User login
The secret I’ll take to my grave: Doc reveals
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
An internist will never forget the dark secret his patient revealed during a routine visit – or the grim aftermath.
The patient, who had a progressive, incurable neurological condition, confided that he planned to kill himself. The patient intended to conceal the true manner and make the death look natural.
“[He planned to do it] very carefully at home so no one would know,” said the internist, who remains anonymous. “[He shared] the methods he would use.”
Perhaps more shocking than the patient’s confession was the physician’s response.
“He did not require my help to do what he planned, and I did not try to stop him,” said the internist. “I reported his death as ‘natural causes’ and never told anyone.”
An ob.gyn., for instance, wrote about struggling with whether to tell a father that his newborn baby was not his genetic child. The newborn had a blood type that made it impossible for the father to be biologically related to the infant, the anonymous doctor wrote.
“I told the wife who then informed me she had a lover,” the ob.gyn. said. “I never told the husband.”
It’s uncertain whether carrying the burden of such hidden knowledge affected the physicians involved in these cases. However, in general, secrets can weigh heavily on the minds of those who keep them and can contribute to stress, said Malia Mason, PhD, a psychologist and dean of research at Columbia Business School in New York. Holding onto secrets can cause depression and anxiety, research shows. The more often people think about the secret, the greater the impact, according to a recent study coauthored by Dr. Mason.
“Keeping a secret diminishes well-being,” Dr. Mason said. “It makes people feel socially distant. It lowers relationship satisfaction, and it leads people to feel inauthentic. The reason that secrets do this is because people think about them all the time. The more you think about it, the more you see these consequences.”
Feelings that stem from a secret depend on the content. The more immoral a secret is thought to be, the more people feel ashamed, according to a 2021 analysis of thousands of secrets, reported by Michael L. Slepian, PhD, and Alex Koch, PhD. However, secrets more related to a person’s profession are often internalized differently, the study found. The more a secret fell higher on the profession/goal-oriented dimension, the more people felt they had insight into the secret, according to the analysis. For example, having clear thinking about the secret and/or knowing how to handle it.
“The more shame participants felt from their secret, the more they indicated the secret hurt their well-being,” Dr. Slepian and Dr. Koch wrote in the study. “The more insight participants felt they had into their secret, the less they indicated the secret hurt their well-being.”
Suspicious deaths exposed after investigations
The internist’s account of keeping his patient’s suicide a secret raises many questions, such as how the patient masked his manner of death. The internist did not share any more details about the incident.
Suicides are among the most challenging manners of deaths to certify, according to James Gill, MD, a pathologist and president of the National Association of Medical Examiners. Death investigators must demonstrate intent, meaning the individuals caused the injury to intentionally harm themselves. Fewer than half of people who die by suicide leave a note, Dr. Gill said, so investigators can’t rely on the absence or the presence of a note in making their determination.
A decedent who had cancer or a severe neurological disorder presents further challenges, said Dr. Gill, who serves as chief medical examiner for the state of Connecticut.
“These [deaths] may not be unexpected and may not be reported to the medical examiner/coroner,” Dr. Gill said. “If there is no suspicion and the treating doctor is willing to sign the death certificate, the death will not come under the jurisdiction of the medical examiner.”
Dr. Gill recalled a death his colleague once investigated that appeared to be natural but emerged as something else after a deeper look.
A woman with metastatic breast cancer was about to be discharged from a hospital into hospice the next morning. The night before, she had a “going away” party with friends who came to visit her in the hospital. Shortly after the friends left, the woman was found dead. Because of her condition, she could have died at any time, Dr. Gill said, but she also had a history of depression and hospital staff were suspicious. The death was reported to the medical examiner’s office.
Toxicology testing found markedly elevated concentrations of phenytoin and pentobarbital, neither of which were prescribed during her hospital stay. Dr. Gill said it turned out that the woman and her friends worked at a veterinarian’s office, and the medication they used to euthanize dogs was a combination of phenytoin and pentobarbital.
“The death was certified as a homicide because of the direct actions of another, but a reasonable argument could be made for suicide,” Dr. Gill said.
In a similar case reported in the journal Science & Justice, a 64-year-old cardiologist was found lifeless by his wife after he collapsed near the stairs of his home. Next to his body was a bottle of whiskey and two cups, one that appeared to be used for the alcohol and one with a yellowish liquid smelling of honey. The wife reported that her husband always drank whiskey with honey before bed. The death was initially classified as natural, but after vehement protest by the family, a forensic autopsy was performed.
Prior to the autopsy, death investigators learned the decedent, who was a well-known and successful practitioner in his community, had Parkinson’s disease. At times, he could not sign his prescriptions because of the increasing tremor in his hands, according to the case study. Investigators learned the patient’s mother had also suffered from Parkinson’s, and that her son had witnessed her decline.
The autopsy revealed only nonspecific lesions such as acute stasis of the viscera, moderate pulmonary and cerebral edema, and moderate generalized atheromatosis. Histological examinations did not yield any unusual findings.
An analysis of the beverage containers detected pentobarbital in the yellowish syrup residue of the second cup. Testing of the doctor’s peripheral blood revealed the presence of a metabolite of pentobarbital, ethanol, and traces of phenobarbital. In addition, a urine analysis showed the presence of venlafaxine, an antidepressant, as well as the benzophenone of lorazepam, a sedating benzodiazepine, and metoclopramide, an antiemetic.
Lead author C. Brandt-Casadevall, MD, and colleagues wrote that the levels were clearly compatible with a scenario of a pentobarbital overdose with a lethal outcome.
“... It is obvious that the victim attempted to hide his suicide from his family circle,” Dr. Brandt-Casadevall and colleagues wrote. “Thus, we obtained no evidence indicating that he might have spoken at any point of putting an end to his life. There was no written note. The victim did not wait to be alone at home. Instead, he committed his act in a routine situation: his wife was watching television late at night and he was upstairs, presumably going to sleep. Thus, he had one to two hours at his disposal, and he ingested a very fast-acting drug which would make any attempt at reanimation impossible, even after a brief period of time. This may have induced the physician in charge to believe that the cause of death was cardiac origin, a likely hypothesis given the age of the victim.”
What to do when a terminally ill patient talks suicide
When a terminally ill patient expresses the desire to end his or her life, it’s important to understand that desire is often a result of existential suffering, a sense of hopelessness, and lack of social support, said Lynn A. Jansen, PhD, a bioethicist at the University of Arizona in Tucson.
“The duty of beneficence requires that physicians attempt to provide the support and care that is needed,” said Dr. Jansen. “Here, interdisciplinary teamwork is important and should be utilized. Physicians should refer patients to professionals, such as social workers, pastoral care, psychologists, etc., who are better able to address these issues.”
The rate of desire for a hastened death among terminally ill patients ranges from 17% to 45%, depending on the population studied and how the desire is evaluated, according to an analysis in the Primary Care Companion to the Journal of Clinical Psychiatry. In one study, 14% of about 130 palliative care patients with cancer had a strong desire to quicken the dying process.
In addition, patients with neurologic disorders have a significantly higher suicide rate than that of those without neurologic disorders, a recent JAMA study found. About 1 in 150 patients diagnosed with a neurological disorder dies by suicide, the analysis determined.
A tricky point to remember is that a desire by a terminally ill patient to hasten his or her death by suicide should not be taken by itself to indicate depression, Dr. Jansen noted.
“In principle, such patients can make an autonomous decision to end their lives,” she said. “However, the expression of such a desire is very often associated with depression and forms of suffering that can be effectively addressed by the health care team.”
Physicians can also explore other avenues with the patient such as palliative care or making sure adequate pain relief is available, added Robert Klitzman, MD, professor of psychiatry and academic director of the master of science in bioethics program at Columbia University, New York.
“If they are saying it’s because they are distressed, ethically, a doctor can and should find ways to decrease their distress,” he said.
Of course, those who practice in the U.S. jurisdictions that have physician-assisted-dying laws have different legal and ethical elements to consider. Physicians in these areas have no ethical duty to participate in the process, Dr. Jansen said, but they have a duty to refer patients who express a desire to pursue physician aid-in-dying to another provider who can assist them.
Physician aid-in-dying laws vary somewhat so it’s important that physicians in these areas be aware of their specific statute, Dr. Klitzman said. California, Colorado, Hawaii, Maine, New Jersey, New Mexico, Oregon, Vermont, Washington, and the District of Columbia have these laws.
“In these states, if a terminally ill patient says they don’t want to live anymore, a physician would first decide if this is a result of depression or if it’s a request for physician aid-in-dying,” he said. “Even then, in most cases, the patient would be evaluated by not one, but two different health professionals at two different points. We want to see if it is a consistent decision that the person has made that they want physician aid-in-dying, and not just that they’ve had a bad day or a setback in their treatment.”
In the case of the internist who told no one of his patient’s suicide plan, Dr. Klitzman said he would have dug deeper into the patient’s mindset.
“Not knowing anything about the patient or the doctor, I would have responded differently,” he said. “I think a physician should address why a patient feels that way. They may feel their pain is unbearable, and we potentially offer more pain relief. Maybe the patient shows evidence of having depression, which may be treatable [with medication]. The patient would then feel better and be able to spend quality time with family and loved ones, make sure their affairs are in order, and have a chance to say goodbye.”
A version of this article first appeared on Medscape.com.
NIH to study COVID vaccine booster in people with autoimmune disease
In the wake of the Centers for Disease Control and Prevention’s recommendation for a third COVID-19 mRNA vaccine dose for immunocompromised people and the Food and Drug Administration’s authorization of the third dose, the according to an announcement.
The investigators of the trial, called COVID‐19 Booster Vaccine in Autoimmune Disease Non‐Responders, also want to determine if pausing immunosuppressive therapy for autoimmune disease improves the antibody response to an extra dose of a COVID-19 vaccine.
The trial will specifically look at the effects of mycophenolate mofetil (MMF) or mycophenolic acid (MPA), and methotrexate (MTX), or receipt of B cell–depletion therapy such as rituximab within the past 12 months on immune response to a booster dose in people with systemic lupus erythematosus, rheumatoid arthritis, multiple sclerosis, systemic sclerosis, or pemphigus. They have to have either no serologic response to their initial COVID-19 vaccine regimen or a suboptimal response, defined as a Roche Elecsys Anti-SARS-CoV-2 S (RBD) result greater than or equal to 50 U/mL.
The results of studies conducted in solid-organ transplant recipients who take immunosuppressants showed that an extra dose of vaccine could improve the immune response to the vaccine in many of the individuals, which suggests that the same approach might work in people with autoimmune disease who need treatment with immunosuppressive drugs. Improving the immune response of people with autoimmune disease to COVID-19 vaccines is important because higher rates of severe COVID-19 and death have been reported in this group of patients than in the general population, and it is unclear whether this is attributable to the autoimmune disease, the immunosuppressive medications taken to treat it, or both.
The open-label trial, conducted by the NIAID-funded Autoimmunity Centers of Excellence, aims to enroll 600 people aged 18 years and older with those conditions at 15-20 sites in the United States.
Because medications commonly taken by people with these conditions have been associated with poorer immune responses to vaccines, the trial will randomize the following two cohorts to stop or continue taking their immunosuppressive medication(s) or stop them before and after the booster according to protocol:
- Cohort 1 includes people who are taking MMF or MPA, without additional B cell–depleting medications or MTX.
- Cohort 2 includes people who are taking MTX without additional B cell–depleting medications or MMF/MPA.
A third, nonrandomized cohort consists of people who have received B cell–depletion therapy within the past 12 months regardless of whether they are also taking MMF/MPA or MTX.
Besides the cohort-specific exclusions, other rheumatic disease medications, including biologics, are allowed in the groups.
The primary outcome of the trial is the proportion of participants who have a protective antibody response at week 4. Secondary outcomes will examine various antibody responses at intervals, changes in disease activity across autoimmune diseases, adverse events, and SARS-CoV-2 infections out to 48 weeks.
Study participants will be followed for a total of 13 months. Preliminary results are expected in November 2021, according to the National Institutes of Health.
The trial is being led by Judith James, MD, PhD; Meggan Mackay, MD, MS; Dinesh Khanna, MBBS, MSc; and Amit Bar-Or, MD.
In the wake of the Centers for Disease Control and Prevention’s recommendation for a third COVID-19 mRNA vaccine dose for immunocompromised people and the Food and Drug Administration’s authorization of the third dose, the according to an announcement.
The investigators of the trial, called COVID‐19 Booster Vaccine in Autoimmune Disease Non‐Responders, also want to determine if pausing immunosuppressive therapy for autoimmune disease improves the antibody response to an extra dose of a COVID-19 vaccine.
The trial will specifically look at the effects of mycophenolate mofetil (MMF) or mycophenolic acid (MPA), and methotrexate (MTX), or receipt of B cell–depletion therapy such as rituximab within the past 12 months on immune response to a booster dose in people with systemic lupus erythematosus, rheumatoid arthritis, multiple sclerosis, systemic sclerosis, or pemphigus. They have to have either no serologic response to their initial COVID-19 vaccine regimen or a suboptimal response, defined as a Roche Elecsys Anti-SARS-CoV-2 S (RBD) result greater than or equal to 50 U/mL.
The results of studies conducted in solid-organ transplant recipients who take immunosuppressants showed that an extra dose of vaccine could improve the immune response to the vaccine in many of the individuals, which suggests that the same approach might work in people with autoimmune disease who need treatment with immunosuppressive drugs. Improving the immune response of people with autoimmune disease to COVID-19 vaccines is important because higher rates of severe COVID-19 and death have been reported in this group of patients than in the general population, and it is unclear whether this is attributable to the autoimmune disease, the immunosuppressive medications taken to treat it, or both.
The open-label trial, conducted by the NIAID-funded Autoimmunity Centers of Excellence, aims to enroll 600 people aged 18 years and older with those conditions at 15-20 sites in the United States.
Because medications commonly taken by people with these conditions have been associated with poorer immune responses to vaccines, the trial will randomize the following two cohorts to stop or continue taking their immunosuppressive medication(s) or stop them before and after the booster according to protocol:
- Cohort 1 includes people who are taking MMF or MPA, without additional B cell–depleting medications or MTX.
- Cohort 2 includes people who are taking MTX without additional B cell–depleting medications or MMF/MPA.
A third, nonrandomized cohort consists of people who have received B cell–depletion therapy within the past 12 months regardless of whether they are also taking MMF/MPA or MTX.
Besides the cohort-specific exclusions, other rheumatic disease medications, including biologics, are allowed in the groups.
The primary outcome of the trial is the proportion of participants who have a protective antibody response at week 4. Secondary outcomes will examine various antibody responses at intervals, changes in disease activity across autoimmune diseases, adverse events, and SARS-CoV-2 infections out to 48 weeks.
Study participants will be followed for a total of 13 months. Preliminary results are expected in November 2021, according to the National Institutes of Health.
The trial is being led by Judith James, MD, PhD; Meggan Mackay, MD, MS; Dinesh Khanna, MBBS, MSc; and Amit Bar-Or, MD.
In the wake of the Centers for Disease Control and Prevention’s recommendation for a third COVID-19 mRNA vaccine dose for immunocompromised people and the Food and Drug Administration’s authorization of the third dose, the according to an announcement.
The investigators of the trial, called COVID‐19 Booster Vaccine in Autoimmune Disease Non‐Responders, also want to determine if pausing immunosuppressive therapy for autoimmune disease improves the antibody response to an extra dose of a COVID-19 vaccine.
The trial will specifically look at the effects of mycophenolate mofetil (MMF) or mycophenolic acid (MPA), and methotrexate (MTX), or receipt of B cell–depletion therapy such as rituximab within the past 12 months on immune response to a booster dose in people with systemic lupus erythematosus, rheumatoid arthritis, multiple sclerosis, systemic sclerosis, or pemphigus. They have to have either no serologic response to their initial COVID-19 vaccine regimen or a suboptimal response, defined as a Roche Elecsys Anti-SARS-CoV-2 S (RBD) result greater than or equal to 50 U/mL.
The results of studies conducted in solid-organ transplant recipients who take immunosuppressants showed that an extra dose of vaccine could improve the immune response to the vaccine in many of the individuals, which suggests that the same approach might work in people with autoimmune disease who need treatment with immunosuppressive drugs. Improving the immune response of people with autoimmune disease to COVID-19 vaccines is important because higher rates of severe COVID-19 and death have been reported in this group of patients than in the general population, and it is unclear whether this is attributable to the autoimmune disease, the immunosuppressive medications taken to treat it, or both.
The open-label trial, conducted by the NIAID-funded Autoimmunity Centers of Excellence, aims to enroll 600 people aged 18 years and older with those conditions at 15-20 sites in the United States.
Because medications commonly taken by people with these conditions have been associated with poorer immune responses to vaccines, the trial will randomize the following two cohorts to stop or continue taking their immunosuppressive medication(s) or stop them before and after the booster according to protocol:
- Cohort 1 includes people who are taking MMF or MPA, without additional B cell–depleting medications or MTX.
- Cohort 2 includes people who are taking MTX without additional B cell–depleting medications or MMF/MPA.
A third, nonrandomized cohort consists of people who have received B cell–depletion therapy within the past 12 months regardless of whether they are also taking MMF/MPA or MTX.
Besides the cohort-specific exclusions, other rheumatic disease medications, including biologics, are allowed in the groups.
The primary outcome of the trial is the proportion of participants who have a protective antibody response at week 4. Secondary outcomes will examine various antibody responses at intervals, changes in disease activity across autoimmune diseases, adverse events, and SARS-CoV-2 infections out to 48 weeks.
Study participants will be followed for a total of 13 months. Preliminary results are expected in November 2021, according to the National Institutes of Health.
The trial is being led by Judith James, MD, PhD; Meggan Mackay, MD, MS; Dinesh Khanna, MBBS, MSc; and Amit Bar-Or, MD.
Pups for veterans with PTSD: Biden signs PAWS act into law
Service members with posttraumatic stress disorder and other mental health conditions may eventually have expanded access to service dogs through legislation recently signed into law by President Joseph R. Biden.

The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (HR 1448) orders the Department of Veterans Affairs to begin a pilot program that over the course of 5 years will examine the utility and effectiveness of service dogs for improving the mental health of military veterans.
The legislation does not set a specific start date for the pilot program, but Rory Diamond, CEO of K9s for Warriors, a nonprofit organization based in Ponte Vedra, Fla., noted that K9s for Warriors and other organizations will be pushing the VA to start in 2022.
“We commend the White House for supporting this bill as a critical step in combating veteran suicide, and we’re confident in the path ahead for service dogs ultimately becoming a covered VA benefit to veterans with PTSD,” Mr. Diamond said in a statement provided to this news organization.
“For servicemembers relying on task-trained service dogs for PTSD, the HR 1448 is a giant leap towards supporting veterans and their service dogs in an equitable way,” Canine Companions, a national nonprofit organization that trains and provides service dogs, said in its own statement.
“It might mean the difference between having a veteran who won’t be here tomorrow and having one that will,” the group added.
Invisible wounds of war
In another statement, Bill McCabe, legislative affairs director at the Enlisted Association, said that “now, more than ever, veterans suffering from invisible wounds of war need access to trained service dogs, which have been scientifically proven to help alleviate symptoms of posttraumatic stress,” as well as traumatic brain injuries (TBIs) and military sexual trauma.
“We thank President Biden for recognizing veterans need every possible option when seeking mental health treatments, and look forward to working with the Department of Veterans Affairs to implement this important program,” Mr. McCabe said.
A recent VA report showed that in 2014, 40% of veterans had mental health conditions such as PTSD and substance use. An average of 20 veterans per day died by suicide that year.
Veterans with problems regarding mobility, hearing, and sight, as well as some mental health problems, have been eligible to have costs of veterinary care for service dogs paid by the VA, although the VA has not paid for the training of the animals.
The PAWS Act, which was bipartisan legislation introduced by U.S. Senators Thom Tillis (R-N.C.), Kyrsten Sinema (D-Ariz.), Kevin Cramer (R-N.D.), and Dianne Feinstein (D-Calif.), aims to expand eligibility to those with any mental health problems.
For at least a decade, various service dog and veterans’ organizations have pushed to have the VA expand the service dog benefit. This new law is a “first step,” said Mr. Diamond. “We had to kick open the door,” he said, adding that “the VA has essentially said no for almost 15 years.”
Mr. Diamond noted that there is “overwhelming” evidence showing that service dogs improve quality of life and reduce distress for veterans with PTSD and other diagnoses.
‘No excuse’
Results from a VA study showed that suicidal ideation was reduced in veterans who were paired with service dogs, compared with veterans paired with emotional support dogs. The study, which was made public in March, found no reduction in overall disability, according to a report by Military.com.
K9s for Warriors cites numerous other studies, published in peer-reviewed journals, that have shown that service dogs reduce PTSD symptoms, especially hypervigilance.
“There really is no excuse not to have the VA engaged in helping veterans suffering from posttraumatic stress who are extremely high risk of suicide to get a lifesaving service dog,” Mr. Diamond said.
His organization has paired 700 veterans suffering from TBI, PTSD, or military sexual trauma with a service dog. The organization provides a 3-week training program for the veteran and his or her dog.
Although about 200 of the graduates have been eligible to receive coverage from the VA for veterinary care for the dogs, it requires a lot of paperwork, and the criteria for who can be certified to receive that benefit are somewhat vague, Mr. Diamond noted.
Under current policy, the dog and veteran must have successfully completed a training program offered by an organization accredited by Assistance Dogs International or the International Guide Dog Federation.
The new pilot program will enable eligible veterans to receive dog training instruction from accredited nonprofit service dog training organizations, and it will give them the opportunity to adopt a dog that they actively assisted in training.
A version of this article first appeared on Medscape.com.
Service members with posttraumatic stress disorder and other mental health conditions may eventually have expanded access to service dogs through legislation recently signed into law by President Joseph R. Biden.
The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (HR 1448) orders the Department of Veterans Affairs to begin a pilot program that over the course of 5 years will examine the utility and effectiveness of service dogs for improving the mental health of military veterans.
The legislation does not set a specific start date for the pilot program, but Rory Diamond, CEO of K9s for Warriors, a nonprofit organization based in Ponte Vedra, Fla., noted that K9s for Warriors and other organizations will be pushing the VA to start in 2022.
“We commend the White House for supporting this bill as a critical step in combating veteran suicide, and we’re confident in the path ahead for service dogs ultimately becoming a covered VA benefit to veterans with PTSD,” Mr. Diamond said in a statement provided to this news organization.
“For servicemembers relying on task-trained service dogs for PTSD, the HR 1448 is a giant leap towards supporting veterans and their service dogs in an equitable way,” Canine Companions, a national nonprofit organization that trains and provides service dogs, said in its own statement.
“It might mean the difference between having a veteran who won’t be here tomorrow and having one that will,” the group added.
Invisible wounds of war
In another statement, Bill McCabe, legislative affairs director at the Enlisted Association, said that “now, more than ever, veterans suffering from invisible wounds of war need access to trained service dogs, which have been scientifically proven to help alleviate symptoms of posttraumatic stress,” as well as traumatic brain injuries (TBIs) and military sexual trauma.
“We thank President Biden for recognizing veterans need every possible option when seeking mental health treatments, and look forward to working with the Department of Veterans Affairs to implement this important program,” Mr. McCabe said.
A recent VA report showed that in 2014, 40% of veterans had mental health conditions such as PTSD and substance use. An average of 20 veterans per day died by suicide that year.
Veterans with problems regarding mobility, hearing, and sight, as well as some mental health problems, have been eligible to have costs of veterinary care for service dogs paid by the VA, although the VA has not paid for the training of the animals.
The PAWS Act, which was bipartisan legislation introduced by U.S. Senators Thom Tillis (R-N.C.), Kyrsten Sinema (D-Ariz.), Kevin Cramer (R-N.D.), and Dianne Feinstein (D-Calif.), aims to expand eligibility to those with any mental health problems.
For at least a decade, various service dog and veterans’ organizations have pushed to have the VA expand the service dog benefit. This new law is a “first step,” said Mr. Diamond. “We had to kick open the door,” he said, adding that “the VA has essentially said no for almost 15 years.”
Mr. Diamond noted that there is “overwhelming” evidence showing that service dogs improve quality of life and reduce distress for veterans with PTSD and other diagnoses.
‘No excuse’
Results from a VA study showed that suicidal ideation was reduced in veterans who were paired with service dogs, compared with veterans paired with emotional support dogs. The study, which was made public in March, found no reduction in overall disability, according to a report by Military.com.
K9s for Warriors cites numerous other studies, published in peer-reviewed journals, that have shown that service dogs reduce PTSD symptoms, especially hypervigilance.
“There really is no excuse not to have the VA engaged in helping veterans suffering from posttraumatic stress who are extremely high risk of suicide to get a lifesaving service dog,” Mr. Diamond said.
His organization has paired 700 veterans suffering from TBI, PTSD, or military sexual trauma with a service dog. The organization provides a 3-week training program for the veteran and his or her dog.
Although about 200 of the graduates have been eligible to receive coverage from the VA for veterinary care for the dogs, it requires a lot of paperwork, and the criteria for who can be certified to receive that benefit are somewhat vague, Mr. Diamond noted.
Under current policy, the dog and veteran must have successfully completed a training program offered by an organization accredited by Assistance Dogs International or the International Guide Dog Federation.
The new pilot program will enable eligible veterans to receive dog training instruction from accredited nonprofit service dog training organizations, and it will give them the opportunity to adopt a dog that they actively assisted in training.
A version of this article first appeared on Medscape.com.
Service members with posttraumatic stress disorder and other mental health conditions may eventually have expanded access to service dogs through legislation recently signed into law by President Joseph R. Biden.
The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (HR 1448) orders the Department of Veterans Affairs to begin a pilot program that over the course of 5 years will examine the utility and effectiveness of service dogs for improving the mental health of military veterans.
The legislation does not set a specific start date for the pilot program, but Rory Diamond, CEO of K9s for Warriors, a nonprofit organization based in Ponte Vedra, Fla., noted that K9s for Warriors and other organizations will be pushing the VA to start in 2022.
“We commend the White House for supporting this bill as a critical step in combating veteran suicide, and we’re confident in the path ahead for service dogs ultimately becoming a covered VA benefit to veterans with PTSD,” Mr. Diamond said in a statement provided to this news organization.
“For servicemembers relying on task-trained service dogs for PTSD, the HR 1448 is a giant leap towards supporting veterans and their service dogs in an equitable way,” Canine Companions, a national nonprofit organization that trains and provides service dogs, said in its own statement.
“It might mean the difference between having a veteran who won’t be here tomorrow and having one that will,” the group added.
Invisible wounds of war
In another statement, Bill McCabe, legislative affairs director at the Enlisted Association, said that “now, more than ever, veterans suffering from invisible wounds of war need access to trained service dogs, which have been scientifically proven to help alleviate symptoms of posttraumatic stress,” as well as traumatic brain injuries (TBIs) and military sexual trauma.
“We thank President Biden for recognizing veterans need every possible option when seeking mental health treatments, and look forward to working with the Department of Veterans Affairs to implement this important program,” Mr. McCabe said.
A recent VA report showed that in 2014, 40% of veterans had mental health conditions such as PTSD and substance use. An average of 20 veterans per day died by suicide that year.
Veterans with problems regarding mobility, hearing, and sight, as well as some mental health problems, have been eligible to have costs of veterinary care for service dogs paid by the VA, although the VA has not paid for the training of the animals.
The PAWS Act, which was bipartisan legislation introduced by U.S. Senators Thom Tillis (R-N.C.), Kyrsten Sinema (D-Ariz.), Kevin Cramer (R-N.D.), and Dianne Feinstein (D-Calif.), aims to expand eligibility to those with any mental health problems.
For at least a decade, various service dog and veterans’ organizations have pushed to have the VA expand the service dog benefit. This new law is a “first step,” said Mr. Diamond. “We had to kick open the door,” he said, adding that “the VA has essentially said no for almost 15 years.”
Mr. Diamond noted that there is “overwhelming” evidence showing that service dogs improve quality of life and reduce distress for veterans with PTSD and other diagnoses.
‘No excuse’
Results from a VA study showed that suicidal ideation was reduced in veterans who were paired with service dogs, compared with veterans paired with emotional support dogs. The study, which was made public in March, found no reduction in overall disability, according to a report by Military.com.
K9s for Warriors cites numerous other studies, published in peer-reviewed journals, that have shown that service dogs reduce PTSD symptoms, especially hypervigilance.
“There really is no excuse not to have the VA engaged in helping veterans suffering from posttraumatic stress who are extremely high risk of suicide to get a lifesaving service dog,” Mr. Diamond said.
His organization has paired 700 veterans suffering from TBI, PTSD, or military sexual trauma with a service dog. The organization provides a 3-week training program for the veteran and his or her dog.
Although about 200 of the graduates have been eligible to receive coverage from the VA for veterinary care for the dogs, it requires a lot of paperwork, and the criteria for who can be certified to receive that benefit are somewhat vague, Mr. Diamond noted.
Under current policy, the dog and veteran must have successfully completed a training program offered by an organization accredited by Assistance Dogs International or the International Guide Dog Federation.
The new pilot program will enable eligible veterans to receive dog training instruction from accredited nonprofit service dog training organizations, and it will give them the opportunity to adopt a dog that they actively assisted in training.
A version of this article first appeared on Medscape.com.
After five fatal overdoses, doctor sentenced for unlawful prescriptions; more
Doctor sentenced for unlawful prescriptions leading to five patient deaths
Darrel R. Rinehart, MD, was sentenced to 3 years in prison in June 2021 for unlawfully distributing controlled substances, primarily opioids, out of his clinic in Columbia, Tenn. Five of his patients who received prescriptions died of fatal overdoses within a year, according to the Indianapolis Star. Dr. Rinehart agreed to leave Tennessee to avoid punishment in that state before setting up his Indiana clinic.
Dr. Rinehart, 66, admitted to distributing Schedule II controlled substances to four different patients without legitimate medical purpose on 18 occasions between December 2014 and December 2015. He also admitted to knowingly distributing hydrocodone, also a Schedule II controlled substance, in January 2016 to a patient who did not have any health issues justifying the prescription. His medical license has been revoked.
Judge approves $15 million settlement in patient’s sexual assault
An incapacitated woman at Hacienda Healthcare, a long-term care center in Phoenix, Ariz., gave birth in late 2018 after being raped by one of the nursing staff, according to Insurance Journal. In June 2021, a judge approved a $15 million settlement in a lawsuit by the woman’s parents against Phillip E. Gear Jr., MD, the woman’s caregiver for 26 years at the center. The woman had been in a vegetative state at Hacienda Healthcare since childhood, and the judge ruled that she had been the victim of numerous sexual assaults prior to the birth.
The pregnancy was discovered when an employee was changing the garments of the then 29-year-old victim and saw that she was delivering a child. Employees told police they had no idea the woman was pregnant. Police have said that DNA from Nathan Sutherland, a licensed practical nurse who worked at Hacienda and has since given up his nursing license, matched a genetic sample taken from the woman’s son.
The woman’s parents, who care for her son, also sued the state of Arizona and another doctor, Thanh Nguyen, MD, who cared for their daughter. Arizona, which contracts with companies like Hacienda to provide services to people with developmental disabilities, settled last year for $7.5 million. Both Hacienda and Dr. Nguyen, who cared for the woman in the months before the birth, settled for undisclosed amounts.
The insurer for Dr. Gear, who died in late 2020, said it has no obligation to pay the amount, arguing that the doctor’s policy didn’t cover claims arising from a sexual act. The insurer also argued that Dr. Gear wasn’t the woman’s primary care physician when she gave birth and couldn’t be held responsible for sexual assault.
The judge declared the $15 million settlement reasonable, concluding that Dr. Gear’s treatment of the woman had fallen below the standard of care, which included failing to examine her regularly and to diagnose her pregnancy. Requests by the woman’s mother to have exclusively female employees tend to her were not followed, as shown by medical records.
Doctor fired for contributing to suffering and death of prisoners
Washington’s prison system will pay $3.25 million and has fired the medical director of one of its facilities, stemming from the death of an inmate.
John Kleutsch, a 57-year-old prisoner, died in late 2018 of septic shock, acute pancreatitis, and a perforated intestine caused by an improperly treated abdominal wound, according to the Seattle Times. A lawsuit filed by his wife, Julia Kleutsch, said that the staff offered him only Tylenol for his pain and that Julia Barnett, MD, the former prison medical director, refused to take him to a hospital.
Dr. Barnett, whose medical license has been indefinitely suspended, was fired in 2019 after an internal investigation found that her medical care and supervision contributed to the suffering and deaths of several men in the prison, including Mr. Kleutsch.
Mr. Kleutsch, imprisoned for child molestation, was recovering from outpatient cancer surgery and sent back to the prison infirmary to recover. The lawsuit says that Mr. Kleutsch asked staff for help when his abdominal wound became excruciatingly painful, puffy, and oozing, and that at least one nurse asked Dr. Barnett to transfer him to a hospital, but she refused. Dr. Kleutsch’s causes of death were conditions never diagnosed at the prison.
Plaintiff attorney Marta O’Brien called the case “one of the worst medical malpractice cases I have encountered” and said it showed “a systemic failure” by the Department of Corrections.
SNF pays $11 million to resolve Medicare fraud allegations
SavaSeniorCare (Sava) and related entities agreed to pay $11.2 million in May 2021 to resolve allegations that they violated the False Claims Act by making their skilled nursing facilities (SNFs) bill Medicare for rehabilitation therapy services that were not reasonable, necessary, or skilled. The payment was also to resolve allegations that Sava billed the Medicare and Medicaid programs for substandard skilled nursing services, according to the U.S. Department of Justice. Sava is based in Georgia but owns and operates SNFs across the country.
The government filed a complaint against Sava in 2015, alleging that between October 2008 and September 2012, Sava intentionally submitted false claims for rehabilitation therapy services as a result of a systematic effort to increase its Medicare and Medicaid billings. The claim alleged that Sava exerted significant pressure on its SNFs to meet unrealistic financial goals, resulting in the provision of medically unreasonable, unnecessary, or unskilled services to Medicare patients. Sava also allegedly sought to increase its Medicare payments by delaying the discharge of patients from its facilities, even though the patients were medically ready to be discharged.
Additionally, the government alleged that some of Sava’s nursing services failed to meet federal standards of care, including failing to have sufficient staffing at certain facilities, failing to follow appropriate pressure ulcer and falls protocols, and failing to appropriately administer medications.
A version of this article first appeared on Medscape.com.
Doctor sentenced for unlawful prescriptions leading to five patient deaths
Darrel R. Rinehart, MD, was sentenced to 3 years in prison in June 2021 for unlawfully distributing controlled substances, primarily opioids, out of his clinic in Columbia, Tenn. Five of his patients who received prescriptions died of fatal overdoses within a year, according to the Indianapolis Star. Dr. Rinehart agreed to leave Tennessee to avoid punishment in that state before setting up his Indiana clinic.
Dr. Rinehart, 66, admitted to distributing Schedule II controlled substances to four different patients without legitimate medical purpose on 18 occasions between December 2014 and December 2015. He also admitted to knowingly distributing hydrocodone, also a Schedule II controlled substance, in January 2016 to a patient who did not have any health issues justifying the prescription. His medical license has been revoked.
Judge approves $15 million settlement in patient’s sexual assault
An incapacitated woman at Hacienda Healthcare, a long-term care center in Phoenix, Ariz., gave birth in late 2018 after being raped by one of the nursing staff, according to Insurance Journal. In June 2021, a judge approved a $15 million settlement in a lawsuit by the woman’s parents against Phillip E. Gear Jr., MD, the woman’s caregiver for 26 years at the center. The woman had been in a vegetative state at Hacienda Healthcare since childhood, and the judge ruled that she had been the victim of numerous sexual assaults prior to the birth.
The pregnancy was discovered when an employee was changing the garments of the then 29-year-old victim and saw that she was delivering a child. Employees told police they had no idea the woman was pregnant. Police have said that DNA from Nathan Sutherland, a licensed practical nurse who worked at Hacienda and has since given up his nursing license, matched a genetic sample taken from the woman’s son.
The woman’s parents, who care for her son, also sued the state of Arizona and another doctor, Thanh Nguyen, MD, who cared for their daughter. Arizona, which contracts with companies like Hacienda to provide services to people with developmental disabilities, settled last year for $7.5 million. Both Hacienda and Dr. Nguyen, who cared for the woman in the months before the birth, settled for undisclosed amounts.
The insurer for Dr. Gear, who died in late 2020, said it has no obligation to pay the amount, arguing that the doctor’s policy didn’t cover claims arising from a sexual act. The insurer also argued that Dr. Gear wasn’t the woman’s primary care physician when she gave birth and couldn’t be held responsible for sexual assault.
The judge declared the $15 million settlement reasonable, concluding that Dr. Gear’s treatment of the woman had fallen below the standard of care, which included failing to examine her regularly and to diagnose her pregnancy. Requests by the woman’s mother to have exclusively female employees tend to her were not followed, as shown by medical records.
Doctor fired for contributing to suffering and death of prisoners
Washington’s prison system will pay $3.25 million and has fired the medical director of one of its facilities, stemming from the death of an inmate.
John Kleutsch, a 57-year-old prisoner, died in late 2018 of septic shock, acute pancreatitis, and a perforated intestine caused by an improperly treated abdominal wound, according to the Seattle Times. A lawsuit filed by his wife, Julia Kleutsch, said that the staff offered him only Tylenol for his pain and that Julia Barnett, MD, the former prison medical director, refused to take him to a hospital.
Dr. Barnett, whose medical license has been indefinitely suspended, was fired in 2019 after an internal investigation found that her medical care and supervision contributed to the suffering and deaths of several men in the prison, including Mr. Kleutsch.
Mr. Kleutsch, imprisoned for child molestation, was recovering from outpatient cancer surgery and sent back to the prison infirmary to recover. The lawsuit says that Mr. Kleutsch asked staff for help when his abdominal wound became excruciatingly painful, puffy, and oozing, and that at least one nurse asked Dr. Barnett to transfer him to a hospital, but she refused. Dr. Kleutsch’s causes of death were conditions never diagnosed at the prison.
Plaintiff attorney Marta O’Brien called the case “one of the worst medical malpractice cases I have encountered” and said it showed “a systemic failure” by the Department of Corrections.
SNF pays $11 million to resolve Medicare fraud allegations
SavaSeniorCare (Sava) and related entities agreed to pay $11.2 million in May 2021 to resolve allegations that they violated the False Claims Act by making their skilled nursing facilities (SNFs) bill Medicare for rehabilitation therapy services that were not reasonable, necessary, or skilled. The payment was also to resolve allegations that Sava billed the Medicare and Medicaid programs for substandard skilled nursing services, according to the U.S. Department of Justice. Sava is based in Georgia but owns and operates SNFs across the country.
The government filed a complaint against Sava in 2015, alleging that between October 2008 and September 2012, Sava intentionally submitted false claims for rehabilitation therapy services as a result of a systematic effort to increase its Medicare and Medicaid billings. The claim alleged that Sava exerted significant pressure on its SNFs to meet unrealistic financial goals, resulting in the provision of medically unreasonable, unnecessary, or unskilled services to Medicare patients. Sava also allegedly sought to increase its Medicare payments by delaying the discharge of patients from its facilities, even though the patients were medically ready to be discharged.
Additionally, the government alleged that some of Sava’s nursing services failed to meet federal standards of care, including failing to have sufficient staffing at certain facilities, failing to follow appropriate pressure ulcer and falls protocols, and failing to appropriately administer medications.
A version of this article first appeared on Medscape.com.
Doctor sentenced for unlawful prescriptions leading to five patient deaths
Darrel R. Rinehart, MD, was sentenced to 3 years in prison in June 2021 for unlawfully distributing controlled substances, primarily opioids, out of his clinic in Columbia, Tenn. Five of his patients who received prescriptions died of fatal overdoses within a year, according to the Indianapolis Star. Dr. Rinehart agreed to leave Tennessee to avoid punishment in that state before setting up his Indiana clinic.
Dr. Rinehart, 66, admitted to distributing Schedule II controlled substances to four different patients without legitimate medical purpose on 18 occasions between December 2014 and December 2015. He also admitted to knowingly distributing hydrocodone, also a Schedule II controlled substance, in January 2016 to a patient who did not have any health issues justifying the prescription. His medical license has been revoked.
Judge approves $15 million settlement in patient’s sexual assault
An incapacitated woman at Hacienda Healthcare, a long-term care center in Phoenix, Ariz., gave birth in late 2018 after being raped by one of the nursing staff, according to Insurance Journal. In June 2021, a judge approved a $15 million settlement in a lawsuit by the woman’s parents against Phillip E. Gear Jr., MD, the woman’s caregiver for 26 years at the center. The woman had been in a vegetative state at Hacienda Healthcare since childhood, and the judge ruled that she had been the victim of numerous sexual assaults prior to the birth.
The pregnancy was discovered when an employee was changing the garments of the then 29-year-old victim and saw that she was delivering a child. Employees told police they had no idea the woman was pregnant. Police have said that DNA from Nathan Sutherland, a licensed practical nurse who worked at Hacienda and has since given up his nursing license, matched a genetic sample taken from the woman’s son.
The woman’s parents, who care for her son, also sued the state of Arizona and another doctor, Thanh Nguyen, MD, who cared for their daughter. Arizona, which contracts with companies like Hacienda to provide services to people with developmental disabilities, settled last year for $7.5 million. Both Hacienda and Dr. Nguyen, who cared for the woman in the months before the birth, settled for undisclosed amounts.
The insurer for Dr. Gear, who died in late 2020, said it has no obligation to pay the amount, arguing that the doctor’s policy didn’t cover claims arising from a sexual act. The insurer also argued that Dr. Gear wasn’t the woman’s primary care physician when she gave birth and couldn’t be held responsible for sexual assault.
The judge declared the $15 million settlement reasonable, concluding that Dr. Gear’s treatment of the woman had fallen below the standard of care, which included failing to examine her regularly and to diagnose her pregnancy. Requests by the woman’s mother to have exclusively female employees tend to her were not followed, as shown by medical records.
Doctor fired for contributing to suffering and death of prisoners
Washington’s prison system will pay $3.25 million and has fired the medical director of one of its facilities, stemming from the death of an inmate.
John Kleutsch, a 57-year-old prisoner, died in late 2018 of septic shock, acute pancreatitis, and a perforated intestine caused by an improperly treated abdominal wound, according to the Seattle Times. A lawsuit filed by his wife, Julia Kleutsch, said that the staff offered him only Tylenol for his pain and that Julia Barnett, MD, the former prison medical director, refused to take him to a hospital.
Dr. Barnett, whose medical license has been indefinitely suspended, was fired in 2019 after an internal investigation found that her medical care and supervision contributed to the suffering and deaths of several men in the prison, including Mr. Kleutsch.
Mr. Kleutsch, imprisoned for child molestation, was recovering from outpatient cancer surgery and sent back to the prison infirmary to recover. The lawsuit says that Mr. Kleutsch asked staff for help when his abdominal wound became excruciatingly painful, puffy, and oozing, and that at least one nurse asked Dr. Barnett to transfer him to a hospital, but she refused. Dr. Kleutsch’s causes of death were conditions never diagnosed at the prison.
Plaintiff attorney Marta O’Brien called the case “one of the worst medical malpractice cases I have encountered” and said it showed “a systemic failure” by the Department of Corrections.
SNF pays $11 million to resolve Medicare fraud allegations
SavaSeniorCare (Sava) and related entities agreed to pay $11.2 million in May 2021 to resolve allegations that they violated the False Claims Act by making their skilled nursing facilities (SNFs) bill Medicare for rehabilitation therapy services that were not reasonable, necessary, or skilled. The payment was also to resolve allegations that Sava billed the Medicare and Medicaid programs for substandard skilled nursing services, according to the U.S. Department of Justice. Sava is based in Georgia but owns and operates SNFs across the country.
The government filed a complaint against Sava in 2015, alleging that between October 2008 and September 2012, Sava intentionally submitted false claims for rehabilitation therapy services as a result of a systematic effort to increase its Medicare and Medicaid billings. The claim alleged that Sava exerted significant pressure on its SNFs to meet unrealistic financial goals, resulting in the provision of medically unreasonable, unnecessary, or unskilled services to Medicare patients. Sava also allegedly sought to increase its Medicare payments by delaying the discharge of patients from its facilities, even though the patients were medically ready to be discharged.
Additionally, the government alleged that some of Sava’s nursing services failed to meet federal standards of care, including failing to have sufficient staffing at certain facilities, failing to follow appropriate pressure ulcer and falls protocols, and failing to appropriately administer medications.
A version of this article first appeared on Medscape.com.
Pandemic unveils growing suicide crisis for communities of color
This story is a collaboration between KHN and “Science Friday.”
Rafiah Maxie has been a licensed clinical social worker in the Chicago area for a decade. Throughout that time, she’d viewed suicide as a problem most prevalent among middle-aged white men.
Until May 27, 2020.
That day, Maxie’s 19-year-old son, Jamal Clay – who loved playing the trumpet and participating in theater, who would help her unload groceries from the car and raise funds for the March of the Dimes – killed himself in their garage.
“Now I cannot blink without seeing my son hanging,” said Maxie, who is Black.
Clay’s death, along with the suicides of more than 100 other Black residents in Illinois last year, has led locals to call for new prevention efforts focused on Black communities. In 2020, during the pandemic’s first year, suicides among White residents decreased compared with previous years, while they increased among Black residents, according to state data.
But this is not a local problem. Nor is it limited to the pandemic.
Interviews with a dozen suicide researchers, data collected from states across the country, and a review of decades of research revealed that suicide is a growing crisis for communities of color – one that plagued them well before the pandemic and has only been exacerbated since.
Overall suicide rates in the U.S. decreased in 2019 and 2020. National and local studies attribute the trend to a drop among White Americans, who make up the majority of suicide deaths. Meanwhile, rates for Black, Hispanic, and Asian Americans – though lower than those of their white peers – continued to climb in many states. (Suicide rates have been consistently high for Native Americans.)
“COVID created more transparency regarding what we already knew was happening,” said Sonyia Richardson, a licensed clinical social worker who focuses on serving people of color, and assistant professor at the University of North Carolina–Charlotte, where she researches suicide. When you put the suicide rates of all communities in one bucket, “that bucket says it’s getting better and what we’re doing is working,” she said. “But that’s not the case for communities of color.”
Losing generations
Although the suicide rate is highest among middle-aged White men, young people of color are emerging as particularly at risk.
Research shows Black kids younger than 13 die by suicide at nearly twice the rate of White kids and, over time, their suicide rates have grown even as rates have decreased for White children. Among teenagers and young adults, suicide deaths have increased more than 45% for Black Americans and about 40% for Asian Americans in the 7 years ending in 2019. Other concerning trends in suicide attempts date to the ’90s.
“We have to pay attention now because if you’re out of the first decade of life and think life is not worth pursuing, that’s a signal to say something is going really wrong.”
These statistics also refute traditional ideas that suicide doesn’t happen in certain ethnic or minority populations because they’re “protected” and “resilient” or the “model minority,” said Kiara Alvarez, a researcher and psychologist at Massachusetts General Hospital who focuses on suicide among Hispanic and immigrant populations.
Although these groups may have had low suicide rates historically, that’s changing, she said.
Paul Chin lost his 17-year-old brother, Chris, to suicide in 2009. A poem Chris wrote in high school about his heritage has left Chin, 8 years his senior, wondering if his brother struggled to feel accepted in the U.S., despite being born and raised in New York.
Growing up, Asian Americans weren’t represented in lessons at school or in pop culture, said Chin, now 37. Even in clinical research on suicide as well as other health topics, kids like Chris are underrepresented, with less than 1% of federal research funding focused on Asian Americans.
It wasn’t until the pandemic, and the concurrent rise in hate crimes against Asian Americans, that Chin saw national attention on the community’s mental health. He hopes the interest is not short-lived.
Suicide is the leading cause of death for Asian Americans ages 15 to 24, yet “that doesn’t get enough attention,” Chin said. “It’s important to continue to share these stories.”
Kathy Williams, who is Black, has been on a similar mission since her 15-year-old son, Torian Graves, died by suicide in 1996. People didn’t talk about suicide in the Black community then, she said. So she started raising the topic at her church in Durham, N.C., and in local schools. She wanted Black families to know the warning signs and society at large to recognize the seriousness of the problem.
The pandemic may have highlighted this, Williams said, but “it has always happened. Always.”
Pandemic sheds light on the triggers
Pinpointing the root causes of rising suicide within communities of color has proved difficult. How much stems from mental illness? How much from socioeconomic changes like job losses or social isolation? Now, COVID-19 may offer some clues.
Recent decades have been marked by growing economic instability, a widening racial wealth gap, and more public attention on police killings of unarmed Black and Brown people, said Michael Lindsey, executive director of the New York University McSilver Institute for Poverty Policy and Research.
With social media, youths face racism on more fronts than their parents did, said Leslie Adams, assistant professor in the department of mental health at Johns Hopkins Bloomberg School of Public Health.
Each of these factors has been shown to affect suicide risk. For example, experiencing racism and sexism together is linked to a threefold increase in suicidal thoughts for Asian American women, said Brian Keum, assistant professor at UCLA, based on preliminary research findings.
COVID-19 intensified these hardships among communities of color, with disproportionate numbers of lost loved ones, lost jobs, and lost housing. The murder of George Floyd prompted widespread racial unrest, and Asian Americans saw an increase in hate crimes.
At the same time, studies in Connecticut and Maryland found that suicide rates rose within these populations and dropped for their White counterparts.
“It’s not just a problem within the person, but societal issues that need to be addressed,” said Shari Jager-Hyman, assistant professor of psychiatry at the University of Pennsylvania.
Lessons from Texas
In Texas, COVID-19 hit Hispanics especially hard. As of July 2021, they accounted for 45% of all COVID-19 deaths and disproportionately lost jobs. Individuals living in the U.S. without authorization were generally not eligible for unemployment benefits or federal stimulus checks.
During this time, suicide deaths among Hispanic Texans climbed from 847 deaths in 2019 to 962 deaths in 2020, according to preliminary state data. Suicide deaths rose for Black Texans and residents classified as “other” races or ethnicities, but decreased for White Texans.
The numbers didn’t surprise Marc Mendiola. The 20-year-old grew up in a majority-Hispanic community on the south side of San Antonio. Even before the pandemic, he often heard classmates say they were suicidal. Many faced dire finances at home, sometimes living without electricity, food, or water. Those who sought mental health treatment often found services prohibitively expensive or inaccessible because they weren’t offered in Spanish.
“These are conditions the community has always been in,” Mendiola said. “But with the pandemic, it’s even worse.”
Four years ago, Mendiola and his classmates at South San High School began advocating for mental health services. In late 2019, just months before COVID-19 struck, their vision became reality. Six community agencies partnered to offer free services to students and their families across three school districts.
Richard Davidson, chief operating officer of Family Service, one of the groups in the collaborative, said the number of students discussing economic stressors has been on the rise since April 2020. More than 90% of the students who received services in the first half of 2021 were Hispanic, and nearly 10% reported thoughts of suicide or self-harm, program data show. None died by suicide.
Many students are so worried about what’s for dinner the next day that they’re not able to see a future beyond that, Davidson said. That’s when suicide can feel like a viable option.
“One of the things we do is help them see … that despite this situation now, you can create a vision for your future,” Davidson said.
A good future
Researchers say the promise of a good future is often overlooked in suicide prevention, perhaps because achieving it is so challenging. It requires economic and social growth and breaking systemic barriers.
Tevis Simon works to address all those fronts. As a child in West Baltimore, Simon, who is Black, faced poverty and trauma. As an adult, she attempted suicide three times. But now she shares her story with youths across the city to inspire them to overcome challenges. She also talks to politicians, law enforcement agencies, and public policy officials about their responsibilities.
“We can’t not talk about race,” said Simon, 43. “We can’t not talk about systematic oppression. We cannot not talk about these conditions that affect our mental well-being and our feeling and desire to live.”
For Jamal Clay in Illinois, the systemic barriers started early. Before his suicide last year, he had tried to harm himself when he was 12 and the victim of bullies. At that time, he was hospitalized for a few days and told to follow up with outpatient therapy, said his mother, Maxie.
But it was difficult to find therapists who accepted Medicaid, she said. When Maxie finally found one, there was a 60-day wait. Other therapists canceled appointments, she said.
“So we worked on our own,” Maxie said, relying on church and community. Her son seemed to improve. “We thought we closed that chapter in our lives.”
But when the pandemic hit, everything got worse, she said. Clay came home from college and worked at an Amazon warehouse. On drives to and from work, he was frequently pulled over by police. He stopped wearing hats so officers would consider him less intimidating, Maxie said.
“He felt uncomfortable being out in the street,” she said.
Maxie is still trying to make sense of what happened the day Clay died. But she’s found meaning in starting a nonprofit called Soul Survivors of Chicago. Through the organization, she provides education, scholarships and shoes – including Jamal’s old ones – to those impacted by violence, suicide, and trauma.
“My son won’t be able to have a first interview in [those] shoes. He won’t be able to have a nice jump shot or go to church or even meet his wife,” Maxie said.
But she hopes his shoes will carry someone else to a good future.
[Editor’s note: For the purposes of this story, “people of color” or “communities of color” refers to any racial or ethnic populations whose members do not identify as White, including those who are multiracial. Hispanics can be of any race or combination of races.]
KHN senior correspondent JoNel Aleccia contributed to this report. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
This story is a collaboration between KHN and “Science Friday.”
Rafiah Maxie has been a licensed clinical social worker in the Chicago area for a decade. Throughout that time, she’d viewed suicide as a problem most prevalent among middle-aged white men.
Until May 27, 2020.
That day, Maxie’s 19-year-old son, Jamal Clay – who loved playing the trumpet and participating in theater, who would help her unload groceries from the car and raise funds for the March of the Dimes – killed himself in their garage.
“Now I cannot blink without seeing my son hanging,” said Maxie, who is Black.
Clay’s death, along with the suicides of more than 100 other Black residents in Illinois last year, has led locals to call for new prevention efforts focused on Black communities. In 2020, during the pandemic’s first year, suicides among White residents decreased compared with previous years, while they increased among Black residents, according to state data.
But this is not a local problem. Nor is it limited to the pandemic.
Interviews with a dozen suicide researchers, data collected from states across the country, and a review of decades of research revealed that suicide is a growing crisis for communities of color – one that plagued them well before the pandemic and has only been exacerbated since.
Overall suicide rates in the U.S. decreased in 2019 and 2020. National and local studies attribute the trend to a drop among White Americans, who make up the majority of suicide deaths. Meanwhile, rates for Black, Hispanic, and Asian Americans – though lower than those of their white peers – continued to climb in many states. (Suicide rates have been consistently high for Native Americans.)
“COVID created more transparency regarding what we already knew was happening,” said Sonyia Richardson, a licensed clinical social worker who focuses on serving people of color, and assistant professor at the University of North Carolina–Charlotte, where she researches suicide. When you put the suicide rates of all communities in one bucket, “that bucket says it’s getting better and what we’re doing is working,” she said. “But that’s not the case for communities of color.”
Losing generations
Although the suicide rate is highest among middle-aged White men, young people of color are emerging as particularly at risk.
Research shows Black kids younger than 13 die by suicide at nearly twice the rate of White kids and, over time, their suicide rates have grown even as rates have decreased for White children. Among teenagers and young adults, suicide deaths have increased more than 45% for Black Americans and about 40% for Asian Americans in the 7 years ending in 2019. Other concerning trends in suicide attempts date to the ’90s.
“We have to pay attention now because if you’re out of the first decade of life and think life is not worth pursuing, that’s a signal to say something is going really wrong.”
These statistics also refute traditional ideas that suicide doesn’t happen in certain ethnic or minority populations because they’re “protected” and “resilient” or the “model minority,” said Kiara Alvarez, a researcher and psychologist at Massachusetts General Hospital who focuses on suicide among Hispanic and immigrant populations.
Although these groups may have had low suicide rates historically, that’s changing, she said.
Paul Chin lost his 17-year-old brother, Chris, to suicide in 2009. A poem Chris wrote in high school about his heritage has left Chin, 8 years his senior, wondering if his brother struggled to feel accepted in the U.S., despite being born and raised in New York.
Growing up, Asian Americans weren’t represented in lessons at school or in pop culture, said Chin, now 37. Even in clinical research on suicide as well as other health topics, kids like Chris are underrepresented, with less than 1% of federal research funding focused on Asian Americans.
It wasn’t until the pandemic, and the concurrent rise in hate crimes against Asian Americans, that Chin saw national attention on the community’s mental health. He hopes the interest is not short-lived.
Suicide is the leading cause of death for Asian Americans ages 15 to 24, yet “that doesn’t get enough attention,” Chin said. “It’s important to continue to share these stories.”
Kathy Williams, who is Black, has been on a similar mission since her 15-year-old son, Torian Graves, died by suicide in 1996. People didn’t talk about suicide in the Black community then, she said. So she started raising the topic at her church in Durham, N.C., and in local schools. She wanted Black families to know the warning signs and society at large to recognize the seriousness of the problem.
The pandemic may have highlighted this, Williams said, but “it has always happened. Always.”
Pandemic sheds light on the triggers
Pinpointing the root causes of rising suicide within communities of color has proved difficult. How much stems from mental illness? How much from socioeconomic changes like job losses or social isolation? Now, COVID-19 may offer some clues.
Recent decades have been marked by growing economic instability, a widening racial wealth gap, and more public attention on police killings of unarmed Black and Brown people, said Michael Lindsey, executive director of the New York University McSilver Institute for Poverty Policy and Research.
With social media, youths face racism on more fronts than their parents did, said Leslie Adams, assistant professor in the department of mental health at Johns Hopkins Bloomberg School of Public Health.
Each of these factors has been shown to affect suicide risk. For example, experiencing racism and sexism together is linked to a threefold increase in suicidal thoughts for Asian American women, said Brian Keum, assistant professor at UCLA, based on preliminary research findings.
COVID-19 intensified these hardships among communities of color, with disproportionate numbers of lost loved ones, lost jobs, and lost housing. The murder of George Floyd prompted widespread racial unrest, and Asian Americans saw an increase in hate crimes.
At the same time, studies in Connecticut and Maryland found that suicide rates rose within these populations and dropped for their White counterparts.
“It’s not just a problem within the person, but societal issues that need to be addressed,” said Shari Jager-Hyman, assistant professor of psychiatry at the University of Pennsylvania.
Lessons from Texas
In Texas, COVID-19 hit Hispanics especially hard. As of July 2021, they accounted for 45% of all COVID-19 deaths and disproportionately lost jobs. Individuals living in the U.S. without authorization were generally not eligible for unemployment benefits or federal stimulus checks.
During this time, suicide deaths among Hispanic Texans climbed from 847 deaths in 2019 to 962 deaths in 2020, according to preliminary state data. Suicide deaths rose for Black Texans and residents classified as “other” races or ethnicities, but decreased for White Texans.
The numbers didn’t surprise Marc Mendiola. The 20-year-old grew up in a majority-Hispanic community on the south side of San Antonio. Even before the pandemic, he often heard classmates say they were suicidal. Many faced dire finances at home, sometimes living without electricity, food, or water. Those who sought mental health treatment often found services prohibitively expensive or inaccessible because they weren’t offered in Spanish.
“These are conditions the community has always been in,” Mendiola said. “But with the pandemic, it’s even worse.”
Four years ago, Mendiola and his classmates at South San High School began advocating for mental health services. In late 2019, just months before COVID-19 struck, their vision became reality. Six community agencies partnered to offer free services to students and their families across three school districts.
Richard Davidson, chief operating officer of Family Service, one of the groups in the collaborative, said the number of students discussing economic stressors has been on the rise since April 2020. More than 90% of the students who received services in the first half of 2021 were Hispanic, and nearly 10% reported thoughts of suicide or self-harm, program data show. None died by suicide.
Many students are so worried about what’s for dinner the next day that they’re not able to see a future beyond that, Davidson said. That’s when suicide can feel like a viable option.
“One of the things we do is help them see … that despite this situation now, you can create a vision for your future,” Davidson said.
A good future
Researchers say the promise of a good future is often overlooked in suicide prevention, perhaps because achieving it is so challenging. It requires economic and social growth and breaking systemic barriers.
Tevis Simon works to address all those fronts. As a child in West Baltimore, Simon, who is Black, faced poverty and trauma. As an adult, she attempted suicide three times. But now she shares her story with youths across the city to inspire them to overcome challenges. She also talks to politicians, law enforcement agencies, and public policy officials about their responsibilities.
“We can’t not talk about race,” said Simon, 43. “We can’t not talk about systematic oppression. We cannot not talk about these conditions that affect our mental well-being and our feeling and desire to live.”
For Jamal Clay in Illinois, the systemic barriers started early. Before his suicide last year, he had tried to harm himself when he was 12 and the victim of bullies. At that time, he was hospitalized for a few days and told to follow up with outpatient therapy, said his mother, Maxie.
But it was difficult to find therapists who accepted Medicaid, she said. When Maxie finally found one, there was a 60-day wait. Other therapists canceled appointments, she said.
“So we worked on our own,” Maxie said, relying on church and community. Her son seemed to improve. “We thought we closed that chapter in our lives.”
But when the pandemic hit, everything got worse, she said. Clay came home from college and worked at an Amazon warehouse. On drives to and from work, he was frequently pulled over by police. He stopped wearing hats so officers would consider him less intimidating, Maxie said.
“He felt uncomfortable being out in the street,” she said.
Maxie is still trying to make sense of what happened the day Clay died. But she’s found meaning in starting a nonprofit called Soul Survivors of Chicago. Through the organization, she provides education, scholarships and shoes – including Jamal’s old ones – to those impacted by violence, suicide, and trauma.
“My son won’t be able to have a first interview in [those] shoes. He won’t be able to have a nice jump shot or go to church or even meet his wife,” Maxie said.
But she hopes his shoes will carry someone else to a good future.
[Editor’s note: For the purposes of this story, “people of color” or “communities of color” refers to any racial or ethnic populations whose members do not identify as White, including those who are multiracial. Hispanics can be of any race or combination of races.]
KHN senior correspondent JoNel Aleccia contributed to this report. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
This story is a collaboration between KHN and “Science Friday.”
Rafiah Maxie has been a licensed clinical social worker in the Chicago area for a decade. Throughout that time, she’d viewed suicide as a problem most prevalent among middle-aged white men.
Until May 27, 2020.
That day, Maxie’s 19-year-old son, Jamal Clay – who loved playing the trumpet and participating in theater, who would help her unload groceries from the car and raise funds for the March of the Dimes – killed himself in their garage.
“Now I cannot blink without seeing my son hanging,” said Maxie, who is Black.
Clay’s death, along with the suicides of more than 100 other Black residents in Illinois last year, has led locals to call for new prevention efforts focused on Black communities. In 2020, during the pandemic’s first year, suicides among White residents decreased compared with previous years, while they increased among Black residents, according to state data.
But this is not a local problem. Nor is it limited to the pandemic.
Interviews with a dozen suicide researchers, data collected from states across the country, and a review of decades of research revealed that suicide is a growing crisis for communities of color – one that plagued them well before the pandemic and has only been exacerbated since.
Overall suicide rates in the U.S. decreased in 2019 and 2020. National and local studies attribute the trend to a drop among White Americans, who make up the majority of suicide deaths. Meanwhile, rates for Black, Hispanic, and Asian Americans – though lower than those of their white peers – continued to climb in many states. (Suicide rates have been consistently high for Native Americans.)
“COVID created more transparency regarding what we already knew was happening,” said Sonyia Richardson, a licensed clinical social worker who focuses on serving people of color, and assistant professor at the University of North Carolina–Charlotte, where she researches suicide. When you put the suicide rates of all communities in one bucket, “that bucket says it’s getting better and what we’re doing is working,” she said. “But that’s not the case for communities of color.”
Losing generations
Although the suicide rate is highest among middle-aged White men, young people of color are emerging as particularly at risk.
Research shows Black kids younger than 13 die by suicide at nearly twice the rate of White kids and, over time, their suicide rates have grown even as rates have decreased for White children. Among teenagers and young adults, suicide deaths have increased more than 45% for Black Americans and about 40% for Asian Americans in the 7 years ending in 2019. Other concerning trends in suicide attempts date to the ’90s.
“We have to pay attention now because if you’re out of the first decade of life and think life is not worth pursuing, that’s a signal to say something is going really wrong.”
These statistics also refute traditional ideas that suicide doesn’t happen in certain ethnic or minority populations because they’re “protected” and “resilient” or the “model minority,” said Kiara Alvarez, a researcher and psychologist at Massachusetts General Hospital who focuses on suicide among Hispanic and immigrant populations.
Although these groups may have had low suicide rates historically, that’s changing, she said.
Paul Chin lost his 17-year-old brother, Chris, to suicide in 2009. A poem Chris wrote in high school about his heritage has left Chin, 8 years his senior, wondering if his brother struggled to feel accepted in the U.S., despite being born and raised in New York.
Growing up, Asian Americans weren’t represented in lessons at school or in pop culture, said Chin, now 37. Even in clinical research on suicide as well as other health topics, kids like Chris are underrepresented, with less than 1% of federal research funding focused on Asian Americans.
It wasn’t until the pandemic, and the concurrent rise in hate crimes against Asian Americans, that Chin saw national attention on the community’s mental health. He hopes the interest is not short-lived.
Suicide is the leading cause of death for Asian Americans ages 15 to 24, yet “that doesn’t get enough attention,” Chin said. “It’s important to continue to share these stories.”
Kathy Williams, who is Black, has been on a similar mission since her 15-year-old son, Torian Graves, died by suicide in 1996. People didn’t talk about suicide in the Black community then, she said. So she started raising the topic at her church in Durham, N.C., and in local schools. She wanted Black families to know the warning signs and society at large to recognize the seriousness of the problem.
The pandemic may have highlighted this, Williams said, but “it has always happened. Always.”
Pandemic sheds light on the triggers
Pinpointing the root causes of rising suicide within communities of color has proved difficult. How much stems from mental illness? How much from socioeconomic changes like job losses or social isolation? Now, COVID-19 may offer some clues.
Recent decades have been marked by growing economic instability, a widening racial wealth gap, and more public attention on police killings of unarmed Black and Brown people, said Michael Lindsey, executive director of the New York University McSilver Institute for Poverty Policy and Research.
With social media, youths face racism on more fronts than their parents did, said Leslie Adams, assistant professor in the department of mental health at Johns Hopkins Bloomberg School of Public Health.
Each of these factors has been shown to affect suicide risk. For example, experiencing racism and sexism together is linked to a threefold increase in suicidal thoughts for Asian American women, said Brian Keum, assistant professor at UCLA, based on preliminary research findings.
COVID-19 intensified these hardships among communities of color, with disproportionate numbers of lost loved ones, lost jobs, and lost housing. The murder of George Floyd prompted widespread racial unrest, and Asian Americans saw an increase in hate crimes.
At the same time, studies in Connecticut and Maryland found that suicide rates rose within these populations and dropped for their White counterparts.
“It’s not just a problem within the person, but societal issues that need to be addressed,” said Shari Jager-Hyman, assistant professor of psychiatry at the University of Pennsylvania.
Lessons from Texas
In Texas, COVID-19 hit Hispanics especially hard. As of July 2021, they accounted for 45% of all COVID-19 deaths and disproportionately lost jobs. Individuals living in the U.S. without authorization were generally not eligible for unemployment benefits or federal stimulus checks.
During this time, suicide deaths among Hispanic Texans climbed from 847 deaths in 2019 to 962 deaths in 2020, according to preliminary state data. Suicide deaths rose for Black Texans and residents classified as “other” races or ethnicities, but decreased for White Texans.
The numbers didn’t surprise Marc Mendiola. The 20-year-old grew up in a majority-Hispanic community on the south side of San Antonio. Even before the pandemic, he often heard classmates say they were suicidal. Many faced dire finances at home, sometimes living without electricity, food, or water. Those who sought mental health treatment often found services prohibitively expensive or inaccessible because they weren’t offered in Spanish.
“These are conditions the community has always been in,” Mendiola said. “But with the pandemic, it’s even worse.”
Four years ago, Mendiola and his classmates at South San High School began advocating for mental health services. In late 2019, just months before COVID-19 struck, their vision became reality. Six community agencies partnered to offer free services to students and their families across three school districts.
Richard Davidson, chief operating officer of Family Service, one of the groups in the collaborative, said the number of students discussing economic stressors has been on the rise since April 2020. More than 90% of the students who received services in the first half of 2021 were Hispanic, and nearly 10% reported thoughts of suicide or self-harm, program data show. None died by suicide.
Many students are so worried about what’s for dinner the next day that they’re not able to see a future beyond that, Davidson said. That’s when suicide can feel like a viable option.
“One of the things we do is help them see … that despite this situation now, you can create a vision for your future,” Davidson said.
A good future
Researchers say the promise of a good future is often overlooked in suicide prevention, perhaps because achieving it is so challenging. It requires economic and social growth and breaking systemic barriers.
Tevis Simon works to address all those fronts. As a child in West Baltimore, Simon, who is Black, faced poverty and trauma. As an adult, she attempted suicide three times. But now she shares her story with youths across the city to inspire them to overcome challenges. She also talks to politicians, law enforcement agencies, and public policy officials about their responsibilities.
“We can’t not talk about race,” said Simon, 43. “We can’t not talk about systematic oppression. We cannot not talk about these conditions that affect our mental well-being and our feeling and desire to live.”
For Jamal Clay in Illinois, the systemic barriers started early. Before his suicide last year, he had tried to harm himself when he was 12 and the victim of bullies. At that time, he was hospitalized for a few days and told to follow up with outpatient therapy, said his mother, Maxie.
But it was difficult to find therapists who accepted Medicaid, she said. When Maxie finally found one, there was a 60-day wait. Other therapists canceled appointments, she said.
“So we worked on our own,” Maxie said, relying on church and community. Her son seemed to improve. “We thought we closed that chapter in our lives.”
But when the pandemic hit, everything got worse, she said. Clay came home from college and worked at an Amazon warehouse. On drives to and from work, he was frequently pulled over by police. He stopped wearing hats so officers would consider him less intimidating, Maxie said.
“He felt uncomfortable being out in the street,” she said.
Maxie is still trying to make sense of what happened the day Clay died. But she’s found meaning in starting a nonprofit called Soul Survivors of Chicago. Through the organization, she provides education, scholarships and shoes – including Jamal’s old ones – to those impacted by violence, suicide, and trauma.
“My son won’t be able to have a first interview in [those] shoes. He won’t be able to have a nice jump shot or go to church or even meet his wife,” Maxie said.
But she hopes his shoes will carry someone else to a good future.
[Editor’s note: For the purposes of this story, “people of color” or “communities of color” refers to any racial or ethnic populations whose members do not identify as White, including those who are multiracial. Hispanics can be of any race or combination of races.]
KHN senior correspondent JoNel Aleccia contributed to this report. KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
A hot dog a day takes 36 minutes away
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”

Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.

Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?

You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”
Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.
Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?
You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”
Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.
Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?
You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.

Healing Haiti: The emotional trauma of repeat crises
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Fauci corrects prediction on when pandemic will be under control
The United States could get the COVID-19 pandemic under control by the spring of 2022 if enough Americans become vaccinated, Anthony S. Fauci, MD, said.
Speaking to Anderson Cooper on CNN, Dr. Fauci corrected the timeline he gave in an interview earlier with Mary Louise Kelly of NPR.
In the NPR interview, he had said that if “the overwhelming majority of the people vaccinated, I think as we get into the fall and the winter, we could start to really get some good control over this as we get into 2022.”
Dr. Fauci told Mr. Cooper that he listened to a recording of the NPR interview later and realized his mistake.
“I meant to say the spring of 2022,” Dr. Fauci told CNN. “I misspoke. My bad.”
Dr. Fauci, the head of the National Institute of Allergy and Infectious Diseases and the chief White House medical adviser, said the pandemic will be under control when the large majority of Americans have gotten vaccinated or been infected with COVID-19 and recovered, which offers some protection against the virus.
People who have been infected and recovered should still get vaccinated, he said.
“The degree of protection you could induce in someone who’s been infected and then recovered and then vaccinated is an enormous increase in the degree of protection,” Dr. Fauci said.
“I think we can get a degree of overall blanket protection of the community that as we get into the early part of 2022 ... we could start getting back to a degree of normality.”
A version of this article first appeared on WebMD.com.
The United States could get the COVID-19 pandemic under control by the spring of 2022 if enough Americans become vaccinated, Anthony S. Fauci, MD, said.
Speaking to Anderson Cooper on CNN, Dr. Fauci corrected the timeline he gave in an interview earlier with Mary Louise Kelly of NPR.
In the NPR interview, he had said that if “the overwhelming majority of the people vaccinated, I think as we get into the fall and the winter, we could start to really get some good control over this as we get into 2022.”
Dr. Fauci told Mr. Cooper that he listened to a recording of the NPR interview later and realized his mistake.
“I meant to say the spring of 2022,” Dr. Fauci told CNN. “I misspoke. My bad.”
Dr. Fauci, the head of the National Institute of Allergy and Infectious Diseases and the chief White House medical adviser, said the pandemic will be under control when the large majority of Americans have gotten vaccinated or been infected with COVID-19 and recovered, which offers some protection against the virus.
People who have been infected and recovered should still get vaccinated, he said.
“The degree of protection you could induce in someone who’s been infected and then recovered and then vaccinated is an enormous increase in the degree of protection,” Dr. Fauci said.
“I think we can get a degree of overall blanket protection of the community that as we get into the early part of 2022 ... we could start getting back to a degree of normality.”
A version of this article first appeared on WebMD.com.
The United States could get the COVID-19 pandemic under control by the spring of 2022 if enough Americans become vaccinated, Anthony S. Fauci, MD, said.
Speaking to Anderson Cooper on CNN, Dr. Fauci corrected the timeline he gave in an interview earlier with Mary Louise Kelly of NPR.
In the NPR interview, he had said that if “the overwhelming majority of the people vaccinated, I think as we get into the fall and the winter, we could start to really get some good control over this as we get into 2022.”
Dr. Fauci told Mr. Cooper that he listened to a recording of the NPR interview later and realized his mistake.
“I meant to say the spring of 2022,” Dr. Fauci told CNN. “I misspoke. My bad.”
Dr. Fauci, the head of the National Institute of Allergy and Infectious Diseases and the chief White House medical adviser, said the pandemic will be under control when the large majority of Americans have gotten vaccinated or been infected with COVID-19 and recovered, which offers some protection against the virus.
People who have been infected and recovered should still get vaccinated, he said.
“The degree of protection you could induce in someone who’s been infected and then recovered and then vaccinated is an enormous increase in the degree of protection,” Dr. Fauci said.
“I think we can get a degree of overall blanket protection of the community that as we get into the early part of 2022 ... we could start getting back to a degree of normality.”
A version of this article first appeared on WebMD.com.
Children and COVID: New cases soar to near-record level
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
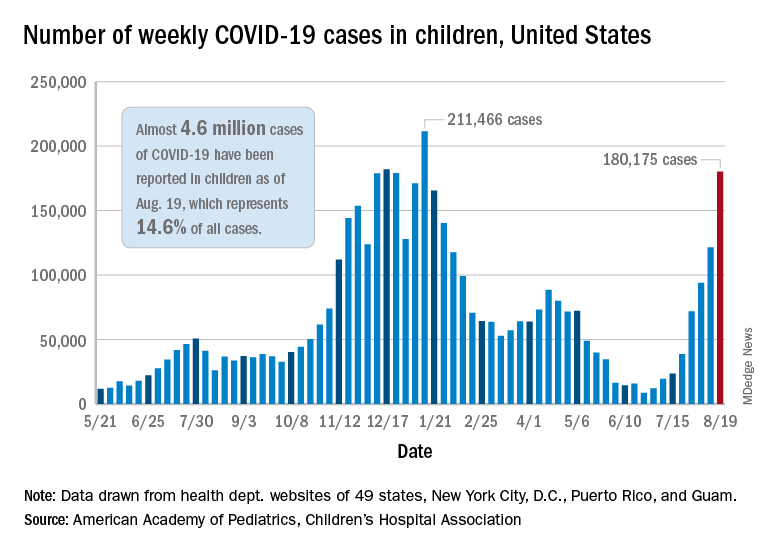
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.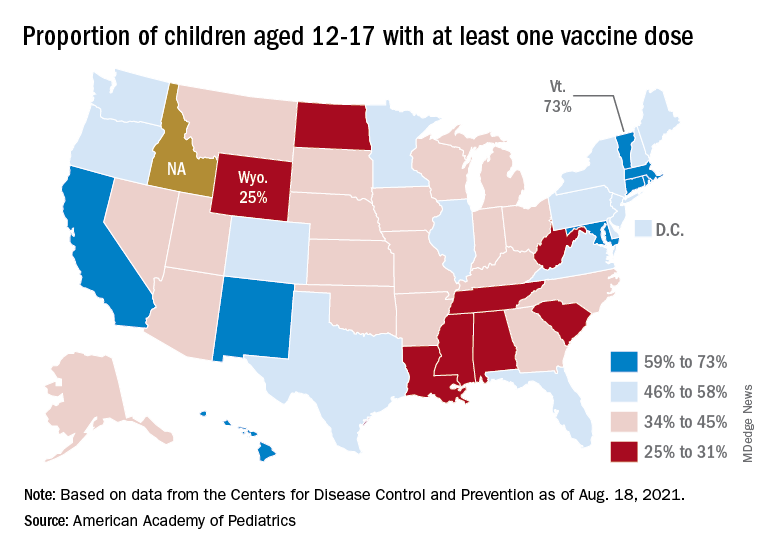
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Family physician Joseph E. Scherger champions lifestyle change
Joseph E. Scherger, MD, MPH, is a family physician of 40 years and an avid runner who has carried over his passion for fitness and nutrition into treating patients.

He achieved this through moving to practicing functional medicine a decade ago.
According to Dr. Scherger, functional medicine “shifts the whole approach [to family medicine], recognizing that people’s chronic diseases, like hypertension and diabetes, are completely reversible, and the reason why is because they’re caused by what we eat and how we live.”
Practicing functional medicine continues to make working exciting for Dr. Scherger, he says.
“Now that I’ve shifted into nutrition and lifestyle, I feel like I’m a healer, you know? I’m not just refilling prescriptions anymore,” he said.
The burden of disease brought about by bad nutrition and our profit-hungry food industry is staggering, explained Dr. Scherger, As such, he encourages his patients to adopt lifestyle and nutritional changes that allow the body to become healthy again.
Dr. Scherger’s shift into lifestyle-oriented medicine reflects his own experiences with healthy living, and how it has impacted his life.
“I’m 70 years old, and I’m still running, and I feel the same as when I was 40 or 50.” He has completed 40 marathons, ten 50K and five 50-mile ultramarathon trail runs, and, although retired from long-distance running, he is currently training for an upcoming 5K Thanksgiving turkey trot with his 6-year-old grandson. “He loves it. He’s faster than I am, I have trouble keeping up with him,” he confessed.
Earlier days of career
“I’ve been very blessed to have a career that kept changing every 5-10 years,” he said. “I’ve been able to evolve in a way of shifting my interests from one area to another,” he said.
Dr. Scherger has held many positions in the medical field, from serving in the National Health Service Corps in Dixon, Calif., as a migrant health physician during 1978-1980, to being chair of graduate medical education at Eisenhower Medical Center in Rancho Mirage, Calif., from 2009 to 2015. In between, he taught at the University of California, Davis, and served as founding dean of the Florida State University College of Medicine.
Originally from Ohio, Dr. Scherger was born in 1950 in the small town of Delphos. He graduated from the University of Dayton in 1971 before attending medical school at University of California, Los Angeles, for 4 years. He then completed a family medicine residency and a masters in public health at the University of Washington, Seattle, in 1978.
A resident of the Golden State for 50 years now, Dr. Scherger describes himself as a “true Californian.” Currently, he is in practice at Eisenhower Health in La Quinta, Calif., where he is a core faculty member in the family medicine residency program. He is also a physician under the health center’s Primary Care 365 program, which offers patients regular communication with and increased access to their physicians, emphasizing on telemedicine. He also founded Restore Health – Disease Reversal, a wellness center in Indian Wells, Calif., that focuses on improving patients’ health through changes in nutrition and lifestyle.
Within his medical practice, Dr. Scherger is seen by colleagues as a doctor who not only advocates for his patients, but also goes above and beyond to solve their problems.
“He’s a leader, an advocate, and he inspires others to do what they do,” said Julia L. Martin, MD, a fellow family medicine practitioner who has been working with Dr. Scherger at the Eisenhower Medical Center for the past 5 years. “Being a physician is a very challenging role. You need to be patient and understanding in trying to investigate what the patient wants and work through that to try to find the solution. Dr. Scherger is really good at that.”
Inspiration for writing
Apart from his roles as a physician and faculty member, Dr. Scherger is also an author of two books: “40 Years in Family Medicine” (Scotts Valley, Calif.: CreateSpace, 2014) and “Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness” (Scotts Valley, Calif.: CreateSpace, 2015). He admits to not being a naturally gifted writer, and is more intrinsically skilled at speaking. When he was in medical school, however, a mentor told him that the written word is eternal, and this left a deep impression on him.
“When I think of something that’s worth writing about, that I think will be a contribution to my field, I don’t hesitate to begin to write and develop,” said Dr. Scherger. “ I’ve done some research that I’m proud of, but most of [my writings] are hopefully thoughtful essays to help move my field along, and it’s enormously satisfying to make these contributions.”
Awards and other contributions to family medicine
Dr. Scherger’s contributions to the field of family medicine have been recognized continuously over his career.
He has served on the board of directors of the American Academy of Family Physicians and the American Board of Family Medicine. He is also the recipient of numerous awards, such as being chosen as Family Physician of the Year by the American Academy of Family Physicians and the California Academy of Family Physicians in 1989. From 1988 to 1991, he was a fellow in the Kellogg National Fellowship Program.
While he has managed to reinvent his own practice and medical focus, Dr. Scherger is also concerned with the need to remodel the current state of primary care and family medicine. Regarding challenges facing the field, he mentions the burnout faced by many doctors.
Nowadays, the work of family medicine includes much more than those common acute illnesses – it includes preventive medicine, chronic illness management and mental health counseling. “Yet, somehow, the whole economic and schedule model is based on brief visits,” said Dr. Scherger. “I think the most common reason that a lot of family doctors are burned out is that they’re expected to see so many people a day, and they know they don’t have enough time to do a really good job.”
He elaborated: “The real challenge now for family practice is to be re-engineered to be for the modern age, and not be still stuck in a ‘make an appointment, come and get it’ model of care, which is outdated. So I’ve been working a long time in trying to reinvent primary care. And, you know, it’s hard to make those changes, and it’s still a work in progress.”
One of the ways Dr. Scherger has been working on the primary care model is to help redesign it for the computer age. He started doing telemedicine and online care in 1997, even though other doctors gave him pushback for doing so at the time. Today, in his practice, half of his patients are remote, and under Eisenhower’s Primary Care 365 service, he uses telemedicine to its fullest potential.
Dr. Martin calls Dr. Scherger an “innovator,” adding: “He really tries to find what works for a solution, in different ways – not just one cookie cutter way.”
Despite nearly 50 years of being a doctor, the profession has not gotten any less rewarding for Dr. Scherger, who says he does not intend to retire as long as he is any good at it.
“My mother always said, ‘Joe, your life should be dedicated to making the world a better place.’ I really took that to heart and realized that my greatest joy is to help other people.”
Joseph E. Scherger, MD, MPH, is a family physician of 40 years and an avid runner who has carried over his passion for fitness and nutrition into treating patients.
He achieved this through moving to practicing functional medicine a decade ago.
According to Dr. Scherger, functional medicine “shifts the whole approach [to family medicine], recognizing that people’s chronic diseases, like hypertension and diabetes, are completely reversible, and the reason why is because they’re caused by what we eat and how we live.”
Practicing functional medicine continues to make working exciting for Dr. Scherger, he says.
“Now that I’ve shifted into nutrition and lifestyle, I feel like I’m a healer, you know? I’m not just refilling prescriptions anymore,” he said.
The burden of disease brought about by bad nutrition and our profit-hungry food industry is staggering, explained Dr. Scherger, As such, he encourages his patients to adopt lifestyle and nutritional changes that allow the body to become healthy again.
Dr. Scherger’s shift into lifestyle-oriented medicine reflects his own experiences with healthy living, and how it has impacted his life.
“I’m 70 years old, and I’m still running, and I feel the same as when I was 40 or 50.” He has completed 40 marathons, ten 50K and five 50-mile ultramarathon trail runs, and, although retired from long-distance running, he is currently training for an upcoming 5K Thanksgiving turkey trot with his 6-year-old grandson. “He loves it. He’s faster than I am, I have trouble keeping up with him,” he confessed.
Earlier days of career
“I’ve been very blessed to have a career that kept changing every 5-10 years,” he said. “I’ve been able to evolve in a way of shifting my interests from one area to another,” he said.
Dr. Scherger has held many positions in the medical field, from serving in the National Health Service Corps in Dixon, Calif., as a migrant health physician during 1978-1980, to being chair of graduate medical education at Eisenhower Medical Center in Rancho Mirage, Calif., from 2009 to 2015. In between, he taught at the University of California, Davis, and served as founding dean of the Florida State University College of Medicine.
Originally from Ohio, Dr. Scherger was born in 1950 in the small town of Delphos. He graduated from the University of Dayton in 1971 before attending medical school at University of California, Los Angeles, for 4 years. He then completed a family medicine residency and a masters in public health at the University of Washington, Seattle, in 1978.
A resident of the Golden State for 50 years now, Dr. Scherger describes himself as a “true Californian.” Currently, he is in practice at Eisenhower Health in La Quinta, Calif., where he is a core faculty member in the family medicine residency program. He is also a physician under the health center’s Primary Care 365 program, which offers patients regular communication with and increased access to their physicians, emphasizing on telemedicine. He also founded Restore Health – Disease Reversal, a wellness center in Indian Wells, Calif., that focuses on improving patients’ health through changes in nutrition and lifestyle.
Within his medical practice, Dr. Scherger is seen by colleagues as a doctor who not only advocates for his patients, but also goes above and beyond to solve their problems.
“He’s a leader, an advocate, and he inspires others to do what they do,” said Julia L. Martin, MD, a fellow family medicine practitioner who has been working with Dr. Scherger at the Eisenhower Medical Center for the past 5 years. “Being a physician is a very challenging role. You need to be patient and understanding in trying to investigate what the patient wants and work through that to try to find the solution. Dr. Scherger is really good at that.”
Inspiration for writing
Apart from his roles as a physician and faculty member, Dr. Scherger is also an author of two books: “40 Years in Family Medicine” (Scotts Valley, Calif.: CreateSpace, 2014) and “Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness” (Scotts Valley, Calif.: CreateSpace, 2015). He admits to not being a naturally gifted writer, and is more intrinsically skilled at speaking. When he was in medical school, however, a mentor told him that the written word is eternal, and this left a deep impression on him.
“When I think of something that’s worth writing about, that I think will be a contribution to my field, I don’t hesitate to begin to write and develop,” said Dr. Scherger. “ I’ve done some research that I’m proud of, but most of [my writings] are hopefully thoughtful essays to help move my field along, and it’s enormously satisfying to make these contributions.”
Awards and other contributions to family medicine
Dr. Scherger’s contributions to the field of family medicine have been recognized continuously over his career.
He has served on the board of directors of the American Academy of Family Physicians and the American Board of Family Medicine. He is also the recipient of numerous awards, such as being chosen as Family Physician of the Year by the American Academy of Family Physicians and the California Academy of Family Physicians in 1989. From 1988 to 1991, he was a fellow in the Kellogg National Fellowship Program.
While he has managed to reinvent his own practice and medical focus, Dr. Scherger is also concerned with the need to remodel the current state of primary care and family medicine. Regarding challenges facing the field, he mentions the burnout faced by many doctors.
Nowadays, the work of family medicine includes much more than those common acute illnesses – it includes preventive medicine, chronic illness management and mental health counseling. “Yet, somehow, the whole economic and schedule model is based on brief visits,” said Dr. Scherger. “I think the most common reason that a lot of family doctors are burned out is that they’re expected to see so many people a day, and they know they don’t have enough time to do a really good job.”
He elaborated: “The real challenge now for family practice is to be re-engineered to be for the modern age, and not be still stuck in a ‘make an appointment, come and get it’ model of care, which is outdated. So I’ve been working a long time in trying to reinvent primary care. And, you know, it’s hard to make those changes, and it’s still a work in progress.”
One of the ways Dr. Scherger has been working on the primary care model is to help redesign it for the computer age. He started doing telemedicine and online care in 1997, even though other doctors gave him pushback for doing so at the time. Today, in his practice, half of his patients are remote, and under Eisenhower’s Primary Care 365 service, he uses telemedicine to its fullest potential.
Dr. Martin calls Dr. Scherger an “innovator,” adding: “He really tries to find what works for a solution, in different ways – not just one cookie cutter way.”
Despite nearly 50 years of being a doctor, the profession has not gotten any less rewarding for Dr. Scherger, who says he does not intend to retire as long as he is any good at it.
“My mother always said, ‘Joe, your life should be dedicated to making the world a better place.’ I really took that to heart and realized that my greatest joy is to help other people.”
Joseph E. Scherger, MD, MPH, is a family physician of 40 years and an avid runner who has carried over his passion for fitness and nutrition into treating patients.
He achieved this through moving to practicing functional medicine a decade ago.
According to Dr. Scherger, functional medicine “shifts the whole approach [to family medicine], recognizing that people’s chronic diseases, like hypertension and diabetes, are completely reversible, and the reason why is because they’re caused by what we eat and how we live.”
Practicing functional medicine continues to make working exciting for Dr. Scherger, he says.
“Now that I’ve shifted into nutrition and lifestyle, I feel like I’m a healer, you know? I’m not just refilling prescriptions anymore,” he said.
The burden of disease brought about by bad nutrition and our profit-hungry food industry is staggering, explained Dr. Scherger, As such, he encourages his patients to adopt lifestyle and nutritional changes that allow the body to become healthy again.
Dr. Scherger’s shift into lifestyle-oriented medicine reflects his own experiences with healthy living, and how it has impacted his life.
“I’m 70 years old, and I’m still running, and I feel the same as when I was 40 or 50.” He has completed 40 marathons, ten 50K and five 50-mile ultramarathon trail runs, and, although retired from long-distance running, he is currently training for an upcoming 5K Thanksgiving turkey trot with his 6-year-old grandson. “He loves it. He’s faster than I am, I have trouble keeping up with him,” he confessed.
Earlier days of career
“I’ve been very blessed to have a career that kept changing every 5-10 years,” he said. “I’ve been able to evolve in a way of shifting my interests from one area to another,” he said.
Dr. Scherger has held many positions in the medical field, from serving in the National Health Service Corps in Dixon, Calif., as a migrant health physician during 1978-1980, to being chair of graduate medical education at Eisenhower Medical Center in Rancho Mirage, Calif., from 2009 to 2015. In between, he taught at the University of California, Davis, and served as founding dean of the Florida State University College of Medicine.
Originally from Ohio, Dr. Scherger was born in 1950 in the small town of Delphos. He graduated from the University of Dayton in 1971 before attending medical school at University of California, Los Angeles, for 4 years. He then completed a family medicine residency and a masters in public health at the University of Washington, Seattle, in 1978.
A resident of the Golden State for 50 years now, Dr. Scherger describes himself as a “true Californian.” Currently, he is in practice at Eisenhower Health in La Quinta, Calif., where he is a core faculty member in the family medicine residency program. He is also a physician under the health center’s Primary Care 365 program, which offers patients regular communication with and increased access to their physicians, emphasizing on telemedicine. He also founded Restore Health – Disease Reversal, a wellness center in Indian Wells, Calif., that focuses on improving patients’ health through changes in nutrition and lifestyle.
Within his medical practice, Dr. Scherger is seen by colleagues as a doctor who not only advocates for his patients, but also goes above and beyond to solve their problems.
“He’s a leader, an advocate, and he inspires others to do what they do,” said Julia L. Martin, MD, a fellow family medicine practitioner who has been working with Dr. Scherger at the Eisenhower Medical Center for the past 5 years. “Being a physician is a very challenging role. You need to be patient and understanding in trying to investigate what the patient wants and work through that to try to find the solution. Dr. Scherger is really good at that.”
Inspiration for writing
Apart from his roles as a physician and faculty member, Dr. Scherger is also an author of two books: “40 Years in Family Medicine” (Scotts Valley, Calif.: CreateSpace, 2014) and “Lean and Fit: A Doctor’s Journey to Healthy Nutrition and Greater Wellness” (Scotts Valley, Calif.: CreateSpace, 2015). He admits to not being a naturally gifted writer, and is more intrinsically skilled at speaking. When he was in medical school, however, a mentor told him that the written word is eternal, and this left a deep impression on him.
“When I think of something that’s worth writing about, that I think will be a contribution to my field, I don’t hesitate to begin to write and develop,” said Dr. Scherger. “ I’ve done some research that I’m proud of, but most of [my writings] are hopefully thoughtful essays to help move my field along, and it’s enormously satisfying to make these contributions.”
Awards and other contributions to family medicine
Dr. Scherger’s contributions to the field of family medicine have been recognized continuously over his career.
He has served on the board of directors of the American Academy of Family Physicians and the American Board of Family Medicine. He is also the recipient of numerous awards, such as being chosen as Family Physician of the Year by the American Academy of Family Physicians and the California Academy of Family Physicians in 1989. From 1988 to 1991, he was a fellow in the Kellogg National Fellowship Program.
While he has managed to reinvent his own practice and medical focus, Dr. Scherger is also concerned with the need to remodel the current state of primary care and family medicine. Regarding challenges facing the field, he mentions the burnout faced by many doctors.
Nowadays, the work of family medicine includes much more than those common acute illnesses – it includes preventive medicine, chronic illness management and mental health counseling. “Yet, somehow, the whole economic and schedule model is based on brief visits,” said Dr. Scherger. “I think the most common reason that a lot of family doctors are burned out is that they’re expected to see so many people a day, and they know they don’t have enough time to do a really good job.”
He elaborated: “The real challenge now for family practice is to be re-engineered to be for the modern age, and not be still stuck in a ‘make an appointment, come and get it’ model of care, which is outdated. So I’ve been working a long time in trying to reinvent primary care. And, you know, it’s hard to make those changes, and it’s still a work in progress.”
One of the ways Dr. Scherger has been working on the primary care model is to help redesign it for the computer age. He started doing telemedicine and online care in 1997, even though other doctors gave him pushback for doing so at the time. Today, in his practice, half of his patients are remote, and under Eisenhower’s Primary Care 365 service, he uses telemedicine to its fullest potential.
Dr. Martin calls Dr. Scherger an “innovator,” adding: “He really tries to find what works for a solution, in different ways – not just one cookie cutter way.”
Despite nearly 50 years of being a doctor, the profession has not gotten any less rewarding for Dr. Scherger, who says he does not intend to retire as long as he is any good at it.
“My mother always said, ‘Joe, your life should be dedicated to making the world a better place.’ I really took that to heart and realized that my greatest joy is to help other people.”