User login
Diagnosis at a Glance: Cases in Dermatology
Case 1

A 65-year-old woman presents to the urgent care center with several growths inside a tattoo on her left leg that developed several weeks before presentation. Patient states she has had the tattoo for approximately 15 years, but had a revision done to the original artwork at a local tattoo parlor 4 months ago; she noted that the skin lesions appeared one month after this revision, have rapidly increased in size, and are occasionally pruritic.
Patient has a medical history of breast cancer, for which she was diagnosed and treated at age 50 years, and she is also a cigarette smoker. She denies a prior history of skin cancer. Physical examination reveals scattered exophytic nodules, with the largest nodule measuring 1.2 cm in diameter.
What is your diagnosis?
Case 2

A 48-year-old woman presents to the urgent care center with dermatitis around her nose and mouth, which she states has been progressing in severity over the past several months and is at times pruritic. She had been treating the site twice daily with topical betamethasone diproprionate cream and had also been on intermittent doses of oral corticosteroids. Physical examination reveals a pronounced erythematous papulopustular eruption of the affected areas. The rash did not involve her neck, forehead, or scalp.
What is your diagnosis?
Mr Himmelsbach is a nurse practitioner at berks Plastic Surgery in Wyomissing, Pennsylvania. Dr Schleicher, editor of “diagnosis at a Glance,” is director of the dermdOX center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s college in Wilkes-barre, Pennsylvania; an associate professor of medicine at the commonwealth medical college in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania in Philadelphia. He is also a member of the emerGeNcY medIcINe editorial board. Ms Remaley is a physician assistant at reading dermatology Associates in reading, Pennsylvania.
Answer
Case 1
Biopsy of the two largest lesions revealed keratoacanthoma (KA); excisional surgeries were subsequently performed on the other lesions. KAs originate within pilosebaceous glands and are classified as a variant of invasive squamous cell carcinoma. The lesions are characterized by rapid growth, potential for spontaneous involution, and low incidence of metastatic spread. Although KAs have been linked to chronic tar exposure in industrial workers, they more commonly occur in cigarette smokers and in a significant percentage of metastatic melanoma patients treated with BRAF inhibitors. KA developing in a tattoo is a rare occurrence, and the association in this case with recent tattoo ink application is an intriguing one.
Case 2
Steroid-induced facial dermatitis manifests as an eruption of papules and pustules on an erythematous scaling base classically involving the nasolabial folds and perioral area. A clear zone may be present around the vermillion border. This rash is caused by prolonged treatment of blemishes or rashes with mid-to-high potency topical corticosteroids. During treatment, the complexion initially improves but then gradually worsens. Upon discontinuation of corticosteroid therapy, a rebound flare ensues, often triggering resumption of the precipitating medication. Management is difficult, though most cases respond to substitution with a low-potency corticosteroid followed by application of either pimecrolimus or a sulfur-containing lotion. 32
Case 1
A 65-year-old woman presents to the urgent care center with several growths inside a tattoo on her left leg that developed several weeks before presentation. Patient states she has had the tattoo for approximately 15 years, but had a revision done to the original artwork at a local tattoo parlor 4 months ago; she noted that the skin lesions appeared one month after this revision, have rapidly increased in size, and are occasionally pruritic.
Patient has a medical history of breast cancer, for which she was diagnosed and treated at age 50 years, and she is also a cigarette smoker. She denies a prior history of skin cancer. Physical examination reveals scattered exophytic nodules, with the largest nodule measuring 1.2 cm in diameter.
What is your diagnosis?
Case 2
A 48-year-old woman presents to the urgent care center with dermatitis around her nose and mouth, which she states has been progressing in severity over the past several months and is at times pruritic. She had been treating the site twice daily with topical betamethasone diproprionate cream and had also been on intermittent doses of oral corticosteroids. Physical examination reveals a pronounced erythematous papulopustular eruption of the affected areas. The rash did not involve her neck, forehead, or scalp.
What is your diagnosis?
Mr Himmelsbach is a nurse practitioner at berks Plastic Surgery in Wyomissing, Pennsylvania. Dr Schleicher, editor of “diagnosis at a Glance,” is director of the dermdOX center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s college in Wilkes-barre, Pennsylvania; an associate professor of medicine at the commonwealth medical college in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania in Philadelphia. He is also a member of the emerGeNcY medIcINe editorial board. Ms Remaley is a physician assistant at reading dermatology Associates in reading, Pennsylvania.
Answer
Case 1
Biopsy of the two largest lesions revealed keratoacanthoma (KA); excisional surgeries were subsequently performed on the other lesions. KAs originate within pilosebaceous glands and are classified as a variant of invasive squamous cell carcinoma. The lesions are characterized by rapid growth, potential for spontaneous involution, and low incidence of metastatic spread. Although KAs have been linked to chronic tar exposure in industrial workers, they more commonly occur in cigarette smokers and in a significant percentage of metastatic melanoma patients treated with BRAF inhibitors. KA developing in a tattoo is a rare occurrence, and the association in this case with recent tattoo ink application is an intriguing one.
Case 2
Steroid-induced facial dermatitis manifests as an eruption of papules and pustules on an erythematous scaling base classically involving the nasolabial folds and perioral area. A clear zone may be present around the vermillion border. This rash is caused by prolonged treatment of blemishes or rashes with mid-to-high potency topical corticosteroids. During treatment, the complexion initially improves but then gradually worsens. Upon discontinuation of corticosteroid therapy, a rebound flare ensues, often triggering resumption of the precipitating medication. Management is difficult, though most cases respond to substitution with a low-potency corticosteroid followed by application of either pimecrolimus or a sulfur-containing lotion. 32
Case 1
A 65-year-old woman presents to the urgent care center with several growths inside a tattoo on her left leg that developed several weeks before presentation. Patient states she has had the tattoo for approximately 15 years, but had a revision done to the original artwork at a local tattoo parlor 4 months ago; she noted that the skin lesions appeared one month after this revision, have rapidly increased in size, and are occasionally pruritic.
Patient has a medical history of breast cancer, for which she was diagnosed and treated at age 50 years, and she is also a cigarette smoker. She denies a prior history of skin cancer. Physical examination reveals scattered exophytic nodules, with the largest nodule measuring 1.2 cm in diameter.
What is your diagnosis?
Case 2
A 48-year-old woman presents to the urgent care center with dermatitis around her nose and mouth, which she states has been progressing in severity over the past several months and is at times pruritic. She had been treating the site twice daily with topical betamethasone diproprionate cream and had also been on intermittent doses of oral corticosteroids. Physical examination reveals a pronounced erythematous papulopustular eruption of the affected areas. The rash did not involve her neck, forehead, or scalp.
What is your diagnosis?
Mr Himmelsbach is a nurse practitioner at berks Plastic Surgery in Wyomissing, Pennsylvania. Dr Schleicher, editor of “diagnosis at a Glance,” is director of the dermdOX center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s college in Wilkes-barre, Pennsylvania; an associate professor of medicine at the commonwealth medical college in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania in Philadelphia. He is also a member of the emerGeNcY medIcINe editorial board. Ms Remaley is a physician assistant at reading dermatology Associates in reading, Pennsylvania.
Answer
Case 1
Biopsy of the two largest lesions revealed keratoacanthoma (KA); excisional surgeries were subsequently performed on the other lesions. KAs originate within pilosebaceous glands and are classified as a variant of invasive squamous cell carcinoma. The lesions are characterized by rapid growth, potential for spontaneous involution, and low incidence of metastatic spread. Although KAs have been linked to chronic tar exposure in industrial workers, they more commonly occur in cigarette smokers and in a significant percentage of metastatic melanoma patients treated with BRAF inhibitors. KA developing in a tattoo is a rare occurrence, and the association in this case with recent tattoo ink application is an intriguing one.
Case 2
Steroid-induced facial dermatitis manifests as an eruption of papules and pustules on an erythematous scaling base classically involving the nasolabial folds and perioral area. A clear zone may be present around the vermillion border. This rash is caused by prolonged treatment of blemishes or rashes with mid-to-high potency topical corticosteroids. During treatment, the complexion initially improves but then gradually worsens. Upon discontinuation of corticosteroid therapy, a rebound flare ensues, often triggering resumption of the precipitating medication. Management is difficult, though most cases respond to substitution with a low-potency corticosteroid followed by application of either pimecrolimus or a sulfur-containing lotion. 32

Treatment in the face of uncertainty following traumatic anhydrous ammonia exposure
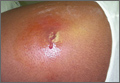
JD is a previously healthy 33-year-old white man, married and father of 2 children, who, while working as an agronomist, was inadvertently exposed to anhydrous ammonia. His only recollection of the event was a "puff of smoke” and the smell of ammonia. He lost consciousness almost immediately and awoke several days later in the intensive care unit. He was blind. Over the days that followed, he regained central vision; however, the loss of peripheral vision in all fields persisted. He said that upon first waking in the morning, he could "only see shadows.” For the rest of the day, he had “tunnel vision.” Ophthalmology and neurology evaluations uncovered no obvious reasons for the persistent vision loss.
The patient also complained of mild headache and discomfort behind his eyes for which he was taking aspirin. The discomfort behind his left eye was worse than on the right. He remained on disability following his work injury, and began to feel increasingly distressed and hopeless. His wife noted he was uncharacteristically irritable with her and the children, and that he had vivid nightmares and said he could smell ammonia. He also had trouble keeping up his yard because of the agitation and anxiety he experienced in approaching his workshed and equipment on the property.
A month later, an ophthalmologist reexamined JD and, again, found no cause for the ocular abnormality and suggested artificial tears for dry eyes. Two months later, he saw an optometrist, who documented constricted visual fields and referred JD to a second ophthalmologist. This consultant suggested possible brain injury and doubted it was psychosomatic in nature. He referred the patient to a neurologist. The neurologist found no organic explanation for his vision loss. He suspected a somatoform disorder and told JD his vision should recover. JD and his wife initially declined the neurologist’s idea of a neuroophthalmology consultation, but eventually agreed. The neuro-ophthalmologist also suspected a functional disturbance as the cause for visual impairment; and he required the patient to stop driving a motor vehicle until his vision improved.
The patient was subsequently referred for psychological evaluation. When initially seen by a psychologist and a family medicine resident, JD was working as a farmhand to make ends meet.

Effects of ammonia exposure
Ammonia is a water-soluble, colorless gas—an alkaloid with a unique odor. In the past, most exposures were related to its use as a fertilizer, as was the case with JD. In recent years, it has also been used to illegally manufacture methamphetamine, which has led to ammonia accidents and increased exposures.1-3
Systems commonly injured are the respiratory tract, ocular system, skin, and gastrointestinal tract (only if ingested).2
Ammonia destroys the mucosal barrier of the respiratory tract, causing loss of cilia, edema, and smooth muscle contraction.3,4 Long-term effects include chronic cough or hoarseness, obstructive or restrictive airway disease, reactive airway disease, or bronchiectasis.1,3
The extent of ocular injury is related to the degree of ammonia exposure. In mild cases, there is eye irritation, increased tear production, a sensation of stinging or burning, and perhaps conjunctivitis or spasmodic winking. The patient may also experience photophobia.1,3,4 In more severe cases, there may be corneal ulcerations, iritis, anterior or posterior synechia, opacification of the cornea, cataracts, glaucoma, atrophy of the retina, or severe pain.1,3 Blindness may occur, temporarily or permanently.4 This complete or partial vision loss is secondary to physical damage that can be seen during an ophthalmologic examination.1,4
Skin injuries can range from a mild erythematous rash to a full thickness burn with bullae and even denudation.1 Long-term effects include scarring or dermatitis.3
Our patient had respiratory and skin symptoms that fit with classic ammonia exposure (respiratory distress requiring intubation, rash). His initial blindness was consistent with ammonia exposure; however, his subsequent peripheral loss was inconsistent with known reaction to ammonia.

Causes of acute visual loss
Vision loss can be caused by injury to the media of the eye (cornea, lens, etc), the retina, or the neural visual pathways. It may also have a psychogenic component.5 Media-related causes of acute vision loss include keratitis or uveitis, edema of the cornea, blood in the anterior chamber (hyphema), disturbance of the lens, or hemorrhage into the vitreous.5,6 Retinal causes include occlusion of the central retinal artery or vein, detachment of the retina, or acute maculopathy.5-8 Neurologic causes include injury to the optic nerve itself (normally monocular) or defects in the chiasmal or retrochiasmal regions (causing partial loss in both eyes).5,9 If all of the above possibilities have been ruled out, consider psychogenic contribution to visual loss.5 Often this diagnosis is called “functional vision loss,” which can include feigning visual loss for secondary gain or subjective blindness as is seen with a somatoform disorder (eg, conversion disorder).
JD had bilateral peripheral vision loss of both the medial and lateral visual fields with macular sparing bilaterally. But he had an otherwise normal physical examination. At this point, the neurologist suspected conversion disorder, while one ophthalmologist thought a neuropathic disorder was responsible.
The neurologist had, early on, recognized that JD was significantly distressed by the accident and encouraged a psychological consultation. With the absence of identifiable ophthalmologic pathology, the patient reluctantly accepted this referral.
The psychologist, aided by family medicine residents, entertained the diagnoses of Post-Traumatic Stress Disorder (PTSD) and somatoform disorders, particularly conversion. PTSD is unique among psychiatric diagnoses in that a patient must meet all 6 DSM V criteria:10
• exposure to a traumatic event involving actual or threatened death or serious injury
• recollections, dreams, or hallucinations in which the trauma is re-experienced
• avoidance of stimuli associated with the trauma
• persistent symptoms of increased arousal (eg, irritability, agitation)
• symptoms and behavior that last for longer than one month
• distress that is clinically significant.
He met the criteria for a PTSD diagnosis and likely would benefit from treatment for it. However, sensory loss related to PTSD alone would be unusual, perhaps as unusual as peripheral vision loss secondary to ammonia exposure. Other factors needed to be explored.
Conversion disorders consist of disorders of movement, such as seizures or paralysis, or disorders of sensations, such as numbness or blindness. These may be episodic or sustained and have acute or chronic onset.11
Psychological factors are judged to be associated with the symptom or deficit because conflicts or other stressors precede the initiation or exacerbation of the symptom or deficit. This was possible in JD, but a degree of uncertainty lingered because he did not exhibit behavior typically seen with factitious disorder, and performance anxiety could conceivably account for the outcome on his vision tests.
In general, he could meet the criteria for conversion disorder, but questions remained. The biggest question is whether the accident resulting in PTSD is the cause of the psychological stress, or is the peripheral vision loss the source of the psychological stress, which would mean it is not a conversion disorder?
Treatment of visual defects
As is the case in many disorders, a definitive diagnosis of the cause of vision loss is not necessary to begin treatment. When you suspect a somatoform disorder including conversion, start therapy and treat the symptoms as “real.”12 Tell the patient that no specific treatment will completely resolve the symptoms, but that it can help.13 Whether the primary cause is neurologic or conversion based, there is often some spontaneous recovery of vision that occurs between 2 weeks and 3 or more months.14 Peripheral field defects have a guarded prognosis, although an extensive rehabilitation program may improve the vision fields somewhat.15-18
Conversion disorders effectively respond to cognitive behavioral therapy (CBT) including gradual exposure to anxiety triggers.19 Rehabilitation for neurologic damage based on remodeling of pathways responds to a similar gradual exercise or exposure to the lost function. Since these interventions are similar processes, a definitive diagnosis was unnecessary in JD’s case. A proprietary visual rehabilitation therapy program is available17 that exposes the patient to visual field activity that requires a cognitive reaction.15 This treatment facilitates recovery even into the sixth month of therapy.16 However, the cost of the software is approximately $6000 and is not yet covered by insurance.15
JD could not afford the commercially available programmed therapy. Therefore, we introduced an alternative treatment plan to challenge the transitional zone. With this plan, JD would play video games for 30 minutes at least twice a week, and preferably daily. He sat close enough to the television so that the transitional zone was approximately 1 to 2 inches from the peripheral portion of the television screen. The game was an action-packed video in which the peripheral portion of the screen was important (such as in first-person shooter games). He was to continue staring at the center of the screen during play in order to truly exercise the peripheral vision. Every day, he reassessed where the transitional zone was located and adjusted his seating accordingly. JD practiced this at least once a day and found that he had to sit closer and closer to the television screen to allow the transitional zone to remain in the screen’s periphery.
The patient, being very motivated, also developed treatments that worked well. He would stare at a blank white wall approximately 2 feet away, focusing on one location. One of his family members would take a laser pointer and start very far away, then slowly move the light closer to the patient’s center of vision. JD would tell his family member when he could see the light and they would move on to a different portion of his visual field.
After 3 months, we retested JD’s vision, which showed great improvement. JD felt he had significant improvement in his vision. The ophthalmologist retested JD about 2 months later and he passed a visual test well enough to obtain a modified driving license so he could return to his work as an agronomist.
Treatment of PTSD
Therapy for PTSD is complex and best approached with a long-term, multifaceted plan.20 Both pharmacotherapy and psychotherapy can be considered for initial treatment; however, no placebo-controlled randomized trials comparing the 2 modalities have been conducted. Combination therapy can also be employed.
Drug therapy, particularly selective serotonin reuptake inhibitors (SSRIs), has been shown to be generally effective in ameliorating positive symptoms associated with PTSD, such as nightmares and flashbacks. But they are less effective at treating negative symptoms such as withdrawal and avoidance.21,22
There is no clinical evidence to support the use of anxiolytics such as benzodiazepines in treating PTSD-specific symptoms. One small study did find a significant reduction in anxiety with alprazolam compared with placebo; however, the response was modest, and specific PTSD symptoms were unchanged.2 Given the high prevalence of comorbid substance abuse in PTSD, benzodiazepines are best avoided since evidence for their effectiveness is lacking.23
Both CBT and eye movement desensitization and reprocessing (EMDR) can be effective therapy for PTSD.24 Both modalities center on desensitization through exposure to traumatic recollections and symptom triggers.
The CBT approach we used focused on JD’s phobic reaction to ammonia that prevented his return to work. First, he listened to relaxation CDs to practice deep breathing and relaxation techniques. Once he was familiar with the techniques, he practiced them in the presence of the shed that contained ammonia products, which was a trigger for his anxiety. At first he was only able to approach the shed while using the breathing exercises to calm his anxiety. Over several weeks, he became more comfortable moving closer to the shed, and he eventually stepped into the shed and began staying for longer periods of time. The course of therapy took several months, but by the end of the sessions he was able to perform necessary tasks in the he was able to perform necessary tasks in the shed with only mild anxiety.
He also suffered from persistent troubling nightmares that significantly affected his sleep and led to physical symptoms of headache and vomiting. These, too, were overcome with the CBT approach.25 We instructed him to immediately write down as much as he could recall of a nightmare upon waking from it. During the following day, he re-read the dream and attempted to re-experience it while using the relaxation techniques to temper anxiety. Over several months of therapy, his nightmares lessened and eventually stopped.
On the last day of therapy, JD reported he had 3 job offers and 2 more interviews lined up, and that he was excited about his opportunities. We congratulated him on his visual recovery and applauded him for his hard work.
Discussion
While it is possible that JD spontaneously recovered his vision loss, it’s more likely that treatment can be credited, given that he did not improve in the 6 months prior to treatment and that his condition resolved over the 3-month rehabilitation period.
Research that guides practice must necessarily limit variables, but real-life patients often have multiple variables complicating both diagnosis and treatment. Our patient is a graphic example. He was exposed to anhydrous ammonia with its multiple physiologic sequelae and it was a traumatic event leading to additional sequelae. Furthermore, his inability to perform his job and fulfill social obligations contributed to his impairment.
JD’s referral to a neural-ophthalmologist did not provide a definitive diagnosis. He then followed up on a referral to the local residency clinic, where the family physician/psychologist team treats patients from a biopsychosocial perspective. Although physicians feel most comfortable when they arrive at a specific diagnosis with a specific evidence-based treatment that predicts a good outcome, this case yielded no definitive diagnosis. Instead, the psychologist and family physician relied on general research findings showing that in the context of traumatic injury or illness followed by debilitating anxiety symptoms, desensitization and rehabilitation provide the best chance of improvement. This shift in treatment approach very likely was responsible for the patient’s improvement.
This approach had the added benefit of helping the patient feel empowered. When JD a and family physician, he was frustrated that no explanation had been found for his problem. As a result, he feared that nothing could be done. When told that a rehabilitation and gradual exposure approach would likely help him, even if we were uncertain of the absolute cause, he became an eager participant in his treatment. He also embraced the idea that it wasn’t up to the doctors alone to improve his condition, but that he could be an active participant. In our view, his enthusiastic efforts contributed to the ultimate treatment outcome.
Often family physicians think they should refer these “complicated” patients to other specialists. However, for patients with combined psychological and physiological pathologies, we believe there are no better experts than family physicians. Properly trained family physicians could have treated this patient without the aid of a psychologist. Other patients who can benefit from this type of integrated biopsychosocial rehabilitation include those with chronic fatigue syndrome, chronic low back pain, and debilitating epilepsy.26-28
1. Lessenger JE. Anhydrous ammonia injuries. J Agromedicine. 1996;3:191-203.
2. Souther L, Small-Johnson J, Messing R. A description of agricultural releases of anhydrous ammonia in Minnesota. Chem Health Safety. 2000;7:16-22.
3. Welch A. Exposing the dangers of anhydrous ammonia. Nurse Pract. 2006;31:40-45.
4. Makarovsky I, Markel G, Dushnitsky T, et al. Ammonia—when something smells wrong. Isr Med Assoc J. 2008;10:537-543.
5. Leveque T. Approach to the adult with acute persistent visual loss. In: UpToDate, Trobe J (ed), UpToDate, Waltham, MA, 2013.
6. Morgan A, Hemphill RR. Acute visual change. Emerg Med Clin North Am. 1998;16:825-843,vii.
7. Beran DI, Murphy-Lavoie H. Acute, painless vision loss. J La State Med Soc. 2009;161:214-216, 218-223.
8. Vortmann M, Schneider JI. Acute monocular vision loss. Emerg Med Clin North Am. 2008;26:73-96.
9. Chamberlain MC, Chalmers L. Acute binocular blindness. Can- cer. 2007;109:1851-1854.
10. American Psychiatric Association. Diagnostic and Statistical Manual. 5th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2013.
11. Aybek S, Kanaan RA, David AS. The neuropsychiatry of conversion disorder. Curr Opin Psychiatry. 2008;21:275-280.
12. Stone J, Vuilleumier P, Friedman JH. Conversion disorder: separating “how” from “why.” Neurology. 2010;74:190-191.
13. Tocchio SL. Treatment of conversion disorder. A clinical and holistic approach. J Psychosoc Nurs Ment Health Serv. 2009; 47:42-49.
14. Mueller I, Gall C, Kasten E, et al. Long-term learning of visual functions in patients after brain damage. Behav Brain Res. 2008;191:32-42.
15. Glisson CC. Capturing the benefit of vision restoration therapy. Curr Opin Ophthalmol. 2006;17:504-508.
16. Marshall RS, Chmayssani M, O’Brien KA, et al. Visual field expansion after visual restoration therapy. Clin Rehabil. 2010;24: 1027-1035.
17. Mueller I, Mast H, Sabel BA. Recovery of visual field defects: a large clinical observational study using vision restoration therapy. Restor Neurol Neurosci. 2007;25:563-572.
18. Romano JG, Schulz P, Kenkel S, et al. Visual field changes after a rehabilitation intervention: vision restoration therapy. J Neurol Sci. 2008;273:70-74.
19. Allen LA, Woolfolk RL. Cognitive behavioral therapy for somatoform disorders. Psychiatr Clin North Am. 2010;33:579-593.
20. Cukor J, Olden M, Lee F, et al. Evidence-based treatments for PTSD, new directions, and special challenges. Ann N Y Acad Sci. 2010;1208:82-89.
21. Meltzer-Brody S, Connor K, Churchill E, et al. Symptom-specific effects of fluoxetine in PTSD. Intl Clin Psychopharmacol. 2000;15:227-231.
22. Stein DJ, Ipser JC, Seedat S. Pharmacotherapy for post traumatic stress disorder. Cochrane Database Syst Rev. 2006(1):CD002795.
23. Braun P, Greenberg D, Dasberg H, et al. Core symptoms of post-traumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry. 1990;51:236-238.
24. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder. Cochrane Database Syst Rev. 2007(3): CD003388.
25. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6:389-401.
26. Reid SF, Chalder T, Cleare A, et al. Chronic fatigue syndrome. Clin Evid (Online). 2008 Aug 28;2008:1101.
27. Hall H, McIntosh G. Low back pain (chronic) Clin Evid (Online). 2008 Oct 1;2008:1116.
28. Prevedini A,Presti G,Ragitti E, et al.Acceptance and commitment Therapy (ACT): the foundation of the therapeutic model and an overview of its contribution to the treatment of patients with chronic physical diseases. G Ital Med Lav Ergon. 2011;33(1suppl A):A53-63.
JD is a previously healthy 33-year-old white man, married and father of 2 children, who, while working as an agronomist, was inadvertently exposed to anhydrous ammonia. His only recollection of the event was a "puff of smoke” and the smell of ammonia. He lost consciousness almost immediately and awoke several days later in the intensive care unit. He was blind. Over the days that followed, he regained central vision; however, the loss of peripheral vision in all fields persisted. He said that upon first waking in the morning, he could "only see shadows.” For the rest of the day, he had “tunnel vision.” Ophthalmology and neurology evaluations uncovered no obvious reasons for the persistent vision loss.
The patient also complained of mild headache and discomfort behind his eyes for which he was taking aspirin. The discomfort behind his left eye was worse than on the right. He remained on disability following his work injury, and began to feel increasingly distressed and hopeless. His wife noted he was uncharacteristically irritable with her and the children, and that he had vivid nightmares and said he could smell ammonia. He also had trouble keeping up his yard because of the agitation and anxiety he experienced in approaching his workshed and equipment on the property.
A month later, an ophthalmologist reexamined JD and, again, found no cause for the ocular abnormality and suggested artificial tears for dry eyes. Two months later, he saw an optometrist, who documented constricted visual fields and referred JD to a second ophthalmologist. This consultant suggested possible brain injury and doubted it was psychosomatic in nature. He referred the patient to a neurologist. The neurologist found no organic explanation for his vision loss. He suspected a somatoform disorder and told JD his vision should recover. JD and his wife initially declined the neurologist’s idea of a neuroophthalmology consultation, but eventually agreed. The neuro-ophthalmologist also suspected a functional disturbance as the cause for visual impairment; and he required the patient to stop driving a motor vehicle until his vision improved.
The patient was subsequently referred for psychological evaluation. When initially seen by a psychologist and a family medicine resident, JD was working as a farmhand to make ends meet.
Effects of ammonia exposure
Ammonia is a water-soluble, colorless gas—an alkaloid with a unique odor. In the past, most exposures were related to its use as a fertilizer, as was the case with JD. In recent years, it has also been used to illegally manufacture methamphetamine, which has led to ammonia accidents and increased exposures.1-3
Systems commonly injured are the respiratory tract, ocular system, skin, and gastrointestinal tract (only if ingested).2
Ammonia destroys the mucosal barrier of the respiratory tract, causing loss of cilia, edema, and smooth muscle contraction.3,4 Long-term effects include chronic cough or hoarseness, obstructive or restrictive airway disease, reactive airway disease, or bronchiectasis.1,3
The extent of ocular injury is related to the degree of ammonia exposure. In mild cases, there is eye irritation, increased tear production, a sensation of stinging or burning, and perhaps conjunctivitis or spasmodic winking. The patient may also experience photophobia.1,3,4 In more severe cases, there may be corneal ulcerations, iritis, anterior or posterior synechia, opacification of the cornea, cataracts, glaucoma, atrophy of the retina, or severe pain.1,3 Blindness may occur, temporarily or permanently.4 This complete or partial vision loss is secondary to physical damage that can be seen during an ophthalmologic examination.1,4
Skin injuries can range from a mild erythematous rash to a full thickness burn with bullae and even denudation.1 Long-term effects include scarring or dermatitis.3
Our patient had respiratory and skin symptoms that fit with classic ammonia exposure (respiratory distress requiring intubation, rash). His initial blindness was consistent with ammonia exposure; however, his subsequent peripheral loss was inconsistent with known reaction to ammonia.
Causes of acute visual loss
Vision loss can be caused by injury to the media of the eye (cornea, lens, etc), the retina, or the neural visual pathways. It may also have a psychogenic component.5 Media-related causes of acute vision loss include keratitis or uveitis, edema of the cornea, blood in the anterior chamber (hyphema), disturbance of the lens, or hemorrhage into the vitreous.5,6 Retinal causes include occlusion of the central retinal artery or vein, detachment of the retina, or acute maculopathy.5-8 Neurologic causes include injury to the optic nerve itself (normally monocular) or defects in the chiasmal or retrochiasmal regions (causing partial loss in both eyes).5,9 If all of the above possibilities have been ruled out, consider psychogenic contribution to visual loss.5 Often this diagnosis is called “functional vision loss,” which can include feigning visual loss for secondary gain or subjective blindness as is seen with a somatoform disorder (eg, conversion disorder).
JD had bilateral peripheral vision loss of both the medial and lateral visual fields with macular sparing bilaterally. But he had an otherwise normal physical examination. At this point, the neurologist suspected conversion disorder, while one ophthalmologist thought a neuropathic disorder was responsible.
The neurologist had, early on, recognized that JD was significantly distressed by the accident and encouraged a psychological consultation. With the absence of identifiable ophthalmologic pathology, the patient reluctantly accepted this referral.
The psychologist, aided by family medicine residents, entertained the diagnoses of Post-Traumatic Stress Disorder (PTSD) and somatoform disorders, particularly conversion. PTSD is unique among psychiatric diagnoses in that a patient must meet all 6 DSM V criteria:10
• exposure to a traumatic event involving actual or threatened death or serious injury
• recollections, dreams, or hallucinations in which the trauma is re-experienced
• avoidance of stimuli associated with the trauma
• persistent symptoms of increased arousal (eg, irritability, agitation)
• symptoms and behavior that last for longer than one month
• distress that is clinically significant.
He met the criteria for a PTSD diagnosis and likely would benefit from treatment for it. However, sensory loss related to PTSD alone would be unusual, perhaps as unusual as peripheral vision loss secondary to ammonia exposure. Other factors needed to be explored.
Conversion disorders consist of disorders of movement, such as seizures or paralysis, or disorders of sensations, such as numbness or blindness. These may be episodic or sustained and have acute or chronic onset.11
Psychological factors are judged to be associated with the symptom or deficit because conflicts or other stressors precede the initiation or exacerbation of the symptom or deficit. This was possible in JD, but a degree of uncertainty lingered because he did not exhibit behavior typically seen with factitious disorder, and performance anxiety could conceivably account for the outcome on his vision tests.
In general, he could meet the criteria for conversion disorder, but questions remained. The biggest question is whether the accident resulting in PTSD is the cause of the psychological stress, or is the peripheral vision loss the source of the psychological stress, which would mean it is not a conversion disorder?
Treatment of visual defects
As is the case in many disorders, a definitive diagnosis of the cause of vision loss is not necessary to begin treatment. When you suspect a somatoform disorder including conversion, start therapy and treat the symptoms as “real.”12 Tell the patient that no specific treatment will completely resolve the symptoms, but that it can help.13 Whether the primary cause is neurologic or conversion based, there is often some spontaneous recovery of vision that occurs between 2 weeks and 3 or more months.14 Peripheral field defects have a guarded prognosis, although an extensive rehabilitation program may improve the vision fields somewhat.15-18
Conversion disorders effectively respond to cognitive behavioral therapy (CBT) including gradual exposure to anxiety triggers.19 Rehabilitation for neurologic damage based on remodeling of pathways responds to a similar gradual exercise or exposure to the lost function. Since these interventions are similar processes, a definitive diagnosis was unnecessary in JD’s case. A proprietary visual rehabilitation therapy program is available17 that exposes the patient to visual field activity that requires a cognitive reaction.15 This treatment facilitates recovery even into the sixth month of therapy.16 However, the cost of the software is approximately $6000 and is not yet covered by insurance.15
JD could not afford the commercially available programmed therapy. Therefore, we introduced an alternative treatment plan to challenge the transitional zone. With this plan, JD would play video games for 30 minutes at least twice a week, and preferably daily. He sat close enough to the television so that the transitional zone was approximately 1 to 2 inches from the peripheral portion of the television screen. The game was an action-packed video in which the peripheral portion of the screen was important (such as in first-person shooter games). He was to continue staring at the center of the screen during play in order to truly exercise the peripheral vision. Every day, he reassessed where the transitional zone was located and adjusted his seating accordingly. JD practiced this at least once a day and found that he had to sit closer and closer to the television screen to allow the transitional zone to remain in the screen’s periphery.
The patient, being very motivated, also developed treatments that worked well. He would stare at a blank white wall approximately 2 feet away, focusing on one location. One of his family members would take a laser pointer and start very far away, then slowly move the light closer to the patient’s center of vision. JD would tell his family member when he could see the light and they would move on to a different portion of his visual field.
After 3 months, we retested JD’s vision, which showed great improvement. JD felt he had significant improvement in his vision. The ophthalmologist retested JD about 2 months later and he passed a visual test well enough to obtain a modified driving license so he could return to his work as an agronomist.
Treatment of PTSD
Therapy for PTSD is complex and best approached with a long-term, multifaceted plan.20 Both pharmacotherapy and psychotherapy can be considered for initial treatment; however, no placebo-controlled randomized trials comparing the 2 modalities have been conducted. Combination therapy can also be employed.
Drug therapy, particularly selective serotonin reuptake inhibitors (SSRIs), has been shown to be generally effective in ameliorating positive symptoms associated with PTSD, such as nightmares and flashbacks. But they are less effective at treating negative symptoms such as withdrawal and avoidance.21,22
There is no clinical evidence to support the use of anxiolytics such as benzodiazepines in treating PTSD-specific symptoms. One small study did find a significant reduction in anxiety with alprazolam compared with placebo; however, the response was modest, and specific PTSD symptoms were unchanged.2 Given the high prevalence of comorbid substance abuse in PTSD, benzodiazepines are best avoided since evidence for their effectiveness is lacking.23
Both CBT and eye movement desensitization and reprocessing (EMDR) can be effective therapy for PTSD.24 Both modalities center on desensitization through exposure to traumatic recollections and symptom triggers.
The CBT approach we used focused on JD’s phobic reaction to ammonia that prevented his return to work. First, he listened to relaxation CDs to practice deep breathing and relaxation techniques. Once he was familiar with the techniques, he practiced them in the presence of the shed that contained ammonia products, which was a trigger for his anxiety. At first he was only able to approach the shed while using the breathing exercises to calm his anxiety. Over several weeks, he became more comfortable moving closer to the shed, and he eventually stepped into the shed and began staying for longer periods of time. The course of therapy took several months, but by the end of the sessions he was able to perform necessary tasks in the he was able to perform necessary tasks in the shed with only mild anxiety.
He also suffered from persistent troubling nightmares that significantly affected his sleep and led to physical symptoms of headache and vomiting. These, too, were overcome with the CBT approach.25 We instructed him to immediately write down as much as he could recall of a nightmare upon waking from it. During the following day, he re-read the dream and attempted to re-experience it while using the relaxation techniques to temper anxiety. Over several months of therapy, his nightmares lessened and eventually stopped.
On the last day of therapy, JD reported he had 3 job offers and 2 more interviews lined up, and that he was excited about his opportunities. We congratulated him on his visual recovery and applauded him for his hard work.
Discussion
While it is possible that JD spontaneously recovered his vision loss, it’s more likely that treatment can be credited, given that he did not improve in the 6 months prior to treatment and that his condition resolved over the 3-month rehabilitation period.
Research that guides practice must necessarily limit variables, but real-life patients often have multiple variables complicating both diagnosis and treatment. Our patient is a graphic example. He was exposed to anhydrous ammonia with its multiple physiologic sequelae and it was a traumatic event leading to additional sequelae. Furthermore, his inability to perform his job and fulfill social obligations contributed to his impairment.
JD’s referral to a neural-ophthalmologist did not provide a definitive diagnosis. He then followed up on a referral to the local residency clinic, where the family physician/psychologist team treats patients from a biopsychosocial perspective. Although physicians feel most comfortable when they arrive at a specific diagnosis with a specific evidence-based treatment that predicts a good outcome, this case yielded no definitive diagnosis. Instead, the psychologist and family physician relied on general research findings showing that in the context of traumatic injury or illness followed by debilitating anxiety symptoms, desensitization and rehabilitation provide the best chance of improvement. This shift in treatment approach very likely was responsible for the patient’s improvement.
This approach had the added benefit of helping the patient feel empowered. When JD a and family physician, he was frustrated that no explanation had been found for his problem. As a result, he feared that nothing could be done. When told that a rehabilitation and gradual exposure approach would likely help him, even if we were uncertain of the absolute cause, he became an eager participant in his treatment. He also embraced the idea that it wasn’t up to the doctors alone to improve his condition, but that he could be an active participant. In our view, his enthusiastic efforts contributed to the ultimate treatment outcome.
Often family physicians think they should refer these “complicated” patients to other specialists. However, for patients with combined psychological and physiological pathologies, we believe there are no better experts than family physicians. Properly trained family physicians could have treated this patient without the aid of a psychologist. Other patients who can benefit from this type of integrated biopsychosocial rehabilitation include those with chronic fatigue syndrome, chronic low back pain, and debilitating epilepsy.26-28
JD is a previously healthy 33-year-old white man, married and father of 2 children, who, while working as an agronomist, was inadvertently exposed to anhydrous ammonia. His only recollection of the event was a "puff of smoke” and the smell of ammonia. He lost consciousness almost immediately and awoke several days later in the intensive care unit. He was blind. Over the days that followed, he regained central vision; however, the loss of peripheral vision in all fields persisted. He said that upon first waking in the morning, he could "only see shadows.” For the rest of the day, he had “tunnel vision.” Ophthalmology and neurology evaluations uncovered no obvious reasons for the persistent vision loss.
The patient also complained of mild headache and discomfort behind his eyes for which he was taking aspirin. The discomfort behind his left eye was worse than on the right. He remained on disability following his work injury, and began to feel increasingly distressed and hopeless. His wife noted he was uncharacteristically irritable with her and the children, and that he had vivid nightmares and said he could smell ammonia. He also had trouble keeping up his yard because of the agitation and anxiety he experienced in approaching his workshed and equipment on the property.
A month later, an ophthalmologist reexamined JD and, again, found no cause for the ocular abnormality and suggested artificial tears for dry eyes. Two months later, he saw an optometrist, who documented constricted visual fields and referred JD to a second ophthalmologist. This consultant suggested possible brain injury and doubted it was psychosomatic in nature. He referred the patient to a neurologist. The neurologist found no organic explanation for his vision loss. He suspected a somatoform disorder and told JD his vision should recover. JD and his wife initially declined the neurologist’s idea of a neuroophthalmology consultation, but eventually agreed. The neuro-ophthalmologist also suspected a functional disturbance as the cause for visual impairment; and he required the patient to stop driving a motor vehicle until his vision improved.
The patient was subsequently referred for psychological evaluation. When initially seen by a psychologist and a family medicine resident, JD was working as a farmhand to make ends meet.
Effects of ammonia exposure
Ammonia is a water-soluble, colorless gas—an alkaloid with a unique odor. In the past, most exposures were related to its use as a fertilizer, as was the case with JD. In recent years, it has also been used to illegally manufacture methamphetamine, which has led to ammonia accidents and increased exposures.1-3
Systems commonly injured are the respiratory tract, ocular system, skin, and gastrointestinal tract (only if ingested).2
Ammonia destroys the mucosal barrier of the respiratory tract, causing loss of cilia, edema, and smooth muscle contraction.3,4 Long-term effects include chronic cough or hoarseness, obstructive or restrictive airway disease, reactive airway disease, or bronchiectasis.1,3
The extent of ocular injury is related to the degree of ammonia exposure. In mild cases, there is eye irritation, increased tear production, a sensation of stinging or burning, and perhaps conjunctivitis or spasmodic winking. The patient may also experience photophobia.1,3,4 In more severe cases, there may be corneal ulcerations, iritis, anterior or posterior synechia, opacification of the cornea, cataracts, glaucoma, atrophy of the retina, or severe pain.1,3 Blindness may occur, temporarily or permanently.4 This complete or partial vision loss is secondary to physical damage that can be seen during an ophthalmologic examination.1,4
Skin injuries can range from a mild erythematous rash to a full thickness burn with bullae and even denudation.1 Long-term effects include scarring or dermatitis.3
Our patient had respiratory and skin symptoms that fit with classic ammonia exposure (respiratory distress requiring intubation, rash). His initial blindness was consistent with ammonia exposure; however, his subsequent peripheral loss was inconsistent with known reaction to ammonia.
Causes of acute visual loss
Vision loss can be caused by injury to the media of the eye (cornea, lens, etc), the retina, or the neural visual pathways. It may also have a psychogenic component.5 Media-related causes of acute vision loss include keratitis or uveitis, edema of the cornea, blood in the anterior chamber (hyphema), disturbance of the lens, or hemorrhage into the vitreous.5,6 Retinal causes include occlusion of the central retinal artery or vein, detachment of the retina, or acute maculopathy.5-8 Neurologic causes include injury to the optic nerve itself (normally monocular) or defects in the chiasmal or retrochiasmal regions (causing partial loss in both eyes).5,9 If all of the above possibilities have been ruled out, consider psychogenic contribution to visual loss.5 Often this diagnosis is called “functional vision loss,” which can include feigning visual loss for secondary gain or subjective blindness as is seen with a somatoform disorder (eg, conversion disorder).
JD had bilateral peripheral vision loss of both the medial and lateral visual fields with macular sparing bilaterally. But he had an otherwise normal physical examination. At this point, the neurologist suspected conversion disorder, while one ophthalmologist thought a neuropathic disorder was responsible.
The neurologist had, early on, recognized that JD was significantly distressed by the accident and encouraged a psychological consultation. With the absence of identifiable ophthalmologic pathology, the patient reluctantly accepted this referral.
The psychologist, aided by family medicine residents, entertained the diagnoses of Post-Traumatic Stress Disorder (PTSD) and somatoform disorders, particularly conversion. PTSD is unique among psychiatric diagnoses in that a patient must meet all 6 DSM V criteria:10
• exposure to a traumatic event involving actual or threatened death or serious injury
• recollections, dreams, or hallucinations in which the trauma is re-experienced
• avoidance of stimuli associated with the trauma
• persistent symptoms of increased arousal (eg, irritability, agitation)
• symptoms and behavior that last for longer than one month
• distress that is clinically significant.
He met the criteria for a PTSD diagnosis and likely would benefit from treatment for it. However, sensory loss related to PTSD alone would be unusual, perhaps as unusual as peripheral vision loss secondary to ammonia exposure. Other factors needed to be explored.
Conversion disorders consist of disorders of movement, such as seizures or paralysis, or disorders of sensations, such as numbness or blindness. These may be episodic or sustained and have acute or chronic onset.11
Psychological factors are judged to be associated with the symptom or deficit because conflicts or other stressors precede the initiation or exacerbation of the symptom or deficit. This was possible in JD, but a degree of uncertainty lingered because he did not exhibit behavior typically seen with factitious disorder, and performance anxiety could conceivably account for the outcome on his vision tests.
In general, he could meet the criteria for conversion disorder, but questions remained. The biggest question is whether the accident resulting in PTSD is the cause of the psychological stress, or is the peripheral vision loss the source of the psychological stress, which would mean it is not a conversion disorder?
Treatment of visual defects
As is the case in many disorders, a definitive diagnosis of the cause of vision loss is not necessary to begin treatment. When you suspect a somatoform disorder including conversion, start therapy and treat the symptoms as “real.”12 Tell the patient that no specific treatment will completely resolve the symptoms, but that it can help.13 Whether the primary cause is neurologic or conversion based, there is often some spontaneous recovery of vision that occurs between 2 weeks and 3 or more months.14 Peripheral field defects have a guarded prognosis, although an extensive rehabilitation program may improve the vision fields somewhat.15-18
Conversion disorders effectively respond to cognitive behavioral therapy (CBT) including gradual exposure to anxiety triggers.19 Rehabilitation for neurologic damage based on remodeling of pathways responds to a similar gradual exercise or exposure to the lost function. Since these interventions are similar processes, a definitive diagnosis was unnecessary in JD’s case. A proprietary visual rehabilitation therapy program is available17 that exposes the patient to visual field activity that requires a cognitive reaction.15 This treatment facilitates recovery even into the sixth month of therapy.16 However, the cost of the software is approximately $6000 and is not yet covered by insurance.15
JD could not afford the commercially available programmed therapy. Therefore, we introduced an alternative treatment plan to challenge the transitional zone. With this plan, JD would play video games for 30 minutes at least twice a week, and preferably daily. He sat close enough to the television so that the transitional zone was approximately 1 to 2 inches from the peripheral portion of the television screen. The game was an action-packed video in which the peripheral portion of the screen was important (such as in first-person shooter games). He was to continue staring at the center of the screen during play in order to truly exercise the peripheral vision. Every day, he reassessed where the transitional zone was located and adjusted his seating accordingly. JD practiced this at least once a day and found that he had to sit closer and closer to the television screen to allow the transitional zone to remain in the screen’s periphery.
The patient, being very motivated, also developed treatments that worked well. He would stare at a blank white wall approximately 2 feet away, focusing on one location. One of his family members would take a laser pointer and start very far away, then slowly move the light closer to the patient’s center of vision. JD would tell his family member when he could see the light and they would move on to a different portion of his visual field.
After 3 months, we retested JD’s vision, which showed great improvement. JD felt he had significant improvement in his vision. The ophthalmologist retested JD about 2 months later and he passed a visual test well enough to obtain a modified driving license so he could return to his work as an agronomist.
Treatment of PTSD
Therapy for PTSD is complex and best approached with a long-term, multifaceted plan.20 Both pharmacotherapy and psychotherapy can be considered for initial treatment; however, no placebo-controlled randomized trials comparing the 2 modalities have been conducted. Combination therapy can also be employed.
Drug therapy, particularly selective serotonin reuptake inhibitors (SSRIs), has been shown to be generally effective in ameliorating positive symptoms associated with PTSD, such as nightmares and flashbacks. But they are less effective at treating negative symptoms such as withdrawal and avoidance.21,22
There is no clinical evidence to support the use of anxiolytics such as benzodiazepines in treating PTSD-specific symptoms. One small study did find a significant reduction in anxiety with alprazolam compared with placebo; however, the response was modest, and specific PTSD symptoms were unchanged.2 Given the high prevalence of comorbid substance abuse in PTSD, benzodiazepines are best avoided since evidence for their effectiveness is lacking.23
Both CBT and eye movement desensitization and reprocessing (EMDR) can be effective therapy for PTSD.24 Both modalities center on desensitization through exposure to traumatic recollections and symptom triggers.
The CBT approach we used focused on JD’s phobic reaction to ammonia that prevented his return to work. First, he listened to relaxation CDs to practice deep breathing and relaxation techniques. Once he was familiar with the techniques, he practiced them in the presence of the shed that contained ammonia products, which was a trigger for his anxiety. At first he was only able to approach the shed while using the breathing exercises to calm his anxiety. Over several weeks, he became more comfortable moving closer to the shed, and he eventually stepped into the shed and began staying for longer periods of time. The course of therapy took several months, but by the end of the sessions he was able to perform necessary tasks in the he was able to perform necessary tasks in the shed with only mild anxiety.
He also suffered from persistent troubling nightmares that significantly affected his sleep and led to physical symptoms of headache and vomiting. These, too, were overcome with the CBT approach.25 We instructed him to immediately write down as much as he could recall of a nightmare upon waking from it. During the following day, he re-read the dream and attempted to re-experience it while using the relaxation techniques to temper anxiety. Over several months of therapy, his nightmares lessened and eventually stopped.
On the last day of therapy, JD reported he had 3 job offers and 2 more interviews lined up, and that he was excited about his opportunities. We congratulated him on his visual recovery and applauded him for his hard work.
Discussion
While it is possible that JD spontaneously recovered his vision loss, it’s more likely that treatment can be credited, given that he did not improve in the 6 months prior to treatment and that his condition resolved over the 3-month rehabilitation period.
Research that guides practice must necessarily limit variables, but real-life patients often have multiple variables complicating both diagnosis and treatment. Our patient is a graphic example. He was exposed to anhydrous ammonia with its multiple physiologic sequelae and it was a traumatic event leading to additional sequelae. Furthermore, his inability to perform his job and fulfill social obligations contributed to his impairment.
JD’s referral to a neural-ophthalmologist did not provide a definitive diagnosis. He then followed up on a referral to the local residency clinic, where the family physician/psychologist team treats patients from a biopsychosocial perspective. Although physicians feel most comfortable when they arrive at a specific diagnosis with a specific evidence-based treatment that predicts a good outcome, this case yielded no definitive diagnosis. Instead, the psychologist and family physician relied on general research findings showing that in the context of traumatic injury or illness followed by debilitating anxiety symptoms, desensitization and rehabilitation provide the best chance of improvement. This shift in treatment approach very likely was responsible for the patient’s improvement.
This approach had the added benefit of helping the patient feel empowered. When JD a and family physician, he was frustrated that no explanation had been found for his problem. As a result, he feared that nothing could be done. When told that a rehabilitation and gradual exposure approach would likely help him, even if we were uncertain of the absolute cause, he became an eager participant in his treatment. He also embraced the idea that it wasn’t up to the doctors alone to improve his condition, but that he could be an active participant. In our view, his enthusiastic efforts contributed to the ultimate treatment outcome.
Often family physicians think they should refer these “complicated” patients to other specialists. However, for patients with combined psychological and physiological pathologies, we believe there are no better experts than family physicians. Properly trained family physicians could have treated this patient without the aid of a psychologist. Other patients who can benefit from this type of integrated biopsychosocial rehabilitation include those with chronic fatigue syndrome, chronic low back pain, and debilitating epilepsy.26-28
1. Lessenger JE. Anhydrous ammonia injuries. J Agromedicine. 1996;3:191-203.
2. Souther L, Small-Johnson J, Messing R. A description of agricultural releases of anhydrous ammonia in Minnesota. Chem Health Safety. 2000;7:16-22.
3. Welch A. Exposing the dangers of anhydrous ammonia. Nurse Pract. 2006;31:40-45.
4. Makarovsky I, Markel G, Dushnitsky T, et al. Ammonia—when something smells wrong. Isr Med Assoc J. 2008;10:537-543.
5. Leveque T. Approach to the adult with acute persistent visual loss. In: UpToDate, Trobe J (ed), UpToDate, Waltham, MA, 2013.
6. Morgan A, Hemphill RR. Acute visual change. Emerg Med Clin North Am. 1998;16:825-843,vii.
7. Beran DI, Murphy-Lavoie H. Acute, painless vision loss. J La State Med Soc. 2009;161:214-216, 218-223.
8. Vortmann M, Schneider JI. Acute monocular vision loss. Emerg Med Clin North Am. 2008;26:73-96.
9. Chamberlain MC, Chalmers L. Acute binocular blindness. Can- cer. 2007;109:1851-1854.
10. American Psychiatric Association. Diagnostic and Statistical Manual. 5th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2013.
11. Aybek S, Kanaan RA, David AS. The neuropsychiatry of conversion disorder. Curr Opin Psychiatry. 2008;21:275-280.
12. Stone J, Vuilleumier P, Friedman JH. Conversion disorder: separating “how” from “why.” Neurology. 2010;74:190-191.
13. Tocchio SL. Treatment of conversion disorder. A clinical and holistic approach. J Psychosoc Nurs Ment Health Serv. 2009; 47:42-49.
14. Mueller I, Gall C, Kasten E, et al. Long-term learning of visual functions in patients after brain damage. Behav Brain Res. 2008;191:32-42.
15. Glisson CC. Capturing the benefit of vision restoration therapy. Curr Opin Ophthalmol. 2006;17:504-508.
16. Marshall RS, Chmayssani M, O’Brien KA, et al. Visual field expansion after visual restoration therapy. Clin Rehabil. 2010;24: 1027-1035.
17. Mueller I, Mast H, Sabel BA. Recovery of visual field defects: a large clinical observational study using vision restoration therapy. Restor Neurol Neurosci. 2007;25:563-572.
18. Romano JG, Schulz P, Kenkel S, et al. Visual field changes after a rehabilitation intervention: vision restoration therapy. J Neurol Sci. 2008;273:70-74.
19. Allen LA, Woolfolk RL. Cognitive behavioral therapy for somatoform disorders. Psychiatr Clin North Am. 2010;33:579-593.
20. Cukor J, Olden M, Lee F, et al. Evidence-based treatments for PTSD, new directions, and special challenges. Ann N Y Acad Sci. 2010;1208:82-89.
21. Meltzer-Brody S, Connor K, Churchill E, et al. Symptom-specific effects of fluoxetine in PTSD. Intl Clin Psychopharmacol. 2000;15:227-231.
22. Stein DJ, Ipser JC, Seedat S. Pharmacotherapy for post traumatic stress disorder. Cochrane Database Syst Rev. 2006(1):CD002795.
23. Braun P, Greenberg D, Dasberg H, et al. Core symptoms of post-traumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry. 1990;51:236-238.
24. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder. Cochrane Database Syst Rev. 2007(3): CD003388.
25. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6:389-401.
26. Reid SF, Chalder T, Cleare A, et al. Chronic fatigue syndrome. Clin Evid (Online). 2008 Aug 28;2008:1101.
27. Hall H, McIntosh G. Low back pain (chronic) Clin Evid (Online). 2008 Oct 1;2008:1116.
28. Prevedini A,Presti G,Ragitti E, et al.Acceptance and commitment Therapy (ACT): the foundation of the therapeutic model and an overview of its contribution to the treatment of patients with chronic physical diseases. G Ital Med Lav Ergon. 2011;33(1suppl A):A53-63.
1. Lessenger JE. Anhydrous ammonia injuries. J Agromedicine. 1996;3:191-203.
2. Souther L, Small-Johnson J, Messing R. A description of agricultural releases of anhydrous ammonia in Minnesota. Chem Health Safety. 2000;7:16-22.
3. Welch A. Exposing the dangers of anhydrous ammonia. Nurse Pract. 2006;31:40-45.
4. Makarovsky I, Markel G, Dushnitsky T, et al. Ammonia—when something smells wrong. Isr Med Assoc J. 2008;10:537-543.
5. Leveque T. Approach to the adult with acute persistent visual loss. In: UpToDate, Trobe J (ed), UpToDate, Waltham, MA, 2013.
6. Morgan A, Hemphill RR. Acute visual change. Emerg Med Clin North Am. 1998;16:825-843,vii.
7. Beran DI, Murphy-Lavoie H. Acute, painless vision loss. J La State Med Soc. 2009;161:214-216, 218-223.
8. Vortmann M, Schneider JI. Acute monocular vision loss. Emerg Med Clin North Am. 2008;26:73-96.
9. Chamberlain MC, Chalmers L. Acute binocular blindness. Can- cer. 2007;109:1851-1854.
10. American Psychiatric Association. Diagnostic and Statistical Manual. 5th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2013.
11. Aybek S, Kanaan RA, David AS. The neuropsychiatry of conversion disorder. Curr Opin Psychiatry. 2008;21:275-280.
12. Stone J, Vuilleumier P, Friedman JH. Conversion disorder: separating “how” from “why.” Neurology. 2010;74:190-191.
13. Tocchio SL. Treatment of conversion disorder. A clinical and holistic approach. J Psychosoc Nurs Ment Health Serv. 2009; 47:42-49.
14. Mueller I, Gall C, Kasten E, et al. Long-term learning of visual functions in patients after brain damage. Behav Brain Res. 2008;191:32-42.
15. Glisson CC. Capturing the benefit of vision restoration therapy. Curr Opin Ophthalmol. 2006;17:504-508.
16. Marshall RS, Chmayssani M, O’Brien KA, et al. Visual field expansion after visual restoration therapy. Clin Rehabil. 2010;24: 1027-1035.
17. Mueller I, Mast H, Sabel BA. Recovery of visual field defects: a large clinical observational study using vision restoration therapy. Restor Neurol Neurosci. 2007;25:563-572.
18. Romano JG, Schulz P, Kenkel S, et al. Visual field changes after a rehabilitation intervention: vision restoration therapy. J Neurol Sci. 2008;273:70-74.
19. Allen LA, Woolfolk RL. Cognitive behavioral therapy for somatoform disorders. Psychiatr Clin North Am. 2010;33:579-593.
20. Cukor J, Olden M, Lee F, et al. Evidence-based treatments for PTSD, new directions, and special challenges. Ann N Y Acad Sci. 2010;1208:82-89.
21. Meltzer-Brody S, Connor K, Churchill E, et al. Symptom-specific effects of fluoxetine in PTSD. Intl Clin Psychopharmacol. 2000;15:227-231.
22. Stein DJ, Ipser JC, Seedat S. Pharmacotherapy for post traumatic stress disorder. Cochrane Database Syst Rev. 2006(1):CD002795.
23. Braun P, Greenberg D, Dasberg H, et al. Core symptoms of post-traumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry. 1990;51:236-238.
24. Bisson J, Andrew M. Psychological treatment of post-traumatic stress disorder. Cochrane Database Syst Rev. 2007(3): CD003388.
25. Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults. J Clin Sleep Med. 2010;6:389-401.
26. Reid SF, Chalder T, Cleare A, et al. Chronic fatigue syndrome. Clin Evid (Online). 2008 Aug 28;2008:1101.
27. Hall H, McIntosh G. Low back pain (chronic) Clin Evid (Online). 2008 Oct 1;2008:1116.
28. Prevedini A,Presti G,Ragitti E, et al.Acceptance and commitment Therapy (ACT): the foundation of the therapeutic model and an overview of its contribution to the treatment of patients with chronic physical diseases. G Ital Med Lav Ergon. 2011;33(1suppl A):A53-63.
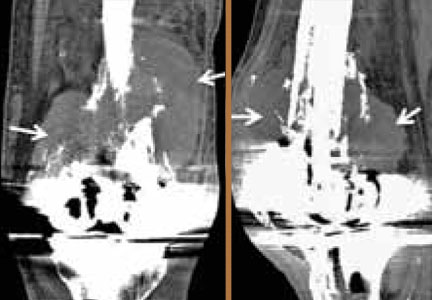
Patient-Specific Imaging and Missed Tumors: A Catastrophic Outcome
Urolithiasis in a Patient With HIV Receiving Atazanavir
Phialophora verrucosa as a Cause of Deep Infection Following Total Knee Arthroplasty
Osteolytic Psuedotumor After Cemented Total Knee Arthroplasty

Acute Compartment Syndrome Following Distal Biceps Tendon Rupture in an Otherwise Healthy Male

Strategies for Treating Scoliosis in Children With Spinal Muscular Atrophy

Case Studies in ToxicologyNeonatal Seizure: Sepsis or Toxic Syndrome?
Neonatal Seizure: Sepsis or Toxic Syndrome?
A mother presents to the ED with her 4-day-old daughter after noting abnormal jerking movements of the neonate's upper extremities. She states the baby has had watery stools for the past day, but has been tolerating bottle formula feeds without vomiting and having appropriate urinary output. The patient was born full-term via normal spontaneous vaginal delivery, with Apgar scores of 8 at 1 minute and 9 at 5 minutes. The postdelivery course was uncomplicated, and both mother and baby were discharged home 2 days after delivery.
Initial vital signs are: heart rate, 135 beats/min; respiratory rate (RR), 48 breaths/min; and temperature, 98.7°F; blood glucose was normal. On physical examination, the baby is awake and well-appearing, with a nonbulging anterior fontanelle, soft, supple neck, and flexed and symmetrically mobile extremities. Moro, suck, rooting, and grasp reflexes are all intact. No abnormal movements are noted. The remainder of the examination is unremarkable.
Do the jerking movements indicate a focal seizure? What could cause these movements in a neonate?
As the length of the postpartum hospital stay has decreased over the past 20 years, EDs have experienced an increase in neonatal visits for conditions that traditionally manifested in newborn nurseries. While most presentations are for benign reasons (eg, issues related to feeding, irritability), patients with concerning conditions, including central nervous system (CNS) abnormalities, may also initially present to the ED. Causes of such clinical findings may be structural (eg, cerebral malformations, subdural hematomas, herpes encephalitis) and/or metabolic (eg, hypoglycemia, hypocalcemia, inborn errors). Many early-onset neonatal seizures are benign and resolve by several months of age, but it is essential to identify those that are consequential and treatable.
Case Continuation
In the evaluation of the neonatal patient with suspected seizure, it is important to take a detailed maternal and labor history, and to consider a broad differential in the face of nonspecific findings. In this case, the patient's mother disclosed a personal history of chronic pain, for which she took buprenorphine 2 mg orally in the morning and 4 mg orally at bedtime (total daily dose of 6mg/day) throughout her pregnancy.
How does drug withdrawal present in the neonate?
Neonatal abstinence syndrome (NAS) is the clinical syndrome of withdrawal in a newborn exposed in utero to drugs capable of inducing dependence. Agents associated with NAS include opioids, benzodiazepines, ethanol, selective serotonin reuptake inhibitors (SSRIs), mood stabilizers, and nicotine.1,2
Over the past decade, there has been a 330% rise in the diagnosis of opioid-related NAS alone.3 In response to this increase, the US Food and Drug Administration recently added a black-box warning to all extended-release/long-acting opioid preparations detailing this risk.4
Presenting symptoms of NAS are protean, differ from patient to patient, and are a function of drug type, duration, and amount of drug exposure. NAS may mimic other severe life-threatening conditions such as those previously noted, and the inability to obtain an adequate symptom-based medical history from a neonate further complicates the diagnosis. Before making a diagnosis of NAS, other conditions should be carefully considered in the differential.
Take Home Points |
|
Neonatal opioid withdrawal manifests primarily with CNS and gastrointestinal (GI) effects since there are high concentrations of opioid receptors in these areas. Although clinical findings are generally similar among opioid agents, the onset and duration following abstinence varies—largely based on individual drug half-life; this helps to differentiate between opioid agents. For example, while babies exposed to heroin in utero present with signs of NAS within 24 hours of birth, those exposed to buprenorphine or methadone tend to present 2 to 6 days after delivery.1 Between 55% to 94% of neonates with in-utero opioid exposure develop NAS.5

Select Serotonin Reuptake Inhibitors
SSRIs have also been associated with a neonatal syndrome, and largely involve similar signs and symptoms as NAS. Although the specific etiology is not clear, it has been suggested that this syndrome is the result of serotonin toxicity rather than withdrawal; as such, it is often referred to as "serotonin discontinuation syndrome." Clinical findings occur from several hours to several days after birth and usually resolve within 1 to 2 weeks.6
Cocaine Exposure
In-utero cocaine exposure is also associated with neurobehavioral abnormalities in neonates although a withdrawal syndrome is less clearly defined. Findings, however, are consistent with NAS and include increased irritability, tremors, and high-pitched cry—most frequently occurring between 24 and 48 hours postdelivery.6
Neonatal Alcohol Withdrawal Syndrome
Neonatal alcohol withdrawal syndrome, particularly in fetuses exposed to alcohol during the last trimester, is distinct from fetal alcohol syndrome (FAS). The latter is associated with typical dysmorphic features, growth deficiencies, and CNS findings reflective of permanent neurologic sequelae. Neonatal alcohol withdrawal presents with CNS findings similar to those listed for other in-utero exposures—eg, increased irritability, tremors, nystagmus hyperactive reflexes.7
Screening for NAS: The Finnegan Scale
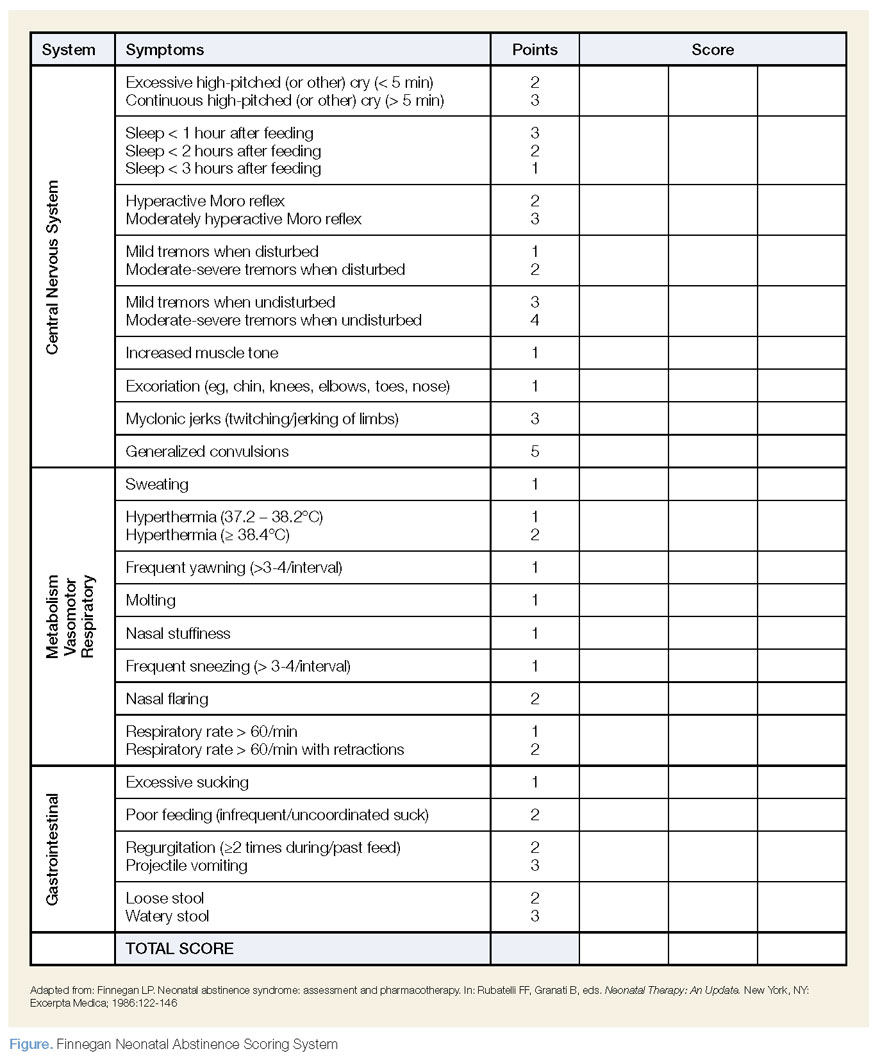
The Finnegan Neonatal Abstinence Scoring System is one of the most commonly employed and validated tools used to screen for NAS. It comprises a 31-item scale, listing the clinical signs and symptoms of NAS, which are scored by severity and organized by system to include neurologic, metabolic, vasomotor, respiratory, and GI disturbances (Figure). Point allocation is based on mild, moderate, or severe symptoms as follows:
- Mild findings (eg, sweating, fever <101°F mottling, nasal stuffiness) each score 1 point.
- Moderate findings (eg, high-pitched cry, hyperactive moro reflex, increased muscle tone, fever >101°F, increased RR >60 with retractions, poor feeding, loose stools) each score 2 points.
- Severe findings (eg, myoclonic jerks, generalized convulsions, projectile vomiting, watery stools) each score 3 points.
While each of the above are independently nonspecific, the constellation of findings, together with the appropriate history, provide for a clinical diagnosis. The Finnegan Scale is therefore designed not only to aid in diagnosis, but also to quantify the severity of NAS and guide management.
Screening for NAS begins at birth in neonates with known in-utero exposure (ie, when risk of NAS is high) or at the time of initial presentation in other circumstances. Scoring is performed every 4 hours; the first two or three scores will determine the need for pharmacotherapy (see Table).
| Table |
Pharmacotherapy is indicated in the following Finnegan scoring scenarios: |
|
|
|
How is NAS treated?
The two main goals of management in the treatment of opioid-related NAS are to relieve the signs and symptoms of withdrawal and to prevent complications (eg, fever, weight loss, seizures). Therapy should begin with nonpharmacologic measures that minimize excess external stimuli, such as swaddling, gentle handling, and minimizing noise and light. To prevent weight loss, small hypercaloric feeds may be helpful. If pharmacologic treatment is indicated, oral opioid replacement with morphine is considered by many to be the drug of choice. Oral morphine dosing may be guided by NAS severity based on the Finnegan score; alternatively, initial dosing at 0.1 mg/kg orally every 4 hours has also been recommended.1
Other agents, such methadone 0.1 mg/kg orally every 12 hours and buprenorphine 15.9 mcg/kg divided in three doses orally, may also be used. In patients whose symptoms persist despite opioid treatment, use of adjuncts such as phenobarbital and clonidine may be indicated.
Case Conclusion
The patient was admitted to the neonatal intensive care unit where she appropriately underwent a sepsis workup. Laboratory evaluation, including blood and urine cultures, was obtained. A brain ultrasound was unremarkable, and since lumbar puncture was unsuccessful, the patient was started empirically on meningitis doses of the cefotaxime, vancomycin, and acyclovir.
An initial Finnegan score was calculated. With the exception of soft stools, there were no other persistent symptoms, and patient did not achieve a score indicating a need for pharmacologic management. After 48 hours, she remained afebrile and soft stools resolved. All laboratory values, including cultures, were unremarkable. The patient was discharged on hospital day 3, with a scheduled well-baby follow-up appointment.
Dr Laskowski is a medical toxicology fellow in the department of emergency medicine at New York University Langone Medical Center. Dr Nelson, editor of "Case Studies in Toxicology," is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
- Cramton RE, Gruchala NE. Babies breaking bad: neonatal and iatrogenic withdrawal syndromes. Curr Opin Pediatr. 2013;25(4): 532-542.
- Kraft WK, Dysart K, Greenspan JS, Gibson E, Kaltenbach K, Ehrlich ME. Revised dose schema of sublingual buprenorphine in the treatment of the neonatal opioid abstinence syndrome. Addiction. 2011;106(3):574-580. http://dx.doi.org/10.1111/j.1360-0443.2010.03170.x Accessed October 24, 2013.
- Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. JAMA. 2012;307(18):1934-40.
- New safety measures announced for extended-release and long-acting opioids. US Food and Drug Administration Web site. www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm363722.htm. Accessed October 24, 2013.
- Burgos AE, Burke BL Jr. Neonatal abstinence syndrome. NeoReviews. 2009;10(5):e222-e228. http://dx.doi.org/10.1542/neo.10-5-e222. Accessed October 24, 2013.
- Hudak ML, Tan RC. Committee on Drugs. Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540-e560.
- Coles CD, Smith IE, Fernhoff PM, Falek A. Neonatal ethanol withdrawal: Characteristics in clinically normal nondysmorphic neonates. J Pediatr. 1984;105(3):445-451.
A mother presents to the ED with her 4-day-old daughter after noting abnormal jerking movements of the neonate's upper extremities. She states the baby has had watery stools for the past day, but has been tolerating bottle formula feeds without vomiting and having appropriate urinary output. The patient was born full-term via normal spontaneous vaginal delivery, with Apgar scores of 8 at 1 minute and 9 at 5 minutes. The postdelivery course was uncomplicated, and both mother and baby were discharged home 2 days after delivery.
Initial vital signs are: heart rate, 135 beats/min; respiratory rate (RR), 48 breaths/min; and temperature, 98.7°F; blood glucose was normal. On physical examination, the baby is awake and well-appearing, with a nonbulging anterior fontanelle, soft, supple neck, and flexed and symmetrically mobile extremities. Moro, suck, rooting, and grasp reflexes are all intact. No abnormal movements are noted. The remainder of the examination is unremarkable.
Do the jerking movements indicate a focal seizure? What could cause these movements in a neonate?
As the length of the postpartum hospital stay has decreased over the past 20 years, EDs have experienced an increase in neonatal visits for conditions that traditionally manifested in newborn nurseries. While most presentations are for benign reasons (eg, issues related to feeding, irritability), patients with concerning conditions, including central nervous system (CNS) abnormalities, may also initially present to the ED. Causes of such clinical findings may be structural (eg, cerebral malformations, subdural hematomas, herpes encephalitis) and/or metabolic (eg, hypoglycemia, hypocalcemia, inborn errors). Many early-onset neonatal seizures are benign and resolve by several months of age, but it is essential to identify those that are consequential and treatable.
Case Continuation
In the evaluation of the neonatal patient with suspected seizure, it is important to take a detailed maternal and labor history, and to consider a broad differential in the face of nonspecific findings. In this case, the patient's mother disclosed a personal history of chronic pain, for which she took buprenorphine 2 mg orally in the morning and 4 mg orally at bedtime (total daily dose of 6mg/day) throughout her pregnancy.
How does drug withdrawal present in the neonate?
Neonatal abstinence syndrome (NAS) is the clinical syndrome of withdrawal in a newborn exposed in utero to drugs capable of inducing dependence. Agents associated with NAS include opioids, benzodiazepines, ethanol, selective serotonin reuptake inhibitors (SSRIs), mood stabilizers, and nicotine.1,2
Over the past decade, there has been a 330% rise in the diagnosis of opioid-related NAS alone.3 In response to this increase, the US Food and Drug Administration recently added a black-box warning to all extended-release/long-acting opioid preparations detailing this risk.4
Presenting symptoms of NAS are protean, differ from patient to patient, and are a function of drug type, duration, and amount of drug exposure. NAS may mimic other severe life-threatening conditions such as those previously noted, and the inability to obtain an adequate symptom-based medical history from a neonate further complicates the diagnosis. Before making a diagnosis of NAS, other conditions should be carefully considered in the differential.
Take Home Points |
|
Neonatal opioid withdrawal manifests primarily with CNS and gastrointestinal (GI) effects since there are high concentrations of opioid receptors in these areas. Although clinical findings are generally similar among opioid agents, the onset and duration following abstinence varies—largely based on individual drug half-life; this helps to differentiate between opioid agents. For example, while babies exposed to heroin in utero present with signs of NAS within 24 hours of birth, those exposed to buprenorphine or methadone tend to present 2 to 6 days after delivery.1 Between 55% to 94% of neonates with in-utero opioid exposure develop NAS.5
Select Serotonin Reuptake Inhibitors
SSRIs have also been associated with a neonatal syndrome, and largely involve similar signs and symptoms as NAS. Although the specific etiology is not clear, it has been suggested that this syndrome is the result of serotonin toxicity rather than withdrawal; as such, it is often referred to as "serotonin discontinuation syndrome." Clinical findings occur from several hours to several days after birth and usually resolve within 1 to 2 weeks.6
Cocaine Exposure
In-utero cocaine exposure is also associated with neurobehavioral abnormalities in neonates although a withdrawal syndrome is less clearly defined. Findings, however, are consistent with NAS and include increased irritability, tremors, and high-pitched cry—most frequently occurring between 24 and 48 hours postdelivery.6
Neonatal Alcohol Withdrawal Syndrome
Neonatal alcohol withdrawal syndrome, particularly in fetuses exposed to alcohol during the last trimester, is distinct from fetal alcohol syndrome (FAS). The latter is associated with typical dysmorphic features, growth deficiencies, and CNS findings reflective of permanent neurologic sequelae. Neonatal alcohol withdrawal presents with CNS findings similar to those listed for other in-utero exposures—eg, increased irritability, tremors, nystagmus hyperactive reflexes.7
Screening for NAS: The Finnegan Scale
The Finnegan Neonatal Abstinence Scoring System is one of the most commonly employed and validated tools used to screen for NAS. It comprises a 31-item scale, listing the clinical signs and symptoms of NAS, which are scored by severity and organized by system to include neurologic, metabolic, vasomotor, respiratory, and GI disturbances (Figure). Point allocation is based on mild, moderate, or severe symptoms as follows:
- Mild findings (eg, sweating, fever <101°F mottling, nasal stuffiness) each score 1 point.
- Moderate findings (eg, high-pitched cry, hyperactive moro reflex, increased muscle tone, fever >101°F, increased RR >60 with retractions, poor feeding, loose stools) each score 2 points.
- Severe findings (eg, myoclonic jerks, generalized convulsions, projectile vomiting, watery stools) each score 3 points.
While each of the above are independently nonspecific, the constellation of findings, together with the appropriate history, provide for a clinical diagnosis. The Finnegan Scale is therefore designed not only to aid in diagnosis, but also to quantify the severity of NAS and guide management.
Screening for NAS begins at birth in neonates with known in-utero exposure (ie, when risk of NAS is high) or at the time of initial presentation in other circumstances. Scoring is performed every 4 hours; the first two or three scores will determine the need for pharmacotherapy (see Table).
| Table |
Pharmacotherapy is indicated in the following Finnegan scoring scenarios: |
|
|
|
How is NAS treated?
The two main goals of management in the treatment of opioid-related NAS are to relieve the signs and symptoms of withdrawal and to prevent complications (eg, fever, weight loss, seizures). Therapy should begin with nonpharmacologic measures that minimize excess external stimuli, such as swaddling, gentle handling, and minimizing noise and light. To prevent weight loss, small hypercaloric feeds may be helpful. If pharmacologic treatment is indicated, oral opioid replacement with morphine is considered by many to be the drug of choice. Oral morphine dosing may be guided by NAS severity based on the Finnegan score; alternatively, initial dosing at 0.1 mg/kg orally every 4 hours has also been recommended.1
Other agents, such methadone 0.1 mg/kg orally every 12 hours and buprenorphine 15.9 mcg/kg divided in three doses orally, may also be used. In patients whose symptoms persist despite opioid treatment, use of adjuncts such as phenobarbital and clonidine may be indicated.
Case Conclusion
The patient was admitted to the neonatal intensive care unit where she appropriately underwent a sepsis workup. Laboratory evaluation, including blood and urine cultures, was obtained. A brain ultrasound was unremarkable, and since lumbar puncture was unsuccessful, the patient was started empirically on meningitis doses of the cefotaxime, vancomycin, and acyclovir.
An initial Finnegan score was calculated. With the exception of soft stools, there were no other persistent symptoms, and patient did not achieve a score indicating a need for pharmacologic management. After 48 hours, she remained afebrile and soft stools resolved. All laboratory values, including cultures, were unremarkable. The patient was discharged on hospital day 3, with a scheduled well-baby follow-up appointment.
Dr Laskowski is a medical toxicology fellow in the department of emergency medicine at New York University Langone Medical Center. Dr Nelson, editor of "Case Studies in Toxicology," is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
A mother presents to the ED with her 4-day-old daughter after noting abnormal jerking movements of the neonate's upper extremities. She states the baby has had watery stools for the past day, but has been tolerating bottle formula feeds without vomiting and having appropriate urinary output. The patient was born full-term via normal spontaneous vaginal delivery, with Apgar scores of 8 at 1 minute and 9 at 5 minutes. The postdelivery course was uncomplicated, and both mother and baby were discharged home 2 days after delivery.
Initial vital signs are: heart rate, 135 beats/min; respiratory rate (RR), 48 breaths/min; and temperature, 98.7°F; blood glucose was normal. On physical examination, the baby is awake and well-appearing, with a nonbulging anterior fontanelle, soft, supple neck, and flexed and symmetrically mobile extremities. Moro, suck, rooting, and grasp reflexes are all intact. No abnormal movements are noted. The remainder of the examination is unremarkable.
Do the jerking movements indicate a focal seizure? What could cause these movements in a neonate?
As the length of the postpartum hospital stay has decreased over the past 20 years, EDs have experienced an increase in neonatal visits for conditions that traditionally manifested in newborn nurseries. While most presentations are for benign reasons (eg, issues related to feeding, irritability), patients with concerning conditions, including central nervous system (CNS) abnormalities, may also initially present to the ED. Causes of such clinical findings may be structural (eg, cerebral malformations, subdural hematomas, herpes encephalitis) and/or metabolic (eg, hypoglycemia, hypocalcemia, inborn errors). Many early-onset neonatal seizures are benign and resolve by several months of age, but it is essential to identify those that are consequential and treatable.
Case Continuation
In the evaluation of the neonatal patient with suspected seizure, it is important to take a detailed maternal and labor history, and to consider a broad differential in the face of nonspecific findings. In this case, the patient's mother disclosed a personal history of chronic pain, for which she took buprenorphine 2 mg orally in the morning and 4 mg orally at bedtime (total daily dose of 6mg/day) throughout her pregnancy.
How does drug withdrawal present in the neonate?
Neonatal abstinence syndrome (NAS) is the clinical syndrome of withdrawal in a newborn exposed in utero to drugs capable of inducing dependence. Agents associated with NAS include opioids, benzodiazepines, ethanol, selective serotonin reuptake inhibitors (SSRIs), mood stabilizers, and nicotine.1,2
Over the past decade, there has been a 330% rise in the diagnosis of opioid-related NAS alone.3 In response to this increase, the US Food and Drug Administration recently added a black-box warning to all extended-release/long-acting opioid preparations detailing this risk.4
Presenting symptoms of NAS are protean, differ from patient to patient, and are a function of drug type, duration, and amount of drug exposure. NAS may mimic other severe life-threatening conditions such as those previously noted, and the inability to obtain an adequate symptom-based medical history from a neonate further complicates the diagnosis. Before making a diagnosis of NAS, other conditions should be carefully considered in the differential.
Take Home Points |
|
Neonatal opioid withdrawal manifests primarily with CNS and gastrointestinal (GI) effects since there are high concentrations of opioid receptors in these areas. Although clinical findings are generally similar among opioid agents, the onset and duration following abstinence varies—largely based on individual drug half-life; this helps to differentiate between opioid agents. For example, while babies exposed to heroin in utero present with signs of NAS within 24 hours of birth, those exposed to buprenorphine or methadone tend to present 2 to 6 days after delivery.1 Between 55% to 94% of neonates with in-utero opioid exposure develop NAS.5
Select Serotonin Reuptake Inhibitors
SSRIs have also been associated with a neonatal syndrome, and largely involve similar signs and symptoms as NAS. Although the specific etiology is not clear, it has been suggested that this syndrome is the result of serotonin toxicity rather than withdrawal; as such, it is often referred to as "serotonin discontinuation syndrome." Clinical findings occur from several hours to several days after birth and usually resolve within 1 to 2 weeks.6
Cocaine Exposure
In-utero cocaine exposure is also associated with neurobehavioral abnormalities in neonates although a withdrawal syndrome is less clearly defined. Findings, however, are consistent with NAS and include increased irritability, tremors, and high-pitched cry—most frequently occurring between 24 and 48 hours postdelivery.6
Neonatal Alcohol Withdrawal Syndrome
Neonatal alcohol withdrawal syndrome, particularly in fetuses exposed to alcohol during the last trimester, is distinct from fetal alcohol syndrome (FAS). The latter is associated with typical dysmorphic features, growth deficiencies, and CNS findings reflective of permanent neurologic sequelae. Neonatal alcohol withdrawal presents with CNS findings similar to those listed for other in-utero exposures—eg, increased irritability, tremors, nystagmus hyperactive reflexes.7
Screening for NAS: The Finnegan Scale
The Finnegan Neonatal Abstinence Scoring System is one of the most commonly employed and validated tools used to screen for NAS. It comprises a 31-item scale, listing the clinical signs and symptoms of NAS, which are scored by severity and organized by system to include neurologic, metabolic, vasomotor, respiratory, and GI disturbances (Figure). Point allocation is based on mild, moderate, or severe symptoms as follows:
- Mild findings (eg, sweating, fever <101°F mottling, nasal stuffiness) each score 1 point.
- Moderate findings (eg, high-pitched cry, hyperactive moro reflex, increased muscle tone, fever >101°F, increased RR >60 with retractions, poor feeding, loose stools) each score 2 points.
- Severe findings (eg, myoclonic jerks, generalized convulsions, projectile vomiting, watery stools) each score 3 points.
While each of the above are independently nonspecific, the constellation of findings, together with the appropriate history, provide for a clinical diagnosis. The Finnegan Scale is therefore designed not only to aid in diagnosis, but also to quantify the severity of NAS and guide management.
Screening for NAS begins at birth in neonates with known in-utero exposure (ie, when risk of NAS is high) or at the time of initial presentation in other circumstances. Scoring is performed every 4 hours; the first two or three scores will determine the need for pharmacotherapy (see Table).
| Table |
Pharmacotherapy is indicated in the following Finnegan scoring scenarios: |
|
|
|
How is NAS treated?
The two main goals of management in the treatment of opioid-related NAS are to relieve the signs and symptoms of withdrawal and to prevent complications (eg, fever, weight loss, seizures). Therapy should begin with nonpharmacologic measures that minimize excess external stimuli, such as swaddling, gentle handling, and minimizing noise and light. To prevent weight loss, small hypercaloric feeds may be helpful. If pharmacologic treatment is indicated, oral opioid replacement with morphine is considered by many to be the drug of choice. Oral morphine dosing may be guided by NAS severity based on the Finnegan score; alternatively, initial dosing at 0.1 mg/kg orally every 4 hours has also been recommended.1
Other agents, such methadone 0.1 mg/kg orally every 12 hours and buprenorphine 15.9 mcg/kg divided in three doses orally, may also be used. In patients whose symptoms persist despite opioid treatment, use of adjuncts such as phenobarbital and clonidine may be indicated.
Case Conclusion
The patient was admitted to the neonatal intensive care unit where she appropriately underwent a sepsis workup. Laboratory evaluation, including blood and urine cultures, was obtained. A brain ultrasound was unremarkable, and since lumbar puncture was unsuccessful, the patient was started empirically on meningitis doses of the cefotaxime, vancomycin, and acyclovir.
An initial Finnegan score was calculated. With the exception of soft stools, there were no other persistent symptoms, and patient did not achieve a score indicating a need for pharmacologic management. After 48 hours, she remained afebrile and soft stools resolved. All laboratory values, including cultures, were unremarkable. The patient was discharged on hospital day 3, with a scheduled well-baby follow-up appointment.
Dr Laskowski is a medical toxicology fellow in the department of emergency medicine at New York University Langone Medical Center. Dr Nelson, editor of "Case Studies in Toxicology," is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
- Cramton RE, Gruchala NE. Babies breaking bad: neonatal and iatrogenic withdrawal syndromes. Curr Opin Pediatr. 2013;25(4): 532-542.
- Kraft WK, Dysart K, Greenspan JS, Gibson E, Kaltenbach K, Ehrlich ME. Revised dose schema of sublingual buprenorphine in the treatment of the neonatal opioid abstinence syndrome. Addiction. 2011;106(3):574-580. http://dx.doi.org/10.1111/j.1360-0443.2010.03170.x Accessed October 24, 2013.
- Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. JAMA. 2012;307(18):1934-40.
- New safety measures announced for extended-release and long-acting opioids. US Food and Drug Administration Web site. www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm363722.htm. Accessed October 24, 2013.
- Burgos AE, Burke BL Jr. Neonatal abstinence syndrome. NeoReviews. 2009;10(5):e222-e228. http://dx.doi.org/10.1542/neo.10-5-e222. Accessed October 24, 2013.
- Hudak ML, Tan RC. Committee on Drugs. Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540-e560.
- Coles CD, Smith IE, Fernhoff PM, Falek A. Neonatal ethanol withdrawal: Characteristics in clinically normal nondysmorphic neonates. J Pediatr. 1984;105(3):445-451.
- Cramton RE, Gruchala NE. Babies breaking bad: neonatal and iatrogenic withdrawal syndromes. Curr Opin Pediatr. 2013;25(4): 532-542.
- Kraft WK, Dysart K, Greenspan JS, Gibson E, Kaltenbach K, Ehrlich ME. Revised dose schema of sublingual buprenorphine in the treatment of the neonatal opioid abstinence syndrome. Addiction. 2011;106(3):574-580. http://dx.doi.org/10.1111/j.1360-0443.2010.03170.x Accessed October 24, 2013.
- Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. JAMA. 2012;307(18):1934-40.
- New safety measures announced for extended-release and long-acting opioids. US Food and Drug Administration Web site. www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm363722.htm. Accessed October 24, 2013.
- Burgos AE, Burke BL Jr. Neonatal abstinence syndrome. NeoReviews. 2009;10(5):e222-e228. http://dx.doi.org/10.1542/neo.10-5-e222. Accessed October 24, 2013.
- Hudak ML, Tan RC. Committee on Drugs. Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540-e560.
- Coles CD, Smith IE, Fernhoff PM, Falek A. Neonatal ethanol withdrawal: Characteristics in clinically normal nondysmorphic neonates. J Pediatr. 1984;105(3):445-451.
Neonatal Seizure: Sepsis or Toxic Syndrome?
Neonatal Seizure: Sepsis or Toxic Syndrome?
A practical guide to community-acquired MRSA
› Treat a simple cutaneous abscess from a methicillin-resistant Staphylococcus
aureus (MRSA) infection with incision and drainage alone. A
› Treat minor MRSA skin lesions in children with mupirocin. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A 21-year-old man seeks care at his family physician (FP)’s office for a painful, draining lesion that’s been on his left thigh for 5 days. He reports that he was bitten by a spider during one of his weekly football games with his fraternity brothers, but doesn’t recall seeing a spider. He has been applying an over-the-counter topical antibiotic without any improvement, and reports that the area of redness has tripled in size within the last 24 hours.
His past medical history is unremarkable except for an allergy to sulfa drugs that was discovered during treatment for a skin infection 2 years ago. He takes no regular medications.
The patient is afebrile and in no distress. The skin overlying his left thigh has a 1 cm oozing lesion with pus evident and surrounding erythema. The wound is warm and tender to the touch.
Based on the patient’s history, the FP suspects methicillin-resistant Staphylococcus aureus (MRSA) and obtains a swab for bacterial culture and sensitivities.
What the surveillance data tell us about MRSA
MRSA infections—a subset of staph infections that are resistant to beta-lactam antibiotics and cephalosporins—continue to be a major source of infection in the community.1 The prevalence of both community-acquired (CA) and hospital acquired (HA) MRSA infections worldwide has continued to grow despite improvements in controlling nosocomial spread.2,3 Data from the early 2000s found an approximate 1% to 2% MRSA colonization rate in the United States, but other countries have had rates as high as 50%.3 Rates across countries have consistently been higher in children and adolescents. A recent surveillance study suggests a decline in the incidence of the most serious types of MRSA infections in major metropolitan areas, the significance of which is still under investigation.4
CA-MRSA and HA-MRSA have different in vitro sensitivities to antimicrobials, different virulence factors, and different epidemiologic profiles.
CA-MRSA occurs in people who have not been recently hospitalized or had any recent medical procedures. These infections usually develop on skin and soft tissue. CA-MRSA typically contains the genes for the Panton-Valentine Leukocidin (PVL) toxin, which is a virulence factor that leads to increased interleukin-8 secretion and skin necrosis.5,6 In addition, CA-MRSA usually does not have genes associated with multidrug-resistant strains.
HA-MRSA occurs in people who have recently been hospitalized, had recent medical procedures, or have been treated in a longterm care setting. HA-MRSA is associated with multidrug-resistant strains; however, it usually does not have the genes for PVL toxin.7
Factors that put patients at risk for CA-MRSA skin infections
As many as 90% of CA-MRSA infections present as skin and soft tissue infections (SSTIs) that have the potential to become invasive if not managed appropriately.3,8 There are a number of factors that put patients at risk for these SSTIs (TABLE 1)7-9—chief among them, intrafamilial or close contact transmission. People living in close quarters with colonized individuals are 14 times more likely to be carriers than a matched unexposed population.9 Similarly, other environments that typically involve close quarters or overcrowding, including military installations, prisons, long-term care facilities, and daycare centers, generally see higher rates of MRSA colonization.10
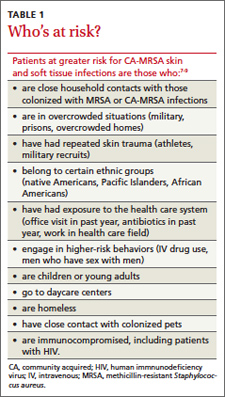
Researchers also hypothesize that repeated skin trauma is another risk factor for CA-MRSA SSTIs. This may explain the increased rates of CA-MRSA infections seen in athletes and military recruits undergoing basic training, as they are prone to skin abrasions.8 Certain ethnic groups have a higher prevalence of CA-MRSA infections as well, including Native Americans, Pacific Islanders, and African Americans.9,11 It is not entirely clear if there is anything unique predisposing these populations to MRSA or if this might be attributed to living in tight communities with close household contacts.
High-risk groups that have elevated rates of CA-MRSA SSTIs and are more likely to be carriers include intravenous drug users, men who have sex with men, immunocompromised individuals (including those with human immunodeficiency virus), and the homeless.8,9 Several studies have also reported higher rates of MRSA colonization and CA-MRSA infections in individuals who have come into contact with the health care system. A meta-analysis indicated that nasal swabs taken from patients at health care facilities were 2.35 times more likely to be positive for MRSA than those taken from individuals as nonhealth care locations.9 Risk factors such as antibiotic use or one or more physician visits in the past year have been associated with higher rates of infections, as well.2
Diagnosis requires careful history and exam
Community-acquired MRSA SSTIs are often diagnosed based on the patient’s history and risk factors, along with physical exam findings. Common findings include single or multiple erythematous pustules, furuncles, carbuncles, cellulitis, and abscesses. Patients may confuse the initial lesion with an insect or spider bite,12 as occurred with the patient in our opening scenario.
If purulent drainage is present, perform a swab for culture and sensitivity to confirm the diagnosis of MRSA and assist in antibiotic selection.13 If a patient with an SSTI does not respond to beta-lactam antibiotics, consider MRSA until proven otherwise.
Once confirmed by microbiological assessment, follow Centers for Disease Control and Prevention guidelines to differentiate CA-MRSA from HA-MRSA.14 It is important to distinguish between the two, as patients with HA-MRSA are at greater risk for antibiotic failure and progression to more invasive infections.
Confirmation of a CA-MRSA infection requires all of the following criteria:14
• Diagnosis was made in the outpatient setting or by positive culture within 48 hours of admission to the hospital
• No history of MRSA infection or colonization
• No history in the past year of hospitalization; admission to a skilled nursing facility or hospice; dialysis; or surgery
• No permanent indwelling catheters or medical devices that go through the skin.
Confirmation of an HA-MRSA infection requires at least one of the following criteria:14
• It occurs more than 48 hours after admission to the hospital.
• There is a prior history of MRSA infection or colonization.
• There is a history in the past year of hospitalization; admission to a skilled
nursing facility, nursing home, or hospice; dialysis; or surgery.
• The presence of any indwelling catheter or medical device that passes through the skin into the body.
Rely on evidence-based treatment protocols
In 2011, the Infectious Disease Society of America (IDSA) published consensus guidelines for CA-MRSA to assist with evidencebased decision making. Primary treatment of cutaneous abscesses remains incision and drainage alone without antibiotics, except under certain circumstances (TABLE 2).13 The guidelines recommend antibiotic treatment with empiric coverage for CA-MRSA when purulent cellulitis exists. However, if cellulitis exists without purulence or abscess formation, antibiotic coverage for CA-MRSA is not encouraged for initial treatment.13
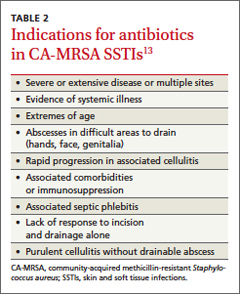
Empiric antibiotic coverage for uncomplicated CA-MRSA SSTIs managed in the outpatient setting should include clindamycin, trimethoprim/sulfamethoxazole (TMPSMX), a tetracycline, or linezolid for 5 to 10 days. Factors including cost, patient age and comorbidities, drug allergies, and local resistance patterns should guide the initial antibiotic you choose. TMP-SMX and tetracyclines are relatively inexpensive (<$20), clindamycin is more costly, and linezolid is often costprohibitive as standard treatment.
Do not prescribe tetracyclines for children younger than 8 years of age because of the risk of permanent tooth discoloration. Clindamycin is the only category “B” antibiotic in the group that can be used during pregnancy, and renal impairment needs to be taken into consideration with TMP-SMX and linezolid. For very minor skin lesions in children, mupirocin 2% topical ointment appears to be the therapy of choice.13
Although IDSA has not provided strong recommendations about treatment of asymptomatic close household contacts, this may be considered as another means of attempting to control the spread of MRSA in the community.
Provide patient education. Patient education is paramount to successful treatment and prevention. Explain to patients that people living in close quarters with individuals who already have the bacteria on the skin are far more likely to be carriers. Overcrowding situations that pose a risk include military installations, prisons, long-term care facilities, athletic teams, and daycare centers.
To prevent MRSA, encourage patients to wash their hands often and shower regularly, especially after exercise. Also keep cuts, scrapes, and wounds clean and covered until they heal. Avoid sharing personal items, such as towel and razors.
Finally, remind patients to get care early if they think they may be infected. Symptoms suggestive of MRSA include a red, swollen, painful area on the skin that may look like a spider bite. The area may contain pus and be accompanied by a fever.
Provide close outpatient follow-up within a few days of initiating therapy to document clinical response and aid in further decision-making. Signs of more extensive cellulitis may signal a need for a change of antibiotics or parenteral therapy. Similarly, joint or bone pain underlying areas of cellulitis, significant myalgias or muscle pain out of proportion to exam, or systemic symptoms such as fever, chills, nausea, or lethargy might indicate more extensive infection requiring inpatient treatment.
How to manage recurrent infections
Management of recurrent CA-MRSA SSTIs in the outpatient setting poses a challenge. Following successful treatment of active infection, you may want to attempt decolonization in select patients. Those with repeated MRSA infections despite adequate hygiene measures or with a high probability of reexposure to colonized close contacts may be treated, although the evidence supporting such protocols is lacking.8,13
Acceptable procedures described by IDSA include nasal mupirocin twice daily for 5 to 10 days, mupirocin plus topical antiseptic solution (eg, chlorhexidine, triclosan, or povidone-iodine) for 5 to 14 days, or mupirocin plus dilute bleach baths (1 teaspoon bleach/gallon of water) twice weekly for 15 minutes over 3 months.13 Although antibiotics are generally only recommended for active infection, the combination of rifampin and an antibiotic with MRSA coverage may be used for 1 to 2 weeks in cases of recurrent infections despite recommended hygiene and topical decolonization measures.13,15,16 Rifampin is not recommended as monotherapy for MRSA infection or decolonization.13
Unfortunately, even in cases where eradication is initially successful, about half of those with subsequent negative MRSA cultures will test positive before the end of a year.16 With recurrent or severe infections or immunocompromised patients, it’s advisable to consider an infectious disease consult.
CASE › The patient’s lesion did not require incision as it was already draining. He received a prescription for doxycycline hyclate 100 mg BID for 7 days (since there was evidence of rapidly progressing cellulitis) and was instructed to return to the clinic in 48 hours.
When he returned to the clinic, the patient stated that the pain had improved and the wound was no longer oozing. Culture results confirmed MR SA sensitive to TMP-SMX, doxycycline, and clindamycin. Examination showed improved erythema, a dry wound, and no pain on palpation. He was given a patient information handout on MRSA infection and advised to return to the clinic if the wound did not completely heal within the next 7 days.
1. Özel G, Aslan V, Bahar Erdem G, et al. Comparison of oxacillin, cefoxitin, ceftizoxime, and moxalactam disk diffusion methods for detection of methicillin susceptibility in staphylococci. Mikrobiyol Bul. 2011;45:258-265.
2. Crum NF, Lee RU, Thornton SA, et al. Fifteen-year study of the changing epidemiology of methicillin-resistant Staphylococcus aureus. Am J Med. 2006;119:943-951.
3. Skov R, Christiansen K, Dancer SJ, et al. Update on the prevention and control of community-acquired meticillin-resistant Staphylococcus aureus (CA-MRSA). Int J Antimicrob Agents. 2012;39:193-200.
4. Dantes R, Mu Y, Belflower R, et al. National burden of invasive methicillin-resistant Staphylococcus aureus infections, United States, 2011. JAMA Intern Med. September 16, 2013. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1738718. Accessed October 15, 2013.
5. Kawaguchiya M, Urushibara N, Kuwahara O, et al. Molecular characteristics of community-acquired methicillin-resistant Staphylococcus aureus in Hokkaido, northern main island of Japan: identification of sequence types 6 and 59 Panton-Valentine leucocidin-positive community-acquired methicillin-resistant Staphylococcus aureus. Microb Drug Resist. 2011;17:241-250.
6. Wiener-Kronish JP, Pittet JF. Therapies against virulence products of Staphylococcus aureus and Pseudomonas aeruginosa. Semin Respir Crit Care Med. 2011;32:228-235.
7. Hansra NK, Shinkai K. Cutaneous community-acquired and hospital-acquired methicillin-resistant Staphylococcus aureus. Dermatol Ther. 2011;24:263-272.
8. Elston DM. Community-acquired methicillin-resistant Staphylococcus aureus. J Am Acad Dermatol. 2007;56:1-16; quiz 17-20.
9. Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-139.
10. Gorwitz RJ. A review of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infections. Pediatr Infect Dis J. 2008;27:1-7.
11. Klevens RM, Morrison MA, Nadle J, et al; Active Bacterial Core Surveillance (ABCs) MRSA Investigators. Invasive methicillinresistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.
12. NeVille-Swensen M, Clayton M. Outpatient management of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infection. J Pediatr Health Care. 2011;25:308-315.
13. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285-292.
14. Diagnosis and testing for MRSA infections. Centers for Disease Control and Infection Web site. Available at: http://www.cdc.gov/mrsa/diagnosis/index.html. Accessed September 30, 2013.
15. Buehlmann M, Frei R, Fenner L, et al. Highly effective regimen for decolonization of methicillin-resistant Staphylococcus aureus carriers. Infect Control Hosp Epidemiol. 2008;29:510-516.
16. Simor AE, Phillips E, McGeer A, et al. Randomized controlled trial of chlorhexidine gluconate for washing, intranasal mupirocin, and rifampin and doxycycline versus no treatment for the eradication of methicillin-resistant Staphylococcus aureus colonization. Clin Infect Dis. 2007;44:178-185.
› Treat a simple cutaneous abscess from a methicillin-resistant Staphylococcus
aureus (MRSA) infection with incision and drainage alone. A
› Treat minor MRSA skin lesions in children with mupirocin. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A 21-year-old man seeks care at his family physician (FP)’s office for a painful, draining lesion that’s been on his left thigh for 5 days. He reports that he was bitten by a spider during one of his weekly football games with his fraternity brothers, but doesn’t recall seeing a spider. He has been applying an over-the-counter topical antibiotic without any improvement, and reports that the area of redness has tripled in size within the last 24 hours.
His past medical history is unremarkable except for an allergy to sulfa drugs that was discovered during treatment for a skin infection 2 years ago. He takes no regular medications.
The patient is afebrile and in no distress. The skin overlying his left thigh has a 1 cm oozing lesion with pus evident and surrounding erythema. The wound is warm and tender to the touch.
Based on the patient’s history, the FP suspects methicillin-resistant Staphylococcus aureus (MRSA) and obtains a swab for bacterial culture and sensitivities.
What the surveillance data tell us about MRSA
MRSA infections—a subset of staph infections that are resistant to beta-lactam antibiotics and cephalosporins—continue to be a major source of infection in the community.1 The prevalence of both community-acquired (CA) and hospital acquired (HA) MRSA infections worldwide has continued to grow despite improvements in controlling nosocomial spread.2,3 Data from the early 2000s found an approximate 1% to 2% MRSA colonization rate in the United States, but other countries have had rates as high as 50%.3 Rates across countries have consistently been higher in children and adolescents. A recent surveillance study suggests a decline in the incidence of the most serious types of MRSA infections in major metropolitan areas, the significance of which is still under investigation.4
CA-MRSA and HA-MRSA have different in vitro sensitivities to antimicrobials, different virulence factors, and different epidemiologic profiles.
CA-MRSA occurs in people who have not been recently hospitalized or had any recent medical procedures. These infections usually develop on skin and soft tissue. CA-MRSA typically contains the genes for the Panton-Valentine Leukocidin (PVL) toxin, which is a virulence factor that leads to increased interleukin-8 secretion and skin necrosis.5,6 In addition, CA-MRSA usually does not have genes associated with multidrug-resistant strains.
HA-MRSA occurs in people who have recently been hospitalized, had recent medical procedures, or have been treated in a longterm care setting. HA-MRSA is associated with multidrug-resistant strains; however, it usually does not have the genes for PVL toxin.7
Factors that put patients at risk for CA-MRSA skin infections
As many as 90% of CA-MRSA infections present as skin and soft tissue infections (SSTIs) that have the potential to become invasive if not managed appropriately.3,8 There are a number of factors that put patients at risk for these SSTIs (TABLE 1)7-9—chief among them, intrafamilial or close contact transmission. People living in close quarters with colonized individuals are 14 times more likely to be carriers than a matched unexposed population.9 Similarly, other environments that typically involve close quarters or overcrowding, including military installations, prisons, long-term care facilities, and daycare centers, generally see higher rates of MRSA colonization.10
Researchers also hypothesize that repeated skin trauma is another risk factor for CA-MRSA SSTIs. This may explain the increased rates of CA-MRSA infections seen in athletes and military recruits undergoing basic training, as they are prone to skin abrasions.8 Certain ethnic groups have a higher prevalence of CA-MRSA infections as well, including Native Americans, Pacific Islanders, and African Americans.9,11 It is not entirely clear if there is anything unique predisposing these populations to MRSA or if this might be attributed to living in tight communities with close household contacts.
High-risk groups that have elevated rates of CA-MRSA SSTIs and are more likely to be carriers include intravenous drug users, men who have sex with men, immunocompromised individuals (including those with human immunodeficiency virus), and the homeless.8,9 Several studies have also reported higher rates of MRSA colonization and CA-MRSA infections in individuals who have come into contact with the health care system. A meta-analysis indicated that nasal swabs taken from patients at health care facilities were 2.35 times more likely to be positive for MRSA than those taken from individuals as nonhealth care locations.9 Risk factors such as antibiotic use or one or more physician visits in the past year have been associated with higher rates of infections, as well.2
Diagnosis requires careful history and exam
Community-acquired MRSA SSTIs are often diagnosed based on the patient’s history and risk factors, along with physical exam findings. Common findings include single or multiple erythematous pustules, furuncles, carbuncles, cellulitis, and abscesses. Patients may confuse the initial lesion with an insect or spider bite,12 as occurred with the patient in our opening scenario.
If purulent drainage is present, perform a swab for culture and sensitivity to confirm the diagnosis of MRSA and assist in antibiotic selection.13 If a patient with an SSTI does not respond to beta-lactam antibiotics, consider MRSA until proven otherwise.
Once confirmed by microbiological assessment, follow Centers for Disease Control and Prevention guidelines to differentiate CA-MRSA from HA-MRSA.14 It is important to distinguish between the two, as patients with HA-MRSA are at greater risk for antibiotic failure and progression to more invasive infections.
Confirmation of a CA-MRSA infection requires all of the following criteria:14
• Diagnosis was made in the outpatient setting or by positive culture within 48 hours of admission to the hospital
• No history of MRSA infection or colonization
• No history in the past year of hospitalization; admission to a skilled nursing facility or hospice; dialysis; or surgery
• No permanent indwelling catheters or medical devices that go through the skin.
Confirmation of an HA-MRSA infection requires at least one of the following criteria:14
• It occurs more than 48 hours after admission to the hospital.
• There is a prior history of MRSA infection or colonization.
• There is a history in the past year of hospitalization; admission to a skilled
nursing facility, nursing home, or hospice; dialysis; or surgery.
• The presence of any indwelling catheter or medical device that passes through the skin into the body.
Rely on evidence-based treatment protocols
In 2011, the Infectious Disease Society of America (IDSA) published consensus guidelines for CA-MRSA to assist with evidencebased decision making. Primary treatment of cutaneous abscesses remains incision and drainage alone without antibiotics, except under certain circumstances (TABLE 2).13 The guidelines recommend antibiotic treatment with empiric coverage for CA-MRSA when purulent cellulitis exists. However, if cellulitis exists without purulence or abscess formation, antibiotic coverage for CA-MRSA is not encouraged for initial treatment.13
Empiric antibiotic coverage for uncomplicated CA-MRSA SSTIs managed in the outpatient setting should include clindamycin, trimethoprim/sulfamethoxazole (TMPSMX), a tetracycline, or linezolid for 5 to 10 days. Factors including cost, patient age and comorbidities, drug allergies, and local resistance patterns should guide the initial antibiotic you choose. TMP-SMX and tetracyclines are relatively inexpensive (<$20), clindamycin is more costly, and linezolid is often costprohibitive as standard treatment.
Do not prescribe tetracyclines for children younger than 8 years of age because of the risk of permanent tooth discoloration. Clindamycin is the only category “B” antibiotic in the group that can be used during pregnancy, and renal impairment needs to be taken into consideration with TMP-SMX and linezolid. For very minor skin lesions in children, mupirocin 2% topical ointment appears to be the therapy of choice.13
Although IDSA has not provided strong recommendations about treatment of asymptomatic close household contacts, this may be considered as another means of attempting to control the spread of MRSA in the community.
Provide patient education. Patient education is paramount to successful treatment and prevention. Explain to patients that people living in close quarters with individuals who already have the bacteria on the skin are far more likely to be carriers. Overcrowding situations that pose a risk include military installations, prisons, long-term care facilities, athletic teams, and daycare centers.
To prevent MRSA, encourage patients to wash their hands often and shower regularly, especially after exercise. Also keep cuts, scrapes, and wounds clean and covered until they heal. Avoid sharing personal items, such as towel and razors.
Finally, remind patients to get care early if they think they may be infected. Symptoms suggestive of MRSA include a red, swollen, painful area on the skin that may look like a spider bite. The area may contain pus and be accompanied by a fever.
Provide close outpatient follow-up within a few days of initiating therapy to document clinical response and aid in further decision-making. Signs of more extensive cellulitis may signal a need for a change of antibiotics or parenteral therapy. Similarly, joint or bone pain underlying areas of cellulitis, significant myalgias or muscle pain out of proportion to exam, or systemic symptoms such as fever, chills, nausea, or lethargy might indicate more extensive infection requiring inpatient treatment.
How to manage recurrent infections
Management of recurrent CA-MRSA SSTIs in the outpatient setting poses a challenge. Following successful treatment of active infection, you may want to attempt decolonization in select patients. Those with repeated MRSA infections despite adequate hygiene measures or with a high probability of reexposure to colonized close contacts may be treated, although the evidence supporting such protocols is lacking.8,13
Acceptable procedures described by IDSA include nasal mupirocin twice daily for 5 to 10 days, mupirocin plus topical antiseptic solution (eg, chlorhexidine, triclosan, or povidone-iodine) for 5 to 14 days, or mupirocin plus dilute bleach baths (1 teaspoon bleach/gallon of water) twice weekly for 15 minutes over 3 months.13 Although antibiotics are generally only recommended for active infection, the combination of rifampin and an antibiotic with MRSA coverage may be used for 1 to 2 weeks in cases of recurrent infections despite recommended hygiene and topical decolonization measures.13,15,16 Rifampin is not recommended as monotherapy for MRSA infection or decolonization.13
Unfortunately, even in cases where eradication is initially successful, about half of those with subsequent negative MRSA cultures will test positive before the end of a year.16 With recurrent or severe infections or immunocompromised patients, it’s advisable to consider an infectious disease consult.
CASE › The patient’s lesion did not require incision as it was already draining. He received a prescription for doxycycline hyclate 100 mg BID for 7 days (since there was evidence of rapidly progressing cellulitis) and was instructed to return to the clinic in 48 hours.
When he returned to the clinic, the patient stated that the pain had improved and the wound was no longer oozing. Culture results confirmed MR SA sensitive to TMP-SMX, doxycycline, and clindamycin. Examination showed improved erythema, a dry wound, and no pain on palpation. He was given a patient information handout on MRSA infection and advised to return to the clinic if the wound did not completely heal within the next 7 days.
› Treat a simple cutaneous abscess from a methicillin-resistant Staphylococcus
aureus (MRSA) infection with incision and drainage alone. A
› Treat minor MRSA skin lesions in children with mupirocin. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A 21-year-old man seeks care at his family physician (FP)’s office for a painful, draining lesion that’s been on his left thigh for 5 days. He reports that he was bitten by a spider during one of his weekly football games with his fraternity brothers, but doesn’t recall seeing a spider. He has been applying an over-the-counter topical antibiotic without any improvement, and reports that the area of redness has tripled in size within the last 24 hours.
His past medical history is unremarkable except for an allergy to sulfa drugs that was discovered during treatment for a skin infection 2 years ago. He takes no regular medications.
The patient is afebrile and in no distress. The skin overlying his left thigh has a 1 cm oozing lesion with pus evident and surrounding erythema. The wound is warm and tender to the touch.
Based on the patient’s history, the FP suspects methicillin-resistant Staphylococcus aureus (MRSA) and obtains a swab for bacterial culture and sensitivities.
What the surveillance data tell us about MRSA
MRSA infections—a subset of staph infections that are resistant to beta-lactam antibiotics and cephalosporins—continue to be a major source of infection in the community.1 The prevalence of both community-acquired (CA) and hospital acquired (HA) MRSA infections worldwide has continued to grow despite improvements in controlling nosocomial spread.2,3 Data from the early 2000s found an approximate 1% to 2% MRSA colonization rate in the United States, but other countries have had rates as high as 50%.3 Rates across countries have consistently been higher in children and adolescents. A recent surveillance study suggests a decline in the incidence of the most serious types of MRSA infections in major metropolitan areas, the significance of which is still under investigation.4
CA-MRSA and HA-MRSA have different in vitro sensitivities to antimicrobials, different virulence factors, and different epidemiologic profiles.
CA-MRSA occurs in people who have not been recently hospitalized or had any recent medical procedures. These infections usually develop on skin and soft tissue. CA-MRSA typically contains the genes for the Panton-Valentine Leukocidin (PVL) toxin, which is a virulence factor that leads to increased interleukin-8 secretion and skin necrosis.5,6 In addition, CA-MRSA usually does not have genes associated with multidrug-resistant strains.
HA-MRSA occurs in people who have recently been hospitalized, had recent medical procedures, or have been treated in a longterm care setting. HA-MRSA is associated with multidrug-resistant strains; however, it usually does not have the genes for PVL toxin.7
Factors that put patients at risk for CA-MRSA skin infections
As many as 90% of CA-MRSA infections present as skin and soft tissue infections (SSTIs) that have the potential to become invasive if not managed appropriately.3,8 There are a number of factors that put patients at risk for these SSTIs (TABLE 1)7-9—chief among them, intrafamilial or close contact transmission. People living in close quarters with colonized individuals are 14 times more likely to be carriers than a matched unexposed population.9 Similarly, other environments that typically involve close quarters or overcrowding, including military installations, prisons, long-term care facilities, and daycare centers, generally see higher rates of MRSA colonization.10
Researchers also hypothesize that repeated skin trauma is another risk factor for CA-MRSA SSTIs. This may explain the increased rates of CA-MRSA infections seen in athletes and military recruits undergoing basic training, as they are prone to skin abrasions.8 Certain ethnic groups have a higher prevalence of CA-MRSA infections as well, including Native Americans, Pacific Islanders, and African Americans.9,11 It is not entirely clear if there is anything unique predisposing these populations to MRSA or if this might be attributed to living in tight communities with close household contacts.
High-risk groups that have elevated rates of CA-MRSA SSTIs and are more likely to be carriers include intravenous drug users, men who have sex with men, immunocompromised individuals (including those with human immunodeficiency virus), and the homeless.8,9 Several studies have also reported higher rates of MRSA colonization and CA-MRSA infections in individuals who have come into contact with the health care system. A meta-analysis indicated that nasal swabs taken from patients at health care facilities were 2.35 times more likely to be positive for MRSA than those taken from individuals as nonhealth care locations.9 Risk factors such as antibiotic use or one or more physician visits in the past year have been associated with higher rates of infections, as well.2
Diagnosis requires careful history and exam
Community-acquired MRSA SSTIs are often diagnosed based on the patient’s history and risk factors, along with physical exam findings. Common findings include single or multiple erythematous pustules, furuncles, carbuncles, cellulitis, and abscesses. Patients may confuse the initial lesion with an insect or spider bite,12 as occurred with the patient in our opening scenario.
If purulent drainage is present, perform a swab for culture and sensitivity to confirm the diagnosis of MRSA and assist in antibiotic selection.13 If a patient with an SSTI does not respond to beta-lactam antibiotics, consider MRSA until proven otherwise.
Once confirmed by microbiological assessment, follow Centers for Disease Control and Prevention guidelines to differentiate CA-MRSA from HA-MRSA.14 It is important to distinguish between the two, as patients with HA-MRSA are at greater risk for antibiotic failure and progression to more invasive infections.
Confirmation of a CA-MRSA infection requires all of the following criteria:14
• Diagnosis was made in the outpatient setting or by positive culture within 48 hours of admission to the hospital
• No history of MRSA infection or colonization
• No history in the past year of hospitalization; admission to a skilled nursing facility or hospice; dialysis; or surgery
• No permanent indwelling catheters or medical devices that go through the skin.
Confirmation of an HA-MRSA infection requires at least one of the following criteria:14
• It occurs more than 48 hours after admission to the hospital.
• There is a prior history of MRSA infection or colonization.
• There is a history in the past year of hospitalization; admission to a skilled
nursing facility, nursing home, or hospice; dialysis; or surgery.
• The presence of any indwelling catheter or medical device that passes through the skin into the body.
Rely on evidence-based treatment protocols
In 2011, the Infectious Disease Society of America (IDSA) published consensus guidelines for CA-MRSA to assist with evidencebased decision making. Primary treatment of cutaneous abscesses remains incision and drainage alone without antibiotics, except under certain circumstances (TABLE 2).13 The guidelines recommend antibiotic treatment with empiric coverage for CA-MRSA when purulent cellulitis exists. However, if cellulitis exists without purulence or abscess formation, antibiotic coverage for CA-MRSA is not encouraged for initial treatment.13
Empiric antibiotic coverage for uncomplicated CA-MRSA SSTIs managed in the outpatient setting should include clindamycin, trimethoprim/sulfamethoxazole (TMPSMX), a tetracycline, or linezolid for 5 to 10 days. Factors including cost, patient age and comorbidities, drug allergies, and local resistance patterns should guide the initial antibiotic you choose. TMP-SMX and tetracyclines are relatively inexpensive (<$20), clindamycin is more costly, and linezolid is often costprohibitive as standard treatment.
Do not prescribe tetracyclines for children younger than 8 years of age because of the risk of permanent tooth discoloration. Clindamycin is the only category “B” antibiotic in the group that can be used during pregnancy, and renal impairment needs to be taken into consideration with TMP-SMX and linezolid. For very minor skin lesions in children, mupirocin 2% topical ointment appears to be the therapy of choice.13
Although IDSA has not provided strong recommendations about treatment of asymptomatic close household contacts, this may be considered as another means of attempting to control the spread of MRSA in the community.
Provide patient education. Patient education is paramount to successful treatment and prevention. Explain to patients that people living in close quarters with individuals who already have the bacteria on the skin are far more likely to be carriers. Overcrowding situations that pose a risk include military installations, prisons, long-term care facilities, athletic teams, and daycare centers.
To prevent MRSA, encourage patients to wash their hands often and shower regularly, especially after exercise. Also keep cuts, scrapes, and wounds clean and covered until they heal. Avoid sharing personal items, such as towel and razors.
Finally, remind patients to get care early if they think they may be infected. Symptoms suggestive of MRSA include a red, swollen, painful area on the skin that may look like a spider bite. The area may contain pus and be accompanied by a fever.
Provide close outpatient follow-up within a few days of initiating therapy to document clinical response and aid in further decision-making. Signs of more extensive cellulitis may signal a need for a change of antibiotics or parenteral therapy. Similarly, joint or bone pain underlying areas of cellulitis, significant myalgias or muscle pain out of proportion to exam, or systemic symptoms such as fever, chills, nausea, or lethargy might indicate more extensive infection requiring inpatient treatment.
How to manage recurrent infections
Management of recurrent CA-MRSA SSTIs in the outpatient setting poses a challenge. Following successful treatment of active infection, you may want to attempt decolonization in select patients. Those with repeated MRSA infections despite adequate hygiene measures or with a high probability of reexposure to colonized close contacts may be treated, although the evidence supporting such protocols is lacking.8,13
Acceptable procedures described by IDSA include nasal mupirocin twice daily for 5 to 10 days, mupirocin plus topical antiseptic solution (eg, chlorhexidine, triclosan, or povidone-iodine) for 5 to 14 days, or mupirocin plus dilute bleach baths (1 teaspoon bleach/gallon of water) twice weekly for 15 minutes over 3 months.13 Although antibiotics are generally only recommended for active infection, the combination of rifampin and an antibiotic with MRSA coverage may be used for 1 to 2 weeks in cases of recurrent infections despite recommended hygiene and topical decolonization measures.13,15,16 Rifampin is not recommended as monotherapy for MRSA infection or decolonization.13
Unfortunately, even in cases where eradication is initially successful, about half of those with subsequent negative MRSA cultures will test positive before the end of a year.16 With recurrent or severe infections or immunocompromised patients, it’s advisable to consider an infectious disease consult.
CASE › The patient’s lesion did not require incision as it was already draining. He received a prescription for doxycycline hyclate 100 mg BID for 7 days (since there was evidence of rapidly progressing cellulitis) and was instructed to return to the clinic in 48 hours.
When he returned to the clinic, the patient stated that the pain had improved and the wound was no longer oozing. Culture results confirmed MR SA sensitive to TMP-SMX, doxycycline, and clindamycin. Examination showed improved erythema, a dry wound, and no pain on palpation. He was given a patient information handout on MRSA infection and advised to return to the clinic if the wound did not completely heal within the next 7 days.
1. Özel G, Aslan V, Bahar Erdem G, et al. Comparison of oxacillin, cefoxitin, ceftizoxime, and moxalactam disk diffusion methods for detection of methicillin susceptibility in staphylococci. Mikrobiyol Bul. 2011;45:258-265.
2. Crum NF, Lee RU, Thornton SA, et al. Fifteen-year study of the changing epidemiology of methicillin-resistant Staphylococcus aureus. Am J Med. 2006;119:943-951.
3. Skov R, Christiansen K, Dancer SJ, et al. Update on the prevention and control of community-acquired meticillin-resistant Staphylococcus aureus (CA-MRSA). Int J Antimicrob Agents. 2012;39:193-200.
4. Dantes R, Mu Y, Belflower R, et al. National burden of invasive methicillin-resistant Staphylococcus aureus infections, United States, 2011. JAMA Intern Med. September 16, 2013. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1738718. Accessed October 15, 2013.
5. Kawaguchiya M, Urushibara N, Kuwahara O, et al. Molecular characteristics of community-acquired methicillin-resistant Staphylococcus aureus in Hokkaido, northern main island of Japan: identification of sequence types 6 and 59 Panton-Valentine leucocidin-positive community-acquired methicillin-resistant Staphylococcus aureus. Microb Drug Resist. 2011;17:241-250.
6. Wiener-Kronish JP, Pittet JF. Therapies against virulence products of Staphylococcus aureus and Pseudomonas aeruginosa. Semin Respir Crit Care Med. 2011;32:228-235.
7. Hansra NK, Shinkai K. Cutaneous community-acquired and hospital-acquired methicillin-resistant Staphylococcus aureus. Dermatol Ther. 2011;24:263-272.
8. Elston DM. Community-acquired methicillin-resistant Staphylococcus aureus. J Am Acad Dermatol. 2007;56:1-16; quiz 17-20.
9. Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-139.
10. Gorwitz RJ. A review of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infections. Pediatr Infect Dis J. 2008;27:1-7.
11. Klevens RM, Morrison MA, Nadle J, et al; Active Bacterial Core Surveillance (ABCs) MRSA Investigators. Invasive methicillinresistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.
12. NeVille-Swensen M, Clayton M. Outpatient management of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infection. J Pediatr Health Care. 2011;25:308-315.
13. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285-292.
14. Diagnosis and testing for MRSA infections. Centers for Disease Control and Infection Web site. Available at: http://www.cdc.gov/mrsa/diagnosis/index.html. Accessed September 30, 2013.
15. Buehlmann M, Frei R, Fenner L, et al. Highly effective regimen for decolonization of methicillin-resistant Staphylococcus aureus carriers. Infect Control Hosp Epidemiol. 2008;29:510-516.
16. Simor AE, Phillips E, McGeer A, et al. Randomized controlled trial of chlorhexidine gluconate for washing, intranasal mupirocin, and rifampin and doxycycline versus no treatment for the eradication of methicillin-resistant Staphylococcus aureus colonization. Clin Infect Dis. 2007;44:178-185.
1. Özel G, Aslan V, Bahar Erdem G, et al. Comparison of oxacillin, cefoxitin, ceftizoxime, and moxalactam disk diffusion methods for detection of methicillin susceptibility in staphylococci. Mikrobiyol Bul. 2011;45:258-265.
2. Crum NF, Lee RU, Thornton SA, et al. Fifteen-year study of the changing epidemiology of methicillin-resistant Staphylococcus aureus. Am J Med. 2006;119:943-951.
3. Skov R, Christiansen K, Dancer SJ, et al. Update on the prevention and control of community-acquired meticillin-resistant Staphylococcus aureus (CA-MRSA). Int J Antimicrob Agents. 2012;39:193-200.
4. Dantes R, Mu Y, Belflower R, et al. National burden of invasive methicillin-resistant Staphylococcus aureus infections, United States, 2011. JAMA Intern Med. September 16, 2013. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1738718. Accessed October 15, 2013.
5. Kawaguchiya M, Urushibara N, Kuwahara O, et al. Molecular characteristics of community-acquired methicillin-resistant Staphylococcus aureus in Hokkaido, northern main island of Japan: identification of sequence types 6 and 59 Panton-Valentine leucocidin-positive community-acquired methicillin-resistant Staphylococcus aureus. Microb Drug Resist. 2011;17:241-250.
6. Wiener-Kronish JP, Pittet JF. Therapies against virulence products of Staphylococcus aureus and Pseudomonas aeruginosa. Semin Respir Crit Care Med. 2011;32:228-235.
7. Hansra NK, Shinkai K. Cutaneous community-acquired and hospital-acquired methicillin-resistant Staphylococcus aureus. Dermatol Ther. 2011;24:263-272.
8. Elston DM. Community-acquired methicillin-resistant Staphylococcus aureus. J Am Acad Dermatol. 2007;56:1-16; quiz 17-20.
9. Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-139.
10. Gorwitz RJ. A review of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infections. Pediatr Infect Dis J. 2008;27:1-7.
11. Klevens RM, Morrison MA, Nadle J, et al; Active Bacterial Core Surveillance (ABCs) MRSA Investigators. Invasive methicillinresistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.
12. NeVille-Swensen M, Clayton M. Outpatient management of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infection. J Pediatr Health Care. 2011;25:308-315.
13. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285-292.
14. Diagnosis and testing for MRSA infections. Centers for Disease Control and Infection Web site. Available at: http://www.cdc.gov/mrsa/diagnosis/index.html. Accessed September 30, 2013.
15. Buehlmann M, Frei R, Fenner L, et al. Highly effective regimen for decolonization of methicillin-resistant Staphylococcus aureus carriers. Infect Control Hosp Epidemiol. 2008;29:510-516.
16. Simor AE, Phillips E, McGeer A, et al. Randomized controlled trial of chlorhexidine gluconate for washing, intranasal mupirocin, and rifampin and doxycycline versus no treatment for the eradication of methicillin-resistant Staphylococcus aureus colonization. Clin Infect Dis. 2007;44:178-185.