User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Novel mutation may be unrecognized cause of sudden infant death
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A previously healthy infant who survived sudden cardiac arrest at home was later found to have a de novo likely pathogenic genetic mutation in the SOS1 gene, which might be an unrecognized cause of sudden infant death, report clinicians from Missouri.
SOS1 gene variants are associated with Noonan syndrome, a genetic disorder that affects the RAS/MAPK signaling pathway. However, on presentation, the infant had none of the usual structural cardiac findings typical of Noonan syndrome, such as valvular disease or hypertrophic cardiomyopathy.
“To date, this is the first case reported of a ventricular fibrillation arrest in a patient with a RASopathy-related variant prior to development of the typically associated structural cardiac phenotype and may represent a previously unrecognized etiology of sudden death during infancy,” write Christopher W. Follansbee, MD, and Lindsey Malloy-Walton, DO, from the Ward Family Heart Center, Children’s Mercy Kansas City, and the University of Missouri School of Medicine.
“Genetic testing in cases of unexplained aborted or sudden cardiac deaths, even in previously healthy children, can be valuable in establishing a diagnosis, determining the prognosis, and assessing risk to family members,” they add in a news release.
Dr. Follansbee and Dr. Malloy-Walton describe the case in a report published in the August issue of HeartRhythm Case Reports.
Case details
The case involved a 2-month-old girl who did not wake up as usual for her morning feeding. Her mother found her limp, pale, and having difficulty breathing.
When emergency medical services arrived, the infant had no pulse. Cardiopulmonary resuscitation was initiated and an external defibrillator revealed coarse ventricular fibrillation. An initial shock of 10 J was given with conversion to an atrial rhythm with aberrant ventricular conduction.
The infant developed increasing frequency of ectopy before degenerating to ventricular fibrillation. A second shock with 20 J was unsuccessful, but a third shock of 20 J successfully converted the rhythm to sinus with aberrant ventricular conduction and atrial ectopy with return of spontaneous circulation.
In the ICU, the infant displayed incessant, nonsustained ectopic atrial tachycardia, with rapid episodes of ectopic atrial tachycardia with ventricular rates up to 300 beats per minute in the setting of seizure activity, they report.
With intravenous lorazepam, seizure activity resolved and treatment with amiodarone boluses led to transient establishment of sinus rhythm.
The QTc was noted to be above 500 ms and Brugada positioning of leads was unrevealing, the authors note.
Transthoracic echocardiogram showed a structurally normal heart with normal valve morphology and a patent foramen ovale with left-to-right flow. The initial ejection fraction was 49%. There was no evidence of ventricular hypertrophy, dilation, or noncompaction.
The infant was started on an esmolol infusion titrated to 225 μg/kg per min with frequent, nonsustained breakthrough of ectopic atrial tachycardia. Over the next 24 hours, the QTc interval normalized with normal T-wave morphology.
A procainamide challenge was negative. Cardiac MRI revealed normalization of ventricular function.
The genetics team was called in and a standard three-generation family history was obtained. An older sibling, 2 years of age, had no known medical conditions. The child’s paternal grandfather had died of a presumed myocardial infarction in his 50s, but no autopsy had been performed.
There was no family history of congenital heart disease, arrhythmia, sudden death, cardiomyopathy, recurrent syncope, congenital deafness, seizure, miscarriage, or developmental delay. Electrocardiograms obtained on the parents were normal.
Genetic testing using a comprehensive arrhythmia and cardiomyopathy next-generation sequencing panel revealed a de novo likely pathogenetic variant of the SOS1 gene associated with Noonan syndrome.
Given the aborted sudden cardiac death, the patient underwent dual-chamber epicardial implantable cardioverter-defibrillator implantation prior to discharge.
Dr. Follansbee and Dr. Malloy-Walton say a limitation to the case report is the lack of definitive association of the SOS1 variant with the presentation.
However, knowing the infant has the SOS1 variant and a history of aborted sudden death will allow for “monitoring and early intervention on typical manifestations of Noonan syndrome as the patient grows,” they say.
This research had no specific funding. Dr. Follansbee and Dr. Malloy-Walton have disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
One-third in U.S. had been infected by SARS-CoV-2 through 2020: Study
, according to a modeling study published Aug. 26 online in Nature.
Jeffrey Shaman, PhD, professor in the department of environmental health sciences and director of the climate and health program at the Columbia University Mailman School of Public Health, New York City, and colleagues developed a model to simulate how SARS-CoV-2 was transmitted within and between all 3,142 counties in the United States.
In their model, the researchers considered migration data between counties, the observed case numbers, and estimates of infections based on the number of people who test positive for SARS-CoV-2 antibodies.
The United States had the highest number of confirmed COVID-19 cases and deaths in the world during 2020. More than 19.6 million cases were reported by the end of the year.
But the authors point out that “69% of the population remained susceptible to viral infection.”
The researchers also studied the ascertainment rate, or the ratio of detected cases to the number of confirmed cases. Nationally, that value increased from 11.3% in March 2020 to 24.5% in December 2020.
That’s one of the biggest pandemic lessons from the data, Dr. Shaman said: “It is vitally important when there is an outbreak and you’re counting cases that there are many more people infected in your community who are contagious than reported cases. Each individual is infectious for multiple days, and there are many more unreported cases.”
That applies now with the Delta variant, he said.
“Vaccinated people who get infected with the Delta variant are part of the transmission chain,” he said.
Fatality rates dropped
Some of the data were very positive, Dr. Shaman told this news organization. The infection fatality rate fell from 0.77% in April to 0.31% in December. The authors suggest that that may be because of improvements in diagnosis and treatment, patient care, and reduced disease severity.
However, the fatality rate was still nearly four times as high as the estimated fatality rate for seasonal influenza (0.08%) and the 2009 influenza pandemic (0.0076%), the authors point out.
Joe K. Gerald, MD, PhD, associate professor and program director of public health policy and management at the University of Arizona, Tucson, told this news organization that this article helps confirm that COVID is much deadlier than the flu and that the intensity of the response has been appropriate.
“We should be willing to invest a lot more in mitigating COVID-19 than seasonal influenza because it has much greater consequences,” he said.
The numbers emphasize that testing must improve.
“We didn’t have enough tests available, and they weren’t easily accessible. For much of the year we were flying in the dark,” Dr. Gerald said.
The number of tests has increased this year, he acknowledged, but testing still lags. “We just can’t miss this many infections or diagnoses and hope to gain control,” he said.
The study also points out the huge variation by state and by county in infections and deaths, and that variation continues. Gerald noted that the varied numbers make it difficult for some regions to accept broader mandates, because the threat from COVID-19 appears very different where they are.
“We have to think about regions, how many people are susceptible, and what the testing capacity is,” he said. “States and even counties should have some leeway to make some important public health decisions, because local conditions are going to differ at different points in time.”
‘We have not turned the corner’
Jill Foster, MD, a pediatric infectious disease physician at the University of Minnesota Medical School, Minneapolis, said in an interview that the study adds evidence: “We have not turned the corner on COVID-19 and are nowhere near herd immunity – if it exists for SARS-CoV-2.”
She said the numbers presented are particularly concerning in regard to how many people were susceptible and were actively able to infect others: “Much higher than most people imagined and very much higher than their comparison, influenza.
“There are still more people susceptible than we had believed,” Dr. Foster added. “If the pattern continues where the Delta variant infects a significant portion of those vaccinated, the number of people susceptible rises even higher than was predicted.”
She said that it is reassuring that the analysis shows a decrease in case fatality and said the finding supports the common opinion that medicine is better able to fight the disease.
“However,” she said, “the optimism is tempered by acknowledging that in order to benefit from these advances, we must not overwhelm the facilities where patients are cared for so that optimal care can be delivered.”
Dr. Foster said these numbers represent a warning that COVID should be treated as a continuing threat.
“We need to acknowledge that there is COVID-19 infection simmering and periodically erupting throughout the country,” she said. “It is not monolithic and varies by geography and seasons in ways that are difficult to predict other than at any given time there is likely more infection present than we are identifying and more people susceptible to infection than we have calculated.”
The authors and Dr. Gerald have disclosed no relevant financial relationships. Dr. Foster has received clinical trials funding from Moderna.
A version of this article first appeared on Medscape.com.
, according to a modeling study published Aug. 26 online in Nature.
Jeffrey Shaman, PhD, professor in the department of environmental health sciences and director of the climate and health program at the Columbia University Mailman School of Public Health, New York City, and colleagues developed a model to simulate how SARS-CoV-2 was transmitted within and between all 3,142 counties in the United States.
In their model, the researchers considered migration data between counties, the observed case numbers, and estimates of infections based on the number of people who test positive for SARS-CoV-2 antibodies.
The United States had the highest number of confirmed COVID-19 cases and deaths in the world during 2020. More than 19.6 million cases were reported by the end of the year.
But the authors point out that “69% of the population remained susceptible to viral infection.”
The researchers also studied the ascertainment rate, or the ratio of detected cases to the number of confirmed cases. Nationally, that value increased from 11.3% in March 2020 to 24.5% in December 2020.
That’s one of the biggest pandemic lessons from the data, Dr. Shaman said: “It is vitally important when there is an outbreak and you’re counting cases that there are many more people infected in your community who are contagious than reported cases. Each individual is infectious for multiple days, and there are many more unreported cases.”
That applies now with the Delta variant, he said.
“Vaccinated people who get infected with the Delta variant are part of the transmission chain,” he said.
Fatality rates dropped
Some of the data were very positive, Dr. Shaman told this news organization. The infection fatality rate fell from 0.77% in April to 0.31% in December. The authors suggest that that may be because of improvements in diagnosis and treatment, patient care, and reduced disease severity.
However, the fatality rate was still nearly four times as high as the estimated fatality rate for seasonal influenza (0.08%) and the 2009 influenza pandemic (0.0076%), the authors point out.
Joe K. Gerald, MD, PhD, associate professor and program director of public health policy and management at the University of Arizona, Tucson, told this news organization that this article helps confirm that COVID is much deadlier than the flu and that the intensity of the response has been appropriate.
“We should be willing to invest a lot more in mitigating COVID-19 than seasonal influenza because it has much greater consequences,” he said.
The numbers emphasize that testing must improve.
“We didn’t have enough tests available, and they weren’t easily accessible. For much of the year we were flying in the dark,” Dr. Gerald said.
The number of tests has increased this year, he acknowledged, but testing still lags. “We just can’t miss this many infections or diagnoses and hope to gain control,” he said.
The study also points out the huge variation by state and by county in infections and deaths, and that variation continues. Gerald noted that the varied numbers make it difficult for some regions to accept broader mandates, because the threat from COVID-19 appears very different where they are.
“We have to think about regions, how many people are susceptible, and what the testing capacity is,” he said. “States and even counties should have some leeway to make some important public health decisions, because local conditions are going to differ at different points in time.”
‘We have not turned the corner’
Jill Foster, MD, a pediatric infectious disease physician at the University of Minnesota Medical School, Minneapolis, said in an interview that the study adds evidence: “We have not turned the corner on COVID-19 and are nowhere near herd immunity – if it exists for SARS-CoV-2.”
She said the numbers presented are particularly concerning in regard to how many people were susceptible and were actively able to infect others: “Much higher than most people imagined and very much higher than their comparison, influenza.
“There are still more people susceptible than we had believed,” Dr. Foster added. “If the pattern continues where the Delta variant infects a significant portion of those vaccinated, the number of people susceptible rises even higher than was predicted.”
She said that it is reassuring that the analysis shows a decrease in case fatality and said the finding supports the common opinion that medicine is better able to fight the disease.
“However,” she said, “the optimism is tempered by acknowledging that in order to benefit from these advances, we must not overwhelm the facilities where patients are cared for so that optimal care can be delivered.”
Dr. Foster said these numbers represent a warning that COVID should be treated as a continuing threat.
“We need to acknowledge that there is COVID-19 infection simmering and periodically erupting throughout the country,” she said. “It is not monolithic and varies by geography and seasons in ways that are difficult to predict other than at any given time there is likely more infection present than we are identifying and more people susceptible to infection than we have calculated.”
The authors and Dr. Gerald have disclosed no relevant financial relationships. Dr. Foster has received clinical trials funding from Moderna.
A version of this article first appeared on Medscape.com.
, according to a modeling study published Aug. 26 online in Nature.
Jeffrey Shaman, PhD, professor in the department of environmental health sciences and director of the climate and health program at the Columbia University Mailman School of Public Health, New York City, and colleagues developed a model to simulate how SARS-CoV-2 was transmitted within and between all 3,142 counties in the United States.
In their model, the researchers considered migration data between counties, the observed case numbers, and estimates of infections based on the number of people who test positive for SARS-CoV-2 antibodies.
The United States had the highest number of confirmed COVID-19 cases and deaths in the world during 2020. More than 19.6 million cases were reported by the end of the year.
But the authors point out that “69% of the population remained susceptible to viral infection.”
The researchers also studied the ascertainment rate, or the ratio of detected cases to the number of confirmed cases. Nationally, that value increased from 11.3% in March 2020 to 24.5% in December 2020.
That’s one of the biggest pandemic lessons from the data, Dr. Shaman said: “It is vitally important when there is an outbreak and you’re counting cases that there are many more people infected in your community who are contagious than reported cases. Each individual is infectious for multiple days, and there are many more unreported cases.”
That applies now with the Delta variant, he said.
“Vaccinated people who get infected with the Delta variant are part of the transmission chain,” he said.
Fatality rates dropped
Some of the data were very positive, Dr. Shaman told this news organization. The infection fatality rate fell from 0.77% in April to 0.31% in December. The authors suggest that that may be because of improvements in diagnosis and treatment, patient care, and reduced disease severity.
However, the fatality rate was still nearly four times as high as the estimated fatality rate for seasonal influenza (0.08%) and the 2009 influenza pandemic (0.0076%), the authors point out.
Joe K. Gerald, MD, PhD, associate professor and program director of public health policy and management at the University of Arizona, Tucson, told this news organization that this article helps confirm that COVID is much deadlier than the flu and that the intensity of the response has been appropriate.
“We should be willing to invest a lot more in mitigating COVID-19 than seasonal influenza because it has much greater consequences,” he said.
The numbers emphasize that testing must improve.
“We didn’t have enough tests available, and they weren’t easily accessible. For much of the year we were flying in the dark,” Dr. Gerald said.
The number of tests has increased this year, he acknowledged, but testing still lags. “We just can’t miss this many infections or diagnoses and hope to gain control,” he said.
The study also points out the huge variation by state and by county in infections and deaths, and that variation continues. Gerald noted that the varied numbers make it difficult for some regions to accept broader mandates, because the threat from COVID-19 appears very different where they are.
“We have to think about regions, how many people are susceptible, and what the testing capacity is,” he said. “States and even counties should have some leeway to make some important public health decisions, because local conditions are going to differ at different points in time.”
‘We have not turned the corner’
Jill Foster, MD, a pediatric infectious disease physician at the University of Minnesota Medical School, Minneapolis, said in an interview that the study adds evidence: “We have not turned the corner on COVID-19 and are nowhere near herd immunity – if it exists for SARS-CoV-2.”
She said the numbers presented are particularly concerning in regard to how many people were susceptible and were actively able to infect others: “Much higher than most people imagined and very much higher than their comparison, influenza.
“There are still more people susceptible than we had believed,” Dr. Foster added. “If the pattern continues where the Delta variant infects a significant portion of those vaccinated, the number of people susceptible rises even higher than was predicted.”
She said that it is reassuring that the analysis shows a decrease in case fatality and said the finding supports the common opinion that medicine is better able to fight the disease.
“However,” she said, “the optimism is tempered by acknowledging that in order to benefit from these advances, we must not overwhelm the facilities where patients are cared for so that optimal care can be delivered.”
Dr. Foster said these numbers represent a warning that COVID should be treated as a continuing threat.
“We need to acknowledge that there is COVID-19 infection simmering and periodically erupting throughout the country,” she said. “It is not monolithic and varies by geography and seasons in ways that are difficult to predict other than at any given time there is likely more infection present than we are identifying and more people susceptible to infection than we have calculated.”
The authors and Dr. Gerald have disclosed no relevant financial relationships. Dr. Foster has received clinical trials funding from Moderna.
A version of this article first appeared on Medscape.com.
A hot dog a day takes 36 minutes away
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”

Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.

Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?

You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”
Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.
Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?
You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.
The death ‘dog’
Imagine you’re out in your backyard managing the grill for a big family barbecue. You’ve got a dazzling assortment of meat assorted on your fancy new propane grill, all charring nicely. Naturally, the hot dogs finish first, and as you pull them off, you figure you’ll help yourself to one now. After all, you are the chef, you deserve a reward. But, as you bite into your smoking hot sandwich, a cold, bony finger taps you on the shoulder. You turn and come face to face with the Grim Reaper. “YOU JUST LOST 36 MINUTES,” Death says. “ALSO, MAY I HAVE ONE OF THOSE? THEY LOOK DELICIOUS.”
Nonplussed and moving automatically, you scoop up another hot dog and place it in a bun. “WITH KETCHUP PLEASE,” Death says. “I NEVER CARED FOR MUSTARD.”
“I don’t understand,” you say. “Surely I won’t die at a family barbecue.”
“DO NOT CALL ME SHIRLEY,” Death says. “AND YOU WILL NOT. IT’S PART OF MY NEW CONTRACT.”
A new study, published in Nature Food, found that a person may lose up to 36 minutes for every hot dog consumed. Researchers from the University of Michigan analyzed nearly 6,000 different foods using a new nutritional index to quantify their health effects in minutes of healthy life lost or gained. Eating a serving of nuts adds an extra 26 minutes of life. The researchers determined that replacing just 10% of daily caloric intake from beef and processed foods with fruits, vegetables, and nuts can add 48 minutes per day. It would also reduce the daily carbon footprint by 33%.
“So you go around to everyone eating bad food and tell them how much life they’ve lost?” you ask when the Grim Reaper finishes his story. “Sounds like a drag.”
“IT IS. WE’VE HAD TO HIRE NEW BLOOD.” Death chuckles at its own bad pun. “NOW IF YOU’LL EXCUSE ME, I MUST CHASTISE A MAN IN FLORIDA FOR EATING A WELL-DONE STEAK.”
More stress, less sex
As the world becomes a more stressful place, the human population could face a 50% drop by the end of the century.
Think of stress as a one-two punch to the libido and human fertility. The more people are stressed out, the less likely they are to have quality interactions with others. Many of us would rather be alone with our wine and cheese to watch our favorite show.
Researchers have found that high stress levels have been known to drop sperm count, ovulation, and sexual activity. Guess what? There has been a 50% decrease in sperm counts over the last 50 years. That’s the second punch. But let’s not forget, the times are changing.
“Changes in reproductive behavior that contribute to the population drop include more young couples choosing to be ‘child-free,’ people having fewer children, and couples waiting longer to start families,” said Alexander Suvorov, PhD, of the University of Massachusetts, the paper’s author.
Let’s summarize: The more stress we’re dealing with, the less people want to deal with each other.
Who would have thought the future would be less fun?
‘You are not a horse. You are not a cow. Seriously, y’all. Stop it.’
WARNING: The following descriptions of COVID-19–related insanity may be offensive to some readers.
Greetings, ladies and gentlemen! Welcome to the first round of Pandemic Pandemonium. Let’s get right to the action.
This week’s preshow match-off involves face mask woes. The first comes to us from Alabama, where a woman wore a space helmet to a school board meeting to protest mask mandates. The second comes from Australia, in the form of mischievous magpies. We will explain.
It is not uncommon for magpies to attack those who come too close to their nests in the spring, or “swooping season,” as it’s affectionately called. The magpies are smart enough to recognize the faces of people they see regularly and not attack; however, it’s feared that mask wearing will change this.
While you’re chewing on that exciting appetizer, let’s take a look at our main course, which has a distinct governmental flavor. Jeff Landry is the attorney general of Louisiana, and, like our space-helmet wearer, he’s not a fan of mask mandates. According to Business Insider, Mr. Landry “drafted and distributed sample letters intended to help parents evade mask-wearing ordinances and COVID-19 vaccination requirements for their children in schools.”
Up against him is the Food and Drug Administration’s Twitter account. In an unrelated matter, the agency tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” This was in response to people using the nonhuman forms of ivermectin to treat very human COVID-19.
Well, there you have it. Who will win tonight’s exciting edition of Pandemic Pandemonium? The first reader to contact us gets to decide the fate of these worthy contestants.
From venomous poison to heart drug
It’s not likely that anyone who sees a giant, venomous spider is thinking, “Hey! That thing could save my life!” It’s usually quite the opposite. Honestly, we would run away from just about any spider. But what if one of the deadliest spiders in the world could also save you from dying of a heart attack?
You probably don’t believe us, right? That’s fair, but the deadly Fraser Island (K’gari) funnel web spider, might also be the most helpful. Investigators from the University of Queensland in Australia have found a way to extract a molecule from the spider’s venom that might help stop damage from heart attacks and may even preserve hearts being used for transplants. “The Hi1a protein from spider venom blocks acid-sensing ion channels in the heart, so the death message is blocked, cell death is reduced, and we see improved heart cell survival,” Nathan Palpant, PhD, of the university, noted in a written statement.
No one has ever developed a drug to stop the “death signal,” so maybe it’s time to befriend spiders instead of running away from them in horror. Just leave the venom extraction to the professionals.

Young Black and White athletes differ in how they recover from concussions
, according to a new study on racial differences in concussion recovery.
“The findings from this study provide novel evidence that the recovery experience following sport-related concussion likely differs between Black and White athletes, and understanding these differences may serve to provide better and more personalized intervention and management strategies,” wrote lead author Aaron M. Yengo-Kahn, MD, of Vanderbilt University Medical Center in Nashville, Tenn. The study was published in the Journal of Neurosurgery: Pediatrics.
To assess how postconcussion experiences and recovery time differ among young White and Black athletes, the researchers launched a retrospective cohort study of youths between the ages of 12 and 23 from the middle Tennessee, northern Alabama, and southern Kentucky regions who had been treated for sport-related concussion. Using data from the Vanderbilt Sports Concussion Center’s outcome registry, they examined the records of 247 student-athletes, 211 of whom were White and 36 of whom were Black.
The majority of the athletes were male – 58% of the White group and 78% of the Black group – and their average age across groups was roughly 16 years. Thirty-three percent of the Black athletes were on public insurance, compared with just 6% of the White athletes, and 41% of the Black athletes lived in low–median income areas while 55% of the White athletes lived in areas with a high median income. Approximately 90% of each group played contact sports.
The median time to symptom resolution was 21 days (interquartile range, 10.5-61.0) for White athletes but just 12.3 days (IQR, 6.8-28.0) for Black athletes. Multivariable regression confirmed that Black athletes reached asymptomatic status sooner than White athletes (hazard ratio, 1.497; 95% confidence interval, 1.014-2.209; P = .042). “The observed shorter symptom resolution among the Black athletes may be explained by a complex interplay among race, concussion knowledge, attitudes toward sport-related concussion, reporting behavior, and sociodemographic disparities,” the authors noted.
The median time until returning to school post injury was 2 school days (IQR, 0-5) for White athletes and 0 school days (IQR, 0-2) for Black athletes. After multivariable analysis, being Black was indeed associated with returning to school sooner, compared with being White (HR, 1.522; 95% CI, 1.02-2,27; P = .040). Being Black was also associated with being less likely to a report a change in daily activity post concussion (odds ratio, 0.368; 95% CI, 0.136-0.996; P = .049).
Adding race to research
To make headway toward understanding race’s impact on concussion research, the authors proposed three immediate steps: Work directly with schools instead of clinics or emergency departments, match the diversity of study cohorts with the racial makeup of the surrounding community, and consider race as a covariate during study design.
“In our work with concussions, there is very little reported on race or racism or how racism affects how patients are navigating these spaces,” said coauthor Jessica Wallace, PhD, of the department of health science at the University of Alabama in Tuscaloosa, Ala., in an interview. “But we have so many athletes at the youth level, adolescent level, even the collegiate level; it’s such a diverse array of patients. We need to have data representative of all of our groups so that we know where we need to be intentional about reducing disparities and closing gaps.”
Dr. Wallace, who recently authored a study on the underreporting of concussions among Black and White high school athletes, emphasized the need for concussion research to be a true collaboration across disciplines.
“I approach this work from this public health and athletic training lens, whereas a lot of my collaborators are in neurosurgery and neurology,” she said. “Moving forward, we as a scientific clinical community have to do interdisciplinary work and be very intentional about how we go about closing these gaps. We have to recognize that there are differences in knowledge and in care, and they’re unacceptable, and we have to work collaboratively in providing resources to communities equitably to decrease them.”
The authors acknowledged their study’s limitations, including the retrospective nature of the study, using zip codes to determine median household income, and an unbalanced number of White and Black athletes. They did add, however, that the ratio of participants “generally aligns with census data in the surrounding metropolitan and county areas.” That said, they also surmised that the scarcity of Black athletes could indicate a deeper disparity in health care system usage and asked future researchers to “consider enrolling athletes directly from schools rather than from within the concussion clinic only.”
Dr. Yengo-Kahn disclosed holding a compensated position on the scientific advisory board of BlinkTBI, but the authors noted that the company had no role in the study and its products were not used. No other conflicts of interest were reported.
, according to a new study on racial differences in concussion recovery.
“The findings from this study provide novel evidence that the recovery experience following sport-related concussion likely differs between Black and White athletes, and understanding these differences may serve to provide better and more personalized intervention and management strategies,” wrote lead author Aaron M. Yengo-Kahn, MD, of Vanderbilt University Medical Center in Nashville, Tenn. The study was published in the Journal of Neurosurgery: Pediatrics.
To assess how postconcussion experiences and recovery time differ among young White and Black athletes, the researchers launched a retrospective cohort study of youths between the ages of 12 and 23 from the middle Tennessee, northern Alabama, and southern Kentucky regions who had been treated for sport-related concussion. Using data from the Vanderbilt Sports Concussion Center’s outcome registry, they examined the records of 247 student-athletes, 211 of whom were White and 36 of whom were Black.
The majority of the athletes were male – 58% of the White group and 78% of the Black group – and their average age across groups was roughly 16 years. Thirty-three percent of the Black athletes were on public insurance, compared with just 6% of the White athletes, and 41% of the Black athletes lived in low–median income areas while 55% of the White athletes lived in areas with a high median income. Approximately 90% of each group played contact sports.
The median time to symptom resolution was 21 days (interquartile range, 10.5-61.0) for White athletes but just 12.3 days (IQR, 6.8-28.0) for Black athletes. Multivariable regression confirmed that Black athletes reached asymptomatic status sooner than White athletes (hazard ratio, 1.497; 95% confidence interval, 1.014-2.209; P = .042). “The observed shorter symptom resolution among the Black athletes may be explained by a complex interplay among race, concussion knowledge, attitudes toward sport-related concussion, reporting behavior, and sociodemographic disparities,” the authors noted.
The median time until returning to school post injury was 2 school days (IQR, 0-5) for White athletes and 0 school days (IQR, 0-2) for Black athletes. After multivariable analysis, being Black was indeed associated with returning to school sooner, compared with being White (HR, 1.522; 95% CI, 1.02-2,27; P = .040). Being Black was also associated with being less likely to a report a change in daily activity post concussion (odds ratio, 0.368; 95% CI, 0.136-0.996; P = .049).
Adding race to research
To make headway toward understanding race’s impact on concussion research, the authors proposed three immediate steps: Work directly with schools instead of clinics or emergency departments, match the diversity of study cohorts with the racial makeup of the surrounding community, and consider race as a covariate during study design.
“In our work with concussions, there is very little reported on race or racism or how racism affects how patients are navigating these spaces,” said coauthor Jessica Wallace, PhD, of the department of health science at the University of Alabama in Tuscaloosa, Ala., in an interview. “But we have so many athletes at the youth level, adolescent level, even the collegiate level; it’s such a diverse array of patients. We need to have data representative of all of our groups so that we know where we need to be intentional about reducing disparities and closing gaps.”
Dr. Wallace, who recently authored a study on the underreporting of concussions among Black and White high school athletes, emphasized the need for concussion research to be a true collaboration across disciplines.
“I approach this work from this public health and athletic training lens, whereas a lot of my collaborators are in neurosurgery and neurology,” she said. “Moving forward, we as a scientific clinical community have to do interdisciplinary work and be very intentional about how we go about closing these gaps. We have to recognize that there are differences in knowledge and in care, and they’re unacceptable, and we have to work collaboratively in providing resources to communities equitably to decrease them.”
The authors acknowledged their study’s limitations, including the retrospective nature of the study, using zip codes to determine median household income, and an unbalanced number of White and Black athletes. They did add, however, that the ratio of participants “generally aligns with census data in the surrounding metropolitan and county areas.” That said, they also surmised that the scarcity of Black athletes could indicate a deeper disparity in health care system usage and asked future researchers to “consider enrolling athletes directly from schools rather than from within the concussion clinic only.”
Dr. Yengo-Kahn disclosed holding a compensated position on the scientific advisory board of BlinkTBI, but the authors noted that the company had no role in the study and its products were not used. No other conflicts of interest were reported.
, according to a new study on racial differences in concussion recovery.
“The findings from this study provide novel evidence that the recovery experience following sport-related concussion likely differs between Black and White athletes, and understanding these differences may serve to provide better and more personalized intervention and management strategies,” wrote lead author Aaron M. Yengo-Kahn, MD, of Vanderbilt University Medical Center in Nashville, Tenn. The study was published in the Journal of Neurosurgery: Pediatrics.
To assess how postconcussion experiences and recovery time differ among young White and Black athletes, the researchers launched a retrospective cohort study of youths between the ages of 12 and 23 from the middle Tennessee, northern Alabama, and southern Kentucky regions who had been treated for sport-related concussion. Using data from the Vanderbilt Sports Concussion Center’s outcome registry, they examined the records of 247 student-athletes, 211 of whom were White and 36 of whom were Black.
The majority of the athletes were male – 58% of the White group and 78% of the Black group – and their average age across groups was roughly 16 years. Thirty-three percent of the Black athletes were on public insurance, compared with just 6% of the White athletes, and 41% of the Black athletes lived in low–median income areas while 55% of the White athletes lived in areas with a high median income. Approximately 90% of each group played contact sports.
The median time to symptom resolution was 21 days (interquartile range, 10.5-61.0) for White athletes but just 12.3 days (IQR, 6.8-28.0) for Black athletes. Multivariable regression confirmed that Black athletes reached asymptomatic status sooner than White athletes (hazard ratio, 1.497; 95% confidence interval, 1.014-2.209; P = .042). “The observed shorter symptom resolution among the Black athletes may be explained by a complex interplay among race, concussion knowledge, attitudes toward sport-related concussion, reporting behavior, and sociodemographic disparities,” the authors noted.
The median time until returning to school post injury was 2 school days (IQR, 0-5) for White athletes and 0 school days (IQR, 0-2) for Black athletes. After multivariable analysis, being Black was indeed associated with returning to school sooner, compared with being White (HR, 1.522; 95% CI, 1.02-2,27; P = .040). Being Black was also associated with being less likely to a report a change in daily activity post concussion (odds ratio, 0.368; 95% CI, 0.136-0.996; P = .049).
Adding race to research
To make headway toward understanding race’s impact on concussion research, the authors proposed three immediate steps: Work directly with schools instead of clinics or emergency departments, match the diversity of study cohorts with the racial makeup of the surrounding community, and consider race as a covariate during study design.
“In our work with concussions, there is very little reported on race or racism or how racism affects how patients are navigating these spaces,” said coauthor Jessica Wallace, PhD, of the department of health science at the University of Alabama in Tuscaloosa, Ala., in an interview. “But we have so many athletes at the youth level, adolescent level, even the collegiate level; it’s such a diverse array of patients. We need to have data representative of all of our groups so that we know where we need to be intentional about reducing disparities and closing gaps.”
Dr. Wallace, who recently authored a study on the underreporting of concussions among Black and White high school athletes, emphasized the need for concussion research to be a true collaboration across disciplines.
“I approach this work from this public health and athletic training lens, whereas a lot of my collaborators are in neurosurgery and neurology,” she said. “Moving forward, we as a scientific clinical community have to do interdisciplinary work and be very intentional about how we go about closing these gaps. We have to recognize that there are differences in knowledge and in care, and they’re unacceptable, and we have to work collaboratively in providing resources to communities equitably to decrease them.”
The authors acknowledged their study’s limitations, including the retrospective nature of the study, using zip codes to determine median household income, and an unbalanced number of White and Black athletes. They did add, however, that the ratio of participants “generally aligns with census data in the surrounding metropolitan and county areas.” That said, they also surmised that the scarcity of Black athletes could indicate a deeper disparity in health care system usage and asked future researchers to “consider enrolling athletes directly from schools rather than from within the concussion clinic only.”
Dr. Yengo-Kahn disclosed holding a compensated position on the scientific advisory board of BlinkTBI, but the authors noted that the company had no role in the study and its products were not used. No other conflicts of interest were reported.
FROM THE JOURNAL OF NEUROSURGERY: PEDIATRICS
Healing Haiti: The emotional trauma of repeat crises
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Steeve Verdieu was at his workstation in his bedroom when the shaking started the morning of Aug. 14. He jumped under his desk and held on as a 7.2-magnitude earthquake tore through his childhood home in southern Haiti.
Mr. Verdieu, 25, said all he could think about was 2010, when a strong earthquake hit the country and left more than 200,000 people dead.
“Most of these adults that are in their mid-20s and 30s have vivid memories,” according to John Fitts, assistant director of Sent To Serve. He started working in the nonprofit sector in Haiti after the 2010 earthquake.
“I can’t even relate to it,” Mr. Fitts said. “If you didn’t live through it, you cannot relate.”
Mr. Verdieu emerged to find his family alive and his home in crumbles.
“In the neighborhood, we have only one child who died the day of the earthquake, but mentally, everybody feels bad,” he said. “Also, we are really frustrated right now because it tends to rain, and everybody is outside right now. So, we are a little bit afraid.”
Mr. Verdieu said that his community has not seen or heard of government authorities coming to offer guidance on next steps.
So, he started posting photos and videos to his Twitter account to seek help.
Surviving to heal
Many Haitians are forced to quickly turn the page after major crises, said Mr. Fitts.
“Survival overrides emotional shock,” he said. “They’re not going to have time. They’re not going to think emotional wellness at this point. It’s not addressed because they don’t have the opportunity to address it. So, it gets buried.”
More rural areas of Haiti were hit hardest by the recent earthquake, which killed over 2,000 people.
Many people were left without shelter and had limited access to food, clean drinking water, and medical help for those severely injured.
But current problems in Haiti, like shaky leadership after the recent assassination of the country’s president, left many people with no direction on what to do next.
With no information coming in, many, like Mr. Verdieu, took to social media or tried calling family and friends to find help on their own.
Having access to basic needs, like food and water, lessens the emotional trauma after these types of disasters, according to Betty Jean, a licensed professional counselor and global mental health and trauma consultant.
“When there is a crisis like an earthquake, the number one thing people need is a sense of safety and that there are entities that are concerned about their overall well-being,” said Ms. Jean, who is Haitian. “The emotional and mental support that we have to provide to people begins first with attending to those primary needs.”
But that’s not always possible in Haiti, mostly because of poor infrastructure, according to Caleb Lucien, founder of Hosean International Ministries.
“For example, the earthquake took place in the south of Haiti,” said Mr. Lucien, who is Haitian. “There has been some gang violence blocking passage from Port-au-Prince [the capital] to the south. Because of the gang fighting, it has been difficult to take the risk of traveling by road. So, airplanes from the capital city have been trying to get supplies there.”
More than resilient
Haitians are usually applauded for their inner strength to keep pushing amid crises. But it’s important to understand that there is often grief behind their resiliency, according to Ms. Jean.
“Sometimes I struggle with that word,” she said. “When I say resilient, I mean they will survive. But we are talking about a traumatized people. I definitely believe the people of Haiti are a people that have PTSD. The Haitian people have not yet fully healed from the first earthquake. I don’t think there was time. And many Haitians are suffering silently right now.”
The trauma shows itself in various ways, said Wilford Marous, entrepreneur and founder of the Haitian Chamber of Commerce in Great Britain.
“I went traveling in Europe with some colleagues of mine to attend some conferences, and one of them, who is Haitian, refused to sleep in a building because he believed it was too high,” he said. “He still had this fear of the earthquake.”
Children are often most affected, Mr. Fitts said.
“They don’t know what to do with it,” he said. “Their parents are not there necessarily to give them the emotional support that they need because they’re just trying to survive when things like this happen. So, a lot of things don’t get addressed and they’re taught early on to move on.”
Hosean International Ministries evacuated 1,500 people after the earthquake in 2010, and 750 of them were kids. The group stayed on the charity’s campground, and children had the chance to continue their education through its school system.
“Kids had issues sleeping,” Mr. Lucien said. “They are dealing with the loss of their loved ones. Some of them lost their moms. Some lost their brothers and sisters. So, we had to work with them and try to get them through that process.”
The charity offered children and their parents counseling sessions to lessen some of the emotional impact after the earthquake.
Common trauma responses
But keep in mind that symptoms like depression and sleeplessness would be common for most people going through mental health crises, such as major natural disasters or war, said Guglielmo Schininà, head of mental health and psychosocial support at the International Organization for Migration.
“It’s important not to jump to conclusions with diagnoses for mental illness or disorders,” Mr. Schininà said. In other situations, psychological effects like these could be symptoms of mental disorders. But in this situation, these are just normal reactions.”
Alongside trauma from natural disasters, many Haitians are angry about the chaos in the country, given the number of resources brought to Haiti over the past decade, according to Ms. Jean.
“We should have had better infrastructure, better roads, lights, emergency plans, trauma hospitals,” she said. “The resources were there.”
The constant lack of safety and security within the country can have ugly outcomes, she said.
“A lot of the political instability, rebels, gang activity, and war within those in politics has been because oppositions feel that those who are in power have not done a very good job of upgrading the Haitian lifestyle,” Ms. Jean said.
Unity and public togetherness are key in times like these, Mr. Marous said. He suggests finding creative ways to promote widespread healing.
“Even if it’s trying to start some sort of healing process through the media,” he said. “Having someone talk to the population, even on TV, 1 hour in the morning. That might be a way to offer some sort of help to the population at large.”
Strategic rebuilding
Haitians across the world are rallying together to keep spirits high, while also helping with recovery efforts, Ms. Jean said.
“We have to step in for the morale of the young people,” she said. “They’re tired. They’re hungry. They want to be cared for. So, our role in the diaspora is really critical in helping Haitians come out of this very traumatic time.”
Hosean International Ministries is organizing and sending supplies to parts of Haiti hardest hit by the earthquake. The ministry is also helping to rebuild some of the homes destroyed by the earthquake.
It’s important to keep in mind lessons learned from past recovery efforts, said Mr. Lucien.
“What we need to do is work with local leaders, asking them exactly what it is that they need,” he said. “The tendency is to rush and say what you’re going to bring. People brought things in 2010 that were not needed. Look for people on the ground, and work with them to provide the help.”
“My call to the international community is how can we come alongside of this resilient nation to alleviate some of the pressure,” Jean said. “But whether or not the help comes, I do believe the Haitian people, yet again, will rise day to day, until we restore and rebuild again.”
This is certainly true for Mr. Verdieu.
He has already launched an online campaign to rebuild his home.
A version of this article first appeared on WebMD.com.
Study informs about risks of discontinuing meds in JIA
Flares are modest in preliminary data.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.

The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
Flares are modest in preliminary data.
Flares are modest in preliminary data.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.
The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
Many but not all children with juvenile idiopathic arthritis (JIA) can regain remission after stopping and then restarting treatment, according to preliminary data from the ongoing Recapture-JIA study that were presented in a symposium sponsored by the Rheumatology Research Foundation.
The aim of this study is to evaluate the risks of discontinuing treatment after a period when JIA has been well controlled. Such data are of increasing interest to parents now that many children with JIA are achieving sustained periods of remission, according to Sarah Ringold, MD, a pediatric rheumatologist and associate professor of pediatrics at Seattle Children’s Hospital.
In follow-up so far, “recapture rates range from 50% to 76%” depending on type of JIA, reported Dr. Ringold, who said that patients with systemic JIA have so far been the most likely to achieve a good response when treatment is restarted.
The study is being conducted through the Childhood Arthritis and Rheumatology Research Alliance, which has 71 participating centers and has accrued data on more than 10,000 children with rheumatic diseases. For the study, the researchers identified 384 children with JIA who were already enrolled in the CARRA registry and had discontinued medications and then subsequently restarted them, and they also enrolled a prospective cohort of patients new to the registry who presented with flare after discontinuing their medication. Dr. Ringold reported on 64 of the patients in the prospective cohort.
Median time to flare: 219 days
Of findings so far, disease recurrence after discontinuation has been generally characterized by flares “of moderate activity” several months to more than a year after treatment discontinuation, according to Dr. Ringold, who emphasized repeatedly that these data are preliminary. The median time to a flare after treatment discontinuation was approximately 7 months (219 days).
In the combined cohorts, the median age at onset of JIA was 4 years. The median age at time of discontinuation was 9 years. More than half (55%) were taking a conventional disease-modifying antirheumatic drug (DMARD) and 35% were taking a tumor necrosis factor inhibitor at the time that their therapy was discontinued.
Most JIA types are represented. The most common form is rheumatoid factor–negative oligoarticular JIA. The main outcome looked the rate of clinically inactive disease at 6 months in children who had discontinued therapy after a period of remission. They defined clinically inactive disease as a Physician’s Global Assessment of less than 1 and an active joint count of 0.
Systemic JIA recapture rate at 6 months: 76%
At the time of disease flare after treatment discontinuation across both the retrospective and prospective cohorts, the median clinical Juvenile Arthritis Disease Activity Score based on 10 joints (cJADAS10; score range of 0-30) was 3.5. The recapture rate to clinically inactive disease at 6 months was 76% in those with systemic JIA and 50% in those with rheumatoid factor–positive polyarticular JIA. Other subtypes fell within this range. Rates of inactive disease at 6 months according to cJADAS10 score were lower, ranging from 26% with enthesitis-related arthritis/juvenile psoriatic arthritis to 57% with systemic JIA.
About 40% of those who restarted on therapy after a flare took the same medication again. About one-third of patients were restarted on glucocorticoids, mostly involving injections to inflamed joints, and data are not yet in about whether these were restarted alone or with other drugs, according to Dr. Ringold.
The final analysis of this study will explore clinical and laboratory variables associated with disease recapture. In the prospective cohort, which did not reach its planned enrollment of 150 children because the COVID pandemic, a broad array of these variables was evaluated at baseline.
Numerous studies have already looked at predictors of sustained remission after stopping medications of JIA, according to Dr. Ringold, but she said that there is relatively little information about outcomes in children who stop medications, flare, and are retreated. Other experts agree.
“We know little about how successfully DMARDs can be discontinued and used again after a disease flare,” reported Jens Klotsche, MD, a researcher at the German Rheumatism Research Center, which is part of the Leibniz Institute in Berlin. Dr. Klotsche, who is an author of a recent study that found etanercept effective for retreatment when children with JIA had discontinued therapy, agreed that “data from large cohort studies are necessary to support the treatment decisions by clinicians, parents, and patients.”
JIA recurrence risk is unclear
In a systematic review published 2 years ago, rates of flare following discontinuation of treatment for JIA were relatively high, but there were some limitations to this analysis, according to the lead author, Olha Halyabar, MD, a pediatric rheumatologist at Boston Children’s Hospital.
“The data in our systematic review showed that overall quality of evidence was low, with large variations and sometimes very different conclusions,” Dr. Halyabar said in an interview. She believes that the data generated by the CARRA analysis will be valuable, particularly in evaluating outcomes across subtypes.
“Even though, at this point, [previously published] reports indicate overall high rates of recurrence (>50% for some JIA subtypes), there are some encouraging studies from early treat-to-target strategies,” she said, adding that large datasets like those from CARRA offer an opportunity to gather data likely to be clinically useful.
Dr. Ringold cautioned that there are some limitations to the CARRA analysis, including some missing data from the retrospective cohort. She also pointed out that patients have been assessed at routine clinical visits rather than at standardized intervals, introducing a potential for bias.
For parents concerned about the costs, inconvenience, and side effects from sustained JIA treatment once remission is achieved, data from CARRA will allow clinicians to provide evidence-based counseling on balancing the risks of discontinuing therapy, including the likelihood of regaining remission when disease returns, against the goals of stopping treatment.
“Parents are having more conversations about when to stop medications,” Dr. Ringold said. She indicated that these data should be helpful for providing guidance.
Dr. Ringold, Dr. Klotsche, and Dr. Halyabar reported having no potential conflicts of interest.
FROM RHEUMATOLOGY RESEARCH FOUNDATION SUMMER SERIES
New recommendations address ME/CFS diagnosis and management
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.

The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.
The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.
The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
FROM THE MAYO CLINIC PROCEEDINGS
AHA targets rising prevalence of obstructive sleep apnea in children
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.

The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.
The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
Obstructive sleep apnea is becoming more common in children and adolescents as the prevalence of obesity increases, but it may also be a preventable risk factor for cardiovascular disease, according to a new scientific statement from the American Heart Association.
The statement focuses on the links between OSA and CVD risk factors in children and adolescents, and reviews diagnostic strategies and treatments. The writing committee reported that 1%-6% of children and adolescents have OSA, as do up to 60% of adolescents considered obese.
The statement was created by the AHA’s Atherosclerosis, Hypertension, and Obesity in the Young subcommittee of the Council on Cardiovascular Disease in the Young and was published online in the Journal of the American Heart Association.
Carissa M. Baker-Smith, MD, chair of the writing group chair and director of pediatric preventive cardiology at Nemours Cardiac Center, Alfred I. duPont Hospital for Children, Wilmington, Del., explained the rationale for issuing the statement at this time, noting that the relationship between OSA and CVD in adults is well documented.
“There has been less focus on the importance of recognizing and treating sleep apnea in youth,” she said in an interview. “Thus, we felt that it was vitally important to get the word out to parents and to providers that paying attention to the quality and duration of your child’s sleep is vitally important to a child’s long-term heart health. Risk factors for heart disease, when present in childhood, can persist into adulthood.”
Clarity on polysomnography
For making the diagnosis of OSA in children, the statement provides clarity on the use of polysomnography and the role of the apnea-hypopnea index, which is lower in children with OSA than in adults. “One controversy, or at least as I saw it, was whether or not polysomnography testing is always required to make the diagnosis of OSA and before proceeding with tonsil and adenoid removal among children for whom enlarged tonsils and adenoids are present,” Dr. Baker-Smith said. “Polysomnography testing is not always needed before an ear, nose, and throat surgeon may recommend surgery.”
The statement also noted that history and physical examination may not yield enough reliable information to distinguish OSA from snoring.
In areas where sleep laboratories that work with children aren’t available, alternative tests such as daytime nap polysomnography, nocturnal oximetry, and nocturnal video recording may be used – with a caveat. “These alternative tests have weaker positive and negative predictive values when compared with polysomnography,” the writing committee noted. Home sleep apnea tests aren’t recommended in children. Questionnaires “are useful as screening, but not as diagnostic tools.”
Pediatric patients being evaluated for OSA should also be screened for hypertension and metabolic syndrome, as well as central nervous system and behavioral disorders. Diagnosing OSA in children and adolescents requires “a high index of suspicion,” the committee wrote.
Pediatricians and pediatric cardiologists should exercise that high index of suspicion when receiving referrals for cardiac evaluations for attention deficit hyperactivity disorder medication, Dr. Baker-Smith said. “Take the time to ask about a child’s sleep – snoring, apnea, etc. – especially if the child has obesity, difficulty focusing during the day, and if there is evidence of systemic hypertension or other signs of metabolic syndrome,” she said.
Risk factors for OSA in children
The statement also reviewed risk factors for OSA, among them obesity, particularly among children younger than 6 years. Other risk factors include upper and lower airway disease, hypotonia, parental history of hyperplasia of the adenoids and tonsils, craniofacial malformations, and neuromuscular disorders. However, the committee cited “limited data” to support that children with congenital heart disease may be at greater risk for OSA and sleep-disordered breathing (SDB).
Black children are at significantly greater risk, and socioeconomic factors “may be potential confounders,” the committee stated. Other risk factors include allergic rhinitis and sickle cell disease.
But the statement underscores that “obesity is the main risk factor” for OSA in children and adolescents, and that the presence of increased inflammation may explain this relationship. Steroids may alleviate these symptoms, even in nonobese children, and removal of the adenoids or tonsils is an option to reduce inflammation in children with OSA.
“Obesity is a significant risk factor for sleep disturbances and obstructive sleep apnea, and the severity of sleep apnea may be improved by weight-loss interventions, which then improves metabolic syndrome factors such as insulin sensitivity,” Dr. Baker-Smith said. “We need to increase awareness about how the rising prevalence of obesity may be impacting sleep quality in kids and recognize sleep-disordered breathing as something that could contribute to risks for hypertension and later cardiovascular disease.”
Children in whom OSA is suspected should also undergo screening for metabolic syndrome, and central nervous system and behavioral disorders.
Cardiovascular risks
The statement explores the connection between cardiovascular complications and SDB and OSA in depth.
“Inadequate sleep duration of < 5 hours per night in children and adolescents has been linked to an increased risk of hypertension and is also associated with an increased prevalence of obesity,” the committee wrote.
However, the statement left one question hanging: whether OSA alone or obesity cause higher BP in younger patients with OSA. But the committee concluded that BP levels increase with the severity of OSA, although the effects can vary with age. OSA in children peaks between ages 2 and 8, corresponding to the peak prevalence of hypertrophy of the tonsils and adenoids. Children aged 10-11 with more severe OSA may have BP dysregulation, while older adolescents develop higher sustained BP. Obesity may be a confounder for daytime BP elevations, while nighttime hypertension depends less on obesity and more on OSA severity.
“OSA is associated with abnormal BP in youth and, in particular, higher nighttime blood pressures and loss of the normal decline in BP that should occur during sleep,” Dr. Baker-Smith said. “Children with OSA appear to have higher BP than controls during both sleep and wake times, and BP levels increase with increasing severity of OSA.”
Nonetheless, children with OSA are at greater risk for other cardiovascular problems. Left ventricular hypertrophy may be a secondary outcome. “The presence of obstructive sleep apnea in children is associated with an 11-fold increased risk for LVH in children, a relationship not seen in the presence of primary snoring alone,” Dr. Baker-Smith said.
Dr. Baker-Smith had no relevant disclosures. Coauthor Amal Isaiah, MD, is coinventor of an imaging system for sleep apnea and receives royalties from the University of Maryland. The other coauthors have no relevant financial relationships to disclose.
FROM JOURNAL OF THE AMERICAN HEART ASSOCIATION
Not so fast food
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.

The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.
The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
As long as I can remember, children have been notoriously wasteful when dining in school cafeterias. Even those children who bring their own food often return home in the afternoon with their lunches half eaten. Not surprisingly, the food tossed out is often the healthier portion of the meal. Schools have tried a variety of strategies to curb this wastage, including using volunteer student monitors to police and encourage ecologically based recycling.
The authors of a recent study published on JAMA Network Open observed that when elementary and middle-school students were allowed a 20-minute seated lunch period they consumed more food and there was significantly less waste of fruits and vegetable compared with when the students’ lunch period was limited to 10 minutes. Interestingly, there was no difference in the beverage and entrée consumption when the lunch period was doubled.
The authors postulate that younger children may not have acquired the dexterity to feed themselves optimally in the shorter lunch period. I’m not sure I buy that argument. It may be simply that the children ate and drank their favorites first and needed a bit more time to allow their little guts to move things along. But, regardless of the explanation, the investigators’ observations deserve further study.
When I was in high school our lunch period was a full hour, which allowed me to make the half mile walk to home and back to eat a home-prepared meal. The noon hour was when school clubs and committees met and there was a full schedule of diversions to fill out the hour. I don’t recall the seated portion of the lunch period having any time restriction.
By the time my own children were in middle school, lunch periods lasted no longer than 20 minutes. I was not surprised to learn from this recent study that in some schools the seated lunch period has been shortened to 10 minutes. In some cases the truncated lunch periods are a response to space and time limitations. I fear that occasionally, educators and administrators have found it so difficult to keep young children who are accustomed to watching television while they eat engaged that the periods have been shortened to minimize the chaos.
Here in Maine, the governor has just announced plans to offer free breakfast and lunch to every student in response to a federal initiative. If we intend to make nutrition a cornerstone of the educational process this study from the University of Illinois at Urbana-Champaign suggests that we must do more than simply provide the food at no cost. We must somehow carve out more time in the day for the children to eat a healthy diet.
But, where is this time going to come from? Many school systems have already cannibalized physical education to the point that most children are not getting a healthy amount of exercise. It is unfortunate that we have come to expect public school systems to solve all of our societal ills and compensate for less-than-healthy home environments. But that is the reality. If we think nutrition and physical activity are important components of our children’s educations then we must make the time necessary to provide them.
Will this mean longer school days? And will those longer days cost money? You bet they will, but that may be the price we have to pay for healthier, better educated children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Children and COVID: New cases soar to near-record level
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
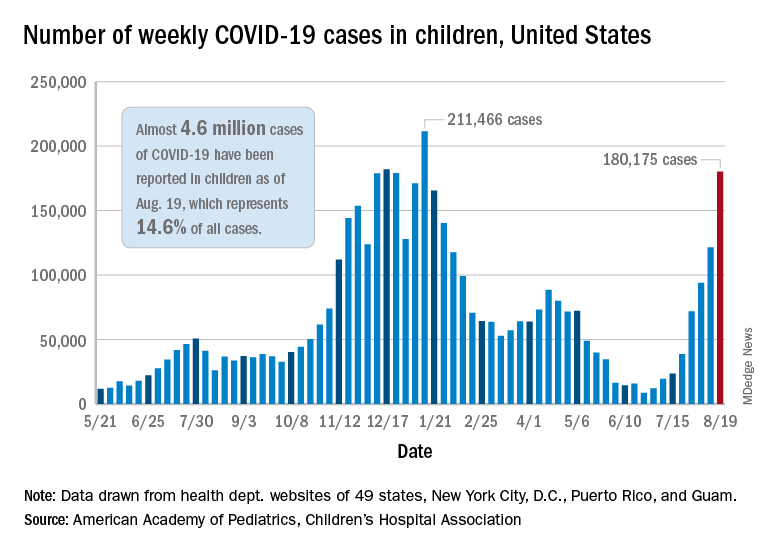
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.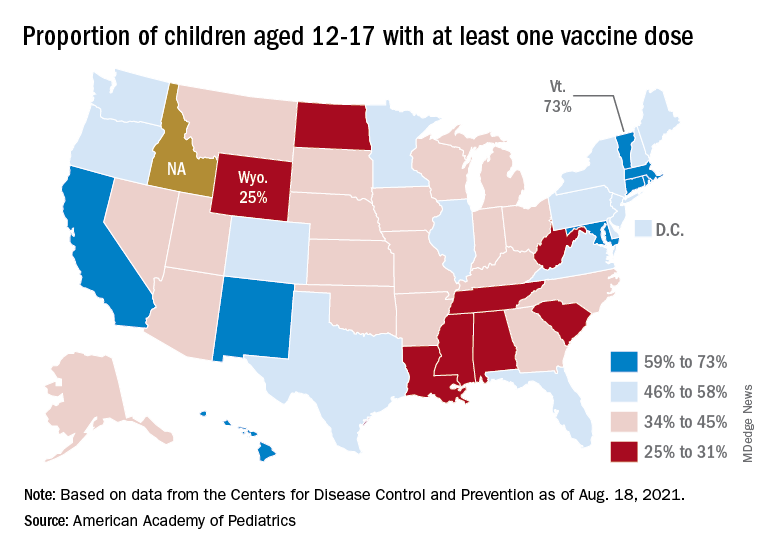
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.
Weekly cases of COVID-19 in children jumped by nearly 50% in the United States, posting the highest count since hitting a pandemic high back in mid-January, a new report shows.
The latest weekly figure represents a 48% increase over the previous week and an increase of over 2,000% in the 8 weeks since the national count dropped to a low of 8,500 cases for the week of June 18-24, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
Vaccinations, in the meantime, appear to be headed in the opposite direction. Vaccine initiations were down for the second consecutive week, falling by 18% among 12- to 15-year-olds and by 15% in those aged 16-17 years, according to data from the Centers for Disease Control and Prevention.
Nationally, about 47% of children aged 12-15 and 56% of those aged 16-17 have received at least one dose of COVID vaccine as of Aug. 23, with 34% and 44%, respectively, reaching full vaccination. The total number of children with at least one dose is 11.6 million, including a relatively small number (about 200,000) of children under age 12 years, the CDC said on its COVID Data Tracker.
At the state level, vaccination is a source of considerable disparity. In Vermont, 73% of children aged 12-17 had received at least one dose by Aug. 18, and 63% were fully vaccinated. In Wyoming, however, just 25% of children had received at least one dose (17% are fully vaccinated), while Alabama has a lowest-in-the-nation full vaccination rate of 14%, based on a separate AAP analysis of CDC data.
There are seven states in which over 60% of 12- to 17-year-olds have at least started the vaccine regimen and five states where less than 30% have received at least one dose, the AAP noted.
Back on the incidence side of the pandemic, Mississippi and Hawaii had the largest increases in new cases over the past 2 weeks, followed by Florida and West Virginia. Cumulative figures show that California has had the most cases overall in children (550,337), Vermont has the highest proportion of all cases in children (22.9%), and Rhode Island has the highest rate of cases per 100,000 (10,636), the AAP and CHA said in the joint report based on data from 49 states, the District of Columbia, New York City, Puerto Rico, and Guam.
Add up all those jurisdictions, and it works out to 4.6 million children infected with SARS-CoV-2 as of Aug. 19, with children representing 14.6% of all cases since the start of the pandemic. There have been over 18,000 hospitalizations so far, which is just 2.3% of the total for all ages in the 23 states (and New York City) that are reporting such data on their health department websites, the AAP and CHA said.
The number of COVID-related deaths in children is now 402 after the largest 1-week increase (24) since late May of 2020, when the AAP/CHA coverage began. Mortality data by age are available from 44 states, New York City, Puerto Rico, and Guam.