User login
Children and COVID: New cases topped 200,000 after 3 weeks of declines
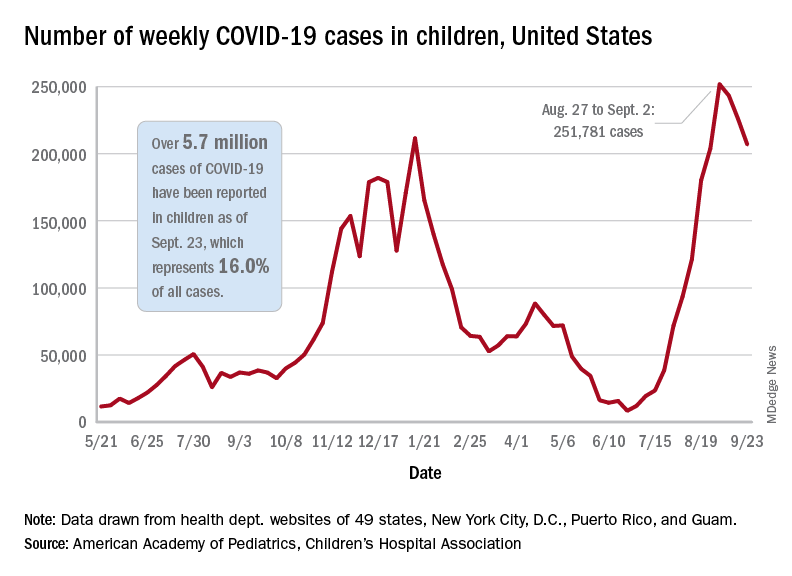
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Polyethylene glycol linked to rare allergic reactions seen with mRNA COVID-19 vaccines
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VA to Provide Services to Veterans With ‘Don’t Ask, Don’t Tell’ Discharges
The US Department of Veterans Affairs (VA) has issued a new policy statement to help ensure that active-duty service members who were discharged for their sexual orientation under the Don’t Ask, Don’t Tell policy will be able to receive full VA benefits.
“[A] great injustice was remedied and a tremendous weight was finally lifted off the shoulders of tens of thousands of dedicated American service members,” President Biden said on September 20 as the country commemorated the 10th anniversary of the repeal of “Don’t Ask, Don’t Tell,” the policy that barred lesbian, gay, bisexual, transgender, and queer (LGBTQ+) service members from serving openly.
Prior to DADT, if active-duty service members spoke out about their sexual orientation, they ran the risk of being hounded, shunned, in some cases assaulted, and discharged. If they kept it a secret, they felt they were living a lie, unable to be their whole selves. More than 100,000 were discharged because of their sexual orientation or gender identity.
Although Don’t Ask, Don’t Tell was a “compromise” law that purposed to protect them, LGBTQ+ service members were still at risk for harassment and abuse. Nor did the law protect them from discharge. Some 14,000 LGBTQ+ service members were discharged while DADT was in effect. And those who received “other than honorable” (OTH) discharges could be excluded from receiving services and benefits.
The 2011 repeal followed a “hard-fought battle,” said a release from the Human Rights Campaign, which led a coalition of members, supporters, elected officials, 70+ organizations, and 20,000 veterans to get the law overturned. HRC staff coordinated grassroots efforts and sent 19 million e-mails to members and supporters, in turn generating an “unprecedented” 625,000 e-mails and 50,000 handwritten letters to members of Congress.
After the repeal, the VA began the long process of inclusion for LGBTQ+ veterans. “At VA, we continuously work not only to meet the needs of LGBTQ+ veterans, but also to address ongoing issues that LGBTQ+ veterans face as a result of the military’s decades-long official policy of homophobia and transphobia,” Kayla Williams, assistant secretary for public affairs in VA’s Office of Public and Intergovernmental Affairs wrote in the Secretary’s blog.
The VA “recognizes that the trauma caused by the military’s decades-long policy of discrimination against LGBTQ+ people cannot be undone in a few short months,” she continued, but the Biden administration and Secretary McDonough are “taking the steps necessary to begin addressing the pain that such policies have created.”
President Biden, in his remarks, noted that as a US Senator, he had supported allowing service members to serve openly and, as Vice President, championed the repeal. He said, “I am honored to be Commander-in-Chief of the strongest and most inclusive military in our nation’s history. Today, our military doesn’t just welcome LGBTQ+ service members—it is led at the highest levels by brave LGBTQ+ veterans, including Under Secretary of the Air Force Gina Ortiz Jones and Assistant Secretary of Defense for Readiness Shawn Skelly, who served under Don’t Ask, Don’t Tell. I was gratified to appoint the first openly gay Senate-confirmed Cabinet member, Secretary Pete Buttigieg, a lieutenant in the U.S. Navy Reserve and Afghanistan veteran who joined the military under the Don’t Ask, Don’t Tell policy. And during my first week in office, I proudly delivered on my pledge to repeal the discriminatory ban on open service by patriotic transgender service members.”
In early September, Rep. Chris Pappas (D-NH), a member of the House Veterans Affairs Committee and Co-Chair of the Equality Caucus, reintroduced the SERVE (Securing the Rights our Veterans Earned) Act. The act, which is co-sponsored by Reps. Mike Levin (D-CA), Kathleen Rice (D-NY), Anthony Brown (D-MD), and Jackie Speier (D-CA), would ensure LGBTQ+ veterans who received an OTH or Entry-Level Separation discharge solely due to sexual orientation or gender identity are afforded the VA benefits they rightfully earned, including access to VA healthcare, and education, burial and memorial services, and home loans. The act includes veterans who were issued “blue discharges” during World War II and veterans discharged under former President Trump’s ban on transgender service members. The legislation has been endorsed by the Congressional LGBTQ+ Equality Caucus and is supported by more than 45 representatives.
There are processes for those veterans through which they can have their discharge papers and separation statuses reviewed and modified, Pappas said in a release, but “it can take months for the changes to take effect, and many of these veterans do not even realize they are eligible.”
Earlier this year, Veterans Affairs Secretary Denis McDonough made it a priority to ensure that LGBTQ+ veterans have the same level of access to VA care and services that all other veterans have. Among other things, he established a task force to examine how VA policies hinder or prohibit access to care and services and remove barriers that transgender veterans face in accessing gender-affirming care.
The VA is also taking steps, Williams noted, to clarify VA policy for veterans who were given OTH discharges based on homosexual conduct, gender identity or HIV status. Under this newly issued guidance, VA adjudicators shall find that all discharged service members whose separation was due to sexual orientation, gender identity or HIV status are considered “Veterans” who may be eligible for VA benefits, like VR&E, home loan guaranty, compensation and pension, health care, homeless program and/or burial benefits, so long as the record does not implicate a statutory or regulatory bar to benefits.
The policy statement does not represent a change in law, as veterans who were discharged under DADT alone have been generally eligible for benefits under current statute and regulation. However, it reiterates what constitutes eligibility for benefits under law. In addition, every Character of Discharge case that is initially considered for denial will also get a second look before that action is taken.
“Given that large numbers of LGBTQ+ veterans who were affected by previous homophobic and transphobic policies have not applied for a discharge upgrade due to the perception that the process could be onerous,” Williams wrote, “we are hopeful that this policy statement encourages more of them to contact VA to determine their eligibility for care and services.”
Today, according to the Human Right Campaign, nearly 6.1% of US military personnel self-identify as LGBTQ. Williams, herself a bisexual veteran, said she chose to present as straight during the push to repeal DADT. “I could talk credibly about how the lack of sufficient Arabic linguists harmed our effectiveness downrange, and my own identity seemed irrelevant. It took many years for me to shed the toxic legacy of having served under DADT and come back out of the closet; I’m proud to recognize this anniversary as my authentic self.”
The US Department of Veterans Affairs (VA) has issued a new policy statement to help ensure that active-duty service members who were discharged for their sexual orientation under the Don’t Ask, Don’t Tell policy will be able to receive full VA benefits.
“[A] great injustice was remedied and a tremendous weight was finally lifted off the shoulders of tens of thousands of dedicated American service members,” President Biden said on September 20 as the country commemorated the 10th anniversary of the repeal of “Don’t Ask, Don’t Tell,” the policy that barred lesbian, gay, bisexual, transgender, and queer (LGBTQ+) service members from serving openly.
Prior to DADT, if active-duty service members spoke out about their sexual orientation, they ran the risk of being hounded, shunned, in some cases assaulted, and discharged. If they kept it a secret, they felt they were living a lie, unable to be their whole selves. More than 100,000 were discharged because of their sexual orientation or gender identity.
Although Don’t Ask, Don’t Tell was a “compromise” law that purposed to protect them, LGBTQ+ service members were still at risk for harassment and abuse. Nor did the law protect them from discharge. Some 14,000 LGBTQ+ service members were discharged while DADT was in effect. And those who received “other than honorable” (OTH) discharges could be excluded from receiving services and benefits.
The 2011 repeal followed a “hard-fought battle,” said a release from the Human Rights Campaign, which led a coalition of members, supporters, elected officials, 70+ organizations, and 20,000 veterans to get the law overturned. HRC staff coordinated grassroots efforts and sent 19 million e-mails to members and supporters, in turn generating an “unprecedented” 625,000 e-mails and 50,000 handwritten letters to members of Congress.
After the repeal, the VA began the long process of inclusion for LGBTQ+ veterans. “At VA, we continuously work not only to meet the needs of LGBTQ+ veterans, but also to address ongoing issues that LGBTQ+ veterans face as a result of the military’s decades-long official policy of homophobia and transphobia,” Kayla Williams, assistant secretary for public affairs in VA’s Office of Public and Intergovernmental Affairs wrote in the Secretary’s blog.
The VA “recognizes that the trauma caused by the military’s decades-long policy of discrimination against LGBTQ+ people cannot be undone in a few short months,” she continued, but the Biden administration and Secretary McDonough are “taking the steps necessary to begin addressing the pain that such policies have created.”
President Biden, in his remarks, noted that as a US Senator, he had supported allowing service members to serve openly and, as Vice President, championed the repeal. He said, “I am honored to be Commander-in-Chief of the strongest and most inclusive military in our nation’s history. Today, our military doesn’t just welcome LGBTQ+ service members—it is led at the highest levels by brave LGBTQ+ veterans, including Under Secretary of the Air Force Gina Ortiz Jones and Assistant Secretary of Defense for Readiness Shawn Skelly, who served under Don’t Ask, Don’t Tell. I was gratified to appoint the first openly gay Senate-confirmed Cabinet member, Secretary Pete Buttigieg, a lieutenant in the U.S. Navy Reserve and Afghanistan veteran who joined the military under the Don’t Ask, Don’t Tell policy. And during my first week in office, I proudly delivered on my pledge to repeal the discriminatory ban on open service by patriotic transgender service members.”
In early September, Rep. Chris Pappas (D-NH), a member of the House Veterans Affairs Committee and Co-Chair of the Equality Caucus, reintroduced the SERVE (Securing the Rights our Veterans Earned) Act. The act, which is co-sponsored by Reps. Mike Levin (D-CA), Kathleen Rice (D-NY), Anthony Brown (D-MD), and Jackie Speier (D-CA), would ensure LGBTQ+ veterans who received an OTH or Entry-Level Separation discharge solely due to sexual orientation or gender identity are afforded the VA benefits they rightfully earned, including access to VA healthcare, and education, burial and memorial services, and home loans. The act includes veterans who were issued “blue discharges” during World War II and veterans discharged under former President Trump’s ban on transgender service members. The legislation has been endorsed by the Congressional LGBTQ+ Equality Caucus and is supported by more than 45 representatives.
There are processes for those veterans through which they can have their discharge papers and separation statuses reviewed and modified, Pappas said in a release, but “it can take months for the changes to take effect, and many of these veterans do not even realize they are eligible.”
Earlier this year, Veterans Affairs Secretary Denis McDonough made it a priority to ensure that LGBTQ+ veterans have the same level of access to VA care and services that all other veterans have. Among other things, he established a task force to examine how VA policies hinder or prohibit access to care and services and remove barriers that transgender veterans face in accessing gender-affirming care.
The VA is also taking steps, Williams noted, to clarify VA policy for veterans who were given OTH discharges based on homosexual conduct, gender identity or HIV status. Under this newly issued guidance, VA adjudicators shall find that all discharged service members whose separation was due to sexual orientation, gender identity or HIV status are considered “Veterans” who may be eligible for VA benefits, like VR&E, home loan guaranty, compensation and pension, health care, homeless program and/or burial benefits, so long as the record does not implicate a statutory or regulatory bar to benefits.
The policy statement does not represent a change in law, as veterans who were discharged under DADT alone have been generally eligible for benefits under current statute and regulation. However, it reiterates what constitutes eligibility for benefits under law. In addition, every Character of Discharge case that is initially considered for denial will also get a second look before that action is taken.
“Given that large numbers of LGBTQ+ veterans who were affected by previous homophobic and transphobic policies have not applied for a discharge upgrade due to the perception that the process could be onerous,” Williams wrote, “we are hopeful that this policy statement encourages more of them to contact VA to determine their eligibility for care and services.”
Today, according to the Human Right Campaign, nearly 6.1% of US military personnel self-identify as LGBTQ. Williams, herself a bisexual veteran, said she chose to present as straight during the push to repeal DADT. “I could talk credibly about how the lack of sufficient Arabic linguists harmed our effectiveness downrange, and my own identity seemed irrelevant. It took many years for me to shed the toxic legacy of having served under DADT and come back out of the closet; I’m proud to recognize this anniversary as my authentic self.”
The US Department of Veterans Affairs (VA) has issued a new policy statement to help ensure that active-duty service members who were discharged for their sexual orientation under the Don’t Ask, Don’t Tell policy will be able to receive full VA benefits.
“[A] great injustice was remedied and a tremendous weight was finally lifted off the shoulders of tens of thousands of dedicated American service members,” President Biden said on September 20 as the country commemorated the 10th anniversary of the repeal of “Don’t Ask, Don’t Tell,” the policy that barred lesbian, gay, bisexual, transgender, and queer (LGBTQ+) service members from serving openly.
Prior to DADT, if active-duty service members spoke out about their sexual orientation, they ran the risk of being hounded, shunned, in some cases assaulted, and discharged. If they kept it a secret, they felt they were living a lie, unable to be their whole selves. More than 100,000 were discharged because of their sexual orientation or gender identity.
Although Don’t Ask, Don’t Tell was a “compromise” law that purposed to protect them, LGBTQ+ service members were still at risk for harassment and abuse. Nor did the law protect them from discharge. Some 14,000 LGBTQ+ service members were discharged while DADT was in effect. And those who received “other than honorable” (OTH) discharges could be excluded from receiving services and benefits.
The 2011 repeal followed a “hard-fought battle,” said a release from the Human Rights Campaign, which led a coalition of members, supporters, elected officials, 70+ organizations, and 20,000 veterans to get the law overturned. HRC staff coordinated grassroots efforts and sent 19 million e-mails to members and supporters, in turn generating an “unprecedented” 625,000 e-mails and 50,000 handwritten letters to members of Congress.
After the repeal, the VA began the long process of inclusion for LGBTQ+ veterans. “At VA, we continuously work not only to meet the needs of LGBTQ+ veterans, but also to address ongoing issues that LGBTQ+ veterans face as a result of the military’s decades-long official policy of homophobia and transphobia,” Kayla Williams, assistant secretary for public affairs in VA’s Office of Public and Intergovernmental Affairs wrote in the Secretary’s blog.
The VA “recognizes that the trauma caused by the military’s decades-long policy of discrimination against LGBTQ+ people cannot be undone in a few short months,” she continued, but the Biden administration and Secretary McDonough are “taking the steps necessary to begin addressing the pain that such policies have created.”
President Biden, in his remarks, noted that as a US Senator, he had supported allowing service members to serve openly and, as Vice President, championed the repeal. He said, “I am honored to be Commander-in-Chief of the strongest and most inclusive military in our nation’s history. Today, our military doesn’t just welcome LGBTQ+ service members—it is led at the highest levels by brave LGBTQ+ veterans, including Under Secretary of the Air Force Gina Ortiz Jones and Assistant Secretary of Defense for Readiness Shawn Skelly, who served under Don’t Ask, Don’t Tell. I was gratified to appoint the first openly gay Senate-confirmed Cabinet member, Secretary Pete Buttigieg, a lieutenant in the U.S. Navy Reserve and Afghanistan veteran who joined the military under the Don’t Ask, Don’t Tell policy. And during my first week in office, I proudly delivered on my pledge to repeal the discriminatory ban on open service by patriotic transgender service members.”
In early September, Rep. Chris Pappas (D-NH), a member of the House Veterans Affairs Committee and Co-Chair of the Equality Caucus, reintroduced the SERVE (Securing the Rights our Veterans Earned) Act. The act, which is co-sponsored by Reps. Mike Levin (D-CA), Kathleen Rice (D-NY), Anthony Brown (D-MD), and Jackie Speier (D-CA), would ensure LGBTQ+ veterans who received an OTH or Entry-Level Separation discharge solely due to sexual orientation or gender identity are afforded the VA benefits they rightfully earned, including access to VA healthcare, and education, burial and memorial services, and home loans. The act includes veterans who were issued “blue discharges” during World War II and veterans discharged under former President Trump’s ban on transgender service members. The legislation has been endorsed by the Congressional LGBTQ+ Equality Caucus and is supported by more than 45 representatives.
There are processes for those veterans through which they can have their discharge papers and separation statuses reviewed and modified, Pappas said in a release, but “it can take months for the changes to take effect, and many of these veterans do not even realize they are eligible.”
Earlier this year, Veterans Affairs Secretary Denis McDonough made it a priority to ensure that LGBTQ+ veterans have the same level of access to VA care and services that all other veterans have. Among other things, he established a task force to examine how VA policies hinder or prohibit access to care and services and remove barriers that transgender veterans face in accessing gender-affirming care.
The VA is also taking steps, Williams noted, to clarify VA policy for veterans who were given OTH discharges based on homosexual conduct, gender identity or HIV status. Under this newly issued guidance, VA adjudicators shall find that all discharged service members whose separation was due to sexual orientation, gender identity or HIV status are considered “Veterans” who may be eligible for VA benefits, like VR&E, home loan guaranty, compensation and pension, health care, homeless program and/or burial benefits, so long as the record does not implicate a statutory or regulatory bar to benefits.
The policy statement does not represent a change in law, as veterans who were discharged under DADT alone have been generally eligible for benefits under current statute and regulation. However, it reiterates what constitutes eligibility for benefits under law. In addition, every Character of Discharge case that is initially considered for denial will also get a second look before that action is taken.
“Given that large numbers of LGBTQ+ veterans who were affected by previous homophobic and transphobic policies have not applied for a discharge upgrade due to the perception that the process could be onerous,” Williams wrote, “we are hopeful that this policy statement encourages more of them to contact VA to determine their eligibility for care and services.”
Today, according to the Human Right Campaign, nearly 6.1% of US military personnel self-identify as LGBTQ. Williams, herself a bisexual veteran, said she chose to present as straight during the push to repeal DADT. “I could talk credibly about how the lack of sufficient Arabic linguists harmed our effectiveness downrange, and my own identity seemed irrelevant. It took many years for me to shed the toxic legacy of having served under DADT and come back out of the closet; I’m proud to recognize this anniversary as my authentic self.”
Physical activity paradoxically tied to higher coronary calcium
new observational data suggest.
In a prospective cohort study of Korean men and women 18 years and older, participants who were the most physically active had the fastest progression of their coronary artery calcium (CAC) scores at 5 years, compared with those who were the least physically active.
“People who exercise may have an increase in their coronary calcium levels, but this is not necessarily bad news. This may mean that atherosclerotic lesions in the coronary arteries are becoming more stable and less dangerous, but we need additional research to understand these changes,” Eliseo Guallar, MD, PhD, professor, Johns Hopkins Bloomberg School of Public Health, Baltimore, the study’s corresponding author, said in an interview.
This paradoxical effect notwithstanding, doctors should continue to advise their patients to follow the physical activity guidelines for Americans that were published in 2018, Dr. Guallar said.
“Physical activity is a key component of a healthy lifestyle. Our analysis can be useful, however, if someone starts exercising and sees that his or her coronary calcium score goes up,” he said.
The study is published online September 20 in Heart.
The degree of build-up of calcium deposits in the coronary arteries is used to determine future cardiovascular disease risk and to guide treatment to prevent myocardial infarction and stroke. A CAC score of at least 100 Agatston units indicates that treatment with statins is warranted, the researchers write.
In the current study, investigators — led by Ki-Chul Sung, MD, Sungkyunkwan University School of Medicine, Seoul, Korea, and Yun Soo Hong, MD, Johns Hopkins Bloomberg School of Public Health, Baltimore — explored the link between different degrees of physical activity and the progression of CAC scores in healthy adults.
“While physical activity improves a wide array of cardiovascular and metabolic biomarkers, endurance athletes were more likely to have a coronary artery calcium (CAC) score >300 Agatston units or coronary plaques compared with sedentary men with a similar risk profile. It is not clear if exercise may itself be associated with calcification of the arteries,” the authors write.
The researchers studied 25,485 participants (22,741 men and 2,744 women) who were part of the Kangbuk Samsung Health Study. All were free of cardiovascular disease at study entry and underwent comprehensive health screening exams at one of two major health centers in Seoul and Suwon, South Korea, between March 1, 2011, and December 31, 2017.
At each exam, participants filled out a questionnaire that included questions on medical and family history, smoking habits, alcohol intake, and education level.
Participants were also quizzed at baseline about their physical activity, using the Korean version of the International Physical Activity Questionnaire Short Form (IPAQ-SF).
On the basis of that, they were categorized into one of three categories: inactive; moderately active, defined as at least 3 days of vigorous-intensity activity for at least 20 min/day or at least 5 days of moderate-intensity activity or walking for at least 30 min/ day or at least 5 days of any combination of walking and moderate- or vigorous-intensity activities, attaining at least 600 MET-min/week; or health-enhancing physically active (HEPA), defined as at least 3 days of vigorous-intensity activity, attaining at least 1,500 MET-min/week or 7 days of any combination of walking or moderate- or vigorous-intensity activities, attaining at least 3000 MET-min/week.
Of the study participants, 47% were classified as inactive, 38% as moderately active, and 15% as HEPA.
Those who were more physically active tended to be older and less likely to smoke than less physically active participants. They also had lower total cholesterol, more hypertension, and existing evidence of calcium deposits in their coronary arteries.
A graded association between physical activity level and the prevalence and progression of coronary artery calcification was seen, irrespective of CAC scores at the start of monitoring.
At baseline, the estimated adjusted average baseline CAC scores in inactive participants was 9.45 (95% CI, 8.76 - 10.14), in moderately active participants was 10.20 (95% CI, 9.40 - 11.00), and in HEPA participants was 12.04 (95% CI, 10.81 - 13.26).
Compared with the least active participants, the estimated adjusted 5-year average increases in CAC was 3.20 (95% CI, 0.72 - 5.69) in moderately active participants and 8.16 (95% CI, 4.80 - 11.53) in HEPA participants.
A higher level of physical activity was associated with faster progression of CAC scores, both in participants with CAC score of 0 at baseline and in those with prevalent CAC.
The authors note there are several limitations to consider when interpreting their findings. These include the absence of an objective assessment of physical activity, the inability to evaluate the association between physical activity and CAC levels with incident cardiovascular events because of a lack of data, and the lack of information on incident myocardial infarction, stroke, CAC density, or volume.
Physical activity might increase coronary atherosclerosis through mechanical stress and vessel wall injury of coronary arteries; physiologic responses during exercise, such as increased blood pressure; increased parathyroid hormone levels; and changes in coronary hemodynamics and inflammation. “In addition, other factors, such as diet, vitamins, and minerals, may change with physical activity,” the authors write.
“The second possibility is that physical activity may increase CAC scores without increasing cardiovascular disease risk,” they write.
“The cardiovascular benefits of physical activity are unquestionable,” the authors emphasize, adding that the national guidelines recommend at least 150 to 300 minutes per week of moderate-intensity or 75 to 150 minutes per week of vigorous-intensity aerobic physical activity.
“Patients and physicians, however, need to consider that engaging in physical activity may accelerate the progression of coronary calcium, possibly due to plaque healing, stabilization and calcification,” they conclude.
Dr. Guallar added: “We would like to link our research to clinical outcomes, so that we can really be sure that the increase in coronary calcium scores does not imply an increase in risk.”
“Do these findings mean that we should stop using coronary artery calcium scores to assess coronary artery disease?” ask Gaurav Gulsin, MD, and Alastair James Moss, MD, University of Leicester, United Kingdom, in an accompanying editorial.
The study highlights the complexity of interpreting CAC scores in patients who have implemented recommendations for physical activity or started statin therapy, they note.
“While proponents would argue that it is an effective tool to screen for subclinical atherosclerosis in asymptomatic individuals, clinicians should be cautious regarding the overuse of this test in otherwise healthy individuals. The coronary artery calcium paradox should not result in paradoxical care for our patients,” Dr. Gulsin and Dr. Moss conclude.
Dr. Sung, Dr. Hong, and the other study authors report no relevant financial relationships. The British Heart Foundation provides funding support for Dr. Gulsin and Dr. Moss.
A version of this article first appeared on Medscape.com.
new observational data suggest.
In a prospective cohort study of Korean men and women 18 years and older, participants who were the most physically active had the fastest progression of their coronary artery calcium (CAC) scores at 5 years, compared with those who were the least physically active.
“People who exercise may have an increase in their coronary calcium levels, but this is not necessarily bad news. This may mean that atherosclerotic lesions in the coronary arteries are becoming more stable and less dangerous, but we need additional research to understand these changes,” Eliseo Guallar, MD, PhD, professor, Johns Hopkins Bloomberg School of Public Health, Baltimore, the study’s corresponding author, said in an interview.
This paradoxical effect notwithstanding, doctors should continue to advise their patients to follow the physical activity guidelines for Americans that were published in 2018, Dr. Guallar said.
“Physical activity is a key component of a healthy lifestyle. Our analysis can be useful, however, if someone starts exercising and sees that his or her coronary calcium score goes up,” he said.
The study is published online September 20 in Heart.
The degree of build-up of calcium deposits in the coronary arteries is used to determine future cardiovascular disease risk and to guide treatment to prevent myocardial infarction and stroke. A CAC score of at least 100 Agatston units indicates that treatment with statins is warranted, the researchers write.
In the current study, investigators — led by Ki-Chul Sung, MD, Sungkyunkwan University School of Medicine, Seoul, Korea, and Yun Soo Hong, MD, Johns Hopkins Bloomberg School of Public Health, Baltimore — explored the link between different degrees of physical activity and the progression of CAC scores in healthy adults.
“While physical activity improves a wide array of cardiovascular and metabolic biomarkers, endurance athletes were more likely to have a coronary artery calcium (CAC) score >300 Agatston units or coronary plaques compared with sedentary men with a similar risk profile. It is not clear if exercise may itself be associated with calcification of the arteries,” the authors write.
The researchers studied 25,485 participants (22,741 men and 2,744 women) who were part of the Kangbuk Samsung Health Study. All were free of cardiovascular disease at study entry and underwent comprehensive health screening exams at one of two major health centers in Seoul and Suwon, South Korea, between March 1, 2011, and December 31, 2017.
At each exam, participants filled out a questionnaire that included questions on medical and family history, smoking habits, alcohol intake, and education level.
Participants were also quizzed at baseline about their physical activity, using the Korean version of the International Physical Activity Questionnaire Short Form (IPAQ-SF).
On the basis of that, they were categorized into one of three categories: inactive; moderately active, defined as at least 3 days of vigorous-intensity activity for at least 20 min/day or at least 5 days of moderate-intensity activity or walking for at least 30 min/ day or at least 5 days of any combination of walking and moderate- or vigorous-intensity activities, attaining at least 600 MET-min/week; or health-enhancing physically active (HEPA), defined as at least 3 days of vigorous-intensity activity, attaining at least 1,500 MET-min/week or 7 days of any combination of walking or moderate- or vigorous-intensity activities, attaining at least 3000 MET-min/week.
Of the study participants, 47% were classified as inactive, 38% as moderately active, and 15% as HEPA.
Those who were more physically active tended to be older and less likely to smoke than less physically active participants. They also had lower total cholesterol, more hypertension, and existing evidence of calcium deposits in their coronary arteries.
A graded association between physical activity level and the prevalence and progression of coronary artery calcification was seen, irrespective of CAC scores at the start of monitoring.
At baseline, the estimated adjusted average baseline CAC scores in inactive participants was 9.45 (95% CI, 8.76 - 10.14), in moderately active participants was 10.20 (95% CI, 9.40 - 11.00), and in HEPA participants was 12.04 (95% CI, 10.81 - 13.26).
Compared with the least active participants, the estimated adjusted 5-year average increases in CAC was 3.20 (95% CI, 0.72 - 5.69) in moderately active participants and 8.16 (95% CI, 4.80 - 11.53) in HEPA participants.
A higher level of physical activity was associated with faster progression of CAC scores, both in participants with CAC score of 0 at baseline and in those with prevalent CAC.
The authors note there are several limitations to consider when interpreting their findings. These include the absence of an objective assessment of physical activity, the inability to evaluate the association between physical activity and CAC levels with incident cardiovascular events because of a lack of data, and the lack of information on incident myocardial infarction, stroke, CAC density, or volume.
Physical activity might increase coronary atherosclerosis through mechanical stress and vessel wall injury of coronary arteries; physiologic responses during exercise, such as increased blood pressure; increased parathyroid hormone levels; and changes in coronary hemodynamics and inflammation. “In addition, other factors, such as diet, vitamins, and minerals, may change with physical activity,” the authors write.
“The second possibility is that physical activity may increase CAC scores without increasing cardiovascular disease risk,” they write.
“The cardiovascular benefits of physical activity are unquestionable,” the authors emphasize, adding that the national guidelines recommend at least 150 to 300 minutes per week of moderate-intensity or 75 to 150 minutes per week of vigorous-intensity aerobic physical activity.
“Patients and physicians, however, need to consider that engaging in physical activity may accelerate the progression of coronary calcium, possibly due to plaque healing, stabilization and calcification,” they conclude.
Dr. Guallar added: “We would like to link our research to clinical outcomes, so that we can really be sure that the increase in coronary calcium scores does not imply an increase in risk.”
“Do these findings mean that we should stop using coronary artery calcium scores to assess coronary artery disease?” ask Gaurav Gulsin, MD, and Alastair James Moss, MD, University of Leicester, United Kingdom, in an accompanying editorial.
The study highlights the complexity of interpreting CAC scores in patients who have implemented recommendations for physical activity or started statin therapy, they note.
“While proponents would argue that it is an effective tool to screen for subclinical atherosclerosis in asymptomatic individuals, clinicians should be cautious regarding the overuse of this test in otherwise healthy individuals. The coronary artery calcium paradox should not result in paradoxical care for our patients,” Dr. Gulsin and Dr. Moss conclude.
Dr. Sung, Dr. Hong, and the other study authors report no relevant financial relationships. The British Heart Foundation provides funding support for Dr. Gulsin and Dr. Moss.
A version of this article first appeared on Medscape.com.
new observational data suggest.
In a prospective cohort study of Korean men and women 18 years and older, participants who were the most physically active had the fastest progression of their coronary artery calcium (CAC) scores at 5 years, compared with those who were the least physically active.
“People who exercise may have an increase in their coronary calcium levels, but this is not necessarily bad news. This may mean that atherosclerotic lesions in the coronary arteries are becoming more stable and less dangerous, but we need additional research to understand these changes,” Eliseo Guallar, MD, PhD, professor, Johns Hopkins Bloomberg School of Public Health, Baltimore, the study’s corresponding author, said in an interview.
This paradoxical effect notwithstanding, doctors should continue to advise their patients to follow the physical activity guidelines for Americans that were published in 2018, Dr. Guallar said.
“Physical activity is a key component of a healthy lifestyle. Our analysis can be useful, however, if someone starts exercising and sees that his or her coronary calcium score goes up,” he said.
The study is published online September 20 in Heart.
The degree of build-up of calcium deposits in the coronary arteries is used to determine future cardiovascular disease risk and to guide treatment to prevent myocardial infarction and stroke. A CAC score of at least 100 Agatston units indicates that treatment with statins is warranted, the researchers write.
In the current study, investigators — led by Ki-Chul Sung, MD, Sungkyunkwan University School of Medicine, Seoul, Korea, and Yun Soo Hong, MD, Johns Hopkins Bloomberg School of Public Health, Baltimore — explored the link between different degrees of physical activity and the progression of CAC scores in healthy adults.
“While physical activity improves a wide array of cardiovascular and metabolic biomarkers, endurance athletes were more likely to have a coronary artery calcium (CAC) score >300 Agatston units or coronary plaques compared with sedentary men with a similar risk profile. It is not clear if exercise may itself be associated with calcification of the arteries,” the authors write.
The researchers studied 25,485 participants (22,741 men and 2,744 women) who were part of the Kangbuk Samsung Health Study. All were free of cardiovascular disease at study entry and underwent comprehensive health screening exams at one of two major health centers in Seoul and Suwon, South Korea, between March 1, 2011, and December 31, 2017.
At each exam, participants filled out a questionnaire that included questions on medical and family history, smoking habits, alcohol intake, and education level.
Participants were also quizzed at baseline about their physical activity, using the Korean version of the International Physical Activity Questionnaire Short Form (IPAQ-SF).
On the basis of that, they were categorized into one of three categories: inactive; moderately active, defined as at least 3 days of vigorous-intensity activity for at least 20 min/day or at least 5 days of moderate-intensity activity or walking for at least 30 min/ day or at least 5 days of any combination of walking and moderate- or vigorous-intensity activities, attaining at least 600 MET-min/week; or health-enhancing physically active (HEPA), defined as at least 3 days of vigorous-intensity activity, attaining at least 1,500 MET-min/week or 7 days of any combination of walking or moderate- or vigorous-intensity activities, attaining at least 3000 MET-min/week.
Of the study participants, 47% were classified as inactive, 38% as moderately active, and 15% as HEPA.
Those who were more physically active tended to be older and less likely to smoke than less physically active participants. They also had lower total cholesterol, more hypertension, and existing evidence of calcium deposits in their coronary arteries.
A graded association between physical activity level and the prevalence and progression of coronary artery calcification was seen, irrespective of CAC scores at the start of monitoring.
At baseline, the estimated adjusted average baseline CAC scores in inactive participants was 9.45 (95% CI, 8.76 - 10.14), in moderately active participants was 10.20 (95% CI, 9.40 - 11.00), and in HEPA participants was 12.04 (95% CI, 10.81 - 13.26).
Compared with the least active participants, the estimated adjusted 5-year average increases in CAC was 3.20 (95% CI, 0.72 - 5.69) in moderately active participants and 8.16 (95% CI, 4.80 - 11.53) in HEPA participants.
A higher level of physical activity was associated with faster progression of CAC scores, both in participants with CAC score of 0 at baseline and in those with prevalent CAC.
The authors note there are several limitations to consider when interpreting their findings. These include the absence of an objective assessment of physical activity, the inability to evaluate the association between physical activity and CAC levels with incident cardiovascular events because of a lack of data, and the lack of information on incident myocardial infarction, stroke, CAC density, or volume.
Physical activity might increase coronary atherosclerosis through mechanical stress and vessel wall injury of coronary arteries; physiologic responses during exercise, such as increased blood pressure; increased parathyroid hormone levels; and changes in coronary hemodynamics and inflammation. “In addition, other factors, such as diet, vitamins, and minerals, may change with physical activity,” the authors write.
“The second possibility is that physical activity may increase CAC scores without increasing cardiovascular disease risk,” they write.
“The cardiovascular benefits of physical activity are unquestionable,” the authors emphasize, adding that the national guidelines recommend at least 150 to 300 minutes per week of moderate-intensity or 75 to 150 minutes per week of vigorous-intensity aerobic physical activity.
“Patients and physicians, however, need to consider that engaging in physical activity may accelerate the progression of coronary calcium, possibly due to plaque healing, stabilization and calcification,” they conclude.
Dr. Guallar added: “We would like to link our research to clinical outcomes, so that we can really be sure that the increase in coronary calcium scores does not imply an increase in risk.”
“Do these findings mean that we should stop using coronary artery calcium scores to assess coronary artery disease?” ask Gaurav Gulsin, MD, and Alastair James Moss, MD, University of Leicester, United Kingdom, in an accompanying editorial.
The study highlights the complexity of interpreting CAC scores in patients who have implemented recommendations for physical activity or started statin therapy, they note.
“While proponents would argue that it is an effective tool to screen for subclinical atherosclerosis in asymptomatic individuals, clinicians should be cautious regarding the overuse of this test in otherwise healthy individuals. The coronary artery calcium paradox should not result in paradoxical care for our patients,” Dr. Gulsin and Dr. Moss conclude.
Dr. Sung, Dr. Hong, and the other study authors report no relevant financial relationships. The British Heart Foundation provides funding support for Dr. Gulsin and Dr. Moss.
A version of this article first appeared on Medscape.com.
Top questions answered about COVID-19 boosters for your patients
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.

Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.
Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.
Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
Doctors preyed on homeless for slip-and-fall schemes; more
a story in the New York Daily News, among other news outlets, indicates.
In the latest iteration of this age-old practice, a team of attorneys and doctors allegedly recruited more than 400 New York City inhabitants, many of whom were homeless or addicted to drugs, over the course of 5 years to participate in their scam.
These people, who were often desperate for money, were coached to claim they’d tripped and fallen over one of the many obstacles pedestrians encounter in the city — sidewalk cracks, potholes, open or protruding cellar doors, and the like. The participant would be cajoled into signing his or her name to a fraudulent suit. Over the years, the scam netted the bosses more than $31 million from city businesses and their insurance companies.
In some cases, to add authenticity to the swindle, the scammers convinced the so-called victims to undergo an operation, promising them up to $1,500 to go under the knife.
Accused by the U.S. Attorney’s Office of masterminding the slip-and-fall operation were two attorneys, George Constantine and Marc Elefant, and a pair of doctors, Andrew Dowd, MD, an orthopedic surgeon, and Sady Ribeiro, MD, a pain management specialist and surgeon.
According to the charges, Mr. Constantine and Mr. Elefant filed lawsuits — either together or separately, though the report isn’t clear — on behalf of hundreds of people who took part in the scheme. Dr. Dowd and Dr. Ribeiro also profited handsomely, according to authorities. Dr. Dowd, they say, earned roughly $9,500 per surgery. Dr. Ribeiro is accused of treating nearly 200 participants during the con and of often paying kickbacks to them to drum up additional referrals.
If convicted on all charges, including mail and wire fraud, each of the defendants could face up to 20 years in prison.
This isn’t the first time such a scheme has been hatched and carried out in New York City.
In May 2020, three men were sentenced to prison for their involvement in a similar slip-and-fall operation that took place between 2013 and 2018. (Their sentencing followed an earlier conviction for conspiracy to commit mail and wire fraud.)
Like the most recent scheme, the one that began in 2013 preyed on the hopeless. “The whole essence of this conspiracy is to find the down-and-out, find the desperate, find the homeless,” the sentencing judge said at the time. “No person who has a job and education and can support his or her family even minimally is going to say, ‘Oh, I’ll undergo unnecessary back surgery for a thousand dollars.’ These people were vulnerable and desperate.”
Sales reps in the OR — helpful or harmful?
Although medical device makers insist that the practice of placing sales reps in operating rooms (ORs) has proven beneficial to surgeons over the years, others claim it has contributed to unwanted outcomes, according to a report published in Kaiser Health News.
In May 2018, for instance, Cristina Martinez underwent what was supposed to be a routine spinal implant procedure. In the course of the operation, her Houston-based spine surgeon discovered that the implant he was about to insert in her back was larger than the one he had intended to use. Under different circumstances, the device maker’s sales representative who was present in the OR that day might have been able to supply the smaller implant. But the rep didn’t have one available, so the surgeon proceeded with the operation using the larger plastic disk.
Four days later, in another procedure, the surgeon removed that disk and replaced it with one that was the correct size. Ms. Martinez has claimed that she awakened from the second procedure in pain, the result of nerve damage that she says led to loss of feeling in her left leg.
In a suit against the doctor, the device maker, and its distributor and sales reps, Ms. Martinez alleges that her injuries were the direct result of their negligence in not having the proper disk available during the initial operation.
The defendants have each denied any wrongdoing.
The accused spine surgeon submitted to the court his operating notes, which reportedly say that he had depended on a company distributor and its sales reps to provide “all lengths available” of the implant. In another filing, he contends that the “small area of leg numbness experienced by Ms. Martinez was a known complication of the first surgery...and was not the result of any alleged negligence.”
The device maker also denies any wrongdoing. In its filings, it claims that sales reps initially ordered a sterile kit that included implants ranging from 50 mm to 55 mm in length. The kit, says the manufacturer, was duly shipped to Houston, but the surgeon replaced the original implant with a 40-mm version during Ms. Martinez’ reoperation.
A trial is scheduled for this November.
But was the Houston incident typical?
Device makers argue that having sales reps in the OR makes sense: Well trained, they offer surgeons vital technical guidance in the use of products that are often complex.
Kaiser Health News says its investigation found otherwise. This practice and others “have been blamed for contributing to serious patient harm in thousands of medical malpractice, product liability, and whistleblower lawsuits filed over the past decade,” it reports.
The list of allegations is long: Some patients say they were injured because sales reps sold or delivered either the wrong-size implant or a defective one. Others say that in their communications with doctors, device makers were shown to have been less than truthful about the safety and durability of their products.
Currently, more than 28,000 suits have been consolidated into six multi-district federal cases. Most involve patients who claim injury after receiving hip implants. Some of the procedures required painful reoperations.
Other court actions cite device makers for other misdeeds, including keeping federal regulators in the dark about potentially dangerous product defects and plying surgeons with millions of dollars in illegal kickbacks.
Device makers have denied these and other allegations. Many of their cases have been settled confidentially.
This high-risk specialty found a way to lower its claim rates
Ob.gyns. who undergo training that simulates team interactions during a high-acuity clinical case face fewer malpractice claims afterward, according to a study published in August in Obstetrics and Gynecology.
Researchers examined the claim rates of 292 ob.gyns. who had undergone one or more such training simulations from 2002 to 2019. To gauge the effect of simulation training on the rate of medical malpractice claims, the researchers compared pretraining rates with posttraining rates. Because participants were insured by the same carrier, the team had access to the relevant claims data as well as the doctors’ durations of coverage.
The investigators assessed claim rates for the period 2002 to 2019 (the full study period), as well as rates for 2-year and 1-year participation.
Researchers found a nonsignificant drop in claim rates for doctors in the 1-year group. The drop was greater for those in the 2-year group; it decreased from 9.2 to 5.4 claims per 100 physician coverage years. (A coverage year is defined as 12 months of indemnity protection.)
For doctors who took part for the entire study period — and were therefore more likely to be among the nearly 20% of doctors who attended three or more training sessions — postsimulation claim rates dropped significantly, from 11.2 to 5.7 per 100 physician coverage years. (Attendance in more than one simulation session correlated with a greater reduction in claim rates.)
“We observed a significant reduction in malpractice claim rates after simulation training,” the researchers concluded. “Wider use of simulation training within obstetrics and gynecology should be considered.”
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
a story in the New York Daily News, among other news outlets, indicates.
In the latest iteration of this age-old practice, a team of attorneys and doctors allegedly recruited more than 400 New York City inhabitants, many of whom were homeless or addicted to drugs, over the course of 5 years to participate in their scam.
These people, who were often desperate for money, were coached to claim they’d tripped and fallen over one of the many obstacles pedestrians encounter in the city — sidewalk cracks, potholes, open or protruding cellar doors, and the like. The participant would be cajoled into signing his or her name to a fraudulent suit. Over the years, the scam netted the bosses more than $31 million from city businesses and their insurance companies.
In some cases, to add authenticity to the swindle, the scammers convinced the so-called victims to undergo an operation, promising them up to $1,500 to go under the knife.
Accused by the U.S. Attorney’s Office of masterminding the slip-and-fall operation were two attorneys, George Constantine and Marc Elefant, and a pair of doctors, Andrew Dowd, MD, an orthopedic surgeon, and Sady Ribeiro, MD, a pain management specialist and surgeon.
According to the charges, Mr. Constantine and Mr. Elefant filed lawsuits — either together or separately, though the report isn’t clear — on behalf of hundreds of people who took part in the scheme. Dr. Dowd and Dr. Ribeiro also profited handsomely, according to authorities. Dr. Dowd, they say, earned roughly $9,500 per surgery. Dr. Ribeiro is accused of treating nearly 200 participants during the con and of often paying kickbacks to them to drum up additional referrals.
If convicted on all charges, including mail and wire fraud, each of the defendants could face up to 20 years in prison.
This isn’t the first time such a scheme has been hatched and carried out in New York City.
In May 2020, three men were sentenced to prison for their involvement in a similar slip-and-fall operation that took place between 2013 and 2018. (Their sentencing followed an earlier conviction for conspiracy to commit mail and wire fraud.)
Like the most recent scheme, the one that began in 2013 preyed on the hopeless. “The whole essence of this conspiracy is to find the down-and-out, find the desperate, find the homeless,” the sentencing judge said at the time. “No person who has a job and education and can support his or her family even minimally is going to say, ‘Oh, I’ll undergo unnecessary back surgery for a thousand dollars.’ These people were vulnerable and desperate.”
Sales reps in the OR — helpful or harmful?
Although medical device makers insist that the practice of placing sales reps in operating rooms (ORs) has proven beneficial to surgeons over the years, others claim it has contributed to unwanted outcomes, according to a report published in Kaiser Health News.
In May 2018, for instance, Cristina Martinez underwent what was supposed to be a routine spinal implant procedure. In the course of the operation, her Houston-based spine surgeon discovered that the implant he was about to insert in her back was larger than the one he had intended to use. Under different circumstances, the device maker’s sales representative who was present in the OR that day might have been able to supply the smaller implant. But the rep didn’t have one available, so the surgeon proceeded with the operation using the larger plastic disk.
Four days later, in another procedure, the surgeon removed that disk and replaced it with one that was the correct size. Ms. Martinez has claimed that she awakened from the second procedure in pain, the result of nerve damage that she says led to loss of feeling in her left leg.
In a suit against the doctor, the device maker, and its distributor and sales reps, Ms. Martinez alleges that her injuries were the direct result of their negligence in not having the proper disk available during the initial operation.
The defendants have each denied any wrongdoing.
The accused spine surgeon submitted to the court his operating notes, which reportedly say that he had depended on a company distributor and its sales reps to provide “all lengths available” of the implant. In another filing, he contends that the “small area of leg numbness experienced by Ms. Martinez was a known complication of the first surgery...and was not the result of any alleged negligence.”
The device maker also denies any wrongdoing. In its filings, it claims that sales reps initially ordered a sterile kit that included implants ranging from 50 mm to 55 mm in length. The kit, says the manufacturer, was duly shipped to Houston, but the surgeon replaced the original implant with a 40-mm version during Ms. Martinez’ reoperation.
A trial is scheduled for this November.
But was the Houston incident typical?
Device makers argue that having sales reps in the OR makes sense: Well trained, they offer surgeons vital technical guidance in the use of products that are often complex.
Kaiser Health News says its investigation found otherwise. This practice and others “have been blamed for contributing to serious patient harm in thousands of medical malpractice, product liability, and whistleblower lawsuits filed over the past decade,” it reports.
The list of allegations is long: Some patients say they were injured because sales reps sold or delivered either the wrong-size implant or a defective one. Others say that in their communications with doctors, device makers were shown to have been less than truthful about the safety and durability of their products.
Currently, more than 28,000 suits have been consolidated into six multi-district federal cases. Most involve patients who claim injury after receiving hip implants. Some of the procedures required painful reoperations.
Other court actions cite device makers for other misdeeds, including keeping federal regulators in the dark about potentially dangerous product defects and plying surgeons with millions of dollars in illegal kickbacks.
Device makers have denied these and other allegations. Many of their cases have been settled confidentially.
This high-risk specialty found a way to lower its claim rates
Ob.gyns. who undergo training that simulates team interactions during a high-acuity clinical case face fewer malpractice claims afterward, according to a study published in August in Obstetrics and Gynecology.
Researchers examined the claim rates of 292 ob.gyns. who had undergone one or more such training simulations from 2002 to 2019. To gauge the effect of simulation training on the rate of medical malpractice claims, the researchers compared pretraining rates with posttraining rates. Because participants were insured by the same carrier, the team had access to the relevant claims data as well as the doctors’ durations of coverage.
The investigators assessed claim rates for the period 2002 to 2019 (the full study period), as well as rates for 2-year and 1-year participation.
Researchers found a nonsignificant drop in claim rates for doctors in the 1-year group. The drop was greater for those in the 2-year group; it decreased from 9.2 to 5.4 claims per 100 physician coverage years. (A coverage year is defined as 12 months of indemnity protection.)
For doctors who took part for the entire study period — and were therefore more likely to be among the nearly 20% of doctors who attended three or more training sessions — postsimulation claim rates dropped significantly, from 11.2 to 5.7 per 100 physician coverage years. (Attendance in more than one simulation session correlated with a greater reduction in claim rates.)
“We observed a significant reduction in malpractice claim rates after simulation training,” the researchers concluded. “Wider use of simulation training within obstetrics and gynecology should be considered.”
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
a story in the New York Daily News, among other news outlets, indicates.
In the latest iteration of this age-old practice, a team of attorneys and doctors allegedly recruited more than 400 New York City inhabitants, many of whom were homeless or addicted to drugs, over the course of 5 years to participate in their scam.
These people, who were often desperate for money, were coached to claim they’d tripped and fallen over one of the many obstacles pedestrians encounter in the city — sidewalk cracks, potholes, open or protruding cellar doors, and the like. The participant would be cajoled into signing his or her name to a fraudulent suit. Over the years, the scam netted the bosses more than $31 million from city businesses and their insurance companies.
In some cases, to add authenticity to the swindle, the scammers convinced the so-called victims to undergo an operation, promising them up to $1,500 to go under the knife.
Accused by the U.S. Attorney’s Office of masterminding the slip-and-fall operation were two attorneys, George Constantine and Marc Elefant, and a pair of doctors, Andrew Dowd, MD, an orthopedic surgeon, and Sady Ribeiro, MD, a pain management specialist and surgeon.
According to the charges, Mr. Constantine and Mr. Elefant filed lawsuits — either together or separately, though the report isn’t clear — on behalf of hundreds of people who took part in the scheme. Dr. Dowd and Dr. Ribeiro also profited handsomely, according to authorities. Dr. Dowd, they say, earned roughly $9,500 per surgery. Dr. Ribeiro is accused of treating nearly 200 participants during the con and of often paying kickbacks to them to drum up additional referrals.
If convicted on all charges, including mail and wire fraud, each of the defendants could face up to 20 years in prison.
This isn’t the first time such a scheme has been hatched and carried out in New York City.
In May 2020, three men were sentenced to prison for their involvement in a similar slip-and-fall operation that took place between 2013 and 2018. (Their sentencing followed an earlier conviction for conspiracy to commit mail and wire fraud.)
Like the most recent scheme, the one that began in 2013 preyed on the hopeless. “The whole essence of this conspiracy is to find the down-and-out, find the desperate, find the homeless,” the sentencing judge said at the time. “No person who has a job and education and can support his or her family even minimally is going to say, ‘Oh, I’ll undergo unnecessary back surgery for a thousand dollars.’ These people were vulnerable and desperate.”
Sales reps in the OR — helpful or harmful?
Although medical device makers insist that the practice of placing sales reps in operating rooms (ORs) has proven beneficial to surgeons over the years, others claim it has contributed to unwanted outcomes, according to a report published in Kaiser Health News.
In May 2018, for instance, Cristina Martinez underwent what was supposed to be a routine spinal implant procedure. In the course of the operation, her Houston-based spine surgeon discovered that the implant he was about to insert in her back was larger than the one he had intended to use. Under different circumstances, the device maker’s sales representative who was present in the OR that day might have been able to supply the smaller implant. But the rep didn’t have one available, so the surgeon proceeded with the operation using the larger plastic disk.
Four days later, in another procedure, the surgeon removed that disk and replaced it with one that was the correct size. Ms. Martinez has claimed that she awakened from the second procedure in pain, the result of nerve damage that she says led to loss of feeling in her left leg.
In a suit against the doctor, the device maker, and its distributor and sales reps, Ms. Martinez alleges that her injuries were the direct result of their negligence in not having the proper disk available during the initial operation.
The defendants have each denied any wrongdoing.
The accused spine surgeon submitted to the court his operating notes, which reportedly say that he had depended on a company distributor and its sales reps to provide “all lengths available” of the implant. In another filing, he contends that the “small area of leg numbness experienced by Ms. Martinez was a known complication of the first surgery...and was not the result of any alleged negligence.”
The device maker also denies any wrongdoing. In its filings, it claims that sales reps initially ordered a sterile kit that included implants ranging from 50 mm to 55 mm in length. The kit, says the manufacturer, was duly shipped to Houston, but the surgeon replaced the original implant with a 40-mm version during Ms. Martinez’ reoperation.
A trial is scheduled for this November.
But was the Houston incident typical?
Device makers argue that having sales reps in the OR makes sense: Well trained, they offer surgeons vital technical guidance in the use of products that are often complex.
Kaiser Health News says its investigation found otherwise. This practice and others “have been blamed for contributing to serious patient harm in thousands of medical malpractice, product liability, and whistleblower lawsuits filed over the past decade,” it reports.
The list of allegations is long: Some patients say they were injured because sales reps sold or delivered either the wrong-size implant or a defective one. Others say that in their communications with doctors, device makers were shown to have been less than truthful about the safety and durability of their products.
Currently, more than 28,000 suits have been consolidated into six multi-district federal cases. Most involve patients who claim injury after receiving hip implants. Some of the procedures required painful reoperations.
Other court actions cite device makers for other misdeeds, including keeping federal regulators in the dark about potentially dangerous product defects and plying surgeons with millions of dollars in illegal kickbacks.
Device makers have denied these and other allegations. Many of their cases have been settled confidentially.
This high-risk specialty found a way to lower its claim rates
Ob.gyns. who undergo training that simulates team interactions during a high-acuity clinical case face fewer malpractice claims afterward, according to a study published in August in Obstetrics and Gynecology.
Researchers examined the claim rates of 292 ob.gyns. who had undergone one or more such training simulations from 2002 to 2019. To gauge the effect of simulation training on the rate of medical malpractice claims, the researchers compared pretraining rates with posttraining rates. Because participants were insured by the same carrier, the team had access to the relevant claims data as well as the doctors’ durations of coverage.
The investigators assessed claim rates for the period 2002 to 2019 (the full study period), as well as rates for 2-year and 1-year participation.
Researchers found a nonsignificant drop in claim rates for doctors in the 1-year group. The drop was greater for those in the 2-year group; it decreased from 9.2 to 5.4 claims per 100 physician coverage years. (A coverage year is defined as 12 months of indemnity protection.)
For doctors who took part for the entire study period — and were therefore more likely to be among the nearly 20% of doctors who attended three or more training sessions — postsimulation claim rates dropped significantly, from 11.2 to 5.7 per 100 physician coverage years. (Attendance in more than one simulation session correlated with a greater reduction in claim rates.)
“We observed a significant reduction in malpractice claim rates after simulation training,” the researchers concluded. “Wider use of simulation training within obstetrics and gynecology should be considered.”
The content contained in this article is for informational purposes only and does not constitute legal advice. Reliance on any information provided in this article is solely at your own risk.
A version of this article first appeared on Medscape.com.
ACOG amicus brief supports case against Mississippi abortion ban
The American College of Obstetricians and Gynecologists (ACOG), took a prominent stand in the battle over abortion legislation by filing an amicus brief to the United States Supreme Court in the case of Dobbs v. Jackson Women’s Health Organization, according to a statement from ACOG issued on Sept. 21.
The case, filed by Thomas E. Dobbs, MD, state health officer of the Mississippi Department of Health, and others, appeals the decision by the U.S. Court of Appeals for the Fifth Circuit to throw out Mississippi’s law banning abortion after 15 weeks of pregnancy.*
ACOG’s amicus brief, which was signed by 24 additional medical organizations, including the American Medical Association, “represents an unprecedented level of support from a diverse group of physicians, nurses, and other health care professionals, which demonstrates the concrete medical consensus of opposition to abortion restriction legislation such as the law at the heart of Dobbs v. Jackson,” according to the ACOG statement.
The brief explains how the ban goes against not only the ability of health professionals to provide safe and essential care, but also goes against scientific evidence and medical ethics. “By preventing clinicians from providing patients with necessary medical care, the ban represents gross interference in the patient-clinician relationship,” according to the ACOG brief.
Potential implications if the ban is upheld include health risks to pregnant women at or near 15 weeks’ gestation, who might be forced to travel out of state, attempt self-induced abortion, or carry a pregnancy to term, according to the brief.
“Each of these outcomes increases the likelihood of negative consequences to a woman’s physical and psychological health that could be avoided if care were available,” according to the brief.
The brief also emphasizes that the ban will have a disproportionate effect on women who are already at risk for being medically underserved and who make up a majority of women seeking abortion: women of color, women in rural areas, and women with limited financial resources.
“This law is an example of harmful legislative interference into the practice of medicine,” said ACOG President J. Martin Tucker, MD, FACOG, on behalf of ACOG, in the statement.
“The outcome of this case could overturn decades of legal precedent that safeguards safe, legal abortion before viability, and the consequences of this case have national implications,” said Maureen G. Phipps, MD, MPH, CEO of ACOG, in an interview, as reported by ACOG press person Kate Connors.
“If the court does not strike down this law, clinicians in states across the country may face similar restrictions in their ability to provide necessary, evidence-based medical care,” Dr. Phipps explained. “If states are allowed to create new laws that further restrict abortion access, patients and families across the country will suffer,” she said.
“We hope that the Supreme Court will respond to the arguments of our brief and to the remarkable medical consensus represented by 25 organization signing the brief,” Dr. Phipps said. “We will continue educating and working through the judicial system in support of our patients’ access to evidence-based care and in opposition to legislative interference in the practice of medicine,” she emphasized.
Other medical organizations that signed the brief in support of the case against the Mississippi abortion ban included the American Academy of Pediatrics, the American Association of Family Physicians, the American College of Nurse Midwives, the American College of Physicians, the American Psychological Association, the American Society for Reproductive Medicine, the Association of Women’s Health, Obstetric and Neonatal Nurses, the American Medical Women’s Association, the Council of University Chairs of Obstetrics and Gynecology, the National Association of Nurse Practitioners in Women’s Health, the North American Society for Pediatric and Adolescent Gynecology, the Society of OB/GYN Hospitalists, and the Society of Family Planning.
*This story was updated on 10/7/2021.
The American College of Obstetricians and Gynecologists (ACOG), took a prominent stand in the battle over abortion legislation by filing an amicus brief to the United States Supreme Court in the case of Dobbs v. Jackson Women’s Health Organization, according to a statement from ACOG issued on Sept. 21.
The case, filed by Thomas E. Dobbs, MD, state health officer of the Mississippi Department of Health, and others, appeals the decision by the U.S. Court of Appeals for the Fifth Circuit to throw out Mississippi’s law banning abortion after 15 weeks of pregnancy.*
ACOG’s amicus brief, which was signed by 24 additional medical organizations, including the American Medical Association, “represents an unprecedented level of support from a diverse group of physicians, nurses, and other health care professionals, which demonstrates the concrete medical consensus of opposition to abortion restriction legislation such as the law at the heart of Dobbs v. Jackson,” according to the ACOG statement.
The brief explains how the ban goes against not only the ability of health professionals to provide safe and essential care, but also goes against scientific evidence and medical ethics. “By preventing clinicians from providing patients with necessary medical care, the ban represents gross interference in the patient-clinician relationship,” according to the ACOG brief.
Potential implications if the ban is upheld include health risks to pregnant women at or near 15 weeks’ gestation, who might be forced to travel out of state, attempt self-induced abortion, or carry a pregnancy to term, according to the brief.
“Each of these outcomes increases the likelihood of negative consequences to a woman’s physical and psychological health that could be avoided if care were available,” according to the brief.
The brief also emphasizes that the ban will have a disproportionate effect on women who are already at risk for being medically underserved and who make up a majority of women seeking abortion: women of color, women in rural areas, and women with limited financial resources.
“This law is an example of harmful legislative interference into the practice of medicine,” said ACOG President J. Martin Tucker, MD, FACOG, on behalf of ACOG, in the statement.
“The outcome of this case could overturn decades of legal precedent that safeguards safe, legal abortion before viability, and the consequences of this case have national implications,” said Maureen G. Phipps, MD, MPH, CEO of ACOG, in an interview, as reported by ACOG press person Kate Connors.
“If the court does not strike down this law, clinicians in states across the country may face similar restrictions in their ability to provide necessary, evidence-based medical care,” Dr. Phipps explained. “If states are allowed to create new laws that further restrict abortion access, patients and families across the country will suffer,” she said.
“We hope that the Supreme Court will respond to the arguments of our brief and to the remarkable medical consensus represented by 25 organization signing the brief,” Dr. Phipps said. “We will continue educating and working through the judicial system in support of our patients’ access to evidence-based care and in opposition to legislative interference in the practice of medicine,” she emphasized.
Other medical organizations that signed the brief in support of the case against the Mississippi abortion ban included the American Academy of Pediatrics, the American Association of Family Physicians, the American College of Nurse Midwives, the American College of Physicians, the American Psychological Association, the American Society for Reproductive Medicine, the Association of Women’s Health, Obstetric and Neonatal Nurses, the American Medical Women’s Association, the Council of University Chairs of Obstetrics and Gynecology, the National Association of Nurse Practitioners in Women’s Health, the North American Society for Pediatric and Adolescent Gynecology, the Society of OB/GYN Hospitalists, and the Society of Family Planning.
*This story was updated on 10/7/2021.
The American College of Obstetricians and Gynecologists (ACOG), took a prominent stand in the battle over abortion legislation by filing an amicus brief to the United States Supreme Court in the case of Dobbs v. Jackson Women’s Health Organization, according to a statement from ACOG issued on Sept. 21.
The case, filed by Thomas E. Dobbs, MD, state health officer of the Mississippi Department of Health, and others, appeals the decision by the U.S. Court of Appeals for the Fifth Circuit to throw out Mississippi’s law banning abortion after 15 weeks of pregnancy.*
ACOG’s amicus brief, which was signed by 24 additional medical organizations, including the American Medical Association, “represents an unprecedented level of support from a diverse group of physicians, nurses, and other health care professionals, which demonstrates the concrete medical consensus of opposition to abortion restriction legislation such as the law at the heart of Dobbs v. Jackson,” according to the ACOG statement.
The brief explains how the ban goes against not only the ability of health professionals to provide safe and essential care, but also goes against scientific evidence and medical ethics. “By preventing clinicians from providing patients with necessary medical care, the ban represents gross interference in the patient-clinician relationship,” according to the ACOG brief.
Potential implications if the ban is upheld include health risks to pregnant women at or near 15 weeks’ gestation, who might be forced to travel out of state, attempt self-induced abortion, or carry a pregnancy to term, according to the brief.
“Each of these outcomes increases the likelihood of negative consequences to a woman’s physical and psychological health that could be avoided if care were available,” according to the brief.
The brief also emphasizes that the ban will have a disproportionate effect on women who are already at risk for being medically underserved and who make up a majority of women seeking abortion: women of color, women in rural areas, and women with limited financial resources.
“This law is an example of harmful legislative interference into the practice of medicine,” said ACOG President J. Martin Tucker, MD, FACOG, on behalf of ACOG, in the statement.
“The outcome of this case could overturn decades of legal precedent that safeguards safe, legal abortion before viability, and the consequences of this case have national implications,” said Maureen G. Phipps, MD, MPH, CEO of ACOG, in an interview, as reported by ACOG press person Kate Connors.
“If the court does not strike down this law, clinicians in states across the country may face similar restrictions in their ability to provide necessary, evidence-based medical care,” Dr. Phipps explained. “If states are allowed to create new laws that further restrict abortion access, patients and families across the country will suffer,” she said.
“We hope that the Supreme Court will respond to the arguments of our brief and to the remarkable medical consensus represented by 25 organization signing the brief,” Dr. Phipps said. “We will continue educating and working through the judicial system in support of our patients’ access to evidence-based care and in opposition to legislative interference in the practice of medicine,” she emphasized.
Other medical organizations that signed the brief in support of the case against the Mississippi abortion ban included the American Academy of Pediatrics, the American Association of Family Physicians, the American College of Nurse Midwives, the American College of Physicians, the American Psychological Association, the American Society for Reproductive Medicine, the Association of Women’s Health, Obstetric and Neonatal Nurses, the American Medical Women’s Association, the Council of University Chairs of Obstetrics and Gynecology, the National Association of Nurse Practitioners in Women’s Health, the North American Society for Pediatric and Adolescent Gynecology, the Society of OB/GYN Hospitalists, and the Society of Family Planning.
*This story was updated on 10/7/2021.
COVID-19 a rare trigger for Guillain-Barré syndrome
Although Guillain-Barré syndrome may rarely follow a recent infection with SARS-CoV-2, a strong relationship of GBS with the novel coronavirus is unlikely, say researchers with the International GBS Outcome Study (IGOS) consortium.
“Our study shows that COVID-19 may precede Guillain-Barré syndrome in rare cases, but the existence of a true association or causal relation still needs to be established,” Bart Jacobs, MD, PhD, department of neurology and immunology, Erasmus Medical Center and University Medical Center, both in Rotterdam, the Netherlands, said in a statement.
The study was published online in the journal Brain.
No uptick in pandemic cases
Since the beginning of the pandemic, there are reports of more than 90 GBS diagnoses following a possible COVID-19 infection. However, it remains unclear whether COVID-19 is another potential infectious trigger or whether the reported cases are coincidental.
To investigate further, Dr. Jacobs and the IGOS consortium reviewed 49 patients (median age, 56 years) with GBS who were added to their ongoing prospective observational cohort study between Jan. 30 and May 30, 2020.
The patients came from China, Denmark, France, Greece, Italy, Japan, the Netherlands, Spain, Switzerland, and the United Kingdom.
Of the 49 GBS patients, 8 (16%) had a confirmed and 3 (6%) had a probable SARS-CoV-2 infection; 15 had possible SARS-CoV-2 infection, 21 had no suspicion of SARS-CoV-2 infection, and 2 were “unclassifiable.”
Of the 11 patients with confirmed/probable SARS-CoV-2 infection, 9 had no serological evidence of any other recent preceding infection known to be associated with GBS.
The other two had serological evidence of a recent Campylobacter jejuni infection, which could have played a role in GBS onset, the researchers noted.
Most patients with a confirmed/probable SARS-CoV-2 infection had a sensorimotor GBS variant (73%), although Miller Fisher syndrome–GBS overlap (18%) and an ataxic variant (9%) were also found.
All patients with a confirmed/probable SARS-CoV-2 infection had a severe form of GBS. Common early neurologic features were facial weakness (64%), sensory deficits (82%), and autonomic dysfunction (64%), although not significantly different, compared with the other patients.
All eight patients who underwent nerve conduction study had a demyelinating subtype, which was more frequent than in the other GBS patients (47%; P = .012) as well as historical region and age-matched controls included in the IGOS cohort before the pandemic (52%, P = .016).
The median time from the onset of SARS-CoV-2 infection to neurologic symptoms was 16 days and ranged from 12 to 22 days.
More research needed
The researchers noted that the 22% frequency of a preceding SARS-CoV-2 infection in this study population was “higher than estimates of the contemporaneous background prevalence of SARS-CoV-2, which may be a result of recruitment bias during the pandemic, but could also indicate that GBS may rarely follow a recent SARS-CoV-2 infection.”
Importantly, however, they did not find more patients diagnosed with GBS during the first 4 months of the pandemic, compared with previous years, “suggesting that a strong association between SARS-CoV-2 and GBS is unlikely.”
“Should SARS-CoV-2 indeed be able to trigger GBS, our data are consistent with a postinfectious disease mechanism rather than direct viral invasion,” they noted, adding that the study was not designed to quantify a causative link between GBS and SARS-CoV-2.
“An unbiased multicenter, international, case-control study is needed to determine whether there is an association or not,” they wrote.
The IGOS is financially supported by the GBS-CIDP Foundation International, Gain, Erasmus MC University Medical Center Rotterdam, Glasgow University, CSL Behring, Grifols, Annexon and Hansa Biopharma. Dr. Jacobs received grants from Grifols, CSL-Behring, Annexon, Prinses Beatrix Spierfonds, Hansa Biopharma, and GBS-CIDP Foundation International and is on the global medical advisory board of the GBS CIDP Foundation International.
A version of this article first appeared on Medscape.com.
Although Guillain-Barré syndrome may rarely follow a recent infection with SARS-CoV-2, a strong relationship of GBS with the novel coronavirus is unlikely, say researchers with the International GBS Outcome Study (IGOS) consortium.
“Our study shows that COVID-19 may precede Guillain-Barré syndrome in rare cases, but the existence of a true association or causal relation still needs to be established,” Bart Jacobs, MD, PhD, department of neurology and immunology, Erasmus Medical Center and University Medical Center, both in Rotterdam, the Netherlands, said in a statement.
The study was published online in the journal Brain.
No uptick in pandemic cases
Since the beginning of the pandemic, there are reports of more than 90 GBS diagnoses following a possible COVID-19 infection. However, it remains unclear whether COVID-19 is another potential infectious trigger or whether the reported cases are coincidental.
To investigate further, Dr. Jacobs and the IGOS consortium reviewed 49 patients (median age, 56 years) with GBS who were added to their ongoing prospective observational cohort study between Jan. 30 and May 30, 2020.
The patients came from China, Denmark, France, Greece, Italy, Japan, the Netherlands, Spain, Switzerland, and the United Kingdom.
Of the 49 GBS patients, 8 (16%) had a confirmed and 3 (6%) had a probable SARS-CoV-2 infection; 15 had possible SARS-CoV-2 infection, 21 had no suspicion of SARS-CoV-2 infection, and 2 were “unclassifiable.”
Of the 11 patients with confirmed/probable SARS-CoV-2 infection, 9 had no serological evidence of any other recent preceding infection known to be associated with GBS.
The other two had serological evidence of a recent Campylobacter jejuni infection, which could have played a role in GBS onset, the researchers noted.
Most patients with a confirmed/probable SARS-CoV-2 infection had a sensorimotor GBS variant (73%), although Miller Fisher syndrome–GBS overlap (18%) and an ataxic variant (9%) were also found.
All patients with a confirmed/probable SARS-CoV-2 infection had a severe form of GBS. Common early neurologic features were facial weakness (64%), sensory deficits (82%), and autonomic dysfunction (64%), although not significantly different, compared with the other patients.
All eight patients who underwent nerve conduction study had a demyelinating subtype, which was more frequent than in the other GBS patients (47%; P = .012) as well as historical region and age-matched controls included in the IGOS cohort before the pandemic (52%, P = .016).
The median time from the onset of SARS-CoV-2 infection to neurologic symptoms was 16 days and ranged from 12 to 22 days.
More research needed
The researchers noted that the 22% frequency of a preceding SARS-CoV-2 infection in this study population was “higher than estimates of the contemporaneous background prevalence of SARS-CoV-2, which may be a result of recruitment bias during the pandemic, but could also indicate that GBS may rarely follow a recent SARS-CoV-2 infection.”
Importantly, however, they did not find more patients diagnosed with GBS during the first 4 months of the pandemic, compared with previous years, “suggesting that a strong association between SARS-CoV-2 and GBS is unlikely.”
“Should SARS-CoV-2 indeed be able to trigger GBS, our data are consistent with a postinfectious disease mechanism rather than direct viral invasion,” they noted, adding that the study was not designed to quantify a causative link between GBS and SARS-CoV-2.
“An unbiased multicenter, international, case-control study is needed to determine whether there is an association or not,” they wrote.
The IGOS is financially supported by the GBS-CIDP Foundation International, Gain, Erasmus MC University Medical Center Rotterdam, Glasgow University, CSL Behring, Grifols, Annexon and Hansa Biopharma. Dr. Jacobs received grants from Grifols, CSL-Behring, Annexon, Prinses Beatrix Spierfonds, Hansa Biopharma, and GBS-CIDP Foundation International and is on the global medical advisory board of the GBS CIDP Foundation International.
A version of this article first appeared on Medscape.com.
Although Guillain-Barré syndrome may rarely follow a recent infection with SARS-CoV-2, a strong relationship of GBS with the novel coronavirus is unlikely, say researchers with the International GBS Outcome Study (IGOS) consortium.
“Our study shows that COVID-19 may precede Guillain-Barré syndrome in rare cases, but the existence of a true association or causal relation still needs to be established,” Bart Jacobs, MD, PhD, department of neurology and immunology, Erasmus Medical Center and University Medical Center, both in Rotterdam, the Netherlands, said in a statement.
The study was published online in the journal Brain.
No uptick in pandemic cases
Since the beginning of the pandemic, there are reports of more than 90 GBS diagnoses following a possible COVID-19 infection. However, it remains unclear whether COVID-19 is another potential infectious trigger or whether the reported cases are coincidental.
To investigate further, Dr. Jacobs and the IGOS consortium reviewed 49 patients (median age, 56 years) with GBS who were added to their ongoing prospective observational cohort study between Jan. 30 and May 30, 2020.
The patients came from China, Denmark, France, Greece, Italy, Japan, the Netherlands, Spain, Switzerland, and the United Kingdom.
Of the 49 GBS patients, 8 (16%) had a confirmed and 3 (6%) had a probable SARS-CoV-2 infection; 15 had possible SARS-CoV-2 infection, 21 had no suspicion of SARS-CoV-2 infection, and 2 were “unclassifiable.”
Of the 11 patients with confirmed/probable SARS-CoV-2 infection, 9 had no serological evidence of any other recent preceding infection known to be associated with GBS.
The other two had serological evidence of a recent Campylobacter jejuni infection, which could have played a role in GBS onset, the researchers noted.
Most patients with a confirmed/probable SARS-CoV-2 infection had a sensorimotor GBS variant (73%), although Miller Fisher syndrome–GBS overlap (18%) and an ataxic variant (9%) were also found.
All patients with a confirmed/probable SARS-CoV-2 infection had a severe form of GBS. Common early neurologic features were facial weakness (64%), sensory deficits (82%), and autonomic dysfunction (64%), although not significantly different, compared with the other patients.
All eight patients who underwent nerve conduction study had a demyelinating subtype, which was more frequent than in the other GBS patients (47%; P = .012) as well as historical region and age-matched controls included in the IGOS cohort before the pandemic (52%, P = .016).
The median time from the onset of SARS-CoV-2 infection to neurologic symptoms was 16 days and ranged from 12 to 22 days.
More research needed
The researchers noted that the 22% frequency of a preceding SARS-CoV-2 infection in this study population was “higher than estimates of the contemporaneous background prevalence of SARS-CoV-2, which may be a result of recruitment bias during the pandemic, but could also indicate that GBS may rarely follow a recent SARS-CoV-2 infection.”
Importantly, however, they did not find more patients diagnosed with GBS during the first 4 months of the pandemic, compared with previous years, “suggesting that a strong association between SARS-CoV-2 and GBS is unlikely.”
“Should SARS-CoV-2 indeed be able to trigger GBS, our data are consistent with a postinfectious disease mechanism rather than direct viral invasion,” they noted, adding that the study was not designed to quantify a causative link between GBS and SARS-CoV-2.
“An unbiased multicenter, international, case-control study is needed to determine whether there is an association or not,” they wrote.
The IGOS is financially supported by the GBS-CIDP Foundation International, Gain, Erasmus MC University Medical Center Rotterdam, Glasgow University, CSL Behring, Grifols, Annexon and Hansa Biopharma. Dr. Jacobs received grants from Grifols, CSL-Behring, Annexon, Prinses Beatrix Spierfonds, Hansa Biopharma, and GBS-CIDP Foundation International and is on the global medical advisory board of the GBS CIDP Foundation International.
A version of this article first appeared on Medscape.com.
CDC chief overrules panel, OKs boosters for health care workers
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.
Remdesivir sharply cuts COVID hospitalization risk, Gilead says
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.