User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Full-time, part-time, FTE: Know the differences
The wholesale to them. While rules vary from state to state, some generalizations can be made.

Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.

Alcohol problems linked to legal performance-enhancement products
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.

In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.
In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
Adolescent alcohol use among boys was prospectively associated with use of legal performance-enhancing substances in young adulthood, based on prospective cohort data from more than 12,000 individuals, wrote Kyle T. Ganson, PhD, MSW, of the University of Toronto, and colleagues.
In addition, legal use of performance-enhancing substances (PES) among young men was associated with increased risk of alcohol use problems.
Although previous studies have shown a range of adverse effects associated with the use of anabolic-androgenic steroid derivatives (defined as illegal PES), the possible adverse effects of legal PES (defined in this report as protein powders, creatine monohydrate, dehydroepiandrostenedione, and amino acids) have not been well studied, the researchers wrote.
In a study published in Pediatrics, the researchers reviewed data from 12,133 young adults aged 18-26 years who were part of the National Longitudinal Study of Adolescent to Adult Health from 1994 to 2008.
Overall, 16% of young men and 1% of young women reported using legal PES in the past year. Among men, legal PES use was prospectively associated with increased risk of a range of alcohol-related problem behaviors including binge drinking (adjusted odds ratio, 1.35), injurious and risky behaviors (aOR, 1.78), legal problems (aOR, 1.52), reduced activities and socializing (aOR, 1.91), and problems with emotional or physical health (aOR, 1.44).
Legal PES use among young adult women was associated with an increased risk of emotional or physical health problems (aOR, 3.00).
Adolescent impact
Between adolescence and young adulthood (an average of 7 years’ follow-up), alcohol use was prospectively associated with legal PES use in young men (OR, 1.39), but neither cigarette smoking nor marijuana use in adolescence was associated with later use of legal PES. Among young women, no type of adolescent substance use was prospectively associated with later use of legal PES.
“To date, legal PES have not been largely considered as part of the spectrum of substances used among adolescents, have not been subject to the same regulatory scrutiny as other substances known to be linked to subsequent substance use and are freely available over the counter to adolescents,” Dr. Ganson and associates noted.
“Clearly, the robust reciprocal temporal relationship between substance use and legal PES suggests that each may serve as a gateway for the other,” they wrote.
The study findings were limited by several factors including the inability to identify outcomes associated with variable PES components, incomplete data collection on several drinking-related risk behaviors, and inability to analyze prospective use of illegal or other substances associated with use of legal PES, the researchers wrote.
However, “these results provide further evidence in support of the gateway theory and prospective health risk behaviors associated with legal PES and substance use,” they wrote.
The data may inform policy on the additional regulation of legal PES use in minors. In the meantime, “it is important for medical providers and clinicians to assess problematic alcohol use and drinking-related risk behaviors among young adult men who have previously used legal PES,” Dr. Ganson and associates concluded.
Challenges to clinicians
An important point to recognize is that PES is a misleading term, Steven Cuff, MD, of the Ohio State University, Columbus, and Michele LaBotz, MD, of Tufts University, Boston, wrote in an accompanying editorial. “Most legal supplements marketed for athletic performance enhancement are ineffective at increasing muscle mass or athletic performance beyond what can be achieved through appropriate nutrition and training,” they emphasized. The current study findings suggest that “legal PES should be integrated into the gateway hypothesis regarding patterns and progression of substance use through adolescence and early adulthood,” and support discouragement of any PES use among adolescents and young adults.
Even legal PES can be dangerous because of the lack of oversight of dietary supplements by the Food and Drug Administration. “There is widespread evidence that many over-the-counter dietary supplements lack stated ingredients, contain unlabeled ingredients (including potential allergens), or are contaminated with impurities or illegal or dangerous substances, such as steroids and stimulants,” the editorialists emphasized.
In addition, the association found in the study between muscle dysphoria and both PES use and substance use disorders, notably alcohol-related morbidity, highlights the need for a proactive approach by pediatricians to minimize the risk, they noted.
“For pediatricians uncomfortable with initiating discussions on PES use with their patients, an American Academy of Pediatrics–supported role-play simulation is available,” they concluded.
The study is important because “PES use is ubiquitous among adolescents and young adults,” Dr. LaBotz said in an interview. “Although it is widely believed that PES use serves as a likely ‘gateway’ to use of anabolic steroids and other substances, this is one of the very few studies that explores this relationship. Their findings that alcohol use appears to correlate with subsequent use of PES, and that PES use appears to correlate with future alcohol-related issues, suggest that this is not a simple linear progression of problematic behavior.”
Dr. LaBotz added that she was not surprised by the study findings, and emphasized that pediatric health care providers should be aware of the association between PES and alcohol use. “PES screening should be incorporated into screening done for alcohol and other substance use. This appears to be particularly true for athletes and other subpopulations who are at higher risk for problematic alcohol use.”
She said much of PES use is driven by the desire by young men for a muscular appearance, but more research is needed on young women. “In the past, this was a goal primarily associated with males, but females have become increasingly interested in achieving muscularity as well, which suggests an increasing risk of PES use among females as compared to earlier reports. We need updated data on patterns, prevalence and consequences of PES use in females.”
In addition, “although preparticipation physical examination forms include screening questions for PES use among athletes, further information is needed on how to incorporate PES into substance use screening that is performed in a general pediatric population, such as including athletes and nonathletes,” Dr. LaBotz said.
The study was supported by the National Institutes of Health and by grants to one of the coauthors from the Pediatric Scientist Development Program funded by the American Academy of Pediatrics and the American Pediatric Society, as well as the American Heart Association Career Development Award. The researchers had no financial conflicts to disclose. Dr. Cuff and Dr. LaBotz had no financial conflicts to disclose.
SOURCE: Ganson KT et al. Pediatrics. 2020 Sep. doi: 10.1542/peds.2020-0409.
FROM PEDIATRICS
COVID-19 vaccine hesitancy ‘somewhat understandable,’ expert says
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Flexibility, innovation key to practice management during pandemic
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.

“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.
“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.
“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
FROM AAP 2020
COVID-19 and the superspreaders: Teens
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.

According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Pediatric fractures shift during pandemic
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New lupus classification criteria perform well in children, young adults
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
FROM ARTHRITIS CARE & RESEARCH
Teen affective disorders raise risk for midlife acute MI
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.

The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
FROM ESC CONGRESS 2020
One measure of child COVID-19 may be trending downward
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
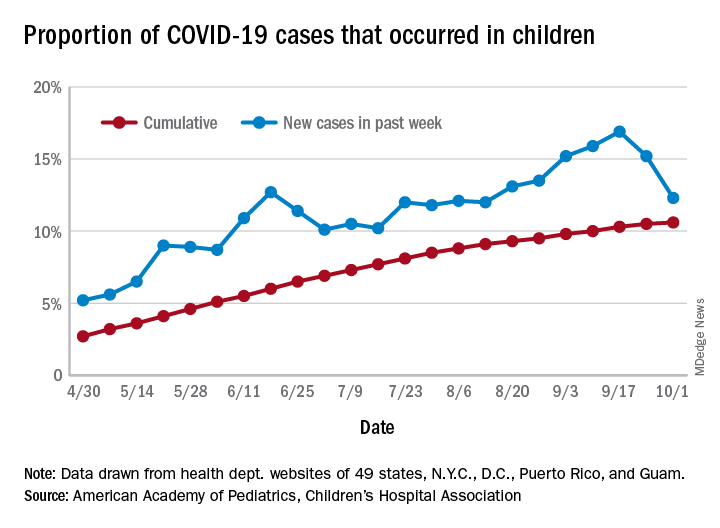
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
CMS gives hospitals 14 weeks to start daily COVID, flu reports
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.