User login
Is HIV criminalization the No. 1 barrier to ending the epidemic?
For many people, being told that they are HIV positive is no longer a death sentence. But for Robert Suttle, a Black gay man and social justice educator, it is a life sentence.
Unexpectedly caught up in the HIV criminalization web at the age of 30, Mr. Suttle spent 6 months in a Louisiana state prison for a consensual sexual relationship with an adult partner. The crime? Not disclosing his HIV-positive status, a charge that Mr. Suttle says is untrue.
“I did disclose my status to my partner; however, I can’t really answer how they might have received it,” he said.
Today, at the age of 42, Mr. Suttle still carries the indelible stain of a conviction and of being a registered sex offender. “After their diagnosis, criminal charge, and/or conviction, many people think they’re done – either ‘I’ve gotten out of prison’ or ‘I’m still on probation’ – whatever the case may be,” he explained. “But we’re still living out these collateral consequences, be it with housing, moving to another state, or finding a job.”
The same is true for HIV-positive people who are charged and tried but manage to dodge prison for one reason or another. Monique Howell, a straight, 40-year-old former army soldier and single mother of five children, said that she was afraid to disclose her HIV status to a sexual partner but did advise him to wear a condom.* She points to her DD14 discharge papers (i.e., forms that verify that someone served in the military) that were issued when her military duty was rescinded following the dismissal of her court case.
“I was going to reenlist, but I got in trouble,” she said. She explained that although a DD14 separation helps to ensure that she can receive benefits and care, the papers were issued with a caveat stating “serious offense,” an indelible stain that, like Mr. Suttle’s, will follow her for the rest of her life.
Laws criminalize myths and misconceptions
HIV criminalization laws subject persons whose behaviors may expose others to HIV to felony or misdemeanor charges. Depending on the state, they can carry prison terms ranging from less than 10 years to life, according to the Centers for Disease Control and Prevention.
Originally enacted at the height of the AIDS epidemic in 1986, when fear was rampant and hundreds were dying, the laws were intended to reduce HIV transmission. But they’ve had unintended consequences: Amplifying stigmatization and discrimination and perpetuating HIV myths and misconceptions, including how HIV is transmitted.
Decades of scientific advances challenge the most basic reasoning behind laws (for example, that transmission is possible via biting or spitting or through a single sexual act, which studies have shown poses a risk as low as 0%-1.4%). In addition, few laws reflect one of the most important HIV research findings of the past decade: undetectable equals untransmittable, meaning that the virus cannot be sexually transmitted by people who are taking antiretroviral therapy and whose viral loads are undetectable.
In most of these cases, individuals who are positive for HIV are charged and punished for unintentional exposure, not deliberate intent to harm. Moreover, for the charge to stick, sexual partners don’t need to have acquired the virus or prove the transmission source if they do become HIV positive.
Ms. Howell noted that it was the Army that brought the charges against her, not her sexual partner at that time (who, incidentally, tested negative). He even testified on her behalf at the trial. “I’ll never forget it,” she said. “He said, ‘I don’t want anything to happen to Monique; even if you put her behind bars, she’s still HIV-positive and she’s still got those children. She told me to get a condom, and I chose not to.’ ”
Criminal vs. clinical fallout
In 2018, 20 scientists across the world issued a consensus statement underscoring the fact that HIV criminalization laws are based on fallacies and faulty science. The statement (which remains one of the most accessed in the Journal of the International AIDS Society) also points out that 33 countries (including the United States) use general criminal statutes such as attempted murder or reckless endangerment to lengthen sentences when people with HIV commit crimes.
When the laws were created, “many were the equivalent [to general criminal laws], because HIV was seen as a death sentence,” explained Chris Beyrer MD, MPH, professor of public health and human rights at Johns Hopkins Bloomberg School of Public Health, Baltimore. “So, failure to disclose your status, to wear a condom was seen as risking someone else’s life, which is no longer the case,” he added.
In fact, “from the perspective of the kinds of impact that these laws have had on transmission, or risk, or behavior, what you find is that they really have no public health benefit and they have real public harms,” said Dr. Beyrer.
Claire Farel, MD, assistant professor and medical director of the UNC Infectious Diseases Clinic at the University of North Carolina at Chapel Hill, concurs. “Because of the criminalization undercurrent, there are people who don’t get tested, meaning that they are at risk for worse health outcomes, such as cancer, vascular disease, and of course HIV-related poor outcomes, including progression to AIDS.”
Farel also points to the residual stigma associated with HIV. “Much of this is inextricable from that surrounding homophobia, especially among young men of color who have sex with men. It opens up a larger conversation that a lot of people don’t want to engage in,” she said.
Laws broaden existing disparities even further
The CDC released a study June 4 showing substantial declines in the overall incidence of HIV in the United States, with an important caveat: There’s been a worsening disparity in cases. Access to care and engagement with care remain poor among certain populations. For example, Black individuals accounted for 41% of new HIV infections in 2019, but they represent only 12% of the U.S. population; Hispanic/Latinx persons accounted for 29% of new infections, although they represent only 17% of the entire population.
The same is true for HIV criminalization: In 2020, more than 50% of defendants were people of color, according to U.S. case data collated by the HIV Justice Network.
Still, the momentum to change these antiquated laws is gaining speed. In May, the Illinois State Senate passed a bill repealing HIV criminalization, and this past March, Virginia’s Governor Ralph Northam signed a bill lowering HIV-related criminalization charges from a felony to a misdemeanor and changing the wording of its law to include both intent and transmission.** California, Colorado, Iowa, Michigan, Nevada, and North Carolina have also modernized or repealed their laws.
Ending the U.S. HIV epidemic: Patients first
Without true HIV criminalization reform, efforts to change the public and clinical mindset regarding HIV from its being a highly stigmatized disease to a preventable, treatable infection are likely to fall short. Dr. Beyrer emphasized that the onus lies with the scientific and activist communities working together. “I don’t know how you can end the epidemic if you are still stigmatizing the people who are actually acquiring these infections,” he said.
There are steps that patients can take while these forces push for change.
“As people first process their diagnosis, they need to learn as much about HIV and the science behind it as possible,” advised Mr. Suttle. He said that to protect oneself, it’s essential to learn about HIV criminalization and the laws in one’s state.
“Find someone you can trust, starting with your medical provider if possible, and if you have a significant other, bring that person to your appointments so they can see that you are in care and doing all that you can do to lower viral loads and protect others,” he added.
Ms. Howell said that although people should be in treatment and care, attitudes also need to change on the clinician side. “We’re just given these meds, told to take them, and are sent on our merry ways, but they don’t tell us how to live our lives properly; nobody grabs us and says, hey, these are the laws and you need to know this or that.”
When a person who is HIV positive does get caught up in the system, if possible, that person should consult an attorney who understands these laws. Mr. Suttle suggested reaching out to organizations in the movement to end HIV criminalization (e.g., the Sero Project, the Center for HIV Law and Policy, or the Positive Women’s Network) for further support, help with cases (including providing experts to testify), social services, and other resources. Mr. Suttle also encourages people who need help and direction to reach out to him directly at rsuttle2000@gmail.com.
Forty years ago, the CDC published its first report of an illness in five healthy gay men living in Los Angeles. The first cases in women were reported shortly thereafter. Over the years, there have been many scientific advances in prevention and treatment. But as Dr. Beyrer aptly noted in an editorial published January 2021 in The Lancet HIV, “time has not lessened the sting of the early decades of AIDS.”
“We should not have to be afraid of who we are because we are HIV positive,” said Ms. Howell.
Dr. Farel, Mr. Suttle, and Ms. Howell report no relevant financial relationships. Dr. Beyrer has a consulting agreement with Merck.
A version of this article first appeared on Medscape.com.
*Correction, 6/14/2021: An earlier version of this story misstated Ms. Howell's age. She is 40.
**Correction, 6/14/2021: An earlier version of this story misspelled Gov. Northam's name.
For many people, being told that they are HIV positive is no longer a death sentence. But for Robert Suttle, a Black gay man and social justice educator, it is a life sentence.
Unexpectedly caught up in the HIV criminalization web at the age of 30, Mr. Suttle spent 6 months in a Louisiana state prison for a consensual sexual relationship with an adult partner. The crime? Not disclosing his HIV-positive status, a charge that Mr. Suttle says is untrue.
“I did disclose my status to my partner; however, I can’t really answer how they might have received it,” he said.
Today, at the age of 42, Mr. Suttle still carries the indelible stain of a conviction and of being a registered sex offender. “After their diagnosis, criminal charge, and/or conviction, many people think they’re done – either ‘I’ve gotten out of prison’ or ‘I’m still on probation’ – whatever the case may be,” he explained. “But we’re still living out these collateral consequences, be it with housing, moving to another state, or finding a job.”
The same is true for HIV-positive people who are charged and tried but manage to dodge prison for one reason or another. Monique Howell, a straight, 40-year-old former army soldier and single mother of five children, said that she was afraid to disclose her HIV status to a sexual partner but did advise him to wear a condom.* She points to her DD14 discharge papers (i.e., forms that verify that someone served in the military) that were issued when her military duty was rescinded following the dismissal of her court case.
“I was going to reenlist, but I got in trouble,” she said. She explained that although a DD14 separation helps to ensure that she can receive benefits and care, the papers were issued with a caveat stating “serious offense,” an indelible stain that, like Mr. Suttle’s, will follow her for the rest of her life.
Laws criminalize myths and misconceptions
HIV criminalization laws subject persons whose behaviors may expose others to HIV to felony or misdemeanor charges. Depending on the state, they can carry prison terms ranging from less than 10 years to life, according to the Centers for Disease Control and Prevention.
Originally enacted at the height of the AIDS epidemic in 1986, when fear was rampant and hundreds were dying, the laws were intended to reduce HIV transmission. But they’ve had unintended consequences: Amplifying stigmatization and discrimination and perpetuating HIV myths and misconceptions, including how HIV is transmitted.
Decades of scientific advances challenge the most basic reasoning behind laws (for example, that transmission is possible via biting or spitting or through a single sexual act, which studies have shown poses a risk as low as 0%-1.4%). In addition, few laws reflect one of the most important HIV research findings of the past decade: undetectable equals untransmittable, meaning that the virus cannot be sexually transmitted by people who are taking antiretroviral therapy and whose viral loads are undetectable.
In most of these cases, individuals who are positive for HIV are charged and punished for unintentional exposure, not deliberate intent to harm. Moreover, for the charge to stick, sexual partners don’t need to have acquired the virus or prove the transmission source if they do become HIV positive.
Ms. Howell noted that it was the Army that brought the charges against her, not her sexual partner at that time (who, incidentally, tested negative). He even testified on her behalf at the trial. “I’ll never forget it,” she said. “He said, ‘I don’t want anything to happen to Monique; even if you put her behind bars, she’s still HIV-positive and she’s still got those children. She told me to get a condom, and I chose not to.’ ”
Criminal vs. clinical fallout
In 2018, 20 scientists across the world issued a consensus statement underscoring the fact that HIV criminalization laws are based on fallacies and faulty science. The statement (which remains one of the most accessed in the Journal of the International AIDS Society) also points out that 33 countries (including the United States) use general criminal statutes such as attempted murder or reckless endangerment to lengthen sentences when people with HIV commit crimes.
When the laws were created, “many were the equivalent [to general criminal laws], because HIV was seen as a death sentence,” explained Chris Beyrer MD, MPH, professor of public health and human rights at Johns Hopkins Bloomberg School of Public Health, Baltimore. “So, failure to disclose your status, to wear a condom was seen as risking someone else’s life, which is no longer the case,” he added.
In fact, “from the perspective of the kinds of impact that these laws have had on transmission, or risk, or behavior, what you find is that they really have no public health benefit and they have real public harms,” said Dr. Beyrer.
Claire Farel, MD, assistant professor and medical director of the UNC Infectious Diseases Clinic at the University of North Carolina at Chapel Hill, concurs. “Because of the criminalization undercurrent, there are people who don’t get tested, meaning that they are at risk for worse health outcomes, such as cancer, vascular disease, and of course HIV-related poor outcomes, including progression to AIDS.”
Farel also points to the residual stigma associated with HIV. “Much of this is inextricable from that surrounding homophobia, especially among young men of color who have sex with men. It opens up a larger conversation that a lot of people don’t want to engage in,” she said.
Laws broaden existing disparities even further
The CDC released a study June 4 showing substantial declines in the overall incidence of HIV in the United States, with an important caveat: There’s been a worsening disparity in cases. Access to care and engagement with care remain poor among certain populations. For example, Black individuals accounted for 41% of new HIV infections in 2019, but they represent only 12% of the U.S. population; Hispanic/Latinx persons accounted for 29% of new infections, although they represent only 17% of the entire population.
The same is true for HIV criminalization: In 2020, more than 50% of defendants were people of color, according to U.S. case data collated by the HIV Justice Network.
Still, the momentum to change these antiquated laws is gaining speed. In May, the Illinois State Senate passed a bill repealing HIV criminalization, and this past March, Virginia’s Governor Ralph Northam signed a bill lowering HIV-related criminalization charges from a felony to a misdemeanor and changing the wording of its law to include both intent and transmission.** California, Colorado, Iowa, Michigan, Nevada, and North Carolina have also modernized or repealed their laws.
Ending the U.S. HIV epidemic: Patients first
Without true HIV criminalization reform, efforts to change the public and clinical mindset regarding HIV from its being a highly stigmatized disease to a preventable, treatable infection are likely to fall short. Dr. Beyrer emphasized that the onus lies with the scientific and activist communities working together. “I don’t know how you can end the epidemic if you are still stigmatizing the people who are actually acquiring these infections,” he said.
There are steps that patients can take while these forces push for change.
“As people first process their diagnosis, they need to learn as much about HIV and the science behind it as possible,” advised Mr. Suttle. He said that to protect oneself, it’s essential to learn about HIV criminalization and the laws in one’s state.
“Find someone you can trust, starting with your medical provider if possible, and if you have a significant other, bring that person to your appointments so they can see that you are in care and doing all that you can do to lower viral loads and protect others,” he added.
Ms. Howell said that although people should be in treatment and care, attitudes also need to change on the clinician side. “We’re just given these meds, told to take them, and are sent on our merry ways, but they don’t tell us how to live our lives properly; nobody grabs us and says, hey, these are the laws and you need to know this or that.”
When a person who is HIV positive does get caught up in the system, if possible, that person should consult an attorney who understands these laws. Mr. Suttle suggested reaching out to organizations in the movement to end HIV criminalization (e.g., the Sero Project, the Center for HIV Law and Policy, or the Positive Women’s Network) for further support, help with cases (including providing experts to testify), social services, and other resources. Mr. Suttle also encourages people who need help and direction to reach out to him directly at rsuttle2000@gmail.com.
Forty years ago, the CDC published its first report of an illness in five healthy gay men living in Los Angeles. The first cases in women were reported shortly thereafter. Over the years, there have been many scientific advances in prevention and treatment. But as Dr. Beyrer aptly noted in an editorial published January 2021 in The Lancet HIV, “time has not lessened the sting of the early decades of AIDS.”
“We should not have to be afraid of who we are because we are HIV positive,” said Ms. Howell.
Dr. Farel, Mr. Suttle, and Ms. Howell report no relevant financial relationships. Dr. Beyrer has a consulting agreement with Merck.
A version of this article first appeared on Medscape.com.
*Correction, 6/14/2021: An earlier version of this story misstated Ms. Howell's age. She is 40.
**Correction, 6/14/2021: An earlier version of this story misspelled Gov. Northam's name.
For many people, being told that they are HIV positive is no longer a death sentence. But for Robert Suttle, a Black gay man and social justice educator, it is a life sentence.
Unexpectedly caught up in the HIV criminalization web at the age of 30, Mr. Suttle spent 6 months in a Louisiana state prison for a consensual sexual relationship with an adult partner. The crime? Not disclosing his HIV-positive status, a charge that Mr. Suttle says is untrue.
“I did disclose my status to my partner; however, I can’t really answer how they might have received it,” he said.
Today, at the age of 42, Mr. Suttle still carries the indelible stain of a conviction and of being a registered sex offender. “After their diagnosis, criminal charge, and/or conviction, many people think they’re done – either ‘I’ve gotten out of prison’ or ‘I’m still on probation’ – whatever the case may be,” he explained. “But we’re still living out these collateral consequences, be it with housing, moving to another state, or finding a job.”
The same is true for HIV-positive people who are charged and tried but manage to dodge prison for one reason or another. Monique Howell, a straight, 40-year-old former army soldier and single mother of five children, said that she was afraid to disclose her HIV status to a sexual partner but did advise him to wear a condom.* She points to her DD14 discharge papers (i.e., forms that verify that someone served in the military) that were issued when her military duty was rescinded following the dismissal of her court case.
“I was going to reenlist, but I got in trouble,” she said. She explained that although a DD14 separation helps to ensure that she can receive benefits and care, the papers were issued with a caveat stating “serious offense,” an indelible stain that, like Mr. Suttle’s, will follow her for the rest of her life.
Laws criminalize myths and misconceptions
HIV criminalization laws subject persons whose behaviors may expose others to HIV to felony or misdemeanor charges. Depending on the state, they can carry prison terms ranging from less than 10 years to life, according to the Centers for Disease Control and Prevention.
Originally enacted at the height of the AIDS epidemic in 1986, when fear was rampant and hundreds were dying, the laws were intended to reduce HIV transmission. But they’ve had unintended consequences: Amplifying stigmatization and discrimination and perpetuating HIV myths and misconceptions, including how HIV is transmitted.
Decades of scientific advances challenge the most basic reasoning behind laws (for example, that transmission is possible via biting or spitting or through a single sexual act, which studies have shown poses a risk as low as 0%-1.4%). In addition, few laws reflect one of the most important HIV research findings of the past decade: undetectable equals untransmittable, meaning that the virus cannot be sexually transmitted by people who are taking antiretroviral therapy and whose viral loads are undetectable.
In most of these cases, individuals who are positive for HIV are charged and punished for unintentional exposure, not deliberate intent to harm. Moreover, for the charge to stick, sexual partners don’t need to have acquired the virus or prove the transmission source if they do become HIV positive.
Ms. Howell noted that it was the Army that brought the charges against her, not her sexual partner at that time (who, incidentally, tested negative). He even testified on her behalf at the trial. “I’ll never forget it,” she said. “He said, ‘I don’t want anything to happen to Monique; even if you put her behind bars, she’s still HIV-positive and she’s still got those children. She told me to get a condom, and I chose not to.’ ”
Criminal vs. clinical fallout
In 2018, 20 scientists across the world issued a consensus statement underscoring the fact that HIV criminalization laws are based on fallacies and faulty science. The statement (which remains one of the most accessed in the Journal of the International AIDS Society) also points out that 33 countries (including the United States) use general criminal statutes such as attempted murder or reckless endangerment to lengthen sentences when people with HIV commit crimes.
When the laws were created, “many were the equivalent [to general criminal laws], because HIV was seen as a death sentence,” explained Chris Beyrer MD, MPH, professor of public health and human rights at Johns Hopkins Bloomberg School of Public Health, Baltimore. “So, failure to disclose your status, to wear a condom was seen as risking someone else’s life, which is no longer the case,” he added.
In fact, “from the perspective of the kinds of impact that these laws have had on transmission, or risk, or behavior, what you find is that they really have no public health benefit and they have real public harms,” said Dr. Beyrer.
Claire Farel, MD, assistant professor and medical director of the UNC Infectious Diseases Clinic at the University of North Carolina at Chapel Hill, concurs. “Because of the criminalization undercurrent, there are people who don’t get tested, meaning that they are at risk for worse health outcomes, such as cancer, vascular disease, and of course HIV-related poor outcomes, including progression to AIDS.”
Farel also points to the residual stigma associated with HIV. “Much of this is inextricable from that surrounding homophobia, especially among young men of color who have sex with men. It opens up a larger conversation that a lot of people don’t want to engage in,” she said.
Laws broaden existing disparities even further
The CDC released a study June 4 showing substantial declines in the overall incidence of HIV in the United States, with an important caveat: There’s been a worsening disparity in cases. Access to care and engagement with care remain poor among certain populations. For example, Black individuals accounted for 41% of new HIV infections in 2019, but they represent only 12% of the U.S. population; Hispanic/Latinx persons accounted for 29% of new infections, although they represent only 17% of the entire population.
The same is true for HIV criminalization: In 2020, more than 50% of defendants were people of color, according to U.S. case data collated by the HIV Justice Network.
Still, the momentum to change these antiquated laws is gaining speed. In May, the Illinois State Senate passed a bill repealing HIV criminalization, and this past March, Virginia’s Governor Ralph Northam signed a bill lowering HIV-related criminalization charges from a felony to a misdemeanor and changing the wording of its law to include both intent and transmission.** California, Colorado, Iowa, Michigan, Nevada, and North Carolina have also modernized or repealed their laws.
Ending the U.S. HIV epidemic: Patients first
Without true HIV criminalization reform, efforts to change the public and clinical mindset regarding HIV from its being a highly stigmatized disease to a preventable, treatable infection are likely to fall short. Dr. Beyrer emphasized that the onus lies with the scientific and activist communities working together. “I don’t know how you can end the epidemic if you are still stigmatizing the people who are actually acquiring these infections,” he said.
There are steps that patients can take while these forces push for change.
“As people first process their diagnosis, they need to learn as much about HIV and the science behind it as possible,” advised Mr. Suttle. He said that to protect oneself, it’s essential to learn about HIV criminalization and the laws in one’s state.
“Find someone you can trust, starting with your medical provider if possible, and if you have a significant other, bring that person to your appointments so they can see that you are in care and doing all that you can do to lower viral loads and protect others,” he added.
Ms. Howell said that although people should be in treatment and care, attitudes also need to change on the clinician side. “We’re just given these meds, told to take them, and are sent on our merry ways, but they don’t tell us how to live our lives properly; nobody grabs us and says, hey, these are the laws and you need to know this or that.”
When a person who is HIV positive does get caught up in the system, if possible, that person should consult an attorney who understands these laws. Mr. Suttle suggested reaching out to organizations in the movement to end HIV criminalization (e.g., the Sero Project, the Center for HIV Law and Policy, or the Positive Women’s Network) for further support, help with cases (including providing experts to testify), social services, and other resources. Mr. Suttle also encourages people who need help and direction to reach out to him directly at rsuttle2000@gmail.com.
Forty years ago, the CDC published its first report of an illness in five healthy gay men living in Los Angeles. The first cases in women were reported shortly thereafter. Over the years, there have been many scientific advances in prevention and treatment. But as Dr. Beyrer aptly noted in an editorial published January 2021 in The Lancet HIV, “time has not lessened the sting of the early decades of AIDS.”
“We should not have to be afraid of who we are because we are HIV positive,” said Ms. Howell.
Dr. Farel, Mr. Suttle, and Ms. Howell report no relevant financial relationships. Dr. Beyrer has a consulting agreement with Merck.
A version of this article first appeared on Medscape.com.
*Correction, 6/14/2021: An earlier version of this story misstated Ms. Howell's age. She is 40.
**Correction, 6/14/2021: An earlier version of this story misspelled Gov. Northam's name.
Zero-burnout practices often solo, physician-owned
according to an analysis published June 7 in Health Affairs.
The findings may have particular significance in an era when more physicians are being employed by hospitals and health systems, says lead author Samuel T. Edwards, MD, an assistant professor of medicine at Oregon Health & Science University, Portland.
“Market forces and various reform efforts have driven practices to consolidate, and we certainly see some signal here that burnout might be a potential negative consequence of that,” said Dr. Edwards, who is also a staff physician in internal medicine at the Veterans Affairs Portland Health Care System.
30% of practices reported zero burnout
Dr. Edwards told this news organization that he was surprised that 30% of the practices surveyed for this analysis reported zero burnout – meaning no member of the practice reported burnout – because reports of burnout are so pervasive in medicine.
For comparison, in 13% of practices surveyed, more than 40% of practice members reported burnout.
Burnout was assessed with a five-point measure that correlates with the emotional exhaustion scale of the Maslach Burnout Inventory.
It was also surprising, Dr. Edwards said, that practices with some of the heaviest workloads – solo practitioners juggling large numbers of patients, insurance plans, and regulatory requirements – were much more likely than larger practices to report zero burnout.
In this study, solo practices were 5.3 times as likely as practices with 6 to 10 clinicians to report zero burnout (95% confidence interval, 1.25-22.6).
The researchers found no link between burnout and patient volume or the proportion of patients with Medicaid insurance.
“People assume that working harder is associated with more burnout, and there are lots of studies that say that’s true. But in our study, it appears that people work really hard in some settings and are not burned out,” Dr. Edwards said.
He says in small offices, there may be a stronger sense of agency, a sense that everyone is on the same team, and there may be stronger relationships with patients.
The study included survey data from 715 small- to medium-size primary care practices in the United States that participated in the Agency for Healthcare Research and Quality’s EvidenceNOW quality improvement initiative between September 2015 and June 2017.
Zero-burnout practices shared several traits. They were more likely to have “a strong practice culture – one in which teamwork, communication, psychological safety, mindfulness of others, facilitative leadership, and understanding that people make and can learn from mistakes were among the key attributes,” Dr. Edwards and colleagues write.
Burnout higher with ACO participation
Organizations that participated in ACOs and other external primary care transformation projects were more likely to have high burnout rates. Specifically, 29% of these practices reported zero burnout, versus 53% that reported high rates of burnout.
Dr. Edwards said the reasons for that are unclear in this cross-sectional study, but there seemed to be an indication that getting involved in too many demonstration projects might be associated with burnout. He noted that participants in this study were already involved in the EvidenceNOW initiative.
Factors regarding electronic health records (EHRs) were not tied to burnout in this study. Dr. Edwards said they surveyed for both satisfaction with EHRs and EHR features and whether they were linked to zero burnout.
He speculates that this may indicate that by now, practices have adapted to using EHRs, though they continue to be a source of frustration for individual clinicians.
Debora Goetz Goldberg, PhD, MHA, MBA, associate professor at George Mason University, McLean, Virginia, told this news organization that she has found similar results in her research of primary care practices and burnout. She found that health system–owned practices had higher levels of burnout.
“We thought that probably was related to less autonomy and decision-making authority,” she said.
She pointed out that Dr. Edwards and colleagues found that physicians who had more “adaptive reserves” were more likely to have zero burnout. Her research found a similar association.
Such organizations, she explained, have a higher level of organizational development and a culture of innovation. They are more comfortable with change and adapt well.
“They are characterized by teamwork, strong communication, and a culture of learning,” she said.
By contrast, burnout may be higher in health system–owned practices because clinicians may feel they have less control over their work environment and feel a loss of autonomy, according to Dr. Goldberg.
“Moral distress,” which can happen when an individual’s professional values don’t line up with an organization’s values, may also play a part, she said. Physicians may be required to see more patients than they feel they can serve well in a day, for instance.
Reducing burnout may take building a more collaborative leadership style, she said.
No link between burnout and patient volume
The current research also highlighted leadership style as a potential driver of burnout.
Dr. Edwards and colleagues found that one of the strongest associations was between facilitative leadership and low burnout. Zero burnout is associated with participatory decision-making.
“Interestingly, we saw that that kind of leadership could exist in multiple settings,” he said. Health care professionals in smaller practices might know each other better and have a shared mission, but shared decision making can also exist in larger practices, he said.
Higher burnout was associated with traditional leadership models that are hierarchical and that operate with a command-and-control structure, according to the study.
The data may have implications for strategies regarding both the smallest and largest practices.
Initiatives that help small practices remain strong are valuable, especially for communities that depend on those practices, Dr. Edwards said.
The researchers give as an example the funding of primary care practice extension networks, which provide support similar to agricultural extension programs for farmers.
At the same time, “having agency at the practice level about how things work is really important in reducing burnout. So in a large system, finding ways to promote agency at the most local level possible can really help with burnout,” he said.
Dr. Edwards said his team controlled for the fact that mathematically, it’s more likely zero burnout would be reported in a solo practice than in a larger practice.
Every practice in this study, he said, had to have at least three persons who responded to the survey, and responses had to represent three roles – a clinician, a nonclinician staff member, and a clinical staff member. The response rate also had to be 50% within the practice, he explained.
All authors are supported by the Agency for Healthcare Research and Quality. Dr. Edwards was also supported by the Department of Veterans Affairs Health Services Research and Development. Dr. Goldberg has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to an analysis published June 7 in Health Affairs.
The findings may have particular significance in an era when more physicians are being employed by hospitals and health systems, says lead author Samuel T. Edwards, MD, an assistant professor of medicine at Oregon Health & Science University, Portland.
“Market forces and various reform efforts have driven practices to consolidate, and we certainly see some signal here that burnout might be a potential negative consequence of that,” said Dr. Edwards, who is also a staff physician in internal medicine at the Veterans Affairs Portland Health Care System.
30% of practices reported zero burnout
Dr. Edwards told this news organization that he was surprised that 30% of the practices surveyed for this analysis reported zero burnout – meaning no member of the practice reported burnout – because reports of burnout are so pervasive in medicine.
For comparison, in 13% of practices surveyed, more than 40% of practice members reported burnout.
Burnout was assessed with a five-point measure that correlates with the emotional exhaustion scale of the Maslach Burnout Inventory.
It was also surprising, Dr. Edwards said, that practices with some of the heaviest workloads – solo practitioners juggling large numbers of patients, insurance plans, and regulatory requirements – were much more likely than larger practices to report zero burnout.
In this study, solo practices were 5.3 times as likely as practices with 6 to 10 clinicians to report zero burnout (95% confidence interval, 1.25-22.6).
The researchers found no link between burnout and patient volume or the proportion of patients with Medicaid insurance.
“People assume that working harder is associated with more burnout, and there are lots of studies that say that’s true. But in our study, it appears that people work really hard in some settings and are not burned out,” Dr. Edwards said.
He says in small offices, there may be a stronger sense of agency, a sense that everyone is on the same team, and there may be stronger relationships with patients.
The study included survey data from 715 small- to medium-size primary care practices in the United States that participated in the Agency for Healthcare Research and Quality’s EvidenceNOW quality improvement initiative between September 2015 and June 2017.
Zero-burnout practices shared several traits. They were more likely to have “a strong practice culture – one in which teamwork, communication, psychological safety, mindfulness of others, facilitative leadership, and understanding that people make and can learn from mistakes were among the key attributes,” Dr. Edwards and colleagues write.
Burnout higher with ACO participation
Organizations that participated in ACOs and other external primary care transformation projects were more likely to have high burnout rates. Specifically, 29% of these practices reported zero burnout, versus 53% that reported high rates of burnout.
Dr. Edwards said the reasons for that are unclear in this cross-sectional study, but there seemed to be an indication that getting involved in too many demonstration projects might be associated with burnout. He noted that participants in this study were already involved in the EvidenceNOW initiative.
Factors regarding electronic health records (EHRs) were not tied to burnout in this study. Dr. Edwards said they surveyed for both satisfaction with EHRs and EHR features and whether they were linked to zero burnout.
He speculates that this may indicate that by now, practices have adapted to using EHRs, though they continue to be a source of frustration for individual clinicians.
Debora Goetz Goldberg, PhD, MHA, MBA, associate professor at George Mason University, McLean, Virginia, told this news organization that she has found similar results in her research of primary care practices and burnout. She found that health system–owned practices had higher levels of burnout.
“We thought that probably was related to less autonomy and decision-making authority,” she said.
She pointed out that Dr. Edwards and colleagues found that physicians who had more “adaptive reserves” were more likely to have zero burnout. Her research found a similar association.
Such organizations, she explained, have a higher level of organizational development and a culture of innovation. They are more comfortable with change and adapt well.
“They are characterized by teamwork, strong communication, and a culture of learning,” she said.
By contrast, burnout may be higher in health system–owned practices because clinicians may feel they have less control over their work environment and feel a loss of autonomy, according to Dr. Goldberg.
“Moral distress,” which can happen when an individual’s professional values don’t line up with an organization’s values, may also play a part, she said. Physicians may be required to see more patients than they feel they can serve well in a day, for instance.
Reducing burnout may take building a more collaborative leadership style, she said.
No link between burnout and patient volume
The current research also highlighted leadership style as a potential driver of burnout.
Dr. Edwards and colleagues found that one of the strongest associations was between facilitative leadership and low burnout. Zero burnout is associated with participatory decision-making.
“Interestingly, we saw that that kind of leadership could exist in multiple settings,” he said. Health care professionals in smaller practices might know each other better and have a shared mission, but shared decision making can also exist in larger practices, he said.
Higher burnout was associated with traditional leadership models that are hierarchical and that operate with a command-and-control structure, according to the study.
The data may have implications for strategies regarding both the smallest and largest practices.
Initiatives that help small practices remain strong are valuable, especially for communities that depend on those practices, Dr. Edwards said.
The researchers give as an example the funding of primary care practice extension networks, which provide support similar to agricultural extension programs for farmers.
At the same time, “having agency at the practice level about how things work is really important in reducing burnout. So in a large system, finding ways to promote agency at the most local level possible can really help with burnout,” he said.
Dr. Edwards said his team controlled for the fact that mathematically, it’s more likely zero burnout would be reported in a solo practice than in a larger practice.
Every practice in this study, he said, had to have at least three persons who responded to the survey, and responses had to represent three roles – a clinician, a nonclinician staff member, and a clinical staff member. The response rate also had to be 50% within the practice, he explained.
All authors are supported by the Agency for Healthcare Research and Quality. Dr. Edwards was also supported by the Department of Veterans Affairs Health Services Research and Development. Dr. Goldberg has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to an analysis published June 7 in Health Affairs.
The findings may have particular significance in an era when more physicians are being employed by hospitals and health systems, says lead author Samuel T. Edwards, MD, an assistant professor of medicine at Oregon Health & Science University, Portland.
“Market forces and various reform efforts have driven practices to consolidate, and we certainly see some signal here that burnout might be a potential negative consequence of that,” said Dr. Edwards, who is also a staff physician in internal medicine at the Veterans Affairs Portland Health Care System.
30% of practices reported zero burnout
Dr. Edwards told this news organization that he was surprised that 30% of the practices surveyed for this analysis reported zero burnout – meaning no member of the practice reported burnout – because reports of burnout are so pervasive in medicine.
For comparison, in 13% of practices surveyed, more than 40% of practice members reported burnout.
Burnout was assessed with a five-point measure that correlates with the emotional exhaustion scale of the Maslach Burnout Inventory.
It was also surprising, Dr. Edwards said, that practices with some of the heaviest workloads – solo practitioners juggling large numbers of patients, insurance plans, and regulatory requirements – were much more likely than larger practices to report zero burnout.
In this study, solo practices were 5.3 times as likely as practices with 6 to 10 clinicians to report zero burnout (95% confidence interval, 1.25-22.6).
The researchers found no link between burnout and patient volume or the proportion of patients with Medicaid insurance.
“People assume that working harder is associated with more burnout, and there are lots of studies that say that’s true. But in our study, it appears that people work really hard in some settings and are not burned out,” Dr. Edwards said.
He says in small offices, there may be a stronger sense of agency, a sense that everyone is on the same team, and there may be stronger relationships with patients.
The study included survey data from 715 small- to medium-size primary care practices in the United States that participated in the Agency for Healthcare Research and Quality’s EvidenceNOW quality improvement initiative between September 2015 and June 2017.
Zero-burnout practices shared several traits. They were more likely to have “a strong practice culture – one in which teamwork, communication, psychological safety, mindfulness of others, facilitative leadership, and understanding that people make and can learn from mistakes were among the key attributes,” Dr. Edwards and colleagues write.
Burnout higher with ACO participation
Organizations that participated in ACOs and other external primary care transformation projects were more likely to have high burnout rates. Specifically, 29% of these practices reported zero burnout, versus 53% that reported high rates of burnout.
Dr. Edwards said the reasons for that are unclear in this cross-sectional study, but there seemed to be an indication that getting involved in too many demonstration projects might be associated with burnout. He noted that participants in this study were already involved in the EvidenceNOW initiative.
Factors regarding electronic health records (EHRs) were not tied to burnout in this study. Dr. Edwards said they surveyed for both satisfaction with EHRs and EHR features and whether they were linked to zero burnout.
He speculates that this may indicate that by now, practices have adapted to using EHRs, though they continue to be a source of frustration for individual clinicians.
Debora Goetz Goldberg, PhD, MHA, MBA, associate professor at George Mason University, McLean, Virginia, told this news organization that she has found similar results in her research of primary care practices and burnout. She found that health system–owned practices had higher levels of burnout.
“We thought that probably was related to less autonomy and decision-making authority,” she said.
She pointed out that Dr. Edwards and colleagues found that physicians who had more “adaptive reserves” were more likely to have zero burnout. Her research found a similar association.
Such organizations, she explained, have a higher level of organizational development and a culture of innovation. They are more comfortable with change and adapt well.
“They are characterized by teamwork, strong communication, and a culture of learning,” she said.
By contrast, burnout may be higher in health system–owned practices because clinicians may feel they have less control over their work environment and feel a loss of autonomy, according to Dr. Goldberg.
“Moral distress,” which can happen when an individual’s professional values don’t line up with an organization’s values, may also play a part, she said. Physicians may be required to see more patients than they feel they can serve well in a day, for instance.
Reducing burnout may take building a more collaborative leadership style, she said.
No link between burnout and patient volume
The current research also highlighted leadership style as a potential driver of burnout.
Dr. Edwards and colleagues found that one of the strongest associations was between facilitative leadership and low burnout. Zero burnout is associated with participatory decision-making.
“Interestingly, we saw that that kind of leadership could exist in multiple settings,” he said. Health care professionals in smaller practices might know each other better and have a shared mission, but shared decision making can also exist in larger practices, he said.
Higher burnout was associated with traditional leadership models that are hierarchical and that operate with a command-and-control structure, according to the study.
The data may have implications for strategies regarding both the smallest and largest practices.
Initiatives that help small practices remain strong are valuable, especially for communities that depend on those practices, Dr. Edwards said.
The researchers give as an example the funding of primary care practice extension networks, which provide support similar to agricultural extension programs for farmers.
At the same time, “having agency at the practice level about how things work is really important in reducing burnout. So in a large system, finding ways to promote agency at the most local level possible can really help with burnout,” he said.
Dr. Edwards said his team controlled for the fact that mathematically, it’s more likely zero burnout would be reported in a solo practice than in a larger practice.
Every practice in this study, he said, had to have at least three persons who responded to the survey, and responses had to represent three roles – a clinician, a nonclinician staff member, and a clinical staff member. The response rate also had to be 50% within the practice, he explained.
All authors are supported by the Agency for Healthcare Research and Quality. Dr. Edwards was also supported by the Department of Veterans Affairs Health Services Research and Development. Dr. Goldberg has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The pandemic changed smokers, but farming didn’t change humans
Pandemic smoking: More or less?
The COVID-19 pandemic has changed a lot of habits in people, for better or worse. Some people may have turned to food and alcohol for comfort, while others started on health kicks to emerge from the ordeal as new people. Well, the same can be said about smokers.

New evidence comes from a survey conducted from May to July 2020 of 694 current and former smokers with an average age of 53 years. All had been hospitalized prior to the pandemic and had previously participated in clinical trials to for smoking cessation in Boston, Nashville, and Pittsburgh hospitals.
Researchers found that 32% of participants smoked more, 37% smoked less, and 31% made no change in their smoking habits. By the time of the survey, 28% of former smokers had relapsed. Although 68% of the participants believed smoking increased the risk of getting COVID-19, that still didn’t stop some people from smoking more. Why?
Respondents “might have increased their smoking due to stress and boredom. On the other hand, the fear of catching COVID might have led them to cut down or quit smoking,” said lead author Nancy A. Rigotti, MD. “Even before the pandemic, tobacco smoking was the leading preventable cause of death in the United States. COVID-19 has given smokers yet another good reason to stop smoking.”
This creates an opportunity for physicians to preach the gospel to smokers about their vulnerability to respiratory disease in hopes of getting them to quit for good. We just wish the same could be said for all of our excessive pandemic online shopping.
3,000 years and just one pair of genomes to wear
Men and women are different. We’ll give you a moment to pick your jaw off the ground.
It makes sense though, the sexes being different, especially when you look at the broader animal kingdom. The males and females of many species are slightly different when it comes to size and shape, but there’s a big question that literally only anthropologists have asked: Were human males and females more different in the past than they are today?

To be more specific, some scientists believe that males and females grew more similar when humans shifted from a hunter-gatherer lifestyle to a farming-based lifestyle, as agriculture encouraged a more equitable division of labor. Others believe that the differences come down to random chance.
Researchers from Penn State University analyzed genomic data from over 350,000 males and females stored in the UK Biobank and looked at the recent (within the last ~3,000 years; post-agriculture adoption in Britain) evolutionary histories of these loci. Height, body mass, hip circumference, body fat percentage, and waist circumference were analyzed, and while there were thousands of differences in the genomes, only one trait occurred more frequently during that time period: Females gained a significantly higher body fat content than males.
It’s a sad day then for the millions of people who were big fans of the “farming caused men and women to become more similar” theory. Count the LOTME crew among them. Be honest: Wouldn’t life be so much simpler if men and women were exactly the same? Just think about it, no more arguments about leaving the toilet seat up. It’d be worth it just for that.
Proteins don’t lie
Research published in Open Biology shows that the human brain contains 14,315 different proteins. The team conducting that study wanted to find out which organ was the most similar to the old brain box, so they did protein counts for the 32 other major tissue types, including heart, salivary gland, lung, spleen, and endometrium.
The tissue with the most proteins in common with the center of human intelligence? You’re thinking it has to be colon at this point, right? We were sure it was going to be colon, but it’s not.
The winner, with 13,442 shared proteins, is the testes. The testes have 15,687 proteins, of which 85.7% are shared with the brain. The researchers, sadly, did not provide protein counts for the other tissue types, but we bet colon was a close second.
Dreaming about COVID?
We thought we were the only ones who have been having crazy dreams lately. Each one seems crazier and more vivid than the one before. Have you been having weird dreams lately?

This is likely your brain’s coping mechanism to handle your pandemic stress, according to Dr. Erik Hoel of Tufts University. Dreams that are crazy and scary might make real life seem lighter and simpler. He calls it the “overfitted brain hypothesis.”
“It is their very strangeness that gives them their biological function,” Dr. Hoel said. It literally makes you feel like COVID-19 and lockdowns aren’t as scary as they seem.
We always knew our minds were powerful things. Apparently, your brain gets tired of everyday familiarity just like you do, and it creates crazy dreams to keep things interesting.
Just remember: That recurring dream that you’re back in college and missing 10 assignments is there to help you, not scare you! Even though it is pretty scary.
Pandemic smoking: More or less?
The COVID-19 pandemic has changed a lot of habits in people, for better or worse. Some people may have turned to food and alcohol for comfort, while others started on health kicks to emerge from the ordeal as new people. Well, the same can be said about smokers.
New evidence comes from a survey conducted from May to July 2020 of 694 current and former smokers with an average age of 53 years. All had been hospitalized prior to the pandemic and had previously participated in clinical trials to for smoking cessation in Boston, Nashville, and Pittsburgh hospitals.
Researchers found that 32% of participants smoked more, 37% smoked less, and 31% made no change in their smoking habits. By the time of the survey, 28% of former smokers had relapsed. Although 68% of the participants believed smoking increased the risk of getting COVID-19, that still didn’t stop some people from smoking more. Why?
Respondents “might have increased their smoking due to stress and boredom. On the other hand, the fear of catching COVID might have led them to cut down or quit smoking,” said lead author Nancy A. Rigotti, MD. “Even before the pandemic, tobacco smoking was the leading preventable cause of death in the United States. COVID-19 has given smokers yet another good reason to stop smoking.”
This creates an opportunity for physicians to preach the gospel to smokers about their vulnerability to respiratory disease in hopes of getting them to quit for good. We just wish the same could be said for all of our excessive pandemic online shopping.
3,000 years and just one pair of genomes to wear
Men and women are different. We’ll give you a moment to pick your jaw off the ground.
It makes sense though, the sexes being different, especially when you look at the broader animal kingdom. The males and females of many species are slightly different when it comes to size and shape, but there’s a big question that literally only anthropologists have asked: Were human males and females more different in the past than they are today?
To be more specific, some scientists believe that males and females grew more similar when humans shifted from a hunter-gatherer lifestyle to a farming-based lifestyle, as agriculture encouraged a more equitable division of labor. Others believe that the differences come down to random chance.
Researchers from Penn State University analyzed genomic data from over 350,000 males and females stored in the UK Biobank and looked at the recent (within the last ~3,000 years; post-agriculture adoption in Britain) evolutionary histories of these loci. Height, body mass, hip circumference, body fat percentage, and waist circumference were analyzed, and while there were thousands of differences in the genomes, only one trait occurred more frequently during that time period: Females gained a significantly higher body fat content than males.
It’s a sad day then for the millions of people who were big fans of the “farming caused men and women to become more similar” theory. Count the LOTME crew among them. Be honest: Wouldn’t life be so much simpler if men and women were exactly the same? Just think about it, no more arguments about leaving the toilet seat up. It’d be worth it just for that.
Proteins don’t lie
Research published in Open Biology shows that the human brain contains 14,315 different proteins. The team conducting that study wanted to find out which organ was the most similar to the old brain box, so they did protein counts for the 32 other major tissue types, including heart, salivary gland, lung, spleen, and endometrium.
The tissue with the most proteins in common with the center of human intelligence? You’re thinking it has to be colon at this point, right? We were sure it was going to be colon, but it’s not.
The winner, with 13,442 shared proteins, is the testes. The testes have 15,687 proteins, of which 85.7% are shared with the brain. The researchers, sadly, did not provide protein counts for the other tissue types, but we bet colon was a close second.
Dreaming about COVID?
We thought we were the only ones who have been having crazy dreams lately. Each one seems crazier and more vivid than the one before. Have you been having weird dreams lately?
This is likely your brain’s coping mechanism to handle your pandemic stress, according to Dr. Erik Hoel of Tufts University. Dreams that are crazy and scary might make real life seem lighter and simpler. He calls it the “overfitted brain hypothesis.”
“It is their very strangeness that gives them their biological function,” Dr. Hoel said. It literally makes you feel like COVID-19 and lockdowns aren’t as scary as they seem.
We always knew our minds were powerful things. Apparently, your brain gets tired of everyday familiarity just like you do, and it creates crazy dreams to keep things interesting.
Just remember: That recurring dream that you’re back in college and missing 10 assignments is there to help you, not scare you! Even though it is pretty scary.
Pandemic smoking: More or less?
The COVID-19 pandemic has changed a lot of habits in people, for better or worse. Some people may have turned to food and alcohol for comfort, while others started on health kicks to emerge from the ordeal as new people. Well, the same can be said about smokers.
New evidence comes from a survey conducted from May to July 2020 of 694 current and former smokers with an average age of 53 years. All had been hospitalized prior to the pandemic and had previously participated in clinical trials to for smoking cessation in Boston, Nashville, and Pittsburgh hospitals.
Researchers found that 32% of participants smoked more, 37% smoked less, and 31% made no change in their smoking habits. By the time of the survey, 28% of former smokers had relapsed. Although 68% of the participants believed smoking increased the risk of getting COVID-19, that still didn’t stop some people from smoking more. Why?
Respondents “might have increased their smoking due to stress and boredom. On the other hand, the fear of catching COVID might have led them to cut down or quit smoking,” said lead author Nancy A. Rigotti, MD. “Even before the pandemic, tobacco smoking was the leading preventable cause of death in the United States. COVID-19 has given smokers yet another good reason to stop smoking.”
This creates an opportunity for physicians to preach the gospel to smokers about their vulnerability to respiratory disease in hopes of getting them to quit for good. We just wish the same could be said for all of our excessive pandemic online shopping.
3,000 years and just one pair of genomes to wear
Men and women are different. We’ll give you a moment to pick your jaw off the ground.
It makes sense though, the sexes being different, especially when you look at the broader animal kingdom. The males and females of many species are slightly different when it comes to size and shape, but there’s a big question that literally only anthropologists have asked: Were human males and females more different in the past than they are today?
To be more specific, some scientists believe that males and females grew more similar when humans shifted from a hunter-gatherer lifestyle to a farming-based lifestyle, as agriculture encouraged a more equitable division of labor. Others believe that the differences come down to random chance.
Researchers from Penn State University analyzed genomic data from over 350,000 males and females stored in the UK Biobank and looked at the recent (within the last ~3,000 years; post-agriculture adoption in Britain) evolutionary histories of these loci. Height, body mass, hip circumference, body fat percentage, and waist circumference were analyzed, and while there were thousands of differences in the genomes, only one trait occurred more frequently during that time period: Females gained a significantly higher body fat content than males.
It’s a sad day then for the millions of people who were big fans of the “farming caused men and women to become more similar” theory. Count the LOTME crew among them. Be honest: Wouldn’t life be so much simpler if men and women were exactly the same? Just think about it, no more arguments about leaving the toilet seat up. It’d be worth it just for that.
Proteins don’t lie
Research published in Open Biology shows that the human brain contains 14,315 different proteins. The team conducting that study wanted to find out which organ was the most similar to the old brain box, so they did protein counts for the 32 other major tissue types, including heart, salivary gland, lung, spleen, and endometrium.
The tissue with the most proteins in common with the center of human intelligence? You’re thinking it has to be colon at this point, right? We were sure it was going to be colon, but it’s not.
The winner, with 13,442 shared proteins, is the testes. The testes have 15,687 proteins, of which 85.7% are shared with the brain. The researchers, sadly, did not provide protein counts for the other tissue types, but we bet colon was a close second.
Dreaming about COVID?
We thought we were the only ones who have been having crazy dreams lately. Each one seems crazier and more vivid than the one before. Have you been having weird dreams lately?
This is likely your brain’s coping mechanism to handle your pandemic stress, according to Dr. Erik Hoel of Tufts University. Dreams that are crazy and scary might make real life seem lighter and simpler. He calls it the “overfitted brain hypothesis.”
“It is their very strangeness that gives them their biological function,” Dr. Hoel said. It literally makes you feel like COVID-19 and lockdowns aren’t as scary as they seem.
We always knew our minds were powerful things. Apparently, your brain gets tired of everyday familiarity just like you do, and it creates crazy dreams to keep things interesting.
Just remember: That recurring dream that you’re back in college and missing 10 assignments is there to help you, not scare you! Even though it is pretty scary.
By the numbers: Children and COVID-19 prevention
Over 6.3 million doses of COVID-19 vaccine have been administered to children aged 12-17 years as of June 7, according to data from the Centers for Disease Control and Prevention.
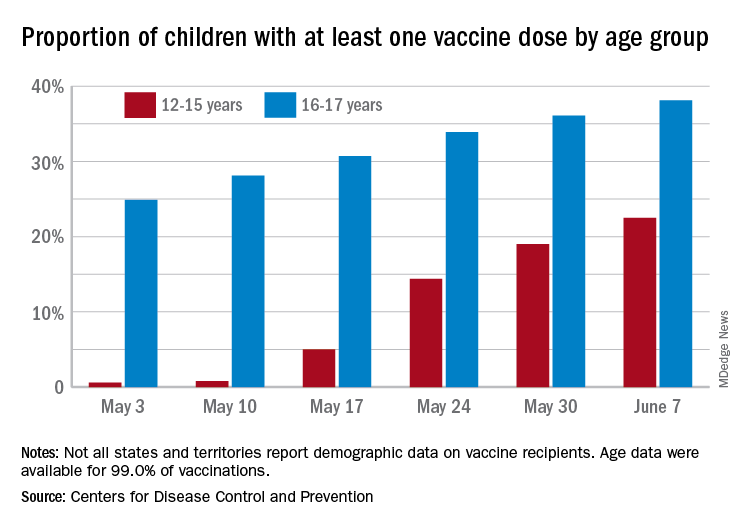
The latest results from the CDC’s COVID Data Tracker show that , with the corresponding figures for vaccine completion coming in at 4.1% and 26.4%. Compared with a week earlier, those numbers are up by 15.4% (one dose) and 486% (completion) for the younger group and by 4.7% and 8.6%, respectively, for the older children.
Children aged 12-15 represented 17.9% of all persons who initiated vaccination in the last 14 days up to June 7, while children aged 16-17 made up 4.8% of vaccine initiation over that period. The 25- to 39-year-olds, at 23.7% of all vaccine initiators, were the only group ahead of those aged 12-15, and the 50- to 64-year-olds were just behind at 17.7%, the CDC data show.
Both groups of children were on the low side, however, when it came to vaccine completion in the last 14 days, with those aged 12-15 at 6.7% of the total and those aged 16-17 years at 4.3%. The only age groups lower than that were ≥75 at 3.5% and <12 at 0.2%, and the highest share of vaccine completion was 26.0% for those aged 25-39, which also happens to be the group with the largest share of the U.S. population (20.5%), the CDC said.
People considered fully vaccinated are those who have received the second dose of a two-dose series or one dose of a single-shot vaccine, but children under age 18 years are eligible only for the Pfizer-BioNTech version, the CDC noted.
Meanwhile, back on the incidence side of the COVID-19 pandemic, the number of new cases in U.S. children for the week ending June 3 was at its lowest point (16,281) since mid-June of 2020, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Cases among children now total 3.99 million, which represents 14.1% of cases among all ages, a proportion that hasn’t increased since mid-May, which hasn’t happened since the two groups started keeping track in mid-April of 2020 in the 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam that report such data by age.
Less encouraging was the CDC’s report that “COVID-19-associated hospitalization rates among adolescents ages 12-17 years increased during March and April, following declines in January and February 2021.”
Children have been experiencing much lower rates of severe disease than those of adults throughout the pandemic, the CDC pointed out, but “recent increases in COVID-19-associated hospitalization rates and the potential for severe disease in adolescents reinforce the importance of continued prevention strategies, including vaccination and the correct and consistent use of masks in those who are not yet fully vaccinated.”
Over 6.3 million doses of COVID-19 vaccine have been administered to children aged 12-17 years as of June 7, according to data from the Centers for Disease Control and Prevention.
The latest results from the CDC’s COVID Data Tracker show that , with the corresponding figures for vaccine completion coming in at 4.1% and 26.4%. Compared with a week earlier, those numbers are up by 15.4% (one dose) and 486% (completion) for the younger group and by 4.7% and 8.6%, respectively, for the older children.
Children aged 12-15 represented 17.9% of all persons who initiated vaccination in the last 14 days up to June 7, while children aged 16-17 made up 4.8% of vaccine initiation over that period. The 25- to 39-year-olds, at 23.7% of all vaccine initiators, were the only group ahead of those aged 12-15, and the 50- to 64-year-olds were just behind at 17.7%, the CDC data show.
Both groups of children were on the low side, however, when it came to vaccine completion in the last 14 days, with those aged 12-15 at 6.7% of the total and those aged 16-17 years at 4.3%. The only age groups lower than that were ≥75 at 3.5% and <12 at 0.2%, and the highest share of vaccine completion was 26.0% for those aged 25-39, which also happens to be the group with the largest share of the U.S. population (20.5%), the CDC said.
People considered fully vaccinated are those who have received the second dose of a two-dose series or one dose of a single-shot vaccine, but children under age 18 years are eligible only for the Pfizer-BioNTech version, the CDC noted.
Meanwhile, back on the incidence side of the COVID-19 pandemic, the number of new cases in U.S. children for the week ending June 3 was at its lowest point (16,281) since mid-June of 2020, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Cases among children now total 3.99 million, which represents 14.1% of cases among all ages, a proportion that hasn’t increased since mid-May, which hasn’t happened since the two groups started keeping track in mid-April of 2020 in the 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam that report such data by age.
Less encouraging was the CDC’s report that “COVID-19-associated hospitalization rates among adolescents ages 12-17 years increased during March and April, following declines in January and February 2021.”
Children have been experiencing much lower rates of severe disease than those of adults throughout the pandemic, the CDC pointed out, but “recent increases in COVID-19-associated hospitalization rates and the potential for severe disease in adolescents reinforce the importance of continued prevention strategies, including vaccination and the correct and consistent use of masks in those who are not yet fully vaccinated.”
Over 6.3 million doses of COVID-19 vaccine have been administered to children aged 12-17 years as of June 7, according to data from the Centers for Disease Control and Prevention.
The latest results from the CDC’s COVID Data Tracker show that , with the corresponding figures for vaccine completion coming in at 4.1% and 26.4%. Compared with a week earlier, those numbers are up by 15.4% (one dose) and 486% (completion) for the younger group and by 4.7% and 8.6%, respectively, for the older children.
Children aged 12-15 represented 17.9% of all persons who initiated vaccination in the last 14 days up to June 7, while children aged 16-17 made up 4.8% of vaccine initiation over that period. The 25- to 39-year-olds, at 23.7% of all vaccine initiators, were the only group ahead of those aged 12-15, and the 50- to 64-year-olds were just behind at 17.7%, the CDC data show.
Both groups of children were on the low side, however, when it came to vaccine completion in the last 14 days, with those aged 12-15 at 6.7% of the total and those aged 16-17 years at 4.3%. The only age groups lower than that were ≥75 at 3.5% and <12 at 0.2%, and the highest share of vaccine completion was 26.0% for those aged 25-39, which also happens to be the group with the largest share of the U.S. population (20.5%), the CDC said.
People considered fully vaccinated are those who have received the second dose of a two-dose series or one dose of a single-shot vaccine, but children under age 18 years are eligible only for the Pfizer-BioNTech version, the CDC noted.
Meanwhile, back on the incidence side of the COVID-19 pandemic, the number of new cases in U.S. children for the week ending June 3 was at its lowest point (16,281) since mid-June of 2020, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Cases among children now total 3.99 million, which represents 14.1% of cases among all ages, a proportion that hasn’t increased since mid-May, which hasn’t happened since the two groups started keeping track in mid-April of 2020 in the 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam that report such data by age.
Less encouraging was the CDC’s report that “COVID-19-associated hospitalization rates among adolescents ages 12-17 years increased during March and April, following declines in January and February 2021.”
Children have been experiencing much lower rates of severe disease than those of adults throughout the pandemic, the CDC pointed out, but “recent increases in COVID-19-associated hospitalization rates and the potential for severe disease in adolescents reinforce the importance of continued prevention strategies, including vaccination and the correct and consistent use of masks in those who are not yet fully vaccinated.”
NIAID advances universal flu vaccine candidate into phase 1 trial
Last month, U.S. government researchers began a test of an experimental influenza vaccine that they hope will provide long-lasting immunity against multiple strains of the virus. Their project adds to the many approaches that have been tried in the decades-long quest for a universal flu shot.
For the first time, the National Institute of Allergy and Infectious Diseases (NIAID) is testing an investigational flu vaccine, known as FluMos-v1, on people. Researchers in recent years have targeted the stalk or stem of an influenza surface protein called hemagglutinin (HA) in trying to develop better flu vaccines. NIAID said FluMos-v1 is designed to spark production of antibodies against the HA protein from different virus strains, which could make it superior to vaccines now available, NIAID said.
“It could be longer lasting than the traditional flu vaccine and give us what we call super seasonal protection that might go beyond just one flu season to next year’s or the year after, or offer additional protection in a pandemic setting,” Alicia T. Widge, MD, of NIAID’s Vaccine Research Center, who is the principal investigator of the trial, said in an interview.
The phase 1 study (NCT04896086) aims to enroll 35 participants, 15 of whom will receive a single intramuscular injection of a comparator treatment, Flucelvax, which has already been approved by the U.S. Food and Drug Administration. The FluMos-v1 group will start with five participants who will receive one 20-μg dose. If no safety problems emerge at that dosage, another 15 volunteers will receive one 60-μg dose of the investigational vaccine.
The incorporation of a comparator group in the phase 1 study may help investigators get an early idea of how well FluMos-v1 compares to a marketed product, Dr. Widge said. The test will be carried out through the National Institutes of Health Clinical Center.
‘Renaissance’ of flu-vaccine research?
Currently, flu vaccines are reformulated each year in an attempt to match the dominant strain for the upcoming season, an effort that often falls notably short. The estimated vaccine effectiveness rate in the United States has ranged from a low of 19% to a high of 60% in recent years, according to the Centers for Disease Control and Prevention.
Scientists have been working for decades on a universal flu vaccine that would offer better results but haven’t yet identified the right strategy to outwit mutations in the virus. Recent setbacks include BiondVax Pharmaceuticals’ October 2020 announcement of a failed phase 3 trial of its experimental M-001 universal flu vaccine candidate.
But advances in understanding the immune system may set the stage for a “renaissance” in efforts to develop a universal flu vaccine, Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, said in an interview.
The COVID-19 pandemic has spurred greater interest in the need to develop a universal flu vaccine, he said. Dr. Osterholm said he is “more optimistic now than ever” about the chances for developing vaccines that can fend off multiple strains over longer periods, although the goal of a shot that can ward off influenza in all cases may remain elusive.
“How good can we make them? Will they ever be really universal? Will they have long periods of protection? I don’t think any of us know that yet,” Dr. Osterholm said. “But this is not the influenza vaccine world of 5 or 7 years ago.”
The mRNA technology used to develop the world’s first approved COVID-19 vaccines, for example, may be applied against influenza, Dr. Osterholm said.
In January 2021, Moderna announced plans to test three development candidates for a seasonal influenza vaccine and aims to start a phase 1 study this year. In an April interview on CNBC’s Squawk Box program, Moderna’s chief executive, Stephané Bancel, spoke about the company’s plans to eventually create a combination vaccine for SARS-Cov-2 and flu viruses.
SARS-CoV-2 “is not going away.” Like flu, this virus will persist and change forms, Ms. Bancel said. Creating a flu shot that outperforms the existing ones would boost confidence in influenza vaccines, which many people now skip, Ms. Bancel said. People might someday be able to get a combination of this more effective flu shot with a COVID-19 vaccine booster in their local pharmacies.
“You can take one dose and then have a nice winter,” Ms. Bancel said of Moderna’s goal for a combination vaccine.
A version of this article first appeared on Medscape.com.
Last month, U.S. government researchers began a test of an experimental influenza vaccine that they hope will provide long-lasting immunity against multiple strains of the virus. Their project adds to the many approaches that have been tried in the decades-long quest for a universal flu shot.
For the first time, the National Institute of Allergy and Infectious Diseases (NIAID) is testing an investigational flu vaccine, known as FluMos-v1, on people. Researchers in recent years have targeted the stalk or stem of an influenza surface protein called hemagglutinin (HA) in trying to develop better flu vaccines. NIAID said FluMos-v1 is designed to spark production of antibodies against the HA protein from different virus strains, which could make it superior to vaccines now available, NIAID said.
“It could be longer lasting than the traditional flu vaccine and give us what we call super seasonal protection that might go beyond just one flu season to next year’s or the year after, or offer additional protection in a pandemic setting,” Alicia T. Widge, MD, of NIAID’s Vaccine Research Center, who is the principal investigator of the trial, said in an interview.
The phase 1 study (NCT04896086) aims to enroll 35 participants, 15 of whom will receive a single intramuscular injection of a comparator treatment, Flucelvax, which has already been approved by the U.S. Food and Drug Administration. The FluMos-v1 group will start with five participants who will receive one 20-μg dose. If no safety problems emerge at that dosage, another 15 volunteers will receive one 60-μg dose of the investigational vaccine.
The incorporation of a comparator group in the phase 1 study may help investigators get an early idea of how well FluMos-v1 compares to a marketed product, Dr. Widge said. The test will be carried out through the National Institutes of Health Clinical Center.
‘Renaissance’ of flu-vaccine research?
Currently, flu vaccines are reformulated each year in an attempt to match the dominant strain for the upcoming season, an effort that often falls notably short. The estimated vaccine effectiveness rate in the United States has ranged from a low of 19% to a high of 60% in recent years, according to the Centers for Disease Control and Prevention.
Scientists have been working for decades on a universal flu vaccine that would offer better results but haven’t yet identified the right strategy to outwit mutations in the virus. Recent setbacks include BiondVax Pharmaceuticals’ October 2020 announcement of a failed phase 3 trial of its experimental M-001 universal flu vaccine candidate.
But advances in understanding the immune system may set the stage for a “renaissance” in efforts to develop a universal flu vaccine, Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, said in an interview.
The COVID-19 pandemic has spurred greater interest in the need to develop a universal flu vaccine, he said. Dr. Osterholm said he is “more optimistic now than ever” about the chances for developing vaccines that can fend off multiple strains over longer periods, although the goal of a shot that can ward off influenza in all cases may remain elusive.
“How good can we make them? Will they ever be really universal? Will they have long periods of protection? I don’t think any of us know that yet,” Dr. Osterholm said. “But this is not the influenza vaccine world of 5 or 7 years ago.”
The mRNA technology used to develop the world’s first approved COVID-19 vaccines, for example, may be applied against influenza, Dr. Osterholm said.
In January 2021, Moderna announced plans to test three development candidates for a seasonal influenza vaccine and aims to start a phase 1 study this year. In an April interview on CNBC’s Squawk Box program, Moderna’s chief executive, Stephané Bancel, spoke about the company’s plans to eventually create a combination vaccine for SARS-Cov-2 and flu viruses.
SARS-CoV-2 “is not going away.” Like flu, this virus will persist and change forms, Ms. Bancel said. Creating a flu shot that outperforms the existing ones would boost confidence in influenza vaccines, which many people now skip, Ms. Bancel said. People might someday be able to get a combination of this more effective flu shot with a COVID-19 vaccine booster in their local pharmacies.
“You can take one dose and then have a nice winter,” Ms. Bancel said of Moderna’s goal for a combination vaccine.
A version of this article first appeared on Medscape.com.
Last month, U.S. government researchers began a test of an experimental influenza vaccine that they hope will provide long-lasting immunity against multiple strains of the virus. Their project adds to the many approaches that have been tried in the decades-long quest for a universal flu shot.
For the first time, the National Institute of Allergy and Infectious Diseases (NIAID) is testing an investigational flu vaccine, known as FluMos-v1, on people. Researchers in recent years have targeted the stalk or stem of an influenza surface protein called hemagglutinin (HA) in trying to develop better flu vaccines. NIAID said FluMos-v1 is designed to spark production of antibodies against the HA protein from different virus strains, which could make it superior to vaccines now available, NIAID said.
“It could be longer lasting than the traditional flu vaccine and give us what we call super seasonal protection that might go beyond just one flu season to next year’s or the year after, or offer additional protection in a pandemic setting,” Alicia T. Widge, MD, of NIAID’s Vaccine Research Center, who is the principal investigator of the trial, said in an interview.
The phase 1 study (NCT04896086) aims to enroll 35 participants, 15 of whom will receive a single intramuscular injection of a comparator treatment, Flucelvax, which has already been approved by the U.S. Food and Drug Administration. The FluMos-v1 group will start with five participants who will receive one 20-μg dose. If no safety problems emerge at that dosage, another 15 volunteers will receive one 60-μg dose of the investigational vaccine.
The incorporation of a comparator group in the phase 1 study may help investigators get an early idea of how well FluMos-v1 compares to a marketed product, Dr. Widge said. The test will be carried out through the National Institutes of Health Clinical Center.
‘Renaissance’ of flu-vaccine research?
Currently, flu vaccines are reformulated each year in an attempt to match the dominant strain for the upcoming season, an effort that often falls notably short. The estimated vaccine effectiveness rate in the United States has ranged from a low of 19% to a high of 60% in recent years, according to the Centers for Disease Control and Prevention.
Scientists have been working for decades on a universal flu vaccine that would offer better results but haven’t yet identified the right strategy to outwit mutations in the virus. Recent setbacks include BiondVax Pharmaceuticals’ October 2020 announcement of a failed phase 3 trial of its experimental M-001 universal flu vaccine candidate.
But advances in understanding the immune system may set the stage for a “renaissance” in efforts to develop a universal flu vaccine, Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, said in an interview.
The COVID-19 pandemic has spurred greater interest in the need to develop a universal flu vaccine, he said. Dr. Osterholm said he is “more optimistic now than ever” about the chances for developing vaccines that can fend off multiple strains over longer periods, although the goal of a shot that can ward off influenza in all cases may remain elusive.
“How good can we make them? Will they ever be really universal? Will they have long periods of protection? I don’t think any of us know that yet,” Dr. Osterholm said. “But this is not the influenza vaccine world of 5 or 7 years ago.”
The mRNA technology used to develop the world’s first approved COVID-19 vaccines, for example, may be applied against influenza, Dr. Osterholm said.
In January 2021, Moderna announced plans to test three development candidates for a seasonal influenza vaccine and aims to start a phase 1 study this year. In an April interview on CNBC’s Squawk Box program, Moderna’s chief executive, Stephané Bancel, spoke about the company’s plans to eventually create a combination vaccine for SARS-Cov-2 and flu viruses.
SARS-CoV-2 “is not going away.” Like flu, this virus will persist and change forms, Ms. Bancel said. Creating a flu shot that outperforms the existing ones would boost confidence in influenza vaccines, which many people now skip, Ms. Bancel said. People might someday be able to get a combination of this more effective flu shot with a COVID-19 vaccine booster in their local pharmacies.
“You can take one dose and then have a nice winter,” Ms. Bancel said of Moderna’s goal for a combination vaccine.
A version of this article first appeared on Medscape.com.
Improving emergency care for children living outside of urban areas
A new physician workforce study documents that almost all clinically active pediatric emergency physicians in the United States – 99% of them – work in urban areas, and that those who do practice in rural areas are significantly older and closer to retirement age.
The portrait of approximately 2,400 self-identified pediatric emergency medicine (EM) physicians may be unsurprising given the overall propensity of physicians – including board-certified general emergency physicians – to practice in urban areas. Even so, it underscores a decades-long concern that many children do not have access to optimal pediatric emergency care.
And the findings highlight the need, the authors say, to keep pressing to improve emergency care for a population of children with “a mortality rate that is already higher than that of its suburban and urban peers (JAMA Network Open 2021;4[5]:e2110084).”
Emergent care of pediatric patients is well within the scope of practice for physicians with training and board certification in general EM, but children and adolescents have different clinical needs and “there are high-stakes scenarios [in children] that we [as emergency physicians] don’t get exposed to as often because we’re not in a children’s hospital or we just don’t have that additional level of training,” said Christopher L. Bennett, MD, MA, of the department of emergency medicine at Stanford University and lead author of the study.
Researchers have documented that some emergency physicians have some discomfort in caring for very ill pediatric patients, he and his coauthors wrote.
Children account for more than 20% of annual ED visits, and most children who seek emergency care in the United States – upwards of 80% – present to general emergency departments. Yet the vast majority of these EDs care for fewer than 14-15 children a day.
With such low pediatric volume, “there will never be pediatric emergency medicine physicians in the rural hospitals in [our] health care system,” said Kathleen M. Brown, MD, medical director for quality and safety of the Emergency Medicine and Trauma Center at Children’s National Medical Center in Washington.
Redistribution “is not a practical solution, and we’ve known that for a long time,” said Dr. Brown, past chairperson of the American College of Emergency Physicians’ pediatric emergency medicine committee. “That’s why national efforts have focused on better preparing the general emergency department and making sure the hospital workforce is ready to take care of children ... to manage and stabilize [them] and recognize when they need more definitive care.”
Continuing efforts to increase “pediatric readiness” in general EDs is one of the recommendations issued by the American Academy of Pediatrics, ACEP, and Emergency Nurses Association in its most recent joint policy statement on emergency care for children, published in May (Pediatrics 2021;147[5]:e2021050787). A 2018 joint policy statement detailed the resources – medications, equipment, policies, and education – necessary for EDs to provide effective pediatric care (Pediatrics 2018;142[5]:e20182459).
There is some evidence that pediatric readiness has improved and that EDs with higher readiness scores may have better pediatric outcomes and lower mortality, said Dr. Brown, a coauthor of both policy statements. (One study cited in the 2018 policy statement, for example, found that children with extremity immobilization and a pain score of 5 or greater had faster management of their pain and decreased exposure to radiation when they were treated in a better-prepared facility than in a facility with less readiness.)
Yet many hospitals still do not have designated pediatric emergency care coordinators (PECCs) – roles that are widely believed to be central to pediatric readiness. PECCs (physicians and nurses) were recommended in 2006 by the then-Institute of Medicine and have been advocated by the AAP, ACEP, and other organizations.
According to 2013 data from the National Pediatric Readiness Project (NPRP), launched that year by the AAP, ACEP, ENA, and the federal Emergency Medical Services for Children program of the Health Resources and Services Administration, at least 15% of EDs lacked at least 1 piece of recommended equipment, and 81% reported barriers to pediatric emergency care guidelines. The NPRP is currently conducting an updated assessment, Dr. Brown said.
Some experts have proposed a different kind of solution – one in which American Board of Pediatrics–certified pediatric EM physicians would care for selective adult patients with common disease patterns who present to rural EDs, in addition to children. They might provide direct patient care across several hospitals in a region, while also addressing quality improvement and assisting EPs and other providers in the region on pediatric care issues.
The proposal, published in May 2020, comes from the 13-member special subcommittee of the ACEP committee on PEM that was tasked with exploring strategies to improve access to emergency pediatric expertise and disaster preparedness in all settings. The proposal was endorsed by the ACEP board of directors, said Jim Homme, MD, a coauthor of the paper (JACEP Open 2020;1:1520-6.)
“We’re saying, look at the ped-trained pediatric emergency provider more broadly. They can actually successfully care for a broader patient population and make it financially feasible ... [for that physician] to be a part of the system,” said Dr. Homme, program director of the emergency medicine residency at the Mayo Clinic College of Medicine and Science in Rochester, Minn.
“The benefit would be not only having the expertise to see children, but to train up other individuals in the institution, and be advocates for the care of children,” he said.
“We’re not saying we want a pediatrics-trained EM physician in every site so that every child would be seen by one – that’s not the goal,” Dr. Homme said. “The goal is to distribute them more broadly than they currently are, and in doing so, make available the other benefits besides direct patient care.”
Most of the physicians in the United States who identify as pediatric EM physicians have completed either a pediatrics or EM residency, followed by a pediatric EM fellowship. It is much more common to have primary training in pediatrics than in EM, said Dr. Homme and Dr. Bennett. A small number of physicians, like Dr. Homme, are dually trained in pediatrics and EM through the completion of two residencies. Dr. Bennett’s workforce study used the American Medical Association Physician Masterfile database and identified 2,403 clinically active pediatric EPs – 5% of all clinically active emergency physicians. Those practicing in rural areas had a median age of 59, compared with a median age of 46 in urban areas. More than half of the pediatric EPs – 68% – reported having pediatric EM board certification.
Three states – Montana, South Dakota, and Wyoming – had no pediatric EMs at all, Dr. Bennett noted.
Readiness in rural Oregon, New England
Torree McGowan, MD, an emergency physician with the St. Charles Health System in Oregon, works in small critical access hospitals in the rural towns of Madras and Prineville, each several hours by ground to the nearest pediatric hospital. She said she feels well equipped to care for children through her training (a rotation in a pediatric ICU and several months working in pediatric EDs) and through her ongoing work with pediatric patients. Children and adolescents comprise about 20%-30% of her volume.
She sees more pediatric illness – children with respiratory syncytial virus who need respiratory support, for instance, and children with severe asthma or diabetic ketoacidosis – than pediatric trauma. When she faces questions, uncertainties, or wants confirmation of a decision, she consults by phone with pediatric subspecialists.
“I don’t take care of kids on vasopressor drips on a regular basis [for instance],” said Dr. McGowan, who sits on ACEP’s disaster preparedness committee and is an Air Force veteran. “But I know the basics and can phone a colleague to be sure I’m doing it correctly. The ability to outreach is there.”
Telemedicine is valuable, she said, but there may also be value in working alongside a pediatric EM physician. One of her EP colleagues is fellowship-trained in ultrasonography and “leads us in training and quality control,” Dr. McGowan said. “And if she’s on shift with you she’ll teach you all about ultrasound. There’s probably utility in having a pediatric EP who does that as well. But incentivizing that and taking them away from the pediatric hospital is a paradigm shift.”
Either way, she said, “being able to bring that expertise out of urban centers, whether it’s to a hospital group like ours or whether it’s by telemedicine, is really, really helpful.”
Her group does not have official PECCs, but the joint policy statements by AAP/ACEP/ENA on pediatric readiness and the “whole pediatric readiness effort’ have been valuable in “driving conversations” with administrators about needs such as purchasing pediatric-sized video laryngoscope blades and other equipment needed for pediatric emergencies, however infrequently they may occur, Dr. McGowan said.
In New England, researchers leading a grassroots regional intervention to establish a PECC in every ED in the region have reported an increased prevalence of “pediatric champions” from less than 30% 5 years ago to greater than 90% in 2019, investigators have reported (Pediatr Emerg Care. 2021. doi: 10.1097/PEC.0000000000002456).
The initiative involved individual outreach to leaders of each ED – largely through phone and e-mail appeals – and collaboration among the State Emergency Medical Services for Children agencies and ACEP and ENA state chapters. The researchers are currently investigating the direct impact of PECCs on patient outcomes.
More on regionalization of ped-trained EPs
Dr. Bennett sees telemedicine as a primary part of improving pediatric emergency care. “I think that’s where things are going to go in pediatric emergency medicine,” he said, especially in the wake of COVID-19: “I don’t see how it’s not going to become much more common.”
Dr. Homme maintains that a broader integration of ABP-certified pediatric EM physicians into underserved regions would advance ED preparedness in a way that telemedicine, or even the appointment of PECCs, does not, said Dr. Homme.
Institutions would need to acknowledge that many of the current restrictions on pediatric EM physicians’ scope of practice are based on arbitrary age cut-offs, and their leaders would need to expand hospital-defined privileges to better align with training and capabilities, he said. Local credentialing provisions and other policies would also need to be adjusted.
Pediatric EM physicians spend at least 4 months of their graduate EM training in an adult ED, and there is significant overlap in the core competencies and the procedures considered essential for practice between pediatric EM fellowship programs and EM programs, Dr. Homme and his coauthors wrote in their proposal. “The pandemic really reinforced this concept,” Dr. Homme said. “As the number of patients in pediatric EDs plummeted, many of the ped-trained providers had to pivot and help care for adults. ... It worked great.”
The broader integration of pediatrics-trained pediatric EM physicians fits well, he believes, with current workforce dynamics. “There aren’t enough individuals coming out of an EM background and doing that subspecialty training to have any hope that they’d be able to cover these underserved areas,” he said. “And the academic pediatric workforce is getting kind of saturated. So having additional employment opportunities would be great.”
Dr. Homme pursued an EM residency after pediatrics training (rather than a pediatric EM fellowship) because he did not want to be limited geographically and because, while he wanted to focus on children, he also “wanted to be available to a larger population.”
He believes that some pediatrics-trained pediatric EM physicians would choose rural practice options, and hopes that the proposal will gain traction. Some EPs will be opposed, he said, and some pediatrics-trained EPs will not interested, “but if we can find people open to the idea on both sides, I think we can really move the needle in the direction we’re trying to, which is to disseminate an area of expertise into areas that just don’t have it.”
A new physician workforce study documents that almost all clinically active pediatric emergency physicians in the United States – 99% of them – work in urban areas, and that those who do practice in rural areas are significantly older and closer to retirement age.
The portrait of approximately 2,400 self-identified pediatric emergency medicine (EM) physicians may be unsurprising given the overall propensity of physicians – including board-certified general emergency physicians – to practice in urban areas. Even so, it underscores a decades-long concern that many children do not have access to optimal pediatric emergency care.
And the findings highlight the need, the authors say, to keep pressing to improve emergency care for a population of children with “a mortality rate that is already higher than that of its suburban and urban peers (JAMA Network Open 2021;4[5]:e2110084).”
Emergent care of pediatric patients is well within the scope of practice for physicians with training and board certification in general EM, but children and adolescents have different clinical needs and “there are high-stakes scenarios [in children] that we [as emergency physicians] don’t get exposed to as often because we’re not in a children’s hospital or we just don’t have that additional level of training,” said Christopher L. Bennett, MD, MA, of the department of emergency medicine at Stanford University and lead author of the study.
Researchers have documented that some emergency physicians have some discomfort in caring for very ill pediatric patients, he and his coauthors wrote.
Children account for more than 20% of annual ED visits, and most children who seek emergency care in the United States – upwards of 80% – present to general emergency departments. Yet the vast majority of these EDs care for fewer than 14-15 children a day.
With such low pediatric volume, “there will never be pediatric emergency medicine physicians in the rural hospitals in [our] health care system,” said Kathleen M. Brown, MD, medical director for quality and safety of the Emergency Medicine and Trauma Center at Children’s National Medical Center in Washington.
Redistribution “is not a practical solution, and we’ve known that for a long time,” said Dr. Brown, past chairperson of the American College of Emergency Physicians’ pediatric emergency medicine committee. “That’s why national efforts have focused on better preparing the general emergency department and making sure the hospital workforce is ready to take care of children ... to manage and stabilize [them] and recognize when they need more definitive care.”
Continuing efforts to increase “pediatric readiness” in general EDs is one of the recommendations issued by the American Academy of Pediatrics, ACEP, and Emergency Nurses Association in its most recent joint policy statement on emergency care for children, published in May (Pediatrics 2021;147[5]:e2021050787). A 2018 joint policy statement detailed the resources – medications, equipment, policies, and education – necessary for EDs to provide effective pediatric care (Pediatrics 2018;142[5]:e20182459).
There is some evidence that pediatric readiness has improved and that EDs with higher readiness scores may have better pediatric outcomes and lower mortality, said Dr. Brown, a coauthor of both policy statements. (One study cited in the 2018 policy statement, for example, found that children with extremity immobilization and a pain score of 5 or greater had faster management of their pain and decreased exposure to radiation when they were treated in a better-prepared facility than in a facility with less readiness.)
Yet many hospitals still do not have designated pediatric emergency care coordinators (PECCs) – roles that are widely believed to be central to pediatric readiness. PECCs (physicians and nurses) were recommended in 2006 by the then-Institute of Medicine and have been advocated by the AAP, ACEP, and other organizations.
According to 2013 data from the National Pediatric Readiness Project (NPRP), launched that year by the AAP, ACEP, ENA, and the federal Emergency Medical Services for Children program of the Health Resources and Services Administration, at least 15% of EDs lacked at least 1 piece of recommended equipment, and 81% reported barriers to pediatric emergency care guidelines. The NPRP is currently conducting an updated assessment, Dr. Brown said.
Some experts have proposed a different kind of solution – one in which American Board of Pediatrics–certified pediatric EM physicians would care for selective adult patients with common disease patterns who present to rural EDs, in addition to children. They might provide direct patient care across several hospitals in a region, while also addressing quality improvement and assisting EPs and other providers in the region on pediatric care issues.
The proposal, published in May 2020, comes from the 13-member special subcommittee of the ACEP committee on PEM that was tasked with exploring strategies to improve access to emergency pediatric expertise and disaster preparedness in all settings. The proposal was endorsed by the ACEP board of directors, said Jim Homme, MD, a coauthor of the paper (JACEP Open 2020;1:1520-6.)
“We’re saying, look at the ped-trained pediatric emergency provider more broadly. They can actually successfully care for a broader patient population and make it financially feasible ... [for that physician] to be a part of the system,” said Dr. Homme, program director of the emergency medicine residency at the Mayo Clinic College of Medicine and Science in Rochester, Minn.
“The benefit would be not only having the expertise to see children, but to train up other individuals in the institution, and be advocates for the care of children,” he said.
“We’re not saying we want a pediatrics-trained EM physician in every site so that every child would be seen by one – that’s not the goal,” Dr. Homme said. “The goal is to distribute them more broadly than they currently are, and in doing so, make available the other benefits besides direct patient care.”
Most of the physicians in the United States who identify as pediatric EM physicians have completed either a pediatrics or EM residency, followed by a pediatric EM fellowship. It is much more common to have primary training in pediatrics than in EM, said Dr. Homme and Dr. Bennett. A small number of physicians, like Dr. Homme, are dually trained in pediatrics and EM through the completion of two residencies. Dr. Bennett’s workforce study used the American Medical Association Physician Masterfile database and identified 2,403 clinically active pediatric EPs – 5% of all clinically active emergency physicians. Those practicing in rural areas had a median age of 59, compared with a median age of 46 in urban areas. More than half of the pediatric EPs – 68% – reported having pediatric EM board certification.
Three states – Montana, South Dakota, and Wyoming – had no pediatric EMs at all, Dr. Bennett noted.
Readiness in rural Oregon, New England
Torree McGowan, MD, an emergency physician with the St. Charles Health System in Oregon, works in small critical access hospitals in the rural towns of Madras and Prineville, each several hours by ground to the nearest pediatric hospital. She said she feels well equipped to care for children through her training (a rotation in a pediatric ICU and several months working in pediatric EDs) and through her ongoing work with pediatric patients. Children and adolescents comprise about 20%-30% of her volume.
She sees more pediatric illness – children with respiratory syncytial virus who need respiratory support, for instance, and children with severe asthma or diabetic ketoacidosis – than pediatric trauma. When she faces questions, uncertainties, or wants confirmation of a decision, she consults by phone with pediatric subspecialists.
“I don’t take care of kids on vasopressor drips on a regular basis [for instance],” said Dr. McGowan, who sits on ACEP’s disaster preparedness committee and is an Air Force veteran. “But I know the basics and can phone a colleague to be sure I’m doing it correctly. The ability to outreach is there.”
Telemedicine is valuable, she said, but there may also be value in working alongside a pediatric EM physician. One of her EP colleagues is fellowship-trained in ultrasonography and “leads us in training and quality control,” Dr. McGowan said. “And if she’s on shift with you she’ll teach you all about ultrasound. There’s probably utility in having a pediatric EP who does that as well. But incentivizing that and taking them away from the pediatric hospital is a paradigm shift.”
Either way, she said, “being able to bring that expertise out of urban centers, whether it’s to a hospital group like ours or whether it’s by telemedicine, is really, really helpful.”
Her group does not have official PECCs, but the joint policy statements by AAP/ACEP/ENA on pediatric readiness and the “whole pediatric readiness effort’ have been valuable in “driving conversations” with administrators about needs such as purchasing pediatric-sized video laryngoscope blades and other equipment needed for pediatric emergencies, however infrequently they may occur, Dr. McGowan said.
In New England, researchers leading a grassroots regional intervention to establish a PECC in every ED in the region have reported an increased prevalence of “pediatric champions” from less than 30% 5 years ago to greater than 90% in 2019, investigators have reported (Pediatr Emerg Care. 2021. doi: 10.1097/PEC.0000000000002456).
The initiative involved individual outreach to leaders of each ED – largely through phone and e-mail appeals – and collaboration among the State Emergency Medical Services for Children agencies and ACEP and ENA state chapters. The researchers are currently investigating the direct impact of PECCs on patient outcomes.
More on regionalization of ped-trained EPs
Dr. Bennett sees telemedicine as a primary part of improving pediatric emergency care. “I think that’s where things are going to go in pediatric emergency medicine,” he said, especially in the wake of COVID-19: “I don’t see how it’s not going to become much more common.”
Dr. Homme maintains that a broader integration of ABP-certified pediatric EM physicians into underserved regions would advance ED preparedness in a way that telemedicine, or even the appointment of PECCs, does not, said Dr. Homme.
Institutions would need to acknowledge that many of the current restrictions on pediatric EM physicians’ scope of practice are based on arbitrary age cut-offs, and their leaders would need to expand hospital-defined privileges to better align with training and capabilities, he said. Local credentialing provisions and other policies would also need to be adjusted.
Pediatric EM physicians spend at least 4 months of their graduate EM training in an adult ED, and there is significant overlap in the core competencies and the procedures considered essential for practice between pediatric EM fellowship programs and EM programs, Dr. Homme and his coauthors wrote in their proposal. “The pandemic really reinforced this concept,” Dr. Homme said. “As the number of patients in pediatric EDs plummeted, many of the ped-trained providers had to pivot and help care for adults. ... It worked great.”
The broader integration of pediatrics-trained pediatric EM physicians fits well, he believes, with current workforce dynamics. “There aren’t enough individuals coming out of an EM background and doing that subspecialty training to have any hope that they’d be able to cover these underserved areas,” he said. “And the academic pediatric workforce is getting kind of saturated. So having additional employment opportunities would be great.”
Dr. Homme pursued an EM residency after pediatrics training (rather than a pediatric EM fellowship) because he did not want to be limited geographically and because, while he wanted to focus on children, he also “wanted to be available to a larger population.”
He believes that some pediatrics-trained pediatric EM physicians would choose rural practice options, and hopes that the proposal will gain traction. Some EPs will be opposed, he said, and some pediatrics-trained EPs will not interested, “but if we can find people open to the idea on both sides, I think we can really move the needle in the direction we’re trying to, which is to disseminate an area of expertise into areas that just don’t have it.”
A new physician workforce study documents that almost all clinically active pediatric emergency physicians in the United States – 99% of them – work in urban areas, and that those who do practice in rural areas are significantly older and closer to retirement age.
The portrait of approximately 2,400 self-identified pediatric emergency medicine (EM) physicians may be unsurprising given the overall propensity of physicians – including board-certified general emergency physicians – to practice in urban areas. Even so, it underscores a decades-long concern that many children do not have access to optimal pediatric emergency care.
And the findings highlight the need, the authors say, to keep pressing to improve emergency care for a population of children with “a mortality rate that is already higher than that of its suburban and urban peers (JAMA Network Open 2021;4[5]:e2110084).”
Emergent care of pediatric patients is well within the scope of practice for physicians with training and board certification in general EM, but children and adolescents have different clinical needs and “there are high-stakes scenarios [in children] that we [as emergency physicians] don’t get exposed to as often because we’re not in a children’s hospital or we just don’t have that additional level of training,” said Christopher L. Bennett, MD, MA, of the department of emergency medicine at Stanford University and lead author of the study.
Researchers have documented that some emergency physicians have some discomfort in caring for very ill pediatric patients, he and his coauthors wrote.
Children account for more than 20% of annual ED visits, and most children who seek emergency care in the United States – upwards of 80% – present to general emergency departments. Yet the vast majority of these EDs care for fewer than 14-15 children a day.
With such low pediatric volume, “there will never be pediatric emergency medicine physicians in the rural hospitals in [our] health care system,” said Kathleen M. Brown, MD, medical director for quality and safety of the Emergency Medicine and Trauma Center at Children’s National Medical Center in Washington.
Redistribution “is not a practical solution, and we’ve known that for a long time,” said Dr. Brown, past chairperson of the American College of Emergency Physicians’ pediatric emergency medicine committee. “That’s why national efforts have focused on better preparing the general emergency department and making sure the hospital workforce is ready to take care of children ... to manage and stabilize [them] and recognize when they need more definitive care.”
Continuing efforts to increase “pediatric readiness” in general EDs is one of the recommendations issued by the American Academy of Pediatrics, ACEP, and Emergency Nurses Association in its most recent joint policy statement on emergency care for children, published in May (Pediatrics 2021;147[5]:e2021050787). A 2018 joint policy statement detailed the resources – medications, equipment, policies, and education – necessary for EDs to provide effective pediatric care (Pediatrics 2018;142[5]:e20182459).
There is some evidence that pediatric readiness has improved and that EDs with higher readiness scores may have better pediatric outcomes and lower mortality, said Dr. Brown, a coauthor of both policy statements. (One study cited in the 2018 policy statement, for example, found that children with extremity immobilization and a pain score of 5 or greater had faster management of their pain and decreased exposure to radiation when they were treated in a better-prepared facility than in a facility with less readiness.)
Yet many hospitals still do not have designated pediatric emergency care coordinators (PECCs) – roles that are widely believed to be central to pediatric readiness. PECCs (physicians and nurses) were recommended in 2006 by the then-Institute of Medicine and have been advocated by the AAP, ACEP, and other organizations.
According to 2013 data from the National Pediatric Readiness Project (NPRP), launched that year by the AAP, ACEP, ENA, and the federal Emergency Medical Services for Children program of the Health Resources and Services Administration, at least 15% of EDs lacked at least 1 piece of recommended equipment, and 81% reported barriers to pediatric emergency care guidelines. The NPRP is currently conducting an updated assessment, Dr. Brown said.
Some experts have proposed a different kind of solution – one in which American Board of Pediatrics–certified pediatric EM physicians would care for selective adult patients with common disease patterns who present to rural EDs, in addition to children. They might provide direct patient care across several hospitals in a region, while also addressing quality improvement and assisting EPs and other providers in the region on pediatric care issues.
The proposal, published in May 2020, comes from the 13-member special subcommittee of the ACEP committee on PEM that was tasked with exploring strategies to improve access to emergency pediatric expertise and disaster preparedness in all settings. The proposal was endorsed by the ACEP board of directors, said Jim Homme, MD, a coauthor of the paper (JACEP Open 2020;1:1520-6.)
“We’re saying, look at the ped-trained pediatric emergency provider more broadly. They can actually successfully care for a broader patient population and make it financially feasible ... [for that physician] to be a part of the system,” said Dr. Homme, program director of the emergency medicine residency at the Mayo Clinic College of Medicine and Science in Rochester, Minn.
“The benefit would be not only having the expertise to see children, but to train up other individuals in the institution, and be advocates for the care of children,” he said.
“We’re not saying we want a pediatrics-trained EM physician in every site so that every child would be seen by one – that’s not the goal,” Dr. Homme said. “The goal is to distribute them more broadly than they currently are, and in doing so, make available the other benefits besides direct patient care.”
Most of the physicians in the United States who identify as pediatric EM physicians have completed either a pediatrics or EM residency, followed by a pediatric EM fellowship. It is much more common to have primary training in pediatrics than in EM, said Dr. Homme and Dr. Bennett. A small number of physicians, like Dr. Homme, are dually trained in pediatrics and EM through the completion of two residencies. Dr. Bennett’s workforce study used the American Medical Association Physician Masterfile database and identified 2,403 clinically active pediatric EPs – 5% of all clinically active emergency physicians. Those practicing in rural areas had a median age of 59, compared with a median age of 46 in urban areas. More than half of the pediatric EPs – 68% – reported having pediatric EM board certification.
Three states – Montana, South Dakota, and Wyoming – had no pediatric EMs at all, Dr. Bennett noted.
Readiness in rural Oregon, New England
Torree McGowan, MD, an emergency physician with the St. Charles Health System in Oregon, works in small critical access hospitals in the rural towns of Madras and Prineville, each several hours by ground to the nearest pediatric hospital. She said she feels well equipped to care for children through her training (a rotation in a pediatric ICU and several months working in pediatric EDs) and through her ongoing work with pediatric patients. Children and adolescents comprise about 20%-30% of her volume.
She sees more pediatric illness – children with respiratory syncytial virus who need respiratory support, for instance, and children with severe asthma or diabetic ketoacidosis – than pediatric trauma. When she faces questions, uncertainties, or wants confirmation of a decision, she consults by phone with pediatric subspecialists.
“I don’t take care of kids on vasopressor drips on a regular basis [for instance],” said Dr. McGowan, who sits on ACEP’s disaster preparedness committee and is an Air Force veteran. “But I know the basics and can phone a colleague to be sure I’m doing it correctly. The ability to outreach is there.”
Telemedicine is valuable, she said, but there may also be value in working alongside a pediatric EM physician. One of her EP colleagues is fellowship-trained in ultrasonography and “leads us in training and quality control,” Dr. McGowan said. “And if she’s on shift with you she’ll teach you all about ultrasound. There’s probably utility in having a pediatric EP who does that as well. But incentivizing that and taking them away from the pediatric hospital is a paradigm shift.”
Either way, she said, “being able to bring that expertise out of urban centers, whether it’s to a hospital group like ours or whether it’s by telemedicine, is really, really helpful.”
Her group does not have official PECCs, but the joint policy statements by AAP/ACEP/ENA on pediatric readiness and the “whole pediatric readiness effort’ have been valuable in “driving conversations” with administrators about needs such as purchasing pediatric-sized video laryngoscope blades and other equipment needed for pediatric emergencies, however infrequently they may occur, Dr. McGowan said.
In New England, researchers leading a grassroots regional intervention to establish a PECC in every ED in the region have reported an increased prevalence of “pediatric champions” from less than 30% 5 years ago to greater than 90% in 2019, investigators have reported (Pediatr Emerg Care. 2021. doi: 10.1097/PEC.0000000000002456).
The initiative involved individual outreach to leaders of each ED – largely through phone and e-mail appeals – and collaboration among the State Emergency Medical Services for Children agencies and ACEP and ENA state chapters. The researchers are currently investigating the direct impact of PECCs on patient outcomes.
More on regionalization of ped-trained EPs
Dr. Bennett sees telemedicine as a primary part of improving pediatric emergency care. “I think that’s where things are going to go in pediatric emergency medicine,” he said, especially in the wake of COVID-19: “I don’t see how it’s not going to become much more common.”
Dr. Homme maintains that a broader integration of ABP-certified pediatric EM physicians into underserved regions would advance ED preparedness in a way that telemedicine, or even the appointment of PECCs, does not, said Dr. Homme.
Institutions would need to acknowledge that many of the current restrictions on pediatric EM physicians’ scope of practice are based on arbitrary age cut-offs, and their leaders would need to expand hospital-defined privileges to better align with training and capabilities, he said. Local credentialing provisions and other policies would also need to be adjusted.
Pediatric EM physicians spend at least 4 months of their graduate EM training in an adult ED, and there is significant overlap in the core competencies and the procedures considered essential for practice between pediatric EM fellowship programs and EM programs, Dr. Homme and his coauthors wrote in their proposal. “The pandemic really reinforced this concept,” Dr. Homme said. “As the number of patients in pediatric EDs plummeted, many of the ped-trained providers had to pivot and help care for adults. ... It worked great.”
The broader integration of pediatrics-trained pediatric EM physicians fits well, he believes, with current workforce dynamics. “There aren’t enough individuals coming out of an EM background and doing that subspecialty training to have any hope that they’d be able to cover these underserved areas,” he said. “And the academic pediatric workforce is getting kind of saturated. So having additional employment opportunities would be great.”
Dr. Homme pursued an EM residency after pediatrics training (rather than a pediatric EM fellowship) because he did not want to be limited geographically and because, while he wanted to focus on children, he also “wanted to be available to a larger population.”
He believes that some pediatrics-trained pediatric EM physicians would choose rural practice options, and hopes that the proposal will gain traction. Some EPs will be opposed, he said, and some pediatrics-trained EPs will not interested, “but if we can find people open to the idea on both sides, I think we can really move the needle in the direction we’re trying to, which is to disseminate an area of expertise into areas that just don’t have it.”
CRC screening guidelines: 45 is the new 50, and 85 is the new 75
Build a better mousetrap, and the world will beat a path to your door. Find an accurate, completely noninvasive method for colorectal cancer screening and you’ll probably win the Nobel Prize for Medicine or Physiology.
But until then, we’ll have to make do with colonoscopy, fecal immunochemical testing (FIT), and other messy but necessary means for preventing full-blown CRC and reducing the risk of CRC morbidity and mortality. And start turning to them earlier in patients’ lives.
The U.S. Preventive Services Task Force (USPSTF) has issued an update of its 2016 recommendations for CRC screening, for the first time advising that screening for all average-risk adults begin at age 45. This new recommendation is in line with the guidelines issued by the American Cancer Society, which were updated in 2018, to reflect the inescapable truth that CRC is increasingly being diagnosed at a younger age.
Not to be left out, the U.S. Multi-Society Task Force (MSTF) – which represents the American College of Gastroenterology, the American Gastroenterological Association, and the American Society for Gastrointestinal Endoscopy – issued a statement supporting lowering the age of initial screening in normal-risk adults to 45, and promised that an update of the 2017 guidelines would include the new recommendation.
Recommendations influence reimbursement
Guidelines are often honored as much in the breach as in the observance, but those issued by the USPSTF have unique sway, according to Sonia S. Kupfer, MD, of the section of gastroenterology, hepatology, and nutrition at the University of Chicago, and colleagues.
“While other guidelines have recommended this younger age, the USPSTF guidelines directly inform insurance coverage and waiving of cost sharing as part of federal law,” they wrote in an editorial accompanying the USPSTF guideline statement in the Journal of the American Medical Association.
Although the USPSTF rated its recommendation on starting at age 45 a ‘B’ level – indicating a moderate certainty of moderate benefit – it’s an important step, Dr. Kupfer said in an interview.
“The big advantage here is that we may be able to make a dent in this early-onset colorectal cancer, which, having seen many of these patients, is very alarming, and they don’t always seem to have classic risk factors,” she said. “So, getting them when we can potentially prevent cancer by taking out polyps, or even getting them in an earlier stage, certainly will be beneficial.”
The MSTF also considered recommending 45 as the starting age for normal-risk patients in its 2017 guidelines, noted Douglas Rex, MD, who was chair of the committee that drew up those guidelines, as well as director of endoscopy at Indiana University Hospital in Indianapolis.
“Since that time there has been more evidence, and there’s also some empiric evidence, about the yield of screening in the 45- to 49-year-old age group,” he said in an interview.
The one that gets done
Although the various guidelines differ in specifics, all are in agreement on the general proposition that colonoscopy is the gold standard for screening and detecting the presence of polyps, adenomas, and CRC.
But as USPSTF member Martha Kubik, PhD, RN, director of the George Mason University School of Nursing in Fairfax, Va., said in a statement: “The right test is the one that gets done.”
Gastroenterologists acknowledge that despite its efficacy, colonoscopy is an invasive procedure involving meticulous and unpleasant and/or uncomfortable bowel prep, sedation, and significant time requirements.
In the theory that something is better than nothing, with clinical evidence of varying degrees of quality, the USPSTF recommends the following procedures or tests for average-risk adults:
- Colonoscopy screening every 10 years.
- every 10 years plus annual FIT.
- CT colonography every 5 years.
- High-sensitivity guaiac fecal occult blood test (gFOBT; Hemoccult II) or FIT every year.
- Stool DNA-FIT (Cologuard) every 1 to 3 years.
The Food and Drug Administration also recently approved an artificial intelligence device designed for use with an endoscope, which its manufacturer says can help clinicians detect gastrointestinal lesions they might otherwise miss. This is not a new screening method, but rather an enhancement of existing ones. It neither diagnoses lesions nor recommends treatments, and is not intended to take the place of laboratory sampling.
“I think artificial intelligence is poised to make colonoscopy more effective,” Dr. Rex said. “In the first five trials that we’ve seen, the average increase in the adenoma detection rate has been 11%, and for each 1% gain in the adenoma detection rate, patients have about a 3% decline in their risk of getting cancer after a colonoscopy and about a 5% decline in their risk for fatal cancer. Those are the largest gains that we’ve seen from a technology.”
Different evidence, varied outcomes
Despite the recommendations, a quick dive into the morass of evidence from multiple studies featured in the updated USPSTF guidelines shows that not all screening methods are created equal.
A single colonoscopy, for example, has been shown in large cohort studies to be associated with a 68% reduction in CRC mortality vs. no screening, compared with a 26% reduction with flexible sigmoidoscopy performed every 3-5 years, 22% reduction with Hemoccult II, and 10% with FIT every 2 years.
The USPSTF investigators did not find any studies evaluating the effectiveness of CT colonography, high-sensitivity gFOBT, stool DNA with or without FIT, or serum tests on CRC incidence, CRC mortality, or both.
The two visualization methods for which studies were available, colonoscopy and CT colonography, were generally comparable in sensitivity and specificity for detecting and correctly identifying adenomas 6 mm and larger, although colonography had higher sensitivity for CRC than colonoscopy.
When performed in two to nine annual or biennial rounds, gFOBT was associated with a reduction of CRC-specific mortality of 9% after 19.5 years and 22% at 30 years, compared with no screening.
In observational studies, screening colonoscopy and FIT were both associated with lower risk of CRC incidence or mortality, compared with no screening.
When to stop?
The major guidelines are all in agreement that once an individual reaches age 75, the decision about whether to continue screening should be made on a case-by-case basis, depending on the patient’s overall health, relative risks, and life expectancy.
But if a study published 2 days after the release of the USPSTF guidelines is any indication, just as 45 is the new 50 for starting screening, 85 may be the new 75 for stopping it.
As researchers from Mass General Cancer Center in Boston reported in JAMA Oncology, screening endoscopy for persons older than 75 in otherwise good health can reduce the risk for CRC incidence and CRC-related death by approximately 40%.
The researchers also found, however, that screening did not provide a significant survival benefit for individuals older than 75 with cardiovascular disease, diabetes, or three or more other health conditions.
“Until now, there really weren’t clear data to help us decide whether patients should be screened after age 75,” coinvestigator Andrew T. Chan. MD, MPH, a gastroenterologist and chief of the clinical and translational epidemiology unit at Mass General, said in a statement. “Current guidance was largely based on modeling and extrapolation of studies conducted in other age groups, and not on solid data to show whether screening was actually helpful in an older population.”
In an interview, Dr. Chan said that while the recommendation to screen older adults has to be tailored to individual risk factors, “it should help to provide more confidence for clinicians and patients.”
“I think this is particularly important, because we know that the population as a whole is aging, so more and more people are in this category of over the age of 75, and it’s not an infrequent issue in the clinic as to what to continue with respect to preventative interventions,” he said.
Dr. Kupfer said that the findings by Dr. Chan and colleagues are largely in keeping with guideline recommendations.
“We factor in a lot of different things, including comorbidities, in making the decision to continue screening up to age 85. Certainly, physiological age and chronological age aren’t always the same, so not every 75-year-old is going to be in the same boat,” she said.
“The risk goes up as people get older, but there starts to be competing mortality at some point, and if you have to do a colonoscopy there are obviously issues related to sedation that, as someone gets older, we have to take into consideration,” she added.
Patients frequently confuse screening with surveillance, Dr. Rex said, and he has had patients tell him: “I hear you don’t do these anymore on people over the age of 75.”
“But that’s not true,” Dr. Rex emphasized.
“Screening is generally considered appropriate even up to the age of 85, but between 75 and 85 it should be considered on an individual basis, and there are several considerations there,” Dr. Rex said. “One is whether a patient has ever been screened before. The second is how they were screened. Third is their life expectancy and how many comorbidities they have. And fourth is their personal feelings about it and interest in it.”
He pointed out that the false-positive rate of stool DNA-FIT tests increases with age, and that for older patients who were previously screened, a standard FIT test may be a more appropriate.
So doc, what should I do?
Multiple guidelines, levels of evidence, different screening methods with varying efficacy, individual risk factors – how can clinicians make sense of all these data at the practice level?
“Any modality can be used for screening. Colorectal cancer screening can be done in a number of different ways, and I think that sometimes gets lost in the shuffle, and the thought becomes that everybody has to get a colonoscopy at 45, but there are certainly other tests,” Dr. Kupfer said.
“This just reminds us that we should be thinking about ways we can be doing screening on a population basis, so that we make sure there is equity,” she said.
It’s also important to remember that patients with familial CRC syndromes should begin screening at an even earlier age than average-risk adults, she emphasized.
“To really make a dent in early-onset colorectal cancer, we have to continue to take an active case-finding approach,” she said.
Dr. Rex noted that despite minor differences, the major guidelines are all similar in their initial statements that screening works.
“We’ve still got 50,000 people a year dying from colorectal cancer, lots more than that of new cases,” he said. “If you look at a single factor contributing to that the most, it’s that a lot of the American public is not getting screened at all – it can be up to 40% of the population, depending on what state you’re in.”
Although there are a variety of screening methods available, there are few studies directly comparing them, leaving clinicians at the practice level with the task of presenting all or some of them to patients.
“What the Multi-Society Task Force says that is different, and I think that they get right, is that we don’t have any data [indicating] that offering five, six, or seven options increases the chance of screening – there’s really no evidence that going past two does,” Dr. Rex said.
“The list of options also includes things that nobody actually does,” he added. “For example, flexible sigmoidoscopy has dropped off the map, and FIT has largely replaced guaiac-based testing, even high-sensitivity guaiac. Nobody is really doing CT colonography. The three tests that are being used are colonoscopy, FIT, and [stool DNA-FIT].”
Dr. Rex said that he favors sequential offers, presenting colonoscopy first, emphasizing the benefits for higher-risk patients, and if the patients refuse, offering a fecal-based test.
“Minimizing the number of options makes the conversation feasible, and it’s still very responsible,” he said.
Dr. Kupfer has performed collaborative research with Myriad Genetic Laboratories. She is an editorial advisory board member for GI & Hepatology News from MDedge, part of the Medscape Professional Network. Dr. Rex serves or served as a consultant for Olympus Corporation; Boston Scientific; Medtronic; and Aries; and received research support from Endo-Aid; Olympus Corporation; and Medivators. He has ownership in ai4gi. He is an editorial board member for Medscape Gastroenterology. Dr. Chan has served as a consultant to Pfizer, Bayer AG, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated June 8, 2021.
Build a better mousetrap, and the world will beat a path to your door. Find an accurate, completely noninvasive method for colorectal cancer screening and you’ll probably win the Nobel Prize for Medicine or Physiology.
But until then, we’ll have to make do with colonoscopy, fecal immunochemical testing (FIT), and other messy but necessary means for preventing full-blown CRC and reducing the risk of CRC morbidity and mortality. And start turning to them earlier in patients’ lives.
The U.S. Preventive Services Task Force (USPSTF) has issued an update of its 2016 recommendations for CRC screening, for the first time advising that screening for all average-risk adults begin at age 45. This new recommendation is in line with the guidelines issued by the American Cancer Society, which were updated in 2018, to reflect the inescapable truth that CRC is increasingly being diagnosed at a younger age.
Not to be left out, the U.S. Multi-Society Task Force (MSTF) – which represents the American College of Gastroenterology, the American Gastroenterological Association, and the American Society for Gastrointestinal Endoscopy – issued a statement supporting lowering the age of initial screening in normal-risk adults to 45, and promised that an update of the 2017 guidelines would include the new recommendation.
Recommendations influence reimbursement
Guidelines are often honored as much in the breach as in the observance, but those issued by the USPSTF have unique sway, according to Sonia S. Kupfer, MD, of the section of gastroenterology, hepatology, and nutrition at the University of Chicago, and colleagues.
“While other guidelines have recommended this younger age, the USPSTF guidelines directly inform insurance coverage and waiving of cost sharing as part of federal law,” they wrote in an editorial accompanying the USPSTF guideline statement in the Journal of the American Medical Association.
Although the USPSTF rated its recommendation on starting at age 45 a ‘B’ level – indicating a moderate certainty of moderate benefit – it’s an important step, Dr. Kupfer said in an interview.
“The big advantage here is that we may be able to make a dent in this early-onset colorectal cancer, which, having seen many of these patients, is very alarming, and they don’t always seem to have classic risk factors,” she said. “So, getting them when we can potentially prevent cancer by taking out polyps, or even getting them in an earlier stage, certainly will be beneficial.”
The MSTF also considered recommending 45 as the starting age for normal-risk patients in its 2017 guidelines, noted Douglas Rex, MD, who was chair of the committee that drew up those guidelines, as well as director of endoscopy at Indiana University Hospital in Indianapolis.
“Since that time there has been more evidence, and there’s also some empiric evidence, about the yield of screening in the 45- to 49-year-old age group,” he said in an interview.
The one that gets done
Although the various guidelines differ in specifics, all are in agreement on the general proposition that colonoscopy is the gold standard for screening and detecting the presence of polyps, adenomas, and CRC.
But as USPSTF member Martha Kubik, PhD, RN, director of the George Mason University School of Nursing in Fairfax, Va., said in a statement: “The right test is the one that gets done.”
Gastroenterologists acknowledge that despite its efficacy, colonoscopy is an invasive procedure involving meticulous and unpleasant and/or uncomfortable bowel prep, sedation, and significant time requirements.
In the theory that something is better than nothing, with clinical evidence of varying degrees of quality, the USPSTF recommends the following procedures or tests for average-risk adults:
- Colonoscopy screening every 10 years.
- every 10 years plus annual FIT.
- CT colonography every 5 years.
- High-sensitivity guaiac fecal occult blood test (gFOBT; Hemoccult II) or FIT every year.
- Stool DNA-FIT (Cologuard) every 1 to 3 years.
The Food and Drug Administration also recently approved an artificial intelligence device designed for use with an endoscope, which its manufacturer says can help clinicians detect gastrointestinal lesions they might otherwise miss. This is not a new screening method, but rather an enhancement of existing ones. It neither diagnoses lesions nor recommends treatments, and is not intended to take the place of laboratory sampling.
“I think artificial intelligence is poised to make colonoscopy more effective,” Dr. Rex said. “In the first five trials that we’ve seen, the average increase in the adenoma detection rate has been 11%, and for each 1% gain in the adenoma detection rate, patients have about a 3% decline in their risk of getting cancer after a colonoscopy and about a 5% decline in their risk for fatal cancer. Those are the largest gains that we’ve seen from a technology.”
Different evidence, varied outcomes
Despite the recommendations, a quick dive into the morass of evidence from multiple studies featured in the updated USPSTF guidelines shows that not all screening methods are created equal.
A single colonoscopy, for example, has been shown in large cohort studies to be associated with a 68% reduction in CRC mortality vs. no screening, compared with a 26% reduction with flexible sigmoidoscopy performed every 3-5 years, 22% reduction with Hemoccult II, and 10% with FIT every 2 years.
The USPSTF investigators did not find any studies evaluating the effectiveness of CT colonography, high-sensitivity gFOBT, stool DNA with or without FIT, or serum tests on CRC incidence, CRC mortality, or both.
The two visualization methods for which studies were available, colonoscopy and CT colonography, were generally comparable in sensitivity and specificity for detecting and correctly identifying adenomas 6 mm and larger, although colonography had higher sensitivity for CRC than colonoscopy.
When performed in two to nine annual or biennial rounds, gFOBT was associated with a reduction of CRC-specific mortality of 9% after 19.5 years and 22% at 30 years, compared with no screening.
In observational studies, screening colonoscopy and FIT were both associated with lower risk of CRC incidence or mortality, compared with no screening.
When to stop?
The major guidelines are all in agreement that once an individual reaches age 75, the decision about whether to continue screening should be made on a case-by-case basis, depending on the patient’s overall health, relative risks, and life expectancy.
But if a study published 2 days after the release of the USPSTF guidelines is any indication, just as 45 is the new 50 for starting screening, 85 may be the new 75 for stopping it.
As researchers from Mass General Cancer Center in Boston reported in JAMA Oncology, screening endoscopy for persons older than 75 in otherwise good health can reduce the risk for CRC incidence and CRC-related death by approximately 40%.
The researchers also found, however, that screening did not provide a significant survival benefit for individuals older than 75 with cardiovascular disease, diabetes, or three or more other health conditions.
“Until now, there really weren’t clear data to help us decide whether patients should be screened after age 75,” coinvestigator Andrew T. Chan. MD, MPH, a gastroenterologist and chief of the clinical and translational epidemiology unit at Mass General, said in a statement. “Current guidance was largely based on modeling and extrapolation of studies conducted in other age groups, and not on solid data to show whether screening was actually helpful in an older population.”
In an interview, Dr. Chan said that while the recommendation to screen older adults has to be tailored to individual risk factors, “it should help to provide more confidence for clinicians and patients.”
“I think this is particularly important, because we know that the population as a whole is aging, so more and more people are in this category of over the age of 75, and it’s not an infrequent issue in the clinic as to what to continue with respect to preventative interventions,” he said.
Dr. Kupfer said that the findings by Dr. Chan and colleagues are largely in keeping with guideline recommendations.
“We factor in a lot of different things, including comorbidities, in making the decision to continue screening up to age 85. Certainly, physiological age and chronological age aren’t always the same, so not every 75-year-old is going to be in the same boat,” she said.
“The risk goes up as people get older, but there starts to be competing mortality at some point, and if you have to do a colonoscopy there are obviously issues related to sedation that, as someone gets older, we have to take into consideration,” she added.
Patients frequently confuse screening with surveillance, Dr. Rex said, and he has had patients tell him: “I hear you don’t do these anymore on people over the age of 75.”
“But that’s not true,” Dr. Rex emphasized.
“Screening is generally considered appropriate even up to the age of 85, but between 75 and 85 it should be considered on an individual basis, and there are several considerations there,” Dr. Rex said. “One is whether a patient has ever been screened before. The second is how they were screened. Third is their life expectancy and how many comorbidities they have. And fourth is their personal feelings about it and interest in it.”
He pointed out that the false-positive rate of stool DNA-FIT tests increases with age, and that for older patients who were previously screened, a standard FIT test may be a more appropriate.
So doc, what should I do?
Multiple guidelines, levels of evidence, different screening methods with varying efficacy, individual risk factors – how can clinicians make sense of all these data at the practice level?
“Any modality can be used for screening. Colorectal cancer screening can be done in a number of different ways, and I think that sometimes gets lost in the shuffle, and the thought becomes that everybody has to get a colonoscopy at 45, but there are certainly other tests,” Dr. Kupfer said.
“This just reminds us that we should be thinking about ways we can be doing screening on a population basis, so that we make sure there is equity,” she said.
It’s also important to remember that patients with familial CRC syndromes should begin screening at an even earlier age than average-risk adults, she emphasized.
“To really make a dent in early-onset colorectal cancer, we have to continue to take an active case-finding approach,” she said.
Dr. Rex noted that despite minor differences, the major guidelines are all similar in their initial statements that screening works.
“We’ve still got 50,000 people a year dying from colorectal cancer, lots more than that of new cases,” he said. “If you look at a single factor contributing to that the most, it’s that a lot of the American public is not getting screened at all – it can be up to 40% of the population, depending on what state you’re in.”
Although there are a variety of screening methods available, there are few studies directly comparing them, leaving clinicians at the practice level with the task of presenting all or some of them to patients.
“What the Multi-Society Task Force says that is different, and I think that they get right, is that we don’t have any data [indicating] that offering five, six, or seven options increases the chance of screening – there’s really no evidence that going past two does,” Dr. Rex said.
“The list of options also includes things that nobody actually does,” he added. “For example, flexible sigmoidoscopy has dropped off the map, and FIT has largely replaced guaiac-based testing, even high-sensitivity guaiac. Nobody is really doing CT colonography. The three tests that are being used are colonoscopy, FIT, and [stool DNA-FIT].”
Dr. Rex said that he favors sequential offers, presenting colonoscopy first, emphasizing the benefits for higher-risk patients, and if the patients refuse, offering a fecal-based test.
“Minimizing the number of options makes the conversation feasible, and it’s still very responsible,” he said.
Dr. Kupfer has performed collaborative research with Myriad Genetic Laboratories. She is an editorial advisory board member for GI & Hepatology News from MDedge, part of the Medscape Professional Network. Dr. Rex serves or served as a consultant for Olympus Corporation; Boston Scientific; Medtronic; and Aries; and received research support from Endo-Aid; Olympus Corporation; and Medivators. He has ownership in ai4gi. He is an editorial board member for Medscape Gastroenterology. Dr. Chan has served as a consultant to Pfizer, Bayer AG, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated June 8, 2021.
Build a better mousetrap, and the world will beat a path to your door. Find an accurate, completely noninvasive method for colorectal cancer screening and you’ll probably win the Nobel Prize for Medicine or Physiology.
But until then, we’ll have to make do with colonoscopy, fecal immunochemical testing (FIT), and other messy but necessary means for preventing full-blown CRC and reducing the risk of CRC morbidity and mortality. And start turning to them earlier in patients’ lives.
The U.S. Preventive Services Task Force (USPSTF) has issued an update of its 2016 recommendations for CRC screening, for the first time advising that screening for all average-risk adults begin at age 45. This new recommendation is in line with the guidelines issued by the American Cancer Society, which were updated in 2018, to reflect the inescapable truth that CRC is increasingly being diagnosed at a younger age.
Not to be left out, the U.S. Multi-Society Task Force (MSTF) – which represents the American College of Gastroenterology, the American Gastroenterological Association, and the American Society for Gastrointestinal Endoscopy – issued a statement supporting lowering the age of initial screening in normal-risk adults to 45, and promised that an update of the 2017 guidelines would include the new recommendation.
Recommendations influence reimbursement
Guidelines are often honored as much in the breach as in the observance, but those issued by the USPSTF have unique sway, according to Sonia S. Kupfer, MD, of the section of gastroenterology, hepatology, and nutrition at the University of Chicago, and colleagues.
“While other guidelines have recommended this younger age, the USPSTF guidelines directly inform insurance coverage and waiving of cost sharing as part of federal law,” they wrote in an editorial accompanying the USPSTF guideline statement in the Journal of the American Medical Association.
Although the USPSTF rated its recommendation on starting at age 45 a ‘B’ level – indicating a moderate certainty of moderate benefit – it’s an important step, Dr. Kupfer said in an interview.
“The big advantage here is that we may be able to make a dent in this early-onset colorectal cancer, which, having seen many of these patients, is very alarming, and they don’t always seem to have classic risk factors,” she said. “So, getting them when we can potentially prevent cancer by taking out polyps, or even getting them in an earlier stage, certainly will be beneficial.”
The MSTF also considered recommending 45 as the starting age for normal-risk patients in its 2017 guidelines, noted Douglas Rex, MD, who was chair of the committee that drew up those guidelines, as well as director of endoscopy at Indiana University Hospital in Indianapolis.
“Since that time there has been more evidence, and there’s also some empiric evidence, about the yield of screening in the 45- to 49-year-old age group,” he said in an interview.
The one that gets done
Although the various guidelines differ in specifics, all are in agreement on the general proposition that colonoscopy is the gold standard for screening and detecting the presence of polyps, adenomas, and CRC.
But as USPSTF member Martha Kubik, PhD, RN, director of the George Mason University School of Nursing in Fairfax, Va., said in a statement: “The right test is the one that gets done.”
Gastroenterologists acknowledge that despite its efficacy, colonoscopy is an invasive procedure involving meticulous and unpleasant and/or uncomfortable bowel prep, sedation, and significant time requirements.
In the theory that something is better than nothing, with clinical evidence of varying degrees of quality, the USPSTF recommends the following procedures or tests for average-risk adults:
- Colonoscopy screening every 10 years.
- every 10 years plus annual FIT.
- CT colonography every 5 years.
- High-sensitivity guaiac fecal occult blood test (gFOBT; Hemoccult II) or FIT every year.
- Stool DNA-FIT (Cologuard) every 1 to 3 years.
The Food and Drug Administration also recently approved an artificial intelligence device designed for use with an endoscope, which its manufacturer says can help clinicians detect gastrointestinal lesions they might otherwise miss. This is not a new screening method, but rather an enhancement of existing ones. It neither diagnoses lesions nor recommends treatments, and is not intended to take the place of laboratory sampling.
“I think artificial intelligence is poised to make colonoscopy more effective,” Dr. Rex said. “In the first five trials that we’ve seen, the average increase in the adenoma detection rate has been 11%, and for each 1% gain in the adenoma detection rate, patients have about a 3% decline in their risk of getting cancer after a colonoscopy and about a 5% decline in their risk for fatal cancer. Those are the largest gains that we’ve seen from a technology.”
Different evidence, varied outcomes
Despite the recommendations, a quick dive into the morass of evidence from multiple studies featured in the updated USPSTF guidelines shows that not all screening methods are created equal.
A single colonoscopy, for example, has been shown in large cohort studies to be associated with a 68% reduction in CRC mortality vs. no screening, compared with a 26% reduction with flexible sigmoidoscopy performed every 3-5 years, 22% reduction with Hemoccult II, and 10% with FIT every 2 years.
The USPSTF investigators did not find any studies evaluating the effectiveness of CT colonography, high-sensitivity gFOBT, stool DNA with or without FIT, or serum tests on CRC incidence, CRC mortality, or both.
The two visualization methods for which studies were available, colonoscopy and CT colonography, were generally comparable in sensitivity and specificity for detecting and correctly identifying adenomas 6 mm and larger, although colonography had higher sensitivity for CRC than colonoscopy.
When performed in two to nine annual or biennial rounds, gFOBT was associated with a reduction of CRC-specific mortality of 9% after 19.5 years and 22% at 30 years, compared with no screening.
In observational studies, screening colonoscopy and FIT were both associated with lower risk of CRC incidence or mortality, compared with no screening.
When to stop?
The major guidelines are all in agreement that once an individual reaches age 75, the decision about whether to continue screening should be made on a case-by-case basis, depending on the patient’s overall health, relative risks, and life expectancy.
But if a study published 2 days after the release of the USPSTF guidelines is any indication, just as 45 is the new 50 for starting screening, 85 may be the new 75 for stopping it.
As researchers from Mass General Cancer Center in Boston reported in JAMA Oncology, screening endoscopy for persons older than 75 in otherwise good health can reduce the risk for CRC incidence and CRC-related death by approximately 40%.
The researchers also found, however, that screening did not provide a significant survival benefit for individuals older than 75 with cardiovascular disease, diabetes, or three or more other health conditions.
“Until now, there really weren’t clear data to help us decide whether patients should be screened after age 75,” coinvestigator Andrew T. Chan. MD, MPH, a gastroenterologist and chief of the clinical and translational epidemiology unit at Mass General, said in a statement. “Current guidance was largely based on modeling and extrapolation of studies conducted in other age groups, and not on solid data to show whether screening was actually helpful in an older population.”
In an interview, Dr. Chan said that while the recommendation to screen older adults has to be tailored to individual risk factors, “it should help to provide more confidence for clinicians and patients.”
“I think this is particularly important, because we know that the population as a whole is aging, so more and more people are in this category of over the age of 75, and it’s not an infrequent issue in the clinic as to what to continue with respect to preventative interventions,” he said.
Dr. Kupfer said that the findings by Dr. Chan and colleagues are largely in keeping with guideline recommendations.
“We factor in a lot of different things, including comorbidities, in making the decision to continue screening up to age 85. Certainly, physiological age and chronological age aren’t always the same, so not every 75-year-old is going to be in the same boat,” she said.
“The risk goes up as people get older, but there starts to be competing mortality at some point, and if you have to do a colonoscopy there are obviously issues related to sedation that, as someone gets older, we have to take into consideration,” she added.
Patients frequently confuse screening with surveillance, Dr. Rex said, and he has had patients tell him: “I hear you don’t do these anymore on people over the age of 75.”
“But that’s not true,” Dr. Rex emphasized.
“Screening is generally considered appropriate even up to the age of 85, but between 75 and 85 it should be considered on an individual basis, and there are several considerations there,” Dr. Rex said. “One is whether a patient has ever been screened before. The second is how they were screened. Third is their life expectancy and how many comorbidities they have. And fourth is their personal feelings about it and interest in it.”
He pointed out that the false-positive rate of stool DNA-FIT tests increases with age, and that for older patients who were previously screened, a standard FIT test may be a more appropriate.
So doc, what should I do?
Multiple guidelines, levels of evidence, different screening methods with varying efficacy, individual risk factors – how can clinicians make sense of all these data at the practice level?
“Any modality can be used for screening. Colorectal cancer screening can be done in a number of different ways, and I think that sometimes gets lost in the shuffle, and the thought becomes that everybody has to get a colonoscopy at 45, but there are certainly other tests,” Dr. Kupfer said.
“This just reminds us that we should be thinking about ways we can be doing screening on a population basis, so that we make sure there is equity,” she said.
It’s also important to remember that patients with familial CRC syndromes should begin screening at an even earlier age than average-risk adults, she emphasized.
“To really make a dent in early-onset colorectal cancer, we have to continue to take an active case-finding approach,” she said.
Dr. Rex noted that despite minor differences, the major guidelines are all similar in their initial statements that screening works.
“We’ve still got 50,000 people a year dying from colorectal cancer, lots more than that of new cases,” he said. “If you look at a single factor contributing to that the most, it’s that a lot of the American public is not getting screened at all – it can be up to 40% of the population, depending on what state you’re in.”
Although there are a variety of screening methods available, there are few studies directly comparing them, leaving clinicians at the practice level with the task of presenting all or some of them to patients.
“What the Multi-Society Task Force says that is different, and I think that they get right, is that we don’t have any data [indicating] that offering five, six, or seven options increases the chance of screening – there’s really no evidence that going past two does,” Dr. Rex said.
“The list of options also includes things that nobody actually does,” he added. “For example, flexible sigmoidoscopy has dropped off the map, and FIT has largely replaced guaiac-based testing, even high-sensitivity guaiac. Nobody is really doing CT colonography. The three tests that are being used are colonoscopy, FIT, and [stool DNA-FIT].”
Dr. Rex said that he favors sequential offers, presenting colonoscopy first, emphasizing the benefits for higher-risk patients, and if the patients refuse, offering a fecal-based test.
“Minimizing the number of options makes the conversation feasible, and it’s still very responsible,” he said.
Dr. Kupfer has performed collaborative research with Myriad Genetic Laboratories. She is an editorial advisory board member for GI & Hepatology News from MDedge, part of the Medscape Professional Network. Dr. Rex serves or served as a consultant for Olympus Corporation; Boston Scientific; Medtronic; and Aries; and received research support from Endo-Aid; Olympus Corporation; and Medivators. He has ownership in ai4gi. He is an editorial board member for Medscape Gastroenterology. Dr. Chan has served as a consultant to Pfizer, Bayer AG, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated June 8, 2021.
Physician convicted in buprenorphine scheme faces up to 20 years in prison
A West Virginia physician faces up to 20 years in prison in the wake of his conviction by a federal jury for illegally distributing buprenorphine.
The jury convicted Sriramloo Kesari, MD, 78, of Charleston, for distributing buprenorphine outside the scope of medical practice, according to a U.S. Department of Justice statement.
Investigators from the Drug Enforcement Administration presented evidence at the trial that Dr. Kesari, a general practitioner, operated a cash-only business selling buprenorphine prescriptions.
Federal prosecutors said that the physician signed prescriptions, which were then distributed by an employee in exchange for cash. Dr. Kesari was often absent, at times physically located in California, according to the federal government.
Prosecutors indicted the West Virginia physician in September 2019 as part of an “opioid strikeforce takedown” in Ohio, Virginia, and West Virginia that resulted in charges against 13 individuals, including 11 physicians.
Dr. Kesari’s attorneys filed motions during the course of the lengthy case showing that psychiatric and neurological exams indicated that the physician was cognitively impaired.
Based on that evidence and the federal indictment, the West Virginia Board of Medicine suspended Dr. Kesari’s license in February 2020, stating that he is not “mentally and/or physically fit to practice medicine and surgery with reasonable skill and safety.”
Dr. Kesari was first licensed in West Virginia in 1979. In 1987, the Board of Medicine placed Dr. Kesari on a 3-year probation because of his failure to keep records for patients for whom he was prescribing controlled substances.
However, within a few months, the Board changed the probation order to allow Dr. Kesari to write prescriptions for schedule II and III substances in the Boone Hospital emergency room where he continued to work.
The physician had no other disciplinary actions until his license suspension, but the Board lists settlement of four malpractice cases and the dismissal of a fifth between 1986 and 2001.
A version of this article first appeared on Medscape.com.
A West Virginia physician faces up to 20 years in prison in the wake of his conviction by a federal jury for illegally distributing buprenorphine.
The jury convicted Sriramloo Kesari, MD, 78, of Charleston, for distributing buprenorphine outside the scope of medical practice, according to a U.S. Department of Justice statement.
Investigators from the Drug Enforcement Administration presented evidence at the trial that Dr. Kesari, a general practitioner, operated a cash-only business selling buprenorphine prescriptions.
Federal prosecutors said that the physician signed prescriptions, which were then distributed by an employee in exchange for cash. Dr. Kesari was often absent, at times physically located in California, according to the federal government.
Prosecutors indicted the West Virginia physician in September 2019 as part of an “opioid strikeforce takedown” in Ohio, Virginia, and West Virginia that resulted in charges against 13 individuals, including 11 physicians.
Dr. Kesari’s attorneys filed motions during the course of the lengthy case showing that psychiatric and neurological exams indicated that the physician was cognitively impaired.
Based on that evidence and the federal indictment, the West Virginia Board of Medicine suspended Dr. Kesari’s license in February 2020, stating that he is not “mentally and/or physically fit to practice medicine and surgery with reasonable skill and safety.”
Dr. Kesari was first licensed in West Virginia in 1979. In 1987, the Board of Medicine placed Dr. Kesari on a 3-year probation because of his failure to keep records for patients for whom he was prescribing controlled substances.
However, within a few months, the Board changed the probation order to allow Dr. Kesari to write prescriptions for schedule II and III substances in the Boone Hospital emergency room where he continued to work.
The physician had no other disciplinary actions until his license suspension, but the Board lists settlement of four malpractice cases and the dismissal of a fifth between 1986 and 2001.
A version of this article first appeared on Medscape.com.
A West Virginia physician faces up to 20 years in prison in the wake of his conviction by a federal jury for illegally distributing buprenorphine.
The jury convicted Sriramloo Kesari, MD, 78, of Charleston, for distributing buprenorphine outside the scope of medical practice, according to a U.S. Department of Justice statement.
Investigators from the Drug Enforcement Administration presented evidence at the trial that Dr. Kesari, a general practitioner, operated a cash-only business selling buprenorphine prescriptions.
Federal prosecutors said that the physician signed prescriptions, which were then distributed by an employee in exchange for cash. Dr. Kesari was often absent, at times physically located in California, according to the federal government.
Prosecutors indicted the West Virginia physician in September 2019 as part of an “opioid strikeforce takedown” in Ohio, Virginia, and West Virginia that resulted in charges against 13 individuals, including 11 physicians.
Dr. Kesari’s attorneys filed motions during the course of the lengthy case showing that psychiatric and neurological exams indicated that the physician was cognitively impaired.
Based on that evidence and the federal indictment, the West Virginia Board of Medicine suspended Dr. Kesari’s license in February 2020, stating that he is not “mentally and/or physically fit to practice medicine and surgery with reasonable skill and safety.”
Dr. Kesari was first licensed in West Virginia in 1979. In 1987, the Board of Medicine placed Dr. Kesari on a 3-year probation because of his failure to keep records for patients for whom he was prescribing controlled substances.
However, within a few months, the Board changed the probation order to allow Dr. Kesari to write prescriptions for schedule II and III substances in the Boone Hospital emergency room where he continued to work.
The physician had no other disciplinary actions until his license suspension, but the Board lists settlement of four malpractice cases and the dismissal of a fifth between 1986 and 2001.
A version of this article first appeared on Medscape.com.
Child suicides drive Colorado hospital to declare state of emergency
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.

From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.

The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by

However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.
From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.
The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by
However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
On May 25, Jena Hausmann, CEO of Children’s Hospital Colorado, Aurora, declared a state of emergency in youth mental health in response to an astronomical increase in pediatric mental health cases, including suicide, which has overwhelmed the institution.
From April 2019 to April 2021, the demand for pediatric behavioral health treatment at the hospital system increased by 90%. In Colorado, suicide is now the number one cause of death among youth and occurs in children as young as 10 years of age.
“Now we are seeing our pediatric emergency departments and our inpatient units overrun with kids attempting suicide and suffering from other forms of major mental health illness,” Dr. Hausmann said in a press release.
“We had to draw attention to what we’re seeing in our hospital and our community on an everyday basis – an unprecedented number of suicidal children who need acute treatment for behavioral health problems – and when I say ‘unprecedented,’ I’m serious – I’ve been in pediatrics for two decades and have never seen anything like this before,” David Brumbaugh, MD, a pediatric gastroenterologist and chief medical officer for Children’s Colorado, told this news organization.
Christine Crawford, MD, associate medical director of the National Alliance on Mental Illness, stated in an interview that she “commends the CEO of the hospital for making this announcement, because it is outrageous to see what is happening with more and more children with significant psychiatric symptoms who are not getting adequate care.”
Jenna Glover, PhD, child psychologist and director of psychology training at Children’s Hospital, said that during the past decade, there has been a steady increase in depression, anxiety, and suicide among youth in Colorado. Suicide, she added, is now the number one cause of death in youth, “so we were already in a state of crisis.” She added that COVID-19 was “the straw that broke the camel’s back.”
“In January to April of this year, behavioral health ED visits to Children’s Hospital were 72% higher than they were 2 years ago at this time,” she said. “Colorado Springs had a 145% increase for ED behavioral health visits during the first 4 months of 2021, compared to the first 4 months of 2020.”
COVID’s impact
Other problems that have been “skyrocketing” in youth are self-harm, substance use, and eating disorders. Younger children are experiencing an increase in behavioral problems, including developmental regression, such as tantrums, and problems with sleeping, toileting, and eating, Dr. Glover noted.
The youth mental health crisis has mushroomed, although social distancing requirements are now beginning to ease and we are in the “home stretch of the pandemic,” Dr. Brumbaugh said.
One possible reason “is that we took kids out of their normal routines, social circles, friendships, etc., for 12 months, and that was the limit of their physiological or mental resistance, and they got to the end of their rope,” he speculated.
Dr. Glover said, “Kids are burned out, and although they’re asking to return to their life, they don’t feel they have the resources. They feel so behind; they don’t know how to catch up.”
Dr. Brumbaugh said that there are not enough child psychiatrists to provide outpatient services or enough inpatient beds for children in crisis.
“This is an unacceptable situation. We would never allow a child with leukemia or appendicitis to go several weeks without treatment,” he said.
Community donors have come forward, enabling an anticipated 50% increase in Children’s Hospital’s mental health outpatient, inpatient, and day services by March 2022.
“On a hospital level, we are continuing to do things to expand access to care, like opening units that provide different levels of care for patients with psychiatric problems, as well as expanding into areas that are more rural,” Dr. Glover said.
However, the “blueprint is not in action yet, and a lot of money still needs to be allocated. A workforce has to be created, because there are not enough clinicians to fill these roles,” she added.
Chronic underfunding
Dr. Brumbaugh said Colorado has always had a “relatively underfunded behavioral health system for kids.” A 2021 report by
However, Dr. Glover noted that Colorado is “not exceptional.” The increased vulnerability to youth mental illness and suicide is characteristic of other mountain states, which have larger rural areas, less access to care, and increased access to guns, she said.
Mass shootings may have amped up stress levels. “For some kids, this is happening in their schools or towns, and they feel traumatized and unsafe,” Dr. Glover added.
Dr. Crawford, who is an assistant professor of psychiatry at Boston University, also pointed out that the mental health crisis in youth is not unique to Colorado.
“Throughout the country, we’ve seen these colliding pandemics – inadequate mental health resources for children and COVID-19, which exacerbated the existing mental health crisis,” she said.
“The pandemic led to an increase in telehealth services, making individual and group psychotherapy available to kids in areas that never had access to these before, which is a ‘silver lining’ of the pandemic,” Dr. Glover said.
Dr. Crawford is “encouraged that we are having more conversations about pediatric mental health, because the pandemic amplified what was already going on and made it impossible to ignore.”
Screening is essential
Screening for mental health problems should be at the top of the mind of pediatricians and other clinicians who work with children, Dr. Glover said.
“Pediatricians are in the best place to catch potentially suicidal kids, because they are more likely to see these kids than therapists,” she noted.
She suggested using a rapid screen for depression, such as the Patient Health Questionnaire-9 (PHQ-9) modified for adolescents. Parents can also fill out a PHQ-9 for younger children and even for themselves.
“Depression, anxiety, and suicidality affect the whole family, so screening for these conditions in adults will benefit the children too,” she said. Teachers should also “be aware of what depression and anxiety symptoms look like in kids, because sometimes they can manifest more as irritability,” Dr. Glover added.
Policymakers and insurers need to prioritize pediatric mental health when determining allocation of health care, said Dr. Crawford.
“Financial incentives should be provided for hospitals to want to reserve beds for psychiatric patients, and in the outpatient setting, we also need to look at the payment structure of psychiatric visits,” she added.
Many psychiatrists do not want to accept insurance because of the increased bureaucracy and low reimbursement rates of insurance companies, and families cannot afford to pay out of pocket, “so we really need to look at the insurance issue at a policy level,” Dr. Crawford said.
Dr. Brumbaugh, Dr. Glover, and Dr. Crawford have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Noses can be electronic, and toilets can be smart
Cancer loses … by a nose
Since the human nose is unpredictable at best, we’ve learned to rely on animals for our detailed nozzle needs. But researchers have found the next best thing to man’s best friend to accurately identify cancers.
A team at the University of Pennsylvania has developed an electronic olfaction, or “e-nose,” that has a 95% accuracy rate in distinguishing benign and malignant pancreatic and ovarian cancer cells from a single blood sample. How?
The e-nose system is equipped with nanosensors that are able to detect the volatile organic compounds (VOCs) emitted by cells in a blood sample. Not only does this create an opportunity for an easier, noninvasive screening practice, but it’s fast. The e-nose can distinguish VOCs from healthy to cancerous blood cells in 20 minutes or less and is just as effective in picking up on early- and late-stage cancers.

The investigators hope that this innovative technology can pave the way for similar devices with other uses. Thanks to the e-nose, a handheld device is in development that may be able to sniff out the signature odor of people with COVID-19.
That’s one smart schnoz.
Do you think this is a (food) game?
Dieting and eating healthy is tough, even during the best of times, and it has not been the best of times. With all respect to Charles Dickens, it’s been the worst of times, full stop. Millions of people have spent the past year sitting around their homes doing nothing, and it’s only natural that many would let their discipline slide.
Naturally, the solution to unhealthy eating habits is to sit down and play with your phone. No, that’s not the joke, the Food Trainer app, available on all cellular devices near you, is designed to encourage healthy eating by turning it into a game of sorts. When users open the app, they’re presented with images of food, and they’re trained to tap on images of healthy food and pass on images of unhealthy ones. The process takes less than 5 minutes.
It sounds really simple, but in a study of more than 1,000 people, consumption of junk food fell by 1 point on an 8-point scale (ranging from four times per day to zero to one time per month), participants lost about half a kilogram (a little over one pound), and more healthy food was eaten. Those who used the app more regularly, along the lines of 10 times per month or more, saw greater benefits.

The authors did acknowledge that those who used the app more may have been more motivated to lose weight anyway, which perhaps limits the overall benefit, but reviews on Google Play were overall quite positive, and if there’s one great truth in this world, it’s that Internet reviewers are almost impossible to please. So perhaps this app is worth looking into if you’re like the LOTME staff and you’re up at the top end of that 8-point scale. What, pizza is delicious, who wouldn’t eat it four times a day? And you can also get it from your phone!
It’s time for a little mass kickin’
The universe, scientists tell us, is a big place. Really big. Chromosomes, scientists tell us, are small. Really small. But despite this very fundamental difference, the universe and chromosomes share a deep, dark secret: unexplained mass.
This being a medical publication, we’ll start with chromosomes. A group of researchers measured their mass with x-rays for the first time and found that “the 46 chromosomes in each of our cells weigh 242 picograms (trillionths of a gram). This is heavier than we would expect, and, if replicated, points to unexplained excess mass in chromosomes,” Ian K. Robinson, PhD, said in a written statement.
We’re not just talking about a bit of a beer belly here. “The chromosomes were about 20 times heavier than the DNA they contained,” according to the investigators.
Now to the universe. Here’s what CERN, the European Council for Nuclear Research, has to say about the mass of the universe: “Galaxies in our universe … are rotating with such speed that the gravity generated by their observable matter could not possibly hold them together. … which leads scientists to believe that something we cannot see is at work. They think something we have yet to detect directly is giving these galaxies extra mass.”
But wait, there’s more! “The matter we know and that makes up all stars and galaxies only accounts for 5% of the content of the universe!”
So chromosomes are about 20 times heavier than the DNA they contain, and the universe is about 20 times heavier than the matter that can be seen. Interesting.
We are, of course, happy to share this news with our readers, but there is one catch: Don’t tell Neil deGrasse Tyson. He’ll want to reclassify our genetic solar system into 45 chromosomes and one dwarf chromosome.
A photo finish for the Smart Toilet
We know that poop can tell us a lot about our health, but new research by scientists at Duke University is really on a roll. Their Smart Toilet has been created to help people keep an eye on their bowel health. The device takes pictures of poop after it is flushed and can tell whether the consistency is loose, bloody, or normal.
The Smart Toilet can really help people with issues such as irritable bowel syndrome and inflammatory bowel disease by helping them, and their doctors, keep tabs on their poop. “Typically, gastroenterologists have to rely on patient self-reported information about their stool to help determine the cause of their gastrointestinal health issues, which can be very unreliable,” study lead author Deborah Fisher said.

Not many people look too closely at their poop before it’s flushed, so the fecal photos can make a big difference. The Smart Toilet is installed into the pipes of a toilet and does its thing when the toilet is flushed, so there doesn’t seem to be much work on the patient’s end. Other than the, um, you know, usual work from the patient’s end.
Cancer loses … by a nose
Since the human nose is unpredictable at best, we’ve learned to rely on animals for our detailed nozzle needs. But researchers have found the next best thing to man’s best friend to accurately identify cancers.
A team at the University of Pennsylvania has developed an electronic olfaction, or “e-nose,” that has a 95% accuracy rate in distinguishing benign and malignant pancreatic and ovarian cancer cells from a single blood sample. How?
The e-nose system is equipped with nanosensors that are able to detect the volatile organic compounds (VOCs) emitted by cells in a blood sample. Not only does this create an opportunity for an easier, noninvasive screening practice, but it’s fast. The e-nose can distinguish VOCs from healthy to cancerous blood cells in 20 minutes or less and is just as effective in picking up on early- and late-stage cancers.
The investigators hope that this innovative technology can pave the way for similar devices with other uses. Thanks to the e-nose, a handheld device is in development that may be able to sniff out the signature odor of people with COVID-19.
That’s one smart schnoz.
Do you think this is a (food) game?
Dieting and eating healthy is tough, even during the best of times, and it has not been the best of times. With all respect to Charles Dickens, it’s been the worst of times, full stop. Millions of people have spent the past year sitting around their homes doing nothing, and it’s only natural that many would let their discipline slide.
Naturally, the solution to unhealthy eating habits is to sit down and play with your phone. No, that’s not the joke, the Food Trainer app, available on all cellular devices near you, is designed to encourage healthy eating by turning it into a game of sorts. When users open the app, they’re presented with images of food, and they’re trained to tap on images of healthy food and pass on images of unhealthy ones. The process takes less than 5 minutes.
It sounds really simple, but in a study of more than 1,000 people, consumption of junk food fell by 1 point on an 8-point scale (ranging from four times per day to zero to one time per month), participants lost about half a kilogram (a little over one pound), and more healthy food was eaten. Those who used the app more regularly, along the lines of 10 times per month or more, saw greater benefits.
The authors did acknowledge that those who used the app more may have been more motivated to lose weight anyway, which perhaps limits the overall benefit, but reviews on Google Play were overall quite positive, and if there’s one great truth in this world, it’s that Internet reviewers are almost impossible to please. So perhaps this app is worth looking into if you’re like the LOTME staff and you’re up at the top end of that 8-point scale. What, pizza is delicious, who wouldn’t eat it four times a day? And you can also get it from your phone!
It’s time for a little mass kickin’
The universe, scientists tell us, is a big place. Really big. Chromosomes, scientists tell us, are small. Really small. But despite this very fundamental difference, the universe and chromosomes share a deep, dark secret: unexplained mass.
This being a medical publication, we’ll start with chromosomes. A group of researchers measured their mass with x-rays for the first time and found that “the 46 chromosomes in each of our cells weigh 242 picograms (trillionths of a gram). This is heavier than we would expect, and, if replicated, points to unexplained excess mass in chromosomes,” Ian K. Robinson, PhD, said in a written statement.
We’re not just talking about a bit of a beer belly here. “The chromosomes were about 20 times heavier than the DNA they contained,” according to the investigators.
Now to the universe. Here’s what CERN, the European Council for Nuclear Research, has to say about the mass of the universe: “Galaxies in our universe … are rotating with such speed that the gravity generated by their observable matter could not possibly hold them together. … which leads scientists to believe that something we cannot see is at work. They think something we have yet to detect directly is giving these galaxies extra mass.”
But wait, there’s more! “The matter we know and that makes up all stars and galaxies only accounts for 5% of the content of the universe!”
So chromosomes are about 20 times heavier than the DNA they contain, and the universe is about 20 times heavier than the matter that can be seen. Interesting.
We are, of course, happy to share this news with our readers, but there is one catch: Don’t tell Neil deGrasse Tyson. He’ll want to reclassify our genetic solar system into 45 chromosomes and one dwarf chromosome.
A photo finish for the Smart Toilet
We know that poop can tell us a lot about our health, but new research by scientists at Duke University is really on a roll. Their Smart Toilet has been created to help people keep an eye on their bowel health. The device takes pictures of poop after it is flushed and can tell whether the consistency is loose, bloody, or normal.
The Smart Toilet can really help people with issues such as irritable bowel syndrome and inflammatory bowel disease by helping them, and their doctors, keep tabs on their poop. “Typically, gastroenterologists have to rely on patient self-reported information about their stool to help determine the cause of their gastrointestinal health issues, which can be very unreliable,” study lead author Deborah Fisher said.
Not many people look too closely at their poop before it’s flushed, so the fecal photos can make a big difference. The Smart Toilet is installed into the pipes of a toilet and does its thing when the toilet is flushed, so there doesn’t seem to be much work on the patient’s end. Other than the, um, you know, usual work from the patient’s end.
Cancer loses … by a nose
Since the human nose is unpredictable at best, we’ve learned to rely on animals for our detailed nozzle needs. But researchers have found the next best thing to man’s best friend to accurately identify cancers.
A team at the University of Pennsylvania has developed an electronic olfaction, or “e-nose,” that has a 95% accuracy rate in distinguishing benign and malignant pancreatic and ovarian cancer cells from a single blood sample. How?
The e-nose system is equipped with nanosensors that are able to detect the volatile organic compounds (VOCs) emitted by cells in a blood sample. Not only does this create an opportunity for an easier, noninvasive screening practice, but it’s fast. The e-nose can distinguish VOCs from healthy to cancerous blood cells in 20 minutes or less and is just as effective in picking up on early- and late-stage cancers.
The investigators hope that this innovative technology can pave the way for similar devices with other uses. Thanks to the e-nose, a handheld device is in development that may be able to sniff out the signature odor of people with COVID-19.
That’s one smart schnoz.
Do you think this is a (food) game?
Dieting and eating healthy is tough, even during the best of times, and it has not been the best of times. With all respect to Charles Dickens, it’s been the worst of times, full stop. Millions of people have spent the past year sitting around their homes doing nothing, and it’s only natural that many would let their discipline slide.
Naturally, the solution to unhealthy eating habits is to sit down and play with your phone. No, that’s not the joke, the Food Trainer app, available on all cellular devices near you, is designed to encourage healthy eating by turning it into a game of sorts. When users open the app, they’re presented with images of food, and they’re trained to tap on images of healthy food and pass on images of unhealthy ones. The process takes less than 5 minutes.
It sounds really simple, but in a study of more than 1,000 people, consumption of junk food fell by 1 point on an 8-point scale (ranging from four times per day to zero to one time per month), participants lost about half a kilogram (a little over one pound), and more healthy food was eaten. Those who used the app more regularly, along the lines of 10 times per month or more, saw greater benefits.
The authors did acknowledge that those who used the app more may have been more motivated to lose weight anyway, which perhaps limits the overall benefit, but reviews on Google Play were overall quite positive, and if there’s one great truth in this world, it’s that Internet reviewers are almost impossible to please. So perhaps this app is worth looking into if you’re like the LOTME staff and you’re up at the top end of that 8-point scale. What, pizza is delicious, who wouldn’t eat it four times a day? And you can also get it from your phone!
It’s time for a little mass kickin’
The universe, scientists tell us, is a big place. Really big. Chromosomes, scientists tell us, are small. Really small. But despite this very fundamental difference, the universe and chromosomes share a deep, dark secret: unexplained mass.
This being a medical publication, we’ll start with chromosomes. A group of researchers measured their mass with x-rays for the first time and found that “the 46 chromosomes in each of our cells weigh 242 picograms (trillionths of a gram). This is heavier than we would expect, and, if replicated, points to unexplained excess mass in chromosomes,” Ian K. Robinson, PhD, said in a written statement.
We’re not just talking about a bit of a beer belly here. “The chromosomes were about 20 times heavier than the DNA they contained,” according to the investigators.
Now to the universe. Here’s what CERN, the European Council for Nuclear Research, has to say about the mass of the universe: “Galaxies in our universe … are rotating with such speed that the gravity generated by their observable matter could not possibly hold them together. … which leads scientists to believe that something we cannot see is at work. They think something we have yet to detect directly is giving these galaxies extra mass.”
But wait, there’s more! “The matter we know and that makes up all stars and galaxies only accounts for 5% of the content of the universe!”
So chromosomes are about 20 times heavier than the DNA they contain, and the universe is about 20 times heavier than the matter that can be seen. Interesting.
We are, of course, happy to share this news with our readers, but there is one catch: Don’t tell Neil deGrasse Tyson. He’ll want to reclassify our genetic solar system into 45 chromosomes and one dwarf chromosome.
A photo finish for the Smart Toilet
We know that poop can tell us a lot about our health, but new research by scientists at Duke University is really on a roll. Their Smart Toilet has been created to help people keep an eye on their bowel health. The device takes pictures of poop after it is flushed and can tell whether the consistency is loose, bloody, or normal.
The Smart Toilet can really help people with issues such as irritable bowel syndrome and inflammatory bowel disease by helping them, and their doctors, keep tabs on their poop. “Typically, gastroenterologists have to rely on patient self-reported information about their stool to help determine the cause of their gastrointestinal health issues, which can be very unreliable,” study lead author Deborah Fisher said.
Not many people look too closely at their poop before it’s flushed, so the fecal photos can make a big difference. The Smart Toilet is installed into the pipes of a toilet and does its thing when the toilet is flushed, so there doesn’t seem to be much work on the patient’s end. Other than the, um, you know, usual work from the patient’s end.