User login
‘Like a coin flip’: Assay denies some cancer patients new drug
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
Recent treatment advances brighten prospects for intracerebral hemorrhage patients
LOS ANGELES – Intracerebral hemorrhage (ICH) appears to be not nearly as uniformly devastating to patients as its reputation suggests. Recent study results documented unexpectedly decent recovery prospects for hemorrhagic stroke patients assessed after 1 year who were earlier considered moderately severe or severely disabled based on their 30-day status. And these data provide further support for the growing impression among clinicians that a way forward for improving outcomes even more is with a “gentle” surgical intervention designed to substantially reduce ICH clot volume.
“Historically, there’s been a lot of nihilism around these patients. Intracerebral hemorrhage has always been the deadliest stroke type, but one of the great advances of the past 10-20 years is that ICH survival has improved. Patients do better than we used to think,” said Kevin N. Sheth, MD, professor of neurology and neurosurgery, and chief of neurocritical care and emergency neurology at Yale University in New Haven, Conn. “Even though ICH remains a difficult disease, this change has two big implications,” Dr. Sheth said in an interview during the International Stroke Conference sponsored by the American Heart Association. First, increased ICH survival offers an opportunity to expand the reach of recent management advances through quality improvement programs that emphasize new strategies that work better and incentivize delivery of these successful strategies to more patients.
The second implication is simply a growing number of ICH survivors, expanding the population of patients who stand to gain from these new management strategies. Dr. Sheth is working with the Get With the Guidelines – Stroke program, a quality-improvement program begun in 2003 and until now aimed at patients with acute ischemic stroke, to develop a 15-site pilot program planned to start in 2020 that will begin implementing and studying a Get With the Guidelines – Stroke quality-improvement program focused on patients with an ICH. The current conception of a quality measurement and improvement program like Get with the Guidelines – Stroke for patients with ICH stems from an important, earlier milestone in the emergence of effective ICH treatments, the 2018 publication of performance measures for ICH care that identified nine key management steps for assessing quality of care and documented the evidence behind them.
“Evidence for optimal treatment of ICH has lagged behind that for ischemic stroke, and consequently, metrics specific to ICH care have not been widely promulgated,” said the authors of the 2018 ICH performance measures, a panel that included Dr. Sheth. “However, numerous more recent studies and clinical trials of various medical and surgical interventions for ICH have been published and form the basis of evidence-based guidelines for the management of ICH,” they explained.
MISTIE III showcases better ICH outcomes
Perhaps the most dramatic recent evidence of brighter prospects for ICH patients came in data collected during the MISTIE III (Minimally Invasive Surgery with Thrombolysis in Intracerebral Hemorrhage Evacuation III) trial, which randomized 506 ICH patients with a hematoma of at least 30 mL to standard care or to a “gentle” clot-reduction protocol using a small-bore catheter placed with stereotactic guidance to both evacuate clot and introduce a serial infusion of alteplase into the clot to try to shrink its volume to less than 15 mL. The study’s results showed a neutral effect for the primary outcome, the incidence of recovery to a modified Rankin Scale (mRS) score of 0-3 at 1 year after entry, which occurred in 45% of the surgically treated patients and 41% of the controls in a modified intention-to-treat analysis that included 499 of the randomized patients, a difference that did not reach statistical significance.
However, when the analysis focused on the 146 of 247 patients (59%) randomized to surgical plus lytic intervention who underwent the procedure and actually had their clot volume reduced to 15 mL or less per protocol, the adjusted incidence of the primary endpoint was double that of patients who underwent the procedure but failed to have their residual clot reduced to this size. A similar doubling of good outcomes occurred when MISTIE patients had their residual clot cut to 20 mL or less, compared with those who didn’t reach this, with the differences in both analyses statistically significant. The actual rates showed patients with clot cut to 15 mL or less having a 53% rate of a mRS score of 0-3 after 1 year, compared with 33% of patients who received the intervention but had their residual clot remain above 15 mL.
The MISTIE III investigators looked at their data to try to get better insight into the outcome of all “poor prognosis” patients in the study regardless of their treatment arm assignment, and how patients and their family members made decisions for withdrawal of life-sustaining therapy. In MISTIE III, 61 patients had withdrawal of life-sustaining treatment (WoLST), with more than 40% of the WoLST occurring with patients randomized to the intervention arm including 10 patients treated to a residual clot volume of 15 mL or less. To quantify the disease severity in these 61 patients, the researchers applied a six-item formula at 30 days after the stroke, a metric their 2019 report described in detail. They then used these severity scores to identify 104 matched patients who were alive at 30 days and remained on life-sustaining treatment to see their 1-year outcomes. At 30 days, the 104 matched patients included 82 (79%) with a mRS score of 5 (severe disability) and 22 patients (21%) with a mRS score of 4 (moderately severe disability). Overall, an mRS score of 4 or 5 was quite prevalent 30 days after the stroke, with 87% of the patients treated with the MISTIE intervention and 90% of the control patients having this degree of disability at 30 days.
When the MISTIE III investigators followed these patients for a year, they made an unexpected finding: A substantial incidence of patients whose condition had improved since day 30. One year out, 40 (39%) of these 104 patients had improved to a mRS score of 1-3, including 10 (10%) with a mRS score of 1 or 2. Another indicator of the reasonable outcome many of these patients achieved was that after 1 year 69% were living at home.

“Our data show that many ICH subjects with clinical factors that suggest ‘poor prognosis,’ when given time, can achieve a favorable outcome and return home,” concluded Noeleen Ostapkovich, who presented these results at the Stroke Conference.
She cited these findings as potentially helpful for refining the information given to patients and families on the prognosis for ICH patients at about 30 days after their event, the usual time for assessment. “These patients looked like they weren’t going to do well after 30 days, but by 365 days they had improved physically and in their ability to care for themselves at home,” noted Ms. Ostapkovich, a researcher in the Brain Injury Outcomes Clinical Trial Coordinating Center of Johns Hopkins University in Baltimore.
A message for acute-care clinicians
She and her colleagues highlighted the implications these new findings have for clinical decision making in the first weeks after an ICH.
“Acute-care physicians see these patients at day 30, not at day 365, so it’s important that they have a clear picture of what these patients could look like a year later. It’s an important message,” Ms. Ostapkovich said in an interview.
In fact, a colleague of hers at Johns Hopkins ran an analysis that looked at factors that contributed to families opting for WoLST for 61 of the MISTIE III patients, and found that 38 family groups (62%) cited the anticipated outcome of the patient in a dependent state as their primary reason for opting for WoLST, Lourdes J. Carhuapoma reported in a separate talk at the conference.

“The main message is that many patients with significant ICH did well and recovered despite having very poor prognostic factors at 30 days, but it took more time. A concern is that the [prognostic] information families receive may be wrong. There is a disconnect,” between what families get told to expect and what actually happens, said Ms. Carhuapoma, an acute care nurse practitioner at Johns Hopkins.
“When physicians, nurses, and family members get together” to discuss ICH patients like these after 30 days, “they see the glass as empty. But the real message is that the glass is half full,” summed up Daniel F. Hanley, MD, lead investigator of MISTIE III and professor of neurology at Johns Hopkins. “These data show a large amount of improvement between 30 and 180 days.” The 104 patients with exclusively mRS scores of 4 or 5 at day 30 had a 30% incidence of improvement to an mRS score of 2 or 3 after 180 days, on their way to a 39% rate of mRS scores of 1-3 at 1 year.

An additional analysis that has not yet been presented showed that the “strongest predictor” of whether or not patients who presented with a mRS score of 4 or 5 after 30 days improved their status at 1 year was if their residual hematoma volume shrank to 15 mL or less, Dr. Hanley said in an interview. “It’s not rocket science. If you had to choose between a 45-mL hematoma and less than 15 mL, which would you choose? What’s new here is how this recovery can play out,” taking 180 days or longer in some patients to become apparent.
More evidence needed to prove MISTIE’s hypothesis
According to Dr. Hanley, the MISTIE III findings have begun to influence practice despite its neutral primary finding, with more attention being paid to reducing residual clot volume following an ICH. And evidence continues to mount that more aggressive minimization of hematoma size can have an important effect on outcomes. For example, another study presented at the conference assessed the incremental change in prognostic accuracy when the ICH score, a five-item formula for estimating the prognosis of an ICH patient, substituted a precise quantification of residual hematoma volume rather than the original, dichotomous entry for either a hematoma volume of 30 mL or greater, or less than 30 mL, and when the severity score also quantified intraventricular hemorrhage (IVH) volume rather than simply designating IVH as present or absent.
Using data from 933 patients who had been enrolled in either MISTIE III or in another study of hematoma volume reduction, CLEAR III, the analysis showed that including specific quantification of both residual ICH volume as well as residual IVH volume improved the area under the receiver operating characteristic curve of the ICH score as a prognostic assessment from 0.70 to 0.75 in the intervention arms of the two trials, and from 0.60 to 0.68 in the two combined control arms, Adam de Havenon, MD, reported in a talk at the conference. “These data show that quantifying ICH and IVH volume improves mortality prognostication,” concluded Dr. de Havenon, a vascular and stroke neurologist at the University of Utah in Salt Lake City.

Furthermore, it’s “certainly evidence for the importance of volume reduction,” he said during discussion of his talk. “The MISTIE procedure can reset patients” so that their outcomes become more like patients with much smaller clot volumes even if they start with large hematomas. “In our experience, if the volume is reduced to 5 mL, there is real benefit regardless of how big the clot was initially,” Dr. de Havenon said.
But the neutral result for the MISTIE III primary endpoint will, for the time being, hobble application of this concept and keep the MISTIE intervention from rising to a level I recommendation until greater evidence for its efficacy comes out.
“It’s been known for many years that clot size matters when it comes to ICH. The MISTIE team has made a very compelling case that [reducing clot volume] is a very reasonable hypothesis, but we must continue to acquire data that can confirm it,” Dr. Sheth commented.
Dr. Sheth’s institution receives research funding from Novartis and Bard for studies that Dr. Sheth helps run. The MISTIE III study received the alteplase used in the study at no cost from Genentech. Ms. Ostapkovich and Ms. Carhuapoma had no disclosures. Dr. Hanley has received personal fees from BrainScope, Medtronic, Neurotrope, Op2Lysis, and Portola. Dr. de Havenon has received research funding from Regeneron.
LOS ANGELES – Intracerebral hemorrhage (ICH) appears to be not nearly as uniformly devastating to patients as its reputation suggests. Recent study results documented unexpectedly decent recovery prospects for hemorrhagic stroke patients assessed after 1 year who were earlier considered moderately severe or severely disabled based on their 30-day status. And these data provide further support for the growing impression among clinicians that a way forward for improving outcomes even more is with a “gentle” surgical intervention designed to substantially reduce ICH clot volume.
“Historically, there’s been a lot of nihilism around these patients. Intracerebral hemorrhage has always been the deadliest stroke type, but one of the great advances of the past 10-20 years is that ICH survival has improved. Patients do better than we used to think,” said Kevin N. Sheth, MD, professor of neurology and neurosurgery, and chief of neurocritical care and emergency neurology at Yale University in New Haven, Conn. “Even though ICH remains a difficult disease, this change has two big implications,” Dr. Sheth said in an interview during the International Stroke Conference sponsored by the American Heart Association. First, increased ICH survival offers an opportunity to expand the reach of recent management advances through quality improvement programs that emphasize new strategies that work better and incentivize delivery of these successful strategies to more patients.
The second implication is simply a growing number of ICH survivors, expanding the population of patients who stand to gain from these new management strategies. Dr. Sheth is working with the Get With the Guidelines – Stroke program, a quality-improvement program begun in 2003 and until now aimed at patients with acute ischemic stroke, to develop a 15-site pilot program planned to start in 2020 that will begin implementing and studying a Get With the Guidelines – Stroke quality-improvement program focused on patients with an ICH. The current conception of a quality measurement and improvement program like Get with the Guidelines – Stroke for patients with ICH stems from an important, earlier milestone in the emergence of effective ICH treatments, the 2018 publication of performance measures for ICH care that identified nine key management steps for assessing quality of care and documented the evidence behind them.
“Evidence for optimal treatment of ICH has lagged behind that for ischemic stroke, and consequently, metrics specific to ICH care have not been widely promulgated,” said the authors of the 2018 ICH performance measures, a panel that included Dr. Sheth. “However, numerous more recent studies and clinical trials of various medical and surgical interventions for ICH have been published and form the basis of evidence-based guidelines for the management of ICH,” they explained.
MISTIE III showcases better ICH outcomes
Perhaps the most dramatic recent evidence of brighter prospects for ICH patients came in data collected during the MISTIE III (Minimally Invasive Surgery with Thrombolysis in Intracerebral Hemorrhage Evacuation III) trial, which randomized 506 ICH patients with a hematoma of at least 30 mL to standard care or to a “gentle” clot-reduction protocol using a small-bore catheter placed with stereotactic guidance to both evacuate clot and introduce a serial infusion of alteplase into the clot to try to shrink its volume to less than 15 mL. The study’s results showed a neutral effect for the primary outcome, the incidence of recovery to a modified Rankin Scale (mRS) score of 0-3 at 1 year after entry, which occurred in 45% of the surgically treated patients and 41% of the controls in a modified intention-to-treat analysis that included 499 of the randomized patients, a difference that did not reach statistical significance.
However, when the analysis focused on the 146 of 247 patients (59%) randomized to surgical plus lytic intervention who underwent the procedure and actually had their clot volume reduced to 15 mL or less per protocol, the adjusted incidence of the primary endpoint was double that of patients who underwent the procedure but failed to have their residual clot reduced to this size. A similar doubling of good outcomes occurred when MISTIE patients had their residual clot cut to 20 mL or less, compared with those who didn’t reach this, with the differences in both analyses statistically significant. The actual rates showed patients with clot cut to 15 mL or less having a 53% rate of a mRS score of 0-3 after 1 year, compared with 33% of patients who received the intervention but had their residual clot remain above 15 mL.
The MISTIE III investigators looked at their data to try to get better insight into the outcome of all “poor prognosis” patients in the study regardless of their treatment arm assignment, and how patients and their family members made decisions for withdrawal of life-sustaining therapy. In MISTIE III, 61 patients had withdrawal of life-sustaining treatment (WoLST), with more than 40% of the WoLST occurring with patients randomized to the intervention arm including 10 patients treated to a residual clot volume of 15 mL or less. To quantify the disease severity in these 61 patients, the researchers applied a six-item formula at 30 days after the stroke, a metric their 2019 report described in detail. They then used these severity scores to identify 104 matched patients who were alive at 30 days and remained on life-sustaining treatment to see their 1-year outcomes. At 30 days, the 104 matched patients included 82 (79%) with a mRS score of 5 (severe disability) and 22 patients (21%) with a mRS score of 4 (moderately severe disability). Overall, an mRS score of 4 or 5 was quite prevalent 30 days after the stroke, with 87% of the patients treated with the MISTIE intervention and 90% of the control patients having this degree of disability at 30 days.
When the MISTIE III investigators followed these patients for a year, they made an unexpected finding: A substantial incidence of patients whose condition had improved since day 30. One year out, 40 (39%) of these 104 patients had improved to a mRS score of 1-3, including 10 (10%) with a mRS score of 1 or 2. Another indicator of the reasonable outcome many of these patients achieved was that after 1 year 69% were living at home.
“Our data show that many ICH subjects with clinical factors that suggest ‘poor prognosis,’ when given time, can achieve a favorable outcome and return home,” concluded Noeleen Ostapkovich, who presented these results at the Stroke Conference.
She cited these findings as potentially helpful for refining the information given to patients and families on the prognosis for ICH patients at about 30 days after their event, the usual time for assessment. “These patients looked like they weren’t going to do well after 30 days, but by 365 days they had improved physically and in their ability to care for themselves at home,” noted Ms. Ostapkovich, a researcher in the Brain Injury Outcomes Clinical Trial Coordinating Center of Johns Hopkins University in Baltimore.
A message for acute-care clinicians
She and her colleagues highlighted the implications these new findings have for clinical decision making in the first weeks after an ICH.
“Acute-care physicians see these patients at day 30, not at day 365, so it’s important that they have a clear picture of what these patients could look like a year later. It’s an important message,” Ms. Ostapkovich said in an interview.
In fact, a colleague of hers at Johns Hopkins ran an analysis that looked at factors that contributed to families opting for WoLST for 61 of the MISTIE III patients, and found that 38 family groups (62%) cited the anticipated outcome of the patient in a dependent state as their primary reason for opting for WoLST, Lourdes J. Carhuapoma reported in a separate talk at the conference.
“The main message is that many patients with significant ICH did well and recovered despite having very poor prognostic factors at 30 days, but it took more time. A concern is that the [prognostic] information families receive may be wrong. There is a disconnect,” between what families get told to expect and what actually happens, said Ms. Carhuapoma, an acute care nurse practitioner at Johns Hopkins.
“When physicians, nurses, and family members get together” to discuss ICH patients like these after 30 days, “they see the glass as empty. But the real message is that the glass is half full,” summed up Daniel F. Hanley, MD, lead investigator of MISTIE III and professor of neurology at Johns Hopkins. “These data show a large amount of improvement between 30 and 180 days.” The 104 patients with exclusively mRS scores of 4 or 5 at day 30 had a 30% incidence of improvement to an mRS score of 2 or 3 after 180 days, on their way to a 39% rate of mRS scores of 1-3 at 1 year.
An additional analysis that has not yet been presented showed that the “strongest predictor” of whether or not patients who presented with a mRS score of 4 or 5 after 30 days improved their status at 1 year was if their residual hematoma volume shrank to 15 mL or less, Dr. Hanley said in an interview. “It’s not rocket science. If you had to choose between a 45-mL hematoma and less than 15 mL, which would you choose? What’s new here is how this recovery can play out,” taking 180 days or longer in some patients to become apparent.
More evidence needed to prove MISTIE’s hypothesis
According to Dr. Hanley, the MISTIE III findings have begun to influence practice despite its neutral primary finding, with more attention being paid to reducing residual clot volume following an ICH. And evidence continues to mount that more aggressive minimization of hematoma size can have an important effect on outcomes. For example, another study presented at the conference assessed the incremental change in prognostic accuracy when the ICH score, a five-item formula for estimating the prognosis of an ICH patient, substituted a precise quantification of residual hematoma volume rather than the original, dichotomous entry for either a hematoma volume of 30 mL or greater, or less than 30 mL, and when the severity score also quantified intraventricular hemorrhage (IVH) volume rather than simply designating IVH as present or absent.
Using data from 933 patients who had been enrolled in either MISTIE III or in another study of hematoma volume reduction, CLEAR III, the analysis showed that including specific quantification of both residual ICH volume as well as residual IVH volume improved the area under the receiver operating characteristic curve of the ICH score as a prognostic assessment from 0.70 to 0.75 in the intervention arms of the two trials, and from 0.60 to 0.68 in the two combined control arms, Adam de Havenon, MD, reported in a talk at the conference. “These data show that quantifying ICH and IVH volume improves mortality prognostication,” concluded Dr. de Havenon, a vascular and stroke neurologist at the University of Utah in Salt Lake City.
Furthermore, it’s “certainly evidence for the importance of volume reduction,” he said during discussion of his talk. “The MISTIE procedure can reset patients” so that their outcomes become more like patients with much smaller clot volumes even if they start with large hematomas. “In our experience, if the volume is reduced to 5 mL, there is real benefit regardless of how big the clot was initially,” Dr. de Havenon said.
But the neutral result for the MISTIE III primary endpoint will, for the time being, hobble application of this concept and keep the MISTIE intervention from rising to a level I recommendation until greater evidence for its efficacy comes out.
“It’s been known for many years that clot size matters when it comes to ICH. The MISTIE team has made a very compelling case that [reducing clot volume] is a very reasonable hypothesis, but we must continue to acquire data that can confirm it,” Dr. Sheth commented.
Dr. Sheth’s institution receives research funding from Novartis and Bard for studies that Dr. Sheth helps run. The MISTIE III study received the alteplase used in the study at no cost from Genentech. Ms. Ostapkovich and Ms. Carhuapoma had no disclosures. Dr. Hanley has received personal fees from BrainScope, Medtronic, Neurotrope, Op2Lysis, and Portola. Dr. de Havenon has received research funding from Regeneron.
LOS ANGELES – Intracerebral hemorrhage (ICH) appears to be not nearly as uniformly devastating to patients as its reputation suggests. Recent study results documented unexpectedly decent recovery prospects for hemorrhagic stroke patients assessed after 1 year who were earlier considered moderately severe or severely disabled based on their 30-day status. And these data provide further support for the growing impression among clinicians that a way forward for improving outcomes even more is with a “gentle” surgical intervention designed to substantially reduce ICH clot volume.
“Historically, there’s been a lot of nihilism around these patients. Intracerebral hemorrhage has always been the deadliest stroke type, but one of the great advances of the past 10-20 years is that ICH survival has improved. Patients do better than we used to think,” said Kevin N. Sheth, MD, professor of neurology and neurosurgery, and chief of neurocritical care and emergency neurology at Yale University in New Haven, Conn. “Even though ICH remains a difficult disease, this change has two big implications,” Dr. Sheth said in an interview during the International Stroke Conference sponsored by the American Heart Association. First, increased ICH survival offers an opportunity to expand the reach of recent management advances through quality improvement programs that emphasize new strategies that work better and incentivize delivery of these successful strategies to more patients.
The second implication is simply a growing number of ICH survivors, expanding the population of patients who stand to gain from these new management strategies. Dr. Sheth is working with the Get With the Guidelines – Stroke program, a quality-improvement program begun in 2003 and until now aimed at patients with acute ischemic stroke, to develop a 15-site pilot program planned to start in 2020 that will begin implementing and studying a Get With the Guidelines – Stroke quality-improvement program focused on patients with an ICH. The current conception of a quality measurement and improvement program like Get with the Guidelines – Stroke for patients with ICH stems from an important, earlier milestone in the emergence of effective ICH treatments, the 2018 publication of performance measures for ICH care that identified nine key management steps for assessing quality of care and documented the evidence behind them.
“Evidence for optimal treatment of ICH has lagged behind that for ischemic stroke, and consequently, metrics specific to ICH care have not been widely promulgated,” said the authors of the 2018 ICH performance measures, a panel that included Dr. Sheth. “However, numerous more recent studies and clinical trials of various medical and surgical interventions for ICH have been published and form the basis of evidence-based guidelines for the management of ICH,” they explained.
MISTIE III showcases better ICH outcomes
Perhaps the most dramatic recent evidence of brighter prospects for ICH patients came in data collected during the MISTIE III (Minimally Invasive Surgery with Thrombolysis in Intracerebral Hemorrhage Evacuation III) trial, which randomized 506 ICH patients with a hematoma of at least 30 mL to standard care or to a “gentle” clot-reduction protocol using a small-bore catheter placed with stereotactic guidance to both evacuate clot and introduce a serial infusion of alteplase into the clot to try to shrink its volume to less than 15 mL. The study’s results showed a neutral effect for the primary outcome, the incidence of recovery to a modified Rankin Scale (mRS) score of 0-3 at 1 year after entry, which occurred in 45% of the surgically treated patients and 41% of the controls in a modified intention-to-treat analysis that included 499 of the randomized patients, a difference that did not reach statistical significance.
However, when the analysis focused on the 146 of 247 patients (59%) randomized to surgical plus lytic intervention who underwent the procedure and actually had their clot volume reduced to 15 mL or less per protocol, the adjusted incidence of the primary endpoint was double that of patients who underwent the procedure but failed to have their residual clot reduced to this size. A similar doubling of good outcomes occurred when MISTIE patients had their residual clot cut to 20 mL or less, compared with those who didn’t reach this, with the differences in both analyses statistically significant. The actual rates showed patients with clot cut to 15 mL or less having a 53% rate of a mRS score of 0-3 after 1 year, compared with 33% of patients who received the intervention but had their residual clot remain above 15 mL.
The MISTIE III investigators looked at their data to try to get better insight into the outcome of all “poor prognosis” patients in the study regardless of their treatment arm assignment, and how patients and their family members made decisions for withdrawal of life-sustaining therapy. In MISTIE III, 61 patients had withdrawal of life-sustaining treatment (WoLST), with more than 40% of the WoLST occurring with patients randomized to the intervention arm including 10 patients treated to a residual clot volume of 15 mL or less. To quantify the disease severity in these 61 patients, the researchers applied a six-item formula at 30 days after the stroke, a metric their 2019 report described in detail. They then used these severity scores to identify 104 matched patients who were alive at 30 days and remained on life-sustaining treatment to see their 1-year outcomes. At 30 days, the 104 matched patients included 82 (79%) with a mRS score of 5 (severe disability) and 22 patients (21%) with a mRS score of 4 (moderately severe disability). Overall, an mRS score of 4 or 5 was quite prevalent 30 days after the stroke, with 87% of the patients treated with the MISTIE intervention and 90% of the control patients having this degree of disability at 30 days.
When the MISTIE III investigators followed these patients for a year, they made an unexpected finding: A substantial incidence of patients whose condition had improved since day 30. One year out, 40 (39%) of these 104 patients had improved to a mRS score of 1-3, including 10 (10%) with a mRS score of 1 or 2. Another indicator of the reasonable outcome many of these patients achieved was that after 1 year 69% were living at home.
“Our data show that many ICH subjects with clinical factors that suggest ‘poor prognosis,’ when given time, can achieve a favorable outcome and return home,” concluded Noeleen Ostapkovich, who presented these results at the Stroke Conference.
She cited these findings as potentially helpful for refining the information given to patients and families on the prognosis for ICH patients at about 30 days after their event, the usual time for assessment. “These patients looked like they weren’t going to do well after 30 days, but by 365 days they had improved physically and in their ability to care for themselves at home,” noted Ms. Ostapkovich, a researcher in the Brain Injury Outcomes Clinical Trial Coordinating Center of Johns Hopkins University in Baltimore.
A message for acute-care clinicians
She and her colleagues highlighted the implications these new findings have for clinical decision making in the first weeks after an ICH.
“Acute-care physicians see these patients at day 30, not at day 365, so it’s important that they have a clear picture of what these patients could look like a year later. It’s an important message,” Ms. Ostapkovich said in an interview.
In fact, a colleague of hers at Johns Hopkins ran an analysis that looked at factors that contributed to families opting for WoLST for 61 of the MISTIE III patients, and found that 38 family groups (62%) cited the anticipated outcome of the patient in a dependent state as their primary reason for opting for WoLST, Lourdes J. Carhuapoma reported in a separate talk at the conference.
“The main message is that many patients with significant ICH did well and recovered despite having very poor prognostic factors at 30 days, but it took more time. A concern is that the [prognostic] information families receive may be wrong. There is a disconnect,” between what families get told to expect and what actually happens, said Ms. Carhuapoma, an acute care nurse practitioner at Johns Hopkins.
“When physicians, nurses, and family members get together” to discuss ICH patients like these after 30 days, “they see the glass as empty. But the real message is that the glass is half full,” summed up Daniel F. Hanley, MD, lead investigator of MISTIE III and professor of neurology at Johns Hopkins. “These data show a large amount of improvement between 30 and 180 days.” The 104 patients with exclusively mRS scores of 4 or 5 at day 30 had a 30% incidence of improvement to an mRS score of 2 or 3 after 180 days, on their way to a 39% rate of mRS scores of 1-3 at 1 year.
An additional analysis that has not yet been presented showed that the “strongest predictor” of whether or not patients who presented with a mRS score of 4 or 5 after 30 days improved their status at 1 year was if their residual hematoma volume shrank to 15 mL or less, Dr. Hanley said in an interview. “It’s not rocket science. If you had to choose between a 45-mL hematoma and less than 15 mL, which would you choose? What’s new here is how this recovery can play out,” taking 180 days or longer in some patients to become apparent.
More evidence needed to prove MISTIE’s hypothesis
According to Dr. Hanley, the MISTIE III findings have begun to influence practice despite its neutral primary finding, with more attention being paid to reducing residual clot volume following an ICH. And evidence continues to mount that more aggressive minimization of hematoma size can have an important effect on outcomes. For example, another study presented at the conference assessed the incremental change in prognostic accuracy when the ICH score, a five-item formula for estimating the prognosis of an ICH patient, substituted a precise quantification of residual hematoma volume rather than the original, dichotomous entry for either a hematoma volume of 30 mL or greater, or less than 30 mL, and when the severity score also quantified intraventricular hemorrhage (IVH) volume rather than simply designating IVH as present or absent.
Using data from 933 patients who had been enrolled in either MISTIE III or in another study of hematoma volume reduction, CLEAR III, the analysis showed that including specific quantification of both residual ICH volume as well as residual IVH volume improved the area under the receiver operating characteristic curve of the ICH score as a prognostic assessment from 0.70 to 0.75 in the intervention arms of the two trials, and from 0.60 to 0.68 in the two combined control arms, Adam de Havenon, MD, reported in a talk at the conference. “These data show that quantifying ICH and IVH volume improves mortality prognostication,” concluded Dr. de Havenon, a vascular and stroke neurologist at the University of Utah in Salt Lake City.
Furthermore, it’s “certainly evidence for the importance of volume reduction,” he said during discussion of his talk. “The MISTIE procedure can reset patients” so that their outcomes become more like patients with much smaller clot volumes even if they start with large hematomas. “In our experience, if the volume is reduced to 5 mL, there is real benefit regardless of how big the clot was initially,” Dr. de Havenon said.
But the neutral result for the MISTIE III primary endpoint will, for the time being, hobble application of this concept and keep the MISTIE intervention from rising to a level I recommendation until greater evidence for its efficacy comes out.
“It’s been known for many years that clot size matters when it comes to ICH. The MISTIE team has made a very compelling case that [reducing clot volume] is a very reasonable hypothesis, but we must continue to acquire data that can confirm it,” Dr. Sheth commented.
Dr. Sheth’s institution receives research funding from Novartis and Bard for studies that Dr. Sheth helps run. The MISTIE III study received the alteplase used in the study at no cost from Genentech. Ms. Ostapkovich and Ms. Carhuapoma had no disclosures. Dr. Hanley has received personal fees from BrainScope, Medtronic, Neurotrope, Op2Lysis, and Portola. Dr. de Havenon has received research funding from Regeneron.
REPORTING FROM ISC 2020
CDC expert answers top COVID-19 questions
With new developments daily and lingering uncertainty about COVID-19, questions about testing and treatment for the coronavirus are at the forefront.
To address these top questions, Jay C. Butler, MD, deputy director for infectious diseases at the Centers for Disease Control and Prevention, sat down with JAMA editor Howard Bauchner, MD, to discuss the latest data on COVID-19 and to outline updated guidance from the agency. The following question-and-answer session was part of a live stream interview hosted by JAMA on March 16, 2020. The questions have been edited for length and clarity.
What test is being used to identify COVID-19?
In the United States, the most common and widely available test is the RT-polymerase chain reaction (rRT-PCR), which over the past few weeks has become available at public health labs across the country, Dr. Butler said during the JAMA interview. Capacity for the test is now possible in all 50 states and in Washington, D.C.
“More recently, there’s been a number of commercial labs that have come online to be able to do the testing,” Dr. Butler said. “Additionally, a number of academic centers are now able to run [Food and Drug Administration]–approved testing using slightly different PCR platforms.”
How accurate is the test?
Dr. Butler called PCR the “gold standard,” for testing COVID-19, and said it’s safe to say the test’s likelihood of identifying infection or past infection is extremely high. However, data on test sensitivity is limited.
“This may be frustrating to those of us who really like to know specifics of how to interpret the test results, but it’s important to keep in mind, we’re talking about a virus that we didn’t know existed 3 months ago,” he said.
At what point does a person with coronavirus test positive?
When exactly a test becomes positive is an unknown, Dr. Butler said. The assumption is that a patient who tests positive is more likely to be infectious, and data suggest the level of infectiousness is greatest after the onset of symptoms.
“There is at least some anecdotal reports that suggest that transmission could occur before onset of symptoms, but the data is still very limited,” he said. “Of course that has big implications in terms of how well we can really slow the spread of the virus.”
Who should get tested?
Dr. Butler said the focus should be individuals who are symptomatic with evidence of respiratory tract infection. People who are concerned about the virus and want a test are not the target.
“It’s important when talking to patients to help them to understand, this is different than a test for HIV or hepatitis C, where much of the message is: ‘Please get tested.’ ” he said. “This a situation where we’re trying to diagnose an acute infection. We do have a resource that may become limited again as some of the equipment required for running the test or collecting the specimen may come into short supply, so we want to focus on those people who are symptomatic and particularly on people who may be at higher risk of more severe illness.”
If a previously infected patient tests negative, can they still shed virus?
The CDC is currently analyzing how a negative PCR test relates to viral load, according to Dr. Butler. He added there have been situations in which a patient has twice tested negative for the virus, but a third swab resulted in a weakly positive result.
“It’s not clear if those are people who are actually infectious,” he said. “The PCR is detecting viral RNA, it doesn’t necessarily indicate there is viable virus present in the respiratory tract. So in general, I think it is safe to go back to work, but a positive test in a situation like that can be very difficult to interpret because we think it probably doesn’t reflect infectivity, but we don’t know for sure.”
Do we have an adequate supply of tests in the United States?
The CDC has addressed supply concerns by broadening the number of PCR platforms that can be used to run COVID-19 analyses, Dr. Butler said. Expansion of these platforms has been one way the government is furthering testing options and enabling consumer labs and academic centers to contribute to testing.
When can people who test positive go back to work?
The CDC is still researching that question and reviewing the data, Dr. Butler said. The current recommendation is that a patient who tests positive is considered clear to return to work after two negative tests at least 24 hours apart, following the resolution of symptoms. The CDC has not yet made an official recommendation on an exact time frame, but the CDC is considering a 14-day minimum of quarantine.
“The one caveat I’ll add is that someone who is a health care worker, even if they have resolved symptoms, it’s still a good idea to wear a surgical mask [when they return to work], just as an extra precaution.”
What do we know about immunity? Can patients get reinfected?
Long-term immunity after exposure and infection is virtually unknown, Dr. Butler said. Investigators know those with COVID-19 have an antibody response, but whether that is protective or not, is unclear. In regard to older coronaviruses, such as those that cause colds, patients generally develop an antibody response and may have a period of immunity, but that immunity eventually wanes and reinfection can occur.
What is the latest on therapies?
A number of trials are underway in China and in the United States to test possible therapies for COVID-19, Dr. Butler said. One of the candidate drugs is the broad spectrum antiviral drug remdesivir, which was developed for the treatment of the Ebola virus. Additionally, the National Institutes of Health is studying the potential for monoclonal antibodies to treat COVID-19.
“Of course these are drugs not yet FDA approved,” he said. “We all want to have them in our toolbox as soon as possible, but we want to make sure these drugs are going to benefit and not harm, and that they really do have the utility that we hope for.”
Is there specific guidance for healthcare workers about COVID-19?
Health care workers have a much higher likelihood of being exposed or exposing others who are at high risk of severe infection, Dr. Butler said. That’s why, if a health care worker becomes infected and recovers, it’s still important to take extra precautions when going back to work, such as wearing a mask.
“These are recommendations that are in-draft,” he said. “I want to be clear, I’m floating concepts out there that people can consider. ... I recognize as a former infection control medical director at a hospital that sometimes you have to adapt those guidelines based on your local conditions.”
With new developments daily and lingering uncertainty about COVID-19, questions about testing and treatment for the coronavirus are at the forefront.
To address these top questions, Jay C. Butler, MD, deputy director for infectious diseases at the Centers for Disease Control and Prevention, sat down with JAMA editor Howard Bauchner, MD, to discuss the latest data on COVID-19 and to outline updated guidance from the agency. The following question-and-answer session was part of a live stream interview hosted by JAMA on March 16, 2020. The questions have been edited for length and clarity.
What test is being used to identify COVID-19?
In the United States, the most common and widely available test is the RT-polymerase chain reaction (rRT-PCR), which over the past few weeks has become available at public health labs across the country, Dr. Butler said during the JAMA interview. Capacity for the test is now possible in all 50 states and in Washington, D.C.
“More recently, there’s been a number of commercial labs that have come online to be able to do the testing,” Dr. Butler said. “Additionally, a number of academic centers are now able to run [Food and Drug Administration]–approved testing using slightly different PCR platforms.”
How accurate is the test?
Dr. Butler called PCR the “gold standard,” for testing COVID-19, and said it’s safe to say the test’s likelihood of identifying infection or past infection is extremely high. However, data on test sensitivity is limited.
“This may be frustrating to those of us who really like to know specifics of how to interpret the test results, but it’s important to keep in mind, we’re talking about a virus that we didn’t know existed 3 months ago,” he said.
At what point does a person with coronavirus test positive?
When exactly a test becomes positive is an unknown, Dr. Butler said. The assumption is that a patient who tests positive is more likely to be infectious, and data suggest the level of infectiousness is greatest after the onset of symptoms.
“There is at least some anecdotal reports that suggest that transmission could occur before onset of symptoms, but the data is still very limited,” he said. “Of course that has big implications in terms of how well we can really slow the spread of the virus.”
Who should get tested?
Dr. Butler said the focus should be individuals who are symptomatic with evidence of respiratory tract infection. People who are concerned about the virus and want a test are not the target.
“It’s important when talking to patients to help them to understand, this is different than a test for HIV or hepatitis C, where much of the message is: ‘Please get tested.’ ” he said. “This a situation where we’re trying to diagnose an acute infection. We do have a resource that may become limited again as some of the equipment required for running the test or collecting the specimen may come into short supply, so we want to focus on those people who are symptomatic and particularly on people who may be at higher risk of more severe illness.”
If a previously infected patient tests negative, can they still shed virus?
The CDC is currently analyzing how a negative PCR test relates to viral load, according to Dr. Butler. He added there have been situations in which a patient has twice tested negative for the virus, but a third swab resulted in a weakly positive result.
“It’s not clear if those are people who are actually infectious,” he said. “The PCR is detecting viral RNA, it doesn’t necessarily indicate there is viable virus present in the respiratory tract. So in general, I think it is safe to go back to work, but a positive test in a situation like that can be very difficult to interpret because we think it probably doesn’t reflect infectivity, but we don’t know for sure.”
Do we have an adequate supply of tests in the United States?
The CDC has addressed supply concerns by broadening the number of PCR platforms that can be used to run COVID-19 analyses, Dr. Butler said. Expansion of these platforms has been one way the government is furthering testing options and enabling consumer labs and academic centers to contribute to testing.
When can people who test positive go back to work?
The CDC is still researching that question and reviewing the data, Dr. Butler said. The current recommendation is that a patient who tests positive is considered clear to return to work after two negative tests at least 24 hours apart, following the resolution of symptoms. The CDC has not yet made an official recommendation on an exact time frame, but the CDC is considering a 14-day minimum of quarantine.
“The one caveat I’ll add is that someone who is a health care worker, even if they have resolved symptoms, it’s still a good idea to wear a surgical mask [when they return to work], just as an extra precaution.”
What do we know about immunity? Can patients get reinfected?
Long-term immunity after exposure and infection is virtually unknown, Dr. Butler said. Investigators know those with COVID-19 have an antibody response, but whether that is protective or not, is unclear. In regard to older coronaviruses, such as those that cause colds, patients generally develop an antibody response and may have a period of immunity, but that immunity eventually wanes and reinfection can occur.
What is the latest on therapies?
A number of trials are underway in China and in the United States to test possible therapies for COVID-19, Dr. Butler said. One of the candidate drugs is the broad spectrum antiviral drug remdesivir, which was developed for the treatment of the Ebola virus. Additionally, the National Institutes of Health is studying the potential for monoclonal antibodies to treat COVID-19.
“Of course these are drugs not yet FDA approved,” he said. “We all want to have them in our toolbox as soon as possible, but we want to make sure these drugs are going to benefit and not harm, and that they really do have the utility that we hope for.”
Is there specific guidance for healthcare workers about COVID-19?
Health care workers have a much higher likelihood of being exposed or exposing others who are at high risk of severe infection, Dr. Butler said. That’s why, if a health care worker becomes infected and recovers, it’s still important to take extra precautions when going back to work, such as wearing a mask.
“These are recommendations that are in-draft,” he said. “I want to be clear, I’m floating concepts out there that people can consider. ... I recognize as a former infection control medical director at a hospital that sometimes you have to adapt those guidelines based on your local conditions.”
With new developments daily and lingering uncertainty about COVID-19, questions about testing and treatment for the coronavirus are at the forefront.
To address these top questions, Jay C. Butler, MD, deputy director for infectious diseases at the Centers for Disease Control and Prevention, sat down with JAMA editor Howard Bauchner, MD, to discuss the latest data on COVID-19 and to outline updated guidance from the agency. The following question-and-answer session was part of a live stream interview hosted by JAMA on March 16, 2020. The questions have been edited for length and clarity.
What test is being used to identify COVID-19?
In the United States, the most common and widely available test is the RT-polymerase chain reaction (rRT-PCR), which over the past few weeks has become available at public health labs across the country, Dr. Butler said during the JAMA interview. Capacity for the test is now possible in all 50 states and in Washington, D.C.
“More recently, there’s been a number of commercial labs that have come online to be able to do the testing,” Dr. Butler said. “Additionally, a number of academic centers are now able to run [Food and Drug Administration]–approved testing using slightly different PCR platforms.”
How accurate is the test?
Dr. Butler called PCR the “gold standard,” for testing COVID-19, and said it’s safe to say the test’s likelihood of identifying infection or past infection is extremely high. However, data on test sensitivity is limited.
“This may be frustrating to those of us who really like to know specifics of how to interpret the test results, but it’s important to keep in mind, we’re talking about a virus that we didn’t know existed 3 months ago,” he said.
At what point does a person with coronavirus test positive?
When exactly a test becomes positive is an unknown, Dr. Butler said. The assumption is that a patient who tests positive is more likely to be infectious, and data suggest the level of infectiousness is greatest after the onset of symptoms.
“There is at least some anecdotal reports that suggest that transmission could occur before onset of symptoms, but the data is still very limited,” he said. “Of course that has big implications in terms of how well we can really slow the spread of the virus.”
Who should get tested?
Dr. Butler said the focus should be individuals who are symptomatic with evidence of respiratory tract infection. People who are concerned about the virus and want a test are not the target.
“It’s important when talking to patients to help them to understand, this is different than a test for HIV or hepatitis C, where much of the message is: ‘Please get tested.’ ” he said. “This a situation where we’re trying to diagnose an acute infection. We do have a resource that may become limited again as some of the equipment required for running the test or collecting the specimen may come into short supply, so we want to focus on those people who are symptomatic and particularly on people who may be at higher risk of more severe illness.”
If a previously infected patient tests negative, can they still shed virus?
The CDC is currently analyzing how a negative PCR test relates to viral load, according to Dr. Butler. He added there have been situations in which a patient has twice tested negative for the virus, but a third swab resulted in a weakly positive result.
“It’s not clear if those are people who are actually infectious,” he said. “The PCR is detecting viral RNA, it doesn’t necessarily indicate there is viable virus present in the respiratory tract. So in general, I think it is safe to go back to work, but a positive test in a situation like that can be very difficult to interpret because we think it probably doesn’t reflect infectivity, but we don’t know for sure.”
Do we have an adequate supply of tests in the United States?
The CDC has addressed supply concerns by broadening the number of PCR platforms that can be used to run COVID-19 analyses, Dr. Butler said. Expansion of these platforms has been one way the government is furthering testing options and enabling consumer labs and academic centers to contribute to testing.
When can people who test positive go back to work?
The CDC is still researching that question and reviewing the data, Dr. Butler said. The current recommendation is that a patient who tests positive is considered clear to return to work after two negative tests at least 24 hours apart, following the resolution of symptoms. The CDC has not yet made an official recommendation on an exact time frame, but the CDC is considering a 14-day minimum of quarantine.
“The one caveat I’ll add is that someone who is a health care worker, even if they have resolved symptoms, it’s still a good idea to wear a surgical mask [when they return to work], just as an extra precaution.”
What do we know about immunity? Can patients get reinfected?
Long-term immunity after exposure and infection is virtually unknown, Dr. Butler said. Investigators know those with COVID-19 have an antibody response, but whether that is protective or not, is unclear. In regard to older coronaviruses, such as those that cause colds, patients generally develop an antibody response and may have a period of immunity, but that immunity eventually wanes and reinfection can occur.
What is the latest on therapies?
A number of trials are underway in China and in the United States to test possible therapies for COVID-19, Dr. Butler said. One of the candidate drugs is the broad spectrum antiviral drug remdesivir, which was developed for the treatment of the Ebola virus. Additionally, the National Institutes of Health is studying the potential for monoclonal antibodies to treat COVID-19.
“Of course these are drugs not yet FDA approved,” he said. “We all want to have them in our toolbox as soon as possible, but we want to make sure these drugs are going to benefit and not harm, and that they really do have the utility that we hope for.”
Is there specific guidance for healthcare workers about COVID-19?
Health care workers have a much higher likelihood of being exposed or exposing others who are at high risk of severe infection, Dr. Butler said. That’s why, if a health care worker becomes infected and recovers, it’s still important to take extra precautions when going back to work, such as wearing a mask.
“These are recommendations that are in-draft,” he said. “I want to be clear, I’m floating concepts out there that people can consider. ... I recognize as a former infection control medical director at a hospital that sometimes you have to adapt those guidelines based on your local conditions.”
ESC says continue hypertension meds despite COVID-19 concern
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
The European Society of Cardiology (ESC) has issued a statement urging physicians and patients to continue treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), in light of a newly described theory that those agents could increase the risk of developing COVID-19 and/or worsen its severity.
The concern arises from the observation that the new coronavirus SARS-CoV-2 causing COVID-19 binds to angiotensin-converting enzyme 2 (ACE2) to infect cells, and both ACE inhibitors and ARBs increase ACE2 levels.
This mechanism has been theorized as a possible risk factor for facilitating the acquisition of COVID-19 infection and worsening its severity. However, paradoxically, it has also been hypothesized to protect against acute lung injury from the disease.
Meanwhile, a Lancet Respiratory Medicine article was published March 11 entitled, “Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection?”
“We ... hypothesize that diabetes and hypertension treatment with ACE2-stimulating drugs increases the risk of developing severe and fatal COVID-19,” said the authors.
This prompted some media coverage in the United Kingdom and “social media-related amplification,” leading to concern and, in some cases, discontinuation of the drugs by patients.
But on March 13, the ESC Council on Hypertension dismissed the concerns as entirely speculative, in a statement posted to the ESC website.
It said that the council “strongly recommend that physicians and patients should continue treatment with their usual antihypertensive therapy because there is no clinical or scientific evidence to suggest that treatment with ACE inhibitors or ARBs should be discontinued because of the COVID-19 infection.”
The statement, signed by Council Chair Professor Giovanni de Simone, MD, on behalf of the nucleus members, also says that in regard to the theorized protective effect against serious lung complications in individuals with COVID-19, the data come only from animal, and not human, studies.
“Speculation about the safety of ACE-inhibitor or ARB treatment in relation to COVID-19 does not have a sound scientific basis or evidence to support it,” the ESC panel concludes.
This article first appeared on Medscape.com.
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
The European Society of Cardiology (ESC) has issued a statement urging physicians and patients to continue treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), in light of a newly described theory that those agents could increase the risk of developing COVID-19 and/or worsen its severity.
The concern arises from the observation that the new coronavirus SARS-CoV-2 causing COVID-19 binds to angiotensin-converting enzyme 2 (ACE2) to infect cells, and both ACE inhibitors and ARBs increase ACE2 levels.
This mechanism has been theorized as a possible risk factor for facilitating the acquisition of COVID-19 infection and worsening its severity. However, paradoxically, it has also been hypothesized to protect against acute lung injury from the disease.
Meanwhile, a Lancet Respiratory Medicine article was published March 11 entitled, “Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection?”
“We ... hypothesize that diabetes and hypertension treatment with ACE2-stimulating drugs increases the risk of developing severe and fatal COVID-19,” said the authors.
This prompted some media coverage in the United Kingdom and “social media-related amplification,” leading to concern and, in some cases, discontinuation of the drugs by patients.
But on March 13, the ESC Council on Hypertension dismissed the concerns as entirely speculative, in a statement posted to the ESC website.
It said that the council “strongly recommend that physicians and patients should continue treatment with their usual antihypertensive therapy because there is no clinical or scientific evidence to suggest that treatment with ACE inhibitors or ARBs should be discontinued because of the COVID-19 infection.”
The statement, signed by Council Chair Professor Giovanni de Simone, MD, on behalf of the nucleus members, also says that in regard to the theorized protective effect against serious lung complications in individuals with COVID-19, the data come only from animal, and not human, studies.
“Speculation about the safety of ACE-inhibitor or ARB treatment in relation to COVID-19 does not have a sound scientific basis or evidence to support it,” the ESC panel concludes.
This article first appeared on Medscape.com.
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
The European Society of Cardiology (ESC) has issued a statement urging physicians and patients to continue treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), in light of a newly described theory that those agents could increase the risk of developing COVID-19 and/or worsen its severity.
The concern arises from the observation that the new coronavirus SARS-CoV-2 causing COVID-19 binds to angiotensin-converting enzyme 2 (ACE2) to infect cells, and both ACE inhibitors and ARBs increase ACE2 levels.
This mechanism has been theorized as a possible risk factor for facilitating the acquisition of COVID-19 infection and worsening its severity. However, paradoxically, it has also been hypothesized to protect against acute lung injury from the disease.
Meanwhile, a Lancet Respiratory Medicine article was published March 11 entitled, “Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection?”
“We ... hypothesize that diabetes and hypertension treatment with ACE2-stimulating drugs increases the risk of developing severe and fatal COVID-19,” said the authors.
This prompted some media coverage in the United Kingdom and “social media-related amplification,” leading to concern and, in some cases, discontinuation of the drugs by patients.
But on March 13, the ESC Council on Hypertension dismissed the concerns as entirely speculative, in a statement posted to the ESC website.
It said that the council “strongly recommend that physicians and patients should continue treatment with their usual antihypertensive therapy because there is no clinical or scientific evidence to suggest that treatment with ACE inhibitors or ARBs should be discontinued because of the COVID-19 infection.”
The statement, signed by Council Chair Professor Giovanni de Simone, MD, on behalf of the nucleus members, also says that in regard to the theorized protective effect against serious lung complications in individuals with COVID-19, the data come only from animal, and not human, studies.
“Speculation about the safety of ACE-inhibitor or ARB treatment in relation to COVID-19 does not have a sound scientific basis or evidence to support it,” the ESC panel concludes.
This article first appeared on Medscape.com.
Here’s what ICUs are putting up against COVID-19
As COVID-19 spreads across the United States, it is important to understand the extent of the nation’s ICU resources, according to the Society of Critical Care Medicine. The SCCM has updated its statistics on the resources available to care for what could become “an overwhelming number of critically ill patients, many of whom may require mechanical ventilation,” the society said in a blog post on March 13.
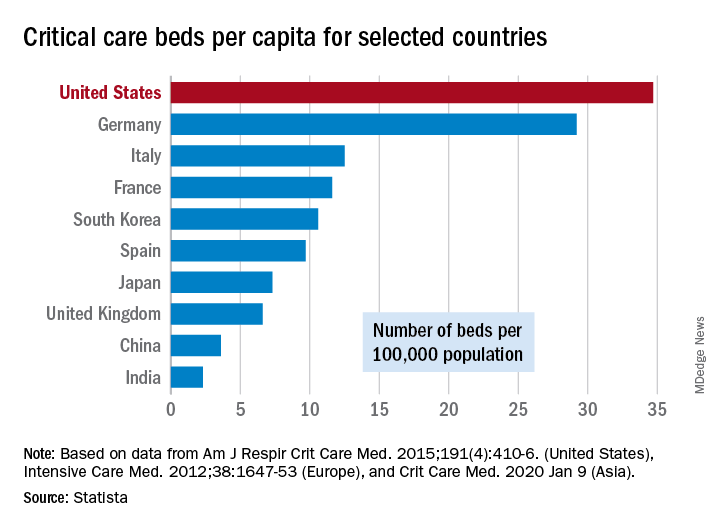
That overwhelming number was considered at an American Hospital Association webinar in February: Investigators projected that 4.8 million patients could be hospitalized with COVID-19, of whom 1.9 million would be admitted to ICUs and 960,000 would require ventilator support, Neil A. Halpern, MD, director of the critical care center at Memorial Sloan Kettering Cancer Center, New York, and Kay See Tan, PhD, of the hospital’s department of epidemiology and biostatistics, reported in that post.
As far as critical care beds are concerned, the United States is in better shape than are other countries dealing with the coronavirus. The United States’ 34.7 critical care beds per 100,000 population put it a good bit ahead of Germany, which has 29.2 beds per 100,000, while other countries in both Europe and Asia are well behind, Dr. Halpern and Dr. Tan noted.
More recent data from the AHA show that just over half of its registered community hospitals deliver ICU services and have at least 10 acute care beds and one ICU bed, they reported.
Those 2,704 hospitals have nearly 535,000 acute care beds, of which almost 97,000 are ICU beds. Almost 71% of those ICU beds are for adults, with the rest located in neonatal and pediatric units, data from an AHA 2018 survey show.
Since patients with COVID-19 are most often admitted to ICUs with severe hypoxic respiratory failure, the nation’s supply of ventilators also may be tested. U.S. acute care hospitals own about 62,000 full-featured mechanical ventilators and almost 99,000 older ventilators that “may not be capable of adequately supporting patients with severe acute respiratory failure,” Dr. Halpern and Dr. Tan said.
As U.S. hospitals reach the crisis levels anticipated in the COVID-19 pandemic, staffing shortages can be expected as well. Almost half (48%) of acute care hospitals have no intensivists, so “other physicians (e.g., pulmonologists, surgeons, anesthesiologists, etc) may be pressed into service as outpatient clinics and elective surgery are suspended,” they wrote.
The blog post includes a tiered staffing strategy that the SCCM “encourages hospitals to adopt in pandemic situations such as COVID-19.”
As COVID-19 spreads across the United States, it is important to understand the extent of the nation’s ICU resources, according to the Society of Critical Care Medicine. The SCCM has updated its statistics on the resources available to care for what could become “an overwhelming number of critically ill patients, many of whom may require mechanical ventilation,” the society said in a blog post on March 13.
That overwhelming number was considered at an American Hospital Association webinar in February: Investigators projected that 4.8 million patients could be hospitalized with COVID-19, of whom 1.9 million would be admitted to ICUs and 960,000 would require ventilator support, Neil A. Halpern, MD, director of the critical care center at Memorial Sloan Kettering Cancer Center, New York, and Kay See Tan, PhD, of the hospital’s department of epidemiology and biostatistics, reported in that post.
As far as critical care beds are concerned, the United States is in better shape than are other countries dealing with the coronavirus. The United States’ 34.7 critical care beds per 100,000 population put it a good bit ahead of Germany, which has 29.2 beds per 100,000, while other countries in both Europe and Asia are well behind, Dr. Halpern and Dr. Tan noted.
More recent data from the AHA show that just over half of its registered community hospitals deliver ICU services and have at least 10 acute care beds and one ICU bed, they reported.
Those 2,704 hospitals have nearly 535,000 acute care beds, of which almost 97,000 are ICU beds. Almost 71% of those ICU beds are for adults, with the rest located in neonatal and pediatric units, data from an AHA 2018 survey show.
Since patients with COVID-19 are most often admitted to ICUs with severe hypoxic respiratory failure, the nation’s supply of ventilators also may be tested. U.S. acute care hospitals own about 62,000 full-featured mechanical ventilators and almost 99,000 older ventilators that “may not be capable of adequately supporting patients with severe acute respiratory failure,” Dr. Halpern and Dr. Tan said.
As U.S. hospitals reach the crisis levels anticipated in the COVID-19 pandemic, staffing shortages can be expected as well. Almost half (48%) of acute care hospitals have no intensivists, so “other physicians (e.g., pulmonologists, surgeons, anesthesiologists, etc) may be pressed into service as outpatient clinics and elective surgery are suspended,” they wrote.
The blog post includes a tiered staffing strategy that the SCCM “encourages hospitals to adopt in pandemic situations such as COVID-19.”
As COVID-19 spreads across the United States, it is important to understand the extent of the nation’s ICU resources, according to the Society of Critical Care Medicine. The SCCM has updated its statistics on the resources available to care for what could become “an overwhelming number of critically ill patients, many of whom may require mechanical ventilation,” the society said in a blog post on March 13.
That overwhelming number was considered at an American Hospital Association webinar in February: Investigators projected that 4.8 million patients could be hospitalized with COVID-19, of whom 1.9 million would be admitted to ICUs and 960,000 would require ventilator support, Neil A. Halpern, MD, director of the critical care center at Memorial Sloan Kettering Cancer Center, New York, and Kay See Tan, PhD, of the hospital’s department of epidemiology and biostatistics, reported in that post.
As far as critical care beds are concerned, the United States is in better shape than are other countries dealing with the coronavirus. The United States’ 34.7 critical care beds per 100,000 population put it a good bit ahead of Germany, which has 29.2 beds per 100,000, while other countries in both Europe and Asia are well behind, Dr. Halpern and Dr. Tan noted.
More recent data from the AHA show that just over half of its registered community hospitals deliver ICU services and have at least 10 acute care beds and one ICU bed, they reported.
Those 2,704 hospitals have nearly 535,000 acute care beds, of which almost 97,000 are ICU beds. Almost 71% of those ICU beds are for adults, with the rest located in neonatal and pediatric units, data from an AHA 2018 survey show.
Since patients with COVID-19 are most often admitted to ICUs with severe hypoxic respiratory failure, the nation’s supply of ventilators also may be tested. U.S. acute care hospitals own about 62,000 full-featured mechanical ventilators and almost 99,000 older ventilators that “may not be capable of adequately supporting patients with severe acute respiratory failure,” Dr. Halpern and Dr. Tan said.
As U.S. hospitals reach the crisis levels anticipated in the COVID-19 pandemic, staffing shortages can be expected as well. Almost half (48%) of acute care hospitals have no intensivists, so “other physicians (e.g., pulmonologists, surgeons, anesthesiologists, etc) may be pressed into service as outpatient clinics and elective surgery are suspended,” they wrote.
The blog post includes a tiered staffing strategy that the SCCM “encourages hospitals to adopt in pandemic situations such as COVID-19.”
So you have a COVID-19 patient: How do you treat them?
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
Clinicians are working out how to manage patients with or suspected of having COVID-19.
“Over the past couple of weeks, we’ve been preparing for the oncoming onslaught of patients,” said Lillian Wu, MD, of the HealthPoint network in the Seattle area of greater King County and president elect of the Washington Academy of Family Physicians.
Step One: Triage
The first step, Wu says, is careful triage.
When patients call one of the 17 clinics in the HealthPoint system, nurses gauge how sick they are. High fever? Shortness of breath? Do they have a chronic illness, such as diabetes, cardiovascular disease, or a lung condition, that increases risk for infection and complications?
“If a patient has mild symptoms, we ask them to stay home or to check back in 24 hours, or we’ll reach out to them. For moderate symptoms, we ask them to come in, and [we] clearly mark on the schedule that it is a respiratory patient, who will be sent to a separate area. If the patient is severe, we don’t even see them and send them directly to the hospital to the ER,” Wu told Medscape Medical News.
These categories parallel the World Health Organization’s designations of uncomplicated illness, mild pneumonia, severe pneumonia, acute respiratory distress syndrome, sepsis, and septic shock. The Centers for Disease Control and Prevention (CDC) advises case by case regarding decisions as to outpatient or inpatient assignment.
“Patients who pass the initial phone triage are given masks, separated, and sent to different parts of the clinic or are required to wait in their cars until it’s time to be seen,” Wu said.
Step 2: Hospital Arrival
Once at the hospital, the CDC’s interim guidance kicks in.
“Any patient with fever, cough, and shortness of breath presenting with a history of travel to countries with high ongoing transmission or a credible history of exposure should be promptly evaluated for COVID-19,” said Raghavendra Tirupathi, MD, medical director, Keystone Infectious Diseases/HIV; chair in infection prevention, Summit Health; and clinical assistant professor of medicine, Penn State School of Medicine, Hershey, Pennsylvania.
“We recommend obtaining baseline CBC with differential, basic metabolic panel, liver function tests, and procalcitonin. Clues for COVID-19 include leukopenia, seen in 30% to 45% of patients, and lymphocytopenia, seen in 85% of the patients in the case series from China,” Tirupathi said. He uses a respiratory virus polymerase chain reaction panel to rule out other pathogens.
Wu concurs. “This is the one time we are grateful when someone tests positive for the flu! If flu is negative and other common respiratory infections are negative, then we do a COVID-19 test,” she said.
But test results may be delayed. “At the University of Washington, it takes 8 hours, but commercial labs take up to 4 days,” Wu said. All patients with respiratory symptoms are treated as persons under investigation, for whom isolation precautions are required. In addition, for these patients, use of personal protective equipment by caregivers is required.
For suspected pneumonia, the American College of Radiography recommends chest CT to identify peripheral basal ground-glass opacities characteristic of COVID-19.
However, diagnosis should be based on detection of SARS-CoV-2, because chest images for COVID-19 are nonspecific – associated signs can also be seen in H1N1 influenza, SARS, and MERS.
Step 3: Supportive Care
Once a patient is admitted, supportive care entails “maintaining fluid status and nutrition and supporting physiological functions until we heal. It’s treating complications and organ support, whether that means providing supplementary oxygen all the way to ventilator support, and just waiting it out. If a patient progresses to acute respiratory distress syndrome, it becomes tougher,” said David Liebers, MD, chief medical officer and an infectious disease specialist at Ellis Medicine in Schenectady, New York.
Efforts are ramping up to develop therapeutics. Remdesivir, an investigational antiviral drug developed to treat Ebola and Marburg hemorrhagic fevers, shows activity against SARS-CoV-2 in vitro.
Remdesivir has been used in a few patients on a compassionate-use basis outside of a clinical trial setting. “It’s a nucleotide analogue, and like other drugs of that class, it disrupts nucleic acid production. Some data suggest that it might have some efficacy,” Liebers said.
Antibiotics are reserved for patients suspected of having concomitant bacterial or fungal infections. Liebers said clinicians should be alerted to “the big three” signs of secondary infection – fever, elevated white blood cell count, and lactic acidosis. Immunosuppressed patients are at elevated risk for secondary infection.
Step 4: Managing Complications
Patients do die of COVID-19, mostly through an inability to ventilate, even when supported with oxygen, Liebers told Medscape Medical News. (According to Tirupathi, “The studies from China indicate that from 6%-10% of patients needed ventilators.”)
Liebers continued, “Others may develop sepsis or a syndrome of multisystem organ failure with renal and endothelial collapse, making it difficult to maintain blood pressure. Like with so many pathologies, it is a vicious circle in which everything gets overworked. Off-and-on treatments can sometimes break the cycle: supplementary oxygen, giving red blood cells, dialysis. We support those functions while waiting for healing to occur.”
A facility’s airborne-infection isolation rooms may become filled to capacity, but that isn’t critical, Liebers said. “Airborne precautions are standard to contain measles, tuberculosis, chickenpox, and herpes zoster, in which very small particles spread in the air,” he said.
Consensus is growing that SARS-CoV-2 spreads in large droplets, he added. Private rooms and closed doors may suffice.
Step 5: Discharge
Liebers said that as of now, the million-dollar question regards criteria for discharge.
Patients who clinically improve are sent home with instructions to remain in isolation. They may be tested again for virus before or after discharge.
Liebers and Wu pointed to the experience at EvergreenHealth Medical Center, in Kirkland, Washington, as guidance from the trenches. “They’re the ones who are learning firsthand and passing the experience along to everyone else,” Wu said.
“The situation is unprecedented,” said Liebers, who, like many others, has barely slept these past weeks. “We’re swimming in murky water right now.”
The epidemic in the United States is still months from peaking, Wu emphasized. “There is no vaccine, and many cases are subclinical. COVID-19 has to spread through the country before it infects a critical mass of people who will develop immunity. It’s too late to contain.”
Added Liebers, “It’s a constantly changing situation, and we are still being surprised – not that this wasn’t predicted.”
This article first appeared on Medscape.com.
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
Clinicians are working out how to manage patients with or suspected of having COVID-19.
“Over the past couple of weeks, we’ve been preparing for the oncoming onslaught of patients,” said Lillian Wu, MD, of the HealthPoint network in the Seattle area of greater King County and president elect of the Washington Academy of Family Physicians.
Step One: Triage
The first step, Wu says, is careful triage.
When patients call one of the 17 clinics in the HealthPoint system, nurses gauge how sick they are. High fever? Shortness of breath? Do they have a chronic illness, such as diabetes, cardiovascular disease, or a lung condition, that increases risk for infection and complications?
“If a patient has mild symptoms, we ask them to stay home or to check back in 24 hours, or we’ll reach out to them. For moderate symptoms, we ask them to come in, and [we] clearly mark on the schedule that it is a respiratory patient, who will be sent to a separate area. If the patient is severe, we don’t even see them and send them directly to the hospital to the ER,” Wu told Medscape Medical News.
These categories parallel the World Health Organization’s designations of uncomplicated illness, mild pneumonia, severe pneumonia, acute respiratory distress syndrome, sepsis, and septic shock. The Centers for Disease Control and Prevention (CDC) advises case by case regarding decisions as to outpatient or inpatient assignment.
“Patients who pass the initial phone triage are given masks, separated, and sent to different parts of the clinic or are required to wait in their cars until it’s time to be seen,” Wu said.
Step 2: Hospital Arrival
Once at the hospital, the CDC’s interim guidance kicks in.
“Any patient with fever, cough, and shortness of breath presenting with a history of travel to countries with high ongoing transmission or a credible history of exposure should be promptly evaluated for COVID-19,” said Raghavendra Tirupathi, MD, medical director, Keystone Infectious Diseases/HIV; chair in infection prevention, Summit Health; and clinical assistant professor of medicine, Penn State School of Medicine, Hershey, Pennsylvania.
“We recommend obtaining baseline CBC with differential, basic metabolic panel, liver function tests, and procalcitonin. Clues for COVID-19 include leukopenia, seen in 30% to 45% of patients, and lymphocytopenia, seen in 85% of the patients in the case series from China,” Tirupathi said. He uses a respiratory virus polymerase chain reaction panel to rule out other pathogens.
Wu concurs. “This is the one time we are grateful when someone tests positive for the flu! If flu is negative and other common respiratory infections are negative, then we do a COVID-19 test,” she said.
But test results may be delayed. “At the University of Washington, it takes 8 hours, but commercial labs take up to 4 days,” Wu said. All patients with respiratory symptoms are treated as persons under investigation, for whom isolation precautions are required. In addition, for these patients, use of personal protective equipment by caregivers is required.
For suspected pneumonia, the American College of Radiography recommends chest CT to identify peripheral basal ground-glass opacities characteristic of COVID-19.
However, diagnosis should be based on detection of SARS-CoV-2, because chest images for COVID-19 are nonspecific – associated signs can also be seen in H1N1 influenza, SARS, and MERS.
Step 3: Supportive Care
Once a patient is admitted, supportive care entails “maintaining fluid status and nutrition and supporting physiological functions until we heal. It’s treating complications and organ support, whether that means providing supplementary oxygen all the way to ventilator support, and just waiting it out. If a patient progresses to acute respiratory distress syndrome, it becomes tougher,” said David Liebers, MD, chief medical officer and an infectious disease specialist at Ellis Medicine in Schenectady, New York.
Efforts are ramping up to develop therapeutics. Remdesivir, an investigational antiviral drug developed to treat Ebola and Marburg hemorrhagic fevers, shows activity against SARS-CoV-2 in vitro.
Remdesivir has been used in a few patients on a compassionate-use basis outside of a clinical trial setting. “It’s a nucleotide analogue, and like other drugs of that class, it disrupts nucleic acid production. Some data suggest that it might have some efficacy,” Liebers said.
Antibiotics are reserved for patients suspected of having concomitant bacterial or fungal infections. Liebers said clinicians should be alerted to “the big three” signs of secondary infection – fever, elevated white blood cell count, and lactic acidosis. Immunosuppressed patients are at elevated risk for secondary infection.
Step 4: Managing Complications
Patients do die of COVID-19, mostly through an inability to ventilate, even when supported with oxygen, Liebers told Medscape Medical News. (According to Tirupathi, “The studies from China indicate that from 6%-10% of patients needed ventilators.”)
Liebers continued, “Others may develop sepsis or a syndrome of multisystem organ failure with renal and endothelial collapse, making it difficult to maintain blood pressure. Like with so many pathologies, it is a vicious circle in which everything gets overworked. Off-and-on treatments can sometimes break the cycle: supplementary oxygen, giving red blood cells, dialysis. We support those functions while waiting for healing to occur.”
A facility’s airborne-infection isolation rooms may become filled to capacity, but that isn’t critical, Liebers said. “Airborne precautions are standard to contain measles, tuberculosis, chickenpox, and herpes zoster, in which very small particles spread in the air,” he said.
Consensus is growing that SARS-CoV-2 spreads in large droplets, he added. Private rooms and closed doors may suffice.
Step 5: Discharge
Liebers said that as of now, the million-dollar question regards criteria for discharge.
Patients who clinically improve are sent home with instructions to remain in isolation. They may be tested again for virus before or after discharge.
Liebers and Wu pointed to the experience at EvergreenHealth Medical Center, in Kirkland, Washington, as guidance from the trenches. “They’re the ones who are learning firsthand and passing the experience along to everyone else,” Wu said.
“The situation is unprecedented,” said Liebers, who, like many others, has barely slept these past weeks. “We’re swimming in murky water right now.”
The epidemic in the United States is still months from peaking, Wu emphasized. “There is no vaccine, and many cases are subclinical. COVID-19 has to spread through the country before it infects a critical mass of people who will develop immunity. It’s too late to contain.”
Added Liebers, “It’s a constantly changing situation, and we are still being surprised – not that this wasn’t predicted.”
This article first appeared on Medscape.com.
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
Clinicians are working out how to manage patients with or suspected of having COVID-19.
“Over the past couple of weeks, we’ve been preparing for the oncoming onslaught of patients,” said Lillian Wu, MD, of the HealthPoint network in the Seattle area of greater King County and president elect of the Washington Academy of Family Physicians.
Step One: Triage
The first step, Wu says, is careful triage.
When patients call one of the 17 clinics in the HealthPoint system, nurses gauge how sick they are. High fever? Shortness of breath? Do they have a chronic illness, such as diabetes, cardiovascular disease, or a lung condition, that increases risk for infection and complications?
“If a patient has mild symptoms, we ask them to stay home or to check back in 24 hours, or we’ll reach out to them. For moderate symptoms, we ask them to come in, and [we] clearly mark on the schedule that it is a respiratory patient, who will be sent to a separate area. If the patient is severe, we don’t even see them and send them directly to the hospital to the ER,” Wu told Medscape Medical News.
These categories parallel the World Health Organization’s designations of uncomplicated illness, mild pneumonia, severe pneumonia, acute respiratory distress syndrome, sepsis, and septic shock. The Centers for Disease Control and Prevention (CDC) advises case by case regarding decisions as to outpatient or inpatient assignment.
“Patients who pass the initial phone triage are given masks, separated, and sent to different parts of the clinic or are required to wait in their cars until it’s time to be seen,” Wu said.
Step 2: Hospital Arrival
Once at the hospital, the CDC’s interim guidance kicks in.
“Any patient with fever, cough, and shortness of breath presenting with a history of travel to countries with high ongoing transmission or a credible history of exposure should be promptly evaluated for COVID-19,” said Raghavendra Tirupathi, MD, medical director, Keystone Infectious Diseases/HIV; chair in infection prevention, Summit Health; and clinical assistant professor of medicine, Penn State School of Medicine, Hershey, Pennsylvania.
“We recommend obtaining baseline CBC with differential, basic metabolic panel, liver function tests, and procalcitonin. Clues for COVID-19 include leukopenia, seen in 30% to 45% of patients, and lymphocytopenia, seen in 85% of the patients in the case series from China,” Tirupathi said. He uses a respiratory virus polymerase chain reaction panel to rule out other pathogens.
Wu concurs. “This is the one time we are grateful when someone tests positive for the flu! If flu is negative and other common respiratory infections are negative, then we do a COVID-19 test,” she said.
But test results may be delayed. “At the University of Washington, it takes 8 hours, but commercial labs take up to 4 days,” Wu said. All patients with respiratory symptoms are treated as persons under investigation, for whom isolation precautions are required. In addition, for these patients, use of personal protective equipment by caregivers is required.
For suspected pneumonia, the American College of Radiography recommends chest CT to identify peripheral basal ground-glass opacities characteristic of COVID-19.
However, diagnosis should be based on detection of SARS-CoV-2, because chest images for COVID-19 are nonspecific – associated signs can also be seen in H1N1 influenza, SARS, and MERS.
Step 3: Supportive Care
Once a patient is admitted, supportive care entails “maintaining fluid status and nutrition and supporting physiological functions until we heal. It’s treating complications and organ support, whether that means providing supplementary oxygen all the way to ventilator support, and just waiting it out. If a patient progresses to acute respiratory distress syndrome, it becomes tougher,” said David Liebers, MD, chief medical officer and an infectious disease specialist at Ellis Medicine in Schenectady, New York.
Efforts are ramping up to develop therapeutics. Remdesivir, an investigational antiviral drug developed to treat Ebola and Marburg hemorrhagic fevers, shows activity against SARS-CoV-2 in vitro.
Remdesivir has been used in a few patients on a compassionate-use basis outside of a clinical trial setting. “It’s a nucleotide analogue, and like other drugs of that class, it disrupts nucleic acid production. Some data suggest that it might have some efficacy,” Liebers said.
Antibiotics are reserved for patients suspected of having concomitant bacterial or fungal infections. Liebers said clinicians should be alerted to “the big three” signs of secondary infection – fever, elevated white blood cell count, and lactic acidosis. Immunosuppressed patients are at elevated risk for secondary infection.
Step 4: Managing Complications
Patients do die of COVID-19, mostly through an inability to ventilate, even when supported with oxygen, Liebers told Medscape Medical News. (According to Tirupathi, “The studies from China indicate that from 6%-10% of patients needed ventilators.”)
Liebers continued, “Others may develop sepsis or a syndrome of multisystem organ failure with renal and endothelial collapse, making it difficult to maintain blood pressure. Like with so many pathologies, it is a vicious circle in which everything gets overworked. Off-and-on treatments can sometimes break the cycle: supplementary oxygen, giving red blood cells, dialysis. We support those functions while waiting for healing to occur.”
A facility’s airborne-infection isolation rooms may become filled to capacity, but that isn’t critical, Liebers said. “Airborne precautions are standard to contain measles, tuberculosis, chickenpox, and herpes zoster, in which very small particles spread in the air,” he said.
Consensus is growing that SARS-CoV-2 spreads in large droplets, he added. Private rooms and closed doors may suffice.
Step 5: Discharge
Liebers said that as of now, the million-dollar question regards criteria for discharge.
Patients who clinically improve are sent home with instructions to remain in isolation. They may be tested again for virus before or after discharge.
Liebers and Wu pointed to the experience at EvergreenHealth Medical Center, in Kirkland, Washington, as guidance from the trenches. “They’re the ones who are learning firsthand and passing the experience along to everyone else,” Wu said.
“The situation is unprecedented,” said Liebers, who, like many others, has barely slept these past weeks. “We’re swimming in murky water right now.”
The epidemic in the United States is still months from peaking, Wu emphasized. “There is no vaccine, and many cases are subclinical. COVID-19 has to spread through the country before it infects a critical mass of people who will develop immunity. It’s too late to contain.”
Added Liebers, “It’s a constantly changing situation, and we are still being surprised – not that this wasn’t predicted.”
This article first appeared on Medscape.com.
President declares national emergency for COVID-19, ramps up testing capability
President Donald Trump has declared a national emergency to allow for additional resources to combat the COVID-19 pandemic and announced increased testing capacity in partnership with private industry.
During a March 13 press conference, the president said the declaration would “open up access to up to $50 billion” for states and territories in combating the spread of the disease.
He also called on all states to “set up emergency operation centers, effective immediately” and for every hospital “to activate its emergency preparedness plan so that they can meet the needs of Americans everywhere.”
Additionally, he said the declaration will confer broad new authority on the Department of Health & Human Services Secretary Alex Azar that will allow him to “immediately waive provisions of applicable laws and regulations to give doctors, all hospitals, and health care providers maximum flexibility to respond to the virus and care for patients.”
Some of the powers he highlighted included the ability to waive laws to enable telehealth; to waive certain federal license requirements to allow doctors licensed in one state to offer services in other states; the ability to waive limits on beds in critical access hospitals; and to waive rules that hinder hospitals from hiring additional physicians.
The president also announced that more testing capacity will be made available within the next week, in partnership with private industry.
“We want to make sure that those who need a test can get a test very safely, quickly, and conveniently, but we don’t want people to take a test if we feel that they shouldn’t be doing it,” he said.
To help make that determination, a website, developed with Google, is expected to be launched the weekend of March 13 to will allow individuals to input their symptoms and risk factors to help determine if they should be tested. If certain criteria are met, the website will provide locations for drive-through testing facilities. Individuals will be tested using a nasal swab and will receive results within 24-36 hours.
The testing is being done in partnership with retailers, including Target and Walmart (who are providing parking lot space for the pop-up testing facilities) and testing companies LabCorp and Quest Diagnostics.
The new test was developed by Roche and just received emergency use authorization from the Food and Drug Administration.
“We therefore expect up to a half-million additional tests will be available early next week,” President Trump said, adding that testing locations will “probably” be announced on Sunday, March 15.
A second application for a new test, submitted by Thermo Fisher, is currently under review at the FDA and is expected to be approved within the next 24 hours, he said. This would add an additional 1.4 million tests in the next week and 5 million within a month, according to the president.
President Donald Trump has declared a national emergency to allow for additional resources to combat the COVID-19 pandemic and announced increased testing capacity in partnership with private industry.
During a March 13 press conference, the president said the declaration would “open up access to up to $50 billion” for states and territories in combating the spread of the disease.
He also called on all states to “set up emergency operation centers, effective immediately” and for every hospital “to activate its emergency preparedness plan so that they can meet the needs of Americans everywhere.”
Additionally, he said the declaration will confer broad new authority on the Department of Health & Human Services Secretary Alex Azar that will allow him to “immediately waive provisions of applicable laws and regulations to give doctors, all hospitals, and health care providers maximum flexibility to respond to the virus and care for patients.”
Some of the powers he highlighted included the ability to waive laws to enable telehealth; to waive certain federal license requirements to allow doctors licensed in one state to offer services in other states; the ability to waive limits on beds in critical access hospitals; and to waive rules that hinder hospitals from hiring additional physicians.
The president also announced that more testing capacity will be made available within the next week, in partnership with private industry.
“We want to make sure that those who need a test can get a test very safely, quickly, and conveniently, but we don’t want people to take a test if we feel that they shouldn’t be doing it,” he said.
To help make that determination, a website, developed with Google, is expected to be launched the weekend of March 13 to will allow individuals to input their symptoms and risk factors to help determine if they should be tested. If certain criteria are met, the website will provide locations for drive-through testing facilities. Individuals will be tested using a nasal swab and will receive results within 24-36 hours.
The testing is being done in partnership with retailers, including Target and Walmart (who are providing parking lot space for the pop-up testing facilities) and testing companies LabCorp and Quest Diagnostics.
The new test was developed by Roche and just received emergency use authorization from the Food and Drug Administration.
“We therefore expect up to a half-million additional tests will be available early next week,” President Trump said, adding that testing locations will “probably” be announced on Sunday, March 15.
A second application for a new test, submitted by Thermo Fisher, is currently under review at the FDA and is expected to be approved within the next 24 hours, he said. This would add an additional 1.4 million tests in the next week and 5 million within a month, according to the president.
President Donald Trump has declared a national emergency to allow for additional resources to combat the COVID-19 pandemic and announced increased testing capacity in partnership with private industry.
During a March 13 press conference, the president said the declaration would “open up access to up to $50 billion” for states and territories in combating the spread of the disease.
He also called on all states to “set up emergency operation centers, effective immediately” and for every hospital “to activate its emergency preparedness plan so that they can meet the needs of Americans everywhere.”
Additionally, he said the declaration will confer broad new authority on the Department of Health & Human Services Secretary Alex Azar that will allow him to “immediately waive provisions of applicable laws and regulations to give doctors, all hospitals, and health care providers maximum flexibility to respond to the virus and care for patients.”
Some of the powers he highlighted included the ability to waive laws to enable telehealth; to waive certain federal license requirements to allow doctors licensed in one state to offer services in other states; the ability to waive limits on beds in critical access hospitals; and to waive rules that hinder hospitals from hiring additional physicians.
The president also announced that more testing capacity will be made available within the next week, in partnership with private industry.
“We want to make sure that those who need a test can get a test very safely, quickly, and conveniently, but we don’t want people to take a test if we feel that they shouldn’t be doing it,” he said.
To help make that determination, a website, developed with Google, is expected to be launched the weekend of March 13 to will allow individuals to input their symptoms and risk factors to help determine if they should be tested. If certain criteria are met, the website will provide locations for drive-through testing facilities. Individuals will be tested using a nasal swab and will receive results within 24-36 hours.
The testing is being done in partnership with retailers, including Target and Walmart (who are providing parking lot space for the pop-up testing facilities) and testing companies LabCorp and Quest Diagnostics.
The new test was developed by Roche and just received emergency use authorization from the Food and Drug Administration.
“We therefore expect up to a half-million additional tests will be available early next week,” President Trump said, adding that testing locations will “probably” be announced on Sunday, March 15.
A second application for a new test, submitted by Thermo Fisher, is currently under review at the FDA and is expected to be approved within the next 24 hours, he said. This would add an additional 1.4 million tests in the next week and 5 million within a month, according to the president.
Your medical conference is canceled. Now what?
Khadija Hafidh, MD, was already booked on a 14-hour, direct flight from Dubai to Los Angeles, when the American College of Physicians (ACP) announced it was canceling its internal medicine meeting scheduled for April.

Canceling her hotel reservation was not a problem, and she was assured a refund for the conference fee, but her airline ticket was another matter, said Dr. Hafidh, an internist and diabetologist with the Dubai Health Authority.
“The airline I booked my ticket with is willing to waive the change fees, but will deduct a cancellation fee if I choose not to take the trip,” Dr. Hafidh said in an interview. “The cancellation fees is $300. A bit steep I must admit.”
Dr. Hafidh now faces a dilemma: Lose the $300 and cancel, or change her flight dates to June for the American Diabetes Association meeting in Chicago.
“But then again, we aren’t sure if that meeting will take place,” Dr. Hafidh said. “A few weeks ago I thought this whole thing was just a storm in a tea cup. However when it was declared a pandemic yesterday, it brought about another dimension.”
More than 25 medical meetings and conferences across the globe have been canceled or postponed because of COVID-19 concerns. The sudden cancellations have caused reservation woes and travel headaches for thousands of physicians who planned to attend the meetings. Some societies are considering the idea of virtual conferences, while other associations have scrapped their meetings until next year.
For physicians facing a canceled conference, the most likely question is, what now? Read on for tips and suggestions.
Reservation refunds vary
Refunds on airfare because of conference cancellations differ, depending on the airline and where you were traveling. Some airlines, such as United Airlines, have waived all change fees for tickets issued March 3, 2020, through March 31, 2020, and passengers can change their dates for up to 12 months after the ticket was issued.
Full refunds often depend on whether your ticket was nonrefundable when purchased. Many airlines, such as Delta, are providing full refunds if the airline canceled your flight. JetBlue is waiving all change and cancellation fees for customers scheduled to travel March 10, 2020, through April 30, 2020.
Las Vegas–based dermatologist H.L. Greenberg, MD, was satisfied with the credit he received from Southwest Airlines after the American Academy of Dermatology (AAD) canceled its Denver meeting. He and his staff were looking forward to the gathering, but he noted that the meeting would likely have been limited, even if it had take place as scheduled.

“I am disappointed that I won’t be able to meet with colleagues and industry to explore what the latest advances and interests are in dermatology,” he said. “Because many academic institutions were forbidding their faculty from traveling, the content of the meeting was going to be severely diminished. It’s just a rough time for everyone.”
Meanwhile, Asa Radix, MD, PhD, a New York–based internist, received a full refund for his Amtrak ticket to Boston when the Conference on Retroviruses and Opportunistic Infections (CROI) scheduled for early March was converted to a virtual meeting. Dr. Radix, senior director of research and education at the Callen-Lorde Community Health Center in New York, left another meeting in Brazil early to get to the Boston conference, he said.
“I was packed, but really that was a minor inconvenience,” he said in an interview. “I appreciate that they prioritized health concerns and changed to a virtual meeting. I received full refunds, no issues whatsoever. [It was] really great since I had no travel insurance.”
Check with your individual airline or train line for information about ticket refunds and credits. Many airlines are currently making special accommodations because of COVID-19. If your flight was covered by trip insurance, also called travel assistance, you are generally protected against unforeseen financial losses such as cancellations. The U.S. Department of Transportation provides this general online resource about airline refunds.
Hotel refunds probable
Most meeting organizations who have made the decision to cancel or postpone a conference also have canceled block hotel reservations reserved for the meeting. Medical associations are not directly refunding the hotel costs, but the majority of hotels are refunding reservations with no questions asked. Physicians interviewed for this story all reported no trouble getting refunds for their hotel reservations. However, attendees who did not book a hotel in official housing blocks should contact the hotel directly to cancel.
What about registration fees?
In response to COVID-19 cancellations, most conference leaders are refunding registration fees in full for both attendees and exhibitors. The refund may not be automatic, some associations such as ACP and the American College of Obstetricians and Gynecologists state it may take up to 45 days for the funds to be credited, depending on the payment used.
If the conference you planned to attend was postponed, the registration fee may be assigned to the new meeting dates and the money may not be refunded. Registration fees for the Minimally Invasive Surgery Symposium, for example, delayed until an unconfirmed date, and for the European Association of Urology (EAU) meeting, postponed until July, will be automatically credited to the rescheduled meeting, according to the websites. If attendees cannot attend the rescheduled EAU meeting, the association will not provide a refund and the registration will not apply to the 2021 meeting, according to its website. However, the group is providing registrants with a free access code for the EAU20 Resource Centre, which contains websites of sessions and scientific content.
A number of physicians have expressed disappointment with the EAU’s postponement on social media. On Twitter, some doctors wrote that the rescheduled dates were bad timing, while others lamented the refund refusal.
The EAU said it regrets that some delegates will experience financial losses, but that the organization has already experienced a significant outlay that cannot be recovered including venue, logistics, travel, and accommodation costs.
"We are doing what we can to absorb costs, but we need to be realistic about what is affordable; should the organization have to refund all or even most registrations, it would significantly jeopardize the viability of the organization," the EAU said in a statement. "These are difficult times, not only for the EAU, but on a global scale. Where there are specific cases of hardship or very extenuating financial circumstances, we will be willing to review individual cases. So far, we believe that we have done what we can do to meet the conflicting demands presented by the postponement of the congress, but this is a situation which changes from day to day, and we need to continuously evaluate what might be the best course of action." *
Contact your medical association directly for details on postponements.
What if I’m a presenter?
In an attempt to save the hard work and time that planners and presenters have invested into now-canceled meetings, some conferences are moving to a digital format. The Conference on Retroviruses and Opportunistic Infections (CROI) was the first to convert its in-person conference to a virtual meeting, held from March 8 to 11, 2020. At-home attendees logged onto CROI’s digital platform to hear plenaries, oral abstracts, themed discussion sessions, and symposia.
Dr. Radix was one of many CROI speakers who changed his presentation on HIV prevalence among transgender men to a virtual format.
“We were provided with detailed instructions from CROI about how to do this,” said Dr. Radix, who tweeted about the experience. “For my presentation, I used the video option in PowerPoint; it seemed the most straightforward and didn’t require buying additional software. It was fairly easy to follow the instructions to create the video but it was disappointing to present to an empty room.”
Matthew Spinelli, MD, an HIV researcher with the University of California, San Francisco, who also presented virtually, said it was remarkable that CROI leaders were able to put together the virtual program in such a short time. He delivered his presentation on the accuracy of a real-time urine tenofovir test using PowerPoint and a podcast microphone.

“It seemed to work pretty well,” he said in an interview. “It’s not the same as being there in person, there’s a lot of networking and chance conversations that happen when you’re all in the same place, but it was the right decision to cancel. If I have to be at home or at work doing social distancing, this was the best possible way of doing it.”
Following in CROI’s footsteps, the National Kidney Foundation’s spring conference has moved to a live virtual conference. The 2020 Healthcare Information and Management Systems Society (HIMSS) global health conference also will move to a digital format. Other societies are considering similar virtual options. Check with your meeting website for more details on digital options and attendee access.
*The article was updated on 03/16/2020.
Khadija Hafidh, MD, was already booked on a 14-hour, direct flight from Dubai to Los Angeles, when the American College of Physicians (ACP) announced it was canceling its internal medicine meeting scheduled for April.
Canceling her hotel reservation was not a problem, and she was assured a refund for the conference fee, but her airline ticket was another matter, said Dr. Hafidh, an internist and diabetologist with the Dubai Health Authority.
“The airline I booked my ticket with is willing to waive the change fees, but will deduct a cancellation fee if I choose not to take the trip,” Dr. Hafidh said in an interview. “The cancellation fees is $300. A bit steep I must admit.”
Dr. Hafidh now faces a dilemma: Lose the $300 and cancel, or change her flight dates to June for the American Diabetes Association meeting in Chicago.
“But then again, we aren’t sure if that meeting will take place,” Dr. Hafidh said. “A few weeks ago I thought this whole thing was just a storm in a tea cup. However when it was declared a pandemic yesterday, it brought about another dimension.”
More than 25 medical meetings and conferences across the globe have been canceled or postponed because of COVID-19 concerns. The sudden cancellations have caused reservation woes and travel headaches for thousands of physicians who planned to attend the meetings. Some societies are considering the idea of virtual conferences, while other associations have scrapped their meetings until next year.
For physicians facing a canceled conference, the most likely question is, what now? Read on for tips and suggestions.
Reservation refunds vary
Refunds on airfare because of conference cancellations differ, depending on the airline and where you were traveling. Some airlines, such as United Airlines, have waived all change fees for tickets issued March 3, 2020, through March 31, 2020, and passengers can change their dates for up to 12 months after the ticket was issued.
Full refunds often depend on whether your ticket was nonrefundable when purchased. Many airlines, such as Delta, are providing full refunds if the airline canceled your flight. JetBlue is waiving all change and cancellation fees for customers scheduled to travel March 10, 2020, through April 30, 2020.
Las Vegas–based dermatologist H.L. Greenberg, MD, was satisfied with the credit he received from Southwest Airlines after the American Academy of Dermatology (AAD) canceled its Denver meeting. He and his staff were looking forward to the gathering, but he noted that the meeting would likely have been limited, even if it had take place as scheduled.
“I am disappointed that I won’t be able to meet with colleagues and industry to explore what the latest advances and interests are in dermatology,” he said. “Because many academic institutions were forbidding their faculty from traveling, the content of the meeting was going to be severely diminished. It’s just a rough time for everyone.”
Meanwhile, Asa Radix, MD, PhD, a New York–based internist, received a full refund for his Amtrak ticket to Boston when the Conference on Retroviruses and Opportunistic Infections (CROI) scheduled for early March was converted to a virtual meeting. Dr. Radix, senior director of research and education at the Callen-Lorde Community Health Center in New York, left another meeting in Brazil early to get to the Boston conference, he said.
“I was packed, but really that was a minor inconvenience,” he said in an interview. “I appreciate that they prioritized health concerns and changed to a virtual meeting. I received full refunds, no issues whatsoever. [It was] really great since I had no travel insurance.”
Check with your individual airline or train line for information about ticket refunds and credits. Many airlines are currently making special accommodations because of COVID-19. If your flight was covered by trip insurance, also called travel assistance, you are generally protected against unforeseen financial losses such as cancellations. The U.S. Department of Transportation provides this general online resource about airline refunds.
Hotel refunds probable
Most meeting organizations who have made the decision to cancel or postpone a conference also have canceled block hotel reservations reserved for the meeting. Medical associations are not directly refunding the hotel costs, but the majority of hotels are refunding reservations with no questions asked. Physicians interviewed for this story all reported no trouble getting refunds for their hotel reservations. However, attendees who did not book a hotel in official housing blocks should contact the hotel directly to cancel.
What about registration fees?
In response to COVID-19 cancellations, most conference leaders are refunding registration fees in full for both attendees and exhibitors. The refund may not be automatic, some associations such as ACP and the American College of Obstetricians and Gynecologists state it may take up to 45 days for the funds to be credited, depending on the payment used.
If the conference you planned to attend was postponed, the registration fee may be assigned to the new meeting dates and the money may not be refunded. Registration fees for the Minimally Invasive Surgery Symposium, for example, delayed until an unconfirmed date, and for the European Association of Urology (EAU) meeting, postponed until July, will be automatically credited to the rescheduled meeting, according to the websites. If attendees cannot attend the rescheduled EAU meeting, the association will not provide a refund and the registration will not apply to the 2021 meeting, according to its website. However, the group is providing registrants with a free access code for the EAU20 Resource Centre, which contains websites of sessions and scientific content.
A number of physicians have expressed disappointment with the EAU’s postponement on social media. On Twitter, some doctors wrote that the rescheduled dates were bad timing, while others lamented the refund refusal.
The EAU said it regrets that some delegates will experience financial losses, but that the organization has already experienced a significant outlay that cannot be recovered including venue, logistics, travel, and accommodation costs.
"We are doing what we can to absorb costs, but we need to be realistic about what is affordable; should the organization have to refund all or even most registrations, it would significantly jeopardize the viability of the organization," the EAU said in a statement. "These are difficult times, not only for the EAU, but on a global scale. Where there are specific cases of hardship or very extenuating financial circumstances, we will be willing to review individual cases. So far, we believe that we have done what we can do to meet the conflicting demands presented by the postponement of the congress, but this is a situation which changes from day to day, and we need to continuously evaluate what might be the best course of action." *
Contact your medical association directly for details on postponements.
What if I’m a presenter?
In an attempt to save the hard work and time that planners and presenters have invested into now-canceled meetings, some conferences are moving to a digital format. The Conference on Retroviruses and Opportunistic Infections (CROI) was the first to convert its in-person conference to a virtual meeting, held from March 8 to 11, 2020. At-home attendees logged onto CROI’s digital platform to hear plenaries, oral abstracts, themed discussion sessions, and symposia.
Dr. Radix was one of many CROI speakers who changed his presentation on HIV prevalence among transgender men to a virtual format.
“We were provided with detailed instructions from CROI about how to do this,” said Dr. Radix, who tweeted about the experience. “For my presentation, I used the video option in PowerPoint; it seemed the most straightforward and didn’t require buying additional software. It was fairly easy to follow the instructions to create the video but it was disappointing to present to an empty room.”
Matthew Spinelli, MD, an HIV researcher with the University of California, San Francisco, who also presented virtually, said it was remarkable that CROI leaders were able to put together the virtual program in such a short time. He delivered his presentation on the accuracy of a real-time urine tenofovir test using PowerPoint and a podcast microphone.
“It seemed to work pretty well,” he said in an interview. “It’s not the same as being there in person, there’s a lot of networking and chance conversations that happen when you’re all in the same place, but it was the right decision to cancel. If I have to be at home or at work doing social distancing, this was the best possible way of doing it.”
Following in CROI’s footsteps, the National Kidney Foundation’s spring conference has moved to a live virtual conference. The 2020 Healthcare Information and Management Systems Society (HIMSS) global health conference also will move to a digital format. Other societies are considering similar virtual options. Check with your meeting website for more details on digital options and attendee access.
*The article was updated on 03/16/2020.
Khadija Hafidh, MD, was already booked on a 14-hour, direct flight from Dubai to Los Angeles, when the American College of Physicians (ACP) announced it was canceling its internal medicine meeting scheduled for April.
Canceling her hotel reservation was not a problem, and she was assured a refund for the conference fee, but her airline ticket was another matter, said Dr. Hafidh, an internist and diabetologist with the Dubai Health Authority.
“The airline I booked my ticket with is willing to waive the change fees, but will deduct a cancellation fee if I choose not to take the trip,” Dr. Hafidh said in an interview. “The cancellation fees is $300. A bit steep I must admit.”
Dr. Hafidh now faces a dilemma: Lose the $300 and cancel, or change her flight dates to June for the American Diabetes Association meeting in Chicago.
“But then again, we aren’t sure if that meeting will take place,” Dr. Hafidh said. “A few weeks ago I thought this whole thing was just a storm in a tea cup. However when it was declared a pandemic yesterday, it brought about another dimension.”
More than 25 medical meetings and conferences across the globe have been canceled or postponed because of COVID-19 concerns. The sudden cancellations have caused reservation woes and travel headaches for thousands of physicians who planned to attend the meetings. Some societies are considering the idea of virtual conferences, while other associations have scrapped their meetings until next year.
For physicians facing a canceled conference, the most likely question is, what now? Read on for tips and suggestions.
Reservation refunds vary
Refunds on airfare because of conference cancellations differ, depending on the airline and where you were traveling. Some airlines, such as United Airlines, have waived all change fees for tickets issued March 3, 2020, through March 31, 2020, and passengers can change their dates for up to 12 months after the ticket was issued.
Full refunds often depend on whether your ticket was nonrefundable when purchased. Many airlines, such as Delta, are providing full refunds if the airline canceled your flight. JetBlue is waiving all change and cancellation fees for customers scheduled to travel March 10, 2020, through April 30, 2020.
Las Vegas–based dermatologist H.L. Greenberg, MD, was satisfied with the credit he received from Southwest Airlines after the American Academy of Dermatology (AAD) canceled its Denver meeting. He and his staff were looking forward to the gathering, but he noted that the meeting would likely have been limited, even if it had take place as scheduled.
“I am disappointed that I won’t be able to meet with colleagues and industry to explore what the latest advances and interests are in dermatology,” he said. “Because many academic institutions were forbidding their faculty from traveling, the content of the meeting was going to be severely diminished. It’s just a rough time for everyone.”
Meanwhile, Asa Radix, MD, PhD, a New York–based internist, received a full refund for his Amtrak ticket to Boston when the Conference on Retroviruses and Opportunistic Infections (CROI) scheduled for early March was converted to a virtual meeting. Dr. Radix, senior director of research and education at the Callen-Lorde Community Health Center in New York, left another meeting in Brazil early to get to the Boston conference, he said.
“I was packed, but really that was a minor inconvenience,” he said in an interview. “I appreciate that they prioritized health concerns and changed to a virtual meeting. I received full refunds, no issues whatsoever. [It was] really great since I had no travel insurance.”
Check with your individual airline or train line for information about ticket refunds and credits. Many airlines are currently making special accommodations because of COVID-19. If your flight was covered by trip insurance, also called travel assistance, you are generally protected against unforeseen financial losses such as cancellations. The U.S. Department of Transportation provides this general online resource about airline refunds.
Hotel refunds probable
Most meeting organizations who have made the decision to cancel or postpone a conference also have canceled block hotel reservations reserved for the meeting. Medical associations are not directly refunding the hotel costs, but the majority of hotels are refunding reservations with no questions asked. Physicians interviewed for this story all reported no trouble getting refunds for their hotel reservations. However, attendees who did not book a hotel in official housing blocks should contact the hotel directly to cancel.
What about registration fees?
In response to COVID-19 cancellations, most conference leaders are refunding registration fees in full for both attendees and exhibitors. The refund may not be automatic, some associations such as ACP and the American College of Obstetricians and Gynecologists state it may take up to 45 days for the funds to be credited, depending on the payment used.
If the conference you planned to attend was postponed, the registration fee may be assigned to the new meeting dates and the money may not be refunded. Registration fees for the Minimally Invasive Surgery Symposium, for example, delayed until an unconfirmed date, and for the European Association of Urology (EAU) meeting, postponed until July, will be automatically credited to the rescheduled meeting, according to the websites. If attendees cannot attend the rescheduled EAU meeting, the association will not provide a refund and the registration will not apply to the 2021 meeting, according to its website. However, the group is providing registrants with a free access code for the EAU20 Resource Centre, which contains websites of sessions and scientific content.
A number of physicians have expressed disappointment with the EAU’s postponement on social media. On Twitter, some doctors wrote that the rescheduled dates were bad timing, while others lamented the refund refusal.
The EAU said it regrets that some delegates will experience financial losses, but that the organization has already experienced a significant outlay that cannot be recovered including venue, logistics, travel, and accommodation costs.
"We are doing what we can to absorb costs, but we need to be realistic about what is affordable; should the organization have to refund all or even most registrations, it would significantly jeopardize the viability of the organization," the EAU said in a statement. "These are difficult times, not only for the EAU, but on a global scale. Where there are specific cases of hardship or very extenuating financial circumstances, we will be willing to review individual cases. So far, we believe that we have done what we can do to meet the conflicting demands presented by the postponement of the congress, but this is a situation which changes from day to day, and we need to continuously evaluate what might be the best course of action." *
Contact your medical association directly for details on postponements.
What if I’m a presenter?
In an attempt to save the hard work and time that planners and presenters have invested into now-canceled meetings, some conferences are moving to a digital format. The Conference on Retroviruses and Opportunistic Infections (CROI) was the first to convert its in-person conference to a virtual meeting, held from March 8 to 11, 2020. At-home attendees logged onto CROI’s digital platform to hear plenaries, oral abstracts, themed discussion sessions, and symposia.
Dr. Radix was one of many CROI speakers who changed his presentation on HIV prevalence among transgender men to a virtual format.
“We were provided with detailed instructions from CROI about how to do this,” said Dr. Radix, who tweeted about the experience. “For my presentation, I used the video option in PowerPoint; it seemed the most straightforward and didn’t require buying additional software. It was fairly easy to follow the instructions to create the video but it was disappointing to present to an empty room.”
Matthew Spinelli, MD, an HIV researcher with the University of California, San Francisco, who also presented virtually, said it was remarkable that CROI leaders were able to put together the virtual program in such a short time. He delivered his presentation on the accuracy of a real-time urine tenofovir test using PowerPoint and a podcast microphone.
“It seemed to work pretty well,” he said in an interview. “It’s not the same as being there in person, there’s a lot of networking and chance conversations that happen when you’re all in the same place, but it was the right decision to cancel. If I have to be at home or at work doing social distancing, this was the best possible way of doing it.”
Following in CROI’s footsteps, the National Kidney Foundation’s spring conference has moved to a live virtual conference. The 2020 Healthcare Information and Management Systems Society (HIMSS) global health conference also will move to a digital format. Other societies are considering similar virtual options. Check with your meeting website for more details on digital options and attendee access.
*The article was updated on 03/16/2020.
Scientific community ‘shocked’ by loss of MIND diet pioneer
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
Martha Clare Morris, ScD, a pioneer in research linking nutrition to brain health and a creator of the breakthrough MIND diet, has died of cancer at the age of 64.
Morris was a professor in the Department of Internal Medicine, assistant provost of community research, and director of the Rush Institute for Healthy Aging at Rush University, in Chicago, Illinois. She was also a director of the internal medicine department’s Section of Community Epidemiology.
Long-time friend and colleague Julie A. Schneider, MD, the Deborah R. and Edgar D. Jannotta Presidential Professor of Pathology and Neurological Sciences, Rush University Medical Center, described Morris as creative, passionate, and adventurous.
Her death was “a shock” to the scientific community, Schneider told Medscape Medical News.
“It’s a tragic loss in so many ways,” said Schneider, who is also associate director of the Rush Alzheimer’s Disease Center. She was a very well-respected nutritional epidemiologist and was passionate about her work; she had just so much unwavering commitment to it.
Diet, said Schneider, is “notoriously a hard thing to study” because “it’s so intertwined with lifestyle” and other factors that create “barriers” to conducting such research.
But Morris had a unique and creative talent for filtering out what might be the individual contribution of a particular modifiable risk factor, said Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, who also knew Morris both personally and professionally.
“Humble” trailblazer
Morris’s pioneering research examined the connection between nutrition and the prevention of cognitive decline. Taking results from this research, she developed the MIND diet – a hybrid of the Mediterranean diet and the Dietary Approaches to Stop Hypertension – along with colleagues at both Rush and Harvard Universities.
The MIND diet – an acronym for Mediterranean-DASH Intervention for Neurodegenerative Delay – emphasizes brain-healthy foods, including leafy green vegetables, nuts, berries, chicken, fish, whole grains, beans, olive oil, and moderate amounts of red wine. The diet limits consumption of red meat, butter, margarine, and processed foods.
In 2015, Morris published her initial findings on the MIND diet in Alzheimer’s and Dementia. Reported by Medscape Medical News at that time, the study showed that the diet protected cardiovascular health and slowed cognitive decline in older individuals.
The excitement around the findings inspired Morris to write “Diet for the Mind,” which was published in 2017. The book summarizes the benefits of the MIND diet and includes brain-healthy recipes created by her daughter Laura, who is a chef. Despite many accolades, Morris was “humble” about this project, said Schneider.
“This was not about publicity and trying to get a book out; she wanted to see if this diet really was going to change people’s lives. She wanted to bring it into the community,” she said.
Proud legacy
Since 2017, Morris had led a large clinical trial of the effectiveness of the MIND diet in preventing cognitive decline. The first study of its kind, the trial received a $14.5 million grant from the National Institutes of Health (NIH). Results of this study are expected in 2021.
The MIND diet was ranked among the top 10 diets for five consecutive years in US News and World Report.
Morris’s nutrition-related research went beyond diets and examined the impact of individual nutrients. One of her studies, published in 2018 and reported by Medscape Medical News, suggested that the presence of folate, phylloquinone, and lutein – nutrients found in relatively large amounts in green leafy vegetables – may account for why consuming a daily serving of these vegetables slows cognitive decline.
One of the most recent studies from Morris’ group, published in January 2020 and reported by Medscape Medical News at that time, provided the first evidence that dietary flavonols, which are found in many fruits and vegetables, are associated with a significantly reduced risk for dementia.
What Morris did so well was to “look at the big picture” and “think about commonalities that cross nutritional components” of diets such as MIND, DASH, the Mediterranean diet, and the Nordic diet, which is similar to the Mediterranean diet but highlights local foods such as fish from Nordic regions, Snyder told Medscape Medical News.
Morris was instrumental in getting the Alzheimer’s Association’s US POINTER (US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk) study off the ground. The 2-year clinical trial is testing whether combining a healthy diet with exercise, cognitive and social stimulation, and the management of cardiovascular conditions protects cognitive function in older adults who are at increased risk for cognitive decline.
This study will be part of her legacy, said Snyder.
“She will be remembered for her perseverance to get us to a place where we can be looking at nutrition as a modifiable risk factor and now testing it in trials that she helped to set up,” she said.
Even before her involvement with US POINTER, Morris had long been an active volunteer for the Alzheimer’s Association, said Snyder.
“She contributed significant time and expertise as we looked at the state of the evidence around nutrition and other lifestyle and behavioral interventions.”
We’ll ‘always have Paris’
While Morris was “truly passionate” about diet and health “both professionally and personally,” she also had a fun side, said Schneider. She remembers she and Morris had a chance meeting in Paris, where they spent an entire day going to museums and restaurants and just talking about life and their travels. To the end, they joked they would “always have Paris,” said Schneider.
She was also a loyal friend. Morris threw a baby shower when Schneider was pregnant, organizing every detail, despite her extremely busy schedule.
Family was another of Morris’s passions. Snyder recalls Morris’s face lighting up when she talked about her children and grandchildren. She also remembers her friend’s zest for life. “She had an energy that was contagious.”
Morris also loved the outdoors and was a keen adventurer. She once trained for weeks before a long bike trip with her daughter and would take a helicopter to access remote backcountry on hiking excursions.
“She wanted to try everything,” said Schneider.
An author or contributor to more than 80 articles in peer-reviewed journals, Morris also served two terms (from 2011 to 2013) as chair of the NIH’s Neurological, Aging and Musculoskeletal Epidemiology Study Section.
She left behind multiple grants for various studies. One unique study, said Schneider, investigated the relationship between iron and other metals in the brain and the neuropathology of Alzheimer disease.
“She was really in the prime of her career,” noted Schneider. “She had so much left to give and to offer, so this is tremendously sad.”
According to news reports, Morris (nee Chinn) grew up in Homewood, Illinois, and earned bachelor’s and master’s degrees in sociology from the University of Iowa in Iowa City, where she met her husband, James Morris. The two married in 1978 and had three children.
Morris completed a doctorate in epidemiology at the Harvard School of Public Health. James died in 2012, also from cancer. Morris passed away peacefully at her home on February 15.
WHO declares COVID-19 outbreak a pandemic
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
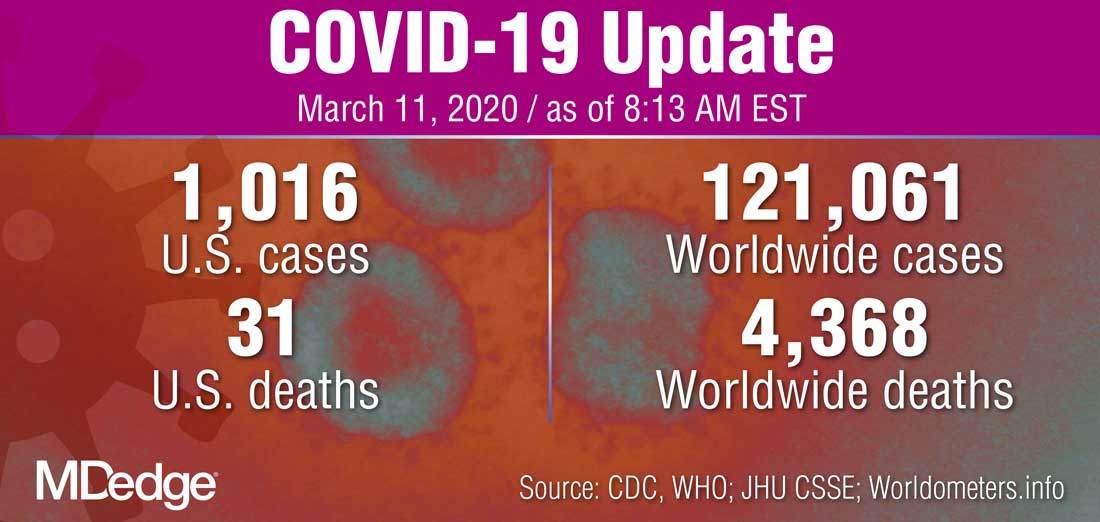
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.
The World Health Organization has formally declared the COVID-19 outbreak a pandemic.
“WHO has been assessing this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction,” WHO Director-General Tedros Adhanom Ghebreyesus said during a March 11 press briefing. “We therefore made the assessment that COVID-19 can be characterized as a pandemic.”
He noted that this is the first time a coronavirus has been seen as a pandemic.
The Director-General cautioned that just looking at the number of countries affected, 114 countries, “does not tell the full story. ... We cannot say this loudly enough, or clearly enough, or often enough: All countries can still change the course of this pandemic.”
He reiterated the need for a whole-of-government and a whole-of-society approach to dealing with this, including taking precautions such as isolating, testing, and treating every case and tracing every contact, as well as readying hospitals and health care professionals.
“Let’s look out for each other, because we need each other,” he said.