User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Parkinson’s disease could be hiding behind those nightmares
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.

For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.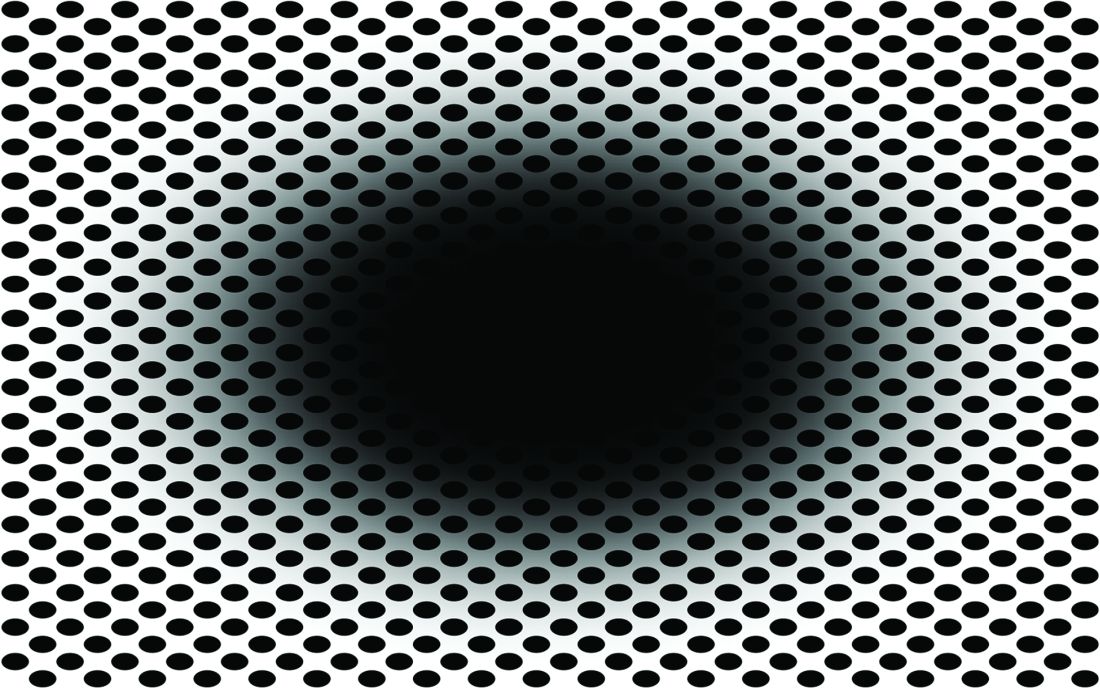
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Pregnant women with monkeypox advised to have C-section
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
FROM ULTRASOUND IN OBSTETRICS & GYNECOLOGY
In utero COVID exposure tied to developmental differences in infants
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
suggests a small-scale analysis that points to the need for further study and monitoring during pregnancy.
The study included 24 pregnant women, half of whom had COVID-19 during pregnancy, and their offspring. It showed impairments at 6 weeks of age on the social interactive dimension of a neonatal assessment.
“Not all babies born to mothers infected with COVID show neurodevelopmental differences, but our data show that their risk is increased in comparison to those not exposed to COVID in the womb. We need a bigger study to confirm the exact extent of the difference,” said lead researcher Rosa Ayesa Arriola, PhD, Valdecilla Research Institute (IDIVAL), Hospital Universitario Marqués de Valdecilla, Santander, Spain, in a release.
The findings were presented at the virtual European Psychiatric Association 2022 Congress.
Differing responses to cuddling
Coauthor Águeda Castro Quintas, PhD student, Network Centre for Biomedical Research in Mental Health, University of Barcelona, explained that the tests showed the children born to mothers who had COVID-19 during pregnancy reacted “slightly differently to being held, or cuddled.”
“We need to note that these are preliminary results, but this is part of a project following a larger sample of 100 mothers and their babies,” she added. The authors plan to compare their results with those from a similar study.
The group will also monitor infant language and motor development aged between 18 and 42 months.
“This is an ongoing project, and we are at an early stage,” Ms. Castro Quintas said. “We don’t know if these effects will result in any longer-term issues,” but longer-term observation “may help us understand this.”
“Of course, in babies who are so young, there are several things we just can’t measure, such as language skills or cognition,” added coinvestigator Nerea San Martín González, department of evolutionary biology, ecology and environmental sciences, University of Barcelona.
While emphasizing the need for larger sample sizes, she said that “in the meantime, we need to stress the importance of medical monitoring to facilitate a healthy pregnancy.”
The researchers note that the consequences of the COVID-19 pandemic for the newborns of affected mothers remain “unknown.”
However, previous studies of other infections during pregnancy suggest that offspring could be “especially vulnerable,”as the pathophysiological mechanisms of the infection, such as cytokine storms and microcoagulation, “could clearly compromise fetal neurodevelopment.”
To investigate further, they examined the neurodevelopment of infants born both immediately before and during the COVID-19 pandemic, from 2017 to 2021.
Twenty-one women who had COVID-19 during pregnancy were matched with 21 healthy controls. They were studied both during pregnancy and in the postpartum period, completing hormonal and other biochemical tests, salivary tests, movement assessments, and psychological questionnaires, adjusted for various factors.
The team also administered the Brazelton Neonatal Behavioural Assessment Scale (NBAS) to the offspring at 6 weeks of age to evaluate neurologic, social, and behavioral aspects of function.
“We have been especially sensitive in how we have conducted these tests,” said Ms. Castro Quintas. “Each mother and baby were closely examined by clinicians with expert training in the field and in the tests.”
Among those offspring exposed to COVID-19 during pregnancy, there was a significant decrease in scores on the social interactive dimension of the NBAS, particularly if infection occurred before week 20 of gestation.
Other NBAS subscales were not associated with maternal COVID-19 during pregnancy.
More research needed
Commenting on the findings, Livio Provenzi, PhD, a psychologist and researcher in developmental psychobiology at the University of Pavia (Italy), noted there is a “great need” to study the direct and indirect effect of the COVID-19 pandemic on parents and their children. “Pregnancy is a period of life which shapes much of our subsequent development, and exposure to adversity in pregnancy can leave long-lasting biological footprints.”
Dr. Provenzi, who was not involved in the study, added in the release that the findings reinforce “evidence of epigenetic alterations in infants born from mothers exposed to pandemic-related stress during pregnancy.
“It shows we need more large-scale, international research to allow us to understand the developmental effects of this health emergency and to deliver better quality of care to parents and infants.”
The study was funded by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III through the University of Barcelona multicenter project and the Government of Cantabria. No relevant financial relationships were declared.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
‘Medical maximizers’ dole out unneeded antibiotics for ASB
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FDA approves dupilumab for children with eczema aged 6 months to 5 years
The whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
The approval, announced on June 7, 2022, makes dupilumab (Dupixent), an interleukin-4 receptor alpha antagonist, the first biologic available in the United States to treat uncontrolled moderate to severe atopic dermatitis in this age group. In this age group, it is administered subcutaneously every 4 weeks. Dupilumab remains the only biologic treatment approved for patients aged 6 years and older for this indication.
Approval was based on data from a 16-week pivotal phase 3 trial that evaluated the efficacy and safety of dupilumab added to standard of care topical corticosteroids (TCS) in children aged 6 months to 5 years with uncontrolled moderate to severe atopic dermatitis. The trial’s principal investigator, Amy S. Paller, MD, professor and chair of dermatology at Northwestern University, Chicago, and colleagues, found that, at 16 weeks, 28% of patients who were treated with dupilumab, added to low-potency TCS, met the primary endpoint of clear or almost clear skin, compared with 4% of those who received low-potency TCS alone (P < .0001).
In addition, patients who received the combined treatment experienced a 70% average improvement in disease severity from baseline, compared with a 20% improvement among those in the TCS-only group (P < .0001). They also experienced a 49% improvement in itch, compared with a 2% improvement among their counterparts in the TCS-only group (P < .0001).
Outside of the United States, the study’s coprimary endpoint was achievement of 75% or greater improvement in overall disease severity. More than half of the patients who received combined treatment (53%) met this endpoint, compared with 11% in the TCS-only group (P < .0001), according to the company.
Safety results were generally consistent with the safety profile of dupilumab in atopic dermatitis for patients aged 6 years and older. The most common adverse events that were more commonly observed with dupilumab included conjunctivitis (5% vs 0% in the placebo group) and herpes viral infections (6% vs. 5% in the placebo group). Among those on dupilumab, ages 6 months to 5 years, hand,foot, and mouth disease was reported in 5% and skin papilloma were reported in 2%, but these cases did not lead to discontinuation of treatment, according to the company release.
A version of this article first appeared on Medscape.com.
The whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
The approval, announced on June 7, 2022, makes dupilumab (Dupixent), an interleukin-4 receptor alpha antagonist, the first biologic available in the United States to treat uncontrolled moderate to severe atopic dermatitis in this age group. In this age group, it is administered subcutaneously every 4 weeks. Dupilumab remains the only biologic treatment approved for patients aged 6 years and older for this indication.
Approval was based on data from a 16-week pivotal phase 3 trial that evaluated the efficacy and safety of dupilumab added to standard of care topical corticosteroids (TCS) in children aged 6 months to 5 years with uncontrolled moderate to severe atopic dermatitis. The trial’s principal investigator, Amy S. Paller, MD, professor and chair of dermatology at Northwestern University, Chicago, and colleagues, found that, at 16 weeks, 28% of patients who were treated with dupilumab, added to low-potency TCS, met the primary endpoint of clear or almost clear skin, compared with 4% of those who received low-potency TCS alone (P < .0001).
In addition, patients who received the combined treatment experienced a 70% average improvement in disease severity from baseline, compared with a 20% improvement among those in the TCS-only group (P < .0001). They also experienced a 49% improvement in itch, compared with a 2% improvement among their counterparts in the TCS-only group (P < .0001).
Outside of the United States, the study’s coprimary endpoint was achievement of 75% or greater improvement in overall disease severity. More than half of the patients who received combined treatment (53%) met this endpoint, compared with 11% in the TCS-only group (P < .0001), according to the company.
Safety results were generally consistent with the safety profile of dupilumab in atopic dermatitis for patients aged 6 years and older. The most common adverse events that were more commonly observed with dupilumab included conjunctivitis (5% vs 0% in the placebo group) and herpes viral infections (6% vs. 5% in the placebo group). Among those on dupilumab, ages 6 months to 5 years, hand,foot, and mouth disease was reported in 5% and skin papilloma were reported in 2%, but these cases did not lead to discontinuation of treatment, according to the company release.
A version of this article first appeared on Medscape.com.
The whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable.
The approval, announced on June 7, 2022, makes dupilumab (Dupixent), an interleukin-4 receptor alpha antagonist, the first biologic available in the United States to treat uncontrolled moderate to severe atopic dermatitis in this age group. In this age group, it is administered subcutaneously every 4 weeks. Dupilumab remains the only biologic treatment approved for patients aged 6 years and older for this indication.
Approval was based on data from a 16-week pivotal phase 3 trial that evaluated the efficacy and safety of dupilumab added to standard of care topical corticosteroids (TCS) in children aged 6 months to 5 years with uncontrolled moderate to severe atopic dermatitis. The trial’s principal investigator, Amy S. Paller, MD, professor and chair of dermatology at Northwestern University, Chicago, and colleagues, found that, at 16 weeks, 28% of patients who were treated with dupilumab, added to low-potency TCS, met the primary endpoint of clear or almost clear skin, compared with 4% of those who received low-potency TCS alone (P < .0001).
In addition, patients who received the combined treatment experienced a 70% average improvement in disease severity from baseline, compared with a 20% improvement among those in the TCS-only group (P < .0001). They also experienced a 49% improvement in itch, compared with a 2% improvement among their counterparts in the TCS-only group (P < .0001).
Outside of the United States, the study’s coprimary endpoint was achievement of 75% or greater improvement in overall disease severity. More than half of the patients who received combined treatment (53%) met this endpoint, compared with 11% in the TCS-only group (P < .0001), according to the company.
Safety results were generally consistent with the safety profile of dupilumab in atopic dermatitis for patients aged 6 years and older. The most common adverse events that were more commonly observed with dupilumab included conjunctivitis (5% vs 0% in the placebo group) and herpes viral infections (6% vs. 5% in the placebo group). Among those on dupilumab, ages 6 months to 5 years, hand,foot, and mouth disease was reported in 5% and skin papilloma were reported in 2%, but these cases did not lead to discontinuation of treatment, according to the company release.
A version of this article first appeared on Medscape.com.
Substance use the main cause of physician license actions
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
FROM JAMA
Children and COVID: Cases down, start of vaccinations near
The first decline in COVID-19 cases among children since early April may have been holiday related, but the shortened week also brought news about vaccination for the youngest children.
The Food and Drug Administration has accepted Pfizer’s application for a COVID-19 vaccine for children under age 5, so vaccination could begin as early as June 21, according to White House COVID-19 response coordinator Ashish Jha, MD.
“We know that many, many parents are eager to vaccinate their youngest kids and it’s important to do this right,” Dr. Jha said at a White House press briefing June 2. “We expect that vaccinations will begin in earnest as early as June 21 and really roll on throughout that week.”
Decline may just be underreporting
Over on the incidence side of the pandemic, “Testing and reporting may have been affected by the holiday weekend [since] states may change their reporting schedules, which may cause irregularities in trends,” the American Academy of Pediatrics and the Children’s Hospital association said in their latest COVID report.
The decline in new cases was not spread uniformly across the four major regions of the United States. The count actually went up in the West for the week of May 27 to June 2, while the South saw the largest decline. The Midwest and Northeast, meanwhile, saw new cases drop for the second straight week, the AAP and CHA said.
The cumulative number of COVID-19 cases in children was up to 13.45 million as of June 2, with children representing 18.9% of all cases since the start of the pandemic, according to the two organizations. The Centers for Disease Control and Prevention reported figures of 13.14 million and 17.5% on June 6.
The AAP/CHA estimates, however, are based on state data that have become increasingly hard to obtain and subject to inconsistency. “Shortages of COVID-19 tests during surges and the increasing use of COVID-19 home tests likely affect the undercounting of COVID-19 cases,” they noted, and “at times when COVID-19 transmission is low, states might reduce the frequency information is updated.”
Vaccinations held steady over the holiday
The ongoing vaccination effort in children aged 5 years and older did not show a Memorial Day drop-off, as initial vaccinations held at 43,000 in 5- to 11-year-olds and at 27,000 in 12- to 17-year-olds for a second consecutive week. That number has ranged from 34,000 to 70,000 for the younger children and from 25,000 to 47,000 for the older group since mid-March, the AAP said in a separate weekly report.
Despite weekly vaccine initiations that have been roughly double those of the older children for months, the 5- to 11-year-olds are still only at 36.0% coverage with at least one dose, compared with 69.5% for the 12- to-17-year-olds. Full vaccination for the two age groups comes in at 29.3% and 59.6%, respectively, as of June 6, according to the CDC’s COVID Data Tracker.
The first decline in COVID-19 cases among children since early April may have been holiday related, but the shortened week also brought news about vaccination for the youngest children.
The Food and Drug Administration has accepted Pfizer’s application for a COVID-19 vaccine for children under age 5, so vaccination could begin as early as June 21, according to White House COVID-19 response coordinator Ashish Jha, MD.
“We know that many, many parents are eager to vaccinate their youngest kids and it’s important to do this right,” Dr. Jha said at a White House press briefing June 2. “We expect that vaccinations will begin in earnest as early as June 21 and really roll on throughout that week.”
Decline may just be underreporting
Over on the incidence side of the pandemic, “Testing and reporting may have been affected by the holiday weekend [since] states may change their reporting schedules, which may cause irregularities in trends,” the American Academy of Pediatrics and the Children’s Hospital association said in their latest COVID report.
The decline in new cases was not spread uniformly across the four major regions of the United States. The count actually went up in the West for the week of May 27 to June 2, while the South saw the largest decline. The Midwest and Northeast, meanwhile, saw new cases drop for the second straight week, the AAP and CHA said.
The cumulative number of COVID-19 cases in children was up to 13.45 million as of June 2, with children representing 18.9% of all cases since the start of the pandemic, according to the two organizations. The Centers for Disease Control and Prevention reported figures of 13.14 million and 17.5% on June 6.
The AAP/CHA estimates, however, are based on state data that have become increasingly hard to obtain and subject to inconsistency. “Shortages of COVID-19 tests during surges and the increasing use of COVID-19 home tests likely affect the undercounting of COVID-19 cases,” they noted, and “at times when COVID-19 transmission is low, states might reduce the frequency information is updated.”
Vaccinations held steady over the holiday
The ongoing vaccination effort in children aged 5 years and older did not show a Memorial Day drop-off, as initial vaccinations held at 43,000 in 5- to 11-year-olds and at 27,000 in 12- to 17-year-olds for a second consecutive week. That number has ranged from 34,000 to 70,000 for the younger children and from 25,000 to 47,000 for the older group since mid-March, the AAP said in a separate weekly report.
Despite weekly vaccine initiations that have been roughly double those of the older children for months, the 5- to 11-year-olds are still only at 36.0% coverage with at least one dose, compared with 69.5% for the 12- to-17-year-olds. Full vaccination for the two age groups comes in at 29.3% and 59.6%, respectively, as of June 6, according to the CDC’s COVID Data Tracker.
The first decline in COVID-19 cases among children since early April may have been holiday related, but the shortened week also brought news about vaccination for the youngest children.
The Food and Drug Administration has accepted Pfizer’s application for a COVID-19 vaccine for children under age 5, so vaccination could begin as early as June 21, according to White House COVID-19 response coordinator Ashish Jha, MD.
“We know that many, many parents are eager to vaccinate their youngest kids and it’s important to do this right,” Dr. Jha said at a White House press briefing June 2. “We expect that vaccinations will begin in earnest as early as June 21 and really roll on throughout that week.”
Decline may just be underreporting
Over on the incidence side of the pandemic, “Testing and reporting may have been affected by the holiday weekend [since] states may change their reporting schedules, which may cause irregularities in trends,” the American Academy of Pediatrics and the Children’s Hospital association said in their latest COVID report.
The decline in new cases was not spread uniformly across the four major regions of the United States. The count actually went up in the West for the week of May 27 to June 2, while the South saw the largest decline. The Midwest and Northeast, meanwhile, saw new cases drop for the second straight week, the AAP and CHA said.
The cumulative number of COVID-19 cases in children was up to 13.45 million as of June 2, with children representing 18.9% of all cases since the start of the pandemic, according to the two organizations. The Centers for Disease Control and Prevention reported figures of 13.14 million and 17.5% on June 6.
The AAP/CHA estimates, however, are based on state data that have become increasingly hard to obtain and subject to inconsistency. “Shortages of COVID-19 tests during surges and the increasing use of COVID-19 home tests likely affect the undercounting of COVID-19 cases,” they noted, and “at times when COVID-19 transmission is low, states might reduce the frequency information is updated.”
Vaccinations held steady over the holiday
The ongoing vaccination effort in children aged 5 years and older did not show a Memorial Day drop-off, as initial vaccinations held at 43,000 in 5- to 11-year-olds and at 27,000 in 12- to 17-year-olds for a second consecutive week. That number has ranged from 34,000 to 70,000 for the younger children and from 25,000 to 47,000 for the older group since mid-March, the AAP said in a separate weekly report.
Despite weekly vaccine initiations that have been roughly double those of the older children for months, the 5- to 11-year-olds are still only at 36.0% coverage with at least one dose, compared with 69.5% for the 12- to-17-year-olds. Full vaccination for the two age groups comes in at 29.3% and 59.6%, respectively, as of June 6, according to the CDC’s COVID Data Tracker.
Cochlear implants benefit deaf children with developmental delays
Deaf babies and toddlers with developmental delays may benefit significantly from receiving cochlear implants over hearing aids.
A new study, published in the journal Pediatrics, pushes against the notion that children with low nonverbal cognition and adaptive functioning skills won’t improve if given cochlear implants. Some insurers cover hearing aids for children with developmental disorders but not the implants, which can cost between $60,000 and $100,000 per ear.
“We were surprised [by] the large magnitude of the improvements, not only in quality of life, but also in cognition, ability to function in daily living situations, and speech and language,” lead author John S. Oghalai, MD, of the University of Southern California, Los Angeles, told this news organization. “Remember, these are children with substantial developmental delays. Any improvements are incredibly important and meaningful.”
All children with severe hearing loss should be referred for cochlear implant evaluation, “regardless of the presence of other disabilities,” Dr. Oghalai said. “The younger this referral happens, the better the outcomes will be.”
Dr. Oghalai and his colleagues reviewed data from 204 children approximately 1-3 years old with hearing aids receiving treatment in Texas and California. Of these, 138 received a cochlear implant and had normal cognitive skills and social competence (referred to as adaptive behavior). Another 37 received a cochlear implant and also met criteria for early developmental impairment (EDI), defined by measures of nonverbal cognitive scores and adaptive functioning.
A third group of 29 children with EDI continued with hearing aids without a cochlear implant.
The children were evaluated annually for 1-5 years, with the average follow-up of 2 years. At baseline, no significant differences were noted between the children with EDI who received implants and those who did not on cognition, language, auditory skills, or measures of parental or child stress.
Overall, children who received implants scored higher on cognitive and social measures than those who continued using hearing aids.
Compared with children with EDI who received implants, children without EDI who received implants had significantly higher developmental scores by the study’s end (P ≤ .001), whereas children with EDI who did not receive implants had significantly lower scores (P ≤ .04).
Children who received implants, and their parents, also experienced less stress than those who did not receive the devices, according to the researchers.
Dr. Oghalai and colleagues also measured developmental trajectories for each cohort. Children without delays who received implants had the best outcomes, but those with EDI who received implants had better outcomes than those with EDI and hearing aids.
Findings ‘overdue’
“This study is overdue,” Howard Francis, MD, chair of the department of head and neck surgery & communication sciences at Duke University, Durham, N.C., told this news organization.
Dr. Francis called the new research “reasonably powered and designed,” and said it “documents benefits in the cognitive, language, and patient-child relationship domains” in children who received cochlear implants “compared to children with similar levels of developmental delay whose hearing loss was treated using hearing aids.”
However, “larger studies will be needed to account for potential effects of older age at intervention in the hearing aid group,” he said. Socioeconomic effects are a topic for future research as well, Dr. Francis added.
The researchers initially wanted to perform a controlled clinical trial. However, by the time they secured funding, health insurance policy had changed to cover cochlear implants for children without EDI because of demonstrated benefits shown in studies.
They also were unable to determine the reasons for families’ decisions to choose implants or hearing aids and were unable to assess the impact of insurance on the choice of implantation. But they did find that families with insurers who would cover implants often did choose the devices. Children were also followed for an average of 2 years, so long-term outcomes are unknown.
Despite these limitations, the results support the value of cochlear implantation in children with disabilities and developmental delays, and it should be discussed with parents, the researchers concluded.
“Cochlear implants are just a tool; they do not provide speech and language,” Dr. Oghalai said. “Any child with severe hearing loss requires significant therapy and education via sign language, auditory-verbal therapy, or both. Making the decision about what type of therapy to do is personal, and it depends upon the family and the options that are available to them in their community.”
The study was funded by the National Institutes of Health. The researchers and Dr. Francis have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Deaf babies and toddlers with developmental delays may benefit significantly from receiving cochlear implants over hearing aids.
A new study, published in the journal Pediatrics, pushes against the notion that children with low nonverbal cognition and adaptive functioning skills won’t improve if given cochlear implants. Some insurers cover hearing aids for children with developmental disorders but not the implants, which can cost between $60,000 and $100,000 per ear.
“We were surprised [by] the large magnitude of the improvements, not only in quality of life, but also in cognition, ability to function in daily living situations, and speech and language,” lead author John S. Oghalai, MD, of the University of Southern California, Los Angeles, told this news organization. “Remember, these are children with substantial developmental delays. Any improvements are incredibly important and meaningful.”
All children with severe hearing loss should be referred for cochlear implant evaluation, “regardless of the presence of other disabilities,” Dr. Oghalai said. “The younger this referral happens, the better the outcomes will be.”
Dr. Oghalai and his colleagues reviewed data from 204 children approximately 1-3 years old with hearing aids receiving treatment in Texas and California. Of these, 138 received a cochlear implant and had normal cognitive skills and social competence (referred to as adaptive behavior). Another 37 received a cochlear implant and also met criteria for early developmental impairment (EDI), defined by measures of nonverbal cognitive scores and adaptive functioning.
A third group of 29 children with EDI continued with hearing aids without a cochlear implant.
The children were evaluated annually for 1-5 years, with the average follow-up of 2 years. At baseline, no significant differences were noted between the children with EDI who received implants and those who did not on cognition, language, auditory skills, or measures of parental or child stress.
Overall, children who received implants scored higher on cognitive and social measures than those who continued using hearing aids.
Compared with children with EDI who received implants, children without EDI who received implants had significantly higher developmental scores by the study’s end (P ≤ .001), whereas children with EDI who did not receive implants had significantly lower scores (P ≤ .04).
Children who received implants, and their parents, also experienced less stress than those who did not receive the devices, according to the researchers.
Dr. Oghalai and colleagues also measured developmental trajectories for each cohort. Children without delays who received implants had the best outcomes, but those with EDI who received implants had better outcomes than those with EDI and hearing aids.
Findings ‘overdue’
“This study is overdue,” Howard Francis, MD, chair of the department of head and neck surgery & communication sciences at Duke University, Durham, N.C., told this news organization.
Dr. Francis called the new research “reasonably powered and designed,” and said it “documents benefits in the cognitive, language, and patient-child relationship domains” in children who received cochlear implants “compared to children with similar levels of developmental delay whose hearing loss was treated using hearing aids.”
However, “larger studies will be needed to account for potential effects of older age at intervention in the hearing aid group,” he said. Socioeconomic effects are a topic for future research as well, Dr. Francis added.
The researchers initially wanted to perform a controlled clinical trial. However, by the time they secured funding, health insurance policy had changed to cover cochlear implants for children without EDI because of demonstrated benefits shown in studies.
They also were unable to determine the reasons for families’ decisions to choose implants or hearing aids and were unable to assess the impact of insurance on the choice of implantation. But they did find that families with insurers who would cover implants often did choose the devices. Children were also followed for an average of 2 years, so long-term outcomes are unknown.
Despite these limitations, the results support the value of cochlear implantation in children with disabilities and developmental delays, and it should be discussed with parents, the researchers concluded.
“Cochlear implants are just a tool; they do not provide speech and language,” Dr. Oghalai said. “Any child with severe hearing loss requires significant therapy and education via sign language, auditory-verbal therapy, or both. Making the decision about what type of therapy to do is personal, and it depends upon the family and the options that are available to them in their community.”
The study was funded by the National Institutes of Health. The researchers and Dr. Francis have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Deaf babies and toddlers with developmental delays may benefit significantly from receiving cochlear implants over hearing aids.
A new study, published in the journal Pediatrics, pushes against the notion that children with low nonverbal cognition and adaptive functioning skills won’t improve if given cochlear implants. Some insurers cover hearing aids for children with developmental disorders but not the implants, which can cost between $60,000 and $100,000 per ear.
“We were surprised [by] the large magnitude of the improvements, not only in quality of life, but also in cognition, ability to function in daily living situations, and speech and language,” lead author John S. Oghalai, MD, of the University of Southern California, Los Angeles, told this news organization. “Remember, these are children with substantial developmental delays. Any improvements are incredibly important and meaningful.”
All children with severe hearing loss should be referred for cochlear implant evaluation, “regardless of the presence of other disabilities,” Dr. Oghalai said. “The younger this referral happens, the better the outcomes will be.”
Dr. Oghalai and his colleagues reviewed data from 204 children approximately 1-3 years old with hearing aids receiving treatment in Texas and California. Of these, 138 received a cochlear implant and had normal cognitive skills and social competence (referred to as adaptive behavior). Another 37 received a cochlear implant and also met criteria for early developmental impairment (EDI), defined by measures of nonverbal cognitive scores and adaptive functioning.
A third group of 29 children with EDI continued with hearing aids without a cochlear implant.
The children were evaluated annually for 1-5 years, with the average follow-up of 2 years. At baseline, no significant differences were noted between the children with EDI who received implants and those who did not on cognition, language, auditory skills, or measures of parental or child stress.
Overall, children who received implants scored higher on cognitive and social measures than those who continued using hearing aids.
Compared with children with EDI who received implants, children without EDI who received implants had significantly higher developmental scores by the study’s end (P ≤ .001), whereas children with EDI who did not receive implants had significantly lower scores (P ≤ .04).
Children who received implants, and their parents, also experienced less stress than those who did not receive the devices, according to the researchers.
Dr. Oghalai and colleagues also measured developmental trajectories for each cohort. Children without delays who received implants had the best outcomes, but those with EDI who received implants had better outcomes than those with EDI and hearing aids.
Findings ‘overdue’
“This study is overdue,” Howard Francis, MD, chair of the department of head and neck surgery & communication sciences at Duke University, Durham, N.C., told this news organization.
Dr. Francis called the new research “reasonably powered and designed,” and said it “documents benefits in the cognitive, language, and patient-child relationship domains” in children who received cochlear implants “compared to children with similar levels of developmental delay whose hearing loss was treated using hearing aids.”
However, “larger studies will be needed to account for potential effects of older age at intervention in the hearing aid group,” he said. Socioeconomic effects are a topic for future research as well, Dr. Francis added.
The researchers initially wanted to perform a controlled clinical trial. However, by the time they secured funding, health insurance policy had changed to cover cochlear implants for children without EDI because of demonstrated benefits shown in studies.
They also were unable to determine the reasons for families’ decisions to choose implants or hearing aids and were unable to assess the impact of insurance on the choice of implantation. But they did find that families with insurers who would cover implants often did choose the devices. Children were also followed for an average of 2 years, so long-term outcomes are unknown.
Despite these limitations, the results support the value of cochlear implantation in children with disabilities and developmental delays, and it should be discussed with parents, the researchers concluded.
“Cochlear implants are just a tool; they do not provide speech and language,” Dr. Oghalai said. “Any child with severe hearing loss requires significant therapy and education via sign language, auditory-verbal therapy, or both. Making the decision about what type of therapy to do is personal, and it depends upon the family and the options that are available to them in their community.”
The study was funded by the National Institutes of Health. The researchers and Dr. Francis have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PEDIATRICS
Social activities may offset psychosis risk in poor communities
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.

The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”

Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Is benzophenone safe in skin care? Part 2: Environmental effects
Although it has been . DiNardo and Downs point out that BP-3 has been linked to contact and photocontact allergies in humans and implicated as a potential endocrine disruptor. They add that it can yield deleterious by-products when reacting with chlorine in swimming pools and wastewater treatment plants and can cause additional side effects in humans who ingest fish.1 This column will focus on recent studies, mainly on the role of benzophenones in sunscreen agents that pose considerable risks to waterways and marine life, with concomitant effects on the food chain.
Environmental effects of BPs and legislative responses
Various UV filters, including BP-3, octinoxate, octocrylene, and ethylhexyl salicylate, are thought to pose considerable peril to the marine environment.2,3 In particular, BP-3 has been demonstrated to provoke coral reef bleaching in vitro, leading to ossification and deforming DNA in the larval stage.3,4
According to a 2018 report, BP-3 is believed to be present in approximately two thirds of organic sunscreens used in the United States.3 In addition, several studies have revealed that detectable levels of organic sunscreen ingredients, including BP-3, have been identified in coastal waters around the globe, including Hawaii and the U.S. Virgin Islands.4-8
A surfeit of tourists has been blamed in part, given that an estimated 25% of applied sunscreen is eliminated within 20 minutes of entering the water and thought to release about 4,000-6,000 tons/year into the surrounding coral reefs.9,10 In Hawaii in particular, sewage contamination of the waterways has resulted from wastewater treatment facilities ill-equipped to filter out organic substances such as BP-3 and octinoxate.10,11 In light of such circumstances, the use of sunscreens containing BP-3 and octinoxate have been restricted in Hawaii, particularly in proximity to beaches, since Jan. 1, 2021, because of their apparent environmental impact.10
The exposure of coral to these compounds is believed to result in bleaching because of impaired membrane integrity and photosynthetic pigment loss in the zooxanthellae that coral releases.9,10 Coral and the algae zooxanthellae have a symbiotic relationship, Siller et al. explain, with the coral delivering protection and components essential for photosynthesis and the algae ultimately serving as nutrients for the coral.10 Stress endured by coral is believed to cause algae to detach, rendering coral more vulnerable to disease and less viable overall.10
In 2016, Downs et al. showed that four out of five sampled locations had detectable levels of BP-3 (100 pp trillion) with a fifth tested site measured at 19.2 pp billion.4
In 2019, Sirois acknowledges the problem of coral bleaching around the world but speculates that banning sunscreen ingredients for this purpose will delude people that such a measure will reverse the decline of coral and may lead to the unintended consequence of lower use of sunscreens. Sirois adds that a more comprehensive investigation of the multiple causes of coral reef bleaching is warranted, as are deeper examinations of studies using higher concentrations of sunscreen ingredients in artificial conditions.12

In the same year, Raffa et al. discussed the impending ban in Hawaii of the two sunscreen ingredients (BP-3 and octinoxate) to help preserve coral reefs. In so doing, they detailed the natural and human-induced harm to coral reefs, including pollution, fishing practices, overall impact of global climate change, and alterations in ocean temperature and chemistry. The implication is that sunscreen ingredients, which help prevent sun damage in users, are not the only causes of harm to coral reefs. Nevertheless, they point out that concentration estimates and mechanism studies buttress the argument that sunscreen ingredients contribute to coral bleaching. Still, the ban in Hawaii is thought to be a trend. Opponents of the ban are concerned that human skin cancers will rise in such circumstances. Alternative chemical sunscreens are being investigated, and physical sunscreens have emerged as the go-to recommendation.13
Notably, oxybenzone has been virtually replaced in the European Union with other UV filters with broad-spectrum action, but the majority of such filters have not yet been approved for use in the United States by the Food and Drug Administration.3
Food chain implications
BP-3 and other UV filters have been investigated for their effects on fish and mammals. Schneider and Lim illustrate that BP-3 is among the frequently used organic UV filters (along with 4-methylbenzylidene camphor, octocrylene, and octinoxate [ethylhexyl methoxycinnamate]) found in most water sources in the world, as well as multiple fish species.2 Cod liver in Norway, for instance, was found to contain octocrylene in 80% of cod, with BP-3 identified in 50% of the sample. BP-3 and octinoxate were also found in white fish.2,14 In laboratory studies, BP-3 in particular has been found in high concentrations in rainbow trout and Japanese rice fish (medaka), causing reduced egg production and hatchlings in females and increased vitellogenin protein production in males, suggesting potential feminization.2,15
Schneider and Lim note that standard wastewater treatment approaches cannot address this issue and the presence of such contaminants in fish can pose dangerous ramifications in the food chain. They assert that, despite relatively low concentrations in the fish, bioaccumulation and biomagnification present the potential for chemicals accumulating over time and becoming more deleterious as such ingredients travel up the food chain. As higher-chain organisms absorb higher concentrations of the chemicals not broken down in the lower-chain organisms, though, there have not yet been reports of adverse effects of biomagnification in humans.2
BP-3 has been found by Brausch and Rand to have bioaccumulated in fish at higher levels than the ambient water, however.1,2,16 Schneider and Lim present these issues as relevant to the sun protection discussion, while advocating for dermatologists to continue to counsel wise sun-protective behaviors.2
Conclusion
While calls for additional research are necessary and encouraging, I think human, and likely environmental, health would be better protected by the use of inorganic sunscreens in general and near or in coastal waterways. In light of legislative actions, in particular, it is important for dermatologists to intervene to ensure that patients do not engage in riskier behaviors in the sun in areas facing imminent organic sunscreen bans.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at dermnews@mdedge.com.
References
1. DiNardo JC and Downs CA. J Cosmet Dermatol. 2018 Feb;17(1):15-9.
2. Schneider SL and Lim HW. J Am Acad Dermatol. 2019 Jan;80(1):266-71.
3. Yeager DG and Lim HW. Dermatol Clin. 2019 Apr;37(2):149-57.
4. Downs CA et al. Arch Environ Contam Toxicol 2016 Feb;70(2):265-88.
5. Sánchez Rodríguez A et al. Chemosphere. 2015 Jul;131:85-90.
6. Tovar-Sánchez A et al. PLoS One. 2013 Jun 5;8(6):e65451.
7. Danovaro R and Corinaldesi C. Microb Ecol. 2003 Feb;45(2):109-18.
8. Daughton CG and Ternes TA. Environ Health Perspect. 1999 Dec;107 Suppl 6:907-38.
9. Danovaro R et al. Environ Health Perspect. 2008 Apr;116(4):441-7.
10. Siller A et al. Plast Surg Nur. 2019 Oct/Dec;39(4):157-60.
11. Ramos S et al. Sci Total Environ. 2015 Sep 1;526:278-311.
12. Sirois J. Sci Total Environ. 2019 Jul 15;674:211-2.
13. Raffa RB et al. J Clin Pharm Ther. 2019 Feb;44(1):134-9.
14. Langford KH et al. Environ Int. 2015 Jul;80:1-7.
15. Coronado M et al. Aquat Toxicol. 2008 Nov 21;90(3):182-7.
16. Brausch JM and Rand GM. Chemosphere. 2011 Mar;82(11):1518-32.
Although it has been . DiNardo and Downs point out that BP-3 has been linked to contact and photocontact allergies in humans and implicated as a potential endocrine disruptor. They add that it can yield deleterious by-products when reacting with chlorine in swimming pools and wastewater treatment plants and can cause additional side effects in humans who ingest fish.1 This column will focus on recent studies, mainly on the role of benzophenones in sunscreen agents that pose considerable risks to waterways and marine life, with concomitant effects on the food chain.
Environmental effects of BPs and legislative responses
Various UV filters, including BP-3, octinoxate, octocrylene, and ethylhexyl salicylate, are thought to pose considerable peril to the marine environment.2,3 In particular, BP-3 has been demonstrated to provoke coral reef bleaching in vitro, leading to ossification and deforming DNA in the larval stage.3,4
According to a 2018 report, BP-3 is believed to be present in approximately two thirds of organic sunscreens used in the United States.3 In addition, several studies have revealed that detectable levels of organic sunscreen ingredients, including BP-3, have been identified in coastal waters around the globe, including Hawaii and the U.S. Virgin Islands.4-8
A surfeit of tourists has been blamed in part, given that an estimated 25% of applied sunscreen is eliminated within 20 minutes of entering the water and thought to release about 4,000-6,000 tons/year into the surrounding coral reefs.9,10 In Hawaii in particular, sewage contamination of the waterways has resulted from wastewater treatment facilities ill-equipped to filter out organic substances such as BP-3 and octinoxate.10,11 In light of such circumstances, the use of sunscreens containing BP-3 and octinoxate have been restricted in Hawaii, particularly in proximity to beaches, since Jan. 1, 2021, because of their apparent environmental impact.10
The exposure of coral to these compounds is believed to result in bleaching because of impaired membrane integrity and photosynthetic pigment loss in the zooxanthellae that coral releases.9,10 Coral and the algae zooxanthellae have a symbiotic relationship, Siller et al. explain, with the coral delivering protection and components essential for photosynthesis and the algae ultimately serving as nutrients for the coral.10 Stress endured by coral is believed to cause algae to detach, rendering coral more vulnerable to disease and less viable overall.10
In 2016, Downs et al. showed that four out of five sampled locations had detectable levels of BP-3 (100 pp trillion) with a fifth tested site measured at 19.2 pp billion.4
In 2019, Sirois acknowledges the problem of coral bleaching around the world but speculates that banning sunscreen ingredients for this purpose will delude people that such a measure will reverse the decline of coral and may lead to the unintended consequence of lower use of sunscreens. Sirois adds that a more comprehensive investigation of the multiple causes of coral reef bleaching is warranted, as are deeper examinations of studies using higher concentrations of sunscreen ingredients in artificial conditions.12
In the same year, Raffa et al. discussed the impending ban in Hawaii of the two sunscreen ingredients (BP-3 and octinoxate) to help preserve coral reefs. In so doing, they detailed the natural and human-induced harm to coral reefs, including pollution, fishing practices, overall impact of global climate change, and alterations in ocean temperature and chemistry. The implication is that sunscreen ingredients, which help prevent sun damage in users, are not the only causes of harm to coral reefs. Nevertheless, they point out that concentration estimates and mechanism studies buttress the argument that sunscreen ingredients contribute to coral bleaching. Still, the ban in Hawaii is thought to be a trend. Opponents of the ban are concerned that human skin cancers will rise in such circumstances. Alternative chemical sunscreens are being investigated, and physical sunscreens have emerged as the go-to recommendation.13
Notably, oxybenzone has been virtually replaced in the European Union with other UV filters with broad-spectrum action, but the majority of such filters have not yet been approved for use in the United States by the Food and Drug Administration.3
Food chain implications
BP-3 and other UV filters have been investigated for their effects on fish and mammals. Schneider and Lim illustrate that BP-3 is among the frequently used organic UV filters (along with 4-methylbenzylidene camphor, octocrylene, and octinoxate [ethylhexyl methoxycinnamate]) found in most water sources in the world, as well as multiple fish species.2 Cod liver in Norway, for instance, was found to contain octocrylene in 80% of cod, with BP-3 identified in 50% of the sample. BP-3 and octinoxate were also found in white fish.2,14 In laboratory studies, BP-3 in particular has been found in high concentrations in rainbow trout and Japanese rice fish (medaka), causing reduced egg production and hatchlings in females and increased vitellogenin protein production in males, suggesting potential feminization.2,15
Schneider and Lim note that standard wastewater treatment approaches cannot address this issue and the presence of such contaminants in fish can pose dangerous ramifications in the food chain. They assert that, despite relatively low concentrations in the fish, bioaccumulation and biomagnification present the potential for chemicals accumulating over time and becoming more deleterious as such ingredients travel up the food chain. As higher-chain organisms absorb higher concentrations of the chemicals not broken down in the lower-chain organisms, though, there have not yet been reports of adverse effects of biomagnification in humans.2
BP-3 has been found by Brausch and Rand to have bioaccumulated in fish at higher levels than the ambient water, however.1,2,16 Schneider and Lim present these issues as relevant to the sun protection discussion, while advocating for dermatologists to continue to counsel wise sun-protective behaviors.2
Conclusion
While calls for additional research are necessary and encouraging, I think human, and likely environmental, health would be better protected by the use of inorganic sunscreens in general and near or in coastal waterways. In light of legislative actions, in particular, it is important for dermatologists to intervene to ensure that patients do not engage in riskier behaviors in the sun in areas facing imminent organic sunscreen bans.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at dermnews@mdedge.com.
References
1. DiNardo JC and Downs CA. J Cosmet Dermatol. 2018 Feb;17(1):15-9.
2. Schneider SL and Lim HW. J Am Acad Dermatol. 2019 Jan;80(1):266-71.
3. Yeager DG and Lim HW. Dermatol Clin. 2019 Apr;37(2):149-57.
4. Downs CA et al. Arch Environ Contam Toxicol 2016 Feb;70(2):265-88.
5. Sánchez Rodríguez A et al. Chemosphere. 2015 Jul;131:85-90.
6. Tovar-Sánchez A et al. PLoS One. 2013 Jun 5;8(6):e65451.
7. Danovaro R and Corinaldesi C. Microb Ecol. 2003 Feb;45(2):109-18.
8. Daughton CG and Ternes TA. Environ Health Perspect. 1999 Dec;107 Suppl 6:907-38.
9. Danovaro R et al. Environ Health Perspect. 2008 Apr;116(4):441-7.
10. Siller A et al. Plast Surg Nur. 2019 Oct/Dec;39(4):157-60.
11. Ramos S et al. Sci Total Environ. 2015 Sep 1;526:278-311.
12. Sirois J. Sci Total Environ. 2019 Jul 15;674:211-2.
13. Raffa RB et al. J Clin Pharm Ther. 2019 Feb;44(1):134-9.
14. Langford KH et al. Environ Int. 2015 Jul;80:1-7.
15. Coronado M et al. Aquat Toxicol. 2008 Nov 21;90(3):182-7.
16. Brausch JM and Rand GM. Chemosphere. 2011 Mar;82(11):1518-32.
Although it has been . DiNardo and Downs point out that BP-3 has been linked to contact and photocontact allergies in humans and implicated as a potential endocrine disruptor. They add that it can yield deleterious by-products when reacting with chlorine in swimming pools and wastewater treatment plants and can cause additional side effects in humans who ingest fish.1 This column will focus on recent studies, mainly on the role of benzophenones in sunscreen agents that pose considerable risks to waterways and marine life, with concomitant effects on the food chain.
Environmental effects of BPs and legislative responses
Various UV filters, including BP-3, octinoxate, octocrylene, and ethylhexyl salicylate, are thought to pose considerable peril to the marine environment.2,3 In particular, BP-3 has been demonstrated to provoke coral reef bleaching in vitro, leading to ossification and deforming DNA in the larval stage.3,4
According to a 2018 report, BP-3 is believed to be present in approximately two thirds of organic sunscreens used in the United States.3 In addition, several studies have revealed that detectable levels of organic sunscreen ingredients, including BP-3, have been identified in coastal waters around the globe, including Hawaii and the U.S. Virgin Islands.4-8
A surfeit of tourists has been blamed in part, given that an estimated 25% of applied sunscreen is eliminated within 20 minutes of entering the water and thought to release about 4,000-6,000 tons/year into the surrounding coral reefs.9,10 In Hawaii in particular, sewage contamination of the waterways has resulted from wastewater treatment facilities ill-equipped to filter out organic substances such as BP-3 and octinoxate.10,11 In light of such circumstances, the use of sunscreens containing BP-3 and octinoxate have been restricted in Hawaii, particularly in proximity to beaches, since Jan. 1, 2021, because of their apparent environmental impact.10
The exposure of coral to these compounds is believed to result in bleaching because of impaired membrane integrity and photosynthetic pigment loss in the zooxanthellae that coral releases.9,10 Coral and the algae zooxanthellae have a symbiotic relationship, Siller et al. explain, with the coral delivering protection and components essential for photosynthesis and the algae ultimately serving as nutrients for the coral.10 Stress endured by coral is believed to cause algae to detach, rendering coral more vulnerable to disease and less viable overall.10
In 2016, Downs et al. showed that four out of five sampled locations had detectable levels of BP-3 (100 pp trillion) with a fifth tested site measured at 19.2 pp billion.4
In 2019, Sirois acknowledges the problem of coral bleaching around the world but speculates that banning sunscreen ingredients for this purpose will delude people that such a measure will reverse the decline of coral and may lead to the unintended consequence of lower use of sunscreens. Sirois adds that a more comprehensive investigation of the multiple causes of coral reef bleaching is warranted, as are deeper examinations of studies using higher concentrations of sunscreen ingredients in artificial conditions.12
In the same year, Raffa et al. discussed the impending ban in Hawaii of the two sunscreen ingredients (BP-3 and octinoxate) to help preserve coral reefs. In so doing, they detailed the natural and human-induced harm to coral reefs, including pollution, fishing practices, overall impact of global climate change, and alterations in ocean temperature and chemistry. The implication is that sunscreen ingredients, which help prevent sun damage in users, are not the only causes of harm to coral reefs. Nevertheless, they point out that concentration estimates and mechanism studies buttress the argument that sunscreen ingredients contribute to coral bleaching. Still, the ban in Hawaii is thought to be a trend. Opponents of the ban are concerned that human skin cancers will rise in such circumstances. Alternative chemical sunscreens are being investigated, and physical sunscreens have emerged as the go-to recommendation.13
Notably, oxybenzone has been virtually replaced in the European Union with other UV filters with broad-spectrum action, but the majority of such filters have not yet been approved for use in the United States by the Food and Drug Administration.3
Food chain implications
BP-3 and other UV filters have been investigated for their effects on fish and mammals. Schneider and Lim illustrate that BP-3 is among the frequently used organic UV filters (along with 4-methylbenzylidene camphor, octocrylene, and octinoxate [ethylhexyl methoxycinnamate]) found in most water sources in the world, as well as multiple fish species.2 Cod liver in Norway, for instance, was found to contain octocrylene in 80% of cod, with BP-3 identified in 50% of the sample. BP-3 and octinoxate were also found in white fish.2,14 In laboratory studies, BP-3 in particular has been found in high concentrations in rainbow trout and Japanese rice fish (medaka), causing reduced egg production and hatchlings in females and increased vitellogenin protein production in males, suggesting potential feminization.2,15
Schneider and Lim note that standard wastewater treatment approaches cannot address this issue and the presence of such contaminants in fish can pose dangerous ramifications in the food chain. They assert that, despite relatively low concentrations in the fish, bioaccumulation and biomagnification present the potential for chemicals accumulating over time and becoming more deleterious as such ingredients travel up the food chain. As higher-chain organisms absorb higher concentrations of the chemicals not broken down in the lower-chain organisms, though, there have not yet been reports of adverse effects of biomagnification in humans.2
BP-3 has been found by Brausch and Rand to have bioaccumulated in fish at higher levels than the ambient water, however.1,2,16 Schneider and Lim present these issues as relevant to the sun protection discussion, while advocating for dermatologists to continue to counsel wise sun-protective behaviors.2
Conclusion
While calls for additional research are necessary and encouraging, I think human, and likely environmental, health would be better protected by the use of inorganic sunscreens in general and near or in coastal waterways. In light of legislative actions, in particular, it is important for dermatologists to intervene to ensure that patients do not engage in riskier behaviors in the sun in areas facing imminent organic sunscreen bans.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at dermnews@mdedge.com.
References
1. DiNardo JC and Downs CA. J Cosmet Dermatol. 2018 Feb;17(1):15-9.
2. Schneider SL and Lim HW. J Am Acad Dermatol. 2019 Jan;80(1):266-71.
3. Yeager DG and Lim HW. Dermatol Clin. 2019 Apr;37(2):149-57.
4. Downs CA et al. Arch Environ Contam Toxicol 2016 Feb;70(2):265-88.
5. Sánchez Rodríguez A et al. Chemosphere. 2015 Jul;131:85-90.
6. Tovar-Sánchez A et al. PLoS One. 2013 Jun 5;8(6):e65451.
7. Danovaro R and Corinaldesi C. Microb Ecol. 2003 Feb;45(2):109-18.
8. Daughton CG and Ternes TA. Environ Health Perspect. 1999 Dec;107 Suppl 6:907-38.
9. Danovaro R et al. Environ Health Perspect. 2008 Apr;116(4):441-7.
10. Siller A et al. Plast Surg Nur. 2019 Oct/Dec;39(4):157-60.
11. Ramos S et al. Sci Total Environ. 2015 Sep 1;526:278-311.
12. Sirois J. Sci Total Environ. 2019 Jul 15;674:211-2.
13. Raffa RB et al. J Clin Pharm Ther. 2019 Feb;44(1):134-9.
14. Langford KH et al. Environ Int. 2015 Jul;80:1-7.
15. Coronado M et al. Aquat Toxicol. 2008 Nov 21;90(3):182-7.
16. Brausch JM and Rand GM. Chemosphere. 2011 Mar;82(11):1518-32.