User login
Children and COVID: Weekly cases top 95,000, admissions continue to rise
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.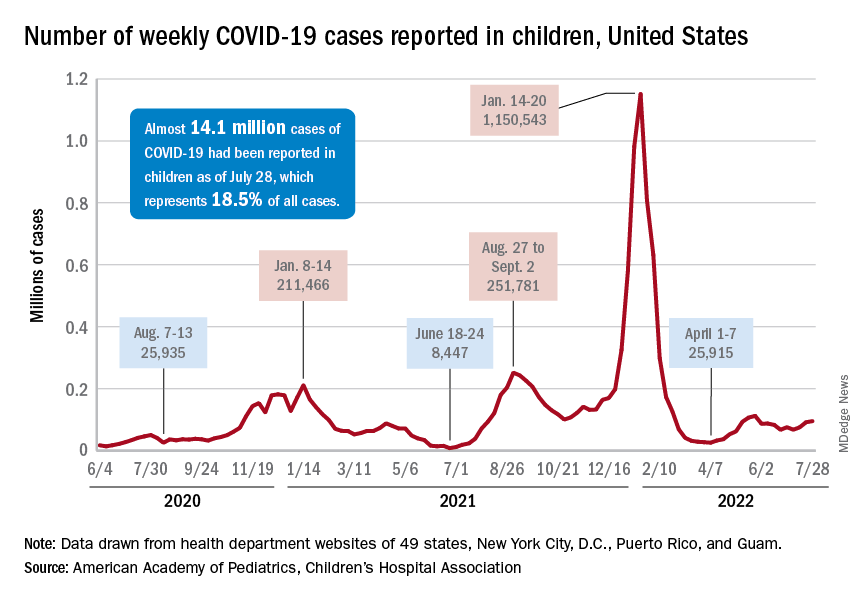
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.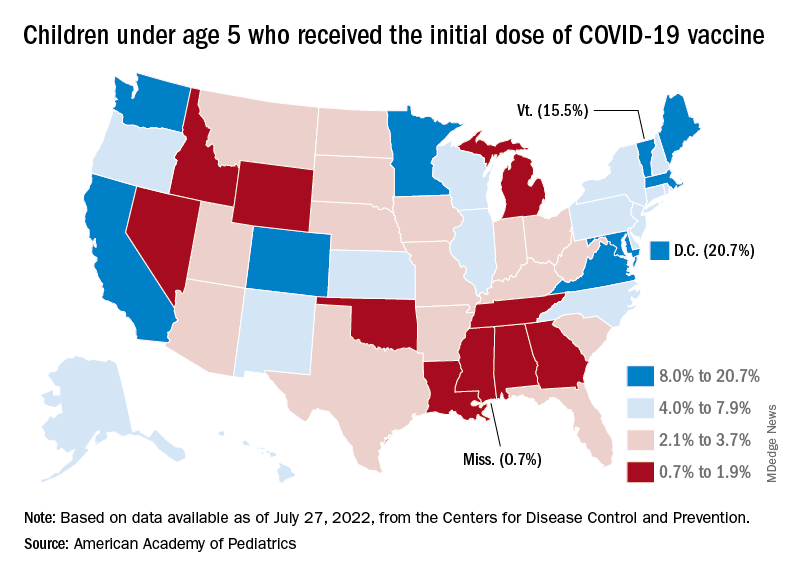
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
Malpractice lawyer gloats at win, then puts foot in mouth
During the closing arguments in a $10 million malpractice trial, attorney Robert McKenna III told jurors the claims against his client, a gastroenterologist, were baseless and equivalent to “extortion.” The patient’s family blamed the gastroenterologist for their father’s death, alleging the doctor perforated his colon during insertion of a feeding tube.
“I take pride in what I do, and I’ve got to tell you, in the 30 years I have been doing this, I have never seen a more insulting, factually devoid presentation in my entire career,” Mr. McKenna said, according to court transcripts. “On the strength of this evidence, they want you to award them $10 million. Welcome to America. Welcome to the personal injury machine, the personal injury industrial complex.”
After less than 30 minutes of deliberation, jurors returned a 12-0 verdict in favor of the physician.
However, Mr. McKenna, from Huntington Beach, Calif., described the case very differently to his staff in a celebration video, which he never expected to become public.
In the video, posted on Twitter and Instagram, Mr. McKenna bragged about how his legal team convinced jurors to doubt the patient’s official cause of death. He said the lawsuit involved a guy “that was probably negligently killed, but we kind of made it look like other people did it.”
“We actually had a death certificate that said he died the very way the plaintiff said he died, and we had to say, ‘No, you really shouldn’t believe what that death certificate says, or the coroner from the Orange County coroner’s office ... who says that it’s right,’” Mr. McKenna said in the video.
The 26-minute verdict was the fastest he’s ever received, Mr. McKenna says in the video, encouraging his partner to ring the firm’s victory bell.
“Overcoming all of those hurdles, we managed to sock three lawyers in the face,” Mr. McKenna said, referring to the plaintiffs’ lawyers.
The video of Mr. McKenna’s remarks is now in wide circulation after having been posted to online attorney forums, Instagram, where it’s been viewed more than 8,000 times, and Twitter, where views have reached over 3,000.
Jorge Ledezma, an Orange County, Calif., attorney who represented the patient’s family in the case, said the remarks make it appear as if Mr. McKenna tricked the jury.
“It was a drastic change from the comments he made to the jury during his closing arguments,” Mr. Ledezma said. “But the video is more important for what he doesn’t say. He doesn’t say his client did everything properly. He doesn’t say our case didn’t have any merit. He doesn’t say his client was a good doctor. Clearly, what he told the jury and what he believes are the exact opposite of each other.”
Mr. McKenna did not return multiple messages seeking comment for this story. In a statement to the LA Times, Mr. McKenna said his remarks were “intended purely as an internal briefing to our staff, using shorthand phrases which might understandably cause confusion for a lay audience unfamiliar with the case at hand, and the law in general.”
“I have expressed my apologies to my client, opposing counsel, and both the medical and legal communities,” Mr. McKenna said in the statement to the LA Times. “However, nothing about my remarks should call into question our very transparent trial strategy or the jury’s verdict in favor of my client.”
What happened to the patient?
Enrique Garcia Sanchez, 49, arrived at the critical care unit at South Coast Global Medical Center in Santa Ana, Calif., on Nov. 5, 2017, complaining of abdominal pain. He was diagnosed with acute pancreatitis, acute hypokalemia, and alcohol abuse, and transferred to the ICU, according to the family’s legal complaint.
Mr. Sanchez had a positive D-Dimer test, indicating a probable blood clot, and he appeared to be experiencing septic shock caused by pancreatitis, according to the complaint. By Nov. 17, Mr. Sanchez was suffering from respiratory failure and severe hypoxemia, and as a result, he was sedated. In addition, his abdomen was described as distended with decreased bowel sounds, according to court documents.
On. Nov. 18, a gastrointestinal specialist was consulted because of Mr. Sanchez’s prolonged intubation and oropharyngeal dysphagia, according to the lawsuit. On Nov. 21, air was leaking from Mr. Sanchez’s breathing tube with diffuse infiltration noted on the right side, and pneumonia.
Mr. Sanchez was eventually unable to swallow, and the gastroenterologist inserted a percutaneous endoscopic gastrostomy (PEG) tube, according to court records.
Mr. Sanchez’s condition worsened, and he developed respiratory distress, hypotension, and weakness during dialysis. On Dec. 9, 2017, physicians noted he had a bacterial infection, and he was later intubated on vent support because of progressive respiratory failure. Additionally, an internist reported that “fecal material” was observed per the PEG tube. Mr. Sanchez’s white blood cell count continued to rise, and his condition deteriorated. Mr. Sanchez died on Dec. 31, 2017.
A death certificate concluded that Mr. Sanchez died from complications of a PEG tube that perforated his colon, according to Mr. Ledezma. The plaintiffs’ legal team argued the gastroenterologist breached the standard of care by failing to ensure the tube was placed properly and failing to remedy the error after leakage was noted.
“Mr. Garcia died because of a misplaced PEG tube that perforated the colon, resulting in peritonitis and sepsis,” attorney Jose Robles said during his closing arguments. “Mr. Garcia had ascites, a contraindication for PEG tube placement. He had ileus, a contraindication for PEG tube placement. The standard of care requires that [the gastroenterologist] conduct a proper workup to confirm that a PEG tube placement can be done appropriately and safely.”
Mr. McKenna argued the gastroenterologist was not at fault for the patient’s death, and that complications from his pancreatitis ultimately killed him. During the trial, physicians who cared for Mr. Sanchez testified the patient had a less than 50% chance of survival.
“What he had was end-stage catastrophic [pancreatitis] that was affecting his organ system and aspiration pneumonia that made it impossible for him to try to breathe on his own,” Mr. McKenna said during closing arguments. “The man ... had a catastrophic injury that ate most of his pancreas. That is not a survivable event.”
Attorney faces backlash from legal community
Since his celebratory remarks were posted online, Mr. McKenna has faced much backlash, particularly from the legal community.
@mgvolada tweeted, “As an attorney I am revolted and I hope sanctions follow ... this is why people hate attorneys.”
@stevewieland, who identified himself as a trial lawyer, wrote he would not feel good about winning such a case.
“No wonder we get no love from the public,” he tweeted.
“Let’s see how the Court of Appeals thinks about your braggadocio and how this makes lawyers appear to the public,” tweeted @Stephen60134955, a self-identified attorney.
Mr. McKenna’s license remains active and in good standing with no disciplinary actions, according to the State Bar of California website.
Mr. Ledezma has filed a motion for a new trial, and a hearing on the motion is scheduled for Aug. 4, 2022. The motion was filed primarily because of issues during the trial, what Mr. Ledezma described as “inflammatory closing arguments,” and in small part, Mr. McKenna’s video remarks, he said.
If the motion is denied, the plaintiffs will move forward with an appeal, he said.
A version of this article first appeared on Medscape.com.
During the closing arguments in a $10 million malpractice trial, attorney Robert McKenna III told jurors the claims against his client, a gastroenterologist, were baseless and equivalent to “extortion.” The patient’s family blamed the gastroenterologist for their father’s death, alleging the doctor perforated his colon during insertion of a feeding tube.
“I take pride in what I do, and I’ve got to tell you, in the 30 years I have been doing this, I have never seen a more insulting, factually devoid presentation in my entire career,” Mr. McKenna said, according to court transcripts. “On the strength of this evidence, they want you to award them $10 million. Welcome to America. Welcome to the personal injury machine, the personal injury industrial complex.”
After less than 30 minutes of deliberation, jurors returned a 12-0 verdict in favor of the physician.
However, Mr. McKenna, from Huntington Beach, Calif., described the case very differently to his staff in a celebration video, which he never expected to become public.
In the video, posted on Twitter and Instagram, Mr. McKenna bragged about how his legal team convinced jurors to doubt the patient’s official cause of death. He said the lawsuit involved a guy “that was probably negligently killed, but we kind of made it look like other people did it.”
“We actually had a death certificate that said he died the very way the plaintiff said he died, and we had to say, ‘No, you really shouldn’t believe what that death certificate says, or the coroner from the Orange County coroner’s office ... who says that it’s right,’” Mr. McKenna said in the video.
The 26-minute verdict was the fastest he’s ever received, Mr. McKenna says in the video, encouraging his partner to ring the firm’s victory bell.
“Overcoming all of those hurdles, we managed to sock three lawyers in the face,” Mr. McKenna said, referring to the plaintiffs’ lawyers.
The video of Mr. McKenna’s remarks is now in wide circulation after having been posted to online attorney forums, Instagram, where it’s been viewed more than 8,000 times, and Twitter, where views have reached over 3,000.
Jorge Ledezma, an Orange County, Calif., attorney who represented the patient’s family in the case, said the remarks make it appear as if Mr. McKenna tricked the jury.
“It was a drastic change from the comments he made to the jury during his closing arguments,” Mr. Ledezma said. “But the video is more important for what he doesn’t say. He doesn’t say his client did everything properly. He doesn’t say our case didn’t have any merit. He doesn’t say his client was a good doctor. Clearly, what he told the jury and what he believes are the exact opposite of each other.”
Mr. McKenna did not return multiple messages seeking comment for this story. In a statement to the LA Times, Mr. McKenna said his remarks were “intended purely as an internal briefing to our staff, using shorthand phrases which might understandably cause confusion for a lay audience unfamiliar with the case at hand, and the law in general.”
“I have expressed my apologies to my client, opposing counsel, and both the medical and legal communities,” Mr. McKenna said in the statement to the LA Times. “However, nothing about my remarks should call into question our very transparent trial strategy or the jury’s verdict in favor of my client.”
What happened to the patient?
Enrique Garcia Sanchez, 49, arrived at the critical care unit at South Coast Global Medical Center in Santa Ana, Calif., on Nov. 5, 2017, complaining of abdominal pain. He was diagnosed with acute pancreatitis, acute hypokalemia, and alcohol abuse, and transferred to the ICU, according to the family’s legal complaint.
Mr. Sanchez had a positive D-Dimer test, indicating a probable blood clot, and he appeared to be experiencing septic shock caused by pancreatitis, according to the complaint. By Nov. 17, Mr. Sanchez was suffering from respiratory failure and severe hypoxemia, and as a result, he was sedated. In addition, his abdomen was described as distended with decreased bowel sounds, according to court documents.
On. Nov. 18, a gastrointestinal specialist was consulted because of Mr. Sanchez’s prolonged intubation and oropharyngeal dysphagia, according to the lawsuit. On Nov. 21, air was leaking from Mr. Sanchez’s breathing tube with diffuse infiltration noted on the right side, and pneumonia.
Mr. Sanchez was eventually unable to swallow, and the gastroenterologist inserted a percutaneous endoscopic gastrostomy (PEG) tube, according to court records.
Mr. Sanchez’s condition worsened, and he developed respiratory distress, hypotension, and weakness during dialysis. On Dec. 9, 2017, physicians noted he had a bacterial infection, and he was later intubated on vent support because of progressive respiratory failure. Additionally, an internist reported that “fecal material” was observed per the PEG tube. Mr. Sanchez’s white blood cell count continued to rise, and his condition deteriorated. Mr. Sanchez died on Dec. 31, 2017.
A death certificate concluded that Mr. Sanchez died from complications of a PEG tube that perforated his colon, according to Mr. Ledezma. The plaintiffs’ legal team argued the gastroenterologist breached the standard of care by failing to ensure the tube was placed properly and failing to remedy the error after leakage was noted.
“Mr. Garcia died because of a misplaced PEG tube that perforated the colon, resulting in peritonitis and sepsis,” attorney Jose Robles said during his closing arguments. “Mr. Garcia had ascites, a contraindication for PEG tube placement. He had ileus, a contraindication for PEG tube placement. The standard of care requires that [the gastroenterologist] conduct a proper workup to confirm that a PEG tube placement can be done appropriately and safely.”
Mr. McKenna argued the gastroenterologist was not at fault for the patient’s death, and that complications from his pancreatitis ultimately killed him. During the trial, physicians who cared for Mr. Sanchez testified the patient had a less than 50% chance of survival.
“What he had was end-stage catastrophic [pancreatitis] that was affecting his organ system and aspiration pneumonia that made it impossible for him to try to breathe on his own,” Mr. McKenna said during closing arguments. “The man ... had a catastrophic injury that ate most of his pancreas. That is not a survivable event.”
Attorney faces backlash from legal community
Since his celebratory remarks were posted online, Mr. McKenna has faced much backlash, particularly from the legal community.
@mgvolada tweeted, “As an attorney I am revolted and I hope sanctions follow ... this is why people hate attorneys.”
@stevewieland, who identified himself as a trial lawyer, wrote he would not feel good about winning such a case.
“No wonder we get no love from the public,” he tweeted.
“Let’s see how the Court of Appeals thinks about your braggadocio and how this makes lawyers appear to the public,” tweeted @Stephen60134955, a self-identified attorney.
Mr. McKenna’s license remains active and in good standing with no disciplinary actions, according to the State Bar of California website.
Mr. Ledezma has filed a motion for a new trial, and a hearing on the motion is scheduled for Aug. 4, 2022. The motion was filed primarily because of issues during the trial, what Mr. Ledezma described as “inflammatory closing arguments,” and in small part, Mr. McKenna’s video remarks, he said.
If the motion is denied, the plaintiffs will move forward with an appeal, he said.
A version of this article first appeared on Medscape.com.
During the closing arguments in a $10 million malpractice trial, attorney Robert McKenna III told jurors the claims against his client, a gastroenterologist, were baseless and equivalent to “extortion.” The patient’s family blamed the gastroenterologist for their father’s death, alleging the doctor perforated his colon during insertion of a feeding tube.
“I take pride in what I do, and I’ve got to tell you, in the 30 years I have been doing this, I have never seen a more insulting, factually devoid presentation in my entire career,” Mr. McKenna said, according to court transcripts. “On the strength of this evidence, they want you to award them $10 million. Welcome to America. Welcome to the personal injury machine, the personal injury industrial complex.”
After less than 30 minutes of deliberation, jurors returned a 12-0 verdict in favor of the physician.
However, Mr. McKenna, from Huntington Beach, Calif., described the case very differently to his staff in a celebration video, which he never expected to become public.
In the video, posted on Twitter and Instagram, Mr. McKenna bragged about how his legal team convinced jurors to doubt the patient’s official cause of death. He said the lawsuit involved a guy “that was probably negligently killed, but we kind of made it look like other people did it.”
“We actually had a death certificate that said he died the very way the plaintiff said he died, and we had to say, ‘No, you really shouldn’t believe what that death certificate says, or the coroner from the Orange County coroner’s office ... who says that it’s right,’” Mr. McKenna said in the video.
The 26-minute verdict was the fastest he’s ever received, Mr. McKenna says in the video, encouraging his partner to ring the firm’s victory bell.
“Overcoming all of those hurdles, we managed to sock three lawyers in the face,” Mr. McKenna said, referring to the plaintiffs’ lawyers.
The video of Mr. McKenna’s remarks is now in wide circulation after having been posted to online attorney forums, Instagram, where it’s been viewed more than 8,000 times, and Twitter, where views have reached over 3,000.
Jorge Ledezma, an Orange County, Calif., attorney who represented the patient’s family in the case, said the remarks make it appear as if Mr. McKenna tricked the jury.
“It was a drastic change from the comments he made to the jury during his closing arguments,” Mr. Ledezma said. “But the video is more important for what he doesn’t say. He doesn’t say his client did everything properly. He doesn’t say our case didn’t have any merit. He doesn’t say his client was a good doctor. Clearly, what he told the jury and what he believes are the exact opposite of each other.”
Mr. McKenna did not return multiple messages seeking comment for this story. In a statement to the LA Times, Mr. McKenna said his remarks were “intended purely as an internal briefing to our staff, using shorthand phrases which might understandably cause confusion for a lay audience unfamiliar with the case at hand, and the law in general.”
“I have expressed my apologies to my client, opposing counsel, and both the medical and legal communities,” Mr. McKenna said in the statement to the LA Times. “However, nothing about my remarks should call into question our very transparent trial strategy or the jury’s verdict in favor of my client.”
What happened to the patient?
Enrique Garcia Sanchez, 49, arrived at the critical care unit at South Coast Global Medical Center in Santa Ana, Calif., on Nov. 5, 2017, complaining of abdominal pain. He was diagnosed with acute pancreatitis, acute hypokalemia, and alcohol abuse, and transferred to the ICU, according to the family’s legal complaint.
Mr. Sanchez had a positive D-Dimer test, indicating a probable blood clot, and he appeared to be experiencing septic shock caused by pancreatitis, according to the complaint. By Nov. 17, Mr. Sanchez was suffering from respiratory failure and severe hypoxemia, and as a result, he was sedated. In addition, his abdomen was described as distended with decreased bowel sounds, according to court documents.
On. Nov. 18, a gastrointestinal specialist was consulted because of Mr. Sanchez’s prolonged intubation and oropharyngeal dysphagia, according to the lawsuit. On Nov. 21, air was leaking from Mr. Sanchez’s breathing tube with diffuse infiltration noted on the right side, and pneumonia.
Mr. Sanchez was eventually unable to swallow, and the gastroenterologist inserted a percutaneous endoscopic gastrostomy (PEG) tube, according to court records.
Mr. Sanchez’s condition worsened, and he developed respiratory distress, hypotension, and weakness during dialysis. On Dec. 9, 2017, physicians noted he had a bacterial infection, and he was later intubated on vent support because of progressive respiratory failure. Additionally, an internist reported that “fecal material” was observed per the PEG tube. Mr. Sanchez’s white blood cell count continued to rise, and his condition deteriorated. Mr. Sanchez died on Dec. 31, 2017.
A death certificate concluded that Mr. Sanchez died from complications of a PEG tube that perforated his colon, according to Mr. Ledezma. The plaintiffs’ legal team argued the gastroenterologist breached the standard of care by failing to ensure the tube was placed properly and failing to remedy the error after leakage was noted.
“Mr. Garcia died because of a misplaced PEG tube that perforated the colon, resulting in peritonitis and sepsis,” attorney Jose Robles said during his closing arguments. “Mr. Garcia had ascites, a contraindication for PEG tube placement. He had ileus, a contraindication for PEG tube placement. The standard of care requires that [the gastroenterologist] conduct a proper workup to confirm that a PEG tube placement can be done appropriately and safely.”
Mr. McKenna argued the gastroenterologist was not at fault for the patient’s death, and that complications from his pancreatitis ultimately killed him. During the trial, physicians who cared for Mr. Sanchez testified the patient had a less than 50% chance of survival.
“What he had was end-stage catastrophic [pancreatitis] that was affecting his organ system and aspiration pneumonia that made it impossible for him to try to breathe on his own,” Mr. McKenna said during closing arguments. “The man ... had a catastrophic injury that ate most of his pancreas. That is not a survivable event.”
Attorney faces backlash from legal community
Since his celebratory remarks were posted online, Mr. McKenna has faced much backlash, particularly from the legal community.
@mgvolada tweeted, “As an attorney I am revolted and I hope sanctions follow ... this is why people hate attorneys.”
@stevewieland, who identified himself as a trial lawyer, wrote he would not feel good about winning such a case.
“No wonder we get no love from the public,” he tweeted.
“Let’s see how the Court of Appeals thinks about your braggadocio and how this makes lawyers appear to the public,” tweeted @Stephen60134955, a self-identified attorney.
Mr. McKenna’s license remains active and in good standing with no disciplinary actions, according to the State Bar of California website.
Mr. Ledezma has filed a motion for a new trial, and a hearing on the motion is scheduled for Aug. 4, 2022. The motion was filed primarily because of issues during the trial, what Mr. Ledezma described as “inflammatory closing arguments,” and in small part, Mr. McKenna’s video remarks, he said.
If the motion is denied, the plaintiffs will move forward with an appeal, he said.
A version of this article first appeared on Medscape.com.
How doctors are weighing the legal risks of abortion care
The names of the doctors in this story have been changed at their request because of fear of legal repercussions and/or professional retaliation.
When an Ohio ob.gyn. had a patient in need of an abortion in July 2022, he knew he had to move quickly.
Daniel, who also sees patients at an abortion clinic, was treating a woman who came in for an abortion around 5 weeks into her pregnancy. And after going through the mandatory waiting periods, the required ultrasounds at each appointment, the consent process, and the options counseling, she was set for a surgical abortion the following Monday.
But on Monday, pre-op tests showed that her blood pressure was very high, posing a serious health risk if Daniel proceeded with the surgery.
Before the Supreme Court overturned Roe v. Wade in June, Daniel would have sent the patient home with instructions on how to lower her blood pressure over time. But the patient now had just four days to show the necessary improvement.
In this case, everything worked out. The patient returned Thursday and was able to have the procedure. But this is just one of the many day-to-day medical decisions abortion providers are now having to make with the changing legal risks being as top-of-mind to doctors as the safety of their patients.
Daniel said he doesn’t want the Ohio abortion law to change the way he communicates with his patients. As far as he knows, it’s still legal to talk to patients about self-managed abortions, as long as everything is unbiased and clearly stated, he says.
“But I don’t think I would get a lot of institutional support to have those conversations with patients because of the perceived legal liability,” says Daniel. “I will still have those conversations, but I’m not going to tell my employer that I’m having them and I’m not going to document them in the chart.”
Daniel is aware that having these kinds of discussions, or entertaining the possibility of omitting certain information from patient records, runs the risk of legal and professional consequences. Enforcement of these rules is foggy, too.
Under the Ohio law, if a fellow staff member suspects you of violating a law, you could be reported to a supervisor or licensing body. Abortion providers are aware they must be cautious about what they say because anti-abortion activitists, posing as patients, have secretly recorded conversations in the past, Daniel says.
Enforcement: The past, present, and future legal risks
Before Roe, enforcement of illegal abortion was spotty, says Mary Ziegler, JD, a professor at Florida State University College of Law, who specializes in the legal history of reproductive rights. At the start of the late 19th century, the doctors who provided illegal abortions would, in most cases, be prosecuted if a patient died as a result of the procedure.
A doctor in Ashland, Pa., named Robert Spencer was known for providing abortions in the small mining town where he practiced in the 1920s. He was reportedly arrested three times – once after a patient died as a result of abortion complications – but was ultimately acquitted.
For many doctors performing abortions at the time, “it was very much a kind of roll of the dice,” Ms. Ziegler says. “There was a sense that these laws were not enforced very much.”
Carole Joffe, PhD, a sociologist with expertise in reproductive health, recalls that there were very few doctors arrested, given the sheer number of abortions that were performed. The American College of Obstetricians and Gynecologists estimates that, in the years leading up to the original Roe decision, about 1.2 million women in the U.S. had illegal abortions – a number that exceeds today’s estimates.
Among the most notable cases of a doctor being detained was the arrest of gynecologist Jane Hodgson, MD, in 1970. Dr. Hodgson intentionally violated Minnesota law, which prohibited all abortions except in cases that were life-threatening to the patient.
After performing an abortion on a patient who had contracted rubella, also known as German measles, Dr. Hodgson was arrested, sentenced to 30 days in jail, and put on a year-long probation. She did not end up serving any time in jail, and her conviction was overturned after the Roe decision in 1973.
Now, the abortion restrictions being passed in many states have authorized much more sweeping penalties than those that existed in the pre-Roe era. According to Joffe, there is one key reason why we can anticipate more doctor arrests now.
“There simply was not the modern anti-abortion movement that we have come to know,” she says. “In the old days, there was not that much legal surveillance, and things were very unsafe. Fast forward to the present, we have much safer options now – like medication abortion pills – but we have a very different legal environment.”
Carmel Shachar, JD, MPH, a law and health policy expert at Harvard Law School, also expects that we will see more frequent prosecutions of doctors who provide abortion.
“There’s so much more data available through medical record-keeping and information generated by our phones and internet searches, that I think it would be much harder for a physician to fly under the radar,” Ms. Shachar says.
Also, Ms. Shachar emphasizes the power of prosecutorial discretion in abortion cases, where one prosecutor may choose to apply a law much more aggressively than another prosecutor in the next county over. Such has been seen in DeKalb County, Ga., which includes parts of Atlanta, where District Attorney Sherry Boston says she plans to use her prosecutorial discretion to address crimes like rape and murder, rather than “potentially investigat[ing] women and doctors for medical decisions,” Bloomberg Law reported. State Sen. Jen Jordan, the Democratic nominee for Georgia attorney general, has also said that, if elected, she would not enforce the state’s new 6-week abortion ban.
Is there a legal path forward for abortion care in states that forbid it?
Robin, an ob.gyn., became a complex family planning fellow in Utah to seek out further medical training and education in abortion care. Her plan was to solidify this as an area of expertise, so that, upon completing her fellowship, she could move back to her home state of Arizona to provide services there.
In Utah, where she currently practices, abortion is banned after 18 weeks. In Arizona, abortion is still allowed up to 24-26 weeks, until a pregnancy reaches “viability” (when a fetus is developed enough that it is able to survive outside the uterus with medical assistance). But new restrictions in Arizona may go into effect as early as September which would prohibit abortions after 15 weeks.
Despite the uncertain future of abortion access in Arizona, Robin still plans on moving there after her fellowship, but she hopes to travel to surrounding states to help provide abortion care where it’s less restricted. Even if she isn’t able to provide abortions at all, she says that there are still ways to help patients get safe, above-board abortions so as not to repeat the dangerous and often gruesome outcomes of self-induced abortions or those done by illegitimate practitioners before Roe.
“One of the roles that I think I can have as a physician is helping people with wraparound care for self-managed abortion,” says Robin. “If they can get the [abortion] pills online, then I can do the ultrasound beforehand, I can do the ultrasound after, I can talk them through it. I can help them with all the aspects of this care, I just can’t give them the pills myself.”
Whether a doctor can be penalized for “aiding and abetting” abortions that happen in different states remains an open question. In Texas, for example, Senate Bill 8 – which took effect Sept. 1, 2021 – not only established a fetal heartbeat law but added language that would allow private citizens to sue anyone who “knowingly engages in conduct that aids or abets the performance or inducement of an abortion” or anyone who even intends to do so.
That’s what happened to Alan Braid, MD, an ob.gyn. based in San Antonio. He confessed in a Washington Post op-ed that he had performed an abortion after cardiac activity had been detected in the pregnancy. Aware of the legal risks, he has since been sued by three people, and those cases are still underway.
But Ms. Ziegler says the chances of a doctor from a progressive state actually getting extradited and prosecuted by a state with restrictive abortion laws is pretty low – not zero, but low.
Like Robin, Natalie – an ob.gyn. in her early 30s – is a complex family planning fellow in Massachusetts. After her fellowship, she wants to return to Texas, where she completed her residency training.
“I’m at the point in my training where everyone starts looking for jobs and figuring out their next steps,” says Natalie. “The Dobbs decision introduced a ton of chaos due to the vagueness in the laws and how they get enforced, and then there’s chaos within institutions themselves and what kind of risk tolerance they have.”
Looking towards her future career path, Natalie says that she would not consider a job at an institution that didn’t allow her to teach abortion care to students, speak publicly about abortion rights, or let her travel outside of Texas to continue providing abortion care. She’s also preemptively seeking legal counsel and general guidance – advice that Ms. Ziegler strongly urges doctors to heed, sooner rather than later.
In states that have strict abortion bans with exceptions for life-threatening cases, there is still a lack of clarity around what is actually considered life-threatening enough to pass as an exception.
“Is it life-threatening in the next 6 hours? 24 hours? Seven days? One month?” Robin asks. “In medicine, we don’t necessarily talk about if something is life-threatening or not, we just say that there’s a high risk of X thing happening in X period of time. What’s the threshold at which that meets legal criteria? Nobody has an answer for that.”
Robin explains that, in her patients who have cancer, a pregnancy wouldn’t “necessarily kill them within the span of the next 9 months, but it could certainly accelerate their disease that could kill them within the next year or two.”
Right now, she says she doesn’t know what she would do if and when she is put in that position as a doctor.
“I didn’t go to medical school and become a doctor to become a felon,” says Robin. “Our goal is to make as many legal changes as we can to protect our patients and then practice as much harm reduction and as much care as we can within the letter of the law.”
A version of this article first appeared on WebMD.com.
The names of the doctors in this story have been changed at their request because of fear of legal repercussions and/or professional retaliation.
When an Ohio ob.gyn. had a patient in need of an abortion in July 2022, he knew he had to move quickly.
Daniel, who also sees patients at an abortion clinic, was treating a woman who came in for an abortion around 5 weeks into her pregnancy. And after going through the mandatory waiting periods, the required ultrasounds at each appointment, the consent process, and the options counseling, she was set for a surgical abortion the following Monday.
But on Monday, pre-op tests showed that her blood pressure was very high, posing a serious health risk if Daniel proceeded with the surgery.
Before the Supreme Court overturned Roe v. Wade in June, Daniel would have sent the patient home with instructions on how to lower her blood pressure over time. But the patient now had just four days to show the necessary improvement.
In this case, everything worked out. The patient returned Thursday and was able to have the procedure. But this is just one of the many day-to-day medical decisions abortion providers are now having to make with the changing legal risks being as top-of-mind to doctors as the safety of their patients.
Daniel said he doesn’t want the Ohio abortion law to change the way he communicates with his patients. As far as he knows, it’s still legal to talk to patients about self-managed abortions, as long as everything is unbiased and clearly stated, he says.
“But I don’t think I would get a lot of institutional support to have those conversations with patients because of the perceived legal liability,” says Daniel. “I will still have those conversations, but I’m not going to tell my employer that I’m having them and I’m not going to document them in the chart.”
Daniel is aware that having these kinds of discussions, or entertaining the possibility of omitting certain information from patient records, runs the risk of legal and professional consequences. Enforcement of these rules is foggy, too.
Under the Ohio law, if a fellow staff member suspects you of violating a law, you could be reported to a supervisor or licensing body. Abortion providers are aware they must be cautious about what they say because anti-abortion activitists, posing as patients, have secretly recorded conversations in the past, Daniel says.
Enforcement: The past, present, and future legal risks
Before Roe, enforcement of illegal abortion was spotty, says Mary Ziegler, JD, a professor at Florida State University College of Law, who specializes in the legal history of reproductive rights. At the start of the late 19th century, the doctors who provided illegal abortions would, in most cases, be prosecuted if a patient died as a result of the procedure.
A doctor in Ashland, Pa., named Robert Spencer was known for providing abortions in the small mining town where he practiced in the 1920s. He was reportedly arrested three times – once after a patient died as a result of abortion complications – but was ultimately acquitted.
For many doctors performing abortions at the time, “it was very much a kind of roll of the dice,” Ms. Ziegler says. “There was a sense that these laws were not enforced very much.”
Carole Joffe, PhD, a sociologist with expertise in reproductive health, recalls that there were very few doctors arrested, given the sheer number of abortions that were performed. The American College of Obstetricians and Gynecologists estimates that, in the years leading up to the original Roe decision, about 1.2 million women in the U.S. had illegal abortions – a number that exceeds today’s estimates.
Among the most notable cases of a doctor being detained was the arrest of gynecologist Jane Hodgson, MD, in 1970. Dr. Hodgson intentionally violated Minnesota law, which prohibited all abortions except in cases that were life-threatening to the patient.
After performing an abortion on a patient who had contracted rubella, also known as German measles, Dr. Hodgson was arrested, sentenced to 30 days in jail, and put on a year-long probation. She did not end up serving any time in jail, and her conviction was overturned after the Roe decision in 1973.
Now, the abortion restrictions being passed in many states have authorized much more sweeping penalties than those that existed in the pre-Roe era. According to Joffe, there is one key reason why we can anticipate more doctor arrests now.
“There simply was not the modern anti-abortion movement that we have come to know,” she says. “In the old days, there was not that much legal surveillance, and things were very unsafe. Fast forward to the present, we have much safer options now – like medication abortion pills – but we have a very different legal environment.”
Carmel Shachar, JD, MPH, a law and health policy expert at Harvard Law School, also expects that we will see more frequent prosecutions of doctors who provide abortion.
“There’s so much more data available through medical record-keeping and information generated by our phones and internet searches, that I think it would be much harder for a physician to fly under the radar,” Ms. Shachar says.
Also, Ms. Shachar emphasizes the power of prosecutorial discretion in abortion cases, where one prosecutor may choose to apply a law much more aggressively than another prosecutor in the next county over. Such has been seen in DeKalb County, Ga., which includes parts of Atlanta, where District Attorney Sherry Boston says she plans to use her prosecutorial discretion to address crimes like rape and murder, rather than “potentially investigat[ing] women and doctors for medical decisions,” Bloomberg Law reported. State Sen. Jen Jordan, the Democratic nominee for Georgia attorney general, has also said that, if elected, she would not enforce the state’s new 6-week abortion ban.
Is there a legal path forward for abortion care in states that forbid it?
Robin, an ob.gyn., became a complex family planning fellow in Utah to seek out further medical training and education in abortion care. Her plan was to solidify this as an area of expertise, so that, upon completing her fellowship, she could move back to her home state of Arizona to provide services there.
In Utah, where she currently practices, abortion is banned after 18 weeks. In Arizona, abortion is still allowed up to 24-26 weeks, until a pregnancy reaches “viability” (when a fetus is developed enough that it is able to survive outside the uterus with medical assistance). But new restrictions in Arizona may go into effect as early as September which would prohibit abortions after 15 weeks.
Despite the uncertain future of abortion access in Arizona, Robin still plans on moving there after her fellowship, but she hopes to travel to surrounding states to help provide abortion care where it’s less restricted. Even if she isn’t able to provide abortions at all, she says that there are still ways to help patients get safe, above-board abortions so as not to repeat the dangerous and often gruesome outcomes of self-induced abortions or those done by illegitimate practitioners before Roe.
“One of the roles that I think I can have as a physician is helping people with wraparound care for self-managed abortion,” says Robin. “If they can get the [abortion] pills online, then I can do the ultrasound beforehand, I can do the ultrasound after, I can talk them through it. I can help them with all the aspects of this care, I just can’t give them the pills myself.”
Whether a doctor can be penalized for “aiding and abetting” abortions that happen in different states remains an open question. In Texas, for example, Senate Bill 8 – which took effect Sept. 1, 2021 – not only established a fetal heartbeat law but added language that would allow private citizens to sue anyone who “knowingly engages in conduct that aids or abets the performance or inducement of an abortion” or anyone who even intends to do so.
That’s what happened to Alan Braid, MD, an ob.gyn. based in San Antonio. He confessed in a Washington Post op-ed that he had performed an abortion after cardiac activity had been detected in the pregnancy. Aware of the legal risks, he has since been sued by three people, and those cases are still underway.
But Ms. Ziegler says the chances of a doctor from a progressive state actually getting extradited and prosecuted by a state with restrictive abortion laws is pretty low – not zero, but low.
Like Robin, Natalie – an ob.gyn. in her early 30s – is a complex family planning fellow in Massachusetts. After her fellowship, she wants to return to Texas, where she completed her residency training.
“I’m at the point in my training where everyone starts looking for jobs and figuring out their next steps,” says Natalie. “The Dobbs decision introduced a ton of chaos due to the vagueness in the laws and how they get enforced, and then there’s chaos within institutions themselves and what kind of risk tolerance they have.”
Looking towards her future career path, Natalie says that she would not consider a job at an institution that didn’t allow her to teach abortion care to students, speak publicly about abortion rights, or let her travel outside of Texas to continue providing abortion care. She’s also preemptively seeking legal counsel and general guidance – advice that Ms. Ziegler strongly urges doctors to heed, sooner rather than later.
In states that have strict abortion bans with exceptions for life-threatening cases, there is still a lack of clarity around what is actually considered life-threatening enough to pass as an exception.
“Is it life-threatening in the next 6 hours? 24 hours? Seven days? One month?” Robin asks. “In medicine, we don’t necessarily talk about if something is life-threatening or not, we just say that there’s a high risk of X thing happening in X period of time. What’s the threshold at which that meets legal criteria? Nobody has an answer for that.”
Robin explains that, in her patients who have cancer, a pregnancy wouldn’t “necessarily kill them within the span of the next 9 months, but it could certainly accelerate their disease that could kill them within the next year or two.”
Right now, she says she doesn’t know what she would do if and when she is put in that position as a doctor.
“I didn’t go to medical school and become a doctor to become a felon,” says Robin. “Our goal is to make as many legal changes as we can to protect our patients and then practice as much harm reduction and as much care as we can within the letter of the law.”
A version of this article first appeared on WebMD.com.
The names of the doctors in this story have been changed at their request because of fear of legal repercussions and/or professional retaliation.
When an Ohio ob.gyn. had a patient in need of an abortion in July 2022, he knew he had to move quickly.
Daniel, who also sees patients at an abortion clinic, was treating a woman who came in for an abortion around 5 weeks into her pregnancy. And after going through the mandatory waiting periods, the required ultrasounds at each appointment, the consent process, and the options counseling, she was set for a surgical abortion the following Monday.
But on Monday, pre-op tests showed that her blood pressure was very high, posing a serious health risk if Daniel proceeded with the surgery.
Before the Supreme Court overturned Roe v. Wade in June, Daniel would have sent the patient home with instructions on how to lower her blood pressure over time. But the patient now had just four days to show the necessary improvement.
In this case, everything worked out. The patient returned Thursday and was able to have the procedure. But this is just one of the many day-to-day medical decisions abortion providers are now having to make with the changing legal risks being as top-of-mind to doctors as the safety of their patients.
Daniel said he doesn’t want the Ohio abortion law to change the way he communicates with his patients. As far as he knows, it’s still legal to talk to patients about self-managed abortions, as long as everything is unbiased and clearly stated, he says.
“But I don’t think I would get a lot of institutional support to have those conversations with patients because of the perceived legal liability,” says Daniel. “I will still have those conversations, but I’m not going to tell my employer that I’m having them and I’m not going to document them in the chart.”
Daniel is aware that having these kinds of discussions, or entertaining the possibility of omitting certain information from patient records, runs the risk of legal and professional consequences. Enforcement of these rules is foggy, too.
Under the Ohio law, if a fellow staff member suspects you of violating a law, you could be reported to a supervisor or licensing body. Abortion providers are aware they must be cautious about what they say because anti-abortion activitists, posing as patients, have secretly recorded conversations in the past, Daniel says.
Enforcement: The past, present, and future legal risks
Before Roe, enforcement of illegal abortion was spotty, says Mary Ziegler, JD, a professor at Florida State University College of Law, who specializes in the legal history of reproductive rights. At the start of the late 19th century, the doctors who provided illegal abortions would, in most cases, be prosecuted if a patient died as a result of the procedure.
A doctor in Ashland, Pa., named Robert Spencer was known for providing abortions in the small mining town where he practiced in the 1920s. He was reportedly arrested three times – once after a patient died as a result of abortion complications – but was ultimately acquitted.
For many doctors performing abortions at the time, “it was very much a kind of roll of the dice,” Ms. Ziegler says. “There was a sense that these laws were not enforced very much.”
Carole Joffe, PhD, a sociologist with expertise in reproductive health, recalls that there were very few doctors arrested, given the sheer number of abortions that were performed. The American College of Obstetricians and Gynecologists estimates that, in the years leading up to the original Roe decision, about 1.2 million women in the U.S. had illegal abortions – a number that exceeds today’s estimates.
Among the most notable cases of a doctor being detained was the arrest of gynecologist Jane Hodgson, MD, in 1970. Dr. Hodgson intentionally violated Minnesota law, which prohibited all abortions except in cases that were life-threatening to the patient.
After performing an abortion on a patient who had contracted rubella, also known as German measles, Dr. Hodgson was arrested, sentenced to 30 days in jail, and put on a year-long probation. She did not end up serving any time in jail, and her conviction was overturned after the Roe decision in 1973.
Now, the abortion restrictions being passed in many states have authorized much more sweeping penalties than those that existed in the pre-Roe era. According to Joffe, there is one key reason why we can anticipate more doctor arrests now.
“There simply was not the modern anti-abortion movement that we have come to know,” she says. “In the old days, there was not that much legal surveillance, and things were very unsafe. Fast forward to the present, we have much safer options now – like medication abortion pills – but we have a very different legal environment.”
Carmel Shachar, JD, MPH, a law and health policy expert at Harvard Law School, also expects that we will see more frequent prosecutions of doctors who provide abortion.
“There’s so much more data available through medical record-keeping and information generated by our phones and internet searches, that I think it would be much harder for a physician to fly under the radar,” Ms. Shachar says.
Also, Ms. Shachar emphasizes the power of prosecutorial discretion in abortion cases, where one prosecutor may choose to apply a law much more aggressively than another prosecutor in the next county over. Such has been seen in DeKalb County, Ga., which includes parts of Atlanta, where District Attorney Sherry Boston says she plans to use her prosecutorial discretion to address crimes like rape and murder, rather than “potentially investigat[ing] women and doctors for medical decisions,” Bloomberg Law reported. State Sen. Jen Jordan, the Democratic nominee for Georgia attorney general, has also said that, if elected, she would not enforce the state’s new 6-week abortion ban.
Is there a legal path forward for abortion care in states that forbid it?
Robin, an ob.gyn., became a complex family planning fellow in Utah to seek out further medical training and education in abortion care. Her plan was to solidify this as an area of expertise, so that, upon completing her fellowship, she could move back to her home state of Arizona to provide services there.
In Utah, where she currently practices, abortion is banned after 18 weeks. In Arizona, abortion is still allowed up to 24-26 weeks, until a pregnancy reaches “viability” (when a fetus is developed enough that it is able to survive outside the uterus with medical assistance). But new restrictions in Arizona may go into effect as early as September which would prohibit abortions after 15 weeks.
Despite the uncertain future of abortion access in Arizona, Robin still plans on moving there after her fellowship, but she hopes to travel to surrounding states to help provide abortion care where it’s less restricted. Even if she isn’t able to provide abortions at all, she says that there are still ways to help patients get safe, above-board abortions so as not to repeat the dangerous and often gruesome outcomes of self-induced abortions or those done by illegitimate practitioners before Roe.
“One of the roles that I think I can have as a physician is helping people with wraparound care for self-managed abortion,” says Robin. “If they can get the [abortion] pills online, then I can do the ultrasound beforehand, I can do the ultrasound after, I can talk them through it. I can help them with all the aspects of this care, I just can’t give them the pills myself.”
Whether a doctor can be penalized for “aiding and abetting” abortions that happen in different states remains an open question. In Texas, for example, Senate Bill 8 – which took effect Sept. 1, 2021 – not only established a fetal heartbeat law but added language that would allow private citizens to sue anyone who “knowingly engages in conduct that aids or abets the performance or inducement of an abortion” or anyone who even intends to do so.
That’s what happened to Alan Braid, MD, an ob.gyn. based in San Antonio. He confessed in a Washington Post op-ed that he had performed an abortion after cardiac activity had been detected in the pregnancy. Aware of the legal risks, he has since been sued by three people, and those cases are still underway.
But Ms. Ziegler says the chances of a doctor from a progressive state actually getting extradited and prosecuted by a state with restrictive abortion laws is pretty low – not zero, but low.
Like Robin, Natalie – an ob.gyn. in her early 30s – is a complex family planning fellow in Massachusetts. After her fellowship, she wants to return to Texas, where she completed her residency training.
“I’m at the point in my training where everyone starts looking for jobs and figuring out their next steps,” says Natalie. “The Dobbs decision introduced a ton of chaos due to the vagueness in the laws and how they get enforced, and then there’s chaos within institutions themselves and what kind of risk tolerance they have.”
Looking towards her future career path, Natalie says that she would not consider a job at an institution that didn’t allow her to teach abortion care to students, speak publicly about abortion rights, or let her travel outside of Texas to continue providing abortion care. She’s also preemptively seeking legal counsel and general guidance – advice that Ms. Ziegler strongly urges doctors to heed, sooner rather than later.
In states that have strict abortion bans with exceptions for life-threatening cases, there is still a lack of clarity around what is actually considered life-threatening enough to pass as an exception.
“Is it life-threatening in the next 6 hours? 24 hours? Seven days? One month?” Robin asks. “In medicine, we don’t necessarily talk about if something is life-threatening or not, we just say that there’s a high risk of X thing happening in X period of time. What’s the threshold at which that meets legal criteria? Nobody has an answer for that.”
Robin explains that, in her patients who have cancer, a pregnancy wouldn’t “necessarily kill them within the span of the next 9 months, but it could certainly accelerate their disease that could kill them within the next year or two.”
Right now, she says she doesn’t know what she would do if and when she is put in that position as a doctor.
“I didn’t go to medical school and become a doctor to become a felon,” says Robin. “Our goal is to make as many legal changes as we can to protect our patients and then practice as much harm reduction and as much care as we can within the letter of the law.”
A version of this article first appeared on WebMD.com.
U.S. clears 786,000 monkeypox vaccine doses for distribution
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
Women with fear of pregnancy call for clinician compassion
Cee Elliot is afraid of pregnancy. The 29-year-old retail manager in Connecticut said she has felt that way since puberty, when she “finally understood” pregnancy and reproduction. Always squeamish around babies and pregnant people, she said, as she learned more about the complications birth can cause, the idea of carrying a child herself became increasingly repulsive.
Later, Ms. Elliot said, she was treated poorly by a partner because of her fears, leading to regular panic attacks. She moved on from that partner, but her fear of pregnancy did not. Along the way, she felt her fears were dismissed by doctors and peers alike.
Tokophobia – a severe fear of childbirth – goes beyond the typical anxieties about birth or pregnancy that women often experience. The condition can intrude on everyday life, crippling social interaction and interrupting regular sleep patterns. Although statistics in the United States don’t exist, as many as 14% of women internationally are thought to have tokophobia.
Although psychiatric treatment focusing on past traumas can help, many women resort to managing the condition themselves. Some seek sterilization, whereas others take multiple forms of contraception simultaneously – combining intrauterine devices and oral birth control, for example, experts said. Some women have sought abortions and some even have attempted suicide rather than face giving birth, according to Leila Frodsham, MbChB, a women’s health expert at King’s College London, who has studied tokophobia.
The International Classification of Diseases added tokophobia to its list of diagnostic codes in 2018. But the Diagnostic and Statistical Manual of Mental Disorders, used by clinicians in the United States, has yet to do the same. Without this designation, some doctors are more inclined to diagnose tokophobia than others, Dr. Frodsham said.
“I think some clinicians struggle to understand how much this condition affects women. There isn’t training in it, and I’d like to see it discussed more,” Dr. Frodsham told this news organization.
Dr. Frodsham said she has seen hundreds of patients seeking help with their fear of pregnancy. Many of these women don’t know that they might have a condition that could benefit from psychiatric treatment.
Tokophobia typically takes two forms: primary, which affects women who have never given birth; and secondary, which stems from a previous traumatic birth experience.
“It’s not the pain of childbirth they are afraid of, but rather their fear comes out of a sense that they lack control over themselves and the situation of being pregnant,” Dr. Frodsham said.
Although the phenomenon has been studied internationally, particularly in Europe, fear of childbirth remains almost entirely unexplored in the United States literature.
One of the only scientific examinations of tokophobia in this country was a 2016 survey of 22 women with the condition by researchers at the University of Michigan, Ann Arbor. Published in the Journal of Obstetric, Gynecology & Neonatal Nursing, the survey found that many of the women expressed concern that their race, gender, or level of income might affect the quality of their care. Some women surveyed said they had experienced traumas directly related to systemic inequalities in the health care system.
Lee Roosevelt, PhD, MPH, CNM, a nurse and midwife and a coauthor of the study, said fear of the health care system, coupled with concern over the loss of bodily autonomy, can foster severe aversion to childbirth. In her experience, she said, clinicians often handle these patients poorly.
“If a woman is making the decision not to have children, we want it to be because she has decided for her, and her body, that it is the right thing,” added Lisa Kane Low, PhD, CNM, professor of obstetrics and gynecology at the University of Michigan, who worked with Dr. Roosevelt on the survey. “She shouldn’t feel the decision is made because she can’t access what she needs or the health care system is unable to provide it.”
Access to midwives, doulas, or therapists trained in trauma counseling can allow women to have a voice in their treatment, Dr. Roosevelt said.
No specific medication exists to treat tokophobia; however, drugs for depression or anxiety sometimes help, Dr. Low said. “Women with tokophobia may not need medication but would benefit from other therapies like desensitization or biobehavioral approaches or combinations of those,” she said.
Treating triggers
According to Dr. Frodsham, women with tokophobia often experience guilt and isolation. They may avoid speaking to women who are pregnant or avoid discussing pregnancy and childbirth, afraid that doing so may trigger their fear.
“They can’t see how they can get close to this catastrophic thing they think is going to happen to them,” she said. “Many of them think they will die.”
Many patients avoid thinking about memories of traumatic events so as to not trigger extreme emotional responses.
Dr. Roosevelt said developing ways to assess and treat tokophobia has become more urgent, since the Supreme Court’s recent decision to overturn Roe v. Wade could lead to more instances of women carrying unwanted pregnancies.
Seeking community
The internet has become a place where women with tokophobia and less severe fears about pregnancy can share their experiences. On the online bulletin board Reddit, r/Tokphobia and r/childfree contain thousands of queries and personal stories about the condition, as well as requests for advice.
Jillian Kilcoyne, who lives in New York and attends college in Michigan, said: “Pregnancy has always freaked me out. A part of me believes it’s a biological injustice that women have to go through such pain and be ignored by the medical community just to give birth.” Ms. Kilcoyne said she has not sought counseling or help from a clinician.
“I’m not sure I even want it,” she told this news organization. “Some people want to get over their phobia because they want families, and others don’t want children at all. I think that those individuals should have the help they need.”
Claudia, a South Carolina resident who asked to be identified only by her first name owing to concerns about her privacy, said her tokophobia began when she started having sex. It grew worse when she developed health conditions that could be exacerbated by pregnancy. She said she stocks up on contraceptives and periodically takes a pregnancy test to ease her nerves.
“This started for me when I realized that having children wasn’t a requirement for life. I didn’t even know there was a name for what I was feeling,” Claudia said in an interview. “So, letting women know they have options, and then not making them feel guilty, or ashamed, is the most important thing. We shouldn’t try to convince women that motherhood is the only, or the correct, path.”
Ms. Elliot urged clinicians to have compassion: “Treat tokophobic patients – especially a pregnant one seeking an abortion – like someone with a life-threatening parasite. Don’t belittle or dismiss them. We’re already going to lose so many lives because of unwanted pregnancies and birth. Don’t add to the number.”
A version of this article first appeared on Medscape.com.
Cee Elliot is afraid of pregnancy. The 29-year-old retail manager in Connecticut said she has felt that way since puberty, when she “finally understood” pregnancy and reproduction. Always squeamish around babies and pregnant people, she said, as she learned more about the complications birth can cause, the idea of carrying a child herself became increasingly repulsive.
Later, Ms. Elliot said, she was treated poorly by a partner because of her fears, leading to regular panic attacks. She moved on from that partner, but her fear of pregnancy did not. Along the way, she felt her fears were dismissed by doctors and peers alike.
Tokophobia – a severe fear of childbirth – goes beyond the typical anxieties about birth or pregnancy that women often experience. The condition can intrude on everyday life, crippling social interaction and interrupting regular sleep patterns. Although statistics in the United States don’t exist, as many as 14% of women internationally are thought to have tokophobia.
Although psychiatric treatment focusing on past traumas can help, many women resort to managing the condition themselves. Some seek sterilization, whereas others take multiple forms of contraception simultaneously – combining intrauterine devices and oral birth control, for example, experts said. Some women have sought abortions and some even have attempted suicide rather than face giving birth, according to Leila Frodsham, MbChB, a women’s health expert at King’s College London, who has studied tokophobia.
The International Classification of Diseases added tokophobia to its list of diagnostic codes in 2018. But the Diagnostic and Statistical Manual of Mental Disorders, used by clinicians in the United States, has yet to do the same. Without this designation, some doctors are more inclined to diagnose tokophobia than others, Dr. Frodsham said.
“I think some clinicians struggle to understand how much this condition affects women. There isn’t training in it, and I’d like to see it discussed more,” Dr. Frodsham told this news organization.
Dr. Frodsham said she has seen hundreds of patients seeking help with their fear of pregnancy. Many of these women don’t know that they might have a condition that could benefit from psychiatric treatment.
Tokophobia typically takes two forms: primary, which affects women who have never given birth; and secondary, which stems from a previous traumatic birth experience.
“It’s not the pain of childbirth they are afraid of, but rather their fear comes out of a sense that they lack control over themselves and the situation of being pregnant,” Dr. Frodsham said.
Although the phenomenon has been studied internationally, particularly in Europe, fear of childbirth remains almost entirely unexplored in the United States literature.
One of the only scientific examinations of tokophobia in this country was a 2016 survey of 22 women with the condition by researchers at the University of Michigan, Ann Arbor. Published in the Journal of Obstetric, Gynecology & Neonatal Nursing, the survey found that many of the women expressed concern that their race, gender, or level of income might affect the quality of their care. Some women surveyed said they had experienced traumas directly related to systemic inequalities in the health care system.
Lee Roosevelt, PhD, MPH, CNM, a nurse and midwife and a coauthor of the study, said fear of the health care system, coupled with concern over the loss of bodily autonomy, can foster severe aversion to childbirth. In her experience, she said, clinicians often handle these patients poorly.
“If a woman is making the decision not to have children, we want it to be because she has decided for her, and her body, that it is the right thing,” added Lisa Kane Low, PhD, CNM, professor of obstetrics and gynecology at the University of Michigan, who worked with Dr. Roosevelt on the survey. “She shouldn’t feel the decision is made because she can’t access what she needs or the health care system is unable to provide it.”
Access to midwives, doulas, or therapists trained in trauma counseling can allow women to have a voice in their treatment, Dr. Roosevelt said.
No specific medication exists to treat tokophobia; however, drugs for depression or anxiety sometimes help, Dr. Low said. “Women with tokophobia may not need medication but would benefit from other therapies like desensitization or biobehavioral approaches or combinations of those,” she said.
Treating triggers
According to Dr. Frodsham, women with tokophobia often experience guilt and isolation. They may avoid speaking to women who are pregnant or avoid discussing pregnancy and childbirth, afraid that doing so may trigger their fear.
“They can’t see how they can get close to this catastrophic thing they think is going to happen to them,” she said. “Many of them think they will die.”
Many patients avoid thinking about memories of traumatic events so as to not trigger extreme emotional responses.
Dr. Roosevelt said developing ways to assess and treat tokophobia has become more urgent, since the Supreme Court’s recent decision to overturn Roe v. Wade could lead to more instances of women carrying unwanted pregnancies.
Seeking community
The internet has become a place where women with tokophobia and less severe fears about pregnancy can share their experiences. On the online bulletin board Reddit, r/Tokphobia and r/childfree contain thousands of queries and personal stories about the condition, as well as requests for advice.
Jillian Kilcoyne, who lives in New York and attends college in Michigan, said: “Pregnancy has always freaked me out. A part of me believes it’s a biological injustice that women have to go through such pain and be ignored by the medical community just to give birth.” Ms. Kilcoyne said she has not sought counseling or help from a clinician.
“I’m not sure I even want it,” she told this news organization. “Some people want to get over their phobia because they want families, and others don’t want children at all. I think that those individuals should have the help they need.”
Claudia, a South Carolina resident who asked to be identified only by her first name owing to concerns about her privacy, said her tokophobia began when she started having sex. It grew worse when she developed health conditions that could be exacerbated by pregnancy. She said she stocks up on contraceptives and periodically takes a pregnancy test to ease her nerves.
“This started for me when I realized that having children wasn’t a requirement for life. I didn’t even know there was a name for what I was feeling,” Claudia said in an interview. “So, letting women know they have options, and then not making them feel guilty, or ashamed, is the most important thing. We shouldn’t try to convince women that motherhood is the only, or the correct, path.”
Ms. Elliot urged clinicians to have compassion: “Treat tokophobic patients – especially a pregnant one seeking an abortion – like someone with a life-threatening parasite. Don’t belittle or dismiss them. We’re already going to lose so many lives because of unwanted pregnancies and birth. Don’t add to the number.”
A version of this article first appeared on Medscape.com.
Cee Elliot is afraid of pregnancy. The 29-year-old retail manager in Connecticut said she has felt that way since puberty, when she “finally understood” pregnancy and reproduction. Always squeamish around babies and pregnant people, she said, as she learned more about the complications birth can cause, the idea of carrying a child herself became increasingly repulsive.
Later, Ms. Elliot said, she was treated poorly by a partner because of her fears, leading to regular panic attacks. She moved on from that partner, but her fear of pregnancy did not. Along the way, she felt her fears were dismissed by doctors and peers alike.
Tokophobia – a severe fear of childbirth – goes beyond the typical anxieties about birth or pregnancy that women often experience. The condition can intrude on everyday life, crippling social interaction and interrupting regular sleep patterns. Although statistics in the United States don’t exist, as many as 14% of women internationally are thought to have tokophobia.
Although psychiatric treatment focusing on past traumas can help, many women resort to managing the condition themselves. Some seek sterilization, whereas others take multiple forms of contraception simultaneously – combining intrauterine devices and oral birth control, for example, experts said. Some women have sought abortions and some even have attempted suicide rather than face giving birth, according to Leila Frodsham, MbChB, a women’s health expert at King’s College London, who has studied tokophobia.
The International Classification of Diseases added tokophobia to its list of diagnostic codes in 2018. But the Diagnostic and Statistical Manual of Mental Disorders, used by clinicians in the United States, has yet to do the same. Without this designation, some doctors are more inclined to diagnose tokophobia than others, Dr. Frodsham said.
“I think some clinicians struggle to understand how much this condition affects women. There isn’t training in it, and I’d like to see it discussed more,” Dr. Frodsham told this news organization.
Dr. Frodsham said she has seen hundreds of patients seeking help with their fear of pregnancy. Many of these women don’t know that they might have a condition that could benefit from psychiatric treatment.
Tokophobia typically takes two forms: primary, which affects women who have never given birth; and secondary, which stems from a previous traumatic birth experience.
“It’s not the pain of childbirth they are afraid of, but rather their fear comes out of a sense that they lack control over themselves and the situation of being pregnant,” Dr. Frodsham said.
Although the phenomenon has been studied internationally, particularly in Europe, fear of childbirth remains almost entirely unexplored in the United States literature.
One of the only scientific examinations of tokophobia in this country was a 2016 survey of 22 women with the condition by researchers at the University of Michigan, Ann Arbor. Published in the Journal of Obstetric, Gynecology & Neonatal Nursing, the survey found that many of the women expressed concern that their race, gender, or level of income might affect the quality of their care. Some women surveyed said they had experienced traumas directly related to systemic inequalities in the health care system.
Lee Roosevelt, PhD, MPH, CNM, a nurse and midwife and a coauthor of the study, said fear of the health care system, coupled with concern over the loss of bodily autonomy, can foster severe aversion to childbirth. In her experience, she said, clinicians often handle these patients poorly.
“If a woman is making the decision not to have children, we want it to be because she has decided for her, and her body, that it is the right thing,” added Lisa Kane Low, PhD, CNM, professor of obstetrics and gynecology at the University of Michigan, who worked with Dr. Roosevelt on the survey. “She shouldn’t feel the decision is made because she can’t access what she needs or the health care system is unable to provide it.”
Access to midwives, doulas, or therapists trained in trauma counseling can allow women to have a voice in their treatment, Dr. Roosevelt said.
No specific medication exists to treat tokophobia; however, drugs for depression or anxiety sometimes help, Dr. Low said. “Women with tokophobia may not need medication but would benefit from other therapies like desensitization or biobehavioral approaches or combinations of those,” she said.
Treating triggers
According to Dr. Frodsham, women with tokophobia often experience guilt and isolation. They may avoid speaking to women who are pregnant or avoid discussing pregnancy and childbirth, afraid that doing so may trigger their fear.
“They can’t see how they can get close to this catastrophic thing they think is going to happen to them,” she said. “Many of them think they will die.”
Many patients avoid thinking about memories of traumatic events so as to not trigger extreme emotional responses.
Dr. Roosevelt said developing ways to assess and treat tokophobia has become more urgent, since the Supreme Court’s recent decision to overturn Roe v. Wade could lead to more instances of women carrying unwanted pregnancies.
Seeking community
The internet has become a place where women with tokophobia and less severe fears about pregnancy can share their experiences. On the online bulletin board Reddit, r/Tokphobia and r/childfree contain thousands of queries and personal stories about the condition, as well as requests for advice.
Jillian Kilcoyne, who lives in New York and attends college in Michigan, said: “Pregnancy has always freaked me out. A part of me believes it’s a biological injustice that women have to go through such pain and be ignored by the medical community just to give birth.” Ms. Kilcoyne said she has not sought counseling or help from a clinician.
“I’m not sure I even want it,” she told this news organization. “Some people want to get over their phobia because they want families, and others don’t want children at all. I think that those individuals should have the help they need.”
Claudia, a South Carolina resident who asked to be identified only by her first name owing to concerns about her privacy, said her tokophobia began when she started having sex. It grew worse when she developed health conditions that could be exacerbated by pregnancy. She said she stocks up on contraceptives and periodically takes a pregnancy test to ease her nerves.
“This started for me when I realized that having children wasn’t a requirement for life. I didn’t even know there was a name for what I was feeling,” Claudia said in an interview. “So, letting women know they have options, and then not making them feel guilty, or ashamed, is the most important thing. We shouldn’t try to convince women that motherhood is the only, or the correct, path.”
Ms. Elliot urged clinicians to have compassion: “Treat tokophobic patients – especially a pregnant one seeking an abortion – like someone with a life-threatening parasite. Don’t belittle or dismiss them. We’re already going to lose so many lives because of unwanted pregnancies and birth. Don’t add to the number.”
A version of this article first appeared on Medscape.com.
To gauge monkeypox spread, researchers eye cases in women
As cases of monkeypox continue to mount in the United States and abroad, infectious disease experts are closely monitoring one group of people in particular: women.

So far, the overwhelming majority of cases of the viral disease have been reported in men who have sex with men. But in recent days, officials have learned of a handful of cases in women – possibly indicating that the outbreak may be widening.
Researchers are keeping close tabs on the proportion of cases in women to “assess whether the outbreak is moving away” from networks of men who have sex with men, where most of the initial cases have been identified, according to a briefing from the UK Health Security Agency (UKHSA).
“There is insufficient evidence to support a change in the transmission dynamics,” the agency said. “However, over the last few weeks the proportion of female cases has been increasing, so this trend needs to be monitored closely.”
A global collaboration of researchers and clinicians recently described 528 cases of monkeypox in 16 countries – but none were in women.
Since data collection for that study ended in June, the research group has confirmed cases in women, said study coauthor John P. Thornhill, MD, PhD, consultant physician in sexual health and HIV and clinical senior lecturer at Barts Health NHS Trust and Queen Mary University of London.
“Cases in women have certainly been reported but are currently far less common,” Dr. Thornhill told this news organization.
Although infections in women have been outliers during the current outbreak, they can be severe when they do occur. Several women in England have been hospitalized with severe symptoms.
A similar pattern has been seen in New York City, where just one woman is among the 639 total cases, according to a July 21 report from the city’s health agency.
Researchers have recently published guidance on monkeypox for ob.gyns., maternal-fetal medicine subspecialists, and people who are pregnant or breastfeeding in anticipation of the possibility of more cases in women.
The Centers for Disease Control and Prevention advises that “pregnant, recently pregnant, and breastfeeding people should be prioritized for medical treatment” of monkeypox if needed.
One monkeypox vaccine, Jynneos, can be offered to people who are pregnant or breastfeeding and are otherwise eligible for vaccination on the basis of confirmed or likely contact with cases, ideally within 4 days of exposure. Some people at high risk for exposure, such as laboratory workers, may receive the vaccine preemptively.
Another vaccine, ACAM2000, is contraindicated in people who are pregnant or breastfeeding, according to the CDC.
Transmission dynamics
Investigators have not yet identified substantial spread of monkeypox beyond men who have sex with men, although transmission among household contacts, including women and children, has been reported.
Most initial infections during the current outbreak occurred during sexual activity. But monkeypox can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC. It also may spread from mother to child in utero.
Infected pets have been known to spread the disease as well. A multistate monkeypox outbreak in the United States in 2003 was linked to pet prairie dogs, including in childcare and school settings. That year, 55% of the 71 cases occurred in female patients.
More testing, higher positivity rates in men
Since May, more men than women in the United Kingdom have undergone testing for monkeypox, with 3,467 tests in men versus 447 tests in women. Among those tested, the positivity rate has been far higher in men than in women, 54% versus 2.2%, respectively.
As of July 20, about 0.65% of U.K. cases with known gender were in women. Two weeks prior, about 0.4% were in women.
In all, 13 monkeypox cases in England have been in women, and four had severe manifestations that required hospitalization, according to the UKHSA.
Globally, more than 16,000 monkeypox cases have been reported, according to the World Health Organization. The agency said that it plans to rename the disease to reduce stigma.
Monkeypox and pregnancy
Ob.gyns. are often on the “front line in terms of identifying people with infectious diseases,” said Denise J. Jamieson, MD, MPH, Emory University, Atlanta. Dr. Jamieson coauthored “A Primer on Monkeypox Virus for Obstetrician-Gynecologists,” published in Obstetrics & Gynecology.
“Obstetricians need to be aware of what infectious diseases are circulating and be aware of what is going on in the community,” she said.
With monkeypox, “it is anybody’s guess as to how widespread this is going to be,” Dr. Jamieson said.
“The initial monkeypox cases in the current outbreak have been predominately but not exclusively among men who have sex with men; enhanced transmission in this group may be facilitated by sexual activity and spread through complex sexual networks,” Dr. Thornhill said. “As the outbreak continues, we will likely see more monkeypox infections” outside that group.
“Those working in sexual health should have a high index of suspicion in all individuals presenting with genital and oral ulcers and those with proctitis,” he added.
During previous monkeypox outbreaks, the chain of household transmissions has been short, typically two or three people, said Chloe M. Orkin, MD, professor of HIV medicine at Queen Mary University of London. Dr. Orkin directs the Sexual Health and HIV All East Research (SHARE) Collaborative, which has worked to compile the international case series.
Though monkeypox has mainly been transmitted among men who have sex with men, not all identify as gay and some may also have female and nonbinary partners, Dr. Orkin said.
“Clinicians should bear this in mind when examining any person,” she said.
A version of this article first appeared on Medscape.com.
As cases of monkeypox continue to mount in the United States and abroad, infectious disease experts are closely monitoring one group of people in particular: women.
So far, the overwhelming majority of cases of the viral disease have been reported in men who have sex with men. But in recent days, officials have learned of a handful of cases in women – possibly indicating that the outbreak may be widening.
Researchers are keeping close tabs on the proportion of cases in women to “assess whether the outbreak is moving away” from networks of men who have sex with men, where most of the initial cases have been identified, according to a briefing from the UK Health Security Agency (UKHSA).
“There is insufficient evidence to support a change in the transmission dynamics,” the agency said. “However, over the last few weeks the proportion of female cases has been increasing, so this trend needs to be monitored closely.”
A global collaboration of researchers and clinicians recently described 528 cases of monkeypox in 16 countries – but none were in women.
Since data collection for that study ended in June, the research group has confirmed cases in women, said study coauthor John P. Thornhill, MD, PhD, consultant physician in sexual health and HIV and clinical senior lecturer at Barts Health NHS Trust and Queen Mary University of London.
“Cases in women have certainly been reported but are currently far less common,” Dr. Thornhill told this news organization.
Although infections in women have been outliers during the current outbreak, they can be severe when they do occur. Several women in England have been hospitalized with severe symptoms.
A similar pattern has been seen in New York City, where just one woman is among the 639 total cases, according to a July 21 report from the city’s health agency.
Researchers have recently published guidance on monkeypox for ob.gyns., maternal-fetal medicine subspecialists, and people who are pregnant or breastfeeding in anticipation of the possibility of more cases in women.
The Centers for Disease Control and Prevention advises that “pregnant, recently pregnant, and breastfeeding people should be prioritized for medical treatment” of monkeypox if needed.
One monkeypox vaccine, Jynneos, can be offered to people who are pregnant or breastfeeding and are otherwise eligible for vaccination on the basis of confirmed or likely contact with cases, ideally within 4 days of exposure. Some people at high risk for exposure, such as laboratory workers, may receive the vaccine preemptively.
Another vaccine, ACAM2000, is contraindicated in people who are pregnant or breastfeeding, according to the CDC.
Transmission dynamics
Investigators have not yet identified substantial spread of monkeypox beyond men who have sex with men, although transmission among household contacts, including women and children, has been reported.
Most initial infections during the current outbreak occurred during sexual activity. But monkeypox can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC. It also may spread from mother to child in utero.
Infected pets have been known to spread the disease as well. A multistate monkeypox outbreak in the United States in 2003 was linked to pet prairie dogs, including in childcare and school settings. That year, 55% of the 71 cases occurred in female patients.
More testing, higher positivity rates in men
Since May, more men than women in the United Kingdom have undergone testing for monkeypox, with 3,467 tests in men versus 447 tests in women. Among those tested, the positivity rate has been far higher in men than in women, 54% versus 2.2%, respectively.
As of July 20, about 0.65% of U.K. cases with known gender were in women. Two weeks prior, about 0.4% were in women.
In all, 13 monkeypox cases in England have been in women, and four had severe manifestations that required hospitalization, according to the UKHSA.
Globally, more than 16,000 monkeypox cases have been reported, according to the World Health Organization. The agency said that it plans to rename the disease to reduce stigma.
Monkeypox and pregnancy
Ob.gyns. are often on the “front line in terms of identifying people with infectious diseases,” said Denise J. Jamieson, MD, MPH, Emory University, Atlanta. Dr. Jamieson coauthored “A Primer on Monkeypox Virus for Obstetrician-Gynecologists,” published in Obstetrics & Gynecology.
“Obstetricians need to be aware of what infectious diseases are circulating and be aware of what is going on in the community,” she said.
With monkeypox, “it is anybody’s guess as to how widespread this is going to be,” Dr. Jamieson said.
“The initial monkeypox cases in the current outbreak have been predominately but not exclusively among men who have sex with men; enhanced transmission in this group may be facilitated by sexual activity and spread through complex sexual networks,” Dr. Thornhill said. “As the outbreak continues, we will likely see more monkeypox infections” outside that group.
“Those working in sexual health should have a high index of suspicion in all individuals presenting with genital and oral ulcers and those with proctitis,” he added.
During previous monkeypox outbreaks, the chain of household transmissions has been short, typically two or three people, said Chloe M. Orkin, MD, professor of HIV medicine at Queen Mary University of London. Dr. Orkin directs the Sexual Health and HIV All East Research (SHARE) Collaborative, which has worked to compile the international case series.
Though monkeypox has mainly been transmitted among men who have sex with men, not all identify as gay and some may also have female and nonbinary partners, Dr. Orkin said.
“Clinicians should bear this in mind when examining any person,” she said.
A version of this article first appeared on Medscape.com.
As cases of monkeypox continue to mount in the United States and abroad, infectious disease experts are closely monitoring one group of people in particular: women.
So far, the overwhelming majority of cases of the viral disease have been reported in men who have sex with men. But in recent days, officials have learned of a handful of cases in women – possibly indicating that the outbreak may be widening.
Researchers are keeping close tabs on the proportion of cases in women to “assess whether the outbreak is moving away” from networks of men who have sex with men, where most of the initial cases have been identified, according to a briefing from the UK Health Security Agency (UKHSA).
“There is insufficient evidence to support a change in the transmission dynamics,” the agency said. “However, over the last few weeks the proportion of female cases has been increasing, so this trend needs to be monitored closely.”
A global collaboration of researchers and clinicians recently described 528 cases of monkeypox in 16 countries – but none were in women.
Since data collection for that study ended in June, the research group has confirmed cases in women, said study coauthor John P. Thornhill, MD, PhD, consultant physician in sexual health and HIV and clinical senior lecturer at Barts Health NHS Trust and Queen Mary University of London.
“Cases in women have certainly been reported but are currently far less common,” Dr. Thornhill told this news organization.
Although infections in women have been outliers during the current outbreak, they can be severe when they do occur. Several women in England have been hospitalized with severe symptoms.
A similar pattern has been seen in New York City, where just one woman is among the 639 total cases, according to a July 21 report from the city’s health agency.
Researchers have recently published guidance on monkeypox for ob.gyns., maternal-fetal medicine subspecialists, and people who are pregnant or breastfeeding in anticipation of the possibility of more cases in women.
The Centers for Disease Control and Prevention advises that “pregnant, recently pregnant, and breastfeeding people should be prioritized for medical treatment” of monkeypox if needed.
One monkeypox vaccine, Jynneos, can be offered to people who are pregnant or breastfeeding and are otherwise eligible for vaccination on the basis of confirmed or likely contact with cases, ideally within 4 days of exposure. Some people at high risk for exposure, such as laboratory workers, may receive the vaccine preemptively.
Another vaccine, ACAM2000, is contraindicated in people who are pregnant or breastfeeding, according to the CDC.
Transmission dynamics
Investigators have not yet identified substantial spread of monkeypox beyond men who have sex with men, although transmission among household contacts, including women and children, has been reported.
Most initial infections during the current outbreak occurred during sexual activity. But monkeypox can spread through any close contact with skin lesions or body fluids and possibly through touching contaminated items like clothing or linens, according to the CDC. It also may spread from mother to child in utero.
Infected pets have been known to spread the disease as well. A multistate monkeypox outbreak in the United States in 2003 was linked to pet prairie dogs, including in childcare and school settings. That year, 55% of the 71 cases occurred in female patients.
More testing, higher positivity rates in men
Since May, more men than women in the United Kingdom have undergone testing for monkeypox, with 3,467 tests in men versus 447 tests in women. Among those tested, the positivity rate has been far higher in men than in women, 54% versus 2.2%, respectively.
As of July 20, about 0.65% of U.K. cases with known gender were in women. Two weeks prior, about 0.4% were in women.
In all, 13 monkeypox cases in England have been in women, and four had severe manifestations that required hospitalization, according to the UKHSA.
Globally, more than 16,000 monkeypox cases have been reported, according to the World Health Organization. The agency said that it plans to rename the disease to reduce stigma.
Monkeypox and pregnancy
Ob.gyns. are often on the “front line in terms of identifying people with infectious diseases,” said Denise J. Jamieson, MD, MPH, Emory University, Atlanta. Dr. Jamieson coauthored “A Primer on Monkeypox Virus for Obstetrician-Gynecologists,” published in Obstetrics & Gynecology.
“Obstetricians need to be aware of what infectious diseases are circulating and be aware of what is going on in the community,” she said.
With monkeypox, “it is anybody’s guess as to how widespread this is going to be,” Dr. Jamieson said.
“The initial monkeypox cases in the current outbreak have been predominately but not exclusively among men who have sex with men; enhanced transmission in this group may be facilitated by sexual activity and spread through complex sexual networks,” Dr. Thornhill said. “As the outbreak continues, we will likely see more monkeypox infections” outside that group.
“Those working in sexual health should have a high index of suspicion in all individuals presenting with genital and oral ulcers and those with proctitis,” he added.
During previous monkeypox outbreaks, the chain of household transmissions has been short, typically two or three people, said Chloe M. Orkin, MD, professor of HIV medicine at Queen Mary University of London. Dr. Orkin directs the Sexual Health and HIV All East Research (SHARE) Collaborative, which has worked to compile the international case series.
Though monkeypox has mainly been transmitted among men who have sex with men, not all identify as gay and some may also have female and nonbinary partners, Dr. Orkin said.
“Clinicians should bear this in mind when examining any person,” she said.
A version of this article first appeared on Medscape.com.
Life and death decisions: What keeps oncologists up at night
It was 2 a.m. And Rebecca Shatsky, MD, could not sleep.
The breast oncologist was thinking about a patient of hers with metastatic cancer.
The patient’s disease had been asymptomatic for some time. Then without warning, her cancer suddenly exploded. Her bone marrow was failing, and her liver was not far behind.
Dr. Shatsky had a treatment plan ready to go but still, she felt uneasy.
“I had to be honest with her that I didn’t know if this plan would work,” says Dr. Shatsky, a medical oncologist at University of California, San Diego (UCSD).
That night, after visiting the patient in the hospital, Dr. Shatsky lay awake going over her next move, making sure it was the right one and hoping it would help keep the disease at bay.
“It’s so much pressure when someone is depending on you to make life or death decisions,” Dr. Shatsky said.
And in the quiet hours of night, these concerns grow louder.
Dr. Shatsky is not alone.
“There’s no off button,” says Aaron Goodman, MD, a hematologist at UCSD Health who goes by “Papa Heme” on Twitter. “I’m always thinking about my patients. Constantly.”
The public rarely gets a glimpse of these private moments. On occasion, oncologists will share a personal story, but more often, insights come from broad research on the ethical, emotional, and psychological toll of practicing medicine.
Many oncologists carry this baggage home with them because they have no other option.
“There is simply no time to process the weight of the day when I’ve got seven more patients who need my full attention before lunch,” Mark Lewis, MD, director, department of gastrointestinal oncology, Intermountain Healthcare, Salt Lake City, Utah. “That is why my processing happens outside of the office, when my brain can be quiet.”
What am I missing?
Dr. Goodman recognizes the gravity of each decision he makes. He pores over every detail of a patient’s scans, lab results, history, and symptoms.
But no matter how many times he checks and rechecks, one question nags at him: What am I missing?
For Dr. Goodman, this exhaustive level of attention is worth it.
“When errors are made, it’s someone’s life,” Dr. Goodman said. “Nothing would have prepared me for this responsibility. Until it lies on you, it’s impossible to understand how much trust patients put into us.”
That trust becomes most apparent for Dr. Goodman when facing a decision about how to treat a patient with acute myeloid leukemia who’s in remission.
Give more chemotherapy to root out the leukemia cells still lurking in the body, and the patient faces a high risk of the cancer returning. Pick stem cell transplant, and the chance of being cured goes up significantly, but the patient could also die within 100 days of the transplant.
“All together, the data show I’m helping patients with a transplant, but for the individual, I could be causing harm. Someone could be living less because of a decision I made,” Dr. Goodman said.
For patients with advanced cancer, oncologists may need to think several moves ahead. Mapping out a patient’s treatment options can feel like a game of chess. Dr. Shatsky is always trying to anticipate how the tumor will behave, what is driving it, and how lifestyle factors may influence a patient’s response in the present and the future.
“It is a mind game,” she says. “Like in chess, I try to outsmart my opponent. But with advanced cancer, there are not necessarily clear-cut guidelines or one way to manage the disease, and I have to do the best I can with drugs I have.”
That’s the art of oncology: Balancing the many knowns and unknowns of a person’s cancer alongside the toxicities of treatment and a patient’s hopes and goals.
Throughout the year, Don Dizon, MD, will see a number of patients with advanced disease. In these instances, the question he often wrestles with is if the patient can’t be cured, whether more treatment will just cause greater harm.
Dr. Dizon recently faced this dilemma with an older patient with metastatic disease who had not done well with an initial treatment regimen. After outlining the risks for more chemotherapy, he explained one option would be to forgo it and simply treat her symptoms.
“It’s an impossible choice,” says Dr. Dizon, director of women’s cancers at Lifespan Cancer Institute and director of medical oncology at Rhode Island Hospital, Providence.
Chemotherapy can provide symptom relief, but it can also be toxic – and patients may be so frail, they can die from more therapy.
“I told my patient, if in your heart, you want to try more therapy, that’s okay. But it’s also okay if you don’t,” Dr. Dizon recalled.
Her response: “You’re supposed to give me the answer.”
However, for patients approaching the end of life, there often is no right answer.
“It’s part of the discomfort you live with as a patient and oncologist, and when I leave the clinic, that’s one thing that follows me home,” Dr. Dizon said. “At the end of the day, I need to look in the mirror and know I did the best I could.”
The difficult conversation
Every Sunday, Dr. Lewis feels the weight of the week ahead. He and his wife, a pediatrician, call it the “Sunday scaries.”
It’s when Dr. Lewis begins thinking about the delicate conversations to come, rehearsing how he’s going to share the news that a person has advanced cancer or that a cancer, once in remission, has returned.
“Before the pandemic, I had 36 people come to a visit where I delivered some very heavy news and it became a Greek chorus of sobbing,” he recalls.
For every oncologist, delivering bad news is an integral part of the job. But after spending months, sometimes years, with a patient and the family, Dr. Lewis knows how to take the temperature of the room – who will likely prefer a more blunt style and who might need a gentler touch.
“The longer you know a patient and family, the better you can gauge the best approach,” Dr. Lewis said. “And for some, you know it’ll be complete devastation no matter what.”
When Jennifer Lycette, MD, prepares for a difficult conversation, she’ll run down all the possible ways it could go. Sometimes her brain will get stuck in a loop, cycling through the different trajectories on repeat.
“For years, I didn’t know how to cope with that,” said Dr. Lycette, medical director at Providence Oncology and Hematology Care Clinic in Seaside, Ore. “I wasn’t taught the tools to cope with that in my medical training. It took midcareer professional coaching that I sought out on my own to learn to remind myself that no matter what the person says, I have the experience and skill set to handle what comes next and to simply be present in the moment with the patient.”
The question that now sits with Dr. Lycette hours after a visit is what she could have done better. She knows from experience how important it is to choose her words carefully.
Early in her career, Dr. Lycette had a patient with stage IV cancer who wanted to know more about the death process. Because most people ask about pain, she assured him that he likely wouldn’t experience too much pain with his type of cancer.
“It will probably be like falling asleep,” said Dr. Lycette, hoping she was offering comfort. “When I saw him next, he told me he hadn’t slept.”
He was afraid that if he did, he wouldn’t wake up.
In that moment, Dr. Lycette realized the power that her words carry and the importance of trying to understand the inner lives of her patients.
Life outside the clinic
Sometimes an oncologist’s late-night ruminations have little to do with cancer itself.
Manali Patel, MD, finds herself worrying if her patients will have enough to eat and whether she will be able to help.
“I was up at 3 a.m. one morning, thinking about how we’re going to fund a project for patients from low-income households who we discovered were experiencing severe food insecurity – what grants we need, what foundations we can work with,” said Dr. Patel, a medical oncologist at Stanford Hospital and Clinics and the VA Palo Alto Health Care System in California.
The past few years of the pandemic have added a new layer of worry for Dr. Patel.
“I don’t want my patients to die from a preventable virus when they’ve already been through so much suffering,” Dr. Patel said.
This thought feeds worries about how her actions outside the clinic could unintentionally harm her patients. Should she go to a big medical conference? A family gathering? The grocery store?
“There are some places you can’t avoid, but these decisions have caused a lot of strife for me,” she said. “The health and safety of our patients – that’s in our wheelhouse – but so many of the policies are outside of our control.”
The inevitable losses and the wins
For patients with metastatic disease, eventually the treatment options will run out.
Dr. Shatsky likes to be up front with patients about that reality: “There will come a day when I will tell you there’s nothing more I can do, and you need to trust that I’m being honest with you and that’s the truth.”
For Dr. Goodman, the devastation that bad news brings patients and families is glaring. He knows there will be no more normalcy in their lives.
“I see a lot of suffering, but I know the suffering happens regardless of whether I see it or not,” Dr. Goodman said.
That’s why holding on to the victories can be so important. Dr. Goodman recalled a young patient who came to him with a 20-cm tumor and is now cured. “Had I not met that individual and done what I had done, he’d be dead, but now he’s going to live his life,” Dr. Goodman said. “But I don’t wake up at 2 a.m. thinking about that.”
Dr. Shatsky gets a lot of joy from the wins – the patients who do really well, the times when she can help a friend or colleagues – and those moments go a long way to outweigh the hurt, worry, and workload.
When dealing with so much gray, “the wins are important, knowing you can make a difference is important,” Dr. Dizon said.
And there’s a delicate balance.
“I think patients want an oncologist who cares and is genuinely invested in their outcomes but not someone who is so sad all the time,” Dr. Lewis said. “When I lose a patient, I still grieve each loss, but I can’t mourn every patient’s death like it’s a family member. Otherwise, I’d break.”
What would you do if you had terminal cancer?
Dr. Dizon recalled how a friend handled the news. She went home and made dinner, he said.
Ultimately, she lived for many years. She saw her kids get married, met her first grandchild, and had time to prepare, something not everyone gets the chance to do.
That’s why it’s important to “do what you normally do as long as you can,” Dr. Dizon said. “Live your life.”
A version of this article first appeared on Medscape.com.
It was 2 a.m. And Rebecca Shatsky, MD, could not sleep.
The breast oncologist was thinking about a patient of hers with metastatic cancer.
The patient’s disease had been asymptomatic for some time. Then without warning, her cancer suddenly exploded. Her bone marrow was failing, and her liver was not far behind.
Dr. Shatsky had a treatment plan ready to go but still, she felt uneasy.
“I had to be honest with her that I didn’t know if this plan would work,” says Dr. Shatsky, a medical oncologist at University of California, San Diego (UCSD).
That night, after visiting the patient in the hospital, Dr. Shatsky lay awake going over her next move, making sure it was the right one and hoping it would help keep the disease at bay.
“It’s so much pressure when someone is depending on you to make life or death decisions,” Dr. Shatsky said.
And in the quiet hours of night, these concerns grow louder.
Dr. Shatsky is not alone.
“There’s no off button,” says Aaron Goodman, MD, a hematologist at UCSD Health who goes by “Papa Heme” on Twitter. “I’m always thinking about my patients. Constantly.”
The public rarely gets a glimpse of these private moments. On occasion, oncologists will share a personal story, but more often, insights come from broad research on the ethical, emotional, and psychological toll of practicing medicine.
Many oncologists carry this baggage home with them because they have no other option.
“There is simply no time to process the weight of the day when I’ve got seven more patients who need my full attention before lunch,” Mark Lewis, MD, director, department of gastrointestinal oncology, Intermountain Healthcare, Salt Lake City, Utah. “That is why my processing happens outside of the office, when my brain can be quiet.”
What am I missing?
Dr. Goodman recognizes the gravity of each decision he makes. He pores over every detail of a patient’s scans, lab results, history, and symptoms.
But no matter how many times he checks and rechecks, one question nags at him: What am I missing?
For Dr. Goodman, this exhaustive level of attention is worth it.
“When errors are made, it’s someone’s life,” Dr. Goodman said. “Nothing would have prepared me for this responsibility. Until it lies on you, it’s impossible to understand how much trust patients put into us.”
That trust becomes most apparent for Dr. Goodman when facing a decision about how to treat a patient with acute myeloid leukemia who’s in remission.
Give more chemotherapy to root out the leukemia cells still lurking in the body, and the patient faces a high risk of the cancer returning. Pick stem cell transplant, and the chance of being cured goes up significantly, but the patient could also die within 100 days of the transplant.
“All together, the data show I’m helping patients with a transplant, but for the individual, I could be causing harm. Someone could be living less because of a decision I made,” Dr. Goodman said.
For patients with advanced cancer, oncologists may need to think several moves ahead. Mapping out a patient’s treatment options can feel like a game of chess. Dr. Shatsky is always trying to anticipate how the tumor will behave, what is driving it, and how lifestyle factors may influence a patient’s response in the present and the future.
“It is a mind game,” she says. “Like in chess, I try to outsmart my opponent. But with advanced cancer, there are not necessarily clear-cut guidelines or one way to manage the disease, and I have to do the best I can with drugs I have.”
That’s the art of oncology: Balancing the many knowns and unknowns of a person’s cancer alongside the toxicities of treatment and a patient’s hopes and goals.
Throughout the year, Don Dizon, MD, will see a number of patients with advanced disease. In these instances, the question he often wrestles with is if the patient can’t be cured, whether more treatment will just cause greater harm.
Dr. Dizon recently faced this dilemma with an older patient with metastatic disease who had not done well with an initial treatment regimen. After outlining the risks for more chemotherapy, he explained one option would be to forgo it and simply treat her symptoms.
“It’s an impossible choice,” says Dr. Dizon, director of women’s cancers at Lifespan Cancer Institute and director of medical oncology at Rhode Island Hospital, Providence.
Chemotherapy can provide symptom relief, but it can also be toxic – and patients may be so frail, they can die from more therapy.
“I told my patient, if in your heart, you want to try more therapy, that’s okay. But it’s also okay if you don’t,” Dr. Dizon recalled.
Her response: “You’re supposed to give me the answer.”
However, for patients approaching the end of life, there often is no right answer.
“It’s part of the discomfort you live with as a patient and oncologist, and when I leave the clinic, that’s one thing that follows me home,” Dr. Dizon said. “At the end of the day, I need to look in the mirror and know I did the best I could.”
The difficult conversation
Every Sunday, Dr. Lewis feels the weight of the week ahead. He and his wife, a pediatrician, call it the “Sunday scaries.”
It’s when Dr. Lewis begins thinking about the delicate conversations to come, rehearsing how he’s going to share the news that a person has advanced cancer or that a cancer, once in remission, has returned.
“Before the pandemic, I had 36 people come to a visit where I delivered some very heavy news and it became a Greek chorus of sobbing,” he recalls.
For every oncologist, delivering bad news is an integral part of the job. But after spending months, sometimes years, with a patient and the family, Dr. Lewis knows how to take the temperature of the room – who will likely prefer a more blunt style and who might need a gentler touch.
“The longer you know a patient and family, the better you can gauge the best approach,” Dr. Lewis said. “And for some, you know it’ll be complete devastation no matter what.”
When Jennifer Lycette, MD, prepares for a difficult conversation, she’ll run down all the possible ways it could go. Sometimes her brain will get stuck in a loop, cycling through the different trajectories on repeat.
“For years, I didn’t know how to cope with that,” said Dr. Lycette, medical director at Providence Oncology and Hematology Care Clinic in Seaside, Ore. “I wasn’t taught the tools to cope with that in my medical training. It took midcareer professional coaching that I sought out on my own to learn to remind myself that no matter what the person says, I have the experience and skill set to handle what comes next and to simply be present in the moment with the patient.”
The question that now sits with Dr. Lycette hours after a visit is what she could have done better. She knows from experience how important it is to choose her words carefully.
Early in her career, Dr. Lycette had a patient with stage IV cancer who wanted to know more about the death process. Because most people ask about pain, she assured him that he likely wouldn’t experience too much pain with his type of cancer.
“It will probably be like falling asleep,” said Dr. Lycette, hoping she was offering comfort. “When I saw him next, he told me he hadn’t slept.”
He was afraid that if he did, he wouldn’t wake up.
In that moment, Dr. Lycette realized the power that her words carry and the importance of trying to understand the inner lives of her patients.
Life outside the clinic
Sometimes an oncologist’s late-night ruminations have little to do with cancer itself.
Manali Patel, MD, finds herself worrying if her patients will have enough to eat and whether she will be able to help.
“I was up at 3 a.m. one morning, thinking about how we’re going to fund a project for patients from low-income households who we discovered were experiencing severe food insecurity – what grants we need, what foundations we can work with,” said Dr. Patel, a medical oncologist at Stanford Hospital and Clinics and the VA Palo Alto Health Care System in California.
The past few years of the pandemic have added a new layer of worry for Dr. Patel.
“I don’t want my patients to die from a preventable virus when they’ve already been through so much suffering,” Dr. Patel said.
This thought feeds worries about how her actions outside the clinic could unintentionally harm her patients. Should she go to a big medical conference? A family gathering? The grocery store?
“There are some places you can’t avoid, but these decisions have caused a lot of strife for me,” she said. “The health and safety of our patients – that’s in our wheelhouse – but so many of the policies are outside of our control.”
The inevitable losses and the wins
For patients with metastatic disease, eventually the treatment options will run out.
Dr. Shatsky likes to be up front with patients about that reality: “There will come a day when I will tell you there’s nothing more I can do, and you need to trust that I’m being honest with you and that’s the truth.”
For Dr. Goodman, the devastation that bad news brings patients and families is glaring. He knows there will be no more normalcy in their lives.
“I see a lot of suffering, but I know the suffering happens regardless of whether I see it or not,” Dr. Goodman said.
That’s why holding on to the victories can be so important. Dr. Goodman recalled a young patient who came to him with a 20-cm tumor and is now cured. “Had I not met that individual and done what I had done, he’d be dead, but now he’s going to live his life,” Dr. Goodman said. “But I don’t wake up at 2 a.m. thinking about that.”
Dr. Shatsky gets a lot of joy from the wins – the patients who do really well, the times when she can help a friend or colleagues – and those moments go a long way to outweigh the hurt, worry, and workload.
When dealing with so much gray, “the wins are important, knowing you can make a difference is important,” Dr. Dizon said.
And there’s a delicate balance.
“I think patients want an oncologist who cares and is genuinely invested in their outcomes but not someone who is so sad all the time,” Dr. Lewis said. “When I lose a patient, I still grieve each loss, but I can’t mourn every patient’s death like it’s a family member. Otherwise, I’d break.”
What would you do if you had terminal cancer?
Dr. Dizon recalled how a friend handled the news. She went home and made dinner, he said.
Ultimately, she lived for many years. She saw her kids get married, met her first grandchild, and had time to prepare, something not everyone gets the chance to do.
That’s why it’s important to “do what you normally do as long as you can,” Dr. Dizon said. “Live your life.”
A version of this article first appeared on Medscape.com.
It was 2 a.m. And Rebecca Shatsky, MD, could not sleep.
The breast oncologist was thinking about a patient of hers with metastatic cancer.
The patient’s disease had been asymptomatic for some time. Then without warning, her cancer suddenly exploded. Her bone marrow was failing, and her liver was not far behind.
Dr. Shatsky had a treatment plan ready to go but still, she felt uneasy.
“I had to be honest with her that I didn’t know if this plan would work,” says Dr. Shatsky, a medical oncologist at University of California, San Diego (UCSD).
That night, after visiting the patient in the hospital, Dr. Shatsky lay awake going over her next move, making sure it was the right one and hoping it would help keep the disease at bay.
“It’s so much pressure when someone is depending on you to make life or death decisions,” Dr. Shatsky said.
And in the quiet hours of night, these concerns grow louder.
Dr. Shatsky is not alone.
“There’s no off button,” says Aaron Goodman, MD, a hematologist at UCSD Health who goes by “Papa Heme” on Twitter. “I’m always thinking about my patients. Constantly.”
The public rarely gets a glimpse of these private moments. On occasion, oncologists will share a personal story, but more often, insights come from broad research on the ethical, emotional, and psychological toll of practicing medicine.
Many oncologists carry this baggage home with them because they have no other option.
“There is simply no time to process the weight of the day when I’ve got seven more patients who need my full attention before lunch,” Mark Lewis, MD, director, department of gastrointestinal oncology, Intermountain Healthcare, Salt Lake City, Utah. “That is why my processing happens outside of the office, when my brain can be quiet.”
What am I missing?
Dr. Goodman recognizes the gravity of each decision he makes. He pores over every detail of a patient’s scans, lab results, history, and symptoms.
But no matter how many times he checks and rechecks, one question nags at him: What am I missing?
For Dr. Goodman, this exhaustive level of attention is worth it.
“When errors are made, it’s someone’s life,” Dr. Goodman said. “Nothing would have prepared me for this responsibility. Until it lies on you, it’s impossible to understand how much trust patients put into us.”
That trust becomes most apparent for Dr. Goodman when facing a decision about how to treat a patient with acute myeloid leukemia who’s in remission.
Give more chemotherapy to root out the leukemia cells still lurking in the body, and the patient faces a high risk of the cancer returning. Pick stem cell transplant, and the chance of being cured goes up significantly, but the patient could also die within 100 days of the transplant.
“All together, the data show I’m helping patients with a transplant, but for the individual, I could be causing harm. Someone could be living less because of a decision I made,” Dr. Goodman said.
For patients with advanced cancer, oncologists may need to think several moves ahead. Mapping out a patient’s treatment options can feel like a game of chess. Dr. Shatsky is always trying to anticipate how the tumor will behave, what is driving it, and how lifestyle factors may influence a patient’s response in the present and the future.
“It is a mind game,” she says. “Like in chess, I try to outsmart my opponent. But with advanced cancer, there are not necessarily clear-cut guidelines or one way to manage the disease, and I have to do the best I can with drugs I have.”
That’s the art of oncology: Balancing the many knowns and unknowns of a person’s cancer alongside the toxicities of treatment and a patient’s hopes and goals.
Throughout the year, Don Dizon, MD, will see a number of patients with advanced disease. In these instances, the question he often wrestles with is if the patient can’t be cured, whether more treatment will just cause greater harm.
Dr. Dizon recently faced this dilemma with an older patient with metastatic disease who had not done well with an initial treatment regimen. After outlining the risks for more chemotherapy, he explained one option would be to forgo it and simply treat her symptoms.
“It’s an impossible choice,” says Dr. Dizon, director of women’s cancers at Lifespan Cancer Institute and director of medical oncology at Rhode Island Hospital, Providence.
Chemotherapy can provide symptom relief, but it can also be toxic – and patients may be so frail, they can die from more therapy.
“I told my patient, if in your heart, you want to try more therapy, that’s okay. But it’s also okay if you don’t,” Dr. Dizon recalled.
Her response: “You’re supposed to give me the answer.”
However, for patients approaching the end of life, there often is no right answer.
“It’s part of the discomfort you live with as a patient and oncologist, and when I leave the clinic, that’s one thing that follows me home,” Dr. Dizon said. “At the end of the day, I need to look in the mirror and know I did the best I could.”
The difficult conversation
Every Sunday, Dr. Lewis feels the weight of the week ahead. He and his wife, a pediatrician, call it the “Sunday scaries.”
It’s when Dr. Lewis begins thinking about the delicate conversations to come, rehearsing how he’s going to share the news that a person has advanced cancer or that a cancer, once in remission, has returned.
“Before the pandemic, I had 36 people come to a visit where I delivered some very heavy news and it became a Greek chorus of sobbing,” he recalls.
For every oncologist, delivering bad news is an integral part of the job. But after spending months, sometimes years, with a patient and the family, Dr. Lewis knows how to take the temperature of the room – who will likely prefer a more blunt style and who might need a gentler touch.
“The longer you know a patient and family, the better you can gauge the best approach,” Dr. Lewis said. “And for some, you know it’ll be complete devastation no matter what.”
When Jennifer Lycette, MD, prepares for a difficult conversation, she’ll run down all the possible ways it could go. Sometimes her brain will get stuck in a loop, cycling through the different trajectories on repeat.
“For years, I didn’t know how to cope with that,” said Dr. Lycette, medical director at Providence Oncology and Hematology Care Clinic in Seaside, Ore. “I wasn’t taught the tools to cope with that in my medical training. It took midcareer professional coaching that I sought out on my own to learn to remind myself that no matter what the person says, I have the experience and skill set to handle what comes next and to simply be present in the moment with the patient.”
The question that now sits with Dr. Lycette hours after a visit is what she could have done better. She knows from experience how important it is to choose her words carefully.
Early in her career, Dr. Lycette had a patient with stage IV cancer who wanted to know more about the death process. Because most people ask about pain, she assured him that he likely wouldn’t experience too much pain with his type of cancer.
“It will probably be like falling asleep,” said Dr. Lycette, hoping she was offering comfort. “When I saw him next, he told me he hadn’t slept.”
He was afraid that if he did, he wouldn’t wake up.
In that moment, Dr. Lycette realized the power that her words carry and the importance of trying to understand the inner lives of her patients.
Life outside the clinic
Sometimes an oncologist’s late-night ruminations have little to do with cancer itself.
Manali Patel, MD, finds herself worrying if her patients will have enough to eat and whether she will be able to help.
“I was up at 3 a.m. one morning, thinking about how we’re going to fund a project for patients from low-income households who we discovered were experiencing severe food insecurity – what grants we need, what foundations we can work with,” said Dr. Patel, a medical oncologist at Stanford Hospital and Clinics and the VA Palo Alto Health Care System in California.
The past few years of the pandemic have added a new layer of worry for Dr. Patel.
“I don’t want my patients to die from a preventable virus when they’ve already been through so much suffering,” Dr. Patel said.
This thought feeds worries about how her actions outside the clinic could unintentionally harm her patients. Should she go to a big medical conference? A family gathering? The grocery store?
“There are some places you can’t avoid, but these decisions have caused a lot of strife for me,” she said. “The health and safety of our patients – that’s in our wheelhouse – but so many of the policies are outside of our control.”
The inevitable losses and the wins
For patients with metastatic disease, eventually the treatment options will run out.
Dr. Shatsky likes to be up front with patients about that reality: “There will come a day when I will tell you there’s nothing more I can do, and you need to trust that I’m being honest with you and that’s the truth.”
For Dr. Goodman, the devastation that bad news brings patients and families is glaring. He knows there will be no more normalcy in their lives.
“I see a lot of suffering, but I know the suffering happens regardless of whether I see it or not,” Dr. Goodman said.
That’s why holding on to the victories can be so important. Dr. Goodman recalled a young patient who came to him with a 20-cm tumor and is now cured. “Had I not met that individual and done what I had done, he’d be dead, but now he’s going to live his life,” Dr. Goodman said. “But I don’t wake up at 2 a.m. thinking about that.”
Dr. Shatsky gets a lot of joy from the wins – the patients who do really well, the times when she can help a friend or colleagues – and those moments go a long way to outweigh the hurt, worry, and workload.
When dealing with so much gray, “the wins are important, knowing you can make a difference is important,” Dr. Dizon said.
And there’s a delicate balance.
“I think patients want an oncologist who cares and is genuinely invested in their outcomes but not someone who is so sad all the time,” Dr. Lewis said. “When I lose a patient, I still grieve each loss, but I can’t mourn every patient’s death like it’s a family member. Otherwise, I’d break.”
What would you do if you had terminal cancer?
Dr. Dizon recalled how a friend handled the news. She went home and made dinner, he said.
Ultimately, she lived for many years. She saw her kids get married, met her first grandchild, and had time to prepare, something not everyone gets the chance to do.
That’s why it’s important to “do what you normally do as long as you can,” Dr. Dizon said. “Live your life.”
A version of this article first appeared on Medscape.com.
RADIANCE II: Positive signal for ultrasound renal denervation
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Top-line results released on July 26 from the RADIANCE II trial show the Paradise ultrasound renal denervation system significantly reduces daytime ambulatory systolic blood pressure, compared with a sham procedure at 2 months in patients with mild to moderate uncontrolled hypertension.
The trial was conducted in 224 patients who were previously treated with up to two medications and were randomized while off medication at more than 60 centers in 8 countries. No further details or results were provided.
The pivotal RADIANCE II trial, required for FDA approval, is the third and largest randomized, sham-controlled study following positive results reported by RADIANCE-HTN SOLO and RADIANCE-HTN TRIO, ReCor Medical and its subsidiary Otsuka Medical Devices noted in the announcement.
The field of renal denervation fell out of favor after the largest trial in 535 patients, SYMPLICITY HTN-3, failed to show a significant reduction in systolic blood pressure at 6 months, compared with sham control in resistant hypertension.
A version of this article first appeared on Medscape.com.
Coming to a pill near you: The exercise molecule
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.

In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.

A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.

Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.
In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.
A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.
Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.
In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.
A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.
Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
A hypogastric nerve-focused approach to nerve-sparing endometriosis surgery
Radical resection of deep infiltrating endometriosis (DIE) or pelvic malignancies can lead to inadvertent damage to the pelvic autonomic nerve bundles, causing urinary dysfunction in up to 41% of cases, as well as anorectal and sexual dysfunction.1 Each of these sequelae can significantly affect the patient’s quality of life.
Nerve-sparing techniques have therefore been a trending topic in gynecologic surgery in the 21st century, starting with papers by Marc Possover, MD, of Switzerland, on the laparoscopic neuronavigation (LANN) technique. In an important 2005 publication, he described how the LANN technique can significantly reduce postoperative functional morbidity in laparoscopic radical pelvic surgery.2

The LANN method utilizes intraoperative neurostimulation to identify and dissect the intrapelvic nerve bundles away from surrounding tissue prior to dissection of the DIE or pelvic malignancies. The nerves are exposed and preserved under direct visualization in a fashion similar to that used to expose and preserve the ureters. Pelvic dissection using the LANN technique is extensive and occurs down to the level of the sacral nerve roots.
Dr. Possover’s 2005 paper and others like it spurred increased awareness of the intrapelvic part of the autonomic nervous system – in particular, the hypogastric nerves, the pelvic splanchnic nerves, and the inferior hypogastric plexus. Across additional published studies, nerve-sparing techniques were shown to be effective in preserving neurologic pelvic functions, with significantly less urinary retention and rectal/sexual dysfunction than seen with traditional laparoscopy techniques.
For example, in a single-center prospective clinical trial reported in 2012, 56 of 65 (86.2%) patients treated with a classical laparoscopic technique for excision of DIE reported neurologic pelvic dysfunctions, compared with 1 of 61 (1.6%) patients treated with a nerve-sparing approach.3
While research has confirmed the importance of nerve-sparing techniques, it also shone light on the reality that the LANN technique is extremely technically challenging and requires a high level of surgical expertise and advanced training. In my teaching of the technique, I also saw that few gynecologic surgeons were able to incorporate the advanced nerve-sparing technique into their practices.
A group consisting of myself and collaborators at the University of Bologna, Italy, and the University of Cambridge, England, recently developed an alternative to the LANN approach that uses the hypogastric nerves as landmarks. The technique requires less dissection and should be technically achievable when the pelvic neuroanatomy and anatomy of the presacral fascia are well understood. The hypogastric nerve is identified and used as a landmark to preserve the deeper autonomic nerve bundles in the pelvis without exposure and without more extensive dissection to the level of the sacral nerve roots.4,5
This hypogastric nerve-based technique will cover the vast majority of radical surgeries for DIE. When more advanced nerve sparing and more extensive dissection is needed for the very deepest levels of disease infiltration, patients can be referred to surgeons with advanced training, comfort, and experience with the LANN technique.
The pelvic neuroanatomy
As described in our video articles published in 2015 in Fertility and Sterility6 and 2019 in the Journal of Minimally Invasive Gynecology,5 the left and right hypogastric nerves are the main sympathetic nerves of the autonomic nervous system in the pelvis. They originate from the superior hypogastric plexus and, at the level of the middle rectal vessels, they join the pelvic sacral splanchnic nerves to form the inferior hypogastric plexus. They are easily identifiable at their origin and are the most superficial and readily identifiable component of the inferior hypogastric plexus.
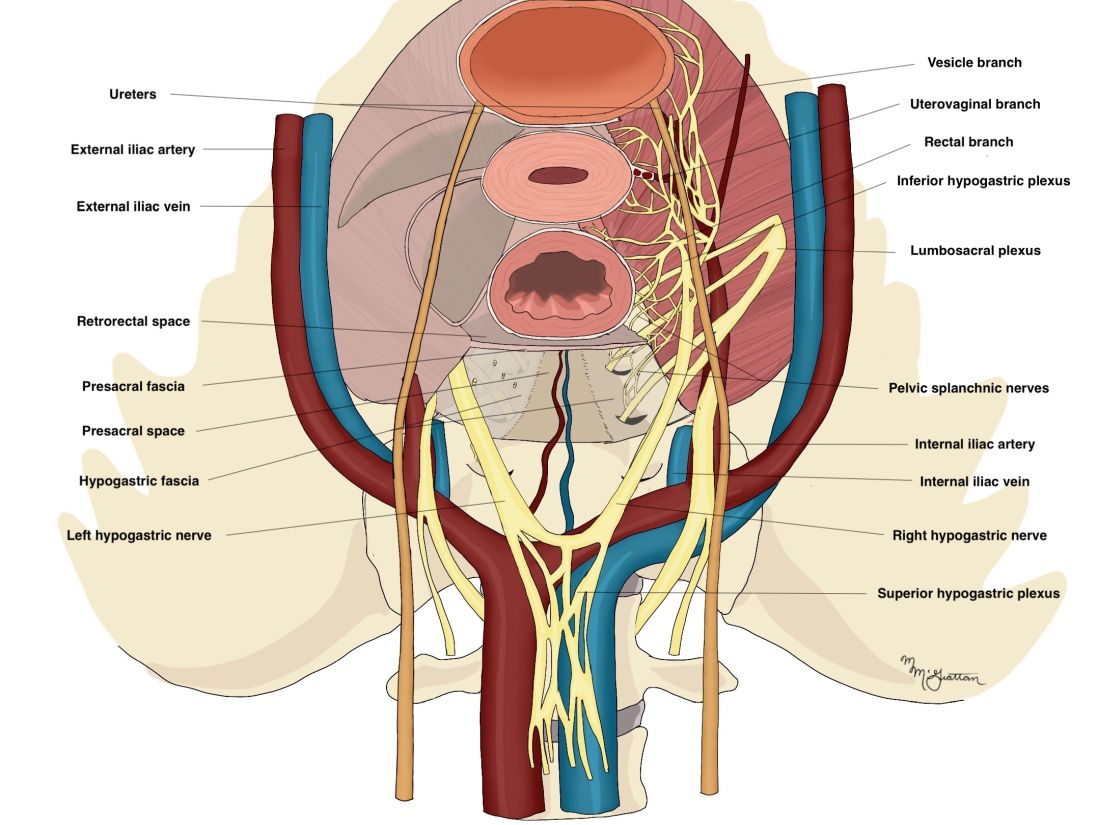
The sympathetic input from the hypogastric nerves causes the internal urethral and anal sphincters to contract, as well as detrusor relaxation and a reduction of peristalsis of the descending colon, sigmoid, and rectum; thus, hypogastric nerve input promotes continence.
The hypogastric nerves also carry afferent signals for pelvic visceral proprioception. Lesion to the hypogastric nerves will usually be subclinical and will put the patient at risk for unnoticeable bladder distension, which usually becomes symptomatic about 7 years after the procedure.7
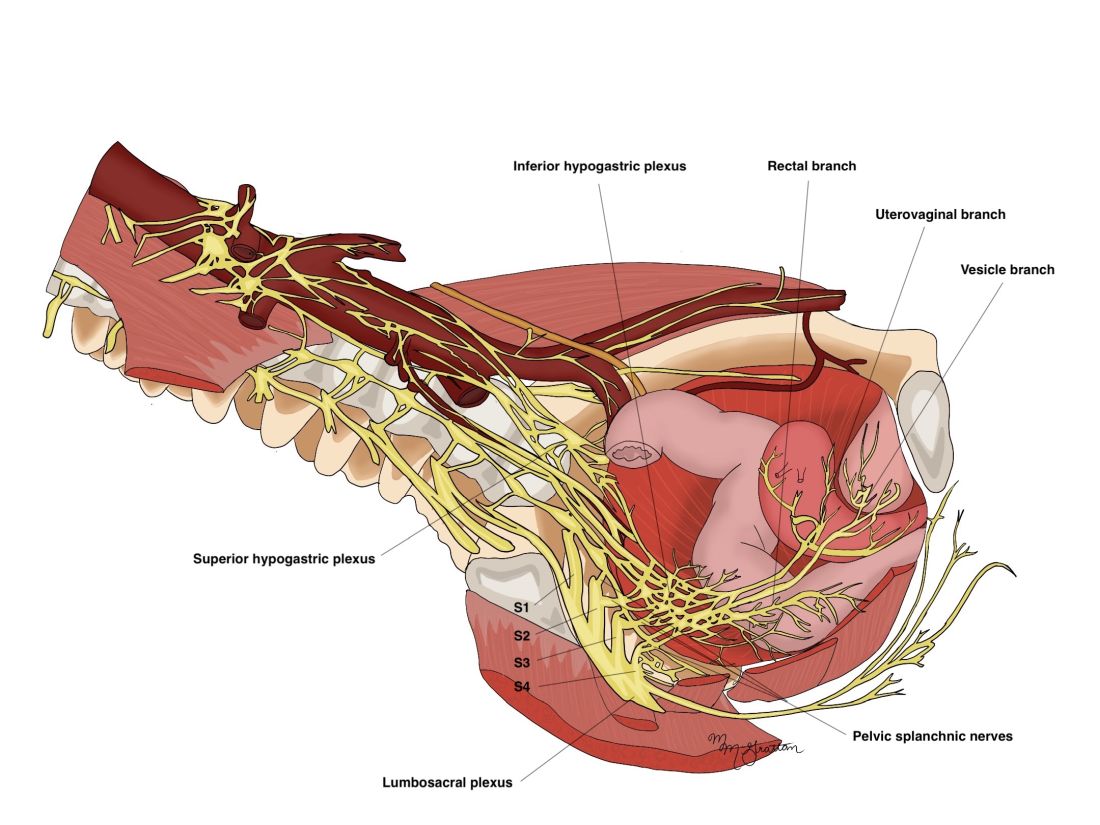
The thin pelvic splanchnic nerves – which merge with the hypogastric nerves into the pararectal fossae to form the inferior hypogastric plexus – arise from nerve roots S2 and S4 and carry all parasympathetic signals to the bladder, rectum, and the sigmoid and left colons. Lesions to these bundles are the main cause of neurogenic urinary retention.
The inferior hypogastric plexi split into the vesical, uterine, and rectal branches, which carry the sympathetic, parasympathetic, and sensory fibers from both the splanchnic and hypogastric nerves. Damage to the inferior hypogastric plexi and/or its branches may induce severe dysfunction to the target organs of the injured fibers.
A focus on the hypogastric nerve
Our approach was developed after we studied the anatomic reliability of the hypogastric nerves through a prospective observational study consisting of measurements during five cadaveric dissections and 10 in-vivo laparoscopic surgeries for rectosigmoid endometriosis.4 We took an interfascial approach to dissection.
Our goal was to clarify the distances between the hypogastric nerves and the ureters, the midsagittal plane, the midcervical plane, and the uterosacral ligaments in each hemipelvis, and in doing so, enable identification of the hypogastric nerves and establish recognizable limits for dissection.
We found quite a bit of variance in the anatomic position and appearance of the hypogastric nerves, but the variances were not very broad. Most notably, the right hypogastric nerve was significantly farther toward the ureter (mean, 14.5 mm; range, 10-25 mm) than the left one (mean, 8.6 mm; range, 7-12 mm).
The ureters were a good landmark for identification of the hypogastric nerves because the nerves were consistently found medially and posteriorly to the ureter at a mean distance of 11.6 mm. Overall, we demonstrated reproducibility in the identification and dissection of the hypogastric nerves using recognizable interfascial planes and anatomic landmarks.4
With good anatomic understanding, a stepwise approach can be taken to identify and preserve the hypogastric nerve and the deeper inferior hypogastric plexus without the need for more extensive dissection.
As shown in our 2019 video, the right hypogastric nerves can be identified transperitoneally in most cases.5 For confirmation, a gentle anterior pulling on the hypogastric nerve causes a caudal movement of the peritoneum overlying the superior hypogastric plexus. (Intermittent pulling on the nerve can also be helpful in localizing the left hypogastric nerve.)
To dissect a hypogastric nerve, the retroperitoneum is opened at the level of the pelvic brim, just inferomedially to the external iliac vessels, and the incision is extended anteriorly, with gentle dissection of the underlying tissue until the ureter is identified.
Once the ureter is identified and lateralized, dissection along the peritoneum is carried deeper and medially into the pelvis until the hypogastric nerve is identified. Lateral to this area are the internal iliac artery, the branching uterine artery, and the obliterated umbilical ligament. In the left hemipelvis, the hypogastric nerve can reliably be found at a mean distance of 8.6 mm from the ureter, while the right one will be found on average 14.5 mm away.
The hypogastric nerves form the posteromedial limit for a safe and simple nerve-sparing dissection. Any dissection posteriorly and laterally to these landmarks should start with the identification of sacral nerve roots and hypogastric nerves.
Dr. Lemos reported that he has no relevant disclosures.
Dr. Lemos is associate professor in the department of obstetrics and gynecology at the University of Toronto.
References
1. Imboden S et al. J Minim Invasive Gynecol. 2021 Aug;28(8):1544-51. doi: 10.1016/j.jmig.2021.01.009.
2. Possover M et al. J Am Coll Surg. 2005;201(6):913-7. doi: 10.1016/j.jamcollsurg.2005.07.006.
3. Ceccaroni M et al. Surg Endosc. 2012;26(7):2029-45. doi: 10.1007/s00464-012-2153-3.
4. Seracchioli R et al. J Minim Invasive Gynecol. 2019;26(7):1340-5. doi: 10.1016/j.jmig.2019.01.010.
5. Zakhari A et al. J Minim Invasive Gynecol. 2020;27(4):813-4. doi: 10.1016/j.jmig.2019.08.001
6. Lemos N et al. Fertil Steril. 2015 Nov;104(5):e11-2. doi: 10.1016/j.fertnstert.2015.07.1138.
7. Possover M. Fertil Steril. 2014 Mar;101(3):754-8. doi: 10.1016/j.fertnstert.2013.12.019.
Radical resection of deep infiltrating endometriosis (DIE) or pelvic malignancies can lead to inadvertent damage to the pelvic autonomic nerve bundles, causing urinary dysfunction in up to 41% of cases, as well as anorectal and sexual dysfunction.1 Each of these sequelae can significantly affect the patient’s quality of life.
Nerve-sparing techniques have therefore been a trending topic in gynecologic surgery in the 21st century, starting with papers by Marc Possover, MD, of Switzerland, on the laparoscopic neuronavigation (LANN) technique. In an important 2005 publication, he described how the LANN technique can significantly reduce postoperative functional morbidity in laparoscopic radical pelvic surgery.2
The LANN method utilizes intraoperative neurostimulation to identify and dissect the intrapelvic nerve bundles away from surrounding tissue prior to dissection of the DIE or pelvic malignancies. The nerves are exposed and preserved under direct visualization in a fashion similar to that used to expose and preserve the ureters. Pelvic dissection using the LANN technique is extensive and occurs down to the level of the sacral nerve roots.
Dr. Possover’s 2005 paper and others like it spurred increased awareness of the intrapelvic part of the autonomic nervous system – in particular, the hypogastric nerves, the pelvic splanchnic nerves, and the inferior hypogastric plexus. Across additional published studies, nerve-sparing techniques were shown to be effective in preserving neurologic pelvic functions, with significantly less urinary retention and rectal/sexual dysfunction than seen with traditional laparoscopy techniques.
For example, in a single-center prospective clinical trial reported in 2012, 56 of 65 (86.2%) patients treated with a classical laparoscopic technique for excision of DIE reported neurologic pelvic dysfunctions, compared with 1 of 61 (1.6%) patients treated with a nerve-sparing approach.3
While research has confirmed the importance of nerve-sparing techniques, it also shone light on the reality that the LANN technique is extremely technically challenging and requires a high level of surgical expertise and advanced training. In my teaching of the technique, I also saw that few gynecologic surgeons were able to incorporate the advanced nerve-sparing technique into their practices.
A group consisting of myself and collaborators at the University of Bologna, Italy, and the University of Cambridge, England, recently developed an alternative to the LANN approach that uses the hypogastric nerves as landmarks. The technique requires less dissection and should be technically achievable when the pelvic neuroanatomy and anatomy of the presacral fascia are well understood. The hypogastric nerve is identified and used as a landmark to preserve the deeper autonomic nerve bundles in the pelvis without exposure and without more extensive dissection to the level of the sacral nerve roots.4,5
This hypogastric nerve-based technique will cover the vast majority of radical surgeries for DIE. When more advanced nerve sparing and more extensive dissection is needed for the very deepest levels of disease infiltration, patients can be referred to surgeons with advanced training, comfort, and experience with the LANN technique.
The pelvic neuroanatomy
As described in our video articles published in 2015 in Fertility and Sterility6 and 2019 in the Journal of Minimally Invasive Gynecology,5 the left and right hypogastric nerves are the main sympathetic nerves of the autonomic nervous system in the pelvis. They originate from the superior hypogastric plexus and, at the level of the middle rectal vessels, they join the pelvic sacral splanchnic nerves to form the inferior hypogastric plexus. They are easily identifiable at their origin and are the most superficial and readily identifiable component of the inferior hypogastric plexus.
The sympathetic input from the hypogastric nerves causes the internal urethral and anal sphincters to contract, as well as detrusor relaxation and a reduction of peristalsis of the descending colon, sigmoid, and rectum; thus, hypogastric nerve input promotes continence.
The hypogastric nerves also carry afferent signals for pelvic visceral proprioception. Lesion to the hypogastric nerves will usually be subclinical and will put the patient at risk for unnoticeable bladder distension, which usually becomes symptomatic about 7 years after the procedure.7
The thin pelvic splanchnic nerves – which merge with the hypogastric nerves into the pararectal fossae to form the inferior hypogastric plexus – arise from nerve roots S2 and S4 and carry all parasympathetic signals to the bladder, rectum, and the sigmoid and left colons. Lesions to these bundles are the main cause of neurogenic urinary retention.
The inferior hypogastric plexi split into the vesical, uterine, and rectal branches, which carry the sympathetic, parasympathetic, and sensory fibers from both the splanchnic and hypogastric nerves. Damage to the inferior hypogastric plexi and/or its branches may induce severe dysfunction to the target organs of the injured fibers.
A focus on the hypogastric nerve
Our approach was developed after we studied the anatomic reliability of the hypogastric nerves through a prospective observational study consisting of measurements during five cadaveric dissections and 10 in-vivo laparoscopic surgeries for rectosigmoid endometriosis.4 We took an interfascial approach to dissection.
Our goal was to clarify the distances between the hypogastric nerves and the ureters, the midsagittal plane, the midcervical plane, and the uterosacral ligaments in each hemipelvis, and in doing so, enable identification of the hypogastric nerves and establish recognizable limits for dissection.
We found quite a bit of variance in the anatomic position and appearance of the hypogastric nerves, but the variances were not very broad. Most notably, the right hypogastric nerve was significantly farther toward the ureter (mean, 14.5 mm; range, 10-25 mm) than the left one (mean, 8.6 mm; range, 7-12 mm).
The ureters were a good landmark for identification of the hypogastric nerves because the nerves were consistently found medially and posteriorly to the ureter at a mean distance of 11.6 mm. Overall, we demonstrated reproducibility in the identification and dissection of the hypogastric nerves using recognizable interfascial planes and anatomic landmarks.4
With good anatomic understanding, a stepwise approach can be taken to identify and preserve the hypogastric nerve and the deeper inferior hypogastric plexus without the need for more extensive dissection.
As shown in our 2019 video, the right hypogastric nerves can be identified transperitoneally in most cases.5 For confirmation, a gentle anterior pulling on the hypogastric nerve causes a caudal movement of the peritoneum overlying the superior hypogastric plexus. (Intermittent pulling on the nerve can also be helpful in localizing the left hypogastric nerve.)
To dissect a hypogastric nerve, the retroperitoneum is opened at the level of the pelvic brim, just inferomedially to the external iliac vessels, and the incision is extended anteriorly, with gentle dissection of the underlying tissue until the ureter is identified.
Once the ureter is identified and lateralized, dissection along the peritoneum is carried deeper and medially into the pelvis until the hypogastric nerve is identified. Lateral to this area are the internal iliac artery, the branching uterine artery, and the obliterated umbilical ligament. In the left hemipelvis, the hypogastric nerve can reliably be found at a mean distance of 8.6 mm from the ureter, while the right one will be found on average 14.5 mm away.
The hypogastric nerves form the posteromedial limit for a safe and simple nerve-sparing dissection. Any dissection posteriorly and laterally to these landmarks should start with the identification of sacral nerve roots and hypogastric nerves.
Dr. Lemos reported that he has no relevant disclosures.
Dr. Lemos is associate professor in the department of obstetrics and gynecology at the University of Toronto.
References
1. Imboden S et al. J Minim Invasive Gynecol. 2021 Aug;28(8):1544-51. doi: 10.1016/j.jmig.2021.01.009.
2. Possover M et al. J Am Coll Surg. 2005;201(6):913-7. doi: 10.1016/j.jamcollsurg.2005.07.006.
3. Ceccaroni M et al. Surg Endosc. 2012;26(7):2029-45. doi: 10.1007/s00464-012-2153-3.
4. Seracchioli R et al. J Minim Invasive Gynecol. 2019;26(7):1340-5. doi: 10.1016/j.jmig.2019.01.010.
5. Zakhari A et al. J Minim Invasive Gynecol. 2020;27(4):813-4. doi: 10.1016/j.jmig.2019.08.001
6. Lemos N et al. Fertil Steril. 2015 Nov;104(5):e11-2. doi: 10.1016/j.fertnstert.2015.07.1138.
7. Possover M. Fertil Steril. 2014 Mar;101(3):754-8. doi: 10.1016/j.fertnstert.2013.12.019.
Radical resection of deep infiltrating endometriosis (DIE) or pelvic malignancies can lead to inadvertent damage to the pelvic autonomic nerve bundles, causing urinary dysfunction in up to 41% of cases, as well as anorectal and sexual dysfunction.1 Each of these sequelae can significantly affect the patient’s quality of life.
Nerve-sparing techniques have therefore been a trending topic in gynecologic surgery in the 21st century, starting with papers by Marc Possover, MD, of Switzerland, on the laparoscopic neuronavigation (LANN) technique. In an important 2005 publication, he described how the LANN technique can significantly reduce postoperative functional morbidity in laparoscopic radical pelvic surgery.2
The LANN method utilizes intraoperative neurostimulation to identify and dissect the intrapelvic nerve bundles away from surrounding tissue prior to dissection of the DIE or pelvic malignancies. The nerves are exposed and preserved under direct visualization in a fashion similar to that used to expose and preserve the ureters. Pelvic dissection using the LANN technique is extensive and occurs down to the level of the sacral nerve roots.
Dr. Possover’s 2005 paper and others like it spurred increased awareness of the intrapelvic part of the autonomic nervous system – in particular, the hypogastric nerves, the pelvic splanchnic nerves, and the inferior hypogastric plexus. Across additional published studies, nerve-sparing techniques were shown to be effective in preserving neurologic pelvic functions, with significantly less urinary retention and rectal/sexual dysfunction than seen with traditional laparoscopy techniques.
For example, in a single-center prospective clinical trial reported in 2012, 56 of 65 (86.2%) patients treated with a classical laparoscopic technique for excision of DIE reported neurologic pelvic dysfunctions, compared with 1 of 61 (1.6%) patients treated with a nerve-sparing approach.3
While research has confirmed the importance of nerve-sparing techniques, it also shone light on the reality that the LANN technique is extremely technically challenging and requires a high level of surgical expertise and advanced training. In my teaching of the technique, I also saw that few gynecologic surgeons were able to incorporate the advanced nerve-sparing technique into their practices.
A group consisting of myself and collaborators at the University of Bologna, Italy, and the University of Cambridge, England, recently developed an alternative to the LANN approach that uses the hypogastric nerves as landmarks. The technique requires less dissection and should be technically achievable when the pelvic neuroanatomy and anatomy of the presacral fascia are well understood. The hypogastric nerve is identified and used as a landmark to preserve the deeper autonomic nerve bundles in the pelvis without exposure and without more extensive dissection to the level of the sacral nerve roots.4,5
This hypogastric nerve-based technique will cover the vast majority of radical surgeries for DIE. When more advanced nerve sparing and more extensive dissection is needed for the very deepest levels of disease infiltration, patients can be referred to surgeons with advanced training, comfort, and experience with the LANN technique.
The pelvic neuroanatomy
As described in our video articles published in 2015 in Fertility and Sterility6 and 2019 in the Journal of Minimally Invasive Gynecology,5 the left and right hypogastric nerves are the main sympathetic nerves of the autonomic nervous system in the pelvis. They originate from the superior hypogastric plexus and, at the level of the middle rectal vessels, they join the pelvic sacral splanchnic nerves to form the inferior hypogastric plexus. They are easily identifiable at their origin and are the most superficial and readily identifiable component of the inferior hypogastric plexus.
The sympathetic input from the hypogastric nerves causes the internal urethral and anal sphincters to contract, as well as detrusor relaxation and a reduction of peristalsis of the descending colon, sigmoid, and rectum; thus, hypogastric nerve input promotes continence.
The hypogastric nerves also carry afferent signals for pelvic visceral proprioception. Lesion to the hypogastric nerves will usually be subclinical and will put the patient at risk for unnoticeable bladder distension, which usually becomes symptomatic about 7 years after the procedure.7
The thin pelvic splanchnic nerves – which merge with the hypogastric nerves into the pararectal fossae to form the inferior hypogastric plexus – arise from nerve roots S2 and S4 and carry all parasympathetic signals to the bladder, rectum, and the sigmoid and left colons. Lesions to these bundles are the main cause of neurogenic urinary retention.
The inferior hypogastric plexi split into the vesical, uterine, and rectal branches, which carry the sympathetic, parasympathetic, and sensory fibers from both the splanchnic and hypogastric nerves. Damage to the inferior hypogastric plexi and/or its branches may induce severe dysfunction to the target organs of the injured fibers.
A focus on the hypogastric nerve
Our approach was developed after we studied the anatomic reliability of the hypogastric nerves through a prospective observational study consisting of measurements during five cadaveric dissections and 10 in-vivo laparoscopic surgeries for rectosigmoid endometriosis.4 We took an interfascial approach to dissection.
Our goal was to clarify the distances between the hypogastric nerves and the ureters, the midsagittal plane, the midcervical plane, and the uterosacral ligaments in each hemipelvis, and in doing so, enable identification of the hypogastric nerves and establish recognizable limits for dissection.
We found quite a bit of variance in the anatomic position and appearance of the hypogastric nerves, but the variances were not very broad. Most notably, the right hypogastric nerve was significantly farther toward the ureter (mean, 14.5 mm; range, 10-25 mm) than the left one (mean, 8.6 mm; range, 7-12 mm).
The ureters were a good landmark for identification of the hypogastric nerves because the nerves were consistently found medially and posteriorly to the ureter at a mean distance of 11.6 mm. Overall, we demonstrated reproducibility in the identification and dissection of the hypogastric nerves using recognizable interfascial planes and anatomic landmarks.4
With good anatomic understanding, a stepwise approach can be taken to identify and preserve the hypogastric nerve and the deeper inferior hypogastric plexus without the need for more extensive dissection.
As shown in our 2019 video, the right hypogastric nerves can be identified transperitoneally in most cases.5 For confirmation, a gentle anterior pulling on the hypogastric nerve causes a caudal movement of the peritoneum overlying the superior hypogastric plexus. (Intermittent pulling on the nerve can also be helpful in localizing the left hypogastric nerve.)
To dissect a hypogastric nerve, the retroperitoneum is opened at the level of the pelvic brim, just inferomedially to the external iliac vessels, and the incision is extended anteriorly, with gentle dissection of the underlying tissue until the ureter is identified.
Once the ureter is identified and lateralized, dissection along the peritoneum is carried deeper and medially into the pelvis until the hypogastric nerve is identified. Lateral to this area are the internal iliac artery, the branching uterine artery, and the obliterated umbilical ligament. In the left hemipelvis, the hypogastric nerve can reliably be found at a mean distance of 8.6 mm from the ureter, while the right one will be found on average 14.5 mm away.
The hypogastric nerves form the posteromedial limit for a safe and simple nerve-sparing dissection. Any dissection posteriorly and laterally to these landmarks should start with the identification of sacral nerve roots and hypogastric nerves.
Dr. Lemos reported that he has no relevant disclosures.
Dr. Lemos is associate professor in the department of obstetrics and gynecology at the University of Toronto.
References
1. Imboden S et al. J Minim Invasive Gynecol. 2021 Aug;28(8):1544-51. doi: 10.1016/j.jmig.2021.01.009.
2. Possover M et al. J Am Coll Surg. 2005;201(6):913-7. doi: 10.1016/j.jamcollsurg.2005.07.006.
3. Ceccaroni M et al. Surg Endosc. 2012;26(7):2029-45. doi: 10.1007/s00464-012-2153-3.
4. Seracchioli R et al. J Minim Invasive Gynecol. 2019;26(7):1340-5. doi: 10.1016/j.jmig.2019.01.010.
5. Zakhari A et al. J Minim Invasive Gynecol. 2020;27(4):813-4. doi: 10.1016/j.jmig.2019.08.001
6. Lemos N et al. Fertil Steril. 2015 Nov;104(5):e11-2. doi: 10.1016/j.fertnstert.2015.07.1138.
7. Possover M. Fertil Steril. 2014 Mar;101(3):754-8. doi: 10.1016/j.fertnstert.2013.12.019.