User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
COVID spikes exacerbate health worker shortages in Rocky Mountains, Great Plains
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
In Montana, pandemic-induced staffing shortages have shuttered a clinic in the state’s capital, led a northwestern regional hospital to ask employees exposed to COVID-19 to continue to work and emptied a health department 400 miles to the east.
“Just one more person out and we wouldn’t be able to keep the surgeries going,” said Dr. Shelly Harkins, MD, chief medical officer of St. Peter’s Health in Helena, a city of roughly 32,000 where cases continue to spread. “When the virus is just all around you, it’s almost impossible to not be deemed a contact at some point. One case can take out a whole team of people in a blink of an eye.”
In North Dakota, where cases per resident are growing faster than any other state, hospitals may once again curtail elective surgeries and possibly seek government aid to hire more nurses if the situation gets worse, North Dakota Hospital Association President Tim Blasl said.
“How long can we run at this rate with the workforce that we have?” Blasl said. “You can have all the licensed beds you want, but if you don’t have anybody to staff those beds, it doesn’t do you any good.”
The northern Rocky Mountains, Great Plains and Upper Midwest are seeing the highest surge of COVID-19 cases in the nation, as some residents have ignored recommendations for curtailing the virus, such as wearing masks and avoiding large gatherings. Montana, Idaho, Utah, Wyoming, North Dakota, South Dakota, Nebraska, Iowa, and Wisconsin have recently ranked among the top 10 U.S. states in confirmed cases per 100,000 residents over a 7-day period, according to an analysis by the New York Times.
Such coronavirus infections – and the quarantines that occur because of them – are exacerbating the health care worker shortage that existed in these states well before the pandemic. Unlike in the nation’s metropolitan hubs, these outbreaks are scattered across hundreds of miles. And even in these states’ biggest cities, the ranks of medical professionals are in short supply. Specialists and registered nurses are sometimes harder to track down than ventilators, N95 masks or hospital beds. Without enough care providers, patients may not be able to get the medical attention they need.
Hospitals have asked staffers to cover extra shifts and learn new skills. They have brought in temporary workers from other parts of the country and transferred some patients to less-crowded hospitals. But, at St. Peter’s Health, if the hospital’s one kidney doctor gets sick or is told to quarantine, Dr. Harkins doesn’t expect to find a backup.
“We make a point to not have excessive staff because we have an obligation to keep the cost of health care down for a community – we just don’t have a lot of slack in our rope,” Dr. Harkins said. “What we don’t account for is a mass exodus of staff for 14 days.”
Some hospitals are already at patient capacity or are nearly there. That’s not just because of the growing number of COVID-19 patients. Elective surgeries have resumed, and medical emergencies don’t pause for a pandemic.
Some Montana hospitals formed agreements with local affiliates early in the pandemic to share staff if one came up short. But now that the disease is spreading fast – and widely – the hope is that their needs don’t peak all at once.
Montana state officials keep a list of primarily in-state volunteer workers ready to travel to towns with shortages of contact tracers, nurses and more. But during a press conference on Oct. 15, Democratic Gov. Steve Bullock said the state had exhausted that database, and its nationwide request for National Guard medical staffing hadn’t brought in new workers.
“If you are a registered nurse, licensed practical nurse, paramedic, EMT, CNA or contact tracer, and are able to join our workforce, please do consider joining our team,” Gov. Bullock said.
This month, Kalispell Regional Medical Center in northwestern Montana even stopped quarantining COVID-exposed staff who remain asymptomatic, a change allowed by Centers for Disease Control and Prevention guidelines for health facilities facing staffing shortages.
“That’s very telling for what staffing is going through right now,” said Andrea Lueck, a registered nurse at the center. “We’re so tight that employees are called off of quarantine.”
Financial pressure early in the pandemic led the hospital to furlough staff, but it had to bring most of them back to work because it needs those bodies more than ever. The regional hub is based in Flathead County, which has recorded the state’s second-highest number of active COVID-19 cases.
Mellody Sharpton, a hospital spokesperson, said hospital workers who are exposed to someone infected with the virus are tested within three to five days and monitored for symptoms. The hospital is also pulling in new workers, with 25 traveling health professionals on hand and another 25 temporary ones on the way.
But Ms. Sharpton said the best way to conserve the hospital’s workforce is to stop the disease surge in the community.
Earlier in the pandemic, Central Montana Medical Center in Lewistown, a town of fewer than 6,000, experienced an exodus of part-time workers or those close to retirement who decided their jobs weren’t worth the risk. The facility recently secured two traveling workers, but both backed out because they couldn’t find housing. And, so far, roughly 40 of the hospital’s 322 employees have missed work for reasons connected to COVID-19.
“We’re at a critical staffing shortage and have been since the beginning of COVID,” said Joanie Slaybaugh, Central Montana Medical Center’s director of human resources. “We’re small enough, everybody feels an obligation to protect themselves and to protect each other. But it doesn’t take much to take out our staff.”
Roosevelt County, where roughly 11,000 live on the northeastern edge of Montana, had one of the nation’s highest rates of new cases as of Oct. 15. But by the end of the month, the county health department will lose half of its registered nurses as one person is about to retire and another was hired through a grant that’s ending. That leaves only one registered nurse aside from its director, Patty Presser. The health department already had to close earlier during the pandemic because of COVID exposure and not enough staffers to cover the gap. Now, if Ms. Presser can’t find nurse replacements in time, she hopes volunteers will step in, though she added they typically stay for only a few weeks.
“I need someone to do immunizations for my community, and you don’t become an immunization nurse in 14 days,” she said. “We don’t have the workforce here to deal with this virus, not even right now, and then I’m going to have my best two people go.”
Back in Helena, Dr. Harkins said St. Peter’s Health had to close a specialty outpatient clinic that treats chronic diseases for two weeks at the end of September because the entire staff had to quarantine.
Now the hospital is considering having doctors take turns spending a week working from home, so that if another wave of quarantines hits in the hospital, at least one untainted person can be brought back to work. But that won’t help for some specialties, like the hospital’s sole kidney doctor.
Every time Dr. Harkins’ phone rings, she said, she takes a breath and hopes it’s not another case that will force a whole division to close.
“Because I think immediately of the hundreds of people that need that service and won’t have it for 14 days,” she said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Evaluating the impact of new pediatric brain tumor classifications
and that will have far-reaching implications for how clinicians diagnose and manage these rare and often debilitating malignancies, a leading European researcher reported at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
“These pediatric neuronal/glioneuronal tumors are quite heterogeneous in terms of the number of different tumors and subclasses of tumors going into these groups, but they have some molecular features in common,” said David T.W. Jones, PhD, of Hopp Children’s Cancer Center in Heidelberg, Germany. “Together they represent quite a sizable portion of all childhood brain tumors, so it’s important to recognize and understand them.”
Dr. Jones noted that updated WHO classifications would add six new descriptions to the category of mixed glioneuronal tumors and one to the list of neuronal tumors. A working group of the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy, known as cIMPACT-NOW, has recommended the expanded classifications for central nervous system tumors.
“The molecular understandings of pediatric neuro-glial tumors are critical in their management,” Roger Packer, MD, senior vice president of the Center for Neuroscience and Behavioral Health at Children’s National in Washington, said in an interview, especially as treatments targeting specific molecular structures emerge. “For those with tumors not amenable to safe, total resections, there’s little evidence that radiation or chemotherapy are effective, and molecular-targeted therapy, guided by the molecular genetic composition, increases the safe use of these new agents.”
Dr. Jones noted that “as a minimum” molecular diagnostics of pediatric low-grade glioneuronal and neuronal tumors should include a BRAF gene mutation and fusion status, as well as FGFR1 mutation plus fusion or rearrangement status.
“Ideally,” he added, “it should also have a broader copy number profile, whether that’s based on sequencing or SNP arrays or DNA methylation rate, a global DNA methylation profile to get those global molecular patterns, and also wider gene and RNA sequence to pick up some of those rarer alterations that may not be covered by targeted BRAF and FGFR1 mutations.”
The updated tumor classification will evolve to include novel tumor classes, as well as links or overlaps between the tumor classes and their characteristic underlying kinetic alterations, he noted. “Some of these profiling measures will actually be required to generate a fully WHO-compatible pathological diagnosis,” Dr. Jones said.
“This group of tumors are now just better molecularly characterized than it was 5 years ago, so in the last few years we’ve really made tremendous progress in understanding what alterations are driving some of these tumors,” he said. “That knowledge is now providing a basis for improved diagnosis and also for starting to plan more targeted treatment strategies.”
But, he added, there’s still a lot to learn about how these oncogenic mechanisms drive tumor pathogenesis. “What is the clinical costs when we really start getting down into defining these distinct molecular groups?” he said. “What are their different responses to treatment depending on different levels, where the MEKi [mitogen-activated protein kinase inhibitor] pathway might be activated and, for example, response to treatment of different subclasses of one tumor?”
Large, collaborative clinical studies will be needed to get those answers, he said.
“There are certainly some therapeutic opportunities arising in this group of tumors now, but in order to really translate those into a clinical benefit, we’re really going to need some careful planning of international studies because of the relative rarity of some of these groups,” he said.
Dr. Jones has no relevant financial relationships to disclose.
and that will have far-reaching implications for how clinicians diagnose and manage these rare and often debilitating malignancies, a leading European researcher reported at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
“These pediatric neuronal/glioneuronal tumors are quite heterogeneous in terms of the number of different tumors and subclasses of tumors going into these groups, but they have some molecular features in common,” said David T.W. Jones, PhD, of Hopp Children’s Cancer Center in Heidelberg, Germany. “Together they represent quite a sizable portion of all childhood brain tumors, so it’s important to recognize and understand them.”
Dr. Jones noted that updated WHO classifications would add six new descriptions to the category of mixed glioneuronal tumors and one to the list of neuronal tumors. A working group of the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy, known as cIMPACT-NOW, has recommended the expanded classifications for central nervous system tumors.
“The molecular understandings of pediatric neuro-glial tumors are critical in their management,” Roger Packer, MD, senior vice president of the Center for Neuroscience and Behavioral Health at Children’s National in Washington, said in an interview, especially as treatments targeting specific molecular structures emerge. “For those with tumors not amenable to safe, total resections, there’s little evidence that radiation or chemotherapy are effective, and molecular-targeted therapy, guided by the molecular genetic composition, increases the safe use of these new agents.”
Dr. Jones noted that “as a minimum” molecular diagnostics of pediatric low-grade glioneuronal and neuronal tumors should include a BRAF gene mutation and fusion status, as well as FGFR1 mutation plus fusion or rearrangement status.
“Ideally,” he added, “it should also have a broader copy number profile, whether that’s based on sequencing or SNP arrays or DNA methylation rate, a global DNA methylation profile to get those global molecular patterns, and also wider gene and RNA sequence to pick up some of those rarer alterations that may not be covered by targeted BRAF and FGFR1 mutations.”
The updated tumor classification will evolve to include novel tumor classes, as well as links or overlaps between the tumor classes and their characteristic underlying kinetic alterations, he noted. “Some of these profiling measures will actually be required to generate a fully WHO-compatible pathological diagnosis,” Dr. Jones said.
“This group of tumors are now just better molecularly characterized than it was 5 years ago, so in the last few years we’ve really made tremendous progress in understanding what alterations are driving some of these tumors,” he said. “That knowledge is now providing a basis for improved diagnosis and also for starting to plan more targeted treatment strategies.”
But, he added, there’s still a lot to learn about how these oncogenic mechanisms drive tumor pathogenesis. “What is the clinical costs when we really start getting down into defining these distinct molecular groups?” he said. “What are their different responses to treatment depending on different levels, where the MEKi [mitogen-activated protein kinase inhibitor] pathway might be activated and, for example, response to treatment of different subclasses of one tumor?”
Large, collaborative clinical studies will be needed to get those answers, he said.
“There are certainly some therapeutic opportunities arising in this group of tumors now, but in order to really translate those into a clinical benefit, we’re really going to need some careful planning of international studies because of the relative rarity of some of these groups,” he said.
Dr. Jones has no relevant financial relationships to disclose.
and that will have far-reaching implications for how clinicians diagnose and manage these rare and often debilitating malignancies, a leading European researcher reported at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year.
“These pediatric neuronal/glioneuronal tumors are quite heterogeneous in terms of the number of different tumors and subclasses of tumors going into these groups, but they have some molecular features in common,” said David T.W. Jones, PhD, of Hopp Children’s Cancer Center in Heidelberg, Germany. “Together they represent quite a sizable portion of all childhood brain tumors, so it’s important to recognize and understand them.”
Dr. Jones noted that updated WHO classifications would add six new descriptions to the category of mixed glioneuronal tumors and one to the list of neuronal tumors. A working group of the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy, known as cIMPACT-NOW, has recommended the expanded classifications for central nervous system tumors.
“The molecular understandings of pediatric neuro-glial tumors are critical in their management,” Roger Packer, MD, senior vice president of the Center for Neuroscience and Behavioral Health at Children’s National in Washington, said in an interview, especially as treatments targeting specific molecular structures emerge. “For those with tumors not amenable to safe, total resections, there’s little evidence that radiation or chemotherapy are effective, and molecular-targeted therapy, guided by the molecular genetic composition, increases the safe use of these new agents.”
Dr. Jones noted that “as a minimum” molecular diagnostics of pediatric low-grade glioneuronal and neuronal tumors should include a BRAF gene mutation and fusion status, as well as FGFR1 mutation plus fusion or rearrangement status.
“Ideally,” he added, “it should also have a broader copy number profile, whether that’s based on sequencing or SNP arrays or DNA methylation rate, a global DNA methylation profile to get those global molecular patterns, and also wider gene and RNA sequence to pick up some of those rarer alterations that may not be covered by targeted BRAF and FGFR1 mutations.”
The updated tumor classification will evolve to include novel tumor classes, as well as links or overlaps between the tumor classes and their characteristic underlying kinetic alterations, he noted. “Some of these profiling measures will actually be required to generate a fully WHO-compatible pathological diagnosis,” Dr. Jones said.
“This group of tumors are now just better molecularly characterized than it was 5 years ago, so in the last few years we’ve really made tremendous progress in understanding what alterations are driving some of these tumors,” he said. “That knowledge is now providing a basis for improved diagnosis and also for starting to plan more targeted treatment strategies.”
But, he added, there’s still a lot to learn about how these oncogenic mechanisms drive tumor pathogenesis. “What is the clinical costs when we really start getting down into defining these distinct molecular groups?” he said. “What are their different responses to treatment depending on different levels, where the MEKi [mitogen-activated protein kinase inhibitor] pathway might be activated and, for example, response to treatment of different subclasses of one tumor?”
Large, collaborative clinical studies will be needed to get those answers, he said.
“There are certainly some therapeutic opportunities arising in this group of tumors now, but in order to really translate those into a clinical benefit, we’re really going to need some careful planning of international studies because of the relative rarity of some of these groups,” he said.
Dr. Jones has no relevant financial relationships to disclose.
FROM CNS-ICNA 2020
Acute flaccid myelitis: More likely missed than diagnosed
and that can result in loss of valuable time to admit patients and begin treatment to get ahead of the virus that may cause the disease.
At the 2020 CNS-ICNA Conjoint Meeting, held virtually this year, Leslie H. Hayes, MD, of Boston Children’s Hospital presented findings of a retrospective case series from 13 institutions in the United States and Canada that determined 78% of patients eventually found to have AFM were initially misdiagnosed. About 62% were given an alternate diagnosis or multiple diagnoses, and 60% did not get a referral for further care or evaluation. The study included 175 children aged 18 years and younger when symptoms first appeared from 2014 to 2018 and who met the Centers for Disease Control and Prevention case definition of AFM.
“As it becomes more evident that AFM outbreaks are driven by enterovirus infections, treatments targeting the viral infection are likely to be most effective very early in the course of disease, necessitating a precise and early diagnosis,” Dr. Hayes said. “Thus awareness is needed to help recognize the signs of symptoms of AFM, particularly among frontline clinicians.”
One reason for misdiagnosis is that AFM has features that overlap with other neuroinflammatory disorders, she said. “In many cases the patients are misdiagnosed as having benign or self-limiting processes that would not prompt the same monitoring and level of care.”
Numbness and prodromal illnesses were associated with misdiagnosis, she said, but otherwise most presenting symptoms were similar between the misdiagnosed and correctly diagnosed patients.
Neurologic disorders with similar features to AFM that the study identified were Guillain-Barré syndrome, spinal cord pathologies such as transverse myelitis, brain pathologies including acute disseminating encephalomyelitis, acute inclusion body encephalitis and stroke, and other neuroinflammatory conditions.
“There were also many patients diagnosed as having processes that in many cases would not prompt inpatient admission, would not involve neurology consultation, and would not be treated in a similar fashion to AFM,” Dr. Hayes said.
Those diagnoses included plexopathy, neuritis, Bell’s palsy, meningoencephalitis, nonspecific infectious illness or parainfectious autoimmune disease, or musculoskeletal problems including toxic or transient synovitis, myositis, fracture or sprain, or torticollis.
“We identified preceding illness and numbness as two features associated with misdiagnosis,” Dr. Hayes said.
“We evaluated illness severity by evaluating the need for invasive and noninvasive ventilation and found that, while not statistically significant, misdiagnosed patients had a trend toward higher need for such respiratory support,” she noted. Specifically, 31.6% of misdiagnosed patients required noninvasive ventilation versus 15.8% of promptly diagnosed patients (P = .06).
Dr. Hayes characterized the rates of ICU admissions between the two groups as not statistically significant: 52.5% and 36.8% for the misdiagnosed and promptly diagnosed groups, respectively (P = .1).
Both groups of patients received intravenous immunoglobulin in similar rates (77.9% and 81.6%, respectively, P = .63), but the misdiagnosed patients were much more likely to receive steroids, 68.2% versus 44.7% (P = .008). That’s likely because steroids are the standard treatment for the neuroinflammatory disorders that they were misdiagnosed with, Dr. Hayes said.
Timely diagnosis and treatment was more of an issue for the misdiagnosed patients; their diagnosis was made on average 5 days after the onset of symptoms versus 3 days (P < .001). “We found that time to treatment, particularly time to IVIg, was significantly longer in the misdiagnosed group,” Dr. Hayes said, at 5 versus 2 days (P < .001).
Dr. Hayes has no relevant financial relationships to disclose.
and that can result in loss of valuable time to admit patients and begin treatment to get ahead of the virus that may cause the disease.
At the 2020 CNS-ICNA Conjoint Meeting, held virtually this year, Leslie H. Hayes, MD, of Boston Children’s Hospital presented findings of a retrospective case series from 13 institutions in the United States and Canada that determined 78% of patients eventually found to have AFM were initially misdiagnosed. About 62% were given an alternate diagnosis or multiple diagnoses, and 60% did not get a referral for further care or evaluation. The study included 175 children aged 18 years and younger when symptoms first appeared from 2014 to 2018 and who met the Centers for Disease Control and Prevention case definition of AFM.
“As it becomes more evident that AFM outbreaks are driven by enterovirus infections, treatments targeting the viral infection are likely to be most effective very early in the course of disease, necessitating a precise and early diagnosis,” Dr. Hayes said. “Thus awareness is needed to help recognize the signs of symptoms of AFM, particularly among frontline clinicians.”
One reason for misdiagnosis is that AFM has features that overlap with other neuroinflammatory disorders, she said. “In many cases the patients are misdiagnosed as having benign or self-limiting processes that would not prompt the same monitoring and level of care.”
Numbness and prodromal illnesses were associated with misdiagnosis, she said, but otherwise most presenting symptoms were similar between the misdiagnosed and correctly diagnosed patients.
Neurologic disorders with similar features to AFM that the study identified were Guillain-Barré syndrome, spinal cord pathologies such as transverse myelitis, brain pathologies including acute disseminating encephalomyelitis, acute inclusion body encephalitis and stroke, and other neuroinflammatory conditions.
“There were also many patients diagnosed as having processes that in many cases would not prompt inpatient admission, would not involve neurology consultation, and would not be treated in a similar fashion to AFM,” Dr. Hayes said.
Those diagnoses included plexopathy, neuritis, Bell’s palsy, meningoencephalitis, nonspecific infectious illness or parainfectious autoimmune disease, or musculoskeletal problems including toxic or transient synovitis, myositis, fracture or sprain, or torticollis.
“We identified preceding illness and numbness as two features associated with misdiagnosis,” Dr. Hayes said.
“We evaluated illness severity by evaluating the need for invasive and noninvasive ventilation and found that, while not statistically significant, misdiagnosed patients had a trend toward higher need for such respiratory support,” she noted. Specifically, 31.6% of misdiagnosed patients required noninvasive ventilation versus 15.8% of promptly diagnosed patients (P = .06).
Dr. Hayes characterized the rates of ICU admissions between the two groups as not statistically significant: 52.5% and 36.8% for the misdiagnosed and promptly diagnosed groups, respectively (P = .1).
Both groups of patients received intravenous immunoglobulin in similar rates (77.9% and 81.6%, respectively, P = .63), but the misdiagnosed patients were much more likely to receive steroids, 68.2% versus 44.7% (P = .008). That’s likely because steroids are the standard treatment for the neuroinflammatory disorders that they were misdiagnosed with, Dr. Hayes said.
Timely diagnosis and treatment was more of an issue for the misdiagnosed patients; their diagnosis was made on average 5 days after the onset of symptoms versus 3 days (P < .001). “We found that time to treatment, particularly time to IVIg, was significantly longer in the misdiagnosed group,” Dr. Hayes said, at 5 versus 2 days (P < .001).
Dr. Hayes has no relevant financial relationships to disclose.
and that can result in loss of valuable time to admit patients and begin treatment to get ahead of the virus that may cause the disease.
At the 2020 CNS-ICNA Conjoint Meeting, held virtually this year, Leslie H. Hayes, MD, of Boston Children’s Hospital presented findings of a retrospective case series from 13 institutions in the United States and Canada that determined 78% of patients eventually found to have AFM were initially misdiagnosed. About 62% were given an alternate diagnosis or multiple diagnoses, and 60% did not get a referral for further care or evaluation. The study included 175 children aged 18 years and younger when symptoms first appeared from 2014 to 2018 and who met the Centers for Disease Control and Prevention case definition of AFM.
“As it becomes more evident that AFM outbreaks are driven by enterovirus infections, treatments targeting the viral infection are likely to be most effective very early in the course of disease, necessitating a precise and early diagnosis,” Dr. Hayes said. “Thus awareness is needed to help recognize the signs of symptoms of AFM, particularly among frontline clinicians.”
One reason for misdiagnosis is that AFM has features that overlap with other neuroinflammatory disorders, she said. “In many cases the patients are misdiagnosed as having benign or self-limiting processes that would not prompt the same monitoring and level of care.”
Numbness and prodromal illnesses were associated with misdiagnosis, she said, but otherwise most presenting symptoms were similar between the misdiagnosed and correctly diagnosed patients.
Neurologic disorders with similar features to AFM that the study identified were Guillain-Barré syndrome, spinal cord pathologies such as transverse myelitis, brain pathologies including acute disseminating encephalomyelitis, acute inclusion body encephalitis and stroke, and other neuroinflammatory conditions.
“There were also many patients diagnosed as having processes that in many cases would not prompt inpatient admission, would not involve neurology consultation, and would not be treated in a similar fashion to AFM,” Dr. Hayes said.
Those diagnoses included plexopathy, neuritis, Bell’s palsy, meningoencephalitis, nonspecific infectious illness or parainfectious autoimmune disease, or musculoskeletal problems including toxic or transient synovitis, myositis, fracture or sprain, or torticollis.
“We identified preceding illness and numbness as two features associated with misdiagnosis,” Dr. Hayes said.
“We evaluated illness severity by evaluating the need for invasive and noninvasive ventilation and found that, while not statistically significant, misdiagnosed patients had a trend toward higher need for such respiratory support,” she noted. Specifically, 31.6% of misdiagnosed patients required noninvasive ventilation versus 15.8% of promptly diagnosed patients (P = .06).
Dr. Hayes characterized the rates of ICU admissions between the two groups as not statistically significant: 52.5% and 36.8% for the misdiagnosed and promptly diagnosed groups, respectively (P = .1).
Both groups of patients received intravenous immunoglobulin in similar rates (77.9% and 81.6%, respectively, P = .63), but the misdiagnosed patients were much more likely to receive steroids, 68.2% versus 44.7% (P = .008). That’s likely because steroids are the standard treatment for the neuroinflammatory disorders that they were misdiagnosed with, Dr. Hayes said.
Timely diagnosis and treatment was more of an issue for the misdiagnosed patients; their diagnosis was made on average 5 days after the onset of symptoms versus 3 days (P < .001). “We found that time to treatment, particularly time to IVIg, was significantly longer in the misdiagnosed group,” Dr. Hayes said, at 5 versus 2 days (P < .001).
Dr. Hayes has no relevant financial relationships to disclose.
FROM CNS-ICNA 2020
Around the world in 24 hours: A snapshot of COVID’s global havoc
Some medical societies feature sessions at their annual meetings that feel like they’re 24 hours long, yet few have the courage to schedule a session that actually runs all day and all night. But the five societies sponsoring the IDWeek conference had that courage. The first 24 hours of the meeting was devoted to the most pressing infectious-disease crisis of the last 100 years: the COVID-19 pandemic. They called it “COVID-19: Chasing the Sun.”
Dr. Fauci predicts a vaccine answer in mid-November
In the first segment, at 10 am Eastern time, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases and the nation’s top infectious-disease expert, began the day by noting that five of the six companies the US invested in to develop a vaccine are conducting phase 3 trials. He said, “we feel confident that we will have an answer likely in mid-November to the beginning of December as to whether we have a safe and effective vaccine”. He added he was “cautiously optimistic” that “we will have a safe and effective vaccine by the end of the year, which we can begin to distribute as we go into 2021.” He highlighted the COVID-19 Prevention Network website for more information on the trials.
Glaring racial health disparities in U.S.
Some of the most glaring health disparities surrounding COVID-19 in the United States were described by Carlos del Rio, MD, professor of medicine at Emory University in Atlanta, Georgia. He pointed out that while white people have about 23 cases per 10,000 population, Blacks have about 62 cases per 10,000, and Latinos have 73 cases per 10,000. While whites don’t see a huge jump in cases until age 80, he said, “among Blacks and Latinos you start seeing that huge increase at a younger age. In fact, starting at age 20, you start seeing a major, major change.”
COVID-19 diagnostics
Audrey Odom John, MD, PhD, chief of pediatric infectious diseases at Children’s Hospital of Philadelphia, is working on a new way of diagnosing COVID-19 infection in children by testing their breath. “We’re really taking advantage of a fundamental biological fact, which is that people stink,” she said. Breath shows the health of the body as a whole, “and it’s easy to see how breath volatiles might arise from a respiratory infection.” Testing breath is easy and inexpensive, which makes it particularly attractive as a potential test globally, she said.
Long-term effects of COVID-19
Post-COVID illness threatens to overwhelm the health system in the United States, even if only 1% of the 8 million people who have been infected have some sort of long-term deficit, “which would be a very conservative estimate,” said John O’Horo, MD, MPH, with the Mayo Clinic in Rochester, Minn. Neurologic dysfunction is going to be a “fairly significant thing to keep an eye on,” he added. Preeti Malani, MD, chief health officer in infectious diseases at the University of Michigan, Ann Arbor, said the emotional aspects of the illness are “striking” and may be the major long-term effect for most patients.
Challenging cases in COVID-19: Through fire and water
In a case presented to panelists during an afternoon session, a Mexican-born woman, 42, presents to urgent care with fever, dyspnea, dry cough, and pleuritic pain, for over a week. Multiple family members have had recent respiratory illness as well. She is obese, on no medications, was not traveling. She’s a nonsmoker and lives in a multigenerational household in the Mission District of San Francisco. Her heart rate is 116, respiratory rate is 36, and her oxygen saturation on room air is 77%. She is admitted to a local hospital and quickly declines, is intubated and started on hydroxychloroquine (HCQ). One day later she is transferred to a hospital for consideration of extracorporeal membrane oxygenation (ECMO).
Panelists were asked a variety of questions about how they would treat this patient. For example, would they continue HCQ? Ravina Kullar, PharmD, MPH, an infectious disease expert from Newport Beach, Calif., answered that she would not continue the HCQ because of lack of evidence and potential harms. Asked whether she would start remdesivir, Dr. Kullar said she would steer her away from that if the patient developed renal failure. Co-moderator Peter Chin-Hong, MD, a medical educator with the University of California, San Francisco, noted that contact tracing will be important as the patient returns to her housing-dense community.
In-hospital infection prevention
The CDC acknowledged aerosol spread of COVID-19 this month, but David Weber, MD, MPH, professor in infectious diseases at the University of North Carolina at Chapel Hill, said, “this does not change anything we need to do in the hospital,” as long as protective pandemic protocols continue to be followed.
There is no evidence, he noted, that SARS-CoV-2 is transmitted far enough that a hospitalized patient could infect people in other rooms or corridors or floors. Opening windows in COVID-19 patients’ rooms is “not an option,” he said, and could be harmful as fungal elements in outside air may introduce new pathogens. The degree to which improved ventilation systems reduce transmission has not been identified and studies are needed to look at that, he said.
Preventing COVID transmission in the community
Mary-Margaret Fill, MD, deputy state epidemiologist in Tennessee, highlighted COVID-19’s spread in prisons. As of mid-October, she said, there are more than 147,000 cases among the U.S. prison population and there have been 1,246 deaths. This translates to a case rate of about 9800 cases per 100,000 people, she said, “double the highest case rate for any state in the country and over three times greater than our national case rate of about 2,500 cases per 100,000 persons.”
Testing varies widely, she noted. For instance, some states test only new prisoners, and some test only when they are symptomatic. One of the strategies to fight this spread is having staff, who go in and out of the community, be assigned to work with only certain groups at a prison. Another is widespread testing of all prisoners. And when prisoners have to leave the prison for care or court dates, a third strategy would be quarantining them upon their return.
COVID-19 vaccines
As the session stretched into the evening in the United States, Mary Marovich, MD, director of vaccine research, AIDS division, with the National Institute of Allergy and Infectious Diseases and the National Institutes of Health, said while each of the government-funded vaccine studies has its own trial, there are standardized objectives for direct comparisons. The studies are being conducted within the same clinical trial networks, and collaborative laboratories apply the same immunoassays and define the infections in the same way. They are all randomized, placebo-controlled trials and all but one have a 30,000-volunteer sample size. She said that while a vaccine is the goal to end the pandemic, monoclonal antibodies, such as those in convalescent plasma, “may serve as a critical bridge.”
The good, the bad, and the ugly during COVID-19 in Latin America
Latin America and the Caribbean are currently the regions hardest hit by COVID-19. Gustavo D. Lopardo, of the Asociacion Panamericana de Infectologia, noted that even before the pandemic Latin America suffered from widespread poverty and inequality. While overcrowding and poverty are determining factors in the spread of the virus, diabetes and obesity – both highly prevalent – are worsening COVID outcomes.
The countries of the region have dealt with asynchronous waves of transmission within their borders by implementing different containment strategies, with dissimilar results. The presenters covered the spectrum of the pandemic, from the “ugly” in Peru, which has the highest mortality rate in the region, to the “good” in Uruguay, where testing is “winning against COVID-19.” Paradoxically, Chile has both the highest cumulative incidence and the lowest case fatality rate of COVID-19 in the region.
In the social and political turmoil imposed by COVID-19, Clóvis Arns da Cunha, MD, president of the Brazilian Society of Infectious Diseases and professor at the Federal University of Paraná, pointed out that “fake news [has become] a public health problem in Brazil” and elsewhere.
Diagnostics and therapeutics in Latin America
Eleven of the 15 countries with the highest death rate in the world are located in Latin America or the Caribbean. Dr. Arns de Cunha pointed out that tests are hard to come by and inadequate diagnostic testing is a major problem. Latin American countries have not been able to compete with the United States and Europe in purchasing polymerase chain reaction test kits from China and South Korea. The test is the best diagnostic tool in the first week of symptoms, but its scale-up has proved to be a challenge in Latin America.
Furthermore, the most sensitive serological markers, CLIA and ECLIA, which perform best after 2 weeks of symptom onset, are not widely available in Latin America where many patients do not have access to the public health system. The detection of silent hypoxemia in symptomatic patients with COVID-19 can save lives; hence, Arns da Cunha praised the program that distributed 100,000 digital oximeters to hundreds of cities in Brazil, targeting vulnerable populations.
The COVID-19 experience in Japan
Takuya Yamagishi, MD, PhD, chief of the Antimicrobial Resistance Research Center at the National Institute of Infectious Diseases in Japan, played an instrumental role in the epidemiological investigation that took place on the Diamond Princess Cruise Ship in February 2020. That COVID-19 outbreak is the largest disease outbreak involving a cruise ship to date, with 712 confirmed COVID-19 cases and 13 deaths.
The ship-based quarantine prompted a massive public health response with unique challenges. In those early days, investigators uncovered important facts about COVID-19 epidemiology, generating hot debates regarding the public health strategy at the time. Notably, the majority of asymptomatically infected persons remained asymptomatic throughout the course of the infection, transmission from asymptomatic cases was almost as likely as transmission from symptomatic cases, and isolation of passengers in their cabins prevented inter-cabin transmission but not intra-cabin transmission.
Swift response in Asia Pacific region
Infectious-disease experts from Taiwan, Singapore, and Australia, who have been at the forefront of clinical care, research, and policy-making, spoke about their experiences.
Taiwan was one of the first countries to adopt a swift response to COVID-19, shortly after they recognized an outbreak of pneumonia of unknown etiology in China and long before the WHO declared a public health emergency, said Ping-Ing Lee, MD, PhD, from the National Taiwan University Children’s Hospital.
The country began onboard health checks on flights from Wuhan as early as Dec. 31, 2019. Dr. Lee attributed Taiwan’s success in prevention and control of COVID-19 to the rigorous use of face masks and environmental disinfection procedures. Regarding the country’s antilockdown stance, he said, “Lockdown may be effective; however, it is associated with a tremendous economic loss.”
In his presentation on remdesivir vs corticosteroids, David Lye, MBBS, said, “I think remdesivir as an antiviral seems to work well given early, but steroids will need to be studied further in terms of its conflicting evidence in multiple well-designed RCTs as well as [their] potential side effects.” He is director of the Infectious Disease Research and Training Office, National Centre for Infectious Diseases, Singapore.
Allen C. Cheng, MBBS, PhD, of Monash University in Melbourne, noted that “control is possible. We seemed to have controlled this twice at the moment with fairly draconian action, but every day does matter.”
China past the first wave
China has already passed the first wave, explained Lei Zhou, MD, of the Chinese Center for Disease Control and Prevention, but there are still some small-scale resurgences. So far a total of four waves have been identified. She also mentioned that contact tracing is intense and highlighted the case of Xinfadi Market in Beijing, the site of an outbreak in June 2020.
Gui-Qiang Wang, MD, from the Department of Infectious Disease, Peking University First Hospital, emphasized the importance of a chest CT for the diagnosis of COVID-19. “In the early stage of the disease, patients may not show any symptoms; however, on CT scan you can see pneumonia. Also, early intervention of high-risk groups and monitoring of warning indicators for disease progression is extremely important,” he said.
“Early antiviral therapy is expected to stop progression, but still needs evaluation,” he said. “Convalescent plasma is safe and effective, but its source is limited; steroid therapy needs to explore appropriate population and timing; and thymosin α is safe, and its effect on outcomes needs large-sample clinical trial.”
Time to Call for an ‘Arab CDC?’
The eastern Mediterranean is geographically, politically, economically, and religiously a very distinct and sensitive region, and “COVID-19 is an added insult to this already frail region of the world,” said Zaid Haddadin, MD, Vanderbilt University Medical Center, Nashville, Tenn.
Poor healthcare and poor public health services are a consequence of weak and fragile governments and infrastructure, the result of war and regional conflicts in many countries. Millions of war refugees live in camps with high population densities and shared facilities, which makes social distancing and community mitigation very challenging. Moreover, the culture includes frequent large social gatherings. Millions of pilgrims visit holy sites in different cities in these countries. There is also movement due to trade and tourism. Travel restrictions are challenging, and there is limited comprehension of precautionary measures.
Najwa Khuri-Bulos, professor of pediatrics and infectious diseases at the University of Jordan, was part of a task force headed by the country’s Ministry of Health. A lockdown was implemented, which helped flatten the curve, but the loosening of restrictions has led to a recent increase in cases. She said, “No country can succeed in controlling spread without the regional collaboration. Perhaps it is time to adopt the call for an Arab CDC.”
Africa is “not out of the woods yet”
The Africa CDC has three key pillars as the foundation for their COVID-19 strategy: preventing transmission, preventing deaths, and preventing social harm, according to Raji Tajudeen, MBBS, FWACP, MPH, head of the agency’s Public Health Institutes and Research Division. Africa, with 1.5 million cases of COVID-19, accounts for 5% of global cases. With a recovery rate of 83% and a case fatality rate of 2.4%, the African continent has fared much better than the rest of the world. “Significant improvements have been made, but we are not out of the woods yet,” he cautioned.
Richard Lessells, PhD, from the University of KwaZulu-Natal, agreed. “Unfortunately, South Africa has not been spared from the worst effects of this pandemic despite what you might read in the press and scientific coverage.” He added, “Over 50% of cases and up to two thirds of the deaths in the African region are coming from South Africa.” A bigger challenge for South Africa has been maintaining essential health services during the COVID-19 pandemic, especially since it is also at the heart of the HIV pandemic. On the brighter side, HIV itself has not emerged as a risk factor for COVID-19 infection or severe disease in South Africa.
Dimie Ogoina, MBBS, FWACP, president of the Nigerian Infectious Diseases Society, stated that COVID-19 has significantly affected access to healthcare in Nigeria, particularly immunizations and antenatal care. Immunization uptake is likely to have dropped by 50% in the country.
Diagnostic pitfalls in COVID-19
Technical errors associated with the SARS-CoV-2 diagnostic pipeline are a major source of variations in diagnosis, explained Jim Huggett, PhD, senior lecturer, analytical microbiology, University of Surrey, Guildford, England. He believes that PCR assays are currently too biased for a single cutoff to be broadly used, and false-positive signals are most likely because of contamination.
Dana Wolf, MD, Clinical Virology Unit, Hadassah Hebrew University Medical Center in Israel, presented a large-scale data analysis of more than 133,000 pooled samples. Such a pooling strategy appeared to be highly efficient for a wide range of prevalence rates (<1% to 6%). “Our empirical evidence strongly projects on the feasibility and benefits of pooling in the current pandemic setting, to enhance continued surveillance, control, and community reopening,” she said.
Corine Geurts van Kessel, MD, PhD, Department of Virology, Erasmus University Rotterdam (the Netherlands), discussing antibodies testing for SARS-CoV-2, pointed out that disease severity can affect testing accuracy. “Reinfection cases tell us that we cannot rely on immunity acquired by natural infection to confer herd immunity,” she said.
Misinformation in the first digital pandemic
The world is not only facing a devastating pandemic, but also an alarming “infodemic” of misinformation. Between January and March 2020, a new COVID-19–related tweet appeared on Twitter every 45 milliseconds. Müge Çevik, MD, MSc, MRCP, an infectious disease clinician, scientist, and science communicator, said that “the greatest challenge for science communication is reaching the audience.”
People have always been skeptical of science reporting by journalists and would rather have scientists communicate with them directly, she noted. Science communication plays a dual role. “On one hand is the need to promote science to a wide audience in order to inform and educate and inspire the next generation of scientists, and on the other hand there is also a need to engage effectively in public dialogue,” she added. Dr. Çevik and colleagues think that “The responsibility of academics should not end with finding the truth. It should end after communicating it.”
Treatment in the ICU
Matteo Bassetti, MD, with the University of Genoa (Italy), who was asked about when to use remdesivir in the intensive care unit and for how long, said, “In the majority of cases, 5 days is probably enough.” However, if there is high viremia, he said, physicians may choose to continue the regimen beyond 5 days. Data show it is important to prescribe this drug for patients with oxygen support in an early phase, within 10 days of the first symptoms, he added. “In the late phase, there is a very limited role for remdesivir, as we know that we are already out of the viremic phase.” He also emphasized that there is no role for hydroxychloroquine or lopinavir-ritonavir.
Breaking the chains of transmission
During the wrap-up session, former US CDC Director Tom Frieden, MD, said, “We’re not even halfway through it” about the pandemic trajectory. “And we have to be very clear that the risk of explosive spread will not end with a vaccine.” He is now president and CEO of Resolve to Save Lives.
Different parts of the world will have very different experiences, Dr. Frieden said, noting that Africa, where 4% of the population is older than 65, has a very different risk level than Europe and the United States, where 10%-20% of people are in older age groups.
“We need a one-two punch,” he noted, first preventing spread, and when it does happen, boxing it in. Mask wearing is essential. “States in the US that mandated universal mask-wearing experienced much more rapid declines (in cases) for every 5 days the mandate was in place.”
Michael Ryan, MD, executive director for the WHO’s Health Emergencies Programme, added, “We need to collectively recommit to winning this game. We know how to break the chains of transmission. We need recommitment to a scientific, societal, and political strategy, and an alliance – a contract – between those entities to try to move us forward.”
This article first appeared on Medscape.com.
Some medical societies feature sessions at their annual meetings that feel like they’re 24 hours long, yet few have the courage to schedule a session that actually runs all day and all night. But the five societies sponsoring the IDWeek conference had that courage. The first 24 hours of the meeting was devoted to the most pressing infectious-disease crisis of the last 100 years: the COVID-19 pandemic. They called it “COVID-19: Chasing the Sun.”
Dr. Fauci predicts a vaccine answer in mid-November
In the first segment, at 10 am Eastern time, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases and the nation’s top infectious-disease expert, began the day by noting that five of the six companies the US invested in to develop a vaccine are conducting phase 3 trials. He said, “we feel confident that we will have an answer likely in mid-November to the beginning of December as to whether we have a safe and effective vaccine”. He added he was “cautiously optimistic” that “we will have a safe and effective vaccine by the end of the year, which we can begin to distribute as we go into 2021.” He highlighted the COVID-19 Prevention Network website for more information on the trials.
Glaring racial health disparities in U.S.
Some of the most glaring health disparities surrounding COVID-19 in the United States were described by Carlos del Rio, MD, professor of medicine at Emory University in Atlanta, Georgia. He pointed out that while white people have about 23 cases per 10,000 population, Blacks have about 62 cases per 10,000, and Latinos have 73 cases per 10,000. While whites don’t see a huge jump in cases until age 80, he said, “among Blacks and Latinos you start seeing that huge increase at a younger age. In fact, starting at age 20, you start seeing a major, major change.”
COVID-19 diagnostics
Audrey Odom John, MD, PhD, chief of pediatric infectious diseases at Children’s Hospital of Philadelphia, is working on a new way of diagnosing COVID-19 infection in children by testing their breath. “We’re really taking advantage of a fundamental biological fact, which is that people stink,” she said. Breath shows the health of the body as a whole, “and it’s easy to see how breath volatiles might arise from a respiratory infection.” Testing breath is easy and inexpensive, which makes it particularly attractive as a potential test globally, she said.
Long-term effects of COVID-19
Post-COVID illness threatens to overwhelm the health system in the United States, even if only 1% of the 8 million people who have been infected have some sort of long-term deficit, “which would be a very conservative estimate,” said John O’Horo, MD, MPH, with the Mayo Clinic in Rochester, Minn. Neurologic dysfunction is going to be a “fairly significant thing to keep an eye on,” he added. Preeti Malani, MD, chief health officer in infectious diseases at the University of Michigan, Ann Arbor, said the emotional aspects of the illness are “striking” and may be the major long-term effect for most patients.
Challenging cases in COVID-19: Through fire and water
In a case presented to panelists during an afternoon session, a Mexican-born woman, 42, presents to urgent care with fever, dyspnea, dry cough, and pleuritic pain, for over a week. Multiple family members have had recent respiratory illness as well. She is obese, on no medications, was not traveling. She’s a nonsmoker and lives in a multigenerational household in the Mission District of San Francisco. Her heart rate is 116, respiratory rate is 36, and her oxygen saturation on room air is 77%. She is admitted to a local hospital and quickly declines, is intubated and started on hydroxychloroquine (HCQ). One day later she is transferred to a hospital for consideration of extracorporeal membrane oxygenation (ECMO).
Panelists were asked a variety of questions about how they would treat this patient. For example, would they continue HCQ? Ravina Kullar, PharmD, MPH, an infectious disease expert from Newport Beach, Calif., answered that she would not continue the HCQ because of lack of evidence and potential harms. Asked whether she would start remdesivir, Dr. Kullar said she would steer her away from that if the patient developed renal failure. Co-moderator Peter Chin-Hong, MD, a medical educator with the University of California, San Francisco, noted that contact tracing will be important as the patient returns to her housing-dense community.
In-hospital infection prevention
The CDC acknowledged aerosol spread of COVID-19 this month, but David Weber, MD, MPH, professor in infectious diseases at the University of North Carolina at Chapel Hill, said, “this does not change anything we need to do in the hospital,” as long as protective pandemic protocols continue to be followed.
There is no evidence, he noted, that SARS-CoV-2 is transmitted far enough that a hospitalized patient could infect people in other rooms or corridors or floors. Opening windows in COVID-19 patients’ rooms is “not an option,” he said, and could be harmful as fungal elements in outside air may introduce new pathogens. The degree to which improved ventilation systems reduce transmission has not been identified and studies are needed to look at that, he said.
Preventing COVID transmission in the community
Mary-Margaret Fill, MD, deputy state epidemiologist in Tennessee, highlighted COVID-19’s spread in prisons. As of mid-October, she said, there are more than 147,000 cases among the U.S. prison population and there have been 1,246 deaths. This translates to a case rate of about 9800 cases per 100,000 people, she said, “double the highest case rate for any state in the country and over three times greater than our national case rate of about 2,500 cases per 100,000 persons.”
Testing varies widely, she noted. For instance, some states test only new prisoners, and some test only when they are symptomatic. One of the strategies to fight this spread is having staff, who go in and out of the community, be assigned to work with only certain groups at a prison. Another is widespread testing of all prisoners. And when prisoners have to leave the prison for care or court dates, a third strategy would be quarantining them upon their return.
COVID-19 vaccines
As the session stretched into the evening in the United States, Mary Marovich, MD, director of vaccine research, AIDS division, with the National Institute of Allergy and Infectious Diseases and the National Institutes of Health, said while each of the government-funded vaccine studies has its own trial, there are standardized objectives for direct comparisons. The studies are being conducted within the same clinical trial networks, and collaborative laboratories apply the same immunoassays and define the infections in the same way. They are all randomized, placebo-controlled trials and all but one have a 30,000-volunteer sample size. She said that while a vaccine is the goal to end the pandemic, monoclonal antibodies, such as those in convalescent plasma, “may serve as a critical bridge.”
The good, the bad, and the ugly during COVID-19 in Latin America
Latin America and the Caribbean are currently the regions hardest hit by COVID-19. Gustavo D. Lopardo, of the Asociacion Panamericana de Infectologia, noted that even before the pandemic Latin America suffered from widespread poverty and inequality. While overcrowding and poverty are determining factors in the spread of the virus, diabetes and obesity – both highly prevalent – are worsening COVID outcomes.
The countries of the region have dealt with asynchronous waves of transmission within their borders by implementing different containment strategies, with dissimilar results. The presenters covered the spectrum of the pandemic, from the “ugly” in Peru, which has the highest mortality rate in the region, to the “good” in Uruguay, where testing is “winning against COVID-19.” Paradoxically, Chile has both the highest cumulative incidence and the lowest case fatality rate of COVID-19 in the region.
In the social and political turmoil imposed by COVID-19, Clóvis Arns da Cunha, MD, president of the Brazilian Society of Infectious Diseases and professor at the Federal University of Paraná, pointed out that “fake news [has become] a public health problem in Brazil” and elsewhere.
Diagnostics and therapeutics in Latin America
Eleven of the 15 countries with the highest death rate in the world are located in Latin America or the Caribbean. Dr. Arns de Cunha pointed out that tests are hard to come by and inadequate diagnostic testing is a major problem. Latin American countries have not been able to compete with the United States and Europe in purchasing polymerase chain reaction test kits from China and South Korea. The test is the best diagnostic tool in the first week of symptoms, but its scale-up has proved to be a challenge in Latin America.
Furthermore, the most sensitive serological markers, CLIA and ECLIA, which perform best after 2 weeks of symptom onset, are not widely available in Latin America where many patients do not have access to the public health system. The detection of silent hypoxemia in symptomatic patients with COVID-19 can save lives; hence, Arns da Cunha praised the program that distributed 100,000 digital oximeters to hundreds of cities in Brazil, targeting vulnerable populations.
The COVID-19 experience in Japan
Takuya Yamagishi, MD, PhD, chief of the Antimicrobial Resistance Research Center at the National Institute of Infectious Diseases in Japan, played an instrumental role in the epidemiological investigation that took place on the Diamond Princess Cruise Ship in February 2020. That COVID-19 outbreak is the largest disease outbreak involving a cruise ship to date, with 712 confirmed COVID-19 cases and 13 deaths.
The ship-based quarantine prompted a massive public health response with unique challenges. In those early days, investigators uncovered important facts about COVID-19 epidemiology, generating hot debates regarding the public health strategy at the time. Notably, the majority of asymptomatically infected persons remained asymptomatic throughout the course of the infection, transmission from asymptomatic cases was almost as likely as transmission from symptomatic cases, and isolation of passengers in their cabins prevented inter-cabin transmission but not intra-cabin transmission.
Swift response in Asia Pacific region
Infectious-disease experts from Taiwan, Singapore, and Australia, who have been at the forefront of clinical care, research, and policy-making, spoke about their experiences.
Taiwan was one of the first countries to adopt a swift response to COVID-19, shortly after they recognized an outbreak of pneumonia of unknown etiology in China and long before the WHO declared a public health emergency, said Ping-Ing Lee, MD, PhD, from the National Taiwan University Children’s Hospital.
The country began onboard health checks on flights from Wuhan as early as Dec. 31, 2019. Dr. Lee attributed Taiwan’s success in prevention and control of COVID-19 to the rigorous use of face masks and environmental disinfection procedures. Regarding the country’s antilockdown stance, he said, “Lockdown may be effective; however, it is associated with a tremendous economic loss.”
In his presentation on remdesivir vs corticosteroids, David Lye, MBBS, said, “I think remdesivir as an antiviral seems to work well given early, but steroids will need to be studied further in terms of its conflicting evidence in multiple well-designed RCTs as well as [their] potential side effects.” He is director of the Infectious Disease Research and Training Office, National Centre for Infectious Diseases, Singapore.
Allen C. Cheng, MBBS, PhD, of Monash University in Melbourne, noted that “control is possible. We seemed to have controlled this twice at the moment with fairly draconian action, but every day does matter.”
China past the first wave
China has already passed the first wave, explained Lei Zhou, MD, of the Chinese Center for Disease Control and Prevention, but there are still some small-scale resurgences. So far a total of four waves have been identified. She also mentioned that contact tracing is intense and highlighted the case of Xinfadi Market in Beijing, the site of an outbreak in June 2020.
Gui-Qiang Wang, MD, from the Department of Infectious Disease, Peking University First Hospital, emphasized the importance of a chest CT for the diagnosis of COVID-19. “In the early stage of the disease, patients may not show any symptoms; however, on CT scan you can see pneumonia. Also, early intervention of high-risk groups and monitoring of warning indicators for disease progression is extremely important,” he said.
“Early antiviral therapy is expected to stop progression, but still needs evaluation,” he said. “Convalescent plasma is safe and effective, but its source is limited; steroid therapy needs to explore appropriate population and timing; and thymosin α is safe, and its effect on outcomes needs large-sample clinical trial.”
Time to Call for an ‘Arab CDC?’
The eastern Mediterranean is geographically, politically, economically, and religiously a very distinct and sensitive region, and “COVID-19 is an added insult to this already frail region of the world,” said Zaid Haddadin, MD, Vanderbilt University Medical Center, Nashville, Tenn.
Poor healthcare and poor public health services are a consequence of weak and fragile governments and infrastructure, the result of war and regional conflicts in many countries. Millions of war refugees live in camps with high population densities and shared facilities, which makes social distancing and community mitigation very challenging. Moreover, the culture includes frequent large social gatherings. Millions of pilgrims visit holy sites in different cities in these countries. There is also movement due to trade and tourism. Travel restrictions are challenging, and there is limited comprehension of precautionary measures.
Najwa Khuri-Bulos, professor of pediatrics and infectious diseases at the University of Jordan, was part of a task force headed by the country’s Ministry of Health. A lockdown was implemented, which helped flatten the curve, but the loosening of restrictions has led to a recent increase in cases. She said, “No country can succeed in controlling spread without the regional collaboration. Perhaps it is time to adopt the call for an Arab CDC.”
Africa is “not out of the woods yet”
The Africa CDC has three key pillars as the foundation for their COVID-19 strategy: preventing transmission, preventing deaths, and preventing social harm, according to Raji Tajudeen, MBBS, FWACP, MPH, head of the agency’s Public Health Institutes and Research Division. Africa, with 1.5 million cases of COVID-19, accounts for 5% of global cases. With a recovery rate of 83% and a case fatality rate of 2.4%, the African continent has fared much better than the rest of the world. “Significant improvements have been made, but we are not out of the woods yet,” he cautioned.
Richard Lessells, PhD, from the University of KwaZulu-Natal, agreed. “Unfortunately, South Africa has not been spared from the worst effects of this pandemic despite what you might read in the press and scientific coverage.” He added, “Over 50% of cases and up to two thirds of the deaths in the African region are coming from South Africa.” A bigger challenge for South Africa has been maintaining essential health services during the COVID-19 pandemic, especially since it is also at the heart of the HIV pandemic. On the brighter side, HIV itself has not emerged as a risk factor for COVID-19 infection or severe disease in South Africa.
Dimie Ogoina, MBBS, FWACP, president of the Nigerian Infectious Diseases Society, stated that COVID-19 has significantly affected access to healthcare in Nigeria, particularly immunizations and antenatal care. Immunization uptake is likely to have dropped by 50% in the country.
Diagnostic pitfalls in COVID-19
Technical errors associated with the SARS-CoV-2 diagnostic pipeline are a major source of variations in diagnosis, explained Jim Huggett, PhD, senior lecturer, analytical microbiology, University of Surrey, Guildford, England. He believes that PCR assays are currently too biased for a single cutoff to be broadly used, and false-positive signals are most likely because of contamination.
Dana Wolf, MD, Clinical Virology Unit, Hadassah Hebrew University Medical Center in Israel, presented a large-scale data analysis of more than 133,000 pooled samples. Such a pooling strategy appeared to be highly efficient for a wide range of prevalence rates (<1% to 6%). “Our empirical evidence strongly projects on the feasibility and benefits of pooling in the current pandemic setting, to enhance continued surveillance, control, and community reopening,” she said.
Corine Geurts van Kessel, MD, PhD, Department of Virology, Erasmus University Rotterdam (the Netherlands), discussing antibodies testing for SARS-CoV-2, pointed out that disease severity can affect testing accuracy. “Reinfection cases tell us that we cannot rely on immunity acquired by natural infection to confer herd immunity,” she said.
Misinformation in the first digital pandemic
The world is not only facing a devastating pandemic, but also an alarming “infodemic” of misinformation. Between January and March 2020, a new COVID-19–related tweet appeared on Twitter every 45 milliseconds. Müge Çevik, MD, MSc, MRCP, an infectious disease clinician, scientist, and science communicator, said that “the greatest challenge for science communication is reaching the audience.”
People have always been skeptical of science reporting by journalists and would rather have scientists communicate with them directly, she noted. Science communication plays a dual role. “On one hand is the need to promote science to a wide audience in order to inform and educate and inspire the next generation of scientists, and on the other hand there is also a need to engage effectively in public dialogue,” she added. Dr. Çevik and colleagues think that “The responsibility of academics should not end with finding the truth. It should end after communicating it.”
Treatment in the ICU
Matteo Bassetti, MD, with the University of Genoa (Italy), who was asked about when to use remdesivir in the intensive care unit and for how long, said, “In the majority of cases, 5 days is probably enough.” However, if there is high viremia, he said, physicians may choose to continue the regimen beyond 5 days. Data show it is important to prescribe this drug for patients with oxygen support in an early phase, within 10 days of the first symptoms, he added. “In the late phase, there is a very limited role for remdesivir, as we know that we are already out of the viremic phase.” He also emphasized that there is no role for hydroxychloroquine or lopinavir-ritonavir.
Breaking the chains of transmission
During the wrap-up session, former US CDC Director Tom Frieden, MD, said, “We’re not even halfway through it” about the pandemic trajectory. “And we have to be very clear that the risk of explosive spread will not end with a vaccine.” He is now president and CEO of Resolve to Save Lives.
Different parts of the world will have very different experiences, Dr. Frieden said, noting that Africa, where 4% of the population is older than 65, has a very different risk level than Europe and the United States, where 10%-20% of people are in older age groups.
“We need a one-two punch,” he noted, first preventing spread, and when it does happen, boxing it in. Mask wearing is essential. “States in the US that mandated universal mask-wearing experienced much more rapid declines (in cases) for every 5 days the mandate was in place.”
Michael Ryan, MD, executive director for the WHO’s Health Emergencies Programme, added, “We need to collectively recommit to winning this game. We know how to break the chains of transmission. We need recommitment to a scientific, societal, and political strategy, and an alliance – a contract – between those entities to try to move us forward.”
This article first appeared on Medscape.com.
Some medical societies feature sessions at their annual meetings that feel like they’re 24 hours long, yet few have the courage to schedule a session that actually runs all day and all night. But the five societies sponsoring the IDWeek conference had that courage. The first 24 hours of the meeting was devoted to the most pressing infectious-disease crisis of the last 100 years: the COVID-19 pandemic. They called it “COVID-19: Chasing the Sun.”
Dr. Fauci predicts a vaccine answer in mid-November
In the first segment, at 10 am Eastern time, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases and the nation’s top infectious-disease expert, began the day by noting that five of the six companies the US invested in to develop a vaccine are conducting phase 3 trials. He said, “we feel confident that we will have an answer likely in mid-November to the beginning of December as to whether we have a safe and effective vaccine”. He added he was “cautiously optimistic” that “we will have a safe and effective vaccine by the end of the year, which we can begin to distribute as we go into 2021.” He highlighted the COVID-19 Prevention Network website for more information on the trials.
Glaring racial health disparities in U.S.
Some of the most glaring health disparities surrounding COVID-19 in the United States were described by Carlos del Rio, MD, professor of medicine at Emory University in Atlanta, Georgia. He pointed out that while white people have about 23 cases per 10,000 population, Blacks have about 62 cases per 10,000, and Latinos have 73 cases per 10,000. While whites don’t see a huge jump in cases until age 80, he said, “among Blacks and Latinos you start seeing that huge increase at a younger age. In fact, starting at age 20, you start seeing a major, major change.”
COVID-19 diagnostics
Audrey Odom John, MD, PhD, chief of pediatric infectious diseases at Children’s Hospital of Philadelphia, is working on a new way of diagnosing COVID-19 infection in children by testing their breath. “We’re really taking advantage of a fundamental biological fact, which is that people stink,” she said. Breath shows the health of the body as a whole, “and it’s easy to see how breath volatiles might arise from a respiratory infection.” Testing breath is easy and inexpensive, which makes it particularly attractive as a potential test globally, she said.
Long-term effects of COVID-19
Post-COVID illness threatens to overwhelm the health system in the United States, even if only 1% of the 8 million people who have been infected have some sort of long-term deficit, “which would be a very conservative estimate,” said John O’Horo, MD, MPH, with the Mayo Clinic in Rochester, Minn. Neurologic dysfunction is going to be a “fairly significant thing to keep an eye on,” he added. Preeti Malani, MD, chief health officer in infectious diseases at the University of Michigan, Ann Arbor, said the emotional aspects of the illness are “striking” and may be the major long-term effect for most patients.
Challenging cases in COVID-19: Through fire and water
In a case presented to panelists during an afternoon session, a Mexican-born woman, 42, presents to urgent care with fever, dyspnea, dry cough, and pleuritic pain, for over a week. Multiple family members have had recent respiratory illness as well. She is obese, on no medications, was not traveling. She’s a nonsmoker and lives in a multigenerational household in the Mission District of San Francisco. Her heart rate is 116, respiratory rate is 36, and her oxygen saturation on room air is 77%. She is admitted to a local hospital and quickly declines, is intubated and started on hydroxychloroquine (HCQ). One day later she is transferred to a hospital for consideration of extracorporeal membrane oxygenation (ECMO).
Panelists were asked a variety of questions about how they would treat this patient. For example, would they continue HCQ? Ravina Kullar, PharmD, MPH, an infectious disease expert from Newport Beach, Calif., answered that she would not continue the HCQ because of lack of evidence and potential harms. Asked whether she would start remdesivir, Dr. Kullar said she would steer her away from that if the patient developed renal failure. Co-moderator Peter Chin-Hong, MD, a medical educator with the University of California, San Francisco, noted that contact tracing will be important as the patient returns to her housing-dense community.
In-hospital infection prevention
The CDC acknowledged aerosol spread of COVID-19 this month, but David Weber, MD, MPH, professor in infectious diseases at the University of North Carolina at Chapel Hill, said, “this does not change anything we need to do in the hospital,” as long as protective pandemic protocols continue to be followed.
There is no evidence, he noted, that SARS-CoV-2 is transmitted far enough that a hospitalized patient could infect people in other rooms or corridors or floors. Opening windows in COVID-19 patients’ rooms is “not an option,” he said, and could be harmful as fungal elements in outside air may introduce new pathogens. The degree to which improved ventilation systems reduce transmission has not been identified and studies are needed to look at that, he said.
Preventing COVID transmission in the community
Mary-Margaret Fill, MD, deputy state epidemiologist in Tennessee, highlighted COVID-19’s spread in prisons. As of mid-October, she said, there are more than 147,000 cases among the U.S. prison population and there have been 1,246 deaths. This translates to a case rate of about 9800 cases per 100,000 people, she said, “double the highest case rate for any state in the country and over three times greater than our national case rate of about 2,500 cases per 100,000 persons.”
Testing varies widely, she noted. For instance, some states test only new prisoners, and some test only when they are symptomatic. One of the strategies to fight this spread is having staff, who go in and out of the community, be assigned to work with only certain groups at a prison. Another is widespread testing of all prisoners. And when prisoners have to leave the prison for care or court dates, a third strategy would be quarantining them upon their return.
COVID-19 vaccines
As the session stretched into the evening in the United States, Mary Marovich, MD, director of vaccine research, AIDS division, with the National Institute of Allergy and Infectious Diseases and the National Institutes of Health, said while each of the government-funded vaccine studies has its own trial, there are standardized objectives for direct comparisons. The studies are being conducted within the same clinical trial networks, and collaborative laboratories apply the same immunoassays and define the infections in the same way. They are all randomized, placebo-controlled trials and all but one have a 30,000-volunteer sample size. She said that while a vaccine is the goal to end the pandemic, monoclonal antibodies, such as those in convalescent plasma, “may serve as a critical bridge.”
The good, the bad, and the ugly during COVID-19 in Latin America
Latin America and the Caribbean are currently the regions hardest hit by COVID-19. Gustavo D. Lopardo, of the Asociacion Panamericana de Infectologia, noted that even before the pandemic Latin America suffered from widespread poverty and inequality. While overcrowding and poverty are determining factors in the spread of the virus, diabetes and obesity – both highly prevalent – are worsening COVID outcomes.
The countries of the region have dealt with asynchronous waves of transmission within their borders by implementing different containment strategies, with dissimilar results. The presenters covered the spectrum of the pandemic, from the “ugly” in Peru, which has the highest mortality rate in the region, to the “good” in Uruguay, where testing is “winning against COVID-19.” Paradoxically, Chile has both the highest cumulative incidence and the lowest case fatality rate of COVID-19 in the region.
In the social and political turmoil imposed by COVID-19, Clóvis Arns da Cunha, MD, president of the Brazilian Society of Infectious Diseases and professor at the Federal University of Paraná, pointed out that “fake news [has become] a public health problem in Brazil” and elsewhere.
Diagnostics and therapeutics in Latin America
Eleven of the 15 countries with the highest death rate in the world are located in Latin America or the Caribbean. Dr. Arns de Cunha pointed out that tests are hard to come by and inadequate diagnostic testing is a major problem. Latin American countries have not been able to compete with the United States and Europe in purchasing polymerase chain reaction test kits from China and South Korea. The test is the best diagnostic tool in the first week of symptoms, but its scale-up has proved to be a challenge in Latin America.
Furthermore, the most sensitive serological markers, CLIA and ECLIA, which perform best after 2 weeks of symptom onset, are not widely available in Latin America where many patients do not have access to the public health system. The detection of silent hypoxemia in symptomatic patients with COVID-19 can save lives; hence, Arns da Cunha praised the program that distributed 100,000 digital oximeters to hundreds of cities in Brazil, targeting vulnerable populations.
The COVID-19 experience in Japan
Takuya Yamagishi, MD, PhD, chief of the Antimicrobial Resistance Research Center at the National Institute of Infectious Diseases in Japan, played an instrumental role in the epidemiological investigation that took place on the Diamond Princess Cruise Ship in February 2020. That COVID-19 outbreak is the largest disease outbreak involving a cruise ship to date, with 712 confirmed COVID-19 cases and 13 deaths.
The ship-based quarantine prompted a massive public health response with unique challenges. In those early days, investigators uncovered important facts about COVID-19 epidemiology, generating hot debates regarding the public health strategy at the time. Notably, the majority of asymptomatically infected persons remained asymptomatic throughout the course of the infection, transmission from asymptomatic cases was almost as likely as transmission from symptomatic cases, and isolation of passengers in their cabins prevented inter-cabin transmission but not intra-cabin transmission.
Swift response in Asia Pacific region
Infectious-disease experts from Taiwan, Singapore, and Australia, who have been at the forefront of clinical care, research, and policy-making, spoke about their experiences.
Taiwan was one of the first countries to adopt a swift response to COVID-19, shortly after they recognized an outbreak of pneumonia of unknown etiology in China and long before the WHO declared a public health emergency, said Ping-Ing Lee, MD, PhD, from the National Taiwan University Children’s Hospital.
The country began onboard health checks on flights from Wuhan as early as Dec. 31, 2019. Dr. Lee attributed Taiwan’s success in prevention and control of COVID-19 to the rigorous use of face masks and environmental disinfection procedures. Regarding the country’s antilockdown stance, he said, “Lockdown may be effective; however, it is associated with a tremendous economic loss.”
In his presentation on remdesivir vs corticosteroids, David Lye, MBBS, said, “I think remdesivir as an antiviral seems to work well given early, but steroids will need to be studied further in terms of its conflicting evidence in multiple well-designed RCTs as well as [their] potential side effects.” He is director of the Infectious Disease Research and Training Office, National Centre for Infectious Diseases, Singapore.
Allen C. Cheng, MBBS, PhD, of Monash University in Melbourne, noted that “control is possible. We seemed to have controlled this twice at the moment with fairly draconian action, but every day does matter.”
China past the first wave
China has already passed the first wave, explained Lei Zhou, MD, of the Chinese Center for Disease Control and Prevention, but there are still some small-scale resurgences. So far a total of four waves have been identified. She also mentioned that contact tracing is intense and highlighted the case of Xinfadi Market in Beijing, the site of an outbreak in June 2020.
Gui-Qiang Wang, MD, from the Department of Infectious Disease, Peking University First Hospital, emphasized the importance of a chest CT for the diagnosis of COVID-19. “In the early stage of the disease, patients may not show any symptoms; however, on CT scan you can see pneumonia. Also, early intervention of high-risk groups and monitoring of warning indicators for disease progression is extremely important,” he said.
“Early antiviral therapy is expected to stop progression, but still needs evaluation,” he said. “Convalescent plasma is safe and effective, but its source is limited; steroid therapy needs to explore appropriate population and timing; and thymosin α is safe, and its effect on outcomes needs large-sample clinical trial.”
Time to Call for an ‘Arab CDC?’
The eastern Mediterranean is geographically, politically, economically, and religiously a very distinct and sensitive region, and “COVID-19 is an added insult to this already frail region of the world,” said Zaid Haddadin, MD, Vanderbilt University Medical Center, Nashville, Tenn.
Poor healthcare and poor public health services are a consequence of weak and fragile governments and infrastructure, the result of war and regional conflicts in many countries. Millions of war refugees live in camps with high population densities and shared facilities, which makes social distancing and community mitigation very challenging. Moreover, the culture includes frequent large social gatherings. Millions of pilgrims visit holy sites in different cities in these countries. There is also movement due to trade and tourism. Travel restrictions are challenging, and there is limited comprehension of precautionary measures.
Najwa Khuri-Bulos, professor of pediatrics and infectious diseases at the University of Jordan, was part of a task force headed by the country’s Ministry of Health. A lockdown was implemented, which helped flatten the curve, but the loosening of restrictions has led to a recent increase in cases. She said, “No country can succeed in controlling spread without the regional collaboration. Perhaps it is time to adopt the call for an Arab CDC.”
Africa is “not out of the woods yet”
The Africa CDC has three key pillars as the foundation for their COVID-19 strategy: preventing transmission, preventing deaths, and preventing social harm, according to Raji Tajudeen, MBBS, FWACP, MPH, head of the agency’s Public Health Institutes and Research Division. Africa, with 1.5 million cases of COVID-19, accounts for 5% of global cases. With a recovery rate of 83% and a case fatality rate of 2.4%, the African continent has fared much better than the rest of the world. “Significant improvements have been made, but we are not out of the woods yet,” he cautioned.
Richard Lessells, PhD, from the University of KwaZulu-Natal, agreed. “Unfortunately, South Africa has not been spared from the worst effects of this pandemic despite what you might read in the press and scientific coverage.” He added, “Over 50% of cases and up to two thirds of the deaths in the African region are coming from South Africa.” A bigger challenge for South Africa has been maintaining essential health services during the COVID-19 pandemic, especially since it is also at the heart of the HIV pandemic. On the brighter side, HIV itself has not emerged as a risk factor for COVID-19 infection or severe disease in South Africa.
Dimie Ogoina, MBBS, FWACP, president of the Nigerian Infectious Diseases Society, stated that COVID-19 has significantly affected access to healthcare in Nigeria, particularly immunizations and antenatal care. Immunization uptake is likely to have dropped by 50% in the country.
Diagnostic pitfalls in COVID-19
Technical errors associated with the SARS-CoV-2 diagnostic pipeline are a major source of variations in diagnosis, explained Jim Huggett, PhD, senior lecturer, analytical microbiology, University of Surrey, Guildford, England. He believes that PCR assays are currently too biased for a single cutoff to be broadly used, and false-positive signals are most likely because of contamination.
Dana Wolf, MD, Clinical Virology Unit, Hadassah Hebrew University Medical Center in Israel, presented a large-scale data analysis of more than 133,000 pooled samples. Such a pooling strategy appeared to be highly efficient for a wide range of prevalence rates (<1% to 6%). “Our empirical evidence strongly projects on the feasibility and benefits of pooling in the current pandemic setting, to enhance continued surveillance, control, and community reopening,” she said.
Corine Geurts van Kessel, MD, PhD, Department of Virology, Erasmus University Rotterdam (the Netherlands), discussing antibodies testing for SARS-CoV-2, pointed out that disease severity can affect testing accuracy. “Reinfection cases tell us that we cannot rely on immunity acquired by natural infection to confer herd immunity,” she said.
Misinformation in the first digital pandemic
The world is not only facing a devastating pandemic, but also an alarming “infodemic” of misinformation. Between January and March 2020, a new COVID-19–related tweet appeared on Twitter every 45 milliseconds. Müge Çevik, MD, MSc, MRCP, an infectious disease clinician, scientist, and science communicator, said that “the greatest challenge for science communication is reaching the audience.”
People have always been skeptical of science reporting by journalists and would rather have scientists communicate with them directly, she noted. Science communication plays a dual role. “On one hand is the need to promote science to a wide audience in order to inform and educate and inspire the next generation of scientists, and on the other hand there is also a need to engage effectively in public dialogue,” she added. Dr. Çevik and colleagues think that “The responsibility of academics should not end with finding the truth. It should end after communicating it.”
Treatment in the ICU
Matteo Bassetti, MD, with the University of Genoa (Italy), who was asked about when to use remdesivir in the intensive care unit and for how long, said, “In the majority of cases, 5 days is probably enough.” However, if there is high viremia, he said, physicians may choose to continue the regimen beyond 5 days. Data show it is important to prescribe this drug for patients with oxygen support in an early phase, within 10 days of the first symptoms, he added. “In the late phase, there is a very limited role for remdesivir, as we know that we are already out of the viremic phase.” He also emphasized that there is no role for hydroxychloroquine or lopinavir-ritonavir.
Breaking the chains of transmission
During the wrap-up session, former US CDC Director Tom Frieden, MD, said, “We’re not even halfway through it” about the pandemic trajectory. “And we have to be very clear that the risk of explosive spread will not end with a vaccine.” He is now president and CEO of Resolve to Save Lives.
Different parts of the world will have very different experiences, Dr. Frieden said, noting that Africa, where 4% of the population is older than 65, has a very different risk level than Europe and the United States, where 10%-20% of people are in older age groups.
“We need a one-two punch,” he noted, first preventing spread, and when it does happen, boxing it in. Mask wearing is essential. “States in the US that mandated universal mask-wearing experienced much more rapid declines (in cases) for every 5 days the mandate was in place.”
Michael Ryan, MD, executive director for the WHO’s Health Emergencies Programme, added, “We need to collectively recommit to winning this game. We know how to break the chains of transmission. We need recommitment to a scientific, societal, and political strategy, and an alliance – a contract – between those entities to try to move us forward.”
This article first appeared on Medscape.com.
FROM IDWEEK 2020
Two-thirds of U.S. teens fail to get needed vaccines
Only 30.6% of American adolescents complete three routinely recommended vaccinations, new research has found, but that number varies widely by state.
The Advisory Committee on Immunization Practices recommends that, by age 17 years, adolescents complete three key immunizations: human papillomavirus (HPV), quadrivalent meningococcal conjugate (MenACWY), and Tdap.
Sara Poston, PharmD, senior director for health outcomes research at GlaxoSmithKline, said at a press conference during IDWeek, an annual scientific meeting on infectious diseases held virtually this year, that her team set out to determine how many teens were completing the vaccinations and how the number varied by state and by behavioral factors.
Completion of the vaccines means getting the HPV series (two doses for people aged 9-14 years at first vaccination or three doses for those aged 15 years or older at first vaccination), completion of the MenACWY series (two doses), and getting a Tdap vaccine (one dose).
Rhode Island has the highest rates
Some states are clearly doing better than others. Idaho had the lowest completion rate (11.3%; 95% confidence interval, 6.9%-18.0%), and Rhode Island had the highest (56.4%; 95% CI, 49.8%-62.8%).
In the 2018 National Immunization Survey–Teen (NIS-Teen), Rhode Island had the highest vaccination coverage rate in the nation for meningococcal vaccine (98.7%) and the second-highest coverage rate for Tdap (96.3%) for adolescents aged 13-17 years. Also in 2018, the state had the highest vaccination rates in the nation for the HPV series for both male and female adolescents 13-17 years of age (78.1%), well above the national average of 51.1%.
Researchers used information from the Centers for Disease Control and Prevention as well as 2015-2018 NIS-Teen data to estimate national and state-level completion rates by age 17. They then combined NIS-Teen data with public state-level data to evaluate what was driving or discouraging completion.
“The good news is, we found some variables that we consider actionable and can be used by states and local health departments to improve the rates,” Dr. Poston said.
Those include encouraging a health care visit at age 16 or 17, provider recommendations to families to get the HPV vaccine, and state-level mandates for the MenACWY vaccine.
Those who had a health care visit at 16 or 17 were more than twice as likely to complete their vaccines (odds ratio, 2.35; 95% CI, 1.80-3.07). Those for whom HPV vaccination had ever been recommended by a health care provider were more than three times as likely to complete their vaccinations (OR, 3.24; 95% CI, 2.76-3.80).
Other factors predictive of completing the vaccines included being Black or Hispanic and having Medicaid insurance.
At the state level, “living in a state with a mandate for the meningococcal ACWY vaccine in elementary or secondary school was also associated with likelihood of vaccination,” Dr. Poston said. Teens in states with mandates were 60% more likely to complete the vaccines than those in states without mandates. (OR, 1.6; 95% CI, 1.2-2.3)
Marielle Fricchione, MD, assistant professor of pediatric infectious diseases at Rush Medical College, Chicago said in an interview, “Teen vaccines are notoriously hard to get into kids because it’s hard to get them back into the office for second doses.”
She said that Illinois is one of the states with a two-dose mandate for MenACWY before entering 6th grade and 12th grade, which has kept vaccination coverage high.
Educating providers on how to recommend HPV vaccination is the biggest vaccine focus, she added.
Schedule next dose at first visit
One thing her department has found successful in HPV completion is scheduling the second dose while the teen is in the office for the first dose.
“Also, you have to recommend it just as strongly for boys as you do for girls, because oropharyngeal cancer is like an epidemic right now for men, and HPV-related oropharyngeal cancer is on an exponential rise,” Dr. Fricchione said.
According to the CDC, HPV is thought to cause 70% of oropharyngeal cancers in the United States.
Equipping providers with statistics on the effectiveness of HPV vaccination in preventing cancer can take away the uneasiness in talking about sexual transmission.
“That really seems to help them give a strong recommendation. It puts them in a data-driven position to talk about the vaccine,” she said. “Once you put that data in front of the providers, they’re floored.”
Research was funded by GlaxoSmithKline. Dr. Poston is employed by GlaxoSmithKline. Dr. Fricchione disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Only 30.6% of American adolescents complete three routinely recommended vaccinations, new research has found, but that number varies widely by state.
The Advisory Committee on Immunization Practices recommends that, by age 17 years, adolescents complete three key immunizations: human papillomavirus (HPV), quadrivalent meningococcal conjugate (MenACWY), and Tdap.
Sara Poston, PharmD, senior director for health outcomes research at GlaxoSmithKline, said at a press conference during IDWeek, an annual scientific meeting on infectious diseases held virtually this year, that her team set out to determine how many teens were completing the vaccinations and how the number varied by state and by behavioral factors.
Completion of the vaccines means getting the HPV series (two doses for people aged 9-14 years at first vaccination or three doses for those aged 15 years or older at first vaccination), completion of the MenACWY series (two doses), and getting a Tdap vaccine (one dose).
Rhode Island has the highest rates
Some states are clearly doing better than others. Idaho had the lowest completion rate (11.3%; 95% confidence interval, 6.9%-18.0%), and Rhode Island had the highest (56.4%; 95% CI, 49.8%-62.8%).
In the 2018 National Immunization Survey–Teen (NIS-Teen), Rhode Island had the highest vaccination coverage rate in the nation for meningococcal vaccine (98.7%) and the second-highest coverage rate for Tdap (96.3%) for adolescents aged 13-17 years. Also in 2018, the state had the highest vaccination rates in the nation for the HPV series for both male and female adolescents 13-17 years of age (78.1%), well above the national average of 51.1%.
Researchers used information from the Centers for Disease Control and Prevention as well as 2015-2018 NIS-Teen data to estimate national and state-level completion rates by age 17. They then combined NIS-Teen data with public state-level data to evaluate what was driving or discouraging completion.
“The good news is, we found some variables that we consider actionable and can be used by states and local health departments to improve the rates,” Dr. Poston said.
Those include encouraging a health care visit at age 16 or 17, provider recommendations to families to get the HPV vaccine, and state-level mandates for the MenACWY vaccine.
Those who had a health care visit at 16 or 17 were more than twice as likely to complete their vaccines (odds ratio, 2.35; 95% CI, 1.80-3.07). Those for whom HPV vaccination had ever been recommended by a health care provider were more than three times as likely to complete their vaccinations (OR, 3.24; 95% CI, 2.76-3.80).
Other factors predictive of completing the vaccines included being Black or Hispanic and having Medicaid insurance.
At the state level, “living in a state with a mandate for the meningococcal ACWY vaccine in elementary or secondary school was also associated with likelihood of vaccination,” Dr. Poston said. Teens in states with mandates were 60% more likely to complete the vaccines than those in states without mandates. (OR, 1.6; 95% CI, 1.2-2.3)
Marielle Fricchione, MD, assistant professor of pediatric infectious diseases at Rush Medical College, Chicago said in an interview, “Teen vaccines are notoriously hard to get into kids because it’s hard to get them back into the office for second doses.”
She said that Illinois is one of the states with a two-dose mandate for MenACWY before entering 6th grade and 12th grade, which has kept vaccination coverage high.
Educating providers on how to recommend HPV vaccination is the biggest vaccine focus, she added.
Schedule next dose at first visit
One thing her department has found successful in HPV completion is scheduling the second dose while the teen is in the office for the first dose.
“Also, you have to recommend it just as strongly for boys as you do for girls, because oropharyngeal cancer is like an epidemic right now for men, and HPV-related oropharyngeal cancer is on an exponential rise,” Dr. Fricchione said.
According to the CDC, HPV is thought to cause 70% of oropharyngeal cancers in the United States.
Equipping providers with statistics on the effectiveness of HPV vaccination in preventing cancer can take away the uneasiness in talking about sexual transmission.
“That really seems to help them give a strong recommendation. It puts them in a data-driven position to talk about the vaccine,” she said. “Once you put that data in front of the providers, they’re floored.”
Research was funded by GlaxoSmithKline. Dr. Poston is employed by GlaxoSmithKline. Dr. Fricchione disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Only 30.6% of American adolescents complete three routinely recommended vaccinations, new research has found, but that number varies widely by state.
The Advisory Committee on Immunization Practices recommends that, by age 17 years, adolescents complete three key immunizations: human papillomavirus (HPV), quadrivalent meningococcal conjugate (MenACWY), and Tdap.
Sara Poston, PharmD, senior director for health outcomes research at GlaxoSmithKline, said at a press conference during IDWeek, an annual scientific meeting on infectious diseases held virtually this year, that her team set out to determine how many teens were completing the vaccinations and how the number varied by state and by behavioral factors.
Completion of the vaccines means getting the HPV series (two doses for people aged 9-14 years at first vaccination or three doses for those aged 15 years or older at first vaccination), completion of the MenACWY series (two doses), and getting a Tdap vaccine (one dose).
Rhode Island has the highest rates
Some states are clearly doing better than others. Idaho had the lowest completion rate (11.3%; 95% confidence interval, 6.9%-18.0%), and Rhode Island had the highest (56.4%; 95% CI, 49.8%-62.8%).
In the 2018 National Immunization Survey–Teen (NIS-Teen), Rhode Island had the highest vaccination coverage rate in the nation for meningococcal vaccine (98.7%) and the second-highest coverage rate for Tdap (96.3%) for adolescents aged 13-17 years. Also in 2018, the state had the highest vaccination rates in the nation for the HPV series for both male and female adolescents 13-17 years of age (78.1%), well above the national average of 51.1%.
Researchers used information from the Centers for Disease Control and Prevention as well as 2015-2018 NIS-Teen data to estimate national and state-level completion rates by age 17. They then combined NIS-Teen data with public state-level data to evaluate what was driving or discouraging completion.
“The good news is, we found some variables that we consider actionable and can be used by states and local health departments to improve the rates,” Dr. Poston said.
Those include encouraging a health care visit at age 16 or 17, provider recommendations to families to get the HPV vaccine, and state-level mandates for the MenACWY vaccine.
Those who had a health care visit at 16 or 17 were more than twice as likely to complete their vaccines (odds ratio, 2.35; 95% CI, 1.80-3.07). Those for whom HPV vaccination had ever been recommended by a health care provider were more than three times as likely to complete their vaccinations (OR, 3.24; 95% CI, 2.76-3.80).
Other factors predictive of completing the vaccines included being Black or Hispanic and having Medicaid insurance.
At the state level, “living in a state with a mandate for the meningococcal ACWY vaccine in elementary or secondary school was also associated with likelihood of vaccination,” Dr. Poston said. Teens in states with mandates were 60% more likely to complete the vaccines than those in states without mandates. (OR, 1.6; 95% CI, 1.2-2.3)
Marielle Fricchione, MD, assistant professor of pediatric infectious diseases at Rush Medical College, Chicago said in an interview, “Teen vaccines are notoriously hard to get into kids because it’s hard to get them back into the office for second doses.”
She said that Illinois is one of the states with a two-dose mandate for MenACWY before entering 6th grade and 12th grade, which has kept vaccination coverage high.
Educating providers on how to recommend HPV vaccination is the biggest vaccine focus, she added.
Schedule next dose at first visit
One thing her department has found successful in HPV completion is scheduling the second dose while the teen is in the office for the first dose.
“Also, you have to recommend it just as strongly for boys as you do for girls, because oropharyngeal cancer is like an epidemic right now for men, and HPV-related oropharyngeal cancer is on an exponential rise,” Dr. Fricchione said.
According to the CDC, HPV is thought to cause 70% of oropharyngeal cancers in the United States.
Equipping providers with statistics on the effectiveness of HPV vaccination in preventing cancer can take away the uneasiness in talking about sexual transmission.
“That really seems to help them give a strong recommendation. It puts them in a data-driven position to talk about the vaccine,” she said. “Once you put that data in front of the providers, they’re floored.”
Research was funded by GlaxoSmithKline. Dr. Poston is employed by GlaxoSmithKline. Dr. Fricchione disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM IDWEEK 2020
Cerebral blood flow may predict children’s recovery from persistent postconcussion symptoms
, according to a study presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. Furthermore, cerebral blood flow at 4-6 weeks predicts recovery during the next 4 weeks in 77% of children.

“This is the first study to examine cerebral blood flow changes in children with persistent postconcussion symptoms,” said Karen Barlow, MBChB, associate professor of biomedical sciences at the University of Queensland in St. Lucia, Australia. “Our findings support the link between neurovascular unit dysfunction and persistent postconcussion symptoms in children, potentially because of injury or dysfunction in the GABAergic interneurons.”
Quantifying cerebral tissue perfusion
At least 25% of children with concussion have persistent postconcussion symptoms at 1 month post injury. Understanding the factors that influence the speed of recovery may help clarify the biology of postconcussion symptoms and suggest new treatments. In previous research, Dr. Barlow and colleagues found that children with early recovery (i.e., recovery by 4 weeks post injury) have decreases in cerebral blood flow, when compared with normal children. Children with persistent symptoms, however, have increases in cerebral blood flow. Dr. Barlow and colleagues conducted a new study to examine how cerebral blood flow changes in children with persistent postconcussion symptoms.
The investigators recruited participants through the randomized controlled Play Game trial, which examined melatonin as a treatment for persistent postconcussion symptoms. Among the exclusion criteria were history of assault, drug or alcohol use, significant past medical or psychiatric history, concussion within the previous 3 months, and use of psychoactive medications.
Children entered the study at 4-8 weeks after injury and received treatment for 4 weeks. Participants underwent 3-D pseudo-continuous arterial spin–labeled MRI before and after the treatment period (i.e., at 5 and 10 weeks post injury). This imaging technique provides a quantitative assessment of cerebral tissue perfusion. “You can do it without manipulating the cerebral circulation, making it particularly useful for research and in children,” said Dr. Barlow.
She and her colleagues evaluated recovery using the Post-Concussion Symptom Inventory. They defined good recovery as a total score at or below baseline at 10 weeks post injury. They considered any children who did not meet this criterion to have poor recovery.
Speed of blood-flow change varied
In all, 124 children were eligible for the study, and 76 had MRIs at both time points. Fourteen participants were excluded because of motion artifacts, slice truncation, and normalization failure. The population’s average age was approximately 14 years. About half of participants were males. The first MRI was performed at 37 days post injury, and the second MRI at around 70 days post injury. Twenty-three children had good recovery.
Children with poor recovery at 10 weeks had higher relative cerebral blood flow, compared with children with good recovery. Treatment group, age, and sex did not affect the changes in relative cerebral blood flow over time. Dr. Barlow and colleagues also measured mean total gray matter cerebral blood flow. Children with poor recovery had higher cerebral blood flow at 5 and 10 weeks post injury, compared with children with good recovery. In addition, cerebral blood flow changed more slowly in participants with poor recovery, compared with those with good recovery. Logistic regression analysis indicated that the mean absolute gray matter cerebral blood flow at 4-6 weeks post injury significantly predicted which children would recover by 10 weeks post injury, with an area under the receiver operating characteristic curve of 77%.
Funders for the study included Alberta Children’s Hospital, the Canadian Institutes of Health Research, and the University of Calgary. Dr. Barlow had no disclosures or conflicts of interest.
SOURCE: Barlow K et al. CNS-ICNA 2020. Abstract PL100.
, according to a study presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. Furthermore, cerebral blood flow at 4-6 weeks predicts recovery during the next 4 weeks in 77% of children.
“This is the first study to examine cerebral blood flow changes in children with persistent postconcussion symptoms,” said Karen Barlow, MBChB, associate professor of biomedical sciences at the University of Queensland in St. Lucia, Australia. “Our findings support the link between neurovascular unit dysfunction and persistent postconcussion symptoms in children, potentially because of injury or dysfunction in the GABAergic interneurons.”
Quantifying cerebral tissue perfusion
At least 25% of children with concussion have persistent postconcussion symptoms at 1 month post injury. Understanding the factors that influence the speed of recovery may help clarify the biology of postconcussion symptoms and suggest new treatments. In previous research, Dr. Barlow and colleagues found that children with early recovery (i.e., recovery by 4 weeks post injury) have decreases in cerebral blood flow, when compared with normal children. Children with persistent symptoms, however, have increases in cerebral blood flow. Dr. Barlow and colleagues conducted a new study to examine how cerebral blood flow changes in children with persistent postconcussion symptoms.
The investigators recruited participants through the randomized controlled Play Game trial, which examined melatonin as a treatment for persistent postconcussion symptoms. Among the exclusion criteria were history of assault, drug or alcohol use, significant past medical or psychiatric history, concussion within the previous 3 months, and use of psychoactive medications.
Children entered the study at 4-8 weeks after injury and received treatment for 4 weeks. Participants underwent 3-D pseudo-continuous arterial spin–labeled MRI before and after the treatment period (i.e., at 5 and 10 weeks post injury). This imaging technique provides a quantitative assessment of cerebral tissue perfusion. “You can do it without manipulating the cerebral circulation, making it particularly useful for research and in children,” said Dr. Barlow.
She and her colleagues evaluated recovery using the Post-Concussion Symptom Inventory. They defined good recovery as a total score at or below baseline at 10 weeks post injury. They considered any children who did not meet this criterion to have poor recovery.
Speed of blood-flow change varied
In all, 124 children were eligible for the study, and 76 had MRIs at both time points. Fourteen participants were excluded because of motion artifacts, slice truncation, and normalization failure. The population’s average age was approximately 14 years. About half of participants were males. The first MRI was performed at 37 days post injury, and the second MRI at around 70 days post injury. Twenty-three children had good recovery.
Children with poor recovery at 10 weeks had higher relative cerebral blood flow, compared with children with good recovery. Treatment group, age, and sex did not affect the changes in relative cerebral blood flow over time. Dr. Barlow and colleagues also measured mean total gray matter cerebral blood flow. Children with poor recovery had higher cerebral blood flow at 5 and 10 weeks post injury, compared with children with good recovery. In addition, cerebral blood flow changed more slowly in participants with poor recovery, compared with those with good recovery. Logistic regression analysis indicated that the mean absolute gray matter cerebral blood flow at 4-6 weeks post injury significantly predicted which children would recover by 10 weeks post injury, with an area under the receiver operating characteristic curve of 77%.
Funders for the study included Alberta Children’s Hospital, the Canadian Institutes of Health Research, and the University of Calgary. Dr. Barlow had no disclosures or conflicts of interest.
SOURCE: Barlow K et al. CNS-ICNA 2020. Abstract PL100.
, according to a study presented at the 2020 CNS-ICNA Conjoint Meeting, held virtually this year. Furthermore, cerebral blood flow at 4-6 weeks predicts recovery during the next 4 weeks in 77% of children.
“This is the first study to examine cerebral blood flow changes in children with persistent postconcussion symptoms,” said Karen Barlow, MBChB, associate professor of biomedical sciences at the University of Queensland in St. Lucia, Australia. “Our findings support the link between neurovascular unit dysfunction and persistent postconcussion symptoms in children, potentially because of injury or dysfunction in the GABAergic interneurons.”
Quantifying cerebral tissue perfusion
At least 25% of children with concussion have persistent postconcussion symptoms at 1 month post injury. Understanding the factors that influence the speed of recovery may help clarify the biology of postconcussion symptoms and suggest new treatments. In previous research, Dr. Barlow and colleagues found that children with early recovery (i.e., recovery by 4 weeks post injury) have decreases in cerebral blood flow, when compared with normal children. Children with persistent symptoms, however, have increases in cerebral blood flow. Dr. Barlow and colleagues conducted a new study to examine how cerebral blood flow changes in children with persistent postconcussion symptoms.
The investigators recruited participants through the randomized controlled Play Game trial, which examined melatonin as a treatment for persistent postconcussion symptoms. Among the exclusion criteria were history of assault, drug or alcohol use, significant past medical or psychiatric history, concussion within the previous 3 months, and use of psychoactive medications.
Children entered the study at 4-8 weeks after injury and received treatment for 4 weeks. Participants underwent 3-D pseudo-continuous arterial spin–labeled MRI before and after the treatment period (i.e., at 5 and 10 weeks post injury). This imaging technique provides a quantitative assessment of cerebral tissue perfusion. “You can do it without manipulating the cerebral circulation, making it particularly useful for research and in children,” said Dr. Barlow.
She and her colleagues evaluated recovery using the Post-Concussion Symptom Inventory. They defined good recovery as a total score at or below baseline at 10 weeks post injury. They considered any children who did not meet this criterion to have poor recovery.
Speed of blood-flow change varied
In all, 124 children were eligible for the study, and 76 had MRIs at both time points. Fourteen participants were excluded because of motion artifacts, slice truncation, and normalization failure. The population’s average age was approximately 14 years. About half of participants were males. The first MRI was performed at 37 days post injury, and the second MRI at around 70 days post injury. Twenty-three children had good recovery.
Children with poor recovery at 10 weeks had higher relative cerebral blood flow, compared with children with good recovery. Treatment group, age, and sex did not affect the changes in relative cerebral blood flow over time. Dr. Barlow and colleagues also measured mean total gray matter cerebral blood flow. Children with poor recovery had higher cerebral blood flow at 5 and 10 weeks post injury, compared with children with good recovery. In addition, cerebral blood flow changed more slowly in participants with poor recovery, compared with those with good recovery. Logistic regression analysis indicated that the mean absolute gray matter cerebral blood flow at 4-6 weeks post injury significantly predicted which children would recover by 10 weeks post injury, with an area under the receiver operating characteristic curve of 77%.
Funders for the study included Alberta Children’s Hospital, the Canadian Institutes of Health Research, and the University of Calgary. Dr. Barlow had no disclosures or conflicts of interest.
SOURCE: Barlow K et al. CNS-ICNA 2020. Abstract PL100.
FROM CNS-ICNA 2020
Twelve end-of-year tax tips: How COVID-19 could lower your tax bite
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.
COVID-19 has had a huge impact on every aspect of physicians’ medical practice, incomes, and business. Although this will probably not end soon, there are some key tax strategies that can help your financial position if you take some important actions by the end of the year.
Some of the ways in which physicians were hard hit include:
- Physicians who are self-employed are facing increased costs for personal protective equipment, cleaning protocols, and new telehealth infrastructure. Many are also facing staffing shortages as employees fall to part-time work or take time off work to care for family members.
- Even physicians working for large hospitals are not isolated from the financial impact of the virus. A recent survey conducted by Medscape concluded that over 60% of physicians in the United States have experienced a decrease in income since the start of the pandemic.
- Saving and investing have been affected: Physicians may expect to see that companies in which they are invested are cutting dividends. Interest rates (CDs, bonds) are lower, and capital gains distributions are reduced this year. Overall, that makes for a fairly grim financial picture.
While taxable income this year has mostly declined, the applicable tax rates overall are low. However, federal, state, and local budget deficits have been skyrocketing owing to the demands of the pandemic. That means, in all likelihood, there will be tax increases in the coming years to cover spending. However, this year’s financial challenges could lend themselves to a unique tax planning scenario that could potentially benefit physicians as they make long-term plans for their investments.
Given these circumstances, these 12 tips can help you to lessen your tax bite this tax season. Many of these tips entail actions that you need to take before Dec. 31, 2020.
1. Coronavirus stimulus rebates
If you have significantly depressed income this year or have lost your job, you may find that you qualify for an Economic Impact Payment, a refundable tax credit on the 2020 tax return. The credit is $1,200 for individuals or $2,400 for joint filers, plus an additional $500 for each qualifying child aged 16 years or younger. You begin to phase out of the credit at an adjusted gross income (AGI) of $75,000 for individuals and $150,000 for joint filers. People who had AGI below these thresholds in 2019 already would have received the credit in advance, but those who now find themselves qualifying will receive the credit when they file their 2020 tax return. No action is needed on your part; your tax preparer will calculate whether you are eligible for the credit when filing your return.
2. Look to accelerate income at lower brackets
With reduced earned income, many physicians will find themselves in significantly lower tax brackets this year. Once you fall below $200,000 for individuals or $250,000 for joint filers, you no longer trigger two additional surcharge taxes. The first is the additional Medicare tax, which is a further 0.9% applied to earned income above those thresholds, on top of ordinary income tax brackets. The second is the Net Investment Income Tax (NIIT), which is an additional 3.8% applied to your investment income on top of capital gains tax brackets.
If you are someone to whom the additional Medicare tax or NIIT no longer applies for 2020, you might consider generating income this year in order to realize the lower tax rates. You could consider selling highly appreciated investments in your taxable portfolio and reinvest the proceeds by repurchasing the same securities, thereby receiving a step-up in cost basis. Remember, when you go to sell securities in retirement, you are only taxed on the gain on the security over your cost basis. By bringing the cost basis up to today’s fair market value, you could be greatly reducing the future tax applied on a sale.
For those with IRA or inherited IRA accounts who also have required minimum distributions (RMDs), you might consider making voluntary withdrawals this year and then reinvesting the proceeds into a savings or taxable account for when you need it. Keep in mind that under the CARES Act, you are no longer required to take RMDs for 2020. However, this action would help avoid being forced to withdraw the amount when you may be at a higher tax bracket. You would need to do this before Dec. 31.
3. Build Roth assets strategies
With reduced incomes and lower marginal tax rates applying to the last dollar of income this year, physicians should carefully consider how to take advantage of current tax rates by building Roth assets. There are a few strategies, including switching 401(k) or 457 contributions from pretax to Roth or performing a backdoor Roth IRA contribution. However, neither is as powerful as converting IRA assets to Roth assets because there is no restriction on conversion amount or income cutoffs.
The goal is to convert enough assets to fill up lower applicable marginal tax brackets while avoiding tax surcharges, where possible. Roth IRA conversions can get you in trouble if you don’t know what to expect, so it’s best to work with a financial advisor or tax professional to give you guidance. For example, Roth conversions can trigger some tax surprises, such as the phaseout for the 199A qualified business income deduction, increased taxation on your Social Security benefits, or higher Income-Related Monthly Adjustment Amount surcharges on Medicare Part B and Part D premiums.
Bear in mind that Roth conversions generate taxable income and cannot be undone once completed. However, paying the lower marginal tax rate today may be a big win when RMDs could push physicians into tax brackets as high as or higher than during their working years.
4. Coronavirus-related distributions
New this year is a penalty-free way to withdraw qualified retirement plan funds for those who are not yet eligible to make penalty-free withdrawals.
Congress introduced the Coronavirus-Related Distribution under the CARES Act. It allows individuals who have been affected by the pandemic to withdraw up to $100,000 before Dec. 31, 2020, without paying the 10% early withdrawal penalty. If you are considering an early retirement because of the pandemic, it may make sense to take this withdrawal while the option lasts and keep the cash available to help fund the gap before the remainder of your retirement plan assets are available penalty free. Keep in mind that this withdrawal generates taxable ordinary income, even though the early withdrawal penalty does not apply. Taking this withdrawal can boost your taxable income bracket, so calculate carefully before you do this.
5. Charitable donations for 2020
There is no shortage of people in need owing to the pandemic. For those who continue to be charitable-minded, a decrease in income may mean you have more opportunity for your regularly recurring charitable donations to decrease your taxes this year. Normally, charitable donations for itemizers are limited to 60% of AGI. However, the CARES Act increased the charitable deduction limit to 100% of AGI for 2020. Even those who claim the standard deduction can take advantage of a new “above-the-line” deduction worth $300 for individuals and $600 for joint filers by making qualified cash donations in 2020. Take special note that the contributions do not apply to donor-advised funds or nonoperating private foundations.
6. Noncash charitable donations
Many physicians are working longer and harder than ever, and for many, that means vacation plans have been placed on hold for the remainder of the year. Don’t let your paid-time-off days go to waste! The IRS now permits leave-based donation programs, which allow employers to make deductible charitable donations for the relief of victims of the COVID-19 pandemic on the basis of the value of the sick, vacation, or personal leave that employees voluntarily forgo. The value of the donation will not be treated as compensation for the employee and will be free of any otherwise applicable Federal Insurance Contributions Act (FICA) taxes, and the employer can deduct the donation as ordinary and necessary business expenses if they meet certain requirements.
7. Claiming 2020 losses on prior tax returns
For self-employed physicians, a wealth of tax planning strategies are available. One of the most significant may be the new provisions under the CARES Act that allow 100% of net operating losses (NOLs) for 3 calendar years of losses – namely 2018, 2019, and 2020 – to be carried back to the prior 5 tax years. Using these NOLs, you may be able to claim a refund for tax returns from prior tax years when there was otherwise a limit on NOLs at 80% of taxable income. If you think this applies to you, it’s wise to meet with your accountant or financial professional to discuss this.
8. Delay payroll taxes where possible
For physicians with employees looking for some cash flow relief, a new payroll tax deferral is available to you this year. Under the CARES Act, employers can delay payment of their 2020 employer payroll tax, namely the 6.2% Social Security tax, with 50% not due until Dec. 31, 2021, and the remainder due Dec. 31, 2022. The deferral will not incur any interest or penalties and is also available to those who are self-employed.
On top of that, a new payroll tax credit was created under the Families First Coronavirus Response Act. Eligible employers can receive this tax credit for the amount of wages they pay to eligible employees who are taking pandemic-related paid family leave or paid sick leave this year. The credit is also available to those who are self-employed. If you think this credit may be applicable to you, it’s worth speaking with your tax preparer about it.
9. Increased business property deductions
The nature of many physician business operations has drastically changed this year. For physicians who already have invested in and implemented new telehealth infrastructure, this can create valuable tax deductions to offset their ordinary income. Businesses may take 100% bonus depreciation on the cost of qualified property both acquired and placed in service after Sept. 27, 2017, and before Jan. 1, 2023. In general, during the last quarter of the year, you should look to decelerate business purchases until after Jan. 1, 2021, to get a deduction in 2021 at a higher marginal tax bracket.
10. Switch to cash accounting instead of accrual accounting
With higher expenses and lower profits, some large practice groups may take a second look to see whether they qualify to switch to cash accounting from accrual accounting to defer taxes. This rule change was adopted back in 2017 to allow small-business taxpayers with average annual gross receipts of $25 million or less in the prior 3 years to use the cash method of accounting. Ultimately, this switch should allow practices to owe the IRS money only after invoices were paid.
11. Physicians looking to sell their unprofitable practices
For physicians looking to make a quick exit from their practice in response to the pandemic, there is some tax relief in the event of a sale at a loss. Certain business owners who sell failed businesses will be able to use up to $50,000 of net losses as individuals or $100,000 as joint filers from the sale to offset ordinary income, current or future, under Internal Revenue Code (IRC) Section 1244. Remember that ordinary income tax rates are much higher than capital gains rates, so you could see some tax relief through a sale. The provision covers shareholders of domestic small-business corporations, both C or S corporations, but not partnerships. You would have to sell the business before Dec. 31 to get this deduction in 2020.
12. Physicians looking to sell their profitable practices
Even self-employed physicians who have managed to maintain profitable practices may be looking for early retirement after the exhaustion of the pandemic. If you own stock in a C corporation engaged in an active trade or business that has not had assets of more than $50 million at any time, you can take advantage of the IRC Section 1202 exemption. Section 1202 provides an exclusion from gain from the sale of stock of either $10 million or 10 times the adjusted basis of the stock, owned at least 5 years, in corporations regarded as “qualified small businesses.” This means you may be able to sell your practice at a gain with a handsome tax shield. Again, to get this tax benefit for April’s tax return, you’d have to engage in this activity before year end.
Regardless of whether the pandemic has placed financial constraints on you this year, tax-savvy opportunities are available to capitalize on your reduced income and lower tax rates. It’s always important to keep in mind not just your taxes in any one given year, but your lifetime tax obligations. Financial advisors and tax planners can perform multiyear tax calculations and recommend ways to manage your tax bracket and help lower your overall lifetime tax obligations.
A version of this article originally appeared on Medscape.com.
Score predicts risk for ventilation in COVID-19 patients
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.

The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.

Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
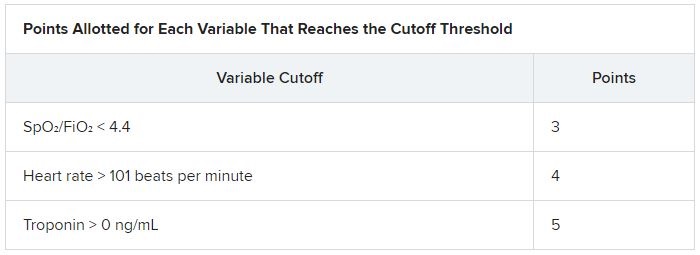
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.
The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.
Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.
The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.
Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
Trump and Biden face off over COVID-19, ACA in final debate
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
COVID-19 a new opportunity for suicide prevention
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.