User login
Another COVID-19 patient to get ivermectin after court order
Another case, another state, another judge ordering a hospital to give a patient a controversial horse deworming drug to treat a severe case of COVID-19.
, according to the Ohio Capital Journal. Judge Gregory Howard’s ruling comes after Mr. Smith’s wife sued to force the hospital to provide the controversial drug to her husband, who has been hospitalized since July 15.
Julie Smith has gotten Fred Wagshul, MD, to agree to administer ivermectin to her husband. Dr. Wagshul is known as a member of a group of doctors who say the Centers for Disease Control and Prevention and the Food and Drug Administration are lying about ivermectin’s usefulness in fighting COVID-19. Both agencies have warned against using the drug to treat COVID-19, saying there is no evidence it works and that it can be dangerous in large amounts.
According to the Ohio Capital Journal, Dr. Wagshul accused the CDC and FDA of engaging in a “conspiracy” to prevent ivermectin’s use.
But Arthur L. Caplan, MD, professor of bioethics at New York University’s Langone Medical Center, said, “it is absurd that this order was issued,” according to an interview in Ars Technica. “If I were these doctors, I simply wouldn’t do it.”
It is not the first time a judge has ordered ivermectin’s use against a hospital’s wishes.
A 68-year-old woman with COVID-19 in an Illinois hospital started receiving the controversial drug in May after her family sued the hospital to have someone administer it.
Nurije Fype’s daughter, Desareta, filed suit against Elmhurst Hospital, part of Edward-Elmhurst Health, asking that her mother receive the treatment, which is approved as an antiparasitic drug but not approved for the treatment of COVID-19. Desareta Fype was granted temporary guardianship of her mother.
The FDA has published guidance titled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19” on its website. The National Institutes of Health said there is not enough data to recommend either for or against its use in treating COVID-19.
But DuPage County Judge James Orel ruled Ms. Fype should be allowed to get the treatment.
Three days later, according to the Daily Herald, the lawyer for the hospital, Joseph Monahan, argued the hospital could not find a hospital-affiliated doctor to administer the ivermectin.
The Herald reported the judge told the hospital to “get out of the way” and allow any board-certified doctor to administer the drug.
When Ms. Fype’s doctor was unable to administer it, the legal team found another doctor, Alan Bain, DO, to do it. Mr. Monahan said Dr. Bain was granted credentials to work at the hospital so he could administer it.
Judge Orel denied a request from Desareta Fype’s lawyer to order the hospital’s nurses to administer further doses. The judge also denied a request to hold the hospital in contempt of court.
A version of this article first appeared on WebMD.com.
Another case, another state, another judge ordering a hospital to give a patient a controversial horse deworming drug to treat a severe case of COVID-19.
, according to the Ohio Capital Journal. Judge Gregory Howard’s ruling comes after Mr. Smith’s wife sued to force the hospital to provide the controversial drug to her husband, who has been hospitalized since July 15.
Julie Smith has gotten Fred Wagshul, MD, to agree to administer ivermectin to her husband. Dr. Wagshul is known as a member of a group of doctors who say the Centers for Disease Control and Prevention and the Food and Drug Administration are lying about ivermectin’s usefulness in fighting COVID-19. Both agencies have warned against using the drug to treat COVID-19, saying there is no evidence it works and that it can be dangerous in large amounts.
According to the Ohio Capital Journal, Dr. Wagshul accused the CDC and FDA of engaging in a “conspiracy” to prevent ivermectin’s use.
But Arthur L. Caplan, MD, professor of bioethics at New York University’s Langone Medical Center, said, “it is absurd that this order was issued,” according to an interview in Ars Technica. “If I were these doctors, I simply wouldn’t do it.”
It is not the first time a judge has ordered ivermectin’s use against a hospital’s wishes.
A 68-year-old woman with COVID-19 in an Illinois hospital started receiving the controversial drug in May after her family sued the hospital to have someone administer it.
Nurije Fype’s daughter, Desareta, filed suit against Elmhurst Hospital, part of Edward-Elmhurst Health, asking that her mother receive the treatment, which is approved as an antiparasitic drug but not approved for the treatment of COVID-19. Desareta Fype was granted temporary guardianship of her mother.
The FDA has published guidance titled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19” on its website. The National Institutes of Health said there is not enough data to recommend either for or against its use in treating COVID-19.
But DuPage County Judge James Orel ruled Ms. Fype should be allowed to get the treatment.
Three days later, according to the Daily Herald, the lawyer for the hospital, Joseph Monahan, argued the hospital could not find a hospital-affiliated doctor to administer the ivermectin.
The Herald reported the judge told the hospital to “get out of the way” and allow any board-certified doctor to administer the drug.
When Ms. Fype’s doctor was unable to administer it, the legal team found another doctor, Alan Bain, DO, to do it. Mr. Monahan said Dr. Bain was granted credentials to work at the hospital so he could administer it.
Judge Orel denied a request from Desareta Fype’s lawyer to order the hospital’s nurses to administer further doses. The judge also denied a request to hold the hospital in contempt of court.
A version of this article first appeared on WebMD.com.
Another case, another state, another judge ordering a hospital to give a patient a controversial horse deworming drug to treat a severe case of COVID-19.
, according to the Ohio Capital Journal. Judge Gregory Howard’s ruling comes after Mr. Smith’s wife sued to force the hospital to provide the controversial drug to her husband, who has been hospitalized since July 15.
Julie Smith has gotten Fred Wagshul, MD, to agree to administer ivermectin to her husband. Dr. Wagshul is known as a member of a group of doctors who say the Centers for Disease Control and Prevention and the Food and Drug Administration are lying about ivermectin’s usefulness in fighting COVID-19. Both agencies have warned against using the drug to treat COVID-19, saying there is no evidence it works and that it can be dangerous in large amounts.
According to the Ohio Capital Journal, Dr. Wagshul accused the CDC and FDA of engaging in a “conspiracy” to prevent ivermectin’s use.
But Arthur L. Caplan, MD, professor of bioethics at New York University’s Langone Medical Center, said, “it is absurd that this order was issued,” according to an interview in Ars Technica. “If I were these doctors, I simply wouldn’t do it.”
It is not the first time a judge has ordered ivermectin’s use against a hospital’s wishes.
A 68-year-old woman with COVID-19 in an Illinois hospital started receiving the controversial drug in May after her family sued the hospital to have someone administer it.
Nurije Fype’s daughter, Desareta, filed suit against Elmhurst Hospital, part of Edward-Elmhurst Health, asking that her mother receive the treatment, which is approved as an antiparasitic drug but not approved for the treatment of COVID-19. Desareta Fype was granted temporary guardianship of her mother.
The FDA has published guidance titled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19” on its website. The National Institutes of Health said there is not enough data to recommend either for or against its use in treating COVID-19.
But DuPage County Judge James Orel ruled Ms. Fype should be allowed to get the treatment.
Three days later, according to the Daily Herald, the lawyer for the hospital, Joseph Monahan, argued the hospital could not find a hospital-affiliated doctor to administer the ivermectin.
The Herald reported the judge told the hospital to “get out of the way” and allow any board-certified doctor to administer the drug.
When Ms. Fype’s doctor was unable to administer it, the legal team found another doctor, Alan Bain, DO, to do it. Mr. Monahan said Dr. Bain was granted credentials to work at the hospital so he could administer it.
Judge Orel denied a request from Desareta Fype’s lawyer to order the hospital’s nurses to administer further doses. The judge also denied a request to hold the hospital in contempt of court.
A version of this article first appeared on WebMD.com.
COVID-clogged ICUs ‘terrify’ those with chronic or emergency illness
Jessica Gosnell, MD, 41, from Portland, Oregon, lives daily with the knowledge that her rare disease — a form of hereditary angioedema — could cause a sudden, severe swelling in her throat that could require quick intubation and land her in an intensive care unit (ICU) for days.
“I’ve been hospitalized for throat swells three times in the last year,” she said in an interview.
Dr. Gosnell no longer practices medicine because of a combination of illnesses, but lives with her husband, Andrew, and two young children, and said they are all “terrified” she will have to go to the hospital amid a COVID-19 surge that had shrunk the number of available ICU beds to 152 from 780 in Oregon as of Aug. 30. Thirty percent of the beds are in use for patients with COVID-19.
She said her life depends on being near hospitals that have ICUs and having access to highly specialized medications, one of which can cost up to $50,000 for the rescue dose.
Her fear has her “literally living bedbound.” In addition to hereditary angioedema, she has Ehlers-Danlos syndrome, which weakens connective tissue. She wears a cervical collar 24/7 to keep from tearing tissues, as any tissue injury can trigger a swell.
Patients worry there won’t be room
As ICU beds in most states are filling with COVID-19 patients as the Delta variant spreads, fears are rising among people like Dr. Gosnell, who have chronic conditions and diseases with unpredictable emergency visits, who worry that if they need emergency care there won’t be room.
As of Aug. 30, in the United States, 79% of ICU beds nationally were in use, 30% of them for COVID-19 patients, according to the U.S. Department of Health and Human Services.
In individual states, the picture is dire. Alabama has fewer than 10% of its ICU beds open across the entire state. In Florida, 93% of ICU beds are filled, 53% of them with COVID patients. In Louisiana, 87% of beds were already in use, 45% of them with COVID patients, just as category 4 hurricane Ida smashed into the coastline on Aug. 29.
News reports have told of people transported and airlifted as hospitals reach capacity.
In Bellville, Tex., U.S. Army veteran Daniel Wilkinson needed advanced care for gallstone pancreatitis that normally would take 30 minutes to treat, his Bellville doctor, Hasan Kakli, MD, told CBS News.
Mr. Wilkinson’s house was three doors from Bellville Hospital, but the hospital was not equipped to treat the condition. Calls to other hospitals found the same answer: no empty ICU beds. After a 7-hour wait on a stretcher, he was airlifted to a Veterans Affairs hospital in Houston, but it was too late. He died on August 22 at age 46.
Dr. Kakli said, “I’ve never lost a patient with this diagnosis. Ever. I’m scared that the next patient I see is someone that I can’t get to where they need to get to. We are playing musical chairs with 100 people and 10 chairs. When the music stops, what happens?”
Also in Texas in August, Joe Valdez, who was shot six times as an unlucky bystander in a domestic dispute, waited for more than a week for surgery at Ben Taub Hospital in Houston, which was over capacity with COVID patients, the Washington Post reported.
Others with chronic diseases fear needing emergency services or even entering a hospital for regular care with the COVID surge.
Nicole Seefeldt, 44, from Easton, Penn., who had a double-lung transplant in 2016, said that she hasn’t been able to see her lung transplant specialists in Philadelphia — an hour-and-a-half drive — for almost 2 years because of fear of contracting COVID. Before the pandemic, she made the trip almost weekly.
“I protect my lungs like they’re children,” she said.
She relies on her local hospital for care, but has put off some needed care, such as a colonoscopy, and has relied on telemedicine because she wants to limit her hospital exposure.
Ms. Seefeldt now faces an eventual kidney transplant, as her kidney function has been reduced to 20%. In the meantime, she worries she will need emergency care for either her lungs or kidneys.
“For those of us who are chronically ill or disabled, what if we have an emergency that is not COVID-related? Are we going to be able to get a bed? Are we going to be able to get treatment? It’s not just COVID patients who come to the [emergency room],” she said.
A pandemic problem
Paul E. Casey, MD, MBA, chief medical officer at Rush University Medical Center in Chicago, said that high vaccination rates in Chicago have helped Rush continue to accommodate both non-COVID and COVID patients in the emergency department.
Though the hospital treated a large volume of COVID patients, “The vast majority of people we see and did see through the pandemic were non-COVID patents,” he said.
Dr. Casey said that in the first wave the hospital noticed a concerning drop in patients coming in for strokes and heart attacks — “things we knew hadn’t gone away.”
And the data backs it up. Over the course of the pandemic, the Centers for Disease Control and Prevention’s National Health Interview Survey found that the percentage of Americans who reported seeing a doctor or health professional fell from 85% at the end of 2019 to about 80% in the first three months of 2021. The survey did not differentiate between in-person visits and telehealth appointments.
Medical practices and patients themselves postponed elective procedures and delayed routine visits during the early months of the crisis.
Patients also reported staying away from hospitals’ emergency departments throughout the pandemic. At the end of 2019, 22% of respondents reported visiting an emergency department in the past year. That dropped to 17% by the end of 2020, and was at 17.7% in the first 3 months of 2021.
Dr. Casey said that, in his hospital’s case, clear messaging became very important to assure patients it was safe to come back. And the message is still critical.
“We want to be loud and clear that patients should continue to seek care for those conditions,” Dr. Casey said. “Deferring healthcare only comes with the long-term sequelae of disease left untreated so we want people to be as proactive in seeking care as they always would be.”
In some cases, fears of entering emergency rooms because of excess patients and risk for infection are keeping some patients from seeking necessary care for minor injuries.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health in Bloomington, said that some of his patients have expressed fears of coming into the hospital for fractures.
Some patients, particularly elderly patients, he said, are having falls and fractures and wearing slings or braces at home rather than going into the hospital for injuries that need immediate attention.
Bones start healing incorrectly, Dr. Rickert said, and the correction becomes much more difficult.
Plea for vaccinations
Dr. Gosnell made a plea posted on her neighborhood news forum for people to get COVID vaccinations.
“It seems to me it’s easy for other people who are not in bodies like mine to take health for granted,” she said. “But there are a lot of us who live in very fragile bodies and our entire life is at the intersection of us and getting healthcare treatment. Small complications to getting treatment can be life altering.”
Dr. Gosnell, Ms. Seefeldt, Dr. Casey, and Dr. Rickert reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jessica Gosnell, MD, 41, from Portland, Oregon, lives daily with the knowledge that her rare disease — a form of hereditary angioedema — could cause a sudden, severe swelling in her throat that could require quick intubation and land her in an intensive care unit (ICU) for days.
“I’ve been hospitalized for throat swells three times in the last year,” she said in an interview.
Dr. Gosnell no longer practices medicine because of a combination of illnesses, but lives with her husband, Andrew, and two young children, and said they are all “terrified” she will have to go to the hospital amid a COVID-19 surge that had shrunk the number of available ICU beds to 152 from 780 in Oregon as of Aug. 30. Thirty percent of the beds are in use for patients with COVID-19.
She said her life depends on being near hospitals that have ICUs and having access to highly specialized medications, one of which can cost up to $50,000 for the rescue dose.
Her fear has her “literally living bedbound.” In addition to hereditary angioedema, she has Ehlers-Danlos syndrome, which weakens connective tissue. She wears a cervical collar 24/7 to keep from tearing tissues, as any tissue injury can trigger a swell.
Patients worry there won’t be room
As ICU beds in most states are filling with COVID-19 patients as the Delta variant spreads, fears are rising among people like Dr. Gosnell, who have chronic conditions and diseases with unpredictable emergency visits, who worry that if they need emergency care there won’t be room.
As of Aug. 30, in the United States, 79% of ICU beds nationally were in use, 30% of them for COVID-19 patients, according to the U.S. Department of Health and Human Services.
In individual states, the picture is dire. Alabama has fewer than 10% of its ICU beds open across the entire state. In Florida, 93% of ICU beds are filled, 53% of them with COVID patients. In Louisiana, 87% of beds were already in use, 45% of them with COVID patients, just as category 4 hurricane Ida smashed into the coastline on Aug. 29.
News reports have told of people transported and airlifted as hospitals reach capacity.
In Bellville, Tex., U.S. Army veteran Daniel Wilkinson needed advanced care for gallstone pancreatitis that normally would take 30 minutes to treat, his Bellville doctor, Hasan Kakli, MD, told CBS News.
Mr. Wilkinson’s house was three doors from Bellville Hospital, but the hospital was not equipped to treat the condition. Calls to other hospitals found the same answer: no empty ICU beds. After a 7-hour wait on a stretcher, he was airlifted to a Veterans Affairs hospital in Houston, but it was too late. He died on August 22 at age 46.
Dr. Kakli said, “I’ve never lost a patient with this diagnosis. Ever. I’m scared that the next patient I see is someone that I can’t get to where they need to get to. We are playing musical chairs with 100 people and 10 chairs. When the music stops, what happens?”
Also in Texas in August, Joe Valdez, who was shot six times as an unlucky bystander in a domestic dispute, waited for more than a week for surgery at Ben Taub Hospital in Houston, which was over capacity with COVID patients, the Washington Post reported.
Others with chronic diseases fear needing emergency services or even entering a hospital for regular care with the COVID surge.
Nicole Seefeldt, 44, from Easton, Penn., who had a double-lung transplant in 2016, said that she hasn’t been able to see her lung transplant specialists in Philadelphia — an hour-and-a-half drive — for almost 2 years because of fear of contracting COVID. Before the pandemic, she made the trip almost weekly.
“I protect my lungs like they’re children,” she said.
She relies on her local hospital for care, but has put off some needed care, such as a colonoscopy, and has relied on telemedicine because she wants to limit her hospital exposure.
Ms. Seefeldt now faces an eventual kidney transplant, as her kidney function has been reduced to 20%. In the meantime, she worries she will need emergency care for either her lungs or kidneys.
“For those of us who are chronically ill or disabled, what if we have an emergency that is not COVID-related? Are we going to be able to get a bed? Are we going to be able to get treatment? It’s not just COVID patients who come to the [emergency room],” she said.
A pandemic problem
Paul E. Casey, MD, MBA, chief medical officer at Rush University Medical Center in Chicago, said that high vaccination rates in Chicago have helped Rush continue to accommodate both non-COVID and COVID patients in the emergency department.
Though the hospital treated a large volume of COVID patients, “The vast majority of people we see and did see through the pandemic were non-COVID patents,” he said.
Dr. Casey said that in the first wave the hospital noticed a concerning drop in patients coming in for strokes and heart attacks — “things we knew hadn’t gone away.”
And the data backs it up. Over the course of the pandemic, the Centers for Disease Control and Prevention’s National Health Interview Survey found that the percentage of Americans who reported seeing a doctor or health professional fell from 85% at the end of 2019 to about 80% in the first three months of 2021. The survey did not differentiate between in-person visits and telehealth appointments.
Medical practices and patients themselves postponed elective procedures and delayed routine visits during the early months of the crisis.
Patients also reported staying away from hospitals’ emergency departments throughout the pandemic. At the end of 2019, 22% of respondents reported visiting an emergency department in the past year. That dropped to 17% by the end of 2020, and was at 17.7% in the first 3 months of 2021.
Dr. Casey said that, in his hospital’s case, clear messaging became very important to assure patients it was safe to come back. And the message is still critical.
“We want to be loud and clear that patients should continue to seek care for those conditions,” Dr. Casey said. “Deferring healthcare only comes with the long-term sequelae of disease left untreated so we want people to be as proactive in seeking care as they always would be.”
In some cases, fears of entering emergency rooms because of excess patients and risk for infection are keeping some patients from seeking necessary care for minor injuries.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health in Bloomington, said that some of his patients have expressed fears of coming into the hospital for fractures.
Some patients, particularly elderly patients, he said, are having falls and fractures and wearing slings or braces at home rather than going into the hospital for injuries that need immediate attention.
Bones start healing incorrectly, Dr. Rickert said, and the correction becomes much more difficult.
Plea for vaccinations
Dr. Gosnell made a plea posted on her neighborhood news forum for people to get COVID vaccinations.
“It seems to me it’s easy for other people who are not in bodies like mine to take health for granted,” she said. “But there are a lot of us who live in very fragile bodies and our entire life is at the intersection of us and getting healthcare treatment. Small complications to getting treatment can be life altering.”
Dr. Gosnell, Ms. Seefeldt, Dr. Casey, and Dr. Rickert reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jessica Gosnell, MD, 41, from Portland, Oregon, lives daily with the knowledge that her rare disease — a form of hereditary angioedema — could cause a sudden, severe swelling in her throat that could require quick intubation and land her in an intensive care unit (ICU) for days.
“I’ve been hospitalized for throat swells three times in the last year,” she said in an interview.
Dr. Gosnell no longer practices medicine because of a combination of illnesses, but lives with her husband, Andrew, and two young children, and said they are all “terrified” she will have to go to the hospital amid a COVID-19 surge that had shrunk the number of available ICU beds to 152 from 780 in Oregon as of Aug. 30. Thirty percent of the beds are in use for patients with COVID-19.
She said her life depends on being near hospitals that have ICUs and having access to highly specialized medications, one of which can cost up to $50,000 for the rescue dose.
Her fear has her “literally living bedbound.” In addition to hereditary angioedema, she has Ehlers-Danlos syndrome, which weakens connective tissue. She wears a cervical collar 24/7 to keep from tearing tissues, as any tissue injury can trigger a swell.
Patients worry there won’t be room
As ICU beds in most states are filling with COVID-19 patients as the Delta variant spreads, fears are rising among people like Dr. Gosnell, who have chronic conditions and diseases with unpredictable emergency visits, who worry that if they need emergency care there won’t be room.
As of Aug. 30, in the United States, 79% of ICU beds nationally were in use, 30% of them for COVID-19 patients, according to the U.S. Department of Health and Human Services.
In individual states, the picture is dire. Alabama has fewer than 10% of its ICU beds open across the entire state. In Florida, 93% of ICU beds are filled, 53% of them with COVID patients. In Louisiana, 87% of beds were already in use, 45% of them with COVID patients, just as category 4 hurricane Ida smashed into the coastline on Aug. 29.
News reports have told of people transported and airlifted as hospitals reach capacity.
In Bellville, Tex., U.S. Army veteran Daniel Wilkinson needed advanced care for gallstone pancreatitis that normally would take 30 minutes to treat, his Bellville doctor, Hasan Kakli, MD, told CBS News.
Mr. Wilkinson’s house was three doors from Bellville Hospital, but the hospital was not equipped to treat the condition. Calls to other hospitals found the same answer: no empty ICU beds. After a 7-hour wait on a stretcher, he was airlifted to a Veterans Affairs hospital in Houston, but it was too late. He died on August 22 at age 46.
Dr. Kakli said, “I’ve never lost a patient with this diagnosis. Ever. I’m scared that the next patient I see is someone that I can’t get to where they need to get to. We are playing musical chairs with 100 people and 10 chairs. When the music stops, what happens?”
Also in Texas in August, Joe Valdez, who was shot six times as an unlucky bystander in a domestic dispute, waited for more than a week for surgery at Ben Taub Hospital in Houston, which was over capacity with COVID patients, the Washington Post reported.
Others with chronic diseases fear needing emergency services or even entering a hospital for regular care with the COVID surge.
Nicole Seefeldt, 44, from Easton, Penn., who had a double-lung transplant in 2016, said that she hasn’t been able to see her lung transplant specialists in Philadelphia — an hour-and-a-half drive — for almost 2 years because of fear of contracting COVID. Before the pandemic, she made the trip almost weekly.
“I protect my lungs like they’re children,” she said.
She relies on her local hospital for care, but has put off some needed care, such as a colonoscopy, and has relied on telemedicine because she wants to limit her hospital exposure.
Ms. Seefeldt now faces an eventual kidney transplant, as her kidney function has been reduced to 20%. In the meantime, she worries she will need emergency care for either her lungs or kidneys.
“For those of us who are chronically ill or disabled, what if we have an emergency that is not COVID-related? Are we going to be able to get a bed? Are we going to be able to get treatment? It’s not just COVID patients who come to the [emergency room],” she said.
A pandemic problem
Paul E. Casey, MD, MBA, chief medical officer at Rush University Medical Center in Chicago, said that high vaccination rates in Chicago have helped Rush continue to accommodate both non-COVID and COVID patients in the emergency department.
Though the hospital treated a large volume of COVID patients, “The vast majority of people we see and did see through the pandemic were non-COVID patents,” he said.
Dr. Casey said that in the first wave the hospital noticed a concerning drop in patients coming in for strokes and heart attacks — “things we knew hadn’t gone away.”
And the data backs it up. Over the course of the pandemic, the Centers for Disease Control and Prevention’s National Health Interview Survey found that the percentage of Americans who reported seeing a doctor or health professional fell from 85% at the end of 2019 to about 80% in the first three months of 2021. The survey did not differentiate between in-person visits and telehealth appointments.
Medical practices and patients themselves postponed elective procedures and delayed routine visits during the early months of the crisis.
Patients also reported staying away from hospitals’ emergency departments throughout the pandemic. At the end of 2019, 22% of respondents reported visiting an emergency department in the past year. That dropped to 17% by the end of 2020, and was at 17.7% in the first 3 months of 2021.
Dr. Casey said that, in his hospital’s case, clear messaging became very important to assure patients it was safe to come back. And the message is still critical.
“We want to be loud and clear that patients should continue to seek care for those conditions,” Dr. Casey said. “Deferring healthcare only comes with the long-term sequelae of disease left untreated so we want people to be as proactive in seeking care as they always would be.”
In some cases, fears of entering emergency rooms because of excess patients and risk for infection are keeping some patients from seeking necessary care for minor injuries.
Jim Rickert, MD, an orthopedic surgeon with Indiana University Health in Bloomington, said that some of his patients have expressed fears of coming into the hospital for fractures.
Some patients, particularly elderly patients, he said, are having falls and fractures and wearing slings or braces at home rather than going into the hospital for injuries that need immediate attention.
Bones start healing incorrectly, Dr. Rickert said, and the correction becomes much more difficult.
Plea for vaccinations
Dr. Gosnell made a plea posted on her neighborhood news forum for people to get COVID vaccinations.
“It seems to me it’s easy for other people who are not in bodies like mine to take health for granted,” she said. “But there are a lot of us who live in very fragile bodies and our entire life is at the intersection of us and getting healthcare treatment. Small complications to getting treatment can be life altering.”
Dr. Gosnell, Ms. Seefeldt, Dr. Casey, and Dr. Rickert reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Two swings, two misses with colchicine, Vascepa in COVID-19
The anti-inflammatory agents colchicine and icosapent ethyl (Vascepa; Amarin) failed to provide substantial benefits in separate randomized COVID-19 trials.
Both were reported at the European Society of Cardiology (ESC) Congress 2021.
The open-label ECLA PHRI COLCOVID trial randomized 1,277 hospitalized adults (mean age 62 years) to usual care alone or with colchicine at a loading dose of 1.5 mg for 2 hours followed by 0.5 mg on day 1 and then 0.5 mg twice daily for 14 days or until discharge.
The investigators hypothesized that colchicine, which is widely used to treat gout and other inflammatory conditions, might modulate the hyperinflammatory syndrome, or cytokine storm, associated with COVID-19.
Results showed that the need for mechanical ventilation or death occurred in 25.0% of patients receiving colchicine and 28.8% with usual care (P = .08).
The coprimary endpoint of death at 28 days was also not significantly different between groups (20.5% vs. 22.2%), principal investigator Rafael Diaz, MD, said in a late-breaking COVID-19 trials session at the congress.
Among the secondary outcomes at 28 days, colchicine significantly reduced the incidence of new intubation or death from respiratory failure from 27.0% to 22.3% (hazard ratio, 0.79; 95% confidence interval, 0.63-0.99) but not mortality from respiratory failure (19.5% vs. 16.8%).
The only important adverse effect was severe diarrhea, which was reported in 11.3% of the colchicine group vs. 4.5% in the control group, said Dr. Diaz, director of Estudios Clínicos Latinoamérica (ECLA), Rosario, Argentina.
The results are consistent with those from the massive RECOVERY trial, which earlier this year stopped enrollment in the colchicine arm for lack of efficacy in patients hospitalized with COVID-19, and COLCORONA, which missed its primary endpoint using colchicine among nonhospitalized adults with COVID-19.
Session chair and COLCORONA principal investigator Jean-Claude Tardif, MD, pointed out that, as clinicians, it’s fairly uncommon to combine systemic steroids with colchicine, which was the case in 92% of patients in ECLA PHRI COLCOVID.

“I think it is an inherent limitation of testing colchicine on top of steroids,” said Dr. Tardif, of the Montreal Heart Institute.
Icosapent ethyl in PREPARE-IT
Dr. Diaz returned in the ESC session to present the results of the PREPARE-IT trial, which tested whether icosapent ethyl – at a loading dose of 8 grams (4 capsules) for the first 3 days and 4 g/d on days 4-60 – could reduce the risk for SARS-CoV-2 infection in 2,041 health care and other public workers in Argentina at high risk for infection (mean age 40.5 years).
Vascepa was approved by the Food and Drug Administration in 2012 for the reduction of elevated triglyceride levels, with an added indication in 2019 to reduce cardiovascular (CV) events in people with elevated triglycerides and established CV disease or diabetes with other CV risk factors.
The rationale for using the high-dose prescription eicosapentaenoic acid (EPA) preparation includes its anti-inflammatory and antithrombotic effects, and that unsaturated fatty acids, especially EPA, might inactivate the enveloped virus, he explained.
Among 1,712 participants followed for up to 60 days, however, the SARS-CoV-2 infection rate was 7.9% with icosapent ethyl vs. 7.1% with a mineral oil placebo (P = .58).
There were also no significant changes from baseline in the icosapent ethyl and placebo groups for the secondary outcomes of high-sensitivity C-reactive protein (0 vs. 0), triglycerides (median –2 mg/dL vs. 7 mg/dL), or Influenza Patient-Reported Outcome (FLU-PRO) questionnaire scores (median 0.01 vs. 0.03).
The use of a mineral oil placebo has been the subject of controversy in previous fish oil trials, but, Dr. Diaz noted, it did not have a significant proinflammatory effect or cause any excess adverse events.
Overall, adverse events were similar between the active and placebo groups, including atrial fibrillation (none), major bleeding (none), minor bleeding (7 events vs. 10 events), gastrointestinal symptoms (6.8% vs. 7.0%), and diarrhea (8.6% vs. 7.7%).
Although it missed the primary endpoint, Dr. Diaz said, “this is the first large, randomized blinded trial to demonstrate excellent safety and tolerability of an 8-gram-per-day loading dose of icosapent ethyl, opening up the potential for acute use in randomized trials of myocardial infarction, acute coronary syndromes, strokes, and revascularization.”
During a discussion of the results, Dr. Diaz said the Delta variant was not present at the time of the analysis and that the second half of the trial will report on whether icosapent ethyl can reduce the risk for hospitalization or death in participants diagnosed with COVID-19.
ECLA PHRI COLCOVID was supported by the Estudios Clínicos Latinoamérica Population Health Research Institute. PREPARE-IT was supported by Estudios Clínicos Latinoamérica with collaboration from Amarin. Dr. Diaz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The anti-inflammatory agents colchicine and icosapent ethyl (Vascepa; Amarin) failed to provide substantial benefits in separate randomized COVID-19 trials.
Both were reported at the European Society of Cardiology (ESC) Congress 2021.
The open-label ECLA PHRI COLCOVID trial randomized 1,277 hospitalized adults (mean age 62 years) to usual care alone or with colchicine at a loading dose of 1.5 mg for 2 hours followed by 0.5 mg on day 1 and then 0.5 mg twice daily for 14 days or until discharge.
The investigators hypothesized that colchicine, which is widely used to treat gout and other inflammatory conditions, might modulate the hyperinflammatory syndrome, or cytokine storm, associated with COVID-19.
Results showed that the need for mechanical ventilation or death occurred in 25.0% of patients receiving colchicine and 28.8% with usual care (P = .08).
The coprimary endpoint of death at 28 days was also not significantly different between groups (20.5% vs. 22.2%), principal investigator Rafael Diaz, MD, said in a late-breaking COVID-19 trials session at the congress.
Among the secondary outcomes at 28 days, colchicine significantly reduced the incidence of new intubation or death from respiratory failure from 27.0% to 22.3% (hazard ratio, 0.79; 95% confidence interval, 0.63-0.99) but not mortality from respiratory failure (19.5% vs. 16.8%).
The only important adverse effect was severe diarrhea, which was reported in 11.3% of the colchicine group vs. 4.5% in the control group, said Dr. Diaz, director of Estudios Clínicos Latinoamérica (ECLA), Rosario, Argentina.
The results are consistent with those from the massive RECOVERY trial, which earlier this year stopped enrollment in the colchicine arm for lack of efficacy in patients hospitalized with COVID-19, and COLCORONA, which missed its primary endpoint using colchicine among nonhospitalized adults with COVID-19.
Session chair and COLCORONA principal investigator Jean-Claude Tardif, MD, pointed out that, as clinicians, it’s fairly uncommon to combine systemic steroids with colchicine, which was the case in 92% of patients in ECLA PHRI COLCOVID.
“I think it is an inherent limitation of testing colchicine on top of steroids,” said Dr. Tardif, of the Montreal Heart Institute.
Icosapent ethyl in PREPARE-IT
Dr. Diaz returned in the ESC session to present the results of the PREPARE-IT trial, which tested whether icosapent ethyl – at a loading dose of 8 grams (4 capsules) for the first 3 days and 4 g/d on days 4-60 – could reduce the risk for SARS-CoV-2 infection in 2,041 health care and other public workers in Argentina at high risk for infection (mean age 40.5 years).
Vascepa was approved by the Food and Drug Administration in 2012 for the reduction of elevated triglyceride levels, with an added indication in 2019 to reduce cardiovascular (CV) events in people with elevated triglycerides and established CV disease or diabetes with other CV risk factors.
The rationale for using the high-dose prescription eicosapentaenoic acid (EPA) preparation includes its anti-inflammatory and antithrombotic effects, and that unsaturated fatty acids, especially EPA, might inactivate the enveloped virus, he explained.
Among 1,712 participants followed for up to 60 days, however, the SARS-CoV-2 infection rate was 7.9% with icosapent ethyl vs. 7.1% with a mineral oil placebo (P = .58).
There were also no significant changes from baseline in the icosapent ethyl and placebo groups for the secondary outcomes of high-sensitivity C-reactive protein (0 vs. 0), triglycerides (median –2 mg/dL vs. 7 mg/dL), or Influenza Patient-Reported Outcome (FLU-PRO) questionnaire scores (median 0.01 vs. 0.03).
The use of a mineral oil placebo has been the subject of controversy in previous fish oil trials, but, Dr. Diaz noted, it did not have a significant proinflammatory effect or cause any excess adverse events.
Overall, adverse events were similar between the active and placebo groups, including atrial fibrillation (none), major bleeding (none), minor bleeding (7 events vs. 10 events), gastrointestinal symptoms (6.8% vs. 7.0%), and diarrhea (8.6% vs. 7.7%).
Although it missed the primary endpoint, Dr. Diaz said, “this is the first large, randomized blinded trial to demonstrate excellent safety and tolerability of an 8-gram-per-day loading dose of icosapent ethyl, opening up the potential for acute use in randomized trials of myocardial infarction, acute coronary syndromes, strokes, and revascularization.”
During a discussion of the results, Dr. Diaz said the Delta variant was not present at the time of the analysis and that the second half of the trial will report on whether icosapent ethyl can reduce the risk for hospitalization or death in participants diagnosed with COVID-19.
ECLA PHRI COLCOVID was supported by the Estudios Clínicos Latinoamérica Population Health Research Institute. PREPARE-IT was supported by Estudios Clínicos Latinoamérica with collaboration from Amarin. Dr. Diaz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The anti-inflammatory agents colchicine and icosapent ethyl (Vascepa; Amarin) failed to provide substantial benefits in separate randomized COVID-19 trials.
Both were reported at the European Society of Cardiology (ESC) Congress 2021.
The open-label ECLA PHRI COLCOVID trial randomized 1,277 hospitalized adults (mean age 62 years) to usual care alone or with colchicine at a loading dose of 1.5 mg for 2 hours followed by 0.5 mg on day 1 and then 0.5 mg twice daily for 14 days or until discharge.
The investigators hypothesized that colchicine, which is widely used to treat gout and other inflammatory conditions, might modulate the hyperinflammatory syndrome, or cytokine storm, associated with COVID-19.
Results showed that the need for mechanical ventilation or death occurred in 25.0% of patients receiving colchicine and 28.8% with usual care (P = .08).
The coprimary endpoint of death at 28 days was also not significantly different between groups (20.5% vs. 22.2%), principal investigator Rafael Diaz, MD, said in a late-breaking COVID-19 trials session at the congress.
Among the secondary outcomes at 28 days, colchicine significantly reduced the incidence of new intubation or death from respiratory failure from 27.0% to 22.3% (hazard ratio, 0.79; 95% confidence interval, 0.63-0.99) but not mortality from respiratory failure (19.5% vs. 16.8%).
The only important adverse effect was severe diarrhea, which was reported in 11.3% of the colchicine group vs. 4.5% in the control group, said Dr. Diaz, director of Estudios Clínicos Latinoamérica (ECLA), Rosario, Argentina.
The results are consistent with those from the massive RECOVERY trial, which earlier this year stopped enrollment in the colchicine arm for lack of efficacy in patients hospitalized with COVID-19, and COLCORONA, which missed its primary endpoint using colchicine among nonhospitalized adults with COVID-19.
Session chair and COLCORONA principal investigator Jean-Claude Tardif, MD, pointed out that, as clinicians, it’s fairly uncommon to combine systemic steroids with colchicine, which was the case in 92% of patients in ECLA PHRI COLCOVID.
“I think it is an inherent limitation of testing colchicine on top of steroids,” said Dr. Tardif, of the Montreal Heart Institute.
Icosapent ethyl in PREPARE-IT
Dr. Diaz returned in the ESC session to present the results of the PREPARE-IT trial, which tested whether icosapent ethyl – at a loading dose of 8 grams (4 capsules) for the first 3 days and 4 g/d on days 4-60 – could reduce the risk for SARS-CoV-2 infection in 2,041 health care and other public workers in Argentina at high risk for infection (mean age 40.5 years).
Vascepa was approved by the Food and Drug Administration in 2012 for the reduction of elevated triglyceride levels, with an added indication in 2019 to reduce cardiovascular (CV) events in people with elevated triglycerides and established CV disease or diabetes with other CV risk factors.
The rationale for using the high-dose prescription eicosapentaenoic acid (EPA) preparation includes its anti-inflammatory and antithrombotic effects, and that unsaturated fatty acids, especially EPA, might inactivate the enveloped virus, he explained.
Among 1,712 participants followed for up to 60 days, however, the SARS-CoV-2 infection rate was 7.9% with icosapent ethyl vs. 7.1% with a mineral oil placebo (P = .58).
There were also no significant changes from baseline in the icosapent ethyl and placebo groups for the secondary outcomes of high-sensitivity C-reactive protein (0 vs. 0), triglycerides (median –2 mg/dL vs. 7 mg/dL), or Influenza Patient-Reported Outcome (FLU-PRO) questionnaire scores (median 0.01 vs. 0.03).
The use of a mineral oil placebo has been the subject of controversy in previous fish oil trials, but, Dr. Diaz noted, it did not have a significant proinflammatory effect or cause any excess adverse events.
Overall, adverse events were similar between the active and placebo groups, including atrial fibrillation (none), major bleeding (none), minor bleeding (7 events vs. 10 events), gastrointestinal symptoms (6.8% vs. 7.0%), and diarrhea (8.6% vs. 7.7%).
Although it missed the primary endpoint, Dr. Diaz said, “this is the first large, randomized blinded trial to demonstrate excellent safety and tolerability of an 8-gram-per-day loading dose of icosapent ethyl, opening up the potential for acute use in randomized trials of myocardial infarction, acute coronary syndromes, strokes, and revascularization.”
During a discussion of the results, Dr. Diaz said the Delta variant was not present at the time of the analysis and that the second half of the trial will report on whether icosapent ethyl can reduce the risk for hospitalization or death in participants diagnosed with COVID-19.
ECLA PHRI COLCOVID was supported by the Estudios Clínicos Latinoamérica Population Health Research Institute. PREPARE-IT was supported by Estudios Clínicos Latinoamérica with collaboration from Amarin. Dr. Diaz reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Deeper dive’ into opioid overdose deaths during COVID pandemic
Opioid overdose deaths were significantly higher during 2020, but occurrences were not homogeneous across nine states. Male deaths were higher than in the 2 previous years in two states, according to a new, granular examination of data collected by researchers at the Massachusetts General Hospital (Mass General), Boston.

The analysis also showed that synthetic opioids such as fentanyl played an outsized role in most of the states that were reviewed. Additional drugs of abuse found in decedents, such as cocaine and psychostimulants, were more prevalent in some states than in others.
The Centers for Disease Control and Prevention used provisional death data in its recent report. It found that opioid-related deaths substantially rose in 2020 and that synthetic opioids were a primary driver.
The current Mass General analysis provides a more timely and detailed dive, senior author Mohammad Jalali, PhD, who is a senior scientist at Mass General’s Institute for Technology Assessment, told this news organization.
The findings, which have not yet been peer reviewed, were published in MedRxiv.
Shifting sands of opioid use disorder
to analyze and project trends and also to be better prepared to address the shifting sands of opioid use disorder in the United States.

They attempted to collect data on confirmed opioid overdose deaths from all 50 states and Washington, D.C. to assess what might have changed during the COVID-19 pandemic. Only nine states provided enough data for the analysis, which has been submitted to a peer reviewed publication.
These states were Alaska, Connecticut, Indiana, Massachusetts, North Carolina, Rhode Island, Colorado, Utah, and Wyoming.
“Drug overdose data are collected and reported more slowly than COVID-19 data,” Dr. Jalali said in a press release. The data reflected a lag time of about 4 to 8 months in Massachusetts and North Carolina to more than a year in Maryland and Ohio, he noted.
The reporting lag “has clouded the understanding of the effects of the COVID-19 pandemic on opioid-related overdose deaths,” said Dr. Jalali.
Commenting on the findings, Brandon Marshall, PhD, associate professor of epidemiology at Brown University, Providence, R.I, said that “the overall pattern of what’s being reported here is not surprising,” given the national trends seen in the CDC data.
“This paper adds a deeper dive into some of the sociodemographic trends that we’re starting to observe in specific states,” Dr. Marshall said.
Also commenting for this news organization, Brian Fuehrlein, MD, PhD, director of the psychiatric emergency department at the VA Connecticut Healthcare System in West Haven, Connecticut, noted that the current study “highlights things that we are currently seeing at VA Connecticut.”
Decrease in heroin, rise in fentanyl
The investigators found a significant reduction in overdose deaths that involved heroin in Alaska, Connecticut, Indiana, Massachusetts, North Carolina, and Rhode Island. That was a new trend for Alaska, Indiana, and Rhode Island, although with only 3 years of data, it’s hard to say whether it will continue, Dr. Jalali noted.

The decrease in heroin involvement seemed to continue a trend previously observed in Colorado, Connecticut, Massachusetts, and North Carolina.
In Connecticut, heroin was involved in 36% of deaths in 2018, 30% in 2019, and 16% in 2020, according to the study.
“We have begun seeing more and more heroin-negative, fentanyl-positive drug screens,” said Dr. Fuehrlein, who is also associate professor of psychiatry at Yale University, New Haven, Conn.
“There is a shift from fentanyl being an adulterant to fentanyl being what is sold and used exclusively,” he added.
In 2020, 92% (n = 887) of deaths in Connecticut involved synthetic opioids, continuing a trend. In Alaska, however, synthetic opioids were involved in 60% (44) of deaths, which is a big jump from 23% (9) in 2018.
Synthetic opioids were involved in the largest percentage of overdoses in all of the states studied. The fewest deaths, 17 (49%), occurred in Wyoming.
Cocaine is also increasingly found in addition to other substances in decedents. In Alaska, about 14% of individuals who overdosed in 2020 also had cocaine in their system, which was a jump from 2% in the prior year.
In Colorado, 19% (94) of those who died also had taken cocaine, up from 13% in 2019. Cocaine was also frequently found in those who died in the northeast: 39% (467) of those who died in Massachusetts, 29% (280) in Connecticut, and 47% (109) in Rhode Island.
There was also an increase in psychostimulants found in those who had died in Massachusetts in 2020.
More male overdoses in 2020
Results also showed that, compared to 2019, significantly more men died from overdoses in 2020 in Colorado (61% vs. 70%, P = .017) and Indiana (62% vs. 70%, P = .026).
This finding was unexpected, said Dr. Marshall, who has observed the same phenomenon in Rhode Island. He is the scientific director of PreventOverdoseRI, Rhode Island’s drug overdose surveillance and information dashboard.
Dr. Marshall and his colleagues conducted a study that also found disproportionate increases in overdoses among men. The findings of that study will be published in September.
“We’re still trying to wrap our head around why that is,” he said. He added that a deeper dive into the Rhode Island data showed that the deaths were increased especially among middle-aged men who had been diagnosed with depression and anxiety.
The same patterns were not seen among women in either Dr. Jalali’s study or his own analysis of the Rhode Island data, said Dr. Marshall.
“That suggests the COVID-19 pandemic impacted men who are at risk for overdose in some particularly severe way,” he noted.
Dr. Fuehrlein said he believes a variety of factors have led to an increase in overdose deaths during the pandemic, including the fact that many patients who would normally seek help avoided care or dropped out of treatment because of COVID fears. In addition, other support systems, such as group therapy and Narcotics Anonymous, were unavailable.
The pandemic increased stress, which can lead to worsening substance use, said Dr. Fuehrlein. He also noted that regular opioid suppliers were often not available, which led some to buy from different dealers, “which can lead to overdose if the fentanyl content is different.”
Identifying at-risk individuals
Dr. Jalali and colleagues note that clinicians and policymakers could use the new study to help identify and treat at-risk individuals.
“Practitioners and policy makers can use our findings to help them anticipate which groups of people might be most affected by opioid overdose and which types of policy interventions might be most effective given each state’s unique situation,” said lead study author Gian-Gabriel P. Garcia, PhD, in a press release. At the time of the study, Dr. Garcia was a postdoctoral fellow at Mass General and Harvard Medical School. He is currently an assistant professor at Georgia Tech, Atlanta.
Dr. Marshall pointed out that Dr. Jalali’s study is also relevant for emergency departments.
ED clinicians “are and will be seeing patients coming in who have no idea they were exposed to an opioid, nevermind fentanyl,” he said. ED clinicians can discuss with patients various harm reduction techniques, including the use of naloxone as well as test strips that can detect fentanyl in the drug supply, he added.
“Given the increasing use of fentanyl, which is very dangerous in overdose, clinicians need to be well versed in a harm reduction/overdose prevention approach to patient care,” Dr. Fuehrlein agreed.
A version of this article first appeared on Medscape.com.
Opioid overdose deaths were significantly higher during 2020, but occurrences were not homogeneous across nine states. Male deaths were higher than in the 2 previous years in two states, according to a new, granular examination of data collected by researchers at the Massachusetts General Hospital (Mass General), Boston.
The analysis also showed that synthetic opioids such as fentanyl played an outsized role in most of the states that were reviewed. Additional drugs of abuse found in decedents, such as cocaine and psychostimulants, were more prevalent in some states than in others.
The Centers for Disease Control and Prevention used provisional death data in its recent report. It found that opioid-related deaths substantially rose in 2020 and that synthetic opioids were a primary driver.
The current Mass General analysis provides a more timely and detailed dive, senior author Mohammad Jalali, PhD, who is a senior scientist at Mass General’s Institute for Technology Assessment, told this news organization.
The findings, which have not yet been peer reviewed, were published in MedRxiv.
Shifting sands of opioid use disorder
to analyze and project trends and also to be better prepared to address the shifting sands of opioid use disorder in the United States.
They attempted to collect data on confirmed opioid overdose deaths from all 50 states and Washington, D.C. to assess what might have changed during the COVID-19 pandemic. Only nine states provided enough data for the analysis, which has been submitted to a peer reviewed publication.
These states were Alaska, Connecticut, Indiana, Massachusetts, North Carolina, Rhode Island, Colorado, Utah, and Wyoming.
“Drug overdose data are collected and reported more slowly than COVID-19 data,” Dr. Jalali said in a press release. The data reflected a lag time of about 4 to 8 months in Massachusetts and North Carolina to more than a year in Maryland and Ohio, he noted.
The reporting lag “has clouded the understanding of the effects of the COVID-19 pandemic on opioid-related overdose deaths,” said Dr. Jalali.
Commenting on the findings, Brandon Marshall, PhD, associate professor of epidemiology at Brown University, Providence, R.I, said that “the overall pattern of what’s being reported here is not surprising,” given the national trends seen in the CDC data.
“This paper adds a deeper dive into some of the sociodemographic trends that we’re starting to observe in specific states,” Dr. Marshall said.
Also commenting for this news organization, Brian Fuehrlein, MD, PhD, director of the psychiatric emergency department at the VA Connecticut Healthcare System in West Haven, Connecticut, noted that the current study “highlights things that we are currently seeing at VA Connecticut.”
Decrease in heroin, rise in fentanyl
The investigators found a significant reduction in overdose deaths that involved heroin in Alaska, Connecticut, Indiana, Massachusetts, North Carolina, and Rhode Island. That was a new trend for Alaska, Indiana, and Rhode Island, although with only 3 years of data, it’s hard to say whether it will continue, Dr. Jalali noted.
The decrease in heroin involvement seemed to continue a trend previously observed in Colorado, Connecticut, Massachusetts, and North Carolina.
In Connecticut, heroin was involved in 36% of deaths in 2018, 30% in 2019, and 16% in 2020, according to the study.
“We have begun seeing more and more heroin-negative, fentanyl-positive drug screens,” said Dr. Fuehrlein, who is also associate professor of psychiatry at Yale University, New Haven, Conn.
“There is a shift from fentanyl being an adulterant to fentanyl being what is sold and used exclusively,” he added.
In 2020, 92% (n = 887) of deaths in Connecticut involved synthetic opioids, continuing a trend. In Alaska, however, synthetic opioids were involved in 60% (44) of deaths, which is a big jump from 23% (9) in 2018.
Synthetic opioids were involved in the largest percentage of overdoses in all of the states studied. The fewest deaths, 17 (49%), occurred in Wyoming.
Cocaine is also increasingly found in addition to other substances in decedents. In Alaska, about 14% of individuals who overdosed in 2020 also had cocaine in their system, which was a jump from 2% in the prior year.
In Colorado, 19% (94) of those who died also had taken cocaine, up from 13% in 2019. Cocaine was also frequently found in those who died in the northeast: 39% (467) of those who died in Massachusetts, 29% (280) in Connecticut, and 47% (109) in Rhode Island.
There was also an increase in psychostimulants found in those who had died in Massachusetts in 2020.
More male overdoses in 2020
Results also showed that, compared to 2019, significantly more men died from overdoses in 2020 in Colorado (61% vs. 70%, P = .017) and Indiana (62% vs. 70%, P = .026).
This finding was unexpected, said Dr. Marshall, who has observed the same phenomenon in Rhode Island. He is the scientific director of PreventOverdoseRI, Rhode Island’s drug overdose surveillance and information dashboard.
Dr. Marshall and his colleagues conducted a study that also found disproportionate increases in overdoses among men. The findings of that study will be published in September.
“We’re still trying to wrap our head around why that is,” he said. He added that a deeper dive into the Rhode Island data showed that the deaths were increased especially among middle-aged men who had been diagnosed with depression and anxiety.
The same patterns were not seen among women in either Dr. Jalali’s study or his own analysis of the Rhode Island data, said Dr. Marshall.
“That suggests the COVID-19 pandemic impacted men who are at risk for overdose in some particularly severe way,” he noted.
Dr. Fuehrlein said he believes a variety of factors have led to an increase in overdose deaths during the pandemic, including the fact that many patients who would normally seek help avoided care or dropped out of treatment because of COVID fears. In addition, other support systems, such as group therapy and Narcotics Anonymous, were unavailable.
The pandemic increased stress, which can lead to worsening substance use, said Dr. Fuehrlein. He also noted that regular opioid suppliers were often not available, which led some to buy from different dealers, “which can lead to overdose if the fentanyl content is different.”
Identifying at-risk individuals
Dr. Jalali and colleagues note that clinicians and policymakers could use the new study to help identify and treat at-risk individuals.
“Practitioners and policy makers can use our findings to help them anticipate which groups of people might be most affected by opioid overdose and which types of policy interventions might be most effective given each state’s unique situation,” said lead study author Gian-Gabriel P. Garcia, PhD, in a press release. At the time of the study, Dr. Garcia was a postdoctoral fellow at Mass General and Harvard Medical School. He is currently an assistant professor at Georgia Tech, Atlanta.
Dr. Marshall pointed out that Dr. Jalali’s study is also relevant for emergency departments.
ED clinicians “are and will be seeing patients coming in who have no idea they were exposed to an opioid, nevermind fentanyl,” he said. ED clinicians can discuss with patients various harm reduction techniques, including the use of naloxone as well as test strips that can detect fentanyl in the drug supply, he added.
“Given the increasing use of fentanyl, which is very dangerous in overdose, clinicians need to be well versed in a harm reduction/overdose prevention approach to patient care,” Dr. Fuehrlein agreed.
A version of this article first appeared on Medscape.com.
Opioid overdose deaths were significantly higher during 2020, but occurrences were not homogeneous across nine states. Male deaths were higher than in the 2 previous years in two states, according to a new, granular examination of data collected by researchers at the Massachusetts General Hospital (Mass General), Boston.
The analysis also showed that synthetic opioids such as fentanyl played an outsized role in most of the states that were reviewed. Additional drugs of abuse found in decedents, such as cocaine and psychostimulants, were more prevalent in some states than in others.
The Centers for Disease Control and Prevention used provisional death data in its recent report. It found that opioid-related deaths substantially rose in 2020 and that synthetic opioids were a primary driver.
The current Mass General analysis provides a more timely and detailed dive, senior author Mohammad Jalali, PhD, who is a senior scientist at Mass General’s Institute for Technology Assessment, told this news organization.
The findings, which have not yet been peer reviewed, were published in MedRxiv.
Shifting sands of opioid use disorder
to analyze and project trends and also to be better prepared to address the shifting sands of opioid use disorder in the United States.
They attempted to collect data on confirmed opioid overdose deaths from all 50 states and Washington, D.C. to assess what might have changed during the COVID-19 pandemic. Only nine states provided enough data for the analysis, which has been submitted to a peer reviewed publication.
These states were Alaska, Connecticut, Indiana, Massachusetts, North Carolina, Rhode Island, Colorado, Utah, and Wyoming.
“Drug overdose data are collected and reported more slowly than COVID-19 data,” Dr. Jalali said in a press release. The data reflected a lag time of about 4 to 8 months in Massachusetts and North Carolina to more than a year in Maryland and Ohio, he noted.
The reporting lag “has clouded the understanding of the effects of the COVID-19 pandemic on opioid-related overdose deaths,” said Dr. Jalali.
Commenting on the findings, Brandon Marshall, PhD, associate professor of epidemiology at Brown University, Providence, R.I, said that “the overall pattern of what’s being reported here is not surprising,” given the national trends seen in the CDC data.
“This paper adds a deeper dive into some of the sociodemographic trends that we’re starting to observe in specific states,” Dr. Marshall said.
Also commenting for this news organization, Brian Fuehrlein, MD, PhD, director of the psychiatric emergency department at the VA Connecticut Healthcare System in West Haven, Connecticut, noted that the current study “highlights things that we are currently seeing at VA Connecticut.”
Decrease in heroin, rise in fentanyl
The investigators found a significant reduction in overdose deaths that involved heroin in Alaska, Connecticut, Indiana, Massachusetts, North Carolina, and Rhode Island. That was a new trend for Alaska, Indiana, and Rhode Island, although with only 3 years of data, it’s hard to say whether it will continue, Dr. Jalali noted.
The decrease in heroin involvement seemed to continue a trend previously observed in Colorado, Connecticut, Massachusetts, and North Carolina.
In Connecticut, heroin was involved in 36% of deaths in 2018, 30% in 2019, and 16% in 2020, according to the study.
“We have begun seeing more and more heroin-negative, fentanyl-positive drug screens,” said Dr. Fuehrlein, who is also associate professor of psychiatry at Yale University, New Haven, Conn.
“There is a shift from fentanyl being an adulterant to fentanyl being what is sold and used exclusively,” he added.
In 2020, 92% (n = 887) of deaths in Connecticut involved synthetic opioids, continuing a trend. In Alaska, however, synthetic opioids were involved in 60% (44) of deaths, which is a big jump from 23% (9) in 2018.
Synthetic opioids were involved in the largest percentage of overdoses in all of the states studied. The fewest deaths, 17 (49%), occurred in Wyoming.
Cocaine is also increasingly found in addition to other substances in decedents. In Alaska, about 14% of individuals who overdosed in 2020 also had cocaine in their system, which was a jump from 2% in the prior year.
In Colorado, 19% (94) of those who died also had taken cocaine, up from 13% in 2019. Cocaine was also frequently found in those who died in the northeast: 39% (467) of those who died in Massachusetts, 29% (280) in Connecticut, and 47% (109) in Rhode Island.
There was also an increase in psychostimulants found in those who had died in Massachusetts in 2020.
More male overdoses in 2020
Results also showed that, compared to 2019, significantly more men died from overdoses in 2020 in Colorado (61% vs. 70%, P = .017) and Indiana (62% vs. 70%, P = .026).
This finding was unexpected, said Dr. Marshall, who has observed the same phenomenon in Rhode Island. He is the scientific director of PreventOverdoseRI, Rhode Island’s drug overdose surveillance and information dashboard.
Dr. Marshall and his colleagues conducted a study that also found disproportionate increases in overdoses among men. The findings of that study will be published in September.
“We’re still trying to wrap our head around why that is,” he said. He added that a deeper dive into the Rhode Island data showed that the deaths were increased especially among middle-aged men who had been diagnosed with depression and anxiety.
The same patterns were not seen among women in either Dr. Jalali’s study or his own analysis of the Rhode Island data, said Dr. Marshall.
“That suggests the COVID-19 pandemic impacted men who are at risk for overdose in some particularly severe way,” he noted.
Dr. Fuehrlein said he believes a variety of factors have led to an increase in overdose deaths during the pandemic, including the fact that many patients who would normally seek help avoided care or dropped out of treatment because of COVID fears. In addition, other support systems, such as group therapy and Narcotics Anonymous, were unavailable.
The pandemic increased stress, which can lead to worsening substance use, said Dr. Fuehrlein. He also noted that regular opioid suppliers were often not available, which led some to buy from different dealers, “which can lead to overdose if the fentanyl content is different.”
Identifying at-risk individuals
Dr. Jalali and colleagues note that clinicians and policymakers could use the new study to help identify and treat at-risk individuals.
“Practitioners and policy makers can use our findings to help them anticipate which groups of people might be most affected by opioid overdose and which types of policy interventions might be most effective given each state’s unique situation,” said lead study author Gian-Gabriel P. Garcia, PhD, in a press release. At the time of the study, Dr. Garcia was a postdoctoral fellow at Mass General and Harvard Medical School. He is currently an assistant professor at Georgia Tech, Atlanta.
Dr. Marshall pointed out that Dr. Jalali’s study is also relevant for emergency departments.
ED clinicians “are and will be seeing patients coming in who have no idea they were exposed to an opioid, nevermind fentanyl,” he said. ED clinicians can discuss with patients various harm reduction techniques, including the use of naloxone as well as test strips that can detect fentanyl in the drug supply, he added.
“Given the increasing use of fentanyl, which is very dangerous in overdose, clinicians need to be well versed in a harm reduction/overdose prevention approach to patient care,” Dr. Fuehrlein agreed.
A version of this article first appeared on Medscape.com.
Children and COVID: Weekly cases top 200,000, vaccinations down
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.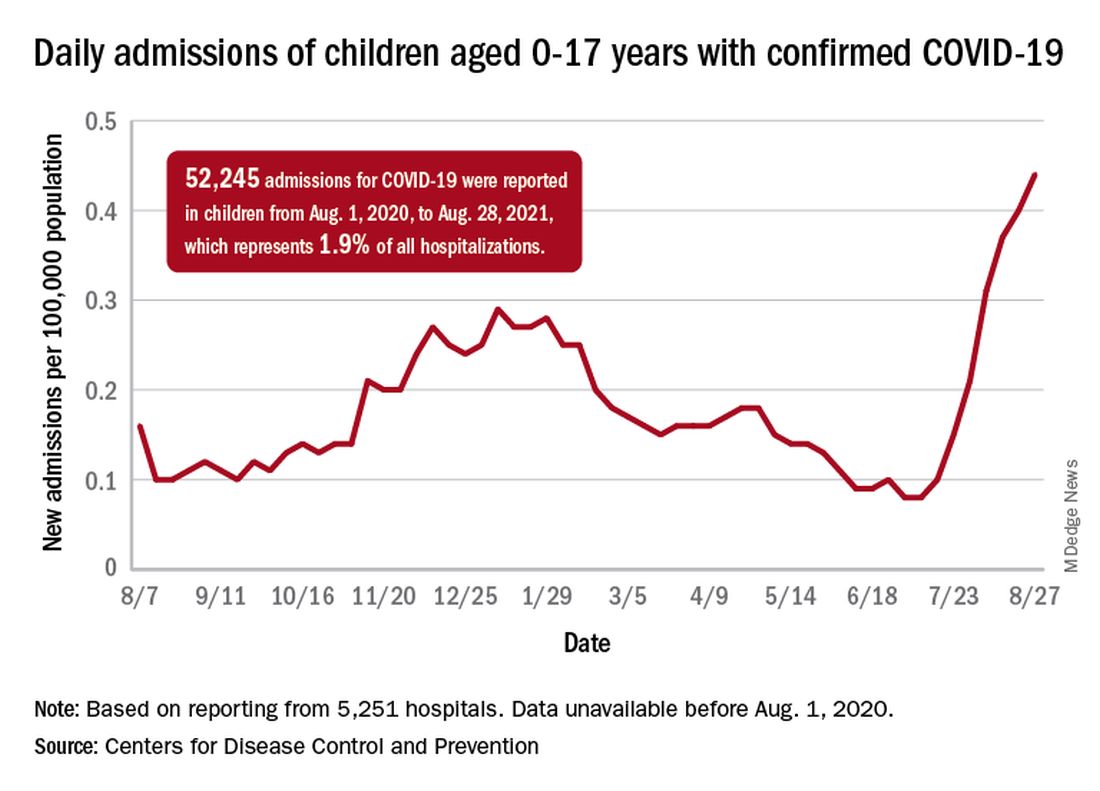
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
Weekly pediatric cases of COVID-19 exceeded 200,000 for just the second time during the pandemic, while new vaccinations in children continued to decline.
The weekly count has now increased for 9 consecutive weeks, during which time it has risen by over 2,300%, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report. Total cases in children number almost 4.8 million since the pandemic started.
Vaccinations in children are following a different trend. Vaccine initiation has dropped 3 weeks in a row for both of the eligible age groups: First doses administered were down by 29% among 12- to 15-year-olds over that span and by 32% in 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
Since vaccination for children aged 12-15 years started in May, 49% had received at least one dose, and just over 36% were fully vaccinated as of Aug. 30. Among children aged 16-17 years, who have been eligible since December, 57.5% had gotten at least one dose of the vaccine and 46% have completed the two-dose regimen. The total number of children with at least one dose, including those under age 12 who are involved in clinical trials, was about 12 million, the CDC said on its COVID Data Tracker.
Hospitalizations are higher than ever
The recent rise in new child cases has been accompanied by an unprecedented increase in hospitalizations. The daily rate in children aged 0-17 years, which did not surpass 0.30 new admissions per 100,000 population during the worst of the winter surge, had risen to 0.45 per 100,000 by Aug. 26. Since July 4, when the new-admission rate was at its low point of 0.07 per 100,000, hospitalizations in children have jumped by 543%, based on data reported to the CDC by 5,251 hospitals.
A total of 52,245 children were admitted with confirmed COVID-19 from Aug. 1, 2020, when the CDC dataset begins, to Aug. 28, 2021. Those children represent 1.9% of all COVID admissions (2.7 million) in the United States over that period, the CDC said.
Total COVID-related deaths in children are up to 425 in the 48 jurisdictions (45 states, New York City, Puerto Rico, and Guam) that provide mortality data by age, the AAP and the CHA said.
Record-high numbers for the previous 2 reporting weeks – 23 deaths during Aug. 20-26 and 24 deaths during Aug. 13-19, when the previous weekly high was 16 – at least partially reflect the recent addition of South Carolina and New Mexico to the AAP/CHA database, as the two states just started reporting age-related data.
FDA OKs IV Briviact for seizures in kids as young as 1 month
All three brivaracetam formulations (tablets, oral solution, and IV) may now be used. The approval marks the first time that the IV formulation will be available for children, the company said in a news release.
The medication is already approved in the United States as monotherapy and adjunctive therapy in adults with epilepsy.
In an open-label follow-up pediatric study, an estimated 71.4% of patients aged 1 month to 17 years with partial-onset seizures remained on brivaracetam therapy at 1 year, and 64.3% did so at 2 years, the company reported.
“We often see children with seizures hospitalized, so it’s important to have a therapy like Briviact IV that can offer rapid administration in an effective dose when needed and does not require titration,” Raman Sankar, MD, PhD, distinguished professor and chief of pediatric neurology, University of California, Los Angeles, said in the release.
“The availability of the oral dose forms also allows continuity of treatment when these young patients are transitioning from hospital to home,” he added.
Safety profile
Dr. Sankar noted that with approval now of both the IV and oral formulations for partial-onset seizures in such young children, “we have a new option that helps meet a critical need in pediatric epilepsy.”
The most common adverse reactions with brivaracetam include somnolence and sedation, dizziness, fatigue, nausea, and vomiting. In the pediatric clinical trials, the safety profile for pediatric patients was similar to adults.
In the adult trials, psychiatric adverse reactions, including nonpsychotic and psychotic symptoms, were reported in approximately 13% of adults taking at least 50 mg/day of brivaracetam compared with 8% taking placebo.
Psychiatric adverse reactions were also observed in open-label pediatric trials and were generally similar to those observed in adults.
Patients should be advised to report these symptoms immediately to a health care professional, the company noted.
A version of this article first appeared on Medscape.com.
All three brivaracetam formulations (tablets, oral solution, and IV) may now be used. The approval marks the first time that the IV formulation will be available for children, the company said in a news release.
The medication is already approved in the United States as monotherapy and adjunctive therapy in adults with epilepsy.
In an open-label follow-up pediatric study, an estimated 71.4% of patients aged 1 month to 17 years with partial-onset seizures remained on brivaracetam therapy at 1 year, and 64.3% did so at 2 years, the company reported.
“We often see children with seizures hospitalized, so it’s important to have a therapy like Briviact IV that can offer rapid administration in an effective dose when needed and does not require titration,” Raman Sankar, MD, PhD, distinguished professor and chief of pediatric neurology, University of California, Los Angeles, said in the release.
“The availability of the oral dose forms also allows continuity of treatment when these young patients are transitioning from hospital to home,” he added.
Safety profile
Dr. Sankar noted that with approval now of both the IV and oral formulations for partial-onset seizures in such young children, “we have a new option that helps meet a critical need in pediatric epilepsy.”
The most common adverse reactions with brivaracetam include somnolence and sedation, dizziness, fatigue, nausea, and vomiting. In the pediatric clinical trials, the safety profile for pediatric patients was similar to adults.
In the adult trials, psychiatric adverse reactions, including nonpsychotic and psychotic symptoms, were reported in approximately 13% of adults taking at least 50 mg/day of brivaracetam compared with 8% taking placebo.
Psychiatric adverse reactions were also observed in open-label pediatric trials and were generally similar to those observed in adults.
Patients should be advised to report these symptoms immediately to a health care professional, the company noted.
A version of this article first appeared on Medscape.com.
All three brivaracetam formulations (tablets, oral solution, and IV) may now be used. The approval marks the first time that the IV formulation will be available for children, the company said in a news release.
The medication is already approved in the United States as monotherapy and adjunctive therapy in adults with epilepsy.
In an open-label follow-up pediatric study, an estimated 71.4% of patients aged 1 month to 17 years with partial-onset seizures remained on brivaracetam therapy at 1 year, and 64.3% did so at 2 years, the company reported.
“We often see children with seizures hospitalized, so it’s important to have a therapy like Briviact IV that can offer rapid administration in an effective dose when needed and does not require titration,” Raman Sankar, MD, PhD, distinguished professor and chief of pediatric neurology, University of California, Los Angeles, said in the release.
“The availability of the oral dose forms also allows continuity of treatment when these young patients are transitioning from hospital to home,” he added.
Safety profile
Dr. Sankar noted that with approval now of both the IV and oral formulations for partial-onset seizures in such young children, “we have a new option that helps meet a critical need in pediatric epilepsy.”
The most common adverse reactions with brivaracetam include somnolence and sedation, dizziness, fatigue, nausea, and vomiting. In the pediatric clinical trials, the safety profile for pediatric patients was similar to adults.
In the adult trials, psychiatric adverse reactions, including nonpsychotic and psychotic symptoms, were reported in approximately 13% of adults taking at least 50 mg/day of brivaracetam compared with 8% taking placebo.
Psychiatric adverse reactions were also observed in open-label pediatric trials and were generally similar to those observed in adults.
Patients should be advised to report these symptoms immediately to a health care professional, the company noted.
A version of this article first appeared on Medscape.com.
CDC panel unanimously backs Pfizer vax, fortifying FDA approval
An independent expert panel within the Centers for Disease Control and Prevention (CDC) has studied the potential benefits and risks of the Pfizer-BioNTech COVID-19 vaccine and voted unanimously to recommend the shots for all Americans ages 16 and older.
The vaccine was fully approved by the U.S. Food and Drug Administration (FDA) last week.
The inoculation is still available to teens ages 12 to 15 under an emergency use authorization from the FDA.
ACIP now sends its recommendation to the CDC Director Rochelle Walensky, MD, for her sign off.
After reviewing the evidence behind the vaccine, panel member Sarah Long, MD, a professor of pediatrics at Drexel University College of Medicine, Philadelphia, said she couldn’t recall another instance where panelists had so much data on which to base their recommendation.
“This vaccine is worthy of the trust of the American people,” she said.
Doctors across the country use vaccines in line with the recommendations made by the ACIP. Their approval typically means that private and government insurers will cover the cost of the shots. In the case of the COVID-19 vaccines, the government is already picking up the tab.
Few surprises
The panel’s independent review of the vaccine’s effectiveness from nine studies held few surprises.
They found the Pfizer vaccine prevented a COVID infection with symptoms about 90%–92% of the time, at least for the first 4 months after the second shot. Protection against hospitalization and death was even higher.
The vaccine was about 89% effective at preventing a COVID infection without symptoms, according to a pooled estimate of five studies.
The data included in the review was updated only through March 13 of this year, however, and does not reflect the impact of further waning of immunity or the impact of the Delta variant.
In making their recommendation, the panel got an update on the safety of the vaccines, which have now been used in the United States for about 9 months.
The rate of anaphylaxis has settled at around five cases for every million shots given, according to the ACIP’s review of the evidence.
Cases of myocarditis and pericarditis were more common after getting a Pfizer-BioNTech vaccine than would be expected to happen naturally in the general population, but the risk was still very rare, and elevated primarily for men younger than age 30.
Out of 17 million second doses of Pfizer-BioNTech vaccines in the United States, there have been 327 confirmed cases of myocarditis reported to the Vaccine Adverse Event Reporting System in people who are younger than age 30. The average hospital stay for a myocarditis cases is 1 to 2 days.
So far, no one in the United States diagnosed with myocarditis after vaccination has died.
What’s more, the risk of myocarditis after vaccination was dwarfed by the risk of myocarditis after a COVID infection. The risk of myocarditis after a COVID infection was 6 to 34 times higher than the risk after receiving an mRNA vaccine.
About 11% of people who get the vaccine experience a serious reaction to the shot, compared with about 3% in the placebo group. Serious reactions were defined as pain; swelling or redness at the injection site that interferes with activity; needing to visit the hospital or ER for pain; tissue necrosis, or having skin slough off; high fever; vomiting that requires hydration; persistent diarrhea; severe headache; or muscle pain/severe joint pain.
“Safe and effective”
After hearing a presentation on the state of the pandemic in the US, some panel members were struck and shaken that 38% of Americans who are eligible are still not fully vaccinated.
Pablo Sanchez, MD, a pediatrician at Nationwide Children’s Hospital in Columbus, Ohio, said, “We’re doing an abysmal job vaccinating the American people. The message has to go out that the vaccines are safe and effective.”
A version of this story first appeared on Medscape.com.
An independent expert panel within the Centers for Disease Control and Prevention (CDC) has studied the potential benefits and risks of the Pfizer-BioNTech COVID-19 vaccine and voted unanimously to recommend the shots for all Americans ages 16 and older.
The vaccine was fully approved by the U.S. Food and Drug Administration (FDA) last week.
The inoculation is still available to teens ages 12 to 15 under an emergency use authorization from the FDA.
ACIP now sends its recommendation to the CDC Director Rochelle Walensky, MD, for her sign off.
After reviewing the evidence behind the vaccine, panel member Sarah Long, MD, a professor of pediatrics at Drexel University College of Medicine, Philadelphia, said she couldn’t recall another instance where panelists had so much data on which to base their recommendation.
“This vaccine is worthy of the trust of the American people,” she said.
Doctors across the country use vaccines in line with the recommendations made by the ACIP. Their approval typically means that private and government insurers will cover the cost of the shots. In the case of the COVID-19 vaccines, the government is already picking up the tab.
Few surprises
The panel’s independent review of the vaccine’s effectiveness from nine studies held few surprises.
They found the Pfizer vaccine prevented a COVID infection with symptoms about 90%–92% of the time, at least for the first 4 months after the second shot. Protection against hospitalization and death was even higher.
The vaccine was about 89% effective at preventing a COVID infection without symptoms, according to a pooled estimate of five studies.
The data included in the review was updated only through March 13 of this year, however, and does not reflect the impact of further waning of immunity or the impact of the Delta variant.
In making their recommendation, the panel got an update on the safety of the vaccines, which have now been used in the United States for about 9 months.
The rate of anaphylaxis has settled at around five cases for every million shots given, according to the ACIP’s review of the evidence.
Cases of myocarditis and pericarditis were more common after getting a Pfizer-BioNTech vaccine than would be expected to happen naturally in the general population, but the risk was still very rare, and elevated primarily for men younger than age 30.
Out of 17 million second doses of Pfizer-BioNTech vaccines in the United States, there have been 327 confirmed cases of myocarditis reported to the Vaccine Adverse Event Reporting System in people who are younger than age 30. The average hospital stay for a myocarditis cases is 1 to 2 days.
So far, no one in the United States diagnosed with myocarditis after vaccination has died.
What’s more, the risk of myocarditis after vaccination was dwarfed by the risk of myocarditis after a COVID infection. The risk of myocarditis after a COVID infection was 6 to 34 times higher than the risk after receiving an mRNA vaccine.
About 11% of people who get the vaccine experience a serious reaction to the shot, compared with about 3% in the placebo group. Serious reactions were defined as pain; swelling or redness at the injection site that interferes with activity; needing to visit the hospital or ER for pain; tissue necrosis, or having skin slough off; high fever; vomiting that requires hydration; persistent diarrhea; severe headache; or muscle pain/severe joint pain.
“Safe and effective”
After hearing a presentation on the state of the pandemic in the US, some panel members were struck and shaken that 38% of Americans who are eligible are still not fully vaccinated.
Pablo Sanchez, MD, a pediatrician at Nationwide Children’s Hospital in Columbus, Ohio, said, “We’re doing an abysmal job vaccinating the American people. The message has to go out that the vaccines are safe and effective.”
A version of this story first appeared on Medscape.com.
An independent expert panel within the Centers for Disease Control and Prevention (CDC) has studied the potential benefits and risks of the Pfizer-BioNTech COVID-19 vaccine and voted unanimously to recommend the shots for all Americans ages 16 and older.
The vaccine was fully approved by the U.S. Food and Drug Administration (FDA) last week.
The inoculation is still available to teens ages 12 to 15 under an emergency use authorization from the FDA.
ACIP now sends its recommendation to the CDC Director Rochelle Walensky, MD, for her sign off.
After reviewing the evidence behind the vaccine, panel member Sarah Long, MD, a professor of pediatrics at Drexel University College of Medicine, Philadelphia, said she couldn’t recall another instance where panelists had so much data on which to base their recommendation.
“This vaccine is worthy of the trust of the American people,” she said.
Doctors across the country use vaccines in line with the recommendations made by the ACIP. Their approval typically means that private and government insurers will cover the cost of the shots. In the case of the COVID-19 vaccines, the government is already picking up the tab.
Few surprises
The panel’s independent review of the vaccine’s effectiveness from nine studies held few surprises.
They found the Pfizer vaccine prevented a COVID infection with symptoms about 90%–92% of the time, at least for the first 4 months after the second shot. Protection against hospitalization and death was even higher.
The vaccine was about 89% effective at preventing a COVID infection without symptoms, according to a pooled estimate of five studies.
The data included in the review was updated only through March 13 of this year, however, and does not reflect the impact of further waning of immunity or the impact of the Delta variant.
In making their recommendation, the panel got an update on the safety of the vaccines, which have now been used in the United States for about 9 months.
The rate of anaphylaxis has settled at around five cases for every million shots given, according to the ACIP’s review of the evidence.
Cases of myocarditis and pericarditis were more common after getting a Pfizer-BioNTech vaccine than would be expected to happen naturally in the general population, but the risk was still very rare, and elevated primarily for men younger than age 30.
Out of 17 million second doses of Pfizer-BioNTech vaccines in the United States, there have been 327 confirmed cases of myocarditis reported to the Vaccine Adverse Event Reporting System in people who are younger than age 30. The average hospital stay for a myocarditis cases is 1 to 2 days.
So far, no one in the United States diagnosed with myocarditis after vaccination has died.
What’s more, the risk of myocarditis after vaccination was dwarfed by the risk of myocarditis after a COVID infection. The risk of myocarditis after a COVID infection was 6 to 34 times higher than the risk after receiving an mRNA vaccine.
About 11% of people who get the vaccine experience a serious reaction to the shot, compared with about 3% in the placebo group. Serious reactions were defined as pain; swelling or redness at the injection site that interferes with activity; needing to visit the hospital or ER for pain; tissue necrosis, or having skin slough off; high fever; vomiting that requires hydration; persistent diarrhea; severe headache; or muscle pain/severe joint pain.
“Safe and effective”
After hearing a presentation on the state of the pandemic in the US, some panel members were struck and shaken that 38% of Americans who are eligible are still not fully vaccinated.
Pablo Sanchez, MD, a pediatrician at Nationwide Children’s Hospital in Columbus, Ohio, said, “We’re doing an abysmal job vaccinating the American people. The message has to go out that the vaccines are safe and effective.”
A version of this story first appeared on Medscape.com.
Advocates seek to reframe masks as a disability accommodation
As governors and legislatures in states such as Texas, Florida, South Carolina, and Arkansas have banned schools and other entities from implementing mask mandates, disability rights advocates have pushed back. In federal civil rights lawsuits, they argue that bans on mask mandates violate antidiscrimination laws protecting people with disabilities.

For unvaccinated and immunosuppressed individuals, masks can provide crucial protection from SARS-CoV-2.
argues Mical Raz, MD, PhD, a professor at the University of Rochester (N.Y.) and a physician at Strong Memorial Hospital, also in Rochester, New York, in an article published in JAMA with coauthor Doron Dorfman, LLB, JSD.
This news organization talked with Dr. Raz about approaching mask requirements as disability accommodation during the COVID-19 pandemic. The following interview was lightly edited for length and clarity.
How did you come to think about mask requirements as a form of disability accommodation?
I saw a tweet from a professor at a university who said they couldn’t ask students about their vaccination status or to wear a mask. All agency was removed from the professor to take care of and protect themselves. I thought, well, that can’t be right. And ostensibly, that would be particularly dangerous for somebody with immunosuppression for whom the vaccine is not adequately protective. So, I called my friend, Doron Dorfman, and asked him to help me think through the legal part of this. We fleshed it out and wrote the article that same night.
How novel is it to view accommodations for people who are immunosuppressed through the lens of disability accommodation?
I think there has not been enough focus during the pandemic on individuals with disabilities or on how disability law can be mobilized during this pandemic to help supplement the public health law. This framework should be used a lot more because it’s good for everybody, not just for individuals with disabilities.
For example, take what’s called the “curb effect.” If you expand sidewalks, yes, it helps individuals who use a wheelchair. But it also helps me as a mom with a stroller. It helps somebody with a shopping cart, or a kid with a bike. If we adopt policies that are inclusive to those who are disadvantaged, it’s good for everybody. We should always strive to be an inclusive society, not just because it’s the right thing to do but because it really makes our society better.
How can mask requirements be used as a form of disability accommodation, as you argue in the JAMA article?
The ADA requires employers to provide reasonable accommodations for disability. In this case, the disability is your immunosuppressive status. We have an abundance of evidence showing individuals who are immunocompromised and vaccinated are still inadequately protected from the SARS-CoV-2 virus. So, there is absolute data to show individuals with immunosuppression have a disability that requires accommodation.
The ADA has a mandate requiring employers to adjust or modify policies in order to accommodate a disability. There are certain situations in which you cannot or do not need to accommodate a disability, when it would fundamentally alter the kind of employment you offer or if it’s an undue burden or hardship. But given that we’ve been wearing masks and working remotely for a year now, arguing that somehow these accommodations are no longer possible seems disingenuous.
In that way, allowing a person who’s immunocompromised to require those around them to mask is a form of modified protective policies. And in this case, those policies line up with a public health good, masking in the face of the highly contagious Delta variant ravaging our country right now.
In your view, can this argument be used in the mask debates happening right now across the country?
This argument can and should be useful for a couple of different lawsuits that are now underway in different states. I hope our article will provide further support for those suits. And I hope in school board hearings, when parents and teachers are talking about their concerns, this could be one way to argue for why we should allow mask mandates in classes. I’ve received emails from parents who said they’re going to bring this article to their school board hearing.
I also hope this could shift the narrative around the pandemic. Instead of focusing on individual responsibility – I got my vaccine shot so I’m fine – let’s focus on how we create an inclusive environment where we protect everybody, including those who cannot be vaccinated because of age or disability, or those who are vaccinated but inadequately protected because of their underlying conditions.
In the JAMA article, you talk about how our pandemic response has focused on individual health and how that individual focus can be ableist. Can you explain that point?
I think this idea that we just make our choices – like whether to get vaccinated or wear a mask, or not – and live with it really perpetuates a highly individualistic and ableist mindset. It doesn’t consider the people I admit to the hospital who are vaccinated but have a heart transplant and didn’t mount the sufficient immune response. Or even the people who chose not to be vaccinated because they were exposed to hours and hours of misinformation on TV.
We like to individualize everything, focusing on personal responsibility and choices, but a pandemic is one of those moments where everybody’s choices affect everybody else. Laying responsibility at the doorstep of each person, rather than thinking about what steps we as a society could be taking, is cheap and politically expedient. There is no public health rationale behind the bans on mask requirements in states like Texas, Iowa, and Florida. These choices are about politics. And the price is always borne by the most disadvantaged among us.
A version of this article first appeared on Medscape.com.
As governors and legislatures in states such as Texas, Florida, South Carolina, and Arkansas have banned schools and other entities from implementing mask mandates, disability rights advocates have pushed back. In federal civil rights lawsuits, they argue that bans on mask mandates violate antidiscrimination laws protecting people with disabilities.
For unvaccinated and immunosuppressed individuals, masks can provide crucial protection from SARS-CoV-2.
argues Mical Raz, MD, PhD, a professor at the University of Rochester (N.Y.) and a physician at Strong Memorial Hospital, also in Rochester, New York, in an article published in JAMA with coauthor Doron Dorfman, LLB, JSD.
This news organization talked with Dr. Raz about approaching mask requirements as disability accommodation during the COVID-19 pandemic. The following interview was lightly edited for length and clarity.
How did you come to think about mask requirements as a form of disability accommodation?
I saw a tweet from a professor at a university who said they couldn’t ask students about their vaccination status or to wear a mask. All agency was removed from the professor to take care of and protect themselves. I thought, well, that can’t be right. And ostensibly, that would be particularly dangerous for somebody with immunosuppression for whom the vaccine is not adequately protective. So, I called my friend, Doron Dorfman, and asked him to help me think through the legal part of this. We fleshed it out and wrote the article that same night.
How novel is it to view accommodations for people who are immunosuppressed through the lens of disability accommodation?
I think there has not been enough focus during the pandemic on individuals with disabilities or on how disability law can be mobilized during this pandemic to help supplement the public health law. This framework should be used a lot more because it’s good for everybody, not just for individuals with disabilities.
For example, take what’s called the “curb effect.” If you expand sidewalks, yes, it helps individuals who use a wheelchair. But it also helps me as a mom with a stroller. It helps somebody with a shopping cart, or a kid with a bike. If we adopt policies that are inclusive to those who are disadvantaged, it’s good for everybody. We should always strive to be an inclusive society, not just because it’s the right thing to do but because it really makes our society better.
How can mask requirements be used as a form of disability accommodation, as you argue in the JAMA article?
The ADA requires employers to provide reasonable accommodations for disability. In this case, the disability is your immunosuppressive status. We have an abundance of evidence showing individuals who are immunocompromised and vaccinated are still inadequately protected from the SARS-CoV-2 virus. So, there is absolute data to show individuals with immunosuppression have a disability that requires accommodation.
The ADA has a mandate requiring employers to adjust or modify policies in order to accommodate a disability. There are certain situations in which you cannot or do not need to accommodate a disability, when it would fundamentally alter the kind of employment you offer or if it’s an undue burden or hardship. But given that we’ve been wearing masks and working remotely for a year now, arguing that somehow these accommodations are no longer possible seems disingenuous.
In that way, allowing a person who’s immunocompromised to require those around them to mask is a form of modified protective policies. And in this case, those policies line up with a public health good, masking in the face of the highly contagious Delta variant ravaging our country right now.
In your view, can this argument be used in the mask debates happening right now across the country?
This argument can and should be useful for a couple of different lawsuits that are now underway in different states. I hope our article will provide further support for those suits. And I hope in school board hearings, when parents and teachers are talking about their concerns, this could be one way to argue for why we should allow mask mandates in classes. I’ve received emails from parents who said they’re going to bring this article to their school board hearing.
I also hope this could shift the narrative around the pandemic. Instead of focusing on individual responsibility – I got my vaccine shot so I’m fine – let’s focus on how we create an inclusive environment where we protect everybody, including those who cannot be vaccinated because of age or disability, or those who are vaccinated but inadequately protected because of their underlying conditions.
In the JAMA article, you talk about how our pandemic response has focused on individual health and how that individual focus can be ableist. Can you explain that point?
I think this idea that we just make our choices – like whether to get vaccinated or wear a mask, or not – and live with it really perpetuates a highly individualistic and ableist mindset. It doesn’t consider the people I admit to the hospital who are vaccinated but have a heart transplant and didn’t mount the sufficient immune response. Or even the people who chose not to be vaccinated because they were exposed to hours and hours of misinformation on TV.
We like to individualize everything, focusing on personal responsibility and choices, but a pandemic is one of those moments where everybody’s choices affect everybody else. Laying responsibility at the doorstep of each person, rather than thinking about what steps we as a society could be taking, is cheap and politically expedient. There is no public health rationale behind the bans on mask requirements in states like Texas, Iowa, and Florida. These choices are about politics. And the price is always borne by the most disadvantaged among us.
A version of this article first appeared on Medscape.com.
As governors and legislatures in states such as Texas, Florida, South Carolina, and Arkansas have banned schools and other entities from implementing mask mandates, disability rights advocates have pushed back. In federal civil rights lawsuits, they argue that bans on mask mandates violate antidiscrimination laws protecting people with disabilities.
For unvaccinated and immunosuppressed individuals, masks can provide crucial protection from SARS-CoV-2.
argues Mical Raz, MD, PhD, a professor at the University of Rochester (N.Y.) and a physician at Strong Memorial Hospital, also in Rochester, New York, in an article published in JAMA with coauthor Doron Dorfman, LLB, JSD.
This news organization talked with Dr. Raz about approaching mask requirements as disability accommodation during the COVID-19 pandemic. The following interview was lightly edited for length and clarity.
How did you come to think about mask requirements as a form of disability accommodation?
I saw a tweet from a professor at a university who said they couldn’t ask students about their vaccination status or to wear a mask. All agency was removed from the professor to take care of and protect themselves. I thought, well, that can’t be right. And ostensibly, that would be particularly dangerous for somebody with immunosuppression for whom the vaccine is not adequately protective. So, I called my friend, Doron Dorfman, and asked him to help me think through the legal part of this. We fleshed it out and wrote the article that same night.
How novel is it to view accommodations for people who are immunosuppressed through the lens of disability accommodation?
I think there has not been enough focus during the pandemic on individuals with disabilities or on how disability law can be mobilized during this pandemic to help supplement the public health law. This framework should be used a lot more because it’s good for everybody, not just for individuals with disabilities.
For example, take what’s called the “curb effect.” If you expand sidewalks, yes, it helps individuals who use a wheelchair. But it also helps me as a mom with a stroller. It helps somebody with a shopping cart, or a kid with a bike. If we adopt policies that are inclusive to those who are disadvantaged, it’s good for everybody. We should always strive to be an inclusive society, not just because it’s the right thing to do but because it really makes our society better.
How can mask requirements be used as a form of disability accommodation, as you argue in the JAMA article?
The ADA requires employers to provide reasonable accommodations for disability. In this case, the disability is your immunosuppressive status. We have an abundance of evidence showing individuals who are immunocompromised and vaccinated are still inadequately protected from the SARS-CoV-2 virus. So, there is absolute data to show individuals with immunosuppression have a disability that requires accommodation.
The ADA has a mandate requiring employers to adjust or modify policies in order to accommodate a disability. There are certain situations in which you cannot or do not need to accommodate a disability, when it would fundamentally alter the kind of employment you offer or if it’s an undue burden or hardship. But given that we’ve been wearing masks and working remotely for a year now, arguing that somehow these accommodations are no longer possible seems disingenuous.
In that way, allowing a person who’s immunocompromised to require those around them to mask is a form of modified protective policies. And in this case, those policies line up with a public health good, masking in the face of the highly contagious Delta variant ravaging our country right now.
In your view, can this argument be used in the mask debates happening right now across the country?
This argument can and should be useful for a couple of different lawsuits that are now underway in different states. I hope our article will provide further support for those suits. And I hope in school board hearings, when parents and teachers are talking about their concerns, this could be one way to argue for why we should allow mask mandates in classes. I’ve received emails from parents who said they’re going to bring this article to their school board hearing.
I also hope this could shift the narrative around the pandemic. Instead of focusing on individual responsibility – I got my vaccine shot so I’m fine – let’s focus on how we create an inclusive environment where we protect everybody, including those who cannot be vaccinated because of age or disability, or those who are vaccinated but inadequately protected because of their underlying conditions.
In the JAMA article, you talk about how our pandemic response has focused on individual health and how that individual focus can be ableist. Can you explain that point?
I think this idea that we just make our choices – like whether to get vaccinated or wear a mask, or not – and live with it really perpetuates a highly individualistic and ableist mindset. It doesn’t consider the people I admit to the hospital who are vaccinated but have a heart transplant and didn’t mount the sufficient immune response. Or even the people who chose not to be vaccinated because they were exposed to hours and hours of misinformation on TV.
We like to individualize everything, focusing on personal responsibility and choices, but a pandemic is one of those moments where everybody’s choices affect everybody else. Laying responsibility at the doorstep of each person, rather than thinking about what steps we as a society could be taking, is cheap and politically expedient. There is no public health rationale behind the bans on mask requirements in states like Texas, Iowa, and Florida. These choices are about politics. And the price is always borne by the most disadvantaged among us.
A version of this article first appeared on Medscape.com.
The secret I’ll take to my grave: Doc reveals
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
MRI is a poor disability predictor in secondary progressive MS
, new research suggests. Analysis from the phase 3 ASCEND trial of nearly 900 patients showed that MRI measures were not associated with worsening of scores on the Expanded Disability Status Scale (EDSS), the most widely used physical outcome measure.
The few associations that were shown between MRI measures and clinical outcomes “were with the newer and possibly more sensitive outcomes” – the Timed 25-Foot Walk (T25FW) and Nine-Hole Peg Test (NHPT), wrote the investigators, led by Marcus W. Koch, MD, PhD, associate professor of neurology in the MS program at the University of Calgary, Canada.
However, “it is unclear if these associations are clinically meaningful,” they added.
Worsening on the NHPT at 48 weeks was associated with a 0.86% loss in normalized brain volume; worsening at 96 weeks was associated with a 1.47% loss.
The findings were published online July 26 in the Multiple Sclerosis Journal.
ASCEND data analysis
Although brain volume loss occurs in all forms of MS, it is believed to be particularly relevant in SPMS. Clinical trials often use MRI measures of brain volume as endpoints, likely on the assumption that these measures indicate worsening disability.
However, brain volume loss proceeds slowly. Changes that occur during the typical 2-year study period may not be associated with significant physical or cognitive disability.
In the current study, investigators examined data from the ASCEND trial, which assessed the use of natalizumab for patients with SPMS, to examine these potential associations. Eligible participants in ASCEND were between ages 18 and 58 years, had had SPMS for 2 or more years, had had disability progression during the previous year, and had an EDSS score between 3.0 and 6.5 at baseline.
Participants underwent gadolinium-enhanced cranial MRI at screening and at 24, 48, 72, and 96 weeks. MRI outcomes included normalized brain volume, normalized cortical gray matter volume, and normalized whole gray matter volume. The ASCEND investigators also examined the number and volume of T2 and contrast-enhancing lesions.
The study’s clinical outcomes included scores on the EDSS, T25FW, and NHPT, which were administered at baseline and every 12 weeks thereafter. Participants also underwent the Symbol Digit Modalities Test (SDMT), which is a cognitive assessment, at baseline and every 4 weeks thereafter. In addition, 3-month confirmed disability progression was measured every 12 weeks.
Few significant associations
The investigators’ analysis included 889 patients (61.9% women; median age, 48 years). The median EDSS score at screening was 6.
Brain volume measures decreased consistently during follow-up. Mean volume loss at 96 weeks was about 1%. In contrast, T2 lesion volume changed little during follow-up. The cumulative number of contrast-enhancing lesions and the cumulative number of new or newly enlarging T2 lesions increased steadily during follow-up.
For an increasing number of participants, scores on the EDSS, NHPT, and T25FW worsened significantly during follow-up. Performance on SDMT, however, changed little. Of all the clinical measures, the NHPT was most consistently associated with MRI measures.
Among patients whose NHPT score worsened at 48 weeks, there was greater loss of normalized brain volume (0.86%, P = .02), normalized cortical gray matter volume (1.15%, P = .03), and normalized whole gray matter volume (1.08%, P = .03) than among those whose NHPT score did not worsen.
Among patients whose NHPT score worsened at 96 weeks, there was greater normalized brain volume loss (1.47%, P = .002), greater increase in T2 lesion volume (4.68%, P = .02), and a greater number of cumulative new or newly enlarging T2 lesions (7.81, P = .03) than those whose NHPT score did not worsen.
After adjusting the data for covariables, the investigators found few significant associations between MRI measures and clinical outcomes. Worsening on the EDSS and SDMT was not associated with any MRI outcome.
Important disability contributors missed
The odds ratio of 3-month confirmed worsening on the T25FW at 96 weeks was 2.25 for patients with more than 10 cumulative new or newly enlarging T2 lesions (P = .03). The OR of 3-month confirmed worsening on the NHPT at 96 weeks was 3.04 for patients with more than 10 such lesions (P = .03).
Greater normalized brain volume loss at 48 weeks was associated with a greater risk for worsening disability on the NHPT at 48 and 96 weeks. For patients with a volume loss greater than 1.5%, the OR of worsening NHPT at 96 weeks was 4.69 (P = .05).
Although previous cross-sectional studies have shown correlations between brain volume and cognitive dysfunction, the current investigators found no association between change in SDMT performance and MRI measures.
From the ASCEND dataset, they found that performance on the SDMT unexpectedly improved with time, perhaps because of a practice effect.
“The SDMT may therefore not adequately reflect the steady cognitive decline that people with SPMS experience,” the investigators wrote.
The lack of association between MRI measures and clinical outcomes may indicate that traditional MRI does not measure important contributors to disability, they noted.
“Although the investigated volume measures in this study are currently the most commonly used in clinical trials, newer MRI metrics such as thalamic or corpus callosum atrophy may have a closer relation to clinical outcome,” they added.
‘Interesting and provocative’
Commenting on the findings, E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children, Toronto, called the study “interesting and provocative.”
“Other studies previously have shown associations between disability and progression, but many have been cross-sectional,” said Dr. Yeh, who was not involved with the research.
The current study is longitudinal and analyzes carefully documented follow-up data from a clinical trial, she noted. However, the 2-year follow-up period was short, considering the pace at which whole brain volume change occurs, Dr. Yeh said.
Some patients with MS have greater brain volume loss than others. Because of this variability, researchers often examine a population’s average brain volume loss. “When you look at averages, it makes it more difficult to understand if the larger brain volume losses are actually associated with change,” said Dr. Yeh.
She noted that because the study population had high EDSS scores at baseline, it is not surprising that the NHPT and the T25FW were more strongly associated with change in brain volume than the EDSS was. Large changes in EDSS score probably did not occur during follow-up, she added.
“We’ll continue to use the EDSS, because it’s what we have,” said Dr. Yeh. However, newer measures, such as the NHPT and the T25FW, may provide better information, she said. Similarly, composite measures of cognition, such as the Brief International Cognitive Assessment for MS, may be superior to the SDMT but take longer to administer.
“We need to look more deeply at which MRI measures are the best for predicting outcome and that correlate well in a short period of time,” said Dr. Yeh.
These measures could include specific regional brain volumes “and more advanced measures that look at axonal injury or axonal loss.” Studies with longer follow-up are also necessary, she concluded.
The investigators and Dr. Yeh have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Analysis from the phase 3 ASCEND trial of nearly 900 patients showed that MRI measures were not associated with worsening of scores on the Expanded Disability Status Scale (EDSS), the most widely used physical outcome measure.
The few associations that were shown between MRI measures and clinical outcomes “were with the newer and possibly more sensitive outcomes” – the Timed 25-Foot Walk (T25FW) and Nine-Hole Peg Test (NHPT), wrote the investigators, led by Marcus W. Koch, MD, PhD, associate professor of neurology in the MS program at the University of Calgary, Canada.
However, “it is unclear if these associations are clinically meaningful,” they added.
Worsening on the NHPT at 48 weeks was associated with a 0.86% loss in normalized brain volume; worsening at 96 weeks was associated with a 1.47% loss.
The findings were published online July 26 in the Multiple Sclerosis Journal.
ASCEND data analysis
Although brain volume loss occurs in all forms of MS, it is believed to be particularly relevant in SPMS. Clinical trials often use MRI measures of brain volume as endpoints, likely on the assumption that these measures indicate worsening disability.
However, brain volume loss proceeds slowly. Changes that occur during the typical 2-year study period may not be associated with significant physical or cognitive disability.
In the current study, investigators examined data from the ASCEND trial, which assessed the use of natalizumab for patients with SPMS, to examine these potential associations. Eligible participants in ASCEND were between ages 18 and 58 years, had had SPMS for 2 or more years, had had disability progression during the previous year, and had an EDSS score between 3.0 and 6.5 at baseline.
Participants underwent gadolinium-enhanced cranial MRI at screening and at 24, 48, 72, and 96 weeks. MRI outcomes included normalized brain volume, normalized cortical gray matter volume, and normalized whole gray matter volume. The ASCEND investigators also examined the number and volume of T2 and contrast-enhancing lesions.
The study’s clinical outcomes included scores on the EDSS, T25FW, and NHPT, which were administered at baseline and every 12 weeks thereafter. Participants also underwent the Symbol Digit Modalities Test (SDMT), which is a cognitive assessment, at baseline and every 4 weeks thereafter. In addition, 3-month confirmed disability progression was measured every 12 weeks.
Few significant associations
The investigators’ analysis included 889 patients (61.9% women; median age, 48 years). The median EDSS score at screening was 6.
Brain volume measures decreased consistently during follow-up. Mean volume loss at 96 weeks was about 1%. In contrast, T2 lesion volume changed little during follow-up. The cumulative number of contrast-enhancing lesions and the cumulative number of new or newly enlarging T2 lesions increased steadily during follow-up.
For an increasing number of participants, scores on the EDSS, NHPT, and T25FW worsened significantly during follow-up. Performance on SDMT, however, changed little. Of all the clinical measures, the NHPT was most consistently associated with MRI measures.
Among patients whose NHPT score worsened at 48 weeks, there was greater loss of normalized brain volume (0.86%, P = .02), normalized cortical gray matter volume (1.15%, P = .03), and normalized whole gray matter volume (1.08%, P = .03) than among those whose NHPT score did not worsen.
Among patients whose NHPT score worsened at 96 weeks, there was greater normalized brain volume loss (1.47%, P = .002), greater increase in T2 lesion volume (4.68%, P = .02), and a greater number of cumulative new or newly enlarging T2 lesions (7.81, P = .03) than those whose NHPT score did not worsen.
After adjusting the data for covariables, the investigators found few significant associations between MRI measures and clinical outcomes. Worsening on the EDSS and SDMT was not associated with any MRI outcome.
Important disability contributors missed
The odds ratio of 3-month confirmed worsening on the T25FW at 96 weeks was 2.25 for patients with more than 10 cumulative new or newly enlarging T2 lesions (P = .03). The OR of 3-month confirmed worsening on the NHPT at 96 weeks was 3.04 for patients with more than 10 such lesions (P = .03).
Greater normalized brain volume loss at 48 weeks was associated with a greater risk for worsening disability on the NHPT at 48 and 96 weeks. For patients with a volume loss greater than 1.5%, the OR of worsening NHPT at 96 weeks was 4.69 (P = .05).
Although previous cross-sectional studies have shown correlations between brain volume and cognitive dysfunction, the current investigators found no association between change in SDMT performance and MRI measures.
From the ASCEND dataset, they found that performance on the SDMT unexpectedly improved with time, perhaps because of a practice effect.
“The SDMT may therefore not adequately reflect the steady cognitive decline that people with SPMS experience,” the investigators wrote.
The lack of association between MRI measures and clinical outcomes may indicate that traditional MRI does not measure important contributors to disability, they noted.
“Although the investigated volume measures in this study are currently the most commonly used in clinical trials, newer MRI metrics such as thalamic or corpus callosum atrophy may have a closer relation to clinical outcome,” they added.
‘Interesting and provocative’
Commenting on the findings, E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children, Toronto, called the study “interesting and provocative.”
“Other studies previously have shown associations between disability and progression, but many have been cross-sectional,” said Dr. Yeh, who was not involved with the research.
The current study is longitudinal and analyzes carefully documented follow-up data from a clinical trial, she noted. However, the 2-year follow-up period was short, considering the pace at which whole brain volume change occurs, Dr. Yeh said.
Some patients with MS have greater brain volume loss than others. Because of this variability, researchers often examine a population’s average brain volume loss. “When you look at averages, it makes it more difficult to understand if the larger brain volume losses are actually associated with change,” said Dr. Yeh.
She noted that because the study population had high EDSS scores at baseline, it is not surprising that the NHPT and the T25FW were more strongly associated with change in brain volume than the EDSS was. Large changes in EDSS score probably did not occur during follow-up, she added.
“We’ll continue to use the EDSS, because it’s what we have,” said Dr. Yeh. However, newer measures, such as the NHPT and the T25FW, may provide better information, she said. Similarly, composite measures of cognition, such as the Brief International Cognitive Assessment for MS, may be superior to the SDMT but take longer to administer.
“We need to look more deeply at which MRI measures are the best for predicting outcome and that correlate well in a short period of time,” said Dr. Yeh.
These measures could include specific regional brain volumes “and more advanced measures that look at axonal injury or axonal loss.” Studies with longer follow-up are also necessary, she concluded.
The investigators and Dr. Yeh have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. Analysis from the phase 3 ASCEND trial of nearly 900 patients showed that MRI measures were not associated with worsening of scores on the Expanded Disability Status Scale (EDSS), the most widely used physical outcome measure.
The few associations that were shown between MRI measures and clinical outcomes “were with the newer and possibly more sensitive outcomes” – the Timed 25-Foot Walk (T25FW) and Nine-Hole Peg Test (NHPT), wrote the investigators, led by Marcus W. Koch, MD, PhD, associate professor of neurology in the MS program at the University of Calgary, Canada.
However, “it is unclear if these associations are clinically meaningful,” they added.
Worsening on the NHPT at 48 weeks was associated with a 0.86% loss in normalized brain volume; worsening at 96 weeks was associated with a 1.47% loss.
The findings were published online July 26 in the Multiple Sclerosis Journal.
ASCEND data analysis
Although brain volume loss occurs in all forms of MS, it is believed to be particularly relevant in SPMS. Clinical trials often use MRI measures of brain volume as endpoints, likely on the assumption that these measures indicate worsening disability.
However, brain volume loss proceeds slowly. Changes that occur during the typical 2-year study period may not be associated with significant physical or cognitive disability.
In the current study, investigators examined data from the ASCEND trial, which assessed the use of natalizumab for patients with SPMS, to examine these potential associations. Eligible participants in ASCEND were between ages 18 and 58 years, had had SPMS for 2 or more years, had had disability progression during the previous year, and had an EDSS score between 3.0 and 6.5 at baseline.
Participants underwent gadolinium-enhanced cranial MRI at screening and at 24, 48, 72, and 96 weeks. MRI outcomes included normalized brain volume, normalized cortical gray matter volume, and normalized whole gray matter volume. The ASCEND investigators also examined the number and volume of T2 and contrast-enhancing lesions.
The study’s clinical outcomes included scores on the EDSS, T25FW, and NHPT, which were administered at baseline and every 12 weeks thereafter. Participants also underwent the Symbol Digit Modalities Test (SDMT), which is a cognitive assessment, at baseline and every 4 weeks thereafter. In addition, 3-month confirmed disability progression was measured every 12 weeks.
Few significant associations
The investigators’ analysis included 889 patients (61.9% women; median age, 48 years). The median EDSS score at screening was 6.
Brain volume measures decreased consistently during follow-up. Mean volume loss at 96 weeks was about 1%. In contrast, T2 lesion volume changed little during follow-up. The cumulative number of contrast-enhancing lesions and the cumulative number of new or newly enlarging T2 lesions increased steadily during follow-up.
For an increasing number of participants, scores on the EDSS, NHPT, and T25FW worsened significantly during follow-up. Performance on SDMT, however, changed little. Of all the clinical measures, the NHPT was most consistently associated with MRI measures.
Among patients whose NHPT score worsened at 48 weeks, there was greater loss of normalized brain volume (0.86%, P = .02), normalized cortical gray matter volume (1.15%, P = .03), and normalized whole gray matter volume (1.08%, P = .03) than among those whose NHPT score did not worsen.
Among patients whose NHPT score worsened at 96 weeks, there was greater normalized brain volume loss (1.47%, P = .002), greater increase in T2 lesion volume (4.68%, P = .02), and a greater number of cumulative new or newly enlarging T2 lesions (7.81, P = .03) than those whose NHPT score did not worsen.
After adjusting the data for covariables, the investigators found few significant associations between MRI measures and clinical outcomes. Worsening on the EDSS and SDMT was not associated with any MRI outcome.
Important disability contributors missed
The odds ratio of 3-month confirmed worsening on the T25FW at 96 weeks was 2.25 for patients with more than 10 cumulative new or newly enlarging T2 lesions (P = .03). The OR of 3-month confirmed worsening on the NHPT at 96 weeks was 3.04 for patients with more than 10 such lesions (P = .03).
Greater normalized brain volume loss at 48 weeks was associated with a greater risk for worsening disability on the NHPT at 48 and 96 weeks. For patients with a volume loss greater than 1.5%, the OR of worsening NHPT at 96 weeks was 4.69 (P = .05).
Although previous cross-sectional studies have shown correlations between brain volume and cognitive dysfunction, the current investigators found no association between change in SDMT performance and MRI measures.
From the ASCEND dataset, they found that performance on the SDMT unexpectedly improved with time, perhaps because of a practice effect.
“The SDMT may therefore not adequately reflect the steady cognitive decline that people with SPMS experience,” the investigators wrote.
The lack of association between MRI measures and clinical outcomes may indicate that traditional MRI does not measure important contributors to disability, they noted.
“Although the investigated volume measures in this study are currently the most commonly used in clinical trials, newer MRI metrics such as thalamic or corpus callosum atrophy may have a closer relation to clinical outcome,” they added.
‘Interesting and provocative’
Commenting on the findings, E. Ann Yeh, MD, director of the Pediatric MS and Neuroinflammatory Disorders Program at the Hospital for Sick Children, Toronto, called the study “interesting and provocative.”
“Other studies previously have shown associations between disability and progression, but many have been cross-sectional,” said Dr. Yeh, who was not involved with the research.
The current study is longitudinal and analyzes carefully documented follow-up data from a clinical trial, she noted. However, the 2-year follow-up period was short, considering the pace at which whole brain volume change occurs, Dr. Yeh said.
Some patients with MS have greater brain volume loss than others. Because of this variability, researchers often examine a population’s average brain volume loss. “When you look at averages, it makes it more difficult to understand if the larger brain volume losses are actually associated with change,” said Dr. Yeh.
She noted that because the study population had high EDSS scores at baseline, it is not surprising that the NHPT and the T25FW were more strongly associated with change in brain volume than the EDSS was. Large changes in EDSS score probably did not occur during follow-up, she added.
“We’ll continue to use the EDSS, because it’s what we have,” said Dr. Yeh. However, newer measures, such as the NHPT and the T25FW, may provide better information, she said. Similarly, composite measures of cognition, such as the Brief International Cognitive Assessment for MS, may be superior to the SDMT but take longer to administer.
“We need to look more deeply at which MRI measures are the best for predicting outcome and that correlate well in a short period of time,” said Dr. Yeh.
These measures could include specific regional brain volumes “and more advanced measures that look at axonal injury or axonal loss.” Studies with longer follow-up are also necessary, she concluded.
The investigators and Dr. Yeh have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From Multiple Sclerosis Journal