User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Poor sleep is linked to cortical amyloid burden
MINNEAPOLIS – People who report feeling more sleepy and less rested have elevated levels of amyloid in regions of the brain that are commonly involved in Alzheimer’s disease, finds a cohort study reported at the annual meeting of the Associated Professional Sleep Societies.
Researchers studied 98 asymptomatic, cognitively healthy late-middle-age adults from the WRAP (Wisconsin Registry for Alzheimer’s Prevention) program, the majority of whom were at elevated risk for the disease because of family history.

Self-reported somnolence, poorer sleep quality, and sleep problems were significantly correlated with higher levels of amyloid deposition in the cortex overall and in four subregions that are typically affected in Alzheimer’s disease (P less than .05).
"It does appear that there is an association between amyloid burden and sleepiness, and that relationship is present in adults who are cognitively healthy but who are at risk of developing Alzheimer’s disease in the future. They are fairly young in terms of amyloid pathology," commented first author Kate Sprecher, a PhD candidate in the neuroscience training program at the University of Wisconsin–Madison. She acknowledged that the findings may differ in a cohort not enriched for people at elevated risk.
"In terms of mechanisms, we can’t say from these data whether sleep is driving amyloid deposition or whether amyloid deposition is disrupting sleep," she added. "Nonetheless, it’s kind of tantalizing that sleep may be a tool that we can use to prevent or delay Alzheimer’s pathology. We may be able to intervene early in the disease, when people are actually able to respond to treatment, because typically, current drugs are targeting later disease, when a great deal of neurodegeneration has already taken place. So sleep may be something that we can target really early."
The investigators plan to further investigate the observed association using objective measures of sleep and obstructive sleep apnea (OSA), according to Ms. Sprecher. "And we’ll do some longitudinal follow-up as well in our cohort to see how sleep changes might relate to actual progression of the disease," she said.
Study participants completed the Medical Outcomes Study (MOS) Sleep Scale and the Epworth Sleepiness Scale (ESS). Amyloid deposition in the brain was measured by positron emission tomography performed with Pittsburgh Compound B.
The participants were 63 years old, on average, and two-thirds were female, reported Ms. Sprecher, who disclosed no conflicts of interest relevant to the research. Overall, 76% had a family history of Alzheimer’s disease, and 34% were positive for the APOE4 allele, which is associated with risk of this disease.
Analyses adjusted for these and other potential confounders showed a correlation (P less than or equal to .05) between somnolence on the MOS Sleep Scale – the average of scores for drowsiness, trouble staying awake, and napping – and the burden of amyloid in the left supramarginal gyrus (correlation [r] = 0.22), the left frontal medial orbital cortex (r = 0.21), and the left frontal inferior orbital cortex (r = 0.21).
Poorer quality of sleep was correlated (P less than or equal to .05) with amyloid burden in the cortex overall (r = 0.25) as well as in the left and right precuneus (r = 0.23 and 0.25), the right supramarginal gyrus (r = 0.23), the left and right frontal medial orbital cortex (r = 0.29 and 0.29), and the left and right frontal inferior orbital cortex (r = 0.26 and 0.25).
Scores on the Sleep Problem Index were also associated with greater burden in some of these cortical areas.
Although ESS scores were significantly correlated with MOS scores, they were not directly correlated with amyloid burden in any of the regions studied.
"This could be because the two questionnaires probe slightly different aspects of sleepiness," Ms. Sprecher proposed in an interview. "The ESS asks how likely you are to fall asleep in several common situations such as while watching TV or driving a car. The MOS asks whether you take naps, feel sleepy during the day, or feel that you get enough sleep at night. Therefore, the MOS may be better at probing how adequate your sleep is, even if you are managing to stay awake during the day."
Ms. Sprecher disclosed no relevant conflicts of interest.
MINNEAPOLIS – People who report feeling more sleepy and less rested have elevated levels of amyloid in regions of the brain that are commonly involved in Alzheimer’s disease, finds a cohort study reported at the annual meeting of the Associated Professional Sleep Societies.
Researchers studied 98 asymptomatic, cognitively healthy late-middle-age adults from the WRAP (Wisconsin Registry for Alzheimer’s Prevention) program, the majority of whom were at elevated risk for the disease because of family history.
Self-reported somnolence, poorer sleep quality, and sleep problems were significantly correlated with higher levels of amyloid deposition in the cortex overall and in four subregions that are typically affected in Alzheimer’s disease (P less than .05).
"It does appear that there is an association between amyloid burden and sleepiness, and that relationship is present in adults who are cognitively healthy but who are at risk of developing Alzheimer’s disease in the future. They are fairly young in terms of amyloid pathology," commented first author Kate Sprecher, a PhD candidate in the neuroscience training program at the University of Wisconsin–Madison. She acknowledged that the findings may differ in a cohort not enriched for people at elevated risk.
"In terms of mechanisms, we can’t say from these data whether sleep is driving amyloid deposition or whether amyloid deposition is disrupting sleep," she added. "Nonetheless, it’s kind of tantalizing that sleep may be a tool that we can use to prevent or delay Alzheimer’s pathology. We may be able to intervene early in the disease, when people are actually able to respond to treatment, because typically, current drugs are targeting later disease, when a great deal of neurodegeneration has already taken place. So sleep may be something that we can target really early."
The investigators plan to further investigate the observed association using objective measures of sleep and obstructive sleep apnea (OSA), according to Ms. Sprecher. "And we’ll do some longitudinal follow-up as well in our cohort to see how sleep changes might relate to actual progression of the disease," she said.
Study participants completed the Medical Outcomes Study (MOS) Sleep Scale and the Epworth Sleepiness Scale (ESS). Amyloid deposition in the brain was measured by positron emission tomography performed with Pittsburgh Compound B.
The participants were 63 years old, on average, and two-thirds were female, reported Ms. Sprecher, who disclosed no conflicts of interest relevant to the research. Overall, 76% had a family history of Alzheimer’s disease, and 34% were positive for the APOE4 allele, which is associated with risk of this disease.
Analyses adjusted for these and other potential confounders showed a correlation (P less than or equal to .05) between somnolence on the MOS Sleep Scale – the average of scores for drowsiness, trouble staying awake, and napping – and the burden of amyloid in the left supramarginal gyrus (correlation [r] = 0.22), the left frontal medial orbital cortex (r = 0.21), and the left frontal inferior orbital cortex (r = 0.21).
Poorer quality of sleep was correlated (P less than or equal to .05) with amyloid burden in the cortex overall (r = 0.25) as well as in the left and right precuneus (r = 0.23 and 0.25), the right supramarginal gyrus (r = 0.23), the left and right frontal medial orbital cortex (r = 0.29 and 0.29), and the left and right frontal inferior orbital cortex (r = 0.26 and 0.25).
Scores on the Sleep Problem Index were also associated with greater burden in some of these cortical areas.
Although ESS scores were significantly correlated with MOS scores, they were not directly correlated with amyloid burden in any of the regions studied.
"This could be because the two questionnaires probe slightly different aspects of sleepiness," Ms. Sprecher proposed in an interview. "The ESS asks how likely you are to fall asleep in several common situations such as while watching TV or driving a car. The MOS asks whether you take naps, feel sleepy during the day, or feel that you get enough sleep at night. Therefore, the MOS may be better at probing how adequate your sleep is, even if you are managing to stay awake during the day."
Ms. Sprecher disclosed no relevant conflicts of interest.
MINNEAPOLIS – People who report feeling more sleepy and less rested have elevated levels of amyloid in regions of the brain that are commonly involved in Alzheimer’s disease, finds a cohort study reported at the annual meeting of the Associated Professional Sleep Societies.
Researchers studied 98 asymptomatic, cognitively healthy late-middle-age adults from the WRAP (Wisconsin Registry for Alzheimer’s Prevention) program, the majority of whom were at elevated risk for the disease because of family history.
Self-reported somnolence, poorer sleep quality, and sleep problems were significantly correlated with higher levels of amyloid deposition in the cortex overall and in four subregions that are typically affected in Alzheimer’s disease (P less than .05).
"It does appear that there is an association between amyloid burden and sleepiness, and that relationship is present in adults who are cognitively healthy but who are at risk of developing Alzheimer’s disease in the future. They are fairly young in terms of amyloid pathology," commented first author Kate Sprecher, a PhD candidate in the neuroscience training program at the University of Wisconsin–Madison. She acknowledged that the findings may differ in a cohort not enriched for people at elevated risk.
"In terms of mechanisms, we can’t say from these data whether sleep is driving amyloid deposition or whether amyloid deposition is disrupting sleep," she added. "Nonetheless, it’s kind of tantalizing that sleep may be a tool that we can use to prevent or delay Alzheimer’s pathology. We may be able to intervene early in the disease, when people are actually able to respond to treatment, because typically, current drugs are targeting later disease, when a great deal of neurodegeneration has already taken place. So sleep may be something that we can target really early."
The investigators plan to further investigate the observed association using objective measures of sleep and obstructive sleep apnea (OSA), according to Ms. Sprecher. "And we’ll do some longitudinal follow-up as well in our cohort to see how sleep changes might relate to actual progression of the disease," she said.
Study participants completed the Medical Outcomes Study (MOS) Sleep Scale and the Epworth Sleepiness Scale (ESS). Amyloid deposition in the brain was measured by positron emission tomography performed with Pittsburgh Compound B.
The participants were 63 years old, on average, and two-thirds were female, reported Ms. Sprecher, who disclosed no conflicts of interest relevant to the research. Overall, 76% had a family history of Alzheimer’s disease, and 34% were positive for the APOE4 allele, which is associated with risk of this disease.
Analyses adjusted for these and other potential confounders showed a correlation (P less than or equal to .05) between somnolence on the MOS Sleep Scale – the average of scores for drowsiness, trouble staying awake, and napping – and the burden of amyloid in the left supramarginal gyrus (correlation [r] = 0.22), the left frontal medial orbital cortex (r = 0.21), and the left frontal inferior orbital cortex (r = 0.21).
Poorer quality of sleep was correlated (P less than or equal to .05) with amyloid burden in the cortex overall (r = 0.25) as well as in the left and right precuneus (r = 0.23 and 0.25), the right supramarginal gyrus (r = 0.23), the left and right frontal medial orbital cortex (r = 0.29 and 0.29), and the left and right frontal inferior orbital cortex (r = 0.26 and 0.25).
Scores on the Sleep Problem Index were also associated with greater burden in some of these cortical areas.
Although ESS scores were significantly correlated with MOS scores, they were not directly correlated with amyloid burden in any of the regions studied.
"This could be because the two questionnaires probe slightly different aspects of sleepiness," Ms. Sprecher proposed in an interview. "The ESS asks how likely you are to fall asleep in several common situations such as while watching TV or driving a car. The MOS asks whether you take naps, feel sleepy during the day, or feel that you get enough sleep at night. Therefore, the MOS may be better at probing how adequate your sleep is, even if you are managing to stay awake during the day."
Ms. Sprecher disclosed no relevant conflicts of interest.
AT SLEEP 2014
Key clinical point: Improved sleep quality might provide protection from Alzheimer’s disease.
Major finding: Self-reported somnolence, poorer sleep quality, and sleep problems were associated with greater amyloid burden in areas of the brain known to be affected by Alzheimer’s disease (P less than .05).
Data source: A cohort study of 98 asymptomatic, cognitively healthy late middle-age adults, the majority at elevated risk for Alzheimer’s disease.
Disclosures: Ms. Sprecher disclosed no relevant conflicts of interest.

VIDEO: How to tell which apnea patients oxygen will help
SAN DIEGO – Some obstructive sleep apnea patients who can’t or won’t use continuous positive airway pressure therapy will benefit from supplemental oxygen therapy, but some won’t – and until now, prolonged testing is needed to tell which patients are which.
Scott A. Sands, Ph.D., and his associates at Brigham and Women’s Hospital, Boston, have found a simpler way to detect which patients would be helped by supplemental oxygen therapy. In a video interview, he describes in simple terms the patient characteristics that he looks for in polysomnography patterns he said at an international conference of the American Thoracic Society. His randomized, controlled trial in 19 patients showed that patients identified by this method did benefit from supplemental oxygen therapy, and their sleep patterns improved.
Dr. Sands reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN DIEGO – Some obstructive sleep apnea patients who can’t or won’t use continuous positive airway pressure therapy will benefit from supplemental oxygen therapy, but some won’t – and until now, prolonged testing is needed to tell which patients are which.
Scott A. Sands, Ph.D., and his associates at Brigham and Women’s Hospital, Boston, have found a simpler way to detect which patients would be helped by supplemental oxygen therapy. In a video interview, he describes in simple terms the patient characteristics that he looks for in polysomnography patterns he said at an international conference of the American Thoracic Society. His randomized, controlled trial in 19 patients showed that patients identified by this method did benefit from supplemental oxygen therapy, and their sleep patterns improved.
Dr. Sands reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SAN DIEGO – Some obstructive sleep apnea patients who can’t or won’t use continuous positive airway pressure therapy will benefit from supplemental oxygen therapy, but some won’t – and until now, prolonged testing is needed to tell which patients are which.
Scott A. Sands, Ph.D., and his associates at Brigham and Women’s Hospital, Boston, have found a simpler way to detect which patients would be helped by supplemental oxygen therapy. In a video interview, he describes in simple terms the patient characteristics that he looks for in polysomnography patterns he said at an international conference of the American Thoracic Society. His randomized, controlled trial in 19 patients showed that patients identified by this method did benefit from supplemental oxygen therapy, and their sleep patterns improved.
Dr. Sands reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
AT ATS 2014

CPAP reduced blood pressure in obese, apneic adults
The use of continuous positive airway pressure modestly reduced blood pressure in two separate studies involving obese patients who had moderate to severe obstructive sleep apnea, according to reports published online June 11 in the New England Journal of Medicine.
In contrast, neither the use of supplemental oxygen in one study nor a weight loss of approximately 7 kg in the other study had a beneficial effect on blood pressure.
In the first study, investigators compared the effects of CPAP against those of nocturnal supplemental oxygen on several markers of cardiovascular risk, including blood pressure. The multicenter study involved cardiology patients aged 45-75 years who either had established coronary heart disease or multiple cardiovascular risk factors, and who also were found to have obstructive sleep apnea when screened for the disorder.

The 318 patients were randomly assigned in equal numbers to receive CPAP plus education in healthy lifestyle and sleep practices, nocturnal supplemental oxygen delivered via cannula plus lifestyle and sleep education, or lifestyle and sleep education alone (the control group) for 12 weeks, said Dr. Daniel J. Gottlieb, of the Veterans Affairs Boston Healthcare System, and his associates.
The mean body mass index was 33.0 kg/m2 in the CPAP group, 34.7 kg/m2 in the supplemental oxygen group, and 33.7 kg/m2 in the education group. Average apnea-hypopnea index scores for the three groups were 25.4, 24.0, and 25.5 events per hour, respectively
At the end of the study, 24-hour mean arterial blood pressure was significantly lower among patients in the CPAP group (87.8 mm Hg) than with oxygen (90.2 mm Hg) or education alone (89.0 mm Hg), a "modest" difference in magnitude that nevertheless has been associated with "a meaningful reduction in cardiovascular risk," the investigators noted.
That benefit was seen even though those patients’ blood pressure was already well controlled by antihypertensive medications and even though their adherence to CPAP was only "average," said Dr. Gottleib, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and his colleagues.
In contrast, mean arterial blood pressure was not significantly different between patients who received supplemental oxygen and the control group, even though the supplemental oxygen did reduce nocturnal hypoxemia and adherence to oxygen therapy was much better than that for CPAP. A further analysis adjusting for potential confounders such as patient age, sex, race, body mass index, and type of antihypertensive medication had no appreciable effect on the results.
"This study offers no support for the common but largely untested clinical practice of providing supplemental oxygen as salvage therapy in patients with obstructive sleep apnea for whom CPAP is problematic," Dr. Gottlieb and his associates reported (N. Engl. J. Med. 2014;370:2276-85 [doi: 10.1056/NEJMoa1306766]).
In the second study, researchers compared the effects of 24 weeks of CPAP alone, weight loss alone, or CPAP plus weight loss in obese adults who had moderate to severe obstructive sleep apnea and elevated C-reactive protein levels. A total of 181 patients underwent randomization, but only 136 completed the study: 48 in the CPAP group, 42 in the weight-loss group, and 46 in the combined-intervention group, said Dr. Julio A. Chirinos, of the Philadelphia Veterans Affairs Medical Center and the University of Pennsylvania, and his associates.
At the conclusion of the intervention, weight loss was similar between the weight-loss–only group (6.8 kg) and the combined-intervention group (7.0 kg), while there was no change in the CPAP-only group.
The study’s primary endpoint was improvement in C-reactive protein levels. There was no significant difference among the three study groups for this outcome. However, the secondary outcome of significantly decreased systolic blood pressure was achieved with the combined intervention (–14.1 mm Hg), compared with weight loss alone (–6.8 mm Hg) or CPAP alone (–3.0 mm Hg).
The combined therapy also improved insulin resistance and serum triglyceride levels, Dr. Chirinos and his associates said (N. Engl. J. Med. 2014;370:2265-75 [doi: 10.1056/NEJMoa1306187]).
"Our study shows that a weight-loss intervention is effective as a central component of the strategies used to improve the cardiovascular risk-factor profile in patients with obesity and obstructive sleep apnea," they added.
Dr. Gottlieb’s study was supported by the National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Research Resources. Philips Respironics donated the equipment used in the study. Dr. Gottlieb reported ties to Philips Respironics and ResMed Corporation, and his associates reported ties to numerous industry sources.
Dr. Chirinos’s study also was supported by the NHLBI. ResMed provided CPAP equipment at no cost but had no role in study design, data accrual or analysis, or manuscript preparation. Dr. Chirinos reported no financial conflicts of interest; his associates reported ties to Boehringer Ingelheim, ConAgra Foods, Novo Nordisk, Nutrisystem, Orexigen, Tate and Lyle, United Health Group, and Weight Watchers.
These studies offer two important considerations to clinicians, noted Dr. Robert C. Basner. First, CPAP may ameliorate hypertension and reduce cardiovascular risk in high-risk obese patients, even when they’re already being treated for hypertension and don’t have the daytime sleepiness that usually characterizes obstructive sleep apnea. Second, weight loss may reduce cardiovascular risks even further when CPAP is prescribed.
But further interpretation of the study findings is limited, Dr. Basner cautioned, because of the relatively low nightly use of CPAP (poor adherence) in the study by Dr. Gottlieb, and because of the wide variability in C-reactive protein values and the unusual statistical handling of those values in the study by Dr. Chirinos.
Dr. Basner is at Columbia University, New York. He was a member of the Data and Safety Monitoring Board of the study performed by Dr. Chirinos. These remarks were taken from his editorial accompanying the two studies (N. Engl. J. Med. 2014;370:2339-41 [doi: 10.1056/NEJMe1404501]).
These studies offer two important considerations to clinicians, noted Dr. Robert C. Basner. First, CPAP may ameliorate hypertension and reduce cardiovascular risk in high-risk obese patients, even when they’re already being treated for hypertension and don’t have the daytime sleepiness that usually characterizes obstructive sleep apnea. Second, weight loss may reduce cardiovascular risks even further when CPAP is prescribed.
But further interpretation of the study findings is limited, Dr. Basner cautioned, because of the relatively low nightly use of CPAP (poor adherence) in the study by Dr. Gottlieb, and because of the wide variability in C-reactive protein values and the unusual statistical handling of those values in the study by Dr. Chirinos.
Dr. Basner is at Columbia University, New York. He was a member of the Data and Safety Monitoring Board of the study performed by Dr. Chirinos. These remarks were taken from his editorial accompanying the two studies (N. Engl. J. Med. 2014;370:2339-41 [doi: 10.1056/NEJMe1404501]).
These studies offer two important considerations to clinicians, noted Dr. Robert C. Basner. First, CPAP may ameliorate hypertension and reduce cardiovascular risk in high-risk obese patients, even when they’re already being treated for hypertension and don’t have the daytime sleepiness that usually characterizes obstructive sleep apnea. Second, weight loss may reduce cardiovascular risks even further when CPAP is prescribed.
But further interpretation of the study findings is limited, Dr. Basner cautioned, because of the relatively low nightly use of CPAP (poor adherence) in the study by Dr. Gottlieb, and because of the wide variability in C-reactive protein values and the unusual statistical handling of those values in the study by Dr. Chirinos.
Dr. Basner is at Columbia University, New York. He was a member of the Data and Safety Monitoring Board of the study performed by Dr. Chirinos. These remarks were taken from his editorial accompanying the two studies (N. Engl. J. Med. 2014;370:2339-41 [doi: 10.1056/NEJMe1404501]).
The use of continuous positive airway pressure modestly reduced blood pressure in two separate studies involving obese patients who had moderate to severe obstructive sleep apnea, according to reports published online June 11 in the New England Journal of Medicine.
In contrast, neither the use of supplemental oxygen in one study nor a weight loss of approximately 7 kg in the other study had a beneficial effect on blood pressure.
In the first study, investigators compared the effects of CPAP against those of nocturnal supplemental oxygen on several markers of cardiovascular risk, including blood pressure. The multicenter study involved cardiology patients aged 45-75 years who either had established coronary heart disease or multiple cardiovascular risk factors, and who also were found to have obstructive sleep apnea when screened for the disorder.
The 318 patients were randomly assigned in equal numbers to receive CPAP plus education in healthy lifestyle and sleep practices, nocturnal supplemental oxygen delivered via cannula plus lifestyle and sleep education, or lifestyle and sleep education alone (the control group) for 12 weeks, said Dr. Daniel J. Gottlieb, of the Veterans Affairs Boston Healthcare System, and his associates.
The mean body mass index was 33.0 kg/m2 in the CPAP group, 34.7 kg/m2 in the supplemental oxygen group, and 33.7 kg/m2 in the education group. Average apnea-hypopnea index scores for the three groups were 25.4, 24.0, and 25.5 events per hour, respectively
At the end of the study, 24-hour mean arterial blood pressure was significantly lower among patients in the CPAP group (87.8 mm Hg) than with oxygen (90.2 mm Hg) or education alone (89.0 mm Hg), a "modest" difference in magnitude that nevertheless has been associated with "a meaningful reduction in cardiovascular risk," the investigators noted.
That benefit was seen even though those patients’ blood pressure was already well controlled by antihypertensive medications and even though their adherence to CPAP was only "average," said Dr. Gottleib, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and his colleagues.
In contrast, mean arterial blood pressure was not significantly different between patients who received supplemental oxygen and the control group, even though the supplemental oxygen did reduce nocturnal hypoxemia and adherence to oxygen therapy was much better than that for CPAP. A further analysis adjusting for potential confounders such as patient age, sex, race, body mass index, and type of antihypertensive medication had no appreciable effect on the results.
"This study offers no support for the common but largely untested clinical practice of providing supplemental oxygen as salvage therapy in patients with obstructive sleep apnea for whom CPAP is problematic," Dr. Gottlieb and his associates reported (N. Engl. J. Med. 2014;370:2276-85 [doi: 10.1056/NEJMoa1306766]).
In the second study, researchers compared the effects of 24 weeks of CPAP alone, weight loss alone, or CPAP plus weight loss in obese adults who had moderate to severe obstructive sleep apnea and elevated C-reactive protein levels. A total of 181 patients underwent randomization, but only 136 completed the study: 48 in the CPAP group, 42 in the weight-loss group, and 46 in the combined-intervention group, said Dr. Julio A. Chirinos, of the Philadelphia Veterans Affairs Medical Center and the University of Pennsylvania, and his associates.
At the conclusion of the intervention, weight loss was similar between the weight-loss–only group (6.8 kg) and the combined-intervention group (7.0 kg), while there was no change in the CPAP-only group.
The study’s primary endpoint was improvement in C-reactive protein levels. There was no significant difference among the three study groups for this outcome. However, the secondary outcome of significantly decreased systolic blood pressure was achieved with the combined intervention (–14.1 mm Hg), compared with weight loss alone (–6.8 mm Hg) or CPAP alone (–3.0 mm Hg).
The combined therapy also improved insulin resistance and serum triglyceride levels, Dr. Chirinos and his associates said (N. Engl. J. Med. 2014;370:2265-75 [doi: 10.1056/NEJMoa1306187]).
"Our study shows that a weight-loss intervention is effective as a central component of the strategies used to improve the cardiovascular risk-factor profile in patients with obesity and obstructive sleep apnea," they added.
Dr. Gottlieb’s study was supported by the National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Research Resources. Philips Respironics donated the equipment used in the study. Dr. Gottlieb reported ties to Philips Respironics and ResMed Corporation, and his associates reported ties to numerous industry sources.
Dr. Chirinos’s study also was supported by the NHLBI. ResMed provided CPAP equipment at no cost but had no role in study design, data accrual or analysis, or manuscript preparation. Dr. Chirinos reported no financial conflicts of interest; his associates reported ties to Boehringer Ingelheim, ConAgra Foods, Novo Nordisk, Nutrisystem, Orexigen, Tate and Lyle, United Health Group, and Weight Watchers.
The use of continuous positive airway pressure modestly reduced blood pressure in two separate studies involving obese patients who had moderate to severe obstructive sleep apnea, according to reports published online June 11 in the New England Journal of Medicine.
In contrast, neither the use of supplemental oxygen in one study nor a weight loss of approximately 7 kg in the other study had a beneficial effect on blood pressure.
In the first study, investigators compared the effects of CPAP against those of nocturnal supplemental oxygen on several markers of cardiovascular risk, including blood pressure. The multicenter study involved cardiology patients aged 45-75 years who either had established coronary heart disease or multiple cardiovascular risk factors, and who also were found to have obstructive sleep apnea when screened for the disorder.
The 318 patients were randomly assigned in equal numbers to receive CPAP plus education in healthy lifestyle and sleep practices, nocturnal supplemental oxygen delivered via cannula plus lifestyle and sleep education, or lifestyle and sleep education alone (the control group) for 12 weeks, said Dr. Daniel J. Gottlieb, of the Veterans Affairs Boston Healthcare System, and his associates.
The mean body mass index was 33.0 kg/m2 in the CPAP group, 34.7 kg/m2 in the supplemental oxygen group, and 33.7 kg/m2 in the education group. Average apnea-hypopnea index scores for the three groups were 25.4, 24.0, and 25.5 events per hour, respectively
At the end of the study, 24-hour mean arterial blood pressure was significantly lower among patients in the CPAP group (87.8 mm Hg) than with oxygen (90.2 mm Hg) or education alone (89.0 mm Hg), a "modest" difference in magnitude that nevertheless has been associated with "a meaningful reduction in cardiovascular risk," the investigators noted.
That benefit was seen even though those patients’ blood pressure was already well controlled by antihypertensive medications and even though their adherence to CPAP was only "average," said Dr. Gottleib, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and his colleagues.
In contrast, mean arterial blood pressure was not significantly different between patients who received supplemental oxygen and the control group, even though the supplemental oxygen did reduce nocturnal hypoxemia and adherence to oxygen therapy was much better than that for CPAP. A further analysis adjusting for potential confounders such as patient age, sex, race, body mass index, and type of antihypertensive medication had no appreciable effect on the results.
"This study offers no support for the common but largely untested clinical practice of providing supplemental oxygen as salvage therapy in patients with obstructive sleep apnea for whom CPAP is problematic," Dr. Gottlieb and his associates reported (N. Engl. J. Med. 2014;370:2276-85 [doi: 10.1056/NEJMoa1306766]).
In the second study, researchers compared the effects of 24 weeks of CPAP alone, weight loss alone, or CPAP plus weight loss in obese adults who had moderate to severe obstructive sleep apnea and elevated C-reactive protein levels. A total of 181 patients underwent randomization, but only 136 completed the study: 48 in the CPAP group, 42 in the weight-loss group, and 46 in the combined-intervention group, said Dr. Julio A. Chirinos, of the Philadelphia Veterans Affairs Medical Center and the University of Pennsylvania, and his associates.
At the conclusion of the intervention, weight loss was similar between the weight-loss–only group (6.8 kg) and the combined-intervention group (7.0 kg), while there was no change in the CPAP-only group.
The study’s primary endpoint was improvement in C-reactive protein levels. There was no significant difference among the three study groups for this outcome. However, the secondary outcome of significantly decreased systolic blood pressure was achieved with the combined intervention (–14.1 mm Hg), compared with weight loss alone (–6.8 mm Hg) or CPAP alone (–3.0 mm Hg).
The combined therapy also improved insulin resistance and serum triglyceride levels, Dr. Chirinos and his associates said (N. Engl. J. Med. 2014;370:2265-75 [doi: 10.1056/NEJMoa1306187]).
"Our study shows that a weight-loss intervention is effective as a central component of the strategies used to improve the cardiovascular risk-factor profile in patients with obesity and obstructive sleep apnea," they added.
Dr. Gottlieb’s study was supported by the National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Research Resources. Philips Respironics donated the equipment used in the study. Dr. Gottlieb reported ties to Philips Respironics and ResMed Corporation, and his associates reported ties to numerous industry sources.
Dr. Chirinos’s study also was supported by the NHLBI. ResMed provided CPAP equipment at no cost but had no role in study design, data accrual or analysis, or manuscript preparation. Dr. Chirinos reported no financial conflicts of interest; his associates reported ties to Boehringer Ingelheim, ConAgra Foods, Novo Nordisk, Nutrisystem, Orexigen, Tate and Lyle, United Health Group, and Weight Watchers.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: Twenty-four-hour mean arterial blood pressure was significantly lower among patients who received CPAP (87.8 mm Hg) than in those who received oxygen (90.2 mm Hg) or education alone (89.0 mm Hg). And significantly decreased systolic blood pressure was achieved with combined weight loss plus CPAP (–14.1 mm Hg), compared with weight loss alone (–6.8 mm Hg) or CPAP alone (–3.0 mm Hg).
Data source: A 12-week, multicenter, randomized clinical trial comparing the effects of CPAP against supplemental oxygen in 318 obese patients with obstructive sleep apnea, and a 24-week randomized clinical trial comparing the effects of CPAP, weight loss, and combined CPAP plus weight loss in 136 obese patients with obstructive sleep apnea.
Disclosures: Dr. Gottlieb’s study was supported by the National Heart, Lung, and Blood Institute (NHLBI) and the National Center for Research Resources. Philips Respironics donated the equipment used in the study. Dr. Gottlieb reported ties to Philips and ResMed. Dr. Chirinos’s study also was supported by the NHLBI. ResMed provided the CPAP equipment at no cost. Dr. Chirinos reported no financial conflicts of interest.

Viral reactivation common in septic patients, study finds
Critically ill patients with sepsis have a markedly higher prevalence of different viruses than do nonseptic critically ill patients and healthy controls, judging from the findings of a study of more than 800 patients.
These findings provide evidence that the reactivation of latent viruses "is extremely common in patients with prolonged sepsis and is consistent with development of immunosuppression," the authors concluded.
For some of the viruses, the levels detected in septic patients were comparable to the levels in organ transplant recipients, "who are pharmacologically immunosuppressed, providing further support that our findings are indicative of clinically relevant immunosuppression," Dr. Anthony Walton, of the department of anesthesiology, Washington University, St. Louis, and his coauthors wrote. The study was published online June 6 in PLoS One (2014;9:e98819 [doi: 10.1371/journal.pone.0098819]).
In what they said is the first study to evaluate the effect of sepsis on "multiple families of viruses," the investigators addressed whether sepsis progresses from a hyperinflammatory phase early in the course of sepsis to an immunosuppressive state, a "controversial hypothesis" for explaining the course of sepsis, they wrote.
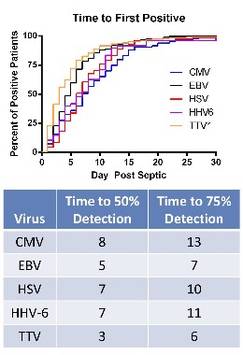
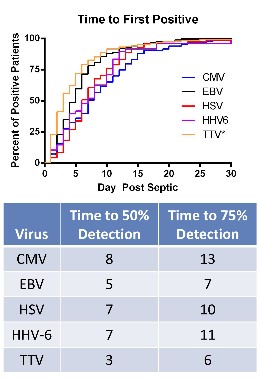
The researchers compared levels of viruses that included cytomegalovirus (CMV), Epstein-Barr virus (EBV), herpes simplex virus (HSV), human herpesvirus 6 (HHV-6), and the anellovirus TTV in whole blood and plasma of 560 critically ill patients with sepsis and 161 critically ill patients who did not have sepsis, who were not immunocompromised at baseline; and 164 healthy, age-matched controls, who were ambulatory and whose blood sample was obtained before elective surgery. The median age of the patients was 63-64 years; the median APACHE II score was 18 in the septic group and 5 in the critically ill, nonseptic group; and the median length of stay in the ICU was 11 days in the septic group and 2 days in the critically ill, nonseptic group. Mortality was 26% among those with sepsis and 6% among the critically ill, nonseptic group.
Among the investigators’ key findings were these:
• CMV seropositivity was detected in about 70% of the patients in the three groups, indicating they had been infected previously. Among these patients, CMV levels were markedly elevated in 24.2% of the septic patients, compared with 1.1% of the critically ill, nonseptic patients and none of the healthy controls.
• EBV was detected in 53.2% of those who were septic, compared with 12.1% of the critically ill, nonseptic patients and 3.6% of the healthy controls.
• HSV was detected in 14.1% of the septic patients, compared with 1.5% of the critically ill, nonseptic patients and none of the healthy controls.
• HHV-6 was detected in 10.4% of those who were septic, compared with less than 1% of the critically ill, nonseptic patients and 3.3% of the healthy controls.
• TTV was detected in almost 78% of the septic patients, close to 64% if the critically ill, nonseptic patients, and 60.1% of the healthy controls, but levels were lower among the latter two groups.
The authors said that it is "likely that viral detection in the setting of sepsis is not due to primary infection but rather to viral reactivation." Almost 43% of those with sepsis had evidence of at least two viruses, which, combined with the "magnitude of viral loads ... provides strong evidence that host immunity is impaired in sepsis," they added.
Among their other findings was that in the septic patients, the detection rate of the viruses increased for all the viruses with increasing number of days spent in the ICU, and septic patients who had CMV detected in the plasma had significantly higher 90-day mortality than did septic patients with no CMV detected.
Limitations of the study include the fact that it does not address whether the increased prevalence of viral reactivation among the septic patients "is merely a marker of impaired immunity or contributes to sepsis morbidity/mortality," they noted. But the implications of their results include the possibility that tracking the viral load of different viruses in septic patients "may be useful as a biomarker of host immunity in sepsis."
The study was funded by the National Institutes of Health. One of the 13 authors is an employee of Biomérieux, a company that is working on a method to monitor levels of different viruses in the blood as an indicator of immune status. No other author disclosures were listed.
The investigators have demonstrated that reactivation of latent viral infections may well contribute to the death of critically ill septic patients. Some of the viral reactivations were associated with secondary fungal infection as well.
Although viral DNA was detected as early as 1 day into sepsis, the bulk of the manifested reactivations occurred over the subsequent 2 weeks. Viral reactivation is a clear marker that the "late" immune suppression of sepsis is a real phenomenon and leads to real sequelae.
Nevertheless, it is not yet clear exactly how this information will become useful in practice, as the cost of daily DNA screening for multiple viruses would be prohibitive, unless high-volume demand drives pricing down. One can see, under that scenario, how viral reactivation could be the signal that immune augmentation therapy is required, and that it might be beneficial. This work is not quite ready for prime time, but it is getting ever closer.
Dr. Steven Q. Simpson is professor of medicine University of Kansas, Kansas City. He is also founder of the Kansas Sepsis Project. He had no disclosures.
The investigators have demonstrated that reactivation of latent viral infections may well contribute to the death of critically ill septic patients. Some of the viral reactivations were associated with secondary fungal infection as well.
Although viral DNA was detected as early as 1 day into sepsis, the bulk of the manifested reactivations occurred over the subsequent 2 weeks. Viral reactivation is a clear marker that the "late" immune suppression of sepsis is a real phenomenon and leads to real sequelae.
Nevertheless, it is not yet clear exactly how this information will become useful in practice, as the cost of daily DNA screening for multiple viruses would be prohibitive, unless high-volume demand drives pricing down. One can see, under that scenario, how viral reactivation could be the signal that immune augmentation therapy is required, and that it might be beneficial. This work is not quite ready for prime time, but it is getting ever closer.
Dr. Steven Q. Simpson is professor of medicine University of Kansas, Kansas City. He is also founder of the Kansas Sepsis Project. He had no disclosures.
The investigators have demonstrated that reactivation of latent viral infections may well contribute to the death of critically ill septic patients. Some of the viral reactivations were associated with secondary fungal infection as well.
Although viral DNA was detected as early as 1 day into sepsis, the bulk of the manifested reactivations occurred over the subsequent 2 weeks. Viral reactivation is a clear marker that the "late" immune suppression of sepsis is a real phenomenon and leads to real sequelae.
Nevertheless, it is not yet clear exactly how this information will become useful in practice, as the cost of daily DNA screening for multiple viruses would be prohibitive, unless high-volume demand drives pricing down. One can see, under that scenario, how viral reactivation could be the signal that immune augmentation therapy is required, and that it might be beneficial. This work is not quite ready for prime time, but it is getting ever closer.
Dr. Steven Q. Simpson is professor of medicine University of Kansas, Kansas City. He is also founder of the Kansas Sepsis Project. He had no disclosures.
Critically ill patients with sepsis have a markedly higher prevalence of different viruses than do nonseptic critically ill patients and healthy controls, judging from the findings of a study of more than 800 patients.
These findings provide evidence that the reactivation of latent viruses "is extremely common in patients with prolonged sepsis and is consistent with development of immunosuppression," the authors concluded.
For some of the viruses, the levels detected in septic patients were comparable to the levels in organ transplant recipients, "who are pharmacologically immunosuppressed, providing further support that our findings are indicative of clinically relevant immunosuppression," Dr. Anthony Walton, of the department of anesthesiology, Washington University, St. Louis, and his coauthors wrote. The study was published online June 6 in PLoS One (2014;9:e98819 [doi: 10.1371/journal.pone.0098819]).
In what they said is the first study to evaluate the effect of sepsis on "multiple families of viruses," the investigators addressed whether sepsis progresses from a hyperinflammatory phase early in the course of sepsis to an immunosuppressive state, a "controversial hypothesis" for explaining the course of sepsis, they wrote.
The researchers compared levels of viruses that included cytomegalovirus (CMV), Epstein-Barr virus (EBV), herpes simplex virus (HSV), human herpesvirus 6 (HHV-6), and the anellovirus TTV in whole blood and plasma of 560 critically ill patients with sepsis and 161 critically ill patients who did not have sepsis, who were not immunocompromised at baseline; and 164 healthy, age-matched controls, who were ambulatory and whose blood sample was obtained before elective surgery. The median age of the patients was 63-64 years; the median APACHE II score was 18 in the septic group and 5 in the critically ill, nonseptic group; and the median length of stay in the ICU was 11 days in the septic group and 2 days in the critically ill, nonseptic group. Mortality was 26% among those with sepsis and 6% among the critically ill, nonseptic group.
Among the investigators’ key findings were these:
• CMV seropositivity was detected in about 70% of the patients in the three groups, indicating they had been infected previously. Among these patients, CMV levels were markedly elevated in 24.2% of the septic patients, compared with 1.1% of the critically ill, nonseptic patients and none of the healthy controls.
• EBV was detected in 53.2% of those who were septic, compared with 12.1% of the critically ill, nonseptic patients and 3.6% of the healthy controls.
• HSV was detected in 14.1% of the septic patients, compared with 1.5% of the critically ill, nonseptic patients and none of the healthy controls.
• HHV-6 was detected in 10.4% of those who were septic, compared with less than 1% of the critically ill, nonseptic patients and 3.3% of the healthy controls.
• TTV was detected in almost 78% of the septic patients, close to 64% if the critically ill, nonseptic patients, and 60.1% of the healthy controls, but levels were lower among the latter two groups.
The authors said that it is "likely that viral detection in the setting of sepsis is not due to primary infection but rather to viral reactivation." Almost 43% of those with sepsis had evidence of at least two viruses, which, combined with the "magnitude of viral loads ... provides strong evidence that host immunity is impaired in sepsis," they added.
Among their other findings was that in the septic patients, the detection rate of the viruses increased for all the viruses with increasing number of days spent in the ICU, and septic patients who had CMV detected in the plasma had significantly higher 90-day mortality than did septic patients with no CMV detected.
Limitations of the study include the fact that it does not address whether the increased prevalence of viral reactivation among the septic patients "is merely a marker of impaired immunity or contributes to sepsis morbidity/mortality," they noted. But the implications of their results include the possibility that tracking the viral load of different viruses in septic patients "may be useful as a biomarker of host immunity in sepsis."
The study was funded by the National Institutes of Health. One of the 13 authors is an employee of Biomérieux, a company that is working on a method to monitor levels of different viruses in the blood as an indicator of immune status. No other author disclosures were listed.
Critically ill patients with sepsis have a markedly higher prevalence of different viruses than do nonseptic critically ill patients and healthy controls, judging from the findings of a study of more than 800 patients.
These findings provide evidence that the reactivation of latent viruses "is extremely common in patients with prolonged sepsis and is consistent with development of immunosuppression," the authors concluded.
For some of the viruses, the levels detected in septic patients were comparable to the levels in organ transplant recipients, "who are pharmacologically immunosuppressed, providing further support that our findings are indicative of clinically relevant immunosuppression," Dr. Anthony Walton, of the department of anesthesiology, Washington University, St. Louis, and his coauthors wrote. The study was published online June 6 in PLoS One (2014;9:e98819 [doi: 10.1371/journal.pone.0098819]).
In what they said is the first study to evaluate the effect of sepsis on "multiple families of viruses," the investigators addressed whether sepsis progresses from a hyperinflammatory phase early in the course of sepsis to an immunosuppressive state, a "controversial hypothesis" for explaining the course of sepsis, they wrote.
The researchers compared levels of viruses that included cytomegalovirus (CMV), Epstein-Barr virus (EBV), herpes simplex virus (HSV), human herpesvirus 6 (HHV-6), and the anellovirus TTV in whole blood and plasma of 560 critically ill patients with sepsis and 161 critically ill patients who did not have sepsis, who were not immunocompromised at baseline; and 164 healthy, age-matched controls, who were ambulatory and whose blood sample was obtained before elective surgery. The median age of the patients was 63-64 years; the median APACHE II score was 18 in the septic group and 5 in the critically ill, nonseptic group; and the median length of stay in the ICU was 11 days in the septic group and 2 days in the critically ill, nonseptic group. Mortality was 26% among those with sepsis and 6% among the critically ill, nonseptic group.
Among the investigators’ key findings were these:
• CMV seropositivity was detected in about 70% of the patients in the three groups, indicating they had been infected previously. Among these patients, CMV levels were markedly elevated in 24.2% of the septic patients, compared with 1.1% of the critically ill, nonseptic patients and none of the healthy controls.
• EBV was detected in 53.2% of those who were septic, compared with 12.1% of the critically ill, nonseptic patients and 3.6% of the healthy controls.
• HSV was detected in 14.1% of the septic patients, compared with 1.5% of the critically ill, nonseptic patients and none of the healthy controls.
• HHV-6 was detected in 10.4% of those who were septic, compared with less than 1% of the critically ill, nonseptic patients and 3.3% of the healthy controls.
• TTV was detected in almost 78% of the septic patients, close to 64% if the critically ill, nonseptic patients, and 60.1% of the healthy controls, but levels were lower among the latter two groups.
The authors said that it is "likely that viral detection in the setting of sepsis is not due to primary infection but rather to viral reactivation." Almost 43% of those with sepsis had evidence of at least two viruses, which, combined with the "magnitude of viral loads ... provides strong evidence that host immunity is impaired in sepsis," they added.
Among their other findings was that in the septic patients, the detection rate of the viruses increased for all the viruses with increasing number of days spent in the ICU, and septic patients who had CMV detected in the plasma had significantly higher 90-day mortality than did septic patients with no CMV detected.
Limitations of the study include the fact that it does not address whether the increased prevalence of viral reactivation among the septic patients "is merely a marker of impaired immunity or contributes to sepsis morbidity/mortality," they noted. But the implications of their results include the possibility that tracking the viral load of different viruses in septic patients "may be useful as a biomarker of host immunity in sepsis."
The study was funded by the National Institutes of Health. One of the 13 authors is an employee of Biomérieux, a company that is working on a method to monitor levels of different viruses in the blood as an indicator of immune status. No other author disclosures were listed.
FROM PLOS ONE
Key clinical point: Reactivation of latent viruses may underlie the development of sepsis in critically ill patients and contribute to their death.
Major finding: Evidence of reactivation with multiple viruses in septic patients – which included almost 43% who were positive for at least two viruses – and the magnitude of viral loads in septic patients indicate that patients with sepsis are immunosuppressed.
Data source: The study compared levels of cytomegalovirus, herpes simplex, and other viruses in 560 critically ill septic patients and 161 critically ill nonseptic patients in intensive care units, and 164 healthy, age-matched controls.
Disclosures: The study was funded by the National Institutes of Health. One of the 13 authors is an employee of Biomérieux, a company that is working on a method to monitor levels of different viruses in the blood as an indicator of immune status. No other author disclosures were listed.
Insomnia with very short sleep duration is a risk factor for cancer
MINNEAPOLIS – People who have the type of insomnia characterized by a sharply shortened duration of sleep are at increased risk for cancer, a longitudinal cohort study showed.
In the study of more than 1,600 adults from the general population, those who reported insomnia and slept 5 hours or less per night as determined by polysomnography had more than double the adjusted cancer risk of their insomnia-free counterparts who slept longer. But the association was no longer significant after depression was controlled for.

"Insomnia with severe short sleep duration is associated with increased risk of cancer, particularly in those with comorbid depression," commented first author Julio Fernandez-Mendoza, Ph.D., of the sleep research and treatment center, department of psychiatry, Penn State College of Medicine, Hershey.
Previous research has established a dose-response relationship between objectively measured sleep duration and other adverse health outcomes, he noted. "For us, basically, objective sleep duration is a biomarker, is an assay, is the best we have right now. ... These findings expand on our previous studies, and it appears that we can continue using this assay to explore the medical morbidity associated with this insomnia phenotype."
In an interview, session cochair Dr. Ruth M. Benca, director of the center for sleep medicine and sleep research at the University of Wisconsin–Madison, commented, "The whole connection between sleep and cancer has now come to the fore with some of the recent studies showing, for example, that sleep apnea seems to be a risk factor for the ultimate development of cancer. And these new data suggest that insomnia, or insomnia and depression, may also play a role. We need more mechanistic studies to understand how those links may work."
The picture is complicated by overlaps between apnea and insomnia, she noted. "People with apnea can have high rates of insomnia, and both insomnia and apnea can be associated with fragmented sleep or insufficient sleep. So is it the insufficient sleep that’s a problem? Do hypoxemia and apnea also contribute? There are some animal studies that suggest that hypoxemia is related to cancer progression."
In the study, the investigators analyzed data from 1,620 individuals in the Penn State cohort who had no history of cancer at baseline. Insomnia was defined as self-reported insomnia present for at least 1 year, and very short sleep duration was defined as 5 hours or less as determined by polysomnography.
After a follow-up of about 15 years, 12.3% of the individuals experienced incident cancer, defined as a cancer diagnosis or death from the disease.
In an analysis adjusted for traditional confounders (sex, age, race, apnea-hypopnea index, body mass index, diabetes, and hypertension), relative to noninsomniacs who slept more than 5 hours nightly, insomniacs who slept 5 hours or less had significant 2.73-fold higher odds of incident cancer.
However, the association was no longer significant after additional adjustment for depression. "This makes sense because we do know very well two things: the strong association of depression with cancer, and second, the strong association of insomnia with depression. They have a lot in common, particularly inflammation. They have in common fatigue also," Dr. Fernandez-Mendoza said at the annual meeting of the Associated Professional Sleep Societies.
Similarly, the association was not significant after additional adjustment for smoking and alcohol use. "That was primarily driven by something that we learned from our natural history papers: Because these are basically behavioral factors, many insomniacs stop smoking or stop using so much alcohol, just related to the sleep hygiene thing," he commented.
The investigators have not yet assessed whether insomnia with very short sleep duration is associated with specific types of cancer, according to Dr. Fernandez-Mendoza.
Of note, insomniacs who slept more than 5 hours did not have elevated odds of cancer. Nor did noninsomniacs who slept 5 hours or less.
Dr. Fernandez-Mendoza disclosed no relevant conflicts of interest.
MINNEAPOLIS – People who have the type of insomnia characterized by a sharply shortened duration of sleep are at increased risk for cancer, a longitudinal cohort study showed.
In the study of more than 1,600 adults from the general population, those who reported insomnia and slept 5 hours or less per night as determined by polysomnography had more than double the adjusted cancer risk of their insomnia-free counterparts who slept longer. But the association was no longer significant after depression was controlled for.
"Insomnia with severe short sleep duration is associated with increased risk of cancer, particularly in those with comorbid depression," commented first author Julio Fernandez-Mendoza, Ph.D., of the sleep research and treatment center, department of psychiatry, Penn State College of Medicine, Hershey.
Previous research has established a dose-response relationship between objectively measured sleep duration and other adverse health outcomes, he noted. "For us, basically, objective sleep duration is a biomarker, is an assay, is the best we have right now. ... These findings expand on our previous studies, and it appears that we can continue using this assay to explore the medical morbidity associated with this insomnia phenotype."
In an interview, session cochair Dr. Ruth M. Benca, director of the center for sleep medicine and sleep research at the University of Wisconsin–Madison, commented, "The whole connection between sleep and cancer has now come to the fore with some of the recent studies showing, for example, that sleep apnea seems to be a risk factor for the ultimate development of cancer. And these new data suggest that insomnia, or insomnia and depression, may also play a role. We need more mechanistic studies to understand how those links may work."
The picture is complicated by overlaps between apnea and insomnia, she noted. "People with apnea can have high rates of insomnia, and both insomnia and apnea can be associated with fragmented sleep or insufficient sleep. So is it the insufficient sleep that’s a problem? Do hypoxemia and apnea also contribute? There are some animal studies that suggest that hypoxemia is related to cancer progression."
In the study, the investigators analyzed data from 1,620 individuals in the Penn State cohort who had no history of cancer at baseline. Insomnia was defined as self-reported insomnia present for at least 1 year, and very short sleep duration was defined as 5 hours or less as determined by polysomnography.
After a follow-up of about 15 years, 12.3% of the individuals experienced incident cancer, defined as a cancer diagnosis or death from the disease.
In an analysis adjusted for traditional confounders (sex, age, race, apnea-hypopnea index, body mass index, diabetes, and hypertension), relative to noninsomniacs who slept more than 5 hours nightly, insomniacs who slept 5 hours or less had significant 2.73-fold higher odds of incident cancer.
However, the association was no longer significant after additional adjustment for depression. "This makes sense because we do know very well two things: the strong association of depression with cancer, and second, the strong association of insomnia with depression. They have a lot in common, particularly inflammation. They have in common fatigue also," Dr. Fernandez-Mendoza said at the annual meeting of the Associated Professional Sleep Societies.
Similarly, the association was not significant after additional adjustment for smoking and alcohol use. "That was primarily driven by something that we learned from our natural history papers: Because these are basically behavioral factors, many insomniacs stop smoking or stop using so much alcohol, just related to the sleep hygiene thing," he commented.
The investigators have not yet assessed whether insomnia with very short sleep duration is associated with specific types of cancer, according to Dr. Fernandez-Mendoza.
Of note, insomniacs who slept more than 5 hours did not have elevated odds of cancer. Nor did noninsomniacs who slept 5 hours or less.
Dr. Fernandez-Mendoza disclosed no relevant conflicts of interest.
MINNEAPOLIS – People who have the type of insomnia characterized by a sharply shortened duration of sleep are at increased risk for cancer, a longitudinal cohort study showed.
In the study of more than 1,600 adults from the general population, those who reported insomnia and slept 5 hours or less per night as determined by polysomnography had more than double the adjusted cancer risk of their insomnia-free counterparts who slept longer. But the association was no longer significant after depression was controlled for.
"Insomnia with severe short sleep duration is associated with increased risk of cancer, particularly in those with comorbid depression," commented first author Julio Fernandez-Mendoza, Ph.D., of the sleep research and treatment center, department of psychiatry, Penn State College of Medicine, Hershey.
Previous research has established a dose-response relationship between objectively measured sleep duration and other adverse health outcomes, he noted. "For us, basically, objective sleep duration is a biomarker, is an assay, is the best we have right now. ... These findings expand on our previous studies, and it appears that we can continue using this assay to explore the medical morbidity associated with this insomnia phenotype."
In an interview, session cochair Dr. Ruth M. Benca, director of the center for sleep medicine and sleep research at the University of Wisconsin–Madison, commented, "The whole connection between sleep and cancer has now come to the fore with some of the recent studies showing, for example, that sleep apnea seems to be a risk factor for the ultimate development of cancer. And these new data suggest that insomnia, or insomnia and depression, may also play a role. We need more mechanistic studies to understand how those links may work."
The picture is complicated by overlaps between apnea and insomnia, she noted. "People with apnea can have high rates of insomnia, and both insomnia and apnea can be associated with fragmented sleep or insufficient sleep. So is it the insufficient sleep that’s a problem? Do hypoxemia and apnea also contribute? There are some animal studies that suggest that hypoxemia is related to cancer progression."
In the study, the investigators analyzed data from 1,620 individuals in the Penn State cohort who had no history of cancer at baseline. Insomnia was defined as self-reported insomnia present for at least 1 year, and very short sleep duration was defined as 5 hours or less as determined by polysomnography.
After a follow-up of about 15 years, 12.3% of the individuals experienced incident cancer, defined as a cancer diagnosis or death from the disease.
In an analysis adjusted for traditional confounders (sex, age, race, apnea-hypopnea index, body mass index, diabetes, and hypertension), relative to noninsomniacs who slept more than 5 hours nightly, insomniacs who slept 5 hours or less had significant 2.73-fold higher odds of incident cancer.
However, the association was no longer significant after additional adjustment for depression. "This makes sense because we do know very well two things: the strong association of depression with cancer, and second, the strong association of insomnia with depression. They have a lot in common, particularly inflammation. They have in common fatigue also," Dr. Fernandez-Mendoza said at the annual meeting of the Associated Professional Sleep Societies.
Similarly, the association was not significant after additional adjustment for smoking and alcohol use. "That was primarily driven by something that we learned from our natural history papers: Because these are basically behavioral factors, many insomniacs stop smoking or stop using so much alcohol, just related to the sleep hygiene thing," he commented.
The investigators have not yet assessed whether insomnia with very short sleep duration is associated with specific types of cancer, according to Dr. Fernandez-Mendoza.
Of note, insomniacs who slept more than 5 hours did not have elevated odds of cancer. Nor did noninsomniacs who slept 5 hours or less.
Dr. Fernandez-Mendoza disclosed no relevant conflicts of interest.
AT SLEEP 2014
Key clinical point: Short sleep duration increases risk of cancer.
Major finding: Insomniacs who slept 5 hours or less nightly had 2.73-fold higher adjusted odds of cancer when compared with noninsomniacs who slept more than 5 hours.
Data source: A longitudinal cohort study of 1,620 individuals from the general population.
Disclosures: Dr. Fernandez-Mendoza disclosed no relevant conflicts of interest.

CPAP compliance similar among patients treated in primary care and sleep clinics
SAN DIEGO – Among patients diagnosed with obstructive sleep apnea, compliance with continuous positive airway pressure devices was similar whether they received treatment in a primary care clinic or in a sleep clinic, results from a Spanish study demonstrated.
However, after 6 months of follow-up, patients who received treatment in a sleep clinic had significantly better Epworth Sleepiness Scale (ESS) scores and ratings of satisfaction, compared with those who received treatment in a primary care clinic.
"OSA affects 4%-6% of the adult population, but only 10% of those with severe disease are treated," Dr. Ferran Barbé said at an international conference of the American Thoracic Society. "In all prevalent and chronic disease, all levels of assistance must be implicated."

In a controlled, noninferiority study, Dr. Barbé and his associates randomized 210 patients diagnosed with obstructive sleep apnea to receive management of continuous positive airway pressure (CPAP) compliance in one of two settings: 100 to one of eight primary care clinics in the region of Lleida, Spain, and 110 to the sleep unit at the University of Lleida. The main outcome was CPAP compliance at 6 months of follow-up. Secondary outcomes included change in the EuroQol scale score, patient satisfaction based on a 10-point visual analog scale, and the change in the ESS score.
The mean age of study participants was 56 years, and 80% were men. CPAP compliance was similar between patients in the sleep clinic group and those in the primary care group (a mean of 5.2 vs. 4.9 hr/day, respectively; P = .28), as was the change in EuroQol scale score (a mean change of 0.17; P = .49). However, patients in the sleep clinic group reported significantly higher rates of satisfaction, compared with their counterparts in the primary care group (a score of 9 vs. 7.5; P less than .001). They also demonstrated significantly greater changes in ESS score (–6.07 vs. –4.09; P = .04).
Overall treatment costs were less expensive in the primary care group, compared with the sleep clinic group.
Primary care physicians "need to reinforce actions that improve self-reported well-being in OSA patients," Dr. Barbé concluded.
The study was supported by the Instituto de Salud Carlos III, the Spanish Society of Pulmonology and Thoracic Surgery, Societat Catalana de Pneumologia, and ALLER (Respiratory Association of Lleida). Dr. Barbé said he had no relevant financial conflicts to disclose.
SAN DIEGO – Among patients diagnosed with obstructive sleep apnea, compliance with continuous positive airway pressure devices was similar whether they received treatment in a primary care clinic or in a sleep clinic, results from a Spanish study demonstrated.
However, after 6 months of follow-up, patients who received treatment in a sleep clinic had significantly better Epworth Sleepiness Scale (ESS) scores and ratings of satisfaction, compared with those who received treatment in a primary care clinic.
"OSA affects 4%-6% of the adult population, but only 10% of those with severe disease are treated," Dr. Ferran Barbé said at an international conference of the American Thoracic Society. "In all prevalent and chronic disease, all levels of assistance must be implicated."
In a controlled, noninferiority study, Dr. Barbé and his associates randomized 210 patients diagnosed with obstructive sleep apnea to receive management of continuous positive airway pressure (CPAP) compliance in one of two settings: 100 to one of eight primary care clinics in the region of Lleida, Spain, and 110 to the sleep unit at the University of Lleida. The main outcome was CPAP compliance at 6 months of follow-up. Secondary outcomes included change in the EuroQol scale score, patient satisfaction based on a 10-point visual analog scale, and the change in the ESS score.
The mean age of study participants was 56 years, and 80% were men. CPAP compliance was similar between patients in the sleep clinic group and those in the primary care group (a mean of 5.2 vs. 4.9 hr/day, respectively; P = .28), as was the change in EuroQol scale score (a mean change of 0.17; P = .49). However, patients in the sleep clinic group reported significantly higher rates of satisfaction, compared with their counterparts in the primary care group (a score of 9 vs. 7.5; P less than .001). They also demonstrated significantly greater changes in ESS score (–6.07 vs. –4.09; P = .04).
Overall treatment costs were less expensive in the primary care group, compared with the sleep clinic group.
Primary care physicians "need to reinforce actions that improve self-reported well-being in OSA patients," Dr. Barbé concluded.
The study was supported by the Instituto de Salud Carlos III, the Spanish Society of Pulmonology and Thoracic Surgery, Societat Catalana de Pneumologia, and ALLER (Respiratory Association of Lleida). Dr. Barbé said he had no relevant financial conflicts to disclose.
SAN DIEGO – Among patients diagnosed with obstructive sleep apnea, compliance with continuous positive airway pressure devices was similar whether they received treatment in a primary care clinic or in a sleep clinic, results from a Spanish study demonstrated.
However, after 6 months of follow-up, patients who received treatment in a sleep clinic had significantly better Epworth Sleepiness Scale (ESS) scores and ratings of satisfaction, compared with those who received treatment in a primary care clinic.
"OSA affects 4%-6% of the adult population, but only 10% of those with severe disease are treated," Dr. Ferran Barbé said at an international conference of the American Thoracic Society. "In all prevalent and chronic disease, all levels of assistance must be implicated."
In a controlled, noninferiority study, Dr. Barbé and his associates randomized 210 patients diagnosed with obstructive sleep apnea to receive management of continuous positive airway pressure (CPAP) compliance in one of two settings: 100 to one of eight primary care clinics in the region of Lleida, Spain, and 110 to the sleep unit at the University of Lleida. The main outcome was CPAP compliance at 6 months of follow-up. Secondary outcomes included change in the EuroQol scale score, patient satisfaction based on a 10-point visual analog scale, and the change in the ESS score.
The mean age of study participants was 56 years, and 80% were men. CPAP compliance was similar between patients in the sleep clinic group and those in the primary care group (a mean of 5.2 vs. 4.9 hr/day, respectively; P = .28), as was the change in EuroQol scale score (a mean change of 0.17; P = .49). However, patients in the sleep clinic group reported significantly higher rates of satisfaction, compared with their counterparts in the primary care group (a score of 9 vs. 7.5; P less than .001). They also demonstrated significantly greater changes in ESS score (–6.07 vs. –4.09; P = .04).
Overall treatment costs were less expensive in the primary care group, compared with the sleep clinic group.
Primary care physicians "need to reinforce actions that improve self-reported well-being in OSA patients," Dr. Barbé concluded.
The study was supported by the Instituto de Salud Carlos III, the Spanish Society of Pulmonology and Thoracic Surgery, Societat Catalana de Pneumologia, and ALLER (Respiratory Association of Lleida). Dr. Barbé said he had no relevant financial conflicts to disclose.
AT ATS 2014
Key clinical point: Among patients with obstructive sleep apnea, compliance with CPAP devices in a primary care clinic setting was similar to that in a sleep clinic setting.
Major finding: CPAP compliance was similar between patients in the sleep clinic group and those in the primary care group (a mean of 5.2 vs. 4.9 hr/day, respectively; P = .28), as was the change in EuroQol scale scores (a mean change of 0.17; P = .49).
Data source: A controlled, noninferiority study of 210 patients diagnosed with obstructive sleep apnea who were randomized to receive management of CPAP compliance in one of two settings: 100 to one of eight primary care clinics in the region of Lleida, Spain, and 110 to the sleep unit at the University of Lleida.
Disclosures: The study was supported by the Instituto de Salud Carlos III, the Spanish Society of Pulmonology and Thoracic Surgery, and the Societat Catalana de Pneumologia. Dr. Barbé said that he had no relevant financial conflicts to disclose.

Two behavioral therapies are on par for alleviating insomnia in cancer survivors
MINNEAPOLIS – Both cognitive behavioral therapy for insomnia and mindfulness-based stress reduction training lessened insomnia in a group of cancer survivors, although the former works faster, new data show.
Investigators compared the two therapies head to head in I-CAN SLEEP (A Comparison of MBSR and CBT for the Treatment of Insomnia in Cancer), a randomized, partially blinded noninferiority trial among 111 adult patients from a tertiary care center in Calgary, Alta., who had nonmetastatic cancer and were at least 1 month out from completion of treatment. The behavioral therapies lasted 8 weeks.

At the end of the behavioral therapy, mindfulness-based stress reduction (MBSR) was inferior to cognitive behavioral therapy for insomnia (CBT-I) in terms of the difference in Insomnia Severity Index. But at 3 months, MBSR met the noninferiority criterion, with the 3.47-point upper bound of the confidence interval for the difference between groups falling within the predefined 4-point threshold (P = .01), Sheila N. Garland, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies. The data were recently published (J. Clin. Oncol. 2014;32:449-57).
Also at 3 months, diary data showed that sleep-onset latency had fallen from baseline by 14 minutes with MBSR and 22 minutes with CBT-I. The groups had a similar reduction in wake after sleep onset of about 35 minutes. Total sleep time increased by 0.73 hours with MBSR and 0.60 hours with CBT-I. Sleep efficiency improved by approximately 8% and 12%. And both therapies achieved a significant reduction in stress and mood disturbance.
"We confirmed that CBT-I produces faster effects and durable effects [when compared with] MBSR, but at 3 months, the two treatments are somewhat comparable and MBSR was not inferior according to our definition," said Dr. Garland of the department of family medicine and community health, University of Pennsylvania, Philadelphia.
"Both treatments were demonstrated to be effective for reducing symptoms of stress and mood disturbance, but I do believe that longer-term follow-up and comparisons are necessary because where CBT-I might be easy to grasp within, say, a 4-week period, mindfulness-based techniques are going to maybe take a little bit longer to incorporate into someone’s life and maybe apply to their sleep. So perhaps more practice is needed before we actually see longer effects."
Importantly, the rate of loss to follow-up at 3 months was 15% with CBT-I but a dramatic 50% with MBSR, with most of this dropout occurring within the first three sessions, noted Dr. Garland. She attributed the latter to the fact that patients were not aware of the specific treatments that were being compared when they agreed to participate in the study, which might have prevented dropout if they did not receive their preferred treatment.
"I actually believe that the blinding may underestimate clinical effectiveness, and this is because these people wouldn’t have normally chosen to practice mindfulness meditation, and that’s an important thing to note in terms of delivering behavioral interventions: people have to be willing, they have to buy into the intervention. So that’s what I think actually contributed to the large dropout," she elaborated. "You would see probably better improvement if they actually chose to go to that intervention. So my intention to blind participants to prevent that preferential dropout ... Well, these results say they are going to drop out anyway.
"This suggests that we should not apply a ‘one-size-fits-all model’ to the treatment of insomnia and emphasizes the need to individualize treatment based on patient characteristics and preferences," she added in an interview.
Session cochair Colin Espie, Ph.D., D.Sc., a professor of sleep medicine in the Nuffield department of clinical neuroscience at the University of Oxford (England), commented, "I think it’s really good to see other treatments being used, particularly in comorbid populations because clearly for people with cancer, sleep is occurring in a particular context and there may be advantages of a mindful approach to your situation in general, of which sleep is a part."
"But I thought there were maybe some design flaws there in that [the patients] maybe didn’t get what they thought was [being offered]. So maybe they thought they’d be getting treatment for insomnia, and it might not be obvious to people that mindfulness was focused on that," he added in an interview.
Dr. Espie also expressed reservations about the small sample size. "I think that to do a noninferiority trial, you need very, very large numbers because you really need to be able to demonstrate that you’ve properly tested the hypothesis and found no difference between those groups. And it was probably quite underpowered from that point of view," he said.
Dr. Garland disclosed no relevant conflicts of interest.
MINNEAPOLIS – Both cognitive behavioral therapy for insomnia and mindfulness-based stress reduction training lessened insomnia in a group of cancer survivors, although the former works faster, new data show.
Investigators compared the two therapies head to head in I-CAN SLEEP (A Comparison of MBSR and CBT for the Treatment of Insomnia in Cancer), a randomized, partially blinded noninferiority trial among 111 adult patients from a tertiary care center in Calgary, Alta., who had nonmetastatic cancer and were at least 1 month out from completion of treatment. The behavioral therapies lasted 8 weeks.
At the end of the behavioral therapy, mindfulness-based stress reduction (MBSR) was inferior to cognitive behavioral therapy for insomnia (CBT-I) in terms of the difference in Insomnia Severity Index. But at 3 months, MBSR met the noninferiority criterion, with the 3.47-point upper bound of the confidence interval for the difference between groups falling within the predefined 4-point threshold (P = .01), Sheila N. Garland, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies. The data were recently published (J. Clin. Oncol. 2014;32:449-57).
Also at 3 months, diary data showed that sleep-onset latency had fallen from baseline by 14 minutes with MBSR and 22 minutes with CBT-I. The groups had a similar reduction in wake after sleep onset of about 35 minutes. Total sleep time increased by 0.73 hours with MBSR and 0.60 hours with CBT-I. Sleep efficiency improved by approximately 8% and 12%. And both therapies achieved a significant reduction in stress and mood disturbance.
"We confirmed that CBT-I produces faster effects and durable effects [when compared with] MBSR, but at 3 months, the two treatments are somewhat comparable and MBSR was not inferior according to our definition," said Dr. Garland of the department of family medicine and community health, University of Pennsylvania, Philadelphia.
"Both treatments were demonstrated to be effective for reducing symptoms of stress and mood disturbance, but I do believe that longer-term follow-up and comparisons are necessary because where CBT-I might be easy to grasp within, say, a 4-week period, mindfulness-based techniques are going to maybe take a little bit longer to incorporate into someone’s life and maybe apply to their sleep. So perhaps more practice is needed before we actually see longer effects."
Importantly, the rate of loss to follow-up at 3 months was 15% with CBT-I but a dramatic 50% with MBSR, with most of this dropout occurring within the first three sessions, noted Dr. Garland. She attributed the latter to the fact that patients were not aware of the specific treatments that were being compared when they agreed to participate in the study, which might have prevented dropout if they did not receive their preferred treatment.
"I actually believe that the blinding may underestimate clinical effectiveness, and this is because these people wouldn’t have normally chosen to practice mindfulness meditation, and that’s an important thing to note in terms of delivering behavioral interventions: people have to be willing, they have to buy into the intervention. So that’s what I think actually contributed to the large dropout," she elaborated. "You would see probably better improvement if they actually chose to go to that intervention. So my intention to blind participants to prevent that preferential dropout ... Well, these results say they are going to drop out anyway.
"This suggests that we should not apply a ‘one-size-fits-all model’ to the treatment of insomnia and emphasizes the need to individualize treatment based on patient characteristics and preferences," she added in an interview.
Session cochair Colin Espie, Ph.D., D.Sc., a professor of sleep medicine in the Nuffield department of clinical neuroscience at the University of Oxford (England), commented, "I think it’s really good to see other treatments being used, particularly in comorbid populations because clearly for people with cancer, sleep is occurring in a particular context and there may be advantages of a mindful approach to your situation in general, of which sleep is a part."
"But I thought there were maybe some design flaws there in that [the patients] maybe didn’t get what they thought was [being offered]. So maybe they thought they’d be getting treatment for insomnia, and it might not be obvious to people that mindfulness was focused on that," he added in an interview.
Dr. Espie also expressed reservations about the small sample size. "I think that to do a noninferiority trial, you need very, very large numbers because you really need to be able to demonstrate that you’ve properly tested the hypothesis and found no difference between those groups. And it was probably quite underpowered from that point of view," he said.
Dr. Garland disclosed no relevant conflicts of interest.
MINNEAPOLIS – Both cognitive behavioral therapy for insomnia and mindfulness-based stress reduction training lessened insomnia in a group of cancer survivors, although the former works faster, new data show.
Investigators compared the two therapies head to head in I-CAN SLEEP (A Comparison of MBSR and CBT for the Treatment of Insomnia in Cancer), a randomized, partially blinded noninferiority trial among 111 adult patients from a tertiary care center in Calgary, Alta., who had nonmetastatic cancer and were at least 1 month out from completion of treatment. The behavioral therapies lasted 8 weeks.
At the end of the behavioral therapy, mindfulness-based stress reduction (MBSR) was inferior to cognitive behavioral therapy for insomnia (CBT-I) in terms of the difference in Insomnia Severity Index. But at 3 months, MBSR met the noninferiority criterion, with the 3.47-point upper bound of the confidence interval for the difference between groups falling within the predefined 4-point threshold (P = .01), Sheila N. Garland, Ph.D., reported at the annual meeting of the Associated Professional Sleep Societies. The data were recently published (J. Clin. Oncol. 2014;32:449-57).
Also at 3 months, diary data showed that sleep-onset latency had fallen from baseline by 14 minutes with MBSR and 22 minutes with CBT-I. The groups had a similar reduction in wake after sleep onset of about 35 minutes. Total sleep time increased by 0.73 hours with MBSR and 0.60 hours with CBT-I. Sleep efficiency improved by approximately 8% and 12%. And both therapies achieved a significant reduction in stress and mood disturbance.
"We confirmed that CBT-I produces faster effects and durable effects [when compared with] MBSR, but at 3 months, the two treatments are somewhat comparable and MBSR was not inferior according to our definition," said Dr. Garland of the department of family medicine and community health, University of Pennsylvania, Philadelphia.
"Both treatments were demonstrated to be effective for reducing symptoms of stress and mood disturbance, but I do believe that longer-term follow-up and comparisons are necessary because where CBT-I might be easy to grasp within, say, a 4-week period, mindfulness-based techniques are going to maybe take a little bit longer to incorporate into someone’s life and maybe apply to their sleep. So perhaps more practice is needed before we actually see longer effects."
Importantly, the rate of loss to follow-up at 3 months was 15% with CBT-I but a dramatic 50% with MBSR, with most of this dropout occurring within the first three sessions, noted Dr. Garland. She attributed the latter to the fact that patients were not aware of the specific treatments that were being compared when they agreed to participate in the study, which might have prevented dropout if they did not receive their preferred treatment.
"I actually believe that the blinding may underestimate clinical effectiveness, and this is because these people wouldn’t have normally chosen to practice mindfulness meditation, and that’s an important thing to note in terms of delivering behavioral interventions: people have to be willing, they have to buy into the intervention. So that’s what I think actually contributed to the large dropout," she elaborated. "You would see probably better improvement if they actually chose to go to that intervention. So my intention to blind participants to prevent that preferential dropout ... Well, these results say they are going to drop out anyway.
"This suggests that we should not apply a ‘one-size-fits-all model’ to the treatment of insomnia and emphasizes the need to individualize treatment based on patient characteristics and preferences," she added in an interview.
Session cochair Colin Espie, Ph.D., D.Sc., a professor of sleep medicine in the Nuffield department of clinical neuroscience at the University of Oxford (England), commented, "I think it’s really good to see other treatments being used, particularly in comorbid populations because clearly for people with cancer, sleep is occurring in a particular context and there may be advantages of a mindful approach to your situation in general, of which sleep is a part."
"But I thought there were maybe some design flaws there in that [the patients] maybe didn’t get what they thought was [being offered]. So maybe they thought they’d be getting treatment for insomnia, and it might not be obvious to people that mindfulness was focused on that," he added in an interview.
Dr. Espie also expressed reservations about the small sample size. "I think that to do a noninferiority trial, you need very, very large numbers because you really need to be able to demonstrate that you’ve properly tested the hypothesis and found no difference between those groups. And it was probably quite underpowered from that point of view," he said.
Dr. Garland disclosed no relevant conflicts of interest.
AT SLEEP 2014
Key clinical point: Two behavioral therapies lessen insomnia in cancer survivors.
Major finding: At 3 months, MBSR was not inferior to CBT-I in terms of scores on the Insomnia Severity Index (P = .01).
Data source: A randomized partially blinded noninferiority trial of 111 cancer survivors with insomnia.
Disclosures: Dr. Garland disclosed no relevant conflicts of interest.

MERS virus can be transmitted from camels to humans, case report shows
A case report on a camel-to-human transmission of Middle East respiratory syndrome coronavirus (MERS-CoV) offers the first conclusive evidence that the virus can be transmitted directly from camels to humans.
The report, published online June 4 in the New England Journal of Medicine (doi:10.1056/NEJMoa1401505) by Esam I. Azhar, Ph.D. and his colleagues at King Abdulaziz University Hospital, in Jeddah, Saudi Arabia, describes a 44-year old Saudi man who, in late October 2013, had applied medicine to the nasal passage of a camel with rhinorrhea.

After becoming ill with respiratory symptoms a week later, he was hospitalized, and investigators visited his stables to collect nasal fluid and blood samples from his animals. Nasal swabs revealed active MERS-CoV infection in one of the nine camels the man owned, and serologic samples from other camels in his herd showed evidence of recent prior infection, at a time when serum screening by immunofluorescence assay had yet to reveal MERS-CoV antibodies in the patient. This meant, the researchers noted, that the camels had been infected before the patient.
Using nasal swab samples, Dr. Azhar and his colleagues carried out reverse-transcriptase–polymerase-chain-reaction detection, isolation, and sequencing of MERS-CoV from the camel with active infection and the patient. Viral isolates from both camel and human were shown to be identical on genetic sequencing. Previously, antibodies cross-reactive to MERS-CoV had been identified in camels, but without isolation and comparison of virus from both animal and human, the camels’ role as reservoirs or intermediate hosts for transmitting the virus to humans could not be confirmed.
In this case, Dr. Azhar and his colleagues wrote in their analysis, "direct cross-species transmission had probably occurred between the two without any intermediate host." The patient died after 2 weeks’ hospitalization, but all of his animals appeared to have cleared the virus following acute infection, suggesting that camels act only as transient hosts of the virus. "The exact reservoir that maintains the virus in its ecologic niche has yet to be identified," the investigators wrote.
None of the study’s authors reported conflicts of interest.
A case report on a camel-to-human transmission of Middle East respiratory syndrome coronavirus (MERS-CoV) offers the first conclusive evidence that the virus can be transmitted directly from camels to humans.
The report, published online June 4 in the New England Journal of Medicine (doi:10.1056/NEJMoa1401505) by Esam I. Azhar, Ph.D. and his colleagues at King Abdulaziz University Hospital, in Jeddah, Saudi Arabia, describes a 44-year old Saudi man who, in late October 2013, had applied medicine to the nasal passage of a camel with rhinorrhea.
After becoming ill with respiratory symptoms a week later, he was hospitalized, and investigators visited his stables to collect nasal fluid and blood samples from his animals. Nasal swabs revealed active MERS-CoV infection in one of the nine camels the man owned, and serologic samples from other camels in his herd showed evidence of recent prior infection, at a time when serum screening by immunofluorescence assay had yet to reveal MERS-CoV antibodies in the patient. This meant, the researchers noted, that the camels had been infected before the patient.
Using nasal swab samples, Dr. Azhar and his colleagues carried out reverse-transcriptase–polymerase-chain-reaction detection, isolation, and sequencing of MERS-CoV from the camel with active infection and the patient. Viral isolates from both camel and human were shown to be identical on genetic sequencing. Previously, antibodies cross-reactive to MERS-CoV had been identified in camels, but without isolation and comparison of virus from both animal and human, the camels’ role as reservoirs or intermediate hosts for transmitting the virus to humans could not be confirmed.
In this case, Dr. Azhar and his colleagues wrote in their analysis, "direct cross-species transmission had probably occurred between the two without any intermediate host." The patient died after 2 weeks’ hospitalization, but all of his animals appeared to have cleared the virus following acute infection, suggesting that camels act only as transient hosts of the virus. "The exact reservoir that maintains the virus in its ecologic niche has yet to be identified," the investigators wrote.
None of the study’s authors reported conflicts of interest.
A case report on a camel-to-human transmission of Middle East respiratory syndrome coronavirus (MERS-CoV) offers the first conclusive evidence that the virus can be transmitted directly from camels to humans.
The report, published online June 4 in the New England Journal of Medicine (doi:10.1056/NEJMoa1401505) by Esam I. Azhar, Ph.D. and his colleagues at King Abdulaziz University Hospital, in Jeddah, Saudi Arabia, describes a 44-year old Saudi man who, in late October 2013, had applied medicine to the nasal passage of a camel with rhinorrhea.
After becoming ill with respiratory symptoms a week later, he was hospitalized, and investigators visited his stables to collect nasal fluid and blood samples from his animals. Nasal swabs revealed active MERS-CoV infection in one of the nine camels the man owned, and serologic samples from other camels in his herd showed evidence of recent prior infection, at a time when serum screening by immunofluorescence assay had yet to reveal MERS-CoV antibodies in the patient. This meant, the researchers noted, that the camels had been infected before the patient.
Using nasal swab samples, Dr. Azhar and his colleagues carried out reverse-transcriptase–polymerase-chain-reaction detection, isolation, and sequencing of MERS-CoV from the camel with active infection and the patient. Viral isolates from both camel and human were shown to be identical on genetic sequencing. Previously, antibodies cross-reactive to MERS-CoV had been identified in camels, but without isolation and comparison of virus from both animal and human, the camels’ role as reservoirs or intermediate hosts for transmitting the virus to humans could not be confirmed.
In this case, Dr. Azhar and his colleagues wrote in their analysis, "direct cross-species transmission had probably occurred between the two without any intermediate host." The patient died after 2 weeks’ hospitalization, but all of his animals appeared to have cleared the virus following acute infection, suggesting that camels act only as transient hosts of the virus. "The exact reservoir that maintains the virus in its ecologic niche has yet to be identified," the investigators wrote.
None of the study’s authors reported conflicts of interest.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE

CBT-I delivered by health educators eased insomnia in older adults
MINNEAPOLIS – Cognitive behavioral therapy tailored for insomnia management and delivered by health educators eased sleep impairment in older adults in a randomized trial of 159 community-dwelling veterans aged 60 years or older with chronic insomnia.
Researchers assigned the veterans to individual cognitive behavioral therapy for insomnia (CBT-I), group CBT-I, or general sleep education and hygiene as a control. The CBT-I combined sleep restriction, stimulus control, and cognitive therapy and was provided by health educators – primarily masters-level professionals – who had weekly telephone access to behavioral sleep medicine specialists. All study groups had five sessions of their assigned treatment over 6 weeks.

CBT-I was associated with better self-reported sleep quality and reduced insomnia symptoms compared with controls 6 months after therapy, according to data presented at the annual meeting of the Associated Professional Sleep Societies. And it worked similarly well whether provided one-on-one or in groups.
"We believe future work is needed to disseminate and implement this and other innovative models of CBT-I ... So it’s very important that there is continued, ongoing work to fine-tune the CBT-I interventions," but particularly in older adults, in whom the risks of episodic or chronic use of sleeping pills may be particularly problematic, said Dr. Cathy A. Alessi, a geriatrician with the VA Greater Los Angeles Healthcare System in North Hills, Calif., and professor of medicine at the David Geffen School of Medicine at UCLA. "We feel strongly that it’s time to get these out into routine practice."
Some parts of the country have few or no sleep medicine specialists, she noted. Thus, the ability to use allied health professionals to deliver this safe and effective treatment should make it available to more patients.
Session cochair Brandy Roane, Ph.D., of the University of North Texas Health Science Center at Fort Worth, noted that the study is helpful in that it provides insight on the feasibility and efficacy of CBT-I in this patient population.
"As our population is aging and we are trying to use more behavioral-based interventions, it is important for us to look at the efficacy. Are they even going to engage in the intervention? Are they going to get lost in it?" asked Dr. Roane.
Do they have age-related inability to understand some of the concepts and do the required cognitive work? And if they are cognitively impaired, will CBT-I be effective? she asked. "Also, are they going to be able to change their behavior in general?"
Importantly, Dr. Roane noted, in addition to its sleep benefits, CBT-I could have a general health and cognitive benefit during the daytime.
The mean age of the veterans in the study was 72 years. They were cognitively healthy, and had no or only mild sleep apnea. But on average, they had six other health conditions in addition to insomnia.
At 6 months, the trial’s primary endpoint, the Pittsburgh Sleep Quality Index score was 7.7 for the control condition, but lower at 5.8 for individual CBT-I (P = .005) and 5.6 for group CBT-I (P = .002). Relative to the control condition, both CBT-I strategies yielded significantly better sleep-onset latency, total wake time, and sleep efficiency as assessed from sleep diaries. Differences in these measures were still significant at 12 months.
The groups were statistically indistinguishable, however, with respect to changes in sleep efficiency as assessed from wrist actigraphy, depressive symptoms, and health-related quality of life.
In related qualitative research, also presented at the meeting (Josephson et al., abstract 0544), the investigators conducted focus groups among the study veterans to get their impressions of the CBT-I model of care, Dr. Alessi noted in an interview.
"Many participants we spoke with preferred behavioral treatment for insomnia over sleeping medications, and were also very receptive to the idea of behavioral treatment being provided by health educators [and others] outside of the mental health setting [as was the case in our study]," she reported. "We also heard compelling anecdotes from participants who described dramatic improvements in their sleep problems, which, for many, had been present for years."
Dr. Alessi disclosed no relevant conflicts of interest.
MINNEAPOLIS – Cognitive behavioral therapy tailored for insomnia management and delivered by health educators eased sleep impairment in older adults in a randomized trial of 159 community-dwelling veterans aged 60 years or older with chronic insomnia.
Researchers assigned the veterans to individual cognitive behavioral therapy for insomnia (CBT-I), group CBT-I, or general sleep education and hygiene as a control. The CBT-I combined sleep restriction, stimulus control, and cognitive therapy and was provided by health educators – primarily masters-level professionals – who had weekly telephone access to behavioral sleep medicine specialists. All study groups had five sessions of their assigned treatment over 6 weeks.
CBT-I was associated with better self-reported sleep quality and reduced insomnia symptoms compared with controls 6 months after therapy, according to data presented at the annual meeting of the Associated Professional Sleep Societies. And it worked similarly well whether provided one-on-one or in groups.
"We believe future work is needed to disseminate and implement this and other innovative models of CBT-I ... So it’s very important that there is continued, ongoing work to fine-tune the CBT-I interventions," but particularly in older adults, in whom the risks of episodic or chronic use of sleeping pills may be particularly problematic, said Dr. Cathy A. Alessi, a geriatrician with the VA Greater Los Angeles Healthcare System in North Hills, Calif., and professor of medicine at the David Geffen School of Medicine at UCLA. "We feel strongly that it’s time to get these out into routine practice."
Some parts of the country have few or no sleep medicine specialists, she noted. Thus, the ability to use allied health professionals to deliver this safe and effective treatment should make it available to more patients.
Session cochair Brandy Roane, Ph.D., of the University of North Texas Health Science Center at Fort Worth, noted that the study is helpful in that it provides insight on the feasibility and efficacy of CBT-I in this patient population.
"As our population is aging and we are trying to use more behavioral-based interventions, it is important for us to look at the efficacy. Are they even going to engage in the intervention? Are they going to get lost in it?" asked Dr. Roane.
Do they have age-related inability to understand some of the concepts and do the required cognitive work? And if they are cognitively impaired, will CBT-I be effective? she asked. "Also, are they going to be able to change their behavior in general?"
Importantly, Dr. Roane noted, in addition to its sleep benefits, CBT-I could have a general health and cognitive benefit during the daytime.
The mean age of the veterans in the study was 72 years. They were cognitively healthy, and had no or only mild sleep apnea. But on average, they had six other health conditions in addition to insomnia.
At 6 months, the trial’s primary endpoint, the Pittsburgh Sleep Quality Index score was 7.7 for the control condition, but lower at 5.8 for individual CBT-I (P = .005) and 5.6 for group CBT-I (P = .002). Relative to the control condition, both CBT-I strategies yielded significantly better sleep-onset latency, total wake time, and sleep efficiency as assessed from sleep diaries. Differences in these measures were still significant at 12 months.
The groups were statistically indistinguishable, however, with respect to changes in sleep efficiency as assessed from wrist actigraphy, depressive symptoms, and health-related quality of life.
In related qualitative research, also presented at the meeting (Josephson et al., abstract 0544), the investigators conducted focus groups among the study veterans to get their impressions of the CBT-I model of care, Dr. Alessi noted in an interview.
"Many participants we spoke with preferred behavioral treatment for insomnia over sleeping medications, and were also very receptive to the idea of behavioral treatment being provided by health educators [and others] outside of the mental health setting [as was the case in our study]," she reported. "We also heard compelling anecdotes from participants who described dramatic improvements in their sleep problems, which, for many, had been present for years."
Dr. Alessi disclosed no relevant conflicts of interest.
MINNEAPOLIS – Cognitive behavioral therapy tailored for insomnia management and delivered by health educators eased sleep impairment in older adults in a randomized trial of 159 community-dwelling veterans aged 60 years or older with chronic insomnia.
Researchers assigned the veterans to individual cognitive behavioral therapy for insomnia (CBT-I), group CBT-I, or general sleep education and hygiene as a control. The CBT-I combined sleep restriction, stimulus control, and cognitive therapy and was provided by health educators – primarily masters-level professionals – who had weekly telephone access to behavioral sleep medicine specialists. All study groups had five sessions of their assigned treatment over 6 weeks.
CBT-I was associated with better self-reported sleep quality and reduced insomnia symptoms compared with controls 6 months after therapy, according to data presented at the annual meeting of the Associated Professional Sleep Societies. And it worked similarly well whether provided one-on-one or in groups.
"We believe future work is needed to disseminate and implement this and other innovative models of CBT-I ... So it’s very important that there is continued, ongoing work to fine-tune the CBT-I interventions," but particularly in older adults, in whom the risks of episodic or chronic use of sleeping pills may be particularly problematic, said Dr. Cathy A. Alessi, a geriatrician with the VA Greater Los Angeles Healthcare System in North Hills, Calif., and professor of medicine at the David Geffen School of Medicine at UCLA. "We feel strongly that it’s time to get these out into routine practice."
Some parts of the country have few or no sleep medicine specialists, she noted. Thus, the ability to use allied health professionals to deliver this safe and effective treatment should make it available to more patients.
Session cochair Brandy Roane, Ph.D., of the University of North Texas Health Science Center at Fort Worth, noted that the study is helpful in that it provides insight on the feasibility and efficacy of CBT-I in this patient population.
"As our population is aging and we are trying to use more behavioral-based interventions, it is important for us to look at the efficacy. Are they even going to engage in the intervention? Are they going to get lost in it?" asked Dr. Roane.
Do they have age-related inability to understand some of the concepts and do the required cognitive work? And if they are cognitively impaired, will CBT-I be effective? she asked. "Also, are they going to be able to change their behavior in general?"
Importantly, Dr. Roane noted, in addition to its sleep benefits, CBT-I could have a general health and cognitive benefit during the daytime.
The mean age of the veterans in the study was 72 years. They were cognitively healthy, and had no or only mild sleep apnea. But on average, they had six other health conditions in addition to insomnia.
At 6 months, the trial’s primary endpoint, the Pittsburgh Sleep Quality Index score was 7.7 for the control condition, but lower at 5.8 for individual CBT-I (P = .005) and 5.6 for group CBT-I (P = .002). Relative to the control condition, both CBT-I strategies yielded significantly better sleep-onset latency, total wake time, and sleep efficiency as assessed from sleep diaries. Differences in these measures were still significant at 12 months.
The groups were statistically indistinguishable, however, with respect to changes in sleep efficiency as assessed from wrist actigraphy, depressive symptoms, and health-related quality of life.
In related qualitative research, also presented at the meeting (Josephson et al., abstract 0544), the investigators conducted focus groups among the study veterans to get their impressions of the CBT-I model of care, Dr. Alessi noted in an interview.
"Many participants we spoke with preferred behavioral treatment for insomnia over sleeping medications, and were also very receptive to the idea of behavioral treatment being provided by health educators [and others] outside of the mental health setting [as was the case in our study]," she reported. "We also heard compelling anecdotes from participants who described dramatic improvements in their sleep problems, which, for many, had been present for years."
Dr. Alessi disclosed no relevant conflicts of interest.
AT SLEEP 2014
Key clinical point: Cognitive behavioral therapy that has been tailored for insomnia treatment was effective in older adults.
Major finding: At 6 months, the Pittsburgh Sleep Quality Index score was 7.7 with general sleep education and hygiene, compared with 5.8 with individual CBT-I (P = .005) and 5.6 with group CBT-I (P = .002).
Data source: A randomized trial among 159 veterans aged 60 years or older with chronic insomnia.
Disclosures: Dr. Alessi disclosed no relevant conflicts of interest.

Novel agent counters sleepiness in narcolepsy patients
MINNEAPOLIS – After 12 weeks of treatment with a novel agent, narcolepsy patients showed an 86% improvement from baseline in scores on the Clinical Global Impression-Change scale, compared with 38% of placebo patients. The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
JZP-110 (formerly ADX-N05), a wake-promoting agent with dopaminergic and noradrenergic activity, reduced symptoms in a phase IIb randomized, double-blind, placebo-controlled trial of 93 patients with narcolepsy, according to Dr. Jed Black of the Stanford (Calif.) Center for Sleep Sciences and Medicine in Redwood City, and a part-time employee of Jazz Pharmaceuticals in Palo Alto.

"This is a wake-promoting agent with a mechanism of action that is somewhat distinct from those that are currently available for treating excessive daytime sleepiness in narcolepsy, with what appears to be a robust and fairly consistent effect across studies to improve alertness ... and also to impact narcolepsy globally," he said.
At week 4, the average change in sleep-onset latency on the Maintenance of Wakefulness Test (MWT) was 9.5 minutes in the active drug group and 1.4 minutes in the placebo group (P less than .0001). The proportion of treatment patients vs. placebo patients with improved Clinical Global Impression – Change scale (CGI-C) scores was 80% vs. 51%, respectively (P = .0066), and Epworth Sleepiness Scale (ESS) scores decreased in the two groups by 5.6 points vs. 2.4 points, respectively (P = .0038).
Additional improvements were noted at 12 weeks, with an average change in sleep-onset latency on the MWT of 12.8 minutes vs. 2.1 minutes (P less than .0001), likely representing a dose response instead of a time-on-treatment response, Dr. Black said.
The researchers randomized 49 patients to placebo and 44 to the active drug. The active drug was initiated at 150 mg/day for 4 weeks, and increased to 300 mg/day for weeks 5-12.
The two primary efficacy endpoints were improvements from baseline in average sleep-onset latency on the MWT and improvements from baseline on the CGI-C; change on the ESS was a secondary endpoint.
The drug might fill an unmet need in narcolepsy patients who do not improve on or cannot tolerate existing treatment options for excessive sleepiness, Dr. Black noted. Additionally, it is not associated with rebound hypersomnia, and limited preclinical data suggest that it may have lower potential for abuse than traditional stimulants, he said.
The study "was exciting in that it presented expanded research on a new wake-promoting compound which likely works differently than currently available wake-promoting agents," session chair Dr. Douglas Kirsch of the Sleep Disorders Service at the Brigham & Women’s Hospital in Boston, said in an interview.
ESS scores fell by 8.5 points in the treatment group vs. 2.5 points in the placebo group (P less than .0001) – putting all of the patients in the active drug group within the normal range
Prolongation of sleep-onset latency with the drug was not affected by whether patients had cataplexy (about a third of cases), said Dr. Black.
Adverse events were more common in the treatment group, and included headache, insomnia, diarrhea, nausea, decreased appetite, anxiety, and irritability. "There was sort of a dose-response on the GI symptoms and...insomnia and also anxiety and irritability," he noted.
Three patients discontinued the drug because of adverse events, compared with two who stopped placebo. Two serious events – acute cholecystitis and conversion disorder (the latter in a patient who had previously experienced this disorder) – occurred in the treatment group, but were deemed unrelated to the drug.
The study was supported by Aerial BioPharma. Dr. Black is a part-time employee of Jazz Pharmaceuticals, which has licensed ADX-N05 from Aerial BioPharma, and other study authors reported associations with the company.
MINNEAPOLIS – After 12 weeks of treatment with a novel agent, narcolepsy patients showed an 86% improvement from baseline in scores on the Clinical Global Impression-Change scale, compared with 38% of placebo patients. The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
JZP-110 (formerly ADX-N05), a wake-promoting agent with dopaminergic and noradrenergic activity, reduced symptoms in a phase IIb randomized, double-blind, placebo-controlled trial of 93 patients with narcolepsy, according to Dr. Jed Black of the Stanford (Calif.) Center for Sleep Sciences and Medicine in Redwood City, and a part-time employee of Jazz Pharmaceuticals in Palo Alto.
"This is a wake-promoting agent with a mechanism of action that is somewhat distinct from those that are currently available for treating excessive daytime sleepiness in narcolepsy, with what appears to be a robust and fairly consistent effect across studies to improve alertness ... and also to impact narcolepsy globally," he said.
At week 4, the average change in sleep-onset latency on the Maintenance of Wakefulness Test (MWT) was 9.5 minutes in the active drug group and 1.4 minutes in the placebo group (P less than .0001). The proportion of treatment patients vs. placebo patients with improved Clinical Global Impression – Change scale (CGI-C) scores was 80% vs. 51%, respectively (P = .0066), and Epworth Sleepiness Scale (ESS) scores decreased in the two groups by 5.6 points vs. 2.4 points, respectively (P = .0038).
Additional improvements were noted at 12 weeks, with an average change in sleep-onset latency on the MWT of 12.8 minutes vs. 2.1 minutes (P less than .0001), likely representing a dose response instead of a time-on-treatment response, Dr. Black said.
The researchers randomized 49 patients to placebo and 44 to the active drug. The active drug was initiated at 150 mg/day for 4 weeks, and increased to 300 mg/day for weeks 5-12.
The two primary efficacy endpoints were improvements from baseline in average sleep-onset latency on the MWT and improvements from baseline on the CGI-C; change on the ESS was a secondary endpoint.
The drug might fill an unmet need in narcolepsy patients who do not improve on or cannot tolerate existing treatment options for excessive sleepiness, Dr. Black noted. Additionally, it is not associated with rebound hypersomnia, and limited preclinical data suggest that it may have lower potential for abuse than traditional stimulants, he said.
The study "was exciting in that it presented expanded research on a new wake-promoting compound which likely works differently than currently available wake-promoting agents," session chair Dr. Douglas Kirsch of the Sleep Disorders Service at the Brigham & Women’s Hospital in Boston, said in an interview.
ESS scores fell by 8.5 points in the treatment group vs. 2.5 points in the placebo group (P less than .0001) – putting all of the patients in the active drug group within the normal range
Prolongation of sleep-onset latency with the drug was not affected by whether patients had cataplexy (about a third of cases), said Dr. Black.
Adverse events were more common in the treatment group, and included headache, insomnia, diarrhea, nausea, decreased appetite, anxiety, and irritability. "There was sort of a dose-response on the GI symptoms and...insomnia and also anxiety and irritability," he noted.
Three patients discontinued the drug because of adverse events, compared with two who stopped placebo. Two serious events – acute cholecystitis and conversion disorder (the latter in a patient who had previously experienced this disorder) – occurred in the treatment group, but were deemed unrelated to the drug.
The study was supported by Aerial BioPharma. Dr. Black is a part-time employee of Jazz Pharmaceuticals, which has licensed ADX-N05 from Aerial BioPharma, and other study authors reported associations with the company.
MINNEAPOLIS – After 12 weeks of treatment with a novel agent, narcolepsy patients showed an 86% improvement from baseline in scores on the Clinical Global Impression-Change scale, compared with 38% of placebo patients. The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
JZP-110 (formerly ADX-N05), a wake-promoting agent with dopaminergic and noradrenergic activity, reduced symptoms in a phase IIb randomized, double-blind, placebo-controlled trial of 93 patients with narcolepsy, according to Dr. Jed Black of the Stanford (Calif.) Center for Sleep Sciences and Medicine in Redwood City, and a part-time employee of Jazz Pharmaceuticals in Palo Alto.
"This is a wake-promoting agent with a mechanism of action that is somewhat distinct from those that are currently available for treating excessive daytime sleepiness in narcolepsy, with what appears to be a robust and fairly consistent effect across studies to improve alertness ... and also to impact narcolepsy globally," he said.
At week 4, the average change in sleep-onset latency on the Maintenance of Wakefulness Test (MWT) was 9.5 minutes in the active drug group and 1.4 minutes in the placebo group (P less than .0001). The proportion of treatment patients vs. placebo patients with improved Clinical Global Impression – Change scale (CGI-C) scores was 80% vs. 51%, respectively (P = .0066), and Epworth Sleepiness Scale (ESS) scores decreased in the two groups by 5.6 points vs. 2.4 points, respectively (P = .0038).
Additional improvements were noted at 12 weeks, with an average change in sleep-onset latency on the MWT of 12.8 minutes vs. 2.1 minutes (P less than .0001), likely representing a dose response instead of a time-on-treatment response, Dr. Black said.
The researchers randomized 49 patients to placebo and 44 to the active drug. The active drug was initiated at 150 mg/day for 4 weeks, and increased to 300 mg/day for weeks 5-12.
The two primary efficacy endpoints were improvements from baseline in average sleep-onset latency on the MWT and improvements from baseline on the CGI-C; change on the ESS was a secondary endpoint.
The drug might fill an unmet need in narcolepsy patients who do not improve on or cannot tolerate existing treatment options for excessive sleepiness, Dr. Black noted. Additionally, it is not associated with rebound hypersomnia, and limited preclinical data suggest that it may have lower potential for abuse than traditional stimulants, he said.
The study "was exciting in that it presented expanded research on a new wake-promoting compound which likely works differently than currently available wake-promoting agents," session chair Dr. Douglas Kirsch of the Sleep Disorders Service at the Brigham & Women’s Hospital in Boston, said in an interview.
ESS scores fell by 8.5 points in the treatment group vs. 2.5 points in the placebo group (P less than .0001) – putting all of the patients in the active drug group within the normal range
Prolongation of sleep-onset latency with the drug was not affected by whether patients had cataplexy (about a third of cases), said Dr. Black.
Adverse events were more common in the treatment group, and included headache, insomnia, diarrhea, nausea, decreased appetite, anxiety, and irritability. "There was sort of a dose-response on the GI symptoms and...insomnia and also anxiety and irritability," he noted.
Three patients discontinued the drug because of adverse events, compared with two who stopped placebo. Two serious events – acute cholecystitis and conversion disorder (the latter in a patient who had previously experienced this disorder) – occurred in the treatment group, but were deemed unrelated to the drug.
The study was supported by Aerial BioPharma. Dr. Black is a part-time employee of Jazz Pharmaceuticals, which has licensed ADX-N05 from Aerial BioPharma, and other study authors reported associations with the company.
AT SLEEP 2014
Key clinical point: The distinct mechanism of action of JZP-110 might provide another option for narcolepsy patients who do not improve on, or cannot tolerate, existing treatments for excessive sleepiness
Major finding: After 12 weeks, average change from baseline in sleep-onset latency on the MWT was 12.8 minutes in treatment group, compared with 2.1 minutes in the placebo group (P less than .0001).
Data source: A phase IIb randomized, double-blind, placebo-controlled trial of 93 patients with narcolepsy.
Disclosures: The study was supported by Aerial BioPharma. Dr. Black is a part-time employee of Jazz Pharmaceuticals, which has licensed ADX-N05 from Aerial BioPharma.
