User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
The anxious patient needs psychosomatic primary care
A balance between fear and relaxation is normal. However, mental dispositions and the continuous influence of environmental stimuli can disrupt this balance. A failure in therapy can often conceal unvoiced fears.

This article is based on the lecture “State of the Art: Treating Anxiety Disorders” by Christian Albus, MD, director of the Clinic and Polyclinic for Psychosomatics and Psychotherapy, University Hospital Cologne (Germany), at the 128th conference of the German Society of Internal Medicine.
Hidden fears
Poor compliance often has a simple cause: The patients are scared. They are afraid of bad news, for example through further investigations. Taking medication regularly reminds them, over and over, of their threatening problem. Those affected rarely speak about these delicate issues of their own volition, said Dr. Albus. But latent fears are no trivial issue.
Cardiac prognosis
A third of those affected by acute coronary syndrome (ACS) subsequently suffer from long-term anxiety disorders. The fear that they will relive their experiences overshadows their zest for life. As a result, signs of clinical depression can be detected in 50% of patients with ACS. Posttraumatic stress disorders have even been observed in up to 30% of patients. Fear also exacerbates the prognosis. Patients suffering from heart attack and subsequent cardiac failure demonstrate a significant correlation between stress and increased mortality.
Self-diagnosis
The fact that we are living in an age of fear is influenced by technological advances. “Dr. Google” is the first source to be consulted for almost half of adults who need their symptoms explained. Well-informed patients improve patient-doctor communication. But unfortunately, many people are becoming addicted to searching for diagnoses and symptoms online. Primarily harmless symptoms are associated with catastrophic diagnoses. Regrettably, Google’s search algorithm also increases this tendency. If someone starts to look for serious diseases, Google will show you these sorts of potential catastrophes on an ever more frequent basis. Google ultimately orients itself around the interests of its users. The result is a spiral of fear that can cause illness.
Cyberchondria
Compulsive searching on the internet for more and more new dangers to health has now developed into its own medical condition, termed cyberchondria. The therapy is strict internet abstinence. The gross exaggeration of health problems by the media also contributes to this. This is because it’s not just sex that sells, but also fear. The current example is long COVID. In the much-cited Gutenberg study, over half of coronavirus patients subsequently exhibited the typical symptoms: fatigue, concentration disorders, and breathing issues. Most media ignore the crucial detail that the same problems were also registered in 40% of the coronavirus-free control group. Dr. Albus pointed out that it’s no wonder that so much fear is being spread by long COVID.
The first step
Responsible medicine must counteract these developments. The first step is actively to address the fear problem. Patients who seem tense benefit enormously from the simple question: “How are you otherwise?” This question may open doors. Suddenly, patients begin to talk about their anxieties and fears. Of course, this approach to patients is time consuming. Still, this time must be taken, said Dr. Albus. In a survey of oncology patients, the majority reported that none of their physicians are ever interested in their emotional state. This is a sign of inadequate care, since psychosomatic primary care should be a standard nowadays in every specialty.
This article was translated from Coliquio.
A balance between fear and relaxation is normal. However, mental dispositions and the continuous influence of environmental stimuli can disrupt this balance. A failure in therapy can often conceal unvoiced fears.
This article is based on the lecture “State of the Art: Treating Anxiety Disorders” by Christian Albus, MD, director of the Clinic and Polyclinic for Psychosomatics and Psychotherapy, University Hospital Cologne (Germany), at the 128th conference of the German Society of Internal Medicine.
Hidden fears
Poor compliance often has a simple cause: The patients are scared. They are afraid of bad news, for example through further investigations. Taking medication regularly reminds them, over and over, of their threatening problem. Those affected rarely speak about these delicate issues of their own volition, said Dr. Albus. But latent fears are no trivial issue.
Cardiac prognosis
A third of those affected by acute coronary syndrome (ACS) subsequently suffer from long-term anxiety disorders. The fear that they will relive their experiences overshadows their zest for life. As a result, signs of clinical depression can be detected in 50% of patients with ACS. Posttraumatic stress disorders have even been observed in up to 30% of patients. Fear also exacerbates the prognosis. Patients suffering from heart attack and subsequent cardiac failure demonstrate a significant correlation between stress and increased mortality.
Self-diagnosis
The fact that we are living in an age of fear is influenced by technological advances. “Dr. Google” is the first source to be consulted for almost half of adults who need their symptoms explained. Well-informed patients improve patient-doctor communication. But unfortunately, many people are becoming addicted to searching for diagnoses and symptoms online. Primarily harmless symptoms are associated with catastrophic diagnoses. Regrettably, Google’s search algorithm also increases this tendency. If someone starts to look for serious diseases, Google will show you these sorts of potential catastrophes on an ever more frequent basis. Google ultimately orients itself around the interests of its users. The result is a spiral of fear that can cause illness.
Cyberchondria
Compulsive searching on the internet for more and more new dangers to health has now developed into its own medical condition, termed cyberchondria. The therapy is strict internet abstinence. The gross exaggeration of health problems by the media also contributes to this. This is because it’s not just sex that sells, but also fear. The current example is long COVID. In the much-cited Gutenberg study, over half of coronavirus patients subsequently exhibited the typical symptoms: fatigue, concentration disorders, and breathing issues. Most media ignore the crucial detail that the same problems were also registered in 40% of the coronavirus-free control group. Dr. Albus pointed out that it’s no wonder that so much fear is being spread by long COVID.
The first step
Responsible medicine must counteract these developments. The first step is actively to address the fear problem. Patients who seem tense benefit enormously from the simple question: “How are you otherwise?” This question may open doors. Suddenly, patients begin to talk about their anxieties and fears. Of course, this approach to patients is time consuming. Still, this time must be taken, said Dr. Albus. In a survey of oncology patients, the majority reported that none of their physicians are ever interested in their emotional state. This is a sign of inadequate care, since psychosomatic primary care should be a standard nowadays in every specialty.
This article was translated from Coliquio.
A balance between fear and relaxation is normal. However, mental dispositions and the continuous influence of environmental stimuli can disrupt this balance. A failure in therapy can often conceal unvoiced fears.
This article is based on the lecture “State of the Art: Treating Anxiety Disorders” by Christian Albus, MD, director of the Clinic and Polyclinic for Psychosomatics and Psychotherapy, University Hospital Cologne (Germany), at the 128th conference of the German Society of Internal Medicine.
Hidden fears
Poor compliance often has a simple cause: The patients are scared. They are afraid of bad news, for example through further investigations. Taking medication regularly reminds them, over and over, of their threatening problem. Those affected rarely speak about these delicate issues of their own volition, said Dr. Albus. But latent fears are no trivial issue.
Cardiac prognosis
A third of those affected by acute coronary syndrome (ACS) subsequently suffer from long-term anxiety disorders. The fear that they will relive their experiences overshadows their zest for life. As a result, signs of clinical depression can be detected in 50% of patients with ACS. Posttraumatic stress disorders have even been observed in up to 30% of patients. Fear also exacerbates the prognosis. Patients suffering from heart attack and subsequent cardiac failure demonstrate a significant correlation between stress and increased mortality.
Self-diagnosis
The fact that we are living in an age of fear is influenced by technological advances. “Dr. Google” is the first source to be consulted for almost half of adults who need their symptoms explained. Well-informed patients improve patient-doctor communication. But unfortunately, many people are becoming addicted to searching for diagnoses and symptoms online. Primarily harmless symptoms are associated with catastrophic diagnoses. Regrettably, Google’s search algorithm also increases this tendency. If someone starts to look for serious diseases, Google will show you these sorts of potential catastrophes on an ever more frequent basis. Google ultimately orients itself around the interests of its users. The result is a spiral of fear that can cause illness.
Cyberchondria
Compulsive searching on the internet for more and more new dangers to health has now developed into its own medical condition, termed cyberchondria. The therapy is strict internet abstinence. The gross exaggeration of health problems by the media also contributes to this. This is because it’s not just sex that sells, but also fear. The current example is long COVID. In the much-cited Gutenberg study, over half of coronavirus patients subsequently exhibited the typical symptoms: fatigue, concentration disorders, and breathing issues. Most media ignore the crucial detail that the same problems were also registered in 40% of the coronavirus-free control group. Dr. Albus pointed out that it’s no wonder that so much fear is being spread by long COVID.
The first step
Responsible medicine must counteract these developments. The first step is actively to address the fear problem. Patients who seem tense benefit enormously from the simple question: “How are you otherwise?” This question may open doors. Suddenly, patients begin to talk about their anxieties and fears. Of course, this approach to patients is time consuming. Still, this time must be taken, said Dr. Albus. In a survey of oncology patients, the majority reported that none of their physicians are ever interested in their emotional state. This is a sign of inadequate care, since psychosomatic primary care should be a standard nowadays in every specialty.
This article was translated from Coliquio.
Distal radial snuffbox technique comes up short in DISCO RADIAL
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Distal radial access is not superior to conventional radial access with regard to radial artery occlusion (RAO) but is a valid alternative for use in percutaneous procedures, according to results of the DISCO RADIAL trial.
The primary endpoint of forearm RAO at discharge was not met, occurring in 0.31% of patients whose radial artery was accessed distally (DRA) at the anatomical snuffbox and in 0.91% of patients with conventional transradial access (TRA) in the intention-to-treat analysis (P = .29).
The DRA group was also twice as likely to crossover to another access point (7.5% vs. 3.7%; P = .002) and to experience radial artery spasm (5.4% vs. 2.7%; P < .015).
“The message first is that if you do a good job with transradial access you can end up with a lower [occlusion] rate,” said coprincipal investigator Adel Aminian, MD, Hôpital Civil Marie Curie, Charleroi, Belgium. “On the other hand, it’s a trade-off between a more demanding puncture for distal radial access but also a simpler hemostatic process, which I think is one of the main advantages of distal radial access.”
The results were presented during the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, and published simultaneously in JACC: Cardiovascular Interventions.
DISCO-RADIAL (Distal Versus Conventional RADIAL Access for Coronary Angiography and Intervention) is the largest trial thus far to compare TRA with the distal radial snuffbox technique, which has shown promise for reducing RAO rates in the recent single-center randomized DAPRAO and ANGIE trials.
The trial was conducted at 15 sites across Europe and Japan in 1,309 patients with an indication for percutaneous coronary procedures using the 6Fr Glidesheath Slender (Terumo). The intention-to-treat population included 657 TRA patients and 650 DRA patients.
The two groups were well matched, with most having a chronic coronary syndrome. Operators had to have performed a minimum of 100 procedures by DRA and follow systematic best practices previously reported by the investigators to prevent RAO, Dr. Aminian said.
The use of DRA did not significantly affect the duration of the coronary procedure (27 minutes vs. 24 minutes with TRA; P = .12) or average radiation dose (1298 mGy vs. 1222 mGy; P = .70).
DRA, however, reduced the need for selective compression devices (88% vs. 99.2%) and shortened the median time to hemostasis from 180 minutes to 153 minutes (P for both < .001).
“These results establish compliance to best practice recommendations for RAO avoidance as a mandatory new reference in transradial practice,” Dr. Aminian concluded. “At the same time, distal radial artery arises as a valid alternative associated with higher crossover rates but with a simpler and shorter hemostasis process.”
A show of hands revealed that about 25% of the audience used distal radial access prior to the presentation but that enthusiasm fell off following the results.
Discussant Hany Eteiba, MD, Glasgow Royal Infirmary, said: “I salute your enthusiasm for presenting a negative trial and you tried to persuade the audience to use the distal radial artery results, but nonetheless.”
Dr. Eteiba said he could see a “potential advantage in the shorter hemostasis time,” and asked whether it might be influencing the rapid turnover for day-case angioplasty.
Dr. Aminian responded that “if you do an angioplasty you have to keep the patient for a certain amount of time, but I think for your nurse work and for the health care resources, having a very short hemostasis time is very interesting. We started with a hemostasis time of 2 hours and now we’ve decreased it to 1 hour and it will decrease even more.”
Session moderator Chaim Lotan, MD, Hadassah-Hebrew University Medical Center, Jerusalem, called DISCO-RADIAL an important study and said, “the question now is what’s the indication in your eyes for using distal radial?”
Dr. Aminian said that one message from the trial is that people who are using transradial access “have to do a better job,” and reminded the audience that RAO rates at many centers are too high, at 10% or upward.
At the same time, Dr. Aminian cautioned that operators wanting to use distal radial access “need to master the technique” or they will “end up with a relatively high failure rate.”
Discussant Eliano Navarese, MD, Nicolaus Copernicus University, Toruń, Poland, said, “I still think that it is a very valid approach, we use it for almost 20 years ... but it is very true, it is very demanding. And the learning curve of 100 cases in the trial maybe needed more cases.”
In an accompanying editorial, Grigorios Tsigkas, MD, PhD, University of Patras, Rio Patras, Greece, and colleagues wrote that the incidence of forearm RAO was “surprisingly low” but could be even lower if the authors administered adequate anticoagulation.
Still, they wrote that distal transradial access “for coronary procedures in combination with the systematic implementation of best practices for RAO prevention may be the final solution against RAO.”
The editorialists suggested that exposure to radiation could be the “main limitation of this novel vascular approach” and that forthcoming trials, such as DOSE, could shed light on this issue.
Increased procedure times in the DISCO RADIAL and ANGIE trials are secondary in stable patients, Dr. Tsigkas said, but could be a limitation in patients presenting with ST-segment elevation myocardial infarction (STEMI). Ongoing research, such as the RESERVE trial from China and a Korean trial, will provide insights into the safety and feasibility of distal transradial access in STEMI.
The study was supported by Terumo Europe. Dr. Aminian reported receiving honoraria or consultation fees from Abbott, Boston Scientific, and Terumo Interventional Systems. Dr. Tsigkas reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EUROPCR 2022
Pancreatic involvement in COVID-19: What do we know?
MADRID – It involves the relationship between COVID-19 and new diagnoses of diabetes and blood glucose disorders, among others, in the post–COVID-19 period. These topics were addressed at the XXXIII National Congress of the Spanish Diabetes Society. They were also the central theme of the inaugural conference, Pancreatic Involvement During COVID-19: From Preclinical Studies to Clinical Relevance, which was led by Alexander Kleger, MD, PhD, head of the department of pancreatology at the Ulm (Germany) University Clinic for Internal Medicine.
The chair of the scientific committee of the congress, Franz Martín, MD, launched the conference by noting that the work of Dr. Kleger and his team has made it possible to ascertain that SARS-CoV-2 can infect pancreatic beta cells that produce insulin. This observation may help in understanding why patients with COVID-19 sometimes experience symptoms related to greater difficulty regulating blood glucose.
“In addition, the German expert and his group have described the abnormalities that occur in beta cells when they are infected by SARS-CoV-2, something especially important, given that knowledge of these abnormalities may be of great importance to understanding the possible appearance of more cases of diabetes in the future,” Dr. Martín added.
“Our data identify the human pancreas as a target of SARS-CoV-2 infection and suggest that pancreatic beta cell involvement could contribute to the metabolic dysregulation seen in COVID-19 patients,” Dr. Kleger pointed out.
In his speech, Dr. Kleger reviewed the evidence on the effects of SARS-CoV-2 that has been garnered since the start of the pandemic, and he presented his research group’s findings on the impact at the pancreatic level.
“Since March 2020, it has been seen that COVID-19 affected the pancreas, and studies published in August of that same year clearly spoke of both a worsening of diabetes and an increase in new cases of this disease diagnosed after SARS-CoV-2 infection. Also, the data showed how hospitalized patients with no previous history of diabetes experienced rapid increases in glucose levels 5 days after admission,” Dr. Kleger said.
Angiotensin-converting enzyme 2
As an example of the pace at which evidence on the pancreatic impact of this virus has been evolving, Dr. Kleger referred to early studies that found no angiotensin-converting enzyme 2 receptor on cells of the endocrine and exocrine pancreas. “To our surprise, in our work, we did observe the obvious presence of angiotensin-converting enzyme 2 specifically expressed in human pancreatic beta cells, something confirmed by other investigations. Another surprising aspect was verifying that the viral infection lasts longer in the pancreas than in the lungs,” said the expert.
These findings caused the researchers to realize that SARS-CoV-2 may be directly or indirectly associated with diabetes. “It is currently the subject of debate whether it may be a direct effect, infecting or directly reaching the pancreatic beta cells, or whether this involvement is a result of the effect of the infection at systemic level, in the context of the cytokine storm and the proinflammatory environment derived from it. Our current challenge is to confirm whether this virus can really replicate in pancreatic beta cells and to assess the possible existence of reinfections, among other aspects,” said Dr. Kleger.
Along with these “developing areas of knowledge,” there are several certainties regarding the link between diabetes and COVID-19. Dr. Kleger summarized the most relevant one. “Preexisting diabetes is known to be a highly prevalent comorbidity seen in 11%-22% of patients and increases the risk of severe disease and mortality.
“SARS-CoV-2 infection has also been shown to affect the exocrine pancreas, manifesting as pancreatitis in 5% of critically ill patients with COVID-19, as well as enlargement of the pancreas and abnormal levels of amylase or lipase in 7.5%-17% of patients.
“Furthermore, it is obvious that SARS-CoV-2 infection produces glycometabolic dysfunction in these patients, with increased hyperglycemia in people with type 2 diabetes and ketoacidosis in 2%-6.4% of patients with and without diabetes.”
After recovery
The most recent research reveals the persistence of this dysregulation long after recovery from COVID-19. “We’ve seen that in a significant proportion of patients, hyperglycemia is maintained for some time; in the specific case of hospitalized patients [without the need for assisted ventilation or other intensive care requirements], for up to more than 2 months after overcoming the illness.
“In the same way, there are studies that have shown that insulin resistance and hyperstimulation of pancreatic beta cells remain at pathological levels in the post–COVID-19 phase. And in line with increased insulin resistance, signs of hyperinflammation have also been detected in these patients.”
Dr. Kleger noted that another research area is the increased incidence of newly diagnosed diabetes after recovery from SARS-CoV-2 infection, “something that seems to be correlated with how severely the disease has been experienced and also depending on whether hospitalization or intensive care was needed. Likewise, retrospective studies have shown that the risk of developing type 2 diabetes is higher in COVID-19 patients, compared with those with other respiratory infections. Regarding the incidence of type 1 diabetes, there is evidence, particularly in the case of children, of a clear correlation between the pandemic waves and the increase in cases.
“Therefore, and in view of this data, we could say that, with regard to the involvement of SARS-CoV-2 in pancreatic beta cells, something is up, but we are not yet able to fully understand what it is. What can be confirmed based on the numerous studies carried out in this regard is that COVID-19 produces a metabolic dysregulation [hyperglycemia, insulin resistance, diabetic ketoacidosis] which in turn favors the development of diabetes in patients with no history of this disease,” said Dr. Kleger.
“Likewise, everything points to the existence of a definitively feasible infection in pancreatic beta cells associated with SARS-CoV-2, but there are still unknown aspects of the physiology that explain this effect that remain the subject of debate and deserve future studies,” he concluded.
Consequences of the pandemic
The experts agreed that, although COVID-19 is no longer at the center of specialist care, it is still a subject of investigation. On the conference’s opening day, an update was made on the approach to diabetes.
Care activity is gradually recovering as the time that professionals devote to COVID-19 care is reduced, “but it will take time to catch up with the care activities not carried out during the pandemic, and, unfortunately, in the coming years, we will see the repercussion of the lack or reduction of care during these years,” stressed the SED chair, Antonio Pérez Pérez, MD, director of endocrinology and nutrition of Hospital de la Santa Creu i Sant Pau, Barcelona.
Dr. Pérez stressed that the pandemic has revealed health system deficiencies in diabetes care. He added that the impact of COVID-19 on diabetes (resulting from the effects of the infection itself or from the inadequacy of prevention, diagnosis, and treatment measures) fostered a deterioration of metabolic control and a delay in the diagnosis of the disease and its complications.
“All this contributes to the fact that we currently continue to see patients with complications, especially in the case of type 2 diabetes, with more serious decompensations and diagnoses in more advanced stages of the disease. This impact has been more significant in older people from disadvantaged areas and with less capacity for self-monitoring and self-adjustment of treatment,” he added.
Describing lessons learned through the experiences accumulated in diabetes care during the pandemic, Dr. Pérez highlighted the push for virtual consultations, accessibility to drugs prescribed in electronic prescriptions, and the use of educational resources online and of telemedicine tools. “The need to invest in the health sector has also been assumed, endowing it with robustness in well-trained health personnel, to promote health education, boost efficient health organization, and invest in innovation aimed at facilitating care.”
Dr. Kleger and Dr. Pérez disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.
MADRID – It involves the relationship between COVID-19 and new diagnoses of diabetes and blood glucose disorders, among others, in the post–COVID-19 period. These topics were addressed at the XXXIII National Congress of the Spanish Diabetes Society. They were also the central theme of the inaugural conference, Pancreatic Involvement During COVID-19: From Preclinical Studies to Clinical Relevance, which was led by Alexander Kleger, MD, PhD, head of the department of pancreatology at the Ulm (Germany) University Clinic for Internal Medicine.
The chair of the scientific committee of the congress, Franz Martín, MD, launched the conference by noting that the work of Dr. Kleger and his team has made it possible to ascertain that SARS-CoV-2 can infect pancreatic beta cells that produce insulin. This observation may help in understanding why patients with COVID-19 sometimes experience symptoms related to greater difficulty regulating blood glucose.
“In addition, the German expert and his group have described the abnormalities that occur in beta cells when they are infected by SARS-CoV-2, something especially important, given that knowledge of these abnormalities may be of great importance to understanding the possible appearance of more cases of diabetes in the future,” Dr. Martín added.
“Our data identify the human pancreas as a target of SARS-CoV-2 infection and suggest that pancreatic beta cell involvement could contribute to the metabolic dysregulation seen in COVID-19 patients,” Dr. Kleger pointed out.
In his speech, Dr. Kleger reviewed the evidence on the effects of SARS-CoV-2 that has been garnered since the start of the pandemic, and he presented his research group’s findings on the impact at the pancreatic level.
“Since March 2020, it has been seen that COVID-19 affected the pancreas, and studies published in August of that same year clearly spoke of both a worsening of diabetes and an increase in new cases of this disease diagnosed after SARS-CoV-2 infection. Also, the data showed how hospitalized patients with no previous history of diabetes experienced rapid increases in glucose levels 5 days after admission,” Dr. Kleger said.
Angiotensin-converting enzyme 2
As an example of the pace at which evidence on the pancreatic impact of this virus has been evolving, Dr. Kleger referred to early studies that found no angiotensin-converting enzyme 2 receptor on cells of the endocrine and exocrine pancreas. “To our surprise, in our work, we did observe the obvious presence of angiotensin-converting enzyme 2 specifically expressed in human pancreatic beta cells, something confirmed by other investigations. Another surprising aspect was verifying that the viral infection lasts longer in the pancreas than in the lungs,” said the expert.
These findings caused the researchers to realize that SARS-CoV-2 may be directly or indirectly associated with diabetes. “It is currently the subject of debate whether it may be a direct effect, infecting or directly reaching the pancreatic beta cells, or whether this involvement is a result of the effect of the infection at systemic level, in the context of the cytokine storm and the proinflammatory environment derived from it. Our current challenge is to confirm whether this virus can really replicate in pancreatic beta cells and to assess the possible existence of reinfections, among other aspects,” said Dr. Kleger.
Along with these “developing areas of knowledge,” there are several certainties regarding the link between diabetes and COVID-19. Dr. Kleger summarized the most relevant one. “Preexisting diabetes is known to be a highly prevalent comorbidity seen in 11%-22% of patients and increases the risk of severe disease and mortality.
“SARS-CoV-2 infection has also been shown to affect the exocrine pancreas, manifesting as pancreatitis in 5% of critically ill patients with COVID-19, as well as enlargement of the pancreas and abnormal levels of amylase or lipase in 7.5%-17% of patients.
“Furthermore, it is obvious that SARS-CoV-2 infection produces glycometabolic dysfunction in these patients, with increased hyperglycemia in people with type 2 diabetes and ketoacidosis in 2%-6.4% of patients with and without diabetes.”
After recovery
The most recent research reveals the persistence of this dysregulation long after recovery from COVID-19. “We’ve seen that in a significant proportion of patients, hyperglycemia is maintained for some time; in the specific case of hospitalized patients [without the need for assisted ventilation or other intensive care requirements], for up to more than 2 months after overcoming the illness.
“In the same way, there are studies that have shown that insulin resistance and hyperstimulation of pancreatic beta cells remain at pathological levels in the post–COVID-19 phase. And in line with increased insulin resistance, signs of hyperinflammation have also been detected in these patients.”
Dr. Kleger noted that another research area is the increased incidence of newly diagnosed diabetes after recovery from SARS-CoV-2 infection, “something that seems to be correlated with how severely the disease has been experienced and also depending on whether hospitalization or intensive care was needed. Likewise, retrospective studies have shown that the risk of developing type 2 diabetes is higher in COVID-19 patients, compared with those with other respiratory infections. Regarding the incidence of type 1 diabetes, there is evidence, particularly in the case of children, of a clear correlation between the pandemic waves and the increase in cases.
“Therefore, and in view of this data, we could say that, with regard to the involvement of SARS-CoV-2 in pancreatic beta cells, something is up, but we are not yet able to fully understand what it is. What can be confirmed based on the numerous studies carried out in this regard is that COVID-19 produces a metabolic dysregulation [hyperglycemia, insulin resistance, diabetic ketoacidosis] which in turn favors the development of diabetes in patients with no history of this disease,” said Dr. Kleger.
“Likewise, everything points to the existence of a definitively feasible infection in pancreatic beta cells associated with SARS-CoV-2, but there are still unknown aspects of the physiology that explain this effect that remain the subject of debate and deserve future studies,” he concluded.
Consequences of the pandemic
The experts agreed that, although COVID-19 is no longer at the center of specialist care, it is still a subject of investigation. On the conference’s opening day, an update was made on the approach to diabetes.
Care activity is gradually recovering as the time that professionals devote to COVID-19 care is reduced, “but it will take time to catch up with the care activities not carried out during the pandemic, and, unfortunately, in the coming years, we will see the repercussion of the lack or reduction of care during these years,” stressed the SED chair, Antonio Pérez Pérez, MD, director of endocrinology and nutrition of Hospital de la Santa Creu i Sant Pau, Barcelona.
Dr. Pérez stressed that the pandemic has revealed health system deficiencies in diabetes care. He added that the impact of COVID-19 on diabetes (resulting from the effects of the infection itself or from the inadequacy of prevention, diagnosis, and treatment measures) fostered a deterioration of metabolic control and a delay in the diagnosis of the disease and its complications.
“All this contributes to the fact that we currently continue to see patients with complications, especially in the case of type 2 diabetes, with more serious decompensations and diagnoses in more advanced stages of the disease. This impact has been more significant in older people from disadvantaged areas and with less capacity for self-monitoring and self-adjustment of treatment,” he added.
Describing lessons learned through the experiences accumulated in diabetes care during the pandemic, Dr. Pérez highlighted the push for virtual consultations, accessibility to drugs prescribed in electronic prescriptions, and the use of educational resources online and of telemedicine tools. “The need to invest in the health sector has also been assumed, endowing it with robustness in well-trained health personnel, to promote health education, boost efficient health organization, and invest in innovation aimed at facilitating care.”
Dr. Kleger and Dr. Pérez disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.
MADRID – It involves the relationship between COVID-19 and new diagnoses of diabetes and blood glucose disorders, among others, in the post–COVID-19 period. These topics were addressed at the XXXIII National Congress of the Spanish Diabetes Society. They were also the central theme of the inaugural conference, Pancreatic Involvement During COVID-19: From Preclinical Studies to Clinical Relevance, which was led by Alexander Kleger, MD, PhD, head of the department of pancreatology at the Ulm (Germany) University Clinic for Internal Medicine.
The chair of the scientific committee of the congress, Franz Martín, MD, launched the conference by noting that the work of Dr. Kleger and his team has made it possible to ascertain that SARS-CoV-2 can infect pancreatic beta cells that produce insulin. This observation may help in understanding why patients with COVID-19 sometimes experience symptoms related to greater difficulty regulating blood glucose.
“In addition, the German expert and his group have described the abnormalities that occur in beta cells when they are infected by SARS-CoV-2, something especially important, given that knowledge of these abnormalities may be of great importance to understanding the possible appearance of more cases of diabetes in the future,” Dr. Martín added.
“Our data identify the human pancreas as a target of SARS-CoV-2 infection and suggest that pancreatic beta cell involvement could contribute to the metabolic dysregulation seen in COVID-19 patients,” Dr. Kleger pointed out.
In his speech, Dr. Kleger reviewed the evidence on the effects of SARS-CoV-2 that has been garnered since the start of the pandemic, and he presented his research group’s findings on the impact at the pancreatic level.
“Since March 2020, it has been seen that COVID-19 affected the pancreas, and studies published in August of that same year clearly spoke of both a worsening of diabetes and an increase in new cases of this disease diagnosed after SARS-CoV-2 infection. Also, the data showed how hospitalized patients with no previous history of diabetes experienced rapid increases in glucose levels 5 days after admission,” Dr. Kleger said.
Angiotensin-converting enzyme 2
As an example of the pace at which evidence on the pancreatic impact of this virus has been evolving, Dr. Kleger referred to early studies that found no angiotensin-converting enzyme 2 receptor on cells of the endocrine and exocrine pancreas. “To our surprise, in our work, we did observe the obvious presence of angiotensin-converting enzyme 2 specifically expressed in human pancreatic beta cells, something confirmed by other investigations. Another surprising aspect was verifying that the viral infection lasts longer in the pancreas than in the lungs,” said the expert.
These findings caused the researchers to realize that SARS-CoV-2 may be directly or indirectly associated with diabetes. “It is currently the subject of debate whether it may be a direct effect, infecting or directly reaching the pancreatic beta cells, or whether this involvement is a result of the effect of the infection at systemic level, in the context of the cytokine storm and the proinflammatory environment derived from it. Our current challenge is to confirm whether this virus can really replicate in pancreatic beta cells and to assess the possible existence of reinfections, among other aspects,” said Dr. Kleger.
Along with these “developing areas of knowledge,” there are several certainties regarding the link between diabetes and COVID-19. Dr. Kleger summarized the most relevant one. “Preexisting diabetes is known to be a highly prevalent comorbidity seen in 11%-22% of patients and increases the risk of severe disease and mortality.
“SARS-CoV-2 infection has also been shown to affect the exocrine pancreas, manifesting as pancreatitis in 5% of critically ill patients with COVID-19, as well as enlargement of the pancreas and abnormal levels of amylase or lipase in 7.5%-17% of patients.
“Furthermore, it is obvious that SARS-CoV-2 infection produces glycometabolic dysfunction in these patients, with increased hyperglycemia in people with type 2 diabetes and ketoacidosis in 2%-6.4% of patients with and without diabetes.”
After recovery
The most recent research reveals the persistence of this dysregulation long after recovery from COVID-19. “We’ve seen that in a significant proportion of patients, hyperglycemia is maintained for some time; in the specific case of hospitalized patients [without the need for assisted ventilation or other intensive care requirements], for up to more than 2 months after overcoming the illness.
“In the same way, there are studies that have shown that insulin resistance and hyperstimulation of pancreatic beta cells remain at pathological levels in the post–COVID-19 phase. And in line with increased insulin resistance, signs of hyperinflammation have also been detected in these patients.”
Dr. Kleger noted that another research area is the increased incidence of newly diagnosed diabetes after recovery from SARS-CoV-2 infection, “something that seems to be correlated with how severely the disease has been experienced and also depending on whether hospitalization or intensive care was needed. Likewise, retrospective studies have shown that the risk of developing type 2 diabetes is higher in COVID-19 patients, compared with those with other respiratory infections. Regarding the incidence of type 1 diabetes, there is evidence, particularly in the case of children, of a clear correlation between the pandemic waves and the increase in cases.
“Therefore, and in view of this data, we could say that, with regard to the involvement of SARS-CoV-2 in pancreatic beta cells, something is up, but we are not yet able to fully understand what it is. What can be confirmed based on the numerous studies carried out in this regard is that COVID-19 produces a metabolic dysregulation [hyperglycemia, insulin resistance, diabetic ketoacidosis] which in turn favors the development of diabetes in patients with no history of this disease,” said Dr. Kleger.
“Likewise, everything points to the existence of a definitively feasible infection in pancreatic beta cells associated with SARS-CoV-2, but there are still unknown aspects of the physiology that explain this effect that remain the subject of debate and deserve future studies,” he concluded.
Consequences of the pandemic
The experts agreed that, although COVID-19 is no longer at the center of specialist care, it is still a subject of investigation. On the conference’s opening day, an update was made on the approach to diabetes.
Care activity is gradually recovering as the time that professionals devote to COVID-19 care is reduced, “but it will take time to catch up with the care activities not carried out during the pandemic, and, unfortunately, in the coming years, we will see the repercussion of the lack or reduction of care during these years,” stressed the SED chair, Antonio Pérez Pérez, MD, director of endocrinology and nutrition of Hospital de la Santa Creu i Sant Pau, Barcelona.
Dr. Pérez stressed that the pandemic has revealed health system deficiencies in diabetes care. He added that the impact of COVID-19 on diabetes (resulting from the effects of the infection itself or from the inadequacy of prevention, diagnosis, and treatment measures) fostered a deterioration of metabolic control and a delay in the diagnosis of the disease and its complications.
“All this contributes to the fact that we currently continue to see patients with complications, especially in the case of type 2 diabetes, with more serious decompensations and diagnoses in more advanced stages of the disease. This impact has been more significant in older people from disadvantaged areas and with less capacity for self-monitoring and self-adjustment of treatment,” he added.
Describing lessons learned through the experiences accumulated in diabetes care during the pandemic, Dr. Pérez highlighted the push for virtual consultations, accessibility to drugs prescribed in electronic prescriptions, and the use of educational resources online and of telemedicine tools. “The need to invest in the health sector has also been assumed, endowing it with robustness in well-trained health personnel, to promote health education, boost efficient health organization, and invest in innovation aimed at facilitating care.”
Dr. Kleger and Dr. Pérez disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com. This article was translated from the Medscape Spanish edition.
AUA 2022: A report from the trenches
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
The annual meeting of the American Urological Association took place recently at the Ernest N. Morial Convention Center in New Orleans. Hundreds of talks and abstracts were presented over the 4 days in New Orleans; below is a summary of what I found to be the key scientific highlights.
1. Updates to the AUA’s guidelines for management of localized kidney cancer
The AUA’s recommendations for the treatment of localized kidney cancer have changed dramatically over the past few decades. Gone are the days of simply removing the entire kidney every time a mass is found. Today, a partial nephrectomy is preferred in most situations.
Our understanding that the prevalence of familial kidney cancer is much higher than previously thought has led to a change in the guidelines regarding which patients should receive genetic counseling. For the first time, the guidelines include the use of adjuvant medical treatment, such as pembrolizumab. A 2021 study in the New England Journal of Medicine showed a survival benefit for patients with high-risk disease who receive such therapies, so it›s not surprising that such treatments are now recommended.
The development of new second- and third-generation gadolinium contrast agents that spare the kidneys has dramatically increased the role for MRIs for patients with severe or even end-stage renal disease. As a result, the guidelines were updated to recommend the use of these agents. The role of a renal biopsy, which has always been limited, given the ability of cross-sectional imaging to diagnosis this disease, has further been constrained and should now be performed only when the results would clearly change a clinical decision, such as whether or not the lesion in question is a metastasis.
2. New and better ureteroscope technology
No one likes kidney stones, not the patient who deals with the incredible pain, nor the surgeon who has to remove them, given that these cases often present in the wee hours of the morning. The preferred surgical approach has changed dramatically over the past decade, moving away from extracorporeal shockwave lithotripsy toward flexible ureteroscope-based technology, which has a higher clearance rate and is more widely and more immediately available. Flexible ureteroscopy has been held back by technological barriers, including limited scope deflection and low laser power. The exceptionally high cost of repair and the tendency of the instruments to break haven’t helped, either. Although single-use ureteroscopes have been available for some time, it wasn’t until the recently introduced second-generation scopes became widely available that they have become popular. These new scopes have small external diameters, great optics, and can easily be used. Newer high-powered lasers and the change from holmium:YAG-based lasers to thulium technology is greatly increasing the size of stones that can be safely addressed ureteroscopically. The cost analysis of single-use technology versus reusable scopes tends to be site dependent but can be appealing in certain situations. Also, on the technology forefront, a new robotically assisted ureteroscope is being introduced that offers the chance for improved intrapelvic mobility and better ergonomics for the surgeon.
3. New options for the treatment of clinically localized prostate cancer
Since the guidelines were last updated in 2017, the definitive management of localized prostate cancer has changed dramatically. Although radical prostatectomy and radiotherapy remain the preferred options for men who choose treatment for their disease, the updated guidelines state that active surveillance is now the preferred approach for men with low-risk cancers.
Although the preferred surveillance protocol is still being debated, the consensus is that almost all men with low-risk disease can be safely monitored for some period. The imaging technology available to monitor patients is also radically changing with the rollout of prostate-specific membrane antigen–based PET technology. The increased sensitivity and specificity of this modality opens the door not only for better up-front staging of newly diagnosed patients with prostate cancer but also may allow clinicians to earlier identify and treat men with metastatic disease. The guidelines for the first time address the use of genetic markers to individualize treatment of men with advanced or metastatic prostate cancer. Exactly which treatments these patients need is still being debated, but the ability to use patient-specific genetic mutation information to customize treatment is potentially groundbreaking.
4. New treatment options for patients with high-grade non–muscle-invasive bladder cancer (NMIBC) refractory to bacille Calmette-Guérin (BCG) therapy
Patients with NMIBC who do not respond to BCG therapy are in a tough position. Cystectomy remains the preferred option as a second-line strategy, but the procedure has a complication rate approaching 30%. Further, many patients are not willing to have their bladder removed because of the life-altering changes that go along with having an urostomy or a neobladder. While intravesical treatments such as valrubicin, docetaxel, or gemcitabine have been available for many years, the success rates of those options are limited. The Food and Drug Administration recently approved the use of the immunotherapy-based treatment pembrolizumab. While none of these options is perfect, the fact that we now have at least some alternatives is a huge step in the right direction.
5. It’s all about the patient: Involving patients in designing the health care delivery system
Although it seems like an obvious concept, patients themselves have traditionally not been involved in designing the health care delivery system on which they rely. Research presented at the AUA shows that many health care outcomes improve when patients are actively involved in the process. For example, Angela Smith, MD, of the University of North Carolina at Chapel Hill, presented a study showing that including patients in the identification of possible research topics helps them feel engaged and more likely to participate in studies. Patients who are involved in advisory councils at the local hospital level are more likely to report having received high-quality care. And surveying patients on the goals of national health care policy helps them feel that the outcomes are more equitable.
As a small-town urologist who spends his days in the trenches of urology, I think the next time my group considers participating in new cancer research, I may talk to the local cancer support group first. If Dr. Smith’s data are correct, not only would our patients be better served, but we would also have an easier time filling the trial!
The 2023 AUA conference is going to be held in Chicago next spring. I hope to see you there!
A version of this article first appeared on Medscape.com.
FROM AUA 2022
SCAI issues guidelines for PFO management, makes case for expansion
The first-ever guidelines for interventional cardiologists using percutaneous patent foramen ovale closure recommend expanding the use of the procedure beyond the Food and Drug Administration–approved indication following PFO-associated ischemic stroke, adding clarification about the use of PFO with anticoagulation and hedging against abuse and overuse of the procedure, said the chair of the guideline writing committee.
“The most important things surrounding these guidelines are to help clinicians and policymakers – third-party payers – to address PFO in patient subsets that were not included in the large randomized clinical trials that led to FDA approval,” said writing group chair Clifford J. Kavinsky, MD, PhD, chief of structural and interventional cardiology at Rush University Medical Center, Chicago.
The Society for Cardiovascular Angiography & Interventions issued the guidelines at its annual scientific sessions meeting in Atlanta and published them simultaneously in the society’s journal.
The guidelines issue strong and conditional recommendations. The former means clinicians should order the intervention for most patients; the latter means decisionmaking is more nuanced and should consider contributing factors.
The guidelines clarify patient selection for PFO closure outside the “pretty narrow” indication the FDA approved, Dr. Kavinsky said, which is for PFO-associated ischemic stroke in patients aged 18-60 years.
“So what about patients who are older than 60? What about patients who had their stroke 10 years ago?” Dr. Kavinsky asked. “Those are issues that were unanswered in the randomized clinical trials.”
The guidelines also refine recommendations about anticoagulation in these patients, including its use after PFO closure in selected patients, Dr. Kavinsky noted. “It’s the opinion of the panel that although anticoagulants may be effective, because of issues of noncompliance, because of issues of interruption of therapy by physicians for a variety of reasons, including surgery or noncompliance, that it is preferable to do a PFO device closure to giving anticoagulant therapy.”
Many of the recommendations cover PFO closure alongside antiplatelet or anticoagulation therapy. Key conditional recommendations for patients who haven’t had a PFO-related stroke are:
- Avoiding its routine use in patients with chronic migraines, prior decompression illness (DCI), thrombophilia, atrial septal aneurysm, transient ischemic attack (TIA), or deep vein thrombosis (DVT).
- Considering PFO closure in patients with platypnea-orthodeoxia syndrome (POS) with no other discernible cause of hypoxia or systemic embolism in whom other embolic causes have been ruled out.
In patients who’ve had a PFO-related stroke, the guidelines strongly recommend PFO closure versus antiplatelet therapy alone, but conditionally, not in patients with atrial fibrillation who’ve had an ischemic stroke. They also conditionally suggest PFO closure rather than long-term antiplatelet therapy alone in PFO stroke patients aged 60 and older, as well as those with thrombophilia already on antiplatelet therapy but not anticoagulation. However, the guidelines make no recommendation on PFO closure based on how much time has passed since the previous stroke.
“Furthermore,” Dr. Kavinsky said, “in patients who require lifelong anticoagulation because of recurrent DVT or recurrent pulmonary emboli or thrombopenia, if they’ve had a PFO-mediated stroke, then it’s our opinion that they should have their PFO closed in addition to taking lifelong anticoagulation because of the same issues of noncompliance and interruption of therapy.” Those are conditional recommendations.
The guideline also checks a box in the FDA labeling that mandated agreement between cardiology and neurology in patient selection. The American Academy of Neurology (AAN) issued its own guideline in 2020 for patients with stroke and PFO. In Europe, the European Society of Cardiology issued two position papers on expanded applications of PFO closure.
The recommendations on when PFO closure shouldn’t be done are noteworthy, Dr. Kavinsky said. “PFOs are present in 25% of the adult population, so the number of patients with PFO is huge and the indication for the FDA is really narrow: to reduce the risk of recurrent stroke in patients with PFO-mediated stroke. So, there’s the tremendous potential for abuse out there, of excessive procedures, of doing unnecessary procedures.”
The guidelines are a follow-up to the operator institutional requirements document SCAI issued in 2019 that set requirements for hospital offering and physicians performing PFO closure, Dr. Kavinsky added.
In an editorial accompanying the published guideline, Robert J. Sommer, MD, and Jamil A. Aboulhosn, MD, wrote that they support the recommendations “which help spotlight and clarify the growing list of potential indications for PFO closure.” They noted that the guidelines panel’s “strong” recommendations were for indications validated by randomized trials and that “conditional” recommendations were based on panelists’ experience and observational data.
“It is critical to recognize that most of these guidelines represent consensus opinion only,” wrote Dr. Sommer, who specializes in adult congenital and pediatric cardiology at Columbia University Irving Medical Center, New York, and Dr. Aboulhosn, an interventional cardiologist at Ronald Reagan University of California, Los Angeles, Medical Center. They emphasized the guidelines’ “heavy emphasis” on shared decisionmaking with patients.
Dr. Kavinsky is a principal investigator for Edwards Lifesciences, W.L. Gore and Associates, Medtronic, and Abbott. Dr. Sommer is a principal investigator and investigator in studies sponsored by W.L. Gore & Associates. Dr. Aboulhosn is a consultant to Abbott Medical.
The first-ever guidelines for interventional cardiologists using percutaneous patent foramen ovale closure recommend expanding the use of the procedure beyond the Food and Drug Administration–approved indication following PFO-associated ischemic stroke, adding clarification about the use of PFO with anticoagulation and hedging against abuse and overuse of the procedure, said the chair of the guideline writing committee.
“The most important things surrounding these guidelines are to help clinicians and policymakers – third-party payers – to address PFO in patient subsets that were not included in the large randomized clinical trials that led to FDA approval,” said writing group chair Clifford J. Kavinsky, MD, PhD, chief of structural and interventional cardiology at Rush University Medical Center, Chicago.
The Society for Cardiovascular Angiography & Interventions issued the guidelines at its annual scientific sessions meeting in Atlanta and published them simultaneously in the society’s journal.
The guidelines issue strong and conditional recommendations. The former means clinicians should order the intervention for most patients; the latter means decisionmaking is more nuanced and should consider contributing factors.
The guidelines clarify patient selection for PFO closure outside the “pretty narrow” indication the FDA approved, Dr. Kavinsky said, which is for PFO-associated ischemic stroke in patients aged 18-60 years.
“So what about patients who are older than 60? What about patients who had their stroke 10 years ago?” Dr. Kavinsky asked. “Those are issues that were unanswered in the randomized clinical trials.”
The guidelines also refine recommendations about anticoagulation in these patients, including its use after PFO closure in selected patients, Dr. Kavinsky noted. “It’s the opinion of the panel that although anticoagulants may be effective, because of issues of noncompliance, because of issues of interruption of therapy by physicians for a variety of reasons, including surgery or noncompliance, that it is preferable to do a PFO device closure to giving anticoagulant therapy.”
Many of the recommendations cover PFO closure alongside antiplatelet or anticoagulation therapy. Key conditional recommendations for patients who haven’t had a PFO-related stroke are:
- Avoiding its routine use in patients with chronic migraines, prior decompression illness (DCI), thrombophilia, atrial septal aneurysm, transient ischemic attack (TIA), or deep vein thrombosis (DVT).
- Considering PFO closure in patients with platypnea-orthodeoxia syndrome (POS) with no other discernible cause of hypoxia or systemic embolism in whom other embolic causes have been ruled out.
In patients who’ve had a PFO-related stroke, the guidelines strongly recommend PFO closure versus antiplatelet therapy alone, but conditionally, not in patients with atrial fibrillation who’ve had an ischemic stroke. They also conditionally suggest PFO closure rather than long-term antiplatelet therapy alone in PFO stroke patients aged 60 and older, as well as those with thrombophilia already on antiplatelet therapy but not anticoagulation. However, the guidelines make no recommendation on PFO closure based on how much time has passed since the previous stroke.
“Furthermore,” Dr. Kavinsky said, “in patients who require lifelong anticoagulation because of recurrent DVT or recurrent pulmonary emboli or thrombopenia, if they’ve had a PFO-mediated stroke, then it’s our opinion that they should have their PFO closed in addition to taking lifelong anticoagulation because of the same issues of noncompliance and interruption of therapy.” Those are conditional recommendations.
The guideline also checks a box in the FDA labeling that mandated agreement between cardiology and neurology in patient selection. The American Academy of Neurology (AAN) issued its own guideline in 2020 for patients with stroke and PFO. In Europe, the European Society of Cardiology issued two position papers on expanded applications of PFO closure.
The recommendations on when PFO closure shouldn’t be done are noteworthy, Dr. Kavinsky said. “PFOs are present in 25% of the adult population, so the number of patients with PFO is huge and the indication for the FDA is really narrow: to reduce the risk of recurrent stroke in patients with PFO-mediated stroke. So, there’s the tremendous potential for abuse out there, of excessive procedures, of doing unnecessary procedures.”
The guidelines are a follow-up to the operator institutional requirements document SCAI issued in 2019 that set requirements for hospital offering and physicians performing PFO closure, Dr. Kavinsky added.
In an editorial accompanying the published guideline, Robert J. Sommer, MD, and Jamil A. Aboulhosn, MD, wrote that they support the recommendations “which help spotlight and clarify the growing list of potential indications for PFO closure.” They noted that the guidelines panel’s “strong” recommendations were for indications validated by randomized trials and that “conditional” recommendations were based on panelists’ experience and observational data.
“It is critical to recognize that most of these guidelines represent consensus opinion only,” wrote Dr. Sommer, who specializes in adult congenital and pediatric cardiology at Columbia University Irving Medical Center, New York, and Dr. Aboulhosn, an interventional cardiologist at Ronald Reagan University of California, Los Angeles, Medical Center. They emphasized the guidelines’ “heavy emphasis” on shared decisionmaking with patients.
Dr. Kavinsky is a principal investigator for Edwards Lifesciences, W.L. Gore and Associates, Medtronic, and Abbott. Dr. Sommer is a principal investigator and investigator in studies sponsored by W.L. Gore & Associates. Dr. Aboulhosn is a consultant to Abbott Medical.
The first-ever guidelines for interventional cardiologists using percutaneous patent foramen ovale closure recommend expanding the use of the procedure beyond the Food and Drug Administration–approved indication following PFO-associated ischemic stroke, adding clarification about the use of PFO with anticoagulation and hedging against abuse and overuse of the procedure, said the chair of the guideline writing committee.
“The most important things surrounding these guidelines are to help clinicians and policymakers – third-party payers – to address PFO in patient subsets that were not included in the large randomized clinical trials that led to FDA approval,” said writing group chair Clifford J. Kavinsky, MD, PhD, chief of structural and interventional cardiology at Rush University Medical Center, Chicago.
The Society for Cardiovascular Angiography & Interventions issued the guidelines at its annual scientific sessions meeting in Atlanta and published them simultaneously in the society’s journal.
The guidelines issue strong and conditional recommendations. The former means clinicians should order the intervention for most patients; the latter means decisionmaking is more nuanced and should consider contributing factors.
The guidelines clarify patient selection for PFO closure outside the “pretty narrow” indication the FDA approved, Dr. Kavinsky said, which is for PFO-associated ischemic stroke in patients aged 18-60 years.
“So what about patients who are older than 60? What about patients who had their stroke 10 years ago?” Dr. Kavinsky asked. “Those are issues that were unanswered in the randomized clinical trials.”
The guidelines also refine recommendations about anticoagulation in these patients, including its use after PFO closure in selected patients, Dr. Kavinsky noted. “It’s the opinion of the panel that although anticoagulants may be effective, because of issues of noncompliance, because of issues of interruption of therapy by physicians for a variety of reasons, including surgery or noncompliance, that it is preferable to do a PFO device closure to giving anticoagulant therapy.”
Many of the recommendations cover PFO closure alongside antiplatelet or anticoagulation therapy. Key conditional recommendations for patients who haven’t had a PFO-related stroke are:
- Avoiding its routine use in patients with chronic migraines, prior decompression illness (DCI), thrombophilia, atrial septal aneurysm, transient ischemic attack (TIA), or deep vein thrombosis (DVT).
- Considering PFO closure in patients with platypnea-orthodeoxia syndrome (POS) with no other discernible cause of hypoxia or systemic embolism in whom other embolic causes have been ruled out.
In patients who’ve had a PFO-related stroke, the guidelines strongly recommend PFO closure versus antiplatelet therapy alone, but conditionally, not in patients with atrial fibrillation who’ve had an ischemic stroke. They also conditionally suggest PFO closure rather than long-term antiplatelet therapy alone in PFO stroke patients aged 60 and older, as well as those with thrombophilia already on antiplatelet therapy but not anticoagulation. However, the guidelines make no recommendation on PFO closure based on how much time has passed since the previous stroke.
“Furthermore,” Dr. Kavinsky said, “in patients who require lifelong anticoagulation because of recurrent DVT or recurrent pulmonary emboli or thrombopenia, if they’ve had a PFO-mediated stroke, then it’s our opinion that they should have their PFO closed in addition to taking lifelong anticoagulation because of the same issues of noncompliance and interruption of therapy.” Those are conditional recommendations.
The guideline also checks a box in the FDA labeling that mandated agreement between cardiology and neurology in patient selection. The American Academy of Neurology (AAN) issued its own guideline in 2020 for patients with stroke and PFO. In Europe, the European Society of Cardiology issued two position papers on expanded applications of PFO closure.
The recommendations on when PFO closure shouldn’t be done are noteworthy, Dr. Kavinsky said. “PFOs are present in 25% of the adult population, so the number of patients with PFO is huge and the indication for the FDA is really narrow: to reduce the risk of recurrent stroke in patients with PFO-mediated stroke. So, there’s the tremendous potential for abuse out there, of excessive procedures, of doing unnecessary procedures.”
The guidelines are a follow-up to the operator institutional requirements document SCAI issued in 2019 that set requirements for hospital offering and physicians performing PFO closure, Dr. Kavinsky added.
In an editorial accompanying the published guideline, Robert J. Sommer, MD, and Jamil A. Aboulhosn, MD, wrote that they support the recommendations “which help spotlight and clarify the growing list of potential indications for PFO closure.” They noted that the guidelines panel’s “strong” recommendations were for indications validated by randomized trials and that “conditional” recommendations were based on panelists’ experience and observational data.
“It is critical to recognize that most of these guidelines represent consensus opinion only,” wrote Dr. Sommer, who specializes in adult congenital and pediatric cardiology at Columbia University Irving Medical Center, New York, and Dr. Aboulhosn, an interventional cardiologist at Ronald Reagan University of California, Los Angeles, Medical Center. They emphasized the guidelines’ “heavy emphasis” on shared decisionmaking with patients.
Dr. Kavinsky is a principal investigator for Edwards Lifesciences, W.L. Gore and Associates, Medtronic, and Abbott. Dr. Sommer is a principal investigator and investigator in studies sponsored by W.L. Gore & Associates. Dr. Aboulhosn is a consultant to Abbott Medical.
FROM SCAI 2022
NAVIGATOR steers uncontrolled asthma toward calmer seas
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.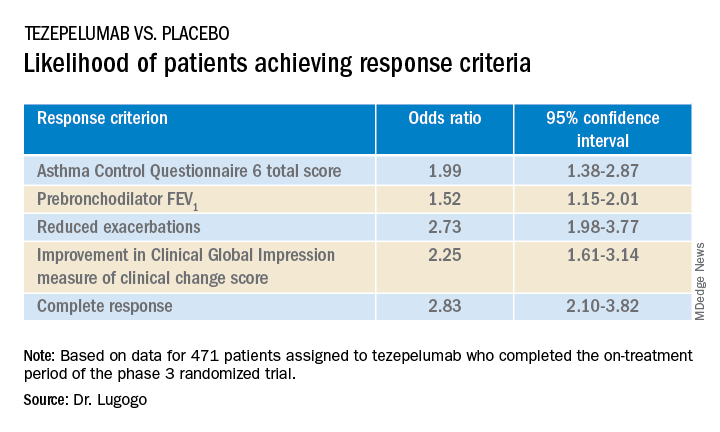
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
AT ATS 2022
New guideline gives active surveillance a boost
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF UROLOGY
Up in smoke: Cannabis-related ED visits increased 18-fold for older Californians
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers in California found an 18-fold increase in the rate of cannabis-related trips to the ED visits among adults over age 65 in the state from 2005 to 2019.
Addressing potential harms of cannabis use among older adults, who face heightened risk for adverse reactions to the substance, “is urgently required,” the researchers reported at the annual meeting of the American Geriatrics Society.
The researchers advised doctors to discuss cannabis use with older patients and screen older adults for cannabis use. Those living with multiple chronic conditions and taking multiple medications are especially likely to be at risk for harm, coinvestigator Benjamin Han, MD, MPH, a geriatrician at the University of California, San Diego, said in an interview.
Dr. Han added that “very little” is understood about the risks and benefits of cannabis use in the elderly, and more studies are needed “so that clinicians can have data-informed discussions with their patients.”
California legalized medical marijuana in 1996 and recreational marijuana in 2016.
The researchers used diagnostic code data from California’s nonmilitary acute care hospitals, collected by the state’s Department of Healthcare Access and Information, to calculate annual rates of cannabis-related visits per 10,000 ED visits.
ED trips up sharply among older adults
Rates of cannabis-related visits increased significantly for all older adult age ranges (P < .001), according to the researchers. Among those aged 65-74 years, the rate increased about 15-fold, from 44.9 per 10,000 visits in 2005 to 714.5 per 100,000 in 2019; for ages 75-84, the rate increased about 22-fold, from 8.4 to 193.9 per 10,000; and for those 85 and older the rate jumped nearly 18-fold, from 2.1 to 39.2 per 10,000.
The greatest increase occurred in visits categorized in diagnostic codes as cannabis abuse and unspecified use. Cannabis dependence and cannabis poisoning accounted for only a small fraction of cases, the investigators found.
The researchers did not have data on specific reasons for a visit, or whether patients had smoked or ingested marijuana products. They also could not discern whether patients had used delta-9-tetrahydrocannabinol, which has psychoactive properties, or cannabidiol, which typically does not have the same mind-altering effects.
Dr. Han said the data may not present a full picture of marijuana-related ED visits. “It is important to recognize that older adults have lived through the very putative language around drug use – including cannabis – as part of the racist war on drugs,” which could lead them to omit having used drugs during the intake process.
A 2017 study linked cannabis use among older adults with more injuries, which in turn led to greater emergency department use. Brian Kaskie, PhD, associate professor in health management and policy at the University of Iowa, Iowa City, said in an interview that the new findings show a state-specific, but alarming trend, and that more research is needed.
“Were these first-time users who were not familiar with anxiety-inducing aspects of cannabis use and took high potency products? Did they complete any education about how to use cannabis?” said Dr. Kaskie, who was not involved in the new study. “Were the ER visits for relatively benign, nonemergent reasons or were these ... visits an outcome of a tragic, harmful event like a car accident or overdose?”
Dr. Han and Dr. Kaskie disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AGS 2022
Tool helps health system cut risky scripts for older adults
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
In the largest implementation yet of the tool, designed by the U.S. Department of Veterans Affairs to decrease the use of potentially inappropriate medications (PIMs), Lifespan, a nonprofit system whose partners include Brown University, Providence, R.I., reported a significant drop in the number of such prescriptions to older adults on discharge from the emergency department (ED).
The number of PIMs among monthly prescriptions fell by roughly 26% at Lifespan’s three adult acute care EDs after the system adopted EQUiPPED – Enhancing Quality of Prescribing Practices for Older Adults Discharged from the Emergency Department. The VA deployed a version of the tool in 2013 to address the lack of training most emergency clinicians receive in the management of geriatric medications.
The model “should be implemented in other states and, with greater replication, could shape national policy regarding quality of care for older adults,” according to the researchers, who reported the results May 12 at the American Geriatrics Society (AGS) 2022 Annual Scientific Meeting, Orlando.
Older adults are three times as likely as younger patients to wind up in an ED because of medication-related harms. This is in part due to the greater number of prescriptions U.S. adults older than 65 years take daily.
A key quality measure
Although the Centers for Medicare & Medicaid Services and other groups have deemed minimizing PIMs an important quality measure, most EDs lack an expert in geriatric prescribing, Elizabeth Goldberg, MD, an associate professor of emergency medicine at Brown University, told this news organization.
With EQUiPPED, clinicians receive access to geriatric medication order sets embedded in electronic health records, individualized benchmark reports, and education about medication safety in older adults. PIMs are defined by the American Geriatrics Society Beers Criteria and include drugs such as proton-pump inhibitors and antipsychotics.
Lifespan’s program involved 362 clinicians who treat about 230,000 patients annually – 40,000 of them aged 65 and older. Dr. Goldberg said implementing the program in such a large population could “really move the needle for older adults” by reducing falls, improving cognitive function, and preventing harm from the use of medication.
She and fellow researchers examined ED prescribing 13 months before and 16 months after they had implemented EQUiPPED, in August and September of 2019. Of clinicians who participated, 48% were attending physicians, 37% were residents, and 34% were advanced practice providers.
PIM prescribing dropped from 8.93% prior to implementation (95% confidence interval: 8.5%-9.36%) to 6.59% after (95% CI: 6.2%-6.98%; P < .001). Before implementation, 1,495 of 16,681 prescribed medications were considered inappropriate, compared with 1,044 of 15,818 medications after, according to the researchers. The biggest declines in prescribing involved antihistamines, muscle relaxants, and benzodiazepines.
Despite the improvements, the system did not meet a goal of reducing PIMs to less than 5%. Dr. Goldberg said educating the large number of clinicians, some of whom rotated in and out of the ED, proved particularly challenging. The COVID-19 pandemic also potentially diverted attention from the quality improvement project, she said.
In addition to its size, the project was notable because it was supported by Blue Cross & Blue Shield of Rhode Island. Dr. Goldberg said obtaining private funding proved to be a quicker and less competitive process than obtaining a government grant. Other institutions interested in running similar studies may need to find insurers that are in the Medicare Advantage market or that have a significant number of younger enrollees with chronic conditions, such as kidney disease, who may benefit from more careful prescribing practices, she said.
The new study builds on previous research, such as a 2017 study that showed that EQUiPPED reduced PIM prescribing at four VA hospitals. Findings from a more recent rollout at three academic health systems suggested that the model might also be effective in targeting the overuse of specific drugs in facilities in which PIM prescribing is already low.
A researcher in those earlier studies, Susan Nicole Hastings, MD, a geriatric medicine specialist at Duke University, Durham, N.C., and the Durham VA Health Care System, told this news organization that Lifespan’s experience supports the idea that “with the right attention to balancing fidelity and tailoring for the new setting, there is tremendous potential for moving successful programs from the VA to other health systems.”
Ann E. Vandenberg, PhD, MPH, a gerontologist at Emory University, Atlanta, said the fragmented nature of the American health care system makes it difficult to disseminate EQUiPPED widely, but interoperability applications that pull data from different electronic health records could help hospital systems to adopt the program without undergoing site-specific customization.
Dr. Hastings and Dr. Vandenberg have received research funding to study EQUiPPED from the Agency for Healthcare Research and Quality. Dr. Hastings also received research funding from the VA.
A version of this article first appeared on Medscape.com.
FROM AGS 2022
Bupivacaine following Mohs surgery reduces opioid use, study finds
An injection of a randomized trial shows.
“Single-dose, in-office bupivacaine administration immediately following reconstructions known to be high risk for pain reduces postoperative narcotic use and acute pain during the time period when our patients have the highest levels of pain,” said first author Vanessa B. Voss, MD, of the University of Missouri–Columbia, who presented the findings at the annual meeting of the American College of Mohs Surgery.

“It was well tolerated, there were no adverse effects, and we recommend the consideration of using this in Mohs micrographic surgery reconstructions that are at the highest risk for pain,” she said.
Recent research has shown that Mohs micrographic surgeons have the highest rates of opioid prescribing of all dermatologists, with about 11% of patients undergoing a Mohs procedure prescribed the drugs for postoperative use, Dr. Voss explained.
Yet, with the ongoing opioid epidemic and even short courses of postoperative opioids placing patients at risk for addiction, the pressure is on to find alternative, nonaddictive strategies for the treatment of acute postoperative pain.
Bupivacaine is commonly used intraoperatively with other types of surgeries to reduce postoperative pain, with a favorable duration of action lasting up to 7 hours, compared with just 2-3 hours with lidocaine. And while its use in Mohs surgery is typically also intraoperative, along with lidocaine, the unique postoperative treatment approach in Mohs surgery has not been well studied, Dr. Voss noted.
To investigate, Dr. Voss and colleagues conducted the prospective, multicenter randomized trial, enrolling 174 patients undergoing Mohs micrographic surgery for skin cancer.
Patients were receiving complex flap reconstructions that have been specifically designated in an American Academy of Dermatology position statement to be high risk for pain following Mohs surgeries, and hence, more likely to involve prescriptions for opioids. These include reconstruction flaps of the scalp, ear, nose or lip, a wedge repair of the ear or lip, or a Mustarde cheek rotation flap.
The mean age of the patients was about 69 years, and about 65% were male. The two groups had no significant differences in demographics, tumor types, or repairs. They were randomized to receive either local injections of bupivacaine 0.5% (with no epinephrine) or placebo with sterile saline injection immediately following the procedure, with the total amount of injection standardized and dependent upon the flap surface area, ranging from 2.5 to 5 cm3.
For postoperative pain, all patients were prescribed acetaminophen 1,000 mg alternating with ibuprofen 400 mg, and tramadol, with instructions to only use tramadol as needed for breakthrough pain.
The reported use of narcotic analgesics by participants was significantly higher among those receiving placebo versus bupivacaine in the first 24 hours following surgery (odds ratio, 2.18; P = .03), as well as in the second 24 hours (OR, 2.18; P = .08) and at 48 hours combined (OR, 2.58; P < .01).
Those in the bupivacaine group also reported lower average pain scores, on a scale of 0-10, during the first 8-hour interval (mean difference, 1.6; P < .001). Importantly, overall, reports of pain medication use and the percentage of patients reporting pain under control were similar between groups, despite lower opioid use in the bupivacaine group.
“The percentage of patients reporting their pain to be under control was similar at all time intervals in both groups, so this means the bupivacaine group had their pain well-controlled despite fewer narcotics, with significant reductions in opioid use,” Dr. Voss noted.
Bupivacaine, though generally regarded as safe, has a reputation for being the most cardiotoxic of the local anesthetic agents; however, there were no such side effects reported in the study. Dr. Voss said the likely explanation is the use of low doses.
“In our study, we had no cardiotoxic effects when using up to 5 cc of 0.5%, which equates to 25 mg per patient,” she explained. This is considered a “very low dose,” since the maximum in the Food and Drug Administration pamphlet for local infiltration is 175 mg per patient every 3 hours, “yet is sufficient for reducing pain/narcotic use.”
She added that “surgeons must be careful to avoid accidental intravascular injection, which could increase risks of systemic toxicity, but this is very rare in the reconstruction settings described.”
Overall, the study suggests a potentially beneficial and unique nonopioid approach that is currently lacking for Mohs procedures associated with a high level of pain. “These findings offer a very effective intervention to reduce postoperative opioid use in this subset of patients,” Dr. Voss told this news organization. “There is not any other intervention that I am aware of to address this, although further study into other long-acting anesthetics may demonstrate similar effects.”

Commenting on the study, Justin J. Leitenberger, MD, session moderator, said that these “data could be impactful for reducing pain as well as the need for opioid medication after dermatologic surgery, both of which would be significant for our patients and public health outcomes.”
Among the challenges in treating pain following Mohs surgeries is that “every patient has a different pain threshold and expectation after surgery,” said Dr. Leitenberger, assistant professor of medicine and dermatology and codirector of dermatologic surgery, Mohs micrographic surgery, and laser and cosmetic surgery at Oregon Health & Science University, Portland.
“Patients undergoing larger repairs in tense areas of skin can experience increased pain and require prescription pain medication,” he said. “Bupivacaine, in this study, shows promise to provide longer lasting pain control from the surgical appointment and easier bridging to nonopioid pain control.”
Regarding the potential cardiotoxicities associated with the drug, Dr. Leitenberger agreed that the risks are low, and added that many surgeons have, in fact, switched to full use of bupivacaine, as opposed to combination with lidocaine, apparently without problems. “This is a small dose locally to the area after a procedure and I agree that the risks are minuscule,” he said.
“Of note, during national lidocaine shortages over the past few years, many practices transitioned to exclusive use of bupivacaine for the entire Mohs procedure, and [anecdotally], this transition did not result in toxicities that were reported,” Dr. Leitenberger said.

Commenting further, Vishal Patel, MD, assistant professor of dermatology and hematology/oncology at George Washington University and director of cutaneous oncology at the GW Cancer Center, both in Washington, also agreed that the benefits appear important. “The benefit from using bupivacaine is encouraging on multiple levels,” he said in an interview.
“Given all that we know about opioids and their negative side effect profile as well as their limited help in cutaneous surgery pain control, the use of long-acting anesthetics is an innovative and reasonable approach to provide pain control in the immediate postoperative window when patients tend to have the most pain,” said Dr. Patel, who is also director of dermatologic surgery at George Washington University.
“After this window, acetaminophen and ibuprofen, which have been shown when used in tandem in an alternating schedule to be superior to opioids, provides an effective pain regimen,” he said. “For larger and more pain-sensitive patients, this appears to be a promising combination.”
Dr. Voss, Dr. Leitenberger, and Dr. Patel have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An injection of a randomized trial shows.
“Single-dose, in-office bupivacaine administration immediately following reconstructions known to be high risk for pain reduces postoperative narcotic use and acute pain during the time period when our patients have the highest levels of pain,” said first author Vanessa B. Voss, MD, of the University of Missouri–Columbia, who presented the findings at the annual meeting of the American College of Mohs Surgery.
“It was well tolerated, there were no adverse effects, and we recommend the consideration of using this in Mohs micrographic surgery reconstructions that are at the highest risk for pain,” she said.
Recent research has shown that Mohs micrographic surgeons have the highest rates of opioid prescribing of all dermatologists, with about 11% of patients undergoing a Mohs procedure prescribed the drugs for postoperative use, Dr. Voss explained.
Yet, with the ongoing opioid epidemic and even short courses of postoperative opioids placing patients at risk for addiction, the pressure is on to find alternative, nonaddictive strategies for the treatment of acute postoperative pain.
Bupivacaine is commonly used intraoperatively with other types of surgeries to reduce postoperative pain, with a favorable duration of action lasting up to 7 hours, compared with just 2-3 hours with lidocaine. And while its use in Mohs surgery is typically also intraoperative, along with lidocaine, the unique postoperative treatment approach in Mohs surgery has not been well studied, Dr. Voss noted.
To investigate, Dr. Voss and colleagues conducted the prospective, multicenter randomized trial, enrolling 174 patients undergoing Mohs micrographic surgery for skin cancer.
Patients were receiving complex flap reconstructions that have been specifically designated in an American Academy of Dermatology position statement to be high risk for pain following Mohs surgeries, and hence, more likely to involve prescriptions for opioids. These include reconstruction flaps of the scalp, ear, nose or lip, a wedge repair of the ear or lip, or a Mustarde cheek rotation flap.
The mean age of the patients was about 69 years, and about 65% were male. The two groups had no significant differences in demographics, tumor types, or repairs. They were randomized to receive either local injections of bupivacaine 0.5% (with no epinephrine) or placebo with sterile saline injection immediately following the procedure, with the total amount of injection standardized and dependent upon the flap surface area, ranging from 2.5 to 5 cm3.
For postoperative pain, all patients were prescribed acetaminophen 1,000 mg alternating with ibuprofen 400 mg, and tramadol, with instructions to only use tramadol as needed for breakthrough pain.
The reported use of narcotic analgesics by participants was significantly higher among those receiving placebo versus bupivacaine in the first 24 hours following surgery (odds ratio, 2.18; P = .03), as well as in the second 24 hours (OR, 2.18; P = .08) and at 48 hours combined (OR, 2.58; P < .01).
Those in the bupivacaine group also reported lower average pain scores, on a scale of 0-10, during the first 8-hour interval (mean difference, 1.6; P < .001). Importantly, overall, reports of pain medication use and the percentage of patients reporting pain under control were similar between groups, despite lower opioid use in the bupivacaine group.
“The percentage of patients reporting their pain to be under control was similar at all time intervals in both groups, so this means the bupivacaine group had their pain well-controlled despite fewer narcotics, with significant reductions in opioid use,” Dr. Voss noted.
Bupivacaine, though generally regarded as safe, has a reputation for being the most cardiotoxic of the local anesthetic agents; however, there were no such side effects reported in the study. Dr. Voss said the likely explanation is the use of low doses.
“In our study, we had no cardiotoxic effects when using up to 5 cc of 0.5%, which equates to 25 mg per patient,” she explained. This is considered a “very low dose,” since the maximum in the Food and Drug Administration pamphlet for local infiltration is 175 mg per patient every 3 hours, “yet is sufficient for reducing pain/narcotic use.”
She added that “surgeons must be careful to avoid accidental intravascular injection, which could increase risks of systemic toxicity, but this is very rare in the reconstruction settings described.”
Overall, the study suggests a potentially beneficial and unique nonopioid approach that is currently lacking for Mohs procedures associated with a high level of pain. “These findings offer a very effective intervention to reduce postoperative opioid use in this subset of patients,” Dr. Voss told this news organization. “There is not any other intervention that I am aware of to address this, although further study into other long-acting anesthetics may demonstrate similar effects.”
Commenting on the study, Justin J. Leitenberger, MD, session moderator, said that these “data could be impactful for reducing pain as well as the need for opioid medication after dermatologic surgery, both of which would be significant for our patients and public health outcomes.”
Among the challenges in treating pain following Mohs surgeries is that “every patient has a different pain threshold and expectation after surgery,” said Dr. Leitenberger, assistant professor of medicine and dermatology and codirector of dermatologic surgery, Mohs micrographic surgery, and laser and cosmetic surgery at Oregon Health & Science University, Portland.
“Patients undergoing larger repairs in tense areas of skin can experience increased pain and require prescription pain medication,” he said. “Bupivacaine, in this study, shows promise to provide longer lasting pain control from the surgical appointment and easier bridging to nonopioid pain control.”
Regarding the potential cardiotoxicities associated with the drug, Dr. Leitenberger agreed that the risks are low, and added that many surgeons have, in fact, switched to full use of bupivacaine, as opposed to combination with lidocaine, apparently without problems. “This is a small dose locally to the area after a procedure and I agree that the risks are minuscule,” he said.
“Of note, during national lidocaine shortages over the past few years, many practices transitioned to exclusive use of bupivacaine for the entire Mohs procedure, and [anecdotally], this transition did not result in toxicities that were reported,” Dr. Leitenberger said.
Commenting further, Vishal Patel, MD, assistant professor of dermatology and hematology/oncology at George Washington University and director of cutaneous oncology at the GW Cancer Center, both in Washington, also agreed that the benefits appear important. “The benefit from using bupivacaine is encouraging on multiple levels,” he said in an interview.
“Given all that we know about opioids and their negative side effect profile as well as their limited help in cutaneous surgery pain control, the use of long-acting anesthetics is an innovative and reasonable approach to provide pain control in the immediate postoperative window when patients tend to have the most pain,” said Dr. Patel, who is also director of dermatologic surgery at George Washington University.
“After this window, acetaminophen and ibuprofen, which have been shown when used in tandem in an alternating schedule to be superior to opioids, provides an effective pain regimen,” he said. “For larger and more pain-sensitive patients, this appears to be a promising combination.”
Dr. Voss, Dr. Leitenberger, and Dr. Patel have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An injection of a randomized trial shows.
“Single-dose, in-office bupivacaine administration immediately following reconstructions known to be high risk for pain reduces postoperative narcotic use and acute pain during the time period when our patients have the highest levels of pain,” said first author Vanessa B. Voss, MD, of the University of Missouri–Columbia, who presented the findings at the annual meeting of the American College of Mohs Surgery.
“It was well tolerated, there were no adverse effects, and we recommend the consideration of using this in Mohs micrographic surgery reconstructions that are at the highest risk for pain,” she said.
Recent research has shown that Mohs micrographic surgeons have the highest rates of opioid prescribing of all dermatologists, with about 11% of patients undergoing a Mohs procedure prescribed the drugs for postoperative use, Dr. Voss explained.
Yet, with the ongoing opioid epidemic and even short courses of postoperative opioids placing patients at risk for addiction, the pressure is on to find alternative, nonaddictive strategies for the treatment of acute postoperative pain.
Bupivacaine is commonly used intraoperatively with other types of surgeries to reduce postoperative pain, with a favorable duration of action lasting up to 7 hours, compared with just 2-3 hours with lidocaine. And while its use in Mohs surgery is typically also intraoperative, along with lidocaine, the unique postoperative treatment approach in Mohs surgery has not been well studied, Dr. Voss noted.
To investigate, Dr. Voss and colleagues conducted the prospective, multicenter randomized trial, enrolling 174 patients undergoing Mohs micrographic surgery for skin cancer.
Patients were receiving complex flap reconstructions that have been specifically designated in an American Academy of Dermatology position statement to be high risk for pain following Mohs surgeries, and hence, more likely to involve prescriptions for opioids. These include reconstruction flaps of the scalp, ear, nose or lip, a wedge repair of the ear or lip, or a Mustarde cheek rotation flap.
The mean age of the patients was about 69 years, and about 65% were male. The two groups had no significant differences in demographics, tumor types, or repairs. They were randomized to receive either local injections of bupivacaine 0.5% (with no epinephrine) or placebo with sterile saline injection immediately following the procedure, with the total amount of injection standardized and dependent upon the flap surface area, ranging from 2.5 to 5 cm3.
For postoperative pain, all patients were prescribed acetaminophen 1,000 mg alternating with ibuprofen 400 mg, and tramadol, with instructions to only use tramadol as needed for breakthrough pain.
The reported use of narcotic analgesics by participants was significantly higher among those receiving placebo versus bupivacaine in the first 24 hours following surgery (odds ratio, 2.18; P = .03), as well as in the second 24 hours (OR, 2.18; P = .08) and at 48 hours combined (OR, 2.58; P < .01).
Those in the bupivacaine group also reported lower average pain scores, on a scale of 0-10, during the first 8-hour interval (mean difference, 1.6; P < .001). Importantly, overall, reports of pain medication use and the percentage of patients reporting pain under control were similar between groups, despite lower opioid use in the bupivacaine group.
“The percentage of patients reporting their pain to be under control was similar at all time intervals in both groups, so this means the bupivacaine group had their pain well-controlled despite fewer narcotics, with significant reductions in opioid use,” Dr. Voss noted.
Bupivacaine, though generally regarded as safe, has a reputation for being the most cardiotoxic of the local anesthetic agents; however, there were no such side effects reported in the study. Dr. Voss said the likely explanation is the use of low doses.
“In our study, we had no cardiotoxic effects when using up to 5 cc of 0.5%, which equates to 25 mg per patient,” she explained. This is considered a “very low dose,” since the maximum in the Food and Drug Administration pamphlet for local infiltration is 175 mg per patient every 3 hours, “yet is sufficient for reducing pain/narcotic use.”
She added that “surgeons must be careful to avoid accidental intravascular injection, which could increase risks of systemic toxicity, but this is very rare in the reconstruction settings described.”
Overall, the study suggests a potentially beneficial and unique nonopioid approach that is currently lacking for Mohs procedures associated with a high level of pain. “These findings offer a very effective intervention to reduce postoperative opioid use in this subset of patients,” Dr. Voss told this news organization. “There is not any other intervention that I am aware of to address this, although further study into other long-acting anesthetics may demonstrate similar effects.”
Commenting on the study, Justin J. Leitenberger, MD, session moderator, said that these “data could be impactful for reducing pain as well as the need for opioid medication after dermatologic surgery, both of which would be significant for our patients and public health outcomes.”
Among the challenges in treating pain following Mohs surgeries is that “every patient has a different pain threshold and expectation after surgery,” said Dr. Leitenberger, assistant professor of medicine and dermatology and codirector of dermatologic surgery, Mohs micrographic surgery, and laser and cosmetic surgery at Oregon Health & Science University, Portland.
“Patients undergoing larger repairs in tense areas of skin can experience increased pain and require prescription pain medication,” he said. “Bupivacaine, in this study, shows promise to provide longer lasting pain control from the surgical appointment and easier bridging to nonopioid pain control.”
Regarding the potential cardiotoxicities associated with the drug, Dr. Leitenberger agreed that the risks are low, and added that many surgeons have, in fact, switched to full use of bupivacaine, as opposed to combination with lidocaine, apparently without problems. “This is a small dose locally to the area after a procedure and I agree that the risks are minuscule,” he said.
“Of note, during national lidocaine shortages over the past few years, many practices transitioned to exclusive use of bupivacaine for the entire Mohs procedure, and [anecdotally], this transition did not result in toxicities that were reported,” Dr. Leitenberger said.
Commenting further, Vishal Patel, MD, assistant professor of dermatology and hematology/oncology at George Washington University and director of cutaneous oncology at the GW Cancer Center, both in Washington, also agreed that the benefits appear important. “The benefit from using bupivacaine is encouraging on multiple levels,” he said in an interview.
“Given all that we know about opioids and their negative side effect profile as well as their limited help in cutaneous surgery pain control, the use of long-acting anesthetics is an innovative and reasonable approach to provide pain control in the immediate postoperative window when patients tend to have the most pain,” said Dr. Patel, who is also director of dermatologic surgery at George Washington University.
“After this window, acetaminophen and ibuprofen, which have been shown when used in tandem in an alternating schedule to be superior to opioids, provides an effective pain regimen,” he said. “For larger and more pain-sensitive patients, this appears to be a promising combination.”
Dr. Voss, Dr. Leitenberger, and Dr. Patel have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACMS 2022