User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Recommending exercise for migraine: Just do it
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
with high-intensity aerobics coming in second, and both beating top-line migraine medications topiramate and amitriptyline, new research suggests.
The new results should encourage clinicians to recommend patients with migraine engage in strength-training exercise whenever possible, study investigator Yohannes W. Woldeamanuel, MD, a physician-scientist and instructor, department of neurology and neurological sciences, Stanford (Calif.) University, told this news organization.
“Exercise is something patients can do all their lives and use it to prevent migraine attacks instead of taking daily medications or repetitive injections that have several adverse effects.”
The findings were published online in the Journal of Headache and Pain.
Head-to-head comparison
Several clinical trials have shown exercise is effective for migraine management, but to date, there have been no head-to-head comparisons of strength training and aerobic exercise, said Dr. Woldeamanuel.
This new study used a systematic review with network meta-analysis (NMA), which compares multiple interventions and ranks the efficacy of each one.
After a literature search, researchers included 21 clinical trials with an exercise regimen arm and a comparison control arm. All study data reported monthly frequency of migraine at baseline and at the end of the intervention.
The total combined sample size was 1,195 patients with migraine, who were a mean age of 35.5 years, with a female-to-male ratio of 6.7:1. All studies used International Classification of Headache Disorders (ICHD) criteria for migraine diagnosis.
The NMA provided 27 pairwise comparisons and 8 indirect comparisons. The pairwise comparisons provided direct evidence between the different interventions.
Researchers combined strength training, including weightlifting, with resistance training. Both modalities target muscles, while aerobic exercise targets cardiovascular health.
The average number of weeks was 9.3, 9.3, and 10.7, and the average number of hours per session for strength/resistance training, high-intensity aerobic exercise, and moderate-intensity aerobic exercise interventions was 50, 56, and 45.3, respectively.
The analysis showed all exercise interventions were more effective than the placebo groups in reducing the frequency of migraine. In terms of ranking, strength training came out on top, with a mean difference in monthly migraine days of −3.55 (95% confidence interval, −6.15 to −0.95) between the active and placebo groups.
Next was high-intensity aerobic exercise (−3.13; 95% CI, −5.28 to −0.97) and moderate-intensity aerobic exercise (−2.18; 95% CI, −3.25 to −1.11), followed by topiramate, placebo, and then amitriptyline.
Strength/resistance training was superior possibly because it targets muscle strengthening, particularly major muscles in the neck and shoulder area, which can be a source of the pain trigger, said Dr. Woldeamanuel. He added neck pain is highly comorbid with migraine.
Interestingly, patients doing exercises that focus on unaffected muscles – for example, squats – still get the benefits of less migraine burden, said Dr. Woldeamanuel.
Training recommendations
Strength training also increases or preserves lean muscle mass, which is associated with reduced migraine frequency. Research shows preservation of lean body mass combats central sensitization in various pain syndromes, said Dr. Woldeamanuel.
The superior effects of high- versus moderate-intensity aerobic exercise may be due to recruitment of endogenous molecules involved in exercise-mediated hypoalgesia (pain reduction).
The most common pathways are the opioid and endocannabinoid systems, although other systems are also likely involved, said Dr. Woldeamanuel. He noted migraine has been linked to a deficiency of both opioidergic and endocannabinoidergic signaling.
Dr. Woldeamanuel commented on the difficulty of comparing exercise interventions for patients with chronic versus episodic migraine, as many studies include both.
However, the two studies with moderate-intensity aerobic exercise exclusively involving patients with chronic migraine showed large effect sizes (Cohen’s d) of 0.80 and 1.10 in reducing monthly headache frequency.
Based on these new results and their own experience, the researchers recommend strength training start with 50% of repetition maximum (RM) with 2-3 sets of 12-15 repetitions three times a week along with 10 minutes of warm-up, stretching, and cool-down, totaling 45-60 minutes per session. Weight/resistance load can then be increased weekly by 5% of RM if the patient is capable of successfully completing three sets.
They also recommend including active recovery days (low-intensity exercise) between training days. All major muscles, including neck, shoulder, and upper limb muscles, should be trained in a rotation.
For high-intensity aerobic exercise, the authors recommend starting with interval training at 55% VO2max (maximum respiratory capacity), or 50% HRmax (maximal heart rate) for 45-60 minutes per session, including 10 minutes of warm-up and cool-down, three times per week. The intensity can then be increased by 5%-10% each week to reach a maximum target of 80%-90% by week 12.
It is best for patients to start with a trainer for guidance and supervision, but once they master the routines, they can do the exercises independently, said Dr. Woldeamanuel.
Managing flare-ups
Headache flare-ups are normal during exercise, which may be caused by “boom and bust cycles” – exercising excessively when feeling good then completely stopping when feeling bad, said Dr. Woldeamanuel. He noted these flare-ups don’t mean “there’s something wrong with the brain or there’s some injury to muscles.”
The best way to manage such flare-ups is to use a pacing strategy that involves “not going overboard on good days and avoiding excessive rest on bad days,” the investigators note.
Dr. Woldeamanuel noted exercise is a lifestyle-based intervention; it not only helps reduce migraine attacks but also helps control other known comorbidities such as obesity and hypertension.
In a comment, Elizabeth Loder, MD, vice-chair, academic affairs, department of neurology, Brigham and Women’s Hospital, and professor of neurology, Harvard Medical School, both in Boston, said, “It’s useful to collect and summarize all of these studies, and to focus on helping patients and doctors understand the possible value of different kinds of exercise.”
The review was “well done,” said Dr. Loder, adding the researchers “have looked carefully at the quality of included studies.”
The study received support from the National Institute of Neurological Disorders and Stroke of the National Institutes of Health. Dr. Woldeamanuel has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF HEADACHE AND PAIN
Highly processed foods ‘as addictive’ as tobacco
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new U.S. study that proposes a set of criteria to assess the addictive potential of some foods.
The research suggests that health care professionals are taking steps toward framing food addiction as a clinical entity in its own right; it currently lacks validated treatment protocols and recognition as a clinical diagnosis.
Meanwhile, other data, reported by researchers at the 2022 Diabetes Professional Care conference in London also add support to the clinical recognition of food addiction.
Clinical psychologist Jen Unwin, PhD, from Southport, England, showed that a 3-month online program of low-carbohydrate diet together with psychoeducational support significantly reduced food addiction symptoms among a varied group of individuals, not all of whom were overweight or had obesity.
Dr. Unwin said her new data represent the first wide-scale clinical audit of its kind, other than a prior report of three patients with food addiction who were successfully treated with a ketogenic diet.
“Food addiction explains so much of what we see in clinical practice, where intelligent people understand what we tell them about the physiology associated with a low-carb diet, and they follow it for a while, but then they relapse,” said Dr. Unwin, explaining the difficulties faced by around 20% of her patients who are considered to have food addiction.
Meanwhile, the authors of the U.S. study, led by Ashley N. Gearhardt, PhD, a psychologist from the University of Michigan, Ann Arbor, wrote that the ability of highly processed foods (HPFs) “to rapidly deliver high doses of refined carbohydrates and/or fat appear key to their addictive potential. Thus, we conclude that HPFs can be considered addictive substances based on scientifically established criteria.”
They asserted that the contribution to preventable deaths by a diet dominated by highly processed foods is comparable with that of tobacco products, and as such, like Dr. Unwin, the authors sought clinical recognition and a more formalized protocol to manage food addiction.
“Understanding whether addiction contributes to HPF intake may lead to new treatments, as preliminary research finds that behavioral and pharmacological interventions that target addictive mechanisms may reduce compulsive HPF intake,” they stated.
The study led by Dr. Gearhardt was published in the journal Addiction, and the study led by Unwin was also recently published in Frontiers in Psychiatry.
Addiction criteria similar to tobacco
HPFs can be associated with an eating phenotype “that reflects the hallmarks of addiction,” said Dr. Gearhardt and coauthors; typically, loss of control over intake, intense cravings, inability to cut down, and continued use despite negative consequences.
Acknowledging the lack of a single addictive agent, they explain that food addiction reflects mechanisms implicated in other addictive disorders such as smoking.
As such, in their study, Dr. Gearhardt and colleagues proposed a set of scientifically based criteria for the evaluation of whether certain foods are addictive. “Specifically, we propose the primary criteria used to resolve one of the last major controversies over whether a substance, tobacco products, was addictive.”
They consider certain foods according to the primary criteria that have stood the test of time after being proposed in 1988 by the U.S. Surgeon General to establish the addictive potential of tobacco: they trigger compulsive use, they have psychoactive effects, and they are reinforcing.
They have updated these criteria to include the ability to trigger urges and cravings, and added that “both these products [tobacco and HPFs] are legal, easily accessible, inexpensive, lack an intoxication syndrome, and are major causes of preventable death.”
For example, with compulsive use, tobacco meets this criterion because evidence suggests that most smokers would like to quit but are unable to do so.
Likewise, wrote Dr. Gearhardt and colleagues, even “in the face of significant diet-related health consequences (e.g., diabetes and cardiovascular disease), the majority of patients are unable to adhere to medically recommended dietary plans that require a reduction in HPF intake.”
Reinforcement, through tobacco use, is demonstrated by its ‘being sufficiently rewarding to maintain self-administration” because of its ability to deliver nicotine, they said, quoting the Surgeon General’s report, and likewise, with food addiction, “both adults and children will self-administer HPFs (e.g., potato chips, candy, and cookies) even when satiated.”
Online group food addiction intervention study
Dr. Unwin and coauthors want people with food addiction to be able to access a validated treatment protocol. Their study aimed to evaluate an online group intervention across multiple sites in the United States, Canada, and the United Kingdom, involving an abstinent, low-carbohydrate diet and biopsychosocial education focused on addiction and recovery in people self-identifying as having food addiction.
“Lots of people with food addiction go to GPs who don’t clinically recognize this, or if they attend addiction services and psychiatry, then they tend to only specialize in drugs, alcohol, and gambling. Eating disorder services are linked but their programs mostly don’t work for a food addict,” Dr. Unwin remarked in an interview.
“We feel running groups, as well as training professionals to run groups, is the best way to manage food addiction,” she said, reflecting on the scale of the problem, with around 10% of adults in the U.K. general population considered to have food addiction. In Dr. Unwin’s study, some people had type 2 diabetes and some overweight/obesity, but she added that some participants were underweight or of normal weight.
Initially, the 103 participants received weekly group (8-24 people) sessions for 10-14 weeks, and then monthly maintenance comprising follow-up that involved coaching participants on how to cope with relapse and get back on track.
Food addiction symptoms were assessed pre- and post program using the modified Yale Food Addiction Scale (mYFAS) 2.0; ICD-10 symptoms of food-related substance use disorder (CRAVED); and mental health well-being measured using the short version of the Warwick Edinburgh Mental Wellbeing scale and body weight.
“The program eliminates processed foods with a personalized, abstinence food plan that involves education around mechanisms involved,” said Dr. Unwin, who explained that processed foods deliver a dopamine high, and in response to this, the brain lowers the number of dopamine receptors to effectively counteract the increase in dopamine. This drop in dopamine receptors explains the depression often associated with food addiction.
Dr. Unwin reported that food addiction symptoms were significantly reduced, with the mYFAS dropping by 1.52, the CRAVED score by 1.53, and body weight by 2.34 kg (5.2 lb). Mental health, as measured by the Warwick Edinburgh Mental Wellbeing scale, improved by 2.37 points.
“We were very interested in mental health and well-being because it impacts so much across our lives, and we saw significant improvements here, but we were less interested in weight because food addicts come in all shapes and sizes with some people underweight,” said Dr. Unwin. “Food addiction symptoms were significantly improved in the group, but we now need to look at the longer-term outcomes.”
Dr. Unwin runs a low-carbohydrate program for type 2 diabetes with her husband David Unwin, MD, who is a GP in Southport, England. She said that they ask patients if they think they have food addiction, and most say they do.
“I always try to explain to patients about the dopamine high, and how this starts the craving which makes people wonder when and where they can find the next sugar hit. Just thinking about the next chocolate bar gets the dopamine running for many people, and the more they tread this path then the worse it gets because the dopamine receptors keep reducing.”
Lorraine Avery, RN, a diabetes nurse specialist for Solent NHS Trust, who attended the DPC conference, welcomed Dr. Unwin’s presentation.
“My concern as a diabetes nurse specialist is that I’m unsure all our patients recognize their food addiction, and there are often more drivers to eating than just the food in front of them,” she said in an interview. “I think there’s an emotional element, too. These people are often ‘yo-yo’ dieters, and they join lots of expert companies to help them lose weight, but these companies want them to regain and re-join their programs,” she said.
“I think there is something about helping patients recognize they have a food addiction and they need to consider that other approaches might be helpful.”
Dr. Unwin reported no relevant financial relationships; some other authors have fee-paying clients with food addiction. Dr. Gearhardt and Ms. Avery reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Consider gaps in access and knowledge in diagnosis and treatment in skin of color
LAS VEGAS – and patients, Susan C. Taylor, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.
Additionally, some disparities occur because of gaps in access to health care, said Dr. Taylor, vice chair, diversity, equity and inclusion, in the department of dermatology at the University of Pennsylvania, Philadelphia, who moderated an expert panel discussion of treatment tips for several common dermatologic conditions in skin of color patients.

Atopic dermatitis angles
Atopic dermatitis (AD) is the fourth most common dermatologic complaint in Black patients, based on data from the United States National Ambulatory Medical Care Survey. Also, data from the National Health and Nutrition Examination Survey show that Black children are nearly twice as likely as White children to develop AD after controlling for socioeconomic factors, Dr. Taylor said.
When Black patients present with AD, “you may not see the erythema,” said Valerie D. Callender, MD, of Howard University, Washington, who presented on AD. Instead, “you may see more follicular and papular presentations.” Erythema and erythroderma can present as shades of violet, gray, or dark brown in patients with rich skin tones, added Dr. Callender, who practices in Glenn Dale, Md.
Consequently, disease severity can be misinterpreted, she said, noting that data suggest that scoring systems such as the Eczema Area and Severity Index and Scoring Atopic Dermatitis underestimate AD severity in dark skin.
As for treatment, skin of color patients with AD are often as bothered by postinflammatory hyperpigmentation (PIH) as by active lesions, so treatment should take these concerns into account, Dr. Callender said. Studies evaluating the effectiveness of AD treatments in diverse populations are limited by lack of representation of racial groups in clinical trials and lack of subset analyses by race.
Acne awareness
An important consideration of acne in skin of color patients is that the acne “might not be red, it might just be darker,” said Andrew F. Alexis, MD, vice-chair for diversity and inclusion in the department of dermatology, and professor of clinical dermatology at Weill Cornell Medicine, New York. A study published in JAMA Dermatology of nearly 30,000 patients with acne from 2007 to 2017 found that non-Hispanic Black patients were more likely than non-Hispanic White patients to see a dermatologist for acne, but Black patients received fewer prescriptions for acne medications than White patients.

The study also showed that Black patients who received prescriptions for acne were more likely to receive topical retinoids and topical antibiotics, and less likely to receive oral antibiotics, spironolactone, or isotretinoin, compared with White patients. Similarly, Asian patients were more likely to receive topical antibiotics and less likely to receive oral antibiotics, compared with White patients.
Other panelists shared some of their best practices for acne in patients with skin of color, including treatment with topical retinoids (for inflammation) and spironolactone, and therapies that address both inflammation and pigmentation, such as salicylic acid and azelaic acid. Dr. Callender also advised asking patients about makeup, as they may not know that many types of makeup used to cover acne are in fact comedogenic.
Melanoma misconceptions
One of the most common misperceptions about melanoma among skin of color patients is that they don’t think they can get it, Dr. Taylor said. Many health care providers don’t think about melanoma in skin of color patients because of the dramatically lower incidence in this population, but as a result, cases may go undiagnosed, and as studies have shown, the mortality rate from melanoma is higher in Black patients.
Consider the palms, soles, nails, and web spaces as possible melanoma sites, Dr. Taylor added.

Educating skin of color patients about melanoma is important, although the incidence is 20 to 30 times lower than in non-Hispanic Whites, said Nada Elbuluk, MD, the founder and director of the University of Southern California Skin of Color Center and Pigmentary Disorders Clinic, Los Angeles. A 2020 editorial published in Cancer Cytopathology pointed out that 1 in 3 Black men or women with a melanoma diagnosis in the United States dies of the disease, compared with 1 in 7 non-Hispanic White men and 1 in 11 non-Hispanic White women with melanoma.
Don’t skip the total body skin exam in these patients, Dr. Elbuluk emphasized. Many patients will only partially undress, and areas such as toes can be missed.
Rosacea review
For patients with skin of color, clinicians need to look for different signs of rosacea than those typically seen in White patients, Dr. Elbuluk said. “The most common presentation of rosacea in skin of color is papulopustular,” and the granulomatous variant.
“These patients will often give you a history of sensitivity to products,” Dr. Elbuluk noted. They may not always have the flushing, but they may report warmth or itching, in addition to product sensitivity.
When considering rosacea in skin of color patients, be sure to have good lighting for close examination, as skin thickening is another subtle sign of rosacea in these patients, she said. Skin thickening “is a very early sign that will present in skin of color with no erythema, so keep that in mind.”
Stinging and burning sensations may be reported by skin of color patients with rosacea. Use patient history to confirm the diagnosis of rosacea, which is often delayed in skin of color patients because of a low index of suspicion, she said.
Psoriasis pointers
Psoriasis in skin of color patients used to be considered rare, “but that is far from true,” Dr. Alexis said. In fact, many cases of psoriasis are undiagnosed or the diagnosis is delayed in these patients.
The panelists noted that current guidelines for psoriasis treatment are based on clinical trials composed mainly of White patients, and do not contain specific recommendations for skin of color patients.
Notably, the morphology, location, and color of psoriasis lesions may be different for patients with darker skin, such as thicker plaques and more scaling over larger areas, they said. Also, skin of color patients may experience long-lasting dyspigmentation from psoriasis lesions that have resolved.
When developing a strategy for psoriasis in skin of color patients, consider not only disease severity, but also comorbidities and medications, response (if any) to prior therapies, patient preferences, and quality of life, the panelists said.
Dr. Callender, Dr. Elbuluk, Dr. Taylor, and Dr. Alexis reported conflicts of interest from numerous sources in industry. MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – and patients, Susan C. Taylor, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.
Additionally, some disparities occur because of gaps in access to health care, said Dr. Taylor, vice chair, diversity, equity and inclusion, in the department of dermatology at the University of Pennsylvania, Philadelphia, who moderated an expert panel discussion of treatment tips for several common dermatologic conditions in skin of color patients.
Atopic dermatitis angles
Atopic dermatitis (AD) is the fourth most common dermatologic complaint in Black patients, based on data from the United States National Ambulatory Medical Care Survey. Also, data from the National Health and Nutrition Examination Survey show that Black children are nearly twice as likely as White children to develop AD after controlling for socioeconomic factors, Dr. Taylor said.
When Black patients present with AD, “you may not see the erythema,” said Valerie D. Callender, MD, of Howard University, Washington, who presented on AD. Instead, “you may see more follicular and papular presentations.” Erythema and erythroderma can present as shades of violet, gray, or dark brown in patients with rich skin tones, added Dr. Callender, who practices in Glenn Dale, Md.
Consequently, disease severity can be misinterpreted, she said, noting that data suggest that scoring systems such as the Eczema Area and Severity Index and Scoring Atopic Dermatitis underestimate AD severity in dark skin.
As for treatment, skin of color patients with AD are often as bothered by postinflammatory hyperpigmentation (PIH) as by active lesions, so treatment should take these concerns into account, Dr. Callender said. Studies evaluating the effectiveness of AD treatments in diverse populations are limited by lack of representation of racial groups in clinical trials and lack of subset analyses by race.
Acne awareness
An important consideration of acne in skin of color patients is that the acne “might not be red, it might just be darker,” said Andrew F. Alexis, MD, vice-chair for diversity and inclusion in the department of dermatology, and professor of clinical dermatology at Weill Cornell Medicine, New York. A study published in JAMA Dermatology of nearly 30,000 patients with acne from 2007 to 2017 found that non-Hispanic Black patients were more likely than non-Hispanic White patients to see a dermatologist for acne, but Black patients received fewer prescriptions for acne medications than White patients.
The study also showed that Black patients who received prescriptions for acne were more likely to receive topical retinoids and topical antibiotics, and less likely to receive oral antibiotics, spironolactone, or isotretinoin, compared with White patients. Similarly, Asian patients were more likely to receive topical antibiotics and less likely to receive oral antibiotics, compared with White patients.
Other panelists shared some of their best practices for acne in patients with skin of color, including treatment with topical retinoids (for inflammation) and spironolactone, and therapies that address both inflammation and pigmentation, such as salicylic acid and azelaic acid. Dr. Callender also advised asking patients about makeup, as they may not know that many types of makeup used to cover acne are in fact comedogenic.
Melanoma misconceptions
One of the most common misperceptions about melanoma among skin of color patients is that they don’t think they can get it, Dr. Taylor said. Many health care providers don’t think about melanoma in skin of color patients because of the dramatically lower incidence in this population, but as a result, cases may go undiagnosed, and as studies have shown, the mortality rate from melanoma is higher in Black patients.
Consider the palms, soles, nails, and web spaces as possible melanoma sites, Dr. Taylor added.
Educating skin of color patients about melanoma is important, although the incidence is 20 to 30 times lower than in non-Hispanic Whites, said Nada Elbuluk, MD, the founder and director of the University of Southern California Skin of Color Center and Pigmentary Disorders Clinic, Los Angeles. A 2020 editorial published in Cancer Cytopathology pointed out that 1 in 3 Black men or women with a melanoma diagnosis in the United States dies of the disease, compared with 1 in 7 non-Hispanic White men and 1 in 11 non-Hispanic White women with melanoma.
Don’t skip the total body skin exam in these patients, Dr. Elbuluk emphasized. Many patients will only partially undress, and areas such as toes can be missed.
Rosacea review
For patients with skin of color, clinicians need to look for different signs of rosacea than those typically seen in White patients, Dr. Elbuluk said. “The most common presentation of rosacea in skin of color is papulopustular,” and the granulomatous variant.
“These patients will often give you a history of sensitivity to products,” Dr. Elbuluk noted. They may not always have the flushing, but they may report warmth or itching, in addition to product sensitivity.
When considering rosacea in skin of color patients, be sure to have good lighting for close examination, as skin thickening is another subtle sign of rosacea in these patients, she said. Skin thickening “is a very early sign that will present in skin of color with no erythema, so keep that in mind.”
Stinging and burning sensations may be reported by skin of color patients with rosacea. Use patient history to confirm the diagnosis of rosacea, which is often delayed in skin of color patients because of a low index of suspicion, she said.
Psoriasis pointers
Psoriasis in skin of color patients used to be considered rare, “but that is far from true,” Dr. Alexis said. In fact, many cases of psoriasis are undiagnosed or the diagnosis is delayed in these patients.
The panelists noted that current guidelines for psoriasis treatment are based on clinical trials composed mainly of White patients, and do not contain specific recommendations for skin of color patients.
Notably, the morphology, location, and color of psoriasis lesions may be different for patients with darker skin, such as thicker plaques and more scaling over larger areas, they said. Also, skin of color patients may experience long-lasting dyspigmentation from psoriasis lesions that have resolved.
When developing a strategy for psoriasis in skin of color patients, consider not only disease severity, but also comorbidities and medications, response (if any) to prior therapies, patient preferences, and quality of life, the panelists said.
Dr. Callender, Dr. Elbuluk, Dr. Taylor, and Dr. Alexis reported conflicts of interest from numerous sources in industry. MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – and patients, Susan C. Taylor, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.
Additionally, some disparities occur because of gaps in access to health care, said Dr. Taylor, vice chair, diversity, equity and inclusion, in the department of dermatology at the University of Pennsylvania, Philadelphia, who moderated an expert panel discussion of treatment tips for several common dermatologic conditions in skin of color patients.
Atopic dermatitis angles
Atopic dermatitis (AD) is the fourth most common dermatologic complaint in Black patients, based on data from the United States National Ambulatory Medical Care Survey. Also, data from the National Health and Nutrition Examination Survey show that Black children are nearly twice as likely as White children to develop AD after controlling for socioeconomic factors, Dr. Taylor said.
When Black patients present with AD, “you may not see the erythema,” said Valerie D. Callender, MD, of Howard University, Washington, who presented on AD. Instead, “you may see more follicular and papular presentations.” Erythema and erythroderma can present as shades of violet, gray, or dark brown in patients with rich skin tones, added Dr. Callender, who practices in Glenn Dale, Md.
Consequently, disease severity can be misinterpreted, she said, noting that data suggest that scoring systems such as the Eczema Area and Severity Index and Scoring Atopic Dermatitis underestimate AD severity in dark skin.
As for treatment, skin of color patients with AD are often as bothered by postinflammatory hyperpigmentation (PIH) as by active lesions, so treatment should take these concerns into account, Dr. Callender said. Studies evaluating the effectiveness of AD treatments in diverse populations are limited by lack of representation of racial groups in clinical trials and lack of subset analyses by race.
Acne awareness
An important consideration of acne in skin of color patients is that the acne “might not be red, it might just be darker,” said Andrew F. Alexis, MD, vice-chair for diversity and inclusion in the department of dermatology, and professor of clinical dermatology at Weill Cornell Medicine, New York. A study published in JAMA Dermatology of nearly 30,000 patients with acne from 2007 to 2017 found that non-Hispanic Black patients were more likely than non-Hispanic White patients to see a dermatologist for acne, but Black patients received fewer prescriptions for acne medications than White patients.
The study also showed that Black patients who received prescriptions for acne were more likely to receive topical retinoids and topical antibiotics, and less likely to receive oral antibiotics, spironolactone, or isotretinoin, compared with White patients. Similarly, Asian patients were more likely to receive topical antibiotics and less likely to receive oral antibiotics, compared with White patients.
Other panelists shared some of their best practices for acne in patients with skin of color, including treatment with topical retinoids (for inflammation) and spironolactone, and therapies that address both inflammation and pigmentation, such as salicylic acid and azelaic acid. Dr. Callender also advised asking patients about makeup, as they may not know that many types of makeup used to cover acne are in fact comedogenic.
Melanoma misconceptions
One of the most common misperceptions about melanoma among skin of color patients is that they don’t think they can get it, Dr. Taylor said. Many health care providers don’t think about melanoma in skin of color patients because of the dramatically lower incidence in this population, but as a result, cases may go undiagnosed, and as studies have shown, the mortality rate from melanoma is higher in Black patients.
Consider the palms, soles, nails, and web spaces as possible melanoma sites, Dr. Taylor added.
Educating skin of color patients about melanoma is important, although the incidence is 20 to 30 times lower than in non-Hispanic Whites, said Nada Elbuluk, MD, the founder and director of the University of Southern California Skin of Color Center and Pigmentary Disorders Clinic, Los Angeles. A 2020 editorial published in Cancer Cytopathology pointed out that 1 in 3 Black men or women with a melanoma diagnosis in the United States dies of the disease, compared with 1 in 7 non-Hispanic White men and 1 in 11 non-Hispanic White women with melanoma.
Don’t skip the total body skin exam in these patients, Dr. Elbuluk emphasized. Many patients will only partially undress, and areas such as toes can be missed.
Rosacea review
For patients with skin of color, clinicians need to look for different signs of rosacea than those typically seen in White patients, Dr. Elbuluk said. “The most common presentation of rosacea in skin of color is papulopustular,” and the granulomatous variant.
“These patients will often give you a history of sensitivity to products,” Dr. Elbuluk noted. They may not always have the flushing, but they may report warmth or itching, in addition to product sensitivity.
When considering rosacea in skin of color patients, be sure to have good lighting for close examination, as skin thickening is another subtle sign of rosacea in these patients, she said. Skin thickening “is a very early sign that will present in skin of color with no erythema, so keep that in mind.”
Stinging and burning sensations may be reported by skin of color patients with rosacea. Use patient history to confirm the diagnosis of rosacea, which is often delayed in skin of color patients because of a low index of suspicion, she said.
Psoriasis pointers
Psoriasis in skin of color patients used to be considered rare, “but that is far from true,” Dr. Alexis said. In fact, many cases of psoriasis are undiagnosed or the diagnosis is delayed in these patients.
The panelists noted that current guidelines for psoriasis treatment are based on clinical trials composed mainly of White patients, and do not contain specific recommendations for skin of color patients.
Notably, the morphology, location, and color of psoriasis lesions may be different for patients with darker skin, such as thicker plaques and more scaling over larger areas, they said. Also, skin of color patients may experience long-lasting dyspigmentation from psoriasis lesions that have resolved.
When developing a strategy for psoriasis in skin of color patients, consider not only disease severity, but also comorbidities and medications, response (if any) to prior therapies, patient preferences, and quality of life, the panelists said.
Dr. Callender, Dr. Elbuluk, Dr. Taylor, and Dr. Alexis reported conflicts of interest from numerous sources in industry. MedscapeLive and this news organization are owned by the same parent company.
AT INNOVATIONS IN DERMATOLOGY
Opt-out HIV testing in EDs can help identify undiagnosed cases
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
The right indoor relative humidity could ward off COVID
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF THE ROYAL SOCIETY INTERFACE
Laser and light devices for acne treatment continue to advance
The calendar year
This was preceded by the FDA clearance of AviClear, marketed by Cutera, in March, and the commercial launch of TheraClearX, marketed by StrataSkin, in July.
“It’s an exciting time to be working with acne,” Fernanda H. Sakamoto, MD, PhD, a dermatologist at the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “We’ll see a lot of people using new devices. I’m looking forward to seeing results in the long term.”

AviClear and the Accure Laser System, marketed by Accure, are both powered by a 1,726-nm laser, but they work differently. AviClear, which was cleared for the treatment of mild, moderate, and severe acne, has a maximum fluence of 30 J/cm2 in single-pulse mode and a maximum fluence of 20 J/cm2 in double-pulse mode. The treatment handpiece has an integrated scanner for delivering treatment spot(s) in an operator-selected pattern. “It’s a little bit lower powered than the Accure and has a maximum pulse energy of 5 joules and a pulse duration of up to 50 milliseconds,” Dr. Sakamoto said. In the treatment of acne, laser and light treatments target the sebaceous gland.
In pivotal data submitted to the FDA, 104 patients with acne who were enrolled at 7 U.S. sites received 304 treatments with AviClear spaced 2-5 weeks apart. Each treatment took about 30 minutes. Treatment success was defined as having at least 50% fewer inflammatory acne lesions 12 weeks after the final treatment visit, compared with baseline. At the week 4 follow-up visit, there were median and mean reductions of 42% and 37%, respectively, in the inflammatory lesion counts from baseline (P < .001). The researchers found that, at the week 4 follow-up visit, 36% of patients had achieved treatment success, which increased to 78% at the 12-week follow-up visit. Treatment was considered safe and tolerable, according to the manufacturer.
The other newcomer device with a 1,726-nm wavelength is the Accure Laser System, which features a smart laser handpiece for real-time thermal monitoring and precise delivery of laser emissions. The device received CE Mark approval in 2020 for the treatment of moderate acne, and on Nov. 22, 2022, the manufacturer announced that it had been cleared by the FDA for the treatment of mild to severe inflammatory acne vulgaris.
Dr. Sakamoto and her Wellman colleagues have been working with five dermatologists to conduct clinical trials of the device: Emil Tanghetti, MD, and Mitchel Goldman, MD, in California; Roy Geronemus, MD, in New York; Joel Cohen, MD, in Colorado; and Daniel Friedmann, MD, in Texas. As of Oct. 2, 2022, more than 50 patients with mild to severe acne were enrolled in four studies and an additional 30 were enrolled in a pilot facial acne trial, Dr. Sakamoto said. In the trials, patients are followed at 4, 8, 12, and 24 weeks post treatment.
Among patients enrolled in the facial acne trial, researchers have observed a 100% responder rate for patients with more than five acne lesions at 4, 8, 12, and 24 weeks post treatment after four monthly treatment sessions. The average lesion reduction at week 12 was 82% and the mean visual analog scale score immediately after treatment was 2.09 out of 10. Each patient received more than 12,000 trigger pulls of energy from the device overall with no adverse events reported. At 12 months, they observed a 90% inflammatory lesion count reduction from baseline and a rapid response to treatment: a 73% reduction achieved after the first two treatment sessions. Histologic studies revealed selective sebaceous gland destruction with no damage to the epidermis, surrounding dermis, or other skin structures.
Dr. Sakamoto emphasized that to date no direct clinical comparisons have been made between the AviClear and Accure devices. “Are all 1,726-nm lasers made equal? That is a question that we have to keep in our mind,” she said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “They are using the same wavelength, but they are different types of lasers.”
For example, the Accure Laser treats to temperature, relies on air cooling, and is targeted to dermatologists and plastic surgeons, while the AviClear treats to fluence, relies on contact cooling, and includes med spas and other nonphysician providers as the target users. “Mathematically, the difference between the two devices is that the Accure can achieve deeper penetration in a single pulse, while the AviClear is a little more superficial,” she said. “Whether that is translated clinically is unknown at this point.”
Dr. Sakamoto also discussed the TheraClearX, which is FDA cleared for the treatment of mild, moderate, and severe acne, including comedonal, pustular, and inflammatory acne vulgaris. The device, which is a new version of the Palomar Acleara, uses a vacuum technique with up to 3 psi pressure in conjunction with broadband light with a wavelength spectrum of 500 nm–1,200 nm delivered through a liquid-cooled, handheld delivery system. The predicate device was the Aesthera Isolaz System. The vacuum extracts buildup of sebaceous material. “At the same time, it takes the blood out of the competing chromophore,” she said. “By doing so, it potentially damages the sebaceous glands and reduces the inflammatory lesions.”
Dr. Sakamoto disclosed that she is the founder of and science advisor for Lightwater Bioscience. She is also a science advisor for Accure Acne and has received portions of patent royalties from Massachusetts General Hospital.
The calendar year
This was preceded by the FDA clearance of AviClear, marketed by Cutera, in March, and the commercial launch of TheraClearX, marketed by StrataSkin, in July.
“It’s an exciting time to be working with acne,” Fernanda H. Sakamoto, MD, PhD, a dermatologist at the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “We’ll see a lot of people using new devices. I’m looking forward to seeing results in the long term.”
AviClear and the Accure Laser System, marketed by Accure, are both powered by a 1,726-nm laser, but they work differently. AviClear, which was cleared for the treatment of mild, moderate, and severe acne, has a maximum fluence of 30 J/cm2 in single-pulse mode and a maximum fluence of 20 J/cm2 in double-pulse mode. The treatment handpiece has an integrated scanner for delivering treatment spot(s) in an operator-selected pattern. “It’s a little bit lower powered than the Accure and has a maximum pulse energy of 5 joules and a pulse duration of up to 50 milliseconds,” Dr. Sakamoto said. In the treatment of acne, laser and light treatments target the sebaceous gland.
In pivotal data submitted to the FDA, 104 patients with acne who were enrolled at 7 U.S. sites received 304 treatments with AviClear spaced 2-5 weeks apart. Each treatment took about 30 minutes. Treatment success was defined as having at least 50% fewer inflammatory acne lesions 12 weeks after the final treatment visit, compared with baseline. At the week 4 follow-up visit, there were median and mean reductions of 42% and 37%, respectively, in the inflammatory lesion counts from baseline (P < .001). The researchers found that, at the week 4 follow-up visit, 36% of patients had achieved treatment success, which increased to 78% at the 12-week follow-up visit. Treatment was considered safe and tolerable, according to the manufacturer.
The other newcomer device with a 1,726-nm wavelength is the Accure Laser System, which features a smart laser handpiece for real-time thermal monitoring and precise delivery of laser emissions. The device received CE Mark approval in 2020 for the treatment of moderate acne, and on Nov. 22, 2022, the manufacturer announced that it had been cleared by the FDA for the treatment of mild to severe inflammatory acne vulgaris.
Dr. Sakamoto and her Wellman colleagues have been working with five dermatologists to conduct clinical trials of the device: Emil Tanghetti, MD, and Mitchel Goldman, MD, in California; Roy Geronemus, MD, in New York; Joel Cohen, MD, in Colorado; and Daniel Friedmann, MD, in Texas. As of Oct. 2, 2022, more than 50 patients with mild to severe acne were enrolled in four studies and an additional 30 were enrolled in a pilot facial acne trial, Dr. Sakamoto said. In the trials, patients are followed at 4, 8, 12, and 24 weeks post treatment.
Among patients enrolled in the facial acne trial, researchers have observed a 100% responder rate for patients with more than five acne lesions at 4, 8, 12, and 24 weeks post treatment after four monthly treatment sessions. The average lesion reduction at week 12 was 82% and the mean visual analog scale score immediately after treatment was 2.09 out of 10. Each patient received more than 12,000 trigger pulls of energy from the device overall with no adverse events reported. At 12 months, they observed a 90% inflammatory lesion count reduction from baseline and a rapid response to treatment: a 73% reduction achieved after the first two treatment sessions. Histologic studies revealed selective sebaceous gland destruction with no damage to the epidermis, surrounding dermis, or other skin structures.
Dr. Sakamoto emphasized that to date no direct clinical comparisons have been made between the AviClear and Accure devices. “Are all 1,726-nm lasers made equal? That is a question that we have to keep in our mind,” she said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “They are using the same wavelength, but they are different types of lasers.”
For example, the Accure Laser treats to temperature, relies on air cooling, and is targeted to dermatologists and plastic surgeons, while the AviClear treats to fluence, relies on contact cooling, and includes med spas and other nonphysician providers as the target users. “Mathematically, the difference between the two devices is that the Accure can achieve deeper penetration in a single pulse, while the AviClear is a little more superficial,” she said. “Whether that is translated clinically is unknown at this point.”
Dr. Sakamoto also discussed the TheraClearX, which is FDA cleared for the treatment of mild, moderate, and severe acne, including comedonal, pustular, and inflammatory acne vulgaris. The device, which is a new version of the Palomar Acleara, uses a vacuum technique with up to 3 psi pressure in conjunction with broadband light with a wavelength spectrum of 500 nm–1,200 nm delivered through a liquid-cooled, handheld delivery system. The predicate device was the Aesthera Isolaz System. The vacuum extracts buildup of sebaceous material. “At the same time, it takes the blood out of the competing chromophore,” she said. “By doing so, it potentially damages the sebaceous glands and reduces the inflammatory lesions.”
Dr. Sakamoto disclosed that she is the founder of and science advisor for Lightwater Bioscience. She is also a science advisor for Accure Acne and has received portions of patent royalties from Massachusetts General Hospital.
The calendar year
This was preceded by the FDA clearance of AviClear, marketed by Cutera, in March, and the commercial launch of TheraClearX, marketed by StrataSkin, in July.
“It’s an exciting time to be working with acne,” Fernanda H. Sakamoto, MD, PhD, a dermatologist at the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston. “We’ll see a lot of people using new devices. I’m looking forward to seeing results in the long term.”
AviClear and the Accure Laser System, marketed by Accure, are both powered by a 1,726-nm laser, but they work differently. AviClear, which was cleared for the treatment of mild, moderate, and severe acne, has a maximum fluence of 30 J/cm2 in single-pulse mode and a maximum fluence of 20 J/cm2 in double-pulse mode. The treatment handpiece has an integrated scanner for delivering treatment spot(s) in an operator-selected pattern. “It’s a little bit lower powered than the Accure and has a maximum pulse energy of 5 joules and a pulse duration of up to 50 milliseconds,” Dr. Sakamoto said. In the treatment of acne, laser and light treatments target the sebaceous gland.
In pivotal data submitted to the FDA, 104 patients with acne who were enrolled at 7 U.S. sites received 304 treatments with AviClear spaced 2-5 weeks apart. Each treatment took about 30 minutes. Treatment success was defined as having at least 50% fewer inflammatory acne lesions 12 weeks after the final treatment visit, compared with baseline. At the week 4 follow-up visit, there were median and mean reductions of 42% and 37%, respectively, in the inflammatory lesion counts from baseline (P < .001). The researchers found that, at the week 4 follow-up visit, 36% of patients had achieved treatment success, which increased to 78% at the 12-week follow-up visit. Treatment was considered safe and tolerable, according to the manufacturer.
The other newcomer device with a 1,726-nm wavelength is the Accure Laser System, which features a smart laser handpiece for real-time thermal monitoring and precise delivery of laser emissions. The device received CE Mark approval in 2020 for the treatment of moderate acne, and on Nov. 22, 2022, the manufacturer announced that it had been cleared by the FDA for the treatment of mild to severe inflammatory acne vulgaris.
Dr. Sakamoto and her Wellman colleagues have been working with five dermatologists to conduct clinical trials of the device: Emil Tanghetti, MD, and Mitchel Goldman, MD, in California; Roy Geronemus, MD, in New York; Joel Cohen, MD, in Colorado; and Daniel Friedmann, MD, in Texas. As of Oct. 2, 2022, more than 50 patients with mild to severe acne were enrolled in four studies and an additional 30 were enrolled in a pilot facial acne trial, Dr. Sakamoto said. In the trials, patients are followed at 4, 8, 12, and 24 weeks post treatment.
Among patients enrolled in the facial acne trial, researchers have observed a 100% responder rate for patients with more than five acne lesions at 4, 8, 12, and 24 weeks post treatment after four monthly treatment sessions. The average lesion reduction at week 12 was 82% and the mean visual analog scale score immediately after treatment was 2.09 out of 10. Each patient received more than 12,000 trigger pulls of energy from the device overall with no adverse events reported. At 12 months, they observed a 90% inflammatory lesion count reduction from baseline and a rapid response to treatment: a 73% reduction achieved after the first two treatment sessions. Histologic studies revealed selective sebaceous gland destruction with no damage to the epidermis, surrounding dermis, or other skin structures.
Dr. Sakamoto emphasized that to date no direct clinical comparisons have been made between the AviClear and Accure devices. “Are all 1,726-nm lasers made equal? That is a question that we have to keep in our mind,” she said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine. “They are using the same wavelength, but they are different types of lasers.”
For example, the Accure Laser treats to temperature, relies on air cooling, and is targeted to dermatologists and plastic surgeons, while the AviClear treats to fluence, relies on contact cooling, and includes med spas and other nonphysician providers as the target users. “Mathematically, the difference between the two devices is that the Accure can achieve deeper penetration in a single pulse, while the AviClear is a little more superficial,” she said. “Whether that is translated clinically is unknown at this point.”
Dr. Sakamoto also discussed the TheraClearX, which is FDA cleared for the treatment of mild, moderate, and severe acne, including comedonal, pustular, and inflammatory acne vulgaris. The device, which is a new version of the Palomar Acleara, uses a vacuum technique with up to 3 psi pressure in conjunction with broadband light with a wavelength spectrum of 500 nm–1,200 nm delivered through a liquid-cooled, handheld delivery system. The predicate device was the Aesthera Isolaz System. The vacuum extracts buildup of sebaceous material. “At the same time, it takes the blood out of the competing chromophore,” she said. “By doing so, it potentially damages the sebaceous glands and reduces the inflammatory lesions.”
Dr. Sakamoto disclosed that she is the founder of and science advisor for Lightwater Bioscience. She is also a science advisor for Accure Acne and has received portions of patent royalties from Massachusetts General Hospital.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE
AAP issues clinical update to cerebral palsy guidelines
Updated clinical guidelines for the early diagnosis and management of cerebral palsy have been issued by the American Academy of Pediatrics.
Coauthored with the American Academy for Cerebral Palsy and Developmental Medicine, the report builds on new evidence for improved care and outcomes since the 2006 consensus guidelines.
Cerebral palsy, the most common neuromotor disorder of childhood, is often accompanied by cognitive impairments, epilepsy, sensory impairments, behavioral problems, communication difficulties, breathing and sleep problems, gastrointestinal and nutritional problems, and bone and orthopedic problems.
In the United States, the estimated prevalence of cerebral palsy ranges from 1.5 to 4 per 1,000 live births.
“Early identification and initiation of evidence-based motor therapies can improve outcomes by taking advantage of the neuroplasticity in the infant brain,” said the guideline authors in an executive summary.
The guideline, published in Pediatrics, is directed to primary care physicians with pediatrics, family practice, or internal medicine training. “It’s a much more comprehensive overview of the important role that primary care providers play in the lifetime care of people with cerebral palsy,” explained Garey Noritz, MD, chair of the 2021-2022 Executive Committee of the Council on Children with Disabilities. Dr. Noritz, a professor of pediatrics at Ohio State University and division chief of the complex health care program at Nationwide Children’s Hospital, both in Columbus, said: “The combined efforts of the primary care physician and specialty providers are needed to achieve the best outcomes.”
The AAP recommends that primary care pediatricians, neonatologists, and other specialists caring for hospitalized newborns recognize those at high risk of cerebral palsy, diagnose them as early as possible, and promptly refer them for therapy. Primary care physicians are advised to identify motor delays early by formalizing standardized developmental surveillance and screening at 9, 18, and 30 months, and to implement family-centered care across multiple specialists.
“If a motor disorder is suspected, primary care physicians should simultaneously begin a medical evaluation, refer to a specialist for definitive diagnosis, and to therapists for treatment,” Dr. Noritz emphasized.
“The earlier any possible movement disorder is recognized and intervention begins, the better a child can develop a gait pattern and work toward living an independent life, said Manish N. Shah, MD, associate professor of pediatric neurosurgery at the University of Texas, Houston, who was not involved in developing the guidelines.
For children in whom physical therapy and medication have not reduced leg spasticity, a minimally invasive spinal procedure can help release contracted tendons and encourage independent walking. The optimal age for selective dorsal rhizotomy is about 4 years, said Dr. Shah, who is director of the Texas Comprehensive Spasticity Center at Children’s Memorial Hermann Hospital in Houston. “You can turn these children into walkers. As adults, they can get jobs, have their own families. It’s life-changing.”
Importantly, the guidelines address the health care disparities leading to a higher prevalence of cerebral palsy in Black children and in those from families with lower socioeconomic status. “Efforts to combat racism and eliminate barriers to culturally sensitive prenatal, perinatal, and later pediatric care may help to improve outcomes for all children with cerebral palsy,” the authors said.
“Every child with cerebral palsy needs an individual plan, but only 30% or 40% are getting interventions,” said Dr. Shah. The updated guidelines could help payers rethink the 15-20 visits a year that are often approved, compared with the 2-3 visits per week that are needed for speech, physical, and occupational therapy, he pointed out.
“Financial issues often compromise the interdisciplinary and coordinated care associated with favorable outcomes in children with cerebral palsy,” said Heidi Feldman, MD, PhD, a developmental and behavioral pediatric specialist at Stanford (Calif.) Medicine Children’s Health’s Johnson Center for Pregnancy and Newborn Services. “With a new guideline, there may be greater willingness to fund these essential services.”
In the meantime, the AAP recommends that pediatricians advise families about available medical, social, and educational services, such as early intervention services, the Title V Maternal and Child Health block grant program, and special education services through the public school system.
Children with cerebral palsy need the same standardized primary care as any child, including the full schedule of recommended vaccinations and vision and hearing testing. They also need to be monitored and treated for the many problems that commonly co-occur, including chronic pain.
When secondary complications arise, the frequency of visits should increase.
Pneumonia, the leading cause of death in children and adolescents with cerebral palsy, can be prevented or minimized through immunization against respiratory diseases and screening for signs and symptoms of aspiration and sleep-disordered breathing.
The AAP also recommends that symptoms or functional declines undergo full investigation into other potential causes.
Since the sedentary lifestyle associated with cerebral palsy is now known to be related to the higher rates of cardiovascular complications in this patient population, the AAP recommends more attention be paid to physical activity and a healthy diet early in life. Pediatricians are advised to help families locate suitable opportunities for adaptive sports and recreation.
Almost 50% of children and adolescents with cerebral palsy have intellectual disability, 60%-80% have difficulty speaking, and about 25% are nonverbal. To address this, pediatricians should maximize the use of augmentative and alternative communication devices and involve experts in speech and language pathology, according to the guidelines.
“Many individuals with cerebral palsy and severe motor limitations have active, creative minds, and may need assistive technology, such as electronic talking devices, to demonstrate that mental life,” said Dr. Feldman. “Primary care clinicians should advocate for assistive technology.”
For challenging behavior, especially in the patient with limited verbal skills, potential nonbehavioral culprits such as constipation, esophageal reflux disease, and musculoskeletal or dental pain must be ruled out.
In the lead-up to adolescence, youth with cerebral palsy must be prepared for puberty, menstruation, and healthy, safe sexual relationships, much like their nonaffected peers. Since a disproportionate number of children with cerebral palsy experience neglect and physical, sexual, and emotional abuse, however, family stressors should be identified and caregivers referred for support services.
For the transition from pediatric to adult health care, the AAP recommends that structured planning begin between 12 and 14 years of age. Before transfer, the pediatrician should prepare a comprehensive medical summary with the input of the patient, parent/guardian, and pediatric subspecialists.
Without a proper handoff, “there is an increased risk of morbidity, medical complications, unnecessary emergency department visits, hospitalizations, and procedures,” the authors warned.
Transitions are likely to run more smoothly when youth are given the opportunity to understand their medical condition and be involved in decisions about their health. With this in mind, the AAP recommends that pediatricians actively discourage overprotective parents from getting in the way of their child developing “maximal independence.”
No potential conflicts of interest were disclosed by the authors, Dr. Shah, or Dr. Feldman.
*This story was updated on Nov. 28, 2022.
Updated clinical guidelines for the early diagnosis and management of cerebral palsy have been issued by the American Academy of Pediatrics.
Coauthored with the American Academy for Cerebral Palsy and Developmental Medicine, the report builds on new evidence for improved care and outcomes since the 2006 consensus guidelines.
Cerebral palsy, the most common neuromotor disorder of childhood, is often accompanied by cognitive impairments, epilepsy, sensory impairments, behavioral problems, communication difficulties, breathing and sleep problems, gastrointestinal and nutritional problems, and bone and orthopedic problems.
In the United States, the estimated prevalence of cerebral palsy ranges from 1.5 to 4 per 1,000 live births.
“Early identification and initiation of evidence-based motor therapies can improve outcomes by taking advantage of the neuroplasticity in the infant brain,” said the guideline authors in an executive summary.
The guideline, published in Pediatrics, is directed to primary care physicians with pediatrics, family practice, or internal medicine training. “It’s a much more comprehensive overview of the important role that primary care providers play in the lifetime care of people with cerebral palsy,” explained Garey Noritz, MD, chair of the 2021-2022 Executive Committee of the Council on Children with Disabilities. Dr. Noritz, a professor of pediatrics at Ohio State University and division chief of the complex health care program at Nationwide Children’s Hospital, both in Columbus, said: “The combined efforts of the primary care physician and specialty providers are needed to achieve the best outcomes.”
The AAP recommends that primary care pediatricians, neonatologists, and other specialists caring for hospitalized newborns recognize those at high risk of cerebral palsy, diagnose them as early as possible, and promptly refer them for therapy. Primary care physicians are advised to identify motor delays early by formalizing standardized developmental surveillance and screening at 9, 18, and 30 months, and to implement family-centered care across multiple specialists.
“If a motor disorder is suspected, primary care physicians should simultaneously begin a medical evaluation, refer to a specialist for definitive diagnosis, and to therapists for treatment,” Dr. Noritz emphasized.
“The earlier any possible movement disorder is recognized and intervention begins, the better a child can develop a gait pattern and work toward living an independent life, said Manish N. Shah, MD, associate professor of pediatric neurosurgery at the University of Texas, Houston, who was not involved in developing the guidelines.
For children in whom physical therapy and medication have not reduced leg spasticity, a minimally invasive spinal procedure can help release contracted tendons and encourage independent walking. The optimal age for selective dorsal rhizotomy is about 4 years, said Dr. Shah, who is director of the Texas Comprehensive Spasticity Center at Children’s Memorial Hermann Hospital in Houston. “You can turn these children into walkers. As adults, they can get jobs, have their own families. It’s life-changing.”
Importantly, the guidelines address the health care disparities leading to a higher prevalence of cerebral palsy in Black children and in those from families with lower socioeconomic status. “Efforts to combat racism and eliminate barriers to culturally sensitive prenatal, perinatal, and later pediatric care may help to improve outcomes for all children with cerebral palsy,” the authors said.
“Every child with cerebral palsy needs an individual plan, but only 30% or 40% are getting interventions,” said Dr. Shah. The updated guidelines could help payers rethink the 15-20 visits a year that are often approved, compared with the 2-3 visits per week that are needed for speech, physical, and occupational therapy, he pointed out.
“Financial issues often compromise the interdisciplinary and coordinated care associated with favorable outcomes in children with cerebral palsy,” said Heidi Feldman, MD, PhD, a developmental and behavioral pediatric specialist at Stanford (Calif.) Medicine Children’s Health’s Johnson Center for Pregnancy and Newborn Services. “With a new guideline, there may be greater willingness to fund these essential services.”
In the meantime, the AAP recommends that pediatricians advise families about available medical, social, and educational services, such as early intervention services, the Title V Maternal and Child Health block grant program, and special education services through the public school system.
Children with cerebral palsy need the same standardized primary care as any child, including the full schedule of recommended vaccinations and vision and hearing testing. They also need to be monitored and treated for the many problems that commonly co-occur, including chronic pain.
When secondary complications arise, the frequency of visits should increase.
Pneumonia, the leading cause of death in children and adolescents with cerebral palsy, can be prevented or minimized through immunization against respiratory diseases and screening for signs and symptoms of aspiration and sleep-disordered breathing.
The AAP also recommends that symptoms or functional declines undergo full investigation into other potential causes.
Since the sedentary lifestyle associated with cerebral palsy is now known to be related to the higher rates of cardiovascular complications in this patient population, the AAP recommends more attention be paid to physical activity and a healthy diet early in life. Pediatricians are advised to help families locate suitable opportunities for adaptive sports and recreation.
Almost 50% of children and adolescents with cerebral palsy have intellectual disability, 60%-80% have difficulty speaking, and about 25% are nonverbal. To address this, pediatricians should maximize the use of augmentative and alternative communication devices and involve experts in speech and language pathology, according to the guidelines.
“Many individuals with cerebral palsy and severe motor limitations have active, creative minds, and may need assistive technology, such as electronic talking devices, to demonstrate that mental life,” said Dr. Feldman. “Primary care clinicians should advocate for assistive technology.”
For challenging behavior, especially in the patient with limited verbal skills, potential nonbehavioral culprits such as constipation, esophageal reflux disease, and musculoskeletal or dental pain must be ruled out.
In the lead-up to adolescence, youth with cerebral palsy must be prepared for puberty, menstruation, and healthy, safe sexual relationships, much like their nonaffected peers. Since a disproportionate number of children with cerebral palsy experience neglect and physical, sexual, and emotional abuse, however, family stressors should be identified and caregivers referred for support services.
For the transition from pediatric to adult health care, the AAP recommends that structured planning begin between 12 and 14 years of age. Before transfer, the pediatrician should prepare a comprehensive medical summary with the input of the patient, parent/guardian, and pediatric subspecialists.
Without a proper handoff, “there is an increased risk of morbidity, medical complications, unnecessary emergency department visits, hospitalizations, and procedures,” the authors warned.
Transitions are likely to run more smoothly when youth are given the opportunity to understand their medical condition and be involved in decisions about their health. With this in mind, the AAP recommends that pediatricians actively discourage overprotective parents from getting in the way of their child developing “maximal independence.”
No potential conflicts of interest were disclosed by the authors, Dr. Shah, or Dr. Feldman.
*This story was updated on Nov. 28, 2022.
Updated clinical guidelines for the early diagnosis and management of cerebral palsy have been issued by the American Academy of Pediatrics.
Coauthored with the American Academy for Cerebral Palsy and Developmental Medicine, the report builds on new evidence for improved care and outcomes since the 2006 consensus guidelines.
Cerebral palsy, the most common neuromotor disorder of childhood, is often accompanied by cognitive impairments, epilepsy, sensory impairments, behavioral problems, communication difficulties, breathing and sleep problems, gastrointestinal and nutritional problems, and bone and orthopedic problems.
In the United States, the estimated prevalence of cerebral palsy ranges from 1.5 to 4 per 1,000 live births.
“Early identification and initiation of evidence-based motor therapies can improve outcomes by taking advantage of the neuroplasticity in the infant brain,” said the guideline authors in an executive summary.
The guideline, published in Pediatrics, is directed to primary care physicians with pediatrics, family practice, or internal medicine training. “It’s a much more comprehensive overview of the important role that primary care providers play in the lifetime care of people with cerebral palsy,” explained Garey Noritz, MD, chair of the 2021-2022 Executive Committee of the Council on Children with Disabilities. Dr. Noritz, a professor of pediatrics at Ohio State University and division chief of the complex health care program at Nationwide Children’s Hospital, both in Columbus, said: “The combined efforts of the primary care physician and specialty providers are needed to achieve the best outcomes.”
The AAP recommends that primary care pediatricians, neonatologists, and other specialists caring for hospitalized newborns recognize those at high risk of cerebral palsy, diagnose them as early as possible, and promptly refer them for therapy. Primary care physicians are advised to identify motor delays early by formalizing standardized developmental surveillance and screening at 9, 18, and 30 months, and to implement family-centered care across multiple specialists.
“If a motor disorder is suspected, primary care physicians should simultaneously begin a medical evaluation, refer to a specialist for definitive diagnosis, and to therapists for treatment,” Dr. Noritz emphasized.
“The earlier any possible movement disorder is recognized and intervention begins, the better a child can develop a gait pattern and work toward living an independent life, said Manish N. Shah, MD, associate professor of pediatric neurosurgery at the University of Texas, Houston, who was not involved in developing the guidelines.
For children in whom physical therapy and medication have not reduced leg spasticity, a minimally invasive spinal procedure can help release contracted tendons and encourage independent walking. The optimal age for selective dorsal rhizotomy is about 4 years, said Dr. Shah, who is director of the Texas Comprehensive Spasticity Center at Children’s Memorial Hermann Hospital in Houston. “You can turn these children into walkers. As adults, they can get jobs, have their own families. It’s life-changing.”
Importantly, the guidelines address the health care disparities leading to a higher prevalence of cerebral palsy in Black children and in those from families with lower socioeconomic status. “Efforts to combat racism and eliminate barriers to culturally sensitive prenatal, perinatal, and later pediatric care may help to improve outcomes for all children with cerebral palsy,” the authors said.
“Every child with cerebral palsy needs an individual plan, but only 30% or 40% are getting interventions,” said Dr. Shah. The updated guidelines could help payers rethink the 15-20 visits a year that are often approved, compared with the 2-3 visits per week that are needed for speech, physical, and occupational therapy, he pointed out.
“Financial issues often compromise the interdisciplinary and coordinated care associated with favorable outcomes in children with cerebral palsy,” said Heidi Feldman, MD, PhD, a developmental and behavioral pediatric specialist at Stanford (Calif.) Medicine Children’s Health’s Johnson Center for Pregnancy and Newborn Services. “With a new guideline, there may be greater willingness to fund these essential services.”
In the meantime, the AAP recommends that pediatricians advise families about available medical, social, and educational services, such as early intervention services, the Title V Maternal and Child Health block grant program, and special education services through the public school system.
Children with cerebral palsy need the same standardized primary care as any child, including the full schedule of recommended vaccinations and vision and hearing testing. They also need to be monitored and treated for the many problems that commonly co-occur, including chronic pain.
When secondary complications arise, the frequency of visits should increase.
Pneumonia, the leading cause of death in children and adolescents with cerebral palsy, can be prevented or minimized through immunization against respiratory diseases and screening for signs and symptoms of aspiration and sleep-disordered breathing.
The AAP also recommends that symptoms or functional declines undergo full investigation into other potential causes.
Since the sedentary lifestyle associated with cerebral palsy is now known to be related to the higher rates of cardiovascular complications in this patient population, the AAP recommends more attention be paid to physical activity and a healthy diet early in life. Pediatricians are advised to help families locate suitable opportunities for adaptive sports and recreation.
Almost 50% of children and adolescents with cerebral palsy have intellectual disability, 60%-80% have difficulty speaking, and about 25% are nonverbal. To address this, pediatricians should maximize the use of augmentative and alternative communication devices and involve experts in speech and language pathology, according to the guidelines.
“Many individuals with cerebral palsy and severe motor limitations have active, creative minds, and may need assistive technology, such as electronic talking devices, to demonstrate that mental life,” said Dr. Feldman. “Primary care clinicians should advocate for assistive technology.”
For challenging behavior, especially in the patient with limited verbal skills, potential nonbehavioral culprits such as constipation, esophageal reflux disease, and musculoskeletal or dental pain must be ruled out.
In the lead-up to adolescence, youth with cerebral palsy must be prepared for puberty, menstruation, and healthy, safe sexual relationships, much like their nonaffected peers. Since a disproportionate number of children with cerebral palsy experience neglect and physical, sexual, and emotional abuse, however, family stressors should be identified and caregivers referred for support services.
For the transition from pediatric to adult health care, the AAP recommends that structured planning begin between 12 and 14 years of age. Before transfer, the pediatrician should prepare a comprehensive medical summary with the input of the patient, parent/guardian, and pediatric subspecialists.
Without a proper handoff, “there is an increased risk of morbidity, medical complications, unnecessary emergency department visits, hospitalizations, and procedures,” the authors warned.
Transitions are likely to run more smoothly when youth are given the opportunity to understand their medical condition and be involved in decisions about their health. With this in mind, the AAP recommends that pediatricians actively discourage overprotective parents from getting in the way of their child developing “maximal independence.”
No potential conflicts of interest were disclosed by the authors, Dr. Shah, or Dr. Feldman.
*This story was updated on Nov. 28, 2022.
FROM PEDIATRICS
Children and COVID: Weekly cases maintain a low-level plateau
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.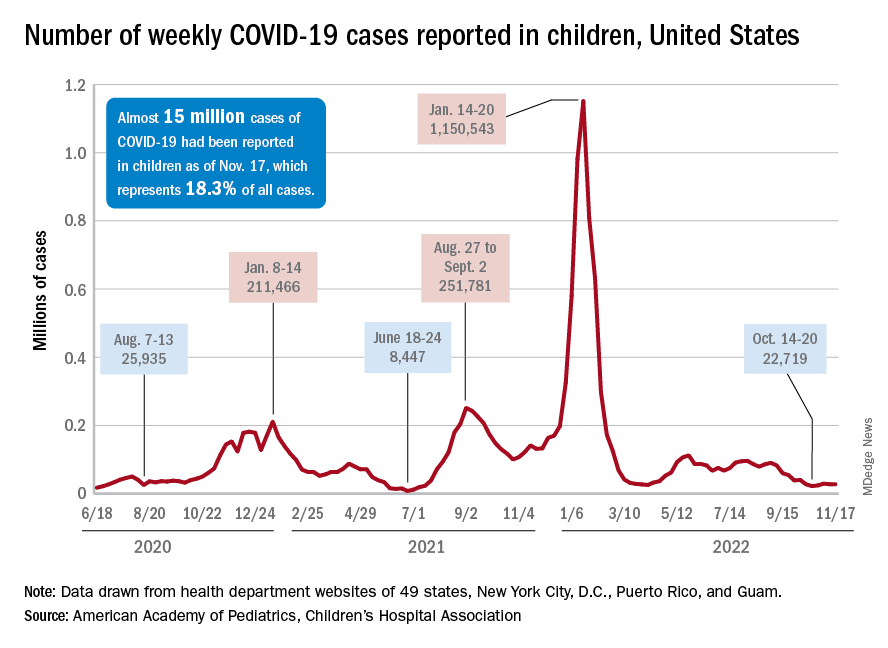
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
Local-level youth suicides reflect mental health care shortages
Rates of youth suicides at the county level increased as mental health professional shortages increased, based on data from more than 5,000 youth suicides across all counties in the United States.
Suicide remains the second leading cause of death among adolescents in the United States, and shortages of pediatric mental health providers are well known, but the association between mental health workforce shortages and youth suicides at the local level has not been well studied, Jennifer A. Hoffmann, MD, of Northwestern University, Chicago, and colleagues wrote.
Previous studies have shown few or no child psychiatrists or child-focused mental health professionals in most counties across the United States, and shortages are more likely in rural and high-poverty counties, the researchers noted.
In a cross-sectional study published in JAMA Pediatrics, the researchers reviewed all youth suicide data from January 2015 to Dec. 31, 2016 using the Centers for Disease Control and Prevention’s Compressed Mortality File. They used a multivariate binomial regression model to examine the association between youth suicide rates and the presence or absence of mental health care. Mental health care shortages were based on data from the U.S. Health Resources and Services Administration’s assessment of the number of mental health professionals relative to the country population and the availability of nearby services. Areas identified as having shortages were designated as Health Professional Shortage Areas (HPSAs) and scored on a severity level of 0-25, with higher scores indicating greater shortages. Approximately two-thirds (67.6%) of the 3,133 counties included in the study met criteria for mental health workforce shortage areas.
The researchers identified 5,034 suicides in youth aged 5-19 years during the study period, for an annual rate of 3.99 per 100,000 individuals. Of these, 72.8% were male and 68.2% were non-Hispanic White.
Overall, a county designation of mental health care shortage was significantly associated with an increased rate of youth suicide (adjusted incidence rate ratio, 1.16) and also increased rate of youth firearm suicide (aIRR, 1.27) after controlling for county and socioeconomic characteristics including the presence of a children’s mental health hospital, the percentage of children without health insurance, median household income, and racial makeup of the county.
The adjusted youth suicide rate increased by 4% for every 1-point increase in the HPSA score in counties with designated mental health workforce shortages.
The adjusted youth suicide rates were higher in counties with a lower median household income, and youth suicides increased with increases in the percentages of uninsured children, the researchers wrote.
“Reducing poverty, addressing social determinants of health, and improving insurance coverage may be considered as components of a multipronged societal strategy to improve child health and reduce youth suicides,” they said. “Efforts are needed to enhance the mental health professional workforce to match current levels of need.” Possible strategies to increase the pediatric mental health workforce may include improving reimbursement and integrating mental health care into primary care and schools by expanding telehealth services.
The study findings were limited by several factors including the potential misclassification of demographics or cause of death, the researchers noted. Other limitations included the inability to assess actual use of mental health services or firearm ownership in a household, and the possible differences between county-level associations and those of a city, neighborhood, or individual.
However, the results indicate that mental health professional workforce shortages were associated with increased youth suicide rates, and the data may inform local-level suicide prevention efforts, they concluded.
Data support the need for early intervention
“It was very important to conduct this study at this time because mental health problems, to include suicidal ideation, continue to increase in adolescents,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “This study reinforces the immense import of sufficient mental health workforce to mitigate this increasing risk of suicide in adolescents.”
Dr. Loper said: “I believe that early intervention, or consistent access to mental health services, can go a very long way in preventing suicide in adolescents.
“I think the primary implications of this study are more relevant at the systems level, and reinforce the necessity of clinicians advocating for policies that address mental health workforce shortages in counties that are underserved,” he added.
However, “One primary barrier to increasing the number of mental health professionals at a local level, and specifically the number of child psychiatrists, is that demand is currently outpacing supply,” said Dr. Loper, a pediatrician and psychiatrist who was not involved in the study. “As the study authors cite, increasing telepsychiatry services and increasing mental health workforce specifically in the primary care setting may help offset these deficiencies,” he noted. Looking ahead, primary prevention of mental health problems by grassroots efforts is vital to stopping the trend in increased youth suicides and more mental health professionals are needed to mitigate the phenomenon of isolation and the degradation of community constructs.
As for additional research, Dr. Loper agreed with the study authors comments on the need for “more granular data” to better understand the correlation between mental health workforce and suicide in adolescents. “Data that captures city or neighborhood statistics related to mental health workforce and adolescent suicide could go a long way in our efforts to continue to better understand this very important correlation.”
The study was supported by an Academic Pediatric Association Young Investigator Award. Dr. Hoffmann disclosed research funding from the U.S. Agency for Healthcare Research and Quality unrelated to the current study. Dr. Loper had no financial conflicts to disclose.
Rates of youth suicides at the county level increased as mental health professional shortages increased, based on data from more than 5,000 youth suicides across all counties in the United States.
Suicide remains the second leading cause of death among adolescents in the United States, and shortages of pediatric mental health providers are well known, but the association between mental health workforce shortages and youth suicides at the local level has not been well studied, Jennifer A. Hoffmann, MD, of Northwestern University, Chicago, and colleagues wrote.
Previous studies have shown few or no child psychiatrists or child-focused mental health professionals in most counties across the United States, and shortages are more likely in rural and high-poverty counties, the researchers noted.
In a cross-sectional study published in JAMA Pediatrics, the researchers reviewed all youth suicide data from January 2015 to Dec. 31, 2016 using the Centers for Disease Control and Prevention’s Compressed Mortality File. They used a multivariate binomial regression model to examine the association between youth suicide rates and the presence or absence of mental health care. Mental health care shortages were based on data from the U.S. Health Resources and Services Administration’s assessment of the number of mental health professionals relative to the country population and the availability of nearby services. Areas identified as having shortages were designated as Health Professional Shortage Areas (HPSAs) and scored on a severity level of 0-25, with higher scores indicating greater shortages. Approximately two-thirds (67.6%) of the 3,133 counties included in the study met criteria for mental health workforce shortage areas.
The researchers identified 5,034 suicides in youth aged 5-19 years during the study period, for an annual rate of 3.99 per 100,000 individuals. Of these, 72.8% were male and 68.2% were non-Hispanic White.
Overall, a county designation of mental health care shortage was significantly associated with an increased rate of youth suicide (adjusted incidence rate ratio, 1.16) and also increased rate of youth firearm suicide (aIRR, 1.27) after controlling for county and socioeconomic characteristics including the presence of a children’s mental health hospital, the percentage of children without health insurance, median household income, and racial makeup of the county.
The adjusted youth suicide rate increased by 4% for every 1-point increase in the HPSA score in counties with designated mental health workforce shortages.
The adjusted youth suicide rates were higher in counties with a lower median household income, and youth suicides increased with increases in the percentages of uninsured children, the researchers wrote.
“Reducing poverty, addressing social determinants of health, and improving insurance coverage may be considered as components of a multipronged societal strategy to improve child health and reduce youth suicides,” they said. “Efforts are needed to enhance the mental health professional workforce to match current levels of need.” Possible strategies to increase the pediatric mental health workforce may include improving reimbursement and integrating mental health care into primary care and schools by expanding telehealth services.
The study findings were limited by several factors including the potential misclassification of demographics or cause of death, the researchers noted. Other limitations included the inability to assess actual use of mental health services or firearm ownership in a household, and the possible differences between county-level associations and those of a city, neighborhood, or individual.
However, the results indicate that mental health professional workforce shortages were associated with increased youth suicide rates, and the data may inform local-level suicide prevention efforts, they concluded.
Data support the need for early intervention
“It was very important to conduct this study at this time because mental health problems, to include suicidal ideation, continue to increase in adolescents,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “This study reinforces the immense import of sufficient mental health workforce to mitigate this increasing risk of suicide in adolescents.”
Dr. Loper said: “I believe that early intervention, or consistent access to mental health services, can go a very long way in preventing suicide in adolescents.
“I think the primary implications of this study are more relevant at the systems level, and reinforce the necessity of clinicians advocating for policies that address mental health workforce shortages in counties that are underserved,” he added.
However, “One primary barrier to increasing the number of mental health professionals at a local level, and specifically the number of child psychiatrists, is that demand is currently outpacing supply,” said Dr. Loper, a pediatrician and psychiatrist who was not involved in the study. “As the study authors cite, increasing telepsychiatry services and increasing mental health workforce specifically in the primary care setting may help offset these deficiencies,” he noted. Looking ahead, primary prevention of mental health problems by grassroots efforts is vital to stopping the trend in increased youth suicides and more mental health professionals are needed to mitigate the phenomenon of isolation and the degradation of community constructs.
As for additional research, Dr. Loper agreed with the study authors comments on the need for “more granular data” to better understand the correlation between mental health workforce and suicide in adolescents. “Data that captures city or neighborhood statistics related to mental health workforce and adolescent suicide could go a long way in our efforts to continue to better understand this very important correlation.”
The study was supported by an Academic Pediatric Association Young Investigator Award. Dr. Hoffmann disclosed research funding from the U.S. Agency for Healthcare Research and Quality unrelated to the current study. Dr. Loper had no financial conflicts to disclose.
Rates of youth suicides at the county level increased as mental health professional shortages increased, based on data from more than 5,000 youth suicides across all counties in the United States.
Suicide remains the second leading cause of death among adolescents in the United States, and shortages of pediatric mental health providers are well known, but the association between mental health workforce shortages and youth suicides at the local level has not been well studied, Jennifer A. Hoffmann, MD, of Northwestern University, Chicago, and colleagues wrote.
Previous studies have shown few or no child psychiatrists or child-focused mental health professionals in most counties across the United States, and shortages are more likely in rural and high-poverty counties, the researchers noted.
In a cross-sectional study published in JAMA Pediatrics, the researchers reviewed all youth suicide data from January 2015 to Dec. 31, 2016 using the Centers for Disease Control and Prevention’s Compressed Mortality File. They used a multivariate binomial regression model to examine the association between youth suicide rates and the presence or absence of mental health care. Mental health care shortages were based on data from the U.S. Health Resources and Services Administration’s assessment of the number of mental health professionals relative to the country population and the availability of nearby services. Areas identified as having shortages were designated as Health Professional Shortage Areas (HPSAs) and scored on a severity level of 0-25, with higher scores indicating greater shortages. Approximately two-thirds (67.6%) of the 3,133 counties included in the study met criteria for mental health workforce shortage areas.
The researchers identified 5,034 suicides in youth aged 5-19 years during the study period, for an annual rate of 3.99 per 100,000 individuals. Of these, 72.8% were male and 68.2% were non-Hispanic White.
Overall, a county designation of mental health care shortage was significantly associated with an increased rate of youth suicide (adjusted incidence rate ratio, 1.16) and also increased rate of youth firearm suicide (aIRR, 1.27) after controlling for county and socioeconomic characteristics including the presence of a children’s mental health hospital, the percentage of children without health insurance, median household income, and racial makeup of the county.
The adjusted youth suicide rate increased by 4% for every 1-point increase in the HPSA score in counties with designated mental health workforce shortages.
The adjusted youth suicide rates were higher in counties with a lower median household income, and youth suicides increased with increases in the percentages of uninsured children, the researchers wrote.
“Reducing poverty, addressing social determinants of health, and improving insurance coverage may be considered as components of a multipronged societal strategy to improve child health and reduce youth suicides,” they said. “Efforts are needed to enhance the mental health professional workforce to match current levels of need.” Possible strategies to increase the pediatric mental health workforce may include improving reimbursement and integrating mental health care into primary care and schools by expanding telehealth services.
The study findings were limited by several factors including the potential misclassification of demographics or cause of death, the researchers noted. Other limitations included the inability to assess actual use of mental health services or firearm ownership in a household, and the possible differences between county-level associations and those of a city, neighborhood, or individual.
However, the results indicate that mental health professional workforce shortages were associated with increased youth suicide rates, and the data may inform local-level suicide prevention efforts, they concluded.
Data support the need for early intervention
“It was very important to conduct this study at this time because mental health problems, to include suicidal ideation, continue to increase in adolescents,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “This study reinforces the immense import of sufficient mental health workforce to mitigate this increasing risk of suicide in adolescents.”
Dr. Loper said: “I believe that early intervention, or consistent access to mental health services, can go a very long way in preventing suicide in adolescents.
“I think the primary implications of this study are more relevant at the systems level, and reinforce the necessity of clinicians advocating for policies that address mental health workforce shortages in counties that are underserved,” he added.
However, “One primary barrier to increasing the number of mental health professionals at a local level, and specifically the number of child psychiatrists, is that demand is currently outpacing supply,” said Dr. Loper, a pediatrician and psychiatrist who was not involved in the study. “As the study authors cite, increasing telepsychiatry services and increasing mental health workforce specifically in the primary care setting may help offset these deficiencies,” he noted. Looking ahead, primary prevention of mental health problems by grassroots efforts is vital to stopping the trend in increased youth suicides and more mental health professionals are needed to mitigate the phenomenon of isolation and the degradation of community constructs.
As for additional research, Dr. Loper agreed with the study authors comments on the need for “more granular data” to better understand the correlation between mental health workforce and suicide in adolescents. “Data that captures city or neighborhood statistics related to mental health workforce and adolescent suicide could go a long way in our efforts to continue to better understand this very important correlation.”
The study was supported by an Academic Pediatric Association Young Investigator Award. Dr. Hoffmann disclosed research funding from the U.S. Agency for Healthcare Research and Quality unrelated to the current study. Dr. Loper had no financial conflicts to disclose.
FROM JAMA PEDIATRICS
Nurse practitioner fined $20k for advertising herself as ‘Doctor Sarah’
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.