User login
Liver Abscess and Metastatic Endophthalmitis
Klebsiella pneumoniae liver abscess is known to be associated with metastatic endophthalmitis,1 although most cases have been clustered in Taiwan, with few reports in the United States.2 The first reported case of Klebsiella liver abscess with endophthalmitis in the United States was in a 38‐year‐old man with a new diagnosis of diabetes, a known risk factor for hematogenous spread of Klebsiella to metastatic sites.3
CASE REPORT
A previously healthy 43‐year old Haitian man presented after experiencing 5 days of right eye pain with associated fever and swelling. The patient denied preceding trauma, manipulation of the eye, contact lens use, or illicit drug use and had no significant medical history. He had moved to the United States from Haiti more than 15 years ago and had not traveled out of the state of Florida since that time.
Physical exam showed tachycardia (rate = 110/min), tachypnea (rate = 20/min), and a temperature of 101.5F. The right eye had injected conjunctiva, a swollen lid, and decreased palpebral fissure, and visual acuity on the left was 20/60, whereas visual acuity on the right was recorded as the ability to count fingers at 3 feet. The remainder of his physical exam was within normal limits including the abdominal exam.
Laboratory data on admission included a white blood cell count of 37,500/L significant for 12% bands, total bilirubin of 2.8 mg/dL, AST of 141 U/L, ALT of 130 U/L, and alkaline phosphatase of 196 U/L. HIV testing was negative, and urine toxicology did not detect the presence of any illicit drugs. Vitreous cultures grew Klebsiella pneumoniae.
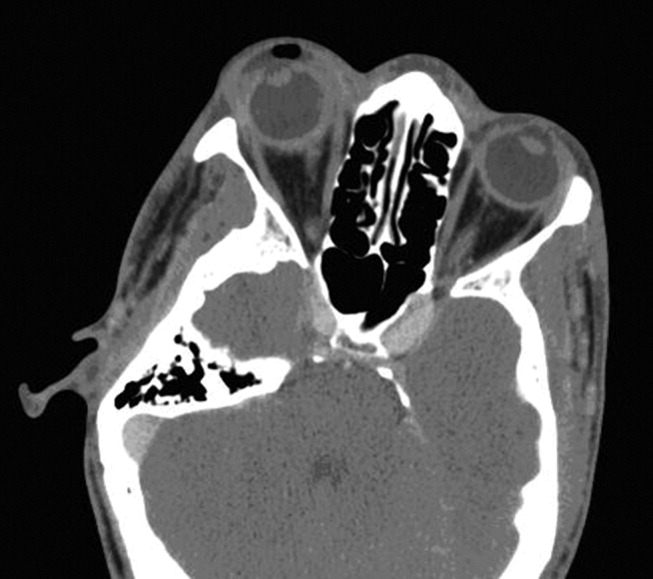
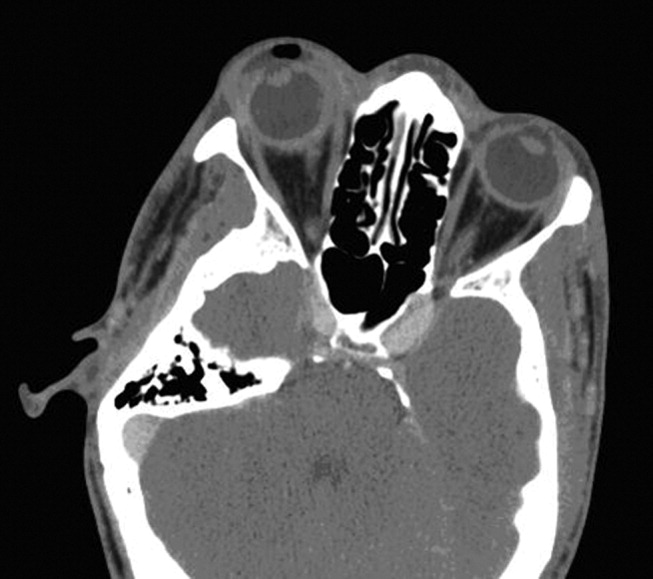
The initial CT scan of the orbit (Fig. 1) showed periorbital swelling and a preseptal collection anterior to the right globe consistent with an abscess. Because of the abnormal results of the liver panel in the presence of the ophthalmologic infection, an abdominal CT was obtained that showed an 11.5 by 8.0 cm lesion involving all segments of the right lobe of the liver with a 0.9‐mm cylindrical extension toward the right hepatic vein.
Percutaneous drainage of the liver abscess was performed, yielding positive cultures for K. pneumoniae. The patient was treated with oral gatifloxacin and intravenous ceftriaxone. Gatifloxacin therapy was chosen for its excellent penetrance into the vitreous.4 Despite antibiotic therapy, a repeat CT scan of the orbit showed further extension of the collection, and the decision was made to drain the abscess and perform right eye enucleation. The patient was discharged home on oral gatifloxacin. A follow‐up abdominal ultrasound 2 weeks after discharge showed complete resolution of the liver abscess.
DISCUSSION
Bacterial endophthalmitis is a rare infection involving the vitreous humor and other deep intraocular structures. It is most commonly exogenous in origin, caused by intraocular surgery, penetrating injury, a corneal ulcer, or periocular infection. Endogenous endophthalmitis occurs when organisms reach the eye hematogenously and accounts for fewer than 6% of all cases of endophthalmitis.5
Klebsiella liver abscesses have been increasing in incidence worldwide and since the mid‐1990s have become a common cause of liver abscess in the United States, along with Escherichia coli. The association with endophthalmitis was first reported in a series of 7 cases from Taiwan in 1986,1 and subsequent East Asian cases have been reported, usually in diabetic patients.6, 7 The association of Klebsiella liver abscesses with endogenous endophthalmitis has been rarely reported in the United States, with review of the literature from 1966 to 2003 revealing only 3 reported cases.2 One of these patients had diabetes, whereas another had beta‐thalassemia with previous splenectomy. Another study looking at only pyogenic liver abscess found biliary disease, hypertension, intraabdominal infection, and diabetes to be the most common underlying or concurrent conditions.8 Our patient did not appear to have any of these risk factors.
Our patient had no known risk factors to promote metastatic spread of the causative organisms. The patient was HIV negative, had no personal or family history of diabetes, and was not found to have elevated glucose levels at any point during admission. Although the ultimate etiology may never be determined, the possibility of undetected malignancy or cardiovascular or inflammatory disease cannot be excluded.
Physicians need to be aware of the global emergence of a hypervirulent strain of K. pneumonia causing liver abscesses and metastatic complications, especially endophthalmitis.9 Mucoviscosity associated gene A (magA) has been found in some liver isolates of K. pneumoniae.10 It has been suggested that as many as one‐third of patients infected with hyperviscous strains of K. pneumoniae will develop an invasive infection.11 Although it is unclear why metastatic endophthalmitis from Klebsiella liver abscess would be more common in East Asia, the magA gene may account for the observed difference. It was not possible to determine if the infectious organism that had infected our patient had the magA gene, although the clinical use of this information may not have changed management because the patient presented with metastatic infection. If this patient's particular organism had tested positive for the magA gene, it might explain why an apparently immunocompetent patient developed metastatic endophthalmitis not simply a liver abscess.
Patients with evidence of endogenous endophthalmitis without clear risk factors should be covered for K. pneumoniae, and extraocular sources should be sought, particularly the liver, even in the absence of diabetes. Early recognition and prompt initiation of antimicrobial therapy is essential if the patient's vision is to be preserved.
- ,,.Klebsiella pneumoniae liver abscess associated with septic endophthalmitis.Arch Intern Med.1986;146:1913–1916.
- ,.Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics.Am J Gastroenterol.2005;100:322–331.
- .Klebsiella pneumoniae liver abscess, endophthalmitis, and meningitis in a man with newly recognized diabetes mellitus.Clin Infect Dis.1999;29:1570–1571.
- ,,.Vitreous and aqueous penetration of orally administered gatifloxacin in humans.Arch Ophthalmol.2003;121:345–350.
- ,,,.Endogenous bacterial endophthalmitis: a 17‐year prospective series and review of 267 reported cases.Surv Ophthalmol.2003;48:403–423.
- ,,, et al.Primary liver abscess due to Klebsiella pneumoniae in Taiwan.Clin Infect Dis.1998;26:1434–1438.
- ,,,,.Septic metastatic lesions of pyogenic liver abscess. Their association with Klebsiella pneumoniae bacteremia in diabetic patients.Arch Intern Med.1991;151:1557–1559.
- ,,,.Pyogenic liver abscess: recent trends in etiology and mortality.Clin Infect Dis.2004;39:1654–1659.
- ,,, et al.A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis?Gut.2002;50:420–424.
- ,,.Liver abscess caused by magA+ Klebsiella pneumoniae in North America.J Clin Microbiol.2005;43:991–992.
- ,,, et al.Clinical implications of hypermucoviscosity phenotype in Klebsiella pneumoniae isolates: association with invasive syndrome in patients with community‐acquired bacteraemia.J Intern Med.2006;259:606–614.
Klebsiella pneumoniae liver abscess is known to be associated with metastatic endophthalmitis,1 although most cases have been clustered in Taiwan, with few reports in the United States.2 The first reported case of Klebsiella liver abscess with endophthalmitis in the United States was in a 38‐year‐old man with a new diagnosis of diabetes, a known risk factor for hematogenous spread of Klebsiella to metastatic sites.3
CASE REPORT
A previously healthy 43‐year old Haitian man presented after experiencing 5 days of right eye pain with associated fever and swelling. The patient denied preceding trauma, manipulation of the eye, contact lens use, or illicit drug use and had no significant medical history. He had moved to the United States from Haiti more than 15 years ago and had not traveled out of the state of Florida since that time.
Physical exam showed tachycardia (rate = 110/min), tachypnea (rate = 20/min), and a temperature of 101.5F. The right eye had injected conjunctiva, a swollen lid, and decreased palpebral fissure, and visual acuity on the left was 20/60, whereas visual acuity on the right was recorded as the ability to count fingers at 3 feet. The remainder of his physical exam was within normal limits including the abdominal exam.
Laboratory data on admission included a white blood cell count of 37,500/L significant for 12% bands, total bilirubin of 2.8 mg/dL, AST of 141 U/L, ALT of 130 U/L, and alkaline phosphatase of 196 U/L. HIV testing was negative, and urine toxicology did not detect the presence of any illicit drugs. Vitreous cultures grew Klebsiella pneumoniae.
The initial CT scan of the orbit (Fig. 1) showed periorbital swelling and a preseptal collection anterior to the right globe consistent with an abscess. Because of the abnormal results of the liver panel in the presence of the ophthalmologic infection, an abdominal CT was obtained that showed an 11.5 by 8.0 cm lesion involving all segments of the right lobe of the liver with a 0.9‐mm cylindrical extension toward the right hepatic vein.
Percutaneous drainage of the liver abscess was performed, yielding positive cultures for K. pneumoniae. The patient was treated with oral gatifloxacin and intravenous ceftriaxone. Gatifloxacin therapy was chosen for its excellent penetrance into the vitreous.4 Despite antibiotic therapy, a repeat CT scan of the orbit showed further extension of the collection, and the decision was made to drain the abscess and perform right eye enucleation. The patient was discharged home on oral gatifloxacin. A follow‐up abdominal ultrasound 2 weeks after discharge showed complete resolution of the liver abscess.
DISCUSSION
Bacterial endophthalmitis is a rare infection involving the vitreous humor and other deep intraocular structures. It is most commonly exogenous in origin, caused by intraocular surgery, penetrating injury, a corneal ulcer, or periocular infection. Endogenous endophthalmitis occurs when organisms reach the eye hematogenously and accounts for fewer than 6% of all cases of endophthalmitis.5
Klebsiella liver abscesses have been increasing in incidence worldwide and since the mid‐1990s have become a common cause of liver abscess in the United States, along with Escherichia coli. The association with endophthalmitis was first reported in a series of 7 cases from Taiwan in 1986,1 and subsequent East Asian cases have been reported, usually in diabetic patients.6, 7 The association of Klebsiella liver abscesses with endogenous endophthalmitis has been rarely reported in the United States, with review of the literature from 1966 to 2003 revealing only 3 reported cases.2 One of these patients had diabetes, whereas another had beta‐thalassemia with previous splenectomy. Another study looking at only pyogenic liver abscess found biliary disease, hypertension, intraabdominal infection, and diabetes to be the most common underlying or concurrent conditions.8 Our patient did not appear to have any of these risk factors.
Our patient had no known risk factors to promote metastatic spread of the causative organisms. The patient was HIV negative, had no personal or family history of diabetes, and was not found to have elevated glucose levels at any point during admission. Although the ultimate etiology may never be determined, the possibility of undetected malignancy or cardiovascular or inflammatory disease cannot be excluded.
Physicians need to be aware of the global emergence of a hypervirulent strain of K. pneumonia causing liver abscesses and metastatic complications, especially endophthalmitis.9 Mucoviscosity associated gene A (magA) has been found in some liver isolates of K. pneumoniae.10 It has been suggested that as many as one‐third of patients infected with hyperviscous strains of K. pneumoniae will develop an invasive infection.11 Although it is unclear why metastatic endophthalmitis from Klebsiella liver abscess would be more common in East Asia, the magA gene may account for the observed difference. It was not possible to determine if the infectious organism that had infected our patient had the magA gene, although the clinical use of this information may not have changed management because the patient presented with metastatic infection. If this patient's particular organism had tested positive for the magA gene, it might explain why an apparently immunocompetent patient developed metastatic endophthalmitis not simply a liver abscess.
Patients with evidence of endogenous endophthalmitis without clear risk factors should be covered for K. pneumoniae, and extraocular sources should be sought, particularly the liver, even in the absence of diabetes. Early recognition and prompt initiation of antimicrobial therapy is essential if the patient's vision is to be preserved.
Klebsiella pneumoniae liver abscess is known to be associated with metastatic endophthalmitis,1 although most cases have been clustered in Taiwan, with few reports in the United States.2 The first reported case of Klebsiella liver abscess with endophthalmitis in the United States was in a 38‐year‐old man with a new diagnosis of diabetes, a known risk factor for hematogenous spread of Klebsiella to metastatic sites.3
CASE REPORT
A previously healthy 43‐year old Haitian man presented after experiencing 5 days of right eye pain with associated fever and swelling. The patient denied preceding trauma, manipulation of the eye, contact lens use, or illicit drug use and had no significant medical history. He had moved to the United States from Haiti more than 15 years ago and had not traveled out of the state of Florida since that time.
Physical exam showed tachycardia (rate = 110/min), tachypnea (rate = 20/min), and a temperature of 101.5F. The right eye had injected conjunctiva, a swollen lid, and decreased palpebral fissure, and visual acuity on the left was 20/60, whereas visual acuity on the right was recorded as the ability to count fingers at 3 feet. The remainder of his physical exam was within normal limits including the abdominal exam.
Laboratory data on admission included a white blood cell count of 37,500/L significant for 12% bands, total bilirubin of 2.8 mg/dL, AST of 141 U/L, ALT of 130 U/L, and alkaline phosphatase of 196 U/L. HIV testing was negative, and urine toxicology did not detect the presence of any illicit drugs. Vitreous cultures grew Klebsiella pneumoniae.
The initial CT scan of the orbit (Fig. 1) showed periorbital swelling and a preseptal collection anterior to the right globe consistent with an abscess. Because of the abnormal results of the liver panel in the presence of the ophthalmologic infection, an abdominal CT was obtained that showed an 11.5 by 8.0 cm lesion involving all segments of the right lobe of the liver with a 0.9‐mm cylindrical extension toward the right hepatic vein.
Percutaneous drainage of the liver abscess was performed, yielding positive cultures for K. pneumoniae. The patient was treated with oral gatifloxacin and intravenous ceftriaxone. Gatifloxacin therapy was chosen for its excellent penetrance into the vitreous.4 Despite antibiotic therapy, a repeat CT scan of the orbit showed further extension of the collection, and the decision was made to drain the abscess and perform right eye enucleation. The patient was discharged home on oral gatifloxacin. A follow‐up abdominal ultrasound 2 weeks after discharge showed complete resolution of the liver abscess.
DISCUSSION
Bacterial endophthalmitis is a rare infection involving the vitreous humor and other deep intraocular structures. It is most commonly exogenous in origin, caused by intraocular surgery, penetrating injury, a corneal ulcer, or periocular infection. Endogenous endophthalmitis occurs when organisms reach the eye hematogenously and accounts for fewer than 6% of all cases of endophthalmitis.5
Klebsiella liver abscesses have been increasing in incidence worldwide and since the mid‐1990s have become a common cause of liver abscess in the United States, along with Escherichia coli. The association with endophthalmitis was first reported in a series of 7 cases from Taiwan in 1986,1 and subsequent East Asian cases have been reported, usually in diabetic patients.6, 7 The association of Klebsiella liver abscesses with endogenous endophthalmitis has been rarely reported in the United States, with review of the literature from 1966 to 2003 revealing only 3 reported cases.2 One of these patients had diabetes, whereas another had beta‐thalassemia with previous splenectomy. Another study looking at only pyogenic liver abscess found biliary disease, hypertension, intraabdominal infection, and diabetes to be the most common underlying or concurrent conditions.8 Our patient did not appear to have any of these risk factors.
Our patient had no known risk factors to promote metastatic spread of the causative organisms. The patient was HIV negative, had no personal or family history of diabetes, and was not found to have elevated glucose levels at any point during admission. Although the ultimate etiology may never be determined, the possibility of undetected malignancy or cardiovascular or inflammatory disease cannot be excluded.
Physicians need to be aware of the global emergence of a hypervirulent strain of K. pneumonia causing liver abscesses and metastatic complications, especially endophthalmitis.9 Mucoviscosity associated gene A (magA) has been found in some liver isolates of K. pneumoniae.10 It has been suggested that as many as one‐third of patients infected with hyperviscous strains of K. pneumoniae will develop an invasive infection.11 Although it is unclear why metastatic endophthalmitis from Klebsiella liver abscess would be more common in East Asia, the magA gene may account for the observed difference. It was not possible to determine if the infectious organism that had infected our patient had the magA gene, although the clinical use of this information may not have changed management because the patient presented with metastatic infection. If this patient's particular organism had tested positive for the magA gene, it might explain why an apparently immunocompetent patient developed metastatic endophthalmitis not simply a liver abscess.
Patients with evidence of endogenous endophthalmitis without clear risk factors should be covered for K. pneumoniae, and extraocular sources should be sought, particularly the liver, even in the absence of diabetes. Early recognition and prompt initiation of antimicrobial therapy is essential if the patient's vision is to be preserved.
- ,,.Klebsiella pneumoniae liver abscess associated with septic endophthalmitis.Arch Intern Med.1986;146:1913–1916.
- ,.Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics.Am J Gastroenterol.2005;100:322–331.
- .Klebsiella pneumoniae liver abscess, endophthalmitis, and meningitis in a man with newly recognized diabetes mellitus.Clin Infect Dis.1999;29:1570–1571.
- ,,.Vitreous and aqueous penetration of orally administered gatifloxacin in humans.Arch Ophthalmol.2003;121:345–350.
- ,,,.Endogenous bacterial endophthalmitis: a 17‐year prospective series and review of 267 reported cases.Surv Ophthalmol.2003;48:403–423.
- ,,, et al.Primary liver abscess due to Klebsiella pneumoniae in Taiwan.Clin Infect Dis.1998;26:1434–1438.
- ,,,,.Septic metastatic lesions of pyogenic liver abscess. Their association with Klebsiella pneumoniae bacteremia in diabetic patients.Arch Intern Med.1991;151:1557–1559.
- ,,,.Pyogenic liver abscess: recent trends in etiology and mortality.Clin Infect Dis.2004;39:1654–1659.
- ,,, et al.A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis?Gut.2002;50:420–424.
- ,,.Liver abscess caused by magA+ Klebsiella pneumoniae in North America.J Clin Microbiol.2005;43:991–992.
- ,,, et al.Clinical implications of hypermucoviscosity phenotype in Klebsiella pneumoniae isolates: association with invasive syndrome in patients with community‐acquired bacteraemia.J Intern Med.2006;259:606–614.
- ,,.Klebsiella pneumoniae liver abscess associated with septic endophthalmitis.Arch Intern Med.1986;146:1913–1916.
- ,.Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics.Am J Gastroenterol.2005;100:322–331.
- .Klebsiella pneumoniae liver abscess, endophthalmitis, and meningitis in a man with newly recognized diabetes mellitus.Clin Infect Dis.1999;29:1570–1571.
- ,,.Vitreous and aqueous penetration of orally administered gatifloxacin in humans.Arch Ophthalmol.2003;121:345–350.
- ,,,.Endogenous bacterial endophthalmitis: a 17‐year prospective series and review of 267 reported cases.Surv Ophthalmol.2003;48:403–423.
- ,,, et al.Primary liver abscess due to Klebsiella pneumoniae in Taiwan.Clin Infect Dis.1998;26:1434–1438.
- ,,,,.Septic metastatic lesions of pyogenic liver abscess. Their association with Klebsiella pneumoniae bacteremia in diabetic patients.Arch Intern Med.1991;151:1557–1559.
- ,,,.Pyogenic liver abscess: recent trends in etiology and mortality.Clin Infect Dis.2004;39:1654–1659.
- ,,, et al.A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis?Gut.2002;50:420–424.
- ,,.Liver abscess caused by magA+ Klebsiella pneumoniae in North America.J Clin Microbiol.2005;43:991–992.
- ,,, et al.Clinical implications of hypermucoviscosity phenotype in Klebsiella pneumoniae isolates: association with invasive syndrome in patients with community‐acquired bacteraemia.J Intern Med.2006;259:606–614.
Measurement of Intraoperative Nerve Conduction Velocities During Anterior Interosseous Nerve Decompression
Dislocation and Instability After Arthroscopic Capsular Release for Refractory Frozen Shoulder
Delayed Rupture of the Flexor Pollicis Longus Tendon After Routine Volar Placement of a T-Plate on the Distal Radius
Acute Calcific Tendinitis of the Hand: 2 Case Reports Involving the Abductor Pollicis Brevis
Traumatic Disruption of Pubis Symphysis With Accompanying Posterior Pelvic Injury After Natural Childbirth
Linezolid‐ and vancomycin‐resistant Enterococcus faecium endocarditis: Successful treatment with tigecycline and daptomycin
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
Enterococci are a leading cause of endocarditis and nosocomial infections. Vancomycin‐resistant enterococci (VRE) emerged in the 1980s and now represent most nosocomial isolates in the United States. The first case of VRE endocarditis was reported in 1996.1 Although increasing enterococcal antibiotic resistance has prompted increasing reliance on newer antibiotics,2 a recent review of VRE endocarditis noted that survival rates were similar to those for vancomycin‐sensitive enterococcal endocarditis.1 Cure was achieved in several patients with bacteriostatic agents in the absence of valve replacement, but no patients were infected with truly linezolid‐resistant organisms. This case of linezolid‐resistant VRE endocarditis represents the first reported cure of infective endocarditis with a tigecycline‐containing regimen.
CASE REPORT
A 62‐year‐old man presented with hypoglycemia and delirium. His medical history included diabetes mellitus, coronary and peripheral arterial disease, and end‐stage renal disease. He had had endocarditis of an unknown type 12 years prior to admission. He had recently developed septic shock because of a Candida parapsilosis, Enterobacter cloacae, and Staphylococcus epidermidis infection of a peripherally inserted central catheter (PICC) and received 14 days of vancomycin, meropenem, and fluconazole administered through a new PICC. This catheter was not removed, and 39 days after completion of the antibiotic therapy, he developed hypoglycemia, which was attributed to weight loss without adjustment of his insulin regimen. He was afebrile; examination revealed a new 3/6 holosystolic murmur radiating to the axilla. There were no other stigmata of infective endocarditis, and his PICC and arteriovenous fistula sites appeared normal. Delirium resolved after administration of intravenous glucose.
E. faecium grew from all 6 initial blood cultures. A transesophageal echocardiogram revealed a new 3‐mm mitral valve vegetation with perforation and severe regurgitation. He had definite endocarditis on the basis of 2 major criteria.3 He was given vancomycin (1 g IV, then administered by levels), then switched to linezolid (600 mg orally every 12 hours), and finally tigecycline (100 mg IV followed by 50 mg IV every 12 hours) plus daptomycin (6 mg/kg IV every 48 hours) as further sensitivity data became available.
The organism was resistant to ampicillin, chloramphenicol, and linezolid (MIC > 20 g/mL), as well as vancomycin (MIC > 50 g/mL), quinupristin/dalfopristin (MIC 2.5 g/mL), and gentamicin (MIC > 200 g/mL), and demonstrated high‐level streptomycin resistance (>2000 g/mL). It was intermediate to doxycycline (MIC 5 g/mL). It was susceptible to daptomycin (MIC 4 g/mL) and tigecycline (MIC 0.06 g/mL).
Blood cultures done on hospital days 1, 4, 6, and 7 (day 1 of tigecycline) were positive, and multiple cultures were negative from day 10 on. Because of the lack of experience with tigecycline in infective endocarditis, unrevascularized left‐main coronary artery disease, and severe mitral regurgitation, the patient was advised to undergo valve replacement and coronary artery bypass surgery after antibiotic therapy. Because he feared surgical complications, he refused and received 70 days of tigecycline plus daptomycin therapy, which was complicated only by nausea. He remained clinically well and had negative blood cultures 16 weeks after completion of therapy.
DISCUSSION
Tigecycline, the first available glycylcycline, is a minocycline‐derived antibiotic that remains active in the presence of the ribosomal modifications and efflux pumps that mediate tetracycline resistance. Thus, it possesses broad‐spectrum bacteriostatic activity, including activity against VRE. A PubMed search revealed no published data about the use of tigecycline for endocarditis in humans. However, tetracyclines have been used to treat endocarditis due to such organisms as Bartonella, Coxiella burnetti, or methicillin‐resistant Staphylococcus aureus (MRSA), frequently for prolonged courses. Tetracyclines were combined with other antibiotics in 5 published cases of VRE endocarditis. All patients survived; 3 were cured with the tetracycline regimen and 2 with other antimicrobials.1 In animal models of endocarditis, tigecycline stabilized vegetation counts of E. faecalis and reduced vegetation counts of MRSA and 1 strain of E. faecium.4
Daptomycin, the first available cyclic lipopeptide, kills by nonlytic depolarization of the bacterial cell membrane. In a recent study, daptomycin was non‐inferior to vancomycin or antistaphylococcal penicillins for S. aureus bacteremia or endocarditis. Although a few patients had left‐sided endocarditis, only 1 of them experienced a successful outcome with daptomycin therapy, and daptomycin displayed a trend toward higher rates of persistent or relapsing infection.5 Less evidence supports the use of daptomycin for serious enterococcal infections.2 One report noted the deaths of 6 of 10 patients treated with daptomycin for VRE bacteremia, including both patients with endocarditis.6 Daptomycin was used successfully in a case of VRE endocarditis in combination with gentamicin and rifampin for 11 weeks1 and at least 6 other reported cases of VRE bacteremia.7, 8
In summary, despite tigecycline's lack of bactericidal activity or proven efficacy in endocarditis, daptomycin's prior performance in VRE bacteremia, and the isolate's borderline daptomycin susceptibility, prolonged combination therapy resulted in a cure of VRE endocarditis. This success extends the experience with using both agents in the treatment of resistant infections. As linezolid‐resistant VRE and other resistant pathogens become more common, the need for research on treatment options becomes more urgent, and familiarity with novel and lesser‐used antibiotics becomes more crucial for hospitalists.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.
- ,.Endocarditis due to vancomycin‐resistant enterococci: case report and review of the literature.Clin Infect Dis.2005;41:1134–1142.
- ,.Approaches to vancomycin resistant enterococci.Curr Opin Infect Dis.2004;17:541–547.
- ,,, et al.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.Clin Infect Dis.2000;4:633–638.
- ,,, et al.Activity and diffusion of tigecycline (GAR‐936) in experimental enterococcal endocarditis.Antimicrob Agents Chemother.2003;47:216–222.
- ,,, et al.Daptomycin versus standard therapy for bacteremia and endocarditis caused by staphylococcus aureus.New Engl J Med.2006;355:653–665.
- ,,.Daptomycin for the treatment of gram‐positive bacteremia and infective endocarditis: a retrospective case series of 31 patients.Pharmacotherapy.2006;26:347–352.
- ,,,,.Daptomycin in the treatment of vancomycin‐resistant Enterococcus faecium bacteremia in neutropenic patients.J Infect.2007;54:567–571.
- ,,,,.Daptomycin for the treatment of vancomycin resistant Enterococcus faecium bacteremia.Scand J Infect Dis.2006;38:290–292.