User login
Delta variant could drive herd immunity threshold over 80%
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
New moms latched on to remote breastfeeding help. Will demand wane as pandemic fades?
Madison Cano knew she wanted to breastfeed her son, Theo. But breastfeeding was painful for her. The skin on her breasts was chafed and blistered last July when she returned home from the hospital. And Theo sometimes screamed during feedings.
Ms. Cano, 30, realized she needed help to get the short- and long-term health benefits of breastfeeding for moms and babies. New studies (Am J Obstet Gynecol. 2021 Mar 26. doi: 10.1016/j.ajog.2021.03.023) also have shown that COVID-vaccinated mothers pass protective antibodies on to their newborns. However, Ms. Cano lives in Montrose in western Colorado, 60 miles away from her lactation counselor, Ali Reynolds, in Grand Junction – and it was during the thick of the pandemic.
She messaged Ms. Reynolds on Facebook and took photos and recorded videos of herself breastfeeding so Reynolds could offer advice and encouragement from afar. It worked. She no longer had pain. Ms. Cano is still breastfeeding Theo, who just turned 1.
“I don’t think I would have understood what was happening and been able to work through it without that resource,” said Ms. Cano.
Support for breastfeeding was upended last year, when it no longer seemed safe to take a baby class at the hospital or invite a nurse into one’s home. Hospitals, lactation counselors, and support groups turned to virtual platforms like Zoom or phone calls. That made lactation support accessible to struggling families during the pandemic, said Danielle Harmon, executive director of the United States Lactation Consultant Association.
Today, although lactation specialists have more options to safely meet in person with families after their COVID-19 vaccinations, many are choosing to continue virtual classes, keeping alive the online communities they created and relying on the technology that worked for many families. Virtual options especially help those in remote areas or those with limited transportation access, breastfeeding experts say.
Right before the pandemic, for example, Sandrine Druon typically had one or two moms attend in-person meetings she held for La Leche League of Longmont at the First Evangelical Lutheran Church or at a Ziggi’s Coffee shop. But because they could no longer meet in person, last June she launched two monthly virtual meetings. Now, an online meeting will typically include 9 or 10 moms. She started an online Spanish-speaking meeting in May and parents joined from their homes in several states and even from other countries. She hopes eventually to have a mix of online and in-person meetings.
The virtual switch hasn’t worked for everyone. Ms. Harmon said the logistics of video support remain difficult, along with privacy concerns on platforms that could be hacked. Other lactation experts noted Black and Hispanic mothers are sometimes still left behind. So lactation specialists are trying to learn from the pandemic on what worked – and what didn’t – to reach all kinds of new parents.
Before the pandemic, 84% of U.S. mothers breastfed at least initially, according to 2019 data from the Centers for Disease Control and Prevention, while Colorado had a 93% rate.
The pandemic hasn’t seemed to change the picture, said Stacy Miller, Colorado’s breastfeeding coordinator for the Special Supplemental Nutrition Program for Women, Infants, and Children, shorthanded as WIC. Citing state birth certificate data, Ms. Miller said preliminary breastfeeding rates among families discharged from Colorado hospitals remained similar in the first quarter of 2021 to rates from 2020 or 2019.
Throughout the pandemic, lactation specialists have tried to offer convenient options for parents. St. Joseph Hospital in Denver launched virtual breastfeeding support groups that still occur today, in addition to breastfeeding help during families’ hospital stays, said Katie Halverstadt, the hospital’s clinical nurse manager of lactation and family education.
Last year in North Carolina, experts adapted an in-person prenatal breastfeeding program to an interactive video platform in English and Spanish. A separate effort on New York’s Long Island successfully converted in-person breastfeeding support to phone and video calls in 2020.
To help support parents in Grand Junction, Colo., Ms. Reynolds expanded her private practice, Valley Lactation, by offering virtual appointments while continuing to see some clients in their homes. That hybrid model continues today, although Ms. Reynolds said the demand for virtual or phone appointments has decreased lately as the country reopens.
Paying out-of-pocket for appointments is a hurdle her clients face, said Ms. Reynolds, but she encourages them to submit claims for telehealth or in-person visits to their health insurance companies for reimbursement. Early in the pandemic, telehealth rules were relaxed to encourage more telephone and virtual appointments – many of which have been covered by insurance.
But insurance coverage for lactation support will likely continue to be an issue independent of whether pandemic telehealth rules expire, Ms. Harmon said. While the Affordable Care Act mandates that insurance companies cover lactation support and supplies, such as breast pumps, Ms. Harmon said reimbursement is often spotty. Mirroring Medicaid, insurance providers often cover services only from licensed providers, she said, but just four states – Georgia, New Mexico, Oregon, and Rhode Island – license lactation consultants.
Experts such as Jennifer Schindler-Ruwisch, an assistant professor at Fairfield (Conn.) University, found the pandemic may have exacerbated breastfeeding barriers for those without access to online technology or translation services, among other things. She published one of the first studies in the United States to examine COVID’s effect on lactation services by collecting experiences from lactation support providers in Connecticut, including many working in WIC programs. For income-eligible WIC families, all breastfeeding classes, peer groups and one-on-one consultations are free.
Birdie Johnson, a doula who provides breastfeeding and other postpartum support to Black families as part of Sacred Seeds Black Doula Collective of Colorado, said virtual support groups during the pandemic also did not meet her clients’ needs for connection and interaction. Social media built communities online, particularly by normalizing breastfeeding struggles among Black parents, she said, but obstacles remained.
“COVID brought our community together and at the same time destroyed it,” Ms. Johnson said.
Black parents in the United States already had lower rates of breastfeeding than Asian or White parents, according to 2017 CDC data, and both Black and Hispanic parents have had lower rates of exclusively breastfeeding their babies at 6 months, which is what the American Academy of Pediatrics recommends. Socioeconomics and lack of workplace support have been found to contribute to the gap. Research also has found Black mothers are more likely than White moms to be introduced to infant formula at hospitals.
A scarcity of Black health care providers in lactation, women’s health and pediatrics is a continuing concern, Ms. Johnson said. In Colorado last year, the Colorado Breastfeeding Coalition, the Center for African American Health, Elephant Circle and Families Forward Resource Center held three training sessions for people of color to become lactation specialists, said Ms. Halverstadt, who chairs the coalition.
Jefferson County, which encompasses much of Denver’s western suburbs, is now training at least a dozen Spanish-speaking community members for lactation certification. In addition to classes, the trainees log clinical hours in breastfeeding support, sometimes during virtual meetings of a Spanish-speaking support group called Cuenta Conmigo Lactancia.
“You are more confident and more at ease with someone who knows your language, your culture and who is part of the community,” said Brenda Rodriguez, a dietitian and certified lactation consultant for Jefferson County Public Health, which reaches roughly 400 breastfeeding families each month through its WIC programs.
Angelica Pereda, a maternal and child health registered nurse, is part of that training program. Ms. Pereda, who is Hispanic and bilingual, gave birth to son Ahmias in April 2020 and struggled with breastfeeding because he could not latch on to her breasts. A lactation consultant could not come into her home during the pandemic, and she was skeptical of virtual consultations because of privacy concerns. So she pumped her breast milk and bottle-fed it to her son.
Her experience gave her newfound empathy for families, and she wants to help other Spanish-speaking parents find solutions – whether in person or virtually.
“There is just not enough breastfeeding support in general, but especially when that support is in a different language,” said Ms. Pereda.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Madison Cano knew she wanted to breastfeed her son, Theo. But breastfeeding was painful for her. The skin on her breasts was chafed and blistered last July when she returned home from the hospital. And Theo sometimes screamed during feedings.
Ms. Cano, 30, realized she needed help to get the short- and long-term health benefits of breastfeeding for moms and babies. New studies (Am J Obstet Gynecol. 2021 Mar 26. doi: 10.1016/j.ajog.2021.03.023) also have shown that COVID-vaccinated mothers pass protective antibodies on to their newborns. However, Ms. Cano lives in Montrose in western Colorado, 60 miles away from her lactation counselor, Ali Reynolds, in Grand Junction – and it was during the thick of the pandemic.
She messaged Ms. Reynolds on Facebook and took photos and recorded videos of herself breastfeeding so Reynolds could offer advice and encouragement from afar. It worked. She no longer had pain. Ms. Cano is still breastfeeding Theo, who just turned 1.
“I don’t think I would have understood what was happening and been able to work through it without that resource,” said Ms. Cano.
Support for breastfeeding was upended last year, when it no longer seemed safe to take a baby class at the hospital or invite a nurse into one’s home. Hospitals, lactation counselors, and support groups turned to virtual platforms like Zoom or phone calls. That made lactation support accessible to struggling families during the pandemic, said Danielle Harmon, executive director of the United States Lactation Consultant Association.
Today, although lactation specialists have more options to safely meet in person with families after their COVID-19 vaccinations, many are choosing to continue virtual classes, keeping alive the online communities they created and relying on the technology that worked for many families. Virtual options especially help those in remote areas or those with limited transportation access, breastfeeding experts say.
Right before the pandemic, for example, Sandrine Druon typically had one or two moms attend in-person meetings she held for La Leche League of Longmont at the First Evangelical Lutheran Church or at a Ziggi’s Coffee shop. But because they could no longer meet in person, last June she launched two monthly virtual meetings. Now, an online meeting will typically include 9 or 10 moms. She started an online Spanish-speaking meeting in May and parents joined from their homes in several states and even from other countries. She hopes eventually to have a mix of online and in-person meetings.
The virtual switch hasn’t worked for everyone. Ms. Harmon said the logistics of video support remain difficult, along with privacy concerns on platforms that could be hacked. Other lactation experts noted Black and Hispanic mothers are sometimes still left behind. So lactation specialists are trying to learn from the pandemic on what worked – and what didn’t – to reach all kinds of new parents.
Before the pandemic, 84% of U.S. mothers breastfed at least initially, according to 2019 data from the Centers for Disease Control and Prevention, while Colorado had a 93% rate.
The pandemic hasn’t seemed to change the picture, said Stacy Miller, Colorado’s breastfeeding coordinator for the Special Supplemental Nutrition Program for Women, Infants, and Children, shorthanded as WIC. Citing state birth certificate data, Ms. Miller said preliminary breastfeeding rates among families discharged from Colorado hospitals remained similar in the first quarter of 2021 to rates from 2020 or 2019.
Throughout the pandemic, lactation specialists have tried to offer convenient options for parents. St. Joseph Hospital in Denver launched virtual breastfeeding support groups that still occur today, in addition to breastfeeding help during families’ hospital stays, said Katie Halverstadt, the hospital’s clinical nurse manager of lactation and family education.
Last year in North Carolina, experts adapted an in-person prenatal breastfeeding program to an interactive video platform in English and Spanish. A separate effort on New York’s Long Island successfully converted in-person breastfeeding support to phone and video calls in 2020.
To help support parents in Grand Junction, Colo., Ms. Reynolds expanded her private practice, Valley Lactation, by offering virtual appointments while continuing to see some clients in their homes. That hybrid model continues today, although Ms. Reynolds said the demand for virtual or phone appointments has decreased lately as the country reopens.
Paying out-of-pocket for appointments is a hurdle her clients face, said Ms. Reynolds, but she encourages them to submit claims for telehealth or in-person visits to their health insurance companies for reimbursement. Early in the pandemic, telehealth rules were relaxed to encourage more telephone and virtual appointments – many of which have been covered by insurance.
But insurance coverage for lactation support will likely continue to be an issue independent of whether pandemic telehealth rules expire, Ms. Harmon said. While the Affordable Care Act mandates that insurance companies cover lactation support and supplies, such as breast pumps, Ms. Harmon said reimbursement is often spotty. Mirroring Medicaid, insurance providers often cover services only from licensed providers, she said, but just four states – Georgia, New Mexico, Oregon, and Rhode Island – license lactation consultants.
Experts such as Jennifer Schindler-Ruwisch, an assistant professor at Fairfield (Conn.) University, found the pandemic may have exacerbated breastfeeding barriers for those without access to online technology or translation services, among other things. She published one of the first studies in the United States to examine COVID’s effect on lactation services by collecting experiences from lactation support providers in Connecticut, including many working in WIC programs. For income-eligible WIC families, all breastfeeding classes, peer groups and one-on-one consultations are free.
Birdie Johnson, a doula who provides breastfeeding and other postpartum support to Black families as part of Sacred Seeds Black Doula Collective of Colorado, said virtual support groups during the pandemic also did not meet her clients’ needs for connection and interaction. Social media built communities online, particularly by normalizing breastfeeding struggles among Black parents, she said, but obstacles remained.
“COVID brought our community together and at the same time destroyed it,” Ms. Johnson said.
Black parents in the United States already had lower rates of breastfeeding than Asian or White parents, according to 2017 CDC data, and both Black and Hispanic parents have had lower rates of exclusively breastfeeding their babies at 6 months, which is what the American Academy of Pediatrics recommends. Socioeconomics and lack of workplace support have been found to contribute to the gap. Research also has found Black mothers are more likely than White moms to be introduced to infant formula at hospitals.
A scarcity of Black health care providers in lactation, women’s health and pediatrics is a continuing concern, Ms. Johnson said. In Colorado last year, the Colorado Breastfeeding Coalition, the Center for African American Health, Elephant Circle and Families Forward Resource Center held three training sessions for people of color to become lactation specialists, said Ms. Halverstadt, who chairs the coalition.
Jefferson County, which encompasses much of Denver’s western suburbs, is now training at least a dozen Spanish-speaking community members for lactation certification. In addition to classes, the trainees log clinical hours in breastfeeding support, sometimes during virtual meetings of a Spanish-speaking support group called Cuenta Conmigo Lactancia.
“You are more confident and more at ease with someone who knows your language, your culture and who is part of the community,” said Brenda Rodriguez, a dietitian and certified lactation consultant for Jefferson County Public Health, which reaches roughly 400 breastfeeding families each month through its WIC programs.
Angelica Pereda, a maternal and child health registered nurse, is part of that training program. Ms. Pereda, who is Hispanic and bilingual, gave birth to son Ahmias in April 2020 and struggled with breastfeeding because he could not latch on to her breasts. A lactation consultant could not come into her home during the pandemic, and she was skeptical of virtual consultations because of privacy concerns. So she pumped her breast milk and bottle-fed it to her son.
Her experience gave her newfound empathy for families, and she wants to help other Spanish-speaking parents find solutions – whether in person or virtually.
“There is just not enough breastfeeding support in general, but especially when that support is in a different language,” said Ms. Pereda.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Madison Cano knew she wanted to breastfeed her son, Theo. But breastfeeding was painful for her. The skin on her breasts was chafed and blistered last July when she returned home from the hospital. And Theo sometimes screamed during feedings.
Ms. Cano, 30, realized she needed help to get the short- and long-term health benefits of breastfeeding for moms and babies. New studies (Am J Obstet Gynecol. 2021 Mar 26. doi: 10.1016/j.ajog.2021.03.023) also have shown that COVID-vaccinated mothers pass protective antibodies on to their newborns. However, Ms. Cano lives in Montrose in western Colorado, 60 miles away from her lactation counselor, Ali Reynolds, in Grand Junction – and it was during the thick of the pandemic.
She messaged Ms. Reynolds on Facebook and took photos and recorded videos of herself breastfeeding so Reynolds could offer advice and encouragement from afar. It worked. She no longer had pain. Ms. Cano is still breastfeeding Theo, who just turned 1.
“I don’t think I would have understood what was happening and been able to work through it without that resource,” said Ms. Cano.
Support for breastfeeding was upended last year, when it no longer seemed safe to take a baby class at the hospital or invite a nurse into one’s home. Hospitals, lactation counselors, and support groups turned to virtual platforms like Zoom or phone calls. That made lactation support accessible to struggling families during the pandemic, said Danielle Harmon, executive director of the United States Lactation Consultant Association.
Today, although lactation specialists have more options to safely meet in person with families after their COVID-19 vaccinations, many are choosing to continue virtual classes, keeping alive the online communities they created and relying on the technology that worked for many families. Virtual options especially help those in remote areas or those with limited transportation access, breastfeeding experts say.
Right before the pandemic, for example, Sandrine Druon typically had one or two moms attend in-person meetings she held for La Leche League of Longmont at the First Evangelical Lutheran Church or at a Ziggi’s Coffee shop. But because they could no longer meet in person, last June she launched two monthly virtual meetings. Now, an online meeting will typically include 9 or 10 moms. She started an online Spanish-speaking meeting in May and parents joined from their homes in several states and even from other countries. She hopes eventually to have a mix of online and in-person meetings.
The virtual switch hasn’t worked for everyone. Ms. Harmon said the logistics of video support remain difficult, along with privacy concerns on platforms that could be hacked. Other lactation experts noted Black and Hispanic mothers are sometimes still left behind. So lactation specialists are trying to learn from the pandemic on what worked – and what didn’t – to reach all kinds of new parents.
Before the pandemic, 84% of U.S. mothers breastfed at least initially, according to 2019 data from the Centers for Disease Control and Prevention, while Colorado had a 93% rate.
The pandemic hasn’t seemed to change the picture, said Stacy Miller, Colorado’s breastfeeding coordinator for the Special Supplemental Nutrition Program for Women, Infants, and Children, shorthanded as WIC. Citing state birth certificate data, Ms. Miller said preliminary breastfeeding rates among families discharged from Colorado hospitals remained similar in the first quarter of 2021 to rates from 2020 or 2019.
Throughout the pandemic, lactation specialists have tried to offer convenient options for parents. St. Joseph Hospital in Denver launched virtual breastfeeding support groups that still occur today, in addition to breastfeeding help during families’ hospital stays, said Katie Halverstadt, the hospital’s clinical nurse manager of lactation and family education.
Last year in North Carolina, experts adapted an in-person prenatal breastfeeding program to an interactive video platform in English and Spanish. A separate effort on New York’s Long Island successfully converted in-person breastfeeding support to phone and video calls in 2020.
To help support parents in Grand Junction, Colo., Ms. Reynolds expanded her private practice, Valley Lactation, by offering virtual appointments while continuing to see some clients in their homes. That hybrid model continues today, although Ms. Reynolds said the demand for virtual or phone appointments has decreased lately as the country reopens.
Paying out-of-pocket for appointments is a hurdle her clients face, said Ms. Reynolds, but she encourages them to submit claims for telehealth or in-person visits to their health insurance companies for reimbursement. Early in the pandemic, telehealth rules were relaxed to encourage more telephone and virtual appointments – many of which have been covered by insurance.
But insurance coverage for lactation support will likely continue to be an issue independent of whether pandemic telehealth rules expire, Ms. Harmon said. While the Affordable Care Act mandates that insurance companies cover lactation support and supplies, such as breast pumps, Ms. Harmon said reimbursement is often spotty. Mirroring Medicaid, insurance providers often cover services only from licensed providers, she said, but just four states – Georgia, New Mexico, Oregon, and Rhode Island – license lactation consultants.
Experts such as Jennifer Schindler-Ruwisch, an assistant professor at Fairfield (Conn.) University, found the pandemic may have exacerbated breastfeeding barriers for those without access to online technology or translation services, among other things. She published one of the first studies in the United States to examine COVID’s effect on lactation services by collecting experiences from lactation support providers in Connecticut, including many working in WIC programs. For income-eligible WIC families, all breastfeeding classes, peer groups and one-on-one consultations are free.
Birdie Johnson, a doula who provides breastfeeding and other postpartum support to Black families as part of Sacred Seeds Black Doula Collective of Colorado, said virtual support groups during the pandemic also did not meet her clients’ needs for connection and interaction. Social media built communities online, particularly by normalizing breastfeeding struggles among Black parents, she said, but obstacles remained.
“COVID brought our community together and at the same time destroyed it,” Ms. Johnson said.
Black parents in the United States already had lower rates of breastfeeding than Asian or White parents, according to 2017 CDC data, and both Black and Hispanic parents have had lower rates of exclusively breastfeeding their babies at 6 months, which is what the American Academy of Pediatrics recommends. Socioeconomics and lack of workplace support have been found to contribute to the gap. Research also has found Black mothers are more likely than White moms to be introduced to infant formula at hospitals.
A scarcity of Black health care providers in lactation, women’s health and pediatrics is a continuing concern, Ms. Johnson said. In Colorado last year, the Colorado Breastfeeding Coalition, the Center for African American Health, Elephant Circle and Families Forward Resource Center held three training sessions for people of color to become lactation specialists, said Ms. Halverstadt, who chairs the coalition.
Jefferson County, which encompasses much of Denver’s western suburbs, is now training at least a dozen Spanish-speaking community members for lactation certification. In addition to classes, the trainees log clinical hours in breastfeeding support, sometimes during virtual meetings of a Spanish-speaking support group called Cuenta Conmigo Lactancia.
“You are more confident and more at ease with someone who knows your language, your culture and who is part of the community,” said Brenda Rodriguez, a dietitian and certified lactation consultant for Jefferson County Public Health, which reaches roughly 400 breastfeeding families each month through its WIC programs.
Angelica Pereda, a maternal and child health registered nurse, is part of that training program. Ms. Pereda, who is Hispanic and bilingual, gave birth to son Ahmias in April 2020 and struggled with breastfeeding because he could not latch on to her breasts. A lactation consultant could not come into her home during the pandemic, and she was skeptical of virtual consultations because of privacy concerns. So she pumped her breast milk and bottle-fed it to her son.
Her experience gave her newfound empathy for families, and she wants to help other Spanish-speaking parents find solutions – whether in person or virtually.
“There is just not enough breastfeeding support in general, but especially when that support is in a different language,” said Ms. Pereda.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Midodrine reduces fainting in young patients
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
FROM ANNALS OF INTERNAL MEDICINE
Diabetes drug’s new weight-loss indication fuels cost-benefit debate
The long list of side effects that follow ads for newer expensive drugs to treat type 2 diabetes sometimes include an unusual warning: They might cause weight loss. That side effect is one that many people – especially those with type 2 diabetes, which is associated with obesity – may desperately want.
So it’s no surprise that some of the same drugs are being reformulated and renamed by manufacturers as a new obesity treatment. No longer limited to the crowded field of treatments for type 2 diabetes, which affects about 10% of Americans, they join the far smaller number of drugs for obesity, which affects 42% of Americans and is ready to be mined for profit.
One that recently hit the market – winning Food and Drug Administration approval in June – is Novo Nordisk’s Wegovy (semaglutide), a higher-dose version of the company’s injectable diabetes drug, Ozempic.
Ozempic’s peppy ads suggest that people who use it might lose weight, but also include a disclaimer: that it “is not a weight-loss drug.” Now – with a new name – it is. And clinical trials showed using it leads to significant weight loss for many patients.
“People who go on this medication lose more weight than with any drug we’ve seen, ever,” said Fatima Cody Stanford, MD, MPH, an obesity medicine specialist at Massachusetts General Hospital and Harvard Medical School, both in Boston, who was not involved with any of the clinical trials.
But that leaves employers and insurers in the uncomfortable position of deciding if it’s worth it.
Wegovy’s monthly wholesale price tag – set at $1,349 – is about 58% more than Ozempic’s, although, the company pointed out, the drug’s injector pens contain more than twice as much of the active ingredient. Studies so far show that patients may need to take it indefinitely to maintain weight loss, translating to a tab that could top $323,000 over 20 years at the current price. Weight-loss treatments are not universally covered by insurance policies.
The arrival of this new class of weight-loss drugs – one from Lilly may soon follow – has created a thicket of issues for those who will pay for them. The decision is complicated by many unknowables concerning their long-term use and whether competition might eventually lower the price.
“The metric we try to use is value,” said James Gelfand, senior vice president for health policy at the ERISA Industry Committee, which represents large, self-insured employers. “If we pay for this drug, how much is this going to cost and how much value will it provide to the beneficiaries?”
Weight-loss treatments have had a lackluster past in this regard, with only modest results. Many employers and insurers likely remember Fen-Phen, a combination of fenfluramine and dexfenfluramine that was pulled from the market in the late 1990s for causing heart valve problems.
New drugs like Wegovy, more effective but also pricier than previous weight-loss treatments, will add more fuel to that debate.
Past treatments were shown to prompt weight loss in the range of 5%-10% of body weight. But many had relatively serious or unpleasant side effects.
Wegovy, however, helped patients lose an average of 15% of their body weight over 68 weeks in the main clinical trial that led to its approval. A comparison group that got a placebo injection lost an average of 2.5% over the same period. On the high end, nearly a third of patients in the treatment group lost 20% or more. Both groups had counseling on diet and exercise.
Side effects, generally considered mild, included nausea, diarrhea, vomiting, and constipation. A few patients developed pancreatitis, a serious inflammation of the pancreas. Like the diabetes medication, the drug carries a warning about a potential risk of a type of thyroid cancer.
Weight loss in those taking Wegovy puts it close to the 20%-25% losses seen with bariatric surgery, said Stanford, and well above the 3%-4% seen with diet and other lifestyle changes alone.
Participants also saw reductions in their waistlines and improvements in their blood pressure and blood sugar levels, which may mean they won’t develop diabetes, said Sean Wharton, MD, an internal medicine specialist and adjunct professor at York University in Toronto who was among the coauthors of the report outlining the results of the first clinical trial on Wegovy.
Since weight loss is known to reduce the risk of heart attack, high blood pressure and diabetes, might the new drug type be worth it?
Covering such treatment would be a sea change for Medicare, which specifically bars coverage for obesity medications or drugs for “anorexia, weight loss, or weight gain,” although it does pay for bariatric surgery. Pharmaceutical companies, patient advocates, and some medical professionals are backing proposed federal legislation to allow coverage. But the legislation, the Treat and Reduce Obesity Act, has not made progress despite being reintroduced every year since 2012, and sponsors are now asking federal officials instead to rewrite existing rules.
Private insurers will have to consider a cost-benefit analysis of adding Wegovy to their list of covered treatments, either broadly or with limits. Obesity was first recognized as a disease by the American Medical Association, easing the path for insurance coverage, in 2013.
“Employers are going to have a bit of a challenge” deciding whether to add the benefit to insurance offerings, said Steve Pearson, founder and president of the Institute for Clinical and Economic Review, which provides cost-benefit analyses of medical treatments but has not yet looked at Wegovy.
The trade-offs are embodied in patients like Phylander Pannell, a 49-year-old Largo, Md., woman who said she lost 65 pounds in a clinical trial of Wegovy. That study gave the drug to all participants for the first 20 weeks, then randomly assigned patients to get either the drug or a placebo for the next 48 weeks to determine what happens when the medication is stopped. Only after the trial ended did she find out she was in the treatment group the entire time.
Her weight fell slowly at first, then ramped up, eventually bringing her 190-pound frame down to about 125. Pains in her joints eased; she felt better all around.
“I definitely feel the drug was it for me,” said Ms. Pannell, who also followed the trial’s guidance on diet and exercise.
The study found that both groups lost weight in the initial 20 weeks, but those who continued to get the drug lost an additional average of 7.9% of their body weight. Those who got a placebo gained back nearly 7%.
After the trial ended, and the COVID-19 pandemic hit, Ms. Pannell regained some weight and is now at 155. She is eager to get back on the medication and hopes her job-based insurance will cover it.
Many employers do cover obesity drugs. For example, about 40% of private employer plans include Novo Nordisk’s once-daily injection called Saxenda on their health plans, said Michael Bachner, Novo Nordisk’s director of media relations.
He said the $1,349-a-month wholesale acquisition price of Wegovy was determined by making it equivalent to that of Saxenda, which is less effective.
Still, that is more than the $851 monthly wholesale price of Ozempic. But, he pointed out, the recommended dosage of Wegovy is more than twice that of Ozempic. Four milligrams come in the Ozempic injector pens for the month, while Wegovy has 9.6.
“There’s more drug in the pen,” Mr. Bachner said. “That drives the price up.”
He added: “This is not a 20-year-old drug that we now have a new indication for and are pricing it higher. It’s a whole different clinical program,” which required new trials.
Now scientists, employers, physicians, and patients will have to decide whether the new drugs are worth it.
Earlier estimates – some commissioned by Novo Nordisk – of the potential cost of adding an obesity drug benefit to Medicare showed an overall reduction in spending when better health from the resulting weight loss was factored in.
Still, those earlier estimates considered much less expensive drugs, including a range of generic and branded drugs costing as little as $7 a month to more than $300, a small fraction of Wegovy’s cost.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
The long list of side effects that follow ads for newer expensive drugs to treat type 2 diabetes sometimes include an unusual warning: They might cause weight loss. That side effect is one that many people – especially those with type 2 diabetes, which is associated with obesity – may desperately want.
So it’s no surprise that some of the same drugs are being reformulated and renamed by manufacturers as a new obesity treatment. No longer limited to the crowded field of treatments for type 2 diabetes, which affects about 10% of Americans, they join the far smaller number of drugs for obesity, which affects 42% of Americans and is ready to be mined for profit.
One that recently hit the market – winning Food and Drug Administration approval in June – is Novo Nordisk’s Wegovy (semaglutide), a higher-dose version of the company’s injectable diabetes drug, Ozempic.
Ozempic’s peppy ads suggest that people who use it might lose weight, but also include a disclaimer: that it “is not a weight-loss drug.” Now – with a new name – it is. And clinical trials showed using it leads to significant weight loss for many patients.
“People who go on this medication lose more weight than with any drug we’ve seen, ever,” said Fatima Cody Stanford, MD, MPH, an obesity medicine specialist at Massachusetts General Hospital and Harvard Medical School, both in Boston, who was not involved with any of the clinical trials.
But that leaves employers and insurers in the uncomfortable position of deciding if it’s worth it.
Wegovy’s monthly wholesale price tag – set at $1,349 – is about 58% more than Ozempic’s, although, the company pointed out, the drug’s injector pens contain more than twice as much of the active ingredient. Studies so far show that patients may need to take it indefinitely to maintain weight loss, translating to a tab that could top $323,000 over 20 years at the current price. Weight-loss treatments are not universally covered by insurance policies.
The arrival of this new class of weight-loss drugs – one from Lilly may soon follow – has created a thicket of issues for those who will pay for them. The decision is complicated by many unknowables concerning their long-term use and whether competition might eventually lower the price.
“The metric we try to use is value,” said James Gelfand, senior vice president for health policy at the ERISA Industry Committee, which represents large, self-insured employers. “If we pay for this drug, how much is this going to cost and how much value will it provide to the beneficiaries?”
Weight-loss treatments have had a lackluster past in this regard, with only modest results. Many employers and insurers likely remember Fen-Phen, a combination of fenfluramine and dexfenfluramine that was pulled from the market in the late 1990s for causing heart valve problems.
New drugs like Wegovy, more effective but also pricier than previous weight-loss treatments, will add more fuel to that debate.
Past treatments were shown to prompt weight loss in the range of 5%-10% of body weight. But many had relatively serious or unpleasant side effects.
Wegovy, however, helped patients lose an average of 15% of their body weight over 68 weeks in the main clinical trial that led to its approval. A comparison group that got a placebo injection lost an average of 2.5% over the same period. On the high end, nearly a third of patients in the treatment group lost 20% or more. Both groups had counseling on diet and exercise.
Side effects, generally considered mild, included nausea, diarrhea, vomiting, and constipation. A few patients developed pancreatitis, a serious inflammation of the pancreas. Like the diabetes medication, the drug carries a warning about a potential risk of a type of thyroid cancer.
Weight loss in those taking Wegovy puts it close to the 20%-25% losses seen with bariatric surgery, said Stanford, and well above the 3%-4% seen with diet and other lifestyle changes alone.
Participants also saw reductions in their waistlines and improvements in their blood pressure and blood sugar levels, which may mean they won’t develop diabetes, said Sean Wharton, MD, an internal medicine specialist and adjunct professor at York University in Toronto who was among the coauthors of the report outlining the results of the first clinical trial on Wegovy.
Since weight loss is known to reduce the risk of heart attack, high blood pressure and diabetes, might the new drug type be worth it?
Covering such treatment would be a sea change for Medicare, which specifically bars coverage for obesity medications or drugs for “anorexia, weight loss, or weight gain,” although it does pay for bariatric surgery. Pharmaceutical companies, patient advocates, and some medical professionals are backing proposed federal legislation to allow coverage. But the legislation, the Treat and Reduce Obesity Act, has not made progress despite being reintroduced every year since 2012, and sponsors are now asking federal officials instead to rewrite existing rules.
Private insurers will have to consider a cost-benefit analysis of adding Wegovy to their list of covered treatments, either broadly or with limits. Obesity was first recognized as a disease by the American Medical Association, easing the path for insurance coverage, in 2013.
“Employers are going to have a bit of a challenge” deciding whether to add the benefit to insurance offerings, said Steve Pearson, founder and president of the Institute for Clinical and Economic Review, which provides cost-benefit analyses of medical treatments but has not yet looked at Wegovy.
The trade-offs are embodied in patients like Phylander Pannell, a 49-year-old Largo, Md., woman who said she lost 65 pounds in a clinical trial of Wegovy. That study gave the drug to all participants for the first 20 weeks, then randomly assigned patients to get either the drug or a placebo for the next 48 weeks to determine what happens when the medication is stopped. Only after the trial ended did she find out she was in the treatment group the entire time.
Her weight fell slowly at first, then ramped up, eventually bringing her 190-pound frame down to about 125. Pains in her joints eased; she felt better all around.
“I definitely feel the drug was it for me,” said Ms. Pannell, who also followed the trial’s guidance on diet and exercise.
The study found that both groups lost weight in the initial 20 weeks, but those who continued to get the drug lost an additional average of 7.9% of their body weight. Those who got a placebo gained back nearly 7%.
After the trial ended, and the COVID-19 pandemic hit, Ms. Pannell regained some weight and is now at 155. She is eager to get back on the medication and hopes her job-based insurance will cover it.
Many employers do cover obesity drugs. For example, about 40% of private employer plans include Novo Nordisk’s once-daily injection called Saxenda on their health plans, said Michael Bachner, Novo Nordisk’s director of media relations.
He said the $1,349-a-month wholesale acquisition price of Wegovy was determined by making it equivalent to that of Saxenda, which is less effective.
Still, that is more than the $851 monthly wholesale price of Ozempic. But, he pointed out, the recommended dosage of Wegovy is more than twice that of Ozempic. Four milligrams come in the Ozempic injector pens for the month, while Wegovy has 9.6.
“There’s more drug in the pen,” Mr. Bachner said. “That drives the price up.”
He added: “This is not a 20-year-old drug that we now have a new indication for and are pricing it higher. It’s a whole different clinical program,” which required new trials.
Now scientists, employers, physicians, and patients will have to decide whether the new drugs are worth it.
Earlier estimates – some commissioned by Novo Nordisk – of the potential cost of adding an obesity drug benefit to Medicare showed an overall reduction in spending when better health from the resulting weight loss was factored in.
Still, those earlier estimates considered much less expensive drugs, including a range of generic and branded drugs costing as little as $7 a month to more than $300, a small fraction of Wegovy’s cost.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
The long list of side effects that follow ads for newer expensive drugs to treat type 2 diabetes sometimes include an unusual warning: They might cause weight loss. That side effect is one that many people – especially those with type 2 diabetes, which is associated with obesity – may desperately want.
So it’s no surprise that some of the same drugs are being reformulated and renamed by manufacturers as a new obesity treatment. No longer limited to the crowded field of treatments for type 2 diabetes, which affects about 10% of Americans, they join the far smaller number of drugs for obesity, which affects 42% of Americans and is ready to be mined for profit.
One that recently hit the market – winning Food and Drug Administration approval in June – is Novo Nordisk’s Wegovy (semaglutide), a higher-dose version of the company’s injectable diabetes drug, Ozempic.
Ozempic’s peppy ads suggest that people who use it might lose weight, but also include a disclaimer: that it “is not a weight-loss drug.” Now – with a new name – it is. And clinical trials showed using it leads to significant weight loss for many patients.
“People who go on this medication lose more weight than with any drug we’ve seen, ever,” said Fatima Cody Stanford, MD, MPH, an obesity medicine specialist at Massachusetts General Hospital and Harvard Medical School, both in Boston, who was not involved with any of the clinical trials.
But that leaves employers and insurers in the uncomfortable position of deciding if it’s worth it.
Wegovy’s monthly wholesale price tag – set at $1,349 – is about 58% more than Ozempic’s, although, the company pointed out, the drug’s injector pens contain more than twice as much of the active ingredient. Studies so far show that patients may need to take it indefinitely to maintain weight loss, translating to a tab that could top $323,000 over 20 years at the current price. Weight-loss treatments are not universally covered by insurance policies.
The arrival of this new class of weight-loss drugs – one from Lilly may soon follow – has created a thicket of issues for those who will pay for them. The decision is complicated by many unknowables concerning their long-term use and whether competition might eventually lower the price.
“The metric we try to use is value,” said James Gelfand, senior vice president for health policy at the ERISA Industry Committee, which represents large, self-insured employers. “If we pay for this drug, how much is this going to cost and how much value will it provide to the beneficiaries?”
Weight-loss treatments have had a lackluster past in this regard, with only modest results. Many employers and insurers likely remember Fen-Phen, a combination of fenfluramine and dexfenfluramine that was pulled from the market in the late 1990s for causing heart valve problems.
New drugs like Wegovy, more effective but also pricier than previous weight-loss treatments, will add more fuel to that debate.
Past treatments were shown to prompt weight loss in the range of 5%-10% of body weight. But many had relatively serious or unpleasant side effects.
Wegovy, however, helped patients lose an average of 15% of their body weight over 68 weeks in the main clinical trial that led to its approval. A comparison group that got a placebo injection lost an average of 2.5% over the same period. On the high end, nearly a third of patients in the treatment group lost 20% or more. Both groups had counseling on diet and exercise.
Side effects, generally considered mild, included nausea, diarrhea, vomiting, and constipation. A few patients developed pancreatitis, a serious inflammation of the pancreas. Like the diabetes medication, the drug carries a warning about a potential risk of a type of thyroid cancer.
Weight loss in those taking Wegovy puts it close to the 20%-25% losses seen with bariatric surgery, said Stanford, and well above the 3%-4% seen with diet and other lifestyle changes alone.
Participants also saw reductions in their waistlines and improvements in their blood pressure and blood sugar levels, which may mean they won’t develop diabetes, said Sean Wharton, MD, an internal medicine specialist and adjunct professor at York University in Toronto who was among the coauthors of the report outlining the results of the first clinical trial on Wegovy.
Since weight loss is known to reduce the risk of heart attack, high blood pressure and diabetes, might the new drug type be worth it?
Covering such treatment would be a sea change for Medicare, which specifically bars coverage for obesity medications or drugs for “anorexia, weight loss, or weight gain,” although it does pay for bariatric surgery. Pharmaceutical companies, patient advocates, and some medical professionals are backing proposed federal legislation to allow coverage. But the legislation, the Treat and Reduce Obesity Act, has not made progress despite being reintroduced every year since 2012, and sponsors are now asking federal officials instead to rewrite existing rules.
Private insurers will have to consider a cost-benefit analysis of adding Wegovy to their list of covered treatments, either broadly or with limits. Obesity was first recognized as a disease by the American Medical Association, easing the path for insurance coverage, in 2013.
“Employers are going to have a bit of a challenge” deciding whether to add the benefit to insurance offerings, said Steve Pearson, founder and president of the Institute for Clinical and Economic Review, which provides cost-benefit analyses of medical treatments but has not yet looked at Wegovy.
The trade-offs are embodied in patients like Phylander Pannell, a 49-year-old Largo, Md., woman who said she lost 65 pounds in a clinical trial of Wegovy. That study gave the drug to all participants for the first 20 weeks, then randomly assigned patients to get either the drug or a placebo for the next 48 weeks to determine what happens when the medication is stopped. Only after the trial ended did she find out she was in the treatment group the entire time.
Her weight fell slowly at first, then ramped up, eventually bringing her 190-pound frame down to about 125. Pains in her joints eased; she felt better all around.
“I definitely feel the drug was it for me,” said Ms. Pannell, who also followed the trial’s guidance on diet and exercise.
The study found that both groups lost weight in the initial 20 weeks, but those who continued to get the drug lost an additional average of 7.9% of their body weight. Those who got a placebo gained back nearly 7%.
After the trial ended, and the COVID-19 pandemic hit, Ms. Pannell regained some weight and is now at 155. She is eager to get back on the medication and hopes her job-based insurance will cover it.
Many employers do cover obesity drugs. For example, about 40% of private employer plans include Novo Nordisk’s once-daily injection called Saxenda on their health plans, said Michael Bachner, Novo Nordisk’s director of media relations.
He said the $1,349-a-month wholesale acquisition price of Wegovy was determined by making it equivalent to that of Saxenda, which is less effective.
Still, that is more than the $851 monthly wholesale price of Ozempic. But, he pointed out, the recommended dosage of Wegovy is more than twice that of Ozempic. Four milligrams come in the Ozempic injector pens for the month, while Wegovy has 9.6.
“There’s more drug in the pen,” Mr. Bachner said. “That drives the price up.”
He added: “This is not a 20-year-old drug that we now have a new indication for and are pricing it higher. It’s a whole different clinical program,” which required new trials.
Now scientists, employers, physicians, and patients will have to decide whether the new drugs are worth it.
Earlier estimates – some commissioned by Novo Nordisk – of the potential cost of adding an obesity drug benefit to Medicare showed an overall reduction in spending when better health from the resulting weight loss was factored in.
Still, those earlier estimates considered much less expensive drugs, including a range of generic and branded drugs costing as little as $7 a month to more than $300, a small fraction of Wegovy’s cost.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
COVID brings evolutionary virologists out of the shadows, into the fight
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.
Doctors’ offices may be hot spot for transmission of respiratory infections
Prior research has examined the issue of hospital-acquired infections. A 2014 study published in the New England Journal of Medicine, for example, found that 4% of hospitalized patients acquired a health care–associated infection during their stay. Furthermore, the Centers for Disease Control and Prevention estimates that, on any given day, one in 31 hospital patients has at least one health care–associated infection. However, researchers for the new study, published in Health Affairs, said evidence about the risk of acquiring respiratory viral infections in medical office settings is limited.
“Hospital-acquired infections has been a problem for a while,” study author Hannah Neprash, PhD, of the department of health policy and management at the University of Minnesota School of Public Health, Minneapolis, said in an interview. “However, there’s never been a similar study of whether a similar phenomenon happens in physician offices. This is especially relevant now when we’re dealing with respiratory infections.”
Methods and results
For the new study, Dr. Neprash and her colleagues analyzed deidentified billing and scheduling data from 2016-2017 for 105,462,600 outpatient visits that occurred at 6,709 office-based primary care practices. They used the World Health Organization case definition for influenzalike illness “to capture cases in which the physician may suspect this illness even if a specific diagnosis code was not present.” Their control conditions included exposure to urinary tract infections and back pain.
Doctor visits were considered unexposed if they were scheduled to start at least 90 minutes before the first influenzalike illness visit of the day. They were considered exposed if they were scheduled to start at the same time or after the first influenzalike illness visit of the day at that practice.
Researchers quantified whether exposed patients were more likely to return with a similar illness in the next 2 weeks, compared with nonexposed patients seen earlier in the day
They found that 2.7 patients per 1,000 returned within 2 weeks with an influenzalike illness.
Patients were more likely to return with influenzalike illness if their visit occurred after an influenzalike illness visit versus before, the researchers said.
The authors of the paper said their new research highlights the importance of infection control in health care settings, including outpatient offices.
Where did the exposure occur?
Diego Hijano, MD, MSc, pediatric infectious disease specialist at St. Jude’s Children’s Research Hospital, Memphis, Tenn., said he was not surprised by the findings, but noted that it’s hard to say if the exposure to influenzalike illnesses happened in the office or in the community.
“If you start to see individuals with influenza in your office it’s because [there’s influenza] in the community,” Dr. Hijano explained. “So that means that you will have more patients coming in with influenza.”
To reduce the transmission of infections, Dr. Neprash suggested that doctors’ offices follow the CDC guidelines for indoor conduct, which include masking, washing hands, and “taking appropriate infection control measures.”
So potentially masking within offices is a way to minimize transmission between whatever people are there to be seen when it’s contagious, Dr. Neprash said.
“Telehealth really took off in 2020 and it’s unclear what the state of telehealth will be going forward. [These findings] suggest that there’s a patient safety argument for continuing to enable primary care physicians to provide visits either by phone or by video,” he added.
Dr. Hijano thinks it would be helpful for doctors to separate patients with respiratory illnesses from those without respiratory illnesses.
Driver of transmissions
Dr. Neprash suggested that another driver of these transmissions could be doctors not washing their hands, which is a “notorious issue,” and Dr. Hijano agreed with that statement.
“We did know that the hands of physicians and nurses and care providers are the main driver of infections in the health care setting,” Dr. Hijano explained. “I mean, washing your hands properly between encounters is the single best way that any given health care provider can prevent the spread of infections.”
“We have a unique opportunity with COVID-19 to change how these clinics are operating now,” Dr. Hijano said. “Many clinics are actually asking patients to call ahead of time if you have symptoms of a respiratory illness that could be contagious, and those who are not are still mandating the use of mask and physical distance in the waiting areas and limiting the amount of number of patients in any given hour. So I think that those are really big practices that would kind of make an impact in respiratory illness in terms of decreasing transmission in clinics.”
The authors, who had no conflicts of interest said their hope is that their study will help inform policy for reopening outpatient care settings. Dr. Hijano, who was not involved in the study also had no conflicts.
Prior research has examined the issue of hospital-acquired infections. A 2014 study published in the New England Journal of Medicine, for example, found that 4% of hospitalized patients acquired a health care–associated infection during their stay. Furthermore, the Centers for Disease Control and Prevention estimates that, on any given day, one in 31 hospital patients has at least one health care–associated infection. However, researchers for the new study, published in Health Affairs, said evidence about the risk of acquiring respiratory viral infections in medical office settings is limited.
“Hospital-acquired infections has been a problem for a while,” study author Hannah Neprash, PhD, of the department of health policy and management at the University of Minnesota School of Public Health, Minneapolis, said in an interview. “However, there’s never been a similar study of whether a similar phenomenon happens in physician offices. This is especially relevant now when we’re dealing with respiratory infections.”
Methods and results
For the new study, Dr. Neprash and her colleagues analyzed deidentified billing and scheduling data from 2016-2017 for 105,462,600 outpatient visits that occurred at 6,709 office-based primary care practices. They used the World Health Organization case definition for influenzalike illness “to capture cases in which the physician may suspect this illness even if a specific diagnosis code was not present.” Their control conditions included exposure to urinary tract infections and back pain.
Doctor visits were considered unexposed if they were scheduled to start at least 90 minutes before the first influenzalike illness visit of the day. They were considered exposed if they were scheduled to start at the same time or after the first influenzalike illness visit of the day at that practice.
Researchers quantified whether exposed patients were more likely to return with a similar illness in the next 2 weeks, compared with nonexposed patients seen earlier in the day
They found that 2.7 patients per 1,000 returned within 2 weeks with an influenzalike illness.
Patients were more likely to return with influenzalike illness if their visit occurred after an influenzalike illness visit versus before, the researchers said.
The authors of the paper said their new research highlights the importance of infection control in health care settings, including outpatient offices.
Where did the exposure occur?
Diego Hijano, MD, MSc, pediatric infectious disease specialist at St. Jude’s Children’s Research Hospital, Memphis, Tenn., said he was not surprised by the findings, but noted that it’s hard to say if the exposure to influenzalike illnesses happened in the office or in the community.
“If you start to see individuals with influenza in your office it’s because [there’s influenza] in the community,” Dr. Hijano explained. “So that means that you will have more patients coming in with influenza.”
To reduce the transmission of infections, Dr. Neprash suggested that doctors’ offices follow the CDC guidelines for indoor conduct, which include masking, washing hands, and “taking appropriate infection control measures.”
So potentially masking within offices is a way to minimize transmission between whatever people are there to be seen when it’s contagious, Dr. Neprash said.
“Telehealth really took off in 2020 and it’s unclear what the state of telehealth will be going forward. [These findings] suggest that there’s a patient safety argument for continuing to enable primary care physicians to provide visits either by phone or by video,” he added.
Dr. Hijano thinks it would be helpful for doctors to separate patients with respiratory illnesses from those without respiratory illnesses.
Driver of transmissions
Dr. Neprash suggested that another driver of these transmissions could be doctors not washing their hands, which is a “notorious issue,” and Dr. Hijano agreed with that statement.
“We did know that the hands of physicians and nurses and care providers are the main driver of infections in the health care setting,” Dr. Hijano explained. “I mean, washing your hands properly between encounters is the single best way that any given health care provider can prevent the spread of infections.”
“We have a unique opportunity with COVID-19 to change how these clinics are operating now,” Dr. Hijano said. “Many clinics are actually asking patients to call ahead of time if you have symptoms of a respiratory illness that could be contagious, and those who are not are still mandating the use of mask and physical distance in the waiting areas and limiting the amount of number of patients in any given hour. So I think that those are really big practices that would kind of make an impact in respiratory illness in terms of decreasing transmission in clinics.”
The authors, who had no conflicts of interest said their hope is that their study will help inform policy for reopening outpatient care settings. Dr. Hijano, who was not involved in the study also had no conflicts.
Prior research has examined the issue of hospital-acquired infections. A 2014 study published in the New England Journal of Medicine, for example, found that 4% of hospitalized patients acquired a health care–associated infection during their stay. Furthermore, the Centers for Disease Control and Prevention estimates that, on any given day, one in 31 hospital patients has at least one health care–associated infection. However, researchers for the new study, published in Health Affairs, said evidence about the risk of acquiring respiratory viral infections in medical office settings is limited.
“Hospital-acquired infections has been a problem for a while,” study author Hannah Neprash, PhD, of the department of health policy and management at the University of Minnesota School of Public Health, Minneapolis, said in an interview. “However, there’s never been a similar study of whether a similar phenomenon happens in physician offices. This is especially relevant now when we’re dealing with respiratory infections.”
Methods and results
For the new study, Dr. Neprash and her colleagues analyzed deidentified billing and scheduling data from 2016-2017 for 105,462,600 outpatient visits that occurred at 6,709 office-based primary care practices. They used the World Health Organization case definition for influenzalike illness “to capture cases in which the physician may suspect this illness even if a specific diagnosis code was not present.” Their control conditions included exposure to urinary tract infections and back pain.
Doctor visits were considered unexposed if they were scheduled to start at least 90 minutes before the first influenzalike illness visit of the day. They were considered exposed if they were scheduled to start at the same time or after the first influenzalike illness visit of the day at that practice.
Researchers quantified whether exposed patients were more likely to return with a similar illness in the next 2 weeks, compared with nonexposed patients seen earlier in the day
They found that 2.7 patients per 1,000 returned within 2 weeks with an influenzalike illness.
Patients were more likely to return with influenzalike illness if their visit occurred after an influenzalike illness visit versus before, the researchers said.
The authors of the paper said their new research highlights the importance of infection control in health care settings, including outpatient offices.
Where did the exposure occur?
Diego Hijano, MD, MSc, pediatric infectious disease specialist at St. Jude’s Children’s Research Hospital, Memphis, Tenn., said he was not surprised by the findings, but noted that it’s hard to say if the exposure to influenzalike illnesses happened in the office or in the community.
“If you start to see individuals with influenza in your office it’s because [there’s influenza] in the community,” Dr. Hijano explained. “So that means that you will have more patients coming in with influenza.”
To reduce the transmission of infections, Dr. Neprash suggested that doctors’ offices follow the CDC guidelines for indoor conduct, which include masking, washing hands, and “taking appropriate infection control measures.”
So potentially masking within offices is a way to minimize transmission between whatever people are there to be seen when it’s contagious, Dr. Neprash said.
“Telehealth really took off in 2020 and it’s unclear what the state of telehealth will be going forward. [These findings] suggest that there’s a patient safety argument for continuing to enable primary care physicians to provide visits either by phone or by video,” he added.
Dr. Hijano thinks it would be helpful for doctors to separate patients with respiratory illnesses from those without respiratory illnesses.
Driver of transmissions
Dr. Neprash suggested that another driver of these transmissions could be doctors not washing their hands, which is a “notorious issue,” and Dr. Hijano agreed with that statement.
“We did know that the hands of physicians and nurses and care providers are the main driver of infections in the health care setting,” Dr. Hijano explained. “I mean, washing your hands properly between encounters is the single best way that any given health care provider can prevent the spread of infections.”
“We have a unique opportunity with COVID-19 to change how these clinics are operating now,” Dr. Hijano said. “Many clinics are actually asking patients to call ahead of time if you have symptoms of a respiratory illness that could be contagious, and those who are not are still mandating the use of mask and physical distance in the waiting areas and limiting the amount of number of patients in any given hour. So I think that those are really big practices that would kind of make an impact in respiratory illness in terms of decreasing transmission in clinics.”
The authors, who had no conflicts of interest said their hope is that their study will help inform policy for reopening outpatient care settings. Dr. Hijano, who was not involved in the study also had no conflicts.
FROM HEALTH AFFAIRS
Mental illness admissions: 18-44 is the age of prevalence
More mental and/or substance use disorders are ranked among the top-five diagnoses for hospitalized men and women aged 18-44 years than for any other age group, according to a recent report from the Agency for Healthcare Research and Quality.
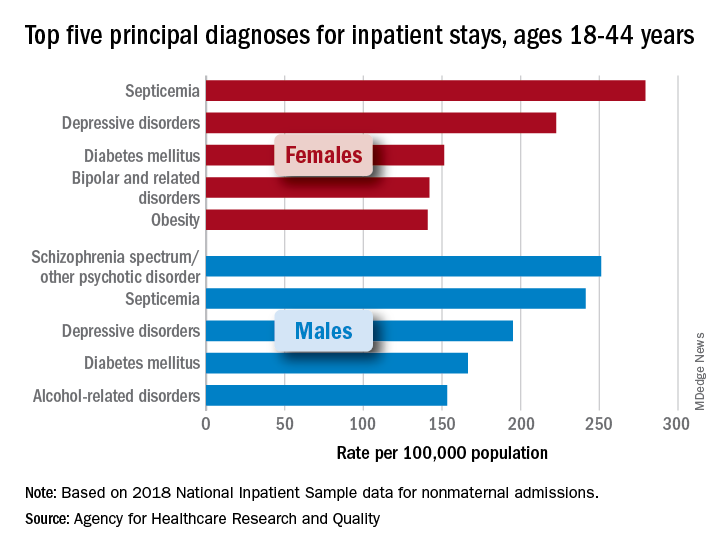
aged 18-44, while depressive disorders were the third-most common (195.0 stays per 100,000) and alcohol-related disorders were fifth at 153.2 per 100,000, Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in an AHRQ statistical brief.
Prevalence was somewhat lower in women aged 18-44 years, with two mental illnesses appearing among the top five nonmaternal diagnoses: Depressive disorders were second at 222.5 stays per 100,000 and bipolar and related disorders were fourth at 142.0 per 100,000. The leading primary diagnosis in women in 2018 was septicemia, which was the most common cause overall in the age group at a rate of 279.3 per 100,000, the investigators reported.
There were no mental and/or substance use disorders in the top five primary diagnoses for any of the other adult age groups – 45-64, 65-74, and ≥75 – included in the report. Septicemia was the leading diagnosis for men in all three groups and for women in two of three (45-64 and ≥75), with osteoarthritis first among women aged 65-74 years, they said.
There was one mental illness among the top-five diagnoses for children under age 18 years, as depressive disorders were the most common reason for stays in girls (176.6 per 100,000 population) and the fifth most common for boys (74.0 per 100,000), said Dr. McDermott of IBM Watson Health and Mr. Roemer of AHRQ.
Septicemia was the leading nonmaternal, nonneonatal diagnosis for all inpatient stays and all ages in 2018 with a rate of 679.5 per 100,000, followed by heart failure (347.9), osteoarthritis (345.5), pneumonia not related to tuberculosis (226.8), and diabetes mellitus (207.8), based on data from the National Inpatient Sample.
Depressive disorders were most common mental health diagnosis in those admitted to hospitals and the 12th most common diagnosis overall; schizophrenia, in 16th place overall, was the only other mental illness among the top 20, the investigators said.
“This information can help establish national health priorities, initiatives, and action plans,” Dr. McDermott and Mr. Roemer wrote, and “at the hospital level, administrators can use diagnosis-related information to inform planning and resource allocation, such as optimizing subspecialty services or units for the care of high-priority conditions.”
More mental and/or substance use disorders are ranked among the top-five diagnoses for hospitalized men and women aged 18-44 years than for any other age group, according to a recent report from the Agency for Healthcare Research and Quality.
aged 18-44, while depressive disorders were the third-most common (195.0 stays per 100,000) and alcohol-related disorders were fifth at 153.2 per 100,000, Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in an AHRQ statistical brief.
Prevalence was somewhat lower in women aged 18-44 years, with two mental illnesses appearing among the top five nonmaternal diagnoses: Depressive disorders were second at 222.5 stays per 100,000 and bipolar and related disorders were fourth at 142.0 per 100,000. The leading primary diagnosis in women in 2018 was septicemia, which was the most common cause overall in the age group at a rate of 279.3 per 100,000, the investigators reported.
There were no mental and/or substance use disorders in the top five primary diagnoses for any of the other adult age groups – 45-64, 65-74, and ≥75 – included in the report. Septicemia was the leading diagnosis for men in all three groups and for women in two of three (45-64 and ≥75), with osteoarthritis first among women aged 65-74 years, they said.
There was one mental illness among the top-five diagnoses for children under age 18 years, as depressive disorders were the most common reason for stays in girls (176.6 per 100,000 population) and the fifth most common for boys (74.0 per 100,000), said Dr. McDermott of IBM Watson Health and Mr. Roemer of AHRQ.
Septicemia was the leading nonmaternal, nonneonatal diagnosis for all inpatient stays and all ages in 2018 with a rate of 679.5 per 100,000, followed by heart failure (347.9), osteoarthritis (345.5), pneumonia not related to tuberculosis (226.8), and diabetes mellitus (207.8), based on data from the National Inpatient Sample.
Depressive disorders were most common mental health diagnosis in those admitted to hospitals and the 12th most common diagnosis overall; schizophrenia, in 16th place overall, was the only other mental illness among the top 20, the investigators said.
“This information can help establish national health priorities, initiatives, and action plans,” Dr. McDermott and Mr. Roemer wrote, and “at the hospital level, administrators can use diagnosis-related information to inform planning and resource allocation, such as optimizing subspecialty services or units for the care of high-priority conditions.”
More mental and/or substance use disorders are ranked among the top-five diagnoses for hospitalized men and women aged 18-44 years than for any other age group, according to a recent report from the Agency for Healthcare Research and Quality.
aged 18-44, while depressive disorders were the third-most common (195.0 stays per 100,000) and alcohol-related disorders were fifth at 153.2 per 100,000, Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in an AHRQ statistical brief.
Prevalence was somewhat lower in women aged 18-44 years, with two mental illnesses appearing among the top five nonmaternal diagnoses: Depressive disorders were second at 222.5 stays per 100,000 and bipolar and related disorders were fourth at 142.0 per 100,000. The leading primary diagnosis in women in 2018 was septicemia, which was the most common cause overall in the age group at a rate of 279.3 per 100,000, the investigators reported.
There were no mental and/or substance use disorders in the top five primary diagnoses for any of the other adult age groups – 45-64, 65-74, and ≥75 – included in the report. Septicemia was the leading diagnosis for men in all three groups and for women in two of three (45-64 and ≥75), with osteoarthritis first among women aged 65-74 years, they said.
There was one mental illness among the top-five diagnoses for children under age 18 years, as depressive disorders were the most common reason for stays in girls (176.6 per 100,000 population) and the fifth most common for boys (74.0 per 100,000), said Dr. McDermott of IBM Watson Health and Mr. Roemer of AHRQ.
Septicemia was the leading nonmaternal, nonneonatal diagnosis for all inpatient stays and all ages in 2018 with a rate of 679.5 per 100,000, followed by heart failure (347.9), osteoarthritis (345.5), pneumonia not related to tuberculosis (226.8), and diabetes mellitus (207.8), based on data from the National Inpatient Sample.
Depressive disorders were most common mental health diagnosis in those admitted to hospitals and the 12th most common diagnosis overall; schizophrenia, in 16th place overall, was the only other mental illness among the top 20, the investigators said.
“This information can help establish national health priorities, initiatives, and action plans,” Dr. McDermott and Mr. Roemer wrote, and “at the hospital level, administrators can use diagnosis-related information to inform planning and resource allocation, such as optimizing subspecialty services or units for the care of high-priority conditions.”
Bronchitis the leader at putting children in the hospital
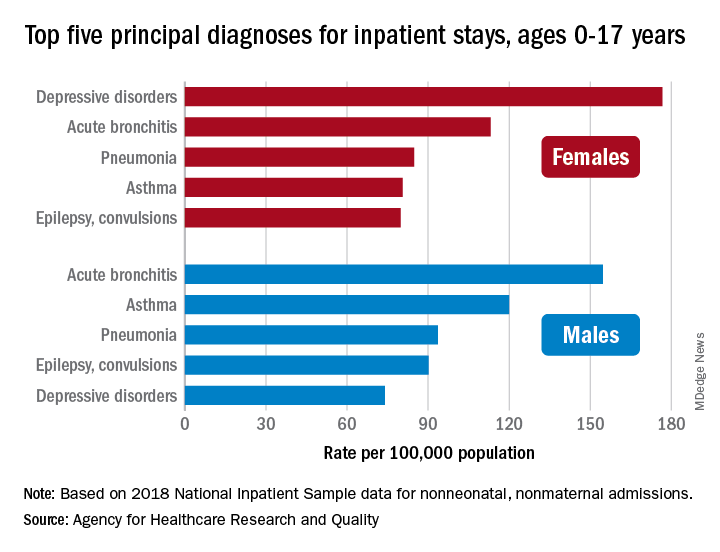
About 7% (99,000) of the 1.47 million nonmaternal, nonneonatal hospital stays in children aged 0-17 years involved a primary diagnosis of acute bronchitis in 2018, representing the leading cause of admissions in boys (154.7 stays per 100,000 population) and the second-leading diagnosis in girls (113.1 stays per 100,000), Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in a statistical brief.
Depressive disorders were the most common primary diagnosis in girls, with a rate of 176.7 stays per 100,000, and the second-leading diagnosis overall, although the rate was less than half that (74.0 per 100,000) in boys. Two other respiratory conditions, asthma and pneumonia, were among the top five for both girls and boys, as was epilepsy, they reported.
The combined rate for all diagnoses was slightly higher for boys, 2,051 per 100,000, compared with 1,922 for girls, they said based on data from the National Inpatient Sample.
“Identifying the most frequent primary conditions for which patients are admitted to the hospital is important to the implementation and improvement of health care delivery, quality initiatives, and health policy,” said Dr. McDermott of IBM Watson Health and Mr. Roemer of the AHRQ.
About 7% (99,000) of the 1.47 million nonmaternal, nonneonatal hospital stays in children aged 0-17 years involved a primary diagnosis of acute bronchitis in 2018, representing the leading cause of admissions in boys (154.7 stays per 100,000 population) and the second-leading diagnosis in girls (113.1 stays per 100,000), Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in a statistical brief.
Depressive disorders were the most common primary diagnosis in girls, with a rate of 176.7 stays per 100,000, and the second-leading diagnosis overall, although the rate was less than half that (74.0 per 100,000) in boys. Two other respiratory conditions, asthma and pneumonia, were among the top five for both girls and boys, as was epilepsy, they reported.
The combined rate for all diagnoses was slightly higher for boys, 2,051 per 100,000, compared with 1,922 for girls, they said based on data from the National Inpatient Sample.
“Identifying the most frequent primary conditions for which patients are admitted to the hospital is important to the implementation and improvement of health care delivery, quality initiatives, and health policy,” said Dr. McDermott of IBM Watson Health and Mr. Roemer of the AHRQ.
About 7% (99,000) of the 1.47 million nonmaternal, nonneonatal hospital stays in children aged 0-17 years involved a primary diagnosis of acute bronchitis in 2018, representing the leading cause of admissions in boys (154.7 stays per 100,000 population) and the second-leading diagnosis in girls (113.1 stays per 100,000), Kimberly W. McDermott, PhD, and Marc Roemer, MS, said in a statistical brief.
Depressive disorders were the most common primary diagnosis in girls, with a rate of 176.7 stays per 100,000, and the second-leading diagnosis overall, although the rate was less than half that (74.0 per 100,000) in boys. Two other respiratory conditions, asthma and pneumonia, were among the top five for both girls and boys, as was epilepsy, they reported.
The combined rate for all diagnoses was slightly higher for boys, 2,051 per 100,000, compared with 1,922 for girls, they said based on data from the National Inpatient Sample.
“Identifying the most frequent primary conditions for which patients are admitted to the hospital is important to the implementation and improvement of health care delivery, quality initiatives, and health policy,” said Dr. McDermott of IBM Watson Health and Mr. Roemer of the AHRQ.
COVID-19 leaves wake of medical debt among U.S. adults
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
Despite the passage of four major relief bills in 2020 and 2021 and federal efforts to offset pandemic- and job-related coverage loss, many people continued to face financial challenges, especially those with a low income and those who are Black or Latino.
The survey, which included responses from 5,450 adults, revealed that 10% of adults aged 19-64 were uninsured during the first half of 2021, a rate lower than what was recorded in 2020 and 2019 in both federal and private surveys. However, uninsured rates were highest among those with low income, those younger than 50 years old, and Black and Latino adults.
For most adults who lost employee health insurance, the coverage gap was relatively brief, with 54% saying their coverage gap lasted 3-4 months. Only 16% of adults said coverage gaps lasted a year or longer.
“The good news is that this survey is suggesting that the coverage losses during the pandemic may have been offset by federal efforts to help people get and maintain health insurance coverage,” lead author Sara Collins, PhD, Commonwealth Fund vice president for health care coverage, access, and tracking, said in an interview.
“The bad news is that a third of Americans continue to struggle with medical bills and medical debt, even among those who have health insurance coverage,” Dr. Collins added.
Indeed, the survey found that about one-third of insured adults reported a medical bill problem or that they were paying off medical debt, as did approximately half of those who were uninsured. Medical debt caused 35% of respondents to use up most or all of their savings to pay it off.
Meanwhile, 27% of adults said medical bills left them unable to pay for necessities such as food, heat, or rent. What surprised Dr. Collins was that 43% of adults said they received a lower credit rating as a result of their medical debt, and 35% said they had taken on more credit card debt to pay off these bills.
“The fact that it’s bleeding over into people’s financial security in terms of their credit scores, I think is something that really needs to be looked at by policymakers,” Dr. Collins said.
When analyzed by race/ethnicity, the researchers found that 55% of Black adults and 44% of Latino/Hispanic adults reported medical bills and debt problems, compared with 32% of White adults. In addition, 47% of those living below the poverty line also reported problems with medical bills.
According to the survey, 45% of respondents were directly affected by the pandemic in at least one of three ways – testing positive or getting sick from COVID-19, losing income, or losing employer coverage – with Black and Latinx adults and those with lower incomes at greater risk.
George Abraham, MD, president of the American College of Physicians, said the Commonwealth Fund’s findings were not surprising because it has always been known that underrepresented populations struggle for access to care because of socioeconomic factors. He said these populations were more vulnerable in terms of more severe infections and disease burden during the pandemic.
“[This study] validates what primary care physicians have been saying all along in regard to our patients’ access to care and their ability to cover health care costs,” said Dr. Abraham, who was not involved with the study. “This will hopefully be an eye-opener and wake-up call that reiterates that we still do not have equitable access to care and vulnerable populations are disproportionately affected.”
He believes that, although people are insured, many of them may contend with medical debt when they fall ill because they can’t afford the premiums.
“Even though they may have been registered for health coverage, they may not have active coverage at the time of illness simply because they weren’t able to make their last premium payments because they’ve been down, because they lost their job, or whatever else,” Dr. Abraham explained. “On paper, they appear to have health care coverage. But in reality, clearly, that coverage does not match their needs or it’s not affordable.”
For Dr. Abraham, the study emphasizes the need to continue support for health care reform, including pricing it so that insurance is available for those with fewer socioeconomic resources.
Yalda Jabbarpour, MD, medical director of the Robert Graham Center for Policy Studies, Washington, said high-deductible health plans need to be “reined in” because they can lead to greater debt, particularly among vulnerable populations.
“Hopefully this will encourage policymakers to look more closely at the problem of medical debt as a contributing factor to financial instability,” Dr. Jabbarpour said. “Federal relief is important, so is expanding access to comprehensive, affordable health care coverage.”
Dr. Collins said there should also be a way to raise awareness of the health care marketplace and coverage options so that people have an easier time getting insured.
A version of this article first appeared on Medscape.com.
As common respiratory viruses resurface, children are at serious risk
Younger children may be vulnerable to the reemergence of common respiratory viruses such as influenza and respiratory syncytial virus (RSV) as COVID-19 restrictions wane, experts say. The impact could be detrimental.
The COVID-19 pandemic and the implementation of preventative measures such as social distancing, travel restrictions, mask use, and shelter in place, reduced the transmission of respiratory viruses, according to the Centers for Disease Control and Prevention. However, because older infants and toddlers have not been exposed to these bugs during the pandemic, they are vulnerable to suffering severe viral infections.
“[We’ve] been in the honeymoon for 18 months,” said Christopher J. Harrison, MD, professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. “We are going to be coming out of the honeymoon and the children who didn’t get sick are going to start packing 2 years’ worth of infections into the next 9 months so there’s going to be twice as many as would be normal.”
The CDC issued a health advisory in June for parts of the southern United States, such as Texas, the Carolinas, and Oklahoma, encouraging broader testing for RSV – a virus that usually causes mild, cold-like symptoms and is the most common cause of bronchiolitis and pneumonia in children – among those who test negative for COVID-19. Virtually all children get an RSV infection by the time they are 2 years old, according to the CDC.
In previous years, RSV usually spread during the fall and spring seasons and usually peaked late December to mid-February. However, there’s been an offseason spike in the common illness this year, with nearly 2,000 confirmed cases each week of July.
Richard J. Webby, PhD, of the infectious diseases department at St. Jude Children’s Research Hospital, Memphis, Tenn., said that although RSV transmits more easily during the winter, the virus is able to thrive during this summer because many children have limited immunity and are more vulnerable to catching the virus than before. Population immunity normally limits a virus to circulating under its most favorable conditions, which is usually the winter. However, because there are a few more “susceptible hosts,” it gives the virus the ability to spread during a time when it typically wouldn’t be able to.
“Now we have a wider range of susceptible kids because they haven’t had that exposure over the past 18 months,” said Dr. Webby, who is on the World Health Organization’s Influenza Vaccine Composition Advisory Team. “It gives the virus more chances to transmit during conditions that are less favorable.”
Dr. Harrison said that, if children continue to take preventative measures such as wearing masks and sanitizing, they can delay catching the RSV – which can be severe in infants and young children – until they’re older and symptoms won’t be as severe.
“The swelling that these viruses cause in the trachea and the bronchial tubes is much bigger in proportion to the overall size of the tubes, so it takes less swelling to clog up the trachea or bronchial tube for the 9-month-old than it does of a 9-year-old,” Dr. Harrison said. “So if a 9-year-old was to get RSV, they’re not going to have nearly the same amount symptoms as the 9-month-old.
Dr. Harrison said delaying RSV in children was never an option before because it’s a virus that’s almost impossible to avoid.
“Hopefully, the mask means that if you get exposed, instead of getting a million virus particles from your classmate or your playmate, you may only get a couple thousand,” Dr. Harrison explained. “And maybe that’s enough that you can fight it off or it may be small enough that you get a mild infection instead of a severe infection.”
A summer surge of RSV has also occurred in Australia. A study published in Clinical Infectious Diseases found that Western Australia saw a 98% reduction in RSV cases. This suggests that COVID-19 restrictions also delayed the RSV season.
Dr. Webby said the lax in penetrative measures against COVID-19 may also affect this upcoming flu season. Usually, around 10%-30% of the population gets infected with the flu each year, but that hasn’t happened the past couple of seasons, he said.
“There might be slightly less overall immunity to these viruses,” Dr. Webby said. “When these viruses do come back, there’s a little bit more room for them to take off.”
Although a severe influenza season rebound this winter is a possibility, Australia continues to experience a historically low flu season. Dr. Harrison, who said the northern hemisphere looks at what’s happening in Australia and the rest of the “southern half of the world because their influenza season is during our summer,” hopes this is an indication that the northern hemisphere will also experience a mild season.
However, there’s no indication of how this upcoming flu season will hit the United States and there isn’t any guidance on what could happen because these historically low levels of respiratory viruses have never happened before, Dr. Webby explained.
He said that, if COVID-19’s delta variant continues to circulate during the fall and winter seasons, it will keep other viruses at low levels. This is because there is rarely a peak of activity of different viruses at the same time.
“When you get infected with the virus, your body’s immune response has this nonspecific reaction that protects you from anything else for a short period of time,” Dr. Webby explained. “When you get a lot of one virus circulating, it’s really hard for these other viruses to get into that population and sort of set off an epidemic of their own.”
To prepare for an unsure influenza season, Dr. Harrison suggests making the influenza vaccine available in August as opposed to October.
Dr. Harrison and Dr. Webby reported no conflicts of interest.
Younger children may be vulnerable to the reemergence of common respiratory viruses such as influenza and respiratory syncytial virus (RSV) as COVID-19 restrictions wane, experts say. The impact could be detrimental.
The COVID-19 pandemic and the implementation of preventative measures such as social distancing, travel restrictions, mask use, and shelter in place, reduced the transmission of respiratory viruses, according to the Centers for Disease Control and Prevention. However, because older infants and toddlers have not been exposed to these bugs during the pandemic, they are vulnerable to suffering severe viral infections.
“[We’ve] been in the honeymoon for 18 months,” said Christopher J. Harrison, MD, professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. “We are going to be coming out of the honeymoon and the children who didn’t get sick are going to start packing 2 years’ worth of infections into the next 9 months so there’s going to be twice as many as would be normal.”
The CDC issued a health advisory in June for parts of the southern United States, such as Texas, the Carolinas, and Oklahoma, encouraging broader testing for RSV – a virus that usually causes mild, cold-like symptoms and is the most common cause of bronchiolitis and pneumonia in children – among those who test negative for COVID-19. Virtually all children get an RSV infection by the time they are 2 years old, according to the CDC.
In previous years, RSV usually spread during the fall and spring seasons and usually peaked late December to mid-February. However, there’s been an offseason spike in the common illness this year, with nearly 2,000 confirmed cases each week of July.
Richard J. Webby, PhD, of the infectious diseases department at St. Jude Children’s Research Hospital, Memphis, Tenn., said that although RSV transmits more easily during the winter, the virus is able to thrive during this summer because many children have limited immunity and are more vulnerable to catching the virus than before. Population immunity normally limits a virus to circulating under its most favorable conditions, which is usually the winter. However, because there are a few more “susceptible hosts,” it gives the virus the ability to spread during a time when it typically wouldn’t be able to.
“Now we have a wider range of susceptible kids because they haven’t had that exposure over the past 18 months,” said Dr. Webby, who is on the World Health Organization’s Influenza Vaccine Composition Advisory Team. “It gives the virus more chances to transmit during conditions that are less favorable.”
Dr. Harrison said that, if children continue to take preventative measures such as wearing masks and sanitizing, they can delay catching the RSV – which can be severe in infants and young children – until they’re older and symptoms won’t be as severe.
“The swelling that these viruses cause in the trachea and the bronchial tubes is much bigger in proportion to the overall size of the tubes, so it takes less swelling to clog up the trachea or bronchial tube for the 9-month-old than it does of a 9-year-old,” Dr. Harrison said. “So if a 9-year-old was to get RSV, they’re not going to have nearly the same amount symptoms as the 9-month-old.
Dr. Harrison said delaying RSV in children was never an option before because it’s a virus that’s almost impossible to avoid.
“Hopefully, the mask means that if you get exposed, instead of getting a million virus particles from your classmate or your playmate, you may only get a couple thousand,” Dr. Harrison explained. “And maybe that’s enough that you can fight it off or it may be small enough that you get a mild infection instead of a severe infection.”
A summer surge of RSV has also occurred in Australia. A study published in Clinical Infectious Diseases found that Western Australia saw a 98% reduction in RSV cases. This suggests that COVID-19 restrictions also delayed the RSV season.
Dr. Webby said the lax in penetrative measures against COVID-19 may also affect this upcoming flu season. Usually, around 10%-30% of the population gets infected with the flu each year, but that hasn’t happened the past couple of seasons, he said.
“There might be slightly less overall immunity to these viruses,” Dr. Webby said. “When these viruses do come back, there’s a little bit more room for them to take off.”
Although a severe influenza season rebound this winter is a possibility, Australia continues to experience a historically low flu season. Dr. Harrison, who said the northern hemisphere looks at what’s happening in Australia and the rest of the “southern half of the world because their influenza season is during our summer,” hopes this is an indication that the northern hemisphere will also experience a mild season.
However, there’s no indication of how this upcoming flu season will hit the United States and there isn’t any guidance on what could happen because these historically low levels of respiratory viruses have never happened before, Dr. Webby explained.
He said that, if COVID-19’s delta variant continues to circulate during the fall and winter seasons, it will keep other viruses at low levels. This is because there is rarely a peak of activity of different viruses at the same time.
“When you get infected with the virus, your body’s immune response has this nonspecific reaction that protects you from anything else for a short period of time,” Dr. Webby explained. “When you get a lot of one virus circulating, it’s really hard for these other viruses to get into that population and sort of set off an epidemic of their own.”
To prepare for an unsure influenza season, Dr. Harrison suggests making the influenza vaccine available in August as opposed to October.
Dr. Harrison and Dr. Webby reported no conflicts of interest.
Younger children may be vulnerable to the reemergence of common respiratory viruses such as influenza and respiratory syncytial virus (RSV) as COVID-19 restrictions wane, experts say. The impact could be detrimental.
The COVID-19 pandemic and the implementation of preventative measures such as social distancing, travel restrictions, mask use, and shelter in place, reduced the transmission of respiratory viruses, according to the Centers for Disease Control and Prevention. However, because older infants and toddlers have not been exposed to these bugs during the pandemic, they are vulnerable to suffering severe viral infections.
“[We’ve] been in the honeymoon for 18 months,” said Christopher J. Harrison, MD, professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. “We are going to be coming out of the honeymoon and the children who didn’t get sick are going to start packing 2 years’ worth of infections into the next 9 months so there’s going to be twice as many as would be normal.”
The CDC issued a health advisory in June for parts of the southern United States, such as Texas, the Carolinas, and Oklahoma, encouraging broader testing for RSV – a virus that usually causes mild, cold-like symptoms and is the most common cause of bronchiolitis and pneumonia in children – among those who test negative for COVID-19. Virtually all children get an RSV infection by the time they are 2 years old, according to the CDC.
In previous years, RSV usually spread during the fall and spring seasons and usually peaked late December to mid-February. However, there’s been an offseason spike in the common illness this year, with nearly 2,000 confirmed cases each week of July.
Richard J. Webby, PhD, of the infectious diseases department at St. Jude Children’s Research Hospital, Memphis, Tenn., said that although RSV transmits more easily during the winter, the virus is able to thrive during this summer because many children have limited immunity and are more vulnerable to catching the virus than before. Population immunity normally limits a virus to circulating under its most favorable conditions, which is usually the winter. However, because there are a few more “susceptible hosts,” it gives the virus the ability to spread during a time when it typically wouldn’t be able to.
“Now we have a wider range of susceptible kids because they haven’t had that exposure over the past 18 months,” said Dr. Webby, who is on the World Health Organization’s Influenza Vaccine Composition Advisory Team. “It gives the virus more chances to transmit during conditions that are less favorable.”
Dr. Harrison said that, if children continue to take preventative measures such as wearing masks and sanitizing, they can delay catching the RSV – which can be severe in infants and young children – until they’re older and symptoms won’t be as severe.
“The swelling that these viruses cause in the trachea and the bronchial tubes is much bigger in proportion to the overall size of the tubes, so it takes less swelling to clog up the trachea or bronchial tube for the 9-month-old than it does of a 9-year-old,” Dr. Harrison said. “So if a 9-year-old was to get RSV, they’re not going to have nearly the same amount symptoms as the 9-month-old.
Dr. Harrison said delaying RSV in children was never an option before because it’s a virus that’s almost impossible to avoid.
“Hopefully, the mask means that if you get exposed, instead of getting a million virus particles from your classmate or your playmate, you may only get a couple thousand,” Dr. Harrison explained. “And maybe that’s enough that you can fight it off or it may be small enough that you get a mild infection instead of a severe infection.”
A summer surge of RSV has also occurred in Australia. A study published in Clinical Infectious Diseases found that Western Australia saw a 98% reduction in RSV cases. This suggests that COVID-19 restrictions also delayed the RSV season.
Dr. Webby said the lax in penetrative measures against COVID-19 may also affect this upcoming flu season. Usually, around 10%-30% of the population gets infected with the flu each year, but that hasn’t happened the past couple of seasons, he said.
“There might be slightly less overall immunity to these viruses,” Dr. Webby said. “When these viruses do come back, there’s a little bit more room for them to take off.”
Although a severe influenza season rebound this winter is a possibility, Australia continues to experience a historically low flu season. Dr. Harrison, who said the northern hemisphere looks at what’s happening in Australia and the rest of the “southern half of the world because their influenza season is during our summer,” hopes this is an indication that the northern hemisphere will also experience a mild season.
However, there’s no indication of how this upcoming flu season will hit the United States and there isn’t any guidance on what could happen because these historically low levels of respiratory viruses have never happened before, Dr. Webby explained.
He said that, if COVID-19’s delta variant continues to circulate during the fall and winter seasons, it will keep other viruses at low levels. This is because there is rarely a peak of activity of different viruses at the same time.
“When you get infected with the virus, your body’s immune response has this nonspecific reaction that protects you from anything else for a short period of time,” Dr. Webby explained. “When you get a lot of one virus circulating, it’s really hard for these other viruses to get into that population and sort of set off an epidemic of their own.”
To prepare for an unsure influenza season, Dr. Harrison suggests making the influenza vaccine available in August as opposed to October.
Dr. Harrison and Dr. Webby reported no conflicts of interest.