User login
Patients with mental illness a priority for COVID vaccine, experts say
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Fertility delay varied with contraceptive method in study
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
FROM THE BMJ
Biden plan to lower Medicare eligibility age to 60 faces hostility from hospitals
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Search for a snakebite drug might lead to a COVID treatment, too
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
New eGFR equation ‘less biased’ by age, kidney function; some disagree
The European Kidney Function Consortium (EKFC) equation surpasses existing equations by “resulting in generally lower bias across the spectrum of age and kidney function,” its developers wrote in an article published online Nov. 9 in Annals of Internal Medicine.
“The new EKFC equation may have helpful properties and perform better in estimating GFR, compared with the current KDIGO [Kidney Disease: Improving Global Outcomes]-recommended equations,” they added.
The primary KDIGO-recommended equation in its most recent guideline was the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, designed for adults, and a companion equation, the CKiD, covers children and adolescents.
“Key in our [new] equation is the adjustment for differences in serum creatinine generation between children and adults, or between men and women,” lead author Hans Pottel, PhD, KU Leuven (Belgium), said in an interview.
In an accompanying editorial, Andrew M. Levey, MD, and associates wrote: “We agree that a single eGFR equation that can be used in children and adults and performs well in the transition from adolescence to young adulthood is a worthy goal.”
“But the claim of equivalent or superior performance, compared with the CKD-EPI equation is not conclusive,” claimed Dr. Levey, who led the research team that developed the CKD-EPI equation, and coauthors.
Dr. Levey is professor of medicine at Tufts University, Boston.
What’s new is Q
Dr. Pottel and codevelopers devised what they call Q values: age- and sex-dependent median creatinine levels in normal individuals.
Q values act to “normalize or rescale creatinine before entering it into the equation, because we know that creatinine generation is different” based on factors that include age, sex, and muscle mass.
The EKFC equation extends the CKD-EPI equation and first eGFR equation by using Q values and applying across age ranges, like the full-age spectrum (FAS) equation, first reported in 2016 by a team led by Dr. Pottel.
“Although the FAS equation was designed to overcome the challenge in measuring GFR in patients transitioning from adolescence to adult nephrology care, it also underestimates GFR at low serum creatinine values and in patients with chronic kidney disease,” wrote Dr. Pottel and coauthors.
Hence, their intent to tweak the FAS equation to overcome this limitation and create the EKFC equation.
“The new equation combines the strengths of the CKD-EPI and FAS equations,” they woite.
However, “we acknowledge that lack of precision is still a major problem with all eGFR equations,” including the new EKFC, they added.
Editorialists dispute better performance of EKFC over CKD-EPI
In their editorial, Dr. Levey and coauthors noted the EKFC equations and other adapted equations in development “represent a conceptual advance over the FAS equations,” but they dispute the claims of better performance, compared with the CKD-EPI.
“We compared the performance of the EKFC and CKD-EPI equations in a different, large external validation population of Black and non-Black adults,” the external population used to validate the CKD-EPI equation, the editorialists reported.
The upshot was “our results did not confirm the author’s conclusions” about the EKFC equation.
In response, Dr. Pottel highlighted that the EKFC equation is currently not designed for use in Black patients.
“With its derivation and validation now reported in the new article, the EKFC equation is fully validated and ready for routine use in Whites,” he said. “We plan to evaluate and possibly fine tune our equation for its application in other ethnicities.”
Regarding the inferior performance, compared with the CKD-EPI equation in the non-Black population tested by the editorialists, Dr. Pottel cited “calibration issues for serum creatinine” that some experts have found in the datasets compiled by developers of the CKI-EPI equation that could limit the utility of these data.
Still room for improvement; app hopefully coming next year
Dr. Pottel and coauthors developed and validated the EKFC equation with data from 19,629 patients drawn from 13 cohorts. This included 11,251 patients from seven cohorts for development and internal validation, and 8378 from six cohorts for external validation. The EKFC effort received endorsement from the European Renal Association–European Dialysis and Transplant Association.
However, “We acknowledge that there is still room for improvement,” Dr. Pottel said.
Although the new report presents the EKFC equations (actually two slightly different equations depending on whether a patient’s serum creatinine is higher or lower than the relevant Q value), most potential users will likely find the equations easier to work with once they’re in an app form that allows someone to simply plug in age, sex, and serum creatinine level. That app currently doesn’t exist but is coming soon, promised Dr. Pottel.
“I hope to have an electronic tool by the beginning of 2021,” he said. “I have to find a programmer who can do this for me.”
The EKFC project has received no commercial funding. Dr. Pottel reported no relevant financial relationships. Dr. Levey has reported receiving research funding from AstraZeneca.
A version of this article originally appeared on Medscape.com.
The European Kidney Function Consortium (EKFC) equation surpasses existing equations by “resulting in generally lower bias across the spectrum of age and kidney function,” its developers wrote in an article published online Nov. 9 in Annals of Internal Medicine.
“The new EKFC equation may have helpful properties and perform better in estimating GFR, compared with the current KDIGO [Kidney Disease: Improving Global Outcomes]-recommended equations,” they added.
The primary KDIGO-recommended equation in its most recent guideline was the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, designed for adults, and a companion equation, the CKiD, covers children and adolescents.
“Key in our [new] equation is the adjustment for differences in serum creatinine generation between children and adults, or between men and women,” lead author Hans Pottel, PhD, KU Leuven (Belgium), said in an interview.
In an accompanying editorial, Andrew M. Levey, MD, and associates wrote: “We agree that a single eGFR equation that can be used in children and adults and performs well in the transition from adolescence to young adulthood is a worthy goal.”
“But the claim of equivalent or superior performance, compared with the CKD-EPI equation is not conclusive,” claimed Dr. Levey, who led the research team that developed the CKD-EPI equation, and coauthors.
Dr. Levey is professor of medicine at Tufts University, Boston.
What’s new is Q
Dr. Pottel and codevelopers devised what they call Q values: age- and sex-dependent median creatinine levels in normal individuals.
Q values act to “normalize or rescale creatinine before entering it into the equation, because we know that creatinine generation is different” based on factors that include age, sex, and muscle mass.
The EKFC equation extends the CKD-EPI equation and first eGFR equation by using Q values and applying across age ranges, like the full-age spectrum (FAS) equation, first reported in 2016 by a team led by Dr. Pottel.
“Although the FAS equation was designed to overcome the challenge in measuring GFR in patients transitioning from adolescence to adult nephrology care, it also underestimates GFR at low serum creatinine values and in patients with chronic kidney disease,” wrote Dr. Pottel and coauthors.
Hence, their intent to tweak the FAS equation to overcome this limitation and create the EKFC equation.
“The new equation combines the strengths of the CKD-EPI and FAS equations,” they woite.
However, “we acknowledge that lack of precision is still a major problem with all eGFR equations,” including the new EKFC, they added.
Editorialists dispute better performance of EKFC over CKD-EPI
In their editorial, Dr. Levey and coauthors noted the EKFC equations and other adapted equations in development “represent a conceptual advance over the FAS equations,” but they dispute the claims of better performance, compared with the CKD-EPI.
“We compared the performance of the EKFC and CKD-EPI equations in a different, large external validation population of Black and non-Black adults,” the external population used to validate the CKD-EPI equation, the editorialists reported.
The upshot was “our results did not confirm the author’s conclusions” about the EKFC equation.
In response, Dr. Pottel highlighted that the EKFC equation is currently not designed for use in Black patients.
“With its derivation and validation now reported in the new article, the EKFC equation is fully validated and ready for routine use in Whites,” he said. “We plan to evaluate and possibly fine tune our equation for its application in other ethnicities.”
Regarding the inferior performance, compared with the CKD-EPI equation in the non-Black population tested by the editorialists, Dr. Pottel cited “calibration issues for serum creatinine” that some experts have found in the datasets compiled by developers of the CKI-EPI equation that could limit the utility of these data.
Still room for improvement; app hopefully coming next year
Dr. Pottel and coauthors developed and validated the EKFC equation with data from 19,629 patients drawn from 13 cohorts. This included 11,251 patients from seven cohorts for development and internal validation, and 8378 from six cohorts for external validation. The EKFC effort received endorsement from the European Renal Association–European Dialysis and Transplant Association.
However, “We acknowledge that there is still room for improvement,” Dr. Pottel said.
Although the new report presents the EKFC equations (actually two slightly different equations depending on whether a patient’s serum creatinine is higher or lower than the relevant Q value), most potential users will likely find the equations easier to work with once they’re in an app form that allows someone to simply plug in age, sex, and serum creatinine level. That app currently doesn’t exist but is coming soon, promised Dr. Pottel.
“I hope to have an electronic tool by the beginning of 2021,” he said. “I have to find a programmer who can do this for me.”
The EKFC project has received no commercial funding. Dr. Pottel reported no relevant financial relationships. Dr. Levey has reported receiving research funding from AstraZeneca.
A version of this article originally appeared on Medscape.com.
The European Kidney Function Consortium (EKFC) equation surpasses existing equations by “resulting in generally lower bias across the spectrum of age and kidney function,” its developers wrote in an article published online Nov. 9 in Annals of Internal Medicine.
“The new EKFC equation may have helpful properties and perform better in estimating GFR, compared with the current KDIGO [Kidney Disease: Improving Global Outcomes]-recommended equations,” they added.
The primary KDIGO-recommended equation in its most recent guideline was the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, designed for adults, and a companion equation, the CKiD, covers children and adolescents.
“Key in our [new] equation is the adjustment for differences in serum creatinine generation between children and adults, or between men and women,” lead author Hans Pottel, PhD, KU Leuven (Belgium), said in an interview.
In an accompanying editorial, Andrew M. Levey, MD, and associates wrote: “We agree that a single eGFR equation that can be used in children and adults and performs well in the transition from adolescence to young adulthood is a worthy goal.”
“But the claim of equivalent or superior performance, compared with the CKD-EPI equation is not conclusive,” claimed Dr. Levey, who led the research team that developed the CKD-EPI equation, and coauthors.
Dr. Levey is professor of medicine at Tufts University, Boston.
What’s new is Q
Dr. Pottel and codevelopers devised what they call Q values: age- and sex-dependent median creatinine levels in normal individuals.
Q values act to “normalize or rescale creatinine before entering it into the equation, because we know that creatinine generation is different” based on factors that include age, sex, and muscle mass.
The EKFC equation extends the CKD-EPI equation and first eGFR equation by using Q values and applying across age ranges, like the full-age spectrum (FAS) equation, first reported in 2016 by a team led by Dr. Pottel.
“Although the FAS equation was designed to overcome the challenge in measuring GFR in patients transitioning from adolescence to adult nephrology care, it also underestimates GFR at low serum creatinine values and in patients with chronic kidney disease,” wrote Dr. Pottel and coauthors.
Hence, their intent to tweak the FAS equation to overcome this limitation and create the EKFC equation.
“The new equation combines the strengths of the CKD-EPI and FAS equations,” they woite.
However, “we acknowledge that lack of precision is still a major problem with all eGFR equations,” including the new EKFC, they added.
Editorialists dispute better performance of EKFC over CKD-EPI
In their editorial, Dr. Levey and coauthors noted the EKFC equations and other adapted equations in development “represent a conceptual advance over the FAS equations,” but they dispute the claims of better performance, compared with the CKD-EPI.
“We compared the performance of the EKFC and CKD-EPI equations in a different, large external validation population of Black and non-Black adults,” the external population used to validate the CKD-EPI equation, the editorialists reported.
The upshot was “our results did not confirm the author’s conclusions” about the EKFC equation.
In response, Dr. Pottel highlighted that the EKFC equation is currently not designed for use in Black patients.
“With its derivation and validation now reported in the new article, the EKFC equation is fully validated and ready for routine use in Whites,” he said. “We plan to evaluate and possibly fine tune our equation for its application in other ethnicities.”
Regarding the inferior performance, compared with the CKD-EPI equation in the non-Black population tested by the editorialists, Dr. Pottel cited “calibration issues for serum creatinine” that some experts have found in the datasets compiled by developers of the CKI-EPI equation that could limit the utility of these data.
Still room for improvement; app hopefully coming next year
Dr. Pottel and coauthors developed and validated the EKFC equation with data from 19,629 patients drawn from 13 cohorts. This included 11,251 patients from seven cohorts for development and internal validation, and 8378 from six cohorts for external validation. The EKFC effort received endorsement from the European Renal Association–European Dialysis and Transplant Association.
However, “We acknowledge that there is still room for improvement,” Dr. Pottel said.
Although the new report presents the EKFC equations (actually two slightly different equations depending on whether a patient’s serum creatinine is higher or lower than the relevant Q value), most potential users will likely find the equations easier to work with once they’re in an app form that allows someone to simply plug in age, sex, and serum creatinine level. That app currently doesn’t exist but is coming soon, promised Dr. Pottel.
“I hope to have an electronic tool by the beginning of 2021,” he said. “I have to find a programmer who can do this for me.”
The EKFC project has received no commercial funding. Dr. Pottel reported no relevant financial relationships. Dr. Levey has reported receiving research funding from AstraZeneca.
A version of this article originally appeared on Medscape.com.
Great Barrington coauthor backs off strict reliance on herd immunity
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
A coauthor of the Great Barrington Declaration says that he and colleagues have never argued against using mitigation strategies to keep COVID-19 from spreading, and that critics have mischaracterized the document as a “let it rip” strategy.
Jay Bhattacharya, MD, PhD, a professor and public health policy expert in infectious diseases at Stanford University in California, spoke on a JAMA Livestream debate on November 6. Marc Lipsitch, MD, an epidemiology professor at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts, represented the 6900 signatories of the John Snow Memorandum, a rebuttal to the Great Barrington document.
The Great Barrington approach of “Focused Protection” advocates isolation and protection of people who are most vulnerable to COVID-19 while avoiding what they characterize as lockdowns. “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the document reads.
The Infectious Diseases Society of America (IDSA) and its HIV Medicine Association denounced the declaration, as reported by Medscape Medical News, and the World Health Organization (WHO) Director General Tedros Adhanom Ghebreyesus called the proposal “unethical.” But the idea has gained some traction at the White House, where Coronavirus Task Force Member and Stanford professor Scott Atlas, MD, has been advising President Donald J. Trump.
On the JAMA debate, Bhattacharya said, “I think all of the mitigation measures are really important,” listing social distancing, hand washing, and masks when distancing is not possible as chief among those strategies for the less vulnerable. “I don’t want to create infections intentionally, but I want us to allow people to go back to their lives as best they can, understanding of the risks they are taking when they do it,” he said, claiming that 99.95% of the population will survive infection.
“The harmful lockdowns are worse for many, many people,” Bhattacharya said.
“I think Jay is moving towards a middle ground which is not really what the Great Barrington Declaration seems to promote,” countered Lipsitch. The declaration does not say use masks or social distance, he said. “It just says we need to go back to a normal life.”
Bhattacharya’s statements to JAMA mean that “maybe we are approaching some common ground,” Lipsitch said.
Definition of a lockdown
Both men were asked to give their definition of a “lockdown.” To Lipsitch, it means people are not allowed out except for essential services and that most businesses are closed, with exceptions for those deemed essential.
Bhattacharya, however, said he views that as a quarantine. Lockdowns “are what we’re currently doing,” he said. Schools, churches, businesses, and arts and culture organizations are shuttered, and “almost every aspect of society is restricted in some way,” Bhattacharya said.
He blamed these lockdowns for most of the excess deaths over and above the COVID-19 deaths and said they had failed to control the pandemic.
Lipsitch said that “it feels to me that Jay is describing as lockdown everything that causes harm, even when it’s not locked down.” He noted that the country was truly closed down for 2 months or so in the spring.
“All of these harms I agree are real,” said Lipsitch. “But they are because the normal life of our society is being interfered with by viral transmission and by people’s inability to live their normal lives.”
Closures and lockdowns are essential to delaying cases and deaths, said Lipsitch. “A case today is worse than a case tomorrow and a lot worse than a case 6 months from now,” he said, noting that a vaccine or improved therapeutics could evolve.
“Delay is not nothing,” Lipsitch added. “It’s actually the goal as I see it, and as the John Snow memo says, we want to keep the virus under control in such a way as that the vulnerable people are not at risk.”
He predicted that cases will continue to grow exponentially because the nation is “not even close to herd immunity.” And, if intensive care units fill up, “there will be a responsive lockdown,” he said, adding that he did not endorse that as a general matter or favor it as a default position.
Bhattacharya claimed that Sweden has tallied only 1800 excess deaths since the pandemic began. “That’s lockdown harm avoided,” he said, advocating a similar strategy for the United States. But, infections have been on the rise in Sweden, and the nation has a higher COVID-19 death rate — with 6000 deaths — than other Nordic countries.
“If we keep this policy of lockdown we will have the same kind of outcomes we’ve already had — high excess deaths and sort of indifferent control of COVID,” Bhattacharya said.
“We’re still going to have misery and death going forward until we reach a point where there’s sufficient immunity either though a vaccine or through natural infection,” he said.
This article first appeared on Medscape.com.
Hospitals poised to launch first COVID-19 vaccines in clinicians
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
At first, when news spread of a 28-year-old doctor on the COVID-19 front lines in Brazil who died after receiving an experimental vaccine, doubts arose about the safety of one of the most promising coronavirus vaccine candidates. But then the story flipped. Although the vaccine maker wouldn’t confirm it, the doctor appeared to have been in the control group and had received a dose of an established meningitis vaccine. The danger came from exposure to the coronavirus itself.
That tragedy underscores the ongoing risk of COVID-19 to healthcare workers, who have been designated by US advisory panels as part of phase 1A – the first to receive doses of any approved vaccine. The Centers for Disease Control and Prevention (CDC) recently reported that 6% of adults hospitalized with COVID from March to May were healthcare workers. The report was based on surveillance data from 13 states. The average age of the patients was 49 years. The agency set a November 15 vaccination “readiness date” for jurisdictions, such as state health departments, even though a vaccine isn’t likely to be authorized by then.
As hospitals scramble to prepare, their watchword is flexibility. They don’t yet know how many initial doses they will get, of which vaccine, or in what time frame. They have a sophisticated infrastructure to deliver flu vaccines each fall, but that framework doesn’t align with the likely scenarios of limited supply, additional reporting requirements, two-dose regimens, and differing storage needs.
“Healthcare organizations have consistently risen to the challenge. I wholeheartedly believe in their potential to do this,” Anna Legreid Dopp, PharmD, senior director of quality improvement and guidelines for the American Society of Health-System Pharmacists, told Medscape Medical News.
Healthcare workers won’t face a vaccine mandate
Even after months of caring for COVID patients, most clinicians remain vulnerable to infection – at work and in their communities. That was what occupational medicine physician Kevin Smith, MD, realized when his health system, Toledo, Ohio–based ProMedica, offered antibody testing to all its 50,000 employees. About 2% of the 6933 tests given came back positive, he says.
Yet many physicians, nurses, and other healthcare workers share the public’s skepticism about the safety and effectiveness of a vaccine that receives swift US Food and Drug Administration (FDA) approval for emergency use. About half of nurses (47%) and almost 1 in 3 physicians (30%) say that they don’t want to get the vaccine when it first becomes available or that they’re unsure about vaccination, according to a Medscape survey.
Because vaccination of healthcare workers will set the stage for public acceptance of the vaccine, hospital epidemiologists are concerned. “We know that there will be some hesitancy in the healthcare workforce, just as there will be in the broader public,” said Marci Drees, MD, chief infection prevention officer and hospital epidemiologist for ChristianaCare in Newark, Delaware, and liaison from the Society for Healthcare Epidemiology of America to the CDC’s Advisory Committee on Immunization Practices.* “I do not think we can expect anyone to be vaccinated if we’re not willing to vaccinate ourselves.”
Healthcare workers are typically required to receive a range of vaccines, including measles, mumps, and rubella (MMR) and pertussis shots. Each year, close to half of US healthcare workers receive a flu vaccine under a workplace mandate. But COVID-19 will be different. The FDA requires anyone given products under an emergency use authorization (EUA) to receive information about risks and benefits and to have the option to decline. Hospitals instead will rely on education as they offer a novel vaccine (or more than one) that will have a minimum effectiveness of 50%.
ProMedica doesn’t require employees to be vaccinated against flu, but employees who decline must get a note from a doctor indicating that they have talked about the risks and benefits of the vaccine. A similar approach may be used with a COVID-19 vaccine, in which employees may be required to learn about the vaccine before they decline, Smith says. “I do believe some people will say they don’t want to get it,” he added.
Like colleagues across the country, Smith is identifying healthcare workers who are involved in direct care of COVID-19 patients and are at highest risk for exposure. Even within the top tier, those performing the riskiest tasks, such as respiratory therapists who provide breathing treatments that spread aerosols and droplets, will be tagged as a priority group, he says. Healthcare workers who spend the most time in proximity to COVID patients, such as nurses in a COVID unit, also are likely to get the first doses, he says.
Swirl, don’t shake, the vaccine
Hospitals are adept at ramping up vaccination campaigns. For example, last year, Vanderbilt University Medical Center, in Nashville, Tennessee, vaccinated nearly 16,000 employees against influenza in their 1-day “Flulapalooza” event. The medical center even earned a Guinness world record in 2011 at the first Flulapalooza for giving the most vaccinations ever within 8 hours.
The 10th anniversary of the event was canceled this year because of COVID restrictions. Instead, nurses, pharmacists, and other clinicians pitched in to vaccinate their coworkers against influenza. Now, plans for COVID-19 vaccination move forward amid uncertainty.
Instead of holding a mass event, “the delivery mechanisms will need to be more targeted and focused,” said Lori Rolando, MD, MPH, director of the Vanderbilt Occupational Health Clinic. In the CDC’s most recent version of its vaccination program “playbook,” the agency recommends giving the vaccines in an area that allows people to remain 6 feet apart and for them to wait for 15 minutes after receiving the shot to make sure they don’t faint, a potential risk common to almost all vaccines.
That’s the easy part. Planning becomes more complex, given the uncertainty as to which vaccines will receive approval and which one a hospital will receive.
If the Pfizer/BioNTech vaccine receives EUA in 2020, about 10 to 20 million doses could be available in November and 20 to 30 million doses in December. The ultracold containers used to ship the vaccines have to be replenished with dry ice within 24 hours of receipt and every 5 days thereafter. Hospitals will need temperature probes to monitor storage in the containers. The five-dose vials can be refrigerated before administering, but only for 5 days. The product must be diluted, and it then must be used within 6 hours.
The Moderna vaccine will be somewhat less plentiful at first. About 10 million doses are expected in November and 15 million doses by the end of December. The 10-dose vials are stored in a freezer. Once they are placed in a refrigerator to thaw, they have to be used within 7 days, and once they’re removed from the refrigerator, they have to be used within 12 hours. The pharmacist or other vaccinator must swirl – but not shake! – the vial before delivering a dose, according to the CDC playbook.
As more information emerges about the vaccines, instructions may change, and Smith is steeled for shifting scenarios. “These are all draft plans. We’re going to modify as we go along,” he says.
The Pfizer vaccine requires a second dose at 21 days, and the Moderna vaccine targets the second dose at 28 days. In addition to using information systems to track vaccinations and any adverse effects, hospitals will give employees a card indicating what vaccine they received, the date it was administered, and the date on which they need to return. (At this point, the time frame for the second dose doesn’t appear to be flexible.)
Regardless of the vaccine, one message stays the same: COVID precautions must continue. That means mask wearing, social distancing, and hand washing – practices that also must be followed by healthcare workers who test positive for naturally acquired antibodies.
“I don’t think anyone expects the COVID vaccine to be 100% effective at preventing COVID,” says Rolando. “So all of the other tools in our toolbox are going to need to be continued to be used as well.”
*Correction, 11/12/20: An earlier version of this article misstated the name of Dr. Drees' institution.
This article first appeared on Medscape.com.
United States adds nearly 74,000 more children with COVID-19
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
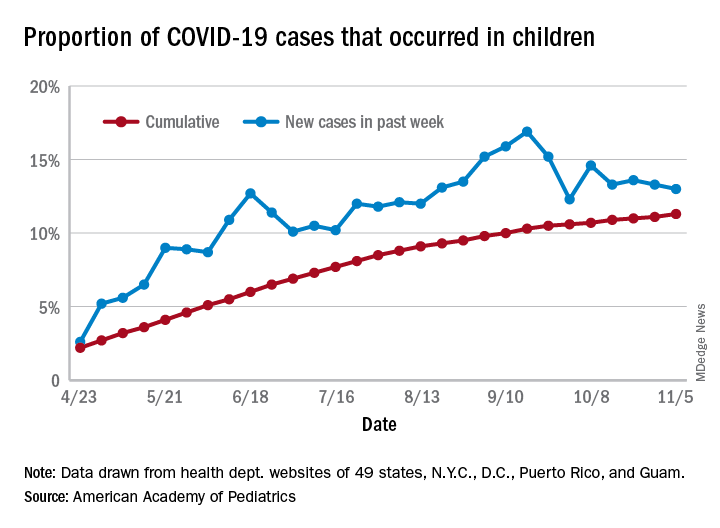
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
The new weekly high for COVID-19 cases in children announced last week has been surpassed already, as the United States experienced almost 74,000 new pediatric cases for the week ending Nov. 5, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The total number of COVID-19 cases in children is now 927,518 in 49 states, the District of Columbia, New York City, Puerto Rico, and Guam, the AAP and CHA said in their weekly report.
Cumulatively, children represent 11.3% of all COVID-19 cases in those jurisdictions, up from 11.1% a week ago. For just the past week, those 73,883 children represent 13.0% of the 567,672 new cases reported among all ages. That proportion peaked at 16.9% in mid-September, the AAP/CHA data show.
Dropping down to the state level, cumulative proportions as of Nov. 5 range from 5.2% in New Jersey to 23.3% in Wyoming, with 11 other states over 15%. California has had more cases, 100,856, than any other state, and Vermont the fewest at 329, the AAP and CHA said.
The national rate per 100,000 children is now 1,232, up from 1,134 the previous week and more than doubled since mid-August (582.2 per 100,000 on Aug. 20). North Dakota’s rate of 3,990 per 100,000 children is the highest of any state (South Dakota is next at 2,779), while Vermont is again the lowest at 245 per 100,000, based on data collected from state health department websites.
Two COVID-19–related deaths in children were reported during the week ending Nov. 5, bringing the total to 123 but leaving the overall proportion of deaths in children unchanged at 0.06% of all deaths. Texas has reported the most COVID-19 deaths in children with 29, while 15 states have recorded no deaths so far (mortality data in children reported by 42 states and New York City), the AAP and CHA said.
Five pediatric heart health practices that may be unnecessary
the American Academy of Pediatrics explained in guidance released Nov. 2.
The AAP Section on Cardiology and Cardiac Surgery developed the recommendations as part of the Choosing Wisely campaign after reviewing evidence pertaining to practices common during pediatric visits, such as routinely ordering an electrocardiogram (ECG) as part of a sports exam.
The guidance lets physicians know what is not necessary or not indicated, with noted exceptions, Christopher S. Snyder, MD, chair of the section, said in an interview.
In all cases, family history is key, said Dr. Snyder, who is also chief of the division of pediatric cardiology at University Hospitals Cleveland Medical Center. That means taking the time necessary to ask about aunts, uncles, and all first-degree relatives, not just asking the single question of whether a patient has a family history of cardiac problems.
The following are the targeted practices and the AAP’s guidance on each.
ECG for sports participation
A screening ECG should not be ordered as part of a routine sports entry examination in otherwise healthy patients who have no symptoms and no personal or family history of cardiac disease, the committee says.
Some medical societies argue that all children who participate in sports should have an ECG, but, Dr. Snyder said, “Currently there are no data that support that, especially in the United States.”
ECGs often yield false positive findings, he noted: “About 10% of them will say the child is a little abnormal.”
That can be a particular problem in places with few or no pediatric cardiologists because kids can become sidelined from sports without access to experts who could clear them.
“In the U.S.,” he said, “we believe that the preparticipation physical exam and screening, which is routine for all high school athletes for sure and most athletes who compete in sports, is currently good enough.”
However, he warned, patients with a family history of heart disease need to see a pediatric cardiologist and “those patients need an ECG.”
The test is not perfect, though, he noted: “You could get your screening, go home, get a fever, COVID, something like that, and come back and have myocarditis and drop dead.”
ECG before ADHD therapy
Similarly, a screening ECG is not routinely needed before initiating therapy for ADHD in asymptomatic, otherwise healthy children who have no personal or family history of cardiac disease, according to the new guidance.
Dr. Snyder said that it has become routine for children to undergo an ECG before ADHD therapy, but evidence doesn’t support the practice, and with the rise in the number of ADHD diagnoses, the tests have increasingly become a burden.
Twenty years ago, the prevalence of ADHD was 3%-4%, Dr. Snyder said. It is now almost threefold higher.
The AAP committee points out that, when ECG abnormalities are identified, they rarely lead to a change in ADHD therapy. Additionally, the typical stimulants used to treat ADHD “have never shown any major effect on the heart,” Dr. Snyder said.
“Black box warnings have been put on these medications, but nothing has been found in the very routine stimulants in normal, routine doses to warrant an ECG,” he said.
Echocardiogram for syncope
The committee says routine use of echocardiograms for children with syncope is unnecessary unless a child has a concerning history or ECG abnormalities.
Most patient who have true syncope or are passing out or fainting are diagnosed through thorough family history, Dr. Snyder said.
“The vast majority of those need an ECG to rule out one other cause that can do this and a physical exam. If those things are normal, there really is no indication to do an echocardiogram,” he said.
“If the patient passes out while they’re running, they pass out doing strenuous exercise, or they pass out for 10-15 minutes as opposed to 20 seconds – those are the ones that need a thorough cardiac workup. But routine passing out, waking up in seconds, those do not.”
Echocardiogram for chest pain
Children with chest pain do not need an echocardiogram unless an ECG is abnormal or the patient has a concerning history, according to the new recommendations.
Too often, Dr. Snyder said, providers treat kids as they would adults.
“Often it comes down to what you learn in medical school,” Dr. Snyder said. “In medical school, we have 6 weeks of cardiology and we had 1 hour of pediatric cardiology.”
That younger patients will clog their arteries with fatty foods and high lipids “is really exceptionally rare,” Dr. Snyder said.
Chest pain “rarely, if ever” means heart attack in younger children, he added.
A thorough history and complete physical exam are critical, “without jumping immediately to an echocardiogram, which 99.9% of the time is going to be normal,” he said.
Troponins for chest pain
In addition, a typical workup for pediatric chest pain need not include evaluating troponins unless there is a concerning history or ECG abnormalities.
Snyder notes that kids with chest pain are often brought to emergency departments that are not pediatric specific, and thus clinicians turn to the standard treatment for adults with chest pain: ECG and troponin.
“The reason we in pediatric cardiology don’t love this is that troponins tend not to be specific just for heart in kids,” Dr. Snyder said. “If someone has anginal chest pain – shortness of breath, chest pain doing anything and everything, [chest pain that] occurs when they’re exercising, feels like an elephant standing on their chest – then we do encourage troponins on those patients.”
The guidance discourages ordering troponins without careful consideration of the patient’s age and condition, he said.
This list was developed by faculty in Pediatric Cardiology at University Hospitals in Cleveland. It was revised and approved by the AAP Section on Cardiology and Cardiac Surgery and the AAP Executive Committee.
A version of this article originally appeared on Medscape.com.
the American Academy of Pediatrics explained in guidance released Nov. 2.
The AAP Section on Cardiology and Cardiac Surgery developed the recommendations as part of the Choosing Wisely campaign after reviewing evidence pertaining to practices common during pediatric visits, such as routinely ordering an electrocardiogram (ECG) as part of a sports exam.
The guidance lets physicians know what is not necessary or not indicated, with noted exceptions, Christopher S. Snyder, MD, chair of the section, said in an interview.
In all cases, family history is key, said Dr. Snyder, who is also chief of the division of pediatric cardiology at University Hospitals Cleveland Medical Center. That means taking the time necessary to ask about aunts, uncles, and all first-degree relatives, not just asking the single question of whether a patient has a family history of cardiac problems.
The following are the targeted practices and the AAP’s guidance on each.
ECG for sports participation
A screening ECG should not be ordered as part of a routine sports entry examination in otherwise healthy patients who have no symptoms and no personal or family history of cardiac disease, the committee says.
Some medical societies argue that all children who participate in sports should have an ECG, but, Dr. Snyder said, “Currently there are no data that support that, especially in the United States.”
ECGs often yield false positive findings, he noted: “About 10% of them will say the child is a little abnormal.”
That can be a particular problem in places with few or no pediatric cardiologists because kids can become sidelined from sports without access to experts who could clear them.
“In the U.S.,” he said, “we believe that the preparticipation physical exam and screening, which is routine for all high school athletes for sure and most athletes who compete in sports, is currently good enough.”
However, he warned, patients with a family history of heart disease need to see a pediatric cardiologist and “those patients need an ECG.”
The test is not perfect, though, he noted: “You could get your screening, go home, get a fever, COVID, something like that, and come back and have myocarditis and drop dead.”
ECG before ADHD therapy
Similarly, a screening ECG is not routinely needed before initiating therapy for ADHD in asymptomatic, otherwise healthy children who have no personal or family history of cardiac disease, according to the new guidance.
Dr. Snyder said that it has become routine for children to undergo an ECG before ADHD therapy, but evidence doesn’t support the practice, and with the rise in the number of ADHD diagnoses, the tests have increasingly become a burden.
Twenty years ago, the prevalence of ADHD was 3%-4%, Dr. Snyder said. It is now almost threefold higher.
The AAP committee points out that, when ECG abnormalities are identified, they rarely lead to a change in ADHD therapy. Additionally, the typical stimulants used to treat ADHD “have never shown any major effect on the heart,” Dr. Snyder said.
“Black box warnings have been put on these medications, but nothing has been found in the very routine stimulants in normal, routine doses to warrant an ECG,” he said.
Echocardiogram for syncope
The committee says routine use of echocardiograms for children with syncope is unnecessary unless a child has a concerning history or ECG abnormalities.
Most patient who have true syncope or are passing out or fainting are diagnosed through thorough family history, Dr. Snyder said.
“The vast majority of those need an ECG to rule out one other cause that can do this and a physical exam. If those things are normal, there really is no indication to do an echocardiogram,” he said.
“If the patient passes out while they’re running, they pass out doing strenuous exercise, or they pass out for 10-15 minutes as opposed to 20 seconds – those are the ones that need a thorough cardiac workup. But routine passing out, waking up in seconds, those do not.”
Echocardiogram for chest pain
Children with chest pain do not need an echocardiogram unless an ECG is abnormal or the patient has a concerning history, according to the new recommendations.
Too often, Dr. Snyder said, providers treat kids as they would adults.
“Often it comes down to what you learn in medical school,” Dr. Snyder said. “In medical school, we have 6 weeks of cardiology and we had 1 hour of pediatric cardiology.”
That younger patients will clog their arteries with fatty foods and high lipids “is really exceptionally rare,” Dr. Snyder said.
Chest pain “rarely, if ever” means heart attack in younger children, he added.
A thorough history and complete physical exam are critical, “without jumping immediately to an echocardiogram, which 99.9% of the time is going to be normal,” he said.
Troponins for chest pain
In addition, a typical workup for pediatric chest pain need not include evaluating troponins unless there is a concerning history or ECG abnormalities.
Snyder notes that kids with chest pain are often brought to emergency departments that are not pediatric specific, and thus clinicians turn to the standard treatment for adults with chest pain: ECG and troponin.
“The reason we in pediatric cardiology don’t love this is that troponins tend not to be specific just for heart in kids,” Dr. Snyder said. “If someone has anginal chest pain – shortness of breath, chest pain doing anything and everything, [chest pain that] occurs when they’re exercising, feels like an elephant standing on their chest – then we do encourage troponins on those patients.”
The guidance discourages ordering troponins without careful consideration of the patient’s age and condition, he said.
This list was developed by faculty in Pediatric Cardiology at University Hospitals in Cleveland. It was revised and approved by the AAP Section on Cardiology and Cardiac Surgery and the AAP Executive Committee.
A version of this article originally appeared on Medscape.com.
the American Academy of Pediatrics explained in guidance released Nov. 2.
The AAP Section on Cardiology and Cardiac Surgery developed the recommendations as part of the Choosing Wisely campaign after reviewing evidence pertaining to practices common during pediatric visits, such as routinely ordering an electrocardiogram (ECG) as part of a sports exam.
The guidance lets physicians know what is not necessary or not indicated, with noted exceptions, Christopher S. Snyder, MD, chair of the section, said in an interview.
In all cases, family history is key, said Dr. Snyder, who is also chief of the division of pediatric cardiology at University Hospitals Cleveland Medical Center. That means taking the time necessary to ask about aunts, uncles, and all first-degree relatives, not just asking the single question of whether a patient has a family history of cardiac problems.
The following are the targeted practices and the AAP’s guidance on each.
ECG for sports participation
A screening ECG should not be ordered as part of a routine sports entry examination in otherwise healthy patients who have no symptoms and no personal or family history of cardiac disease, the committee says.
Some medical societies argue that all children who participate in sports should have an ECG, but, Dr. Snyder said, “Currently there are no data that support that, especially in the United States.”
ECGs often yield false positive findings, he noted: “About 10% of them will say the child is a little abnormal.”
That can be a particular problem in places with few or no pediatric cardiologists because kids can become sidelined from sports without access to experts who could clear them.
“In the U.S.,” he said, “we believe that the preparticipation physical exam and screening, which is routine for all high school athletes for sure and most athletes who compete in sports, is currently good enough.”
However, he warned, patients with a family history of heart disease need to see a pediatric cardiologist and “those patients need an ECG.”
The test is not perfect, though, he noted: “You could get your screening, go home, get a fever, COVID, something like that, and come back and have myocarditis and drop dead.”
ECG before ADHD therapy
Similarly, a screening ECG is not routinely needed before initiating therapy for ADHD in asymptomatic, otherwise healthy children who have no personal or family history of cardiac disease, according to the new guidance.
Dr. Snyder said that it has become routine for children to undergo an ECG before ADHD therapy, but evidence doesn’t support the practice, and with the rise in the number of ADHD diagnoses, the tests have increasingly become a burden.
Twenty years ago, the prevalence of ADHD was 3%-4%, Dr. Snyder said. It is now almost threefold higher.
The AAP committee points out that, when ECG abnormalities are identified, they rarely lead to a change in ADHD therapy. Additionally, the typical stimulants used to treat ADHD “have never shown any major effect on the heart,” Dr. Snyder said.
“Black box warnings have been put on these medications, but nothing has been found in the very routine stimulants in normal, routine doses to warrant an ECG,” he said.
Echocardiogram for syncope
The committee says routine use of echocardiograms for children with syncope is unnecessary unless a child has a concerning history or ECG abnormalities.
Most patient who have true syncope or are passing out or fainting are diagnosed through thorough family history, Dr. Snyder said.
“The vast majority of those need an ECG to rule out one other cause that can do this and a physical exam. If those things are normal, there really is no indication to do an echocardiogram,” he said.
“If the patient passes out while they’re running, they pass out doing strenuous exercise, or they pass out for 10-15 minutes as opposed to 20 seconds – those are the ones that need a thorough cardiac workup. But routine passing out, waking up in seconds, those do not.”
Echocardiogram for chest pain
Children with chest pain do not need an echocardiogram unless an ECG is abnormal or the patient has a concerning history, according to the new recommendations.
Too often, Dr. Snyder said, providers treat kids as they would adults.
“Often it comes down to what you learn in medical school,” Dr. Snyder said. “In medical school, we have 6 weeks of cardiology and we had 1 hour of pediatric cardiology.”
That younger patients will clog their arteries with fatty foods and high lipids “is really exceptionally rare,” Dr. Snyder said.
Chest pain “rarely, if ever” means heart attack in younger children, he added.
A thorough history and complete physical exam are critical, “without jumping immediately to an echocardiogram, which 99.9% of the time is going to be normal,” he said.
Troponins for chest pain
In addition, a typical workup for pediatric chest pain need not include evaluating troponins unless there is a concerning history or ECG abnormalities.
Snyder notes that kids with chest pain are often brought to emergency departments that are not pediatric specific, and thus clinicians turn to the standard treatment for adults with chest pain: ECG and troponin.
“The reason we in pediatric cardiology don’t love this is that troponins tend not to be specific just for heart in kids,” Dr. Snyder said. “If someone has anginal chest pain – shortness of breath, chest pain doing anything and everything, [chest pain that] occurs when they’re exercising, feels like an elephant standing on their chest – then we do encourage troponins on those patients.”
The guidance discourages ordering troponins without careful consideration of the patient’s age and condition, he said.
This list was developed by faculty in Pediatric Cardiology at University Hospitals in Cleveland. It was revised and approved by the AAP Section on Cardiology and Cardiac Surgery and the AAP Executive Committee.
A version of this article originally appeared on Medscape.com.
Proposed Medicare rule would expand CGM coverage
A new proposed rule from the Centers for Medicare & Medicaid Services (CMS) would expand coverage for continuous glucose monitors (CGMs) under Medicare to include devices that aren’t approved for making treatment decisions.
If accepted, the proposed rule would classify all approved CGMs as durable medical equipment under Medicare Part B and establish payment amounts for all related supplies. The move primarily affects Medtronic’s Guardian Connect System, which has not been approved by the U.S. Food and Drug Administration to replace the need for fingersticks in determining insulin or other glucose-lowering medication dosing.
Two other CGM systems, the Dexcom G6 and Abbott Libre, have “therapeutic” indications and are, therefore, already covered under Medicare, as is the combined insulin pump–CGM Tandem Diabetes Care Control-IQ Technology system.
According to a CMS statement, “CGMs that are not approved for use in making diabetes treatment decisions can be used to alert beneficiaries about potentially dangerous glucose levels while they sleep and that they should further test their glucose levels using a blood glucose monitor. ... This proposal would give Medicare beneficiaries and their physicians a wider range of technology and devices to choose from in managing diabetes.”
Sean Salmon, executive vice president and president of the Diabetes Group at Medtronic said in an interview that the company is “very encouraged” by the proposal. “Importantly, the proposed rule would enable continuity of therapy for people on Medtronic insulin pumps aging into Medicare – including Medtronic hybrid closed loop systems, which automatically adjust insulin delivery based on readings from the integrated CGM.”
The type 1 diabetes research and advocacy organization JDRF also applauded the proposed rule, noting in a statement, “CGM technology can be an integral component of artificial pancreas systems and important on its own to significantly improve diabetes management and enable users to avoid potential crises and risks for long-term complications. JDRF is heartened by this proposed change as it has long advocated for coverage, affordability and choice of all therapies to help ensure people with T1D have what they need to survive.”
The proposal is part of a broader set of proposed changes to Medicare Durable Medical Equipment, Prosthetics, Orthotic Devices and Supplies (DMEPOS) coverage and payment policies. Comments on the entire document can be submitted through Jan. 4, 2021 to the Federal Register.
A new proposed rule from the Centers for Medicare & Medicaid Services (CMS) would expand coverage for continuous glucose monitors (CGMs) under Medicare to include devices that aren’t approved for making treatment decisions.
If accepted, the proposed rule would classify all approved CGMs as durable medical equipment under Medicare Part B and establish payment amounts for all related supplies. The move primarily affects Medtronic’s Guardian Connect System, which has not been approved by the U.S. Food and Drug Administration to replace the need for fingersticks in determining insulin or other glucose-lowering medication dosing.
Two other CGM systems, the Dexcom G6 and Abbott Libre, have “therapeutic” indications and are, therefore, already covered under Medicare, as is the combined insulin pump–CGM Tandem Diabetes Care Control-IQ Technology system.
According to a CMS statement, “CGMs that are not approved for use in making diabetes treatment decisions can be used to alert beneficiaries about potentially dangerous glucose levels while they sleep and that they should further test their glucose levels using a blood glucose monitor. ... This proposal would give Medicare beneficiaries and their physicians a wider range of technology and devices to choose from in managing diabetes.”
Sean Salmon, executive vice president and president of the Diabetes Group at Medtronic said in an interview that the company is “very encouraged” by the proposal. “Importantly, the proposed rule would enable continuity of therapy for people on Medtronic insulin pumps aging into Medicare – including Medtronic hybrid closed loop systems, which automatically adjust insulin delivery based on readings from the integrated CGM.”
The type 1 diabetes research and advocacy organization JDRF also applauded the proposed rule, noting in a statement, “CGM technology can be an integral component of artificial pancreas systems and important on its own to significantly improve diabetes management and enable users to avoid potential crises and risks for long-term complications. JDRF is heartened by this proposed change as it has long advocated for coverage, affordability and choice of all therapies to help ensure people with T1D have what they need to survive.”
The proposal is part of a broader set of proposed changes to Medicare Durable Medical Equipment, Prosthetics, Orthotic Devices and Supplies (DMEPOS) coverage and payment policies. Comments on the entire document can be submitted through Jan. 4, 2021 to the Federal Register.
A new proposed rule from the Centers for Medicare & Medicaid Services (CMS) would expand coverage for continuous glucose monitors (CGMs) under Medicare to include devices that aren’t approved for making treatment decisions.
If accepted, the proposed rule would classify all approved CGMs as durable medical equipment under Medicare Part B and establish payment amounts for all related supplies. The move primarily affects Medtronic’s Guardian Connect System, which has not been approved by the U.S. Food and Drug Administration to replace the need for fingersticks in determining insulin or other glucose-lowering medication dosing.
Two other CGM systems, the Dexcom G6 and Abbott Libre, have “therapeutic” indications and are, therefore, already covered under Medicare, as is the combined insulin pump–CGM Tandem Diabetes Care Control-IQ Technology system.
According to a CMS statement, “CGMs that are not approved for use in making diabetes treatment decisions can be used to alert beneficiaries about potentially dangerous glucose levels while they sleep and that they should further test their glucose levels using a blood glucose monitor. ... This proposal would give Medicare beneficiaries and their physicians a wider range of technology and devices to choose from in managing diabetes.”
Sean Salmon, executive vice president and president of the Diabetes Group at Medtronic said in an interview that the company is “very encouraged” by the proposal. “Importantly, the proposed rule would enable continuity of therapy for people on Medtronic insulin pumps aging into Medicare – including Medtronic hybrid closed loop systems, which automatically adjust insulin delivery based on readings from the integrated CGM.”
The type 1 diabetes research and advocacy organization JDRF also applauded the proposed rule, noting in a statement, “CGM technology can be an integral component of artificial pancreas systems and important on its own to significantly improve diabetes management and enable users to avoid potential crises and risks for long-term complications. JDRF is heartened by this proposed change as it has long advocated for coverage, affordability and choice of all therapies to help ensure people with T1D have what they need to survive.”
The proposal is part of a broader set of proposed changes to Medicare Durable Medical Equipment, Prosthetics, Orthotic Devices and Supplies (DMEPOS) coverage and payment policies. Comments on the entire document can be submitted through Jan. 4, 2021 to the Federal Register.