User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Pneumonia-related readmissions plummeted under QI initiative
AUSTIN, TEX. – A multidisciplinary intervention, including implementation of a diagnostic scoring system and daily interdepartmental meetings to review cases, significantly decreased readmission rates for patients at a tertiary care center who were discharged with a diagnosis of pneumonia.
From November 2012 to January 2013 – a 3-month period after implementation of the quality improvement (QI) initiative – the all-cause readmission rates among 227 patients discharged with a diagnosis of pneumonia declined by 7.5 percentage points, compared with the all-cause readmission rates among 236 patients discharged during the same period in the prior year, before implementation of the initiative (from 20.7% to 13.2%), Dr. Hussein Hussein, a fellow at the University of Oklahoma Health Sciences Center, Oklahoma City, reported at the annual meeting of the American College of Chest Physicians.
A similar reduction was seen for pneumonia-related readmissions, which declined from 10.5% to 3% during the same period, said Dr. Hussein, who was with Yale New Haven Hospital, New Haven, Conn., at the time the research was conducted.

Further, after implementation of the scoring system – a modified Clinical Pulmonary Infection Score (MCPIS) calculated based on patient temperature, white blood cell count, sputum cultures, oxygen requirements, and radiographic appearance, which was administered at admission and again at 32 hours – the accuracy of pneumonia diagnoses appeared to improve; the mean MCPIS scores among patients with a discharge diagnosis of pneumonia increased significantly after implementation (from 4 to 6); the proportion of patients considered unlikely to have pneumonia decreased from 42.6% to 3.6%; the proportion considered to probably have pneumonia decreased from 31.9% to 17.9%; and the number deemed likely to have pneumonia increased from 25.5% to 78.6%.
All of the changes were statistically significant, and the improved accuracy of diagnosis was likely a result of provider education that led to increased use of sputum cultures, Dr. Hussein noted.
Pneumonia is the second most common discharge diagnosis among Medicare beneficiaries, and nearly 20% of these patients are readmitted within 30 days at a cost exceeding $17 billion annually.
“This is why the Centers for Medicare & Medicaid Services is penalizing poor-performing hospitals with high rates of readmission,” he said.
The MCPIS was implemented in 2012 as a quality improvement tool. Based on the scores, patients were categorized as unlikely to have pneumonia (score of 3 or less), probably having pneumonia (score of 4-5), and likely to have pneumonia (score of 6 or greater). The daily meetings during which patients admitted with pneumonia were reviewed, involved participation of physicians from different medical divisions and representatives from nursing, social work, and continuing care.
The primary goal of these rounds was to ensure timely follow-up after discharge, Dr. Hussein explained, adding that if the diagnosis was felt to be incorrect, the case was discussed with the team that was caring for the patient.
To assess the effects of this intervention, he and his colleagues conducted a retrospective chart review of all patients discharged with a diagnosis of pneumonia during each of the two assessment periods.
“Our multidisciplinary intervention resulted in a significant decrease in readmission rates in patients discharged with a diagnosis of pneumonia, as well as improvement in the accuracy of diagnosis,” he said.
Dr. Hussein reported having no disclosures.
AUSTIN, TEX. – A multidisciplinary intervention, including implementation of a diagnostic scoring system and daily interdepartmental meetings to review cases, significantly decreased readmission rates for patients at a tertiary care center who were discharged with a diagnosis of pneumonia.
From November 2012 to January 2013 – a 3-month period after implementation of the quality improvement (QI) initiative – the all-cause readmission rates among 227 patients discharged with a diagnosis of pneumonia declined by 7.5 percentage points, compared with the all-cause readmission rates among 236 patients discharged during the same period in the prior year, before implementation of the initiative (from 20.7% to 13.2%), Dr. Hussein Hussein, a fellow at the University of Oklahoma Health Sciences Center, Oklahoma City, reported at the annual meeting of the American College of Chest Physicians.
A similar reduction was seen for pneumonia-related readmissions, which declined from 10.5% to 3% during the same period, said Dr. Hussein, who was with Yale New Haven Hospital, New Haven, Conn., at the time the research was conducted.
Further, after implementation of the scoring system – a modified Clinical Pulmonary Infection Score (MCPIS) calculated based on patient temperature, white blood cell count, sputum cultures, oxygen requirements, and radiographic appearance, which was administered at admission and again at 32 hours – the accuracy of pneumonia diagnoses appeared to improve; the mean MCPIS scores among patients with a discharge diagnosis of pneumonia increased significantly after implementation (from 4 to 6); the proportion of patients considered unlikely to have pneumonia decreased from 42.6% to 3.6%; the proportion considered to probably have pneumonia decreased from 31.9% to 17.9%; and the number deemed likely to have pneumonia increased from 25.5% to 78.6%.
All of the changes were statistically significant, and the improved accuracy of diagnosis was likely a result of provider education that led to increased use of sputum cultures, Dr. Hussein noted.
Pneumonia is the second most common discharge diagnosis among Medicare beneficiaries, and nearly 20% of these patients are readmitted within 30 days at a cost exceeding $17 billion annually.
“This is why the Centers for Medicare & Medicaid Services is penalizing poor-performing hospitals with high rates of readmission,” he said.
The MCPIS was implemented in 2012 as a quality improvement tool. Based on the scores, patients were categorized as unlikely to have pneumonia (score of 3 or less), probably having pneumonia (score of 4-5), and likely to have pneumonia (score of 6 or greater). The daily meetings during which patients admitted with pneumonia were reviewed, involved participation of physicians from different medical divisions and representatives from nursing, social work, and continuing care.
The primary goal of these rounds was to ensure timely follow-up after discharge, Dr. Hussein explained, adding that if the diagnosis was felt to be incorrect, the case was discussed with the team that was caring for the patient.
To assess the effects of this intervention, he and his colleagues conducted a retrospective chart review of all patients discharged with a diagnosis of pneumonia during each of the two assessment periods.
“Our multidisciplinary intervention resulted in a significant decrease in readmission rates in patients discharged with a diagnosis of pneumonia, as well as improvement in the accuracy of diagnosis,” he said.
Dr. Hussein reported having no disclosures.
AUSTIN, TEX. – A multidisciplinary intervention, including implementation of a diagnostic scoring system and daily interdepartmental meetings to review cases, significantly decreased readmission rates for patients at a tertiary care center who were discharged with a diagnosis of pneumonia.
From November 2012 to January 2013 – a 3-month period after implementation of the quality improvement (QI) initiative – the all-cause readmission rates among 227 patients discharged with a diagnosis of pneumonia declined by 7.5 percentage points, compared with the all-cause readmission rates among 236 patients discharged during the same period in the prior year, before implementation of the initiative (from 20.7% to 13.2%), Dr. Hussein Hussein, a fellow at the University of Oklahoma Health Sciences Center, Oklahoma City, reported at the annual meeting of the American College of Chest Physicians.
A similar reduction was seen for pneumonia-related readmissions, which declined from 10.5% to 3% during the same period, said Dr. Hussein, who was with Yale New Haven Hospital, New Haven, Conn., at the time the research was conducted.
Further, after implementation of the scoring system – a modified Clinical Pulmonary Infection Score (MCPIS) calculated based on patient temperature, white blood cell count, sputum cultures, oxygen requirements, and radiographic appearance, which was administered at admission and again at 32 hours – the accuracy of pneumonia diagnoses appeared to improve; the mean MCPIS scores among patients with a discharge diagnosis of pneumonia increased significantly after implementation (from 4 to 6); the proportion of patients considered unlikely to have pneumonia decreased from 42.6% to 3.6%; the proportion considered to probably have pneumonia decreased from 31.9% to 17.9%; and the number deemed likely to have pneumonia increased from 25.5% to 78.6%.
All of the changes were statistically significant, and the improved accuracy of diagnosis was likely a result of provider education that led to increased use of sputum cultures, Dr. Hussein noted.
Pneumonia is the second most common discharge diagnosis among Medicare beneficiaries, and nearly 20% of these patients are readmitted within 30 days at a cost exceeding $17 billion annually.
“This is why the Centers for Medicare & Medicaid Services is penalizing poor-performing hospitals with high rates of readmission,” he said.
The MCPIS was implemented in 2012 as a quality improvement tool. Based on the scores, patients were categorized as unlikely to have pneumonia (score of 3 or less), probably having pneumonia (score of 4-5), and likely to have pneumonia (score of 6 or greater). The daily meetings during which patients admitted with pneumonia were reviewed, involved participation of physicians from different medical divisions and representatives from nursing, social work, and continuing care.
The primary goal of these rounds was to ensure timely follow-up after discharge, Dr. Hussein explained, adding that if the diagnosis was felt to be incorrect, the case was discussed with the team that was caring for the patient.
To assess the effects of this intervention, he and his colleagues conducted a retrospective chart review of all patients discharged with a diagnosis of pneumonia during each of the two assessment periods.
“Our multidisciplinary intervention resulted in a significant decrease in readmission rates in patients discharged with a diagnosis of pneumonia, as well as improvement in the accuracy of diagnosis,” he said.
Dr. Hussein reported having no disclosures.
Key clinical point: A scoring system and multidisciplinary effort improved pneumonia patient readmission rates and diagnostic accuracy.
Major finding: All-cause and pneumonia-related readmission rates declined from 20.7% to 13.2%, and from 10.5% to 3%, respectively.
Data source: A retrospective review of the charts of 463 patients.
Disclosures: Dr. Hussein reported having no disclosures.

LAMA/LABA combo tops fluticasone/salmeterol in moderate/severe COPD
AUSTIN, TEX.– Once daily combination treatment with umeclidinium and vilanterol was more effective than twice-daily combination treatment with fluticasone and salmeterol in patients with moderate to severe chronic obstructive pulmonary disease in two 12-week double-blind, parallel-group double-dummy studies.
In the two multicenter studies, 706 and 697 patients, respectively, were randomized to receive either 62.5 mcg of the long-acting muscarinic antagonist (LAMA) umeclidinium and 25 mcg of the long-acting beta-2 agonist (LABA) vilanterol – a recently approved combination bronchodilator maintenance treatment for COPD – or a combination of 250 mcg of the inhaled corticosteroid (ICS) fluticasone and 50 mcg of the LABA salmeterol, which is also indicated as a maintenance therapy for COPD.
The patients in the LAMA/LABA groups, who were treated once daily for 12 weeks, had significantly greater improvements on all lung function measures, compared with those in the ICS/LABA groups, who were treated twice daily, Dr. James F. Donohue of the University of North Carolina at Chapel Hill reported at the annual meeting of the American College of Chest Physicians.
In the first study, the improvement from baseline to day 84 (the primary study endpoint) in 0- to 24-hour weighted mean forced expiratory volume in 1 second (FEV1) was 165 mL for the LAMA/LABA group, compared with 91 mL in the ICS/LABA group. In the second study, the improvement in the two groups was 213 mL and 112 mL.
The LAMA/LABA combination also improved trough FEV1 on day 85 by 82 mL and 98 mL more than did the ICS/LABA combination in the two studies, respectively.
Both combinations provided clinically meaningful improvements in dyspnea and quality of life scores, Dr. Donohue said.
Adverse events occurred during treatment in a similar proportion of patients in both treatment groups in both studies: 26% and 27% in the LAMA/LABA and ICS/LABA patients in the first study, and 30% and 31%, respectively, in the second study. The most common adverse events were headache and nasopharyngitis.
In the first study, serious adverse events occurred in 2% of the LAMA/LABA patients and 3% of ICS/LABA patients, and in 3% and 4% of patients in the second study.
One death occurred in the ICS/LABA group in the first study, but it was not considered study related. Five deaths occurred in the second study, including two in the LAMA/LABA patients and three in the ICS/LABA patients. One of the deaths in the ICS/LABA group was because of pneumonia and was reported as drug related by the investigator.
No new safety signals were detected in these studies, Dr. Donohue said.
Patients in both studies had FEV1 between 30% and 70%, and had not experienced a COPD exacerbation within the previous year. The LAMA/LABA therapy was delivered via Ellipta inhaler, and the ICS/LABA therapy was delivered via Diskus inhaler.
The Food and Drug Administration approved umeclidinium/vilanterol combination therapy (Anoro Ellipta) in December 2013, the first LAMA/LABA therapy approved in the United States. Dr. Donohue and his colleagues conducted the pivotal regulatory trial of the drug combination, which was published in July 2013 (Respir. Med. 2013;107:1538-46).
The current trials represent an effort to determine where the treatment fits into the armamentarium for treating patients with COPD, he said.
The “really robust findings as befits two bronchodilators” suggest umeclidinium/vilanterol combination therapy is an effective treatment option that provides greater lung function than fluticasone/salmeterol for moderate to severe COPD in patients with infrequent exacerbations, Dr. Donohue said.
GSK, which developed the umeclidinium/vilanterol combination product with Theravance, funded the studies. Dr. Donohue reported receiving consultant fees and/or serving on an advisory committee for Almirall, AstraZeneca, Boehringer Ingelheim, Dey, Elevation Pharmaceutical, Forest Laboratories, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Pfizer, and Sunovion. He has also served as a member of drug safety monitoring boards for the National Institutes of Health, Novartis, Otsuda, Pearl, and Teva.
AUSTIN, TEX.– Once daily combination treatment with umeclidinium and vilanterol was more effective than twice-daily combination treatment with fluticasone and salmeterol in patients with moderate to severe chronic obstructive pulmonary disease in two 12-week double-blind, parallel-group double-dummy studies.
In the two multicenter studies, 706 and 697 patients, respectively, were randomized to receive either 62.5 mcg of the long-acting muscarinic antagonist (LAMA) umeclidinium and 25 mcg of the long-acting beta-2 agonist (LABA) vilanterol – a recently approved combination bronchodilator maintenance treatment for COPD – or a combination of 250 mcg of the inhaled corticosteroid (ICS) fluticasone and 50 mcg of the LABA salmeterol, which is also indicated as a maintenance therapy for COPD.
The patients in the LAMA/LABA groups, who were treated once daily for 12 weeks, had significantly greater improvements on all lung function measures, compared with those in the ICS/LABA groups, who were treated twice daily, Dr. James F. Donohue of the University of North Carolina at Chapel Hill reported at the annual meeting of the American College of Chest Physicians.
In the first study, the improvement from baseline to day 84 (the primary study endpoint) in 0- to 24-hour weighted mean forced expiratory volume in 1 second (FEV1) was 165 mL for the LAMA/LABA group, compared with 91 mL in the ICS/LABA group. In the second study, the improvement in the two groups was 213 mL and 112 mL.
The LAMA/LABA combination also improved trough FEV1 on day 85 by 82 mL and 98 mL more than did the ICS/LABA combination in the two studies, respectively.
Both combinations provided clinically meaningful improvements in dyspnea and quality of life scores, Dr. Donohue said.
Adverse events occurred during treatment in a similar proportion of patients in both treatment groups in both studies: 26% and 27% in the LAMA/LABA and ICS/LABA patients in the first study, and 30% and 31%, respectively, in the second study. The most common adverse events were headache and nasopharyngitis.
In the first study, serious adverse events occurred in 2% of the LAMA/LABA patients and 3% of ICS/LABA patients, and in 3% and 4% of patients in the second study.
One death occurred in the ICS/LABA group in the first study, but it was not considered study related. Five deaths occurred in the second study, including two in the LAMA/LABA patients and three in the ICS/LABA patients. One of the deaths in the ICS/LABA group was because of pneumonia and was reported as drug related by the investigator.
No new safety signals were detected in these studies, Dr. Donohue said.
Patients in both studies had FEV1 between 30% and 70%, and had not experienced a COPD exacerbation within the previous year. The LAMA/LABA therapy was delivered via Ellipta inhaler, and the ICS/LABA therapy was delivered via Diskus inhaler.
The Food and Drug Administration approved umeclidinium/vilanterol combination therapy (Anoro Ellipta) in December 2013, the first LAMA/LABA therapy approved in the United States. Dr. Donohue and his colleagues conducted the pivotal regulatory trial of the drug combination, which was published in July 2013 (Respir. Med. 2013;107:1538-46).
The current trials represent an effort to determine where the treatment fits into the armamentarium for treating patients with COPD, he said.
The “really robust findings as befits two bronchodilators” suggest umeclidinium/vilanterol combination therapy is an effective treatment option that provides greater lung function than fluticasone/salmeterol for moderate to severe COPD in patients with infrequent exacerbations, Dr. Donohue said.
GSK, which developed the umeclidinium/vilanterol combination product with Theravance, funded the studies. Dr. Donohue reported receiving consultant fees and/or serving on an advisory committee for Almirall, AstraZeneca, Boehringer Ingelheim, Dey, Elevation Pharmaceutical, Forest Laboratories, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Pfizer, and Sunovion. He has also served as a member of drug safety monitoring boards for the National Institutes of Health, Novartis, Otsuda, Pearl, and Teva.
AUSTIN, TEX.– Once daily combination treatment with umeclidinium and vilanterol was more effective than twice-daily combination treatment with fluticasone and salmeterol in patients with moderate to severe chronic obstructive pulmonary disease in two 12-week double-blind, parallel-group double-dummy studies.
In the two multicenter studies, 706 and 697 patients, respectively, were randomized to receive either 62.5 mcg of the long-acting muscarinic antagonist (LAMA) umeclidinium and 25 mcg of the long-acting beta-2 agonist (LABA) vilanterol – a recently approved combination bronchodilator maintenance treatment for COPD – or a combination of 250 mcg of the inhaled corticosteroid (ICS) fluticasone and 50 mcg of the LABA salmeterol, which is also indicated as a maintenance therapy for COPD.
The patients in the LAMA/LABA groups, who were treated once daily for 12 weeks, had significantly greater improvements on all lung function measures, compared with those in the ICS/LABA groups, who were treated twice daily, Dr. James F. Donohue of the University of North Carolina at Chapel Hill reported at the annual meeting of the American College of Chest Physicians.
In the first study, the improvement from baseline to day 84 (the primary study endpoint) in 0- to 24-hour weighted mean forced expiratory volume in 1 second (FEV1) was 165 mL for the LAMA/LABA group, compared with 91 mL in the ICS/LABA group. In the second study, the improvement in the two groups was 213 mL and 112 mL.
The LAMA/LABA combination also improved trough FEV1 on day 85 by 82 mL and 98 mL more than did the ICS/LABA combination in the two studies, respectively.
Both combinations provided clinically meaningful improvements in dyspnea and quality of life scores, Dr. Donohue said.
Adverse events occurred during treatment in a similar proportion of patients in both treatment groups in both studies: 26% and 27% in the LAMA/LABA and ICS/LABA patients in the first study, and 30% and 31%, respectively, in the second study. The most common adverse events were headache and nasopharyngitis.
In the first study, serious adverse events occurred in 2% of the LAMA/LABA patients and 3% of ICS/LABA patients, and in 3% and 4% of patients in the second study.
One death occurred in the ICS/LABA group in the first study, but it was not considered study related. Five deaths occurred in the second study, including two in the LAMA/LABA patients and three in the ICS/LABA patients. One of the deaths in the ICS/LABA group was because of pneumonia and was reported as drug related by the investigator.
No new safety signals were detected in these studies, Dr. Donohue said.
Patients in both studies had FEV1 between 30% and 70%, and had not experienced a COPD exacerbation within the previous year. The LAMA/LABA therapy was delivered via Ellipta inhaler, and the ICS/LABA therapy was delivered via Diskus inhaler.
The Food and Drug Administration approved umeclidinium/vilanterol combination therapy (Anoro Ellipta) in December 2013, the first LAMA/LABA therapy approved in the United States. Dr. Donohue and his colleagues conducted the pivotal regulatory trial of the drug combination, which was published in July 2013 (Respir. Med. 2013;107:1538-46).
The current trials represent an effort to determine where the treatment fits into the armamentarium for treating patients with COPD, he said.
The “really robust findings as befits two bronchodilators” suggest umeclidinium/vilanterol combination therapy is an effective treatment option that provides greater lung function than fluticasone/salmeterol for moderate to severe COPD in patients with infrequent exacerbations, Dr. Donohue said.
GSK, which developed the umeclidinium/vilanterol combination product with Theravance, funded the studies. Dr. Donohue reported receiving consultant fees and/or serving on an advisory committee for Almirall, AstraZeneca, Boehringer Ingelheim, Dey, Elevation Pharmaceutical, Forest Laboratories, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Pfizer, and Sunovion. He has also served as a member of drug safety monitoring boards for the National Institutes of Health, Novartis, Otsuda, Pearl, and Teva.
AT CHEST 2014
Key clinical point: Umeclidinium/vilanterol is an effective treatment option for moderate to severe COPD patients with infrequent exacerbations.
Major finding: The improvement in 0- to 24-hour weighted mean FEV1 on day 84 with LAMA/LABA vs. ICS/LABA was 165 mL vs. 91 mL and 213 mL vs. 112 mL in two randomized trials, respectively.
Data source: Two randomized double-blind, parallel-group double-dummy studies involving 706 and 697 patients.
Disclosures: GSK, which developed the umeclidinium/vilanterol combination product with Theravance, funded the studies. Dr. Donohue reported receiving consultant fees and/or serving on an advisory committee for Almirall, AstraZeneca, Boehringer Ingelheim, Dey, Elevation Pharmaceutical, Forest Laboratories, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Pfizer, and Sunovion. He has also served as a member of drug safety monitoring boards for the National Institutes of Health, Novartis, Otsuda, Pearl, and Teva.
Post-PCV13 findings prompt continued surveillance
PHILADELPHIA – Invasive pneumococcal infections declined by 42% in 2011, compared with 2007-2009, the years after the introduction of the 13-valent pneumococcal conjugate vaccine, according to an analysis of data from eight U.S. children’s hospitals.
Infections continued to decline – by 48% overall – 2-3 years after full implementation of the vaccine. Declines were seen in the rates of bacteremia, pneumonia, and mastoiditis, but the rates of pneumococcal meningitis in the latter years remained unchanged, with an increasing proportion of cases occurring among children with invasive disease.

The most common 13-valent pneumococcal conjugate vaccine (PCV13) serotypes causing invasive pneumococcal infections in 2011 were 19A and 7F. The declines in invasive infections in 2012 and 2013 were mainly because of declines in serotype 19A and 7F isolates, which decreased by 58% and 54%, respectively, but serotype 3 isolates remained at pre-PCV13 levels, Dr. Sheldon L. Kaplan of Baylor College of Medicine and Texas Children’s Hospital, in Houston, reported at an annual scientific meeting on infectious diseases.
“We had 29 children with invasive pneumococcal disease caused by a PCV13 serotype [in 2012-2013]. All but one were a 19A or serotype 3,” he said at thecombined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nine children with serotype 19A isolates, and 4 with serotype 3 isolates had received at least two doses of PCV13 prior to developing infections. In 2013, 3 of 12 children with 19A isolates had received four PCV13 doses prior to developing serotype 19A infections.
Only three serotype 1-, 7-, and 19F-related invasive infections occurred during the study period, and no serotype 5–related infections occurred.
In 2012-2013, non-PCV13 serotypes – mainly 33F and 22F – accounted for 71% of isolates, Dr. Kaplan said.
Of note, 45% of children at the eight hospitals that are part of the U.S. Pediatric Multicenter Pneumococcal Surveillance Study Group – which has been conducting pneumococcal surveillance since 1993 – had an underlying condition during 2011-2013, compared with 37% in 2007-2009. The difference was statistically significant, Dr. Kaplan said, noting that malignancies were the most common type of underlying condition, followed by central nervous system disorders, genetic disorder, cardiovascular disorders, and renal disorders.
Non-PCV13 serotypes accounted for 78% of isolates from children with underlying conditions, he said.
Mortality was 0.8% (5 of 626) in 2007-2009, and 3.7% (13 of 352) in 2011-2013. Of the 13 children who died in 2011-2013, 10 had a non-PCV13 serotype, and 9 had an underlying condition, Dr. Kaplan said.
Almost all (99%) of non–central nervous system infections in 2011-2013 were susceptible to penicillin and ceftriaxone.
“Continued surveillance is warranted, especially to monitor non-PCV13 serotypes associated with invasive pneumococcal disease,” he said.
As for pneumococcal meningitis, rates decreased significantly after the introduction of PCV7, but the proportion among children with invasive pneumococcal disease increased by 67% over time, accounting for 12% of cases during 2007-2009, compared with 20% of cases during 2011-2013, according to Dr. Liset Olarte, also of Baylor College of Medicine and Texas Children’s Hospital.
The proportion decreased by 21% among children younger than 24 months, but increased significantly in those aged 24 to 59 months, she noted.
Clinical data showed that in 2007-2009, 19A, 7F, and 3 were the most common serotypes associated with pneumococcal meningitis in the eight hospitals in the surveillance study group. In 2011-13, 19A remained the most common serotype, followed by non-PCV13 serotypes 35B and 22F. Overall, non-PCV13 serotypes causing pneumococcal meningitis increased in both number of cases (24 to 49) and proportion of cases (46% to 73%) after PCV13 introduction.
“In our study, only the change in serotype 7F was statistically significant,” said Dr. Olarte.
The proportion of isolates that were non-susceptible to penicillin did not change significantly from 2007-2009 to 2011-2013 (26% and 25%, respectively), but the proportion nonsusceptible to ceftriaxone, and thus requiring vancomycin for treatment, decreased significantly – by 77% – from 13% to 3%.
All of the isolates with a ceftriaxone minimum inhibitory concentration of 1 mcg/mL or greater and penicillin minimum inhibitory concentration of 2 mcg/mL or greater were serotype 19A, Dr. Olarte said.
Mortality did not change significantly during the study period, but there was a marked, significant increase in hemiparesis cases, from 1% to 12%, after introduction of PCV13. However, this increase was not associated with any particular serotype.
Additionally, subdural empyema on neuroimaging increased from 1% to 16%, but was not associated with any particular serotype and was not associated with the cases of hemiparesis.
Overall, 52% of survivors had some sort of neurologic sequelae at the time of discharge, but there were no differences in terms of specific sequelae between the two groups.
The rates of morbidity and mortality for pneumococcal meningitis remain substantial and have not changed significantly since introduction of PCV13, Dr. Olarte said.
However, if the number of cephalosporin nonsusceptible pneumococci isolated from children with meningitis continues to decrease, modification of empiric antibiotic selection for suspected bacterial meningitis might be considered in the future, therefore ongoing surveillance is warranted, she said.
The studies were partially supported by Pfizer. The authors reported having no other disclosures.
PHILADELPHIA – Invasive pneumococcal infections declined by 42% in 2011, compared with 2007-2009, the years after the introduction of the 13-valent pneumococcal conjugate vaccine, according to an analysis of data from eight U.S. children’s hospitals.
Infections continued to decline – by 48% overall – 2-3 years after full implementation of the vaccine. Declines were seen in the rates of bacteremia, pneumonia, and mastoiditis, but the rates of pneumococcal meningitis in the latter years remained unchanged, with an increasing proportion of cases occurring among children with invasive disease.
The most common 13-valent pneumococcal conjugate vaccine (PCV13) serotypes causing invasive pneumococcal infections in 2011 were 19A and 7F. The declines in invasive infections in 2012 and 2013 were mainly because of declines in serotype 19A and 7F isolates, which decreased by 58% and 54%, respectively, but serotype 3 isolates remained at pre-PCV13 levels, Dr. Sheldon L. Kaplan of Baylor College of Medicine and Texas Children’s Hospital, in Houston, reported at an annual scientific meeting on infectious diseases.
“We had 29 children with invasive pneumococcal disease caused by a PCV13 serotype [in 2012-2013]. All but one were a 19A or serotype 3,” he said at thecombined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nine children with serotype 19A isolates, and 4 with serotype 3 isolates had received at least two doses of PCV13 prior to developing infections. In 2013, 3 of 12 children with 19A isolates had received four PCV13 doses prior to developing serotype 19A infections.
Only three serotype 1-, 7-, and 19F-related invasive infections occurred during the study period, and no serotype 5–related infections occurred.
In 2012-2013, non-PCV13 serotypes – mainly 33F and 22F – accounted for 71% of isolates, Dr. Kaplan said.
Of note, 45% of children at the eight hospitals that are part of the U.S. Pediatric Multicenter Pneumococcal Surveillance Study Group – which has been conducting pneumococcal surveillance since 1993 – had an underlying condition during 2011-2013, compared with 37% in 2007-2009. The difference was statistically significant, Dr. Kaplan said, noting that malignancies were the most common type of underlying condition, followed by central nervous system disorders, genetic disorder, cardiovascular disorders, and renal disorders.
Non-PCV13 serotypes accounted for 78% of isolates from children with underlying conditions, he said.
Mortality was 0.8% (5 of 626) in 2007-2009, and 3.7% (13 of 352) in 2011-2013. Of the 13 children who died in 2011-2013, 10 had a non-PCV13 serotype, and 9 had an underlying condition, Dr. Kaplan said.
Almost all (99%) of non–central nervous system infections in 2011-2013 were susceptible to penicillin and ceftriaxone.
“Continued surveillance is warranted, especially to monitor non-PCV13 serotypes associated with invasive pneumococcal disease,” he said.
As for pneumococcal meningitis, rates decreased significantly after the introduction of PCV7, but the proportion among children with invasive pneumococcal disease increased by 67% over time, accounting for 12% of cases during 2007-2009, compared with 20% of cases during 2011-2013, according to Dr. Liset Olarte, also of Baylor College of Medicine and Texas Children’s Hospital.
The proportion decreased by 21% among children younger than 24 months, but increased significantly in those aged 24 to 59 months, she noted.
Clinical data showed that in 2007-2009, 19A, 7F, and 3 were the most common serotypes associated with pneumococcal meningitis in the eight hospitals in the surveillance study group. In 2011-13, 19A remained the most common serotype, followed by non-PCV13 serotypes 35B and 22F. Overall, non-PCV13 serotypes causing pneumococcal meningitis increased in both number of cases (24 to 49) and proportion of cases (46% to 73%) after PCV13 introduction.
“In our study, only the change in serotype 7F was statistically significant,” said Dr. Olarte.
The proportion of isolates that were non-susceptible to penicillin did not change significantly from 2007-2009 to 2011-2013 (26% and 25%, respectively), but the proportion nonsusceptible to ceftriaxone, and thus requiring vancomycin for treatment, decreased significantly – by 77% – from 13% to 3%.
All of the isolates with a ceftriaxone minimum inhibitory concentration of 1 mcg/mL or greater and penicillin minimum inhibitory concentration of 2 mcg/mL or greater were serotype 19A, Dr. Olarte said.
Mortality did not change significantly during the study period, but there was a marked, significant increase in hemiparesis cases, from 1% to 12%, after introduction of PCV13. However, this increase was not associated with any particular serotype.
Additionally, subdural empyema on neuroimaging increased from 1% to 16%, but was not associated with any particular serotype and was not associated with the cases of hemiparesis.
Overall, 52% of survivors had some sort of neurologic sequelae at the time of discharge, but there were no differences in terms of specific sequelae between the two groups.
The rates of morbidity and mortality for pneumococcal meningitis remain substantial and have not changed significantly since introduction of PCV13, Dr. Olarte said.
However, if the number of cephalosporin nonsusceptible pneumococci isolated from children with meningitis continues to decrease, modification of empiric antibiotic selection for suspected bacterial meningitis might be considered in the future, therefore ongoing surveillance is warranted, she said.
The studies were partially supported by Pfizer. The authors reported having no other disclosures.
PHILADELPHIA – Invasive pneumococcal infections declined by 42% in 2011, compared with 2007-2009, the years after the introduction of the 13-valent pneumococcal conjugate vaccine, according to an analysis of data from eight U.S. children’s hospitals.
Infections continued to decline – by 48% overall – 2-3 years after full implementation of the vaccine. Declines were seen in the rates of bacteremia, pneumonia, and mastoiditis, but the rates of pneumococcal meningitis in the latter years remained unchanged, with an increasing proportion of cases occurring among children with invasive disease.
The most common 13-valent pneumococcal conjugate vaccine (PCV13) serotypes causing invasive pneumococcal infections in 2011 were 19A and 7F. The declines in invasive infections in 2012 and 2013 were mainly because of declines in serotype 19A and 7F isolates, which decreased by 58% and 54%, respectively, but serotype 3 isolates remained at pre-PCV13 levels, Dr. Sheldon L. Kaplan of Baylor College of Medicine and Texas Children’s Hospital, in Houston, reported at an annual scientific meeting on infectious diseases.
“We had 29 children with invasive pneumococcal disease caused by a PCV13 serotype [in 2012-2013]. All but one were a 19A or serotype 3,” he said at thecombined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nine children with serotype 19A isolates, and 4 with serotype 3 isolates had received at least two doses of PCV13 prior to developing infections. In 2013, 3 of 12 children with 19A isolates had received four PCV13 doses prior to developing serotype 19A infections.
Only three serotype 1-, 7-, and 19F-related invasive infections occurred during the study period, and no serotype 5–related infections occurred.
In 2012-2013, non-PCV13 serotypes – mainly 33F and 22F – accounted for 71% of isolates, Dr. Kaplan said.
Of note, 45% of children at the eight hospitals that are part of the U.S. Pediatric Multicenter Pneumococcal Surveillance Study Group – which has been conducting pneumococcal surveillance since 1993 – had an underlying condition during 2011-2013, compared with 37% in 2007-2009. The difference was statistically significant, Dr. Kaplan said, noting that malignancies were the most common type of underlying condition, followed by central nervous system disorders, genetic disorder, cardiovascular disorders, and renal disorders.
Non-PCV13 serotypes accounted for 78% of isolates from children with underlying conditions, he said.
Mortality was 0.8% (5 of 626) in 2007-2009, and 3.7% (13 of 352) in 2011-2013. Of the 13 children who died in 2011-2013, 10 had a non-PCV13 serotype, and 9 had an underlying condition, Dr. Kaplan said.
Almost all (99%) of non–central nervous system infections in 2011-2013 were susceptible to penicillin and ceftriaxone.
“Continued surveillance is warranted, especially to monitor non-PCV13 serotypes associated with invasive pneumococcal disease,” he said.
As for pneumococcal meningitis, rates decreased significantly after the introduction of PCV7, but the proportion among children with invasive pneumococcal disease increased by 67% over time, accounting for 12% of cases during 2007-2009, compared with 20% of cases during 2011-2013, according to Dr. Liset Olarte, also of Baylor College of Medicine and Texas Children’s Hospital.
The proportion decreased by 21% among children younger than 24 months, but increased significantly in those aged 24 to 59 months, she noted.
Clinical data showed that in 2007-2009, 19A, 7F, and 3 were the most common serotypes associated with pneumococcal meningitis in the eight hospitals in the surveillance study group. In 2011-13, 19A remained the most common serotype, followed by non-PCV13 serotypes 35B and 22F. Overall, non-PCV13 serotypes causing pneumococcal meningitis increased in both number of cases (24 to 49) and proportion of cases (46% to 73%) after PCV13 introduction.
“In our study, only the change in serotype 7F was statistically significant,” said Dr. Olarte.
The proportion of isolates that were non-susceptible to penicillin did not change significantly from 2007-2009 to 2011-2013 (26% and 25%, respectively), but the proportion nonsusceptible to ceftriaxone, and thus requiring vancomycin for treatment, decreased significantly – by 77% – from 13% to 3%.
All of the isolates with a ceftriaxone minimum inhibitory concentration of 1 mcg/mL or greater and penicillin minimum inhibitory concentration of 2 mcg/mL or greater were serotype 19A, Dr. Olarte said.
Mortality did not change significantly during the study period, but there was a marked, significant increase in hemiparesis cases, from 1% to 12%, after introduction of PCV13. However, this increase was not associated with any particular serotype.
Additionally, subdural empyema on neuroimaging increased from 1% to 16%, but was not associated with any particular serotype and was not associated with the cases of hemiparesis.
Overall, 52% of survivors had some sort of neurologic sequelae at the time of discharge, but there were no differences in terms of specific sequelae between the two groups.
The rates of morbidity and mortality for pneumococcal meningitis remain substantial and have not changed significantly since introduction of PCV13, Dr. Olarte said.
However, if the number of cephalosporin nonsusceptible pneumococci isolated from children with meningitis continues to decrease, modification of empiric antibiotic selection for suspected bacterial meningitis might be considered in the future, therefore ongoing surveillance is warranted, she said.
The studies were partially supported by Pfizer. The authors reported having no other disclosures.
Key clinical point: PCV13 has had a beneficial effect on the rates of invasive pneumococcal infection, but continued surveillance is warranted.
Major finding: Invasive pneumococcal infections have declined by 48% since introduction of PCV13, but rates of pneumococcal meningitis remain unchanged.
Data source: Analyses of data from the eight children’s hospitals in the U.S. Pediatric Multicenter Pneumococcal Surveillance Study Group.
Disclosures: The studies were partially supported by Pfizer. The authors reported having no other disclosures.

Shorter screen developed for pediatric obstructive sleep apnea
Pediatricians can use a short, simple questionnaire to screen children for obstructive sleep apnea, according to a study of children and parents referred to a sleep center for screening.
While the shorter tool is not as sensitive as longer questionnaires, it is faster and easier to use, allowing primary caregivers to screen more children.

About 1%-4% of children are affected by obstructive sleep apnea (OSA), an underdiagnosed condition that can have significant effects on a child’s behavior, performance, and health.
The researchers, led by Dr. Gili Kadmon of the Schneider Children’s Medical Center, Petach Tikva, Israel, developed the IF SLEEPY screen of eight yes/no questions that investigate a child’s snoring, breathing problems during sleep, daytime irritability, sleepiness, moods, concentration problems, and other issues. The screen was given to parents of 150 children aged 3-17 years who had been referred to a sleep center in Toronto. Children aged 7 years or older were also asked to answer a modified questionnaire. Only children who were eligible for a sleep study were included in the sample (Int. J. Pediatr. Otorhinolaryngol. 2014 Oct 7. [doi: 10.1016/j.ijporl.2014.09.018]).
A comparison of the parents’ questionnaire scores with their child’s apnea-hypopnea index obtained during a subsequent overnight polysomnographic study found that the screen had a 78% sensitivity for mild to severe obstructive sleep apnea (OSA) cases, with a 40% specificity. The children’s responses were less sensitive, but more specific (45% and 52%, respectively).
To improve the screen’s specificity, the researchers dropped a question about concentration, creating the I SLEEPY version, which resulted in sensitivity and specificity scores for the parent answers of 76% and 55%, respectively. A third version (I’M SLEEPY) added a measure of the child’s body mass index, which resulted in parent scores that were 82% sensitive and 50% specific.
The new screens’ sensitivities and specificities are lower than those of the three longer pediatric OSA screens currently available. Those screens have 40 or more items, and can yield sensitivities and specificities as high as 91% and 88%. However, the authors suggest that a 1-minute screen with a mnemonic name is better suited for a primary care setting. They report they are currently developing a study of the screen in general pediatric clinics. The authors reported having no disclosures.
Pediatricians can use a short, simple questionnaire to screen children for obstructive sleep apnea, according to a study of children and parents referred to a sleep center for screening.
While the shorter tool is not as sensitive as longer questionnaires, it is faster and easier to use, allowing primary caregivers to screen more children.
About 1%-4% of children are affected by obstructive sleep apnea (OSA), an underdiagnosed condition that can have significant effects on a child’s behavior, performance, and health.
The researchers, led by Dr. Gili Kadmon of the Schneider Children’s Medical Center, Petach Tikva, Israel, developed the IF SLEEPY screen of eight yes/no questions that investigate a child’s snoring, breathing problems during sleep, daytime irritability, sleepiness, moods, concentration problems, and other issues. The screen was given to parents of 150 children aged 3-17 years who had been referred to a sleep center in Toronto. Children aged 7 years or older were also asked to answer a modified questionnaire. Only children who were eligible for a sleep study were included in the sample (Int. J. Pediatr. Otorhinolaryngol. 2014 Oct 7. [doi: 10.1016/j.ijporl.2014.09.018]).
A comparison of the parents’ questionnaire scores with their child’s apnea-hypopnea index obtained during a subsequent overnight polysomnographic study found that the screen had a 78% sensitivity for mild to severe obstructive sleep apnea (OSA) cases, with a 40% specificity. The children’s responses were less sensitive, but more specific (45% and 52%, respectively).
To improve the screen’s specificity, the researchers dropped a question about concentration, creating the I SLEEPY version, which resulted in sensitivity and specificity scores for the parent answers of 76% and 55%, respectively. A third version (I’M SLEEPY) added a measure of the child’s body mass index, which resulted in parent scores that were 82% sensitive and 50% specific.
The new screens’ sensitivities and specificities are lower than those of the three longer pediatric OSA screens currently available. Those screens have 40 or more items, and can yield sensitivities and specificities as high as 91% and 88%. However, the authors suggest that a 1-minute screen with a mnemonic name is better suited for a primary care setting. They report they are currently developing a study of the screen in general pediatric clinics. The authors reported having no disclosures.
Pediatricians can use a short, simple questionnaire to screen children for obstructive sleep apnea, according to a study of children and parents referred to a sleep center for screening.
While the shorter tool is not as sensitive as longer questionnaires, it is faster and easier to use, allowing primary caregivers to screen more children.
About 1%-4% of children are affected by obstructive sleep apnea (OSA), an underdiagnosed condition that can have significant effects on a child’s behavior, performance, and health.
The researchers, led by Dr. Gili Kadmon of the Schneider Children’s Medical Center, Petach Tikva, Israel, developed the IF SLEEPY screen of eight yes/no questions that investigate a child’s snoring, breathing problems during sleep, daytime irritability, sleepiness, moods, concentration problems, and other issues. The screen was given to parents of 150 children aged 3-17 years who had been referred to a sleep center in Toronto. Children aged 7 years or older were also asked to answer a modified questionnaire. Only children who were eligible for a sleep study were included in the sample (Int. J. Pediatr. Otorhinolaryngol. 2014 Oct 7. [doi: 10.1016/j.ijporl.2014.09.018]).
A comparison of the parents’ questionnaire scores with their child’s apnea-hypopnea index obtained during a subsequent overnight polysomnographic study found that the screen had a 78% sensitivity for mild to severe obstructive sleep apnea (OSA) cases, with a 40% specificity. The children’s responses were less sensitive, but more specific (45% and 52%, respectively).
To improve the screen’s specificity, the researchers dropped a question about concentration, creating the I SLEEPY version, which resulted in sensitivity and specificity scores for the parent answers of 76% and 55%, respectively. A third version (I’M SLEEPY) added a measure of the child’s body mass index, which resulted in parent scores that were 82% sensitive and 50% specific.
The new screens’ sensitivities and specificities are lower than those of the three longer pediatric OSA screens currently available. Those screens have 40 or more items, and can yield sensitivities and specificities as high as 91% and 88%. However, the authors suggest that a 1-minute screen with a mnemonic name is better suited for a primary care setting. They report they are currently developing a study of the screen in general pediatric clinics. The authors reported having no disclosures.
FROM THE INTERNATIONAL JOURNAL OF PEDIATRIC OTORHINOLARYNGOLOGY
Key clinical point: A new screening questionnaire for sleep apnea in children is easier to use than longer questionnaires, though less sensitive and specific.
Major finding: An eight-question screening tool for pediatric obstructive sleep apnea had 78% sensitivity and 40% specificity for mild to severe OSA.
Data source: A screening trial using a new shortened questionnaire followed by a sleep study of 150 children referred to a sleep clinic.
Disclosures: The authors reported having no disclosures.

Guidelines for children’s bronchiolitis treatment issued by AAP
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.

The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
These guidelines, written with clarity, give incredibly direct and helpful direction on the diagnosis and treatment of bronchiolitis. It is great that they are coming out now, prior to RSV season. Bronchiolitis is a clinical diagnosis and these guidelines reaffirm that there is not usually any need for x-ray or laboratory confirmation of the diagnosis. The guidelines are primarily important for clarifying, based on the evidence, that many commonly used treatments, including albuterol, epinephrine, and steroids are not recommended for treatment of bronchiolitis as they are simply not helpful.
The guidance on administration of palivizumab is also important. It should not be administered in infants with a gestational age of > 29 weeks, and it should be reserved for infants in the first year of life who had a gestational age < 32 weeks and who had hemodynamically significant heart disease or chronic lung disease of prematurity.
Neil Skolnik, M.D., is the associate director of the family medicine program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.
The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
The main treatment for bronchiolitis in young children should be support and observation, according to new clinical practice guidelines for diagnosing, managing, and preventing bronchiolitis.
The guidelines apply to children aged 1-23 months and emphasize clinical diagnosis and no medications except nebulized hypertonic saline for infants hospitalized with bronchiolitis, wrote Dr. Shawn L. Ralston, Dr. Allan S. Lieberthal, and their associates (Pediatrics 2014 October 27 [doi:10.1542/peds.2014-2742]). These guidelines update and replace the ones issued by the American Academy of Pediatrics in 2006 (Pediatrics 2006 118:1774-93). The findings are based on a review of the evidence in the Cochrane Library, Medline, and the Cumulative Index of Nursing and Allied Health Literature (CINAHL) from 2004 through May 2014.
The most notable change to these updated guidelines, according to Dr. Lieberthal, is the preventive recommendation for palivizumab, which is now not indicated for children born at 29 weeks’ gestation or older unless they have hemodynamically significant heart disease or chronic lung disease of prematurity (those born at less than 32 weeks’ gestation who needed at least 21% oxygen for their first month). Infants who qualify for prophylactic palivizumab should receive five monthly doses during respiratory syncytial virus season.
Dr. Lieberthal noted in an interview that several other recommendations state that certain treatments should not be used at all rather than simply not being routinely used. These include albuterol, epinephrine, corticosteroids, chest physiotherapy, and antibiotics.
“Bronchiolitis is a self-limited viral illness,” he said. Because it is diagnosed by signs and symptoms, no lab tests, oximetry, imaging, or other tests are needed, and treatment involves only support and observation. “None of the treatments that have been tested have been shown to affect the outcome of the illness,” said Dr. Lieberthal, who practices general pediatrics and clinical pediatric pulmonology at Kaiser-Permanente in Panorama City, Calif.
Dr. Ralston noted in an interview that a new recommendation exists for using hypertonic saline to children who are hospitalized for bronchiolitis (although not in the emergency department), but the evidence for it is weak and its therapeutic value limited.
“This medication appears to have a slow onset and to provide a favorable response only in settings where patients are hospitalized for longer than is typical in most U.S. hospitals, as most of the studies were performed outside the U.S.,” said Dr. Ralston, a pediatrician at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The guidelines also note that clinicians “may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90%” in children, although the evidence for this recommendation is also weak. Children should receive nasogastric or intravenous fluids if they cannot maintain oral hydration.
Parents should be advised that children who avoid secondhand tobacco smoke and are exclusively breastfed for at least 6 months have a reduced risk of bronchiolitis. Further, anyone caring for a child with bronchiolitis should disinfect their hands using an alcohol-based rub or soap and water after direct contact with the child and the child’s immediate environment.
Dr. Ralston said that important points stressed in both this recommendation and in the previous one include clinical diagnosis and avoiding exposure to tobacco smoke to reduce children’s risk of bronchiolitis.
“This guideline is mostly about what you shouldn’t do for the disease since because of the high volume of disease bronchiolitis represents a major area of unnecessary medical intervention in children,” she said. “We know that the vast majority of children will suffer only side effects from the medications or testing typically used in bronchiolitis care.”
Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.
FROM PEDIATRICS
Key clinical point: Bronchiolitis should be diagnosed clinically and treated with support.
Major finding: Most treatments should not be administered because outcomes are not improved.
Data source: The findings are based on a review of the evidence in the Cochrane Library, Medline, and CINAHL from 2004 through May 2014.
Disclosures: Funding was provided by the American Academy of Pediatrics with travel support from the American Academy of Family Physicians, the American College of Chest Physicians, the American Thoracic Society, and the American College of Emergency Physicians for their representatives.

Short-course TB therapy fails in three international trials
Three different short-course treatment regimens for tuberculosis failed to show noninferiority to the standard 6-month course in separate phase III randomized clinical trials, even though the experimental regimens produced a more rapid decline in bacterial load, as expected, according to reports published online Oct. 23 in the New England Journal of Medicine.
The main reason that the short-course (4-month) approaches failed to measure up to standard treatment was that, despite their greater bactericidal activity, the rate of relapse was excessive after treatment was completed.

Researchers undertook these large international trials because the data from several phase II and murine studies had been so promising: replacing either the isoniazid or the ethambutol in the standard anti-TB regimen with a fluoroquinolone appeared to permit shortening of the treatment period without sacrificing efficacy. But the consistently negative results from these phase III studies clearly demonstrate that this approach is not effective.
The first trial involved 1,931 adults with newly diagnosed and untreated Mycobacterium tuberculosis infection who were treated in South Africa, India, Tanzania, Kenya, Thailand, Malaysia, Zambia, China, and Mexico. These patients were randomly assigned to receive the standard regimen of isoniazid, rifampin, pyrazinamide, and ethambutol for 8 weeks, followed by 18 weeks of isoniazid plus rifampin (control group, 640 participants); or an experimental regimen in which ethambutol was replaced by moxifloxacin for 17 weeks, followed by 9 weeks of placebo (655 participants); or an experimental regimen in which isoniazid was replaced by moxifloxacin in the same way (636 participants), said Dr. Stephen H. Gillespie of the University of St. Andrews (England) and University College London and his associates.
Patients in the two experimental groups converted to culture-negative status more rapidly than did those in the control group. However, in a per-protocol analysis, 92% of the control group achieved a favorable final outcome, compared with only 85% and 80% of the experimental groups, respectively. Results of a modified intention-to-treat analysis and of more than 20 sensitivity analyses showed the same pattern. At the end of active treatment, only 12 patients in the control group had a relapse of TB infection, compared with 64 patients and 46 patients, respectively, in the experimental groups, Dr. Gillespie and his colleagues said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1407426]).
The second trial was an open-label noninferiority study involving 1,836 patients in Benin, Guinea, Kenya, Senegal, and South Africa. They were randomly assigned to standard 6-month treatment (919 control subjects) or an experimental treatment in which gatifloxacin was substituted for ethambutol and the course of therapy was shortened to 4 months (917 patients), said Dr. Corinne S. Merle of the London School of Hygiene and Tropical Medicine and her associates.
The primary efficacy endpoint, the percentage of patients with an unfavorable outcome after 24 months, was 17.2% in the control group and 21.0% in the experimental group, a significant difference. In particular, more than twice as many patients in the experimental group (14.6%) had a relapse than in the control group (7.1%). As with Dr. Gillespie’s study, Dr. Merle’s study failed to show that the short-course regimen was noninferior to the standard regimen. Again, “the expectations raised by [phase I and II trials] were not borne out in this phase III trial,” they said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1315817]).
The third trial, involving 827 patients in South Africa, Zimbabwe, Botswana, and Zambia, compared the standard control regimen against a 4-month regimen in which isoniazid was replaced by moxifloxacin and a 6-month regimen in which isoniazid was replaced by moxifloxacin, said Dr. Amina Jindani of St. George’s University of London and University College London and her associates.
In the per-protocol analysis, unfavorable outcomes occurred in 4.9% of the control group and 3.2% of the 6-month experimental group, compared with 18.2% of the short-course experimental group. The corresponding figures for the intention-to-treat analysis were 14.4%, 13.7%, and 26.9%, respectively.
Again, this discrepancy was attributed primarily to the significantly higher relapse rate in the short-course, compared with the control treatments – 26 cases with 4 months of treatment vs. 5 cases each with 6 months, Dr. Jindani and her associates said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1314210]).
Although the studies described here have established the capacity for large, multicenter trials across disease-endemic countries, the design and selection of future experimental regimens will need to incorporate a triage process that can mitigate risks while enabling the accelerated development of much-needed treatment-shortening therapies. The disconnect between the phase II data that motivated these trials and the phase III results reinforces the idea that small sample sizes limit the utility of short trials in predicting the success of treatment-shortening regimens.
As these three trials have confirmed, our understanding of the science underlying positive clinical outcomes remains rudimentary. It’s time to go back to basics.
Digby F. Warner, Ph.D., and Valerie Mizrahi, Ph.D., are in the molecular mycobacteriology research unit at the Institute of Infectious Disease and Molecular Medicine, Cape Town and in the department of clinical laboratory sciences at the University of Cape Town, both in South Africa. Dr. Warner reported receiving funding from the South African Medical Research Council, Medical Research Foundation South Africa, and Wellcome Trust. Dr. Mizrahi reported funding from the European & Developing Countries Clinical Trials Partnership, the Bill and Melinda Gates Foundation, the Wellcome Trust, and USAID. Dr. Mizrahi also serves on the scientific advisory committee of the Global Alliance for TB Drug Development, which supported Dr. Gillespie’s study. This comment is excerpted from an editorial by Dr. Warner and Dr. Mizrahi that accompanied the three reports (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMe1410977]).
Although the studies described here have established the capacity for large, multicenter trials across disease-endemic countries, the design and selection of future experimental regimens will need to incorporate a triage process that can mitigate risks while enabling the accelerated development of much-needed treatment-shortening therapies. The disconnect between the phase II data that motivated these trials and the phase III results reinforces the idea that small sample sizes limit the utility of short trials in predicting the success of treatment-shortening regimens.
As these three trials have confirmed, our understanding of the science underlying positive clinical outcomes remains rudimentary. It’s time to go back to basics.
Digby F. Warner, Ph.D., and Valerie Mizrahi, Ph.D., are in the molecular mycobacteriology research unit at the Institute of Infectious Disease and Molecular Medicine, Cape Town and in the department of clinical laboratory sciences at the University of Cape Town, both in South Africa. Dr. Warner reported receiving funding from the South African Medical Research Council, Medical Research Foundation South Africa, and Wellcome Trust. Dr. Mizrahi reported funding from the European & Developing Countries Clinical Trials Partnership, the Bill and Melinda Gates Foundation, the Wellcome Trust, and USAID. Dr. Mizrahi also serves on the scientific advisory committee of the Global Alliance for TB Drug Development, which supported Dr. Gillespie’s study. This comment is excerpted from an editorial by Dr. Warner and Dr. Mizrahi that accompanied the three reports (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMe1410977]).
Although the studies described here have established the capacity for large, multicenter trials across disease-endemic countries, the design and selection of future experimental regimens will need to incorporate a triage process that can mitigate risks while enabling the accelerated development of much-needed treatment-shortening therapies. The disconnect between the phase II data that motivated these trials and the phase III results reinforces the idea that small sample sizes limit the utility of short trials in predicting the success of treatment-shortening regimens.
As these three trials have confirmed, our understanding of the science underlying positive clinical outcomes remains rudimentary. It’s time to go back to basics.
Digby F. Warner, Ph.D., and Valerie Mizrahi, Ph.D., are in the molecular mycobacteriology research unit at the Institute of Infectious Disease and Molecular Medicine, Cape Town and in the department of clinical laboratory sciences at the University of Cape Town, both in South Africa. Dr. Warner reported receiving funding from the South African Medical Research Council, Medical Research Foundation South Africa, and Wellcome Trust. Dr. Mizrahi reported funding from the European & Developing Countries Clinical Trials Partnership, the Bill and Melinda Gates Foundation, the Wellcome Trust, and USAID. Dr. Mizrahi also serves on the scientific advisory committee of the Global Alliance for TB Drug Development, which supported Dr. Gillespie’s study. This comment is excerpted from an editorial by Dr. Warner and Dr. Mizrahi that accompanied the three reports (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMe1410977]).
Three different short-course treatment regimens for tuberculosis failed to show noninferiority to the standard 6-month course in separate phase III randomized clinical trials, even though the experimental regimens produced a more rapid decline in bacterial load, as expected, according to reports published online Oct. 23 in the New England Journal of Medicine.
The main reason that the short-course (4-month) approaches failed to measure up to standard treatment was that, despite their greater bactericidal activity, the rate of relapse was excessive after treatment was completed.
Researchers undertook these large international trials because the data from several phase II and murine studies had been so promising: replacing either the isoniazid or the ethambutol in the standard anti-TB regimen with a fluoroquinolone appeared to permit shortening of the treatment period without sacrificing efficacy. But the consistently negative results from these phase III studies clearly demonstrate that this approach is not effective.
The first trial involved 1,931 adults with newly diagnosed and untreated Mycobacterium tuberculosis infection who were treated in South Africa, India, Tanzania, Kenya, Thailand, Malaysia, Zambia, China, and Mexico. These patients were randomly assigned to receive the standard regimen of isoniazid, rifampin, pyrazinamide, and ethambutol for 8 weeks, followed by 18 weeks of isoniazid plus rifampin (control group, 640 participants); or an experimental regimen in which ethambutol was replaced by moxifloxacin for 17 weeks, followed by 9 weeks of placebo (655 participants); or an experimental regimen in which isoniazid was replaced by moxifloxacin in the same way (636 participants), said Dr. Stephen H. Gillespie of the University of St. Andrews (England) and University College London and his associates.
Patients in the two experimental groups converted to culture-negative status more rapidly than did those in the control group. However, in a per-protocol analysis, 92% of the control group achieved a favorable final outcome, compared with only 85% and 80% of the experimental groups, respectively. Results of a modified intention-to-treat analysis and of more than 20 sensitivity analyses showed the same pattern. At the end of active treatment, only 12 patients in the control group had a relapse of TB infection, compared with 64 patients and 46 patients, respectively, in the experimental groups, Dr. Gillespie and his colleagues said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1407426]).
The second trial was an open-label noninferiority study involving 1,836 patients in Benin, Guinea, Kenya, Senegal, and South Africa. They were randomly assigned to standard 6-month treatment (919 control subjects) or an experimental treatment in which gatifloxacin was substituted for ethambutol and the course of therapy was shortened to 4 months (917 patients), said Dr. Corinne S. Merle of the London School of Hygiene and Tropical Medicine and her associates.
The primary efficacy endpoint, the percentage of patients with an unfavorable outcome after 24 months, was 17.2% in the control group and 21.0% in the experimental group, a significant difference. In particular, more than twice as many patients in the experimental group (14.6%) had a relapse than in the control group (7.1%). As with Dr. Gillespie’s study, Dr. Merle’s study failed to show that the short-course regimen was noninferior to the standard regimen. Again, “the expectations raised by [phase I and II trials] were not borne out in this phase III trial,” they said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1315817]).
The third trial, involving 827 patients in South Africa, Zimbabwe, Botswana, and Zambia, compared the standard control regimen against a 4-month regimen in which isoniazid was replaced by moxifloxacin and a 6-month regimen in which isoniazid was replaced by moxifloxacin, said Dr. Amina Jindani of St. George’s University of London and University College London and her associates.
In the per-protocol analysis, unfavorable outcomes occurred in 4.9% of the control group and 3.2% of the 6-month experimental group, compared with 18.2% of the short-course experimental group. The corresponding figures for the intention-to-treat analysis were 14.4%, 13.7%, and 26.9%, respectively.
Again, this discrepancy was attributed primarily to the significantly higher relapse rate in the short-course, compared with the control treatments – 26 cases with 4 months of treatment vs. 5 cases each with 6 months, Dr. Jindani and her associates said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1314210]).
Three different short-course treatment regimens for tuberculosis failed to show noninferiority to the standard 6-month course in separate phase III randomized clinical trials, even though the experimental regimens produced a more rapid decline in bacterial load, as expected, according to reports published online Oct. 23 in the New England Journal of Medicine.
The main reason that the short-course (4-month) approaches failed to measure up to standard treatment was that, despite their greater bactericidal activity, the rate of relapse was excessive after treatment was completed.
Researchers undertook these large international trials because the data from several phase II and murine studies had been so promising: replacing either the isoniazid or the ethambutol in the standard anti-TB regimen with a fluoroquinolone appeared to permit shortening of the treatment period without sacrificing efficacy. But the consistently negative results from these phase III studies clearly demonstrate that this approach is not effective.
The first trial involved 1,931 adults with newly diagnosed and untreated Mycobacterium tuberculosis infection who were treated in South Africa, India, Tanzania, Kenya, Thailand, Malaysia, Zambia, China, and Mexico. These patients were randomly assigned to receive the standard regimen of isoniazid, rifampin, pyrazinamide, and ethambutol for 8 weeks, followed by 18 weeks of isoniazid plus rifampin (control group, 640 participants); or an experimental regimen in which ethambutol was replaced by moxifloxacin for 17 weeks, followed by 9 weeks of placebo (655 participants); or an experimental regimen in which isoniazid was replaced by moxifloxacin in the same way (636 participants), said Dr. Stephen H. Gillespie of the University of St. Andrews (England) and University College London and his associates.
Patients in the two experimental groups converted to culture-negative status more rapidly than did those in the control group. However, in a per-protocol analysis, 92% of the control group achieved a favorable final outcome, compared with only 85% and 80% of the experimental groups, respectively. Results of a modified intention-to-treat analysis and of more than 20 sensitivity analyses showed the same pattern. At the end of active treatment, only 12 patients in the control group had a relapse of TB infection, compared with 64 patients and 46 patients, respectively, in the experimental groups, Dr. Gillespie and his colleagues said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1407426]).
The second trial was an open-label noninferiority study involving 1,836 patients in Benin, Guinea, Kenya, Senegal, and South Africa. They were randomly assigned to standard 6-month treatment (919 control subjects) or an experimental treatment in which gatifloxacin was substituted for ethambutol and the course of therapy was shortened to 4 months (917 patients), said Dr. Corinne S. Merle of the London School of Hygiene and Tropical Medicine and her associates.
The primary efficacy endpoint, the percentage of patients with an unfavorable outcome after 24 months, was 17.2% in the control group and 21.0% in the experimental group, a significant difference. In particular, more than twice as many patients in the experimental group (14.6%) had a relapse than in the control group (7.1%). As with Dr. Gillespie’s study, Dr. Merle’s study failed to show that the short-course regimen was noninferior to the standard regimen. Again, “the expectations raised by [phase I and II trials] were not borne out in this phase III trial,” they said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1315817]).
The third trial, involving 827 patients in South Africa, Zimbabwe, Botswana, and Zambia, compared the standard control regimen against a 4-month regimen in which isoniazid was replaced by moxifloxacin and a 6-month regimen in which isoniazid was replaced by moxifloxacin, said Dr. Amina Jindani of St. George’s University of London and University College London and her associates.
In the per-protocol analysis, unfavorable outcomes occurred in 4.9% of the control group and 3.2% of the 6-month experimental group, compared with 18.2% of the short-course experimental group. The corresponding figures for the intention-to-treat analysis were 14.4%, 13.7%, and 26.9%, respectively.
Again, this discrepancy was attributed primarily to the significantly higher relapse rate in the short-course, compared with the control treatments – 26 cases with 4 months of treatment vs. 5 cases each with 6 months, Dr. Jindani and her associates said (N. Engl. J. Med. 2014 Oct. 23 [doi:10.1056/NEJMoa1314210]).
Key clinical point: Shortening tuberculosis treatment to 4 months is not proven to be effective in three phase III studies.
Major finding: Relapse was seen in more than twice as many patients (14.6%) receiving treatment in which gatifloxacin was substituted for ethambutol and the course of therapy was shortened to 4 months in lieu of the standard 6-month treatment (7.1%).
Data source: An open-label noninferiority study involving 1,836 patients.
Disclosures: The researchers reported no relevant financial conflicts.
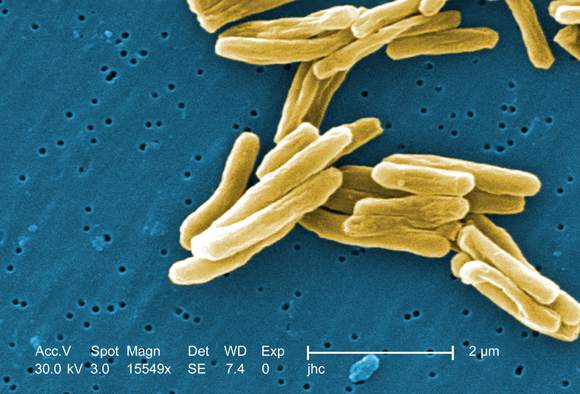
Pediatric ID hospitalizations down after vaccine introductions
PHILADELPHIA– Infectious diseases played a primary role in 16% of pediatric hospitalizations between 1997 and 2009, and remain a leading cause of pediatric hospitalizations and health care expenditures, but the proportion of hospitalizations associated with an infectious disease declined by 18% during the study period, according to an analysis of the Kids’ Inpatient Database.

Periods of decline were temporally associated with the introduction of pneumococcal and rotavirus vaccines, Chris Stockmann of the University of Utah Health Sciences Center, Salt Lake City, reported at an annual scientific meeting on infectious diseases.
Infectious diseases were second only to newborn deliveries as a cause of pediatric hospitalizations during the study period, Mr. Stockmann said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The burden was highest among children under age 5 years, who accounted for about 75% of all infectious disease hospitalizations; those under age 3 months accounted for 15%.
Eight diagnoses accounted for more than 80% of the hospitalizations. The most common were pneumonia and bronchiolitis, followed by urinary tract infections, other upper respiratory tract infections, intestinal infections, other viral infections, sepsis, and meningitis. Respiratory infections accounted for about two-thirds of all hospitalizations, he said.
Pneumonia was the leading cause of hospitalizations across all age groups. The second leading cause was bronchiolitis in those under age 5 years, and UTI in those aged 5 years and older.
“A smattering of other conditions, including intestinal infections, viral infections, and meningitis, also make an appearance in the top 4,” he said.
Over time, pneumonia, bronchiolitis, and other upper respiratory tract infections decreased by 15% to 30%, and the intestinal infection rate was nearly halved.
The decrease in pneumonia hospitalizations coincided with the introduction of the 7-valent pneumococcal conjugate vaccine in 2000, and the introduction of the rotavirus vaccine in 2007. The introduction of these vaccines also was associated with a reduction in intestinal infection hospitalizations, he said.
During the study period, the overall charge for all infectious disease hospitalizations was $4.3 billion per year nationally. At the patient level, the mean charge was just under $15,000, and the mean length of stay was just over 3 days, Mr. Stockmann said.
Total hospital charges were driven by pneumonia and bronchiolitis, but at the individual patient level, sepsis and meningitis were the most expensive conditions, he noted.
The data for this analysis were derived from the National Inpatient Survey’s Kids’ Inpatient Database (KID), owned and operated by the Agency for Healthcare Research and Quality, and maintained by the Healthcare Cost and Utilization Project. Currently, 3,500 hospitals in 44 states contribute data to KID, which is released every 3 years; data for this study were available for 1997, 2000, 2003, 2006, and 2009 and were weighted with a complex survey design to more than 36 million discharges nationwide.
The findings underscore the need for additional efforts to reduce the burden of pediatric respiratory tract infections, Mr. Stockmann said. “We would posit that respiratory viral vaccines may play a key role in that,” he said.
Mr. Stockmann reported having no disclosures.
PHILADELPHIA– Infectious diseases played a primary role in 16% of pediatric hospitalizations between 1997 and 2009, and remain a leading cause of pediatric hospitalizations and health care expenditures, but the proportion of hospitalizations associated with an infectious disease declined by 18% during the study period, according to an analysis of the Kids’ Inpatient Database.
Periods of decline were temporally associated with the introduction of pneumococcal and rotavirus vaccines, Chris Stockmann of the University of Utah Health Sciences Center, Salt Lake City, reported at an annual scientific meeting on infectious diseases.
Infectious diseases were second only to newborn deliveries as a cause of pediatric hospitalizations during the study period, Mr. Stockmann said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The burden was highest among children under age 5 years, who accounted for about 75% of all infectious disease hospitalizations; those under age 3 months accounted for 15%.
Eight diagnoses accounted for more than 80% of the hospitalizations. The most common were pneumonia and bronchiolitis, followed by urinary tract infections, other upper respiratory tract infections, intestinal infections, other viral infections, sepsis, and meningitis. Respiratory infections accounted for about two-thirds of all hospitalizations, he said.
Pneumonia was the leading cause of hospitalizations across all age groups. The second leading cause was bronchiolitis in those under age 5 years, and UTI in those aged 5 years and older.
“A smattering of other conditions, including intestinal infections, viral infections, and meningitis, also make an appearance in the top 4,” he said.
Over time, pneumonia, bronchiolitis, and other upper respiratory tract infections decreased by 15% to 30%, and the intestinal infection rate was nearly halved.
The decrease in pneumonia hospitalizations coincided with the introduction of the 7-valent pneumococcal conjugate vaccine in 2000, and the introduction of the rotavirus vaccine in 2007. The introduction of these vaccines also was associated with a reduction in intestinal infection hospitalizations, he said.
During the study period, the overall charge for all infectious disease hospitalizations was $4.3 billion per year nationally. At the patient level, the mean charge was just under $15,000, and the mean length of stay was just over 3 days, Mr. Stockmann said.
Total hospital charges were driven by pneumonia and bronchiolitis, but at the individual patient level, sepsis and meningitis were the most expensive conditions, he noted.
The data for this analysis were derived from the National Inpatient Survey’s Kids’ Inpatient Database (KID), owned and operated by the Agency for Healthcare Research and Quality, and maintained by the Healthcare Cost and Utilization Project. Currently, 3,500 hospitals in 44 states contribute data to KID, which is released every 3 years; data for this study were available for 1997, 2000, 2003, 2006, and 2009 and were weighted with a complex survey design to more than 36 million discharges nationwide.
The findings underscore the need for additional efforts to reduce the burden of pediatric respiratory tract infections, Mr. Stockmann said. “We would posit that respiratory viral vaccines may play a key role in that,” he said.
Mr. Stockmann reported having no disclosures.
PHILADELPHIA– Infectious diseases played a primary role in 16% of pediatric hospitalizations between 1997 and 2009, and remain a leading cause of pediatric hospitalizations and health care expenditures, but the proportion of hospitalizations associated with an infectious disease declined by 18% during the study period, according to an analysis of the Kids’ Inpatient Database.
Periods of decline were temporally associated with the introduction of pneumococcal and rotavirus vaccines, Chris Stockmann of the University of Utah Health Sciences Center, Salt Lake City, reported at an annual scientific meeting on infectious diseases.
Infectious diseases were second only to newborn deliveries as a cause of pediatric hospitalizations during the study period, Mr. Stockmann said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The burden was highest among children under age 5 years, who accounted for about 75% of all infectious disease hospitalizations; those under age 3 months accounted for 15%.
Eight diagnoses accounted for more than 80% of the hospitalizations. The most common were pneumonia and bronchiolitis, followed by urinary tract infections, other upper respiratory tract infections, intestinal infections, other viral infections, sepsis, and meningitis. Respiratory infections accounted for about two-thirds of all hospitalizations, he said.
Pneumonia was the leading cause of hospitalizations across all age groups. The second leading cause was bronchiolitis in those under age 5 years, and UTI in those aged 5 years and older.
“A smattering of other conditions, including intestinal infections, viral infections, and meningitis, also make an appearance in the top 4,” he said.
Over time, pneumonia, bronchiolitis, and other upper respiratory tract infections decreased by 15% to 30%, and the intestinal infection rate was nearly halved.
The decrease in pneumonia hospitalizations coincided with the introduction of the 7-valent pneumococcal conjugate vaccine in 2000, and the introduction of the rotavirus vaccine in 2007. The introduction of these vaccines also was associated with a reduction in intestinal infection hospitalizations, he said.
During the study period, the overall charge for all infectious disease hospitalizations was $4.3 billion per year nationally. At the patient level, the mean charge was just under $15,000, and the mean length of stay was just over 3 days, Mr. Stockmann said.
Total hospital charges were driven by pneumonia and bronchiolitis, but at the individual patient level, sepsis and meningitis were the most expensive conditions, he noted.
The data for this analysis were derived from the National Inpatient Survey’s Kids’ Inpatient Database (KID), owned and operated by the Agency for Healthcare Research and Quality, and maintained by the Healthcare Cost and Utilization Project. Currently, 3,500 hospitals in 44 states contribute data to KID, which is released every 3 years; data for this study were available for 1997, 2000, 2003, 2006, and 2009 and were weighted with a complex survey design to more than 36 million discharges nationwide.
The findings underscore the need for additional efforts to reduce the burden of pediatric respiratory tract infections, Mr. Stockmann said. “We would posit that respiratory viral vaccines may play a key role in that,” he said.
Mr. Stockmann reported having no disclosures.
Key clinical point: Pneumococcal and rotavirus vaccine introductions have been associated with decreases in the rate of pediatric infectious disease hospitalizations.
Major finding: Pediatric infectious disease hospitalizations declined by 18% between 1997 and 2009.
Data source: An analysis of the Kids’ Inpatient Database weighted to 36.3 million discharges.
Disclosures: Mr. Stockmann reported having no disclosures.

ID CONSULT: Influenza virus and pneumococci dance together
Most practitioners know that the flu vaccine has been proven to reduce the frequency of middle ear infections, sinusitis, and pneumonia. However, how that happens is not as clear. My group has been studying the details of the interaction between flu virus and pneumococci to unravel the steps in the dance between the flu virus and the pneumococcus in the nasopharynx that results in significant respiratory diseases. Pneumococci live in the posterior part of the nose and upper pharynx as commensal bacteria in all of us, harmlessly present in relatively low numbers. The bacteria are so common that studies to detect pneumococci in the nasopharynx discover their presence in up to 80% of infants and young children, and about 20% of adults at any one time. The bacteria are harmless in patients that have a competent immune system unless an intercurrent viral upper respiratory infection (URI) occurs.
The trigger in pathogenesis of pneumococcal infections is a viral URI, and particularly influenza infection. The combination of pneumococci and flu in the nose can cause compromise in all four aspects of host defense: 1) structural change, 2) physiologic change, 3) innate immunity change, and 4) adaptive immunity change. Structural change is swelling of the nasal passageways, Eustachian tube, osteomeatal sinus pathway, and tracheobronchial tree. Physiologic change is increased mucus production and reduced cilia beat, resulting in stasis of thickened mucus in the respiratory tree. Thus the stage is set for compromise in the immune response.

Innate immunity basically translates to the response of neutrophils, macrophages, and lymphocytes that are resident in the respiratory pathways or migrate there in response to signals from the site of infection that a problem is brewing. To start the process of innate immunity, chemicals are released from resident epithelial cells, lymphocytes, and neutrophils/macrophages. The chemicals are called cytokines and chemokines. The viruses enter the epithelial cells of the nasopharynx and tracheobronchial tree, and leave a change on the surface of the epithelial cells that alerts lymphocytes to kill and destroy those cells harboring virus. Neutrophils and macrophages ingest the bacteria by recognizing surface proteins on the bacteria that are foreign. Sometimes that is all that is needed, and the host clears the infection. But sometimes the innate response is not enough.
The innate response is good and bad. The bad part is that the release of the cytokines and chemokines and the migration of immune cells to the site of infection results in the release of even more cytokines and chemokines that cause increased inflammation. Microbes love inflammation. The inflammation caused by the virus, such as flu virus, creates a very favorable environment for the pneumococci. So the pneumococci start to reproduce in abundance. Then when the secretions of the nose are swept into the Eustachian tube and middle ear or the sinus drainage pathways and then to the sinuses or into the trachea and bronchi and then the lungs, we see the clinical manifestations of acute otitis media, sinusitis, or pneumonia. The innate response failed.
The adaptive response – as the word implies – is when the immune cells recognize and adapt to the presence of foreign microbes by recognizing their presence, migrating to lymph nodes and spleen, communicating with each other, and consequently multiplying into great numbers. The interaction between the immune cells – T cells and B cells – in the lymph node and migration back to the site of infection takes a few days to occur (3-5 days) if the host has prior immunity from prior infections or vaccination. If there is no prior immunity and no vaccination, then it takes 10-14 days for the adaptive immunity response to kick in and clear the infection. During that extra time, the pneumococci are gaining in numbers, causing more inflammation, and we see those clinical signs of fever, redness, and swelling at the site of infection, and pain.
So influenza can cause all of the events above by itself, but when the virus dances with the pneumococci, and the pneumococci benefit from the partnership, that is the most frequent cause of acute otitis media, sinusitis, and pneumonia. And all of that could have been prevented in most of our patients if they only got their annual flu vaccine.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. The study was supported by a National Institutes of Health grant. Dr. Pichichero said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Most practitioners know that the flu vaccine has been proven to reduce the frequency of middle ear infections, sinusitis, and pneumonia. However, how that happens is not as clear. My group has been studying the details of the interaction between flu virus and pneumococci to unravel the steps in the dance between the flu virus and the pneumococcus in the nasopharynx that results in significant respiratory diseases. Pneumococci live in the posterior part of the nose and upper pharynx as commensal bacteria in all of us, harmlessly present in relatively low numbers. The bacteria are so common that studies to detect pneumococci in the nasopharynx discover their presence in up to 80% of infants and young children, and about 20% of adults at any one time. The bacteria are harmless in patients that have a competent immune system unless an intercurrent viral upper respiratory infection (URI) occurs.
The trigger in pathogenesis of pneumococcal infections is a viral URI, and particularly influenza infection. The combination of pneumococci and flu in the nose can cause compromise in all four aspects of host defense: 1) structural change, 2) physiologic change, 3) innate immunity change, and 4) adaptive immunity change. Structural change is swelling of the nasal passageways, Eustachian tube, osteomeatal sinus pathway, and tracheobronchial tree. Physiologic change is increased mucus production and reduced cilia beat, resulting in stasis of thickened mucus in the respiratory tree. Thus the stage is set for compromise in the immune response.
Innate immunity basically translates to the response of neutrophils, macrophages, and lymphocytes that are resident in the respiratory pathways or migrate there in response to signals from the site of infection that a problem is brewing. To start the process of innate immunity, chemicals are released from resident epithelial cells, lymphocytes, and neutrophils/macrophages. The chemicals are called cytokines and chemokines. The viruses enter the epithelial cells of the nasopharynx and tracheobronchial tree, and leave a change on the surface of the epithelial cells that alerts lymphocytes to kill and destroy those cells harboring virus. Neutrophils and macrophages ingest the bacteria by recognizing surface proteins on the bacteria that are foreign. Sometimes that is all that is needed, and the host clears the infection. But sometimes the innate response is not enough.
The innate response is good and bad. The bad part is that the release of the cytokines and chemokines and the migration of immune cells to the site of infection results in the release of even more cytokines and chemokines that cause increased inflammation. Microbes love inflammation. The inflammation caused by the virus, such as flu virus, creates a very favorable environment for the pneumococci. So the pneumococci start to reproduce in abundance. Then when the secretions of the nose are swept into the Eustachian tube and middle ear or the sinus drainage pathways and then to the sinuses or into the trachea and bronchi and then the lungs, we see the clinical manifestations of acute otitis media, sinusitis, or pneumonia. The innate response failed.
The adaptive response – as the word implies – is when the immune cells recognize and adapt to the presence of foreign microbes by recognizing their presence, migrating to lymph nodes and spleen, communicating with each other, and consequently multiplying into great numbers. The interaction between the immune cells – T cells and B cells – in the lymph node and migration back to the site of infection takes a few days to occur (3-5 days) if the host has prior immunity from prior infections or vaccination. If there is no prior immunity and no vaccination, then it takes 10-14 days for the adaptive immunity response to kick in and clear the infection. During that extra time, the pneumococci are gaining in numbers, causing more inflammation, and we see those clinical signs of fever, redness, and swelling at the site of infection, and pain.
So influenza can cause all of the events above by itself, but when the virus dances with the pneumococci, and the pneumococci benefit from the partnership, that is the most frequent cause of acute otitis media, sinusitis, and pneumonia. And all of that could have been prevented in most of our patients if they only got their annual flu vaccine.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. The study was supported by a National Institutes of Health grant. Dr. Pichichero said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Most practitioners know that the flu vaccine has been proven to reduce the frequency of middle ear infections, sinusitis, and pneumonia. However, how that happens is not as clear. My group has been studying the details of the interaction between flu virus and pneumococci to unravel the steps in the dance between the flu virus and the pneumococcus in the nasopharynx that results in significant respiratory diseases. Pneumococci live in the posterior part of the nose and upper pharynx as commensal bacteria in all of us, harmlessly present in relatively low numbers. The bacteria are so common that studies to detect pneumococci in the nasopharynx discover their presence in up to 80% of infants and young children, and about 20% of adults at any one time. The bacteria are harmless in patients that have a competent immune system unless an intercurrent viral upper respiratory infection (URI) occurs.
The trigger in pathogenesis of pneumococcal infections is a viral URI, and particularly influenza infection. The combination of pneumococci and flu in the nose can cause compromise in all four aspects of host defense: 1) structural change, 2) physiologic change, 3) innate immunity change, and 4) adaptive immunity change. Structural change is swelling of the nasal passageways, Eustachian tube, osteomeatal sinus pathway, and tracheobronchial tree. Physiologic change is increased mucus production and reduced cilia beat, resulting in stasis of thickened mucus in the respiratory tree. Thus the stage is set for compromise in the immune response.
Innate immunity basically translates to the response of neutrophils, macrophages, and lymphocytes that are resident in the respiratory pathways or migrate there in response to signals from the site of infection that a problem is brewing. To start the process of innate immunity, chemicals are released from resident epithelial cells, lymphocytes, and neutrophils/macrophages. The chemicals are called cytokines and chemokines. The viruses enter the epithelial cells of the nasopharynx and tracheobronchial tree, and leave a change on the surface of the epithelial cells that alerts lymphocytes to kill and destroy those cells harboring virus. Neutrophils and macrophages ingest the bacteria by recognizing surface proteins on the bacteria that are foreign. Sometimes that is all that is needed, and the host clears the infection. But sometimes the innate response is not enough.
The innate response is good and bad. The bad part is that the release of the cytokines and chemokines and the migration of immune cells to the site of infection results in the release of even more cytokines and chemokines that cause increased inflammation. Microbes love inflammation. The inflammation caused by the virus, such as flu virus, creates a very favorable environment for the pneumococci. So the pneumococci start to reproduce in abundance. Then when the secretions of the nose are swept into the Eustachian tube and middle ear or the sinus drainage pathways and then to the sinuses or into the trachea and bronchi and then the lungs, we see the clinical manifestations of acute otitis media, sinusitis, or pneumonia. The innate response failed.
The adaptive response – as the word implies – is when the immune cells recognize and adapt to the presence of foreign microbes by recognizing their presence, migrating to lymph nodes and spleen, communicating with each other, and consequently multiplying into great numbers. The interaction between the immune cells – T cells and B cells – in the lymph node and migration back to the site of infection takes a few days to occur (3-5 days) if the host has prior immunity from prior infections or vaccination. If there is no prior immunity and no vaccination, then it takes 10-14 days for the adaptive immunity response to kick in and clear the infection. During that extra time, the pneumococci are gaining in numbers, causing more inflammation, and we see those clinical signs of fever, redness, and swelling at the site of infection, and pain.
So influenza can cause all of the events above by itself, but when the virus dances with the pneumococci, and the pneumococci benefit from the partnership, that is the most frequent cause of acute otitis media, sinusitis, and pneumonia. And all of that could have been prevented in most of our patients if they only got their annual flu vaccine.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. The study was supported by a National Institutes of Health grant. Dr. Pichichero said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.

Measure associated with LOS in infants with bronchiolitis
SAN DIEGO – Children with a high bronchiolitis risk of admission score are more likely to require longer hospital stays, results from a single-center study showed.
“There’s no tool in the published literature we’re aware of that helps you predict how long a child with bronchiolitis will need to be in the hospital for,” Dr. Matko Marlais said in an interview at the annual meeting of the American Academy of Pediatrics. Such information would be helpful, he continued, because “if the child is quite well, but they still need admission we might decide to put them on the observation ward for 24 hours. But if they’re really unwell, we might decide to put them in the hospital ward as an inpatient. It’s helpful to make that decision at the point of the emergency room triage.”
The 5-point bronchiolitis risk of admission score (BRAS) was developed as a way to help predict the requirement for admission in infants with acute bronchiolitis, and it was validated with this outcome in mind. Points are assigned on the association between the infant and certain factors including duration of symptoms, respiratory rate, heart rate, oxygen saturation, and age at presentation (Arch. Dis. Child. 2011;96:648-52). In an effort to determine whether use of BRAS in the emergency room is able to predict the level of care and length of hospital stay in infants with acute bronchiolitis, Dr. Marlais and his associates evaluated the medical records of all infants who presented to the department of pediatric emergency medicine at Chelsea and Westminster Hospital, London, with the condition during a 12-month period. The analysis was limited to infants up to 1 year of age who required hospitalization.
Clinicians applied the BRAS at the point of emergency room triage and extracted data for each patient from a review of clinical notes, including clinical features at presentation, length of resultant hospital stay, and level of care required (supportive care or noninvasive ventilation via nasal continuous positive airway pressure [CPAP]). The researchers used Spearman Rank correlation coefficient to determine if the BRAS was correlated with the length of hospital stay.
Dr. Marlais reported findings from 163 infants included in the analysis. Of these, 54% were male and their mean age at presentation was 18 weeks. The majority of infants (83%) only required supportive care during their admission, while 17% required noninvasive ventilation via nasal CPAP.
The mean hospital length of stay was 3 days, with a range of 1-30 days. The researchers found that the bronchiolitis risk of admission score was correlated with length of hospital stay (correlation coefficient of 0.47; P< .0001). They also observed that infants who required noninvasive ventilation via CPAP had a significantly higher BRAS, compared with those who required only supportive care (a mean score of 4.14 vs. 3.01, respectively; P< .0001).
“The child with the highest score in this cohort is much more likely to need a hospital stay for 3, 4 or 5 days rather than a child with a lower score,” said Dr. Marlais of the hospital. The association “helps us in managing their flow through the hospital and in giving the parents a bit of an indication as to how long they’ll need to be in the hospital.”
While he characterized the findings as “fairly expected,” he acknowledged certain limitations of the study, including the fact that BRAS “wasn’t developed with [hospital] length of stay as the outcome in mind. It was developed to predict the need for hospital admission. Technically, we would need to develop a new score looking at the predictive factors specifically for length of stay. We haven’t done that.”
Dr. Marlais reported having no relevant financial disclosures.
On Twitter @dougbrunk
SAN DIEGO – Children with a high bronchiolitis risk of admission score are more likely to require longer hospital stays, results from a single-center study showed.
“There’s no tool in the published literature we’re aware of that helps you predict how long a child with bronchiolitis will need to be in the hospital for,” Dr. Matko Marlais said in an interview at the annual meeting of the American Academy of Pediatrics. Such information would be helpful, he continued, because “if the child is quite well, but they still need admission we might decide to put them on the observation ward for 24 hours. But if they’re really unwell, we might decide to put them in the hospital ward as an inpatient. It’s helpful to make that decision at the point of the emergency room triage.”
The 5-point bronchiolitis risk of admission score (BRAS) was developed as a way to help predict the requirement for admission in infants with acute bronchiolitis, and it was validated with this outcome in mind. Points are assigned on the association between the infant and certain factors including duration of symptoms, respiratory rate, heart rate, oxygen saturation, and age at presentation (Arch. Dis. Child. 2011;96:648-52). In an effort to determine whether use of BRAS in the emergency room is able to predict the level of care and length of hospital stay in infants with acute bronchiolitis, Dr. Marlais and his associates evaluated the medical records of all infants who presented to the department of pediatric emergency medicine at Chelsea and Westminster Hospital, London, with the condition during a 12-month period. The analysis was limited to infants up to 1 year of age who required hospitalization.
Clinicians applied the BRAS at the point of emergency room triage and extracted data for each patient from a review of clinical notes, including clinical features at presentation, length of resultant hospital stay, and level of care required (supportive care or noninvasive ventilation via nasal continuous positive airway pressure [CPAP]). The researchers used Spearman Rank correlation coefficient to determine if the BRAS was correlated with the length of hospital stay.
Dr. Marlais reported findings from 163 infants included in the analysis. Of these, 54% were male and their mean age at presentation was 18 weeks. The majority of infants (83%) only required supportive care during their admission, while 17% required noninvasive ventilation via nasal CPAP.
The mean hospital length of stay was 3 days, with a range of 1-30 days. The researchers found that the bronchiolitis risk of admission score was correlated with length of hospital stay (correlation coefficient of 0.47; P< .0001). They also observed that infants who required noninvasive ventilation via CPAP had a significantly higher BRAS, compared with those who required only supportive care (a mean score of 4.14 vs. 3.01, respectively; P< .0001).
“The child with the highest score in this cohort is much more likely to need a hospital stay for 3, 4 or 5 days rather than a child with a lower score,” said Dr. Marlais of the hospital. The association “helps us in managing their flow through the hospital and in giving the parents a bit of an indication as to how long they’ll need to be in the hospital.”
While he characterized the findings as “fairly expected,” he acknowledged certain limitations of the study, including the fact that BRAS “wasn’t developed with [hospital] length of stay as the outcome in mind. It was developed to predict the need for hospital admission. Technically, we would need to develop a new score looking at the predictive factors specifically for length of stay. We haven’t done that.”
Dr. Marlais reported having no relevant financial disclosures.
On Twitter @dougbrunk
SAN DIEGO – Children with a high bronchiolitis risk of admission score are more likely to require longer hospital stays, results from a single-center study showed.
“There’s no tool in the published literature we’re aware of that helps you predict how long a child with bronchiolitis will need to be in the hospital for,” Dr. Matko Marlais said in an interview at the annual meeting of the American Academy of Pediatrics. Such information would be helpful, he continued, because “if the child is quite well, but they still need admission we might decide to put them on the observation ward for 24 hours. But if they’re really unwell, we might decide to put them in the hospital ward as an inpatient. It’s helpful to make that decision at the point of the emergency room triage.”
The 5-point bronchiolitis risk of admission score (BRAS) was developed as a way to help predict the requirement for admission in infants with acute bronchiolitis, and it was validated with this outcome in mind. Points are assigned on the association between the infant and certain factors including duration of symptoms, respiratory rate, heart rate, oxygen saturation, and age at presentation (Arch. Dis. Child. 2011;96:648-52). In an effort to determine whether use of BRAS in the emergency room is able to predict the level of care and length of hospital stay in infants with acute bronchiolitis, Dr. Marlais and his associates evaluated the medical records of all infants who presented to the department of pediatric emergency medicine at Chelsea and Westminster Hospital, London, with the condition during a 12-month period. The analysis was limited to infants up to 1 year of age who required hospitalization.
Clinicians applied the BRAS at the point of emergency room triage and extracted data for each patient from a review of clinical notes, including clinical features at presentation, length of resultant hospital stay, and level of care required (supportive care or noninvasive ventilation via nasal continuous positive airway pressure [CPAP]). The researchers used Spearman Rank correlation coefficient to determine if the BRAS was correlated with the length of hospital stay.
Dr. Marlais reported findings from 163 infants included in the analysis. Of these, 54% were male and their mean age at presentation was 18 weeks. The majority of infants (83%) only required supportive care during their admission, while 17% required noninvasive ventilation via nasal CPAP.
The mean hospital length of stay was 3 days, with a range of 1-30 days. The researchers found that the bronchiolitis risk of admission score was correlated with length of hospital stay (correlation coefficient of 0.47; P< .0001). They also observed that infants who required noninvasive ventilation via CPAP had a significantly higher BRAS, compared with those who required only supportive care (a mean score of 4.14 vs. 3.01, respectively; P< .0001).
“The child with the highest score in this cohort is much more likely to need a hospital stay for 3, 4 or 5 days rather than a child with a lower score,” said Dr. Marlais of the hospital. The association “helps us in managing their flow through the hospital and in giving the parents a bit of an indication as to how long they’ll need to be in the hospital.”
While he characterized the findings as “fairly expected,” he acknowledged certain limitations of the study, including the fact that BRAS “wasn’t developed with [hospital] length of stay as the outcome in mind. It was developed to predict the need for hospital admission. Technically, we would need to develop a new score looking at the predictive factors specifically for length of stay. We haven’t done that.”
Dr. Marlais reported having no relevant financial disclosures.
On Twitter @dougbrunk
AT THE AAP NATIONAL CONFERENCE
Key clinical point: Length of hospital stay is associated with a bronchiolitis risk of admission score (BRAS).
Major finding: In infants with acute bronchiolitis, the BRAS was associated with length of hospital stay (correlation coefficient of .047; P < .0001).
Data source: A review of 163 infants who presented to the department of pediatric emergency medicine at Chelsea and Westminster Hospital, London, with acute bronchiolitis during a 12-month period.
Disclosures: Dr. Marlais reported having no relevant financial disclosures.
Study IDs factors linked to bronchodilator use in bronchiolitis
SAN DIEGO – Key factors associated with the use of bronchodilators in young children hospitalized with bronchiolitis include older age and wheezing and hypoxia upon admission, results from a single-center study showed.
Although the American Academy of Pediatrics does not endorse the routine use of bronchodilators in the treatment of children hospitalized with bronchiolitis (Pediatrics 2006;118:1774-93), “there is substantial variability in the management of bronchiolitis, including the usage of bronchodilators,” researchers led by Dr. Janet Schairer wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. A recent Cochrane report showed that bronchodilators do not decrease length of hospitalization or reduce the time to illness resolution (Cochrane Database Syst. Rev. 2014; 6:CD001266).

In an effort to determine which demographic and clinical factors are associated with the use of bronchodilators in the treatment of children hospitalized with bronchiolitis, Dr. Schairer and her associates reviewed the medical records of 232 children aged 2 weeks to 24 months who were hospitalized with the condition at Jersey Shore University Medical Center, Neptune, N.J., from October 2009 until September 2012. Data analysis included multivariate regression models to identify variables that were associated with administration of bronchodilators.
Of the 232 children, 120 (51.7%) received bronchodilators and 112 (48.3%) did not. The researchers observed no difference in bronchodilator use among patients with risk factors for asthma, including family history of asthma, personal history of wheezing or eczema, and smoke exposure. “That surprised us,” Dr. Schairer of the division of general pediatrics at the medical center, said in an interview.
Compared with children who did not receive bronchodilators, those who did were older (a mean of 6.5 vs. 4.5 months, respectively; P less than .01); and at hospital admission had a higher prevalence of wheezing (45% vs. 19.6%; P less than .0001); diminished air exchange (10.8% vs. 2.7%; P less than .02), and hypoxia (38.3% vs. 25%; P less than .03). Other treatments administered to those who did and did not receive bronchodilators included nebulized 3% saline (37.9% vs. 36.5%), systemic steroids (10.9% vs. 0%), and antibiotics (45% vs. 33%).
Regression analysis revealed that the use of bronchodilators increased with older age (odds ratio, 0.89), and with oxygen requirement (OR, 1.15) or wheezing (OR, 1.23) at the time of admission. No association between bronchodilator use and length of hospitalization was observed (P > .05).
“Widespread implementation of the AAP guidelines for treatment of children with bronchiolitis is required for reduction of unnecessary use of bronchodilators in hospitalized patients,” Dr. Schairer and her associates concluded in the abstract. “Research to assess which, if any, demographic and clinical factors are associated with response to bronchodilator therapy is needed to further guide physicians in the treatment of bronchiolitis.”
She acknowledged certain limitations of the study, including its single-center design and relatively small cohort size.
Dr. Schairer reported having no financial disclosures.
On Twitter @dougbrunk
SAN DIEGO – Key factors associated with the use of bronchodilators in young children hospitalized with bronchiolitis include older age and wheezing and hypoxia upon admission, results from a single-center study showed.
Although the American Academy of Pediatrics does not endorse the routine use of bronchodilators in the treatment of children hospitalized with bronchiolitis (Pediatrics 2006;118:1774-93), “there is substantial variability in the management of bronchiolitis, including the usage of bronchodilators,” researchers led by Dr. Janet Schairer wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. A recent Cochrane report showed that bronchodilators do not decrease length of hospitalization or reduce the time to illness resolution (Cochrane Database Syst. Rev. 2014; 6:CD001266).
In an effort to determine which demographic and clinical factors are associated with the use of bronchodilators in the treatment of children hospitalized with bronchiolitis, Dr. Schairer and her associates reviewed the medical records of 232 children aged 2 weeks to 24 months who were hospitalized with the condition at Jersey Shore University Medical Center, Neptune, N.J., from October 2009 until September 2012. Data analysis included multivariate regression models to identify variables that were associated with administration of bronchodilators.
Of the 232 children, 120 (51.7%) received bronchodilators and 112 (48.3%) did not. The researchers observed no difference in bronchodilator use among patients with risk factors for asthma, including family history of asthma, personal history of wheezing or eczema, and smoke exposure. “That surprised us,” Dr. Schairer of the division of general pediatrics at the medical center, said in an interview.
Compared with children who did not receive bronchodilators, those who did were older (a mean of 6.5 vs. 4.5 months, respectively; P less than .01); and at hospital admission had a higher prevalence of wheezing (45% vs. 19.6%; P less than .0001); diminished air exchange (10.8% vs. 2.7%; P less than .02), and hypoxia (38.3% vs. 25%; P less than .03). Other treatments administered to those who did and did not receive bronchodilators included nebulized 3% saline (37.9% vs. 36.5%), systemic steroids (10.9% vs. 0%), and antibiotics (45% vs. 33%).
Regression analysis revealed that the use of bronchodilators increased with older age (odds ratio, 0.89), and with oxygen requirement (OR, 1.15) or wheezing (OR, 1.23) at the time of admission. No association between bronchodilator use and length of hospitalization was observed (P > .05).
“Widespread implementation of the AAP guidelines for treatment of children with bronchiolitis is required for reduction of unnecessary use of bronchodilators in hospitalized patients,” Dr. Schairer and her associates concluded in the abstract. “Research to assess which, if any, demographic and clinical factors are associated with response to bronchodilator therapy is needed to further guide physicians in the treatment of bronchiolitis.”
She acknowledged certain limitations of the study, including its single-center design and relatively small cohort size.
Dr. Schairer reported having no financial disclosures.
On Twitter @dougbrunk
SAN DIEGO – Key factors associated with the use of bronchodilators in young children hospitalized with bronchiolitis include older age and wheezing and hypoxia upon admission, results from a single-center study showed.
Although the American Academy of Pediatrics does not endorse the routine use of bronchodilators in the treatment of children hospitalized with bronchiolitis (Pediatrics 2006;118:1774-93), “there is substantial variability in the management of bronchiolitis, including the usage of bronchodilators,” researchers led by Dr. Janet Schairer wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. A recent Cochrane report showed that bronchodilators do not decrease length of hospitalization or reduce the time to illness resolution (Cochrane Database Syst. Rev. 2014; 6:CD001266).
In an effort to determine which demographic and clinical factors are associated with the use of bronchodilators in the treatment of children hospitalized with bronchiolitis, Dr. Schairer and her associates reviewed the medical records of 232 children aged 2 weeks to 24 months who were hospitalized with the condition at Jersey Shore University Medical Center, Neptune, N.J., from October 2009 until September 2012. Data analysis included multivariate regression models to identify variables that were associated with administration of bronchodilators.
Of the 232 children, 120 (51.7%) received bronchodilators and 112 (48.3%) did not. The researchers observed no difference in bronchodilator use among patients with risk factors for asthma, including family history of asthma, personal history of wheezing or eczema, and smoke exposure. “That surprised us,” Dr. Schairer of the division of general pediatrics at the medical center, said in an interview.
Compared with children who did not receive bronchodilators, those who did were older (a mean of 6.5 vs. 4.5 months, respectively; P less than .01); and at hospital admission had a higher prevalence of wheezing (45% vs. 19.6%; P less than .0001); diminished air exchange (10.8% vs. 2.7%; P less than .02), and hypoxia (38.3% vs. 25%; P less than .03). Other treatments administered to those who did and did not receive bronchodilators included nebulized 3% saline (37.9% vs. 36.5%), systemic steroids (10.9% vs. 0%), and antibiotics (45% vs. 33%).
Regression analysis revealed that the use of bronchodilators increased with older age (odds ratio, 0.89), and with oxygen requirement (OR, 1.15) or wheezing (OR, 1.23) at the time of admission. No association between bronchodilator use and length of hospitalization was observed (P > .05).
“Widespread implementation of the AAP guidelines for treatment of children with bronchiolitis is required for reduction of unnecessary use of bronchodilators in hospitalized patients,” Dr. Schairer and her associates concluded in the abstract. “Research to assess which, if any, demographic and clinical factors are associated with response to bronchodilator therapy is needed to further guide physicians in the treatment of bronchiolitis.”
She acknowledged certain limitations of the study, including its single-center design and relatively small cohort size.
Dr. Schairer reported having no financial disclosures.
On Twitter @dougbrunk
AT THE AAP NATIONAL CONFERENCE
Key clinical point: Bronchodilator use by young children hospitalized with bronchiolitis had no effect on duration of hospitalization.
Major finding: Compared with children who did not receive bronchodilators, those who did were older (a mean of 6.5 vs. 4.5 months, respectively; P less than .01); and at hospital admission had a higher prevalence of wheezing (45% vs. 19.6%; P less than .0001); diminished air exchange (10.8% vs. 2.7%; P less than .02), and hypoxia (38.3% vs. 25%; P less than .03).
Data source: A review of 232 children aged 2 weeks to 24 months who were hospitalized with bronchiolitis at Jersey Shore University Medical Center, Neptune, N.J., from October 2009 until September 2012.
Disclosures: Dr. Schairer reported having no financial disclosures.
