User login
Tibial Plateau "Kissing Lesion" From a Proud Osteochondral Autograft
Nausea, fever, and weight loss
• Order blood cultures for febrile patients who are suspected IV drug users. Doing so is wise because of the high morbidity and mortality associated with infectious endocarditis.
• Consider the possibility of a false-positive monospot test in patients who have leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, or rubella.
CASE A 27-year-old man came into our emergency department (ED) with a 1½ week history of profound nausea, vomiting, diarrhea, intermittent fevers, and weight loss of 15 pounds. At the urging of his mother, he had recently visited a new family physician to investigate a 3- to 4-month history of fatigue and anorexia. According to the patient, the blood work done by the FP was normal, but since that visit things had gotten worse.
The patient denied any ill contacts or recent travel. He said he had no headache, neck stiffness, sore throat, cough, dysuria, back pain, rash, focal numbness, or weakness. His past medical history was significant for prescription drug abuse, and he was now on buprenorphine and naloxone (Suboxone) treatment. He initially denied IV drug use, but later acknowledged it after the discovery of syringes and heroin among his personal belongings.
On physical exam he appeared cachectic and tremulous. His temperature was 101.4°F; heart rate 139 beats per minute, blood pressure 83/43 mm Hg, and SpO2 93%. His pupils were small, conjunctiva pale, and sclera white. His oropharynx was without lesions. The rest of his physical exam was unremarkable.
Laboratory results in the ED revealed a white blood cell count of 14,600 cells/mcL, platelets 85,000/mcL, hemoglobin 11.8 g/dL, and creatinine 2.04 mg/dL. He had a positive monospot test. We sent out blood and urine cultures, as well as human immunodeficiency virus (HIV) and Epstein-Barr virus (EBV) serologies. Imaging included a chest x-ray, which showed possible nonsegmental or mild perihilar airspace disease.
The patient was admitted to the hospital for sepsis with associated acute kidney injury, dehydration, and weight loss.
Although the patient had a positive monospot test, the severity of the clinical picture did not fully match that of infectious mononucleosis. Also, it seemed curious to us that a high-risk patient would contract EBV for the first time at age 27.
Given the patient’s clinical presentation and the fact that he was an IV drug user, we suspected HIV infection. But an HIV-1 RNA quantitative PCR test came back negative.
What is the Most Likely Explanation for his Condition?
Infectious endocarditis
Our patient was admitted to the telemetry unit, given aggressive IV hydration, and started empirically on vancomycin secondary to the risk for infectious endocarditis (IE). On hospital Day 1, the patient’s blood cultures returned positive for methicillin-sensitive Staphylococcus aureus and an echocardiogram revealed a large tricuspid vegetation (FIGURE 1).
IE is relatively common in IV drug users, affecting up to 2% to 5% of this population each year in the United States.1 Onset of symptoms is usually acute, and in many cases, there is no heart murmur or peripheral stigmata of IE.1
Blood cultures are positive in 69% to 97% of cases of IE,2 with more than 50% caused by S aureus.3 The most common valve infected is the tricuspid valve (30%-70%), especially when related to IV drug use.1 More than half of IV drug users with tricuspid IE will have extracardiac infections, most often occurring in the lungs, bone, kidneys, and brain.3
Because of the high morbidity and mortality associated with IE, physicians caring for febrile patients who are suspected IV drug users should order blood cultures. Three blood draws should be taken, at 30-minute intervals, from separate venipuncture sites.4 Positive cultures should be followed by an echocardiogram to rule out IE. For severely ill patients, empiric antibiotics should be started.4
FIGURE 1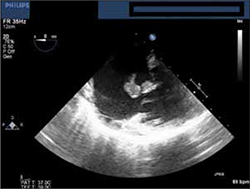
Echocardiogram reveals tricuspid vegetation
Treatment is complicated for IV drug users
Treatment for IE is with IV antibiotics. This can be complicated in the case of an IV drug user, as he or she may be unwilling to remain hospitalized for the duration of treatment. In addition, there are ethical concerns about sending such patients into the community with an indwelling IV.
Cardiac surgery is a possibility. Complications of IE that warrant surgery include repeated septic emboli with large vegetation, heart failure secondary to aortic or mitral-valve regurgitation, persistent fever after 8 days of appropriate antibiotic therapy, infection with certain difficult-to-cure microorganisms, and perivalvular abscess development.5
FIGURE 2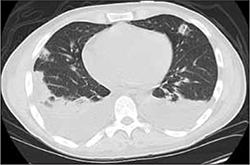
Chest CT shows pulmonary emboli
Successful valve repair for our patient
Our patient’s hospital course was complicated by the development of pulmonary septic emboli (FIGURE 2) and persistent fever. He underwent a successful tricuspid valve repair and was discharged with a peripheral IV to a skilled nursing facility to complete a 6-week course of IV cefazolin.
The cause of the misdirect? We believe the monospot test was either a false-positive result or a persistent positive result from an infection earlier in the year. (False-positives occur rarely, but have been reported in patients with leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, and rubella.6)
Our patient had an uneventful recovery at the skilled nursing facility and returned home after the completion of his antibiotics. The patient was counseled to enter a drug treatment program, but at the time of discharge from the skilled nursing facility, had not made the arrangements.
CORRESPONDENCE
Christopher Bernheisel, MD, Director, Family Medicine Inpatient Service, The University of Cincinnati, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; bernheiseljfp@me.com
1. Sande MA, Lee BL, Mills J, et al. Endocarditis in intravenous drug users. In: Kaye D, ed. Infective endocarditis. 1st ed. New York, NY: Raven Press; 1992:345-359.
2. Cannady PB Jr, Sanford JP. Negative blood cultures in infective endocarditis: a review. South Med J. 1976;69:1420-1424.
3. Mathew J, Addai T, Anand A, et al. Clinical features, site of involvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch Intern Med. 1995;155:1641-1648.
4. Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis of the European Society of Cardiology. Eur Heart J. 2009;30:2369-2413.
5. Horstkotte D, Follath F, Gutschik E, et al. Guidelines on prevention, diagnosis and treatment of infective endocarditis executive summary; the task force on infective endocarditis of the European Society of Cardiology. Eur Heart J. 2004;25:267-276.
6. Schumacher HR, Austin RM, Stass SA. False-positive serology in infectious mononucleosis. Lancet. 1979;1:722.
• Order blood cultures for febrile patients who are suspected IV drug users. Doing so is wise because of the high morbidity and mortality associated with infectious endocarditis.
• Consider the possibility of a false-positive monospot test in patients who have leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, or rubella.
CASE A 27-year-old man came into our emergency department (ED) with a 1½ week history of profound nausea, vomiting, diarrhea, intermittent fevers, and weight loss of 15 pounds. At the urging of his mother, he had recently visited a new family physician to investigate a 3- to 4-month history of fatigue and anorexia. According to the patient, the blood work done by the FP was normal, but since that visit things had gotten worse.
The patient denied any ill contacts or recent travel. He said he had no headache, neck stiffness, sore throat, cough, dysuria, back pain, rash, focal numbness, or weakness. His past medical history was significant for prescription drug abuse, and he was now on buprenorphine and naloxone (Suboxone) treatment. He initially denied IV drug use, but later acknowledged it after the discovery of syringes and heroin among his personal belongings.
On physical exam he appeared cachectic and tremulous. His temperature was 101.4°F; heart rate 139 beats per minute, blood pressure 83/43 mm Hg, and SpO2 93%. His pupils were small, conjunctiva pale, and sclera white. His oropharynx was without lesions. The rest of his physical exam was unremarkable.
Laboratory results in the ED revealed a white blood cell count of 14,600 cells/mcL, platelets 85,000/mcL, hemoglobin 11.8 g/dL, and creatinine 2.04 mg/dL. He had a positive monospot test. We sent out blood and urine cultures, as well as human immunodeficiency virus (HIV) and Epstein-Barr virus (EBV) serologies. Imaging included a chest x-ray, which showed possible nonsegmental or mild perihilar airspace disease.
The patient was admitted to the hospital for sepsis with associated acute kidney injury, dehydration, and weight loss.
Although the patient had a positive monospot test, the severity of the clinical picture did not fully match that of infectious mononucleosis. Also, it seemed curious to us that a high-risk patient would contract EBV for the first time at age 27.
Given the patient’s clinical presentation and the fact that he was an IV drug user, we suspected HIV infection. But an HIV-1 RNA quantitative PCR test came back negative.
What is the Most Likely Explanation for his Condition?
Infectious endocarditis
Our patient was admitted to the telemetry unit, given aggressive IV hydration, and started empirically on vancomycin secondary to the risk for infectious endocarditis (IE). On hospital Day 1, the patient’s blood cultures returned positive for methicillin-sensitive Staphylococcus aureus and an echocardiogram revealed a large tricuspid vegetation (FIGURE 1).
IE is relatively common in IV drug users, affecting up to 2% to 5% of this population each year in the United States.1 Onset of symptoms is usually acute, and in many cases, there is no heart murmur or peripheral stigmata of IE.1
Blood cultures are positive in 69% to 97% of cases of IE,2 with more than 50% caused by S aureus.3 The most common valve infected is the tricuspid valve (30%-70%), especially when related to IV drug use.1 More than half of IV drug users with tricuspid IE will have extracardiac infections, most often occurring in the lungs, bone, kidneys, and brain.3
Because of the high morbidity and mortality associated with IE, physicians caring for febrile patients who are suspected IV drug users should order blood cultures. Three blood draws should be taken, at 30-minute intervals, from separate venipuncture sites.4 Positive cultures should be followed by an echocardiogram to rule out IE. For severely ill patients, empiric antibiotics should be started.4
FIGURE 1
Echocardiogram reveals tricuspid vegetation
Treatment is complicated for IV drug users
Treatment for IE is with IV antibiotics. This can be complicated in the case of an IV drug user, as he or she may be unwilling to remain hospitalized for the duration of treatment. In addition, there are ethical concerns about sending such patients into the community with an indwelling IV.
Cardiac surgery is a possibility. Complications of IE that warrant surgery include repeated septic emboli with large vegetation, heart failure secondary to aortic or mitral-valve regurgitation, persistent fever after 8 days of appropriate antibiotic therapy, infection with certain difficult-to-cure microorganisms, and perivalvular abscess development.5
FIGURE 2
Chest CT shows pulmonary emboli
Successful valve repair for our patient
Our patient’s hospital course was complicated by the development of pulmonary septic emboli (FIGURE 2) and persistent fever. He underwent a successful tricuspid valve repair and was discharged with a peripheral IV to a skilled nursing facility to complete a 6-week course of IV cefazolin.
The cause of the misdirect? We believe the monospot test was either a false-positive result or a persistent positive result from an infection earlier in the year. (False-positives occur rarely, but have been reported in patients with leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, and rubella.6)
Our patient had an uneventful recovery at the skilled nursing facility and returned home after the completion of his antibiotics. The patient was counseled to enter a drug treatment program, but at the time of discharge from the skilled nursing facility, had not made the arrangements.
CORRESPONDENCE
Christopher Bernheisel, MD, Director, Family Medicine Inpatient Service, The University of Cincinnati, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; bernheiseljfp@me.com
• Order blood cultures for febrile patients who are suspected IV drug users. Doing so is wise because of the high morbidity and mortality associated with infectious endocarditis.
• Consider the possibility of a false-positive monospot test in patients who have leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, or rubella.
CASE A 27-year-old man came into our emergency department (ED) with a 1½ week history of profound nausea, vomiting, diarrhea, intermittent fevers, and weight loss of 15 pounds. At the urging of his mother, he had recently visited a new family physician to investigate a 3- to 4-month history of fatigue and anorexia. According to the patient, the blood work done by the FP was normal, but since that visit things had gotten worse.
The patient denied any ill contacts or recent travel. He said he had no headache, neck stiffness, sore throat, cough, dysuria, back pain, rash, focal numbness, or weakness. His past medical history was significant for prescription drug abuse, and he was now on buprenorphine and naloxone (Suboxone) treatment. He initially denied IV drug use, but later acknowledged it after the discovery of syringes and heroin among his personal belongings.
On physical exam he appeared cachectic and tremulous. His temperature was 101.4°F; heart rate 139 beats per minute, blood pressure 83/43 mm Hg, and SpO2 93%. His pupils were small, conjunctiva pale, and sclera white. His oropharynx was without lesions. The rest of his physical exam was unremarkable.
Laboratory results in the ED revealed a white blood cell count of 14,600 cells/mcL, platelets 85,000/mcL, hemoglobin 11.8 g/dL, and creatinine 2.04 mg/dL. He had a positive monospot test. We sent out blood and urine cultures, as well as human immunodeficiency virus (HIV) and Epstein-Barr virus (EBV) serologies. Imaging included a chest x-ray, which showed possible nonsegmental or mild perihilar airspace disease.
The patient was admitted to the hospital for sepsis with associated acute kidney injury, dehydration, and weight loss.
Although the patient had a positive monospot test, the severity of the clinical picture did not fully match that of infectious mononucleosis. Also, it seemed curious to us that a high-risk patient would contract EBV for the first time at age 27.
Given the patient’s clinical presentation and the fact that he was an IV drug user, we suspected HIV infection. But an HIV-1 RNA quantitative PCR test came back negative.
What is the Most Likely Explanation for his Condition?
Infectious endocarditis
Our patient was admitted to the telemetry unit, given aggressive IV hydration, and started empirically on vancomycin secondary to the risk for infectious endocarditis (IE). On hospital Day 1, the patient’s blood cultures returned positive for methicillin-sensitive Staphylococcus aureus and an echocardiogram revealed a large tricuspid vegetation (FIGURE 1).
IE is relatively common in IV drug users, affecting up to 2% to 5% of this population each year in the United States.1 Onset of symptoms is usually acute, and in many cases, there is no heart murmur or peripheral stigmata of IE.1
Blood cultures are positive in 69% to 97% of cases of IE,2 with more than 50% caused by S aureus.3 The most common valve infected is the tricuspid valve (30%-70%), especially when related to IV drug use.1 More than half of IV drug users with tricuspid IE will have extracardiac infections, most often occurring in the lungs, bone, kidneys, and brain.3
Because of the high morbidity and mortality associated with IE, physicians caring for febrile patients who are suspected IV drug users should order blood cultures. Three blood draws should be taken, at 30-minute intervals, from separate venipuncture sites.4 Positive cultures should be followed by an echocardiogram to rule out IE. For severely ill patients, empiric antibiotics should be started.4
FIGURE 1
Echocardiogram reveals tricuspid vegetation
Treatment is complicated for IV drug users
Treatment for IE is with IV antibiotics. This can be complicated in the case of an IV drug user, as he or she may be unwilling to remain hospitalized for the duration of treatment. In addition, there are ethical concerns about sending such patients into the community with an indwelling IV.
Cardiac surgery is a possibility. Complications of IE that warrant surgery include repeated septic emboli with large vegetation, heart failure secondary to aortic or mitral-valve regurgitation, persistent fever after 8 days of appropriate antibiotic therapy, infection with certain difficult-to-cure microorganisms, and perivalvular abscess development.5
FIGURE 2
Chest CT shows pulmonary emboli
Successful valve repair for our patient
Our patient’s hospital course was complicated by the development of pulmonary septic emboli (FIGURE 2) and persistent fever. He underwent a successful tricuspid valve repair and was discharged with a peripheral IV to a skilled nursing facility to complete a 6-week course of IV cefazolin.
The cause of the misdirect? We believe the monospot test was either a false-positive result or a persistent positive result from an infection earlier in the year. (False-positives occur rarely, but have been reported in patients with leukemia, lymphoma, pancreatic cancer, systemic lupus erythematosus, HIV infection, and rubella.6)
Our patient had an uneventful recovery at the skilled nursing facility and returned home after the completion of his antibiotics. The patient was counseled to enter a drug treatment program, but at the time of discharge from the skilled nursing facility, had not made the arrangements.
CORRESPONDENCE
Christopher Bernheisel, MD, Director, Family Medicine Inpatient Service, The University of Cincinnati, 2123 Auburn Avenue, Suite 340, Cincinnati, OH 45219; bernheiseljfp@me.com
1. Sande MA, Lee BL, Mills J, et al. Endocarditis in intravenous drug users. In: Kaye D, ed. Infective endocarditis. 1st ed. New York, NY: Raven Press; 1992:345-359.
2. Cannady PB Jr, Sanford JP. Negative blood cultures in infective endocarditis: a review. South Med J. 1976;69:1420-1424.
3. Mathew J, Addai T, Anand A, et al. Clinical features, site of involvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch Intern Med. 1995;155:1641-1648.
4. Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis of the European Society of Cardiology. Eur Heart J. 2009;30:2369-2413.
5. Horstkotte D, Follath F, Gutschik E, et al. Guidelines on prevention, diagnosis and treatment of infective endocarditis executive summary; the task force on infective endocarditis of the European Society of Cardiology. Eur Heart J. 2004;25:267-276.
6. Schumacher HR, Austin RM, Stass SA. False-positive serology in infectious mononucleosis. Lancet. 1979;1:722.
1. Sande MA, Lee BL, Mills J, et al. Endocarditis in intravenous drug users. In: Kaye D, ed. Infective endocarditis. 1st ed. New York, NY: Raven Press; 1992:345-359.
2. Cannady PB Jr, Sanford JP. Negative blood cultures in infective endocarditis: a review. South Med J. 1976;69:1420-1424.
3. Mathew J, Addai T, Anand A, et al. Clinical features, site of involvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch Intern Med. 1995;155:1641-1648.
4. Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis of the European Society of Cardiology. Eur Heart J. 2009;30:2369-2413.
5. Horstkotte D, Follath F, Gutschik E, et al. Guidelines on prevention, diagnosis and treatment of infective endocarditis executive summary; the task force on infective endocarditis of the European Society of Cardiology. Eur Heart J. 2004;25:267-276.
6. Schumacher HR, Austin RM, Stass SA. False-positive serology in infectious mononucleosis. Lancet. 1979;1:722.
A case of lung cancer and hypercoagulability, complicated by suspected heparin-induced thrombocytopenia
Heparin-induced thrombocytopenia (HIT) is a life-threatening disorder that follows exposure to unfractionated heparin or (less commonly) low-molecular-weight heparin (LMWH). Patients classically present with a low platelet count (< 150,000 cells/mm3) or a relative decrease of 50% or more from baseline, although the fall may be less (eg, 30%–40%) in some patients.Thrombotic complications develop in approximately 20%–50% of patients.
HIT is caused by antibodies against complexes of platelet factor 4 and heparin.These antibodies are present in nearly all patients who receive a clinical diagnosis of the disorder and are also known to cause disease in animals.However,they are also present in many patients who have been exposed to heparin in various clinical settings but who do not develop clinical manifestations. It is uncertain why complications occur in some patients but not in others.1 We present a 73-year-old man who developed thrombocytopenia after starting LMWH and who has newly diagnosed adenocarcinoma of the lungs with extensive arterial and venous thrombosis and a negative serology for HIT.
Case presentation
A 73-year-old man presented to the emergency department after waking up in the morning with right-sided vague weakness and an inability to get out of bed. He had a history of right parietal stroke 1 month before the current presentation, when he was diagnosed with an aortic arch atheroma and started on warfarin. (At that time, CT scan of the head showed a right posterior temporoparietal lobe infarct in the posterior right middle cerebral artery distribution, and MRI of the brain and magnetic resonance angiography showed acute or subacute infarction in the distribution of the posterior division of the right middle cerebral artery, likely embolic, and tiny acute infarctions in the left frontal lobe.) This patient had been admitted 5 days prior to the current presentation for right lower extremity deep vein thrombosis (DVT) and was discharged after being prescribed enoxaparin (60 mg subcutaneously every 12 hours) and warfarin as per international normalized ratio (INR) daily.
Also included in the medical history was supraventricular tachycardia status post ablation, non–ST elevation myocardial infarction (NSTEMI), hypertension, hyperlipidemia, and macular degeneration. He had no surgical history. The patient had a family history of coronary artery disease. He had an extensive smoking history up until the day of admission. His medications on admission included atorvastatin (Lipitor; 20 mg daily), warfarin daily as per INR, enoxaparin (60 mg subcutaneously every 12 hours), amlodipine (5 mg daily), and aspirin (81 mg daily).
Pertinent initial laboratory results on admission were as follows: hemoglobin, 12.9 g/dL; white blood cell count, 8.6 ×109/L; platelet count, 183,000 cells/ mm3; INR, 1.2; and initial troponin level, negative.His admission chest x-ray showed a 4.5 cm × 5.5 cm lobulated density in the right hilum, suspicious for a hilar or subcarinal mass. Initial peripheral blood smear showed an isolated platelet decrease with increased size and no schistocytes. Initial CT of the head on admission showed no evidence of acute transcortical infarction and no definite evidence of acute intracranial hemorrhage but did show interval evolution of the right middle cerebral artery and left watershed distribution infarctions, with a probable small region of laminar necrosis in the right parietal lobe.
Clinical Course
The patient was initially thought to have had a transient ischemic attack causing aphasia, confusion, and rightsided weakness. He was started on therapeutic anticoagulation with dalteparin (Fragmin; 12,000 U subcutaneously daily),and enoxaparin was discontinued. The following day,his platelet count was 86,000 cells/mm3,down from an admission platelet count of 183,000 cells/mm3. A subsequent MRI of the brain showed a new hemorrhagic area in the right parietal infarct. The decision was made to stop anticoagulation, even though he had an embolic source from his aortic arch atheroma and lower extremity DVT.
The patient then underwent inferior vena cava (IVC) filter placement to prevent pulmonary thromboembolism and was transferred to the medical service due to low platelet count and an episode of nine beats of ventricular tachycardia. Subsequently, his troponin level was found to be elevated > 12 ng/mL, without significant electrocardiographic changes. He was diagnosed as having NSTEMI. Given his conversion from an ischemic to hemorrhagic CNS infarct and decrease in platelet count after LMWH exposure, HIT became a concern, and both anticoagulation and antiplatelet agents were held. The patient’s platelet count continued to trend downward over the next 3 days to a low of 27,000 cells/mm3. An HIT panel was negative by both immunologic and functional assays.
A CT scan of the brain 3 days after admission to monitor the hemorrhagic infarct showed multiple evolving infarcts and a new left occipital hemorrhagic infarct. The following day, a repeat CT scan of the head showed mulatiple evolving infarcts of varying ages, some with hemorrhage, and a mild interval increase in the previously described left medial parietal and left occipital lobe infarcts.
With worsening of his hemorrhagic infarct, along with his low platelet count and negative HIT panel,the decision was made to transfuse 2 units of platelets. His platelet count increased to 64,000 cells/mm3 after transfusion, subsequently dropping to 44,000 cells/mm3. However, during this time, the patient began to have worsening right lower extremity pain and left upper quadrant abdominal pain.
A CT scan of the thorax showed multifocal right hilar adenopathy suspicious for malignancy, either metastatic or representing a central lung carcinoma. It also showed nonocclusive segmental and possibly subsegmental pulmonary emboli in the right lower and middle lobes, as well as hypodense areas in the spleen, suggestive of areas of splenic infarction. Echocardiography showed an ejection fraction of 60%–70%, diastolic dysfunction, mildly elevated pulmonary artery pressure, and no evidence of patent foramen ovale.A cardiac stress test showed no reversible defects and an ejection fraction of 63%.
Risk of further bleeding into the brain was thought to be too great to initiate anticoagulation despite the CT thorax findings. The neurologist recommended waiting 2 weeks post hemorrhagic infarction before beginning anticoagulation. Antiphospholipid antibody syndrome was ruled out, with a negative lupus anticoagulant and anticardiolipin antibody. Also, negative blood cultures, normal fibrinogen levels, and normal haptoglobin levels ruled out disseminated intravascular coagulation. D-dimer was elevated but nonspecific, secondary to malignancy and multiple infarcts. He was started on aspirin (81 mg daily) 9 days after admission.
The patient had a repeat CT scan of the thorax and CT scan of the abdomen and pelvis due to continued abdominal pain. The CT scans showed multiple subsegmental pulmonary emboli, greatest in the right lower lobe, some of which were new since the prior study; continued evidence of multifocal splenic infarction (Figure 3); and multiple right and left kidney infarcts.
The patient then underwent endobronchial ultrasound (EBUS)-guided biopsy of his right hilar adenopathy to confirm the diagnosis of suspected malignancy. After the procedure, he developed right upper quadrant pleuritic pain with a low-grade fever. A repeat CT scan of the thorax showed a marked increase in the extent of the right lower lobe pulmonary emboli, with a new small embolus noted in the anterior segment of the right upper lobe. There was a thrombus inferior to the IVC filter, with probable mild extension of a thrombus superior to the filter as well, and again multiple splenic and bilateral renal infarcts.
With progression of thrombosis and now post EBUS, anticoagulation was initiated with argatroban and warfarin. His D-dimer was followed daily and remained high, despite therapeutic anticoagulation with warfarin. Given the persistently elevated D-dimer, the hematologist recommended discontinuing warfarin and starting fondaparinux (Arixtra) subcutaneously. His platelet count improved to a range of 156,000 cells/mm3 to 181,000 cells/mm3, even before the initiation of chemotherapy.
Follow-up
HIT was suspected clinically by classic drop in platelet count but was negative on enzyme-linked immunosorbent assay (ELISA) and serotonin release assay (SRA). The patient has been maintained on fondaparinux for anticoagulation, avoiding heparin. Factor V Leiden and lupus anticoagulant were negative.
Fondaparinux was discontinued after 3 months, and the patient presented again with swelling of his right lower extremity. Ultrasonography of the right lower extremity redemonstrated an occlusive thrombus in the peripheral portion of the right femoaral vein and throughout the right peroneal vein. The patient was restarted on fondaparinux (7.5 mg subcutaneously daily). During this follow-up, his platelet count ranged from 134,000 cells/mm3 to 193,000 cells/mm3.
Regarding management of nonsmall cell lung carcinoma of the left upper lobe (stains positive for TTF- 1 [thyroid transcription factor-1], CK7, and CK20; weakly positive for CK5/6; and negative for P63) with metastasis to bone and adrenal glands, he received 4 cycles of paclitaxel/carboplatin, with improved disease. A repeat CT of the chest, abdomen, and pelvis after chemotherapy showed improvement in mediastinal and hilar lymphadenopathy, resolution of extensive right lower lobe pulmonary consolidation, resolution of right-sided effusion, and no evidence of metastatic malignancy in the abdomen or pelvis and no osseous metastasis.
He was started on maintenance therapy with pemetrexed (Alimta), which was continued for 4 months, until repeat CT revealed progressive disease. He then received 4 cycles of vinorelbine. He had progression-free survival of 7 months from first-line chemotherapy and stable disease for 7 months after 4 cycles of vinorelbine.
Discussion
In summary, we have a 73-year-old man admitted with a hemorrhagbic infarct, NSTEMI, and recently diagnosed right lower extremity DVT with a decreasing platelet count in the setting of LMWH. Throughout the hospital course, he had worsening hemorrhagic infarcts, preventing proper anticoagulation for his progressive thromboembolic events in the lungs, spleen, kidneys, and legs. Incidentally, he was also found to have a mass on a chest x-ray, later identified by biopsy as adenocarcinoma.
Given that the 4T scoring system for HIT showed a high probability with 8 points—identified by a platelet count fall > 50%, a platelet nadir > 20,000 cells/mm3, clear onset between days 5 and 14 with exposure to heparin/LMWH, new thrombosis, and no apparent cause of thrombocytopenia—suspicion for HIT remained high. Both functional and immunologic assays were negative for HIT, when repeated 2 weeks apart. The assays for laboratory diagnosis of HIT are immunologic, done by ELISA with a sensitivity of > 95% and a specificity of 50%–89%, and functional, done by SRA with a sensitivity > 90% and a specificity > 90%.2 As neither assay is 100% sensitive and specific, we still had a high clinical suspicion for HIT.
The HIT diagnostics in the presence of other comorbid states that may also induce thrombocytopenia represent a specific clinical problem. Despite increasing awareness of the clinical features of HIT, laboratory detection of the pathogenic HIT antibodies remains central to diagnosis. 4–6 This is because thrombocytopenia during heparin anticoagulation does not necessarily indicate HIT. Indeed, several other disorders complicated by thrombosis and thrombocytopenia during or shortly following heparin treatment strongly resemble HIT.These “pseudo-HIT”disorders7,8 (eg, cancer, sepsis, disseminated intravascular coagulation, pulmonary embolism, antiphospholipid syndrome) can reliably be distinguished from HIT by negative results using sensitive tests for HIT antibodies.
Thrombosis is strongly associated with HIT, with an incidence of 50%– 67%.9,10 The most common complication of HIT is venous thrombosis (DVT being the most frequent, followed by pulmonary embolism).9,11 Arterial thrombosis commonly presents as limb ischemia followed by cerebral vascular accident and myocardial infarction. Our patient had DVT followed by NSTEMI, cerebral vascular accident, and pulmonary embolism. He also had splenic and renal infarctions, which are rare in HIT. A literature review revealed, in abstract form, a retrospective study from a single institution showing a high incidence of thrombosis in a patient with a high 4T score and negative SRAs.12
The most common causes of thrombocytopenia in cancer are related to cancer treatment and bone marrow invasion by tumor cells. Chemotherapy and radiation therapy are damaging to the bone marrow and can cause severe myelosuppression, which results in lowering of platelet counts as well as white and red blood cell counts. It commonly occurs in patients with leukemia and lymphoma, but there are many other cancer types that can spread to bone marrow. Other causes of thrombocytopenia in cancer include the syndrome of disseminated intravascular coagulation and thrombotic microangiopathy.13
Nonbacterial thrombotic endocarditis (NBTE) is a disease characterized by the presence of vegetations on cardiac valves, consisting of fibrin and platelet aggregates devoid of inflammation or bacteria. NBTE has increasingly been recognized as a condition associated with numerous diseases and a potentially life-threatening source of thromboembolism. NBTE is not a common entity; however, it is frequently underestimated, probably due to underlying diseases (cancer, autoimmune disorders, HIV). NBTE is difficult to diagnose and relies on strong clinical suspicion. NBTE is also difficult to manage, and each case should be individually managed by identifying and treating the underlying pathology.14 Even though our patient had thromboembolism, there was no evidence of vegetations on cardiac valves by transthoracic or transesophageal echocardiography.
Trousseau’s syndrome is a paraneoplastic syndrome characterized by hypercoagulability related to malignancy. Coagulation abnormalities may include disseminated intravascular coagulation, pulmonary embolism, various types of gangrene, thrombotic endocarditis, arterial thrombosis, and embolic stoke.15 We considered this with our patient; however, a literature review showed no cases of Trousseau’s syndrome associated with thrombocytopenia, although concurrent Trousseau’s syndrome and HIT could not be excluded.
In summary, we need to consider all the above differential diagnoses in a patient presenting with thrombocytopenia and thrombosis. Treatment relies on clinical correlation of all the findings and supporting data.
1. Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. N Engl J Med 2006;355:809–817.
2. Cuker A, Crowther MA. 2009 Clinical Practice Guideline on the Evaluation andManagement of Heparin-Induced Thrombocytopenia (HIT). American Society of Hematology Quick Reference. http://www.hematology. org/Practice/Guidelines/2934.aspx. Accessed May 6, 2011.
3. Antonijevic NM, Radovanovic N, Obradovic S, et al. Obstacles in the diagnostics and therapy of heparin-induced thrombocytopenia. Srp Arh Celok Lek 2010;138(suppl 1):69–73.
4. Warkentin TE, Chong BH, Greinacher A.Heparin induced thrombocytopenia: towards consensus. Thromb Haemost 1998;79:1–7.
5. Warkentin TE. Heparin-induced thrombocytopenia: a clinicopathologic syndrome.
Thromb Haemost 1999; 82:439–447. 6. Warkentin TE, Greinacher A. Laboratory testing for heparin-induced thrombocytopenia.J Thromb Thrombolysis 2000:10(suppl 1):35–45.
7. Warkentin TE. Pseudo-heparin-induced thrombocytopenia. In: Warkentin TE, Greinacher A, eds. Heparin-Induced Thrombocytopenia. New York: Marcel Dekker, Inc.; 2000:245–260.
8. Warkentin TE. Venous limb gangrene (VLG) complicating warfarin treatment of deep-vein thrombosis (DVT) in metastatic carcinoma (abstract). Blood 1999;94(suppl 1):114b.
9. Warkentin TE, Kelton JG. A 14-year study of heparin-induced thrombocytopenia. Am J Med 1996;101:502–507.
10. Greinacher A, Volpe H, Janssens U, et al. Recombinant hirudin (lepirudin) provides safe and effective anticoagulation in patients with heparin-induced thrombocytopenia: a prospective study. Circulation 1999;99:73–80.
11. Nand S, Wong W, Yuen B, et al. Heparin induced thrombocytopenia with thrombosis: incidence, analysis of risk factors, and clinical outcomes in 108 consecutive patients treated at a single institution. Am J Hematol 1997;56:12–16.
12. Hueser C, Patel AJ, Allan JN. Incidence of thrombosis in serotonin release assay negative patients and correlation with pretest heparin- induced thrombocytopenia scoring system. Blood 2008;112:1816.
13. Prandoni P, Falanga A, Piccioli A. Cancer, thrombosis and heparin-induced thrombocytopenia. Thromb Res 2007;120(suppl 2):S137–S140.
14. Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis. Eur J Cardiothoracic Surg 2007;32:696– 701.
15. Lim BR, Henry DH. Stroke syndrome secondary to hypercoagulability of lung cancer. Commun Oncol 2008;5:595–596.
Heparin-induced thrombocytopenia (HIT) is a life-threatening disorder that follows exposure to unfractionated heparin or (less commonly) low-molecular-weight heparin (LMWH). Patients classically present with a low platelet count (< 150,000 cells/mm3) or a relative decrease of 50% or more from baseline, although the fall may be less (eg, 30%–40%) in some patients.Thrombotic complications develop in approximately 20%–50% of patients.
HIT is caused by antibodies against complexes of platelet factor 4 and heparin.These antibodies are present in nearly all patients who receive a clinical diagnosis of the disorder and are also known to cause disease in animals.However,they are also present in many patients who have been exposed to heparin in various clinical settings but who do not develop clinical manifestations. It is uncertain why complications occur in some patients but not in others.1 We present a 73-year-old man who developed thrombocytopenia after starting LMWH and who has newly diagnosed adenocarcinoma of the lungs with extensive arterial and venous thrombosis and a negative serology for HIT.
Case presentation
A 73-year-old man presented to the emergency department after waking up in the morning with right-sided vague weakness and an inability to get out of bed. He had a history of right parietal stroke 1 month before the current presentation, when he was diagnosed with an aortic arch atheroma and started on warfarin. (At that time, CT scan of the head showed a right posterior temporoparietal lobe infarct in the posterior right middle cerebral artery distribution, and MRI of the brain and magnetic resonance angiography showed acute or subacute infarction in the distribution of the posterior division of the right middle cerebral artery, likely embolic, and tiny acute infarctions in the left frontal lobe.) This patient had been admitted 5 days prior to the current presentation for right lower extremity deep vein thrombosis (DVT) and was discharged after being prescribed enoxaparin (60 mg subcutaneously every 12 hours) and warfarin as per international normalized ratio (INR) daily.
Also included in the medical history was supraventricular tachycardia status post ablation, non–ST elevation myocardial infarction (NSTEMI), hypertension, hyperlipidemia, and macular degeneration. He had no surgical history. The patient had a family history of coronary artery disease. He had an extensive smoking history up until the day of admission. His medications on admission included atorvastatin (Lipitor; 20 mg daily), warfarin daily as per INR, enoxaparin (60 mg subcutaneously every 12 hours), amlodipine (5 mg daily), and aspirin (81 mg daily).
Pertinent initial laboratory results on admission were as follows: hemoglobin, 12.9 g/dL; white blood cell count, 8.6 ×109/L; platelet count, 183,000 cells/ mm3; INR, 1.2; and initial troponin level, negative.His admission chest x-ray showed a 4.5 cm × 5.5 cm lobulated density in the right hilum, suspicious for a hilar or subcarinal mass. Initial peripheral blood smear showed an isolated platelet decrease with increased size and no schistocytes. Initial CT of the head on admission showed no evidence of acute transcortical infarction and no definite evidence of acute intracranial hemorrhage but did show interval evolution of the right middle cerebral artery and left watershed distribution infarctions, with a probable small region of laminar necrosis in the right parietal lobe.
Clinical Course
The patient was initially thought to have had a transient ischemic attack causing aphasia, confusion, and rightsided weakness. He was started on therapeutic anticoagulation with dalteparin (Fragmin; 12,000 U subcutaneously daily),and enoxaparin was discontinued. The following day,his platelet count was 86,000 cells/mm3,down from an admission platelet count of 183,000 cells/mm3. A subsequent MRI of the brain showed a new hemorrhagic area in the right parietal infarct. The decision was made to stop anticoagulation, even though he had an embolic source from his aortic arch atheroma and lower extremity DVT.
The patient then underwent inferior vena cava (IVC) filter placement to prevent pulmonary thromboembolism and was transferred to the medical service due to low platelet count and an episode of nine beats of ventricular tachycardia. Subsequently, his troponin level was found to be elevated > 12 ng/mL, without significant electrocardiographic changes. He was diagnosed as having NSTEMI. Given his conversion from an ischemic to hemorrhagic CNS infarct and decrease in platelet count after LMWH exposure, HIT became a concern, and both anticoagulation and antiplatelet agents were held. The patient’s platelet count continued to trend downward over the next 3 days to a low of 27,000 cells/mm3. An HIT panel was negative by both immunologic and functional assays.
A CT scan of the brain 3 days after admission to monitor the hemorrhagic infarct showed multiple evolving infarcts and a new left occipital hemorrhagic infarct. The following day, a repeat CT scan of the head showed mulatiple evolving infarcts of varying ages, some with hemorrhage, and a mild interval increase in the previously described left medial parietal and left occipital lobe infarcts.
With worsening of his hemorrhagic infarct, along with his low platelet count and negative HIT panel,the decision was made to transfuse 2 units of platelets. His platelet count increased to 64,000 cells/mm3 after transfusion, subsequently dropping to 44,000 cells/mm3. However, during this time, the patient began to have worsening right lower extremity pain and left upper quadrant abdominal pain.
A CT scan of the thorax showed multifocal right hilar adenopathy suspicious for malignancy, either metastatic or representing a central lung carcinoma. It also showed nonocclusive segmental and possibly subsegmental pulmonary emboli in the right lower and middle lobes, as well as hypodense areas in the spleen, suggestive of areas of splenic infarction. Echocardiography showed an ejection fraction of 60%–70%, diastolic dysfunction, mildly elevated pulmonary artery pressure, and no evidence of patent foramen ovale.A cardiac stress test showed no reversible defects and an ejection fraction of 63%.
Risk of further bleeding into the brain was thought to be too great to initiate anticoagulation despite the CT thorax findings. The neurologist recommended waiting 2 weeks post hemorrhagic infarction before beginning anticoagulation. Antiphospholipid antibody syndrome was ruled out, with a negative lupus anticoagulant and anticardiolipin antibody. Also, negative blood cultures, normal fibrinogen levels, and normal haptoglobin levels ruled out disseminated intravascular coagulation. D-dimer was elevated but nonspecific, secondary to malignancy and multiple infarcts. He was started on aspirin (81 mg daily) 9 days after admission.
The patient had a repeat CT scan of the thorax and CT scan of the abdomen and pelvis due to continued abdominal pain. The CT scans showed multiple subsegmental pulmonary emboli, greatest in the right lower lobe, some of which were new since the prior study; continued evidence of multifocal splenic infarction (Figure 3); and multiple right and left kidney infarcts.
The patient then underwent endobronchial ultrasound (EBUS)-guided biopsy of his right hilar adenopathy to confirm the diagnosis of suspected malignancy. After the procedure, he developed right upper quadrant pleuritic pain with a low-grade fever. A repeat CT scan of the thorax showed a marked increase in the extent of the right lower lobe pulmonary emboli, with a new small embolus noted in the anterior segment of the right upper lobe. There was a thrombus inferior to the IVC filter, with probable mild extension of a thrombus superior to the filter as well, and again multiple splenic and bilateral renal infarcts.
With progression of thrombosis and now post EBUS, anticoagulation was initiated with argatroban and warfarin. His D-dimer was followed daily and remained high, despite therapeutic anticoagulation with warfarin. Given the persistently elevated D-dimer, the hematologist recommended discontinuing warfarin and starting fondaparinux (Arixtra) subcutaneously. His platelet count improved to a range of 156,000 cells/mm3 to 181,000 cells/mm3, even before the initiation of chemotherapy.
Follow-up
HIT was suspected clinically by classic drop in platelet count but was negative on enzyme-linked immunosorbent assay (ELISA) and serotonin release assay (SRA). The patient has been maintained on fondaparinux for anticoagulation, avoiding heparin. Factor V Leiden and lupus anticoagulant were negative.
Fondaparinux was discontinued after 3 months, and the patient presented again with swelling of his right lower extremity. Ultrasonography of the right lower extremity redemonstrated an occlusive thrombus in the peripheral portion of the right femoaral vein and throughout the right peroneal vein. The patient was restarted on fondaparinux (7.5 mg subcutaneously daily). During this follow-up, his platelet count ranged from 134,000 cells/mm3 to 193,000 cells/mm3.
Regarding management of nonsmall cell lung carcinoma of the left upper lobe (stains positive for TTF- 1 [thyroid transcription factor-1], CK7, and CK20; weakly positive for CK5/6; and negative for P63) with metastasis to bone and adrenal glands, he received 4 cycles of paclitaxel/carboplatin, with improved disease. A repeat CT of the chest, abdomen, and pelvis after chemotherapy showed improvement in mediastinal and hilar lymphadenopathy, resolution of extensive right lower lobe pulmonary consolidation, resolution of right-sided effusion, and no evidence of metastatic malignancy in the abdomen or pelvis and no osseous metastasis.
He was started on maintenance therapy with pemetrexed (Alimta), which was continued for 4 months, until repeat CT revealed progressive disease. He then received 4 cycles of vinorelbine. He had progression-free survival of 7 months from first-line chemotherapy and stable disease for 7 months after 4 cycles of vinorelbine.
Discussion
In summary, we have a 73-year-old man admitted with a hemorrhagbic infarct, NSTEMI, and recently diagnosed right lower extremity DVT with a decreasing platelet count in the setting of LMWH. Throughout the hospital course, he had worsening hemorrhagic infarcts, preventing proper anticoagulation for his progressive thromboembolic events in the lungs, spleen, kidneys, and legs. Incidentally, he was also found to have a mass on a chest x-ray, later identified by biopsy as adenocarcinoma.
Given that the 4T scoring system for HIT showed a high probability with 8 points—identified by a platelet count fall > 50%, a platelet nadir > 20,000 cells/mm3, clear onset between days 5 and 14 with exposure to heparin/LMWH, new thrombosis, and no apparent cause of thrombocytopenia—suspicion for HIT remained high. Both functional and immunologic assays were negative for HIT, when repeated 2 weeks apart. The assays for laboratory diagnosis of HIT are immunologic, done by ELISA with a sensitivity of > 95% and a specificity of 50%–89%, and functional, done by SRA with a sensitivity > 90% and a specificity > 90%.2 As neither assay is 100% sensitive and specific, we still had a high clinical suspicion for HIT.
The HIT diagnostics in the presence of other comorbid states that may also induce thrombocytopenia represent a specific clinical problem. Despite increasing awareness of the clinical features of HIT, laboratory detection of the pathogenic HIT antibodies remains central to diagnosis. 4–6 This is because thrombocytopenia during heparin anticoagulation does not necessarily indicate HIT. Indeed, several other disorders complicated by thrombosis and thrombocytopenia during or shortly following heparin treatment strongly resemble HIT.These “pseudo-HIT”disorders7,8 (eg, cancer, sepsis, disseminated intravascular coagulation, pulmonary embolism, antiphospholipid syndrome) can reliably be distinguished from HIT by negative results using sensitive tests for HIT antibodies.
Thrombosis is strongly associated with HIT, with an incidence of 50%– 67%.9,10 The most common complication of HIT is venous thrombosis (DVT being the most frequent, followed by pulmonary embolism).9,11 Arterial thrombosis commonly presents as limb ischemia followed by cerebral vascular accident and myocardial infarction. Our patient had DVT followed by NSTEMI, cerebral vascular accident, and pulmonary embolism. He also had splenic and renal infarctions, which are rare in HIT. A literature review revealed, in abstract form, a retrospective study from a single institution showing a high incidence of thrombosis in a patient with a high 4T score and negative SRAs.12
The most common causes of thrombocytopenia in cancer are related to cancer treatment and bone marrow invasion by tumor cells. Chemotherapy and radiation therapy are damaging to the bone marrow and can cause severe myelosuppression, which results in lowering of platelet counts as well as white and red blood cell counts. It commonly occurs in patients with leukemia and lymphoma, but there are many other cancer types that can spread to bone marrow. Other causes of thrombocytopenia in cancer include the syndrome of disseminated intravascular coagulation and thrombotic microangiopathy.13
Nonbacterial thrombotic endocarditis (NBTE) is a disease characterized by the presence of vegetations on cardiac valves, consisting of fibrin and platelet aggregates devoid of inflammation or bacteria. NBTE has increasingly been recognized as a condition associated with numerous diseases and a potentially life-threatening source of thromboembolism. NBTE is not a common entity; however, it is frequently underestimated, probably due to underlying diseases (cancer, autoimmune disorders, HIV). NBTE is difficult to diagnose and relies on strong clinical suspicion. NBTE is also difficult to manage, and each case should be individually managed by identifying and treating the underlying pathology.14 Even though our patient had thromboembolism, there was no evidence of vegetations on cardiac valves by transthoracic or transesophageal echocardiography.
Trousseau’s syndrome is a paraneoplastic syndrome characterized by hypercoagulability related to malignancy. Coagulation abnormalities may include disseminated intravascular coagulation, pulmonary embolism, various types of gangrene, thrombotic endocarditis, arterial thrombosis, and embolic stoke.15 We considered this with our patient; however, a literature review showed no cases of Trousseau’s syndrome associated with thrombocytopenia, although concurrent Trousseau’s syndrome and HIT could not be excluded.
In summary, we need to consider all the above differential diagnoses in a patient presenting with thrombocytopenia and thrombosis. Treatment relies on clinical correlation of all the findings and supporting data.
Heparin-induced thrombocytopenia (HIT) is a life-threatening disorder that follows exposure to unfractionated heparin or (less commonly) low-molecular-weight heparin (LMWH). Patients classically present with a low platelet count (< 150,000 cells/mm3) or a relative decrease of 50% or more from baseline, although the fall may be less (eg, 30%–40%) in some patients.Thrombotic complications develop in approximately 20%–50% of patients.
HIT is caused by antibodies against complexes of platelet factor 4 and heparin.These antibodies are present in nearly all patients who receive a clinical diagnosis of the disorder and are also known to cause disease in animals.However,they are also present in many patients who have been exposed to heparin in various clinical settings but who do not develop clinical manifestations. It is uncertain why complications occur in some patients but not in others.1 We present a 73-year-old man who developed thrombocytopenia after starting LMWH and who has newly diagnosed adenocarcinoma of the lungs with extensive arterial and venous thrombosis and a negative serology for HIT.
Case presentation
A 73-year-old man presented to the emergency department after waking up in the morning with right-sided vague weakness and an inability to get out of bed. He had a history of right parietal stroke 1 month before the current presentation, when he was diagnosed with an aortic arch atheroma and started on warfarin. (At that time, CT scan of the head showed a right posterior temporoparietal lobe infarct in the posterior right middle cerebral artery distribution, and MRI of the brain and magnetic resonance angiography showed acute or subacute infarction in the distribution of the posterior division of the right middle cerebral artery, likely embolic, and tiny acute infarctions in the left frontal lobe.) This patient had been admitted 5 days prior to the current presentation for right lower extremity deep vein thrombosis (DVT) and was discharged after being prescribed enoxaparin (60 mg subcutaneously every 12 hours) and warfarin as per international normalized ratio (INR) daily.
Also included in the medical history was supraventricular tachycardia status post ablation, non–ST elevation myocardial infarction (NSTEMI), hypertension, hyperlipidemia, and macular degeneration. He had no surgical history. The patient had a family history of coronary artery disease. He had an extensive smoking history up until the day of admission. His medications on admission included atorvastatin (Lipitor; 20 mg daily), warfarin daily as per INR, enoxaparin (60 mg subcutaneously every 12 hours), amlodipine (5 mg daily), and aspirin (81 mg daily).
Pertinent initial laboratory results on admission were as follows: hemoglobin, 12.9 g/dL; white blood cell count, 8.6 ×109/L; platelet count, 183,000 cells/ mm3; INR, 1.2; and initial troponin level, negative.His admission chest x-ray showed a 4.5 cm × 5.5 cm lobulated density in the right hilum, suspicious for a hilar or subcarinal mass. Initial peripheral blood smear showed an isolated platelet decrease with increased size and no schistocytes. Initial CT of the head on admission showed no evidence of acute transcortical infarction and no definite evidence of acute intracranial hemorrhage but did show interval evolution of the right middle cerebral artery and left watershed distribution infarctions, with a probable small region of laminar necrosis in the right parietal lobe.
Clinical Course
The patient was initially thought to have had a transient ischemic attack causing aphasia, confusion, and rightsided weakness. He was started on therapeutic anticoagulation with dalteparin (Fragmin; 12,000 U subcutaneously daily),and enoxaparin was discontinued. The following day,his platelet count was 86,000 cells/mm3,down from an admission platelet count of 183,000 cells/mm3. A subsequent MRI of the brain showed a new hemorrhagic area in the right parietal infarct. The decision was made to stop anticoagulation, even though he had an embolic source from his aortic arch atheroma and lower extremity DVT.
The patient then underwent inferior vena cava (IVC) filter placement to prevent pulmonary thromboembolism and was transferred to the medical service due to low platelet count and an episode of nine beats of ventricular tachycardia. Subsequently, his troponin level was found to be elevated > 12 ng/mL, without significant electrocardiographic changes. He was diagnosed as having NSTEMI. Given his conversion from an ischemic to hemorrhagic CNS infarct and decrease in platelet count after LMWH exposure, HIT became a concern, and both anticoagulation and antiplatelet agents were held. The patient’s platelet count continued to trend downward over the next 3 days to a low of 27,000 cells/mm3. An HIT panel was negative by both immunologic and functional assays.
A CT scan of the brain 3 days after admission to monitor the hemorrhagic infarct showed multiple evolving infarcts and a new left occipital hemorrhagic infarct. The following day, a repeat CT scan of the head showed mulatiple evolving infarcts of varying ages, some with hemorrhage, and a mild interval increase in the previously described left medial parietal and left occipital lobe infarcts.
With worsening of his hemorrhagic infarct, along with his low platelet count and negative HIT panel,the decision was made to transfuse 2 units of platelets. His platelet count increased to 64,000 cells/mm3 after transfusion, subsequently dropping to 44,000 cells/mm3. However, during this time, the patient began to have worsening right lower extremity pain and left upper quadrant abdominal pain.
A CT scan of the thorax showed multifocal right hilar adenopathy suspicious for malignancy, either metastatic or representing a central lung carcinoma. It also showed nonocclusive segmental and possibly subsegmental pulmonary emboli in the right lower and middle lobes, as well as hypodense areas in the spleen, suggestive of areas of splenic infarction. Echocardiography showed an ejection fraction of 60%–70%, diastolic dysfunction, mildly elevated pulmonary artery pressure, and no evidence of patent foramen ovale.A cardiac stress test showed no reversible defects and an ejection fraction of 63%.
Risk of further bleeding into the brain was thought to be too great to initiate anticoagulation despite the CT thorax findings. The neurologist recommended waiting 2 weeks post hemorrhagic infarction before beginning anticoagulation. Antiphospholipid antibody syndrome was ruled out, with a negative lupus anticoagulant and anticardiolipin antibody. Also, negative blood cultures, normal fibrinogen levels, and normal haptoglobin levels ruled out disseminated intravascular coagulation. D-dimer was elevated but nonspecific, secondary to malignancy and multiple infarcts. He was started on aspirin (81 mg daily) 9 days after admission.
The patient had a repeat CT scan of the thorax and CT scan of the abdomen and pelvis due to continued abdominal pain. The CT scans showed multiple subsegmental pulmonary emboli, greatest in the right lower lobe, some of which were new since the prior study; continued evidence of multifocal splenic infarction (Figure 3); and multiple right and left kidney infarcts.
The patient then underwent endobronchial ultrasound (EBUS)-guided biopsy of his right hilar adenopathy to confirm the diagnosis of suspected malignancy. After the procedure, he developed right upper quadrant pleuritic pain with a low-grade fever. A repeat CT scan of the thorax showed a marked increase in the extent of the right lower lobe pulmonary emboli, with a new small embolus noted in the anterior segment of the right upper lobe. There was a thrombus inferior to the IVC filter, with probable mild extension of a thrombus superior to the filter as well, and again multiple splenic and bilateral renal infarcts.
With progression of thrombosis and now post EBUS, anticoagulation was initiated with argatroban and warfarin. His D-dimer was followed daily and remained high, despite therapeutic anticoagulation with warfarin. Given the persistently elevated D-dimer, the hematologist recommended discontinuing warfarin and starting fondaparinux (Arixtra) subcutaneously. His platelet count improved to a range of 156,000 cells/mm3 to 181,000 cells/mm3, even before the initiation of chemotherapy.
Follow-up
HIT was suspected clinically by classic drop in platelet count but was negative on enzyme-linked immunosorbent assay (ELISA) and serotonin release assay (SRA). The patient has been maintained on fondaparinux for anticoagulation, avoiding heparin. Factor V Leiden and lupus anticoagulant were negative.
Fondaparinux was discontinued after 3 months, and the patient presented again with swelling of his right lower extremity. Ultrasonography of the right lower extremity redemonstrated an occlusive thrombus in the peripheral portion of the right femoaral vein and throughout the right peroneal vein. The patient was restarted on fondaparinux (7.5 mg subcutaneously daily). During this follow-up, his platelet count ranged from 134,000 cells/mm3 to 193,000 cells/mm3.
Regarding management of nonsmall cell lung carcinoma of the left upper lobe (stains positive for TTF- 1 [thyroid transcription factor-1], CK7, and CK20; weakly positive for CK5/6; and negative for P63) with metastasis to bone and adrenal glands, he received 4 cycles of paclitaxel/carboplatin, with improved disease. A repeat CT of the chest, abdomen, and pelvis after chemotherapy showed improvement in mediastinal and hilar lymphadenopathy, resolution of extensive right lower lobe pulmonary consolidation, resolution of right-sided effusion, and no evidence of metastatic malignancy in the abdomen or pelvis and no osseous metastasis.
He was started on maintenance therapy with pemetrexed (Alimta), which was continued for 4 months, until repeat CT revealed progressive disease. He then received 4 cycles of vinorelbine. He had progression-free survival of 7 months from first-line chemotherapy and stable disease for 7 months after 4 cycles of vinorelbine.
Discussion
In summary, we have a 73-year-old man admitted with a hemorrhagbic infarct, NSTEMI, and recently diagnosed right lower extremity DVT with a decreasing platelet count in the setting of LMWH. Throughout the hospital course, he had worsening hemorrhagic infarcts, preventing proper anticoagulation for his progressive thromboembolic events in the lungs, spleen, kidneys, and legs. Incidentally, he was also found to have a mass on a chest x-ray, later identified by biopsy as adenocarcinoma.
Given that the 4T scoring system for HIT showed a high probability with 8 points—identified by a platelet count fall > 50%, a platelet nadir > 20,000 cells/mm3, clear onset between days 5 and 14 with exposure to heparin/LMWH, new thrombosis, and no apparent cause of thrombocytopenia—suspicion for HIT remained high. Both functional and immunologic assays were negative for HIT, when repeated 2 weeks apart. The assays for laboratory diagnosis of HIT are immunologic, done by ELISA with a sensitivity of > 95% and a specificity of 50%–89%, and functional, done by SRA with a sensitivity > 90% and a specificity > 90%.2 As neither assay is 100% sensitive and specific, we still had a high clinical suspicion for HIT.
The HIT diagnostics in the presence of other comorbid states that may also induce thrombocytopenia represent a specific clinical problem. Despite increasing awareness of the clinical features of HIT, laboratory detection of the pathogenic HIT antibodies remains central to diagnosis. 4–6 This is because thrombocytopenia during heparin anticoagulation does not necessarily indicate HIT. Indeed, several other disorders complicated by thrombosis and thrombocytopenia during or shortly following heparin treatment strongly resemble HIT.These “pseudo-HIT”disorders7,8 (eg, cancer, sepsis, disseminated intravascular coagulation, pulmonary embolism, antiphospholipid syndrome) can reliably be distinguished from HIT by negative results using sensitive tests for HIT antibodies.
Thrombosis is strongly associated with HIT, with an incidence of 50%– 67%.9,10 The most common complication of HIT is venous thrombosis (DVT being the most frequent, followed by pulmonary embolism).9,11 Arterial thrombosis commonly presents as limb ischemia followed by cerebral vascular accident and myocardial infarction. Our patient had DVT followed by NSTEMI, cerebral vascular accident, and pulmonary embolism. He also had splenic and renal infarctions, which are rare in HIT. A literature review revealed, in abstract form, a retrospective study from a single institution showing a high incidence of thrombosis in a patient with a high 4T score and negative SRAs.12
The most common causes of thrombocytopenia in cancer are related to cancer treatment and bone marrow invasion by tumor cells. Chemotherapy and radiation therapy are damaging to the bone marrow and can cause severe myelosuppression, which results in lowering of platelet counts as well as white and red blood cell counts. It commonly occurs in patients with leukemia and lymphoma, but there are many other cancer types that can spread to bone marrow. Other causes of thrombocytopenia in cancer include the syndrome of disseminated intravascular coagulation and thrombotic microangiopathy.13
Nonbacterial thrombotic endocarditis (NBTE) is a disease characterized by the presence of vegetations on cardiac valves, consisting of fibrin and platelet aggregates devoid of inflammation or bacteria. NBTE has increasingly been recognized as a condition associated with numerous diseases and a potentially life-threatening source of thromboembolism. NBTE is not a common entity; however, it is frequently underestimated, probably due to underlying diseases (cancer, autoimmune disorders, HIV). NBTE is difficult to diagnose and relies on strong clinical suspicion. NBTE is also difficult to manage, and each case should be individually managed by identifying and treating the underlying pathology.14 Even though our patient had thromboembolism, there was no evidence of vegetations on cardiac valves by transthoracic or transesophageal echocardiography.
Trousseau’s syndrome is a paraneoplastic syndrome characterized by hypercoagulability related to malignancy. Coagulation abnormalities may include disseminated intravascular coagulation, pulmonary embolism, various types of gangrene, thrombotic endocarditis, arterial thrombosis, and embolic stoke.15 We considered this with our patient; however, a literature review showed no cases of Trousseau’s syndrome associated with thrombocytopenia, although concurrent Trousseau’s syndrome and HIT could not be excluded.
In summary, we need to consider all the above differential diagnoses in a patient presenting with thrombocytopenia and thrombosis. Treatment relies on clinical correlation of all the findings and supporting data.
1. Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. N Engl J Med 2006;355:809–817.
2. Cuker A, Crowther MA. 2009 Clinical Practice Guideline on the Evaluation andManagement of Heparin-Induced Thrombocytopenia (HIT). American Society of Hematology Quick Reference. http://www.hematology. org/Practice/Guidelines/2934.aspx. Accessed May 6, 2011.
3. Antonijevic NM, Radovanovic N, Obradovic S, et al. Obstacles in the diagnostics and therapy of heparin-induced thrombocytopenia. Srp Arh Celok Lek 2010;138(suppl 1):69–73.
4. Warkentin TE, Chong BH, Greinacher A.Heparin induced thrombocytopenia: towards consensus. Thromb Haemost 1998;79:1–7.
5. Warkentin TE. Heparin-induced thrombocytopenia: a clinicopathologic syndrome.
Thromb Haemost 1999; 82:439–447. 6. Warkentin TE, Greinacher A. Laboratory testing for heparin-induced thrombocytopenia.J Thromb Thrombolysis 2000:10(suppl 1):35–45.
7. Warkentin TE. Pseudo-heparin-induced thrombocytopenia. In: Warkentin TE, Greinacher A, eds. Heparin-Induced Thrombocytopenia. New York: Marcel Dekker, Inc.; 2000:245–260.
8. Warkentin TE. Venous limb gangrene (VLG) complicating warfarin treatment of deep-vein thrombosis (DVT) in metastatic carcinoma (abstract). Blood 1999;94(suppl 1):114b.
9. Warkentin TE, Kelton JG. A 14-year study of heparin-induced thrombocytopenia. Am J Med 1996;101:502–507.
10. Greinacher A, Volpe H, Janssens U, et al. Recombinant hirudin (lepirudin) provides safe and effective anticoagulation in patients with heparin-induced thrombocytopenia: a prospective study. Circulation 1999;99:73–80.
11. Nand S, Wong W, Yuen B, et al. Heparin induced thrombocytopenia with thrombosis: incidence, analysis of risk factors, and clinical outcomes in 108 consecutive patients treated at a single institution. Am J Hematol 1997;56:12–16.
12. Hueser C, Patel AJ, Allan JN. Incidence of thrombosis in serotonin release assay negative patients and correlation with pretest heparin- induced thrombocytopenia scoring system. Blood 2008;112:1816.
13. Prandoni P, Falanga A, Piccioli A. Cancer, thrombosis and heparin-induced thrombocytopenia. Thromb Res 2007;120(suppl 2):S137–S140.
14. Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis. Eur J Cardiothoracic Surg 2007;32:696– 701.
15. Lim BR, Henry DH. Stroke syndrome secondary to hypercoagulability of lung cancer. Commun Oncol 2008;5:595–596.
1. Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. N Engl J Med 2006;355:809–817.
2. Cuker A, Crowther MA. 2009 Clinical Practice Guideline on the Evaluation andManagement of Heparin-Induced Thrombocytopenia (HIT). American Society of Hematology Quick Reference. http://www.hematology. org/Practice/Guidelines/2934.aspx. Accessed May 6, 2011.
3. Antonijevic NM, Radovanovic N, Obradovic S, et al. Obstacles in the diagnostics and therapy of heparin-induced thrombocytopenia. Srp Arh Celok Lek 2010;138(suppl 1):69–73.
4. Warkentin TE, Chong BH, Greinacher A.Heparin induced thrombocytopenia: towards consensus. Thromb Haemost 1998;79:1–7.
5. Warkentin TE. Heparin-induced thrombocytopenia: a clinicopathologic syndrome.
Thromb Haemost 1999; 82:439–447. 6. Warkentin TE, Greinacher A. Laboratory testing for heparin-induced thrombocytopenia.J Thromb Thrombolysis 2000:10(suppl 1):35–45.
7. Warkentin TE. Pseudo-heparin-induced thrombocytopenia. In: Warkentin TE, Greinacher A, eds. Heparin-Induced Thrombocytopenia. New York: Marcel Dekker, Inc.; 2000:245–260.
8. Warkentin TE. Venous limb gangrene (VLG) complicating warfarin treatment of deep-vein thrombosis (DVT) in metastatic carcinoma (abstract). Blood 1999;94(suppl 1):114b.
9. Warkentin TE, Kelton JG. A 14-year study of heparin-induced thrombocytopenia. Am J Med 1996;101:502–507.
10. Greinacher A, Volpe H, Janssens U, et al. Recombinant hirudin (lepirudin) provides safe and effective anticoagulation in patients with heparin-induced thrombocytopenia: a prospective study. Circulation 1999;99:73–80.
11. Nand S, Wong W, Yuen B, et al. Heparin induced thrombocytopenia with thrombosis: incidence, analysis of risk factors, and clinical outcomes in 108 consecutive patients treated at a single institution. Am J Hematol 1997;56:12–16.
12. Hueser C, Patel AJ, Allan JN. Incidence of thrombosis in serotonin release assay negative patients and correlation with pretest heparin- induced thrombocytopenia scoring system. Blood 2008;112:1816.
13. Prandoni P, Falanga A, Piccioli A. Cancer, thrombosis and heparin-induced thrombocytopenia. Thromb Res 2007;120(suppl 2):S137–S140.
14. Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis. Eur J Cardiothoracic Surg 2007;32:696– 701.
15. Lim BR, Henry DH. Stroke syndrome secondary to hypercoagulability of lung cancer. Commun Oncol 2008;5:595–596.