User login
The VA Goes Its Own Way on Aducanumab
In the Veterans Health Administration (VHA), the current prevalence of veterans with dementia is estimated to be about 10%.1 A 2013 report from the VHA Office of Policy and Planning projected a 22% increase in patients with dementia between 2020 and 2033. That increase amounts to between 276,000 and 335,000 additional veterans enrolled in the US Department of Veterans Affairs (VA) health care.2 Of course, these alarming statistics can in no way begin to convey the devastating biopsychosocial impact of Alzheimer disease and other dementias on veterans and their families. In many cases, veterans’ service to their country resulted in injuries and illnesses that increased the risk that they would develop dementia, such as traumatic brain injuries and posttraumatic stress disorder.3
Confronted with these concerning statistics, why didn’t VA Pharmacy Benefits Management (PBM) follow the US Food and Drug Administration (FDA) approval of aduncanumab-avwa for patients with dementia? Instead, PBM issued a monograph in July 2021 that recommended against providing aduncanumab-avwa to patients with Alzheimer dementia (mild or otherwise) or mild cognitive impairment, “given the lack of evidence of a robust and meaningful clinical benefit and the known safety signal.”4
In this editorial, I examine the reasons for the PBM recommendation, explain how the VA denial of approval for this new drug for dementia contravened that of the FDA and the ethical implications of this decision for veterans with dementia and the health care professionals (HCPs) who treat them.
The VA PBM national drug monographs are scientific reviews of clinical data supporting the potential inclusion of new medications in the VHA formulary.Aducanumab-avwa is a human monoclonal antibody. Its mechanism of action is to stimulate clearance of β-amyloid plaques from the brains of patients with Alzheimer disease. β-amyloid is a protein byproduct of amyloid precursor protein. Abnormal levels of β-amyloid build up in the brain of a patient with Alzheimer disease, forming clumps that disrupt neuronal connections that enable information transmission and other functions contributing to the death of brain cells.5
The FDA approved aducanumab on June 7, 2021, through the accelerated approval pathway.6 Drugs approved through the regular pathway must show a clinical benefit. Because detecting and demonstrating clinical benefit through research can be a lengthy process, in 1992 the FDA initiated the accelerated approval pathway. This alternative regulatory option permits the agency to approve a drug that “filled an unmet medical need” for a serious or life-threatening condition based on a surrogate endpoint.7 Examples of such endpoints are laboratory values, imaging evidence, physical signs, or other objective findings that are believed to predict a clinical benefit. In 2012, the FDA Safety Innovations Act expanded the basis for approval to an intermediate clinical endpoint: a measure of a therapeutic effect that demonstrates a “reasonable likelihood” of predicting clinical benefit.7
The FDA, unlike the PBM, found that aducanumab “provided a meaningful therapeutic advantage over existing treatments.” The FDA underscored that unlike other medications currently available to treat Alzheimer dementias that target symptoms, aducanumab acts on the underlying neurophysiology and neuropathology of the disease based on the decrease in β-amyloid plaques in participants in 2 large clinical trials. The FDA approved the drug for the treatment of patients with either mild cognitive impairment or in the mild state of Alzheimer dementia.
From the time of its announcement, the FDA decision to approve the drug was controversial and criticized in both professional articles and the news media. A particular poignant charge by Largent and Lynch was that the FDA had exploited the desperation of vulnerable patients with dementia and their families willing to try medications with unclear value and uncertain risk precisely because they believed they had no other viable options.8 Critics charged that the FDA took the unusual step of overruling the recommendations of a council of its senior advisors, claiming that there was insufficient evidence for approval; that there was a potential conflict of interest between the agency and the pharmaceutical industry; and that the FDA inappropriately used the accelerated approval pathway.9 In August 2021, in response to these critiques, the Office of the Inspector General announced that it would review the process the agency used in approving the drug.10 Nor was the VA alone in its refusal: The Centers for Medicare and Medicaid (CMS) has proposed to cover the drug for its beneficiaries enrolled in CMS-endorsed clinical trials with the caveat that the drug’s manufacturer, Biogen, must continue to conduct studies on the safety and effectiveness of the drug.11
Why did VHA come to a different scientific conclusion than that of the FDA? In reviewing the data from the 2 major studies, PBM did not find that this surrogate endpoint of reduction in β-amyloid plaques was a valid measure of a meaningful clinical benefit. Further, this lack of valid therapeutic change could not outweigh the risks of the amyloid-related imaging abnormalities (ARIA) in research participants. ARIA include cerebral vasogenic edema, effusions in sulci, microhemorrhages in the brain, and/or localized superficial siderosis. These findings are thought to be the result of the antibody binding to β-amyloid deposits that in turn increase cerebrovascular permeability.5
Thus, in not approving aducanumab, PBM and VHA leadership acted on the core bioethical principles of beneficence and nonmaleficence to prevent harms that proportionally outweighed benefits. Another ethical consideration for the VHA was that of distributive justice given the expense of the medication and the VHA obligation to be responsible stewards of public resources. At the time of the VHA decision, a year’s worth of aducanumab cost about $56,000: In December 2021, the manufacturer announced a dramatic decrease in the drug’s price.12 Although it may seem that fairness requires the VHA to provide any possible treatment for veterans whose cognitive impairment is in part an adverse effect of their time in uniform, a stronger counter argument is that the same high safety and scientific standard should be used for the approval of medications for patients with dementia as for any other disorder.
Among VHA HCPs and their patients with new and early diagnosed mild cognitive impairment or mild dementia, what is lacking in PBM’s clinical ethics analysis is the important principle of autonomy. PBM did carve out a space for the use of the drug in “highly selected patients by experts and centers that have the necessary diagnostic and management expertise.”5 The series of safety standards that must be met along with monitoring for the drug to be prescribed is PBM’s effort to obtain an equilibrium between preventing harm while respecting professional judgment and patient choice. PBM and VHA will reconsider its criteria if research shows improved effectiveness and safety. As with most debated decisions, for some patients and HCPs that balancing act may not have gone far enough, yet many believe that VHA for now is on the right side of the controversy.
1. Williamson V, Stevelink SAM, Greenberg K, Greenberg N. Prevalence of mental health disorders in elderly U.S. military veterans: a metaanalysis and systematic review. Am J Geriatr Psychiatry. 2018;26:534-545. doi:10.1016/j.jagp.2017.11.001
2. US Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. Projections of the prevalence and incidence of dementias. Updated November 5, 2021. Accessed March 20, 2022. www.va.gov/geriatrics/GEC_Data_Reports.asp
3. Zhu CW, Sano M. Demographic, health, and exposure risks associated with cognitive loss, Alzheimer’s disease and other dementias in US military veterans. Front Psychiatry. 2021;12:610334. doi:10.3389/fpsyt.2021.610334
4. VHA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Aducanumab-avwa (ADUHELM) National Drug Monograph. Published July 2021. Accessed March 20, 2022. https://www.pbm.va.gov/PBM/clinicalguidance/drugmonographs/Aducanumab_ADUHELM_monograph_508.pdf
5. National Institutes of Health, National Institute on Aging. What happens to the brain in Alzheimer’s disease? Updated May 16, 2017. Accessed March 20, 2022. https://www.nia.nih.gov/health/what-happens-brain-alzheimers-disease
6. US Food and Drug Administration. FDA grants accelerated approval for Alzheimer’s drug. News release. Published June 7, 2021. Accessed March 21, 2022. https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-drug
7. US Food and Drug Administration. Accelerated approval. Updated January 4, 2018. Accessed March 21,2022.https://www.fda.gov/patients/fast-track-breakthrough-therapy-accelerated-approval-priority-review/accelerated-approval
8. Largent EL, Peterson E, Lynch HF. FDA approval and the ethics of desperation. JAMA Intern Med. 2021;181(12):1555-1556. doi:10.1001/jamainternmed.2021.6045
9. Belluck P, Kaplan S, Robbins R. How an unproven Alzheimer’s drug got approved. New York Times, Updated October 21, 2021. Accessed March 21, 2022. https://www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html
10. US Department of Health and Human Services, Office of the Inspector General. Review of the FDA’s accelerated approval pathway. Accessed March 20, 2022. https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000608.asp
11. Centers for Medicare and Medicaid Services. Monoclonal antibodies directed against amyloid for the treatment of Alzheimer’s disease decision summary. Published January 11, 2022. Accessed March 21, 2022. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=305
12. Gleckman H. What’s behind Biogen’s move to cut prices on its controversial Alzheimer’s drug alduhelm. Forbes. Published December 23, 2021. Accessed March 21,2022. https://www.forbes.com/sites/howardgleckman/2021/12/23/whats-behind-biogens-move-to-cut-prices-on-its-controversial-alzheimers-drug-aduhelm/?sh=498c6a235154
In the Veterans Health Administration (VHA), the current prevalence of veterans with dementia is estimated to be about 10%.1 A 2013 report from the VHA Office of Policy and Planning projected a 22% increase in patients with dementia between 2020 and 2033. That increase amounts to between 276,000 and 335,000 additional veterans enrolled in the US Department of Veterans Affairs (VA) health care.2 Of course, these alarming statistics can in no way begin to convey the devastating biopsychosocial impact of Alzheimer disease and other dementias on veterans and their families. In many cases, veterans’ service to their country resulted in injuries and illnesses that increased the risk that they would develop dementia, such as traumatic brain injuries and posttraumatic stress disorder.3
Confronted with these concerning statistics, why didn’t VA Pharmacy Benefits Management (PBM) follow the US Food and Drug Administration (FDA) approval of aduncanumab-avwa for patients with dementia? Instead, PBM issued a monograph in July 2021 that recommended against providing aduncanumab-avwa to patients with Alzheimer dementia (mild or otherwise) or mild cognitive impairment, “given the lack of evidence of a robust and meaningful clinical benefit and the known safety signal.”4
In this editorial, I examine the reasons for the PBM recommendation, explain how the VA denial of approval for this new drug for dementia contravened that of the FDA and the ethical implications of this decision for veterans with dementia and the health care professionals (HCPs) who treat them.
The VA PBM national drug monographs are scientific reviews of clinical data supporting the potential inclusion of new medications in the VHA formulary.Aducanumab-avwa is a human monoclonal antibody. Its mechanism of action is to stimulate clearance of β-amyloid plaques from the brains of patients with Alzheimer disease. β-amyloid is a protein byproduct of amyloid precursor protein. Abnormal levels of β-amyloid build up in the brain of a patient with Alzheimer disease, forming clumps that disrupt neuronal connections that enable information transmission and other functions contributing to the death of brain cells.5
The FDA approved aducanumab on June 7, 2021, through the accelerated approval pathway.6 Drugs approved through the regular pathway must show a clinical benefit. Because detecting and demonstrating clinical benefit through research can be a lengthy process, in 1992 the FDA initiated the accelerated approval pathway. This alternative regulatory option permits the agency to approve a drug that “filled an unmet medical need” for a serious or life-threatening condition based on a surrogate endpoint.7 Examples of such endpoints are laboratory values, imaging evidence, physical signs, or other objective findings that are believed to predict a clinical benefit. In 2012, the FDA Safety Innovations Act expanded the basis for approval to an intermediate clinical endpoint: a measure of a therapeutic effect that demonstrates a “reasonable likelihood” of predicting clinical benefit.7
The FDA, unlike the PBM, found that aducanumab “provided a meaningful therapeutic advantage over existing treatments.” The FDA underscored that unlike other medications currently available to treat Alzheimer dementias that target symptoms, aducanumab acts on the underlying neurophysiology and neuropathology of the disease based on the decrease in β-amyloid plaques in participants in 2 large clinical trials. The FDA approved the drug for the treatment of patients with either mild cognitive impairment or in the mild state of Alzheimer dementia.
From the time of its announcement, the FDA decision to approve the drug was controversial and criticized in both professional articles and the news media. A particular poignant charge by Largent and Lynch was that the FDA had exploited the desperation of vulnerable patients with dementia and their families willing to try medications with unclear value and uncertain risk precisely because they believed they had no other viable options.8 Critics charged that the FDA took the unusual step of overruling the recommendations of a council of its senior advisors, claiming that there was insufficient evidence for approval; that there was a potential conflict of interest between the agency and the pharmaceutical industry; and that the FDA inappropriately used the accelerated approval pathway.9 In August 2021, in response to these critiques, the Office of the Inspector General announced that it would review the process the agency used in approving the drug.10 Nor was the VA alone in its refusal: The Centers for Medicare and Medicaid (CMS) has proposed to cover the drug for its beneficiaries enrolled in CMS-endorsed clinical trials with the caveat that the drug’s manufacturer, Biogen, must continue to conduct studies on the safety and effectiveness of the drug.11
Why did VHA come to a different scientific conclusion than that of the FDA? In reviewing the data from the 2 major studies, PBM did not find that this surrogate endpoint of reduction in β-amyloid plaques was a valid measure of a meaningful clinical benefit. Further, this lack of valid therapeutic change could not outweigh the risks of the amyloid-related imaging abnormalities (ARIA) in research participants. ARIA include cerebral vasogenic edema, effusions in sulci, microhemorrhages in the brain, and/or localized superficial siderosis. These findings are thought to be the result of the antibody binding to β-amyloid deposits that in turn increase cerebrovascular permeability.5
Thus, in not approving aducanumab, PBM and VHA leadership acted on the core bioethical principles of beneficence and nonmaleficence to prevent harms that proportionally outweighed benefits. Another ethical consideration for the VHA was that of distributive justice given the expense of the medication and the VHA obligation to be responsible stewards of public resources. At the time of the VHA decision, a year’s worth of aducanumab cost about $56,000: In December 2021, the manufacturer announced a dramatic decrease in the drug’s price.12 Although it may seem that fairness requires the VHA to provide any possible treatment for veterans whose cognitive impairment is in part an adverse effect of their time in uniform, a stronger counter argument is that the same high safety and scientific standard should be used for the approval of medications for patients with dementia as for any other disorder.
Among VHA HCPs and their patients with new and early diagnosed mild cognitive impairment or mild dementia, what is lacking in PBM’s clinical ethics analysis is the important principle of autonomy. PBM did carve out a space for the use of the drug in “highly selected patients by experts and centers that have the necessary diagnostic and management expertise.”5 The series of safety standards that must be met along with monitoring for the drug to be prescribed is PBM’s effort to obtain an equilibrium between preventing harm while respecting professional judgment and patient choice. PBM and VHA will reconsider its criteria if research shows improved effectiveness and safety. As with most debated decisions, for some patients and HCPs that balancing act may not have gone far enough, yet many believe that VHA for now is on the right side of the controversy.
In the Veterans Health Administration (VHA), the current prevalence of veterans with dementia is estimated to be about 10%.1 A 2013 report from the VHA Office of Policy and Planning projected a 22% increase in patients with dementia between 2020 and 2033. That increase amounts to between 276,000 and 335,000 additional veterans enrolled in the US Department of Veterans Affairs (VA) health care.2 Of course, these alarming statistics can in no way begin to convey the devastating biopsychosocial impact of Alzheimer disease and other dementias on veterans and their families. In many cases, veterans’ service to their country resulted in injuries and illnesses that increased the risk that they would develop dementia, such as traumatic brain injuries and posttraumatic stress disorder.3
Confronted with these concerning statistics, why didn’t VA Pharmacy Benefits Management (PBM) follow the US Food and Drug Administration (FDA) approval of aduncanumab-avwa for patients with dementia? Instead, PBM issued a monograph in July 2021 that recommended against providing aduncanumab-avwa to patients with Alzheimer dementia (mild or otherwise) or mild cognitive impairment, “given the lack of evidence of a robust and meaningful clinical benefit and the known safety signal.”4
In this editorial, I examine the reasons for the PBM recommendation, explain how the VA denial of approval for this new drug for dementia contravened that of the FDA and the ethical implications of this decision for veterans with dementia and the health care professionals (HCPs) who treat them.
The VA PBM national drug monographs are scientific reviews of clinical data supporting the potential inclusion of new medications in the VHA formulary.Aducanumab-avwa is a human monoclonal antibody. Its mechanism of action is to stimulate clearance of β-amyloid plaques from the brains of patients with Alzheimer disease. β-amyloid is a protein byproduct of amyloid precursor protein. Abnormal levels of β-amyloid build up in the brain of a patient with Alzheimer disease, forming clumps that disrupt neuronal connections that enable information transmission and other functions contributing to the death of brain cells.5
The FDA approved aducanumab on June 7, 2021, through the accelerated approval pathway.6 Drugs approved through the regular pathway must show a clinical benefit. Because detecting and demonstrating clinical benefit through research can be a lengthy process, in 1992 the FDA initiated the accelerated approval pathway. This alternative regulatory option permits the agency to approve a drug that “filled an unmet medical need” for a serious or life-threatening condition based on a surrogate endpoint.7 Examples of such endpoints are laboratory values, imaging evidence, physical signs, or other objective findings that are believed to predict a clinical benefit. In 2012, the FDA Safety Innovations Act expanded the basis for approval to an intermediate clinical endpoint: a measure of a therapeutic effect that demonstrates a “reasonable likelihood” of predicting clinical benefit.7
The FDA, unlike the PBM, found that aducanumab “provided a meaningful therapeutic advantage over existing treatments.” The FDA underscored that unlike other medications currently available to treat Alzheimer dementias that target symptoms, aducanumab acts on the underlying neurophysiology and neuropathology of the disease based on the decrease in β-amyloid plaques in participants in 2 large clinical trials. The FDA approved the drug for the treatment of patients with either mild cognitive impairment or in the mild state of Alzheimer dementia.
From the time of its announcement, the FDA decision to approve the drug was controversial and criticized in both professional articles and the news media. A particular poignant charge by Largent and Lynch was that the FDA had exploited the desperation of vulnerable patients with dementia and their families willing to try medications with unclear value and uncertain risk precisely because they believed they had no other viable options.8 Critics charged that the FDA took the unusual step of overruling the recommendations of a council of its senior advisors, claiming that there was insufficient evidence for approval; that there was a potential conflict of interest between the agency and the pharmaceutical industry; and that the FDA inappropriately used the accelerated approval pathway.9 In August 2021, in response to these critiques, the Office of the Inspector General announced that it would review the process the agency used in approving the drug.10 Nor was the VA alone in its refusal: The Centers for Medicare and Medicaid (CMS) has proposed to cover the drug for its beneficiaries enrolled in CMS-endorsed clinical trials with the caveat that the drug’s manufacturer, Biogen, must continue to conduct studies on the safety and effectiveness of the drug.11
Why did VHA come to a different scientific conclusion than that of the FDA? In reviewing the data from the 2 major studies, PBM did not find that this surrogate endpoint of reduction in β-amyloid plaques was a valid measure of a meaningful clinical benefit. Further, this lack of valid therapeutic change could not outweigh the risks of the amyloid-related imaging abnormalities (ARIA) in research participants. ARIA include cerebral vasogenic edema, effusions in sulci, microhemorrhages in the brain, and/or localized superficial siderosis. These findings are thought to be the result of the antibody binding to β-amyloid deposits that in turn increase cerebrovascular permeability.5
Thus, in not approving aducanumab, PBM and VHA leadership acted on the core bioethical principles of beneficence and nonmaleficence to prevent harms that proportionally outweighed benefits. Another ethical consideration for the VHA was that of distributive justice given the expense of the medication and the VHA obligation to be responsible stewards of public resources. At the time of the VHA decision, a year’s worth of aducanumab cost about $56,000: In December 2021, the manufacturer announced a dramatic decrease in the drug’s price.12 Although it may seem that fairness requires the VHA to provide any possible treatment for veterans whose cognitive impairment is in part an adverse effect of their time in uniform, a stronger counter argument is that the same high safety and scientific standard should be used for the approval of medications for patients with dementia as for any other disorder.
Among VHA HCPs and their patients with new and early diagnosed mild cognitive impairment or mild dementia, what is lacking in PBM’s clinical ethics analysis is the important principle of autonomy. PBM did carve out a space for the use of the drug in “highly selected patients by experts and centers that have the necessary diagnostic and management expertise.”5 The series of safety standards that must be met along with monitoring for the drug to be prescribed is PBM’s effort to obtain an equilibrium between preventing harm while respecting professional judgment and patient choice. PBM and VHA will reconsider its criteria if research shows improved effectiveness and safety. As with most debated decisions, for some patients and HCPs that balancing act may not have gone far enough, yet many believe that VHA for now is on the right side of the controversy.
1. Williamson V, Stevelink SAM, Greenberg K, Greenberg N. Prevalence of mental health disorders in elderly U.S. military veterans: a metaanalysis and systematic review. Am J Geriatr Psychiatry. 2018;26:534-545. doi:10.1016/j.jagp.2017.11.001
2. US Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. Projections of the prevalence and incidence of dementias. Updated November 5, 2021. Accessed March 20, 2022. www.va.gov/geriatrics/GEC_Data_Reports.asp
3. Zhu CW, Sano M. Demographic, health, and exposure risks associated with cognitive loss, Alzheimer’s disease and other dementias in US military veterans. Front Psychiatry. 2021;12:610334. doi:10.3389/fpsyt.2021.610334
4. VHA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Aducanumab-avwa (ADUHELM) National Drug Monograph. Published July 2021. Accessed March 20, 2022. https://www.pbm.va.gov/PBM/clinicalguidance/drugmonographs/Aducanumab_ADUHELM_monograph_508.pdf
5. National Institutes of Health, National Institute on Aging. What happens to the brain in Alzheimer’s disease? Updated May 16, 2017. Accessed March 20, 2022. https://www.nia.nih.gov/health/what-happens-brain-alzheimers-disease
6. US Food and Drug Administration. FDA grants accelerated approval for Alzheimer’s drug. News release. Published June 7, 2021. Accessed March 21, 2022. https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-drug
7. US Food and Drug Administration. Accelerated approval. Updated January 4, 2018. Accessed March 21,2022.https://www.fda.gov/patients/fast-track-breakthrough-therapy-accelerated-approval-priority-review/accelerated-approval
8. Largent EL, Peterson E, Lynch HF. FDA approval and the ethics of desperation. JAMA Intern Med. 2021;181(12):1555-1556. doi:10.1001/jamainternmed.2021.6045
9. Belluck P, Kaplan S, Robbins R. How an unproven Alzheimer’s drug got approved. New York Times, Updated October 21, 2021. Accessed March 21, 2022. https://www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html
10. US Department of Health and Human Services, Office of the Inspector General. Review of the FDA’s accelerated approval pathway. Accessed March 20, 2022. https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000608.asp
11. Centers for Medicare and Medicaid Services. Monoclonal antibodies directed against amyloid for the treatment of Alzheimer’s disease decision summary. Published January 11, 2022. Accessed March 21, 2022. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=305
12. Gleckman H. What’s behind Biogen’s move to cut prices on its controversial Alzheimer’s drug alduhelm. Forbes. Published December 23, 2021. Accessed March 21,2022. https://www.forbes.com/sites/howardgleckman/2021/12/23/whats-behind-biogens-move-to-cut-prices-on-its-controversial-alzheimers-drug-aduhelm/?sh=498c6a235154
1. Williamson V, Stevelink SAM, Greenberg K, Greenberg N. Prevalence of mental health disorders in elderly U.S. military veterans: a metaanalysis and systematic review. Am J Geriatr Psychiatry. 2018;26:534-545. doi:10.1016/j.jagp.2017.11.001
2. US Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. Projections of the prevalence and incidence of dementias. Updated November 5, 2021. Accessed March 20, 2022. www.va.gov/geriatrics/GEC_Data_Reports.asp
3. Zhu CW, Sano M. Demographic, health, and exposure risks associated with cognitive loss, Alzheimer’s disease and other dementias in US military veterans. Front Psychiatry. 2021;12:610334. doi:10.3389/fpsyt.2021.610334
4. VHA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Aducanumab-avwa (ADUHELM) National Drug Monograph. Published July 2021. Accessed March 20, 2022. https://www.pbm.va.gov/PBM/clinicalguidance/drugmonographs/Aducanumab_ADUHELM_monograph_508.pdf
5. National Institutes of Health, National Institute on Aging. What happens to the brain in Alzheimer’s disease? Updated May 16, 2017. Accessed March 20, 2022. https://www.nia.nih.gov/health/what-happens-brain-alzheimers-disease
6. US Food and Drug Administration. FDA grants accelerated approval for Alzheimer’s drug. News release. Published June 7, 2021. Accessed March 21, 2022. https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-drug
7. US Food and Drug Administration. Accelerated approval. Updated January 4, 2018. Accessed March 21,2022.https://www.fda.gov/patients/fast-track-breakthrough-therapy-accelerated-approval-priority-review/accelerated-approval
8. Largent EL, Peterson E, Lynch HF. FDA approval and the ethics of desperation. JAMA Intern Med. 2021;181(12):1555-1556. doi:10.1001/jamainternmed.2021.6045
9. Belluck P, Kaplan S, Robbins R. How an unproven Alzheimer’s drug got approved. New York Times, Updated October 21, 2021. Accessed March 21, 2022. https://www.nytimes.com/2021/07/19/health/alzheimers-drug-aduhelm-fda.html
10. US Department of Health and Human Services, Office of the Inspector General. Review of the FDA’s accelerated approval pathway. Accessed March 20, 2022. https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000608.asp
11. Centers for Medicare and Medicaid Services. Monoclonal antibodies directed against amyloid for the treatment of Alzheimer’s disease decision summary. Published January 11, 2022. Accessed March 21, 2022. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=305
12. Gleckman H. What’s behind Biogen’s move to cut prices on its controversial Alzheimer’s drug alduhelm. Forbes. Published December 23, 2021. Accessed March 21,2022. https://www.forbes.com/sites/howardgleckman/2021/12/23/whats-behind-biogens-move-to-cut-prices-on-its-controversial-alzheimers-drug-aduhelm/?sh=498c6a235154
When Are Inpatient and Emergency Dermatologic Consultations Appropriate?
There are limited clinical data concerning inpatient and emergency department (ED) dermatologic consultations. The indications for these consultations vary widely, but in one study (N=271), it was found that 21% of inpatient consultations were for contact dermatitis and 10% were for drug eruptions.1 In the same study, 77% of patients who required a dermatology consultation eventually were given a different diagnosis or change in treatment after consultation. For example, of all consultations for suspected cellulitis, only 10% were confirmed after dermatology evaluation.1
Hospitalists and emergency physicians continue to struggle with the assessment of dermatologic conditions, often consulting dermatology whenever a patient has a “rash” or skin concern. Dermatology is still not emphasized in medical education and often is taught to most medical students in an abbreviated fashion, which results in physicians feeling ill-equipped to deal with any dermatologic condition—either mundane or potentially life-threatening. A study in 2016 showed that a monthly lecture series given to hospitalists over the course of 5 years did not improve diagnostic accuracy in patients who were admitted with skin manifestations.2 This further shows that there is a need for dermatologic experts in the hospital.
We need to develop better guidelines for physicians in the ED and on inpatient units to guide them on appropriate use of dermatologic consultation outside the ambulatory office and the clinic. A 2013 study showed that patients often were discharged immediately after a dermatologic consultation, furthering our hypothesis that many inpatient consultations can be delayed until after discharge.3
In an era in which medical costs are soaring and there is constant surveillance for ways to reduce costs without impairing quality of care, limiting unnecessary specialty consultations should be embraced. In 2009, $1.8 billion in Medicare claims was paid for dermatology-related admissions.3 A substantial savings to Medicare consulting fees for certain diagnoses, such as cellulitis or contact dermatitis, could be realized if patients were referred for outpatient assessment and treatment. In a study of 271 consultations, 54 patients also had a skin biopsy, which further increases dollars spent on inpatient care and is (usually) something that can be performed in the outpatient setting.1 In another study, the more common recommended treatments were topical corticosteroids and supportive educational measures for patients and hospital staff,3 which further substantiates that most dermatology consultations are not truly emergent and can wait for outpatient consultation.
In addition, we are dealing with the COVID-19 pandemic in our hospitals and EDs. Many physicians, including dermatologists, would prefer to avoid unnecessary exposure to SARS-CoV-2 on inpatient units and in the ED. It certainly would be preferable to require consultants to come in to evaluate patients only when they truly need to be seen while in the hospital.
There also is limited dermatology training in other specialties, and the dermatology team can help fill this gap with educational programs and one-on-one teaching. Hospital teams have signaled this need, but there has been limited success with multiple teaching opportunities.4
We believe that this need for inpatient dermatology services can be filled with the newer subspecialty of hospital dermatology, which is not commonly present at most hospitals; a reason why the subspecialty has not been more popular is that there are few available data in the form of randomized clinical trials that can guide inpatient dermatologists with the care of rare hospital skin diseases.5 Having a dermatologic hospitalist available might allow for patients to be seen more readily, which ultimately will save lives and health care dollars and would increase real-time teaching and education for house staff, nursing, and attendings at the bedside.
In a 2018 article,6 it was postulated that quicker diagnosis of pseudocellulitis and initiation of antibiotics to treat this condition would save the US health care system $210 million annually. We believe that pseudocellulitis would be best evaluated by inpatient dermatology teams, thereby avoiding costly dermatologic consultations, at an average rate of $138.89.6
Morbilliform drug eruptions are among the most common skin conditions seen in the hospital; approximately 95% of cases are an uncomplicated reaction to a medication or virus. Data show that many of these consultations might be unnecessary.7
Our institution (Hackensack University Medical Center, New Jersey) is a tertiary hospital that also is connected with a major cancer center. Given this connection, skin eruptions due to chemotherapy and radiation are common. The treatment of drug eruptions, graft-vs-host disease, and other oncologic or drug-related eruptions should be within the scope of practice of our hospitalists, but these cases frequently involve dermatologic consultation.
We constructed a consultation flowchart (Figure) to help guide the triage of patients in need of dermatologic evaluation by inpatient teams and possibly to avoid unnecessary consultation fees. The manner in which this—or any flowchart or teaching aid—is conveyed to hospital personnel is critical so that these tools are not perceived as patronizing or confrontational. In our flowchart, we list emergent dermatologic conditions that we believe are appropriate for dermatology consultation including erythrodermic psoriasis, bullous pemphigoid flare, and Stevens-Johnson syndrome/toxic epidermal necrolysis.

We believe that the flowchart can educate inpatient medical teams about appropriate dermatology consultation. Use of the flowchart also may decrease unnecessary consultations, which ultimately will lower health care spending overall.
- Davila M, Christenson LJ, Sontheimer RD. Epidemiology and outcomes of dermatology in-patient consultations in a Midwestern U.S. university hospital. Dermatol Online J. 2010;16:12.
- Beshay A, Liu M, Fox L, et al. Inpatient dermatology consultative programs: a continued need, tools for needs assessment for curriculum development, and a call for new methods of teaching. J Am Acad Dermatol. 2016;74:769-771. doi:10.1016/j.jaad.2015.11.017
- Hu L, Haynes H, Ferrazza D, et al. Impact of specialist consultations on inpatient admissions for dermatology-specific and related DRGs. J Gen Intern Med. 2013;28:1477-1482. doi:10.1007/s11606-013-2440-2
- Faletsky A, Han JJ, Mostaghimi A. Inpatient dermatology best practice strategies for educating and relaying findings to colleagues. Curr Dermatol Rep. 2020;9:256-260. doi:10.1007/s13671-020-00317-y
- Fox LP. Hospital dermatology, introduction. Semin Cutan Med Surg. 2017;36:1-2. doi:10.12788/j.sder.2017.015
- Li D, Xia FD, Khosravi H, et al. Outcomes of early dermatology consultation for inpatients diagnosed with cellulitis. JAMA Dermatol. 2018;154:537-543. doi:10.1001/jamadermatol.2017.6197
- Biesbroeck LK, Shinohara MM. Inpatient consultative dermatology. Med Clin North Am. 2015;99:1349-1364. doi:10.1016/j.mcna.2015.06.004
There are limited clinical data concerning inpatient and emergency department (ED) dermatologic consultations. The indications for these consultations vary widely, but in one study (N=271), it was found that 21% of inpatient consultations were for contact dermatitis and 10% were for drug eruptions.1 In the same study, 77% of patients who required a dermatology consultation eventually were given a different diagnosis or change in treatment after consultation. For example, of all consultations for suspected cellulitis, only 10% were confirmed after dermatology evaluation.1
Hospitalists and emergency physicians continue to struggle with the assessment of dermatologic conditions, often consulting dermatology whenever a patient has a “rash” or skin concern. Dermatology is still not emphasized in medical education and often is taught to most medical students in an abbreviated fashion, which results in physicians feeling ill-equipped to deal with any dermatologic condition—either mundane or potentially life-threatening. A study in 2016 showed that a monthly lecture series given to hospitalists over the course of 5 years did not improve diagnostic accuracy in patients who were admitted with skin manifestations.2 This further shows that there is a need for dermatologic experts in the hospital.
We need to develop better guidelines for physicians in the ED and on inpatient units to guide them on appropriate use of dermatologic consultation outside the ambulatory office and the clinic. A 2013 study showed that patients often were discharged immediately after a dermatologic consultation, furthering our hypothesis that many inpatient consultations can be delayed until after discharge.3
In an era in which medical costs are soaring and there is constant surveillance for ways to reduce costs without impairing quality of care, limiting unnecessary specialty consultations should be embraced. In 2009, $1.8 billion in Medicare claims was paid for dermatology-related admissions.3 A substantial savings to Medicare consulting fees for certain diagnoses, such as cellulitis or contact dermatitis, could be realized if patients were referred for outpatient assessment and treatment. In a study of 271 consultations, 54 patients also had a skin biopsy, which further increases dollars spent on inpatient care and is (usually) something that can be performed in the outpatient setting.1 In another study, the more common recommended treatments were topical corticosteroids and supportive educational measures for patients and hospital staff,3 which further substantiates that most dermatology consultations are not truly emergent and can wait for outpatient consultation.
In addition, we are dealing with the COVID-19 pandemic in our hospitals and EDs. Many physicians, including dermatologists, would prefer to avoid unnecessary exposure to SARS-CoV-2 on inpatient units and in the ED. It certainly would be preferable to require consultants to come in to evaluate patients only when they truly need to be seen while in the hospital.
There also is limited dermatology training in other specialties, and the dermatology team can help fill this gap with educational programs and one-on-one teaching. Hospital teams have signaled this need, but there has been limited success with multiple teaching opportunities.4
We believe that this need for inpatient dermatology services can be filled with the newer subspecialty of hospital dermatology, which is not commonly present at most hospitals; a reason why the subspecialty has not been more popular is that there are few available data in the form of randomized clinical trials that can guide inpatient dermatologists with the care of rare hospital skin diseases.5 Having a dermatologic hospitalist available might allow for patients to be seen more readily, which ultimately will save lives and health care dollars and would increase real-time teaching and education for house staff, nursing, and attendings at the bedside.
In a 2018 article,6 it was postulated that quicker diagnosis of pseudocellulitis and initiation of antibiotics to treat this condition would save the US health care system $210 million annually. We believe that pseudocellulitis would be best evaluated by inpatient dermatology teams, thereby avoiding costly dermatologic consultations, at an average rate of $138.89.6
Morbilliform drug eruptions are among the most common skin conditions seen in the hospital; approximately 95% of cases are an uncomplicated reaction to a medication or virus. Data show that many of these consultations might be unnecessary.7
Our institution (Hackensack University Medical Center, New Jersey) is a tertiary hospital that also is connected with a major cancer center. Given this connection, skin eruptions due to chemotherapy and radiation are common. The treatment of drug eruptions, graft-vs-host disease, and other oncologic or drug-related eruptions should be within the scope of practice of our hospitalists, but these cases frequently involve dermatologic consultation.
We constructed a consultation flowchart (Figure) to help guide the triage of patients in need of dermatologic evaluation by inpatient teams and possibly to avoid unnecessary consultation fees. The manner in which this—or any flowchart or teaching aid—is conveyed to hospital personnel is critical so that these tools are not perceived as patronizing or confrontational. In our flowchart, we list emergent dermatologic conditions that we believe are appropriate for dermatology consultation including erythrodermic psoriasis, bullous pemphigoid flare, and Stevens-Johnson syndrome/toxic epidermal necrolysis.
We believe that the flowchart can educate inpatient medical teams about appropriate dermatology consultation. Use of the flowchart also may decrease unnecessary consultations, which ultimately will lower health care spending overall.
There are limited clinical data concerning inpatient and emergency department (ED) dermatologic consultations. The indications for these consultations vary widely, but in one study (N=271), it was found that 21% of inpatient consultations were for contact dermatitis and 10% were for drug eruptions.1 In the same study, 77% of patients who required a dermatology consultation eventually were given a different diagnosis or change in treatment after consultation. For example, of all consultations for suspected cellulitis, only 10% were confirmed after dermatology evaluation.1
Hospitalists and emergency physicians continue to struggle with the assessment of dermatologic conditions, often consulting dermatology whenever a patient has a “rash” or skin concern. Dermatology is still not emphasized in medical education and often is taught to most medical students in an abbreviated fashion, which results in physicians feeling ill-equipped to deal with any dermatologic condition—either mundane or potentially life-threatening. A study in 2016 showed that a monthly lecture series given to hospitalists over the course of 5 years did not improve diagnostic accuracy in patients who were admitted with skin manifestations.2 This further shows that there is a need for dermatologic experts in the hospital.
We need to develop better guidelines for physicians in the ED and on inpatient units to guide them on appropriate use of dermatologic consultation outside the ambulatory office and the clinic. A 2013 study showed that patients often were discharged immediately after a dermatologic consultation, furthering our hypothesis that many inpatient consultations can be delayed until after discharge.3
In an era in which medical costs are soaring and there is constant surveillance for ways to reduce costs without impairing quality of care, limiting unnecessary specialty consultations should be embraced. In 2009, $1.8 billion in Medicare claims was paid for dermatology-related admissions.3 A substantial savings to Medicare consulting fees for certain diagnoses, such as cellulitis or contact dermatitis, could be realized if patients were referred for outpatient assessment and treatment. In a study of 271 consultations, 54 patients also had a skin biopsy, which further increases dollars spent on inpatient care and is (usually) something that can be performed in the outpatient setting.1 In another study, the more common recommended treatments were topical corticosteroids and supportive educational measures for patients and hospital staff,3 which further substantiates that most dermatology consultations are not truly emergent and can wait for outpatient consultation.
In addition, we are dealing with the COVID-19 pandemic in our hospitals and EDs. Many physicians, including dermatologists, would prefer to avoid unnecessary exposure to SARS-CoV-2 on inpatient units and in the ED. It certainly would be preferable to require consultants to come in to evaluate patients only when they truly need to be seen while in the hospital.
There also is limited dermatology training in other specialties, and the dermatology team can help fill this gap with educational programs and one-on-one teaching. Hospital teams have signaled this need, but there has been limited success with multiple teaching opportunities.4
We believe that this need for inpatient dermatology services can be filled with the newer subspecialty of hospital dermatology, which is not commonly present at most hospitals; a reason why the subspecialty has not been more popular is that there are few available data in the form of randomized clinical trials that can guide inpatient dermatologists with the care of rare hospital skin diseases.5 Having a dermatologic hospitalist available might allow for patients to be seen more readily, which ultimately will save lives and health care dollars and would increase real-time teaching and education for house staff, nursing, and attendings at the bedside.
In a 2018 article,6 it was postulated that quicker diagnosis of pseudocellulitis and initiation of antibiotics to treat this condition would save the US health care system $210 million annually. We believe that pseudocellulitis would be best evaluated by inpatient dermatology teams, thereby avoiding costly dermatologic consultations, at an average rate of $138.89.6
Morbilliform drug eruptions are among the most common skin conditions seen in the hospital; approximately 95% of cases are an uncomplicated reaction to a medication or virus. Data show that many of these consultations might be unnecessary.7
Our institution (Hackensack University Medical Center, New Jersey) is a tertiary hospital that also is connected with a major cancer center. Given this connection, skin eruptions due to chemotherapy and radiation are common. The treatment of drug eruptions, graft-vs-host disease, and other oncologic or drug-related eruptions should be within the scope of practice of our hospitalists, but these cases frequently involve dermatologic consultation.
We constructed a consultation flowchart (Figure) to help guide the triage of patients in need of dermatologic evaluation by inpatient teams and possibly to avoid unnecessary consultation fees. The manner in which this—or any flowchart or teaching aid—is conveyed to hospital personnel is critical so that these tools are not perceived as patronizing or confrontational. In our flowchart, we list emergent dermatologic conditions that we believe are appropriate for dermatology consultation including erythrodermic psoriasis, bullous pemphigoid flare, and Stevens-Johnson syndrome/toxic epidermal necrolysis.
We believe that the flowchart can educate inpatient medical teams about appropriate dermatology consultation. Use of the flowchart also may decrease unnecessary consultations, which ultimately will lower health care spending overall.
- Davila M, Christenson LJ, Sontheimer RD. Epidemiology and outcomes of dermatology in-patient consultations in a Midwestern U.S. university hospital. Dermatol Online J. 2010;16:12.
- Beshay A, Liu M, Fox L, et al. Inpatient dermatology consultative programs: a continued need, tools for needs assessment for curriculum development, and a call for new methods of teaching. J Am Acad Dermatol. 2016;74:769-771. doi:10.1016/j.jaad.2015.11.017
- Hu L, Haynes H, Ferrazza D, et al. Impact of specialist consultations on inpatient admissions for dermatology-specific and related DRGs. J Gen Intern Med. 2013;28:1477-1482. doi:10.1007/s11606-013-2440-2
- Faletsky A, Han JJ, Mostaghimi A. Inpatient dermatology best practice strategies for educating and relaying findings to colleagues. Curr Dermatol Rep. 2020;9:256-260. doi:10.1007/s13671-020-00317-y
- Fox LP. Hospital dermatology, introduction. Semin Cutan Med Surg. 2017;36:1-2. doi:10.12788/j.sder.2017.015
- Li D, Xia FD, Khosravi H, et al. Outcomes of early dermatology consultation for inpatients diagnosed with cellulitis. JAMA Dermatol. 2018;154:537-543. doi:10.1001/jamadermatol.2017.6197
- Biesbroeck LK, Shinohara MM. Inpatient consultative dermatology. Med Clin North Am. 2015;99:1349-1364. doi:10.1016/j.mcna.2015.06.004
- Davila M, Christenson LJ, Sontheimer RD. Epidemiology and outcomes of dermatology in-patient consultations in a Midwestern U.S. university hospital. Dermatol Online J. 2010;16:12.
- Beshay A, Liu M, Fox L, et al. Inpatient dermatology consultative programs: a continued need, tools for needs assessment for curriculum development, and a call for new methods of teaching. J Am Acad Dermatol. 2016;74:769-771. doi:10.1016/j.jaad.2015.11.017
- Hu L, Haynes H, Ferrazza D, et al. Impact of specialist consultations on inpatient admissions for dermatology-specific and related DRGs. J Gen Intern Med. 2013;28:1477-1482. doi:10.1007/s11606-013-2440-2
- Faletsky A, Han JJ, Mostaghimi A. Inpatient dermatology best practice strategies for educating and relaying findings to colleagues. Curr Dermatol Rep. 2020;9:256-260. doi:10.1007/s13671-020-00317-y
- Fox LP. Hospital dermatology, introduction. Semin Cutan Med Surg. 2017;36:1-2. doi:10.12788/j.sder.2017.015
- Li D, Xia FD, Khosravi H, et al. Outcomes of early dermatology consultation for inpatients diagnosed with cellulitis. JAMA Dermatol. 2018;154:537-543. doi:10.1001/jamadermatol.2017.6197
- Biesbroeck LK, Shinohara MM. Inpatient consultative dermatology. Med Clin North Am. 2015;99:1349-1364. doi:10.1016/j.mcna.2015.06.004
Practice Points
- Primary inpatient teams should call patients’ insurance companies to verify in-network dermatologists for eventual outpatient follow-up.
- Chronic skin problems (eg, psoriasis, hidradenitis suppurativa) are better cared for in an outpatient setting due to the necessity for follow-up reassessments.
- There remains a need to fill knowledge gaps for common inpatient dermatologic problems that do not necessitate consultations, such as morbilliform drug rash and other chronic and unchanged dermatoses.
Residency Roundup: Introducing a New Partnership Between Cutis and the APD-RPDS
We are excited to announce a new partnership between Cutis and the Association of Professors of Dermatology Residency Program Directors Section (APD-RPDS). The new APD-RPDS column Residency Roundup will contain quarterly communications and submissions that we hope will facilitate greater dissemination of information that is useful to the dermatology teaching community.
The APD is a group of academic dermatologists whose membership comprises chairs, chiefs, residency and fellowship program directors, and teaching faculty. Each fall, the group convenes in Chicago, Illinois, for a 2-day meeting centered around departmental and program leadership with a focus on education. The APD-RPDS was formed in 2020 and is led by a steering committee of 9 members, including our current Chair, Ilana S. Rosman, MD (Washington University School of Medicine, St. Louis, Missouri), and Vice Chair, Jo-Ann M. Latkowski, MD (New York University, New York). Committee members are elected from and by the APD membership and must serve in program leadership at their home programs. The APD-RPDS helps plan and coordinate breakout sessions and lectures at the annual APD meeting, which typically relate to program director duties, changing policies within the American Board of Dermatology or Accreditation Council for Graduate Medical Education, ideas for future growth, and changes in our specialty and in resident education. Members of the APD-RPDS have access to the APD listserv, a valuable resource for discussing issues affecting residency training. We also have work groups led by our members, which include diversity, equity, and inclusion; resource development; communications; and the annual survey. To join the APD, the RPDS, and/or any of our workgroups, please reach out to us or visit the APD website (https://www.dermatologyprofessors.org).
We look forward to welcoming and expediently reviewing members’ submissions to the new Residency Roundup column falling into 2 principal categories within the scope of dermatologic recruitment, didactic education, and clinical training. The first category will feature novel tools, programs, and platforms to improve dermatology training through collaboration. This could entail a description of a new platform designed for sharing resources among programs and specialties to enhance learning for trainees and faculty alike. For example, if a database is created that contains prerecorded lectures pertaining to alopecia, a potential article submission might introduce the database and provide information on what topics are covered and how to access these lectures for readers worldwide. Likewise, if a new technology emerges that allows for easier collaboration among programs, a possible submission would introduce the technology and discuss its potential benefits to trainees, faculty, and practicing dermatologists.
Secondly and more commonly, we anticipate the Residency Roundup column will feature articles that delve into the critical issues and challenges currently impacting recruitment, training, and administration in dermatology residency programs. Specific topics may include but are not limited to recruitment of underrepresented in medicine applicants to dermatology, technological advances to improve teaching methods within training programs, surveys delving into the dermatology match process, and educational gaps or future directions in the specialty. The column occasionally may be used to disseminate information from our section of the APD, including consensus statements or editorials related to changes implemented in the dermatology residency application process. A prospective editorial on this subject could explore varying viewpoints of implemented and proposed changes as well as the reasons behind the changes.
Our group is collaborative, and our aim is to improve education, equity, management of program director responsibilities, and the dermatology application process for programs and applicants alike. With your input, experience, and varied perspectives, we look forward to moving the field of dermatology to a better future by working together.
We are excited to announce a new partnership between Cutis and the Association of Professors of Dermatology Residency Program Directors Section (APD-RPDS). The new APD-RPDS column Residency Roundup will contain quarterly communications and submissions that we hope will facilitate greater dissemination of information that is useful to the dermatology teaching community.
The APD is a group of academic dermatologists whose membership comprises chairs, chiefs, residency and fellowship program directors, and teaching faculty. Each fall, the group convenes in Chicago, Illinois, for a 2-day meeting centered around departmental and program leadership with a focus on education. The APD-RPDS was formed in 2020 and is led by a steering committee of 9 members, including our current Chair, Ilana S. Rosman, MD (Washington University School of Medicine, St. Louis, Missouri), and Vice Chair, Jo-Ann M. Latkowski, MD (New York University, New York). Committee members are elected from and by the APD membership and must serve in program leadership at their home programs. The APD-RPDS helps plan and coordinate breakout sessions and lectures at the annual APD meeting, which typically relate to program director duties, changing policies within the American Board of Dermatology or Accreditation Council for Graduate Medical Education, ideas for future growth, and changes in our specialty and in resident education. Members of the APD-RPDS have access to the APD listserv, a valuable resource for discussing issues affecting residency training. We also have work groups led by our members, which include diversity, equity, and inclusion; resource development; communications; and the annual survey. To join the APD, the RPDS, and/or any of our workgroups, please reach out to us or visit the APD website (https://www.dermatologyprofessors.org).
We look forward to welcoming and expediently reviewing members’ submissions to the new Residency Roundup column falling into 2 principal categories within the scope of dermatologic recruitment, didactic education, and clinical training. The first category will feature novel tools, programs, and platforms to improve dermatology training through collaboration. This could entail a description of a new platform designed for sharing resources among programs and specialties to enhance learning for trainees and faculty alike. For example, if a database is created that contains prerecorded lectures pertaining to alopecia, a potential article submission might introduce the database and provide information on what topics are covered and how to access these lectures for readers worldwide. Likewise, if a new technology emerges that allows for easier collaboration among programs, a possible submission would introduce the technology and discuss its potential benefits to trainees, faculty, and practicing dermatologists.
Secondly and more commonly, we anticipate the Residency Roundup column will feature articles that delve into the critical issues and challenges currently impacting recruitment, training, and administration in dermatology residency programs. Specific topics may include but are not limited to recruitment of underrepresented in medicine applicants to dermatology, technological advances to improve teaching methods within training programs, surveys delving into the dermatology match process, and educational gaps or future directions in the specialty. The column occasionally may be used to disseminate information from our section of the APD, including consensus statements or editorials related to changes implemented in the dermatology residency application process. A prospective editorial on this subject could explore varying viewpoints of implemented and proposed changes as well as the reasons behind the changes.
Our group is collaborative, and our aim is to improve education, equity, management of program director responsibilities, and the dermatology application process for programs and applicants alike. With your input, experience, and varied perspectives, we look forward to moving the field of dermatology to a better future by working together.
We are excited to announce a new partnership between Cutis and the Association of Professors of Dermatology Residency Program Directors Section (APD-RPDS). The new APD-RPDS column Residency Roundup will contain quarterly communications and submissions that we hope will facilitate greater dissemination of information that is useful to the dermatology teaching community.
The APD is a group of academic dermatologists whose membership comprises chairs, chiefs, residency and fellowship program directors, and teaching faculty. Each fall, the group convenes in Chicago, Illinois, for a 2-day meeting centered around departmental and program leadership with a focus on education. The APD-RPDS was formed in 2020 and is led by a steering committee of 9 members, including our current Chair, Ilana S. Rosman, MD (Washington University School of Medicine, St. Louis, Missouri), and Vice Chair, Jo-Ann M. Latkowski, MD (New York University, New York). Committee members are elected from and by the APD membership and must serve in program leadership at their home programs. The APD-RPDS helps plan and coordinate breakout sessions and lectures at the annual APD meeting, which typically relate to program director duties, changing policies within the American Board of Dermatology or Accreditation Council for Graduate Medical Education, ideas for future growth, and changes in our specialty and in resident education. Members of the APD-RPDS have access to the APD listserv, a valuable resource for discussing issues affecting residency training. We also have work groups led by our members, which include diversity, equity, and inclusion; resource development; communications; and the annual survey. To join the APD, the RPDS, and/or any of our workgroups, please reach out to us or visit the APD website (https://www.dermatologyprofessors.org).
We look forward to welcoming and expediently reviewing members’ submissions to the new Residency Roundup column falling into 2 principal categories within the scope of dermatologic recruitment, didactic education, and clinical training. The first category will feature novel tools, programs, and platforms to improve dermatology training through collaboration. This could entail a description of a new platform designed for sharing resources among programs and specialties to enhance learning for trainees and faculty alike. For example, if a database is created that contains prerecorded lectures pertaining to alopecia, a potential article submission might introduce the database and provide information on what topics are covered and how to access these lectures for readers worldwide. Likewise, if a new technology emerges that allows for easier collaboration among programs, a possible submission would introduce the technology and discuss its potential benefits to trainees, faculty, and practicing dermatologists.
Secondly and more commonly, we anticipate the Residency Roundup column will feature articles that delve into the critical issues and challenges currently impacting recruitment, training, and administration in dermatology residency programs. Specific topics may include but are not limited to recruitment of underrepresented in medicine applicants to dermatology, technological advances to improve teaching methods within training programs, surveys delving into the dermatology match process, and educational gaps or future directions in the specialty. The column occasionally may be used to disseminate information from our section of the APD, including consensus statements or editorials related to changes implemented in the dermatology residency application process. A prospective editorial on this subject could explore varying viewpoints of implemented and proposed changes as well as the reasons behind the changes.
Our group is collaborative, and our aim is to improve education, equity, management of program director responsibilities, and the dermatology application process for programs and applicants alike. With your input, experience, and varied perspectives, we look forward to moving the field of dermatology to a better future by working together.
We all struggle with the unwritten rules of medical culture
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
There is a two-lane bridge in my town. It is quaint and picturesque, and when we first moved here, I would gaze out at the water as I drove, letting my mind wander along with the seagulls drifting alongside the car. Until one day, crossing back over, I passed a school bus stopped in the other lane, and instead of waving back, the driver gave me such a fierce look of disapproval I felt like I’d been to the principal’s office. What had I done?
I started paying more attention to the pattern of the other cars on the bridge. Although it appeared to be a standard two-lane width, the lanes weren’t quite wide enough if a school bus or large truck needed to cross at the same time as a car coming from the opposite direction. They had to wait until the other lane was clear. It was an unwritten rule of the town that if you saw a school bus on the other side, you stopped your car and yielded the bridge to the bus. It took me weeks to figure this out. When I did, I felt like I finally belonged in the community. Before, I’d been an outsider.
This got me thinking about culture. Every place has its unwritten rules, whether a community or a workplace. But how do we know the culture of a place? It’s pretty much impossible until we experience it for ourselves.
When I did figure out the bridge, I had a little bit of anger, to be honest. How was I supposed to know about the lanes? There weren’t any signs. Geez.
Now, when I approach the bridge, I don’t even think about it. I know what to do if I see a bus coming.
But sometimes I remember that time of confusion before I deciphered the unwritten rule. I still have a twinge of guilt for having done something wrong, even though it hadn’t been my fault.
It reminded me of a memory from medical training. I was an MS4, and my ER rotation was in a busy county hospital with a level I trauma center. To say that the place was chaotic would be an understatement.
On the first morning, I was shown the chart rack (yes, this was back in the day of paper charts). Charts were placed in the order that patients arrived. Med students and residents were to take a chart in chronological order, go triage and assess the patient, and then find an attending. Once finished, you put the chart back on the rack and picked up the next one. This was the extent of my orientation to the ER.
The days and weeks of the rotation flew by. It was a busy and exciting time. By the end of the month, I’d come to feel a part of the team.
Until one day, after finishing discharging a patient, an attending asked me, “Where’s the billing sheet?”
I had no idea what she was talking about. No one had ever shown me a billing sheet. But by this point, as an MS4, I knew well that if an attending asked you something you didn’t know the answer to, you shouldn’t just say that you didn’t know. You should try to figure out if you could at least approximate an answer first.
As I scrambled in my mind to figure out what she was asking me, she took one look at the apprehension in my eyes and asked again, raising her voice, “You haven’t been doing the billing sheets?”
I thought back to the first day of the rotation. The cursory 30-second orientation. Chart rack. Take one. See the patient. Put it back. See the next patient. Nothing about billing sheets.
“No,” I said. “No one ever told me about – ”
But the attending didn’t care that I hadn’t been instructed on the billing sheets. She ripped into me, yelling about how she couldn’t believe I’d been working there the entire month and was not doing the billing sheets. She showed me what they were and where they were supposed to be going and, in front of the whole staff, treated me like not only the biggest idiot she’d ever worked with but that the hospital had ever seen.
As she berated me, I thought about all the patients I’d seen that month. All the billing sheets I hadn’t placed in the pile. All the attendings who hadn’t gotten credit for the patients they’d staffed with me.
But how could I have known? I wanted to ask. How could I have known if nobody showed me or told me?
It was like the bridge. I was in a new environment and somehow expected to know the rules without anyone telling me; and when I didn’t know, people treated me like I’d done it the wrong way on purpose.
I didn’t end up saying anything more to that attending. What could I have said? She had already unleashed a mountain of her pent-up anger at me.
What I did decide in that moment was that I would never be an attending like that.
Like the bridge, this memory years later can still make me feel guilt and shame for doing something wrong. Even though it wasn’t my fault.
I was thinking about this recently with the Match. Thousands of freshly graduated medical students embarking on their new positions as interns in teaching hospitals across the country.
If someone treats you poorly for not knowing something, you are not an idiot. You’ve worked incredibly hard to get where you are, and you deserve to be there.
For attendings and more senior trainees, remember what it was like to be starting in a new place. We all make mistakes, and often it’s simply because of a lack of information.
Trainees shouldn’t have to suffer and be made to feel like outsiders until they figure out the unwritten rules of the place. They belong.
Dr. Lycette is medical director of Providence Oncology and Hematology Care Clinic, Seaside, Ore. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
The importance of treating insomnia in psychiatric illness
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6

Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6
Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
Data suggests this symptom, defined as chronic sleep onset and/or sleep continuity problems associated with impaired daytime functioning, is common in psychiatric illnesses, and can worsen their course.2
The incidence of psychiatric illness in patients with insomnia is estimated at near 50%, with the highest rates found in mood disorders such as depression and bipolar disorder, as well as anxiety disorders.3 In patients with diagnosed major depressive disorder, insomnia rates can approach 90%.4-6
Insomnia has been identified as a risk factor for development of mental illness, including doubling the risk of major depressive disorder and tripling the risk of any depressive or anxiety disorder.7,8 It can also significantly increase the risk of alcohol abuse and psychosis.8
Sleep disturbances can worsen symptoms of diagnosed mental illness, including substance abuse, mood and psychotic disorders.9-10 In one study, nearly 75% of patients with a diagnosis of schizophrenia or bipolar spectrum disorder had at least one type of sleep disturbance (insomnia, hypersomnia, or delayed sleep phase).10 This was almost twice the rate in healthy controls. Importantly, compared with well-rested subjects with mental illness in this study, sleep-disordered participants had higher rates of negative and depressive symptoms on the Positive and Negative Syndrome Scale, as well as significantly lower function via the global assessment of functioning.11,12
Additional data suggests simply being awake during the night (00:00-05:59) elevates risk of suicide. The mean incident rate of completed suicide in one study was a striking four times the rate noted during daytime hours (06:00-23:59 ) (P < .001).13
Although insomnia symptoms can resolve after relief from a particular life stressor, as many as half of patients with more severe symptoms develop a chronic course.14 This then leads to an extended use of many types of sedative-hypnotics designed and studied primarily for short-term use.15 In a survey reviewing national use of prescription drugs for insomnia, as many as 20% of individuals use a medication to target insomnia in a given month.16
Fortunately, despite the many challenges posed by COVID-19, particularly for those with psychiatric illness and limited access to care, telehealth has become more readily available. Additionally, digital versions of evidence-based treatments specifically for sleep problems, such as cognitive-behavioral therapy for insomnia (CBT-I), are regularly being developed.
The benefits of CBT-I have been demonstrated repeatedly and it is recommended as the first line treatment for insomnia by the Clinical Guidelines of the American Academy of Sleep Medicine, the Centers for Disease Control and Prevention, and the National Institutes of Health.17-21 Studies suggest benefits persist long-term, even after completing the therapy sessions, which differ in durability from medication choices.18
One group that may be particularly suited for treatment with CBT-I is women with insomnia during pregnancy or the postpartum period. In these women, options for treatment may be limited by risk of medication during breastfeeding, as well as difficulty traveling to a physician’s or therapist’s office to receive psychotherapy. However, two recent studies evaluated the use of digital CBT-I to treat insomnia during pregnancy and in the postpartum period, respectively.22-23
In both studies,the same group of women with insomnia diagnosed during pregnancy were given six weekly 20-minute sessions of digital CBT-I or standard treatment for insomnia, including medication and psychotherapy per their usual provider.
By study end, the pregnant women receiving the CBT-I intervention not only had significantly improved severity of insomnia, they also experienced improved depression and anxiety symptoms, and a decrease in the use of prescription or over-the-counter sleep aides, compared with the standard treatment group, lowering the fetal exposure to medication during pregnancy.22
In the more recent study, the same group was followed for 6 months post partum.23 Results were again notable, with the women who received CBT-I reporting significantly less insomnia, as well as significantly lower rates of probable major depression at 3 and 6 months (18% vs. 4%, 10% vs. 0%, respectively.) They also exhibited lower rates of moderate to severe anxiety (17% vs. 4%) at 3 months, compared with those receiving standard care. With as many as one in seven women suffering from postpartum depression, these findings represent a substantial public health benefit.
In summary, insomnia is a critical area of focus for any provider diagnosing and treating psychiatric illness. Attempts to optimize sleep, whether through CBT-I or other psychotherapy approaches, or evidence-based medications dosed for appropriate lengths and at safe doses, should be a part of most, if not all, clinical encounters.
Dr. Reid is a board-certified psychiatrist and award-winning medical educator with a private practice in Philadelphia, as well as a clinical faculty role at the University of Pennsylvania, also in Philadelphia. She attended medical school at Columbia University, New York, and completed her psychiatry residency at the University of California, Los Angeles. Dr. Reid is a regular contributor to Psychology Today with her blog, “Think Like a Shrink,” and writes and podcasts as The Reflective Doc.
References
1. Voitsidis P et al. Psychiatry Res. 2020 Jul;289:113076. doi: 10.1016/j.psychres.2020.113076.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, Va.: American Psychiatric Publishing, 2013.
3. Ford DE and Kamerow DB. JAMA. 1989;262(11):1479-84. doi: 10.1001/jama.1989.03430110069030.
4. Ohayon MM and Roth T. J Psychiatr Res. Jan-Feb 2003;37(1):9-15. doi: 10.1016/s0022-3956(02)00052-3.
5. Seow LSE et al. J Ment Health. 2016 Dec;25(6):492-9. doi: 10.3109/09638237.2015.1124390.
6. Thase ME. J Clin Psychiatry. 1999;60 Suppl 17:28-31; discussion 46-8.
7. Baglioni C et al. J Affect Disord. 2011 Dec;135(1-3):10-9. doi: 10.1016/j.jad.2011.01.011.
8. Hertenstein E et al. Sleep Med Rev. 2019 Feb;43:96-105. doi: 10.1016/j.smrv.2018.10.006.
9. Brower KJ et al. Medical Hypotheses. 2010;74(5):928-33. doi: 10.1016/j.mehy.2009.10.020.
10. Laskemoen JF et al. Compr Psychiatry. 2019 May;91:6-12. doi: 10.1016/j.comppsych.2019.02.006.
11. Kay SR et al. Schizophr Bull. 1987;13(2):261-76. doi: 10.1093/schbul/13.2.261.
12. Hall R. Psychosomatics. May-Jun 1995;36(3):267-75. doi: 10.1016/S0033-3182(95)71666-8.
13. Perlis ML et al. J Clin Psychiatry. 2016 Jun;77(6):e726-33. doi: 10.4088/JCP.15m10131.
14. Morin CM et al. Arch Intern Med. 2009 Mar 9. doi: 10.1001/archinternmed.2008.610.
15. Cheung J et al. Sleep Med Clin. 2019 Jun;14(2):253-65. doi: 10.1016/j.jsmc.2019.01.006.
16. Bertisch SM et al. Sleep. 2014 Feb 1. doi: 10.5665/sleep.3410.
17. Okajima I et al. Sleep Biol Rhythms. 2010 Nov 28. doi: 10.1111/j.1479-8425.2010.00481.x.
18. Trauer JM et al. Ann Intern Med. 2015 Aug 4. doi: 10.7326/M14-2841.
19. Edinger J et al. J Clin Sleep Med. 2021 Feb 1. doi: 10.5664/jcsm.8986.
20. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/sleep/for-clinicians.html.
21. National Institutes of Health. Sleep Health. https://www.nhlbi.nih.gov/health-topics/education-and-awareness/sleep-health.
22. Felder JN et al. JAMA Psychiatry. 2020;77(5):484-92. doi:10.1001/jamapsychiatry.2019.4491.
23. Felder JN et al. Sleep. 2022 Feb 14. doi: 10.1093/sleep/zsab280.
Breast cancer therapy toxicities: Education and communication
This transcript of a video roundtable, which is available on Medscape.com, has been edited for clarity.
Hope S. Rugo, MD: Hello. I’m Hope Rugo, a breast medical oncologist from the University of California, San Francisco. I’m joined here by three of my friends and colleagues to discuss the toxicity of new agents in the treatment of breast cancer. Fatima, do you want to start by introducing yourself?
Fatima F. Cardoso, MD: Sure. Hello, everyone. I’m Fatima Cardoso, a breast medical oncologist in Lisbon, Portugal.
Dr. Rugo: Sheila.
Sheila Pettiford: Hi, I’m Sheila Pettiford. I am a metastatic [breast cancer] patient and have been for almost 8 years in April. I used to live in Philadelphia, Pennsylvania, but moved to Delaware in the last couple of years during the pandemic. I’m happy to be here.
Dr. Rugo: Julia.
Julia Maués: Hi, everyone. I also am a person living with metastatic breast cancer. I was diagnosed in 2013, so it’s going to be 9 years, also in April.
Effective monitoring and management of side effects: A team effort
Dr. Rugo: We have an amazing group and an international representation, which is also really nice because we get different perspectives. What we’re going to talk about is important to providers and patients across the board. With the host of new agents for the treatment of breast cancer – most of which have really moved us forward in terms of having effective treatment options – we’ve also been faced with a lot of new toxicities or side effects that we haven’t seen before or that we might not have expected from the specific agent.
Those toxicities across the board include side effects that are quite familiar to us, like low blood counts, but we may not advise people well enough about other side effects such as mouth sores, inflammation of the lungs, immune toxicities, and skin toxicities.
Fatima, do you want to start and talk about how we can think about these toxicities and address them?
Dr. Cardoso: Sure. Thank you. From the health care provider point of view, what I would highlight is to educate. Educate before we start the treatment. It’s very important to inform the patient but in a balanced way, so we don’t overexaggerate certain types of side effects or underestimate certain types of side effects.
It’s very important because an informed patient will be attentive to the types of side effects that can happen. Also, teach the patient when it is a [cause for] alarm or something for which they might need to contact their health care team and when that’s not the case. I think this is one crucial topic.
The other one is to monitor. Find ways how to best communicate between the patient and the health care team but in a way that you can monitor, so you can act very early on. Most of these new side effects, if you act early on, will not become severe. It is very important to know about them and to act early on.
I believe there is something important that we don’t think about all the time, and that is prophylaxis. Do not be shy about using prophylactic measures, be it for the mouth sores, nausea and vomiting, diarrhea, and other things that really impact the quality of life of patients. Those, to start, are my three major points of attention for health care professionals.
Dr. Rugo: I think that’s so incredibly important – the comments that you’ve made – and also that prevention and prophylaxis are so important. You don’t want to have a patient have diarrhea in the middle of the night and not have any antipropulsive agents at home. Just as a very straightforward example, it’s really important.
Also, the ability to know what you should be looking for and how you can manage it [is important]. There are many examples of times when, even with some education, providers may not have communicated well to the patient. Then the patient is surprised and unhappy with the situation and unable to manage it.
The importance of education
Sheila, your comments on this from the patient perspective are so important. How important is the education piece, and how do you manage the fear of side effects vs actually managing the side effects that might be caused by the treatment you’re taking?
Ms. Pettiford: Thank you for that question. I really think it’s a dance. It’s a dance between the patient and the health care team. Yes, education is absolutely important. However, the health care professionals have to establish a relationship of trust with the patient. My own circumstances were that – and I was very fortunate in that my oncologist, who I chose just by looking and not by a recommendation – I did find an oncologist who listened to me.
When it came time for me to deal with a new medication, the education she provided me was sufficient because of the fact that there was a lot of listening that had gone on prior to the new medicine being given to me. I trusted what I was hearing, and it felt like there was a balanced situation that came about from what I was being told. I could look it up, too.
There still is that part of the patient who will be participating in the process, as well. They can still look up things, and that’s one of the downfalls of the information age we are in. It is a dance. I just want to go back to that. There’s a dance between the patient and the health care providers.
Dr. Rugo: Julia, from the patient’s side, how do you balance the benefits you might get from a treatment versus the side effects and how best to manage them?
Ms. Maués: I think it’s interesting that when we talk with our doctors, and especially when we read about a certain treatment, the attention is focused on the very severe and unlikely side effects that a drug has. We don’t talk as much about the side effects that are most likely to happen and will affect us but may not be life threatening.
Especially for those of us with metastatic cancer who are going to ideally be on a drug for a very long time, we’re then faced with low-grade nausea for the rest of our lives. That’s not okay either, right? I think it’s important to talk about all of the levels of toxicities and everything that can be done to avoid this.
Communication is key
Ms. Pettiford: I just want to add something that Dr. Cardoso said about monitoring that is absolutely important. We’re in a day and time when it’s very difficult to get someone on the telephone, but we do have digital charts and other ways that monitoring can take place. I was at a large teaching university, and I had to go monthly for my treatments. Every month, there were questions that were asked about my life and my condition. I could always get in contact with somebody through the digital chart.
Dr. Rugo: That’s an incredibly important comment, Sheila, about communication and how patients can feel like they have someone to go to in real time who can help manage things. Fatima, I’m interested in your comment on that.
Also, just to go to the next step, which is that when we see data reported on clinical trials and how the agent we’ve added or substituted is better than the standard, the toxicity tables are side effects that occur in at least 10% or more patients and sometimes even 20%. Then they’re graded, where often the division is grade 3 or greater. That may not actually reflect much about what the individual patient experience is. How do we interpret these data? Communication and interpretation?
Dr. Cardoso: Absolutely. I always call attention that perhaps, since we focus so much on grade 3 and 4 [side effects], that is the reason why we don’t see in the usual reporting differences quality of life between treatments. Quality of life is affected also significantly by grade 2 side effects. Or, like Julia was mentioning, even grade 1, if they are persistent, will eventually affect your quality of life.
Sometimes, like I was saying, don’t underestimate – it’s a little bit like that. We focus on explaining, “Look, this new immunotherapy can give you all these different side effects.” But then we forget to say: “Oh, by the way, it may also give you some nausea.” Actually, the nausea will affect the patient’s quality of life. I think that’s why it is so important to balance the way we provide the information.
I would like also to take on what Sheila said that sometimes too much information is not very helpful. That’s why sometimes we have to go stepwise. The first time you’re about to start the treatment, advise [the patient] on the most frequent side effects. Later on, you have time to say: “Okay, by the way, this can also give a rare side effect. This is what you should look for. If you have it, please contact your health care team.”
I think the most difficult part, at least from my experience, is for patients to understand what is really a sign of a severe side effect and what is normal for that type of treatment. Some of the new ways of communicating, like using some patient-reported outcome (PRO) apps, actually help the patient by saying, “This that you are feeling is normal. It can wait for your next appointment. This that you are feeling, it’s better if you try to reach your health care team right away. Or, this is an urgent thing and go to the emergency room near you.”
For this kind of triage, there are now new apps that can help. I think this is the most difficult part because when you are a patient, you don’t know if what you are feeling is actually a sign of something very severe or if it’s normal for the type of treatment you are receiving.
Dr. Rugo: I think that’s so important, and these new PRO apps may help with this. Of course, nothing substitutes for talking in the end if you’re confused or it doesn’t fit into whatever’s in that paradigm. I think it’s important.
Best practices in focusing on the individual patient
Julia, what do you think the best way of educating the patient is when you’re going to start a new treatment? You might be newly diagnosed with cancer or you might have had cancer for a number of years. You’re going to start a new treatment. What’s the best way to know what to look for and how to manage it?
Ms. Maués: I think the key here is that everyone’s different, so have that conversation, the doctor and the patient, about what the best way [of education] is for that specific person. Do they want a flyer listing all of the side effects? Do they want a link to a video they can watch and understand? Do they want someone to come in and give an extra explanation about things? Everyone learns so differently, and I think it’s really hard to assume there’s one way that all patients will understand.
I think the PRO apps are great, and also another benefit is that you keep track of your side effects. Sometimes we don’t even remember well. When did you have nausea? Was it in the morning? Was it in the evening? Is it every day? If you track it with these apps, then you will have the data stored there in the form to answer those questions.
Dr. Cardoso: There was recently a publication – I found it quite interesting – from Lesley Fallowfield’s group saying that the majority of patients would better absorb the information if it is not just text, but if it somehow has a video component, an image, or an infographic that would help them memorize a little bit more information.
Dr. Rugo: There’s been a move toward trying to make videos because the amount of education that’s needed on the providers’ side from our nurses and advanced practice providers may be overwhelming, so things might get missed. The idea of having videos to get everybody on the same page is very popular right now for this reason, and Lesley’s work is really groundbreaking.
Sheila, what do you think is the best way to communicate information?
Ms. Pettiford: Well, I definitely think it’s important for the doctors to recognize, as Julia said, that everyone is different, and all their patients are different. They could come with the same exact subtype of whatever cancer they have – in this situation, breast cancer – and still have so many different reactions. It’s so important for everybody on the health care team to listen to what the patient says because the patient is the one who is living with the illness and knows their body, hopefully.
It’s just one of those things. It’s not a one-size-fits-all situation. You give the standards, but I think it’s important to offer various ways of communicating to a patient because some people are visual. Some people want an overwhelming amount of information so they can sort through it. Then, you have some people who just want the bullet points. Again, it is important not to try to do it as a one-size-fits-all type thing.
Dr. Rugo: Yes, that’s such a good point. I’m always struck by the fact that some patients are totally on top of it and listen to it all, and then other people, we just can’t get them to even call in regarding their side effects. In some ways, it’s frightening for people to call in with issues. Maybe they’re afraid they won’t get the treatment, or that it is related to their cancer progressing, too. Trying to meet people on their own level is a real challenge and an important one.
We talked about education for providers. Fatima, how should we be best educating for these new drugs and new side effects? So many different manifestations can occur, and as we talked about, they might be quite uncommon. We just want people to keep their ears up for any kind of unusual toxicity we see. We all know that the presentation of efficacy data is not adequate for education.
Dr. Cardoso: When we present a new treatment, we focus usually on efficacy, right? Then we say a few things about safety, particularly if there is a new or a severe side effect, but we don’t go through details on how to best manage this in clinical practice.
Anecdotally, I remember that I contacted you because I was going to start using a new treatment and you had some experience. I asked, “What about nausea and vomiting? What do you do for prophylaxis?” I couldn’t find it anywhere in the manuscripts or the presentations. I think we need to focus a little bit more on practical tips. If you are about to start this new treatment, what you should think about and not just the very severe and rare side effects?
Of course, as health care professionals, we need to keep this in our minds. For example, with immunotherapy, side effects can often occur even after stopping the treatment. For other types of new treatments, we need to gain knowledge about endocrinology, for example, which is something that oncologists wouldn’t have to deal with that often in the past. Now, new skills are needed.
It’s also what makes our profession so exciting. There’s always something new to learn, and I like to look at it from that perspective. It’s not boring at all. We are always learning new things.
Dr. Rugo: Indeed. Certainly, you and I have worked together on trying to encourage our pharmaceutical colleagues to publish these papers alongside their urgency of distributing the efficacy data and publishing the papers on efficacy, and also to do a nitty-gritty review of safety and talk about management strategies. I’m really pleased that there seems to be a little more focus on that earlier now in the drug process – although still not early enough – but it’s getting there. That’s a good thing.
Ms. Pettiford: Julia, you mentioned earlier how important it is for the individual patient’s quality of life to understand how these side effects can affect them. It really is one of those things in which we have to make personal decisions. What might be good for one person in terms of what happens with side effects, and their ability to function might not work with someone else.
If you are a person who’s dealing with metastatic disease who has children, a household, a dog, and a cat to take care of, what I can handle being that I’m a single person is not what they can handle. That’s all a part of the education piece. That’s all part of the teamwork. That’s all part of the communication process. It all comes into play.
Dr. Rugo: That’s such an incredibly important point. As we’re wrapping up, it would be great if everybody had some points to make that pulled together some of our conversation. Julia, do you want to start?
Ms. Maués: Yes, I was going to add specifically about the topic you were just discussing, with all that an oncologist’s team has to know and all the different areas of our health being affected by these new treatments. One tip for patients and their teams is that the other providers around the patients may not be as informed about the disease and the treatments they are on. Sometimes we patients end up getting information that isn’t up to date with the latest drugs and things like that.
When we do talk with someone about our issues, make sure they are informed about the new drugs. For example, we often have skin issues. There are dermatologists that work with cancer patients often, and they’re very informed about the side effects that come with these drugs. There are others who never see these sorts of issues and may assume it’s something completely different.
I usually just go to doctors that my oncologist’s team collaborates with and gets referrals from because they send their patients to these doctors often. These are doctors that see cancer patients. We’re a very unique group.
Dr. Rugo: That’s a really good point. I have the same thing. We all have a little stable of people we refer to for various issues that we can reach on speed dial.
The importance of diversity in clinical trials to obtain the most useful outcomes
Fatima, there’s recently been, appropriately so, more of a push to try and evaluate side effects by racial and ethnic subgroups. I think we’re still pretty crummy at it, but we are making some progress. How important is that to you when you think about patients and managing them?
Dr. Cardoso: I think this is quite important. One area of research that is underused, really, is all the new genomics and sequencing technologies to understand why people react differently to the same treatment. Why is it that for some people, either for ethnic or other reasons, you have a different metabolism or something else that justifies a very high rate of side effects from a certain treatment, whereas in other regions of the world this doesn’t happen?
Not to go into these new drugs, but when using a very old drug like a taxane, I found a difference in reaction between the Portuguese patients and the Belgian patients, the two countries where I’ve worked. I even found that the cause might be genetic because the Portuguese living in Belgium reacted differently than the Belgians themselves.
Maybe there is something in the genetics that justifies the type of side effects that you have. I make a plea also for us to dedicate research to understanding why certain side effects are related to race and others are related to maybe some other types of genetic alterations that will lead to an increased side effect.
Dr. Rugo: Sheila, comments?
Ms. Pettiford: That is just excellent. It’s excellent to even consider it because it is so obvious. To me, it’s an obvious situation because there are things that are underneath the skin that we don’t understand. We have to take that into consideration when we are dealing with all these wonderful – I call them miracle – drugs that have come about in the last 20 years.
There still is much more to be done, and I try to participate in any type of organization that’s encouraging diversity in clinical trials because you need to have people of all different ethnicities in order for us to get to these answers. It’s fascinating that you found this out, doctor.
The patient-centered dosing initiative
Ms. Maués: I have the pleasure of being a member of a patient-led initiative called the Patient-Centered Dosing Initiative (PCDI). We are highlighting the discussion around dosages of drugs, especially in the metastatic setting. Metastatic breast cancer is what we’re focusing on, although it could apply to any type of cancer. We are advised by a number of wonderful, world-renowned physicians, Dr. Rugo being one of them. Anne Loeser, the leader of our group, has spoken at ASCO about this topic of dosage. What we’re seeing is that the dosage determination for oncology drugs is still done in the same way it used to be done decades ago and mostly with the curative intent of early-stage disease — metastatic cancer patients back then really didn’t live long at all. What we’re seeing right now is people with metastatic breast cancer that are able to, in some cases, live a long life managing their disease.
Patients are put on doses that are too high for them to be able to manage the side effects, and then they end up having to go off the drug, which means they have lost one of the tools in their toolbox. So, what we like to say about dosing is that, for metastatic cancer patients, it’s a marathon and not a sprint. If we throw all the poison at the patient from the very beginning, they won’t be able to take this for a very long time. And in the metastatic setting, the goal is to stay on each therapy for as long as possible. If we burn one of the cards early on, you have to move on to the next one. This is finite because at some point, there are not enough drugs that can help a particular patient. The PCDI is really getting a lot of visibility with the FDA and experts. People are talking more about dosages, and the FDA is now providing guidance for pharmaceutical companies to study different dosages in the clinical trials from the very beginning. This initiative is almost 3 years old, and we have made a tremendous impact since then.
Dr. Rugo: I think this is an incredibly important area moving forward, and thankfully, there’s so much interest now in not only promoting diversity, enrollment in trials, and education to promote diversity but also in looking at differences in efficacy and side effects.
I’ll just thank everybody for your contributions and amazing perspectives in this incredibly important area. As we move forward with better agents, we need to also make sure we’re understanding what the side effects are, managing them, and hearing the voices of our patients. Thanks very much.
Ms. Pettiford: Thank you so much.
Dr. Cardoso: Thank you.
Ms. Maués: Thank you.
Editor’s note: Our panelists would like to highlight these points:
- The patient and the health care team must build trust with each other.
- African Americans have historical reasons for not trusting the health care industry. Much outreach is still needed.
- Inform and educate before the start of treatment and during the treatment.
- Be balanced and do not underestimate common side effects or overestimate rare ones. Adapt the amount and the detail of the information to the wishes of the individual patient. Offer various methods of delivery (e.g., videos, pamphlets, fact sheets).
- Patients will research their condition and treatments online. Instead of trying to stop this, help them find the best sources.
- Patients will connect with others in the patient community and learn from each other’s experiences. Keep in mind that everyone is different, and decisions should always be made together with the medical team.
- Monitor patients regularly, especially during the first few treatment cycles.
- Use different forms of communication between the patient and health care providers (e.g., apps, digital charts, oncology nurses/nurse navigators, responsive oncologists, different forms of telemedicine), but don’t forget to speak directly with the patient.
- The use of new PRO apps can be very useful to help patients differentiate between urgent and nonurgent signs and symptoms.
- As much as possible, use preventive/prophylactic measures, namely for nausea, vomiting, diarrhea/constipation, and mucositis.
- Be aware of late side effects, especially with immunotherapy.
- Don’t forget that grade 1-2 side effects can substantially impact quality of life, particularly if they are persistent.
- Consider quality-of-life issues for each patient. What is acceptable for one patient may not be for another.
- Learn how to manage new and specific side effects (e.g., endocrine, skin related, pneumonitis).
- Keep an open dialogue about treatment and side effects. Things can change, and there are different ways to address issues such as medications for side effects and dosing changes.
- Listen to your patient and respond in a timely fashion.
- Ethnicity and genetics should be studied as a factor for individual side effects. Standard industry dosages of a new anticancer medication might not be as effective in one ethnic group as another due to the lack of diversity in clinical trials.
- Medications with hard-to-manage or dangerous side effects may be counterproductive regardless of effectiveness.
- Cancer treatment varies vastly depending on region and type of treatment facility. There are many unmet needs in rural areas because of lack of oncology personnel, finances, transportation, etc.
Dr. Rugo is a professor in the department of medicine, University of California San Francisco Comprehensive Cancer Center; director, Breast Oncology and Clinical Trials Education, Cancer Infusion Services, UCSF Helen Diller Family Comprehensive Cancer Center, San Francisco. Dr. Cardoso is director, breast unit, Champalimaud Clinical Centre, Lisbon. Financial disclosures for both Dr. Rugo and Dr. Cardoso are available on Medscape.com, where this article first appeared. Julia Maués is a patient in Washington. She has disclosed no relevant financial relationships. Sheila Pettiford is a patient in Middletown, Del. She has disclosed no relevant financial relationships.
This transcript of a video roundtable, which is available on Medscape.com, has been edited for clarity.
Hope S. Rugo, MD: Hello. I’m Hope Rugo, a breast medical oncologist from the University of California, San Francisco. I’m joined here by three of my friends and colleagues to discuss the toxicity of new agents in the treatment of breast cancer. Fatima, do you want to start by introducing yourself?
Fatima F. Cardoso, MD: Sure. Hello, everyone. I’m Fatima Cardoso, a breast medical oncologist in Lisbon, Portugal.
Dr. Rugo: Sheila.
Sheila Pettiford: Hi, I’m Sheila Pettiford. I am a metastatic [breast cancer] patient and have been for almost 8 years in April. I used to live in Philadelphia, Pennsylvania, but moved to Delaware in the last couple of years during the pandemic. I’m happy to be here.
Dr. Rugo: Julia.
Julia Maués: Hi, everyone. I also am a person living with metastatic breast cancer. I was diagnosed in 2013, so it’s going to be 9 years, also in April.
Effective monitoring and management of side effects: A team effort
Dr. Rugo: We have an amazing group and an international representation, which is also really nice because we get different perspectives. What we’re going to talk about is important to providers and patients across the board. With the host of new agents for the treatment of breast cancer – most of which have really moved us forward in terms of having effective treatment options – we’ve also been faced with a lot of new toxicities or side effects that we haven’t seen before or that we might not have expected from the specific agent.
Those toxicities across the board include side effects that are quite familiar to us, like low blood counts, but we may not advise people well enough about other side effects such as mouth sores, inflammation of the lungs, immune toxicities, and skin toxicities.
Fatima, do you want to start and talk about how we can think about these toxicities and address them?
Dr. Cardoso: Sure. Thank you. From the health care provider point of view, what I would highlight is to educate. Educate before we start the treatment. It’s very important to inform the patient but in a balanced way, so we don’t overexaggerate certain types of side effects or underestimate certain types of side effects.
It’s very important because an informed patient will be attentive to the types of side effects that can happen. Also, teach the patient when it is a [cause for] alarm or something for which they might need to contact their health care team and when that’s not the case. I think this is one crucial topic.
The other one is to monitor. Find ways how to best communicate between the patient and the health care team but in a way that you can monitor, so you can act very early on. Most of these new side effects, if you act early on, will not become severe. It is very important to know about them and to act early on.
I believe there is something important that we don’t think about all the time, and that is prophylaxis. Do not be shy about using prophylactic measures, be it for the mouth sores, nausea and vomiting, diarrhea, and other things that really impact the quality of life of patients. Those, to start, are my three major points of attention for health care professionals.
Dr. Rugo: I think that’s so incredibly important – the comments that you’ve made – and also that prevention and prophylaxis are so important. You don’t want to have a patient have diarrhea in the middle of the night and not have any antipropulsive agents at home. Just as a very straightforward example, it’s really important.
Also, the ability to know what you should be looking for and how you can manage it [is important]. There are many examples of times when, even with some education, providers may not have communicated well to the patient. Then the patient is surprised and unhappy with the situation and unable to manage it.
The importance of education
Sheila, your comments on this from the patient perspective are so important. How important is the education piece, and how do you manage the fear of side effects vs actually managing the side effects that might be caused by the treatment you’re taking?
Ms. Pettiford: Thank you for that question. I really think it’s a dance. It’s a dance between the patient and the health care team. Yes, education is absolutely important. However, the health care professionals have to establish a relationship of trust with the patient. My own circumstances were that – and I was very fortunate in that my oncologist, who I chose just by looking and not by a recommendation – I did find an oncologist who listened to me.
When it came time for me to deal with a new medication, the education she provided me was sufficient because of the fact that there was a lot of listening that had gone on prior to the new medicine being given to me. I trusted what I was hearing, and it felt like there was a balanced situation that came about from what I was being told. I could look it up, too.
There still is that part of the patient who will be participating in the process, as well. They can still look up things, and that’s one of the downfalls of the information age we are in. It is a dance. I just want to go back to that. There’s a dance between the patient and the health care providers.
Dr. Rugo: Julia, from the patient’s side, how do you balance the benefits you might get from a treatment versus the side effects and how best to manage them?
Ms. Maués: I think it’s interesting that when we talk with our doctors, and especially when we read about a certain treatment, the attention is focused on the very severe and unlikely side effects that a drug has. We don’t talk as much about the side effects that are most likely to happen and will affect us but may not be life threatening.
Especially for those of us with metastatic cancer who are going to ideally be on a drug for a very long time, we’re then faced with low-grade nausea for the rest of our lives. That’s not okay either, right? I think it’s important to talk about all of the levels of toxicities and everything that can be done to avoid this.
Communication is key
Ms. Pettiford: I just want to add something that Dr. Cardoso said about monitoring that is absolutely important. We’re in a day and time when it’s very difficult to get someone on the telephone, but we do have digital charts and other ways that monitoring can take place. I was at a large teaching university, and I had to go monthly for my treatments. Every month, there were questions that were asked about my life and my condition. I could always get in contact with somebody through the digital chart.
Dr. Rugo: That’s an incredibly important comment, Sheila, about communication and how patients can feel like they have someone to go to in real time who can help manage things. Fatima, I’m interested in your comment on that.
Also, just to go to the next step, which is that when we see data reported on clinical trials and how the agent we’ve added or substituted is better than the standard, the toxicity tables are side effects that occur in at least 10% or more patients and sometimes even 20%. Then they’re graded, where often the division is grade 3 or greater. That may not actually reflect much about what the individual patient experience is. How do we interpret these data? Communication and interpretation?
Dr. Cardoso: Absolutely. I always call attention that perhaps, since we focus so much on grade 3 and 4 [side effects], that is the reason why we don’t see in the usual reporting differences quality of life between treatments. Quality of life is affected also significantly by grade 2 side effects. Or, like Julia was mentioning, even grade 1, if they are persistent, will eventually affect your quality of life.
Sometimes, like I was saying, don’t underestimate – it’s a little bit like that. We focus on explaining, “Look, this new immunotherapy can give you all these different side effects.” But then we forget to say: “Oh, by the way, it may also give you some nausea.” Actually, the nausea will affect the patient’s quality of life. I think that’s why it is so important to balance the way we provide the information.
I would like also to take on what Sheila said that sometimes too much information is not very helpful. That’s why sometimes we have to go stepwise. The first time you’re about to start the treatment, advise [the patient] on the most frequent side effects. Later on, you have time to say: “Okay, by the way, this can also give a rare side effect. This is what you should look for. If you have it, please contact your health care team.”
I think the most difficult part, at least from my experience, is for patients to understand what is really a sign of a severe side effect and what is normal for that type of treatment. Some of the new ways of communicating, like using some patient-reported outcome (PRO) apps, actually help the patient by saying, “This that you are feeling is normal. It can wait for your next appointment. This that you are feeling, it’s better if you try to reach your health care team right away. Or, this is an urgent thing and go to the emergency room near you.”
For this kind of triage, there are now new apps that can help. I think this is the most difficult part because when you are a patient, you don’t know if what you are feeling is actually a sign of something very severe or if it’s normal for the type of treatment you are receiving.
Dr. Rugo: I think that’s so important, and these new PRO apps may help with this. Of course, nothing substitutes for talking in the end if you’re confused or it doesn’t fit into whatever’s in that paradigm. I think it’s important.
Best practices in focusing on the individual patient
Julia, what do you think the best way of educating the patient is when you’re going to start a new treatment? You might be newly diagnosed with cancer or you might have had cancer for a number of years. You’re going to start a new treatment. What’s the best way to know what to look for and how to manage it?
Ms. Maués: I think the key here is that everyone’s different, so have that conversation, the doctor and the patient, about what the best way [of education] is for that specific person. Do they want a flyer listing all of the side effects? Do they want a link to a video they can watch and understand? Do they want someone to come in and give an extra explanation about things? Everyone learns so differently, and I think it’s really hard to assume there’s one way that all patients will understand.
I think the PRO apps are great, and also another benefit is that you keep track of your side effects. Sometimes we don’t even remember well. When did you have nausea? Was it in the morning? Was it in the evening? Is it every day? If you track it with these apps, then you will have the data stored there in the form to answer those questions.
Dr. Cardoso: There was recently a publication – I found it quite interesting – from Lesley Fallowfield’s group saying that the majority of patients would better absorb the information if it is not just text, but if it somehow has a video component, an image, or an infographic that would help them memorize a little bit more information.
Dr. Rugo: There’s been a move toward trying to make videos because the amount of education that’s needed on the providers’ side from our nurses and advanced practice providers may be overwhelming, so things might get missed. The idea of having videos to get everybody on the same page is very popular right now for this reason, and Lesley’s work is really groundbreaking.
Sheila, what do you think is the best way to communicate information?
Ms. Pettiford: Well, I definitely think it’s important for the doctors to recognize, as Julia said, that everyone is different, and all their patients are different. They could come with the same exact subtype of whatever cancer they have – in this situation, breast cancer – and still have so many different reactions. It’s so important for everybody on the health care team to listen to what the patient says because the patient is the one who is living with the illness and knows their body, hopefully.
It’s just one of those things. It’s not a one-size-fits-all situation. You give the standards, but I think it’s important to offer various ways of communicating to a patient because some people are visual. Some people want an overwhelming amount of information so they can sort through it. Then, you have some people who just want the bullet points. Again, it is important not to try to do it as a one-size-fits-all type thing.
Dr. Rugo: Yes, that’s such a good point. I’m always struck by the fact that some patients are totally on top of it and listen to it all, and then other people, we just can’t get them to even call in regarding their side effects. In some ways, it’s frightening for people to call in with issues. Maybe they’re afraid they won’t get the treatment, or that it is related to their cancer progressing, too. Trying to meet people on their own level is a real challenge and an important one.
We talked about education for providers. Fatima, how should we be best educating for these new drugs and new side effects? So many different manifestations can occur, and as we talked about, they might be quite uncommon. We just want people to keep their ears up for any kind of unusual toxicity we see. We all know that the presentation of efficacy data is not adequate for education.
Dr. Cardoso: When we present a new treatment, we focus usually on efficacy, right? Then we say a few things about safety, particularly if there is a new or a severe side effect, but we don’t go through details on how to best manage this in clinical practice.
Anecdotally, I remember that I contacted you because I was going to start using a new treatment and you had some experience. I asked, “What about nausea and vomiting? What do you do for prophylaxis?” I couldn’t find it anywhere in the manuscripts or the presentations. I think we need to focus a little bit more on practical tips. If you are about to start this new treatment, what you should think about and not just the very severe and rare side effects?
Of course, as health care professionals, we need to keep this in our minds. For example, with immunotherapy, side effects can often occur even after stopping the treatment. For other types of new treatments, we need to gain knowledge about endocrinology, for example, which is something that oncologists wouldn’t have to deal with that often in the past. Now, new skills are needed.
It’s also what makes our profession so exciting. There’s always something new to learn, and I like to look at it from that perspective. It’s not boring at all. We are always learning new things.
Dr. Rugo: Indeed. Certainly, you and I have worked together on trying to encourage our pharmaceutical colleagues to publish these papers alongside their urgency of distributing the efficacy data and publishing the papers on efficacy, and also to do a nitty-gritty review of safety and talk about management strategies. I’m really pleased that there seems to be a little more focus on that earlier now in the drug process – although still not early enough – but it’s getting there. That’s a good thing.
Ms. Pettiford: Julia, you mentioned earlier how important it is for the individual patient’s quality of life to understand how these side effects can affect them. It really is one of those things in which we have to make personal decisions. What might be good for one person in terms of what happens with side effects, and their ability to function might not work with someone else.
If you are a person who’s dealing with metastatic disease who has children, a household, a dog, and a cat to take care of, what I can handle being that I’m a single person is not what they can handle. That’s all a part of the education piece. That’s all part of the teamwork. That’s all part of the communication process. It all comes into play.
Dr. Rugo: That’s such an incredibly important point. As we’re wrapping up, it would be great if everybody had some points to make that pulled together some of our conversation. Julia, do you want to start?
Ms. Maués: Yes, I was going to add specifically about the topic you were just discussing, with all that an oncologist’s team has to know and all the different areas of our health being affected by these new treatments. One tip for patients and their teams is that the other providers around the patients may not be as informed about the disease and the treatments they are on. Sometimes we patients end up getting information that isn’t up to date with the latest drugs and things like that.
When we do talk with someone about our issues, make sure they are informed about the new drugs. For example, we often have skin issues. There are dermatologists that work with cancer patients often, and they’re very informed about the side effects that come with these drugs. There are others who never see these sorts of issues and may assume it’s something completely different.
I usually just go to doctors that my oncologist’s team collaborates with and gets referrals from because they send their patients to these doctors often. These are doctors that see cancer patients. We’re a very unique group.
Dr. Rugo: That’s a really good point. I have the same thing. We all have a little stable of people we refer to for various issues that we can reach on speed dial.
The importance of diversity in clinical trials to obtain the most useful outcomes
Fatima, there’s recently been, appropriately so, more of a push to try and evaluate side effects by racial and ethnic subgroups. I think we’re still pretty crummy at it, but we are making some progress. How important is that to you when you think about patients and managing them?
Dr. Cardoso: I think this is quite important. One area of research that is underused, really, is all the new genomics and sequencing technologies to understand why people react differently to the same treatment. Why is it that for some people, either for ethnic or other reasons, you have a different metabolism or something else that justifies a very high rate of side effects from a certain treatment, whereas in other regions of the world this doesn’t happen?
Not to go into these new drugs, but when using a very old drug like a taxane, I found a difference in reaction between the Portuguese patients and the Belgian patients, the two countries where I’ve worked. I even found that the cause might be genetic because the Portuguese living in Belgium reacted differently than the Belgians themselves.
Maybe there is something in the genetics that justifies the type of side effects that you have. I make a plea also for us to dedicate research to understanding why certain side effects are related to race and others are related to maybe some other types of genetic alterations that will lead to an increased side effect.
Dr. Rugo: Sheila, comments?
Ms. Pettiford: That is just excellent. It’s excellent to even consider it because it is so obvious. To me, it’s an obvious situation because there are things that are underneath the skin that we don’t understand. We have to take that into consideration when we are dealing with all these wonderful – I call them miracle – drugs that have come about in the last 20 years.
There still is much more to be done, and I try to participate in any type of organization that’s encouraging diversity in clinical trials because you need to have people of all different ethnicities in order for us to get to these answers. It’s fascinating that you found this out, doctor.
The patient-centered dosing initiative
Ms. Maués: I have the pleasure of being a member of a patient-led initiative called the Patient-Centered Dosing Initiative (PCDI). We are highlighting the discussion around dosages of drugs, especially in the metastatic setting. Metastatic breast cancer is what we’re focusing on, although it could apply to any type of cancer. We are advised by a number of wonderful, world-renowned physicians, Dr. Rugo being one of them. Anne Loeser, the leader of our group, has spoken at ASCO about this topic of dosage. What we’re seeing is that the dosage determination for oncology drugs is still done in the same way it used to be done decades ago and mostly with the curative intent of early-stage disease — metastatic cancer patients back then really didn’t live long at all. What we’re seeing right now is people with metastatic breast cancer that are able to, in some cases, live a long life managing their disease.
Patients are put on doses that are too high for them to be able to manage the side effects, and then they end up having to go off the drug, which means they have lost one of the tools in their toolbox. So, what we like to say about dosing is that, for metastatic cancer patients, it’s a marathon and not a sprint. If we throw all the poison at the patient from the very beginning, they won’t be able to take this for a very long time. And in the metastatic setting, the goal is to stay on each therapy for as long as possible. If we burn one of the cards early on, you have to move on to the next one. This is finite because at some point, there are not enough drugs that can help a particular patient. The PCDI is really getting a lot of visibility with the FDA and experts. People are talking more about dosages, and the FDA is now providing guidance for pharmaceutical companies to study different dosages in the clinical trials from the very beginning. This initiative is almost 3 years old, and we have made a tremendous impact since then.
Dr. Rugo: I think this is an incredibly important area moving forward, and thankfully, there’s so much interest now in not only promoting diversity, enrollment in trials, and education to promote diversity but also in looking at differences in efficacy and side effects.
I’ll just thank everybody for your contributions and amazing perspectives in this incredibly important area. As we move forward with better agents, we need to also make sure we’re understanding what the side effects are, managing them, and hearing the voices of our patients. Thanks very much.
Ms. Pettiford: Thank you so much.
Dr. Cardoso: Thank you.
Ms. Maués: Thank you.
Editor’s note: Our panelists would like to highlight these points:
- The patient and the health care team must build trust with each other.
- African Americans have historical reasons for not trusting the health care industry. Much outreach is still needed.
- Inform and educate before the start of treatment and during the treatment.
- Be balanced and do not underestimate common side effects or overestimate rare ones. Adapt the amount and the detail of the information to the wishes of the individual patient. Offer various methods of delivery (e.g., videos, pamphlets, fact sheets).
- Patients will research their condition and treatments online. Instead of trying to stop this, help them find the best sources.
- Patients will connect with others in the patient community and learn from each other’s experiences. Keep in mind that everyone is different, and decisions should always be made together with the medical team.
- Monitor patients regularly, especially during the first few treatment cycles.
- Use different forms of communication between the patient and health care providers (e.g., apps, digital charts, oncology nurses/nurse navigators, responsive oncologists, different forms of telemedicine), but don’t forget to speak directly with the patient.
- The use of new PRO apps can be very useful to help patients differentiate between urgent and nonurgent signs and symptoms.
- As much as possible, use preventive/prophylactic measures, namely for nausea, vomiting, diarrhea/constipation, and mucositis.
- Be aware of late side effects, especially with immunotherapy.
- Don’t forget that grade 1-2 side effects can substantially impact quality of life, particularly if they are persistent.
- Consider quality-of-life issues for each patient. What is acceptable for one patient may not be for another.
- Learn how to manage new and specific side effects (e.g., endocrine, skin related, pneumonitis).
- Keep an open dialogue about treatment and side effects. Things can change, and there are different ways to address issues such as medications for side effects and dosing changes.
- Listen to your patient and respond in a timely fashion.
- Ethnicity and genetics should be studied as a factor for individual side effects. Standard industry dosages of a new anticancer medication might not be as effective in one ethnic group as another due to the lack of diversity in clinical trials.
- Medications with hard-to-manage or dangerous side effects may be counterproductive regardless of effectiveness.
- Cancer treatment varies vastly depending on region and type of treatment facility. There are many unmet needs in rural areas because of lack of oncology personnel, finances, transportation, etc.
Dr. Rugo is a professor in the department of medicine, University of California San Francisco Comprehensive Cancer Center; director, Breast Oncology and Clinical Trials Education, Cancer Infusion Services, UCSF Helen Diller Family Comprehensive Cancer Center, San Francisco. Dr. Cardoso is director, breast unit, Champalimaud Clinical Centre, Lisbon. Financial disclosures for both Dr. Rugo and Dr. Cardoso are available on Medscape.com, where this article first appeared. Julia Maués is a patient in Washington. She has disclosed no relevant financial relationships. Sheila Pettiford is a patient in Middletown, Del. She has disclosed no relevant financial relationships.
This transcript of a video roundtable, which is available on Medscape.com, has been edited for clarity.
Hope S. Rugo, MD: Hello. I’m Hope Rugo, a breast medical oncologist from the University of California, San Francisco. I’m joined here by three of my friends and colleagues to discuss the toxicity of new agents in the treatment of breast cancer. Fatima, do you want to start by introducing yourself?
Fatima F. Cardoso, MD: Sure. Hello, everyone. I’m Fatima Cardoso, a breast medical oncologist in Lisbon, Portugal.
Dr. Rugo: Sheila.
Sheila Pettiford: Hi, I’m Sheila Pettiford. I am a metastatic [breast cancer] patient and have been for almost 8 years in April. I used to live in Philadelphia, Pennsylvania, but moved to Delaware in the last couple of years during the pandemic. I’m happy to be here.
Dr. Rugo: Julia.
Julia Maués: Hi, everyone. I also am a person living with metastatic breast cancer. I was diagnosed in 2013, so it’s going to be 9 years, also in April.
Effective monitoring and management of side effects: A team effort
Dr. Rugo: We have an amazing group and an international representation, which is also really nice because we get different perspectives. What we’re going to talk about is important to providers and patients across the board. With the host of new agents for the treatment of breast cancer – most of which have really moved us forward in terms of having effective treatment options – we’ve also been faced with a lot of new toxicities or side effects that we haven’t seen before or that we might not have expected from the specific agent.
Those toxicities across the board include side effects that are quite familiar to us, like low blood counts, but we may not advise people well enough about other side effects such as mouth sores, inflammation of the lungs, immune toxicities, and skin toxicities.
Fatima, do you want to start and talk about how we can think about these toxicities and address them?
Dr. Cardoso: Sure. Thank you. From the health care provider point of view, what I would highlight is to educate. Educate before we start the treatment. It’s very important to inform the patient but in a balanced way, so we don’t overexaggerate certain types of side effects or underestimate certain types of side effects.
It’s very important because an informed patient will be attentive to the types of side effects that can happen. Also, teach the patient when it is a [cause for] alarm or something for which they might need to contact their health care team and when that’s not the case. I think this is one crucial topic.
The other one is to monitor. Find ways how to best communicate between the patient and the health care team but in a way that you can monitor, so you can act very early on. Most of these new side effects, if you act early on, will not become severe. It is very important to know about them and to act early on.
I believe there is something important that we don’t think about all the time, and that is prophylaxis. Do not be shy about using prophylactic measures, be it for the mouth sores, nausea and vomiting, diarrhea, and other things that really impact the quality of life of patients. Those, to start, are my three major points of attention for health care professionals.
Dr. Rugo: I think that’s so incredibly important – the comments that you’ve made – and also that prevention and prophylaxis are so important. You don’t want to have a patient have diarrhea in the middle of the night and not have any antipropulsive agents at home. Just as a very straightforward example, it’s really important.
Also, the ability to know what you should be looking for and how you can manage it [is important]. There are many examples of times when, even with some education, providers may not have communicated well to the patient. Then the patient is surprised and unhappy with the situation and unable to manage it.
The importance of education
Sheila, your comments on this from the patient perspective are so important. How important is the education piece, and how do you manage the fear of side effects vs actually managing the side effects that might be caused by the treatment you’re taking?
Ms. Pettiford: Thank you for that question. I really think it’s a dance. It’s a dance between the patient and the health care team. Yes, education is absolutely important. However, the health care professionals have to establish a relationship of trust with the patient. My own circumstances were that – and I was very fortunate in that my oncologist, who I chose just by looking and not by a recommendation – I did find an oncologist who listened to me.
When it came time for me to deal with a new medication, the education she provided me was sufficient because of the fact that there was a lot of listening that had gone on prior to the new medicine being given to me. I trusted what I was hearing, and it felt like there was a balanced situation that came about from what I was being told. I could look it up, too.
There still is that part of the patient who will be participating in the process, as well. They can still look up things, and that’s one of the downfalls of the information age we are in. It is a dance. I just want to go back to that. There’s a dance between the patient and the health care providers.
Dr. Rugo: Julia, from the patient’s side, how do you balance the benefits you might get from a treatment versus the side effects and how best to manage them?
Ms. Maués: I think it’s interesting that when we talk with our doctors, and especially when we read about a certain treatment, the attention is focused on the very severe and unlikely side effects that a drug has. We don’t talk as much about the side effects that are most likely to happen and will affect us but may not be life threatening.
Especially for those of us with metastatic cancer who are going to ideally be on a drug for a very long time, we’re then faced with low-grade nausea for the rest of our lives. That’s not okay either, right? I think it’s important to talk about all of the levels of toxicities and everything that can be done to avoid this.
Communication is key
Ms. Pettiford: I just want to add something that Dr. Cardoso said about monitoring that is absolutely important. We’re in a day and time when it’s very difficult to get someone on the telephone, but we do have digital charts and other ways that monitoring can take place. I was at a large teaching university, and I had to go monthly for my treatments. Every month, there were questions that were asked about my life and my condition. I could always get in contact with somebody through the digital chart.
Dr. Rugo: That’s an incredibly important comment, Sheila, about communication and how patients can feel like they have someone to go to in real time who can help manage things. Fatima, I’m interested in your comment on that.
Also, just to go to the next step, which is that when we see data reported on clinical trials and how the agent we’ve added or substituted is better than the standard, the toxicity tables are side effects that occur in at least 10% or more patients and sometimes even 20%. Then they’re graded, where often the division is grade 3 or greater. That may not actually reflect much about what the individual patient experience is. How do we interpret these data? Communication and interpretation?
Dr. Cardoso: Absolutely. I always call attention that perhaps, since we focus so much on grade 3 and 4 [side effects], that is the reason why we don’t see in the usual reporting differences quality of life between treatments. Quality of life is affected also significantly by grade 2 side effects. Or, like Julia was mentioning, even grade 1, if they are persistent, will eventually affect your quality of life.
Sometimes, like I was saying, don’t underestimate – it’s a little bit like that. We focus on explaining, “Look, this new immunotherapy can give you all these different side effects.” But then we forget to say: “Oh, by the way, it may also give you some nausea.” Actually, the nausea will affect the patient’s quality of life. I think that’s why it is so important to balance the way we provide the information.
I would like also to take on what Sheila said that sometimes too much information is not very helpful. That’s why sometimes we have to go stepwise. The first time you’re about to start the treatment, advise [the patient] on the most frequent side effects. Later on, you have time to say: “Okay, by the way, this can also give a rare side effect. This is what you should look for. If you have it, please contact your health care team.”
I think the most difficult part, at least from my experience, is for patients to understand what is really a sign of a severe side effect and what is normal for that type of treatment. Some of the new ways of communicating, like using some patient-reported outcome (PRO) apps, actually help the patient by saying, “This that you are feeling is normal. It can wait for your next appointment. This that you are feeling, it’s better if you try to reach your health care team right away. Or, this is an urgent thing and go to the emergency room near you.”
For this kind of triage, there are now new apps that can help. I think this is the most difficult part because when you are a patient, you don’t know if what you are feeling is actually a sign of something very severe or if it’s normal for the type of treatment you are receiving.
Dr. Rugo: I think that’s so important, and these new PRO apps may help with this. Of course, nothing substitutes for talking in the end if you’re confused or it doesn’t fit into whatever’s in that paradigm. I think it’s important.
Best practices in focusing on the individual patient
Julia, what do you think the best way of educating the patient is when you’re going to start a new treatment? You might be newly diagnosed with cancer or you might have had cancer for a number of years. You’re going to start a new treatment. What’s the best way to know what to look for and how to manage it?
Ms. Maués: I think the key here is that everyone’s different, so have that conversation, the doctor and the patient, about what the best way [of education] is for that specific person. Do they want a flyer listing all of the side effects? Do they want a link to a video they can watch and understand? Do they want someone to come in and give an extra explanation about things? Everyone learns so differently, and I think it’s really hard to assume there’s one way that all patients will understand.
I think the PRO apps are great, and also another benefit is that you keep track of your side effects. Sometimes we don’t even remember well. When did you have nausea? Was it in the morning? Was it in the evening? Is it every day? If you track it with these apps, then you will have the data stored there in the form to answer those questions.
Dr. Cardoso: There was recently a publication – I found it quite interesting – from Lesley Fallowfield’s group saying that the majority of patients would better absorb the information if it is not just text, but if it somehow has a video component, an image, or an infographic that would help them memorize a little bit more information.
Dr. Rugo: There’s been a move toward trying to make videos because the amount of education that’s needed on the providers’ side from our nurses and advanced practice providers may be overwhelming, so things might get missed. The idea of having videos to get everybody on the same page is very popular right now for this reason, and Lesley’s work is really groundbreaking.
Sheila, what do you think is the best way to communicate information?
Ms. Pettiford: Well, I definitely think it’s important for the doctors to recognize, as Julia said, that everyone is different, and all their patients are different. They could come with the same exact subtype of whatever cancer they have – in this situation, breast cancer – and still have so many different reactions. It’s so important for everybody on the health care team to listen to what the patient says because the patient is the one who is living with the illness and knows their body, hopefully.
It’s just one of those things. It’s not a one-size-fits-all situation. You give the standards, but I think it’s important to offer various ways of communicating to a patient because some people are visual. Some people want an overwhelming amount of information so they can sort through it. Then, you have some people who just want the bullet points. Again, it is important not to try to do it as a one-size-fits-all type thing.
Dr. Rugo: Yes, that’s such a good point. I’m always struck by the fact that some patients are totally on top of it and listen to it all, and then other people, we just can’t get them to even call in regarding their side effects. In some ways, it’s frightening for people to call in with issues. Maybe they’re afraid they won’t get the treatment, or that it is related to their cancer progressing, too. Trying to meet people on their own level is a real challenge and an important one.
We talked about education for providers. Fatima, how should we be best educating for these new drugs and new side effects? So many different manifestations can occur, and as we talked about, they might be quite uncommon. We just want people to keep their ears up for any kind of unusual toxicity we see. We all know that the presentation of efficacy data is not adequate for education.
Dr. Cardoso: When we present a new treatment, we focus usually on efficacy, right? Then we say a few things about safety, particularly if there is a new or a severe side effect, but we don’t go through details on how to best manage this in clinical practice.
Anecdotally, I remember that I contacted you because I was going to start using a new treatment and you had some experience. I asked, “What about nausea and vomiting? What do you do for prophylaxis?” I couldn’t find it anywhere in the manuscripts or the presentations. I think we need to focus a little bit more on practical tips. If you are about to start this new treatment, what you should think about and not just the very severe and rare side effects?
Of course, as health care professionals, we need to keep this in our minds. For example, with immunotherapy, side effects can often occur even after stopping the treatment. For other types of new treatments, we need to gain knowledge about endocrinology, for example, which is something that oncologists wouldn’t have to deal with that often in the past. Now, new skills are needed.
It’s also what makes our profession so exciting. There’s always something new to learn, and I like to look at it from that perspective. It’s not boring at all. We are always learning new things.
Dr. Rugo: Indeed. Certainly, you and I have worked together on trying to encourage our pharmaceutical colleagues to publish these papers alongside their urgency of distributing the efficacy data and publishing the papers on efficacy, and also to do a nitty-gritty review of safety and talk about management strategies. I’m really pleased that there seems to be a little more focus on that earlier now in the drug process – although still not early enough – but it’s getting there. That’s a good thing.
Ms. Pettiford: Julia, you mentioned earlier how important it is for the individual patient’s quality of life to understand how these side effects can affect them. It really is one of those things in which we have to make personal decisions. What might be good for one person in terms of what happens with side effects, and their ability to function might not work with someone else.
If you are a person who’s dealing with metastatic disease who has children, a household, a dog, and a cat to take care of, what I can handle being that I’m a single person is not what they can handle. That’s all a part of the education piece. That’s all part of the teamwork. That’s all part of the communication process. It all comes into play.
Dr. Rugo: That’s such an incredibly important point. As we’re wrapping up, it would be great if everybody had some points to make that pulled together some of our conversation. Julia, do you want to start?
Ms. Maués: Yes, I was going to add specifically about the topic you were just discussing, with all that an oncologist’s team has to know and all the different areas of our health being affected by these new treatments. One tip for patients and their teams is that the other providers around the patients may not be as informed about the disease and the treatments they are on. Sometimes we patients end up getting information that isn’t up to date with the latest drugs and things like that.
When we do talk with someone about our issues, make sure they are informed about the new drugs. For example, we often have skin issues. There are dermatologists that work with cancer patients often, and they’re very informed about the side effects that come with these drugs. There are others who never see these sorts of issues and may assume it’s something completely different.
I usually just go to doctors that my oncologist’s team collaborates with and gets referrals from because they send their patients to these doctors often. These are doctors that see cancer patients. We’re a very unique group.
Dr. Rugo: That’s a really good point. I have the same thing. We all have a little stable of people we refer to for various issues that we can reach on speed dial.
The importance of diversity in clinical trials to obtain the most useful outcomes
Fatima, there’s recently been, appropriately so, more of a push to try and evaluate side effects by racial and ethnic subgroups. I think we’re still pretty crummy at it, but we are making some progress. How important is that to you when you think about patients and managing them?
Dr. Cardoso: I think this is quite important. One area of research that is underused, really, is all the new genomics and sequencing technologies to understand why people react differently to the same treatment. Why is it that for some people, either for ethnic or other reasons, you have a different metabolism or something else that justifies a very high rate of side effects from a certain treatment, whereas in other regions of the world this doesn’t happen?
Not to go into these new drugs, but when using a very old drug like a taxane, I found a difference in reaction between the Portuguese patients and the Belgian patients, the two countries where I’ve worked. I even found that the cause might be genetic because the Portuguese living in Belgium reacted differently than the Belgians themselves.
Maybe there is something in the genetics that justifies the type of side effects that you have. I make a plea also for us to dedicate research to understanding why certain side effects are related to race and others are related to maybe some other types of genetic alterations that will lead to an increased side effect.
Dr. Rugo: Sheila, comments?
Ms. Pettiford: That is just excellent. It’s excellent to even consider it because it is so obvious. To me, it’s an obvious situation because there are things that are underneath the skin that we don’t understand. We have to take that into consideration when we are dealing with all these wonderful – I call them miracle – drugs that have come about in the last 20 years.
There still is much more to be done, and I try to participate in any type of organization that’s encouraging diversity in clinical trials because you need to have people of all different ethnicities in order for us to get to these answers. It’s fascinating that you found this out, doctor.
The patient-centered dosing initiative
Ms. Maués: I have the pleasure of being a member of a patient-led initiative called the Patient-Centered Dosing Initiative (PCDI). We are highlighting the discussion around dosages of drugs, especially in the metastatic setting. Metastatic breast cancer is what we’re focusing on, although it could apply to any type of cancer. We are advised by a number of wonderful, world-renowned physicians, Dr. Rugo being one of them. Anne Loeser, the leader of our group, has spoken at ASCO about this topic of dosage. What we’re seeing is that the dosage determination for oncology drugs is still done in the same way it used to be done decades ago and mostly with the curative intent of early-stage disease — metastatic cancer patients back then really didn’t live long at all. What we’re seeing right now is people with metastatic breast cancer that are able to, in some cases, live a long life managing their disease.
Patients are put on doses that are too high for them to be able to manage the side effects, and then they end up having to go off the drug, which means they have lost one of the tools in their toolbox. So, what we like to say about dosing is that, for metastatic cancer patients, it’s a marathon and not a sprint. If we throw all the poison at the patient from the very beginning, they won’t be able to take this for a very long time. And in the metastatic setting, the goal is to stay on each therapy for as long as possible. If we burn one of the cards early on, you have to move on to the next one. This is finite because at some point, there are not enough drugs that can help a particular patient. The PCDI is really getting a lot of visibility with the FDA and experts. People are talking more about dosages, and the FDA is now providing guidance for pharmaceutical companies to study different dosages in the clinical trials from the very beginning. This initiative is almost 3 years old, and we have made a tremendous impact since then.
Dr. Rugo: I think this is an incredibly important area moving forward, and thankfully, there’s so much interest now in not only promoting diversity, enrollment in trials, and education to promote diversity but also in looking at differences in efficacy and side effects.
I’ll just thank everybody for your contributions and amazing perspectives in this incredibly important area. As we move forward with better agents, we need to also make sure we’re understanding what the side effects are, managing them, and hearing the voices of our patients. Thanks very much.
Ms. Pettiford: Thank you so much.
Dr. Cardoso: Thank you.
Ms. Maués: Thank you.
Editor’s note: Our panelists would like to highlight these points:
- The patient and the health care team must build trust with each other.
- African Americans have historical reasons for not trusting the health care industry. Much outreach is still needed.
- Inform and educate before the start of treatment and during the treatment.
- Be balanced and do not underestimate common side effects or overestimate rare ones. Adapt the amount and the detail of the information to the wishes of the individual patient. Offer various methods of delivery (e.g., videos, pamphlets, fact sheets).
- Patients will research their condition and treatments online. Instead of trying to stop this, help them find the best sources.
- Patients will connect with others in the patient community and learn from each other’s experiences. Keep in mind that everyone is different, and decisions should always be made together with the medical team.
- Monitor patients regularly, especially during the first few treatment cycles.
- Use different forms of communication between the patient and health care providers (e.g., apps, digital charts, oncology nurses/nurse navigators, responsive oncologists, different forms of telemedicine), but don’t forget to speak directly with the patient.
- The use of new PRO apps can be very useful to help patients differentiate between urgent and nonurgent signs and symptoms.
- As much as possible, use preventive/prophylactic measures, namely for nausea, vomiting, diarrhea/constipation, and mucositis.
- Be aware of late side effects, especially with immunotherapy.
- Don’t forget that grade 1-2 side effects can substantially impact quality of life, particularly if they are persistent.
- Consider quality-of-life issues for each patient. What is acceptable for one patient may not be for another.
- Learn how to manage new and specific side effects (e.g., endocrine, skin related, pneumonitis).
- Keep an open dialogue about treatment and side effects. Things can change, and there are different ways to address issues such as medications for side effects and dosing changes.
- Listen to your patient and respond in a timely fashion.
- Ethnicity and genetics should be studied as a factor for individual side effects. Standard industry dosages of a new anticancer medication might not be as effective in one ethnic group as another due to the lack of diversity in clinical trials.
- Medications with hard-to-manage or dangerous side effects may be counterproductive regardless of effectiveness.
- Cancer treatment varies vastly depending on region and type of treatment facility. There are many unmet needs in rural areas because of lack of oncology personnel, finances, transportation, etc.
Dr. Rugo is a professor in the department of medicine, University of California San Francisco Comprehensive Cancer Center; director, Breast Oncology and Clinical Trials Education, Cancer Infusion Services, UCSF Helen Diller Family Comprehensive Cancer Center, San Francisco. Dr. Cardoso is director, breast unit, Champalimaud Clinical Centre, Lisbon. Financial disclosures for both Dr. Rugo and Dr. Cardoso are available on Medscape.com, where this article first appeared. Julia Maués is a patient in Washington. She has disclosed no relevant financial relationships. Sheila Pettiford is a patient in Middletown, Del. She has disclosed no relevant financial relationships.
Give patients can’ts but also can do’s
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.

Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.
Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
On his last shift in the last hockey game of the regular season, our 14-year-old grandson broke his arm. Although this was his first fracture, the rest of the nuclear family has had ample experience with orthopedic trauma over the last year, both planned and unplanned.
As I drove Peter and my daughter-in-law to his first postsetting and casting appointment I told him how sorry I was that he had been told “no contact sports for the next 3 months.” This was a tough pill for a kid eager to begin his first high school lacrosse season. Then I asked him what the doctor had told him he could do in the way of activity.
Based on personal and professional experience I was not surprised when he told me that no one had suggested things he could be doing. In fact, being a cautious and thoughtful kid, he was concerned about what he should be doing around the house let alone any athletic activities. It turns out he wasn’t even lifting his laptop computer with two hands because some nurse had told him not to lift anything over 2 pounds.
I told him “Peter, even some of the most experienced doctors focus on the ‘can’ts’ and forget to tell you the ‘cans’ and ‘shoulds.’ While you’re in the waiting room make up a mental list of what you would like to be doing that you aren’t.”
As he climbed back in the car for the ride home I asked how the visit went. The x-ray showed good alignment and the doctor was pleased. But, as I predicted, they were already on the launch pad to the receptionist to make a follow-up appointment without the physician uttering a single word about what activities he could resume. Always a very coachable kid, Peter piped up with the list he had created in the waiting room and was relieved to hear that he could do anything as long as it didn’t hurt. In fact, the doctor encouraged him to use his fingers because it might speed the healing.
Not every patient, regardless of age, is as cautious as my grandson and in some circumstances the physician must err on the side of emphasizing the “don’ts.” However, in my experience, too many physicians forget to include a generous list of “can do’s” in their visit closing discussions. This oversight is a mistake for several reasons.
First, and maybe most importantly, even a brief discussion of “can do’s” can soften the depressing message that the patient will not be able to do things he or she enjoys. I can’t quote the references but I am sure there is plenty of evidence that depression slows the healing process.
Second, and this is particularly true in older patients with orthopedic problems – failure to include a plan for return to activity can hinder recovery. I can recall more than a few patients who were seen in the emergency department and diagnosed with sprains but not given even the simplest instructions on how to begin moving the injured joint. When they finally returned to see me we had to begin the painful and unnecessary project of thawing a frozen joint.
Fortunately, we have evolved past the era when best rest was near the top of the list of our recommended remedies. However, there still remains a bias against activity in some situations. The most recent example is the evolving strategies for the management of concussion. There is some evidence that involving the patient in a return to activity plan may shorten the time to recovery. The myth about brain rest has been slow to die.
Finally, providing the patient with a personalized list of “can do’s” makes good business sense because it can head off those time-gobbling call backs that tie up you and your office staff. As an experienced physician, you have probably learned the most frequently asked “Can Jason do ... ?” questions. Make your own list and give the patient your answers. An ounce of anticipatory guidance is worth hours on the telephone or sorting through the email inbox.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
COVID-19 and the psychiatrist/psychoanalyst: My experience
COVID-19 affected all aspects of psychiatric care. As a psychiatrist who is also a psychoanalyst, I faced some unique challenges to caring for my patients during the pandemic. In this article, I describe how COVID-19 impacted my practice, and how I adjusted to ensure that my patients received the best possible care.
The loss of ‘normal’
Our recognition of the loss was not immediate since no one knew what to expect. From March 11, 2020 through the end of the warm weather, when we could be outdoors, personal life was still gratifying. There was even a new spirit of togetherness in my neighborhood, with people seamlessly cooperating by crossing the street to avoid getting too close to one another, practicing proper social distancing in the grocery line, and smiling at everyone.
November 2020 through Spring 2021 was an unprecedented period of no socialization and spending time exclusively with my husband. By the end, I was finally aware of the exhaustion I felt trying to work with patients via phone and video sessions. Beyond that, we were (and still are) conducting administrative meetings and national organization meetings by video.
Spring 2021 until the arrival of cold weather felt more relaxed, as socializing outside again became possible. But from Winter 2021 to now has been a weary repeat of isolation, and a realization that my work life might never go back to “normal.” I would have to make peace with various sorts of losses of gratification in my work.
Life before COVID-19
I am a psychiatrist and psychoanalyst in a group private practice near the University of Cincinnati Medical Center. As a former full-time faculty member there, I maintain some teaching and supervision of residents. I typically see patients from 8:30 AM until 6:30 PM, and for years have had an average of 5 patients in psychoanalysis on the couch for 3 to 4 sessions per week. I see some psychotherapy patients weekly or twice a week and have some hours for new diagnostic evaluations and medication management. In addition, as a faculty member of the Cincinnati Psychoanalytic Institute, I take part in several committees, teach in the psychotherapy program and psychoanalytic training program, and supervise students and candidates. Most weeks, I see between 35 and 40 patients, with 4 to 6 weeks of vacation time per year.
Major changes with the onset of the pandemic
Once the threat from COVID-19 became clear in March 2020, I thought through my options. My office comprises 5 professional offices, a waiting room, and an administrative area. Our administrative assistant and 1 or 2 practitioners were in the office with me most days. We maintained appropriate distance from each another and wore masks in common areas. The practice group was exemplary in immediately setting up safe practices. I learned a few colleagues were seeing patients outside using lawn chairs in the back of our lot where there was some privacy, but many stopped coming to the building altogether.
I felt real sadness having to tell patients I could no longer see them in my office. However, I was relieved to find how quickly many patients made an immediate transition to telephone or video sessions. Since I was alone in my office and not distracted by barking dogs, ringing doorbells, or loud lawnmowers, I continued to come to the office, and never switched to working from home.
Since I was not vis-à-vis with patients on the couch, those sessions shifted to the telephone. I offered psychotherapy patients the option of video sessions via the Health Insurance Portability and Accountability Act–compliant Doximity app (doxy.me) or telephone, and found that approximately 75% preferred video. When I used the telephone, I used a professional-grade headset, which made it less onerous than being tied to a receiver, and I occasionally used the speaker option. I also installed a desk platform that allows me to raise and lower my computer from sitting to standing height.
I worried a great deal about patients I felt would do poorly with video or telephone sessions: older adults who found comfort in human contact that was sometimes curative, less well-integrated individuals who needed real contact in order to feel there was a treatment process, those with serious mental illnesses who needed reassurance at their reality-testing, and new patients who I couldn’t fully assess without in-person meetings.
In the beginning of the pandemic, as we were still learning about the virus, nothing seemed safe. We were washing our hands constantly, afraid to touch doorknobs, mail, or groceries. Thankfully, we learned that COVID-19 transmission occurs primarily through inhalation of droplets and particles containing the virus.1 Masks, good ventilation, and adequate distance from others considerably cut infection rates. By January 2021, the availability of a vaccine made an enormous difference in vulnerability to severe illness.
When I stopped seeing patients in my office, I set up the conference room that had doors on either end so I could sit on one end of a table and have the patient at the other end, keeping about 8 feet between us. I also kept a fan blowing air away from me and parallel to the patient. After each session, I opened both doors to allow for full ventilation of the room. This provided a solution for the patients I knew I needed to meet with in person.
Continue to: Case examples: How it worked...
Case examples: How it worked
The following case examples illustrate how I provided care during this time. To protect patient anonymity, these vignettes are composites.
Psychotherapy patients
Established patients in psychotherapy have seemed to work well with video or telephone sessions. The video option added a new element I never appreciated: seeing patients in their homes or cars allowed me to gain a new set of impressions about them. The use of technology is clearly another element I would not have identified before. Less technically adept older patients are likely to join a video session with only the top of their head visible, or with insufficient lighting. In some cases, I coached patients to rearrange their computer so I could see their faces, but only if it seemed that doing so would not cause them greater distress.
Ms. A, age 74, is a widow who retired from a high-level professional position 5 years ago. She was brought to the hospital due to ongoing anxiety, especially about her health. Ms. A maintained a wide range of relationships with friends, colleagues she mentored, and neighbors who provided a satisfying social network, and she continued to contribute to her field via scholarly writing projects. Before the pandemic, she found occasional sessions helpful in putting her health fears into perspective. When the pandemic led her to isolate at home, Ms. A became anxious and depressed to an unprecedented extent. Video sessions were unsatisfying, and she was terrified of taking tranquilizers or other medications. Once COVID-19 vaccinations became available and both she and I received both doses, we switched to meeting in the conference room every 2 to 3 weeks, with considerably better results.
Mr. B, age 41, is a single male who I diagnosed with schizophrenia at age 19 when he developed paranoid delusions and auditory hallucinations. Mr. B was not interested in taking antipsychotic medications, and his situation did not improve even when he did try taking them. He volunteered at a local emergency department doing odd jobs—moving gurneys, cleaning rooms, hauling boxes of supplies—for many years, and had always been employed in jobs such as grocery stocking or janitorial work that did not involve extensive interactions with people. He repeatedly enrolled in programs that would provide a skill such as phlebotomy or medical billing, only to find that he was never hired for such work. We talked once a month for 30 minutes about his frustrations trying to find women to date and marry, and how he was repeatedly taken advantage of (one “date” from an escort service took him to an ATM and got him to withdraw most of the money in his account).
Coincident with COVID-19, Mr. B’s father died from widespread metastatic cancer. His father had been Mr. B’s guide, friend, payee for Social Security Disability Insurance funds, and source of advice. To provide humane and somewhat effective treatment, I saw Mr. B in the conference room. His capacity to express grief and distress at the loss of his father has been impressive, as has his initiative in finding a grief group to attend, which he has done consistently.
Several patients who had been seeing me for weekly psychotherapy chose not to continue, many without specifically informing me of their decision. I understood the situation was in flux, and it would not be clear to anyone what to expect for the future. To avoid pressuring anyone, I chose not to contact patients to inquire about their plans.
Ms. C, age 50, is a professional with 3 children whose marriage had been highly dissatisfying for years, and she was now ready to investigate it. She was very successful in her career, having taken on a leadership role in her firm and earning a high income, while her husband was erratic, unreliable, and self-absorbed. Though he was well-educated and competent in his field, he could not maintain employment in a corporate environment and worked as a consultant with relatively little success. Along with the hours she spent working, Ms. C took responsibility for the family finances, was the chief wage earner, managed the needs of their children, made sure meals were prepared, and took on many other responsibilities.
Continue to: Case examples: How it worked (cont.)...
We agreed to a weekly session that fit Ms. C’s schedule, and she seemed able to relax and talk about herself. I found Ms. C quite likeable and enjoyed meeting with her, though I worried about whether we would need a greater intensity to get at the reasons such a successful and intelligent woman would fear setting limits with her husband or even considering ending the relationship. The reasons were clear as we put together the story of her early life, but conviction only develops with full emotional awareness (transference provides this in psychoanalysis).
The pandemic started approximately 18 months into our work, and Ms. C disappeared. She called my administrative assistant to cancel further appointments but did not ask to speak with me directly. While I knew this might represent resistance, I also felt unwilling to pressure Ms. C if she chose not to continue. I remain hopeful that I will hear from her once again; if not, I will send a note by mail to say that I enjoyed working with her, am happy to see her again, and hope she found some benefit from our work.
Mr. D contacted me for psychotherapy following the death of his father, who I had seen as a patient many years earlier. I was aware of the likely impact of his father’s outsized personality and emotional dysregulation on Mr. D and agreed to meet with him. He had taken over the family business and had made it an even greater success, but had trouble feeling confident about setting limits with employees who he knew took advantage of his avoidance.
Mr. D and I met weekly for several months and then moved to every other week, a form of resistance I expected as we got closer to his feeling pain. At the same time, I recognize that many patients use this tactic to “dose” themselves with the intensity they can tolerate, and Mr. D was quite observant and able to pick up themes where we’d left off.
When the pandemic shut down office visits, Mr. D immediately agreed to video sessions, which he has continued at roughly the same frequency. While I miss sitting with him, we continue to make progress towards his goal of learning to see himself as able to compete with his father.
Psychoanalysis patients
I found that patients in psychoanalysis had no trouble with the transition to telephone sessions, and the intensity of the work was not diluted. In some ways, audio-only communication is more intimate and might encourage patients to talk about topics they may not have otherwise brought up. I have not seen any evidence of less progress among these patients.
Dr. E, age 45, is a divorced physician who began psychoanalysis 3 times per week on the couch in 2018 for problems with frustration and confusion about his career, his identity as a father, and intense loneliness. He had worked up to 80 hours per week to earn as much money as he could, but also to avoid time at home with his then-wife and young children. The lack of time to recover led him to hate his work, left no time for social connections, and led to binges of heavy drinking. Our work had begun to allow him to develop a narrative about his early life that had never been considered, and to identify patterns of repetition of old defensive strategies that had never served him well.
At the onset of the pandemic, I told Dr. E that we would have to switch to telephone sessions, and he agreed immediately. In fact, he came to prefer telephone work since it spared him the 2 hours per day he had spent coming to my office. While I found it less satisfying than working in person, we have continued the same schedule and with the same intensity and trajectory established before the pandemic.
Continue to: Working with new patients...
Working with new patients
Seeing new patients for diagnostic evaluation is always best done in person, because the information I gain from the patient’s appearance, clothing, demeanor, gait, postures, gesturing, and facial expressions (among other elements) gives me important impressions I miss with video or telephone. In many cases, patients gain a sense of who I am from sitting in my office, and using the conference room eliminates that benefit. I attempted to create a warm environment in the conference room by obtaining lamps that produce warmer indirect light and hanging artwork that reflects my tastes. There are clocks in places that allow me and my patient to keep track of time. In meeting new patients by video, I get some impressions about their surroundings that add to the information I get through our interview. I have done many diagnostic evaluations during the pandemic and gotten treatments (whether medication, psychotherapy, or both) underway without discernible problems in the outcomes. Patients who started with me in person have mostly wanted to continue with in-person meetings, but as many have told me, interspersed video sessions save them travel time.
What about vaccination?
Once COVID-19 vaccinations were widely available, I assumed patients would be as eager to get them as I had been. When I began asking patients about whether they had gotten their vaccines, I was surprised to hear that a few were not going to get vaccinated, clearly based on political views and misinformation about the danger of vaccines. (The topic of political beliefs and their impact on psychological treatment is beyond the scope of this commentary.) I tried to counter obvious misinformation, repeated my recommendation that the patient get vaccinated, and then turned to other topics. I later decided to tell all patients that vaccination was required to enter the office. Only 1 patient who had been coming to the office dropped out, and she eventually returned to meeting by video.
COVID-19’s toll on the therapist
While the first several months of the pandemic were so full of uncertainty about the future, once vaccinations were available, it seemed cause for hope of a return to normalcy. As time went on, however, it became clear that normal was still a long way off. With vaccine refusal and new variants upending my naïve view that we were near the end, I began to feel aware of the impact this had on me, and began to focus on self-care (Box). I had always seen myself as unusually lucky to have a full practice, a supportive partnership with my husband, grown children who didn’t need me to homeschool them, a strong social network of friends who could share the burden and cheer each other up at outdoor gatherings, and a wonderful group of siblings and in-laws (all in different cities) who stayed in touch via video calls and quarantined in advance of getting together in someone’s home.
Box
Self-care has always been a requirement of doing psychotherapeutic work, and I encourage practitioners to be sure they are attending to themselves. We can’t be effective as listeners, empathizers, diagnosticians, and problem-solvers if we ourselves aren’t healthy. We evaluate our patients in terms of mood, outlook, sleep, appetite, energy, motivation, and energy; we also investigate their capacity for relationships that are sustaining. Self-care is the same, taking care of both our physical and relationship beings. Getting enough sleep, exercising daily, cooking healthy meals, and making time to relax are all ways of caring for our physical identities that should have been in place before COVID-19. Making personal time for ourselves in the face of constant demands for time from patients, colleagues, partners, children, parents, siblings, and friends never happens without the resolve to do it. As a psychiatrist who is used to sitting for up to 10 hours per day, I strongly recommend making a daily habit of walking, running, biking, or using an elliptical trainer, treadmill, or stationary bike for 30 minutes or more. Sleep is necessary for adequate concentration and attention to patient after patient. If you have trouble sleeping, talk with your doctor about remedies. If you use a sleep aid, I strongly recommend alternating medications so you don’t develop tolerance to any of them. Plan your food and cooking ahead of time so you aren’t tempted to order out. If you cook simple meals yourself (ideally with your partner helping or in range so you can chat), you will consume fewer calories, less sodium, and more nutrients. Even if you have a spouse and young children at home, work out a plan with your partner that allows each of you time for exercise or to recoup after a long day with patients. Babysitters allow you to take the time to be with each other that is necessary to sustaining a connection. Think about time for sexual intimacy if that has dropped off the calendar. Relationships with others, such as parents, siblings and their families, and friends are invaluable. The time spent with others might seem inconsequential, but is critical to our internal sense of security, even in the face of external disorder.
Staying busy and engaged with my practice, spouse, family, and friends kept sadness away most of the time. But I surprised myself a few months ago when I sat down to reflect and check in with myself. I felt enormous loss, resentment, and exhaustion at the privations of the pandemic: every trip to the grocery story felt dangerous. I hadn’t seen the inside of a concert hall, movie theater, restaurant, or museum in nearly 2 years. Travel for meetings and visits to family and friends and various adventures had been abruptly stopped. I lost both parents (not to COVID-19) during 2020; both were older adults living in senior communities that could not allow visitors. The usual grieving process would include attending services at my synagogue where I could say Kaddish for them, and video services were simply not tolerable.
Most of us have become experts at video meetings and likely have come to despise them. While our Institute has always held classes with some out-of-town students joining by video, with a very sophisticated system that provides excellent sound and visual fidelity, teaching entirely by video is another matter. I now teach students I have never met in person and might not recognize if I passed them in public. The art of creating discussion around a table is much more difficult on a computer screen. The first class I taught to residents during the pandemic was completely disorienting as I faced a wall of black screens with names and silence. Each student had turned off their camera and muted their microphone, so I was lecturing to a computer. That never happened again after I insisted on seeing everyone’s face and hearing their voices.
Thankfully, my usual experience of a long day seeing patients followed by chatting while cooking dinner with my husband and walking the dogs before settling down to read didn’t change. But the pleasure of sitting with patients was replaced by the daily grind of figuring out who will need a video link, who will be on the telephone, and who will come to the office, and it doesn’t feel the same. Again, in the big picture, I realize how fortunate I have been, but it’s been a big change in the world of the psychotherapist.
1. Centers for Disease Control and Prevention. COVID-19 frequently asked questions. Accessed March 8, 2022. https://www.cdc.gov/coronavirus/2019-ncov/faq.html#Spread
COVID-19 affected all aspects of psychiatric care. As a psychiatrist who is also a psychoanalyst, I faced some unique challenges to caring for my patients during the pandemic. In this article, I describe how COVID-19 impacted my practice, and how I adjusted to ensure that my patients received the best possible care.
The loss of ‘normal’
Our recognition of the loss was not immediate since no one knew what to expect. From March 11, 2020 through the end of the warm weather, when we could be outdoors, personal life was still gratifying. There was even a new spirit of togetherness in my neighborhood, with people seamlessly cooperating by crossing the street to avoid getting too close to one another, practicing proper social distancing in the grocery line, and smiling at everyone.
November 2020 through Spring 2021 was an unprecedented period of no socialization and spending time exclusively with my husband. By the end, I was finally aware of the exhaustion I felt trying to work with patients via phone and video sessions. Beyond that, we were (and still are) conducting administrative meetings and national organization meetings by video.
Spring 2021 until the arrival of cold weather felt more relaxed, as socializing outside again became possible. But from Winter 2021 to now has been a weary repeat of isolation, and a realization that my work life might never go back to “normal.” I would have to make peace with various sorts of losses of gratification in my work.
Life before COVID-19
I am a psychiatrist and psychoanalyst in a group private practice near the University of Cincinnati Medical Center. As a former full-time faculty member there, I maintain some teaching and supervision of residents. I typically see patients from 8:30 AM until 6:30 PM, and for years have had an average of 5 patients in psychoanalysis on the couch for 3 to 4 sessions per week. I see some psychotherapy patients weekly or twice a week and have some hours for new diagnostic evaluations and medication management. In addition, as a faculty member of the Cincinnati Psychoanalytic Institute, I take part in several committees, teach in the psychotherapy program and psychoanalytic training program, and supervise students and candidates. Most weeks, I see between 35 and 40 patients, with 4 to 6 weeks of vacation time per year.
Major changes with the onset of the pandemic
Once the threat from COVID-19 became clear in March 2020, I thought through my options. My office comprises 5 professional offices, a waiting room, and an administrative area. Our administrative assistant and 1 or 2 practitioners were in the office with me most days. We maintained appropriate distance from each another and wore masks in common areas. The practice group was exemplary in immediately setting up safe practices. I learned a few colleagues were seeing patients outside using lawn chairs in the back of our lot where there was some privacy, but many stopped coming to the building altogether.
I felt real sadness having to tell patients I could no longer see them in my office. However, I was relieved to find how quickly many patients made an immediate transition to telephone or video sessions. Since I was alone in my office and not distracted by barking dogs, ringing doorbells, or loud lawnmowers, I continued to come to the office, and never switched to working from home.
Since I was not vis-à-vis with patients on the couch, those sessions shifted to the telephone. I offered psychotherapy patients the option of video sessions via the Health Insurance Portability and Accountability Act–compliant Doximity app (doxy.me) or telephone, and found that approximately 75% preferred video. When I used the telephone, I used a professional-grade headset, which made it less onerous than being tied to a receiver, and I occasionally used the speaker option. I also installed a desk platform that allows me to raise and lower my computer from sitting to standing height.
I worried a great deal about patients I felt would do poorly with video or telephone sessions: older adults who found comfort in human contact that was sometimes curative, less well-integrated individuals who needed real contact in order to feel there was a treatment process, those with serious mental illnesses who needed reassurance at their reality-testing, and new patients who I couldn’t fully assess without in-person meetings.
In the beginning of the pandemic, as we were still learning about the virus, nothing seemed safe. We were washing our hands constantly, afraid to touch doorknobs, mail, or groceries. Thankfully, we learned that COVID-19 transmission occurs primarily through inhalation of droplets and particles containing the virus.1 Masks, good ventilation, and adequate distance from others considerably cut infection rates. By January 2021, the availability of a vaccine made an enormous difference in vulnerability to severe illness.
When I stopped seeing patients in my office, I set up the conference room that had doors on either end so I could sit on one end of a table and have the patient at the other end, keeping about 8 feet between us. I also kept a fan blowing air away from me and parallel to the patient. After each session, I opened both doors to allow for full ventilation of the room. This provided a solution for the patients I knew I needed to meet with in person.
Continue to: Case examples: How it worked...
Case examples: How it worked
The following case examples illustrate how I provided care during this time. To protect patient anonymity, these vignettes are composites.
Psychotherapy patients
Established patients in psychotherapy have seemed to work well with video or telephone sessions. The video option added a new element I never appreciated: seeing patients in their homes or cars allowed me to gain a new set of impressions about them. The use of technology is clearly another element I would not have identified before. Less technically adept older patients are likely to join a video session with only the top of their head visible, or with insufficient lighting. In some cases, I coached patients to rearrange their computer so I could see their faces, but only if it seemed that doing so would not cause them greater distress.
Ms. A, age 74, is a widow who retired from a high-level professional position 5 years ago. She was brought to the hospital due to ongoing anxiety, especially about her health. Ms. A maintained a wide range of relationships with friends, colleagues she mentored, and neighbors who provided a satisfying social network, and she continued to contribute to her field via scholarly writing projects. Before the pandemic, she found occasional sessions helpful in putting her health fears into perspective. When the pandemic led her to isolate at home, Ms. A became anxious and depressed to an unprecedented extent. Video sessions were unsatisfying, and she was terrified of taking tranquilizers or other medications. Once COVID-19 vaccinations became available and both she and I received both doses, we switched to meeting in the conference room every 2 to 3 weeks, with considerably better results.
Mr. B, age 41, is a single male who I diagnosed with schizophrenia at age 19 when he developed paranoid delusions and auditory hallucinations. Mr. B was not interested in taking antipsychotic medications, and his situation did not improve even when he did try taking them. He volunteered at a local emergency department doing odd jobs—moving gurneys, cleaning rooms, hauling boxes of supplies—for many years, and had always been employed in jobs such as grocery stocking or janitorial work that did not involve extensive interactions with people. He repeatedly enrolled in programs that would provide a skill such as phlebotomy or medical billing, only to find that he was never hired for such work. We talked once a month for 30 minutes about his frustrations trying to find women to date and marry, and how he was repeatedly taken advantage of (one “date” from an escort service took him to an ATM and got him to withdraw most of the money in his account).
Coincident with COVID-19, Mr. B’s father died from widespread metastatic cancer. His father had been Mr. B’s guide, friend, payee for Social Security Disability Insurance funds, and source of advice. To provide humane and somewhat effective treatment, I saw Mr. B in the conference room. His capacity to express grief and distress at the loss of his father has been impressive, as has his initiative in finding a grief group to attend, which he has done consistently.
Several patients who had been seeing me for weekly psychotherapy chose not to continue, many without specifically informing me of their decision. I understood the situation was in flux, and it would not be clear to anyone what to expect for the future. To avoid pressuring anyone, I chose not to contact patients to inquire about their plans.
Ms. C, age 50, is a professional with 3 children whose marriage had been highly dissatisfying for years, and she was now ready to investigate it. She was very successful in her career, having taken on a leadership role in her firm and earning a high income, while her husband was erratic, unreliable, and self-absorbed. Though he was well-educated and competent in his field, he could not maintain employment in a corporate environment and worked as a consultant with relatively little success. Along with the hours she spent working, Ms. C took responsibility for the family finances, was the chief wage earner, managed the needs of their children, made sure meals were prepared, and took on many other responsibilities.
Continue to: Case examples: How it worked (cont.)...
We agreed to a weekly session that fit Ms. C’s schedule, and she seemed able to relax and talk about herself. I found Ms. C quite likeable and enjoyed meeting with her, though I worried about whether we would need a greater intensity to get at the reasons such a successful and intelligent woman would fear setting limits with her husband or even considering ending the relationship. The reasons were clear as we put together the story of her early life, but conviction only develops with full emotional awareness (transference provides this in psychoanalysis).
The pandemic started approximately 18 months into our work, and Ms. C disappeared. She called my administrative assistant to cancel further appointments but did not ask to speak with me directly. While I knew this might represent resistance, I also felt unwilling to pressure Ms. C if she chose not to continue. I remain hopeful that I will hear from her once again; if not, I will send a note by mail to say that I enjoyed working with her, am happy to see her again, and hope she found some benefit from our work.
Mr. D contacted me for psychotherapy following the death of his father, who I had seen as a patient many years earlier. I was aware of the likely impact of his father’s outsized personality and emotional dysregulation on Mr. D and agreed to meet with him. He had taken over the family business and had made it an even greater success, but had trouble feeling confident about setting limits with employees who he knew took advantage of his avoidance.
Mr. D and I met weekly for several months and then moved to every other week, a form of resistance I expected as we got closer to his feeling pain. At the same time, I recognize that many patients use this tactic to “dose” themselves with the intensity they can tolerate, and Mr. D was quite observant and able to pick up themes where we’d left off.
When the pandemic shut down office visits, Mr. D immediately agreed to video sessions, which he has continued at roughly the same frequency. While I miss sitting with him, we continue to make progress towards his goal of learning to see himself as able to compete with his father.
Psychoanalysis patients
I found that patients in psychoanalysis had no trouble with the transition to telephone sessions, and the intensity of the work was not diluted. In some ways, audio-only communication is more intimate and might encourage patients to talk about topics they may not have otherwise brought up. I have not seen any evidence of less progress among these patients.
Dr. E, age 45, is a divorced physician who began psychoanalysis 3 times per week on the couch in 2018 for problems with frustration and confusion about his career, his identity as a father, and intense loneliness. He had worked up to 80 hours per week to earn as much money as he could, but also to avoid time at home with his then-wife and young children. The lack of time to recover led him to hate his work, left no time for social connections, and led to binges of heavy drinking. Our work had begun to allow him to develop a narrative about his early life that had never been considered, and to identify patterns of repetition of old defensive strategies that had never served him well.
At the onset of the pandemic, I told Dr. E that we would have to switch to telephone sessions, and he agreed immediately. In fact, he came to prefer telephone work since it spared him the 2 hours per day he had spent coming to my office. While I found it less satisfying than working in person, we have continued the same schedule and with the same intensity and trajectory established before the pandemic.
Continue to: Working with new patients...
Working with new patients
Seeing new patients for diagnostic evaluation is always best done in person, because the information I gain from the patient’s appearance, clothing, demeanor, gait, postures, gesturing, and facial expressions (among other elements) gives me important impressions I miss with video or telephone. In many cases, patients gain a sense of who I am from sitting in my office, and using the conference room eliminates that benefit. I attempted to create a warm environment in the conference room by obtaining lamps that produce warmer indirect light and hanging artwork that reflects my tastes. There are clocks in places that allow me and my patient to keep track of time. In meeting new patients by video, I get some impressions about their surroundings that add to the information I get through our interview. I have done many diagnostic evaluations during the pandemic and gotten treatments (whether medication, psychotherapy, or both) underway without discernible problems in the outcomes. Patients who started with me in person have mostly wanted to continue with in-person meetings, but as many have told me, interspersed video sessions save them travel time.
What about vaccination?
Once COVID-19 vaccinations were widely available, I assumed patients would be as eager to get them as I had been. When I began asking patients about whether they had gotten their vaccines, I was surprised to hear that a few were not going to get vaccinated, clearly based on political views and misinformation about the danger of vaccines. (The topic of political beliefs and their impact on psychological treatment is beyond the scope of this commentary.) I tried to counter obvious misinformation, repeated my recommendation that the patient get vaccinated, and then turned to other topics. I later decided to tell all patients that vaccination was required to enter the office. Only 1 patient who had been coming to the office dropped out, and she eventually returned to meeting by video.
COVID-19’s toll on the therapist
While the first several months of the pandemic were so full of uncertainty about the future, once vaccinations were available, it seemed cause for hope of a return to normalcy. As time went on, however, it became clear that normal was still a long way off. With vaccine refusal and new variants upending my naïve view that we were near the end, I began to feel aware of the impact this had on me, and began to focus on self-care (Box). I had always seen myself as unusually lucky to have a full practice, a supportive partnership with my husband, grown children who didn’t need me to homeschool them, a strong social network of friends who could share the burden and cheer each other up at outdoor gatherings, and a wonderful group of siblings and in-laws (all in different cities) who stayed in touch via video calls and quarantined in advance of getting together in someone’s home.
Box
Self-care has always been a requirement of doing psychotherapeutic work, and I encourage practitioners to be sure they are attending to themselves. We can’t be effective as listeners, empathizers, diagnosticians, and problem-solvers if we ourselves aren’t healthy. We evaluate our patients in terms of mood, outlook, sleep, appetite, energy, motivation, and energy; we also investigate their capacity for relationships that are sustaining. Self-care is the same, taking care of both our physical and relationship beings. Getting enough sleep, exercising daily, cooking healthy meals, and making time to relax are all ways of caring for our physical identities that should have been in place before COVID-19. Making personal time for ourselves in the face of constant demands for time from patients, colleagues, partners, children, parents, siblings, and friends never happens without the resolve to do it. As a psychiatrist who is used to sitting for up to 10 hours per day, I strongly recommend making a daily habit of walking, running, biking, or using an elliptical trainer, treadmill, or stationary bike for 30 minutes or more. Sleep is necessary for adequate concentration and attention to patient after patient. If you have trouble sleeping, talk with your doctor about remedies. If you use a sleep aid, I strongly recommend alternating medications so you don’t develop tolerance to any of them. Plan your food and cooking ahead of time so you aren’t tempted to order out. If you cook simple meals yourself (ideally with your partner helping or in range so you can chat), you will consume fewer calories, less sodium, and more nutrients. Even if you have a spouse and young children at home, work out a plan with your partner that allows each of you time for exercise or to recoup after a long day with patients. Babysitters allow you to take the time to be with each other that is necessary to sustaining a connection. Think about time for sexual intimacy if that has dropped off the calendar. Relationships with others, such as parents, siblings and their families, and friends are invaluable. The time spent with others might seem inconsequential, but is critical to our internal sense of security, even in the face of external disorder.
Staying busy and engaged with my practice, spouse, family, and friends kept sadness away most of the time. But I surprised myself a few months ago when I sat down to reflect and check in with myself. I felt enormous loss, resentment, and exhaustion at the privations of the pandemic: every trip to the grocery story felt dangerous. I hadn’t seen the inside of a concert hall, movie theater, restaurant, or museum in nearly 2 years. Travel for meetings and visits to family and friends and various adventures had been abruptly stopped. I lost both parents (not to COVID-19) during 2020; both were older adults living in senior communities that could not allow visitors. The usual grieving process would include attending services at my synagogue where I could say Kaddish for them, and video services were simply not tolerable.
Most of us have become experts at video meetings and likely have come to despise them. While our Institute has always held classes with some out-of-town students joining by video, with a very sophisticated system that provides excellent sound and visual fidelity, teaching entirely by video is another matter. I now teach students I have never met in person and might not recognize if I passed them in public. The art of creating discussion around a table is much more difficult on a computer screen. The first class I taught to residents during the pandemic was completely disorienting as I faced a wall of black screens with names and silence. Each student had turned off their camera and muted their microphone, so I was lecturing to a computer. That never happened again after I insisted on seeing everyone’s face and hearing their voices.
Thankfully, my usual experience of a long day seeing patients followed by chatting while cooking dinner with my husband and walking the dogs before settling down to read didn’t change. But the pleasure of sitting with patients was replaced by the daily grind of figuring out who will need a video link, who will be on the telephone, and who will come to the office, and it doesn’t feel the same. Again, in the big picture, I realize how fortunate I have been, but it’s been a big change in the world of the psychotherapist.
COVID-19 affected all aspects of psychiatric care. As a psychiatrist who is also a psychoanalyst, I faced some unique challenges to caring for my patients during the pandemic. In this article, I describe how COVID-19 impacted my practice, and how I adjusted to ensure that my patients received the best possible care.
The loss of ‘normal’
Our recognition of the loss was not immediate since no one knew what to expect. From March 11, 2020 through the end of the warm weather, when we could be outdoors, personal life was still gratifying. There was even a new spirit of togetherness in my neighborhood, with people seamlessly cooperating by crossing the street to avoid getting too close to one another, practicing proper social distancing in the grocery line, and smiling at everyone.
November 2020 through Spring 2021 was an unprecedented period of no socialization and spending time exclusively with my husband. By the end, I was finally aware of the exhaustion I felt trying to work with patients via phone and video sessions. Beyond that, we were (and still are) conducting administrative meetings and national organization meetings by video.
Spring 2021 until the arrival of cold weather felt more relaxed, as socializing outside again became possible. But from Winter 2021 to now has been a weary repeat of isolation, and a realization that my work life might never go back to “normal.” I would have to make peace with various sorts of losses of gratification in my work.
Life before COVID-19
I am a psychiatrist and psychoanalyst in a group private practice near the University of Cincinnati Medical Center. As a former full-time faculty member there, I maintain some teaching and supervision of residents. I typically see patients from 8:30 AM until 6:30 PM, and for years have had an average of 5 patients in psychoanalysis on the couch for 3 to 4 sessions per week. I see some psychotherapy patients weekly or twice a week and have some hours for new diagnostic evaluations and medication management. In addition, as a faculty member of the Cincinnati Psychoanalytic Institute, I take part in several committees, teach in the psychotherapy program and psychoanalytic training program, and supervise students and candidates. Most weeks, I see between 35 and 40 patients, with 4 to 6 weeks of vacation time per year.
Major changes with the onset of the pandemic
Once the threat from COVID-19 became clear in March 2020, I thought through my options. My office comprises 5 professional offices, a waiting room, and an administrative area. Our administrative assistant and 1 or 2 practitioners were in the office with me most days. We maintained appropriate distance from each another and wore masks in common areas. The practice group was exemplary in immediately setting up safe practices. I learned a few colleagues were seeing patients outside using lawn chairs in the back of our lot where there was some privacy, but many stopped coming to the building altogether.
I felt real sadness having to tell patients I could no longer see them in my office. However, I was relieved to find how quickly many patients made an immediate transition to telephone or video sessions. Since I was alone in my office and not distracted by barking dogs, ringing doorbells, or loud lawnmowers, I continued to come to the office, and never switched to working from home.
Since I was not vis-à-vis with patients on the couch, those sessions shifted to the telephone. I offered psychotherapy patients the option of video sessions via the Health Insurance Portability and Accountability Act–compliant Doximity app (doxy.me) or telephone, and found that approximately 75% preferred video. When I used the telephone, I used a professional-grade headset, which made it less onerous than being tied to a receiver, and I occasionally used the speaker option. I also installed a desk platform that allows me to raise and lower my computer from sitting to standing height.
I worried a great deal about patients I felt would do poorly with video or telephone sessions: older adults who found comfort in human contact that was sometimes curative, less well-integrated individuals who needed real contact in order to feel there was a treatment process, those with serious mental illnesses who needed reassurance at their reality-testing, and new patients who I couldn’t fully assess without in-person meetings.
In the beginning of the pandemic, as we were still learning about the virus, nothing seemed safe. We were washing our hands constantly, afraid to touch doorknobs, mail, or groceries. Thankfully, we learned that COVID-19 transmission occurs primarily through inhalation of droplets and particles containing the virus.1 Masks, good ventilation, and adequate distance from others considerably cut infection rates. By January 2021, the availability of a vaccine made an enormous difference in vulnerability to severe illness.
When I stopped seeing patients in my office, I set up the conference room that had doors on either end so I could sit on one end of a table and have the patient at the other end, keeping about 8 feet between us. I also kept a fan blowing air away from me and parallel to the patient. After each session, I opened both doors to allow for full ventilation of the room. This provided a solution for the patients I knew I needed to meet with in person.
Continue to: Case examples: How it worked...
Case examples: How it worked
The following case examples illustrate how I provided care during this time. To protect patient anonymity, these vignettes are composites.
Psychotherapy patients
Established patients in psychotherapy have seemed to work well with video or telephone sessions. The video option added a new element I never appreciated: seeing patients in their homes or cars allowed me to gain a new set of impressions about them. The use of technology is clearly another element I would not have identified before. Less technically adept older patients are likely to join a video session with only the top of their head visible, or with insufficient lighting. In some cases, I coached patients to rearrange their computer so I could see their faces, but only if it seemed that doing so would not cause them greater distress.
Ms. A, age 74, is a widow who retired from a high-level professional position 5 years ago. She was brought to the hospital due to ongoing anxiety, especially about her health. Ms. A maintained a wide range of relationships with friends, colleagues she mentored, and neighbors who provided a satisfying social network, and she continued to contribute to her field via scholarly writing projects. Before the pandemic, she found occasional sessions helpful in putting her health fears into perspective. When the pandemic led her to isolate at home, Ms. A became anxious and depressed to an unprecedented extent. Video sessions were unsatisfying, and she was terrified of taking tranquilizers or other medications. Once COVID-19 vaccinations became available and both she and I received both doses, we switched to meeting in the conference room every 2 to 3 weeks, with considerably better results.
Mr. B, age 41, is a single male who I diagnosed with schizophrenia at age 19 when he developed paranoid delusions and auditory hallucinations. Mr. B was not interested in taking antipsychotic medications, and his situation did not improve even when he did try taking them. He volunteered at a local emergency department doing odd jobs—moving gurneys, cleaning rooms, hauling boxes of supplies—for many years, and had always been employed in jobs such as grocery stocking or janitorial work that did not involve extensive interactions with people. He repeatedly enrolled in programs that would provide a skill such as phlebotomy or medical billing, only to find that he was never hired for such work. We talked once a month for 30 minutes about his frustrations trying to find women to date and marry, and how he was repeatedly taken advantage of (one “date” from an escort service took him to an ATM and got him to withdraw most of the money in his account).
Coincident with COVID-19, Mr. B’s father died from widespread metastatic cancer. His father had been Mr. B’s guide, friend, payee for Social Security Disability Insurance funds, and source of advice. To provide humane and somewhat effective treatment, I saw Mr. B in the conference room. His capacity to express grief and distress at the loss of his father has been impressive, as has his initiative in finding a grief group to attend, which he has done consistently.
Several patients who had been seeing me for weekly psychotherapy chose not to continue, many without specifically informing me of their decision. I understood the situation was in flux, and it would not be clear to anyone what to expect for the future. To avoid pressuring anyone, I chose not to contact patients to inquire about their plans.
Ms. C, age 50, is a professional with 3 children whose marriage had been highly dissatisfying for years, and she was now ready to investigate it. She was very successful in her career, having taken on a leadership role in her firm and earning a high income, while her husband was erratic, unreliable, and self-absorbed. Though he was well-educated and competent in his field, he could not maintain employment in a corporate environment and worked as a consultant with relatively little success. Along with the hours she spent working, Ms. C took responsibility for the family finances, was the chief wage earner, managed the needs of their children, made sure meals were prepared, and took on many other responsibilities.
Continue to: Case examples: How it worked (cont.)...
We agreed to a weekly session that fit Ms. C’s schedule, and she seemed able to relax and talk about herself. I found Ms. C quite likeable and enjoyed meeting with her, though I worried about whether we would need a greater intensity to get at the reasons such a successful and intelligent woman would fear setting limits with her husband or even considering ending the relationship. The reasons were clear as we put together the story of her early life, but conviction only develops with full emotional awareness (transference provides this in psychoanalysis).
The pandemic started approximately 18 months into our work, and Ms. C disappeared. She called my administrative assistant to cancel further appointments but did not ask to speak with me directly. While I knew this might represent resistance, I also felt unwilling to pressure Ms. C if she chose not to continue. I remain hopeful that I will hear from her once again; if not, I will send a note by mail to say that I enjoyed working with her, am happy to see her again, and hope she found some benefit from our work.
Mr. D contacted me for psychotherapy following the death of his father, who I had seen as a patient many years earlier. I was aware of the likely impact of his father’s outsized personality and emotional dysregulation on Mr. D and agreed to meet with him. He had taken over the family business and had made it an even greater success, but had trouble feeling confident about setting limits with employees who he knew took advantage of his avoidance.
Mr. D and I met weekly for several months and then moved to every other week, a form of resistance I expected as we got closer to his feeling pain. At the same time, I recognize that many patients use this tactic to “dose” themselves with the intensity they can tolerate, and Mr. D was quite observant and able to pick up themes where we’d left off.
When the pandemic shut down office visits, Mr. D immediately agreed to video sessions, which he has continued at roughly the same frequency. While I miss sitting with him, we continue to make progress towards his goal of learning to see himself as able to compete with his father.
Psychoanalysis patients
I found that patients in psychoanalysis had no trouble with the transition to telephone sessions, and the intensity of the work was not diluted. In some ways, audio-only communication is more intimate and might encourage patients to talk about topics they may not have otherwise brought up. I have not seen any evidence of less progress among these patients.
Dr. E, age 45, is a divorced physician who began psychoanalysis 3 times per week on the couch in 2018 for problems with frustration and confusion about his career, his identity as a father, and intense loneliness. He had worked up to 80 hours per week to earn as much money as he could, but also to avoid time at home with his then-wife and young children. The lack of time to recover led him to hate his work, left no time for social connections, and led to binges of heavy drinking. Our work had begun to allow him to develop a narrative about his early life that had never been considered, and to identify patterns of repetition of old defensive strategies that had never served him well.
At the onset of the pandemic, I told Dr. E that we would have to switch to telephone sessions, and he agreed immediately. In fact, he came to prefer telephone work since it spared him the 2 hours per day he had spent coming to my office. While I found it less satisfying than working in person, we have continued the same schedule and with the same intensity and trajectory established before the pandemic.
Continue to: Working with new patients...
Working with new patients
Seeing new patients for diagnostic evaluation is always best done in person, because the information I gain from the patient’s appearance, clothing, demeanor, gait, postures, gesturing, and facial expressions (among other elements) gives me important impressions I miss with video or telephone. In many cases, patients gain a sense of who I am from sitting in my office, and using the conference room eliminates that benefit. I attempted to create a warm environment in the conference room by obtaining lamps that produce warmer indirect light and hanging artwork that reflects my tastes. There are clocks in places that allow me and my patient to keep track of time. In meeting new patients by video, I get some impressions about their surroundings that add to the information I get through our interview. I have done many diagnostic evaluations during the pandemic and gotten treatments (whether medication, psychotherapy, or both) underway without discernible problems in the outcomes. Patients who started with me in person have mostly wanted to continue with in-person meetings, but as many have told me, interspersed video sessions save them travel time.
What about vaccination?
Once COVID-19 vaccinations were widely available, I assumed patients would be as eager to get them as I had been. When I began asking patients about whether they had gotten their vaccines, I was surprised to hear that a few were not going to get vaccinated, clearly based on political views and misinformation about the danger of vaccines. (The topic of political beliefs and their impact on psychological treatment is beyond the scope of this commentary.) I tried to counter obvious misinformation, repeated my recommendation that the patient get vaccinated, and then turned to other topics. I later decided to tell all patients that vaccination was required to enter the office. Only 1 patient who had been coming to the office dropped out, and she eventually returned to meeting by video.
COVID-19’s toll on the therapist
While the first several months of the pandemic were so full of uncertainty about the future, once vaccinations were available, it seemed cause for hope of a return to normalcy. As time went on, however, it became clear that normal was still a long way off. With vaccine refusal and new variants upending my naïve view that we were near the end, I began to feel aware of the impact this had on me, and began to focus on self-care (Box). I had always seen myself as unusually lucky to have a full practice, a supportive partnership with my husband, grown children who didn’t need me to homeschool them, a strong social network of friends who could share the burden and cheer each other up at outdoor gatherings, and a wonderful group of siblings and in-laws (all in different cities) who stayed in touch via video calls and quarantined in advance of getting together in someone’s home.
Box
Self-care has always been a requirement of doing psychotherapeutic work, and I encourage practitioners to be sure they are attending to themselves. We can’t be effective as listeners, empathizers, diagnosticians, and problem-solvers if we ourselves aren’t healthy. We evaluate our patients in terms of mood, outlook, sleep, appetite, energy, motivation, and energy; we also investigate their capacity for relationships that are sustaining. Self-care is the same, taking care of both our physical and relationship beings. Getting enough sleep, exercising daily, cooking healthy meals, and making time to relax are all ways of caring for our physical identities that should have been in place before COVID-19. Making personal time for ourselves in the face of constant demands for time from patients, colleagues, partners, children, parents, siblings, and friends never happens without the resolve to do it. As a psychiatrist who is used to sitting for up to 10 hours per day, I strongly recommend making a daily habit of walking, running, biking, or using an elliptical trainer, treadmill, or stationary bike for 30 minutes or more. Sleep is necessary for adequate concentration and attention to patient after patient. If you have trouble sleeping, talk with your doctor about remedies. If you use a sleep aid, I strongly recommend alternating medications so you don’t develop tolerance to any of them. Plan your food and cooking ahead of time so you aren’t tempted to order out. If you cook simple meals yourself (ideally with your partner helping or in range so you can chat), you will consume fewer calories, less sodium, and more nutrients. Even if you have a spouse and young children at home, work out a plan with your partner that allows each of you time for exercise or to recoup after a long day with patients. Babysitters allow you to take the time to be with each other that is necessary to sustaining a connection. Think about time for sexual intimacy if that has dropped off the calendar. Relationships with others, such as parents, siblings and their families, and friends are invaluable. The time spent with others might seem inconsequential, but is critical to our internal sense of security, even in the face of external disorder.
Staying busy and engaged with my practice, spouse, family, and friends kept sadness away most of the time. But I surprised myself a few months ago when I sat down to reflect and check in with myself. I felt enormous loss, resentment, and exhaustion at the privations of the pandemic: every trip to the grocery story felt dangerous. I hadn’t seen the inside of a concert hall, movie theater, restaurant, or museum in nearly 2 years. Travel for meetings and visits to family and friends and various adventures had been abruptly stopped. I lost both parents (not to COVID-19) during 2020; both were older adults living in senior communities that could not allow visitors. The usual grieving process would include attending services at my synagogue where I could say Kaddish for them, and video services were simply not tolerable.
Most of us have become experts at video meetings and likely have come to despise them. While our Institute has always held classes with some out-of-town students joining by video, with a very sophisticated system that provides excellent sound and visual fidelity, teaching entirely by video is another matter. I now teach students I have never met in person and might not recognize if I passed them in public. The art of creating discussion around a table is much more difficult on a computer screen. The first class I taught to residents during the pandemic was completely disorienting as I faced a wall of black screens with names and silence. Each student had turned off their camera and muted their microphone, so I was lecturing to a computer. That never happened again after I insisted on seeing everyone’s face and hearing their voices.
Thankfully, my usual experience of a long day seeing patients followed by chatting while cooking dinner with my husband and walking the dogs before settling down to read didn’t change. But the pleasure of sitting with patients was replaced by the daily grind of figuring out who will need a video link, who will be on the telephone, and who will come to the office, and it doesn’t feel the same. Again, in the big picture, I realize how fortunate I have been, but it’s been a big change in the world of the psychotherapist.
1. Centers for Disease Control and Prevention. COVID-19 frequently asked questions. Accessed March 8, 2022. https://www.cdc.gov/coronavirus/2019-ncov/faq.html#Spread
1. Centers for Disease Control and Prevention. COVID-19 frequently asked questions. Accessed March 8, 2022. https://www.cdc.gov/coronavirus/2019-ncov/faq.html#Spread

Sexual activity alters the microbiome, with potential psychiatric implications
Evidence is strong that sexual partners transmit microbiota (bacteria, viruses, fungi, protozoa, and archaea) to each other. While microbial flora are abundant in the gastrointestinal tract, they are also present in the vagina, penis, urethra, mouth, and skin.1 For better or worse, sexual contact of all types means that participants will acquire each other’s microbiota.
The 39 trillion microbiota in the body (which exceed the 30 trillion cells in the body) are commensal and influence both the larger brain in the skull and the smaller enteric brain in the gut. The microbiota and their microbiome genes (1,000 times larger than the human genome) have been linked to depression, anxiety, psychosis, and autism.2-4 They produce 90% of the body’s serotonin, as well as catecholamines (norepinephrine, epinephrine, dopamine), make hormones (eg, cortisol), and modulate the immune system. Microbiota have several important functions, including food digestion, synthesis of vitamins, autoimmunity, hypothalamic-pituitary-adrenal axis regulation, and CNS modulation.
Consequences of dysbiosis
Everyone should be concerned about maintaining a healthy diversity of microbiota in their body, with a predominance of beneficial bacteria such as Lactobacillus and Bacteroides, and avoiding acquiring pathogenic bacteria such as Gardnerella, Prevotella, and Atopobium. Sexual activity involving a partner with unhealthy microbiota may increase the risk of dysbiosis, defined as a reduction in microbiota diversity, including a loss of beneficial bacteria and a rise in harmful bacteria.
Dysbiosis is associated with multiple symptoms, including5:
- brain “fog,” irritability, mood changes, and anxiety
- bloating, loss of intestinal permeability, and insufficient reclamation of nutrients
- congestion of certain organs, such as the liver, gallbladder, and pancreas
- production of antigen-antibody complexes in response to chemicals in partially digested food
- aggravation of inflammatory disorders such as migraine, arthritis, and autoimmune disorders.
Apart from intimate sexual contact, simply sharing a household with someone leads to sharing of gut microflora. Persons who live together, whether genetically related or not, have similar microbiota. Compared with people living in separate households, cohabiting human pairs, dog pairs, and human-dog pairs share most of their microbiota (especially in the skin).
A consequence of acquiring pathogenic microbiota in the vagina is bacterial vaginosis (BV), which is not an infection but an ecologic imbalance in the composition of the vaginal microbiota. BV is caused by a significant decline in the beneficial vaginal Lactobacillus and a marked increase in the non-Lactobacillus taxa (especially Gardnerella and Atopobium).6 It can last for a least 1 week after sexual intercourse. BV is rare or absent among virgins. For a male partner, penile microbiota changes significantly after unprotected sex.6
Pathogenic bacteria can be cultivated from the glans, the coronal sulcus, and the prepuce, as well as from the penile skin, semen, urethra, and urine.6 Diverse bacteria exist in human semen, regardless if the male is fertile or infertile.7Anaerococcus is a biomarker for low sperm quality. Many of the semen bacteria are also found in the vagina of women with BV.7 Semen is a medium for the transmission of bacteria and viruses between men and women, and can contribute to sexually transmitted diseases.8
There are approximately 21 million cases of BV in the United States each year, and BV can also increase the risk of HIV and poor obstetric outcomes.9 The microbiota in the penile skin and urethra in males who have monogamous relationships with females are very similar to the vaginal microbiota of their female partner.
Consequences of BV include:
- decrease in hydrogen peroxide–producing bacilli
- prevalence of anaerobic bacteria (Prevotella, Gardnerella, and Atopobium)
- alkalinization, fishy odor, and gray-white vaginal discharge
- increase in the rate of pelvic inflammatory disease, ectopic pregnancy, endometriosis, preterm birth, and tubal factor infertility.9
Circumcision decreases the risk of BV. There is an increased rate of BV bacterial taxa in men with extramarital affairs and in women with multiple partners. Both oral and vaginal sex increase the abundance of Lactobacillus in the male oral and penile microbiota. Gingivitis has also been reported after oral sex.10
A link to psychiatric disorders
Given that all forms of sexual contact (vaginal, oral, anal, or skin) can transmit microbiota bidirectionally between partners, it is vital to practice safe sex and consider a monogamous relationship rather than indiscriminate promiscuity. Unfortunately, certain psychiatric disorders, such as bipolar disorder, are associated with hypersexuality and multiple partners, which may disrupt the microbiota. This can further disrupt the diversity of an individual’s microbiome and may put them at risk for mood, anxiety, and other psychiatric disorders. Another problem is sexually transmitted infections such as gonorrhea or syphilis require antibiotic therapy. It is well established that antibiotics kill both the bad pathogenic and the good nonpathogenic microbiota, further exacerbating dysbiosis and leading to disruptions in the microbiota-gut-brain (MGB) axis, which then results in psychiatric disorders.
The MGB axis modulates neurological processes via the vagus nerve, the major “highway” connecting the gut and brain for bidirectional traffic. The MGB axis produces microbial metabolites and immune factors that can lead to changes in brain neurotransmitters as well as neuroinflammation and psychiatric symptoms such as depression and anxiety.5
Many researchers are focusing on how to exploit the microbiome to develop novel therapeutic strategies, and encouraging advances are emerging.5 But the exact mechanisms by which the gut microbiome can impact mental health is still a work in progress. It is highly likely that dysbiosis is associated with mood and anxiety symptoms.
The bottom line: Sexual activity—whether it is heavy kissing, vaginal intercourse, oral sex, anal sex, or extensive skin contact—can lead to the exchange of microbiota. If an individual has dysbiosis, that could impact the mental health of their sexual partner(s). This raises the question of whether counseling patients about avoiding indiscriminate sex and practicing safe sex is as important for mental health as diet and exercise counseling is for physical health.
1. Reid G, Younes JA, Van der Mei HC, et al. Microbiota restoration: natural and supplemented recovery of human microbial communities. Nat Rev Microbiol. 2011;9(1):27-38.
2. Cryan JF, Dinan TG. Mind-altering microorganisms: the impact of the gut microbiota on brain and behaviour. Nat Rev Neurosci. 2012;13(10):701-712.
3. Peirce JM, Alviña K. The role of inflammation and the gut microbiome in depression and anxiety. J Neurosci Res. 2019;97(10):1223-1241.
4. Yolken R, Prandovszky E, Severance EG, et al. The oropharyngeal microbiome is altered in individuals with schizophrenia and mania. Schizophr Res. 2021;234:51-57.
5. Capuco A, Urits I, Hasoon J, et al. Current perspectives on gut microbiome dysbiosis and depression. Adv Ther. 2020;37(4):1328-1346.
6. Zozaya M, Ferris MJ, Siren JD, et al. Bacterial communities in penile skin, male urethra, and vagina of heterosexual couples with and without bacterial vaginosis. Microbiome. 2016;4:16. doi:10.1186/s40168-016-0161-6
7. Hou D, Zhou X, Zhong X, et al. Microbiota of the seminal fluid from healthy and infertile men. Fertil Steril. 2013;100(5):1261-1269.
8. Gallo MF, Warner L, King CC, et al. Association between semen exposure and incident bacterial vaginosis. Infect Dis Obstet Gynecol. 2011;2011:842652.
9. Liu CM, Hungate BA, Tobian AA, et al. Penile microbiota and female partner bacterial vaginosis in Rakai, Uganda. mBio. 2015;6(3):e00589. doi:10.1128/mBio.00589-15
10. Carda-Diéguez M, Cárdenas N, Aparicio M, et al. Variations in vaginal, penile, and oral microbiota after sexual intercourse: a case report. Front Med. 2019;6:178. doi:10.3389/fmed.2019.00178
Evidence is strong that sexual partners transmit microbiota (bacteria, viruses, fungi, protozoa, and archaea) to each other. While microbial flora are abundant in the gastrointestinal tract, they are also present in the vagina, penis, urethra, mouth, and skin.1 For better or worse, sexual contact of all types means that participants will acquire each other’s microbiota.
The 39 trillion microbiota in the body (which exceed the 30 trillion cells in the body) are commensal and influence both the larger brain in the skull and the smaller enteric brain in the gut. The microbiota and their microbiome genes (1,000 times larger than the human genome) have been linked to depression, anxiety, psychosis, and autism.2-4 They produce 90% of the body’s serotonin, as well as catecholamines (norepinephrine, epinephrine, dopamine), make hormones (eg, cortisol), and modulate the immune system. Microbiota have several important functions, including food digestion, synthesis of vitamins, autoimmunity, hypothalamic-pituitary-adrenal axis regulation, and CNS modulation.
Consequences of dysbiosis
Everyone should be concerned about maintaining a healthy diversity of microbiota in their body, with a predominance of beneficial bacteria such as Lactobacillus and Bacteroides, and avoiding acquiring pathogenic bacteria such as Gardnerella, Prevotella, and Atopobium. Sexual activity involving a partner with unhealthy microbiota may increase the risk of dysbiosis, defined as a reduction in microbiota diversity, including a loss of beneficial bacteria and a rise in harmful bacteria.
Dysbiosis is associated with multiple symptoms, including5:
- brain “fog,” irritability, mood changes, and anxiety
- bloating, loss of intestinal permeability, and insufficient reclamation of nutrients
- congestion of certain organs, such as the liver, gallbladder, and pancreas
- production of antigen-antibody complexes in response to chemicals in partially digested food
- aggravation of inflammatory disorders such as migraine, arthritis, and autoimmune disorders.
Apart from intimate sexual contact, simply sharing a household with someone leads to sharing of gut microflora. Persons who live together, whether genetically related or not, have similar microbiota. Compared with people living in separate households, cohabiting human pairs, dog pairs, and human-dog pairs share most of their microbiota (especially in the skin).
A consequence of acquiring pathogenic microbiota in the vagina is bacterial vaginosis (BV), which is not an infection but an ecologic imbalance in the composition of the vaginal microbiota. BV is caused by a significant decline in the beneficial vaginal Lactobacillus and a marked increase in the non-Lactobacillus taxa (especially Gardnerella and Atopobium).6 It can last for a least 1 week after sexual intercourse. BV is rare or absent among virgins. For a male partner, penile microbiota changes significantly after unprotected sex.6
Pathogenic bacteria can be cultivated from the glans, the coronal sulcus, and the prepuce, as well as from the penile skin, semen, urethra, and urine.6 Diverse bacteria exist in human semen, regardless if the male is fertile or infertile.7Anaerococcus is a biomarker for low sperm quality. Many of the semen bacteria are also found in the vagina of women with BV.7 Semen is a medium for the transmission of bacteria and viruses between men and women, and can contribute to sexually transmitted diseases.8
There are approximately 21 million cases of BV in the United States each year, and BV can also increase the risk of HIV and poor obstetric outcomes.9 The microbiota in the penile skin and urethra in males who have monogamous relationships with females are very similar to the vaginal microbiota of their female partner.
Consequences of BV include:
- decrease in hydrogen peroxide–producing bacilli
- prevalence of anaerobic bacteria (Prevotella, Gardnerella, and Atopobium)
- alkalinization, fishy odor, and gray-white vaginal discharge
- increase in the rate of pelvic inflammatory disease, ectopic pregnancy, endometriosis, preterm birth, and tubal factor infertility.9
Circumcision decreases the risk of BV. There is an increased rate of BV bacterial taxa in men with extramarital affairs and in women with multiple partners. Both oral and vaginal sex increase the abundance of Lactobacillus in the male oral and penile microbiota. Gingivitis has also been reported after oral sex.10
A link to psychiatric disorders
Given that all forms of sexual contact (vaginal, oral, anal, or skin) can transmit microbiota bidirectionally between partners, it is vital to practice safe sex and consider a monogamous relationship rather than indiscriminate promiscuity. Unfortunately, certain psychiatric disorders, such as bipolar disorder, are associated with hypersexuality and multiple partners, which may disrupt the microbiota. This can further disrupt the diversity of an individual’s microbiome and may put them at risk for mood, anxiety, and other psychiatric disorders. Another problem is sexually transmitted infections such as gonorrhea or syphilis require antibiotic therapy. It is well established that antibiotics kill both the bad pathogenic and the good nonpathogenic microbiota, further exacerbating dysbiosis and leading to disruptions in the microbiota-gut-brain (MGB) axis, which then results in psychiatric disorders.
The MGB axis modulates neurological processes via the vagus nerve, the major “highway” connecting the gut and brain for bidirectional traffic. The MGB axis produces microbial metabolites and immune factors that can lead to changes in brain neurotransmitters as well as neuroinflammation and psychiatric symptoms such as depression and anxiety.5
Many researchers are focusing on how to exploit the microbiome to develop novel therapeutic strategies, and encouraging advances are emerging.5 But the exact mechanisms by which the gut microbiome can impact mental health is still a work in progress. It is highly likely that dysbiosis is associated with mood and anxiety symptoms.
The bottom line: Sexual activity—whether it is heavy kissing, vaginal intercourse, oral sex, anal sex, or extensive skin contact—can lead to the exchange of microbiota. If an individual has dysbiosis, that could impact the mental health of their sexual partner(s). This raises the question of whether counseling patients about avoiding indiscriminate sex and practicing safe sex is as important for mental health as diet and exercise counseling is for physical health.
Evidence is strong that sexual partners transmit microbiota (bacteria, viruses, fungi, protozoa, and archaea) to each other. While microbial flora are abundant in the gastrointestinal tract, they are also present in the vagina, penis, urethra, mouth, and skin.1 For better or worse, sexual contact of all types means that participants will acquire each other’s microbiota.
The 39 trillion microbiota in the body (which exceed the 30 trillion cells in the body) are commensal and influence both the larger brain in the skull and the smaller enteric brain in the gut. The microbiota and their microbiome genes (1,000 times larger than the human genome) have been linked to depression, anxiety, psychosis, and autism.2-4 They produce 90% of the body’s serotonin, as well as catecholamines (norepinephrine, epinephrine, dopamine), make hormones (eg, cortisol), and modulate the immune system. Microbiota have several important functions, including food digestion, synthesis of vitamins, autoimmunity, hypothalamic-pituitary-adrenal axis regulation, and CNS modulation.
Consequences of dysbiosis
Everyone should be concerned about maintaining a healthy diversity of microbiota in their body, with a predominance of beneficial bacteria such as Lactobacillus and Bacteroides, and avoiding acquiring pathogenic bacteria such as Gardnerella, Prevotella, and Atopobium. Sexual activity involving a partner with unhealthy microbiota may increase the risk of dysbiosis, defined as a reduction in microbiota diversity, including a loss of beneficial bacteria and a rise in harmful bacteria.
Dysbiosis is associated with multiple symptoms, including5:
- brain “fog,” irritability, mood changes, and anxiety
- bloating, loss of intestinal permeability, and insufficient reclamation of nutrients
- congestion of certain organs, such as the liver, gallbladder, and pancreas
- production of antigen-antibody complexes in response to chemicals in partially digested food
- aggravation of inflammatory disorders such as migraine, arthritis, and autoimmune disorders.
Apart from intimate sexual contact, simply sharing a household with someone leads to sharing of gut microflora. Persons who live together, whether genetically related or not, have similar microbiota. Compared with people living in separate households, cohabiting human pairs, dog pairs, and human-dog pairs share most of their microbiota (especially in the skin).
A consequence of acquiring pathogenic microbiota in the vagina is bacterial vaginosis (BV), which is not an infection but an ecologic imbalance in the composition of the vaginal microbiota. BV is caused by a significant decline in the beneficial vaginal Lactobacillus and a marked increase in the non-Lactobacillus taxa (especially Gardnerella and Atopobium).6 It can last for a least 1 week after sexual intercourse. BV is rare or absent among virgins. For a male partner, penile microbiota changes significantly after unprotected sex.6
Pathogenic bacteria can be cultivated from the glans, the coronal sulcus, and the prepuce, as well as from the penile skin, semen, urethra, and urine.6 Diverse bacteria exist in human semen, regardless if the male is fertile or infertile.7Anaerococcus is a biomarker for low sperm quality. Many of the semen bacteria are also found in the vagina of women with BV.7 Semen is a medium for the transmission of bacteria and viruses between men and women, and can contribute to sexually transmitted diseases.8
There are approximately 21 million cases of BV in the United States each year, and BV can also increase the risk of HIV and poor obstetric outcomes.9 The microbiota in the penile skin and urethra in males who have monogamous relationships with females are very similar to the vaginal microbiota of their female partner.
Consequences of BV include:
- decrease in hydrogen peroxide–producing bacilli
- prevalence of anaerobic bacteria (Prevotella, Gardnerella, and Atopobium)
- alkalinization, fishy odor, and gray-white vaginal discharge
- increase in the rate of pelvic inflammatory disease, ectopic pregnancy, endometriosis, preterm birth, and tubal factor infertility.9
Circumcision decreases the risk of BV. There is an increased rate of BV bacterial taxa in men with extramarital affairs and in women with multiple partners. Both oral and vaginal sex increase the abundance of Lactobacillus in the male oral and penile microbiota. Gingivitis has also been reported after oral sex.10
A link to psychiatric disorders
Given that all forms of sexual contact (vaginal, oral, anal, or skin) can transmit microbiota bidirectionally between partners, it is vital to practice safe sex and consider a monogamous relationship rather than indiscriminate promiscuity. Unfortunately, certain psychiatric disorders, such as bipolar disorder, are associated with hypersexuality and multiple partners, which may disrupt the microbiota. This can further disrupt the diversity of an individual’s microbiome and may put them at risk for mood, anxiety, and other psychiatric disorders. Another problem is sexually transmitted infections such as gonorrhea or syphilis require antibiotic therapy. It is well established that antibiotics kill both the bad pathogenic and the good nonpathogenic microbiota, further exacerbating dysbiosis and leading to disruptions in the microbiota-gut-brain (MGB) axis, which then results in psychiatric disorders.
The MGB axis modulates neurological processes via the vagus nerve, the major “highway” connecting the gut and brain for bidirectional traffic. The MGB axis produces microbial metabolites and immune factors that can lead to changes in brain neurotransmitters as well as neuroinflammation and psychiatric symptoms such as depression and anxiety.5
Many researchers are focusing on how to exploit the microbiome to develop novel therapeutic strategies, and encouraging advances are emerging.5 But the exact mechanisms by which the gut microbiome can impact mental health is still a work in progress. It is highly likely that dysbiosis is associated with mood and anxiety symptoms.
The bottom line: Sexual activity—whether it is heavy kissing, vaginal intercourse, oral sex, anal sex, or extensive skin contact—can lead to the exchange of microbiota. If an individual has dysbiosis, that could impact the mental health of their sexual partner(s). This raises the question of whether counseling patients about avoiding indiscriminate sex and practicing safe sex is as important for mental health as diet and exercise counseling is for physical health.
1. Reid G, Younes JA, Van der Mei HC, et al. Microbiota restoration: natural and supplemented recovery of human microbial communities. Nat Rev Microbiol. 2011;9(1):27-38.
2. Cryan JF, Dinan TG. Mind-altering microorganisms: the impact of the gut microbiota on brain and behaviour. Nat Rev Neurosci. 2012;13(10):701-712.
3. Peirce JM, Alviña K. The role of inflammation and the gut microbiome in depression and anxiety. J Neurosci Res. 2019;97(10):1223-1241.
4. Yolken R, Prandovszky E, Severance EG, et al. The oropharyngeal microbiome is altered in individuals with schizophrenia and mania. Schizophr Res. 2021;234:51-57.
5. Capuco A, Urits I, Hasoon J, et al. Current perspectives on gut microbiome dysbiosis and depression. Adv Ther. 2020;37(4):1328-1346.
6. Zozaya M, Ferris MJ, Siren JD, et al. Bacterial communities in penile skin, male urethra, and vagina of heterosexual couples with and without bacterial vaginosis. Microbiome. 2016;4:16. doi:10.1186/s40168-016-0161-6
7. Hou D, Zhou X, Zhong X, et al. Microbiota of the seminal fluid from healthy and infertile men. Fertil Steril. 2013;100(5):1261-1269.
8. Gallo MF, Warner L, King CC, et al. Association between semen exposure and incident bacterial vaginosis. Infect Dis Obstet Gynecol. 2011;2011:842652.
9. Liu CM, Hungate BA, Tobian AA, et al. Penile microbiota and female partner bacterial vaginosis in Rakai, Uganda. mBio. 2015;6(3):e00589. doi:10.1128/mBio.00589-15
10. Carda-Diéguez M, Cárdenas N, Aparicio M, et al. Variations in vaginal, penile, and oral microbiota after sexual intercourse: a case report. Front Med. 2019;6:178. doi:10.3389/fmed.2019.00178
1. Reid G, Younes JA, Van der Mei HC, et al. Microbiota restoration: natural and supplemented recovery of human microbial communities. Nat Rev Microbiol. 2011;9(1):27-38.
2. Cryan JF, Dinan TG. Mind-altering microorganisms: the impact of the gut microbiota on brain and behaviour. Nat Rev Neurosci. 2012;13(10):701-712.
3. Peirce JM, Alviña K. The role of inflammation and the gut microbiome in depression and anxiety. J Neurosci Res. 2019;97(10):1223-1241.
4. Yolken R, Prandovszky E, Severance EG, et al. The oropharyngeal microbiome is altered in individuals with schizophrenia and mania. Schizophr Res. 2021;234:51-57.
5. Capuco A, Urits I, Hasoon J, et al. Current perspectives on gut microbiome dysbiosis and depression. Adv Ther. 2020;37(4):1328-1346.
6. Zozaya M, Ferris MJ, Siren JD, et al. Bacterial communities in penile skin, male urethra, and vagina of heterosexual couples with and without bacterial vaginosis. Microbiome. 2016;4:16. doi:10.1186/s40168-016-0161-6
7. Hou D, Zhou X, Zhong X, et al. Microbiota of the seminal fluid from healthy and infertile men. Fertil Steril. 2013;100(5):1261-1269.
8. Gallo MF, Warner L, King CC, et al. Association between semen exposure and incident bacterial vaginosis. Infect Dis Obstet Gynecol. 2011;2011:842652.
9. Liu CM, Hungate BA, Tobian AA, et al. Penile microbiota and female partner bacterial vaginosis in Rakai, Uganda. mBio. 2015;6(3):e00589. doi:10.1128/mBio.00589-15
10. Carda-Diéguez M, Cárdenas N, Aparicio M, et al. Variations in vaginal, penile, and oral microbiota after sexual intercourse: a case report. Front Med. 2019;6:178. doi:10.3389/fmed.2019.00178
Treatment augmentation strategies for OCD: A review of 8 studies
Obsessive-compulsive disorder (OCD) is a chronic, debilitating neuropsychiatric disorder that affects 1% to 3% of the population worldwide.1,2 Together, serotonin reuptake inhibitors (SRIs) and cognitive-behavior therapy (CBT) are considered the first-line treatment for OCD.3 In children and adults, CBT is considered at least as effective as pharmacotherapy.4 Despite being an effective treatment, CBT continues to have barriers to its widespread use, including limited availability of trained CBT therapists, delayed clinical response, and high costs.5
Only approximately one-half of patients with OCD respond to SRI therapy, and a considerable percentage (30% to 40%) show significant residual symptoms even after multiple trials of SRIs.6-8 In addition, SRIs may have adverse effects (eg, sexual dysfunction, gastrointestinal symptoms) that impair patient adherence to these medications.9 Therefore, finding better treatment options is important for managing patients with OCD.
Augmentation strategies are recommended for patients who show partial response to SRI treatment or poor response to multiple SRIs. Augmentation typically includes incorporating additional medications with the primary drug with the goal of boosting the therapeutic efficacy of the primary drug. Typically, these additional medications have different mechanisms of action. However, there are no large-scale randomized controlled trials (RCTs) to inform treatment augmentation after first-line treatments for OCD produce suboptimal outcomes. The available evidence is predominantly based on small-scale RCTs, open-label trials, and case series.
In this article, we review the evidence for treatment augmentation strategies for OCD and summarize 8 studies that show promising results (Table10-17). We focus only on pharmacologic agents and do not include other biological interventions, such as repetitive transcranial magnetic stimulation over supplementary motor area, ablative neurosurgery, or deep brain stimulation.
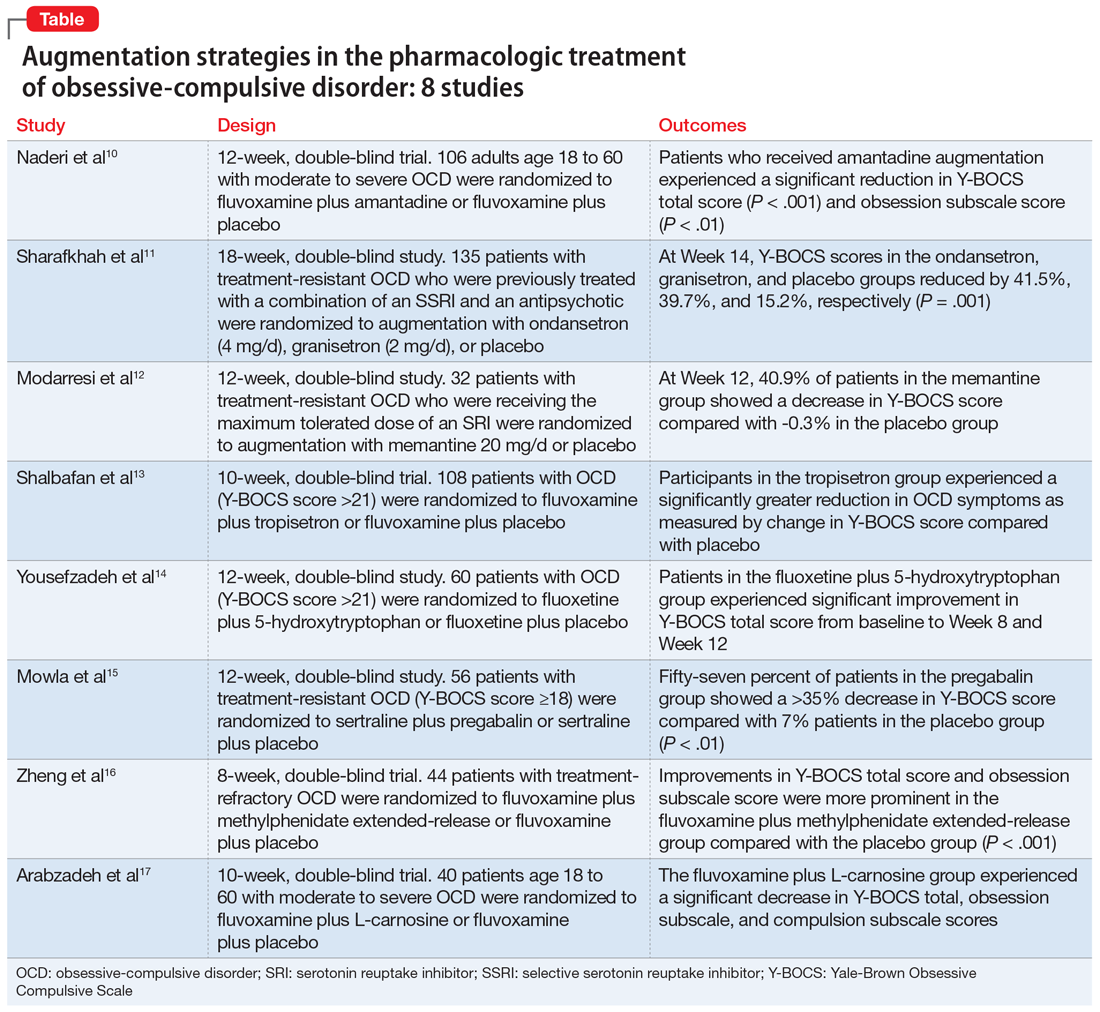
Continue to: Reference 1...
1. Naderi S, Faghih H , Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessivecompulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/ pcn.12803
Numerous studies support the role of glutamate dysregulation in the pathophysiology of OCD. Cortico-striato-thalamo-cortical (CSTC) abnormalities play a major role in the pathophysiology of OCD as suggested by neuroimaging research studies that indicate glutamate is the fundamental neurotransmitter of the CSTC circuit. Dysregulation of glutamatergic signaling within this circuit has been linked to OCD. Patients with OCD have been found to have an increase of glutamate in the CSF. As a result, medications that affect glutamate levels can be used to treat patients with OCD who do not respond to first-line agents. In patients already taking SRIs, augmentation of glutamate-modulating medications can reduce OCD symptoms. As an uncompetitive antagonist of the N-methyl-
Naderi et al10 evaluated amantadine as augmentative therapy to fluvoxamine for treating patients with moderate to severe OCD.
Study design
- This 12-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of amantadine as an augmentative agent to fluvoxamine in 106 patients age 18 to 60 with moderate to severe OCD.
- Participants met DSM-5 criteria for OCD and had a Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score >21. Participants were excluded if they had any substance dependence; an IQ <70; any other Axis I mental disorder; any serious cardiac, renal, or hepatic disease; had received psychotropic medications during the last 6 weeks, were pregnant or breastfeeding, or had rising liver transaminases to 3 times the upper limit of normal or higher.
- Participants received fluvoxamine 100 mg twice daily plus amantadine 100 mg/d, or fluvoxamine 100 mg twice daily plus placebo. All patients received fluvoxamine 100 mg/d for 28 days followed by 200 mg/d for the remainder of the trial.
- The primary outcome measure was difference in Y-BOCS total scores between the amantadine and placebo groups. The secondary outcome was the difference in Y-BOCS obsession and compulsion subscale scores.
Outcomes
- Patients who received amantadine augmentation experienced a significant reduction in Y-BOCS total score (P < .001) and obsession subscale score (P < .01).
- The amantadine group showed good tolerability and safety. There were no clinically significant adverse effects.
- Amantadine is an effective adjuvant to fluvoxamine for reducing OCD symptoms.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
2. Sharafkhah M, Aghakarim Alamdar M, Massoudifar A, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222- 233. doi:10.1097/YIC.0000000000000267
Although selective serotonin reuptake inhibitors (SSRIs) are considered a first-line treatment when teamed with CBT and antipsychotic augmentation, symptom resolution is not always achieved, and treatment resistance is a common problem. Sharafkhah et al11 compared the efficacy of ondansetron and granisetron augmentation specifically for patients with treatment-resistant OCD.
Study Design
- In this 18-week, randomized, double-blind, placebo-controlled study, 135 patients with treatment-resistant OCD who were previously treated with a combination of an SSRI and an antipsychotic received augmentation with ondansetron (n = 45, 4 mg/d), granisetron (n = 45, 2 mg/d), or placebo.
- Patients were rated using Y-BOCS every 2 weeks during phase I (intervention period), which lasted 14 weeks. After completing the intervention, patients were followed for 4 more weeks during phase II (discontinuation period).
- The aim of this study was to determine the safety, efficacy, and tolerability of ondansetron vs granisetron as augmentation for patients with treatment-resistant OCD. A secondary aim was to determine the rate of relapse of OCD symptoms after discontinuing ondansetron as compared with granisetron at 4 weeks after intervention.
Outcomes
- At Week 14, the reductions in Y-BOCS scores in the ondansetron, granisetron, and placebo groups were 41.5%, 39.7%, and 15.2%, respectively (P = .001). The reduction in Y-BOCS score in the ondansetron and granisetron groups was significantly greater than placebo at all phase I visits.
- Complete response was higher in the ondansetron group compared with the granisetron group (P = .041).
- Y-BOCS scores increased in both the ondansetron and granisetron groups during the discontinuation phase, but OCD symptoms were not significantly exacerbated.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
3. Modarresi A, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitorrefractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-120268
Increased glutamate levels in CSF, glutamatergic overactivity, and polymorphisms of genes coding the NMDA receptor have been shown to contribute to the occurrence of OCD. Memantine is a noncompetitive antagonist of the NMDA receptor. Various control trials have shown augmentation with memantine 5 mg/d to 20 mg/d significantly reduced symptom severity in patients with moderate to severe OCD. Modarresi et al12 evaluated memantine as a treatment option for patients with severe OCD who did not respond to SRI monotherapy.
Study design
- This 12-week, double-blind, randomized, placebo-controlled trial evaluated the efficacy of memantine augmentation in 32 patients age 18 to 40 who met DSM-5 criteria for OCD, had a Y-BOCS score ≥24, and no psychiatric comorbidity. Participants had not responded to ≥3 adequate trials (minimum 3 months) of SRI therapy, 1 of which was clomipramine.
- Individuals were excluded if they were undergoing CBT; had an additional anxiety disorder, mood disorder, or current drug or alcohol use disorder, or any systemic disorder; had a history of seizures; were pregnant or breastfeeding; or had a history of memantine use.
- Participants already receiving the maximum tolerated dose of an SRI received augmentation with memantine 20 mg/d or placebo.
- The primary outcome measure was change in Y-BOCS score from baseline. The secondary outcome was the number of individuals who achieved treatment response (defined as ≥35% reduction in Y-BOCS score).
Continue to: Outcomes...
Outcomes
- There was a statistically significant difference in Y-BOCS score in patients treated with memantine at Week 8 and Week 12 vs those who received placebo. By Week 8, 17.2% of patients in the memantine group showed a decrease in Y-BOCS score, compared with -0.8% patients in the placebo group. The difference became more significant by Week 12, with 40.9% in the memantine group showing a decrease in Y-BOCS score vs -0.3% in the placebo group. This resulted in 73.3% of patients achieving treatment response.
- Eight weeks of memantine augmentation was necessary to observe a significant improvement in OCD symptoms, and 12 weeks was needed for treatment response.
- The mean Y-BOCS total score decreased significantly in the memantine group from Week 4 to Week 8 (16.8%) and again from Week 8 to Week 12 (28.5%).
- The memantine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- Memantine augmentation in patients with severe OCD who do not respond to an SRI is effective and well-tolerated.
4. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407- 1414. doi:10.1177/0269881119878177
Studies have demonstrated the involvement of the amygdala, medial and lateral orbitofrontal cortex, and dorsal anterior cingulate cortex in OCD. Additionally, studies have also investigated the role of serotonin, dopamine, and glutamate system dysregulation in the pathology of OCD.
The 5-HT3 receptors are ligand-gated ion channels found in the prefrontal cortex, amygdala, and hippocampus. Studies of 5-HT3 receptor antagonists such as ondansetron and granisetron have shown beneficial results in augmentation with SSRIs for patients with OCD.11 Tropisetron, a 5-HT3 receptor antagonist, is highly lipophilic and able to cross the blood brain barrier. It also has dopamine-inhibiting properties that could have benefits in OCD management. Shalbafan et al13 evaluated the efficacy of tropisetron augmentation to fluvoxamine for patients with OCD.
Study design
- In a 10-week, randomized, double-blind, placebo-controlled, parallel-group trial, 108 individuals age 18 to 60 who met DSM-5 criteria for OCD and had a Y-BOCS score >21 received fluvoxamine plus tropisetron or fluvoxamine plus placebo. A total of 48 (44.4%) participants in each group completed the trial. Participants were evaluated using the Y-BOCS scale at baseline and at Week 4 and Week 10.
- The primary outcome was decrease in total Y-BOCS score from baseline to Week 10. The secondary outcome was the difference in change in Y-BOCS obsession and compulsion subscale scores between the groups.
Outcomes
- The Y-BOCS total score was not significantly different between the 2 groups (P = .975). Repeated measures analysis of variance determined a significant effect for time in both tropisetron and placebo groups (Greenhouse-Geisser F [2.72–2303.84] = 152.25, P < .001; and Greenhouse-Geisser F [1.37–1736.81] = 75.57, P < .001, respectively). At Week 10, 35 participants in the tropisetron group and 19 participants in the placebo group were complete responders.
- The baseline Y-BOCS obsession and compulsion subscales did not significantly differ between treatment groups.
Conclusion
- Compared with participants in the placebo group, those in the tropisetron group experienced a significantly greater reduction in OCD symptoms as measured by Y-BOCS score. More participants in the tropisetron group experienced complete response and remission.
- This study demonstrated that compared with placebo, when administered as augmentation with fluvoxamine, tropisetron can have beneficial effects for patients with OCD.
Continue to: Reference 5...
5. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a doubleblind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254- 262. doi:10.1097/YIC.0000000000000321
Nutraceuticals such as glycine, milk thistle, myoinositol, and serotonin (5-hydroxytryptophan) have been proposed as augmentation options for OCD. Yousefzadeh et al14 investigated the effectiveness of using 5-hydroxytryptophan in treating OCD.
Study design
- In a 12-week, randomized, double-blind study, 60 patients who met DSM-5 criteria for moderate to severe OCD (Y-BOCS score >21) were randomly assigned to receive fluoxetine plus 5-hydroxytryptophan 100 mg twice daily or fluoxetine plus placebo.
- All patients were administered fluoxetine 20 mg/d for the first 4 weeks of the study followed by fluoxetine 60 mg/d for the remainder of the trial.
- Symptoms were assessed using the Y-BOCS at baseline, Week 4, Week 8, and Week 12.
- The primary outcome measure was the difference between the 2 groups in change in Y-BOCS total score from baseline to the end of the trial. Secondary outcome measures were the differences in the Y-BOCS obsession and compulsion subscale scores from baseline to Week 12.
Outcomes
- Compared to the placebo group, the 5-hydroxytryptophan group experienced a statistically significant greater improvement in Y-BOCS total score from baseline to Week 8 (P = .002) and Week 12 (P < .001).
- General linear model repeated measure showed significant effects for time × treatment interaction on Y-BOCS total (F = 12.07, df = 2.29, P < .001), obsession subscale (F = 8.25, df = 1.91, P = .001), and compulsion subscale scores (F = 6.64, df = 2.01, P = .002).
- The 5-hydroxytryptophan group demonstrated higher partial and complete treatment response rates (P = .032 and P = .001, respectively) as determined by change in Y-BOCS total score.
- The 5-hydroxytryptophan group showed a significant improvement from baseline to Week 12 in Y-BOCS obsession subscale score (5.23 ± 2.33 vs 3.53 ± 2.13, P = .009).
- There was a significant change from baseline to the end of the trial in the Y-BOCS compulsion subscale score (3.88 ± 2.04 vs 2.30 ± 1.37, P = .002).
Conclusion
- This trial demonstrated the potential benefits of 5-hydroxytryptophan in combination with fluoxetine for patients with OCD.
6. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
Glutamatergic dysfunction has been identified as a potential cause of OCD. Studies have found elevated levels of glutamatergic transmission in the cortical-striatal-thalamic circuit of the brain and elevated glutamate concentration in the CSF in patients with OCD. Pregabalin has multiple mechanisms of action that inhibit the release of glutamate. Mowla et al15 evaluated pregabalin as an augmentation treatment for resistant OCD.
Study design
- This 12-week, double-blind, placebo-controlled clinical trial evaluated the efficacy of adjunctive pregabalin in 56 patients who met DSM-5 criteria for OCD and had not responded to ≥12 weeks of treatment with an adequate and stable dose of sertraline (baseline Y-BOCS score ≥18).
- Individuals who had other major psychiatric disorders, major medical problems, were pregnant, or had past substance or alcohol abuse were excluded.
- Participants were randomly assigned to receive sertraline plus pregabalin (n = 28) or sertraline plus placebo (n = 28). Mean sertraline dosage was 256.5 mg/d; range was 100 mg/d to 300 mg/d. Pregabalin was started at 75 mg/d and increased by 75 mg increments weekly. The mean dosage was 185.9 mg/d; range was 75 mg/d to 225 mg/d.
- The primary outcome measure was change in Y-BOCS score. A decrease >35% in Y-BOCS score was considered a significant response rate.
Outcomes
- There was a statistically significant decrease in Y-BOCS score in patients who received pregabalin. In the pregabalin group, 57.14% of patients (n = 16) showed a >35% decrease in Y-BOCS score compared with 7.14% of patients (n = 2) in the placebo group (P < .01).
- The pregabalin group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- In patients with treatment-resistant OCD who did not respond to sertraline monotherapy, augmentation with pregabalin significantly decreases Y-BOCS scores compared with placebo.
Continue to: Reference 7...
7. Zheng H, Jia F, Han H, et al. Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebocontrolled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro. 2018.12.010
Recent evidence suggests dysregulation of serotonin and dopamine in patients with OCD. Methylphenidate is a dopamine and norepinephrine inhibitor and releaser. A limited number of studies have suggested stimulants might be useful for OCD patients. Zheng et al16 conducted a pilot trial to determine whether methylphenidate augmentation may be of benefit in the management of outpatients with OCD.
Study design
- In an 8-week, double-blind, randomized, placebo-controlled trial, 44 patients (29 [66%] men, with a mean [SD] age of 24.7 [6]) with treatment-refractory OCD were randomized to receive fluvoxamine 250 mg/d plus methylphenidate extended-release (MPH-ER) 36 mg/d or fluvoxamine 250 mg/d plus placebo. The MPH-ER dose was 18 mg/d for the first 4 weeks and 36 mg/d for the rest of the trial.
- Biweekly assessments consisted of scores on the Y-BOCS, Hamilton Depression Rating Scale (HDRS), and Hamilton Anxiety Rating Scale (HAM-A).
- The primary outcomes were improvement in Y-BOCS score and the clinical response rate. Secondary outcomes included a change in score on the Y-BOCS subscales, HARS, and HAM-A. Data were analyzed with the intention-to-treat sample.
Outcomes
- Forty-one patients finished the trial. The baseline Y-BOCS total scores and subscale scores did not differ significantly between the 2 groups.
- Improvements in Y-BOCS total score and obsession subscale score were more prominent in the fluvoxamine plus MPH-ER group compared with the placebo group (P < .001).
- HDRS score decreased in both the placebo and MPH-ER groups. HAM-A scores decreased significantly in the MPH-ER plus fluvoxamine group compared with the placebo group.
Conclusion
- This study demonstrated that the combination of fluvoxamine and MPH-ER produces a higher and faster response rate than fluvoxamine plus placebo in patients with OCD.
8. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
Glutamate dysregulation is implicated in the pathogenesis of OCD. Glutamate-modulating agents have been used to treat OCD. Studies have shown L-carnosine has a neuroprotective role via its modulatory effect on glutamate. Arabzadeh et al17 evaluated the efficacy of L-carnosine as an adjuvant to fluvoxamine for treating OCD.
Study design
- This 10-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy of adjunctive L-carnosine in 40 patients age 18 to 60 who met DSM-5 criteria for OCD and had moderate to severe OCD (Y-BOCS score ≥21).
- Individuals with any other DSM-5 major psychiatric disorders, serious medical or neurologic illness, substance dependence (other than caffeine or nicotine), mental retardation (based on clinical judgment), were pregnant or breastfeeding, had any contraindication for the use of L‐carnosine or fluvoxamine, or received any psychotropic drugs in the previous 6 weeks were excluded.
- Participants received fluvoxamine 100 mg/d for the first 4 weeks and 200 mg/d for the next 6 weeks plus either L-carnosine 500 mg twice daily or placebo. This dosage of L-carnosine was chosen because previously it had been tolerated and effective.
- The primary outcome measure was difference in Y-BOCS total scores. Secondary outcomes were differences in Y-BOCS obsession and compulsion subscale scores and differences in change in score on Y-BOCS total and subscale scores from baseline.
Outcomes
- The L-carnosine group experienced a significant decrease in Y-BOCS total score (P < .001), obsession subscale score (P < .01), and compulsion subscale score (P < .01).
- The group that received fluvoxamine plus L-carnosine also experienced a more complete response (P = .03).
- The L-carnosine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- L-carnosine significantly reduces OCD symptoms when used as an adjuvant to fluvoxamine.
1. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
2. Ruscio AM, Stein DJ, Chiu WT, et al. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63.
3. Eddy KT, Dutra L, Bradley, R, et al. A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev. 2004;24(8):1011-1030.
4. Franklin ME, Foa EB. Treatment of obsessive compulsive disorder. Annu Rev Clin Psychol. 2011;7:229-243.
5. Koran LM, Hanna GL, Hollander E, et al. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 Suppl):5-53.
6. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375-391.
7. Pallanti S, Hollander E, Bienstock C, et al. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. 2002;5(2):181-191.
8. Atmaca M. Treatment-refractory obsessive compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2016;70:127-133.
9. Barth M, Kriston L, Klostermann S, et al. Efficacy of selective serotonin reuptake inhibitors and adverse events: meta-regression and mediation analysis of placebo-controlled trials. Br J Psychiatry. 2016;208(2):114-119.
10. NaderiS, Faghih H, Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/pcn.12803
11. SharafkhahM, Aghakarim Alamdar M, MassoudifarA, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222-233. doi:10.1097/YIC.0000000000000267
12. ModarresiA, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-12026
13. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407-1414. doi:10.1177/0269881119878177
14. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254-262. doi:10.1097/YIC.0000000000000321
15. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
16. Zheng H, Jia F, Han H, et al.Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebo-controlled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro.2018.12.010
17. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
Obsessive-compulsive disorder (OCD) is a chronic, debilitating neuropsychiatric disorder that affects 1% to 3% of the population worldwide.1,2 Together, serotonin reuptake inhibitors (SRIs) and cognitive-behavior therapy (CBT) are considered the first-line treatment for OCD.3 In children and adults, CBT is considered at least as effective as pharmacotherapy.4 Despite being an effective treatment, CBT continues to have barriers to its widespread use, including limited availability of trained CBT therapists, delayed clinical response, and high costs.5
Only approximately one-half of patients with OCD respond to SRI therapy, and a considerable percentage (30% to 40%) show significant residual symptoms even after multiple trials of SRIs.6-8 In addition, SRIs may have adverse effects (eg, sexual dysfunction, gastrointestinal symptoms) that impair patient adherence to these medications.9 Therefore, finding better treatment options is important for managing patients with OCD.
Augmentation strategies are recommended for patients who show partial response to SRI treatment or poor response to multiple SRIs. Augmentation typically includes incorporating additional medications with the primary drug with the goal of boosting the therapeutic efficacy of the primary drug. Typically, these additional medications have different mechanisms of action. However, there are no large-scale randomized controlled trials (RCTs) to inform treatment augmentation after first-line treatments for OCD produce suboptimal outcomes. The available evidence is predominantly based on small-scale RCTs, open-label trials, and case series.
In this article, we review the evidence for treatment augmentation strategies for OCD and summarize 8 studies that show promising results (Table10-17). We focus only on pharmacologic agents and do not include other biological interventions, such as repetitive transcranial magnetic stimulation over supplementary motor area, ablative neurosurgery, or deep brain stimulation.
Continue to: Reference 1...
1. Naderi S, Faghih H , Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessivecompulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/ pcn.12803
Numerous studies support the role of glutamate dysregulation in the pathophysiology of OCD. Cortico-striato-thalamo-cortical (CSTC) abnormalities play a major role in the pathophysiology of OCD as suggested by neuroimaging research studies that indicate glutamate is the fundamental neurotransmitter of the CSTC circuit. Dysregulation of glutamatergic signaling within this circuit has been linked to OCD. Patients with OCD have been found to have an increase of glutamate in the CSF. As a result, medications that affect glutamate levels can be used to treat patients with OCD who do not respond to first-line agents. In patients already taking SRIs, augmentation of glutamate-modulating medications can reduce OCD symptoms. As an uncompetitive antagonist of the N-methyl-
Naderi et al10 evaluated amantadine as augmentative therapy to fluvoxamine for treating patients with moderate to severe OCD.
Study design
- This 12-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of amantadine as an augmentative agent to fluvoxamine in 106 patients age 18 to 60 with moderate to severe OCD.
- Participants met DSM-5 criteria for OCD and had a Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score >21. Participants were excluded if they had any substance dependence; an IQ <70; any other Axis I mental disorder; any serious cardiac, renal, or hepatic disease; had received psychotropic medications during the last 6 weeks, were pregnant or breastfeeding, or had rising liver transaminases to 3 times the upper limit of normal or higher.
- Participants received fluvoxamine 100 mg twice daily plus amantadine 100 mg/d, or fluvoxamine 100 mg twice daily plus placebo. All patients received fluvoxamine 100 mg/d for 28 days followed by 200 mg/d for the remainder of the trial.
- The primary outcome measure was difference in Y-BOCS total scores between the amantadine and placebo groups. The secondary outcome was the difference in Y-BOCS obsession and compulsion subscale scores.
Outcomes
- Patients who received amantadine augmentation experienced a significant reduction in Y-BOCS total score (P < .001) and obsession subscale score (P < .01).
- The amantadine group showed good tolerability and safety. There were no clinically significant adverse effects.
- Amantadine is an effective adjuvant to fluvoxamine for reducing OCD symptoms.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
2. Sharafkhah M, Aghakarim Alamdar M, Massoudifar A, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222- 233. doi:10.1097/YIC.0000000000000267
Although selective serotonin reuptake inhibitors (SSRIs) are considered a first-line treatment when teamed with CBT and antipsychotic augmentation, symptom resolution is not always achieved, and treatment resistance is a common problem. Sharafkhah et al11 compared the efficacy of ondansetron and granisetron augmentation specifically for patients with treatment-resistant OCD.
Study Design
- In this 18-week, randomized, double-blind, placebo-controlled study, 135 patients with treatment-resistant OCD who were previously treated with a combination of an SSRI and an antipsychotic received augmentation with ondansetron (n = 45, 4 mg/d), granisetron (n = 45, 2 mg/d), or placebo.
- Patients were rated using Y-BOCS every 2 weeks during phase I (intervention period), which lasted 14 weeks. After completing the intervention, patients were followed for 4 more weeks during phase II (discontinuation period).
- The aim of this study was to determine the safety, efficacy, and tolerability of ondansetron vs granisetron as augmentation for patients with treatment-resistant OCD. A secondary aim was to determine the rate of relapse of OCD symptoms after discontinuing ondansetron as compared with granisetron at 4 weeks after intervention.
Outcomes
- At Week 14, the reductions in Y-BOCS scores in the ondansetron, granisetron, and placebo groups were 41.5%, 39.7%, and 15.2%, respectively (P = .001). The reduction in Y-BOCS score in the ondansetron and granisetron groups was significantly greater than placebo at all phase I visits.
- Complete response was higher in the ondansetron group compared with the granisetron group (P = .041).
- Y-BOCS scores increased in both the ondansetron and granisetron groups during the discontinuation phase, but OCD symptoms were not significantly exacerbated.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
3. Modarresi A, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitorrefractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-120268
Increased glutamate levels in CSF, glutamatergic overactivity, and polymorphisms of genes coding the NMDA receptor have been shown to contribute to the occurrence of OCD. Memantine is a noncompetitive antagonist of the NMDA receptor. Various control trials have shown augmentation with memantine 5 mg/d to 20 mg/d significantly reduced symptom severity in patients with moderate to severe OCD. Modarresi et al12 evaluated memantine as a treatment option for patients with severe OCD who did not respond to SRI monotherapy.
Study design
- This 12-week, double-blind, randomized, placebo-controlled trial evaluated the efficacy of memantine augmentation in 32 patients age 18 to 40 who met DSM-5 criteria for OCD, had a Y-BOCS score ≥24, and no psychiatric comorbidity. Participants had not responded to ≥3 adequate trials (minimum 3 months) of SRI therapy, 1 of which was clomipramine.
- Individuals were excluded if they were undergoing CBT; had an additional anxiety disorder, mood disorder, or current drug or alcohol use disorder, or any systemic disorder; had a history of seizures; were pregnant or breastfeeding; or had a history of memantine use.
- Participants already receiving the maximum tolerated dose of an SRI received augmentation with memantine 20 mg/d or placebo.
- The primary outcome measure was change in Y-BOCS score from baseline. The secondary outcome was the number of individuals who achieved treatment response (defined as ≥35% reduction in Y-BOCS score).
Continue to: Outcomes...
Outcomes
- There was a statistically significant difference in Y-BOCS score in patients treated with memantine at Week 8 and Week 12 vs those who received placebo. By Week 8, 17.2% of patients in the memantine group showed a decrease in Y-BOCS score, compared with -0.8% patients in the placebo group. The difference became more significant by Week 12, with 40.9% in the memantine group showing a decrease in Y-BOCS score vs -0.3% in the placebo group. This resulted in 73.3% of patients achieving treatment response.
- Eight weeks of memantine augmentation was necessary to observe a significant improvement in OCD symptoms, and 12 weeks was needed for treatment response.
- The mean Y-BOCS total score decreased significantly in the memantine group from Week 4 to Week 8 (16.8%) and again from Week 8 to Week 12 (28.5%).
- The memantine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- Memantine augmentation in patients with severe OCD who do not respond to an SRI is effective and well-tolerated.
4. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407- 1414. doi:10.1177/0269881119878177
Studies have demonstrated the involvement of the amygdala, medial and lateral orbitofrontal cortex, and dorsal anterior cingulate cortex in OCD. Additionally, studies have also investigated the role of serotonin, dopamine, and glutamate system dysregulation in the pathology of OCD.
The 5-HT3 receptors are ligand-gated ion channels found in the prefrontal cortex, amygdala, and hippocampus. Studies of 5-HT3 receptor antagonists such as ondansetron and granisetron have shown beneficial results in augmentation with SSRIs for patients with OCD.11 Tropisetron, a 5-HT3 receptor antagonist, is highly lipophilic and able to cross the blood brain barrier. It also has dopamine-inhibiting properties that could have benefits in OCD management. Shalbafan et al13 evaluated the efficacy of tropisetron augmentation to fluvoxamine for patients with OCD.
Study design
- In a 10-week, randomized, double-blind, placebo-controlled, parallel-group trial, 108 individuals age 18 to 60 who met DSM-5 criteria for OCD and had a Y-BOCS score >21 received fluvoxamine plus tropisetron or fluvoxamine plus placebo. A total of 48 (44.4%) participants in each group completed the trial. Participants were evaluated using the Y-BOCS scale at baseline and at Week 4 and Week 10.
- The primary outcome was decrease in total Y-BOCS score from baseline to Week 10. The secondary outcome was the difference in change in Y-BOCS obsession and compulsion subscale scores between the groups.
Outcomes
- The Y-BOCS total score was not significantly different between the 2 groups (P = .975). Repeated measures analysis of variance determined a significant effect for time in both tropisetron and placebo groups (Greenhouse-Geisser F [2.72–2303.84] = 152.25, P < .001; and Greenhouse-Geisser F [1.37–1736.81] = 75.57, P < .001, respectively). At Week 10, 35 participants in the tropisetron group and 19 participants in the placebo group were complete responders.
- The baseline Y-BOCS obsession and compulsion subscales did not significantly differ between treatment groups.
Conclusion
- Compared with participants in the placebo group, those in the tropisetron group experienced a significantly greater reduction in OCD symptoms as measured by Y-BOCS score. More participants in the tropisetron group experienced complete response and remission.
- This study demonstrated that compared with placebo, when administered as augmentation with fluvoxamine, tropisetron can have beneficial effects for patients with OCD.
Continue to: Reference 5...
5. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a doubleblind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254- 262. doi:10.1097/YIC.0000000000000321
Nutraceuticals such as glycine, milk thistle, myoinositol, and serotonin (5-hydroxytryptophan) have been proposed as augmentation options for OCD. Yousefzadeh et al14 investigated the effectiveness of using 5-hydroxytryptophan in treating OCD.
Study design
- In a 12-week, randomized, double-blind study, 60 patients who met DSM-5 criteria for moderate to severe OCD (Y-BOCS score >21) were randomly assigned to receive fluoxetine plus 5-hydroxytryptophan 100 mg twice daily or fluoxetine plus placebo.
- All patients were administered fluoxetine 20 mg/d for the first 4 weeks of the study followed by fluoxetine 60 mg/d for the remainder of the trial.
- Symptoms were assessed using the Y-BOCS at baseline, Week 4, Week 8, and Week 12.
- The primary outcome measure was the difference between the 2 groups in change in Y-BOCS total score from baseline to the end of the trial. Secondary outcome measures were the differences in the Y-BOCS obsession and compulsion subscale scores from baseline to Week 12.
Outcomes
- Compared to the placebo group, the 5-hydroxytryptophan group experienced a statistically significant greater improvement in Y-BOCS total score from baseline to Week 8 (P = .002) and Week 12 (P < .001).
- General linear model repeated measure showed significant effects for time × treatment interaction on Y-BOCS total (F = 12.07, df = 2.29, P < .001), obsession subscale (F = 8.25, df = 1.91, P = .001), and compulsion subscale scores (F = 6.64, df = 2.01, P = .002).
- The 5-hydroxytryptophan group demonstrated higher partial and complete treatment response rates (P = .032 and P = .001, respectively) as determined by change in Y-BOCS total score.
- The 5-hydroxytryptophan group showed a significant improvement from baseline to Week 12 in Y-BOCS obsession subscale score (5.23 ± 2.33 vs 3.53 ± 2.13, P = .009).
- There was a significant change from baseline to the end of the trial in the Y-BOCS compulsion subscale score (3.88 ± 2.04 vs 2.30 ± 1.37, P = .002).
Conclusion
- This trial demonstrated the potential benefits of 5-hydroxytryptophan in combination with fluoxetine for patients with OCD.
6. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
Glutamatergic dysfunction has been identified as a potential cause of OCD. Studies have found elevated levels of glutamatergic transmission in the cortical-striatal-thalamic circuit of the brain and elevated glutamate concentration in the CSF in patients with OCD. Pregabalin has multiple mechanisms of action that inhibit the release of glutamate. Mowla et al15 evaluated pregabalin as an augmentation treatment for resistant OCD.
Study design
- This 12-week, double-blind, placebo-controlled clinical trial evaluated the efficacy of adjunctive pregabalin in 56 patients who met DSM-5 criteria for OCD and had not responded to ≥12 weeks of treatment with an adequate and stable dose of sertraline (baseline Y-BOCS score ≥18).
- Individuals who had other major psychiatric disorders, major medical problems, were pregnant, or had past substance or alcohol abuse were excluded.
- Participants were randomly assigned to receive sertraline plus pregabalin (n = 28) or sertraline plus placebo (n = 28). Mean sertraline dosage was 256.5 mg/d; range was 100 mg/d to 300 mg/d. Pregabalin was started at 75 mg/d and increased by 75 mg increments weekly. The mean dosage was 185.9 mg/d; range was 75 mg/d to 225 mg/d.
- The primary outcome measure was change in Y-BOCS score. A decrease >35% in Y-BOCS score was considered a significant response rate.
Outcomes
- There was a statistically significant decrease in Y-BOCS score in patients who received pregabalin. In the pregabalin group, 57.14% of patients (n = 16) showed a >35% decrease in Y-BOCS score compared with 7.14% of patients (n = 2) in the placebo group (P < .01).
- The pregabalin group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- In patients with treatment-resistant OCD who did not respond to sertraline monotherapy, augmentation with pregabalin significantly decreases Y-BOCS scores compared with placebo.
Continue to: Reference 7...
7. Zheng H, Jia F, Han H, et al. Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebocontrolled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro. 2018.12.010
Recent evidence suggests dysregulation of serotonin and dopamine in patients with OCD. Methylphenidate is a dopamine and norepinephrine inhibitor and releaser. A limited number of studies have suggested stimulants might be useful for OCD patients. Zheng et al16 conducted a pilot trial to determine whether methylphenidate augmentation may be of benefit in the management of outpatients with OCD.
Study design
- In an 8-week, double-blind, randomized, placebo-controlled trial, 44 patients (29 [66%] men, with a mean [SD] age of 24.7 [6]) with treatment-refractory OCD were randomized to receive fluvoxamine 250 mg/d plus methylphenidate extended-release (MPH-ER) 36 mg/d or fluvoxamine 250 mg/d plus placebo. The MPH-ER dose was 18 mg/d for the first 4 weeks and 36 mg/d for the rest of the trial.
- Biweekly assessments consisted of scores on the Y-BOCS, Hamilton Depression Rating Scale (HDRS), and Hamilton Anxiety Rating Scale (HAM-A).
- The primary outcomes were improvement in Y-BOCS score and the clinical response rate. Secondary outcomes included a change in score on the Y-BOCS subscales, HARS, and HAM-A. Data were analyzed with the intention-to-treat sample.
Outcomes
- Forty-one patients finished the trial. The baseline Y-BOCS total scores and subscale scores did not differ significantly between the 2 groups.
- Improvements in Y-BOCS total score and obsession subscale score were more prominent in the fluvoxamine plus MPH-ER group compared with the placebo group (P < .001).
- HDRS score decreased in both the placebo and MPH-ER groups. HAM-A scores decreased significantly in the MPH-ER plus fluvoxamine group compared with the placebo group.
Conclusion
- This study demonstrated that the combination of fluvoxamine and MPH-ER produces a higher and faster response rate than fluvoxamine plus placebo in patients with OCD.
8. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
Glutamate dysregulation is implicated in the pathogenesis of OCD. Glutamate-modulating agents have been used to treat OCD. Studies have shown L-carnosine has a neuroprotective role via its modulatory effect on glutamate. Arabzadeh et al17 evaluated the efficacy of L-carnosine as an adjuvant to fluvoxamine for treating OCD.
Study design
- This 10-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy of adjunctive L-carnosine in 40 patients age 18 to 60 who met DSM-5 criteria for OCD and had moderate to severe OCD (Y-BOCS score ≥21).
- Individuals with any other DSM-5 major psychiatric disorders, serious medical or neurologic illness, substance dependence (other than caffeine or nicotine), mental retardation (based on clinical judgment), were pregnant or breastfeeding, had any contraindication for the use of L‐carnosine or fluvoxamine, or received any psychotropic drugs in the previous 6 weeks were excluded.
- Participants received fluvoxamine 100 mg/d for the first 4 weeks and 200 mg/d for the next 6 weeks plus either L-carnosine 500 mg twice daily or placebo. This dosage of L-carnosine was chosen because previously it had been tolerated and effective.
- The primary outcome measure was difference in Y-BOCS total scores. Secondary outcomes were differences in Y-BOCS obsession and compulsion subscale scores and differences in change in score on Y-BOCS total and subscale scores from baseline.
Outcomes
- The L-carnosine group experienced a significant decrease in Y-BOCS total score (P < .001), obsession subscale score (P < .01), and compulsion subscale score (P < .01).
- The group that received fluvoxamine plus L-carnosine also experienced a more complete response (P = .03).
- The L-carnosine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- L-carnosine significantly reduces OCD symptoms when used as an adjuvant to fluvoxamine.
Obsessive-compulsive disorder (OCD) is a chronic, debilitating neuropsychiatric disorder that affects 1% to 3% of the population worldwide.1,2 Together, serotonin reuptake inhibitors (SRIs) and cognitive-behavior therapy (CBT) are considered the first-line treatment for OCD.3 In children and adults, CBT is considered at least as effective as pharmacotherapy.4 Despite being an effective treatment, CBT continues to have barriers to its widespread use, including limited availability of trained CBT therapists, delayed clinical response, and high costs.5
Only approximately one-half of patients with OCD respond to SRI therapy, and a considerable percentage (30% to 40%) show significant residual symptoms even after multiple trials of SRIs.6-8 In addition, SRIs may have adverse effects (eg, sexual dysfunction, gastrointestinal symptoms) that impair patient adherence to these medications.9 Therefore, finding better treatment options is important for managing patients with OCD.
Augmentation strategies are recommended for patients who show partial response to SRI treatment or poor response to multiple SRIs. Augmentation typically includes incorporating additional medications with the primary drug with the goal of boosting the therapeutic efficacy of the primary drug. Typically, these additional medications have different mechanisms of action. However, there are no large-scale randomized controlled trials (RCTs) to inform treatment augmentation after first-line treatments for OCD produce suboptimal outcomes. The available evidence is predominantly based on small-scale RCTs, open-label trials, and case series.
In this article, we review the evidence for treatment augmentation strategies for OCD and summarize 8 studies that show promising results (Table10-17). We focus only on pharmacologic agents and do not include other biological interventions, such as repetitive transcranial magnetic stimulation over supplementary motor area, ablative neurosurgery, or deep brain stimulation.
Continue to: Reference 1...
1. Naderi S, Faghih H , Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessivecompulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/ pcn.12803
Numerous studies support the role of glutamate dysregulation in the pathophysiology of OCD. Cortico-striato-thalamo-cortical (CSTC) abnormalities play a major role in the pathophysiology of OCD as suggested by neuroimaging research studies that indicate glutamate is the fundamental neurotransmitter of the CSTC circuit. Dysregulation of glutamatergic signaling within this circuit has been linked to OCD. Patients with OCD have been found to have an increase of glutamate in the CSF. As a result, medications that affect glutamate levels can be used to treat patients with OCD who do not respond to first-line agents. In patients already taking SRIs, augmentation of glutamate-modulating medications can reduce OCD symptoms. As an uncompetitive antagonist of the N-methyl-
Naderi et al10 evaluated amantadine as augmentative therapy to fluvoxamine for treating patients with moderate to severe OCD.
Study design
- This 12-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of amantadine as an augmentative agent to fluvoxamine in 106 patients age 18 to 60 with moderate to severe OCD.
- Participants met DSM-5 criteria for OCD and had a Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score >21. Participants were excluded if they had any substance dependence; an IQ <70; any other Axis I mental disorder; any serious cardiac, renal, or hepatic disease; had received psychotropic medications during the last 6 weeks, were pregnant or breastfeeding, or had rising liver transaminases to 3 times the upper limit of normal or higher.
- Participants received fluvoxamine 100 mg twice daily plus amantadine 100 mg/d, or fluvoxamine 100 mg twice daily plus placebo. All patients received fluvoxamine 100 mg/d for 28 days followed by 200 mg/d for the remainder of the trial.
- The primary outcome measure was difference in Y-BOCS total scores between the amantadine and placebo groups. The secondary outcome was the difference in Y-BOCS obsession and compulsion subscale scores.
Outcomes
- Patients who received amantadine augmentation experienced a significant reduction in Y-BOCS total score (P < .001) and obsession subscale score (P < .01).
- The amantadine group showed good tolerability and safety. There were no clinically significant adverse effects.
- Amantadine is an effective adjuvant to fluvoxamine for reducing OCD symptoms.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
2. Sharafkhah M, Aghakarim Alamdar M, Massoudifar A, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222- 233. doi:10.1097/YIC.0000000000000267
Although selective serotonin reuptake inhibitors (SSRIs) are considered a first-line treatment when teamed with CBT and antipsychotic augmentation, symptom resolution is not always achieved, and treatment resistance is a common problem. Sharafkhah et al11 compared the efficacy of ondansetron and granisetron augmentation specifically for patients with treatment-resistant OCD.
Study Design
- In this 18-week, randomized, double-blind, placebo-controlled study, 135 patients with treatment-resistant OCD who were previously treated with a combination of an SSRI and an antipsychotic received augmentation with ondansetron (n = 45, 4 mg/d), granisetron (n = 45, 2 mg/d), or placebo.
- Patients were rated using Y-BOCS every 2 weeks during phase I (intervention period), which lasted 14 weeks. After completing the intervention, patients were followed for 4 more weeks during phase II (discontinuation period).
- The aim of this study was to determine the safety, efficacy, and tolerability of ondansetron vs granisetron as augmentation for patients with treatment-resistant OCD. A secondary aim was to determine the rate of relapse of OCD symptoms after discontinuing ondansetron as compared with granisetron at 4 weeks after intervention.
Outcomes
- At Week 14, the reductions in Y-BOCS scores in the ondansetron, granisetron, and placebo groups were 41.5%, 39.7%, and 15.2%, respectively (P = .001). The reduction in Y-BOCS score in the ondansetron and granisetron groups was significantly greater than placebo at all phase I visits.
- Complete response was higher in the ondansetron group compared with the granisetron group (P = .041).
- Y-BOCS scores increased in both the ondansetron and granisetron groups during the discontinuation phase, but OCD symptoms were not significantly exacerbated.
Conclusion
- Ondansetron and granisetron can be beneficial as an augmentation strategy for patients with treatment-resistant OCD.
3. Modarresi A, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitorrefractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-120268
Increased glutamate levels in CSF, glutamatergic overactivity, and polymorphisms of genes coding the NMDA receptor have been shown to contribute to the occurrence of OCD. Memantine is a noncompetitive antagonist of the NMDA receptor. Various control trials have shown augmentation with memantine 5 mg/d to 20 mg/d significantly reduced symptom severity in patients with moderate to severe OCD. Modarresi et al12 evaluated memantine as a treatment option for patients with severe OCD who did not respond to SRI monotherapy.
Study design
- This 12-week, double-blind, randomized, placebo-controlled trial evaluated the efficacy of memantine augmentation in 32 patients age 18 to 40 who met DSM-5 criteria for OCD, had a Y-BOCS score ≥24, and no psychiatric comorbidity. Participants had not responded to ≥3 adequate trials (minimum 3 months) of SRI therapy, 1 of which was clomipramine.
- Individuals were excluded if they were undergoing CBT; had an additional anxiety disorder, mood disorder, or current drug or alcohol use disorder, or any systemic disorder; had a history of seizures; were pregnant or breastfeeding; or had a history of memantine use.
- Participants already receiving the maximum tolerated dose of an SRI received augmentation with memantine 20 mg/d or placebo.
- The primary outcome measure was change in Y-BOCS score from baseline. The secondary outcome was the number of individuals who achieved treatment response (defined as ≥35% reduction in Y-BOCS score).
Continue to: Outcomes...
Outcomes
- There was a statistically significant difference in Y-BOCS score in patients treated with memantine at Week 8 and Week 12 vs those who received placebo. By Week 8, 17.2% of patients in the memantine group showed a decrease in Y-BOCS score, compared with -0.8% patients in the placebo group. The difference became more significant by Week 12, with 40.9% in the memantine group showing a decrease in Y-BOCS score vs -0.3% in the placebo group. This resulted in 73.3% of patients achieving treatment response.
- Eight weeks of memantine augmentation was necessary to observe a significant improvement in OCD symptoms, and 12 weeks was needed for treatment response.
- The mean Y-BOCS total score decreased significantly in the memantine group from Week 4 to Week 8 (16.8%) and again from Week 8 to Week 12 (28.5%).
- The memantine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- Memantine augmentation in patients with severe OCD who do not respond to an SRI is effective and well-tolerated.
4. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407- 1414. doi:10.1177/0269881119878177
Studies have demonstrated the involvement of the amygdala, medial and lateral orbitofrontal cortex, and dorsal anterior cingulate cortex in OCD. Additionally, studies have also investigated the role of serotonin, dopamine, and glutamate system dysregulation in the pathology of OCD.
The 5-HT3 receptors are ligand-gated ion channels found in the prefrontal cortex, amygdala, and hippocampus. Studies of 5-HT3 receptor antagonists such as ondansetron and granisetron have shown beneficial results in augmentation with SSRIs for patients with OCD.11 Tropisetron, a 5-HT3 receptor antagonist, is highly lipophilic and able to cross the blood brain barrier. It also has dopamine-inhibiting properties that could have benefits in OCD management. Shalbafan et al13 evaluated the efficacy of tropisetron augmentation to fluvoxamine for patients with OCD.
Study design
- In a 10-week, randomized, double-blind, placebo-controlled, parallel-group trial, 108 individuals age 18 to 60 who met DSM-5 criteria for OCD and had a Y-BOCS score >21 received fluvoxamine plus tropisetron or fluvoxamine plus placebo. A total of 48 (44.4%) participants in each group completed the trial. Participants were evaluated using the Y-BOCS scale at baseline and at Week 4 and Week 10.
- The primary outcome was decrease in total Y-BOCS score from baseline to Week 10. The secondary outcome was the difference in change in Y-BOCS obsession and compulsion subscale scores between the groups.
Outcomes
- The Y-BOCS total score was not significantly different between the 2 groups (P = .975). Repeated measures analysis of variance determined a significant effect for time in both tropisetron and placebo groups (Greenhouse-Geisser F [2.72–2303.84] = 152.25, P < .001; and Greenhouse-Geisser F [1.37–1736.81] = 75.57, P < .001, respectively). At Week 10, 35 participants in the tropisetron group and 19 participants in the placebo group were complete responders.
- The baseline Y-BOCS obsession and compulsion subscales did not significantly differ between treatment groups.
Conclusion
- Compared with participants in the placebo group, those in the tropisetron group experienced a significantly greater reduction in OCD symptoms as measured by Y-BOCS score. More participants in the tropisetron group experienced complete response and remission.
- This study demonstrated that compared with placebo, when administered as augmentation with fluvoxamine, tropisetron can have beneficial effects for patients with OCD.
Continue to: Reference 5...
5. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a doubleblind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254- 262. doi:10.1097/YIC.0000000000000321
Nutraceuticals such as glycine, milk thistle, myoinositol, and serotonin (5-hydroxytryptophan) have been proposed as augmentation options for OCD. Yousefzadeh et al14 investigated the effectiveness of using 5-hydroxytryptophan in treating OCD.
Study design
- In a 12-week, randomized, double-blind study, 60 patients who met DSM-5 criteria for moderate to severe OCD (Y-BOCS score >21) were randomly assigned to receive fluoxetine plus 5-hydroxytryptophan 100 mg twice daily or fluoxetine plus placebo.
- All patients were administered fluoxetine 20 mg/d for the first 4 weeks of the study followed by fluoxetine 60 mg/d for the remainder of the trial.
- Symptoms were assessed using the Y-BOCS at baseline, Week 4, Week 8, and Week 12.
- The primary outcome measure was the difference between the 2 groups in change in Y-BOCS total score from baseline to the end of the trial. Secondary outcome measures were the differences in the Y-BOCS obsession and compulsion subscale scores from baseline to Week 12.
Outcomes
- Compared to the placebo group, the 5-hydroxytryptophan group experienced a statistically significant greater improvement in Y-BOCS total score from baseline to Week 8 (P = .002) and Week 12 (P < .001).
- General linear model repeated measure showed significant effects for time × treatment interaction on Y-BOCS total (F = 12.07, df = 2.29, P < .001), obsession subscale (F = 8.25, df = 1.91, P = .001), and compulsion subscale scores (F = 6.64, df = 2.01, P = .002).
- The 5-hydroxytryptophan group demonstrated higher partial and complete treatment response rates (P = .032 and P = .001, respectively) as determined by change in Y-BOCS total score.
- The 5-hydroxytryptophan group showed a significant improvement from baseline to Week 12 in Y-BOCS obsession subscale score (5.23 ± 2.33 vs 3.53 ± 2.13, P = .009).
- There was a significant change from baseline to the end of the trial in the Y-BOCS compulsion subscale score (3.88 ± 2.04 vs 2.30 ± 1.37, P = .002).
Conclusion
- This trial demonstrated the potential benefits of 5-hydroxytryptophan in combination with fluoxetine for patients with OCD.
6. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
Glutamatergic dysfunction has been identified as a potential cause of OCD. Studies have found elevated levels of glutamatergic transmission in the cortical-striatal-thalamic circuit of the brain and elevated glutamate concentration in the CSF in patients with OCD. Pregabalin has multiple mechanisms of action that inhibit the release of glutamate. Mowla et al15 evaluated pregabalin as an augmentation treatment for resistant OCD.
Study design
- This 12-week, double-blind, placebo-controlled clinical trial evaluated the efficacy of adjunctive pregabalin in 56 patients who met DSM-5 criteria for OCD and had not responded to ≥12 weeks of treatment with an adequate and stable dose of sertraline (baseline Y-BOCS score ≥18).
- Individuals who had other major psychiatric disorders, major medical problems, were pregnant, or had past substance or alcohol abuse were excluded.
- Participants were randomly assigned to receive sertraline plus pregabalin (n = 28) or sertraline plus placebo (n = 28). Mean sertraline dosage was 256.5 mg/d; range was 100 mg/d to 300 mg/d. Pregabalin was started at 75 mg/d and increased by 75 mg increments weekly. The mean dosage was 185.9 mg/d; range was 75 mg/d to 225 mg/d.
- The primary outcome measure was change in Y-BOCS score. A decrease >35% in Y-BOCS score was considered a significant response rate.
Outcomes
- There was a statistically significant decrease in Y-BOCS score in patients who received pregabalin. In the pregabalin group, 57.14% of patients (n = 16) showed a >35% decrease in Y-BOCS score compared with 7.14% of patients (n = 2) in the placebo group (P < .01).
- The pregabalin group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- In patients with treatment-resistant OCD who did not respond to sertraline monotherapy, augmentation with pregabalin significantly decreases Y-BOCS scores compared with placebo.
Continue to: Reference 7...
7. Zheng H, Jia F, Han H, et al. Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebocontrolled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro. 2018.12.010
Recent evidence suggests dysregulation of serotonin and dopamine in patients with OCD. Methylphenidate is a dopamine and norepinephrine inhibitor and releaser. A limited number of studies have suggested stimulants might be useful for OCD patients. Zheng et al16 conducted a pilot trial to determine whether methylphenidate augmentation may be of benefit in the management of outpatients with OCD.
Study design
- In an 8-week, double-blind, randomized, placebo-controlled trial, 44 patients (29 [66%] men, with a mean [SD] age of 24.7 [6]) with treatment-refractory OCD were randomized to receive fluvoxamine 250 mg/d plus methylphenidate extended-release (MPH-ER) 36 mg/d or fluvoxamine 250 mg/d plus placebo. The MPH-ER dose was 18 mg/d for the first 4 weeks and 36 mg/d for the rest of the trial.
- Biweekly assessments consisted of scores on the Y-BOCS, Hamilton Depression Rating Scale (HDRS), and Hamilton Anxiety Rating Scale (HAM-A).
- The primary outcomes were improvement in Y-BOCS score and the clinical response rate. Secondary outcomes included a change in score on the Y-BOCS subscales, HARS, and HAM-A. Data were analyzed with the intention-to-treat sample.
Outcomes
- Forty-one patients finished the trial. The baseline Y-BOCS total scores and subscale scores did not differ significantly between the 2 groups.
- Improvements in Y-BOCS total score and obsession subscale score were more prominent in the fluvoxamine plus MPH-ER group compared with the placebo group (P < .001).
- HDRS score decreased in both the placebo and MPH-ER groups. HAM-A scores decreased significantly in the MPH-ER plus fluvoxamine group compared with the placebo group.
Conclusion
- This study demonstrated that the combination of fluvoxamine and MPH-ER produces a higher and faster response rate than fluvoxamine plus placebo in patients with OCD.
8. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
Glutamate dysregulation is implicated in the pathogenesis of OCD. Glutamate-modulating agents have been used to treat OCD. Studies have shown L-carnosine has a neuroprotective role via its modulatory effect on glutamate. Arabzadeh et al17 evaluated the efficacy of L-carnosine as an adjuvant to fluvoxamine for treating OCD.
Study design
- This 10-week, randomized, double-blind, placebo-controlled trial evaluated the efficacy of adjunctive L-carnosine in 40 patients age 18 to 60 who met DSM-5 criteria for OCD and had moderate to severe OCD (Y-BOCS score ≥21).
- Individuals with any other DSM-5 major psychiatric disorders, serious medical or neurologic illness, substance dependence (other than caffeine or nicotine), mental retardation (based on clinical judgment), were pregnant or breastfeeding, had any contraindication for the use of L‐carnosine or fluvoxamine, or received any psychotropic drugs in the previous 6 weeks were excluded.
- Participants received fluvoxamine 100 mg/d for the first 4 weeks and 200 mg/d for the next 6 weeks plus either L-carnosine 500 mg twice daily or placebo. This dosage of L-carnosine was chosen because previously it had been tolerated and effective.
- The primary outcome measure was difference in Y-BOCS total scores. Secondary outcomes were differences in Y-BOCS obsession and compulsion subscale scores and differences in change in score on Y-BOCS total and subscale scores from baseline.
Outcomes
- The L-carnosine group experienced a significant decrease in Y-BOCS total score (P < .001), obsession subscale score (P < .01), and compulsion subscale score (P < .01).
- The group that received fluvoxamine plus L-carnosine also experienced a more complete response (P = .03).
- The L-carnosine group showed good tolerability and safety. There were no clinically significant adverse effects.
Conclusion
- L-carnosine significantly reduces OCD symptoms when used as an adjuvant to fluvoxamine.
1. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
2. Ruscio AM, Stein DJ, Chiu WT, et al. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63.
3. Eddy KT, Dutra L, Bradley, R, et al. A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev. 2004;24(8):1011-1030.
4. Franklin ME, Foa EB. Treatment of obsessive compulsive disorder. Annu Rev Clin Psychol. 2011;7:229-243.
5. Koran LM, Hanna GL, Hollander E, et al. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 Suppl):5-53.
6. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375-391.
7. Pallanti S, Hollander E, Bienstock C, et al. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. 2002;5(2):181-191.
8. Atmaca M. Treatment-refractory obsessive compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2016;70:127-133.
9. Barth M, Kriston L, Klostermann S, et al. Efficacy of selective serotonin reuptake inhibitors and adverse events: meta-regression and mediation analysis of placebo-controlled trials. Br J Psychiatry. 2016;208(2):114-119.
10. NaderiS, Faghih H, Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/pcn.12803
11. SharafkhahM, Aghakarim Alamdar M, MassoudifarA, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222-233. doi:10.1097/YIC.0000000000000267
12. ModarresiA, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-12026
13. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407-1414. doi:10.1177/0269881119878177
14. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254-262. doi:10.1097/YIC.0000000000000321
15. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
16. Zheng H, Jia F, Han H, et al.Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebo-controlled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro.2018.12.010
17. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
1. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
2. Ruscio AM, Stein DJ, Chiu WT, et al. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63.
3. Eddy KT, Dutra L, Bradley, R, et al. A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev. 2004;24(8):1011-1030.
4. Franklin ME, Foa EB. Treatment of obsessive compulsive disorder. Annu Rev Clin Psychol. 2011;7:229-243.
5. Koran LM, Hanna GL, Hollander E, et al. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 Suppl):5-53.
6. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375-391.
7. Pallanti S, Hollander E, Bienstock C, et al. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. 2002;5(2):181-191.
8. Atmaca M. Treatment-refractory obsessive compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2016;70:127-133.
9. Barth M, Kriston L, Klostermann S, et al. Efficacy of selective serotonin reuptake inhibitors and adverse events: meta-regression and mediation analysis of placebo-controlled trials. Br J Psychiatry. 2016;208(2):114-119.
10. NaderiS, Faghih H, Aqamolaei A, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. 2019;73(4):169-174. doi:10.1111/pcn.12803
11. SharafkhahM, Aghakarim Alamdar M, MassoudifarA, et al. Comparing the efficacy of ondansetron and granisetron augmentation in treatment-resistant obsessive-compulsive disorder: a randomized double-blind placebo-controlled study. Int Clin Psychopharmacol. 2019;34(5):222-233. doi:10.1097/YIC.0000000000000267
12. ModarresiA, Sayyah M, Razooghi S, et al. Memantine augmentation improves symptoms in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder: a randomized controlled trial. Pharmacopsychiatry. 2018;51(6):263-269. doi:10.1055/s-0043-12026
13. Shalbafan M, Malekpour F, Tadayon Najafabadi B, et al. Fluvoxamine combination therapy with tropisetron for obsessive-compulsive disorder patients: a placebo-controlled, randomized clinical trial. J Psychopharmacol. 2019;33(11):1407-1414. doi:10.1177/0269881119878177
14. Yousefzadeh F, Sahebolzamani E, Sadri A, et al. 5-Hydroxytryptophan as adjuvant therapy in treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Int Clin Psychopharmacol. 2020;35(5):254-262. doi:10.1097/YIC.0000000000000321
15. Mowla A, Ghaedsharaf M. Pregabalin augmentation for resistant obsessive-compulsive disorder: a double-blind placebo-controlled clinical trial. CNS Spectr. 2020;25(4):552-556. doi:10.1017/S1092852919001500
16. Zheng H, Jia F, Han H, et al.Combined fluvoxamine and extended-release methylphenidate improved treatment response compared to fluvoxamine alone in patients with treatment-refractory obsessive-compulsive disorder: a randomized double-blind, placebo-controlled study. Eur Neuropsychopharmacol. 2019;29(3):397-404. doi:10.1016/j.euroneuro.2018.12.010
17. Arabzadeh S, Shahhossenie M, Mesgarpour B, et al. L-carnosine as an adjuvant to fluvoxamine in treatment of obsessive compulsive disorder: a randomized double-blind study. Hum Psychopharmacol. 2017;32(4). doi:10.1002/hup.2584
