User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Topical gel for epidermolysis bullosa shows ongoing benefit
GLASGOW, Scotland – the phase 3 safety and efficacy study of the treatment.
Over 200 patients from the trial, including 105 who began treatment with a control gel, continued taking oleogel-S10 after 90 days. The current interim analysis at 12 months indicates there was a 55% reduction in the proportion of the body affected, compared with baseline.
Moreover, reductions in skin activity scores seen in the double-blind phase of the trial were maintained during the open-label extension. About 6% of patients experienced adverse events that led to withdrawal from the study.
The results show that oleogel-S10 was associated with “accelerated wound healing,” said study presenter Tracey Cunningham, MD, chief medical officer, Amryt Pharmaceuticals DAC, Dublin, which is developing the topical agent. “There were no new safety signals with this longer exposure to oleogel-S10, and patients had sustained improvement in wound burden,” she added.
The research was presented at the British Association of Dermatologists (BAD) 2022 Annual Meeting on July 6.
In April, European Medicines Agency recommended approval of oleogel-S10 for the treatment of partial-thickness skin wounds associated with dystrophic and junctional EB for patients aged 6 months and older.
However, just a month earlier, the U.S. Food and Drug Administration declined to approve the topical agent for use in EB, even after it extended its review by 3 months to include additional analyses of data previously submitted by the company.
In the post-presentation discussion, Dr. Cunningham said that the FDA had “not been satisfied at this point with the information that we have given them,” adding, “We don’t agree with the decision, and we will be appealing.”
Raman K. Madan, MD, a dermatologist at Northwell Health, Huntington, New York, who was not involved in the study, said that the reductions in wound healing seen in the study are “meaningful” and that the numbers represent a “big breakthrough.”
He told this news organization that there are “very few products on the market” for EB and that having an option for patients “would be amazing.”
“The big issue here would be cost and coverage for patients,” he said. If approved, “hopefully” it will be affordable, he added.
Dr. Madan noted that from his perspective, the majority of the reactions to the topical gel were “mild,” and there are “a lot of confounding factors” underlying the number of serious adverse events. “These patients with epidermolysis are prone to some of these issues regardless of treatment,” he said.
During her presentation, Dr. Cunningham noted that EB is a rare, debilitating condition that is characterized by varying degrees of skin fragility, blisters, and impaired wound healing that in turn lead to serious complications that affect quality of life.
While wound management is a “fundamental priority” for patients living with EB, she said, there is a “high, unmet” clinical need.
To those ends, EASE was the largest randomized controlled phase 3 efficacy and safety study in EB. In the study, 252 patients were allocated to receive oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing.
The double-blind phase of the trial met its primary endpoint: A higher proportion of patients who were given oleogel-S10 achieved first complete closure of the EB target wound by day 45, compared with patients who were given control gel, at 41.3% versus 28.9%. This equated to a relative risk of wound closure by day 45 of 1.44, or an odds ratio of 1.84 (P = .013).
However, as reported at the time by this news organization, the difference in time to wound healing by day 90 between the two patient groups was not statistically significant (P = .302), with 50.5% of oleogel-S10 patients achieving wound closure, versus 43.9% of those in the control group.
Dr. Cunningham discussed the open-label extension, which involved 205 patients from the double-blind phase (mean age, of 16.3 years) treated with oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing for 24 months.
In presenting the results of the first 12 months of the open-label extension, she said that oleogel-S10 led to “consistent” reductions in the body surface area percentage (BSAP) affected by EB. The overall reduction from baseline was 55% after receiving treatment for 15 months.
Between day 90 and month 12 of the open-label extension, the absolute BSAP was reduced from 7.4% to 5.4% for patients who had received oleogel-S10 from the start of the study. For those who started in the control group and then switched to the oleogel-S10 arm during the open-label extension, the reduction was from 8.3% to 6.4%.
Dr. Cunningham pointed out that a 1% reduction in BSAP equates approximately to the palmar surface of the hand.
Scores on the Epidermolysis Bullosa Disease Activity and Scarring Index (EBDASI) Skin activity subscale indicated that the reductions achieved in the double-blind phase of the trial were maintained.
Among patients who received oleogel-S10 from the start of the trial, EBDASI Skin scores were reduced from 19.6 at baseline to 13.5 at 12 months’ follow-up in the open-label extension. The reduction was from 19.6 to 13.5 for those who began the trial taking control gel.
Dr. Cunningham showed that adverse events of any grade were seen in 72.0% of patients who began taking oleogel-S10 at the start of the trial and in 69.5% of those who began the trial taking control gel.
Serious adverse events were recorded in 23.0% and 20.0% of patients, respectively, while 6.0% of those who initially received oleogel-S10 and 6.7% of those initially assigned to control gel experienced adverse events that led to study withdrawal during the open-label phase.
The most frequently reported adverse events in the open-label extension were wound complications, seen in 39.5% of patients; anemia, seen in 14.1%; wound infection, seen in 9.3%; pyrexia, seen in 8.3%; and pruritus, seen in 5.9%. No more details regarding adverse events were provided.
The study was funded by Amryt Pharmaceuticals DAC. Dr. Cunningham is an employee of Amryt Pharmaceuticals. No other relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
GLASGOW, Scotland – the phase 3 safety and efficacy study of the treatment.
Over 200 patients from the trial, including 105 who began treatment with a control gel, continued taking oleogel-S10 after 90 days. The current interim analysis at 12 months indicates there was a 55% reduction in the proportion of the body affected, compared with baseline.
Moreover, reductions in skin activity scores seen in the double-blind phase of the trial were maintained during the open-label extension. About 6% of patients experienced adverse events that led to withdrawal from the study.
The results show that oleogel-S10 was associated with “accelerated wound healing,” said study presenter Tracey Cunningham, MD, chief medical officer, Amryt Pharmaceuticals DAC, Dublin, which is developing the topical agent. “There were no new safety signals with this longer exposure to oleogel-S10, and patients had sustained improvement in wound burden,” she added.
The research was presented at the British Association of Dermatologists (BAD) 2022 Annual Meeting on July 6.
In April, European Medicines Agency recommended approval of oleogel-S10 for the treatment of partial-thickness skin wounds associated with dystrophic and junctional EB for patients aged 6 months and older.
However, just a month earlier, the U.S. Food and Drug Administration declined to approve the topical agent for use in EB, even after it extended its review by 3 months to include additional analyses of data previously submitted by the company.
In the post-presentation discussion, Dr. Cunningham said that the FDA had “not been satisfied at this point with the information that we have given them,” adding, “We don’t agree with the decision, and we will be appealing.”
Raman K. Madan, MD, a dermatologist at Northwell Health, Huntington, New York, who was not involved in the study, said that the reductions in wound healing seen in the study are “meaningful” and that the numbers represent a “big breakthrough.”
He told this news organization that there are “very few products on the market” for EB and that having an option for patients “would be amazing.”
“The big issue here would be cost and coverage for patients,” he said. If approved, “hopefully” it will be affordable, he added.
Dr. Madan noted that from his perspective, the majority of the reactions to the topical gel were “mild,” and there are “a lot of confounding factors” underlying the number of serious adverse events. “These patients with epidermolysis are prone to some of these issues regardless of treatment,” he said.
During her presentation, Dr. Cunningham noted that EB is a rare, debilitating condition that is characterized by varying degrees of skin fragility, blisters, and impaired wound healing that in turn lead to serious complications that affect quality of life.
While wound management is a “fundamental priority” for patients living with EB, she said, there is a “high, unmet” clinical need.
To those ends, EASE was the largest randomized controlled phase 3 efficacy and safety study in EB. In the study, 252 patients were allocated to receive oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing.
The double-blind phase of the trial met its primary endpoint: A higher proportion of patients who were given oleogel-S10 achieved first complete closure of the EB target wound by day 45, compared with patients who were given control gel, at 41.3% versus 28.9%. This equated to a relative risk of wound closure by day 45 of 1.44, or an odds ratio of 1.84 (P = .013).
However, as reported at the time by this news organization, the difference in time to wound healing by day 90 between the two patient groups was not statistically significant (P = .302), with 50.5% of oleogel-S10 patients achieving wound closure, versus 43.9% of those in the control group.
Dr. Cunningham discussed the open-label extension, which involved 205 patients from the double-blind phase (mean age, of 16.3 years) treated with oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing for 24 months.
In presenting the results of the first 12 months of the open-label extension, she said that oleogel-S10 led to “consistent” reductions in the body surface area percentage (BSAP) affected by EB. The overall reduction from baseline was 55% after receiving treatment for 15 months.
Between day 90 and month 12 of the open-label extension, the absolute BSAP was reduced from 7.4% to 5.4% for patients who had received oleogel-S10 from the start of the study. For those who started in the control group and then switched to the oleogel-S10 arm during the open-label extension, the reduction was from 8.3% to 6.4%.
Dr. Cunningham pointed out that a 1% reduction in BSAP equates approximately to the palmar surface of the hand.
Scores on the Epidermolysis Bullosa Disease Activity and Scarring Index (EBDASI) Skin activity subscale indicated that the reductions achieved in the double-blind phase of the trial were maintained.
Among patients who received oleogel-S10 from the start of the trial, EBDASI Skin scores were reduced from 19.6 at baseline to 13.5 at 12 months’ follow-up in the open-label extension. The reduction was from 19.6 to 13.5 for those who began the trial taking control gel.
Dr. Cunningham showed that adverse events of any grade were seen in 72.0% of patients who began taking oleogel-S10 at the start of the trial and in 69.5% of those who began the trial taking control gel.
Serious adverse events were recorded in 23.0% and 20.0% of patients, respectively, while 6.0% of those who initially received oleogel-S10 and 6.7% of those initially assigned to control gel experienced adverse events that led to study withdrawal during the open-label phase.
The most frequently reported adverse events in the open-label extension were wound complications, seen in 39.5% of patients; anemia, seen in 14.1%; wound infection, seen in 9.3%; pyrexia, seen in 8.3%; and pruritus, seen in 5.9%. No more details regarding adverse events were provided.
The study was funded by Amryt Pharmaceuticals DAC. Dr. Cunningham is an employee of Amryt Pharmaceuticals. No other relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
GLASGOW, Scotland – the phase 3 safety and efficacy study of the treatment.
Over 200 patients from the trial, including 105 who began treatment with a control gel, continued taking oleogel-S10 after 90 days. The current interim analysis at 12 months indicates there was a 55% reduction in the proportion of the body affected, compared with baseline.
Moreover, reductions in skin activity scores seen in the double-blind phase of the trial were maintained during the open-label extension. About 6% of patients experienced adverse events that led to withdrawal from the study.
The results show that oleogel-S10 was associated with “accelerated wound healing,” said study presenter Tracey Cunningham, MD, chief medical officer, Amryt Pharmaceuticals DAC, Dublin, which is developing the topical agent. “There were no new safety signals with this longer exposure to oleogel-S10, and patients had sustained improvement in wound burden,” she added.
The research was presented at the British Association of Dermatologists (BAD) 2022 Annual Meeting on July 6.
In April, European Medicines Agency recommended approval of oleogel-S10 for the treatment of partial-thickness skin wounds associated with dystrophic and junctional EB for patients aged 6 months and older.
However, just a month earlier, the U.S. Food and Drug Administration declined to approve the topical agent for use in EB, even after it extended its review by 3 months to include additional analyses of data previously submitted by the company.
In the post-presentation discussion, Dr. Cunningham said that the FDA had “not been satisfied at this point with the information that we have given them,” adding, “We don’t agree with the decision, and we will be appealing.”
Raman K. Madan, MD, a dermatologist at Northwell Health, Huntington, New York, who was not involved in the study, said that the reductions in wound healing seen in the study are “meaningful” and that the numbers represent a “big breakthrough.”
He told this news organization that there are “very few products on the market” for EB and that having an option for patients “would be amazing.”
“The big issue here would be cost and coverage for patients,” he said. If approved, “hopefully” it will be affordable, he added.
Dr. Madan noted that from his perspective, the majority of the reactions to the topical gel were “mild,” and there are “a lot of confounding factors” underlying the number of serious adverse events. “These patients with epidermolysis are prone to some of these issues regardless of treatment,” he said.
During her presentation, Dr. Cunningham noted that EB is a rare, debilitating condition that is characterized by varying degrees of skin fragility, blisters, and impaired wound healing that in turn lead to serious complications that affect quality of life.
While wound management is a “fundamental priority” for patients living with EB, she said, there is a “high, unmet” clinical need.
To those ends, EASE was the largest randomized controlled phase 3 efficacy and safety study in EB. In the study, 252 patients were allocated to receive oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing.
The double-blind phase of the trial met its primary endpoint: A higher proportion of patients who were given oleogel-S10 achieved first complete closure of the EB target wound by day 45, compared with patients who were given control gel, at 41.3% versus 28.9%. This equated to a relative risk of wound closure by day 45 of 1.44, or an odds ratio of 1.84 (P = .013).
However, as reported at the time by this news organization, the difference in time to wound healing by day 90 between the two patient groups was not statistically significant (P = .302), with 50.5% of oleogel-S10 patients achieving wound closure, versus 43.9% of those in the control group.
Dr. Cunningham discussed the open-label extension, which involved 205 patients from the double-blind phase (mean age, of 16.3 years) treated with oleogel-S10 or control gel plus standard-of-care nonadhesive wound dressing for 24 months.
In presenting the results of the first 12 months of the open-label extension, she said that oleogel-S10 led to “consistent” reductions in the body surface area percentage (BSAP) affected by EB. The overall reduction from baseline was 55% after receiving treatment for 15 months.
Between day 90 and month 12 of the open-label extension, the absolute BSAP was reduced from 7.4% to 5.4% for patients who had received oleogel-S10 from the start of the study. For those who started in the control group and then switched to the oleogel-S10 arm during the open-label extension, the reduction was from 8.3% to 6.4%.
Dr. Cunningham pointed out that a 1% reduction in BSAP equates approximately to the palmar surface of the hand.
Scores on the Epidermolysis Bullosa Disease Activity and Scarring Index (EBDASI) Skin activity subscale indicated that the reductions achieved in the double-blind phase of the trial were maintained.
Among patients who received oleogel-S10 from the start of the trial, EBDASI Skin scores were reduced from 19.6 at baseline to 13.5 at 12 months’ follow-up in the open-label extension. The reduction was from 19.6 to 13.5 for those who began the trial taking control gel.
Dr. Cunningham showed that adverse events of any grade were seen in 72.0% of patients who began taking oleogel-S10 at the start of the trial and in 69.5% of those who began the trial taking control gel.
Serious adverse events were recorded in 23.0% and 20.0% of patients, respectively, while 6.0% of those who initially received oleogel-S10 and 6.7% of those initially assigned to control gel experienced adverse events that led to study withdrawal during the open-label phase.
The most frequently reported adverse events in the open-label extension were wound complications, seen in 39.5% of patients; anemia, seen in 14.1%; wound infection, seen in 9.3%; pyrexia, seen in 8.3%; and pruritus, seen in 5.9%. No more details regarding adverse events were provided.
The study was funded by Amryt Pharmaceuticals DAC. Dr. Cunningham is an employee of Amryt Pharmaceuticals. No other relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
Children and COVID: Vaccination a harder sell in the summer
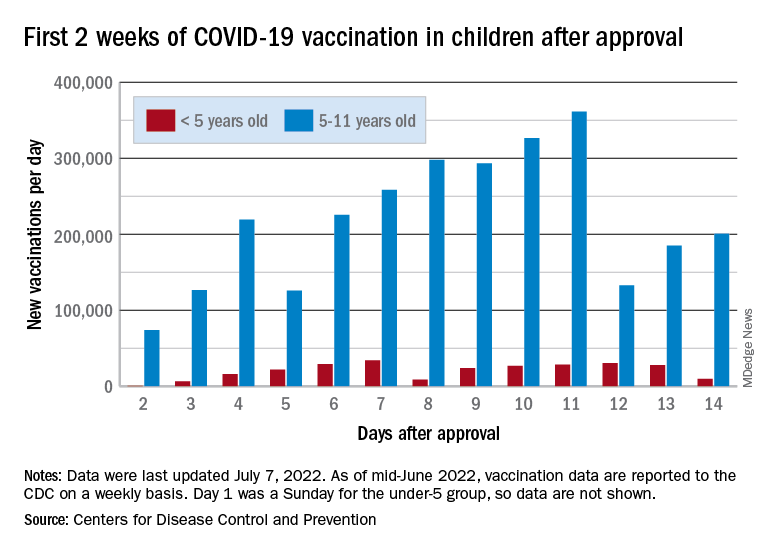
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.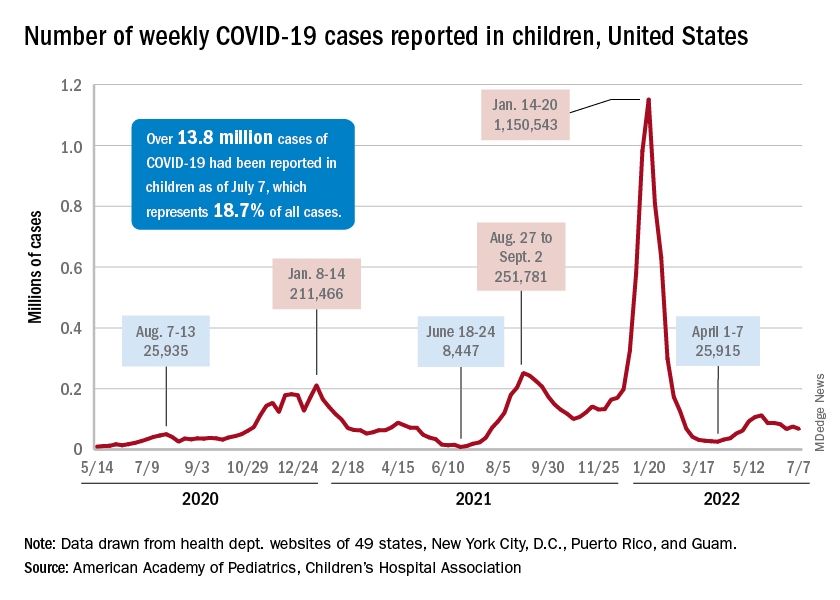
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
The COVID-19 vaccination effort in the youngest children has begun much more slowly than the most recent rollout for older children, according to the Centers for Disease Control and Prevention.
in early November of 2021, based on CDC data last updated on July 7.
That approval, of course, came between the Delta and Omicron surges, when awareness was higher. The low initial uptake among those under age 5, however, was not unexpected by the Biden administration. “That number in and of itself is very much in line with our expectation, and we’re eager to continue working closely with partners to build on this start,” a senior administration official told ABC News.
With approval of the vaccine occurring after the school year was over, parents’ thoughts have been focused more on vacations and less on vaccinations. “Even before these vaccines officially became available, this was going to be a different rollout; it was going to take more time,” the official explained.
Incidence measures continue on different paths
New COVID-19 cases dropped during the latest reporting week (July 1-7), returning to the downward trend that began in late May and then stopped for 1 week (June 24-30), when cases were up by 12.4%, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Children also represent a smaller share of cases, probably because of underreporting. “There has been a notable decline in the portion of reported weekly COVID-19 cases that are children,” the two groups said in their weekly COVID report. Although “cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases.”
Other measures, however, have been rising slowly but steadily since the spring. New admissions of patients aged 0-17 years with confirmed COVID, which were down to 0.13 per 100,000 population in early April, had climbed to 0.39 per 100,000 by July 7, the CDC said on its COVID Data Tracker.
Emergency department visits continue to show the same upward trend, despite a small decline in early June. A COVID diagnosis was involved in just 0.5% of ED visits in children aged 0-11 years on March 26, but by July 6 the rate was 4.7%. Increases were not as high among older children: From 0.3% on March 26 to 2.5% on July 6 for those aged 12-15 and from 0.3% to 2.4% for 16- and 17-year-olds, according to the CDC.
Childhood type 1 diabetes tests suggested at ages 2 and 6
, new data suggest.
Both genetic screening and islet-cell autoantibody screening for type 1 diabetes risk have become less expensive in recent years. Nonetheless, as of now, most children who receive such screening do so through programs that screen relatives of people who already have the condition, such as the global TrialNet program.
Some in the type 1 diabetes field have urged wider screening, with the rationale that knowledge of increased risk can prepare families to recognize the early signs of hyperglycemia and seek medical help to prevent the onset of diabetic ketoacidosis.
Moreover, potential therapies to prevent or delay type 1 diabetes are currently in development, including the anti-CD3 monoclonal antibody teplizumab (Tzield, Provention Bio).
However, given that the incidence of type 1 diabetes is about 1 in 300 children, any population-wide screening program would need to be implemented in the most efficient and cost-effective way possible with limited numbers of tests, say Mohamed Ghalwash, PhD, of the Center for Computational Health, IBM Research, Yorktown Heights, N.Y., and colleagues.
Results from their analysis of nearly 25,000 children from five prospective cohorts in Europe and the United States were published online in Lancet Diabetes & Endocrinology.
Screening in kids feasible, but may need geographic tweaking
“Our results show that initial screening for islet autoantibodies at two ages (2 years and 6 years) is sensitive and efficient for public health translation but might require adjustment by country on the basis of population-specific disease characteristics,” Dr. Ghalwash and colleagues write.
In an accompanying editorial, pediatric endocrinologist Maria J. Redondo, MD, PhD, writes: “This study is timely because recent successes in preventing type 1 diabetes highlight the need to identify the best candidates for intervention ... This paper constitutes an important contribution to the literature.”
However, Dr. Redondo, of Baylor College of Medicine and Texas Children’s Hospital, Houston, also cautioned: “It remains to be seen whether Dr. Ghalwash and colleagues’ strategy could work in the general population, because all the participants in the combined dataset had genetic risk factors for the disease or a relative with type 1 diabetes, in whom performance is expected to be higher.”
She also noted that most participants were of northern European ancestry and that it is unknown whether the same or a similar screening strategy could be applied to individuals older than 15 years, in whom preclinical type 1 diabetes progresses more slowly.
Two-time childhood screening yielded high sensitivity, specificity
The data from a total of 24,662 participants were pooled from five prospective cohorts from Finland (DIPP), Germany (BABYDIAB), Sweden (DiPiS), and the United States (DAISY and DEW-IT).
All were at elevated risk for type 1 diabetes based on human leukocyte antigen (HLA) genotyping, and some had first-degree relatives with the condition. Participants were screened annually for three type 1 diabetes–associated autoantibodies up to age 15 years or the onset of type 1 diabetes.
During follow-up, 672 children developed type 1 diabetes by age 15 years and 6,050 did not. (The rest hadn’t yet reached age 15 years or type 1 diabetes onset.) The median age at first appearance of islet autoantibodies was 4.5 years.
A two-age screening strategy at 2 years and 6 years was more sensitive than screening at just one age, with a sensitivity of 82% and a positive predictive value of 79% for the development of type 1 diabetes by age 15 years.
The predictive value increased with the number of autoantibodies tested. For example, a single islet autoantibody at age 2 years indicated a 4-year risk of developing type 1 diabetes by age 5.99 years of 31%, while multiple antibody positivity at age 2 years carried a 4-year risk of 55%.
By age 6 years, the risk over the next 9 years was 39% if the test had been negative at age 2 years and 70% if the test had been positive at 2 years. But overall, a 6-year-old with multiple autoantibodies had an overall 83% risk of type 1 diabetes regardless of the test result at 2 years.
The predictive performance of sensitivity by age differed by country, suggesting that the optimal ages for autoantibody testing might differ by geographic region, Dr. Ghalwash and colleagues say.
Dr. Redondo commented, “The model might require adaptation to local factors that affect the progression and prevalence of type 1 diabetes.” And, she added, “important aspects, such as screening cost, global access, acceptability, and follow-up support will need to be addressed for this strategy to be a viable public health option.”
The study was funded by JDRF. Dr. Ghalwash and another author are employees of IBM. A third author was a JDRF employee when the research was done and is now an employee of Janssen Research and Development. Dr. Redondo has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new data suggest.
Both genetic screening and islet-cell autoantibody screening for type 1 diabetes risk have become less expensive in recent years. Nonetheless, as of now, most children who receive such screening do so through programs that screen relatives of people who already have the condition, such as the global TrialNet program.
Some in the type 1 diabetes field have urged wider screening, with the rationale that knowledge of increased risk can prepare families to recognize the early signs of hyperglycemia and seek medical help to prevent the onset of diabetic ketoacidosis.
Moreover, potential therapies to prevent or delay type 1 diabetes are currently in development, including the anti-CD3 monoclonal antibody teplizumab (Tzield, Provention Bio).
However, given that the incidence of type 1 diabetes is about 1 in 300 children, any population-wide screening program would need to be implemented in the most efficient and cost-effective way possible with limited numbers of tests, say Mohamed Ghalwash, PhD, of the Center for Computational Health, IBM Research, Yorktown Heights, N.Y., and colleagues.
Results from their analysis of nearly 25,000 children from five prospective cohorts in Europe and the United States were published online in Lancet Diabetes & Endocrinology.
Screening in kids feasible, but may need geographic tweaking
“Our results show that initial screening for islet autoantibodies at two ages (2 years and 6 years) is sensitive and efficient for public health translation but might require adjustment by country on the basis of population-specific disease characteristics,” Dr. Ghalwash and colleagues write.
In an accompanying editorial, pediatric endocrinologist Maria J. Redondo, MD, PhD, writes: “This study is timely because recent successes in preventing type 1 diabetes highlight the need to identify the best candidates for intervention ... This paper constitutes an important contribution to the literature.”
However, Dr. Redondo, of Baylor College of Medicine and Texas Children’s Hospital, Houston, also cautioned: “It remains to be seen whether Dr. Ghalwash and colleagues’ strategy could work in the general population, because all the participants in the combined dataset had genetic risk factors for the disease or a relative with type 1 diabetes, in whom performance is expected to be higher.”
She also noted that most participants were of northern European ancestry and that it is unknown whether the same or a similar screening strategy could be applied to individuals older than 15 years, in whom preclinical type 1 diabetes progresses more slowly.
Two-time childhood screening yielded high sensitivity, specificity
The data from a total of 24,662 participants were pooled from five prospective cohorts from Finland (DIPP), Germany (BABYDIAB), Sweden (DiPiS), and the United States (DAISY and DEW-IT).
All were at elevated risk for type 1 diabetes based on human leukocyte antigen (HLA) genotyping, and some had first-degree relatives with the condition. Participants were screened annually for three type 1 diabetes–associated autoantibodies up to age 15 years or the onset of type 1 diabetes.
During follow-up, 672 children developed type 1 diabetes by age 15 years and 6,050 did not. (The rest hadn’t yet reached age 15 years or type 1 diabetes onset.) The median age at first appearance of islet autoantibodies was 4.5 years.
A two-age screening strategy at 2 years and 6 years was more sensitive than screening at just one age, with a sensitivity of 82% and a positive predictive value of 79% for the development of type 1 diabetes by age 15 years.
The predictive value increased with the number of autoantibodies tested. For example, a single islet autoantibody at age 2 years indicated a 4-year risk of developing type 1 diabetes by age 5.99 years of 31%, while multiple antibody positivity at age 2 years carried a 4-year risk of 55%.
By age 6 years, the risk over the next 9 years was 39% if the test had been negative at age 2 years and 70% if the test had been positive at 2 years. But overall, a 6-year-old with multiple autoantibodies had an overall 83% risk of type 1 diabetes regardless of the test result at 2 years.
The predictive performance of sensitivity by age differed by country, suggesting that the optimal ages for autoantibody testing might differ by geographic region, Dr. Ghalwash and colleagues say.
Dr. Redondo commented, “The model might require adaptation to local factors that affect the progression and prevalence of type 1 diabetes.” And, she added, “important aspects, such as screening cost, global access, acceptability, and follow-up support will need to be addressed for this strategy to be a viable public health option.”
The study was funded by JDRF. Dr. Ghalwash and another author are employees of IBM. A third author was a JDRF employee when the research was done and is now an employee of Janssen Research and Development. Dr. Redondo has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new data suggest.
Both genetic screening and islet-cell autoantibody screening for type 1 diabetes risk have become less expensive in recent years. Nonetheless, as of now, most children who receive such screening do so through programs that screen relatives of people who already have the condition, such as the global TrialNet program.
Some in the type 1 diabetes field have urged wider screening, with the rationale that knowledge of increased risk can prepare families to recognize the early signs of hyperglycemia and seek medical help to prevent the onset of diabetic ketoacidosis.
Moreover, potential therapies to prevent or delay type 1 diabetes are currently in development, including the anti-CD3 monoclonal antibody teplizumab (Tzield, Provention Bio).
However, given that the incidence of type 1 diabetes is about 1 in 300 children, any population-wide screening program would need to be implemented in the most efficient and cost-effective way possible with limited numbers of tests, say Mohamed Ghalwash, PhD, of the Center for Computational Health, IBM Research, Yorktown Heights, N.Y., and colleagues.
Results from their analysis of nearly 25,000 children from five prospective cohorts in Europe and the United States were published online in Lancet Diabetes & Endocrinology.
Screening in kids feasible, but may need geographic tweaking
“Our results show that initial screening for islet autoantibodies at two ages (2 years and 6 years) is sensitive and efficient for public health translation but might require adjustment by country on the basis of population-specific disease characteristics,” Dr. Ghalwash and colleagues write.
In an accompanying editorial, pediatric endocrinologist Maria J. Redondo, MD, PhD, writes: “This study is timely because recent successes in preventing type 1 diabetes highlight the need to identify the best candidates for intervention ... This paper constitutes an important contribution to the literature.”
However, Dr. Redondo, of Baylor College of Medicine and Texas Children’s Hospital, Houston, also cautioned: “It remains to be seen whether Dr. Ghalwash and colleagues’ strategy could work in the general population, because all the participants in the combined dataset had genetic risk factors for the disease or a relative with type 1 diabetes, in whom performance is expected to be higher.”
She also noted that most participants were of northern European ancestry and that it is unknown whether the same or a similar screening strategy could be applied to individuals older than 15 years, in whom preclinical type 1 diabetes progresses more slowly.
Two-time childhood screening yielded high sensitivity, specificity
The data from a total of 24,662 participants were pooled from five prospective cohorts from Finland (DIPP), Germany (BABYDIAB), Sweden (DiPiS), and the United States (DAISY and DEW-IT).
All were at elevated risk for type 1 diabetes based on human leukocyte antigen (HLA) genotyping, and some had first-degree relatives with the condition. Participants were screened annually for three type 1 diabetes–associated autoantibodies up to age 15 years or the onset of type 1 diabetes.
During follow-up, 672 children developed type 1 diabetes by age 15 years and 6,050 did not. (The rest hadn’t yet reached age 15 years or type 1 diabetes onset.) The median age at first appearance of islet autoantibodies was 4.5 years.
A two-age screening strategy at 2 years and 6 years was more sensitive than screening at just one age, with a sensitivity of 82% and a positive predictive value of 79% for the development of type 1 diabetes by age 15 years.
The predictive value increased with the number of autoantibodies tested. For example, a single islet autoantibody at age 2 years indicated a 4-year risk of developing type 1 diabetes by age 5.99 years of 31%, while multiple antibody positivity at age 2 years carried a 4-year risk of 55%.
By age 6 years, the risk over the next 9 years was 39% if the test had been negative at age 2 years and 70% if the test had been positive at 2 years. But overall, a 6-year-old with multiple autoantibodies had an overall 83% risk of type 1 diabetes regardless of the test result at 2 years.
The predictive performance of sensitivity by age differed by country, suggesting that the optimal ages for autoantibody testing might differ by geographic region, Dr. Ghalwash and colleagues say.
Dr. Redondo commented, “The model might require adaptation to local factors that affect the progression and prevalence of type 1 diabetes.” And, she added, “important aspects, such as screening cost, global access, acceptability, and follow-up support will need to be addressed for this strategy to be a viable public health option.”
The study was funded by JDRF. Dr. Ghalwash and another author are employees of IBM. A third author was a JDRF employee when the research was done and is now an employee of Janssen Research and Development. Dr. Redondo has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM LANCET DIABETES & ENDOCRINOLOGY
Social media in the lives of adolescents
Adolescence is a time of growing autonomy fueled by puberty, intellectual development, and identity formation. Social media engages adolescents by giving them easy access to (semi) private communication with peers, the ability to safely explore their sexuality, and easily investigate issues of intellectual curiosity, as they move from childhood to older adolescence. Social media facilitates the creation of a teenager’s own world, separate and distinct from adult concern or scrutiny. It is clearly compelling for adolescents, but we are in the early days of understanding the effect of various types of digital activities on the health and well-being of youth. There is evidence that for some, the addictive potential of these applications is potent, exacerbating or triggering mood, anxiety, and eating disorder symptoms. Their drive to explore their identity and relationships and their immature capacity to regulate emotions and behaviors make the risks of overuse substantial. But it would be impossible (and probably socially very costly) to simply avoid social media. So how to discuss its healthy use with your patients and their parents?
The data
Social media are digital communication platforms that allow users to build a public profile and then accumulate a network of followers, and follow other users, based on shared interests. They include FaceBook, Instagram, Snapchat, YouTube, and Twitter. Surveys demonstrated that 90% of U.S. adolescents use social media, with 75% having at least one social media profile and over half visiting social media sites at least once daily. Adolescents spend over 7 hours daily on their phones, not including time devoted to online schoolwork, and 8- to 12-year-olds are not far behind at almost 5 hours of daily phone use. On average, 39% of adolescent screen time is spent on passive consumption, 26% on social media, 25% on interactive activities (browsing the web, interactive video gaming) and 3% on content creation (coding, etc). There was considerable variability in survey results, and differences between genders, with boys engaged in video games almost eight times as often as girls, and girls in social media nearly twice as often as boys.1
The research
There is a growing body of research devoted to understanding the effects of all of this digital activity on youth health and well-being.

A large, longitudinal study of Canadian 13- to 17-year-olds found that time spent on social media or watching television was strongly associated with depressive and anxiety symptoms, with a robust dose-response relationship.2 However, causality is not clear, as anxious, shy, and depressed adolescents may use more social media as a consequence of their mood. Interestingly, there was no such relationship with mood and anxiety symptoms and time spent on video games.3 For youth with depression and anxiety, time spent on social media has been strongly associated with increased levels of self-reported distress, self-injury and suicidality, but again, causality is hard to prove.
One very large study from the United Kingdom (including more than 10,000 participants), demonstrated a strong relationship between time spent on social media and severity of depressive symptoms, with a more pronounced effect in girls than in boys.4 Many more nuanced studies have demonstrated that excessive time spent on social media, the presence of an addictive pattern of use, and the degree to which an adolescent’s sense of well-being is connected to social media are the variables that strongly predict an association with worsening depressive or anxiety symptoms.5
Several studies have demonstrated that low to moderate use of social media, and use to gather information and make plans were associated with better scores of emotional self-regulation and lower rates of depressive symptoms in teens.6 It seems safe to say that social media can be useful and fun, but that too much can be bad for you. So help your adolescent patients to expand their perspective on its use by discussing it with them.
Make them curious about quantity
Most teens feel they do not have enough time for all of the things they need to do, so invite them to play detective by using their phone’s applications that can track their time spent online and in different apps.

Remind them that these apps were designed to be so engaging that for some addiction is a real problem. As with tobacco, addiction is the business model by which these companies earn advertising dollars. Indeed, adolescents are the target demographic, as they are most sensitive to social rewards and are the most valuable audience for advertisers. Engage their natural suspicion of authority by pointing out that with every hour on Insta, someone else is making a lot of money. They get to choose how they want to relax, connect with friends, and explore the world, so help them to be aware of how these apps are designed to keep them from choosing.
Raise awareness of vulnerability
Adolescents who have attention-deficit/hyperactivity disorder already have difficulty with impulse control and with shifting their attention to less engaging activities. Adolescents with anxiety are prone to avoid stressful situations, but still hunger for knowledge and connections. Adolescents with depression are managing low motivation and self-esteem, and the rewards of social media may keep them from exercise and actual social engagement that are critical to their treatment. Youth with eating disorders are especially prone to critical comparison of themselves to others, feeding their distorted body images. Help your patients with these common illnesses to be aware of how social media may make their treatment harder, rather than being the source of relief it may feel like.
Protect their health
For all young people, too much time spent in virtual activities and passive media consumption may not leave enough time to explore potential interests, talents, or relationships. These are important activities throughout life, but they are the central developmental tasks of adolescence. They also need 8-10 hours of sleep nightly and regular exercise. And of course, they have homework! Help them to think about how to use their time wisely to support satisfying relationships and activities, with time for relaxation and good health.
Keep parents in the room for these discussions
State that most of us have difficulty putting down our phones. Children and teens need adults who model striving for balance in all areas of choice. Just as we try to teach them to make good choices about food, getting excellent nutrition while still valuing taste and pleasure, we can talk about how to balance virtual activities with actual activities, work with play, and effort with relaxation. You can help expand your young patients’ self-awareness, acknowledge the fun and utility of their digital time, and enhance their sense of how we must all learn how to put screens down sometimes. In so doing, you can help families to ensure that they are engaging with the digital tools and toys available to all of us in ways that can support their health and well-being.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Geena Davis Institute on Gender and Media. The Common Sense Census: Media Use by Teens and Tweens, 2015.
2. Abi-Jaoude E et al. CMAJ 2020;192(6):E136-41.
3. Boers E et al. Can J Psychiatry. 2020 Mar;65(3):206-8.
4. Kelly Y et al. EClinicalMedicine. 2019 Jan 4;6:59-68.
5. Vidal C et al. Int Rev Psychiatry. 2020 May;32(3):235-53.
6. Coyne SM et al. J Res Adolescence. 2019;29(4):897-907.
Adolescence is a time of growing autonomy fueled by puberty, intellectual development, and identity formation. Social media engages adolescents by giving them easy access to (semi) private communication with peers, the ability to safely explore their sexuality, and easily investigate issues of intellectual curiosity, as they move from childhood to older adolescence. Social media facilitates the creation of a teenager’s own world, separate and distinct from adult concern or scrutiny. It is clearly compelling for adolescents, but we are in the early days of understanding the effect of various types of digital activities on the health and well-being of youth. There is evidence that for some, the addictive potential of these applications is potent, exacerbating or triggering mood, anxiety, and eating disorder symptoms. Their drive to explore their identity and relationships and their immature capacity to regulate emotions and behaviors make the risks of overuse substantial. But it would be impossible (and probably socially very costly) to simply avoid social media. So how to discuss its healthy use with your patients and their parents?
The data
Social media are digital communication platforms that allow users to build a public profile and then accumulate a network of followers, and follow other users, based on shared interests. They include FaceBook, Instagram, Snapchat, YouTube, and Twitter. Surveys demonstrated that 90% of U.S. adolescents use social media, with 75% having at least one social media profile and over half visiting social media sites at least once daily. Adolescents spend over 7 hours daily on their phones, not including time devoted to online schoolwork, and 8- to 12-year-olds are not far behind at almost 5 hours of daily phone use. On average, 39% of adolescent screen time is spent on passive consumption, 26% on social media, 25% on interactive activities (browsing the web, interactive video gaming) and 3% on content creation (coding, etc). There was considerable variability in survey results, and differences between genders, with boys engaged in video games almost eight times as often as girls, and girls in social media nearly twice as often as boys.1
The research
There is a growing body of research devoted to understanding the effects of all of this digital activity on youth health and well-being.
A large, longitudinal study of Canadian 13- to 17-year-olds found that time spent on social media or watching television was strongly associated with depressive and anxiety symptoms, with a robust dose-response relationship.2 However, causality is not clear, as anxious, shy, and depressed adolescents may use more social media as a consequence of their mood. Interestingly, there was no such relationship with mood and anxiety symptoms and time spent on video games.3 For youth with depression and anxiety, time spent on social media has been strongly associated with increased levels of self-reported distress, self-injury and suicidality, but again, causality is hard to prove.
One very large study from the United Kingdom (including more than 10,000 participants), demonstrated a strong relationship between time spent on social media and severity of depressive symptoms, with a more pronounced effect in girls than in boys.4 Many more nuanced studies have demonstrated that excessive time spent on social media, the presence of an addictive pattern of use, and the degree to which an adolescent’s sense of well-being is connected to social media are the variables that strongly predict an association with worsening depressive or anxiety symptoms.5
Several studies have demonstrated that low to moderate use of social media, and use to gather information and make plans were associated with better scores of emotional self-regulation and lower rates of depressive symptoms in teens.6 It seems safe to say that social media can be useful and fun, but that too much can be bad for you. So help your adolescent patients to expand their perspective on its use by discussing it with them.
Make them curious about quantity
Most teens feel they do not have enough time for all of the things they need to do, so invite them to play detective by using their phone’s applications that can track their time spent online and in different apps.
Remind them that these apps were designed to be so engaging that for some addiction is a real problem. As with tobacco, addiction is the business model by which these companies earn advertising dollars. Indeed, adolescents are the target demographic, as they are most sensitive to social rewards and are the most valuable audience for advertisers. Engage their natural suspicion of authority by pointing out that with every hour on Insta, someone else is making a lot of money. They get to choose how they want to relax, connect with friends, and explore the world, so help them to be aware of how these apps are designed to keep them from choosing.
Raise awareness of vulnerability
Adolescents who have attention-deficit/hyperactivity disorder already have difficulty with impulse control and with shifting their attention to less engaging activities. Adolescents with anxiety are prone to avoid stressful situations, but still hunger for knowledge and connections. Adolescents with depression are managing low motivation and self-esteem, and the rewards of social media may keep them from exercise and actual social engagement that are critical to their treatment. Youth with eating disorders are especially prone to critical comparison of themselves to others, feeding their distorted body images. Help your patients with these common illnesses to be aware of how social media may make their treatment harder, rather than being the source of relief it may feel like.
Protect their health
For all young people, too much time spent in virtual activities and passive media consumption may not leave enough time to explore potential interests, talents, or relationships. These are important activities throughout life, but they are the central developmental tasks of adolescence. They also need 8-10 hours of sleep nightly and regular exercise. And of course, they have homework! Help them to think about how to use their time wisely to support satisfying relationships and activities, with time for relaxation and good health.
Keep parents in the room for these discussions
State that most of us have difficulty putting down our phones. Children and teens need adults who model striving for balance in all areas of choice. Just as we try to teach them to make good choices about food, getting excellent nutrition while still valuing taste and pleasure, we can talk about how to balance virtual activities with actual activities, work with play, and effort with relaxation. You can help expand your young patients’ self-awareness, acknowledge the fun and utility of their digital time, and enhance their sense of how we must all learn how to put screens down sometimes. In so doing, you can help families to ensure that they are engaging with the digital tools and toys available to all of us in ways that can support their health and well-being.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Geena Davis Institute on Gender and Media. The Common Sense Census: Media Use by Teens and Tweens, 2015.
2. Abi-Jaoude E et al. CMAJ 2020;192(6):E136-41.
3. Boers E et al. Can J Psychiatry. 2020 Mar;65(3):206-8.
4. Kelly Y et al. EClinicalMedicine. 2019 Jan 4;6:59-68.
5. Vidal C et al. Int Rev Psychiatry. 2020 May;32(3):235-53.
6. Coyne SM et al. J Res Adolescence. 2019;29(4):897-907.
Adolescence is a time of growing autonomy fueled by puberty, intellectual development, and identity formation. Social media engages adolescents by giving them easy access to (semi) private communication with peers, the ability to safely explore their sexuality, and easily investigate issues of intellectual curiosity, as they move from childhood to older adolescence. Social media facilitates the creation of a teenager’s own world, separate and distinct from adult concern or scrutiny. It is clearly compelling for adolescents, but we are in the early days of understanding the effect of various types of digital activities on the health and well-being of youth. There is evidence that for some, the addictive potential of these applications is potent, exacerbating or triggering mood, anxiety, and eating disorder symptoms. Their drive to explore their identity and relationships and their immature capacity to regulate emotions and behaviors make the risks of overuse substantial. But it would be impossible (and probably socially very costly) to simply avoid social media. So how to discuss its healthy use with your patients and their parents?
The data
Social media are digital communication platforms that allow users to build a public profile and then accumulate a network of followers, and follow other users, based on shared interests. They include FaceBook, Instagram, Snapchat, YouTube, and Twitter. Surveys demonstrated that 90% of U.S. adolescents use social media, with 75% having at least one social media profile and over half visiting social media sites at least once daily. Adolescents spend over 7 hours daily on their phones, not including time devoted to online schoolwork, and 8- to 12-year-olds are not far behind at almost 5 hours of daily phone use. On average, 39% of adolescent screen time is spent on passive consumption, 26% on social media, 25% on interactive activities (browsing the web, interactive video gaming) and 3% on content creation (coding, etc). There was considerable variability in survey results, and differences between genders, with boys engaged in video games almost eight times as often as girls, and girls in social media nearly twice as often as boys.1
The research
There is a growing body of research devoted to understanding the effects of all of this digital activity on youth health and well-being.
A large, longitudinal study of Canadian 13- to 17-year-olds found that time spent on social media or watching television was strongly associated with depressive and anxiety symptoms, with a robust dose-response relationship.2 However, causality is not clear, as anxious, shy, and depressed adolescents may use more social media as a consequence of their mood. Interestingly, there was no such relationship with mood and anxiety symptoms and time spent on video games.3 For youth with depression and anxiety, time spent on social media has been strongly associated with increased levels of self-reported distress, self-injury and suicidality, but again, causality is hard to prove.
One very large study from the United Kingdom (including more than 10,000 participants), demonstrated a strong relationship between time spent on social media and severity of depressive symptoms, with a more pronounced effect in girls than in boys.4 Many more nuanced studies have demonstrated that excessive time spent on social media, the presence of an addictive pattern of use, and the degree to which an adolescent’s sense of well-being is connected to social media are the variables that strongly predict an association with worsening depressive or anxiety symptoms.5
Several studies have demonstrated that low to moderate use of social media, and use to gather information and make plans were associated with better scores of emotional self-regulation and lower rates of depressive symptoms in teens.6 It seems safe to say that social media can be useful and fun, but that too much can be bad for you. So help your adolescent patients to expand their perspective on its use by discussing it with them.
Make them curious about quantity
Most teens feel they do not have enough time for all of the things they need to do, so invite them to play detective by using their phone’s applications that can track their time spent online and in different apps.
Remind them that these apps were designed to be so engaging that for some addiction is a real problem. As with tobacco, addiction is the business model by which these companies earn advertising dollars. Indeed, adolescents are the target demographic, as they are most sensitive to social rewards and are the most valuable audience for advertisers. Engage their natural suspicion of authority by pointing out that with every hour on Insta, someone else is making a lot of money. They get to choose how they want to relax, connect with friends, and explore the world, so help them to be aware of how these apps are designed to keep them from choosing.
Raise awareness of vulnerability
Adolescents who have attention-deficit/hyperactivity disorder already have difficulty with impulse control and with shifting their attention to less engaging activities. Adolescents with anxiety are prone to avoid stressful situations, but still hunger for knowledge and connections. Adolescents with depression are managing low motivation and self-esteem, and the rewards of social media may keep them from exercise and actual social engagement that are critical to their treatment. Youth with eating disorders are especially prone to critical comparison of themselves to others, feeding their distorted body images. Help your patients with these common illnesses to be aware of how social media may make their treatment harder, rather than being the source of relief it may feel like.
Protect their health
For all young people, too much time spent in virtual activities and passive media consumption may not leave enough time to explore potential interests, talents, or relationships. These are important activities throughout life, but they are the central developmental tasks of adolescence. They also need 8-10 hours of sleep nightly and regular exercise. And of course, they have homework! Help them to think about how to use their time wisely to support satisfying relationships and activities, with time for relaxation and good health.
Keep parents in the room for these discussions
State that most of us have difficulty putting down our phones. Children and teens need adults who model striving for balance in all areas of choice. Just as we try to teach them to make good choices about food, getting excellent nutrition while still valuing taste and pleasure, we can talk about how to balance virtual activities with actual activities, work with play, and effort with relaxation. You can help expand your young patients’ self-awareness, acknowledge the fun and utility of their digital time, and enhance their sense of how we must all learn how to put screens down sometimes. In so doing, you can help families to ensure that they are engaging with the digital tools and toys available to all of us in ways that can support their health and well-being.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Geena Davis Institute on Gender and Media. The Common Sense Census: Media Use by Teens and Tweens, 2015.
2. Abi-Jaoude E et al. CMAJ 2020;192(6):E136-41.
3. Boers E et al. Can J Psychiatry. 2020 Mar;65(3):206-8.
4. Kelly Y et al. EClinicalMedicine. 2019 Jan 4;6:59-68.
5. Vidal C et al. Int Rev Psychiatry. 2020 May;32(3):235-53.
6. Coyne SM et al. J Res Adolescence. 2019;29(4):897-907.
Inflation and health care: The prognosis for doctors
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Long COVID-19 in children and adolescents: What do we know?
Among scientists, the existence of long COVID-19 in children and adolescents has been the subject of debate.
Published by a Mexican multidisciplinary group in Scientific Reports, the first study is a systematic review and meta-analysis. It identified mood symptoms as the most prevalent clinical manifestations of long COVID-19 in children and adolescents. These symptoms included sadness, tension, anger, depression, and anxiety (16.50%); fatigue (9.66%); and sleep disorders (8.42%).
The second study, LongCOVIDKidsDK, was conducted in Denmark. It compared 11,000 children younger than 14 years who had tested positive for COVID-19 with 33,000 children who had no history of COVID-19. The study was published in The Lancet Child and Adolescent Health.
Definitions are changing
In their meta-analysis, the researchers estimated the prevalence and counted signs and symptoms of long COVID-19, as defined by the United Kingdom’s National Institute for Health and Care Excellence. Long COVID-19 was defined as the presence of one or more symptoms more than 4 weeks after SARS-CoV-2 infection. For search terms, the researchers used “COVID-19,” “COVID,” “SARSCOV-2,” “coronavirus,” “long COVID,” “postCOVID,” “PASC,” “long-haulers,” “prolonged,” “post-acute,” “persistent,” “convalescent,” “sequelae,” and “postviral.”
Of the 8,373 citations returned by the search as of Feb. 10, 2022, 21 prospective studies, 2 of them on preprint servers, met the authors’ selection criteria. Those studies included a total of 80,071 children and adolescents younger than 18 years.
In the meta-analysis, the prevalence of long COVID-19 among children and adolescents was reported to be 25.24% (95% confidence interval, 18.17-33.02; I2, 99.61%), regardless of whether the case had been asymptomatic, mild, moderate, severe, or serious. For patients who had been hospitalized, the prevalence was 29.19% (95% CI, 17.83-41.98; I2, 80.84%).
These numbers, while striking, are not the focus of the study, according to first author Sandra Lopez-Leon, MD, PhD, associate professor of pharmacoepidemiology at Rutgers University, New Brunswick, N.J. “It’s important that we don’t focus on that 25%,” she said in an interview. “It’s a disease that we’re learning about, we’re at a time when the definitions are still changing, and, depending on when it is measured, a different number will be given. The message we want to give is that long COVID-19 exists, it’s happening in children and adolescents, and patients need this recognition. And also to show that it can affect the whole body.”
The study showed that the children and adolescents who presented with SARS-CoV-2 infection were at higher risk of subsequent long dyspnea, anosmia/ageusia, or fever, compared with control persons.
In total, in the studies that were included, more than 40 long-term clinical manifestations associated with COVID-19 in the pediatric population were identified.
The most common symptoms among children aged 0-3 years were mood swings, skin rashes, and stomachaches. In 4- to 11-year-olds, the most common symptoms were mood swings, trouble remembering or concentrating, and skin rashes. In 12- to 14-year-olds, they were fatigue, mood swings, and trouble remembering or concentrating. These data are based on parent responses.
The list of signs and symptoms also includes headache, respiratory symptoms, cognitive symptoms (such as decreased concentration, learning difficulties, confusion, and memory loss), loss of appetite, and smell disorder (hyposmia, anosmia, hyperosmia, parosmia, and phantom smell).
In the studies, the prevalence of the following symptoms was less than 5%: hyperhidrosis, chest pain, dizziness, cough, myalgia/arthralgia, changes in body weight, taste disorder, otalgia (tinnitus, ear pain, vertigo), ophthalmologic symptoms (conjunctivitis, dry eye, blurred vision, photophobia, pain), dermatologic symptoms (dry skin, itchy skin, rashes, hives, hair loss), urinary symptoms, abdominal pain, throat pain, chest tightness, variations in heart rate, palpitations, constipation, dysphonia, fever, diarrhea, vomiting/nausea, menstrual changes, neurological abnormalities, speech disorders, and dysphagia.
The authors made it clear that the frequency and severity of these symptoms can fluctuate from one patient to another.
“The meta-analysis is important because it brings together 21 studies selected from more than 8,000 articles – and in them, a large number of children – to study the most common manifestations of long COVID-19,” Gabriela Ensinck, MD, head of the infectious diseases department at the Víctor J. Vilela Children’s Hospital in Rosario, Argentina, told this news organization. Dr. Ensinck did not participate in the study. “The important thing here is that long COVID-19 exists in pediatrics. And that it is a prolongation of signs or symptoms over time, a time for which there is no single definition.”
“It’s a snapshot of all the symptoms that can remain after COVID-19,” Dr. Lopez-Leon explained. “The meta-analysis seeks to see if there’s an association between having had COVID-19 and having the symptoms, but at no time does it speak of causality.”
The prevalence of symptoms largely depends on the time since the onset of acute COVID-19. Most symptoms improve over time. In the studies that were included in the meta-analysis, the follow-up time varied between 1 and 13 months. It is important to understand what symptoms are associated with each period after the onset of infection, the authors said.
Danish parent survey
The Danish study LongCOVIDKidsDK followed the World Health Organization criteria for long COVID-19 and included children and adolescents aged 0-14 years who received a diagnosis of COVID-19 and who experienced symptoms that lasted at least 2 months.
Between July 20, 2021, and Sept. 15, 2021, a questionnaire was sent to 38,152 case patients and 147,212 control persons. Of this group, 10,997 (28.8%) case patients and 33,016 (22.4%) control persons answered the survey.
Children who had been diagnosed with SARS-CoV-2 infection were more likely to experience long-lasting symptoms than children who had never been diagnosed. Approximately one-third of children with a positive SARS-CoV-2 test experienced symptoms that were not present before infection. Children who experienced long-lasting symptoms included 40% of children diagnosed with COVID-19 and 27% of control persons aged 0-3 years, 38% of case patients and 34% of control persons aged 4-11 years, and 46% of case patients and 41% of control persons aged 12-14 years.
Interestingly, those diagnosed with COVID-19 reported fewer psychological and social problems than those in the control group. Among the oldest (aged 12-14 years), quality of life scores were higher and anxiety scores were lower for those who had tested positive for SARS-CoV-2.
More information needed
Given the diversity of symptoms in the meta-analysis and the LongCOVIDKidsDK study, a multidisciplinary approach is imperative. Dr. Lopez-Leon suggests that there is a need to raise awareness among parents, clinicians, researchers, and the health system about the conditions that can occur after COVID-19. Clinicians must better understand the sequelae to provide targeted care and treatment. The authors of the Danish study recommend establishing clinics for long COVID-19 with multispecialty care.
Maren J. Heilskov Rytter, PhD, associate professor of clinical medicine at the University of Copenhagen, wrote an editorial in The Lancet Child and Adolescent Health about the Danish study. Until it is clarified whether SARS-CoV-2 does indeed cause persistent symptoms, she wrote, “it seems excessive and premature to establish specific multidisciplinary clinics for children with long COVID-19.”
Dr. Rytter highlighted the difficulty of interpreting LongCOVIDKidsDK data, owing to recall bias, the failure to exclude other causes of symptoms in the cases analyzed, and the number of symptoms in the control persons. In addition, the data analyzed in Denmark are of limited clinical relevance, she said, given a greater presence of mild symptoms and, paradoxically, a higher quality of life.
She concluded, “In the majority of children with nonspecific symptoms after COVID-19, the symptoms presented are more likely to have been caused by something other than COVID-19, and if they are related to COVID-19, they are likely to go away over time.”
Dr. Ensinck, who is coauthor of the Argentine Ministry of Health’s guide for long COVID-19 monitoring for children and adolescents and who represented the Infectious Diseases Committee of the Argentine Society of Pediatrics, highlighted another aspect of the problem. “What should be taken into account in these data is to see how much the confinement contributed. Children are the ones who suffered the most in the period in which schools were closed; they could not meet their peers, they had sick relatives, they felt fear. … all this must be taken into account.”
There is as yet no agreement on how to define and diagnose long COVID-19 in adults, a population that has been studied more closely. Part of the problem is that long COVID-19 has been linked to more than 200 symptoms, which can range in severity from inconvenient to debilitating, can last for months or years, and can recur, sometimes months after apparent recovery. Thus, there are still disparate answers to basic questions about the syndrome’s frequency and its effects on vaccination, reinfection, and the latest variant of SARS-CoV-2.
This article has been translated from the Medscape Spanish edition. A version appeared on Medscape.com.
Among scientists, the existence of long COVID-19 in children and adolescents has been the subject of debate.
Published by a Mexican multidisciplinary group in Scientific Reports, the first study is a systematic review and meta-analysis. It identified mood symptoms as the most prevalent clinical manifestations of long COVID-19 in children and adolescents. These symptoms included sadness, tension, anger, depression, and anxiety (16.50%); fatigue (9.66%); and sleep disorders (8.42%).
The second study, LongCOVIDKidsDK, was conducted in Denmark. It compared 11,000 children younger than 14 years who had tested positive for COVID-19 with 33,000 children who had no history of COVID-19. The study was published in The Lancet Child and Adolescent Health.
Definitions are changing
In their meta-analysis, the researchers estimated the prevalence and counted signs and symptoms of long COVID-19, as defined by the United Kingdom’s National Institute for Health and Care Excellence. Long COVID-19 was defined as the presence of one or more symptoms more than 4 weeks after SARS-CoV-2 infection. For search terms, the researchers used “COVID-19,” “COVID,” “SARSCOV-2,” “coronavirus,” “long COVID,” “postCOVID,” “PASC,” “long-haulers,” “prolonged,” “post-acute,” “persistent,” “convalescent,” “sequelae,” and “postviral.”
Of the 8,373 citations returned by the search as of Feb. 10, 2022, 21 prospective studies, 2 of them on preprint servers, met the authors’ selection criteria. Those studies included a total of 80,071 children and adolescents younger than 18 years.
In the meta-analysis, the prevalence of long COVID-19 among children and adolescents was reported to be 25.24% (95% confidence interval, 18.17-33.02; I2, 99.61%), regardless of whether the case had been asymptomatic, mild, moderate, severe, or serious. For patients who had been hospitalized, the prevalence was 29.19% (95% CI, 17.83-41.98; I2, 80.84%).
These numbers, while striking, are not the focus of the study, according to first author Sandra Lopez-Leon, MD, PhD, associate professor of pharmacoepidemiology at Rutgers University, New Brunswick, N.J. “It’s important that we don’t focus on that 25%,” she said in an interview. “It’s a disease that we’re learning about, we’re at a time when the definitions are still changing, and, depending on when it is measured, a different number will be given. The message we want to give is that long COVID-19 exists, it’s happening in children and adolescents, and patients need this recognition. And also to show that it can affect the whole body.”
The study showed that the children and adolescents who presented with SARS-CoV-2 infection were at higher risk of subsequent long dyspnea, anosmia/ageusia, or fever, compared with control persons.
In total, in the studies that were included, more than 40 long-term clinical manifestations associated with COVID-19 in the pediatric population were identified.
The most common symptoms among children aged 0-3 years were mood swings, skin rashes, and stomachaches. In 4- to 11-year-olds, the most common symptoms were mood swings, trouble remembering or concentrating, and skin rashes. In 12- to 14-year-olds, they were fatigue, mood swings, and trouble remembering or concentrating. These data are based on parent responses.
The list of signs and symptoms also includes headache, respiratory symptoms, cognitive symptoms (such as decreased concentration, learning difficulties, confusion, and memory loss), loss of appetite, and smell disorder (hyposmia, anosmia, hyperosmia, parosmia, and phantom smell).
In the studies, the prevalence of the following symptoms was less than 5%: hyperhidrosis, chest pain, dizziness, cough, myalgia/arthralgia, changes in body weight, taste disorder, otalgia (tinnitus, ear pain, vertigo), ophthalmologic symptoms (conjunctivitis, dry eye, blurred vision, photophobia, pain), dermatologic symptoms (dry skin, itchy skin, rashes, hives, hair loss), urinary symptoms, abdominal pain, throat pain, chest tightness, variations in heart rate, palpitations, constipation, dysphonia, fever, diarrhea, vomiting/nausea, menstrual changes, neurological abnormalities, speech disorders, and dysphagia.
The authors made it clear that the frequency and severity of these symptoms can fluctuate from one patient to another.
“The meta-analysis is important because it brings together 21 studies selected from more than 8,000 articles – and in them, a large number of children – to study the most common manifestations of long COVID-19,” Gabriela Ensinck, MD, head of the infectious diseases department at the Víctor J. Vilela Children’s Hospital in Rosario, Argentina, told this news organization. Dr. Ensinck did not participate in the study. “The important thing here is that long COVID-19 exists in pediatrics. And that it is a prolongation of signs or symptoms over time, a time for which there is no single definition.”
“It’s a snapshot of all the symptoms that can remain after COVID-19,” Dr. Lopez-Leon explained. “The meta-analysis seeks to see if there’s an association between having had COVID-19 and having the symptoms, but at no time does it speak of causality.”
The prevalence of symptoms largely depends on the time since the onset of acute COVID-19. Most symptoms improve over time. In the studies that were included in the meta-analysis, the follow-up time varied between 1 and 13 months. It is important to understand what symptoms are associated with each period after the onset of infection, the authors said.
Danish parent survey
The Danish study LongCOVIDKidsDK followed the World Health Organization criteria for long COVID-19 and included children and adolescents aged 0-14 years who received a diagnosis of COVID-19 and who experienced symptoms that lasted at least 2 months.
Between July 20, 2021, and Sept. 15, 2021, a questionnaire was sent to 38,152 case patients and 147,212 control persons. Of this group, 10,997 (28.8%) case patients and 33,016 (22.4%) control persons answered the survey.
Children who had been diagnosed with SARS-CoV-2 infection were more likely to experience long-lasting symptoms than children who had never been diagnosed. Approximately one-third of children with a positive SARS-CoV-2 test experienced symptoms that were not present before infection. Children who experienced long-lasting symptoms included 40% of children diagnosed with COVID-19 and 27% of control persons aged 0-3 years, 38% of case patients and 34% of control persons aged 4-11 years, and 46% of case patients and 41% of control persons aged 12-14 years.
Interestingly, those diagnosed with COVID-19 reported fewer psychological and social problems than those in the control group. Among the oldest (aged 12-14 years), quality of life scores were higher and anxiety scores were lower for those who had tested positive for SARS-CoV-2.
More information needed
Given the diversity of symptoms in the meta-analysis and the LongCOVIDKidsDK study, a multidisciplinary approach is imperative. Dr. Lopez-Leon suggests that there is a need to raise awareness among parents, clinicians, researchers, and the health system about the conditions that can occur after COVID-19. Clinicians must better understand the sequelae to provide targeted care and treatment. The authors of the Danish study recommend establishing clinics for long COVID-19 with multispecialty care.
Maren J. Heilskov Rytter, PhD, associate professor of clinical medicine at the University of Copenhagen, wrote an editorial in The Lancet Child and Adolescent Health about the Danish study. Until it is clarified whether SARS-CoV-2 does indeed cause persistent symptoms, she wrote, “it seems excessive and premature to establish specific multidisciplinary clinics for children with long COVID-19.”
Dr. Rytter highlighted the difficulty of interpreting LongCOVIDKidsDK data, owing to recall bias, the failure to exclude other causes of symptoms in the cases analyzed, and the number of symptoms in the control persons. In addition, the data analyzed in Denmark are of limited clinical relevance, she said, given a greater presence of mild symptoms and, paradoxically, a higher quality of life.
She concluded, “In the majority of children with nonspecific symptoms after COVID-19, the symptoms presented are more likely to have been caused by something other than COVID-19, and if they are related to COVID-19, they are likely to go away over time.”
Dr. Ensinck, who is coauthor of the Argentine Ministry of Health’s guide for long COVID-19 monitoring for children and adolescents and who represented the Infectious Diseases Committee of the Argentine Society of Pediatrics, highlighted another aspect of the problem. “What should be taken into account in these data is to see how much the confinement contributed. Children are the ones who suffered the most in the period in which schools were closed; they could not meet their peers, they had sick relatives, they felt fear. … all this must be taken into account.”
There is as yet no agreement on how to define and diagnose long COVID-19 in adults, a population that has been studied more closely. Part of the problem is that long COVID-19 has been linked to more than 200 symptoms, which can range in severity from inconvenient to debilitating, can last for months or years, and can recur, sometimes months after apparent recovery. Thus, there are still disparate answers to basic questions about the syndrome’s frequency and its effects on vaccination, reinfection, and the latest variant of SARS-CoV-2.
This article has been translated from the Medscape Spanish edition. A version appeared on Medscape.com.
Among scientists, the existence of long COVID-19 in children and adolescents has been the subject of debate.
Published by a Mexican multidisciplinary group in Scientific Reports, the first study is a systematic review and meta-analysis. It identified mood symptoms as the most prevalent clinical manifestations of long COVID-19 in children and adolescents. These symptoms included sadness, tension, anger, depression, and anxiety (16.50%); fatigue (9.66%); and sleep disorders (8.42%).
The second study, LongCOVIDKidsDK, was conducted in Denmark. It compared 11,000 children younger than 14 years who had tested positive for COVID-19 with 33,000 children who had no history of COVID-19. The study was published in The Lancet Child and Adolescent Health.
Definitions are changing
In their meta-analysis, the researchers estimated the prevalence and counted signs and symptoms of long COVID-19, as defined by the United Kingdom’s National Institute for Health and Care Excellence. Long COVID-19 was defined as the presence of one or more symptoms more than 4 weeks after SARS-CoV-2 infection. For search terms, the researchers used “COVID-19,” “COVID,” “SARSCOV-2,” “coronavirus,” “long COVID,” “postCOVID,” “PASC,” “long-haulers,” “prolonged,” “post-acute,” “persistent,” “convalescent,” “sequelae,” and “postviral.”
Of the 8,373 citations returned by the search as of Feb. 10, 2022, 21 prospective studies, 2 of them on preprint servers, met the authors’ selection criteria. Those studies included a total of 80,071 children and adolescents younger than 18 years.
In the meta-analysis, the prevalence of long COVID-19 among children and adolescents was reported to be 25.24% (95% confidence interval, 18.17-33.02; I2, 99.61%), regardless of whether the case had been asymptomatic, mild, moderate, severe, or serious. For patients who had been hospitalized, the prevalence was 29.19% (95% CI, 17.83-41.98; I2, 80.84%).
These numbers, while striking, are not the focus of the study, according to first author Sandra Lopez-Leon, MD, PhD, associate professor of pharmacoepidemiology at Rutgers University, New Brunswick, N.J. “It’s important that we don’t focus on that 25%,” she said in an interview. “It’s a disease that we’re learning about, we’re at a time when the definitions are still changing, and, depending on when it is measured, a different number will be given. The message we want to give is that long COVID-19 exists, it’s happening in children and adolescents, and patients need this recognition. And also to show that it can affect the whole body.”
The study showed that the children and adolescents who presented with SARS-CoV-2 infection were at higher risk of subsequent long dyspnea, anosmia/ageusia, or fever, compared with control persons.
In total, in the studies that were included, more than 40 long-term clinical manifestations associated with COVID-19 in the pediatric population were identified.
The most common symptoms among children aged 0-3 years were mood swings, skin rashes, and stomachaches. In 4- to 11-year-olds, the most common symptoms were mood swings, trouble remembering or concentrating, and skin rashes. In 12- to 14-year-olds, they were fatigue, mood swings, and trouble remembering or concentrating. These data are based on parent responses.
The list of signs and symptoms also includes headache, respiratory symptoms, cognitive symptoms (such as decreased concentration, learning difficulties, confusion, and memory loss), loss of appetite, and smell disorder (hyposmia, anosmia, hyperosmia, parosmia, and phantom smell).
In the studies, the prevalence of the following symptoms was less than 5%: hyperhidrosis, chest pain, dizziness, cough, myalgia/arthralgia, changes in body weight, taste disorder, otalgia (tinnitus, ear pain, vertigo), ophthalmologic symptoms (conjunctivitis, dry eye, blurred vision, photophobia, pain), dermatologic symptoms (dry skin, itchy skin, rashes, hives, hair loss), urinary symptoms, abdominal pain, throat pain, chest tightness, variations in heart rate, palpitations, constipation, dysphonia, fever, diarrhea, vomiting/nausea, menstrual changes, neurological abnormalities, speech disorders, and dysphagia.
The authors made it clear that the frequency and severity of these symptoms can fluctuate from one patient to another.
“The meta-analysis is important because it brings together 21 studies selected from more than 8,000 articles – and in them, a large number of children – to study the most common manifestations of long COVID-19,” Gabriela Ensinck, MD, head of the infectious diseases department at the Víctor J. Vilela Children’s Hospital in Rosario, Argentina, told this news organization. Dr. Ensinck did not participate in the study. “The important thing here is that long COVID-19 exists in pediatrics. And that it is a prolongation of signs or symptoms over time, a time for which there is no single definition.”
“It’s a snapshot of all the symptoms that can remain after COVID-19,” Dr. Lopez-Leon explained. “The meta-analysis seeks to see if there’s an association between having had COVID-19 and having the symptoms, but at no time does it speak of causality.”
The prevalence of symptoms largely depends on the time since the onset of acute COVID-19. Most symptoms improve over time. In the studies that were included in the meta-analysis, the follow-up time varied between 1 and 13 months. It is important to understand what symptoms are associated with each period after the onset of infection, the authors said.
Danish parent survey
The Danish study LongCOVIDKidsDK followed the World Health Organization criteria for long COVID-19 and included children and adolescents aged 0-14 years who received a diagnosis of COVID-19 and who experienced symptoms that lasted at least 2 months.
Between July 20, 2021, and Sept. 15, 2021, a questionnaire was sent to 38,152 case patients and 147,212 control persons. Of this group, 10,997 (28.8%) case patients and 33,016 (22.4%) control persons answered the survey.
Children who had been diagnosed with SARS-CoV-2 infection were more likely to experience long-lasting symptoms than children who had never been diagnosed. Approximately one-third of children with a positive SARS-CoV-2 test experienced symptoms that were not present before infection. Children who experienced long-lasting symptoms included 40% of children diagnosed with COVID-19 and 27% of control persons aged 0-3 years, 38% of case patients and 34% of control persons aged 4-11 years, and 46% of case patients and 41% of control persons aged 12-14 years.
Interestingly, those diagnosed with COVID-19 reported fewer psychological and social problems than those in the control group. Among the oldest (aged 12-14 years), quality of life scores were higher and anxiety scores were lower for those who had tested positive for SARS-CoV-2.
More information needed
Given the diversity of symptoms in the meta-analysis and the LongCOVIDKidsDK study, a multidisciplinary approach is imperative. Dr. Lopez-Leon suggests that there is a need to raise awareness among parents, clinicians, researchers, and the health system about the conditions that can occur after COVID-19. Clinicians must better understand the sequelae to provide targeted care and treatment. The authors of the Danish study recommend establishing clinics for long COVID-19 with multispecialty care.
Maren J. Heilskov Rytter, PhD, associate professor of clinical medicine at the University of Copenhagen, wrote an editorial in The Lancet Child and Adolescent Health about the Danish study. Until it is clarified whether SARS-CoV-2 does indeed cause persistent symptoms, she wrote, “it seems excessive and premature to establish specific multidisciplinary clinics for children with long COVID-19.”
Dr. Rytter highlighted the difficulty of interpreting LongCOVIDKidsDK data, owing to recall bias, the failure to exclude other causes of symptoms in the cases analyzed, and the number of symptoms in the control persons. In addition, the data analyzed in Denmark are of limited clinical relevance, she said, given a greater presence of mild symptoms and, paradoxically, a higher quality of life.
She concluded, “In the majority of children with nonspecific symptoms after COVID-19, the symptoms presented are more likely to have been caused by something other than COVID-19, and if they are related to COVID-19, they are likely to go away over time.”
Dr. Ensinck, who is coauthor of the Argentine Ministry of Health’s guide for long COVID-19 monitoring for children and adolescents and who represented the Infectious Diseases Committee of the Argentine Society of Pediatrics, highlighted another aspect of the problem. “What should be taken into account in these data is to see how much the confinement contributed. Children are the ones who suffered the most in the period in which schools were closed; they could not meet their peers, they had sick relatives, they felt fear. … all this must be taken into account.”
There is as yet no agreement on how to define and diagnose long COVID-19 in adults, a population that has been studied more closely. Part of the problem is that long COVID-19 has been linked to more than 200 symptoms, which can range in severity from inconvenient to debilitating, can last for months or years, and can recur, sometimes months after apparent recovery. Thus, there are still disparate answers to basic questions about the syndrome’s frequency and its effects on vaccination, reinfection, and the latest variant of SARS-CoV-2.
This article has been translated from the Medscape Spanish edition. A version appeared on Medscape.com.
FROM SCIENTIFIC REPORTS AND THE LANCET CHILD AND ADOLESCENT HEALTH
Eczema causes substantial burden for many infants and preschoolers
INDIANAPOLIS – . Those are key findings from a large international web-based survey that was presented during a poster session at the annual meeting of the Society for Pediatric Dermatology.
“Improved knowledge of the AD-related burden may help reinforce the medical need in the pediatric population and contribute to better and earlier adequate management of the disease,” authors led by Stephan Weidinger , MD, PhD, vice head of the department of dermatology at University Hospital Schleswig-Holstein, Kiel, Germany, wrote in the abstract.
For the study, Dr. Weidinger and colleagues evaluated 1,486 infants and preschoolers with AD aged 6 months to under 6 years, who participated in the Epidemiology of Children with Atopic Dermatitis Reporting on their Experience (EPI-CARE), an international, cross-sectional, web-based survey of children and adolescents. The study population resided in 18 countries from five regions of the world, including North America, Latin America, Europe, Middle East/Eurasia, and East Asia. Parents or guardians answered all questions for infants/preschoolers younger than 4 years of age, while preschoolers aged 4 to younger than 6 years were asked to answer questions related to the impact of AD on their health-related quality of life.
AD severity was assessed using Patient Global Assessment (PtGA), where parents or guardians described their child’s eczema severity over the last week as mild, moderate, or severe. The researchers stratified outcomes by geographic region and AD severity, which included the following atopic comorbidities: worst itch, worst skin pain, and overall sleep disturbance in the past 24 hours as measured by the 0-10 numeric rating scale, where higher scores indicate worse severity; eczema-related hospitalization in the past 12 months; and frequency and average duration of flares over the past month.
The mean age of the study participants was 3 years and 61.6% had mild disease. The most common atopic comorbidities were hay fever, asthma, and seasonal allergies, and the incidence of atopic comorbidities increased with increasing AD severity. One or more atopic comorbidities was reported in 88.3% of patients with mild AD, compared with 92.1% of those with moderate disease and 95.8% of those with severe disease. In addition, infants and preschoolers with moderate or severe AD had worse itch, skin pain, and sleep disturbances over the past 24 hours, compared with those who had mild AD.
More than half of infants and preschoolers with severe AD (54.1%) were reported to have been hospitalized in the past 12 months (this ranged from 30.2% to 71.3% across regions), as did 35% of patients with moderate AD and 32.1% of those with mild AD. In addition, 50.6% of infants and preschoolers with severe AD had more than two flares in the past month, compared with 18.1% of those with moderate AD and 6.3% of those with mild disease.
In other findings, 50.7% of infants and preschoolers with severe AD had flares than lasted an average of 2 or more weeks, compared with 20.8% of those with moderate disease and 10% of those with mild disease. Also, 78.3% of preschoolers aged 4 to less than 6 years had missed one or more days of school in the previous 4 weeks: a mean of 5.1 days among those with mild AD, a mean of 7.3 days among those with moderate AD, and a mean of 12.1 days among those with severe disease.
Raj J. Chovatiya MD, PhD, of the department of dermatology at Northwestern University, Chicago, who was asked to comment on the study, said that infants and preschoolers remain an understudied group despite the high prevalence of AD in this age range. “The results of this study demonstrate a substantial burden of disease in this population, particularly among those with more severe disease,” said Dr. Chovatiya, who also directs the university’s Center for Eczema and Itch. “This includes longer and more frequent AD flares as well as high rates of inpatient hospitalization. These findings suggest that additional research is needed to better characterize disease burden and optimize outcomes for young children with AD.”
The study was funded by Regeneron Pharmaceuticals and Sanofi. Dr. Weidinger and other coauthors reported having received institutional research grants and consulting fees from many pharmaceutical companies that manufacture drugs used for the treatment of psoriasis and eczema.
Dr. Chovatiya disclosed that he has served as an advisory board member, consultant, speaker, and/or investigator for AbbVie, Arcutis, Arena, Beiersdorf, Bristol Myers Squibb, Dermavant, Eli Lilly, EPI Health, Incyte, L’Oréal, the National Eczema Association, Pfizer, Regeneron, Sanofi, and UCB.
INDIANAPOLIS – . Those are key findings from a large international web-based survey that was presented during a poster session at the annual meeting of the Society for Pediatric Dermatology.
“Improved knowledge of the AD-related burden may help reinforce the medical need in the pediatric population and contribute to better and earlier adequate management of the disease,” authors led by Stephan Weidinger , MD, PhD, vice head of the department of dermatology at University Hospital Schleswig-Holstein, Kiel, Germany, wrote in the abstract.
For the study, Dr. Weidinger and colleagues evaluated 1,486 infants and preschoolers with AD aged 6 months to under 6 years, who participated in the Epidemiology of Children with Atopic Dermatitis Reporting on their Experience (EPI-CARE), an international, cross-sectional, web-based survey of children and adolescents. The study population resided in 18 countries from five regions of the world, including North America, Latin America, Europe, Middle East/Eurasia, and East Asia. Parents or guardians answered all questions for infants/preschoolers younger than 4 years of age, while preschoolers aged 4 to younger than 6 years were asked to answer questions related to the impact of AD on their health-related quality of life.
AD severity was assessed using Patient Global Assessment (PtGA), where parents or guardians described their child’s eczema severity over the last week as mild, moderate, or severe. The researchers stratified outcomes by geographic region and AD severity, which included the following atopic comorbidities: worst itch, worst skin pain, and overall sleep disturbance in the past 24 hours as measured by the 0-10 numeric rating scale, where higher scores indicate worse severity; eczema-related hospitalization in the past 12 months; and frequency and average duration of flares over the past month.
The mean age of the study participants was 3 years and 61.6% had mild disease. The most common atopic comorbidities were hay fever, asthma, and seasonal allergies, and the incidence of atopic comorbidities increased with increasing AD severity. One or more atopic comorbidities was reported in 88.3% of patients with mild AD, compared with 92.1% of those with moderate disease and 95.8% of those with severe disease. In addition, infants and preschoolers with moderate or severe AD had worse itch, skin pain, and sleep disturbances over the past 24 hours, compared with those who had mild AD.
More than half of infants and preschoolers with severe AD (54.1%) were reported to have been hospitalized in the past 12 months (this ranged from 30.2% to 71.3% across regions), as did 35% of patients with moderate AD and 32.1% of those with mild AD. In addition, 50.6% of infants and preschoolers with severe AD had more than two flares in the past month, compared with 18.1% of those with moderate AD and 6.3% of those with mild disease.
In other findings, 50.7% of infants and preschoolers with severe AD had flares than lasted an average of 2 or more weeks, compared with 20.8% of those with moderate disease and 10% of those with mild disease. Also, 78.3% of preschoolers aged 4 to less than 6 years had missed one or more days of school in the previous 4 weeks: a mean of 5.1 days among those with mild AD, a mean of 7.3 days among those with moderate AD, and a mean of 12.1 days among those with severe disease.
Raj J. Chovatiya MD, PhD, of the department of dermatology at Northwestern University, Chicago, who was asked to comment on the study, said that infants and preschoolers remain an understudied group despite the high prevalence of AD in this age range. “The results of this study demonstrate a substantial burden of disease in this population, particularly among those with more severe disease,” said Dr. Chovatiya, who also directs the university’s Center for Eczema and Itch. “This includes longer and more frequent AD flares as well as high rates of inpatient hospitalization. These findings suggest that additional research is needed to better characterize disease burden and optimize outcomes for young children with AD.”
The study was funded by Regeneron Pharmaceuticals and Sanofi. Dr. Weidinger and other coauthors reported having received institutional research grants and consulting fees from many pharmaceutical companies that manufacture drugs used for the treatment of psoriasis and eczema.
Dr. Chovatiya disclosed that he has served as an advisory board member, consultant, speaker, and/or investigator for AbbVie, Arcutis, Arena, Beiersdorf, Bristol Myers Squibb, Dermavant, Eli Lilly, EPI Health, Incyte, L’Oréal, the National Eczema Association, Pfizer, Regeneron, Sanofi, and UCB.
INDIANAPOLIS – . Those are key findings from a large international web-based survey that was presented during a poster session at the annual meeting of the Society for Pediatric Dermatology.
“Improved knowledge of the AD-related burden may help reinforce the medical need in the pediatric population and contribute to better and earlier adequate management of the disease,” authors led by Stephan Weidinger , MD, PhD, vice head of the department of dermatology at University Hospital Schleswig-Holstein, Kiel, Germany, wrote in the abstract.
For the study, Dr. Weidinger and colleagues evaluated 1,486 infants and preschoolers with AD aged 6 months to under 6 years, who participated in the Epidemiology of Children with Atopic Dermatitis Reporting on their Experience (EPI-CARE), an international, cross-sectional, web-based survey of children and adolescents. The study population resided in 18 countries from five regions of the world, including North America, Latin America, Europe, Middle East/Eurasia, and East Asia. Parents or guardians answered all questions for infants/preschoolers younger than 4 years of age, while preschoolers aged 4 to younger than 6 years were asked to answer questions related to the impact of AD on their health-related quality of life.
AD severity was assessed using Patient Global Assessment (PtGA), where parents or guardians described their child’s eczema severity over the last week as mild, moderate, or severe. The researchers stratified outcomes by geographic region and AD severity, which included the following atopic comorbidities: worst itch, worst skin pain, and overall sleep disturbance in the past 24 hours as measured by the 0-10 numeric rating scale, where higher scores indicate worse severity; eczema-related hospitalization in the past 12 months; and frequency and average duration of flares over the past month.
The mean age of the study participants was 3 years and 61.6% had mild disease. The most common atopic comorbidities were hay fever, asthma, and seasonal allergies, and the incidence of atopic comorbidities increased with increasing AD severity. One or more atopic comorbidities was reported in 88.3% of patients with mild AD, compared with 92.1% of those with moderate disease and 95.8% of those with severe disease. In addition, infants and preschoolers with moderate or severe AD had worse itch, skin pain, and sleep disturbances over the past 24 hours, compared with those who had mild AD.
More than half of infants and preschoolers with severe AD (54.1%) were reported to have been hospitalized in the past 12 months (this ranged from 30.2% to 71.3% across regions), as did 35% of patients with moderate AD and 32.1% of those with mild AD. In addition, 50.6% of infants and preschoolers with severe AD had more than two flares in the past month, compared with 18.1% of those with moderate AD and 6.3% of those with mild disease.
In other findings, 50.7% of infants and preschoolers with severe AD had flares than lasted an average of 2 or more weeks, compared with 20.8% of those with moderate disease and 10% of those with mild disease. Also, 78.3% of preschoolers aged 4 to less than 6 years had missed one or more days of school in the previous 4 weeks: a mean of 5.1 days among those with mild AD, a mean of 7.3 days among those with moderate AD, and a mean of 12.1 days among those with severe disease.
Raj J. Chovatiya MD, PhD, of the department of dermatology at Northwestern University, Chicago, who was asked to comment on the study, said that infants and preschoolers remain an understudied group despite the high prevalence of AD in this age range. “The results of this study demonstrate a substantial burden of disease in this population, particularly among those with more severe disease,” said Dr. Chovatiya, who also directs the university’s Center for Eczema and Itch. “This includes longer and more frequent AD flares as well as high rates of inpatient hospitalization. These findings suggest that additional research is needed to better characterize disease burden and optimize outcomes for young children with AD.”
The study was funded by Regeneron Pharmaceuticals and Sanofi. Dr. Weidinger and other coauthors reported having received institutional research grants and consulting fees from many pharmaceutical companies that manufacture drugs used for the treatment of psoriasis and eczema.
Dr. Chovatiya disclosed that he has served as an advisory board member, consultant, speaker, and/or investigator for AbbVie, Arcutis, Arena, Beiersdorf, Bristol Myers Squibb, Dermavant, Eli Lilly, EPI Health, Incyte, L’Oréal, the National Eczema Association, Pfizer, Regeneron, Sanofi, and UCB.
AT SPD 2022
Gender surgeons on TikTok, Instagram: Appropriate or not?
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.
A woman wearing purple surgical scrubs stares into a camera, looking frustrated, but doesn’t speak. Superimposed over her head is the text “just realized I only get to Yeet 4 Teets next week,” and a crying emoji. Rain appears to drip down over her while “Stan” by Eminem plays in the background.
That October 2020 TikTok by Sidhbh Gallagher, MD, a Miami-based plastic surgeon known as @gendersurgeon, had almost 10,000 likes and was tagged #topsurgery, #masculoplasty, #ftm, and #transman, among other hashtags.
“What health check do I have to get in preparation for teetus deletus?” is the question in another Dr. Gallagher TikTok. Dr. Gallagher is a prolific user of social media with over 268K TikTok followers and over 44K Instagram followers. Another Dr. Gallagher TikTok account, @thevagicianmd, has some 7K followers.
Another cosmetic surgeon, Tony Mangubat, MD, known as @Tikdoctony to his more than 200K followers, uses similar hashtags – like #teetusdeleetus – in his TikToks.
Clearly not medical terms, hashtags like #yeettheteet and #teetusdeletus are often used by the transgender community. The posts by Dr. Gallagher and Dr. Mangubat are part of an ever-growing wave of social media activity by medical professionals.
Plastic surgeons have never been shy about advertising their work – and many have taken to social media to do so, including showing before and after photos. A 2020 study published in Plastic and Reconstructive Surgery found that the majority of such surgeons, especially those in private practice, use social media.
especially to a younger-skewing audience.
Because of the limits on pornography and nudity of social media platforms, most social media posts by gender surgeons are about female-to-male (FTM) mastectomies, the fastest-growing transgender procedure.
The American Society of Plastic Surgeons (ASPS) started separately tracking gender-affirmation procedures in 2015. That year, members reported doing 1,360 FTM procedures.
In 2020, the ASPS further separated procedures into additional categories. That year – when many surgeries were postponed because of the COVID-19 pandemic – FTM mastectomies grew by 15%, with 8,548 procedures performed, a far greater number than for any other transgender surgery, and a sixfold increase in the number of procedures done in 2015.
‘Gimmicky,’ but building community
Surgeons interviewed for this article said they use social media primarily to connect with patients and to educate in a light-hearted way.
While Dr. Gallagher acknowledges that using #teetusdeletus is “kind of gimmicky,” she said she doesn’t view it as unprofessional because she is “using the words of the community I serve.” Many of her patients have seen a medical professional “who just didn’t understand what it is to have gender dysphoria, didn’t understand what it is to be trans, so going from that experience to somebody who uses the same language as the community uses can be quite a comfortable experience,” she said in an interview.
Dr. Mangubat, a Seattle-area plastic surgeon who has been doing mastectomies for trans male patients since 1988, said he tailors his TikToks to that group. He likes TikTok – which he started using in early 2021 – because it has rules against bullying, swearing, and pornography, he told this news organization.
“It’s really not ... advertising ... it’s a community-building platform,” said Dr. Mangubat. “If you build community, people will trust you, and if you provide good accurate information, then people will be safer,” he said.
But, “I’m not telling them to come to me,” he stressed.
He always appears in scrubs and doesn’t do music, doesn’t dance, and doesn’t post before and after photos, but he still gets thousands – or sometimes hundreds of thousands – of likes.
His mission, he said, is to answer the community’s questions. “We’re reaching patients that have had their top surgery, that are going to have their top surgery, that are looking for how to get top surgery, that are just starting on testosterone, that haven’t started on testosterone – it’s the whole spectrum of patients,” said Dr. Mangubat.
Risks downplayed?
Other surgeons have expressed concern about ethical boundaries and the tendency of social media posts to downplay risks of what are life-changing procedures.
A 2020 study of YouTube videos on top surgery, for instance, concluded that “there were no unbiased videos by board-certified plastic surgeons explaining the risks, benefits, treatment options, and alternatives to surgery.”
Alison Clayton, MBBS, an Australian psychiatrist, said that social media posts can create false expectations because they emphasize style over substance, omit risks, and can create an unwarranted sense of trust in the doctor that can spill over into the physician-patient relationship.
Dr. Clayton also believes that “the gender-affirming surgical procedures being offered to these youth have a scant empirical evidence base for benefits to psychological health and well-being.”
It is known that a number of those who transition, using either opposite sex hormones and/or surgical procedures, later have regret and “detransition,” but statistics are lacking. It is also a controversial area, with many detransitioners saying they didn’t get appropriate care and weren’t properly assessed before being given hormones or heading to surgery.
Most of the gender surgeons interviewed for this article said they see almost “zero” regret if proper mental health evaluations are performed before surgery, and they added, the procedures can relieve dysphoria.
Nevertheless, posts should not be “all fun and games,” said Josef Hadeed, MD, chair of the ASPS Patient Safety Committee and Public Education Committee and a member of its Social Media Subcommittee.
“When someone makes a decision to undergo a surgical procedure, they should be very aware there are some risks and potentially serious risks involved,” he told this news organization.
The ASPS “wants members to use social media in a judicious manner” in a way that educates the public and encourages patients to learn about a procedure and to consult with board-certified plastic surgeons, said Dr. Hadeed.
The Beverly Hills, Calif.–based surgeon does gender-affirmation procedures himself and uses Instagram, on which he has 53.4K followers, to educate patients and highlight his work using before and after photos.
“I like to think I do it in a very tasteful way,” Dr. Hadeed said. “It’s not in a way that’s sort of suggestive to patients, including minors, that this is something they need to get done, because if they are thinking about getting it done there is a lengthy process that they have to go through before they even set foot in our office.”
And he said “it may be inappropriate” to use certain hashtags or terminology, “even if it does ‘speak’ to the patients. Professionally, plastic surgeons should maintain a higher standard and maintain that even with their social media.”
Marci Bowers, MD, a gynecologic surgeon who performs gender-affirming procedures, and who is transgender herself, agreed.
“Some of the posts out there seem sensational, distasteful, and risk compromising patient confidentiality,” Dr. Bowers said in an interview.
“Much of this seemed to cross the line of good taste and appropriateness,” added Dr. Bowers, who is the incoming president of the World Professional Association for Transgender Health (WPATH). “Creating an idealized video without addressing risk is inappropriate and misleading,” she stressed.
“These surgeons would perhaps better serve their clients by focusing on and improving their clinical care,” she added.
Dr. Bowers said that although WPATH has not addressed social media use in the past, its ethics committee will be taking on the topic this year.
Social media posts about gender-affirming procedures “don’t usually talk about the barriers, they don’t talk about bad outcomes, they tend to just focus on success stories,” said Gwendolyn P. Quinn, MD, a bioethicist, and Livia S. Wan, MD, professor of obstetrics and gynecology at the NYU Grossman School of Medicine.
But she also sees some positives. The posts can help normalize gender-affirming surgery, and post-procedure photos might “help people realize that they can’t just have everything exactly the way they want it to be,” said Dr. Quinn.
Does social media influence or educate?
Studies have documented the power of social media to influence desire and decisionmaking, especially when it comes to cosmetic surgery.
“The use of social media creates a vague area between patient confidentiality and entertainment,” writes Nisha Gupta and colleagues of the UCLA David Geffen School of Medicine in a review published in the Aesthetic Surgery Journal.
While social media use is on the rise by plastic surgeons and has the potential to educate, it has also “compromised the integrity of the doctor-patient relationship,” they add.
Surgeons can use tools to place themselves higher in searches, and patients might assume that those who have hundreds of thousands of followers “are the most qualified or trusted, although this is not always the case,” they note.
Markus Rach, PhD, a researcher with the University of Applied Sciences and Arts Northwestern Switzerland, analyzed the impact of TikTok’s plastic surgery content on how adolescents perceived themselves and how it influenced their decision to have a procedure.
Most TikTok users are under age 24, and #plasticsurgery has a huge viewership with some 3.8 billion views at the time of publication, said Dr. Rach. He found that influencers tended to make adolescents feel bad and want surgery but that plastic surgeons had a moderating effect on both negative feelings and the intent to get surgery.
Dr. Bowers said that, despite her concerns, she does not “believe social media influences like TikTok and Facebook create artificial demand.”
However, Dr. Mangubat said social media can make plastic surgery seem enticing. “It can happen, and it does happen,” he said, but he added that’s true for any cosmetic procedure, not just gender-affirming surgery.
The pitfall with social media is that “patients are being sold a vision of themselves that may or may not be possible,” he observed.
Dr. Quinn worries less about people being talked into a procedure and more about those who don’t want surgery.
“There are people who identify as transgender but do not feel the need to change any parts of their body,” she said. “And that should be okay.”
Concerns about minors
New guidance from WPATH, their Standards of Care (SOC) 8 – the first update in 10 years – are due to be published this month. As reported by this news organization, and as stated in the draft of the SOC 8 published for comment in December 2021, the organization has recommended lowering the age for “top” surgery from 18 to 15 years.
Dr. Clayton has concerns about young people with gender dysphoria, who she says are “often vulnerable youth, many of whom have comorbid psychiatric and neurodevelopmental disorders.”
“This may contribute to a greater vulnerability of this population to undue influence,” added Dr. Clayton.
Sean Devitt, MD, and Jeffrey M. Kenkel, MD, of the University of Texas Southwestern Medical Center, Dallas, expressed concern that social media posts by plastic surgeons could be especially dangerous for young people.
“Given that the prefrontal cortex, which is largely responsible for impulse control, is not fully developed until the age of 25, is it ethical to allow younger patients to make life-lasting decisions under the guise of education?” they ask in a commentary on the review by Ms. Gupta and colleagues about plastic surgeons’ use of social media. The review did not focus on gender-affirmation procedures.
Many surgeons – but not all – steer clear of genital (“bottom”) surgeries in minors. However, bilateral mastectomies are being performed in those as young as age 13 based on surgeons’ risk-benefit calculus for the patient.
A study, published in May in the Annals of Plastic Surgery, showed there was a 13-fold increase in the number of bilateral mastectomies performed on under-18s between January 2013 and the end of July 2020. Of the 209 minors (age 12-17) who had the surgery, two (0.95%) expressed regret by the time of follow-up, at 3 and 7 years post-operatively, but neither had reversal surgery.
A small 2018 study, published in JAMA Pediatrics, among trans males who had top surgery found high rates of satisfaction, though one of the 68 patients reported experiencing regret “sometimes.” The mean age of patients in the surgical group was 19 years and the youngest patient was 14.
“Most of us who practice heavily in this field will make exceptions, not for genital surgery but typically for top surgery,” said Dr. Gallagher, who added that she operates on one minor [under 18] a month, while doing some 400-500 gender-affirmative surgeries a year. For some patients, “doing nothing isn’t necessarily a no-harm option,” said Dr. Gallagher.
“Arbitrarily picking the age of 18 and sentencing that patient to another year of dysphoria” might not be the best risk-benefit calculus, she said.
Dr. Mangubat agrees, especially if, for example, a trans man develops double D breasts by age 14. “You’ve sentenced them to 4 years of misery” before they can get insurance coverage, he said. His youngest top surgery patient was age 15. He said the person’s family, mental health professional, and primary care physician were all in favor of the procedure.
Dr. Mangubat also noted that some insurers, such as Kaiser Permanente, now cover bilateral mastectomy starting at age 16.
Dr. Quinn, the bioethicist, said not every minor or young adult is equipped to make the best long-term decisions.
She works with younger patients who have cancer, for example, and said her suggestions that they consider fertility preservation are often met with protestations “that they will never have children.”
The same issue arises with transgender patients. They may not want to think about having children or issues such as breast feeding while in their teens or early 20s. “But you know from your experience that they may feel differently in 10 years, but they’re just not in the mind frame to think about it,” said Dr. Quinn.
Some young people may accurately never want children, said Dr. Quinn, “but there is a lack of maturity shown when a person just shuts down a conversation and won’t even listen to infertility threats and potential preservation options.”
Concerns about regret?
Dr. Gallagher said she follows the WPATH standards, which require mental health evaluations, and as a result, “the risk of regret is incredibly low.”
However, one of Dr. Gallagher’s patients who detransitioned, Grace, who goes by @HormoneHangover on social media, said she has taken umbrage at some of the Miami surgeon’s TikToks, including one, “Why might some patients feel sad after surgery ... despite wanting it for so long??”
“This is actually not uncommon with ANY kind of surgery, but it’s temporary!” said the TikTok text. Dr. Gallagher is wearing a red dress and heels and flips her hair while the text scrolls above her.
But to Grace, the TikTok “really bothered me, because sometimes there is regret, and I think that sort of advertising paints a falsely rosy picture,” she said in an interview.
And it is emblematic of what she feels was Dr. Gallagher’s “breezy” approach to explaining the procedure to her. “The surgery itself was a shocking experience for me,” she said. “The physical experience was very jarring. It was very disturbing in a way I hadn’t anticipated or understood in advance,” said Grace.
Dr. Mangubat, who does 100 bilateral mastectomies in trans patients a year, said he goes to great lengths to ensure his patients are good candidates. Everyone – even those who self-pay – must have counseling, and if the individual seems to be considering the surgery because it’s “trendy,” he steers clear.
“If they’re not serious about it, I don’t want to operate on them,” said Dr. Mangubat. “There have been maybe two patients who have come back” to detransition, he said.
Dr. Hadeed also said he has not seen regret. He attributes this to his vetting process, which includes investigating the background of the mental health professionals who write support letters.
“We’ve turned away a lot of patients from our office either because of inadequate letters or because the person writing the letter just doesn’t really have any proper credentials,” he said.
Is social media use by plastic surgeons the new normal?
With so many plastic surgeons – including those who perform transgender procedures – using social media, it may increasingly be just part of doing business.
“Undoubtedly gender surgery teams will have a greater presence on social media in the future,” write Alireza Hamidian Jahromi, MD, and a colleague of the plastic surgery department at Rush University Medical Center, Chicago, in a letter published in Plastic and Reconstructive Surgery.
Kyle R. Latack, MD, and colleagues at the University of Southern California and the University of Michigan, have studied the use of social media by the transgender community and write that they believe “there should be an increased effort to develop high-quality and unbiased resources for patient education that can be made [available] on social media.”
Dr. Gallagher said TikTok helped her erase fear. “A bilateral mastectomy is a scary surgery for an 18-year-old or a 20-year-old,” she said, “but they have to do it for their well-being.”
“That is a criticism I’ve heard – that I seek to minimize it or that I’m flippant about it,” said Dr. Gallagher.
For “top surgery the risk profile is pretty low,” she said, “so what I try to do is educate people that it’s maybe not as scary a procedure as they think.”
Dr. Mangubat, however, is concerned about some of what he sees, especially the explosion of surgeons offering gender-affirming procedures. “Now everybody wants a piece of it,” he said.
“Let’s face it, it’s money now. You get paid for doing this surgery. Hospitals get paid a lot of money for their operating rooms for doing the surgery,” said Dr. Mangubat. “There are some surgeons who believe the transgender community is just another market.”
A version of this article first appeared on Medscape.com.
Depression screens do not reduce suicidal acts in teens: Study
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PREVENTIVE MEDICINE
Nocturnal sleep key to successful kindergarten adjustment
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics

Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics
Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics
Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
FROM PEDIATRICS