User login
Case Studies in Toxicology: The Acclaimed Zombie-Apocalypse Drug—Is it Just an Illusion?
Dr Takematsu is a senior fellow of medical toxicology, department of emergency medicine, New York University School of Medicine and New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at New York University School of Medicine and New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.

Case
A 50-year-old man with a 16-year history of injection heroin abuse presented to the ED complaining of ulcerative lesions on his right arm, which he stated had become worse over the past 3 months. He claimed the skin lesions, which involved his entire right arm, had grown “wider and deeper” since he started using the drug “Krokodil.” He further noted that he obtained the product from four different drug suppliers but did not know how it was prepared.
On presentation, his vital signs were: blood pressure, 135/78 mm Hg; heart rate, 92 beats/minute; respiratory rate, 14 breaths/minute; temperature, 98.2˚ F. Oxygen saturation was 100% on room air. Physical examination of the right arm was notable for broad ulcers that exposed fat tissue and muscle and involved the entire forearm circumferentially (Figure 1). There were no signs of acute infection such as erythema, warmth, or abscess formation. The remainder of the physical examination was unremarkable.
What is Krokodil?
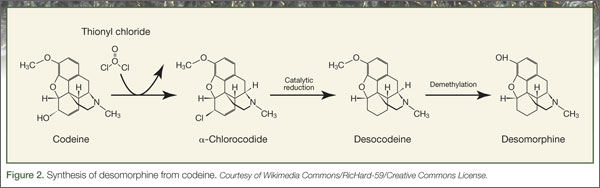
The name Krokodil is derived from the Russian word for crocodile, and stems from the greenish, severely damaged “crocodile-like” skin lesions purportedly caused by subcutaneous injection of this opioid derivative. Krokodil is not a specific drug but rather it describes the product derived from an attempt to synthesize desomorphine, the core ingredient. Desomorphine is a short-acting opioid analogue that has a reported potency eight to 10 times greater than morphine (Figure 2).
Also called “Russian Magic,” Krokodil has been used in Russia since 2003 following the country’s major restrictions on the importation of heroin. Since desomorphine can be synthesized from codeine, which was available in over-the-counter medications in Russia until 2012, drug users have turned to it as an inexpensive heroin substitute. (The average cost of a codeine-containing product is about 120 Rubles [$4.00] per 10-pack.1)
The chemical process of synthesizing desomorphine typically involves mixing one to five packs of codeine-based analgesics1 with a solvent (eg, paint thinner, gasoline), along with iodine and red phosphorous, which can be obtained from the striking pads of matchboxes.2 This produces a yield equivalent to 500 Rubles of heroin, making it an attractive alternative to low-income drug users.1 However, the yields are poor, and the starting products vary based on the codeine source. No systemic analysis of Krokodil has been performed to assess the purity and concentration of desomorphine in the resulting product.
What are the risks of using Krokodil?
Krokodil is typically self-administered by either intravenous (IV) or subcutaneous (“skin-popping”) injection. Solvents and contaminants in the product can damage tissue with which they come into contact. Thus, IV use of this product causes venous scarring and collapse3; when venous access is exhausted, or following infiltration, the subcutaneous route may lead to necrosis and ulceration of the skin. These lesions are said to be used by illicit drug users as a “shooter’s patch” to inject drugs,4 leading to further skin damage. In addition to the local dermal effects, systemic inflammation results from the dissemination of the components of the product, causing neurological, solid-organ, and other effects.
Has Krokodil reached the United States?
Because of the horrifying appearance of the skin lesions, Krokodil has been called by many descriptive names such as the “flesh-eating drug” and “zombie-apocalypse drug,” which in turn has led to somewhat sensationalistic media reporting. There is, however, no clear evidence of entry of desomorphine or of Krokodil use in the United States, and most authorities feel either is unlikely to occur. This speculation is supported by the low cost and easy availability of heroin in the United States compared to Russia. Of note, although Russia banned the nonprescription sale of products containing codeine in November 2012, the ban has had minimal impact on the rate of necrotic skin lesions.
To date, none of the so-called cases of Krokodil-associated lesions reported in the United States have confirmatory analytical testing, and diagnoses have been based primarily on history or morphological features of the wound. Furthermore, no reference laboratories in the United States have identified desomorphine in any of their tested samples. Since the skin lesions are not pathognomonic of Krokodil use and share morphologic features with all forms of subcutaneous drug use, analytical confirmation is critical to identifying this as an emerging drug trend. Therefore, users of product sold or brewed as Krokodil may develop skin lesions regardless of desomorphine content due to contaminants in the injected product.
What causes the skin lesions?
Desomorphine itself is not likely the cause of the skin lesions. In its pure form, there is no reason to expect this compound would induce any specific changes in the skin that would lead to necrosis. In fact, similar chemical syntheses of desomorphine produced in other countries, such as in the Czech Republic and New Zealand, have not led to analogous skin lesions. Ulcerative skin damage is most likely caused by the inflammatory contaminants in Krokodil. Injection of solvents and other chemicals into the subcutaneous space lead to skin damage and provide a bed for the development of indolent infections. This mechanism is similar to that leading to epidemics, in which similar lesions have been associated with black-tar heroin injection and drug contamination with Bacillus anthracis.5,6
Some people, however, point out the severity of the skin lesions associated with the use of Krokodil compared to other injection drugs. This may be related to the need for frequent administration of Krokodil due to its short duration of action, in turn leading to repeated exposure to the impure solvents.
Treatment of associated lesions involves wound care, including debridement, topical care, and antibiotics; amputation may be required in severe cases.
Case conclusion
The patient in this case was taken to the operating room for debridement of the right arm. The pathology results of the tissue showed ulceration, abscess, acute and chronic inflamed granulation tissue, fibrosis, and necrosis. A magnetic resonance image of the arm showed no signs of osteomyelitis. A blood sample sent for analysis was negative for desomorphine. The patient was stable after the surgery, and was discharged with follow-up instructions and referral for drug abuse counseling.
- Grund JP, Latypov A, Harris M. Breaking worse: The emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. Int J Drug Policy. 2013;24(4):265-274.
- Gahr M, Freudenmann RW, Hiemke C, Gunst IM, Connemann BJ, Schönfeldt-Lecuona C. Desomorphine goes “crocodile.” J Addict Dis. 2012;31(4):407-412.
- Pieper B, Kirsner RS, Templin TN, Birk TJ. Injection drug use: an understudied cause of venous disease. Arch Dermatol. 2007;143(10):1305-1309.
- Iyer S, Subramanian P, Pabari A. A devastating complication of “skin popping.” Surgeon. 2011;9(5):295-297.
- Dunbar NM, Harruff RC. Necrotizing fasciitis: manifestations, microbiology and connection with black tar heroin. J Forensic Sci. 2007;52(4):920-923.
- Grunow R, Klee SR, Beyer W, et al. Anthrax among heroin users in Europe possibly caused by same Bacillus anthracis strain since 2000. E Euro Surveill. 2013;18(13):pii=20437.
Dr Takematsu is a senior fellow of medical toxicology, department of emergency medicine, New York University School of Medicine and New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at New York University School of Medicine and New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
Case
A 50-year-old man with a 16-year history of injection heroin abuse presented to the ED complaining of ulcerative lesions on his right arm, which he stated had become worse over the past 3 months. He claimed the skin lesions, which involved his entire right arm, had grown “wider and deeper” since he started using the drug “Krokodil.” He further noted that he obtained the product from four different drug suppliers but did not know how it was prepared.
On presentation, his vital signs were: blood pressure, 135/78 mm Hg; heart rate, 92 beats/minute; respiratory rate, 14 breaths/minute; temperature, 98.2˚ F. Oxygen saturation was 100% on room air. Physical examination of the right arm was notable for broad ulcers that exposed fat tissue and muscle and involved the entire forearm circumferentially (Figure 1). There were no signs of acute infection such as erythema, warmth, or abscess formation. The remainder of the physical examination was unremarkable.
What is Krokodil?
The name Krokodil is derived from the Russian word for crocodile, and stems from the greenish, severely damaged “crocodile-like” skin lesions purportedly caused by subcutaneous injection of this opioid derivative. Krokodil is not a specific drug but rather it describes the product derived from an attempt to synthesize desomorphine, the core ingredient. Desomorphine is a short-acting opioid analogue that has a reported potency eight to 10 times greater than morphine (Figure 2).
Also called “Russian Magic,” Krokodil has been used in Russia since 2003 following the country’s major restrictions on the importation of heroin. Since desomorphine can be synthesized from codeine, which was available in over-the-counter medications in Russia until 2012, drug users have turned to it as an inexpensive heroin substitute. (The average cost of a codeine-containing product is about 120 Rubles [$4.00] per 10-pack.1)
The chemical process of synthesizing desomorphine typically involves mixing one to five packs of codeine-based analgesics1 with a solvent (eg, paint thinner, gasoline), along with iodine and red phosphorous, which can be obtained from the striking pads of matchboxes.2 This produces a yield equivalent to 500 Rubles of heroin, making it an attractive alternative to low-income drug users.1 However, the yields are poor, and the starting products vary based on the codeine source. No systemic analysis of Krokodil has been performed to assess the purity and concentration of desomorphine in the resulting product.
What are the risks of using Krokodil?
Krokodil is typically self-administered by either intravenous (IV) or subcutaneous (“skin-popping”) injection. Solvents and contaminants in the product can damage tissue with which they come into contact. Thus, IV use of this product causes venous scarring and collapse3; when venous access is exhausted, or following infiltration, the subcutaneous route may lead to necrosis and ulceration of the skin. These lesions are said to be used by illicit drug users as a “shooter’s patch” to inject drugs,4 leading to further skin damage. In addition to the local dermal effects, systemic inflammation results from the dissemination of the components of the product, causing neurological, solid-organ, and other effects.
Has Krokodil reached the United States?
Because of the horrifying appearance of the skin lesions, Krokodil has been called by many descriptive names such as the “flesh-eating drug” and “zombie-apocalypse drug,” which in turn has led to somewhat sensationalistic media reporting. There is, however, no clear evidence of entry of desomorphine or of Krokodil use in the United States, and most authorities feel either is unlikely to occur. This speculation is supported by the low cost and easy availability of heroin in the United States compared to Russia. Of note, although Russia banned the nonprescription sale of products containing codeine in November 2012, the ban has had minimal impact on the rate of necrotic skin lesions.
To date, none of the so-called cases of Krokodil-associated lesions reported in the United States have confirmatory analytical testing, and diagnoses have been based primarily on history or morphological features of the wound. Furthermore, no reference laboratories in the United States have identified desomorphine in any of their tested samples. Since the skin lesions are not pathognomonic of Krokodil use and share morphologic features with all forms of subcutaneous drug use, analytical confirmation is critical to identifying this as an emerging drug trend. Therefore, users of product sold or brewed as Krokodil may develop skin lesions regardless of desomorphine content due to contaminants in the injected product.
What causes the skin lesions?
Desomorphine itself is not likely the cause of the skin lesions. In its pure form, there is no reason to expect this compound would induce any specific changes in the skin that would lead to necrosis. In fact, similar chemical syntheses of desomorphine produced in other countries, such as in the Czech Republic and New Zealand, have not led to analogous skin lesions. Ulcerative skin damage is most likely caused by the inflammatory contaminants in Krokodil. Injection of solvents and other chemicals into the subcutaneous space lead to skin damage and provide a bed for the development of indolent infections. This mechanism is similar to that leading to epidemics, in which similar lesions have been associated with black-tar heroin injection and drug contamination with Bacillus anthracis.5,6
Some people, however, point out the severity of the skin lesions associated with the use of Krokodil compared to other injection drugs. This may be related to the need for frequent administration of Krokodil due to its short duration of action, in turn leading to repeated exposure to the impure solvents.
Treatment of associated lesions involves wound care, including debridement, topical care, and antibiotics; amputation may be required in severe cases.
Case conclusion
The patient in this case was taken to the operating room for debridement of the right arm. The pathology results of the tissue showed ulceration, abscess, acute and chronic inflamed granulation tissue, fibrosis, and necrosis. A magnetic resonance image of the arm showed no signs of osteomyelitis. A blood sample sent for analysis was negative for desomorphine. The patient was stable after the surgery, and was discharged with follow-up instructions and referral for drug abuse counseling.
Dr Takematsu is a senior fellow of medical toxicology, department of emergency medicine, New York University School of Medicine and New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at New York University School of Medicine and New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
Case
A 50-year-old man with a 16-year history of injection heroin abuse presented to the ED complaining of ulcerative lesions on his right arm, which he stated had become worse over the past 3 months. He claimed the skin lesions, which involved his entire right arm, had grown “wider and deeper” since he started using the drug “Krokodil.” He further noted that he obtained the product from four different drug suppliers but did not know how it was prepared.
On presentation, his vital signs were: blood pressure, 135/78 mm Hg; heart rate, 92 beats/minute; respiratory rate, 14 breaths/minute; temperature, 98.2˚ F. Oxygen saturation was 100% on room air. Physical examination of the right arm was notable for broad ulcers that exposed fat tissue and muscle and involved the entire forearm circumferentially (Figure 1). There were no signs of acute infection such as erythema, warmth, or abscess formation. The remainder of the physical examination was unremarkable.
What is Krokodil?
The name Krokodil is derived from the Russian word for crocodile, and stems from the greenish, severely damaged “crocodile-like” skin lesions purportedly caused by subcutaneous injection of this opioid derivative. Krokodil is not a specific drug but rather it describes the product derived from an attempt to synthesize desomorphine, the core ingredient. Desomorphine is a short-acting opioid analogue that has a reported potency eight to 10 times greater than morphine (Figure 2).
Also called “Russian Magic,” Krokodil has been used in Russia since 2003 following the country’s major restrictions on the importation of heroin. Since desomorphine can be synthesized from codeine, which was available in over-the-counter medications in Russia until 2012, drug users have turned to it as an inexpensive heroin substitute. (The average cost of a codeine-containing product is about 120 Rubles [$4.00] per 10-pack.1)
The chemical process of synthesizing desomorphine typically involves mixing one to five packs of codeine-based analgesics1 with a solvent (eg, paint thinner, gasoline), along with iodine and red phosphorous, which can be obtained from the striking pads of matchboxes.2 This produces a yield equivalent to 500 Rubles of heroin, making it an attractive alternative to low-income drug users.1 However, the yields are poor, and the starting products vary based on the codeine source. No systemic analysis of Krokodil has been performed to assess the purity and concentration of desomorphine in the resulting product.
What are the risks of using Krokodil?
Krokodil is typically self-administered by either intravenous (IV) or subcutaneous (“skin-popping”) injection. Solvents and contaminants in the product can damage tissue with which they come into contact. Thus, IV use of this product causes venous scarring and collapse3; when venous access is exhausted, or following infiltration, the subcutaneous route may lead to necrosis and ulceration of the skin. These lesions are said to be used by illicit drug users as a “shooter’s patch” to inject drugs,4 leading to further skin damage. In addition to the local dermal effects, systemic inflammation results from the dissemination of the components of the product, causing neurological, solid-organ, and other effects.
Has Krokodil reached the United States?
Because of the horrifying appearance of the skin lesions, Krokodil has been called by many descriptive names such as the “flesh-eating drug” and “zombie-apocalypse drug,” which in turn has led to somewhat sensationalistic media reporting. There is, however, no clear evidence of entry of desomorphine or of Krokodil use in the United States, and most authorities feel either is unlikely to occur. This speculation is supported by the low cost and easy availability of heroin in the United States compared to Russia. Of note, although Russia banned the nonprescription sale of products containing codeine in November 2012, the ban has had minimal impact on the rate of necrotic skin lesions.
To date, none of the so-called cases of Krokodil-associated lesions reported in the United States have confirmatory analytical testing, and diagnoses have been based primarily on history or morphological features of the wound. Furthermore, no reference laboratories in the United States have identified desomorphine in any of their tested samples. Since the skin lesions are not pathognomonic of Krokodil use and share morphologic features with all forms of subcutaneous drug use, analytical confirmation is critical to identifying this as an emerging drug trend. Therefore, users of product sold or brewed as Krokodil may develop skin lesions regardless of desomorphine content due to contaminants in the injected product.
What causes the skin lesions?
Desomorphine itself is not likely the cause of the skin lesions. In its pure form, there is no reason to expect this compound would induce any specific changes in the skin that would lead to necrosis. In fact, similar chemical syntheses of desomorphine produced in other countries, such as in the Czech Republic and New Zealand, have not led to analogous skin lesions. Ulcerative skin damage is most likely caused by the inflammatory contaminants in Krokodil. Injection of solvents and other chemicals into the subcutaneous space lead to skin damage and provide a bed for the development of indolent infections. This mechanism is similar to that leading to epidemics, in which similar lesions have been associated with black-tar heroin injection and drug contamination with Bacillus anthracis.5,6
Some people, however, point out the severity of the skin lesions associated with the use of Krokodil compared to other injection drugs. This may be related to the need for frequent administration of Krokodil due to its short duration of action, in turn leading to repeated exposure to the impure solvents.
Treatment of associated lesions involves wound care, including debridement, topical care, and antibiotics; amputation may be required in severe cases.
Case conclusion
The patient in this case was taken to the operating room for debridement of the right arm. The pathology results of the tissue showed ulceration, abscess, acute and chronic inflamed granulation tissue, fibrosis, and necrosis. A magnetic resonance image of the arm showed no signs of osteomyelitis. A blood sample sent for analysis was negative for desomorphine. The patient was stable after the surgery, and was discharged with follow-up instructions and referral for drug abuse counseling.
- Grund JP, Latypov A, Harris M. Breaking worse: The emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. Int J Drug Policy. 2013;24(4):265-274.
- Gahr M, Freudenmann RW, Hiemke C, Gunst IM, Connemann BJ, Schönfeldt-Lecuona C. Desomorphine goes “crocodile.” J Addict Dis. 2012;31(4):407-412.
- Pieper B, Kirsner RS, Templin TN, Birk TJ. Injection drug use: an understudied cause of venous disease. Arch Dermatol. 2007;143(10):1305-1309.
- Iyer S, Subramanian P, Pabari A. A devastating complication of “skin popping.” Surgeon. 2011;9(5):295-297.
- Dunbar NM, Harruff RC. Necrotizing fasciitis: manifestations, microbiology and connection with black tar heroin. J Forensic Sci. 2007;52(4):920-923.
- Grunow R, Klee SR, Beyer W, et al. Anthrax among heroin users in Europe possibly caused by same Bacillus anthracis strain since 2000. E Euro Surveill. 2013;18(13):pii=20437.
- Grund JP, Latypov A, Harris M. Breaking worse: The emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. Int J Drug Policy. 2013;24(4):265-274.
- Gahr M, Freudenmann RW, Hiemke C, Gunst IM, Connemann BJ, Schönfeldt-Lecuona C. Desomorphine goes “crocodile.” J Addict Dis. 2012;31(4):407-412.
- Pieper B, Kirsner RS, Templin TN, Birk TJ. Injection drug use: an understudied cause of venous disease. Arch Dermatol. 2007;143(10):1305-1309.
- Iyer S, Subramanian P, Pabari A. A devastating complication of “skin popping.” Surgeon. 2011;9(5):295-297.
- Dunbar NM, Harruff RC. Necrotizing fasciitis: manifestations, microbiology and connection with black tar heroin. J Forensic Sci. 2007;52(4):920-923.
- Grunow R, Klee SR, Beyer W, et al. Anthrax among heroin users in Europe possibly caused by same Bacillus anthracis strain since 2000. E Euro Surveill. 2013;18(13):pii=20437.

Diagnosis at a Glance
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
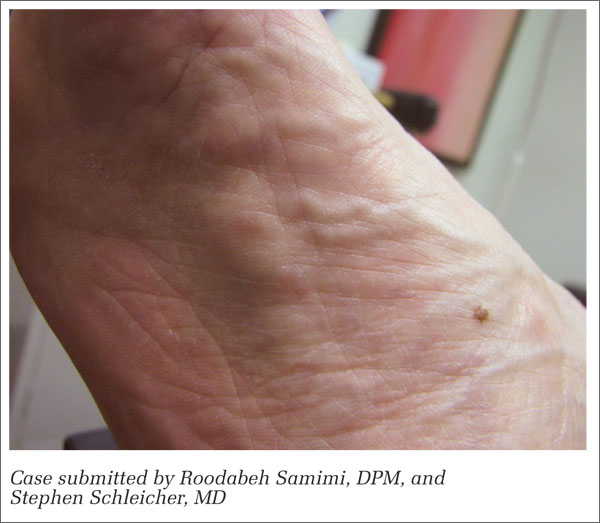
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2

A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2
A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2
A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.

A Case of Malignant Transformation of Myositis Ossificans
Necrotizing Fasciitis: Diagnosis and Management in the ED
Necrotizing fasciitis is a rare but lifethreatening soft-tissue infection. Its presentation is characterized by rapidly spreading inflammation and resultant death—both of the surrounding soft tissue and fascial planes. Prompt recognition and aggressive treatment are paramount to avoid fatality, and appropriate management in the ED is essential to a successful outcome. As the following case illustrates, a high index of suspicion and multidisciplinary approach, including applicable imaging studies, result in timely diagnosis and treatment.
Case
A 60-year-old woman with a medical history of childhood Lyme disease, asthma, high cholesterol, and seasonal allergies, presented to the ED with a 3-day history of left hip and thigh pain, general malaise, decreased appetite, nausea, myalgia, and increased lethargy. She reported difficulty with weight-bearing on her left leg but denied any recent leg trauma or falls. Patient also had a 3-year history of intermittent hip pain, which she treated with ibuprofen. Three weeks prior to presentation, she had undergone an invasive dental procedure in preparation for a root canal. She later developed a fever of 102° F and had taken ibuprofen two-and-a-half hours prior to arrival at our institution.
Initial vital signs on physical examination were: blood pressure (BP) 71/37 mm Hg; heart rate (HR), 98 beats/minute; respiratory rate, 18 breaths/minute; temperature, 98.5° F. Oxygen saturation was 100% on room air. Patient was awake and alert but extremely pale and sluggish. Her head, ears, nose, and throat; pulmonary; cardiac; and abdominal examinations were normal. On physical examination, the skin overlying her left hip and thigh was grossly unremarkable, and no previous incision sites or areas of trauma were observed throughout the left lower extremity. No obvious signs of infection or erythema were noted; however, an area of warmth was felt on the lateral aspect of the left thigh but did not extend beyond the knee. Patient was able to flex her left hip approximately 30° and only complained of pain to the lateral aspect of the upper leg with passive internal and external rotation. Heel strike was negative, and knee examination was negative for pathology. The right lower extremity was unremarkable.


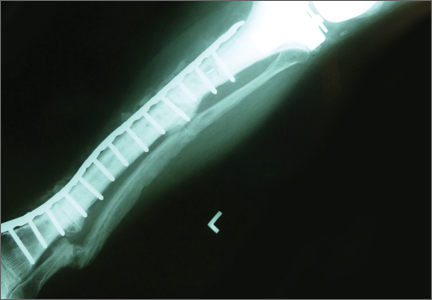
A plain radiograph of the pelvis and left hip showed soft-tissue swelling but no bony pathology or fracture (Figure 1). There was no visual evidence of subcutaneous gas, and chest radiograph was negative for any active disease. Based on the clinical picture of septic shock due to possible septic arthritis, emergent magnetic resonance imaging (MRI) of the left hip and thigh was performed without contrast (Figures 2 and 3). Extensive edema was noted diffusely throughout patient’s left gluteus medius muscle and vastus latera lis muscle; no loculated fluid collection was noted. The edema was concentrated around the proximal left thigh but extended to the level of the knee. The left hip was free of any fluid collection, ruling-out septic arthritis. Based on these MRI findings, a computed tomography scan was ordered, which showed no fluid collection in the pelvis and abdomen (Figure 4).


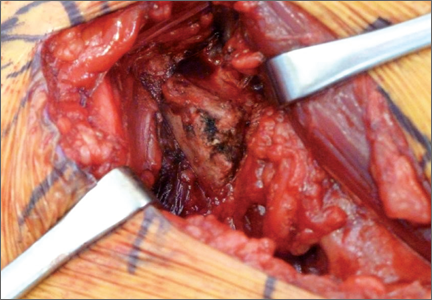
Patient was continued on an antibiotic regimen of IV vancomycin, clindamycin, and piperacillin-tazobactam. Vasopressor support was gradually reduced and respiratory support weaned until both were finally discontinued on postoperative day 2. Soon thereafter, she was transferred to the surgical floor. Negative pressure wound vacuum-assisted closure therapy was applied to the left thigh and was maintained for one week.
The operative cultures were positive for group A Streptococcus (GAS) pyogenes. Upon discharge, antibiotic regimen was adjusted and limited to oral amoxicillin-clavulanate for 14 days until completion. After a 2-week hospital stay, patient was transferred to an acute rehabilitation facility in stable condition and remained there for one week. Follow up was maintained for a total of 6 months, during which time she had no lasting effects from either illness or resultant interventions other than cosmetic concerns from the surgical wounds. In a follow-up phone discussion with patient 10 months after recovery, she reported that she had returned to work as a registered nurse and had been without any functional disability or discomfort.
Discussion
Originally described by Hippocrates in the 5th century as a complication of erysipelas, necrotizing fasciitis later became known as the “malignant ulcer.” It was subsequently described in the United States in 1871 as “hospital gangrene” by Confederate surgeon Joseph Jones.1-3 In 1952, the name was later modified to necrotizing fasciitis by Wilson.4
Today, necrotizing fasciitis is an uncommon disease process, yet one that must be recognized and treated immediately. If not dealt with promptly and aggressively, the virulent and toxin-producing bacteria— most commonly GAS pyogenes— will cause severe systemic toxicity and may lead to death.5
Incidences and Outcomes
According to the US Centers for Disease Control and Prevention (CDC), about 9,000 to 11,500 cases of invasive GAS disease occur each year in the United States, resulting in approximately 1,000 to 1,800 deaths annually. Necrotizing fasciitis comprises an average of 6% to 7% (540- 805) of these invasive cases per year.6
The incidence of necrotizing fasciitis rose sharply in the mid-1980s to the early 1990s but has remained steady over the past 10 years, with 2012 CDC statistics reporting 72 cases per 32,777,740 persons through its voluntary surveillance program. This extrapolates to an estimated 686 cases of GAS-associated necrotizing fasciitis in the United States, with a reported mortality rate of 20% to 25%.7
The highest incidence of disease occurs in the elderly and in patients with diabetes, immunosuppression, and peripheral vascular disease. In children, varicella infection is a known risk factor.8
Other risk factors include obesity, alcohol use, malnutrition, and smoking, as well as corticosteroid use and chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs). Despite the large number of predisposing factors that have been identified, half of all cases of necrotizing fasciitis occur in healthy individuals.9-14
Etiology
Necrotizing fasciitis is thought to be caused by at least two distinct bacteriologic entities. Type I is considered polymicrobial, with Bacteriodes, Clostridium, and Peptostreptococcus, in combination with anaerobic Streptococcus (other than GAS) and Enterobacteriaceae (eg, Escherichia coli, Klebsiella), being the most common infecting species. Type II causative agents include GAS and other β-hemolytic streptococci— alone or with other species of Staphylococcus aureus, including methicillin- resistant S aureus.8 In rare instances, the causative agent is fungal.
Treatment
In a review of patient medical records, Wong et al15 demonstrated that prompt recognition and surgical management of necrotizing fasciitis (ie, within 24 hours of presentation) resulted in improved outcomes. Since the particular causative agent of necrotizing fasciitis in each case is usually unknown, initial treatment should include broad-spectrum IV antibiotics— which are active against grampositive, gram-negative, and anaerobic bacteria—with special consideration for GAS and Clostridium (Table). It is not recommended that initial empiric therapy include antifungals. In this case, the patient was in the OR within 10 hours from presentation, was started immediately on antibiotic regimens for hospital-specific sepsis, and was given appropriate resuscitative measures.
Hyperbaric oxygen therapy is mentioned in the literature as an adjunct to surgery and antibiotics in the treatment of necrotizing fasciitis. Acting as a bactericidal/ bacteriostatic agent against anaerobic bacteria by increasing formation of free oxygen radicals, this therapy is thought to restore the bacterial killing capacity of leukocytes in a hypoxic wound by increasing oxygen tension. Treatment with hyperbaric oxygen may also better define necrotic tissue, facilitating more precise amputation and debridement. Although there are no randomized controlled studies in humans, several authors have shown a reduction in mortality and morbidity with the use of hyperbaric oxygen therapy, in conjunction with early antibiotic and surgical treatment, in animal models and in retrospective studies of patients. 19 When available, hyperbaric oxygen can be initiated once antibiotics have been started and debridement has been performed. The use of hyperbaric oxygen therapy should not delay definitive surgical debridement.
Our case demonstrates a true surgical emergency—one that was appropriately managed with a multidisciplinary team approach. A high index of suspicion by the examining ED staff and surgical consultants led to supportive measures to maintain the patient’s vital signs and ultimately her life. Despite having no clear etiology for the cause of necrotizing fasciitis, we believe it may have resulted from the patient’s prior dental work or chronic NSAID use. Although there is no causal relationship, reports suggest that NSAIDs may prevent prompt recognition and accelerate the infection by altering its initial presentation.20 The patient reported no recent use of anti-inflammatory medication in association with her pain—only for fever.
This report also underscores the importance of urgent MRI in the ED setting. In addition to helping exclude other diagnoses involving the hip joint, MRI provided a roadmap for debridement of active infection. Moreover, the test eliminated the need to explore the left hip joint as well as the risk of seeding a sterile space.21
Conclusion

- Descamps V, Aitken J, Lee MG. Hippocrates on necrotising fasciitis [letter]. Lancet. 1994; 344(8921):556.
- Jones J. Investigations upon the nature, causes, and treatments of hospital gangrene as it prevailed in the Confederate armies 1861-1865. In: Hastings HF, ed. US Sanitary Commission, Surgical memoirs of the War of Rebellion. New York, New York: Riverside; 1871:146-170.
- Loudon I. Necrotising fasciitis, hospital gangrene, and phagedena. Lancet. 1994;344(8934):1416-1419.
- Wilson B. Necrotizing fasciitis. Am Surg. 1952;18(4):416-431.
- Green RJ, Dafoe DC, Raffin TA. Necrotizing fasciitis. Chest. 1996;110(1):219-229.
- Necrotizing fasciitis: A Rare Disease, Especially for the Healthy. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/Features/NecrotizingFasciitis/. Accessed January 2, 2014.
- ABCs report: group A Streptococcus, 2012-provisional. Active Bacterial Core Surveillance (ABCs): Emerging Infections Program Network. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/abcs/reports-findings/survreports/gas12.html. Accessed January 2, 2014.
- Stevens, DL, Baddour, LM. Necrotizing soft tissue infections. UpToDate Web site. http://www.uptodate.com/contents/necrotizing-soft-tissue-infections. Accessed January 2, 2014.
- Bellapianta J, Ljungquist K, Tobin E, Uhl R. Necrotizing Fasciitis. J Am Acad Orthop Surg. 2009;17(3):174-182.
- Childers BJ, Potyondy LD, Nachreiner R, et al. Necrotizing fasciitis: A fourteen-year retrospective study of 163 consecutive patients. Am Surg. 2002;68(2):109-116.
- Dufel S, Martino M. Simple cellulitis or a more serious infection? J Fam Pract. 2006;55(5):396-400.
- Lamagni TL, Neal S, Keshishian C, et al. Severe Streptococcus pyogenes infections, United Kingdom, 2003-2004. Emerg Infect Dis. 2008;14(2):202-209.
- Sharkawy A, Low D, Saginur R, et al. Severe group A streptococcal soft-tissue infections in Ontario: 1992-1996. Clin Infect Dis. 2002;34(4):454-460.
- Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987; 206(5):661-665.
- Wong CH, Chang HC, Pasupathy S, Khin LW, Tan JL, Low CO. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A(8):1454-1460.
- Khan, AT, Tahmeedullah, Obajdullah. Treatment of necrotizing fasciitis with quinolones. J Coll Physicians Surg Pak. 2003;13(11): 649-652.
- Schwartz, RA. Necrotizing fasciitis empiric therapy. Medscape Web site. http://emedicine.medscape.com/
article/2012058-overview. Accessed January 2, 2014. - Stevens, DL, Bisno, AL, Chambers, HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis. 2005;41(10):1373-1406.
- Mechem, CC, Manaker, S. Hyperbaric oxygen therapy. UpToDate Web site. http://www.uptodate.com/contents/hyperbaric-oxygen-therapy?source=search_result&search=Mechem%2C+C.+Crawford%2C++Manaker%2C+Scott.+Hyperbaric+Oxygen+Therapy.&selectedTitle=8%7E91. Accessed January 2, 2014.
- Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal anti-inflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82(4):225-235.
- Tang WM, Wong JW, Wong LL, Leong JC. Streptococcal necrotizing myositis: the role of magnetic resonance imaging. A case report. J Bone Joint Surg Am. 2001;83-A(11):1723-1726.
Necrotizing fasciitis is a rare but lifethreatening soft-tissue infection. Its presentation is characterized by rapidly spreading inflammation and resultant death—both of the surrounding soft tissue and fascial planes. Prompt recognition and aggressive treatment are paramount to avoid fatality, and appropriate management in the ED is essential to a successful outcome. As the following case illustrates, a high index of suspicion and multidisciplinary approach, including applicable imaging studies, result in timely diagnosis and treatment.
Case
A 60-year-old woman with a medical history of childhood Lyme disease, asthma, high cholesterol, and seasonal allergies, presented to the ED with a 3-day history of left hip and thigh pain, general malaise, decreased appetite, nausea, myalgia, and increased lethargy. She reported difficulty with weight-bearing on her left leg but denied any recent leg trauma or falls. Patient also had a 3-year history of intermittent hip pain, which she treated with ibuprofen. Three weeks prior to presentation, she had undergone an invasive dental procedure in preparation for a root canal. She later developed a fever of 102° F and had taken ibuprofen two-and-a-half hours prior to arrival at our institution.
Initial vital signs on physical examination were: blood pressure (BP) 71/37 mm Hg; heart rate (HR), 98 beats/minute; respiratory rate, 18 breaths/minute; temperature, 98.5° F. Oxygen saturation was 100% on room air. Patient was awake and alert but extremely pale and sluggish. Her head, ears, nose, and throat; pulmonary; cardiac; and abdominal examinations were normal. On physical examination, the skin overlying her left hip and thigh was grossly unremarkable, and no previous incision sites or areas of trauma were observed throughout the left lower extremity. No obvious signs of infection or erythema were noted; however, an area of warmth was felt on the lateral aspect of the left thigh but did not extend beyond the knee. Patient was able to flex her left hip approximately 30° and only complained of pain to the lateral aspect of the upper leg with passive internal and external rotation. Heel strike was negative, and knee examination was negative for pathology. The right lower extremity was unremarkable.
A plain radiograph of the pelvis and left hip showed soft-tissue swelling but no bony pathology or fracture (Figure 1). There was no visual evidence of subcutaneous gas, and chest radiograph was negative for any active disease. Based on the clinical picture of septic shock due to possible septic arthritis, emergent magnetic resonance imaging (MRI) of the left hip and thigh was performed without contrast (Figures 2 and 3). Extensive edema was noted diffusely throughout patient’s left gluteus medius muscle and vastus latera lis muscle; no loculated fluid collection was noted. The edema was concentrated around the proximal left thigh but extended to the level of the knee. The left hip was free of any fluid collection, ruling-out septic arthritis. Based on these MRI findings, a computed tomography scan was ordered, which showed no fluid collection in the pelvis and abdomen (Figure 4).
Patient was continued on an antibiotic regimen of IV vancomycin, clindamycin, and piperacillin-tazobactam. Vasopressor support was gradually reduced and respiratory support weaned until both were finally discontinued on postoperative day 2. Soon thereafter, she was transferred to the surgical floor. Negative pressure wound vacuum-assisted closure therapy was applied to the left thigh and was maintained for one week.
The operative cultures were positive for group A Streptococcus (GAS) pyogenes. Upon discharge, antibiotic regimen was adjusted and limited to oral amoxicillin-clavulanate for 14 days until completion. After a 2-week hospital stay, patient was transferred to an acute rehabilitation facility in stable condition and remained there for one week. Follow up was maintained for a total of 6 months, during which time she had no lasting effects from either illness or resultant interventions other than cosmetic concerns from the surgical wounds. In a follow-up phone discussion with patient 10 months after recovery, she reported that she had returned to work as a registered nurse and had been without any functional disability or discomfort.
Discussion
Originally described by Hippocrates in the 5th century as a complication of erysipelas, necrotizing fasciitis later became known as the “malignant ulcer.” It was subsequently described in the United States in 1871 as “hospital gangrene” by Confederate surgeon Joseph Jones.1-3 In 1952, the name was later modified to necrotizing fasciitis by Wilson.4
Today, necrotizing fasciitis is an uncommon disease process, yet one that must be recognized and treated immediately. If not dealt with promptly and aggressively, the virulent and toxin-producing bacteria— most commonly GAS pyogenes— will cause severe systemic toxicity and may lead to death.5
Incidences and Outcomes
According to the US Centers for Disease Control and Prevention (CDC), about 9,000 to 11,500 cases of invasive GAS disease occur each year in the United States, resulting in approximately 1,000 to 1,800 deaths annually. Necrotizing fasciitis comprises an average of 6% to 7% (540- 805) of these invasive cases per year.6
The incidence of necrotizing fasciitis rose sharply in the mid-1980s to the early 1990s but has remained steady over the past 10 years, with 2012 CDC statistics reporting 72 cases per 32,777,740 persons through its voluntary surveillance program. This extrapolates to an estimated 686 cases of GAS-associated necrotizing fasciitis in the United States, with a reported mortality rate of 20% to 25%.7
The highest incidence of disease occurs in the elderly and in patients with diabetes, immunosuppression, and peripheral vascular disease. In children, varicella infection is a known risk factor.8
Other risk factors include obesity, alcohol use, malnutrition, and smoking, as well as corticosteroid use and chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs). Despite the large number of predisposing factors that have been identified, half of all cases of necrotizing fasciitis occur in healthy individuals.9-14
Etiology
Necrotizing fasciitis is thought to be caused by at least two distinct bacteriologic entities. Type I is considered polymicrobial, with Bacteriodes, Clostridium, and Peptostreptococcus, in combination with anaerobic Streptococcus (other than GAS) and Enterobacteriaceae (eg, Escherichia coli, Klebsiella), being the most common infecting species. Type II causative agents include GAS and other β-hemolytic streptococci— alone or with other species of Staphylococcus aureus, including methicillin- resistant S aureus.8 In rare instances, the causative agent is fungal.
Treatment
In a review of patient medical records, Wong et al15 demonstrated that prompt recognition and surgical management of necrotizing fasciitis (ie, within 24 hours of presentation) resulted in improved outcomes. Since the particular causative agent of necrotizing fasciitis in each case is usually unknown, initial treatment should include broad-spectrum IV antibiotics— which are active against grampositive, gram-negative, and anaerobic bacteria—with special consideration for GAS and Clostridium (Table). It is not recommended that initial empiric therapy include antifungals. In this case, the patient was in the OR within 10 hours from presentation, was started immediately on antibiotic regimens for hospital-specific sepsis, and was given appropriate resuscitative measures.
Hyperbaric oxygen therapy is mentioned in the literature as an adjunct to surgery and antibiotics in the treatment of necrotizing fasciitis. Acting as a bactericidal/ bacteriostatic agent against anaerobic bacteria by increasing formation of free oxygen radicals, this therapy is thought to restore the bacterial killing capacity of leukocytes in a hypoxic wound by increasing oxygen tension. Treatment with hyperbaric oxygen may also better define necrotic tissue, facilitating more precise amputation and debridement. Although there are no randomized controlled studies in humans, several authors have shown a reduction in mortality and morbidity with the use of hyperbaric oxygen therapy, in conjunction with early antibiotic and surgical treatment, in animal models and in retrospective studies of patients. 19 When available, hyperbaric oxygen can be initiated once antibiotics have been started and debridement has been performed. The use of hyperbaric oxygen therapy should not delay definitive surgical debridement.
Our case demonstrates a true surgical emergency—one that was appropriately managed with a multidisciplinary team approach. A high index of suspicion by the examining ED staff and surgical consultants led to supportive measures to maintain the patient’s vital signs and ultimately her life. Despite having no clear etiology for the cause of necrotizing fasciitis, we believe it may have resulted from the patient’s prior dental work or chronic NSAID use. Although there is no causal relationship, reports suggest that NSAIDs may prevent prompt recognition and accelerate the infection by altering its initial presentation.20 The patient reported no recent use of anti-inflammatory medication in association with her pain—only for fever.
This report also underscores the importance of urgent MRI in the ED setting. In addition to helping exclude other diagnoses involving the hip joint, MRI provided a roadmap for debridement of active infection. Moreover, the test eliminated the need to explore the left hip joint as well as the risk of seeding a sterile space.21
Conclusion
Necrotizing fasciitis is a rare but lifethreatening soft-tissue infection. Its presentation is characterized by rapidly spreading inflammation and resultant death—both of the surrounding soft tissue and fascial planes. Prompt recognition and aggressive treatment are paramount to avoid fatality, and appropriate management in the ED is essential to a successful outcome. As the following case illustrates, a high index of suspicion and multidisciplinary approach, including applicable imaging studies, result in timely diagnosis and treatment.
Case
A 60-year-old woman with a medical history of childhood Lyme disease, asthma, high cholesterol, and seasonal allergies, presented to the ED with a 3-day history of left hip and thigh pain, general malaise, decreased appetite, nausea, myalgia, and increased lethargy. She reported difficulty with weight-bearing on her left leg but denied any recent leg trauma or falls. Patient also had a 3-year history of intermittent hip pain, which she treated with ibuprofen. Three weeks prior to presentation, she had undergone an invasive dental procedure in preparation for a root canal. She later developed a fever of 102° F and had taken ibuprofen two-and-a-half hours prior to arrival at our institution.
Initial vital signs on physical examination were: blood pressure (BP) 71/37 mm Hg; heart rate (HR), 98 beats/minute; respiratory rate, 18 breaths/minute; temperature, 98.5° F. Oxygen saturation was 100% on room air. Patient was awake and alert but extremely pale and sluggish. Her head, ears, nose, and throat; pulmonary; cardiac; and abdominal examinations were normal. On physical examination, the skin overlying her left hip and thigh was grossly unremarkable, and no previous incision sites or areas of trauma were observed throughout the left lower extremity. No obvious signs of infection or erythema were noted; however, an area of warmth was felt on the lateral aspect of the left thigh but did not extend beyond the knee. Patient was able to flex her left hip approximately 30° and only complained of pain to the lateral aspect of the upper leg with passive internal and external rotation. Heel strike was negative, and knee examination was negative for pathology. The right lower extremity was unremarkable.
A plain radiograph of the pelvis and left hip showed soft-tissue swelling but no bony pathology or fracture (Figure 1). There was no visual evidence of subcutaneous gas, and chest radiograph was negative for any active disease. Based on the clinical picture of septic shock due to possible septic arthritis, emergent magnetic resonance imaging (MRI) of the left hip and thigh was performed without contrast (Figures 2 and 3). Extensive edema was noted diffusely throughout patient’s left gluteus medius muscle and vastus latera lis muscle; no loculated fluid collection was noted. The edema was concentrated around the proximal left thigh but extended to the level of the knee. The left hip was free of any fluid collection, ruling-out septic arthritis. Based on these MRI findings, a computed tomography scan was ordered, which showed no fluid collection in the pelvis and abdomen (Figure 4).
Patient was continued on an antibiotic regimen of IV vancomycin, clindamycin, and piperacillin-tazobactam. Vasopressor support was gradually reduced and respiratory support weaned until both were finally discontinued on postoperative day 2. Soon thereafter, she was transferred to the surgical floor. Negative pressure wound vacuum-assisted closure therapy was applied to the left thigh and was maintained for one week.
The operative cultures were positive for group A Streptococcus (GAS) pyogenes. Upon discharge, antibiotic regimen was adjusted and limited to oral amoxicillin-clavulanate for 14 days until completion. After a 2-week hospital stay, patient was transferred to an acute rehabilitation facility in stable condition and remained there for one week. Follow up was maintained for a total of 6 months, during which time she had no lasting effects from either illness or resultant interventions other than cosmetic concerns from the surgical wounds. In a follow-up phone discussion with patient 10 months after recovery, she reported that she had returned to work as a registered nurse and had been without any functional disability or discomfort.
Discussion
Originally described by Hippocrates in the 5th century as a complication of erysipelas, necrotizing fasciitis later became known as the “malignant ulcer.” It was subsequently described in the United States in 1871 as “hospital gangrene” by Confederate surgeon Joseph Jones.1-3 In 1952, the name was later modified to necrotizing fasciitis by Wilson.4
Today, necrotizing fasciitis is an uncommon disease process, yet one that must be recognized and treated immediately. If not dealt with promptly and aggressively, the virulent and toxin-producing bacteria— most commonly GAS pyogenes— will cause severe systemic toxicity and may lead to death.5
Incidences and Outcomes
According to the US Centers for Disease Control and Prevention (CDC), about 9,000 to 11,500 cases of invasive GAS disease occur each year in the United States, resulting in approximately 1,000 to 1,800 deaths annually. Necrotizing fasciitis comprises an average of 6% to 7% (540- 805) of these invasive cases per year.6
The incidence of necrotizing fasciitis rose sharply in the mid-1980s to the early 1990s but has remained steady over the past 10 years, with 2012 CDC statistics reporting 72 cases per 32,777,740 persons through its voluntary surveillance program. This extrapolates to an estimated 686 cases of GAS-associated necrotizing fasciitis in the United States, with a reported mortality rate of 20% to 25%.7
The highest incidence of disease occurs in the elderly and in patients with diabetes, immunosuppression, and peripheral vascular disease. In children, varicella infection is a known risk factor.8
Other risk factors include obesity, alcohol use, malnutrition, and smoking, as well as corticosteroid use and chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs). Despite the large number of predisposing factors that have been identified, half of all cases of necrotizing fasciitis occur in healthy individuals.9-14
Etiology
Necrotizing fasciitis is thought to be caused by at least two distinct bacteriologic entities. Type I is considered polymicrobial, with Bacteriodes, Clostridium, and Peptostreptococcus, in combination with anaerobic Streptococcus (other than GAS) and Enterobacteriaceae (eg, Escherichia coli, Klebsiella), being the most common infecting species. Type II causative agents include GAS and other β-hemolytic streptococci— alone or with other species of Staphylococcus aureus, including methicillin- resistant S aureus.8 In rare instances, the causative agent is fungal.
Treatment
In a review of patient medical records, Wong et al15 demonstrated that prompt recognition and surgical management of necrotizing fasciitis (ie, within 24 hours of presentation) resulted in improved outcomes. Since the particular causative agent of necrotizing fasciitis in each case is usually unknown, initial treatment should include broad-spectrum IV antibiotics— which are active against grampositive, gram-negative, and anaerobic bacteria—with special consideration for GAS and Clostridium (Table). It is not recommended that initial empiric therapy include antifungals. In this case, the patient was in the OR within 10 hours from presentation, was started immediately on antibiotic regimens for hospital-specific sepsis, and was given appropriate resuscitative measures.
Hyperbaric oxygen therapy is mentioned in the literature as an adjunct to surgery and antibiotics in the treatment of necrotizing fasciitis. Acting as a bactericidal/ bacteriostatic agent against anaerobic bacteria by increasing formation of free oxygen radicals, this therapy is thought to restore the bacterial killing capacity of leukocytes in a hypoxic wound by increasing oxygen tension. Treatment with hyperbaric oxygen may also better define necrotic tissue, facilitating more precise amputation and debridement. Although there are no randomized controlled studies in humans, several authors have shown a reduction in mortality and morbidity with the use of hyperbaric oxygen therapy, in conjunction with early antibiotic and surgical treatment, in animal models and in retrospective studies of patients. 19 When available, hyperbaric oxygen can be initiated once antibiotics have been started and debridement has been performed. The use of hyperbaric oxygen therapy should not delay definitive surgical debridement.
Our case demonstrates a true surgical emergency—one that was appropriately managed with a multidisciplinary team approach. A high index of suspicion by the examining ED staff and surgical consultants led to supportive measures to maintain the patient’s vital signs and ultimately her life. Despite having no clear etiology for the cause of necrotizing fasciitis, we believe it may have resulted from the patient’s prior dental work or chronic NSAID use. Although there is no causal relationship, reports suggest that NSAIDs may prevent prompt recognition and accelerate the infection by altering its initial presentation.20 The patient reported no recent use of anti-inflammatory medication in association with her pain—only for fever.
This report also underscores the importance of urgent MRI in the ED setting. In addition to helping exclude other diagnoses involving the hip joint, MRI provided a roadmap for debridement of active infection. Moreover, the test eliminated the need to explore the left hip joint as well as the risk of seeding a sterile space.21
Conclusion
- Descamps V, Aitken J, Lee MG. Hippocrates on necrotising fasciitis [letter]. Lancet. 1994; 344(8921):556.
- Jones J. Investigations upon the nature, causes, and treatments of hospital gangrene as it prevailed in the Confederate armies 1861-1865. In: Hastings HF, ed. US Sanitary Commission, Surgical memoirs of the War of Rebellion. New York, New York: Riverside; 1871:146-170.
- Loudon I. Necrotising fasciitis, hospital gangrene, and phagedena. Lancet. 1994;344(8934):1416-1419.
- Wilson B. Necrotizing fasciitis. Am Surg. 1952;18(4):416-431.
- Green RJ, Dafoe DC, Raffin TA. Necrotizing fasciitis. Chest. 1996;110(1):219-229.
- Necrotizing fasciitis: A Rare Disease, Especially for the Healthy. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/Features/NecrotizingFasciitis/. Accessed January 2, 2014.
- ABCs report: group A Streptococcus, 2012-provisional. Active Bacterial Core Surveillance (ABCs): Emerging Infections Program Network. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/abcs/reports-findings/survreports/gas12.html. Accessed January 2, 2014.
- Stevens, DL, Baddour, LM. Necrotizing soft tissue infections. UpToDate Web site. http://www.uptodate.com/contents/necrotizing-soft-tissue-infections. Accessed January 2, 2014.
- Bellapianta J, Ljungquist K, Tobin E, Uhl R. Necrotizing Fasciitis. J Am Acad Orthop Surg. 2009;17(3):174-182.
- Childers BJ, Potyondy LD, Nachreiner R, et al. Necrotizing fasciitis: A fourteen-year retrospective study of 163 consecutive patients. Am Surg. 2002;68(2):109-116.
- Dufel S, Martino M. Simple cellulitis or a more serious infection? J Fam Pract. 2006;55(5):396-400.
- Lamagni TL, Neal S, Keshishian C, et al. Severe Streptococcus pyogenes infections, United Kingdom, 2003-2004. Emerg Infect Dis. 2008;14(2):202-209.
- Sharkawy A, Low D, Saginur R, et al. Severe group A streptococcal soft-tissue infections in Ontario: 1992-1996. Clin Infect Dis. 2002;34(4):454-460.
- Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987; 206(5):661-665.
- Wong CH, Chang HC, Pasupathy S, Khin LW, Tan JL, Low CO. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A(8):1454-1460.
- Khan, AT, Tahmeedullah, Obajdullah. Treatment of necrotizing fasciitis with quinolones. J Coll Physicians Surg Pak. 2003;13(11): 649-652.
- Schwartz, RA. Necrotizing fasciitis empiric therapy. Medscape Web site. http://emedicine.medscape.com/
article/2012058-overview. Accessed January 2, 2014. - Stevens, DL, Bisno, AL, Chambers, HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis. 2005;41(10):1373-1406.
- Mechem, CC, Manaker, S. Hyperbaric oxygen therapy. UpToDate Web site. http://www.uptodate.com/contents/hyperbaric-oxygen-therapy?source=search_result&search=Mechem%2C+C.+Crawford%2C++Manaker%2C+Scott.+Hyperbaric+Oxygen+Therapy.&selectedTitle=8%7E91. Accessed January 2, 2014.
- Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal anti-inflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82(4):225-235.
- Tang WM, Wong JW, Wong LL, Leong JC. Streptococcal necrotizing myositis: the role of magnetic resonance imaging. A case report. J Bone Joint Surg Am. 2001;83-A(11):1723-1726.
- Descamps V, Aitken J, Lee MG. Hippocrates on necrotising fasciitis [letter]. Lancet. 1994; 344(8921):556.
- Jones J. Investigations upon the nature, causes, and treatments of hospital gangrene as it prevailed in the Confederate armies 1861-1865. In: Hastings HF, ed. US Sanitary Commission, Surgical memoirs of the War of Rebellion. New York, New York: Riverside; 1871:146-170.
- Loudon I. Necrotising fasciitis, hospital gangrene, and phagedena. Lancet. 1994;344(8934):1416-1419.
- Wilson B. Necrotizing fasciitis. Am Surg. 1952;18(4):416-431.
- Green RJ, Dafoe DC, Raffin TA. Necrotizing fasciitis. Chest. 1996;110(1):219-229.
- Necrotizing fasciitis: A Rare Disease, Especially for the Healthy. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/Features/NecrotizingFasciitis/. Accessed January 2, 2014.
- ABCs report: group A Streptococcus, 2012-provisional. Active Bacterial Core Surveillance (ABCs): Emerging Infections Program Network. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/abcs/reports-findings/survreports/gas12.html. Accessed January 2, 2014.
- Stevens, DL, Baddour, LM. Necrotizing soft tissue infections. UpToDate Web site. http://www.uptodate.com/contents/necrotizing-soft-tissue-infections. Accessed January 2, 2014.
- Bellapianta J, Ljungquist K, Tobin E, Uhl R. Necrotizing Fasciitis. J Am Acad Orthop Surg. 2009;17(3):174-182.
- Childers BJ, Potyondy LD, Nachreiner R, et al. Necrotizing fasciitis: A fourteen-year retrospective study of 163 consecutive patients. Am Surg. 2002;68(2):109-116.
- Dufel S, Martino M. Simple cellulitis or a more serious infection? J Fam Pract. 2006;55(5):396-400.
- Lamagni TL, Neal S, Keshishian C, et al. Severe Streptococcus pyogenes infections, United Kingdom, 2003-2004. Emerg Infect Dis. 2008;14(2):202-209.
- Sharkawy A, Low D, Saginur R, et al. Severe group A streptococcal soft-tissue infections in Ontario: 1992-1996. Clin Infect Dis. 2002;34(4):454-460.
- Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987; 206(5):661-665.
- Wong CH, Chang HC, Pasupathy S, Khin LW, Tan JL, Low CO. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A(8):1454-1460.
- Khan, AT, Tahmeedullah, Obajdullah. Treatment of necrotizing fasciitis with quinolones. J Coll Physicians Surg Pak. 2003;13(11): 649-652.
- Schwartz, RA. Necrotizing fasciitis empiric therapy. Medscape Web site. http://emedicine.medscape.com/
article/2012058-overview. Accessed January 2, 2014. - Stevens, DL, Bisno, AL, Chambers, HF, et al. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of soft-tissue infections. Clin Infect Dis. 2005;41(10):1373-1406.
- Mechem, CC, Manaker, S. Hyperbaric oxygen therapy. UpToDate Web site. http://www.uptodate.com/contents/hyperbaric-oxygen-therapy?source=search_result&search=Mechem%2C+C.+Crawford%2C++Manaker%2C+Scott.+Hyperbaric+Oxygen+Therapy.&selectedTitle=8%7E91. Accessed January 2, 2014.
- Aronoff DM, Bloch KC. Assessing the relationship between the use of nonsteroidal anti-inflammatory drugs and necrotizing fasciitis caused by group A streptococcus. Medicine (Baltimore). 2003;82(4):225-235.
- Tang WM, Wong JW, Wong LL, Leong JC. Streptococcal necrotizing myositis: the role of magnetic resonance imaging. A case report. J Bone Joint Surg Am. 2001;83-A(11):1723-1726.

Swollen Tongue in an Immune-Compromised Host
Total Knee Arthroplasty With Concurrent Femoral and Tibial Osteotomies in Osteogenesis Imperfecta
Symptomatic Hip Impingement Due to Exostosis Associated With Supra-Acetabular Pelvic External Fixator Pin
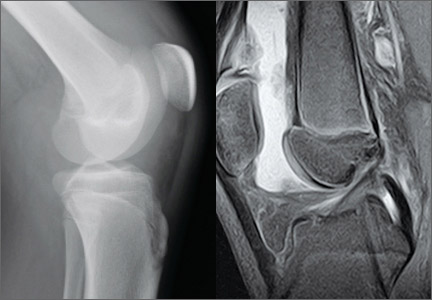
Subacute Superior Patellar Pole Sleeve Fracture
Nausea, blurry vision, hallucinations—Dx?
THE CASE
A 55-year-old Asian woman was brought to the emergency department by her husband, with symptoms of nausea, blurry vision, headache, and hallucinations. Her husband told us that he and his wife had flown to New Orleans to embark on a Caribbean cruise 5 days earlier. The next morning—their first full day on the ship—his wife became nauseous and her vision was blurred. She went to the ship’s doctor, who treated her for motion sickness.
On Day 3, she developed a right-sided headache at the back of her head and neck. The patient refused to go to the hospital at the first Mexican port and waited until the ship arrived in Belize. She was taken ashore for a computed tomography (CT) scan, which was negative. She stayed the night in the hospital.
The next day, the patient developed weakness and numbness in her left arm. She was seen by a neurologist and given amitriptyline, and underwent a second CT scan. When this scan, too, was read as negative, she and her husband flew home to Phoenix and sought care at our emergency department. There, the patient had a third CT scan, which showed temporal edema suggestive of encephalitis.
A neurologist performed a lumbar puncture and found nonspecific pleocytosis in the spinal fluid. The patient was started on aggressive antiviral therapy, including intravenous acyclovir, as well as steroids, but she showed no improvement. The symptoms continued, and the patient had vivid hallucinations: She reported seeing mermaids waving in the windows and children running around the hospital halls and ceilings.
An extensive serological workup followed, and was negative for: cytomegalovirus, dengue virus, West Nile virus, Lyme disease, coxsackievirus, syphilis, Cryptococcus, Coccidioides, mumps, measles, antinuclear antibodies, lupus, malaria, and herpes simplex virus.
THE DIAGNOSIS
After ruling out the other possible etiologies, and noting that the patient had eaten fish the day before the symptoms developed, the hospitalist, neurologist, and infectious disease specialist agreed that the most likely diagnosis was ciguatera poisoning. A literature search revealed the recommended treatment: a mannitol infusion of a 20% solution, 1 g/kg, with a piggyback of 250 mL over 30 minutes,1 every 6 hours as needed.
A dramatic improvement
The patient’s headache and arm weakness improved within 24 hours of receiving the mannitol. Her mental status improved as well as the blurry vision.
Two days later, the patient received a second mannitol infusion and was discharged the next day, although she still had mild weakness in her left arm and lingering hallucinations. A 2-week follow-up appointment with the neurologist was scheduled so that she could have a third mannitol treatment for her persistent visual changes.
DISCUSSION
Ciguatera poisoning—a little-known marine toxin
Ciguatera toxin is a lipid-soluble, heat-stable marine toxin2 made by dinoflagellates such as Gambierdiscus toxicus in tropical and subtropical waters. Larger fish eat the herbivore fish that have eaten the dinoflagellates and the toxin bioaccumulates until it reaches large predatory fish like barracuda, grouper, snapper, and sea bass.3 Although the toxin is harmless to fish, it can cause serious gastrointestinal (GI), neurological, and cardiovascular symptoms in humans. Cold allodynia—ie, cold stimuli experienced as painful or hot—is considered pathognomonic.
Although the condition is rare, the incidence is on the rise. There were an estimated 20,000 cases of ciguatera poisoning worldwide in 1997,4 and >100,000 cases in 2010.5 In addition, the Centers for Disease Control and Prevention reported 14 “ciguatoxin” outbreaks in the United States between 2009 and 2010.6-8 The endemic area of ciguatera seems to be spreading, as well. Once confined to fish caught in tropical waters like the Caribbean, ciguatera-laden fish have been caught off the coast of South Carolina and North Carolina.9
A triad of symptoms
Patients with ciguatera poisoning may present with the following triad of symptoms:
• GI problems (nausea, vomiting, diarrhea), which usually occur one to 2 days postexposure,
• neurological symptoms (hallucinations, headache, ataxia), which typically occur 2 to 4 days postexposure, and
• cardiovascular symptoms (bradycardia, hypotension), which are the least common and typically occur only in severe cases.10
Our patient’s eating history and onset of symptoms suggested that she ingested the ciguatera toxin in New Orleans the night before leaving on the cruise, yet she did not experience cold allodynia. Her medical treatment was prolonged, with multiple exclusion tests resulting in a 19-day hospital stay.
No consensus regarding Tx
The medical management of this rare condition is still in its infancy, and there is no consensus regarding treatment.11 In addition, while there are specific assays for fish tissue,12 there appears to be no diagnostic test for humans.
Our patient’s immediate response to a mannitol infusion was consistent with other reported cases of ciguatera poisonings.1 However, mannitol therapy came into question in 2002, when a randomized trial comparing it with normal saline for ciguatera poisoning found that both provided immediate symptom relief.11
THE TAKEAWAY
As tropical fish exports reach new markets and world travel increases, the number of ciguatera cases is likely to continue to rise. The lack of both a specific diagnostic test and an evidence-based treatment highlights the importance of taking a thorough food history—and considering this unusual toxin, as well as more common foodborne pathogens—in patients who present with GI and neurological symptoms.
1. Palafox N, Jain L, Pinano A, et al. Successful treatment of ciguatera fish poisoning with intravenous mannitol. JAMA. 1988;259:2740-2742.
2. Swift AEB, Swift TR. Ciguatera. Clin Toxicol. 1993;31:1-29.
3. Eastaugh J, Shepherd, S. Infectious and toxic syndromes from fish and shellfish consumption. A review. Arch Intern Med. 1989;149:1735-1740.
4. Lipp EK, Rose JB. The role of seafood in foodborne diseases in the United States of America. Rev Sci Tech. 1997;16:620-640.
5. Schoemaker R, House D, Ryan J. Defining the neurotoxin derived illness chronic ciguatera using markers of chronic systemic inflammatory disturbances: a case/control study. Neurotoxicol Teratol. 2010;32:633-639.
6. Hall AJ, Wikswo ME, Manikonda K, et al. Acute gastroenteritis surveillance through the national outbreak reporting system, United States. Emerg Infect Dis. 2013;19:1305-1309.
7. Pennotti R, Scallan E, Backer L, et al. Ciguatera and scombroid fish poisoning in the United States. Foodborne Pathogens Dis. 2013;10:1059-1066.
8. Centers for Disease Control and Prevention (CDC). Surveillance for foodborne disease outbreaks—United States, 2009-2010. MMWR Morb Mortal Wkly Rep. 2013;62:41-47.
9. Centers for Disease Control and Prevention (CDC). Cluster of ciguatera fish poisoning—North Carolina, 2007. MMWR Morb Mortal Wkly Rep. 2009;58:283-285.
10. Morris JG Jr, Lewin P, Hargrett N, et al. Clinical features of ciguatera fish poisoning: a study of the disease in the US Virgin Islands. Arch Intern Med. 1982;142:1090-1092.
11. Schnorf H, Taurarii M, Cundy T. Ciguatera fish poisoning: A double-blind randomized trial of mannitol therapy. Neurology. 2002;58:873-880.
12. Hokama Y, Nishimura K, Takenaka W, et al. Simplified solidphase membrane immunobead assay (MIA) with monoclonal anti-ciguatoxin antibody (MAb-CTX) for detection of ciguatoxin and related polyether toxins. J Nat Toxins. 1998;7:1-21.
THE CASE
A 55-year-old Asian woman was brought to the emergency department by her husband, with symptoms of nausea, blurry vision, headache, and hallucinations. Her husband told us that he and his wife had flown to New Orleans to embark on a Caribbean cruise 5 days earlier. The next morning—their first full day on the ship—his wife became nauseous and her vision was blurred. She went to the ship’s doctor, who treated her for motion sickness.
On Day 3, she developed a right-sided headache at the back of her head and neck. The patient refused to go to the hospital at the first Mexican port and waited until the ship arrived in Belize. She was taken ashore for a computed tomography (CT) scan, which was negative. She stayed the night in the hospital.
The next day, the patient developed weakness and numbness in her left arm. She was seen by a neurologist and given amitriptyline, and underwent a second CT scan. When this scan, too, was read as negative, she and her husband flew home to Phoenix and sought care at our emergency department. There, the patient had a third CT scan, which showed temporal edema suggestive of encephalitis.
A neurologist performed a lumbar puncture and found nonspecific pleocytosis in the spinal fluid. The patient was started on aggressive antiviral therapy, including intravenous acyclovir, as well as steroids, but she showed no improvement. The symptoms continued, and the patient had vivid hallucinations: She reported seeing mermaids waving in the windows and children running around the hospital halls and ceilings.
An extensive serological workup followed, and was negative for: cytomegalovirus, dengue virus, West Nile virus, Lyme disease, coxsackievirus, syphilis, Cryptococcus, Coccidioides, mumps, measles, antinuclear antibodies, lupus, malaria, and herpes simplex virus.
THE DIAGNOSIS
After ruling out the other possible etiologies, and noting that the patient had eaten fish the day before the symptoms developed, the hospitalist, neurologist, and infectious disease specialist agreed that the most likely diagnosis was ciguatera poisoning. A literature search revealed the recommended treatment: a mannitol infusion of a 20% solution, 1 g/kg, with a piggyback of 250 mL over 30 minutes,1 every 6 hours as needed.
A dramatic improvement
The patient’s headache and arm weakness improved within 24 hours of receiving the mannitol. Her mental status improved as well as the blurry vision.
Two days later, the patient received a second mannitol infusion and was discharged the next day, although she still had mild weakness in her left arm and lingering hallucinations. A 2-week follow-up appointment with the neurologist was scheduled so that she could have a third mannitol treatment for her persistent visual changes.
DISCUSSION
Ciguatera poisoning—a little-known marine toxin
Ciguatera toxin is a lipid-soluble, heat-stable marine toxin2 made by dinoflagellates such as Gambierdiscus toxicus in tropical and subtropical waters. Larger fish eat the herbivore fish that have eaten the dinoflagellates and the toxin bioaccumulates until it reaches large predatory fish like barracuda, grouper, snapper, and sea bass.3 Although the toxin is harmless to fish, it can cause serious gastrointestinal (GI), neurological, and cardiovascular symptoms in humans. Cold allodynia—ie, cold stimuli experienced as painful or hot—is considered pathognomonic.
Although the condition is rare, the incidence is on the rise. There were an estimated 20,000 cases of ciguatera poisoning worldwide in 1997,4 and >100,000 cases in 2010.5 In addition, the Centers for Disease Control and Prevention reported 14 “ciguatoxin” outbreaks in the United States between 2009 and 2010.6-8 The endemic area of ciguatera seems to be spreading, as well. Once confined to fish caught in tropical waters like the Caribbean, ciguatera-laden fish have been caught off the coast of South Carolina and North Carolina.9
A triad of symptoms
Patients with ciguatera poisoning may present with the following triad of symptoms:
• GI problems (nausea, vomiting, diarrhea), which usually occur one to 2 days postexposure,
• neurological symptoms (hallucinations, headache, ataxia), which typically occur 2 to 4 days postexposure, and
• cardiovascular symptoms (bradycardia, hypotension), which are the least common and typically occur only in severe cases.10
Our patient’s eating history and onset of symptoms suggested that she ingested the ciguatera toxin in New Orleans the night before leaving on the cruise, yet she did not experience cold allodynia. Her medical treatment was prolonged, with multiple exclusion tests resulting in a 19-day hospital stay.
No consensus regarding Tx
The medical management of this rare condition is still in its infancy, and there is no consensus regarding treatment.11 In addition, while there are specific assays for fish tissue,12 there appears to be no diagnostic test for humans.
Our patient’s immediate response to a mannitol infusion was consistent with other reported cases of ciguatera poisonings.1 However, mannitol therapy came into question in 2002, when a randomized trial comparing it with normal saline for ciguatera poisoning found that both provided immediate symptom relief.11
THE TAKEAWAY
As tropical fish exports reach new markets and world travel increases, the number of ciguatera cases is likely to continue to rise. The lack of both a specific diagnostic test and an evidence-based treatment highlights the importance of taking a thorough food history—and considering this unusual toxin, as well as more common foodborne pathogens—in patients who present with GI and neurological symptoms.
THE CASE
A 55-year-old Asian woman was brought to the emergency department by her husband, with symptoms of nausea, blurry vision, headache, and hallucinations. Her husband told us that he and his wife had flown to New Orleans to embark on a Caribbean cruise 5 days earlier. The next morning—their first full day on the ship—his wife became nauseous and her vision was blurred. She went to the ship’s doctor, who treated her for motion sickness.
On Day 3, she developed a right-sided headache at the back of her head and neck. The patient refused to go to the hospital at the first Mexican port and waited until the ship arrived in Belize. She was taken ashore for a computed tomography (CT) scan, which was negative. She stayed the night in the hospital.
The next day, the patient developed weakness and numbness in her left arm. She was seen by a neurologist and given amitriptyline, and underwent a second CT scan. When this scan, too, was read as negative, she and her husband flew home to Phoenix and sought care at our emergency department. There, the patient had a third CT scan, which showed temporal edema suggestive of encephalitis.
A neurologist performed a lumbar puncture and found nonspecific pleocytosis in the spinal fluid. The patient was started on aggressive antiviral therapy, including intravenous acyclovir, as well as steroids, but she showed no improvement. The symptoms continued, and the patient had vivid hallucinations: She reported seeing mermaids waving in the windows and children running around the hospital halls and ceilings.
An extensive serological workup followed, and was negative for: cytomegalovirus, dengue virus, West Nile virus, Lyme disease, coxsackievirus, syphilis, Cryptococcus, Coccidioides, mumps, measles, antinuclear antibodies, lupus, malaria, and herpes simplex virus.
THE DIAGNOSIS
After ruling out the other possible etiologies, and noting that the patient had eaten fish the day before the symptoms developed, the hospitalist, neurologist, and infectious disease specialist agreed that the most likely diagnosis was ciguatera poisoning. A literature search revealed the recommended treatment: a mannitol infusion of a 20% solution, 1 g/kg, with a piggyback of 250 mL over 30 minutes,1 every 6 hours as needed.
A dramatic improvement
The patient’s headache and arm weakness improved within 24 hours of receiving the mannitol. Her mental status improved as well as the blurry vision.
Two days later, the patient received a second mannitol infusion and was discharged the next day, although she still had mild weakness in her left arm and lingering hallucinations. A 2-week follow-up appointment with the neurologist was scheduled so that she could have a third mannitol treatment for her persistent visual changes.
DISCUSSION
Ciguatera poisoning—a little-known marine toxin
Ciguatera toxin is a lipid-soluble, heat-stable marine toxin2 made by dinoflagellates such as Gambierdiscus toxicus in tropical and subtropical waters. Larger fish eat the herbivore fish that have eaten the dinoflagellates and the toxin bioaccumulates until it reaches large predatory fish like barracuda, grouper, snapper, and sea bass.3 Although the toxin is harmless to fish, it can cause serious gastrointestinal (GI), neurological, and cardiovascular symptoms in humans. Cold allodynia—ie, cold stimuli experienced as painful or hot—is considered pathognomonic.
Although the condition is rare, the incidence is on the rise. There were an estimated 20,000 cases of ciguatera poisoning worldwide in 1997,4 and >100,000 cases in 2010.5 In addition, the Centers for Disease Control and Prevention reported 14 “ciguatoxin” outbreaks in the United States between 2009 and 2010.6-8 The endemic area of ciguatera seems to be spreading, as well. Once confined to fish caught in tropical waters like the Caribbean, ciguatera-laden fish have been caught off the coast of South Carolina and North Carolina.9
A triad of symptoms
Patients with ciguatera poisoning may present with the following triad of symptoms:
• GI problems (nausea, vomiting, diarrhea), which usually occur one to 2 days postexposure,
• neurological symptoms (hallucinations, headache, ataxia), which typically occur 2 to 4 days postexposure, and
• cardiovascular symptoms (bradycardia, hypotension), which are the least common and typically occur only in severe cases.10
Our patient’s eating history and onset of symptoms suggested that she ingested the ciguatera toxin in New Orleans the night before leaving on the cruise, yet she did not experience cold allodynia. Her medical treatment was prolonged, with multiple exclusion tests resulting in a 19-day hospital stay.
No consensus regarding Tx
The medical management of this rare condition is still in its infancy, and there is no consensus regarding treatment.11 In addition, while there are specific assays for fish tissue,12 there appears to be no diagnostic test for humans.
Our patient’s immediate response to a mannitol infusion was consistent with other reported cases of ciguatera poisonings.1 However, mannitol therapy came into question in 2002, when a randomized trial comparing it with normal saline for ciguatera poisoning found that both provided immediate symptom relief.11
THE TAKEAWAY
As tropical fish exports reach new markets and world travel increases, the number of ciguatera cases is likely to continue to rise. The lack of both a specific diagnostic test and an evidence-based treatment highlights the importance of taking a thorough food history—and considering this unusual toxin, as well as more common foodborne pathogens—in patients who present with GI and neurological symptoms.
1. Palafox N, Jain L, Pinano A, et al. Successful treatment of ciguatera fish poisoning with intravenous mannitol. JAMA. 1988;259:2740-2742.
2. Swift AEB, Swift TR. Ciguatera. Clin Toxicol. 1993;31:1-29.
3. Eastaugh J, Shepherd, S. Infectious and toxic syndromes from fish and shellfish consumption. A review. Arch Intern Med. 1989;149:1735-1740.
4. Lipp EK, Rose JB. The role of seafood in foodborne diseases in the United States of America. Rev Sci Tech. 1997;16:620-640.
5. Schoemaker R, House D, Ryan J. Defining the neurotoxin derived illness chronic ciguatera using markers of chronic systemic inflammatory disturbances: a case/control study. Neurotoxicol Teratol. 2010;32:633-639.
6. Hall AJ, Wikswo ME, Manikonda K, et al. Acute gastroenteritis surveillance through the national outbreak reporting system, United States. Emerg Infect Dis. 2013;19:1305-1309.
7. Pennotti R, Scallan E, Backer L, et al. Ciguatera and scombroid fish poisoning in the United States. Foodborne Pathogens Dis. 2013;10:1059-1066.
8. Centers for Disease Control and Prevention (CDC). Surveillance for foodborne disease outbreaks—United States, 2009-2010. MMWR Morb Mortal Wkly Rep. 2013;62:41-47.
9. Centers for Disease Control and Prevention (CDC). Cluster of ciguatera fish poisoning—North Carolina, 2007. MMWR Morb Mortal Wkly Rep. 2009;58:283-285.
10. Morris JG Jr, Lewin P, Hargrett N, et al. Clinical features of ciguatera fish poisoning: a study of the disease in the US Virgin Islands. Arch Intern Med. 1982;142:1090-1092.
11. Schnorf H, Taurarii M, Cundy T. Ciguatera fish poisoning: A double-blind randomized trial of mannitol therapy. Neurology. 2002;58:873-880.
12. Hokama Y, Nishimura K, Takenaka W, et al. Simplified solidphase membrane immunobead assay (MIA) with monoclonal anti-ciguatoxin antibody (MAb-CTX) for detection of ciguatoxin and related polyether toxins. J Nat Toxins. 1998;7:1-21.
1. Palafox N, Jain L, Pinano A, et al. Successful treatment of ciguatera fish poisoning with intravenous mannitol. JAMA. 1988;259:2740-2742.
2. Swift AEB, Swift TR. Ciguatera. Clin Toxicol. 1993;31:1-29.
3. Eastaugh J, Shepherd, S. Infectious and toxic syndromes from fish and shellfish consumption. A review. Arch Intern Med. 1989;149:1735-1740.
4. Lipp EK, Rose JB. The role of seafood in foodborne diseases in the United States of America. Rev Sci Tech. 1997;16:620-640.
5. Schoemaker R, House D, Ryan J. Defining the neurotoxin derived illness chronic ciguatera using markers of chronic systemic inflammatory disturbances: a case/control study. Neurotoxicol Teratol. 2010;32:633-639.
6. Hall AJ, Wikswo ME, Manikonda K, et al. Acute gastroenteritis surveillance through the national outbreak reporting system, United States. Emerg Infect Dis. 2013;19:1305-1309.
7. Pennotti R, Scallan E, Backer L, et al. Ciguatera and scombroid fish poisoning in the United States. Foodborne Pathogens Dis. 2013;10:1059-1066.
8. Centers for Disease Control and Prevention (CDC). Surveillance for foodborne disease outbreaks—United States, 2009-2010. MMWR Morb Mortal Wkly Rep. 2013;62:41-47.
9. Centers for Disease Control and Prevention (CDC). Cluster of ciguatera fish poisoning—North Carolina, 2007. MMWR Morb Mortal Wkly Rep. 2009;58:283-285.
10. Morris JG Jr, Lewin P, Hargrett N, et al. Clinical features of ciguatera fish poisoning: a study of the disease in the US Virgin Islands. Arch Intern Med. 1982;142:1090-1092.
11. Schnorf H, Taurarii M, Cundy T. Ciguatera fish poisoning: A double-blind randomized trial of mannitol therapy. Neurology. 2002;58:873-880.
12. Hokama Y, Nishimura K, Takenaka W, et al. Simplified solidphase membrane immunobead assay (MIA) with monoclonal anti-ciguatoxin antibody (MAb-CTX) for detection of ciguatoxin and related polyether toxins. J Nat Toxins. 1998;7:1-21.

Case Studies in Toxicology: Tiny Bubbles (Or, the Dangers of Cleaning Your Fruit)
Case
A previously healthy 32-year-old man presented to the ED after unintentionally ingesting a mouthful of concentrated (35%) hydrogen peroxide (H2O2) from an unmarked bottle he kept in his refrigerator. Upon realizing his error, he immediately drank a liter of water, which promptly induced vomiting. In the ED, the patient complained of mild throat and chest discomfort as well as “abdominal fullness.”
His initial vital signs were: blood pressure, 140/92 mm Hg; heart rate, 93 beats/minute; respiratory rate, 18 breaths/minute; temperature, 96.4° F. Oxygen saturation was 98% on room air. Physical examination revealed tenderness in the epigastric region with no peritoneal findings. Oropharynx and chest examination were normal, and standard laboratory investigations were all within normal limits.
What are the potential exposures to hydrogen peroxide?
Hydrogen peroxide is a colorless and odorless liquid. Solutions with concentrations ranging from 3% to 5% have many household applications, including use as a wound disinfectant and dentifrice; dilute solutions are also utilized for similar purposes in the hospital setting. Industrial-strength H2O2 (concentrations of 10% to 35%) is employed to bleach textiles and paper, and higher concentrations (70% to 90%) are used as an oxygen source for rocket engines.
Consumer application of concentrated H2O2 solutions has become increasingly common. Some, like this patient, clean the surfaces of fruits and vegetables with H2O2 to decrease transmission of bacteria during cutting.1 More concerning, however, is the purported medicinal benefits of ingesting “food-grade” (35%) H2O2 mixed with water—touted on many Internet sites as a treatment for illnesses such as emphysema, cancer, anemia, and HIV.2 Sometimes referred to as “hyperoxygenation therapy,” this so-called treatment has not been approved by the US Food and Drug Administration for any such purpose.3 When diluted sufficiently, this concoction is not harmful but unlikely to provide any health benefits.
Dr Lucyk is a fellow of medical toxicology in the department of emergency medicine at the New York University School of Medicine and the New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
What are the toxic effects of concentrated hydrogen peroxide?
Injury from concentrated H2O2 consumption is primarily from either direct caustic injury or the embolic obstruction of blood flow. Following ingestion, the enzyme catalase metabolizes the breakdown of H2O2 in accordance with the following equation: 2H2O2(aq) → 2H2O(l) + O2(g) + heat. A single milliliter of 35% H2O2 results in the liberation of 100 mL of O2. (The more common 3% household solution generates 10 mL of oxygen per 1 ml of H2O2.) The creation of a large intragastric pressure gradient from the liberation of gas, coupled with the caustic and exothermic injury of the bowel mucosa, may contribute to the movement of oxygen through epithelial interstices into the circulation.In addition, and perhaps more importantly, absorption of intact H2O2 with subsequent metabolism by catalase in the blood liberates oxygen directly within the vasculature. Oxygen bubbles may coalesce in blood circulation and occlude vascular flow. In canine studies, elevated oxygen tension in the portal venous system led to cessation of mesenteric flow in arteries and veins, though the mechanism of action is unclear.4 Furthermore, coalescence of bubbles can lead to disruption of bowel-cell architecture, fibrin plugging of capillaries, venous thrombosis, and infarction of tissues.4
Cases of cardiac and cerebral gas embolism have been reported, and present similarly to patients with diving-related decompression injuries (eg, stroke-like syndromes).5,6 The proposed mechanism for these latter effects involves the metabolism of H2O2 in the systemic circulation with production of oxygen bubbles. In the presence of an atrial septal defect, bubbles may move from the right atrium to the arterial circulation.7
Toxicity and death from H2O2 exposure associated with the historical treatment of inspissated meconium,4 as well as the irrigation of wounds,8 has been reported in the medical literature. Ingestion of a 3% solution is generally benign, resulting at worst in gastrointestinal symptoms or throat irritation.9 Rarely does significant toxicity occur at this low concentration,5 with the vast majority of such cases involving concentrated solutions of 35%.
Case continuation
Case 2

Based on this patient’s continued symptoms, an abdominal radiograph was obtained to assess the presence of portal venous air. Although radiographic findings were normal, continued abdominal examination findings warranted a subsequent abdominal computed tomography (CT) scan, which revealed the presence of extensive air throughout the portal venous system (Figure.).
Do all patients presenting with H2O2 ingestion require imaging to assess for the presence of portal venous air?

Reportedly, ingestion of as little as a “sip” or “mouthful” of 35% H2O2 has resulted in venous and arterial gas embolism,6 occasionally with severe consequences, but no current consensus guidelines exist regarding imaging requirements. Some toxicologists and hyperbaric physicians believe that the presence of portal venous air does not adversely impact a patient’s prognosis or necessitate treatment, and therefore a workup is unnecessary. Others, however, suggest that the presence of portal venous air indicates oversaturation of oxygen in the blood, placing the patient at increased risk for cardiac and cerebral air embolism. Neither one of these theories is well supported in the literature. Although practice patterns vary by institution, it is reasonable that all patients presenting with abdominal complaints after ingestion of H2O2 undergo CT imaging to assess for portal venous air.
If portal venous air is detected, do patients require hyperbaric oxygen therapy?
The management of patients with portal venous gas following H2O2
Hyperbaric therapy increases the amount of oxygen that can be dissolved in the blood, thereby decreasing bubble formation and allowing transport of dissolved oxygen to the lungs where it can be exhaled. Some patients with portal venous air experience significant pain and portal venous hypertension, which may respond rapidly to this therapy.10 Based on available literature, hyperbaric therapy is reasonable for patients with significant abdominal pain and portal venous air following H2O2 ingestion; less controversial is the role of hyperbaric therapy in those with cerebral air embolism. Multiple case reports of patients with significant neurologic findings demonstrate resolution of symptoms following hyperbaric therapy.6
Case conclusion
Hyperbaric oxygen therapy was recommended for the patient in this case, but transfer to a hyperbaric facility was not possible. He was instead admitted to the hospital for continuous monitoring. Over the next 12 hours, his symptoms gradually resolved, and a repeat CT scan the following day showed complete resolution of the portal venous gas. The patient was subsequently discharged without any sequelae.
- Ukuku DO, Bari ML, Kawamoto S, Isshiki K. Use of hydrogen peroxide in combination with nisin, sodium lactate and citric acid for reducing transfer of bacterial pathogens from whole melon surfaces to fresh-cut pieces. Int J Food Microbiol. 2005;104(2):225-233.
- 35% H2O2 hydrogen peroxide food grade certified benefits. The One Minute Miracle Web site. http:// www.theoneminutemiracleinc.com/pages/h2o2- benefits/. Accessed November 20, 2013.
- FDA warns consumers against drinking high-strength hydrogen peroxide for medicinal use: ingestion can lead to serious health risk and death [news release]. Silver Spring, MD: US Food and Drug Administration; July 27, 2006. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ 2006/ucm108701.htm. Accessed November 20, 2013.
- Shaw A, Cooperman A, Fusco J. Gas embolism produced by hydrogen peroxide. N Engl J Med. 1967;277(5):238-241.
- Cina SJ, Downs JC, Conradi SE. Hydrogen peroxide: a source of lethal oxygen embolism. Case report and review of the literature. Am J Forensic Med Pathol. 1994;15(1):44-50.
- Rider SP, Jackson SB, Rusyniak DE. Cerebral air gas embolism from concentrated hydrogen peroxide ingestion. Clin Toxicol (Phila). 2008;46(9):815-818.
- French LK, Horowitz BZ, McKeown NJ. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clin Toxicol (Phila). 2010;48(6):533-538.
- Bassan MM, Dudai M, Shalev O. Near-fatal systemic oxygen embolism due to wound irrigation with hydrogen peroxide. Postgrad Med J. 1982;58(681):448-450.
- Henry MC, Wheeler J, Mofenson HC, et al. Hydrogen peroxide 3% exposures. J Toxicol Clin Toxicol. 1996;34(3):323-327.
- Papafragkou S, Gasparyan A, Batista R, Scott P. Treatment of portal venous gas embolism with hyperbaric oxygen after accidental ingestion of hydrogen peroxide: a case report and review of the literature. J Emerg Med. 2012;43(1):e21-e23.
Case
A previously healthy 32-year-old man presented to the ED after unintentionally ingesting a mouthful of concentrated (35%) hydrogen peroxide (H2O2) from an unmarked bottle he kept in his refrigerator. Upon realizing his error, he immediately drank a liter of water, which promptly induced vomiting. In the ED, the patient complained of mild throat and chest discomfort as well as “abdominal fullness.”
His initial vital signs were: blood pressure, 140/92 mm Hg; heart rate, 93 beats/minute; respiratory rate, 18 breaths/minute; temperature, 96.4° F. Oxygen saturation was 98% on room air. Physical examination revealed tenderness in the epigastric region with no peritoneal findings. Oropharynx and chest examination were normal, and standard laboratory investigations were all within normal limits.
What are the potential exposures to hydrogen peroxide?
Hydrogen peroxide is a colorless and odorless liquid. Solutions with concentrations ranging from 3% to 5% have many household applications, including use as a wound disinfectant and dentifrice; dilute solutions are also utilized for similar purposes in the hospital setting. Industrial-strength H2O2 (concentrations of 10% to 35%) is employed to bleach textiles and paper, and higher concentrations (70% to 90%) are used as an oxygen source for rocket engines.
Consumer application of concentrated H2O2 solutions has become increasingly common. Some, like this patient, clean the surfaces of fruits and vegetables with H2O2 to decrease transmission of bacteria during cutting.1 More concerning, however, is the purported medicinal benefits of ingesting “food-grade” (35%) H2O2 mixed with water—touted on many Internet sites as a treatment for illnesses such as emphysema, cancer, anemia, and HIV.2 Sometimes referred to as “hyperoxygenation therapy,” this so-called treatment has not been approved by the US Food and Drug Administration for any such purpose.3 When diluted sufficiently, this concoction is not harmful but unlikely to provide any health benefits.
Dr Lucyk is a fellow of medical toxicology in the department of emergency medicine at the New York University School of Medicine and the New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
What are the toxic effects of concentrated hydrogen peroxide?
Injury from concentrated H2O2 consumption is primarily from either direct caustic injury or the embolic obstruction of blood flow. Following ingestion, the enzyme catalase metabolizes the breakdown of H2O2 in accordance with the following equation: 2H2O2(aq) → 2H2O(l) + O2(g) + heat. A single milliliter of 35% H2O2 results in the liberation of 100 mL of O2. (The more common 3% household solution generates 10 mL of oxygen per 1 ml of H2O2.) The creation of a large intragastric pressure gradient from the liberation of gas, coupled with the caustic and exothermic injury of the bowel mucosa, may contribute to the movement of oxygen through epithelial interstices into the circulation.In addition, and perhaps more importantly, absorption of intact H2O2 with subsequent metabolism by catalase in the blood liberates oxygen directly within the vasculature. Oxygen bubbles may coalesce in blood circulation and occlude vascular flow. In canine studies, elevated oxygen tension in the portal venous system led to cessation of mesenteric flow in arteries and veins, though the mechanism of action is unclear.4 Furthermore, coalescence of bubbles can lead to disruption of bowel-cell architecture, fibrin plugging of capillaries, venous thrombosis, and infarction of tissues.4
Cases of cardiac and cerebral gas embolism have been reported, and present similarly to patients with diving-related decompression injuries (eg, stroke-like syndromes).5,6 The proposed mechanism for these latter effects involves the metabolism of H2O2 in the systemic circulation with production of oxygen bubbles. In the presence of an atrial septal defect, bubbles may move from the right atrium to the arterial circulation.7
Toxicity and death from H2O2 exposure associated with the historical treatment of inspissated meconium,4 as well as the irrigation of wounds,8 has been reported in the medical literature. Ingestion of a 3% solution is generally benign, resulting at worst in gastrointestinal symptoms or throat irritation.9 Rarely does significant toxicity occur at this low concentration,5 with the vast majority of such cases involving concentrated solutions of 35%.
Case continuation
Case 2
Based on this patient’s continued symptoms, an abdominal radiograph was obtained to assess the presence of portal venous air. Although radiographic findings were normal, continued abdominal examination findings warranted a subsequent abdominal computed tomography (CT) scan, which revealed the presence of extensive air throughout the portal venous system (Figure.).
Do all patients presenting with H2O2 ingestion require imaging to assess for the presence of portal venous air?
Reportedly, ingestion of as little as a “sip” or “mouthful” of 35% H2O2 has resulted in venous and arterial gas embolism,6 occasionally with severe consequences, but no current consensus guidelines exist regarding imaging requirements. Some toxicologists and hyperbaric physicians believe that the presence of portal venous air does not adversely impact a patient’s prognosis or necessitate treatment, and therefore a workup is unnecessary. Others, however, suggest that the presence of portal venous air indicates oversaturation of oxygen in the blood, placing the patient at increased risk for cardiac and cerebral air embolism. Neither one of these theories is well supported in the literature. Although practice patterns vary by institution, it is reasonable that all patients presenting with abdominal complaints after ingestion of H2O2 undergo CT imaging to assess for portal venous air.
If portal venous air is detected, do patients require hyperbaric oxygen therapy?
The management of patients with portal venous gas following H2O2
Hyperbaric therapy increases the amount of oxygen that can be dissolved in the blood, thereby decreasing bubble formation and allowing transport of dissolved oxygen to the lungs where it can be exhaled. Some patients with portal venous air experience significant pain and portal venous hypertension, which may respond rapidly to this therapy.10 Based on available literature, hyperbaric therapy is reasonable for patients with significant abdominal pain and portal venous air following H2O2 ingestion; less controversial is the role of hyperbaric therapy in those with cerebral air embolism. Multiple case reports of patients with significant neurologic findings demonstrate resolution of symptoms following hyperbaric therapy.6
Case conclusion
Hyperbaric oxygen therapy was recommended for the patient in this case, but transfer to a hyperbaric facility was not possible. He was instead admitted to the hospital for continuous monitoring. Over the next 12 hours, his symptoms gradually resolved, and a repeat CT scan the following day showed complete resolution of the portal venous gas. The patient was subsequently discharged without any sequelae.
Case
A previously healthy 32-year-old man presented to the ED after unintentionally ingesting a mouthful of concentrated (35%) hydrogen peroxide (H2O2) from an unmarked bottle he kept in his refrigerator. Upon realizing his error, he immediately drank a liter of water, which promptly induced vomiting. In the ED, the patient complained of mild throat and chest discomfort as well as “abdominal fullness.”
His initial vital signs were: blood pressure, 140/92 mm Hg; heart rate, 93 beats/minute; respiratory rate, 18 breaths/minute; temperature, 96.4° F. Oxygen saturation was 98% on room air. Physical examination revealed tenderness in the epigastric region with no peritoneal findings. Oropharynx and chest examination were normal, and standard laboratory investigations were all within normal limits.
What are the potential exposures to hydrogen peroxide?
Hydrogen peroxide is a colorless and odorless liquid. Solutions with concentrations ranging from 3% to 5% have many household applications, including use as a wound disinfectant and dentifrice; dilute solutions are also utilized for similar purposes in the hospital setting. Industrial-strength H2O2 (concentrations of 10% to 35%) is employed to bleach textiles and paper, and higher concentrations (70% to 90%) are used as an oxygen source for rocket engines.
Consumer application of concentrated H2O2 solutions has become increasingly common. Some, like this patient, clean the surfaces of fruits and vegetables with H2O2 to decrease transmission of bacteria during cutting.1 More concerning, however, is the purported medicinal benefits of ingesting “food-grade” (35%) H2O2 mixed with water—touted on many Internet sites as a treatment for illnesses such as emphysema, cancer, anemia, and HIV.2 Sometimes referred to as “hyperoxygenation therapy,” this so-called treatment has not been approved by the US Food and Drug Administration for any such purpose.3 When diluted sufficiently, this concoction is not harmful but unlikely to provide any health benefits.
Dr Lucyk is a fellow of medical toxicology in the department of emergency medicine at the New York University School of Medicine and the New York City Poison Control Center. Dr Nelson, editor of “Case Studies in Toxicology,” is a professor in the department of emergency medicine and director of the medical toxicology fellowship program at the New York University School of Medicine and the New York City Poison Control Center. He is also associate editor, toxicology, of the EMERGENCY MEDICINE editorial board.
What are the toxic effects of concentrated hydrogen peroxide?
Injury from concentrated H2O2 consumption is primarily from either direct caustic injury or the embolic obstruction of blood flow. Following ingestion, the enzyme catalase metabolizes the breakdown of H2O2 in accordance with the following equation: 2H2O2(aq) → 2H2O(l) + O2(g) + heat. A single milliliter of 35% H2O2 results in the liberation of 100 mL of O2. (The more common 3% household solution generates 10 mL of oxygen per 1 ml of H2O2.) The creation of a large intragastric pressure gradient from the liberation of gas, coupled with the caustic and exothermic injury of the bowel mucosa, may contribute to the movement of oxygen through epithelial interstices into the circulation.In addition, and perhaps more importantly, absorption of intact H2O2 with subsequent metabolism by catalase in the blood liberates oxygen directly within the vasculature. Oxygen bubbles may coalesce in blood circulation and occlude vascular flow. In canine studies, elevated oxygen tension in the portal venous system led to cessation of mesenteric flow in arteries and veins, though the mechanism of action is unclear.4 Furthermore, coalescence of bubbles can lead to disruption of bowel-cell architecture, fibrin plugging of capillaries, venous thrombosis, and infarction of tissues.4
Cases of cardiac and cerebral gas embolism have been reported, and present similarly to patients with diving-related decompression injuries (eg, stroke-like syndromes).5,6 The proposed mechanism for these latter effects involves the metabolism of H2O2 in the systemic circulation with production of oxygen bubbles. In the presence of an atrial septal defect, bubbles may move from the right atrium to the arterial circulation.7
Toxicity and death from H2O2 exposure associated with the historical treatment of inspissated meconium,4 as well as the irrigation of wounds,8 has been reported in the medical literature. Ingestion of a 3% solution is generally benign, resulting at worst in gastrointestinal symptoms or throat irritation.9 Rarely does significant toxicity occur at this low concentration,5 with the vast majority of such cases involving concentrated solutions of 35%.
Case continuation
Case 2
Based on this patient’s continued symptoms, an abdominal radiograph was obtained to assess the presence of portal venous air. Although radiographic findings were normal, continued abdominal examination findings warranted a subsequent abdominal computed tomography (CT) scan, which revealed the presence of extensive air throughout the portal venous system (Figure.).
Do all patients presenting with H2O2 ingestion require imaging to assess for the presence of portal venous air?
Reportedly, ingestion of as little as a “sip” or “mouthful” of 35% H2O2 has resulted in venous and arterial gas embolism,6 occasionally with severe consequences, but no current consensus guidelines exist regarding imaging requirements. Some toxicologists and hyperbaric physicians believe that the presence of portal venous air does not adversely impact a patient’s prognosis or necessitate treatment, and therefore a workup is unnecessary. Others, however, suggest that the presence of portal venous air indicates oversaturation of oxygen in the blood, placing the patient at increased risk for cardiac and cerebral air embolism. Neither one of these theories is well supported in the literature. Although practice patterns vary by institution, it is reasonable that all patients presenting with abdominal complaints after ingestion of H2O2 undergo CT imaging to assess for portal venous air.
If portal venous air is detected, do patients require hyperbaric oxygen therapy?
The management of patients with portal venous gas following H2O2
Hyperbaric therapy increases the amount of oxygen that can be dissolved in the blood, thereby decreasing bubble formation and allowing transport of dissolved oxygen to the lungs where it can be exhaled. Some patients with portal venous air experience significant pain and portal venous hypertension, which may respond rapidly to this therapy.10 Based on available literature, hyperbaric therapy is reasonable for patients with significant abdominal pain and portal venous air following H2O2 ingestion; less controversial is the role of hyperbaric therapy in those with cerebral air embolism. Multiple case reports of patients with significant neurologic findings demonstrate resolution of symptoms following hyperbaric therapy.6
Case conclusion
Hyperbaric oxygen therapy was recommended for the patient in this case, but transfer to a hyperbaric facility was not possible. He was instead admitted to the hospital for continuous monitoring. Over the next 12 hours, his symptoms gradually resolved, and a repeat CT scan the following day showed complete resolution of the portal venous gas. The patient was subsequently discharged without any sequelae.
- Ukuku DO, Bari ML, Kawamoto S, Isshiki K. Use of hydrogen peroxide in combination with nisin, sodium lactate and citric acid for reducing transfer of bacterial pathogens from whole melon surfaces to fresh-cut pieces. Int J Food Microbiol. 2005;104(2):225-233.
- 35% H2O2 hydrogen peroxide food grade certified benefits. The One Minute Miracle Web site. http:// www.theoneminutemiracleinc.com/pages/h2o2- benefits/. Accessed November 20, 2013.
- FDA warns consumers against drinking high-strength hydrogen peroxide for medicinal use: ingestion can lead to serious health risk and death [news release]. Silver Spring, MD: US Food and Drug Administration; July 27, 2006. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ 2006/ucm108701.htm. Accessed November 20, 2013.
- Shaw A, Cooperman A, Fusco J. Gas embolism produced by hydrogen peroxide. N Engl J Med. 1967;277(5):238-241.
- Cina SJ, Downs JC, Conradi SE. Hydrogen peroxide: a source of lethal oxygen embolism. Case report and review of the literature. Am J Forensic Med Pathol. 1994;15(1):44-50.
- Rider SP, Jackson SB, Rusyniak DE. Cerebral air gas embolism from concentrated hydrogen peroxide ingestion. Clin Toxicol (Phila). 2008;46(9):815-818.
- French LK, Horowitz BZ, McKeown NJ. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clin Toxicol (Phila). 2010;48(6):533-538.
- Bassan MM, Dudai M, Shalev O. Near-fatal systemic oxygen embolism due to wound irrigation with hydrogen peroxide. Postgrad Med J. 1982;58(681):448-450.
- Henry MC, Wheeler J, Mofenson HC, et al. Hydrogen peroxide 3% exposures. J Toxicol Clin Toxicol. 1996;34(3):323-327.
- Papafragkou S, Gasparyan A, Batista R, Scott P. Treatment of portal venous gas embolism with hyperbaric oxygen after accidental ingestion of hydrogen peroxide: a case report and review of the literature. J Emerg Med. 2012;43(1):e21-e23.
- Ukuku DO, Bari ML, Kawamoto S, Isshiki K. Use of hydrogen peroxide in combination with nisin, sodium lactate and citric acid for reducing transfer of bacterial pathogens from whole melon surfaces to fresh-cut pieces. Int J Food Microbiol. 2005;104(2):225-233.
- 35% H2O2 hydrogen peroxide food grade certified benefits. The One Minute Miracle Web site. http:// www.theoneminutemiracleinc.com/pages/h2o2- benefits/. Accessed November 20, 2013.
- FDA warns consumers against drinking high-strength hydrogen peroxide for medicinal use: ingestion can lead to serious health risk and death [news release]. Silver Spring, MD: US Food and Drug Administration; July 27, 2006. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ 2006/ucm108701.htm. Accessed November 20, 2013.
- Shaw A, Cooperman A, Fusco J. Gas embolism produced by hydrogen peroxide. N Engl J Med. 1967;277(5):238-241.
- Cina SJ, Downs JC, Conradi SE. Hydrogen peroxide: a source of lethal oxygen embolism. Case report and review of the literature. Am J Forensic Med Pathol. 1994;15(1):44-50.
- Rider SP, Jackson SB, Rusyniak DE. Cerebral air gas embolism from concentrated hydrogen peroxide ingestion. Clin Toxicol (Phila). 2008;46(9):815-818.
- French LK, Horowitz BZ, McKeown NJ. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clin Toxicol (Phila). 2010;48(6):533-538.
- Bassan MM, Dudai M, Shalev O. Near-fatal systemic oxygen embolism due to wound irrigation with hydrogen peroxide. Postgrad Med J. 1982;58(681):448-450.
- Henry MC, Wheeler J, Mofenson HC, et al. Hydrogen peroxide 3% exposures. J Toxicol Clin Toxicol. 1996;34(3):323-327.
- Papafragkou S, Gasparyan A, Batista R, Scott P. Treatment of portal venous gas embolism with hyperbaric oxygen after accidental ingestion of hydrogen peroxide: a case report and review of the literature. J Emerg Med. 2012;43(1):e21-e23.
