User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Costs are keeping Americans out of the doctor’s office
The cost of health care is keeping more Americans from seeing a doctor, even as the number of individuals with insurance coverage increases, according to a new study.
“Despite short-term gains owing to the [Affordable Care Act], over the past 20 years the portion of adults aged 18-64 years unable to see a physician owing to the cost increased, mostly because of an increase among persons with insurance,” Laura Hawks, MD, of Cambridge (Mass.) Health Alliance and Harvard Medical School in Boston and colleagues wrote in a new research report published in JAMA Internal Medicine.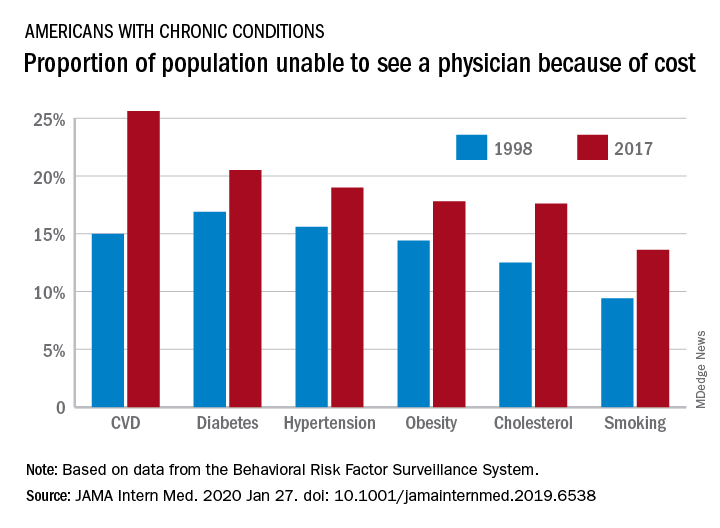
“In 2017, nearly one-fifth of individuals with any chronic condition (diabetes, obesity, or cardiovascular disease) said they were unable to see a physician owing to cost,” they continued.
Researchers examined 20 years of data (January 1998 through December 2017) from the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System to identify trends in unmet need for physician and preventive services.
Among adults aged 18-64 years who responded to the survey in 1998 and 2017, uninsurance decreased by 2.1 percentage points, falling from 16.9% to 14.8%. But at the same time, the portion of adults who were unable to see a physician because of cost rose by 2.7 percentage points, from 11.4% to 15.7%. Looking specifically at adults who had insurance coverage, the researchers found that cost was a barrier for 11.5% of them in 2017, up from 7.1% in 1998.
These results come against a backdrop of growing medical costs, increasing deductibles and copayments, an increasing use of cost containment measures like prior authorization, and narrow provider networks in the wake of the transition to value-based payment structures, the authors noted.
“Our finding that financial access to physician care worsened is concerning,” Dr. Hawks and her colleagues wrote. “Persons with conditions such as diabetes, hypertension, cardiovascular disease, and poor health status risk substantial harms if they forgo physician care. Financial barriers to care have been associated with increased hospitalizations and worse health outcomes in patients with cardiovascular disease and hypertension and increased morbidity among patients with diabetes.”
One of the trends highlighted by the study authors is the growing number of employers offering plans with a high deductible.
“Enrollment in a high-deductible health plan, which has become increasingly common in the last decade, a trend uninterrupted by the ACA, is associated with forgoing needed care, especially among those of lower socioeconomic status,” the authors wrote. “Other changes in insurance benefit design, such as imposing tiered copayments and coinsurance obligations, eliminating coverage for some services (e.g., eyeglasses) and narrowing provider networks (which can force some patients to go out-of-network for care) may also have undermined the affordability of care.”
There was some positive news among the findings, however.
“The main encouraging finding from our analysis is the increase in the proportion of persons – both insured and uninsured – receiving cholesterol checks and flu shots,” Dr. Hawk and her colleagues wrote, adding that this increase “may be attributable to the increasing implementation of quality metrics, financial incentives, and improved systems for the delivery of these services.”
However, not all preventive services that had cost barriers eliminated under the ACA saw improvement, such as cancer screening. They note that the proportion of women who did not receive mammography increased during the study period and then plateaued, but did not improve following the implementation of the ACA. The authors described the reasons for this as “unclear.”
Dr. Hawks received funding support from an Institutional National Research Service award and from Cambridge Health Alliance, her employer. Other authors reported membership in Physicians for a National Health Program.
SOURCE: Hawks L et al. JAMA Intern Med. 2020 Jan 27. doi: 10.1001/jamainternmed.2019.6538.
The cost of health care is keeping more Americans from seeing a doctor, even as the number of individuals with insurance coverage increases, according to a new study.
“Despite short-term gains owing to the [Affordable Care Act], over the past 20 years the portion of adults aged 18-64 years unable to see a physician owing to the cost increased, mostly because of an increase among persons with insurance,” Laura Hawks, MD, of Cambridge (Mass.) Health Alliance and Harvard Medical School in Boston and colleagues wrote in a new research report published in JAMA Internal Medicine.
“In 2017, nearly one-fifth of individuals with any chronic condition (diabetes, obesity, or cardiovascular disease) said they were unable to see a physician owing to cost,” they continued.
Researchers examined 20 years of data (January 1998 through December 2017) from the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System to identify trends in unmet need for physician and preventive services.
Among adults aged 18-64 years who responded to the survey in 1998 and 2017, uninsurance decreased by 2.1 percentage points, falling from 16.9% to 14.8%. But at the same time, the portion of adults who were unable to see a physician because of cost rose by 2.7 percentage points, from 11.4% to 15.7%. Looking specifically at adults who had insurance coverage, the researchers found that cost was a barrier for 11.5% of them in 2017, up from 7.1% in 1998.
These results come against a backdrop of growing medical costs, increasing deductibles and copayments, an increasing use of cost containment measures like prior authorization, and narrow provider networks in the wake of the transition to value-based payment structures, the authors noted.
“Our finding that financial access to physician care worsened is concerning,” Dr. Hawks and her colleagues wrote. “Persons with conditions such as diabetes, hypertension, cardiovascular disease, and poor health status risk substantial harms if they forgo physician care. Financial barriers to care have been associated with increased hospitalizations and worse health outcomes in patients with cardiovascular disease and hypertension and increased morbidity among patients with diabetes.”
One of the trends highlighted by the study authors is the growing number of employers offering plans with a high deductible.
“Enrollment in a high-deductible health plan, which has become increasingly common in the last decade, a trend uninterrupted by the ACA, is associated with forgoing needed care, especially among those of lower socioeconomic status,” the authors wrote. “Other changes in insurance benefit design, such as imposing tiered copayments and coinsurance obligations, eliminating coverage for some services (e.g., eyeglasses) and narrowing provider networks (which can force some patients to go out-of-network for care) may also have undermined the affordability of care.”
There was some positive news among the findings, however.
“The main encouraging finding from our analysis is the increase in the proportion of persons – both insured and uninsured – receiving cholesterol checks and flu shots,” Dr. Hawk and her colleagues wrote, adding that this increase “may be attributable to the increasing implementation of quality metrics, financial incentives, and improved systems for the delivery of these services.”
However, not all preventive services that had cost barriers eliminated under the ACA saw improvement, such as cancer screening. They note that the proportion of women who did not receive mammography increased during the study period and then plateaued, but did not improve following the implementation of the ACA. The authors described the reasons for this as “unclear.”
Dr. Hawks received funding support from an Institutional National Research Service award and from Cambridge Health Alliance, her employer. Other authors reported membership in Physicians for a National Health Program.
SOURCE: Hawks L et al. JAMA Intern Med. 2020 Jan 27. doi: 10.1001/jamainternmed.2019.6538.
The cost of health care is keeping more Americans from seeing a doctor, even as the number of individuals with insurance coverage increases, according to a new study.
“Despite short-term gains owing to the [Affordable Care Act], over the past 20 years the portion of adults aged 18-64 years unable to see a physician owing to the cost increased, mostly because of an increase among persons with insurance,” Laura Hawks, MD, of Cambridge (Mass.) Health Alliance and Harvard Medical School in Boston and colleagues wrote in a new research report published in JAMA Internal Medicine.
“In 2017, nearly one-fifth of individuals with any chronic condition (diabetes, obesity, or cardiovascular disease) said they were unable to see a physician owing to cost,” they continued.
Researchers examined 20 years of data (January 1998 through December 2017) from the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System to identify trends in unmet need for physician and preventive services.
Among adults aged 18-64 years who responded to the survey in 1998 and 2017, uninsurance decreased by 2.1 percentage points, falling from 16.9% to 14.8%. But at the same time, the portion of adults who were unable to see a physician because of cost rose by 2.7 percentage points, from 11.4% to 15.7%. Looking specifically at adults who had insurance coverage, the researchers found that cost was a barrier for 11.5% of them in 2017, up from 7.1% in 1998.
These results come against a backdrop of growing medical costs, increasing deductibles and copayments, an increasing use of cost containment measures like prior authorization, and narrow provider networks in the wake of the transition to value-based payment structures, the authors noted.
“Our finding that financial access to physician care worsened is concerning,” Dr. Hawks and her colleagues wrote. “Persons with conditions such as diabetes, hypertension, cardiovascular disease, and poor health status risk substantial harms if they forgo physician care. Financial barriers to care have been associated with increased hospitalizations and worse health outcomes in patients with cardiovascular disease and hypertension and increased morbidity among patients with diabetes.”
One of the trends highlighted by the study authors is the growing number of employers offering plans with a high deductible.
“Enrollment in a high-deductible health plan, which has become increasingly common in the last decade, a trend uninterrupted by the ACA, is associated with forgoing needed care, especially among those of lower socioeconomic status,” the authors wrote. “Other changes in insurance benefit design, such as imposing tiered copayments and coinsurance obligations, eliminating coverage for some services (e.g., eyeglasses) and narrowing provider networks (which can force some patients to go out-of-network for care) may also have undermined the affordability of care.”
There was some positive news among the findings, however.
“The main encouraging finding from our analysis is the increase in the proportion of persons – both insured and uninsured – receiving cholesterol checks and flu shots,” Dr. Hawk and her colleagues wrote, adding that this increase “may be attributable to the increasing implementation of quality metrics, financial incentives, and improved systems for the delivery of these services.”
However, not all preventive services that had cost barriers eliminated under the ACA saw improvement, such as cancer screening. They note that the proportion of women who did not receive mammography increased during the study period and then plateaued, but did not improve following the implementation of the ACA. The authors described the reasons for this as “unclear.”
Dr. Hawks received funding support from an Institutional National Research Service award and from Cambridge Health Alliance, her employer. Other authors reported membership in Physicians for a National Health Program.
SOURCE: Hawks L et al. JAMA Intern Med. 2020 Jan 27. doi: 10.1001/jamainternmed.2019.6538.
FROM JAMA INTERNAL MEDICINE
Journal editors seek more complete disclosure from authors
A group of leading medical journal editors is seeking to improve the completeness and transparency of financial disclosure reporting with a proposed new disclosure form that puts more onus on readers to decide whether relationships and activities should influence how they view published papers.
The proposed changes are described in an editorial published simultaneously today in the Annals of Internal Medicine, British Medical Journal, Journal of the American Medical Association, The Lancet, New England Journal of Medicine, and several other journals whose editors are members of the International Committee of Medical Journal Editors (ICMJE).
“While no approach to disclosure will be perfect or foolproof, we hope the changes we propose will help promote transparency and trust,” the editorial stated (Ann Intern Med. 2020 Jan 27. doi: 10.7326/M19-3933).
The ICMJE adopted its currently used electronic form – the “ICMJE Form for the Disclosure of Potential Conflicts of Interest” – 10 years ago in an effort to create some uniformity amidst a patchwork of differing disclosure requirements for authors.
It’s not known how many journals outside of the ICMJE’s member journals routinely use the disclosure form, but the organization’s website houses an extensive list of journals whose editors or publishers have requested to be listed as following the ICMJE’s recommendations for editing, reporting, and publishing, including those concerning disclosures. The ICMJE does not “certify” journals. The full set of recommendations was updated in December 2019.
Most authors are committed to transparent reporting, but “opinions differ over which relationships or activities to report,” the editorial stated.
An author might choose to omit an item that others deem important because of a difference in opinion regarding “relevance,” confusion over definitions, or a simple oversight. Some authors may be “concerned that readers will interpret the listing of any item as a ‘potential conflict of interest’ as indicative of problematic influence and wrongdoing,” the editorial stated.
The revised form, like the current one, asks authors to disclose relationships and activities that are directly related to the reported work, as well as those that are topically related (within the broadly defined field addressed in the work). But unlike the current form, the new version provides a checklist of relationships and activities and asks authors to check ‘yes’ or ‘no’ for each one (and to name them when the answer is ‘yes’).
Items in the checklist include grants, payments/honoraria for lectures, patents issued or planned, stock/stock options, and leadership or fiduciary roles in committees, boards, or societies.
The proposed new form makes no mention of “potential conflicts of interest” or “relevancy,” per say. Authors aren’t asked to determine what might be interpreted as a potential conflict of interest, but instead are asked for a “complete listing” of what readers may find “pertinent” to their work.
“We’re trying to move away from calling everything a [potential] ‘conflict,’ ” Darren B. Taichman, MD, PhD, secretary of ICMJE and executive editor of the Annals of Internal Medicine, said in an interview. “We want to remove for authors the concern or stigma, if you will, that anything listed on a form implies that there is something wrong, because that’s just not true. … We want readers to decide what relationships are important as they interpret the work.”
Dr. Taichman said in the interview that the ICMJE’s updating of the form was more a function of “good housekeeping” and continuous appreciation of disclosure as an important issue, rather than any one specific issue, such as concern over a “relevancy” approach to disclosures.
The ICMJE is seeking feedback about its proposed form, which is available with a link for providing comments, at www.icmje.org.
Broader national efforts
Editors and others have been increasingly moving, however, toward asking for more complete disclosures where authors aren’t asked to judge “relevancy” and where readers can make decisions on their own. The American Society of Clinical Oncology, which produces the Journal of Clinical Oncology (JCO) as well as practice guidelines and continuing medical education programs, moved about 5 years ago to a system of general disclosure that asks physicians and others to disclose all financial interests and industry relationships, with no qualifiers.
Earlier in January 2020, the Accreditation Council for Continuing Medical Education issued proposed revisions to its Standards for Integrity and Independence in Accredited Continuing Education. These revisions, which are open for comment, require CME providers to collect disclosure information about all financial relationships of speakers and presenters. It’s up to the CME provider to then determine which relationships are relevant, according to the proposed document.
More change is on the way, as disclosure issues are being deliberated nationally in the wake of a highly publicized disclosure failure at Memorial Sloan Kettering Cancer Center in 2018. Chief medical officer José Baselga, MD, PhD, failed to report millions of dollars of industry payments and ownership interests in journal articles he wrote or cowrote over several years.
In February 2019, leaders from journals, academia, medical societies, and other institutions gathered in Washington for a closed-door meeting to hash out various disclosure related issues.
Hosted by the Association of American Medical Colleges and cosponsored by Memorial Sloan Kettering Cancer Center, ASCO, JAMA, and the Council of Medical Specialty Societies, the meeting led to a series of working groups that are creating additional recommendations “due out soon in 2020,” Heather Pierce, senior director of science policy and regulatory counsel for the AAMC, said in an interview.
Among the questions being discussed: What disclosures should be verified and who should do so? How can disclosures be made more complete and easier for researchers? And, “most importantly,” said Ms. Pierce, how can policy requirements across each of these sectors be aligned so that there’s more coordination and oversight – and with it, public trust?
Some critics of current disclosure policies have called for more reporting of compensation amounts, and Ms. Pierce said that this has been part of cross-sector discussions.
The ICMJE’s proposed form invites, but does not require, authors to indicate what payments were made to them or their institutions. “Part of this is due to the fact that it’s hard to define, let alone agree on, what’s an important amount,” Dr. Taichman said.
A push for registries
The ICMJE is also aiming to make the disclosure process more efficient for authors – and to eliminate inconsistent and incomplete disclosures – by accepting disclosures from web-based repositories, according to the editorial. Repositories allow authors to maintain an inventory of their relationships and activities and then create electronic disclosures that are tailored to the requirements of the ICMJE, medical societies, and other entities.
The AAMC-run repository, called Convey, is consistent with ICMJE reporting requirements and other criteria (e.g., there are no fees for individuals to enter, store, or export their data), but the development of other repositories may be helpful “for meeting regional, linguistic, and regulatory needs” of authors across the world, the editorial stated.
The Annals of Internal Medicine and the New England Journal of Medicine are both currently collecting disclosures through Convey. The platform was born from discussions that followed a 2009 Institute of Medicine report on conflicts of interest.
Signers of the ICMJE editorial include representatives of the National Library of Medicine and the World Association of Medical Editors, in addition to editors in chief and other leaders of the ICMJE member journals.
A group of leading medical journal editors is seeking to improve the completeness and transparency of financial disclosure reporting with a proposed new disclosure form that puts more onus on readers to decide whether relationships and activities should influence how they view published papers.
The proposed changes are described in an editorial published simultaneously today in the Annals of Internal Medicine, British Medical Journal, Journal of the American Medical Association, The Lancet, New England Journal of Medicine, and several other journals whose editors are members of the International Committee of Medical Journal Editors (ICMJE).
“While no approach to disclosure will be perfect or foolproof, we hope the changes we propose will help promote transparency and trust,” the editorial stated (Ann Intern Med. 2020 Jan 27. doi: 10.7326/M19-3933).
The ICMJE adopted its currently used electronic form – the “ICMJE Form for the Disclosure of Potential Conflicts of Interest” – 10 years ago in an effort to create some uniformity amidst a patchwork of differing disclosure requirements for authors.
It’s not known how many journals outside of the ICMJE’s member journals routinely use the disclosure form, but the organization’s website houses an extensive list of journals whose editors or publishers have requested to be listed as following the ICMJE’s recommendations for editing, reporting, and publishing, including those concerning disclosures. The ICMJE does not “certify” journals. The full set of recommendations was updated in December 2019.
Most authors are committed to transparent reporting, but “opinions differ over which relationships or activities to report,” the editorial stated.
An author might choose to omit an item that others deem important because of a difference in opinion regarding “relevance,” confusion over definitions, or a simple oversight. Some authors may be “concerned that readers will interpret the listing of any item as a ‘potential conflict of interest’ as indicative of problematic influence and wrongdoing,” the editorial stated.
The revised form, like the current one, asks authors to disclose relationships and activities that are directly related to the reported work, as well as those that are topically related (within the broadly defined field addressed in the work). But unlike the current form, the new version provides a checklist of relationships and activities and asks authors to check ‘yes’ or ‘no’ for each one (and to name them when the answer is ‘yes’).
Items in the checklist include grants, payments/honoraria for lectures, patents issued or planned, stock/stock options, and leadership or fiduciary roles in committees, boards, or societies.
The proposed new form makes no mention of “potential conflicts of interest” or “relevancy,” per say. Authors aren’t asked to determine what might be interpreted as a potential conflict of interest, but instead are asked for a “complete listing” of what readers may find “pertinent” to their work.
“We’re trying to move away from calling everything a [potential] ‘conflict,’ ” Darren B. Taichman, MD, PhD, secretary of ICMJE and executive editor of the Annals of Internal Medicine, said in an interview. “We want to remove for authors the concern or stigma, if you will, that anything listed on a form implies that there is something wrong, because that’s just not true. … We want readers to decide what relationships are important as they interpret the work.”
Dr. Taichman said in the interview that the ICMJE’s updating of the form was more a function of “good housekeeping” and continuous appreciation of disclosure as an important issue, rather than any one specific issue, such as concern over a “relevancy” approach to disclosures.
The ICMJE is seeking feedback about its proposed form, which is available with a link for providing comments, at www.icmje.org.
Broader national efforts
Editors and others have been increasingly moving, however, toward asking for more complete disclosures where authors aren’t asked to judge “relevancy” and where readers can make decisions on their own. The American Society of Clinical Oncology, which produces the Journal of Clinical Oncology (JCO) as well as practice guidelines and continuing medical education programs, moved about 5 years ago to a system of general disclosure that asks physicians and others to disclose all financial interests and industry relationships, with no qualifiers.
Earlier in January 2020, the Accreditation Council for Continuing Medical Education issued proposed revisions to its Standards for Integrity and Independence in Accredited Continuing Education. These revisions, which are open for comment, require CME providers to collect disclosure information about all financial relationships of speakers and presenters. It’s up to the CME provider to then determine which relationships are relevant, according to the proposed document.
More change is on the way, as disclosure issues are being deliberated nationally in the wake of a highly publicized disclosure failure at Memorial Sloan Kettering Cancer Center in 2018. Chief medical officer José Baselga, MD, PhD, failed to report millions of dollars of industry payments and ownership interests in journal articles he wrote or cowrote over several years.
In February 2019, leaders from journals, academia, medical societies, and other institutions gathered in Washington for a closed-door meeting to hash out various disclosure related issues.
Hosted by the Association of American Medical Colleges and cosponsored by Memorial Sloan Kettering Cancer Center, ASCO, JAMA, and the Council of Medical Specialty Societies, the meeting led to a series of working groups that are creating additional recommendations “due out soon in 2020,” Heather Pierce, senior director of science policy and regulatory counsel for the AAMC, said in an interview.
Among the questions being discussed: What disclosures should be verified and who should do so? How can disclosures be made more complete and easier for researchers? And, “most importantly,” said Ms. Pierce, how can policy requirements across each of these sectors be aligned so that there’s more coordination and oversight – and with it, public trust?
Some critics of current disclosure policies have called for more reporting of compensation amounts, and Ms. Pierce said that this has been part of cross-sector discussions.
The ICMJE’s proposed form invites, but does not require, authors to indicate what payments were made to them or their institutions. “Part of this is due to the fact that it’s hard to define, let alone agree on, what’s an important amount,” Dr. Taichman said.
A push for registries
The ICMJE is also aiming to make the disclosure process more efficient for authors – and to eliminate inconsistent and incomplete disclosures – by accepting disclosures from web-based repositories, according to the editorial. Repositories allow authors to maintain an inventory of their relationships and activities and then create electronic disclosures that are tailored to the requirements of the ICMJE, medical societies, and other entities.
The AAMC-run repository, called Convey, is consistent with ICMJE reporting requirements and other criteria (e.g., there are no fees for individuals to enter, store, or export their data), but the development of other repositories may be helpful “for meeting regional, linguistic, and regulatory needs” of authors across the world, the editorial stated.
The Annals of Internal Medicine and the New England Journal of Medicine are both currently collecting disclosures through Convey. The platform was born from discussions that followed a 2009 Institute of Medicine report on conflicts of interest.
Signers of the ICMJE editorial include representatives of the National Library of Medicine and the World Association of Medical Editors, in addition to editors in chief and other leaders of the ICMJE member journals.
A group of leading medical journal editors is seeking to improve the completeness and transparency of financial disclosure reporting with a proposed new disclosure form that puts more onus on readers to decide whether relationships and activities should influence how they view published papers.
The proposed changes are described in an editorial published simultaneously today in the Annals of Internal Medicine, British Medical Journal, Journal of the American Medical Association, The Lancet, New England Journal of Medicine, and several other journals whose editors are members of the International Committee of Medical Journal Editors (ICMJE).
“While no approach to disclosure will be perfect or foolproof, we hope the changes we propose will help promote transparency and trust,” the editorial stated (Ann Intern Med. 2020 Jan 27. doi: 10.7326/M19-3933).
The ICMJE adopted its currently used electronic form – the “ICMJE Form for the Disclosure of Potential Conflicts of Interest” – 10 years ago in an effort to create some uniformity amidst a patchwork of differing disclosure requirements for authors.
It’s not known how many journals outside of the ICMJE’s member journals routinely use the disclosure form, but the organization’s website houses an extensive list of journals whose editors or publishers have requested to be listed as following the ICMJE’s recommendations for editing, reporting, and publishing, including those concerning disclosures. The ICMJE does not “certify” journals. The full set of recommendations was updated in December 2019.
Most authors are committed to transparent reporting, but “opinions differ over which relationships or activities to report,” the editorial stated.
An author might choose to omit an item that others deem important because of a difference in opinion regarding “relevance,” confusion over definitions, or a simple oversight. Some authors may be “concerned that readers will interpret the listing of any item as a ‘potential conflict of interest’ as indicative of problematic influence and wrongdoing,” the editorial stated.
The revised form, like the current one, asks authors to disclose relationships and activities that are directly related to the reported work, as well as those that are topically related (within the broadly defined field addressed in the work). But unlike the current form, the new version provides a checklist of relationships and activities and asks authors to check ‘yes’ or ‘no’ for each one (and to name them when the answer is ‘yes’).
Items in the checklist include grants, payments/honoraria for lectures, patents issued or planned, stock/stock options, and leadership or fiduciary roles in committees, boards, or societies.
The proposed new form makes no mention of “potential conflicts of interest” or “relevancy,” per say. Authors aren’t asked to determine what might be interpreted as a potential conflict of interest, but instead are asked for a “complete listing” of what readers may find “pertinent” to their work.
“We’re trying to move away from calling everything a [potential] ‘conflict,’ ” Darren B. Taichman, MD, PhD, secretary of ICMJE and executive editor of the Annals of Internal Medicine, said in an interview. “We want to remove for authors the concern or stigma, if you will, that anything listed on a form implies that there is something wrong, because that’s just not true. … We want readers to decide what relationships are important as they interpret the work.”
Dr. Taichman said in the interview that the ICMJE’s updating of the form was more a function of “good housekeeping” and continuous appreciation of disclosure as an important issue, rather than any one specific issue, such as concern over a “relevancy” approach to disclosures.
The ICMJE is seeking feedback about its proposed form, which is available with a link for providing comments, at www.icmje.org.
Broader national efforts
Editors and others have been increasingly moving, however, toward asking for more complete disclosures where authors aren’t asked to judge “relevancy” and where readers can make decisions on their own. The American Society of Clinical Oncology, which produces the Journal of Clinical Oncology (JCO) as well as practice guidelines and continuing medical education programs, moved about 5 years ago to a system of general disclosure that asks physicians and others to disclose all financial interests and industry relationships, with no qualifiers.
Earlier in January 2020, the Accreditation Council for Continuing Medical Education issued proposed revisions to its Standards for Integrity and Independence in Accredited Continuing Education. These revisions, which are open for comment, require CME providers to collect disclosure information about all financial relationships of speakers and presenters. It’s up to the CME provider to then determine which relationships are relevant, according to the proposed document.
More change is on the way, as disclosure issues are being deliberated nationally in the wake of a highly publicized disclosure failure at Memorial Sloan Kettering Cancer Center in 2018. Chief medical officer José Baselga, MD, PhD, failed to report millions of dollars of industry payments and ownership interests in journal articles he wrote or cowrote over several years.
In February 2019, leaders from journals, academia, medical societies, and other institutions gathered in Washington for a closed-door meeting to hash out various disclosure related issues.
Hosted by the Association of American Medical Colleges and cosponsored by Memorial Sloan Kettering Cancer Center, ASCO, JAMA, and the Council of Medical Specialty Societies, the meeting led to a series of working groups that are creating additional recommendations “due out soon in 2020,” Heather Pierce, senior director of science policy and regulatory counsel for the AAMC, said in an interview.
Among the questions being discussed: What disclosures should be verified and who should do so? How can disclosures be made more complete and easier for researchers? And, “most importantly,” said Ms. Pierce, how can policy requirements across each of these sectors be aligned so that there’s more coordination and oversight – and with it, public trust?
Some critics of current disclosure policies have called for more reporting of compensation amounts, and Ms. Pierce said that this has been part of cross-sector discussions.
The ICMJE’s proposed form invites, but does not require, authors to indicate what payments were made to them or their institutions. “Part of this is due to the fact that it’s hard to define, let alone agree on, what’s an important amount,” Dr. Taichman said.
A push for registries
The ICMJE is also aiming to make the disclosure process more efficient for authors – and to eliminate inconsistent and incomplete disclosures – by accepting disclosures from web-based repositories, according to the editorial. Repositories allow authors to maintain an inventory of their relationships and activities and then create electronic disclosures that are tailored to the requirements of the ICMJE, medical societies, and other entities.
The AAMC-run repository, called Convey, is consistent with ICMJE reporting requirements and other criteria (e.g., there are no fees for individuals to enter, store, or export their data), but the development of other repositories may be helpful “for meeting regional, linguistic, and regulatory needs” of authors across the world, the editorial stated.
The Annals of Internal Medicine and the New England Journal of Medicine are both currently collecting disclosures through Convey. The platform was born from discussions that followed a 2009 Institute of Medicine report on conflicts of interest.
Signers of the ICMJE editorial include representatives of the National Library of Medicine and the World Association of Medical Editors, in addition to editors in chief and other leaders of the ICMJE member journals.
FROM ANNALS OF INTERNAL MEDICINE
Registry data reveal temporal relationship between psoriasis symptoms and PsA onset
ATLANTA – Psoriasis type and patient age at presentation among patients with psoriatic arthritis predict the timing of arthritis symptom synchronicity, according to findings from the Psoriatic Arthritis Registry of Turkey International Database.

However, in those who develop arthritis symptoms first, age at onset is not predictive of psoriatic arthritis (PsA) symptom synchronicity, Umut Kalyoncu, MD, reported at the annual meeting of the American College of Rheumatology.
Of 1,631 patients from the registry, 1,251 had psoriasis first, 71 had arthritis first, and 309 had synchronous onset, which was defined as the onset of both psoriasis and arthritis symptoms within a 12-month period. The time from skin disease to PsA was 155.6 months, –67.4 months, and 1.8 months, among the groups, respectively, and the mean age at PsA onset was similar, ranging from about 41 to 42 years in those who developed arthritis first, said Dr. Kalyoncu, of the department of rheumatology at Hacettepe University, Ankara, Turkey.
However, the mean age of PsA onset among those who developed psoriasis first was 29.4 years, compared with 46.3 years in those who developed arthritis first.
“So there is a really big difference between psoriasis beginning age,” he said.
PsA types also differed by onset symptoms: Axial involvement was more common with arthritis-first onset at 38.0%, compared with 28.8% for psoriasis first and 27.8% for synchronous onset). Oligoarthritis occurred more often with arthritis-first onset (45.1% vs. 30.7% and 29.4%, respectively), and polyarthritis occurred less often with arthritis-first onset (33.8% vs. 49.4% and 47.6%, respectively), he said.
Psoriasis type also differed among the groups: Pustular skin involvement was more common in arthritis-first patients (18.3% vs. 11.9% and 16.5% of psoriasis-first and synchronous-onset patients), scalp lesions as the initial lesion were more common in psoriasis-first patients (48.3% vs. 35.2% of arthritis-first patients and 39.8% of synchronous-onset patients), and genital involvement was present more often in arthritis-first patients (12.7% vs. 6.2% and 4.9% of psoriasis-first and synchronous-onset patients).
Early-onset (type 1) psoriasis was more common in psoriasis-first patients (74% vs. 28.1% and 51.8% of arthritis-first and synchronous-onset patients), whereas late-onset (type 2) psoriasis was more common in arthritis-first patients (71.9% vs. 26.0% and 48.2% for psoriasis-first and synchronous-onset patients).
A family history of psoriasis or PsA was more common in psoriasis-first patients (35.6% vs. 26.3% and 28.2% of arthritis-first and synchronous-onset patients), Dr. Kalyoncu said.
Treatment types did not differ between the groups.
Multiple linear regression analysis for the time elapsed from psoriasis to PsA symptom synchronicity, with all other independent variables set to baseline values, showed an overall intercept interval of 66 months, but with nail involvement, family history, or plaque psoriasis, the interval was extended by 28, 24, and 20 months, respectively. However, the presence of pustular psoriasis decreased the intercept interval by 28 months.
A temporal relationship between the onset of skin psoriasis and PsA is a well-known feature of psoriatic disease, with prior studies showing that the majority of cases involve psoriasis-first onset, Dr. Kalyoncu said, adding that heterogeneity in musculoskeletal and skin involvement is also a known feature.
However, little is known about the role of genetics, he noted.
Therefore, he and his colleagues used the Psoriatic Arthritis Registry of Turkey International Database, which was established in 2014 and now also includes data from patients in Canada and Italy, to explore the associations between disease characteristics and the temporal relationship of skin and musculoskeletal disease.
Based on the findings, age at the onset of psoriasis was the main factor that determined PsA symptom synchronicity, he said.
“We know that HLA-Cw6 is important in genetic susceptibility of psoriatic arthritis, but it is important only for early-onset arthritis, not late-onset psoriasis,” Dr. Kalyoncu said. “So our results make an indirect contribution [to the understanding of] these genetic and immunochemical differences between early-onset and late-onset psoriasis, and we need further future studies about this topic.”
Dr. Kalyoncu reported having no relevant disclosures.
SOURCE: Kalyoncu U et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2854.
ATLANTA – Psoriasis type and patient age at presentation among patients with psoriatic arthritis predict the timing of arthritis symptom synchronicity, according to findings from the Psoriatic Arthritis Registry of Turkey International Database.
However, in those who develop arthritis symptoms first, age at onset is not predictive of psoriatic arthritis (PsA) symptom synchronicity, Umut Kalyoncu, MD, reported at the annual meeting of the American College of Rheumatology.
Of 1,631 patients from the registry, 1,251 had psoriasis first, 71 had arthritis first, and 309 had synchronous onset, which was defined as the onset of both psoriasis and arthritis symptoms within a 12-month period. The time from skin disease to PsA was 155.6 months, –67.4 months, and 1.8 months, among the groups, respectively, and the mean age at PsA onset was similar, ranging from about 41 to 42 years in those who developed arthritis first, said Dr. Kalyoncu, of the department of rheumatology at Hacettepe University, Ankara, Turkey.
However, the mean age of PsA onset among those who developed psoriasis first was 29.4 years, compared with 46.3 years in those who developed arthritis first.
“So there is a really big difference between psoriasis beginning age,” he said.
PsA types also differed by onset symptoms: Axial involvement was more common with arthritis-first onset at 38.0%, compared with 28.8% for psoriasis first and 27.8% for synchronous onset). Oligoarthritis occurred more often with arthritis-first onset (45.1% vs. 30.7% and 29.4%, respectively), and polyarthritis occurred less often with arthritis-first onset (33.8% vs. 49.4% and 47.6%, respectively), he said.
Psoriasis type also differed among the groups: Pustular skin involvement was more common in arthritis-first patients (18.3% vs. 11.9% and 16.5% of psoriasis-first and synchronous-onset patients), scalp lesions as the initial lesion were more common in psoriasis-first patients (48.3% vs. 35.2% of arthritis-first patients and 39.8% of synchronous-onset patients), and genital involvement was present more often in arthritis-first patients (12.7% vs. 6.2% and 4.9% of psoriasis-first and synchronous-onset patients).
Early-onset (type 1) psoriasis was more common in psoriasis-first patients (74% vs. 28.1% and 51.8% of arthritis-first and synchronous-onset patients), whereas late-onset (type 2) psoriasis was more common in arthritis-first patients (71.9% vs. 26.0% and 48.2% for psoriasis-first and synchronous-onset patients).
A family history of psoriasis or PsA was more common in psoriasis-first patients (35.6% vs. 26.3% and 28.2% of arthritis-first and synchronous-onset patients), Dr. Kalyoncu said.
Treatment types did not differ between the groups.
Multiple linear regression analysis for the time elapsed from psoriasis to PsA symptom synchronicity, with all other independent variables set to baseline values, showed an overall intercept interval of 66 months, but with nail involvement, family history, or plaque psoriasis, the interval was extended by 28, 24, and 20 months, respectively. However, the presence of pustular psoriasis decreased the intercept interval by 28 months.
A temporal relationship between the onset of skin psoriasis and PsA is a well-known feature of psoriatic disease, with prior studies showing that the majority of cases involve psoriasis-first onset, Dr. Kalyoncu said, adding that heterogeneity in musculoskeletal and skin involvement is also a known feature.
However, little is known about the role of genetics, he noted.
Therefore, he and his colleagues used the Psoriatic Arthritis Registry of Turkey International Database, which was established in 2014 and now also includes data from patients in Canada and Italy, to explore the associations between disease characteristics and the temporal relationship of skin and musculoskeletal disease.
Based on the findings, age at the onset of psoriasis was the main factor that determined PsA symptom synchronicity, he said.
“We know that HLA-Cw6 is important in genetic susceptibility of psoriatic arthritis, but it is important only for early-onset arthritis, not late-onset psoriasis,” Dr. Kalyoncu said. “So our results make an indirect contribution [to the understanding of] these genetic and immunochemical differences between early-onset and late-onset psoriasis, and we need further future studies about this topic.”
Dr. Kalyoncu reported having no relevant disclosures.
SOURCE: Kalyoncu U et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2854.
ATLANTA – Psoriasis type and patient age at presentation among patients with psoriatic arthritis predict the timing of arthritis symptom synchronicity, according to findings from the Psoriatic Arthritis Registry of Turkey International Database.
However, in those who develop arthritis symptoms first, age at onset is not predictive of psoriatic arthritis (PsA) symptom synchronicity, Umut Kalyoncu, MD, reported at the annual meeting of the American College of Rheumatology.
Of 1,631 patients from the registry, 1,251 had psoriasis first, 71 had arthritis first, and 309 had synchronous onset, which was defined as the onset of both psoriasis and arthritis symptoms within a 12-month period. The time from skin disease to PsA was 155.6 months, –67.4 months, and 1.8 months, among the groups, respectively, and the mean age at PsA onset was similar, ranging from about 41 to 42 years in those who developed arthritis first, said Dr. Kalyoncu, of the department of rheumatology at Hacettepe University, Ankara, Turkey.
However, the mean age of PsA onset among those who developed psoriasis first was 29.4 years, compared with 46.3 years in those who developed arthritis first.
“So there is a really big difference between psoriasis beginning age,” he said.
PsA types also differed by onset symptoms: Axial involvement was more common with arthritis-first onset at 38.0%, compared with 28.8% for psoriasis first and 27.8% for synchronous onset). Oligoarthritis occurred more often with arthritis-first onset (45.1% vs. 30.7% and 29.4%, respectively), and polyarthritis occurred less often with arthritis-first onset (33.8% vs. 49.4% and 47.6%, respectively), he said.
Psoriasis type also differed among the groups: Pustular skin involvement was more common in arthritis-first patients (18.3% vs. 11.9% and 16.5% of psoriasis-first and synchronous-onset patients), scalp lesions as the initial lesion were more common in psoriasis-first patients (48.3% vs. 35.2% of arthritis-first patients and 39.8% of synchronous-onset patients), and genital involvement was present more often in arthritis-first patients (12.7% vs. 6.2% and 4.9% of psoriasis-first and synchronous-onset patients).
Early-onset (type 1) psoriasis was more common in psoriasis-first patients (74% vs. 28.1% and 51.8% of arthritis-first and synchronous-onset patients), whereas late-onset (type 2) psoriasis was more common in arthritis-first patients (71.9% vs. 26.0% and 48.2% for psoriasis-first and synchronous-onset patients).
A family history of psoriasis or PsA was more common in psoriasis-first patients (35.6% vs. 26.3% and 28.2% of arthritis-first and synchronous-onset patients), Dr. Kalyoncu said.
Treatment types did not differ between the groups.
Multiple linear regression analysis for the time elapsed from psoriasis to PsA symptom synchronicity, with all other independent variables set to baseline values, showed an overall intercept interval of 66 months, but with nail involvement, family history, or plaque psoriasis, the interval was extended by 28, 24, and 20 months, respectively. However, the presence of pustular psoriasis decreased the intercept interval by 28 months.
A temporal relationship between the onset of skin psoriasis and PsA is a well-known feature of psoriatic disease, with prior studies showing that the majority of cases involve psoriasis-first onset, Dr. Kalyoncu said, adding that heterogeneity in musculoskeletal and skin involvement is also a known feature.
However, little is known about the role of genetics, he noted.
Therefore, he and his colleagues used the Psoriatic Arthritis Registry of Turkey International Database, which was established in 2014 and now also includes data from patients in Canada and Italy, to explore the associations between disease characteristics and the temporal relationship of skin and musculoskeletal disease.
Based on the findings, age at the onset of psoriasis was the main factor that determined PsA symptom synchronicity, he said.
“We know that HLA-Cw6 is important in genetic susceptibility of psoriatic arthritis, but it is important only for early-onset arthritis, not late-onset psoriasis,” Dr. Kalyoncu said. “So our results make an indirect contribution [to the understanding of] these genetic and immunochemical differences between early-onset and late-onset psoriasis, and we need further future studies about this topic.”
Dr. Kalyoncu reported having no relevant disclosures.
SOURCE: Kalyoncu U et al. Arthritis Rheumatol. 2019;71(suppl 10), Abstract 2854.
REPORTING FROM ACR 2019
In rheumatology, biosimilars are flatlining. Why?
Although biosimilar versions of tumor necrosis factor inhibitors (TNFis) have been available to U.S. rheumatologists and their patients for over 3 years, uptake has thus far been slow.
In an analysis of data from a large commercial payer, the two available biosimilars for infliximab (Remicade) accounted for less than 1% of TNFi prescribing since the first biosimilar to infliximab was approved in 2016.
The study, published in Arthritis & Rheumatology, involved a total of 1.1 million TNFi prescriptions or infusions received by 95,906 patients from 2016 to 2019. Investigators found that uptake of biosimilar infliximab was essentially flat, standing at 0.1% of prescribing in the second quarter of 2017, and topping out at 0.9% in the first quarter of 2019. For branded infliximab, prescribing was also stable, but accounted for about 20% of overall biologic dispensing in each quarter of the period studied.
There are currently two biosimilar medications to the originator infliximab, which is one of five originator biologics available to treat rheumatic diseases in the United States: infliximab-dyyb (Inflectra) and infliximab-abda (Renflexis). The former was approved in 2016 and the latter in 2017, said study author Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston, and her coauthors.

“Our paper reports a disappointingly low uptake of biosimilar infliximab since the first quarter of 2017 using claims data from a large private health plan. The main and maybe the only reason to consider using a biosimilar is cost saving,” said Dr. Kim in an interview. “Our results suggest that current modest cost savings from infliximab biosimilars in the U.S. are not sufficient to promote their widespread use.”
In the payer database study conducted by Dr. Kim and colleagues, the insurer paid similar mean amounts per patient per quarter for originator and biosimilar infliximab in mid-2017 ($8,322 versus $8,656). By the end of 2018, a gap appeared, with the insurer paying a mean quarterly per-patient sum of $8,111 for biosimilar infliximab compared with $9,535 for the branded biologic.
“The lack of market penetration and very modest price reductions for biosimilars have left policymakers, payers, physicians, and the public frustrated, particularly because sales in Europe continue to rapidly expand and robust cost-savings have materialized,” wrote Jinoos Yazdany, MD, MPH, in an editorial accompanying the study.

Dr. Yazdany, professor and chief of the division of rheumatology at the University of California, San Francisco, noted that increased spending on biologics in the United States – which increased by 50% from 2014 to 2018 – has been driven by rising prices as well as increased uptake of biologic therapies.
At least in part, Europe has been able to reap cost savings where the United States hasn’t because fundamental differences in health care reimbursement can ease sweeping biosimilar adoption, Dr. Yazdany noted. “Countries like Denmark and Sweden, using the negotiating and purchasing power of their single-payer systems have instituted a winner-takes-all bidding system,” with Denmark seeing cost savings of up to two-thirds when bidding was combined with mandatory switching, she said.
The continued market dominance of originator infliximab means that savings from biosimilars have thus far amounted to about $91 million, far short of the $1 billion that the Congressional Budget Office had projected for this date, Dr. Yazdany said.
One problem in the adoption of biosimilars by U.S. rheumatologists may have been uneven marketing and pricing across different types of practice, Colin C. Edgerton, MD, a rheumatologist at Low Country Rheumatology in South Carolina and chair of the American College of Rheumatology’s Committee on Rheumatologic Care, said in an interview.

“Rheumatologists have generally developed comfort with biosimilars, although this is not universal. The core message, that all biologics vary and that this is OK, is getting out. In general, rheumatologists also understand the problem with high drug prices and the threat to patient access,” Dr. Edgerton said. But “the early marketing and pricing focus for biosimilars seemed to be on hospitals and facilities, and this did not work effectively for community rheumatologists, where the majority of care is delivered. We have been pleased to see a manufacturer pivot toward community rheumatology where additional efforts need to be made to bend the curve on biosimilar adoption. It is critical for practices with experience using biosimilars to educate peers, and this is where networks of practicing rheumatologists are important.”
In Dr. Yazdany’s editorial, she cited four structural factors impeding biosimilar uptake and downstream savings.
First, she cites ongoing actions by pharmaceutical companies, which create a “patent thicket” that has the effect of fencing off originator biologics from biosimilars long beyond the original 12-year exclusivity period. Supporting the notion that “patent thickets” are a common strategy, Dr. Yazdany noted that almost half of the patent applications that AbbVie has filed for adalimumab (Humira) have come in after the original exclusivity period expired in 2014. Humira’s price has risen 18% yearly during this period.
The complicated role played by pharmacy benefit managers (PBMs) is another factor in slow adoption, said Dr. Yazdany: When manufacturers offer rebates to PBMs, the price of the originator biologic may be less than its biosimilar. Further, manufacturers may sign multiyear rebate agreements just before a biosimilar launch; PBMs are also sometimes threatened with the withdrawal of rebates if they offer biosimilars, she noted.
Third, prescriber inertia may also be at play, Dr. Yazdany noted, not least because patients often see little difference in out-of-pocket costs when they make the switch to a biosimilar – PBM rebates are not necessarily passed on to patients. Payers may not reimburse a biosimilar, or formularies can be built without them, influencing prescribing, and there’s usually no reimbursement incentive for biosimilar prescribing in the nonpublic sector, she said. To the contrary, infusing a drug with a higher price often means higher reimbursement for the administering clinician, since commercial insurance reimbursement is often calculated as a percent of the charge for the drug.
Further contributing to inertia is the extra time required for patient education and writing a new set of orders – all work that can’t be captured for extra reimbursement. Dr. Edgerton said that rheumatologists can talk with patients about the “nocebo effect” relating to biosimilars. “This is a phenomenon in which patients are thought to experience worsening symptoms associated with negative beliefs about biosimilars. There has been a study in Arthritis Care & Research addressing this concern. The authors found that positive framing of biosimilars led to more participants being willing to switch than negative framing. This suggests that clinicians have an important role in informing patients about biosimilars, and addressing hesitancy.”
Finally, Dr. Yazdany pointed out that for a pharmaceutical company pursuing biosimilar approval, the regulatory pathway itself can provide its own set of complications and confusion. Biosimilars are not exact molecular replicas of the originator biologic, and these differences can change efficacy and immunogenicity, and also affect stability. Hence, a company wishing to market a biosimilar has to show the Food and Drug Administration that safety and efficacy aren’t affected by a switch to biosimilar from an originator biologic. Extrapolation from one indication to another can be made – with scientific justification.
Rheumatologists are mindful of the potential differences between biosimilars and the originator biologic, as evinced in a recent position statement from the American College of Rheumatology. The position statement advises that “extrapolation should be pursued with caution,” and asks for clear labeling when biosimilars have been designated “interchangeable” with their biosimilar. Interchangeability can clear the way for pharmacy substitution of a prescribed biologic, though Dr. Yazdany noted that 40 states have passed legislation requiring prescriber notification.
The FDA is currently using postmarketing pharmacovigilance to monitor biosimilar performance in the real world, and a recent systematic review “should provide some reassurance,” wrote Dr. Yazdany, citing the study, which looked at 14,000 patients who had a total of 14 disease indications for biosimilar use. The 90-article review largely found no differences in safety, efficacy, or immunogenicity between originators and their biosimilars. Dr. Yazdany recommended greater openness to incorporating the European experience in the FDA’s ongoing reassessment.
A further way forward can come through tackling the patent thicket with the proposed bipartisan Biologic Patent Transparency Act, which would require publication of biologic patents in a one-stop publicly searchable database. Going further with legislation to address anticompetitive activity by pharmaceutical companies could shorten the runway to biosimilar launching considerably, she noted.
The complicated landscape of PBMs and rebates affects many sectors of health care, and new policy efforts are needed here as well, she said. Reimbursement strategies – and much-needed continuing medical education – can both ease prescriber unfamiliarity with biosimilars and provide incentives for their use, she concluded.
Dr. Kim concurred that change is needed before the United States is likely to reap significant economic benefit from biosimilars. “The uptake of biosimilars and their impact on overall health care cost needs to be reevaluated when we have more biosimilars available in the next 3-4 years. However, for now, it appears that substantial savings achieved in some European countries – for example, Denmark – may not be possible without systemic reform of the U.S. pharmaceutical market,” she said.
Dr. Yazdany is supported by the Alice Betts Endowed Chair in Arthritis Research, the Russel/Engleman Research Center at the University of California, San Francisco, and the National Institutes of Health. She has received independent research grants from Pfizer and Genentech and research consulting fees from Eli Lilly and AstraZeneca.
Dr. Kim’s study was supported by the division of pharmacoepidemiology and pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, and Arnold Ventures. Dr. Kim has received research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Bristol-Myers Squibb, and Roche.
SOURCES: Kim SC et al. Arthritis Rheumatol. 2020 Jan 13. doi: 10.1002/art.41201; Yazdany J. Arthritis Rheumatol. 2020 Jan 10. doi: 10.1002/art.41203.
Although biosimilar versions of tumor necrosis factor inhibitors (TNFis) have been available to U.S. rheumatologists and their patients for over 3 years, uptake has thus far been slow.
In an analysis of data from a large commercial payer, the two available biosimilars for infliximab (Remicade) accounted for less than 1% of TNFi prescribing since the first biosimilar to infliximab was approved in 2016.
The study, published in Arthritis & Rheumatology, involved a total of 1.1 million TNFi prescriptions or infusions received by 95,906 patients from 2016 to 2019. Investigators found that uptake of biosimilar infliximab was essentially flat, standing at 0.1% of prescribing in the second quarter of 2017, and topping out at 0.9% in the first quarter of 2019. For branded infliximab, prescribing was also stable, but accounted for about 20% of overall biologic dispensing in each quarter of the period studied.
There are currently two biosimilar medications to the originator infliximab, which is one of five originator biologics available to treat rheumatic diseases in the United States: infliximab-dyyb (Inflectra) and infliximab-abda (Renflexis). The former was approved in 2016 and the latter in 2017, said study author Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston, and her coauthors.
“Our paper reports a disappointingly low uptake of biosimilar infliximab since the first quarter of 2017 using claims data from a large private health plan. The main and maybe the only reason to consider using a biosimilar is cost saving,” said Dr. Kim in an interview. “Our results suggest that current modest cost savings from infliximab biosimilars in the U.S. are not sufficient to promote their widespread use.”
In the payer database study conducted by Dr. Kim and colleagues, the insurer paid similar mean amounts per patient per quarter for originator and biosimilar infliximab in mid-2017 ($8,322 versus $8,656). By the end of 2018, a gap appeared, with the insurer paying a mean quarterly per-patient sum of $8,111 for biosimilar infliximab compared with $9,535 for the branded biologic.
“The lack of market penetration and very modest price reductions for biosimilars have left policymakers, payers, physicians, and the public frustrated, particularly because sales in Europe continue to rapidly expand and robust cost-savings have materialized,” wrote Jinoos Yazdany, MD, MPH, in an editorial accompanying the study.
Dr. Yazdany, professor and chief of the division of rheumatology at the University of California, San Francisco, noted that increased spending on biologics in the United States – which increased by 50% from 2014 to 2018 – has been driven by rising prices as well as increased uptake of biologic therapies.
At least in part, Europe has been able to reap cost savings where the United States hasn’t because fundamental differences in health care reimbursement can ease sweeping biosimilar adoption, Dr. Yazdany noted. “Countries like Denmark and Sweden, using the negotiating and purchasing power of their single-payer systems have instituted a winner-takes-all bidding system,” with Denmark seeing cost savings of up to two-thirds when bidding was combined with mandatory switching, she said.
The continued market dominance of originator infliximab means that savings from biosimilars have thus far amounted to about $91 million, far short of the $1 billion that the Congressional Budget Office had projected for this date, Dr. Yazdany said.
One problem in the adoption of biosimilars by U.S. rheumatologists may have been uneven marketing and pricing across different types of practice, Colin C. Edgerton, MD, a rheumatologist at Low Country Rheumatology in South Carolina and chair of the American College of Rheumatology’s Committee on Rheumatologic Care, said in an interview.
“Rheumatologists have generally developed comfort with biosimilars, although this is not universal. The core message, that all biologics vary and that this is OK, is getting out. In general, rheumatologists also understand the problem with high drug prices and the threat to patient access,” Dr. Edgerton said. But “the early marketing and pricing focus for biosimilars seemed to be on hospitals and facilities, and this did not work effectively for community rheumatologists, where the majority of care is delivered. We have been pleased to see a manufacturer pivot toward community rheumatology where additional efforts need to be made to bend the curve on biosimilar adoption. It is critical for practices with experience using biosimilars to educate peers, and this is where networks of practicing rheumatologists are important.”
In Dr. Yazdany’s editorial, she cited four structural factors impeding biosimilar uptake and downstream savings.
First, she cites ongoing actions by pharmaceutical companies, which create a “patent thicket” that has the effect of fencing off originator biologics from biosimilars long beyond the original 12-year exclusivity period. Supporting the notion that “patent thickets” are a common strategy, Dr. Yazdany noted that almost half of the patent applications that AbbVie has filed for adalimumab (Humira) have come in after the original exclusivity period expired in 2014. Humira’s price has risen 18% yearly during this period.
The complicated role played by pharmacy benefit managers (PBMs) is another factor in slow adoption, said Dr. Yazdany: When manufacturers offer rebates to PBMs, the price of the originator biologic may be less than its biosimilar. Further, manufacturers may sign multiyear rebate agreements just before a biosimilar launch; PBMs are also sometimes threatened with the withdrawal of rebates if they offer biosimilars, she noted.
Third, prescriber inertia may also be at play, Dr. Yazdany noted, not least because patients often see little difference in out-of-pocket costs when they make the switch to a biosimilar – PBM rebates are not necessarily passed on to patients. Payers may not reimburse a biosimilar, or formularies can be built without them, influencing prescribing, and there’s usually no reimbursement incentive for biosimilar prescribing in the nonpublic sector, she said. To the contrary, infusing a drug with a higher price often means higher reimbursement for the administering clinician, since commercial insurance reimbursement is often calculated as a percent of the charge for the drug.
Further contributing to inertia is the extra time required for patient education and writing a new set of orders – all work that can’t be captured for extra reimbursement. Dr. Edgerton said that rheumatologists can talk with patients about the “nocebo effect” relating to biosimilars. “This is a phenomenon in which patients are thought to experience worsening symptoms associated with negative beliefs about biosimilars. There has been a study in Arthritis Care & Research addressing this concern. The authors found that positive framing of biosimilars led to more participants being willing to switch than negative framing. This suggests that clinicians have an important role in informing patients about biosimilars, and addressing hesitancy.”
Finally, Dr. Yazdany pointed out that for a pharmaceutical company pursuing biosimilar approval, the regulatory pathway itself can provide its own set of complications and confusion. Biosimilars are not exact molecular replicas of the originator biologic, and these differences can change efficacy and immunogenicity, and also affect stability. Hence, a company wishing to market a biosimilar has to show the Food and Drug Administration that safety and efficacy aren’t affected by a switch to biosimilar from an originator biologic. Extrapolation from one indication to another can be made – with scientific justification.
Rheumatologists are mindful of the potential differences between biosimilars and the originator biologic, as evinced in a recent position statement from the American College of Rheumatology. The position statement advises that “extrapolation should be pursued with caution,” and asks for clear labeling when biosimilars have been designated “interchangeable” with their biosimilar. Interchangeability can clear the way for pharmacy substitution of a prescribed biologic, though Dr. Yazdany noted that 40 states have passed legislation requiring prescriber notification.
The FDA is currently using postmarketing pharmacovigilance to monitor biosimilar performance in the real world, and a recent systematic review “should provide some reassurance,” wrote Dr. Yazdany, citing the study, which looked at 14,000 patients who had a total of 14 disease indications for biosimilar use. The 90-article review largely found no differences in safety, efficacy, or immunogenicity between originators and their biosimilars. Dr. Yazdany recommended greater openness to incorporating the European experience in the FDA’s ongoing reassessment.
A further way forward can come through tackling the patent thicket with the proposed bipartisan Biologic Patent Transparency Act, which would require publication of biologic patents in a one-stop publicly searchable database. Going further with legislation to address anticompetitive activity by pharmaceutical companies could shorten the runway to biosimilar launching considerably, she noted.
The complicated landscape of PBMs and rebates affects many sectors of health care, and new policy efforts are needed here as well, she said. Reimbursement strategies – and much-needed continuing medical education – can both ease prescriber unfamiliarity with biosimilars and provide incentives for their use, she concluded.
Dr. Kim concurred that change is needed before the United States is likely to reap significant economic benefit from biosimilars. “The uptake of biosimilars and their impact on overall health care cost needs to be reevaluated when we have more biosimilars available in the next 3-4 years. However, for now, it appears that substantial savings achieved in some European countries – for example, Denmark – may not be possible without systemic reform of the U.S. pharmaceutical market,” she said.
Dr. Yazdany is supported by the Alice Betts Endowed Chair in Arthritis Research, the Russel/Engleman Research Center at the University of California, San Francisco, and the National Institutes of Health. She has received independent research grants from Pfizer and Genentech and research consulting fees from Eli Lilly and AstraZeneca.
Dr. Kim’s study was supported by the division of pharmacoepidemiology and pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, and Arnold Ventures. Dr. Kim has received research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Bristol-Myers Squibb, and Roche.
SOURCES: Kim SC et al. Arthritis Rheumatol. 2020 Jan 13. doi: 10.1002/art.41201; Yazdany J. Arthritis Rheumatol. 2020 Jan 10. doi: 10.1002/art.41203.
Although biosimilar versions of tumor necrosis factor inhibitors (TNFis) have been available to U.S. rheumatologists and their patients for over 3 years, uptake has thus far been slow.
In an analysis of data from a large commercial payer, the two available biosimilars for infliximab (Remicade) accounted for less than 1% of TNFi prescribing since the first biosimilar to infliximab was approved in 2016.
The study, published in Arthritis & Rheumatology, involved a total of 1.1 million TNFi prescriptions or infusions received by 95,906 patients from 2016 to 2019. Investigators found that uptake of biosimilar infliximab was essentially flat, standing at 0.1% of prescribing in the second quarter of 2017, and topping out at 0.9% in the first quarter of 2019. For branded infliximab, prescribing was also stable, but accounted for about 20% of overall biologic dispensing in each quarter of the period studied.
There are currently two biosimilar medications to the originator infliximab, which is one of five originator biologics available to treat rheumatic diseases in the United States: infliximab-dyyb (Inflectra) and infliximab-abda (Renflexis). The former was approved in 2016 and the latter in 2017, said study author Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston, and her coauthors.
“Our paper reports a disappointingly low uptake of biosimilar infliximab since the first quarter of 2017 using claims data from a large private health plan. The main and maybe the only reason to consider using a biosimilar is cost saving,” said Dr. Kim in an interview. “Our results suggest that current modest cost savings from infliximab biosimilars in the U.S. are not sufficient to promote their widespread use.”
In the payer database study conducted by Dr. Kim and colleagues, the insurer paid similar mean amounts per patient per quarter for originator and biosimilar infliximab in mid-2017 ($8,322 versus $8,656). By the end of 2018, a gap appeared, with the insurer paying a mean quarterly per-patient sum of $8,111 for biosimilar infliximab compared with $9,535 for the branded biologic.
“The lack of market penetration and very modest price reductions for biosimilars have left policymakers, payers, physicians, and the public frustrated, particularly because sales in Europe continue to rapidly expand and robust cost-savings have materialized,” wrote Jinoos Yazdany, MD, MPH, in an editorial accompanying the study.
Dr. Yazdany, professor and chief of the division of rheumatology at the University of California, San Francisco, noted that increased spending on biologics in the United States – which increased by 50% from 2014 to 2018 – has been driven by rising prices as well as increased uptake of biologic therapies.
At least in part, Europe has been able to reap cost savings where the United States hasn’t because fundamental differences in health care reimbursement can ease sweeping biosimilar adoption, Dr. Yazdany noted. “Countries like Denmark and Sweden, using the negotiating and purchasing power of their single-payer systems have instituted a winner-takes-all bidding system,” with Denmark seeing cost savings of up to two-thirds when bidding was combined with mandatory switching, she said.
The continued market dominance of originator infliximab means that savings from biosimilars have thus far amounted to about $91 million, far short of the $1 billion that the Congressional Budget Office had projected for this date, Dr. Yazdany said.
One problem in the adoption of biosimilars by U.S. rheumatologists may have been uneven marketing and pricing across different types of practice, Colin C. Edgerton, MD, a rheumatologist at Low Country Rheumatology in South Carolina and chair of the American College of Rheumatology’s Committee on Rheumatologic Care, said in an interview.
“Rheumatologists have generally developed comfort with biosimilars, although this is not universal. The core message, that all biologics vary and that this is OK, is getting out. In general, rheumatologists also understand the problem with high drug prices and the threat to patient access,” Dr. Edgerton said. But “the early marketing and pricing focus for biosimilars seemed to be on hospitals and facilities, and this did not work effectively for community rheumatologists, where the majority of care is delivered. We have been pleased to see a manufacturer pivot toward community rheumatology where additional efforts need to be made to bend the curve on biosimilar adoption. It is critical for practices with experience using biosimilars to educate peers, and this is where networks of practicing rheumatologists are important.”
In Dr. Yazdany’s editorial, she cited four structural factors impeding biosimilar uptake and downstream savings.
First, she cites ongoing actions by pharmaceutical companies, which create a “patent thicket” that has the effect of fencing off originator biologics from biosimilars long beyond the original 12-year exclusivity period. Supporting the notion that “patent thickets” are a common strategy, Dr. Yazdany noted that almost half of the patent applications that AbbVie has filed for adalimumab (Humira) have come in after the original exclusivity period expired in 2014. Humira’s price has risen 18% yearly during this period.
The complicated role played by pharmacy benefit managers (PBMs) is another factor in slow adoption, said Dr. Yazdany: When manufacturers offer rebates to PBMs, the price of the originator biologic may be less than its biosimilar. Further, manufacturers may sign multiyear rebate agreements just before a biosimilar launch; PBMs are also sometimes threatened with the withdrawal of rebates if they offer biosimilars, she noted.
Third, prescriber inertia may also be at play, Dr. Yazdany noted, not least because patients often see little difference in out-of-pocket costs when they make the switch to a biosimilar – PBM rebates are not necessarily passed on to patients. Payers may not reimburse a biosimilar, or formularies can be built without them, influencing prescribing, and there’s usually no reimbursement incentive for biosimilar prescribing in the nonpublic sector, she said. To the contrary, infusing a drug with a higher price often means higher reimbursement for the administering clinician, since commercial insurance reimbursement is often calculated as a percent of the charge for the drug.
Further contributing to inertia is the extra time required for patient education and writing a new set of orders – all work that can’t be captured for extra reimbursement. Dr. Edgerton said that rheumatologists can talk with patients about the “nocebo effect” relating to biosimilars. “This is a phenomenon in which patients are thought to experience worsening symptoms associated with negative beliefs about biosimilars. There has been a study in Arthritis Care & Research addressing this concern. The authors found that positive framing of biosimilars led to more participants being willing to switch than negative framing. This suggests that clinicians have an important role in informing patients about biosimilars, and addressing hesitancy.”
Finally, Dr. Yazdany pointed out that for a pharmaceutical company pursuing biosimilar approval, the regulatory pathway itself can provide its own set of complications and confusion. Biosimilars are not exact molecular replicas of the originator biologic, and these differences can change efficacy and immunogenicity, and also affect stability. Hence, a company wishing to market a biosimilar has to show the Food and Drug Administration that safety and efficacy aren’t affected by a switch to biosimilar from an originator biologic. Extrapolation from one indication to another can be made – with scientific justification.
Rheumatologists are mindful of the potential differences between biosimilars and the originator biologic, as evinced in a recent position statement from the American College of Rheumatology. The position statement advises that “extrapolation should be pursued with caution,” and asks for clear labeling when biosimilars have been designated “interchangeable” with their biosimilar. Interchangeability can clear the way for pharmacy substitution of a prescribed biologic, though Dr. Yazdany noted that 40 states have passed legislation requiring prescriber notification.
The FDA is currently using postmarketing pharmacovigilance to monitor biosimilar performance in the real world, and a recent systematic review “should provide some reassurance,” wrote Dr. Yazdany, citing the study, which looked at 14,000 patients who had a total of 14 disease indications for biosimilar use. The 90-article review largely found no differences in safety, efficacy, or immunogenicity between originators and their biosimilars. Dr. Yazdany recommended greater openness to incorporating the European experience in the FDA’s ongoing reassessment.
A further way forward can come through tackling the patent thicket with the proposed bipartisan Biologic Patent Transparency Act, which would require publication of biologic patents in a one-stop publicly searchable database. Going further with legislation to address anticompetitive activity by pharmaceutical companies could shorten the runway to biosimilar launching considerably, she noted.
The complicated landscape of PBMs and rebates affects many sectors of health care, and new policy efforts are needed here as well, she said. Reimbursement strategies – and much-needed continuing medical education – can both ease prescriber unfamiliarity with biosimilars and provide incentives for their use, she concluded.
Dr. Kim concurred that change is needed before the United States is likely to reap significant economic benefit from biosimilars. “The uptake of biosimilars and their impact on overall health care cost needs to be reevaluated when we have more biosimilars available in the next 3-4 years. However, for now, it appears that substantial savings achieved in some European countries – for example, Denmark – may not be possible without systemic reform of the U.S. pharmaceutical market,” she said.
Dr. Yazdany is supported by the Alice Betts Endowed Chair in Arthritis Research, the Russel/Engleman Research Center at the University of California, San Francisco, and the National Institutes of Health. She has received independent research grants from Pfizer and Genentech and research consulting fees from Eli Lilly and AstraZeneca.
Dr. Kim’s study was supported by the division of pharmacoepidemiology and pharmacoeconomics, department of medicine, Brigham and Women’s Hospital, and Arnold Ventures. Dr. Kim has received research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Bristol-Myers Squibb, and Roche.
SOURCES: Kim SC et al. Arthritis Rheumatol. 2020 Jan 13. doi: 10.1002/art.41201; Yazdany J. Arthritis Rheumatol. 2020 Jan 10. doi: 10.1002/art.41203.
FROM ARTHRITIS & RHEUMATOLOGY
Antimalarial adherence is important for diabetes prevention in lupus
Adhering to antimalarial treatment offers some protection to patients with systemic lupus erythematosus (SLE) from developing type 2 diabetes mellitus (T2DM), according to new research.
Patients who took at least 90% of their prescribed antimalarial doses were 39% less likely to develop T2DM than patients who discontinued antimalarial therapy. Patients who took less than 90% of their prescribed doses but didn’t discontinue treatment were 22% less likely to develop T2DM.
“[O]ur study provides further support for the importance of adherence to antimalarials in SLE by demonstrating protective impacts on T2DM,” Shahrzad Salmasi, PhD, of the University of British Columbia, Vancouver, and colleagues wrote in Arthritis Care & Research.
Dr. Salmasi and colleagues conducted this retrospective study using administrative health data on patients in British Columbia. The researchers analyzed 1,498 patients with SLE. Their mean age was about 44 years, and 91% were women.
The researchers used data on prescription dates and days’ supply to establish antimalarial drug courses and gaps in treatment. A new treatment course occurred when a 90-day gap was exceeded between refills. The researchers calculated the proportion of days covered (PDC) – the total number of days with antimalarials divided by the length of the course – and separated patients into three categories:
- Adherent to treatment – PDC of 0.90 or greater
- Nonadherent – PDC greater than 0 but less than 0.90
- Discontinuer – PDC of 0
The patients had a mean of about 23 antimalarial prescriptions and a mean of about two courses. The mean course duration was 554 days.
At a median follow-up of 4.6 years, there were 140 incident cases of T2DM. The researchers calculated the risk of T2DM among adherent and nonadherent patients, comparing these groups with the discontinuers and adjusting for age, sex, comorbidities, and concomitant medications.
The adjusted hazard ratio for developing T2DM was 0.61 among adherent patients and 0.78 among nonadherent patients.
“This population-based study highlighted that taking less than 90% of the prescribed antimalarials compromises their effect in preventing T2DM in SLE patients,” Dr. Salmasi and colleagues wrote. “Our findings should be used to emphasize the importance of medication adherence in not only treating SLE but also preventing its complications.”
The researchers reported having no conflicts of interest.
SOURCE: Salmasi S et al. Arthritis Care Res. 2020 Jan 21. doi: 10.1002/acr.24147.
Adhering to antimalarial treatment offers some protection to patients with systemic lupus erythematosus (SLE) from developing type 2 diabetes mellitus (T2DM), according to new research.
Patients who took at least 90% of their prescribed antimalarial doses were 39% less likely to develop T2DM than patients who discontinued antimalarial therapy. Patients who took less than 90% of their prescribed doses but didn’t discontinue treatment were 22% less likely to develop T2DM.
“[O]ur study provides further support for the importance of adherence to antimalarials in SLE by demonstrating protective impacts on T2DM,” Shahrzad Salmasi, PhD, of the University of British Columbia, Vancouver, and colleagues wrote in Arthritis Care & Research.
Dr. Salmasi and colleagues conducted this retrospective study using administrative health data on patients in British Columbia. The researchers analyzed 1,498 patients with SLE. Their mean age was about 44 years, and 91% were women.
The researchers used data on prescription dates and days’ supply to establish antimalarial drug courses and gaps in treatment. A new treatment course occurred when a 90-day gap was exceeded between refills. The researchers calculated the proportion of days covered (PDC) – the total number of days with antimalarials divided by the length of the course – and separated patients into three categories:
- Adherent to treatment – PDC of 0.90 or greater
- Nonadherent – PDC greater than 0 but less than 0.90
- Discontinuer – PDC of 0
The patients had a mean of about 23 antimalarial prescriptions and a mean of about two courses. The mean course duration was 554 days.
At a median follow-up of 4.6 years, there were 140 incident cases of T2DM. The researchers calculated the risk of T2DM among adherent and nonadherent patients, comparing these groups with the discontinuers and adjusting for age, sex, comorbidities, and concomitant medications.
The adjusted hazard ratio for developing T2DM was 0.61 among adherent patients and 0.78 among nonadherent patients.
“This population-based study highlighted that taking less than 90% of the prescribed antimalarials compromises their effect in preventing T2DM in SLE patients,” Dr. Salmasi and colleagues wrote. “Our findings should be used to emphasize the importance of medication adherence in not only treating SLE but also preventing its complications.”
The researchers reported having no conflicts of interest.
SOURCE: Salmasi S et al. Arthritis Care Res. 2020 Jan 21. doi: 10.1002/acr.24147.
Adhering to antimalarial treatment offers some protection to patients with systemic lupus erythematosus (SLE) from developing type 2 diabetes mellitus (T2DM), according to new research.
Patients who took at least 90% of their prescribed antimalarial doses were 39% less likely to develop T2DM than patients who discontinued antimalarial therapy. Patients who took less than 90% of their prescribed doses but didn’t discontinue treatment were 22% less likely to develop T2DM.
“[O]ur study provides further support for the importance of adherence to antimalarials in SLE by demonstrating protective impacts on T2DM,” Shahrzad Salmasi, PhD, of the University of British Columbia, Vancouver, and colleagues wrote in Arthritis Care & Research.
Dr. Salmasi and colleagues conducted this retrospective study using administrative health data on patients in British Columbia. The researchers analyzed 1,498 patients with SLE. Their mean age was about 44 years, and 91% were women.
The researchers used data on prescription dates and days’ supply to establish antimalarial drug courses and gaps in treatment. A new treatment course occurred when a 90-day gap was exceeded between refills. The researchers calculated the proportion of days covered (PDC) – the total number of days with antimalarials divided by the length of the course – and separated patients into three categories:
- Adherent to treatment – PDC of 0.90 or greater
- Nonadherent – PDC greater than 0 but less than 0.90
- Discontinuer – PDC of 0
The patients had a mean of about 23 antimalarial prescriptions and a mean of about two courses. The mean course duration was 554 days.
At a median follow-up of 4.6 years, there were 140 incident cases of T2DM. The researchers calculated the risk of T2DM among adherent and nonadherent patients, comparing these groups with the discontinuers and adjusting for age, sex, comorbidities, and concomitant medications.
The adjusted hazard ratio for developing T2DM was 0.61 among adherent patients and 0.78 among nonadherent patients.
“This population-based study highlighted that taking less than 90% of the prescribed antimalarials compromises their effect in preventing T2DM in SLE patients,” Dr. Salmasi and colleagues wrote. “Our findings should be used to emphasize the importance of medication adherence in not only treating SLE but also preventing its complications.”
The researchers reported having no conflicts of interest.
SOURCE: Salmasi S et al. Arthritis Care Res. 2020 Jan 21. doi: 10.1002/acr.24147.
FROM ARTHRITIS CARE & RESEARCH
Actor Alan Alda discusses using empathy as an antidote to burnout
LA JOLLA, CALIF. – Physicians and other medical professionals who routinely foster empathic connections with patients may be helping themselves steer clear of burnout.
That’s what iconic actor Alan Alda suggested during a media briefing at Scripps Research on Jan. 16, 2020.
“There’s a tremendous pressure on doctors now to have shorter and shorter visits with their patients,” said the 83-year-old Mr. Alda, who received the Public Welfare Medal from the National Academy of Sciences in 2016 for his work as a champion of science. “A lot of that time is taken up with recording on a computer, which can only put pressure on the doctor.”
Practicing empathy, he continued, “kind of opens people up to one another, which inspirits them.”
Mr. Alda appeared on the research campus to announce that Scripps Research will serve as the new West Coast home of Alda Communication Training, which will work in tandem with the Alan Alda Center for Communicating Science at Stony Brook (N.Y.) University, a nonprofit organization that Mr. Alda helped found in 2009.
“This will be a center where people can come to get training in effective communication,” Mr. Alda, who is the winner of six Emmy Awards and six Golden Globe awards, told an audience of scientists and medical professionals prior to the media briefing.
“It’s an experiential kind of training,” he explained. “We don’t give tips. We don’t give lectures. We put you through exercises that are fun and actually make you laugh, but turn you into a better communicator, so you’re better able to connect to the people you’re talking to.”
During a question-and-answer session, Mr. Alda opened up about his Parkinson’s disease, which he said was diagnosed about 5 years ago. In 2018, he decided to speak publicly about his diagnosis for the first time.
“The reason was that I wanted to communicate to people who had recently been diagnosed not to believe or give into the stereotype that, when you get a diagnosis, your life is over,” said Mr. Alda, who played army surgeon “Hawkeye” Pierce on the TV series “M*A*S*H.”
“Under the burden of that belief, some people won’t tell their family or workplace colleagues,” he said. “There are exercises you can do and medications you can take to prolong the time it takes before Parkinson’s gets much more serious. It’s not to diminish the fact that it can get really bad; but to think that your life is over as soon as you get a diagnosis is wrong.”
The first 2-day training session at Scripps Research will be held in June 2020. Additional sessions are scheduled to take place in October and December. Registration is available at aldacommunicationtraining.com/workshops.
LA JOLLA, CALIF. – Physicians and other medical professionals who routinely foster empathic connections with patients may be helping themselves steer clear of burnout.
That’s what iconic actor Alan Alda suggested during a media briefing at Scripps Research on Jan. 16, 2020.
“There’s a tremendous pressure on doctors now to have shorter and shorter visits with their patients,” said the 83-year-old Mr. Alda, who received the Public Welfare Medal from the National Academy of Sciences in 2016 for his work as a champion of science. “A lot of that time is taken up with recording on a computer, which can only put pressure on the doctor.”
Practicing empathy, he continued, “kind of opens people up to one another, which inspirits them.”
Mr. Alda appeared on the research campus to announce that Scripps Research will serve as the new West Coast home of Alda Communication Training, which will work in tandem with the Alan Alda Center for Communicating Science at Stony Brook (N.Y.) University, a nonprofit organization that Mr. Alda helped found in 2009.
“This will be a center where people can come to get training in effective communication,” Mr. Alda, who is the winner of six Emmy Awards and six Golden Globe awards, told an audience of scientists and medical professionals prior to the media briefing.
“It’s an experiential kind of training,” he explained. “We don’t give tips. We don’t give lectures. We put you through exercises that are fun and actually make you laugh, but turn you into a better communicator, so you’re better able to connect to the people you’re talking to.”
During a question-and-answer session, Mr. Alda opened up about his Parkinson’s disease, which he said was diagnosed about 5 years ago. In 2018, he decided to speak publicly about his diagnosis for the first time.
“The reason was that I wanted to communicate to people who had recently been diagnosed not to believe or give into the stereotype that, when you get a diagnosis, your life is over,” said Mr. Alda, who played army surgeon “Hawkeye” Pierce on the TV series “M*A*S*H.”
“Under the burden of that belief, some people won’t tell their family or workplace colleagues,” he said. “There are exercises you can do and medications you can take to prolong the time it takes before Parkinson’s gets much more serious. It’s not to diminish the fact that it can get really bad; but to think that your life is over as soon as you get a diagnosis is wrong.”
The first 2-day training session at Scripps Research will be held in June 2020. Additional sessions are scheduled to take place in October and December. Registration is available at aldacommunicationtraining.com/workshops.
LA JOLLA, CALIF. – Physicians and other medical professionals who routinely foster empathic connections with patients may be helping themselves steer clear of burnout.
That’s what iconic actor Alan Alda suggested during a media briefing at Scripps Research on Jan. 16, 2020.
“There’s a tremendous pressure on doctors now to have shorter and shorter visits with their patients,” said the 83-year-old Mr. Alda, who received the Public Welfare Medal from the National Academy of Sciences in 2016 for his work as a champion of science. “A lot of that time is taken up with recording on a computer, which can only put pressure on the doctor.”
Practicing empathy, he continued, “kind of opens people up to one another, which inspirits them.”
Mr. Alda appeared on the research campus to announce that Scripps Research will serve as the new West Coast home of Alda Communication Training, which will work in tandem with the Alan Alda Center for Communicating Science at Stony Brook (N.Y.) University, a nonprofit organization that Mr. Alda helped found in 2009.
“This will be a center where people can come to get training in effective communication,” Mr. Alda, who is the winner of six Emmy Awards and six Golden Globe awards, told an audience of scientists and medical professionals prior to the media briefing.
“It’s an experiential kind of training,” he explained. “We don’t give tips. We don’t give lectures. We put you through exercises that are fun and actually make you laugh, but turn you into a better communicator, so you’re better able to connect to the people you’re talking to.”
During a question-and-answer session, Mr. Alda opened up about his Parkinson’s disease, which he said was diagnosed about 5 years ago. In 2018, he decided to speak publicly about his diagnosis for the first time.
“The reason was that I wanted to communicate to people who had recently been diagnosed not to believe or give into the stereotype that, when you get a diagnosis, your life is over,” said Mr. Alda, who played army surgeon “Hawkeye” Pierce on the TV series “M*A*S*H.”
“Under the burden of that belief, some people won’t tell their family or workplace colleagues,” he said. “There are exercises you can do and medications you can take to prolong the time it takes before Parkinson’s gets much more serious. It’s not to diminish the fact that it can get really bad; but to think that your life is over as soon as you get a diagnosis is wrong.”
The first 2-day training session at Scripps Research will be held in June 2020. Additional sessions are scheduled to take place in October and December. Registration is available at aldacommunicationtraining.com/workshops.
Apremilast more likely to succeed with moderate psoriatic arthritis activity
new research suggests.

A paper published in Arthritis Care & Research presents a pooled analysis of the PALACE 1-3 studies that included a total of 1,493 patients with active psoriatic arthritis whose disease had resisted treatment with tumor necrosis factor inhibitors or conventional disease-modifying antirheumatic drugs. Participants were randomized either to the oral phosphodiesterase 4 inhibitor apremilast (Otezla) 30 mg twice daily, 20 mg twice daily, or placebo for 24 weeks, after which all patients on placebo were rerandomized to one of the two apremilast doses until 52 weeks.
The analysis focused on 494 patients who were randomized to apremilast 30 mg twice daily at baseline.
At week 16, 40% patients with low disease activity at baseline had achieved remission on their clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) score, compared with 7% of patients with moderate disease activity and 2.1% of patients with high disease activity. The cDAPSA score is calculated as a composite score including swollen and tender joint counts, patient’s assessment of pain, and patient’s global assessment of disease activity, with possible scores from 0 to 154. Based on patients’ cDAPSA score, the researchers defined remission as a score of 4 or less, low disease activity as more than 4 and up to 13, moderate disease activity as more than 13 and up to 27, and high disease activity as greater than 27.
Among patients with moderate disease activity, 29.8% achieved low disease activity by week 16; among patients with high disease activity at baseline, 11.5% achieved low disease activity, and 38.1% achieved moderate disease activity.
The study found that patients who had moderate disease activity at baseline and achieved either low disease activity or remission by week 16 had a 58.9%-88.5% probability of remaining at those treatment targets by week 52. Patients with high disease activity at baseline who achieved low disease activity or remission by week 16 had a 64.3%-77.4% probability of achieving treatment targets by week 52.
Overall, nearly twice as many patients who had moderate disease activity at baseline achieved their treatment targets when compared with those who began with high disease activity (46.9% vs. 24.9%).
Any patient who achieved at least a 30% improvement in cDAPSA score by week 16 had a 63% probability of achieving treatment targets by week 52.
First author Philip J. Mease, MD, from the Swedish Medical Center and the University of Washington, Seattle, and coauthors noted that the absence of treatment response by week 16 should point to the need for a treatment adjustment. “Taken together, these findings provide a framework of reference for the selection and monitoring of patients with the highest likelihood of achieving optimal treatment responses with apremilast in clinical practice,” they wrote.
The authors also commented that their study provided support for the use of clinical Disease Activity Index for Psoriatic Arthritis score to monitor patients treated with apremilast.
The study was sponsored by Celgene. Three authors were employees of Celgene at the time of the study, and nine authors declared a range of consultancies, grants, research, and other support from the pharmaceutical sector, including from Celgene.
SOURCE: Mease P et al. Arthritis Care Res. 2019 Jan 7. doi: 10.1002/acr.24134
new research suggests.
A paper published in Arthritis Care & Research presents a pooled analysis of the PALACE 1-3 studies that included a total of 1,493 patients with active psoriatic arthritis whose disease had resisted treatment with tumor necrosis factor inhibitors or conventional disease-modifying antirheumatic drugs. Participants were randomized either to the oral phosphodiesterase 4 inhibitor apremilast (Otezla) 30 mg twice daily, 20 mg twice daily, or placebo for 24 weeks, after which all patients on placebo were rerandomized to one of the two apremilast doses until 52 weeks.
The analysis focused on 494 patients who were randomized to apremilast 30 mg twice daily at baseline.
At week 16, 40% patients with low disease activity at baseline had achieved remission on their clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) score, compared with 7% of patients with moderate disease activity and 2.1% of patients with high disease activity. The cDAPSA score is calculated as a composite score including swollen and tender joint counts, patient’s assessment of pain, and patient’s global assessment of disease activity, with possible scores from 0 to 154. Based on patients’ cDAPSA score, the researchers defined remission as a score of 4 or less, low disease activity as more than 4 and up to 13, moderate disease activity as more than 13 and up to 27, and high disease activity as greater than 27.
Among patients with moderate disease activity, 29.8% achieved low disease activity by week 16; among patients with high disease activity at baseline, 11.5% achieved low disease activity, and 38.1% achieved moderate disease activity.
The study found that patients who had moderate disease activity at baseline and achieved either low disease activity or remission by week 16 had a 58.9%-88.5% probability of remaining at those treatment targets by week 52. Patients with high disease activity at baseline who achieved low disease activity or remission by week 16 had a 64.3%-77.4% probability of achieving treatment targets by week 52.
Overall, nearly twice as many patients who had moderate disease activity at baseline achieved their treatment targets when compared with those who began with high disease activity (46.9% vs. 24.9%).
Any patient who achieved at least a 30% improvement in cDAPSA score by week 16 had a 63% probability of achieving treatment targets by week 52.
First author Philip J. Mease, MD, from the Swedish Medical Center and the University of Washington, Seattle, and coauthors noted that the absence of treatment response by week 16 should point to the need for a treatment adjustment. “Taken together, these findings provide a framework of reference for the selection and monitoring of patients with the highest likelihood of achieving optimal treatment responses with apremilast in clinical practice,” they wrote.
The authors also commented that their study provided support for the use of clinical Disease Activity Index for Psoriatic Arthritis score to monitor patients treated with apremilast.
The study was sponsored by Celgene. Three authors were employees of Celgene at the time of the study, and nine authors declared a range of consultancies, grants, research, and other support from the pharmaceutical sector, including from Celgene.
SOURCE: Mease P et al. Arthritis Care Res. 2019 Jan 7. doi: 10.1002/acr.24134
new research suggests.
A paper published in Arthritis Care & Research presents a pooled analysis of the PALACE 1-3 studies that included a total of 1,493 patients with active psoriatic arthritis whose disease had resisted treatment with tumor necrosis factor inhibitors or conventional disease-modifying antirheumatic drugs. Participants were randomized either to the oral phosphodiesterase 4 inhibitor apremilast (Otezla) 30 mg twice daily, 20 mg twice daily, or placebo for 24 weeks, after which all patients on placebo were rerandomized to one of the two apremilast doses until 52 weeks.
The analysis focused on 494 patients who were randomized to apremilast 30 mg twice daily at baseline.
At week 16, 40% patients with low disease activity at baseline had achieved remission on their clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) score, compared with 7% of patients with moderate disease activity and 2.1% of patients with high disease activity. The cDAPSA score is calculated as a composite score including swollen and tender joint counts, patient’s assessment of pain, and patient’s global assessment of disease activity, with possible scores from 0 to 154. Based on patients’ cDAPSA score, the researchers defined remission as a score of 4 or less, low disease activity as more than 4 and up to 13, moderate disease activity as more than 13 and up to 27, and high disease activity as greater than 27.
Among patients with moderate disease activity, 29.8% achieved low disease activity by week 16; among patients with high disease activity at baseline, 11.5% achieved low disease activity, and 38.1% achieved moderate disease activity.
The study found that patients who had moderate disease activity at baseline and achieved either low disease activity or remission by week 16 had a 58.9%-88.5% probability of remaining at those treatment targets by week 52. Patients with high disease activity at baseline who achieved low disease activity or remission by week 16 had a 64.3%-77.4% probability of achieving treatment targets by week 52.
Overall, nearly twice as many patients who had moderate disease activity at baseline achieved their treatment targets when compared with those who began with high disease activity (46.9% vs. 24.9%).
Any patient who achieved at least a 30% improvement in cDAPSA score by week 16 had a 63% probability of achieving treatment targets by week 52.
First author Philip J. Mease, MD, from the Swedish Medical Center and the University of Washington, Seattle, and coauthors noted that the absence of treatment response by week 16 should point to the need for a treatment adjustment. “Taken together, these findings provide a framework of reference for the selection and monitoring of patients with the highest likelihood of achieving optimal treatment responses with apremilast in clinical practice,” they wrote.
The authors also commented that their study provided support for the use of clinical Disease Activity Index for Psoriatic Arthritis score to monitor patients treated with apremilast.
The study was sponsored by Celgene. Three authors were employees of Celgene at the time of the study, and nine authors declared a range of consultancies, grants, research, and other support from the pharmaceutical sector, including from Celgene.
SOURCE: Mease P et al. Arthritis Care Res. 2019 Jan 7. doi: 10.1002/acr.24134
FROM ARTHRITIS CARE & RESEARCH
February 2020
Subacute cutaneous lupus erythematosus
Subacute cutaneous lupus erythematosus (SCLE) is a type of cutaneous lupus erythematosus that may occur independently of or in combination with systemic lupus erythematosus. About 10%-15% of patients with SCLE will develop systemic lupus erythematosus. White females are more typically affected.
SCLE lesions often present as scaly, annular, or polycyclic scaly patches and plaques with central clearing. They may appear psoriasiform. They heal without atrophy or scarring but may leave dyspigmentation. Follicular plugging is absent. Lesions generally occur on sun exposed areas such as the neck, V of the chest, and upper extremities. Up to 75% of patients may exhibit associated symptoms such as photosensitivity, oral ulcers, and arthritis. Less than 20% of patients will develop internal disease, including nephritis and pulmonary disease. Symptoms of Sjögren’s syndrome and SCLE may overlap in some patients, and will portend higher risk for internal disease.
The differential diagnosis includes eczema, psoriasis, dermatophytosis, granuloma annulare, and erythema annulare centrifugum. Histology reveals epidermal atrophy and keratinocyte apoptosis, with a superficial and perivascular lymphohistiocytic infiltrate in the upper dermis. Interface changes at the dermal-epidermal junction can be seen. Direct immunofluorescence of lesional skin is positive in one-third of cases, often revealing granular deposits of IgG and IgM at the dermal-epidermal junction and around hair follicles (called the lupus-band test). Serology in SCLE may reveal a positive antinuclear antigen test, as well as positive Ro/SSA antigen. Other lupus serologies such as La/SSB, dsDNA, antihistone, and Sm antibodies may be positive, but are less commonly seen.

Several drugs may cause SCLE, such as hydrochlorothiazide, terbinafine, ACE inhibitors, NSAIDs, calcium-channel blockers, interferons, anticonvulsants, griseofulvin, penicillamine, spironolactone, tumor necrosis factor–alpha inhibitors, and statins. Discontinuing the offending medications may clear the lesions, but not always.
Treatment includes sunscreen and avoidance of sun exposure. Potent topical corticosteroids are helpful. If systemic treatment is indicated, antimalarials are first line.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
Subacute cutaneous lupus erythematosus
Subacute cutaneous lupus erythematosus (SCLE) is a type of cutaneous lupus erythematosus that may occur independently of or in combination with systemic lupus erythematosus. About 10%-15% of patients with SCLE will develop systemic lupus erythematosus. White females are more typically affected.
SCLE lesions often present as scaly, annular, or polycyclic scaly patches and plaques with central clearing. They may appear psoriasiform. They heal without atrophy or scarring but may leave dyspigmentation. Follicular plugging is absent. Lesions generally occur on sun exposed areas such as the neck, V of the chest, and upper extremities. Up to 75% of patients may exhibit associated symptoms such as photosensitivity, oral ulcers, and arthritis. Less than 20% of patients will develop internal disease, including nephritis and pulmonary disease. Symptoms of Sjögren’s syndrome and SCLE may overlap in some patients, and will portend higher risk for internal disease.
The differential diagnosis includes eczema, psoriasis, dermatophytosis, granuloma annulare, and erythema annulare centrifugum. Histology reveals epidermal atrophy and keratinocyte apoptosis, with a superficial and perivascular lymphohistiocytic infiltrate in the upper dermis. Interface changes at the dermal-epidermal junction can be seen. Direct immunofluorescence of lesional skin is positive in one-third of cases, often revealing granular deposits of IgG and IgM at the dermal-epidermal junction and around hair follicles (called the lupus-band test). Serology in SCLE may reveal a positive antinuclear antigen test, as well as positive Ro/SSA antigen. Other lupus serologies such as La/SSB, dsDNA, antihistone, and Sm antibodies may be positive, but are less commonly seen.
Several drugs may cause SCLE, such as hydrochlorothiazide, terbinafine, ACE inhibitors, NSAIDs, calcium-channel blockers, interferons, anticonvulsants, griseofulvin, penicillamine, spironolactone, tumor necrosis factor–alpha inhibitors, and statins. Discontinuing the offending medications may clear the lesions, but not always.
Treatment includes sunscreen and avoidance of sun exposure. Potent topical corticosteroids are helpful. If systemic treatment is indicated, antimalarials are first line.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
Subacute cutaneous lupus erythematosus
Subacute cutaneous lupus erythematosus (SCLE) is a type of cutaneous lupus erythematosus that may occur independently of or in combination with systemic lupus erythematosus. About 10%-15% of patients with SCLE will develop systemic lupus erythematosus. White females are more typically affected.
SCLE lesions often present as scaly, annular, or polycyclic scaly patches and plaques with central clearing. They may appear psoriasiform. They heal without atrophy or scarring but may leave dyspigmentation. Follicular plugging is absent. Lesions generally occur on sun exposed areas such as the neck, V of the chest, and upper extremities. Up to 75% of patients may exhibit associated symptoms such as photosensitivity, oral ulcers, and arthritis. Less than 20% of patients will develop internal disease, including nephritis and pulmonary disease. Symptoms of Sjögren’s syndrome and SCLE may overlap in some patients, and will portend higher risk for internal disease.
The differential diagnosis includes eczema, psoriasis, dermatophytosis, granuloma annulare, and erythema annulare centrifugum. Histology reveals epidermal atrophy and keratinocyte apoptosis, with a superficial and perivascular lymphohistiocytic infiltrate in the upper dermis. Interface changes at the dermal-epidermal junction can be seen. Direct immunofluorescence of lesional skin is positive in one-third of cases, often revealing granular deposits of IgG and IgM at the dermal-epidermal junction and around hair follicles (called the lupus-band test). Serology in SCLE may reveal a positive antinuclear antigen test, as well as positive Ro/SSA antigen. Other lupus serologies such as La/SSB, dsDNA, antihistone, and Sm antibodies may be positive, but are less commonly seen.
Several drugs may cause SCLE, such as hydrochlorothiazide, terbinafine, ACE inhibitors, NSAIDs, calcium-channel blockers, interferons, anticonvulsants, griseofulvin, penicillamine, spironolactone, tumor necrosis factor–alpha inhibitors, and statins. Discontinuing the offending medications may clear the lesions, but not always.
Treatment includes sunscreen and avoidance of sun exposure. Potent topical corticosteroids are helpful. If systemic treatment is indicated, antimalarials are first line.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.

New year, old you
This column should arrive just in time. By this time in February, eighty percent of us will abort what we resolved to do this year. If this was you, it could be considered a catastrophic failure because not only is it a new year, it is a new decade. That’s right, the opportunity to fix the 10-year-imperfect you won’t come again until 2030!

I’m among you. I intended to read fiction daily (starting with “The Great Gatsby,” not “Moby Dick” – I thought I would give myself a fighting chance, but alas ...), to workout at least 5 days every week (I tore my left triangular fibrocartilage complex, so there’s that), to write at least 500 words daily (I’m typing this one-handed: I’m lucky to get 500 letters a day). So I’m out.
If you resolved to do something this year, chances are it was to make a better you: a self-improvement goal such as losing weight, saving more money, or exercising more. According to a Marist Poll, these were the most popular resolutions for 2020. At the bottom of the most-likely-resolutions list were things like “worry less” or “be kinder to others.” These are important goals we’d agree, but we don’t deem them resolution-worthy. Why?
And why do we have New Year’s resolutions in the first place? When I looked into this further, I was surprised by some of the history I discovered.
As far back as the Babylonians, once a year, we’ve tried our best to get better. At the feast of Akitu, the Babylonian new year festival (about March on our modern calendar), people resolved to do a better job of paying debts and returning favors – spin had not been invented, and yoga hadn’t caught on in the Middle East yet. This fundamental desire to be a better human seems hardwired, and long before Bullet Journals we seem to have loved “fresh start” days on the calendar. Yet, we’re doomed to fail, over and over, at least for the last 5,000 or so attempts.
We know so much more now. Put your Nike Renue Fusion shoes next to your bed so you get up and run first thing. Set SMART goals. Sign up for automatic retirement contribution and for automatic, plant-based meal delivery from Blue Apron. (I’ve no conflict of interest in these products).

Good ideas all, but I’m suggesting a different approach: Resolve to do something else this year.
Rather than try the same things we’ve attempted, how about selecting something from the bottom of the Marist Poll list – such as resolving to be more humble. Admit when you don’t know something or don’t understand what’s being discussed. Recognize and acknowledge when you’ve screwed up. Or resolve to be more selfless. Add on someone else’s patient, an extra call without expecting a favor in return, or do what you can to help a curbside consult, even if there is no reward or even a small risk to you. Repay the debt you owe your friends, family, colleagues, staff, and patients.
These things are a little trickier to track, but you can find a way to keep yourself accountable. Add a box to your weekly planner that says “Be humble and kind” and check it off for the next 42 weeks. Good news, March 1 falls on a Sunday this year – let’s call it the feast of Akitu.
Happy New Year! And good luck!
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
This column should arrive just in time. By this time in February, eighty percent of us will abort what we resolved to do this year. If this was you, it could be considered a catastrophic failure because not only is it a new year, it is a new decade. That’s right, the opportunity to fix the 10-year-imperfect you won’t come again until 2030!
I’m among you. I intended to read fiction daily (starting with “The Great Gatsby,” not “Moby Dick” – I thought I would give myself a fighting chance, but alas ...), to workout at least 5 days every week (I tore my left triangular fibrocartilage complex, so there’s that), to write at least 500 words daily (I’m typing this one-handed: I’m lucky to get 500 letters a day). So I’m out.
If you resolved to do something this year, chances are it was to make a better you: a self-improvement goal such as losing weight, saving more money, or exercising more. According to a Marist Poll, these were the most popular resolutions for 2020. At the bottom of the most-likely-resolutions list were things like “worry less” or “be kinder to others.” These are important goals we’d agree, but we don’t deem them resolution-worthy. Why?
And why do we have New Year’s resolutions in the first place? When I looked into this further, I was surprised by some of the history I discovered.
As far back as the Babylonians, once a year, we’ve tried our best to get better. At the feast of Akitu, the Babylonian new year festival (about March on our modern calendar), people resolved to do a better job of paying debts and returning favors – spin had not been invented, and yoga hadn’t caught on in the Middle East yet. This fundamental desire to be a better human seems hardwired, and long before Bullet Journals we seem to have loved “fresh start” days on the calendar. Yet, we’re doomed to fail, over and over, at least for the last 5,000 or so attempts.
We know so much more now. Put your Nike Renue Fusion shoes next to your bed so you get up and run first thing. Set SMART goals. Sign up for automatic retirement contribution and for automatic, plant-based meal delivery from Blue Apron. (I’ve no conflict of interest in these products).
Good ideas all, but I’m suggesting a different approach: Resolve to do something else this year.
Rather than try the same things we’ve attempted, how about selecting something from the bottom of the Marist Poll list – such as resolving to be more humble. Admit when you don’t know something or don’t understand what’s being discussed. Recognize and acknowledge when you’ve screwed up. Or resolve to be more selfless. Add on someone else’s patient, an extra call without expecting a favor in return, or do what you can to help a curbside consult, even if there is no reward or even a small risk to you. Repay the debt you owe your friends, family, colleagues, staff, and patients.
These things are a little trickier to track, but you can find a way to keep yourself accountable. Add a box to your weekly planner that says “Be humble and kind” and check it off for the next 42 weeks. Good news, March 1 falls on a Sunday this year – let’s call it the feast of Akitu.
Happy New Year! And good luck!
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
This column should arrive just in time. By this time in February, eighty percent of us will abort what we resolved to do this year. If this was you, it could be considered a catastrophic failure because not only is it a new year, it is a new decade. That’s right, the opportunity to fix the 10-year-imperfect you won’t come again until 2030!
I’m among you. I intended to read fiction daily (starting with “The Great Gatsby,” not “Moby Dick” – I thought I would give myself a fighting chance, but alas ...), to workout at least 5 days every week (I tore my left triangular fibrocartilage complex, so there’s that), to write at least 500 words daily (I’m typing this one-handed: I’m lucky to get 500 letters a day). So I’m out.
If you resolved to do something this year, chances are it was to make a better you: a self-improvement goal such as losing weight, saving more money, or exercising more. According to a Marist Poll, these were the most popular resolutions for 2020. At the bottom of the most-likely-resolutions list were things like “worry less” or “be kinder to others.” These are important goals we’d agree, but we don’t deem them resolution-worthy. Why?
And why do we have New Year’s resolutions in the first place? When I looked into this further, I was surprised by some of the history I discovered.
As far back as the Babylonians, once a year, we’ve tried our best to get better. At the feast of Akitu, the Babylonian new year festival (about March on our modern calendar), people resolved to do a better job of paying debts and returning favors – spin had not been invented, and yoga hadn’t caught on in the Middle East yet. This fundamental desire to be a better human seems hardwired, and long before Bullet Journals we seem to have loved “fresh start” days on the calendar. Yet, we’re doomed to fail, over and over, at least for the last 5,000 or so attempts.
We know so much more now. Put your Nike Renue Fusion shoes next to your bed so you get up and run first thing. Set SMART goals. Sign up for automatic retirement contribution and for automatic, plant-based meal delivery from Blue Apron. (I’ve no conflict of interest in these products).
Good ideas all, but I’m suggesting a different approach: Resolve to do something else this year.
Rather than try the same things we’ve attempted, how about selecting something from the bottom of the Marist Poll list – such as resolving to be more humble. Admit when you don’t know something or don’t understand what’s being discussed. Recognize and acknowledge when you’ve screwed up. Or resolve to be more selfless. Add on someone else’s patient, an extra call without expecting a favor in return, or do what you can to help a curbside consult, even if there is no reward or even a small risk to you. Repay the debt you owe your friends, family, colleagues, staff, and patients.
These things are a little trickier to track, but you can find a way to keep yourself accountable. Add a box to your weekly planner that says “Be humble and kind” and check it off for the next 42 weeks. Good news, March 1 falls on a Sunday this year – let’s call it the feast of Akitu.
Happy New Year! And good luck!
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.

TNFi treatment shows hint of slowing axial spondyloarthritis radiographic progression
according to an analysis of studies with low risk of bias, but no evidence exists for slowed disease progression at the sacroiliac joint, according to a systematic review and meta-analysis of 24 studies.
The review, conducted by Paras Karmacharya, MBBS, and colleagues at the Mayo Clinic in Rochester, Minn., did not find a significant protective effect overall for tumor necrosis factor inhibitor (TNFi) treatment on radiographic progression of ankylosing spondylitis at the spine at 2 and 4 years. But when the researchers restricted the analysis to six studies of TNFi with low risk of bias, the results were significant for slowing radiographic progression at 4 years or more (modified Stoke Ankylosing Spondylitis Spine Score [mSASSS] difference, –2.17).
NSAIDs did not show any benefit in slowing progression at either the spine or sacroiliac joint over a shorter 2-year time span for which results were available. The single study of secukinumab (Cosentyx) that was included in the analysis did not show a significant difference in radiographic progression over 2 years (mean mSASSS difference, –0.34).
For the few studies that included data on radiographic progression in patients with nonradiographic axial spondyloarthritis, there was no effect seen on the spine with either high or low NSAID use at 2 years and no evidence for an effect of TNFi on progression at the sacroiliac joint.
“Although our study showed a significant effect of TNFi on long-term radiographic progression (in sensitivity analysis), none of the included studies provide prospective, long-term, controlled comparison. Most included studies were judged to have a low risk of bias; however predominance of observational and open-label extensions of randomized, controlled trials limits overall level of evidence,” the authors wrote in Arthritis & Rheumatology.
Any benefits of early treatment on slowing the natural progression of disease might support introducing the treatment early with a treat-to-target strategy, similar to RA, the researchers noted. However, “the current guidelines recommend against this due to lack of evidence.”
The analysis involved 18 studies with TNFi, 8 with NSAIDs, and 1 with secukinumab (3 studies contained data for both NSAIDs and TNFi). The investigators used a change of 2 mSASSS units in 2 years or one new syndesmophyte formation in 2 years as the primary endpoint for radiographic progression.
“Further studies should explore the effect of NSAIDs and biologics alone and in combination in patients with early axial spondyloarthritis; their use in the group with high risk of progression should be evaluated with a follow-up [longer than] 4 years to see if effects are more pronounced over time. Newer measures with higher sensitivity to detect structural changes, such as those based on quantitative low-dose CT should be compared to mSASSS for use in clinical trials,” the researchers concluded.
The work was funded by various grants from the National Institutes of Health. The authors reported no relevant disclosures.
SOURCE: Karmacharya P et al. Arthritis Rheumatol. 2020 Jan 20. doi: 10.1002/art.41206.
according to an analysis of studies with low risk of bias, but no evidence exists for slowed disease progression at the sacroiliac joint, according to a systematic review and meta-analysis of 24 studies.
The review, conducted by Paras Karmacharya, MBBS, and colleagues at the Mayo Clinic in Rochester, Minn., did not find a significant protective effect overall for tumor necrosis factor inhibitor (TNFi) treatment on radiographic progression of ankylosing spondylitis at the spine at 2 and 4 years. But when the researchers restricted the analysis to six studies of TNFi with low risk of bias, the results were significant for slowing radiographic progression at 4 years or more (modified Stoke Ankylosing Spondylitis Spine Score [mSASSS] difference, –2.17).
NSAIDs did not show any benefit in slowing progression at either the spine or sacroiliac joint over a shorter 2-year time span for which results were available. The single study of secukinumab (Cosentyx) that was included in the analysis did not show a significant difference in radiographic progression over 2 years (mean mSASSS difference, –0.34).
For the few studies that included data on radiographic progression in patients with nonradiographic axial spondyloarthritis, there was no effect seen on the spine with either high or low NSAID use at 2 years and no evidence for an effect of TNFi on progression at the sacroiliac joint.
“Although our study showed a significant effect of TNFi on long-term radiographic progression (in sensitivity analysis), none of the included studies provide prospective, long-term, controlled comparison. Most included studies were judged to have a low risk of bias; however predominance of observational and open-label extensions of randomized, controlled trials limits overall level of evidence,” the authors wrote in Arthritis & Rheumatology.
Any benefits of early treatment on slowing the natural progression of disease might support introducing the treatment early with a treat-to-target strategy, similar to RA, the researchers noted. However, “the current guidelines recommend against this due to lack of evidence.”
The analysis involved 18 studies with TNFi, 8 with NSAIDs, and 1 with secukinumab (3 studies contained data for both NSAIDs and TNFi). The investigators used a change of 2 mSASSS units in 2 years or one new syndesmophyte formation in 2 years as the primary endpoint for radiographic progression.
“Further studies should explore the effect of NSAIDs and biologics alone and in combination in patients with early axial spondyloarthritis; their use in the group with high risk of progression should be evaluated with a follow-up [longer than] 4 years to see if effects are more pronounced over time. Newer measures with higher sensitivity to detect structural changes, such as those based on quantitative low-dose CT should be compared to mSASSS for use in clinical trials,” the researchers concluded.
The work was funded by various grants from the National Institutes of Health. The authors reported no relevant disclosures.
SOURCE: Karmacharya P et al. Arthritis Rheumatol. 2020 Jan 20. doi: 10.1002/art.41206.
according to an analysis of studies with low risk of bias, but no evidence exists for slowed disease progression at the sacroiliac joint, according to a systematic review and meta-analysis of 24 studies.
The review, conducted by Paras Karmacharya, MBBS, and colleagues at the Mayo Clinic in Rochester, Minn., did not find a significant protective effect overall for tumor necrosis factor inhibitor (TNFi) treatment on radiographic progression of ankylosing spondylitis at the spine at 2 and 4 years. But when the researchers restricted the analysis to six studies of TNFi with low risk of bias, the results were significant for slowing radiographic progression at 4 years or more (modified Stoke Ankylosing Spondylitis Spine Score [mSASSS] difference, –2.17).
NSAIDs did not show any benefit in slowing progression at either the spine or sacroiliac joint over a shorter 2-year time span for which results were available. The single study of secukinumab (Cosentyx) that was included in the analysis did not show a significant difference in radiographic progression over 2 years (mean mSASSS difference, –0.34).
For the few studies that included data on radiographic progression in patients with nonradiographic axial spondyloarthritis, there was no effect seen on the spine with either high or low NSAID use at 2 years and no evidence for an effect of TNFi on progression at the sacroiliac joint.
“Although our study showed a significant effect of TNFi on long-term radiographic progression (in sensitivity analysis), none of the included studies provide prospective, long-term, controlled comparison. Most included studies were judged to have a low risk of bias; however predominance of observational and open-label extensions of randomized, controlled trials limits overall level of evidence,” the authors wrote in Arthritis & Rheumatology.
Any benefits of early treatment on slowing the natural progression of disease might support introducing the treatment early with a treat-to-target strategy, similar to RA, the researchers noted. However, “the current guidelines recommend against this due to lack of evidence.”
The analysis involved 18 studies with TNFi, 8 with NSAIDs, and 1 with secukinumab (3 studies contained data for both NSAIDs and TNFi). The investigators used a change of 2 mSASSS units in 2 years or one new syndesmophyte formation in 2 years as the primary endpoint for radiographic progression.
“Further studies should explore the effect of NSAIDs and biologics alone and in combination in patients with early axial spondyloarthritis; their use in the group with high risk of progression should be evaluated with a follow-up [longer than] 4 years to see if effects are more pronounced over time. Newer measures with higher sensitivity to detect structural changes, such as those based on quantitative low-dose CT should be compared to mSASSS for use in clinical trials,” the researchers concluded.
The work was funded by various grants from the National Institutes of Health. The authors reported no relevant disclosures.
SOURCE: Karmacharya P et al. Arthritis Rheumatol. 2020 Jan 20. doi: 10.1002/art.41206.
FROM ARTHRITIS & RHEUMATOLOGY