User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Provide support in uncertain times
A sense of safety and stability, both emotional and physical, is crucial in promoting the healthy development of youth. Between the global pandemic, need for social distancing, economic downturn, and increased awareness of racial disparities, for many this sense of stability has been rattled.

School closures have led to a loss of social interaction, challenges to continued academic growth, and, for some students, lack of access to nutrition and increased food insecurity. For students with learning or mental health challenges, closures may have eliminated or significantly reduced desperately needed supports received in school.1 While these trying circumstances have been difficult for many, the transition back to school in the fall also may be challenging because of the uncertainty about what this will look like and possible change in routine. Some students or their families may have anxiety about returning, either because of a history of adverse experiences at school such as bullying, or because of fears about exposure for themselves or others to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The past several months also brought about greater awareness of systemic racial disparities, whether as reflected in health care, education, or the criminal justice system. According to the Centers for Disease Control and Prevention data, Latinx and African-American individuals in the United States have had a threefold greater chance of contracting SARS-CoV-2 and have a twofold greater risk of death, compared with white people in the same communities.2 Other social determinants of health – economic stability, education, social factors such as incarceration and discrimination, and neighborhood factors including access to healthy food – play a role in this vulnerability.

The pandemic has resulted in a need for social distancing, and as a result, isolation. Children and teens exposed to the news may have anxiety about what they see or hear. Additional pressures in the family can include economic uncertainty, loss of employment for the primary wage earner of the household, or stress related to family members being first responders.
Any one of these factors is a potentially significant stressor, so how do we best support youth to help them survive and hopefully thrive during this time?
- It is important to establish a sense of routine; this can help create a sense of stability and safety. Recognizing that circumstances are not the same as they were 5 or 6 months ago, encouraging structure should not come at the cost of preserving connection.
- Note positive behavior and choices made by children and make sure they know it was observed.
- Many children have experienced increased screen time with the lack of structure of the traditional school day or summer camp and extracurricular activities. Limiting screen time and being mindful of its potential impact on mood is prudent.
- Self-care for parents and guardians is important. This time is stressful for the adults of the household, let alone children who are learning self-regulation skills.
- Listen to children’s or teens’ concerns and share information in developmentally appropriate ways. It is okay to not have all of the answers.
- Balance fostering a sense of gratitude with not invalidating a child’s or teen’s experience. Showing empathy during this time is vital. While there may be other soccer seasons, it is normal to experience grief about the loss of experiences during this time.
- Parents and guardians know their children best, so it is prudent for them to be mindful of concerning changes such as an increase in sadness, anxiety, or irritability that negatively impacts daily functioning such as sleeping, eating, or relationships with family and friends.
- Promote social interactions with appropriate safeguards in place. Unfortunately, the number of SARS-CoV-2 infections is increasing in multiple states, and there is the potential to return to some of the previous restrictions. However, encouraging social interaction while following local guidelines and with cautions such as limiting the number of people present, meeting outside, or considering interacting with others who are similarly social distancing can help foster social connection and development.
- Maintain connection digitally when in-person contact is not an option.3 Social groups, places of worship, and other activities have been agile in developing virtual communities. Communication by voice and/or video is thought to be more powerful than by written communication (text, email) alone.4 However, it is important to consider those who may have limited to no access to electronic methods.
- Encourage open communication with children about diversity and bias, and consider how our interactions with others may affect our children’s perspectives.5
- As providers, it is crucial that we address structural and institutional systems that negatively impact the health, safety, and access to care including our Black, indigenous, and people of color (BIPOC) and lesbian, gay, bisexual, transgender/transsexual, queer/questioning, intersex, and allied/asexual/aromantic/agender (LGBTQIA) patients.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. Dr. Strange has no relevant financial disclosures. Email her at pdnews@mdedge.com.
Online resources for parents and families
- Child Mind Institute: Coping With the Coronavirus Crisis: Supporting Your Kids.
- American Psychological Association: Talking with children about discrimination.
- Common Sense Media: Help with determining appropriateness of media for children.
Hotlines
- National Suicide Prevention Hotline: 1-800-273-8255
- GLBT National Hotline: 888-843-4564
- The California Peer-Run Warm Line: 1-855-845-7415
- Trevor Project: 866-488-7386 or text TREVOR to 1-202-304-1200
- Trans Lifeline: 877-565-8860
- Crisis Text Line: Text HOME to 741741
References
1. JAMA Pediatr. 2020 Apr 14. doi: 10.1001/jamapediatrics.2020.1456.
2. CDC: COVID-19 in Racial and Ethnic Minority Groups.
3. JAMA. 2020 Mar 23. doi: 10.1001/jama.2020.4469.
4. JAMA Intern Med. 2020 Apr 10. doi: 10.1001/jamainternmed.2020.1562.
5. American Psychological Association: Talking with children about discrimination.
A sense of safety and stability, both emotional and physical, is crucial in promoting the healthy development of youth. Between the global pandemic, need for social distancing, economic downturn, and increased awareness of racial disparities, for many this sense of stability has been rattled.
School closures have led to a loss of social interaction, challenges to continued academic growth, and, for some students, lack of access to nutrition and increased food insecurity. For students with learning or mental health challenges, closures may have eliminated or significantly reduced desperately needed supports received in school.1 While these trying circumstances have been difficult for many, the transition back to school in the fall also may be challenging because of the uncertainty about what this will look like and possible change in routine. Some students or their families may have anxiety about returning, either because of a history of adverse experiences at school such as bullying, or because of fears about exposure for themselves or others to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The past several months also brought about greater awareness of systemic racial disparities, whether as reflected in health care, education, or the criminal justice system. According to the Centers for Disease Control and Prevention data, Latinx and African-American individuals in the United States have had a threefold greater chance of contracting SARS-CoV-2 and have a twofold greater risk of death, compared with white people in the same communities.2 Other social determinants of health – economic stability, education, social factors such as incarceration and discrimination, and neighborhood factors including access to healthy food – play a role in this vulnerability.
The pandemic has resulted in a need for social distancing, and as a result, isolation. Children and teens exposed to the news may have anxiety about what they see or hear. Additional pressures in the family can include economic uncertainty, loss of employment for the primary wage earner of the household, or stress related to family members being first responders.
Any one of these factors is a potentially significant stressor, so how do we best support youth to help them survive and hopefully thrive during this time?
- It is important to establish a sense of routine; this can help create a sense of stability and safety. Recognizing that circumstances are not the same as they were 5 or 6 months ago, encouraging structure should not come at the cost of preserving connection.
- Note positive behavior and choices made by children and make sure they know it was observed.
- Many children have experienced increased screen time with the lack of structure of the traditional school day or summer camp and extracurricular activities. Limiting screen time and being mindful of its potential impact on mood is prudent.
- Self-care for parents and guardians is important. This time is stressful for the adults of the household, let alone children who are learning self-regulation skills.
- Listen to children’s or teens’ concerns and share information in developmentally appropriate ways. It is okay to not have all of the answers.
- Balance fostering a sense of gratitude with not invalidating a child’s or teen’s experience. Showing empathy during this time is vital. While there may be other soccer seasons, it is normal to experience grief about the loss of experiences during this time.
- Parents and guardians know their children best, so it is prudent for them to be mindful of concerning changes such as an increase in sadness, anxiety, or irritability that negatively impacts daily functioning such as sleeping, eating, or relationships with family and friends.
- Promote social interactions with appropriate safeguards in place. Unfortunately, the number of SARS-CoV-2 infections is increasing in multiple states, and there is the potential to return to some of the previous restrictions. However, encouraging social interaction while following local guidelines and with cautions such as limiting the number of people present, meeting outside, or considering interacting with others who are similarly social distancing can help foster social connection and development.
- Maintain connection digitally when in-person contact is not an option.3 Social groups, places of worship, and other activities have been agile in developing virtual communities. Communication by voice and/or video is thought to be more powerful than by written communication (text, email) alone.4 However, it is important to consider those who may have limited to no access to electronic methods.
- Encourage open communication with children about diversity and bias, and consider how our interactions with others may affect our children’s perspectives.5
- As providers, it is crucial that we address structural and institutional systems that negatively impact the health, safety, and access to care including our Black, indigenous, and people of color (BIPOC) and lesbian, gay, bisexual, transgender/transsexual, queer/questioning, intersex, and allied/asexual/aromantic/agender (LGBTQIA) patients.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. Dr. Strange has no relevant financial disclosures. Email her at pdnews@mdedge.com.
Online resources for parents and families
- Child Mind Institute: Coping With the Coronavirus Crisis: Supporting Your Kids.
- American Psychological Association: Talking with children about discrimination.
- Common Sense Media: Help with determining appropriateness of media for children.
Hotlines
- National Suicide Prevention Hotline: 1-800-273-8255
- GLBT National Hotline: 888-843-4564
- The California Peer-Run Warm Line: 1-855-845-7415
- Trevor Project: 866-488-7386 or text TREVOR to 1-202-304-1200
- Trans Lifeline: 877-565-8860
- Crisis Text Line: Text HOME to 741741
References
1. JAMA Pediatr. 2020 Apr 14. doi: 10.1001/jamapediatrics.2020.1456.
2. CDC: COVID-19 in Racial and Ethnic Minority Groups.
3. JAMA. 2020 Mar 23. doi: 10.1001/jama.2020.4469.
4. JAMA Intern Med. 2020 Apr 10. doi: 10.1001/jamainternmed.2020.1562.
5. American Psychological Association: Talking with children about discrimination.
A sense of safety and stability, both emotional and physical, is crucial in promoting the healthy development of youth. Between the global pandemic, need for social distancing, economic downturn, and increased awareness of racial disparities, for many this sense of stability has been rattled.
School closures have led to a loss of social interaction, challenges to continued academic growth, and, for some students, lack of access to nutrition and increased food insecurity. For students with learning or mental health challenges, closures may have eliminated or significantly reduced desperately needed supports received in school.1 While these trying circumstances have been difficult for many, the transition back to school in the fall also may be challenging because of the uncertainty about what this will look like and possible change in routine. Some students or their families may have anxiety about returning, either because of a history of adverse experiences at school such as bullying, or because of fears about exposure for themselves or others to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The past several months also brought about greater awareness of systemic racial disparities, whether as reflected in health care, education, or the criminal justice system. According to the Centers for Disease Control and Prevention data, Latinx and African-American individuals in the United States have had a threefold greater chance of contracting SARS-CoV-2 and have a twofold greater risk of death, compared with white people in the same communities.2 Other social determinants of health – economic stability, education, social factors such as incarceration and discrimination, and neighborhood factors including access to healthy food – play a role in this vulnerability.
The pandemic has resulted in a need for social distancing, and as a result, isolation. Children and teens exposed to the news may have anxiety about what they see or hear. Additional pressures in the family can include economic uncertainty, loss of employment for the primary wage earner of the household, or stress related to family members being first responders.
Any one of these factors is a potentially significant stressor, so how do we best support youth to help them survive and hopefully thrive during this time?
- It is important to establish a sense of routine; this can help create a sense of stability and safety. Recognizing that circumstances are not the same as they were 5 or 6 months ago, encouraging structure should not come at the cost of preserving connection.
- Note positive behavior and choices made by children and make sure they know it was observed.
- Many children have experienced increased screen time with the lack of structure of the traditional school day or summer camp and extracurricular activities. Limiting screen time and being mindful of its potential impact on mood is prudent.
- Self-care for parents and guardians is important. This time is stressful for the adults of the household, let alone children who are learning self-regulation skills.
- Listen to children’s or teens’ concerns and share information in developmentally appropriate ways. It is okay to not have all of the answers.
- Balance fostering a sense of gratitude with not invalidating a child’s or teen’s experience. Showing empathy during this time is vital. While there may be other soccer seasons, it is normal to experience grief about the loss of experiences during this time.
- Parents and guardians know their children best, so it is prudent for them to be mindful of concerning changes such as an increase in sadness, anxiety, or irritability that negatively impacts daily functioning such as sleeping, eating, or relationships with family and friends.
- Promote social interactions with appropriate safeguards in place. Unfortunately, the number of SARS-CoV-2 infections is increasing in multiple states, and there is the potential to return to some of the previous restrictions. However, encouraging social interaction while following local guidelines and with cautions such as limiting the number of people present, meeting outside, or considering interacting with others who are similarly social distancing can help foster social connection and development.
- Maintain connection digitally when in-person contact is not an option.3 Social groups, places of worship, and other activities have been agile in developing virtual communities. Communication by voice and/or video is thought to be more powerful than by written communication (text, email) alone.4 However, it is important to consider those who may have limited to no access to electronic methods.
- Encourage open communication with children about diversity and bias, and consider how our interactions with others may affect our children’s perspectives.5
- As providers, it is crucial that we address structural and institutional systems that negatively impact the health, safety, and access to care including our Black, indigenous, and people of color (BIPOC) and lesbian, gay, bisexual, transgender/transsexual, queer/questioning, intersex, and allied/asexual/aromantic/agender (LGBTQIA) patients.
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. Dr. Strange has no relevant financial disclosures. Email her at pdnews@mdedge.com.
Online resources for parents and families
- Child Mind Institute: Coping With the Coronavirus Crisis: Supporting Your Kids.
- American Psychological Association: Talking with children about discrimination.
- Common Sense Media: Help with determining appropriateness of media for children.
Hotlines
- National Suicide Prevention Hotline: 1-800-273-8255
- GLBT National Hotline: 888-843-4564
- The California Peer-Run Warm Line: 1-855-845-7415
- Trevor Project: 866-488-7386 or text TREVOR to 1-202-304-1200
- Trans Lifeline: 877-565-8860
- Crisis Text Line: Text HOME to 741741
References
1. JAMA Pediatr. 2020 Apr 14. doi: 10.1001/jamapediatrics.2020.1456.
2. CDC: COVID-19 in Racial and Ethnic Minority Groups.
3. JAMA. 2020 Mar 23. doi: 10.1001/jama.2020.4469.
4. JAMA Intern Med. 2020 Apr 10. doi: 10.1001/jamainternmed.2020.1562.
5. American Psychological Association: Talking with children about discrimination.
Residents, fellows will get minimum 6 weeks leave for caregiving
the American Board of Medical Specialties has announced.
The “ABMS Policy on Parental, Caregiver and Family Leave” announced July 13 was developed after a report from the Accreditation Council for Graduate Medical Education’s Council of Review Committee Residents in June 2019.
Richard E. Hawkins, MD, ABMS President and CEO, said in a statement that “the growing shifts in viewpoints regarding work-life balance and parental roles had a great influence in the creation of this policy, which fosters an environment that supports our trainees’ ability to care not only for patients, but also for themselves and their families.”
Specifically, the time can be taken for birth and care of a newborn, adopting a child, or becoming a foster parent; care of a child, spouse, or parent with a serious health condition; or the trainee’s own serious health condition. The policy applies to member boards with training programs of at least 2 years.
Boards must communicate when a leave will require an official extension to avoid disruptions to a physician’s career trajectory, a delay in starting a fellowship, or moving into a salaried position.
Work/life balance was by far the biggest challenge reported in the Medscape Residents Lifestyle & Happiness Report 2019.
Several member boards had already implemented policies that offered more flexibility without unduly delaying board certification; now ABMS is extending that to all boards.
ABMS says member boards may limit the maximum time away in a single year or level of training and directed member boards to “make reasonable testing accommodations” – for example, by allowing candidates to take an exam provided the candidate completes all training requirements by a certain date.
Kristy Rialon, MD, an author of the ACGME report and assistant professor of surgery at Baylor College of Medicine and the Texas Children’s Hospital, both in Houston, noted the significance of the change in a news release.
“By virtue of their ages, residents and fellows – male and female – often find themselves having and raising children, as well as serving as family members’ caregivers,” Dr. Rialon said. “By adopting more realistic and compassionate approaches, the ABMS member boards will significantly improve the quality of life for residents and fellows. This also will support our female physicians, helping to narrow the gender gap in their career advancement by allowing for greater leave flexibility.”
A Medscape survey published July 15 said work-life balance was the No. 1 concern of female physicians, far outpacing pay.
A version of this article originally appeared on Medscape.com.
the American Board of Medical Specialties has announced.
The “ABMS Policy on Parental, Caregiver and Family Leave” announced July 13 was developed after a report from the Accreditation Council for Graduate Medical Education’s Council of Review Committee Residents in June 2019.
Richard E. Hawkins, MD, ABMS President and CEO, said in a statement that “the growing shifts in viewpoints regarding work-life balance and parental roles had a great influence in the creation of this policy, which fosters an environment that supports our trainees’ ability to care not only for patients, but also for themselves and their families.”
Specifically, the time can be taken for birth and care of a newborn, adopting a child, or becoming a foster parent; care of a child, spouse, or parent with a serious health condition; or the trainee’s own serious health condition. The policy applies to member boards with training programs of at least 2 years.
Boards must communicate when a leave will require an official extension to avoid disruptions to a physician’s career trajectory, a delay in starting a fellowship, or moving into a salaried position.
Work/life balance was by far the biggest challenge reported in the Medscape Residents Lifestyle & Happiness Report 2019.
Several member boards had already implemented policies that offered more flexibility without unduly delaying board certification; now ABMS is extending that to all boards.
ABMS says member boards may limit the maximum time away in a single year or level of training and directed member boards to “make reasonable testing accommodations” – for example, by allowing candidates to take an exam provided the candidate completes all training requirements by a certain date.
Kristy Rialon, MD, an author of the ACGME report and assistant professor of surgery at Baylor College of Medicine and the Texas Children’s Hospital, both in Houston, noted the significance of the change in a news release.
“By virtue of their ages, residents and fellows – male and female – often find themselves having and raising children, as well as serving as family members’ caregivers,” Dr. Rialon said. “By adopting more realistic and compassionate approaches, the ABMS member boards will significantly improve the quality of life for residents and fellows. This also will support our female physicians, helping to narrow the gender gap in their career advancement by allowing for greater leave flexibility.”
A Medscape survey published July 15 said work-life balance was the No. 1 concern of female physicians, far outpacing pay.
A version of this article originally appeared on Medscape.com.
the American Board of Medical Specialties has announced.
The “ABMS Policy on Parental, Caregiver and Family Leave” announced July 13 was developed after a report from the Accreditation Council for Graduate Medical Education’s Council of Review Committee Residents in June 2019.
Richard E. Hawkins, MD, ABMS President and CEO, said in a statement that “the growing shifts in viewpoints regarding work-life balance and parental roles had a great influence in the creation of this policy, which fosters an environment that supports our trainees’ ability to care not only for patients, but also for themselves and their families.”
Specifically, the time can be taken for birth and care of a newborn, adopting a child, or becoming a foster parent; care of a child, spouse, or parent with a serious health condition; or the trainee’s own serious health condition. The policy applies to member boards with training programs of at least 2 years.
Boards must communicate when a leave will require an official extension to avoid disruptions to a physician’s career trajectory, a delay in starting a fellowship, or moving into a salaried position.
Work/life balance was by far the biggest challenge reported in the Medscape Residents Lifestyle & Happiness Report 2019.
Several member boards had already implemented policies that offered more flexibility without unduly delaying board certification; now ABMS is extending that to all boards.
ABMS says member boards may limit the maximum time away in a single year or level of training and directed member boards to “make reasonable testing accommodations” – for example, by allowing candidates to take an exam provided the candidate completes all training requirements by a certain date.
Kristy Rialon, MD, an author of the ACGME report and assistant professor of surgery at Baylor College of Medicine and the Texas Children’s Hospital, both in Houston, noted the significance of the change in a news release.
“By virtue of their ages, residents and fellows – male and female – often find themselves having and raising children, as well as serving as family members’ caregivers,” Dr. Rialon said. “By adopting more realistic and compassionate approaches, the ABMS member boards will significantly improve the quality of life for residents and fellows. This also will support our female physicians, helping to narrow the gender gap in their career advancement by allowing for greater leave flexibility.”
A Medscape survey published July 15 said work-life balance was the No. 1 concern of female physicians, far outpacing pay.
A version of this article originally appeared on Medscape.com.
Ready for PRIME time? Newly ID’d cells predict RA flares
A newly identified circulating cell type may be a reliable marker for impending RA flares. The discovery and description of the cells, which bear a “striking” similarity to synovial fibroblasts, provide important clues to the origins of RA and progressive joint inflammation, investigators say.

By studying longitudinally collected blood samples from four patients with RA over 4 years, Dana E. Orange, MD and colleagues at Rockefeller University, New York, identified a pattern of B-cell activation and expansion of circulating cells that are negative for CD45 and CD31 expression, and positive for PDPN, dubbed preinflammatory mesenchymal or “PRIME” cells.
Expansion of PRIME cells in circulation increased dramatically in the weeks leading up to a flare and decreased during a flare, suggesting the possibility of a serum assay for predicting flares and allowing for early intervention to ameliorate or prevent disabling consequences, the investigators wrote in a study published in the New England Journal of Medicine.
“Our hope is that this will be a diagnostic in the future, but we need to study it in more patients to see how it will perform,” Dr. Orange said in an interview, adding that the cells, if shown to be pathogenic, could also be targets for new therapeutic strategies.
RNA sequencing
Dr. Orange and colleagues discovered the PRIME cells through a novel clinical and technical protocol involving home collection of blood by patients and longitudinal RNA sequencing to study gene expression profiles during times of both disease quiescence and flares, and noticed a distinct pattern of PRIME cell expansion, depletion, and gene expression.
“Looking at their gene expression profiles, they overlapped with fibroblasts that reside in inflamed rheumatoid arthritis synovium, and in an animal model those types of fibroblasts were important for allowing entry of inflammatory infiltrates around the joint,” she said.
PRIME cells may be a precursor of synovial fibroblasts, which have been implicated by some researchers in the spread of RA between joints, Dr. Orange added.
Patients do homework
The investigators began by enrolling four patients, followed for 1-4 years, who met 2010 American College of Rheumatology–European League Against Rheumatism criteria and who were seropositive for anti–cyclic citrullinated peptide antibodies.
They assessed disease activity from patient homes weekly or during escalation of flares up to four times daily, with the Routine Assessment of Patient Index Data 3 (RAPID3) questionnaire, as well as monthly clinic visits. At clinic visits during flares, disease activity was assessed using both the RAPID3 and 28-joint Disease Activity Score.
The patients performed fingerstick blood collection and mailed the samples overnight each week to Rockefeller University, where RNA was extracted and sequenced. The investigators identified gene transcripts that were differentially expressed in blood prior to flares, and compared them with data profiles derived from synovial single-cell RNA sequencing.
To validate the findings, the researchers used flow cytometry and sorted blood-cell RNA sequencing of samples from an additional 19 patients with RA.
They found that a total of 2,613 genes were differentially expressed during a flare, compared with baseline, and that expression of 1,437 of these genes was increased during a flare, with the remaining 1,176 decreased during flares.
Before the storm
Focusing on two flare-antecedent clusters of genes, they identified one cluster of transcripts that increased 2 weeks before a flare, enriched with genes coding for developmental pathways for naive B cells (that is, not yet exposed to antigens) and leukocytes.
The second cluster included gene transcripts that increased during the week before a flare, then decreased over the duration of the flare. Genes in this cluster were enriched for pathways that were unexpected in typical blood specimens, including genes involved in cartilage morphogenesis, endochondral bone growth, and extracellular matrix organization. The gene activity suggested the presence of a mesenchymal cell, they wrote.
The RNA expression profiles of these newly identified PRIME cells were very similar to those of synovial fibroblasts, and the investigators speculated that PRIME cells may be synovial fibroblast precursors.
They proposed a model of RA exacerbation in which PRIME cells become activated by B cells in the weeks immediately preceding a flare, and then migrate out of blood into the synovium.
The investigators are currently investigating “how reproducible this signature is in different flares in patients on different types of background therapy, and then we’re very interested in looking at the upstream triggers of the B cell and the PRIME cell,” Dr. Orange said.
“One of the reasons this is very exciting is that there are these signatures that can be found when patients are clearly asymptomatic but about to flare, and if we can intervene at that time, then the patients won’t have to live through a flare, they won’t have to have that experience,” she said.
Pros and cons
In an editorial accompanying the study, Ellen M. Gravallese, MD, from Brigham and Women’s Hospital in Boston and William H. Robinson, MD, PhD, from Stanford (Calif.) University and the Veterans Affairs Palo Alto (Calif.) Health Care System wrote that the study demonstrates an important method for identifying genetic contributions to many different types of disease.
“Orange and colleagues show that intensively collected longitudinal data from a small sample of patients can be used to identify dysregulated transcriptional signatures that are not recognized by classical cross-sectional studies. This study illustrates the exciting potential of longitudinal genomics to identify key antecedents of disease flares in an approach that may be applicable to the investigation of pathogenic and protective immune responses in a wide range of human diseases,” they wrote.

Rheumatology researcher Christopher D. Buckley, MBBS, DPhil, from the University of Birmingham (England), who was not involved in the study, said that the use of blood samples is both a strength and a weakness of the study.
“Blood is much easier to get than synovial tissue, but synovial tissue is important. If I’m trying to look at the blood and trying to make an inference about what’s going on in the synovium, if I don’t look at the synovium I don’t know what the link between the blood and synovium is,” he said in an interview.
On the plus side, “the big advantage about looking at blood is that you do multiple time points, which is really cool,” he said.
Dr. Buckley is a coauthor of a recent paper in Nature Medicine – published after the study by Dr. Orange and colleagues was accepted by the New England Journal of Medicine – showing that a population of macrophages in synovium was highly predictive of remission in patients with RA, and that therapeutic modulation of these macrophages has the potential as a treatment strategy for RA.
“We are very keen to understand the cellular basis of disease. We’re very good at understanding genes, but genes have to work in cells, and cells make organs, so the cells are critical,” he said.
The paper adds fuel to a controversy that has been raging among rheumatology researchers for more than a decade: the “flying fibroblast” hypothesis, which suggests that fibroblasts can migrate from one joint to another, hence spreading the disease in a manner akin to cancer metastases.
“It’s been quite controversial whether these cells like fibroblasts can exist in the blood, or whether they’re found in sufficient number in the blood,” Dr. Buckley said. “The fact that they have identified these PRIME cells is fascinating, because that’s going to cause us to go back and reinvestigate the whole flying fibroblast story.”

His colleague John Isaacs, MBBS, PhD, from Newcastle (England) University, is principal investigator for the BIO-FLARE study, in which participants with RA stop taking their disease-modifying antirheumatic drugs under close supervision of researchers. The investigators then study the patients looking for flare signals as well as the biology of flares themselves.
“As it happens, our protocols would not pick up this particular cell, because we have not been focusing on the stroma, at least not in peripheral blood. We’ve all been looking at synovium as part of BIO-FLARE,” he said in an interview. “We will be looking for this cell now that we have seen this research, and certainly we would want to replicate.”
He agreed with Dr. Buckley’s observation that the PRIME cell data may revive the flying fibroblast hypothesis. “This is a great paper in a top clinical journal. What isn’t there is mechanism. That’s the thing we’re all going to want to understand now: Where do the cells come from, how do they actually trigger flares, and how do they go down as flare starts?”
Both Dr. Buckley and Dr. Isaacs agreed that the study findings point to important new avenues of research, but also noted that the study was small, involving a total of only 23 patients, and that replication of the findings and elucidation of the mechanism of PRIME cell generation and disposition will be required.
The study was supported by grants from the National Institutes of Health, Simons Foundation, Robertson Foundation, Rheumatology Research Foundation, Bernard and Irene Schwartz Foundation, the Iris and Junming Le Foundation, and Rockefeller University. Dr. Orange disclosed a provisional patent for the discovery of the PRIME cells. Dr. Buckley and Dr. Isaacs reported no relevant conflicts of interest.
SOURCE: Orange DE et al. N Engl J Med. 2020 Jul 15. doi: 10.1056/NEJMoa2004114.
A newly identified circulating cell type may be a reliable marker for impending RA flares. The discovery and description of the cells, which bear a “striking” similarity to synovial fibroblasts, provide important clues to the origins of RA and progressive joint inflammation, investigators say.
By studying longitudinally collected blood samples from four patients with RA over 4 years, Dana E. Orange, MD and colleagues at Rockefeller University, New York, identified a pattern of B-cell activation and expansion of circulating cells that are negative for CD45 and CD31 expression, and positive for PDPN, dubbed preinflammatory mesenchymal or “PRIME” cells.
Expansion of PRIME cells in circulation increased dramatically in the weeks leading up to a flare and decreased during a flare, suggesting the possibility of a serum assay for predicting flares and allowing for early intervention to ameliorate or prevent disabling consequences, the investigators wrote in a study published in the New England Journal of Medicine.
“Our hope is that this will be a diagnostic in the future, but we need to study it in more patients to see how it will perform,” Dr. Orange said in an interview, adding that the cells, if shown to be pathogenic, could also be targets for new therapeutic strategies.
RNA sequencing
Dr. Orange and colleagues discovered the PRIME cells through a novel clinical and technical protocol involving home collection of blood by patients and longitudinal RNA sequencing to study gene expression profiles during times of both disease quiescence and flares, and noticed a distinct pattern of PRIME cell expansion, depletion, and gene expression.
“Looking at their gene expression profiles, they overlapped with fibroblasts that reside in inflamed rheumatoid arthritis synovium, and in an animal model those types of fibroblasts were important for allowing entry of inflammatory infiltrates around the joint,” she said.
PRIME cells may be a precursor of synovial fibroblasts, which have been implicated by some researchers in the spread of RA between joints, Dr. Orange added.
Patients do homework
The investigators began by enrolling four patients, followed for 1-4 years, who met 2010 American College of Rheumatology–European League Against Rheumatism criteria and who were seropositive for anti–cyclic citrullinated peptide antibodies.
They assessed disease activity from patient homes weekly or during escalation of flares up to four times daily, with the Routine Assessment of Patient Index Data 3 (RAPID3) questionnaire, as well as monthly clinic visits. At clinic visits during flares, disease activity was assessed using both the RAPID3 and 28-joint Disease Activity Score.
The patients performed fingerstick blood collection and mailed the samples overnight each week to Rockefeller University, where RNA was extracted and sequenced. The investigators identified gene transcripts that were differentially expressed in blood prior to flares, and compared them with data profiles derived from synovial single-cell RNA sequencing.
To validate the findings, the researchers used flow cytometry and sorted blood-cell RNA sequencing of samples from an additional 19 patients with RA.
They found that a total of 2,613 genes were differentially expressed during a flare, compared with baseline, and that expression of 1,437 of these genes was increased during a flare, with the remaining 1,176 decreased during flares.
Before the storm
Focusing on two flare-antecedent clusters of genes, they identified one cluster of transcripts that increased 2 weeks before a flare, enriched with genes coding for developmental pathways for naive B cells (that is, not yet exposed to antigens) and leukocytes.
The second cluster included gene transcripts that increased during the week before a flare, then decreased over the duration of the flare. Genes in this cluster were enriched for pathways that were unexpected in typical blood specimens, including genes involved in cartilage morphogenesis, endochondral bone growth, and extracellular matrix organization. The gene activity suggested the presence of a mesenchymal cell, they wrote.
The RNA expression profiles of these newly identified PRIME cells were very similar to those of synovial fibroblasts, and the investigators speculated that PRIME cells may be synovial fibroblast precursors.
They proposed a model of RA exacerbation in which PRIME cells become activated by B cells in the weeks immediately preceding a flare, and then migrate out of blood into the synovium.
The investigators are currently investigating “how reproducible this signature is in different flares in patients on different types of background therapy, and then we’re very interested in looking at the upstream triggers of the B cell and the PRIME cell,” Dr. Orange said.
“One of the reasons this is very exciting is that there are these signatures that can be found when patients are clearly asymptomatic but about to flare, and if we can intervene at that time, then the patients won’t have to live through a flare, they won’t have to have that experience,” she said.
Pros and cons
In an editorial accompanying the study, Ellen M. Gravallese, MD, from Brigham and Women’s Hospital in Boston and William H. Robinson, MD, PhD, from Stanford (Calif.) University and the Veterans Affairs Palo Alto (Calif.) Health Care System wrote that the study demonstrates an important method for identifying genetic contributions to many different types of disease.
“Orange and colleagues show that intensively collected longitudinal data from a small sample of patients can be used to identify dysregulated transcriptional signatures that are not recognized by classical cross-sectional studies. This study illustrates the exciting potential of longitudinal genomics to identify key antecedents of disease flares in an approach that may be applicable to the investigation of pathogenic and protective immune responses in a wide range of human diseases,” they wrote.
Rheumatology researcher Christopher D. Buckley, MBBS, DPhil, from the University of Birmingham (England), who was not involved in the study, said that the use of blood samples is both a strength and a weakness of the study.
“Blood is much easier to get than synovial tissue, but synovial tissue is important. If I’m trying to look at the blood and trying to make an inference about what’s going on in the synovium, if I don’t look at the synovium I don’t know what the link between the blood and synovium is,” he said in an interview.
On the plus side, “the big advantage about looking at blood is that you do multiple time points, which is really cool,” he said.
Dr. Buckley is a coauthor of a recent paper in Nature Medicine – published after the study by Dr. Orange and colleagues was accepted by the New England Journal of Medicine – showing that a population of macrophages in synovium was highly predictive of remission in patients with RA, and that therapeutic modulation of these macrophages has the potential as a treatment strategy for RA.
“We are very keen to understand the cellular basis of disease. We’re very good at understanding genes, but genes have to work in cells, and cells make organs, so the cells are critical,” he said.
The paper adds fuel to a controversy that has been raging among rheumatology researchers for more than a decade: the “flying fibroblast” hypothesis, which suggests that fibroblasts can migrate from one joint to another, hence spreading the disease in a manner akin to cancer metastases.
“It’s been quite controversial whether these cells like fibroblasts can exist in the blood, or whether they’re found in sufficient number in the blood,” Dr. Buckley said. “The fact that they have identified these PRIME cells is fascinating, because that’s going to cause us to go back and reinvestigate the whole flying fibroblast story.”
His colleague John Isaacs, MBBS, PhD, from Newcastle (England) University, is principal investigator for the BIO-FLARE study, in which participants with RA stop taking their disease-modifying antirheumatic drugs under close supervision of researchers. The investigators then study the patients looking for flare signals as well as the biology of flares themselves.
“As it happens, our protocols would not pick up this particular cell, because we have not been focusing on the stroma, at least not in peripheral blood. We’ve all been looking at synovium as part of BIO-FLARE,” he said in an interview. “We will be looking for this cell now that we have seen this research, and certainly we would want to replicate.”
He agreed with Dr. Buckley’s observation that the PRIME cell data may revive the flying fibroblast hypothesis. “This is a great paper in a top clinical journal. What isn’t there is mechanism. That’s the thing we’re all going to want to understand now: Where do the cells come from, how do they actually trigger flares, and how do they go down as flare starts?”
Both Dr. Buckley and Dr. Isaacs agreed that the study findings point to important new avenues of research, but also noted that the study was small, involving a total of only 23 patients, and that replication of the findings and elucidation of the mechanism of PRIME cell generation and disposition will be required.
The study was supported by grants from the National Institutes of Health, Simons Foundation, Robertson Foundation, Rheumatology Research Foundation, Bernard and Irene Schwartz Foundation, the Iris and Junming Le Foundation, and Rockefeller University. Dr. Orange disclosed a provisional patent for the discovery of the PRIME cells. Dr. Buckley and Dr. Isaacs reported no relevant conflicts of interest.
SOURCE: Orange DE et al. N Engl J Med. 2020 Jul 15. doi: 10.1056/NEJMoa2004114.
A newly identified circulating cell type may be a reliable marker for impending RA flares. The discovery and description of the cells, which bear a “striking” similarity to synovial fibroblasts, provide important clues to the origins of RA and progressive joint inflammation, investigators say.
By studying longitudinally collected blood samples from four patients with RA over 4 years, Dana E. Orange, MD and colleagues at Rockefeller University, New York, identified a pattern of B-cell activation and expansion of circulating cells that are negative for CD45 and CD31 expression, and positive for PDPN, dubbed preinflammatory mesenchymal or “PRIME” cells.
Expansion of PRIME cells in circulation increased dramatically in the weeks leading up to a flare and decreased during a flare, suggesting the possibility of a serum assay for predicting flares and allowing for early intervention to ameliorate or prevent disabling consequences, the investigators wrote in a study published in the New England Journal of Medicine.
“Our hope is that this will be a diagnostic in the future, but we need to study it in more patients to see how it will perform,” Dr. Orange said in an interview, adding that the cells, if shown to be pathogenic, could also be targets for new therapeutic strategies.
RNA sequencing
Dr. Orange and colleagues discovered the PRIME cells through a novel clinical and technical protocol involving home collection of blood by patients and longitudinal RNA sequencing to study gene expression profiles during times of both disease quiescence and flares, and noticed a distinct pattern of PRIME cell expansion, depletion, and gene expression.
“Looking at their gene expression profiles, they overlapped with fibroblasts that reside in inflamed rheumatoid arthritis synovium, and in an animal model those types of fibroblasts were important for allowing entry of inflammatory infiltrates around the joint,” she said.
PRIME cells may be a precursor of synovial fibroblasts, which have been implicated by some researchers in the spread of RA between joints, Dr. Orange added.
Patients do homework
The investigators began by enrolling four patients, followed for 1-4 years, who met 2010 American College of Rheumatology–European League Against Rheumatism criteria and who were seropositive for anti–cyclic citrullinated peptide antibodies.
They assessed disease activity from patient homes weekly or during escalation of flares up to four times daily, with the Routine Assessment of Patient Index Data 3 (RAPID3) questionnaire, as well as monthly clinic visits. At clinic visits during flares, disease activity was assessed using both the RAPID3 and 28-joint Disease Activity Score.
The patients performed fingerstick blood collection and mailed the samples overnight each week to Rockefeller University, where RNA was extracted and sequenced. The investigators identified gene transcripts that were differentially expressed in blood prior to flares, and compared them with data profiles derived from synovial single-cell RNA sequencing.
To validate the findings, the researchers used flow cytometry and sorted blood-cell RNA sequencing of samples from an additional 19 patients with RA.
They found that a total of 2,613 genes were differentially expressed during a flare, compared with baseline, and that expression of 1,437 of these genes was increased during a flare, with the remaining 1,176 decreased during flares.
Before the storm
Focusing on two flare-antecedent clusters of genes, they identified one cluster of transcripts that increased 2 weeks before a flare, enriched with genes coding for developmental pathways for naive B cells (that is, not yet exposed to antigens) and leukocytes.
The second cluster included gene transcripts that increased during the week before a flare, then decreased over the duration of the flare. Genes in this cluster were enriched for pathways that were unexpected in typical blood specimens, including genes involved in cartilage morphogenesis, endochondral bone growth, and extracellular matrix organization. The gene activity suggested the presence of a mesenchymal cell, they wrote.
The RNA expression profiles of these newly identified PRIME cells were very similar to those of synovial fibroblasts, and the investigators speculated that PRIME cells may be synovial fibroblast precursors.
They proposed a model of RA exacerbation in which PRIME cells become activated by B cells in the weeks immediately preceding a flare, and then migrate out of blood into the synovium.
The investigators are currently investigating “how reproducible this signature is in different flares in patients on different types of background therapy, and then we’re very interested in looking at the upstream triggers of the B cell and the PRIME cell,” Dr. Orange said.
“One of the reasons this is very exciting is that there are these signatures that can be found when patients are clearly asymptomatic but about to flare, and if we can intervene at that time, then the patients won’t have to live through a flare, they won’t have to have that experience,” she said.
Pros and cons
In an editorial accompanying the study, Ellen M. Gravallese, MD, from Brigham and Women’s Hospital in Boston and William H. Robinson, MD, PhD, from Stanford (Calif.) University and the Veterans Affairs Palo Alto (Calif.) Health Care System wrote that the study demonstrates an important method for identifying genetic contributions to many different types of disease.
“Orange and colleagues show that intensively collected longitudinal data from a small sample of patients can be used to identify dysregulated transcriptional signatures that are not recognized by classical cross-sectional studies. This study illustrates the exciting potential of longitudinal genomics to identify key antecedents of disease flares in an approach that may be applicable to the investigation of pathogenic and protective immune responses in a wide range of human diseases,” they wrote.
Rheumatology researcher Christopher D. Buckley, MBBS, DPhil, from the University of Birmingham (England), who was not involved in the study, said that the use of blood samples is both a strength and a weakness of the study.
“Blood is much easier to get than synovial tissue, but synovial tissue is important. If I’m trying to look at the blood and trying to make an inference about what’s going on in the synovium, if I don’t look at the synovium I don’t know what the link between the blood and synovium is,” he said in an interview.
On the plus side, “the big advantage about looking at blood is that you do multiple time points, which is really cool,” he said.
Dr. Buckley is a coauthor of a recent paper in Nature Medicine – published after the study by Dr. Orange and colleagues was accepted by the New England Journal of Medicine – showing that a population of macrophages in synovium was highly predictive of remission in patients with RA, and that therapeutic modulation of these macrophages has the potential as a treatment strategy for RA.
“We are very keen to understand the cellular basis of disease. We’re very good at understanding genes, but genes have to work in cells, and cells make organs, so the cells are critical,” he said.
The paper adds fuel to a controversy that has been raging among rheumatology researchers for more than a decade: the “flying fibroblast” hypothesis, which suggests that fibroblasts can migrate from one joint to another, hence spreading the disease in a manner akin to cancer metastases.
“It’s been quite controversial whether these cells like fibroblasts can exist in the blood, or whether they’re found in sufficient number in the blood,” Dr. Buckley said. “The fact that they have identified these PRIME cells is fascinating, because that’s going to cause us to go back and reinvestigate the whole flying fibroblast story.”
His colleague John Isaacs, MBBS, PhD, from Newcastle (England) University, is principal investigator for the BIO-FLARE study, in which participants with RA stop taking their disease-modifying antirheumatic drugs under close supervision of researchers. The investigators then study the patients looking for flare signals as well as the biology of flares themselves.
“As it happens, our protocols would not pick up this particular cell, because we have not been focusing on the stroma, at least not in peripheral blood. We’ve all been looking at synovium as part of BIO-FLARE,” he said in an interview. “We will be looking for this cell now that we have seen this research, and certainly we would want to replicate.”
He agreed with Dr. Buckley’s observation that the PRIME cell data may revive the flying fibroblast hypothesis. “This is a great paper in a top clinical journal. What isn’t there is mechanism. That’s the thing we’re all going to want to understand now: Where do the cells come from, how do they actually trigger flares, and how do they go down as flare starts?”
Both Dr. Buckley and Dr. Isaacs agreed that the study findings point to important new avenues of research, but also noted that the study was small, involving a total of only 23 patients, and that replication of the findings and elucidation of the mechanism of PRIME cell generation and disposition will be required.
The study was supported by grants from the National Institutes of Health, Simons Foundation, Robertson Foundation, Rheumatology Research Foundation, Bernard and Irene Schwartz Foundation, the Iris and Junming Le Foundation, and Rockefeller University. Dr. Orange disclosed a provisional patent for the discovery of the PRIME cells. Dr. Buckley and Dr. Isaacs reported no relevant conflicts of interest.
SOURCE: Orange DE et al. N Engl J Med. 2020 Jul 15. doi: 10.1056/NEJMoa2004114.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: A newly identified cell type may be predictive of RA flares.
Major finding: Preinflammatory mesenchymal cells were expanded in the week preceding a flare and decreased during the flare.
Study details: A longitudinal observational study of 23 patients with RA.
Disclosures: The study was supported by grants from the National Institutes of Health, Simons Foundation, Robertson Foundation, Rheumatology Research Foundation, Bernard and Irene Schwartz Foundation, the Iris and Junming Le Foundation, and Rockefeller University. Dr. Orange disclosed a provisional patent for the discovery of the preinflammatory mesenchymal cells.
Source: Orange DE et al. N Engl J Med. 2020 Jul 15. doi: 10.1056/NEJMoa2004114.
COVID-19: A primary care perspective
With the COVID-19 pandemic, we are experiencing a once-in-a-100-year event. Dr. Steven A. Schulz, who is serving children on the front line in upstate New York, and I outline some of the challenges primary care pediatricians have been facing and solutions that have succeeded.
Reduction in direct patient care and its consequences

Because of the unknowns of COVID-19, many parents have not wanted to bring their children to a medical office because of fear of contracting SARS-CoV-2. At the same time, pediatricians have restricted in-person visits to prevent spread of SARS-CoV-2 and to help flatten the curve of infection. Use of pediatric medical professional services, compared with last year, dropped by 52% in March 2020 and by 58% in April, according to FAIR Health, a nonprofit organization that manages a database of 31 million claims. This is resulting in decreased immunization rates, which increases concern for secondary spikes of other preventable illnesses; for example, data from the Centers for Disease Control and Prevention showed that, from mid-March to mid-April 2020, physicians in the Vaccines for Children program ordered 2.5 million fewer doses of vaccines and 250,000 fewer doses of measles-containing vaccines, compared with the same period in 2019. Fewer children are being seen for well visits, which means opportunities are lost for adequate monitoring of growth, development, physical wellness, and social determinants of health.
This is occurring at a time when families have been experiencing increased stress in terms of finances, social isolation, finding adequate child care, and serving as parent, teacher, and breadwinner. An increase in injuries is occurring because of inadequate parental supervision because many parents have been distracted while working from home. An increase in cases of severe abuse is occurring because schools, child care providers, physicians, and other mandated reporters in the community have decreased interaction with children. Children’s Hospital Colorado in Colorado Springs saw a 118% increase in the number of trauma cases in its ED between January and April 2020. Some of these were accidental injuries caused by falls or bicycle accidents, but there was a 200% increase in nonaccidental trauma, which was associated with a steep fall in calls to the state’s child abuse hotline. Academic gains are being lost, and there has been worry for a prolonged “summer slide” risk, especially for children living in poverty and children with developmental disabilities.

The COVID-19 pandemic also is affecting physicians and staff. As frontline personnel, we are at risk to contract the virus, and news media reminds us of severe illness and deaths among health care workers. The pandemic is affecting financial viability; estimated revenue of pediatric offices fell by 45% in March 2020 and 48% in April, compared with the previous year, according to FAIR Health. Nurses and staff have been furloughed. Practices have had to apply for grants and Paycheck Protection Program funds while extending credit lines.
Limited testing capability for SARS-CoV-2
Testing for SARS-CoV-2 has been variably available. There have been problems with false positive and especially false negative results (BMJ. 2020 May 12. doi: 10.1136/bmj.m1808).The best specimen collection method has yet to be determined. Blood testing for antibody has been touted, but it remains unclear if there is clinical benefit because a positive result offers no guarantee of immunity, and immunity may quickly wane. Perhaps widespread primary care office–based testing will be in place by the fall, with hope for future reliable point of care results.
Evolving knowledge regarding SARS-CoV-2 and MIS-C
It initially was thought that children were relatively spared from serious illness caused by COVID-19. Then reports of cases of newly identified multisystem inflammatory syndrome of children occurred. It has been unclear how children contribute to the spread of COVID-19 illness, although emerging evidence indicates it is lower than adult transmission. What will happen when children return to school and daycare in the fall?
The challenges have led to creative solutions for how to deliver care.
Adapting to telehealth to provide care
At least for the short term, HIPAA regulations have been relaxed to allow for video visits using platforms such as FaceTime, Skype, Zoom, Doximity, and Doxy.me. Some of these platforms are HIPAA compliant and will be long-term solutions; however, electronic medical record portals allowing for video visits are the more secure option, according to HIPAA.

It has been a learning experience to see what can be accomplished with a video visit. Taking a history and visual examination of injuries and rashes has been possible. Addressing mental health concerns through the video exchange generally has been effective.
However, video visits change the provider-patient interpersonal dynamic and offer only visual exam capabilities, compared with an in-person visit. We cannot look in ears, palpate a liver and spleen, touch and examine a joint or bone, or feel a rash. Video visits also are dependent on the quality of patient Internet access, sufficient data plans, and mutual capabilities to address the inevitable technological glitches on the provider’s end as well. Expanding information technology infrastructure ability and added licensure costs have occurred. Practices and health systems have been working with insurance companies to ensure telephone and video visits are reimbursed on a comparable level to in-office visits.
A new type of office visit and developing appropriate safety plans
Patients must be universally screened prior to arrival during appointment scheduling for well and illness visits. Patients aged older than 2 years and caregivers must wear masks on entering the facility. In many practices, patients are scheduled during specific sick or well visit time slots throughout the day. Waiting rooms chairs need to be spaced for 6-foot social distancing, and cars in the parking lot often serve as waiting rooms until staff can meet patients at the door and take them to the exam room. Alternate entrances, car-side exams, and drive-by and/or tent testing facilities often have become part of the new normal everyday practice. Creating virtual visit time blocks in provider’s schedules has allowed for decreased office congestion. Patients often are checked out from their room, as opposed to waiting in a line at a check out desk. Nurse triage protocols also have been adapted and enhanced to meet needs and concerns.
With the need for summer physicals and many regions opening up, a gradual return toward baseline has been evolving, although some of the twists of a “new normal” will stay in place. The new normal has been for providers and staff to wear surgical masks and face shields; sometimes N95 masks, gloves, and gowns have been needed. Cleaning rooms and equipment between patient visits has become a major, new time-consuming task. Acquiring and maintaining adequate supplies has been a challenge.
Summary
The American Academy of Pediatrics, CDC, and state and local health departments have been providing informative and regular updates, webinars, and best practices guidelines. Pediatricians, community organizations, schools, and mental health professionals have been collaborating, overcoming hurdles, and working together to help mitigate the effects of the pandemic on children, their families, and our communities. Continued education, cooperation, and adaptation will be needed in the months ahead. If there is a silver lining to this pandemic experience, it may be that families have grown closer together as they sheltered in place (and we have grown closer to our own families as well). One day perhaps a child who lived through this pandemic might be asked what it was like, and their recollection might be that it was a wonderful time because their parents stayed home all the time, took care of them, taught them their school work, and took lots of long family walks.
Dr. Schulz is pediatric medical director, Rochester (N.Y.) Regional Health. Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. Dr. Schulz and Dr. Pichichero said they have no relevant financial disclosures. Email them at pdnews@mdedge.com.
This article was updated 7/16/2020.
With the COVID-19 pandemic, we are experiencing a once-in-a-100-year event. Dr. Steven A. Schulz, who is serving children on the front line in upstate New York, and I outline some of the challenges primary care pediatricians have been facing and solutions that have succeeded.
Reduction in direct patient care and its consequences
Because of the unknowns of COVID-19, many parents have not wanted to bring their children to a medical office because of fear of contracting SARS-CoV-2. At the same time, pediatricians have restricted in-person visits to prevent spread of SARS-CoV-2 and to help flatten the curve of infection. Use of pediatric medical professional services, compared with last year, dropped by 52% in March 2020 and by 58% in April, according to FAIR Health, a nonprofit organization that manages a database of 31 million claims. This is resulting in decreased immunization rates, which increases concern for secondary spikes of other preventable illnesses; for example, data from the Centers for Disease Control and Prevention showed that, from mid-March to mid-April 2020, physicians in the Vaccines for Children program ordered 2.5 million fewer doses of vaccines and 250,000 fewer doses of measles-containing vaccines, compared with the same period in 2019. Fewer children are being seen for well visits, which means opportunities are lost for adequate monitoring of growth, development, physical wellness, and social determinants of health.
This is occurring at a time when families have been experiencing increased stress in terms of finances, social isolation, finding adequate child care, and serving as parent, teacher, and breadwinner. An increase in injuries is occurring because of inadequate parental supervision because many parents have been distracted while working from home. An increase in cases of severe abuse is occurring because schools, child care providers, physicians, and other mandated reporters in the community have decreased interaction with children. Children’s Hospital Colorado in Colorado Springs saw a 118% increase in the number of trauma cases in its ED between January and April 2020. Some of these were accidental injuries caused by falls or bicycle accidents, but there was a 200% increase in nonaccidental trauma, which was associated with a steep fall in calls to the state’s child abuse hotline. Academic gains are being lost, and there has been worry for a prolonged “summer slide” risk, especially for children living in poverty and children with developmental disabilities.
The COVID-19 pandemic also is affecting physicians and staff. As frontline personnel, we are at risk to contract the virus, and news media reminds us of severe illness and deaths among health care workers. The pandemic is affecting financial viability; estimated revenue of pediatric offices fell by 45% in March 2020 and 48% in April, compared with the previous year, according to FAIR Health. Nurses and staff have been furloughed. Practices have had to apply for grants and Paycheck Protection Program funds while extending credit lines.
Limited testing capability for SARS-CoV-2
Testing for SARS-CoV-2 has been variably available. There have been problems with false positive and especially false negative results (BMJ. 2020 May 12. doi: 10.1136/bmj.m1808).The best specimen collection method has yet to be determined. Blood testing for antibody has been touted, but it remains unclear if there is clinical benefit because a positive result offers no guarantee of immunity, and immunity may quickly wane. Perhaps widespread primary care office–based testing will be in place by the fall, with hope for future reliable point of care results.
Evolving knowledge regarding SARS-CoV-2 and MIS-C
It initially was thought that children were relatively spared from serious illness caused by COVID-19. Then reports of cases of newly identified multisystem inflammatory syndrome of children occurred. It has been unclear how children contribute to the spread of COVID-19 illness, although emerging evidence indicates it is lower than adult transmission. What will happen when children return to school and daycare in the fall?
The challenges have led to creative solutions for how to deliver care.
Adapting to telehealth to provide care
At least for the short term, HIPAA regulations have been relaxed to allow for video visits using platforms such as FaceTime, Skype, Zoom, Doximity, and Doxy.me. Some of these platforms are HIPAA compliant and will be long-term solutions; however, electronic medical record portals allowing for video visits are the more secure option, according to HIPAA.
It has been a learning experience to see what can be accomplished with a video visit. Taking a history and visual examination of injuries and rashes has been possible. Addressing mental health concerns through the video exchange generally has been effective.
However, video visits change the provider-patient interpersonal dynamic and offer only visual exam capabilities, compared with an in-person visit. We cannot look in ears, palpate a liver and spleen, touch and examine a joint or bone, or feel a rash. Video visits also are dependent on the quality of patient Internet access, sufficient data plans, and mutual capabilities to address the inevitable technological glitches on the provider’s end as well. Expanding information technology infrastructure ability and added licensure costs have occurred. Practices and health systems have been working with insurance companies to ensure telephone and video visits are reimbursed on a comparable level to in-office visits.
A new type of office visit and developing appropriate safety plans
Patients must be universally screened prior to arrival during appointment scheduling for well and illness visits. Patients aged older than 2 years and caregivers must wear masks on entering the facility. In many practices, patients are scheduled during specific sick or well visit time slots throughout the day. Waiting rooms chairs need to be spaced for 6-foot social distancing, and cars in the parking lot often serve as waiting rooms until staff can meet patients at the door and take them to the exam room. Alternate entrances, car-side exams, and drive-by and/or tent testing facilities often have become part of the new normal everyday practice. Creating virtual visit time blocks in provider’s schedules has allowed for decreased office congestion. Patients often are checked out from their room, as opposed to waiting in a line at a check out desk. Nurse triage protocols also have been adapted and enhanced to meet needs and concerns.
With the need for summer physicals and many regions opening up, a gradual return toward baseline has been evolving, although some of the twists of a “new normal” will stay in place. The new normal has been for providers and staff to wear surgical masks and face shields; sometimes N95 masks, gloves, and gowns have been needed. Cleaning rooms and equipment between patient visits has become a major, new time-consuming task. Acquiring and maintaining adequate supplies has been a challenge.
Summary
The American Academy of Pediatrics, CDC, and state and local health departments have been providing informative and regular updates, webinars, and best practices guidelines. Pediatricians, community organizations, schools, and mental health professionals have been collaborating, overcoming hurdles, and working together to help mitigate the effects of the pandemic on children, their families, and our communities. Continued education, cooperation, and adaptation will be needed in the months ahead. If there is a silver lining to this pandemic experience, it may be that families have grown closer together as they sheltered in place (and we have grown closer to our own families as well). One day perhaps a child who lived through this pandemic might be asked what it was like, and their recollection might be that it was a wonderful time because their parents stayed home all the time, took care of them, taught them their school work, and took lots of long family walks.
Dr. Schulz is pediatric medical director, Rochester (N.Y.) Regional Health. Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. Dr. Schulz and Dr. Pichichero said they have no relevant financial disclosures. Email them at pdnews@mdedge.com.
This article was updated 7/16/2020.
With the COVID-19 pandemic, we are experiencing a once-in-a-100-year event. Dr. Steven A. Schulz, who is serving children on the front line in upstate New York, and I outline some of the challenges primary care pediatricians have been facing and solutions that have succeeded.
Reduction in direct patient care and its consequences
Because of the unknowns of COVID-19, many parents have not wanted to bring their children to a medical office because of fear of contracting SARS-CoV-2. At the same time, pediatricians have restricted in-person visits to prevent spread of SARS-CoV-2 and to help flatten the curve of infection. Use of pediatric medical professional services, compared with last year, dropped by 52% in March 2020 and by 58% in April, according to FAIR Health, a nonprofit organization that manages a database of 31 million claims. This is resulting in decreased immunization rates, which increases concern for secondary spikes of other preventable illnesses; for example, data from the Centers for Disease Control and Prevention showed that, from mid-March to mid-April 2020, physicians in the Vaccines for Children program ordered 2.5 million fewer doses of vaccines and 250,000 fewer doses of measles-containing vaccines, compared with the same period in 2019. Fewer children are being seen for well visits, which means opportunities are lost for adequate monitoring of growth, development, physical wellness, and social determinants of health.
This is occurring at a time when families have been experiencing increased stress in terms of finances, social isolation, finding adequate child care, and serving as parent, teacher, and breadwinner. An increase in injuries is occurring because of inadequate parental supervision because many parents have been distracted while working from home. An increase in cases of severe abuse is occurring because schools, child care providers, physicians, and other mandated reporters in the community have decreased interaction with children. Children’s Hospital Colorado in Colorado Springs saw a 118% increase in the number of trauma cases in its ED between January and April 2020. Some of these were accidental injuries caused by falls or bicycle accidents, but there was a 200% increase in nonaccidental trauma, which was associated with a steep fall in calls to the state’s child abuse hotline. Academic gains are being lost, and there has been worry for a prolonged “summer slide” risk, especially for children living in poverty and children with developmental disabilities.
The COVID-19 pandemic also is affecting physicians and staff. As frontline personnel, we are at risk to contract the virus, and news media reminds us of severe illness and deaths among health care workers. The pandemic is affecting financial viability; estimated revenue of pediatric offices fell by 45% in March 2020 and 48% in April, compared with the previous year, according to FAIR Health. Nurses and staff have been furloughed. Practices have had to apply for grants and Paycheck Protection Program funds while extending credit lines.
Limited testing capability for SARS-CoV-2
Testing for SARS-CoV-2 has been variably available. There have been problems with false positive and especially false negative results (BMJ. 2020 May 12. doi: 10.1136/bmj.m1808).The best specimen collection method has yet to be determined. Blood testing for antibody has been touted, but it remains unclear if there is clinical benefit because a positive result offers no guarantee of immunity, and immunity may quickly wane. Perhaps widespread primary care office–based testing will be in place by the fall, with hope for future reliable point of care results.
Evolving knowledge regarding SARS-CoV-2 and MIS-C
It initially was thought that children were relatively spared from serious illness caused by COVID-19. Then reports of cases of newly identified multisystem inflammatory syndrome of children occurred. It has been unclear how children contribute to the spread of COVID-19 illness, although emerging evidence indicates it is lower than adult transmission. What will happen when children return to school and daycare in the fall?
The challenges have led to creative solutions for how to deliver care.
Adapting to telehealth to provide care
At least for the short term, HIPAA regulations have been relaxed to allow for video visits using platforms such as FaceTime, Skype, Zoom, Doximity, and Doxy.me. Some of these platforms are HIPAA compliant and will be long-term solutions; however, electronic medical record portals allowing for video visits are the more secure option, according to HIPAA.
It has been a learning experience to see what can be accomplished with a video visit. Taking a history and visual examination of injuries and rashes has been possible. Addressing mental health concerns through the video exchange generally has been effective.
However, video visits change the provider-patient interpersonal dynamic and offer only visual exam capabilities, compared with an in-person visit. We cannot look in ears, palpate a liver and spleen, touch and examine a joint or bone, or feel a rash. Video visits also are dependent on the quality of patient Internet access, sufficient data plans, and mutual capabilities to address the inevitable technological glitches on the provider’s end as well. Expanding information technology infrastructure ability and added licensure costs have occurred. Practices and health systems have been working with insurance companies to ensure telephone and video visits are reimbursed on a comparable level to in-office visits.
A new type of office visit and developing appropriate safety plans
Patients must be universally screened prior to arrival during appointment scheduling for well and illness visits. Patients aged older than 2 years and caregivers must wear masks on entering the facility. In many practices, patients are scheduled during specific sick or well visit time slots throughout the day. Waiting rooms chairs need to be spaced for 6-foot social distancing, and cars in the parking lot often serve as waiting rooms until staff can meet patients at the door and take them to the exam room. Alternate entrances, car-side exams, and drive-by and/or tent testing facilities often have become part of the new normal everyday practice. Creating virtual visit time blocks in provider’s schedules has allowed for decreased office congestion. Patients often are checked out from their room, as opposed to waiting in a line at a check out desk. Nurse triage protocols also have been adapted and enhanced to meet needs and concerns.
With the need for summer physicals and many regions opening up, a gradual return toward baseline has been evolving, although some of the twists of a “new normal” will stay in place. The new normal has been for providers and staff to wear surgical masks and face shields; sometimes N95 masks, gloves, and gowns have been needed. Cleaning rooms and equipment between patient visits has become a major, new time-consuming task. Acquiring and maintaining adequate supplies has been a challenge.
Summary
The American Academy of Pediatrics, CDC, and state and local health departments have been providing informative and regular updates, webinars, and best practices guidelines. Pediatricians, community organizations, schools, and mental health professionals have been collaborating, overcoming hurdles, and working together to help mitigate the effects of the pandemic on children, their families, and our communities. Continued education, cooperation, and adaptation will be needed in the months ahead. If there is a silver lining to this pandemic experience, it may be that families have grown closer together as they sheltered in place (and we have grown closer to our own families as well). One day perhaps a child who lived through this pandemic might be asked what it was like, and their recollection might be that it was a wonderful time because their parents stayed home all the time, took care of them, taught them their school work, and took lots of long family walks.
Dr. Schulz is pediatric medical director, Rochester (N.Y.) Regional Health. Dr. Pichichero is a specialist in pediatric infectious diseases and director of the Research Institute at Rochester (N.Y.) General Hospital. Dr. Schulz and Dr. Pichichero said they have no relevant financial disclosures. Email them at pdnews@mdedge.com.
This article was updated 7/16/2020.
Move over supplements, here come medical foods
As the Food and Drug Administration focuses on other issues, companies, both big and small, are looking to boost physician and consumer interest in their “medical foods” – products that fall somewhere between drugs and supplements and promise to mitigate symptoms, or even address underlying pathologies, of a range of diseases.
Manufacturers now market an array of medical foods, ranging from powders and capsules for Alzheimer disease to low-protein spaghetti for chronic kidney disease (CKD). The FDA has not been completely absent; it takes a narrow view of what medical conditions qualify for treatment with food products and has warned some manufacturers that their misbranded products are acting more like unapproved drugs.
By the FDA’s definition, medical food is limited to products that provide crucial therapy for patients with inborn errors of metabolism (IEM). An example is specialized baby formula for infants with phenylketonuria. Unlike supplements, medical foods are supposed to be used under the supervision of a physician. This has prompted some sales reps to turn up in the clinic, and most manufacturers have online approval forms for doctors to sign. Manufacturers, advisers, and regulators were interviewed for a closer look at this burgeoning industry.
The market
The global market for medical foods – about $18 billion in 2019 – is expected to grow steadily in the near future. It is drawing more interest, especially in Europe, where medical foods are more accepted by physicians and consumers, Meghan Donnelly, MS, RDN, said in an interview. She is a registered dietitian who conducts physician outreach in the United States for Flavis, a division of Dr. Schär. That company, based in northern Italy, started out targeting IEMs but now also sells gluten-free foods for celiac disease and low-protein foods for CKD.
It is still a niche market in the United States – and isn’t likely to ever approach the size of the supplement market, according to Marcus Charuvastra, the managing director of Targeted Medical Pharma, which markets Theramine capsules for pain management, among many other products. But it could still be a big win for a manufacturer if they get a small slice of a big market, such as for Alzheimer disease.
Defining medical food
According to an update of the Orphan Drug Act in 1988, a medical food is “a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation.” The FDA issued regulations to accompany that law in 1993 but has since only issued a guidance document that is not legally binding.
Medical foods are not drugs and they are not supplements (the latter are intended only for healthy people). The FDA doesn’t require formal approval of a medical food, but, by law, the ingredients must be generally recognized as safe, and manufacturers must follow good manufacturing practices. However, the agency has taken a narrow view of what conditions require medical foods.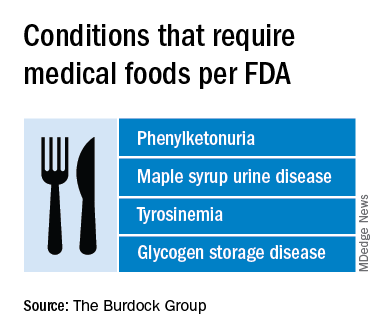
Policing medical foods hasn’t been a priority for the FDA, which is why there has been a proliferation of products that don’t meet the FDA’s view of the statutory definition of medical foods, according to Miriam Guggenheim, a food and drug law attorney in Washington, D.C. The FDA usually takes enforcement action when it sees a risk to the public’s health.
The agency’s stance has led to confusion – among manufacturers, physicians, consumers, and even regulators – making the market a kind of Wild West, according to Paul Hyman, a Washington, D.C.–based attorney who has represented medical food companies.
George A. Burdock, PhD, an Orlando-based regulatory consultant who has worked with medical food makers, believes the FDA will be forced to expand their narrow definition. He foresees a reconsideration of many medical food products in light of an October 2019 White House executive order prohibiting federal agencies from issuing guidance in lieu of rules.
Manufacturers and the FDA differ
One example of a product about which regulators and manufacturers differ is Theramine, which is described as “specially designed to supply the nervous system with the fuel it needs to meet the altered metabolic requirements of chronic pain and inflammatory disorders.”
It is not considered a medical food by the FDA, and the company has had numerous discussions with the agency about their diverging views, according to Mr. Charuvastra. “We’ve had our warning letters and we’ve had our sit downs, and we just had an inspection.”
Targeted Medical Pharma continues to market its products as medical foods but steers away from making any claims that they are like drugs, he said.
Confusion about medical foods has been exposed in the California Workers’ Compensation System by Leslie Wilson, PhD, and colleagues at the University of California, San Francisco. They found that physicians regularly wrote medical food prescriptions for non–FDA-approved uses and that the system reimbursed the majority of the products at a cost of $15.5 million from 2011 to 2013. More than half of these prescriptions were for Theramine.
Dr. Wilson reported that, for most products, no evidence supported effectiveness, and they were frequently mislabeled – for all 36 that were studied, submissions for reimbursement were made using a National Drug Code, an impossibility because medical foods are not drugs, and 14 were labeled “Rx only.”
Big-name companies joining in
The FDA does not keep a list of approved medical foods or manufacturers. Both small businesses and big food companies like Danone, Nestlé, and Abbott are players. Most products are sold online.
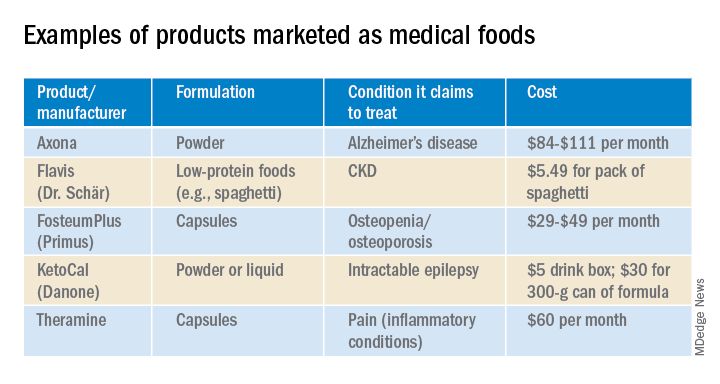
In the United States, Danone’s Nutricia division sells formulas and low-protein foods for IEMs. They also sell Ketocal, a powder or ready-to-drink liquid that is pitched as a balanced medical food to simplify and optimize the ketogenic diet for children with intractable epilepsy. Yet the FDA does not include epilepsy among the conditions that medical foods can treat.
Nestlé sells traditional medical foods for IEMs and also markets a range of what it calls nutritional therapies for such conditions as irritable bowel syndrome and dysphagia.
Nestlé is a minority shareholder in Axona, a product originally developed by Accera (Cerecin as of 2018). Jacquelyn Campo, senior director of global communications at Nestlé Health Sciences, said that the company is not actively involved in the operations management of Cerecin. However, on its website, Nestlé touts Axona, which is only available in the United States, as a “medical food” that “is intended for the clinical dietary management of mild to moderate Alzheimer disease.” The Axona site claims that the main ingredient, caprylic triglyceride, is broken down into ketones that provide fuel to treat cerebral hypometabolism, a precursor to Alzheimer disease. In a 2009 study, daily dosing of a preliminary formulation was associated with improved cognitive performance compared with placebo in patients with mild to moderate Alzheimer disease.
In 2013, the FDA warned Accera that it was misbranding Axona as a medical food and that the therapeutic claims the company was making would make the product an unapproved drug. Ms. Campo said Nestlé is aware of the agency’s warning, but added, “to our knowledge, Cerecin provided answers to the issues raised by the FDA.”
With the goal of getting drug approval, Accera went on to test a tweaked formulation in a 400-patient randomized, placebo-controlled trial called NOURISH AD that ultimately failed. Nevertheless, Axona is still marketed as a medical food. It costs about $100 for a month’s supply.
Repeated requests for comment from Cerecin were not answered. Danielle Schor, an FDA spokesperson, said the agency will not discuss the status of individual products.
More disputes and insurance coverage
Mary Ann DeMarco, executive director of sales and marketing for the Scottsdale, Ariz.–based medical food maker Primus Pharmaceuticals, said the company believes its products fit within the FDA’s medical foods rubric.
These include Fosteum Plus capsules, which it markets “for the clinical dietary management of the metabolic processes of osteopenia and osteoporosis.” The capsules contain a combination of genistein, zinc, calcium, phosphate, vitamin K2, and vitamin D. As proof of effectiveness, the company cites clinical data on some of the ingredients – not the product itself.
Primus has run afoul of the FDA before when it similarly positioned another product, called Limbrel, as a medical food for osteoarthritis. From 2007 to 2017, the FDA received 194 adverse event reports associated with Limbrel, including reports of drug-induced liver injury, pancreatitis, and hypersensitivity pneumonitis. In December 2017, the agency urged Primus to recall Limbrel, a move that it said was “necessary to protect the public health and welfare.” Primus withdrew the product but laid out a defense of Limbrel on a devoted website.
The FDA would not comment any further, said Ms. Schor. Ms. DeMarco said that Primus is working with the FDA to bring Limbrel back to market.
A lack of insurance coverage – even for approved medical foods for IEMs – has frustrated advocates, parents, and manufacturers. They are putting their weight behind the Medical Nutrition Equity Act, which would mandate public and private payer coverage of medical foods for IEMs and digestive conditions such as Crohn disease. That 2019 House bill has 56 cosponsors; there is no Senate companion bill.
“If you can get reimbursement, it really makes the market,” for Primus and the other manufacturers, Mr. Hyman said.
Primus Pharmaceuticals has launched its own campaign, Cover My Medical Foods, to enlist consumers and others to the cause.
Partnering with advocates
Although its low-protein breads, pastas, and baking products are not considered medical foods by the FDA, Dr. Schär is marketing them as such in the United States. They are trying to make a mark in CKD, according to Ms. Donnelly. She added that Dr. Schär has been successful in Europe, where nutrition therapy is more integrated in the health care system.
In 2019, Flavis and the National Kidney Foundation joined forces to raise awareness of nutritional interventions and to build enthusiasm for the Flavis products. The partnership has now ended, mostly because Flavis could no longer afford it, according to Ms. Donnelly.
“Information on diet and nutrition is the most requested subject matter from the NKF,” said Anthony Gucciardo, senior vice president of strategic partnerships at the foundation. The partnership “has never been necessarily about promoting their products per se; it’s promoting a healthy diet and really a diet specific for CKD.”
The NKF developed cobranded materials on low-protein foods for physicians and a teaching tool they could use with patients. Consumers could access nutrition information and a discount on Flavis products on a dedicated webpage. The foundation didn’t describe the low-protein products as medical foods, said Mr. Gucciardo, even if Flavis promoted them as such.
In patients with CKD, dietary management can help prevent the progression to end-stage renal disease. Although Medicare covers medical nutrition therapy – in which patients receive personalized assessments and dietary advice – uptake is abysmally low, according to a 2018 study.
Dr. Burdock thinks low-protein foods for CKD do meet the FDA’s criteria for a medical food but that the agency might not necessarily agree with him. The FDA would not comment.
Physician beware
When it comes to medical foods, the FDA has often looked the other way because the ingredients may already have been proven safe and the danger to an individual or to the public’s health is relatively low, according to Dr. Burdock and Mr. Hyman.
However, if the agency “feels that a medical food will prevent people from seeking medical care or there is potential to defraud the public, it is justified in taking action against the company,” said Dr. Burdock.
According to Dr. Wilson, the pharmacist who reported on the inappropriate medical food prescriptions in the California system, the FDA could help by creating a list of approved medical foods. Physicians should take time to learn about the difference between medical foods and supplements, she said, adding that they should also not hesitate to “question the veracity of the claims for them.”
Ms. Guggenheim believed doctors need to know that, for the most part, these are not FDA-approved products. She emphasized the importance of evaluating the products and looking at the data of their impact on a disease or condition.
“Many of these companies strongly believe that the products work and help people, so clinicians need to be very data driven,” she said.
A version of this article originally appeared on Medscape.com.
As the Food and Drug Administration focuses on other issues, companies, both big and small, are looking to boost physician and consumer interest in their “medical foods” – products that fall somewhere between drugs and supplements and promise to mitigate symptoms, or even address underlying pathologies, of a range of diseases.
Manufacturers now market an array of medical foods, ranging from powders and capsules for Alzheimer disease to low-protein spaghetti for chronic kidney disease (CKD). The FDA has not been completely absent; it takes a narrow view of what medical conditions qualify for treatment with food products and has warned some manufacturers that their misbranded products are acting more like unapproved drugs.
By the FDA’s definition, medical food is limited to products that provide crucial therapy for patients with inborn errors of metabolism (IEM). An example is specialized baby formula for infants with phenylketonuria. Unlike supplements, medical foods are supposed to be used under the supervision of a physician. This has prompted some sales reps to turn up in the clinic, and most manufacturers have online approval forms for doctors to sign. Manufacturers, advisers, and regulators were interviewed for a closer look at this burgeoning industry.
The market
The global market for medical foods – about $18 billion in 2019 – is expected to grow steadily in the near future. It is drawing more interest, especially in Europe, where medical foods are more accepted by physicians and consumers, Meghan Donnelly, MS, RDN, said in an interview. She is a registered dietitian who conducts physician outreach in the United States for Flavis, a division of Dr. Schär. That company, based in northern Italy, started out targeting IEMs but now also sells gluten-free foods for celiac disease and low-protein foods for CKD.
It is still a niche market in the United States – and isn’t likely to ever approach the size of the supplement market, according to Marcus Charuvastra, the managing director of Targeted Medical Pharma, which markets Theramine capsules for pain management, among many other products. But it could still be a big win for a manufacturer if they get a small slice of a big market, such as for Alzheimer disease.
Defining medical food
According to an update of the Orphan Drug Act in 1988, a medical food is “a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation.” The FDA issued regulations to accompany that law in 1993 but has since only issued a guidance document that is not legally binding.
Medical foods are not drugs and they are not supplements (the latter are intended only for healthy people). The FDA doesn’t require formal approval of a medical food, but, by law, the ingredients must be generally recognized as safe, and manufacturers must follow good manufacturing practices. However, the agency has taken a narrow view of what conditions require medical foods.
Policing medical foods hasn’t been a priority for the FDA, which is why there has been a proliferation of products that don’t meet the FDA’s view of the statutory definition of medical foods, according to Miriam Guggenheim, a food and drug law attorney in Washington, D.C. The FDA usually takes enforcement action when it sees a risk to the public’s health.
The agency’s stance has led to confusion – among manufacturers, physicians, consumers, and even regulators – making the market a kind of Wild West, according to Paul Hyman, a Washington, D.C.–based attorney who has represented medical food companies.
George A. Burdock, PhD, an Orlando-based regulatory consultant who has worked with medical food makers, believes the FDA will be forced to expand their narrow definition. He foresees a reconsideration of many medical food products in light of an October 2019 White House executive order prohibiting federal agencies from issuing guidance in lieu of rules.
Manufacturers and the FDA differ
One example of a product about which regulators and manufacturers differ is Theramine, which is described as “specially designed to supply the nervous system with the fuel it needs to meet the altered metabolic requirements of chronic pain and inflammatory disorders.”
It is not considered a medical food by the FDA, and the company has had numerous discussions with the agency about their diverging views, according to Mr. Charuvastra. “We’ve had our warning letters and we’ve had our sit downs, and we just had an inspection.”
Targeted Medical Pharma continues to market its products as medical foods but steers away from making any claims that they are like drugs, he said.
Confusion about medical foods has been exposed in the California Workers’ Compensation System by Leslie Wilson, PhD, and colleagues at the University of California, San Francisco. They found that physicians regularly wrote medical food prescriptions for non–FDA-approved uses and that the system reimbursed the majority of the products at a cost of $15.5 million from 2011 to 2013. More than half of these prescriptions were for Theramine.
Dr. Wilson reported that, for most products, no evidence supported effectiveness, and they were frequently mislabeled – for all 36 that were studied, submissions for reimbursement were made using a National Drug Code, an impossibility because medical foods are not drugs, and 14 were labeled “Rx only.”
Big-name companies joining in
The FDA does not keep a list of approved medical foods or manufacturers. Both small businesses and big food companies like Danone, Nestlé, and Abbott are players. Most products are sold online.
In the United States, Danone’s Nutricia division sells formulas and low-protein foods for IEMs. They also sell Ketocal, a powder or ready-to-drink liquid that is pitched as a balanced medical food to simplify and optimize the ketogenic diet for children with intractable epilepsy. Yet the FDA does not include epilepsy among the conditions that medical foods can treat.
Nestlé sells traditional medical foods for IEMs and also markets a range of what it calls nutritional therapies for such conditions as irritable bowel syndrome and dysphagia.
Nestlé is a minority shareholder in Axona, a product originally developed by Accera (Cerecin as of 2018). Jacquelyn Campo, senior director of global communications at Nestlé Health Sciences, said that the company is not actively involved in the operations management of Cerecin. However, on its website, Nestlé touts Axona, which is only available in the United States, as a “medical food” that “is intended for the clinical dietary management of mild to moderate Alzheimer disease.” The Axona site claims that the main ingredient, caprylic triglyceride, is broken down into ketones that provide fuel to treat cerebral hypometabolism, a precursor to Alzheimer disease. In a 2009 study, daily dosing of a preliminary formulation was associated with improved cognitive performance compared with placebo in patients with mild to moderate Alzheimer disease.
In 2013, the FDA warned Accera that it was misbranding Axona as a medical food and that the therapeutic claims the company was making would make the product an unapproved drug. Ms. Campo said Nestlé is aware of the agency’s warning, but added, “to our knowledge, Cerecin provided answers to the issues raised by the FDA.”
With the goal of getting drug approval, Accera went on to test a tweaked formulation in a 400-patient randomized, placebo-controlled trial called NOURISH AD that ultimately failed. Nevertheless, Axona is still marketed as a medical food. It costs about $100 for a month’s supply.
Repeated requests for comment from Cerecin were not answered. Danielle Schor, an FDA spokesperson, said the agency will not discuss the status of individual products.
More disputes and insurance coverage
Mary Ann DeMarco, executive director of sales and marketing for the Scottsdale, Ariz.–based medical food maker Primus Pharmaceuticals, said the company believes its products fit within the FDA’s medical foods rubric.
These include Fosteum Plus capsules, which it markets “for the clinical dietary management of the metabolic processes of osteopenia and osteoporosis.” The capsules contain a combination of genistein, zinc, calcium, phosphate, vitamin K2, and vitamin D. As proof of effectiveness, the company cites clinical data on some of the ingredients – not the product itself.
Primus has run afoul of the FDA before when it similarly positioned another product, called Limbrel, as a medical food for osteoarthritis. From 2007 to 2017, the FDA received 194 adverse event reports associated with Limbrel, including reports of drug-induced liver injury, pancreatitis, and hypersensitivity pneumonitis. In December 2017, the agency urged Primus to recall Limbrel, a move that it said was “necessary to protect the public health and welfare.” Primus withdrew the product but laid out a defense of Limbrel on a devoted website.
The FDA would not comment any further, said Ms. Schor. Ms. DeMarco said that Primus is working with the FDA to bring Limbrel back to market.
A lack of insurance coverage – even for approved medical foods for IEMs – has frustrated advocates, parents, and manufacturers. They are putting their weight behind the Medical Nutrition Equity Act, which would mandate public and private payer coverage of medical foods for IEMs and digestive conditions such as Crohn disease. That 2019 House bill has 56 cosponsors; there is no Senate companion bill.
“If you can get reimbursement, it really makes the market,” for Primus and the other manufacturers, Mr. Hyman said.
Primus Pharmaceuticals has launched its own campaign, Cover My Medical Foods, to enlist consumers and others to the cause.
Partnering with advocates
Although its low-protein breads, pastas, and baking products are not considered medical foods by the FDA, Dr. Schär is marketing them as such in the United States. They are trying to make a mark in CKD, according to Ms. Donnelly. She added that Dr. Schär has been successful in Europe, where nutrition therapy is more integrated in the health care system.
In 2019, Flavis and the National Kidney Foundation joined forces to raise awareness of nutritional interventions and to build enthusiasm for the Flavis products. The partnership has now ended, mostly because Flavis could no longer afford it, according to Ms. Donnelly.
“Information on diet and nutrition is the most requested subject matter from the NKF,” said Anthony Gucciardo, senior vice president of strategic partnerships at the foundation. The partnership “has never been necessarily about promoting their products per se; it’s promoting a healthy diet and really a diet specific for CKD.”
The NKF developed cobranded materials on low-protein foods for physicians and a teaching tool they could use with patients. Consumers could access nutrition information and a discount on Flavis products on a dedicated webpage. The foundation didn’t describe the low-protein products as medical foods, said Mr. Gucciardo, even if Flavis promoted them as such.
In patients with CKD, dietary management can help prevent the progression to end-stage renal disease. Although Medicare covers medical nutrition therapy – in which patients receive personalized assessments and dietary advice – uptake is abysmally low, according to a 2018 study.
Dr. Burdock thinks low-protein foods for CKD do meet the FDA’s criteria for a medical food but that the agency might not necessarily agree with him. The FDA would not comment.
Physician beware
When it comes to medical foods, the FDA has often looked the other way because the ingredients may already have been proven safe and the danger to an individual or to the public’s health is relatively low, according to Dr. Burdock and Mr. Hyman.
However, if the agency “feels that a medical food will prevent people from seeking medical care or there is potential to defraud the public, it is justified in taking action against the company,” said Dr. Burdock.
According to Dr. Wilson, the pharmacist who reported on the inappropriate medical food prescriptions in the California system, the FDA could help by creating a list of approved medical foods. Physicians should take time to learn about the difference between medical foods and supplements, she said, adding that they should also not hesitate to “question the veracity of the claims for them.”
Ms. Guggenheim believed doctors need to know that, for the most part, these are not FDA-approved products. She emphasized the importance of evaluating the products and looking at the data of their impact on a disease or condition.
“Many of these companies strongly believe that the products work and help people, so clinicians need to be very data driven,” she said.
A version of this article originally appeared on Medscape.com.
As the Food and Drug Administration focuses on other issues, companies, both big and small, are looking to boost physician and consumer interest in their “medical foods” – products that fall somewhere between drugs and supplements and promise to mitigate symptoms, or even address underlying pathologies, of a range of diseases.
Manufacturers now market an array of medical foods, ranging from powders and capsules for Alzheimer disease to low-protein spaghetti for chronic kidney disease (CKD). The FDA has not been completely absent; it takes a narrow view of what medical conditions qualify for treatment with food products and has warned some manufacturers that their misbranded products are acting more like unapproved drugs.
By the FDA’s definition, medical food is limited to products that provide crucial therapy for patients with inborn errors of metabolism (IEM). An example is specialized baby formula for infants with phenylketonuria. Unlike supplements, medical foods are supposed to be used under the supervision of a physician. This has prompted some sales reps to turn up in the clinic, and most manufacturers have online approval forms for doctors to sign. Manufacturers, advisers, and regulators were interviewed for a closer look at this burgeoning industry.
The market
The global market for medical foods – about $18 billion in 2019 – is expected to grow steadily in the near future. It is drawing more interest, especially in Europe, where medical foods are more accepted by physicians and consumers, Meghan Donnelly, MS, RDN, said in an interview. She is a registered dietitian who conducts physician outreach in the United States for Flavis, a division of Dr. Schär. That company, based in northern Italy, started out targeting IEMs but now also sells gluten-free foods for celiac disease and low-protein foods for CKD.
It is still a niche market in the United States – and isn’t likely to ever approach the size of the supplement market, according to Marcus Charuvastra, the managing director of Targeted Medical Pharma, which markets Theramine capsules for pain management, among many other products. But it could still be a big win for a manufacturer if they get a small slice of a big market, such as for Alzheimer disease.
Defining medical food
According to an update of the Orphan Drug Act in 1988, a medical food is “a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation.” The FDA issued regulations to accompany that law in 1993 but has since only issued a guidance document that is not legally binding.
Medical foods are not drugs and they are not supplements (the latter are intended only for healthy people). The FDA doesn’t require formal approval of a medical food, but, by law, the ingredients must be generally recognized as safe, and manufacturers must follow good manufacturing practices. However, the agency has taken a narrow view of what conditions require medical foods.
Policing medical foods hasn’t been a priority for the FDA, which is why there has been a proliferation of products that don’t meet the FDA’s view of the statutory definition of medical foods, according to Miriam Guggenheim, a food and drug law attorney in Washington, D.C. The FDA usually takes enforcement action when it sees a risk to the public’s health.
The agency’s stance has led to confusion – among manufacturers, physicians, consumers, and even regulators – making the market a kind of Wild West, according to Paul Hyman, a Washington, D.C.–based attorney who has represented medical food companies.
George A. Burdock, PhD, an Orlando-based regulatory consultant who has worked with medical food makers, believes the FDA will be forced to expand their narrow definition. He foresees a reconsideration of many medical food products in light of an October 2019 White House executive order prohibiting federal agencies from issuing guidance in lieu of rules.
Manufacturers and the FDA differ
One example of a product about which regulators and manufacturers differ is Theramine, which is described as “specially designed to supply the nervous system with the fuel it needs to meet the altered metabolic requirements of chronic pain and inflammatory disorders.”
It is not considered a medical food by the FDA, and the company has had numerous discussions with the agency about their diverging views, according to Mr. Charuvastra. “We’ve had our warning letters and we’ve had our sit downs, and we just had an inspection.”
Targeted Medical Pharma continues to market its products as medical foods but steers away from making any claims that they are like drugs, he said.
Confusion about medical foods has been exposed in the California Workers’ Compensation System by Leslie Wilson, PhD, and colleagues at the University of California, San Francisco. They found that physicians regularly wrote medical food prescriptions for non–FDA-approved uses and that the system reimbursed the majority of the products at a cost of $15.5 million from 2011 to 2013. More than half of these prescriptions were for Theramine.
Dr. Wilson reported that, for most products, no evidence supported effectiveness, and they were frequently mislabeled – for all 36 that were studied, submissions for reimbursement were made using a National Drug Code, an impossibility because medical foods are not drugs, and 14 were labeled “Rx only.”
Big-name companies joining in
The FDA does not keep a list of approved medical foods or manufacturers. Both small businesses and big food companies like Danone, Nestlé, and Abbott are players. Most products are sold online.
In the United States, Danone’s Nutricia division sells formulas and low-protein foods for IEMs. They also sell Ketocal, a powder or ready-to-drink liquid that is pitched as a balanced medical food to simplify and optimize the ketogenic diet for children with intractable epilepsy. Yet the FDA does not include epilepsy among the conditions that medical foods can treat.
Nestlé sells traditional medical foods for IEMs and also markets a range of what it calls nutritional therapies for such conditions as irritable bowel syndrome and dysphagia.
Nestlé is a minority shareholder in Axona, a product originally developed by Accera (Cerecin as of 2018). Jacquelyn Campo, senior director of global communications at Nestlé Health Sciences, said that the company is not actively involved in the operations management of Cerecin. However, on its website, Nestlé touts Axona, which is only available in the United States, as a “medical food” that “is intended for the clinical dietary management of mild to moderate Alzheimer disease.” The Axona site claims that the main ingredient, caprylic triglyceride, is broken down into ketones that provide fuel to treat cerebral hypometabolism, a precursor to Alzheimer disease. In a 2009 study, daily dosing of a preliminary formulation was associated with improved cognitive performance compared with placebo in patients with mild to moderate Alzheimer disease.
In 2013, the FDA warned Accera that it was misbranding Axona as a medical food and that the therapeutic claims the company was making would make the product an unapproved drug. Ms. Campo said Nestlé is aware of the agency’s warning, but added, “to our knowledge, Cerecin provided answers to the issues raised by the FDA.”
With the goal of getting drug approval, Accera went on to test a tweaked formulation in a 400-patient randomized, placebo-controlled trial called NOURISH AD that ultimately failed. Nevertheless, Axona is still marketed as a medical food. It costs about $100 for a month’s supply.
Repeated requests for comment from Cerecin were not answered. Danielle Schor, an FDA spokesperson, said the agency will not discuss the status of individual products.
More disputes and insurance coverage
Mary Ann DeMarco, executive director of sales and marketing for the Scottsdale, Ariz.–based medical food maker Primus Pharmaceuticals, said the company believes its products fit within the FDA’s medical foods rubric.
These include Fosteum Plus capsules, which it markets “for the clinical dietary management of the metabolic processes of osteopenia and osteoporosis.” The capsules contain a combination of genistein, zinc, calcium, phosphate, vitamin K2, and vitamin D. As proof of effectiveness, the company cites clinical data on some of the ingredients – not the product itself.
Primus has run afoul of the FDA before when it similarly positioned another product, called Limbrel, as a medical food for osteoarthritis. From 2007 to 2017, the FDA received 194 adverse event reports associated with Limbrel, including reports of drug-induced liver injury, pancreatitis, and hypersensitivity pneumonitis. In December 2017, the agency urged Primus to recall Limbrel, a move that it said was “necessary to protect the public health and welfare.” Primus withdrew the product but laid out a defense of Limbrel on a devoted website.
The FDA would not comment any further, said Ms. Schor. Ms. DeMarco said that Primus is working with the FDA to bring Limbrel back to market.
A lack of insurance coverage – even for approved medical foods for IEMs – has frustrated advocates, parents, and manufacturers. They are putting their weight behind the Medical Nutrition Equity Act, which would mandate public and private payer coverage of medical foods for IEMs and digestive conditions such as Crohn disease. That 2019 House bill has 56 cosponsors; there is no Senate companion bill.
“If you can get reimbursement, it really makes the market,” for Primus and the other manufacturers, Mr. Hyman said.
Primus Pharmaceuticals has launched its own campaign, Cover My Medical Foods, to enlist consumers and others to the cause.
Partnering with advocates
Although its low-protein breads, pastas, and baking products are not considered medical foods by the FDA, Dr. Schär is marketing them as such in the United States. They are trying to make a mark in CKD, according to Ms. Donnelly. She added that Dr. Schär has been successful in Europe, where nutrition therapy is more integrated in the health care system.
In 2019, Flavis and the National Kidney Foundation joined forces to raise awareness of nutritional interventions and to build enthusiasm for the Flavis products. The partnership has now ended, mostly because Flavis could no longer afford it, according to Ms. Donnelly.
“Information on diet and nutrition is the most requested subject matter from the NKF,” said Anthony Gucciardo, senior vice president of strategic partnerships at the foundation. The partnership “has never been necessarily about promoting their products per se; it’s promoting a healthy diet and really a diet specific for CKD.”
The NKF developed cobranded materials on low-protein foods for physicians and a teaching tool they could use with patients. Consumers could access nutrition information and a discount on Flavis products on a dedicated webpage. The foundation didn’t describe the low-protein products as medical foods, said Mr. Gucciardo, even if Flavis promoted them as such.
In patients with CKD, dietary management can help prevent the progression to end-stage renal disease. Although Medicare covers medical nutrition therapy – in which patients receive personalized assessments and dietary advice – uptake is abysmally low, according to a 2018 study.
Dr. Burdock thinks low-protein foods for CKD do meet the FDA’s criteria for a medical food but that the agency might not necessarily agree with him. The FDA would not comment.
Physician beware
When it comes to medical foods, the FDA has often looked the other way because the ingredients may already have been proven safe and the danger to an individual or to the public’s health is relatively low, according to Dr. Burdock and Mr. Hyman.
However, if the agency “feels that a medical food will prevent people from seeking medical care or there is potential to defraud the public, it is justified in taking action against the company,” said Dr. Burdock.
According to Dr. Wilson, the pharmacist who reported on the inappropriate medical food prescriptions in the California system, the FDA could help by creating a list of approved medical foods. Physicians should take time to learn about the difference between medical foods and supplements, she said, adding that they should also not hesitate to “question the veracity of the claims for them.”
Ms. Guggenheim believed doctors need to know that, for the most part, these are not FDA-approved products. She emphasized the importance of evaluating the products and looking at the data of their impact on a disease or condition.
“Many of these companies strongly believe that the products work and help people, so clinicians need to be very data driven,” she said.
A version of this article originally appeared on Medscape.com.
How to not miss something

It’s a mad, mad, mad world. In California, we seem bent on swelling our curve. We’d just begun bringing our patients back into the office. We felt safe, back to business. Then air raid sirens again. Retreat to the Underground. Minimize waiting room waiting, convert to telephone and video. Do what we can to protect our patients and people.
As doctors, we’ve gotten proficient at being triage nurses, examining each appointment request, and sorting who should be seen in person and who could be cared for virtually. We do it for every clinic now.
My 11 a.m. patient last Thursday was an 83-year-old Filipino man with at least a 13-year history of hand dermatitis (based on his long electronic medical record). He had plenty of betamethasone refills. There were even photos of his large, brown hands in his chart. Grandpa hands, calloused by tending his garden and scarred from fixing bikes, building sheds, and doing oil changes for any nephew or niece who asked. The most recent uploads showed a bit of fingertip fissuring, some lichenified plaques. Not much different than they looked after planting persimmon trees a decade ago. I called him early that morning to offer a phone appointment. Perhaps I could save him from venturing out.
“I see that you have an appointment with me in a few hours. If you’d like, I might be able to help you by phone instead.” “Oh, thank you, doc,” he replied. “It’s so kind of you to call. But doc, I think maybe it is better if I come in to see you.” “Are you sure?” “Oh, yes. I will be careful.”
He checked in at 10:45. When I walked into the room he was wearing a face mask and a face shield – good job! He also had a cane and U.S. Navy Destroyer hat. And on the bottom left of his plastic shield was a sticker decal of a U.S. Navy Chief Petty Officer, dress blue insignia. His hands looked just like the photos: no purpura, plenty of lentigines. Fissures, calluses, lichenified plaques. I touched them. In the unaffected areas, his skin was remarkably soft. What stories these hands told. “I was 20 years in the Navy, doc,” he said. “I would have stayed longer but my wife, who’s younger, wanted me back home.” He talked about his nine grandchildren, some of whom went on to join the navy too – but as officers, he noted with pride. Now he spends his days caring for his wife; she has dementia. He can’t stay long because she’s in the waiting room and is likely to get confused if alone for too long.
We quickly reviewed good hand care. I ordered clobetasol ointment. He was pleased; that seemed to work years ago and he was glad to have it again.
So, why did he need to come in? Clearly I could have done this remotely. “Thank you so much for seeing me, doc,” as he stood to walk out. “Proper inspections have to be done in person, right?” Yes, I thought. Otherwise, you might miss something.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
It’s a mad, mad, mad world. In California, we seem bent on swelling our curve. We’d just begun bringing our patients back into the office. We felt safe, back to business. Then air raid sirens again. Retreat to the Underground. Minimize waiting room waiting, convert to telephone and video. Do what we can to protect our patients and people.
As doctors, we’ve gotten proficient at being triage nurses, examining each appointment request, and sorting who should be seen in person and who could be cared for virtually. We do it for every clinic now.
My 11 a.m. patient last Thursday was an 83-year-old Filipino man with at least a 13-year history of hand dermatitis (based on his long electronic medical record). He had plenty of betamethasone refills. There were even photos of his large, brown hands in his chart. Grandpa hands, calloused by tending his garden and scarred from fixing bikes, building sheds, and doing oil changes for any nephew or niece who asked. The most recent uploads showed a bit of fingertip fissuring, some lichenified plaques. Not much different than they looked after planting persimmon trees a decade ago. I called him early that morning to offer a phone appointment. Perhaps I could save him from venturing out.
“I see that you have an appointment with me in a few hours. If you’d like, I might be able to help you by phone instead.” “Oh, thank you, doc,” he replied. “It’s so kind of you to call. But doc, I think maybe it is better if I come in to see you.” “Are you sure?” “Oh, yes. I will be careful.”
He checked in at 10:45. When I walked into the room he was wearing a face mask and a face shield – good job! He also had a cane and U.S. Navy Destroyer hat. And on the bottom left of his plastic shield was a sticker decal of a U.S. Navy Chief Petty Officer, dress blue insignia. His hands looked just like the photos: no purpura, plenty of lentigines. Fissures, calluses, lichenified plaques. I touched them. In the unaffected areas, his skin was remarkably soft. What stories these hands told. “I was 20 years in the Navy, doc,” he said. “I would have stayed longer but my wife, who’s younger, wanted me back home.” He talked about his nine grandchildren, some of whom went on to join the navy too – but as officers, he noted with pride. Now he spends his days caring for his wife; she has dementia. He can’t stay long because she’s in the waiting room and is likely to get confused if alone for too long.
We quickly reviewed good hand care. I ordered clobetasol ointment. He was pleased; that seemed to work years ago and he was glad to have it again.
So, why did he need to come in? Clearly I could have done this remotely. “Thank you so much for seeing me, doc,” as he stood to walk out. “Proper inspections have to be done in person, right?” Yes, I thought. Otherwise, you might miss something.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
It’s a mad, mad, mad world. In California, we seem bent on swelling our curve. We’d just begun bringing our patients back into the office. We felt safe, back to business. Then air raid sirens again. Retreat to the Underground. Minimize waiting room waiting, convert to telephone and video. Do what we can to protect our patients and people.
As doctors, we’ve gotten proficient at being triage nurses, examining each appointment request, and sorting who should be seen in person and who could be cared for virtually. We do it for every clinic now.
My 11 a.m. patient last Thursday was an 83-year-old Filipino man with at least a 13-year history of hand dermatitis (based on his long electronic medical record). He had plenty of betamethasone refills. There were even photos of his large, brown hands in his chart. Grandpa hands, calloused by tending his garden and scarred from fixing bikes, building sheds, and doing oil changes for any nephew or niece who asked. The most recent uploads showed a bit of fingertip fissuring, some lichenified plaques. Not much different than they looked after planting persimmon trees a decade ago. I called him early that morning to offer a phone appointment. Perhaps I could save him from venturing out.
“I see that you have an appointment with me in a few hours. If you’d like, I might be able to help you by phone instead.” “Oh, thank you, doc,” he replied. “It’s so kind of you to call. But doc, I think maybe it is better if I come in to see you.” “Are you sure?” “Oh, yes. I will be careful.”
He checked in at 10:45. When I walked into the room he was wearing a face mask and a face shield – good job! He also had a cane and U.S. Navy Destroyer hat. And on the bottom left of his plastic shield was a sticker decal of a U.S. Navy Chief Petty Officer, dress blue insignia. His hands looked just like the photos: no purpura, plenty of lentigines. Fissures, calluses, lichenified plaques. I touched them. In the unaffected areas, his skin was remarkably soft. What stories these hands told. “I was 20 years in the Navy, doc,” he said. “I would have stayed longer but my wife, who’s younger, wanted me back home.” He talked about his nine grandchildren, some of whom went on to join the navy too – but as officers, he noted with pride. Now he spends his days caring for his wife; she has dementia. He can’t stay long because she’s in the waiting room and is likely to get confused if alone for too long.
We quickly reviewed good hand care. I ordered clobetasol ointment. He was pleased; that seemed to work years ago and he was glad to have it again.
So, why did he need to come in? Clearly I could have done this remotely. “Thank you so much for seeing me, doc,” as he stood to walk out. “Proper inspections have to be done in person, right?” Yes, I thought. Otherwise, you might miss something.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
FDA approves Tremfya (guselkumab) for psoriatic arthritis
, according to a July 14 announcement from its manufacturer, Janssen.

The FDA’s approval marks the second indication for guselkumab, which was first approved for adults with plaque psoriasis in 2017.
The agency based its approval on two pivotal phase 3 clinical trials, DISCOVER-1 and DISCOVER-2, which tested the biologic in 1,120 adults with active PsA who were naive to biologics (both trials) or had an inadequate response or intolerance to one or two tumor necrosis factor inhibitors (in about 30% of patients in DISCOVER-1). Part of this pretrial standard treatment could include at least 4 months of Otezla (apremilast), at least 3 months of nonbiologic disease-modifying antirheumatic drugs (DMARDs), or at least 4 weeks of NSAIDs. In both trials, about 58% of patients took methotrexate.
Participants who took guselkumab achieved 20% improvement in American College of Rheumatology response criteria at week 24 at rates of 52% in DISCOVER-1 and 64% in DISCOVER-2, whereas placebo-treated patients had rates of 22% and 33%, respectively.
Guselkumab improved patients’ other symptoms, including skin manifestations of psoriasis, physical functioning, enthesitis, dactylitis, and fatigue, according to the Janssen release.
Guselkumab, a fully human monoclonal antibody that selectively binds to the p19 subunit of IL-23, is administered as a 100-mg subcutaneous injection every 8 weeks, following two starter doses at weeks 0 and 4, and can be used alone or in combination with a conventional DMARD.
In guselkumab clinical trials of patients with PsA, a minority had bronchitis or a decreased neutrophil count, but the safety profile was otherwise generally consistent with what has been seen in patients with plaque psoriasis, according to the company release. Other common side effects described in 1% or more of patients have included upper respiratory infections, headache, injection-site reactions, arthralgia, diarrhea, gastroenteritis, tinea infections, and herpes simplex infections.
, according to a July 14 announcement from its manufacturer, Janssen.
The FDA’s approval marks the second indication for guselkumab, which was first approved for adults with plaque psoriasis in 2017.
The agency based its approval on two pivotal phase 3 clinical trials, DISCOVER-1 and DISCOVER-2, which tested the biologic in 1,120 adults with active PsA who were naive to biologics (both trials) or had an inadequate response or intolerance to one or two tumor necrosis factor inhibitors (in about 30% of patients in DISCOVER-1). Part of this pretrial standard treatment could include at least 4 months of Otezla (apremilast), at least 3 months of nonbiologic disease-modifying antirheumatic drugs (DMARDs), or at least 4 weeks of NSAIDs. In both trials, about 58% of patients took methotrexate.
Participants who took guselkumab achieved 20% improvement in American College of Rheumatology response criteria at week 24 at rates of 52% in DISCOVER-1 and 64% in DISCOVER-2, whereas placebo-treated patients had rates of 22% and 33%, respectively.
Guselkumab improved patients’ other symptoms, including skin manifestations of psoriasis, physical functioning, enthesitis, dactylitis, and fatigue, according to the Janssen release.
Guselkumab, a fully human monoclonal antibody that selectively binds to the p19 subunit of IL-23, is administered as a 100-mg subcutaneous injection every 8 weeks, following two starter doses at weeks 0 and 4, and can be used alone or in combination with a conventional DMARD.
In guselkumab clinical trials of patients with PsA, a minority had bronchitis or a decreased neutrophil count, but the safety profile was otherwise generally consistent with what has been seen in patients with plaque psoriasis, according to the company release. Other common side effects described in 1% or more of patients have included upper respiratory infections, headache, injection-site reactions, arthralgia, diarrhea, gastroenteritis, tinea infections, and herpes simplex infections.
, according to a July 14 announcement from its manufacturer, Janssen.
The FDA’s approval marks the second indication for guselkumab, which was first approved for adults with plaque psoriasis in 2017.
The agency based its approval on two pivotal phase 3 clinical trials, DISCOVER-1 and DISCOVER-2, which tested the biologic in 1,120 adults with active PsA who were naive to biologics (both trials) or had an inadequate response or intolerance to one or two tumor necrosis factor inhibitors (in about 30% of patients in DISCOVER-1). Part of this pretrial standard treatment could include at least 4 months of Otezla (apremilast), at least 3 months of nonbiologic disease-modifying antirheumatic drugs (DMARDs), or at least 4 weeks of NSAIDs. In both trials, about 58% of patients took methotrexate.
Participants who took guselkumab achieved 20% improvement in American College of Rheumatology response criteria at week 24 at rates of 52% in DISCOVER-1 and 64% in DISCOVER-2, whereas placebo-treated patients had rates of 22% and 33%, respectively.
Guselkumab improved patients’ other symptoms, including skin manifestations of psoriasis, physical functioning, enthesitis, dactylitis, and fatigue, according to the Janssen release.
Guselkumab, a fully human monoclonal antibody that selectively binds to the p19 subunit of IL-23, is administered as a 100-mg subcutaneous injection every 8 weeks, following two starter doses at weeks 0 and 4, and can be used alone or in combination with a conventional DMARD.
In guselkumab clinical trials of patients with PsA, a minority had bronchitis or a decreased neutrophil count, but the safety profile was otherwise generally consistent with what has been seen in patients with plaque psoriasis, according to the company release. Other common side effects described in 1% or more of patients have included upper respiratory infections, headache, injection-site reactions, arthralgia, diarrhea, gastroenteritis, tinea infections, and herpes simplex infections.
The public’s trust in science
Having been a bench research scientist 30 years ago, I am flabbergasted at what is and is not currently possible. In a few weeks, scientists sequenced a novel coronavirus and used the genetic sequence to select candidate molecules for a vaccine. But we still can’t reliably say how much protection a cloth mask provides. Worse yet, even if/when we could reliably quantify contagion, it isn’t clear that the public will believe us anyhow.

The good news is that the public worldwide did believe scientists about the threat of a pandemic and the need to flatten the curve. Saving lives has not been about the strength of an antibiotic or the skill in managing a ventilator, but the credibility of medical scientists. The degree of acceptance was variable and subject to a variety of delays caused by regional politicians, but The bad news is that the public’s trust in that scientific advice has waned, the willingness to accept onerous restrictions has fatigued, and the cooperation for maintaining these social changes is evaporating.
I will leave pontificating about the spread of COVID-19 to other experts in other forums. My focus is on the public’s trust in the professionalism of physicians, nurses, medical scientists, and the health care industry as a whole. That trust has been our most valuable tool in fighting the pandemic so far. There have been situations in which weaknesses in modern science have let society down during the pandemic of the century. In my February 2020 column, at the beginning of the outbreak, a month before it was declared a pandemic, when its magnitude was still unclear, I emphasized the importance of having a trusted scientific spokesperson providing timely, accurate information to the public. That, obviously, did not happen in the United States and the degree of the ensuing disaster is still to be revealed.
Scientists have made some wrong decisions about this novel threat. The advice on masks is an illustrative example. For many years, infection control nurses have insisted that medical students wear a mask to protect themselves, even if they were observing rounds from just inside the doorway of a room of a baby with bronchiolitis. The landfills are full of briefly worn surgical masks. Now the story goes: Surgical masks don’t protect staff; they protect others. Changes like that contribute to a credibility gap.
For 3 months, there was conflicting advice about the appropriateness of masks. In early March 2020, some health care workers were disciplined for wearing personal masks. Now, most scientists recommend the public use masks to reduce contagion. Significant subgroups in the U.S. population have refused, mostly to signal their contrarian politics. In June there was an anecdote of a success story from the Show Me state of Missouri, where a mask is credited for preventing an outbreak from a sick hair stylist.
It is hard to find something more reliable than an anecdote. On June 1, a meta-analysis funded by the World Health Organization was published online by Lancet. It supports the idea that masks are beneficial. It is mostly forest plots, so you can try to interpret it yourself. There were 172 observational studies in the systematic review, and the meta-analysis contains 44 relevant comparative studies and 0 randomized controlled trials. Most of those forest plots have an I2 of 75% or worse, which to me indicates that they are not much more reliable than a good anecdote. My primary conclusion was that modern academic science, in an era with a shortage of toilet paper, should convert to printing on soft tissue paper.

It is important to note that the guesstimated overall benefit of cloth masks was a relative risk of 0.30. That benefit is easily nullified if the false security of a mask causes people to congregate together in groups three times larger or for three times more minutes. N95 masks were more effective.
A different article was published in PNAS on June 11. Its senior author was awarded the Nobel Prize in Chemistry in 1995. That article touted the benefits of masks. The article is facing heavy criticism for flaws in methodology and flaws in the peer review process. A long list of signatories have joined a letter asking for the article’s retraction.
This article, when combined with the two instances of prominent articles being retracted in the prior month by the New England Journal of Medicine and The Lancet, is accumulating evidence the peer review system is not working as intended.
There are many heroes in this pandemic, from the frontline health care workers in hotspots to the grocery workers and cleaning staff. There is hope, indeed some faith, that medical scientists in the foreseeable future will provide treatments and a vaccine for this viral plague. This month, the credibility of scientists again plays a major role as communities respond to outbreaks related to reopening the economy. Let’s celebrate the victories, resolve to fix the impure system, and restore a high level of public trust in science. Lives depend on it.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
Having been a bench research scientist 30 years ago, I am flabbergasted at what is and is not currently possible. In a few weeks, scientists sequenced a novel coronavirus and used the genetic sequence to select candidate molecules for a vaccine. But we still can’t reliably say how much protection a cloth mask provides. Worse yet, even if/when we could reliably quantify contagion, it isn’t clear that the public will believe us anyhow.
The good news is that the public worldwide did believe scientists about the threat of a pandemic and the need to flatten the curve. Saving lives has not been about the strength of an antibiotic or the skill in managing a ventilator, but the credibility of medical scientists. The degree of acceptance was variable and subject to a variety of delays caused by regional politicians, but The bad news is that the public’s trust in that scientific advice has waned, the willingness to accept onerous restrictions has fatigued, and the cooperation for maintaining these social changes is evaporating.
I will leave pontificating about the spread of COVID-19 to other experts in other forums. My focus is on the public’s trust in the professionalism of physicians, nurses, medical scientists, and the health care industry as a whole. That trust has been our most valuable tool in fighting the pandemic so far. There have been situations in which weaknesses in modern science have let society down during the pandemic of the century. In my February 2020 column, at the beginning of the outbreak, a month before it was declared a pandemic, when its magnitude was still unclear, I emphasized the importance of having a trusted scientific spokesperson providing timely, accurate information to the public. That, obviously, did not happen in the United States and the degree of the ensuing disaster is still to be revealed.
Scientists have made some wrong decisions about this novel threat. The advice on masks is an illustrative example. For many years, infection control nurses have insisted that medical students wear a mask to protect themselves, even if they were observing rounds from just inside the doorway of a room of a baby with bronchiolitis. The landfills are full of briefly worn surgical masks. Now the story goes: Surgical masks don’t protect staff; they protect others. Changes like that contribute to a credibility gap.
For 3 months, there was conflicting advice about the appropriateness of masks. In early March 2020, some health care workers were disciplined for wearing personal masks. Now, most scientists recommend the public use masks to reduce contagion. Significant subgroups in the U.S. population have refused, mostly to signal their contrarian politics. In June there was an anecdote of a success story from the Show Me state of Missouri, where a mask is credited for preventing an outbreak from a sick hair stylist.
It is hard to find something more reliable than an anecdote. On June 1, a meta-analysis funded by the World Health Organization was published online by Lancet. It supports the idea that masks are beneficial. It is mostly forest plots, so you can try to interpret it yourself. There were 172 observational studies in the systematic review, and the meta-analysis contains 44 relevant comparative studies and 0 randomized controlled trials. Most of those forest plots have an I2 of 75% or worse, which to me indicates that they are not much more reliable than a good anecdote. My primary conclusion was that modern academic science, in an era with a shortage of toilet paper, should convert to printing on soft tissue paper.
It is important to note that the guesstimated overall benefit of cloth masks was a relative risk of 0.30. That benefit is easily nullified if the false security of a mask causes people to congregate together in groups three times larger or for three times more minutes. N95 masks were more effective.
A different article was published in PNAS on June 11. Its senior author was awarded the Nobel Prize in Chemistry in 1995. That article touted the benefits of masks. The article is facing heavy criticism for flaws in methodology and flaws in the peer review process. A long list of signatories have joined a letter asking for the article’s retraction.
This article, when combined with the two instances of prominent articles being retracted in the prior month by the New England Journal of Medicine and The Lancet, is accumulating evidence the peer review system is not working as intended.
There are many heroes in this pandemic, from the frontline health care workers in hotspots to the grocery workers and cleaning staff. There is hope, indeed some faith, that medical scientists in the foreseeable future will provide treatments and a vaccine for this viral plague. This month, the credibility of scientists again plays a major role as communities respond to outbreaks related to reopening the economy. Let’s celebrate the victories, resolve to fix the impure system, and restore a high level of public trust in science. Lives depend on it.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
Having been a bench research scientist 30 years ago, I am flabbergasted at what is and is not currently possible. In a few weeks, scientists sequenced a novel coronavirus and used the genetic sequence to select candidate molecules for a vaccine. But we still can’t reliably say how much protection a cloth mask provides. Worse yet, even if/when we could reliably quantify contagion, it isn’t clear that the public will believe us anyhow.
The good news is that the public worldwide did believe scientists about the threat of a pandemic and the need to flatten the curve. Saving lives has not been about the strength of an antibiotic or the skill in managing a ventilator, but the credibility of medical scientists. The degree of acceptance was variable and subject to a variety of delays caused by regional politicians, but The bad news is that the public’s trust in that scientific advice has waned, the willingness to accept onerous restrictions has fatigued, and the cooperation for maintaining these social changes is evaporating.
I will leave pontificating about the spread of COVID-19 to other experts in other forums. My focus is on the public’s trust in the professionalism of physicians, nurses, medical scientists, and the health care industry as a whole. That trust has been our most valuable tool in fighting the pandemic so far. There have been situations in which weaknesses in modern science have let society down during the pandemic of the century. In my February 2020 column, at the beginning of the outbreak, a month before it was declared a pandemic, when its magnitude was still unclear, I emphasized the importance of having a trusted scientific spokesperson providing timely, accurate information to the public. That, obviously, did not happen in the United States and the degree of the ensuing disaster is still to be revealed.
Scientists have made some wrong decisions about this novel threat. The advice on masks is an illustrative example. For many years, infection control nurses have insisted that medical students wear a mask to protect themselves, even if they were observing rounds from just inside the doorway of a room of a baby with bronchiolitis. The landfills are full of briefly worn surgical masks. Now the story goes: Surgical masks don’t protect staff; they protect others. Changes like that contribute to a credibility gap.
For 3 months, there was conflicting advice about the appropriateness of masks. In early March 2020, some health care workers were disciplined for wearing personal masks. Now, most scientists recommend the public use masks to reduce contagion. Significant subgroups in the U.S. population have refused, mostly to signal their contrarian politics. In June there was an anecdote of a success story from the Show Me state of Missouri, where a mask is credited for preventing an outbreak from a sick hair stylist.
It is hard to find something more reliable than an anecdote. On June 1, a meta-analysis funded by the World Health Organization was published online by Lancet. It supports the idea that masks are beneficial. It is mostly forest plots, so you can try to interpret it yourself. There were 172 observational studies in the systematic review, and the meta-analysis contains 44 relevant comparative studies and 0 randomized controlled trials. Most of those forest plots have an I2 of 75% or worse, which to me indicates that they are not much more reliable than a good anecdote. My primary conclusion was that modern academic science, in an era with a shortage of toilet paper, should convert to printing on soft tissue paper.
It is important to note that the guesstimated overall benefit of cloth masks was a relative risk of 0.30. That benefit is easily nullified if the false security of a mask causes people to congregate together in groups three times larger or for three times more minutes. N95 masks were more effective.
A different article was published in PNAS on June 11. Its senior author was awarded the Nobel Prize in Chemistry in 1995. That article touted the benefits of masks. The article is facing heavy criticism for flaws in methodology and flaws in the peer review process. A long list of signatories have joined a letter asking for the article’s retraction.
This article, when combined with the two instances of prominent articles being retracted in the prior month by the New England Journal of Medicine and The Lancet, is accumulating evidence the peer review system is not working as intended.
There are many heroes in this pandemic, from the frontline health care workers in hotspots to the grocery workers and cleaning staff. There is hope, indeed some faith, that medical scientists in the foreseeable future will provide treatments and a vaccine for this viral plague. This month, the credibility of scientists again plays a major role as communities respond to outbreaks related to reopening the economy. Let’s celebrate the victories, resolve to fix the impure system, and restore a high level of public trust in science. Lives depend on it.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
PASDAS beats DAS28 in measuring psoriatic arthritis treat-to-target success
Measuring success with a treat-to-target strategy in psoriatic arthritis patients proved to be more comprehensive with the Psoriatic Arthritis Disease Activity Score (PASDAS) than it was with the Disease Activity Score in 28 joints (DAS28), according to findings from a prospective cohort study.
Fewer patients had a low disease activity score according to DAS28, and a higher percentage of patients deemed adequately treated according to DAS28 were found to have residual disease activity, compared with the number of patients so categorized according to PASDAS, researcher Michelle Mulder reported in her presentation of the study at the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA).
“PASDAS implementation in a tightly monitored PsA [psoriatic arthritis] cohort suggests relevant residual disease burden, even though DAS28 was measured at every visit previously,” said Ms. Mulder, an MD/PhD student at Sint Maartenskliniek in Nijmegen, The Netherlands.
The presentation was convincing to Philip Helliwell, MD, PhD, who is a professor of clinical rheumatology at Leeds (England) University, and was also one of the developers of PASDAS. “We know it can be used in clinical practice with a certain amount of organization and clinical staff to help you,” he said during another presentation at GRAPPA.
Treat to target is a widely accepted therapeutic strategy. It’s particularly common in rheumatoid arthritis, but increasing evidence suggests that it improves patient outcomes in psoriatic arthritis. DAS28 is frequently used in treat-to-target approaches in rheumatoid arthritis, and often gets applied to psoriatic arthritis since rheumatologists are already comfortable with it, according to Ms. Mulder. “However, DAS28 has shown some limitations when used in psoriatic arthritis. For example, its joint count is limited to only 28 joints, and it does not take all PsA domains into account,” she said.
DAS28 was previously used at Sint Maartenskliniek in combination with psoriatic arthritis–specific assessment recommendations, but the institution opted in 2019 to switch to PASDAS, which was developed by GRAPPA and the European League Against Rheumatism. “To better adhere to international PsA guidelines, we chose to implement PASDAS in our cohort with the assumption that it might improve patient care,” Ms. Mulder said.
With DAS28, clinicians measured the C-reactive protein (CRP) and Patient Global Visual Analog Scale (VAS) domains and were advised to examine 28 joints for tender and swollen joint count domains. Under the PASDAS guidance, clinicians examined 68 joints for tenderness, 66 joints for swelling, CRP, Patient Global VAS, Physician Global VAS, Leeds Enthesitis Index, dactylitis, and the 12-item Short Form Physical Composite Scale. They also examined the skin, nails, and axial disease.
To examine the effects of the switch from DAS28 to PASDAS, the researchers compared outcomes in 855 patients before and after the change during March to December 2019. The mean age of patients was 55 years, and 46% were female. The mean disease duration was 10 years, and the mean PASDAS score was 3.1. A total of 96% of participants were negative for anti-cyclic citrullinated peptide. Overall, 30% had arthritis, 9% had axial disease, 3% had dactylitis, 21% had enthesitis, 51% had skin disease, and 42% had nail disease.
About three-quarters (77.4%) of patients reached the threshold of low disease activity (LDA) according to the DAS28 measure, while 53.1% did so using the PASDAS. High disease activity occurred in 7.8% of patients according to DAS28, compared with 2.7% as measured by PASDAS. Patients who reached only the DAS28 LDA target but not the PASDAS target, compared with patients who reached the LDA target in both measures, had significantly worse counts for swelling in 66 joints (0.7 vs. 0.2; P < .001) and tenderness in 68 joints (2.1 vs. 0.7; P < .001), as well as worse scores for enthesitis (0.5 vs. 0.1; P < .001), dactylitis (4% vs. 1%; P = .005), patient global VAS (44.0 vs. 14.4; P < .001), Health Assessment Questionnaire (0.8 vs. 0.4; P < .001) and Patient Acceptable Symptom State (unacceptable score in 17% vs. 3%; P < .001).
Ms. Mulder acknowledged that PASDAS imposes a significant burden on clinicians, and noted that Sint Maartenskliniek created patient infrastructure to handle the load. “It’s very important that you set up your clinic in a specific way. When the patient comes in, we draw blood immediately and we ask them to fill in the questionnaires, and then they go to a specialized nurse who measures all the different components of the PASDAS. It took a lot of time to train the specialized nurses and to implement the PASDAS score in our electronic health records. After we did those things, it was quite easy because we have this whole setup. It takes time and it is difficult, but it is definitely possible to do it,” Ms. Mulder said during a live Q&A following her prerecorded presentation.
The study received no funding. Ms. Mulder had no relevant financial disclosures. Dr. Helliwell has financial ties to AbbVie, Amgen, Celgen, Galapagos, Janssen, Novartis, Pfizer, and UCB.
SOURCE: Mulder M et al. GRAPPA 2020 Virtual Annual Meeting.
Measuring success with a treat-to-target strategy in psoriatic arthritis patients proved to be more comprehensive with the Psoriatic Arthritis Disease Activity Score (PASDAS) than it was with the Disease Activity Score in 28 joints (DAS28), according to findings from a prospective cohort study.
Fewer patients had a low disease activity score according to DAS28, and a higher percentage of patients deemed adequately treated according to DAS28 were found to have residual disease activity, compared with the number of patients so categorized according to PASDAS, researcher Michelle Mulder reported in her presentation of the study at the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA).
“PASDAS implementation in a tightly monitored PsA [psoriatic arthritis] cohort suggests relevant residual disease burden, even though DAS28 was measured at every visit previously,” said Ms. Mulder, an MD/PhD student at Sint Maartenskliniek in Nijmegen, The Netherlands.
The presentation was convincing to Philip Helliwell, MD, PhD, who is a professor of clinical rheumatology at Leeds (England) University, and was also one of the developers of PASDAS. “We know it can be used in clinical practice with a certain amount of organization and clinical staff to help you,” he said during another presentation at GRAPPA.
Treat to target is a widely accepted therapeutic strategy. It’s particularly common in rheumatoid arthritis, but increasing evidence suggests that it improves patient outcomes in psoriatic arthritis. DAS28 is frequently used in treat-to-target approaches in rheumatoid arthritis, and often gets applied to psoriatic arthritis since rheumatologists are already comfortable with it, according to Ms. Mulder. “However, DAS28 has shown some limitations when used in psoriatic arthritis. For example, its joint count is limited to only 28 joints, and it does not take all PsA domains into account,” she said.
DAS28 was previously used at Sint Maartenskliniek in combination with psoriatic arthritis–specific assessment recommendations, but the institution opted in 2019 to switch to PASDAS, which was developed by GRAPPA and the European League Against Rheumatism. “To better adhere to international PsA guidelines, we chose to implement PASDAS in our cohort with the assumption that it might improve patient care,” Ms. Mulder said.
With DAS28, clinicians measured the C-reactive protein (CRP) and Patient Global Visual Analog Scale (VAS) domains and were advised to examine 28 joints for tender and swollen joint count domains. Under the PASDAS guidance, clinicians examined 68 joints for tenderness, 66 joints for swelling, CRP, Patient Global VAS, Physician Global VAS, Leeds Enthesitis Index, dactylitis, and the 12-item Short Form Physical Composite Scale. They also examined the skin, nails, and axial disease.
To examine the effects of the switch from DAS28 to PASDAS, the researchers compared outcomes in 855 patients before and after the change during March to December 2019. The mean age of patients was 55 years, and 46% were female. The mean disease duration was 10 years, and the mean PASDAS score was 3.1. A total of 96% of participants were negative for anti-cyclic citrullinated peptide. Overall, 30% had arthritis, 9% had axial disease, 3% had dactylitis, 21% had enthesitis, 51% had skin disease, and 42% had nail disease.
About three-quarters (77.4%) of patients reached the threshold of low disease activity (LDA) according to the DAS28 measure, while 53.1% did so using the PASDAS. High disease activity occurred in 7.8% of patients according to DAS28, compared with 2.7% as measured by PASDAS. Patients who reached only the DAS28 LDA target but not the PASDAS target, compared with patients who reached the LDA target in both measures, had significantly worse counts for swelling in 66 joints (0.7 vs. 0.2; P < .001) and tenderness in 68 joints (2.1 vs. 0.7; P < .001), as well as worse scores for enthesitis (0.5 vs. 0.1; P < .001), dactylitis (4% vs. 1%; P = .005), patient global VAS (44.0 vs. 14.4; P < .001), Health Assessment Questionnaire (0.8 vs. 0.4; P < .001) and Patient Acceptable Symptom State (unacceptable score in 17% vs. 3%; P < .001).
Ms. Mulder acknowledged that PASDAS imposes a significant burden on clinicians, and noted that Sint Maartenskliniek created patient infrastructure to handle the load. “It’s very important that you set up your clinic in a specific way. When the patient comes in, we draw blood immediately and we ask them to fill in the questionnaires, and then they go to a specialized nurse who measures all the different components of the PASDAS. It took a lot of time to train the specialized nurses and to implement the PASDAS score in our electronic health records. After we did those things, it was quite easy because we have this whole setup. It takes time and it is difficult, but it is definitely possible to do it,” Ms. Mulder said during a live Q&A following her prerecorded presentation.
The study received no funding. Ms. Mulder had no relevant financial disclosures. Dr. Helliwell has financial ties to AbbVie, Amgen, Celgen, Galapagos, Janssen, Novartis, Pfizer, and UCB.
SOURCE: Mulder M et al. GRAPPA 2020 Virtual Annual Meeting.
Measuring success with a treat-to-target strategy in psoriatic arthritis patients proved to be more comprehensive with the Psoriatic Arthritis Disease Activity Score (PASDAS) than it was with the Disease Activity Score in 28 joints (DAS28), according to findings from a prospective cohort study.
Fewer patients had a low disease activity score according to DAS28, and a higher percentage of patients deemed adequately treated according to DAS28 were found to have residual disease activity, compared with the number of patients so categorized according to PASDAS, researcher Michelle Mulder reported in her presentation of the study at the virtual annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA).
“PASDAS implementation in a tightly monitored PsA [psoriatic arthritis] cohort suggests relevant residual disease burden, even though DAS28 was measured at every visit previously,” said Ms. Mulder, an MD/PhD student at Sint Maartenskliniek in Nijmegen, The Netherlands.
The presentation was convincing to Philip Helliwell, MD, PhD, who is a professor of clinical rheumatology at Leeds (England) University, and was also one of the developers of PASDAS. “We know it can be used in clinical practice with a certain amount of organization and clinical staff to help you,” he said during another presentation at GRAPPA.
Treat to target is a widely accepted therapeutic strategy. It’s particularly common in rheumatoid arthritis, but increasing evidence suggests that it improves patient outcomes in psoriatic arthritis. DAS28 is frequently used in treat-to-target approaches in rheumatoid arthritis, and often gets applied to psoriatic arthritis since rheumatologists are already comfortable with it, according to Ms. Mulder. “However, DAS28 has shown some limitations when used in psoriatic arthritis. For example, its joint count is limited to only 28 joints, and it does not take all PsA domains into account,” she said.
DAS28 was previously used at Sint Maartenskliniek in combination with psoriatic arthritis–specific assessment recommendations, but the institution opted in 2019 to switch to PASDAS, which was developed by GRAPPA and the European League Against Rheumatism. “To better adhere to international PsA guidelines, we chose to implement PASDAS in our cohort with the assumption that it might improve patient care,” Ms. Mulder said.
With DAS28, clinicians measured the C-reactive protein (CRP) and Patient Global Visual Analog Scale (VAS) domains and were advised to examine 28 joints for tender and swollen joint count domains. Under the PASDAS guidance, clinicians examined 68 joints for tenderness, 66 joints for swelling, CRP, Patient Global VAS, Physician Global VAS, Leeds Enthesitis Index, dactylitis, and the 12-item Short Form Physical Composite Scale. They also examined the skin, nails, and axial disease.
To examine the effects of the switch from DAS28 to PASDAS, the researchers compared outcomes in 855 patients before and after the change during March to December 2019. The mean age of patients was 55 years, and 46% were female. The mean disease duration was 10 years, and the mean PASDAS score was 3.1. A total of 96% of participants were negative for anti-cyclic citrullinated peptide. Overall, 30% had arthritis, 9% had axial disease, 3% had dactylitis, 21% had enthesitis, 51% had skin disease, and 42% had nail disease.
About three-quarters (77.4%) of patients reached the threshold of low disease activity (LDA) according to the DAS28 measure, while 53.1% did so using the PASDAS. High disease activity occurred in 7.8% of patients according to DAS28, compared with 2.7% as measured by PASDAS. Patients who reached only the DAS28 LDA target but not the PASDAS target, compared with patients who reached the LDA target in both measures, had significantly worse counts for swelling in 66 joints (0.7 vs. 0.2; P < .001) and tenderness in 68 joints (2.1 vs. 0.7; P < .001), as well as worse scores for enthesitis (0.5 vs. 0.1; P < .001), dactylitis (4% vs. 1%; P = .005), patient global VAS (44.0 vs. 14.4; P < .001), Health Assessment Questionnaire (0.8 vs. 0.4; P < .001) and Patient Acceptable Symptom State (unacceptable score in 17% vs. 3%; P < .001).
Ms. Mulder acknowledged that PASDAS imposes a significant burden on clinicians, and noted that Sint Maartenskliniek created patient infrastructure to handle the load. “It’s very important that you set up your clinic in a specific way. When the patient comes in, we draw blood immediately and we ask them to fill in the questionnaires, and then they go to a specialized nurse who measures all the different components of the PASDAS. It took a lot of time to train the specialized nurses and to implement the PASDAS score in our electronic health records. After we did those things, it was quite easy because we have this whole setup. It takes time and it is difficult, but it is definitely possible to do it,” Ms. Mulder said during a live Q&A following her prerecorded presentation.
The study received no funding. Ms. Mulder had no relevant financial disclosures. Dr. Helliwell has financial ties to AbbVie, Amgen, Celgen, Galapagos, Janssen, Novartis, Pfizer, and UCB.
SOURCE: Mulder M et al. GRAPPA 2020 Virtual Annual Meeting.
FROM GRAPPA 2020 VIRTUAL ANNUAL MEETING
COVID-19 symptoms can linger for months
Clinicians and researchers have focused on the acute phase of COVID-19 infection, but it’s increasingly clear that some recovered patients discharged from acute care need continued monitoring for long-lasting effects, a study has found.
In a research letter published online July 9 in JAMA, Angelo Carfi, MD, and colleagues from the Gemelli Against COVID-19 Post–Acute Care Study Group in Rome, report that
Postdischarge assessments of patients who met criteria for SARS-CoV-2 negativity, including a reverse transcriptase–polymerase chain reaction test, were conducted from April 21 to May 29. Among the results:
- Only 12.6% of the 143 patients were completely free of any COVID-19 symptom
- About 32% of patients had one or two symptoms and 55% had three or more
- None had fever or other signs and symptoms of acute illness
- About 53% of patients still had fatigue, 43.4% had dyspnea, 27.3% had joint pain, and had 21.7% chest pain
- About 44% reported worsened quality of life on the EuroQol visual analog scale.
The sample cohort, assessed in a COVID-19 patient service recently established at the Fondazione Policlinico Universitario Agostino Gemelli had a mean age of 56.5 years and 37% were women. The mean length of hospital stay was 13.5 days. During their hospitalization, 72.7% of patients showed evidence of interstitial pneumonia. Noninvasive ventilation was given to 14.7% of patients and 4.9% received invasive ventilation.
The reality of lingering symptoms has led Dr. Carfi’s clinic to schedule a final “wrap-up visit” for patients after full assessment. “On that occasion the doctor prescribes anything necessary to correct the anomalies found during the full evaluation,” Dr. Carfi, a geriatrician at the Gemelli clinic, said in an interview. “These usually include vitamin supplementation and, in selected cases, a new drug prescription such as a blood thinner if necessary.”
Patients can also enroll in a training program in which breathing status is monitored.
In North America, doctors are also addressing the reality that the road to recovery can be a long and upward one, with persistent symptoms worse than those seen with acute influenza infection. “We see patients who were first diagnosed in March or April and still have symptoms in July,” said Zijian Chen, MD, an endocrinologist and medical director of Mount Sinai Health System’s Center for Post-COVID Care in New York.
“Persistent symptoms are much worse for COVID patients than flu patients. Even flu patients who spent time in the intensive care unit recover fully, and we can optimize their breathing before discharge,” Dr. Chen said in an interview.
As in the Italian study, Dr. Chen sees patients with COVID-19 who have ongoing shortness of breath, some requiring supplemental oxygen, or with persistent chest pain on exertion, blood clotting problems, poor concentration, gastrointestinal distress, and reduced muscle strength and impaired grasping power. He doesn’t rule out permanent lung damage in some. “Even asymptomatic individuals already show lung scarring on imaging,” he said.
The Mount Sinai program provides specialized interdisciplinary management that may include CT scans, endoscopy, and drugs such as respiratory medications or anticoagulants. It also offers training to combat the fatigue and deconditioning caused by the infection, symptoms that are not medically treatable but impact quality of life.
“These patients do get better, but I expect they may still have symptoms requiring monitoring after a year,” Dr. Chen said.
The study received no specific funding. Dr. Carfi and colleagues have disclosed no relevant financial relationships. Dr. Chen has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Clinicians and researchers have focused on the acute phase of COVID-19 infection, but it’s increasingly clear that some recovered patients discharged from acute care need continued monitoring for long-lasting effects, a study has found.
In a research letter published online July 9 in JAMA, Angelo Carfi, MD, and colleagues from the Gemelli Against COVID-19 Post–Acute Care Study Group in Rome, report that
Postdischarge assessments of patients who met criteria for SARS-CoV-2 negativity, including a reverse transcriptase–polymerase chain reaction test, were conducted from April 21 to May 29. Among the results:
- Only 12.6% of the 143 patients were completely free of any COVID-19 symptom
- About 32% of patients had one or two symptoms and 55% had three or more
- None had fever or other signs and symptoms of acute illness
- About 53% of patients still had fatigue, 43.4% had dyspnea, 27.3% had joint pain, and had 21.7% chest pain
- About 44% reported worsened quality of life on the EuroQol visual analog scale.
The sample cohort, assessed in a COVID-19 patient service recently established at the Fondazione Policlinico Universitario Agostino Gemelli had a mean age of 56.5 years and 37% were women. The mean length of hospital stay was 13.5 days. During their hospitalization, 72.7% of patients showed evidence of interstitial pneumonia. Noninvasive ventilation was given to 14.7% of patients and 4.9% received invasive ventilation.
The reality of lingering symptoms has led Dr. Carfi’s clinic to schedule a final “wrap-up visit” for patients after full assessment. “On that occasion the doctor prescribes anything necessary to correct the anomalies found during the full evaluation,” Dr. Carfi, a geriatrician at the Gemelli clinic, said in an interview. “These usually include vitamin supplementation and, in selected cases, a new drug prescription such as a blood thinner if necessary.”
Patients can also enroll in a training program in which breathing status is monitored.
In North America, doctors are also addressing the reality that the road to recovery can be a long and upward one, with persistent symptoms worse than those seen with acute influenza infection. “We see patients who were first diagnosed in March or April and still have symptoms in July,” said Zijian Chen, MD, an endocrinologist and medical director of Mount Sinai Health System’s Center for Post-COVID Care in New York.
“Persistent symptoms are much worse for COVID patients than flu patients. Even flu patients who spent time in the intensive care unit recover fully, and we can optimize their breathing before discharge,” Dr. Chen said in an interview.
As in the Italian study, Dr. Chen sees patients with COVID-19 who have ongoing shortness of breath, some requiring supplemental oxygen, or with persistent chest pain on exertion, blood clotting problems, poor concentration, gastrointestinal distress, and reduced muscle strength and impaired grasping power. He doesn’t rule out permanent lung damage in some. “Even asymptomatic individuals already show lung scarring on imaging,” he said.
The Mount Sinai program provides specialized interdisciplinary management that may include CT scans, endoscopy, and drugs such as respiratory medications or anticoagulants. It also offers training to combat the fatigue and deconditioning caused by the infection, symptoms that are not medically treatable but impact quality of life.
“These patients do get better, but I expect they may still have symptoms requiring monitoring after a year,” Dr. Chen said.
The study received no specific funding. Dr. Carfi and colleagues have disclosed no relevant financial relationships. Dr. Chen has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Clinicians and researchers have focused on the acute phase of COVID-19 infection, but it’s increasingly clear that some recovered patients discharged from acute care need continued monitoring for long-lasting effects, a study has found.
In a research letter published online July 9 in JAMA, Angelo Carfi, MD, and colleagues from the Gemelli Against COVID-19 Post–Acute Care Study Group in Rome, report that
Postdischarge assessments of patients who met criteria for SARS-CoV-2 negativity, including a reverse transcriptase–polymerase chain reaction test, were conducted from April 21 to May 29. Among the results:
- Only 12.6% of the 143 patients were completely free of any COVID-19 symptom
- About 32% of patients had one or two symptoms and 55% had three or more
- None had fever or other signs and symptoms of acute illness
- About 53% of patients still had fatigue, 43.4% had dyspnea, 27.3% had joint pain, and had 21.7% chest pain
- About 44% reported worsened quality of life on the EuroQol visual analog scale.
The sample cohort, assessed in a COVID-19 patient service recently established at the Fondazione Policlinico Universitario Agostino Gemelli had a mean age of 56.5 years and 37% were women. The mean length of hospital stay was 13.5 days. During their hospitalization, 72.7% of patients showed evidence of interstitial pneumonia. Noninvasive ventilation was given to 14.7% of patients and 4.9% received invasive ventilation.
The reality of lingering symptoms has led Dr. Carfi’s clinic to schedule a final “wrap-up visit” for patients after full assessment. “On that occasion the doctor prescribes anything necessary to correct the anomalies found during the full evaluation,” Dr. Carfi, a geriatrician at the Gemelli clinic, said in an interview. “These usually include vitamin supplementation and, in selected cases, a new drug prescription such as a blood thinner if necessary.”
Patients can also enroll in a training program in which breathing status is monitored.
In North America, doctors are also addressing the reality that the road to recovery can be a long and upward one, with persistent symptoms worse than those seen with acute influenza infection. “We see patients who were first diagnosed in March or April and still have symptoms in July,” said Zijian Chen, MD, an endocrinologist and medical director of Mount Sinai Health System’s Center for Post-COVID Care in New York.
“Persistent symptoms are much worse for COVID patients than flu patients. Even flu patients who spent time in the intensive care unit recover fully, and we can optimize their breathing before discharge,” Dr. Chen said in an interview.
As in the Italian study, Dr. Chen sees patients with COVID-19 who have ongoing shortness of breath, some requiring supplemental oxygen, or with persistent chest pain on exertion, blood clotting problems, poor concentration, gastrointestinal distress, and reduced muscle strength and impaired grasping power. He doesn’t rule out permanent lung damage in some. “Even asymptomatic individuals already show lung scarring on imaging,” he said.
The Mount Sinai program provides specialized interdisciplinary management that may include CT scans, endoscopy, and drugs such as respiratory medications or anticoagulants. It also offers training to combat the fatigue and deconditioning caused by the infection, symptoms that are not medically treatable but impact quality of life.
“These patients do get better, but I expect they may still have symptoms requiring monitoring after a year,” Dr. Chen said.
The study received no specific funding. Dr. Carfi and colleagues have disclosed no relevant financial relationships. Dr. Chen has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.