User login
Does rapid weight loss from GLP-1s decrease muscle mass?
Recently, the glucagonlike peptide 1 (GLP-1) receptor agonist semaglutide has changed the obesity treatment landscape. This and other similar medications approaching the market are in high demand because of their ease of use, effectiveness, and lack of interactions with other medications.
Semaglutide is a weekly subcutaneous injection approved by the U.S. Food and Drug Administration for weight loss in conjunction with lifestyle change. It elicits an average weight loss of 15%-18% from baseline in adults with overweight or obesity (body mass index ≥ 27 with at least one obesity-related comorbidity or BMI ≥ 30) in a period of 52-68 weeks (Wilding et al; Rubino et al). Liraglutide is a daily GLP-1 agonist, which is FDA approved for treatment of overweight, with an average weight loss of 8% from treatment start.
Though GLP-1 agonists are very effective for weight loss, questions about side effects have arisen.
Current modalities of weight loss don’t specifically target fat mass (FM), so it is expected that, to a degree, fat-free mass (FFM), including muscle mass, will also be lost along with fat mass.
Loss of muscle mass is associated with an increased risk for lower bone density, fatigue, injuries, and decreased strength. In addition, sarcopenic obesity, a combination of high body fat percentage and low skeletal muscle mass, is concerning in patients older than 65 years and/or postmenopausal patients. Because GLP-1 agonists cause more rapid and sustainable weight loss, compared with intensive behavioral lifestyle therapy, there has been more media attention recently about possible muscle mass loss with GLP-1–agonist use.
However, proper well-rounded approaches to obesity treatment can mitigate the issue of muscle mass loss even when rapid weight loss occurs. When weight loss is achieved with very-low-calorie dietary changes alone (without exercise), it is also associated with significant reductions in lean muscle mass; however, incorporating exercise, preferably resistance training, can mitigate the muscle mass loss. The muscle-preserving effect of exercise is especially prominent in older populations where it is needed most and should be incorporated (Armanento-Villareal et al.; Winter et al.; Batsis and Zagaria; Mason et al.).
Furthermore, studies in rat models demonstrate liraglutide induces myogenesis in myoblasts and protects against muscular atrophy. In human studies, GLP-1 infusion was associated with an improved skeletal and cardiac muscle microvasculature, suggesting that GLP-1 agonists may have some positive effects on the muscle. A 2020 systematic review examined the effect of gradual vs. rapid weight loss and demonstrated no significant difference in muscle loss between the rapid weight-loss group and gradual weight-loss group. Even after gastric bypass surgery, most of the muscle mass loss occurred during the first year, when weight loss is happening. However, after the first year, skeletal muscle was maintained even without introducing additional dietary or exercise interventions.
Age, although a consideration, should not be a discriminating factor against treating obesity. Sarcopenic obesity is a serious risk especially in patients aged 65 years or older, but GLP-1–agonist therapy can be beneficial to prevent muscle atrophy and increase blood flow to skeletal and cardiac muscle. In addition, patients must be encouraged to maintain an appropriate dietary and exercise regimen to treat their obesity. Management of obesity is complex and multifaceted, and patients should understand their responsibility to follow clinician recommendations during this journey to decrease the associated side effects.
Overall, with any level of weight loss achieved with current strategies, a certain amount of muscle mass loss is expected. All efforts to actively preserve muscle mass can prevent too much muscle loss.
Therefore, providers prescribing medications like GLP-1 agonists to treat obesity must also counsel patients about incorporating aerobic exercise and resistance training as part of the treatment plan as well as ensuring they eat a high-protein diet. Generally, resistance training is preferred over aerobic exercise for muscle mass preservation and increased strength, but studies also demonstrate benefit with aerobic exercise.
In the first few visits of initiating obesity treatment, patients should be encouraged to start to incorporate light physical activity as tolerable while starting to make dietary changes to include at least 0.8g/kg/day of protein (Fappi et al.). These initial visits are also an important opportunity for clinicians to ingrain the importance of exercise as part of healthy weight loss. At every visit, physical activity level should be assessed.
Dr. Ahn is a clinical fellow in obesity medicine, Weight Management Center, at Massachusetts General Hospital, Boston. Dr. Singhal is an assistant professor of pediatrics, Harvard Medical School, Boston, and director, Pediatric Program, MGH Weight Center, Massachusetts General Hospital. Dr. Singhal reported that his spouse consults with AstraZeneca, Dilachi Pharma, Eli Lilly, Genetech, Immunomedics, Pfizer, Sanofi, and Novartis.
A version of this article first appeared on Medscape.com.
Recently, the glucagonlike peptide 1 (GLP-1) receptor agonist semaglutide has changed the obesity treatment landscape. This and other similar medications approaching the market are in high demand because of their ease of use, effectiveness, and lack of interactions with other medications.
Semaglutide is a weekly subcutaneous injection approved by the U.S. Food and Drug Administration for weight loss in conjunction with lifestyle change. It elicits an average weight loss of 15%-18% from baseline in adults with overweight or obesity (body mass index ≥ 27 with at least one obesity-related comorbidity or BMI ≥ 30) in a period of 52-68 weeks (Wilding et al; Rubino et al). Liraglutide is a daily GLP-1 agonist, which is FDA approved for treatment of overweight, with an average weight loss of 8% from treatment start.
Though GLP-1 agonists are very effective for weight loss, questions about side effects have arisen.
Current modalities of weight loss don’t specifically target fat mass (FM), so it is expected that, to a degree, fat-free mass (FFM), including muscle mass, will also be lost along with fat mass.
Loss of muscle mass is associated with an increased risk for lower bone density, fatigue, injuries, and decreased strength. In addition, sarcopenic obesity, a combination of high body fat percentage and low skeletal muscle mass, is concerning in patients older than 65 years and/or postmenopausal patients. Because GLP-1 agonists cause more rapid and sustainable weight loss, compared with intensive behavioral lifestyle therapy, there has been more media attention recently about possible muscle mass loss with GLP-1–agonist use.
However, proper well-rounded approaches to obesity treatment can mitigate the issue of muscle mass loss even when rapid weight loss occurs. When weight loss is achieved with very-low-calorie dietary changes alone (without exercise), it is also associated with significant reductions in lean muscle mass; however, incorporating exercise, preferably resistance training, can mitigate the muscle mass loss. The muscle-preserving effect of exercise is especially prominent in older populations where it is needed most and should be incorporated (Armanento-Villareal et al.; Winter et al.; Batsis and Zagaria; Mason et al.).
Furthermore, studies in rat models demonstrate liraglutide induces myogenesis in myoblasts and protects against muscular atrophy. In human studies, GLP-1 infusion was associated with an improved skeletal and cardiac muscle microvasculature, suggesting that GLP-1 agonists may have some positive effects on the muscle. A 2020 systematic review examined the effect of gradual vs. rapid weight loss and demonstrated no significant difference in muscle loss between the rapid weight-loss group and gradual weight-loss group. Even after gastric bypass surgery, most of the muscle mass loss occurred during the first year, when weight loss is happening. However, after the first year, skeletal muscle was maintained even without introducing additional dietary or exercise interventions.
Age, although a consideration, should not be a discriminating factor against treating obesity. Sarcopenic obesity is a serious risk especially in patients aged 65 years or older, but GLP-1–agonist therapy can be beneficial to prevent muscle atrophy and increase blood flow to skeletal and cardiac muscle. In addition, patients must be encouraged to maintain an appropriate dietary and exercise regimen to treat their obesity. Management of obesity is complex and multifaceted, and patients should understand their responsibility to follow clinician recommendations during this journey to decrease the associated side effects.
Overall, with any level of weight loss achieved with current strategies, a certain amount of muscle mass loss is expected. All efforts to actively preserve muscle mass can prevent too much muscle loss.
Therefore, providers prescribing medications like GLP-1 agonists to treat obesity must also counsel patients about incorporating aerobic exercise and resistance training as part of the treatment plan as well as ensuring they eat a high-protein diet. Generally, resistance training is preferred over aerobic exercise for muscle mass preservation and increased strength, but studies also demonstrate benefit with aerobic exercise.
In the first few visits of initiating obesity treatment, patients should be encouraged to start to incorporate light physical activity as tolerable while starting to make dietary changes to include at least 0.8g/kg/day of protein (Fappi et al.). These initial visits are also an important opportunity for clinicians to ingrain the importance of exercise as part of healthy weight loss. At every visit, physical activity level should be assessed.
Dr. Ahn is a clinical fellow in obesity medicine, Weight Management Center, at Massachusetts General Hospital, Boston. Dr. Singhal is an assistant professor of pediatrics, Harvard Medical School, Boston, and director, Pediatric Program, MGH Weight Center, Massachusetts General Hospital. Dr. Singhal reported that his spouse consults with AstraZeneca, Dilachi Pharma, Eli Lilly, Genetech, Immunomedics, Pfizer, Sanofi, and Novartis.
A version of this article first appeared on Medscape.com.
Recently, the glucagonlike peptide 1 (GLP-1) receptor agonist semaglutide has changed the obesity treatment landscape. This and other similar medications approaching the market are in high demand because of their ease of use, effectiveness, and lack of interactions with other medications.
Semaglutide is a weekly subcutaneous injection approved by the U.S. Food and Drug Administration for weight loss in conjunction with lifestyle change. It elicits an average weight loss of 15%-18% from baseline in adults with overweight or obesity (body mass index ≥ 27 with at least one obesity-related comorbidity or BMI ≥ 30) in a period of 52-68 weeks (Wilding et al; Rubino et al). Liraglutide is a daily GLP-1 agonist, which is FDA approved for treatment of overweight, with an average weight loss of 8% from treatment start.
Though GLP-1 agonists are very effective for weight loss, questions about side effects have arisen.
Current modalities of weight loss don’t specifically target fat mass (FM), so it is expected that, to a degree, fat-free mass (FFM), including muscle mass, will also be lost along with fat mass.
Loss of muscle mass is associated with an increased risk for lower bone density, fatigue, injuries, and decreased strength. In addition, sarcopenic obesity, a combination of high body fat percentage and low skeletal muscle mass, is concerning in patients older than 65 years and/or postmenopausal patients. Because GLP-1 agonists cause more rapid and sustainable weight loss, compared with intensive behavioral lifestyle therapy, there has been more media attention recently about possible muscle mass loss with GLP-1–agonist use.
However, proper well-rounded approaches to obesity treatment can mitigate the issue of muscle mass loss even when rapid weight loss occurs. When weight loss is achieved with very-low-calorie dietary changes alone (without exercise), it is also associated with significant reductions in lean muscle mass; however, incorporating exercise, preferably resistance training, can mitigate the muscle mass loss. The muscle-preserving effect of exercise is especially prominent in older populations where it is needed most and should be incorporated (Armanento-Villareal et al.; Winter et al.; Batsis and Zagaria; Mason et al.).
Furthermore, studies in rat models demonstrate liraglutide induces myogenesis in myoblasts and protects against muscular atrophy. In human studies, GLP-1 infusion was associated with an improved skeletal and cardiac muscle microvasculature, suggesting that GLP-1 agonists may have some positive effects on the muscle. A 2020 systematic review examined the effect of gradual vs. rapid weight loss and demonstrated no significant difference in muscle loss between the rapid weight-loss group and gradual weight-loss group. Even after gastric bypass surgery, most of the muscle mass loss occurred during the first year, when weight loss is happening. However, after the first year, skeletal muscle was maintained even without introducing additional dietary or exercise interventions.
Age, although a consideration, should not be a discriminating factor against treating obesity. Sarcopenic obesity is a serious risk especially in patients aged 65 years or older, but GLP-1–agonist therapy can be beneficial to prevent muscle atrophy and increase blood flow to skeletal and cardiac muscle. In addition, patients must be encouraged to maintain an appropriate dietary and exercise regimen to treat their obesity. Management of obesity is complex and multifaceted, and patients should understand their responsibility to follow clinician recommendations during this journey to decrease the associated side effects.
Overall, with any level of weight loss achieved with current strategies, a certain amount of muscle mass loss is expected. All efforts to actively preserve muscle mass can prevent too much muscle loss.
Therefore, providers prescribing medications like GLP-1 agonists to treat obesity must also counsel patients about incorporating aerobic exercise and resistance training as part of the treatment plan as well as ensuring they eat a high-protein diet. Generally, resistance training is preferred over aerobic exercise for muscle mass preservation and increased strength, but studies also demonstrate benefit with aerobic exercise.
In the first few visits of initiating obesity treatment, patients should be encouraged to start to incorporate light physical activity as tolerable while starting to make dietary changes to include at least 0.8g/kg/day of protein (Fappi et al.). These initial visits are also an important opportunity for clinicians to ingrain the importance of exercise as part of healthy weight loss. At every visit, physical activity level should be assessed.
Dr. Ahn is a clinical fellow in obesity medicine, Weight Management Center, at Massachusetts General Hospital, Boston. Dr. Singhal is an assistant professor of pediatrics, Harvard Medical School, Boston, and director, Pediatric Program, MGH Weight Center, Massachusetts General Hospital. Dr. Singhal reported that his spouse consults with AstraZeneca, Dilachi Pharma, Eli Lilly, Genetech, Immunomedics, Pfizer, Sanofi, and Novartis.
A version of this article first appeared on Medscape.com.
Brisk walking: No-cost option for patients to improve cancer outcomes
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
Has the time come to bury BMI in favor of other screening measures?
In 1832, Belgian statistician Adolphe Quetelet introduced the concept of body mass index (BMI) – one’s weight (in kilograms) divided by the square of one’s height (in meters) as a measurement of ideal body weight. Approximately 140 years later, nutritional epidemiologist Ancel Keys proposed the use of BMI as a surrogate marker for evaluating body fat percentage within a population.
For the past 50 years, the scientific and medical communities have relied on BMI as a research and study tool to categorize patients’ weight (that is, severely underweight, underweight, normal weight, overweight, and obesity). The World Health Organization, National Institutes of Health, and U.S. Centers for Disease Control and Prevention use the following BMI weight classifications for adult patients:
- Underweight: BMI < 18.5
- Normal weight: BMI ≥ 18.5 to 24.9
- Overweight: BMI ≥ 25 to 29.9
- Obesity: BMI ≥ 30
Of note, BMI categories for children and adolescents (aged 2-19 years) are based on sex- and age-specific percentiles and will not be addressed in this article.
BMI appears to be a straightforward, easy, and cost-effective way to identify “healthy” weight and assess a patient’s risk for related conditions. For example, studies show that a BMI ≥ 35 kg/m2 correlates to higher prevalence of type 2 diabetes, hypertension, dyslipidemia, and decreased lifespan. At least 13 types of cancer have been linked to obesity, regardless of dietary or physical activity behaviors. While the health dangers associated with BMI ≥ 35 are substantial and difficult to dispute, concerns arise when BMI alone is used to determine healthy weight and disease risk in patients with a BMI of 25-35.
BMI limitations
There are troubling limitations to using BMI alone to assess a patient’s weight and health status. BMI only takes into account a patient’s height and weight, neither of which are sole determinants of health. Moreover, BMI measurements do not distinguish between fat mass and fat-free mass, each of which has very distinct effects on health. High fat mass is associated with an increased risk for disease and mortality, while higher lean body mass correlates with increased physical fitness and longevity. BMI also does not consider age, sex, race, ethnicity, or types of adipose tissue, all of which tremendously influence disease risk across all BMI categories.
Body composition and adipose tissue
Body composition and type of excess adipose tissue better correlate disease risk than does BMI. The World Health Organization defines obesity as having a body fat percentage > 25% for men and > 35% for women. Body composition can be measured by skin-fold thickness, bioelectrical impedance, dual-energy x-ray absorptiometry (DXA), CT, or MRI.
A cross-sectional study by Shah and colleagues) comparing BMI and DXA found that BMI underestimated obesity prevalence. In the study, BMI characterized 26% of participants as obese while DXA (a direct measurement of fat) characterized 64%. Further, 39% of patients categorized as nonobese based on BMI were found to be obese on DXA. Also, BMI misclassified 25% of men and 48% of women in the study. These findings and those of other studies suggest that BMI has a high specificity but low sensitivity for diagnosing obesity, questioning its reliability as a clinical screening tool.
Current guideline recommendations on pharmacologic and surgical treatment options for patients with overweight or obesity, including those of the American Association of Clinical Endocrinology and American College of Endocrinology (AACE/ACE) and the American College of Cardiology/American Heart Association and The Obesity Society (ACC/AHA/TOS), rely on BMI, diminishing their utilization. For example, a recent literature search by Li and associates found that Asian American patients with lower BMIs and BMIs of 25 or 27 are at increased risk for metabolic disease. On the basis of study findings, some organizations recommend considering pharmacotherapy at a lower BMI cutoff of ≥ 25.0 or ≥ 27.5 for Asian people to ensure early treatment intervention in this patient population because guidelines do not recommend pharmacologic treatment unless the BMI is 27 with weight-related complications or 30. Under the current guidelines, a patient of Asian descent has greater disease severity with potentially more complications by the time pharmacotherapy is initiated.
As previously noted, body composition, which requires the use of special equipment (skinfold calipers, DXA, CT, MRI, body impedance scale), best captures the ratio of fat mass to fat-free mass. DXA is frequently used in research studies looking at body composition because of its lower cost, faster time to obtain the study, and ability to measure bone density. MRI has been found to be as accurate as CT for assessing visceral adipose tissue (VAT), skeletal muscle mass, and organ mass, and does not expose patients to ionizing radiation like CT does. MRI clinical use, however, is limited because of its high cost, and it may be problematic for patients with claustrophobia or who are unable to remain immobile for an extended period.
Patients with a high VAT mass, compared with subcutaneous adipose tissue (SAT), are at increased risk for metabolic syndrome, nonalcoholic fatty liver disease, and cardiovascular disease regardless of BMI, underscoring the clinical usefulness of measuring visceral adiposity over BMI.
One of the barriers to implementing VAT assessment in clinical practice is the cost of imaging studies. Fortunately, data suggest that waist circumference and/or waist-to-hip ratio measurements can be a valuable surrogate for VAT measurement. A waist circumference greater than 35 inches (88 cm) or a waist-to-hip ratio greater than 0.8 for women, and greater than 40 inches (102 cm) or a waist-to-hip ratio greater than 0.95 for men, increases metabolic disease risk. Obtaining these measurements requires a tape measure and a few extra minutes and offers more potent data than BMI alone. For example, a large cardiometabolic study found that within each BMI category, increasing gender-specific waist circumferences were associated with significantly higher VAT, liver fat, and a more harmful cardiometabolic risk profile. Men and women with a lower or normal BMI and a high waist circumference are at greatest relative health risk, compared with those with low waist circumference values. Yet, using the BMI alone in these patients would not raise any clinical concern, which is a missed opportunity for cardiometabolic risk reduction.
Biomarkers
Specific biomarkers are closely related to obesity. Leptin and resistin protein levels increase with adipose mass, while adiponectin decreases, probably contributing to insulin resistance. The higher levels of tumor necrosis factor–alpha and interleukin-6 from obesity contribute to chronic inflammation. The combined effect of chronic inflammation and insulin resistance allows greater bioavailability of insulinlike growth factor-1 (IGF-1), which has a role in initiating type 2 diabetes, cardiovascular disease, and cancer. Ideally, measuring these biomarkers could provide more advantageous information than BMI. Unfortunately, for now, the lack of standardized assays and imperfect knowledge of exactly how these biomarkers elicit disease prevents clinical use.
Obesity is a common, highly complex, chronic, and relapsing disease. Thankfully, a number of effective treatments and interventions are available. Although an accurate diagnosis of obesity is essential, underdiagnosed cases and missed opportunities for metabolic disease risk reduction persist. Overdiagnosing obesity, however, has the potential to incur unnecessary health care costs and result in weight bias and stigma.
While BMI is a quick and inexpensive means to assess obesity, by itself it lacks the necessary components for an accurate diagnosis. Particularly for individuals with a normal BMI or less severe overweight/obesity (BMI 27-34.9), other factors must be accounted for, including age, gender, and race. At a minimum, waist circumference should be measured to best risk-stratify and determine treatment intensity. Body composition analysis with BMI calculation refines the diagnosis of obesity.
Finally, clinicians may find best practices by using BMI delta change models. As with so many other clinical measurements, the trajectory tells the most astute story. For example, a patient whose BMI decreased from 45 to 35 may warrant less intensive treatment than a patient whose BMI increased from 26 to 31. Any change in BMI warrants clinical attention. A rapidly or consistently increasing BMI, even within normal range, should prompt clinicians to assess other factors related to obesity and metabolic disease risk (for example, lifestyle factors, waist circumference, blood pressure, cholesterol, diabetes screening) and initiate a conversation about weight management. Similarly, a consistently or rapidly decreasing BMI – even in elevated ranges and particularly with unintentional weight loss – should prompt evaluation.
Although BMI continues to be useful in clinical practice, epidemiology, and research, it should be used in combination with other clinical factors to provide the utmost quality of care.
Dr. Bartfield is assistant professor, obesity medicine specialist, Wake Forest Baptists Medical Center/Atrium Health Weight Management Center, Greensboro, N.C. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
In 1832, Belgian statistician Adolphe Quetelet introduced the concept of body mass index (BMI) – one’s weight (in kilograms) divided by the square of one’s height (in meters) as a measurement of ideal body weight. Approximately 140 years later, nutritional epidemiologist Ancel Keys proposed the use of BMI as a surrogate marker for evaluating body fat percentage within a population.
For the past 50 years, the scientific and medical communities have relied on BMI as a research and study tool to categorize patients’ weight (that is, severely underweight, underweight, normal weight, overweight, and obesity). The World Health Organization, National Institutes of Health, and U.S. Centers for Disease Control and Prevention use the following BMI weight classifications for adult patients:
- Underweight: BMI < 18.5
- Normal weight: BMI ≥ 18.5 to 24.9
- Overweight: BMI ≥ 25 to 29.9
- Obesity: BMI ≥ 30
Of note, BMI categories for children and adolescents (aged 2-19 years) are based on sex- and age-specific percentiles and will not be addressed in this article.
BMI appears to be a straightforward, easy, and cost-effective way to identify “healthy” weight and assess a patient’s risk for related conditions. For example, studies show that a BMI ≥ 35 kg/m2 correlates to higher prevalence of type 2 diabetes, hypertension, dyslipidemia, and decreased lifespan. At least 13 types of cancer have been linked to obesity, regardless of dietary or physical activity behaviors. While the health dangers associated with BMI ≥ 35 are substantial and difficult to dispute, concerns arise when BMI alone is used to determine healthy weight and disease risk in patients with a BMI of 25-35.
BMI limitations
There are troubling limitations to using BMI alone to assess a patient’s weight and health status. BMI only takes into account a patient’s height and weight, neither of which are sole determinants of health. Moreover, BMI measurements do not distinguish between fat mass and fat-free mass, each of which has very distinct effects on health. High fat mass is associated with an increased risk for disease and mortality, while higher lean body mass correlates with increased physical fitness and longevity. BMI also does not consider age, sex, race, ethnicity, or types of adipose tissue, all of which tremendously influence disease risk across all BMI categories.
Body composition and adipose tissue
Body composition and type of excess adipose tissue better correlate disease risk than does BMI. The World Health Organization defines obesity as having a body fat percentage > 25% for men and > 35% for women. Body composition can be measured by skin-fold thickness, bioelectrical impedance, dual-energy x-ray absorptiometry (DXA), CT, or MRI.
A cross-sectional study by Shah and colleagues) comparing BMI and DXA found that BMI underestimated obesity prevalence. In the study, BMI characterized 26% of participants as obese while DXA (a direct measurement of fat) characterized 64%. Further, 39% of patients categorized as nonobese based on BMI were found to be obese on DXA. Also, BMI misclassified 25% of men and 48% of women in the study. These findings and those of other studies suggest that BMI has a high specificity but low sensitivity for diagnosing obesity, questioning its reliability as a clinical screening tool.
Current guideline recommendations on pharmacologic and surgical treatment options for patients with overweight or obesity, including those of the American Association of Clinical Endocrinology and American College of Endocrinology (AACE/ACE) and the American College of Cardiology/American Heart Association and The Obesity Society (ACC/AHA/TOS), rely on BMI, diminishing their utilization. For example, a recent literature search by Li and associates found that Asian American patients with lower BMIs and BMIs of 25 or 27 are at increased risk for metabolic disease. On the basis of study findings, some organizations recommend considering pharmacotherapy at a lower BMI cutoff of ≥ 25.0 or ≥ 27.5 for Asian people to ensure early treatment intervention in this patient population because guidelines do not recommend pharmacologic treatment unless the BMI is 27 with weight-related complications or 30. Under the current guidelines, a patient of Asian descent has greater disease severity with potentially more complications by the time pharmacotherapy is initiated.
As previously noted, body composition, which requires the use of special equipment (skinfold calipers, DXA, CT, MRI, body impedance scale), best captures the ratio of fat mass to fat-free mass. DXA is frequently used in research studies looking at body composition because of its lower cost, faster time to obtain the study, and ability to measure bone density. MRI has been found to be as accurate as CT for assessing visceral adipose tissue (VAT), skeletal muscle mass, and organ mass, and does not expose patients to ionizing radiation like CT does. MRI clinical use, however, is limited because of its high cost, and it may be problematic for patients with claustrophobia or who are unable to remain immobile for an extended period.
Patients with a high VAT mass, compared with subcutaneous adipose tissue (SAT), are at increased risk for metabolic syndrome, nonalcoholic fatty liver disease, and cardiovascular disease regardless of BMI, underscoring the clinical usefulness of measuring visceral adiposity over BMI.
One of the barriers to implementing VAT assessment in clinical practice is the cost of imaging studies. Fortunately, data suggest that waist circumference and/or waist-to-hip ratio measurements can be a valuable surrogate for VAT measurement. A waist circumference greater than 35 inches (88 cm) or a waist-to-hip ratio greater than 0.8 for women, and greater than 40 inches (102 cm) or a waist-to-hip ratio greater than 0.95 for men, increases metabolic disease risk. Obtaining these measurements requires a tape measure and a few extra minutes and offers more potent data than BMI alone. For example, a large cardiometabolic study found that within each BMI category, increasing gender-specific waist circumferences were associated with significantly higher VAT, liver fat, and a more harmful cardiometabolic risk profile. Men and women with a lower or normal BMI and a high waist circumference are at greatest relative health risk, compared with those with low waist circumference values. Yet, using the BMI alone in these patients would not raise any clinical concern, which is a missed opportunity for cardiometabolic risk reduction.
Biomarkers
Specific biomarkers are closely related to obesity. Leptin and resistin protein levels increase with adipose mass, while adiponectin decreases, probably contributing to insulin resistance. The higher levels of tumor necrosis factor–alpha and interleukin-6 from obesity contribute to chronic inflammation. The combined effect of chronic inflammation and insulin resistance allows greater bioavailability of insulinlike growth factor-1 (IGF-1), which has a role in initiating type 2 diabetes, cardiovascular disease, and cancer. Ideally, measuring these biomarkers could provide more advantageous information than BMI. Unfortunately, for now, the lack of standardized assays and imperfect knowledge of exactly how these biomarkers elicit disease prevents clinical use.
Obesity is a common, highly complex, chronic, and relapsing disease. Thankfully, a number of effective treatments and interventions are available. Although an accurate diagnosis of obesity is essential, underdiagnosed cases and missed opportunities for metabolic disease risk reduction persist. Overdiagnosing obesity, however, has the potential to incur unnecessary health care costs and result in weight bias and stigma.
While BMI is a quick and inexpensive means to assess obesity, by itself it lacks the necessary components for an accurate diagnosis. Particularly for individuals with a normal BMI or less severe overweight/obesity (BMI 27-34.9), other factors must be accounted for, including age, gender, and race. At a minimum, waist circumference should be measured to best risk-stratify and determine treatment intensity. Body composition analysis with BMI calculation refines the diagnosis of obesity.
Finally, clinicians may find best practices by using BMI delta change models. As with so many other clinical measurements, the trajectory tells the most astute story. For example, a patient whose BMI decreased from 45 to 35 may warrant less intensive treatment than a patient whose BMI increased from 26 to 31. Any change in BMI warrants clinical attention. A rapidly or consistently increasing BMI, even within normal range, should prompt clinicians to assess other factors related to obesity and metabolic disease risk (for example, lifestyle factors, waist circumference, blood pressure, cholesterol, diabetes screening) and initiate a conversation about weight management. Similarly, a consistently or rapidly decreasing BMI – even in elevated ranges and particularly with unintentional weight loss – should prompt evaluation.
Although BMI continues to be useful in clinical practice, epidemiology, and research, it should be used in combination with other clinical factors to provide the utmost quality of care.
Dr. Bartfield is assistant professor, obesity medicine specialist, Wake Forest Baptists Medical Center/Atrium Health Weight Management Center, Greensboro, N.C. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
In 1832, Belgian statistician Adolphe Quetelet introduced the concept of body mass index (BMI) – one’s weight (in kilograms) divided by the square of one’s height (in meters) as a measurement of ideal body weight. Approximately 140 years later, nutritional epidemiologist Ancel Keys proposed the use of BMI as a surrogate marker for evaluating body fat percentage within a population.
For the past 50 years, the scientific and medical communities have relied on BMI as a research and study tool to categorize patients’ weight (that is, severely underweight, underweight, normal weight, overweight, and obesity). The World Health Organization, National Institutes of Health, and U.S. Centers for Disease Control and Prevention use the following BMI weight classifications for adult patients:
- Underweight: BMI < 18.5
- Normal weight: BMI ≥ 18.5 to 24.9
- Overweight: BMI ≥ 25 to 29.9
- Obesity: BMI ≥ 30
Of note, BMI categories for children and adolescents (aged 2-19 years) are based on sex- and age-specific percentiles and will not be addressed in this article.
BMI appears to be a straightforward, easy, and cost-effective way to identify “healthy” weight and assess a patient’s risk for related conditions. For example, studies show that a BMI ≥ 35 kg/m2 correlates to higher prevalence of type 2 diabetes, hypertension, dyslipidemia, and decreased lifespan. At least 13 types of cancer have been linked to obesity, regardless of dietary or physical activity behaviors. While the health dangers associated with BMI ≥ 35 are substantial and difficult to dispute, concerns arise when BMI alone is used to determine healthy weight and disease risk in patients with a BMI of 25-35.
BMI limitations
There are troubling limitations to using BMI alone to assess a patient’s weight and health status. BMI only takes into account a patient’s height and weight, neither of which are sole determinants of health. Moreover, BMI measurements do not distinguish between fat mass and fat-free mass, each of which has very distinct effects on health. High fat mass is associated with an increased risk for disease and mortality, while higher lean body mass correlates with increased physical fitness and longevity. BMI also does not consider age, sex, race, ethnicity, or types of adipose tissue, all of which tremendously influence disease risk across all BMI categories.
Body composition and adipose tissue
Body composition and type of excess adipose tissue better correlate disease risk than does BMI. The World Health Organization defines obesity as having a body fat percentage > 25% for men and > 35% for women. Body composition can be measured by skin-fold thickness, bioelectrical impedance, dual-energy x-ray absorptiometry (DXA), CT, or MRI.
A cross-sectional study by Shah and colleagues) comparing BMI and DXA found that BMI underestimated obesity prevalence. In the study, BMI characterized 26% of participants as obese while DXA (a direct measurement of fat) characterized 64%. Further, 39% of patients categorized as nonobese based on BMI were found to be obese on DXA. Also, BMI misclassified 25% of men and 48% of women in the study. These findings and those of other studies suggest that BMI has a high specificity but low sensitivity for diagnosing obesity, questioning its reliability as a clinical screening tool.
Current guideline recommendations on pharmacologic and surgical treatment options for patients with overweight or obesity, including those of the American Association of Clinical Endocrinology and American College of Endocrinology (AACE/ACE) and the American College of Cardiology/American Heart Association and The Obesity Society (ACC/AHA/TOS), rely on BMI, diminishing their utilization. For example, a recent literature search by Li and associates found that Asian American patients with lower BMIs and BMIs of 25 or 27 are at increased risk for metabolic disease. On the basis of study findings, some organizations recommend considering pharmacotherapy at a lower BMI cutoff of ≥ 25.0 or ≥ 27.5 for Asian people to ensure early treatment intervention in this patient population because guidelines do not recommend pharmacologic treatment unless the BMI is 27 with weight-related complications or 30. Under the current guidelines, a patient of Asian descent has greater disease severity with potentially more complications by the time pharmacotherapy is initiated.
As previously noted, body composition, which requires the use of special equipment (skinfold calipers, DXA, CT, MRI, body impedance scale), best captures the ratio of fat mass to fat-free mass. DXA is frequently used in research studies looking at body composition because of its lower cost, faster time to obtain the study, and ability to measure bone density. MRI has been found to be as accurate as CT for assessing visceral adipose tissue (VAT), skeletal muscle mass, and organ mass, and does not expose patients to ionizing radiation like CT does. MRI clinical use, however, is limited because of its high cost, and it may be problematic for patients with claustrophobia or who are unable to remain immobile for an extended period.
Patients with a high VAT mass, compared with subcutaneous adipose tissue (SAT), are at increased risk for metabolic syndrome, nonalcoholic fatty liver disease, and cardiovascular disease regardless of BMI, underscoring the clinical usefulness of measuring visceral adiposity over BMI.
One of the barriers to implementing VAT assessment in clinical practice is the cost of imaging studies. Fortunately, data suggest that waist circumference and/or waist-to-hip ratio measurements can be a valuable surrogate for VAT measurement. A waist circumference greater than 35 inches (88 cm) or a waist-to-hip ratio greater than 0.8 for women, and greater than 40 inches (102 cm) or a waist-to-hip ratio greater than 0.95 for men, increases metabolic disease risk. Obtaining these measurements requires a tape measure and a few extra minutes and offers more potent data than BMI alone. For example, a large cardiometabolic study found that within each BMI category, increasing gender-specific waist circumferences were associated with significantly higher VAT, liver fat, and a more harmful cardiometabolic risk profile. Men and women with a lower or normal BMI and a high waist circumference are at greatest relative health risk, compared with those with low waist circumference values. Yet, using the BMI alone in these patients would not raise any clinical concern, which is a missed opportunity for cardiometabolic risk reduction.
Biomarkers
Specific biomarkers are closely related to obesity. Leptin and resistin protein levels increase with adipose mass, while adiponectin decreases, probably contributing to insulin resistance. The higher levels of tumor necrosis factor–alpha and interleukin-6 from obesity contribute to chronic inflammation. The combined effect of chronic inflammation and insulin resistance allows greater bioavailability of insulinlike growth factor-1 (IGF-1), which has a role in initiating type 2 diabetes, cardiovascular disease, and cancer. Ideally, measuring these biomarkers could provide more advantageous information than BMI. Unfortunately, for now, the lack of standardized assays and imperfect knowledge of exactly how these biomarkers elicit disease prevents clinical use.
Obesity is a common, highly complex, chronic, and relapsing disease. Thankfully, a number of effective treatments and interventions are available. Although an accurate diagnosis of obesity is essential, underdiagnosed cases and missed opportunities for metabolic disease risk reduction persist. Overdiagnosing obesity, however, has the potential to incur unnecessary health care costs and result in weight bias and stigma.
While BMI is a quick and inexpensive means to assess obesity, by itself it lacks the necessary components for an accurate diagnosis. Particularly for individuals with a normal BMI or less severe overweight/obesity (BMI 27-34.9), other factors must be accounted for, including age, gender, and race. At a minimum, waist circumference should be measured to best risk-stratify and determine treatment intensity. Body composition analysis with BMI calculation refines the diagnosis of obesity.
Finally, clinicians may find best practices by using BMI delta change models. As with so many other clinical measurements, the trajectory tells the most astute story. For example, a patient whose BMI decreased from 45 to 35 may warrant less intensive treatment than a patient whose BMI increased from 26 to 31. Any change in BMI warrants clinical attention. A rapidly or consistently increasing BMI, even within normal range, should prompt clinicians to assess other factors related to obesity and metabolic disease risk (for example, lifestyle factors, waist circumference, blood pressure, cholesterol, diabetes screening) and initiate a conversation about weight management. Similarly, a consistently or rapidly decreasing BMI – even in elevated ranges and particularly with unintentional weight loss – should prompt evaluation.
Although BMI continues to be useful in clinical practice, epidemiology, and research, it should be used in combination with other clinical factors to provide the utmost quality of care.
Dr. Bartfield is assistant professor, obesity medicine specialist, Wake Forest Baptists Medical Center/Atrium Health Weight Management Center, Greensboro, N.C. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Debate: Initial combination therapy for type 2 diabetes?
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO –
This question was debated by two well-known clinician-researchers in the diabetes world at the recent annual scientific sessions of the American Diabetes Association.
Ralph A. DeFronzo, MD, argued for combination therapy at the time of diagnosis, and David M. Nathan, MD, countered that sequential therapy is a better way to go.
‘The ominous octet’: Addressing multiple underlying defects
Of course, Dr. DeFronzo said, the right agents must be selected. “The drugs we’re going to use as combination at a minimum have to correct the underlying insulin resistance and beta-cell failure, or we are not going to be successful.”
In addition, he said, these drugs should also provide protection against cardiovascular, kidney, and fatty liver disease, because “[managing] diabetes is more than just controlling the glucose.”
Recent U.S. data suggest that half of people with diabetes have a hemoglobin A1c above 7%, and a quarter remain above 8%. “We’re not really doing a very good job in terms of glycemic control,” said Dr. DeFronzo, chief of the diabetes division at University of Texas, San Antonio.
One reason for this failure, he said, is the complex pathophysiology of type 2 diabetes represented by eight major defects, what he called the “ominous octet”: decreased pancreatic insulin secretion, gut incretin effects, glucose uptake in the muscle, increased lipolysis, glucose reabsorption in the kidney, hepatic glucose production, increased glucagon secretion, and neurotransmitter dysfunction.
“There are eight problems, so you’re going to need multiple drugs in combination ... not ones that just lower the A1c.”
And, Dr. DeFronzo said, these drugs “must be started early in the natural history of type 2 diabetes if progressive beta-cell failure is to be prevented.”
He pointed to the United Kingdom Prospective Diabetes Study (UKPDS), in which the sulfonylurea glyburide was used first, followed by metformin. With each drug, the A1c decreased initially but then rose within 3 years. By 15 years, 65% of participants were taking insulin.
More recently, the GRADE study examined the effects of adding four different glucose-lowering agents (glimepiride, sitagliptin, liraglutide, or insulin glargine) in people who hadn’t achieved target A1c with metformin.
“So, by definition, drug number one failed,” he observed.
During the study, all participants showed an initial A1c drop, followed by progressive failure, “again ... showing that stepwise therapy doesn’t work.”
All patients with type 2 diabetes at his center are treated using the “DeFronzo algorithm” consisting of three drug classes: a glucagon-like peptide-1 (GLP-1) agonist, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, and pioglitazone, as each of them targets more than one of the “ominous octet” defects.
“The drugs that clearly do not work on a long-term basis are metformin and sulfonylureas,” he emphasized.
Several studies demonstrate the efficacy of combination therapy, he said. In one, DURATION 8, the combination of exenatide and dapagliflozin was superior to either agent individually in lowering A1c, cardiovascular events, and all-cause mortality over 2 years.
And in the 5-year VERIFY study, early combination therapy with vildagliptin plus metformin proved superior in A1c-lowering to starting patients on metformin and adding vildagliptin later.
Dr. DeFronzo’s own “knock-out punch” study, EDICT, in people with new-onset type 2 diabetes, compared the initial combination of metformin, pioglitazone, and exenatide with conventional sequential add-on therapy with metformin, glipizide, and insulin glargine.
The primary endpoint – the difference in the proportion of patients with A1c less than 6.5% – was 70% versus 29% with combination compared with sequential therapy, a difference “as robust as you can be going against the stepwise approach” at P < .00001, he said.
The combination therapy virtually normalized both insulin sensitivity and beta-cell function, whereas the conventional therapy did neither.
Also from Dr. DeFronzo’s group, in the Qatar study, which compared exenatide plus pioglitazone with basal-bolus insulin in people with about 10 years’ duration of type 2 diabetes and A1c above 7.5% taking sulfonylurea plus metformin, the combination therapy produced an A1c of 6.2% versus 7.1% with insulin.
Dr. DeFronzo pointed to new language added to the ADA Standards of Medical Care in Diabetes in 2022.
While still endorsing stepwise therapy, the document also says that “there are data to support initial combination therapy for more rapid attainment of glycemic targets and longer durability of glycemic effect.” The two references cited are EDICT and VERIFY.
“Finally, the American Diabetes Association has gotten the message,” he concluded.
Sequential therapy: Far more data, lower cost
Dr. Nathan began by pointing out that the ADA Standards of Care continue to advise use of metformin as first-line therapy for type 2 diabetes “because of its high efficacy in lowering A1c, minimal hypoglycemia risk when used as monotherapy, weight neutrality with the potential for modest weight loss, good safety profile, and low cost.”
He emphasized that he was not arguing “against the use of early or even initial combination therapy when there are co-existent morbidities [such as cardiovascular or chronic kidney disease] that merit use of demonstrably effective medications.” But Dr. Nathan pointed out, those patients are not the majority with type 2 diabetes.
He laid out four main arguments for choosing traditional sequential therapy over initial combination therapy. For one, it “enables determination of efficacy of adding individual medications, while initial combination precludes determining benefits of individual drugs.”
Second, traditional sequential therapy allows for assessment of side effects from individual drugs.
“With Dr. DeFronzo’s algorithm you throw everything at them, and if they get nausea, vomiting, or diarrhea, you won’t know which drug it is ... If they get an allergic reaction, you won’t know which medication it is,” observed Dr. Nathan, who is director of the clinical research center and the diabetes center at Massachusetts General Hospital, Boston.
Moreover, he said, traditional sequential therapy “promotes individualization, with selection of drugs, which is something we’re laboring to achieve. Initial combination obviously limits that.”
Further, sequential therapy is “parsimonious and cost-effective, whereas initial combination therapy is expensive, with modest advantages at most.”
And, there are “lots of data” supporting traditional sequential therapy and relatively little for initial combination therapy.
Dr. Nathan added that when he searched the literature for relevant randomized clinical trials, he found 16 investigating initial combination therapy versus monotherapy, but only three that examined combination versus sequential therapy.
“Very few of them, except for EDICT and VERIFY, actually include the sequential therapy that we would use in practice,” he said.
Moreover, he observed, except for the VERIFY study, most are less than half a year in duration. And in VERIFY, there was an initial 20% difference in the proportions of patients with A1c below 7.0%, but by 12 months, that difference had shrunk to just 5%-6%.
“So, looking over time is very important,” Dr. Nathan cautioned. “We really have to be careful ... Six months is barely enough time to see A1c equilibrate ... You really need to study a long-term, chronic, progressive disease like type 2 diabetes over a long enough period of time to be clinically meaningful.”
Dr. Nathan acknowledged to Dr. DeFronzo that the latter’s EDICT study was “well conducted” and “long enough,” and that the researchers did examine monotherapy versus sequential therapy. However, he pointed out that it was a small study with 249 patients and the dropout rate was high, with 58% of patients remaining in the study with triple therapy versus 68% for conventional treatment. “That’s a bit problematic,” Dr. Nathan noted.
At 2 years, the “trivial” difference in A1c was 6.5% with conventional therapy versus 6.0% with triple therapy. “This is all on the very flat complications curve with regard to A1c,” he observed.
Patients treated with sequential therapy with sulfonylurea and insulin had higher rates of hypoglycemia and weight gain, whereas the combination triple therapy group had more gastrointestinal side effects and edema.
However, the most dramatic difference was cost: the average wholesale price for sequential therapy totaled about $85 per month, compared with $1,310 for initial combination therapy. For the approximately 1.5 million patients with new-onset type 2 diabetes in the United States, that difference comes to an additional cost per year of about $22 billion, Dr. Nathan calculated.
“Although current sequential therapy leaves much to be desired ... initial combination therapy has generally only been tested for brief, clinically insufficient periods.
“And therefore, I think sequential therapy is still what is called for,” he concluded. “Well-powered, acceptable-duration studies need to be performed before we can adopt initial/early combination therapy as the standard of care.”
Dr. DeFronzo has reported receiving research support from Boehringer Ingelheim, AstraZeneca, and Merck; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca; and participation on a data safety monitoring board or advisory board for AstraZeneca, Intarcia, Novo Nordisk, and Boehringer Ingelheim. Dr. Nathan has reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Conflicting blood pressure targets: Déjà vu all over again
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stop me if you’ve heard this before. There’s a controversy over blood pressure targets. Some argue for 140/90 mm Hg, others for 130/80 mm Hg, and some super ambitious folks think that we should aim for 120/80 mm Hg. If this sounds familiar, it should. We did it in 2017. It’s unclear what, if anything, we learned from the experience. On the upside, it’s not as bad as it was 100 years ago.
When high blood pressure was a ‘good’ thing
Back then, many believed that you needed higher blood pressure as you got older to push the blood through your progressively stiffened and hardened arteries. Hence the name “essential” hypertension. The concern was that lowering blood pressure would hypoperfuse your organs and be dangerous. In the 1930s, John Hay told an audience at a British Medical Association lecture: “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”
The 1900s were a simpler time when people had fatal strokes in their 50s, and their families were consoled by the knowledge that they had lived a good life.
If our thinking around blood pressure had evolved slightly faster, perhaps President Roosevelt wouldn’t have died of a stroke during World War II as his doctors watched his systolic blood pressure climb above 200 mm Hg and suggested massages and barbiturates to take the edge off.
The current controversy
Not that long ago, 180 mm Hg was considered mild hypertension. Now, we are arguing about a systolic blood pressure of 140 versus 130 mm Hg.
The American Academy of Family Physicians takes the view that 140/90 mm Hg is good enough for most people. Their most recent clinical practice guideline, based primarily on two 2020 Cochrane Reviews of blood pressure targets in patients with and without cardiovascular disease, did not find any mortality benefit for a lower blood pressure threshold.
This puts the AAFP guideline in conflict with the 2017 guideline issued jointly by the American College of Cardiology, American Heart Association, and nine other groups, which recommended a target of 130/80 mm Hg for pretty much everyone. Though they say greater than 140/90 mm Hg should be the threshold for low-risk patients or for starting therapy post stroke, we often forget those nuances. The main point of contention is that the AAFP guideline was looking for a mortality benefit, whereas the ACC/AHA/everyone else guideline was looking at preventing cardiovascular events. The latter guideline was driven mainly by the results of the SPRINT trial. ACC/AHA argue for more aggressive targets to prevent the things that cardiologists care about, namely heart attacks.
The AAFP guideline conceded that more aggressive control will result in fewer myocardial infarctions but warn that it comes with more adverse events. Treating 1,000 patients to this lower target would theoretically prevent four MIs, possibly prevent three strokes, but result in 30 adverse events.
In the end, what we are seeing here is not so much a debate over the evidence as a debate over priorities. Interventions that don’t improve mortality can be questioned in terms of their cost effectiveness. But you probably don’t want to have a heart attack (even a nonfatal one). And you certainly don’t want to have a stroke. However, lower blood pressure targets inevitably require more medications. Notwithstanding the economic costs, the dangers of polypharmacy, medication interactions, side effects, and syncope leading to falls cannot be ignored. Falls are not benign adverse events, especially in older adults.
The counter argument is that physicians are human and often let things slide. Set the target at 140/90 mm Hg, and many physicians won’t jump on a systolic blood pressure of 144 mm Hg. Set the target at 130 mm Hg, and maybe they’ll be more likely to react. There’s a fine line between permissiveness and complacency.
If you zoom out and look at the multitude of blood pressure guidelines, you start to notice an important fact. There is not much daylight between them. There are subtle differences in what constitutes high risk and different definitions of older (older should be defined as 10 years older than the reader’s current age). But otherwise, the blood pressure targets are not that different.
Does that final 10 mm Hg really matter when barriers to care mean that tens of millions in the United States are unaware they have hypertension? Even among those diagnosed, many are either untreated or inadequately treated.
With this context, perhaps the most insightful thing that can be said about the blood pressure guideline controversy is that it’s not all that controversial. We can likely all agree that we need to be better at treating hypertension and that creative solutions to reach underserved communities are necessary.
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating hypertension. We should acknowledge that beyond a certain point any cardiovascular benefit comes at the cost of hypotension and side effects. That tipping point will be different for different groups, and probably at a higher set point in older patients.
Individualizing care isn’t difficult. We do it all the time. We just shouldn’t be letting people walk around with untreated hypertension. It’s not the 1900s anymore.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Is there a link between body image concerns and polycystic ovary syndrome?
This transcript has been edited for clarity.
At ENDO 2023, I presented our systematic review and meta-analysis related to body image concerns in women and individuals with polycystic ovary syndrome (PCOS). PCOS is the most common endocrine condition affecting women worldwide. It’s as common as 10%-15%.
Previously thought to be a benign condition affecting a small proportion of women of reproductive age, it’s changed now. It affects women of all ages, all ethnicities, and throughout the world. Body image concern is an area where one feels uncomfortable with how they look and how they feel. Someone might wonder, why worry about body image concerns? When people have body image concerns, it leads to low self-esteem.
Low self-esteem can lead to depression and anxiety, eventually making you a not-so-productive member of society. Several studies have also shown that body image concerns can lead to eating disorders such as anorexia and bulimia, which can be life threatening. Several studies in the past have shown there is a link between PCOS and body image concerns, but what exactly is the link? We don’t know. How big is the problem? We didn’t know until now.
To answer this, we looked at everything published about PCOS and body image concerns together, be it a randomized study, a cluster study, or any kind of study. We put them all into one place and studied them for evidence. The second objective of our work was that we wanted to share any evidence with the international PCOS guidelines group, who are currently reviewing and revising the guidelines for 2023.
We looked at all the major scientific databases, such as PubMed, PubMed Central, and Medline, for any study that’s been published for polycystic ovary syndrome and body image concerns where they specifically used a validated questionnaire – that’s important, and I’ll come back to that later.
We found 6,221 articles on an initial search. After meticulously looking through all of them, we narrowed it down to 9 articles that were relevant to our work. That’s going from 6,221 articles to 9, which were reviewed by 2 independent researchers. If there was any conflict between them, a third independent researcher resolved the conflict.
We found some studies had used the same questionnaires and some had their own questionnaire. We combined the studies where they used the same questionnaire and we did what we call a meta-analysis. We used their data and combined them to find an additional analysis, which is a combination of the two.
The two most commonly used questionnaires were the Multidimensional Body-Self Relations Questionnaire (MBSRQ) survey and the Body-Esteem Scale for Adolescents and Adults (BESAA). I’m not going into detail, but in simplest terms, the MBSRQ has 69 questions, which breaks down into 5 subscales, and BESAA has 3 subscales, which has 23 questions.
When we combined the results in the MBSRQ questionnaire, women with PCOS fared worse in all the subscales, showing there is a concern about body image in women with PCOS when compared with their colleagues who are healthy and do not have PCOS.
With BESAA, we found a little bit of a mixed picture. There was still a significant difference about weight perception, but how they felt and how they attributed, there was no significant difference. Probably the main reason was that only two studies used it and there was a smaller number of people involved in the study.
Why is this important? We feel that by identifying or diagnosing body image concerns, we will be addressing patient concerns. That is important because we clinicians have our own thoughts of what we need to do to help women with PCOS to prevent long-term risk, but it’s also important to talk to the person sitting in front of you right now. What is their concern?
There’s also been a generational shift where women with PCOS used say, “Oh, I’m worried that I can’t have a kid,” to now say, “I’m worried that I don’t feel well about myself.” We need to address that.
When we shared these findings with the international PCOS guidelines, they said we should probably approach this on an individual case-by-case basis because it will mean that the length of consultation might increase if we spend time with body image concerns.
This is where questionnaires come into play. With a validated questionnaire, a person can complete that before they come into the consultation, thereby minimizing the amount of time spent. If they’re not scoring high on the questionnaire, we don’t need to address that. If they are scoring high, then it can be picked up as a topic to discuss.
As I mentioned, there are a couple of limitations, one being the fewer studies and lower numbers of people in the studies. We need to address this in the future.
Long story short, at the moment, there is evidence to say that body image concerns are quite significantly high in women and individuals with PCOS. This is something we need to address as soon as possible.
We are planning future work to understand how social media comes into play, how society influences body image, and how health care professionals across the world are addressing PCOS and body image concerns. Hopefully, we will be able to share these findings in the near future. Thank you.
Dr. Kempegowda is assistant professor in endocrinology, diabetes, and general medicine at the Institute of Applied Health Research, University of Birmingham, and a consultant in endocrinology, diabetes and acute medicine, Queen Elizabeth Hospital, Birmingham, England, and disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
At ENDO 2023, I presented our systematic review and meta-analysis related to body image concerns in women and individuals with polycystic ovary syndrome (PCOS). PCOS is the most common endocrine condition affecting women worldwide. It’s as common as 10%-15%.
Previously thought to be a benign condition affecting a small proportion of women of reproductive age, it’s changed now. It affects women of all ages, all ethnicities, and throughout the world. Body image concern is an area where one feels uncomfortable with how they look and how they feel. Someone might wonder, why worry about body image concerns? When people have body image concerns, it leads to low self-esteem.
Low self-esteem can lead to depression and anxiety, eventually making you a not-so-productive member of society. Several studies have also shown that body image concerns can lead to eating disorders such as anorexia and bulimia, which can be life threatening. Several studies in the past have shown there is a link between PCOS and body image concerns, but what exactly is the link? We don’t know. How big is the problem? We didn’t know until now.
To answer this, we looked at everything published about PCOS and body image concerns together, be it a randomized study, a cluster study, or any kind of study. We put them all into one place and studied them for evidence. The second objective of our work was that we wanted to share any evidence with the international PCOS guidelines group, who are currently reviewing and revising the guidelines for 2023.
We looked at all the major scientific databases, such as PubMed, PubMed Central, and Medline, for any study that’s been published for polycystic ovary syndrome and body image concerns where they specifically used a validated questionnaire – that’s important, and I’ll come back to that later.
We found 6,221 articles on an initial search. After meticulously looking through all of them, we narrowed it down to 9 articles that were relevant to our work. That’s going from 6,221 articles to 9, which were reviewed by 2 independent researchers. If there was any conflict between them, a third independent researcher resolved the conflict.
We found some studies had used the same questionnaires and some had their own questionnaire. We combined the studies where they used the same questionnaire and we did what we call a meta-analysis. We used their data and combined them to find an additional analysis, which is a combination of the two.
The two most commonly used questionnaires were the Multidimensional Body-Self Relations Questionnaire (MBSRQ) survey and the Body-Esteem Scale for Adolescents and Adults (BESAA). I’m not going into detail, but in simplest terms, the MBSRQ has 69 questions, which breaks down into 5 subscales, and BESAA has 3 subscales, which has 23 questions.
When we combined the results in the MBSRQ questionnaire, women with PCOS fared worse in all the subscales, showing there is a concern about body image in women with PCOS when compared with their colleagues who are healthy and do not have PCOS.
With BESAA, we found a little bit of a mixed picture. There was still a significant difference about weight perception, but how they felt and how they attributed, there was no significant difference. Probably the main reason was that only two studies used it and there was a smaller number of people involved in the study.
Why is this important? We feel that by identifying or diagnosing body image concerns, we will be addressing patient concerns. That is important because we clinicians have our own thoughts of what we need to do to help women with PCOS to prevent long-term risk, but it’s also important to talk to the person sitting in front of you right now. What is their concern?
There’s also been a generational shift where women with PCOS used say, “Oh, I’m worried that I can’t have a kid,” to now say, “I’m worried that I don’t feel well about myself.” We need to address that.
When we shared these findings with the international PCOS guidelines, they said we should probably approach this on an individual case-by-case basis because it will mean that the length of consultation might increase if we spend time with body image concerns.
This is where questionnaires come into play. With a validated questionnaire, a person can complete that before they come into the consultation, thereby minimizing the amount of time spent. If they’re not scoring high on the questionnaire, we don’t need to address that. If they are scoring high, then it can be picked up as a topic to discuss.
As I mentioned, there are a couple of limitations, one being the fewer studies and lower numbers of people in the studies. We need to address this in the future.
Long story short, at the moment, there is evidence to say that body image concerns are quite significantly high in women and individuals with PCOS. This is something we need to address as soon as possible.
We are planning future work to understand how social media comes into play, how society influences body image, and how health care professionals across the world are addressing PCOS and body image concerns. Hopefully, we will be able to share these findings in the near future. Thank you.
Dr. Kempegowda is assistant professor in endocrinology, diabetes, and general medicine at the Institute of Applied Health Research, University of Birmingham, and a consultant in endocrinology, diabetes and acute medicine, Queen Elizabeth Hospital, Birmingham, England, and disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
At ENDO 2023, I presented our systematic review and meta-analysis related to body image concerns in women and individuals with polycystic ovary syndrome (PCOS). PCOS is the most common endocrine condition affecting women worldwide. It’s as common as 10%-15%.
Previously thought to be a benign condition affecting a small proportion of women of reproductive age, it’s changed now. It affects women of all ages, all ethnicities, and throughout the world. Body image concern is an area where one feels uncomfortable with how they look and how they feel. Someone might wonder, why worry about body image concerns? When people have body image concerns, it leads to low self-esteem.
Low self-esteem can lead to depression and anxiety, eventually making you a not-so-productive member of society. Several studies have also shown that body image concerns can lead to eating disorders such as anorexia and bulimia, which can be life threatening. Several studies in the past have shown there is a link between PCOS and body image concerns, but what exactly is the link? We don’t know. How big is the problem? We didn’t know until now.
To answer this, we looked at everything published about PCOS and body image concerns together, be it a randomized study, a cluster study, or any kind of study. We put them all into one place and studied them for evidence. The second objective of our work was that we wanted to share any evidence with the international PCOS guidelines group, who are currently reviewing and revising the guidelines for 2023.
We looked at all the major scientific databases, such as PubMed, PubMed Central, and Medline, for any study that’s been published for polycystic ovary syndrome and body image concerns where they specifically used a validated questionnaire – that’s important, and I’ll come back to that later.
We found 6,221 articles on an initial search. After meticulously looking through all of them, we narrowed it down to 9 articles that were relevant to our work. That’s going from 6,221 articles to 9, which were reviewed by 2 independent researchers. If there was any conflict between them, a third independent researcher resolved the conflict.
We found some studies had used the same questionnaires and some had their own questionnaire. We combined the studies where they used the same questionnaire and we did what we call a meta-analysis. We used their data and combined them to find an additional analysis, which is a combination of the two.
The two most commonly used questionnaires were the Multidimensional Body-Self Relations Questionnaire (MBSRQ) survey and the Body-Esteem Scale for Adolescents and Adults (BESAA). I’m not going into detail, but in simplest terms, the MBSRQ has 69 questions, which breaks down into 5 subscales, and BESAA has 3 subscales, which has 23 questions.
When we combined the results in the MBSRQ questionnaire, women with PCOS fared worse in all the subscales, showing there is a concern about body image in women with PCOS when compared with their colleagues who are healthy and do not have PCOS.
With BESAA, we found a little bit of a mixed picture. There was still a significant difference about weight perception, but how they felt and how they attributed, there was no significant difference. Probably the main reason was that only two studies used it and there was a smaller number of people involved in the study.
Why is this important? We feel that by identifying or diagnosing body image concerns, we will be addressing patient concerns. That is important because we clinicians have our own thoughts of what we need to do to help women with PCOS to prevent long-term risk, but it’s also important to talk to the person sitting in front of you right now. What is their concern?
There’s also been a generational shift where women with PCOS used say, “Oh, I’m worried that I can’t have a kid,” to now say, “I’m worried that I don’t feel well about myself.” We need to address that.
When we shared these findings with the international PCOS guidelines, they said we should probably approach this on an individual case-by-case basis because it will mean that the length of consultation might increase if we spend time with body image concerns.
This is where questionnaires come into play. With a validated questionnaire, a person can complete that before they come into the consultation, thereby minimizing the amount of time spent. If they’re not scoring high on the questionnaire, we don’t need to address that. If they are scoring high, then it can be picked up as a topic to discuss.
As I mentioned, there are a couple of limitations, one being the fewer studies and lower numbers of people in the studies. We need to address this in the future.
Long story short, at the moment, there is evidence to say that body image concerns are quite significantly high in women and individuals with PCOS. This is something we need to address as soon as possible.
We are planning future work to understand how social media comes into play, how society influences body image, and how health care professionals across the world are addressing PCOS and body image concerns. Hopefully, we will be able to share these findings in the near future. Thank you.
Dr. Kempegowda is assistant professor in endocrinology, diabetes, and general medicine at the Institute of Applied Health Research, University of Birmingham, and a consultant in endocrinology, diabetes and acute medicine, Queen Elizabeth Hospital, Birmingham, England, and disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A teenage girl refuses more cancer treatment; her father disagrees
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
The surprising occupations with higher-than-expected ovarian cancer rates
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.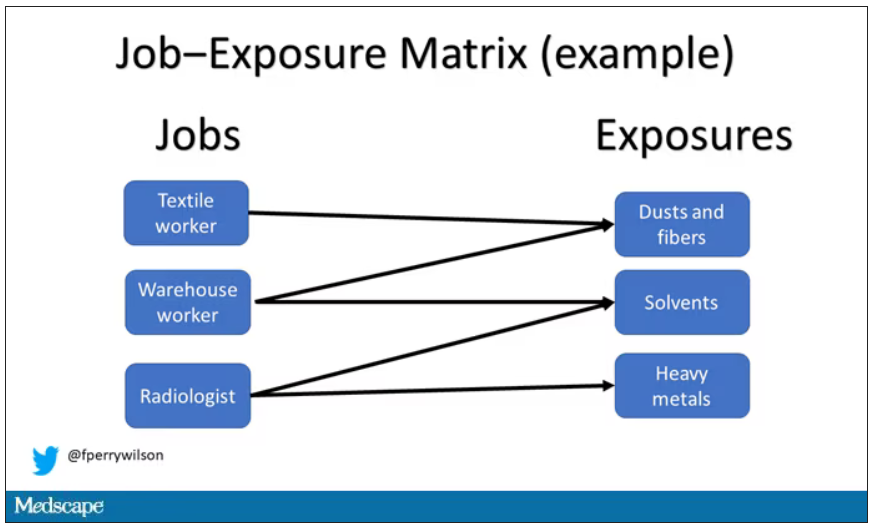
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.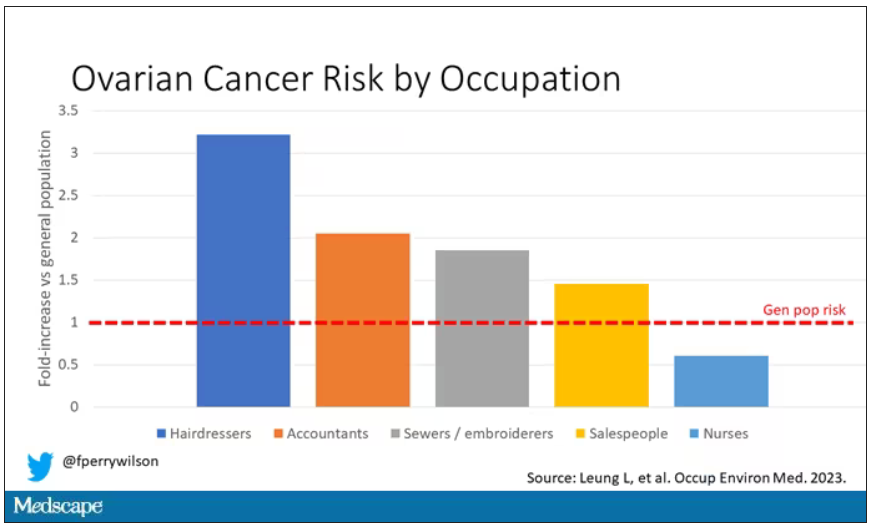
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
‘Body size is not a choice’ and deserves legal protections
Legislators in New York City recently approved a bill specifically prohibiting weight- and height-based discrimination, on par with existing protections for gender, race, sexual orientation, and other personal identities. Other U.S. cities, as well as New York state, are considering similar moves.
Weight-based discrimination in the United States has increased by an estimated 66% over the past decade, putting it on par with the prevalence of racial discrimination. More than 40% of adult Americans and 18% of children report experiencing weight discrimination in employment, school, and/or health care settings – as well as within interpersonal relationships – demonstrating a clear need to have legal protections in place.
For obesity advocates in Canada, the news from New York triggered a moment of reflection to consider how our own advocacy efforts have fared over the years, or not. Just like in the United States, body size and obesity (and appearance in general) are not specifically protected grounds under human rights legislation in Canada (for example, the Canadian Human Rights Act), unlike race, gender, sexual orientation, and religion.
Case law is uneven across the Canadian provinces when it comes to determining whether obesity is even a disease and/or a disability. And despite broad support for anti–weight discrimination policies in Canada (Front Public Health. 2023 Apr 17;11:1060794; Milbank Q. 2015 Dec;93[4]:691-731), years of advocacy at the national and provincial levels have not led to any legislative changes (Ramos Salas Obes Rev. 2017 Nov;18[11]:1323-35; Can J Diabetes. 2015 Apr. doi: 10.1016/j.jcjd.2015.01.009). A 2017 private members bill seeking to add protection for body size to Manitoba’s human rights code was defeated, with many members of the legislature citing enforcement difficulties as the reason for voting down the proposition.
Some obesity advocates have argued that people living with obesity can be protected under the grounds of disability in the Canadian Human Rights Act. To be protected, however, individuals must demonstrate that there is actual or perceived disability relating to their weight or size; yet, many people living with obesity and those who have a higher weight don’t perceive themselves as having a disability.
In our view, the disparate viewpoints on the worthiness of considering body size a human rights issue could be resolved, at least partially, by wider understanding and adoption of the relatively new clinical definition of obesity. This definition holds that obesity is not about size; an obesity diagnosis can be made only when objective clinical investigations identify that excess or abnormal adiposity (fat tissue) impairs health.
While obesity advocates use the clinical definition of obesity, weight and body size proponents disagree that obesity is a chronic disease, and in fact believe that treating it as such can be stigmatizing. In a sense, this can sometimes be true, as not all people with larger bodies have obesity per the new definition but risk being identified as “unhealthy” in the clinical world. Bias, it turns out, can be a two-way street.
Regardless of the advocacy strategy used, it’s clear that specific anti–weight discrimination laws are needed in Canada. One in four Canadian adults report experiencing discrimination in their day-to-day life, with race, gender, age, and weight being the most commonly reported forms. To refuse to protect them against some, but not all, forms of discrimination is itself unjust, and is surely rooted in the age-old misinformed concept that excess weight is the result of laziness, poor food choices, and lack of physical activity, among other moral failings.
Including body size in human rights codes may provide a mechanism to seek legal remedy from discriminatory acts, but it will do little to address rampant weight bias, in the same way that race-based legal protections don’t eradicate racism. And it’s not just the legal community that fails to understand that weight is, by and large, a product of our environment and our genes. Weight bias and stigma are well documented in media, workplaces, the home, and in health care systems.
The solution, in our minds, is meaningful education across all these domains, reinforcing that weight is not a behavior, just as health is not a size. If we truly understand and embrace these concepts, then as a society we may someday recognize that body size is not a choice, just like race, sexual orientation, gender identity, and other individual characteristics. And if it’s not a choice, if it’s not a behavior, then it deserves the same protections.
At the same time, people with obesity deserve to seek evidence-based treatment, just as those at higher weights who experience no weight or adiposity-related health issues deserve not to be identified as having a disease simply because of their size.
If we all follow the science, we might yet turn a common understanding into more equitable outcomes for all.
Dr. Ramos Salas and Mr. Hussey are research consultants for Replica Communications, Hamilton, Ont. She disclosed ties with the Canadian Institutes of Health Research, European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, The Obesity Society, World Obesity, and the World Health Organization. Mr. Hussey disclosed ties with the European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, and the World Health Organization (Nutrition and Food Safety).
A version of this article originally appeared on Medscape.com.
Legislators in New York City recently approved a bill specifically prohibiting weight- and height-based discrimination, on par with existing protections for gender, race, sexual orientation, and other personal identities. Other U.S. cities, as well as New York state, are considering similar moves.
Weight-based discrimination in the United States has increased by an estimated 66% over the past decade, putting it on par with the prevalence of racial discrimination. More than 40% of adult Americans and 18% of children report experiencing weight discrimination in employment, school, and/or health care settings – as well as within interpersonal relationships – demonstrating a clear need to have legal protections in place.
For obesity advocates in Canada, the news from New York triggered a moment of reflection to consider how our own advocacy efforts have fared over the years, or not. Just like in the United States, body size and obesity (and appearance in general) are not specifically protected grounds under human rights legislation in Canada (for example, the Canadian Human Rights Act), unlike race, gender, sexual orientation, and religion.
Case law is uneven across the Canadian provinces when it comes to determining whether obesity is even a disease and/or a disability. And despite broad support for anti–weight discrimination policies in Canada (Front Public Health. 2023 Apr 17;11:1060794; Milbank Q. 2015 Dec;93[4]:691-731), years of advocacy at the national and provincial levels have not led to any legislative changes (Ramos Salas Obes Rev. 2017 Nov;18[11]:1323-35; Can J Diabetes. 2015 Apr. doi: 10.1016/j.jcjd.2015.01.009). A 2017 private members bill seeking to add protection for body size to Manitoba’s human rights code was defeated, with many members of the legislature citing enforcement difficulties as the reason for voting down the proposition.
Some obesity advocates have argued that people living with obesity can be protected under the grounds of disability in the Canadian Human Rights Act. To be protected, however, individuals must demonstrate that there is actual or perceived disability relating to their weight or size; yet, many people living with obesity and those who have a higher weight don’t perceive themselves as having a disability.
In our view, the disparate viewpoints on the worthiness of considering body size a human rights issue could be resolved, at least partially, by wider understanding and adoption of the relatively new clinical definition of obesity. This definition holds that obesity is not about size; an obesity diagnosis can be made only when objective clinical investigations identify that excess or abnormal adiposity (fat tissue) impairs health.
While obesity advocates use the clinical definition of obesity, weight and body size proponents disagree that obesity is a chronic disease, and in fact believe that treating it as such can be stigmatizing. In a sense, this can sometimes be true, as not all people with larger bodies have obesity per the new definition but risk being identified as “unhealthy” in the clinical world. Bias, it turns out, can be a two-way street.
Regardless of the advocacy strategy used, it’s clear that specific anti–weight discrimination laws are needed in Canada. One in four Canadian adults report experiencing discrimination in their day-to-day life, with race, gender, age, and weight being the most commonly reported forms. To refuse to protect them against some, but not all, forms of discrimination is itself unjust, and is surely rooted in the age-old misinformed concept that excess weight is the result of laziness, poor food choices, and lack of physical activity, among other moral failings.
Including body size in human rights codes may provide a mechanism to seek legal remedy from discriminatory acts, but it will do little to address rampant weight bias, in the same way that race-based legal protections don’t eradicate racism. And it’s not just the legal community that fails to understand that weight is, by and large, a product of our environment and our genes. Weight bias and stigma are well documented in media, workplaces, the home, and in health care systems.
The solution, in our minds, is meaningful education across all these domains, reinforcing that weight is not a behavior, just as health is not a size. If we truly understand and embrace these concepts, then as a society we may someday recognize that body size is not a choice, just like race, sexual orientation, gender identity, and other individual characteristics. And if it’s not a choice, if it’s not a behavior, then it deserves the same protections.
At the same time, people with obesity deserve to seek evidence-based treatment, just as those at higher weights who experience no weight or adiposity-related health issues deserve not to be identified as having a disease simply because of their size.
If we all follow the science, we might yet turn a common understanding into more equitable outcomes for all.
Dr. Ramos Salas and Mr. Hussey are research consultants for Replica Communications, Hamilton, Ont. She disclosed ties with the Canadian Institutes of Health Research, European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, The Obesity Society, World Obesity, and the World Health Organization. Mr. Hussey disclosed ties with the European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, and the World Health Organization (Nutrition and Food Safety).
A version of this article originally appeared on Medscape.com.
Legislators in New York City recently approved a bill specifically prohibiting weight- and height-based discrimination, on par with existing protections for gender, race, sexual orientation, and other personal identities. Other U.S. cities, as well as New York state, are considering similar moves.
Weight-based discrimination in the United States has increased by an estimated 66% over the past decade, putting it on par with the prevalence of racial discrimination. More than 40% of adult Americans and 18% of children report experiencing weight discrimination in employment, school, and/or health care settings – as well as within interpersonal relationships – demonstrating a clear need to have legal protections in place.
For obesity advocates in Canada, the news from New York triggered a moment of reflection to consider how our own advocacy efforts have fared over the years, or not. Just like in the United States, body size and obesity (and appearance in general) are not specifically protected grounds under human rights legislation in Canada (for example, the Canadian Human Rights Act), unlike race, gender, sexual orientation, and religion.
Case law is uneven across the Canadian provinces when it comes to determining whether obesity is even a disease and/or a disability. And despite broad support for anti–weight discrimination policies in Canada (Front Public Health. 2023 Apr 17;11:1060794; Milbank Q. 2015 Dec;93[4]:691-731), years of advocacy at the national and provincial levels have not led to any legislative changes (Ramos Salas Obes Rev. 2017 Nov;18[11]:1323-35; Can J Diabetes. 2015 Apr. doi: 10.1016/j.jcjd.2015.01.009). A 2017 private members bill seeking to add protection for body size to Manitoba’s human rights code was defeated, with many members of the legislature citing enforcement difficulties as the reason for voting down the proposition.
Some obesity advocates have argued that people living with obesity can be protected under the grounds of disability in the Canadian Human Rights Act. To be protected, however, individuals must demonstrate that there is actual or perceived disability relating to their weight or size; yet, many people living with obesity and those who have a higher weight don’t perceive themselves as having a disability.
In our view, the disparate viewpoints on the worthiness of considering body size a human rights issue could be resolved, at least partially, by wider understanding and adoption of the relatively new clinical definition of obesity. This definition holds that obesity is not about size; an obesity diagnosis can be made only when objective clinical investigations identify that excess or abnormal adiposity (fat tissue) impairs health.
While obesity advocates use the clinical definition of obesity, weight and body size proponents disagree that obesity is a chronic disease, and in fact believe that treating it as such can be stigmatizing. In a sense, this can sometimes be true, as not all people with larger bodies have obesity per the new definition but risk being identified as “unhealthy” in the clinical world. Bias, it turns out, can be a two-way street.
Regardless of the advocacy strategy used, it’s clear that specific anti–weight discrimination laws are needed in Canada. One in four Canadian adults report experiencing discrimination in their day-to-day life, with race, gender, age, and weight being the most commonly reported forms. To refuse to protect them against some, but not all, forms of discrimination is itself unjust, and is surely rooted in the age-old misinformed concept that excess weight is the result of laziness, poor food choices, and lack of physical activity, among other moral failings.
Including body size in human rights codes may provide a mechanism to seek legal remedy from discriminatory acts, but it will do little to address rampant weight bias, in the same way that race-based legal protections don’t eradicate racism. And it’s not just the legal community that fails to understand that weight is, by and large, a product of our environment and our genes. Weight bias and stigma are well documented in media, workplaces, the home, and in health care systems.
The solution, in our minds, is meaningful education across all these domains, reinforcing that weight is not a behavior, just as health is not a size. If we truly understand and embrace these concepts, then as a society we may someday recognize that body size is not a choice, just like race, sexual orientation, gender identity, and other individual characteristics. And if it’s not a choice, if it’s not a behavior, then it deserves the same protections.
At the same time, people with obesity deserve to seek evidence-based treatment, just as those at higher weights who experience no weight or adiposity-related health issues deserve not to be identified as having a disease simply because of their size.
If we all follow the science, we might yet turn a common understanding into more equitable outcomes for all.
Dr. Ramos Salas and Mr. Hussey are research consultants for Replica Communications, Hamilton, Ont. She disclosed ties with the Canadian Institutes of Health Research, European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, The Obesity Society, World Obesity, and the World Health Organization. Mr. Hussey disclosed ties with the European Association for the Study of Obesity, Novo Nordisk, Obesity Canada, and the World Health Organization (Nutrition and Food Safety).
A version of this article originally appeared on Medscape.com.
As psychiatrists, do we offer hope or do we offer death?
I remember what it was like to be a medical student at a well-known cancer hospital where patients were dying of cancer. In life’s final stages, it was not uncommon for physicians to increase the dose of morphine; it alleviated pain, eased labored breathing, and yes, probably hastened the inevitable for patients who were in their final hours. In these scenarios, no one considered this euthanasia, and no one questioned whether it was the right thing to do.

Fast-forward to 2023 when the act of a physician hastening a patient’s death has become a controversial topic as criteria have expanded. Like all such topics in our polarized society, people aligned on sides, politics and religion rush to the head of the room, legislation is proposed, and words take on new meanings. If you’re in favor of legalization of clinician assistance in a patient’s death, the term is “medical assistance in dying”. If you’re opposed, the term is the more graphic physician-assisted suicide.
The scenario is entirely different from what I saw in my medical school rotations decades ago. It’s no longer an issue of easing the pain and discomfort of patients’ final hours; the question now is whether, faced with a potentially terminal or progressively debilitating physical illness, a patient has the right to determine when, and how, their life will end, and the medical profession is given a role in this.
In many places the bar has been further lowered to incorporate nonterminal conditions, and Belgium and the Netherlands now allow physician-facilitated suicide for psychiatric conditions, a practice that many find reprehensible. In these countries, patients may be provided with medications to ingest, but psychiatrists also administer lethal injections.
While Belgium and the Netherlands were the first countries to legalize physician-facilitated death, it could be argued that Canada has embraced it with the most gusto; physician-assisted suicide has been legal there since 2016.
Canada already has the largest number of physician-assisted deaths of any nation, with 10,064 in 2021 – an increase of 32% from 2020. The Canadian federal government is currently considering adding serious mental illness as an eligible category. If this law passes, the country will have the most liberal assisted-death policy in the world. The Canadian government planned to make serious mental illness an eligible category in March 2023, but in an eleventh-hour announcement, it deferred its decision until March 2024.
In a press release, the government said that the 1-year extension would “provide additional time to prepare for the safe and consistent assessment and provision of MAID in all cases, including where the person’s sole underlying medical condition is a mental illness. It will also allow time for the Government of Canada to fully consider the final report of the Special Joint Committee on MAID, tabled in Parliament on Feb. 15, 2023.”
As a psychiatrist who treats patients with treatment-refractory conditions, I have watched people undergo trial after trial of medications while having psychotherapy, and sometimes transcranial magnetic stimulation or electroconvulsive therapy (ECT). The thing that is sustaining for patients is the hope that they will get better and go on to find meaning and purpose in life, even if it is not in the form they once envisioned.
Where is the line, one wonders, when the patient has not responded to two medications or 12? Must they have ECT before we consider helping them end their lives? Do we try for 6 months or 6 years? What about new research pointing to better medications or psychedelics that are not yet available? According to Canada’s proposed legislation, the patient must be aware that treatment options exist, including facilitated suicide.
Physician-assisted suicide for psychiatric conditions creates a conundrum for psychiatrists. As mental health professionals, we work to prevent suicide and view it as an act that is frequently fueled by depression. Those who are determined to die by their own hand often do. Depression distorts cognition and leads many patients to believe that they would be better off dead and that their loved ones would be better off without them.
These cognitive distortions are part of their illness. So, how do we, as psychiatrists, move from a stance of preventing suicide – using measures such as involuntary treatment when necessary – to being the people who offer and facilitate death for our patients? I’ll leave this for my Canadian colleagues to contemplate, as I live in a state where assisted suicide for any condition remains illegal.
As Canada moves toward facilitating death for serious mental illness, we have to wonder whether racial or socioeconomic factors will play a role. Might those who are poor, who have less access to expensive treatment options and social support, be more likely to request facilitated death? And how do we determine whether patients with serious mental illness are competent to make such a decision or whether it is mental illness that is driving their perception of a future without hope?
As psychiatrists, we often struggle to help our patients overcome the stigma associated with treatments for mental illness. Still, patients often refuse potentially helpful treatments because they worry about the consequences of getting care. These include career repercussions and the disapproval of others. When this legislation is finally passed, will our Canadian colleagues offer it as an option when their patient refuses lithium or antipsychotics, inpatient care, or ECT?
Susan Kalish, MD, is a geriatric and palliative care physician in Boston who favors the availability of facilitated death. She practices in a state where this option is not available.
She told me that she is “in favor of expanding acceptance of, and access to, medical aid in dying for patients who choose to exercise autonomy over their dying process, for those who remain with irremediable suffering, despite provision of optimal palliative care.” However, she added, some countries have lowered the threshold “way too far.”
She noted, “It is complicated and harmful to the general issue of medical aid in dying.”
As psychiatrists, do we offer hope to our most vulnerable patients, or do we offer death? Do we rail against suicide, or do we facilitate it? Do we risk facilitating a patient’s demise when other options are unavailable because of a lack of access to treatment or when social and financial struggles exacerbate a person’s hopelessness? Should we worry that psychiatric euthanasia will turn into a form of eugenics where those who can’t contribute are made to feel that they should bow out? If we, as psychiatrists, aren’t the emissaries of hope, who exactly are we?
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
I remember what it was like to be a medical student at a well-known cancer hospital where patients were dying of cancer. In life’s final stages, it was not uncommon for physicians to increase the dose of morphine; it alleviated pain, eased labored breathing, and yes, probably hastened the inevitable for patients who were in their final hours. In these scenarios, no one considered this euthanasia, and no one questioned whether it was the right thing to do.
Fast-forward to 2023 when the act of a physician hastening a patient’s death has become a controversial topic as criteria have expanded. Like all such topics in our polarized society, people aligned on sides, politics and religion rush to the head of the room, legislation is proposed, and words take on new meanings. If you’re in favor of legalization of clinician assistance in a patient’s death, the term is “medical assistance in dying”. If you’re opposed, the term is the more graphic physician-assisted suicide.
The scenario is entirely different from what I saw in my medical school rotations decades ago. It’s no longer an issue of easing the pain and discomfort of patients’ final hours; the question now is whether, faced with a potentially terminal or progressively debilitating physical illness, a patient has the right to determine when, and how, their life will end, and the medical profession is given a role in this.
In many places the bar has been further lowered to incorporate nonterminal conditions, and Belgium and the Netherlands now allow physician-facilitated suicide for psychiatric conditions, a practice that many find reprehensible. In these countries, patients may be provided with medications to ingest, but psychiatrists also administer lethal injections.
While Belgium and the Netherlands were the first countries to legalize physician-facilitated death, it could be argued that Canada has embraced it with the most gusto; physician-assisted suicide has been legal there since 2016.
Canada already has the largest number of physician-assisted deaths of any nation, with 10,064 in 2021 – an increase of 32% from 2020. The Canadian federal government is currently considering adding serious mental illness as an eligible category. If this law passes, the country will have the most liberal assisted-death policy in the world. The Canadian government planned to make serious mental illness an eligible category in March 2023, but in an eleventh-hour announcement, it deferred its decision until March 2024.
In a press release, the government said that the 1-year extension would “provide additional time to prepare for the safe and consistent assessment and provision of MAID in all cases, including where the person’s sole underlying medical condition is a mental illness. It will also allow time for the Government of Canada to fully consider the final report of the Special Joint Committee on MAID, tabled in Parliament on Feb. 15, 2023.”
As a psychiatrist who treats patients with treatment-refractory conditions, I have watched people undergo trial after trial of medications while having psychotherapy, and sometimes transcranial magnetic stimulation or electroconvulsive therapy (ECT). The thing that is sustaining for patients is the hope that they will get better and go on to find meaning and purpose in life, even if it is not in the form they once envisioned.
Where is the line, one wonders, when the patient has not responded to two medications or 12? Must they have ECT before we consider helping them end their lives? Do we try for 6 months or 6 years? What about new research pointing to better medications or psychedelics that are not yet available? According to Canada’s proposed legislation, the patient must be aware that treatment options exist, including facilitated suicide.
Physician-assisted suicide for psychiatric conditions creates a conundrum for psychiatrists. As mental health professionals, we work to prevent suicide and view it as an act that is frequently fueled by depression. Those who are determined to die by their own hand often do. Depression distorts cognition and leads many patients to believe that they would be better off dead and that their loved ones would be better off without them.
These cognitive distortions are part of their illness. So, how do we, as psychiatrists, move from a stance of preventing suicide – using measures such as involuntary treatment when necessary – to being the people who offer and facilitate death for our patients? I’ll leave this for my Canadian colleagues to contemplate, as I live in a state where assisted suicide for any condition remains illegal.
As Canada moves toward facilitating death for serious mental illness, we have to wonder whether racial or socioeconomic factors will play a role. Might those who are poor, who have less access to expensive treatment options and social support, be more likely to request facilitated death? And how do we determine whether patients with serious mental illness are competent to make such a decision or whether it is mental illness that is driving their perception of a future without hope?
As psychiatrists, we often struggle to help our patients overcome the stigma associated with treatments for mental illness. Still, patients often refuse potentially helpful treatments because they worry about the consequences of getting care. These include career repercussions and the disapproval of others. When this legislation is finally passed, will our Canadian colleagues offer it as an option when their patient refuses lithium or antipsychotics, inpatient care, or ECT?
Susan Kalish, MD, is a geriatric and palliative care physician in Boston who favors the availability of facilitated death. She practices in a state where this option is not available.
She told me that she is “in favor of expanding acceptance of, and access to, medical aid in dying for patients who choose to exercise autonomy over their dying process, for those who remain with irremediable suffering, despite provision of optimal palliative care.” However, she added, some countries have lowered the threshold “way too far.”
She noted, “It is complicated and harmful to the general issue of medical aid in dying.”
As psychiatrists, do we offer hope to our most vulnerable patients, or do we offer death? Do we rail against suicide, or do we facilitate it? Do we risk facilitating a patient’s demise when other options are unavailable because of a lack of access to treatment or when social and financial struggles exacerbate a person’s hopelessness? Should we worry that psychiatric euthanasia will turn into a form of eugenics where those who can’t contribute are made to feel that they should bow out? If we, as psychiatrists, aren’t the emissaries of hope, who exactly are we?
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
I remember what it was like to be a medical student at a well-known cancer hospital where patients were dying of cancer. In life’s final stages, it was not uncommon for physicians to increase the dose of morphine; it alleviated pain, eased labored breathing, and yes, probably hastened the inevitable for patients who were in their final hours. In these scenarios, no one considered this euthanasia, and no one questioned whether it was the right thing to do.
Fast-forward to 2023 when the act of a physician hastening a patient’s death has become a controversial topic as criteria have expanded. Like all such topics in our polarized society, people aligned on sides, politics and religion rush to the head of the room, legislation is proposed, and words take on new meanings. If you’re in favor of legalization of clinician assistance in a patient’s death, the term is “medical assistance in dying”. If you’re opposed, the term is the more graphic physician-assisted suicide.
The scenario is entirely different from what I saw in my medical school rotations decades ago. It’s no longer an issue of easing the pain and discomfort of patients’ final hours; the question now is whether, faced with a potentially terminal or progressively debilitating physical illness, a patient has the right to determine when, and how, their life will end, and the medical profession is given a role in this.
In many places the bar has been further lowered to incorporate nonterminal conditions, and Belgium and the Netherlands now allow physician-facilitated suicide for psychiatric conditions, a practice that many find reprehensible. In these countries, patients may be provided with medications to ingest, but psychiatrists also administer lethal injections.
While Belgium and the Netherlands were the first countries to legalize physician-facilitated death, it could be argued that Canada has embraced it with the most gusto; physician-assisted suicide has been legal there since 2016.
Canada already has the largest number of physician-assisted deaths of any nation, with 10,064 in 2021 – an increase of 32% from 2020. The Canadian federal government is currently considering adding serious mental illness as an eligible category. If this law passes, the country will have the most liberal assisted-death policy in the world. The Canadian government planned to make serious mental illness an eligible category in March 2023, but in an eleventh-hour announcement, it deferred its decision until March 2024.
In a press release, the government said that the 1-year extension would “provide additional time to prepare for the safe and consistent assessment and provision of MAID in all cases, including where the person’s sole underlying medical condition is a mental illness. It will also allow time for the Government of Canada to fully consider the final report of the Special Joint Committee on MAID, tabled in Parliament on Feb. 15, 2023.”
As a psychiatrist who treats patients with treatment-refractory conditions, I have watched people undergo trial after trial of medications while having psychotherapy, and sometimes transcranial magnetic stimulation or electroconvulsive therapy (ECT). The thing that is sustaining for patients is the hope that they will get better and go on to find meaning and purpose in life, even if it is not in the form they once envisioned.
Where is the line, one wonders, when the patient has not responded to two medications or 12? Must they have ECT before we consider helping them end their lives? Do we try for 6 months or 6 years? What about new research pointing to better medications or psychedelics that are not yet available? According to Canada’s proposed legislation, the patient must be aware that treatment options exist, including facilitated suicide.
Physician-assisted suicide for psychiatric conditions creates a conundrum for psychiatrists. As mental health professionals, we work to prevent suicide and view it as an act that is frequently fueled by depression. Those who are determined to die by their own hand often do. Depression distorts cognition and leads many patients to believe that they would be better off dead and that their loved ones would be better off without them.
These cognitive distortions are part of their illness. So, how do we, as psychiatrists, move from a stance of preventing suicide – using measures such as involuntary treatment when necessary – to being the people who offer and facilitate death for our patients? I’ll leave this for my Canadian colleagues to contemplate, as I live in a state where assisted suicide for any condition remains illegal.
As Canada moves toward facilitating death for serious mental illness, we have to wonder whether racial or socioeconomic factors will play a role. Might those who are poor, who have less access to expensive treatment options and social support, be more likely to request facilitated death? And how do we determine whether patients with serious mental illness are competent to make such a decision or whether it is mental illness that is driving their perception of a future without hope?
As psychiatrists, we often struggle to help our patients overcome the stigma associated with treatments for mental illness. Still, patients often refuse potentially helpful treatments because they worry about the consequences of getting care. These include career repercussions and the disapproval of others. When this legislation is finally passed, will our Canadian colleagues offer it as an option when their patient refuses lithium or antipsychotics, inpatient care, or ECT?
Susan Kalish, MD, is a geriatric and palliative care physician in Boston who favors the availability of facilitated death. She practices in a state where this option is not available.
She told me that she is “in favor of expanding acceptance of, and access to, medical aid in dying for patients who choose to exercise autonomy over their dying process, for those who remain with irremediable suffering, despite provision of optimal palliative care.” However, she added, some countries have lowered the threshold “way too far.”
She noted, “It is complicated and harmful to the general issue of medical aid in dying.”
As psychiatrists, do we offer hope to our most vulnerable patients, or do we offer death? Do we rail against suicide, or do we facilitate it? Do we risk facilitating a patient’s demise when other options are unavailable because of a lack of access to treatment or when social and financial struggles exacerbate a person’s hopelessness? Should we worry that psychiatric euthanasia will turn into a form of eugenics where those who can’t contribute are made to feel that they should bow out? If we, as psychiatrists, aren’t the emissaries of hope, who exactly are we?
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.