User login
Will COVID-19 finally trigger action on health disparities?
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Because of stark racial disparities in COVID-19 infection and mortality, the pandemic is being called a “sentinel” and “bellwether” event that should push the United States to finally come to grips with disparities in health care.
When it comes to COVID-19, the pattern is “irrefutable”: Blacks in the United States are being infected with SARS-CoV-2 and are dying of COVID-19 at higher rates than whites, Clyde W. Yancy, MD, Northwestern University, Chicago, wrote in a viewpoint article published online April 15 in JAMA.
According to one recent survey, he noted, the infection rate is threefold higher and the death rate is sixfold higher in predominantly black counties in the United States relative to predominantly white counties.
A sixfold increase in the rate of death for blacks due to a now ubiquitous virus should be deemed “unconscionable” and a moment of “ethical reckoning,” Dr. Yancy wrote.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
The COVID-19 pandemic may be the “bellwether” event that the United States has needed to fully address disparities in health care, Dr. Yancy said.
“Public health is complicated and social reengineering is complex, but change of this magnitude does not happen without a new resolve,” he concluded. “The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event. Certainly, within the broad and powerful economic and legislative engines of the U.S., there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain.”
The question is, he asks, will the nation finally “think differently, and, as has been done in response to other major diseases, declare that a civil society will no longer accept disproportionate suffering?”
Keith C. Ferdinand, MD, Tulane University, New Orleans, doesn’t think so.
In a related editorial published online April 17 in the Journal of the American College of Cardiology, he points out that the 1985 Heckler Report, from the Department of Health and Human Services, documented higher racial/ethnic mortality rates and the need to correct them. This was followed in 2002 by a report from the Institute of Medicine called Unequal Treatment that also underscored health disparities.
Despite some progress, the goal of reducing and eventually eliminating racial/ethnic disparities has not been realized, Dr. Ferdinand said. “I think baked into the consciousness of the American psyche is that there are some people who have and some who have not,” he said in an interview.
“To some extent, some societies at some point become immune. We would not like to think that America, with its sense of egalitarianism, would get to that point, but maybe we have,” said Dr. Ferdinand.
A ‘sentinel event’
He points out that black people are not genetically or biologically predisposed to COVID-19 but are socially prone to coronavirus exposure and are more likely to have comorbid conditions, such as hypertension, diabetes, obesity, and heart disease, that fuel complications.
The “tragic” higher COVID-19 mortality among African Americans and other racial/ethnic minorities confirms “inadequate” efforts on the part of society to eliminate disparities in cardiovascular disease (CVD) and is a “sentinel event,” Dr. Ferdinand wrote.
A sentinel event, as defined by the Joint Commission, is an unexpected occurrence that leads to death or serious physical or psychological injury or the risk thereof, he explained.
“Conventionally identified sentinel events, such as unintended retention of foreign objects and fall-related events, are used to evaluate quality in hospital care. Similarly, disparate [African American] COVID-19 mortality reflects long-standing, unacceptable U.S. racial/ethnic and socioeconomic CVD inequities and unmasks system failures and unacceptable care to be caught and mitigated,” Dr. Ferdinand concluded.
Dr. Yancy and Dr. Ferdinand have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New advocacy group aims to give ‘every physician’ a voice
A new advocacy organization is launching on April 28 to give “every physician” a voice in decisions that affect their professional lives. But this group doesn’t intend to use the top-down approach to decision making seen in many medical societies.
Paul Teirstein, MD, chief of cardiology for Scripps Clinic in La Jolla, Calif., and founder of the new organization United Physicians, said in an interviewit is a nonprofit group that will operate through online participation.
He said
Projects would need the support of a two-thirds majority of United Physicians’ members to proceed with any proposals. Meetings will be held publicly online, Dr. Teirstein explained.
There is a need for a broad-based organization that will respond to the voice of practicing physicians rather than dictate legislative priorities from management ranks, he said.
Dr. Teirstein said he learned how challenging it is to bring physicians together on issues in 2014 in his battles against changes in maintenance of certification rules. The result of his efforts was the National Board of Physicians and Surgeons (NBPAS), set up to provide a means of certification different from the one offered by the American Board of Internal Medicine.
Dr. Teirstein has argued that the approach of ABIM unfairly burdened physicians with a stepped-up schedule of testing and relied on an outdated approach to the practice of medicine.
Physicians busy with their practices feel they lack a unified voice in contesting the growing administrative burden and unproductive federal and state policies, Dr. Teirstein said.
He cited the limited enrollment in the largest physician groups as evidence of how disenfranchised many clinicians feel. There are about 1 million professional active physicians in the United States, according to the nonprofit Kaiser Family Foundation. Yet, even the largest physician group, the American Medical Association, has about 250,000 members, according to its 2018 annual report
“Clearly, most physicians believe they have little voice when it comes to health care decisions,” Dr. Teirstein said. “Our physician associations are governed from the top down. The leaders set the agenda. There may be delegates, but does leadership really listen to the delegates? Do the delegates really listen to the physician community?”
On its website, AMA describes itself as “physicians’ powerful ally in patient care” that works with more than 190 state and specialty medical societies. In recent months, James L. Madara, MD, the group’s chief executive officer, has urged governors to remove obstacles for physicians who want to fill workforce gaps in COVID-19 hot spots, among other actions.
In its annual report, the AMA, which declined to comment for this article, said its membership rose by 3.4% in 2018, double the growth rate of the previous year, thanks to a membership drive.
“The campaign celebrates the powerful work of our physician members and showcases how their individual efforts – along with the AMA – are moving medicine forward,” wrote Dr. Madara and other organization leaders in the report.
What Dr. Teirstein proposes is an inversion of the structure used by other medical societies, in which he says leaders and delegates dictate priorities.
United Physicians will use meetings and votes held by members online to decide which projects to pursue. Fees would be kept nominal, likely about $10 a year, depending on the number of members. Fees would be subject to change on the basis of expenses. The AMA has a sliding fee schedule that tops out with annual dues for physicians in regular practice of $420.
“There are no delegates, no representatives, and no board of directors. We want every physician to join and every physician to vote on every issue,” Dr. Teirstein said.
He stressed that he sees United Physicians as being complementary to the AMA.
“We do not compete with other organizations. Ideally, other organizations will use the platform,” Dr. Teirstein said. “If the AMA is considering a new policy, it can use the United Physicians platform to measure physician support. For example, through online discussions, petitions, and voting, it might learn a proposed policy needs a few tweaks to be accepted by most physicians.”
No compensation
Dr. Teirstein is among physician leaders who in recent years have sought to rally their colleagues to fight back against growing administrative burdens.
In a 2015 article in JAMA that was written with Medscape’s editor in chief, Eric Topol, MD, Dr. Teirstein criticized the ABIM’s drive to have physicians complete tests every 2 years and participate in continuous certification instead of recertifying once a decade, as had been the practice.
Dr. Teirstein formed the NBPAS as an alternative path for certification, with Dr. Topol serving on the board for that organization. Dr. Topol also will serve as a member of the advisory board for Teirstein’s United Physicians.
Dr. Topol wrote an article that appeared in the New Yorker last August that argued for physicians to move beyond the confines of medical societies and seek a path for broad-based activism. He said he intended to challenge medical societies, which, for all the good they do, can sometimes lose focus on that core relationship in favor of the bottom line.
Dr. Topol said in an interview that his colleague’s new project is a “good idea for a democratized platform at a time when physician solidarity is needed more than ever.”
Dr. Teirstein plans to run United Physicians on a volunteer basis. This builds on the approach he has used for NBPAS. He and the directors of the NBPAS will receive no compensation, he said, as was confirmed by the NBPAS.
In contrast, Dr. Madara made about $2.5 million in total compensation for 2018, according to the organization’s Internal Revenue Service filing. Physicians who served as trustees and officials for the AMA that year received annual compensation that ranged from around $60,000 to $291,980, depending on their duties.
“Having volunteer leadership mitigates conflict of interest. It also ensures leadership has a ‘day job’ that keeps them in touch with issues impacting practicing physicians,” Dr. Teirstein said
Start-up costs for United Physicians will be supported by NBPAS, but it will function as a completely independent organization, he added.
In introducing the group, Dr. Teirstein outlined suggestions for proposals it might pursue. These include making hospitals secure adequate supplies of personal protective equipment ahead of health crises such as the COVID-19 pandemic.
His outline also includes suggestions for issues that likely will persist beyond the response to the pandemic.
Dr. Teirstein proposed a project for persuading insurance companies to provide online calendar appointments for peer-to-peer patient preauthorization. Failure of the insurer’s representative to attend would trigger approval of authorization under this proposal. He also suggested a lobbying effort for specific reimbursement for peer-to-peer, patient preauthorization phone calls.
Dr. Teirstein said he hopes most of the proposals will come from physicians who join United Physicians. Still, it is unclear whether United Physicians will succeed. An initial challenge could be in sorting through a barrage of competing ideas submitted to United Physicians.
But Dr. Teirstein appears hopeful about the changes for this experiment in online advocacy. He intends for United Physicians to be a pathway for clinicians to translate their complaints about policies into calls for action, with only a short investment of their time.
“Most of us have wonderful, engrossing jobs. It’s hard to beat helping a patient, and most of us get to do it every day,” Dr. .Teirstein said. “Will we take the 30 seconds required to sign up and become a United Physicians member? Will we spend a little time each week reviewing the issues and voting? I think it’s an experiment worth watching.”
A version of this article originally appeared on Medscape.com.
A new advocacy organization is launching on April 28 to give “every physician” a voice in decisions that affect their professional lives. But this group doesn’t intend to use the top-down approach to decision making seen in many medical societies.
Paul Teirstein, MD, chief of cardiology for Scripps Clinic in La Jolla, Calif., and founder of the new organization United Physicians, said in an interviewit is a nonprofit group that will operate through online participation.
He said
Projects would need the support of a two-thirds majority of United Physicians’ members to proceed with any proposals. Meetings will be held publicly online, Dr. Teirstein explained.
There is a need for a broad-based organization that will respond to the voice of practicing physicians rather than dictate legislative priorities from management ranks, he said.
Dr. Teirstein said he learned how challenging it is to bring physicians together on issues in 2014 in his battles against changes in maintenance of certification rules. The result of his efforts was the National Board of Physicians and Surgeons (NBPAS), set up to provide a means of certification different from the one offered by the American Board of Internal Medicine.
Dr. Teirstein has argued that the approach of ABIM unfairly burdened physicians with a stepped-up schedule of testing and relied on an outdated approach to the practice of medicine.
Physicians busy with their practices feel they lack a unified voice in contesting the growing administrative burden and unproductive federal and state policies, Dr. Teirstein said.
He cited the limited enrollment in the largest physician groups as evidence of how disenfranchised many clinicians feel. There are about 1 million professional active physicians in the United States, according to the nonprofit Kaiser Family Foundation. Yet, even the largest physician group, the American Medical Association, has about 250,000 members, according to its 2018 annual report
“Clearly, most physicians believe they have little voice when it comes to health care decisions,” Dr. Teirstein said. “Our physician associations are governed from the top down. The leaders set the agenda. There may be delegates, but does leadership really listen to the delegates? Do the delegates really listen to the physician community?”
On its website, AMA describes itself as “physicians’ powerful ally in patient care” that works with more than 190 state and specialty medical societies. In recent months, James L. Madara, MD, the group’s chief executive officer, has urged governors to remove obstacles for physicians who want to fill workforce gaps in COVID-19 hot spots, among other actions.
In its annual report, the AMA, which declined to comment for this article, said its membership rose by 3.4% in 2018, double the growth rate of the previous year, thanks to a membership drive.
“The campaign celebrates the powerful work of our physician members and showcases how their individual efforts – along with the AMA – are moving medicine forward,” wrote Dr. Madara and other organization leaders in the report.
What Dr. Teirstein proposes is an inversion of the structure used by other medical societies, in which he says leaders and delegates dictate priorities.
United Physicians will use meetings and votes held by members online to decide which projects to pursue. Fees would be kept nominal, likely about $10 a year, depending on the number of members. Fees would be subject to change on the basis of expenses. The AMA has a sliding fee schedule that tops out with annual dues for physicians in regular practice of $420.
“There are no delegates, no representatives, and no board of directors. We want every physician to join and every physician to vote on every issue,” Dr. Teirstein said.
He stressed that he sees United Physicians as being complementary to the AMA.
“We do not compete with other organizations. Ideally, other organizations will use the platform,” Dr. Teirstein said. “If the AMA is considering a new policy, it can use the United Physicians platform to measure physician support. For example, through online discussions, petitions, and voting, it might learn a proposed policy needs a few tweaks to be accepted by most physicians.”
No compensation
Dr. Teirstein is among physician leaders who in recent years have sought to rally their colleagues to fight back against growing administrative burdens.
In a 2015 article in JAMA that was written with Medscape’s editor in chief, Eric Topol, MD, Dr. Teirstein criticized the ABIM’s drive to have physicians complete tests every 2 years and participate in continuous certification instead of recertifying once a decade, as had been the practice.
Dr. Teirstein formed the NBPAS as an alternative path for certification, with Dr. Topol serving on the board for that organization. Dr. Topol also will serve as a member of the advisory board for Teirstein’s United Physicians.
Dr. Topol wrote an article that appeared in the New Yorker last August that argued for physicians to move beyond the confines of medical societies and seek a path for broad-based activism. He said he intended to challenge medical societies, which, for all the good they do, can sometimes lose focus on that core relationship in favor of the bottom line.
Dr. Topol said in an interview that his colleague’s new project is a “good idea for a democratized platform at a time when physician solidarity is needed more than ever.”
Dr. Teirstein plans to run United Physicians on a volunteer basis. This builds on the approach he has used for NBPAS. He and the directors of the NBPAS will receive no compensation, he said, as was confirmed by the NBPAS.
In contrast, Dr. Madara made about $2.5 million in total compensation for 2018, according to the organization’s Internal Revenue Service filing. Physicians who served as trustees and officials for the AMA that year received annual compensation that ranged from around $60,000 to $291,980, depending on their duties.
“Having volunteer leadership mitigates conflict of interest. It also ensures leadership has a ‘day job’ that keeps them in touch with issues impacting practicing physicians,” Dr. Teirstein said
Start-up costs for United Physicians will be supported by NBPAS, but it will function as a completely independent organization, he added.
In introducing the group, Dr. Teirstein outlined suggestions for proposals it might pursue. These include making hospitals secure adequate supplies of personal protective equipment ahead of health crises such as the COVID-19 pandemic.
His outline also includes suggestions for issues that likely will persist beyond the response to the pandemic.
Dr. Teirstein proposed a project for persuading insurance companies to provide online calendar appointments for peer-to-peer patient preauthorization. Failure of the insurer’s representative to attend would trigger approval of authorization under this proposal. He also suggested a lobbying effort for specific reimbursement for peer-to-peer, patient preauthorization phone calls.
Dr. Teirstein said he hopes most of the proposals will come from physicians who join United Physicians. Still, it is unclear whether United Physicians will succeed. An initial challenge could be in sorting through a barrage of competing ideas submitted to United Physicians.
But Dr. Teirstein appears hopeful about the changes for this experiment in online advocacy. He intends for United Physicians to be a pathway for clinicians to translate their complaints about policies into calls for action, with only a short investment of their time.
“Most of us have wonderful, engrossing jobs. It’s hard to beat helping a patient, and most of us get to do it every day,” Dr. .Teirstein said. “Will we take the 30 seconds required to sign up and become a United Physicians member? Will we spend a little time each week reviewing the issues and voting? I think it’s an experiment worth watching.”
A version of this article originally appeared on Medscape.com.
A new advocacy organization is launching on April 28 to give “every physician” a voice in decisions that affect their professional lives. But this group doesn’t intend to use the top-down approach to decision making seen in many medical societies.
Paul Teirstein, MD, chief of cardiology for Scripps Clinic in La Jolla, Calif., and founder of the new organization United Physicians, said in an interviewit is a nonprofit group that will operate through online participation.
He said
Projects would need the support of a two-thirds majority of United Physicians’ members to proceed with any proposals. Meetings will be held publicly online, Dr. Teirstein explained.
There is a need for a broad-based organization that will respond to the voice of practicing physicians rather than dictate legislative priorities from management ranks, he said.
Dr. Teirstein said he learned how challenging it is to bring physicians together on issues in 2014 in his battles against changes in maintenance of certification rules. The result of his efforts was the National Board of Physicians and Surgeons (NBPAS), set up to provide a means of certification different from the one offered by the American Board of Internal Medicine.
Dr. Teirstein has argued that the approach of ABIM unfairly burdened physicians with a stepped-up schedule of testing and relied on an outdated approach to the practice of medicine.
Physicians busy with their practices feel they lack a unified voice in contesting the growing administrative burden and unproductive federal and state policies, Dr. Teirstein said.
He cited the limited enrollment in the largest physician groups as evidence of how disenfranchised many clinicians feel. There are about 1 million professional active physicians in the United States, according to the nonprofit Kaiser Family Foundation. Yet, even the largest physician group, the American Medical Association, has about 250,000 members, according to its 2018 annual report
“Clearly, most physicians believe they have little voice when it comes to health care decisions,” Dr. Teirstein said. “Our physician associations are governed from the top down. The leaders set the agenda. There may be delegates, but does leadership really listen to the delegates? Do the delegates really listen to the physician community?”
On its website, AMA describes itself as “physicians’ powerful ally in patient care” that works with more than 190 state and specialty medical societies. In recent months, James L. Madara, MD, the group’s chief executive officer, has urged governors to remove obstacles for physicians who want to fill workforce gaps in COVID-19 hot spots, among other actions.
In its annual report, the AMA, which declined to comment for this article, said its membership rose by 3.4% in 2018, double the growth rate of the previous year, thanks to a membership drive.
“The campaign celebrates the powerful work of our physician members and showcases how their individual efforts – along with the AMA – are moving medicine forward,” wrote Dr. Madara and other organization leaders in the report.
What Dr. Teirstein proposes is an inversion of the structure used by other medical societies, in which he says leaders and delegates dictate priorities.
United Physicians will use meetings and votes held by members online to decide which projects to pursue. Fees would be kept nominal, likely about $10 a year, depending on the number of members. Fees would be subject to change on the basis of expenses. The AMA has a sliding fee schedule that tops out with annual dues for physicians in regular practice of $420.
“There are no delegates, no representatives, and no board of directors. We want every physician to join and every physician to vote on every issue,” Dr. Teirstein said.
He stressed that he sees United Physicians as being complementary to the AMA.
“We do not compete with other organizations. Ideally, other organizations will use the platform,” Dr. Teirstein said. “If the AMA is considering a new policy, it can use the United Physicians platform to measure physician support. For example, through online discussions, petitions, and voting, it might learn a proposed policy needs a few tweaks to be accepted by most physicians.”
No compensation
Dr. Teirstein is among physician leaders who in recent years have sought to rally their colleagues to fight back against growing administrative burdens.
In a 2015 article in JAMA that was written with Medscape’s editor in chief, Eric Topol, MD, Dr. Teirstein criticized the ABIM’s drive to have physicians complete tests every 2 years and participate in continuous certification instead of recertifying once a decade, as had been the practice.
Dr. Teirstein formed the NBPAS as an alternative path for certification, with Dr. Topol serving on the board for that organization. Dr. Topol also will serve as a member of the advisory board for Teirstein’s United Physicians.
Dr. Topol wrote an article that appeared in the New Yorker last August that argued for physicians to move beyond the confines of medical societies and seek a path for broad-based activism. He said he intended to challenge medical societies, which, for all the good they do, can sometimes lose focus on that core relationship in favor of the bottom line.
Dr. Topol said in an interview that his colleague’s new project is a “good idea for a democratized platform at a time when physician solidarity is needed more than ever.”
Dr. Teirstein plans to run United Physicians on a volunteer basis. This builds on the approach he has used for NBPAS. He and the directors of the NBPAS will receive no compensation, he said, as was confirmed by the NBPAS.
In contrast, Dr. Madara made about $2.5 million in total compensation for 2018, according to the organization’s Internal Revenue Service filing. Physicians who served as trustees and officials for the AMA that year received annual compensation that ranged from around $60,000 to $291,980, depending on their duties.
“Having volunteer leadership mitigates conflict of interest. It also ensures leadership has a ‘day job’ that keeps them in touch with issues impacting practicing physicians,” Dr. Teirstein said
Start-up costs for United Physicians will be supported by NBPAS, but it will function as a completely independent organization, he added.
In introducing the group, Dr. Teirstein outlined suggestions for proposals it might pursue. These include making hospitals secure adequate supplies of personal protective equipment ahead of health crises such as the COVID-19 pandemic.
His outline also includes suggestions for issues that likely will persist beyond the response to the pandemic.
Dr. Teirstein proposed a project for persuading insurance companies to provide online calendar appointments for peer-to-peer patient preauthorization. Failure of the insurer’s representative to attend would trigger approval of authorization under this proposal. He also suggested a lobbying effort for specific reimbursement for peer-to-peer, patient preauthorization phone calls.
Dr. Teirstein said he hopes most of the proposals will come from physicians who join United Physicians. Still, it is unclear whether United Physicians will succeed. An initial challenge could be in sorting through a barrage of competing ideas submitted to United Physicians.
But Dr. Teirstein appears hopeful about the changes for this experiment in online advocacy. He intends for United Physicians to be a pathway for clinicians to translate their complaints about policies into calls for action, with only a short investment of their time.
“Most of us have wonderful, engrossing jobs. It’s hard to beat helping a patient, and most of us get to do it every day,” Dr. .Teirstein said. “Will we take the 30 seconds required to sign up and become a United Physicians member? Will we spend a little time each week reviewing the issues and voting? I think it’s an experiment worth watching.”
A version of this article originally appeared on Medscape.com.
EHA webinar addresses treating AML patients with COVID-19
A hematologist in Italy shared his personal experience addressing the intersection of COVID-19 and the care of acute myeloid leukemia (AML) patients during a webinar hosted by the European Hematology Association (EHA).

Felicetto Ferrara, MD, of Cardarelli Hospital in Naples, Italy, discussed the main difficulties in administering optimal treatment for AML patients who become infected with SARS-CoV-2.
The major problems include the need to isolate patients while simultaneously allowing for collaboration with pulmonologists and intensivists, the delays in AML treatment caused by COVID-19, and the risk of drug-drug interactions while treating AML patients with COVID-19.
The need to isolate AML patients with COVID-19 is paramount, according to Dr. Ferrara. Isolation can be accomplished, ideally, by the creation of a dedicated COVID-19 unit or, alternatively, with the use of single-patient negative pressure rooms. Dr. Ferrara stressed that all patients with AML should be tested for COVID-19 before admission.
Delaying or reducing AML treatment
Treatment delays are of particular concern, according to Dr. Ferrara, and some patients may require dose reductions, especially for AML treatments that might have a detrimental effect on the immune system.
Decisions must be made as to whether planned approaches to induction or consolidation therapy should be changed, and special concern has to be paid to elderly AML patients, who have the highest risks of bad COVID-19 outcomes.
Specific attention should be paid to patients with acute promyelocytic leukemia as well, according to Dr. Ferrara. These patients are of concern in the COVID-19 era because of their risk of differentiation syndrome, which can induce respiratory distress.
In all cases, autologous or allogeneic stem cell transplant should be deferred until confirmed COVID-19–negative test results are obtained.
Continuing AML treatment
Of particular concern is the fact that, without a standard therapy for COVID-19, many different drugs might be used in treatment efforts. This raises the potential for serious drug-drug interactions with the patient’s AML medications, so close attention should be paid to an individual patient’s medications.
In terms of continuing AML treatment for younger adults (less than 65 years) who are positive for COVID-19, symptomatic and asymptomatic patients should be treated differently, Dr. Ferarra said.
Symptomatic patients should be given hydroxyurea until symptom resolution, and unless urgent, any further AML treatments should be delayed. However, if treatment is needed immediately, it should be given in a COVID-19–dedicated unit.
The restrictions are much looser for young adult asymptomatic COVID-19 patients with AML. Standard induction therapy should be given, with intermediate-dose cytarabine used as consolidation therapy.
Therapy in elderly patients with AML and COVID-19 should be based on symptom status as well, said Dr. Ferrara.
Asymptomatic but otherwise fit elderly patients should have standard induction therapy if they are in the European Leukemia Network favorable genetic subgroup. Asymptomatic elderly patients with high-risk molecular disease can receive venetoclax with a hypomethylating agent.
Symptomatic elderly patients should continue with hydroxyurea until symptom resolution, and any other treatments should be delayed in nonemergency cases.
Relapsed AML patients with COVID-19 should have their treatments postponed until they obtain negative COVID-19 test results whenever possible, Dr. Ferarra said. However, if treatment is necessary, molecularly targeted therapies (gilteritinib, ivosidenib, and enasidenib) are preferable to high-dose chemotherapy.
In all cases, treatment decisions should be made in conjunction with pulmonologists and intensivists, Dr. Ferrera noted.
Webinar moderator Francesco Cerisoli, MD, head of research and mentoring at EHA, highlighted the fact that EHA has published specific recommendations for treating AML patients during the COVID-19 pandemic. The majority of these were discussed by and are aligned with the recommendations presented by Dr. Ferrara.
The EHA webinar contains a disclaimer that the content discussed was based on the personal experiences and opinions of the speakers and that no general, evidence-based guidance could be derived from the discussion. There were no disclosures given.
A hematologist in Italy shared his personal experience addressing the intersection of COVID-19 and the care of acute myeloid leukemia (AML) patients during a webinar hosted by the European Hematology Association (EHA).
Felicetto Ferrara, MD, of Cardarelli Hospital in Naples, Italy, discussed the main difficulties in administering optimal treatment for AML patients who become infected with SARS-CoV-2.
The major problems include the need to isolate patients while simultaneously allowing for collaboration with pulmonologists and intensivists, the delays in AML treatment caused by COVID-19, and the risk of drug-drug interactions while treating AML patients with COVID-19.
The need to isolate AML patients with COVID-19 is paramount, according to Dr. Ferrara. Isolation can be accomplished, ideally, by the creation of a dedicated COVID-19 unit or, alternatively, with the use of single-patient negative pressure rooms. Dr. Ferrara stressed that all patients with AML should be tested for COVID-19 before admission.
Delaying or reducing AML treatment
Treatment delays are of particular concern, according to Dr. Ferrara, and some patients may require dose reductions, especially for AML treatments that might have a detrimental effect on the immune system.
Decisions must be made as to whether planned approaches to induction or consolidation therapy should be changed, and special concern has to be paid to elderly AML patients, who have the highest risks of bad COVID-19 outcomes.
Specific attention should be paid to patients with acute promyelocytic leukemia as well, according to Dr. Ferrara. These patients are of concern in the COVID-19 era because of their risk of differentiation syndrome, which can induce respiratory distress.
In all cases, autologous or allogeneic stem cell transplant should be deferred until confirmed COVID-19–negative test results are obtained.
Continuing AML treatment
Of particular concern is the fact that, without a standard therapy for COVID-19, many different drugs might be used in treatment efforts. This raises the potential for serious drug-drug interactions with the patient’s AML medications, so close attention should be paid to an individual patient’s medications.
In terms of continuing AML treatment for younger adults (less than 65 years) who are positive for COVID-19, symptomatic and asymptomatic patients should be treated differently, Dr. Ferarra said.
Symptomatic patients should be given hydroxyurea until symptom resolution, and unless urgent, any further AML treatments should be delayed. However, if treatment is needed immediately, it should be given in a COVID-19–dedicated unit.
The restrictions are much looser for young adult asymptomatic COVID-19 patients with AML. Standard induction therapy should be given, with intermediate-dose cytarabine used as consolidation therapy.
Therapy in elderly patients with AML and COVID-19 should be based on symptom status as well, said Dr. Ferrara.
Asymptomatic but otherwise fit elderly patients should have standard induction therapy if they are in the European Leukemia Network favorable genetic subgroup. Asymptomatic elderly patients with high-risk molecular disease can receive venetoclax with a hypomethylating agent.
Symptomatic elderly patients should continue with hydroxyurea until symptom resolution, and any other treatments should be delayed in nonemergency cases.
Relapsed AML patients with COVID-19 should have their treatments postponed until they obtain negative COVID-19 test results whenever possible, Dr. Ferarra said. However, if treatment is necessary, molecularly targeted therapies (gilteritinib, ivosidenib, and enasidenib) are preferable to high-dose chemotherapy.
In all cases, treatment decisions should be made in conjunction with pulmonologists and intensivists, Dr. Ferrera noted.
Webinar moderator Francesco Cerisoli, MD, head of research and mentoring at EHA, highlighted the fact that EHA has published specific recommendations for treating AML patients during the COVID-19 pandemic. The majority of these were discussed by and are aligned with the recommendations presented by Dr. Ferrara.
The EHA webinar contains a disclaimer that the content discussed was based on the personal experiences and opinions of the speakers and that no general, evidence-based guidance could be derived from the discussion. There were no disclosures given.
A hematologist in Italy shared his personal experience addressing the intersection of COVID-19 and the care of acute myeloid leukemia (AML) patients during a webinar hosted by the European Hematology Association (EHA).
Felicetto Ferrara, MD, of Cardarelli Hospital in Naples, Italy, discussed the main difficulties in administering optimal treatment for AML patients who become infected with SARS-CoV-2.
The major problems include the need to isolate patients while simultaneously allowing for collaboration with pulmonologists and intensivists, the delays in AML treatment caused by COVID-19, and the risk of drug-drug interactions while treating AML patients with COVID-19.
The need to isolate AML patients with COVID-19 is paramount, according to Dr. Ferrara. Isolation can be accomplished, ideally, by the creation of a dedicated COVID-19 unit or, alternatively, with the use of single-patient negative pressure rooms. Dr. Ferrara stressed that all patients with AML should be tested for COVID-19 before admission.
Delaying or reducing AML treatment
Treatment delays are of particular concern, according to Dr. Ferrara, and some patients may require dose reductions, especially for AML treatments that might have a detrimental effect on the immune system.
Decisions must be made as to whether planned approaches to induction or consolidation therapy should be changed, and special concern has to be paid to elderly AML patients, who have the highest risks of bad COVID-19 outcomes.
Specific attention should be paid to patients with acute promyelocytic leukemia as well, according to Dr. Ferrara. These patients are of concern in the COVID-19 era because of their risk of differentiation syndrome, which can induce respiratory distress.
In all cases, autologous or allogeneic stem cell transplant should be deferred until confirmed COVID-19–negative test results are obtained.
Continuing AML treatment
Of particular concern is the fact that, without a standard therapy for COVID-19, many different drugs might be used in treatment efforts. This raises the potential for serious drug-drug interactions with the patient’s AML medications, so close attention should be paid to an individual patient’s medications.
In terms of continuing AML treatment for younger adults (less than 65 years) who are positive for COVID-19, symptomatic and asymptomatic patients should be treated differently, Dr. Ferarra said.
Symptomatic patients should be given hydroxyurea until symptom resolution, and unless urgent, any further AML treatments should be delayed. However, if treatment is needed immediately, it should be given in a COVID-19–dedicated unit.
The restrictions are much looser for young adult asymptomatic COVID-19 patients with AML. Standard induction therapy should be given, with intermediate-dose cytarabine used as consolidation therapy.
Therapy in elderly patients with AML and COVID-19 should be based on symptom status as well, said Dr. Ferrara.
Asymptomatic but otherwise fit elderly patients should have standard induction therapy if they are in the European Leukemia Network favorable genetic subgroup. Asymptomatic elderly patients with high-risk molecular disease can receive venetoclax with a hypomethylating agent.
Symptomatic elderly patients should continue with hydroxyurea until symptom resolution, and any other treatments should be delayed in nonemergency cases.
Relapsed AML patients with COVID-19 should have their treatments postponed until they obtain negative COVID-19 test results whenever possible, Dr. Ferarra said. However, if treatment is necessary, molecularly targeted therapies (gilteritinib, ivosidenib, and enasidenib) are preferable to high-dose chemotherapy.
In all cases, treatment decisions should be made in conjunction with pulmonologists and intensivists, Dr. Ferrera noted.
Webinar moderator Francesco Cerisoli, MD, head of research and mentoring at EHA, highlighted the fact that EHA has published specific recommendations for treating AML patients during the COVID-19 pandemic. The majority of these were discussed by and are aligned with the recommendations presented by Dr. Ferrara.
The EHA webinar contains a disclaimer that the content discussed was based on the personal experiences and opinions of the speakers and that no general, evidence-based guidance could be derived from the discussion. There were no disclosures given.
Rural ICU capacity could be strained by COVID-19
The nonmetropolitan, largely rural, areas of the United States have fewer ICU beds than do urban areas, but their populations may be at higher risk for COVID-19 complications, according to the Kaiser Family Foundation.
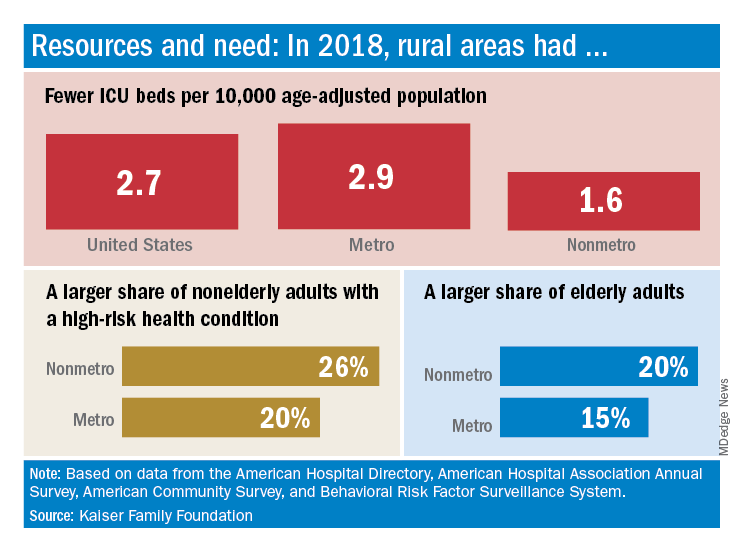
In 2018, the United States had 2.7 ICU beds per 10,000 age-adjusted population, but that number drops to 1.6 beds per 10,000 in nonmetro America and rises to 2.9 per 10,000 in metro areas. Counts for all hospital beds were much closer: 21.6 per 10,000 (rural) and 23.9 per 10,000 (urban), Kaiser investigators reported.
“The novel coronavirus was slower to spread to rural areas in the U.S., but that appears to be changing, with new outbreaks becoming evident in less densely populated parts of the country,” Kendal Orgera and associates said in a recent analysis.
Those rural areas have COVID-19 issues beyond ICU bed counts. Populations in nonmetro areas are less healthy – 26% of adults under age 65 years had a preexisting medical condition in 2018, compared with 20% in metro areas – and older – 20% of people are 65 and older, versus 15% in metro areas, they said.
“If coronavirus continues to spread in rural communities across the U.S., it is possible many [nonmetro] areas will face shortages of ICU beds with limited options to adapt. Patients in rural areas experiencing more severe illnesses may be transferred to hospitals with greater capacity, but if nearby urban areas are also overwhelmed, transfer may not be an option,” Ms. Orgera and associates wrote.
They defined nonmetro counties as those with rural towns of fewer than 2,500 people and/or “urban areas with populations ranging from 2,500 to 49,999 that are not part of larger labor market areas.” The Kaiser analysis involved 2018 data from the American Hospital Association, American Hospital Directory, American Community Survey, and the Behavioral Risk Factor Surveillance System.
The nonmetropolitan, largely rural, areas of the United States have fewer ICU beds than do urban areas, but their populations may be at higher risk for COVID-19 complications, according to the Kaiser Family Foundation.
In 2018, the United States had 2.7 ICU beds per 10,000 age-adjusted population, but that number drops to 1.6 beds per 10,000 in nonmetro America and rises to 2.9 per 10,000 in metro areas. Counts for all hospital beds were much closer: 21.6 per 10,000 (rural) and 23.9 per 10,000 (urban), Kaiser investigators reported.
“The novel coronavirus was slower to spread to rural areas in the U.S., but that appears to be changing, with new outbreaks becoming evident in less densely populated parts of the country,” Kendal Orgera and associates said in a recent analysis.
Those rural areas have COVID-19 issues beyond ICU bed counts. Populations in nonmetro areas are less healthy – 26% of adults under age 65 years had a preexisting medical condition in 2018, compared with 20% in metro areas – and older – 20% of people are 65 and older, versus 15% in metro areas, they said.
“If coronavirus continues to spread in rural communities across the U.S., it is possible many [nonmetro] areas will face shortages of ICU beds with limited options to adapt. Patients in rural areas experiencing more severe illnesses may be transferred to hospitals with greater capacity, but if nearby urban areas are also overwhelmed, transfer may not be an option,” Ms. Orgera and associates wrote.
They defined nonmetro counties as those with rural towns of fewer than 2,500 people and/or “urban areas with populations ranging from 2,500 to 49,999 that are not part of larger labor market areas.” The Kaiser analysis involved 2018 data from the American Hospital Association, American Hospital Directory, American Community Survey, and the Behavioral Risk Factor Surveillance System.
The nonmetropolitan, largely rural, areas of the United States have fewer ICU beds than do urban areas, but their populations may be at higher risk for COVID-19 complications, according to the Kaiser Family Foundation.
In 2018, the United States had 2.7 ICU beds per 10,000 age-adjusted population, but that number drops to 1.6 beds per 10,000 in nonmetro America and rises to 2.9 per 10,000 in metro areas. Counts for all hospital beds were much closer: 21.6 per 10,000 (rural) and 23.9 per 10,000 (urban), Kaiser investigators reported.
“The novel coronavirus was slower to spread to rural areas in the U.S., but that appears to be changing, with new outbreaks becoming evident in less densely populated parts of the country,” Kendal Orgera and associates said in a recent analysis.
Those rural areas have COVID-19 issues beyond ICU bed counts. Populations in nonmetro areas are less healthy – 26% of adults under age 65 years had a preexisting medical condition in 2018, compared with 20% in metro areas – and older – 20% of people are 65 and older, versus 15% in metro areas, they said.
“If coronavirus continues to spread in rural communities across the U.S., it is possible many [nonmetro] areas will face shortages of ICU beds with limited options to adapt. Patients in rural areas experiencing more severe illnesses may be transferred to hospitals with greater capacity, but if nearby urban areas are also overwhelmed, transfer may not be an option,” Ms. Orgera and associates wrote.
They defined nonmetro counties as those with rural towns of fewer than 2,500 people and/or “urban areas with populations ranging from 2,500 to 49,999 that are not part of larger labor market areas.” The Kaiser analysis involved 2018 data from the American Hospital Association, American Hospital Directory, American Community Survey, and the Behavioral Risk Factor Surveillance System.
Undeterred during COVID-19, hospital chaplains transform delivery of spiritual care
The first time that the Rev. Michael Mercier, BCC (a board-certified chaplain), provided spiritual care for a patient hospitalized with COVID-19 in March, he found himself engaged in a bit of soul-searching. Even though he donned a mask, gloves, and gown, he could get no closer than the hospital room doorway to interact with the patient because of infection-control measures.
“It went against all my natural instincts and my experience as a chaplain,” said Rev. Mercier, who serves as director of spiritual care for Rhode Island Hospital, Hasbro Children’s Hospital, Miriam Hospital, and Newport Hospital, which are operated by Lifespan, Rhode Island’s largest health system. “The first instinct is to be physically present in the room with the person who’s dying, to have the family gathered around the bedside.”
Prior to standing in the doorway that day, he’d been on the phone with family members, “just listening to their fear and their anxiety that they could not be with their loved one when their loved one was dying,” he said. “I validated their feelings. I also urged them to work with me and the nurse to bring a phone into the room, hold it to the patient’s ear, and they were able to say their goodbyes and how much they loved the person.”
The patient was a devout Roman Catholic, he added, and the family requested that the Prayer of Commendation and the Apostolic Pardon be performed. Rev. Mercier arranged for a Catholic priest to carry out this request. “The nurse told the patient what was going on, and the priest offered the prayers and the rituals from the doorway,” Rev. Mercier said. “It was a surreal experience. For me, it was almost entirely phone based, and it was mostly with the family because the patient couldn’t talk too much.”

To add to the sense of detachment in a situation like that, doctors, nurses, and chaplains caring for COVID-19 patients are wearing masks and face shields, and sometimes the sickest patients are intubated, which can complicate efforts to communicate. “I’m surprised at how we find the mask as somewhat of a barrier,” said Carolanne B. Hauck, BCC, director of chaplaincy care & education and volunteer services at Lancaster (Pa.) General Hospital, which is part of the Penn Medicine system. “By that I mean, often for us, sitting at the bedside and really being able to see someone’s face and have them see our face – with our masks, that’s just not happening. We’re also having briefer visits when we’re visiting with COVID patients.”
COVID-19 may have quarantined some traditional ways of providing spiritual care, but hospital chaplains are relying on technology more than ever in their efforts to meet the needs of patients and their families, including the use of iPads, FaceTime, and video conferencing programs like Zoom and BlueJeans.
“We’ve used Zoom to talk with family members that live out of state,” Rev. Mercier said. “Most of the time, I get an invitation to join a Zoom meeting, but now I need to become proficient in utilizing Zoom to set up those end-of-life family meetings. There’s a lot of learning on the fly, how to use these technologies in a way that’s helpful for everybody. That’s the biggest thing I’m learning: Connection is connection during this time of high stress and anxiety, and we just have to get creative.”
Despite the “disembodied” nature of technology, patients and their families have expressed gratitude to chaplains for their efforts to facilitate connections between loved ones and to be “a guide on the side,” as Mary Wetsch-Johnson, BCC, put it. She recalled one phone conversation with the daughter of a man with COVID-19 who was placed on comfort measures. “She said her dad was like the dad on the TV series Father Knows Best, just a kind-hearted, loving, wonderful man,” said Ms. Wetsch-Johnson, a chaplain at CHI Franciscan Health, which operates 10 acute-care hospitals in the Puget Sound region of Washington state. “She was able to describe him in a way that I felt like I knew him. She talked about the discord they had in their family and how they’re processing through that, and about her own personal journey with grief and loss. She then asked me for information about funeral homes, and I provided her with information. At the end of it, she said, ‘I did not know that I needed you today, but you are exactly what I needed.’ ”

Hospital chaplains may be using smartphones and other gadgets to communicate with patients and their families more than they did in the pre-COVID-19 world, but their basic job has not changed, said Rabbi Neal J. Loevinger, BCC, director of spiritual care services at Vassar Brothers Medical Center in Poughkeepsie, N.Y., part of a seven-hospital system operated by Nuvance Health. “We offer the hope of a caring presence,” said Rabbi Loevinger, who is also a member of the board of directors for Neshama: Association of Jewish Chaplains. “If someone is in a hole, our job is to climb down into the hole with them and say, ‘We’re going to get out of this hole together.’ We can’t promise that someone’s going to get better. We can’t promise that everything’s going to be all right. What we can promise is that we will not abandon you. We can promise that there will be someone accompanying you in any way we can through this crisis.”
Ms. Hauck remembered a phone conversation with the granddaughter of a patient hospitalized with COVID-19 who was nearing the end of her life. The granddaughter told her a story about how her grandmother and her best friend made a pact with each other that, when one was dying, the other would come to her side and pray the Rosary with her. “The granddaughter got tearful and said, ‘That can’t happen now,’ ” said Ms. Hauck, who oversees a staff of 9 chaplains and 10 per diem chaplains. “I made a promise that I would do my best to be at the bedside and pray the Rosary with her grandmother.”
The nurses were aware of the request, and about a day later, Ms. Hauck received a call at 1 a.m., indicating that the patient was close to dying. She drove to Lancaster General, put on her personal protective equipment, made it to the patient’s bedside, and began to pray the Rosary with her, with a nurse in the room. “The nurse said to me, ‘Carolanne, all of her stats are going up,’ and the patient actually became a little more alert,” she recalled. “We talked a little bit, and I asked, ‘Would you like to pray the Rosary now?’ She shook her head yes, and said, ‘Hail Mary, full of grace ...’ and those were the last words that she spoke. I finished the prayers for her, and then she died. It was very meaningful knowing that I could honor that wish for her, but more importantly, that I could do that for the family, who otherwise would have been at her side saying the Rosary with her. We have a recognition of how hard it is to leave someone at the hospital and not be at their bedside.”

Hospital chaplains are also supporting interdisciplinary teams of physicians, nurses, and other staff, as they navigate the provision of care in the wake of a pandemic. “They are under a great deal of stress – not only from being at work but with all the role changes that have happened in their home life,” Ms. Wetsch-Johnson said. “Some of them now are being the teacher at home and having to care for children. They have a lot that they come in with. My job is to help them so that they can go do their job. Regularly what I do is check in with the units and ask, ‘How are you doing today? What’s going on for you?’ Because people need to know that someone’s there to be with them and walk with them and listen to them.”
In the spirit of being present for their staff, she and her colleagues established “respite rooms” at CHI Franciscan hospitals, where workers can decompress and get recentered before returning to work. “We usually have water and snacks in there for them, and some type of soothing music,” Ms. Wetsch-Johnson said. “There is also literature on breathing exercises and stretching exercises. We’re also inviting people to write little notes of hope and gratitude, and they’re putting those up for each other. It’s important that we keep supporting them as they support the patients. Personally, I also round with our physicians, because they carry a lot with them, just as much as any other staff. I check in with dietary and environmental services. Everybody’s giving in their own unique way; that helps this whole health care system keep going.”

On any given day, it’s not uncommon for hospital staff members to spontaneously pull aside chaplains to vent, pray, or just to talk. “They process their own fears and anxieties about working in this kind of environment,” Rev. Mercier said. “They’re scared for themselves. They think, ‘Could I get the virus? Could I spread the virus to my family?’ Or, they may express the care and concern they have for their patients. Oftentimes, it’s a mixture of both. Those spontaneous conversations are often the most powerful.”
Ms. Hauck noted that some nurses and clinicians at Lancaster General Hospital “are doing work they may have not done before,” she said. “Some of them are experiencing death for the first time, so we help them to navigate that. One of the best things we can do is hear the anxiety they have or the sadness they have when a patient dies. Also, maybe the frustration that they couldn’t do more in some cases and helping them to see that sometimes their best is good enough.”
She recalled one younger patient with COVID-19 who fell seriously ill. “It was really affecting a lot of people on the unit because of the patient’s age,” she said. “When we saw that the patient was getting better and would be discharged, there was such a sense of relief. I’m not sure that patient will ever understand how that helped us. It was comforting to us to know that people are getting better. It is something we celebrate.”
As chaplains adjust to their “new normal,” carving out time for self-care is key. Ms. Hauck and her staff periodically meet on Zoom with a psychotherapist “who understands what we do, asks us really good questions, and reminds us to take care of ourselves,” she said. “Personally, I’m making sure I get my exercise in, I pack a healthy lunch. We do check in with each other. Part of our handoff at every shift provides for an opportunity to debrief about how your day was.”
Rev. Mercier’s self check-in includes deep-breathing meditation and reciting certain prayers throughout the day. “The deep breathing helps me center and refocus with my body, while the prayers remind me of my connection to the Divine,” he said. “It also reminds me that in the midst of the fear and the anxiety, I fear for myself. It’s hard not to be concerned that I could be infected. I have a family at home and could spread this to them. The prayer practices are a reminder to me that it’s okay to feel those fears and anxieties. Sometimes the spiritual practice helps me find that place of acceptance. That enables me to keep moving forward.”
Ms. Wetsch-Johnson described the sense of upendedness caused by the COVID-19 pandemic as a “ripple in the water that’s going to have long-lasting effects on the delivery of health care. People are taking the time to listen to one another. I’ve seen people in all departments be more compassionate with one another. I’ve seen managers go out of their way to make sure their staff are deeply cared for. I think that will have a ripple effect. That’s my hope, that we will continue to be more compassionate, more loving, and more understanding.”
Rabbi Loevinger hopes that even the most reticent physicians remember that chaplains serve as their advocate, too, especially during times of crisis. “This has been a time of unprecedented ethical wrestling in our hospitals, where there’s been a real concern that doctors, nurses, and respiratory therapists are going to be faced with morally distressing situations regarding insufficient PPE, or insufficient ventilator or dialysis machine supply to support everybody that needs to be supported,” he said. “Chaplains are a key part of the process of making ethical decisions, but also supporting physicians who are in distress over [being in] situations they never had imagined. Physicians don’t like to talk about the fact that a lot of the decisions they make are really heartbreaking. But if chaplains understand anything, it’s that being brokenhearted is part of the human condition, and that we can be part of the answer for keeping physicians morally and spiritually grounded in their work. We always invite that conversation.”
For Rev. Mercier, serving in a time of crisis reminds him of the importance of providing care as a team, “not just for patients and families, but for one another,” he said. “One of the lessons we can learn is, how can we build that connection with one another, to support and care for one another? How can we make sure that no one feels alone while working in the hospital?”
He draws inspiration from a saying credited to St. John of the Cross, which reads, “I saw the river through which every soul must pass, and the name of that river is suffering. I saw the boat that carries each soul across that river, and the name of that boat is love.”
“It’s that image that’s sticking with me, not just for myself as a chaplain but for all of my colleagues in the hospital,” said Rev. Mercier, who also pastors Tabernacle Baptist Church in Hope, R.I. “We’re in that river with the patients right now, suffering, and we’re doing our best to help them get to the other side – whatever the other side may look like.”
Correction, 4/30/20: An earlier version of the caption for the photo with Mary Wetsch-Johnson misstated the location. The photo was taken outside St. Elizabeth Hospital in Enumclaw, Wash.
The first time that the Rev. Michael Mercier, BCC (a board-certified chaplain), provided spiritual care for a patient hospitalized with COVID-19 in March, he found himself engaged in a bit of soul-searching. Even though he donned a mask, gloves, and gown, he could get no closer than the hospital room doorway to interact with the patient because of infection-control measures.
“It went against all my natural instincts and my experience as a chaplain,” said Rev. Mercier, who serves as director of spiritual care for Rhode Island Hospital, Hasbro Children’s Hospital, Miriam Hospital, and Newport Hospital, which are operated by Lifespan, Rhode Island’s largest health system. “The first instinct is to be physically present in the room with the person who’s dying, to have the family gathered around the bedside.”
Prior to standing in the doorway that day, he’d been on the phone with family members, “just listening to their fear and their anxiety that they could not be with their loved one when their loved one was dying,” he said. “I validated their feelings. I also urged them to work with me and the nurse to bring a phone into the room, hold it to the patient’s ear, and they were able to say their goodbyes and how much they loved the person.”
The patient was a devout Roman Catholic, he added, and the family requested that the Prayer of Commendation and the Apostolic Pardon be performed. Rev. Mercier arranged for a Catholic priest to carry out this request. “The nurse told the patient what was going on, and the priest offered the prayers and the rituals from the doorway,” Rev. Mercier said. “It was a surreal experience. For me, it was almost entirely phone based, and it was mostly with the family because the patient couldn’t talk too much.”
To add to the sense of detachment in a situation like that, doctors, nurses, and chaplains caring for COVID-19 patients are wearing masks and face shields, and sometimes the sickest patients are intubated, which can complicate efforts to communicate. “I’m surprised at how we find the mask as somewhat of a barrier,” said Carolanne B. Hauck, BCC, director of chaplaincy care & education and volunteer services at Lancaster (Pa.) General Hospital, which is part of the Penn Medicine system. “By that I mean, often for us, sitting at the bedside and really being able to see someone’s face and have them see our face – with our masks, that’s just not happening. We’re also having briefer visits when we’re visiting with COVID patients.”
COVID-19 may have quarantined some traditional ways of providing spiritual care, but hospital chaplains are relying on technology more than ever in their efforts to meet the needs of patients and their families, including the use of iPads, FaceTime, and video conferencing programs like Zoom and BlueJeans.
“We’ve used Zoom to talk with family members that live out of state,” Rev. Mercier said. “Most of the time, I get an invitation to join a Zoom meeting, but now I need to become proficient in utilizing Zoom to set up those end-of-life family meetings. There’s a lot of learning on the fly, how to use these technologies in a way that’s helpful for everybody. That’s the biggest thing I’m learning: Connection is connection during this time of high stress and anxiety, and we just have to get creative.”
Despite the “disembodied” nature of technology, patients and their families have expressed gratitude to chaplains for their efforts to facilitate connections between loved ones and to be “a guide on the side,” as Mary Wetsch-Johnson, BCC, put it. She recalled one phone conversation with the daughter of a man with COVID-19 who was placed on comfort measures. “She said her dad was like the dad on the TV series Father Knows Best, just a kind-hearted, loving, wonderful man,” said Ms. Wetsch-Johnson, a chaplain at CHI Franciscan Health, which operates 10 acute-care hospitals in the Puget Sound region of Washington state. “She was able to describe him in a way that I felt like I knew him. She talked about the discord they had in their family and how they’re processing through that, and about her own personal journey with grief and loss. She then asked me for information about funeral homes, and I provided her with information. At the end of it, she said, ‘I did not know that I needed you today, but you are exactly what I needed.’ ”
Hospital chaplains may be using smartphones and other gadgets to communicate with patients and their families more than they did in the pre-COVID-19 world, but their basic job has not changed, said Rabbi Neal J. Loevinger, BCC, director of spiritual care services at Vassar Brothers Medical Center in Poughkeepsie, N.Y., part of a seven-hospital system operated by Nuvance Health. “We offer the hope of a caring presence,” said Rabbi Loevinger, who is also a member of the board of directors for Neshama: Association of Jewish Chaplains. “If someone is in a hole, our job is to climb down into the hole with them and say, ‘We’re going to get out of this hole together.’ We can’t promise that someone’s going to get better. We can’t promise that everything’s going to be all right. What we can promise is that we will not abandon you. We can promise that there will be someone accompanying you in any way we can through this crisis.”
Ms. Hauck remembered a phone conversation with the granddaughter of a patient hospitalized with COVID-19 who was nearing the end of her life. The granddaughter told her a story about how her grandmother and her best friend made a pact with each other that, when one was dying, the other would come to her side and pray the Rosary with her. “The granddaughter got tearful and said, ‘That can’t happen now,’ ” said Ms. Hauck, who oversees a staff of 9 chaplains and 10 per diem chaplains. “I made a promise that I would do my best to be at the bedside and pray the Rosary with her grandmother.”
The nurses were aware of the request, and about a day later, Ms. Hauck received a call at 1 a.m., indicating that the patient was close to dying. She drove to Lancaster General, put on her personal protective equipment, made it to the patient’s bedside, and began to pray the Rosary with her, with a nurse in the room. “The nurse said to me, ‘Carolanne, all of her stats are going up,’ and the patient actually became a little more alert,” she recalled. “We talked a little bit, and I asked, ‘Would you like to pray the Rosary now?’ She shook her head yes, and said, ‘Hail Mary, full of grace ...’ and those were the last words that she spoke. I finished the prayers for her, and then she died. It was very meaningful knowing that I could honor that wish for her, but more importantly, that I could do that for the family, who otherwise would have been at her side saying the Rosary with her. We have a recognition of how hard it is to leave someone at the hospital and not be at their bedside.”
Hospital chaplains are also supporting interdisciplinary teams of physicians, nurses, and other staff, as they navigate the provision of care in the wake of a pandemic. “They are under a great deal of stress – not only from being at work but with all the role changes that have happened in their home life,” Ms. Wetsch-Johnson said. “Some of them now are being the teacher at home and having to care for children. They have a lot that they come in with. My job is to help them so that they can go do their job. Regularly what I do is check in with the units and ask, ‘How are you doing today? What’s going on for you?’ Because people need to know that someone’s there to be with them and walk with them and listen to them.”
In the spirit of being present for their staff, she and her colleagues established “respite rooms” at CHI Franciscan hospitals, where workers can decompress and get recentered before returning to work. “We usually have water and snacks in there for them, and some type of soothing music,” Ms. Wetsch-Johnson said. “There is also literature on breathing exercises and stretching exercises. We’re also inviting people to write little notes of hope and gratitude, and they’re putting those up for each other. It’s important that we keep supporting them as they support the patients. Personally, I also round with our physicians, because they carry a lot with them, just as much as any other staff. I check in with dietary and environmental services. Everybody’s giving in their own unique way; that helps this whole health care system keep going.”
On any given day, it’s not uncommon for hospital staff members to spontaneously pull aside chaplains to vent, pray, or just to talk. “They process their own fears and anxieties about working in this kind of environment,” Rev. Mercier said. “They’re scared for themselves. They think, ‘Could I get the virus? Could I spread the virus to my family?’ Or, they may express the care and concern they have for their patients. Oftentimes, it’s a mixture of both. Those spontaneous conversations are often the most powerful.”
Ms. Hauck noted that some nurses and clinicians at Lancaster General Hospital “are doing work they may have not done before,” she said. “Some of them are experiencing death for the first time, so we help them to navigate that. One of the best things we can do is hear the anxiety they have or the sadness they have when a patient dies. Also, maybe the frustration that they couldn’t do more in some cases and helping them to see that sometimes their best is good enough.”
She recalled one younger patient with COVID-19 who fell seriously ill. “It was really affecting a lot of people on the unit because of the patient’s age,” she said. “When we saw that the patient was getting better and would be discharged, there was such a sense of relief. I’m not sure that patient will ever understand how that helped us. It was comforting to us to know that people are getting better. It is something we celebrate.”
As chaplains adjust to their “new normal,” carving out time for self-care is key. Ms. Hauck and her staff periodically meet on Zoom with a psychotherapist “who understands what we do, asks us really good questions, and reminds us to take care of ourselves,” she said. “Personally, I’m making sure I get my exercise in, I pack a healthy lunch. We do check in with each other. Part of our handoff at every shift provides for an opportunity to debrief about how your day was.”
Rev. Mercier’s self check-in includes deep-breathing meditation and reciting certain prayers throughout the day. “The deep breathing helps me center and refocus with my body, while the prayers remind me of my connection to the Divine,” he said. “It also reminds me that in the midst of the fear and the anxiety, I fear for myself. It’s hard not to be concerned that I could be infected. I have a family at home and could spread this to them. The prayer practices are a reminder to me that it’s okay to feel those fears and anxieties. Sometimes the spiritual practice helps me find that place of acceptance. That enables me to keep moving forward.”
Ms. Wetsch-Johnson described the sense of upendedness caused by the COVID-19 pandemic as a “ripple in the water that’s going to have long-lasting effects on the delivery of health care. People are taking the time to listen to one another. I’ve seen people in all departments be more compassionate with one another. I’ve seen managers go out of their way to make sure their staff are deeply cared for. I think that will have a ripple effect. That’s my hope, that we will continue to be more compassionate, more loving, and more understanding.”
Rabbi Loevinger hopes that even the most reticent physicians remember that chaplains serve as their advocate, too, especially during times of crisis. “This has been a time of unprecedented ethical wrestling in our hospitals, where there’s been a real concern that doctors, nurses, and respiratory therapists are going to be faced with morally distressing situations regarding insufficient PPE, or insufficient ventilator or dialysis machine supply to support everybody that needs to be supported,” he said. “Chaplains are a key part of the process of making ethical decisions, but also supporting physicians who are in distress over [being in] situations they never had imagined. Physicians don’t like to talk about the fact that a lot of the decisions they make are really heartbreaking. But if chaplains understand anything, it’s that being brokenhearted is part of the human condition, and that we can be part of the answer for keeping physicians morally and spiritually grounded in their work. We always invite that conversation.”
For Rev. Mercier, serving in a time of crisis reminds him of the importance of providing care as a team, “not just for patients and families, but for one another,” he said. “One of the lessons we can learn is, how can we build that connection with one another, to support and care for one another? How can we make sure that no one feels alone while working in the hospital?”
He draws inspiration from a saying credited to St. John of the Cross, which reads, “I saw the river through which every soul must pass, and the name of that river is suffering. I saw the boat that carries each soul across that river, and the name of that boat is love.”
“It’s that image that’s sticking with me, not just for myself as a chaplain but for all of my colleagues in the hospital,” said Rev. Mercier, who also pastors Tabernacle Baptist Church in Hope, R.I. “We’re in that river with the patients right now, suffering, and we’re doing our best to help them get to the other side – whatever the other side may look like.”
Correction, 4/30/20: An earlier version of the caption for the photo with Mary Wetsch-Johnson misstated the location. The photo was taken outside St. Elizabeth Hospital in Enumclaw, Wash.
The first time that the Rev. Michael Mercier, BCC (a board-certified chaplain), provided spiritual care for a patient hospitalized with COVID-19 in March, he found himself engaged in a bit of soul-searching. Even though he donned a mask, gloves, and gown, he could get no closer than the hospital room doorway to interact with the patient because of infection-control measures.
“It went against all my natural instincts and my experience as a chaplain,” said Rev. Mercier, who serves as director of spiritual care for Rhode Island Hospital, Hasbro Children’s Hospital, Miriam Hospital, and Newport Hospital, which are operated by Lifespan, Rhode Island’s largest health system. “The first instinct is to be physically present in the room with the person who’s dying, to have the family gathered around the bedside.”
Prior to standing in the doorway that day, he’d been on the phone with family members, “just listening to their fear and their anxiety that they could not be with their loved one when their loved one was dying,” he said. “I validated their feelings. I also urged them to work with me and the nurse to bring a phone into the room, hold it to the patient’s ear, and they were able to say their goodbyes and how much they loved the person.”
The patient was a devout Roman Catholic, he added, and the family requested that the Prayer of Commendation and the Apostolic Pardon be performed. Rev. Mercier arranged for a Catholic priest to carry out this request. “The nurse told the patient what was going on, and the priest offered the prayers and the rituals from the doorway,” Rev. Mercier said. “It was a surreal experience. For me, it was almost entirely phone based, and it was mostly with the family because the patient couldn’t talk too much.”
To add to the sense of detachment in a situation like that, doctors, nurses, and chaplains caring for COVID-19 patients are wearing masks and face shields, and sometimes the sickest patients are intubated, which can complicate efforts to communicate. “I’m surprised at how we find the mask as somewhat of a barrier,” said Carolanne B. Hauck, BCC, director of chaplaincy care & education and volunteer services at Lancaster (Pa.) General Hospital, which is part of the Penn Medicine system. “By that I mean, often for us, sitting at the bedside and really being able to see someone’s face and have them see our face – with our masks, that’s just not happening. We’re also having briefer visits when we’re visiting with COVID patients.”
COVID-19 may have quarantined some traditional ways of providing spiritual care, but hospital chaplains are relying on technology more than ever in their efforts to meet the needs of patients and their families, including the use of iPads, FaceTime, and video conferencing programs like Zoom and BlueJeans.
“We’ve used Zoom to talk with family members that live out of state,” Rev. Mercier said. “Most of the time, I get an invitation to join a Zoom meeting, but now I need to become proficient in utilizing Zoom to set up those end-of-life family meetings. There’s a lot of learning on the fly, how to use these technologies in a way that’s helpful for everybody. That’s the biggest thing I’m learning: Connection is connection during this time of high stress and anxiety, and we just have to get creative.”
Despite the “disembodied” nature of technology, patients and their families have expressed gratitude to chaplains for their efforts to facilitate connections between loved ones and to be “a guide on the side,” as Mary Wetsch-Johnson, BCC, put it. She recalled one phone conversation with the daughter of a man with COVID-19 who was placed on comfort measures. “She said her dad was like the dad on the TV series Father Knows Best, just a kind-hearted, loving, wonderful man,” said Ms. Wetsch-Johnson, a chaplain at CHI Franciscan Health, which operates 10 acute-care hospitals in the Puget Sound region of Washington state. “She was able to describe him in a way that I felt like I knew him. She talked about the discord they had in their family and how they’re processing through that, and about her own personal journey with grief and loss. She then asked me for information about funeral homes, and I provided her with information. At the end of it, she said, ‘I did not know that I needed you today, but you are exactly what I needed.’ ”
Hospital chaplains may be using smartphones and other gadgets to communicate with patients and their families more than they did in the pre-COVID-19 world, but their basic job has not changed, said Rabbi Neal J. Loevinger, BCC, director of spiritual care services at Vassar Brothers Medical Center in Poughkeepsie, N.Y., part of a seven-hospital system operated by Nuvance Health. “We offer the hope of a caring presence,” said Rabbi Loevinger, who is also a member of the board of directors for Neshama: Association of Jewish Chaplains. “If someone is in a hole, our job is to climb down into the hole with them and say, ‘We’re going to get out of this hole together.’ We can’t promise that someone’s going to get better. We can’t promise that everything’s going to be all right. What we can promise is that we will not abandon you. We can promise that there will be someone accompanying you in any way we can through this crisis.”
Ms. Hauck remembered a phone conversation with the granddaughter of a patient hospitalized with COVID-19 who was nearing the end of her life. The granddaughter told her a story about how her grandmother and her best friend made a pact with each other that, when one was dying, the other would come to her side and pray the Rosary with her. “The granddaughter got tearful and said, ‘That can’t happen now,’ ” said Ms. Hauck, who oversees a staff of 9 chaplains and 10 per diem chaplains. “I made a promise that I would do my best to be at the bedside and pray the Rosary with her grandmother.”
The nurses were aware of the request, and about a day later, Ms. Hauck received a call at 1 a.m., indicating that the patient was close to dying. She drove to Lancaster General, put on her personal protective equipment, made it to the patient’s bedside, and began to pray the Rosary with her, with a nurse in the room. “The nurse said to me, ‘Carolanne, all of her stats are going up,’ and the patient actually became a little more alert,” she recalled. “We talked a little bit, and I asked, ‘Would you like to pray the Rosary now?’ She shook her head yes, and said, ‘Hail Mary, full of grace ...’ and those were the last words that she spoke. I finished the prayers for her, and then she died. It was very meaningful knowing that I could honor that wish for her, but more importantly, that I could do that for the family, who otherwise would have been at her side saying the Rosary with her. We have a recognition of how hard it is to leave someone at the hospital and not be at their bedside.”
Hospital chaplains are also supporting interdisciplinary teams of physicians, nurses, and other staff, as they navigate the provision of care in the wake of a pandemic. “They are under a great deal of stress – not only from being at work but with all the role changes that have happened in their home life,” Ms. Wetsch-Johnson said. “Some of them now are being the teacher at home and having to care for children. They have a lot that they come in with. My job is to help them so that they can go do their job. Regularly what I do is check in with the units and ask, ‘How are you doing today? What’s going on for you?’ Because people need to know that someone’s there to be with them and walk with them and listen to them.”
In the spirit of being present for their staff, she and her colleagues established “respite rooms” at CHI Franciscan hospitals, where workers can decompress and get recentered before returning to work. “We usually have water and snacks in there for them, and some type of soothing music,” Ms. Wetsch-Johnson said. “There is also literature on breathing exercises and stretching exercises. We’re also inviting people to write little notes of hope and gratitude, and they’re putting those up for each other. It’s important that we keep supporting them as they support the patients. Personally, I also round with our physicians, because they carry a lot with them, just as much as any other staff. I check in with dietary and environmental services. Everybody’s giving in their own unique way; that helps this whole health care system keep going.”
On any given day, it’s not uncommon for hospital staff members to spontaneously pull aside chaplains to vent, pray, or just to talk. “They process their own fears and anxieties about working in this kind of environment,” Rev. Mercier said. “They’re scared for themselves. They think, ‘Could I get the virus? Could I spread the virus to my family?’ Or, they may express the care and concern they have for their patients. Oftentimes, it’s a mixture of both. Those spontaneous conversations are often the most powerful.”
Ms. Hauck noted that some nurses and clinicians at Lancaster General Hospital “are doing work they may have not done before,” she said. “Some of them are experiencing death for the first time, so we help them to navigate that. One of the best things we can do is hear the anxiety they have or the sadness they have when a patient dies. Also, maybe the frustration that they couldn’t do more in some cases and helping them to see that sometimes their best is good enough.”
She recalled one younger patient with COVID-19 who fell seriously ill. “It was really affecting a lot of people on the unit because of the patient’s age,” she said. “When we saw that the patient was getting better and would be discharged, there was such a sense of relief. I’m not sure that patient will ever understand how that helped us. It was comforting to us to know that people are getting better. It is something we celebrate.”
As chaplains adjust to their “new normal,” carving out time for self-care is key. Ms. Hauck and her staff periodically meet on Zoom with a psychotherapist “who understands what we do, asks us really good questions, and reminds us to take care of ourselves,” she said. “Personally, I’m making sure I get my exercise in, I pack a healthy lunch. We do check in with each other. Part of our handoff at every shift provides for an opportunity to debrief about how your day was.”
Rev. Mercier’s self check-in includes deep-breathing meditation and reciting certain prayers throughout the day. “The deep breathing helps me center and refocus with my body, while the prayers remind me of my connection to the Divine,” he said. “It also reminds me that in the midst of the fear and the anxiety, I fear for myself. It’s hard not to be concerned that I could be infected. I have a family at home and could spread this to them. The prayer practices are a reminder to me that it’s okay to feel those fears and anxieties. Sometimes the spiritual practice helps me find that place of acceptance. That enables me to keep moving forward.”
Ms. Wetsch-Johnson described the sense of upendedness caused by the COVID-19 pandemic as a “ripple in the water that’s going to have long-lasting effects on the delivery of health care. People are taking the time to listen to one another. I’ve seen people in all departments be more compassionate with one another. I’ve seen managers go out of their way to make sure their staff are deeply cared for. I think that will have a ripple effect. That’s my hope, that we will continue to be more compassionate, more loving, and more understanding.”
Rabbi Loevinger hopes that even the most reticent physicians remember that chaplains serve as their advocate, too, especially during times of crisis. “This has been a time of unprecedented ethical wrestling in our hospitals, where there’s been a real concern that doctors, nurses, and respiratory therapists are going to be faced with morally distressing situations regarding insufficient PPE, or insufficient ventilator or dialysis machine supply to support everybody that needs to be supported,” he said. “Chaplains are a key part of the process of making ethical decisions, but also supporting physicians who are in distress over [being in] situations they never had imagined. Physicians don’t like to talk about the fact that a lot of the decisions they make are really heartbreaking. But if chaplains understand anything, it’s that being brokenhearted is part of the human condition, and that we can be part of the answer for keeping physicians morally and spiritually grounded in their work. We always invite that conversation.”
For Rev. Mercier, serving in a time of crisis reminds him of the importance of providing care as a team, “not just for patients and families, but for one another,” he said. “One of the lessons we can learn is, how can we build that connection with one another, to support and care for one another? How can we make sure that no one feels alone while working in the hospital?”
He draws inspiration from a saying credited to St. John of the Cross, which reads, “I saw the river through which every soul must pass, and the name of that river is suffering. I saw the boat that carries each soul across that river, and the name of that boat is love.”
“It’s that image that’s sticking with me, not just for myself as a chaplain but for all of my colleagues in the hospital,” said Rev. Mercier, who also pastors Tabernacle Baptist Church in Hope, R.I. “We’re in that river with the patients right now, suffering, and we’re doing our best to help them get to the other side – whatever the other side may look like.”
Correction, 4/30/20: An earlier version of the caption for the photo with Mary Wetsch-Johnson misstated the location. The photo was taken outside St. Elizabeth Hospital in Enumclaw, Wash.
COVID-19 registry tracks pregnant women, newborns
A multidisciplinary team of researchers has created a national registry to study how COVID-19 affects pregnant women and their newborns.
“Pregnant women are generally considered healthy, but they are also a vulnerable group, and we currently have no data on COVID-19 in pregnancy,” coprincipal investigator Yalda Afshar, MD, PhD, an ob.gyn. at UCLA Health in Los Angeles, said in an interview.
“We expect this registry to provide data that will be critical in helping to improve care for pregnant women during this global pandemic,” Dr. Afshar, a fellow with UCLA Biodesign, stated in a news release.
The Pregnancy Coronavirus Outcomes Registry is enrolling pregnant women and those who have been pregnant or post partum within the past 6 weeks and who have either received a confirmed diagnosis of COVID-19 or are being evaluated for COVID-19.
Women are being recruited through their health care provider. A study coordinator contacts the participants by telephone. Women can also join the registry on their own without a referral by visiting the registry website.
The registry collects data on COVID-19 symptoms, clinical course, pregnancy, and neonatal outcomes and follows women from enrollment through the second and third trimesters and the postpartum period. The goal is to follow the mothers and babies for up to 1 year.
Hundreds of women already enrolled
Dr. Afshar noted that these kinds of registries often take months to design and to receive funding, but with COVID-19, “there was no time for that. We had to get it up and running ASAP.”
She said the team has been “blown away” by how quickly people have come forward to join the registry. Within 2 weeks of going live, the registry had enrolled more than 400 participants from across the United States. “At this rate, I think we will easily get 1,000 participants in a month or so,” Dr. Afshar said.
“With the global reach of this disease, the findings resulting from this work have the potential to impact millions of lives in an entire generation,” Johnese Spisso, CEO of UCLA Health, said in the news release.
Dr. Afshar noted that, although the impact of COVID-19 on pregnancy remains unknown, history suggests the disease will make some pregnancies and deliveries more challenging. “We know that in previous outbreaks of the regular flu, for example, there have been more deaths and poorer outcomes among pregnant women compared with nonpregnant women.”
Dr. Afshar is overseeing the study with colleagues at the University of California, Los Angeles, and the University of California, San Francisco, where the registry data will be coordinated.
“In addition to gaining a better understanding of the course of the disease, we will investigate disease transmission to determine if it can be passed from a mother to her baby in utero and during the postpartum period, such as in breast milk,” UCSF’s Stephanie Gaw, MD, PhD, who is leading the biospecimen core of the study, said in the release.
Health care providers interested in more information about the registry may send an email to PRIORITYCOVID19@ucsf.edu. A YouTube video on the registry is also available.
Dr. Afshar disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A multidisciplinary team of researchers has created a national registry to study how COVID-19 affects pregnant women and their newborns.
“Pregnant women are generally considered healthy, but they are also a vulnerable group, and we currently have no data on COVID-19 in pregnancy,” coprincipal investigator Yalda Afshar, MD, PhD, an ob.gyn. at UCLA Health in Los Angeles, said in an interview.
“We expect this registry to provide data that will be critical in helping to improve care for pregnant women during this global pandemic,” Dr. Afshar, a fellow with UCLA Biodesign, stated in a news release.
The Pregnancy Coronavirus Outcomes Registry is enrolling pregnant women and those who have been pregnant or post partum within the past 6 weeks and who have either received a confirmed diagnosis of COVID-19 or are being evaluated for COVID-19.
Women are being recruited through their health care provider. A study coordinator contacts the participants by telephone. Women can also join the registry on their own without a referral by visiting the registry website.
The registry collects data on COVID-19 symptoms, clinical course, pregnancy, and neonatal outcomes and follows women from enrollment through the second and third trimesters and the postpartum period. The goal is to follow the mothers and babies for up to 1 year.
Hundreds of women already enrolled
Dr. Afshar noted that these kinds of registries often take months to design and to receive funding, but with COVID-19, “there was no time for that. We had to get it up and running ASAP.”
She said the team has been “blown away” by how quickly people have come forward to join the registry. Within 2 weeks of going live, the registry had enrolled more than 400 participants from across the United States. “At this rate, I think we will easily get 1,000 participants in a month or so,” Dr. Afshar said.
“With the global reach of this disease, the findings resulting from this work have the potential to impact millions of lives in an entire generation,” Johnese Spisso, CEO of UCLA Health, said in the news release.
Dr. Afshar noted that, although the impact of COVID-19 on pregnancy remains unknown, history suggests the disease will make some pregnancies and deliveries more challenging. “We know that in previous outbreaks of the regular flu, for example, there have been more deaths and poorer outcomes among pregnant women compared with nonpregnant women.”
Dr. Afshar is overseeing the study with colleagues at the University of California, Los Angeles, and the University of California, San Francisco, where the registry data will be coordinated.
“In addition to gaining a better understanding of the course of the disease, we will investigate disease transmission to determine if it can be passed from a mother to her baby in utero and during the postpartum period, such as in breast milk,” UCSF’s Stephanie Gaw, MD, PhD, who is leading the biospecimen core of the study, said in the release.
Health care providers interested in more information about the registry may send an email to PRIORITYCOVID19@ucsf.edu. A YouTube video on the registry is also available.
Dr. Afshar disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A multidisciplinary team of researchers has created a national registry to study how COVID-19 affects pregnant women and their newborns.
“Pregnant women are generally considered healthy, but they are also a vulnerable group, and we currently have no data on COVID-19 in pregnancy,” coprincipal investigator Yalda Afshar, MD, PhD, an ob.gyn. at UCLA Health in Los Angeles, said in an interview.
“We expect this registry to provide data that will be critical in helping to improve care for pregnant women during this global pandemic,” Dr. Afshar, a fellow with UCLA Biodesign, stated in a news release.
The Pregnancy Coronavirus Outcomes Registry is enrolling pregnant women and those who have been pregnant or post partum within the past 6 weeks and who have either received a confirmed diagnosis of COVID-19 or are being evaluated for COVID-19.
Women are being recruited through their health care provider. A study coordinator contacts the participants by telephone. Women can also join the registry on their own without a referral by visiting the registry website.
The registry collects data on COVID-19 symptoms, clinical course, pregnancy, and neonatal outcomes and follows women from enrollment through the second and third trimesters and the postpartum period. The goal is to follow the mothers and babies for up to 1 year.
Hundreds of women already enrolled
Dr. Afshar noted that these kinds of registries often take months to design and to receive funding, but with COVID-19, “there was no time for that. We had to get it up and running ASAP.”
She said the team has been “blown away” by how quickly people have come forward to join the registry. Within 2 weeks of going live, the registry had enrolled more than 400 participants from across the United States. “At this rate, I think we will easily get 1,000 participants in a month or so,” Dr. Afshar said.
“With the global reach of this disease, the findings resulting from this work have the potential to impact millions of lives in an entire generation,” Johnese Spisso, CEO of UCLA Health, said in the news release.
Dr. Afshar noted that, although the impact of COVID-19 on pregnancy remains unknown, history suggests the disease will make some pregnancies and deliveries more challenging. “We know that in previous outbreaks of the regular flu, for example, there have been more deaths and poorer outcomes among pregnant women compared with nonpregnant women.”
Dr. Afshar is overseeing the study with colleagues at the University of California, Los Angeles, and the University of California, San Francisco, where the registry data will be coordinated.
“In addition to gaining a better understanding of the course of the disease, we will investigate disease transmission to determine if it can be passed from a mother to her baby in utero and during the postpartum period, such as in breast milk,” UCSF’s Stephanie Gaw, MD, PhD, who is leading the biospecimen core of the study, said in the release.
Health care providers interested in more information about the registry may send an email to PRIORITYCOVID19@ucsf.edu. A YouTube video on the registry is also available.
Dr. Afshar disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 decimates outpatient visits
There has been a massive decline in outpatient office visits as patients have stayed home – likely deferring needed care – because of COVID-19, new research shows.
The number of visits to ambulatory practices dropped by a whopping 60% in mid-March, and continues to be down by at least 50% since early February, according to new data compiled and analyzed by Harvard University and Phreesia, a health care technology company.
Phreesia – which helps medical practices with patient registration, insurance verification, and payments – has data on 50,000 providers in all 50 states; in a typical year, Phreesia tracks 50 million outpatient visits.
The report was published online April 23 by the Commonwealth Fund.
The company captured data on visits from February 1 through April 16. The decline was greatest in New England and the Mid-Atlantic states, where, at the steepest end of the decline in late March, visits were down 66%.
They have rebounded slightly since then but are still down 64%. Practices in the mountain states had the smallest decline, but visits were down by 45% as of April 16.
Many practices have attempted to reach out to patients through telemedicine. As of April 16, about 30% of all visits tracked by Phreesia were provided via telemedicine – by phone or through video. That’s a monumental increase from mid-February, when zero visits were conducted virtually.
However, the Harvard researchers found that telemedicine visits barely made up for the huge decline in office visits.
Decline by specialty
Not surprisingly, declining visits have been steeper in procedure-oriented specialties.
Overall visits – including telemedicine – to ophthalmologists and otolaryngologists had declined by 79% and 75%, respectively, as of the week of April 5. Dermatology saw a 73% decline. Surgery, pulmonology, urology, orthopedics, cardiology, and gastroenterology all experienced declines ranging from 61% to 66%.
Primary care offices, oncology, endocrinology, and obstetrics/gynecology all fared slightly better, with visits down by half. Behavioral health experienced the lowest rate of decline (30%).
School-aged children were skipping care most often. The study showed a 71% drop in visits in 7- to 17-year-olds, and a 59% decline in visits by neonates, infants, and toddlers (up to age 6). Overall, pediatric practices experienced a 62% drop-off in visits.
Nearly two-thirds of Americans over age 65 also stayed away from their doctors. Only half of those aged 18 to 64 reduced their physician visits.
This article first appeared on Medscape.com.
There has been a massive decline in outpatient office visits as patients have stayed home – likely deferring needed care – because of COVID-19, new research shows.
The number of visits to ambulatory practices dropped by a whopping 60% in mid-March, and continues to be down by at least 50% since early February, according to new data compiled and analyzed by Harvard University and Phreesia, a health care technology company.
Phreesia – which helps medical practices with patient registration, insurance verification, and payments – has data on 50,000 providers in all 50 states; in a typical year, Phreesia tracks 50 million outpatient visits.
The report was published online April 23 by the Commonwealth Fund.
The company captured data on visits from February 1 through April 16. The decline was greatest in New England and the Mid-Atlantic states, where, at the steepest end of the decline in late March, visits were down 66%.
They have rebounded slightly since then but are still down 64%. Practices in the mountain states had the smallest decline, but visits were down by 45% as of April 16.
Many practices have attempted to reach out to patients through telemedicine. As of April 16, about 30% of all visits tracked by Phreesia were provided via telemedicine – by phone or through video. That’s a monumental increase from mid-February, when zero visits were conducted virtually.
However, the Harvard researchers found that telemedicine visits barely made up for the huge decline in office visits.
Decline by specialty
Not surprisingly, declining visits have been steeper in procedure-oriented specialties.
Overall visits – including telemedicine – to ophthalmologists and otolaryngologists had declined by 79% and 75%, respectively, as of the week of April 5. Dermatology saw a 73% decline. Surgery, pulmonology, urology, orthopedics, cardiology, and gastroenterology all experienced declines ranging from 61% to 66%.
Primary care offices, oncology, endocrinology, and obstetrics/gynecology all fared slightly better, with visits down by half. Behavioral health experienced the lowest rate of decline (30%).
School-aged children were skipping care most often. The study showed a 71% drop in visits in 7- to 17-year-olds, and a 59% decline in visits by neonates, infants, and toddlers (up to age 6). Overall, pediatric practices experienced a 62% drop-off in visits.
Nearly two-thirds of Americans over age 65 also stayed away from their doctors. Only half of those aged 18 to 64 reduced their physician visits.
This article first appeared on Medscape.com.
There has been a massive decline in outpatient office visits as patients have stayed home – likely deferring needed care – because of COVID-19, new research shows.
The number of visits to ambulatory practices dropped by a whopping 60% in mid-March, and continues to be down by at least 50% since early February, according to new data compiled and analyzed by Harvard University and Phreesia, a health care technology company.
Phreesia – which helps medical practices with patient registration, insurance verification, and payments – has data on 50,000 providers in all 50 states; in a typical year, Phreesia tracks 50 million outpatient visits.
The report was published online April 23 by the Commonwealth Fund.
The company captured data on visits from February 1 through April 16. The decline was greatest in New England and the Mid-Atlantic states, where, at the steepest end of the decline in late March, visits were down 66%.
They have rebounded slightly since then but are still down 64%. Practices in the mountain states had the smallest decline, but visits were down by 45% as of April 16.
Many practices have attempted to reach out to patients through telemedicine. As of April 16, about 30% of all visits tracked by Phreesia were provided via telemedicine – by phone or through video. That’s a monumental increase from mid-February, when zero visits were conducted virtually.
However, the Harvard researchers found that telemedicine visits barely made up for the huge decline in office visits.
Decline by specialty
Not surprisingly, declining visits have been steeper in procedure-oriented specialties.
Overall visits – including telemedicine – to ophthalmologists and otolaryngologists had declined by 79% and 75%, respectively, as of the week of April 5. Dermatology saw a 73% decline. Surgery, pulmonology, urology, orthopedics, cardiology, and gastroenterology all experienced declines ranging from 61% to 66%.
Primary care offices, oncology, endocrinology, and obstetrics/gynecology all fared slightly better, with visits down by half. Behavioral health experienced the lowest rate of decline (30%).
School-aged children were skipping care most often. The study showed a 71% drop in visits in 7- to 17-year-olds, and a 59% decline in visits by neonates, infants, and toddlers (up to age 6). Overall, pediatric practices experienced a 62% drop-off in visits.
Nearly two-thirds of Americans over age 65 also stayed away from their doctors. Only half of those aged 18 to 64 reduced their physician visits.
This article first appeared on Medscape.com.
ASCO panel outlines cancer care challenges during COVID-19 pandemic
The COVID-19 pandemic continues to exact a heavy price on cancer patients, cancer care, and clinical trials, an expert panel reported during a presscast.
“Limited data available thus far are sobering: In Italy, about 20% of COVID-related deaths occurred in people with cancer, and, in China, COVID-19 patients who had cancer were about five times more likely than others to die or be placed on a ventilator in an intensive care unit,” said Howard A “Skip” Burris, MD, president of the American Society of Clinical Oncology and president and CEO of the Sarah Cannon Cancer Institute in Nashville, Tenn.
“We also have little evidence on returning COVID-19 patients with cancer. Physicians have to rely on limited data, anecdotal reports, and their own professional expertise” regarding the extent of increased risk to cancer patients with COVID-19, whether to interrupt or modify treatment, and the effects of cancer on recovery from COVID-19 infection, Dr. Burris said during the ASCO-sponsored online presscast.
Care of COVID-free patients
For cancer patients without COVID-19, the picture is equally dim, with the prospect of delayed surgery, chemotherapy, or screening; shortages of medications and equipment needed for critical care; the shift to telemedicine that may increase patient anxiety; and the potential loss of access to innovative therapies through clinical trials, Dr. Burris said.
“We’re concerned that some hospitals have effectively deemed all cancer surgeries to be elective, requiring them to be postponed. For patients with fast-moving or hard-to-treat cancer, this delay may be devastating,” he said.
Dr. Burris also cited concerns about delayed cancer diagnosis. “In a typical month, roughly 150,000 Americans are diagnosed with cancer. But right now, routine screening visits are postponed, and patients with pain or other warning signs may put off a doctor’s visit because of social distancing,” he said.
The pandemic has also exacerbated shortages of sedatives and opioid analgesics required for intubation and mechanical ventilation of patients.
Trials halted or slowed
Dr. Burris also briefly discussed results of a new survey, which were posted online ahead of publication in JCO Oncology Practice. The survey showed that, of 14 academic and 18 community-based cancer programs, 59.4% reported halting screening and/or enrollment for at least some clinical trials and suspending research-based clinical visits except for those where cancer treatment was delivered.
“Half of respondents reported ceasing research-only blood and/or tissue collections,” the authors of the article reported.
“Trial interruptions are devastating news for thousands of patients; in many cases, clinical trials are the best or only appropriate option for care,” Dr. Burris said.
The article authors, led by David Waterhouse, MD, of Oncology Hematology Care in Cincinnati, pointed to a silver lining in the pandemic cloud in the form of opportunities to improve clinical trials going forward.
“Nearly all respondents (90.3%) identified telehealth visits for participants as a potential improvement to clinical trial conduct, and more than three-quarters (77.4%) indicated that remote patient review of symptoms held similar potential,” the authors wrote.
Other potential improvements included remote site visits from trial sponsors and/or contract research organizations, more efficient study enrollment through secure electronic platforms, direct shipment of oral drugs to patients, remote assessments of adverse events, and streamlined data collection.
Lessons from the front lines
Another member of the presscast panel, Melissa Dillmon, MD, of the Harbin Clinic Cancer Center in Rome, Georgia, described the experience of community oncologists during the pandemic.
Her community, located in northeastern Georgia, experienced a COVID-19 outbreak in early March linked to services at two large churches. Community public health authorities issued a shelter-in-place order before the state government issued stay-at-home guidelines and shuttered all but essential business, some of which were allowed by state order to reopen as of April 24.
Dr. Dillmon’s center began screening patients for COVID-19 symptoms at the door, limited visitors or companions, instituted virtual visits and tumor boards, and set up a cancer treatment triage system that would allow essential surgeries to proceed and most infusions to continue, while delaying the start of chemotherapy when possible.
“We have encouraged patients to continue on treatment, especially if treatment is being given with curative intent, or if the cancer is responding well already to treatment,” she said.
The center, located in a community with a high prevalence of comorbidities and high incidence of lung cancer, has seen a sharp decline in colonoscopies, mammograms, and lung scans as patient shelter in place.
“We have great concerns about patients missing their screening lung scans, as this program has already proven to be finding earlier lung cancers that are curable,” Dr. Dillmon said.
A view from Washington state
Another panel member, Gary Lyman, MD, of the Fred Hutchinson Cancer Research Center in Seattle, described the response by the state of Washington, the initial epicenter of the COVID-19 outbreak in the United States.
Following identification of infections in hospitalized patients and at a nursing home in Kirkland, Washington, “our response, which began in early March and progressed through the second and third week in March at the state level, was to restrict large gatherings; progressively, schools were closed; larger businesses closed; and, by March 23, a stay-at-home policy was implemented, and all nonessential businesses were closed,” Dr. Lyman said.
“We believe, based on what has happened since that time, that this has considerably flattened the curve,” he continued.
Lessons from the Washington experience include the need to plan for a long-term disruption or alteration of cancer care, expand COVID-19 testing to all patients coming into hospitals or major clinics, institute aggressive supportive care measures, prepare for subsequent waves of infection, collect and share data, and, for remote or rural areas, identify lifelines to needed resources, Dr. Lyman said.
ASCO resources
Also speaking at the presscast, Jonathan Marron, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, outlined ASCO’s guidance on allocation of scarce resources during the COVID-19 pandemic.
Richard L. Schilsky, MD, ASCO chief medical officer and executive vice president, outlined community-wide collaborations, data initiatives, and online resources for both clinicians and patients.
The COVID-19 pandemic continues to exact a heavy price on cancer patients, cancer care, and clinical trials, an expert panel reported during a presscast.
“Limited data available thus far are sobering: In Italy, about 20% of COVID-related deaths occurred in people with cancer, and, in China, COVID-19 patients who had cancer were about five times more likely than others to die or be placed on a ventilator in an intensive care unit,” said Howard A “Skip” Burris, MD, president of the American Society of Clinical Oncology and president and CEO of the Sarah Cannon Cancer Institute in Nashville, Tenn.
“We also have little evidence on returning COVID-19 patients with cancer. Physicians have to rely on limited data, anecdotal reports, and their own professional expertise” regarding the extent of increased risk to cancer patients with COVID-19, whether to interrupt or modify treatment, and the effects of cancer on recovery from COVID-19 infection, Dr. Burris said during the ASCO-sponsored online presscast.
Care of COVID-free patients
For cancer patients without COVID-19, the picture is equally dim, with the prospect of delayed surgery, chemotherapy, or screening; shortages of medications and equipment needed for critical care; the shift to telemedicine that may increase patient anxiety; and the potential loss of access to innovative therapies through clinical trials, Dr. Burris said.
“We’re concerned that some hospitals have effectively deemed all cancer surgeries to be elective, requiring them to be postponed. For patients with fast-moving or hard-to-treat cancer, this delay may be devastating,” he said.
Dr. Burris also cited concerns about delayed cancer diagnosis. “In a typical month, roughly 150,000 Americans are diagnosed with cancer. But right now, routine screening visits are postponed, and patients with pain or other warning signs may put off a doctor’s visit because of social distancing,” he said.
The pandemic has also exacerbated shortages of sedatives and opioid analgesics required for intubation and mechanical ventilation of patients.
Trials halted or slowed
Dr. Burris also briefly discussed results of a new survey, which were posted online ahead of publication in JCO Oncology Practice. The survey showed that, of 14 academic and 18 community-based cancer programs, 59.4% reported halting screening and/or enrollment for at least some clinical trials and suspending research-based clinical visits except for those where cancer treatment was delivered.
“Half of respondents reported ceasing research-only blood and/or tissue collections,” the authors of the article reported.
“Trial interruptions are devastating news for thousands of patients; in many cases, clinical trials are the best or only appropriate option for care,” Dr. Burris said.
The article authors, led by David Waterhouse, MD, of Oncology Hematology Care in Cincinnati, pointed to a silver lining in the pandemic cloud in the form of opportunities to improve clinical trials going forward.
“Nearly all respondents (90.3%) identified telehealth visits for participants as a potential improvement to clinical trial conduct, and more than three-quarters (77.4%) indicated that remote patient review of symptoms held similar potential,” the authors wrote.
Other potential improvements included remote site visits from trial sponsors and/or contract research organizations, more efficient study enrollment through secure electronic platforms, direct shipment of oral drugs to patients, remote assessments of adverse events, and streamlined data collection.
Lessons from the front lines
Another member of the presscast panel, Melissa Dillmon, MD, of the Harbin Clinic Cancer Center in Rome, Georgia, described the experience of community oncologists during the pandemic.
Her community, located in northeastern Georgia, experienced a COVID-19 outbreak in early March linked to services at two large churches. Community public health authorities issued a shelter-in-place order before the state government issued stay-at-home guidelines and shuttered all but essential business, some of which were allowed by state order to reopen as of April 24.
Dr. Dillmon’s center began screening patients for COVID-19 symptoms at the door, limited visitors or companions, instituted virtual visits and tumor boards, and set up a cancer treatment triage system that would allow essential surgeries to proceed and most infusions to continue, while delaying the start of chemotherapy when possible.
“We have encouraged patients to continue on treatment, especially if treatment is being given with curative intent, or if the cancer is responding well already to treatment,” she said.
The center, located in a community with a high prevalence of comorbidities and high incidence of lung cancer, has seen a sharp decline in colonoscopies, mammograms, and lung scans as patient shelter in place.
“We have great concerns about patients missing their screening lung scans, as this program has already proven to be finding earlier lung cancers that are curable,” Dr. Dillmon said.
A view from Washington state
Another panel member, Gary Lyman, MD, of the Fred Hutchinson Cancer Research Center in Seattle, described the response by the state of Washington, the initial epicenter of the COVID-19 outbreak in the United States.
Following identification of infections in hospitalized patients and at a nursing home in Kirkland, Washington, “our response, which began in early March and progressed through the second and third week in March at the state level, was to restrict large gatherings; progressively, schools were closed; larger businesses closed; and, by March 23, a stay-at-home policy was implemented, and all nonessential businesses were closed,” Dr. Lyman said.
“We believe, based on what has happened since that time, that this has considerably flattened the curve,” he continued.
Lessons from the Washington experience include the need to plan for a long-term disruption or alteration of cancer care, expand COVID-19 testing to all patients coming into hospitals or major clinics, institute aggressive supportive care measures, prepare for subsequent waves of infection, collect and share data, and, for remote or rural areas, identify lifelines to needed resources, Dr. Lyman said.
ASCO resources
Also speaking at the presscast, Jonathan Marron, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, outlined ASCO’s guidance on allocation of scarce resources during the COVID-19 pandemic.
Richard L. Schilsky, MD, ASCO chief medical officer and executive vice president, outlined community-wide collaborations, data initiatives, and online resources for both clinicians and patients.
The COVID-19 pandemic continues to exact a heavy price on cancer patients, cancer care, and clinical trials, an expert panel reported during a presscast.
“Limited data available thus far are sobering: In Italy, about 20% of COVID-related deaths occurred in people with cancer, and, in China, COVID-19 patients who had cancer were about five times more likely than others to die or be placed on a ventilator in an intensive care unit,” said Howard A “Skip” Burris, MD, president of the American Society of Clinical Oncology and president and CEO of the Sarah Cannon Cancer Institute in Nashville, Tenn.
“We also have little evidence on returning COVID-19 patients with cancer. Physicians have to rely on limited data, anecdotal reports, and their own professional expertise” regarding the extent of increased risk to cancer patients with COVID-19, whether to interrupt or modify treatment, and the effects of cancer on recovery from COVID-19 infection, Dr. Burris said during the ASCO-sponsored online presscast.
Care of COVID-free patients
For cancer patients without COVID-19, the picture is equally dim, with the prospect of delayed surgery, chemotherapy, or screening; shortages of medications and equipment needed for critical care; the shift to telemedicine that may increase patient anxiety; and the potential loss of access to innovative therapies through clinical trials, Dr. Burris said.
“We’re concerned that some hospitals have effectively deemed all cancer surgeries to be elective, requiring them to be postponed. For patients with fast-moving or hard-to-treat cancer, this delay may be devastating,” he said.
Dr. Burris also cited concerns about delayed cancer diagnosis. “In a typical month, roughly 150,000 Americans are diagnosed with cancer. But right now, routine screening visits are postponed, and patients with pain or other warning signs may put off a doctor’s visit because of social distancing,” he said.
The pandemic has also exacerbated shortages of sedatives and opioid analgesics required for intubation and mechanical ventilation of patients.
Trials halted or slowed
Dr. Burris also briefly discussed results of a new survey, which were posted online ahead of publication in JCO Oncology Practice. The survey showed that, of 14 academic and 18 community-based cancer programs, 59.4% reported halting screening and/or enrollment for at least some clinical trials and suspending research-based clinical visits except for those where cancer treatment was delivered.
“Half of respondents reported ceasing research-only blood and/or tissue collections,” the authors of the article reported.
“Trial interruptions are devastating news for thousands of patients; in many cases, clinical trials are the best or only appropriate option for care,” Dr. Burris said.
The article authors, led by David Waterhouse, MD, of Oncology Hematology Care in Cincinnati, pointed to a silver lining in the pandemic cloud in the form of opportunities to improve clinical trials going forward.
“Nearly all respondents (90.3%) identified telehealth visits for participants as a potential improvement to clinical trial conduct, and more than three-quarters (77.4%) indicated that remote patient review of symptoms held similar potential,” the authors wrote.
Other potential improvements included remote site visits from trial sponsors and/or contract research organizations, more efficient study enrollment through secure electronic platforms, direct shipment of oral drugs to patients, remote assessments of adverse events, and streamlined data collection.
Lessons from the front lines
Another member of the presscast panel, Melissa Dillmon, MD, of the Harbin Clinic Cancer Center in Rome, Georgia, described the experience of community oncologists during the pandemic.
Her community, located in northeastern Georgia, experienced a COVID-19 outbreak in early March linked to services at two large churches. Community public health authorities issued a shelter-in-place order before the state government issued stay-at-home guidelines and shuttered all but essential business, some of which were allowed by state order to reopen as of April 24.
Dr. Dillmon’s center began screening patients for COVID-19 symptoms at the door, limited visitors or companions, instituted virtual visits and tumor boards, and set up a cancer treatment triage system that would allow essential surgeries to proceed and most infusions to continue, while delaying the start of chemotherapy when possible.
“We have encouraged patients to continue on treatment, especially if treatment is being given with curative intent, or if the cancer is responding well already to treatment,” she said.
The center, located in a community with a high prevalence of comorbidities and high incidence of lung cancer, has seen a sharp decline in colonoscopies, mammograms, and lung scans as patient shelter in place.
“We have great concerns about patients missing their screening lung scans, as this program has already proven to be finding earlier lung cancers that are curable,” Dr. Dillmon said.
A view from Washington state
Another panel member, Gary Lyman, MD, of the Fred Hutchinson Cancer Research Center in Seattle, described the response by the state of Washington, the initial epicenter of the COVID-19 outbreak in the United States.
Following identification of infections in hospitalized patients and at a nursing home in Kirkland, Washington, “our response, which began in early March and progressed through the second and third week in March at the state level, was to restrict large gatherings; progressively, schools were closed; larger businesses closed; and, by March 23, a stay-at-home policy was implemented, and all nonessential businesses were closed,” Dr. Lyman said.
“We believe, based on what has happened since that time, that this has considerably flattened the curve,” he continued.
Lessons from the Washington experience include the need to plan for a long-term disruption or alteration of cancer care, expand COVID-19 testing to all patients coming into hospitals or major clinics, institute aggressive supportive care measures, prepare for subsequent waves of infection, collect and share data, and, for remote or rural areas, identify lifelines to needed resources, Dr. Lyman said.
ASCO resources
Also speaking at the presscast, Jonathan Marron, MD, of Boston Children’s Hospital and Harvard Medical School, Boston, outlined ASCO’s guidance on allocation of scarce resources during the COVID-19 pandemic.
Richard L. Schilsky, MD, ASCO chief medical officer and executive vice president, outlined community-wide collaborations, data initiatives, and online resources for both clinicians and patients.
COVID-19: Frequently asked clinical questions

Question
How should patients on immunosuppressive therapy be advised during the COVID-19 pandemic?
Answer
In general, those patients who have not tested positive, have not been exposed, and are asymptomatic should continue their medications as prescribed.
The American College of Rheumatology issued a statement on April 14, recommending that stable patients continue their medications. Those with known exposure but without confirmed infection may continue hydroxychloroquine, sulfasalazine, and NSAIDs.
Immunosuppressants, non–IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily. Anti-malarial therapies (hydroxycholoroquine and chloroquine) may be continued and IL-6 inhibitors may be continued in select circumstances.1
The American Academy of Dermatology recommends that the discussion of continuation of biologics be based on a case-by-case basis, citing insufficient evidence to recommend against discontinuation at this time in those patients who have not tested positive. In patients who have tested positive for COVID-19 it is recommended that biologic therapy be suspended until symptoms have resolved.2
Question
Should I continue preventive services during peak COVID-19?
Answer
The Centers for Disease Control and Prevention recommends delaying all elective ambulatory provider visits. In general, preventative services, such as adult immunizations, lipid screening, and cancer screenings, should be delayed. Additionally, the CDC recommends reaching out to patients who are at high risk for complications from respiratory diseases to ensure medication adherence and provide resources if these patients become ill. Facilities can reduce transmission of COVID-19 by triaging and assessing patients through virtual visits through phone calls, video conferences, text-monitoring systems, and other telemedicine tools. Physicians should try to provide routine and chronic care through virtual visits when possible over in-person visits.3

Question
Should I continue to vaccinate my pediatric population during peak COVID-19?
Answer
Practices that schedule separate well visits and sick visits in different sessions or locations can continue to provide well child visits. A practice could, for example, schedule well visits in the morning and sick visits in the afternoon if a single facility is used. These practices should prioritize newborn care and vaccinations of children, especially for those under the age of 24 months.4

Question
Can physicians use telehealth (phone only or audiovisual) to conduct visits with Medicare patients even if they are new patients?
Answer
Effective March 1 through the duration of the pandemic, Medicare will pay physicians for telehealth services at the same rate as an in-office visit. On March 30th, the Centers for Medicare & Medcaid Services announced new policies for physicians and hospitals during the COVID-19 pandemic. These guidelines were updated on April 9.
Audio-only visits are now permitted and the limit on the number of these kinds of visits allowed per month has been waived. Controlled substances can be prescribed via telehealth; however, complying with each state’s individual laws is still required.
Use of any two-way, audiovisual device is permitted. The level of service billed for visits with both audio and visual components is the same as an in-office visit. Telemedicine can be used for both new and existing patients.5
A list of services that may be rendered via telehealth are available on the CMS website.6
It will be important to regularly check the references given, as information on some of these topics is updated frequently.
Dr. Chuong is a second-year resident in the family medicine residency, Dr. Flanagan is a third-year resident, and Dr. Matthews is an intern, all at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at the Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. ACR issues COVID-19 treatment guidance for rheumatic disease patients.
2. American Academy of Dermatology: Guidance on the use of biologic agents during COVID-19 outbreak.
3. Centers for Disease Control and Prevention. Actions to take in response to community transmission of COVID-19.
4. Centers for Disease Control and Prevention. Maintaining childhood immunizations during COVID19 pandemic.
5. Centers for Medicare & Medcaid Services. COVID-19 frequently asked questions (FAQs) on Medicare Fee-for-Service (FFS) billing.
6. Centers for Medicare & Medcaid Services. List of telehealth services.
Question
How should patients on immunosuppressive therapy be advised during the COVID-19 pandemic?
Answer
In general, those patients who have not tested positive, have not been exposed, and are asymptomatic should continue their medications as prescribed.
The American College of Rheumatology issued a statement on April 14, recommending that stable patients continue their medications. Those with known exposure but without confirmed infection may continue hydroxychloroquine, sulfasalazine, and NSAIDs.
Immunosuppressants, non–IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily. Anti-malarial therapies (hydroxycholoroquine and chloroquine) may be continued and IL-6 inhibitors may be continued in select circumstances.1
The American Academy of Dermatology recommends that the discussion of continuation of biologics be based on a case-by-case basis, citing insufficient evidence to recommend against discontinuation at this time in those patients who have not tested positive. In patients who have tested positive for COVID-19 it is recommended that biologic therapy be suspended until symptoms have resolved.2
Question
Should I continue preventive services during peak COVID-19?
Answer
The Centers for Disease Control and Prevention recommends delaying all elective ambulatory provider visits. In general, preventative services, such as adult immunizations, lipid screening, and cancer screenings, should be delayed. Additionally, the CDC recommends reaching out to patients who are at high risk for complications from respiratory diseases to ensure medication adherence and provide resources if these patients become ill. Facilities can reduce transmission of COVID-19 by triaging and assessing patients through virtual visits through phone calls, video conferences, text-monitoring systems, and other telemedicine tools. Physicians should try to provide routine and chronic care through virtual visits when possible over in-person visits.3
Question
Should I continue to vaccinate my pediatric population during peak COVID-19?
Answer
Practices that schedule separate well visits and sick visits in different sessions or locations can continue to provide well child visits. A practice could, for example, schedule well visits in the morning and sick visits in the afternoon if a single facility is used. These practices should prioritize newborn care and vaccinations of children, especially for those under the age of 24 months.4
Question
Can physicians use telehealth (phone only or audiovisual) to conduct visits with Medicare patients even if they are new patients?
Answer
Effective March 1 through the duration of the pandemic, Medicare will pay physicians for telehealth services at the same rate as an in-office visit. On March 30th, the Centers for Medicare & Medcaid Services announced new policies for physicians and hospitals during the COVID-19 pandemic. These guidelines were updated on April 9.
Audio-only visits are now permitted and the limit on the number of these kinds of visits allowed per month has been waived. Controlled substances can be prescribed via telehealth; however, complying with each state’s individual laws is still required.
Use of any two-way, audiovisual device is permitted. The level of service billed for visits with both audio and visual components is the same as an in-office visit. Telemedicine can be used for both new and existing patients.5
A list of services that may be rendered via telehealth are available on the CMS website.6
It will be important to regularly check the references given, as information on some of these topics is updated frequently.
Dr. Chuong is a second-year resident in the family medicine residency, Dr. Flanagan is a third-year resident, and Dr. Matthews is an intern, all at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at the Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. ACR issues COVID-19 treatment guidance for rheumatic disease patients.
2. American Academy of Dermatology: Guidance on the use of biologic agents during COVID-19 outbreak.
3. Centers for Disease Control and Prevention. Actions to take in response to community transmission of COVID-19.
4. Centers for Disease Control and Prevention. Maintaining childhood immunizations during COVID19 pandemic.
5. Centers for Medicare & Medcaid Services. COVID-19 frequently asked questions (FAQs) on Medicare Fee-for-Service (FFS) billing.
6. Centers for Medicare & Medcaid Services. List of telehealth services.
Question
How should patients on immunosuppressive therapy be advised during the COVID-19 pandemic?
Answer
In general, those patients who have not tested positive, have not been exposed, and are asymptomatic should continue their medications as prescribed.
The American College of Rheumatology issued a statement on April 14, recommending that stable patients continue their medications. Those with known exposure but without confirmed infection may continue hydroxychloroquine, sulfasalazine, and NSAIDs.
Immunosuppressants, non–IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily, pending a negative test or after two weeks without symptoms. In patients with confirmed positive COVID-19 infection, sulfasalazine, methotrexate, leflunomide, immunosuppressants, non-IL-6 biologics, and JAK inhibitors should be stopped temporarily. Anti-malarial therapies (hydroxycholoroquine and chloroquine) may be continued and IL-6 inhibitors may be continued in select circumstances.1
The American Academy of Dermatology recommends that the discussion of continuation of biologics be based on a case-by-case basis, citing insufficient evidence to recommend against discontinuation at this time in those patients who have not tested positive. In patients who have tested positive for COVID-19 it is recommended that biologic therapy be suspended until symptoms have resolved.2
Question
Should I continue preventive services during peak COVID-19?
Answer
The Centers for Disease Control and Prevention recommends delaying all elective ambulatory provider visits. In general, preventative services, such as adult immunizations, lipid screening, and cancer screenings, should be delayed. Additionally, the CDC recommends reaching out to patients who are at high risk for complications from respiratory diseases to ensure medication adherence and provide resources if these patients become ill. Facilities can reduce transmission of COVID-19 by triaging and assessing patients through virtual visits through phone calls, video conferences, text-monitoring systems, and other telemedicine tools. Physicians should try to provide routine and chronic care through virtual visits when possible over in-person visits.3
Question
Should I continue to vaccinate my pediatric population during peak COVID-19?
Answer
Practices that schedule separate well visits and sick visits in different sessions or locations can continue to provide well child visits. A practice could, for example, schedule well visits in the morning and sick visits in the afternoon if a single facility is used. These practices should prioritize newborn care and vaccinations of children, especially for those under the age of 24 months.4
Question
Can physicians use telehealth (phone only or audiovisual) to conduct visits with Medicare patients even if they are new patients?
Answer
Effective March 1 through the duration of the pandemic, Medicare will pay physicians for telehealth services at the same rate as an in-office visit. On March 30th, the Centers for Medicare & Medcaid Services announced new policies for physicians and hospitals during the COVID-19 pandemic. These guidelines were updated on April 9.
Audio-only visits are now permitted and the limit on the number of these kinds of visits allowed per month has been waived. Controlled substances can be prescribed via telehealth; however, complying with each state’s individual laws is still required.
Use of any two-way, audiovisual device is permitted. The level of service billed for visits with both audio and visual components is the same as an in-office visit. Telemedicine can be used for both new and existing patients.5
A list of services that may be rendered via telehealth are available on the CMS website.6
It will be important to regularly check the references given, as information on some of these topics is updated frequently.
Dr. Chuong is a second-year resident in the family medicine residency, Dr. Flanagan is a third-year resident, and Dr. Matthews is an intern, all at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at the Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. ACR issues COVID-19 treatment guidance for rheumatic disease patients.
2. American Academy of Dermatology: Guidance on the use of biologic agents during COVID-19 outbreak.
3. Centers for Disease Control and Prevention. Actions to take in response to community transmission of COVID-19.
4. Centers for Disease Control and Prevention. Maintaining childhood immunizations during COVID19 pandemic.
5. Centers for Medicare & Medcaid Services. COVID-19 frequently asked questions (FAQs) on Medicare Fee-for-Service (FFS) billing.
6. Centers for Medicare & Medcaid Services. List of telehealth services.
Global registry collects data on pediatric cancer patients with COVID-19
A week after its launch, a new online registry has information on more than 2 dozen cases of pediatric cancer patients with COVID-19.

The registry, created by St. Jude Children’s Research Hospital in Memphis, Tenn., and the International Society of Paediatric Oncology, is the first global COVID-19 registry for children with cancer.
Clinicians enter cases through an online form, then complete 30- and 60-day follow-up reports via email. St. Jude compiles the data and releases regularly updated summaries, including the number of cases by country and by treatment. Eventually, researchers might be able to apply for access to the raw data for their own projects.
It’s all free of charge, said Carlos Rodriguez-Galindo, MD, chair of the department of global pediatric medicine at St. Jude.
The registry is hosted on a website called “The Global COVID-19 Observatory and Resource Center for Childhood Cancer.” In addition to the registry, the website has a resource library and a discussion forum where clinicians can exchange information.
Other COVID-19 cancer registries have launched recently as well, including registries created by the COVID-19 and Cancer Consortium and the American Society of Clinical Oncology. The idea is to compile and disseminate best practices and other information quickly amid concerns that immunosuppressed cancer patients might be especially vulnerable.
So far, that doesn’t seem to be the case for children. Their relative protection from the disease and serious complications seems to hold even when they have cancer, Dr. Rodriguez-Galindo said.
“When we talk with the people in China” the number of COVID-19 cases in children with cancer is “very small,” he said. There are a couple of reports from Europe finding the same thing, and the severity of COVID-19 also “seems to be lower than you would expect,” he added.
The new registry will help better define the situation, according to Dr. Rodriguez-Galindo.
St. Jude is working with European countries that have their own national pediatric cancer COVID-19 registries to share information. St. Jude’s ties with lower- and middle-income countries, established via the department of global pediatric medicine, should help populate the global registry as well.
Furthermore, international surveys are being planned to gauge the impact of COVID-19 on children with cancer and their access to care.
A week after its launch, a new online registry has information on more than 2 dozen cases of pediatric cancer patients with COVID-19.
The registry, created by St. Jude Children’s Research Hospital in Memphis, Tenn., and the International Society of Paediatric Oncology, is the first global COVID-19 registry for children with cancer.
Clinicians enter cases through an online form, then complete 30- and 60-day follow-up reports via email. St. Jude compiles the data and releases regularly updated summaries, including the number of cases by country and by treatment. Eventually, researchers might be able to apply for access to the raw data for their own projects.
It’s all free of charge, said Carlos Rodriguez-Galindo, MD, chair of the department of global pediatric medicine at St. Jude.
The registry is hosted on a website called “The Global COVID-19 Observatory and Resource Center for Childhood Cancer.” In addition to the registry, the website has a resource library and a discussion forum where clinicians can exchange information.
Other COVID-19 cancer registries have launched recently as well, including registries created by the COVID-19 and Cancer Consortium and the American Society of Clinical Oncology. The idea is to compile and disseminate best practices and other information quickly amid concerns that immunosuppressed cancer patients might be especially vulnerable.
So far, that doesn’t seem to be the case for children. Their relative protection from the disease and serious complications seems to hold even when they have cancer, Dr. Rodriguez-Galindo said.
“When we talk with the people in China” the number of COVID-19 cases in children with cancer is “very small,” he said. There are a couple of reports from Europe finding the same thing, and the severity of COVID-19 also “seems to be lower than you would expect,” he added.
The new registry will help better define the situation, according to Dr. Rodriguez-Galindo.
St. Jude is working with European countries that have their own national pediatric cancer COVID-19 registries to share information. St. Jude’s ties with lower- and middle-income countries, established via the department of global pediatric medicine, should help populate the global registry as well.
Furthermore, international surveys are being planned to gauge the impact of COVID-19 on children with cancer and their access to care.
A week after its launch, a new online registry has information on more than 2 dozen cases of pediatric cancer patients with COVID-19.
The registry, created by St. Jude Children’s Research Hospital in Memphis, Tenn., and the International Society of Paediatric Oncology, is the first global COVID-19 registry for children with cancer.
Clinicians enter cases through an online form, then complete 30- and 60-day follow-up reports via email. St. Jude compiles the data and releases regularly updated summaries, including the number of cases by country and by treatment. Eventually, researchers might be able to apply for access to the raw data for their own projects.
It’s all free of charge, said Carlos Rodriguez-Galindo, MD, chair of the department of global pediatric medicine at St. Jude.
The registry is hosted on a website called “The Global COVID-19 Observatory and Resource Center for Childhood Cancer.” In addition to the registry, the website has a resource library and a discussion forum where clinicians can exchange information.
Other COVID-19 cancer registries have launched recently as well, including registries created by the COVID-19 and Cancer Consortium and the American Society of Clinical Oncology. The idea is to compile and disseminate best practices and other information quickly amid concerns that immunosuppressed cancer patients might be especially vulnerable.
So far, that doesn’t seem to be the case for children. Their relative protection from the disease and serious complications seems to hold even when they have cancer, Dr. Rodriguez-Galindo said.
“When we talk with the people in China” the number of COVID-19 cases in children with cancer is “very small,” he said. There are a couple of reports from Europe finding the same thing, and the severity of COVID-19 also “seems to be lower than you would expect,” he added.
The new registry will help better define the situation, according to Dr. Rodriguez-Galindo.
St. Jude is working with European countries that have their own national pediatric cancer COVID-19 registries to share information. St. Jude’s ties with lower- and middle-income countries, established via the department of global pediatric medicine, should help populate the global registry as well.
Furthermore, international surveys are being planned to gauge the impact of COVID-19 on children with cancer and their access to care.