User login
COVID-19 hospitalizations for 30- to 39-year-olds hit record high
Hospitals are reporting record numbers of COVID-19 patients in their 30s, largely because of the contagious Delta variant, according to The Wall Street Journal.
The rate of new hospitalizations for ages 30-39 reached 2.5 per 100,000 people last week, according to the latest CDC data, which is up from the previous peak of 2 per 100,000 people in January.
What’s more, new hospital admissions for patients in their 30s reached an average of 1,113 a day during the last week, which was up from 908 the week before.
“It means Delta is really bad,” James Lawler, MD, an infectious disease doctor and codirector of the Global Center for Health Security at the University of Nebraska Medical Center, told the newspaper.
People in the age group mostly avoided hospitalization throughout the pandemic because of their relatively good health and young age, the newspaper reported. But in recent weeks, those between ages 30 and 39 are contracting the coronavirus because of their active lifestyle – for many in their 30s, these are prime years for working, parenting, and socializing.
Hospitalizations are mostly among unvaccinated adults, according to the Wall Street Journal. Nationally, less than half of those ages 25-39 are fully vaccinated, compared with 61% of all adults, according to CDC data updated Sunday.
“It loves social mobility,” James Fiorica, MD, chief medical officer of Sarasota Memorial Health Care System in Florida, told the newspaper.
“An unvaccinated 30-year-old can be a perfect carrier,” he said.
On top of that, COVID-19 patients in their 30s are arriving at hospitals with more severe disease than in earlier waves, the Journal reported. At the University of Arkansas for Medical Sciences hospital, for instance, doctors are now monitoring younger patients daily with a scoring system for possible organ failure. That wasn’t necessary earlier in the pandemic for people in their 30s.
“This age group pretty much went unscathed,” Nikhil Meena, MD, director of the hospital’s Medical Intensive Care Unit, told the newspaper.
Now, he said, “they’re all out there doing their thing and getting infected and getting sick enough to be in this hospital.”
A version of this article first appeared on WebMD.com.
Hospitals are reporting record numbers of COVID-19 patients in their 30s, largely because of the contagious Delta variant, according to The Wall Street Journal.
The rate of new hospitalizations for ages 30-39 reached 2.5 per 100,000 people last week, according to the latest CDC data, which is up from the previous peak of 2 per 100,000 people in January.
What’s more, new hospital admissions for patients in their 30s reached an average of 1,113 a day during the last week, which was up from 908 the week before.
“It means Delta is really bad,” James Lawler, MD, an infectious disease doctor and codirector of the Global Center for Health Security at the University of Nebraska Medical Center, told the newspaper.
People in the age group mostly avoided hospitalization throughout the pandemic because of their relatively good health and young age, the newspaper reported. But in recent weeks, those between ages 30 and 39 are contracting the coronavirus because of their active lifestyle – for many in their 30s, these are prime years for working, parenting, and socializing.
Hospitalizations are mostly among unvaccinated adults, according to the Wall Street Journal. Nationally, less than half of those ages 25-39 are fully vaccinated, compared with 61% of all adults, according to CDC data updated Sunday.
“It loves social mobility,” James Fiorica, MD, chief medical officer of Sarasota Memorial Health Care System in Florida, told the newspaper.
“An unvaccinated 30-year-old can be a perfect carrier,” he said.
On top of that, COVID-19 patients in their 30s are arriving at hospitals with more severe disease than in earlier waves, the Journal reported. At the University of Arkansas for Medical Sciences hospital, for instance, doctors are now monitoring younger patients daily with a scoring system for possible organ failure. That wasn’t necessary earlier in the pandemic for people in their 30s.
“This age group pretty much went unscathed,” Nikhil Meena, MD, director of the hospital’s Medical Intensive Care Unit, told the newspaper.
Now, he said, “they’re all out there doing their thing and getting infected and getting sick enough to be in this hospital.”
A version of this article first appeared on WebMD.com.
Hospitals are reporting record numbers of COVID-19 patients in their 30s, largely because of the contagious Delta variant, according to The Wall Street Journal.
The rate of new hospitalizations for ages 30-39 reached 2.5 per 100,000 people last week, according to the latest CDC data, which is up from the previous peak of 2 per 100,000 people in January.
What’s more, new hospital admissions for patients in their 30s reached an average of 1,113 a day during the last week, which was up from 908 the week before.
“It means Delta is really bad,” James Lawler, MD, an infectious disease doctor and codirector of the Global Center for Health Security at the University of Nebraska Medical Center, told the newspaper.
People in the age group mostly avoided hospitalization throughout the pandemic because of their relatively good health and young age, the newspaper reported. But in recent weeks, those between ages 30 and 39 are contracting the coronavirus because of their active lifestyle – for many in their 30s, these are prime years for working, parenting, and socializing.
Hospitalizations are mostly among unvaccinated adults, according to the Wall Street Journal. Nationally, less than half of those ages 25-39 are fully vaccinated, compared with 61% of all adults, according to CDC data updated Sunday.
“It loves social mobility,” James Fiorica, MD, chief medical officer of Sarasota Memorial Health Care System in Florida, told the newspaper.
“An unvaccinated 30-year-old can be a perfect carrier,” he said.
On top of that, COVID-19 patients in their 30s are arriving at hospitals with more severe disease than in earlier waves, the Journal reported. At the University of Arkansas for Medical Sciences hospital, for instance, doctors are now monitoring younger patients daily with a scoring system for possible organ failure. That wasn’t necessary earlier in the pandemic for people in their 30s.
“This age group pretty much went unscathed,” Nikhil Meena, MD, director of the hospital’s Medical Intensive Care Unit, told the newspaper.
Now, he said, “they’re all out there doing their thing and getting infected and getting sick enough to be in this hospital.”
A version of this article first appeared on WebMD.com.
U.S. pediatric hospitals in peril as Delta hits children
Over the course of the pandemic, COVID-19 has been a less serious illness for children than it has been for adults, and that continues to be true. But with the arrival of Delta, the risk for kids is rising, and that’s creating a perilous situation for hospitals across the United States that treat them.
Roughly 1,800 kids were hospitalized with COVID-19 in the United States last week, a 500% increase in the rate of COVID-19 hospitalizations for children since early July, according to data from the Centers for Disease Control and Prevention.
Emerging data from a large study in Canada suggest that children who test positive for COVID-19 during the Delta wave may be more than twice as likely to be hospitalized as they were when previous variants were dominating transmission. The new data support what many pediatric infectious disease experts say they’ve been seeing: Younger kids with more serious symptoms.
That may sound concerning, but keep in mind that the overall risk of hospitalization for kids who have COVID-19 is still very low – about one child for every hundred who test positive for the virus will end up needing hospital care for their symptoms, according to current statistics maintained by the American Academy of Pediatrics.
‘This is different’
At Le Bonheur Children’s Hospital in Memphis, they saw Delta coming.
Since last year, every kid that comes to the emergency department at the hospital gets a screening test for COVID-19.
In past waves, doctors usually found kids who were infected by accident – they tested positive after coming in for some other problem, a broken leg or appendicitis, said Nick Hysmith, MD, medical director of infection prevention at the hospital. But within the last few weeks, kids with fevers, sore throats, coughs, and runny noses started testing positive for COVID-19.
“We have seen our positive numbers go from, you know, close to about 8%-10% jump up to 20%, and then in recent weeks, we can get as high as 26% or 30%,” Dr. Hysmith said. “Then we started seeing kids sick enough to be admitted.”
“Over the last week, we’ve really seen an increase,” he said. As of August 16, the hospital had 24 children with COVID-19 admitted. Seven of the children were in the PICU, and two were on ventilators.
Arkansas Children’s Hospital had 23 young COVID-19 patients, 10 in intensive care, and five on ventilators, as of Friday, according to the Washington Post. At Children’s of Mississippi, the only hospital for kids in that state, 22 youth were hospitalized as of Monday, with three in intensive care as of August 16, according to the hospital. The nonprofit relief organization Samaritan’s Purse is setting up a second field hospital in the basement of Children’s to expand the hospital’s capacity.
“This is different,” Dr. Hysmith said. “What we’re seeing now is previously healthy kids coming in with symptomatic infection.”
This increased virulence is happening at a bad time. Schools around the United States are reopening for in-person classes, some for the first time in more than a year. Eight states have blocked districts from requiring masks, while many more have made them optional.
Children under 12 still have no access to a vaccine, so they are facing increased exposure to a germ that’s become more dangerous with little protection, especially in schools that have eschewed masks.
More than just COVID-19
Then there are the latent effects of the virus to contend with.
“We’re not only seeing more children now with acute SARS-CoV-2 in the hospital, we’re starting also to see an uptick of MISC – or Multisystem Inflammatory Syndrome in Children,” said Charlotte Hobbs, MD, a pediatric infectious disease specialist at Mississippi Children’s Hospital. “We are just beginning to [see] those cases, and we anticipate that’s going to get worse.”
Adding to COVID-19’s misery, another virus is also capitalizing on this increased mixing of kids back into the community. Respiratory syncytial virus (RSV) hospitalizes about 58,000 children under age 5 in the United States each year. The typical RSV season starts in the fall and peaks in February, along with influenza. This year, the RSV season is early, and it is ferocious.
The combination of the two infections is hitting children’s hospitals hard, and it’s layered on top of the indirect effects of the pandemic, such as the increased population of kids and teens who need mental health care in the wake of the crisis.
“It’s all these things happening at the same time,” said Mark Wietecha, CEO of the Children’s Hospital Association. “To have our hospitals this crowded in August is unusual.
And children’s hospitals are grappling with the same workforce shortages as hospitals that treat adults, while their pool of potential staff is much smaller.
“We can’t easily recruit physicians and nurses from adult hospitals in any practical way to staff a kids’ hospital,” Mr. Wietecha said.
Although pediatric doctors and nurses were trained to care for adults before they specialized, clinicians who primarily care for adults typically haven’t been taught how to care for kids.
Clinicians have fewer tools to fight COVID-19 infections in children than are available for adults.
“There have been many studies in terms of therapies and treatments for acute SARS-CoV-2 infection in adults. We have less data and information in children, and on top of that, some of these treatments aren’t even available under an EUA [emergency use authorization] to children: For example, the monoclonal antibodies,” Dr. Hobbs said.
Antibody treatments are being widely deployed to ease the pressure on hospitals that treat adults. But these therapies aren’t available for kids.
That means children’s hospitals could quickly become overwhelmed, especially in areas where community transmission is high, vaccination rates are low, and parents are screaming about masks.
“So we really have this constellation of events that really doesn’t favor children under the age of 12,” Dr. Hobbs said.
“Universal masking shouldn’t be a debate, because it’s the one thing, with adult vaccination, that can be done to protect this vulnerable population,” she said. “This isn’t a political issue. It’s a public health issue. Period.”
A version of this article first appeared on Medscape.com.
Over the course of the pandemic, COVID-19 has been a less serious illness for children than it has been for adults, and that continues to be true. But with the arrival of Delta, the risk for kids is rising, and that’s creating a perilous situation for hospitals across the United States that treat them.
Roughly 1,800 kids were hospitalized with COVID-19 in the United States last week, a 500% increase in the rate of COVID-19 hospitalizations for children since early July, according to data from the Centers for Disease Control and Prevention.
Emerging data from a large study in Canada suggest that children who test positive for COVID-19 during the Delta wave may be more than twice as likely to be hospitalized as they were when previous variants were dominating transmission. The new data support what many pediatric infectious disease experts say they’ve been seeing: Younger kids with more serious symptoms.
That may sound concerning, but keep in mind that the overall risk of hospitalization for kids who have COVID-19 is still very low – about one child for every hundred who test positive for the virus will end up needing hospital care for their symptoms, according to current statistics maintained by the American Academy of Pediatrics.
‘This is different’
At Le Bonheur Children’s Hospital in Memphis, they saw Delta coming.
Since last year, every kid that comes to the emergency department at the hospital gets a screening test for COVID-19.
In past waves, doctors usually found kids who were infected by accident – they tested positive after coming in for some other problem, a broken leg or appendicitis, said Nick Hysmith, MD, medical director of infection prevention at the hospital. But within the last few weeks, kids with fevers, sore throats, coughs, and runny noses started testing positive for COVID-19.
“We have seen our positive numbers go from, you know, close to about 8%-10% jump up to 20%, and then in recent weeks, we can get as high as 26% or 30%,” Dr. Hysmith said. “Then we started seeing kids sick enough to be admitted.”
“Over the last week, we’ve really seen an increase,” he said. As of August 16, the hospital had 24 children with COVID-19 admitted. Seven of the children were in the PICU, and two were on ventilators.
Arkansas Children’s Hospital had 23 young COVID-19 patients, 10 in intensive care, and five on ventilators, as of Friday, according to the Washington Post. At Children’s of Mississippi, the only hospital for kids in that state, 22 youth were hospitalized as of Monday, with three in intensive care as of August 16, according to the hospital. The nonprofit relief organization Samaritan’s Purse is setting up a second field hospital in the basement of Children’s to expand the hospital’s capacity.
“This is different,” Dr. Hysmith said. “What we’re seeing now is previously healthy kids coming in with symptomatic infection.”
This increased virulence is happening at a bad time. Schools around the United States are reopening for in-person classes, some for the first time in more than a year. Eight states have blocked districts from requiring masks, while many more have made them optional.
Children under 12 still have no access to a vaccine, so they are facing increased exposure to a germ that’s become more dangerous with little protection, especially in schools that have eschewed masks.
More than just COVID-19
Then there are the latent effects of the virus to contend with.
“We’re not only seeing more children now with acute SARS-CoV-2 in the hospital, we’re starting also to see an uptick of MISC – or Multisystem Inflammatory Syndrome in Children,” said Charlotte Hobbs, MD, a pediatric infectious disease specialist at Mississippi Children’s Hospital. “We are just beginning to [see] those cases, and we anticipate that’s going to get worse.”
Adding to COVID-19’s misery, another virus is also capitalizing on this increased mixing of kids back into the community. Respiratory syncytial virus (RSV) hospitalizes about 58,000 children under age 5 in the United States each year. The typical RSV season starts in the fall and peaks in February, along with influenza. This year, the RSV season is early, and it is ferocious.
The combination of the two infections is hitting children’s hospitals hard, and it’s layered on top of the indirect effects of the pandemic, such as the increased population of kids and teens who need mental health care in the wake of the crisis.
“It’s all these things happening at the same time,” said Mark Wietecha, CEO of the Children’s Hospital Association. “To have our hospitals this crowded in August is unusual.
And children’s hospitals are grappling with the same workforce shortages as hospitals that treat adults, while their pool of potential staff is much smaller.
“We can’t easily recruit physicians and nurses from adult hospitals in any practical way to staff a kids’ hospital,” Mr. Wietecha said.
Although pediatric doctors and nurses were trained to care for adults before they specialized, clinicians who primarily care for adults typically haven’t been taught how to care for kids.
Clinicians have fewer tools to fight COVID-19 infections in children than are available for adults.
“There have been many studies in terms of therapies and treatments for acute SARS-CoV-2 infection in adults. We have less data and information in children, and on top of that, some of these treatments aren’t even available under an EUA [emergency use authorization] to children: For example, the monoclonal antibodies,” Dr. Hobbs said.
Antibody treatments are being widely deployed to ease the pressure on hospitals that treat adults. But these therapies aren’t available for kids.
That means children’s hospitals could quickly become overwhelmed, especially in areas where community transmission is high, vaccination rates are low, and parents are screaming about masks.
“So we really have this constellation of events that really doesn’t favor children under the age of 12,” Dr. Hobbs said.
“Universal masking shouldn’t be a debate, because it’s the one thing, with adult vaccination, that can be done to protect this vulnerable population,” she said. “This isn’t a political issue. It’s a public health issue. Period.”
A version of this article first appeared on Medscape.com.
Over the course of the pandemic, COVID-19 has been a less serious illness for children than it has been for adults, and that continues to be true. But with the arrival of Delta, the risk for kids is rising, and that’s creating a perilous situation for hospitals across the United States that treat them.
Roughly 1,800 kids were hospitalized with COVID-19 in the United States last week, a 500% increase in the rate of COVID-19 hospitalizations for children since early July, according to data from the Centers for Disease Control and Prevention.
Emerging data from a large study in Canada suggest that children who test positive for COVID-19 during the Delta wave may be more than twice as likely to be hospitalized as they were when previous variants were dominating transmission. The new data support what many pediatric infectious disease experts say they’ve been seeing: Younger kids with more serious symptoms.
That may sound concerning, but keep in mind that the overall risk of hospitalization for kids who have COVID-19 is still very low – about one child for every hundred who test positive for the virus will end up needing hospital care for their symptoms, according to current statistics maintained by the American Academy of Pediatrics.
‘This is different’
At Le Bonheur Children’s Hospital in Memphis, they saw Delta coming.
Since last year, every kid that comes to the emergency department at the hospital gets a screening test for COVID-19.
In past waves, doctors usually found kids who were infected by accident – they tested positive after coming in for some other problem, a broken leg or appendicitis, said Nick Hysmith, MD, medical director of infection prevention at the hospital. But within the last few weeks, kids with fevers, sore throats, coughs, and runny noses started testing positive for COVID-19.
“We have seen our positive numbers go from, you know, close to about 8%-10% jump up to 20%, and then in recent weeks, we can get as high as 26% or 30%,” Dr. Hysmith said. “Then we started seeing kids sick enough to be admitted.”
“Over the last week, we’ve really seen an increase,” he said. As of August 16, the hospital had 24 children with COVID-19 admitted. Seven of the children were in the PICU, and two were on ventilators.
Arkansas Children’s Hospital had 23 young COVID-19 patients, 10 in intensive care, and five on ventilators, as of Friday, according to the Washington Post. At Children’s of Mississippi, the only hospital for kids in that state, 22 youth were hospitalized as of Monday, with three in intensive care as of August 16, according to the hospital. The nonprofit relief organization Samaritan’s Purse is setting up a second field hospital in the basement of Children’s to expand the hospital’s capacity.
“This is different,” Dr. Hysmith said. “What we’re seeing now is previously healthy kids coming in with symptomatic infection.”
This increased virulence is happening at a bad time. Schools around the United States are reopening for in-person classes, some for the first time in more than a year. Eight states have blocked districts from requiring masks, while many more have made them optional.
Children under 12 still have no access to a vaccine, so they are facing increased exposure to a germ that’s become more dangerous with little protection, especially in schools that have eschewed masks.
More than just COVID-19
Then there are the latent effects of the virus to contend with.
“We’re not only seeing more children now with acute SARS-CoV-2 in the hospital, we’re starting also to see an uptick of MISC – or Multisystem Inflammatory Syndrome in Children,” said Charlotte Hobbs, MD, a pediatric infectious disease specialist at Mississippi Children’s Hospital. “We are just beginning to [see] those cases, and we anticipate that’s going to get worse.”
Adding to COVID-19’s misery, another virus is also capitalizing on this increased mixing of kids back into the community. Respiratory syncytial virus (RSV) hospitalizes about 58,000 children under age 5 in the United States each year. The typical RSV season starts in the fall and peaks in February, along with influenza. This year, the RSV season is early, and it is ferocious.
The combination of the two infections is hitting children’s hospitals hard, and it’s layered on top of the indirect effects of the pandemic, such as the increased population of kids and teens who need mental health care in the wake of the crisis.
“It’s all these things happening at the same time,” said Mark Wietecha, CEO of the Children’s Hospital Association. “To have our hospitals this crowded in August is unusual.
And children’s hospitals are grappling with the same workforce shortages as hospitals that treat adults, while their pool of potential staff is much smaller.
“We can’t easily recruit physicians and nurses from adult hospitals in any practical way to staff a kids’ hospital,” Mr. Wietecha said.
Although pediatric doctors and nurses were trained to care for adults before they specialized, clinicians who primarily care for adults typically haven’t been taught how to care for kids.
Clinicians have fewer tools to fight COVID-19 infections in children than are available for adults.
“There have been many studies in terms of therapies and treatments for acute SARS-CoV-2 infection in adults. We have less data and information in children, and on top of that, some of these treatments aren’t even available under an EUA [emergency use authorization] to children: For example, the monoclonal antibodies,” Dr. Hobbs said.
Antibody treatments are being widely deployed to ease the pressure on hospitals that treat adults. But these therapies aren’t available for kids.
That means children’s hospitals could quickly become overwhelmed, especially in areas where community transmission is high, vaccination rates are low, and parents are screaming about masks.
“So we really have this constellation of events that really doesn’t favor children under the age of 12,” Dr. Hobbs said.
“Universal masking shouldn’t be a debate, because it’s the one thing, with adult vaccination, that can be done to protect this vulnerable population,” she said. “This isn’t a political issue. It’s a public health issue. Period.”
A version of this article first appeared on Medscape.com.
U.S. reports record COVID-19 hospitalizations of children
The number of children hospitalized with COVID-19 in the U.S. hit a record high on Aug. 14, with more than 1,900 in hospitals.
Hospitals across the South are running out of beds as the contagious Delta variant spreads, mostly among unvaccinated people. Children make up about 2.4% of the country’s COVID-19 hospitalizations, and those under 12 are particularly vulnerable since they’re not eligible to receive a vaccine.
“This is not last year’s COVID,” Sally Goza, MD, former president of the American Academy of Pediatrics, told CNN on Aug. 14.
“This one is worse, and our children are the ones that are going to be affected by it the most,” she said.
The number of newly hospitalized COVID-19 patients for ages 18-49 also hit record highs during the week of Aug. 9. A fifth of the nation’s hospitalizations are in Florida, where the number of COVID-19 patients hit a record high of 16,100 on Aug. 14. More than 90% of the state’s intensive care unit beds are filled.
More than 90% of the ICU beds in Texas are full as well. On Aug. 13, there were no pediatric ICU beds available in Dallas or the 19 surrounding counties, which means that young patients would be transported father away for care – even Oklahoma City.
“That means if your child’s in a car wreck, if your child has a congenital heart defect or something and needs an ICU bed, or more likely, if they have COVID and need an ICU bed, we don’t have one,” Clay Jenkins, a Dallas County judge, said on Aug. 13.
“Your child will wait for another child to die,” he said.
As children return to classes, educators are talking about the possibility of vaccine mandates. The National Education Association announced its support of mandatory vaccination for its members.
“Our students under 12 can’t get vaccinated,” Becky Pringle, president of the association, told CNN.
“It’s our responsibility to keep them safe,” she said. “Keeping them safe means that everyone who can be vaccinated should be vaccinated.”
The U.S. now has an average of about 129,000 new COVID-19 cases per day, Reuters reported, which has doubled in about 2 weeks. The number of hospitalized patients is at a 6-month high, and about 600 people are dying each day.
Arkansas, Florida, Louisiana, Mississippi, and Oregon have reported record numbers of COVID-19 hospitalizations.
In addition, eight states make up half of all the COVID-19 hospitalizations in the U.S. but only 24% of the nation’s population – Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, Nevada, and Texas. These states have vaccination rates lower than the national average, and their COVID-19 patients account for at least 15% of their overall hospitalizations.
To address the surge in hospitalizations, Oregon Gov. Kate Brown has ordered the deployment of up to 1,500 Oregon National Guard members to help health care workers.
“I know this is not the summer many of us envisioned,” Gov. Brown said Aug. 13. “The harsh and frustrating reality is that the Delta variant has changed everything. Delta is highly contagious, and we must take action now.”
A version of this article first appeared on WebMD.com.
The number of children hospitalized with COVID-19 in the U.S. hit a record high on Aug. 14, with more than 1,900 in hospitals.
Hospitals across the South are running out of beds as the contagious Delta variant spreads, mostly among unvaccinated people. Children make up about 2.4% of the country’s COVID-19 hospitalizations, and those under 12 are particularly vulnerable since they’re not eligible to receive a vaccine.
“This is not last year’s COVID,” Sally Goza, MD, former president of the American Academy of Pediatrics, told CNN on Aug. 14.
“This one is worse, and our children are the ones that are going to be affected by it the most,” she said.
The number of newly hospitalized COVID-19 patients for ages 18-49 also hit record highs during the week of Aug. 9. A fifth of the nation’s hospitalizations are in Florida, where the number of COVID-19 patients hit a record high of 16,100 on Aug. 14. More than 90% of the state’s intensive care unit beds are filled.
More than 90% of the ICU beds in Texas are full as well. On Aug. 13, there were no pediatric ICU beds available in Dallas or the 19 surrounding counties, which means that young patients would be transported father away for care – even Oklahoma City.
“That means if your child’s in a car wreck, if your child has a congenital heart defect or something and needs an ICU bed, or more likely, if they have COVID and need an ICU bed, we don’t have one,” Clay Jenkins, a Dallas County judge, said on Aug. 13.
“Your child will wait for another child to die,” he said.
As children return to classes, educators are talking about the possibility of vaccine mandates. The National Education Association announced its support of mandatory vaccination for its members.
“Our students under 12 can’t get vaccinated,” Becky Pringle, president of the association, told CNN.
“It’s our responsibility to keep them safe,” she said. “Keeping them safe means that everyone who can be vaccinated should be vaccinated.”
The U.S. now has an average of about 129,000 new COVID-19 cases per day, Reuters reported, which has doubled in about 2 weeks. The number of hospitalized patients is at a 6-month high, and about 600 people are dying each day.
Arkansas, Florida, Louisiana, Mississippi, and Oregon have reported record numbers of COVID-19 hospitalizations.
In addition, eight states make up half of all the COVID-19 hospitalizations in the U.S. but only 24% of the nation’s population – Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, Nevada, and Texas. These states have vaccination rates lower than the national average, and their COVID-19 patients account for at least 15% of their overall hospitalizations.
To address the surge in hospitalizations, Oregon Gov. Kate Brown has ordered the deployment of up to 1,500 Oregon National Guard members to help health care workers.
“I know this is not the summer many of us envisioned,” Gov. Brown said Aug. 13. “The harsh and frustrating reality is that the Delta variant has changed everything. Delta is highly contagious, and we must take action now.”
A version of this article first appeared on WebMD.com.
The number of children hospitalized with COVID-19 in the U.S. hit a record high on Aug. 14, with more than 1,900 in hospitals.
Hospitals across the South are running out of beds as the contagious Delta variant spreads, mostly among unvaccinated people. Children make up about 2.4% of the country’s COVID-19 hospitalizations, and those under 12 are particularly vulnerable since they’re not eligible to receive a vaccine.
“This is not last year’s COVID,” Sally Goza, MD, former president of the American Academy of Pediatrics, told CNN on Aug. 14.
“This one is worse, and our children are the ones that are going to be affected by it the most,” she said.
The number of newly hospitalized COVID-19 patients for ages 18-49 also hit record highs during the week of Aug. 9. A fifth of the nation’s hospitalizations are in Florida, where the number of COVID-19 patients hit a record high of 16,100 on Aug. 14. More than 90% of the state’s intensive care unit beds are filled.
More than 90% of the ICU beds in Texas are full as well. On Aug. 13, there were no pediatric ICU beds available in Dallas or the 19 surrounding counties, which means that young patients would be transported father away for care – even Oklahoma City.
“That means if your child’s in a car wreck, if your child has a congenital heart defect or something and needs an ICU bed, or more likely, if they have COVID and need an ICU bed, we don’t have one,” Clay Jenkins, a Dallas County judge, said on Aug. 13.
“Your child will wait for another child to die,” he said.
As children return to classes, educators are talking about the possibility of vaccine mandates. The National Education Association announced its support of mandatory vaccination for its members.
“Our students under 12 can’t get vaccinated,” Becky Pringle, president of the association, told CNN.
“It’s our responsibility to keep them safe,” she said. “Keeping them safe means that everyone who can be vaccinated should be vaccinated.”
The U.S. now has an average of about 129,000 new COVID-19 cases per day, Reuters reported, which has doubled in about 2 weeks. The number of hospitalized patients is at a 6-month high, and about 600 people are dying each day.
Arkansas, Florida, Louisiana, Mississippi, and Oregon have reported record numbers of COVID-19 hospitalizations.
In addition, eight states make up half of all the COVID-19 hospitalizations in the U.S. but only 24% of the nation’s population – Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, Nevada, and Texas. These states have vaccination rates lower than the national average, and their COVID-19 patients account for at least 15% of their overall hospitalizations.
To address the surge in hospitalizations, Oregon Gov. Kate Brown has ordered the deployment of up to 1,500 Oregon National Guard members to help health care workers.
“I know this is not the summer many of us envisioned,” Gov. Brown said Aug. 13. “The harsh and frustrating reality is that the Delta variant has changed everything. Delta is highly contagious, and we must take action now.”
A version of this article first appeared on WebMD.com.
Endocrinologists’ wealth remains steady, despite pandemic
Despite ongoing pandemic-related economic challenges, endocrinologists report stability in their overall wealth in the past year, with more than a third of the specialists having a net worth between $1 million and $5 million, according to the Medscape Endocrinologist Wealth & Debt Report 2021.

The findings regarding wealth and debt among endocrinologists, along with 28 other specialties, were reported as part of Medscape’s Physician Compensation Report 2021, which included nearly 18,000 physicians.
According to the report, endocrinologists had an upswing in their income, compared with the prior year, with average annual earnings of $245,000 versus $236,000 in 2020. The earnings tie them with infectious disease specialists at fourth from the bottom of the list of specialties.
In the latest report, 38% reported a net worth between $1 million and $5 million, down 1% from 39% in last year’s report.
Nine percent of endocrinologists had a net worth of over $5 million, matching last year’s rate.
That puts endocrinologists and rheumatologists near the middle of specialists earning more than $5 million. Dermatologists rank the highest, with 28% worth over $5 million. Allergy and immunology specialists are at the bottom of the list, with just 2%.
Joel Greenwald, MD, a wealth management advisor to physicians based in St. Louis Park, Minn., said the reasons for the stability in wealth are multifactorial.
“The rise in home prices is certainly a factor,” he said. “Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%.
“I’ve seen clients accumulate cash, which has added to their net worth,” Dr. Greenwald added. “They cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on [during lockdowns].”
The percentage of endocrinologists reporting a net worth below $500,000 decreased from 37% in 2020 to 31% for the current report, placing them fifth from the top of the list of specialists with a net worth below $500,000. Family medicine was at the top of the list, at 40%.
Gender disparities in net worth are striking
The gender disparities in net worth among endocrinologists are substantial. Although only 15% of male endocrinologists have a net worth of less than $500,000, that rate is nearly three times higher – 44% – for female endocrinologists.
Twenty-seven percent of male endocrinologists have a net worth between $1 million and $2 million, compared with just 13% among women. Although 14% of men have a net worth of more than $5 million, only 4% of female endocrinologists fall in that category.
Of note, 61% of those who responded to the poll were men; 36% were women.
Expenses, savings
Only 6% of endocrinologists reported being unable to pay their mortgage as a result of the pandemic; 8% said they were unable to pay other bills because of COVID-19.
The vast majority, however – 91% – said the pandemic did not affect their ability to pay bills or their mortgage. U.S. Census Bureau data from last July show that about a quarter of adults (25.3%) missed a mortgage or rent payment because of challenges related to COVID-19.
Approximately three-quarters of endocrinologists (72%) reported having not made any changes to reduce major expenses in 2020, despite the pandemic. About 25% took significant measures to reduce expenses, including refinancing their house or moving to a different home.
Seventeen percent say they are still paying off their school loans, similar to the rate last year.
The report notes that, according to the Association of American Medical Colleges, the average medical school debt for students who graduated in 2019 was $201,490, compared with an average student loan debt for all graduating students in the same year of $28,950.
Although 65% of endocrinologists said they added the same amount to their 401(k) plan in the past year, 28% put less into their fund, and although 53% put the same amount into their taxable savings account, 23% reported not using the taxable savings accounts at all.
Although earnings were steady in the past year, 12% of endocrinologists report having losses from practice problems, compared with 5% the previous year. COVID-19 was the most common cause. The proportion reporting no financial losses declined to 65%, versus 75% in the last report.
A version of this article first appeared on Medscape.com.
Despite ongoing pandemic-related economic challenges, endocrinologists report stability in their overall wealth in the past year, with more than a third of the specialists having a net worth between $1 million and $5 million, according to the Medscape Endocrinologist Wealth & Debt Report 2021.
The findings regarding wealth and debt among endocrinologists, along with 28 other specialties, were reported as part of Medscape’s Physician Compensation Report 2021, which included nearly 18,000 physicians.
According to the report, endocrinologists had an upswing in their income, compared with the prior year, with average annual earnings of $245,000 versus $236,000 in 2020. The earnings tie them with infectious disease specialists at fourth from the bottom of the list of specialties.
In the latest report, 38% reported a net worth between $1 million and $5 million, down 1% from 39% in last year’s report.
Nine percent of endocrinologists had a net worth of over $5 million, matching last year’s rate.
That puts endocrinologists and rheumatologists near the middle of specialists earning more than $5 million. Dermatologists rank the highest, with 28% worth over $5 million. Allergy and immunology specialists are at the bottom of the list, with just 2%.
Joel Greenwald, MD, a wealth management advisor to physicians based in St. Louis Park, Minn., said the reasons for the stability in wealth are multifactorial.
“The rise in home prices is certainly a factor,” he said. “Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%.
“I’ve seen clients accumulate cash, which has added to their net worth,” Dr. Greenwald added. “They cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on [during lockdowns].”
The percentage of endocrinologists reporting a net worth below $500,000 decreased from 37% in 2020 to 31% for the current report, placing them fifth from the top of the list of specialists with a net worth below $500,000. Family medicine was at the top of the list, at 40%.
Gender disparities in net worth are striking
The gender disparities in net worth among endocrinologists are substantial. Although only 15% of male endocrinologists have a net worth of less than $500,000, that rate is nearly three times higher – 44% – for female endocrinologists.
Twenty-seven percent of male endocrinologists have a net worth between $1 million and $2 million, compared with just 13% among women. Although 14% of men have a net worth of more than $5 million, only 4% of female endocrinologists fall in that category.
Of note, 61% of those who responded to the poll were men; 36% were women.
Expenses, savings
Only 6% of endocrinologists reported being unable to pay their mortgage as a result of the pandemic; 8% said they were unable to pay other bills because of COVID-19.
The vast majority, however – 91% – said the pandemic did not affect their ability to pay bills or their mortgage. U.S. Census Bureau data from last July show that about a quarter of adults (25.3%) missed a mortgage or rent payment because of challenges related to COVID-19.
Approximately three-quarters of endocrinologists (72%) reported having not made any changes to reduce major expenses in 2020, despite the pandemic. About 25% took significant measures to reduce expenses, including refinancing their house or moving to a different home.
Seventeen percent say they are still paying off their school loans, similar to the rate last year.
The report notes that, according to the Association of American Medical Colleges, the average medical school debt for students who graduated in 2019 was $201,490, compared with an average student loan debt for all graduating students in the same year of $28,950.
Although 65% of endocrinologists said they added the same amount to their 401(k) plan in the past year, 28% put less into their fund, and although 53% put the same amount into their taxable savings account, 23% reported not using the taxable savings accounts at all.
Although earnings were steady in the past year, 12% of endocrinologists report having losses from practice problems, compared with 5% the previous year. COVID-19 was the most common cause. The proportion reporting no financial losses declined to 65%, versus 75% in the last report.
A version of this article first appeared on Medscape.com.
Despite ongoing pandemic-related economic challenges, endocrinologists report stability in their overall wealth in the past year, with more than a third of the specialists having a net worth between $1 million and $5 million, according to the Medscape Endocrinologist Wealth & Debt Report 2021.
The findings regarding wealth and debt among endocrinologists, along with 28 other specialties, were reported as part of Medscape’s Physician Compensation Report 2021, which included nearly 18,000 physicians.
According to the report, endocrinologists had an upswing in their income, compared with the prior year, with average annual earnings of $245,000 versus $236,000 in 2020. The earnings tie them with infectious disease specialists at fourth from the bottom of the list of specialties.
In the latest report, 38% reported a net worth between $1 million and $5 million, down 1% from 39% in last year’s report.
Nine percent of endocrinologists had a net worth of over $5 million, matching last year’s rate.
That puts endocrinologists and rheumatologists near the middle of specialists earning more than $5 million. Dermatologists rank the highest, with 28% worth over $5 million. Allergy and immunology specialists are at the bottom of the list, with just 2%.
Joel Greenwald, MD, a wealth management advisor to physicians based in St. Louis Park, Minn., said the reasons for the stability in wealth are multifactorial.
“The rise in home prices is certainly a factor,” he said. “Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%.
“I’ve seen clients accumulate cash, which has added to their net worth,” Dr. Greenwald added. “They cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on [during lockdowns].”
The percentage of endocrinologists reporting a net worth below $500,000 decreased from 37% in 2020 to 31% for the current report, placing them fifth from the top of the list of specialists with a net worth below $500,000. Family medicine was at the top of the list, at 40%.
Gender disparities in net worth are striking
The gender disparities in net worth among endocrinologists are substantial. Although only 15% of male endocrinologists have a net worth of less than $500,000, that rate is nearly three times higher – 44% – for female endocrinologists.
Twenty-seven percent of male endocrinologists have a net worth between $1 million and $2 million, compared with just 13% among women. Although 14% of men have a net worth of more than $5 million, only 4% of female endocrinologists fall in that category.
Of note, 61% of those who responded to the poll were men; 36% were women.
Expenses, savings
Only 6% of endocrinologists reported being unable to pay their mortgage as a result of the pandemic; 8% said they were unable to pay other bills because of COVID-19.
The vast majority, however – 91% – said the pandemic did not affect their ability to pay bills or their mortgage. U.S. Census Bureau data from last July show that about a quarter of adults (25.3%) missed a mortgage or rent payment because of challenges related to COVID-19.
Approximately three-quarters of endocrinologists (72%) reported having not made any changes to reduce major expenses in 2020, despite the pandemic. About 25% took significant measures to reduce expenses, including refinancing their house or moving to a different home.
Seventeen percent say they are still paying off their school loans, similar to the rate last year.
The report notes that, according to the Association of American Medical Colleges, the average medical school debt for students who graduated in 2019 was $201,490, compared with an average student loan debt for all graduating students in the same year of $28,950.
Although 65% of endocrinologists said they added the same amount to their 401(k) plan in the past year, 28% put less into their fund, and although 53% put the same amount into their taxable savings account, 23% reported not using the taxable savings accounts at all.
Although earnings were steady in the past year, 12% of endocrinologists report having losses from practice problems, compared with 5% the previous year. COVID-19 was the most common cause. The proportion reporting no financial losses declined to 65%, versus 75% in the last report.
A version of this article first appeared on Medscape.com.
Can a blood-based test predict TNFi nonresponse in RA?
A blood test that uses a patient’s unique genetic signature has shown some ability to predict nonresponse to tumor necrosis factor inhibitors as treatment for rheumatoid arthritis, an observational clinical study has found, but the test’s predictive accuracy was well below 100%.
The test is the blood-based molecular signature response classifier (MSRC) that uses RNA sequencing data based on 23 different biomarkers: 19 RNA transcripts and 4 clinical features. The clinical features are body mass index, gender, patient global assessment, and anticyclic citrullinated protein (anti-CCP) status.
The NETWORK-004 study, published in Rheumatology and Therapy, was able to stratify patients who were likely to respond inadequately to TNFi therapy and could provide patient-specific information to guide therapy choice in RA patients regardless of whether they’ve already been on TNFi therapy. The study evaluated the MSRC test in 504 patients, 391 of whom were treatment naive.
Avoiding ‘fail first’ approach
The idea behind the test is to circumvent the “fail first” approach in finding the right therapy for RA in an individual patient. While the test costs $4,995, Alif Saleh, chief executive officer of Scipher Medicine, which markets the test under the name PrismRA, said in a press release that it has the potential to reduce costs by $19,000 or more per patient per year by avoiding treatments that don’t work. A previous study, which Scipher funded, reported that the test resulted in savings of $7,379 in per-patient costs of ineffective therapy. The same study reported a 25% decrease in costs for ineffective treatments for Medicare-eligible patients.
The price of RA drugs, particularly anti-TNF agents, is hefty and rising. GoodRx has reported that the price of RA drugs increased 92% from 2014 to 2019, and the prices for anti-TNF agents such as etanercept and adalimumab more than doubled in that period. Adalimumab can cost upwards of $84,000 per year while etanercept has a list price of around $72,000 a year. The pharmacy benefit manager WellDyne started covering the test MSRC in February.
Nehad Soloman, MD, a rheumatologist and internist at Midwestern University Arizona College of Osteopathic Medicine in Glendale and a compensated NETWORK-004 investigator, said the MSRC test would be indicated for confirmed RA patients for whom rheumatologists are considering biologic agents, particularly TNFi drugs. “You wouldn’t do it on an RA patient who’s been on several different medications because it doesn’t serve a purpose at that point,” he said.

The potential cost savings may not be the only reason to use the test, Dr. Soloman said. “You don’t want to be dabbling with the wrong drug if there’s another path you can try and save society some money as well as the time and energy it takes to monitor the patients – as well as the patient’s pain,” he said.
How the MSRC test works
The MSRC test detects a signal that’s associated with a high or very high likelihood of inadequate response to TNFi therapies and indicates that the patient is unlikely to achieve low disease activity or remission with TNFi therapies. Response is defined as achieving ACR50 – meaning 50% improvement in American College of Rheumatology response criteria – at 6 months.

Test results are reported on a continuous 1-25 scale, explained Slava Akmaev, PhD, chief technology officer and head of therapeutics at Scipher. “The higher the score, the more likely the patient will have an inadequate response to TNFi therapies and be unable to reach low disease activity; the lower the score, the less likely the patient will have an inadequate response to TNFi therapies,” he said. However, Dr. Akmaev noted that a low score does not ensure a positive response to TNFi therapies.
The MSRC test differs from the multibiomarker disease activity blood test (MBDA; marketed as Vectra by Myriad Genetics) in the number of biomarkers it measures: 19 RNA transcripts vs. 12 serum protein biomarkers in MBDA. The MBDA test is also intended to provide a quantitative, objective measurement of RA disease activity rather than to predict nonresponse to TNFi or other biologics. A number of studies have validated the MBDA test for predicting disease control in RA patients, but not necessarily response to TNFi therapy.
The “high” category threshold of the MSRC test corresponds to an approximate 90% chance of inadequate response to TNFi therapy, or a 10% chance of responding. The “very high” category threshold corresponds to an approximate 95% chance of inadequate response to TNFi therapy, Dr. Akmaev said.
NETWORK-004 used area under the curve (AUC) to measure the accuracy of the MSRC test. An AUC of 1 represents 100% accuracy. Overall, the MSRC had an AUC of 0.64, or 64% accuracy of predicting patients unlikely to respond to TNFi therapy and to achieve ACR50 at 6 months, with an odds ratio of 4.1 (95% confidence interval, 2.0-8.3; P = .0001).
The predictive accuracy went up to 74% with ORs of 3.4-8.8 for additional endpoints at 3 and 6 months (P < .01). Among patients who had already been on TNFi therapy, the predictive accuracy was 83% and associated with ORs of 3.3-26.6 based on ACR, 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP), and Clinical Disease Activity Index (CDAI) metrics.
The investigators also performed an in-cohort cross-validation of the MSRC using baseline blood samples of 245 treatment-naive patients from the CERTAIN study, which yielded a 66% predictive accuracy for the ACR50 outcome at 6 months. Using the 19 RNA transcripts from the test, but not the clinical factors, the predictive accuracy was 62.5%. Using ACR70, CDAI, and DAS28 as measures for 6-month response, the cross-validation analysis of all 23 MSRC features yielded predictive accuracy of 64%-67%.
The study found significant differences in model scores between patients who did and did not have the molecular signal of nonresponse, and the proportion of patients who achieved low disease activity or remission at 6 months based on CDAI and DAS28-CRP measures was greater among those who lacked a molecular signature of nonresponse.
“Those who lack this signature can proceed with TNFi therapy and possibly achieve an increased response rate relative to the unstratified population,” wrote lead study author Stanley B. Cohen, MD, and colleagues.
Daniel E. Furst, MD, emeritus professor at the University of California, Los Angeles, described the design of the NETWORK-004 study as “excellent,” but said that it didn’t overcome potential issues with the MSRC test itself. “The results unfortunately are great for group data but not for individuals, with a predictive area under the curve of 60% to 80%, it really is not that useful,” he said. “Let’s say you’re a patient who’s not doing well, and I do a test and it’s positive; that still means that 20% of the time you will respond.”

He also noted that he coauthored a paper that used decreases in DAS28 to predict nonresponse to certolizumab pegol plus methotrexate with 95% probability in the first 12 weeks of treatment. “That’s closer to what we need,” Dr. Furst said.
However, the MSRC test is a promising sign of where testing for predicting RA therapy is headed, he said. “We are steadily working toward genetic signatures that really are predictive on an individual basis,” Dr. Furst said. “It’s coming; it’s just not here yet.”
Dr. Furst had no relevant financial relationships to disclose. Dr. Soloman is a paid investigator and consultant to Scipher Medicine.
A blood test that uses a patient’s unique genetic signature has shown some ability to predict nonresponse to tumor necrosis factor inhibitors as treatment for rheumatoid arthritis, an observational clinical study has found, but the test’s predictive accuracy was well below 100%.
The test is the blood-based molecular signature response classifier (MSRC) that uses RNA sequencing data based on 23 different biomarkers: 19 RNA transcripts and 4 clinical features. The clinical features are body mass index, gender, patient global assessment, and anticyclic citrullinated protein (anti-CCP) status.
The NETWORK-004 study, published in Rheumatology and Therapy, was able to stratify patients who were likely to respond inadequately to TNFi therapy and could provide patient-specific information to guide therapy choice in RA patients regardless of whether they’ve already been on TNFi therapy. The study evaluated the MSRC test in 504 patients, 391 of whom were treatment naive.
Avoiding ‘fail first’ approach
The idea behind the test is to circumvent the “fail first” approach in finding the right therapy for RA in an individual patient. While the test costs $4,995, Alif Saleh, chief executive officer of Scipher Medicine, which markets the test under the name PrismRA, said in a press release that it has the potential to reduce costs by $19,000 or more per patient per year by avoiding treatments that don’t work. A previous study, which Scipher funded, reported that the test resulted in savings of $7,379 in per-patient costs of ineffective therapy. The same study reported a 25% decrease in costs for ineffective treatments for Medicare-eligible patients.
The price of RA drugs, particularly anti-TNF agents, is hefty and rising. GoodRx has reported that the price of RA drugs increased 92% from 2014 to 2019, and the prices for anti-TNF agents such as etanercept and adalimumab more than doubled in that period. Adalimumab can cost upwards of $84,000 per year while etanercept has a list price of around $72,000 a year. The pharmacy benefit manager WellDyne started covering the test MSRC in February.
Nehad Soloman, MD, a rheumatologist and internist at Midwestern University Arizona College of Osteopathic Medicine in Glendale and a compensated NETWORK-004 investigator, said the MSRC test would be indicated for confirmed RA patients for whom rheumatologists are considering biologic agents, particularly TNFi drugs. “You wouldn’t do it on an RA patient who’s been on several different medications because it doesn’t serve a purpose at that point,” he said.
The potential cost savings may not be the only reason to use the test, Dr. Soloman said. “You don’t want to be dabbling with the wrong drug if there’s another path you can try and save society some money as well as the time and energy it takes to monitor the patients – as well as the patient’s pain,” he said.
How the MSRC test works
The MSRC test detects a signal that’s associated with a high or very high likelihood of inadequate response to TNFi therapies and indicates that the patient is unlikely to achieve low disease activity or remission with TNFi therapies. Response is defined as achieving ACR50 – meaning 50% improvement in American College of Rheumatology response criteria – at 6 months.
Test results are reported on a continuous 1-25 scale, explained Slava Akmaev, PhD, chief technology officer and head of therapeutics at Scipher. “The higher the score, the more likely the patient will have an inadequate response to TNFi therapies and be unable to reach low disease activity; the lower the score, the less likely the patient will have an inadequate response to TNFi therapies,” he said. However, Dr. Akmaev noted that a low score does not ensure a positive response to TNFi therapies.
The MSRC test differs from the multibiomarker disease activity blood test (MBDA; marketed as Vectra by Myriad Genetics) in the number of biomarkers it measures: 19 RNA transcripts vs. 12 serum protein biomarkers in MBDA. The MBDA test is also intended to provide a quantitative, objective measurement of RA disease activity rather than to predict nonresponse to TNFi or other biologics. A number of studies have validated the MBDA test for predicting disease control in RA patients, but not necessarily response to TNFi therapy.
The “high” category threshold of the MSRC test corresponds to an approximate 90% chance of inadequate response to TNFi therapy, or a 10% chance of responding. The “very high” category threshold corresponds to an approximate 95% chance of inadequate response to TNFi therapy, Dr. Akmaev said.
NETWORK-004 used area under the curve (AUC) to measure the accuracy of the MSRC test. An AUC of 1 represents 100% accuracy. Overall, the MSRC had an AUC of 0.64, or 64% accuracy of predicting patients unlikely to respond to TNFi therapy and to achieve ACR50 at 6 months, with an odds ratio of 4.1 (95% confidence interval, 2.0-8.3; P = .0001).
The predictive accuracy went up to 74% with ORs of 3.4-8.8 for additional endpoints at 3 and 6 months (P < .01). Among patients who had already been on TNFi therapy, the predictive accuracy was 83% and associated with ORs of 3.3-26.6 based on ACR, 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP), and Clinical Disease Activity Index (CDAI) metrics.
The investigators also performed an in-cohort cross-validation of the MSRC using baseline blood samples of 245 treatment-naive patients from the CERTAIN study, which yielded a 66% predictive accuracy for the ACR50 outcome at 6 months. Using the 19 RNA transcripts from the test, but not the clinical factors, the predictive accuracy was 62.5%. Using ACR70, CDAI, and DAS28 as measures for 6-month response, the cross-validation analysis of all 23 MSRC features yielded predictive accuracy of 64%-67%.
The study found significant differences in model scores between patients who did and did not have the molecular signal of nonresponse, and the proportion of patients who achieved low disease activity or remission at 6 months based on CDAI and DAS28-CRP measures was greater among those who lacked a molecular signature of nonresponse.
“Those who lack this signature can proceed with TNFi therapy and possibly achieve an increased response rate relative to the unstratified population,” wrote lead study author Stanley B. Cohen, MD, and colleagues.
Daniel E. Furst, MD, emeritus professor at the University of California, Los Angeles, described the design of the NETWORK-004 study as “excellent,” but said that it didn’t overcome potential issues with the MSRC test itself. “The results unfortunately are great for group data but not for individuals, with a predictive area under the curve of 60% to 80%, it really is not that useful,” he said. “Let’s say you’re a patient who’s not doing well, and I do a test and it’s positive; that still means that 20% of the time you will respond.”
He also noted that he coauthored a paper that used decreases in DAS28 to predict nonresponse to certolizumab pegol plus methotrexate with 95% probability in the first 12 weeks of treatment. “That’s closer to what we need,” Dr. Furst said.
However, the MSRC test is a promising sign of where testing for predicting RA therapy is headed, he said. “We are steadily working toward genetic signatures that really are predictive on an individual basis,” Dr. Furst said. “It’s coming; it’s just not here yet.”
Dr. Furst had no relevant financial relationships to disclose. Dr. Soloman is a paid investigator and consultant to Scipher Medicine.
A blood test that uses a patient’s unique genetic signature has shown some ability to predict nonresponse to tumor necrosis factor inhibitors as treatment for rheumatoid arthritis, an observational clinical study has found, but the test’s predictive accuracy was well below 100%.
The test is the blood-based molecular signature response classifier (MSRC) that uses RNA sequencing data based on 23 different biomarkers: 19 RNA transcripts and 4 clinical features. The clinical features are body mass index, gender, patient global assessment, and anticyclic citrullinated protein (anti-CCP) status.
The NETWORK-004 study, published in Rheumatology and Therapy, was able to stratify patients who were likely to respond inadequately to TNFi therapy and could provide patient-specific information to guide therapy choice in RA patients regardless of whether they’ve already been on TNFi therapy. The study evaluated the MSRC test in 504 patients, 391 of whom were treatment naive.
Avoiding ‘fail first’ approach
The idea behind the test is to circumvent the “fail first” approach in finding the right therapy for RA in an individual patient. While the test costs $4,995, Alif Saleh, chief executive officer of Scipher Medicine, which markets the test under the name PrismRA, said in a press release that it has the potential to reduce costs by $19,000 or more per patient per year by avoiding treatments that don’t work. A previous study, which Scipher funded, reported that the test resulted in savings of $7,379 in per-patient costs of ineffective therapy. The same study reported a 25% decrease in costs for ineffective treatments for Medicare-eligible patients.
The price of RA drugs, particularly anti-TNF agents, is hefty and rising. GoodRx has reported that the price of RA drugs increased 92% from 2014 to 2019, and the prices for anti-TNF agents such as etanercept and adalimumab more than doubled in that period. Adalimumab can cost upwards of $84,000 per year while etanercept has a list price of around $72,000 a year. The pharmacy benefit manager WellDyne started covering the test MSRC in February.
Nehad Soloman, MD, a rheumatologist and internist at Midwestern University Arizona College of Osteopathic Medicine in Glendale and a compensated NETWORK-004 investigator, said the MSRC test would be indicated for confirmed RA patients for whom rheumatologists are considering biologic agents, particularly TNFi drugs. “You wouldn’t do it on an RA patient who’s been on several different medications because it doesn’t serve a purpose at that point,” he said.
The potential cost savings may not be the only reason to use the test, Dr. Soloman said. “You don’t want to be dabbling with the wrong drug if there’s another path you can try and save society some money as well as the time and energy it takes to monitor the patients – as well as the patient’s pain,” he said.
How the MSRC test works
The MSRC test detects a signal that’s associated with a high or very high likelihood of inadequate response to TNFi therapies and indicates that the patient is unlikely to achieve low disease activity or remission with TNFi therapies. Response is defined as achieving ACR50 – meaning 50% improvement in American College of Rheumatology response criteria – at 6 months.
Test results are reported on a continuous 1-25 scale, explained Slava Akmaev, PhD, chief technology officer and head of therapeutics at Scipher. “The higher the score, the more likely the patient will have an inadequate response to TNFi therapies and be unable to reach low disease activity; the lower the score, the less likely the patient will have an inadequate response to TNFi therapies,” he said. However, Dr. Akmaev noted that a low score does not ensure a positive response to TNFi therapies.
The MSRC test differs from the multibiomarker disease activity blood test (MBDA; marketed as Vectra by Myriad Genetics) in the number of biomarkers it measures: 19 RNA transcripts vs. 12 serum protein biomarkers in MBDA. The MBDA test is also intended to provide a quantitative, objective measurement of RA disease activity rather than to predict nonresponse to TNFi or other biologics. A number of studies have validated the MBDA test for predicting disease control in RA patients, but not necessarily response to TNFi therapy.
The “high” category threshold of the MSRC test corresponds to an approximate 90% chance of inadequate response to TNFi therapy, or a 10% chance of responding. The “very high” category threshold corresponds to an approximate 95% chance of inadequate response to TNFi therapy, Dr. Akmaev said.
NETWORK-004 used area under the curve (AUC) to measure the accuracy of the MSRC test. An AUC of 1 represents 100% accuracy. Overall, the MSRC had an AUC of 0.64, or 64% accuracy of predicting patients unlikely to respond to TNFi therapy and to achieve ACR50 at 6 months, with an odds ratio of 4.1 (95% confidence interval, 2.0-8.3; P = .0001).
The predictive accuracy went up to 74% with ORs of 3.4-8.8 for additional endpoints at 3 and 6 months (P < .01). Among patients who had already been on TNFi therapy, the predictive accuracy was 83% and associated with ORs of 3.3-26.6 based on ACR, 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP), and Clinical Disease Activity Index (CDAI) metrics.
The investigators also performed an in-cohort cross-validation of the MSRC using baseline blood samples of 245 treatment-naive patients from the CERTAIN study, which yielded a 66% predictive accuracy for the ACR50 outcome at 6 months. Using the 19 RNA transcripts from the test, but not the clinical factors, the predictive accuracy was 62.5%. Using ACR70, CDAI, and DAS28 as measures for 6-month response, the cross-validation analysis of all 23 MSRC features yielded predictive accuracy of 64%-67%.
The study found significant differences in model scores between patients who did and did not have the molecular signal of nonresponse, and the proportion of patients who achieved low disease activity or remission at 6 months based on CDAI and DAS28-CRP measures was greater among those who lacked a molecular signature of nonresponse.
“Those who lack this signature can proceed with TNFi therapy and possibly achieve an increased response rate relative to the unstratified population,” wrote lead study author Stanley B. Cohen, MD, and colleagues.
Daniel E. Furst, MD, emeritus professor at the University of California, Los Angeles, described the design of the NETWORK-004 study as “excellent,” but said that it didn’t overcome potential issues with the MSRC test itself. “The results unfortunately are great for group data but not for individuals, with a predictive area under the curve of 60% to 80%, it really is not that useful,” he said. “Let’s say you’re a patient who’s not doing well, and I do a test and it’s positive; that still means that 20% of the time you will respond.”
He also noted that he coauthored a paper that used decreases in DAS28 to predict nonresponse to certolizumab pegol plus methotrexate with 95% probability in the first 12 weeks of treatment. “That’s closer to what we need,” Dr. Furst said.
However, the MSRC test is a promising sign of where testing for predicting RA therapy is headed, he said. “We are steadily working toward genetic signatures that really are predictive on an individual basis,” Dr. Furst said. “It’s coming; it’s just not here yet.”
Dr. Furst had no relevant financial relationships to disclose. Dr. Soloman is a paid investigator and consultant to Scipher Medicine.
FROM RHEUMATOLOGY AND THERAPY
Survey: Family medicine adds wealth, but higher net worth skews male
.
In early 2020, in a survey done before the pandemic, family physicians reported average earnings of $234,000. In 2021, with months of pandemic behind them, survey data show that family physicians averaged $236,000 in earnings.
“Although many medical offices were closed for a period of time in 2020, some physicians made use of the Paycheck Protection Program; others cut staff, renegotiated leases, switched to telephysician visits, and made other cost-cutting changes that kept earnings on par,” Medscape’s Christine Lehman wrote.
Their net worth – total wealth accounting for all financial assets and debts – did even better in 2021. More family physicians are worth $1 million to $5 million in 2021, compared with last year (38% vs. 33%), more are worth over $5 million (4% vs. 3%), and fewer FPs are worth less than $1 million (60% vs. 65%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely, the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male, female family physicians
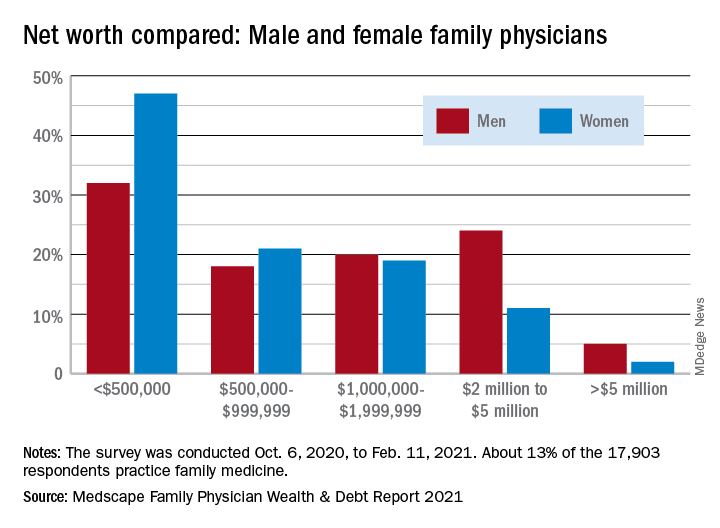
The wealth disparities that exist among family physicians get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: Five percent of male FPs are worth over $5 million versus 2% of females, and 24% of men are worth $2 million to $5 million versus 11% of women, based on data from the 13% of survey respondents (n = 17,903) who practice family medicine.
Zooming out from the world of family practice to the universe of all physicians shows that FPs are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, family medicine at 4%, and dermatology at 28%. Meanwhile, family physicians’ 40% share of those worth under $500,000 is at the high end of a range in which oncologists are lowest at 16%.
Medical school and other debt
Another area where FPs find themselves looking down on most specialties is medical school debt. Only emergency medicine has more physicians (33%) paying off their school loans than family medicine (31%), while infectious disease has the fewest (12%), according to the Medscape survey, which was conducted Oct. 6, 2020, to Feb. 11, 2021.
Larger proportions of family physicians are paying off credit card debt (30%), car loans (44%), and mortgages on primary residences (67%), while 10% said that they are not paying off debts. Nonpayment of those debts was an issue for 9% of FPs who said that they missed payments on mortgages or other bills because of the COVID-19 pandemic. Almost all FPs said that they live either within (48%) or below (46%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-month emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
.
In early 2020, in a survey done before the pandemic, family physicians reported average earnings of $234,000. In 2021, with months of pandemic behind them, survey data show that family physicians averaged $236,000 in earnings.
“Although many medical offices were closed for a period of time in 2020, some physicians made use of the Paycheck Protection Program; others cut staff, renegotiated leases, switched to telephysician visits, and made other cost-cutting changes that kept earnings on par,” Medscape’s Christine Lehman wrote.
Their net worth – total wealth accounting for all financial assets and debts – did even better in 2021. More family physicians are worth $1 million to $5 million in 2021, compared with last year (38% vs. 33%), more are worth over $5 million (4% vs. 3%), and fewer FPs are worth less than $1 million (60% vs. 65%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely, the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male, female family physicians
The wealth disparities that exist among family physicians get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: Five percent of male FPs are worth over $5 million versus 2% of females, and 24% of men are worth $2 million to $5 million versus 11% of women, based on data from the 13% of survey respondents (n = 17,903) who practice family medicine.
Zooming out from the world of family practice to the universe of all physicians shows that FPs are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, family medicine at 4%, and dermatology at 28%. Meanwhile, family physicians’ 40% share of those worth under $500,000 is at the high end of a range in which oncologists are lowest at 16%.
Medical school and other debt
Another area where FPs find themselves looking down on most specialties is medical school debt. Only emergency medicine has more physicians (33%) paying off their school loans than family medicine (31%), while infectious disease has the fewest (12%), according to the Medscape survey, which was conducted Oct. 6, 2020, to Feb. 11, 2021.
Larger proportions of family physicians are paying off credit card debt (30%), car loans (44%), and mortgages on primary residences (67%), while 10% said that they are not paying off debts. Nonpayment of those debts was an issue for 9% of FPs who said that they missed payments on mortgages or other bills because of the COVID-19 pandemic. Almost all FPs said that they live either within (48%) or below (46%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-month emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
.
In early 2020, in a survey done before the pandemic, family physicians reported average earnings of $234,000. In 2021, with months of pandemic behind them, survey data show that family physicians averaged $236,000 in earnings.
“Although many medical offices were closed for a period of time in 2020, some physicians made use of the Paycheck Protection Program; others cut staff, renegotiated leases, switched to telephysician visits, and made other cost-cutting changes that kept earnings on par,” Medscape’s Christine Lehman wrote.
Their net worth – total wealth accounting for all financial assets and debts – did even better in 2021. More family physicians are worth $1 million to $5 million in 2021, compared with last year (38% vs. 33%), more are worth over $5 million (4% vs. 3%), and fewer FPs are worth less than $1 million (60% vs. 65%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely, the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male, female family physicians
The wealth disparities that exist among family physicians get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: Five percent of male FPs are worth over $5 million versus 2% of females, and 24% of men are worth $2 million to $5 million versus 11% of women, based on data from the 13% of survey respondents (n = 17,903) who practice family medicine.
Zooming out from the world of family practice to the universe of all physicians shows that FPs are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, family medicine at 4%, and dermatology at 28%. Meanwhile, family physicians’ 40% share of those worth under $500,000 is at the high end of a range in which oncologists are lowest at 16%.
Medical school and other debt
Another area where FPs find themselves looking down on most specialties is medical school debt. Only emergency medicine has more physicians (33%) paying off their school loans than family medicine (31%), while infectious disease has the fewest (12%), according to the Medscape survey, which was conducted Oct. 6, 2020, to Feb. 11, 2021.
Larger proportions of family physicians are paying off credit card debt (30%), car loans (44%), and mortgages on primary residences (67%), while 10% said that they are not paying off debts. Nonpayment of those debts was an issue for 9% of FPs who said that they missed payments on mortgages or other bills because of the COVID-19 pandemic. Almost all FPs said that they live either within (48%) or below (46%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-month emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
Survey: Internists gain wealth, pay off debt
a Medscape survey shows.
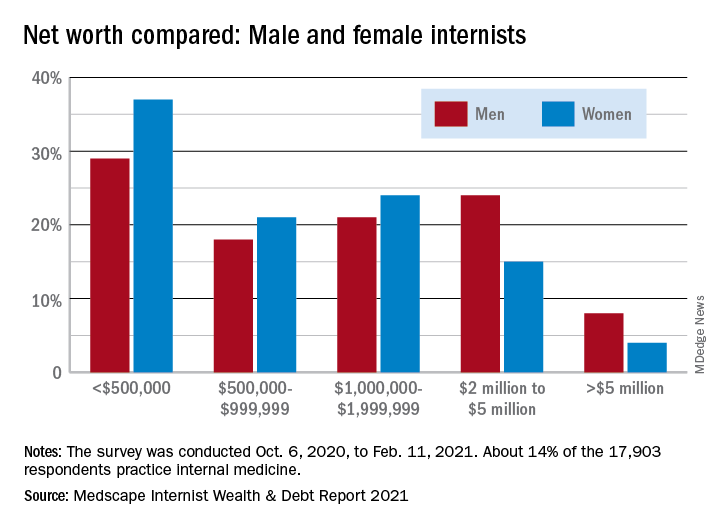
More internists are worth $1 million to $5 million in 2021, compared with last year (42% vs. 37%), more are worth over $5 million (6% vs. 5%), and fewer internists are worth less than $1 million (52% vs. 58%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male and female internists
The wealth disparities that exist among internists get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: 8% of male internists are worth over $5 million versus 4% of females, and 24% of men are worth $2 million to $5 million but only 15% of women, based on data from the 14% of survey respondents (n = 17,903) who practice internal medicine.
Zooming out from the world of internal medicine to the universe of all physicians shows that internists are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, internal medicine at 6%, and dermatology at 28%. Meanwhile, internists’ 33% share of those worth under $500,000 is lower than family medicine’s 40% but higher than oncologists’ 16%.
Medical school and other debt
Continuing the comparison with all specialties, internists are doing somewhat better at paying off school loans. Among those responding to the survey, 20% are still paying off their medical school debt, closer to the low of 12% for infectious disease specialists than the high of 33% for the emergency physicians, according to the Medscape report.
Larger proportions of internists are paying off credit card debt (26%), car loans (35%), and mortgages on primary residences (61%), while 13% said that they are not paying off debts. Nonpayment of those debts was an issue for 11% of internists who said that they missed payments on mortgages or other bills because of the COVID pandemic.
Almost all internists said that they live either within (50%) or below (44%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-months emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
a Medscape survey shows.
More internists are worth $1 million to $5 million in 2021, compared with last year (42% vs. 37%), more are worth over $5 million (6% vs. 5%), and fewer internists are worth less than $1 million (52% vs. 58%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male and female internists
The wealth disparities that exist among internists get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: 8% of male internists are worth over $5 million versus 4% of females, and 24% of men are worth $2 million to $5 million but only 15% of women, based on data from the 14% of survey respondents (n = 17,903) who practice internal medicine.
Zooming out from the world of internal medicine to the universe of all physicians shows that internists are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, internal medicine at 6%, and dermatology at 28%. Meanwhile, internists’ 33% share of those worth under $500,000 is lower than family medicine’s 40% but higher than oncologists’ 16%.
Medical school and other debt
Continuing the comparison with all specialties, internists are doing somewhat better at paying off school loans. Among those responding to the survey, 20% are still paying off their medical school debt, closer to the low of 12% for infectious disease specialists than the high of 33% for the emergency physicians, according to the Medscape report.
Larger proportions of internists are paying off credit card debt (26%), car loans (35%), and mortgages on primary residences (61%), while 13% said that they are not paying off debts. Nonpayment of those debts was an issue for 11% of internists who said that they missed payments on mortgages or other bills because of the COVID pandemic.
Almost all internists said that they live either within (50%) or below (44%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-months emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
a Medscape survey shows.
More internists are worth $1 million to $5 million in 2021, compared with last year (42% vs. 37%), more are worth over $5 million (6% vs. 5%), and fewer internists are worth less than $1 million (52% vs. 58%), according to Medscape’s annual wealth and debt report.
“The rise in home prices is certainly a factor,” Joel Greenwald, MD, CFP, a wealth management adviser for physicians, said in an interview.
“Definitely the rise in the stock market played a large role; the S&P 500 finished the year up over 18%. Finally, I’ve seen clients ... cut back on spending because they were worried about big declines in income and also because there was simply less to spend money on,” said Dr. Greenwald of St. Louis Park, Minn.
Wealth disparities between male and female internists
The wealth disparities that exist among internists get somewhat realigned, however, when viewed through the lens of physician gender. The higher-worth segments of the specialty skew rather heavily male: 8% of male internists are worth over $5 million versus 4% of females, and 24% of men are worth $2 million to $5 million but only 15% of women, based on data from the 14% of survey respondents (n = 17,903) who practice internal medicine.
Zooming out from the world of internal medicine to the universe of all physicians shows that internists are closer to allergists and immunologists than to dermatologists when it comes to share of practitioners with net worth over $5 million. That macro view puts allergy/immunology at 2%, internal medicine at 6%, and dermatology at 28%. Meanwhile, internists’ 33% share of those worth under $500,000 is lower than family medicine’s 40% but higher than oncologists’ 16%.
Medical school and other debt
Continuing the comparison with all specialties, internists are doing somewhat better at paying off school loans. Among those responding to the survey, 20% are still paying off their medical school debt, closer to the low of 12% for infectious disease specialists than the high of 33% for the emergency physicians, according to the Medscape report.
Larger proportions of internists are paying off credit card debt (26%), car loans (35%), and mortgages on primary residences (61%), while 13% said that they are not paying off debts. Nonpayment of those debts was an issue for 11% of internists who said that they missed payments on mortgages or other bills because of the COVID pandemic.
Almost all internists said that they live either within (50%) or below (44%) their means, Medscape reported.
“There are certainly folks who believe that as long as they pay off their credit card each month and contribute to their 401(k) enough to get their employer match, they’re doing okay,” Dr. Greenwald said. “I would say that living within one’s means is having a 3- to 6-months emergency fund; saving at least 20% of gross income toward retirement; adequately funding 529 college accounts; and, for younger docs, paying down high-interest-rate debt at a good clip.”
Novel antidepressant shines in phase 2 trial, but FDA has issues with its NDA
Although a novel investigational drug that combines dextromethorphan and bupropion (AXS-05, Axsome Therapeutics) met its primary and key secondary endpoints in a phase 2 trial of patients with treatment-resistant depression (TRD), the U.S. Food and Drug Administration has voiced some concerns.
In the MERIT study, AXS-05 significantly delayed time to depression relapse compared with placebo (primary endpoint) – with no relapses observed for at least 6 months. It also significantly prevented depression relapse (secondary endpoint), the company said in a news release announcing the topline results.
The drug has been granted breakthrough therapy designations by the FDA for the treatment of major depressive disorder (MDD) and agitation associated with Alzheimer’s disease.
In addition,
However, Axsome stated that the FDA has identified “deficiencies that preclude labeling discussions at this time.”
The company is “attempting to learn the nature of these deficiencies with the goal of addressing them,” Herriot Tabuteau, MD, chief executive officer of Axsome, said in a statement.
However, Dr. Tabuteau acknowledged that this development “may lead to a delay in the potential approval of AXS-05.”
‘Well tolerated’
A total of 44 adults with TRD were enrolled into the MERIT study from the long-term, open-label phase 3 trial of AXS-05.
All patients were in stable remission after treatment with AXS-05 and were randomly assigned to continued treatment with AXS-05 (45 mg dextromethorphan/105 mg bupropion twice daily) or to switch to placebo.
Compared with placebo, AXS-05 significantly delayed time to depression relapse (P = .002) and prevented depression relapse (P = .004).
The novel drug was also well tolerated, with no treatment-emergent adverse events reported in more than one participant in the AXS-05 group, the company said.
One patient treated with AXS-05 did experience gout and bacteremia, but these incidents were deemed unrelated to the medication.
A version of this article first appeared on Medscape.com.
Although a novel investigational drug that combines dextromethorphan and bupropion (AXS-05, Axsome Therapeutics) met its primary and key secondary endpoints in a phase 2 trial of patients with treatment-resistant depression (TRD), the U.S. Food and Drug Administration has voiced some concerns.
In the MERIT study, AXS-05 significantly delayed time to depression relapse compared with placebo (primary endpoint) – with no relapses observed for at least 6 months. It also significantly prevented depression relapse (secondary endpoint), the company said in a news release announcing the topline results.
The drug has been granted breakthrough therapy designations by the FDA for the treatment of major depressive disorder (MDD) and agitation associated with Alzheimer’s disease.
In addition,
However, Axsome stated that the FDA has identified “deficiencies that preclude labeling discussions at this time.”
The company is “attempting to learn the nature of these deficiencies with the goal of addressing them,” Herriot Tabuteau, MD, chief executive officer of Axsome, said in a statement.
However, Dr. Tabuteau acknowledged that this development “may lead to a delay in the potential approval of AXS-05.”
‘Well tolerated’
A total of 44 adults with TRD were enrolled into the MERIT study from the long-term, open-label phase 3 trial of AXS-05.
All patients were in stable remission after treatment with AXS-05 and were randomly assigned to continued treatment with AXS-05 (45 mg dextromethorphan/105 mg bupropion twice daily) or to switch to placebo.
Compared with placebo, AXS-05 significantly delayed time to depression relapse (P = .002) and prevented depression relapse (P = .004).
The novel drug was also well tolerated, with no treatment-emergent adverse events reported in more than one participant in the AXS-05 group, the company said.
One patient treated with AXS-05 did experience gout and bacteremia, but these incidents were deemed unrelated to the medication.
A version of this article first appeared on Medscape.com.
Although a novel investigational drug that combines dextromethorphan and bupropion (AXS-05, Axsome Therapeutics) met its primary and key secondary endpoints in a phase 2 trial of patients with treatment-resistant depression (TRD), the U.S. Food and Drug Administration has voiced some concerns.
In the MERIT study, AXS-05 significantly delayed time to depression relapse compared with placebo (primary endpoint) – with no relapses observed for at least 6 months. It also significantly prevented depression relapse (secondary endpoint), the company said in a news release announcing the topline results.
The drug has been granted breakthrough therapy designations by the FDA for the treatment of major depressive disorder (MDD) and agitation associated with Alzheimer’s disease.
In addition,
However, Axsome stated that the FDA has identified “deficiencies that preclude labeling discussions at this time.”
The company is “attempting to learn the nature of these deficiencies with the goal of addressing them,” Herriot Tabuteau, MD, chief executive officer of Axsome, said in a statement.
However, Dr. Tabuteau acknowledged that this development “may lead to a delay in the potential approval of AXS-05.”
‘Well tolerated’
A total of 44 adults with TRD were enrolled into the MERIT study from the long-term, open-label phase 3 trial of AXS-05.
All patients were in stable remission after treatment with AXS-05 and were randomly assigned to continued treatment with AXS-05 (45 mg dextromethorphan/105 mg bupropion twice daily) or to switch to placebo.
Compared with placebo, AXS-05 significantly delayed time to depression relapse (P = .002) and prevented depression relapse (P = .004).
The novel drug was also well tolerated, with no treatment-emergent adverse events reported in more than one participant in the AXS-05 group, the company said.
One patient treated with AXS-05 did experience gout and bacteremia, but these incidents were deemed unrelated to the medication.
A version of this article first appeared on Medscape.com.
Soccer star med student fled the Taliban, about to be doctor: A Q&A with Nadia Nadim
At the end of 2021, Nadia Nadim will join the tens of thousands of medical students who will exchange their short white coats for the long ones of practicing physicians. Unlike other future doctors, this soon-to-be reconstructive surgeon has also been wearing a uniform that’s more than white. She has donned brightly colored red, purple, or blue jerseys as a striker for teams in the U.S. National Women’s Soccer League and the Danish National football team.
The 33-year-old found her way into medicine after a harrowing childhood. Following the murder of her father by the Taliban, Nadia, her mother, and her four sisters fled Afghanistan in fear for their lives. They sought refuge in Denmark, where Nadia first discovered football [soccer] and a growing call to become a humanitarian activist.
This interview has been edited for length and clarity.
Question: Would you mind telling us a bit about your background and your journey into medicine?
Nadia: I was born in Afghanistan and was raised there until I was 10 years old. Then we had to flee the country because of war. We came to Denmark at the start of sixth grade. At that point, I didn’t really understand the language. I didn’t understand a lot of things. The only thing I kind of knew was math because my mom was teaching us at home.
My mom had always emphasized the importance of education. She said that it can get you out of any situation in your life. If you’re having problems or are in poverty or whatever, education is the key. She was the first kid in her family to get education. No one before her ever went to school, especially not girls.
My mom wanted to become a doctor, but then she got married and her plans changed. She always had this dream and then wanted one of her kids to become a doctor. When I heard that I was like: “Hell no, I’m not gonna. I’m not gonna fulfill your dreams.” My older sister wanted to become a doctor, and I was like: “I’m not gonna become a doctor. I’m gonna do something else. I’m gonna try to become rich.”
I remember in ninth grade, we had this one week where you get to choose what you want to do. I chose to go to the clinic close to our house, not because I had the biggest interest but because it was close and I could sleep in longer.
The week that I was there, I was really surprised. I thought: “Wow, this is really cool to be in the hospital.” I saw some cosmetic operations and eye surgeries. I could see myself in that environment. I love the fact the doctors are able to help people, especially the ones who are really in need. I thought “Maybe I should give this a go.”
So I signed up (for medical school). I got in. I didn’t tell my mom. I told her that I applied to business school and was accepted. She’s was half-heartedly saying: “Oh, I’m so proud of you!” She didn’t really mean it.
I remember being in the first semester and thinking: “I’ve chosen so right.” I loved everything about med school, from the blood to the conversations that you have with your patients. I love it.
Obviously, football is a big part of your life as well. How have you balanced medical training with your work as an athlete on a global stage?
It hasn’t been easy. I did my bachelor’s degree as normal as everyone else because it was possible for me to be in school from 7 a.m. to 3 p.m. My football training was at 6 p.m. It was possible but also really tough.
We have these huge exams in Denmark where you are literally tested on six, seven, or eight big subjects. The failure rate is really high. I was selected for the Danish national team. The time for my exam was literally the same time that I was about to go to camp. I remember there was this lady ... I explained my problem, and she said: “Well, I’m sorry, this is it. You have to make a choice. No one can play football and be a doctor, so I guess you have to make a choice.” I wanted to prove her wrong.
What advice would you have for students who may be in such similar situations, in which they have a counselor or an advisor who isn’t very supportive?
I think there’s always two ways: Either you’re gonna listen and be like “okay, this is it. I give up.” Or, if you’re really passionate about it, you’re gonna go the hard way, which is that you do your thing and then slowly everything is gonna go your way.
I think it’s just about being strong enough to “do you.” I think that’s important. Don’t just give up easily just because you’ve been told: ‘We’ve never done this before. It’s impossible.’ I don’t believe that [impossible] is something that exists. I think if you want to do something, there’s always a way. You just have to find it.
I have never taken no for an answer, I guess. But it’s not gonna be easy.
Given all that is on your plate, how do you avoid burnout?
I love doing active stuff. I have a lot of hobbies. I also enjoy just chilling. If my football allows it, and I’m fresh, I love to do stuff outside like tennis, basketball, and swimming.
I love to watch Bollywood movies, just because I speak Hindi. They have something a bit magical around them, like fairy tale movies. I love to watch Korean dramas. I think I’m always interested in other cultures.
You also have a lot of other projects in the works. Could you tell us briefly about some that you’re currently working on?
One of the things that is really close to my heart and I’m passionate about is volunteer work. You know, the humanitarian organizations that do so much in the world. I’ve been on the receiving hand on the other side. I know that a little tiny help can have a huge impact on your character and your future. That’s probably also one of the reasons I want to be a doctor.
One of the organizations that I work with is the Danish Refugee Council. I have visited refugee camps around the world. I’ve been in Jordan and Kenya, and also Denmark. I’m also ambassador for [United Nations Educational, Scientific, and Cultural Organization] UNESCO’s education for girls. Because, again, I think education is the key to a lot of the problems we do face right now.
For instance, let’s say racism, which is a huge thing. You could probably decrease that by educating people. Ignorance, I think, is a huge factor, the fear that you see among a lot of people because of Islam. It’s just people being ignorant. They don’t know. They just assume or they see a certain group and think that they are the representation for the entire population. All of this ends with education.
If you could educate people, I think a lot of problems would disappear or at least get better. So yeah, I am really busy. But whenever I have a bit of time, I try to use it on making a change.
I started by saying that my mom said education is very important. I think that’s something that my entire family has taken to. My oldest [sister] is a doctor, and then I have two nurses in the family, my youngest sisters. I think a goal is to have a clinic all together.
At the end of 2021, Nadia Nadim will join the tens of thousands of medical students who will exchange their short white coats for the long ones of practicing physicians. Unlike other future doctors, this soon-to-be reconstructive surgeon has also been wearing a uniform that’s more than white. She has donned brightly colored red, purple, or blue jerseys as a striker for teams in the U.S. National Women’s Soccer League and the Danish National football team.
The 33-year-old found her way into medicine after a harrowing childhood. Following the murder of her father by the Taliban, Nadia, her mother, and her four sisters fled Afghanistan in fear for their lives. They sought refuge in Denmark, where Nadia first discovered football [soccer] and a growing call to become a humanitarian activist.
This interview has been edited for length and clarity.
Question: Would you mind telling us a bit about your background and your journey into medicine?
Nadia: I was born in Afghanistan and was raised there until I was 10 years old. Then we had to flee the country because of war. We came to Denmark at the start of sixth grade. At that point, I didn’t really understand the language. I didn’t understand a lot of things. The only thing I kind of knew was math because my mom was teaching us at home.
My mom had always emphasized the importance of education. She said that it can get you out of any situation in your life. If you’re having problems or are in poverty or whatever, education is the key. She was the first kid in her family to get education. No one before her ever went to school, especially not girls.
My mom wanted to become a doctor, but then she got married and her plans changed. She always had this dream and then wanted one of her kids to become a doctor. When I heard that I was like: “Hell no, I’m not gonna. I’m not gonna fulfill your dreams.” My older sister wanted to become a doctor, and I was like: “I’m not gonna become a doctor. I’m gonna do something else. I’m gonna try to become rich.”
I remember in ninth grade, we had this one week where you get to choose what you want to do. I chose to go to the clinic close to our house, not because I had the biggest interest but because it was close and I could sleep in longer.
The week that I was there, I was really surprised. I thought: “Wow, this is really cool to be in the hospital.” I saw some cosmetic operations and eye surgeries. I could see myself in that environment. I love the fact the doctors are able to help people, especially the ones who are really in need. I thought “Maybe I should give this a go.”
So I signed up (for medical school). I got in. I didn’t tell my mom. I told her that I applied to business school and was accepted. She’s was half-heartedly saying: “Oh, I’m so proud of you!” She didn’t really mean it.
I remember being in the first semester and thinking: “I’ve chosen so right.” I loved everything about med school, from the blood to the conversations that you have with your patients. I love it.
Obviously, football is a big part of your life as well. How have you balanced medical training with your work as an athlete on a global stage?
It hasn’t been easy. I did my bachelor’s degree as normal as everyone else because it was possible for me to be in school from 7 a.m. to 3 p.m. My football training was at 6 p.m. It was possible but also really tough.
We have these huge exams in Denmark where you are literally tested on six, seven, or eight big subjects. The failure rate is really high. I was selected for the Danish national team. The time for my exam was literally the same time that I was about to go to camp. I remember there was this lady ... I explained my problem, and she said: “Well, I’m sorry, this is it. You have to make a choice. No one can play football and be a doctor, so I guess you have to make a choice.” I wanted to prove her wrong.
What advice would you have for students who may be in such similar situations, in which they have a counselor or an advisor who isn’t very supportive?
I think there’s always two ways: Either you’re gonna listen and be like “okay, this is it. I give up.” Or, if you’re really passionate about it, you’re gonna go the hard way, which is that you do your thing and then slowly everything is gonna go your way.
I think it’s just about being strong enough to “do you.” I think that’s important. Don’t just give up easily just because you’ve been told: ‘We’ve never done this before. It’s impossible.’ I don’t believe that [impossible] is something that exists. I think if you want to do something, there’s always a way. You just have to find it.
I have never taken no for an answer, I guess. But it’s not gonna be easy.
Given all that is on your plate, how do you avoid burnout?
I love doing active stuff. I have a lot of hobbies. I also enjoy just chilling. If my football allows it, and I’m fresh, I love to do stuff outside like tennis, basketball, and swimming.
I love to watch Bollywood movies, just because I speak Hindi. They have something a bit magical around them, like fairy tale movies. I love to watch Korean dramas. I think I’m always interested in other cultures.
You also have a lot of other projects in the works. Could you tell us briefly about some that you’re currently working on?
One of the things that is really close to my heart and I’m passionate about is volunteer work. You know, the humanitarian organizations that do so much in the world. I’ve been on the receiving hand on the other side. I know that a little tiny help can have a huge impact on your character and your future. That’s probably also one of the reasons I want to be a doctor.
One of the organizations that I work with is the Danish Refugee Council. I have visited refugee camps around the world. I’ve been in Jordan and Kenya, and also Denmark. I’m also ambassador for [United Nations Educational, Scientific, and Cultural Organization] UNESCO’s education for girls. Because, again, I think education is the key to a lot of the problems we do face right now.
For instance, let’s say racism, which is a huge thing. You could probably decrease that by educating people. Ignorance, I think, is a huge factor, the fear that you see among a lot of people because of Islam. It’s just people being ignorant. They don’t know. They just assume or they see a certain group and think that they are the representation for the entire population. All of this ends with education.
If you could educate people, I think a lot of problems would disappear or at least get better. So yeah, I am really busy. But whenever I have a bit of time, I try to use it on making a change.
I started by saying that my mom said education is very important. I think that’s something that my entire family has taken to. My oldest [sister] is a doctor, and then I have two nurses in the family, my youngest sisters. I think a goal is to have a clinic all together.
At the end of 2021, Nadia Nadim will join the tens of thousands of medical students who will exchange their short white coats for the long ones of practicing physicians. Unlike other future doctors, this soon-to-be reconstructive surgeon has also been wearing a uniform that’s more than white. She has donned brightly colored red, purple, or blue jerseys as a striker for teams in the U.S. National Women’s Soccer League and the Danish National football team.
The 33-year-old found her way into medicine after a harrowing childhood. Following the murder of her father by the Taliban, Nadia, her mother, and her four sisters fled Afghanistan in fear for their lives. They sought refuge in Denmark, where Nadia first discovered football [soccer] and a growing call to become a humanitarian activist.
This interview has been edited for length and clarity.
Question: Would you mind telling us a bit about your background and your journey into medicine?
Nadia: I was born in Afghanistan and was raised there until I was 10 years old. Then we had to flee the country because of war. We came to Denmark at the start of sixth grade. At that point, I didn’t really understand the language. I didn’t understand a lot of things. The only thing I kind of knew was math because my mom was teaching us at home.
My mom had always emphasized the importance of education. She said that it can get you out of any situation in your life. If you’re having problems or are in poverty or whatever, education is the key. She was the first kid in her family to get education. No one before her ever went to school, especially not girls.
My mom wanted to become a doctor, but then she got married and her plans changed. She always had this dream and then wanted one of her kids to become a doctor. When I heard that I was like: “Hell no, I’m not gonna. I’m not gonna fulfill your dreams.” My older sister wanted to become a doctor, and I was like: “I’m not gonna become a doctor. I’m gonna do something else. I’m gonna try to become rich.”
I remember in ninth grade, we had this one week where you get to choose what you want to do. I chose to go to the clinic close to our house, not because I had the biggest interest but because it was close and I could sleep in longer.
The week that I was there, I was really surprised. I thought: “Wow, this is really cool to be in the hospital.” I saw some cosmetic operations and eye surgeries. I could see myself in that environment. I love the fact the doctors are able to help people, especially the ones who are really in need. I thought “Maybe I should give this a go.”
So I signed up (for medical school). I got in. I didn’t tell my mom. I told her that I applied to business school and was accepted. She’s was half-heartedly saying: “Oh, I’m so proud of you!” She didn’t really mean it.
I remember being in the first semester and thinking: “I’ve chosen so right.” I loved everything about med school, from the blood to the conversations that you have with your patients. I love it.
Obviously, football is a big part of your life as well. How have you balanced medical training with your work as an athlete on a global stage?
It hasn’t been easy. I did my bachelor’s degree as normal as everyone else because it was possible for me to be in school from 7 a.m. to 3 p.m. My football training was at 6 p.m. It was possible but also really tough.
We have these huge exams in Denmark where you are literally tested on six, seven, or eight big subjects. The failure rate is really high. I was selected for the Danish national team. The time for my exam was literally the same time that I was about to go to camp. I remember there was this lady ... I explained my problem, and she said: “Well, I’m sorry, this is it. You have to make a choice. No one can play football and be a doctor, so I guess you have to make a choice.” I wanted to prove her wrong.
What advice would you have for students who may be in such similar situations, in which they have a counselor or an advisor who isn’t very supportive?
I think there’s always two ways: Either you’re gonna listen and be like “okay, this is it. I give up.” Or, if you’re really passionate about it, you’re gonna go the hard way, which is that you do your thing and then slowly everything is gonna go your way.
I think it’s just about being strong enough to “do you.” I think that’s important. Don’t just give up easily just because you’ve been told: ‘We’ve never done this before. It’s impossible.’ I don’t believe that [impossible] is something that exists. I think if you want to do something, there’s always a way. You just have to find it.
I have never taken no for an answer, I guess. But it’s not gonna be easy.
Given all that is on your plate, how do you avoid burnout?
I love doing active stuff. I have a lot of hobbies. I also enjoy just chilling. If my football allows it, and I’m fresh, I love to do stuff outside like tennis, basketball, and swimming.
I love to watch Bollywood movies, just because I speak Hindi. They have something a bit magical around them, like fairy tale movies. I love to watch Korean dramas. I think I’m always interested in other cultures.
You also have a lot of other projects in the works. Could you tell us briefly about some that you’re currently working on?
One of the things that is really close to my heart and I’m passionate about is volunteer work. You know, the humanitarian organizations that do so much in the world. I’ve been on the receiving hand on the other side. I know that a little tiny help can have a huge impact on your character and your future. That’s probably also one of the reasons I want to be a doctor.
One of the organizations that I work with is the Danish Refugee Council. I have visited refugee camps around the world. I’ve been in Jordan and Kenya, and also Denmark. I’m also ambassador for [United Nations Educational, Scientific, and Cultural Organization] UNESCO’s education for girls. Because, again, I think education is the key to a lot of the problems we do face right now.
For instance, let’s say racism, which is a huge thing. You could probably decrease that by educating people. Ignorance, I think, is a huge factor, the fear that you see among a lot of people because of Islam. It’s just people being ignorant. They don’t know. They just assume or they see a certain group and think that they are the representation for the entire population. All of this ends with education.
If you could educate people, I think a lot of problems would disappear or at least get better. So yeah, I am really busy. But whenever I have a bit of time, I try to use it on making a change.
I started by saying that my mom said education is very important. I think that’s something that my entire family has taken to. My oldest [sister] is a doctor, and then I have two nurses in the family, my youngest sisters. I think a goal is to have a clinic all together.
Why aren’t more women doctors in the top-paying specialties?
Women compose only 6% of orthopedic surgeons, 8% of interventional cardiologists, 10% of urologists, 17% of plastic surgeons, and 18% of otolaryngologists, according to the 2020 Association of American Medical Colleges Physician Specialty Data Report.
Plastic surgeons earn an average of $526,000 annually, which is the highest-paying specialty. Otolaryngologists earn an average of $417,000 annually, and urologists earn $427,000, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Yet, far more women are practicing in specialties that pay less. Women are the majority in pediatrics (64%), ob.gyn. (59%), internal medicine (53%), and endocrinology (51%), the AAMC data show. The exception is dermatology, which pays well and in which 51% are women. The annual average pay is $394,000.
Why are so many women avoiding the top-paying specialties?
Several physician researchers and leaders in the top-paying specialties point to four main factors: Women are attracted to specialties that have more women in faculty and leadership positions, women prioritize work-life balance over pay, women residents may be deterred from the high-paying specialties because of gender discrimination and sexual harassment, and the longer training periods for surgical specialties may be a deterrent for women who want to have children.
Lack of women leaders
The specialties with the most women tend to have the highest proportion of women in leadership positions. For example, obstetrics and gynecology had the highest proportion of women department chairs (24.1%) and vice chairs (38.8). Pediatrics had the highest proportion of women division directors (31.5%) and residency program directors (64.6%), a study shows.
Surgical specialties, on the other hand, may have a harder time attracting female residents, possibly because of a lack of women in leadership positions. A recent study that examined gender differences in attitudes toward surgery training found that women would be more likely to go into surgery if there were more surgical faculty and residents of their same gender.
An analysis of orthopedic residency programs shows that more trainees were drawn to programs that had more female faculty members, including associate professors and women in leadership positions.

Terri Malcolm, MD, a board-certified ob.gyn. and CEO/founder of Master Physician Leaders, said women need to consider whether they want to be a trailblazer in a specialty that has fewer women. “What support systems are in place to accommodate your goals, whether it’s career advancement, having a family, or mentorship? Where can you show up as your whole self and be supported in that?”
Being the only woman in a residency program can be a challenge, said Dr. Malcolm. If the residents and attendings are predominantly men, for example, they may not think about creating a call schedule that takes into account maternity leave or the fact that women tend to be caretakers for their children and parents.
The study of gender differences toward surgery training shows that 75% of women, in comparison with 46% of men, would be more willing to enter surgery if maternity leave and childcare were made available to female residents and attending physicians.
Women want work-life balance
Although both men and women want families, women still shoulder more family and childcare responsibilities. That may explain why women physicians ranked work-life balance first and compensation second in the Medscape Women Physicians 2020 Report: The Issues They Care About.
“My physician colleagues have been and are supportive of intellectual abilities, but I feel they don’t fully understand the uneven distribution of childcare issues on women,” a woman dermatologist commented.

Women may want to work fewer hours or have a more flexible schedule to take care of children. “I can count on one hand the number of women who have a part-time job in orthopedics. It’s very rare, and working part time absolutely is a barrier for someone who wants to be a surgeon,” said Julie Samora, MD, PhD, a researcher and pediatric hand surgeon at Nationwide Children’s Hospital, in Columbus, Ohio. She is also a spokesperson for the American Association of Orthopedic Surgeons.
Preeti Malani, MD, a professor of medicine who specializes in infectious diseases at the University of Michigan, chose to work full-time in academia while raising two children with her husband. In a decade, she rose through the ranks to full professor. “I took the advice of a woman who wanted to recruit me to have a full-time position with maximum flexibility rather than work part time, often for more hours and less pay. I also have tried to build my career so I was not doing all clinical work.”
Her husband is a surgeon at the University of Michigan. His schedule was not flexible, and he was unable to take on family responsibilities, said Dr. Malani. “I knew someone had to be able to grab the kids from daycare or pick them up at school if they were sick.” She also took work home and worked weekends.
Young women physicians in particular are thinking about combining parenting with work – in the Medscape report, that issue ranked third among the issues women care about. Seeing other women doctors navigate that in their particular specialty can have a positive impact.
“When I chose adolescent medicine, I remember working with a doctor in this field who talked about how much she enjoyed raising her kids even as teenagers and how much she was enjoying them as young adults. She seemed so balanced and happy in her family, and it gave me a nice feeling about the field,” said Nancy Dodson, MD, MPH, a pediatrician specializing in adolescent medicine at Pediatrics on Hudson in New York.
Rachel Zhuk, MD, a reproductive psychiatrist in New York, took a break after medical school to spend time with her newborn son. She met a woman who was also a young parent and a psychiatrist. “We were both figuring out parenting together – it was like looking into my future.” That friendship and her desire to have more time with patients influenced her decision to pursue psychiatry instead of internal medicine.
Discrimination and harassment influence specialty choice
Women doctors in the top-paying surgical and other specialties have reported experiencing more discrimination and harassment than men.
Of 927 orthopedic surgeons who responded to an AAOS survey, 66% said they experienced gender discrimination, bullying, sexual harassment, or harassment in the health care workplace. More than twice as many women (81%) experienced these behaviors as men (35%).
“This study shows that women in orthopedic surgery disproportionately experience these negative behaviors, and only a handful of institutions in the United States provide any type of training to prevent them,” said Dr. Samora, the lead author of the AAOS report.
Radiology is another male-dominated field – women represent 26% of all radiologists, the 2020 AAMC specialty report shows. A systematic review shows that 40% of women radiologists experienced gender discrimination at work, compared with 1% of men, and that 47% of women experienced sexual harassment.
Female trainees in surgery have also reported disproportionate rates of discrimination and harassment. Female general surgical residents have experienced more gender discrimination than male residents (65.1% vs. 10.0%) and more sexual harassment than male residents (19.9% vs. 3.9), a national survey indicates.
When medical students are exposed to these behaviors through personal experience, witnessing, or hearing about them, it can affect which specialty they choose. A survey of fourth-year medical students shows that far more women than men reported that exposure to gender discrimination and sexual harassment influenced their specialty choices (45.3% vs. 16.4%) and residency rankings (25.3% vs. 10.9%). Women who chose general surgery were the most likely to experience gender discrimination and sexual harassment during residency selection; women who chose psychiatry were the least likely to experience such behaviors, the report shows.
“If young trainees witness such behaviors in a specific field, they would naturally migrate toward a different specialty,” said Dr. Samora.
Trainees can also be put off by residency directors asking them inappropriate questions. Of nearly 500 female orthopedic surgeons surveyed, 62% reported that they were asked inappropriate questions during their residency interviews. “Inappropriate questions and comments directed toward women during residency interviews are clearly not conducive to women entering the field,” the authors stated. They found that little changed during the study period from 1971 to 2015.
The most frequent inappropriate questions concerned whether the prospective residents would be getting pregnant or raising children during residency and their marital status. One female orthopedic surgeon reported: “I was asked if I have children and was told that it would be too difficult to complete an orthopedic residency with children.”
The interviewers also made frequent comments about the inferiority of women to men. For example, “I was told by one program interviewer that ‘I don’t have a bias about women in medicine, I have a bias about women in orthopedic surgery,’ ” another female orthopedic surgeon commented.
Longer training
Residency training for the top-paying surgical specialties, including orthopedic surgery, plastic surgery, and otolaryngology, lasts 5-6 years. This compares with 3-4 years for the lower-paying specialties, such as pediatrics, internal medicine, and ob.gyn., according to data from the American Medical Association.
Women doctors are in their prime childbearing years during residency. Women who want to start a family will consider whether they want to get pregnant during residency or wait until they finish their training, said Dr. Malcolm.
The vast majority (84%) of 190 female orthopedic surgery trainees who responded to a survey indicated that they did not have children or were pregnant during residency. Nearly half (48%) reported that they had postponed having children because they were in training.
“The longer training is definitely a concerning issue for women of childbearing age. Many professional women are waiting to have children, for multiple reasons, but one major fear is the stigma due to taking time off from work obligations. There is a risk of irritating your peers because they may have to take on more work and cover more calls for you during your absence,” said Dr. Samora.
That fear is not unfounded. At least half of the 190 female orthopedic residents reported that they encountered bias against becoming pregnant during training from both coresidents (60%) and attendings (50%), according to the study.
Another recent survey suggests that pregnant surgical residents face several barriers during their training, including a lack of salary for extended family leave, resentment from fellow residents who need to cover for them during maternity leave, and a lack of formal lactation policies.
A few policy changes by national board organizations, including those in the surgical specialties, may make life a little easier for female trainees to have children, suggested Dr. Samora.
Residents and fellows are now allowed a minimum of 6 weeks away for medical leave or caregiving once during training, without having to use vacation or sick leave and without having to extend their training, the American Board of Medical Specialties has announced.
In addition, the American Board of Orthopaedic Surgery and the American Board of Surgery have enacted policies that allow lactating women to take a break to pump during their board exams.
A version of this article first appeared on Medscape.com.
Women compose only 6% of orthopedic surgeons, 8% of interventional cardiologists, 10% of urologists, 17% of plastic surgeons, and 18% of otolaryngologists, according to the 2020 Association of American Medical Colleges Physician Specialty Data Report.
Plastic surgeons earn an average of $526,000 annually, which is the highest-paying specialty. Otolaryngologists earn an average of $417,000 annually, and urologists earn $427,000, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Yet, far more women are practicing in specialties that pay less. Women are the majority in pediatrics (64%), ob.gyn. (59%), internal medicine (53%), and endocrinology (51%), the AAMC data show. The exception is dermatology, which pays well and in which 51% are women. The annual average pay is $394,000.
Why are so many women avoiding the top-paying specialties?
Several physician researchers and leaders in the top-paying specialties point to four main factors: Women are attracted to specialties that have more women in faculty and leadership positions, women prioritize work-life balance over pay, women residents may be deterred from the high-paying specialties because of gender discrimination and sexual harassment, and the longer training periods for surgical specialties may be a deterrent for women who want to have children.
Lack of women leaders
The specialties with the most women tend to have the highest proportion of women in leadership positions. For example, obstetrics and gynecology had the highest proportion of women department chairs (24.1%) and vice chairs (38.8). Pediatrics had the highest proportion of women division directors (31.5%) and residency program directors (64.6%), a study shows.
Surgical specialties, on the other hand, may have a harder time attracting female residents, possibly because of a lack of women in leadership positions. A recent study that examined gender differences in attitudes toward surgery training found that women would be more likely to go into surgery if there were more surgical faculty and residents of their same gender.
An analysis of orthopedic residency programs shows that more trainees were drawn to programs that had more female faculty members, including associate professors and women in leadership positions.
Terri Malcolm, MD, a board-certified ob.gyn. and CEO/founder of Master Physician Leaders, said women need to consider whether they want to be a trailblazer in a specialty that has fewer women. “What support systems are in place to accommodate your goals, whether it’s career advancement, having a family, or mentorship? Where can you show up as your whole self and be supported in that?”
Being the only woman in a residency program can be a challenge, said Dr. Malcolm. If the residents and attendings are predominantly men, for example, they may not think about creating a call schedule that takes into account maternity leave or the fact that women tend to be caretakers for their children and parents.
The study of gender differences toward surgery training shows that 75% of women, in comparison with 46% of men, would be more willing to enter surgery if maternity leave and childcare were made available to female residents and attending physicians.
Women want work-life balance
Although both men and women want families, women still shoulder more family and childcare responsibilities. That may explain why women physicians ranked work-life balance first and compensation second in the Medscape Women Physicians 2020 Report: The Issues They Care About.
“My physician colleagues have been and are supportive of intellectual abilities, but I feel they don’t fully understand the uneven distribution of childcare issues on women,” a woman dermatologist commented.
Women may want to work fewer hours or have a more flexible schedule to take care of children. “I can count on one hand the number of women who have a part-time job in orthopedics. It’s very rare, and working part time absolutely is a barrier for someone who wants to be a surgeon,” said Julie Samora, MD, PhD, a researcher and pediatric hand surgeon at Nationwide Children’s Hospital, in Columbus, Ohio. She is also a spokesperson for the American Association of Orthopedic Surgeons.
Preeti Malani, MD, a professor of medicine who specializes in infectious diseases at the University of Michigan, chose to work full-time in academia while raising two children with her husband. In a decade, she rose through the ranks to full professor. “I took the advice of a woman who wanted to recruit me to have a full-time position with maximum flexibility rather than work part time, often for more hours and less pay. I also have tried to build my career so I was not doing all clinical work.”
Her husband is a surgeon at the University of Michigan. His schedule was not flexible, and he was unable to take on family responsibilities, said Dr. Malani. “I knew someone had to be able to grab the kids from daycare or pick them up at school if they were sick.” She also took work home and worked weekends.
Young women physicians in particular are thinking about combining parenting with work – in the Medscape report, that issue ranked third among the issues women care about. Seeing other women doctors navigate that in their particular specialty can have a positive impact.
“When I chose adolescent medicine, I remember working with a doctor in this field who talked about how much she enjoyed raising her kids even as teenagers and how much she was enjoying them as young adults. She seemed so balanced and happy in her family, and it gave me a nice feeling about the field,” said Nancy Dodson, MD, MPH, a pediatrician specializing in adolescent medicine at Pediatrics on Hudson in New York.
Rachel Zhuk, MD, a reproductive psychiatrist in New York, took a break after medical school to spend time with her newborn son. She met a woman who was also a young parent and a psychiatrist. “We were both figuring out parenting together – it was like looking into my future.” That friendship and her desire to have more time with patients influenced her decision to pursue psychiatry instead of internal medicine.
Discrimination and harassment influence specialty choice
Women doctors in the top-paying surgical and other specialties have reported experiencing more discrimination and harassment than men.
Of 927 orthopedic surgeons who responded to an AAOS survey, 66% said they experienced gender discrimination, bullying, sexual harassment, or harassment in the health care workplace. More than twice as many women (81%) experienced these behaviors as men (35%).
“This study shows that women in orthopedic surgery disproportionately experience these negative behaviors, and only a handful of institutions in the United States provide any type of training to prevent them,” said Dr. Samora, the lead author of the AAOS report.
Radiology is another male-dominated field – women represent 26% of all radiologists, the 2020 AAMC specialty report shows. A systematic review shows that 40% of women radiologists experienced gender discrimination at work, compared with 1% of men, and that 47% of women experienced sexual harassment.
Female trainees in surgery have also reported disproportionate rates of discrimination and harassment. Female general surgical residents have experienced more gender discrimination than male residents (65.1% vs. 10.0%) and more sexual harassment than male residents (19.9% vs. 3.9), a national survey indicates.
When medical students are exposed to these behaviors through personal experience, witnessing, or hearing about them, it can affect which specialty they choose. A survey of fourth-year medical students shows that far more women than men reported that exposure to gender discrimination and sexual harassment influenced their specialty choices (45.3% vs. 16.4%) and residency rankings (25.3% vs. 10.9%). Women who chose general surgery were the most likely to experience gender discrimination and sexual harassment during residency selection; women who chose psychiatry were the least likely to experience such behaviors, the report shows.
“If young trainees witness such behaviors in a specific field, they would naturally migrate toward a different specialty,” said Dr. Samora.
Trainees can also be put off by residency directors asking them inappropriate questions. Of nearly 500 female orthopedic surgeons surveyed, 62% reported that they were asked inappropriate questions during their residency interviews. “Inappropriate questions and comments directed toward women during residency interviews are clearly not conducive to women entering the field,” the authors stated. They found that little changed during the study period from 1971 to 2015.
The most frequent inappropriate questions concerned whether the prospective residents would be getting pregnant or raising children during residency and their marital status. One female orthopedic surgeon reported: “I was asked if I have children and was told that it would be too difficult to complete an orthopedic residency with children.”
The interviewers also made frequent comments about the inferiority of women to men. For example, “I was told by one program interviewer that ‘I don’t have a bias about women in medicine, I have a bias about women in orthopedic surgery,’ ” another female orthopedic surgeon commented.
Longer training
Residency training for the top-paying surgical specialties, including orthopedic surgery, plastic surgery, and otolaryngology, lasts 5-6 years. This compares with 3-4 years for the lower-paying specialties, such as pediatrics, internal medicine, and ob.gyn., according to data from the American Medical Association.
Women doctors are in their prime childbearing years during residency. Women who want to start a family will consider whether they want to get pregnant during residency or wait until they finish their training, said Dr. Malcolm.
The vast majority (84%) of 190 female orthopedic surgery trainees who responded to a survey indicated that they did not have children or were pregnant during residency. Nearly half (48%) reported that they had postponed having children because they were in training.
“The longer training is definitely a concerning issue for women of childbearing age. Many professional women are waiting to have children, for multiple reasons, but one major fear is the stigma due to taking time off from work obligations. There is a risk of irritating your peers because they may have to take on more work and cover more calls for you during your absence,” said Dr. Samora.
That fear is not unfounded. At least half of the 190 female orthopedic residents reported that they encountered bias against becoming pregnant during training from both coresidents (60%) and attendings (50%), according to the study.
Another recent survey suggests that pregnant surgical residents face several barriers during their training, including a lack of salary for extended family leave, resentment from fellow residents who need to cover for them during maternity leave, and a lack of formal lactation policies.
A few policy changes by national board organizations, including those in the surgical specialties, may make life a little easier for female trainees to have children, suggested Dr. Samora.
Residents and fellows are now allowed a minimum of 6 weeks away for medical leave or caregiving once during training, without having to use vacation or sick leave and without having to extend their training, the American Board of Medical Specialties has announced.
In addition, the American Board of Orthopaedic Surgery and the American Board of Surgery have enacted policies that allow lactating women to take a break to pump during their board exams.
A version of this article first appeared on Medscape.com.
Women compose only 6% of orthopedic surgeons, 8% of interventional cardiologists, 10% of urologists, 17% of plastic surgeons, and 18% of otolaryngologists, according to the 2020 Association of American Medical Colleges Physician Specialty Data Report.
Plastic surgeons earn an average of $526,000 annually, which is the highest-paying specialty. Otolaryngologists earn an average of $417,000 annually, and urologists earn $427,000, according to the Medscape Physician Compensation Report 2021: The Recovery Begins.
Yet, far more women are practicing in specialties that pay less. Women are the majority in pediatrics (64%), ob.gyn. (59%), internal medicine (53%), and endocrinology (51%), the AAMC data show. The exception is dermatology, which pays well and in which 51% are women. The annual average pay is $394,000.
Why are so many women avoiding the top-paying specialties?
Several physician researchers and leaders in the top-paying specialties point to four main factors: Women are attracted to specialties that have more women in faculty and leadership positions, women prioritize work-life balance over pay, women residents may be deterred from the high-paying specialties because of gender discrimination and sexual harassment, and the longer training periods for surgical specialties may be a deterrent for women who want to have children.
Lack of women leaders
The specialties with the most women tend to have the highest proportion of women in leadership positions. For example, obstetrics and gynecology had the highest proportion of women department chairs (24.1%) and vice chairs (38.8). Pediatrics had the highest proportion of women division directors (31.5%) and residency program directors (64.6%), a study shows.
Surgical specialties, on the other hand, may have a harder time attracting female residents, possibly because of a lack of women in leadership positions. A recent study that examined gender differences in attitudes toward surgery training found that women would be more likely to go into surgery if there were more surgical faculty and residents of their same gender.
An analysis of orthopedic residency programs shows that more trainees were drawn to programs that had more female faculty members, including associate professors and women in leadership positions.
Terri Malcolm, MD, a board-certified ob.gyn. and CEO/founder of Master Physician Leaders, said women need to consider whether they want to be a trailblazer in a specialty that has fewer women. “What support systems are in place to accommodate your goals, whether it’s career advancement, having a family, or mentorship? Where can you show up as your whole self and be supported in that?”
Being the only woman in a residency program can be a challenge, said Dr. Malcolm. If the residents and attendings are predominantly men, for example, they may not think about creating a call schedule that takes into account maternity leave or the fact that women tend to be caretakers for their children and parents.
The study of gender differences toward surgery training shows that 75% of women, in comparison with 46% of men, would be more willing to enter surgery if maternity leave and childcare were made available to female residents and attending physicians.
Women want work-life balance
Although both men and women want families, women still shoulder more family and childcare responsibilities. That may explain why women physicians ranked work-life balance first and compensation second in the Medscape Women Physicians 2020 Report: The Issues They Care About.
“My physician colleagues have been and are supportive of intellectual abilities, but I feel they don’t fully understand the uneven distribution of childcare issues on women,” a woman dermatologist commented.
Women may want to work fewer hours or have a more flexible schedule to take care of children. “I can count on one hand the number of women who have a part-time job in orthopedics. It’s very rare, and working part time absolutely is a barrier for someone who wants to be a surgeon,” said Julie Samora, MD, PhD, a researcher and pediatric hand surgeon at Nationwide Children’s Hospital, in Columbus, Ohio. She is also a spokesperson for the American Association of Orthopedic Surgeons.
Preeti Malani, MD, a professor of medicine who specializes in infectious diseases at the University of Michigan, chose to work full-time in academia while raising two children with her husband. In a decade, she rose through the ranks to full professor. “I took the advice of a woman who wanted to recruit me to have a full-time position with maximum flexibility rather than work part time, often for more hours and less pay. I also have tried to build my career so I was not doing all clinical work.”
Her husband is a surgeon at the University of Michigan. His schedule was not flexible, and he was unable to take on family responsibilities, said Dr. Malani. “I knew someone had to be able to grab the kids from daycare or pick them up at school if they were sick.” She also took work home and worked weekends.
Young women physicians in particular are thinking about combining parenting with work – in the Medscape report, that issue ranked third among the issues women care about. Seeing other women doctors navigate that in their particular specialty can have a positive impact.
“When I chose adolescent medicine, I remember working with a doctor in this field who talked about how much she enjoyed raising her kids even as teenagers and how much she was enjoying them as young adults. She seemed so balanced and happy in her family, and it gave me a nice feeling about the field,” said Nancy Dodson, MD, MPH, a pediatrician specializing in adolescent medicine at Pediatrics on Hudson in New York.
Rachel Zhuk, MD, a reproductive psychiatrist in New York, took a break after medical school to spend time with her newborn son. She met a woman who was also a young parent and a psychiatrist. “We were both figuring out parenting together – it was like looking into my future.” That friendship and her desire to have more time with patients influenced her decision to pursue psychiatry instead of internal medicine.
Discrimination and harassment influence specialty choice
Women doctors in the top-paying surgical and other specialties have reported experiencing more discrimination and harassment than men.
Of 927 orthopedic surgeons who responded to an AAOS survey, 66% said they experienced gender discrimination, bullying, sexual harassment, or harassment in the health care workplace. More than twice as many women (81%) experienced these behaviors as men (35%).
“This study shows that women in orthopedic surgery disproportionately experience these negative behaviors, and only a handful of institutions in the United States provide any type of training to prevent them,” said Dr. Samora, the lead author of the AAOS report.
Radiology is another male-dominated field – women represent 26% of all radiologists, the 2020 AAMC specialty report shows. A systematic review shows that 40% of women radiologists experienced gender discrimination at work, compared with 1% of men, and that 47% of women experienced sexual harassment.
Female trainees in surgery have also reported disproportionate rates of discrimination and harassment. Female general surgical residents have experienced more gender discrimination than male residents (65.1% vs. 10.0%) and more sexual harassment than male residents (19.9% vs. 3.9), a national survey indicates.
When medical students are exposed to these behaviors through personal experience, witnessing, or hearing about them, it can affect which specialty they choose. A survey of fourth-year medical students shows that far more women than men reported that exposure to gender discrimination and sexual harassment influenced their specialty choices (45.3% vs. 16.4%) and residency rankings (25.3% vs. 10.9%). Women who chose general surgery were the most likely to experience gender discrimination and sexual harassment during residency selection; women who chose psychiatry were the least likely to experience such behaviors, the report shows.
“If young trainees witness such behaviors in a specific field, they would naturally migrate toward a different specialty,” said Dr. Samora.
Trainees can also be put off by residency directors asking them inappropriate questions. Of nearly 500 female orthopedic surgeons surveyed, 62% reported that they were asked inappropriate questions during their residency interviews. “Inappropriate questions and comments directed toward women during residency interviews are clearly not conducive to women entering the field,” the authors stated. They found that little changed during the study period from 1971 to 2015.
The most frequent inappropriate questions concerned whether the prospective residents would be getting pregnant or raising children during residency and their marital status. One female orthopedic surgeon reported: “I was asked if I have children and was told that it would be too difficult to complete an orthopedic residency with children.”
The interviewers also made frequent comments about the inferiority of women to men. For example, “I was told by one program interviewer that ‘I don’t have a bias about women in medicine, I have a bias about women in orthopedic surgery,’ ” another female orthopedic surgeon commented.
Longer training
Residency training for the top-paying surgical specialties, including orthopedic surgery, plastic surgery, and otolaryngology, lasts 5-6 years. This compares with 3-4 years for the lower-paying specialties, such as pediatrics, internal medicine, and ob.gyn., according to data from the American Medical Association.
Women doctors are in their prime childbearing years during residency. Women who want to start a family will consider whether they want to get pregnant during residency or wait until they finish their training, said Dr. Malcolm.
The vast majority (84%) of 190 female orthopedic surgery trainees who responded to a survey indicated that they did not have children or were pregnant during residency. Nearly half (48%) reported that they had postponed having children because they were in training.
“The longer training is definitely a concerning issue for women of childbearing age. Many professional women are waiting to have children, for multiple reasons, but one major fear is the stigma due to taking time off from work obligations. There is a risk of irritating your peers because they may have to take on more work and cover more calls for you during your absence,” said Dr. Samora.
That fear is not unfounded. At least half of the 190 female orthopedic residents reported that they encountered bias against becoming pregnant during training from both coresidents (60%) and attendings (50%), according to the study.
Another recent survey suggests that pregnant surgical residents face several barriers during their training, including a lack of salary for extended family leave, resentment from fellow residents who need to cover for them during maternity leave, and a lack of formal lactation policies.
A few policy changes by national board organizations, including those in the surgical specialties, may make life a little easier for female trainees to have children, suggested Dr. Samora.
Residents and fellows are now allowed a minimum of 6 weeks away for medical leave or caregiving once during training, without having to use vacation or sick leave and without having to extend their training, the American Board of Medical Specialties has announced.
In addition, the American Board of Orthopaedic Surgery and the American Board of Surgery have enacted policies that allow lactating women to take a break to pump during their board exams.
A version of this article first appeared on Medscape.com.