increased among minority populations compared to Caucasians. New Mexico American Indians are experiencing an epidemic of chronic kidney disease due primarily to the high rates of obesity and diabetes. The present study entitled Home-Based Kidney Care is designed to delay / reduce rates of ESRD by early interventions in CKD. Investigators propose to assess the safety and efficacy of conducting a full-scale study to determine if home based care delivered
by a collaborative team composed of community health workers, the Albuquerque Area Indian Health Board and University of New Mexico faculty will decrease the risk for the development and the progression of CKD.
ID: NCT03179085
Sponsor: University of New Mexico
Location: University of New Mexico, Albuquerque
INcreasing Veteran EngagemeNT to Prevent Diabetes (INVENT)
This study will evaluate a VA MyHealtheVet Secure Messaging intervention that uses different intervention messaging strategies designed to increase engagement in behaviors to prevent type 2 diabetes (T2DM). After completing a baseline survey, participants will be randomly assigned to receive different novel presentations of information about ways to prevent T2DM through both secure messaging and US mail. The investigators will test the 5 presentations that each: (1) represent an innovative approach from behavioral economics or health psychology with great promise to increase engagement in behaviors to prevent T2DM among patients with prediabetes; and (2) have not been tested in this setting.
ID: NCT03403231
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Self-efficacy, Beliefs and Adherence—Pilot and Feasibility Trial of a Pharmacist-led Intervention
This study uses an intervention mixed methods design. The overall purpose is to improve medication adherence and assess the clinical impact on diabetes outcomes among patients with uncontrolled diabetes. We will examine if usual care combined with a clinic-based health literacy/psychosocial support intervention improves medication adherence compared to usual care alone. A randomized controlled trial will be conducted at William S. Middleton Memorial Veterans Hospital in Madison, targeting individuals with
uncontrolled diabetes. The patient-centered health literacy intervention will focus on enhancing patients’ self-efficacy and addressing patients’ negative beliefs in medicine and illness.
ID: NCT03406923
Sponsor: University of Wisconsin, Madison
Location: William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin
Practical Telemedicine to Improve Control and Engagement for Veterans With Clinic-Refractory Diabetes Mellitus (PRACTICE-DM)
Diabetes generates significant morbidity, mortality, and costs within the Veterans Health Administration (VHA). Veterans with persistently poor diabetes control despite clinic-based care are among the highest-risk diabetes patients in VHA, and contribute disproportionately to VHA’s massive burden of diabetes complications and costs. VHA critically needs effective, practical management alternatives for veterans whose diabetes does not respond to clinic-based management. The proposed study will address this need by leveraging VHA’s unique Home Telehealth capacity to deliver comprehensive telemedicine-based management for veterans with persistently poor diabetes control despite clinic-based care. Because this intensive intervention is delivered using only existing Home Telehealth workforce, infrastructure, and technical resources—which are ubiquitous at VHA centers nationwide—it could represent an effective, practical approach to improving outcomes in veterans with PPDM, potentially translating to a substantial reduction in VHA’s diabetes burden.
ID: NCT03520413
Sponsor: VA Office of Research and Development
Locations: Durham VA Medical Center, North Carolina; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Cooking for Health
Type 2 diabetes is a leading cause of morbidity and mortality among American Indians in the US. Although healthy diet is a key component of diabetes management programs, many American Indians face contextual barriers to adopting a healthy diet including: difficulty budgeting for food on low-incomes, low literacy and numeracy when purchasing food, and limited cooking skills. The proposed project will develop, implement, and evaluate a culturally-targeted healthy foods budgeting, purchasing, and cooking skills intervention aimed at improving the cardio-metabolic health of American Indians with type 2 diabetes who live in rural areas.
ID: NCT03699709
Sponsor: University of Washington
Location: Missouri Breaks Industries Research, Eagle Butte, South Dakota
Providing access to clinical trials for native American, veteran, and active-duty military patients can be a challenge, but a significant number of trials are now recruiting from those populations. Many trials explicitly recruit patients from the US Department of Veterans
Affairs (VA), the military, and Indian Health Service. The VA Office of Research and Development alone sponsors more than 480 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of October 24, 2018; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on preventing diabetes mellitus or improving patient care. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials. gov.
Diabetes Prevention Program Outcomes Study (DPPOS)
The Diabetes Prevention Program (DPP) was a multicenter trial examining the ability of an intensive lifestyle or metformin to prevent or delay the development of diabetes in a high risk population due to the presence of impaired glucose tolerance (IGT). The DPP has ended early demonstrating that lifestyle reduced diabetes onset by 58% and metformin reduced diabetes onset by 31%.
ID: NCT00038727
Sponsor: National Institute of Diabetes and Digestive and Kidney Diseases
Location: George Washington University, Rockville, Maryland
Efforts to Improve Diabetes Control
The primary objectives of this study are: (1) test the longterm effectiveness of a peer mentor model on improving glucose control, blood pressure, LDL levels, diabetes mellitus quality of life, and depression scores in a mixed race population of poorly controlled diabetic veterans; (2) test the effectiveness of using former peer mentees as peer mentors as a means of creating a self-sustaining program; and (3) test the effects of becoming a mentor on those who were originally mentees given a growing literature that being a mentor is good for your health. Secondary objectives include: (1) in those randomized to being a mentee, explore mentor characteristics associated with improved HbA1c.
ID: NCT01651117
Sponsor: VA Office of Research and Development
Location: Corporal Michael J. Crescenz VA Medical Center, Philadelphia, Pennsylvania
A Patient-Centered Strategy for Improving Diabetes Prevention in Urban American Indians
The goal of the proposed research is to identify effective patient-centered strategies to prevent diabetes in high-risk populations in real world settings. The investigators will accomplish this by conducting a randomized controlled trial comparing an enhanced Diabetes Prevention Program addressing psychosocial stressors to a standard version in a high-risk population of urban American Indian
and Alaskan Native peoples within a primary care setting.
ID: NCT02266576
Sponsor: Stanford University
Locations: Timpany Center of San Jose State University, California; Stanford University School of Medicine, California
Physical Activity and Participation
Physical activity is the cornerstone of good diabetes management, and yet effective physical activity intervention is not available. The investigators developed a lifestyle intervention based on individual’s home activity patterns. The goal of the study is to test the efficacy of this intervention among veterans with diabetes in a randomized-controlled trial. In addition to physical activity, the investigators will also assess if the intervention will improve social participation among veterans.
ID: NCT02268916
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Caring Others Increasing EngageMent in PACT (CO-IMPACT)
This trial will compare two methods of increasing engagement in care and success in diabetes management, among patients with diabetes with high-risk features, who also have family members involved in their care.
ID: NCT02328326
Sponsor: VA Office of Research and Development
Locations: VA Ann Arbor Healthcare System, Michigan;VA Pittsburgh Healthcare System, Pennsylvania
STEP UP to Avert Amputation in Diabetes (STEP UP)
This study will evaluate a comprehensive tailored behavioral intervention aimed to improve foot self-care and self-monitoring (combined with dermal thermometry) to prevent recurrent ulcers in Veterans at highest risk of amputation. This intervention may be a novel strategy for improving self-care and early detection of foot abnormalities in this at-risk population using psychological theories to target multiple health behaviors simultaneously. This could be an efficient and cost-effective approach to improve diabetes-related foot health behavior, and other risk factors in patients who are vulnerable to devastating consequences related to amputation.
ID: NCT02356848
Sponsor: VA Office of Research and Development
Location: Manhattan Campus of the VA NY Harbor Healthcare System
Physical Activity Behavior Change for Older Adults After Dysvascular Amputation (PABC)
This pilot study will use mobile-health technology to deliver an intervention designed for lasting physical activity behavior change. The study will assess the feasibility of using the Physical Activity Behavior Change (PABC) intervention for Veterans with lower limb amputation. This intervention will be delivered using wrist-worn wearable activity sensors and a home-based tablet computer to allow real-time physical activity feedback and video interface between the participants and the therapist.
ID: NCT02738086
Sponsor: VA Office of Research and Development
Location: Rocky Mountain Regional VA Medical Center, Aurora, Colorado
ForgIng New Paths to Prevent DIabeTes (FINDIT)
This study will evaluate the effects of screening for type 2 diabetes mellitus (T2DM) and brief counseling about screening test results on weight and key health behaviors among veterans with risk factors for T2DM. Study participants will be randomly assigned to 1 of 2 study groups: (1) Blood Test Group; or (2) Brochure Group. Participants in the Blood Test Group will complete a blood test called hemoglobin A1c (HbA1c) which measures average blood sugar levels. Participants will receive brief counseling about the results from their primary care provider or someone authorized to speak on their behalf. Participants randomly selected for the Brochure Group will review a handout from the VA National Center for Health Promotion and Disease Prevention (NCP) on recommended screening tests and immunizations. All participants will be asked to complete a survey prior to study group assignment, immediately after a Primary Care appointment, 3 months after enrollment, and 12 months after enrollment.
ID: NCT02747108
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Using Technology to Share Fitness Goals and Results to Improve Diabetes Outcomes
The investigators will recruit DoD beneficiaries, aged 18 years or older and diagnosed with type 2 diabetes. Patients will be randomized into one of two groups. Group 1 will use a fitness tracker but will not be able to see other participants data and group 2 will use a fitness tracker and will be able to see other members daily and weekly results. Outcome measures will be assessed at baseline, 3 months and 6 months to include hemoglobin A1c, weight, body mass index, blood pressure, and number of hours and days fitness tracker is used. The goal is to see if the group randomized into an online community will have improved activity and outcome measurements compared with those who use the pedometer alone.
ID: NCT02761018
Sponsor: Mike O’Callaghan Military Hospital
Location: Mike O’Callaghan Federal Medical Center, Nellis Air Force Base, Nevada
Healthy Living Partnerships to Prevent Diabetes in Veterans Pilot Study (HELP Vets)
Diabetes and obesity are both major public health concerns and the prevalence of diabetes is even higher in the patient population of the VA. This planning project is designed to adapt a successful weight-loss program for delivery through an existing outpatient clinic to reach local veterans at risk for developing diabetes. The information gathered as a part of this project will be used to plan a larger trial designed to improve the health of veterans by offering them a diabetes prevention program through their usual source of healthcare.
ID: NCT02835495
Sponsor: Wake Forest University Health Sciences
Location: Wake Forest School of Medicine
Mindful Stress Reduction in Diabetes Self-Management Education for Veterans (MindSTRIDE)
The purpose of this study is to see if adding Mindfulness training to diabetes education reduces feelings of stress and makes it easier to adhere to healthy behaviors that improve diabetes outcomes (such as hemoglobin A1c).
ID: NCT02928952
Sponsor: VA Office of Research and Development
Location: VA Pittsburgh Healthcare System University Drive Division, Pittsburgh, Pennsylvania
Improving Diabetes Care Through Effective Personalized Patient Portal Interactions
Patient-facing eHealth technologies are those that connect patients and the healthcare system, and include online patient portals. Although many organizations are adopting patient portals, there is limited understanding of how the different portal features help improve health outcomes. This study is designed to develop and test an intervention to improve adoption and use of patient portal features for diabetes management.
ID: NCT02953262
Sponsor: VA Office of Research and Development
Locations: Edith Nourse Rogers Memorial Veterans Hospital, Bedford, Massachusetts; VA Boston Healthcare System Jamaica Plain Campus, Massachusetts.
Home-Based Kidney Care in Native American’s of New Mexico (HBKC)
People reach end stage renal disease (ESRD) due to progressive chronic kidney disease (CKD), which is associated with increased risk for heart disease and death. The burden of chronic kidney disease is increased among minority populations compared to Caucasians. New Mexico American Indians are experiencing an epidemic of chronic kidney disease due primarily to the high rates of obesity and diabetes. The present study entitled Home-Based Kidney Care is designed to delay / reduce rates of ESRD by early interventions in CKD. Investigators propose to assess the safety and efficacy of conducting a full-scale study to determine if home based care delivered
by a collaborative team composed of community health workers, the Albuquerque Area Indian Health Board and University of New Mexico faculty will decrease the risk for the development and the progression of CKD.
ID: NCT03179085
Sponsor: University of New Mexico
Location: University of New Mexico, Albuquerque
INcreasing Veteran EngagemeNT to Prevent Diabetes (INVENT)
This study will evaluate a VA MyHealtheVet Secure Messaging intervention that uses different intervention messaging strategies designed to increase engagement in behaviors to prevent type 2 diabetes (T2DM). After completing a baseline survey, participants will be randomly assigned to receive different novel presentations of information about ways to prevent T2DM through both secure messaging and US mail. The investigators will test the 5 presentations that each: (1) represent an innovative approach from behavioral economics or health psychology with great promise to increase engagement in behaviors to prevent T2DM among patients with prediabetes; and (2) have not been tested in this setting.
ID: NCT03403231
Sponsor: VA Office of Research and Development
Location: VA Ann Arbor Healthcare System, Michigan
Self-efficacy, Beliefs and Adherence—Pilot and Feasibility Trial of a Pharmacist-led Intervention
This study uses an intervention mixed methods design. The overall purpose is to improve medication adherence and assess the clinical impact on diabetes outcomes among patients with uncontrolled diabetes. We will examine if usual care combined with a clinic-based health literacy/psychosocial support intervention improves medication adherence compared to usual care alone. A randomized controlled trial will be conducted at William S. Middleton Memorial Veterans Hospital in Madison, targeting individuals with
uncontrolled diabetes. The patient-centered health literacy intervention will focus on enhancing patients’ self-efficacy and addressing patients’ negative beliefs in medicine and illness.
ID: NCT03406923
Sponsor: University of Wisconsin, Madison
Location: William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin
Practical Telemedicine to Improve Control and Engagement for Veterans With Clinic-Refractory Diabetes Mellitus (PRACTICE-DM)
Diabetes generates significant morbidity, mortality, and costs within the Veterans Health Administration (VHA). Veterans with persistently poor diabetes control despite clinic-based care are among the highest-risk diabetes patients in VHA, and contribute disproportionately to VHA’s massive burden of diabetes complications and costs. VHA critically needs effective, practical management alternatives for veterans whose diabetes does not respond to clinic-based management. The proposed study will address this need by leveraging VHA’s unique Home Telehealth capacity to deliver comprehensive telemedicine-based management for veterans with persistently poor diabetes control despite clinic-based care. Because this intensive intervention is delivered using only existing Home Telehealth workforce, infrastructure, and technical resources—which are ubiquitous at VHA centers nationwide—it could represent an effective, practical approach to improving outcomes in veterans with PPDM, potentially translating to a substantial reduction in VHA’s diabetes burden.
ID: NCT03520413
Sponsor: VA Office of Research and Development
Locations: Durham VA Medical Center, North Carolina; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Cooking for Health
Type 2 diabetes is a leading cause of morbidity and mortality among American Indians in the US. Although healthy diet is a key component of diabetes management programs, many American Indians face contextual barriers to adopting a healthy diet including: difficulty budgeting for food on low-incomes, low literacy and numeracy when purchasing food, and limited cooking skills. The proposed project will develop, implement, and evaluate a culturally-targeted healthy foods budgeting, purchasing, and cooking skills intervention aimed at improving the cardio-metabolic health of American Indians with type 2 diabetes who live in rural areas.
ID: NCT03699709
Sponsor: University of Washington
Location: Missouri Breaks Industries Research, Eagle Butte, South Dakota
Triple-drug therapy proves effective in CF patients with most common mutation
Reinforcing previous findings, a new study has determined that the next-generation corrector elexacaftor, in combination with tezacaftor and ivacaftor, can effectively treat patients with Phe508del-minimal function genotypes who did not respond to previous cystic fibrosis transmembrane conductance regulator (CFTR) modulator regimens.
“These results provide evidence that , thus addressing the underlying cause of disease in the large majority of patients,” wrote Peter G. Middleton, PhD, of the University of Sydney (Australia) and his coauthors. The study was published in the New England Journal of Medicine.
To further determine if the elexacaftor-tezacaftor-ivacaftor regimen was effective and safe, the researchers launched a randomized, placebo-controlled phase 3 trial of 403 cystic fibrosis patients age 12 or older who had a single Phe508del allele. Patients in the combination group (n = 200) received 200 mg of elexacaftor once daily, 100 mg of tezacaftor once daily, and 150 mg of ivacaftor every 12 hours for 24 weeks. Patients in the other group (n = 203) received matched placebos.
At 14 weeks, patients in the combination group had a change in percentage of predicted forced expiratory volume in 1 second (FEV1) that was 13.8 points higher than the placebo group (95% confidence interval, 12.1-15.4, P less than .001). At 24 weeks, the combination group had a predicted FEV1 difference that was 14.3 percentage points higher (95% confidence interval, 12.7-15.8, P less than .001). The rate of pulmonary exacerbations was 63% lower (rate ratio 0.37; 95% CI, 0.25-0.55, P less than .001) and sweat chloride concentration was 41.8 mmol/L lower (95% CI, –44.4 to –39.3, P less than .001) in the combination group through 24 weeks.
At least one adverse event occurred in 93.1% of patients in the combination group and 96% of patients in the placebo group. Serious adverse events occurred in 28 patients (13.9%) in the combination group and 42 patients (20.9%) in the placebo group. There were no deaths in either group.
The study was funded by Vertex Pharmaceuticals. The authors had disclosures, including receiving personal fees and grants from various pharmaceutical companies and being on the advisory board, owning stock, or being an employee of Vertex Pharmaceuticals.
SOURCE: Middleton PG et al. 2019 Oct 31. N Engl J Med. doi: 10.1056/NEJMoa1908639.
After 30 years, new research from Middleton et al. and others appears to be the breakthrough we’ve been waiting for in treating cystic fibrosis, wrote Francis S. Collins, MD, PhD, of the National Institutes of Health in an accompanying editorial (N Engl J Med. 2019 Oct 31. doi: 10.1056/NEJMe1911602).
As one of the researchers who discovered the cystic fibrosis gene, he acknowledged the 3 decades of work that followed their discovery and the excitement that comes from being able to counter the common Phe508del CFTR mutation that afflicts so many cystic fibrosis patients. “These findings indicate that it may soon be possible to offer safe and effective molecularly targeted therapies to 90% of persons with cystic fibrosis,” he wrote.
“Yet we must not abandon the patients with cystic fibrosis who have null mutations and will not have a response to these drugs,” he added, noting that those challenges remain “substantial” and potentially will involve in vivo somatic-cell gene editing of airway epithelial cells. That said, what once was a dream 30 years ago now appears to be a reality.
Dr. Collins reported being a coinventor of the original patents on the CFTR gene, for which he donated all royalties to the Cystic Fibrosis Foundation.
After 30 years, new research from Middleton et al. and others appears to be the breakthrough we’ve been waiting for in treating cystic fibrosis, wrote Francis S. Collins, MD, PhD, of the National Institutes of Health in an accompanying editorial (N Engl J Med. 2019 Oct 31. doi: 10.1056/NEJMe1911602).
As one of the researchers who discovered the cystic fibrosis gene, he acknowledged the 3 decades of work that followed their discovery and the excitement that comes from being able to counter the common Phe508del CFTR mutation that afflicts so many cystic fibrosis patients. “These findings indicate that it may soon be possible to offer safe and effective molecularly targeted therapies to 90% of persons with cystic fibrosis,” he wrote.
“Yet we must not abandon the patients with cystic fibrosis who have null mutations and will not have a response to these drugs,” he added, noting that those challenges remain “substantial” and potentially will involve in vivo somatic-cell gene editing of airway epithelial cells. That said, what once was a dream 30 years ago now appears to be a reality.
Dr. Collins reported being a coinventor of the original patents on the CFTR gene, for which he donated all royalties to the Cystic Fibrosis Foundation.
After 30 years, new research from Middleton et al. and others appears to be the breakthrough we’ve been waiting for in treating cystic fibrosis, wrote Francis S. Collins, MD, PhD, of the National Institutes of Health in an accompanying editorial (N Engl J Med. 2019 Oct 31. doi: 10.1056/NEJMe1911602).
As one of the researchers who discovered the cystic fibrosis gene, he acknowledged the 3 decades of work that followed their discovery and the excitement that comes from being able to counter the common Phe508del CFTR mutation that afflicts so many cystic fibrosis patients. “These findings indicate that it may soon be possible to offer safe and effective molecularly targeted therapies to 90% of persons with cystic fibrosis,” he wrote.
“Yet we must not abandon the patients with cystic fibrosis who have null mutations and will not have a response to these drugs,” he added, noting that those challenges remain “substantial” and potentially will involve in vivo somatic-cell gene editing of airway epithelial cells. That said, what once was a dream 30 years ago now appears to be a reality.
Dr. Collins reported being a coinventor of the original patents on the CFTR gene, for which he donated all royalties to the Cystic Fibrosis Foundation.
Reinforcing previous findings, a new study has determined that the next-generation corrector elexacaftor, in combination with tezacaftor and ivacaftor, can effectively treat patients with Phe508del-minimal function genotypes who did not respond to previous cystic fibrosis transmembrane conductance regulator (CFTR) modulator regimens.
“These results provide evidence that , thus addressing the underlying cause of disease in the large majority of patients,” wrote Peter G. Middleton, PhD, of the University of Sydney (Australia) and his coauthors. The study was published in the New England Journal of Medicine.
To further determine if the elexacaftor-tezacaftor-ivacaftor regimen was effective and safe, the researchers launched a randomized, placebo-controlled phase 3 trial of 403 cystic fibrosis patients age 12 or older who had a single Phe508del allele. Patients in the combination group (n = 200) received 200 mg of elexacaftor once daily, 100 mg of tezacaftor once daily, and 150 mg of ivacaftor every 12 hours for 24 weeks. Patients in the other group (n = 203) received matched placebos.
At 14 weeks, patients in the combination group had a change in percentage of predicted forced expiratory volume in 1 second (FEV1) that was 13.8 points higher than the placebo group (95% confidence interval, 12.1-15.4, P less than .001). At 24 weeks, the combination group had a predicted FEV1 difference that was 14.3 percentage points higher (95% confidence interval, 12.7-15.8, P less than .001). The rate of pulmonary exacerbations was 63% lower (rate ratio 0.37; 95% CI, 0.25-0.55, P less than .001) and sweat chloride concentration was 41.8 mmol/L lower (95% CI, –44.4 to –39.3, P less than .001) in the combination group through 24 weeks.
At least one adverse event occurred in 93.1% of patients in the combination group and 96% of patients in the placebo group. Serious adverse events occurred in 28 patients (13.9%) in the combination group and 42 patients (20.9%) in the placebo group. There were no deaths in either group.
The study was funded by Vertex Pharmaceuticals. The authors had disclosures, including receiving personal fees and grants from various pharmaceutical companies and being on the advisory board, owning stock, or being an employee of Vertex Pharmaceuticals.
SOURCE: Middleton PG et al. 2019 Oct 31. N Engl J Med. doi: 10.1056/NEJMoa1908639.
Reinforcing previous findings, a new study has determined that the next-generation corrector elexacaftor, in combination with tezacaftor and ivacaftor, can effectively treat patients with Phe508del-minimal function genotypes who did not respond to previous cystic fibrosis transmembrane conductance regulator (CFTR) modulator regimens.
“These results provide evidence that , thus addressing the underlying cause of disease in the large majority of patients,” wrote Peter G. Middleton, PhD, of the University of Sydney (Australia) and his coauthors. The study was published in the New England Journal of Medicine.
To further determine if the elexacaftor-tezacaftor-ivacaftor regimen was effective and safe, the researchers launched a randomized, placebo-controlled phase 3 trial of 403 cystic fibrosis patients age 12 or older who had a single Phe508del allele. Patients in the combination group (n = 200) received 200 mg of elexacaftor once daily, 100 mg of tezacaftor once daily, and 150 mg of ivacaftor every 12 hours for 24 weeks. Patients in the other group (n = 203) received matched placebos.
At 14 weeks, patients in the combination group had a change in percentage of predicted forced expiratory volume in 1 second (FEV1) that was 13.8 points higher than the placebo group (95% confidence interval, 12.1-15.4, P less than .001). At 24 weeks, the combination group had a predicted FEV1 difference that was 14.3 percentage points higher (95% confidence interval, 12.7-15.8, P less than .001). The rate of pulmonary exacerbations was 63% lower (rate ratio 0.37; 95% CI, 0.25-0.55, P less than .001) and sweat chloride concentration was 41.8 mmol/L lower (95% CI, –44.4 to –39.3, P less than .001) in the combination group through 24 weeks.
At least one adverse event occurred in 93.1% of patients in the combination group and 96% of patients in the placebo group. Serious adverse events occurred in 28 patients (13.9%) in the combination group and 42 patients (20.9%) in the placebo group. There were no deaths in either group.
The study was funded by Vertex Pharmaceuticals. The authors had disclosures, including receiving personal fees and grants from various pharmaceutical companies and being on the advisory board, owning stock, or being an employee of Vertex Pharmaceuticals.
SOURCE: Middleton PG et al. 2019 Oct 31. N Engl J Med. doi: 10.1056/NEJMoa1908639.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Vaping-linked lung injury cases near 1,900
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-seven deaths have been confirmed.
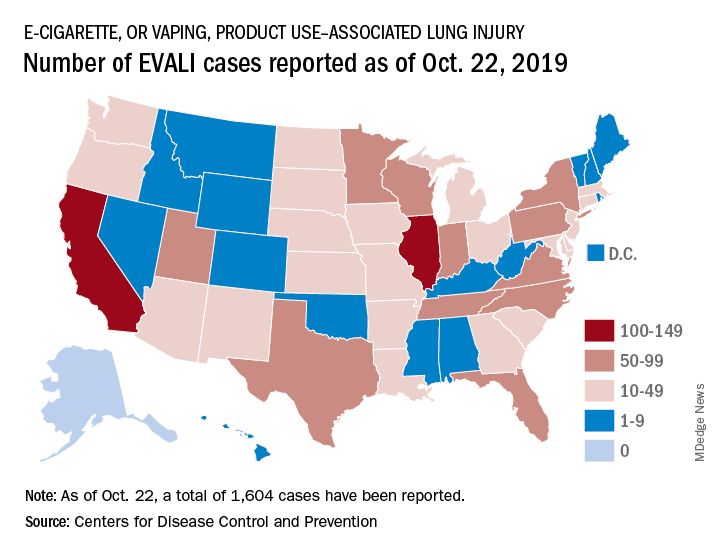
Deaths have occurred in 24 states and the District of Columbia: Alabama, California (3), Connecticut, Delaware, Florida, Georgia (3), Illinois (2), Indiana (3), Kansas (2), Massachusetts, Michigan, Minnesota (3), Mississippi, Missouri, Montana, Nebraska, New Jersey, New York, Oregon (2), Pennsylvania, Tennessee (2), Texas, Utah, and Virginia. As on Oct. 28, the median age of deceased patients was 49 years and ranged from 17 to 75 years.
The CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. It also is validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-seven deaths have been confirmed.
Deaths have occurred in 24 states and the District of Columbia: Alabama, California (3), Connecticut, Delaware, Florida, Georgia (3), Illinois (2), Indiana (3), Kansas (2), Massachusetts, Michigan, Minnesota (3), Mississippi, Missouri, Montana, Nebraska, New Jersey, New York, Oregon (2), Pennsylvania, Tennessee (2), Texas, Utah, and Virginia. As on Oct. 28, the median age of deceased patients was 49 years and ranged from 17 to 75 years.
The CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. It also is validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
according to the latest update provided by the Centers for Disease Control and Prevention. Thirty-seven deaths have been confirmed.
Deaths have occurred in 24 states and the District of Columbia: Alabama, California (3), Connecticut, Delaware, Florida, Georgia (3), Illinois (2), Indiana (3), Kansas (2), Massachusetts, Michigan, Minnesota (3), Mississippi, Missouri, Montana, Nebraska, New Jersey, New York, Oregon (2), Pennsylvania, Tennessee (2), Texas, Utah, and Virginia. As on Oct. 28, the median age of deceased patients was 49 years and ranged from 17 to 75 years.
The CDC is now doing additional testing on available samples for chemical in the bronchoalveolar lavage fluid, blood, or urine, as well as lung biopsy or autopsy specimens. It also is validating methods for aerosol emission testing of case-associated product samples from vaping products and e-liquids.
For more information and resources visit For the Public, For Healthcare Providers, and For State and Local Health Departments pages, as well as the CDC’s Publications and Resources page.
Microbleeds After Brain Injury Predict Worse Disability
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.
KRAS-mutation colon, rectal cancers have distinct survival profiles
SAN FRANCISCO – When it comes to KRAS mutational status, liver metastases originating from left-sided colon tumors have different clinical and survival characteristics from those originating from primary rectal tumors. There was no significant difference in survival between bearers of mutated versus wild-type (WT) KRAS in rectal tumor cases, while there was a significant difference in survival from left-sided colon cases, according to a first-time analysis of the effect of KRAS status in this specific population.
The work was presented at the annual clinical congress of the American College of Surgeons by Neda Amini, MD. “The liver metastasis originating from a rectal tumor might have a different biology than from a primary colon tumor, and we should have stratification according to the primary tumor location in clinical trials testing chemotherapy and targeted agents,” said Dr. Amini, who is a surgical resident at Sinai Hospital of Baltimore, during her presentation of the research.
“I thought that was interesting because most of the studies that have been done look at KRAS mutations in colorectal cancers, and [colon and rectal cancers] are two completely different entities,” said session comoderator Valentine Nfonsam, MD, associate professor of surgery at the University of Arizona, Tucson, in an interview. The findings could also impact clinical practice. “If a patient has rectal cancer, if they have a KRAS mutation, whether you treat them with cetuximab or not, the overall survival doesn’t really change. Whereas for colon cancer patients you really want to make that distinction. You want to truly personalize their therapy, because of the difference in survival in a patient with the KRAS mutation in colon cancer” Dr. Nfonsam said.
“It gets to the heart that there might be different biology between colon cancers and rectal cancers. It’s important to understand the differences in the basic biology, which affects the treatment and the surgery,” said the other comoderator, Jonathan Mitchem, MD, in an interview. Dr. Mitchem is an assistant professor at the University of Missouri–Columbia.
KRAS is common in colorectal cancer, occurring in 30% of cases, and multiple trials have shown it is associated with nonresponse to the epidermal growth factor receptor inhibitors cetuximab or panitumumab. All colorectal cancer patients with liver metastases should be screened for KRAS mutations, according to National Comprehensive Cancer Network guidelines.
The researchers conducted a retrospective analysis of 1,304 patients who underwent curative-intent surgery for colorectal liver metastases at nine institutions between 2000 and 2016. The KRAS mutation rate was similar in the primary colon and rectal tumors (34.2% vs. 30.9%; P = .24). The frequency was highest in right-sided colon tumors (39.4%). There was a statistically significant difference in the frequency of KRAS mutation between primary rectal tumors (30.9%), and left-sided colon tumors (21.1%; P = .001).
There were several differences in clinical characteristics between left-sided colon cancers and rectal cancers. Rectal cancer patients were more likely to be male (73.4% vs. 62.4%; P = .001); more likely to be stage T1-T2 (16.6% vs. 10.6%; P = .012); less likely to have serum carcinoembryonic antigen greater than 100 ng/mL (8.4% vs. 14.1%; P = .018); and less likely to have a liver metastasis under 3 cm (36.1% vs. 49.3%).
There were significant differences between KRAS mutant and KRAS wild-type patients with a colon primary tumor, including greater likelihood of lymph node metastasis in WT (65.2% vs. 55.37%; P = .004), greater likelihood of liver metastasis greater than 3 cm in WT (48.8% versus 39.3%; P = .01), greater likelihood of extrahepatic disease in mutant KRAS (16.3% vs. 10.4%; P = .01), greater likelihood of prehepatic resection chemotherapy in WT (65.5% vs. 56.0%; P = .005), greater likelihood of posthepatic resection chemotherapy in mutant KRAS (64.5% vs. 55.5%; P = .01), and greater likelihood of receiving anti–epidermal growth factor therapy in WT (5.7% vs. 0.3%; P less than .001). The only difference seen in patients with rectal primary tumors was the odds of receiving post-hepatic surgery chemotherapy, which was higher among patients with mutated KRAS (70.8% vs. 59.0%; P = .03).
After a median follow-up of 26.4 months, the 1-, 3-, and 5-year overall survival rates were 88.9%, 62.5%, and 44.5%. Among patients with primary colon cancer, there was a statistically significant lower survival curve in patients with a KRAS mutation overall and in those with left-sided colon tumors (log rank P less than .001 for both), but there was no significant survival difference between mutation bearers and wild-type patients with a primary rectal tumor (log rank P = .53). A multivariate analysis showed an 82% risk of death from KRAS mutation in primary colon cancer (hazard ratio, 1.82; P less than .001), but a univariate analysis showed no significant mortality association in rectal primary tumors (hazard ratio, 1.13; P = .46).
The funding source was not disclosed. The authors had no relevant financial disclosures.
SOURCE: Amini N et al. J Am Coll Surg. 2019 Oct;229(4):Suppl 1, S69-70.
SAN FRANCISCO – When it comes to KRAS mutational status, liver metastases originating from left-sided colon tumors have different clinical and survival characteristics from those originating from primary rectal tumors. There was no significant difference in survival between bearers of mutated versus wild-type (WT) KRAS in rectal tumor cases, while there was a significant difference in survival from left-sided colon cases, according to a first-time analysis of the effect of KRAS status in this specific population.
The work was presented at the annual clinical congress of the American College of Surgeons by Neda Amini, MD. “The liver metastasis originating from a rectal tumor might have a different biology than from a primary colon tumor, and we should have stratification according to the primary tumor location in clinical trials testing chemotherapy and targeted agents,” said Dr. Amini, who is a surgical resident at Sinai Hospital of Baltimore, during her presentation of the research.
“I thought that was interesting because most of the studies that have been done look at KRAS mutations in colorectal cancers, and [colon and rectal cancers] are two completely different entities,” said session comoderator Valentine Nfonsam, MD, associate professor of surgery at the University of Arizona, Tucson, in an interview. The findings could also impact clinical practice. “If a patient has rectal cancer, if they have a KRAS mutation, whether you treat them with cetuximab or not, the overall survival doesn’t really change. Whereas for colon cancer patients you really want to make that distinction. You want to truly personalize their therapy, because of the difference in survival in a patient with the KRAS mutation in colon cancer” Dr. Nfonsam said.
“It gets to the heart that there might be different biology between colon cancers and rectal cancers. It’s important to understand the differences in the basic biology, which affects the treatment and the surgery,” said the other comoderator, Jonathan Mitchem, MD, in an interview. Dr. Mitchem is an assistant professor at the University of Missouri–Columbia.
KRAS is common in colorectal cancer, occurring in 30% of cases, and multiple trials have shown it is associated with nonresponse to the epidermal growth factor receptor inhibitors cetuximab or panitumumab. All colorectal cancer patients with liver metastases should be screened for KRAS mutations, according to National Comprehensive Cancer Network guidelines.
The researchers conducted a retrospective analysis of 1,304 patients who underwent curative-intent surgery for colorectal liver metastases at nine institutions between 2000 and 2016. The KRAS mutation rate was similar in the primary colon and rectal tumors (34.2% vs. 30.9%; P = .24). The frequency was highest in right-sided colon tumors (39.4%). There was a statistically significant difference in the frequency of KRAS mutation between primary rectal tumors (30.9%), and left-sided colon tumors (21.1%; P = .001).
There were several differences in clinical characteristics between left-sided colon cancers and rectal cancers. Rectal cancer patients were more likely to be male (73.4% vs. 62.4%; P = .001); more likely to be stage T1-T2 (16.6% vs. 10.6%; P = .012); less likely to have serum carcinoembryonic antigen greater than 100 ng/mL (8.4% vs. 14.1%; P = .018); and less likely to have a liver metastasis under 3 cm (36.1% vs. 49.3%).
There were significant differences between KRAS mutant and KRAS wild-type patients with a colon primary tumor, including greater likelihood of lymph node metastasis in WT (65.2% vs. 55.37%; P = .004), greater likelihood of liver metastasis greater than 3 cm in WT (48.8% versus 39.3%; P = .01), greater likelihood of extrahepatic disease in mutant KRAS (16.3% vs. 10.4%; P = .01), greater likelihood of prehepatic resection chemotherapy in WT (65.5% vs. 56.0%; P = .005), greater likelihood of posthepatic resection chemotherapy in mutant KRAS (64.5% vs. 55.5%; P = .01), and greater likelihood of receiving anti–epidermal growth factor therapy in WT (5.7% vs. 0.3%; P less than .001). The only difference seen in patients with rectal primary tumors was the odds of receiving post-hepatic surgery chemotherapy, which was higher among patients with mutated KRAS (70.8% vs. 59.0%; P = .03).
After a median follow-up of 26.4 months, the 1-, 3-, and 5-year overall survival rates were 88.9%, 62.5%, and 44.5%. Among patients with primary colon cancer, there was a statistically significant lower survival curve in patients with a KRAS mutation overall and in those with left-sided colon tumors (log rank P less than .001 for both), but there was no significant survival difference between mutation bearers and wild-type patients with a primary rectal tumor (log rank P = .53). A multivariate analysis showed an 82% risk of death from KRAS mutation in primary colon cancer (hazard ratio, 1.82; P less than .001), but a univariate analysis showed no significant mortality association in rectal primary tumors (hazard ratio, 1.13; P = .46).
The funding source was not disclosed. The authors had no relevant financial disclosures.
SOURCE: Amini N et al. J Am Coll Surg. 2019 Oct;229(4):Suppl 1, S69-70.
SAN FRANCISCO – When it comes to KRAS mutational status, liver metastases originating from left-sided colon tumors have different clinical and survival characteristics from those originating from primary rectal tumors. There was no significant difference in survival between bearers of mutated versus wild-type (WT) KRAS in rectal tumor cases, while there was a significant difference in survival from left-sided colon cases, according to a first-time analysis of the effect of KRAS status in this specific population.
The work was presented at the annual clinical congress of the American College of Surgeons by Neda Amini, MD. “The liver metastasis originating from a rectal tumor might have a different biology than from a primary colon tumor, and we should have stratification according to the primary tumor location in clinical trials testing chemotherapy and targeted agents,” said Dr. Amini, who is a surgical resident at Sinai Hospital of Baltimore, during her presentation of the research.
“I thought that was interesting because most of the studies that have been done look at KRAS mutations in colorectal cancers, and [colon and rectal cancers] are two completely different entities,” said session comoderator Valentine Nfonsam, MD, associate professor of surgery at the University of Arizona, Tucson, in an interview. The findings could also impact clinical practice. “If a patient has rectal cancer, if they have a KRAS mutation, whether you treat them with cetuximab or not, the overall survival doesn’t really change. Whereas for colon cancer patients you really want to make that distinction. You want to truly personalize their therapy, because of the difference in survival in a patient with the KRAS mutation in colon cancer” Dr. Nfonsam said.
“It gets to the heart that there might be different biology between colon cancers and rectal cancers. It’s important to understand the differences in the basic biology, which affects the treatment and the surgery,” said the other comoderator, Jonathan Mitchem, MD, in an interview. Dr. Mitchem is an assistant professor at the University of Missouri–Columbia.
KRAS is common in colorectal cancer, occurring in 30% of cases, and multiple trials have shown it is associated with nonresponse to the epidermal growth factor receptor inhibitors cetuximab or panitumumab. All colorectal cancer patients with liver metastases should be screened for KRAS mutations, according to National Comprehensive Cancer Network guidelines.
The researchers conducted a retrospective analysis of 1,304 patients who underwent curative-intent surgery for colorectal liver metastases at nine institutions between 2000 and 2016. The KRAS mutation rate was similar in the primary colon and rectal tumors (34.2% vs. 30.9%; P = .24). The frequency was highest in right-sided colon tumors (39.4%). There was a statistically significant difference in the frequency of KRAS mutation between primary rectal tumors (30.9%), and left-sided colon tumors (21.1%; P = .001).
There were several differences in clinical characteristics between left-sided colon cancers and rectal cancers. Rectal cancer patients were more likely to be male (73.4% vs. 62.4%; P = .001); more likely to be stage T1-T2 (16.6% vs. 10.6%; P = .012); less likely to have serum carcinoembryonic antigen greater than 100 ng/mL (8.4% vs. 14.1%; P = .018); and less likely to have a liver metastasis under 3 cm (36.1% vs. 49.3%).
There were significant differences between KRAS mutant and KRAS wild-type patients with a colon primary tumor, including greater likelihood of lymph node metastasis in WT (65.2% vs. 55.37%; P = .004), greater likelihood of liver metastasis greater than 3 cm in WT (48.8% versus 39.3%; P = .01), greater likelihood of extrahepatic disease in mutant KRAS (16.3% vs. 10.4%; P = .01), greater likelihood of prehepatic resection chemotherapy in WT (65.5% vs. 56.0%; P = .005), greater likelihood of posthepatic resection chemotherapy in mutant KRAS (64.5% vs. 55.5%; P = .01), and greater likelihood of receiving anti–epidermal growth factor therapy in WT (5.7% vs. 0.3%; P less than .001). The only difference seen in patients with rectal primary tumors was the odds of receiving post-hepatic surgery chemotherapy, which was higher among patients with mutated KRAS (70.8% vs. 59.0%; P = .03).
After a median follow-up of 26.4 months, the 1-, 3-, and 5-year overall survival rates were 88.9%, 62.5%, and 44.5%. Among patients with primary colon cancer, there was a statistically significant lower survival curve in patients with a KRAS mutation overall and in those with left-sided colon tumors (log rank P less than .001 for both), but there was no significant survival difference between mutation bearers and wild-type patients with a primary rectal tumor (log rank P = .53). A multivariate analysis showed an 82% risk of death from KRAS mutation in primary colon cancer (hazard ratio, 1.82; P less than .001), but a univariate analysis showed no significant mortality association in rectal primary tumors (hazard ratio, 1.13; P = .46).
The funding source was not disclosed. The authors had no relevant financial disclosures.
SOURCE: Amini N et al. J Am Coll Surg. 2019 Oct;229(4):Suppl 1, S69-70.
REPORTING FROM CLINICAL CONGRESS 2019
Macitentan produces similar results in PAH-SSc and IPAH/HPAH
NEW ORLEANS – Real-world data support the use of macitentan to treat pulmonary arterial hypertension (PAH) associated with connective tissue disease, according to a speaker at the annual meeting of the American College of Chest Physicians.

Outcomes of macitentan (Opsumit) treatment were similar in patients who had PAH associated with systemic sclerosis (PAH-SSc) and patients who had idiopathic PAH (IPAH) or heritable PAH (HPAH), Vallerie McLaughlin, MD, of the University of Michigan, Ann Arbor, said at the meeting.
“Within the limits of a real-world registry, these data add to the growing body of evidence supporting the use of macitentan for treatment in patients with CTD [connective tissue disease],” Dr. McLaughlin said.
She and her colleagues evaluated data from the prospective OPUS registry (NCT02126943) and the retrospective OrPHeUS study (NCT03197688), both of which included patients who were newly started on macitentan.
Dr. McLaughlin presented data on 2,311 patients with IPAH/HPAH and 668 patients with PAH-SSc. She also presented data on patients with PAH-systemic lupus erythematosus and PAH-mixed CTD, but numbers in these groups were small, and outcomes were similar to those in the PAH-SSc group.
Demographic and disease characteristics at the start of macitentan were similar between the IPAH/HPAH and PAH-SSc groups. The median age was 64 years in both groups. The median time from PAH diagnosis was 7.6 months in the IPAH/HPAH group and 8.5 months in the PAH-SSc group.
The median duration of macitentan exposure was 13.4 months in the IPAH/HPAH group and 14.4 months in the PAH-SSc group. The proportion of patients receiving macitentan in combination with other therapies (double or triple combinations) increased from baseline to 6 months in both groups.
Hepatic adverse events occurred in 7.4% of IPAH/HPAH patients and 7.9% of PAH-SSc patients. The most common adverse events among the IPAH/HPAH and PAH-SSc groups in the OPUS registry alone were dyspnea (19% and 26.1%, respectively), peripheral edema (9.8% and 12.4%), fatigue (6.8% and 11.7%), anemia (6.7% and 11.7%), headache (10.2% and 11%), and dizziness (6.7% and 10.7%).
About 39% of patients in both groups discontinued macitentan. Similar proportions in each group discontinued because of adverse events (17% in the IPAH/HPAH group and 18.3% in the PAH-SSc group) and hepatic adverse events (0.2% and 0.7%, respectively).
The proportion of patients with at least one hospitalization was 36.2% in the IPAH/HPAH group and 40.1% in the PAH-SSc group.
The 12-month Kaplan-Meier survival estimate was 92.9% in the IPAH/HPAH group and 91.3% in the PAH-SSc group. The 24-month estimated survival rate was 85.6% and 82.1%, respectively.
The OPUS registry and OrPHeUS study are sponsored by Actelion. Dr. McLaughlin disclosed relationships with Actelion, Acceleron, Bayer, Caremark, CiVi Biopharma, Reata, Sonovie, and United Therapeutics.
SOURCE: McLaughlin V et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.827.
NEW ORLEANS – Real-world data support the use of macitentan to treat pulmonary arterial hypertension (PAH) associated with connective tissue disease, according to a speaker at the annual meeting of the American College of Chest Physicians.
Outcomes of macitentan (Opsumit) treatment were similar in patients who had PAH associated with systemic sclerosis (PAH-SSc) and patients who had idiopathic PAH (IPAH) or heritable PAH (HPAH), Vallerie McLaughlin, MD, of the University of Michigan, Ann Arbor, said at the meeting.
“Within the limits of a real-world registry, these data add to the growing body of evidence supporting the use of macitentan for treatment in patients with CTD [connective tissue disease],” Dr. McLaughlin said.
She and her colleagues evaluated data from the prospective OPUS registry (NCT02126943) and the retrospective OrPHeUS study (NCT03197688), both of which included patients who were newly started on macitentan.
Dr. McLaughlin presented data on 2,311 patients with IPAH/HPAH and 668 patients with PAH-SSc. She also presented data on patients with PAH-systemic lupus erythematosus and PAH-mixed CTD, but numbers in these groups were small, and outcomes were similar to those in the PAH-SSc group.
Demographic and disease characteristics at the start of macitentan were similar between the IPAH/HPAH and PAH-SSc groups. The median age was 64 years in both groups. The median time from PAH diagnosis was 7.6 months in the IPAH/HPAH group and 8.5 months in the PAH-SSc group.
The median duration of macitentan exposure was 13.4 months in the IPAH/HPAH group and 14.4 months in the PAH-SSc group. The proportion of patients receiving macitentan in combination with other therapies (double or triple combinations) increased from baseline to 6 months in both groups.
Hepatic adverse events occurred in 7.4% of IPAH/HPAH patients and 7.9% of PAH-SSc patients. The most common adverse events among the IPAH/HPAH and PAH-SSc groups in the OPUS registry alone were dyspnea (19% and 26.1%, respectively), peripheral edema (9.8% and 12.4%), fatigue (6.8% and 11.7%), anemia (6.7% and 11.7%), headache (10.2% and 11%), and dizziness (6.7% and 10.7%).
About 39% of patients in both groups discontinued macitentan. Similar proportions in each group discontinued because of adverse events (17% in the IPAH/HPAH group and 18.3% in the PAH-SSc group) and hepatic adverse events (0.2% and 0.7%, respectively).
The proportion of patients with at least one hospitalization was 36.2% in the IPAH/HPAH group and 40.1% in the PAH-SSc group.
The 12-month Kaplan-Meier survival estimate was 92.9% in the IPAH/HPAH group and 91.3% in the PAH-SSc group. The 24-month estimated survival rate was 85.6% and 82.1%, respectively.
The OPUS registry and OrPHeUS study are sponsored by Actelion. Dr. McLaughlin disclosed relationships with Actelion, Acceleron, Bayer, Caremark, CiVi Biopharma, Reata, Sonovie, and United Therapeutics.
SOURCE: McLaughlin V et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.827.
NEW ORLEANS – Real-world data support the use of macitentan to treat pulmonary arterial hypertension (PAH) associated with connective tissue disease, according to a speaker at the annual meeting of the American College of Chest Physicians.
Outcomes of macitentan (Opsumit) treatment were similar in patients who had PAH associated with systemic sclerosis (PAH-SSc) and patients who had idiopathic PAH (IPAH) or heritable PAH (HPAH), Vallerie McLaughlin, MD, of the University of Michigan, Ann Arbor, said at the meeting.
“Within the limits of a real-world registry, these data add to the growing body of evidence supporting the use of macitentan for treatment in patients with CTD [connective tissue disease],” Dr. McLaughlin said.
She and her colleagues evaluated data from the prospective OPUS registry (NCT02126943) and the retrospective OrPHeUS study (NCT03197688), both of which included patients who were newly started on macitentan.
Dr. McLaughlin presented data on 2,311 patients with IPAH/HPAH and 668 patients with PAH-SSc. She also presented data on patients with PAH-systemic lupus erythematosus and PAH-mixed CTD, but numbers in these groups were small, and outcomes were similar to those in the PAH-SSc group.
Demographic and disease characteristics at the start of macitentan were similar between the IPAH/HPAH and PAH-SSc groups. The median age was 64 years in both groups. The median time from PAH diagnosis was 7.6 months in the IPAH/HPAH group and 8.5 months in the PAH-SSc group.
The median duration of macitentan exposure was 13.4 months in the IPAH/HPAH group and 14.4 months in the PAH-SSc group. The proportion of patients receiving macitentan in combination with other therapies (double or triple combinations) increased from baseline to 6 months in both groups.
Hepatic adverse events occurred in 7.4% of IPAH/HPAH patients and 7.9% of PAH-SSc patients. The most common adverse events among the IPAH/HPAH and PAH-SSc groups in the OPUS registry alone were dyspnea (19% and 26.1%, respectively), peripheral edema (9.8% and 12.4%), fatigue (6.8% and 11.7%), anemia (6.7% and 11.7%), headache (10.2% and 11%), and dizziness (6.7% and 10.7%).
About 39% of patients in both groups discontinued macitentan. Similar proportions in each group discontinued because of adverse events (17% in the IPAH/HPAH group and 18.3% in the PAH-SSc group) and hepatic adverse events (0.2% and 0.7%, respectively).
The proportion of patients with at least one hospitalization was 36.2% in the IPAH/HPAH group and 40.1% in the PAH-SSc group.
The 12-month Kaplan-Meier survival estimate was 92.9% in the IPAH/HPAH group and 91.3% in the PAH-SSc group. The 24-month estimated survival rate was 85.6% and 82.1%, respectively.
The OPUS registry and OrPHeUS study are sponsored by Actelion. Dr. McLaughlin disclosed relationships with Actelion, Acceleron, Bayer, Caremark, CiVi Biopharma, Reata, Sonovie, and United Therapeutics.
SOURCE: McLaughlin V et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.827.
REPORTING FROM CHEST 2019
Thousands of Emergency-Care Claims Were Denied; Court Rules VA Must Reimburse
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.

Flu vaccine cuts infection severity in kids and adults
WASHINGTON –
During recent U.S. flu seasons, children and adults who contracted influenza despite vaccination had significantly fewer severe infections and infection complications, compared with unimmunized people, according to two separate reports from CDC researchers presented at an annual scientific meeting on infectious diseases.
One of the reports tracked the impact of flu vaccine in children using data that the CDC collected at seven medical centers that participated in the agency’s New Vaccine Surveillance Network, which provided information on children aged 6 months to 17 years who were hospitalized for an acute respiratory illness, including more than 1,700 children during the 2016-2017 flu season and more than 1,900 during the 2017-2018 season. Roughly 10% of these children tested positive for influenza, and the subsequent analysis focused on these cases and compared incidence rates among children who had been vaccinated during the index season and those who had remained unvaccinated.
Combined data from both seasons showed that vaccinated children were 50% less likely to have been hospitalized for an acute influenza infection, compared with unvaccinated kids, a pattern consistently seen both in children aged 6 months to 8 years and in those aged 9-17 years. The pattern of vaccine effectiveness also held regardless of which flu strain caused the infections, reported Angela P. Campbell, MD, a CDC medical officer.
“We saw a nice benefit from vaccination, both in previously healthy children and in those with an underlying medical condition,” a finding that adds to existing evidence of vaccine effectiveness, Dr. Campbell said in a video interview. The results confirmed that flu vaccination does not just prevent infections but also cuts the rate of more severe infections that lead to hospitalization, she explained.
Another CDC study looked at data collected by the agency’s Influenza Hospitalization Surveillance Network from adults at least 18 years old who were hospitalized for a laboratory-confirmed influenza infection during five flu seasons, 2013-2014 through 2017-18. The data, which came from more than 250 acute-care hospitals in 13 states, included more than 43,000 people hospitalized for an identified influenza strain and with a known vaccination history who were not institutionalized and had not received any antiviral treatment.

After propensity-weighted adjustment to create better parity between the vaccinated and unvaccinated patients, the results showed that people 18-64 years old with vaccination had statistically significant decreases in mortality of a relative 36%, need for mechanical ventilation of 34%, pneumonia of 20%, and need for ICU admission of a relative 19%, as well as an 18% drop in average ICU length of stay, Shikha Garg, MD, said at the meeting. The propensity-weighted analysis of data from people at least 65 years old showed statistically significant relative reductions linked with vaccination: 46% reduction in the need for mechanical ventilation, 28% reduction in ICU admissions, and 9% reduction in hospitalized length of stay.
Further analysis of these outcomes by the strains that caused these influenza infections showed that the statistically significant benefits from vaccination were seen only in patients infected with an H1N1 strain. Statistically significant effects on these severe outcomes were not apparent among people infected with the H3N2 or B strains, said Dr. Garg, a medical epidemiologist at the CDC.
“All adults should receive an annual flu vaccination as it can improve outcomes among those who develop influenza despite vaccination,” she concluded.
Results from a third CDC study reported at the meeting examined the importance of two vaccine doses (administered at least 4 weeks apart) given to children aged 6 months to 8 years for the first season they receive flu vaccination, which is the immunization approach for flu recommended by the CDC. The findings from a total of more than 7,500 children immunized during the 2014-2018 seasons showed a clear increment in vaccine protection among kids who received two doses during their first season vaccinated, especially in children who were 2 years old or younger. In that age group, administration of two doses produced vaccine effectiveness of 53% versus a 23% vaccine effectiveness after a single vaccine dose, reported Jessie Chung, a CDC epidemiologist.
WASHINGTON –
During recent U.S. flu seasons, children and adults who contracted influenza despite vaccination had significantly fewer severe infections and infection complications, compared with unimmunized people, according to two separate reports from CDC researchers presented at an annual scientific meeting on infectious diseases.
One of the reports tracked the impact of flu vaccine in children using data that the CDC collected at seven medical centers that participated in the agency’s New Vaccine Surveillance Network, which provided information on children aged 6 months to 17 years who were hospitalized for an acute respiratory illness, including more than 1,700 children during the 2016-2017 flu season and more than 1,900 during the 2017-2018 season. Roughly 10% of these children tested positive for influenza, and the subsequent analysis focused on these cases and compared incidence rates among children who had been vaccinated during the index season and those who had remained unvaccinated.
Combined data from both seasons showed that vaccinated children were 50% less likely to have been hospitalized for an acute influenza infection, compared with unvaccinated kids, a pattern consistently seen both in children aged 6 months to 8 years and in those aged 9-17 years. The pattern of vaccine effectiveness also held regardless of which flu strain caused the infections, reported Angela P. Campbell, MD, a CDC medical officer.
“We saw a nice benefit from vaccination, both in previously healthy children and in those with an underlying medical condition,” a finding that adds to existing evidence of vaccine effectiveness, Dr. Campbell said in a video interview. The results confirmed that flu vaccination does not just prevent infections but also cuts the rate of more severe infections that lead to hospitalization, she explained.
Another CDC study looked at data collected by the agency’s Influenza Hospitalization Surveillance Network from adults at least 18 years old who were hospitalized for a laboratory-confirmed influenza infection during five flu seasons, 2013-2014 through 2017-18. The data, which came from more than 250 acute-care hospitals in 13 states, included more than 43,000 people hospitalized for an identified influenza strain and with a known vaccination history who were not institutionalized and had not received any antiviral treatment.
After propensity-weighted adjustment to create better parity between the vaccinated and unvaccinated patients, the results showed that people 18-64 years old with vaccination had statistically significant decreases in mortality of a relative 36%, need for mechanical ventilation of 34%, pneumonia of 20%, and need for ICU admission of a relative 19%, as well as an 18% drop in average ICU length of stay, Shikha Garg, MD, said at the meeting. The propensity-weighted analysis of data from people at least 65 years old showed statistically significant relative reductions linked with vaccination: 46% reduction in the need for mechanical ventilation, 28% reduction in ICU admissions, and 9% reduction in hospitalized length of stay.
Further analysis of these outcomes by the strains that caused these influenza infections showed that the statistically significant benefits from vaccination were seen only in patients infected with an H1N1 strain. Statistically significant effects on these severe outcomes were not apparent among people infected with the H3N2 or B strains, said Dr. Garg, a medical epidemiologist at the CDC.
“All adults should receive an annual flu vaccination as it can improve outcomes among those who develop influenza despite vaccination,” she concluded.
Results from a third CDC study reported at the meeting examined the importance of two vaccine doses (administered at least 4 weeks apart) given to children aged 6 months to 8 years for the first season they receive flu vaccination, which is the immunization approach for flu recommended by the CDC. The findings from a total of more than 7,500 children immunized during the 2014-2018 seasons showed a clear increment in vaccine protection among kids who received two doses during their first season vaccinated, especially in children who were 2 years old or younger. In that age group, administration of two doses produced vaccine effectiveness of 53% versus a 23% vaccine effectiveness after a single vaccine dose, reported Jessie Chung, a CDC epidemiologist.
WASHINGTON –
During recent U.S. flu seasons, children and adults who contracted influenza despite vaccination had significantly fewer severe infections and infection complications, compared with unimmunized people, according to two separate reports from CDC researchers presented at an annual scientific meeting on infectious diseases.
One of the reports tracked the impact of flu vaccine in children using data that the CDC collected at seven medical centers that participated in the agency’s New Vaccine Surveillance Network, which provided information on children aged 6 months to 17 years who were hospitalized for an acute respiratory illness, including more than 1,700 children during the 2016-2017 flu season and more than 1,900 during the 2017-2018 season. Roughly 10% of these children tested positive for influenza, and the subsequent analysis focused on these cases and compared incidence rates among children who had been vaccinated during the index season and those who had remained unvaccinated.
Combined data from both seasons showed that vaccinated children were 50% less likely to have been hospitalized for an acute influenza infection, compared with unvaccinated kids, a pattern consistently seen both in children aged 6 months to 8 years and in those aged 9-17 years. The pattern of vaccine effectiveness also held regardless of which flu strain caused the infections, reported Angela P. Campbell, MD, a CDC medical officer.
“We saw a nice benefit from vaccination, both in previously healthy children and in those with an underlying medical condition,” a finding that adds to existing evidence of vaccine effectiveness, Dr. Campbell said in a video interview. The results confirmed that flu vaccination does not just prevent infections but also cuts the rate of more severe infections that lead to hospitalization, she explained.
Another CDC study looked at data collected by the agency’s Influenza Hospitalization Surveillance Network from adults at least 18 years old who were hospitalized for a laboratory-confirmed influenza infection during five flu seasons, 2013-2014 through 2017-18. The data, which came from more than 250 acute-care hospitals in 13 states, included more than 43,000 people hospitalized for an identified influenza strain and with a known vaccination history who were not institutionalized and had not received any antiviral treatment.
After propensity-weighted adjustment to create better parity between the vaccinated and unvaccinated patients, the results showed that people 18-64 years old with vaccination had statistically significant decreases in mortality of a relative 36%, need for mechanical ventilation of 34%, pneumonia of 20%, and need for ICU admission of a relative 19%, as well as an 18% drop in average ICU length of stay, Shikha Garg, MD, said at the meeting. The propensity-weighted analysis of data from people at least 65 years old showed statistically significant relative reductions linked with vaccination: 46% reduction in the need for mechanical ventilation, 28% reduction in ICU admissions, and 9% reduction in hospitalized length of stay.
Further analysis of these outcomes by the strains that caused these influenza infections showed that the statistically significant benefits from vaccination were seen only in patients infected with an H1N1 strain. Statistically significant effects on these severe outcomes were not apparent among people infected with the H3N2 or B strains, said Dr. Garg, a medical epidemiologist at the CDC.
“All adults should receive an annual flu vaccination as it can improve outcomes among those who develop influenza despite vaccination,” she concluded.
Results from a third CDC study reported at the meeting examined the importance of two vaccine doses (administered at least 4 weeks apart) given to children aged 6 months to 8 years for the first season they receive flu vaccination, which is the immunization approach for flu recommended by the CDC. The findings from a total of more than 7,500 children immunized during the 2014-2018 seasons showed a clear increment in vaccine protection among kids who received two doses during their first season vaccinated, especially in children who were 2 years old or younger. In that age group, administration of two doses produced vaccine effectiveness of 53% versus a 23% vaccine effectiveness after a single vaccine dose, reported Jessie Chung, a CDC epidemiologist.
REPORTING FROM ID WEEK 2019

Thromboembolic events more likely among CIDP patients with CVAD
AUSTIN, TEX. – Patients with chronic inflammatory demyelinating polyneuropathy (CIDP) who receive intravenous immunoglobulin (IVIg) appear to have an increased risk of thromboembolic events if it is administered with a central venous access device (CVAD) when compared against those without a CVAD, according to a recent study.
Although CVADs can reliably deliver IVIg, they also represent an established risk factor for thromboembolic events, Ami Patel, PhD, a senior epidemiologist at CSL Behring, and colleagues noted on their poster at the annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine.
The results suggest a need for physicians to be vigilant about patients’ potential risk factors for thromboembolic events, Dr. Patel said in an interview. Further research is planned, however, because the current study did not control for other risk factors or explore other possible confounding, she said.
Dr. Patel and her associates analyzed U.S. claims data (IBM/Truven MarketScan) from 2006 to 2018 and included all patients with a CIDP diagnosis claim and a postdiagnosis code for IVIg. A code for CVAD up to 2 months before CIDP diagnosis without removal before IVIg treatment ended determined those with CVAD exposure, and thromboembolic events included any codes related to arterial, venous, or vascular prostheses.
The researchers then compared patients in a case-control fashion, matching each one with a CVAD to five patients of similar demographics without a CVAD. Characteristics used for matching included medical insurance type, prescription data availability, sex, age, geographic region, and years enrolled in the database.
Among 7,447 patients with at least one IVIg claim, 11.8% (n = 882) had CVAD exposure and 88.2% (n = 6,565) did not. Of those without a CVAD, 3,642 patients were matched to patients with CVAD. A quarter (25.4%) of patients with a CVAD had a thromboembolic event, compared with 11.2% of matched patients without CVADs (P less than .0001).
In the year leading up to IVIg therapy, 16.9% of those with a CVAD and 10.9% of matched patients without one had a previous thromboembolic event (P less than .0001). Patients with a CVAD also had significantly higher rates of hypertension (51.9% vs. 45.0% with placebo; P less than .001) and anticoagulation therapy (7.0% vs. 5.2% with placebo; P less than .05). Differences between the groups were not significant for diabetes (26.9% vs. 24.2%) and hyperlipidemia (19.1% vs. 17.8%).
Occlusion and stenosis of the carotid artery was the most common arterial thromboembolic outcome, occurring in 5.3% of those with a CVAD and in 2.8% of those without a CVAD. The most common venous thromboembolic event was acute venous embolism and thrombosis of lower-extremity deep vessels, which occurred in 7% of those with a CVAD and in 1.8% of those without.
The researchers also compared inpatient admissions and emergency department visits among those with and without a CVAD; both rates were higher in patients with a CVAD. Visits to the emergency department occurred at a rate of 0.14 events per month for those with a CVAD (2.01 distinct months with a claim) and 0.09 events per month for those without a CVAD (0.65 distinct months with a claim). Patients with a CVAD had 1.44 months with an inpatient admissions claim, in comparison with 0.41 months among matched patients without a CVAD. Inpatient admission frequency per month was 0.14 for those with a CVAD and 0.08 for those without.
The research was funded by CSL Behring. Dr. Patel and two of the other five authors are employees of CSL Behring.
SOURCE: Patel A et al. AANEM 2019, Abstract 94.
AUSTIN, TEX. – Patients with chronic inflammatory demyelinating polyneuropathy (CIDP) who receive intravenous immunoglobulin (IVIg) appear to have an increased risk of thromboembolic events if it is administered with a central venous access device (CVAD) when compared against those without a CVAD, according to a recent study.
Although CVADs can reliably deliver IVIg, they also represent an established risk factor for thromboembolic events, Ami Patel, PhD, a senior epidemiologist at CSL Behring, and colleagues noted on their poster at the annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine.
The results suggest a need for physicians to be vigilant about patients’ potential risk factors for thromboembolic events, Dr. Patel said in an interview. Further research is planned, however, because the current study did not control for other risk factors or explore other possible confounding, she said.
Dr. Patel and her associates analyzed U.S. claims data (IBM/Truven MarketScan) from 2006 to 2018 and included all patients with a CIDP diagnosis claim and a postdiagnosis code for IVIg. A code for CVAD up to 2 months before CIDP diagnosis without removal before IVIg treatment ended determined those with CVAD exposure, and thromboembolic events included any codes related to arterial, venous, or vascular prostheses.
The researchers then compared patients in a case-control fashion, matching each one with a CVAD to five patients of similar demographics without a CVAD. Characteristics used for matching included medical insurance type, prescription data availability, sex, age, geographic region, and years enrolled in the database.
Among 7,447 patients with at least one IVIg claim, 11.8% (n = 882) had CVAD exposure and 88.2% (n = 6,565) did not. Of those without a CVAD, 3,642 patients were matched to patients with CVAD. A quarter (25.4%) of patients with a CVAD had a thromboembolic event, compared with 11.2% of matched patients without CVADs (P less than .0001).
In the year leading up to IVIg therapy, 16.9% of those with a CVAD and 10.9% of matched patients without one had a previous thromboembolic event (P less than .0001). Patients with a CVAD also had significantly higher rates of hypertension (51.9% vs. 45.0% with placebo; P less than .001) and anticoagulation therapy (7.0% vs. 5.2% with placebo; P less than .05). Differences between the groups were not significant for diabetes (26.9% vs. 24.2%) and hyperlipidemia (19.1% vs. 17.8%).
Occlusion and stenosis of the carotid artery was the most common arterial thromboembolic outcome, occurring in 5.3% of those with a CVAD and in 2.8% of those without a CVAD. The most common venous thromboembolic event was acute venous embolism and thrombosis of lower-extremity deep vessels, which occurred in 7% of those with a CVAD and in 1.8% of those without.
The researchers also compared inpatient admissions and emergency department visits among those with and without a CVAD; both rates were higher in patients with a CVAD. Visits to the emergency department occurred at a rate of 0.14 events per month for those with a CVAD (2.01 distinct months with a claim) and 0.09 events per month for those without a CVAD (0.65 distinct months with a claim). Patients with a CVAD had 1.44 months with an inpatient admissions claim, in comparison with 0.41 months among matched patients without a CVAD. Inpatient admission frequency per month was 0.14 for those with a CVAD and 0.08 for those without.
The research was funded by CSL Behring. Dr. Patel and two of the other five authors are employees of CSL Behring.
SOURCE: Patel A et al. AANEM 2019, Abstract 94.
AUSTIN, TEX. – Patients with chronic inflammatory demyelinating polyneuropathy (CIDP) who receive intravenous immunoglobulin (IVIg) appear to have an increased risk of thromboembolic events if it is administered with a central venous access device (CVAD) when compared against those without a CVAD, according to a recent study.
Although CVADs can reliably deliver IVIg, they also represent an established risk factor for thromboembolic events, Ami Patel, PhD, a senior epidemiologist at CSL Behring, and colleagues noted on their poster at the annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine.
The results suggest a need for physicians to be vigilant about patients’ potential risk factors for thromboembolic events, Dr. Patel said in an interview. Further research is planned, however, because the current study did not control for other risk factors or explore other possible confounding, she said.
Dr. Patel and her associates analyzed U.S. claims data (IBM/Truven MarketScan) from 2006 to 2018 and included all patients with a CIDP diagnosis claim and a postdiagnosis code for IVIg. A code for CVAD up to 2 months before CIDP diagnosis without removal before IVIg treatment ended determined those with CVAD exposure, and thromboembolic events included any codes related to arterial, venous, or vascular prostheses.
The researchers then compared patients in a case-control fashion, matching each one with a CVAD to five patients of similar demographics without a CVAD. Characteristics used for matching included medical insurance type, prescription data availability, sex, age, geographic region, and years enrolled in the database.
Among 7,447 patients with at least one IVIg claim, 11.8% (n = 882) had CVAD exposure and 88.2% (n = 6,565) did not. Of those without a CVAD, 3,642 patients were matched to patients with CVAD. A quarter (25.4%) of patients with a CVAD had a thromboembolic event, compared with 11.2% of matched patients without CVADs (P less than .0001).
In the year leading up to IVIg therapy, 16.9% of those with a CVAD and 10.9% of matched patients without one had a previous thromboembolic event (P less than .0001). Patients with a CVAD also had significantly higher rates of hypertension (51.9% vs. 45.0% with placebo; P less than .001) and anticoagulation therapy (7.0% vs. 5.2% with placebo; P less than .05). Differences between the groups were not significant for diabetes (26.9% vs. 24.2%) and hyperlipidemia (19.1% vs. 17.8%).
Occlusion and stenosis of the carotid artery was the most common arterial thromboembolic outcome, occurring in 5.3% of those with a CVAD and in 2.8% of those without a CVAD. The most common venous thromboembolic event was acute venous embolism and thrombosis of lower-extremity deep vessels, which occurred in 7% of those with a CVAD and in 1.8% of those without.
The researchers also compared inpatient admissions and emergency department visits among those with and without a CVAD; both rates were higher in patients with a CVAD. Visits to the emergency department occurred at a rate of 0.14 events per month for those with a CVAD (2.01 distinct months with a claim) and 0.09 events per month for those without a CVAD (0.65 distinct months with a claim). Patients with a CVAD had 1.44 months with an inpatient admissions claim, in comparison with 0.41 months among matched patients without a CVAD. Inpatient admission frequency per month was 0.14 for those with a CVAD and 0.08 for those without.
The research was funded by CSL Behring. Dr. Patel and two of the other five authors are employees of CSL Behring.
SOURCE: Patel A et al. AANEM 2019, Abstract 94.
REPORTING FROM AANEM 2019