User login
Early heparin treatment linked to lower COVID-19 mortality
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
Early treatment with low-molecular-weight heparin (LMWH) reduces the risk for death in patients with COVID-19, a retrospective cohort study shows.
Heparin could reduce the risk for blood clots, Andrea De Vito, MD, of the unit of infectious diseases at the University of Sassari, Italy, said during his online presentation of the findings at the 31st European Congress of Clinical Microbiology & Infectious Diseases.
“Several studies try to describe the role played by coagulopathies in COVID-19 death,” but the mechanism causing them is still unclear, Dr. De Vito explained.
Some guidelines have suggested heparin as a treatment for hospitalized COVID-19 patients, but few have looked at nonhospitalized patients. In fact, the National Institutes of Health discourages the use of heparin in nonhospitalized COVID-19 patients, and guidance for the home care of COVID-19 patients from the World Health Organization doesn’t mention heparin treatment at all, he said.
To examine the benefits of early heparin – whether administered at home or in the hospital – Dr. De Vito and colleagues looked at a cohort of older adults with COVID-19 who were evaluated or treated at an Italian university hospital.
“Some patients were hospitalized immediately after symptoms onset; other people preferred to call their general practitioner and started the treatment at home,” Dr. De Vito said in an interview. “Other people were hospitalized for worsening of symptoms later in the course of the disease.”
Of the 734 patients, 296 received heparin within 5 days of the onset of symptoms or a positive COVID-19 test. Of the remaining 438 patients, 196 received LMWH treatment later during the disease course, and the rest never received LMWH.
All patients who received early heparin were treated with LMWH 4,000 IU, or 6,000 IU if their body mass index was above 30 kg/m2. This was reduced to 2,000 IU if estimated glomerular filtration rate (eGFR) dropped below 30 mL/min. None of the patients had previously received heparin.
Median age was slightly younger for patients who received early heparin than for those who did not (76.8 vs. 78.5 years).
Other demographic characteristics, such as sex and BMI, were similar in the two groups, as were rates of comorbidities, such as hypertension, cardiovascular disease, diabetes, chronic obstructive pulmonary disease, kidney disease, and neurologic conditions. Also similar were the frequency of symptoms (such as fever, cough, and shortness of breath) and rates of treatment with remdesivir or steroids.
Rates of hospital admission were not significantly different between patients who received early heparin and those who did not (65% vs. 61%). There was also no significant difference in use of a venturi mask (35% vs. 28%), noninvasive ventilation (13% vs. 14%), or intubation (5% vs. 8%).
However, rates of death were significantly lower in patients who received early heparin than in those who did not (13% vs. 25%; P < .0001).
There was a trend toward shorter hospital stays for patients treated with early heparin, but the difference was not significant (median, 10 vs. 13 days; P = .08).
Researchers also conducted a separate analysis of 219 COVID-19 patients who received LMWH at home, regardless of when during their disease course they received it. These patients were significantly less likely to be hospitalized than were patients who did not receive LMWH at home (odds ratio, 0.2; P < .0001).
Comparatively, early heparin treatment had a greater effect on the risk for death and the risk for hospitalization than did other factors.
“Thromboemboli are a major complication of COVID. There is good consensus that hospitalized patients with COVID should receive anticoagulants prophylactically, although the best dose is being studied,” said Judy Stone, MD, an infectious disease physician and journalist who was not involved in the study.
“This study extends those findings of benefit from anticoagulants to nonhospitalized patients, with fewer deaths in those treated with low-molecular-weight heparin,” Dr. Stone told this news organization. “The major limitation is that the study is retrospective and observational. The next step would be to confirm these findings prospectively, randomizing a similar group to LMWH or no anticoagulation.”
Another limitation of the study is that some of the patients lived in nursing homes and might have received care from nurses that eliminated the need for hospitalization, Dr. De Vito added.
The study did not note any external funding. The authors have disclosed no relevant financial relationships. Dr. Stone is a member of the advisory committee for the C-Path CURE Drug Repurposing Collaboratory (CDRC) program and has written for Medscape.
A version of this article first appeared on Medscape.com.
Stop using Neutrogena and Aveeno spray sunscreen, J&J warns
Benzene is not an ingredient of sunscreen, and should not be present in these products. The levels detected were low and would not be expected to have an adverse effect on health, but the company says it is recalling the products anyway “out of an abundance of caution.”
The sunscreen products that have been recalled are:
- NEUTROGENA® Beach Defense® aerosol sunscreen.
- NEUTROGENA® Cool Dry Sport aerosol sunscreen.
- NEUTROGENA® Invisible Daily™ defense aerosol sunscreen.
- NEUTROGENA® Ultra Sheer® aerosol sunscreen.
- AVEENO® Protect + Refresh aerosol sunscreen.
These products were distributed nationwide through a variety of retail stores. Consumers should stop using these products and throw them away, the company said.
At the same time, it emphasized the importance of using alternative sunscreen products to protect the skin from excessive sun exposure, which can lead to skin cancer including melanoma.
Johnson & Johnson has launched an investigation into how benzene got into these products.
One of the company’s other spray sunscreen products, Neutrogena Wet Skin, was not included in the recall.
Recently, benzene was found in 78 widely-used sunscreen products in tests conducted by the online pharmacy and laboratory Valisure. Most of the products were aerosol sprays, and the company called on the Food and Drug Administration to recall them all.
That petition suggested that the finding of benzene was the result of contamination somewhere in the manufacturing process.
“This isn’t a sunscreen issue, it’s a manufacturing issue,” said Adam Friedman, MD, professor and chief of dermatology at George Washington University. “We don’t want those things to be blurred.”
There is a risk that people take away the wrong message from these findings.
“People already have ambivalence about sunscreen, and this is just going to make that worse,” Dr. Friedman said in an interview.
He pointed out that benzene is present in car exhaust, second-hand smoke, and elsewhere. Inhalation exposure has been the primary focus of toxicology investigations, as has exposure from things such as contaminated drinking water – not via topical application. “We don’t know how effectively [benzene] gets through the skin, if it gets absorbed systemically, and how that then behaves downstream,” he noted.
On the other hand, ultraviolet radiation is a well-established carcinogen. Avoiding an effective preventive measure such as sunscreen could prove more harmful than exposure to trace amounts of benzene, he said.
A version of this article first appeared on WebMD.com.
Benzene is not an ingredient of sunscreen, and should not be present in these products. The levels detected were low and would not be expected to have an adverse effect on health, but the company says it is recalling the products anyway “out of an abundance of caution.”
The sunscreen products that have been recalled are:
- NEUTROGENA® Beach Defense® aerosol sunscreen.
- NEUTROGENA® Cool Dry Sport aerosol sunscreen.
- NEUTROGENA® Invisible Daily™ defense aerosol sunscreen.
- NEUTROGENA® Ultra Sheer® aerosol sunscreen.
- AVEENO® Protect + Refresh aerosol sunscreen.
These products were distributed nationwide through a variety of retail stores. Consumers should stop using these products and throw them away, the company said.
At the same time, it emphasized the importance of using alternative sunscreen products to protect the skin from excessive sun exposure, which can lead to skin cancer including melanoma.
Johnson & Johnson has launched an investigation into how benzene got into these products.
One of the company’s other spray sunscreen products, Neutrogena Wet Skin, was not included in the recall.
Recently, benzene was found in 78 widely-used sunscreen products in tests conducted by the online pharmacy and laboratory Valisure. Most of the products were aerosol sprays, and the company called on the Food and Drug Administration to recall them all.
That petition suggested that the finding of benzene was the result of contamination somewhere in the manufacturing process.
“This isn’t a sunscreen issue, it’s a manufacturing issue,” said Adam Friedman, MD, professor and chief of dermatology at George Washington University. “We don’t want those things to be blurred.”
There is a risk that people take away the wrong message from these findings.
“People already have ambivalence about sunscreen, and this is just going to make that worse,” Dr. Friedman said in an interview.
He pointed out that benzene is present in car exhaust, second-hand smoke, and elsewhere. Inhalation exposure has been the primary focus of toxicology investigations, as has exposure from things such as contaminated drinking water – not via topical application. “We don’t know how effectively [benzene] gets through the skin, if it gets absorbed systemically, and how that then behaves downstream,” he noted.
On the other hand, ultraviolet radiation is a well-established carcinogen. Avoiding an effective preventive measure such as sunscreen could prove more harmful than exposure to trace amounts of benzene, he said.
A version of this article first appeared on WebMD.com.
Benzene is not an ingredient of sunscreen, and should not be present in these products. The levels detected were low and would not be expected to have an adverse effect on health, but the company says it is recalling the products anyway “out of an abundance of caution.”
The sunscreen products that have been recalled are:
- NEUTROGENA® Beach Defense® aerosol sunscreen.
- NEUTROGENA® Cool Dry Sport aerosol sunscreen.
- NEUTROGENA® Invisible Daily™ defense aerosol sunscreen.
- NEUTROGENA® Ultra Sheer® aerosol sunscreen.
- AVEENO® Protect + Refresh aerosol sunscreen.
These products were distributed nationwide through a variety of retail stores. Consumers should stop using these products and throw them away, the company said.
At the same time, it emphasized the importance of using alternative sunscreen products to protect the skin from excessive sun exposure, which can lead to skin cancer including melanoma.
Johnson & Johnson has launched an investigation into how benzene got into these products.
One of the company’s other spray sunscreen products, Neutrogena Wet Skin, was not included in the recall.
Recently, benzene was found in 78 widely-used sunscreen products in tests conducted by the online pharmacy and laboratory Valisure. Most of the products were aerosol sprays, and the company called on the Food and Drug Administration to recall them all.
That petition suggested that the finding of benzene was the result of contamination somewhere in the manufacturing process.
“This isn’t a sunscreen issue, it’s a manufacturing issue,” said Adam Friedman, MD, professor and chief of dermatology at George Washington University. “We don’t want those things to be blurred.”
There is a risk that people take away the wrong message from these findings.
“People already have ambivalence about sunscreen, and this is just going to make that worse,” Dr. Friedman said in an interview.
He pointed out that benzene is present in car exhaust, second-hand smoke, and elsewhere. Inhalation exposure has been the primary focus of toxicology investigations, as has exposure from things such as contaminated drinking water – not via topical application. “We don’t know how effectively [benzene] gets through the skin, if it gets absorbed systemically, and how that then behaves downstream,” he noted.
On the other hand, ultraviolet radiation is a well-established carcinogen. Avoiding an effective preventive measure such as sunscreen could prove more harmful than exposure to trace amounts of benzene, he said.
A version of this article first appeared on WebMD.com.
Delta variant infects six vaccinated guests at outdoor wedding
In April, 92 people gathered in Texas for a wedding. To lower the chances of COVID-19 infection, the festivities were held outside under a large, open-air tent. All 92 guests were required to be fully vaccinated.
Despite those precautions, six people tested positive for the coronavirus and one of them died, Forbes magazine reported, citing a preprint published in medRxiv.
Researchers from Baylor College of Medicine said viral sequencing suggests “the strain containing the Delta variant was transmitted to wedding guests from two patients traveling from India. With no history of vaccine failure in these patients, our observations suggest these are true cases of vaccine breakthrough, mediated by the Delta variant.”
Three females and three males aged 53-69 tested positive for COVID-19. Three were overweight, but none had significant comorbidities or a history of failed vaccination.
The first people to get sick were a man and woman who traveled from India, Forbes reported. The man had no health problems, but the woman had diabetes. Both had gotten two doses of the Covaxin BBV152 vaccine before leaving India.
They tested positive for COVID-19 4 days after the wedding, and the man became so ill he was hospitalized. Six days after the wedding, he died, according to Forbes.
Two people who’d gotten the Pfizer/BioNTech vaccine and two people who received the Moderna vaccine interacted with the first two people, and they also tested positive. One of them, a man in his 60s, had to be hospitalized.
Forbes summed it up this way: “While the available COVID-19 vaccines can offer good protection against COVID-19, the protection is not perfect. As long as the pandemic is continuing, it is better to maintain multiple layers of COVID-19 precautions when you can.”
A version of this article first appeared on WebMD.com.
In April, 92 people gathered in Texas for a wedding. To lower the chances of COVID-19 infection, the festivities were held outside under a large, open-air tent. All 92 guests were required to be fully vaccinated.
Despite those precautions, six people tested positive for the coronavirus and one of them died, Forbes magazine reported, citing a preprint published in medRxiv.
Researchers from Baylor College of Medicine said viral sequencing suggests “the strain containing the Delta variant was transmitted to wedding guests from two patients traveling from India. With no history of vaccine failure in these patients, our observations suggest these are true cases of vaccine breakthrough, mediated by the Delta variant.”
Three females and three males aged 53-69 tested positive for COVID-19. Three were overweight, but none had significant comorbidities or a history of failed vaccination.
The first people to get sick were a man and woman who traveled from India, Forbes reported. The man had no health problems, but the woman had diabetes. Both had gotten two doses of the Covaxin BBV152 vaccine before leaving India.
They tested positive for COVID-19 4 days after the wedding, and the man became so ill he was hospitalized. Six days after the wedding, he died, according to Forbes.
Two people who’d gotten the Pfizer/BioNTech vaccine and two people who received the Moderna vaccine interacted with the first two people, and they also tested positive. One of them, a man in his 60s, had to be hospitalized.
Forbes summed it up this way: “While the available COVID-19 vaccines can offer good protection against COVID-19, the protection is not perfect. As long as the pandemic is continuing, it is better to maintain multiple layers of COVID-19 precautions when you can.”
A version of this article first appeared on WebMD.com.
In April, 92 people gathered in Texas for a wedding. To lower the chances of COVID-19 infection, the festivities were held outside under a large, open-air tent. All 92 guests were required to be fully vaccinated.
Despite those precautions, six people tested positive for the coronavirus and one of them died, Forbes magazine reported, citing a preprint published in medRxiv.
Researchers from Baylor College of Medicine said viral sequencing suggests “the strain containing the Delta variant was transmitted to wedding guests from two patients traveling from India. With no history of vaccine failure in these patients, our observations suggest these are true cases of vaccine breakthrough, mediated by the Delta variant.”
Three females and three males aged 53-69 tested positive for COVID-19. Three were overweight, but none had significant comorbidities or a history of failed vaccination.
The first people to get sick were a man and woman who traveled from India, Forbes reported. The man had no health problems, but the woman had diabetes. Both had gotten two doses of the Covaxin BBV152 vaccine before leaving India.
They tested positive for COVID-19 4 days after the wedding, and the man became so ill he was hospitalized. Six days after the wedding, he died, according to Forbes.
Two people who’d gotten the Pfizer/BioNTech vaccine and two people who received the Moderna vaccine interacted with the first two people, and they also tested positive. One of them, a man in his 60s, had to be hospitalized.
Forbes summed it up this way: “While the available COVID-19 vaccines can offer good protection against COVID-19, the protection is not perfect. As long as the pandemic is continuing, it is better to maintain multiple layers of COVID-19 precautions when you can.”
A version of this article first appeared on WebMD.com.
Children and COVID: New vaccinations drop as the case count rises
With only a quarter of all children aged 12-15 years fully vaccinated against COVID-19, first vaccinations continued to drop and new cases for all children rose for the second consecutive week.
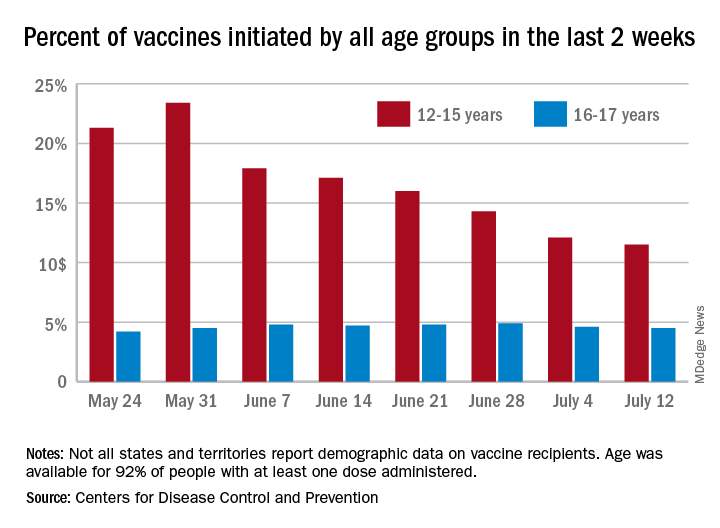
Just under 25% of children aged 12-15 had completed the vaccine regimen as of July 12, and just over one-third (33.5%) had received at least one dose. Meanwhile, that age group represented 11.5% of people who initiated vaccination during the 2 weeks ending July 12, down from 12.1% a week earlier, the Centers for Disease Control and Prevention said. The total number of new vaccinations for the week ending July 12 was just over 201,000, compared with 307,000 for the previous week.
New cases of COVID-19, however, were on the rise in children. The 19,000 new cases reported for the week ending July 8 were up from 12,000 a week earlier and 8,000 the week before that, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That report also shows that children made up 22.3% of all new cases during the week of July 2-8, compared with 16.8% the previous week, and that there were nine deaths in children that same week, the most since March. COVID-related deaths among children total 344 in the 46 jurisdictions (43 states, New York City, Puerto Rico, and Guam) that are reporting such data by age. “It is not possible to standardize more detailed age ranges for children based on what is publicly available from the states,” the two groups noted.
Such data are available from the CDC’s COVID Data Tracker, however, and they show that children aged 16-17 years, who became eligible for COVID vaccination before the younger age group, are further ahead in the process. Among the older children, almost 46% had gotten at least one dose and 37% were fully vaccinated by July 12.
With only a quarter of all children aged 12-15 years fully vaccinated against COVID-19, first vaccinations continued to drop and new cases for all children rose for the second consecutive week.
Just under 25% of children aged 12-15 had completed the vaccine regimen as of July 12, and just over one-third (33.5%) had received at least one dose. Meanwhile, that age group represented 11.5% of people who initiated vaccination during the 2 weeks ending July 12, down from 12.1% a week earlier, the Centers for Disease Control and Prevention said. The total number of new vaccinations for the week ending July 12 was just over 201,000, compared with 307,000 for the previous week.
New cases of COVID-19, however, were on the rise in children. The 19,000 new cases reported for the week ending July 8 were up from 12,000 a week earlier and 8,000 the week before that, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That report also shows that children made up 22.3% of all new cases during the week of July 2-8, compared with 16.8% the previous week, and that there were nine deaths in children that same week, the most since March. COVID-related deaths among children total 344 in the 46 jurisdictions (43 states, New York City, Puerto Rico, and Guam) that are reporting such data by age. “It is not possible to standardize more detailed age ranges for children based on what is publicly available from the states,” the two groups noted.
Such data are available from the CDC’s COVID Data Tracker, however, and they show that children aged 16-17 years, who became eligible for COVID vaccination before the younger age group, are further ahead in the process. Among the older children, almost 46% had gotten at least one dose and 37% were fully vaccinated by July 12.
With only a quarter of all children aged 12-15 years fully vaccinated against COVID-19, first vaccinations continued to drop and new cases for all children rose for the second consecutive week.
Just under 25% of children aged 12-15 had completed the vaccine regimen as of July 12, and just over one-third (33.5%) had received at least one dose. Meanwhile, that age group represented 11.5% of people who initiated vaccination during the 2 weeks ending July 12, down from 12.1% a week earlier, the Centers for Disease Control and Prevention said. The total number of new vaccinations for the week ending July 12 was just over 201,000, compared with 307,000 for the previous week.
New cases of COVID-19, however, were on the rise in children. The 19,000 new cases reported for the week ending July 8 were up from 12,000 a week earlier and 8,000 the week before that, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
That report also shows that children made up 22.3% of all new cases during the week of July 2-8, compared with 16.8% the previous week, and that there were nine deaths in children that same week, the most since March. COVID-related deaths among children total 344 in the 46 jurisdictions (43 states, New York City, Puerto Rico, and Guam) that are reporting such data by age. “It is not possible to standardize more detailed age ranges for children based on what is publicly available from the states,” the two groups noted.
Such data are available from the CDC’s COVID Data Tracker, however, and they show that children aged 16-17 years, who became eligible for COVID vaccination before the younger age group, are further ahead in the process. Among the older children, almost 46% had gotten at least one dose and 37% were fully vaccinated by July 12.
FDA to warn J&J that vaccine can increase Guillain-Barré risk: Media
as early as July 13, according to multiple media reports.
Although the FDA is projected to add the new warning to the labeling for the vaccine, the agency still calculates the benefit of vaccination with the J&J product continues to outweigh the risk. Benefits include protection against the Delta variant and serious COVID-19 outcomes.
More than 100 cases of Guillain-Barré reported to the Vaccine Adverse Event Reporting System, a federal program for reporting vaccine issues, spurred the FDA to act.
Men and people older than 50 appear to be at highest risk, according to reports of a July 12 Centers for Disease Control and Prevention statement. The CDC also revealed that most cases occur about 2 weeks following immunization.
Guillain-Barré syndrome often causes muscle weakness and sometimes temporary paralysis. Most people who develop the rare syndrome recover.
Such was not the case for a 57-year-old man, the New York Times reported July 12. He had a history of both a heart attack and stroke in the previous 4 years and died in April after vaccination with the J&J vaccine and developing Guillain-Barré.
The new warning comes in the wake of a number of setbacks for the company’s COVID-19 vaccine. On April 13, the FDA and CDC both recommended a 10-day pause on administration of the J&J vaccine after reports of rare blood clot events emerged. In mid-June, the FDA requested that Johnson and Johnson discard millions of vaccine doses produced at a manufacturing facility in Baltimore.
The mRNA vaccines from Pfizer/BioNTech and Moderna are not affected by the new FDA warning.
The Biden administration is expected to make a formal announcement of the new warning for the Johnson and Johnson vaccine as early as July 13, the Times reports.
A version of this article first appeared on Medscape.com.
as early as July 13, according to multiple media reports.
Although the FDA is projected to add the new warning to the labeling for the vaccine, the agency still calculates the benefit of vaccination with the J&J product continues to outweigh the risk. Benefits include protection against the Delta variant and serious COVID-19 outcomes.
More than 100 cases of Guillain-Barré reported to the Vaccine Adverse Event Reporting System, a federal program for reporting vaccine issues, spurred the FDA to act.
Men and people older than 50 appear to be at highest risk, according to reports of a July 12 Centers for Disease Control and Prevention statement. The CDC also revealed that most cases occur about 2 weeks following immunization.
Guillain-Barré syndrome often causes muscle weakness and sometimes temporary paralysis. Most people who develop the rare syndrome recover.
Such was not the case for a 57-year-old man, the New York Times reported July 12. He had a history of both a heart attack and stroke in the previous 4 years and died in April after vaccination with the J&J vaccine and developing Guillain-Barré.
The new warning comes in the wake of a number of setbacks for the company’s COVID-19 vaccine. On April 13, the FDA and CDC both recommended a 10-day pause on administration of the J&J vaccine after reports of rare blood clot events emerged. In mid-June, the FDA requested that Johnson and Johnson discard millions of vaccine doses produced at a manufacturing facility in Baltimore.
The mRNA vaccines from Pfizer/BioNTech and Moderna are not affected by the new FDA warning.
The Biden administration is expected to make a formal announcement of the new warning for the Johnson and Johnson vaccine as early as July 13, the Times reports.
A version of this article first appeared on Medscape.com.
as early as July 13, according to multiple media reports.
Although the FDA is projected to add the new warning to the labeling for the vaccine, the agency still calculates the benefit of vaccination with the J&J product continues to outweigh the risk. Benefits include protection against the Delta variant and serious COVID-19 outcomes.
More than 100 cases of Guillain-Barré reported to the Vaccine Adverse Event Reporting System, a federal program for reporting vaccine issues, spurred the FDA to act.
Men and people older than 50 appear to be at highest risk, according to reports of a July 12 Centers for Disease Control and Prevention statement. The CDC also revealed that most cases occur about 2 weeks following immunization.
Guillain-Barré syndrome often causes muscle weakness and sometimes temporary paralysis. Most people who develop the rare syndrome recover.
Such was not the case for a 57-year-old man, the New York Times reported July 12. He had a history of both a heart attack and stroke in the previous 4 years and died in April after vaccination with the J&J vaccine and developing Guillain-Barré.
The new warning comes in the wake of a number of setbacks for the company’s COVID-19 vaccine. On April 13, the FDA and CDC both recommended a 10-day pause on administration of the J&J vaccine after reports of rare blood clot events emerged. In mid-June, the FDA requested that Johnson and Johnson discard millions of vaccine doses produced at a manufacturing facility in Baltimore.
The mRNA vaccines from Pfizer/BioNTech and Moderna are not affected by the new FDA warning.
The Biden administration is expected to make a formal announcement of the new warning for the Johnson and Johnson vaccine as early as July 13, the Times reports.
A version of this article first appeared on Medscape.com.
Standard medical mask can protect wearer from aerosols
A standard medical face mask is more effective at preventing the wearer from inhaling aerosols without causing substantial breathing resistance than various cloth, medical, or respirator masks, new research shows.
“Medical face masks with good filtration efficacies can provide even better protective effects than KN95 respirators,” Christian Sterr, MD, from Philipps University of Marburg (Germany), and colleagues wrote. “FFP2 respirators, on the other hand, could be useful in high-risk situations but require greater breathing effort and therefore physical stress for users.”
Extensive evidence has shown that face masks are an excellent form of source control, preventing infectious people from spreading the SARS-CoV-2 virus into the environment. But evidence has been less clear about how well masks protect the wearer from inhaling particles containing the virus.
The researchers conducted three experiments to test 32 different face masks. The findings were presented at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published online in PLOS One .
First they tested pressure drop, which “relates to how easily air can pass through the material,” said Chris Cappa, PhD, professor of civil and environmental engineering at the University of California, Davis, who was not involved with the study.
“Higher pressure drops mean that there is greater resistance to the air passing through. A higher pressure drop will typically mean breathing through the material will be slightly more challenging, compared to a low pressure drop. There is no relationship between pressure drop and the mask effectiveness,” he said in an interview.
Pressure drop was lowest with type II medical face masks, the typical three-ply surgical masks designed to stop large particles expelled by the wearer from entering the environment, was highest with respirators, including KN95 and FFP2 masks, and varied with the different cloth masks tested.
Next the researchers compared filtration efficacy, which “refers to how well the material removes particles from the air that passes through the mask material,” Dr. Cappa explained. They did this by placing each mask over the opening to an air collector that measured how many particles got through. “A mask that has 100% filtration efficacy will remove all particles from the air that passes through it and 0% means that no particles are removed.”
Cloth masks had the lowest filtration efficacy, at 28%. Certified face masks that met European Standards had a relatively high efficacy, at 70%; for uncertified face masks, filtration efficacy was 63%. As expected, KN95 and FFP2 masks had the highest filtration efficacy, at 94% and 98%, respectively.Finally, the researchers tested as-worn filtration efficacies. They placed each mask on a dummy head with an artificial airway that collected airborne particles. They then pumped a mixture of aerosol particles – ranging in size from 0.3 to 2.0 mcm – and particle-free pressurized air into the air-proof acrylic chamber in which the head was placed.
In this experiment, cloth masks and noncertified face masks were least effective, filtering less than 20% of aerosols. Interestingly, the cloth face mask with the highest filtration on its own (84%) had the lowest filtration efficacy (9%), apparently because of its very high pressure drop (breathing resistance). When more effort is required to breathe through a mask, more air can bypass the filtration system.
Type II medical face masks, however, filtered 47% of aerosols, KN95 masks filtered 41%, and FFP2 masks filtered 65%. Face shields did not prevent the inhalation of any aerosols.
“We know that face shields will only be effective in stopping very large droplets, essentially visible spittle,” Dr. Cappa explained. “Most of the particles that we exhale will travel right around a face shield.”
The “optimal mask effect is a combination of high filter performance and low filter resistance,” which applies to most of the FFP2 and medical type II face masks tested, Dr. Sterr and colleagues wrote. “The type II medical masks in our random sample showed very good as-worn filtration performances with a low additional work of breathing at the same time.”
Although this study showed how well different masks filtered out particles, it could not assess how well different masks prevent actual infection.
“Like any virus, SARS-CoV-2 can only infect people as long as it is viable,” the researchers wrote. “Moreover, a certain number of viable virus particles need to be inhaled to trigger an infection. Thus, the assessed filtration efficacy may differ from the provided protection rate against SARS-CoV-2.”
In addition, particles containing the virus could dry out while going through the mask and become less infectious. “Even a small reduction in inhaled particles might prevent infection or at least lead to a less severe infection,” they noted.
In fact, filtration efficacy does not necessarily indicate how well the mask filters out particles while being worn. “This might be due to the combined effects of mask fit and pressure drop of the mask material and therefore tendency for mask leakage,” the team wrote. “High pressure drop results in higher breathing resistance and therefore supports leakage, especially if combined to a loosely fitting mask.”
These findings are “in line with what we already knew,” Dr. Cappa explained. “Even if the mask material filters out nearly all particles that pass through it, as is the case for high-efficiency masks such as N95 and FFP2, if the mask does not fit well, then it will only provide moderate protection for the wearer.”
Although the findings reaffirm the different levels of filtration provided by various cloth masks, they do not “provide any guidance on which types of cloth masks are better or worse,” he said. But they do show that “medical face masks will generally provide more protection to the wearer.”
It’s not surprising that face shields offer little protection from aerosols, Dr. Cappa said, but they can provide added protection when worn with a mask.
“A face shield could prevent large droplets that might shoot out when a person coughs or sneezes from depositing on a person’s eye,” he pointed out. And it can help “redirect the plume of particles that an infected person exhales, which could be useful in close quarters. However, even then those particles will keep moving around and could be inhaled. A mask can really help to decrease the amount inhaled.”
The study did not use external funding. The authors and Dr. Cappa disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A standard medical face mask is more effective at preventing the wearer from inhaling aerosols without causing substantial breathing resistance than various cloth, medical, or respirator masks, new research shows.
“Medical face masks with good filtration efficacies can provide even better protective effects than KN95 respirators,” Christian Sterr, MD, from Philipps University of Marburg (Germany), and colleagues wrote. “FFP2 respirators, on the other hand, could be useful in high-risk situations but require greater breathing effort and therefore physical stress for users.”
Extensive evidence has shown that face masks are an excellent form of source control, preventing infectious people from spreading the SARS-CoV-2 virus into the environment. But evidence has been less clear about how well masks protect the wearer from inhaling particles containing the virus.
The researchers conducted three experiments to test 32 different face masks. The findings were presented at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published online in PLOS One .
First they tested pressure drop, which “relates to how easily air can pass through the material,” said Chris Cappa, PhD, professor of civil and environmental engineering at the University of California, Davis, who was not involved with the study.
“Higher pressure drops mean that there is greater resistance to the air passing through. A higher pressure drop will typically mean breathing through the material will be slightly more challenging, compared to a low pressure drop. There is no relationship between pressure drop and the mask effectiveness,” he said in an interview.
Pressure drop was lowest with type II medical face masks, the typical three-ply surgical masks designed to stop large particles expelled by the wearer from entering the environment, was highest with respirators, including KN95 and FFP2 masks, and varied with the different cloth masks tested.
Next the researchers compared filtration efficacy, which “refers to how well the material removes particles from the air that passes through the mask material,” Dr. Cappa explained. They did this by placing each mask over the opening to an air collector that measured how many particles got through. “A mask that has 100% filtration efficacy will remove all particles from the air that passes through it and 0% means that no particles are removed.”
Cloth masks had the lowest filtration efficacy, at 28%. Certified face masks that met European Standards had a relatively high efficacy, at 70%; for uncertified face masks, filtration efficacy was 63%. As expected, KN95 and FFP2 masks had the highest filtration efficacy, at 94% and 98%, respectively.Finally, the researchers tested as-worn filtration efficacies. They placed each mask on a dummy head with an artificial airway that collected airborne particles. They then pumped a mixture of aerosol particles – ranging in size from 0.3 to 2.0 mcm – and particle-free pressurized air into the air-proof acrylic chamber in which the head was placed.
In this experiment, cloth masks and noncertified face masks were least effective, filtering less than 20% of aerosols. Interestingly, the cloth face mask with the highest filtration on its own (84%) had the lowest filtration efficacy (9%), apparently because of its very high pressure drop (breathing resistance). When more effort is required to breathe through a mask, more air can bypass the filtration system.
Type II medical face masks, however, filtered 47% of aerosols, KN95 masks filtered 41%, and FFP2 masks filtered 65%. Face shields did not prevent the inhalation of any aerosols.
“We know that face shields will only be effective in stopping very large droplets, essentially visible spittle,” Dr. Cappa explained. “Most of the particles that we exhale will travel right around a face shield.”
The “optimal mask effect is a combination of high filter performance and low filter resistance,” which applies to most of the FFP2 and medical type II face masks tested, Dr. Sterr and colleagues wrote. “The type II medical masks in our random sample showed very good as-worn filtration performances with a low additional work of breathing at the same time.”
Although this study showed how well different masks filtered out particles, it could not assess how well different masks prevent actual infection.
“Like any virus, SARS-CoV-2 can only infect people as long as it is viable,” the researchers wrote. “Moreover, a certain number of viable virus particles need to be inhaled to trigger an infection. Thus, the assessed filtration efficacy may differ from the provided protection rate against SARS-CoV-2.”
In addition, particles containing the virus could dry out while going through the mask and become less infectious. “Even a small reduction in inhaled particles might prevent infection or at least lead to a less severe infection,” they noted.
In fact, filtration efficacy does not necessarily indicate how well the mask filters out particles while being worn. “This might be due to the combined effects of mask fit and pressure drop of the mask material and therefore tendency for mask leakage,” the team wrote. “High pressure drop results in higher breathing resistance and therefore supports leakage, especially if combined to a loosely fitting mask.”
These findings are “in line with what we already knew,” Dr. Cappa explained. “Even if the mask material filters out nearly all particles that pass through it, as is the case for high-efficiency masks such as N95 and FFP2, if the mask does not fit well, then it will only provide moderate protection for the wearer.”
Although the findings reaffirm the different levels of filtration provided by various cloth masks, they do not “provide any guidance on which types of cloth masks are better or worse,” he said. But they do show that “medical face masks will generally provide more protection to the wearer.”
It’s not surprising that face shields offer little protection from aerosols, Dr. Cappa said, but they can provide added protection when worn with a mask.
“A face shield could prevent large droplets that might shoot out when a person coughs or sneezes from depositing on a person’s eye,” he pointed out. And it can help “redirect the plume of particles that an infected person exhales, which could be useful in close quarters. However, even then those particles will keep moving around and could be inhaled. A mask can really help to decrease the amount inhaled.”
The study did not use external funding. The authors and Dr. Cappa disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A standard medical face mask is more effective at preventing the wearer from inhaling aerosols without causing substantial breathing resistance than various cloth, medical, or respirator masks, new research shows.
“Medical face masks with good filtration efficacies can provide even better protective effects than KN95 respirators,” Christian Sterr, MD, from Philipps University of Marburg (Germany), and colleagues wrote. “FFP2 respirators, on the other hand, could be useful in high-risk situations but require greater breathing effort and therefore physical stress for users.”
Extensive evidence has shown that face masks are an excellent form of source control, preventing infectious people from spreading the SARS-CoV-2 virus into the environment. But evidence has been less clear about how well masks protect the wearer from inhaling particles containing the virus.
The researchers conducted three experiments to test 32 different face masks. The findings were presented at the 31st European Congress of Clinical Microbiology & Infectious Diseases and published online in PLOS One .
First they tested pressure drop, which “relates to how easily air can pass through the material,” said Chris Cappa, PhD, professor of civil and environmental engineering at the University of California, Davis, who was not involved with the study.
“Higher pressure drops mean that there is greater resistance to the air passing through. A higher pressure drop will typically mean breathing through the material will be slightly more challenging, compared to a low pressure drop. There is no relationship between pressure drop and the mask effectiveness,” he said in an interview.
Pressure drop was lowest with type II medical face masks, the typical three-ply surgical masks designed to stop large particles expelled by the wearer from entering the environment, was highest with respirators, including KN95 and FFP2 masks, and varied with the different cloth masks tested.
Next the researchers compared filtration efficacy, which “refers to how well the material removes particles from the air that passes through the mask material,” Dr. Cappa explained. They did this by placing each mask over the opening to an air collector that measured how many particles got through. “A mask that has 100% filtration efficacy will remove all particles from the air that passes through it and 0% means that no particles are removed.”
Cloth masks had the lowest filtration efficacy, at 28%. Certified face masks that met European Standards had a relatively high efficacy, at 70%; for uncertified face masks, filtration efficacy was 63%. As expected, KN95 and FFP2 masks had the highest filtration efficacy, at 94% and 98%, respectively.Finally, the researchers tested as-worn filtration efficacies. They placed each mask on a dummy head with an artificial airway that collected airborne particles. They then pumped a mixture of aerosol particles – ranging in size from 0.3 to 2.0 mcm – and particle-free pressurized air into the air-proof acrylic chamber in which the head was placed.
In this experiment, cloth masks and noncertified face masks were least effective, filtering less than 20% of aerosols. Interestingly, the cloth face mask with the highest filtration on its own (84%) had the lowest filtration efficacy (9%), apparently because of its very high pressure drop (breathing resistance). When more effort is required to breathe through a mask, more air can bypass the filtration system.
Type II medical face masks, however, filtered 47% of aerosols, KN95 masks filtered 41%, and FFP2 masks filtered 65%. Face shields did not prevent the inhalation of any aerosols.
“We know that face shields will only be effective in stopping very large droplets, essentially visible spittle,” Dr. Cappa explained. “Most of the particles that we exhale will travel right around a face shield.”
The “optimal mask effect is a combination of high filter performance and low filter resistance,” which applies to most of the FFP2 and medical type II face masks tested, Dr. Sterr and colleagues wrote. “The type II medical masks in our random sample showed very good as-worn filtration performances with a low additional work of breathing at the same time.”
Although this study showed how well different masks filtered out particles, it could not assess how well different masks prevent actual infection.
“Like any virus, SARS-CoV-2 can only infect people as long as it is viable,” the researchers wrote. “Moreover, a certain number of viable virus particles need to be inhaled to trigger an infection. Thus, the assessed filtration efficacy may differ from the provided protection rate against SARS-CoV-2.”
In addition, particles containing the virus could dry out while going through the mask and become less infectious. “Even a small reduction in inhaled particles might prevent infection or at least lead to a less severe infection,” they noted.
In fact, filtration efficacy does not necessarily indicate how well the mask filters out particles while being worn. “This might be due to the combined effects of mask fit and pressure drop of the mask material and therefore tendency for mask leakage,” the team wrote. “High pressure drop results in higher breathing resistance and therefore supports leakage, especially if combined to a loosely fitting mask.”
These findings are “in line with what we already knew,” Dr. Cappa explained. “Even if the mask material filters out nearly all particles that pass through it, as is the case for high-efficiency masks such as N95 and FFP2, if the mask does not fit well, then it will only provide moderate protection for the wearer.”
Although the findings reaffirm the different levels of filtration provided by various cloth masks, they do not “provide any guidance on which types of cloth masks are better or worse,” he said. But they do show that “medical face masks will generally provide more protection to the wearer.”
It’s not surprising that face shields offer little protection from aerosols, Dr. Cappa said, but they can provide added protection when worn with a mask.
“A face shield could prevent large droplets that might shoot out when a person coughs or sneezes from depositing on a person’s eye,” he pointed out. And it can help “redirect the plume of particles that an infected person exhales, which could be useful in close quarters. However, even then those particles will keep moving around and could be inhaled. A mask can really help to decrease the amount inhaled.”
The study did not use external funding. The authors and Dr. Cappa disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA head calls for investigation into agency’s approval of aducanumab (Aduhelm)
After several weeks of outcry and heated debate over the Food and Drug Administration’s controversial approval of the Alzheimer’s drug aducanumab (Aduhelm), the head of the agency is now calling for a federal investigation into its own approval proceedings.

Janet Woodcock, MD, the FDA’s acting commissioner, sent a letter to the Office of the Inspector General on July 9, she announced in a tweet.
Dr. Woodcock is asking for an investigation into questionable meetings and other interactions between Biogen and FDA staff members prior to the drug’s approval that “may have occurred outside of the formal correspondence process.”
The letter explains that concerns around these issues “could undermine the public’s confidence in the FDA’s decision.” Therefore, an independent investigation is needed to determine whether anything occurred that was “inconsistent with FDA policies and procedures.”
Dr. Woodcock noted that she has “tremendous confidence in the integrity of the staff and leadership of the Center for Drug Evaluation and Research” involved in the review process.
However, “FDA is dedicated to scientific integrity, to reviewing data without bias, and to basing its regulatory decisions on data,” she wrote. “You have my personal commitment that the Agency will fully cooperate should your office undertake a review.”
Dr. Woodcock concluded by urging that a review be conducted as soon as possible, noting that “should such a review result in actionable items, you also have my commitment to addressing these issues.”
A version of this article first appeared on Medscape.com.
After several weeks of outcry and heated debate over the Food and Drug Administration’s controversial approval of the Alzheimer’s drug aducanumab (Aduhelm), the head of the agency is now calling for a federal investigation into its own approval proceedings.
Janet Woodcock, MD, the FDA’s acting commissioner, sent a letter to the Office of the Inspector General on July 9, she announced in a tweet.
Dr. Woodcock is asking for an investigation into questionable meetings and other interactions between Biogen and FDA staff members prior to the drug’s approval that “may have occurred outside of the formal correspondence process.”
The letter explains that concerns around these issues “could undermine the public’s confidence in the FDA’s decision.” Therefore, an independent investigation is needed to determine whether anything occurred that was “inconsistent with FDA policies and procedures.”
Dr. Woodcock noted that she has “tremendous confidence in the integrity of the staff and leadership of the Center for Drug Evaluation and Research” involved in the review process.
However, “FDA is dedicated to scientific integrity, to reviewing data without bias, and to basing its regulatory decisions on data,” she wrote. “You have my personal commitment that the Agency will fully cooperate should your office undertake a review.”
Dr. Woodcock concluded by urging that a review be conducted as soon as possible, noting that “should such a review result in actionable items, you also have my commitment to addressing these issues.”
A version of this article first appeared on Medscape.com.
After several weeks of outcry and heated debate over the Food and Drug Administration’s controversial approval of the Alzheimer’s drug aducanumab (Aduhelm), the head of the agency is now calling for a federal investigation into its own approval proceedings.
Janet Woodcock, MD, the FDA’s acting commissioner, sent a letter to the Office of the Inspector General on July 9, she announced in a tweet.
Dr. Woodcock is asking for an investigation into questionable meetings and other interactions between Biogen and FDA staff members prior to the drug’s approval that “may have occurred outside of the formal correspondence process.”
The letter explains that concerns around these issues “could undermine the public’s confidence in the FDA’s decision.” Therefore, an independent investigation is needed to determine whether anything occurred that was “inconsistent with FDA policies and procedures.”
Dr. Woodcock noted that she has “tremendous confidence in the integrity of the staff and leadership of the Center for Drug Evaluation and Research” involved in the review process.
However, “FDA is dedicated to scientific integrity, to reviewing data without bias, and to basing its regulatory decisions on data,” she wrote. “You have my personal commitment that the Agency will fully cooperate should your office undertake a review.”
Dr. Woodcock concluded by urging that a review be conducted as soon as possible, noting that “should such a review result in actionable items, you also have my commitment to addressing these issues.”
A version of this article first appeared on Medscape.com.
Are oncologists liable for pandemic-related treatment delays?
Albuquerque oncologist Barbara McAneny, MD, has a patient in his 30s who experienced rectal bleeding for 6 months in 2020 but didn’t see a physician because he was afraid of catching COVID-19. He hoped it was just hemorrhoids.
When he finally came in to see her recently, Dr. McAneny diagnosed a large colon cancer. She fears the delay could prove fatal. “We’ll do our best to cure him, but I don’t know if he’ll be treatable,” she said. “Six months absolutely can make a difference.”
She and other oncologists around the country are seeing many patients in the past few months with advanced breast, colon, lung, and other cancers who were not diagnosed and treated during the COVID-19 pandemic because the patients didn’t want to come in, or because medical facilities weren’t taking nonemergency or non-COVID patients.
Given that failure to diagnose cancer is among the most common medical malpractice allegations, should oncologists be worried that they are at legal risk?
Pandemic provides ‘safe harbor’
In a March survey done by medical malpractice insurer The Doctors Company, one-third of physicians said they were very concerned or somewhat concerned that malpractice claims related to care during the pandemic will rise.
But in most of these cases, physicians and hospitals have little to worry about in terms of medical malpractice liability, according to veteran plaintiff and defense attorneys and the head of a large medical liability insurer.
“You had people with diseases like cancer not getting care because health care systems were overwhelmed,” said Sean Domnick, JD, a malpractice plaintiff attorney in Boca Raton, Fla. “Will those lead to successful malpractice lawsuits? Most likely not.”
“The risks will be low because it’s hard to pin it on the doctor if the patient didn’t want to come in or facilities weren’t scheduling appointments because of the public health emergency,” said Richard Roberts, MD, JD, a professor of family medicine at the University of Wisconsin–Madison who is also a malpractice defense attorney.
In addition, liability protections enacted in more than 30 states because of the COVID-19 pandemic will help shield clinicians from lawsuits. Those laws generally require allegations of gross negligence or reckless conduct far beyond ordinary negligence, which are hard to prove. But the immunity provisions remain largely untested in the courts, and it’s unclear how they will affect cases involving care for conditions other than COVID-19.
Another helpful factor is the widespread public appreciation of the valiant work by health care professionals throughout the pandemic, though that halo effect could fade over the next several years as malpractice claims from the pandemic period are filed and tried.
“In many circumstances, the pandemic will prove to be a safe harbor for providers,” said Steven Wigrizer, JD, a malpractice plaintiff attorney in Philadelphia. “Jurors will be reluctant to impose liability on providers who were doing their best in a global pandemic the world hadn’t seen in 100 years.”
Risky situations
These predictions from liability experts should reassure physicians who are anxious over reports that many cancer diagnoses were missed as a result of the COVID-19 pandemic.
Still, there are situations where physicians and hospitals could be vulnerable to malpractice claims despite the pandemic conditions. The highest-risk cases are those where patients recognized a potential cancer symptom like a breast lump or rectal bleeding, and tried to visit a doctor’s office or hospital, but were told they couldn’t be seen.
“Those kinds of cases lend themselves to delayed diagnosis claims,” said Richard Anderson, MD, an oncologist who is chairman and CEO of The Doctors Company. “My guess is we will see claims,” though he expects a reduced number arising from 2020 care scenarios, compared with previous years.
So far, his company has seen 20% fewer claims in 2020, which he said isn’t surprising given that the volume of physician and hospital visits plummeted.
Another risky situation is where physicians – particularly primary care physicians but also specialists like gynecologists and urologists – did not inform patients about concerning test results and order a follow-up test or visit. That is dangerous even if the physician did try to schedule a visit but the patient canceled the appointment.
“The jury will ask, ‘What did you do to get the patient back?’ ” said Sean Byrne, JD, a malpractice defense attorney in Richmond, Va. “The provider will say: ‘I’m sure we called.’ But it’s a difficult defense to say the patient didn’t return the call. I need written proof.”
Mr. Domnick said failures to follow up on suspicious test results could produce viable malpractice claims, pandemic or not. “The question becomes to what extent doctors will try to hide behind COVID to explain otherwise run-of-the-mill negligence,” he said. “We’ll have to see how that plays out.”
There are also worries about missed cancer diagnoses during telemedicine visits. “On telemedicine, I can’t feel a lymph node, I can’t palpate a breast mass, and I can’t see if someone’s liver is enlarged,” Dr. McAneny fretted. “I think you’ll get suits because you’ll miss stuff.”
One other area of exposure cited by the experts: Radiologists and pathologists could be sued for missing tumors in reading imaging tests. “The COVID-19 demand on resources has been immense,” Mr. Byrne said. “If that production pressure resulted in any quality loss in testing services, we could see claims.”
Patient protocols provide protection
There’s no question that cancer screenings dropped sharply during the pandemic. In June 2020, the National Cancer Institute estimated there was a 75% decrease in mammograms and colonoscopies during the first few months of the pandemic. It projected that delays in screenings, diagnoses, and treatment likely would result in 10,000 more breast and colorectal cancer deaths than otherwise expected over the next decade.
Delays of even 1 month in treatment for seven common forms of cancer can increase mortality risk by 6%-13%, according to a BMJ study.
While many medical facilities stopped doing preventive screening tests during the height of the pandemic last year, health care professionals still found ways to bring in patients with diagnosed cancers or who were at heightened cancer risk for tests and treatment.
Most facilities convened multidisciplinary tumor boards to decide which patients could wait for treatment, which patients could be maintained on drug therapy, and which ones needed immediate surgery, said Carla Fisher, MD, director of breast surgery at Indiana University, Indianapolis. For breast cancer, they used guidelines from her professional group, the American Society of Breast Surgeons.
Following such protocols for prioritizing patients for treatment during the pandemic should help protect against liability, experts said.
Even if it can be shown that a clinician’s negligence led to delayed diagnosis or treatment of a patient’s cancer, plaintiff attorneys will be wary about filing such claims. That is because it is difficult in most cases to prove that the delay significantly worsened the course of the patient’s disease or the odds of survival. Showing harm may be more possible with certain cancers known to be particularly aggressive.
“The plaintiff attorney will have to get an expert to say that the 3-month delay in getting the patient a mammogram caused her great harm,” said Dr. Roberts. “But it’s hard to calculate that scientifically, and it’s really hard to lay that all on the doctor or health system, because they were supposed to lock down during the pandemic.”
Playing catch-up
With patients now feeling more comfortable about coming in for physician visits, Mr. Byrne urges clinicians to make a special effort to mitigate potential liability arising from the past year. Physicians should carefully review patients’ charts and make sure to catch them up on preventive screenings. Some health systems, like Kaiser Permanente, have been doing proactive patient outreach for cancer screening throughout the pandemic.
“Providers may need to be extra diligent, and consider expanding the exam into a wellness visit and remind patients about cancer surveillance,” he said.
Overall, however, the expert consensus is that physicians should focus on providing the best quality care going forward, and not worry excessively about the care they wish they could have delivered over the past year during the extraordinary pandemic conditions.
“Liability risks will be decreased, because state laws have changed and doctors will be cut some slack, not just by judges and juries but by patients themselves,” Dr. Roberts said. “As you are running down the hall to take care of the next person, don’t be looking over your shoulder or you’ll run into the wall.”
A version of this article first appeared on Medscape.com.
Albuquerque oncologist Barbara McAneny, MD, has a patient in his 30s who experienced rectal bleeding for 6 months in 2020 but didn’t see a physician because he was afraid of catching COVID-19. He hoped it was just hemorrhoids.
When he finally came in to see her recently, Dr. McAneny diagnosed a large colon cancer. She fears the delay could prove fatal. “We’ll do our best to cure him, but I don’t know if he’ll be treatable,” she said. “Six months absolutely can make a difference.”
She and other oncologists around the country are seeing many patients in the past few months with advanced breast, colon, lung, and other cancers who were not diagnosed and treated during the COVID-19 pandemic because the patients didn’t want to come in, or because medical facilities weren’t taking nonemergency or non-COVID patients.
Given that failure to diagnose cancer is among the most common medical malpractice allegations, should oncologists be worried that they are at legal risk?
Pandemic provides ‘safe harbor’
In a March survey done by medical malpractice insurer The Doctors Company, one-third of physicians said they were very concerned or somewhat concerned that malpractice claims related to care during the pandemic will rise.
But in most of these cases, physicians and hospitals have little to worry about in terms of medical malpractice liability, according to veteran plaintiff and defense attorneys and the head of a large medical liability insurer.
“You had people with diseases like cancer not getting care because health care systems were overwhelmed,” said Sean Domnick, JD, a malpractice plaintiff attorney in Boca Raton, Fla. “Will those lead to successful malpractice lawsuits? Most likely not.”
“The risks will be low because it’s hard to pin it on the doctor if the patient didn’t want to come in or facilities weren’t scheduling appointments because of the public health emergency,” said Richard Roberts, MD, JD, a professor of family medicine at the University of Wisconsin–Madison who is also a malpractice defense attorney.
In addition, liability protections enacted in more than 30 states because of the COVID-19 pandemic will help shield clinicians from lawsuits. Those laws generally require allegations of gross negligence or reckless conduct far beyond ordinary negligence, which are hard to prove. But the immunity provisions remain largely untested in the courts, and it’s unclear how they will affect cases involving care for conditions other than COVID-19.
Another helpful factor is the widespread public appreciation of the valiant work by health care professionals throughout the pandemic, though that halo effect could fade over the next several years as malpractice claims from the pandemic period are filed and tried.
“In many circumstances, the pandemic will prove to be a safe harbor for providers,” said Steven Wigrizer, JD, a malpractice plaintiff attorney in Philadelphia. “Jurors will be reluctant to impose liability on providers who were doing their best in a global pandemic the world hadn’t seen in 100 years.”
Risky situations
These predictions from liability experts should reassure physicians who are anxious over reports that many cancer diagnoses were missed as a result of the COVID-19 pandemic.
Still, there are situations where physicians and hospitals could be vulnerable to malpractice claims despite the pandemic conditions. The highest-risk cases are those where patients recognized a potential cancer symptom like a breast lump or rectal bleeding, and tried to visit a doctor’s office or hospital, but were told they couldn’t be seen.
“Those kinds of cases lend themselves to delayed diagnosis claims,” said Richard Anderson, MD, an oncologist who is chairman and CEO of The Doctors Company. “My guess is we will see claims,” though he expects a reduced number arising from 2020 care scenarios, compared with previous years.
So far, his company has seen 20% fewer claims in 2020, which he said isn’t surprising given that the volume of physician and hospital visits plummeted.
Another risky situation is where physicians – particularly primary care physicians but also specialists like gynecologists and urologists – did not inform patients about concerning test results and order a follow-up test or visit. That is dangerous even if the physician did try to schedule a visit but the patient canceled the appointment.
“The jury will ask, ‘What did you do to get the patient back?’ ” said Sean Byrne, JD, a malpractice defense attorney in Richmond, Va. “The provider will say: ‘I’m sure we called.’ But it’s a difficult defense to say the patient didn’t return the call. I need written proof.”
Mr. Domnick said failures to follow up on suspicious test results could produce viable malpractice claims, pandemic or not. “The question becomes to what extent doctors will try to hide behind COVID to explain otherwise run-of-the-mill negligence,” he said. “We’ll have to see how that plays out.”
There are also worries about missed cancer diagnoses during telemedicine visits. “On telemedicine, I can’t feel a lymph node, I can’t palpate a breast mass, and I can’t see if someone’s liver is enlarged,” Dr. McAneny fretted. “I think you’ll get suits because you’ll miss stuff.”
One other area of exposure cited by the experts: Radiologists and pathologists could be sued for missing tumors in reading imaging tests. “The COVID-19 demand on resources has been immense,” Mr. Byrne said. “If that production pressure resulted in any quality loss in testing services, we could see claims.”
Patient protocols provide protection
There’s no question that cancer screenings dropped sharply during the pandemic. In June 2020, the National Cancer Institute estimated there was a 75% decrease in mammograms and colonoscopies during the first few months of the pandemic. It projected that delays in screenings, diagnoses, and treatment likely would result in 10,000 more breast and colorectal cancer deaths than otherwise expected over the next decade.
Delays of even 1 month in treatment for seven common forms of cancer can increase mortality risk by 6%-13%, according to a BMJ study.
While many medical facilities stopped doing preventive screening tests during the height of the pandemic last year, health care professionals still found ways to bring in patients with diagnosed cancers or who were at heightened cancer risk for tests and treatment.
Most facilities convened multidisciplinary tumor boards to decide which patients could wait for treatment, which patients could be maintained on drug therapy, and which ones needed immediate surgery, said Carla Fisher, MD, director of breast surgery at Indiana University, Indianapolis. For breast cancer, they used guidelines from her professional group, the American Society of Breast Surgeons.
Following such protocols for prioritizing patients for treatment during the pandemic should help protect against liability, experts said.
Even if it can be shown that a clinician’s negligence led to delayed diagnosis or treatment of a patient’s cancer, plaintiff attorneys will be wary about filing such claims. That is because it is difficult in most cases to prove that the delay significantly worsened the course of the patient’s disease or the odds of survival. Showing harm may be more possible with certain cancers known to be particularly aggressive.
“The plaintiff attorney will have to get an expert to say that the 3-month delay in getting the patient a mammogram caused her great harm,” said Dr. Roberts. “But it’s hard to calculate that scientifically, and it’s really hard to lay that all on the doctor or health system, because they were supposed to lock down during the pandemic.”
Playing catch-up
With patients now feeling more comfortable about coming in for physician visits, Mr. Byrne urges clinicians to make a special effort to mitigate potential liability arising from the past year. Physicians should carefully review patients’ charts and make sure to catch them up on preventive screenings. Some health systems, like Kaiser Permanente, have been doing proactive patient outreach for cancer screening throughout the pandemic.
“Providers may need to be extra diligent, and consider expanding the exam into a wellness visit and remind patients about cancer surveillance,” he said.
Overall, however, the expert consensus is that physicians should focus on providing the best quality care going forward, and not worry excessively about the care they wish they could have delivered over the past year during the extraordinary pandemic conditions.
“Liability risks will be decreased, because state laws have changed and doctors will be cut some slack, not just by judges and juries but by patients themselves,” Dr. Roberts said. “As you are running down the hall to take care of the next person, don’t be looking over your shoulder or you’ll run into the wall.”
A version of this article first appeared on Medscape.com.
Albuquerque oncologist Barbara McAneny, MD, has a patient in his 30s who experienced rectal bleeding for 6 months in 2020 but didn’t see a physician because he was afraid of catching COVID-19. He hoped it was just hemorrhoids.
When he finally came in to see her recently, Dr. McAneny diagnosed a large colon cancer. She fears the delay could prove fatal. “We’ll do our best to cure him, but I don’t know if he’ll be treatable,” she said. “Six months absolutely can make a difference.”
She and other oncologists around the country are seeing many patients in the past few months with advanced breast, colon, lung, and other cancers who were not diagnosed and treated during the COVID-19 pandemic because the patients didn’t want to come in, or because medical facilities weren’t taking nonemergency or non-COVID patients.
Given that failure to diagnose cancer is among the most common medical malpractice allegations, should oncologists be worried that they are at legal risk?
Pandemic provides ‘safe harbor’
In a March survey done by medical malpractice insurer The Doctors Company, one-third of physicians said they were very concerned or somewhat concerned that malpractice claims related to care during the pandemic will rise.
But in most of these cases, physicians and hospitals have little to worry about in terms of medical malpractice liability, according to veteran plaintiff and defense attorneys and the head of a large medical liability insurer.
“You had people with diseases like cancer not getting care because health care systems were overwhelmed,” said Sean Domnick, JD, a malpractice plaintiff attorney in Boca Raton, Fla. “Will those lead to successful malpractice lawsuits? Most likely not.”
“The risks will be low because it’s hard to pin it on the doctor if the patient didn’t want to come in or facilities weren’t scheduling appointments because of the public health emergency,” said Richard Roberts, MD, JD, a professor of family medicine at the University of Wisconsin–Madison who is also a malpractice defense attorney.
In addition, liability protections enacted in more than 30 states because of the COVID-19 pandemic will help shield clinicians from lawsuits. Those laws generally require allegations of gross negligence or reckless conduct far beyond ordinary negligence, which are hard to prove. But the immunity provisions remain largely untested in the courts, and it’s unclear how they will affect cases involving care for conditions other than COVID-19.
Another helpful factor is the widespread public appreciation of the valiant work by health care professionals throughout the pandemic, though that halo effect could fade over the next several years as malpractice claims from the pandemic period are filed and tried.
“In many circumstances, the pandemic will prove to be a safe harbor for providers,” said Steven Wigrizer, JD, a malpractice plaintiff attorney in Philadelphia. “Jurors will be reluctant to impose liability on providers who were doing their best in a global pandemic the world hadn’t seen in 100 years.”
Risky situations
These predictions from liability experts should reassure physicians who are anxious over reports that many cancer diagnoses were missed as a result of the COVID-19 pandemic.
Still, there are situations where physicians and hospitals could be vulnerable to malpractice claims despite the pandemic conditions. The highest-risk cases are those where patients recognized a potential cancer symptom like a breast lump or rectal bleeding, and tried to visit a doctor’s office or hospital, but were told they couldn’t be seen.
“Those kinds of cases lend themselves to delayed diagnosis claims,” said Richard Anderson, MD, an oncologist who is chairman and CEO of The Doctors Company. “My guess is we will see claims,” though he expects a reduced number arising from 2020 care scenarios, compared with previous years.
So far, his company has seen 20% fewer claims in 2020, which he said isn’t surprising given that the volume of physician and hospital visits plummeted.
Another risky situation is where physicians – particularly primary care physicians but also specialists like gynecologists and urologists – did not inform patients about concerning test results and order a follow-up test or visit. That is dangerous even if the physician did try to schedule a visit but the patient canceled the appointment.
“The jury will ask, ‘What did you do to get the patient back?’ ” said Sean Byrne, JD, a malpractice defense attorney in Richmond, Va. “The provider will say: ‘I’m sure we called.’ But it’s a difficult defense to say the patient didn’t return the call. I need written proof.”
Mr. Domnick said failures to follow up on suspicious test results could produce viable malpractice claims, pandemic or not. “The question becomes to what extent doctors will try to hide behind COVID to explain otherwise run-of-the-mill negligence,” he said. “We’ll have to see how that plays out.”
There are also worries about missed cancer diagnoses during telemedicine visits. “On telemedicine, I can’t feel a lymph node, I can’t palpate a breast mass, and I can’t see if someone’s liver is enlarged,” Dr. McAneny fretted. “I think you’ll get suits because you’ll miss stuff.”
One other area of exposure cited by the experts: Radiologists and pathologists could be sued for missing tumors in reading imaging tests. “The COVID-19 demand on resources has been immense,” Mr. Byrne said. “If that production pressure resulted in any quality loss in testing services, we could see claims.”
Patient protocols provide protection
There’s no question that cancer screenings dropped sharply during the pandemic. In June 2020, the National Cancer Institute estimated there was a 75% decrease in mammograms and colonoscopies during the first few months of the pandemic. It projected that delays in screenings, diagnoses, and treatment likely would result in 10,000 more breast and colorectal cancer deaths than otherwise expected over the next decade.
Delays of even 1 month in treatment for seven common forms of cancer can increase mortality risk by 6%-13%, according to a BMJ study.
While many medical facilities stopped doing preventive screening tests during the height of the pandemic last year, health care professionals still found ways to bring in patients with diagnosed cancers or who were at heightened cancer risk for tests and treatment.
Most facilities convened multidisciplinary tumor boards to decide which patients could wait for treatment, which patients could be maintained on drug therapy, and which ones needed immediate surgery, said Carla Fisher, MD, director of breast surgery at Indiana University, Indianapolis. For breast cancer, they used guidelines from her professional group, the American Society of Breast Surgeons.
Following such protocols for prioritizing patients for treatment during the pandemic should help protect against liability, experts said.
Even if it can be shown that a clinician’s negligence led to delayed diagnosis or treatment of a patient’s cancer, plaintiff attorneys will be wary about filing such claims. That is because it is difficult in most cases to prove that the delay significantly worsened the course of the patient’s disease or the odds of survival. Showing harm may be more possible with certain cancers known to be particularly aggressive.
“The plaintiff attorney will have to get an expert to say that the 3-month delay in getting the patient a mammogram caused her great harm,” said Dr. Roberts. “But it’s hard to calculate that scientifically, and it’s really hard to lay that all on the doctor or health system, because they were supposed to lock down during the pandemic.”
Playing catch-up
With patients now feeling more comfortable about coming in for physician visits, Mr. Byrne urges clinicians to make a special effort to mitigate potential liability arising from the past year. Physicians should carefully review patients’ charts and make sure to catch them up on preventive screenings. Some health systems, like Kaiser Permanente, have been doing proactive patient outreach for cancer screening throughout the pandemic.
“Providers may need to be extra diligent, and consider expanding the exam into a wellness visit and remind patients about cancer surveillance,” he said.
Overall, however, the expert consensus is that physicians should focus on providing the best quality care going forward, and not worry excessively about the care they wish they could have delivered over the past year during the extraordinary pandemic conditions.
“Liability risks will be decreased, because state laws have changed and doctors will be cut some slack, not just by judges and juries but by patients themselves,” Dr. Roberts said. “As you are running down the hall to take care of the next person, don’t be looking over your shoulder or you’ll run into the wall.”
A version of this article first appeared on Medscape.com.
Limited English proficiency linked with less health care in U.S.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.

Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.
Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.
Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
FROM HEALTH AFFAIRS
Mutational signature may reveal underlying link between red meat and CRC
A mechanistic link between red meat consumption and colorectal cancer (CRC) has been identified in the form of an alkylating mutational signature, according to investigators.
This is the first time a colorectal mutational signature has been associated with a component of diet, which demonstrates the value of large-scale molecular epidemiologic studies and suggests potential for early, precision dietary intervention, reported lead author Carino Gurjao, MSc, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston, and colleagues.
“Red meat consumption has been consistently linked to the incidence of colorectal cancer,” the investigators wrote in Cancer Discovery. “The suggested mechanism is mutagenesis through alkylating damage induced by N-nitroso-compounds (NOCs), which are metabolic products of blood heme iron or meat nitrites/nitrates. Nevertheless, this mutational damage is yet to be observed directly in patients’ tumors.”
To this end, the investigators turned to three long-term, large-scale, prospective cohort studies: the Nurses’ Health Studies I and II, and the Health Professionals Follow-up Study. These databases include nearly 300,000 individuals with follow-up dating back as far as 1976. The investigators identified 900 cases of primary, untreated CRC with adequate tissue for analysis, then, for each case, performed whole exome sequencing on both tumor tissue and normal colorectal tissue.
This revealed an alkylating mutational signature previously undescribed in CRC that was significantly associated with consumption of red meat prior to diagnosis, but not other dietary or lifestyle factors. The signature occurred most frequently in tumors and normal crypts in the distal colon and rectum.
According to the investigators, the presence of the alkylating signature in normal colorectal crypts “suggests that mutational changes due to such damage may start to occur early in the path of colorectal carcinogenesis.”
Further analysis showed that tumors harboring common KRAS and PIK3CA driver mutations had the highest levels of alkylating damage, with higher levels predicting worse survival.
“These results ... further implicate the role of red meat in CRC initiation and progression,” the investigators concluded.
Early findings, important implications
Cosenior author Kana Wu, MD, PhD, principal research scientist in the department of nutrition at Harvard School of Public Health, Boston, noted that these are early findings, although they may pave the way toward new dietary recommendations and methods of food production.
“While more detailed analysis needs to be conducted, and our results need to be confirmed in other studies, this study is a promising first step to better understand the biological mechanisms underlying the role of red and processed meats in colorectal cancers,” Dr. Wu said in an interview. “It is important to gain more insight into the biological mechanisms so we can improve dietary guidelines for cancer prevention and guide food reformulation efforts to lower cancer risk.”
For now, Dr. Wu predicted that standing dietary recommendations will remain unchanged.
“This study will not alter current diet recommendations to limit intake of red and processed meats,” Dr. Wu said, referring to similar recommendations across several organizations, including the American Heart Association, the World Cancer Research Fund/American Institute for Cancer Research, and the American Cancer Society.
“For example,” Dr. Wu said, “the WCRF/AICR recommends limiting consumption of red and processed meat to ‘no more than moderate amounts [12-18 ounces per week] of red meat, such as beef, pork, and lamb, and [to] eat little, if any, processed meat.’”
Possible biomarker?
According to Patricia Thompson-Carino, PhD, deputy director of the Stony Brook (N.Y.) Cancer Center, the study provides convincing evidence linking red meat consumption with development of CRC.
“Higher frequency of the signature in the distal colon is compelling for its consistency with epidemiologic evidence,” Dr. Thompson-Carino said in an interview. “Combined with the observed worse survival in patients harboring the signature and association with oncogenic KRAS and PIK3CA driver mutations, this study significantly elevates the biological plausibility that red meat is a modifiable source of NOC mutagenicity and carcinogenesis in humans.”
The signature could be used as a biomarker to detect exposure to NOCs, and susceptibility to CRC, she added.
Still, Dr. Thompson-Carino suggested that more work is needed to fully elucidate underlying mechanisms of action, which are needed to accurately shape dietary guidance.
“Key to advancing red meat dietary recommendations will be understanding the relationships between the new mutation signature and the NOCs derived from red meat and their source, whether endogenous [for example, intestinal N-nitrosation] or exogenous [for example, chemical preservation or charring],” she said. The study was supported by the National Institutes of Health, the Stand Up To Cancer Colorectal Cancer Dream Team Translational Research Grant (coadministered by the American Association for Cancer Research), the Project P Fund, and others. The investigators, Dr. Wu, and Dr. Thompson-Carino reported no conflicts of interest related to this study.
A mechanistic link between red meat consumption and colorectal cancer (CRC) has been identified in the form of an alkylating mutational signature, according to investigators.
This is the first time a colorectal mutational signature has been associated with a component of diet, which demonstrates the value of large-scale molecular epidemiologic studies and suggests potential for early, precision dietary intervention, reported lead author Carino Gurjao, MSc, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston, and colleagues.
“Red meat consumption has been consistently linked to the incidence of colorectal cancer,” the investigators wrote in Cancer Discovery. “The suggested mechanism is mutagenesis through alkylating damage induced by N-nitroso-compounds (NOCs), which are metabolic products of blood heme iron or meat nitrites/nitrates. Nevertheless, this mutational damage is yet to be observed directly in patients’ tumors.”
To this end, the investigators turned to three long-term, large-scale, prospective cohort studies: the Nurses’ Health Studies I and II, and the Health Professionals Follow-up Study. These databases include nearly 300,000 individuals with follow-up dating back as far as 1976. The investigators identified 900 cases of primary, untreated CRC with adequate tissue for analysis, then, for each case, performed whole exome sequencing on both tumor tissue and normal colorectal tissue.
This revealed an alkylating mutational signature previously undescribed in CRC that was significantly associated with consumption of red meat prior to diagnosis, but not other dietary or lifestyle factors. The signature occurred most frequently in tumors and normal crypts in the distal colon and rectum.
According to the investigators, the presence of the alkylating signature in normal colorectal crypts “suggests that mutational changes due to such damage may start to occur early in the path of colorectal carcinogenesis.”
Further analysis showed that tumors harboring common KRAS and PIK3CA driver mutations had the highest levels of alkylating damage, with higher levels predicting worse survival.
“These results ... further implicate the role of red meat in CRC initiation and progression,” the investigators concluded.
Early findings, important implications
Cosenior author Kana Wu, MD, PhD, principal research scientist in the department of nutrition at Harvard School of Public Health, Boston, noted that these are early findings, although they may pave the way toward new dietary recommendations and methods of food production.
“While more detailed analysis needs to be conducted, and our results need to be confirmed in other studies, this study is a promising first step to better understand the biological mechanisms underlying the role of red and processed meats in colorectal cancers,” Dr. Wu said in an interview. “It is important to gain more insight into the biological mechanisms so we can improve dietary guidelines for cancer prevention and guide food reformulation efforts to lower cancer risk.”
For now, Dr. Wu predicted that standing dietary recommendations will remain unchanged.
“This study will not alter current diet recommendations to limit intake of red and processed meats,” Dr. Wu said, referring to similar recommendations across several organizations, including the American Heart Association, the World Cancer Research Fund/American Institute for Cancer Research, and the American Cancer Society.
“For example,” Dr. Wu said, “the WCRF/AICR recommends limiting consumption of red and processed meat to ‘no more than moderate amounts [12-18 ounces per week] of red meat, such as beef, pork, and lamb, and [to] eat little, if any, processed meat.’”
Possible biomarker?
According to Patricia Thompson-Carino, PhD, deputy director of the Stony Brook (N.Y.) Cancer Center, the study provides convincing evidence linking red meat consumption with development of CRC.
“Higher frequency of the signature in the distal colon is compelling for its consistency with epidemiologic evidence,” Dr. Thompson-Carino said in an interview. “Combined with the observed worse survival in patients harboring the signature and association with oncogenic KRAS and PIK3CA driver mutations, this study significantly elevates the biological plausibility that red meat is a modifiable source of NOC mutagenicity and carcinogenesis in humans.”
The signature could be used as a biomarker to detect exposure to NOCs, and susceptibility to CRC, she added.
Still, Dr. Thompson-Carino suggested that more work is needed to fully elucidate underlying mechanisms of action, which are needed to accurately shape dietary guidance.
“Key to advancing red meat dietary recommendations will be understanding the relationships between the new mutation signature and the NOCs derived from red meat and their source, whether endogenous [for example, intestinal N-nitrosation] or exogenous [for example, chemical preservation or charring],” she said. The study was supported by the National Institutes of Health, the Stand Up To Cancer Colorectal Cancer Dream Team Translational Research Grant (coadministered by the American Association for Cancer Research), the Project P Fund, and others. The investigators, Dr. Wu, and Dr. Thompson-Carino reported no conflicts of interest related to this study.
A mechanistic link between red meat consumption and colorectal cancer (CRC) has been identified in the form of an alkylating mutational signature, according to investigators.
This is the first time a colorectal mutational signature has been associated with a component of diet, which demonstrates the value of large-scale molecular epidemiologic studies and suggests potential for early, precision dietary intervention, reported lead author Carino Gurjao, MSc, of the Dana-Farber Cancer Institute and Harvard Medical School, both in Boston, and colleagues.
“Red meat consumption has been consistently linked to the incidence of colorectal cancer,” the investigators wrote in Cancer Discovery. “The suggested mechanism is mutagenesis through alkylating damage induced by N-nitroso-compounds (NOCs), which are metabolic products of blood heme iron or meat nitrites/nitrates. Nevertheless, this mutational damage is yet to be observed directly in patients’ tumors.”
To this end, the investigators turned to three long-term, large-scale, prospective cohort studies: the Nurses’ Health Studies I and II, and the Health Professionals Follow-up Study. These databases include nearly 300,000 individuals with follow-up dating back as far as 1976. The investigators identified 900 cases of primary, untreated CRC with adequate tissue for analysis, then, for each case, performed whole exome sequencing on both tumor tissue and normal colorectal tissue.
This revealed an alkylating mutational signature previously undescribed in CRC that was significantly associated with consumption of red meat prior to diagnosis, but not other dietary or lifestyle factors. The signature occurred most frequently in tumors and normal crypts in the distal colon and rectum.
According to the investigators, the presence of the alkylating signature in normal colorectal crypts “suggests that mutational changes due to such damage may start to occur early in the path of colorectal carcinogenesis.”
Further analysis showed that tumors harboring common KRAS and PIK3CA driver mutations had the highest levels of alkylating damage, with higher levels predicting worse survival.
“These results ... further implicate the role of red meat in CRC initiation and progression,” the investigators concluded.
Early findings, important implications
Cosenior author Kana Wu, MD, PhD, principal research scientist in the department of nutrition at Harvard School of Public Health, Boston, noted that these are early findings, although they may pave the way toward new dietary recommendations and methods of food production.
“While more detailed analysis needs to be conducted, and our results need to be confirmed in other studies, this study is a promising first step to better understand the biological mechanisms underlying the role of red and processed meats in colorectal cancers,” Dr. Wu said in an interview. “It is important to gain more insight into the biological mechanisms so we can improve dietary guidelines for cancer prevention and guide food reformulation efforts to lower cancer risk.”
For now, Dr. Wu predicted that standing dietary recommendations will remain unchanged.
“This study will not alter current diet recommendations to limit intake of red and processed meats,” Dr. Wu said, referring to similar recommendations across several organizations, including the American Heart Association, the World Cancer Research Fund/American Institute for Cancer Research, and the American Cancer Society.
“For example,” Dr. Wu said, “the WCRF/AICR recommends limiting consumption of red and processed meat to ‘no more than moderate amounts [12-18 ounces per week] of red meat, such as beef, pork, and lamb, and [to] eat little, if any, processed meat.’”
Possible biomarker?
According to Patricia Thompson-Carino, PhD, deputy director of the Stony Brook (N.Y.) Cancer Center, the study provides convincing evidence linking red meat consumption with development of CRC.
“Higher frequency of the signature in the distal colon is compelling for its consistency with epidemiologic evidence,” Dr. Thompson-Carino said in an interview. “Combined with the observed worse survival in patients harboring the signature and association with oncogenic KRAS and PIK3CA driver mutations, this study significantly elevates the biological plausibility that red meat is a modifiable source of NOC mutagenicity and carcinogenesis in humans.”
The signature could be used as a biomarker to detect exposure to NOCs, and susceptibility to CRC, she added.
Still, Dr. Thompson-Carino suggested that more work is needed to fully elucidate underlying mechanisms of action, which are needed to accurately shape dietary guidance.
“Key to advancing red meat dietary recommendations will be understanding the relationships between the new mutation signature and the NOCs derived from red meat and their source, whether endogenous [for example, intestinal N-nitrosation] or exogenous [for example, chemical preservation or charring],” she said. The study was supported by the National Institutes of Health, the Stand Up To Cancer Colorectal Cancer Dream Team Translational Research Grant (coadministered by the American Association for Cancer Research), the Project P Fund, and others. The investigators, Dr. Wu, and Dr. Thompson-Carino reported no conflicts of interest related to this study.
FROM CANCER DISCOVERY