User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Hydroxychloroquine use not linked to increased risks for psychiatric events
Key clinical point: Hydroxychloroquine for the treatment of rheumatoid arthritis (RA) does not increase the risks for depression, suicidality, or psychosis compared with sulfasalazine.
Major finding: Hydroxychloroquine use was not associated with risks for depression, acute psychosis, or suicidality compared with sulfasalazine. The hazard ratios [HRs] for short-term risks for depression, acute psychosis, and suicidality were 0.96 (95% confidence interval [CI], 0.79-1.16), 1.03 (95% CI, 0.66-1.60), and 0.94 (95% CI, 0.49-1.77), respectively. The corresponding HRs for long-term risks were 0.94 (95% CI, 0.71-1.26), 0.99 (95% CI, 0.72-1.35), and 0.77 (95% CI, 0.56-1.07), respectively.
Study details: Findings from a multinational network cohort study of RA patients using hydroxychloroquine (n=918,144) and sulfasalazine (n=290,383).
Disclosures: This study was supported by the National Institute for Health Research Oxford Biomedical Research Centre, US National Institutes of Health, US Department of Veterans Affairs, Janssen Research & Development, IQVIA, the Korea Health Technology, and the Korea Health Industry Development Institute. Some of the authors reported personal funding/support from pharmaceutical companies and/or research organizations.
Source: Lane JCE et al. Rheumatology (Oxford). 2020 Dec 25. doi: 10.1093/rheumatology/keaa771.
Key clinical point: Hydroxychloroquine for the treatment of rheumatoid arthritis (RA) does not increase the risks for depression, suicidality, or psychosis compared with sulfasalazine.
Major finding: Hydroxychloroquine use was not associated with risks for depression, acute psychosis, or suicidality compared with sulfasalazine. The hazard ratios [HRs] for short-term risks for depression, acute psychosis, and suicidality were 0.96 (95% confidence interval [CI], 0.79-1.16), 1.03 (95% CI, 0.66-1.60), and 0.94 (95% CI, 0.49-1.77), respectively. The corresponding HRs for long-term risks were 0.94 (95% CI, 0.71-1.26), 0.99 (95% CI, 0.72-1.35), and 0.77 (95% CI, 0.56-1.07), respectively.
Study details: Findings from a multinational network cohort study of RA patients using hydroxychloroquine (n=918,144) and sulfasalazine (n=290,383).
Disclosures: This study was supported by the National Institute for Health Research Oxford Biomedical Research Centre, US National Institutes of Health, US Department of Veterans Affairs, Janssen Research & Development, IQVIA, the Korea Health Technology, and the Korea Health Industry Development Institute. Some of the authors reported personal funding/support from pharmaceutical companies and/or research organizations.
Source: Lane JCE et al. Rheumatology (Oxford). 2020 Dec 25. doi: 10.1093/rheumatology/keaa771.
Key clinical point: Hydroxychloroquine for the treatment of rheumatoid arthritis (RA) does not increase the risks for depression, suicidality, or psychosis compared with sulfasalazine.
Major finding: Hydroxychloroquine use was not associated with risks for depression, acute psychosis, or suicidality compared with sulfasalazine. The hazard ratios [HRs] for short-term risks for depression, acute psychosis, and suicidality were 0.96 (95% confidence interval [CI], 0.79-1.16), 1.03 (95% CI, 0.66-1.60), and 0.94 (95% CI, 0.49-1.77), respectively. The corresponding HRs for long-term risks were 0.94 (95% CI, 0.71-1.26), 0.99 (95% CI, 0.72-1.35), and 0.77 (95% CI, 0.56-1.07), respectively.
Study details: Findings from a multinational network cohort study of RA patients using hydroxychloroquine (n=918,144) and sulfasalazine (n=290,383).
Disclosures: This study was supported by the National Institute for Health Research Oxford Biomedical Research Centre, US National Institutes of Health, US Department of Veterans Affairs, Janssen Research & Development, IQVIA, the Korea Health Technology, and the Korea Health Industry Development Institute. Some of the authors reported personal funding/support from pharmaceutical companies and/or research organizations.
Source: Lane JCE et al. Rheumatology (Oxford). 2020 Dec 25. doi: 10.1093/rheumatology/keaa771.
Increased risk of RA in patients with endometriosis
Key clinical point: Patients with endometriosis are at a significantly higher risk of developing rheumatoid arthritis (RA).
Major finding: The risk of RA was significantly higher in patients with endometriosis (adjusted hazard ratio [aHR], 1.75; 95% confidence interval [CI], 1.27-2.41), those aged 45 years or older (aHR, 1.50; 95% CI, 1.06-2.13), and those with autoimmune disease (aHR, 6.99; 95% CI, 2.84-17.21).
Study details: This 13-year Taiwanese population-based study included 14,463 women with and 14,463 women without endometriosis who were propensity score-matched by age, comorbidities, corticosteroids, nonsteroidal anti-inflammatory drugs, and hormonal medications.
Disclosures: The study was supported by the Chung Shan Medical University’s DryLab Team and grants awarded to Chung Shan Medical University. The authors declared no conflicts of interest.
Source: Xue YH et al. Rheumatology (Oxford). 2020 Dec 17. doi: 10.1093/rheumatology/keaa784.
Key clinical point: Patients with endometriosis are at a significantly higher risk of developing rheumatoid arthritis (RA).
Major finding: The risk of RA was significantly higher in patients with endometriosis (adjusted hazard ratio [aHR], 1.75; 95% confidence interval [CI], 1.27-2.41), those aged 45 years or older (aHR, 1.50; 95% CI, 1.06-2.13), and those with autoimmune disease (aHR, 6.99; 95% CI, 2.84-17.21).
Study details: This 13-year Taiwanese population-based study included 14,463 women with and 14,463 women without endometriosis who were propensity score-matched by age, comorbidities, corticosteroids, nonsteroidal anti-inflammatory drugs, and hormonal medications.
Disclosures: The study was supported by the Chung Shan Medical University’s DryLab Team and grants awarded to Chung Shan Medical University. The authors declared no conflicts of interest.
Source: Xue YH et al. Rheumatology (Oxford). 2020 Dec 17. doi: 10.1093/rheumatology/keaa784.
Key clinical point: Patients with endometriosis are at a significantly higher risk of developing rheumatoid arthritis (RA).
Major finding: The risk of RA was significantly higher in patients with endometriosis (adjusted hazard ratio [aHR], 1.75; 95% confidence interval [CI], 1.27-2.41), those aged 45 years or older (aHR, 1.50; 95% CI, 1.06-2.13), and those with autoimmune disease (aHR, 6.99; 95% CI, 2.84-17.21).
Study details: This 13-year Taiwanese population-based study included 14,463 women with and 14,463 women without endometriosis who were propensity score-matched by age, comorbidities, corticosteroids, nonsteroidal anti-inflammatory drugs, and hormonal medications.
Disclosures: The study was supported by the Chung Shan Medical University’s DryLab Team and grants awarded to Chung Shan Medical University. The authors declared no conflicts of interest.
Source: Xue YH et al. Rheumatology (Oxford). 2020 Dec 17. doi: 10.1093/rheumatology/keaa784.
Efficacy of filgotinib in patients with RA with limited or no methotrexate exposure
Key clinical point: In patients with active rheumatoid arthritis (RA) who had limited or no prior methotrexate (MTX) exposure, filgotinib (FIL) with MTX reduced signs and symptoms of RA and improved physical function with an acceptable safety profile up to 52 weeks.
Major finding: At week 24, significantly higher proportions of patients receiving FIL200 + MTX (81%; P less than .001) and FIL100 + MTX (80%; P = .017) achieved 20% improvement in American College of Rheumatology criteria (ACR20) vs. MTX (71%). Significant improvements in Health Assessment Questionnaire-Disability Index and 28-joint Disease Activity Score with C-reactive protein less than 2.6 were seen at week 24. Adverse event rates through week 52 were comparable between all treatments.
Study details: In this 52-week phase 3 FINCH 3 trial, 1,252 patients with RA were randomly assigned in a 2:1:1:2 ratio to receive filgotinib 200 mg with MTX (FIL200 + MTX), filgotinib 100 mg with MTX (FIL100+MTX), filgotinib 200 mg monotherapy (FIL200), or MTX.
Disclosures: The study was funded by Gilead Sciences, Inc. The lead author reported receiving grant/research support from and serving as a consultant for Celltrion, Galapagos, and Gilead Sciences.
Source: Westhovens R et al. Ann Rheum Dis. 2021 Jan 15. doi: 10.1136/annrheumdis-2020-219213.
Key clinical point: In patients with active rheumatoid arthritis (RA) who had limited or no prior methotrexate (MTX) exposure, filgotinib (FIL) with MTX reduced signs and symptoms of RA and improved physical function with an acceptable safety profile up to 52 weeks.
Major finding: At week 24, significantly higher proportions of patients receiving FIL200 + MTX (81%; P less than .001) and FIL100 + MTX (80%; P = .017) achieved 20% improvement in American College of Rheumatology criteria (ACR20) vs. MTX (71%). Significant improvements in Health Assessment Questionnaire-Disability Index and 28-joint Disease Activity Score with C-reactive protein less than 2.6 were seen at week 24. Adverse event rates through week 52 were comparable between all treatments.
Study details: In this 52-week phase 3 FINCH 3 trial, 1,252 patients with RA were randomly assigned in a 2:1:1:2 ratio to receive filgotinib 200 mg with MTX (FIL200 + MTX), filgotinib 100 mg with MTX (FIL100+MTX), filgotinib 200 mg monotherapy (FIL200), or MTX.
Disclosures: The study was funded by Gilead Sciences, Inc. The lead author reported receiving grant/research support from and serving as a consultant for Celltrion, Galapagos, and Gilead Sciences.
Source: Westhovens R et al. Ann Rheum Dis. 2021 Jan 15. doi: 10.1136/annrheumdis-2020-219213.
Key clinical point: In patients with active rheumatoid arthritis (RA) who had limited or no prior methotrexate (MTX) exposure, filgotinib (FIL) with MTX reduced signs and symptoms of RA and improved physical function with an acceptable safety profile up to 52 weeks.
Major finding: At week 24, significantly higher proportions of patients receiving FIL200 + MTX (81%; P less than .001) and FIL100 + MTX (80%; P = .017) achieved 20% improvement in American College of Rheumatology criteria (ACR20) vs. MTX (71%). Significant improvements in Health Assessment Questionnaire-Disability Index and 28-joint Disease Activity Score with C-reactive protein less than 2.6 were seen at week 24. Adverse event rates through week 52 were comparable between all treatments.
Study details: In this 52-week phase 3 FINCH 3 trial, 1,252 patients with RA were randomly assigned in a 2:1:1:2 ratio to receive filgotinib 200 mg with MTX (FIL200 + MTX), filgotinib 100 mg with MTX (FIL100+MTX), filgotinib 200 mg monotherapy (FIL200), or MTX.
Disclosures: The study was funded by Gilead Sciences, Inc. The lead author reported receiving grant/research support from and serving as a consultant for Celltrion, Galapagos, and Gilead Sciences.
Source: Westhovens R et al. Ann Rheum Dis. 2021 Jan 15. doi: 10.1136/annrheumdis-2020-219213.
CVD and CV risk factors linked to increased dementia risk in patients with RA
Key clinical point: Cardiovascular (CV) disease (CVD) and CV risk factors were risk factors for incident dementia among rheumatoid arthritis (RA) patients between 65 and 74 years of age; however, this risk attenuated with increasing age.
Major finding: Patients with CVD and CV risk factors between 65 and 74 years of age had an increased risk for dementia vs. those without CVD and CV risk factors (adjusted hazard Ratio [aHR], 1.18; 95% confidence interval [CI], 1.04-1.33; aHR, 1.03; 95% CI, 1.00-1.11, respectively). For patients between 75 and 84 years of age, a trend toward an increased risk of dementia was observed with CVD but was not statistically significant (aHR, 1.03; 95% CI, 0.92-1.14). These associations were not observed among patients aged 85 years and older.
Study details: Longitudinal analysis of 56,567 patients with RA using Center for Medicare & Medicaid claims (CMS) data from 2006 to 2014; 11,789 (20.1%) incident cases of dementia were included in the analysis.
Disclosures: The study was supported by I Navarro-Millan’s IPCI award from Weill Cornell Medicine Division of General Internal Medicine. JR Curtis received research support and consulting fees from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Pfizer, Regeneron, Roche, and UCB. SB Lieber reported spousal ownership interests in Cigna, Intuitive Surgical, Inc., Merck, and Pfizer. I Navarro-Millán received consulting fees from Sobi. The remaining authors declared no conflicts of interest.
Source: Sattui SE et al. Semin Arthritis Rheum. 2021 Jan 5. doi: 10.1016/j.semarthrit.2020.09.022.
Key clinical point: Cardiovascular (CV) disease (CVD) and CV risk factors were risk factors for incident dementia among rheumatoid arthritis (RA) patients between 65 and 74 years of age; however, this risk attenuated with increasing age.
Major finding: Patients with CVD and CV risk factors between 65 and 74 years of age had an increased risk for dementia vs. those without CVD and CV risk factors (adjusted hazard Ratio [aHR], 1.18; 95% confidence interval [CI], 1.04-1.33; aHR, 1.03; 95% CI, 1.00-1.11, respectively). For patients between 75 and 84 years of age, a trend toward an increased risk of dementia was observed with CVD but was not statistically significant (aHR, 1.03; 95% CI, 0.92-1.14). These associations were not observed among patients aged 85 years and older.
Study details: Longitudinal analysis of 56,567 patients with RA using Center for Medicare & Medicaid claims (CMS) data from 2006 to 2014; 11,789 (20.1%) incident cases of dementia were included in the analysis.
Disclosures: The study was supported by I Navarro-Millan’s IPCI award from Weill Cornell Medicine Division of General Internal Medicine. JR Curtis received research support and consulting fees from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Pfizer, Regeneron, Roche, and UCB. SB Lieber reported spousal ownership interests in Cigna, Intuitive Surgical, Inc., Merck, and Pfizer. I Navarro-Millán received consulting fees from Sobi. The remaining authors declared no conflicts of interest.
Source: Sattui SE et al. Semin Arthritis Rheum. 2021 Jan 5. doi: 10.1016/j.semarthrit.2020.09.022.
Key clinical point: Cardiovascular (CV) disease (CVD) and CV risk factors were risk factors for incident dementia among rheumatoid arthritis (RA) patients between 65 and 74 years of age; however, this risk attenuated with increasing age.
Major finding: Patients with CVD and CV risk factors between 65 and 74 years of age had an increased risk for dementia vs. those without CVD and CV risk factors (adjusted hazard Ratio [aHR], 1.18; 95% confidence interval [CI], 1.04-1.33; aHR, 1.03; 95% CI, 1.00-1.11, respectively). For patients between 75 and 84 years of age, a trend toward an increased risk of dementia was observed with CVD but was not statistically significant (aHR, 1.03; 95% CI, 0.92-1.14). These associations were not observed among patients aged 85 years and older.
Study details: Longitudinal analysis of 56,567 patients with RA using Center for Medicare & Medicaid claims (CMS) data from 2006 to 2014; 11,789 (20.1%) incident cases of dementia were included in the analysis.
Disclosures: The study was supported by I Navarro-Millan’s IPCI award from Weill Cornell Medicine Division of General Internal Medicine. JR Curtis received research support and consulting fees from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Pfizer, Regeneron, Roche, and UCB. SB Lieber reported spousal ownership interests in Cigna, Intuitive Surgical, Inc., Merck, and Pfizer. I Navarro-Millán received consulting fees from Sobi. The remaining authors declared no conflicts of interest.
Source: Sattui SE et al. Semin Arthritis Rheum. 2021 Jan 5. doi: 10.1016/j.semarthrit.2020.09.022.
Elevated disease activity, cytokine levels linked to diabetes risk in RA
Key clinical point: Higher disease activity and elevated levels of cytokines/chemokines are associated with a greater risk of diabetes mellitus (DM) in patients with rheumatoid arthritis (RA).
Major finding: High Disease activity Score (DAS28)-C reactive protein (CRP) was associated with an increased risk of DM (test for trend: P less than .001). Several cytokines/chemokines analyzed showed independent association with DM risk including interleukin (IL)-1, IL-6, and select macrophage-derived cytokines/chemokines (hazard ratio per standard deviation range, 1.11-1.26). These associations were independent of the DAS28-CRP.
Study details: This longitudinal analysis included 1,866 patients with RA without prevalent DM from Veteran’s Affairs Rheumatoid Arthritis Registry. Thirty cytokines and chemokines were measured in banked serum obtained at the time of enrolment.
Disclosures: No study sponsor was identified. The presenting author has received consulting fees from Bristol-Myers Squibb and Gilead.
Source: Baker JF. Ann Rheum Dis. 2021 Jan 4. doi: 10.1136/annrheumdis-2020-219140
Key clinical point: Higher disease activity and elevated levels of cytokines/chemokines are associated with a greater risk of diabetes mellitus (DM) in patients with rheumatoid arthritis (RA).
Major finding: High Disease activity Score (DAS28)-C reactive protein (CRP) was associated with an increased risk of DM (test for trend: P less than .001). Several cytokines/chemokines analyzed showed independent association with DM risk including interleukin (IL)-1, IL-6, and select macrophage-derived cytokines/chemokines (hazard ratio per standard deviation range, 1.11-1.26). These associations were independent of the DAS28-CRP.
Study details: This longitudinal analysis included 1,866 patients with RA without prevalent DM from Veteran’s Affairs Rheumatoid Arthritis Registry. Thirty cytokines and chemokines were measured in banked serum obtained at the time of enrolment.
Disclosures: No study sponsor was identified. The presenting author has received consulting fees from Bristol-Myers Squibb and Gilead.
Source: Baker JF. Ann Rheum Dis. 2021 Jan 4. doi: 10.1136/annrheumdis-2020-219140
Key clinical point: Higher disease activity and elevated levels of cytokines/chemokines are associated with a greater risk of diabetes mellitus (DM) in patients with rheumatoid arthritis (RA).
Major finding: High Disease activity Score (DAS28)-C reactive protein (CRP) was associated with an increased risk of DM (test for trend: P less than .001). Several cytokines/chemokines analyzed showed independent association with DM risk including interleukin (IL)-1, IL-6, and select macrophage-derived cytokines/chemokines (hazard ratio per standard deviation range, 1.11-1.26). These associations were independent of the DAS28-CRP.
Study details: This longitudinal analysis included 1,866 patients with RA without prevalent DM from Veteran’s Affairs Rheumatoid Arthritis Registry. Thirty cytokines and chemokines were measured in banked serum obtained at the time of enrolment.
Disclosures: No study sponsor was identified. The presenting author has received consulting fees from Bristol-Myers Squibb and Gilead.
Source: Baker JF. Ann Rheum Dis. 2021 Jan 4. doi: 10.1136/annrheumdis-2020-219140
Hydroxychloroquine use not linked to heart failure risk in patients with RA
Key clinical point: Use of hydroxychloroquine (HCQ) is not associated with increased risk of developing heart failure (HF) in patients with rheumatoid arthritis (RA).
Major finding: HCQ cumulative dose was not associated with HF (odds ratio [OR], 0.96 [95% confidence interval (CI), 0.90-1.03] per 100 g). No statistically significant association was found for patients with a cumulative dose of 300 g or more (OR, 0.92; 95% CI, 0.41-2.08). Duration of HCQ use prior to index was not associated with HF (OR, 0.98; 95% CI, 0.91-1.05).
Study details: The data come from a nested case-control study of 143 RA cases diagnosed with HF and 143 non-HF RA controls.
Disclosures: The study was funded by grants from the National Institutes of Health. The authors declared no conflicts of interest.
Source: Sorour AA et al. J Rheumatol. 2021 Jan 15. doi: 10.3899/jrheum.201180
Key clinical point: Use of hydroxychloroquine (HCQ) is not associated with increased risk of developing heart failure (HF) in patients with rheumatoid arthritis (RA).
Major finding: HCQ cumulative dose was not associated with HF (odds ratio [OR], 0.96 [95% confidence interval (CI), 0.90-1.03] per 100 g). No statistically significant association was found for patients with a cumulative dose of 300 g or more (OR, 0.92; 95% CI, 0.41-2.08). Duration of HCQ use prior to index was not associated with HF (OR, 0.98; 95% CI, 0.91-1.05).
Study details: The data come from a nested case-control study of 143 RA cases diagnosed with HF and 143 non-HF RA controls.
Disclosures: The study was funded by grants from the National Institutes of Health. The authors declared no conflicts of interest.
Source: Sorour AA et al. J Rheumatol. 2021 Jan 15. doi: 10.3899/jrheum.201180
Key clinical point: Use of hydroxychloroquine (HCQ) is not associated with increased risk of developing heart failure (HF) in patients with rheumatoid arthritis (RA).
Major finding: HCQ cumulative dose was not associated with HF (odds ratio [OR], 0.96 [95% confidence interval (CI), 0.90-1.03] per 100 g). No statistically significant association was found for patients with a cumulative dose of 300 g or more (OR, 0.92; 95% CI, 0.41-2.08). Duration of HCQ use prior to index was not associated with HF (OR, 0.98; 95% CI, 0.91-1.05).
Study details: The data come from a nested case-control study of 143 RA cases diagnosed with HF and 143 non-HF RA controls.
Disclosures: The study was funded by grants from the National Institutes of Health. The authors declared no conflicts of interest.
Source: Sorour AA et al. J Rheumatol. 2021 Jan 15. doi: 10.3899/jrheum.201180
Maternal autoimmune disease raises children’s risk of ADHD
Maternal autoimmune diseases significantly increased the risk of ADHD in children, based on data from a large cohort study of more than 800,000 mothers and children and a subsequent meta-analysis.
“There is growing evidence that immune-related cells and proteins play a role in brain development and function and that maternal immune activation, including infection, autoimmune disease, and chronic inflammation during pregnancy, increases the risk of neurodevelopmental disorders among children,” wrote Timothy C. Nielsen, MPH, of the University of Sydney, and colleagues.
Previous research has examined a link between maternal autoimmune disorders and autism spectrum disorders in children, but associations with ADHD have not been well studied, they said.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 831,718 mothers and their 831,718 singleton infants in Australia. A total of 12,787 infants were born to mothers with an autoimmune diagnosis; 12,610 of them were matched to 50,440 control infants. ADHD was determined based on prescription for a stimulant treatment or a hospital diagnosis; children with a first ADHD event younger than 3 years were excluded.
In the total cohort of 63,050 infants, the presence of any maternal autoimmune disease was associated with a significantly increased risk of ADHD (hazard ratio, 1.30) as was the presence of several specific conditions: type 1 diabetes (HR, 2.23), psoriasis (HR, 1.66), and rheumatic fever or rheumatic carditis (HR, 1.75).
In addition, the researchers conducted a meta-analysis of the current study and four additional studies that yielded similar results. In the meta-analysis, the risk of ADHD was significantly associated with any maternal autoimmune disease in two studies (HR, 1.20); with maternal type 1 diabetes in four studies (HR, 1.53); with maternal hyperthyroidism in three studies (HR 1.15); and with maternal psoriasis in two studies (HR, 1.31).
Type 1 diabetes (T1D) had the highest HR and was the most often studied condition. However, “the observed association may also be related to nonimmune aspects of T1D, such as glycemic control, as nonautoimmune diabetes has been associated with ADHD among children,” the researchers wrote.
The study findings were limited by several factors, including the lack of outpatient and primary care records to identify maternal autoimmune disease, and lack of data on any medication used to managed diseases during pregnancy, as well as a lack of data on children with ADHD who might not have been treated with medication, the researchers noted. In addition, “given differences in study design and definitions, the pooled HRs presented in the meta-analysis need to be treated cautiously.”
However, the results were strengthened by the hybrid study design and large study population, and were generally consistent with previous research supporting an effect of maternal immune function on fetal neurodevelopment, they noted.
“Our study provides justification for future studies that examine the effect of maternal autoimmune diseases, including biomarkers, condition severity, and management in pregnancy and in the periconception period, on neurodevelopmental disorders in children,” they concluded.
Studies need to explore mechanism of action
The current study, with its hybrid design, adds support to the evidence of an association between any maternal autoimmune disease and ADHD in children, as well as an association between the specific conditions of type 1 diabetes, hyperthyroidism, and psoriasis in mothers and ADHD in children, Søren Dalsgaard, MD, of Aarhus (Denmark) University, wrote in an accompanying editorial.
“Importantly, Nielsen et al. emphasized in their article that, for the many different autoimmune diseases, different underlying mechanisms for the associations with disorders of the central nervous system were likely. They mentioned that, for T1D, low glycemic control may play a role, as type 2 diabetes has been associated with ADHD,” said Dr. Dalsgaard.
“Overall, these mechanisms are thought to include shared genetic and environmental risk factors or direct effects of maternal autoantibodies or cytokines crossing the placenta and altering the fetal immune response, which in turns leads to changes in the central nervous system,” Dr. Dalsgaard explained. However, the current study and previous studies have not identified the mechanisms to explain the association between ADHD in children and maternal autoimmune disease.
“To understand more about these associations, future studies should include researchers and data from different scientific disciplines, such as epidemiology, animal modeling, genetics, and neuroimmunology,” he concluded.
Association is not causality
Overall, the study findings add to the evidence of a correlation between autoimmune diseases and neurologic disease, said Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., in an interview. “Anything that might contribute to behavioral problems is worth investigating.” However, it is important to remember that association is not causation.

“There is some literature and evidence that autoimmune disease is associated with mental health issues, but the mechanisms of action are unknown,” said Dr. Lessin. ADHD is highly heritable, so the association may be caused by a similar genetic predisposition, or it may be something related to autoimmunity that is impacting the fetus by passing through the placenta.
The current study’s strengths include the large size and hybrid design, but limitations such as the identification of ADHD based on medication prescriptions may have led to underreporting, and identifying maternal autoimmune disease via inpatient hospital diagnosis could have selected for more severe disease, he said.
From a clinical standpoint, the study suggests a correlation that should be noted in a family history and potentially used to inform a diagnosis, especially in cases of type 1 diabetes where the association was strongest, Dr. Lessin said. The findings also support the value of further research to look for mechanisms that might explain whether the association between autoimmune disease and ADHD is autoimmune system causality or shared genetic susceptibility.
The study received no outside funding. One coauthor disclosed receiving grants from the National Blood Authority Australia and the Australian National Health and Medical Research Council during the conduct of the study. Dr. Dalsgaard had no financial conflicts to disclose. Dr. Lessin disclosed serving as editor of the ADHD toolkit for the American Academy of Pediatrics and coauthor of the current ADHD clinical guidelines. He also serves in advisory capacity to Cognoa, a company involved in diagnosis of autism, and Corium/KemPharm, companies involved in the development of ADHD treatments.
Maternal autoimmune diseases significantly increased the risk of ADHD in children, based on data from a large cohort study of more than 800,000 mothers and children and a subsequent meta-analysis.
“There is growing evidence that immune-related cells and proteins play a role in brain development and function and that maternal immune activation, including infection, autoimmune disease, and chronic inflammation during pregnancy, increases the risk of neurodevelopmental disorders among children,” wrote Timothy C. Nielsen, MPH, of the University of Sydney, and colleagues.
Previous research has examined a link between maternal autoimmune disorders and autism spectrum disorders in children, but associations with ADHD have not been well studied, they said.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 831,718 mothers and their 831,718 singleton infants in Australia. A total of 12,787 infants were born to mothers with an autoimmune diagnosis; 12,610 of them were matched to 50,440 control infants. ADHD was determined based on prescription for a stimulant treatment or a hospital diagnosis; children with a first ADHD event younger than 3 years were excluded.
In the total cohort of 63,050 infants, the presence of any maternal autoimmune disease was associated with a significantly increased risk of ADHD (hazard ratio, 1.30) as was the presence of several specific conditions: type 1 diabetes (HR, 2.23), psoriasis (HR, 1.66), and rheumatic fever or rheumatic carditis (HR, 1.75).
In addition, the researchers conducted a meta-analysis of the current study and four additional studies that yielded similar results. In the meta-analysis, the risk of ADHD was significantly associated with any maternal autoimmune disease in two studies (HR, 1.20); with maternal type 1 diabetes in four studies (HR, 1.53); with maternal hyperthyroidism in three studies (HR 1.15); and with maternal psoriasis in two studies (HR, 1.31).
Type 1 diabetes (T1D) had the highest HR and was the most often studied condition. However, “the observed association may also be related to nonimmune aspects of T1D, such as glycemic control, as nonautoimmune diabetes has been associated with ADHD among children,” the researchers wrote.
The study findings were limited by several factors, including the lack of outpatient and primary care records to identify maternal autoimmune disease, and lack of data on any medication used to managed diseases during pregnancy, as well as a lack of data on children with ADHD who might not have been treated with medication, the researchers noted. In addition, “given differences in study design and definitions, the pooled HRs presented in the meta-analysis need to be treated cautiously.”
However, the results were strengthened by the hybrid study design and large study population, and were generally consistent with previous research supporting an effect of maternal immune function on fetal neurodevelopment, they noted.
“Our study provides justification for future studies that examine the effect of maternal autoimmune diseases, including biomarkers, condition severity, and management in pregnancy and in the periconception period, on neurodevelopmental disorders in children,” they concluded.
Studies need to explore mechanism of action
The current study, with its hybrid design, adds support to the evidence of an association between any maternal autoimmune disease and ADHD in children, as well as an association between the specific conditions of type 1 diabetes, hyperthyroidism, and psoriasis in mothers and ADHD in children, Søren Dalsgaard, MD, of Aarhus (Denmark) University, wrote in an accompanying editorial.
“Importantly, Nielsen et al. emphasized in their article that, for the many different autoimmune diseases, different underlying mechanisms for the associations with disorders of the central nervous system were likely. They mentioned that, for T1D, low glycemic control may play a role, as type 2 diabetes has been associated with ADHD,” said Dr. Dalsgaard.
“Overall, these mechanisms are thought to include shared genetic and environmental risk factors or direct effects of maternal autoantibodies or cytokines crossing the placenta and altering the fetal immune response, which in turns leads to changes in the central nervous system,” Dr. Dalsgaard explained. However, the current study and previous studies have not identified the mechanisms to explain the association between ADHD in children and maternal autoimmune disease.
“To understand more about these associations, future studies should include researchers and data from different scientific disciplines, such as epidemiology, animal modeling, genetics, and neuroimmunology,” he concluded.
Association is not causality
Overall, the study findings add to the evidence of a correlation between autoimmune diseases and neurologic disease, said Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., in an interview. “Anything that might contribute to behavioral problems is worth investigating.” However, it is important to remember that association is not causation.
“There is some literature and evidence that autoimmune disease is associated with mental health issues, but the mechanisms of action are unknown,” said Dr. Lessin. ADHD is highly heritable, so the association may be caused by a similar genetic predisposition, or it may be something related to autoimmunity that is impacting the fetus by passing through the placenta.
The current study’s strengths include the large size and hybrid design, but limitations such as the identification of ADHD based on medication prescriptions may have led to underreporting, and identifying maternal autoimmune disease via inpatient hospital diagnosis could have selected for more severe disease, he said.
From a clinical standpoint, the study suggests a correlation that should be noted in a family history and potentially used to inform a diagnosis, especially in cases of type 1 diabetes where the association was strongest, Dr. Lessin said. The findings also support the value of further research to look for mechanisms that might explain whether the association between autoimmune disease and ADHD is autoimmune system causality or shared genetic susceptibility.
The study received no outside funding. One coauthor disclosed receiving grants from the National Blood Authority Australia and the Australian National Health and Medical Research Council during the conduct of the study. Dr. Dalsgaard had no financial conflicts to disclose. Dr. Lessin disclosed serving as editor of the ADHD toolkit for the American Academy of Pediatrics and coauthor of the current ADHD clinical guidelines. He also serves in advisory capacity to Cognoa, a company involved in diagnosis of autism, and Corium/KemPharm, companies involved in the development of ADHD treatments.
Maternal autoimmune diseases significantly increased the risk of ADHD in children, based on data from a large cohort study of more than 800,000 mothers and children and a subsequent meta-analysis.
“There is growing evidence that immune-related cells and proteins play a role in brain development and function and that maternal immune activation, including infection, autoimmune disease, and chronic inflammation during pregnancy, increases the risk of neurodevelopmental disorders among children,” wrote Timothy C. Nielsen, MPH, of the University of Sydney, and colleagues.
Previous research has examined a link between maternal autoimmune disorders and autism spectrum disorders in children, but associations with ADHD have not been well studied, they said.
In a population-based cohort study published in JAMA Pediatrics, the researchers identified 831,718 mothers and their 831,718 singleton infants in Australia. A total of 12,787 infants were born to mothers with an autoimmune diagnosis; 12,610 of them were matched to 50,440 control infants. ADHD was determined based on prescription for a stimulant treatment or a hospital diagnosis; children with a first ADHD event younger than 3 years were excluded.
In the total cohort of 63,050 infants, the presence of any maternal autoimmune disease was associated with a significantly increased risk of ADHD (hazard ratio, 1.30) as was the presence of several specific conditions: type 1 diabetes (HR, 2.23), psoriasis (HR, 1.66), and rheumatic fever or rheumatic carditis (HR, 1.75).
In addition, the researchers conducted a meta-analysis of the current study and four additional studies that yielded similar results. In the meta-analysis, the risk of ADHD was significantly associated with any maternal autoimmune disease in two studies (HR, 1.20); with maternal type 1 diabetes in four studies (HR, 1.53); with maternal hyperthyroidism in three studies (HR 1.15); and with maternal psoriasis in two studies (HR, 1.31).
Type 1 diabetes (T1D) had the highest HR and was the most often studied condition. However, “the observed association may also be related to nonimmune aspects of T1D, such as glycemic control, as nonautoimmune diabetes has been associated with ADHD among children,” the researchers wrote.
The study findings were limited by several factors, including the lack of outpatient and primary care records to identify maternal autoimmune disease, and lack of data on any medication used to managed diseases during pregnancy, as well as a lack of data on children with ADHD who might not have been treated with medication, the researchers noted. In addition, “given differences in study design and definitions, the pooled HRs presented in the meta-analysis need to be treated cautiously.”
However, the results were strengthened by the hybrid study design and large study population, and were generally consistent with previous research supporting an effect of maternal immune function on fetal neurodevelopment, they noted.
“Our study provides justification for future studies that examine the effect of maternal autoimmune diseases, including biomarkers, condition severity, and management in pregnancy and in the periconception period, on neurodevelopmental disorders in children,” they concluded.
Studies need to explore mechanism of action
The current study, with its hybrid design, adds support to the evidence of an association between any maternal autoimmune disease and ADHD in children, as well as an association between the specific conditions of type 1 diabetes, hyperthyroidism, and psoriasis in mothers and ADHD in children, Søren Dalsgaard, MD, of Aarhus (Denmark) University, wrote in an accompanying editorial.
“Importantly, Nielsen et al. emphasized in their article that, for the many different autoimmune diseases, different underlying mechanisms for the associations with disorders of the central nervous system were likely. They mentioned that, for T1D, low glycemic control may play a role, as type 2 diabetes has been associated with ADHD,” said Dr. Dalsgaard.
“Overall, these mechanisms are thought to include shared genetic and environmental risk factors or direct effects of maternal autoantibodies or cytokines crossing the placenta and altering the fetal immune response, which in turns leads to changes in the central nervous system,” Dr. Dalsgaard explained. However, the current study and previous studies have not identified the mechanisms to explain the association between ADHD in children and maternal autoimmune disease.
“To understand more about these associations, future studies should include researchers and data from different scientific disciplines, such as epidemiology, animal modeling, genetics, and neuroimmunology,” he concluded.
Association is not causality
Overall, the study findings add to the evidence of a correlation between autoimmune diseases and neurologic disease, said Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., in an interview. “Anything that might contribute to behavioral problems is worth investigating.” However, it is important to remember that association is not causation.
“There is some literature and evidence that autoimmune disease is associated with mental health issues, but the mechanisms of action are unknown,” said Dr. Lessin. ADHD is highly heritable, so the association may be caused by a similar genetic predisposition, or it may be something related to autoimmunity that is impacting the fetus by passing through the placenta.
The current study’s strengths include the large size and hybrid design, but limitations such as the identification of ADHD based on medication prescriptions may have led to underreporting, and identifying maternal autoimmune disease via inpatient hospital diagnosis could have selected for more severe disease, he said.
From a clinical standpoint, the study suggests a correlation that should be noted in a family history and potentially used to inform a diagnosis, especially in cases of type 1 diabetes where the association was strongest, Dr. Lessin said. The findings also support the value of further research to look for mechanisms that might explain whether the association between autoimmune disease and ADHD is autoimmune system causality or shared genetic susceptibility.
The study received no outside funding. One coauthor disclosed receiving grants from the National Blood Authority Australia and the Australian National Health and Medical Research Council during the conduct of the study. Dr. Dalsgaard had no financial conflicts to disclose. Dr. Lessin disclosed serving as editor of the ADHD toolkit for the American Academy of Pediatrics and coauthor of the current ADHD clinical guidelines. He also serves in advisory capacity to Cognoa, a company involved in diagnosis of autism, and Corium/KemPharm, companies involved in the development of ADHD treatments.
FROM JAMA PEDIATRICS
Meta-analysis finds much less lupus than expected
The prevalence of systemic lupus erythematosus (SLE) appears to be much lower than previously believed and may pose “a potential risk to research funding for the disease,” according to results of a meta-analysis involving a network of population-based registries.
“When we started this study, a widely cited lupus statistic was that approximately 1.5 million Americans were affected. Our meta-analysis found the actual prevalence to be slightly more than 200,000: a number that approaches the [Food and Drug Administration’s] definition of a rare disease,” Emily Somers, PhD, ScM, senior author and associate professor of rheumatology and environmental health sciences at the University of Michigan, Ann Arbor, said in a written statement.
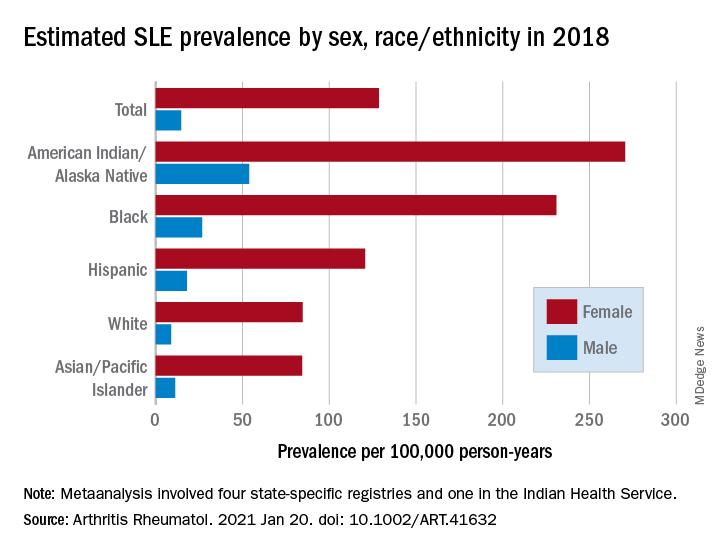
Their estimates, published online in Arthritis & Rheumatology, put the overall SLE prevalence in the United States at 72.8 per 100,000 person-years in 2018, with nearly nine times more females affected (128.7 cases per 100,000) than males (14.6 per 100,000). Race and ethnicity also play a role, as prevalence was highest among American Indian/Alaska Native and Black females, with Hispanic females lower but still higher than White and Asian/Pacific Islander females, Peter M. Izmirly, MD, MSc, of New York University, the lead author, and associates said.
SLE prevalence was distributed similarly in men, although there was a greater relative margin between American Indians/Alaska Natives (53.8 cases per 100,000 person-years) and Blacks (26.7 per 100,000), and Asians/Pacific Islanders were higher than Whites (11.2 vs. 8.9), the investigators reported.
The meta-analysis leveraged data from the Centers for Disease Control and Prevention’s national lupus registries, which include four state-specific SLE registries and a fifth in the Indian Health Service. All cases of SLE occurred in 2002-2009, and the data were age adjusted to the 2000 U.S. population and separately extrapolated to the 2018 U.S. Census population, they explained.
The analysis was funded by cooperative agreements between the New York City Department of Health and Mental Hygiene and New York University, and the CDC and National Institute of Health.
The prevalence of systemic lupus erythematosus (SLE) appears to be much lower than previously believed and may pose “a potential risk to research funding for the disease,” according to results of a meta-analysis involving a network of population-based registries.
“When we started this study, a widely cited lupus statistic was that approximately 1.5 million Americans were affected. Our meta-analysis found the actual prevalence to be slightly more than 200,000: a number that approaches the [Food and Drug Administration’s] definition of a rare disease,” Emily Somers, PhD, ScM, senior author and associate professor of rheumatology and environmental health sciences at the University of Michigan, Ann Arbor, said in a written statement.
Their estimates, published online in Arthritis & Rheumatology, put the overall SLE prevalence in the United States at 72.8 per 100,000 person-years in 2018, with nearly nine times more females affected (128.7 cases per 100,000) than males (14.6 per 100,000). Race and ethnicity also play a role, as prevalence was highest among American Indian/Alaska Native and Black females, with Hispanic females lower but still higher than White and Asian/Pacific Islander females, Peter M. Izmirly, MD, MSc, of New York University, the lead author, and associates said.
SLE prevalence was distributed similarly in men, although there was a greater relative margin between American Indians/Alaska Natives (53.8 cases per 100,000 person-years) and Blacks (26.7 per 100,000), and Asians/Pacific Islanders were higher than Whites (11.2 vs. 8.9), the investigators reported.
The meta-analysis leveraged data from the Centers for Disease Control and Prevention’s national lupus registries, which include four state-specific SLE registries and a fifth in the Indian Health Service. All cases of SLE occurred in 2002-2009, and the data were age adjusted to the 2000 U.S. population and separately extrapolated to the 2018 U.S. Census population, they explained.
The analysis was funded by cooperative agreements between the New York City Department of Health and Mental Hygiene and New York University, and the CDC and National Institute of Health.
The prevalence of systemic lupus erythematosus (SLE) appears to be much lower than previously believed and may pose “a potential risk to research funding for the disease,” according to results of a meta-analysis involving a network of population-based registries.
“When we started this study, a widely cited lupus statistic was that approximately 1.5 million Americans were affected. Our meta-analysis found the actual prevalence to be slightly more than 200,000: a number that approaches the [Food and Drug Administration’s] definition of a rare disease,” Emily Somers, PhD, ScM, senior author and associate professor of rheumatology and environmental health sciences at the University of Michigan, Ann Arbor, said in a written statement.
Their estimates, published online in Arthritis & Rheumatology, put the overall SLE prevalence in the United States at 72.8 per 100,000 person-years in 2018, with nearly nine times more females affected (128.7 cases per 100,000) than males (14.6 per 100,000). Race and ethnicity also play a role, as prevalence was highest among American Indian/Alaska Native and Black females, with Hispanic females lower but still higher than White and Asian/Pacific Islander females, Peter M. Izmirly, MD, MSc, of New York University, the lead author, and associates said.
SLE prevalence was distributed similarly in men, although there was a greater relative margin between American Indians/Alaska Natives (53.8 cases per 100,000 person-years) and Blacks (26.7 per 100,000), and Asians/Pacific Islanders were higher than Whites (11.2 vs. 8.9), the investigators reported.
The meta-analysis leveraged data from the Centers for Disease Control and Prevention’s national lupus registries, which include four state-specific SLE registries and a fifth in the Indian Health Service. All cases of SLE occurred in 2002-2009, and the data were age adjusted to the 2000 U.S. population and separately extrapolated to the 2018 U.S. Census population, they explained.
The analysis was funded by cooperative agreements between the New York City Department of Health and Mental Hygiene and New York University, and the CDC and National Institute of Health.
FROM ARTHRITIS & RHEUMATOLOGY
Can the U.S. keep COVID-19 variants in check? Here’s what it takes
The COVID-19 variants that have emerged in the United Kingdom, Brazil, South Africa and now Southern California are eliciting two notably distinct responses from U.S. public health officials.

First, broad concern. A variant that wreaked havoc in the United Kingdom, leading to a spike in cases and hospitalizations, is surfacing in a growing number of places in the United States. During the week of Jan. 24, another worrisome variant seen in Brazil surfaced in Minnesota. If these or other strains significantly change the way the virus transmits and attacks the body, as scientists fear they might, they could cause yet another prolonged surge in illness and death in the U.S., even as cases have begun to plateau and vaccines are rolling out.
On the other hand, variants aren’t novel or even uncommon in viral illnesses. The viruses that trigger common colds and flus regularly evolve. Even if a mutated strain of SARS-CoV-2, the virus that causes COVID-19, makes it more contagious or makes people sicker,
The problem is that the U.S. has struggled with every step of its public health response in its first year of battle against COVID-19. And that raises the question of whether the nation will devote the attention and resources needed to outflank the virus as it evolves.
Researchers are quick to stress that a coronavirus mutation in itself is no cause for alarm. In the course of making millions and billions of copies as part of the infection process, small changes to a virus’s genome happen all the time as a function of evolutionary biology.
“The word ‘variant’ and the word ‘mutation’ have these scary connotations, and they aren’t necessarily scary,” said Kelly Wroblewski, director of infectious disease programs for the Association of Public Health Laboratories.
When a mutation rings public health alarms, it’s typically because it has combined with other mutations and, collectively, changed how the virus behaves. At that point, it may be named a variant. A variant can make a virus spread faster, or more easily jump between species. It can make a virus more successful at making people sicker, or change how our immune systems respond.
SARS-CoV-2 has been mutating for as long as we’ve known about it; mutations were identified by scientists throughout 2020. Though relevant scientifically – mutations can actually be helpful, acting like a fingerprint that allows scientists to track a virus’s spread – the identified strains mostly carried little concern for public health.
Then came the end of the year, when several variants began drawing scrutiny. One of the most concerning, first detected in the United Kingdom, appears to make the virus more transmissible. Emerging evidence suggests it also could be deadlier, though scientists are still debating that.
We know more about the U.K. variant than others not because it’s necessarily worse, but because the British have one of the best virus surveillance programs in the world, said William Hanage, PhD, an epidemiologist and a professor at Harvard University.
By contrast, the U.S. has one of the weakest genomic surveillance programs of any rich country, Dr. Hanage said. “As it is, people like me cobble together partnerships with places and try and beg them” for samples, he said on a recent call with reporters.
Other variant strains were identified in South Africa and Brazil, and they share some mutations with the U.K. variant. That those changes evolved independently in several parts of the world suggests they might present an evolutionary advantage for the virus. Yet another strain was recently identified in Southern California and flagged due to its increasing presence in hard-hit cities like Los Angeles.
The Southern California strain was detected because a team of researchers at Cedars-Sinai, a hospital and research center in Los Angeles, has unfettered access to patient samples. They were able to see that the strain made up a growing share of cases at the hospital in recent weeks, as well as among the limited number of other samples haphazardly collected at a network of labs in the region.
Not only does the U.S. do less genomic sequencing than most wealthy countries, but it also does its surveillance by happenstance. That means it takes longer to detect new strains and draw conclusions about them. It’s not yet clear, for example, whether that Southern California strain was truly worthy of a press release.
Vast swaths of America’s privatized and decentralized system of health care aren’t set up to send samples to public health or academic labs. “I’m more concerned about the systems to detect variants than I am these particular variants,” said Mark Pandori, PhD, director of Nevada’s public health laboratory and associate professor at the University of Nevada-Reno School of Medicine.
Limited genomic surveillance of viruses is yet another side effect of a fragmented and underfunded public health system that’s struggled to test, track contacts and get COVID-19 under control throughout the pandemic, Ms. Wroblewski said.
The nation’s public health infrastructure, generally funded on a disease-by-disease basis, has decent systems set up to sequence flu, foodborne illnesses and tuberculosis, but there has been no national strategy on COVID-19. “To look for variants, it needs to be a national picture if it’s going to be done well,” Ms. Wroblewski said.
The Biden administration has outlined a strategy for a national response to COVID-19, which includes expanded surveillance for variants.
So far, vaccines for COVID-19 appear to protect against the known variants. Moderna has said its vaccine is effective against the U.K. and South African strains, though it yields fewer antibodies in the face of the latter. The company is working to develop a revised dose of the vaccine that could be added to the current two-shot regimen as a precaution.
But a lot of damage can be done in the time it will take to roll out the current vaccine, let alone an update.
Even with limited sampling, the U.K. variant has been detected in more than two dozen U.S. states, and the Centers for Disease Control and Prevention has warned it could be the predominant strain in the U.S. by March. When it took off in the United Kingdom at the end of last year, it caused a swell in cases, overwhelmed hospitals, and led to a holiday lockdown. Whether the U.S. faces the same fate could depend on which strains it is competing against, and how the public behaves in the weeks ahead.
Already risky interactions among people could, on average, get a little riskier. Many researchers are calling for better masks and better indoor ventilation. But any updates on recommendations likely would play at the margins. Even if variants spread more easily, the same recommendations public health experts have been espousing for months – masking, physical distancing, and limiting time indoors with others – will be the best way to ward them off, said Kirsten Bibbins-Domingo, MD, a physician and professor at the University of California, San Francisco.
“It’s very unsexy what the solutions are,” Dr. Bibbins-Domingo said. “But we need everyone to do them.”
That doesn’t make the task simple. Masking remains controversial in many states, and the public’s patience for maintaining physical distance has worn thin.
Adding to the concerns: Though case numbers stabilized in many parts of the U.S. in January, they have stabilized at rates many times what they were during previous periods in the pandemic or in other parts of the world. Having all that virus in so many bodies creates more opportunities for new mutations and new variants to emerge.
“If we keep letting this thing sneak around, it’s going to get around all the measures we take against it, and that’s the worst possible thing,” said Nevada’s Dr. Pandori.
Compared with less virulent strains, a more contagious variant likely will require that more people be vaccinated before a community can see the benefits of widespread immunity. It’s a bleak outlook for a nation already falling behind in the race to vaccinate enough people to bring the pandemic under control.
“When your best solution is to ask people to do the things that they don’t like to do anyway, that’s very scary,” said Dr. Bibbins-Domingo.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
The COVID-19 variants that have emerged in the United Kingdom, Brazil, South Africa and now Southern California are eliciting two notably distinct responses from U.S. public health officials.
First, broad concern. A variant that wreaked havoc in the United Kingdom, leading to a spike in cases and hospitalizations, is surfacing in a growing number of places in the United States. During the week of Jan. 24, another worrisome variant seen in Brazil surfaced in Minnesota. If these or other strains significantly change the way the virus transmits and attacks the body, as scientists fear they might, they could cause yet another prolonged surge in illness and death in the U.S., even as cases have begun to plateau and vaccines are rolling out.
On the other hand, variants aren’t novel or even uncommon in viral illnesses. The viruses that trigger common colds and flus regularly evolve. Even if a mutated strain of SARS-CoV-2, the virus that causes COVID-19, makes it more contagious or makes people sicker,
The problem is that the U.S. has struggled with every step of its public health response in its first year of battle against COVID-19. And that raises the question of whether the nation will devote the attention and resources needed to outflank the virus as it evolves.
Researchers are quick to stress that a coronavirus mutation in itself is no cause for alarm. In the course of making millions and billions of copies as part of the infection process, small changes to a virus’s genome happen all the time as a function of evolutionary biology.
“The word ‘variant’ and the word ‘mutation’ have these scary connotations, and they aren’t necessarily scary,” said Kelly Wroblewski, director of infectious disease programs for the Association of Public Health Laboratories.
When a mutation rings public health alarms, it’s typically because it has combined with other mutations and, collectively, changed how the virus behaves. At that point, it may be named a variant. A variant can make a virus spread faster, or more easily jump between species. It can make a virus more successful at making people sicker, or change how our immune systems respond.
SARS-CoV-2 has been mutating for as long as we’ve known about it; mutations were identified by scientists throughout 2020. Though relevant scientifically – mutations can actually be helpful, acting like a fingerprint that allows scientists to track a virus’s spread – the identified strains mostly carried little concern for public health.
Then came the end of the year, when several variants began drawing scrutiny. One of the most concerning, first detected in the United Kingdom, appears to make the virus more transmissible. Emerging evidence suggests it also could be deadlier, though scientists are still debating that.
We know more about the U.K. variant than others not because it’s necessarily worse, but because the British have one of the best virus surveillance programs in the world, said William Hanage, PhD, an epidemiologist and a professor at Harvard University.
By contrast, the U.S. has one of the weakest genomic surveillance programs of any rich country, Dr. Hanage said. “As it is, people like me cobble together partnerships with places and try and beg them” for samples, he said on a recent call with reporters.
Other variant strains were identified in South Africa and Brazil, and they share some mutations with the U.K. variant. That those changes evolved independently in several parts of the world suggests they might present an evolutionary advantage for the virus. Yet another strain was recently identified in Southern California and flagged due to its increasing presence in hard-hit cities like Los Angeles.
The Southern California strain was detected because a team of researchers at Cedars-Sinai, a hospital and research center in Los Angeles, has unfettered access to patient samples. They were able to see that the strain made up a growing share of cases at the hospital in recent weeks, as well as among the limited number of other samples haphazardly collected at a network of labs in the region.
Not only does the U.S. do less genomic sequencing than most wealthy countries, but it also does its surveillance by happenstance. That means it takes longer to detect new strains and draw conclusions about them. It’s not yet clear, for example, whether that Southern California strain was truly worthy of a press release.
Vast swaths of America’s privatized and decentralized system of health care aren’t set up to send samples to public health or academic labs. “I’m more concerned about the systems to detect variants than I am these particular variants,” said Mark Pandori, PhD, director of Nevada’s public health laboratory and associate professor at the University of Nevada-Reno School of Medicine.
Limited genomic surveillance of viruses is yet another side effect of a fragmented and underfunded public health system that’s struggled to test, track contacts and get COVID-19 under control throughout the pandemic, Ms. Wroblewski said.
The nation’s public health infrastructure, generally funded on a disease-by-disease basis, has decent systems set up to sequence flu, foodborne illnesses and tuberculosis, but there has been no national strategy on COVID-19. “To look for variants, it needs to be a national picture if it’s going to be done well,” Ms. Wroblewski said.
The Biden administration has outlined a strategy for a national response to COVID-19, which includes expanded surveillance for variants.
So far, vaccines for COVID-19 appear to protect against the known variants. Moderna has said its vaccine is effective against the U.K. and South African strains, though it yields fewer antibodies in the face of the latter. The company is working to develop a revised dose of the vaccine that could be added to the current two-shot regimen as a precaution.
But a lot of damage can be done in the time it will take to roll out the current vaccine, let alone an update.
Even with limited sampling, the U.K. variant has been detected in more than two dozen U.S. states, and the Centers for Disease Control and Prevention has warned it could be the predominant strain in the U.S. by March. When it took off in the United Kingdom at the end of last year, it caused a swell in cases, overwhelmed hospitals, and led to a holiday lockdown. Whether the U.S. faces the same fate could depend on which strains it is competing against, and how the public behaves in the weeks ahead.
Already risky interactions among people could, on average, get a little riskier. Many researchers are calling for better masks and better indoor ventilation. But any updates on recommendations likely would play at the margins. Even if variants spread more easily, the same recommendations public health experts have been espousing for months – masking, physical distancing, and limiting time indoors with others – will be the best way to ward them off, said Kirsten Bibbins-Domingo, MD, a physician and professor at the University of California, San Francisco.
“It’s very unsexy what the solutions are,” Dr. Bibbins-Domingo said. “But we need everyone to do them.”
That doesn’t make the task simple. Masking remains controversial in many states, and the public’s patience for maintaining physical distance has worn thin.
Adding to the concerns: Though case numbers stabilized in many parts of the U.S. in January, they have stabilized at rates many times what they were during previous periods in the pandemic or in other parts of the world. Having all that virus in so many bodies creates more opportunities for new mutations and new variants to emerge.
“If we keep letting this thing sneak around, it’s going to get around all the measures we take against it, and that’s the worst possible thing,” said Nevada’s Dr. Pandori.
Compared with less virulent strains, a more contagious variant likely will require that more people be vaccinated before a community can see the benefits of widespread immunity. It’s a bleak outlook for a nation already falling behind in the race to vaccinate enough people to bring the pandemic under control.
“When your best solution is to ask people to do the things that they don’t like to do anyway, that’s very scary,” said Dr. Bibbins-Domingo.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
The COVID-19 variants that have emerged in the United Kingdom, Brazil, South Africa and now Southern California are eliciting two notably distinct responses from U.S. public health officials.
First, broad concern. A variant that wreaked havoc in the United Kingdom, leading to a spike in cases and hospitalizations, is surfacing in a growing number of places in the United States. During the week of Jan. 24, another worrisome variant seen in Brazil surfaced in Minnesota. If these or other strains significantly change the way the virus transmits and attacks the body, as scientists fear they might, they could cause yet another prolonged surge in illness and death in the U.S., even as cases have begun to plateau and vaccines are rolling out.
On the other hand, variants aren’t novel or even uncommon in viral illnesses. The viruses that trigger common colds and flus regularly evolve. Even if a mutated strain of SARS-CoV-2, the virus that causes COVID-19, makes it more contagious or makes people sicker,
The problem is that the U.S. has struggled with every step of its public health response in its first year of battle against COVID-19. And that raises the question of whether the nation will devote the attention and resources needed to outflank the virus as it evolves.
Researchers are quick to stress that a coronavirus mutation in itself is no cause for alarm. In the course of making millions and billions of copies as part of the infection process, small changes to a virus’s genome happen all the time as a function of evolutionary biology.
“The word ‘variant’ and the word ‘mutation’ have these scary connotations, and they aren’t necessarily scary,” said Kelly Wroblewski, director of infectious disease programs for the Association of Public Health Laboratories.
When a mutation rings public health alarms, it’s typically because it has combined with other mutations and, collectively, changed how the virus behaves. At that point, it may be named a variant. A variant can make a virus spread faster, or more easily jump between species. It can make a virus more successful at making people sicker, or change how our immune systems respond.
SARS-CoV-2 has been mutating for as long as we’ve known about it; mutations were identified by scientists throughout 2020. Though relevant scientifically – mutations can actually be helpful, acting like a fingerprint that allows scientists to track a virus’s spread – the identified strains mostly carried little concern for public health.
Then came the end of the year, when several variants began drawing scrutiny. One of the most concerning, first detected in the United Kingdom, appears to make the virus more transmissible. Emerging evidence suggests it also could be deadlier, though scientists are still debating that.
We know more about the U.K. variant than others not because it’s necessarily worse, but because the British have one of the best virus surveillance programs in the world, said William Hanage, PhD, an epidemiologist and a professor at Harvard University.
By contrast, the U.S. has one of the weakest genomic surveillance programs of any rich country, Dr. Hanage said. “As it is, people like me cobble together partnerships with places and try and beg them” for samples, he said on a recent call with reporters.
Other variant strains were identified in South Africa and Brazil, and they share some mutations with the U.K. variant. That those changes evolved independently in several parts of the world suggests they might present an evolutionary advantage for the virus. Yet another strain was recently identified in Southern California and flagged due to its increasing presence in hard-hit cities like Los Angeles.
The Southern California strain was detected because a team of researchers at Cedars-Sinai, a hospital and research center in Los Angeles, has unfettered access to patient samples. They were able to see that the strain made up a growing share of cases at the hospital in recent weeks, as well as among the limited number of other samples haphazardly collected at a network of labs in the region.
Not only does the U.S. do less genomic sequencing than most wealthy countries, but it also does its surveillance by happenstance. That means it takes longer to detect new strains and draw conclusions about them. It’s not yet clear, for example, whether that Southern California strain was truly worthy of a press release.
Vast swaths of America’s privatized and decentralized system of health care aren’t set up to send samples to public health or academic labs. “I’m more concerned about the systems to detect variants than I am these particular variants,” said Mark Pandori, PhD, director of Nevada’s public health laboratory and associate professor at the University of Nevada-Reno School of Medicine.
Limited genomic surveillance of viruses is yet another side effect of a fragmented and underfunded public health system that’s struggled to test, track contacts and get COVID-19 under control throughout the pandemic, Ms. Wroblewski said.
The nation’s public health infrastructure, generally funded on a disease-by-disease basis, has decent systems set up to sequence flu, foodborne illnesses and tuberculosis, but there has been no national strategy on COVID-19. “To look for variants, it needs to be a national picture if it’s going to be done well,” Ms. Wroblewski said.
The Biden administration has outlined a strategy for a national response to COVID-19, which includes expanded surveillance for variants.
So far, vaccines for COVID-19 appear to protect against the known variants. Moderna has said its vaccine is effective against the U.K. and South African strains, though it yields fewer antibodies in the face of the latter. The company is working to develop a revised dose of the vaccine that could be added to the current two-shot regimen as a precaution.
But a lot of damage can be done in the time it will take to roll out the current vaccine, let alone an update.
Even with limited sampling, the U.K. variant has been detected in more than two dozen U.S. states, and the Centers for Disease Control and Prevention has warned it could be the predominant strain in the U.S. by March. When it took off in the United Kingdom at the end of last year, it caused a swell in cases, overwhelmed hospitals, and led to a holiday lockdown. Whether the U.S. faces the same fate could depend on which strains it is competing against, and how the public behaves in the weeks ahead.
Already risky interactions among people could, on average, get a little riskier. Many researchers are calling for better masks and better indoor ventilation. But any updates on recommendations likely would play at the margins. Even if variants spread more easily, the same recommendations public health experts have been espousing for months – masking, physical distancing, and limiting time indoors with others – will be the best way to ward them off, said Kirsten Bibbins-Domingo, MD, a physician and professor at the University of California, San Francisco.
“It’s very unsexy what the solutions are,” Dr. Bibbins-Domingo said. “But we need everyone to do them.”
That doesn’t make the task simple. Masking remains controversial in many states, and the public’s patience for maintaining physical distance has worn thin.
Adding to the concerns: Though case numbers stabilized in many parts of the U.S. in January, they have stabilized at rates many times what they were during previous periods in the pandemic or in other parts of the world. Having all that virus in so many bodies creates more opportunities for new mutations and new variants to emerge.
“If we keep letting this thing sneak around, it’s going to get around all the measures we take against it, and that’s the worst possible thing,” said Nevada’s Dr. Pandori.
Compared with less virulent strains, a more contagious variant likely will require that more people be vaccinated before a community can see the benefits of widespread immunity. It’s a bleak outlook for a nation already falling behind in the race to vaccinate enough people to bring the pandemic under control.
“When your best solution is to ask people to do the things that they don’t like to do anyway, that’s very scary,” said Dr. Bibbins-Domingo.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
Physician offices should have bigger role in vaccine rollout: MGMA
Physician offices, which have been deemphasized in the COVID-19 vaccine rollout, should have a more prominent role in the effort going forward, said the Medical Group Management Association in a letter sent to President Joe Biden on Jan. 26.
“Due to our members’ role as community providers, we ask that the Administration include medical group practices in COVID-19 vaccine distribution strategies moving forward,” Halee Fischer-Wright, MD, president and CEO of MGMA, stated in the letter.
“Current vaccine efforts are haphazard at best and appear to rely on a passive first come first served approach with the public rushing to sign up for vaccines when scant supply becomes available,” MGMA noted. “This favors patients who can advocate for themselves or have family members able to do the same. Yet medical group practices already have patient relationships and experience vaccinating patients for influenza and other conditions.”
Moreover, physician practices have data on patient demographics, preexisting conditions, and risk factors. This is valuable information not available to hospitals, pharmacies, and state health departments, MGMA said.
“Furthermore, in a time of uncertainty and misinformation, patients are looking to their own physicians as a trusted source for information on vaccine safety and efficacy,” the letter stated. “Physician group practices can and should play a significant role in vaccine education.”
Despite these advantages of vaccinating patients in doctors’ offices, MGMA pointed out that “states have largely not leveraged physician practices in vaccine rollout efforts.”
In an MGMA survey conducted last week, 85% of independent practices and 45% of hospital- or health system–owned practices that sought COVID-19 vaccine for their patients were unable to obtain any. Of the practices able to get vaccine supplies, the majority said they had received only enough to vaccinate 1% or less of their patients.
Susan R. Bailey, MD, president of the American Medical Association commented in an interview that, “once enough supplies are available, we encourage the administration to ensure physician practices have an adequate supply of COVID-19 vaccines to vaccinate their patients. Physician practices will be an integral part of the vaccine administration process. Physicians are a trusted source of information for patients and their direct conversations and recommendations for patients to get vaccinated will help address hesitancy and result in more people getting vaccinated.”
Many groups, MGMA said, had been approved by their states to distribute the vaccine but received little or no inventory. Practice phone lines have been “flooded” by patients wanting to know why their physicians can’t vaccinate them.
Programs vary by state
In an interview, Dr. Fischer-Wright said that most practices want to vaccinate their patients. But only some states have set up programs that allow them to apply for the COVID-19 vaccines. “Most of our practices that were eligible for vaccination have applied for it,” she added.
The New York State Health Department is taking a different approach, according to Dial Hewlett Jr., MD, medical director for disease control services with the Westchester County Department of Health in White Plains, N.Y.. The state health department has designated specific sites across New York as vaccination hubs; in Westchester County, the hub is the Westchester Medical Center. When the hospital receives a vaccine shipment, it distributes some of it to smaller sites such as the county health department, which includes a vaccination clinic.
“So far, they haven’t gotten to the point where they’re distributing to pharmacies or doctors’ offices,” Dr. Hewlett said in an interview.
Right now, he said, the chief limiting factor is vaccine supply. When that expands, he said, physician offices will likely get more vaccine doses.
Both Dr. Hewlett and Dr. Fischer-Wright pointed out that physician offices are limited because they aren’t able to store the Pfizer vaccine, which requires ultracold freezers. “But now that we have the Moderna vaccine, 50% of the 200 million doses that have been promised can be delivered in a physician office,” said Dr. Fischer-Wright.
So why haven’t practices received more vaccine? Besides the inadequate supply across the nation, Dr. Fischer-Wright said, there have been difficulties in getting the vaccine to physician offices. Some MGMA members, she added, did receive vaccine supplies immediately. “These were independent practices that had over 200 physicians.”
Dr. Hewlett noted that some smaller practices have complained to the county department that they couldn’t obtain vaccine because they lacked the clout to compete with larger groups. “They’re not ordering enough product to make it a priority for whoever is involved with the distribution.”
Another problem – evident in the results of MGMA’s recent poll – is that health care systems that have vaccine supplies are sharing them with their own practices before they make any available to community practices.
“If you’re working for Northwell Health, you probably won’t have the kinds of challenges that the small mom-and-pop practice would have,” Dr. Hewlett said.
Overcoming vaccine hesitancy
More than a quarter of the U.S. population has indicated they are hesitant to get the COVID-19 vaccine. This is an area where Dr. Fischer-Wright believes physicians can help immensely.
“The benefit of having that type of activity occur in the physician office is that it’s a place where physicians have already established trust with patients,” she said. “And one of the reasons why some people don’t want a shot is that they don’t trust the vaccine. Having a human being that you have a relationship with provide you with the pros and cons is very compelling to get people to make an alternative choice.”
Physicians and their staff will also need to be educated before they administer the vaccine, Dr. Hewlett noted. “There will have to be education on the handling of the vaccine, but I think that can easily be done. Many practices have physician assistants and nurse practitioners who have been doing a lot of vaccinations in the office setting.”
Complex logistics
Based on the experience of his department’s vaccination clinic, which has been giving COVID-19 shots since Jan. 5, Dr. Hewlett said private practices have a lot to consider before they launch their own vaccination efforts.
To begin with, he said, “it’s a tricky situation with these vaccines that require two doses.” Before his clinic makes an appointment to vaccinate a patient, the scheduler has to make sure that the patient can return in 21 or 28 days, depending on whether they’re getting the Pfizer or Moderna vaccine.
“It’s difficult if they can’t show up 28 days after that date because we expect the same number of people to show up 28 days later for their second dose,” he said. “This is quite different from a standard medical practice. There aren’t too many situations where a person has to come back to the office after 28 days or 21 days.”
While the Centers for Disease Control and Prevention recently said the immunization schedule can be more flexible, Dr. Hewlett added, his clinic prefers to get patients back on the recommended schedule to make sure the vaccine will be maximally effective.
The clinic also has to follow state regulations requiring that all vaccines it receives be administered within a week of receipt. Right now, the clinic is open 6 days a week, giving about 300-400 shots a day. Each morning, a clerk records how many doses were administered the previous day, along with the lot numbers – and all data must be reported to the state.
The operation is fairly labor intensive. The clinic has a staff of about 30 people, most of whom are now engaged full time in the COVID-19 vaccination effort.
“We have people who check patients in and who screen to make sure no one has COVID symptoms. Other people escort patients to the vaccination stations. We have about 15 nurse practitioners and public health nurses who give the shots, and we have to make sure they’re accounting for every dose that’s given. And we have to make sure everybody getting a dose meets the eligibility criteria for shots,” he said. “We also have an area where patients are watched for 15 minutes after they’re vaccinated. Then there’s a group of five data entry people who locate appointment slots 28 days from today.”
It’s all still “a work in progress,” Dr. Hewlett said, but the staff who give COVID-19 shots and the patients who receive them are gratified to be making a difference.
A version of this article first appeared on Medscape.com.
Physician offices, which have been deemphasized in the COVID-19 vaccine rollout, should have a more prominent role in the effort going forward, said the Medical Group Management Association in a letter sent to President Joe Biden on Jan. 26.
“Due to our members’ role as community providers, we ask that the Administration include medical group practices in COVID-19 vaccine distribution strategies moving forward,” Halee Fischer-Wright, MD, president and CEO of MGMA, stated in the letter.
“Current vaccine efforts are haphazard at best and appear to rely on a passive first come first served approach with the public rushing to sign up for vaccines when scant supply becomes available,” MGMA noted. “This favors patients who can advocate for themselves or have family members able to do the same. Yet medical group practices already have patient relationships and experience vaccinating patients for influenza and other conditions.”
Moreover, physician practices have data on patient demographics, preexisting conditions, and risk factors. This is valuable information not available to hospitals, pharmacies, and state health departments, MGMA said.
“Furthermore, in a time of uncertainty and misinformation, patients are looking to their own physicians as a trusted source for information on vaccine safety and efficacy,” the letter stated. “Physician group practices can and should play a significant role in vaccine education.”
Despite these advantages of vaccinating patients in doctors’ offices, MGMA pointed out that “states have largely not leveraged physician practices in vaccine rollout efforts.”
In an MGMA survey conducted last week, 85% of independent practices and 45% of hospital- or health system–owned practices that sought COVID-19 vaccine for their patients were unable to obtain any. Of the practices able to get vaccine supplies, the majority said they had received only enough to vaccinate 1% or less of their patients.
Susan R. Bailey, MD, president of the American Medical Association commented in an interview that, “once enough supplies are available, we encourage the administration to ensure physician practices have an adequate supply of COVID-19 vaccines to vaccinate their patients. Physician practices will be an integral part of the vaccine administration process. Physicians are a trusted source of information for patients and their direct conversations and recommendations for patients to get vaccinated will help address hesitancy and result in more people getting vaccinated.”
Many groups, MGMA said, had been approved by their states to distribute the vaccine but received little or no inventory. Practice phone lines have been “flooded” by patients wanting to know why their physicians can’t vaccinate them.
Programs vary by state
In an interview, Dr. Fischer-Wright said that most practices want to vaccinate their patients. But only some states have set up programs that allow them to apply for the COVID-19 vaccines. “Most of our practices that were eligible for vaccination have applied for it,” she added.
The New York State Health Department is taking a different approach, according to Dial Hewlett Jr., MD, medical director for disease control services with the Westchester County Department of Health in White Plains, N.Y.. The state health department has designated specific sites across New York as vaccination hubs; in Westchester County, the hub is the Westchester Medical Center. When the hospital receives a vaccine shipment, it distributes some of it to smaller sites such as the county health department, which includes a vaccination clinic.
“So far, they haven’t gotten to the point where they’re distributing to pharmacies or doctors’ offices,” Dr. Hewlett said in an interview.
Right now, he said, the chief limiting factor is vaccine supply. When that expands, he said, physician offices will likely get more vaccine doses.
Both Dr. Hewlett and Dr. Fischer-Wright pointed out that physician offices are limited because they aren’t able to store the Pfizer vaccine, which requires ultracold freezers. “But now that we have the Moderna vaccine, 50% of the 200 million doses that have been promised can be delivered in a physician office,” said Dr. Fischer-Wright.
So why haven’t practices received more vaccine? Besides the inadequate supply across the nation, Dr. Fischer-Wright said, there have been difficulties in getting the vaccine to physician offices. Some MGMA members, she added, did receive vaccine supplies immediately. “These were independent practices that had over 200 physicians.”
Dr. Hewlett noted that some smaller practices have complained to the county department that they couldn’t obtain vaccine because they lacked the clout to compete with larger groups. “They’re not ordering enough product to make it a priority for whoever is involved with the distribution.”
Another problem – evident in the results of MGMA’s recent poll – is that health care systems that have vaccine supplies are sharing them with their own practices before they make any available to community practices.
“If you’re working for Northwell Health, you probably won’t have the kinds of challenges that the small mom-and-pop practice would have,” Dr. Hewlett said.
Overcoming vaccine hesitancy
More than a quarter of the U.S. population has indicated they are hesitant to get the COVID-19 vaccine. This is an area where Dr. Fischer-Wright believes physicians can help immensely.
“The benefit of having that type of activity occur in the physician office is that it’s a place where physicians have already established trust with patients,” she said. “And one of the reasons why some people don’t want a shot is that they don’t trust the vaccine. Having a human being that you have a relationship with provide you with the pros and cons is very compelling to get people to make an alternative choice.”
Physicians and their staff will also need to be educated before they administer the vaccine, Dr. Hewlett noted. “There will have to be education on the handling of the vaccine, but I think that can easily be done. Many practices have physician assistants and nurse practitioners who have been doing a lot of vaccinations in the office setting.”
Complex logistics
Based on the experience of his department’s vaccination clinic, which has been giving COVID-19 shots since Jan. 5, Dr. Hewlett said private practices have a lot to consider before they launch their own vaccination efforts.
To begin with, he said, “it’s a tricky situation with these vaccines that require two doses.” Before his clinic makes an appointment to vaccinate a patient, the scheduler has to make sure that the patient can return in 21 or 28 days, depending on whether they’re getting the Pfizer or Moderna vaccine.
“It’s difficult if they can’t show up 28 days after that date because we expect the same number of people to show up 28 days later for their second dose,” he said. “This is quite different from a standard medical practice. There aren’t too many situations where a person has to come back to the office after 28 days or 21 days.”
While the Centers for Disease Control and Prevention recently said the immunization schedule can be more flexible, Dr. Hewlett added, his clinic prefers to get patients back on the recommended schedule to make sure the vaccine will be maximally effective.
The clinic also has to follow state regulations requiring that all vaccines it receives be administered within a week of receipt. Right now, the clinic is open 6 days a week, giving about 300-400 shots a day. Each morning, a clerk records how many doses were administered the previous day, along with the lot numbers – and all data must be reported to the state.
The operation is fairly labor intensive. The clinic has a staff of about 30 people, most of whom are now engaged full time in the COVID-19 vaccination effort.
“We have people who check patients in and who screen to make sure no one has COVID symptoms. Other people escort patients to the vaccination stations. We have about 15 nurse practitioners and public health nurses who give the shots, and we have to make sure they’re accounting for every dose that’s given. And we have to make sure everybody getting a dose meets the eligibility criteria for shots,” he said. “We also have an area where patients are watched for 15 minutes after they’re vaccinated. Then there’s a group of five data entry people who locate appointment slots 28 days from today.”
It’s all still “a work in progress,” Dr. Hewlett said, but the staff who give COVID-19 shots and the patients who receive them are gratified to be making a difference.
A version of this article first appeared on Medscape.com.
Physician offices, which have been deemphasized in the COVID-19 vaccine rollout, should have a more prominent role in the effort going forward, said the Medical Group Management Association in a letter sent to President Joe Biden on Jan. 26.
“Due to our members’ role as community providers, we ask that the Administration include medical group practices in COVID-19 vaccine distribution strategies moving forward,” Halee Fischer-Wright, MD, president and CEO of MGMA, stated in the letter.
“Current vaccine efforts are haphazard at best and appear to rely on a passive first come first served approach with the public rushing to sign up for vaccines when scant supply becomes available,” MGMA noted. “This favors patients who can advocate for themselves or have family members able to do the same. Yet medical group practices already have patient relationships and experience vaccinating patients for influenza and other conditions.”
Moreover, physician practices have data on patient demographics, preexisting conditions, and risk factors. This is valuable information not available to hospitals, pharmacies, and state health departments, MGMA said.
“Furthermore, in a time of uncertainty and misinformation, patients are looking to their own physicians as a trusted source for information on vaccine safety and efficacy,” the letter stated. “Physician group practices can and should play a significant role in vaccine education.”
Despite these advantages of vaccinating patients in doctors’ offices, MGMA pointed out that “states have largely not leveraged physician practices in vaccine rollout efforts.”
In an MGMA survey conducted last week, 85% of independent practices and 45% of hospital- or health system–owned practices that sought COVID-19 vaccine for their patients were unable to obtain any. Of the practices able to get vaccine supplies, the majority said they had received only enough to vaccinate 1% or less of their patients.
Susan R. Bailey, MD, president of the American Medical Association commented in an interview that, “once enough supplies are available, we encourage the administration to ensure physician practices have an adequate supply of COVID-19 vaccines to vaccinate their patients. Physician practices will be an integral part of the vaccine administration process. Physicians are a trusted source of information for patients and their direct conversations and recommendations for patients to get vaccinated will help address hesitancy and result in more people getting vaccinated.”
Many groups, MGMA said, had been approved by their states to distribute the vaccine but received little or no inventory. Practice phone lines have been “flooded” by patients wanting to know why their physicians can’t vaccinate them.
Programs vary by state
In an interview, Dr. Fischer-Wright said that most practices want to vaccinate their patients. But only some states have set up programs that allow them to apply for the COVID-19 vaccines. “Most of our practices that were eligible for vaccination have applied for it,” she added.
The New York State Health Department is taking a different approach, according to Dial Hewlett Jr., MD, medical director for disease control services with the Westchester County Department of Health in White Plains, N.Y.. The state health department has designated specific sites across New York as vaccination hubs; in Westchester County, the hub is the Westchester Medical Center. When the hospital receives a vaccine shipment, it distributes some of it to smaller sites such as the county health department, which includes a vaccination clinic.
“So far, they haven’t gotten to the point where they’re distributing to pharmacies or doctors’ offices,” Dr. Hewlett said in an interview.
Right now, he said, the chief limiting factor is vaccine supply. When that expands, he said, physician offices will likely get more vaccine doses.
Both Dr. Hewlett and Dr. Fischer-Wright pointed out that physician offices are limited because they aren’t able to store the Pfizer vaccine, which requires ultracold freezers. “But now that we have the Moderna vaccine, 50% of the 200 million doses that have been promised can be delivered in a physician office,” said Dr. Fischer-Wright.
So why haven’t practices received more vaccine? Besides the inadequate supply across the nation, Dr. Fischer-Wright said, there have been difficulties in getting the vaccine to physician offices. Some MGMA members, she added, did receive vaccine supplies immediately. “These were independent practices that had over 200 physicians.”
Dr. Hewlett noted that some smaller practices have complained to the county department that they couldn’t obtain vaccine because they lacked the clout to compete with larger groups. “They’re not ordering enough product to make it a priority for whoever is involved with the distribution.”
Another problem – evident in the results of MGMA’s recent poll – is that health care systems that have vaccine supplies are sharing them with their own practices before they make any available to community practices.
“If you’re working for Northwell Health, you probably won’t have the kinds of challenges that the small mom-and-pop practice would have,” Dr. Hewlett said.
Overcoming vaccine hesitancy
More than a quarter of the U.S. population has indicated they are hesitant to get the COVID-19 vaccine. This is an area where Dr. Fischer-Wright believes physicians can help immensely.
“The benefit of having that type of activity occur in the physician office is that it’s a place where physicians have already established trust with patients,” she said. “And one of the reasons why some people don’t want a shot is that they don’t trust the vaccine. Having a human being that you have a relationship with provide you with the pros and cons is very compelling to get people to make an alternative choice.”
Physicians and their staff will also need to be educated before they administer the vaccine, Dr. Hewlett noted. “There will have to be education on the handling of the vaccine, but I think that can easily be done. Many practices have physician assistants and nurse practitioners who have been doing a lot of vaccinations in the office setting.”
Complex logistics
Based on the experience of his department’s vaccination clinic, which has been giving COVID-19 shots since Jan. 5, Dr. Hewlett said private practices have a lot to consider before they launch their own vaccination efforts.
To begin with, he said, “it’s a tricky situation with these vaccines that require two doses.” Before his clinic makes an appointment to vaccinate a patient, the scheduler has to make sure that the patient can return in 21 or 28 days, depending on whether they’re getting the Pfizer or Moderna vaccine.
“It’s difficult if they can’t show up 28 days after that date because we expect the same number of people to show up 28 days later for their second dose,” he said. “This is quite different from a standard medical practice. There aren’t too many situations where a person has to come back to the office after 28 days or 21 days.”
While the Centers for Disease Control and Prevention recently said the immunization schedule can be more flexible, Dr. Hewlett added, his clinic prefers to get patients back on the recommended schedule to make sure the vaccine will be maximally effective.
The clinic also has to follow state regulations requiring that all vaccines it receives be administered within a week of receipt. Right now, the clinic is open 6 days a week, giving about 300-400 shots a day. Each morning, a clerk records how many doses were administered the previous day, along with the lot numbers – and all data must be reported to the state.
The operation is fairly labor intensive. The clinic has a staff of about 30 people, most of whom are now engaged full time in the COVID-19 vaccination effort.
“We have people who check patients in and who screen to make sure no one has COVID symptoms. Other people escort patients to the vaccination stations. We have about 15 nurse practitioners and public health nurses who give the shots, and we have to make sure they’re accounting for every dose that’s given. And we have to make sure everybody getting a dose meets the eligibility criteria for shots,” he said. “We also have an area where patients are watched for 15 minutes after they’re vaccinated. Then there’s a group of five data entry people who locate appointment slots 28 days from today.”
It’s all still “a work in progress,” Dr. Hewlett said, but the staff who give COVID-19 shots and the patients who receive them are gratified to be making a difference.
A version of this article first appeared on Medscape.com.