User login
Ultrasound, cardiac CT valuable in COVID-19 assessment
As if the management of patients with severe COVID-19 infections is not complicated enough, an estimated 50%-60% of patients admitted to an ICU with the disease will have some form of cardiovascular involvement, which further increases their already high risk for morbidity and mortality.

Multimodality cardiovascular imaging, chosen wisely, can both help to direct management of cardiovascular complications associated with COVID-19 and lessen risk of exposure of health care workers to SARS-CoV-2, said members of an expert panel from the American College of Cardiology Cardiovascular Imaging Leadership Council.
“When we face a patient with known or suspected COVID-19, it’s not like any other disease because we face potential exposure risk to personnel doing imaging studies and also to other patients,” corresponding author Marcelo F. Di Carli, MD, of Brigham and Women’s Hospital Boston said in an interview.
“Any imaging study that is being considered should be performed only if we think it will help us make a change in the way that we’re going to treat that particular patient. This is true for imaging in any disease – why would you do an imaging study that will make no difference in treatment? – but the stakes are even higher in COVID-19,” he said.
The panel’s recommendations for cardiovascular imaging in patients with COVID-19 are outlined in a guidance document published online in the Journal of the American College of Cardiology.
Testing and biomarkers
The guidance begins by highlighting the importance of diagnostic testing for COVID-19 infection and the use of universal precautions for health care personnel performing imaging studies, as well as disinfection of imaging equipment and rooms after each use.
Circulating biomarkers that measure end-organ stress or injury, inflammation, hypoperfusion, and activation of thrombosis/hemostasis pathways may be prognostically useful, but “almost none of the widely measured biomarkers represent a specific trigger for imaging outside of that supported by clinical judgment,” the guidance states.
In contrast, low to moderate, nonrising concentrations of markers for myocardial stress, such as B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP), or of myocardial injury, such as cardiac troponins (cTn), may be helpful for excluding the need for imaging.
“Importantly, clinicians should be aware that most patients with abnormal BNP/NT-proBNP or cTn do not have acute heart failure or myocardial infarction; and rise in concentration of either class of biomarker presumably reflects complex processes including direct myocardial stress/injury related to systemic illness,” the panel members wrote.
Oldies but goodies
“One thing that we found out in our review of the literature and in our experiences in our own work settings is that cardiac ultrasound plays a huge role in this disease – like in any disease – but this one in particular,” Dr. Di Carli said. “One of the most feared complications in COVID-19 leads to inflammation of the heart muscle, which then leads to heart dysfunction. And of course cardiac ultrasound, because of its portability, can be performed at bedside to help clinicians ascertain an abnormality in the heart.”
Cardiac CT is also extremely helpful for determining whether patients with ECG findings suggestive of infarction have suffered an actual thrombotic event.
“These patients may best be served by a noninvasive study as compared to an invasive coronary angiogram,” he said.
Clinical scenarios
Cardiologists may be called in to consult on the evaluation of possible cardiogenic components of pulmonary abnormalities in patients who present with dyspnea and chest x-rays showing airspace or interstitial infiltrates suggestive of pneumonia, the authors noted.
“Clinicians will rely on history, physical exam, ECG [electrocardiogram] and biomarkers, and recent cardiac imaging tests if available. Underlying cardiac history including [coronary artery disease], cardiomyopathy, heart failure, and arrhythmia should be sought, and frequent contributors to decompensation should be eliminated,” they wrote.
For patients with suspected cardiac injury, either point-of-care ultrasound or limited echocardiography can be used for the initial evaluation, with additional, more advanced technologies called into play for specific clinical scenarios outlined in the guidance.
For example, the guidance recommends that patients with chest pain and abnormal ECG readings with clinical concern for ST-elevation acute coronary syndrome or high clinical risk for in-hospital mortality from conditions such as cardiogenic shock, dynamic ST-segment changes, or left ventricular ejection fraction less than 40% thought to be caused by non–ST-elevation myocardial infarction be referred for emergent coronary angiography and reperfusion.
In contrast, in patients with chest pain and abnormal ECG but equivocal symptoms, atypical or equivocal ECG abnormalities, or late presentations, point-of-care ultrasound or limited echocardiogram could be used to look for regional wall motion abnormalities and left ventricular ejection fraction, whereas in patients with chest pain and ST-elevation without clear evidence of ST-elevation myocardial infarction, coronary CT angiography can help to rule out ACS and point to alternate diagnoses, the authors said.
The guidance also offers recommendations for imaging in patients with hemodynamic instability (shock or hypotension), patients with new left ventricular dysfunction in the absence of shock or hypotension, and patients with subacute and chronic-phase disease.
Development of the guidance document was supported by the ACC. Dr. Di Carli disclosed institutional grant support from Gilead Sciences and Spectrum Dynamics, and consulting income from Janssen and Bayer.
SOURCE: Rudski L et al. J Am Coll Cardiol. 2020 Jul 22. doi: 10.1016/j.jacc.2020.06.080.
As if the management of patients with severe COVID-19 infections is not complicated enough, an estimated 50%-60% of patients admitted to an ICU with the disease will have some form of cardiovascular involvement, which further increases their already high risk for morbidity and mortality.
Multimodality cardiovascular imaging, chosen wisely, can both help to direct management of cardiovascular complications associated with COVID-19 and lessen risk of exposure of health care workers to SARS-CoV-2, said members of an expert panel from the American College of Cardiology Cardiovascular Imaging Leadership Council.
“When we face a patient with known or suspected COVID-19, it’s not like any other disease because we face potential exposure risk to personnel doing imaging studies and also to other patients,” corresponding author Marcelo F. Di Carli, MD, of Brigham and Women’s Hospital Boston said in an interview.
“Any imaging study that is being considered should be performed only if we think it will help us make a change in the way that we’re going to treat that particular patient. This is true for imaging in any disease – why would you do an imaging study that will make no difference in treatment? – but the stakes are even higher in COVID-19,” he said.
The panel’s recommendations for cardiovascular imaging in patients with COVID-19 are outlined in a guidance document published online in the Journal of the American College of Cardiology.
Testing and biomarkers
The guidance begins by highlighting the importance of diagnostic testing for COVID-19 infection and the use of universal precautions for health care personnel performing imaging studies, as well as disinfection of imaging equipment and rooms after each use.
Circulating biomarkers that measure end-organ stress or injury, inflammation, hypoperfusion, and activation of thrombosis/hemostasis pathways may be prognostically useful, but “almost none of the widely measured biomarkers represent a specific trigger for imaging outside of that supported by clinical judgment,” the guidance states.
In contrast, low to moderate, nonrising concentrations of markers for myocardial stress, such as B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP), or of myocardial injury, such as cardiac troponins (cTn), may be helpful for excluding the need for imaging.
“Importantly, clinicians should be aware that most patients with abnormal BNP/NT-proBNP or cTn do not have acute heart failure or myocardial infarction; and rise in concentration of either class of biomarker presumably reflects complex processes including direct myocardial stress/injury related to systemic illness,” the panel members wrote.
Oldies but goodies
“One thing that we found out in our review of the literature and in our experiences in our own work settings is that cardiac ultrasound plays a huge role in this disease – like in any disease – but this one in particular,” Dr. Di Carli said. “One of the most feared complications in COVID-19 leads to inflammation of the heart muscle, which then leads to heart dysfunction. And of course cardiac ultrasound, because of its portability, can be performed at bedside to help clinicians ascertain an abnormality in the heart.”
Cardiac CT is also extremely helpful for determining whether patients with ECG findings suggestive of infarction have suffered an actual thrombotic event.
“These patients may best be served by a noninvasive study as compared to an invasive coronary angiogram,” he said.
Clinical scenarios
Cardiologists may be called in to consult on the evaluation of possible cardiogenic components of pulmonary abnormalities in patients who present with dyspnea and chest x-rays showing airspace or interstitial infiltrates suggestive of pneumonia, the authors noted.
“Clinicians will rely on history, physical exam, ECG [electrocardiogram] and biomarkers, and recent cardiac imaging tests if available. Underlying cardiac history including [coronary artery disease], cardiomyopathy, heart failure, and arrhythmia should be sought, and frequent contributors to decompensation should be eliminated,” they wrote.
For patients with suspected cardiac injury, either point-of-care ultrasound or limited echocardiography can be used for the initial evaluation, with additional, more advanced technologies called into play for specific clinical scenarios outlined in the guidance.
For example, the guidance recommends that patients with chest pain and abnormal ECG readings with clinical concern for ST-elevation acute coronary syndrome or high clinical risk for in-hospital mortality from conditions such as cardiogenic shock, dynamic ST-segment changes, or left ventricular ejection fraction less than 40% thought to be caused by non–ST-elevation myocardial infarction be referred for emergent coronary angiography and reperfusion.
In contrast, in patients with chest pain and abnormal ECG but equivocal symptoms, atypical or equivocal ECG abnormalities, or late presentations, point-of-care ultrasound or limited echocardiogram could be used to look for regional wall motion abnormalities and left ventricular ejection fraction, whereas in patients with chest pain and ST-elevation without clear evidence of ST-elevation myocardial infarction, coronary CT angiography can help to rule out ACS and point to alternate diagnoses, the authors said.
The guidance also offers recommendations for imaging in patients with hemodynamic instability (shock or hypotension), patients with new left ventricular dysfunction in the absence of shock or hypotension, and patients with subacute and chronic-phase disease.
Development of the guidance document was supported by the ACC. Dr. Di Carli disclosed institutional grant support from Gilead Sciences and Spectrum Dynamics, and consulting income from Janssen and Bayer.
SOURCE: Rudski L et al. J Am Coll Cardiol. 2020 Jul 22. doi: 10.1016/j.jacc.2020.06.080.
As if the management of patients with severe COVID-19 infections is not complicated enough, an estimated 50%-60% of patients admitted to an ICU with the disease will have some form of cardiovascular involvement, which further increases their already high risk for morbidity and mortality.
Multimodality cardiovascular imaging, chosen wisely, can both help to direct management of cardiovascular complications associated with COVID-19 and lessen risk of exposure of health care workers to SARS-CoV-2, said members of an expert panel from the American College of Cardiology Cardiovascular Imaging Leadership Council.
“When we face a patient with known or suspected COVID-19, it’s not like any other disease because we face potential exposure risk to personnel doing imaging studies and also to other patients,” corresponding author Marcelo F. Di Carli, MD, of Brigham and Women’s Hospital Boston said in an interview.
“Any imaging study that is being considered should be performed only if we think it will help us make a change in the way that we’re going to treat that particular patient. This is true for imaging in any disease – why would you do an imaging study that will make no difference in treatment? – but the stakes are even higher in COVID-19,” he said.
The panel’s recommendations for cardiovascular imaging in patients with COVID-19 are outlined in a guidance document published online in the Journal of the American College of Cardiology.
Testing and biomarkers
The guidance begins by highlighting the importance of diagnostic testing for COVID-19 infection and the use of universal precautions for health care personnel performing imaging studies, as well as disinfection of imaging equipment and rooms after each use.
Circulating biomarkers that measure end-organ stress or injury, inflammation, hypoperfusion, and activation of thrombosis/hemostasis pathways may be prognostically useful, but “almost none of the widely measured biomarkers represent a specific trigger for imaging outside of that supported by clinical judgment,” the guidance states.
In contrast, low to moderate, nonrising concentrations of markers for myocardial stress, such as B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP), or of myocardial injury, such as cardiac troponins (cTn), may be helpful for excluding the need for imaging.
“Importantly, clinicians should be aware that most patients with abnormal BNP/NT-proBNP or cTn do not have acute heart failure or myocardial infarction; and rise in concentration of either class of biomarker presumably reflects complex processes including direct myocardial stress/injury related to systemic illness,” the panel members wrote.
Oldies but goodies
“One thing that we found out in our review of the literature and in our experiences in our own work settings is that cardiac ultrasound plays a huge role in this disease – like in any disease – but this one in particular,” Dr. Di Carli said. “One of the most feared complications in COVID-19 leads to inflammation of the heart muscle, which then leads to heart dysfunction. And of course cardiac ultrasound, because of its portability, can be performed at bedside to help clinicians ascertain an abnormality in the heart.”
Cardiac CT is also extremely helpful for determining whether patients with ECG findings suggestive of infarction have suffered an actual thrombotic event.
“These patients may best be served by a noninvasive study as compared to an invasive coronary angiogram,” he said.
Clinical scenarios
Cardiologists may be called in to consult on the evaluation of possible cardiogenic components of pulmonary abnormalities in patients who present with dyspnea and chest x-rays showing airspace or interstitial infiltrates suggestive of pneumonia, the authors noted.
“Clinicians will rely on history, physical exam, ECG [electrocardiogram] and biomarkers, and recent cardiac imaging tests if available. Underlying cardiac history including [coronary artery disease], cardiomyopathy, heart failure, and arrhythmia should be sought, and frequent contributors to decompensation should be eliminated,” they wrote.
For patients with suspected cardiac injury, either point-of-care ultrasound or limited echocardiography can be used for the initial evaluation, with additional, more advanced technologies called into play for specific clinical scenarios outlined in the guidance.
For example, the guidance recommends that patients with chest pain and abnormal ECG readings with clinical concern for ST-elevation acute coronary syndrome or high clinical risk for in-hospital mortality from conditions such as cardiogenic shock, dynamic ST-segment changes, or left ventricular ejection fraction less than 40% thought to be caused by non–ST-elevation myocardial infarction be referred for emergent coronary angiography and reperfusion.
In contrast, in patients with chest pain and abnormal ECG but equivocal symptoms, atypical or equivocal ECG abnormalities, or late presentations, point-of-care ultrasound or limited echocardiogram could be used to look for regional wall motion abnormalities and left ventricular ejection fraction, whereas in patients with chest pain and ST-elevation without clear evidence of ST-elevation myocardial infarction, coronary CT angiography can help to rule out ACS and point to alternate diagnoses, the authors said.
The guidance also offers recommendations for imaging in patients with hemodynamic instability (shock or hypotension), patients with new left ventricular dysfunction in the absence of shock or hypotension, and patients with subacute and chronic-phase disease.
Development of the guidance document was supported by the ACC. Dr. Di Carli disclosed institutional grant support from Gilead Sciences and Spectrum Dynamics, and consulting income from Janssen and Bayer.
SOURCE: Rudski L et al. J Am Coll Cardiol. 2020 Jul 22. doi: 10.1016/j.jacc.2020.06.080.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Combination therapy quells COVID-19 cytokine storm
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.

Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.
Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.
Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
One-third of outpatients with COVID-19 are unwell weeks later
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
Rapid drop of antibodies seen in those with mild COVID-19
The research was conducted by F. Javier Ibarrondo, PhD, and colleagues and was published online on July 21 in a letter to the editor of the New England Journal of Medicine. Ibarrondo is associate researcher at the University of California, Los Angeles. (The original letter incorrectly calculated the half-life at 73 days.)
Coauthor Otto Yang, MD, professor of medicine in the division of infectious diseases at UCLA, told Medscape Medical News that the rapidity in the antibody drop at 5 weeks “is striking compared to other infections.”
The phenomenon has been suspected and has been observed before but had not been quantified.
“Our paper is the first to put firm numbers on the dropping of antibodies after early infection,” he said.
The researchers evaluated 34 people (average age, 43 years) who had recovered from mild COVID-19 and had referred themselves to UCLA for observational research.
Previous report also found a quick fade
As Medscape Medical News reported, a previous study from China that was published in Nature Medicine also found that the antibodies fade quickly.
Interpreting the meaning of the current research comes with a few caveats, Dr. Yang said.
“One is that we don’t know for sure that antibodies are what protect people from getting infected,” he said. Although it’s a reasonable assumption, he said, that’s not always the case.
Another caveat is that even if antibodies do protect, the tests being used to measure them – including the test that was used in this study – may not measure them the right way, and it is not yet known how many antibodies are needed for protection, he explained.
The UCLA researchers used an enzyme-linked immunosorbent assay to detect anti–SARS-CoV-2 spike receptor–binding domain immunoglobulin G concentrations.
“No reason for anybody to be getting an antibody test medically”
The study provides further proof that “[t]here’s no reason for anybody to be getting an antibody test medically right now,” Dr. Yang said.
Additionally, “FDA-approved tests are not approved for quantitative measures, only qualitative,” he continued. He noted that the findings may have implications with respect to herd immunity.
“Herd immunity depends on a lot of people having immunity to the infection all at the same time. If infection is followed by only brief protection from infection, the natural infection is not going to reach herd immunity,” he explained.
Buddy Creech, MD, MPH, associate professor of pediatrics and director of the Vanderbilt Vaccine Research Program in Nashville, Tenn., pointed out that antibodies “are just part of the story.”
“When we make an immune response to any germ,” he said, “we not only make an immune response for the time being but for the future. The next time we’re exposed, we can call into action B cells and T cells who have been there and done that.”
So even though the antibodies fade over time, other arms of the immune system are being trained for future action, he said.
Herd immunity does not require that populations have a huge level of antibodies that remains forever, he explained.
“It requires that in general, we’re not going to get infected as easily, and we’re not going to have disease as easily, and we’re not going to transmit the virus for as long,” he said.
Dr. Creech said he and others researching COVID-19 find that studies that show that antibodies fade quickly provide more proof “that this coronavirus is going to be here to stay unless we can take care of it through very effective treatments to take it from potentially fatal disease to one that is nothing more than a cold” or until a vaccine is developed.
He noted there are four other coronaviruses in widespread circulation every year that “amount to about 25% of the common cold.”
This study may help narrow the window as to when convalescent plasma – plasma that is taken from people who have recovered from COVID-19 and that is used to help people who are acutely ill with the disease – will be most effective, Dr. Creech explained. He said the results suggest that it is important that plasma be collected within the first couple of months after recovery so as to capture the most antibodies.
This study is important as another snapshot “so we understand the differences between severe and mild disease, so we can study it over time, so we have all the tools we need as we start these pivotal vaccine studies to make sure we’re making the right immune response for the right duration of time so we can put an end to this pandemic,” Dr. Creech concluded.
The study was supported by grants from the AIDS Healthcare Foundation, the Doris Duke Charitable Foundation, the National Institutes of Health, the James B. Pendleton Charitable Trust, and the McCarthy Family Foundation. A coauthor reports receiving grants from Gilead outside the submitted work. Dr. Creech has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The research was conducted by F. Javier Ibarrondo, PhD, and colleagues and was published online on July 21 in a letter to the editor of the New England Journal of Medicine. Ibarrondo is associate researcher at the University of California, Los Angeles. (The original letter incorrectly calculated the half-life at 73 days.)
Coauthor Otto Yang, MD, professor of medicine in the division of infectious diseases at UCLA, told Medscape Medical News that the rapidity in the antibody drop at 5 weeks “is striking compared to other infections.”
The phenomenon has been suspected and has been observed before but had not been quantified.
“Our paper is the first to put firm numbers on the dropping of antibodies after early infection,” he said.
The researchers evaluated 34 people (average age, 43 years) who had recovered from mild COVID-19 and had referred themselves to UCLA for observational research.
Previous report also found a quick fade
As Medscape Medical News reported, a previous study from China that was published in Nature Medicine also found that the antibodies fade quickly.
Interpreting the meaning of the current research comes with a few caveats, Dr. Yang said.
“One is that we don’t know for sure that antibodies are what protect people from getting infected,” he said. Although it’s a reasonable assumption, he said, that’s not always the case.
Another caveat is that even if antibodies do protect, the tests being used to measure them – including the test that was used in this study – may not measure them the right way, and it is not yet known how many antibodies are needed for protection, he explained.
The UCLA researchers used an enzyme-linked immunosorbent assay to detect anti–SARS-CoV-2 spike receptor–binding domain immunoglobulin G concentrations.
“No reason for anybody to be getting an antibody test medically”
The study provides further proof that “[t]here’s no reason for anybody to be getting an antibody test medically right now,” Dr. Yang said.
Additionally, “FDA-approved tests are not approved for quantitative measures, only qualitative,” he continued. He noted that the findings may have implications with respect to herd immunity.
“Herd immunity depends on a lot of people having immunity to the infection all at the same time. If infection is followed by only brief protection from infection, the natural infection is not going to reach herd immunity,” he explained.
Buddy Creech, MD, MPH, associate professor of pediatrics and director of the Vanderbilt Vaccine Research Program in Nashville, Tenn., pointed out that antibodies “are just part of the story.”
“When we make an immune response to any germ,” he said, “we not only make an immune response for the time being but for the future. The next time we’re exposed, we can call into action B cells and T cells who have been there and done that.”
So even though the antibodies fade over time, other arms of the immune system are being trained for future action, he said.
Herd immunity does not require that populations have a huge level of antibodies that remains forever, he explained.
“It requires that in general, we’re not going to get infected as easily, and we’re not going to have disease as easily, and we’re not going to transmit the virus for as long,” he said.
Dr. Creech said he and others researching COVID-19 find that studies that show that antibodies fade quickly provide more proof “that this coronavirus is going to be here to stay unless we can take care of it through very effective treatments to take it from potentially fatal disease to one that is nothing more than a cold” or until a vaccine is developed.
He noted there are four other coronaviruses in widespread circulation every year that “amount to about 25% of the common cold.”
This study may help narrow the window as to when convalescent plasma – plasma that is taken from people who have recovered from COVID-19 and that is used to help people who are acutely ill with the disease – will be most effective, Dr. Creech explained. He said the results suggest that it is important that plasma be collected within the first couple of months after recovery so as to capture the most antibodies.
This study is important as another snapshot “so we understand the differences between severe and mild disease, so we can study it over time, so we have all the tools we need as we start these pivotal vaccine studies to make sure we’re making the right immune response for the right duration of time so we can put an end to this pandemic,” Dr. Creech concluded.
The study was supported by grants from the AIDS Healthcare Foundation, the Doris Duke Charitable Foundation, the National Institutes of Health, the James B. Pendleton Charitable Trust, and the McCarthy Family Foundation. A coauthor reports receiving grants from Gilead outside the submitted work. Dr. Creech has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The research was conducted by F. Javier Ibarrondo, PhD, and colleagues and was published online on July 21 in a letter to the editor of the New England Journal of Medicine. Ibarrondo is associate researcher at the University of California, Los Angeles. (The original letter incorrectly calculated the half-life at 73 days.)
Coauthor Otto Yang, MD, professor of medicine in the division of infectious diseases at UCLA, told Medscape Medical News that the rapidity in the antibody drop at 5 weeks “is striking compared to other infections.”
The phenomenon has been suspected and has been observed before but had not been quantified.
“Our paper is the first to put firm numbers on the dropping of antibodies after early infection,” he said.
The researchers evaluated 34 people (average age, 43 years) who had recovered from mild COVID-19 and had referred themselves to UCLA for observational research.
Previous report also found a quick fade
As Medscape Medical News reported, a previous study from China that was published in Nature Medicine also found that the antibodies fade quickly.
Interpreting the meaning of the current research comes with a few caveats, Dr. Yang said.
“One is that we don’t know for sure that antibodies are what protect people from getting infected,” he said. Although it’s a reasonable assumption, he said, that’s not always the case.
Another caveat is that even if antibodies do protect, the tests being used to measure them – including the test that was used in this study – may not measure them the right way, and it is not yet known how many antibodies are needed for protection, he explained.
The UCLA researchers used an enzyme-linked immunosorbent assay to detect anti–SARS-CoV-2 spike receptor–binding domain immunoglobulin G concentrations.
“No reason for anybody to be getting an antibody test medically”
The study provides further proof that “[t]here’s no reason for anybody to be getting an antibody test medically right now,” Dr. Yang said.
Additionally, “FDA-approved tests are not approved for quantitative measures, only qualitative,” he continued. He noted that the findings may have implications with respect to herd immunity.
“Herd immunity depends on a lot of people having immunity to the infection all at the same time. If infection is followed by only brief protection from infection, the natural infection is not going to reach herd immunity,” he explained.
Buddy Creech, MD, MPH, associate professor of pediatrics and director of the Vanderbilt Vaccine Research Program in Nashville, Tenn., pointed out that antibodies “are just part of the story.”
“When we make an immune response to any germ,” he said, “we not only make an immune response for the time being but for the future. The next time we’re exposed, we can call into action B cells and T cells who have been there and done that.”
So even though the antibodies fade over time, other arms of the immune system are being trained for future action, he said.
Herd immunity does not require that populations have a huge level of antibodies that remains forever, he explained.
“It requires that in general, we’re not going to get infected as easily, and we’re not going to have disease as easily, and we’re not going to transmit the virus for as long,” he said.
Dr. Creech said he and others researching COVID-19 find that studies that show that antibodies fade quickly provide more proof “that this coronavirus is going to be here to stay unless we can take care of it through very effective treatments to take it from potentially fatal disease to one that is nothing more than a cold” or until a vaccine is developed.
He noted there are four other coronaviruses in widespread circulation every year that “amount to about 25% of the common cold.”
This study may help narrow the window as to when convalescent plasma – plasma that is taken from people who have recovered from COVID-19 and that is used to help people who are acutely ill with the disease – will be most effective, Dr. Creech explained. He said the results suggest that it is important that plasma be collected within the first couple of months after recovery so as to capture the most antibodies.
This study is important as another snapshot “so we understand the differences between severe and mild disease, so we can study it over time, so we have all the tools we need as we start these pivotal vaccine studies to make sure we’re making the right immune response for the right duration of time so we can put an end to this pandemic,” Dr. Creech concluded.
The study was supported by grants from the AIDS Healthcare Foundation, the Doris Duke Charitable Foundation, the National Institutes of Health, the James B. Pendleton Charitable Trust, and the McCarthy Family Foundation. A coauthor reports receiving grants from Gilead outside the submitted work. Dr. Creech has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Is the presence of enanthem a clue for COVID-19?
Larger studies should explore and confirm this association, the study’s authors and other experts suggested.
Dermatologists are already aware of the connection between enanthem and viral etiology. “As seen with other viral infections, we wondered if COVID-19 could produce enanthem in addition to skin rash exanthem,” one of the study author’s, Juan Jiménez-Cauhe, MD, a dermatologist with Hospital Universitario Ramon y Cajal, Madrid, said in an interview. He and his colleagues summarized their findings in a research letter in JAMA Dermatology.
They examined the oral cavity of 21 COVID-19 patients at a tertiary care hospital who also had a skin rash from March 30 to April 8. They classified enanthems into four categories: petechial, macular, macular with petechiae, or erythematovesicular. Six of the patients presented with oral lesions, all of them located in the palate; in one patient, the enanthem was macular, it was petechial in two patients and was macular with petechiae in three patients. The six patients ranged between the ages of 40 and 69 years; four were women.
Petechial or vesicular patterns are often associated with viral infections. In this particular study, the investigators did not observe vesicular lesions.
On average, mucocutaneous lesions appeared about 12 days after the onset of COVID-19 symptoms. “Interestingly, this latency was shorter in patients with petechial enanthem, compared with those with a macular lesion with petechiae appearance,” the authors wrote.
This shorter time might suggest an association for SARS-CoV-2, said Dr. Jiménez-Cauhe. Strong cough may have also caused petechial lesions on the palate, but it’s unlikely, as they appeared close in time to COVID-19 symptoms. It’s also unlikely that any drugs caused the lesions, as drug rashes can take 2-3 weeks to appear.

This fits in line with other evidence of broader skin manifestations appearing at the same time or after COVID-19, Esther Freeman, MD, said in an interview. Dr. Freeman, director of global health dermatology at Massachusetts General Hospital, Boston, is the principal investigator of the COVID-19 Dermatology Registry, a collaboration of the American Academy of Dermatology and International League of Dermatological Societies.
The study’s small cohort made it difficult to establish a solid association between the oral lesions and SARS-CoV-2. “However, the presence of enanthem in a patient with a skin rash is a useful finding that suggests a viral etiology rather than a drug reaction. This is particularly useful in COVID-19 patients, who were receiving many drugs as part of the treatment,” Dr. Jimenez-Cauhe said. Future studies should assess whether the presence of enanthem and exanthem lead physicians to consider SARS-CoV-2 as possible agents, ruling out infection with a blood or nasopharyngeal test.
This study adds to the growing body of knowledge on cutaneous and mucocutaneous findings associated with SARS-CoV-2 infection, Jules Lipoff, MD, of the department of dermatology, University of Pennsylvania, Philadelphia, said in an interview. “One challenge in evaluating these findings is that these findings are nonspecific, and medication reactions can often cause similar rashes, such as morbilliform eruptions that can be associated with both viruses and medications.”

Enanthems, as the study authors noted, are more specific to viral infections and are less commonly associated with medication reactions. “So, even though this is a small case series with significant limitations, it does add more evidence that COVID-19 is directly responsible for findings in the skin and mucous membranes,” said Dr. Lipoff.
Dr. Freeman noted that the study may also encourage clinicians to look in a patient’s mouth when assessing for SARS-CoV-2. Additional research should examine these data in a larger population.
Several studies by Dr. Freeman, Dr. Lipoff, and others strongly suggest that SARS-CoV-2 has a spectrum of associated dermatologic manifestations. One evaluated perniolike skin lesions (J Am Acad Dermatol. 2020 Aug; 83[2]:486-92). The other was a case series from the COVID-19 registry that examined 716 cases of new-onset dermatologic symptoms in patients from 31 countries with confirmed/suspected SARS-CoV-2 (J Am Acad Dermatol. 2020 Jul 2;S0190-9622[20]32126-5.).
The authors of the report had no disclosures.
SOURCE: Jimenez-Cauhe J et al. JAMA Dermatol. 2020 Jul 15. doi: 10.1001/jamadermatol.2020.2550.
Larger studies should explore and confirm this association, the study’s authors and other experts suggested.
Dermatologists are already aware of the connection between enanthem and viral etiology. “As seen with other viral infections, we wondered if COVID-19 could produce enanthem in addition to skin rash exanthem,” one of the study author’s, Juan Jiménez-Cauhe, MD, a dermatologist with Hospital Universitario Ramon y Cajal, Madrid, said in an interview. He and his colleagues summarized their findings in a research letter in JAMA Dermatology.
They examined the oral cavity of 21 COVID-19 patients at a tertiary care hospital who also had a skin rash from March 30 to April 8. They classified enanthems into four categories: petechial, macular, macular with petechiae, or erythematovesicular. Six of the patients presented with oral lesions, all of them located in the palate; in one patient, the enanthem was macular, it was petechial in two patients and was macular with petechiae in three patients. The six patients ranged between the ages of 40 and 69 years; four were women.
Petechial or vesicular patterns are often associated with viral infections. In this particular study, the investigators did not observe vesicular lesions.
On average, mucocutaneous lesions appeared about 12 days after the onset of COVID-19 symptoms. “Interestingly, this latency was shorter in patients with petechial enanthem, compared with those with a macular lesion with petechiae appearance,” the authors wrote.
This shorter time might suggest an association for SARS-CoV-2, said Dr. Jiménez-Cauhe. Strong cough may have also caused petechial lesions on the palate, but it’s unlikely, as they appeared close in time to COVID-19 symptoms. It’s also unlikely that any drugs caused the lesions, as drug rashes can take 2-3 weeks to appear.
This fits in line with other evidence of broader skin manifestations appearing at the same time or after COVID-19, Esther Freeman, MD, said in an interview. Dr. Freeman, director of global health dermatology at Massachusetts General Hospital, Boston, is the principal investigator of the COVID-19 Dermatology Registry, a collaboration of the American Academy of Dermatology and International League of Dermatological Societies.
The study’s small cohort made it difficult to establish a solid association between the oral lesions and SARS-CoV-2. “However, the presence of enanthem in a patient with a skin rash is a useful finding that suggests a viral etiology rather than a drug reaction. This is particularly useful in COVID-19 patients, who were receiving many drugs as part of the treatment,” Dr. Jimenez-Cauhe said. Future studies should assess whether the presence of enanthem and exanthem lead physicians to consider SARS-CoV-2 as possible agents, ruling out infection with a blood or nasopharyngeal test.
This study adds to the growing body of knowledge on cutaneous and mucocutaneous findings associated with SARS-CoV-2 infection, Jules Lipoff, MD, of the department of dermatology, University of Pennsylvania, Philadelphia, said in an interview. “One challenge in evaluating these findings is that these findings are nonspecific, and medication reactions can often cause similar rashes, such as morbilliform eruptions that can be associated with both viruses and medications.”
Enanthems, as the study authors noted, are more specific to viral infections and are less commonly associated with medication reactions. “So, even though this is a small case series with significant limitations, it does add more evidence that COVID-19 is directly responsible for findings in the skin and mucous membranes,” said Dr. Lipoff.
Dr. Freeman noted that the study may also encourage clinicians to look in a patient’s mouth when assessing for SARS-CoV-2. Additional research should examine these data in a larger population.
Several studies by Dr. Freeman, Dr. Lipoff, and others strongly suggest that SARS-CoV-2 has a spectrum of associated dermatologic manifestations. One evaluated perniolike skin lesions (J Am Acad Dermatol. 2020 Aug; 83[2]:486-92). The other was a case series from the COVID-19 registry that examined 716 cases of new-onset dermatologic symptoms in patients from 31 countries with confirmed/suspected SARS-CoV-2 (J Am Acad Dermatol. 2020 Jul 2;S0190-9622[20]32126-5.).
The authors of the report had no disclosures.
SOURCE: Jimenez-Cauhe J et al. JAMA Dermatol. 2020 Jul 15. doi: 10.1001/jamadermatol.2020.2550.
Larger studies should explore and confirm this association, the study’s authors and other experts suggested.
Dermatologists are already aware of the connection between enanthem and viral etiology. “As seen with other viral infections, we wondered if COVID-19 could produce enanthem in addition to skin rash exanthem,” one of the study author’s, Juan Jiménez-Cauhe, MD, a dermatologist with Hospital Universitario Ramon y Cajal, Madrid, said in an interview. He and his colleagues summarized their findings in a research letter in JAMA Dermatology.
They examined the oral cavity of 21 COVID-19 patients at a tertiary care hospital who also had a skin rash from March 30 to April 8. They classified enanthems into four categories: petechial, macular, macular with petechiae, or erythematovesicular. Six of the patients presented with oral lesions, all of them located in the palate; in one patient, the enanthem was macular, it was petechial in two patients and was macular with petechiae in three patients. The six patients ranged between the ages of 40 and 69 years; four were women.
Petechial or vesicular patterns are often associated with viral infections. In this particular study, the investigators did not observe vesicular lesions.
On average, mucocutaneous lesions appeared about 12 days after the onset of COVID-19 symptoms. “Interestingly, this latency was shorter in patients with petechial enanthem, compared with those with a macular lesion with petechiae appearance,” the authors wrote.
This shorter time might suggest an association for SARS-CoV-2, said Dr. Jiménez-Cauhe. Strong cough may have also caused petechial lesions on the palate, but it’s unlikely, as they appeared close in time to COVID-19 symptoms. It’s also unlikely that any drugs caused the lesions, as drug rashes can take 2-3 weeks to appear.
This fits in line with other evidence of broader skin manifestations appearing at the same time or after COVID-19, Esther Freeman, MD, said in an interview. Dr. Freeman, director of global health dermatology at Massachusetts General Hospital, Boston, is the principal investigator of the COVID-19 Dermatology Registry, a collaboration of the American Academy of Dermatology and International League of Dermatological Societies.
The study’s small cohort made it difficult to establish a solid association between the oral lesions and SARS-CoV-2. “However, the presence of enanthem in a patient with a skin rash is a useful finding that suggests a viral etiology rather than a drug reaction. This is particularly useful in COVID-19 patients, who were receiving many drugs as part of the treatment,” Dr. Jimenez-Cauhe said. Future studies should assess whether the presence of enanthem and exanthem lead physicians to consider SARS-CoV-2 as possible agents, ruling out infection with a blood or nasopharyngeal test.
This study adds to the growing body of knowledge on cutaneous and mucocutaneous findings associated with SARS-CoV-2 infection, Jules Lipoff, MD, of the department of dermatology, University of Pennsylvania, Philadelphia, said in an interview. “One challenge in evaluating these findings is that these findings are nonspecific, and medication reactions can often cause similar rashes, such as morbilliform eruptions that can be associated with both viruses and medications.”
Enanthems, as the study authors noted, are more specific to viral infections and are less commonly associated with medication reactions. “So, even though this is a small case series with significant limitations, it does add more evidence that COVID-19 is directly responsible for findings in the skin and mucous membranes,” said Dr. Lipoff.
Dr. Freeman noted that the study may also encourage clinicians to look in a patient’s mouth when assessing for SARS-CoV-2. Additional research should examine these data in a larger population.
Several studies by Dr. Freeman, Dr. Lipoff, and others strongly suggest that SARS-CoV-2 has a spectrum of associated dermatologic manifestations. One evaluated perniolike skin lesions (J Am Acad Dermatol. 2020 Aug; 83[2]:486-92). The other was a case series from the COVID-19 registry that examined 716 cases of new-onset dermatologic symptoms in patients from 31 countries with confirmed/suspected SARS-CoV-2 (J Am Acad Dermatol. 2020 Jul 2;S0190-9622[20]32126-5.).
The authors of the report had no disclosures.
SOURCE: Jimenez-Cauhe J et al. JAMA Dermatol. 2020 Jul 15. doi: 10.1001/jamadermatol.2020.2550.
FROM JAMA DERMATOLOGY
Non–COVID-19 VA Hospital Admissions Drop During the Pandemic
Anecdotal reports have suggested that people have been less likely to go to the hospital for emergencies during the COVID-19 pandemic. Findings from a study by 2 physicians at Mount Sinai in New York now provide support for that: Between March 11 and April 21, 2020, 42% fewer patients were admitted to US Department of Veterans Affairs (VA) inpatient facilities when compared with the preceding 6 weeks.
The researchers analyzed data from the VA Corporate Data Warehouse and examined at trends during the first 16 weeks of 2019 and 2020 for 6 common emergency conditions: stroke, myocardial infarction, heart failure, chronic obstructive pulmonary disease (COPD), appendicitis, and pneumonia. Strikingly, the number of patients admitted dropped from 77,624 in weeks 5 to 10 of 2020 to 45,155 in weeks 11 to 16.
The number of patients admitted for stroke declined by 52%; myocardial infarction, 40%; COPD, 48%; heart failure, 49%; and appendicitis, 57%. By contrast, the number of patients admitted overall and for each condition did not decline during the same weeks in 2019. Admissions for pneumonia dropped during weeks 11 to 16 by 14% in 2019 and 28% in 2020. When patients who tested positive for COVID-19 were excluded, however, pneumonia admissions decreased by 46%. Of patients who were admitted during weeks 11 to 16 of 2020, 2,458 had tested positive for COVID-19 during weeks 5 to 10.
The authers contend that the marked drop in admissions is unlikely to be attributable to a reduction in disease incidence. Rather, they theorize that many patients may be avoiding hospitals out of fear of becoming infected with SARS-CoV-2. These data “should raise serious concerns,” the authors say, about the well-being and health outcomes of the patients who aren’t getting the emergency or inpatient care they need.
Anecdotal reports have suggested that people have been less likely to go to the hospital for emergencies during the COVID-19 pandemic. Findings from a study by 2 physicians at Mount Sinai in New York now provide support for that: Between March 11 and April 21, 2020, 42% fewer patients were admitted to US Department of Veterans Affairs (VA) inpatient facilities when compared with the preceding 6 weeks.
The researchers analyzed data from the VA Corporate Data Warehouse and examined at trends during the first 16 weeks of 2019 and 2020 for 6 common emergency conditions: stroke, myocardial infarction, heart failure, chronic obstructive pulmonary disease (COPD), appendicitis, and pneumonia. Strikingly, the number of patients admitted dropped from 77,624 in weeks 5 to 10 of 2020 to 45,155 in weeks 11 to 16.
The number of patients admitted for stroke declined by 52%; myocardial infarction, 40%; COPD, 48%; heart failure, 49%; and appendicitis, 57%. By contrast, the number of patients admitted overall and for each condition did not decline during the same weeks in 2019. Admissions for pneumonia dropped during weeks 11 to 16 by 14% in 2019 and 28% in 2020. When patients who tested positive for COVID-19 were excluded, however, pneumonia admissions decreased by 46%. Of patients who were admitted during weeks 11 to 16 of 2020, 2,458 had tested positive for COVID-19 during weeks 5 to 10.
The authers contend that the marked drop in admissions is unlikely to be attributable to a reduction in disease incidence. Rather, they theorize that many patients may be avoiding hospitals out of fear of becoming infected with SARS-CoV-2. These data “should raise serious concerns,” the authors say, about the well-being and health outcomes of the patients who aren’t getting the emergency or inpatient care they need.
Anecdotal reports have suggested that people have been less likely to go to the hospital for emergencies during the COVID-19 pandemic. Findings from a study by 2 physicians at Mount Sinai in New York now provide support for that: Between March 11 and April 21, 2020, 42% fewer patients were admitted to US Department of Veterans Affairs (VA) inpatient facilities when compared with the preceding 6 weeks.
The researchers analyzed data from the VA Corporate Data Warehouse and examined at trends during the first 16 weeks of 2019 and 2020 for 6 common emergency conditions: stroke, myocardial infarction, heart failure, chronic obstructive pulmonary disease (COPD), appendicitis, and pneumonia. Strikingly, the number of patients admitted dropped from 77,624 in weeks 5 to 10 of 2020 to 45,155 in weeks 11 to 16.
The number of patients admitted for stroke declined by 52%; myocardial infarction, 40%; COPD, 48%; heart failure, 49%; and appendicitis, 57%. By contrast, the number of patients admitted overall and for each condition did not decline during the same weeks in 2019. Admissions for pneumonia dropped during weeks 11 to 16 by 14% in 2019 and 28% in 2020. When patients who tested positive for COVID-19 were excluded, however, pneumonia admissions decreased by 46%. Of patients who were admitted during weeks 11 to 16 of 2020, 2,458 had tested positive for COVID-19 during weeks 5 to 10.
The authers contend that the marked drop in admissions is unlikely to be attributable to a reduction in disease incidence. Rather, they theorize that many patients may be avoiding hospitals out of fear of becoming infected with SARS-CoV-2. These data “should raise serious concerns,” the authors say, about the well-being and health outcomes of the patients who aren’t getting the emergency or inpatient care they need.
Internists’ use of ultrasound can reduce radiology referrals
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.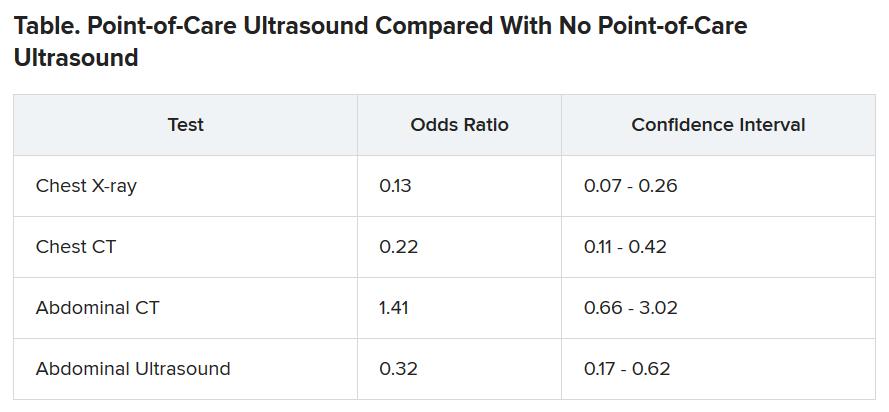
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FDA approves low-sodium treatment option for narcolepsy
Xywav is a novel oxybate product with a unique composition of cations, resulting in 92% less sodium than sodium oxybate (Xyrem, Jazz Pharmaceuticals) at the recommended dosage range of 6 to 9 grams, the company said in a news release.
The FDA approved the drug based on a phase 3 trial involving 201 patients who had narcolepsy with cataplexy.
As reported by Medscape Medical News from the World Sleep 2019 meeting, Xywav demonstrated highly statistically significant differences (P < .0001) in weekly number of cataplexy attacks (primary efficacy endpoint) and Epworth Sleepiness Scale scores (key secondary outcome) vs placebo.
“Based on the efficacy demonstrated in the clinical program, the approval of Xywav is important for people living with cataplexy or EDS associated with narcolepsy,” lead investigator Richard K. Bogan, MD, said in the company’s news release.
He noted that the average American consumes too much sodium. “Excess sodium intake has been linked with increases in blood pressure, hypertension, stroke, and other cardiovascular disease,” said Dr. Bogan, associate clinical professor at the University of South Carolina School of Medicine, Columbia.
“Xywav makes it possible for patients to have a lower-sodium oxybate treatment option. This may help patients taking sodium oxybate better align with daily sodium intake recommendations, including those by the American Heart Association,” he added.
The overall safety profile of Xywav is in line with sodium oxybate, the company said. The most common adverse reactions in adults, occurring in at least 5% of participants, were headache, nausea, dizziness, decreased appetite, parasomnia, diarrhea, hyperhidrosis (excessive sweating), anxiety, and vomiting.
Xywav has a boxed warning as a CNS depressant and for its potential for abuse and misuse. As a result, the drug is only available through a Risk Evaluation and Mitigation Strategy (REMS) program.
The US Drug Enforcement Agency has designated Xywav as a schedule III drug, meaning it has a moderate to low potential for physical and psychological dependence.
The company plans to launch Xywav by the end of the year. Full prescribing information and a medication guide are available online.
This article first appeared on Medscape.com.
Xywav is a novel oxybate product with a unique composition of cations, resulting in 92% less sodium than sodium oxybate (Xyrem, Jazz Pharmaceuticals) at the recommended dosage range of 6 to 9 grams, the company said in a news release.
The FDA approved the drug based on a phase 3 trial involving 201 patients who had narcolepsy with cataplexy.
As reported by Medscape Medical News from the World Sleep 2019 meeting, Xywav demonstrated highly statistically significant differences (P < .0001) in weekly number of cataplexy attacks (primary efficacy endpoint) and Epworth Sleepiness Scale scores (key secondary outcome) vs placebo.
“Based on the efficacy demonstrated in the clinical program, the approval of Xywav is important for people living with cataplexy or EDS associated with narcolepsy,” lead investigator Richard K. Bogan, MD, said in the company’s news release.
He noted that the average American consumes too much sodium. “Excess sodium intake has been linked with increases in blood pressure, hypertension, stroke, and other cardiovascular disease,” said Dr. Bogan, associate clinical professor at the University of South Carolina School of Medicine, Columbia.
“Xywav makes it possible for patients to have a lower-sodium oxybate treatment option. This may help patients taking sodium oxybate better align with daily sodium intake recommendations, including those by the American Heart Association,” he added.
The overall safety profile of Xywav is in line with sodium oxybate, the company said. The most common adverse reactions in adults, occurring in at least 5% of participants, were headache, nausea, dizziness, decreased appetite, parasomnia, diarrhea, hyperhidrosis (excessive sweating), anxiety, and vomiting.
Xywav has a boxed warning as a CNS depressant and for its potential for abuse and misuse. As a result, the drug is only available through a Risk Evaluation and Mitigation Strategy (REMS) program.
The US Drug Enforcement Agency has designated Xywav as a schedule III drug, meaning it has a moderate to low potential for physical and psychological dependence.
The company plans to launch Xywav by the end of the year. Full prescribing information and a medication guide are available online.
This article first appeared on Medscape.com.
Xywav is a novel oxybate product with a unique composition of cations, resulting in 92% less sodium than sodium oxybate (Xyrem, Jazz Pharmaceuticals) at the recommended dosage range of 6 to 9 grams, the company said in a news release.
The FDA approved the drug based on a phase 3 trial involving 201 patients who had narcolepsy with cataplexy.
As reported by Medscape Medical News from the World Sleep 2019 meeting, Xywav demonstrated highly statistically significant differences (P < .0001) in weekly number of cataplexy attacks (primary efficacy endpoint) and Epworth Sleepiness Scale scores (key secondary outcome) vs placebo.
“Based on the efficacy demonstrated in the clinical program, the approval of Xywav is important for people living with cataplexy or EDS associated with narcolepsy,” lead investigator Richard K. Bogan, MD, said in the company’s news release.
He noted that the average American consumes too much sodium. “Excess sodium intake has been linked with increases in blood pressure, hypertension, stroke, and other cardiovascular disease,” said Dr. Bogan, associate clinical professor at the University of South Carolina School of Medicine, Columbia.
“Xywav makes it possible for patients to have a lower-sodium oxybate treatment option. This may help patients taking sodium oxybate better align with daily sodium intake recommendations, including those by the American Heart Association,” he added.
The overall safety profile of Xywav is in line with sodium oxybate, the company said. The most common adverse reactions in adults, occurring in at least 5% of participants, were headache, nausea, dizziness, decreased appetite, parasomnia, diarrhea, hyperhidrosis (excessive sweating), anxiety, and vomiting.
Xywav has a boxed warning as a CNS depressant and for its potential for abuse and misuse. As a result, the drug is only available through a Risk Evaluation and Mitigation Strategy (REMS) program.
The US Drug Enforcement Agency has designated Xywav as a schedule III drug, meaning it has a moderate to low potential for physical and psychological dependence.
The company plans to launch Xywav by the end of the year. Full prescribing information and a medication guide are available online.
This article first appeared on Medscape.com.
Medics with ‘long COVID’ call for clinical recognition
Thousands of coronavirus patients risk going without treatment and support for debilitating symptoms lasting months because of a lack of awareness of ‘long COVID’, according to a group formed by clinicians with extended serious after-effects of the virus.
Many members of the 100-strong Facebook group UK doctors: COVID “Long tail” have been unable to work for weeks after failing to recover from an episode of COVID-19. They warn of the need for clinical recognition of “long COVID,” along with systems to log symptoms and manage patients in the community. Without this, there could be major consequences for return to work across all professions, as well as implications for disease prevention.
‘Weird symptoms’
Three of the group: Dr Amali Lokugamage, consultant obstetrician at the Whittington Hospital; Dr Sharon Taylor, child psychiatrist at St Mary’s Hospital London, and Dr Clare Rayner, a retired occupational health physician and lecturer at the University of Manchester, have highlighted their concerns in The BMJ and on social media groups. They say colleagues are observing a range of symptoms of long COVID in their practices.
These include cardiac, gut and respiratory symptoms, skin manifestations, neurological and psychiatric symptoms, severe fatigue, and relapsing fevers, sometimes continuing for more than 16 weeks, and which they say go well beyond definitions of chronic fatigue. The authors are also aware of a pattern of symptom clusters recurring every third or fourth day, which in some cases are so severe that people are having to take extended periods of sick leave.
Writing in The BMJ the authors say: “Concerns have been raised about the lack of awareness among NHS doctors, nurses, paramedics, and other healthcare professionals with regard to the prolonged, varied, and weird symptoms [of COVID-19].”
Speaking to Medscape News UK, Dr. Clare Rayner said: “We see a huge need that is not being met, because these cases are just not being seen in hospital. All the attention has been on the acute illness.”
She pointed to the urgent need for government planning for a surge in people requiring support to return to work following long-term COVID-19 symptoms. According to occupational health research, only 10-40% of people who take 6 weeks off work return to work, dropping to 5%-10% after an absence of 6 months.
In her own case, she is recovering after 4 months of illness, including a hospital admission with gut symptoms and dehydration, and 2 weeks of social service home support. She has experienced a range of relapsing and remitting symptoms, which she describes as ‘bizarre and coming in phases’.
Stimulating recovery
The recently-announced NHS portal for COVID-19 patients has been welcomed by the authors as an opportunity for long-standing symptoms to reach the medical and Government radar. But Dr Taylor believes it should have been set up from the start with input from patients with symptoms, to make sure that any support provided reflects the nature of the problems experienced.
In her case, as a previously regular gym attender with a resting heart rate in the 50s, she has now been diagnosed as having multi-organ disease affecting her heart, spleen, lung, and autonomic system. She has fluid on the lungs and heart, and suffers from continuous chest pain and oxygen desaturation when lying down. She has not been able to work since she contracted COVID-19 in March.
“COVID patients with the chronic form of the disease need to be involved in research right from the start to ensure the right questions are asked - not just those who have had acute disease,” she insists to Medscape News UK. “We need to gather evidence, to inform the development of a multi-disciplinary approach and a range of rehabilitation options depending on the organs involved.
“The focus needs to be on stimulating recovery and preventing development of chronic problems. We still don’t know if those with chronic COVID disease are infectious, how long their prolonged cardio-respiratory and neurological complications will last, and crucially whether treatment will reduce the duration of their problems. The worry is that left unattended, these patients may develop irreversible damage leading to chronic illness.”
General practice
GPs have been at the forefront of management of the long-standing consequences of COVID-19. In its recent report General practice in the post-COVID world, the Royal College of General Practitioners highlights the need for urgent government planning and funding to prepare general practice services for facilitating the recovery of local communities.
The report calls on the four governments of the UK each to produce a comprehensive plan to support GPs in managing the longer-term effects of COVID-19 in the community, including costed proposals for additional funding for general practice; workforce solutions; reductions in regulatory burdens and ‘red tape’; a systematic approach for identifying patients most likely to need primary care support, and proposals for how health inequalities will be minimized to ensure all patients have access to the necessary post-COVID-19 care.
RCGP Chair Professor Martin Marshall said: “COVID-19 will leave a lingering and difficult legacy and it is GPs working with patients in their communities who will be picking up the pieces.”
One issue is the lack of a reliable estimate of the prevalence of post viral symptoms for other viruses, let alone for COVID-19. Even a 1% chance of long-term problems amongst survivors would suggest 2500 with a need for extra support, but experience with post-viral syndrome generally suggests the prevalence may be more like 3%.
The BMA has been carrying out tracker surveys of its own members at 2-week intervals since March. The most recent, involving more than 5000 doctors, indicated that around 30% of doctors who believed they’d had COVID-19 were still experiencing physical symptoms they thought were caused by the virus, 21% had taken sick leave, and a further 9% had taken annual leave to deal with ongoing symptoms.
Dr David Strain, chair of the BMA medical academic staff committee and clinical senior lecturer at the University of Exeter Medical School, has a particular interest in the after-effects of COVID-19. He said it was becoming evident that the virus was leaving a lasting legacy with a significant number of people, even younger ones.
He told Medscape News UK: “Once COVID-19 enters the nervous system, the lasting symptoms on people can range from a mild loss of sense of smell or taste, to more severe symptoms such as difficulties in concentration. A small number have also been left with chronic fatigue syndrome, which is poorly understood, and can be difficult to treat. This does not appear to be dependent on the initial severity of COVID-19 symptoms.
“Currently, it is impossible to predict the prevalence of longer-lasting effects. A full assessment of COVID-19’s impact will only be possible once people return to work on a regular basis and the effect on their physical health becomes evident. Of the doctors in the BMA survey who had experienced COVID-19, 15% took sick leave beyond their acute illness, and another 6% used annual leave allowance to extend their recovery time.
“Clearly, more research will be needed into the long-term consequences of COVID-19 and the future treatments needed to deal with them.”
Further research
The National Institute for Health Research (NIHR) has called for applications for research to enhance understanding and management of the health and social care consequences of the global COVID-19 pandemic beyond the acute phase, with a particular focus on ‘health outcomes, public health, social care and health service delivery and to mitigate the impact of subsequent phases and aftermath’.
The authors of The BMJ article stress the wide-ranging nature of ‘long COVID’ symptoms and warn of the dangers of treating them for research purposes under the banner of chronic fatigue. They say: “These wide-ranging, unusual, and potentially very serious symptoms can be anxiety-provoking, particularly secondary to a virus that has only been known to the world for 8 months and which we have barely begun to understand. However, it is dismissive solely to attribute such symptoms to anxiety in the thousands of patients like ourselves who have attended hospital or general practice with chronic COVID-19.”
This article first appeared on Medscape.com.
Thousands of coronavirus patients risk going without treatment and support for debilitating symptoms lasting months because of a lack of awareness of ‘long COVID’, according to a group formed by clinicians with extended serious after-effects of the virus.
Many members of the 100-strong Facebook group UK doctors: COVID “Long tail” have been unable to work for weeks after failing to recover from an episode of COVID-19. They warn of the need for clinical recognition of “long COVID,” along with systems to log symptoms and manage patients in the community. Without this, there could be major consequences for return to work across all professions, as well as implications for disease prevention.
‘Weird symptoms’
Three of the group: Dr Amali Lokugamage, consultant obstetrician at the Whittington Hospital; Dr Sharon Taylor, child psychiatrist at St Mary’s Hospital London, and Dr Clare Rayner, a retired occupational health physician and lecturer at the University of Manchester, have highlighted their concerns in The BMJ and on social media groups. They say colleagues are observing a range of symptoms of long COVID in their practices.
These include cardiac, gut and respiratory symptoms, skin manifestations, neurological and psychiatric symptoms, severe fatigue, and relapsing fevers, sometimes continuing for more than 16 weeks, and which they say go well beyond definitions of chronic fatigue. The authors are also aware of a pattern of symptom clusters recurring every third or fourth day, which in some cases are so severe that people are having to take extended periods of sick leave.
Writing in The BMJ the authors say: “Concerns have been raised about the lack of awareness among NHS doctors, nurses, paramedics, and other healthcare professionals with regard to the prolonged, varied, and weird symptoms [of COVID-19].”
Speaking to Medscape News UK, Dr. Clare Rayner said: “We see a huge need that is not being met, because these cases are just not being seen in hospital. All the attention has been on the acute illness.”
She pointed to the urgent need for government planning for a surge in people requiring support to return to work following long-term COVID-19 symptoms. According to occupational health research, only 10-40% of people who take 6 weeks off work return to work, dropping to 5%-10% after an absence of 6 months.
In her own case, she is recovering after 4 months of illness, including a hospital admission with gut symptoms and dehydration, and 2 weeks of social service home support. She has experienced a range of relapsing and remitting symptoms, which she describes as ‘bizarre and coming in phases’.
Stimulating recovery
The recently-announced NHS portal for COVID-19 patients has been welcomed by the authors as an opportunity for long-standing symptoms to reach the medical and Government radar. But Dr Taylor believes it should have been set up from the start with input from patients with symptoms, to make sure that any support provided reflects the nature of the problems experienced.
In her case, as a previously regular gym attender with a resting heart rate in the 50s, she has now been diagnosed as having multi-organ disease affecting her heart, spleen, lung, and autonomic system. She has fluid on the lungs and heart, and suffers from continuous chest pain and oxygen desaturation when lying down. She has not been able to work since she contracted COVID-19 in March.
“COVID patients with the chronic form of the disease need to be involved in research right from the start to ensure the right questions are asked - not just those who have had acute disease,” she insists to Medscape News UK. “We need to gather evidence, to inform the development of a multi-disciplinary approach and a range of rehabilitation options depending on the organs involved.
“The focus needs to be on stimulating recovery and preventing development of chronic problems. We still don’t know if those with chronic COVID disease are infectious, how long their prolonged cardio-respiratory and neurological complications will last, and crucially whether treatment will reduce the duration of their problems. The worry is that left unattended, these patients may develop irreversible damage leading to chronic illness.”
General practice
GPs have been at the forefront of management of the long-standing consequences of COVID-19. In its recent report General practice in the post-COVID world, the Royal College of General Practitioners highlights the need for urgent government planning and funding to prepare general practice services for facilitating the recovery of local communities.
The report calls on the four governments of the UK each to produce a comprehensive plan to support GPs in managing the longer-term effects of COVID-19 in the community, including costed proposals for additional funding for general practice; workforce solutions; reductions in regulatory burdens and ‘red tape’; a systematic approach for identifying patients most likely to need primary care support, and proposals for how health inequalities will be minimized to ensure all patients have access to the necessary post-COVID-19 care.
RCGP Chair Professor Martin Marshall said: “COVID-19 will leave a lingering and difficult legacy and it is GPs working with patients in their communities who will be picking up the pieces.”
One issue is the lack of a reliable estimate of the prevalence of post viral symptoms for other viruses, let alone for COVID-19. Even a 1% chance of long-term problems amongst survivors would suggest 2500 with a need for extra support, but experience with post-viral syndrome generally suggests the prevalence may be more like 3%.
The BMA has been carrying out tracker surveys of its own members at 2-week intervals since March. The most recent, involving more than 5000 doctors, indicated that around 30% of doctors who believed they’d had COVID-19 were still experiencing physical symptoms they thought were caused by the virus, 21% had taken sick leave, and a further 9% had taken annual leave to deal with ongoing symptoms.
Dr David Strain, chair of the BMA medical academic staff committee and clinical senior lecturer at the University of Exeter Medical School, has a particular interest in the after-effects of COVID-19. He said it was becoming evident that the virus was leaving a lasting legacy with a significant number of people, even younger ones.
He told Medscape News UK: “Once COVID-19 enters the nervous system, the lasting symptoms on people can range from a mild loss of sense of smell or taste, to more severe symptoms such as difficulties in concentration. A small number have also been left with chronic fatigue syndrome, which is poorly understood, and can be difficult to treat. This does not appear to be dependent on the initial severity of COVID-19 symptoms.
“Currently, it is impossible to predict the prevalence of longer-lasting effects. A full assessment of COVID-19’s impact will only be possible once people return to work on a regular basis and the effect on their physical health becomes evident. Of the doctors in the BMA survey who had experienced COVID-19, 15% took sick leave beyond their acute illness, and another 6% used annual leave allowance to extend their recovery time.
“Clearly, more research will be needed into the long-term consequences of COVID-19 and the future treatments needed to deal with them.”
Further research
The National Institute for Health Research (NIHR) has called for applications for research to enhance understanding and management of the health and social care consequences of the global COVID-19 pandemic beyond the acute phase, with a particular focus on ‘health outcomes, public health, social care and health service delivery and to mitigate the impact of subsequent phases and aftermath’.
The authors of The BMJ article stress the wide-ranging nature of ‘long COVID’ symptoms and warn of the dangers of treating them for research purposes under the banner of chronic fatigue. They say: “These wide-ranging, unusual, and potentially very serious symptoms can be anxiety-provoking, particularly secondary to a virus that has only been known to the world for 8 months and which we have barely begun to understand. However, it is dismissive solely to attribute such symptoms to anxiety in the thousands of patients like ourselves who have attended hospital or general practice with chronic COVID-19.”
This article first appeared on Medscape.com.
Thousands of coronavirus patients risk going without treatment and support for debilitating symptoms lasting months because of a lack of awareness of ‘long COVID’, according to a group formed by clinicians with extended serious after-effects of the virus.
Many members of the 100-strong Facebook group UK doctors: COVID “Long tail” have been unable to work for weeks after failing to recover from an episode of COVID-19. They warn of the need for clinical recognition of “long COVID,” along with systems to log symptoms and manage patients in the community. Without this, there could be major consequences for return to work across all professions, as well as implications for disease prevention.
‘Weird symptoms’
Three of the group: Dr Amali Lokugamage, consultant obstetrician at the Whittington Hospital; Dr Sharon Taylor, child psychiatrist at St Mary’s Hospital London, and Dr Clare Rayner, a retired occupational health physician and lecturer at the University of Manchester, have highlighted their concerns in The BMJ and on social media groups. They say colleagues are observing a range of symptoms of long COVID in their practices.
These include cardiac, gut and respiratory symptoms, skin manifestations, neurological and psychiatric symptoms, severe fatigue, and relapsing fevers, sometimes continuing for more than 16 weeks, and which they say go well beyond definitions of chronic fatigue. The authors are also aware of a pattern of symptom clusters recurring every third or fourth day, which in some cases are so severe that people are having to take extended periods of sick leave.
Writing in The BMJ the authors say: “Concerns have been raised about the lack of awareness among NHS doctors, nurses, paramedics, and other healthcare professionals with regard to the prolonged, varied, and weird symptoms [of COVID-19].”
Speaking to Medscape News UK, Dr. Clare Rayner said: “We see a huge need that is not being met, because these cases are just not being seen in hospital. All the attention has been on the acute illness.”
She pointed to the urgent need for government planning for a surge in people requiring support to return to work following long-term COVID-19 symptoms. According to occupational health research, only 10-40% of people who take 6 weeks off work return to work, dropping to 5%-10% after an absence of 6 months.
In her own case, she is recovering after 4 months of illness, including a hospital admission with gut symptoms and dehydration, and 2 weeks of social service home support. She has experienced a range of relapsing and remitting symptoms, which she describes as ‘bizarre and coming in phases’.
Stimulating recovery
The recently-announced NHS portal for COVID-19 patients has been welcomed by the authors as an opportunity for long-standing symptoms to reach the medical and Government radar. But Dr Taylor believes it should have been set up from the start with input from patients with symptoms, to make sure that any support provided reflects the nature of the problems experienced.
In her case, as a previously regular gym attender with a resting heart rate in the 50s, she has now been diagnosed as having multi-organ disease affecting her heart, spleen, lung, and autonomic system. She has fluid on the lungs and heart, and suffers from continuous chest pain and oxygen desaturation when lying down. She has not been able to work since she contracted COVID-19 in March.
“COVID patients with the chronic form of the disease need to be involved in research right from the start to ensure the right questions are asked - not just those who have had acute disease,” she insists to Medscape News UK. “We need to gather evidence, to inform the development of a multi-disciplinary approach and a range of rehabilitation options depending on the organs involved.
“The focus needs to be on stimulating recovery and preventing development of chronic problems. We still don’t know if those with chronic COVID disease are infectious, how long their prolonged cardio-respiratory and neurological complications will last, and crucially whether treatment will reduce the duration of their problems. The worry is that left unattended, these patients may develop irreversible damage leading to chronic illness.”
General practice
GPs have been at the forefront of management of the long-standing consequences of COVID-19. In its recent report General practice in the post-COVID world, the Royal College of General Practitioners highlights the need for urgent government planning and funding to prepare general practice services for facilitating the recovery of local communities.
The report calls on the four governments of the UK each to produce a comprehensive plan to support GPs in managing the longer-term effects of COVID-19 in the community, including costed proposals for additional funding for general practice; workforce solutions; reductions in regulatory burdens and ‘red tape’; a systematic approach for identifying patients most likely to need primary care support, and proposals for how health inequalities will be minimized to ensure all patients have access to the necessary post-COVID-19 care.
RCGP Chair Professor Martin Marshall said: “COVID-19 will leave a lingering and difficult legacy and it is GPs working with patients in their communities who will be picking up the pieces.”
One issue is the lack of a reliable estimate of the prevalence of post viral symptoms for other viruses, let alone for COVID-19. Even a 1% chance of long-term problems amongst survivors would suggest 2500 with a need for extra support, but experience with post-viral syndrome generally suggests the prevalence may be more like 3%.
The BMA has been carrying out tracker surveys of its own members at 2-week intervals since March. The most recent, involving more than 5000 doctors, indicated that around 30% of doctors who believed they’d had COVID-19 were still experiencing physical symptoms they thought were caused by the virus, 21% had taken sick leave, and a further 9% had taken annual leave to deal with ongoing symptoms.
Dr David Strain, chair of the BMA medical academic staff committee and clinical senior lecturer at the University of Exeter Medical School, has a particular interest in the after-effects of COVID-19. He said it was becoming evident that the virus was leaving a lasting legacy with a significant number of people, even younger ones.
He told Medscape News UK: “Once COVID-19 enters the nervous system, the lasting symptoms on people can range from a mild loss of sense of smell or taste, to more severe symptoms such as difficulties in concentration. A small number have also been left with chronic fatigue syndrome, which is poorly understood, and can be difficult to treat. This does not appear to be dependent on the initial severity of COVID-19 symptoms.
“Currently, it is impossible to predict the prevalence of longer-lasting effects. A full assessment of COVID-19’s impact will only be possible once people return to work on a regular basis and the effect on their physical health becomes evident. Of the doctors in the BMA survey who had experienced COVID-19, 15% took sick leave beyond their acute illness, and another 6% used annual leave allowance to extend their recovery time.
“Clearly, more research will be needed into the long-term consequences of COVID-19 and the future treatments needed to deal with them.”
Further research
The National Institute for Health Research (NIHR) has called for applications for research to enhance understanding and management of the health and social care consequences of the global COVID-19 pandemic beyond the acute phase, with a particular focus on ‘health outcomes, public health, social care and health service delivery and to mitigate the impact of subsequent phases and aftermath’.
The authors of The BMJ article stress the wide-ranging nature of ‘long COVID’ symptoms and warn of the dangers of treating them for research purposes under the banner of chronic fatigue. They say: “These wide-ranging, unusual, and potentially very serious symptoms can be anxiety-provoking, particularly secondary to a virus that has only been known to the world for 8 months and which we have barely begun to understand. However, it is dismissive solely to attribute such symptoms to anxiety in the thousands of patients like ourselves who have attended hospital or general practice with chronic COVID-19.”
This article first appeared on Medscape.com.
Quitting smoking after MI has huge benefits in young adults
Young adult smokers who stop smoking in the first year after an initial myocardial infarction are far less likely to die over the next 10 years than their peers who continue to smoke. Yet nearly two-thirds keep smoking after the event, according to new data from the Partners YOUNG-MI Registry.
“Smoking is one of the most common risk factors for developing an MI at a young age. ... This reinforces the need to have more young individuals avoid, or quit, the use of tobacco,” Ron Blankstein, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, said in an interview.
Yet, the finding that 62% of young adults continue to smoke 1 year after MI points to an “enormous need for better smoking cessation efforts following a heart attack,” he said.
“Powerful” message for clinicians
“This study joins an incredibly powerful body of evidence that says if you quit smoking, you’re going to live longer,” said Michael Fiore, MD, MPH, MBA, director of the University of Wisconsin Center for Tobacco Research and Intervention, Madison, who wasn’t involved in the study.
“As physicians, there is nothing we can do that will have a greater impact for our patients than quitting smoking. The study is a powerful call for clinicians to intervene with their patients that smoke – both if you have an MI or if you don’t,” Dr. Fiore told this news organization.
The study involved 2,072 individuals 50 years or younger (median age, 45 years; 81% male) who were hospitalized for an initial MI at two large academic medical centers in Boston. Of these, 33.9% were never-smokers, 13.6% were former smokers, and 52.5% were smokers at the time of their MI.
During a median follow-up of 10.2 years, those who quit smoking had a significantly lower rate of death from any cause (unadjusted hazard ratio, 0.35; 95% confidence interval, 0.19-0.63; P < .001) and a cardiovascular cause (HR, 0.29; 95% CI, 0.11-0.79; P = .02), relative to those who continued to smoke.
The results remained statistically significant in a propensity-matched analysis for both all-cause (HR, 0.30; 95% CI, 0.16-0.56; P < .001) and CV mortality (HR, 0.19; 95% CI, 0.06-0.56; P = .003).
“Although patients who quit smoking were similar to those who continued to smoke with respect to their baseline characteristics, smoking cessation was associated with an approximate 70%-80% reduction in all-cause and CV mortality,” the authors note in their article, published online July 8 in JAMA Network Open.
They say it’s also noteworthy that long-term death rates of never-smokers and former smokers who quit before the MI were nearly identical.
‘A failure of our health care system’
The bottom line, said Dr. Blankstein, is that it is “never too late to quit, and those who experience an MI should do so right away. Our health care system must help promote such efforts, as there is immense room for improvement.”
Dr. Fiore said: “When I see an article like this, it just reminds me that, if you’re really thinking about staying healthy, there is nothing better you can do to improve the quality and longevity of your life than quitting smoking.”
The observation that many patients continue to smoke after MI is a “failure of our health care system, and it’s an individual failure in that these individuals are not able to overcome their powerful nicotine dependence. It’s an unfortunate occurrence that’s resulting in unnecessary deaths,” said Dr. Fiore.
There is no “magic bullet” to overcome nicotine addiction, but there are approved treatments that can “substantially boost quit rates,” he noted.
The two most effective smoking-cessation treatments are varenicline (Chantix) and combination nicotine replacement therapy, a patch combined ideally with nicotine mini lozenges, particularly when combined with some brief counseling, said Fiore.
He encourages cardiologists to get their patients to commit to quitting and then link them to resources such as 1-800-QUIT-NOW or SmokeFree.gov.
Funding for the study was provided by grants from the National Heart, Lung, and Blood Institute. Dr. Blankstein reported receiving research support from Amgen and Astellas. Dr. Fiore had no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Young adult smokers who stop smoking in the first year after an initial myocardial infarction are far less likely to die over the next 10 years than their peers who continue to smoke. Yet nearly two-thirds keep smoking after the event, according to new data from the Partners YOUNG-MI Registry.
“Smoking is one of the most common risk factors for developing an MI at a young age. ... This reinforces the need to have more young individuals avoid, or quit, the use of tobacco,” Ron Blankstein, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, said in an interview.
Yet, the finding that 62% of young adults continue to smoke 1 year after MI points to an “enormous need for better smoking cessation efforts following a heart attack,” he said.
“Powerful” message for clinicians
“This study joins an incredibly powerful body of evidence that says if you quit smoking, you’re going to live longer,” said Michael Fiore, MD, MPH, MBA, director of the University of Wisconsin Center for Tobacco Research and Intervention, Madison, who wasn’t involved in the study.
“As physicians, there is nothing we can do that will have a greater impact for our patients than quitting smoking. The study is a powerful call for clinicians to intervene with their patients that smoke – both if you have an MI or if you don’t,” Dr. Fiore told this news organization.
The study involved 2,072 individuals 50 years or younger (median age, 45 years; 81% male) who were hospitalized for an initial MI at two large academic medical centers in Boston. Of these, 33.9% were never-smokers, 13.6% were former smokers, and 52.5% were smokers at the time of their MI.
During a median follow-up of 10.2 years, those who quit smoking had a significantly lower rate of death from any cause (unadjusted hazard ratio, 0.35; 95% confidence interval, 0.19-0.63; P < .001) and a cardiovascular cause (HR, 0.29; 95% CI, 0.11-0.79; P = .02), relative to those who continued to smoke.
The results remained statistically significant in a propensity-matched analysis for both all-cause (HR, 0.30; 95% CI, 0.16-0.56; P < .001) and CV mortality (HR, 0.19; 95% CI, 0.06-0.56; P = .003).
“Although patients who quit smoking were similar to those who continued to smoke with respect to their baseline characteristics, smoking cessation was associated with an approximate 70%-80% reduction in all-cause and CV mortality,” the authors note in their article, published online July 8 in JAMA Network Open.
They say it’s also noteworthy that long-term death rates of never-smokers and former smokers who quit before the MI were nearly identical.
‘A failure of our health care system’
The bottom line, said Dr. Blankstein, is that it is “never too late to quit, and those who experience an MI should do so right away. Our health care system must help promote such efforts, as there is immense room for improvement.”
Dr. Fiore said: “When I see an article like this, it just reminds me that, if you’re really thinking about staying healthy, there is nothing better you can do to improve the quality and longevity of your life than quitting smoking.”
The observation that many patients continue to smoke after MI is a “failure of our health care system, and it’s an individual failure in that these individuals are not able to overcome their powerful nicotine dependence. It’s an unfortunate occurrence that’s resulting in unnecessary deaths,” said Dr. Fiore.
There is no “magic bullet” to overcome nicotine addiction, but there are approved treatments that can “substantially boost quit rates,” he noted.
The two most effective smoking-cessation treatments are varenicline (Chantix) and combination nicotine replacement therapy, a patch combined ideally with nicotine mini lozenges, particularly when combined with some brief counseling, said Fiore.
He encourages cardiologists to get their patients to commit to quitting and then link them to resources such as 1-800-QUIT-NOW or SmokeFree.gov.
Funding for the study was provided by grants from the National Heart, Lung, and Blood Institute. Dr. Blankstein reported receiving research support from Amgen and Astellas. Dr. Fiore had no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Young adult smokers who stop smoking in the first year after an initial myocardial infarction are far less likely to die over the next 10 years than their peers who continue to smoke. Yet nearly two-thirds keep smoking after the event, according to new data from the Partners YOUNG-MI Registry.
“Smoking is one of the most common risk factors for developing an MI at a young age. ... This reinforces the need to have more young individuals avoid, or quit, the use of tobacco,” Ron Blankstein, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, said in an interview.
Yet, the finding that 62% of young adults continue to smoke 1 year after MI points to an “enormous need for better smoking cessation efforts following a heart attack,” he said.
“Powerful” message for clinicians
“This study joins an incredibly powerful body of evidence that says if you quit smoking, you’re going to live longer,” said Michael Fiore, MD, MPH, MBA, director of the University of Wisconsin Center for Tobacco Research and Intervention, Madison, who wasn’t involved in the study.
“As physicians, there is nothing we can do that will have a greater impact for our patients than quitting smoking. The study is a powerful call for clinicians to intervene with their patients that smoke – both if you have an MI or if you don’t,” Dr. Fiore told this news organization.
The study involved 2,072 individuals 50 years or younger (median age, 45 years; 81% male) who were hospitalized for an initial MI at two large academic medical centers in Boston. Of these, 33.9% were never-smokers, 13.6% were former smokers, and 52.5% were smokers at the time of their MI.
During a median follow-up of 10.2 years, those who quit smoking had a significantly lower rate of death from any cause (unadjusted hazard ratio, 0.35; 95% confidence interval, 0.19-0.63; P < .001) and a cardiovascular cause (HR, 0.29; 95% CI, 0.11-0.79; P = .02), relative to those who continued to smoke.
The results remained statistically significant in a propensity-matched analysis for both all-cause (HR, 0.30; 95% CI, 0.16-0.56; P < .001) and CV mortality (HR, 0.19; 95% CI, 0.06-0.56; P = .003).
“Although patients who quit smoking were similar to those who continued to smoke with respect to their baseline characteristics, smoking cessation was associated with an approximate 70%-80% reduction in all-cause and CV mortality,” the authors note in their article, published online July 8 in JAMA Network Open.
They say it’s also noteworthy that long-term death rates of never-smokers and former smokers who quit before the MI were nearly identical.
‘A failure of our health care system’
The bottom line, said Dr. Blankstein, is that it is “never too late to quit, and those who experience an MI should do so right away. Our health care system must help promote such efforts, as there is immense room for improvement.”
Dr. Fiore said: “When I see an article like this, it just reminds me that, if you’re really thinking about staying healthy, there is nothing better you can do to improve the quality and longevity of your life than quitting smoking.”
The observation that many patients continue to smoke after MI is a “failure of our health care system, and it’s an individual failure in that these individuals are not able to overcome their powerful nicotine dependence. It’s an unfortunate occurrence that’s resulting in unnecessary deaths,” said Dr. Fiore.
There is no “magic bullet” to overcome nicotine addiction, but there are approved treatments that can “substantially boost quit rates,” he noted.
The two most effective smoking-cessation treatments are varenicline (Chantix) and combination nicotine replacement therapy, a patch combined ideally with nicotine mini lozenges, particularly when combined with some brief counseling, said Fiore.
He encourages cardiologists to get their patients to commit to quitting and then link them to resources such as 1-800-QUIT-NOW or SmokeFree.gov.
Funding for the study was provided by grants from the National Heart, Lung, and Blood Institute. Dr. Blankstein reported receiving research support from Amgen and Astellas. Dr. Fiore had no relevant disclosures.
A version of this article originally appeared on Medscape.com.