User login
Lung cancer screening, early diagnosis still lower among blacks, Hispanics
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
SAN FRANCISCO – A review of lung cancer cases in New York suggests that 2011 guidelines issued by the National Comprehensive Cancer Network (NCCN) have made little difference in addressing ethnic and socioeconomic disparities in lung cancer diagnosis. The review showed some progress; however, . The researchers also found a reduced incidence of lung cancer only in whites.
The guidelines call for CT screening for smokers aged 55-74 years that have a 30 pack-year history within the past 15 years and were based on a lung cancer screening trial showing that annual low-dose CT led to a 20% reduction in lung cancer deaths, compared with chest x-ray (N Eng J Med. 2011;365:395-409).
Nonwhites “aren’t always exposed to screening opportunities, and may be taken care of by providers who haven’t necessarily bought into screening or aren’t necessarily aware of it. So the downstream effects of the lack of access to screening hurts them doubly, because they’re diagnosed later and they also have disparities in access to treatment,” said Elizabeth David, MD, in an interview. Dr. David is an associate professor of surgery of University of Southern California, Los Angeles. She comoderated a session at the annual congress of the American College of Surgeons, where the research was presented.
The findings underscore the need to get the word out to primary care providers in all communities that catching lung cancer early can make all the difference to patients. “The more we can do to talk about lung cancer as a treatable disease and a cancer that can become a chronically managed medical problem for patients, rather than a death sentence, which it has the misperception of being, the more we can encourage people to seek treatment when they have a symptom, instead of being afraid and doing nothing,” said Dr. David.
The researchers considered metropolitan New York to be a good test case to examine the impact of the screening guidelines since it is socioeconomically and racially diverse. “New York presents a microcosm of what’s going on nationally in other urban areas,” said Tamar Nobel, MD, from Mount Sinai Hospital, New York, who presented the study.
The researchers analyzed records from the New York State Cancer Registry from the period 2008-201 and compared that with data from 2012-2015 (total, n = 18,284). The incidence of lung cancer declined among whites from the first period to the second, at an average annual percent change of –1.5% (95% confidence interval, –1.0% to –2.0%). A similar result was seen in Hispanics (–1.7%; 95% CI, –0.4% to –2.9%), but not among blacks (–1.2%; not significant). There was an increase among Asians/Pacific Islanders (+1.4%; 95% CI, 0.6% to 2.2%).
There were also inequalities when it came to the odds of a stage I diagnosis. Although the percentages increased in whites (+3.5%; 95% CI, 0.6%-6.4%) and blacks (+6.0%; 95% CI, 2.3%-9.7%), the median percentage was higher among whites (27.6% versus 18.2%; no overlap among 95% CIs; odds ratio, 0.62; 95% CI, 0.56-0.68). Hispanics and Asians/Pacific Islanders experienced no significant changes in their odds of a stage I diagnosis, and both groups remained significantly less likely than whites to be diagnosed with stage I disease (OR, 0.72 and 0.86, respectively, both significant).
No funding was disclosed. Dr. David and Dr. Nobel have no relevant financial disclosures.
SOURCE: Nobel T et al. ACS Clinical Congress 2019. Abstract, doi: 10.1016/j.jamcollsurg.2019.08.607.
REPORTING FROM CLINICAL CONGRESS 2019
Tide beginning to turn on vaccine hesitancy
NEW ORLEANS –

The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
NEW ORLEANS –
The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
NEW ORLEANS –
The shift began with the measles outbreak in Southern California in late 2014, he said. According to the Centers for Disease Control and Prevention, 125 measles cases with rash that occurred between Dec. 28, 2014, and Feb. 8, 2015, were confirmed in U.S. residents. Of these, 100 were California residents (MMWR. 2015 Feb 20;64[06];153-4).
“This outbreak spread ultimately to 25 states and involved 189 people,” Dr. Offit said at the annual meeting of the American Academy of Pediatrics. “It was in the news almost every day. As a consequence, there were measles outbreaks in New York, New Jersey, Florida, Oregon, and Texas, and Washington, which began to turn the public sentiment against the antivaccine movement.”
Even longstanding skeptics are changing their tune. Dr. Offit, professor of pediatrics in the division of infectious diseases at the Children’s Hospital of Philadelphia, cited a recent study from the Autism Science Foundation which found that 85% of parents of children with autism spectrum disorder don’t believe that vaccines cause the condition. “Although there will be parents who continue to believe that vaccines cause autism, most parents of children with autism don’t believe that,” he said. “Also, it’s a little hard to make your case that vaccines are dangerous and that you shouldn’t get them in the midst of outbreaks.”
Perhaps the greatest pushback against antivaccination efforts has been made in the legal arena. In 2019 alone, legislators in California banned parents from not vaccinating their kids because of personal beliefs, while lawmakers in New York repealed the religious exemption to vaccinate, those in Maine repealed the religious and philosophical exemption, those in New Jersey required detailed written explanation for religious exemption, and those in Washington State repealed the philosophical exemption for the MMR vaccine.
Pushback also is apparent on various social media platforms. For example, Dr. Offit said, Pinterest restricts vaccine search results to curb the spread of misinformation, YouTube removes ads from antivaccine channels, Amazon Prime has pulled antivaccination documentaries from its video service, and Facebook has taken steps to curb misinformation about vaccines. “With outbreaks and with children suffering, the media and public sentiment has largely turned against those who are vehemently against vaccines,” he said. “I’m talking about an angry, politically connected, lawyer-backed group of people who are conspiracy theorists, [those] who no matter what you say, they’re going to believe there’s a conspiracy theory to hurt their children and not believe you. When that group becomes big enough and you start to see outbreaks like we’ve seen, then it becomes an issue. That’s where it comes down to legislation. Is it your inalienable right as a U.S. citizen to allow your child to catch and transmit a potentially fatal infection? That’s what we’re struggling with now.”
When meeting with parents who are skeptical about vaccines or refuse their children to have them, Dr. Offit advises clinicians to “go down swinging” in favor of vaccination. He shared how his wife, Bonnie, a pediatrician who practices in suburban Philadelphia, counsels parents who raise such concerns. “The way she handled it initially was to do the best she could to eventually get people vaccinated,” he said. “She was successful about one-quarter of the time. Then she drew a line. She started saying to parents, ‘Look; don’t put me in a position where you are asking me to practice substandard care. I can’t send them out of this room knowing that there’s more measles out there, knowing that there’s mumps out there, knowing that there’s whooping cough out there, knowing that there’s pneumococcus and varicella out there. If this child leaves this office and is hurt by any of those viruses or bacteria and I knew I could have done something to prevent it, I couldn’t live with myself. If you’re going to let this child out without being vaccinated I can’t see you anymore because I’m responsible for the health of this child.’ With that [approach], she has been far more successful. Because at some level, if you continue to see that patient, you’re tacitly agreeing that it’s okay to [not vaccinate].”
In 2000, Dr. Offit and colleagues created the Vaccine Education Center at Children’s Hospital of Philadelphia, which provides complete, up-to-date, and reliable information about vaccines to parents and clinicians. It summarizes the purpose of each vaccine, and the relative risks and benefits in easy-to-read language. The CDC also maintains updated information about vaccines and immunizations on its web site. For his part, Dr. Offit tells parents that passing on an opportunity to vaccinate their child is not a risk-free choice. “If you choose not to get a vaccine you probably will get away with it, but you might not,” he said. “You are playing a game of Russian roulette. It may not be five empty chambers and one bullet, but maybe it’s 100,000 empty chambers and one bullet. There’s a bullet there.”
Dr. Offit reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM AAP 2019
Lung cancer on the decline, but still higher among men than women
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
according to the Centers for Disease Control and Prevention.
![]()
From 2007 to 2016, rates dropped among both sexes in metropolitan and nonmetropolitan areas, according to Mary Elizabeth O’Neil, MPH, and colleagues. Their report is in Morbidity and Mortality Weekly Report (MMWR Morb Mortal Wkly Rep. 2019 Nov 8;68[44];993-8). But lung cancer incidence in 2016 was still 40% higher among men than among women, said Ms. O’Neil, an epidemiologist at the CDC.
Rather than narrowly focusing on the “just stop smoking” message, “a comprehensive approach to lung cancer prevention and control includes such population-based strategies as screening for tobacco dependence, promoting tobacco cessation, implementing comprehensive smoke-free laws, testing all homes for radon and using proven methods to lower high radon levels, and reducing exposure to lung carcinogens such as asbestos.” According to the authors of the report, “increasing the implementation of these strategies, particularly among persons living in nonmetropolitan counties, might help to reduce disparities in the decline of lung cancer incidence.”
The recommendation is based on data extracted from the U.S. Cancer Statistics Database for 2007-2016. The data cover 97% of the population.
In nonmetropolitan counties in 2007, incidence rates among men were 60% higher (99 vs. 61 per 100,000). Although rates decreased in both sexes, they were still elevated compared with women in 2016 (82 vs. 58 per 100,000; 40%).
Over the 10-year period, the rate declined more among men than among women (–2.9% vs. –1.5%) in metropolitan areas. The pattern repeated in nonmetropolitan areas (–2.1% and –0.5%, respectively).
There were different declines in different age groups by region, the authors noted.
Men aged 45-54 years in metropolitan areas experienced the largest decline (–5.2%).
Among women, the largest decline occurred in metropolitan areas among those aged 35-44 years (–5%). In nonmetropolitan areas, women in this age group experienced a 3.6% decline and women aged 65-74 years, a 1.3% decline.
Among persons aged 35-54 years, incidence rates in nonmetropolitan and metropolitan counties did not differ by sex but were higher in nonmetropolitan counties than in metropolitan counties.
There were also overall changes in smoking patterns. According to 2017 data from the National Health Interview Survey data, more adults in metropolitan areas than nonmetropolitan areas smoked (23% versus 13%) but fewer had tried to quit (50% vs. 56%). Successful quitting attempts also were lower (5% vs. 9%).
Although it is a large contributing factor, smoking is not the only risk factor for lung cancer, the authors wrote. About 10%-15% of lung cancer patients have never smoked tobacco. Nonsmoked tobacco products and second-hand exposure to cigarette smoke are risks, as are indoor radon and asbestos exposure.
Clinicians can help improve this scenario by screening at each office visit, the authors said. The recommendation is based on U.S. Preventive Services Task Force guidance.
“Lung cancer screening is recommended for adults at high risk for developing lung cancer because of their age and cigarette smoking history. Screening efforts can identify lung cancer in its early stages and provide an important opportunity to promote tobacco smoking cessation.”
However, lack of insurance among residents of nonmetropolitan areas may hamper access to these services, they said. In those regions, “a higher percentage of residents aged less than 65 years report being uninsured compared with those in metropolitan areas.”
SOURCE: O’Neil ME et al. MMWR Morb Mortal Wkly Rep. 2019 Nov 8: 68(44);993-8.
FROM MMWR
Dupilumab effective in early- and late-onset asthma
NEW ORLEANS – A new analysis suggests

Dupilumab may be more effective in reducing severe asthma exacerbations in patients with late-onset asthma, but the drug’s effect on lung function appeared the same regardless of asthma onset. Nicola Hanania, MD, of Baylor College of Medicine in Houston presented these results at the annual meeting of the American College of Chest Physicians.
Dr. Hanania and colleagues conducted a subanalysis of the LIBERTY ASTHMA QUEST study (NCT02414854). Previous data from this study showed that patients with uncontrolled, moderate to severe asthma who received dupilumab had fewer exacerbations and better lung function than did patients who received placebo (N Engl J Med. 2018;378:2486-96).
In their subanalysis, Dr. Hanania and his colleagues evaluated the efficacy of dupilumab, given at 200 mg or 300 mg every 2 weeks, in patients with early-onset asthma (at 40 years of age or younger) and late-onset asthma (at 41 years or older). The analysis included 919 patients with early-onset asthma who received dupilumab and 450 early-onset patients who received placebo. There were 345 patients with late-onset asthma who received dupilumab and 188 late-onset patients who received placebo.
Exacerbations
Dupilumab significantly reduced the adjusted annualized severe exacerbation rates during the 52-week treatment period. Significant reductions occurred in both early- and late-onset patients, though reductions were greater in the late-onset group.
In early-onset patients, dupilumab reduced severe exacerbations by 38% when given at 200 mg and by 37% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients, dupilumab reduced exacerbations by 64% and 69%, respectively (P less than .001 vs. placebo).
Dr. Hanania said it isn’t clear why late-onset patients appear to derive more benefit with regard to exacerbations. It may be because these patients have more comorbidities or because they aren’t using their inhalers correctly. The researchers are investigating these possibilities.
Dr. Hanania went on to note that reductions in exacerbation rates were greatest in patients with elevated blood eosinophils (150 cells/mcL or greater) or fractional exhaled nitric oxide (FeNO; 25 ppb or greater).
In patients with early-onset asthma and elevated eosinophils, dupilumab reduced severe exacerbations by 50% when given at 200 mg and by 55% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated eosinophils, dupilumab reduced exacerbations by 65% and 73%, respectively (P less than .001 vs. placebo).
In patients with early-onset asthma and elevated FeNO, dupilumab reduced severe exacerbations by 56% when given at 200 mg and by 52% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated FeNO, dupilumab reduced exacerbations by 79% and 71%, respectively (P less than .001 vs. placebo).
Lung function
Dupilumab also improved prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), compared with placebo, with similar results in early- and late-onset patients.
In early-onset patients, the P values were less than .001 for both doses of dupilumab at weeks 12 and 52. In late-onset patients, the P values were less than .001 for the 300-mg dose at week 12 and the 200-mg dose at week 52, less than .01 for the 200-mg dose at week 12, and less than .05 for the 300-mg dose at week 52.
The effects of dupilumab on pre-BD FEV1 were greatest in patients with elevated eosinophils or FeNO. At week 12, the P value was less than .001 for both doses of dupilumab in early-onset patients with elevated eosinophils or FeNO. The P value was less than .01 for both doses in late-onset patients with elevated eosinophils. And the P value was less than .001 for both doses in late-onset patients with elevated FeNO.
This research was sponsored by Sanofi and Regeneron. Dr. Hanania disclosed relationships with Genentech, Novartis, AstraZeneca, Boehringer Ingelheim, GSK, Regeneron, and Sanofi.
SOURCE: Hanania N et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.870.
NEW ORLEANS – A new analysis suggests
Dupilumab may be more effective in reducing severe asthma exacerbations in patients with late-onset asthma, but the drug’s effect on lung function appeared the same regardless of asthma onset. Nicola Hanania, MD, of Baylor College of Medicine in Houston presented these results at the annual meeting of the American College of Chest Physicians.
Dr. Hanania and colleagues conducted a subanalysis of the LIBERTY ASTHMA QUEST study (NCT02414854). Previous data from this study showed that patients with uncontrolled, moderate to severe asthma who received dupilumab had fewer exacerbations and better lung function than did patients who received placebo (N Engl J Med. 2018;378:2486-96).
In their subanalysis, Dr. Hanania and his colleagues evaluated the efficacy of dupilumab, given at 200 mg or 300 mg every 2 weeks, in patients with early-onset asthma (at 40 years of age or younger) and late-onset asthma (at 41 years or older). The analysis included 919 patients with early-onset asthma who received dupilumab and 450 early-onset patients who received placebo. There were 345 patients with late-onset asthma who received dupilumab and 188 late-onset patients who received placebo.
Exacerbations
Dupilumab significantly reduced the adjusted annualized severe exacerbation rates during the 52-week treatment period. Significant reductions occurred in both early- and late-onset patients, though reductions were greater in the late-onset group.
In early-onset patients, dupilumab reduced severe exacerbations by 38% when given at 200 mg and by 37% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients, dupilumab reduced exacerbations by 64% and 69%, respectively (P less than .001 vs. placebo).
Dr. Hanania said it isn’t clear why late-onset patients appear to derive more benefit with regard to exacerbations. It may be because these patients have more comorbidities or because they aren’t using their inhalers correctly. The researchers are investigating these possibilities.
Dr. Hanania went on to note that reductions in exacerbation rates were greatest in patients with elevated blood eosinophils (150 cells/mcL or greater) or fractional exhaled nitric oxide (FeNO; 25 ppb or greater).
In patients with early-onset asthma and elevated eosinophils, dupilumab reduced severe exacerbations by 50% when given at 200 mg and by 55% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated eosinophils, dupilumab reduced exacerbations by 65% and 73%, respectively (P less than .001 vs. placebo).
In patients with early-onset asthma and elevated FeNO, dupilumab reduced severe exacerbations by 56% when given at 200 mg and by 52% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated FeNO, dupilumab reduced exacerbations by 79% and 71%, respectively (P less than .001 vs. placebo).
Lung function
Dupilumab also improved prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), compared with placebo, with similar results in early- and late-onset patients.
In early-onset patients, the P values were less than .001 for both doses of dupilumab at weeks 12 and 52. In late-onset patients, the P values were less than .001 for the 300-mg dose at week 12 and the 200-mg dose at week 52, less than .01 for the 200-mg dose at week 12, and less than .05 for the 300-mg dose at week 52.
The effects of dupilumab on pre-BD FEV1 were greatest in patients with elevated eosinophils or FeNO. At week 12, the P value was less than .001 for both doses of dupilumab in early-onset patients with elevated eosinophils or FeNO. The P value was less than .01 for both doses in late-onset patients with elevated eosinophils. And the P value was less than .001 for both doses in late-onset patients with elevated FeNO.
This research was sponsored by Sanofi and Regeneron. Dr. Hanania disclosed relationships with Genentech, Novartis, AstraZeneca, Boehringer Ingelheim, GSK, Regeneron, and Sanofi.
SOURCE: Hanania N et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.870.
NEW ORLEANS – A new analysis suggests
Dupilumab may be more effective in reducing severe asthma exacerbations in patients with late-onset asthma, but the drug’s effect on lung function appeared the same regardless of asthma onset. Nicola Hanania, MD, of Baylor College of Medicine in Houston presented these results at the annual meeting of the American College of Chest Physicians.
Dr. Hanania and colleagues conducted a subanalysis of the LIBERTY ASTHMA QUEST study (NCT02414854). Previous data from this study showed that patients with uncontrolled, moderate to severe asthma who received dupilumab had fewer exacerbations and better lung function than did patients who received placebo (N Engl J Med. 2018;378:2486-96).
In their subanalysis, Dr. Hanania and his colleagues evaluated the efficacy of dupilumab, given at 200 mg or 300 mg every 2 weeks, in patients with early-onset asthma (at 40 years of age or younger) and late-onset asthma (at 41 years or older). The analysis included 919 patients with early-onset asthma who received dupilumab and 450 early-onset patients who received placebo. There were 345 patients with late-onset asthma who received dupilumab and 188 late-onset patients who received placebo.
Exacerbations
Dupilumab significantly reduced the adjusted annualized severe exacerbation rates during the 52-week treatment period. Significant reductions occurred in both early- and late-onset patients, though reductions were greater in the late-onset group.
In early-onset patients, dupilumab reduced severe exacerbations by 38% when given at 200 mg and by 37% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients, dupilumab reduced exacerbations by 64% and 69%, respectively (P less than .001 vs. placebo).
Dr. Hanania said it isn’t clear why late-onset patients appear to derive more benefit with regard to exacerbations. It may be because these patients have more comorbidities or because they aren’t using their inhalers correctly. The researchers are investigating these possibilities.
Dr. Hanania went on to note that reductions in exacerbation rates were greatest in patients with elevated blood eosinophils (150 cells/mcL or greater) or fractional exhaled nitric oxide (FeNO; 25 ppb or greater).
In patients with early-onset asthma and elevated eosinophils, dupilumab reduced severe exacerbations by 50% when given at 200 mg and by 55% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated eosinophils, dupilumab reduced exacerbations by 65% and 73%, respectively (P less than .001 vs. placebo).
In patients with early-onset asthma and elevated FeNO, dupilumab reduced severe exacerbations by 56% when given at 200 mg and by 52% when given at 300 mg (P less than .001 vs. placebo). In late-onset patients with elevated FeNO, dupilumab reduced exacerbations by 79% and 71%, respectively (P less than .001 vs. placebo).
Lung function
Dupilumab also improved prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), compared with placebo, with similar results in early- and late-onset patients.
In early-onset patients, the P values were less than .001 for both doses of dupilumab at weeks 12 and 52. In late-onset patients, the P values were less than .001 for the 300-mg dose at week 12 and the 200-mg dose at week 52, less than .01 for the 200-mg dose at week 12, and less than .05 for the 300-mg dose at week 52.
The effects of dupilumab on pre-BD FEV1 were greatest in patients with elevated eosinophils or FeNO. At week 12, the P value was less than .001 for both doses of dupilumab in early-onset patients with elevated eosinophils or FeNO. The P value was less than .01 for both doses in late-onset patients with elevated eosinophils. And the P value was less than .001 for both doses in late-onset patients with elevated FeNO.
This research was sponsored by Sanofi and Regeneron. Dr. Hanania disclosed relationships with Genentech, Novartis, AstraZeneca, Boehringer Ingelheim, GSK, Regeneron, and Sanofi.
SOURCE: Hanania N et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.870.
REPORTING FROM CHEST 2019
Measles infection linked to impaired ‘immune memory’
Infection with the measles virus appears to reduce immunity to other pathogens, according to a paper published in Science.

The hypothesis that the measles virus could cause “immunological amnesia” by impairing immune memory is supported by early research showing children with measles had negative cutaneous tuberculin reactions after having previously tested positive.
“Subsequent studies have shown decreased interferon signaling, skewed cytokine responses, lymphopenia, and suppression of lymphocyte proliferation shortly after infection,” wrote Michael Mina, MD, from Brigham and Women’s Hospital in Boston, and coauthors.
“Given the variation in the degree of immune repertoire modulation we observed, we anticipate that future risk of morbidity and mortality after measles would not be homogeneous but would be skewed toward individuals with the most severe elimination of immunological memory,” they wrote. “These findings underscore the crucial need for continued widespread vaccination.”
In this study, researchers compared the levels of around 400 pathogen-specific antibodies in blood samples from 77 unvaccinated children, taken before and 2 months after natural measles infection, with 5 unvaccinated children who did not contract measles. A total of 34 the children experienced mild measles, and 43 had severe measles.
They found that the samples taken after measles infection showed “substantial” reductions in the number of pathogen epitopes, compared with the samples from children who did not get infected with measles.
This amounted to approximately a 20% mean reduction in overall diversity or size of the antibody repertoire. However, in children who experienced severe measles, there was a median loss of 40% (range, 11%-62%) of antibody repertoire, compared with a median of 33% (range, 12%-73%) range in children who experienced mild infection. Meanwhile, the control subjects retained approximately 90% of their antibody repertoire over a similar or longer time period. Some children lost up to 70% of antibodies for specific pathogens.
The study did find increases in measles virus–specific antigens in children both after measles infection and MMR vaccination. However the authors did not detect any changes in total IgG, IgA, or IgM levels.
Dr. Mina and associates wrote.
They also noted that controls who received the MMR vaccine showed a marked increase in overall antibody repertoire.
In a separate investigation reported in Science Immunology, Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles to determine if B-cell impairment can lead to measles-associated immunosuppression. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IgVH-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B-cell frequencies in measles patients recovered to levels before infection, they had significant changes in IgVH-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IgVH-J genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IgVH genes, Dr. Petrova and associates reported.
The study by Mina et al. was supported by grants from various U.S., European, and Finnish foundations and national organizations. Some of the coauthors had relationships with biotechnology and pharmaceutical companies, and three reported a patent holding related to technology used in the study. The study by Petrova et al. was funded by grants to the investigators from various Indonesian and German organizations and the Wellcome Trust. The authors reported no conflicts of interest.
SOURCES: Mina M et al. Science. 2019 Nov 1;366:599-606; Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125.
As a result of reduced vaccination, after decades of decline, the number of worldwide cases of measles has increased by nearly 300% since 2018. Epidemiologic evidence has associated measles infections with increases in morbidity and mortality for as long as 5 years after the infection and suggests that, in the prevaccine era, measles virus may have been associated with up to 50% of all childhood deaths, mostly because of nonmeasles infections. Measles replication in immune cells has been hypothesized to impair immune memory, potentially causing what some scientists call “immunological amnesia.”A measles virus receptor, called CD150/ SLAMF1, is highly expressed on memory T, B, and plasma cells. Measles virus gains entry to these immune memory cells using that receptor and kills the cells.

The scientists stated that it could take months or years to return the immune repertoire back to baseline. During the rebuilding process, children would be at increased risk for infectious diseases they had previously experienced.
In a second outstanding paper, Petrova et al. in Science Immunology studied B cells before and after measles infection, and identified two immunologic consequences: The naive B-cell pool was depleted, leading to a return to immunologic immaturity, and the memory B-cell pool was depleted, resulting in compromised immune memory to previously encountered pathogens.
Thus, the link between measles infections and increased susceptibility to other infections and increased deaths from nonmeasles infectious diseases in the aftermath of measles has been revealed. This information adds new data to share with parents who consider refusing measles vaccination. The risks are far greater than getting measles.
Michael E. Pichichero, MD, is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He was asked to comment on the articles. Dr. Pichichero has no conflicts to declare.
As a result of reduced vaccination, after decades of decline, the number of worldwide cases of measles has increased by nearly 300% since 2018. Epidemiologic evidence has associated measles infections with increases in morbidity and mortality for as long as 5 years after the infection and suggests that, in the prevaccine era, measles virus may have been associated with up to 50% of all childhood deaths, mostly because of nonmeasles infections. Measles replication in immune cells has been hypothesized to impair immune memory, potentially causing what some scientists call “immunological amnesia.”A measles virus receptor, called CD150/ SLAMF1, is highly expressed on memory T, B, and plasma cells. Measles virus gains entry to these immune memory cells using that receptor and kills the cells.
The scientists stated that it could take months or years to return the immune repertoire back to baseline. During the rebuilding process, children would be at increased risk for infectious diseases they had previously experienced.
In a second outstanding paper, Petrova et al. in Science Immunology studied B cells before and after measles infection, and identified two immunologic consequences: The naive B-cell pool was depleted, leading to a return to immunologic immaturity, and the memory B-cell pool was depleted, resulting in compromised immune memory to previously encountered pathogens.
Thus, the link between measles infections and increased susceptibility to other infections and increased deaths from nonmeasles infectious diseases in the aftermath of measles has been revealed. This information adds new data to share with parents who consider refusing measles vaccination. The risks are far greater than getting measles.
Michael E. Pichichero, MD, is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He was asked to comment on the articles. Dr. Pichichero has no conflicts to declare.
As a result of reduced vaccination, after decades of decline, the number of worldwide cases of measles has increased by nearly 300% since 2018. Epidemiologic evidence has associated measles infections with increases in morbidity and mortality for as long as 5 years after the infection and suggests that, in the prevaccine era, measles virus may have been associated with up to 50% of all childhood deaths, mostly because of nonmeasles infections. Measles replication in immune cells has been hypothesized to impair immune memory, potentially causing what some scientists call “immunological amnesia.”A measles virus receptor, called CD150/ SLAMF1, is highly expressed on memory T, B, and plasma cells. Measles virus gains entry to these immune memory cells using that receptor and kills the cells.
The scientists stated that it could take months or years to return the immune repertoire back to baseline. During the rebuilding process, children would be at increased risk for infectious diseases they had previously experienced.
In a second outstanding paper, Petrova et al. in Science Immunology studied B cells before and after measles infection, and identified two immunologic consequences: The naive B-cell pool was depleted, leading to a return to immunologic immaturity, and the memory B-cell pool was depleted, resulting in compromised immune memory to previously encountered pathogens.
Thus, the link between measles infections and increased susceptibility to other infections and increased deaths from nonmeasles infectious diseases in the aftermath of measles has been revealed. This information adds new data to share with parents who consider refusing measles vaccination. The risks are far greater than getting measles.
Michael E. Pichichero, MD, is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. He was asked to comment on the articles. Dr. Pichichero has no conflicts to declare.
Infection with the measles virus appears to reduce immunity to other pathogens, according to a paper published in Science.
The hypothesis that the measles virus could cause “immunological amnesia” by impairing immune memory is supported by early research showing children with measles had negative cutaneous tuberculin reactions after having previously tested positive.
“Subsequent studies have shown decreased interferon signaling, skewed cytokine responses, lymphopenia, and suppression of lymphocyte proliferation shortly after infection,” wrote Michael Mina, MD, from Brigham and Women’s Hospital in Boston, and coauthors.
“Given the variation in the degree of immune repertoire modulation we observed, we anticipate that future risk of morbidity and mortality after measles would not be homogeneous but would be skewed toward individuals with the most severe elimination of immunological memory,” they wrote. “These findings underscore the crucial need for continued widespread vaccination.”
In this study, researchers compared the levels of around 400 pathogen-specific antibodies in blood samples from 77 unvaccinated children, taken before and 2 months after natural measles infection, with 5 unvaccinated children who did not contract measles. A total of 34 the children experienced mild measles, and 43 had severe measles.
They found that the samples taken after measles infection showed “substantial” reductions in the number of pathogen epitopes, compared with the samples from children who did not get infected with measles.
This amounted to approximately a 20% mean reduction in overall diversity or size of the antibody repertoire. However, in children who experienced severe measles, there was a median loss of 40% (range, 11%-62%) of antibody repertoire, compared with a median of 33% (range, 12%-73%) range in children who experienced mild infection. Meanwhile, the control subjects retained approximately 90% of their antibody repertoire over a similar or longer time period. Some children lost up to 70% of antibodies for specific pathogens.
The study did find increases in measles virus–specific antigens in children both after measles infection and MMR vaccination. However the authors did not detect any changes in total IgG, IgA, or IgM levels.
Dr. Mina and associates wrote.
They also noted that controls who received the MMR vaccine showed a marked increase in overall antibody repertoire.
In a separate investigation reported in Science Immunology, Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles to determine if B-cell impairment can lead to measles-associated immunosuppression. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IgVH-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B-cell frequencies in measles patients recovered to levels before infection, they had significant changes in IgVH-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IgVH-J genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IgVH genes, Dr. Petrova and associates reported.
The study by Mina et al. was supported by grants from various U.S., European, and Finnish foundations and national organizations. Some of the coauthors had relationships with biotechnology and pharmaceutical companies, and three reported a patent holding related to technology used in the study. The study by Petrova et al. was funded by grants to the investigators from various Indonesian and German organizations and the Wellcome Trust. The authors reported no conflicts of interest.
SOURCES: Mina M et al. Science. 2019 Nov 1;366:599-606; Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125.
Infection with the measles virus appears to reduce immunity to other pathogens, according to a paper published in Science.
The hypothesis that the measles virus could cause “immunological amnesia” by impairing immune memory is supported by early research showing children with measles had negative cutaneous tuberculin reactions after having previously tested positive.
“Subsequent studies have shown decreased interferon signaling, skewed cytokine responses, lymphopenia, and suppression of lymphocyte proliferation shortly after infection,” wrote Michael Mina, MD, from Brigham and Women’s Hospital in Boston, and coauthors.
“Given the variation in the degree of immune repertoire modulation we observed, we anticipate that future risk of morbidity and mortality after measles would not be homogeneous but would be skewed toward individuals with the most severe elimination of immunological memory,” they wrote. “These findings underscore the crucial need for continued widespread vaccination.”
In this study, researchers compared the levels of around 400 pathogen-specific antibodies in blood samples from 77 unvaccinated children, taken before and 2 months after natural measles infection, with 5 unvaccinated children who did not contract measles. A total of 34 the children experienced mild measles, and 43 had severe measles.
They found that the samples taken after measles infection showed “substantial” reductions in the number of pathogen epitopes, compared with the samples from children who did not get infected with measles.
This amounted to approximately a 20% mean reduction in overall diversity or size of the antibody repertoire. However, in children who experienced severe measles, there was a median loss of 40% (range, 11%-62%) of antibody repertoire, compared with a median of 33% (range, 12%-73%) range in children who experienced mild infection. Meanwhile, the control subjects retained approximately 90% of their antibody repertoire over a similar or longer time period. Some children lost up to 70% of antibodies for specific pathogens.
The study did find increases in measles virus–specific antigens in children both after measles infection and MMR vaccination. However the authors did not detect any changes in total IgG, IgA, or IgM levels.
Dr. Mina and associates wrote.
They also noted that controls who received the MMR vaccine showed a marked increase in overall antibody repertoire.
In a separate investigation reported in Science Immunology, Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles to determine if B-cell impairment can lead to measles-associated immunosuppression. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IgVH-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B-cell frequencies in measles patients recovered to levels before infection, they had significant changes in IgVH-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IgVH-J genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IgVH genes, Dr. Petrova and associates reported.
The study by Mina et al. was supported by grants from various U.S., European, and Finnish foundations and national organizations. Some of the coauthors had relationships with biotechnology and pharmaceutical companies, and three reported a patent holding related to technology used in the study. The study by Petrova et al. was funded by grants to the investigators from various Indonesian and German organizations and the Wellcome Trust. The authors reported no conflicts of interest.
SOURCES: Mina M et al. Science. 2019 Nov 1;366:599-606; Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125.
FROM SCIENCE
Student vapers make mint the most popular Juul flavor
according to data from the 2019 Monitoring the Future study.
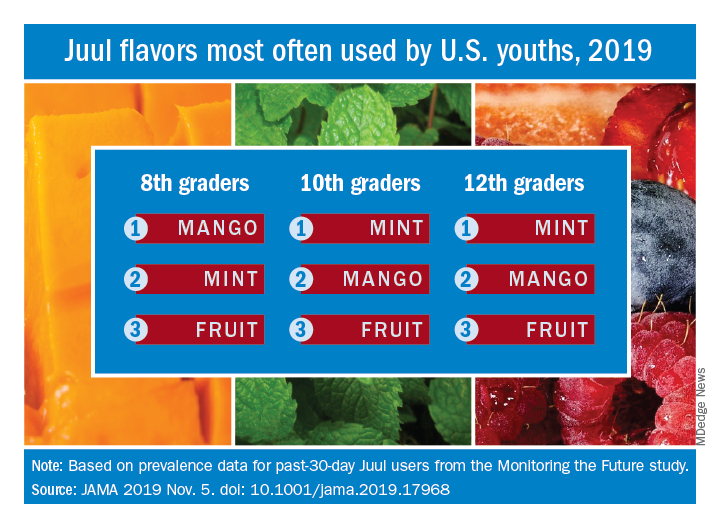
Almost half (47.1%) of the 12th graders who had used Juul e-cigarettes in the past 30 days reported that mint was the flavor they most often used, compared with 23.8% for mango and 8.6% for fruit, which is a combination of flavors, Adam M. Leventhal, PhD, of the University of Southern California, Los Angeles, and associates wrote in JAMA.
Mint was also the flavor most often used by 10th graders (43.5%), with mango again second at 27.3%, and fruit third at 10.8%. Eighth-grade students switched mango (33.5%) and mint (29.2%) but had fruit third again at 16.0%, the investigators reported, based on data for 1,739 respondents to the Monitoring the Future survey who had used a vaping product within the past 30 days.
Juul has suspended sales of four – mango, fruit, creme, and cucumber – of its original eight flavors, Dr. Leventhal and associates noted, and e-cigarette flavors other than tobacco, menthol, and mint have been prohibited by some local municipalities.
“The current findings raise uncertainty whether regulations or sales suspensions that exempt mint flavors are optimal strategies for reducing youth e-cigarette use,” they wrote.
As this article was being written, the Wall Street Journal had just reported that the Food and Drug Administration will ban mint and all other e-cigarette flavors except tobacco and menthol.
SOURCE: Leventhal AM et al. JAMA. 2019 Nov 5. doi: 10.1001/jama.2019.17968.
according to data from the 2019 Monitoring the Future study.
Almost half (47.1%) of the 12th graders who had used Juul e-cigarettes in the past 30 days reported that mint was the flavor they most often used, compared with 23.8% for mango and 8.6% for fruit, which is a combination of flavors, Adam M. Leventhal, PhD, of the University of Southern California, Los Angeles, and associates wrote in JAMA.
Mint was also the flavor most often used by 10th graders (43.5%), with mango again second at 27.3%, and fruit third at 10.8%. Eighth-grade students switched mango (33.5%) and mint (29.2%) but had fruit third again at 16.0%, the investigators reported, based on data for 1,739 respondents to the Monitoring the Future survey who had used a vaping product within the past 30 days.
Juul has suspended sales of four – mango, fruit, creme, and cucumber – of its original eight flavors, Dr. Leventhal and associates noted, and e-cigarette flavors other than tobacco, menthol, and mint have been prohibited by some local municipalities.
“The current findings raise uncertainty whether regulations or sales suspensions that exempt mint flavors are optimal strategies for reducing youth e-cigarette use,” they wrote.
As this article was being written, the Wall Street Journal had just reported that the Food and Drug Administration will ban mint and all other e-cigarette flavors except tobacco and menthol.
SOURCE: Leventhal AM et al. JAMA. 2019 Nov 5. doi: 10.1001/jama.2019.17968.
according to data from the 2019 Monitoring the Future study.
Almost half (47.1%) of the 12th graders who had used Juul e-cigarettes in the past 30 days reported that mint was the flavor they most often used, compared with 23.8% for mango and 8.6% for fruit, which is a combination of flavors, Adam M. Leventhal, PhD, of the University of Southern California, Los Angeles, and associates wrote in JAMA.
Mint was also the flavor most often used by 10th graders (43.5%), with mango again second at 27.3%, and fruit third at 10.8%. Eighth-grade students switched mango (33.5%) and mint (29.2%) but had fruit third again at 16.0%, the investigators reported, based on data for 1,739 respondents to the Monitoring the Future survey who had used a vaping product within the past 30 days.
Juul has suspended sales of four – mango, fruit, creme, and cucumber – of its original eight flavors, Dr. Leventhal and associates noted, and e-cigarette flavors other than tobacco, menthol, and mint have been prohibited by some local municipalities.
“The current findings raise uncertainty whether regulations or sales suspensions that exempt mint flavors are optimal strategies for reducing youth e-cigarette use,” they wrote.
As this article was being written, the Wall Street Journal had just reported that the Food and Drug Administration will ban mint and all other e-cigarette flavors except tobacco and menthol.
SOURCE: Leventhal AM et al. JAMA. 2019 Nov 5. doi: 10.1001/jama.2019.17968.
FROM JAMA
Robotic bronchoscopy beat standard techniques for targeting lung nodules
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
NEW ORLEANS –
A prospective study in a cadaver model showed that robotic bronchoscopy targeted nodules more effectively than electromagnetic navigation or an ultrathin bronchoscope with radial endobronchial ultrasound (UTB-rEBUS).
“This is really the first study to randomize, blind, and compare procedural outcomes between existing technologies in advanced bronchoscopy,” said Lonny Yarmus, DO, of Johns Hopkins Medicine in Baltimore.
Dr. Yarmus described this study, PRECISION-1, at the annual meeting of the American Society of Chest Physicians. The study was designed to compare the following:
- UTB-rEBUS (3.0 mm outer diameter and 1.7 mm working channel).
- Electromagnetic navigation bronchoscopy (Superdimension version 7.1).
- Robotic bronchoscopy (3.5 mm outer diameter and 2.0-mm working channel).
With all methods, a 21-gauge needle was used. For each nodule, UTB-rEBUS was done first to eliminate potential localization bias. The subsequent order of electromagnetic navigation and robotic bronchoscopy was determined based on block randomization.
Eight bronchoscopists performed a total of 60 procedures using each of the methods to target 20 nodules implanted in cadavers. The nodules were distributed across all lobes, 80% were in the outer third of the lung, and 50% had a positive bronchus sign on computed tomography (CT). The mean nodule size was 16.5 plus or minus 1.5 mm.
The study’s primary endpoint was the ability to localize and puncture target nodules within a maximum of three attempts per method. This includes center, peripheral, and distal punctures of nodules. Cone-beam CT was used to confirm that needles punctured the target lesions. The bronchoscopists were blinded to cone-beam CT results, and a blinded, independent investigator assessed whether nodule punctures were successful. The primary endpoint was met in 25% of UTB-rEBUS procedures, 45% of electromagnetic navigation procedures, and 80% of robotic bronchoscopy procedures.
The study’s secondary endpoint was localization success, which was defined as navigation to within needle biopsy distance of the nodule. This includes center, peripheral, and distal punctures of nodules, as well as adjacent punctures (touching the nodule but not within it). The secondary endpoint was met in 35% of UTB-rEBUS procedures, 65% of electromagnetic navigation procedures, and 90% of robotic bronchoscopy procedures.
The researchers also assessed successful navigation, which was defined as the provider localizing with software or radial ultrasound and passing the needle to make a biopsy attempt. Navigation was successful in 65% of UTB-rEBUS procedures, 85% of electromagnetic navigation procedures, and 100% of robotic bronchoscopy procedures.
“Utilization of robotic bronchoscopy with shape-sensing technology can significantly increase the ability to localize and puncture lesions when compared with standard existing technologies,” Dr. Yarmus said in closing.
He did note that this research was done in a cadaveric model, so “prospective, randomized, and comparative in vivo studies are needed.”
This study was funded by the Association of Interventional Pulmonary Program Directors. Dr. Yarmus disclosed government and societal funding and relationships with Boston Scientific, Veran, Medtronic, Intuitive, Auris, Erbe, Olympus, BD, Rocket, Ambu, Inspire Medical, and AstraZeneca.
SOURCE: Yarmus L et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.311.
REPORTING FROM CHEST 2019
Inhaled nitric oxide improves activity in pulmonary fibrosis patients at risk of PH
NEW ORLEANS – In patients with interstitial lung diseases at risk of pulmonary hypertension, inhaled nitric oxide produced meaningful improvements in activity that have been maintained over the long term, an investigator reported here.
Inhaled nitric oxide, which improved moderate to vigorous physical activity by 34% versus placebo in an 8-week controlled trial, has demonstrated long-term maintenance of activity parameters in open-label extension data, presented at the annual meeting of the American College of Chest Physicians.

The treatment was safe and well tolerated in this cohort of subjects at risk of pulmonary hypertension associated with pulmonary fibrosis (PH-PF), said Steven D. Nathan, MD, director of the advanced lung disease and lung transplant program at Inova Fairfax (Va.) Hospital.
The findings to date suggest inhaled nitric oxide (iNO) is a potentially effective treatment option for patients at risk for pulmonary hypertension, which is associated with poor outcomes in various forms of interstitial lung disease, Dr. Nathan said in his presentation, adding that a second cohort of PH-PF patients has been fully recruited and continue to be followed.
“Hopefully, once we show that iNO is positive and validate what we’ve seen with cohort one, then we’ll be moving on to cohort three, which will be a pivotal phase 3 clinical study with actigraphy activity–monitoring being the primary endpoint, and that has been agreed upon by the Food and Drug Administration,” he said.
The actigraph device used in the study, worn on the wrist of the nondominant arm, continuously measures patient movement in acceleration units and allows for categorization of intensity, from sedentary to vigorous, Dr. Nathan explained in this presentation.
“To me, actigraphy activity–monitoring is kind of a step beyond the 6-minute walk test,” he said. “We get a sense of how [patients] might function, based on the 6-minute walk test, but what actigraphy gives us is actually how they do function once they leave the clinic. So I think this is emerging as a very viable and valuable endpoint in clinical trials.”
Dr. Nathan reported on 23 patients with a variety of pulmonary fibrotic interstitial lung diseases randomized to receive iNO 30 mcg/kg based on their ideal body weight (IBW) per hour, and 18 who were randomized to placebo, for 8 weeks of blinded treatment. After that, patients from both arms transitioned to open-label treatment, stepping up to 45 mcg/kg IBW/hr for at least 8 weeks, and then to 75 mcg/kg IBW/hr.
After the 8 weeks of blinded treatment, activity as measured by actigraphy was maintained in the patients receiving iNO, and decreased in the placebo arm (P = .05), according to Dr. Nathan, who added that this difference was largely driven by changes in levels of moderate to vigorous physical activity, which improved in the treatment arm, while declining substantially in the placebo arm.
Clinically significant improvements in moderate to vigorous physical activity were seen in 23.1% of patients in the treatment arm and 0% of the placebo arm, while clinically significant declines in that measure were seen in 38.5% of the treatment group versus 71.4% of the placebo group.
Data from the open-label extension phase, which included a total of 18 patients, show that activity was “well maintained” over a total of 20 weeks, with patients formerly in the placebo arm demonstrating levels of activity comparable to what was achieved in the patients randomized to treatment: “We felt like this supports the clinical efficacy of the nitric oxide effect, that the placebo arm started to behave like the treatment arm,” Dr. Nathan said.
Some adverse events were reported in the study, but none were felt to be attributable to the iNO, according to Dr. Nathan.
Dr. Nathan provided disclosures related to Roche-Genentech, Boehringer Ingelheim, Promedior, Bellerophon, and United Therapeutics.
SOURCE: Nathan SD et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.308.
NEW ORLEANS – In patients with interstitial lung diseases at risk of pulmonary hypertension, inhaled nitric oxide produced meaningful improvements in activity that have been maintained over the long term, an investigator reported here.
Inhaled nitric oxide, which improved moderate to vigorous physical activity by 34% versus placebo in an 8-week controlled trial, has demonstrated long-term maintenance of activity parameters in open-label extension data, presented at the annual meeting of the American College of Chest Physicians.
The treatment was safe and well tolerated in this cohort of subjects at risk of pulmonary hypertension associated with pulmonary fibrosis (PH-PF), said Steven D. Nathan, MD, director of the advanced lung disease and lung transplant program at Inova Fairfax (Va.) Hospital.
The findings to date suggest inhaled nitric oxide (iNO) is a potentially effective treatment option for patients at risk for pulmonary hypertension, which is associated with poor outcomes in various forms of interstitial lung disease, Dr. Nathan said in his presentation, adding that a second cohort of PH-PF patients has been fully recruited and continue to be followed.
“Hopefully, once we show that iNO is positive and validate what we’ve seen with cohort one, then we’ll be moving on to cohort three, which will be a pivotal phase 3 clinical study with actigraphy activity–monitoring being the primary endpoint, and that has been agreed upon by the Food and Drug Administration,” he said.
The actigraph device used in the study, worn on the wrist of the nondominant arm, continuously measures patient movement in acceleration units and allows for categorization of intensity, from sedentary to vigorous, Dr. Nathan explained in this presentation.
“To me, actigraphy activity–monitoring is kind of a step beyond the 6-minute walk test,” he said. “We get a sense of how [patients] might function, based on the 6-minute walk test, but what actigraphy gives us is actually how they do function once they leave the clinic. So I think this is emerging as a very viable and valuable endpoint in clinical trials.”
Dr. Nathan reported on 23 patients with a variety of pulmonary fibrotic interstitial lung diseases randomized to receive iNO 30 mcg/kg based on their ideal body weight (IBW) per hour, and 18 who were randomized to placebo, for 8 weeks of blinded treatment. After that, patients from both arms transitioned to open-label treatment, stepping up to 45 mcg/kg IBW/hr for at least 8 weeks, and then to 75 mcg/kg IBW/hr.
After the 8 weeks of blinded treatment, activity as measured by actigraphy was maintained in the patients receiving iNO, and decreased in the placebo arm (P = .05), according to Dr. Nathan, who added that this difference was largely driven by changes in levels of moderate to vigorous physical activity, which improved in the treatment arm, while declining substantially in the placebo arm.
Clinically significant improvements in moderate to vigorous physical activity were seen in 23.1% of patients in the treatment arm and 0% of the placebo arm, while clinically significant declines in that measure were seen in 38.5% of the treatment group versus 71.4% of the placebo group.
Data from the open-label extension phase, which included a total of 18 patients, show that activity was “well maintained” over a total of 20 weeks, with patients formerly in the placebo arm demonstrating levels of activity comparable to what was achieved in the patients randomized to treatment: “We felt like this supports the clinical efficacy of the nitric oxide effect, that the placebo arm started to behave like the treatment arm,” Dr. Nathan said.
Some adverse events were reported in the study, but none were felt to be attributable to the iNO, according to Dr. Nathan.
Dr. Nathan provided disclosures related to Roche-Genentech, Boehringer Ingelheim, Promedior, Bellerophon, and United Therapeutics.
SOURCE: Nathan SD et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.308.
NEW ORLEANS – In patients with interstitial lung diseases at risk of pulmonary hypertension, inhaled nitric oxide produced meaningful improvements in activity that have been maintained over the long term, an investigator reported here.
Inhaled nitric oxide, which improved moderate to vigorous physical activity by 34% versus placebo in an 8-week controlled trial, has demonstrated long-term maintenance of activity parameters in open-label extension data, presented at the annual meeting of the American College of Chest Physicians.
The treatment was safe and well tolerated in this cohort of subjects at risk of pulmonary hypertension associated with pulmonary fibrosis (PH-PF), said Steven D. Nathan, MD, director of the advanced lung disease and lung transplant program at Inova Fairfax (Va.) Hospital.
The findings to date suggest inhaled nitric oxide (iNO) is a potentially effective treatment option for patients at risk for pulmonary hypertension, which is associated with poor outcomes in various forms of interstitial lung disease, Dr. Nathan said in his presentation, adding that a second cohort of PH-PF patients has been fully recruited and continue to be followed.
“Hopefully, once we show that iNO is positive and validate what we’ve seen with cohort one, then we’ll be moving on to cohort three, which will be a pivotal phase 3 clinical study with actigraphy activity–monitoring being the primary endpoint, and that has been agreed upon by the Food and Drug Administration,” he said.
The actigraph device used in the study, worn on the wrist of the nondominant arm, continuously measures patient movement in acceleration units and allows for categorization of intensity, from sedentary to vigorous, Dr. Nathan explained in this presentation.
“To me, actigraphy activity–monitoring is kind of a step beyond the 6-minute walk test,” he said. “We get a sense of how [patients] might function, based on the 6-minute walk test, but what actigraphy gives us is actually how they do function once they leave the clinic. So I think this is emerging as a very viable and valuable endpoint in clinical trials.”
Dr. Nathan reported on 23 patients with a variety of pulmonary fibrotic interstitial lung diseases randomized to receive iNO 30 mcg/kg based on their ideal body weight (IBW) per hour, and 18 who were randomized to placebo, for 8 weeks of blinded treatment. After that, patients from both arms transitioned to open-label treatment, stepping up to 45 mcg/kg IBW/hr for at least 8 weeks, and then to 75 mcg/kg IBW/hr.
After the 8 weeks of blinded treatment, activity as measured by actigraphy was maintained in the patients receiving iNO, and decreased in the placebo arm (P = .05), according to Dr. Nathan, who added that this difference was largely driven by changes in levels of moderate to vigorous physical activity, which improved in the treatment arm, while declining substantially in the placebo arm.
Clinically significant improvements in moderate to vigorous physical activity were seen in 23.1% of patients in the treatment arm and 0% of the placebo arm, while clinically significant declines in that measure were seen in 38.5% of the treatment group versus 71.4% of the placebo group.
Data from the open-label extension phase, which included a total of 18 patients, show that activity was “well maintained” over a total of 20 weeks, with patients formerly in the placebo arm demonstrating levels of activity comparable to what was achieved in the patients randomized to treatment: “We felt like this supports the clinical efficacy of the nitric oxide effect, that the placebo arm started to behave like the treatment arm,” Dr. Nathan said.
Some adverse events were reported in the study, but none were felt to be attributable to the iNO, according to Dr. Nathan.
Dr. Nathan provided disclosures related to Roche-Genentech, Boehringer Ingelheim, Promedior, Bellerophon, and United Therapeutics.
SOURCE: Nathan SD et al. CHEST 2019. Abstract, doi: 10.1016/j.chest.2019.08.308.
REPORTING FROM CHEST 2019
Fluoroscopic system can improve targeting of lung lesions
NEW ORLEANS – A novel according to an industry-sponsored, prospective study.

The system, which incorporates fluoroscopic navigation, increased the percentage of cases in which the target overlapped with the lesion, from 60% to 83%. The percentage of cases without any target overlap decreased from 32% to 5%.
“Tomosynthesis-based fluoroscopic navigation … improves the three-dimensional convergence between the virtual target and the actual target,” said Krish Bhadra, MD, of CHI Memorial Medical Group in Chattanooga, Tenn.
Dr. Bhadra presented results with this system at the annual meeting of the American College of Chest Physicians.
He and his colleagues conducted a study of Medtronic’s superDimension navigation system (version 7.2), which provides real-time imaging with three-dimensional fluoroscopy. The system has a “local registration” feature, which uses fluoroscopy and an algorithm to update the virtual target location during the procedure. This allows the user to reposition the catheter based on the location of the lesion.
The researchers tested the system in 50 patients from two centers (NCT03585959). Patients’ lesions had to be larger than 10 mm, not visible endobronchially, and not reachable by convex endobronchial ultrasound. Lesions within 10 mm of the diaphragm were excluded.
The median lesion size was 17.0 mm, 61.2% were smaller than 20 mm, 65.3% were in the upper lobe, and 53.1% had a bronchus sign present. The median distance from lesion to pleura was 5.9 mm.
Dr. Bhadra said the system performed as designed in all cases, and the protocol-defined technical success rate was 95.9% (47/49). Local registration was attempted in 49 patients and was successful in 47 patients (95.9%). In the unsuccessful cases, local registration was not completed based on the system design because the correction distance was greater than 3.0 cm.
The study’s primary endpoint was three-dimensional overlap of the virtual target and the actual lesion, as confirmed by cone-beam computed tomography. Success was defined as greater than 0% overlap after location correction. Target overlap was achieved in 59.6% (28/47) of cases before local registration and 83.0% (39/47) of cases after.
There were six cases in which local registration was successful, but these subjects weren’t evaluable because of failed procedure recording. When those subjects were excluded, target overlap was achieved in 95.1% (39/41) of cases after local registration.
The median percent overlap between the virtual target and the actual lesion was 11.4% before local registration and 32.8% after. The percentage of cases without any target overlap decreased from 31.7% (13/41) before local registration to 4.9% (2/41) after.
Focusing on the two cases without target overlap, Dr. Bhadra noted that he was able to get a biopsy that proved a malignancy in one of those patients. In the other patient, Dr. Bhadra was able to identify features of organizing pneumonia.
“Even though we did not have overlap, we must have been close enough that we were able to get malignant tissue in one [patient] and features of organizing pneumonia in a patient who’s got no history of organizing pneumonia,” Dr. Bhadra said.
He and his colleagues did not evaluate diagnostic yield in this study, but they did assess complications up to 7 days after the procedure.
The team reported one case of pneumothorax, but the patient didn’t require a chest tube. Additionally, there were two cases of bronchopulmonary hemorrhage, but the patients didn’t require any interventions.
This study was sponsored by Medtronic. Dr. Bhadra disclosed relationships with Medtronic, Boston Scientific, BodyVision, Auris Surgical Robotics, Intuitive Surgical, Veracyte, Biodesix, Merit Medical Endotek, and Johnson & Johnson.
SOURCE: Bhadra K et al. CHEST 2019. doi: 10.1016/j.chest.2019.08.314.
NEW ORLEANS – A novel according to an industry-sponsored, prospective study.
The system, which incorporates fluoroscopic navigation, increased the percentage of cases in which the target overlapped with the lesion, from 60% to 83%. The percentage of cases without any target overlap decreased from 32% to 5%.
“Tomosynthesis-based fluoroscopic navigation … improves the three-dimensional convergence between the virtual target and the actual target,” said Krish Bhadra, MD, of CHI Memorial Medical Group in Chattanooga, Tenn.
Dr. Bhadra presented results with this system at the annual meeting of the American College of Chest Physicians.
He and his colleagues conducted a study of Medtronic’s superDimension navigation system (version 7.2), which provides real-time imaging with three-dimensional fluoroscopy. The system has a “local registration” feature, which uses fluoroscopy and an algorithm to update the virtual target location during the procedure. This allows the user to reposition the catheter based on the location of the lesion.
The researchers tested the system in 50 patients from two centers (NCT03585959). Patients’ lesions had to be larger than 10 mm, not visible endobronchially, and not reachable by convex endobronchial ultrasound. Lesions within 10 mm of the diaphragm were excluded.
The median lesion size was 17.0 mm, 61.2% were smaller than 20 mm, 65.3% were in the upper lobe, and 53.1% had a bronchus sign present. The median distance from lesion to pleura was 5.9 mm.
Dr. Bhadra said the system performed as designed in all cases, and the protocol-defined technical success rate was 95.9% (47/49). Local registration was attempted in 49 patients and was successful in 47 patients (95.9%). In the unsuccessful cases, local registration was not completed based on the system design because the correction distance was greater than 3.0 cm.
The study’s primary endpoint was three-dimensional overlap of the virtual target and the actual lesion, as confirmed by cone-beam computed tomography. Success was defined as greater than 0% overlap after location correction. Target overlap was achieved in 59.6% (28/47) of cases before local registration and 83.0% (39/47) of cases after.
There were six cases in which local registration was successful, but these subjects weren’t evaluable because of failed procedure recording. When those subjects were excluded, target overlap was achieved in 95.1% (39/41) of cases after local registration.
The median percent overlap between the virtual target and the actual lesion was 11.4% before local registration and 32.8% after. The percentage of cases without any target overlap decreased from 31.7% (13/41) before local registration to 4.9% (2/41) after.
Focusing on the two cases without target overlap, Dr. Bhadra noted that he was able to get a biopsy that proved a malignancy in one of those patients. In the other patient, Dr. Bhadra was able to identify features of organizing pneumonia.
“Even though we did not have overlap, we must have been close enough that we were able to get malignant tissue in one [patient] and features of organizing pneumonia in a patient who’s got no history of organizing pneumonia,” Dr. Bhadra said.
He and his colleagues did not evaluate diagnostic yield in this study, but they did assess complications up to 7 days after the procedure.
The team reported one case of pneumothorax, but the patient didn’t require a chest tube. Additionally, there were two cases of bronchopulmonary hemorrhage, but the patients didn’t require any interventions.
This study was sponsored by Medtronic. Dr. Bhadra disclosed relationships with Medtronic, Boston Scientific, BodyVision, Auris Surgical Robotics, Intuitive Surgical, Veracyte, Biodesix, Merit Medical Endotek, and Johnson & Johnson.
SOURCE: Bhadra K et al. CHEST 2019. doi: 10.1016/j.chest.2019.08.314.
NEW ORLEANS – A novel according to an industry-sponsored, prospective study.
The system, which incorporates fluoroscopic navigation, increased the percentage of cases in which the target overlapped with the lesion, from 60% to 83%. The percentage of cases without any target overlap decreased from 32% to 5%.
“Tomosynthesis-based fluoroscopic navigation … improves the three-dimensional convergence between the virtual target and the actual target,” said Krish Bhadra, MD, of CHI Memorial Medical Group in Chattanooga, Tenn.
Dr. Bhadra presented results with this system at the annual meeting of the American College of Chest Physicians.
He and his colleagues conducted a study of Medtronic’s superDimension navigation system (version 7.2), which provides real-time imaging with three-dimensional fluoroscopy. The system has a “local registration” feature, which uses fluoroscopy and an algorithm to update the virtual target location during the procedure. This allows the user to reposition the catheter based on the location of the lesion.
The researchers tested the system in 50 patients from two centers (NCT03585959). Patients’ lesions had to be larger than 10 mm, not visible endobronchially, and not reachable by convex endobronchial ultrasound. Lesions within 10 mm of the diaphragm were excluded.
The median lesion size was 17.0 mm, 61.2% were smaller than 20 mm, 65.3% were in the upper lobe, and 53.1% had a bronchus sign present. The median distance from lesion to pleura was 5.9 mm.
Dr. Bhadra said the system performed as designed in all cases, and the protocol-defined technical success rate was 95.9% (47/49). Local registration was attempted in 49 patients and was successful in 47 patients (95.9%). In the unsuccessful cases, local registration was not completed based on the system design because the correction distance was greater than 3.0 cm.
The study’s primary endpoint was three-dimensional overlap of the virtual target and the actual lesion, as confirmed by cone-beam computed tomography. Success was defined as greater than 0% overlap after location correction. Target overlap was achieved in 59.6% (28/47) of cases before local registration and 83.0% (39/47) of cases after.
There were six cases in which local registration was successful, but these subjects weren’t evaluable because of failed procedure recording. When those subjects were excluded, target overlap was achieved in 95.1% (39/41) of cases after local registration.
The median percent overlap between the virtual target and the actual lesion was 11.4% before local registration and 32.8% after. The percentage of cases without any target overlap decreased from 31.7% (13/41) before local registration to 4.9% (2/41) after.
Focusing on the two cases without target overlap, Dr. Bhadra noted that he was able to get a biopsy that proved a malignancy in one of those patients. In the other patient, Dr. Bhadra was able to identify features of organizing pneumonia.
“Even though we did not have overlap, we must have been close enough that we were able to get malignant tissue in one [patient] and features of organizing pneumonia in a patient who’s got no history of organizing pneumonia,” Dr. Bhadra said.
He and his colleagues did not evaluate diagnostic yield in this study, but they did assess complications up to 7 days after the procedure.
The team reported one case of pneumothorax, but the patient didn’t require a chest tube. Additionally, there were two cases of bronchopulmonary hemorrhage, but the patients didn’t require any interventions.
This study was sponsored by Medtronic. Dr. Bhadra disclosed relationships with Medtronic, Boston Scientific, BodyVision, Auris Surgical Robotics, Intuitive Surgical, Veracyte, Biodesix, Merit Medical Endotek, and Johnson & Johnson.
SOURCE: Bhadra K et al. CHEST 2019. doi: 10.1016/j.chest.2019.08.314.
REPORTING FROM CHEST 2019
Measles causes B-cell changes, leading to ‘immune amnesia’
“Our findings provide a biological explanation for the observed increase in childhood mortality and secondary infections several years after an episode of measles,” said Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors. The study was published in Science Immunology.
To determine if B-cell impairment can lead to measles-associated immunosuppression, the researchers investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IGHV-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B cell frequencies in measles patients recovered to levels before infection, they had significant changes in IGHV-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IGHV genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IGHV genes, Dr. Petrova and associates said.
Finally, the researchers confirmed a hypothesis about the depletion of B memory cell clones during measles and a repopulation of new cells with less clonal expansion. The frequency of individual IGHV-J gene combinations before infection was correlated with a reduction after infection, “with the most frequent combinations undergoing the most marked depletion” and the result being an increase in genetic diversity.
To further test their findings, the researchers vaccinated two groups of four ferrets with live-attenuated influenza vaccine (LAIV) and at 4 weeks infected one of the groups with canine distemper virus (CDV), a surrogate for MeV. At 14 weeks after vaccination, the uninfected group maintained high levels of influenza-specific neutralizing antibodies while the infected group saw impaired B cells and a subsequent reduction in neutralizing antibodies.
Understanding the impact of measles on the immune system
“How measles infection has such a long-lasting deleterious effect on the immune system while allowing robust immunity against itself has been a burning immunological question,” Duane R. Wesemann, MD, PhD, of Brigham and Women’s Hospital in Boston, said in an accompanying editorial. The research from Petrova et al. begins to answer that question.
Among the observations he found most interesting was how “post-measles memory cells were more diverse than the pre-measles memory pool,” despite expectations that measles immunity would be dominant. He speculated that the void in memory cells is filled by a set of clones binding to unidentified or nonnative antigens, which may bring polyclonal diversity into B memory cells.
More research is needed to determine just what these findings mean, including looking beyond memory cell depletion and focusing on the impact of immature immunoglobulin repertoires in naive cells. But his broad takeaway is that measles remains both a public health concern and an opportunity to understand how the human body counters disease.
“The unique relationship measles has with the human immune system,” he said, “can illuminate aspects of its inner workings.”
The study was funded by grants to the investigators the Indonesian Endowment Fund for Education, the Wellcome Trust, the German Centre for Infection Research, the Collaborative Research Centre of the German Research Foundation, the German Ministry of Health, and the Royal Society. The authors declared no conflicts of interest. Dr. Wesemann reported receiving support from National Institutes of Health grants and an award from the Burroughs Wellcome Fund; he also reports being a consultant for OpenBiome.
SOURCE: Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125; Wesemann DR. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aaz4195.
“Our findings provide a biological explanation for the observed increase in childhood mortality and secondary infections several years after an episode of measles,” said Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors. The study was published in Science Immunology.
To determine if B-cell impairment can lead to measles-associated immunosuppression, the researchers investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IGHV-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B cell frequencies in measles patients recovered to levels before infection, they had significant changes in IGHV-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IGHV genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IGHV genes, Dr. Petrova and associates said.
Finally, the researchers confirmed a hypothesis about the depletion of B memory cell clones during measles and a repopulation of new cells with less clonal expansion. The frequency of individual IGHV-J gene combinations before infection was correlated with a reduction after infection, “with the most frequent combinations undergoing the most marked depletion” and the result being an increase in genetic diversity.
To further test their findings, the researchers vaccinated two groups of four ferrets with live-attenuated influenza vaccine (LAIV) and at 4 weeks infected one of the groups with canine distemper virus (CDV), a surrogate for MeV. At 14 weeks after vaccination, the uninfected group maintained high levels of influenza-specific neutralizing antibodies while the infected group saw impaired B cells and a subsequent reduction in neutralizing antibodies.
Understanding the impact of measles on the immune system
“How measles infection has such a long-lasting deleterious effect on the immune system while allowing robust immunity against itself has been a burning immunological question,” Duane R. Wesemann, MD, PhD, of Brigham and Women’s Hospital in Boston, said in an accompanying editorial. The research from Petrova et al. begins to answer that question.
Among the observations he found most interesting was how “post-measles memory cells were more diverse than the pre-measles memory pool,” despite expectations that measles immunity would be dominant. He speculated that the void in memory cells is filled by a set of clones binding to unidentified or nonnative antigens, which may bring polyclonal diversity into B memory cells.
More research is needed to determine just what these findings mean, including looking beyond memory cell depletion and focusing on the impact of immature immunoglobulin repertoires in naive cells. But his broad takeaway is that measles remains both a public health concern and an opportunity to understand how the human body counters disease.
“The unique relationship measles has with the human immune system,” he said, “can illuminate aspects of its inner workings.”
The study was funded by grants to the investigators the Indonesian Endowment Fund for Education, the Wellcome Trust, the German Centre for Infection Research, the Collaborative Research Centre of the German Research Foundation, the German Ministry of Health, and the Royal Society. The authors declared no conflicts of interest. Dr. Wesemann reported receiving support from National Institutes of Health grants and an award from the Burroughs Wellcome Fund; he also reports being a consultant for OpenBiome.
SOURCE: Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125; Wesemann DR. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aaz4195.
“Our findings provide a biological explanation for the observed increase in childhood mortality and secondary infections several years after an episode of measles,” said Velislava N. Petrova, PhD, of the Wellcome Sanger Institute in Cambridge, England, and coauthors. The study was published in Science Immunology.
To determine if B-cell impairment can lead to measles-associated immunosuppression, the researchers investigated genetic changes in 26 unvaccinated children from the Netherlands who previously had measles. Their antibody genes were sequenced before any symptoms of measles developed and roughly 40 days after rash. Two control groups also were sequenced accordingly: vaccinated adults and three unvaccinated children from the same community who were not infected with measles.
Naive B cells from individuals in the vaccinated and uninfected control groups showed high correlation of immunoglobulin heavy chain (IGHV-J) gene frequencies across time periods (R2 = 0.96 and 0.92, respectively) but no significant differences in gene expression (P greater than .05). At the same time, although B cell frequencies in measles patients recovered to levels before infection, they had significant changes in IGHV-J gene frequencies (P = .01) and decreased correlation in gene expression (R2 = 0.78).
In addition, individuals in the control groups had “a stable genetic composition of B memory cells” but no significant changes in the third complementarity-determining region (CDR3) lengths or mutational frequency of IGHV genes (P greater than .05). B memory cells in measles patients, however, showed increases in mutational frequency (P = .0008) and a reduction in CDR3 length (P = .017) of IGHV genes, Dr. Petrova and associates said.
Finally, the researchers confirmed a hypothesis about the depletion of B memory cell clones during measles and a repopulation of new cells with less clonal expansion. The frequency of individual IGHV-J gene combinations before infection was correlated with a reduction after infection, “with the most frequent combinations undergoing the most marked depletion” and the result being an increase in genetic diversity.
To further test their findings, the researchers vaccinated two groups of four ferrets with live-attenuated influenza vaccine (LAIV) and at 4 weeks infected one of the groups with canine distemper virus (CDV), a surrogate for MeV. At 14 weeks after vaccination, the uninfected group maintained high levels of influenza-specific neutralizing antibodies while the infected group saw impaired B cells and a subsequent reduction in neutralizing antibodies.
Understanding the impact of measles on the immune system
“How measles infection has such a long-lasting deleterious effect on the immune system while allowing robust immunity against itself has been a burning immunological question,” Duane R. Wesemann, MD, PhD, of Brigham and Women’s Hospital in Boston, said in an accompanying editorial. The research from Petrova et al. begins to answer that question.
Among the observations he found most interesting was how “post-measles memory cells were more diverse than the pre-measles memory pool,” despite expectations that measles immunity would be dominant. He speculated that the void in memory cells is filled by a set of clones binding to unidentified or nonnative antigens, which may bring polyclonal diversity into B memory cells.
More research is needed to determine just what these findings mean, including looking beyond memory cell depletion and focusing on the impact of immature immunoglobulin repertoires in naive cells. But his broad takeaway is that measles remains both a public health concern and an opportunity to understand how the human body counters disease.
“The unique relationship measles has with the human immune system,” he said, “can illuminate aspects of its inner workings.”
The study was funded by grants to the investigators the Indonesian Endowment Fund for Education, the Wellcome Trust, the German Centre for Infection Research, the Collaborative Research Centre of the German Research Foundation, the German Ministry of Health, and the Royal Society. The authors declared no conflicts of interest. Dr. Wesemann reported receiving support from National Institutes of Health grants and an award from the Burroughs Wellcome Fund; he also reports being a consultant for OpenBiome.
SOURCE: Petrova VN et al. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aay6125; Wesemann DR. Sci Immunol. 2019 Nov 1. doi: 10.1126/sciimmunol.aaz4195.
FROM SCIENCE IMMUNOTHERAPY