User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Progestin-only contraceptives may promote breast pain in adolescent macromastia patients
Key clinical point: Use of progestin-only contraception was associated with greater breast hypertrophy and pain in adolescents with macromastia.
Major finding: Compared to controls, macromastia patients who used progestin-only contraceptives were 500% more likely to report breast pain (odds ratio 4.94); macromastia patients who used progestin-only contraception also had significantly more breast tissue resected during mammaplasty and greater musculoskeletal pain.
Study details: The data come from a retrospective study of 378 macromastia patients aged 12 to 21 years and 378 controls; 5.3% of macromastia patients and 28.0% of controls used progestin-only contraception.
Disclosures: The study was supported in part by the Plastic Surgery Foundation. The researchers had no financial conflicts to disclose.
Source: Nuzzi LC et al. Plast Reconstr Surg Glob Open. 2021 Feb 12. doi: 10.1097/GOX.0000000000003421.
Key clinical point: Use of progestin-only contraception was associated with greater breast hypertrophy and pain in adolescents with macromastia.
Major finding: Compared to controls, macromastia patients who used progestin-only contraceptives were 500% more likely to report breast pain (odds ratio 4.94); macromastia patients who used progestin-only contraception also had significantly more breast tissue resected during mammaplasty and greater musculoskeletal pain.
Study details: The data come from a retrospective study of 378 macromastia patients aged 12 to 21 years and 378 controls; 5.3% of macromastia patients and 28.0% of controls used progestin-only contraception.
Disclosures: The study was supported in part by the Plastic Surgery Foundation. The researchers had no financial conflicts to disclose.
Source: Nuzzi LC et al. Plast Reconstr Surg Glob Open. 2021 Feb 12. doi: 10.1097/GOX.0000000000003421.
Key clinical point: Use of progestin-only contraception was associated with greater breast hypertrophy and pain in adolescents with macromastia.
Major finding: Compared to controls, macromastia patients who used progestin-only contraceptives were 500% more likely to report breast pain (odds ratio 4.94); macromastia patients who used progestin-only contraception also had significantly more breast tissue resected during mammaplasty and greater musculoskeletal pain.
Study details: The data come from a retrospective study of 378 macromastia patients aged 12 to 21 years and 378 controls; 5.3% of macromastia patients and 28.0% of controls used progestin-only contraception.
Disclosures: The study was supported in part by the Plastic Surgery Foundation. The researchers had no financial conflicts to disclose.
Source: Nuzzi LC et al. Plast Reconstr Surg Glob Open. 2021 Feb 12. doi: 10.1097/GOX.0000000000003421.
Exercise may mitigate arterial stiffness from oral contraceptive use
Key clinical point: Among healthy young women taking oral contraceptives, pulse wave velocity was lower in active women compared with inactive women, suggesting that physical activity may mitigate the risk of arterial stiffness associated with OC use.
Major finding: Pulse wave velocity as an indicator of arterial stiffness was similar in oral contraceptive users and non-users, however, PWV was significantly lower in active women vs. inactive women (5.4 ms -1 vs. 6.3 ms -1).
Study details: The data come from a cross-sectional study of 49 healthy young women with an average age of 21.9 years, divided into four groups (inactive vs. active, OC use vs. non-OC use).
Disclosures: The study was supported in part by the European Union and the New Aquitaine region through the Habisan program (CPER-FEDER). The researchers had no financial conflicts to disclose.
Source: Enea C et al. Int J Environ Res Public Health. 2021 Mar 25. doi: 10.3390/ijerph18073393.
Key clinical point: Among healthy young women taking oral contraceptives, pulse wave velocity was lower in active women compared with inactive women, suggesting that physical activity may mitigate the risk of arterial stiffness associated with OC use.
Major finding: Pulse wave velocity as an indicator of arterial stiffness was similar in oral contraceptive users and non-users, however, PWV was significantly lower in active women vs. inactive women (5.4 ms -1 vs. 6.3 ms -1).
Study details: The data come from a cross-sectional study of 49 healthy young women with an average age of 21.9 years, divided into four groups (inactive vs. active, OC use vs. non-OC use).
Disclosures: The study was supported in part by the European Union and the New Aquitaine region through the Habisan program (CPER-FEDER). The researchers had no financial conflicts to disclose.
Source: Enea C et al. Int J Environ Res Public Health. 2021 Mar 25. doi: 10.3390/ijerph18073393.
Key clinical point: Among healthy young women taking oral contraceptives, pulse wave velocity was lower in active women compared with inactive women, suggesting that physical activity may mitigate the risk of arterial stiffness associated with OC use.
Major finding: Pulse wave velocity as an indicator of arterial stiffness was similar in oral contraceptive users and non-users, however, PWV was significantly lower in active women vs. inactive women (5.4 ms -1 vs. 6.3 ms -1).
Study details: The data come from a cross-sectional study of 49 healthy young women with an average age of 21.9 years, divided into four groups (inactive vs. active, OC use vs. non-OC use).
Disclosures: The study was supported in part by the European Union and the New Aquitaine region through the Habisan program (CPER-FEDER). The researchers had no financial conflicts to disclose.
Source: Enea C et al. Int J Environ Res Public Health. 2021 Mar 25. doi: 10.3390/ijerph18073393.
Preimplantation genetic testing for aneuploidy
Why does the debate linger after 30 years?
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.

Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at obnews@mdedge.com.
Why does the debate linger after 30 years?
Why does the debate linger after 30 years?
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.
Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at obnews@mdedge.com.
The holy grail of assisted reproductive technology (ART) is the delivery of a healthy child. From the world’s first successful ART cycle of in vitro fertilization in 1978 (3 years later in the United States), the goal of every cycle is to provide the woman with an embryo that has the highest potential for implantation and, ultimately, a single live birth.
Embryo aneuploidy is a major factor in the success of human reproduction. As women age, aneuploidy is reported in less than 30% of women aged younger than 35 years but rises to 90% for those in their mid-40s. Intuitively and through randomized, controlled trials, chromosome testing of embryos is a reasonable approach toward improved cycle outcomes and allows for the transfer of a single euploid embryo.
Recently, the phrase “add-ons” has entered the vernacular of editorials on IVF. These additional procedures are offered to patients with the expectation of improving results, yet many have not been supported by rigorous scientifically controlled research trials, e.g., endometrial scratch, embryo glue, and time-lapse imaging of embryos. Where does preimplantation genetic testing (PGT) belong in the IVF armamentarium and why, after 30 years, are there two diametrically opposed views on its benefit? (We will not address testing for single gene defects or chromosome structural rearrangements.)
How did we get here?
The first iteration of PGT used fluorescence in situ hybridization to not only identify X-linked recessive diseases (Hum Genet. 1992;89:18-22) but also the most common chromosome disorders (13, 18, 21, X, Y) by removing one to two blastomere cells from a day 3 embryo (six- to eight-cell stage). Despite wide enthusiasm, the technique was eventually determined to reduce implantation by nearly 40% and was abandoned; presumably impairing the embryo by removing up to one-third of its make-up.
Because of extended embryo culture to the blastocyst stage along with the improved cryopreservation process of vitrification, the next generation of embryo analysis surfaced, what we now refer to as PGT 2.0. Currently, approximately five to six cells from the outer embryo trophectoderm are removed and sent to a specialized laboratory for 24-chromosome screening while the biopsied embryos are cryopreserved. Outcome data (aneuploidy rates, mosaicism) have been influenced by the evolution of genetic platforms – from array comparative genome hybridization to single-nucleotide polymorphism array, to quantitative polymerase chain reaction, to next-generation sequencing (NGS). The newest platform, NGS with high resolution, provides the most extensive degree of analysis by detecting unbalanced translocations and a low cut-off percentage for mosaicism (20%). The clinical error rate is approximately 1%-2%, improved from the 2%-4% of earlier techniques.
The phenomenon of mosaicism describes two distinct cell lines in one embryo (typically one normal and one abnormal) and is defined based on the percentage of mosaicism – currently, the lower limit is 20%. Embryos with less than 20%-30% mosaicism are considered euploid and those greater than 70%-80% are aneuploid. Of note, clinics that do not request the reporting of mosaicism can result in the potential discarding of embryos labeled as aneuploid that would otherwise have potentially resulted in a live birth. The higher the cut-off value for designating mosaicism, the lower the false-positive rate (declaring an embryo aneuploid when euploid). While there is no safe degree of mosaicism, most transfers have resulted in chromosomally normal infants despite a lower implantation rate and higher miscarriage rate.
Current status
The greatest advantage of PGT for aneuploidy (PGT-A) is its increase in promoting a single embryo transfer. Medical evidence supports pregnancy outcomes equivalent from a single euploid embryo transfer versus a double “untested” embryo transfer.
Only a handful of randomized, controlled trials have evaluated the efficacy of PGT-A. Outcomes have favored improved live birth rates; however, criticism exists for enrolling only good prognosis patients given their high likelihood of developing blastocyst embryos to biopsy. The only trial that used an “intention to treat” protocol (rather than randomization at the time of biopsy) did not demonstrate any difference in live birth or miscarriage comparing embryo selection by PGT-A versus embryo morphology alone. However, post hoc analysis did show a benefit with PGT-A in the 35- to 40-year-old age group, not in the less than 35-year-old group. All other trials demonstrated a reduction in miscarriage with PGT-A but only as a secondary outcome.
The medical literature does not support PGT-A to manage patients with recurrent pregnancy loss and there is no evidence for improvement in women aged less than 35 years or egg donors (F&S Reports. 2021;2:36-42). PGT-A has been effective in patients wishing family balancing.
Controversy
Enthusiasm for PGT-A is countered by lingering concerns. Trophectoderm cells are not in 100% concordance with the inner cell mass, which presumably explains the reports of chromosomally normal live births from the transfer of aneuploid embryos. Biopsy techniques among embryologists are not standardized. As a result, damage to the embryo has been raised as a possible explanation for equivalent pregnancy rates in studies showing no superiority of PGT-A in pregnancy outcome, although this point has recently been refuted.
PGT-A also embraces the “blast-or-bust” credo whereby no embryo transfer occurs unless a blastocyst embryo develops. This continues to beg the unanswerable question – would a woman who did not develop a blastocyst embryo for potential biopsy still conceive if she underwent a day 3 cleavage stage embryo transfer?
Future
Exciting iterations are encroaching for PGT 3.0. One method is blastocyst fluid aspiration to obtain DNA suitable for analysis by molecular genetic methods. Another is noninvasive PGT whereby spent media from the embryo is analyzed using cell-free DNA. Concordance with inner cell mass is reasonably good (approximately 85%) but needs to improve. A major advantage is the biopsy skill set among embryologists is eliminated. A criticism of noninvasive PGT is the risk of false-positive results from contamination of aneuploid cell secretion by physiologic apoptotic cells. Confined placental mosaicism can also increase aneuploidy in cell-free DNA thereby contributing to false positives.
Conclusion
PGT-A is robust technology that appears to benefit women aged above 35 years but not the general infertile population. Error rates must be consistent among laboratories and be lowered. Regarding mosaic embryos, the American Society for Reproductive Medicine guidelines recommend offering another egg retrieval if only mosaic embryos are available and to only consider mosaic embryo transfer following extensive genetic counseling. Long-term effects of PGT-A on children are lacking. The Cochrane Database concluded there was insufficient evidence to make PGT-A routine.
So, the debate is clear and ongoing – universal versus discretionary use of PGT-A? As in all things of life, one size does not fit all, and PGT-A is no exception.
Dr. Trolice is director of Fertility CARE – The IVF Center in Winter Park, Fla., and professor of obstetrics and gynecology at the University of Central Florida, Orlando. Contact him at obnews@mdedge.com.
Plastic IUD placement instruments prevent uterine perforations
Key clinical point: In a biomechanical ex vivo analysis, metal uterine sounds caused uterine perforation, but the manufacturer’s plastic intrauterine device placement rod did not.
Major finding: The lowest mean maximum force generated for IUD placement was 12.3 Newtons with the levonorgestrel intrauterine system placement instrument, followed by 14.1 Newtons with the copper T380A intrauterine device placement instrument 14.1 Newtons; the highest mean maximum force of 17.9 N occurred with the metal sound (P < 0.01).
Study details: The data come from 16 premenopausal women with benign conditions who provided hysterectomy sections at a single center.
Disclosures: The study was funded indirectly through grants to the University of Utah from Bayer, Bioceptive, Sebela, Medicines 360, Merck, and Cooper Surgical. Lead author Dr. Duncan had no financial conflicts to disclose.
Source: Duncan J et al. BMC Womens Health. 2021 Apr 7. doi: 10.1186/s12905-021-01285-6.
Key clinical point: In a biomechanical ex vivo analysis, metal uterine sounds caused uterine perforation, but the manufacturer’s plastic intrauterine device placement rod did not.
Major finding: The lowest mean maximum force generated for IUD placement was 12.3 Newtons with the levonorgestrel intrauterine system placement instrument, followed by 14.1 Newtons with the copper T380A intrauterine device placement instrument 14.1 Newtons; the highest mean maximum force of 17.9 N occurred with the metal sound (P < 0.01).
Study details: The data come from 16 premenopausal women with benign conditions who provided hysterectomy sections at a single center.
Disclosures: The study was funded indirectly through grants to the University of Utah from Bayer, Bioceptive, Sebela, Medicines 360, Merck, and Cooper Surgical. Lead author Dr. Duncan had no financial conflicts to disclose.
Source: Duncan J et al. BMC Womens Health. 2021 Apr 7. doi: 10.1186/s12905-021-01285-6.
Key clinical point: In a biomechanical ex vivo analysis, metal uterine sounds caused uterine perforation, but the manufacturer’s plastic intrauterine device placement rod did not.
Major finding: The lowest mean maximum force generated for IUD placement was 12.3 Newtons with the levonorgestrel intrauterine system placement instrument, followed by 14.1 Newtons with the copper T380A intrauterine device placement instrument 14.1 Newtons; the highest mean maximum force of 17.9 N occurred with the metal sound (P < 0.01).
Study details: The data come from 16 premenopausal women with benign conditions who provided hysterectomy sections at a single center.
Disclosures: The study was funded indirectly through grants to the University of Utah from Bayer, Bioceptive, Sebela, Medicines 360, Merck, and Cooper Surgical. Lead author Dr. Duncan had no financial conflicts to disclose.
Source: Duncan J et al. BMC Womens Health. 2021 Apr 7. doi: 10.1186/s12905-021-01285-6.
Oral contraceptive use shows no impact on later heart failure risk
Key clinical point: Use of oral contraceptives by women of reproductive age was not associated with increased risk of heart failure later in life, but the potential impact of different formulations and dosages deserves further research.
Major finding: Over an average of 12 years’ follow-up, the researchers identified 138 incident cases of heart failure. The incidence of heart failure was not significantly associated with heart failure in multivariate analysis (hazard ratio 0.96); however, any OC use was positively associated with left ventricular end-diastolic mass (P = 0.006) and stroke volume (P = 0.01 and P = 0.005 for left and right ventricles, respectively).
Study details: The data come from a retrospective study of 3,594 women with an average age of 62 years who were enrolled in the Multi‐Ethnic Study of Atherosclerosis and could provide data on oral contraceptive use.
Disclosures: The study was supported by the Guangdong Peak Project, the Science and Technology Planning Project of Guangdong Province, Natural Science Foundation of Guangdong Province, and the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
Source: Luo D et al. ESC Heart Fail. 2021 Apr 9. doi: 10.1002/ehf2.13328.
Key clinical point: Use of oral contraceptives by women of reproductive age was not associated with increased risk of heart failure later in life, but the potential impact of different formulations and dosages deserves further research.
Major finding: Over an average of 12 years’ follow-up, the researchers identified 138 incident cases of heart failure. The incidence of heart failure was not significantly associated with heart failure in multivariate analysis (hazard ratio 0.96); however, any OC use was positively associated with left ventricular end-diastolic mass (P = 0.006) and stroke volume (P = 0.01 and P = 0.005 for left and right ventricles, respectively).
Study details: The data come from a retrospective study of 3,594 women with an average age of 62 years who were enrolled in the Multi‐Ethnic Study of Atherosclerosis and could provide data on oral contraceptive use.
Disclosures: The study was supported by the Guangdong Peak Project, the Science and Technology Planning Project of Guangdong Province, Natural Science Foundation of Guangdong Province, and the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
Source: Luo D et al. ESC Heart Fail. 2021 Apr 9. doi: 10.1002/ehf2.13328.
Key clinical point: Use of oral contraceptives by women of reproductive age was not associated with increased risk of heart failure later in life, but the potential impact of different formulations and dosages deserves further research.
Major finding: Over an average of 12 years’ follow-up, the researchers identified 138 incident cases of heart failure. The incidence of heart failure was not significantly associated with heart failure in multivariate analysis (hazard ratio 0.96); however, any OC use was positively associated with left ventricular end-diastolic mass (P = 0.006) and stroke volume (P = 0.01 and P = 0.005 for left and right ventricles, respectively).
Study details: The data come from a retrospective study of 3,594 women with an average age of 62 years who were enrolled in the Multi‐Ethnic Study of Atherosclerosis and could provide data on oral contraceptive use.
Disclosures: The study was supported by the Guangdong Peak Project, the Science and Technology Planning Project of Guangdong Province, Natural Science Foundation of Guangdong Province, and the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
Source: Luo D et al. ESC Heart Fail. 2021 Apr 9. doi: 10.1002/ehf2.13328.
More signs COVID shots are safe for pregnant women
As the U.S. races to vaccinate millions of people against the coronavirus, pregnant women face the extra challenge of not knowing whether the vaccines are safe for them or their unborn babies.
None of the recent COVID-19 vaccine trials, including those for Pfizer, Moderna, and Johnson & Johnson, enrolled pregnant or breastfeeding women because they consider them a high-risk group.
That was despite the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists asking that pregnant and breastfeeding women be included in trials. The Food and Drug Administration even included pregnant women in the COVID-19 vaccine emergency use authorization (EUA) because of their higher risk of having a more severe disease.
Despite that lack of clinical trial data, more and more smaller studies are suggesting that the vaccines are safe for both mother and child.
Pfizer is now studying its two-dose vaccine in 4,000 pregnant and breastfeeding women to see how safe, tolerated, and robust their immune response is. Researchers will also look at how safe the vaccine is for infants and whether mothers pass along antibodies to children. But the preliminary results won’t be available until the end of the year, a Pfizer spokesperson says.
Without that information, pregnant women are less likely to get vaccinated, according to a large international survey. Less than 45% of pregnant women in the United States said they intended to get vaccinated even when they were told the vaccine was safe and 90% effective. That figure rises to 52% of pregnant women in 16 countries, including the United States, compared with 74% of nonpregnant women willing to be vaccinated. The findings were published online March 1, 2021, in the European Journal of Epidemiology.
The vaccine-hesitant pregnant women in the international study were most concerned that the COVID-19 vaccine could harm their developing fetuses, a worry related to the lack of clinical evidence in pregnant women, said lead researcher Julia Wu, ScD, an epidemiologist at the Harvard School of Public Health’s Human Immunomics Initiative in Boston.
The information vacuum also increases the chances that “people will fall victim to misinformation campaigns like the one on social media that claims that the COVID-19 vaccine causes infertility,” Dr. Wu said. This unfounded claim has deterred some women of childbearing age from getting the vaccine.
Deciding to get vaccinated
Frontline health care professionals were in the first group eligible to receive the vaccine in December 2020. “All of us who were pregnant ... had to decide whether to wait for the data, because we don’t know what the risks are, or go ahead and get it [the vaccine]. We had been dealing with the pandemic for months and were afraid of being exposed to the virus and infecting family members,” said Jacqueline Parchem, MD, a maternal-fetal medicine specialist at the University of Texas Health Science Center, Houston.
Given the lack of safety data, the CDC guidance to pregnant women has been to consult with their doctors and that it’s a personal choice. The Center for Disease Control and Prevention’s latest vaccine guidance said that “there is no evidence that antibodies formed from COVID-19 vaccination cause any problem with pregnancy, including the development of the placenta.”
The CDC is monitoring vaccinated people through its v-safe program and reported on April 12 that more than 86,000 v-safe participants said they were pregnant when they were vaccinated.
Health care workers who were nursing their infants when they were eligible for the vaccine faced a similar dilemma as pregnant women – they lacked the data on them to make a truly informed decision.
“I was nervous about the vaccine side effects for myself and whether my son Bennett, who was about a year old, would experience any of these himself,” said Christa Carrig, a labor and delivery nurse at Massachusetts General Hospital in Boston, who was breastfeeding at the time.
She and Dr. Parchem know that pregnant women with COVID-19 are more likely to have severe illness and complications such as high blood pressure and preterm delivery. “Pregnancy takes a toll on the body. When a woman gets COVID-19 and that insult is added, women who were otherwise young and healthy get much sicker than you would expect,” said Ms. Carrig.
“As a high-risk pregnancy specialist, I know that, with COVID, that babies don’t do well when moms are sick,” said Dr. Parchem.
Pregnant women accounted for more than 84,629 cases of COVID-19 and 95 deaths in the United States between Jan. 22 last year and April 12 this year, according to the CDC COVID data tracker.
Dr. Parchem and Ms. Carrig decided to get vaccinated because of their high risk of exposure to COVID-19 at work. After the second dose, Ms. Carrig reported chills but Bennett had no side effects from breastfeeding. Dr. Parchem, who delivered a healthy baby boy in February, reported no side effects other than a sore arm.
“There’s also a psychological benefit to returning to some sense of normalcy,” said Dr. Parchem. “My mother was finally able to visit us to see the new baby after we were all vaccinated. This was the first visit in more than a year.”
New study results
Ms. Carrig was one of 131 vaccinated hospital workers in the Boston area who took part in the first study to profile the immune response in pregnant and breastfeeding women and compare it with both nonpregnant and pregnant women who had COVID-19.
The study was not designed to evaluate the safety of the vaccines or whether they prevent COVID-19 illness and hospitalizations. That is the role of the large vaccine trials, the authors said.
The participants were aged 18-45 years and received both doses of either Pfizer or Moderna vaccines during one of their trimesters. They provided blood and/or breast milk samples after each vaccine dose, 2-6 weeks after the last dose, and at delivery for the 10 who gave birth during the study.
The vaccines produced a similar strong antibody response among the pregnant/breastfeeding women and nonpregnant women. Their antibody levels were much higher than those found in the pregnant women who had COVID-19, the researchers reported on March 25, 2021, in the American Journal of Obstetrics and Gynecology.
“This is important because a lot of people tend to think once they’ve had COVID-19, they are protected from the virus. This finding suggests that the vaccines produce a stronger antibody response than the infection itself, and this might be important for long-lasting protection against COVID-19,” said Dr. Parchem.
The study also addressed whether newborns benefit from the antibodies produced by their mothers. “In the 10 women who delivered, we detected antibodies in their umbilical cords and breast milk,” says Andrea Edlow, MD, lead researcher and a maternal-fetal medicine specialist at Massachusetts General Hospital.
Newborns are particularly vulnerable to respiratory infections because they have small airways and their immune systems are underdeveloped. These infections can be lethal early in life.
“The public health strategy is to vaccinate mothers against respiratory viruses, bacteria, and parasites that neonates up to 6 months are exposed to. Influenza and pertussis (whooping cough) are two examples of vaccines that we give mothers that we know transfer [antibodies] across the umbilical cord,” said Dr. Edlow.
But this “passive transfer immunity” is different from active immunity, when the body produces its own antibody immune response, she explains.
A different study, also published in March, confirmed that antibodies were transferred from 27 vaccinated pregnant mothers to their infants when they delivered. A new finding was that the women who were vaccinated with both doses and earlier in their third semester passed on more antibodies than the women who were vaccinated later or with only one dose.
Impact of the studies
The Society for Maternal-Fetal Medicine updated its guidance on counseling pregnant and lactating patients about the COVID-19 vaccines to include Dr. Edlow’s study.
“We were struck by how much pregnant and breastfeeding women want to participate in research and to help others in the same situation make decisions. I hope this will be an example to drug companies doing research on new vaccines in the future – that they should not be left behind and can make decisions themselves whether to participate after weighing the risks and benefits,” said Dr. Edlow.
She continues to enroll more vaccinated women in her study in the Boston area, including non–health care workers who have asked to take part.
“It was worth getting vaccinated and participating in the study. I know that I have antibodies and it worked and that I passed them on to Bennett. Also, I know that all the information is available for other women who are questioning whether to get vaccinated or not,” said Ms. Carrig.
Dr. Parchem is also taking part in the CDC’s v-safe pregnancy registry, which is collecting health and safety data on vaccinated pregnant women.
Before she was vaccinated, Dr. Parchem said, “my advice was very measured because we lacked data either saying that it definitely works or showing that it was unsafe. Now that we have this data supporting the benefits, I feel more confident in recommending the vaccines.”
A version of this article first appeared on Medscape.com.
As the U.S. races to vaccinate millions of people against the coronavirus, pregnant women face the extra challenge of not knowing whether the vaccines are safe for them or their unborn babies.
None of the recent COVID-19 vaccine trials, including those for Pfizer, Moderna, and Johnson & Johnson, enrolled pregnant or breastfeeding women because they consider them a high-risk group.
That was despite the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists asking that pregnant and breastfeeding women be included in trials. The Food and Drug Administration even included pregnant women in the COVID-19 vaccine emergency use authorization (EUA) because of their higher risk of having a more severe disease.
Despite that lack of clinical trial data, more and more smaller studies are suggesting that the vaccines are safe for both mother and child.
Pfizer is now studying its two-dose vaccine in 4,000 pregnant and breastfeeding women to see how safe, tolerated, and robust their immune response is. Researchers will also look at how safe the vaccine is for infants and whether mothers pass along antibodies to children. But the preliminary results won’t be available until the end of the year, a Pfizer spokesperson says.
Without that information, pregnant women are less likely to get vaccinated, according to a large international survey. Less than 45% of pregnant women in the United States said they intended to get vaccinated even when they were told the vaccine was safe and 90% effective. That figure rises to 52% of pregnant women in 16 countries, including the United States, compared with 74% of nonpregnant women willing to be vaccinated. The findings were published online March 1, 2021, in the European Journal of Epidemiology.
The vaccine-hesitant pregnant women in the international study were most concerned that the COVID-19 vaccine could harm their developing fetuses, a worry related to the lack of clinical evidence in pregnant women, said lead researcher Julia Wu, ScD, an epidemiologist at the Harvard School of Public Health’s Human Immunomics Initiative in Boston.
The information vacuum also increases the chances that “people will fall victim to misinformation campaigns like the one on social media that claims that the COVID-19 vaccine causes infertility,” Dr. Wu said. This unfounded claim has deterred some women of childbearing age from getting the vaccine.
Deciding to get vaccinated
Frontline health care professionals were in the first group eligible to receive the vaccine in December 2020. “All of us who were pregnant ... had to decide whether to wait for the data, because we don’t know what the risks are, or go ahead and get it [the vaccine]. We had been dealing with the pandemic for months and were afraid of being exposed to the virus and infecting family members,” said Jacqueline Parchem, MD, a maternal-fetal medicine specialist at the University of Texas Health Science Center, Houston.
Given the lack of safety data, the CDC guidance to pregnant women has been to consult with their doctors and that it’s a personal choice. The Center for Disease Control and Prevention’s latest vaccine guidance said that “there is no evidence that antibodies formed from COVID-19 vaccination cause any problem with pregnancy, including the development of the placenta.”
The CDC is monitoring vaccinated people through its v-safe program and reported on April 12 that more than 86,000 v-safe participants said they were pregnant when they were vaccinated.
Health care workers who were nursing their infants when they were eligible for the vaccine faced a similar dilemma as pregnant women – they lacked the data on them to make a truly informed decision.
“I was nervous about the vaccine side effects for myself and whether my son Bennett, who was about a year old, would experience any of these himself,” said Christa Carrig, a labor and delivery nurse at Massachusetts General Hospital in Boston, who was breastfeeding at the time.
She and Dr. Parchem know that pregnant women with COVID-19 are more likely to have severe illness and complications such as high blood pressure and preterm delivery. “Pregnancy takes a toll on the body. When a woman gets COVID-19 and that insult is added, women who were otherwise young and healthy get much sicker than you would expect,” said Ms. Carrig.
“As a high-risk pregnancy specialist, I know that, with COVID, that babies don’t do well when moms are sick,” said Dr. Parchem.
Pregnant women accounted for more than 84,629 cases of COVID-19 and 95 deaths in the United States between Jan. 22 last year and April 12 this year, according to the CDC COVID data tracker.
Dr. Parchem and Ms. Carrig decided to get vaccinated because of their high risk of exposure to COVID-19 at work. After the second dose, Ms. Carrig reported chills but Bennett had no side effects from breastfeeding. Dr. Parchem, who delivered a healthy baby boy in February, reported no side effects other than a sore arm.
“There’s also a psychological benefit to returning to some sense of normalcy,” said Dr. Parchem. “My mother was finally able to visit us to see the new baby after we were all vaccinated. This was the first visit in more than a year.”
New study results
Ms. Carrig was one of 131 vaccinated hospital workers in the Boston area who took part in the first study to profile the immune response in pregnant and breastfeeding women and compare it with both nonpregnant and pregnant women who had COVID-19.
The study was not designed to evaluate the safety of the vaccines or whether they prevent COVID-19 illness and hospitalizations. That is the role of the large vaccine trials, the authors said.
The participants were aged 18-45 years and received both doses of either Pfizer or Moderna vaccines during one of their trimesters. They provided blood and/or breast milk samples after each vaccine dose, 2-6 weeks after the last dose, and at delivery for the 10 who gave birth during the study.
The vaccines produced a similar strong antibody response among the pregnant/breastfeeding women and nonpregnant women. Their antibody levels were much higher than those found in the pregnant women who had COVID-19, the researchers reported on March 25, 2021, in the American Journal of Obstetrics and Gynecology.
“This is important because a lot of people tend to think once they’ve had COVID-19, they are protected from the virus. This finding suggests that the vaccines produce a stronger antibody response than the infection itself, and this might be important for long-lasting protection against COVID-19,” said Dr. Parchem.
The study also addressed whether newborns benefit from the antibodies produced by their mothers. “In the 10 women who delivered, we detected antibodies in their umbilical cords and breast milk,” says Andrea Edlow, MD, lead researcher and a maternal-fetal medicine specialist at Massachusetts General Hospital.
Newborns are particularly vulnerable to respiratory infections because they have small airways and their immune systems are underdeveloped. These infections can be lethal early in life.
“The public health strategy is to vaccinate mothers against respiratory viruses, bacteria, and parasites that neonates up to 6 months are exposed to. Influenza and pertussis (whooping cough) are two examples of vaccines that we give mothers that we know transfer [antibodies] across the umbilical cord,” said Dr. Edlow.
But this “passive transfer immunity” is different from active immunity, when the body produces its own antibody immune response, she explains.
A different study, also published in March, confirmed that antibodies were transferred from 27 vaccinated pregnant mothers to their infants when they delivered. A new finding was that the women who were vaccinated with both doses and earlier in their third semester passed on more antibodies than the women who were vaccinated later or with only one dose.
Impact of the studies
The Society for Maternal-Fetal Medicine updated its guidance on counseling pregnant and lactating patients about the COVID-19 vaccines to include Dr. Edlow’s study.
“We were struck by how much pregnant and breastfeeding women want to participate in research and to help others in the same situation make decisions. I hope this will be an example to drug companies doing research on new vaccines in the future – that they should not be left behind and can make decisions themselves whether to participate after weighing the risks and benefits,” said Dr. Edlow.
She continues to enroll more vaccinated women in her study in the Boston area, including non–health care workers who have asked to take part.
“It was worth getting vaccinated and participating in the study. I know that I have antibodies and it worked and that I passed them on to Bennett. Also, I know that all the information is available for other women who are questioning whether to get vaccinated or not,” said Ms. Carrig.
Dr. Parchem is also taking part in the CDC’s v-safe pregnancy registry, which is collecting health and safety data on vaccinated pregnant women.
Before she was vaccinated, Dr. Parchem said, “my advice was very measured because we lacked data either saying that it definitely works or showing that it was unsafe. Now that we have this data supporting the benefits, I feel more confident in recommending the vaccines.”
A version of this article first appeared on Medscape.com.
As the U.S. races to vaccinate millions of people against the coronavirus, pregnant women face the extra challenge of not knowing whether the vaccines are safe for them or their unborn babies.
None of the recent COVID-19 vaccine trials, including those for Pfizer, Moderna, and Johnson & Johnson, enrolled pregnant or breastfeeding women because they consider them a high-risk group.
That was despite the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists asking that pregnant and breastfeeding women be included in trials. The Food and Drug Administration even included pregnant women in the COVID-19 vaccine emergency use authorization (EUA) because of their higher risk of having a more severe disease.
Despite that lack of clinical trial data, more and more smaller studies are suggesting that the vaccines are safe for both mother and child.
Pfizer is now studying its two-dose vaccine in 4,000 pregnant and breastfeeding women to see how safe, tolerated, and robust their immune response is. Researchers will also look at how safe the vaccine is for infants and whether mothers pass along antibodies to children. But the preliminary results won’t be available until the end of the year, a Pfizer spokesperson says.
Without that information, pregnant women are less likely to get vaccinated, according to a large international survey. Less than 45% of pregnant women in the United States said they intended to get vaccinated even when they were told the vaccine was safe and 90% effective. That figure rises to 52% of pregnant women in 16 countries, including the United States, compared with 74% of nonpregnant women willing to be vaccinated. The findings were published online March 1, 2021, in the European Journal of Epidemiology.
The vaccine-hesitant pregnant women in the international study were most concerned that the COVID-19 vaccine could harm their developing fetuses, a worry related to the lack of clinical evidence in pregnant women, said lead researcher Julia Wu, ScD, an epidemiologist at the Harvard School of Public Health’s Human Immunomics Initiative in Boston.
The information vacuum also increases the chances that “people will fall victim to misinformation campaigns like the one on social media that claims that the COVID-19 vaccine causes infertility,” Dr. Wu said. This unfounded claim has deterred some women of childbearing age from getting the vaccine.
Deciding to get vaccinated
Frontline health care professionals were in the first group eligible to receive the vaccine in December 2020. “All of us who were pregnant ... had to decide whether to wait for the data, because we don’t know what the risks are, or go ahead and get it [the vaccine]. We had been dealing with the pandemic for months and were afraid of being exposed to the virus and infecting family members,” said Jacqueline Parchem, MD, a maternal-fetal medicine specialist at the University of Texas Health Science Center, Houston.
Given the lack of safety data, the CDC guidance to pregnant women has been to consult with their doctors and that it’s a personal choice. The Center for Disease Control and Prevention’s latest vaccine guidance said that “there is no evidence that antibodies formed from COVID-19 vaccination cause any problem with pregnancy, including the development of the placenta.”
The CDC is monitoring vaccinated people through its v-safe program and reported on April 12 that more than 86,000 v-safe participants said they were pregnant when they were vaccinated.
Health care workers who were nursing their infants when they were eligible for the vaccine faced a similar dilemma as pregnant women – they lacked the data on them to make a truly informed decision.
“I was nervous about the vaccine side effects for myself and whether my son Bennett, who was about a year old, would experience any of these himself,” said Christa Carrig, a labor and delivery nurse at Massachusetts General Hospital in Boston, who was breastfeeding at the time.
She and Dr. Parchem know that pregnant women with COVID-19 are more likely to have severe illness and complications such as high blood pressure and preterm delivery. “Pregnancy takes a toll on the body. When a woman gets COVID-19 and that insult is added, women who were otherwise young and healthy get much sicker than you would expect,” said Ms. Carrig.
“As a high-risk pregnancy specialist, I know that, with COVID, that babies don’t do well when moms are sick,” said Dr. Parchem.
Pregnant women accounted for more than 84,629 cases of COVID-19 and 95 deaths in the United States between Jan. 22 last year and April 12 this year, according to the CDC COVID data tracker.
Dr. Parchem and Ms. Carrig decided to get vaccinated because of their high risk of exposure to COVID-19 at work. After the second dose, Ms. Carrig reported chills but Bennett had no side effects from breastfeeding. Dr. Parchem, who delivered a healthy baby boy in February, reported no side effects other than a sore arm.
“There’s also a psychological benefit to returning to some sense of normalcy,” said Dr. Parchem. “My mother was finally able to visit us to see the new baby after we were all vaccinated. This was the first visit in more than a year.”
New study results
Ms. Carrig was one of 131 vaccinated hospital workers in the Boston area who took part in the first study to profile the immune response in pregnant and breastfeeding women and compare it with both nonpregnant and pregnant women who had COVID-19.
The study was not designed to evaluate the safety of the vaccines or whether they prevent COVID-19 illness and hospitalizations. That is the role of the large vaccine trials, the authors said.
The participants were aged 18-45 years and received both doses of either Pfizer or Moderna vaccines during one of their trimesters. They provided blood and/or breast milk samples after each vaccine dose, 2-6 weeks after the last dose, and at delivery for the 10 who gave birth during the study.
The vaccines produced a similar strong antibody response among the pregnant/breastfeeding women and nonpregnant women. Their antibody levels were much higher than those found in the pregnant women who had COVID-19, the researchers reported on March 25, 2021, in the American Journal of Obstetrics and Gynecology.
“This is important because a lot of people tend to think once they’ve had COVID-19, they are protected from the virus. This finding suggests that the vaccines produce a stronger antibody response than the infection itself, and this might be important for long-lasting protection against COVID-19,” said Dr. Parchem.
The study also addressed whether newborns benefit from the antibodies produced by their mothers. “In the 10 women who delivered, we detected antibodies in their umbilical cords and breast milk,” says Andrea Edlow, MD, lead researcher and a maternal-fetal medicine specialist at Massachusetts General Hospital.
Newborns are particularly vulnerable to respiratory infections because they have small airways and their immune systems are underdeveloped. These infections can be lethal early in life.
“The public health strategy is to vaccinate mothers against respiratory viruses, bacteria, and parasites that neonates up to 6 months are exposed to. Influenza and pertussis (whooping cough) are two examples of vaccines that we give mothers that we know transfer [antibodies] across the umbilical cord,” said Dr. Edlow.
But this “passive transfer immunity” is different from active immunity, when the body produces its own antibody immune response, she explains.
A different study, also published in March, confirmed that antibodies were transferred from 27 vaccinated pregnant mothers to their infants when they delivered. A new finding was that the women who were vaccinated with both doses and earlier in their third semester passed on more antibodies than the women who were vaccinated later or with only one dose.
Impact of the studies
The Society for Maternal-Fetal Medicine updated its guidance on counseling pregnant and lactating patients about the COVID-19 vaccines to include Dr. Edlow’s study.
“We were struck by how much pregnant and breastfeeding women want to participate in research and to help others in the same situation make decisions. I hope this will be an example to drug companies doing research on new vaccines in the future – that they should not be left behind and can make decisions themselves whether to participate after weighing the risks and benefits,” said Dr. Edlow.
She continues to enroll more vaccinated women in her study in the Boston area, including non–health care workers who have asked to take part.
“It was worth getting vaccinated and participating in the study. I know that I have antibodies and it worked and that I passed them on to Bennett. Also, I know that all the information is available for other women who are questioning whether to get vaccinated or not,” said Ms. Carrig.
Dr. Parchem is also taking part in the CDC’s v-safe pregnancy registry, which is collecting health and safety data on vaccinated pregnant women.
Before she was vaccinated, Dr. Parchem said, “my advice was very measured because we lacked data either saying that it definitely works or showing that it was unsafe. Now that we have this data supporting the benefits, I feel more confident in recommending the vaccines.”
A version of this article first appeared on Medscape.com.
Helpful giant rodents and our old friend, the hookworm
Rat-ting out coronavirus
Did you know there is a possibility that giant rodents could rat out coronavirus? Not many people are keen on the presence of a 3-foot-long African giant pouched rat, but they have already been trained to sniff out diseases that are dangerous to humans, such as brucellosis and tuberculosis, according to researchers at the University of Glasgow.

Professor Dan Haydon and his associates believe there is a good possibility that the rats can be trained to sniff out COVID-19. Dogs have been helpful in sniffing for COVID-19 at airports and are being trained to detect it through armpit sweat, making detection of the virus easier for travelers and staff. Even robots have gotten into the COVID-19 detecting act.
Since African giant pouched rats can grow to be the size of a small dog and “are easily tamed as companion animals,” it seems likely that they have the potential to do the same. That is, sniffing for COVID-19, not appearing at your local airport. That’s still gross.
Stay healthy, get a parasite bestie
The key to health could actually be swimming around in your gut. Researchers from University College London have found that a parasitic worm could be the answer to longevity and avoidance of chronic diseases.
The seeming immunity from inflammatory diseases such as arthritis, diabetes, and multiple sclerosis may come from helminth parasites, or hookworms – parasites that have been coexisting harmlessly with the human body for thousands of years. The investigators went so far as to call them “old friends,” but the kind that you rarely see at reunions or call up for a favor.
As a result of modern sanitation and improved hygiene, humans and hookworms are seeing much less of each other, which may be a factor in the rise of “aging-associated inflammation” such as COVID-19 symptoms, they suggested. So is there a way to get these old friends back?
“Restorative hookworm treatments” could help with heart disease or dementia, according to the investigators, but maybe you’re not totally on board with getting an actual parasite in your system. We get it. There are helminth-derived proteins that have already been tested to get the job done.
Maybe old friends really do make the best friends.
I love the smell of microbe-infected aerosols in the morning
Have you gone into a public restroom and just stood around for a while appreciating the fine aromas? No? You haven’t? You do your business and get out? Well, it’s a good thing you act like a normal person, because the aerosols released when toilets flush can contain all sorts of nasty bacteria and viruses.

The authors of a new study published in Physics of Fluids came to this groundbreaking conclusion by going to a public bathroom, sticking particle counters above a urinal and a toilet, and letting them sit for a while. After 3 hours and 100 flushes, the ambient level of particles 0.3-3 mcm in diameter had increased dramatically, with particles sized 0.5-1 mcm particularly prone to lingering. For those particles, the level from baseline increased by over 200%.
This is a major concern, the researchers said, because the sort of microbes that are expelled through feces, urine, and vomit can include some pretty nasty things. Ebola, noroviruses that can cause food poisoning, and even good old SARS-CoV-2 can be expelled from the body but remain viable for a time in these aerosols. The researchers recommended improving the ventilation systems in restrooms so that aerosols don’t hang around for hours at a time. Plus, it might make the place not smell like a, uh, public restroom.
Not to question the research and the people behind it, but we’re not sure how necessary it was to give people another reason not to hang out in a place where hundreds, if not thousands, of people come to relieve themselves. There’s a reason we’re supposed to “stop and smell the roses” and not “stop and smell the public bathroom.”
World ends not with a bang but with a cheeseburger
Speaking of old sayings, one of our favorites, “You are what you eat,” may offer a culinary explanation for those who do enjoy the ambiance of a fine, aerosol-infested public restroom.
That explanation involves the high-calorie, high-fat smorgasbord known as the Western diet and some mice who were forced to consume it. Those mice, it turns out, were more anxious and less cognitively advanced than their counterparts who were not eating “highly palatable, energy dense foods (e.g., high saturated fat, high sugar) that are commonly consumed by humans,” according to the authors of a recent literature review.
“Consumption of a Western diet is related to poorer cognitive performance across the lifespan,” the investigators said, adding that consumption of a Western diet “during critical early life stages of development has negative consequences on various cognitive abilities later in adulthood.”
To show their appreciation for the sacrifices these brave test subjects had made in the name of science, the scientists released the Western diet–addled rodents from captivity. Not only did they survive and thrive in the wilds of darkest suburbia, but within 6 months almost half of them were running for Congress.
Rat-ting out coronavirus
Did you know there is a possibility that giant rodents could rat out coronavirus? Not many people are keen on the presence of a 3-foot-long African giant pouched rat, but they have already been trained to sniff out diseases that are dangerous to humans, such as brucellosis and tuberculosis, according to researchers at the University of Glasgow.
Professor Dan Haydon and his associates believe there is a good possibility that the rats can be trained to sniff out COVID-19. Dogs have been helpful in sniffing for COVID-19 at airports and are being trained to detect it through armpit sweat, making detection of the virus easier for travelers and staff. Even robots have gotten into the COVID-19 detecting act.
Since African giant pouched rats can grow to be the size of a small dog and “are easily tamed as companion animals,” it seems likely that they have the potential to do the same. That is, sniffing for COVID-19, not appearing at your local airport. That’s still gross.
Stay healthy, get a parasite bestie
The key to health could actually be swimming around in your gut. Researchers from University College London have found that a parasitic worm could be the answer to longevity and avoidance of chronic diseases.
The seeming immunity from inflammatory diseases such as arthritis, diabetes, and multiple sclerosis may come from helminth parasites, or hookworms – parasites that have been coexisting harmlessly with the human body for thousands of years. The investigators went so far as to call them “old friends,” but the kind that you rarely see at reunions or call up for a favor.
As a result of modern sanitation and improved hygiene, humans and hookworms are seeing much less of each other, which may be a factor in the rise of “aging-associated inflammation” such as COVID-19 symptoms, they suggested. So is there a way to get these old friends back?
“Restorative hookworm treatments” could help with heart disease or dementia, according to the investigators, but maybe you’re not totally on board with getting an actual parasite in your system. We get it. There are helminth-derived proteins that have already been tested to get the job done.
Maybe old friends really do make the best friends.
I love the smell of microbe-infected aerosols in the morning
Have you gone into a public restroom and just stood around for a while appreciating the fine aromas? No? You haven’t? You do your business and get out? Well, it’s a good thing you act like a normal person, because the aerosols released when toilets flush can contain all sorts of nasty bacteria and viruses.
The authors of a new study published in Physics of Fluids came to this groundbreaking conclusion by going to a public bathroom, sticking particle counters above a urinal and a toilet, and letting them sit for a while. After 3 hours and 100 flushes, the ambient level of particles 0.3-3 mcm in diameter had increased dramatically, with particles sized 0.5-1 mcm particularly prone to lingering. For those particles, the level from baseline increased by over 200%.
This is a major concern, the researchers said, because the sort of microbes that are expelled through feces, urine, and vomit can include some pretty nasty things. Ebola, noroviruses that can cause food poisoning, and even good old SARS-CoV-2 can be expelled from the body but remain viable for a time in these aerosols. The researchers recommended improving the ventilation systems in restrooms so that aerosols don’t hang around for hours at a time. Plus, it might make the place not smell like a, uh, public restroom.
Not to question the research and the people behind it, but we’re not sure how necessary it was to give people another reason not to hang out in a place where hundreds, if not thousands, of people come to relieve themselves. There’s a reason we’re supposed to “stop and smell the roses” and not “stop and smell the public bathroom.”
World ends not with a bang but with a cheeseburger
Speaking of old sayings, one of our favorites, “You are what you eat,” may offer a culinary explanation for those who do enjoy the ambiance of a fine, aerosol-infested public restroom.
That explanation involves the high-calorie, high-fat smorgasbord known as the Western diet and some mice who were forced to consume it. Those mice, it turns out, were more anxious and less cognitively advanced than their counterparts who were not eating “highly palatable, energy dense foods (e.g., high saturated fat, high sugar) that are commonly consumed by humans,” according to the authors of a recent literature review.
“Consumption of a Western diet is related to poorer cognitive performance across the lifespan,” the investigators said, adding that consumption of a Western diet “during critical early life stages of development has negative consequences on various cognitive abilities later in adulthood.”
To show their appreciation for the sacrifices these brave test subjects had made in the name of science, the scientists released the Western diet–addled rodents from captivity. Not only did they survive and thrive in the wilds of darkest suburbia, but within 6 months almost half of them were running for Congress.
Rat-ting out coronavirus
Did you know there is a possibility that giant rodents could rat out coronavirus? Not many people are keen on the presence of a 3-foot-long African giant pouched rat, but they have already been trained to sniff out diseases that are dangerous to humans, such as brucellosis and tuberculosis, according to researchers at the University of Glasgow.
Professor Dan Haydon and his associates believe there is a good possibility that the rats can be trained to sniff out COVID-19. Dogs have been helpful in sniffing for COVID-19 at airports and are being trained to detect it through armpit sweat, making detection of the virus easier for travelers and staff. Even robots have gotten into the COVID-19 detecting act.
Since African giant pouched rats can grow to be the size of a small dog and “are easily tamed as companion animals,” it seems likely that they have the potential to do the same. That is, sniffing for COVID-19, not appearing at your local airport. That’s still gross.
Stay healthy, get a parasite bestie
The key to health could actually be swimming around in your gut. Researchers from University College London have found that a parasitic worm could be the answer to longevity and avoidance of chronic diseases.
The seeming immunity from inflammatory diseases such as arthritis, diabetes, and multiple sclerosis may come from helminth parasites, or hookworms – parasites that have been coexisting harmlessly with the human body for thousands of years. The investigators went so far as to call them “old friends,” but the kind that you rarely see at reunions or call up for a favor.
As a result of modern sanitation and improved hygiene, humans and hookworms are seeing much less of each other, which may be a factor in the rise of “aging-associated inflammation” such as COVID-19 symptoms, they suggested. So is there a way to get these old friends back?
“Restorative hookworm treatments” could help with heart disease or dementia, according to the investigators, but maybe you’re not totally on board with getting an actual parasite in your system. We get it. There are helminth-derived proteins that have already been tested to get the job done.
Maybe old friends really do make the best friends.
I love the smell of microbe-infected aerosols in the morning
Have you gone into a public restroom and just stood around for a while appreciating the fine aromas? No? You haven’t? You do your business and get out? Well, it’s a good thing you act like a normal person, because the aerosols released when toilets flush can contain all sorts of nasty bacteria and viruses.
The authors of a new study published in Physics of Fluids came to this groundbreaking conclusion by going to a public bathroom, sticking particle counters above a urinal and a toilet, and letting them sit for a while. After 3 hours and 100 flushes, the ambient level of particles 0.3-3 mcm in diameter had increased dramatically, with particles sized 0.5-1 mcm particularly prone to lingering. For those particles, the level from baseline increased by over 200%.
This is a major concern, the researchers said, because the sort of microbes that are expelled through feces, urine, and vomit can include some pretty nasty things. Ebola, noroviruses that can cause food poisoning, and even good old SARS-CoV-2 can be expelled from the body but remain viable for a time in these aerosols. The researchers recommended improving the ventilation systems in restrooms so that aerosols don’t hang around for hours at a time. Plus, it might make the place not smell like a, uh, public restroom.
Not to question the research and the people behind it, but we’re not sure how necessary it was to give people another reason not to hang out in a place where hundreds, if not thousands, of people come to relieve themselves. There’s a reason we’re supposed to “stop and smell the roses” and not “stop and smell the public bathroom.”
World ends not with a bang but with a cheeseburger
Speaking of old sayings, one of our favorites, “You are what you eat,” may offer a culinary explanation for those who do enjoy the ambiance of a fine, aerosol-infested public restroom.
That explanation involves the high-calorie, high-fat smorgasbord known as the Western diet and some mice who were forced to consume it. Those mice, it turns out, were more anxious and less cognitively advanced than their counterparts who were not eating “highly palatable, energy dense foods (e.g., high saturated fat, high sugar) that are commonly consumed by humans,” according to the authors of a recent literature review.
“Consumption of a Western diet is related to poorer cognitive performance across the lifespan,” the investigators said, adding that consumption of a Western diet “during critical early life stages of development has negative consequences on various cognitive abilities later in adulthood.”
To show their appreciation for the sacrifices these brave test subjects had made in the name of science, the scientists released the Western diet–addled rodents from captivity. Not only did they survive and thrive in the wilds of darkest suburbia, but within 6 months almost half of them were running for Congress.

The neurology of long-haul COVID-19
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.

Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.

Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.
Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.
Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.
Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.
Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
FROM AAN 2021
US methods of delivery, a snapshot
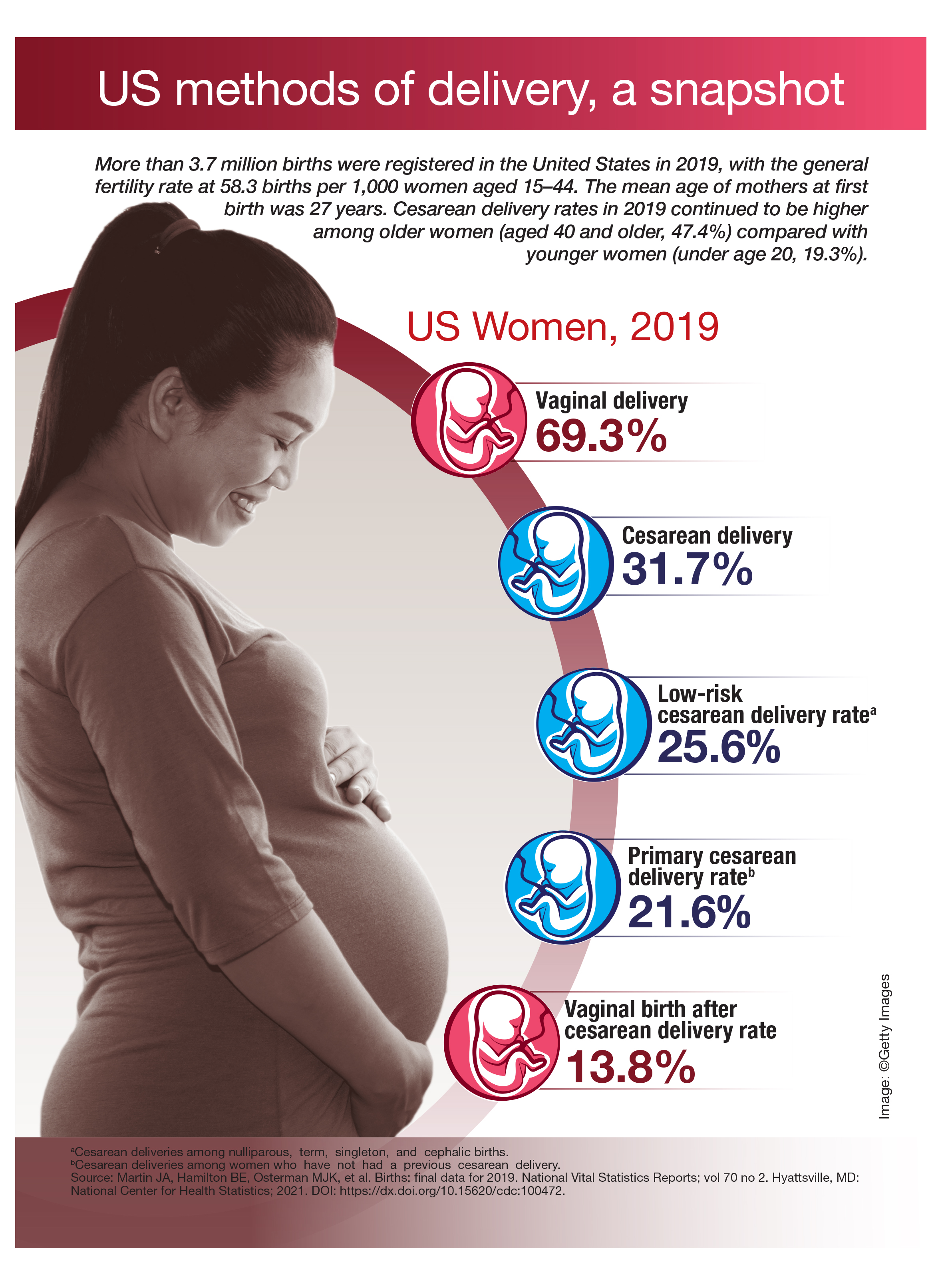
PTSD linked to ischemic heart disease
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.
A study using data from Veterans Health Administration (VHA) electronic medical records shows a significant association between posttraumatic stress disorder (PTSD) among female veterans and an increased risk for incident ischemic heart disease (IHD).
The increased risk for IHD was highest among women younger than 40 with PTSD, and among racial and ethnic minorities.
“These women have been emerging as important targets for cardiovascular prevention, and our study suggests that PTSD may be an important psychosocial risk factor for IHD in these individuals,” wrote the researchers, led by Ramin Ebrahimi, MD, department of medicine, cardiology section, Veterans Affairs Greater Los Angeles Health Care System. “With the number of women veterans growing, it is critical to appreciate the health care needs of this relatively young and diverse patient population.”
The study results also have “important implications for earlier and more aggressive IHD risk assessment, monitoring and management in vulnerable women veterans,” they added. “Indeed, our findings support recent calls for cardiovascular risk screening in younger individuals and for the need to harness a broad range of clinicians who routinely treat younger women to maximize prevention efforts.”
The article was published online in JAMA Cardiology on March 17.
Increasing number of VHA users
“As an interventional cardiologist and the director of the cardiac catheterization laboratory, I noticed a significant number of the patients referred to the cath lab carried a diagnosis of posttraumatic stress disorder,” Dr. Ebrahimi said in an interview. “This intrigued me and started my journey into trying to understand how psychiatric disorders in general, and PTSD, may impact/interact with cardiovascular disorders,” he added.
The number of female veterans in the military has been increasing, and they now make up about 10% of the 20 million American veterans; that number is projected to exceed 2.2 million in the next 20 years, the authors wrote. Female veterans are also the fastest growing group of users of the VHA, they added.
IHD is the leading cause of death in women in the United States, despite the advancements in prevention and treatment. Although women are twice as likely to develop PTSD as are men, and it is even more likely in female veterans, much of the research has predominately been on male veterans, the authors wrote.
For this retrospective study, which used data from the VHA Corporate Data Warehouse, the authors examined a cohort of female veterans who were 18 years or older who had used the VHA health care system between Jan. 1, 2000, and Dec. 31, 2017.
Of the 828,997 female veterans, 151,030 had PTSD. Women excluded from the study were those who did not have any clinical encounters after their index visit, participants who had a diagnosis of IHD at or before the index visit, and those with incident IHD within 90 days of the index visit, allowing time between a PTSD diagnosis and IHD.
Propensity score matching on age at index visit, the number of previous visits, and the presence of traditional and female-specific cardiovascular risk factors, as well as mental and physical health conditions, was conducted to identify female veterans ever diagnosed with PTSD, who were matched in a 1:2 ratio to those never diagnosed with PTSD. In all, 132,923 women with PTSD and 265,846 women without PTSD were included, and data were analyzed for the period of Oct. 1, 2018, to Oct. 30, 2020.
IHD was defined as new-onset coronary artery disease, angina, or myocardial infarction–based ICD-9 and ICD-10 diagnostic codes. Age, race, and ethnicity were self-reported.
The analytic sample consisted of relatively young female veterans (mean [SD] age at baseline, 40.1 [12.2] years) of various races (White, 57.6%; Black, 29.8%) and ethnicities, the authors reported.
Of the 9,940 women who experienced incident IHD during follow-up, 5,559 did not have PTSD (2.1% of the overall population examined) and 4,381 had PTSD (3.3%). PTSD was significantly associated with an increased risk for IHD. Over the median follow-up of 4.9 years, female veterans with PTSD had a 44% higher rate of developing incident IHD compared with the female veterans without PTSD (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.38-1.50).
In addition, those with PTSD who developed IHD were younger at diagnosis (mean [SD] age, 55.5 [9.7]) than were patients without PTSD (mean [SD] age, 57.8 [10.7]). Effect sizes were largest in the group younger than 40 years (HR, 1.72; 95% CI, 1.55-1.90) and decreased for older participants (HR for those ≥60 years, 1.24; 95% CI, 1.12-1.38)
The authors found a 49% to 66% increase in risk for IHD associated with PTSD in Black women (HR, 1.49; 95% CI, 1.38-1.62) and those identified as non-White and non-Black (HR, 1.66; 95%, 1.33-2.08).
Women of all ethnic groups with PTSD were at higher risk of developing IHD, but this was especially true for Hispanic/Latina women (HR, 1.50; 95% CI 1.22-1.84), they noted.
The authors reported some limitations to their findings. The analytic sample could result in a lower ascertainment of certain conditions, such as psychiatric disorders, they wrote. Substance disorders were low in this study, possibly because of the younger age of female veterans in the sample. Because this study used VHA electronic medical records data, medical care outside of the VHA that was not paid for by the VHA could not be considered.
In addition, although this study used a large sample of female veterans, the findings cannot be generalized to female veterans outside of the VHA system, nonveteran women, or men, the researchers wrote.
A call to action
In an accompanying comment, Beth E. Cohen, MD, of the University of California, San Francisco, and the San Francisco Veterans Affairs Health Care System, points out that the physical implications for psychosocial conditions, including depression and PTSD, have been recognized for quite some time. For example, results of the INTERHEART case-control study of 30,000 people showed stress, depression, and stressful life events accounted for one-third the population-attributable risk for myocardial infarction.
As was also noted by Dr. Ebrahimi and colleagues, much of the current research has been on male veterans, yet types of trauma differ among genders; women experience higher rates of military sexual trauma but lower rates of combat trauma, Dr. Cohen wrote. The PTSD symptoms, trajectory, and biological effects can differ for women and men, as can the pathogenesis, presentation, and outcomes of cardiovascular disease (CVD).
These findings, she said, “are an important extension of the prior literature and represent the largest study in female veterans to date. Although methods differ across studies, the magnitude of risk associated with PTSD was consistent with that found in prior studies of male veterans and nonveteran samples.”
The assessment of age-specific risk is also a strength of the study, “and has implications for clinical practice, because PTSD-associated risk was greatest in a younger group in whom CVD may be overlooked.”
Dr. Cohen addressed the limitations outlined by the authors, including ascertainment bias, severity of PTSD symptoms, and their chronicity, but added that “even in the context of these limitations, this study illustrates the importance of PTSD to the health of women veterans and the additional work needed to reduce their CVD risk.”
Clinical questions remain, she added. Screens for PTSD are widely used in the VHA, yet no studies have examined whether screening or early detection decrease CVD risk. In addition, no evidence suggests that screening for or treatment of PTSD improves cardiovascular outcomes.
“Given the challenges of answering these questions in observational studies, it will be important to incorporate measures of CVD risk and outcomes in trials of behavioral and medical therapies for patients with PTSD,” she wrote.
She added that collaborations among multidisciplinary patient care teams will be important. “The findings of this study represent a call to action for this important work to understand the cardiovascular effects of PTSD and improve the health and well-being of women veterans,” Dr. Cohen concluded.
This research was supported by Investigator-Initiated Research Award from the Department of Defense U.S. Army Medical Research and Material Command Congressionally Directed Medical Research Programs (Dr. Ebrahimi) and in part by grants from the VA Informatics and Computing Infrastructure and the Offices of Research and Development at the Northport, Durham, and Greater Los Angeles Veterans Affairs medical centers. Dr. Ebrahimi reported receiving grants from the Department of Defense during the conduct of the study. Disclosures for other authors are available in the paper. Dr. Cohen reports no disclosures.
A version of this article first appeared on Medscape.com.