User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Your patients are rotting their teeth with vaping
Primary care physicians, and especially pediatricians, should consider telling their patients about the long-term oral health problems associated with vaping.
A new study found that patients who use vapes were at a higher risk of developing tooth decay and periodontal disease.
Vapes were introduced to the U.S. market in 2006 as an alternative to conventional cigarettes and have become widely popular among youth. According to a 2022 survey from the U.S. Centers for Disease Control and Prevention, 2.55 million middle and high school students in this country reported using the devices in the previous 30 days.
The new study, published in the Journal of the American Dental Association, expands on an initial case series published in 2020 of patients who reported use of vapes and who had severe dental decay. Karina Irusa, BDS, assistant professor of comprehensive care at Tufts University, Boston, and lead author of the case series, wanted to investigate whether her initial findings would apply to a large population of vape users.
For the new study, Dr. Irusa and colleagues collected data on 13,216 patients aged 16-40 who attended Tufts dental clinics between 2019 and 2021. All patients had received a diagnosis of tooth decay, had a tooth decay risk assessment on record, and had answered “yes” or “no” to use of vapes in a health history questionnaire.
Patients had records on file of varying types of dental lesions, cavities filled within the previous 3 years, heavy plaque on teeth, inadequate brushing and flushing, and a self-report of recreational drug use and frequent snacking. If patients had these factors on their file, they were at high risk of developing decay that leads to cavities.
The study found that 79% of patients who responded “yes” to being a current user of vapes were at high risk for dental decay, compared with 60% of those who did not report using the devices.
Materials in the vaping liquids further cause an inflammatory response that disrupts an individual’s internal microbiome, according to numerous studies.
“All the ingredients of vaping are surely a recipe for overgrowth of cavities causing bacteria,” said Jennifer Genuardi, MD, an internist and pediatrician at federally qualified community health center Urban Health Plan, in New York, who was not involved in the study.
Dr. Irusa said information on patient’s vaping habits should be included in routine dental and medical history questionnaires as part of their overall electronic health record.
“Decay in its severe form not only affects one’s ability to eat but affects facial aesthetics and self-esteem as well,” Dr. Irusa said.
Dr. Genuardi called the findings unsurprising.
“We are learning daily more and more about the dangers of vaping,” Dr. Genuardi said. “There’s a focus of today’s research on the effect of actions on our microbiome and the subsequent effects on our health.”
Dr. Genuardi also said many of her teenage patients do not enjoy dental visits or having cavities filled, which could serve as a useful deterrent to vaping for a demographic that has been targeted with marketing from vape manufacturers.
“Cavity formation and the experience of having cavities filled is an experience teens can identify with, so this to me seems like perhaps an even more effective angle to try to curb this unhealthy behavior of vaping,” Dr. Genuardi said.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Primary care physicians, and especially pediatricians, should consider telling their patients about the long-term oral health problems associated with vaping.
A new study found that patients who use vapes were at a higher risk of developing tooth decay and periodontal disease.
Vapes were introduced to the U.S. market in 2006 as an alternative to conventional cigarettes and have become widely popular among youth. According to a 2022 survey from the U.S. Centers for Disease Control and Prevention, 2.55 million middle and high school students in this country reported using the devices in the previous 30 days.
The new study, published in the Journal of the American Dental Association, expands on an initial case series published in 2020 of patients who reported use of vapes and who had severe dental decay. Karina Irusa, BDS, assistant professor of comprehensive care at Tufts University, Boston, and lead author of the case series, wanted to investigate whether her initial findings would apply to a large population of vape users.
For the new study, Dr. Irusa and colleagues collected data on 13,216 patients aged 16-40 who attended Tufts dental clinics between 2019 and 2021. All patients had received a diagnosis of tooth decay, had a tooth decay risk assessment on record, and had answered “yes” or “no” to use of vapes in a health history questionnaire.
Patients had records on file of varying types of dental lesions, cavities filled within the previous 3 years, heavy plaque on teeth, inadequate brushing and flushing, and a self-report of recreational drug use and frequent snacking. If patients had these factors on their file, they were at high risk of developing decay that leads to cavities.
The study found that 79% of patients who responded “yes” to being a current user of vapes were at high risk for dental decay, compared with 60% of those who did not report using the devices.
Materials in the vaping liquids further cause an inflammatory response that disrupts an individual’s internal microbiome, according to numerous studies.
“All the ingredients of vaping are surely a recipe for overgrowth of cavities causing bacteria,” said Jennifer Genuardi, MD, an internist and pediatrician at federally qualified community health center Urban Health Plan, in New York, who was not involved in the study.
Dr. Irusa said information on patient’s vaping habits should be included in routine dental and medical history questionnaires as part of their overall electronic health record.
“Decay in its severe form not only affects one’s ability to eat but affects facial aesthetics and self-esteem as well,” Dr. Irusa said.
Dr. Genuardi called the findings unsurprising.
“We are learning daily more and more about the dangers of vaping,” Dr. Genuardi said. “There’s a focus of today’s research on the effect of actions on our microbiome and the subsequent effects on our health.”
Dr. Genuardi also said many of her teenage patients do not enjoy dental visits or having cavities filled, which could serve as a useful deterrent to vaping for a demographic that has been targeted with marketing from vape manufacturers.
“Cavity formation and the experience of having cavities filled is an experience teens can identify with, so this to me seems like perhaps an even more effective angle to try to curb this unhealthy behavior of vaping,” Dr. Genuardi said.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Primary care physicians, and especially pediatricians, should consider telling their patients about the long-term oral health problems associated with vaping.
A new study found that patients who use vapes were at a higher risk of developing tooth decay and periodontal disease.
Vapes were introduced to the U.S. market in 2006 as an alternative to conventional cigarettes and have become widely popular among youth. According to a 2022 survey from the U.S. Centers for Disease Control and Prevention, 2.55 million middle and high school students in this country reported using the devices in the previous 30 days.
The new study, published in the Journal of the American Dental Association, expands on an initial case series published in 2020 of patients who reported use of vapes and who had severe dental decay. Karina Irusa, BDS, assistant professor of comprehensive care at Tufts University, Boston, and lead author of the case series, wanted to investigate whether her initial findings would apply to a large population of vape users.
For the new study, Dr. Irusa and colleagues collected data on 13,216 patients aged 16-40 who attended Tufts dental clinics between 2019 and 2021. All patients had received a diagnosis of tooth decay, had a tooth decay risk assessment on record, and had answered “yes” or “no” to use of vapes in a health history questionnaire.
Patients had records on file of varying types of dental lesions, cavities filled within the previous 3 years, heavy plaque on teeth, inadequate brushing and flushing, and a self-report of recreational drug use and frequent snacking. If patients had these factors on their file, they were at high risk of developing decay that leads to cavities.
The study found that 79% of patients who responded “yes” to being a current user of vapes were at high risk for dental decay, compared with 60% of those who did not report using the devices.
Materials in the vaping liquids further cause an inflammatory response that disrupts an individual’s internal microbiome, according to numerous studies.
“All the ingredients of vaping are surely a recipe for overgrowth of cavities causing bacteria,” said Jennifer Genuardi, MD, an internist and pediatrician at federally qualified community health center Urban Health Plan, in New York, who was not involved in the study.
Dr. Irusa said information on patient’s vaping habits should be included in routine dental and medical history questionnaires as part of their overall electronic health record.
“Decay in its severe form not only affects one’s ability to eat but affects facial aesthetics and self-esteem as well,” Dr. Irusa said.
Dr. Genuardi called the findings unsurprising.
“We are learning daily more and more about the dangers of vaping,” Dr. Genuardi said. “There’s a focus of today’s research on the effect of actions on our microbiome and the subsequent effects on our health.”
Dr. Genuardi also said many of her teenage patients do not enjoy dental visits or having cavities filled, which could serve as a useful deterrent to vaping for a demographic that has been targeted with marketing from vape manufacturers.
“Cavity formation and the experience of having cavities filled is an experience teens can identify with, so this to me seems like perhaps an even more effective angle to try to curb this unhealthy behavior of vaping,” Dr. Genuardi said.
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN DENTAL ASSOCIATION
Rates of health care use after bariatric surgery in teens
Researchers found significantly lower rates of both emergency department (ED) use and hospitalization 5 years after sleeve gastrectomy compared with gastric bypass, and similarly low rates of adverse events.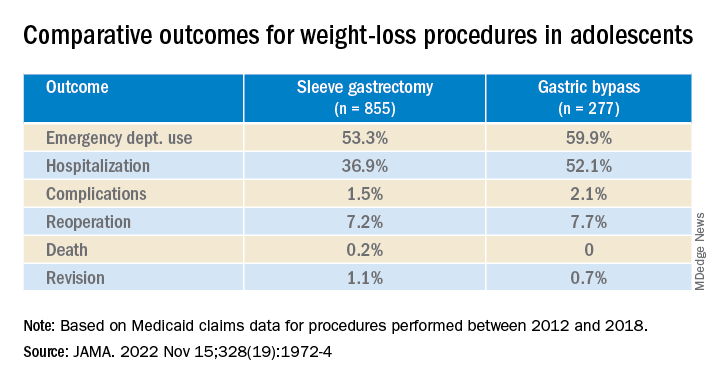
The study, by researchers with the department of surgery and Center for Health Outcomes and Policy, University of Michigan, Ann Arbor, was published in JAMA.
Studies have shown that sleeve gastrectomy and gastric bypass both lead to significant weight loss and are associated with low complication rates among adolescents with severe obesity.
Until now, however, comparative outcomes for these two weight-loss procedures have not been described for adolescents insured by Medicaid, the largest insurer of adolescents in the United States.
Using Medicaid claims data, Ryan Howard, MD, and colleagues identified 855 adolescents who underwent sleeve gastrectomy and 277 who underwent Roux-en-Y gastric bypass between 2012 and 2018.
Adolescents in both groups were about 18 years old on average at the time of surgery, and about three-quarters were female.
Sleeve gastrectomy became more common over the study period. The annual percentage of sleeve gastrectomy relative to gastric bypass increased from 48.8% in 2012 to 82.6% in 2018.
There was no significant difference in rates of complications (P = .31) or reoperation (P = .78), defined as abdominal operation potentially related to the index procedure, including biliary procedures and abdominal wall, internal, and paraesophageal hernia repair.
Researchers also found no difference between sleeve gastrectomy and gastric bypass in rates of death (P = .42) or revision (P = .63), which included any operation that directly modified the index procedure.
The results “may help inform the treatment of severe obesity in adolescents insured by Medicaid, although future studies should also evaluate long-term weight loss and comorbidity resolution in this population,” Dr. Howard and colleagues write.
They caution that their analysis is subject to selection bias because patient characteristics may influence the choice of procedure, although appropriate statistical adjustment was used.
Other limitations include the small sample size, which increases the possibility of type II error; the relatively short follow-up period; and the inability to directly attribute outcomes to the index procedure.
Funding for the study was provided by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers found significantly lower rates of both emergency department (ED) use and hospitalization 5 years after sleeve gastrectomy compared with gastric bypass, and similarly low rates of adverse events.
The study, by researchers with the department of surgery and Center for Health Outcomes and Policy, University of Michigan, Ann Arbor, was published in JAMA.
Studies have shown that sleeve gastrectomy and gastric bypass both lead to significant weight loss and are associated with low complication rates among adolescents with severe obesity.
Until now, however, comparative outcomes for these two weight-loss procedures have not been described for adolescents insured by Medicaid, the largest insurer of adolescents in the United States.
Using Medicaid claims data, Ryan Howard, MD, and colleagues identified 855 adolescents who underwent sleeve gastrectomy and 277 who underwent Roux-en-Y gastric bypass between 2012 and 2018.
Adolescents in both groups were about 18 years old on average at the time of surgery, and about three-quarters were female.
Sleeve gastrectomy became more common over the study period. The annual percentage of sleeve gastrectomy relative to gastric bypass increased from 48.8% in 2012 to 82.6% in 2018.
There was no significant difference in rates of complications (P = .31) or reoperation (P = .78), defined as abdominal operation potentially related to the index procedure, including biliary procedures and abdominal wall, internal, and paraesophageal hernia repair.
Researchers also found no difference between sleeve gastrectomy and gastric bypass in rates of death (P = .42) or revision (P = .63), which included any operation that directly modified the index procedure.
The results “may help inform the treatment of severe obesity in adolescents insured by Medicaid, although future studies should also evaluate long-term weight loss and comorbidity resolution in this population,” Dr. Howard and colleagues write.
They caution that their analysis is subject to selection bias because patient characteristics may influence the choice of procedure, although appropriate statistical adjustment was used.
Other limitations include the small sample size, which increases the possibility of type II error; the relatively short follow-up period; and the inability to directly attribute outcomes to the index procedure.
Funding for the study was provided by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers found significantly lower rates of both emergency department (ED) use and hospitalization 5 years after sleeve gastrectomy compared with gastric bypass, and similarly low rates of adverse events.
The study, by researchers with the department of surgery and Center for Health Outcomes and Policy, University of Michigan, Ann Arbor, was published in JAMA.
Studies have shown that sleeve gastrectomy and gastric bypass both lead to significant weight loss and are associated with low complication rates among adolescents with severe obesity.
Until now, however, comparative outcomes for these two weight-loss procedures have not been described for adolescents insured by Medicaid, the largest insurer of adolescents in the United States.
Using Medicaid claims data, Ryan Howard, MD, and colleagues identified 855 adolescents who underwent sleeve gastrectomy and 277 who underwent Roux-en-Y gastric bypass between 2012 and 2018.
Adolescents in both groups were about 18 years old on average at the time of surgery, and about three-quarters were female.
Sleeve gastrectomy became more common over the study period. The annual percentage of sleeve gastrectomy relative to gastric bypass increased from 48.8% in 2012 to 82.6% in 2018.
There was no significant difference in rates of complications (P = .31) or reoperation (P = .78), defined as abdominal operation potentially related to the index procedure, including biliary procedures and abdominal wall, internal, and paraesophageal hernia repair.
Researchers also found no difference between sleeve gastrectomy and gastric bypass in rates of death (P = .42) or revision (P = .63), which included any operation that directly modified the index procedure.
The results “may help inform the treatment of severe obesity in adolescents insured by Medicaid, although future studies should also evaluate long-term weight loss and comorbidity resolution in this population,” Dr. Howard and colleagues write.
They caution that their analysis is subject to selection bias because patient characteristics may influence the choice of procedure, although appropriate statistical adjustment was used.
Other limitations include the small sample size, which increases the possibility of type II error; the relatively short follow-up period; and the inability to directly attribute outcomes to the index procedure.
Funding for the study was provided by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
More work needed to optimize STI screening in primary care settings
TAMPA – Boosting screening for sexually transmitted infections in primary care settings could help alleviate some of the barriers to optimal testing and treatment, a new quality improvement initiative suggests.
Many primary care doctors are challenged for time and send people to other health care settings, such as a local health department or a clinic that specializes in STI diagnosis and treatment, said Wendy Kays, DNP, APRN, AGNP-BC, AAHIVS, a nurse practitioner and researcher at Care Resource, Miami.
However, for multiple reasons, many patients do not follow up and are not screened or treated, Dr. Kays said at the Association of Nurses in AIDS Care annual meeting. Some people can afford the copay to see a primary care provider, for example, but do not have the resources to pay for a second clinical visit or laboratory testing.
In other instances, transportation can be a problem. “People, especially in the neighborhood where we are located, depend a lot on buses to go to their primary care,” Dr. Kays told this news organization. But “follow-up is very important. It can promote early treatment and prevent the spread of disease.”
Primary care is critical as a gateway into health care that could help address low rates of STI screening, she said. There is also evidence that STIs are on the rise because of the COVID-19 pandemic.
If more primary care doctors tested and treated STIs using standardized Centers for Disease Control and Prevention guidelines, patients would not have to make a trip to another location, Dr. Kays said.
“The primary health setting … is actually the perfect place to get your screening,” said Jimmie Leckliter, MSN-Ed, RN, PHN, in an interview. He was not affiliated with the presentation. “I’m a former ER nurse, and a lot of people are using the ER as primary care, and it’s not really set up to do that screening.”
Mr. Leckliter suggested that primary care doctors incorporate some questions about sexual health during a regular head-to-toe checkup and ask questions in a very clinical, nonjudgmental way.
He also acknowledged that for some physicians it can be uncomfortable to raise the issues. “Unfortunately, I think in our society, talking to people about sex is taboo, and people become uncomfortable. We need to be able to learn to put our biases aside and treat our patients. That’s what our job is, added Mr. Leckliter, an adjunct faculty member at the College of the Desert’s School of Nursing and Allied Health Programs, Palm Springs, Calif.
Clinicians should be aware of the stigma associated with sending a person to an STD clinic for further workup, Mr. Leckliter advised. “You have to look at the stigma in the community in which you’re located. It makes a big difference,” he said. “Is it mainly a Latino or African American community?”
Compliance was a challenge
Dr. Kays and colleague performed a quality improvement project focused on implementing the CDC’s STI treatment guidelines at Care Resource. One goal was to educate a multidisciplinary team on the importance of screening in the primary care setting. The clientele at Care Resource consists primarily of underprivileged minorities, including the Latino, Black, gay, and transgender communities.
Six health care providers participated – two medical doctors and four advanced-practice providers. They evaluated patient charts from the electronic health record system 4 weeks before the intervention and 4 weeks after.
The education had a positive impact, the researchers reported, even though three providers were compliant with the CDC-recommended screening protocol and three others were not.
The quality improvement initiative had some limitations, Dr. Kays noted. “The hope is that the [quality improvement] process will continue moving forward, and early diagnosis and treatment of STIs will be standardized in this primary care practice.”
An evidence-based tool to screen for STIs in primary care is “crucial,” she added. Using a standardized, evidence-based protocol in primary care “can create positive change in patients’ outcomes.”
The study was independently supported. Dr. Kays and Mr. Leckliter report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – Boosting screening for sexually transmitted infections in primary care settings could help alleviate some of the barriers to optimal testing and treatment, a new quality improvement initiative suggests.
Many primary care doctors are challenged for time and send people to other health care settings, such as a local health department or a clinic that specializes in STI diagnosis and treatment, said Wendy Kays, DNP, APRN, AGNP-BC, AAHIVS, a nurse practitioner and researcher at Care Resource, Miami.
However, for multiple reasons, many patients do not follow up and are not screened or treated, Dr. Kays said at the Association of Nurses in AIDS Care annual meeting. Some people can afford the copay to see a primary care provider, for example, but do not have the resources to pay for a second clinical visit or laboratory testing.
In other instances, transportation can be a problem. “People, especially in the neighborhood where we are located, depend a lot on buses to go to their primary care,” Dr. Kays told this news organization. But “follow-up is very important. It can promote early treatment and prevent the spread of disease.”
Primary care is critical as a gateway into health care that could help address low rates of STI screening, she said. There is also evidence that STIs are on the rise because of the COVID-19 pandemic.
If more primary care doctors tested and treated STIs using standardized Centers for Disease Control and Prevention guidelines, patients would not have to make a trip to another location, Dr. Kays said.
“The primary health setting … is actually the perfect place to get your screening,” said Jimmie Leckliter, MSN-Ed, RN, PHN, in an interview. He was not affiliated with the presentation. “I’m a former ER nurse, and a lot of people are using the ER as primary care, and it’s not really set up to do that screening.”
Mr. Leckliter suggested that primary care doctors incorporate some questions about sexual health during a regular head-to-toe checkup and ask questions in a very clinical, nonjudgmental way.
He also acknowledged that for some physicians it can be uncomfortable to raise the issues. “Unfortunately, I think in our society, talking to people about sex is taboo, and people become uncomfortable. We need to be able to learn to put our biases aside and treat our patients. That’s what our job is, added Mr. Leckliter, an adjunct faculty member at the College of the Desert’s School of Nursing and Allied Health Programs, Palm Springs, Calif.
Clinicians should be aware of the stigma associated with sending a person to an STD clinic for further workup, Mr. Leckliter advised. “You have to look at the stigma in the community in which you’re located. It makes a big difference,” he said. “Is it mainly a Latino or African American community?”
Compliance was a challenge
Dr. Kays and colleague performed a quality improvement project focused on implementing the CDC’s STI treatment guidelines at Care Resource. One goal was to educate a multidisciplinary team on the importance of screening in the primary care setting. The clientele at Care Resource consists primarily of underprivileged minorities, including the Latino, Black, gay, and transgender communities.
Six health care providers participated – two medical doctors and four advanced-practice providers. They evaluated patient charts from the electronic health record system 4 weeks before the intervention and 4 weeks after.
The education had a positive impact, the researchers reported, even though three providers were compliant with the CDC-recommended screening protocol and three others were not.
The quality improvement initiative had some limitations, Dr. Kays noted. “The hope is that the [quality improvement] process will continue moving forward, and early diagnosis and treatment of STIs will be standardized in this primary care practice.”
An evidence-based tool to screen for STIs in primary care is “crucial,” she added. Using a standardized, evidence-based protocol in primary care “can create positive change in patients’ outcomes.”
The study was independently supported. Dr. Kays and Mr. Leckliter report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – Boosting screening for sexually transmitted infections in primary care settings could help alleviate some of the barriers to optimal testing and treatment, a new quality improvement initiative suggests.
Many primary care doctors are challenged for time and send people to other health care settings, such as a local health department or a clinic that specializes in STI diagnosis and treatment, said Wendy Kays, DNP, APRN, AGNP-BC, AAHIVS, a nurse practitioner and researcher at Care Resource, Miami.
However, for multiple reasons, many patients do not follow up and are not screened or treated, Dr. Kays said at the Association of Nurses in AIDS Care annual meeting. Some people can afford the copay to see a primary care provider, for example, but do not have the resources to pay for a second clinical visit or laboratory testing.
In other instances, transportation can be a problem. “People, especially in the neighborhood where we are located, depend a lot on buses to go to their primary care,” Dr. Kays told this news organization. But “follow-up is very important. It can promote early treatment and prevent the spread of disease.”
Primary care is critical as a gateway into health care that could help address low rates of STI screening, she said. There is also evidence that STIs are on the rise because of the COVID-19 pandemic.
If more primary care doctors tested and treated STIs using standardized Centers for Disease Control and Prevention guidelines, patients would not have to make a trip to another location, Dr. Kays said.
“The primary health setting … is actually the perfect place to get your screening,” said Jimmie Leckliter, MSN-Ed, RN, PHN, in an interview. He was not affiliated with the presentation. “I’m a former ER nurse, and a lot of people are using the ER as primary care, and it’s not really set up to do that screening.”
Mr. Leckliter suggested that primary care doctors incorporate some questions about sexual health during a regular head-to-toe checkup and ask questions in a very clinical, nonjudgmental way.
He also acknowledged that for some physicians it can be uncomfortable to raise the issues. “Unfortunately, I think in our society, talking to people about sex is taboo, and people become uncomfortable. We need to be able to learn to put our biases aside and treat our patients. That’s what our job is, added Mr. Leckliter, an adjunct faculty member at the College of the Desert’s School of Nursing and Allied Health Programs, Palm Springs, Calif.
Clinicians should be aware of the stigma associated with sending a person to an STD clinic for further workup, Mr. Leckliter advised. “You have to look at the stigma in the community in which you’re located. It makes a big difference,” he said. “Is it mainly a Latino or African American community?”
Compliance was a challenge
Dr. Kays and colleague performed a quality improvement project focused on implementing the CDC’s STI treatment guidelines at Care Resource. One goal was to educate a multidisciplinary team on the importance of screening in the primary care setting. The clientele at Care Resource consists primarily of underprivileged minorities, including the Latino, Black, gay, and transgender communities.
Six health care providers participated – two medical doctors and four advanced-practice providers. They evaluated patient charts from the electronic health record system 4 weeks before the intervention and 4 weeks after.
The education had a positive impact, the researchers reported, even though three providers were compliant with the CDC-recommended screening protocol and three others were not.
The quality improvement initiative had some limitations, Dr. Kays noted. “The hope is that the [quality improvement] process will continue moving forward, and early diagnosis and treatment of STIs will be standardized in this primary care practice.”
An evidence-based tool to screen for STIs in primary care is “crucial,” she added. Using a standardized, evidence-based protocol in primary care “can create positive change in patients’ outcomes.”
The study was independently supported. Dr. Kays and Mr. Leckliter report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Just 8 minutes of exercise a day is all you need
according to a new study in the European Heart Journal.
Just 54 minutes of vigorous exercise per week provides the most bang for your buck, researchers found, lowering the risk of early death from any cause by 36%, and your chances of getting heart disease by 35%.
Scientists examined data from fitness trackers worn by more than 71,000 people studied in the United Kingdom, then analyzed their health over the next several years.
While more time spent exercising unsurprisingly led to better health, the protective effects of exercise start to plateau after a certain point, according to the study.
A tough, short workout improves blood pressure, shrinks artery-clogging plaques, and boosts your overall fitness.
Vigorous exercise helps your body adapt better than moderate exercise does, leading to more notable benefits, says study author Matthew Ahmadi, PhD, a postdoctoral research fellow at the University of Sydney.
“Collectively, these will lower a person’s risk of cardiovascular disease. Exercise can also lower body inflammation, which will in turn lower the risk for certain cancers,” he says.
The CDC recommends at least 150 minutes of “moderate intensity” exercise each week, such as walking at a brisk pace. Or you could spend 75 minutes each week doing vigorous exercise, like running, it says. The CDC also recommends muscle strengthening activities, like lifting weights, at least 2 days per week.
But only 54% of Americans actually manage to get their 150 minutes of aerobic activity in each week, according to the most recent data from the National Center for Health Statistics. Even fewer – just 24% – also squeeze in the two recommended strength workouts.
So 8 minutes a day instead of 30 minutes could persuade busy people to get the exercise they need.
“Lack of time is one of the main reasons people have reported for not engaging in exercise,” says Dr. Ahmadi.
Vigorous exercise doesn’t mean you have to run, bike, or lift weights. Scientists consider a physical activity “vigorous” if it’s greater than 6 times your resting metabolic rate, or MET. That includes all kinds of strenuous movement, including dancing in a nightclub or carrying groceries upstairs.
“All of these activities are equally beneficial,” says Dr. Ahmadi.
He recommends aiming for 2-minute bouts of a heart-pumping activity, spread throughout the day for the most benefit in the least amount of time. If you wear a smartwatch or other device that tracks your heart rate, you’ll be above the threshold if your heart is pumping at 77% or more of your max heart rate (which most fitness trackers help you calculate).
No smartwatch? “The easiest way a person can infer if they are doing vigorous activity is if they are breathing hard enough that it’s difficult to have a conversation or speak in a full sentence while doing the activity,” Dr. Ahmadi says. In other words, if you’re huffing and puffing, then you’re in the zone.
A version of this article first appeared on WebMD.com.
according to a new study in the European Heart Journal.
Just 54 minutes of vigorous exercise per week provides the most bang for your buck, researchers found, lowering the risk of early death from any cause by 36%, and your chances of getting heart disease by 35%.
Scientists examined data from fitness trackers worn by more than 71,000 people studied in the United Kingdom, then analyzed their health over the next several years.
While more time spent exercising unsurprisingly led to better health, the protective effects of exercise start to plateau after a certain point, according to the study.
A tough, short workout improves blood pressure, shrinks artery-clogging plaques, and boosts your overall fitness.
Vigorous exercise helps your body adapt better than moderate exercise does, leading to more notable benefits, says study author Matthew Ahmadi, PhD, a postdoctoral research fellow at the University of Sydney.
“Collectively, these will lower a person’s risk of cardiovascular disease. Exercise can also lower body inflammation, which will in turn lower the risk for certain cancers,” he says.
The CDC recommends at least 150 minutes of “moderate intensity” exercise each week, such as walking at a brisk pace. Or you could spend 75 minutes each week doing vigorous exercise, like running, it says. The CDC also recommends muscle strengthening activities, like lifting weights, at least 2 days per week.
But only 54% of Americans actually manage to get their 150 minutes of aerobic activity in each week, according to the most recent data from the National Center for Health Statistics. Even fewer – just 24% – also squeeze in the two recommended strength workouts.
So 8 minutes a day instead of 30 minutes could persuade busy people to get the exercise they need.
“Lack of time is one of the main reasons people have reported for not engaging in exercise,” says Dr. Ahmadi.
Vigorous exercise doesn’t mean you have to run, bike, or lift weights. Scientists consider a physical activity “vigorous” if it’s greater than 6 times your resting metabolic rate, or MET. That includes all kinds of strenuous movement, including dancing in a nightclub or carrying groceries upstairs.
“All of these activities are equally beneficial,” says Dr. Ahmadi.
He recommends aiming for 2-minute bouts of a heart-pumping activity, spread throughout the day for the most benefit in the least amount of time. If you wear a smartwatch or other device that tracks your heart rate, you’ll be above the threshold if your heart is pumping at 77% or more of your max heart rate (which most fitness trackers help you calculate).
No smartwatch? “The easiest way a person can infer if they are doing vigorous activity is if they are breathing hard enough that it’s difficult to have a conversation or speak in a full sentence while doing the activity,” Dr. Ahmadi says. In other words, if you’re huffing and puffing, then you’re in the zone.
A version of this article first appeared on WebMD.com.
according to a new study in the European Heart Journal.
Just 54 minutes of vigorous exercise per week provides the most bang for your buck, researchers found, lowering the risk of early death from any cause by 36%, and your chances of getting heart disease by 35%.
Scientists examined data from fitness trackers worn by more than 71,000 people studied in the United Kingdom, then analyzed their health over the next several years.
While more time spent exercising unsurprisingly led to better health, the protective effects of exercise start to plateau after a certain point, according to the study.
A tough, short workout improves blood pressure, shrinks artery-clogging plaques, and boosts your overall fitness.
Vigorous exercise helps your body adapt better than moderate exercise does, leading to more notable benefits, says study author Matthew Ahmadi, PhD, a postdoctoral research fellow at the University of Sydney.
“Collectively, these will lower a person’s risk of cardiovascular disease. Exercise can also lower body inflammation, which will in turn lower the risk for certain cancers,” he says.
The CDC recommends at least 150 minutes of “moderate intensity” exercise each week, such as walking at a brisk pace. Or you could spend 75 minutes each week doing vigorous exercise, like running, it says. The CDC also recommends muscle strengthening activities, like lifting weights, at least 2 days per week.
But only 54% of Americans actually manage to get their 150 minutes of aerobic activity in each week, according to the most recent data from the National Center for Health Statistics. Even fewer – just 24% – also squeeze in the two recommended strength workouts.
So 8 minutes a day instead of 30 minutes could persuade busy people to get the exercise they need.
“Lack of time is one of the main reasons people have reported for not engaging in exercise,” says Dr. Ahmadi.
Vigorous exercise doesn’t mean you have to run, bike, or lift weights. Scientists consider a physical activity “vigorous” if it’s greater than 6 times your resting metabolic rate, or MET. That includes all kinds of strenuous movement, including dancing in a nightclub or carrying groceries upstairs.
“All of these activities are equally beneficial,” says Dr. Ahmadi.
He recommends aiming for 2-minute bouts of a heart-pumping activity, spread throughout the day for the most benefit in the least amount of time. If you wear a smartwatch or other device that tracks your heart rate, you’ll be above the threshold if your heart is pumping at 77% or more of your max heart rate (which most fitness trackers help you calculate).
No smartwatch? “The easiest way a person can infer if they are doing vigorous activity is if they are breathing hard enough that it’s difficult to have a conversation or speak in a full sentence while doing the activity,” Dr. Ahmadi says. In other words, if you’re huffing and puffing, then you’re in the zone.
A version of this article first appeared on WebMD.com.
FROM EUROPEAN HEART JOURNAL
Brepocitinib improves symptoms of mild to moderate AD in phase 2b trial
compared with a group that received vehicle, in a recently published study..
The investigators said that brepocitinib, an investigational dual tyrosine kinase 2 (TYK2) and Janus kinase 1 (JAK1) inhibitor, was effective and well tolerated in patients with mild to moderate AD based on improvements in multiple measures, including Eczema Area and Severity Index (EASI) total score and Investigator Global Assessment (IGA) responder rates. Brepocitinib also reduced pruritus symptoms as early as 2 days after the start of treatment, they noted.
“This study supports the further evaluation of topical brepocitinib as a novel treatment for mild to moderate AD,” Megan N. Landis, MD, of the department of medicine at the University of Louisville (Ky.) and colleagues wrote in the study published in the British Journal of Dermatology.
They evaluated brepocitinib in a phase 2b, double-blind, dose-ranging study where 292 patients were randomized to receive brepocitinib once daily (brepocitinib 0.1%, 0.3%, 1.0%, 3.0%) or twice daily (brepocitinib 0.3%, 1.0%), or vehicle for 6 weeks. At 6 weeks, the researchers assessed EASI total score as a primary outcome, an IGA score of 0 or 1 as a secondary outcome. The mean age of the patients was 40 years (range, 13-74), almost 60% were White, 17.5% were Black, and about 20% were Asian.
Compared with the corresponding once-daily vehicle group (least squares mean reduction of –44.4; 90% confidence interval, –57.3 to –31.6) and the twice-daily vehicle group (LSM, –47.6; 90% CI, –57.5 to –37.7) , the brepocitinib 1% once-daily group (LSM, –70.1; 90% CI, –82.1 to –58.0) and twice-daily group (LSM, –75.0; 90% CI, –83.8 to –66.2) had significant percentage reductions in EASI total score compared with baseline at 6 weeks. Patients in the other brepocitinib dose groups had nonsignificant reductions in EASI from baseline.
Regarding secondary outcomes, a significantly higher percentage of patients in five of the six active treatment groups achieved an IGA score of 0 or 1 and at least a 2-point reduction in IGA score in the once-daily brepocitinib 0.1% group (29.7%; 90% CI, 18.5%-43.3%), 0.3% group (33.3%; 90% CI, 21.3%-47.0%), 1.0% group (40.5%; 90% CI, 28.0%-54.4%), 3.0% group (44.4%; 90% CI, 30.2%-59.1%), and brepocitinib 0.3% twice-daily group (33.3%; 90% CI, 21.3%-47.0%) compared with the once-daily (10.8%; 90% CI, 4.8%-22.2%) and twice-daily (13.9%; 90% CI, 6.9%-25.4%) vehicle groups.
The study authors noted that 37.0% of patients overall experienced treatment-emergent adverse events (TEAEs), with most TEAEs occurring in the once-daily vehicle (48.6%), twice-daily vehicle (47.2%), and brepocitinib 0.1% (45.9%) groups. Adverse events were not considered dose dependent, and no group had any serious TEAEs or deaths.
Nasopharyngitis and worsening AD were the most common TEAEs reported, with about 8% of those in the vehicle groups experiencing worsening AD.
Brepocitinib is also currently being developed as a treatment for dermatomyositis, systemic lupus erythematosus, hidradenitis suppurativa, and noninfectious uveitis by Priovant Therapeutics, a company founded by Pfizer and Roivant Sciences.
In September 2021, the Food and Drug Administration approved topical ruxolitinib cream for the treatment of patients with mild to moderate atopic dermatitis aged 12 years and older, the first topical JAK inhibitor approved for AD.
This study was sponsored by Pfizer. The authors reported personal and institutional relationships in the form of investigator positions, fees, honoraria, research grants, employee positions, and holding stock or shares for a variety of pharmaceutical, life science, and biotechnology companies.
compared with a group that received vehicle, in a recently published study..
The investigators said that brepocitinib, an investigational dual tyrosine kinase 2 (TYK2) and Janus kinase 1 (JAK1) inhibitor, was effective and well tolerated in patients with mild to moderate AD based on improvements in multiple measures, including Eczema Area and Severity Index (EASI) total score and Investigator Global Assessment (IGA) responder rates. Brepocitinib also reduced pruritus symptoms as early as 2 days after the start of treatment, they noted.
“This study supports the further evaluation of topical brepocitinib as a novel treatment for mild to moderate AD,” Megan N. Landis, MD, of the department of medicine at the University of Louisville (Ky.) and colleagues wrote in the study published in the British Journal of Dermatology.
They evaluated brepocitinib in a phase 2b, double-blind, dose-ranging study where 292 patients were randomized to receive brepocitinib once daily (brepocitinib 0.1%, 0.3%, 1.0%, 3.0%) or twice daily (brepocitinib 0.3%, 1.0%), or vehicle for 6 weeks. At 6 weeks, the researchers assessed EASI total score as a primary outcome, an IGA score of 0 or 1 as a secondary outcome. The mean age of the patients was 40 years (range, 13-74), almost 60% were White, 17.5% were Black, and about 20% were Asian.
Compared with the corresponding once-daily vehicle group (least squares mean reduction of –44.4; 90% confidence interval, –57.3 to –31.6) and the twice-daily vehicle group (LSM, –47.6; 90% CI, –57.5 to –37.7) , the brepocitinib 1% once-daily group (LSM, –70.1; 90% CI, –82.1 to –58.0) and twice-daily group (LSM, –75.0; 90% CI, –83.8 to –66.2) had significant percentage reductions in EASI total score compared with baseline at 6 weeks. Patients in the other brepocitinib dose groups had nonsignificant reductions in EASI from baseline.
Regarding secondary outcomes, a significantly higher percentage of patients in five of the six active treatment groups achieved an IGA score of 0 or 1 and at least a 2-point reduction in IGA score in the once-daily brepocitinib 0.1% group (29.7%; 90% CI, 18.5%-43.3%), 0.3% group (33.3%; 90% CI, 21.3%-47.0%), 1.0% group (40.5%; 90% CI, 28.0%-54.4%), 3.0% group (44.4%; 90% CI, 30.2%-59.1%), and brepocitinib 0.3% twice-daily group (33.3%; 90% CI, 21.3%-47.0%) compared with the once-daily (10.8%; 90% CI, 4.8%-22.2%) and twice-daily (13.9%; 90% CI, 6.9%-25.4%) vehicle groups.
The study authors noted that 37.0% of patients overall experienced treatment-emergent adverse events (TEAEs), with most TEAEs occurring in the once-daily vehicle (48.6%), twice-daily vehicle (47.2%), and brepocitinib 0.1% (45.9%) groups. Adverse events were not considered dose dependent, and no group had any serious TEAEs or deaths.
Nasopharyngitis and worsening AD were the most common TEAEs reported, with about 8% of those in the vehicle groups experiencing worsening AD.
Brepocitinib is also currently being developed as a treatment for dermatomyositis, systemic lupus erythematosus, hidradenitis suppurativa, and noninfectious uveitis by Priovant Therapeutics, a company founded by Pfizer and Roivant Sciences.
In September 2021, the Food and Drug Administration approved topical ruxolitinib cream for the treatment of patients with mild to moderate atopic dermatitis aged 12 years and older, the first topical JAK inhibitor approved for AD.
This study was sponsored by Pfizer. The authors reported personal and institutional relationships in the form of investigator positions, fees, honoraria, research grants, employee positions, and holding stock or shares for a variety of pharmaceutical, life science, and biotechnology companies.
compared with a group that received vehicle, in a recently published study..
The investigators said that brepocitinib, an investigational dual tyrosine kinase 2 (TYK2) and Janus kinase 1 (JAK1) inhibitor, was effective and well tolerated in patients with mild to moderate AD based on improvements in multiple measures, including Eczema Area and Severity Index (EASI) total score and Investigator Global Assessment (IGA) responder rates. Brepocitinib also reduced pruritus symptoms as early as 2 days after the start of treatment, they noted.
“This study supports the further evaluation of topical brepocitinib as a novel treatment for mild to moderate AD,” Megan N. Landis, MD, of the department of medicine at the University of Louisville (Ky.) and colleagues wrote in the study published in the British Journal of Dermatology.
They evaluated brepocitinib in a phase 2b, double-blind, dose-ranging study where 292 patients were randomized to receive brepocitinib once daily (brepocitinib 0.1%, 0.3%, 1.0%, 3.0%) or twice daily (brepocitinib 0.3%, 1.0%), or vehicle for 6 weeks. At 6 weeks, the researchers assessed EASI total score as a primary outcome, an IGA score of 0 or 1 as a secondary outcome. The mean age of the patients was 40 years (range, 13-74), almost 60% were White, 17.5% were Black, and about 20% were Asian.
Compared with the corresponding once-daily vehicle group (least squares mean reduction of –44.4; 90% confidence interval, –57.3 to –31.6) and the twice-daily vehicle group (LSM, –47.6; 90% CI, –57.5 to –37.7) , the brepocitinib 1% once-daily group (LSM, –70.1; 90% CI, –82.1 to –58.0) and twice-daily group (LSM, –75.0; 90% CI, –83.8 to –66.2) had significant percentage reductions in EASI total score compared with baseline at 6 weeks. Patients in the other brepocitinib dose groups had nonsignificant reductions in EASI from baseline.
Regarding secondary outcomes, a significantly higher percentage of patients in five of the six active treatment groups achieved an IGA score of 0 or 1 and at least a 2-point reduction in IGA score in the once-daily brepocitinib 0.1% group (29.7%; 90% CI, 18.5%-43.3%), 0.3% group (33.3%; 90% CI, 21.3%-47.0%), 1.0% group (40.5%; 90% CI, 28.0%-54.4%), 3.0% group (44.4%; 90% CI, 30.2%-59.1%), and brepocitinib 0.3% twice-daily group (33.3%; 90% CI, 21.3%-47.0%) compared with the once-daily (10.8%; 90% CI, 4.8%-22.2%) and twice-daily (13.9%; 90% CI, 6.9%-25.4%) vehicle groups.
The study authors noted that 37.0% of patients overall experienced treatment-emergent adverse events (TEAEs), with most TEAEs occurring in the once-daily vehicle (48.6%), twice-daily vehicle (47.2%), and brepocitinib 0.1% (45.9%) groups. Adverse events were not considered dose dependent, and no group had any serious TEAEs or deaths.
Nasopharyngitis and worsening AD were the most common TEAEs reported, with about 8% of those in the vehicle groups experiencing worsening AD.
Brepocitinib is also currently being developed as a treatment for dermatomyositis, systemic lupus erythematosus, hidradenitis suppurativa, and noninfectious uveitis by Priovant Therapeutics, a company founded by Pfizer and Roivant Sciences.
In September 2021, the Food and Drug Administration approved topical ruxolitinib cream for the treatment of patients with mild to moderate atopic dermatitis aged 12 years and older, the first topical JAK inhibitor approved for AD.
This study was sponsored by Pfizer. The authors reported personal and institutional relationships in the form of investigator positions, fees, honoraria, research grants, employee positions, and holding stock or shares for a variety of pharmaceutical, life science, and biotechnology companies.
FROM BRITISH JOURNAL OF DERMATOLOGY
More vaccinated people dying of COVID as fewer get booster shots
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
Don’t call me ‘Dr.,’ say some physicians – but most prefer the title
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Study supports banning probiotics from the ICU
NASHVILLE, TENN. – Supported by several cases series, according to new findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
According to data presented by Scott Mayer, MD, chief resident at HealthONE Denver, which is part of the HCA Healthcare chain of hospitals, the risk is increased by any probiotic exposure. However, the risk is particularly acute for powdered formulations, presumably because powder more easily disseminates to contaminate central venous catheters.
“We think that probiotics should be eliminated entirely from the ICU. If not, we encourage eliminating the powder formulations,” said Dr. Mayer, who led the study.
The data linking probiotics to ICU bacteremia were drawn from 23,533 ICU admissions over a 5-year period in the HCA hospital database. Bacteremia proven to be probiotic-related was uncommon (0.37%), but the consequences were serious.
For those with probiotic-related bacteremia, the mortality rate was 25.6% or essentially twofold greater than the 13.5% mortality rate among those without probiotic bacteremia. An odds ratio drawn from a regression analysis confirmed a significant difference (OR, 2.23; 95% confidence interval, 1.30-3.71; P < .01).
“The absolute risk of mortality is modest but not insignificant,” said Dr. Mayer. This suggests one probiotic-related mortality for about every 200 patients taking a probiotic in the ICU.
These deaths occur without any clear compensatory benefit from taking probiotics, according to Dr. Mayer. There is a long list of potential benefits from probiotics that might be relevant to patients in the ICU, particularly prophylaxis for Clostridioides difficile infection, but also including a variety of gastrointestinal disorders, such as irritable bowel syndrome; however, none of these are firmly established in general, and particularly for patients in the ICU.
“The American College of Gastroenterology currently recommends against probiotics for the prevention of C. diff.,” Dr. Mayer said. Although the American Gastroenterological Association has issued a “conditional recommendation” for prevention of C. diff. infection with probiotics, Dr. Mayer pointed out this is qualified by a “low quality of evidence” and it is not specific to the ICU setting.
“The evidence for benefit is weak or nonexistent, but the risks are real,” Dr. Mayer said.
To confirm that probiotic-associated ICU bacteremias in the HCA hospital database were, in fact, related to probiotics being taken by patients at time of admission, Dr. Mayer evaluated the record of each of the 86 patients with probiotic bacteremia–associated mortality.
“I identified the organism that grew from the blood cultures to confirm that it was contained in the probiotic the patient was taking,” explained Dr. Mayer, who said this information was available in the electronic medical records.
The risk of probiotic-associated bacteremia in ICU patients was consistent with a series of case series that prompted the study. Dr. Mayer explained that he became interested when he encountered patients on his ICU rounds who were taking probiotics. He knew very little about these agents and explored the medical literature to see what evidence was available.
“I found several case reports of ICU patients with probiotic-associated infections, several of which were suspected of being associated with contamination of the central lines,” Dr. Mayer said. In one case, the patient was not taking a probiotic, but a patient in an adjacent bed was receiving a powdered probiotic that was implicated. This prompted suspicion that the cause was central-line contamination.
This was evaluated in the HCA ICU database and also found to be a significant risk. Among the 67 patients in whom a capsule or tablet was used, the rate of probiotic-associated bacteremia was 0.33%. For those in which the probiotic was a powdered formulation, the rate was 0.76%, a significant difference (P < .01).
Dr. Mayer acknowledged that these data do not rule out all potential benefits from probiotics in the ICU. He believes an obstacle to proving benefit has been the heterogeneity of available products, which are likely to be relevant to any therapeutic role, including prevention of C. diff. infection.
“There are now a large number of products available, and they contain a large variety of strains of organisms, so this has been a difficult area to study,” he said. However, he maintains it is prudent at this point to avoid probiotics in the ICU because the risks are not confined to the patient making this choice.
“My concern is not just the lack of evidence of benefit relative to the risk for the patient but the potential for probiotics in the ICU to place other patients at risk,” Dr. Mayer said.
Others have also noted the potential benefits of probiotics in the ICU, but the promise remains elusive. In a 2018 review article published in the Journal of Emergency and Critical Care Medicine, the authors evaluated a series of potential applications of probiotics in critically ill patients. These included treatment of ventilator-associated pneumonia (VAP), catheter-associated urinary tract infections (CAUTI), and surgical-site infections (SSI). For each, the data were negative or inconclusive.
Over the 4 years that have passed since the review was published, several trials have further explored the potential benefits of probiotics in the ICU but none have changed this basic conclusion. For example, a 2021 multinational trial, published in The Lancet, randomized more than 2,600 patients to probiotics or placebo and showed no effect on VAP incidence (21.9% vs. 21.3%).
The lead author of the 2018 review, Heather A. Vitko, PhD, an associate professor in the department of acute and tertiary care, University of Pittsburgh School of Nursing, also emphasized that the potential for benefit cannot be considered without the potential for risk. She, like Dr. Mayer, cited the case studies implicating probiotics in systemic infections.
For administration, probiotic capsules or sachets “often need to be opened for administration through a feeding tube,” she noted. The risk of contamination comes from both the air and contaminated hands, the latter of which “can cause a translocation to a central line catheter where the microbes have direct entry into the systemic circulation.”
She did not call for a ban of probiotics in the ICU, but she did recommend “a precautionary approach,” encouraging clinicians to “distinguish between reality [of what has been proven] and what is presented in the marketing of antibiotics.”
Dr. Mayer and Dr. Vitko have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NASHVILLE, TENN. – Supported by several cases series, according to new findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
According to data presented by Scott Mayer, MD, chief resident at HealthONE Denver, which is part of the HCA Healthcare chain of hospitals, the risk is increased by any probiotic exposure. However, the risk is particularly acute for powdered formulations, presumably because powder more easily disseminates to contaminate central venous catheters.
“We think that probiotics should be eliminated entirely from the ICU. If not, we encourage eliminating the powder formulations,” said Dr. Mayer, who led the study.
The data linking probiotics to ICU bacteremia were drawn from 23,533 ICU admissions over a 5-year period in the HCA hospital database. Bacteremia proven to be probiotic-related was uncommon (0.37%), but the consequences were serious.
For those with probiotic-related bacteremia, the mortality rate was 25.6% or essentially twofold greater than the 13.5% mortality rate among those without probiotic bacteremia. An odds ratio drawn from a regression analysis confirmed a significant difference (OR, 2.23; 95% confidence interval, 1.30-3.71; P < .01).
“The absolute risk of mortality is modest but not insignificant,” said Dr. Mayer. This suggests one probiotic-related mortality for about every 200 patients taking a probiotic in the ICU.
These deaths occur without any clear compensatory benefit from taking probiotics, according to Dr. Mayer. There is a long list of potential benefits from probiotics that might be relevant to patients in the ICU, particularly prophylaxis for Clostridioides difficile infection, but also including a variety of gastrointestinal disorders, such as irritable bowel syndrome; however, none of these are firmly established in general, and particularly for patients in the ICU.
“The American College of Gastroenterology currently recommends against probiotics for the prevention of C. diff.,” Dr. Mayer said. Although the American Gastroenterological Association has issued a “conditional recommendation” for prevention of C. diff. infection with probiotics, Dr. Mayer pointed out this is qualified by a “low quality of evidence” and it is not specific to the ICU setting.
“The evidence for benefit is weak or nonexistent, but the risks are real,” Dr. Mayer said.
To confirm that probiotic-associated ICU bacteremias in the HCA hospital database were, in fact, related to probiotics being taken by patients at time of admission, Dr. Mayer evaluated the record of each of the 86 patients with probiotic bacteremia–associated mortality.
“I identified the organism that grew from the blood cultures to confirm that it was contained in the probiotic the patient was taking,” explained Dr. Mayer, who said this information was available in the electronic medical records.
The risk of probiotic-associated bacteremia in ICU patients was consistent with a series of case series that prompted the study. Dr. Mayer explained that he became interested when he encountered patients on his ICU rounds who were taking probiotics. He knew very little about these agents and explored the medical literature to see what evidence was available.
“I found several case reports of ICU patients with probiotic-associated infections, several of which were suspected of being associated with contamination of the central lines,” Dr. Mayer said. In one case, the patient was not taking a probiotic, but a patient in an adjacent bed was receiving a powdered probiotic that was implicated. This prompted suspicion that the cause was central-line contamination.
This was evaluated in the HCA ICU database and also found to be a significant risk. Among the 67 patients in whom a capsule or tablet was used, the rate of probiotic-associated bacteremia was 0.33%. For those in which the probiotic was a powdered formulation, the rate was 0.76%, a significant difference (P < .01).
Dr. Mayer acknowledged that these data do not rule out all potential benefits from probiotics in the ICU. He believes an obstacle to proving benefit has been the heterogeneity of available products, which are likely to be relevant to any therapeutic role, including prevention of C. diff. infection.
“There are now a large number of products available, and they contain a large variety of strains of organisms, so this has been a difficult area to study,” he said. However, he maintains it is prudent at this point to avoid probiotics in the ICU because the risks are not confined to the patient making this choice.
“My concern is not just the lack of evidence of benefit relative to the risk for the patient but the potential for probiotics in the ICU to place other patients at risk,” Dr. Mayer said.
Others have also noted the potential benefits of probiotics in the ICU, but the promise remains elusive. In a 2018 review article published in the Journal of Emergency and Critical Care Medicine, the authors evaluated a series of potential applications of probiotics in critically ill patients. These included treatment of ventilator-associated pneumonia (VAP), catheter-associated urinary tract infections (CAUTI), and surgical-site infections (SSI). For each, the data were negative or inconclusive.
Over the 4 years that have passed since the review was published, several trials have further explored the potential benefits of probiotics in the ICU but none have changed this basic conclusion. For example, a 2021 multinational trial, published in The Lancet, randomized more than 2,600 patients to probiotics or placebo and showed no effect on VAP incidence (21.9% vs. 21.3%).
The lead author of the 2018 review, Heather A. Vitko, PhD, an associate professor in the department of acute and tertiary care, University of Pittsburgh School of Nursing, also emphasized that the potential for benefit cannot be considered without the potential for risk. She, like Dr. Mayer, cited the case studies implicating probiotics in systemic infections.
For administration, probiotic capsules or sachets “often need to be opened for administration through a feeding tube,” she noted. The risk of contamination comes from both the air and contaminated hands, the latter of which “can cause a translocation to a central line catheter where the microbes have direct entry into the systemic circulation.”
She did not call for a ban of probiotics in the ICU, but she did recommend “a precautionary approach,” encouraging clinicians to “distinguish between reality [of what has been proven] and what is presented in the marketing of antibiotics.”
Dr. Mayer and Dr. Vitko have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NASHVILLE, TENN. – Supported by several cases series, according to new findings presented at the annual meeting of the American College of Chest Physicians (CHEST).
According to data presented by Scott Mayer, MD, chief resident at HealthONE Denver, which is part of the HCA Healthcare chain of hospitals, the risk is increased by any probiotic exposure. However, the risk is particularly acute for powdered formulations, presumably because powder more easily disseminates to contaminate central venous catheters.
“We think that probiotics should be eliminated entirely from the ICU. If not, we encourage eliminating the powder formulations,” said Dr. Mayer, who led the study.
The data linking probiotics to ICU bacteremia were drawn from 23,533 ICU admissions over a 5-year period in the HCA hospital database. Bacteremia proven to be probiotic-related was uncommon (0.37%), but the consequences were serious.
For those with probiotic-related bacteremia, the mortality rate was 25.6% or essentially twofold greater than the 13.5% mortality rate among those without probiotic bacteremia. An odds ratio drawn from a regression analysis confirmed a significant difference (OR, 2.23; 95% confidence interval, 1.30-3.71; P < .01).
“The absolute risk of mortality is modest but not insignificant,” said Dr. Mayer. This suggests one probiotic-related mortality for about every 200 patients taking a probiotic in the ICU.
These deaths occur without any clear compensatory benefit from taking probiotics, according to Dr. Mayer. There is a long list of potential benefits from probiotics that might be relevant to patients in the ICU, particularly prophylaxis for Clostridioides difficile infection, but also including a variety of gastrointestinal disorders, such as irritable bowel syndrome; however, none of these are firmly established in general, and particularly for patients in the ICU.
“The American College of Gastroenterology currently recommends against probiotics for the prevention of C. diff.,” Dr. Mayer said. Although the American Gastroenterological Association has issued a “conditional recommendation” for prevention of C. diff. infection with probiotics, Dr. Mayer pointed out this is qualified by a “low quality of evidence” and it is not specific to the ICU setting.
“The evidence for benefit is weak or nonexistent, but the risks are real,” Dr. Mayer said.
To confirm that probiotic-associated ICU bacteremias in the HCA hospital database were, in fact, related to probiotics being taken by patients at time of admission, Dr. Mayer evaluated the record of each of the 86 patients with probiotic bacteremia–associated mortality.
“I identified the organism that grew from the blood cultures to confirm that it was contained in the probiotic the patient was taking,” explained Dr. Mayer, who said this information was available in the electronic medical records.
The risk of probiotic-associated bacteremia in ICU patients was consistent with a series of case series that prompted the study. Dr. Mayer explained that he became interested when he encountered patients on his ICU rounds who were taking probiotics. He knew very little about these agents and explored the medical literature to see what evidence was available.
“I found several case reports of ICU patients with probiotic-associated infections, several of which were suspected of being associated with contamination of the central lines,” Dr. Mayer said. In one case, the patient was not taking a probiotic, but a patient in an adjacent bed was receiving a powdered probiotic that was implicated. This prompted suspicion that the cause was central-line contamination.
This was evaluated in the HCA ICU database and also found to be a significant risk. Among the 67 patients in whom a capsule or tablet was used, the rate of probiotic-associated bacteremia was 0.33%. For those in which the probiotic was a powdered formulation, the rate was 0.76%, a significant difference (P < .01).
Dr. Mayer acknowledged that these data do not rule out all potential benefits from probiotics in the ICU. He believes an obstacle to proving benefit has been the heterogeneity of available products, which are likely to be relevant to any therapeutic role, including prevention of C. diff. infection.
“There are now a large number of products available, and they contain a large variety of strains of organisms, so this has been a difficult area to study,” he said. However, he maintains it is prudent at this point to avoid probiotics in the ICU because the risks are not confined to the patient making this choice.
“My concern is not just the lack of evidence of benefit relative to the risk for the patient but the potential for probiotics in the ICU to place other patients at risk,” Dr. Mayer said.
Others have also noted the potential benefits of probiotics in the ICU, but the promise remains elusive. In a 2018 review article published in the Journal of Emergency and Critical Care Medicine, the authors evaluated a series of potential applications of probiotics in critically ill patients. These included treatment of ventilator-associated pneumonia (VAP), catheter-associated urinary tract infections (CAUTI), and surgical-site infections (SSI). For each, the data were negative or inconclusive.
Over the 4 years that have passed since the review was published, several trials have further explored the potential benefits of probiotics in the ICU but none have changed this basic conclusion. For example, a 2021 multinational trial, published in The Lancet, randomized more than 2,600 patients to probiotics or placebo and showed no effect on VAP incidence (21.9% vs. 21.3%).
The lead author of the 2018 review, Heather A. Vitko, PhD, an associate professor in the department of acute and tertiary care, University of Pittsburgh School of Nursing, also emphasized that the potential for benefit cannot be considered without the potential for risk. She, like Dr. Mayer, cited the case studies implicating probiotics in systemic infections.
For administration, probiotic capsules or sachets “often need to be opened for administration through a feeding tube,” she noted. The risk of contamination comes from both the air and contaminated hands, the latter of which “can cause a translocation to a central line catheter where the microbes have direct entry into the systemic circulation.”
She did not call for a ban of probiotics in the ICU, but she did recommend “a precautionary approach,” encouraging clinicians to “distinguish between reality [of what has been proven] and what is presented in the marketing of antibiotics.”
Dr. Mayer and Dr. Vitko have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CHEST 2022
Recommending exercise for migraine: Just do it
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF HEADACHE AND PAIN
Highly processed foods ‘as addictive’ as tobacco
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.