User login
Annual reviewers list
We deeply appreciate the involvement of our reviewers who made the Journal of Hospital Medicine so successful in its first year. Listed below are the many reviewers and volume of their contributions. They have our sincere gratitude.
Reviewed 4 or More Articles
Eric Alper (6)
David Anthony (4)
Vineet Arora (4)
Thomas E. Baudendistel (11)
Daniel J. Brotman (7)
Vincent W. Chiang (5)
Eugene Shu‐Sen Chu (5)
Gurpreet Dhaliwal (7)
Lorenzo Di Francesco (4)
Andras Fenyves (4)
Stacy Fischer (5)
Kathlyn Fletcher (5)
Philip H. Goodman (4)
Carolyn Gould (4)
Jeffrey L. Greenwald (6)
Lakshmi Halasyamani (4)
Brian Harte (13)
Christopher P. Landrigan (5)
Peter K. Lindenauer (4)
Greg Maynard (7)
Sylvia Cheney McKean (4)
Thomas Aquinas Murphy (4)
James C. Pile (9)
Thomas Price (4)
Sumant Ranji (8)
Bradley Allen Sharpe (4)
Jason Stein (7)
Robin Tricoles (9)
Guillermo E. Umpierrez (5)
Arpana Vidyarthi (6)
Heidi Wald (7)
David Wesorick (4)
Reviewed 3 Articles
Ron G. Angus
Paul Aronowitz
Vanitha Bala
Jennifer Best
Cynthia Jean Brown
Gregory Bump
Hugo Quinny Cheng
Eva Chittenden
Eric Coleman
Curtiss B. Cook
Edward Etchells
Alan John Forster
Roma Y. Gianchandani
Leslie W. Hall
Jennifer Hanrahan
Amir K. Jaffer
Peter John Kaboli
Jennifer Kapo
Dennis Manning
Constantine Manthous
Janet Nagamine
Kevin J. O'Leary
Brian Michael Pate
Robert C. Pendleton
Jeffrey Lawrence Schnipper
Hasan Shabbir
James Edwin Stone
Chad Whelan
Audrey Young
Reviewed 2 Articles
Drew Abernathy
Stephen J. Bekanich
Paul Cantey
Kerry Cho
Patrick Conway
Jasminka Criley
Catherine Curley
Jennifer Daru
Catherine F. Decker
Andrew Paul DeFilippis
Daniel J. DiBona
Mark Earnest
Douglas Einstadter
Margaret Fang
Jonathan M. Flacker
Bradley Evan Flansbaum
Michael Frankel
Jeffrey Glasheen
Amir H. Hamrahian
Karen E. Hauer
Eric Edwin Howell
Carlos Manuel Isada
Christopher Seoung Kim
Sunil Kripalani
Jean S. Kutner
Cindy Lai
Janet Larson
David Likosky
David Ling
Michelle Magee
Navneet Majhail
Michael Matheny
George Mathew
Govardhanan Nagaiah
James Newman
Christopher Ohl
Shawn Ralston
Daniel A. Rauch
John James Ross
Joel Rubenstein
David Schulman
Kaveh G. Shojania
Gregory Randall Smith Jr.
Peter Youngers Watson
Chad T. Whelan
Neil Winawer
Scott Wright
Reviewed 1 Article
Adebola Adesanya
Nasim Afsarmanesh
Richard Keith Albert
Mel L. Anderson, III
Wendy Artrong
Thomas W. Barrett
David Bar‐Shain
Marc Baskin
Brent Beasley
Thomas Bookwalter
Susan S. Braithwaite
Beril Caker
Douglas Carlson
Alison Chantal Caviness
Steven L. Cohn
Yvette Marie Cua
Russ Cucina
Ethan Ulysses Cumbler
Mellar Davis
Allan S. Detsky
Jeffrey Randolph Dichter
Thomas Donner
Daniel David Dressler
Erin Egan
Matthew Eisen
Kenneth Richard Epstein
Leslie Fall
Shaun Uiglas Frost
Michael Sebastian Galin
Matthew Garber
Rajesh Garg
Raminder Singh Gill
Jackie Glover
Adrienne Green
Paul Hain
Braden Hale
Sajeev Handa
Julie Hauer
Michael Heisler
Jeanne M. Huddleston
Alan J. Hunter
Kevin Hwang
Brian Jack
Ian Harold Jenkins
Kurien John
Daniel Johnson
Todd Joyner
Deepa Kabirdas
Allen Kachalia
Abel Ngo Kho
Steven Jay Kravet
Marco Aurelio Ladino
Robert Lash
Joshua Lee
Sei Lee
Arthur Jefferson Lesesne
Marcia Levetown
Luci Leykum
Joshua David Liberman
Jonathan Mansbach
Brian Markoff
David Meltzer
Anna Leco Merca
Barbara Messinger‐Rapport
Gregory Misky
William Moran
Brahmajee Nallamothu
Theore Elliott Nash
Heather Nye
Timothy O'Brien
Bruce Ovbiagele
Thomas Andrew Owens
Mary Pak
Steven Zvi Pantilat
Vikas Parekh
Kimberly Rask
Michael Rothberg
Hilary F. Ryder
Wael Saber
Sanjay Saint
Rene Salazar
Kaycee Sink
N. Smith
Malathi Srinivasin
Raj Srivastava
Erin Stucky
Alexander Turchin
Bobbak Vahid
Robert Wachter
Robert L. Wears
Howard Weitz
Winthrop Whitcomb
Mark V. Williams
Sherrie Williams
David Woods
We deeply appreciate the involvement of our reviewers who made the Journal of Hospital Medicine so successful in its first year. Listed below are the many reviewers and volume of their contributions. They have our sincere gratitude.
Reviewed 4 or More Articles
Eric Alper (6)
David Anthony (4)
Vineet Arora (4)
Thomas E. Baudendistel (11)
Daniel J. Brotman (7)
Vincent W. Chiang (5)
Eugene Shu‐Sen Chu (5)
Gurpreet Dhaliwal (7)
Lorenzo Di Francesco (4)
Andras Fenyves (4)
Stacy Fischer (5)
Kathlyn Fletcher (5)
Philip H. Goodman (4)
Carolyn Gould (4)
Jeffrey L. Greenwald (6)
Lakshmi Halasyamani (4)
Brian Harte (13)
Christopher P. Landrigan (5)
Peter K. Lindenauer (4)
Greg Maynard (7)
Sylvia Cheney McKean (4)
Thomas Aquinas Murphy (4)
James C. Pile (9)
Thomas Price (4)
Sumant Ranji (8)
Bradley Allen Sharpe (4)
Jason Stein (7)
Robin Tricoles (9)
Guillermo E. Umpierrez (5)
Arpana Vidyarthi (6)
Heidi Wald (7)
David Wesorick (4)
Reviewed 3 Articles
Ron G. Angus
Paul Aronowitz
Vanitha Bala
Jennifer Best
Cynthia Jean Brown
Gregory Bump
Hugo Quinny Cheng
Eva Chittenden
Eric Coleman
Curtiss B. Cook
Edward Etchells
Alan John Forster
Roma Y. Gianchandani
Leslie W. Hall
Jennifer Hanrahan
Amir K. Jaffer
Peter John Kaboli
Jennifer Kapo
Dennis Manning
Constantine Manthous
Janet Nagamine
Kevin J. O'Leary
Brian Michael Pate
Robert C. Pendleton
Jeffrey Lawrence Schnipper
Hasan Shabbir
James Edwin Stone
Chad Whelan
Audrey Young
Reviewed 2 Articles
Drew Abernathy
Stephen J. Bekanich
Paul Cantey
Kerry Cho
Patrick Conway
Jasminka Criley
Catherine Curley
Jennifer Daru
Catherine F. Decker
Andrew Paul DeFilippis
Daniel J. DiBona
Mark Earnest
Douglas Einstadter
Margaret Fang
Jonathan M. Flacker
Bradley Evan Flansbaum
Michael Frankel
Jeffrey Glasheen
Amir H. Hamrahian
Karen E. Hauer
Eric Edwin Howell
Carlos Manuel Isada
Christopher Seoung Kim
Sunil Kripalani
Jean S. Kutner
Cindy Lai
Janet Larson
David Likosky
David Ling
Michelle Magee
Navneet Majhail
Michael Matheny
George Mathew
Govardhanan Nagaiah
James Newman
Christopher Ohl
Shawn Ralston
Daniel A. Rauch
John James Ross
Joel Rubenstein
David Schulman
Kaveh G. Shojania
Gregory Randall Smith Jr.
Peter Youngers Watson
Chad T. Whelan
Neil Winawer
Scott Wright
Reviewed 1 Article
Adebola Adesanya
Nasim Afsarmanesh
Richard Keith Albert
Mel L. Anderson, III
Wendy Artrong
Thomas W. Barrett
David Bar‐Shain
Marc Baskin
Brent Beasley
Thomas Bookwalter
Susan S. Braithwaite
Beril Caker
Douglas Carlson
Alison Chantal Caviness
Steven L. Cohn
Yvette Marie Cua
Russ Cucina
Ethan Ulysses Cumbler
Mellar Davis
Allan S. Detsky
Jeffrey Randolph Dichter
Thomas Donner
Daniel David Dressler
Erin Egan
Matthew Eisen
Kenneth Richard Epstein
Leslie Fall
Shaun Uiglas Frost
Michael Sebastian Galin
Matthew Garber
Rajesh Garg
Raminder Singh Gill
Jackie Glover
Adrienne Green
Paul Hain
Braden Hale
Sajeev Handa
Julie Hauer
Michael Heisler
Jeanne M. Huddleston
Alan J. Hunter
Kevin Hwang
Brian Jack
Ian Harold Jenkins
Kurien John
Daniel Johnson
Todd Joyner
Deepa Kabirdas
Allen Kachalia
Abel Ngo Kho
Steven Jay Kravet
Marco Aurelio Ladino
Robert Lash
Joshua Lee
Sei Lee
Arthur Jefferson Lesesne
Marcia Levetown
Luci Leykum
Joshua David Liberman
Jonathan Mansbach
Brian Markoff
David Meltzer
Anna Leco Merca
Barbara Messinger‐Rapport
Gregory Misky
William Moran
Brahmajee Nallamothu
Theore Elliott Nash
Heather Nye
Timothy O'Brien
Bruce Ovbiagele
Thomas Andrew Owens
Mary Pak
Steven Zvi Pantilat
Vikas Parekh
Kimberly Rask
Michael Rothberg
Hilary F. Ryder
Wael Saber
Sanjay Saint
Rene Salazar
Kaycee Sink
N. Smith
Malathi Srinivasin
Raj Srivastava
Erin Stucky
Alexander Turchin
Bobbak Vahid
Robert Wachter
Robert L. Wears
Howard Weitz
Winthrop Whitcomb
Mark V. Williams
Sherrie Williams
David Woods
We deeply appreciate the involvement of our reviewers who made the Journal of Hospital Medicine so successful in its first year. Listed below are the many reviewers and volume of their contributions. They have our sincere gratitude.
Reviewed 4 or More Articles
Eric Alper (6)
David Anthony (4)
Vineet Arora (4)
Thomas E. Baudendistel (11)
Daniel J. Brotman (7)
Vincent W. Chiang (5)
Eugene Shu‐Sen Chu (5)
Gurpreet Dhaliwal (7)
Lorenzo Di Francesco (4)
Andras Fenyves (4)
Stacy Fischer (5)
Kathlyn Fletcher (5)
Philip H. Goodman (4)
Carolyn Gould (4)
Jeffrey L. Greenwald (6)
Lakshmi Halasyamani (4)
Brian Harte (13)
Christopher P. Landrigan (5)
Peter K. Lindenauer (4)
Greg Maynard (7)
Sylvia Cheney McKean (4)
Thomas Aquinas Murphy (4)
James C. Pile (9)
Thomas Price (4)
Sumant Ranji (8)
Bradley Allen Sharpe (4)
Jason Stein (7)
Robin Tricoles (9)
Guillermo E. Umpierrez (5)
Arpana Vidyarthi (6)
Heidi Wald (7)
David Wesorick (4)
Reviewed 3 Articles
Ron G. Angus
Paul Aronowitz
Vanitha Bala
Jennifer Best
Cynthia Jean Brown
Gregory Bump
Hugo Quinny Cheng
Eva Chittenden
Eric Coleman
Curtiss B. Cook
Edward Etchells
Alan John Forster
Roma Y. Gianchandani
Leslie W. Hall
Jennifer Hanrahan
Amir K. Jaffer
Peter John Kaboli
Jennifer Kapo
Dennis Manning
Constantine Manthous
Janet Nagamine
Kevin J. O'Leary
Brian Michael Pate
Robert C. Pendleton
Jeffrey Lawrence Schnipper
Hasan Shabbir
James Edwin Stone
Chad Whelan
Audrey Young
Reviewed 2 Articles
Drew Abernathy
Stephen J. Bekanich
Paul Cantey
Kerry Cho
Patrick Conway
Jasminka Criley
Catherine Curley
Jennifer Daru
Catherine F. Decker
Andrew Paul DeFilippis
Daniel J. DiBona
Mark Earnest
Douglas Einstadter
Margaret Fang
Jonathan M. Flacker
Bradley Evan Flansbaum
Michael Frankel
Jeffrey Glasheen
Amir H. Hamrahian
Karen E. Hauer
Eric Edwin Howell
Carlos Manuel Isada
Christopher Seoung Kim
Sunil Kripalani
Jean S. Kutner
Cindy Lai
Janet Larson
David Likosky
David Ling
Michelle Magee
Navneet Majhail
Michael Matheny
George Mathew
Govardhanan Nagaiah
James Newman
Christopher Ohl
Shawn Ralston
Daniel A. Rauch
John James Ross
Joel Rubenstein
David Schulman
Kaveh G. Shojania
Gregory Randall Smith Jr.
Peter Youngers Watson
Chad T. Whelan
Neil Winawer
Scott Wright
Reviewed 1 Article
Adebola Adesanya
Nasim Afsarmanesh
Richard Keith Albert
Mel L. Anderson, III
Wendy Artrong
Thomas W. Barrett
David Bar‐Shain
Marc Baskin
Brent Beasley
Thomas Bookwalter
Susan S. Braithwaite
Beril Caker
Douglas Carlson
Alison Chantal Caviness
Steven L. Cohn
Yvette Marie Cua
Russ Cucina
Ethan Ulysses Cumbler
Mellar Davis
Allan S. Detsky
Jeffrey Randolph Dichter
Thomas Donner
Daniel David Dressler
Erin Egan
Matthew Eisen
Kenneth Richard Epstein
Leslie Fall
Shaun Uiglas Frost
Michael Sebastian Galin
Matthew Garber
Rajesh Garg
Raminder Singh Gill
Jackie Glover
Adrienne Green
Paul Hain
Braden Hale
Sajeev Handa
Julie Hauer
Michael Heisler
Jeanne M. Huddleston
Alan J. Hunter
Kevin Hwang
Brian Jack
Ian Harold Jenkins
Kurien John
Daniel Johnson
Todd Joyner
Deepa Kabirdas
Allen Kachalia
Abel Ngo Kho
Steven Jay Kravet
Marco Aurelio Ladino
Robert Lash
Joshua Lee
Sei Lee
Arthur Jefferson Lesesne
Marcia Levetown
Luci Leykum
Joshua David Liberman
Jonathan Mansbach
Brian Markoff
David Meltzer
Anna Leco Merca
Barbara Messinger‐Rapport
Gregory Misky
William Moran
Brahmajee Nallamothu
Theore Elliott Nash
Heather Nye
Timothy O'Brien
Bruce Ovbiagele
Thomas Andrew Owens
Mary Pak
Steven Zvi Pantilat
Vikas Parekh
Kimberly Rask
Michael Rothberg
Hilary F. Ryder
Wael Saber
Sanjay Saint
Rene Salazar
Kaycee Sink
N. Smith
Malathi Srinivasin
Raj Srivastava
Erin Stucky
Alexander Turchin
Bobbak Vahid
Robert Wachter
Robert L. Wears
Howard Weitz
Winthrop Whitcomb
Mark V. Williams
Sherrie Williams
David Woods
Fixed‐dose, subcutaneous, unfractionated heparin effective for VTE
-
CLINICAL QUESTION: How safe and effective is fixed‐dose subcutaneous unfractionated heparin in the treatment of venous thromboembolism?
-
BOTTOM LINE: In this study, fixed‐dose weight‐adjusted unfractionated heparin (UFH) administered subcutaneously was as safe and effective as low‐molecular‐weight heparin (LMWH) in the treatment of venous thromboembolism (VTE). Estimated drug costs for a 6‐day course are $712 for LMWH and $37 for UFH. Most clinicians will want to see similar results from at least 1 additional well‐done clinical trial, including more patients with symptomatic pulmonary embolism, before routinely treating VTE with subcutaneous UFH. (LOE = 1b)
-
REFERENCE: Kearon C, Ginsberg JS, Julian JA, et al, for the Fixed‐Dose Heparin (FIDO) Investigators. Comparison of fixed‐dose weight‐adjusted unfractionated heparin and low‐molecular‐weight heparin for acute treatment of venous thromboembolism. JAMA 2006;296:935‐942.
-
STUDY DESIGN: Randomized controlled trial (single‐blinded)
-
FUNDING: Foundation
-
SETTING: Outpatient (any)
-
ALLOCATION: Concealed
-
SYNOPSIS: These investigators randomly assigned (concealed allocation assignment) 708 patients, 18 years or older, with acute VTE to subcutaneous UFH (initial dose of 333 U/kg, followed by a fixed dose of 250 U/kg every 12 hours) or LMWH (dalteparin or enoxaparin, 100 IU/kg every 12 hours). The dose of subcutaneous UFH remained fixed for individual patients and was not changed during treatment as a result of anticoagulation profiles. The diagnosis of VTE included patients with acute deep vein thrombosis of the legs (81%) or symptomatic pulmonary embolism (19%). Oral warfarin was usually started on the same day as heparin in both groups and continued for a minimum of 3 months with doses adjusted to achieve an international normalized ratio (INR) of between 2.0 and 3.0. Heparin was continued for at least 5 days and until the INR was 2.0 or higher for 2 consecutive days. Individuals unaware of treatment group assignment assessed all outcomes, including study eligibility criteria. Follow‐up occurred for more than 98% of subjects for 3 months. All eligible and consenting patients underwent final data analysis. The risk of recurrent VTE in the first 3 months after treatment was not significantly different between patients in the UFH group (3.8%) and those in the LMWH group (3.4%). The risk of major bleeding during the first 10 days of treatment was also similar between the UFH group (1.1%) and LMWH group (1.4%). Approximately 70% of patients in both groups received treatment entirely out of hospital. Overall, there were 18 deaths in the UFH group and 22 deaths in the LMWH group (difference not significant). Adverse events were unrelated to whether subjects were subtherapeutic or supratherapeutic.
-
CLINICAL QUESTION: How safe and effective is fixed‐dose subcutaneous unfractionated heparin in the treatment of venous thromboembolism?
-
BOTTOM LINE: In this study, fixed‐dose weight‐adjusted unfractionated heparin (UFH) administered subcutaneously was as safe and effective as low‐molecular‐weight heparin (LMWH) in the treatment of venous thromboembolism (VTE). Estimated drug costs for a 6‐day course are $712 for LMWH and $37 for UFH. Most clinicians will want to see similar results from at least 1 additional well‐done clinical trial, including more patients with symptomatic pulmonary embolism, before routinely treating VTE with subcutaneous UFH. (LOE = 1b)
-
REFERENCE: Kearon C, Ginsberg JS, Julian JA, et al, for the Fixed‐Dose Heparin (FIDO) Investigators. Comparison of fixed‐dose weight‐adjusted unfractionated heparin and low‐molecular‐weight heparin for acute treatment of venous thromboembolism. JAMA 2006;296:935‐942.
-
STUDY DESIGN: Randomized controlled trial (single‐blinded)
-
FUNDING: Foundation
-
SETTING: Outpatient (any)
-
ALLOCATION: Concealed
-
SYNOPSIS: These investigators randomly assigned (concealed allocation assignment) 708 patients, 18 years or older, with acute VTE to subcutaneous UFH (initial dose of 333 U/kg, followed by a fixed dose of 250 U/kg every 12 hours) or LMWH (dalteparin or enoxaparin, 100 IU/kg every 12 hours). The dose of subcutaneous UFH remained fixed for individual patients and was not changed during treatment as a result of anticoagulation profiles. The diagnosis of VTE included patients with acute deep vein thrombosis of the legs (81%) or symptomatic pulmonary embolism (19%). Oral warfarin was usually started on the same day as heparin in both groups and continued for a minimum of 3 months with doses adjusted to achieve an international normalized ratio (INR) of between 2.0 and 3.0. Heparin was continued for at least 5 days and until the INR was 2.0 or higher for 2 consecutive days. Individuals unaware of treatment group assignment assessed all outcomes, including study eligibility criteria. Follow‐up occurred for more than 98% of subjects for 3 months. All eligible and consenting patients underwent final data analysis. The risk of recurrent VTE in the first 3 months after treatment was not significantly different between patients in the UFH group (3.8%) and those in the LMWH group (3.4%). The risk of major bleeding during the first 10 days of treatment was also similar between the UFH group (1.1%) and LMWH group (1.4%). Approximately 70% of patients in both groups received treatment entirely out of hospital. Overall, there were 18 deaths in the UFH group and 22 deaths in the LMWH group (difference not significant). Adverse events were unrelated to whether subjects were subtherapeutic or supratherapeutic.
-
CLINICAL QUESTION: How safe and effective is fixed‐dose subcutaneous unfractionated heparin in the treatment of venous thromboembolism?
-
BOTTOM LINE: In this study, fixed‐dose weight‐adjusted unfractionated heparin (UFH) administered subcutaneously was as safe and effective as low‐molecular‐weight heparin (LMWH) in the treatment of venous thromboembolism (VTE). Estimated drug costs for a 6‐day course are $712 for LMWH and $37 for UFH. Most clinicians will want to see similar results from at least 1 additional well‐done clinical trial, including more patients with symptomatic pulmonary embolism, before routinely treating VTE with subcutaneous UFH. (LOE = 1b)
-
REFERENCE: Kearon C, Ginsberg JS, Julian JA, et al, for the Fixed‐Dose Heparin (FIDO) Investigators. Comparison of fixed‐dose weight‐adjusted unfractionated heparin and low‐molecular‐weight heparin for acute treatment of venous thromboembolism. JAMA 2006;296:935‐942.
-
STUDY DESIGN: Randomized controlled trial (single‐blinded)
-
FUNDING: Foundation
-
SETTING: Outpatient (any)
-
ALLOCATION: Concealed
-
SYNOPSIS: These investigators randomly assigned (concealed allocation assignment) 708 patients, 18 years or older, with acute VTE to subcutaneous UFH (initial dose of 333 U/kg, followed by a fixed dose of 250 U/kg every 12 hours) or LMWH (dalteparin or enoxaparin, 100 IU/kg every 12 hours). The dose of subcutaneous UFH remained fixed for individual patients and was not changed during treatment as a result of anticoagulation profiles. The diagnosis of VTE included patients with acute deep vein thrombosis of the legs (81%) or symptomatic pulmonary embolism (19%). Oral warfarin was usually started on the same day as heparin in both groups and continued for a minimum of 3 months with doses adjusted to achieve an international normalized ratio (INR) of between 2.0 and 3.0. Heparin was continued for at least 5 days and until the INR was 2.0 or higher for 2 consecutive days. Individuals unaware of treatment group assignment assessed all outcomes, including study eligibility criteria. Follow‐up occurred for more than 98% of subjects for 3 months. All eligible and consenting patients underwent final data analysis. The risk of recurrent VTE in the first 3 months after treatment was not significantly different between patients in the UFH group (3.8%) and those in the LMWH group (3.4%). The risk of major bleeding during the first 10 days of treatment was also similar between the UFH group (1.1%) and LMWH group (1.4%). Approximately 70% of patients in both groups received treatment entirely out of hospital. Overall, there were 18 deaths in the UFH group and 22 deaths in the LMWH group (difference not significant). Adverse events were unrelated to whether subjects were subtherapeutic or supratherapeutic.
Disseminated histoplasmosis
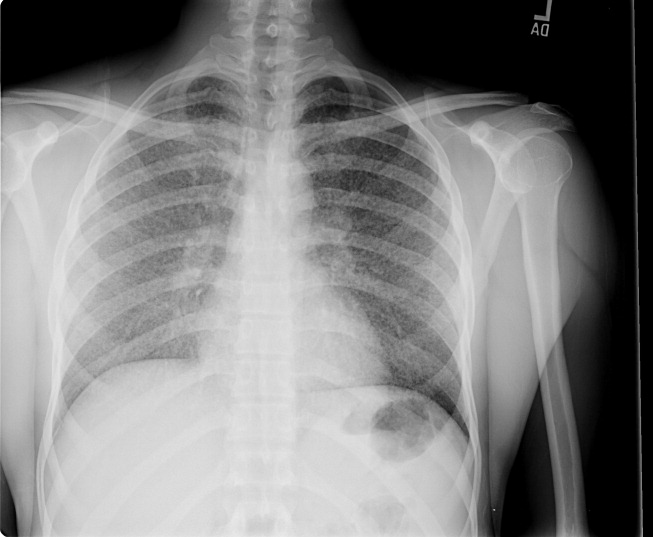
A previously healthy 27‐year‐old El Salvadoran immigrant presented with a 2‐week history of cough, fever, rigors, prostration, anorexia, weight loss, and scant hemoptysis. Physical examination revealed a thin, febrile, toxic‐appearing man in respiratory distress with bibasilar rales and scattered wheezes. Laboratory data showed a sodium of 126 mEq/L, lactate dehydrogenase of 617 U/L, ferritin of 3570 ng/mL, and liver test abnormalities suggestive of cholestasis. Chest film (Fig. 1) and computed tomography (Fig. 2) demonstrated a diffuse miliary air space pattern. Sputum smears for mycobacterium tuberculosis were negative. A urine histoplasmosis antigen level was markedly positive (7.6 EIA units), and bone marrow cultures eventually grew Histoplasma capsulatum. The HIV test result was positive, and his CD4 count was 34 cells/mm3. He was successfully treated with liposomal amphotericin B followed by itraconazole.
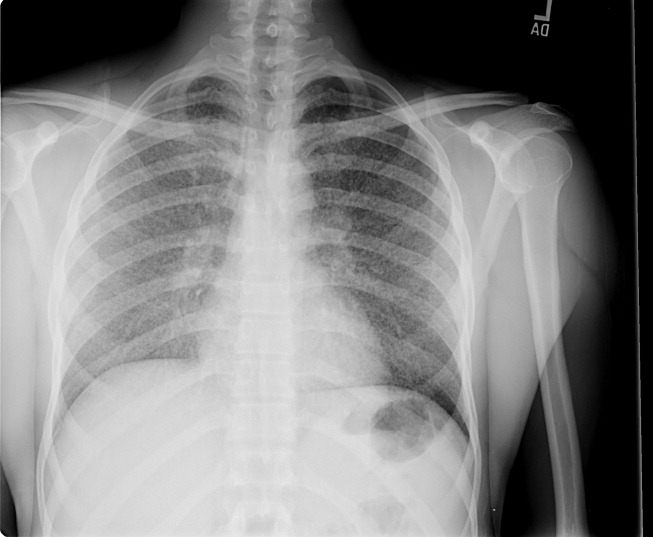
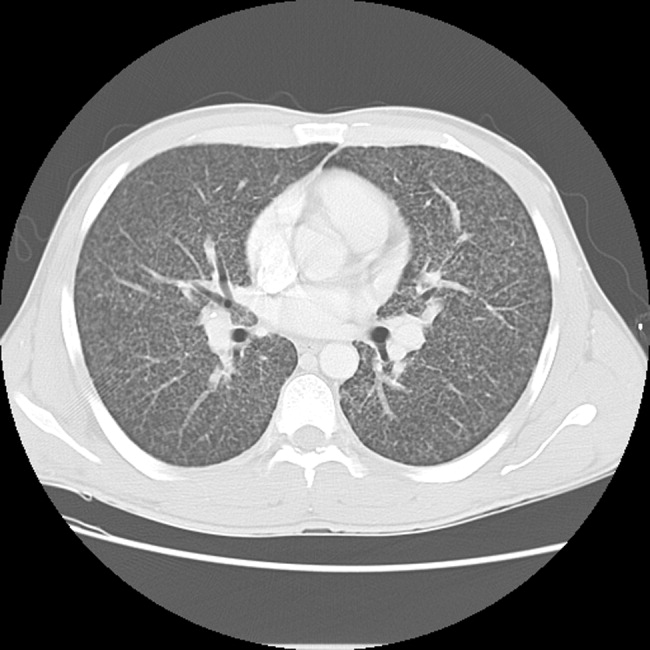
Histoplasmosis is the most prevalent endemic mycosis in Latin America. Most infections are asymptomatic or self‐limited, but immunodeficient individuals may develop acute pulmonary or severe, progressive disseminated infection, usually from reactivation of latent disease. Although nonspecific, the serum lactate dehydrogenase and ferritin levels are often markedly elevated. Chest imaging may be normal or show a diffuse reticulonodular pattern (with nodules less than 3 mm in diameter), indistinguishable from miliary tuberculosis. In HIV‐infected individuals, disseminated histoplasmosis usually develops when the CD4 count is less than 75 cells/mm3. Treatment is generally lifelong.
A previously healthy 27‐year‐old El Salvadoran immigrant presented with a 2‐week history of cough, fever, rigors, prostration, anorexia, weight loss, and scant hemoptysis. Physical examination revealed a thin, febrile, toxic‐appearing man in respiratory distress with bibasilar rales and scattered wheezes. Laboratory data showed a sodium of 126 mEq/L, lactate dehydrogenase of 617 U/L, ferritin of 3570 ng/mL, and liver test abnormalities suggestive of cholestasis. Chest film (Fig. 1) and computed tomography (Fig. 2) demonstrated a diffuse miliary air space pattern. Sputum smears for mycobacterium tuberculosis were negative. A urine histoplasmosis antigen level was markedly positive (7.6 EIA units), and bone marrow cultures eventually grew Histoplasma capsulatum. The HIV test result was positive, and his CD4 count was 34 cells/mm3. He was successfully treated with liposomal amphotericin B followed by itraconazole.
Histoplasmosis is the most prevalent endemic mycosis in Latin America. Most infections are asymptomatic or self‐limited, but immunodeficient individuals may develop acute pulmonary or severe, progressive disseminated infection, usually from reactivation of latent disease. Although nonspecific, the serum lactate dehydrogenase and ferritin levels are often markedly elevated. Chest imaging may be normal or show a diffuse reticulonodular pattern (with nodules less than 3 mm in diameter), indistinguishable from miliary tuberculosis. In HIV‐infected individuals, disseminated histoplasmosis usually develops when the CD4 count is less than 75 cells/mm3. Treatment is generally lifelong.
A previously healthy 27‐year‐old El Salvadoran immigrant presented with a 2‐week history of cough, fever, rigors, prostration, anorexia, weight loss, and scant hemoptysis. Physical examination revealed a thin, febrile, toxic‐appearing man in respiratory distress with bibasilar rales and scattered wheezes. Laboratory data showed a sodium of 126 mEq/L, lactate dehydrogenase of 617 U/L, ferritin of 3570 ng/mL, and liver test abnormalities suggestive of cholestasis. Chest film (Fig. 1) and computed tomography (Fig. 2) demonstrated a diffuse miliary air space pattern. Sputum smears for mycobacterium tuberculosis were negative. A urine histoplasmosis antigen level was markedly positive (7.6 EIA units), and bone marrow cultures eventually grew Histoplasma capsulatum. The HIV test result was positive, and his CD4 count was 34 cells/mm3. He was successfully treated with liposomal amphotericin B followed by itraconazole.
Histoplasmosis is the most prevalent endemic mycosis in Latin America. Most infections are asymptomatic or self‐limited, but immunodeficient individuals may develop acute pulmonary or severe, progressive disseminated infection, usually from reactivation of latent disease. Although nonspecific, the serum lactate dehydrogenase and ferritin levels are often markedly elevated. Chest imaging may be normal or show a diffuse reticulonodular pattern (with nodules less than 3 mm in diameter), indistinguishable from miliary tuberculosis. In HIV‐infected individuals, disseminated histoplasmosis usually develops when the CD4 count is less than 75 cells/mm3. Treatment is generally lifelong.
At Home

It was 8 p.m. on a cold Minnesota night, and my vision was obscured by flurries of snow and decomposing wiper blades. I was late for home. When I arrived, 11 sets of eyes turned toward me. (Twelve, really, counting my boxer Chocky Locky). They were sitting in the dining room, and the evening meal had just started. I washed quickly and took my seat at the table.
We have a large dining table that seats 12, but our current dish service—due to an unforeseen disaster—has only 11 settings. Thus, our service was at its maximum capacity. Tonight’s crowd included my wife and me, a grandmother, four offspring of various genders and a female teenager of unknown origin, a male preteen well-known to the household, and two young females who had sat at the table before.
As per standard operating procedure, each person at the table began to speak at the same time. Eventually order was established, though this was at best a transitory phenomenon. We received reports on each participant’s day, with highlights of lunch hour mayhem, recess riots, and general curricular boredom.
I began to question the unknown teen: name, age, place of origin, habits, and so on, but my history taking was interrupted. My younger son wanted to relay the results of an important test he had taken. He had passed and was now certified to use punctuation. I turned to resume my history taking, but made the important physical exam observation of intense eye rolling on the part of my daughter and her friend. This is a well-known physical finding in this age group and one that generally signals a pre-seizure threshold that I did not want to further induce.
After an intense nutritional session that included all major food groups and several minor ones, there were several short, unscheduled presentations. The grandmother gave a long and interesting family history with highlights of a great-great grandfather, who had been a freelance horse thief for both the Polish and Russian armies, and his son, who had been—alternatively—a gambler, a rabbi, a communist, and a union organizer.
After this history lesson, we received a fascinating report from one of my male offspring entitled, “proper placement of the hand and axillae, combined with repetitive flapping movements of the arm, to elicit an auditory stimulus similar to flatulence.” Much hilarity ensued.

It was unclear whose turn it was to clear the table. The schedule was not available, and several of the offspring cited work limits they would hate to see abused. Eventually the job was done with only minimal threats of withdrawal of privileges. As I prepared to resume my reading, a call went out for transportation services. It was time to discharge one of the visiting children to her abode. I was happy to decrease the numbers in house, though I would have been happier to see our numbers go even lower. Our length of stay seemed to be rising daily. As I attempted to initiate the transportation home, I realized we had to go through the checklist. Do you have your scarf, your gloves, and your shoes? Did you have a good time? I considered a policy of no readmission in 30 days, but it was voted down in a team meeting.
I returned from transportation duties, and I sat quietly for a moment and looked at the Times and the Post-Bulletin. These were papers I had been waiting to review—especially the comics. But something always seems to come up when one has papers to review. My youngest daughter and her friends needed my guidance on an art project. I had hoped they would see one, do one, teach one, but I had to repeatedly sketch the face outlines for them to color.
As I sat down again to the papers, the doorbell rang. Nobody else appeared to be on doorbell duty, so I went to the front of the house. There was a young man in a white shirt and black tie. He was proselytizing for a religious group. I informed him that our house had adopted a “no religious rep policy.” This helps us to avoid being unduly influenced by reps, though I must admit I still use my Taoist pen. It’s a Zen-Pen: one side writes, the other doesn’t.
Finally, I returned to my seat. At that point, the room plunged into darkness. A moment of panic. Quickly, I took my own pulse, a technique I had learned from the medical literature. Once calmed, I went through the differential. The power might be out for the whole city or just the house. Perhaps a fuse had blown from one too many electronic entertainment devices. Or maybe mice had chewed through a power cable. As I pondered my next course of diagnostic action and reviewed my alternatives in an evidence-based and allorhythmic approach, I auscultated a series of breath sounds that might be interpreted as gasps or giggles.
I intuitively realized that it was a severe case of “little girls playing a joke on Dad by switching off the light.” I had two choices. The first was to be crabby and bellow for them to quit playing with the switch. I felt this to be a harsh choice with bad potential side effects. Instead, I ducked under the table and silently hid. When proper lighting was restored, they were amazed to see I had vanished, and when they came to investigate, I revealed myself and uttered the key phrase: “Boo!” A riotous wrestling match ensued, which led to the injury of a family heirloom and my spine.
It was time for bed, despite my elder son’s complaint of a type of chronic insomnia only remediable by late-night cartoon observation. Evening reading began. Such important journals as Click Clack Moo, P.J. Funnybunny Camps Out, and the Stinky Cheese Man and Other Fairly Stupid Tales were on the agenda.
As I drifted off to sleep, the phone rang. It was a wrong number. Several hours later, an emergency call for supplemental H2O was answered. Two hours after that, I awoke to a hideous scream; it was a nightmare. My alarm rang at 6:15, and I jumped from bed refreshed. No, that’s a lie. I stumbled from bed after hitting the snooze button four times. Morning nutrition rounds were a stale toaster pastry and coffee. Team Newman noted that there were last-minute reports not finished for school and preparation for a day of testing.
I drove to work exhausted after a night of Home. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
It was 8 p.m. on a cold Minnesota night, and my vision was obscured by flurries of snow and decomposing wiper blades. I was late for home. When I arrived, 11 sets of eyes turned toward me. (Twelve, really, counting my boxer Chocky Locky). They were sitting in the dining room, and the evening meal had just started. I washed quickly and took my seat at the table.
We have a large dining table that seats 12, but our current dish service—due to an unforeseen disaster—has only 11 settings. Thus, our service was at its maximum capacity. Tonight’s crowd included my wife and me, a grandmother, four offspring of various genders and a female teenager of unknown origin, a male preteen well-known to the household, and two young females who had sat at the table before.
As per standard operating procedure, each person at the table began to speak at the same time. Eventually order was established, though this was at best a transitory phenomenon. We received reports on each participant’s day, with highlights of lunch hour mayhem, recess riots, and general curricular boredom.
I began to question the unknown teen: name, age, place of origin, habits, and so on, but my history taking was interrupted. My younger son wanted to relay the results of an important test he had taken. He had passed and was now certified to use punctuation. I turned to resume my history taking, but made the important physical exam observation of intense eye rolling on the part of my daughter and her friend. This is a well-known physical finding in this age group and one that generally signals a pre-seizure threshold that I did not want to further induce.
After an intense nutritional session that included all major food groups and several minor ones, there were several short, unscheduled presentations. The grandmother gave a long and interesting family history with highlights of a great-great grandfather, who had been a freelance horse thief for both the Polish and Russian armies, and his son, who had been—alternatively—a gambler, a rabbi, a communist, and a union organizer.
After this history lesson, we received a fascinating report from one of my male offspring entitled, “proper placement of the hand and axillae, combined with repetitive flapping movements of the arm, to elicit an auditory stimulus similar to flatulence.” Much hilarity ensued.
It was unclear whose turn it was to clear the table. The schedule was not available, and several of the offspring cited work limits they would hate to see abused. Eventually the job was done with only minimal threats of withdrawal of privileges. As I prepared to resume my reading, a call went out for transportation services. It was time to discharge one of the visiting children to her abode. I was happy to decrease the numbers in house, though I would have been happier to see our numbers go even lower. Our length of stay seemed to be rising daily. As I attempted to initiate the transportation home, I realized we had to go through the checklist. Do you have your scarf, your gloves, and your shoes? Did you have a good time? I considered a policy of no readmission in 30 days, but it was voted down in a team meeting.
I returned from transportation duties, and I sat quietly for a moment and looked at the Times and the Post-Bulletin. These were papers I had been waiting to review—especially the comics. But something always seems to come up when one has papers to review. My youngest daughter and her friends needed my guidance on an art project. I had hoped they would see one, do one, teach one, but I had to repeatedly sketch the face outlines for them to color.
As I sat down again to the papers, the doorbell rang. Nobody else appeared to be on doorbell duty, so I went to the front of the house. There was a young man in a white shirt and black tie. He was proselytizing for a religious group. I informed him that our house had adopted a “no religious rep policy.” This helps us to avoid being unduly influenced by reps, though I must admit I still use my Taoist pen. It’s a Zen-Pen: one side writes, the other doesn’t.
Finally, I returned to my seat. At that point, the room plunged into darkness. A moment of panic. Quickly, I took my own pulse, a technique I had learned from the medical literature. Once calmed, I went through the differential. The power might be out for the whole city or just the house. Perhaps a fuse had blown from one too many electronic entertainment devices. Or maybe mice had chewed through a power cable. As I pondered my next course of diagnostic action and reviewed my alternatives in an evidence-based and allorhythmic approach, I auscultated a series of breath sounds that might be interpreted as gasps or giggles.
I intuitively realized that it was a severe case of “little girls playing a joke on Dad by switching off the light.” I had two choices. The first was to be crabby and bellow for them to quit playing with the switch. I felt this to be a harsh choice with bad potential side effects. Instead, I ducked under the table and silently hid. When proper lighting was restored, they were amazed to see I had vanished, and when they came to investigate, I revealed myself and uttered the key phrase: “Boo!” A riotous wrestling match ensued, which led to the injury of a family heirloom and my spine.
It was time for bed, despite my elder son’s complaint of a type of chronic insomnia only remediable by late-night cartoon observation. Evening reading began. Such important journals as Click Clack Moo, P.J. Funnybunny Camps Out, and the Stinky Cheese Man and Other Fairly Stupid Tales were on the agenda.
As I drifted off to sleep, the phone rang. It was a wrong number. Several hours later, an emergency call for supplemental H2O was answered. Two hours after that, I awoke to a hideous scream; it was a nightmare. My alarm rang at 6:15, and I jumped from bed refreshed. No, that’s a lie. I stumbled from bed after hitting the snooze button four times. Morning nutrition rounds were a stale toaster pastry and coffee. Team Newman noted that there were last-minute reports not finished for school and preparation for a day of testing.
I drove to work exhausted after a night of Home. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
It was 8 p.m. on a cold Minnesota night, and my vision was obscured by flurries of snow and decomposing wiper blades. I was late for home. When I arrived, 11 sets of eyes turned toward me. (Twelve, really, counting my boxer Chocky Locky). They were sitting in the dining room, and the evening meal had just started. I washed quickly and took my seat at the table.
We have a large dining table that seats 12, but our current dish service—due to an unforeseen disaster—has only 11 settings. Thus, our service was at its maximum capacity. Tonight’s crowd included my wife and me, a grandmother, four offspring of various genders and a female teenager of unknown origin, a male preteen well-known to the household, and two young females who had sat at the table before.
As per standard operating procedure, each person at the table began to speak at the same time. Eventually order was established, though this was at best a transitory phenomenon. We received reports on each participant’s day, with highlights of lunch hour mayhem, recess riots, and general curricular boredom.
I began to question the unknown teen: name, age, place of origin, habits, and so on, but my history taking was interrupted. My younger son wanted to relay the results of an important test he had taken. He had passed and was now certified to use punctuation. I turned to resume my history taking, but made the important physical exam observation of intense eye rolling on the part of my daughter and her friend. This is a well-known physical finding in this age group and one that generally signals a pre-seizure threshold that I did not want to further induce.
After an intense nutritional session that included all major food groups and several minor ones, there were several short, unscheduled presentations. The grandmother gave a long and interesting family history with highlights of a great-great grandfather, who had been a freelance horse thief for both the Polish and Russian armies, and his son, who had been—alternatively—a gambler, a rabbi, a communist, and a union organizer.
After this history lesson, we received a fascinating report from one of my male offspring entitled, “proper placement of the hand and axillae, combined with repetitive flapping movements of the arm, to elicit an auditory stimulus similar to flatulence.” Much hilarity ensued.
It was unclear whose turn it was to clear the table. The schedule was not available, and several of the offspring cited work limits they would hate to see abused. Eventually the job was done with only minimal threats of withdrawal of privileges. As I prepared to resume my reading, a call went out for transportation services. It was time to discharge one of the visiting children to her abode. I was happy to decrease the numbers in house, though I would have been happier to see our numbers go even lower. Our length of stay seemed to be rising daily. As I attempted to initiate the transportation home, I realized we had to go through the checklist. Do you have your scarf, your gloves, and your shoes? Did you have a good time? I considered a policy of no readmission in 30 days, but it was voted down in a team meeting.
I returned from transportation duties, and I sat quietly for a moment and looked at the Times and the Post-Bulletin. These were papers I had been waiting to review—especially the comics. But something always seems to come up when one has papers to review. My youngest daughter and her friends needed my guidance on an art project. I had hoped they would see one, do one, teach one, but I had to repeatedly sketch the face outlines for them to color.
As I sat down again to the papers, the doorbell rang. Nobody else appeared to be on doorbell duty, so I went to the front of the house. There was a young man in a white shirt and black tie. He was proselytizing for a religious group. I informed him that our house had adopted a “no religious rep policy.” This helps us to avoid being unduly influenced by reps, though I must admit I still use my Taoist pen. It’s a Zen-Pen: one side writes, the other doesn’t.
Finally, I returned to my seat. At that point, the room plunged into darkness. A moment of panic. Quickly, I took my own pulse, a technique I had learned from the medical literature. Once calmed, I went through the differential. The power might be out for the whole city or just the house. Perhaps a fuse had blown from one too many electronic entertainment devices. Or maybe mice had chewed through a power cable. As I pondered my next course of diagnostic action and reviewed my alternatives in an evidence-based and allorhythmic approach, I auscultated a series of breath sounds that might be interpreted as gasps or giggles.
I intuitively realized that it was a severe case of “little girls playing a joke on Dad by switching off the light.” I had two choices. The first was to be crabby and bellow for them to quit playing with the switch. I felt this to be a harsh choice with bad potential side effects. Instead, I ducked under the table and silently hid. When proper lighting was restored, they were amazed to see I had vanished, and when they came to investigate, I revealed myself and uttered the key phrase: “Boo!” A riotous wrestling match ensued, which led to the injury of a family heirloom and my spine.
It was time for bed, despite my elder son’s complaint of a type of chronic insomnia only remediable by late-night cartoon observation. Evening reading began. Such important journals as Click Clack Moo, P.J. Funnybunny Camps Out, and the Stinky Cheese Man and Other Fairly Stupid Tales were on the agenda.
As I drifted off to sleep, the phone rang. It was a wrong number. Several hours later, an emergency call for supplemental H2O was answered. Two hours after that, I awoke to a hideous scream; it was a nightmare. My alarm rang at 6:15, and I jumped from bed refreshed. No, that’s a lie. I stumbled from bed after hitting the snooze button four times. Morning nutrition rounds were a stale toaster pastry and coffee. Team Newman noted that there were last-minute reports not finished for school and preparation for a day of testing.
I drove to work exhausted after a night of Home. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
The Hospitalist-Patient Conundrum

Hospitalist-patient continuity is primarily a function of the number of consecutive days worked by a hospitalist, but the way new referrals are distributed can also affect continuity. This month, I will discuss both.
For my first few years as a hospitalist in the late 1980s and early 1990s, my one partner and I generally worked a schedule of 21 days on and seven days off. While I wouldn’t recommend that anyone try that today, it wasn’t as bad as you might think, because our patient volumes weren’t terribly high and, on about a third of the worked days, I was done shortly after lunch.
While working that schedule, I became aware of its benefit to hospitalist-patient continuity. I can remember many patients with hospital stays of more than two weeks whom I saw every day myself. As you might imagine, my partner and I talked periodically about working fewer than 21 days at a stretch and handing a service over to one another more frequently. But we were concerned that this would make us inefficient because more of our worked days would involve getting to know a new list of patients. In effect, we’d work more hours without an increase in income or patient volume.
While still working the 21-day schedule, I came to know another practice and was stunned that these doctors had taken essentially the opposite approach to scheduling. They worked 24-hour shifts on site and never worked more than one shift at a time. (If your shifts are 24-hours long, you probably can’t or shouldn’t work more than one at a time.) This schedule meant that a patient would see a different hospitalist each day. I couldn’t believe that either the patients or the hospitalists would think this was a reasonable thing to do, but the doctors were convinced it worked well. Later I learned that this group had been started by an emergency medicine practice, and it seems they had made the mistake of inserting an emergency department (ED) physician schedule into a hospitalist practice—and 24-hour shifts for ED doctors were more common then than now.
So, early in my career, the first two schedules I became acquainted with sat on opposite ends of a continuum that has since been filled in by many other options. Both the practice I was part of and the 24-hour-shift practice abandoned their original schedules within a few years and moved on to other alternatives. In fact, I have since worked nearly every schedule you can imagine, including the seven-on/seven-off schedule, which I think is a suboptimal choice for most groups. (See August 2006 “Career Management,” p. 9.) With each variation in my work schedule, I’ve thought a lot about its effect on continuity.
While there isn’t a great deal of research to prove it, improved continuity is probably associated with improvements in things like:
- Quality care and safety;
- Patient satisfaction (and probably hospitalist satisfaction also);
- Hospital resource utilization; and
- Hospitalist efficiency.
When hospitalists design a schedule, I recommend that the doctors think first about what will allow them a sustainable lifestyle while ensuring the necessary coverage—for some practices, this means keeping a doctor in the hospital around the clock. Ideally, they will come up with several options that satisfy these two metrics. In many cases, the option that results in the best continuity is the one they should choose.
While the number of consecutive days of work is the most important variable in determining continuity, the way a group distributes new referrals can also have an effect. If a hospitalist doesn’t take on any new referrals on the day before starting a series of days off, there will be fewer patients to hand over to the doctor who takes over the next day. If every member of the practice is exempted from taking on new patients on the day before rotating off, then fewer patients will have a new hospitalist, which means continuity is better. Another way to think of this is that new referrals are “frontloaded” into the earlier days a hospitalist works in each series, and no new patients are assigned on the last day—or maybe more—of a hospitalist’s consecutive days of work.
In my experience, most groups try to distribute patients equally to each doctor each day. This means that a doctor who will be off starting tomorrow takes the standard portion of new referrals to the practice today. The fact that all of those patients will be turned over to a new hospitalist tomorrow, however, adversely affects continuity.
Note that exempting a group member from taking on new patients on the last day of a rotation means that the doctors can’t all rotate on and off on the same day. For example, if a group has four doctors working each day, and all rotate off on the same day—a common practice—then of course it is impossible to exempt all the doctors from new referrals on the day before going off. Instead, it will work best if only one doctor rotates on or off at a time. That leaves all the other doctors available to accept new referrals, while exempting the one about to rotate off.
This approach has benefits that go beyond improving continuity. It means a hospitalist’s workload the day before rotating off will be lighter than on other days. This provides extra time to “tee the patient up” for the next hospitalist—maybe write a more detailed note or dictate a discharge summary in anticipation of the patient leaving the next day—and/or it means a shorter day of work, assuming the doctors can leave the hospital when their work is done and aren’t required to stay around until the end of a pre-defined shift. This shorter day can mean an opportunity to do things like scheduling a flight to vacation late on the last day of work rather than the next morning, which might mean an extra day out of town.
And if a doctor isn’t assigned any new patients on the day prior to rotating off, there will be fewer patients to get to know for the doctor coming in the next day. The first day back on service will be less stressful and, arguably, more efficient.
A principle benefit of having all hospitalists switch on the same day is that the system quickly becomes transparent to the hospital staff. They learn that every Monday—or whatever day is decided upon—all of the hospitalists are getting to know patients for the first time and will probably round much more slowly. Many important processes, such as discharges, may be delayed until later in the day. If only one hospitalist switches at a time, hospital staff will have a hard time keeping up. Any inefficiencies caused by the switch will be spread over many days, however, and this may make it easier to handle. And if patients are teed up better for the new hospitalist and there are fewer patients on the list, the inefficiency that is caused by a new doctor getting to know the patients can be offset by the smaller number of patients. That means, for example, that discharges are much less likely to be delayed because of the smaller patient load on the doctor’s first day on service.
Up to this point I’ve been discussing continuity during a single admission. What about continuity from one admission to the next? Nearly all groups assign patients based on when they are admitted, and the hospitalist who cared for the patient during a prior admission may have little influence on which hospitalist admits them this time. If a patient is readmitted within a week or two, and the previous attending hospitalist is working, some groups will try to pair them once again through a bounce-back system.
It’s worth thinking about whether your group could make an effort to always have the same hospitalist care for a patient unless that physician is off—even if the admissions are months apart. This system would mean that on first admission to the practice a patient would be assigned to the hospitalist who is up next. In this way, each hospitalist in the group would develop his or her own panel of patients. This would be particularly valuable for patients who are admitted frequently; however, it would be difficult for a doctor to control how labor-intensive his patient panel might become. One person might have the bad luck to collect far more medically and socially complex patients than others in the group, and workloads might become unbalanced, making the whole group less efficient. I’m hopeful that a group will come up with a way to overcome these problems and create a workable system of good continuity from one admission to the next, but, as far as I’m aware, no group is doing this now. If you have a workable system, please let me know.
One group I worked with years ago addressed continuity from one admission to the next by using a system that matched each hospitalist with a panel of referring doctors. For example, the same hospitalist would always admit the patients “belonging to” a cadre of primary care physicians (PCPs), and another hospitalist in the group would always admit patients from another set of PCPs. The patient would see the same hospitalist each admission, and the hospitalist could develop a close working relationship with the panel of PCPs. The hospitalist and the PCP became familiar with each other’s practice styles, schedules, and days off, and memorized one another’s phone and fax numbers, the names of office and support staff, and so on, making for a very smooth working relationship that could benefit patient care. If the assigned hospitalist was off when a particular PCP’s patient needed admission, then a partner would provide interim care and turn the patient over when that hospitalist returned.
As you can imagine, this can be a difficult system to implement because there are many days on which a patient might be hospitalized when the assigned hospitalist is not around. Additionally, it is nearly impossible to divide PCPs and their patients equitably so that each hospitalist has a reasonable workload and patient complexity. I can imagine this group meeting periodically to match hospitalists and PCPs in a fashion similar to a fantasy football draft: “I’ll take PCP Smith and Williams from you, if you take PCP Wilson off my hands.”
I’m interested in hearing any additional ideas groups have developed to facilitate good continuity. The number of consecutive days worked by each hospitalist and the way new patients are assigned are significant ways to influence continuity, but there may be others that we should all keep in mind. And remember, maximizing continuity is not only good for patients; it enables the hospitalist practice to function more efficiently because it minimizes the number of new patients each hospitalist will have to get to know. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Hospitalist-patient continuity is primarily a function of the number of consecutive days worked by a hospitalist, but the way new referrals are distributed can also affect continuity. This month, I will discuss both.
For my first few years as a hospitalist in the late 1980s and early 1990s, my one partner and I generally worked a schedule of 21 days on and seven days off. While I wouldn’t recommend that anyone try that today, it wasn’t as bad as you might think, because our patient volumes weren’t terribly high and, on about a third of the worked days, I was done shortly after lunch.
While working that schedule, I became aware of its benefit to hospitalist-patient continuity. I can remember many patients with hospital stays of more than two weeks whom I saw every day myself. As you might imagine, my partner and I talked periodically about working fewer than 21 days at a stretch and handing a service over to one another more frequently. But we were concerned that this would make us inefficient because more of our worked days would involve getting to know a new list of patients. In effect, we’d work more hours without an increase in income or patient volume.
While still working the 21-day schedule, I came to know another practice and was stunned that these doctors had taken essentially the opposite approach to scheduling. They worked 24-hour shifts on site and never worked more than one shift at a time. (If your shifts are 24-hours long, you probably can’t or shouldn’t work more than one at a time.) This schedule meant that a patient would see a different hospitalist each day. I couldn’t believe that either the patients or the hospitalists would think this was a reasonable thing to do, but the doctors were convinced it worked well. Later I learned that this group had been started by an emergency medicine practice, and it seems they had made the mistake of inserting an emergency department (ED) physician schedule into a hospitalist practice—and 24-hour shifts for ED doctors were more common then than now.
So, early in my career, the first two schedules I became acquainted with sat on opposite ends of a continuum that has since been filled in by many other options. Both the practice I was part of and the 24-hour-shift practice abandoned their original schedules within a few years and moved on to other alternatives. In fact, I have since worked nearly every schedule you can imagine, including the seven-on/seven-off schedule, which I think is a suboptimal choice for most groups. (See August 2006 “Career Management,” p. 9.) With each variation in my work schedule, I’ve thought a lot about its effect on continuity.
While there isn’t a great deal of research to prove it, improved continuity is probably associated with improvements in things like:
- Quality care and safety;
- Patient satisfaction (and probably hospitalist satisfaction also);
- Hospital resource utilization; and
- Hospitalist efficiency.
When hospitalists design a schedule, I recommend that the doctors think first about what will allow them a sustainable lifestyle while ensuring the necessary coverage—for some practices, this means keeping a doctor in the hospital around the clock. Ideally, they will come up with several options that satisfy these two metrics. In many cases, the option that results in the best continuity is the one they should choose.
While the number of consecutive days of work is the most important variable in determining continuity, the way a group distributes new referrals can also have an effect. If a hospitalist doesn’t take on any new referrals on the day before starting a series of days off, there will be fewer patients to hand over to the doctor who takes over the next day. If every member of the practice is exempted from taking on new patients on the day before rotating off, then fewer patients will have a new hospitalist, which means continuity is better. Another way to think of this is that new referrals are “frontloaded” into the earlier days a hospitalist works in each series, and no new patients are assigned on the last day—or maybe more—of a hospitalist’s consecutive days of work.
In my experience, most groups try to distribute patients equally to each doctor each day. This means that a doctor who will be off starting tomorrow takes the standard portion of new referrals to the practice today. The fact that all of those patients will be turned over to a new hospitalist tomorrow, however, adversely affects continuity.
Note that exempting a group member from taking on new patients on the last day of a rotation means that the doctors can’t all rotate on and off on the same day. For example, if a group has four doctors working each day, and all rotate off on the same day—a common practice—then of course it is impossible to exempt all the doctors from new referrals on the day before going off. Instead, it will work best if only one doctor rotates on or off at a time. That leaves all the other doctors available to accept new referrals, while exempting the one about to rotate off.
This approach has benefits that go beyond improving continuity. It means a hospitalist’s workload the day before rotating off will be lighter than on other days. This provides extra time to “tee the patient up” for the next hospitalist—maybe write a more detailed note or dictate a discharge summary in anticipation of the patient leaving the next day—and/or it means a shorter day of work, assuming the doctors can leave the hospital when their work is done and aren’t required to stay around until the end of a pre-defined shift. This shorter day can mean an opportunity to do things like scheduling a flight to vacation late on the last day of work rather than the next morning, which might mean an extra day out of town.
And if a doctor isn’t assigned any new patients on the day prior to rotating off, there will be fewer patients to get to know for the doctor coming in the next day. The first day back on service will be less stressful and, arguably, more efficient.
A principle benefit of having all hospitalists switch on the same day is that the system quickly becomes transparent to the hospital staff. They learn that every Monday—or whatever day is decided upon—all of the hospitalists are getting to know patients for the first time and will probably round much more slowly. Many important processes, such as discharges, may be delayed until later in the day. If only one hospitalist switches at a time, hospital staff will have a hard time keeping up. Any inefficiencies caused by the switch will be spread over many days, however, and this may make it easier to handle. And if patients are teed up better for the new hospitalist and there are fewer patients on the list, the inefficiency that is caused by a new doctor getting to know the patients can be offset by the smaller number of patients. That means, for example, that discharges are much less likely to be delayed because of the smaller patient load on the doctor’s first day on service.
Up to this point I’ve been discussing continuity during a single admission. What about continuity from one admission to the next? Nearly all groups assign patients based on when they are admitted, and the hospitalist who cared for the patient during a prior admission may have little influence on which hospitalist admits them this time. If a patient is readmitted within a week or two, and the previous attending hospitalist is working, some groups will try to pair them once again through a bounce-back system.
It’s worth thinking about whether your group could make an effort to always have the same hospitalist care for a patient unless that physician is off—even if the admissions are months apart. This system would mean that on first admission to the practice a patient would be assigned to the hospitalist who is up next. In this way, each hospitalist in the group would develop his or her own panel of patients. This would be particularly valuable for patients who are admitted frequently; however, it would be difficult for a doctor to control how labor-intensive his patient panel might become. One person might have the bad luck to collect far more medically and socially complex patients than others in the group, and workloads might become unbalanced, making the whole group less efficient. I’m hopeful that a group will come up with a way to overcome these problems and create a workable system of good continuity from one admission to the next, but, as far as I’m aware, no group is doing this now. If you have a workable system, please let me know.
One group I worked with years ago addressed continuity from one admission to the next by using a system that matched each hospitalist with a panel of referring doctors. For example, the same hospitalist would always admit the patients “belonging to” a cadre of primary care physicians (PCPs), and another hospitalist in the group would always admit patients from another set of PCPs. The patient would see the same hospitalist each admission, and the hospitalist could develop a close working relationship with the panel of PCPs. The hospitalist and the PCP became familiar with each other’s practice styles, schedules, and days off, and memorized one another’s phone and fax numbers, the names of office and support staff, and so on, making for a very smooth working relationship that could benefit patient care. If the assigned hospitalist was off when a particular PCP’s patient needed admission, then a partner would provide interim care and turn the patient over when that hospitalist returned.
As you can imagine, this can be a difficult system to implement because there are many days on which a patient might be hospitalized when the assigned hospitalist is not around. Additionally, it is nearly impossible to divide PCPs and their patients equitably so that each hospitalist has a reasonable workload and patient complexity. I can imagine this group meeting periodically to match hospitalists and PCPs in a fashion similar to a fantasy football draft: “I’ll take PCP Smith and Williams from you, if you take PCP Wilson off my hands.”
I’m interested in hearing any additional ideas groups have developed to facilitate good continuity. The number of consecutive days worked by each hospitalist and the way new patients are assigned are significant ways to influence continuity, but there may be others that we should all keep in mind. And remember, maximizing continuity is not only good for patients; it enables the hospitalist practice to function more efficiently because it minimizes the number of new patients each hospitalist will have to get to know. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Hospitalist-patient continuity is primarily a function of the number of consecutive days worked by a hospitalist, but the way new referrals are distributed can also affect continuity. This month, I will discuss both.
For my first few years as a hospitalist in the late 1980s and early 1990s, my one partner and I generally worked a schedule of 21 days on and seven days off. While I wouldn’t recommend that anyone try that today, it wasn’t as bad as you might think, because our patient volumes weren’t terribly high and, on about a third of the worked days, I was done shortly after lunch.
While working that schedule, I became aware of its benefit to hospitalist-patient continuity. I can remember many patients with hospital stays of more than two weeks whom I saw every day myself. As you might imagine, my partner and I talked periodically about working fewer than 21 days at a stretch and handing a service over to one another more frequently. But we were concerned that this would make us inefficient because more of our worked days would involve getting to know a new list of patients. In effect, we’d work more hours without an increase in income or patient volume.
While still working the 21-day schedule, I came to know another practice and was stunned that these doctors had taken essentially the opposite approach to scheduling. They worked 24-hour shifts on site and never worked more than one shift at a time. (If your shifts are 24-hours long, you probably can’t or shouldn’t work more than one at a time.) This schedule meant that a patient would see a different hospitalist each day. I couldn’t believe that either the patients or the hospitalists would think this was a reasonable thing to do, but the doctors were convinced it worked well. Later I learned that this group had been started by an emergency medicine practice, and it seems they had made the mistake of inserting an emergency department (ED) physician schedule into a hospitalist practice—and 24-hour shifts for ED doctors were more common then than now.
So, early in my career, the first two schedules I became acquainted with sat on opposite ends of a continuum that has since been filled in by many other options. Both the practice I was part of and the 24-hour-shift practice abandoned their original schedules within a few years and moved on to other alternatives. In fact, I have since worked nearly every schedule you can imagine, including the seven-on/seven-off schedule, which I think is a suboptimal choice for most groups. (See August 2006 “Career Management,” p. 9.) With each variation in my work schedule, I’ve thought a lot about its effect on continuity.
While there isn’t a great deal of research to prove it, improved continuity is probably associated with improvements in things like:
- Quality care and safety;
- Patient satisfaction (and probably hospitalist satisfaction also);
- Hospital resource utilization; and
- Hospitalist efficiency.
When hospitalists design a schedule, I recommend that the doctors think first about what will allow them a sustainable lifestyle while ensuring the necessary coverage—for some practices, this means keeping a doctor in the hospital around the clock. Ideally, they will come up with several options that satisfy these two metrics. In many cases, the option that results in the best continuity is the one they should choose.
While the number of consecutive days of work is the most important variable in determining continuity, the way a group distributes new referrals can also have an effect. If a hospitalist doesn’t take on any new referrals on the day before starting a series of days off, there will be fewer patients to hand over to the doctor who takes over the next day. If every member of the practice is exempted from taking on new patients on the day before rotating off, then fewer patients will have a new hospitalist, which means continuity is better. Another way to think of this is that new referrals are “frontloaded” into the earlier days a hospitalist works in each series, and no new patients are assigned on the last day—or maybe more—of a hospitalist’s consecutive days of work.
In my experience, most groups try to distribute patients equally to each doctor each day. This means that a doctor who will be off starting tomorrow takes the standard portion of new referrals to the practice today. The fact that all of those patients will be turned over to a new hospitalist tomorrow, however, adversely affects continuity.
Note that exempting a group member from taking on new patients on the last day of a rotation means that the doctors can’t all rotate on and off on the same day. For example, if a group has four doctors working each day, and all rotate off on the same day—a common practice—then of course it is impossible to exempt all the doctors from new referrals on the day before going off. Instead, it will work best if only one doctor rotates on or off at a time. That leaves all the other doctors available to accept new referrals, while exempting the one about to rotate off.
This approach has benefits that go beyond improving continuity. It means a hospitalist’s workload the day before rotating off will be lighter than on other days. This provides extra time to “tee the patient up” for the next hospitalist—maybe write a more detailed note or dictate a discharge summary in anticipation of the patient leaving the next day—and/or it means a shorter day of work, assuming the doctors can leave the hospital when their work is done and aren’t required to stay around until the end of a pre-defined shift. This shorter day can mean an opportunity to do things like scheduling a flight to vacation late on the last day of work rather than the next morning, which might mean an extra day out of town.
And if a doctor isn’t assigned any new patients on the day prior to rotating off, there will be fewer patients to get to know for the doctor coming in the next day. The first day back on service will be less stressful and, arguably, more efficient.
A principle benefit of having all hospitalists switch on the same day is that the system quickly becomes transparent to the hospital staff. They learn that every Monday—or whatever day is decided upon—all of the hospitalists are getting to know patients for the first time and will probably round much more slowly. Many important processes, such as discharges, may be delayed until later in the day. If only one hospitalist switches at a time, hospital staff will have a hard time keeping up. Any inefficiencies caused by the switch will be spread over many days, however, and this may make it easier to handle. And if patients are teed up better for the new hospitalist and there are fewer patients on the list, the inefficiency that is caused by a new doctor getting to know the patients can be offset by the smaller number of patients. That means, for example, that discharges are much less likely to be delayed because of the smaller patient load on the doctor’s first day on service.
Up to this point I’ve been discussing continuity during a single admission. What about continuity from one admission to the next? Nearly all groups assign patients based on when they are admitted, and the hospitalist who cared for the patient during a prior admission may have little influence on which hospitalist admits them this time. If a patient is readmitted within a week or two, and the previous attending hospitalist is working, some groups will try to pair them once again through a bounce-back system.
It’s worth thinking about whether your group could make an effort to always have the same hospitalist care for a patient unless that physician is off—even if the admissions are months apart. This system would mean that on first admission to the practice a patient would be assigned to the hospitalist who is up next. In this way, each hospitalist in the group would develop his or her own panel of patients. This would be particularly valuable for patients who are admitted frequently; however, it would be difficult for a doctor to control how labor-intensive his patient panel might become. One person might have the bad luck to collect far more medically and socially complex patients than others in the group, and workloads might become unbalanced, making the whole group less efficient. I’m hopeful that a group will come up with a way to overcome these problems and create a workable system of good continuity from one admission to the next, but, as far as I’m aware, no group is doing this now. If you have a workable system, please let me know.
One group I worked with years ago addressed continuity from one admission to the next by using a system that matched each hospitalist with a panel of referring doctors. For example, the same hospitalist would always admit the patients “belonging to” a cadre of primary care physicians (PCPs), and another hospitalist in the group would always admit patients from another set of PCPs. The patient would see the same hospitalist each admission, and the hospitalist could develop a close working relationship with the panel of PCPs. The hospitalist and the PCP became familiar with each other’s practice styles, schedules, and days off, and memorized one another’s phone and fax numbers, the names of office and support staff, and so on, making for a very smooth working relationship that could benefit patient care. If the assigned hospitalist was off when a particular PCP’s patient needed admission, then a partner would provide interim care and turn the patient over when that hospitalist returned.
As you can imagine, this can be a difficult system to implement because there are many days on which a patient might be hospitalized when the assigned hospitalist is not around. Additionally, it is nearly impossible to divide PCPs and their patients equitably so that each hospitalist has a reasonable workload and patient complexity. I can imagine this group meeting periodically to match hospitalists and PCPs in a fashion similar to a fantasy football draft: “I’ll take PCP Smith and Williams from you, if you take PCP Wilson off my hands.”
I’m interested in hearing any additional ideas groups have developed to facilitate good continuity. The number of consecutive days worked by each hospitalist and the way new patients are assigned are significant ways to influence continuity, but there may be others that we should all keep in mind. And remember, maximizing continuity is not only good for patients; it enables the hospitalist practice to function more efficiently because it minimizes the number of new patients each hospitalist will have to get to know. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
The Business of Hospitalists
In March 2005, the Association of American Medical Colleges announced that America will face a shortage of between 85,000 and 200,000 physicians by 2020. The U.S. population is growing faster than the number of new physicians entering the workforce. How big the shortfall will be has been argued since last year, but most pundits expect there to be too few physicians—in total—to take care of the burgeoning population, especially the elderly.
If a shortage of physicians is to be anticipated, what effect might this have on hospitals and hospitalists?
Where Does the Number Come From?
The debate about the range of the projected shortfall of 85,000 to 200,000 physicians reflects several differing assumptions. All estimates are based on the ratio of physicians to the overall population. Different estimates are based on distinctive models for the necessary staffing of the medical enterprise. For example, prepaid medical groups that serve large populations of patients (e.g., Kaiser Permanente) have physician-per-capita ratios of up to 20% less than fee-for-service environments. A larger elderly population will likely demand more medical services per capita. So, the estimate of a shortfall depends on the model of medical care for 2020 anticipated to be predominant in 2020 and a calculation of usage rate per capita for services—again, especially among the elderly.
Work/life balance choices that recent medical school graduates make also add to the uncertainty of predictions concerning the relative size of the shortage in total and by specialty. Young men and women graduating today increasingly express a preference for reduced or more manageable hours of work per week, sometimes opting for shift work or other forms of more predictable workload. There is also an understanding that women physicians tend to work part-time in some stages of their career—especially when they are trying to balance the demands of starting and raising a young family. Many of their male spouses are making similar choices.
The Specialty Nature of the Shortfall
A relative shortfall in available physicians relates to the specialty choice of new residency graduates. From 1996 to 2002, for example, certain specialties experienced increases in the number of applicants to residency programs, such as anesthesiology, dermatology, and radiology; whereas, other specialties saw reduced demand for training slots, such as in family practice and general surgery. For example, U.S. medical school seniors filled 89% of the general surgery residency slots available in 1996, but only 75% of the available slots in 2002.
The relative number of physicians in certain geographies will also be affected by the attractiveness of that particular area of the country or practice location and style, such as rural versus urban or suburban.
Physicians’ retirement rates generate different estimates, too. Currently, 18% of physicians in the United States are older than 65—compared with 12.6% of the overall population. In certain states, the percentage of physicians older than 65 is substantially higher, in some cases more than 20%. Different analysts generate different expectations about how many physicians over age 65 will leave the workforce. The number of hours that doctors practice and their decisions about when they will retire, based on their personal financial circumstances, are quite varied. This makes calculations of the shortfall to be anticipated subject to a variety of interpretations
Substitution
There is a debate also over the question of substitution. If there are too few physicians in the United States, will a shortfall in supply be made up by increasing numbers of foreign medical graduates or by other non-physician practitioners?
New foreign medical graduates may make up perhaps as many as 6,000 positions nationally. This will not make up for the shortfall of between 3,000 and 10,000 per year of additional physicians who need to graduate and enter the workforce.
Substitution by non-physician practitioners will mitigate some of the effects of the shortfall. We can anticipate that the use of nurse practitioners, physician assistants, nurses, and health educators will increase in situations where they can substitute for lower intensity medical care—especially in primary care settings, outpatient environments, and as adjuncts to care delivered by proceduralists and surgeons of many types. This will make some difference in the overall expectation for reduced availability of physicians.
Given all of these inputs, all projections point to a shortage of physicians, but none of the analyses agree on the absolute size.
The Effects of the Shortage
In any event, the projected shortage will affect how hospitals support their various service lines and, thus, will impact on the work performed by hospitalists, intensivists, and other physicians who support that work in hospitals. Hospitals anticipate this effect at the intersection of the shortage with increasing demands for rapid throughput, thorough and safe care for patients, and accountability for clearly specified clinical outcomes. Hospitals are already worrying about how to staff neurosurgery, cardiology, and general surgery positions. Changes in how primary care is delivered will affect where patient referrals come from and hospitals’ relationship with their specialist physicians.
How Will a Shortage Affect Hospitalists?
Increasing demand for services: With fewer physicians choosing general or primary care practice, hospitalists will find increasing demand for their services as coverage for acute care. Fewer primary care physicians will be able to afford the luxury of inpatient practice and gravitate toward highly efficient outpatient office-based practice while referring acute care to their hospitalist colleagues and specialists to pick up the slack for specific procedures, hospital follow-up care and return on discharge.
Hospitalists will be responsible then for a larger population of inpatients, providing for comprehensive care management in coordinating the services for all the care needs of many different types of diagnoses.
Increasing span of influence: In addition, there will be increasing demand by procedure-oriented physicians for hospitalist coverage to improve their efficiency in providing acute specialty care. Some of this demand may spill into single-specialty outpatient and focused freestanding hospital environments. Hospitalists will be pulled to cover specialists, who find their efficiency and the volume of work required prohibits them from providing comprehensive inpatient care for complex patients. They will prefer to focus on procedural interventions. Orthopedic surgery, cardiac surgery, neurosurgery, and cardiology, in particular, are likely to be new clients for hospitalist services.
Increasing emphasis on multidisciplinary care: Given the demand for evidence-based outcomes, hospitalists will provide physician input into clinical care design for a greater variety of patients in an increasing span of clinical service lines. This will put a demand on hospitalists for skills related to teamwork, leadership, and management in group environments. It will also require hospitalists to become broadly knowledgeable about the skills and contributions of all other potential care providers.
The New Medical Staff
The looming physician shortage in the United States will significantly affect the demand for and the variety and scope of work that hospitalists perform. The number of medical specialties dependent on hospitalist services will broaden. And hospitals will turn to hospitalists as their primary medical staff partners, responsible for the majority of medical staff functions and responsibilities. TH
Mike Guthrie, MD, is executive in residence at the University of Colorado (Denver) School of Business, Program in Health Administration, and a faculty member of SHM’s Leadership Academy.
In March 2005, the Association of American Medical Colleges announced that America will face a shortage of between 85,000 and 200,000 physicians by 2020. The U.S. population is growing faster than the number of new physicians entering the workforce. How big the shortfall will be has been argued since last year, but most pundits expect there to be too few physicians—in total—to take care of the burgeoning population, especially the elderly.
If a shortage of physicians is to be anticipated, what effect might this have on hospitals and hospitalists?
Where Does the Number Come From?
The debate about the range of the projected shortfall of 85,000 to 200,000 physicians reflects several differing assumptions. All estimates are based on the ratio of physicians to the overall population. Different estimates are based on distinctive models for the necessary staffing of the medical enterprise. For example, prepaid medical groups that serve large populations of patients (e.g., Kaiser Permanente) have physician-per-capita ratios of up to 20% less than fee-for-service environments. A larger elderly population will likely demand more medical services per capita. So, the estimate of a shortfall depends on the model of medical care for 2020 anticipated to be predominant in 2020 and a calculation of usage rate per capita for services—again, especially among the elderly.
Work/life balance choices that recent medical school graduates make also add to the uncertainty of predictions concerning the relative size of the shortage in total and by specialty. Young men and women graduating today increasingly express a preference for reduced or more manageable hours of work per week, sometimes opting for shift work or other forms of more predictable workload. There is also an understanding that women physicians tend to work part-time in some stages of their career—especially when they are trying to balance the demands of starting and raising a young family. Many of their male spouses are making similar choices.
The Specialty Nature of the Shortfall
A relative shortfall in available physicians relates to the specialty choice of new residency graduates. From 1996 to 2002, for example, certain specialties experienced increases in the number of applicants to residency programs, such as anesthesiology, dermatology, and radiology; whereas, other specialties saw reduced demand for training slots, such as in family practice and general surgery. For example, U.S. medical school seniors filled 89% of the general surgery residency slots available in 1996, but only 75% of the available slots in 2002.
The relative number of physicians in certain geographies will also be affected by the attractiveness of that particular area of the country or practice location and style, such as rural versus urban or suburban.
Physicians’ retirement rates generate different estimates, too. Currently, 18% of physicians in the United States are older than 65—compared with 12.6% of the overall population. In certain states, the percentage of physicians older than 65 is substantially higher, in some cases more than 20%. Different analysts generate different expectations about how many physicians over age 65 will leave the workforce. The number of hours that doctors practice and their decisions about when they will retire, based on their personal financial circumstances, are quite varied. This makes calculations of the shortfall to be anticipated subject to a variety of interpretations
Substitution
There is a debate also over the question of substitution. If there are too few physicians in the United States, will a shortfall in supply be made up by increasing numbers of foreign medical graduates or by other non-physician practitioners?
New foreign medical graduates may make up perhaps as many as 6,000 positions nationally. This will not make up for the shortfall of between 3,000 and 10,000 per year of additional physicians who need to graduate and enter the workforce.
Substitution by non-physician practitioners will mitigate some of the effects of the shortfall. We can anticipate that the use of nurse practitioners, physician assistants, nurses, and health educators will increase in situations where they can substitute for lower intensity medical care—especially in primary care settings, outpatient environments, and as adjuncts to care delivered by proceduralists and surgeons of many types. This will make some difference in the overall expectation for reduced availability of physicians.
Given all of these inputs, all projections point to a shortage of physicians, but none of the analyses agree on the absolute size.
The Effects of the Shortage
In any event, the projected shortage will affect how hospitals support their various service lines and, thus, will impact on the work performed by hospitalists, intensivists, and other physicians who support that work in hospitals. Hospitals anticipate this effect at the intersection of the shortage with increasing demands for rapid throughput, thorough and safe care for patients, and accountability for clearly specified clinical outcomes. Hospitals are already worrying about how to staff neurosurgery, cardiology, and general surgery positions. Changes in how primary care is delivered will affect where patient referrals come from and hospitals’ relationship with their specialist physicians.
How Will a Shortage Affect Hospitalists?
Increasing demand for services: With fewer physicians choosing general or primary care practice, hospitalists will find increasing demand for their services as coverage for acute care. Fewer primary care physicians will be able to afford the luxury of inpatient practice and gravitate toward highly efficient outpatient office-based practice while referring acute care to their hospitalist colleagues and specialists to pick up the slack for specific procedures, hospital follow-up care and return on discharge.
Hospitalists will be responsible then for a larger population of inpatients, providing for comprehensive care management in coordinating the services for all the care needs of many different types of diagnoses.
Increasing span of influence: In addition, there will be increasing demand by procedure-oriented physicians for hospitalist coverage to improve their efficiency in providing acute specialty care. Some of this demand may spill into single-specialty outpatient and focused freestanding hospital environments. Hospitalists will be pulled to cover specialists, who find their efficiency and the volume of work required prohibits them from providing comprehensive inpatient care for complex patients. They will prefer to focus on procedural interventions. Orthopedic surgery, cardiac surgery, neurosurgery, and cardiology, in particular, are likely to be new clients for hospitalist services.
Increasing emphasis on multidisciplinary care: Given the demand for evidence-based outcomes, hospitalists will provide physician input into clinical care design for a greater variety of patients in an increasing span of clinical service lines. This will put a demand on hospitalists for skills related to teamwork, leadership, and management in group environments. It will also require hospitalists to become broadly knowledgeable about the skills and contributions of all other potential care providers.
The New Medical Staff
The looming physician shortage in the United States will significantly affect the demand for and the variety and scope of work that hospitalists perform. The number of medical specialties dependent on hospitalist services will broaden. And hospitals will turn to hospitalists as their primary medical staff partners, responsible for the majority of medical staff functions and responsibilities. TH
Mike Guthrie, MD, is executive in residence at the University of Colorado (Denver) School of Business, Program in Health Administration, and a faculty member of SHM’s Leadership Academy.
In March 2005, the Association of American Medical Colleges announced that America will face a shortage of between 85,000 and 200,000 physicians by 2020. The U.S. population is growing faster than the number of new physicians entering the workforce. How big the shortfall will be has been argued since last year, but most pundits expect there to be too few physicians—in total—to take care of the burgeoning population, especially the elderly.
If a shortage of physicians is to be anticipated, what effect might this have on hospitals and hospitalists?
Where Does the Number Come From?
The debate about the range of the projected shortfall of 85,000 to 200,000 physicians reflects several differing assumptions. All estimates are based on the ratio of physicians to the overall population. Different estimates are based on distinctive models for the necessary staffing of the medical enterprise. For example, prepaid medical groups that serve large populations of patients (e.g., Kaiser Permanente) have physician-per-capita ratios of up to 20% less than fee-for-service environments. A larger elderly population will likely demand more medical services per capita. So, the estimate of a shortfall depends on the model of medical care for 2020 anticipated to be predominant in 2020 and a calculation of usage rate per capita for services—again, especially among the elderly.
Work/life balance choices that recent medical school graduates make also add to the uncertainty of predictions concerning the relative size of the shortage in total and by specialty. Young men and women graduating today increasingly express a preference for reduced or more manageable hours of work per week, sometimes opting for shift work or other forms of more predictable workload. There is also an understanding that women physicians tend to work part-time in some stages of their career—especially when they are trying to balance the demands of starting and raising a young family. Many of their male spouses are making similar choices.
The Specialty Nature of the Shortfall
A relative shortfall in available physicians relates to the specialty choice of new residency graduates. From 1996 to 2002, for example, certain specialties experienced increases in the number of applicants to residency programs, such as anesthesiology, dermatology, and radiology; whereas, other specialties saw reduced demand for training slots, such as in family practice and general surgery. For example, U.S. medical school seniors filled 89% of the general surgery residency slots available in 1996, but only 75% of the available slots in 2002.
The relative number of physicians in certain geographies will also be affected by the attractiveness of that particular area of the country or practice location and style, such as rural versus urban or suburban.
Physicians’ retirement rates generate different estimates, too. Currently, 18% of physicians in the United States are older than 65—compared with 12.6% of the overall population. In certain states, the percentage of physicians older than 65 is substantially higher, in some cases more than 20%. Different analysts generate different expectations about how many physicians over age 65 will leave the workforce. The number of hours that doctors practice and their decisions about when they will retire, based on their personal financial circumstances, are quite varied. This makes calculations of the shortfall to be anticipated subject to a variety of interpretations
Substitution
There is a debate also over the question of substitution. If there are too few physicians in the United States, will a shortfall in supply be made up by increasing numbers of foreign medical graduates or by other non-physician practitioners?
New foreign medical graduates may make up perhaps as many as 6,000 positions nationally. This will not make up for the shortfall of between 3,000 and 10,000 per year of additional physicians who need to graduate and enter the workforce.
Substitution by non-physician practitioners will mitigate some of the effects of the shortfall. We can anticipate that the use of nurse practitioners, physician assistants, nurses, and health educators will increase in situations where they can substitute for lower intensity medical care—especially in primary care settings, outpatient environments, and as adjuncts to care delivered by proceduralists and surgeons of many types. This will make some difference in the overall expectation for reduced availability of physicians.
Given all of these inputs, all projections point to a shortage of physicians, but none of the analyses agree on the absolute size.
The Effects of the Shortage
In any event, the projected shortage will affect how hospitals support their various service lines and, thus, will impact on the work performed by hospitalists, intensivists, and other physicians who support that work in hospitals. Hospitals anticipate this effect at the intersection of the shortage with increasing demands for rapid throughput, thorough and safe care for patients, and accountability for clearly specified clinical outcomes. Hospitals are already worrying about how to staff neurosurgery, cardiology, and general surgery positions. Changes in how primary care is delivered will affect where patient referrals come from and hospitals’ relationship with their specialist physicians.
How Will a Shortage Affect Hospitalists?
Increasing demand for services: With fewer physicians choosing general or primary care practice, hospitalists will find increasing demand for their services as coverage for acute care. Fewer primary care physicians will be able to afford the luxury of inpatient practice and gravitate toward highly efficient outpatient office-based practice while referring acute care to their hospitalist colleagues and specialists to pick up the slack for specific procedures, hospital follow-up care and return on discharge.
Hospitalists will be responsible then for a larger population of inpatients, providing for comprehensive care management in coordinating the services for all the care needs of many different types of diagnoses.
Increasing span of influence: In addition, there will be increasing demand by procedure-oriented physicians for hospitalist coverage to improve their efficiency in providing acute specialty care. Some of this demand may spill into single-specialty outpatient and focused freestanding hospital environments. Hospitalists will be pulled to cover specialists, who find their efficiency and the volume of work required prohibits them from providing comprehensive inpatient care for complex patients. They will prefer to focus on procedural interventions. Orthopedic surgery, cardiac surgery, neurosurgery, and cardiology, in particular, are likely to be new clients for hospitalist services.
Increasing emphasis on multidisciplinary care: Given the demand for evidence-based outcomes, hospitalists will provide physician input into clinical care design for a greater variety of patients in an increasing span of clinical service lines. This will put a demand on hospitalists for skills related to teamwork, leadership, and management in group environments. It will also require hospitalists to become broadly knowledgeable about the skills and contributions of all other potential care providers.
The New Medical Staff
The looming physician shortage in the United States will significantly affect the demand for and the variety and scope of work that hospitalists perform. The number of medical specialties dependent on hospitalist services will broaden. And hospitals will turn to hospitalists as their primary medical staff partners, responsible for the majority of medical staff functions and responsibilities. TH
Mike Guthrie, MD, is executive in residence at the University of Colorado (Denver) School of Business, Program in Health Administration, and a faculty member of SHM’s Leadership Academy.
In the Literature

Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
Hospital Quality for AMI: Process Measures and Their Relationship with Short-term Mortality
Bradley EH, Herrin J, Elbel B, et al. Hospital quality for acute myocardial infarction: correlation among process measures and relationship with short-term mortality. JAMA. 2006 Jul 5;296(1):72-78.
Background
The Centers for Medicare and Medicaid Services (CMS) and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) monitor and publicly report hospital performance in the treatment of acute myocardial infarction (AMI). Core process measures are considered an indicator of quality of care, but little is known about how these measures affect outcomes (mortality). Five of the seven core measures for AMI assess medication prescription practices; the other two measures are counseling on smoking cessation and timely reperfusion therapy.
Inferences about a hospital’s quality of care for AMI are created by measuring the hospital’s success at performing these measures. No previous study had evaluated a possible correlation between performance on these measures and short-term mortality. The authors of this study used National Registry of Myocardial Infarction (NRMI) and CMS databases to determine the association between hospital performance on AMI process measures and hospital-specific, risk-standardized, 30-day mortality rates.
Methods
A cross-sectional study was performed using hospitals that reported AMI discharges to the NRMI from January 2002 through March 2003. Hospitals had to report a minimum of 10 eligible patients. Hospital performance on core measures was recorded: beta-blocker on admission, beta-blocker on dismissal, aspirin on admission, aspirin on dismissal, angiotensin-converting enzyme inhibitor (ACE) prescription on dismissal, smoking cessation counseling for smokers during admission, and time to reperfusion therapy. Risk-standardized, 30-day, all-cause mortality rates were calculated for each hospital using CMS Medicare claims for patients ages 66 and older with AMI. The primary analysis determined the association of hospital-specific, risk-standardized, 30-day mortality rates with hospital performance on the core process measures.
Results
The most successfully completed core process measure for AMI was aspirin on admission. A mean of 86.4% of participating hospitals completed this measure. The core process measure for AMI that was the least frequently documented was smoking cessation counseling; a mean of 13.9% of participating hospitals completed this measure. Notably, timely reperfusion therapy for AMI—fibrinolytic therapy within 30 minutes of arrival or percutaneous intervention within 120 minutes of arrival—was completed by only 54.5% (mean) of participating hospitals.
Each core process measure had a statistically significant but small correlation with the risk-standardized, 30-day mortality rate (explaining between 0.1% and 3.3% of variance in mortality). Of the 180 hospitals in the top quintile of risk-standardized, 30-day mortality rates, only 31% were in the top quintile of the core process measures. A composite model of all seven core process measures determined that these measures could only explain 6% of the hospital-level variation in risk-standardized, 30-day mortality rates. Secondary analyses did not differ substantially.
Conclusions
In this study, each core process measure for AMI showed a modest correlation with 30-day mortality, but accounted for only 6% of 30-day mortality. This finding highlights the fact that continued measurement of these processes is valuable, but a hospital’s short-term mortality rates for AMI cannot be reliably inferred from performance on publicly reported process measures. These measures are weighted more toward long-term outcome measures. There is a need for new research to define and study new AMI process measures that can explain more of the variance in both short- and long-term outcomes.
Clopidogrel and Aspirin versus Aspirin Alone for the Prevention of Atherothrombotic Events
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006 Apr 20;354(16):1706-1717.
Background
Atherothrombotic disorders of the circulatory system are the leading cause of death and disability in the world. Low-dose aspirin has been shown to reduce ischemic event in populations above a certain risk threshold; however, aspirin alone may be insufficient treatment to prevent ischemic events in high-risk patients. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce ischemic events in patients with unstable angina, non-ST segment elevation and ST segment elevation myocardial infarction, as well as in those undergoing angioplasty and stenting.
Methods
This was a prospective, multicenter, randomized, double-blind, placebo-controlled study of the efficacy and safety of aspirin plus clopidogrel in comparison with aspirin plus placebo in patients at high risk for a cardiovascular event. Patients included in the study were 45 or older and had one of the following: multiple atherothrombotic risk factors, documented coronary artery disease, documented cerebrovascular disease, or documented symptomatic peripheral vascular disease. The primary efficacy endpoint was the first occurrence of myocardial infarction (MI), stroke, or death from cardiovascular causes. The primary safety endpoint was severe bleeding.
Results
A total of 15,603 patients were enrolled in the study. Treatment was permanently discontinued by 20.4% in the clopidogrel group as compared with 18.2% in the placebo group (P<0.001). A total of 4.8% of patients in the clopidogrel group and 4.9% in the placebo group discontinued treatment because of an adverse event (P=0.67). Other than the treatment medications, concomitant medication use was similar in both groups. A median follow-up of 28 months revealed that the rates of primary efficacy events in the clopidogrel and placebo group were similar (6.8% versus 7.3%, P=0.22, respectively). The rate of primary safety events was 1.7% in the clopidogrel group and 1.3% in the placebo group, P=0.09.
Conclusions
This trial enrolled patients who either had established atherothrombotic disease or were at high risk for such disease and found that there was no significant benefit associated with the use of clopidogrel plus aspirin compared to aspirin alone in reducing myocardial infarction, stroke, or cardiovascular death. The risk of moderate or severe bleeding in symptomatic patients was higher in the clopidogrel plus aspirin group than in the aspirin plus placebo group. Overall, these findings do not support the use of dual antiplatelet therapy across this broad patient population.
D-Dimer in the Diagnosis of Pulmonary Embolism
Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006 Jun 6;144(11):812-821.
Background
The clinical usefulness of the D-dimer test in the diagnosis of pulmonary embolism (PE) has been previously studied. In patients with suspected PE, it may be safe to omit additional diagnostic testing if a patient has a negative D-dimer test; however, this approach has never been evaluated in a randomized, controlled trial.
The investigators in this trial studied two subgroups of patients with suspected PE and a negative D-dimer: patients with a low clinical probability of PE and those with a moderate or high clinical probability of PE who had a non-diagnostic ventilation perfusion scan (VQ scan) and no proximal deep vein thrombosis on venous ultrasonography. The hypothesis was that patients with a negative D-dimer who do not have further testing for PE won’t have a higher frequency of venous thromboembolism during follow-up than patients who undergo routine diagnostic testing.
Methods
Before any diagnostic testing, patients were assigned a probability score, using the Wells Criteria, to categorize the probability of PE as low or moderate to high.
Patients with low probability Wells scores: D-dimer testing was done on all patients with a low clinical probability of PE. Patients with a negative D-dimer were randomly assigned either to no additional diagnostic testing and no anticoagulation treatment or to additional diagnostic testing with an initial VQ scan. If the VQ scan was negative, then PE was excluded. If the VQ scan showed one or more segmental perfusion defects that were normally ventilated, then the scan was considered diagnostic for PE. If there were perfusion defects that did not meet the criteria for a high probability scan, then the scan was considered non-diagnostic. Patients with non-diagnostic scans underwent ultrasonography of the proximal veins of the legs. If deep vein thrombosis was present, PE was diagnosed. If ultrasonography was normal, the test was repeated after seven and 14 days. In all patients with a positive D-dimer, a VQ scan was performed.
Patients with moderate to high probability Wells scores: A VQ scan was performed on all patients with a moderate to high probability for PE. Patients with high probability scans were treated; patients with normal scans were not treated. Patients with non-diagnostic scans and normal venous ultrasonography were randomly assigned to receive either no additional testing or serial ultrasonography.
Outcomes: All patients were followed for six months for the development of venous thromboembolism after initial diagnostic testing.
Results
The study enrolled 1,126 patients. Overall, 160 patients (14.2%) had PE diagnosed at initial presentation or by venous ultrasonography. Of 952 patients who did not receive an initial diagnosis of PE, 11 (1.2%) had PE diagnosed at follow-up.
Patients with low probability Wells scores: Low clinical probability was present in 670 patients (60%). In patients with low clinical probability of PE, 373 (56%) had negative D-dimer tests and 297 (44%) had positive D-dimer tests. Of the 373 patients with low probability and negative D-dimer results, 187 were randomized to no additional testing and 186 received a VQ scan. The frequency of venous thromboembolism at six-month follow-up was similar in these two groups (-0.5% [CI, -3.0% to 1.6%]). Three patients with negative D-dimer tests were diagnosed with PE by VQ scan. Results were fairly complete (five patients without a six-month follow-up in the no additional testing group and one without a follow-up in the VQ scan group).
Twenty-four patients with low clinical probability and positive D-dimer results (n=297) were diagnosed with PE. Three patients did not complete the six-month follow-up. Of the remaining 294 patients, five patients had venous thromboembolism at six months.
Patients with moderate to high probability Wells scores: There were 456 patients (40%) had moderate or high clinical probability for PE. Each of these patients had a VQ scan. Non-diagnostic VQ scans and normal venous ultrasonography were performed on 226 patients. Of these 226 patients, 86 had a negative D-dimer and 140 had a positive D-dimer. Of the 86 patients with negative VQ scans, normal venous ultrasonography, and a negative D-dimer, 83 were randomly assigned to no additional testing or serial venous ultrasonography (42 and 41 respectively). At six months follow-up, one patient assigned to no additional testing had venous thromboembolism, and no patients in the additional testing group had venous thromboembolism.
Conclusions
The results of this trial suggest that it is safe to withhold additional diagnostic testing in patients with suspected PE, low pretest clinical probability, and a negative D-dimer test. Even in patients with moderate to high pretest clinical probability, a non-diagnostic VQ scan, and normal venous ultrasonography, only one patient with a negative D-dimer had a venous thromboembolic event at six months follow-up. The assay used for this study was an erythrocyte agglutination SimpliRED assay. Reported sensitivity is approximately 90%, and specificity is approximately 75%. To the readers, it should be noted that the authors defined a low probability Wells score as 4 rather than 1.5 or lower.
Efficacy and Safety of Inhaled Insulin Therapy in Adults with Diabetes Mellitus
Ceglia L, Lau J, Pittas AG. Meta-analysis: efficacy and safety of inhaled insulin therapy in adults with diabetes mellitus. Ann Intern Med. 2006 Nov 7;145(9):665-675.
Background
Despite its effectiveness in attaining glycemic control, there is considerable resistance to insulin use by patients and healthcare providers, primarily because of the need for subcutaneous injection. In January 2006, the U.S. Food and Drug Administration (FDA) approved the first formulation of inhaled insulin for clinical use in nonsmoking adults with type 1 or type 2 diabetes and no pulmonary disease. The authors of this paper present a systematic review to examine the efficacy, safety, and patient acceptability of inhaled insulin.
Methods
The authors conducted a search of MEDLINE to find English-language, randomized, controlled trials of inhaled insulin in nonpregnant adults with diabetes. To find unpublished studies, the authors reviewed the briefing document on Exubera powder for oral inhalation (Pfizer Inc., New York). An abstract was included if it reported original data from controlled trials in patients with type 1 or 2 diabetes and hemoglobin A1C outcomes for patients receiving inhaled insulin versus outcomes for a comparison group (subcutaneous insulin or oral hypoglycemics). Studies with less than 12 weeks duration were excluded because no comparison could be made regarding glycemic efficacy. For glycemic efficacy, the primary outcome was the treatment group difference in hemoglobin A1C from baseline. Secondary outcome was the proportion of patients with hemoglobin A1C levels less than 7%. To evaluate safety, the primary outcomes were severe hypoglycemia (glucose ≤36 mg/dL), cough, and treatment group difference in pulmonary function variables.
Results
Sixteen trials involving a total of 4,023 patients met inclusion criteria. Seven trials compared inhaled insulin with various subcutaneous insulin regimens in patients with type 1 diabetes. Nine trials compared inhaled insulin with subcutaneous insulin or oral hypoglycemic agents in patients with type 2 diabetes. Inhaled insulin was given with meals and titrated according to study-specific glucose goals. Subcutaneous insulin was titrated to the same specific goals. Doses of oral hypoglycemic agents were adjusted for glycemic targets in only two of the nine trials. The combined data from the studies demonstrated a small but statistically significant decrease in the levels of baseline hemoglobin A1C levels in favor of subcutaneous insulin (weighted mean difference 0.08%, [CI 0.03% to 0.14%]) in patients with type 1 or type 2 diabetes. The greatest advantage of subcutaneous insulin was noted in the study with the longest duration (104 weeks). There was no difference between the study groups in studies with duration of 24 weeks or less. Patients with type 1 or type 2 diabetes taking inhaled insulin were no more likely to achieve hemoglobin A1C levels less than 7% than those using subcutaneous insulin.
The combined data from studies comparing inhaled insulin to oral hypoglycemic agents in patients with type 2 diabetes showed that inhaled insulin lowered hemoglobin A1C levels more effectively (weighted mean difference -1.04%, [CI -1.59% to -0.49%]). In studies in which the oral hypoglycemic agents were titrated, inhaled insulin still lowered baseline hemoglobin A1C levels but to a lesser degree (weighted mean difference -0.20%, [CI - 0.34% to -0.07%]). Patients with type 2 diabetes taking inhaled insulin were more likely to achieve hemoglobin A1C levels less than 7% than those taking oral agents.
There was no difference in episodes of severe hypoglycemia in patients using inhaled insulin compared to those using subcutaneous insulin. A higher proportion of patients using inhaled insulin reported at least one episode of severe hypoglycemia compared to those using oral agents (risk ratio, 3.06 [CI 1.03 to 9.07]; 9.4% versus 3.5%, respectively).
With respect to pulmonary safety, all trials selected patients without histories of pulmonary problems and with at least six months of nonsmoking status. Pulmonary safety was assessed by self-reported symptoms and by pulmonary function tests. The most common pulmonary symptom associated with inhaled insulin was nonproductive cough. This symptom was reported more frequently compared to patients using subcutaneous insulin or oral agents (risk ratio, 3.52 [CI 2.23 to 5.56]; 16.9% versus 5.0%). Cough was noted early in the treatment course and diminished in frequency over time. Patients receiving inhaled insulin had a greater decrease in FEV1 (forced expiratory volume in the first second) from baseline than the comparator group (weighted mean difference, -0.031 L [CI-0.043 L to -0.020 L]). This decrease progressed slowly over the first six months but stabilized in studies of up to two years’ duration.
Only four trials reported data on overall patient satisfaction for inhaled insulin versus subcutaneous insulin. All trials reported a statistically significant increase in overall patient satisfaction with inhaled insulin over subcutaneous insulin. Patients randomly assigned to inhaled insulin were more likely to continue taking inhaled insulin than to switch back to subcutaneous insulin.
Conclusions
This meta-analysis showed that inhaled insulin is comparable to subcutaneous insulin in lowering hemoglobin A1C levels in patients with type 1 or type 2 diabetes. The proportion of patients reaching a target hemoglobin A1C of less than 7% was much lower in the studies in this meta-analysis as compared to levels in trials of intensive subcutaneous insulin therapy.
It’s more difficult to compare inhaled insulin with oral hypoglycemic agents because most studies involving oral agents used fixed dosing with different types of oral agents. There was a three-fold risk of severe hypoglycemia in patients using inhaled insulin compared to those using oral hypoglycemic agents. This is probably due to overall improved glycemic control in the inhaled insulin group. Cough was more common in the inhaled insulin groups, and there were small decreases in FEV1, but these did not progress over two years. The potential for pulmonary toxicity with long-term administration has not been evaluated and deserves further study.
Read Your Patients
Translate the following statement into plain English:*
“It is fruitless to become lachrymose over precipitately departed lacteal fluid.”1
If these words made you pause—even for a moment—you now have an inkling of what people of limited literacy confront when they deal with the healthcare system.
Health literacy is best defined as a patient’s ability to read, comprehend, and act on medical instructions and to make appropriate health-related decisions.2,3 It is closely related to, although not absolutely dependent upon, one’s overall level of literacy—and literacy problems are surprisingly widespread. According to the National Assessment of Adult Literacy (NAAL), a survey of more than 19,000 adults conducted in 2003 by the National Center for Educational Statistics and published in 2006, 36% of American adults have nothing more than basic or below basic literacy. People in these two categories might be able to sign their names, decipher a bus schedule, or read very simple instructions telling them what they can and cannot eat before a medical test, but they cannot read a juror information pamphlet, much less an informed consent form. Another recent survey suggested that about one-third of adults in public hospitals read at or below a sixth-grade level.4
Components of Health Literacy
Several components figure into a person’s ability to manage his health and engage the healthcare system. Literacy limitations can impair any or all of these factors, which include:
- Health promotion: reading and understanding product labels or articles in newspapers;
- Health protection: reading and understanding applications for insurance or following sanitary precautions in the workplace;
- Disease prevention and screening: obtaining information about flu shots and blood pressure maintenance;
- Ability to access care and navigate the system: determining the most appropriate healthcare provider to call when a problem arises or filling out forms correctly; and
- Routine care and maintenance: testing blood glucose and getting regular checkups.1
Health literacy is further complicated by the fact that it can fluctuate in the same individual at different times and under different circumstances. For example, you might have no trouble deciphering the sentence at the beginning of this article if you feel well and are reading it in your office, living room, study, or some other familiar and comfortable environment. Now imagine that you’re ill and sitting in a noisy, chaotic emergency department, with a sheaf of other forms and papers to plow through. Suddenly the statement above may not be as easy to interpret.
“We must leave behind the notion of ‘illiterates,’ ” says Lakshmi Halasyamani, MD, chair of the Hospital Quality and Patient Safety Committee for SHM. “A person may not normally have a literacy problem, but they may be overwhelmed by the medical terminology, or they simply may not feel well enough to comprehend immediately everything the doctor says to them.”
The changing nature of healthcare may exacerbate the problem. Thirty years ago, only 650 drugs were available, and the average hospital stay for a myocardial infarction was four to six weeks. Today, there are more than 10,000 prescription drugs alone, and the typical stay for a heart attack is two to four days. As healthcare grows increasingly fragmented and complex, doctors have less time than ever to explain things and answer questions for their patients. Nevertheless, patients are expected to shoulder an ever-greater portion of the responsibility for their care and to live with conditions like diabetes or congestive heart failure, which require aggressive and detailed management.5 This is a challenge for even the most highly educated person; for someone whose literacy skills are fragile, the task can seem hopeless.
In addition to its medical and emotional consequences, limited health literacy is estimated to cost U.S. society $50 to $73 billion per year.6
Who Is Most Likely to Have Literacy Problems?
In general, “the likelihood of low literacy increases in racial and ethnic minority groups, patients with language barriers, and those with low educational achievement,” says Benjamin Powers, MD, associate professor of general internal medicine at Duke University and a physician at the Durham Veterans Affairs Medical Center in North Carolina.
It’s no surprise that literacy overall, and health literacy specifically, correlate so closely with education and especially with the lack of a high school degree. What is perhaps more surprising is that educational achievement alone does not necessarily guarantee good health literacy.
“Even high school graduates may have trouble,” says Mark Williams, MD. In addition to being a professor of medicine and director of the hospital medicine unit at Emory University School of Medicine in Atlanta, Dr. Williams is the editor of the Journal of Hospital Medicine and has studied health literacy problems for years. “Some highly literate people may have problems reading or absorbing health-related information if they’re sick and not feeling well.”
These people are not illiterate in the conventional sense, but they may have inadequate functional health literacy skills, at least in certain settings.
Age is another risk factor. In one survey of Medicare enrollees, at least one-third of people age 65 or older had some degree of health illiteracy, Dr. Williams says. As with so many other skills, proficient reading requires regular practice, and people tend to read less as they age, so their literacy skills may decline. “It’s especially a problem for the ‘oldest old,’ people who are 75 years old or more,” he explains.
Language and cultural differences also enter into the equation. A patient may be well educated and able to articulate in her own language (perhaps even able to converse well in English under normal circumstances), but may be unfamiliar with medical terminology. Put her in a situation in which she feels ill, flustered, and disoriented, and her communication skills may deteriorate even more, says Dr. Halasyamani.
In short, health literacy consists of many components, including “an emotional overlay, information overload, and cultural overload. All of these factor into the patients’ ability to understand what we tell them,” says Barbara DeBuono, MD, MPH, senior medical advisor on U.S. Public Health and Policy at Pfizer Pharmaceuticals.
Issues Unique to Hospitalists
There are also a few issues unique to hospitalists and their patients, warns Dr. DeBuono, who is also on the board of the Partnership for Clear Health Communication (See “Ask Me 3,” at right.) “Hospitalists don’t necessarily have a long-term relationship with these patients, so they have to make a quick assessment of the patient’s ability to understand and absorb information. Then they have to determine the best way to communicate that information, and, when necessary, change their communication strategy to fit the circumstances.”
In addition, she says, “hospital patients usually are more complicated than patients seen in an office practice. They may have chronic conditions and several comorbidities, and the information and discharge instructions the physicians give them can be pretty complex.”
Indeed, “a patient may come in thinking she had no issues and leave the hospital with four or five complaints. We’ve rocked her world, and that can be overwhelming for even the most motivated person,” says Dr. Halasyamani, who cautions that any chronic illness that requires a significant amount of ongoing self-care, such as diabetes or heart failure, can tax a patient’s ability to completely understand her situation and coordinate her care effectively.
Fragmented Care
Patients with multiple and complex morbidities also are likely to be cared for by several physicians, who prescribe numerous drugs, tests, and procedures, and who don’t necessarily know what the other members of the care team are doing. Even highly sophisticated people can get the feeling that they’re caught in an ever-changing kaleidoscope of medical visits and jargon, in which the various fragments never coalesce into a comprehensible whole. As Dr. Powers and coauthor Hayden Bosworth, PhD, wrote in a recent editorial: “ … there may be specific physician and health system organizational factors that exacerbate or mitigate the impact of low literacy. Literacy may matter more for patients who are cared for in a chaotic and discontinuous system that is not organized around delivering high quality care in a multidisciplinary setting.”7
This is more than a subjective impression: There is evidence supporting the importance of coordinated care for people of limited literacy skills. Dr. Powers and Bosworth recently compared the impact of low literacy on blood pressure control in patients in the Veterans Affairs (VA) system and those who attended local community clinics.
“Although the prevalence of low literacy was high in both populations, there was a significant association with low literacy and poor blood pressure control in the community clinics but not the VA,” Dr. Powers tells The Hospitalist. “In other words, literacy seemed to be an important predictor of good blood pressure control in one healthcare setting but not in another.”
In hospitals, “the frequency of handoffs among doctors, nurses, caseworkers, and social workers may all contribute to the fragmented nature of a patient’s care,” warns Dr. Halasyamani. This may be exacerbated even further should the patient have the misfortune to be admitted during a transitional period, such as a weekend or the end of the month when staff members rotate.
Red Flags
Literacy limitations are easy to miss: Patients rarely announce that they can’t read forms or comprehend a clinician’s instructions. “Just asking, ‘Do you understand?’ rarely works, because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively,” says Dr. Williams.
Usually, the clues are subtle. “Most physicians do encounter such patients, but we’re not trained to detect literacy problems and respond appropriately,” says Sunil Kripalani, MD, MSc, who, like Dr. Williams, is an Emory University hospitalist with a special interest in patient literacy issues. Dr. Kripalani suggests looking for red flags, including:
- Vague or evasive answers to questions. For example, “the patient who is taking a host of medications but can’t name them or tell you what time of day he’s supposed to take them;”
- Few, if any, questions or discussions of concerns: “Patients with limited literacy are less prone to ask questions, and the questions they do ask may not be as deep as those asked by a patient with greater literacy skills. The patient may use very simple terminology and not integrate any of the concepts discussed during the appointment;” and
- Missed appointments and repeated crises and hospitalizations resulting from the patient’s inability to read appointment cards or manage his illness. “Limited literacy skills may be a contributor to the exacerbations that put the patient in the hospital,” says Dr. Kripalani.
A patient with few family or social connections is also cause for concern, adds Dr. Halasyamani: “Lack of social support means there’s not another set of eyes and ears taking in the information.” Yet another red flag to her is the patient who cannot describe his plans for pursuing his care at home.
When patients have their medications with them, Dr. Williams asks how they take them. Those who can read simply look at the label, but a patient with literacy problems must open the bottle and look at the pills to identify them.
Solutions
How can physicians ensure that these patients understand and can follow instructions? Perhaps the easiest and most effective way is the “teach-back” approach, in which you ask the patient to repeat or teach back to you what you’ve just explained to him. For example, you might have him show you how to use an asthma inhaler or how to measure his blood glucose. In this way, you can rapidly assess and correct any deficiencies in the patient’s understanding.
“I’ve seen it take less than 90 seconds for physicians to confirm patient understanding in the context of a clinical visit,” says Dr. Kripalani.
A related technique that might help save time is to resist the temptation to tell the patient too much in a single visit. “Don’t try to give the patient too much information,” he advises. “People can process and retain maybe three nuggets of information at a time, so tell the patient the three most important things and then confirm their understanding of those three things.”
Dr. DeBuono suggests using visual aids like pictures or cartoons to help get important points across. If written material is necessary, have it printed in large type, which might appear less daunting than a page covered in dense, tiny print.
Above all, never embarrass a patient by bluntly asking him if he can read. “Explore the issue sensitively and respectfully,” Dr. Williams says. “Ask if they ever struggle with written materials or what the best way is for them to learn.” Adds Dr. DeBuono, “just by being sensitive to the fact that the patient may not understand is half the game.” TH
Norra MacReady is a medical journalist based in Southern California.
*“There’s no use crying over spilt milk.”
References
- Rudd RE. Literacy and implications for navigating health care. Harvard School of Public Health: Health Literacy Website. Slide 20. 2002. Available at www.hsph.harvard.edu/healthliteracy/slides/2002/2002_01.html. Last accessed December 1, 2006.
- Schillinger D, Grumbach K, Piette J, et al. Association of health literacy with diabetes outcomes. JAMA. 2002 Jul 24;288(4):475-482.
- Paasche-Orlow MK, Schillinger D, Greene SM, et al. How health care systems can begin to address the challenge of limited literacy. J Gen Intern Med. 2006 Aug;21(8):884-887.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006 Jul 27;355(4):339-341. Erratum in N Engl J Med. 2006 Sept 7;355(10):1076.
- Williams MV. Recognizing and overcoming inadequate health literacy, a barrier to care. Cleve Clin J Med. 2002 May;69(5):415-418.
- Weiss BD. Health literacy: a manual for clinicians [American Medical Association Web site]. American Medical Association Foundation and the American Medical Association, 2003. Available at: www.ama-assn.org/ama1/pub/upload/mm/367/healthlitclinicians.pdf. Last accessed December 16, 2006.
- Powers BJ, Bosworth HB. Revisiting literacy and adherence: future clinical and research directions. J Gen Intern Med. 2006;21:1341-1342.
Just asking, “Do you understand?” rarely works because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively.—Mark Williams, MD, professor of medicine and director of the hospital medicine unit at Emory University School of Medicine, Atlanta.
Translate the following statement into plain English:*
“It is fruitless to become lachrymose over precipitately departed lacteal fluid.”1
If these words made you pause—even for a moment—you now have an inkling of what people of limited literacy confront when they deal with the healthcare system.
Health literacy is best defined as a patient’s ability to read, comprehend, and act on medical instructions and to make appropriate health-related decisions.2,3 It is closely related to, although not absolutely dependent upon, one’s overall level of literacy—and literacy problems are surprisingly widespread. According to the National Assessment of Adult Literacy (NAAL), a survey of more than 19,000 adults conducted in 2003 by the National Center for Educational Statistics and published in 2006, 36% of American adults have nothing more than basic or below basic literacy. People in these two categories might be able to sign their names, decipher a bus schedule, or read very simple instructions telling them what they can and cannot eat before a medical test, but they cannot read a juror information pamphlet, much less an informed consent form. Another recent survey suggested that about one-third of adults in public hospitals read at or below a sixth-grade level.4
Components of Health Literacy
Several components figure into a person’s ability to manage his health and engage the healthcare system. Literacy limitations can impair any or all of these factors, which include:
- Health promotion: reading and understanding product labels or articles in newspapers;
- Health protection: reading and understanding applications for insurance or following sanitary precautions in the workplace;
- Disease prevention and screening: obtaining information about flu shots and blood pressure maintenance;
- Ability to access care and navigate the system: determining the most appropriate healthcare provider to call when a problem arises or filling out forms correctly; and
- Routine care and maintenance: testing blood glucose and getting regular checkups.1
Health literacy is further complicated by the fact that it can fluctuate in the same individual at different times and under different circumstances. For example, you might have no trouble deciphering the sentence at the beginning of this article if you feel well and are reading it in your office, living room, study, or some other familiar and comfortable environment. Now imagine that you’re ill and sitting in a noisy, chaotic emergency department, with a sheaf of other forms and papers to plow through. Suddenly the statement above may not be as easy to interpret.
“We must leave behind the notion of ‘illiterates,’ ” says Lakshmi Halasyamani, MD, chair of the Hospital Quality and Patient Safety Committee for SHM. “A person may not normally have a literacy problem, but they may be overwhelmed by the medical terminology, or they simply may not feel well enough to comprehend immediately everything the doctor says to them.”
The changing nature of healthcare may exacerbate the problem. Thirty years ago, only 650 drugs were available, and the average hospital stay for a myocardial infarction was four to six weeks. Today, there are more than 10,000 prescription drugs alone, and the typical stay for a heart attack is two to four days. As healthcare grows increasingly fragmented and complex, doctors have less time than ever to explain things and answer questions for their patients. Nevertheless, patients are expected to shoulder an ever-greater portion of the responsibility for their care and to live with conditions like diabetes or congestive heart failure, which require aggressive and detailed management.5 This is a challenge for even the most highly educated person; for someone whose literacy skills are fragile, the task can seem hopeless.
In addition to its medical and emotional consequences, limited health literacy is estimated to cost U.S. society $50 to $73 billion per year.6
Who Is Most Likely to Have Literacy Problems?
In general, “the likelihood of low literacy increases in racial and ethnic minority groups, patients with language barriers, and those with low educational achievement,” says Benjamin Powers, MD, associate professor of general internal medicine at Duke University and a physician at the Durham Veterans Affairs Medical Center in North Carolina.
It’s no surprise that literacy overall, and health literacy specifically, correlate so closely with education and especially with the lack of a high school degree. What is perhaps more surprising is that educational achievement alone does not necessarily guarantee good health literacy.
“Even high school graduates may have trouble,” says Mark Williams, MD. In addition to being a professor of medicine and director of the hospital medicine unit at Emory University School of Medicine in Atlanta, Dr. Williams is the editor of the Journal of Hospital Medicine and has studied health literacy problems for years. “Some highly literate people may have problems reading or absorbing health-related information if they’re sick and not feeling well.”
These people are not illiterate in the conventional sense, but they may have inadequate functional health literacy skills, at least in certain settings.
Age is another risk factor. In one survey of Medicare enrollees, at least one-third of people age 65 or older had some degree of health illiteracy, Dr. Williams says. As with so many other skills, proficient reading requires regular practice, and people tend to read less as they age, so their literacy skills may decline. “It’s especially a problem for the ‘oldest old,’ people who are 75 years old or more,” he explains.
Language and cultural differences also enter into the equation. A patient may be well educated and able to articulate in her own language (perhaps even able to converse well in English under normal circumstances), but may be unfamiliar with medical terminology. Put her in a situation in which she feels ill, flustered, and disoriented, and her communication skills may deteriorate even more, says Dr. Halasyamani.
In short, health literacy consists of many components, including “an emotional overlay, information overload, and cultural overload. All of these factor into the patients’ ability to understand what we tell them,” says Barbara DeBuono, MD, MPH, senior medical advisor on U.S. Public Health and Policy at Pfizer Pharmaceuticals.
Issues Unique to Hospitalists
There are also a few issues unique to hospitalists and their patients, warns Dr. DeBuono, who is also on the board of the Partnership for Clear Health Communication (See “Ask Me 3,” at right.) “Hospitalists don’t necessarily have a long-term relationship with these patients, so they have to make a quick assessment of the patient’s ability to understand and absorb information. Then they have to determine the best way to communicate that information, and, when necessary, change their communication strategy to fit the circumstances.”
In addition, she says, “hospital patients usually are more complicated than patients seen in an office practice. They may have chronic conditions and several comorbidities, and the information and discharge instructions the physicians give them can be pretty complex.”
Indeed, “a patient may come in thinking she had no issues and leave the hospital with four or five complaints. We’ve rocked her world, and that can be overwhelming for even the most motivated person,” says Dr. Halasyamani, who cautions that any chronic illness that requires a significant amount of ongoing self-care, such as diabetes or heart failure, can tax a patient’s ability to completely understand her situation and coordinate her care effectively.
Fragmented Care
Patients with multiple and complex morbidities also are likely to be cared for by several physicians, who prescribe numerous drugs, tests, and procedures, and who don’t necessarily know what the other members of the care team are doing. Even highly sophisticated people can get the feeling that they’re caught in an ever-changing kaleidoscope of medical visits and jargon, in which the various fragments never coalesce into a comprehensible whole. As Dr. Powers and coauthor Hayden Bosworth, PhD, wrote in a recent editorial: “ … there may be specific physician and health system organizational factors that exacerbate or mitigate the impact of low literacy. Literacy may matter more for patients who are cared for in a chaotic and discontinuous system that is not organized around delivering high quality care in a multidisciplinary setting.”7
This is more than a subjective impression: There is evidence supporting the importance of coordinated care for people of limited literacy skills. Dr. Powers and Bosworth recently compared the impact of low literacy on blood pressure control in patients in the Veterans Affairs (VA) system and those who attended local community clinics.
“Although the prevalence of low literacy was high in both populations, there was a significant association with low literacy and poor blood pressure control in the community clinics but not the VA,” Dr. Powers tells The Hospitalist. “In other words, literacy seemed to be an important predictor of good blood pressure control in one healthcare setting but not in another.”
In hospitals, “the frequency of handoffs among doctors, nurses, caseworkers, and social workers may all contribute to the fragmented nature of a patient’s care,” warns Dr. Halasyamani. This may be exacerbated even further should the patient have the misfortune to be admitted during a transitional period, such as a weekend or the end of the month when staff members rotate.
Red Flags
Literacy limitations are easy to miss: Patients rarely announce that they can’t read forms or comprehend a clinician’s instructions. “Just asking, ‘Do you understand?’ rarely works, because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively,” says Dr. Williams.
Usually, the clues are subtle. “Most physicians do encounter such patients, but we’re not trained to detect literacy problems and respond appropriately,” says Sunil Kripalani, MD, MSc, who, like Dr. Williams, is an Emory University hospitalist with a special interest in patient literacy issues. Dr. Kripalani suggests looking for red flags, including:
- Vague or evasive answers to questions. For example, “the patient who is taking a host of medications but can’t name them or tell you what time of day he’s supposed to take them;”
- Few, if any, questions or discussions of concerns: “Patients with limited literacy are less prone to ask questions, and the questions they do ask may not be as deep as those asked by a patient with greater literacy skills. The patient may use very simple terminology and not integrate any of the concepts discussed during the appointment;” and
- Missed appointments and repeated crises and hospitalizations resulting from the patient’s inability to read appointment cards or manage his illness. “Limited literacy skills may be a contributor to the exacerbations that put the patient in the hospital,” says Dr. Kripalani.
A patient with few family or social connections is also cause for concern, adds Dr. Halasyamani: “Lack of social support means there’s not another set of eyes and ears taking in the information.” Yet another red flag to her is the patient who cannot describe his plans for pursuing his care at home.
When patients have their medications with them, Dr. Williams asks how they take them. Those who can read simply look at the label, but a patient with literacy problems must open the bottle and look at the pills to identify them.
Solutions
How can physicians ensure that these patients understand and can follow instructions? Perhaps the easiest and most effective way is the “teach-back” approach, in which you ask the patient to repeat or teach back to you what you’ve just explained to him. For example, you might have him show you how to use an asthma inhaler or how to measure his blood glucose. In this way, you can rapidly assess and correct any deficiencies in the patient’s understanding.
“I’ve seen it take less than 90 seconds for physicians to confirm patient understanding in the context of a clinical visit,” says Dr. Kripalani.
A related technique that might help save time is to resist the temptation to tell the patient too much in a single visit. “Don’t try to give the patient too much information,” he advises. “People can process and retain maybe three nuggets of information at a time, so tell the patient the three most important things and then confirm their understanding of those three things.”
Dr. DeBuono suggests using visual aids like pictures or cartoons to help get important points across. If written material is necessary, have it printed in large type, which might appear less daunting than a page covered in dense, tiny print.
Above all, never embarrass a patient by bluntly asking him if he can read. “Explore the issue sensitively and respectfully,” Dr. Williams says. “Ask if they ever struggle with written materials or what the best way is for them to learn.” Adds Dr. DeBuono, “just by being sensitive to the fact that the patient may not understand is half the game.” TH
Norra MacReady is a medical journalist based in Southern California.
*“There’s no use crying over spilt milk.”
References
- Rudd RE. Literacy and implications for navigating health care. Harvard School of Public Health: Health Literacy Website. Slide 20. 2002. Available at www.hsph.harvard.edu/healthliteracy/slides/2002/2002_01.html. Last accessed December 1, 2006.
- Schillinger D, Grumbach K, Piette J, et al. Association of health literacy with diabetes outcomes. JAMA. 2002 Jul 24;288(4):475-482.
- Paasche-Orlow MK, Schillinger D, Greene SM, et al. How health care systems can begin to address the challenge of limited literacy. J Gen Intern Med. 2006 Aug;21(8):884-887.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006 Jul 27;355(4):339-341. Erratum in N Engl J Med. 2006 Sept 7;355(10):1076.
- Williams MV. Recognizing and overcoming inadequate health literacy, a barrier to care. Cleve Clin J Med. 2002 May;69(5):415-418.
- Weiss BD. Health literacy: a manual for clinicians [American Medical Association Web site]. American Medical Association Foundation and the American Medical Association, 2003. Available at: www.ama-assn.org/ama1/pub/upload/mm/367/healthlitclinicians.pdf. Last accessed December 16, 2006.
- Powers BJ, Bosworth HB. Revisiting literacy and adherence: future clinical and research directions. J Gen Intern Med. 2006;21:1341-1342.
Just asking, “Do you understand?” rarely works because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively.—Mark Williams, MD, professor of medicine and director of the hospital medicine unit at Emory University School of Medicine, Atlanta.
Translate the following statement into plain English:*
“It is fruitless to become lachrymose over precipitately departed lacteal fluid.”1
If these words made you pause—even for a moment—you now have an inkling of what people of limited literacy confront when they deal with the healthcare system.
Health literacy is best defined as a patient’s ability to read, comprehend, and act on medical instructions and to make appropriate health-related decisions.2,3 It is closely related to, although not absolutely dependent upon, one’s overall level of literacy—and literacy problems are surprisingly widespread. According to the National Assessment of Adult Literacy (NAAL), a survey of more than 19,000 adults conducted in 2003 by the National Center for Educational Statistics and published in 2006, 36% of American adults have nothing more than basic or below basic literacy. People in these two categories might be able to sign their names, decipher a bus schedule, or read very simple instructions telling them what they can and cannot eat before a medical test, but they cannot read a juror information pamphlet, much less an informed consent form. Another recent survey suggested that about one-third of adults in public hospitals read at or below a sixth-grade level.4
Components of Health Literacy
Several components figure into a person’s ability to manage his health and engage the healthcare system. Literacy limitations can impair any or all of these factors, which include:
- Health promotion: reading and understanding product labels or articles in newspapers;
- Health protection: reading and understanding applications for insurance or following sanitary precautions in the workplace;
- Disease prevention and screening: obtaining information about flu shots and blood pressure maintenance;
- Ability to access care and navigate the system: determining the most appropriate healthcare provider to call when a problem arises or filling out forms correctly; and
- Routine care and maintenance: testing blood glucose and getting regular checkups.1
Health literacy is further complicated by the fact that it can fluctuate in the same individual at different times and under different circumstances. For example, you might have no trouble deciphering the sentence at the beginning of this article if you feel well and are reading it in your office, living room, study, or some other familiar and comfortable environment. Now imagine that you’re ill and sitting in a noisy, chaotic emergency department, with a sheaf of other forms and papers to plow through. Suddenly the statement above may not be as easy to interpret.
“We must leave behind the notion of ‘illiterates,’ ” says Lakshmi Halasyamani, MD, chair of the Hospital Quality and Patient Safety Committee for SHM. “A person may not normally have a literacy problem, but they may be overwhelmed by the medical terminology, or they simply may not feel well enough to comprehend immediately everything the doctor says to them.”
The changing nature of healthcare may exacerbate the problem. Thirty years ago, only 650 drugs were available, and the average hospital stay for a myocardial infarction was four to six weeks. Today, there are more than 10,000 prescription drugs alone, and the typical stay for a heart attack is two to four days. As healthcare grows increasingly fragmented and complex, doctors have less time than ever to explain things and answer questions for their patients. Nevertheless, patients are expected to shoulder an ever-greater portion of the responsibility for their care and to live with conditions like diabetes or congestive heart failure, which require aggressive and detailed management.5 This is a challenge for even the most highly educated person; for someone whose literacy skills are fragile, the task can seem hopeless.
In addition to its medical and emotional consequences, limited health literacy is estimated to cost U.S. society $50 to $73 billion per year.6
Who Is Most Likely to Have Literacy Problems?
In general, “the likelihood of low literacy increases in racial and ethnic minority groups, patients with language barriers, and those with low educational achievement,” says Benjamin Powers, MD, associate professor of general internal medicine at Duke University and a physician at the Durham Veterans Affairs Medical Center in North Carolina.
It’s no surprise that literacy overall, and health literacy specifically, correlate so closely with education and especially with the lack of a high school degree. What is perhaps more surprising is that educational achievement alone does not necessarily guarantee good health literacy.
“Even high school graduates may have trouble,” says Mark Williams, MD. In addition to being a professor of medicine and director of the hospital medicine unit at Emory University School of Medicine in Atlanta, Dr. Williams is the editor of the Journal of Hospital Medicine and has studied health literacy problems for years. “Some highly literate people may have problems reading or absorbing health-related information if they’re sick and not feeling well.”
These people are not illiterate in the conventional sense, but they may have inadequate functional health literacy skills, at least in certain settings.
Age is another risk factor. In one survey of Medicare enrollees, at least one-third of people age 65 or older had some degree of health illiteracy, Dr. Williams says. As with so many other skills, proficient reading requires regular practice, and people tend to read less as they age, so their literacy skills may decline. “It’s especially a problem for the ‘oldest old,’ people who are 75 years old or more,” he explains.
Language and cultural differences also enter into the equation. A patient may be well educated and able to articulate in her own language (perhaps even able to converse well in English under normal circumstances), but may be unfamiliar with medical terminology. Put her in a situation in which she feels ill, flustered, and disoriented, and her communication skills may deteriorate even more, says Dr. Halasyamani.
In short, health literacy consists of many components, including “an emotional overlay, information overload, and cultural overload. All of these factor into the patients’ ability to understand what we tell them,” says Barbara DeBuono, MD, MPH, senior medical advisor on U.S. Public Health and Policy at Pfizer Pharmaceuticals.
Issues Unique to Hospitalists
There are also a few issues unique to hospitalists and their patients, warns Dr. DeBuono, who is also on the board of the Partnership for Clear Health Communication (See “Ask Me 3,” at right.) “Hospitalists don’t necessarily have a long-term relationship with these patients, so they have to make a quick assessment of the patient’s ability to understand and absorb information. Then they have to determine the best way to communicate that information, and, when necessary, change their communication strategy to fit the circumstances.”
In addition, she says, “hospital patients usually are more complicated than patients seen in an office practice. They may have chronic conditions and several comorbidities, and the information and discharge instructions the physicians give them can be pretty complex.”
Indeed, “a patient may come in thinking she had no issues and leave the hospital with four or five complaints. We’ve rocked her world, and that can be overwhelming for even the most motivated person,” says Dr. Halasyamani, who cautions that any chronic illness that requires a significant amount of ongoing self-care, such as diabetes or heart failure, can tax a patient’s ability to completely understand her situation and coordinate her care effectively.
Fragmented Care
Patients with multiple and complex morbidities also are likely to be cared for by several physicians, who prescribe numerous drugs, tests, and procedures, and who don’t necessarily know what the other members of the care team are doing. Even highly sophisticated people can get the feeling that they’re caught in an ever-changing kaleidoscope of medical visits and jargon, in which the various fragments never coalesce into a comprehensible whole. As Dr. Powers and coauthor Hayden Bosworth, PhD, wrote in a recent editorial: “ … there may be specific physician and health system organizational factors that exacerbate or mitigate the impact of low literacy. Literacy may matter more for patients who are cared for in a chaotic and discontinuous system that is not organized around delivering high quality care in a multidisciplinary setting.”7
This is more than a subjective impression: There is evidence supporting the importance of coordinated care for people of limited literacy skills. Dr. Powers and Bosworth recently compared the impact of low literacy on blood pressure control in patients in the Veterans Affairs (VA) system and those who attended local community clinics.
“Although the prevalence of low literacy was high in both populations, there was a significant association with low literacy and poor blood pressure control in the community clinics but not the VA,” Dr. Powers tells The Hospitalist. “In other words, literacy seemed to be an important predictor of good blood pressure control in one healthcare setting but not in another.”
In hospitals, “the frequency of handoffs among doctors, nurses, caseworkers, and social workers may all contribute to the fragmented nature of a patient’s care,” warns Dr. Halasyamani. This may be exacerbated even further should the patient have the misfortune to be admitted during a transitional period, such as a weekend or the end of the month when staff members rotate.
Red Flags
Literacy limitations are easy to miss: Patients rarely announce that they can’t read forms or comprehend a clinician’s instructions. “Just asking, ‘Do you understand?’ rarely works, because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively,” says Dr. Williams.
Usually, the clues are subtle. “Most physicians do encounter such patients, but we’re not trained to detect literacy problems and respond appropriately,” says Sunil Kripalani, MD, MSc, who, like Dr. Williams, is an Emory University hospitalist with a special interest in patient literacy issues. Dr. Kripalani suggests looking for red flags, including:
- Vague or evasive answers to questions. For example, “the patient who is taking a host of medications but can’t name them or tell you what time of day he’s supposed to take them;”
- Few, if any, questions or discussions of concerns: “Patients with limited literacy are less prone to ask questions, and the questions they do ask may not be as deep as those asked by a patient with greater literacy skills. The patient may use very simple terminology and not integrate any of the concepts discussed during the appointment;” and
- Missed appointments and repeated crises and hospitalizations resulting from the patient’s inability to read appointment cards or manage his illness. “Limited literacy skills may be a contributor to the exacerbations that put the patient in the hospital,” says Dr. Kripalani.
A patient with few family or social connections is also cause for concern, adds Dr. Halasyamani: “Lack of social support means there’s not another set of eyes and ears taking in the information.” Yet another red flag to her is the patient who cannot describe his plans for pursuing his care at home.
When patients have their medications with them, Dr. Williams asks how they take them. Those who can read simply look at the label, but a patient with literacy problems must open the bottle and look at the pills to identify them.
Solutions
How can physicians ensure that these patients understand and can follow instructions? Perhaps the easiest and most effective way is the “teach-back” approach, in which you ask the patient to repeat or teach back to you what you’ve just explained to him. For example, you might have him show you how to use an asthma inhaler or how to measure his blood glucose. In this way, you can rapidly assess and correct any deficiencies in the patient’s understanding.
“I’ve seen it take less than 90 seconds for physicians to confirm patient understanding in the context of a clinical visit,” says Dr. Kripalani.
A related technique that might help save time is to resist the temptation to tell the patient too much in a single visit. “Don’t try to give the patient too much information,” he advises. “People can process and retain maybe three nuggets of information at a time, so tell the patient the three most important things and then confirm their understanding of those three things.”
Dr. DeBuono suggests using visual aids like pictures or cartoons to help get important points across. If written material is necessary, have it printed in large type, which might appear less daunting than a page covered in dense, tiny print.
Above all, never embarrass a patient by bluntly asking him if he can read. “Explore the issue sensitively and respectfully,” Dr. Williams says. “Ask if they ever struggle with written materials or what the best way is for them to learn.” Adds Dr. DeBuono, “just by being sensitive to the fact that the patient may not understand is half the game.” TH
Norra MacReady is a medical journalist based in Southern California.
*“There’s no use crying over spilt milk.”
References
- Rudd RE. Literacy and implications for navigating health care. Harvard School of Public Health: Health Literacy Website. Slide 20. 2002. Available at www.hsph.harvard.edu/healthliteracy/slides/2002/2002_01.html. Last accessed December 1, 2006.
- Schillinger D, Grumbach K, Piette J, et al. Association of health literacy with diabetes outcomes. JAMA. 2002 Jul 24;288(4):475-482.
- Paasche-Orlow MK, Schillinger D, Greene SM, et al. How health care systems can begin to address the challenge of limited literacy. J Gen Intern Med. 2006 Aug;21(8):884-887.
- Marcus EN. The silent epidemic—the health effects of illiteracy. N Engl J Med. 2006 Jul 27;355(4):339-341. Erratum in N Engl J Med. 2006 Sept 7;355(10):1076.
- Williams MV. Recognizing and overcoming inadequate health literacy, a barrier to care. Cleve Clin J Med. 2002 May;69(5):415-418.
- Weiss BD. Health literacy: a manual for clinicians [American Medical Association Web site]. American Medical Association Foundation and the American Medical Association, 2003. Available at: www.ama-assn.org/ama1/pub/upload/mm/367/healthlitclinicians.pdf. Last accessed December 16, 2006.
- Powers BJ, Bosworth HB. Revisiting literacy and adherence: future clinical and research directions. J Gen Intern Med. 2006;21:1341-1342.
Just asking, “Do you understand?” rarely works because the patient may just nod yes. Physicians need to assess the patient’s comprehension proactively.—Mark Williams, MD, professor of medicine and director of the hospital medicine unit at Emory University School of Medicine, Atlanta.
Get Smart
In YOU: The Smart Patient: An Insider's Handbook for Getting the Best Treatment, authors Michael F. Roizen, MD, and Mehmet C. Oz, MD, well-credentialed celebrity physicians, tell the reader that being a smart patient may make the difference between good and poor care and may even save your life. Everyone can be a “medical detective,” they suggest, seeking and supplying the facts that providers and administrators need in order to avoid errors or mix-ups.
The Joint Commission Resources, a collaborator on this publication, announces on its Web site that this book “empowers patients” (www.jcrinc.com/generic.asp?durki=11727&site=11&return=405.). Dr. Oz, in a Web post to customers who might purchase the book, puts it this way: “[T]he Joint Commission, our nation’s healthcare safety advocate, approached us to help with a big problem. Medical errors cost us 98,000 lives per year, and the Joint Commission could not squash this crazily large number without pulling in the biggest ally of all, the Smart Patient.” It’s a “scary statistic,” but true, he writes, “You have a two in five chance of being affected by a major medical complication in your life.” (For more information on the book, visit www.amazon.com/YOU-Insiders-Handbook-Getting-Treatment/dp/0743293010.)
The Hospitalist asked some hospitalists what they would recommend to a friend or relative headed for a hospital stay. Do they have any tips that only an insider would know? As might be expected, some of their advice echoes that already available in print, in broadcasts, and on the Web. And some things that were mentioned in these publications were also on our hospitalists’ list, including bringing along statistics, dates, and other healthcare specifics that might be crucial to providers. In fact, Drs. Roizen and Oz recommend assembling a thorough health history and bringing two copies of it to hospital admission—one especially for “the admitting nurse who welcomes you to your bed.”
Assume Nothing
In their book chapter on hospital stays, Drs. Oz and Roizen emphasize that patients and their visitors should keep an eye out to make certain hospital staff wash their hands and give the patient the right treatments, tests, and medications. “It’s astounding the amount of diligence you and your family will have to exercise during a hospital stay,” a reader-reviewer writes on the book’s Web page on the Amazon.com site. Some of the warnings posted in a book excerpt at the Joint Commission on Accreditation of Healthcare Organizations (JCAHO)’s site include “Don’t touch that remote!” and “wear rubber gloves” if you do want to watch TV. Readers are told that “a study found that the TV remote control is one of the most germ-infested things in a hospital room.”
Patients are also cautioned to “insist on being scanned,” to “insist on a clean stethoscope,” and to keep “an industrial-sized jug of alcohol hand-sanitizing gel” by the bed. In fact, the authors write: “Stethoscopes are filthy from being used on several patients an hour. Most doc[tor]s now wash their stethoscopes with alcohol between patients, but we’d always ask.” Our hospitalists agreed.
Ian Jenkins, MD, a hospitalist with the University of California at San Diego, would tell his friends and family to remind providers to wash their hands. “Don’t let anyone touch you unless you’ve seen them wash or gel their hands correctly—and their stethoscopes, too.”
Drs. Oz and Roizen say, “You might even post a sign that reads ‘Thank You for Washing Your Hands’ as a gentle reminder.”
Trust your intuition, one hospitalist tells people facing hospitalization. “If you sense that something is awry, it probably is,” says Jeanne Farnan, MD, a hospitalist scholar at The University of Chicago Hospitals. “Discuss concerns with physicians/nurses. Write down your questions in case they come to you spontaneously.”
On the other hand, she tells friends and relatives, “Patients, when asked questions, will often respond, ‘it’s in my chart.’ We often don't have access to a primary MD’s notes/chart, and not all documentation is pristine. When we are asking questions regarding your medical history, it is only to provide you with the best care—not to be a nuisance.”
Be Selective about Your Providers and Hospital
One recommendation from JCAHO’s patient education Web pages is a section entitled “Finding Dr. Right.” “Choose wisely and you could rest easy for many years to come,” it says.
Sandeep Sachdeva, MD, lead hospitalist at Swedish Medical Center’s Stroke Program and clinical instructor at the University of Washington at Seattle, says this may apply even to a patient’s relationship with a hospitalist.
“Sometimes patients come in and tell us their stories [about how providers treat them]. It’s just amazing; I think patients who have family members providing close supervision seem to get better care than somebody [who] is not asking questions,” he says. “And some care providers find questions intimidating, but the patient should not get discouraged by that. … If they feel that the care provider is not listening to them or not being attentive to them, they can always have a recourse: They can talk to the supervisor of that provider or somebody else [to get] a different provider. Patients sometimes have the fear that if they speak up against somebody that their care might be jeopardized.”
Dr. Sachdeva advises friends and relatives that they talk to the nursing supervisor or ask for the physician supervisor or an administrative person or social worker so that they get the attention they need.
Dr. Jenkins agrees. “Informed consent” is one of his tips for friends and family: “If your doctor won't talk to you about the risks and benefits of your treatments, and alternatives to them, you need a new doctor.”
Our hospitalists suggest being discriminating, savvy, and proactive:
- “Find one hospital you are comfortable with, [where] your family physician is on staff, and use it exclusively if possible,” says David M. Grace, MD, a hospitalist with The Schumacher Group in Lafayette, La. “By utilizing one hospital, all of your previous records and test results are immediately available when needed. Often this translates into a much shorter hospitalization as there are no delays in obtaining old records, and it minimizes the chance of duplicate tests/procedures being performed.”
- “Know who your doctors are [and] what their role is, and understand their input into your healthcare,” says Dr. Farnan, who is extensively involved in medical residents’ training. And “be cognizant of the physician work hours,” she advises. “We often have families who demand to speak with ‘their’ doctor at all hours of the early morning and night.” She tells friends and relatives, “I think more patients need to understand the nature [and] structure of the system [and] what kind of information a covering physician can provide. If the family of the patient has questions [and] wants to speak with the primary MD, it may be best to attempt in the daytime when the primary service is more likely to be present.”
- “Know the full names, and preferably [the] phone numbers, of all your outpatient physicians,” says Dr. Grace. “One area will often have multiple doctors with the same last name, and, frequently, records need to be requested from them. Up-to-date contact information on your physicians helps us request the right records from the right physicians with minimal delay.”
What to Bring to the Hospital
Some hospital Web sites advise patients on what to bring with them for their hospital stay, suggesting everything from your own robe, slippers, pajamas, or nightgown to an advance directive. Definitely, the latter is an important point.
“Whether it’s an elective or emergent admission,” says Dr. Grace, “there are a few things [you] can do to ensure [your] hospitalization is as safe, efficient, and productive as possible,” he tells friends and relatives. Among them, he says, is to “have a Living Will or advance directives completed, ensure the hospital has a copy, and discuss your wishes with your family prior to admission. Clear and concise plans, coupled with good family awareness, will help ensure your wishes and values are honored appropriately.”
And, as several of his hospitalist colleagues suggest, “Bring all of the medications you are currently using, including any over-the-counter medicines and herbs or homeopathic treatments. It’s imperative that physicians know what medications you are taking [because] many cannot be stopped abruptly, and [they may] have interactions with medications you may receive in the hospital.”
In addition, “know what medications you’re truly allergic to [e.g., hives, swelling, breathing problems],” Dr. Grace advises, “and which medications you have had side effects from [e.g., stomach upset, sleepiness, and so on]. Many patients confuse the two. Occasionally the best or only option involves using medications with potential unwanted side effects. Rarely do we use medications to which the patient has a true allergy.”
Communication: The Key to the Hospital Kingdom
Dr. Sachdeva recommends being ready to communicate even before going to the hospital. “In the case of an emergency admission,” he says, “they should have all their information readily available because at the time for a needed hospitalization, they may be sick and confused.” Have it “on their person” or in “an easily identifiable place,” he says, and, like his colleagues, he reiterates that this information should include a list of medications, problems, doctors, and phone numbers, along with a list of patient advocates and their phone numbers.
“Most of the time, patients are able to notify a family member, but if that doesn’t happen, then the ER can notify the appropriate person to be present to supervise and oversee the care from a patient perspective,” he says.
Communication was mentioned by all the hospitalists we interviewed. “Be prepared to ask questions and take an active role in your healthcare,” says Dr. Grace. “Ask your nurse what each medication you receive is and what it’s for. Ensure you know what medications to continue taking when you return home and which ones to stop. If you don’t understand your diagnosis, prognosis, or treatment plan, make sure you ask.”
One hospitalist’s advice pertained to the patient’s and family’s behavior and is based on an experience in her own family: “Be really nice to everybody,” Alison Holmes, MD, a hospitalist with Concord Hospital, Concord, N.H., advises friends and family. “This is hard to do when you’re sick and scared, but it’s incredibly important.”
Dr. Holmes speaks of her own parents’ experience: “My mother was admitted to the hospital for pneumonia about a year ago. She had very long wait in the emergency room. My father got very upset and called me and said, ‘Oh, they were so angry at me, I was yelling at everybody.’
“That won’t get you anywhere!” I told him. “That will get you worse care.” I asked, “Where is she now?” and he said, ‘Oh, she’s still in the emergency room,’ and I said, “You’re at home? You left her there?” Dr. Holmes then advised her father to return to the hospital right away.
Finally, all the hospitalists we interviewed emphasized that they would tell their family members to designate a point person for communication. And you can’t assume that that would be their doctor son or daughter, even if they happened to be in the same locale.
“When possible, don’t stay in the hospital alone,” says Dr. Holmes. “Try to always have a family member present so that there is someone available for questions. It’s not always clear where [the physician] can reach someone or how far away [that person is]. It can take a little coordination and multiple people to do it,” she says.
Also, Dr. Farnan points out, “It is often difficult [because of time limitations] for [physicians] to repeat the same information to multiple family members.”
All patients, but especially the elderly, says Dr. Sachdeva, should have a patient advocate with them at the hospital. If they don’t have family close by, they should have “a close friend or neighbor who is willing to take on that job, someone who can be there in the room and ask these questions: What medicine are you giving me? What’s the next step? What are the options?”
Dr. Sachdeva advises relatives that they might be distressed or unable to focus, so having a healthy advocate with them may be extremely important, “the difference between life and death,” although, no doubt, he’d leave that last comment out of his advice to family. “Because a lot of the time, it is not that we don’t try to do a good job, but it’s just [that] the advocate might bring something to our attention that we might not have otherwise noticed.” TH
Andrea Sattinger has been writing for The Hospitalist since 2005.
In YOU: The Smart Patient: An Insider's Handbook for Getting the Best Treatment, authors Michael F. Roizen, MD, and Mehmet C. Oz, MD, well-credentialed celebrity physicians, tell the reader that being a smart patient may make the difference between good and poor care and may even save your life. Everyone can be a “medical detective,” they suggest, seeking and supplying the facts that providers and administrators need in order to avoid errors or mix-ups.
The Joint Commission Resources, a collaborator on this publication, announces on its Web site that this book “empowers patients” (www.jcrinc.com/generic.asp?durki=11727&site=11&return=405.). Dr. Oz, in a Web post to customers who might purchase the book, puts it this way: “[T]he Joint Commission, our nation’s healthcare safety advocate, approached us to help with a big problem. Medical errors cost us 98,000 lives per year, and the Joint Commission could not squash this crazily large number without pulling in the biggest ally of all, the Smart Patient.” It’s a “scary statistic,” but true, he writes, “You have a two in five chance of being affected by a major medical complication in your life.” (For more information on the book, visit www.amazon.com/YOU-Insiders-Handbook-Getting-Treatment/dp/0743293010.)
The Hospitalist asked some hospitalists what they would recommend to a friend or relative headed for a hospital stay. Do they have any tips that only an insider would know? As might be expected, some of their advice echoes that already available in print, in broadcasts, and on the Web. And some things that were mentioned in these publications were also on our hospitalists’ list, including bringing along statistics, dates, and other healthcare specifics that might be crucial to providers. In fact, Drs. Roizen and Oz recommend assembling a thorough health history and bringing two copies of it to hospital admission—one especially for “the admitting nurse who welcomes you to your bed.”
Assume Nothing
In their book chapter on hospital stays, Drs. Oz and Roizen emphasize that patients and their visitors should keep an eye out to make certain hospital staff wash their hands and give the patient the right treatments, tests, and medications. “It’s astounding the amount of diligence you and your family will have to exercise during a hospital stay,” a reader-reviewer writes on the book’s Web page on the Amazon.com site. Some of the warnings posted in a book excerpt at the Joint Commission on Accreditation of Healthcare Organizations (JCAHO)’s site include “Don’t touch that remote!” and “wear rubber gloves” if you do want to watch TV. Readers are told that “a study found that the TV remote control is one of the most germ-infested things in a hospital room.”
Patients are also cautioned to “insist on being scanned,” to “insist on a clean stethoscope,” and to keep “an industrial-sized jug of alcohol hand-sanitizing gel” by the bed. In fact, the authors write: “Stethoscopes are filthy from being used on several patients an hour. Most doc[tor]s now wash their stethoscopes with alcohol between patients, but we’d always ask.” Our hospitalists agreed.
Ian Jenkins, MD, a hospitalist with the University of California at San Diego, would tell his friends and family to remind providers to wash their hands. “Don’t let anyone touch you unless you’ve seen them wash or gel their hands correctly—and their stethoscopes, too.”
Drs. Oz and Roizen say, “You might even post a sign that reads ‘Thank You for Washing Your Hands’ as a gentle reminder.”
Trust your intuition, one hospitalist tells people facing hospitalization. “If you sense that something is awry, it probably is,” says Jeanne Farnan, MD, a hospitalist scholar at The University of Chicago Hospitals. “Discuss concerns with physicians/nurses. Write down your questions in case they come to you spontaneously.”
On the other hand, she tells friends and relatives, “Patients, when asked questions, will often respond, ‘it’s in my chart.’ We often don't have access to a primary MD’s notes/chart, and not all documentation is pristine. When we are asking questions regarding your medical history, it is only to provide you with the best care—not to be a nuisance.”
Be Selective about Your Providers and Hospital
One recommendation from JCAHO’s patient education Web pages is a section entitled “Finding Dr. Right.” “Choose wisely and you could rest easy for many years to come,” it says.
Sandeep Sachdeva, MD, lead hospitalist at Swedish Medical Center’s Stroke Program and clinical instructor at the University of Washington at Seattle, says this may apply even to a patient’s relationship with a hospitalist.
“Sometimes patients come in and tell us their stories [about how providers treat them]. It’s just amazing; I think patients who have family members providing close supervision seem to get better care than somebody [who] is not asking questions,” he says. “And some care providers find questions intimidating, but the patient should not get discouraged by that. … If they feel that the care provider is not listening to them or not being attentive to them, they can always have a recourse: They can talk to the supervisor of that provider or somebody else [to get] a different provider. Patients sometimes have the fear that if they speak up against somebody that their care might be jeopardized.”
Dr. Sachdeva advises friends and relatives that they talk to the nursing supervisor or ask for the physician supervisor or an administrative person or social worker so that they get the attention they need.
Dr. Jenkins agrees. “Informed consent” is one of his tips for friends and family: “If your doctor won't talk to you about the risks and benefits of your treatments, and alternatives to them, you need a new doctor.”
Our hospitalists suggest being discriminating, savvy, and proactive:
- “Find one hospital you are comfortable with, [where] your family physician is on staff, and use it exclusively if possible,” says David M. Grace, MD, a hospitalist with The Schumacher Group in Lafayette, La. “By utilizing one hospital, all of your previous records and test results are immediately available when needed. Often this translates into a much shorter hospitalization as there are no delays in obtaining old records, and it minimizes the chance of duplicate tests/procedures being performed.”
- “Know who your doctors are [and] what their role is, and understand their input into your healthcare,” says Dr. Farnan, who is extensively involved in medical residents’ training. And “be cognizant of the physician work hours,” she advises. “We often have families who demand to speak with ‘their’ doctor at all hours of the early morning and night.” She tells friends and relatives, “I think more patients need to understand the nature [and] structure of the system [and] what kind of information a covering physician can provide. If the family of the patient has questions [and] wants to speak with the primary MD, it may be best to attempt in the daytime when the primary service is more likely to be present.”
- “Know the full names, and preferably [the] phone numbers, of all your outpatient physicians,” says Dr. Grace. “One area will often have multiple doctors with the same last name, and, frequently, records need to be requested from them. Up-to-date contact information on your physicians helps us request the right records from the right physicians with minimal delay.”
What to Bring to the Hospital
Some hospital Web sites advise patients on what to bring with them for their hospital stay, suggesting everything from your own robe, slippers, pajamas, or nightgown to an advance directive. Definitely, the latter is an important point.
“Whether it’s an elective or emergent admission,” says Dr. Grace, “there are a few things [you] can do to ensure [your] hospitalization is as safe, efficient, and productive as possible,” he tells friends and relatives. Among them, he says, is to “have a Living Will or advance directives completed, ensure the hospital has a copy, and discuss your wishes with your family prior to admission. Clear and concise plans, coupled with good family awareness, will help ensure your wishes and values are honored appropriately.”
And, as several of his hospitalist colleagues suggest, “Bring all of the medications you are currently using, including any over-the-counter medicines and herbs or homeopathic treatments. It’s imperative that physicians know what medications you are taking [because] many cannot be stopped abruptly, and [they may] have interactions with medications you may receive in the hospital.”
In addition, “know what medications you’re truly allergic to [e.g., hives, swelling, breathing problems],” Dr. Grace advises, “and which medications you have had side effects from [e.g., stomach upset, sleepiness, and so on]. Many patients confuse the two. Occasionally the best or only option involves using medications with potential unwanted side effects. Rarely do we use medications to which the patient has a true allergy.”
Communication: The Key to the Hospital Kingdom
Dr. Sachdeva recommends being ready to communicate even before going to the hospital. “In the case of an emergency admission,” he says, “they should have all their information readily available because at the time for a needed hospitalization, they may be sick and confused.” Have it “on their person” or in “an easily identifiable place,” he says, and, like his colleagues, he reiterates that this information should include a list of medications, problems, doctors, and phone numbers, along with a list of patient advocates and their phone numbers.
“Most of the time, patients are able to notify a family member, but if that doesn’t happen, then the ER can notify the appropriate person to be present to supervise and oversee the care from a patient perspective,” he says.
Communication was mentioned by all the hospitalists we interviewed. “Be prepared to ask questions and take an active role in your healthcare,” says Dr. Grace. “Ask your nurse what each medication you receive is and what it’s for. Ensure you know what medications to continue taking when you return home and which ones to stop. If you don’t understand your diagnosis, prognosis, or treatment plan, make sure you ask.”
One hospitalist’s advice pertained to the patient’s and family’s behavior and is based on an experience in her own family: “Be really nice to everybody,” Alison Holmes, MD, a hospitalist with Concord Hospital, Concord, N.H., advises friends and family. “This is hard to do when you’re sick and scared, but it’s incredibly important.”
Dr. Holmes speaks of her own parents’ experience: “My mother was admitted to the hospital for pneumonia about a year ago. She had very long wait in the emergency room. My father got very upset and called me and said, ‘Oh, they were so angry at me, I was yelling at everybody.’
“That won’t get you anywhere!” I told him. “That will get you worse care.” I asked, “Where is she now?” and he said, ‘Oh, she’s still in the emergency room,’ and I said, “You’re at home? You left her there?” Dr. Holmes then advised her father to return to the hospital right away.
Finally, all the hospitalists we interviewed emphasized that they would tell their family members to designate a point person for communication. And you can’t assume that that would be their doctor son or daughter, even if they happened to be in the same locale.
“When possible, don’t stay in the hospital alone,” says Dr. Holmes. “Try to always have a family member present so that there is someone available for questions. It’s not always clear where [the physician] can reach someone or how far away [that person is]. It can take a little coordination and multiple people to do it,” she says.
Also, Dr. Farnan points out, “It is often difficult [because of time limitations] for [physicians] to repeat the same information to multiple family members.”
All patients, but especially the elderly, says Dr. Sachdeva, should have a patient advocate with them at the hospital. If they don’t have family close by, they should have “a close friend or neighbor who is willing to take on that job, someone who can be there in the room and ask these questions: What medicine are you giving me? What’s the next step? What are the options?”
Dr. Sachdeva advises relatives that they might be distressed or unable to focus, so having a healthy advocate with them may be extremely important, “the difference between life and death,” although, no doubt, he’d leave that last comment out of his advice to family. “Because a lot of the time, it is not that we don’t try to do a good job, but it’s just [that] the advocate might bring something to our attention that we might not have otherwise noticed.” TH
Andrea Sattinger has been writing for The Hospitalist since 2005.
In YOU: The Smart Patient: An Insider's Handbook for Getting the Best Treatment, authors Michael F. Roizen, MD, and Mehmet C. Oz, MD, well-credentialed celebrity physicians, tell the reader that being a smart patient may make the difference between good and poor care and may even save your life. Everyone can be a “medical detective,” they suggest, seeking and supplying the facts that providers and administrators need in order to avoid errors or mix-ups.
The Joint Commission Resources, a collaborator on this publication, announces on its Web site that this book “empowers patients” (www.jcrinc.com/generic.asp?durki=11727&site=11&return=405.). Dr. Oz, in a Web post to customers who might purchase the book, puts it this way: “[T]he Joint Commission, our nation’s healthcare safety advocate, approached us to help with a big problem. Medical errors cost us 98,000 lives per year, and the Joint Commission could not squash this crazily large number without pulling in the biggest ally of all, the Smart Patient.” It’s a “scary statistic,” but true, he writes, “You have a two in five chance of being affected by a major medical complication in your life.” (For more information on the book, visit www.amazon.com/YOU-Insiders-Handbook-Getting-Treatment/dp/0743293010.)
The Hospitalist asked some hospitalists what they would recommend to a friend or relative headed for a hospital stay. Do they have any tips that only an insider would know? As might be expected, some of their advice echoes that already available in print, in broadcasts, and on the Web. And some things that were mentioned in these publications were also on our hospitalists’ list, including bringing along statistics, dates, and other healthcare specifics that might be crucial to providers. In fact, Drs. Roizen and Oz recommend assembling a thorough health history and bringing two copies of it to hospital admission—one especially for “the admitting nurse who welcomes you to your bed.”
Assume Nothing
In their book chapter on hospital stays, Drs. Oz and Roizen emphasize that patients and their visitors should keep an eye out to make certain hospital staff wash their hands and give the patient the right treatments, tests, and medications. “It’s astounding the amount of diligence you and your family will have to exercise during a hospital stay,” a reader-reviewer writes on the book’s Web page on the Amazon.com site. Some of the warnings posted in a book excerpt at the Joint Commission on Accreditation of Healthcare Organizations (JCAHO)’s site include “Don’t touch that remote!” and “wear rubber gloves” if you do want to watch TV. Readers are told that “a study found that the TV remote control is one of the most germ-infested things in a hospital room.”
Patients are also cautioned to “insist on being scanned,” to “insist on a clean stethoscope,” and to keep “an industrial-sized jug of alcohol hand-sanitizing gel” by the bed. In fact, the authors write: “Stethoscopes are filthy from being used on several patients an hour. Most doc[tor]s now wash their stethoscopes with alcohol between patients, but we’d always ask.” Our hospitalists agreed.
Ian Jenkins, MD, a hospitalist with the University of California at San Diego, would tell his friends and family to remind providers to wash their hands. “Don’t let anyone touch you unless you’ve seen them wash or gel their hands correctly—and their stethoscopes, too.”
Drs. Oz and Roizen say, “You might even post a sign that reads ‘Thank You for Washing Your Hands’ as a gentle reminder.”
Trust your intuition, one hospitalist tells people facing hospitalization. “If you sense that something is awry, it probably is,” says Jeanne Farnan, MD, a hospitalist scholar at The University of Chicago Hospitals. “Discuss concerns with physicians/nurses. Write down your questions in case they come to you spontaneously.”
On the other hand, she tells friends and relatives, “Patients, when asked questions, will often respond, ‘it’s in my chart.’ We often don't have access to a primary MD’s notes/chart, and not all documentation is pristine. When we are asking questions regarding your medical history, it is only to provide you with the best care—not to be a nuisance.”
Be Selective about Your Providers and Hospital
One recommendation from JCAHO’s patient education Web pages is a section entitled “Finding Dr. Right.” “Choose wisely and you could rest easy for many years to come,” it says.
Sandeep Sachdeva, MD, lead hospitalist at Swedish Medical Center’s Stroke Program and clinical instructor at the University of Washington at Seattle, says this may apply even to a patient’s relationship with a hospitalist.
“Sometimes patients come in and tell us their stories [about how providers treat them]. It’s just amazing; I think patients who have family members providing close supervision seem to get better care than somebody [who] is not asking questions,” he says. “And some care providers find questions intimidating, but the patient should not get discouraged by that. … If they feel that the care provider is not listening to them or not being attentive to them, they can always have a recourse: They can talk to the supervisor of that provider or somebody else [to get] a different provider. Patients sometimes have the fear that if they speak up against somebody that their care might be jeopardized.”
Dr. Sachdeva advises friends and relatives that they talk to the nursing supervisor or ask for the physician supervisor or an administrative person or social worker so that they get the attention they need.
Dr. Jenkins agrees. “Informed consent” is one of his tips for friends and family: “If your doctor won't talk to you about the risks and benefits of your treatments, and alternatives to them, you need a new doctor.”
Our hospitalists suggest being discriminating, savvy, and proactive:
- “Find one hospital you are comfortable with, [where] your family physician is on staff, and use it exclusively if possible,” says David M. Grace, MD, a hospitalist with The Schumacher Group in Lafayette, La. “By utilizing one hospital, all of your previous records and test results are immediately available when needed. Often this translates into a much shorter hospitalization as there are no delays in obtaining old records, and it minimizes the chance of duplicate tests/procedures being performed.”
- “Know who your doctors are [and] what their role is, and understand their input into your healthcare,” says Dr. Farnan, who is extensively involved in medical residents’ training. And “be cognizant of the physician work hours,” she advises. “We often have families who demand to speak with ‘their’ doctor at all hours of the early morning and night.” She tells friends and relatives, “I think more patients need to understand the nature [and] structure of the system [and] what kind of information a covering physician can provide. If the family of the patient has questions [and] wants to speak with the primary MD, it may be best to attempt in the daytime when the primary service is more likely to be present.”
- “Know the full names, and preferably [the] phone numbers, of all your outpatient physicians,” says Dr. Grace. “One area will often have multiple doctors with the same last name, and, frequently, records need to be requested from them. Up-to-date contact information on your physicians helps us request the right records from the right physicians with minimal delay.”
What to Bring to the Hospital
Some hospital Web sites advise patients on what to bring with them for their hospital stay, suggesting everything from your own robe, slippers, pajamas, or nightgown to an advance directive. Definitely, the latter is an important point.
“Whether it’s an elective or emergent admission,” says Dr. Grace, “there are a few things [you] can do to ensure [your] hospitalization is as safe, efficient, and productive as possible,” he tells friends and relatives. Among them, he says, is to “have a Living Will or advance directives completed, ensure the hospital has a copy, and discuss your wishes with your family prior to admission. Clear and concise plans, coupled with good family awareness, will help ensure your wishes and values are honored appropriately.”
And, as several of his hospitalist colleagues suggest, “Bring all of the medications you are currently using, including any over-the-counter medicines and herbs or homeopathic treatments. It’s imperative that physicians know what medications you are taking [because] many cannot be stopped abruptly, and [they may] have interactions with medications you may receive in the hospital.”
In addition, “know what medications you’re truly allergic to [e.g., hives, swelling, breathing problems],” Dr. Grace advises, “and which medications you have had side effects from [e.g., stomach upset, sleepiness, and so on]. Many patients confuse the two. Occasionally the best or only option involves using medications with potential unwanted side effects. Rarely do we use medications to which the patient has a true allergy.”
Communication: The Key to the Hospital Kingdom
Dr. Sachdeva recommends being ready to communicate even before going to the hospital. “In the case of an emergency admission,” he says, “they should have all their information readily available because at the time for a needed hospitalization, they may be sick and confused.” Have it “on their person” or in “an easily identifiable place,” he says, and, like his colleagues, he reiterates that this information should include a list of medications, problems, doctors, and phone numbers, along with a list of patient advocates and their phone numbers.
“Most of the time, patients are able to notify a family member, but if that doesn’t happen, then the ER can notify the appropriate person to be present to supervise and oversee the care from a patient perspective,” he says.
Communication was mentioned by all the hospitalists we interviewed. “Be prepared to ask questions and take an active role in your healthcare,” says Dr. Grace. “Ask your nurse what each medication you receive is and what it’s for. Ensure you know what medications to continue taking when you return home and which ones to stop. If you don’t understand your diagnosis, prognosis, or treatment plan, make sure you ask.”
One hospitalist’s advice pertained to the patient’s and family’s behavior and is based on an experience in her own family: “Be really nice to everybody,” Alison Holmes, MD, a hospitalist with Concord Hospital, Concord, N.H., advises friends and family. “This is hard to do when you’re sick and scared, but it’s incredibly important.”
Dr. Holmes speaks of her own parents’ experience: “My mother was admitted to the hospital for pneumonia about a year ago. She had very long wait in the emergency room. My father got very upset and called me and said, ‘Oh, they were so angry at me, I was yelling at everybody.’
“That won’t get you anywhere!” I told him. “That will get you worse care.” I asked, “Where is she now?” and he said, ‘Oh, she’s still in the emergency room,’ and I said, “You’re at home? You left her there?” Dr. Holmes then advised her father to return to the hospital right away.
Finally, all the hospitalists we interviewed emphasized that they would tell their family members to designate a point person for communication. And you can’t assume that that would be their doctor son or daughter, even if they happened to be in the same locale.
“When possible, don’t stay in the hospital alone,” says Dr. Holmes. “Try to always have a family member present so that there is someone available for questions. It’s not always clear where [the physician] can reach someone or how far away [that person is]. It can take a little coordination and multiple people to do it,” she says.
Also, Dr. Farnan points out, “It is often difficult [because of time limitations] for [physicians] to repeat the same information to multiple family members.”
All patients, but especially the elderly, says Dr. Sachdeva, should have a patient advocate with them at the hospital. If they don’t have family close by, they should have “a close friend or neighbor who is willing to take on that job, someone who can be there in the room and ask these questions: What medicine are you giving me? What’s the next step? What are the options?”
Dr. Sachdeva advises relatives that they might be distressed or unable to focus, so having a healthy advocate with them may be extremely important, “the difference between life and death,” although, no doubt, he’d leave that last comment out of his advice to family. “Because a lot of the time, it is not that we don’t try to do a good job, but it’s just [that] the advocate might bring something to our attention that we might not have otherwise noticed.” TH
Andrea Sattinger has been writing for The Hospitalist since 2005.
IT for HM
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
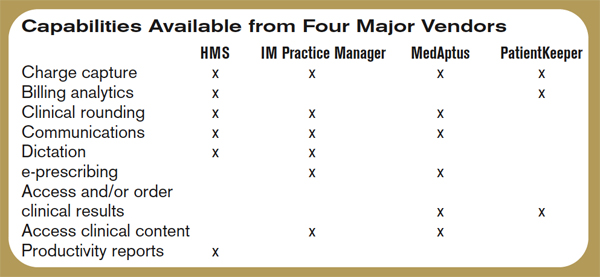
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.