User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Gender-affirming surgeries nearly tripled between 2016 and 2019: Study
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).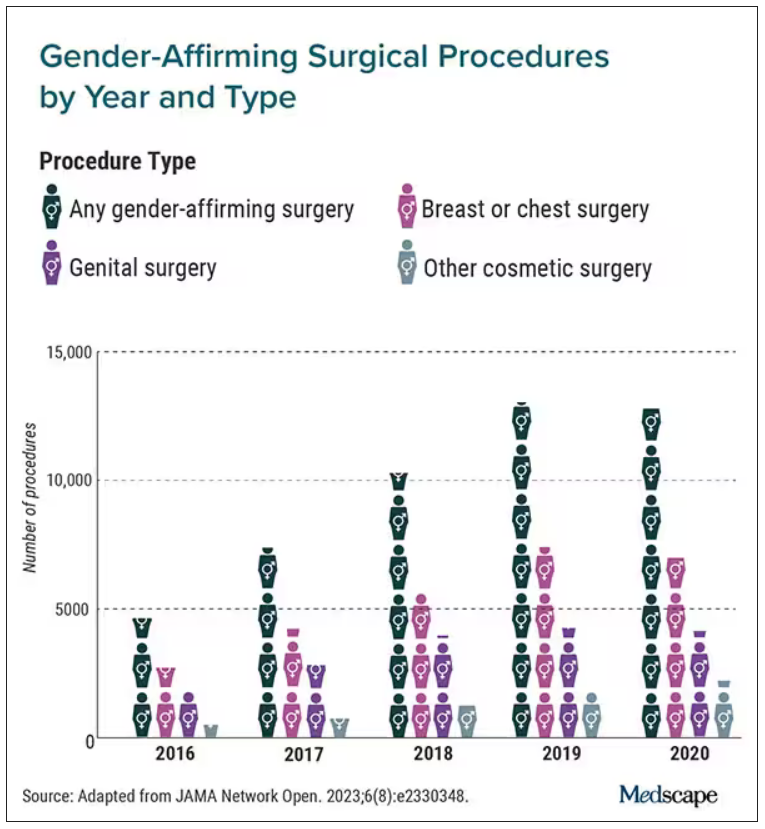
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Medicare announces 10 drugs targeted for price cuts in 2026
People on Medicare may in 2026 see prices drop for 10 medicines, including pricey diabetes, cancer, blood clot, and arthritis treatments, if advocates for federal drug-price negotiations can implement their plans amid tough opposition.
It’s unclear at this time, though, how these negotiations will play out. The Chamber of Commerce has sided with pharmaceutical companies in bids to block direct Medicare negotiation of drug prices. Many influential Republicans in Congress oppose this plan, which has deep support from both Democrats and AARP.
While facing strong opposition to negotiations, the Centers for Medicare & Medicaid Services sought in its announcement to illustrate the high costs of the selected medicines.
CMS provided data on total Part D costs for selected medicines for the period from June 2022 to May 2023, along with tallies of the number of people taking these drugs. The 10 selected medicines are as follows:
- Eliquis (generic name: apixaban), used to prevent and treat serious blood clots. It is taken by about 3.7 million people through Part D plans. The estimated cost is $16.4 billion.
- Jardiance (generic name: empagliflozin), used for diabetes and heart failure. It is taken by almost 1.6 million people through Part D plans. The estimated cost is $7.06 billion.
- Xarelto (generic name: rivaroxaban), used for blood clots. It is taken by about 1.3 million people through Part D plans. The estimated cost is $6 billion.
- Januvia (generic name: sitagliptin), used for diabetes. It is taken by about 869,00 people through Part D plans. The estimated cost is $4.1 billion.
- Farxiga (generic name: dapagliflozin), used for diabetes, heart failure, and chronic kidney disease. It is taken by about 799,000 people through Part D plans. The estimated cost is almost $3.3 billion.
- Entresto (generic name: sacubitril/valsartan), used to treat heart failure. It is taken by 587,000 people through Part D plans. The estimated cost is $2.9 billion.
- Enbrel( generic name: etanercept), used for rheumatoid arthritis, psoriasis, and psoriatic arthritis. It is taken by 48,000 people through Part D plans. The estimated cost is $2.8 billion.
- Imbruvica (generic name: ibrutinib), used to treat some blood cancers. It is taken by about 20,000 people in Part D plans. The estimated cost is $2.7 billion.
- Stelara (generic name: ustekinumab), used to treat plaque psoriasis, psoriatic arthritis, or certain bowel conditions (Crohn’s disease, ulcerative colitis). It is used by about 22,000 people through Part D plans. The estimated cost is $2.6 billion.
- Fiasp; Fiasp FlexTouch; Fiasp PenFill; NovoLog; NovoLog FlexPen; NovoLog PenFill. These are forms of insulin used to treat diabetes. They are used by about 777,000 people through Part D plans. The estimated cost is $2.6 billion.
A vocal critic of Medicare drug negotiations, Joel White, president of the Council for Affordable Health Coverage, called the announcement of the 10 drugs selected for negotiation “a hollow victory lap.” A former Republican staffer on the House Ways and Means Committee, Mr. White aided with the development of the Medicare Part D plans and has kept tabs on the pharmacy programs since its launch in 2006.
“No one’s costs will go down now or for years because of this announcement” about Part D negotiations, Mr. White said in a statement.
According to its website, CAHC includes among its members the American Academy of Ophthalmology as well as some patient groups, drugmakers, such as Johnson & Johnson, and insurers and industry groups, such as the National Association of Manufacturers.
Separately, the influential Chamber of Commerce is making a strong push to at least delay the implementation of the Medicare Part D drug negotiations. On Aug. 28, the chamber released a letter sent to the Biden administration, raising concerns about a “rush” to implement the provisions of the Inflation Reduction Act.
The chamber also has filed suit to challenge the drug negotiation provisions of the Inflation Reduction Act, requesting that the court issue a preliminary injunction by Oct. 1, 2023.
Other pending legal challenges to direct Medicare drug negotiations include suits filed by Merck, Bristol-Myers Squibb, Johnson & Johnson, Boehringer Ingelheim, and AstraZeneca, according to an email from Pharmaceutical Research and Manufacturers of America. PhRMA also said it is a party to a case.
In addition, the three congressional Republicans with most direct influence over Medicare policy issued on Aug. 29 a joint statement outlining their objections to the planned negotiations on drug prices.
This drug-negotiation proposal is “an unworkable, legally dubious scheme that will lead to higher prices for new drugs coming to market, stifle the development of new cures, and destroy jobs,” said House Energy and Commerce Committee Chair Cathy McMorris Rodgers (R-Wash.), House Ways and Means Committee Chair Jason Smith (R-Mo.), and Senate Finance Committee Ranking Member Mike Crapo (R-Idaho).
Democrats were equally firm and vocal in their support of the negotiations. Senate Finance Chairman Ron Wyden (D-Ore.) issued a statement on Aug. 29 that said the release of the list of the 10 drugs selected for Medicare drug negotiations is part of a “seismic shift in the relationship between Big Pharma, the federal government, and seniors who are counting on lower prices.
“I will be following the negotiation process closely and will fight any attempt by Big Pharma to undo or undermine the progress that’s been made,” Mr. Wyden said.
In addition, AARP issued a statement of its continued support for Medicare drug negotiations.
“The No. 1 reason seniors skip or ration their prescriptions is because they can’t afford them. This must stop,” said AARP executive vice president and chief advocacy and engagement officer Nancy LeaMond in the statement. “The big drug companies and their allies continue suing to overturn the Medicare drug price negotiation program to keep up their price gouging. We can’t allow seniors to be Big Pharma’s cash machine anymore.”
A version of this article first appeared on Medscape.com.
People on Medicare may in 2026 see prices drop for 10 medicines, including pricey diabetes, cancer, blood clot, and arthritis treatments, if advocates for federal drug-price negotiations can implement their plans amid tough opposition.
It’s unclear at this time, though, how these negotiations will play out. The Chamber of Commerce has sided with pharmaceutical companies in bids to block direct Medicare negotiation of drug prices. Many influential Republicans in Congress oppose this plan, which has deep support from both Democrats and AARP.
While facing strong opposition to negotiations, the Centers for Medicare & Medicaid Services sought in its announcement to illustrate the high costs of the selected medicines.
CMS provided data on total Part D costs for selected medicines for the period from June 2022 to May 2023, along with tallies of the number of people taking these drugs. The 10 selected medicines are as follows:
- Eliquis (generic name: apixaban), used to prevent and treat serious blood clots. It is taken by about 3.7 million people through Part D plans. The estimated cost is $16.4 billion.
- Jardiance (generic name: empagliflozin), used for diabetes and heart failure. It is taken by almost 1.6 million people through Part D plans. The estimated cost is $7.06 billion.
- Xarelto (generic name: rivaroxaban), used for blood clots. It is taken by about 1.3 million people through Part D plans. The estimated cost is $6 billion.
- Januvia (generic name: sitagliptin), used for diabetes. It is taken by about 869,00 people through Part D plans. The estimated cost is $4.1 billion.
- Farxiga (generic name: dapagliflozin), used for diabetes, heart failure, and chronic kidney disease. It is taken by about 799,000 people through Part D plans. The estimated cost is almost $3.3 billion.
- Entresto (generic name: sacubitril/valsartan), used to treat heart failure. It is taken by 587,000 people through Part D plans. The estimated cost is $2.9 billion.
- Enbrel( generic name: etanercept), used for rheumatoid arthritis, psoriasis, and psoriatic arthritis. It is taken by 48,000 people through Part D plans. The estimated cost is $2.8 billion.
- Imbruvica (generic name: ibrutinib), used to treat some blood cancers. It is taken by about 20,000 people in Part D plans. The estimated cost is $2.7 billion.
- Stelara (generic name: ustekinumab), used to treat plaque psoriasis, psoriatic arthritis, or certain bowel conditions (Crohn’s disease, ulcerative colitis). It is used by about 22,000 people through Part D plans. The estimated cost is $2.6 billion.
- Fiasp; Fiasp FlexTouch; Fiasp PenFill; NovoLog; NovoLog FlexPen; NovoLog PenFill. These are forms of insulin used to treat diabetes. They are used by about 777,000 people through Part D plans. The estimated cost is $2.6 billion.
A vocal critic of Medicare drug negotiations, Joel White, president of the Council for Affordable Health Coverage, called the announcement of the 10 drugs selected for negotiation “a hollow victory lap.” A former Republican staffer on the House Ways and Means Committee, Mr. White aided with the development of the Medicare Part D plans and has kept tabs on the pharmacy programs since its launch in 2006.
“No one’s costs will go down now or for years because of this announcement” about Part D negotiations, Mr. White said in a statement.
According to its website, CAHC includes among its members the American Academy of Ophthalmology as well as some patient groups, drugmakers, such as Johnson & Johnson, and insurers and industry groups, such as the National Association of Manufacturers.
Separately, the influential Chamber of Commerce is making a strong push to at least delay the implementation of the Medicare Part D drug negotiations. On Aug. 28, the chamber released a letter sent to the Biden administration, raising concerns about a “rush” to implement the provisions of the Inflation Reduction Act.
The chamber also has filed suit to challenge the drug negotiation provisions of the Inflation Reduction Act, requesting that the court issue a preliminary injunction by Oct. 1, 2023.
Other pending legal challenges to direct Medicare drug negotiations include suits filed by Merck, Bristol-Myers Squibb, Johnson & Johnson, Boehringer Ingelheim, and AstraZeneca, according to an email from Pharmaceutical Research and Manufacturers of America. PhRMA also said it is a party to a case.
In addition, the three congressional Republicans with most direct influence over Medicare policy issued on Aug. 29 a joint statement outlining their objections to the planned negotiations on drug prices.
This drug-negotiation proposal is “an unworkable, legally dubious scheme that will lead to higher prices for new drugs coming to market, stifle the development of new cures, and destroy jobs,” said House Energy and Commerce Committee Chair Cathy McMorris Rodgers (R-Wash.), House Ways and Means Committee Chair Jason Smith (R-Mo.), and Senate Finance Committee Ranking Member Mike Crapo (R-Idaho).
Democrats were equally firm and vocal in their support of the negotiations. Senate Finance Chairman Ron Wyden (D-Ore.) issued a statement on Aug. 29 that said the release of the list of the 10 drugs selected for Medicare drug negotiations is part of a “seismic shift in the relationship between Big Pharma, the federal government, and seniors who are counting on lower prices.
“I will be following the negotiation process closely and will fight any attempt by Big Pharma to undo or undermine the progress that’s been made,” Mr. Wyden said.
In addition, AARP issued a statement of its continued support for Medicare drug negotiations.
“The No. 1 reason seniors skip or ration their prescriptions is because they can’t afford them. This must stop,” said AARP executive vice president and chief advocacy and engagement officer Nancy LeaMond in the statement. “The big drug companies and their allies continue suing to overturn the Medicare drug price negotiation program to keep up their price gouging. We can’t allow seniors to be Big Pharma’s cash machine anymore.”
A version of this article first appeared on Medscape.com.
People on Medicare may in 2026 see prices drop for 10 medicines, including pricey diabetes, cancer, blood clot, and arthritis treatments, if advocates for federal drug-price negotiations can implement their plans amid tough opposition.
It’s unclear at this time, though, how these negotiations will play out. The Chamber of Commerce has sided with pharmaceutical companies in bids to block direct Medicare negotiation of drug prices. Many influential Republicans in Congress oppose this plan, which has deep support from both Democrats and AARP.
While facing strong opposition to negotiations, the Centers for Medicare & Medicaid Services sought in its announcement to illustrate the high costs of the selected medicines.
CMS provided data on total Part D costs for selected medicines for the period from June 2022 to May 2023, along with tallies of the number of people taking these drugs. The 10 selected medicines are as follows:
- Eliquis (generic name: apixaban), used to prevent and treat serious blood clots. It is taken by about 3.7 million people through Part D plans. The estimated cost is $16.4 billion.
- Jardiance (generic name: empagliflozin), used for diabetes and heart failure. It is taken by almost 1.6 million people through Part D plans. The estimated cost is $7.06 billion.
- Xarelto (generic name: rivaroxaban), used for blood clots. It is taken by about 1.3 million people through Part D plans. The estimated cost is $6 billion.
- Januvia (generic name: sitagliptin), used for diabetes. It is taken by about 869,00 people through Part D plans. The estimated cost is $4.1 billion.
- Farxiga (generic name: dapagliflozin), used for diabetes, heart failure, and chronic kidney disease. It is taken by about 799,000 people through Part D plans. The estimated cost is almost $3.3 billion.
- Entresto (generic name: sacubitril/valsartan), used to treat heart failure. It is taken by 587,000 people through Part D plans. The estimated cost is $2.9 billion.
- Enbrel( generic name: etanercept), used for rheumatoid arthritis, psoriasis, and psoriatic arthritis. It is taken by 48,000 people through Part D plans. The estimated cost is $2.8 billion.
- Imbruvica (generic name: ibrutinib), used to treat some blood cancers. It is taken by about 20,000 people in Part D plans. The estimated cost is $2.7 billion.
- Stelara (generic name: ustekinumab), used to treat plaque psoriasis, psoriatic arthritis, or certain bowel conditions (Crohn’s disease, ulcerative colitis). It is used by about 22,000 people through Part D plans. The estimated cost is $2.6 billion.
- Fiasp; Fiasp FlexTouch; Fiasp PenFill; NovoLog; NovoLog FlexPen; NovoLog PenFill. These are forms of insulin used to treat diabetes. They are used by about 777,000 people through Part D plans. The estimated cost is $2.6 billion.
A vocal critic of Medicare drug negotiations, Joel White, president of the Council for Affordable Health Coverage, called the announcement of the 10 drugs selected for negotiation “a hollow victory lap.” A former Republican staffer on the House Ways and Means Committee, Mr. White aided with the development of the Medicare Part D plans and has kept tabs on the pharmacy programs since its launch in 2006.
“No one’s costs will go down now or for years because of this announcement” about Part D negotiations, Mr. White said in a statement.
According to its website, CAHC includes among its members the American Academy of Ophthalmology as well as some patient groups, drugmakers, such as Johnson & Johnson, and insurers and industry groups, such as the National Association of Manufacturers.
Separately, the influential Chamber of Commerce is making a strong push to at least delay the implementation of the Medicare Part D drug negotiations. On Aug. 28, the chamber released a letter sent to the Biden administration, raising concerns about a “rush” to implement the provisions of the Inflation Reduction Act.
The chamber also has filed suit to challenge the drug negotiation provisions of the Inflation Reduction Act, requesting that the court issue a preliminary injunction by Oct. 1, 2023.
Other pending legal challenges to direct Medicare drug negotiations include suits filed by Merck, Bristol-Myers Squibb, Johnson & Johnson, Boehringer Ingelheim, and AstraZeneca, according to an email from Pharmaceutical Research and Manufacturers of America. PhRMA also said it is a party to a case.
In addition, the three congressional Republicans with most direct influence over Medicare policy issued on Aug. 29 a joint statement outlining their objections to the planned negotiations on drug prices.
This drug-negotiation proposal is “an unworkable, legally dubious scheme that will lead to higher prices for new drugs coming to market, stifle the development of new cures, and destroy jobs,” said House Energy and Commerce Committee Chair Cathy McMorris Rodgers (R-Wash.), House Ways and Means Committee Chair Jason Smith (R-Mo.), and Senate Finance Committee Ranking Member Mike Crapo (R-Idaho).
Democrats were equally firm and vocal in their support of the negotiations. Senate Finance Chairman Ron Wyden (D-Ore.) issued a statement on Aug. 29 that said the release of the list of the 10 drugs selected for Medicare drug negotiations is part of a “seismic shift in the relationship between Big Pharma, the federal government, and seniors who are counting on lower prices.
“I will be following the negotiation process closely and will fight any attempt by Big Pharma to undo or undermine the progress that’s been made,” Mr. Wyden said.
In addition, AARP issued a statement of its continued support for Medicare drug negotiations.
“The No. 1 reason seniors skip or ration their prescriptions is because they can’t afford them. This must stop,” said AARP executive vice president and chief advocacy and engagement officer Nancy LeaMond in the statement. “The big drug companies and their allies continue suing to overturn the Medicare drug price negotiation program to keep up their price gouging. We can’t allow seniors to be Big Pharma’s cash machine anymore.”
A version of this article first appeared on Medscape.com.
CTE common among young athletes in largest brain donor study
Analysis of brain tissue from athletes who were exposed to RHIs and died before the age of 30 revealed neuropathological evidence of shrinkage of the brain and microscopic changes that indicate a breach of the blood-brain barrier. The case series also identified the first known American female athlete with CTE.
Nearly all of those with CTE had a mild form of the disease and 71% played only at the amateur level in youth, high school, or college sports.
“A lot of people think CTE is a result of high-level, professional play such as football, ice hockey, and boxing, but it can affect amateur athletes and can affect people at a young age,” lead author Ann McKee, MD, professor of neurology and pathology and director of the Chronic Traumatic Encephalopathy Center at Boston University, said in an interview.
The findings were published online in JAMA Neurology.
A rare look
Brain donation at younger ages is rare, so most of what is known about CTE comes from studies in older athletes.
“We’ve always known that young people could develop this disease early after just amateur high school, youth, and college exposure, but this is the largest study of donor brains at this age,” Dr. McKee said.
The case series included 152 brains of athletes who played contact sports, experienced RHIs, and died before age 30. The tissues are part of the Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE) Brain Bank and were donated between February 2008 and September 2022.
Researchers reviewed the donors’ medical records and conducted retrospective interviews with the donors’ next of kin to assess cognitive symptoms, mood disturbances, and neurobehavioral issues.
Donors died between the ages of 13 and 29 years, 92.8% were male and 73% were White. In 57.2% of the cases, suicide was the cause of death, with no difference between those with or without CTE.
CTE was neuropathologically diagnosed in 41.4% of athletes, using diagnostic criteria developed by the National Institute of Neurological Disorders and Stroke.
More than 95% had mild CTE. Diagnosis was associated with older age (mean difference, 3.92 years; P < .001) and significantly more years of exposure to contact sports (11.6 vs. 8.8 years).
Among those with CTE, 71.4% played amateur sports, including football (60.9%), soccer (17.2%), hockey (7.8%), and wrestling (7%).
The cohort includes the first known American female athlete with CTE. Recruiting female brain donors has always been a challenge, Dr. McKee said. In this study, females comprised about 7% of the entire cohort and tended to be younger and play fewer years of a sport, compared with their male counterparts. All of that could lower their risk for CTE, Dr. McKee said.
“We don’t have enough brain donations to make any comments about differences between the genders, but we’ve always known that women can develop CTE,” she said. “It’s been reported after domestic violence and in an autistic woman who was a headbanger, so it was just a matter of time before we found our first case.”
Early stage of CTE?
Neuropathological analysis revealed neuronal p-tau aggregates in all CTE cases, a hallmark of the disease.
Young athletes with CTE had significantly more ventricular dilatation, suggesting atrophy or shrinkage of the brain, and more cavum septum pellucidum.
“I was surprised that even at this very young age group we could see structural changes to the gross pathology,” Dr. McKee said.
Investigators also found evidence of perivascular macrophages in the deep white matter, a microscopic change that correlated with CTE and years of play and indicates a breach of the blood-brain barrier that could allow pro-inflammatory molecules to enter the brain, setting up a neuroinflammatory response.
“Neuroinflammation is a very early change after repetitive head impacts, as well as in CTE,” Dr. McKee said. “This may be one of the mechanisms by which the inflammation starts, meaning microvascular injury might be an integral part of the pathogenesis of CTE.”
A message for clinicians
All athletes had symptoms of mood and neurobehavioral dysfunction common in people with RHIs. There were no significant differences in those clinical symptoms based on CTE diagnosis, which is likely related to the retrospective nature of the clinical evaluations, Dr. McKee said.
While the study leaves many questions about CTE in younger athletes unanswered, there is a message for clinicians and for patients in the findings, she said.
For clinicians, it’s important to note that “this young population of amateur athletes can be very symptomatic, and in all likelihood, a lot of these symptoms are reversible with proper care and management,” Dr. McKee said.
“For individual athletes, it’s important to note that 58% of this cohort did not have CTE, so just because you have these symptoms is not an indication that you have a neurodegenerative disease,” she added.
The study was funded by Andlinger Foundation, the National Football League, Mac Parkman Foundation, National Operating Committee on Standards for Athletic Equipment, and the Nick and Lynn Buoniconti Foundation, World Wrestling Entertainment, Alzheimer’s Association, National Institutes of Health, Concussion Legacy Foundation, U.S. Department of Defense and the U.S. Department of Veterans Affairs. Dr. McKee is a member of the Mackey-White Health and Safety Committee of the National Football League Players Association and reported receiving grants from the NIH and Department of Veteran Affairs and other funding from the Buoniconti Foundation and Mac Parkman Foundation during the conduct of the study.
A version of this article appeared on Medscape.com.
Analysis of brain tissue from athletes who were exposed to RHIs and died before the age of 30 revealed neuropathological evidence of shrinkage of the brain and microscopic changes that indicate a breach of the blood-brain barrier. The case series also identified the first known American female athlete with CTE.
Nearly all of those with CTE had a mild form of the disease and 71% played only at the amateur level in youth, high school, or college sports.
“A lot of people think CTE is a result of high-level, professional play such as football, ice hockey, and boxing, but it can affect amateur athletes and can affect people at a young age,” lead author Ann McKee, MD, professor of neurology and pathology and director of the Chronic Traumatic Encephalopathy Center at Boston University, said in an interview.
The findings were published online in JAMA Neurology.
A rare look
Brain donation at younger ages is rare, so most of what is known about CTE comes from studies in older athletes.
“We’ve always known that young people could develop this disease early after just amateur high school, youth, and college exposure, but this is the largest study of donor brains at this age,” Dr. McKee said.
The case series included 152 brains of athletes who played contact sports, experienced RHIs, and died before age 30. The tissues are part of the Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE) Brain Bank and were donated between February 2008 and September 2022.
Researchers reviewed the donors’ medical records and conducted retrospective interviews with the donors’ next of kin to assess cognitive symptoms, mood disturbances, and neurobehavioral issues.
Donors died between the ages of 13 and 29 years, 92.8% were male and 73% were White. In 57.2% of the cases, suicide was the cause of death, with no difference between those with or without CTE.
CTE was neuropathologically diagnosed in 41.4% of athletes, using diagnostic criteria developed by the National Institute of Neurological Disorders and Stroke.
More than 95% had mild CTE. Diagnosis was associated with older age (mean difference, 3.92 years; P < .001) and significantly more years of exposure to contact sports (11.6 vs. 8.8 years).
Among those with CTE, 71.4% played amateur sports, including football (60.9%), soccer (17.2%), hockey (7.8%), and wrestling (7%).
The cohort includes the first known American female athlete with CTE. Recruiting female brain donors has always been a challenge, Dr. McKee said. In this study, females comprised about 7% of the entire cohort and tended to be younger and play fewer years of a sport, compared with their male counterparts. All of that could lower their risk for CTE, Dr. McKee said.
“We don’t have enough brain donations to make any comments about differences between the genders, but we’ve always known that women can develop CTE,” she said. “It’s been reported after domestic violence and in an autistic woman who was a headbanger, so it was just a matter of time before we found our first case.”
Early stage of CTE?
Neuropathological analysis revealed neuronal p-tau aggregates in all CTE cases, a hallmark of the disease.
Young athletes with CTE had significantly more ventricular dilatation, suggesting atrophy or shrinkage of the brain, and more cavum septum pellucidum.
“I was surprised that even at this very young age group we could see structural changes to the gross pathology,” Dr. McKee said.
Investigators also found evidence of perivascular macrophages in the deep white matter, a microscopic change that correlated with CTE and years of play and indicates a breach of the blood-brain barrier that could allow pro-inflammatory molecules to enter the brain, setting up a neuroinflammatory response.
“Neuroinflammation is a very early change after repetitive head impacts, as well as in CTE,” Dr. McKee said. “This may be one of the mechanisms by which the inflammation starts, meaning microvascular injury might be an integral part of the pathogenesis of CTE.”
A message for clinicians
All athletes had symptoms of mood and neurobehavioral dysfunction common in people with RHIs. There were no significant differences in those clinical symptoms based on CTE diagnosis, which is likely related to the retrospective nature of the clinical evaluations, Dr. McKee said.
While the study leaves many questions about CTE in younger athletes unanswered, there is a message for clinicians and for patients in the findings, she said.
For clinicians, it’s important to note that “this young population of amateur athletes can be very symptomatic, and in all likelihood, a lot of these symptoms are reversible with proper care and management,” Dr. McKee said.
“For individual athletes, it’s important to note that 58% of this cohort did not have CTE, so just because you have these symptoms is not an indication that you have a neurodegenerative disease,” she added.
The study was funded by Andlinger Foundation, the National Football League, Mac Parkman Foundation, National Operating Committee on Standards for Athletic Equipment, and the Nick and Lynn Buoniconti Foundation, World Wrestling Entertainment, Alzheimer’s Association, National Institutes of Health, Concussion Legacy Foundation, U.S. Department of Defense and the U.S. Department of Veterans Affairs. Dr. McKee is a member of the Mackey-White Health and Safety Committee of the National Football League Players Association and reported receiving grants from the NIH and Department of Veteran Affairs and other funding from the Buoniconti Foundation and Mac Parkman Foundation during the conduct of the study.
A version of this article appeared on Medscape.com.
Analysis of brain tissue from athletes who were exposed to RHIs and died before the age of 30 revealed neuropathological evidence of shrinkage of the brain and microscopic changes that indicate a breach of the blood-brain barrier. The case series also identified the first known American female athlete with CTE.
Nearly all of those with CTE had a mild form of the disease and 71% played only at the amateur level in youth, high school, or college sports.
“A lot of people think CTE is a result of high-level, professional play such as football, ice hockey, and boxing, but it can affect amateur athletes and can affect people at a young age,” lead author Ann McKee, MD, professor of neurology and pathology and director of the Chronic Traumatic Encephalopathy Center at Boston University, said in an interview.
The findings were published online in JAMA Neurology.
A rare look
Brain donation at younger ages is rare, so most of what is known about CTE comes from studies in older athletes.
“We’ve always known that young people could develop this disease early after just amateur high school, youth, and college exposure, but this is the largest study of donor brains at this age,” Dr. McKee said.
The case series included 152 brains of athletes who played contact sports, experienced RHIs, and died before age 30. The tissues are part of the Understanding Neurologic Injury and Traumatic Encephalopathy (UNITE) Brain Bank and were donated between February 2008 and September 2022.
Researchers reviewed the donors’ medical records and conducted retrospective interviews with the donors’ next of kin to assess cognitive symptoms, mood disturbances, and neurobehavioral issues.
Donors died between the ages of 13 and 29 years, 92.8% were male and 73% were White. In 57.2% of the cases, suicide was the cause of death, with no difference between those with or without CTE.
CTE was neuropathologically diagnosed in 41.4% of athletes, using diagnostic criteria developed by the National Institute of Neurological Disorders and Stroke.
More than 95% had mild CTE. Diagnosis was associated with older age (mean difference, 3.92 years; P < .001) and significantly more years of exposure to contact sports (11.6 vs. 8.8 years).
Among those with CTE, 71.4% played amateur sports, including football (60.9%), soccer (17.2%), hockey (7.8%), and wrestling (7%).
The cohort includes the first known American female athlete with CTE. Recruiting female brain donors has always been a challenge, Dr. McKee said. In this study, females comprised about 7% of the entire cohort and tended to be younger and play fewer years of a sport, compared with their male counterparts. All of that could lower their risk for CTE, Dr. McKee said.
“We don’t have enough brain donations to make any comments about differences between the genders, but we’ve always known that women can develop CTE,” she said. “It’s been reported after domestic violence and in an autistic woman who was a headbanger, so it was just a matter of time before we found our first case.”
Early stage of CTE?
Neuropathological analysis revealed neuronal p-tau aggregates in all CTE cases, a hallmark of the disease.
Young athletes with CTE had significantly more ventricular dilatation, suggesting atrophy or shrinkage of the brain, and more cavum septum pellucidum.
“I was surprised that even at this very young age group we could see structural changes to the gross pathology,” Dr. McKee said.
Investigators also found evidence of perivascular macrophages in the deep white matter, a microscopic change that correlated with CTE and years of play and indicates a breach of the blood-brain barrier that could allow pro-inflammatory molecules to enter the brain, setting up a neuroinflammatory response.
“Neuroinflammation is a very early change after repetitive head impacts, as well as in CTE,” Dr. McKee said. “This may be one of the mechanisms by which the inflammation starts, meaning microvascular injury might be an integral part of the pathogenesis of CTE.”
A message for clinicians
All athletes had symptoms of mood and neurobehavioral dysfunction common in people with RHIs. There were no significant differences in those clinical symptoms based on CTE diagnosis, which is likely related to the retrospective nature of the clinical evaluations, Dr. McKee said.
While the study leaves many questions about CTE in younger athletes unanswered, there is a message for clinicians and for patients in the findings, she said.
For clinicians, it’s important to note that “this young population of amateur athletes can be very symptomatic, and in all likelihood, a lot of these symptoms are reversible with proper care and management,” Dr. McKee said.
“For individual athletes, it’s important to note that 58% of this cohort did not have CTE, so just because you have these symptoms is not an indication that you have a neurodegenerative disease,” she added.
The study was funded by Andlinger Foundation, the National Football League, Mac Parkman Foundation, National Operating Committee on Standards for Athletic Equipment, and the Nick and Lynn Buoniconti Foundation, World Wrestling Entertainment, Alzheimer’s Association, National Institutes of Health, Concussion Legacy Foundation, U.S. Department of Defense and the U.S. Department of Veterans Affairs. Dr. McKee is a member of the Mackey-White Health and Safety Committee of the National Football League Players Association and reported receiving grants from the NIH and Department of Veteran Affairs and other funding from the Buoniconti Foundation and Mac Parkman Foundation during the conduct of the study.
A version of this article appeared on Medscape.com.
Severe COVID may cause long-term cellular changes: Study
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
FROM CELL
Cruel summer for medical students and Taylor Swift fans
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Number of people with long COVID could be vastly underestimated
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
FROM NEUROLOGY, NEUROIMMUNOLOGY & NEUROINFLAMMATION
AAP’s hearing test clinical update is the first since 2009
The update is the first since 2009.
The AAP’s clinical report was published online in Pediatrics.
Charles Bower, MD, with the department of otolaryngology at Arkansas Children’s Hospital in Little Rock, led the research team representing AAP’s Committee on Practice and Ambulatory Medicine, section on otolaryngology and head and neck surgery.
The report details how primary care clinicians can detect changes in hearing status by age.
Eliminating terms such as ‘failed’ or ‘impairment’
A key change in this report is that it no longer uses terms such as “loss,” “failed,” or “impairment,” “to reflect that children who are deaf or hard of hearing (D/HH) are equal, healthy, and whole,” the authors wrote.
The report’s recommendations are based on the literature and engagement with deaf and hard of hearing professionals and partner organizations, such as the National Association of the Deaf, working with the AAP Early Hearing Detection and Intervention program.
Birth to 5 a critical time
The authors noted that early medical support for hearing is especially important between birth and 5 years of age. That span is a critical time for brain and language development.
Parents and caregivers are often the first to notice a child’s inattention or erratic responses to sound, they wrote, and it’s important to address these concerns with a pediatrician even if the child has passed a newborn hearing test after birth.
Among recommendations in the update:
- All children should have an objective, evidence-based risk assessment for changes in hearing.
- Children at all ages should have prompt screening if there is clinical or caregiver concern about hearing.
- A child who screens positive for atypical hearing in one or both ears should be referred to an audiologist for diagnostic consultation and testing.
- Because standard testing for children with developmental or behavioral health conditions may be impossible or inaccurate, referral may be more appropriate to audiology for electrophysiological hearing testing using auditory brainstem response (ABR) with sedation.
- To prevent false negatives and to avoid delays in identification, access to language, and support, screening tests should not be repeated more than once before referral to audiology.
Additional recommendations
The report authors pointed out that genetic causes may affect hearing and may show up beyond the newborn period.
They wrote that congenital cytomegalovirus (cCMV) infection is the most common infectious cause of childhood sensorineural hearing change and accounts for 25% of deaf and hard of hearing children at age 4.
Meningitis and otitis media also are leading causes of a change in hearing.
Judith E.C. Lieu, MD, MSPH, professor, program director and vice-chair for education in the department of otolaryngology and head and neck surgery at Washington University in St. Louis, who was not part of the research team, said screening recommendations have not changed much in the update, but she highlighted some points.
She noted that tympanometry is not listed as a method of hearing screening in primary care.
“I agree that tympanogram is not a hearing screening. It is an adjunct to look at middle ear function, but that doesn’t necessarily mean it looks for hearing,” she said.
Dr. Lieu says she does take issue with the stated length of one of the tests in the paper. She said she is concerned that the pure-tone audiometry test for ages 4 through adolescence is listed as taking 30 minutes in a primary care setting. She said she worries that pediatricians will be put off by reading that it is a 30-minute test.
“Honestly, in my experience, it doesn’t take 30 minutes. Maybe 10 minutes,” she said. “I don’t know any pediatrician who could devote 30 minutes to one screening test.”
Development milestones have been adjusted
Also different in these recommendations are the developmental and speech milestones updated according to the most recent AAP information, Dr. Lieu said. Though the new milestones don’t change by much, they are important to note, she said, such as updated guidance on when to be concerned about speech delay.
She said she wished the guidance included more about hearing loss in older children.
The report authors stated that about 1 to 3 per 1,000 children have atypical hearing at birth and similar numbers become deaf or hard of hearing later in childhood.
But Dr. Lieu says that statistic may give the wrong impression about frequency of atypical hearing.
“Hearing loss increases during childhood,” she pointed out. “By the time they hit about age 18, about 15% of kids have some kind of hearing loss.”
“I don’t think it’s made clear to pediatricians that this is not 1 or 2 in a thousand children – this happens much more frequently,” she said.
The report authors and Dr. Lieu report no relevant financial relationships.
The update is the first since 2009.
The AAP’s clinical report was published online in Pediatrics.
Charles Bower, MD, with the department of otolaryngology at Arkansas Children’s Hospital in Little Rock, led the research team representing AAP’s Committee on Practice and Ambulatory Medicine, section on otolaryngology and head and neck surgery.
The report details how primary care clinicians can detect changes in hearing status by age.
Eliminating terms such as ‘failed’ or ‘impairment’
A key change in this report is that it no longer uses terms such as “loss,” “failed,” or “impairment,” “to reflect that children who are deaf or hard of hearing (D/HH) are equal, healthy, and whole,” the authors wrote.
The report’s recommendations are based on the literature and engagement with deaf and hard of hearing professionals and partner organizations, such as the National Association of the Deaf, working with the AAP Early Hearing Detection and Intervention program.
Birth to 5 a critical time
The authors noted that early medical support for hearing is especially important between birth and 5 years of age. That span is a critical time for brain and language development.
Parents and caregivers are often the first to notice a child’s inattention or erratic responses to sound, they wrote, and it’s important to address these concerns with a pediatrician even if the child has passed a newborn hearing test after birth.
Among recommendations in the update:
- All children should have an objective, evidence-based risk assessment for changes in hearing.
- Children at all ages should have prompt screening if there is clinical or caregiver concern about hearing.
- A child who screens positive for atypical hearing in one or both ears should be referred to an audiologist for diagnostic consultation and testing.
- Because standard testing for children with developmental or behavioral health conditions may be impossible or inaccurate, referral may be more appropriate to audiology for electrophysiological hearing testing using auditory brainstem response (ABR) with sedation.
- To prevent false negatives and to avoid delays in identification, access to language, and support, screening tests should not be repeated more than once before referral to audiology.
Additional recommendations
The report authors pointed out that genetic causes may affect hearing and may show up beyond the newborn period.
They wrote that congenital cytomegalovirus (cCMV) infection is the most common infectious cause of childhood sensorineural hearing change and accounts for 25% of deaf and hard of hearing children at age 4.
Meningitis and otitis media also are leading causes of a change in hearing.
Judith E.C. Lieu, MD, MSPH, professor, program director and vice-chair for education in the department of otolaryngology and head and neck surgery at Washington University in St. Louis, who was not part of the research team, said screening recommendations have not changed much in the update, but she highlighted some points.
She noted that tympanometry is not listed as a method of hearing screening in primary care.
“I agree that tympanogram is not a hearing screening. It is an adjunct to look at middle ear function, but that doesn’t necessarily mean it looks for hearing,” she said.
Dr. Lieu says she does take issue with the stated length of one of the tests in the paper. She said she is concerned that the pure-tone audiometry test for ages 4 through adolescence is listed as taking 30 minutes in a primary care setting. She said she worries that pediatricians will be put off by reading that it is a 30-minute test.
“Honestly, in my experience, it doesn’t take 30 minutes. Maybe 10 minutes,” she said. “I don’t know any pediatrician who could devote 30 minutes to one screening test.”
Development milestones have been adjusted
Also different in these recommendations are the developmental and speech milestones updated according to the most recent AAP information, Dr. Lieu said. Though the new milestones don’t change by much, they are important to note, she said, such as updated guidance on when to be concerned about speech delay.
She said she wished the guidance included more about hearing loss in older children.
The report authors stated that about 1 to 3 per 1,000 children have atypical hearing at birth and similar numbers become deaf or hard of hearing later in childhood.
But Dr. Lieu says that statistic may give the wrong impression about frequency of atypical hearing.
“Hearing loss increases during childhood,” she pointed out. “By the time they hit about age 18, about 15% of kids have some kind of hearing loss.”
“I don’t think it’s made clear to pediatricians that this is not 1 or 2 in a thousand children – this happens much more frequently,” she said.
The report authors and Dr. Lieu report no relevant financial relationships.
The update is the first since 2009.
The AAP’s clinical report was published online in Pediatrics.
Charles Bower, MD, with the department of otolaryngology at Arkansas Children’s Hospital in Little Rock, led the research team representing AAP’s Committee on Practice and Ambulatory Medicine, section on otolaryngology and head and neck surgery.
The report details how primary care clinicians can detect changes in hearing status by age.
Eliminating terms such as ‘failed’ or ‘impairment’
A key change in this report is that it no longer uses terms such as “loss,” “failed,” or “impairment,” “to reflect that children who are deaf or hard of hearing (D/HH) are equal, healthy, and whole,” the authors wrote.
The report’s recommendations are based on the literature and engagement with deaf and hard of hearing professionals and partner organizations, such as the National Association of the Deaf, working with the AAP Early Hearing Detection and Intervention program.
Birth to 5 a critical time
The authors noted that early medical support for hearing is especially important between birth and 5 years of age. That span is a critical time for brain and language development.
Parents and caregivers are often the first to notice a child’s inattention or erratic responses to sound, they wrote, and it’s important to address these concerns with a pediatrician even if the child has passed a newborn hearing test after birth.
Among recommendations in the update:
- All children should have an objective, evidence-based risk assessment for changes in hearing.
- Children at all ages should have prompt screening if there is clinical or caregiver concern about hearing.
- A child who screens positive for atypical hearing in one or both ears should be referred to an audiologist for diagnostic consultation and testing.
- Because standard testing for children with developmental or behavioral health conditions may be impossible or inaccurate, referral may be more appropriate to audiology for electrophysiological hearing testing using auditory brainstem response (ABR) with sedation.
- To prevent false negatives and to avoid delays in identification, access to language, and support, screening tests should not be repeated more than once before referral to audiology.
Additional recommendations
The report authors pointed out that genetic causes may affect hearing and may show up beyond the newborn period.
They wrote that congenital cytomegalovirus (cCMV) infection is the most common infectious cause of childhood sensorineural hearing change and accounts for 25% of deaf and hard of hearing children at age 4.
Meningitis and otitis media also are leading causes of a change in hearing.
Judith E.C. Lieu, MD, MSPH, professor, program director and vice-chair for education in the department of otolaryngology and head and neck surgery at Washington University in St. Louis, who was not part of the research team, said screening recommendations have not changed much in the update, but she highlighted some points.
She noted that tympanometry is not listed as a method of hearing screening in primary care.
“I agree that tympanogram is not a hearing screening. It is an adjunct to look at middle ear function, but that doesn’t necessarily mean it looks for hearing,” she said.
Dr. Lieu says she does take issue with the stated length of one of the tests in the paper. She said she is concerned that the pure-tone audiometry test for ages 4 through adolescence is listed as taking 30 minutes in a primary care setting. She said she worries that pediatricians will be put off by reading that it is a 30-minute test.
“Honestly, in my experience, it doesn’t take 30 minutes. Maybe 10 minutes,” she said. “I don’t know any pediatrician who could devote 30 minutes to one screening test.”
Development milestones have been adjusted
Also different in these recommendations are the developmental and speech milestones updated according to the most recent AAP information, Dr. Lieu said. Though the new milestones don’t change by much, they are important to note, she said, such as updated guidance on when to be concerned about speech delay.
She said she wished the guidance included more about hearing loss in older children.
The report authors stated that about 1 to 3 per 1,000 children have atypical hearing at birth and similar numbers become deaf or hard of hearing later in childhood.
But Dr. Lieu says that statistic may give the wrong impression about frequency of atypical hearing.
“Hearing loss increases during childhood,” she pointed out. “By the time they hit about age 18, about 15% of kids have some kind of hearing loss.”
“I don’t think it’s made clear to pediatricians that this is not 1 or 2 in a thousand children – this happens much more frequently,” she said.
The report authors and Dr. Lieu report no relevant financial relationships.
FROM PEDIATRICS
National Practitioner Data Bank should go public, group says
arguing that extra public scrutiny could pressure state medical boards to be more aggressive watchdogs.
Public Citizen’s report includes an analysis of how frequently medical boards sanctioned physicians in 2019, 2020, and 2021. These sanctions include license revocations, suspensions, voluntary surrenders of licenses, and limitations on practice while under investigation.
The report used data from the National Practitioner Data Bank (NPDB), a federal repository of reports about state licensure, discipline, and certification actions as well as medical malpractice payments. The database is closed to the public, but hospitals, malpractice insurers, and investigators can query it.
According to Public Citizen’s calculations, states most likely to take serious disciplinary action against physicians were:
- Michigan: 1.74 serious disciplinary actions per 1,000 physicians per year
- Ohio: 1.61
- North Dakota: 1.60
- Colorado: 1.55
- Arizona: 1.53
- The states least likely to do so were:
- Nevada: 0.24 serious disciplinary actions per 1,000 physicians per year
- New Hampshire: 0.25
- Georgia: 0.27
- Indiana: 0.28
- Nebraska: 0.32
- California, the largest U.S. state by both population and number of physicians, landed near the middle, ranking 27th with a rate of 0.83 serious actions per 1,000 physicians, Public Citizen said.
“There is no evidence that physicians in any state are, overall, more or less likely to be incompetent or miscreant than the physicians in any other state,” said Robert Oshel, PhD, a former NPDB associate director for research and an author of the report.
The differences instead reflect variations in boards’ enforcement of medical practice laws, domination of licensing boards by physicians, and inadequate budgets, he noted.
Public Citizen said Congress should change federal law to let members of the public get information from the NPDB to do a background check on physicians whom they are considering seeing or are already seeing. This would not only help individuals but also would spur state licensing boards to do their own checks with the NPDB, the group said.
“If licensing boards routinely queried the NPDB, they would not be faulted by the public and state legislators for not knowing about malpractice payments or disciplinary actions affecting their licensees and therefore not taking reasonable actions concerning their licensees found to have poor records,” the report said.
Questioning NPDB access for consumers
Michelle Mello, JD, PhD, a professor of law and health policy at Stanford (Calif.) University, has studied the current applications of the NPDB. In 2019, she published an article in The New England Journal of Medicine examining changes in practice patterns for clinicians who faced multiple malpractice claims.
Dr. Mello questioned what benefit consumers would get from direct access to the NPDB’s information.
“It provides almost no context for the information it reports, making it even harder for patients to make sense of what they see there,” Dr. Mello said in an interview.
Hospitals are already required to routinely query the NPDB. This legal requirement should be expanded to include licensing boards, which the report called “the last line of defense for the public from incompetent and miscreant physicians,” Public Citizen said.
“Ideally, this amendment should include free continuous query access by medical boards for all their licensees,” the report said. “In the absence of any action by Congress, individual state legislatures should require their licensing boards to query all their licensees or enroll in continuous query, as a few states already do.”
The Federation of State Medical Boards agreed with some of the other suggestions Public Citizen offered in the report. The two concur on the need for increased funding to state medical boards to ensure that they have adequate resources and staffing to fulfill their duties, FSMB said in a statement.
But FSMB disagreed with Public Citizens’ approach to ranking boards, saying it could mislead. The report lacks context about how boards’ funding and authority vary, Humayun Chaudhry, DO, FSMB’s chief executive officer, said. He also questioned the decision to focus only on serious disciplinary actions.
“The Public Citizen report does not take into account the wide range of disciplinary steps boards can take such as letters of reprimand or fines, which are often enough to stop problem behaviors – preempting further problems in the future,” Dr. Chaudhry said.
D.C. gets worst rating
The District of Columbia earned the worst mark in the Public Citizen ranking, holding the 51st spot, the same place it held in the group’s similar ranking on actions taken in the 2017-2019 period. There were 0.19 serious disciplinary actions per 1,000 physicians a year in Washington, Public Citizen said.
In an email to this news organization, Dr. Oshel said that the Public Citizen analysis focused on the number of licensed physicians in each state and D.C. that can be obtained and compared reliably. It avoided using the term “practicing physicians” owing in part to doubts about the reliability of these counts, he said.
As many as 20% of physicians nationwide are focused primarily on work outside of clinical care, Dr. Oshel estimated. In D.C., perhaps 40% of physicians may fall into this category. Of the more than 13,700 physicians licensed in D.C., there may be only about 8,126 actively practicing, according to Dr. Oshel.
But even using that lower estimate of practicing physicians would only raise D.C.’s ranking to 46, signaling a need for stepped-up enforcement, Dr. Oshel said.
“[Whether it’s] 46th or 51st, both are bad,” Dr. Oshel said.
A version of this article first appeared on Medscape.com.
arguing that extra public scrutiny could pressure state medical boards to be more aggressive watchdogs.
Public Citizen’s report includes an analysis of how frequently medical boards sanctioned physicians in 2019, 2020, and 2021. These sanctions include license revocations, suspensions, voluntary surrenders of licenses, and limitations on practice while under investigation.
The report used data from the National Practitioner Data Bank (NPDB), a federal repository of reports about state licensure, discipline, and certification actions as well as medical malpractice payments. The database is closed to the public, but hospitals, malpractice insurers, and investigators can query it.
According to Public Citizen’s calculations, states most likely to take serious disciplinary action against physicians were:
- Michigan: 1.74 serious disciplinary actions per 1,000 physicians per year
- Ohio: 1.61
- North Dakota: 1.60
- Colorado: 1.55
- Arizona: 1.53
- The states least likely to do so were:
- Nevada: 0.24 serious disciplinary actions per 1,000 physicians per year
- New Hampshire: 0.25
- Georgia: 0.27
- Indiana: 0.28
- Nebraska: 0.32
- California, the largest U.S. state by both population and number of physicians, landed near the middle, ranking 27th with a rate of 0.83 serious actions per 1,000 physicians, Public Citizen said.
“There is no evidence that physicians in any state are, overall, more or less likely to be incompetent or miscreant than the physicians in any other state,” said Robert Oshel, PhD, a former NPDB associate director for research and an author of the report.
The differences instead reflect variations in boards’ enforcement of medical practice laws, domination of licensing boards by physicians, and inadequate budgets, he noted.
Public Citizen said Congress should change federal law to let members of the public get information from the NPDB to do a background check on physicians whom they are considering seeing or are already seeing. This would not only help individuals but also would spur state licensing boards to do their own checks with the NPDB, the group said.
“If licensing boards routinely queried the NPDB, they would not be faulted by the public and state legislators for not knowing about malpractice payments or disciplinary actions affecting their licensees and therefore not taking reasonable actions concerning their licensees found to have poor records,” the report said.
Questioning NPDB access for consumers
Michelle Mello, JD, PhD, a professor of law and health policy at Stanford (Calif.) University, has studied the current applications of the NPDB. In 2019, she published an article in The New England Journal of Medicine examining changes in practice patterns for clinicians who faced multiple malpractice claims.
Dr. Mello questioned what benefit consumers would get from direct access to the NPDB’s information.
“It provides almost no context for the information it reports, making it even harder for patients to make sense of what they see there,” Dr. Mello said in an interview.
Hospitals are already required to routinely query the NPDB. This legal requirement should be expanded to include licensing boards, which the report called “the last line of defense for the public from incompetent and miscreant physicians,” Public Citizen said.
“Ideally, this amendment should include free continuous query access by medical boards for all their licensees,” the report said. “In the absence of any action by Congress, individual state legislatures should require their licensing boards to query all their licensees or enroll in continuous query, as a few states already do.”
The Federation of State Medical Boards agreed with some of the other suggestions Public Citizen offered in the report. The two concur on the need for increased funding to state medical boards to ensure that they have adequate resources and staffing to fulfill their duties, FSMB said in a statement.
But FSMB disagreed with Public Citizens’ approach to ranking boards, saying it could mislead. The report lacks context about how boards’ funding and authority vary, Humayun Chaudhry, DO, FSMB’s chief executive officer, said. He also questioned the decision to focus only on serious disciplinary actions.
“The Public Citizen report does not take into account the wide range of disciplinary steps boards can take such as letters of reprimand or fines, which are often enough to stop problem behaviors – preempting further problems in the future,” Dr. Chaudhry said.
D.C. gets worst rating
The District of Columbia earned the worst mark in the Public Citizen ranking, holding the 51st spot, the same place it held in the group’s similar ranking on actions taken in the 2017-2019 period. There were 0.19 serious disciplinary actions per 1,000 physicians a year in Washington, Public Citizen said.
In an email to this news organization, Dr. Oshel said that the Public Citizen analysis focused on the number of licensed physicians in each state and D.C. that can be obtained and compared reliably. It avoided using the term “practicing physicians” owing in part to doubts about the reliability of these counts, he said.
As many as 20% of physicians nationwide are focused primarily on work outside of clinical care, Dr. Oshel estimated. In D.C., perhaps 40% of physicians may fall into this category. Of the more than 13,700 physicians licensed in D.C., there may be only about 8,126 actively practicing, according to Dr. Oshel.
But even using that lower estimate of practicing physicians would only raise D.C.’s ranking to 46, signaling a need for stepped-up enforcement, Dr. Oshel said.
“[Whether it’s] 46th or 51st, both are bad,” Dr. Oshel said.
A version of this article first appeared on Medscape.com.
arguing that extra public scrutiny could pressure state medical boards to be more aggressive watchdogs.
Public Citizen’s report includes an analysis of how frequently medical boards sanctioned physicians in 2019, 2020, and 2021. These sanctions include license revocations, suspensions, voluntary surrenders of licenses, and limitations on practice while under investigation.
The report used data from the National Practitioner Data Bank (NPDB), a federal repository of reports about state licensure, discipline, and certification actions as well as medical malpractice payments. The database is closed to the public, but hospitals, malpractice insurers, and investigators can query it.
According to Public Citizen’s calculations, states most likely to take serious disciplinary action against physicians were:
- Michigan: 1.74 serious disciplinary actions per 1,000 physicians per year
- Ohio: 1.61
- North Dakota: 1.60
- Colorado: 1.55
- Arizona: 1.53
- The states least likely to do so were:
- Nevada: 0.24 serious disciplinary actions per 1,000 physicians per year
- New Hampshire: 0.25
- Georgia: 0.27
- Indiana: 0.28
- Nebraska: 0.32
- California, the largest U.S. state by both population and number of physicians, landed near the middle, ranking 27th with a rate of 0.83 serious actions per 1,000 physicians, Public Citizen said.
“There is no evidence that physicians in any state are, overall, more or less likely to be incompetent or miscreant than the physicians in any other state,” said Robert Oshel, PhD, a former NPDB associate director for research and an author of the report.
The differences instead reflect variations in boards’ enforcement of medical practice laws, domination of licensing boards by physicians, and inadequate budgets, he noted.
Public Citizen said Congress should change federal law to let members of the public get information from the NPDB to do a background check on physicians whom they are considering seeing or are already seeing. This would not only help individuals but also would spur state licensing boards to do their own checks with the NPDB, the group said.
“If licensing boards routinely queried the NPDB, they would not be faulted by the public and state legislators for not knowing about malpractice payments or disciplinary actions affecting their licensees and therefore not taking reasonable actions concerning their licensees found to have poor records,” the report said.
Questioning NPDB access for consumers
Michelle Mello, JD, PhD, a professor of law and health policy at Stanford (Calif.) University, has studied the current applications of the NPDB. In 2019, she published an article in The New England Journal of Medicine examining changes in practice patterns for clinicians who faced multiple malpractice claims.
Dr. Mello questioned what benefit consumers would get from direct access to the NPDB’s information.
“It provides almost no context for the information it reports, making it even harder for patients to make sense of what they see there,” Dr. Mello said in an interview.
Hospitals are already required to routinely query the NPDB. This legal requirement should be expanded to include licensing boards, which the report called “the last line of defense for the public from incompetent and miscreant physicians,” Public Citizen said.
“Ideally, this amendment should include free continuous query access by medical boards for all their licensees,” the report said. “In the absence of any action by Congress, individual state legislatures should require their licensing boards to query all their licensees or enroll in continuous query, as a few states already do.”
The Federation of State Medical Boards agreed with some of the other suggestions Public Citizen offered in the report. The two concur on the need for increased funding to state medical boards to ensure that they have adequate resources and staffing to fulfill their duties, FSMB said in a statement.
But FSMB disagreed with Public Citizens’ approach to ranking boards, saying it could mislead. The report lacks context about how boards’ funding and authority vary, Humayun Chaudhry, DO, FSMB’s chief executive officer, said. He also questioned the decision to focus only on serious disciplinary actions.
“The Public Citizen report does not take into account the wide range of disciplinary steps boards can take such as letters of reprimand or fines, which are often enough to stop problem behaviors – preempting further problems in the future,” Dr. Chaudhry said.
D.C. gets worst rating
The District of Columbia earned the worst mark in the Public Citizen ranking, holding the 51st spot, the same place it held in the group’s similar ranking on actions taken in the 2017-2019 period. There were 0.19 serious disciplinary actions per 1,000 physicians a year in Washington, Public Citizen said.
In an email to this news organization, Dr. Oshel said that the Public Citizen analysis focused on the number of licensed physicians in each state and D.C. that can be obtained and compared reliably. It avoided using the term “practicing physicians” owing in part to doubts about the reliability of these counts, he said.
As many as 20% of physicians nationwide are focused primarily on work outside of clinical care, Dr. Oshel estimated. In D.C., perhaps 40% of physicians may fall into this category. Of the more than 13,700 physicians licensed in D.C., there may be only about 8,126 actively practicing, according to Dr. Oshel.
But even using that lower estimate of practicing physicians would only raise D.C.’s ranking to 46, signaling a need for stepped-up enforcement, Dr. Oshel said.
“[Whether it’s] 46th or 51st, both are bad,” Dr. Oshel said.
A version of this article first appeared on Medscape.com.
New COVID strain may evade vaccines, alarming health officials
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
First guidelines developed for childhood eosinophilic GI disorders beyond eosinophilic esophagitis
The limited scope and depth of existing literature on childhood eosinophilic gastrointestinal disorders (EGIDs) beyond eosinophilic esophagitis (EoE) spurred an international group of researchers and clinicians to develop the first clinical practice guidelines for diagnosing and treating these rare conditions.
They were developed jointly by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition.
Non-EoE EGIDs are rare chronic inflammatory disorders of the gastrointestinal tract, estimated at less than 200,000 cases annually in the United States, with unknown long-term consequences, Glenn Furuta, MD, professor of pediatrics at the University of Colorado at Denver and section head of gastroenterology at Children’s Hospital Colorado, both in Aurora, said in an interview
“There are many unmet needs. Research has been limited and has not progressed at the pace we want it to,” added Dr. Furuta, who is corresponding author of the guidelines.
The guidelines were published online in the Journal of Pediatric Gastroenterology & Nutrition, by lead author Alexandra Papadopoulou, MD, division of gastroenterology and hepatology, first department of pediatrics, University of Athens, and Children’s Hospital Agia Sofia, also in Athens, and colleagues.
With these, we provide guidance for clinicians to better understand the conditions and also how to diagnose and initiate care for patients with these rare diseases, said Dr. Furuta.
Difficult-to-diagnose conditions
Guideline development involved a working group of 26 pediatric gastroenterologists, adult gastroenterologists, allergists/immunologists, and pathologists from 16 countries across five continents. The consensus document includes 34 statements based on available evidence and 41 recommendations based on expert opinion and best clinical practices. In cases where the supporting evidence was weak but agreement was strong, the authors issued conditional recommendations.
The guidelines subdivide the non-EoE EGIDs according to inflammation location: eosinophilic gastritis, eosinophilic duodenitis (EoD), eosinophilic colitis, and eosinophilic enteritis. The latter can be further subdivided into EoD, eosinophilic jejunitis, and eosinophilic ileitis.
Non-EoE EGIDs are hard to diagnose because symptoms are relatively nonspecific and may include abdominal pain, vomiting, diarrhea, and bloody stools, all of which could have any number of underlying causes, Dr. Furuta said.
If you are treating a patient who is not getting better with such symptoms as persisting infections, acid-related problems, significant bleeding leading to anemia, intestinal perforation or obstruction, or low serum protein leading to swelling, then you should think that something else is going on that requires more of an evaluation, Dr. Furuta noted.
Patients with personal or family histories of eosinophilic or allergic disease should raise greater suspicion, Dr. Furuta said. “The next step requires an endoscopy and biopsy.”
Awareness of non-EoE EGIDs has been higher among pediatric gastroenterologists than among those treating adult disease because pediatric gastroenterologists have always obtained biopsies of the intestinal tract, Dr. Furuta noted.
The guidelines recommend that diagnosis of non-EoE EGIDs in children and adolescents must include signs or symptoms of gastrointestinal dysfunction, dense eosinophilic infiltrates found in mucosal or full-thickness biopsies above organ-specific threshold values included in the document, and absence of other diseases associated with GI mucosal eosinophilic inflammation.
Individualized treatment
The authors noted that the strength of recommendations varies with the often-modest availability of randomized controlled trial data on treatment efficacy.
For example, they recommended that systemic steroids be considered to induce remission but only conditionally recommend topical steroids. They conditionally recommend consideration of empiric elimination diets and conditionally recommend against using food allergy testing to guide diet.
The choice of treatment should be individualized on the basis of the affected GI segment, severity of the disease, patient characteristics, and family resources and capabilities, the authors wrote.
“We’ve provided guidance on how to care for patients based on the consensus of experts who have the necessary experience and knowledge base,” Dr. Furuta said. “Our ability to say: ‘Here are the established treatments,’ is lacking, though. We need research studies to verify that our recommended approaches are indeed correct.”
The authors conditionally recommended that treatment goals include achieving symptom resolution, improving gross endoscopic and histologic abnormalities, promoting normal childhood growth and development, and preventing disease complications.
No pediatric study has determined the natural history of non-EoE EGIDs, and no study of maintenance therapy has been conducted, the authors noted.
For this reason, they conditionally recommended that the clinical decision to continue therapy should be discussed with patients and their parents/caregivers, and those discussions include the benefits and risk of long-term treatment, its cost, and its impact on health-related quality of life.
A starting point for patient management
In a comment, Vincent Mukkada, MD, professor of pediatrics at the University of Cincinnati and an attending physician in gastroenterology, hepatology, and nutrition at Cincinnati Children’s Hospital and Medical Center, observed that, though improved awareness among pediatric gastroenterologists may account for some of the increase in GI eosinophil disease, the incidence is also likely growing.
“We’re looking for them much more,” said Dr. Mukkada.
“But I also think they’re increasing, just like all other atopic diseases. We’re not sure why,” he added.
“The hope is that these guidelines will allow nonsubspecialized gastroenterologists and allergists feel comfortable to at least start on the journey of managing these patients. And, for pediatricians who learn that their patient has received a non-EoE EGID diagnosis, they can go to the summary figures in this one document and very quickly get an overview of the disease and its course,” Dr. Mukkada said.
Guideline development was funded by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology and Nutrition. The authors and Dr. Mukkada reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The limited scope and depth of existing literature on childhood eosinophilic gastrointestinal disorders (EGIDs) beyond eosinophilic esophagitis (EoE) spurred an international group of researchers and clinicians to develop the first clinical practice guidelines for diagnosing and treating these rare conditions.
They were developed jointly by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition.
Non-EoE EGIDs are rare chronic inflammatory disorders of the gastrointestinal tract, estimated at less than 200,000 cases annually in the United States, with unknown long-term consequences, Glenn Furuta, MD, professor of pediatrics at the University of Colorado at Denver and section head of gastroenterology at Children’s Hospital Colorado, both in Aurora, said in an interview
“There are many unmet needs. Research has been limited and has not progressed at the pace we want it to,” added Dr. Furuta, who is corresponding author of the guidelines.
The guidelines were published online in the Journal of Pediatric Gastroenterology & Nutrition, by lead author Alexandra Papadopoulou, MD, division of gastroenterology and hepatology, first department of pediatrics, University of Athens, and Children’s Hospital Agia Sofia, also in Athens, and colleagues.
With these, we provide guidance for clinicians to better understand the conditions and also how to diagnose and initiate care for patients with these rare diseases, said Dr. Furuta.
Difficult-to-diagnose conditions
Guideline development involved a working group of 26 pediatric gastroenterologists, adult gastroenterologists, allergists/immunologists, and pathologists from 16 countries across five continents. The consensus document includes 34 statements based on available evidence and 41 recommendations based on expert opinion and best clinical practices. In cases where the supporting evidence was weak but agreement was strong, the authors issued conditional recommendations.
The guidelines subdivide the non-EoE EGIDs according to inflammation location: eosinophilic gastritis, eosinophilic duodenitis (EoD), eosinophilic colitis, and eosinophilic enteritis. The latter can be further subdivided into EoD, eosinophilic jejunitis, and eosinophilic ileitis.
Non-EoE EGIDs are hard to diagnose because symptoms are relatively nonspecific and may include abdominal pain, vomiting, diarrhea, and bloody stools, all of which could have any number of underlying causes, Dr. Furuta said.
If you are treating a patient who is not getting better with such symptoms as persisting infections, acid-related problems, significant bleeding leading to anemia, intestinal perforation or obstruction, or low serum protein leading to swelling, then you should think that something else is going on that requires more of an evaluation, Dr. Furuta noted.
Patients with personal or family histories of eosinophilic or allergic disease should raise greater suspicion, Dr. Furuta said. “The next step requires an endoscopy and biopsy.”
Awareness of non-EoE EGIDs has been higher among pediatric gastroenterologists than among those treating adult disease because pediatric gastroenterologists have always obtained biopsies of the intestinal tract, Dr. Furuta noted.
The guidelines recommend that diagnosis of non-EoE EGIDs in children and adolescents must include signs or symptoms of gastrointestinal dysfunction, dense eosinophilic infiltrates found in mucosal or full-thickness biopsies above organ-specific threshold values included in the document, and absence of other diseases associated with GI mucosal eosinophilic inflammation.
Individualized treatment
The authors noted that the strength of recommendations varies with the often-modest availability of randomized controlled trial data on treatment efficacy.
For example, they recommended that systemic steroids be considered to induce remission but only conditionally recommend topical steroids. They conditionally recommend consideration of empiric elimination diets and conditionally recommend against using food allergy testing to guide diet.
The choice of treatment should be individualized on the basis of the affected GI segment, severity of the disease, patient characteristics, and family resources and capabilities, the authors wrote.
“We’ve provided guidance on how to care for patients based on the consensus of experts who have the necessary experience and knowledge base,” Dr. Furuta said. “Our ability to say: ‘Here are the established treatments,’ is lacking, though. We need research studies to verify that our recommended approaches are indeed correct.”
The authors conditionally recommended that treatment goals include achieving symptom resolution, improving gross endoscopic and histologic abnormalities, promoting normal childhood growth and development, and preventing disease complications.
No pediatric study has determined the natural history of non-EoE EGIDs, and no study of maintenance therapy has been conducted, the authors noted.
For this reason, they conditionally recommended that the clinical decision to continue therapy should be discussed with patients and their parents/caregivers, and those discussions include the benefits and risk of long-term treatment, its cost, and its impact on health-related quality of life.
A starting point for patient management
In a comment, Vincent Mukkada, MD, professor of pediatrics at the University of Cincinnati and an attending physician in gastroenterology, hepatology, and nutrition at Cincinnati Children’s Hospital and Medical Center, observed that, though improved awareness among pediatric gastroenterologists may account for some of the increase in GI eosinophil disease, the incidence is also likely growing.
“We’re looking for them much more,” said Dr. Mukkada.
“But I also think they’re increasing, just like all other atopic diseases. We’re not sure why,” he added.
“The hope is that these guidelines will allow nonsubspecialized gastroenterologists and allergists feel comfortable to at least start on the journey of managing these patients. And, for pediatricians who learn that their patient has received a non-EoE EGID diagnosis, they can go to the summary figures in this one document and very quickly get an overview of the disease and its course,” Dr. Mukkada said.
Guideline development was funded by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology and Nutrition. The authors and Dr. Mukkada reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The limited scope and depth of existing literature on childhood eosinophilic gastrointestinal disorders (EGIDs) beyond eosinophilic esophagitis (EoE) spurred an international group of researchers and clinicians to develop the first clinical practice guidelines for diagnosing and treating these rare conditions.
They were developed jointly by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition.
Non-EoE EGIDs are rare chronic inflammatory disorders of the gastrointestinal tract, estimated at less than 200,000 cases annually in the United States, with unknown long-term consequences, Glenn Furuta, MD, professor of pediatrics at the University of Colorado at Denver and section head of gastroenterology at Children’s Hospital Colorado, both in Aurora, said in an interview
“There are many unmet needs. Research has been limited and has not progressed at the pace we want it to,” added Dr. Furuta, who is corresponding author of the guidelines.
The guidelines were published online in the Journal of Pediatric Gastroenterology & Nutrition, by lead author Alexandra Papadopoulou, MD, division of gastroenterology and hepatology, first department of pediatrics, University of Athens, and Children’s Hospital Agia Sofia, also in Athens, and colleagues.
With these, we provide guidance for clinicians to better understand the conditions and also how to diagnose and initiate care for patients with these rare diseases, said Dr. Furuta.
Difficult-to-diagnose conditions
Guideline development involved a working group of 26 pediatric gastroenterologists, adult gastroenterologists, allergists/immunologists, and pathologists from 16 countries across five continents. The consensus document includes 34 statements based on available evidence and 41 recommendations based on expert opinion and best clinical practices. In cases where the supporting evidence was weak but agreement was strong, the authors issued conditional recommendations.
The guidelines subdivide the non-EoE EGIDs according to inflammation location: eosinophilic gastritis, eosinophilic duodenitis (EoD), eosinophilic colitis, and eosinophilic enteritis. The latter can be further subdivided into EoD, eosinophilic jejunitis, and eosinophilic ileitis.
Non-EoE EGIDs are hard to diagnose because symptoms are relatively nonspecific and may include abdominal pain, vomiting, diarrhea, and bloody stools, all of which could have any number of underlying causes, Dr. Furuta said.
If you are treating a patient who is not getting better with such symptoms as persisting infections, acid-related problems, significant bleeding leading to anemia, intestinal perforation or obstruction, or low serum protein leading to swelling, then you should think that something else is going on that requires more of an evaluation, Dr. Furuta noted.
Patients with personal or family histories of eosinophilic or allergic disease should raise greater suspicion, Dr. Furuta said. “The next step requires an endoscopy and biopsy.”
Awareness of non-EoE EGIDs has been higher among pediatric gastroenterologists than among those treating adult disease because pediatric gastroenterologists have always obtained biopsies of the intestinal tract, Dr. Furuta noted.
The guidelines recommend that diagnosis of non-EoE EGIDs in children and adolescents must include signs or symptoms of gastrointestinal dysfunction, dense eosinophilic infiltrates found in mucosal or full-thickness biopsies above organ-specific threshold values included in the document, and absence of other diseases associated with GI mucosal eosinophilic inflammation.
Individualized treatment
The authors noted that the strength of recommendations varies with the often-modest availability of randomized controlled trial data on treatment efficacy.
For example, they recommended that systemic steroids be considered to induce remission but only conditionally recommend topical steroids. They conditionally recommend consideration of empiric elimination diets and conditionally recommend against using food allergy testing to guide diet.
The choice of treatment should be individualized on the basis of the affected GI segment, severity of the disease, patient characteristics, and family resources and capabilities, the authors wrote.
“We’ve provided guidance on how to care for patients based on the consensus of experts who have the necessary experience and knowledge base,” Dr. Furuta said. “Our ability to say: ‘Here are the established treatments,’ is lacking, though. We need research studies to verify that our recommended approaches are indeed correct.”
The authors conditionally recommended that treatment goals include achieving symptom resolution, improving gross endoscopic and histologic abnormalities, promoting normal childhood growth and development, and preventing disease complications.
No pediatric study has determined the natural history of non-EoE EGIDs, and no study of maintenance therapy has been conducted, the authors noted.
For this reason, they conditionally recommended that the clinical decision to continue therapy should be discussed with patients and their parents/caregivers, and those discussions include the benefits and risk of long-term treatment, its cost, and its impact on health-related quality of life.
A starting point for patient management
In a comment, Vincent Mukkada, MD, professor of pediatrics at the University of Cincinnati and an attending physician in gastroenterology, hepatology, and nutrition at Cincinnati Children’s Hospital and Medical Center, observed that, though improved awareness among pediatric gastroenterologists may account for some of the increase in GI eosinophil disease, the incidence is also likely growing.
“We’re looking for them much more,” said Dr. Mukkada.
“But I also think they’re increasing, just like all other atopic diseases. We’re not sure why,” he added.
“The hope is that these guidelines will allow nonsubspecialized gastroenterologists and allergists feel comfortable to at least start on the journey of managing these patients. And, for pediatricians who learn that their patient has received a non-EoE EGID diagnosis, they can go to the summary figures in this one document and very quickly get an overview of the disease and its course,” Dr. Mukkada said.
Guideline development was funded by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology and Nutrition. The authors and Dr. Mukkada reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF PEDIATRIC GASTROENTEROLOGY & NUTRITION