User login
Update from the Public Policy Committee
The Public Policy Committee has spent a great deal of time in recent months learning about the current reimbursement issues facing hospitalists. It is our belief that hospitalists bring something unique to the bedside that is not being recognized by our current payor system. This recognition will be a long-term project for the committee, but we have a number of short-term goals. The short-term goals are to educate our membership about using the currently available codes to optimize their practice; working with payors or intermediaries; and negotiating with the facilities to receive remuneration. We will investigate the possibility of coordinating with pilot projects being conducted by the Center for Medicare and Medicaid Services. These pilots may be able to demonstrate further the value of having a hospitalist manage the care of the hospitalized patient. We monitor closely any proposed changes in the Medicare fee schedule and work to preserve the current schedule as much as possible. However, longer term, we need to identify and design a model that rewards hospitalists for the quality and efficiency that they bring to their patients and facilities.
This may involve working with a number of other organizations as our allies. To this end, the Public Policy Committee recommended, and the SHM Board approved, that SHM’s government affairs contractor, Medical Advocacy Services, Inc. (MASI), draft a White Paper regarding the consideration of hospitalists as a specialty. Organizations draft such papers to thoroughly examine a particular topic. White Papers are typically used as an advocacy tool and can be presented to other organizations and to policymakers to make the case for a policy. The committee will work with MASI during the writing process, and a final paper will be released in 2005.
The Public Policy Committee also recently updated SHM’s “Guiding Principles,” which outline SHM’s position on numerous current health policy issues. The principles were first drafted by MASI and the Public Policy Committee in 2003. They enable MASI and me to make quick decisions on whether or not to sign SHM onto joint letters to Congress or the Administration. They cover areas such as medical liability, regulatory relief, and access to care. The principles will be particularly useful as health issues arise when the 109th Congress convenes in January. The updated Guiding Principles, approved by the Board in October, can be viewed on the SHM Advocacy Web site, under “Where We Stand.” We will update them regularly to address emerging and evolving issue areas.
For more information about SHM’s public policy positions, please visit the Advocacy section of the SHM Web site at www.hospitalmedicine.org.
The Public Policy Committee has spent a great deal of time in recent months learning about the current reimbursement issues facing hospitalists. It is our belief that hospitalists bring something unique to the bedside that is not being recognized by our current payor system. This recognition will be a long-term project for the committee, but we have a number of short-term goals. The short-term goals are to educate our membership about using the currently available codes to optimize their practice; working with payors or intermediaries; and negotiating with the facilities to receive remuneration. We will investigate the possibility of coordinating with pilot projects being conducted by the Center for Medicare and Medicaid Services. These pilots may be able to demonstrate further the value of having a hospitalist manage the care of the hospitalized patient. We monitor closely any proposed changes in the Medicare fee schedule and work to preserve the current schedule as much as possible. However, longer term, we need to identify and design a model that rewards hospitalists for the quality and efficiency that they bring to their patients and facilities.
This may involve working with a number of other organizations as our allies. To this end, the Public Policy Committee recommended, and the SHM Board approved, that SHM’s government affairs contractor, Medical Advocacy Services, Inc. (MASI), draft a White Paper regarding the consideration of hospitalists as a specialty. Organizations draft such papers to thoroughly examine a particular topic. White Papers are typically used as an advocacy tool and can be presented to other organizations and to policymakers to make the case for a policy. The committee will work with MASI during the writing process, and a final paper will be released in 2005.
The Public Policy Committee also recently updated SHM’s “Guiding Principles,” which outline SHM’s position on numerous current health policy issues. The principles were first drafted by MASI and the Public Policy Committee in 2003. They enable MASI and me to make quick decisions on whether or not to sign SHM onto joint letters to Congress or the Administration. They cover areas such as medical liability, regulatory relief, and access to care. The principles will be particularly useful as health issues arise when the 109th Congress convenes in January. The updated Guiding Principles, approved by the Board in October, can be viewed on the SHM Advocacy Web site, under “Where We Stand.” We will update them regularly to address emerging and evolving issue areas.
For more information about SHM’s public policy positions, please visit the Advocacy section of the SHM Web site at www.hospitalmedicine.org.
The Public Policy Committee has spent a great deal of time in recent months learning about the current reimbursement issues facing hospitalists. It is our belief that hospitalists bring something unique to the bedside that is not being recognized by our current payor system. This recognition will be a long-term project for the committee, but we have a number of short-term goals. The short-term goals are to educate our membership about using the currently available codes to optimize their practice; working with payors or intermediaries; and negotiating with the facilities to receive remuneration. We will investigate the possibility of coordinating with pilot projects being conducted by the Center for Medicare and Medicaid Services. These pilots may be able to demonstrate further the value of having a hospitalist manage the care of the hospitalized patient. We monitor closely any proposed changes in the Medicare fee schedule and work to preserve the current schedule as much as possible. However, longer term, we need to identify and design a model that rewards hospitalists for the quality and efficiency that they bring to their patients and facilities.
This may involve working with a number of other organizations as our allies. To this end, the Public Policy Committee recommended, and the SHM Board approved, that SHM’s government affairs contractor, Medical Advocacy Services, Inc. (MASI), draft a White Paper regarding the consideration of hospitalists as a specialty. Organizations draft such papers to thoroughly examine a particular topic. White Papers are typically used as an advocacy tool and can be presented to other organizations and to policymakers to make the case for a policy. The committee will work with MASI during the writing process, and a final paper will be released in 2005.
The Public Policy Committee also recently updated SHM’s “Guiding Principles,” which outline SHM’s position on numerous current health policy issues. The principles were first drafted by MASI and the Public Policy Committee in 2003. They enable MASI and me to make quick decisions on whether or not to sign SHM onto joint letters to Congress or the Administration. They cover areas such as medical liability, regulatory relief, and access to care. The principles will be particularly useful as health issues arise when the 109th Congress convenes in January. The updated Guiding Principles, approved by the Board in October, can be viewed on the SHM Advocacy Web site, under “Where We Stand.” We will update them regularly to address emerging and evolving issue areas.
For more information about SHM’s public policy positions, please visit the Advocacy section of the SHM Web site at www.hospitalmedicine.org.
Practice Guidelines for the Management of Bacterial Meningitis
Enter text here
Enter text here
Enter text here
Rates, Predictors, and Outcomes of Major Hemorrhage in Patients with Atrial Fibrillation
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
The Fountain of Youth
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion


This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
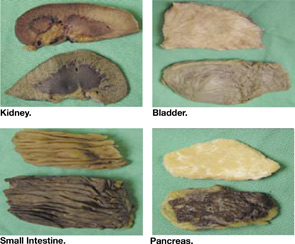
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
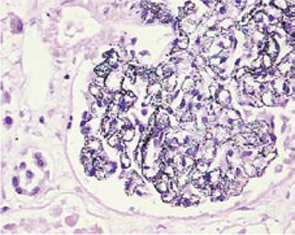
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Involuntary commitment, ‘false’ memories
Self-proclaimed ‘exorcist’ claims he was improperly committed
Court of claims (NY)
In response to a 911 call, police arrested a man who, the caller said, was trying to choke and stab an individual. Upon his arrest, the man claimed that he was an exorcist. He justified his attack by alleging that his victim was a medium for demons and spirits.
The suspect was taken to a psychiatric hospital; staff decided that he endangered himself and others and should be committed. During his commitment, he was restrained and forcibly given medication.
The man later sued the hospital for intentional infliction of emotional distress and malpractice. He charged that the hospital denied him the right to a court hearing after he was admitted.
The court dismissed the case. The court noted that the plaintiff did not present expert testimony to support his emotional distress claim.
Dr. Grant’s observations
Involuntary commitment. Although the standards for involuntary commitment vary from state to state, some general principles apply.
A patient who endangers himself or others may be held for varying periods until a court hearing can be arranged. State law determines how long someone can be held before a court-ordered commitment. Although the patient has a right to a court hearing, the state is not obligated to conduct that hearing sooner than is determined by state law. Clinicians need to learn the laws governing involuntary commitment in the states in which they practice.
Patients who are involuntarily committed are not required to accept treatment, however. Competent adults generally must give informed consent to treatment, but this rule is usually suspended in an emergency. When a patient is a danger to self or others, that person can be restrained and medicated against his or her will for as long as the emergency lasts. In such cases, the clinician should clearly document:
- indications for using restraint and forced medication (include a detailed assessment of the patient’s dangerous behaviors)
- the patient’s response to previous behavioral approaches or treatments
- grounds for believing that the patient’s refusal of other interventions is clearly a product of the illness.
Patient: psychiatrists planted false memories, gave wrong diagnosis
Green County (WI) circuit court
A 55-year-old woman was seen in a hospital clinic’s weight-loss program and developed anxiety symptoms as she reached normal weight. Her psychologist assigned her to read a book about surviving incest, which focused on repressed memories that surface during recovery. The woman then received hypnosis from a psychiatrist who was not trained as a hypnotist.
During the hypnosis sessions, the patient reported “remembering” past instances of abuse that she had not previously recalled. The psychiatrist guided her to relive or reenact one event, in which she reported remembering being anally raped. The patient became more depressed and required hospitalization. Another psychiatrist, who took over the case when the first psychiatrist left the clinic, diagnosed the patient as having multiple personality disorder.
The patient later questioned the diagnosis and came to believe that her treatment had been inappropriate and that the memories had been planted. The patient, once a registered nurse, is now disabled.
In court, the jury heard:
- charges of negligence against the treating physicians on behalf of the woman and her son, who was briefly treated by the original psychiatrist
- charges that neither the psychiatrists nor the clinic obtained informed consent before treating the woman or her son.
- The jury decided for the physician, clinic, and hospital on all charges.
Dr. Grant’s observations
This case involves several complex and controversial areas in psychiatry: recovered memory, multiple personality disorder, and use of hypnosis. Although the jury found for the physician, clinic, and hospital, these areas provide fertile ground for lawsuits, many of which are successful.
The case involved two distinct legal causes of action:
- negligent care
- lack of informed consent.
Recovered memory. The veracity of recovered memory has been vigorously debated.1 Because the credibility of recovered memory cannot be established, the clinician should clearly state in the chart that the past incident the patient reports during therapy may not have happened. The clinician also must avoid imposing his or her beliefs on the patient (such as assuming that patients with eating disorders have been sexually abused) or advocating for action on the patient’s part.
Hypnosis used to recover memories of abuse may be particularly complex legally.2 A clinician using hypnosis may jeopardize therapeutic disinterest by interjecting suggestions—often without realizing that he or she is doing so.
To avoid negligence claims, clinicians should stay within their areas of competence when treating patients. If hypnosis is deemed clinically necessary, a clinician not trained in hypnosis should refer the patient to a certified clinical hypnotist.
Multiple personality disorder is included in DSM-IV-TR as dissociative identity disorder, but approximately one-third of psychiatrists question whether this is a legitimate diagnosis.3 Clearly documenting the basis for this—or any—diagnosis may help the clinician avoid a lawsuit or defend against a negligence charge.
Informed consent. Failure to inform patients about the risks associated with recovered memories is one of the most common allegations against clinicians in recovered memory cases.
Canterbury v. Spence, the landmark case of informed consent, offers some guidance. The court found that the clinician must provide reasonable disclosure of:
- therapy alternatives open to the patient
- goals expected to be achieved
- the risks involved with recovering memories.4
Some have proposed that clinicians should disclose the risk of recovering false memories of sexual and physical abuse before starting treatment.5 The clinician should then clearly document this disclosure.
1. Pope HG, Jr. Psychology astray: Fallacies in studies of repressed memory and childhood trauma. Boca Raton, FL: Upton Books, 1997.
2. Borawick v. Shay. 68 F3d 597 (2d Cir. 1995).
3. Pope HG, Jr, Oliva PS, Hudson JI, et al. Attitudes toward DSM-IV dissociative disorders diagnoses among board-certified American psychiatrists. Am J Psychiatry 1999;156:321-3.
4. Canterbury v. Spence. 464 F2d 775 (DC Cir 1972).
5. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29:138-47.
Self-proclaimed ‘exorcist’ claims he was improperly committed
Court of claims (NY)
In response to a 911 call, police arrested a man who, the caller said, was trying to choke and stab an individual. Upon his arrest, the man claimed that he was an exorcist. He justified his attack by alleging that his victim was a medium for demons and spirits.
The suspect was taken to a psychiatric hospital; staff decided that he endangered himself and others and should be committed. During his commitment, he was restrained and forcibly given medication.
The man later sued the hospital for intentional infliction of emotional distress and malpractice. He charged that the hospital denied him the right to a court hearing after he was admitted.
The court dismissed the case. The court noted that the plaintiff did not present expert testimony to support his emotional distress claim.
Dr. Grant’s observations
Involuntary commitment. Although the standards for involuntary commitment vary from state to state, some general principles apply.
A patient who endangers himself or others may be held for varying periods until a court hearing can be arranged. State law determines how long someone can be held before a court-ordered commitment. Although the patient has a right to a court hearing, the state is not obligated to conduct that hearing sooner than is determined by state law. Clinicians need to learn the laws governing involuntary commitment in the states in which they practice.
Patients who are involuntarily committed are not required to accept treatment, however. Competent adults generally must give informed consent to treatment, but this rule is usually suspended in an emergency. When a patient is a danger to self or others, that person can be restrained and medicated against his or her will for as long as the emergency lasts. In such cases, the clinician should clearly document:
- indications for using restraint and forced medication (include a detailed assessment of the patient’s dangerous behaviors)
- the patient’s response to previous behavioral approaches or treatments
- grounds for believing that the patient’s refusal of other interventions is clearly a product of the illness.
Patient: psychiatrists planted false memories, gave wrong diagnosis
Green County (WI) circuit court
A 55-year-old woman was seen in a hospital clinic’s weight-loss program and developed anxiety symptoms as she reached normal weight. Her psychologist assigned her to read a book about surviving incest, which focused on repressed memories that surface during recovery. The woman then received hypnosis from a psychiatrist who was not trained as a hypnotist.
During the hypnosis sessions, the patient reported “remembering” past instances of abuse that she had not previously recalled. The psychiatrist guided her to relive or reenact one event, in which she reported remembering being anally raped. The patient became more depressed and required hospitalization. Another psychiatrist, who took over the case when the first psychiatrist left the clinic, diagnosed the patient as having multiple personality disorder.
The patient later questioned the diagnosis and came to believe that her treatment had been inappropriate and that the memories had been planted. The patient, once a registered nurse, is now disabled.
In court, the jury heard:
- charges of negligence against the treating physicians on behalf of the woman and her son, who was briefly treated by the original psychiatrist
- charges that neither the psychiatrists nor the clinic obtained informed consent before treating the woman or her son.
- The jury decided for the physician, clinic, and hospital on all charges.
Dr. Grant’s observations
This case involves several complex and controversial areas in psychiatry: recovered memory, multiple personality disorder, and use of hypnosis. Although the jury found for the physician, clinic, and hospital, these areas provide fertile ground for lawsuits, many of which are successful.
The case involved two distinct legal causes of action:
- negligent care
- lack of informed consent.
Recovered memory. The veracity of recovered memory has been vigorously debated.1 Because the credibility of recovered memory cannot be established, the clinician should clearly state in the chart that the past incident the patient reports during therapy may not have happened. The clinician also must avoid imposing his or her beliefs on the patient (such as assuming that patients with eating disorders have been sexually abused) or advocating for action on the patient’s part.
Hypnosis used to recover memories of abuse may be particularly complex legally.2 A clinician using hypnosis may jeopardize therapeutic disinterest by interjecting suggestions—often without realizing that he or she is doing so.
To avoid negligence claims, clinicians should stay within their areas of competence when treating patients. If hypnosis is deemed clinically necessary, a clinician not trained in hypnosis should refer the patient to a certified clinical hypnotist.
Multiple personality disorder is included in DSM-IV-TR as dissociative identity disorder, but approximately one-third of psychiatrists question whether this is a legitimate diagnosis.3 Clearly documenting the basis for this—or any—diagnosis may help the clinician avoid a lawsuit or defend against a negligence charge.
Informed consent. Failure to inform patients about the risks associated with recovered memories is one of the most common allegations against clinicians in recovered memory cases.
Canterbury v. Spence, the landmark case of informed consent, offers some guidance. The court found that the clinician must provide reasonable disclosure of:
- therapy alternatives open to the patient
- goals expected to be achieved
- the risks involved with recovering memories.4
Some have proposed that clinicians should disclose the risk of recovering false memories of sexual and physical abuse before starting treatment.5 The clinician should then clearly document this disclosure.
Self-proclaimed ‘exorcist’ claims he was improperly committed
Court of claims (NY)
In response to a 911 call, police arrested a man who, the caller said, was trying to choke and stab an individual. Upon his arrest, the man claimed that he was an exorcist. He justified his attack by alleging that his victim was a medium for demons and spirits.
The suspect was taken to a psychiatric hospital; staff decided that he endangered himself and others and should be committed. During his commitment, he was restrained and forcibly given medication.
The man later sued the hospital for intentional infliction of emotional distress and malpractice. He charged that the hospital denied him the right to a court hearing after he was admitted.
The court dismissed the case. The court noted that the plaintiff did not present expert testimony to support his emotional distress claim.
Dr. Grant’s observations
Involuntary commitment. Although the standards for involuntary commitment vary from state to state, some general principles apply.
A patient who endangers himself or others may be held for varying periods until a court hearing can be arranged. State law determines how long someone can be held before a court-ordered commitment. Although the patient has a right to a court hearing, the state is not obligated to conduct that hearing sooner than is determined by state law. Clinicians need to learn the laws governing involuntary commitment in the states in which they practice.
Patients who are involuntarily committed are not required to accept treatment, however. Competent adults generally must give informed consent to treatment, but this rule is usually suspended in an emergency. When a patient is a danger to self or others, that person can be restrained and medicated against his or her will for as long as the emergency lasts. In such cases, the clinician should clearly document:
- indications for using restraint and forced medication (include a detailed assessment of the patient’s dangerous behaviors)
- the patient’s response to previous behavioral approaches or treatments
- grounds for believing that the patient’s refusal of other interventions is clearly a product of the illness.
Patient: psychiatrists planted false memories, gave wrong diagnosis
Green County (WI) circuit court
A 55-year-old woman was seen in a hospital clinic’s weight-loss program and developed anxiety symptoms as she reached normal weight. Her psychologist assigned her to read a book about surviving incest, which focused on repressed memories that surface during recovery. The woman then received hypnosis from a psychiatrist who was not trained as a hypnotist.
During the hypnosis sessions, the patient reported “remembering” past instances of abuse that she had not previously recalled. The psychiatrist guided her to relive or reenact one event, in which she reported remembering being anally raped. The patient became more depressed and required hospitalization. Another psychiatrist, who took over the case when the first psychiatrist left the clinic, diagnosed the patient as having multiple personality disorder.
The patient later questioned the diagnosis and came to believe that her treatment had been inappropriate and that the memories had been planted. The patient, once a registered nurse, is now disabled.
In court, the jury heard:
- charges of negligence against the treating physicians on behalf of the woman and her son, who was briefly treated by the original psychiatrist
- charges that neither the psychiatrists nor the clinic obtained informed consent before treating the woman or her son.
- The jury decided for the physician, clinic, and hospital on all charges.
Dr. Grant’s observations
This case involves several complex and controversial areas in psychiatry: recovered memory, multiple personality disorder, and use of hypnosis. Although the jury found for the physician, clinic, and hospital, these areas provide fertile ground for lawsuits, many of which are successful.
The case involved two distinct legal causes of action:
- negligent care
- lack of informed consent.
Recovered memory. The veracity of recovered memory has been vigorously debated.1 Because the credibility of recovered memory cannot be established, the clinician should clearly state in the chart that the past incident the patient reports during therapy may not have happened. The clinician also must avoid imposing his or her beliefs on the patient (such as assuming that patients with eating disorders have been sexually abused) or advocating for action on the patient’s part.
Hypnosis used to recover memories of abuse may be particularly complex legally.2 A clinician using hypnosis may jeopardize therapeutic disinterest by interjecting suggestions—often without realizing that he or she is doing so.
To avoid negligence claims, clinicians should stay within their areas of competence when treating patients. If hypnosis is deemed clinically necessary, a clinician not trained in hypnosis should refer the patient to a certified clinical hypnotist.
Multiple personality disorder is included in DSM-IV-TR as dissociative identity disorder, but approximately one-third of psychiatrists question whether this is a legitimate diagnosis.3 Clearly documenting the basis for this—or any—diagnosis may help the clinician avoid a lawsuit or defend against a negligence charge.
Informed consent. Failure to inform patients about the risks associated with recovered memories is one of the most common allegations against clinicians in recovered memory cases.
Canterbury v. Spence, the landmark case of informed consent, offers some guidance. The court found that the clinician must provide reasonable disclosure of:
- therapy alternatives open to the patient
- goals expected to be achieved
- the risks involved with recovering memories.4
Some have proposed that clinicians should disclose the risk of recovering false memories of sexual and physical abuse before starting treatment.5 The clinician should then clearly document this disclosure.
1. Pope HG, Jr. Psychology astray: Fallacies in studies of repressed memory and childhood trauma. Boca Raton, FL: Upton Books, 1997.
2. Borawick v. Shay. 68 F3d 597 (2d Cir. 1995).
3. Pope HG, Jr, Oliva PS, Hudson JI, et al. Attitudes toward DSM-IV dissociative disorders diagnoses among board-certified American psychiatrists. Am J Psychiatry 1999;156:321-3.
4. Canterbury v. Spence. 464 F2d 775 (DC Cir 1972).
5. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29:138-47.
1. Pope HG, Jr. Psychology astray: Fallacies in studies of repressed memory and childhood trauma. Boca Raton, FL: Upton Books, 1997.
2. Borawick v. Shay. 68 F3d 597 (2d Cir. 1995).
3. Pope HG, Jr, Oliva PS, Hudson JI, et al. Attitudes toward DSM-IV dissociative disorders diagnoses among board-certified American psychiatrists. Am J Psychiatry 1999;156:321-3.
4. Canterbury v. Spence. 464 F2d 775 (DC Cir 1972).
5. Cannell J, Hudson JI, Pope HG, Jr. Standards for informed consent in recovered memory therapy. J Am Acad Psychiatry Law 2001;29:138-47.
Liability in patient suicide
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
Clinical psychiatrists often find it hard to evaluate suicide risk and understand their potential legal liability. Prevalence of suicidality compounds this challenge: Up to one-third of the general population in the United States have suicidal thoughts at some point.1 Although most people who consider suicide do not act on those thoughts, 51% of psychiatrists report having had a patient who committed suicide.2
Because patient suicide risk is real, psychiatrists often worry about malpractice claims. Although post-suicide lawsuits account for the largest number of malpractice suits against psychiatrists,3,4 a psychiatrist’s risk of being sued for malpractice is still quite low.3 Even when sued, clinicians win up to 80% of cases.3
Still, with malpractice claims increasing overall, clinicians should understand their potential liability in preventing suicide and the basic principles behind a malpractice claim.
Patient jumps from window after suicide watch is called off
Los Angeles County (CA) superior court
A 24-year-old man was hospitalized after attempting suicide by ingesting prescription pills and alcohol. He was admitted to the general medical floor with a 24-hour sitter to guard against additional suicide attempts. When the psychiatrist tried to evaluate him, he found the patient unresponsive because of the pills’ effects.
The next day, the psychiatrist evaluated the patient and recommended that the patient be transferred to the psychiatric unit and that the sitter be continued. Four hours later, without a further evaluation, the psychiatrist recommended moving the patient to another room and canceling the sitter.
The next day, the patient jumped from his sixth-floor hospital room window. He sustained traumatic brain injury.
The patient’s guardian ad litem argued that discontinuing the sitter was negligent. The defendant argued that discontinuation was within the parameters of proper care.
- The jury found for the defense.
Patient commits suicide hours after ER discharge
Lake County (IL) circuit court
A 36-year-old man was being treated by a psychiatrist for major depressive disorder. The patient owned several guns for hunting and target shooting and had a state-issued firearm owner’s identification card.
In October 2003, the patient presented to the emergency room and was examined by a mental health assessment staff. The psychiatrist recommended voluntary admission to the psychiatric unit for 23 hours.
The patient’s father discouraged the admission and stated that the patient could lose his gun owner’s card as a result. The patient was subsequently discharged. Within 24 hours after discharge, the patient shot himself in the chest and died.
The deceased’s estate argued that the psychiatrist should have admitted the patient involuntarily. The psychiatrist claimed no obligation to involuntary admission and argued that the patient did not meet criteria typically used for such admission.
- The jury found for the defense.
Doctor’s hanging attempt in hospital causes permanent brain damage
Morris County (NJ) district court
A cardiologist was admitted to the hospital’s psychiatric unit after decompensating. While hospitalized, he attempted suicide by hanging in a clinic bathroom. He suffered permanent brain injury as a result of the hanging. Because the injury left him in a childlike state, he required constant care.
The patient’s attorney argued that hospital personnel knew he was suicidal yet did not adequately supervise him. The attorney also argued that the injury cost his client $5 million in lost income.
The defense reported that the hospital had placed the patient on suicide watch and that staff checked him every 5 minutes. The defense also argued that the bathroom where the suicide was attempted was impossible to monitor.
- The jury found for the defense.
Dr. Grant’s observations
To win a malpractice claim, the injured party must show four things:
Duty to care for the patient existed based on the provider’s relationship with the patient. Whether on a hospital floor or in the emergency room, once a doctor-patient relationship has been established, the provider agrees to provide non-negligent care.
Negligence. The physician or hospital personnel acted negligently and violated the duty of care. This concept is based upon a “standard of care” —ie, what other psychiatrists would do in this situation.
Harm. Even if someone has acted negligently, a malpractice case cannot go forward if no harm has been suffered.
Causation. The negligent act caused the harm.
The defendants most likely won the cases cited above because the injured parties could not establish negligence. Clinicians are not negligent for merely failing to predict suicide, as the inability to predict suicide has been demonstrated.5,6 Clinicians, however, must follow the profession’s standard of care, assess the relative degree of risk, and form a treatment and safety plan consistent with that risk.4
Based on relevant case law, the following actions can decrease the risk of patient suicide—and a resultant malpractice claim:
- Conduct a comprehensive evaluation of the patient and his or her suicide risk. Ask about:
- Consider hospitalizing at-risk patients. If you decide against hospitalization, provide a comprehensive safety plan. In the gun owner’s case, such a plan would include arranging with the family to remove firearms. Implement additional anti-suicide precautions, such as more-intensive outpatient therapy or involving family members in treatment.
- Document suicide risk assessment and the reasons for your treatment decisions. Juries may interpret lack of documented information in the patient’s favor.
- Design a treatment plan for hospitalized patients to reduce suicide risk. Consider the patient’s reaction to constant surveillance. For example, checking a paranoid patient every 5 minutes may be more therapeutic than a constant watch while providing adequate safety. Thoroughly document your reasons behind the plan.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
1. Hirschfeld RMA, Russell JM. Assessment and treatment of suicidal patients. N Engl J Med 1997;337:910-5.
2. Chemtob CM, Hamada RS, Bauer GB, et al. Patient suicide: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
3. Baerger DR. Risk management with the suicidal patient: lessons from case law. Prof Psychol Res Pract 2001;32:359-66.
4. Packman WL, O’Connor Pennuto T, Bongar B, Orthwein J. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
5. Pokorny AD. Prediction of suicide in psychiatric patients. Arch Gen Psychiatry 1983;40:249-57.
6. Pokorny AD. Suicide prediction revisited. Suicide Life Threat Behav 1993;23:1-10.
7. Bell v. New York City Health and Hospitals Corp., 456 NYS 2d 787 (App. Div. 1982).
8. Simon RI. The suicidal patient. In: Lifson LE, Simon SI (eds). The mental health practitioner and the law: A comprehensive handbook. Cambridge, MA: Harvard University Press, 1998;166-86.
Suicidal patient jumps from building after protesting hospital discharge
Hudson County (NJ) superior court
A 44-year-old man with bipolar disorder and a history of suicidal behavior was hospitalized after telling the treating psychiatrist he had suicidal thoughts. Approximately 3 weeks later, the psychiatrist informed the patient he would be discharged.
Despite his objections, the patient was discharged 4 days later with the psychiatrist’s approval. This occurred even though the patient was found to be suicidal when he was evaluated that day by an in-hospital social services agency.
Two days later, the patient jumped from a 4-story building and sustained permanent partial paralysis. Subsequent treatments included spinal rod insertion, laminectomy, skin grafts, and 3 months’ rehabilitation.
The patient sued the psychiatrist for negligence for both the discharge and for inadequate medication management. The suit claimed that the prescribed mood stabilizer was dosed below therapeutic serum levels and that the psychiatrist switched the patient’s adjunctive antidepressant too close to his discharge date to determine its efficacy.
- The case was settled for $1 million.
Inappropriate drug therapy blamed for inducing fatal heart failure
Kings County (CA) superior court
A patient with severe mental illness died of congestive heart failure (CHF), and his three minor children argued that their father’s medications caused his death.
The patient’s surgeon and family practitioner observed that he had a history of acute psychosis and was taking haloperidol. He was also being treated for schizophrenia and bipolar disorder and was living in a group home. The patient was diagnosed with diabetes in 1998.
In 2000, a group home staff member observed ankle swelling and foam around the patient’s mouth. The consulting psychiatrist reduced the mood stabilizer dosage. The family physician subsequently saw the patient for complaints of cough, wheeze, dizziness, and foam on the mouth. Neither physician acknowledged the foam.
The patient was found dead the next day. Autopsy showed that he died of drug intoxication; toxicology studies showed that serum levels of two psychotropic medications were elevated.
The plaintiffs argued that the psychiatrist’s mismanagement of the psychotropics led to the patient’s death, and that the family practitioner failed to test for CHF. The psychiatrist argued that the drug levels were necessary to control the patient’s mental illness. The family practitioner questioned the autopsy conclusion and stated that relevant diagnostic studies were not ordered because the patient’s presentation was atypical for CHF.
- The jury settled in the defense’s favor.
Unattended patient sustains brain injury in attempted suicide
Unnamed county (MN) district court
A patient was hospitalized in the psychiatric unit with a diagnosis of major depressive disorder, suicidal ideation, and a defined suicide plan. The hospital psychiatrist ordered a suicide watch.
Three days after admission, hospital staff allowed the patient to use the psychiatric unit’s exercise equipment. When left unsupervised in the exercise room, the patient attempted suicide by hanging. Staff discovered and resuscitated the patient, but the hanging attempt resulted in severe anoxic brain injury, which caused permanent and total disability.
- The case was settled out of court for $2.75 million.
Bipolar teen attacks mother with knife; family blames misdiagnosis
Tarrant County (TX) district court
A 14-year-old boy was being treated in early 2000 by a psychiatric group for depression and hyperactivity, for which he was prescribed methylphenidate and paroxetine. Later that year, he became agitated and attacked his mother with a knife. He was arrested and charged with assault with a deadly weapon.
The plaintiff sued the psychiatrists for failure to diagnose his bipolar condition and showed that prescribing paroxetine without a mood stabilizer is contraindicated in bipolar patients. The defendants argued that the patient did not have bipolar disorder when the medications were prescribed.
- The jury found no negligence. Claims by the plaintiff’s mother were dismissed.
Hudson County (NJ) superior court
A 44-year-old man with bipolar disorder and a history of suicidal behavior was hospitalized after telling the treating psychiatrist he had suicidal thoughts. Approximately 3 weeks later, the psychiatrist informed the patient he would be discharged.
Despite his objections, the patient was discharged 4 days later with the psychiatrist’s approval. This occurred even though the patient was found to be suicidal when he was evaluated that day by an in-hospital social services agency.
Two days later, the patient jumped from a 4-story building and sustained permanent partial paralysis. Subsequent treatments included spinal rod insertion, laminectomy, skin grafts, and 3 months’ rehabilitation.
The patient sued the psychiatrist for negligence for both the discharge and for inadequate medication management. The suit claimed that the prescribed mood stabilizer was dosed below therapeutic serum levels and that the psychiatrist switched the patient’s adjunctive antidepressant too close to his discharge date to determine its efficacy.
- The case was settled for $1 million.
Inappropriate drug therapy blamed for inducing fatal heart failure
Kings County (CA) superior court
A patient with severe mental illness died of congestive heart failure (CHF), and his three minor children argued that their father’s medications caused his death.
The patient’s surgeon and family practitioner observed that he had a history of acute psychosis and was taking haloperidol. He was also being treated for schizophrenia and bipolar disorder and was living in a group home. The patient was diagnosed with diabetes in 1998.
In 2000, a group home staff member observed ankle swelling and foam around the patient’s mouth. The consulting psychiatrist reduced the mood stabilizer dosage. The family physician subsequently saw the patient for complaints of cough, wheeze, dizziness, and foam on the mouth. Neither physician acknowledged the foam.
The patient was found dead the next day. Autopsy showed that he died of drug intoxication; toxicology studies showed that serum levels of two psychotropic medications were elevated.
The plaintiffs argued that the psychiatrist’s mismanagement of the psychotropics led to the patient’s death, and that the family practitioner failed to test for CHF. The psychiatrist argued that the drug levels were necessary to control the patient’s mental illness. The family practitioner questioned the autopsy conclusion and stated that relevant diagnostic studies were not ordered because the patient’s presentation was atypical for CHF.
- The jury settled in the defense’s favor.
Unattended patient sustains brain injury in attempted suicide
Unnamed county (MN) district court
A patient was hospitalized in the psychiatric unit with a diagnosis of major depressive disorder, suicidal ideation, and a defined suicide plan. The hospital psychiatrist ordered a suicide watch.
Three days after admission, hospital staff allowed the patient to use the psychiatric unit’s exercise equipment. When left unsupervised in the exercise room, the patient attempted suicide by hanging. Staff discovered and resuscitated the patient, but the hanging attempt resulted in severe anoxic brain injury, which caused permanent and total disability.
- The case was settled out of court for $2.75 million.
Bipolar teen attacks mother with knife; family blames misdiagnosis
Tarrant County (TX) district court
A 14-year-old boy was being treated in early 2000 by a psychiatric group for depression and hyperactivity, for which he was prescribed methylphenidate and paroxetine. Later that year, he became agitated and attacked his mother with a knife. He was arrested and charged with assault with a deadly weapon.
The plaintiff sued the psychiatrists for failure to diagnose his bipolar condition and showed that prescribing paroxetine without a mood stabilizer is contraindicated in bipolar patients. The defendants argued that the patient did not have bipolar disorder when the medications were prescribed.
- The jury found no negligence. Claims by the plaintiff’s mother were dismissed.
Hudson County (NJ) superior court
A 44-year-old man with bipolar disorder and a history of suicidal behavior was hospitalized after telling the treating psychiatrist he had suicidal thoughts. Approximately 3 weeks later, the psychiatrist informed the patient he would be discharged.
Despite his objections, the patient was discharged 4 days later with the psychiatrist’s approval. This occurred even though the patient was found to be suicidal when he was evaluated that day by an in-hospital social services agency.
Two days later, the patient jumped from a 4-story building and sustained permanent partial paralysis. Subsequent treatments included spinal rod insertion, laminectomy, skin grafts, and 3 months’ rehabilitation.
The patient sued the psychiatrist for negligence for both the discharge and for inadequate medication management. The suit claimed that the prescribed mood stabilizer was dosed below therapeutic serum levels and that the psychiatrist switched the patient’s adjunctive antidepressant too close to his discharge date to determine its efficacy.
- The case was settled for $1 million.
Inappropriate drug therapy blamed for inducing fatal heart failure
Kings County (CA) superior court
A patient with severe mental illness died of congestive heart failure (CHF), and his three minor children argued that their father’s medications caused his death.
The patient’s surgeon and family practitioner observed that he had a history of acute psychosis and was taking haloperidol. He was also being treated for schizophrenia and bipolar disorder and was living in a group home. The patient was diagnosed with diabetes in 1998.
In 2000, a group home staff member observed ankle swelling and foam around the patient’s mouth. The consulting psychiatrist reduced the mood stabilizer dosage. The family physician subsequently saw the patient for complaints of cough, wheeze, dizziness, and foam on the mouth. Neither physician acknowledged the foam.
The patient was found dead the next day. Autopsy showed that he died of drug intoxication; toxicology studies showed that serum levels of two psychotropic medications were elevated.
The plaintiffs argued that the psychiatrist’s mismanagement of the psychotropics led to the patient’s death, and that the family practitioner failed to test for CHF. The psychiatrist argued that the drug levels were necessary to control the patient’s mental illness. The family practitioner questioned the autopsy conclusion and stated that relevant diagnostic studies were not ordered because the patient’s presentation was atypical for CHF.
- The jury settled in the defense’s favor.
Unattended patient sustains brain injury in attempted suicide
Unnamed county (MN) district court
A patient was hospitalized in the psychiatric unit with a diagnosis of major depressive disorder, suicidal ideation, and a defined suicide plan. The hospital psychiatrist ordered a suicide watch.
Three days after admission, hospital staff allowed the patient to use the psychiatric unit’s exercise equipment. When left unsupervised in the exercise room, the patient attempted suicide by hanging. Staff discovered and resuscitated the patient, but the hanging attempt resulted in severe anoxic brain injury, which caused permanent and total disability.
- The case was settled out of court for $2.75 million.
Bipolar teen attacks mother with knife; family blames misdiagnosis
Tarrant County (TX) district court
A 14-year-old boy was being treated in early 2000 by a psychiatric group for depression and hyperactivity, for which he was prescribed methylphenidate and paroxetine. Later that year, he became agitated and attacked his mother with a knife. He was arrested and charged with assault with a deadly weapon.
The plaintiff sued the psychiatrists for failure to diagnose his bipolar condition and showed that prescribing paroxetine without a mood stabilizer is contraindicated in bipolar patients. The defendants argued that the patient did not have bipolar disorder when the medications were prescribed.
- The jury found no negligence. Claims by the plaintiff’s mother were dismissed.