User login
EMR System Shortage Means HM Opportunity
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
Less than 8% of U.S. hospitals have electronic medical record (EMR) systems in at least one clinical unit, and only 1.5% have a comprehensive system in all of their units, according to a March 25 report on the New England Journal of Medicine's Web site. The news isn't all bad: One hospitalist and information technology (IT) expert views this study as an opportunity for HM to push for EMR programs in their institutions.
Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass., says the environment for EMR initiatives is especially ripe given the government’s recent commitment of nearly $20 billion in stimulus funding for health IT implementation over the next six years.
The stimulus financing won't be available until fiscal 2011, but Dr. Stanley says the timeline gives hospitalists time to negotiate an EMR system that could work across their institutions. He adds that keeping lines of communication open between specialists is just as important as maintaining a productive dialogue between physicians and the staff that implement the software programs.
"Every doctor wants their information their way," Dr. Stanley says. "And this is a really difficult reflex for a lot of doctors. When you enter these political negotiations, you have to try to get doctors to understand that perfection on a small scale sometimes results in big problems on the large scale. If everybody is willing to compromise just a little bit, you can find a happy medium. As a hospitalist, it puts you in a nice political middle ground."
Avoid the “Urgent Trap”
“The important task rarely must be done today, or even this week. … But the urgent task calls for instant action. … The momentary appeal of these tasks seems irresistible and important, and they devour our energy. But in the light of time’s perspective, their deceptive prominence fades; with a sense of loss we recall the vital tasks we pushed aside. We realize we’ve become slaves to the tyranny of the urgent.” 1
—Charles Hummel

A few months ago, on one of my presidential travels, I met a young hospitalist who was overwhelmed. Thirty-year-old Emily had finished her residency in a good program just six months before. She had been a good resident, even winning an award as Resident of the Year. She was married with a young child at home and had recently moved to a new city, which was about 500 miles from her and her husband’s families. Her husband was staying at home to care for their child. They had chosen to move to this city because of its ideal climate and abundance of outdoor activities. The city had several HM opportunities, and Emily had chosen the one with the largest, most mature program. Everything seemed perfect at the start of her new job, but within a few months, she was overwhelmed, which led her to thoughts of quitting or moving to a program across the city to improve her lot.
One could naturally think that this was just a hospitalist in transition, from residency to attending. She was dealing with a lot of professional and personal issues, and maybe she had just not found her groove yet. And this was certainly true. Professionally, she was dealing with about a 20-patient-a-day workload. She had volunteered for two hospital committees and was serving as a physician champion for a UTI bundle the hospital was rolling out. The program was not short-staffed, but it did foster a culture of finishing your work before going home, and Emily was consistently staying one or two hours beyond her eight- to 12-hour shifts.
When I asked her about the specifics of her HM program, she had few complaints. The program had several night hospitalists, so she was grateful for the lack of night call. They also had fellows from an academic medical center helping with weekend admissions, so weekend call was once every six weeks. The monthly hours required by the program were reasonable. She got along with the group and hospital leadership; her salary was competitive and, in fact, guaranteed the first two years. At that time, she would graduate to a modified-productivity system based on a combination of work RVUs and quality metrics.
Yet Emily clearly was overwhelmed and contemplating a resignation.
As I talked with her, I started working through the differential diagnosis like any physician would. Knowing that the source of many hospitalist issues is the program itself, I worked through the various pillars of hospitalist satisfaction as demonstrated in SHM’s white paper on career satisfaction: reward/recognition, workload schedule, community/environment, and autonomy control.2 There seemed to be minor issues in some of the areas but nothing significant.
I then jumped to job fit and attempted to get a rough estimate of job control. Once again, minor issues. Emily did not appear to have a major disconnect between her desire for control and the control she currently had in her work.
So, being the persistent diagnostician, I asked her what she thought she needed. She immediately said, “Six more hours in a day!” And then, as I talked with her some more, the problem became apparent. She was a victim of what Charles Hummel described in 1967 as the “Tyranny of the Urgent.”1
Hummel was not the first to describe being overwhelmed by the small things of the day, nor will he be the last. Steven Covey, David Allen, and many others have made entire careers describing effective time-management techniques to control the small things. The core problem is that each of us starts the day with a plan, but we are sidetracked by many small tasks. At a given moment, the tasks appear to need an inconsequential amount of our time; however, they add up to significant amounts of time over the course of a day. Thus, we are detracted from accomplishing the core plan for the day—or the week or the month.
Hummel, a Christian writer, is not for everyone, but his discussion about the delirious enticement of completing a task that is thrown in front you was extremely insightful. I particularly like his reference to the demands and interruptions of the telephone. And Hummel was writing about this before e-mail, cell phones, televisions in public places, and instant messaging were prevalent.
On one hand, HM is perfectly synergistic with the tyranny of the urgent. Patients don’t get sick on a schedule. Codes and RRT calls occur suddenly. Families arrive at the hospital and can’t be ignored. Admissions and consults sprout up and orders need to be written. The list goes on.
As hospitalists, we must seek to prioritize what is important. We must actively choose to do this one thing rather than the million other tasks thrown at us. I am not saying to ignore patient care, but take a careful look at what you can control.
As I talked with Emily, I discovered she constantly checked her e-mail throughout the day, even on days she wasn’t working. She never sat down and took a lunch, even for 20 minutes. She hadn’t taken a family vacation, even for a short weekend, mainly because of what she described as work demands. She also told me that she enjoyed reading novels but had not read a single book since starting her new job.
As I spoke with Emily, I pointed out some of the things she was telling me. Soon, she started to slow down and think a little. I coached her to limit herself in the next two years to one quality improvement activity or committee. I also suggested she simply use the next two professional years to learn how to become an attending. I told her to read and continue to become comfortable with decision-making as a hospitalist—all else professionally should take a back seat.
Personally, I coached her to eliminate some of the daily distractions, specifically the overuse of her e-mail. I suggested she ask the nurses to avoid interrupting her when she is writing a note; take a regular lunch with a colleague; leave work on time.
In the end, each of us needs to decide what is important and discover how we should spend our time. Of course, we need to fix the practice issues so HM can thrive, but each of us needs to do a personal assessment, discover (or maybe rediscover) what is important, budget our time, and follow through. If we do, we will all be better off.
Thank you for allowing me to serve as your president. TH
Dr. Cawley is SHM president.
References
1. Hummel, Charles E. Tyranny of the Urgent. Downers Grove, Ill.: Intervarsity Press; 1967.
2. A challenge for a new specialty: a white paper on hospitalist career satisfaction. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed March 2, 2009.
“The important task rarely must be done today, or even this week. … But the urgent task calls for instant action. … The momentary appeal of these tasks seems irresistible and important, and they devour our energy. But in the light of time’s perspective, their deceptive prominence fades; with a sense of loss we recall the vital tasks we pushed aside. We realize we’ve become slaves to the tyranny of the urgent.” 1
—Charles Hummel
A few months ago, on one of my presidential travels, I met a young hospitalist who was overwhelmed. Thirty-year-old Emily had finished her residency in a good program just six months before. She had been a good resident, even winning an award as Resident of the Year. She was married with a young child at home and had recently moved to a new city, which was about 500 miles from her and her husband’s families. Her husband was staying at home to care for their child. They had chosen to move to this city because of its ideal climate and abundance of outdoor activities. The city had several HM opportunities, and Emily had chosen the one with the largest, most mature program. Everything seemed perfect at the start of her new job, but within a few months, she was overwhelmed, which led her to thoughts of quitting or moving to a program across the city to improve her lot.
One could naturally think that this was just a hospitalist in transition, from residency to attending. She was dealing with a lot of professional and personal issues, and maybe she had just not found her groove yet. And this was certainly true. Professionally, she was dealing with about a 20-patient-a-day workload. She had volunteered for two hospital committees and was serving as a physician champion for a UTI bundle the hospital was rolling out. The program was not short-staffed, but it did foster a culture of finishing your work before going home, and Emily was consistently staying one or two hours beyond her eight- to 12-hour shifts.
When I asked her about the specifics of her HM program, she had few complaints. The program had several night hospitalists, so she was grateful for the lack of night call. They also had fellows from an academic medical center helping with weekend admissions, so weekend call was once every six weeks. The monthly hours required by the program were reasonable. She got along with the group and hospital leadership; her salary was competitive and, in fact, guaranteed the first two years. At that time, she would graduate to a modified-productivity system based on a combination of work RVUs and quality metrics.
Yet Emily clearly was overwhelmed and contemplating a resignation.
As I talked with her, I started working through the differential diagnosis like any physician would. Knowing that the source of many hospitalist issues is the program itself, I worked through the various pillars of hospitalist satisfaction as demonstrated in SHM’s white paper on career satisfaction: reward/recognition, workload schedule, community/environment, and autonomy control.2 There seemed to be minor issues in some of the areas but nothing significant.
I then jumped to job fit and attempted to get a rough estimate of job control. Once again, minor issues. Emily did not appear to have a major disconnect between her desire for control and the control she currently had in her work.
So, being the persistent diagnostician, I asked her what she thought she needed. She immediately said, “Six more hours in a day!” And then, as I talked with her some more, the problem became apparent. She was a victim of what Charles Hummel described in 1967 as the “Tyranny of the Urgent.”1
Hummel was not the first to describe being overwhelmed by the small things of the day, nor will he be the last. Steven Covey, David Allen, and many others have made entire careers describing effective time-management techniques to control the small things. The core problem is that each of us starts the day with a plan, but we are sidetracked by many small tasks. At a given moment, the tasks appear to need an inconsequential amount of our time; however, they add up to significant amounts of time over the course of a day. Thus, we are detracted from accomplishing the core plan for the day—or the week or the month.
Hummel, a Christian writer, is not for everyone, but his discussion about the delirious enticement of completing a task that is thrown in front you was extremely insightful. I particularly like his reference to the demands and interruptions of the telephone. And Hummel was writing about this before e-mail, cell phones, televisions in public places, and instant messaging were prevalent.
On one hand, HM is perfectly synergistic with the tyranny of the urgent. Patients don’t get sick on a schedule. Codes and RRT calls occur suddenly. Families arrive at the hospital and can’t be ignored. Admissions and consults sprout up and orders need to be written. The list goes on.
As hospitalists, we must seek to prioritize what is important. We must actively choose to do this one thing rather than the million other tasks thrown at us. I am not saying to ignore patient care, but take a careful look at what you can control.
As I talked with Emily, I discovered she constantly checked her e-mail throughout the day, even on days she wasn’t working. She never sat down and took a lunch, even for 20 minutes. She hadn’t taken a family vacation, even for a short weekend, mainly because of what she described as work demands. She also told me that she enjoyed reading novels but had not read a single book since starting her new job.
As I spoke with Emily, I pointed out some of the things she was telling me. Soon, she started to slow down and think a little. I coached her to limit herself in the next two years to one quality improvement activity or committee. I also suggested she simply use the next two professional years to learn how to become an attending. I told her to read and continue to become comfortable with decision-making as a hospitalist—all else professionally should take a back seat.
Personally, I coached her to eliminate some of the daily distractions, specifically the overuse of her e-mail. I suggested she ask the nurses to avoid interrupting her when she is writing a note; take a regular lunch with a colleague; leave work on time.
In the end, each of us needs to decide what is important and discover how we should spend our time. Of course, we need to fix the practice issues so HM can thrive, but each of us needs to do a personal assessment, discover (or maybe rediscover) what is important, budget our time, and follow through. If we do, we will all be better off.
Thank you for allowing me to serve as your president. TH
Dr. Cawley is SHM president.
References
1. Hummel, Charles E. Tyranny of the Urgent. Downers Grove, Ill.: Intervarsity Press; 1967.
2. A challenge for a new specialty: a white paper on hospitalist career satisfaction. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed March 2, 2009.
“The important task rarely must be done today, or even this week. … But the urgent task calls for instant action. … The momentary appeal of these tasks seems irresistible and important, and they devour our energy. But in the light of time’s perspective, their deceptive prominence fades; with a sense of loss we recall the vital tasks we pushed aside. We realize we’ve become slaves to the tyranny of the urgent.” 1
—Charles Hummel
A few months ago, on one of my presidential travels, I met a young hospitalist who was overwhelmed. Thirty-year-old Emily had finished her residency in a good program just six months before. She had been a good resident, even winning an award as Resident of the Year. She was married with a young child at home and had recently moved to a new city, which was about 500 miles from her and her husband’s families. Her husband was staying at home to care for their child. They had chosen to move to this city because of its ideal climate and abundance of outdoor activities. The city had several HM opportunities, and Emily had chosen the one with the largest, most mature program. Everything seemed perfect at the start of her new job, but within a few months, she was overwhelmed, which led her to thoughts of quitting or moving to a program across the city to improve her lot.
One could naturally think that this was just a hospitalist in transition, from residency to attending. She was dealing with a lot of professional and personal issues, and maybe she had just not found her groove yet. And this was certainly true. Professionally, she was dealing with about a 20-patient-a-day workload. She had volunteered for two hospital committees and was serving as a physician champion for a UTI bundle the hospital was rolling out. The program was not short-staffed, but it did foster a culture of finishing your work before going home, and Emily was consistently staying one or two hours beyond her eight- to 12-hour shifts.
When I asked her about the specifics of her HM program, she had few complaints. The program had several night hospitalists, so she was grateful for the lack of night call. They also had fellows from an academic medical center helping with weekend admissions, so weekend call was once every six weeks. The monthly hours required by the program were reasonable. She got along with the group and hospital leadership; her salary was competitive and, in fact, guaranteed the first two years. At that time, she would graduate to a modified-productivity system based on a combination of work RVUs and quality metrics.
Yet Emily clearly was overwhelmed and contemplating a resignation.
As I talked with her, I started working through the differential diagnosis like any physician would. Knowing that the source of many hospitalist issues is the program itself, I worked through the various pillars of hospitalist satisfaction as demonstrated in SHM’s white paper on career satisfaction: reward/recognition, workload schedule, community/environment, and autonomy control.2 There seemed to be minor issues in some of the areas but nothing significant.
I then jumped to job fit and attempted to get a rough estimate of job control. Once again, minor issues. Emily did not appear to have a major disconnect between her desire for control and the control she currently had in her work.
So, being the persistent diagnostician, I asked her what she thought she needed. She immediately said, “Six more hours in a day!” And then, as I talked with her some more, the problem became apparent. She was a victim of what Charles Hummel described in 1967 as the “Tyranny of the Urgent.”1
Hummel was not the first to describe being overwhelmed by the small things of the day, nor will he be the last. Steven Covey, David Allen, and many others have made entire careers describing effective time-management techniques to control the small things. The core problem is that each of us starts the day with a plan, but we are sidetracked by many small tasks. At a given moment, the tasks appear to need an inconsequential amount of our time; however, they add up to significant amounts of time over the course of a day. Thus, we are detracted from accomplishing the core plan for the day—or the week or the month.
Hummel, a Christian writer, is not for everyone, but his discussion about the delirious enticement of completing a task that is thrown in front you was extremely insightful. I particularly like his reference to the demands and interruptions of the telephone. And Hummel was writing about this before e-mail, cell phones, televisions in public places, and instant messaging were prevalent.
On one hand, HM is perfectly synergistic with the tyranny of the urgent. Patients don’t get sick on a schedule. Codes and RRT calls occur suddenly. Families arrive at the hospital and can’t be ignored. Admissions and consults sprout up and orders need to be written. The list goes on.
As hospitalists, we must seek to prioritize what is important. We must actively choose to do this one thing rather than the million other tasks thrown at us. I am not saying to ignore patient care, but take a careful look at what you can control.
As I talked with Emily, I discovered she constantly checked her e-mail throughout the day, even on days she wasn’t working. She never sat down and took a lunch, even for 20 minutes. She hadn’t taken a family vacation, even for a short weekend, mainly because of what she described as work demands. She also told me that she enjoyed reading novels but had not read a single book since starting her new job.
As I spoke with Emily, I pointed out some of the things she was telling me. Soon, she started to slow down and think a little. I coached her to limit herself in the next two years to one quality improvement activity or committee. I also suggested she simply use the next two professional years to learn how to become an attending. I told her to read and continue to become comfortable with decision-making as a hospitalist—all else professionally should take a back seat.
Personally, I coached her to eliminate some of the daily distractions, specifically the overuse of her e-mail. I suggested she ask the nurses to avoid interrupting her when she is writing a note; take a regular lunch with a colleague; leave work on time.
In the end, each of us needs to decide what is important and discover how we should spend our time. Of course, we need to fix the practice issues so HM can thrive, but each of us needs to do a personal assessment, discover (or maybe rediscover) what is important, budget our time, and follow through. If we do, we will all be better off.
Thank you for allowing me to serve as your president. TH
Dr. Cawley is SHM president.
References
1. Hummel, Charles E. Tyranny of the Urgent. Downers Grove, Ill.: Intervarsity Press; 1967.
2. A challenge for a new specialty: a white paper on hospitalist career satisfaction. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed March 2, 2009.
Stimulus Clarification

Let’s begin with a couple of clinical questions:
Scenario One: You are discharging a 70-year-old man admitted five days earlier with community-acquired pneumonia (CAP). He has diabetes, class II heart failure, hyperlipidemia, and hypertension. He can perform daily activities, is off oxygen, and is doing well on oral antibiotics. His heart failure and blood pressure are under control, but his finger-stick blood sugars are consistently high (140-190 mg/dL) throughout his stay. You discharge him on his outpatient medication regimen. His next scheduled follow-up appointment is in four weeks.
When would you have him see his primary-care provider?
a. In two days;
b. In one week;
c. In two weeks; or
d. In four weeks.

Scenario Two: You admit a 70-year-old diabetic woman with atypical chest pain. She has described her pain, which is localized under her left breast, as “burning.” It occurred at rest and did not change with activity or eating. It improved about two hours after receiving an antacid. Her EKG and three troponins are normal. Her LDL cholesterol is 125 mg/dL. She is a former smoker and her blood pressure is controlled through use of lisinopril.
What do you do?
a. Order an exercise stress test;
b. Order a dobutamine stress echo;
c. Refer the patient to cardiology; or
d. Discharge the patient to home and have her follow up if she has further symptoms.
Answers:
Scenario One: We don’t know.
Scenario Two: We don’t know.
Healthcare Rationing?
Within hours of President Obama’s signing of the new economic stimulus package, I received an e-mail from my dad, who had read online that the new legislation would result in healthcare rationing. Having followed this issue relatively closely, I was puzzled by how the stimulus plan’s direct impact on healthcare—$87 billion for Medicaid, $25 billion for extension of COBRA medical insurance, $10 billion for the National Institutes of Health (NIH), nearly $20 billion for information technology infrastructure, and $1 billion for comparative effectiveness research (CER)—could be interpreted as the rationing of healthcare.
A quick peek at the Internet revealed the answer. A handful of bloggers clearly were interpreting the combination of Obama’s pledge to reduce healthcare costs and the billion-dollar appropriation for CER to mean the government would use the results of this research to limit care based on cost-effectiveness. In other words, a bureaucrat would decide if an elderly patient would receive a hip replacement based on whether it made fiscal sense.
So is healthcare rationing Obama’s solution to healthcare reform?
More Equals Less
There is great variability in the care provided throughout the U.S. There are well-known disparities—within age, race, and sex, for example—but there are also less apparent disparities. Medicare beneficiaries matched for severity of illness receive vastly different care based solely upon where they live. In 2003, per capita healthcare spending was $5,278, $5,661, and $11,350 for patients living in Portland, Oregon; Seattle; and Miami, respectively. That equates to about $125,000 additional lifetime healthcare costs for a 65-year-old treated in Miami compared with the same 65-year-old in Portland.1
And what does the Miamian get for the added cost? The results are surprisingly counterintuitive. It turns out that chronically ill elderly patients treated in more-resource-intense parts of the country do not have improved survival, quality of life, or access to care compared with those in less-resource-intense parts of the country. In fact, across most of these variables, the outcomes appear worse the more we do.2
Discover What Works
The focus in medicine has been to improve outcomes and control costs through the application of evidence-based medicine. The idea is that we can improve outcomes if everyone would just follow the clinical guidelines for an individual disease state. This has become the primary focus of pay for performance and the Joint Commission’s mandates on quality indicators, such as early antibiotics in pneumonia care.
This is sound thinking, until you realize that the vast majority of the decisions we have no definitive answer. For example, BMJ Clinical Evidence estimates that of the 2,500 treatments used for a variety of clinical problems, only 36% of them were deemed “beneficial” or “likely to be beneficial,” while 46% were of unknown benefit.3 In the absence of evidence, we are forced to use our clinical judgment, a surprisingly scary proposition when affordable, high-quality care is the goal.
This clinical judgment is what policymakers refer to as discretionary decision-making. The problem is that there is great variability in what experienced, prudent physicians judge to be appropriate. Recently, 1,275 physicians were asked about their decision-making around clinical scenarios with variable levels of evidential support. When asked when they would recommend a routine follow-up visit for a patient with well-controlled hypertension, 47% of physicians in high-resource-use areas (e.g., Miami), compared with 9% of physicians in low-resource-use areas (e.g., Portland), would recommend followup within three months compared with after three months. Management of an elderly clinic patient with new-onset chest pain was met with similar levels of variability in cardiac testing, referral to cardiology, and admission to the hospital between the higher- and lower-resource areas.
Those results contrasted with the consistent use across all spending groups for relatively proven modalities, such as mammographic screening in patients 50 to 70 years old.4 When the definitive answer isn’t available, we are left to use our clinical judgment, which often results in overuse of resources without benefit, and possibly harm.
We need to augment our focus on adherence to current guidelines with the discovery necessary to develop future guidelines. This requires that we move toward better information about what works and what doesn’t.
Enter the Obama administration’s commitment of significant resources to NIH research and comparative effectiveness research. The former allows for continued discovery of new technologies, while the latter informs clinicians about which technologies work the best for a particular clinical disease state.
Coordinating Fragmented Care
As hospitalists, our daily to-do lists are riddled with the consequences of fragmented care. We spend hours trying to track down primary-care physicians, finding test results from outside facilities, and coordinating complex care with multiple providers across multiple continuums. This results in inefficient and costly hospitalist systems, repetition of expensive tests, and overall worse patient outcomes. Thus, the stimulus bill’s push will be to build information technology (IT) infrastructure, such as electronic medical records, with the goal of making safer, more efficient systems that improve outcomes while cutting costs.
While the devil will be in the details—and with medical IT, the details can be daunting—I think this is a wise investment in our future.
We must get healthcare costs under control and improve the quality of care. There are myriad thoughts and proposals on how to accomplish this. The new administration is betting that discovery and technology will provide the answer to what to do with an acute-chest-pain patient and, in turn, the brewing healthcare crisis in America. That doesn’t sound like healthcare rationing to me, Dad. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.
References
1. Wennberg DE, Fisher ES, Skinner JS, Bronner KK. Extending the PFP agenda, part 2: How Medicare can reduce waste and improve the care of the chronically ill. Health Affairs. 2007;26:1575-1585.
2. Fischer ES, Wennberg, JE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138:288-298.
3. How much do we know? British Medical Journal Web site. Available at: http://clinical evidence.bmj.com/ceweb/about/knowledge.jsp. Accessed Feb. 24, 2009.
4. Sirovich B, Gallahger PM, Wennberg DE, Fisher ES. Discretionary decision-making by primary care physicians and the cost of U.S. healthcare. Health Affairs. 2008;27:813-823.
Let’s begin with a couple of clinical questions:
Scenario One: You are discharging a 70-year-old man admitted five days earlier with community-acquired pneumonia (CAP). He has diabetes, class II heart failure, hyperlipidemia, and hypertension. He can perform daily activities, is off oxygen, and is doing well on oral antibiotics. His heart failure and blood pressure are under control, but his finger-stick blood sugars are consistently high (140-190 mg/dL) throughout his stay. You discharge him on his outpatient medication regimen. His next scheduled follow-up appointment is in four weeks.
When would you have him see his primary-care provider?
a. In two days;
b. In one week;
c. In two weeks; or
d. In four weeks.
Scenario Two: You admit a 70-year-old diabetic woman with atypical chest pain. She has described her pain, which is localized under her left breast, as “burning.” It occurred at rest and did not change with activity or eating. It improved about two hours after receiving an antacid. Her EKG and three troponins are normal. Her LDL cholesterol is 125 mg/dL. She is a former smoker and her blood pressure is controlled through use of lisinopril.
What do you do?
a. Order an exercise stress test;
b. Order a dobutamine stress echo;
c. Refer the patient to cardiology; or
d. Discharge the patient to home and have her follow up if she has further symptoms.
Answers:
Scenario One: We don’t know.
Scenario Two: We don’t know.
Healthcare Rationing?
Within hours of President Obama’s signing of the new economic stimulus package, I received an e-mail from my dad, who had read online that the new legislation would result in healthcare rationing. Having followed this issue relatively closely, I was puzzled by how the stimulus plan’s direct impact on healthcare—$87 billion for Medicaid, $25 billion for extension of COBRA medical insurance, $10 billion for the National Institutes of Health (NIH), nearly $20 billion for information technology infrastructure, and $1 billion for comparative effectiveness research (CER)—could be interpreted as the rationing of healthcare.
A quick peek at the Internet revealed the answer. A handful of bloggers clearly were interpreting the combination of Obama’s pledge to reduce healthcare costs and the billion-dollar appropriation for CER to mean the government would use the results of this research to limit care based on cost-effectiveness. In other words, a bureaucrat would decide if an elderly patient would receive a hip replacement based on whether it made fiscal sense.
So is healthcare rationing Obama’s solution to healthcare reform?
More Equals Less
There is great variability in the care provided throughout the U.S. There are well-known disparities—within age, race, and sex, for example—but there are also less apparent disparities. Medicare beneficiaries matched for severity of illness receive vastly different care based solely upon where they live. In 2003, per capita healthcare spending was $5,278, $5,661, and $11,350 for patients living in Portland, Oregon; Seattle; and Miami, respectively. That equates to about $125,000 additional lifetime healthcare costs for a 65-year-old treated in Miami compared with the same 65-year-old in Portland.1
And what does the Miamian get for the added cost? The results are surprisingly counterintuitive. It turns out that chronically ill elderly patients treated in more-resource-intense parts of the country do not have improved survival, quality of life, or access to care compared with those in less-resource-intense parts of the country. In fact, across most of these variables, the outcomes appear worse the more we do.2
Discover What Works
The focus in medicine has been to improve outcomes and control costs through the application of evidence-based medicine. The idea is that we can improve outcomes if everyone would just follow the clinical guidelines for an individual disease state. This has become the primary focus of pay for performance and the Joint Commission’s mandates on quality indicators, such as early antibiotics in pneumonia care.
This is sound thinking, until you realize that the vast majority of the decisions we have no definitive answer. For example, BMJ Clinical Evidence estimates that of the 2,500 treatments used for a variety of clinical problems, only 36% of them were deemed “beneficial” or “likely to be beneficial,” while 46% were of unknown benefit.3 In the absence of evidence, we are forced to use our clinical judgment, a surprisingly scary proposition when affordable, high-quality care is the goal.
This clinical judgment is what policymakers refer to as discretionary decision-making. The problem is that there is great variability in what experienced, prudent physicians judge to be appropriate. Recently, 1,275 physicians were asked about their decision-making around clinical scenarios with variable levels of evidential support. When asked when they would recommend a routine follow-up visit for a patient with well-controlled hypertension, 47% of physicians in high-resource-use areas (e.g., Miami), compared with 9% of physicians in low-resource-use areas (e.g., Portland), would recommend followup within three months compared with after three months. Management of an elderly clinic patient with new-onset chest pain was met with similar levels of variability in cardiac testing, referral to cardiology, and admission to the hospital between the higher- and lower-resource areas.
Those results contrasted with the consistent use across all spending groups for relatively proven modalities, such as mammographic screening in patients 50 to 70 years old.4 When the definitive answer isn’t available, we are left to use our clinical judgment, which often results in overuse of resources without benefit, and possibly harm.
We need to augment our focus on adherence to current guidelines with the discovery necessary to develop future guidelines. This requires that we move toward better information about what works and what doesn’t.
Enter the Obama administration’s commitment of significant resources to NIH research and comparative effectiveness research. The former allows for continued discovery of new technologies, while the latter informs clinicians about which technologies work the best for a particular clinical disease state.
Coordinating Fragmented Care
As hospitalists, our daily to-do lists are riddled with the consequences of fragmented care. We spend hours trying to track down primary-care physicians, finding test results from outside facilities, and coordinating complex care with multiple providers across multiple continuums. This results in inefficient and costly hospitalist systems, repetition of expensive tests, and overall worse patient outcomes. Thus, the stimulus bill’s push will be to build information technology (IT) infrastructure, such as electronic medical records, with the goal of making safer, more efficient systems that improve outcomes while cutting costs.
While the devil will be in the details—and with medical IT, the details can be daunting—I think this is a wise investment in our future.
We must get healthcare costs under control and improve the quality of care. There are myriad thoughts and proposals on how to accomplish this. The new administration is betting that discovery and technology will provide the answer to what to do with an acute-chest-pain patient and, in turn, the brewing healthcare crisis in America. That doesn’t sound like healthcare rationing to me, Dad. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.
References
1. Wennberg DE, Fisher ES, Skinner JS, Bronner KK. Extending the PFP agenda, part 2: How Medicare can reduce waste and improve the care of the chronically ill. Health Affairs. 2007;26:1575-1585.
2. Fischer ES, Wennberg, JE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138:288-298.
3. How much do we know? British Medical Journal Web site. Available at: http://clinical evidence.bmj.com/ceweb/about/knowledge.jsp. Accessed Feb. 24, 2009.
4. Sirovich B, Gallahger PM, Wennberg DE, Fisher ES. Discretionary decision-making by primary care physicians and the cost of U.S. healthcare. Health Affairs. 2008;27:813-823.
Let’s begin with a couple of clinical questions:
Scenario One: You are discharging a 70-year-old man admitted five days earlier with community-acquired pneumonia (CAP). He has diabetes, class II heart failure, hyperlipidemia, and hypertension. He can perform daily activities, is off oxygen, and is doing well on oral antibiotics. His heart failure and blood pressure are under control, but his finger-stick blood sugars are consistently high (140-190 mg/dL) throughout his stay. You discharge him on his outpatient medication regimen. His next scheduled follow-up appointment is in four weeks.
When would you have him see his primary-care provider?
a. In two days;
b. In one week;
c. In two weeks; or
d. In four weeks.
Scenario Two: You admit a 70-year-old diabetic woman with atypical chest pain. She has described her pain, which is localized under her left breast, as “burning.” It occurred at rest and did not change with activity or eating. It improved about two hours after receiving an antacid. Her EKG and three troponins are normal. Her LDL cholesterol is 125 mg/dL. She is a former smoker and her blood pressure is controlled through use of lisinopril.
What do you do?
a. Order an exercise stress test;
b. Order a dobutamine stress echo;
c. Refer the patient to cardiology; or
d. Discharge the patient to home and have her follow up if she has further symptoms.
Answers:
Scenario One: We don’t know.
Scenario Two: We don’t know.
Healthcare Rationing?
Within hours of President Obama’s signing of the new economic stimulus package, I received an e-mail from my dad, who had read online that the new legislation would result in healthcare rationing. Having followed this issue relatively closely, I was puzzled by how the stimulus plan’s direct impact on healthcare—$87 billion for Medicaid, $25 billion for extension of COBRA medical insurance, $10 billion for the National Institutes of Health (NIH), nearly $20 billion for information technology infrastructure, and $1 billion for comparative effectiveness research (CER)—could be interpreted as the rationing of healthcare.
A quick peek at the Internet revealed the answer. A handful of bloggers clearly were interpreting the combination of Obama’s pledge to reduce healthcare costs and the billion-dollar appropriation for CER to mean the government would use the results of this research to limit care based on cost-effectiveness. In other words, a bureaucrat would decide if an elderly patient would receive a hip replacement based on whether it made fiscal sense.
So is healthcare rationing Obama’s solution to healthcare reform?
More Equals Less
There is great variability in the care provided throughout the U.S. There are well-known disparities—within age, race, and sex, for example—but there are also less apparent disparities. Medicare beneficiaries matched for severity of illness receive vastly different care based solely upon where they live. In 2003, per capita healthcare spending was $5,278, $5,661, and $11,350 for patients living in Portland, Oregon; Seattle; and Miami, respectively. That equates to about $125,000 additional lifetime healthcare costs for a 65-year-old treated in Miami compared with the same 65-year-old in Portland.1
And what does the Miamian get for the added cost? The results are surprisingly counterintuitive. It turns out that chronically ill elderly patients treated in more-resource-intense parts of the country do not have improved survival, quality of life, or access to care compared with those in less-resource-intense parts of the country. In fact, across most of these variables, the outcomes appear worse the more we do.2
Discover What Works
The focus in medicine has been to improve outcomes and control costs through the application of evidence-based medicine. The idea is that we can improve outcomes if everyone would just follow the clinical guidelines for an individual disease state. This has become the primary focus of pay for performance and the Joint Commission’s mandates on quality indicators, such as early antibiotics in pneumonia care.
This is sound thinking, until you realize that the vast majority of the decisions we have no definitive answer. For example, BMJ Clinical Evidence estimates that of the 2,500 treatments used for a variety of clinical problems, only 36% of them were deemed “beneficial” or “likely to be beneficial,” while 46% were of unknown benefit.3 In the absence of evidence, we are forced to use our clinical judgment, a surprisingly scary proposition when affordable, high-quality care is the goal.
This clinical judgment is what policymakers refer to as discretionary decision-making. The problem is that there is great variability in what experienced, prudent physicians judge to be appropriate. Recently, 1,275 physicians were asked about their decision-making around clinical scenarios with variable levels of evidential support. When asked when they would recommend a routine follow-up visit for a patient with well-controlled hypertension, 47% of physicians in high-resource-use areas (e.g., Miami), compared with 9% of physicians in low-resource-use areas (e.g., Portland), would recommend followup within three months compared with after three months. Management of an elderly clinic patient with new-onset chest pain was met with similar levels of variability in cardiac testing, referral to cardiology, and admission to the hospital between the higher- and lower-resource areas.
Those results contrasted with the consistent use across all spending groups for relatively proven modalities, such as mammographic screening in patients 50 to 70 years old.4 When the definitive answer isn’t available, we are left to use our clinical judgment, which often results in overuse of resources without benefit, and possibly harm.
We need to augment our focus on adherence to current guidelines with the discovery necessary to develop future guidelines. This requires that we move toward better information about what works and what doesn’t.
Enter the Obama administration’s commitment of significant resources to NIH research and comparative effectiveness research. The former allows for continued discovery of new technologies, while the latter informs clinicians about which technologies work the best for a particular clinical disease state.
Coordinating Fragmented Care
As hospitalists, our daily to-do lists are riddled with the consequences of fragmented care. We spend hours trying to track down primary-care physicians, finding test results from outside facilities, and coordinating complex care with multiple providers across multiple continuums. This results in inefficient and costly hospitalist systems, repetition of expensive tests, and overall worse patient outcomes. Thus, the stimulus bill’s push will be to build information technology (IT) infrastructure, such as electronic medical records, with the goal of making safer, more efficient systems that improve outcomes while cutting costs.
While the devil will be in the details—and with medical IT, the details can be daunting—I think this is a wise investment in our future.
We must get healthcare costs under control and improve the quality of care. There are myriad thoughts and proposals on how to accomplish this. The new administration is betting that discovery and technology will provide the answer to what to do with an acute-chest-pain patient and, in turn, the brewing healthcare crisis in America. That doesn’t sound like healthcare rationing to me, Dad. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of hospital medicine and the hospitalist training program, and as associate program director of the Internal Medicine Residency Program.
References
1. Wennberg DE, Fisher ES, Skinner JS, Bronner KK. Extending the PFP agenda, part 2: How Medicare can reduce waste and improve the care of the chronically ill. Health Affairs. 2007;26:1575-1585.
2. Fischer ES, Wennberg, JE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138:288-298.
3. How much do we know? British Medical Journal Web site. Available at: http://clinical evidence.bmj.com/ceweb/about/knowledge.jsp. Accessed Feb. 24, 2009.
4. Sirovich B, Gallahger PM, Wennberg DE, Fisher ES. Discretionary decision-making by primary care physicians and the cost of U.S. healthcare. Health Affairs. 2008;27:813-823.
Top o’ the Morning

In the what-have-you-done-for-me-lately category, many hospitalists are expected to really ramp up their efforts to improve their hospital’s throughput. So many hospital executives, who not long ago were dazzled by impressive reductions in lengths of stay and cost per case attributable to hospitalists, seem to have turned their attention to discharging patients early in the day. To some hospitalists who still expect gratitude for things done in the past, it seems terribly unfair that administrators now expect us to attend to this new metric. And, by the way, don’t let discharging patients early in the day interfere with improvements in quality metrics, patient satisfaction, and documentation.
Because of these increasing demands on hospitalists, we might feel sorry for ourselves. I do sometimes. But I also know that if we became hospital executives—and some of us have—we would expect the same of hospitalists in our institutions.
I’m struck by how often hospitalists, particularly those not in leadership positions, fail to understand why it matters so much to the execs that discharge orders are written early in the day. For them, I’ll try to provide a brief explanation.
Why It Matters
An increasing number of hospitals are operating with all of their staffed beds fully occupied. Many end up with patients boarding in the ED or ICU because no “regular” beds are available. And hospitals really suffer financially when they have to cancel elective admissions, such as surgeries, because no beds are available for the patient postop.
Hospitals could build more beds to increase their capacity, but that requires a long time and something along the lines of $1 million per bed. Where could they get the financing in today’s market? The other option is to shorten the length of time a patient occupies a bed so that more patients can be served using the existing inventory.
In nearly every hospital, the biggest bed crunch occurs in the afternoon. This is the time patients are ready to leave the post-anesthesia care unit or ED and move to their “floor” bed. If patients being discharged that day haven’t left yet, gridlock occurs. Costs of the gridlock are spread throughout the hospital, notably in the ED, which suffers because of the resulting increased lengths of stay and reduced throughput. This isn’t just an economic issue for the hospital; patients are adversely affected, too.
Even if your hospital has spare beds, early discharge still matters. If the discharge day isn’t managed well and patients routinely leave late in the afternoon, the hospital will have to spend more on evening-shift nursing staff.
It makes sense to look at every step that must occur prior to a patient vacating their room on the day of discharge. The time that the doctor actually writes the discharge order is one of the most critical, rate-limiting steps in the discharge process, so helpful executives suggest we organize our rounds to see the potential discharges first, then get around to seeing the patients who are really sick. I think most hospitalists, including me, find it really difficult to do this. If you’re in this category, you might consider starting your rounds earlier in the day.
Consider Rounding Earlier
Starting rounds earlier is usually an unpopular idea. Many groups refuse to consider it. If you are in a group that works day (rounding) shifts with specified start and stop times, coming in before the start of your shift to begin rounding is just donating uncompensated time to the practice. That is one of many reasons I think it is best for most practices to avoid specified start and stop times for their day shifts. Instead, I think it is reasonable for each doctor to decide when to start and stop work each day depending on the workload. So on days you have a higher-than-usual number of expected discharges or sick patients, you would probably choose to start earlier. And when patient volumes are low, you might choose to start later. The same is true of when you choose to leave for the day. Choosing to start earlier in the day should mean that you can wrap things up earlier on most days.
For a lot of hospitalists, routinely starting rounds earlier would be OK as long as they can finish earlier. But there are some for whom this is really tough or impossible, such as those who need to take their kids to school before work each morning. Rounding early won’t do any good if the hospital doesn’t ensure test results and other information is available early.
A practice could choose to undertake an initiative as simple as the following steps to support improvements in writing most discharge orders early in the day:
- Encourage starting rounds earlier (e.g., 7 a.m.) on most days;
- Whenever possible, prepare discharge summaries the day before;
- As often as possible, write in the order section “probable discharge tomorrow” one day before planned discharges;
- Keep routine morning conferences, such as signout, as short as possible; move it to later in the day, or eliminate it entirely, if feasible; and
- If you have routine, sit-down rounds with case managers each morning, think about whether they get in the way of early-in-the-day discharges. If so, consider moving them to the afternoons, and focus on discussing the next day’s potential discharges rather than discharges for the current day.
Consider establishing targets for each of these metrics and audit performance compared with a historical baseline. For example, the goal might be that the “probable discharge tomorrow” order appears the day before discharge in 50% of hospitalist patients, and the discharge summary is prepared the day before in 30%. These things help ensure other hospital staff members realize discharge is possible or likely and can significantly reduce discharges that are a surprise to nurses and others.
There is nothing magic about the bulleted protocol above. I’m offering it as only one potential idea to improve throughput, and you might want to pursue an entirely different strategy.
The Flip Side
Two closely related issues come up when working on getting discharge orders written early in the day. The first is that some late-afternoon discharges are in reality very early discharges that might have otherwise waited until the next day. It is important to stress that not all discharge orders are written early, and that hospitalists should not hold on to patients who could be discharged late in the day and instead release them the next morning to make their statistics look better.
The other related point is that a declining length of stay and discharging early in the day begin to compete with each other at some point. From a bed management perspective, the theoretical optimal length of stay means discharging patients the moment they are ready and not waiting until the next morning. This means discharging around the clock without regard to the time of day, and that would look terrible when analyzed from the perspective of the portion of discharge orders written early in the day—not to mention it would be very unpleasant for patients asked to leave at night. So I’m not suggesting that we should be discharging patients around the clock, but I just want to point out the tension between length of stay and writing discharge orders early in the day. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospital practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official SHM position.
In the what-have-you-done-for-me-lately category, many hospitalists are expected to really ramp up their efforts to improve their hospital’s throughput. So many hospital executives, who not long ago were dazzled by impressive reductions in lengths of stay and cost per case attributable to hospitalists, seem to have turned their attention to discharging patients early in the day. To some hospitalists who still expect gratitude for things done in the past, it seems terribly unfair that administrators now expect us to attend to this new metric. And, by the way, don’t let discharging patients early in the day interfere with improvements in quality metrics, patient satisfaction, and documentation.
Because of these increasing demands on hospitalists, we might feel sorry for ourselves. I do sometimes. But I also know that if we became hospital executives—and some of us have—we would expect the same of hospitalists in our institutions.
I’m struck by how often hospitalists, particularly those not in leadership positions, fail to understand why it matters so much to the execs that discharge orders are written early in the day. For them, I’ll try to provide a brief explanation.
Why It Matters
An increasing number of hospitals are operating with all of their staffed beds fully occupied. Many end up with patients boarding in the ED or ICU because no “regular” beds are available. And hospitals really suffer financially when they have to cancel elective admissions, such as surgeries, because no beds are available for the patient postop.
Hospitals could build more beds to increase their capacity, but that requires a long time and something along the lines of $1 million per bed. Where could they get the financing in today’s market? The other option is to shorten the length of time a patient occupies a bed so that more patients can be served using the existing inventory.
In nearly every hospital, the biggest bed crunch occurs in the afternoon. This is the time patients are ready to leave the post-anesthesia care unit or ED and move to their “floor” bed. If patients being discharged that day haven’t left yet, gridlock occurs. Costs of the gridlock are spread throughout the hospital, notably in the ED, which suffers because of the resulting increased lengths of stay and reduced throughput. This isn’t just an economic issue for the hospital; patients are adversely affected, too.
Even if your hospital has spare beds, early discharge still matters. If the discharge day isn’t managed well and patients routinely leave late in the afternoon, the hospital will have to spend more on evening-shift nursing staff.
It makes sense to look at every step that must occur prior to a patient vacating their room on the day of discharge. The time that the doctor actually writes the discharge order is one of the most critical, rate-limiting steps in the discharge process, so helpful executives suggest we organize our rounds to see the potential discharges first, then get around to seeing the patients who are really sick. I think most hospitalists, including me, find it really difficult to do this. If you’re in this category, you might consider starting your rounds earlier in the day.
Consider Rounding Earlier
Starting rounds earlier is usually an unpopular idea. Many groups refuse to consider it. If you are in a group that works day (rounding) shifts with specified start and stop times, coming in before the start of your shift to begin rounding is just donating uncompensated time to the practice. That is one of many reasons I think it is best for most practices to avoid specified start and stop times for their day shifts. Instead, I think it is reasonable for each doctor to decide when to start and stop work each day depending on the workload. So on days you have a higher-than-usual number of expected discharges or sick patients, you would probably choose to start earlier. And when patient volumes are low, you might choose to start later. The same is true of when you choose to leave for the day. Choosing to start earlier in the day should mean that you can wrap things up earlier on most days.
For a lot of hospitalists, routinely starting rounds earlier would be OK as long as they can finish earlier. But there are some for whom this is really tough or impossible, such as those who need to take their kids to school before work each morning. Rounding early won’t do any good if the hospital doesn’t ensure test results and other information is available early.
A practice could choose to undertake an initiative as simple as the following steps to support improvements in writing most discharge orders early in the day:
- Encourage starting rounds earlier (e.g., 7 a.m.) on most days;
- Whenever possible, prepare discharge summaries the day before;
- As often as possible, write in the order section “probable discharge tomorrow” one day before planned discharges;
- Keep routine morning conferences, such as signout, as short as possible; move it to later in the day, or eliminate it entirely, if feasible; and
- If you have routine, sit-down rounds with case managers each morning, think about whether they get in the way of early-in-the-day discharges. If so, consider moving them to the afternoons, and focus on discussing the next day’s potential discharges rather than discharges for the current day.
Consider establishing targets for each of these metrics and audit performance compared with a historical baseline. For example, the goal might be that the “probable discharge tomorrow” order appears the day before discharge in 50% of hospitalist patients, and the discharge summary is prepared the day before in 30%. These things help ensure other hospital staff members realize discharge is possible or likely and can significantly reduce discharges that are a surprise to nurses and others.
There is nothing magic about the bulleted protocol above. I’m offering it as only one potential idea to improve throughput, and you might want to pursue an entirely different strategy.
The Flip Side
Two closely related issues come up when working on getting discharge orders written early in the day. The first is that some late-afternoon discharges are in reality very early discharges that might have otherwise waited until the next day. It is important to stress that not all discharge orders are written early, and that hospitalists should not hold on to patients who could be discharged late in the day and instead release them the next morning to make their statistics look better.
The other related point is that a declining length of stay and discharging early in the day begin to compete with each other at some point. From a bed management perspective, the theoretical optimal length of stay means discharging patients the moment they are ready and not waiting until the next morning. This means discharging around the clock without regard to the time of day, and that would look terrible when analyzed from the perspective of the portion of discharge orders written early in the day—not to mention it would be very unpleasant for patients asked to leave at night. So I’m not suggesting that we should be discharging patients around the clock, but I just want to point out the tension between length of stay and writing discharge orders early in the day. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospital practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official SHM position.
In the what-have-you-done-for-me-lately category, many hospitalists are expected to really ramp up their efforts to improve their hospital’s throughput. So many hospital executives, who not long ago were dazzled by impressive reductions in lengths of stay and cost per case attributable to hospitalists, seem to have turned their attention to discharging patients early in the day. To some hospitalists who still expect gratitude for things done in the past, it seems terribly unfair that administrators now expect us to attend to this new metric. And, by the way, don’t let discharging patients early in the day interfere with improvements in quality metrics, patient satisfaction, and documentation.
Because of these increasing demands on hospitalists, we might feel sorry for ourselves. I do sometimes. But I also know that if we became hospital executives—and some of us have—we would expect the same of hospitalists in our institutions.
I’m struck by how often hospitalists, particularly those not in leadership positions, fail to understand why it matters so much to the execs that discharge orders are written early in the day. For them, I’ll try to provide a brief explanation.
Why It Matters
An increasing number of hospitals are operating with all of their staffed beds fully occupied. Many end up with patients boarding in the ED or ICU because no “regular” beds are available. And hospitals really suffer financially when they have to cancel elective admissions, such as surgeries, because no beds are available for the patient postop.
Hospitals could build more beds to increase their capacity, but that requires a long time and something along the lines of $1 million per bed. Where could they get the financing in today’s market? The other option is to shorten the length of time a patient occupies a bed so that more patients can be served using the existing inventory.
In nearly every hospital, the biggest bed crunch occurs in the afternoon. This is the time patients are ready to leave the post-anesthesia care unit or ED and move to their “floor” bed. If patients being discharged that day haven’t left yet, gridlock occurs. Costs of the gridlock are spread throughout the hospital, notably in the ED, which suffers because of the resulting increased lengths of stay and reduced throughput. This isn’t just an economic issue for the hospital; patients are adversely affected, too.
Even if your hospital has spare beds, early discharge still matters. If the discharge day isn’t managed well and patients routinely leave late in the afternoon, the hospital will have to spend more on evening-shift nursing staff.
It makes sense to look at every step that must occur prior to a patient vacating their room on the day of discharge. The time that the doctor actually writes the discharge order is one of the most critical, rate-limiting steps in the discharge process, so helpful executives suggest we organize our rounds to see the potential discharges first, then get around to seeing the patients who are really sick. I think most hospitalists, including me, find it really difficult to do this. If you’re in this category, you might consider starting your rounds earlier in the day.
Consider Rounding Earlier
Starting rounds earlier is usually an unpopular idea. Many groups refuse to consider it. If you are in a group that works day (rounding) shifts with specified start and stop times, coming in before the start of your shift to begin rounding is just donating uncompensated time to the practice. That is one of many reasons I think it is best for most practices to avoid specified start and stop times for their day shifts. Instead, I think it is reasonable for each doctor to decide when to start and stop work each day depending on the workload. So on days you have a higher-than-usual number of expected discharges or sick patients, you would probably choose to start earlier. And when patient volumes are low, you might choose to start later. The same is true of when you choose to leave for the day. Choosing to start earlier in the day should mean that you can wrap things up earlier on most days.
For a lot of hospitalists, routinely starting rounds earlier would be OK as long as they can finish earlier. But there are some for whom this is really tough or impossible, such as those who need to take their kids to school before work each morning. Rounding early won’t do any good if the hospital doesn’t ensure test results and other information is available early.
A practice could choose to undertake an initiative as simple as the following steps to support improvements in writing most discharge orders early in the day:
- Encourage starting rounds earlier (e.g., 7 a.m.) on most days;
- Whenever possible, prepare discharge summaries the day before;
- As often as possible, write in the order section “probable discharge tomorrow” one day before planned discharges;
- Keep routine morning conferences, such as signout, as short as possible; move it to later in the day, or eliminate it entirely, if feasible; and
- If you have routine, sit-down rounds with case managers each morning, think about whether they get in the way of early-in-the-day discharges. If so, consider moving them to the afternoons, and focus on discussing the next day’s potential discharges rather than discharges for the current day.
Consider establishing targets for each of these metrics and audit performance compared with a historical baseline. For example, the goal might be that the “probable discharge tomorrow” order appears the day before discharge in 50% of hospitalist patients, and the discharge summary is prepared the day before in 30%. These things help ensure other hospital staff members realize discharge is possible or likely and can significantly reduce discharges that are a surprise to nurses and others.
There is nothing magic about the bulleted protocol above. I’m offering it as only one potential idea to improve throughput, and you might want to pursue an entirely different strategy.
The Flip Side
Two closely related issues come up when working on getting discharge orders written early in the day. The first is that some late-afternoon discharges are in reality very early discharges that might have otherwise waited until the next day. It is important to stress that not all discharge orders are written early, and that hospitalists should not hold on to patients who could be discharged late in the day and instead release them the next morning to make their statistics look better.
The other related point is that a declining length of stay and discharging early in the day begin to compete with each other at some point. From a bed management perspective, the theoretical optimal length of stay means discharging patients the moment they are ready and not waiting until the next morning. This means discharging around the clock without regard to the time of day, and that would look terrible when analyzed from the perspective of the portion of discharge orders written early in the day—not to mention it would be very unpleasant for patients asked to leave at night. So I’m not suggesting that we should be discharging patients around the clock, but I just want to point out the tension between length of stay and writing discharge orders early in the day. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospital practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official SHM position.
HM groups should provide informational brochures to admitted patients
HM: A Difference-Maker
The author of a new study that shows 20% of Medicare patient discharges are readmitted within 30 days thinks hospitalists can—and should—take a lead role in reducing those rates by improving patient transitions from hospital to home.
The study, released today in the New England Journal of Medicine, also shows that half of nonsurgical patients are readmitted to the hospital without seeing an outpatient doctor, and the unplanned rehospitalizations cost Medicare $17.4 billion in 2004.
“This is not a problem that is limited to the elderly. Going home after being in the hospital is scary,” says Stephen Jencks, MD, MPh, a psychiatrist who worked for the Centers for Medicare & Medicaid Services for more than 20 years. “We need to treat that transition as being as dangerous as going through the operating room.”
Dr. Jencks thinks HM, because of its full-time presence in hospitals, is positioned to make a difference by working with all levels of hospital staff and maintaining relationships with primary-care physicians.
“Hospitalists should say: We are in the middle of this; we are in a position to do this; and if we don’t, a lot of people will continue to get hurt,” Dr. Jencks says. “I think if they can make the re-hospitalization problem better, they will have a real feather in their cap.”
Researchers found most patients were rehospitalized for conditions other than those they were originally hospitalized for but might have been controlled prior to discharge. Rehospitalization rates varied widely by state: Maryland, New Jersey, Louisiana, Illinois, and Mississippi had rates 45% higher than Idaho, Utah, Oregon, Colorado, and New Mexico.
Study co-author Mark Williams, MD, a professor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, also is leader of SHM’s transitional care mentoring program, Project BOOST.
The authors suggest several steps to reduce rehospitalizations: interventions to optimize the discharge process; sharing readmission information between hospitals; and physician collaboration to ensure follow-up care.
The author of a new study that shows 20% of Medicare patient discharges are readmitted within 30 days thinks hospitalists can—and should—take a lead role in reducing those rates by improving patient transitions from hospital to home.
The study, released today in the New England Journal of Medicine, also shows that half of nonsurgical patients are readmitted to the hospital without seeing an outpatient doctor, and the unplanned rehospitalizations cost Medicare $17.4 billion in 2004.
“This is not a problem that is limited to the elderly. Going home after being in the hospital is scary,” says Stephen Jencks, MD, MPh, a psychiatrist who worked for the Centers for Medicare & Medicaid Services for more than 20 years. “We need to treat that transition as being as dangerous as going through the operating room.”
Dr. Jencks thinks HM, because of its full-time presence in hospitals, is positioned to make a difference by working with all levels of hospital staff and maintaining relationships with primary-care physicians.
“Hospitalists should say: We are in the middle of this; we are in a position to do this; and if we don’t, a lot of people will continue to get hurt,” Dr. Jencks says. “I think if they can make the re-hospitalization problem better, they will have a real feather in their cap.”
Researchers found most patients were rehospitalized for conditions other than those they were originally hospitalized for but might have been controlled prior to discharge. Rehospitalization rates varied widely by state: Maryland, New Jersey, Louisiana, Illinois, and Mississippi had rates 45% higher than Idaho, Utah, Oregon, Colorado, and New Mexico.
Study co-author Mark Williams, MD, a professor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, also is leader of SHM’s transitional care mentoring program, Project BOOST.
The authors suggest several steps to reduce rehospitalizations: interventions to optimize the discharge process; sharing readmission information between hospitals; and physician collaboration to ensure follow-up care.
The author of a new study that shows 20% of Medicare patient discharges are readmitted within 30 days thinks hospitalists can—and should—take a lead role in reducing those rates by improving patient transitions from hospital to home.
The study, released today in the New England Journal of Medicine, also shows that half of nonsurgical patients are readmitted to the hospital without seeing an outpatient doctor, and the unplanned rehospitalizations cost Medicare $17.4 billion in 2004.
“This is not a problem that is limited to the elderly. Going home after being in the hospital is scary,” says Stephen Jencks, MD, MPh, a psychiatrist who worked for the Centers for Medicare & Medicaid Services for more than 20 years. “We need to treat that transition as being as dangerous as going through the operating room.”
Dr. Jencks thinks HM, because of its full-time presence in hospitals, is positioned to make a difference by working with all levels of hospital staff and maintaining relationships with primary-care physicians.
“Hospitalists should say: We are in the middle of this; we are in a position to do this; and if we don’t, a lot of people will continue to get hurt,” Dr. Jencks says. “I think if they can make the re-hospitalization problem better, they will have a real feather in their cap.”
Researchers found most patients were rehospitalized for conditions other than those they were originally hospitalized for but might have been controlled prior to discharge. Rehospitalization rates varied widely by state: Maryland, New Jersey, Louisiana, Illinois, and Mississippi had rates 45% higher than Idaho, Utah, Oregon, Colorado, and New Mexico.
Study co-author Mark Williams, MD, a professor in the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, also is leader of SHM’s transitional care mentoring program, Project BOOST.
The authors suggest several steps to reduce rehospitalizations: interventions to optimize the discharge process; sharing readmission information between hospitals; and physician collaboration to ensure follow-up care.
There Until the End
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
Patients with advanced cancer who have end-of-life conversations with palliative-care physicians have lower treatment costs, according to a March 9 report in the Archives of Internal Medicine (2009;169(5):480-488). Two other articles in the same issue examine dying patients' feelings of abandonment by physicians.
As more hospitalists move into palliative care, these studies confirm that working with patients in their final days is beneficial for the patient and the hospital.
Take a recent case at Meriter Hospital in Madison, Wis.: A ventilated patient in the hospital's ICU had been receiving aggressive treatment until a palliative-care hospitalist was brought in for a consult. The patient could barely communicate because of the tube in his trachea and an inability to raise his arms; however, the hospitalist took the time to understand the patient's wishes.
"It was very clear he [the patient] had had enough," says hospitalist Amanda duPreez, MD, medical director of Meriter's palliative-care team. "He was ready to die. Had we not been invited into that conversation, it would have been several more days."
Dr. DuPreez thinks hospitalists on palliative-care teams are a natural extension of HM's goal to reduce patient length of stay and contribute to fiscal efficiencies.
"First and foremost, how do we help improve the quality of your life?" Dr. duPreez asks. "Just by nature of [asking that question], there are subsequent cost savings. The intent is never to go out and slash costs across the board. It's a natural byproduct of sitting down with your patients and asking where they're at."
Dr. DuPreez's palliative-care team is looking to recruit another hospitalist because its five-member group has seen its consultations nearly double to more than 30 per week.
When Is GI Bleeding Prophylaxis Indicated in Hospitalized Patients?
Case
A 69-year-old man with Type 2 diabetes mellitus and chronic obstructive pulmonary disease is admitted to the ICU with respiratory compromise related to community-acquired pneumonia (CAP), accompanied by delirium, hyperglycemia, and hypovolemia. He responds well to supportive, noninvasive ventilatory therapy, but develops positive stool occult blood testing during the second day in the ICU. Upon clinical improvement, you transfer him to the general medical floor. What is the best strategy for preventing clinically significant gastrointestinal (GI) bleeding during his hospitalization?
Background
Stress-related mucosal disease (SRMD) refers to superficial erosions or focal ulceration of the proximal gastrointestinal mucosa resulting from physiologic demand in acute illness. Multiple factors contribute to its development, including disruption of the protective mucosal barrier, splanchnic vasculature hypoperfusion, and release of inflammatory mediators.1,2 Increasing severity and number of lesions are associated with the propensity for stress-related mucosal bleeding (SRMB). Based on severity, GI hemorrhage can be defined as occult (detected on chemical testing), overt (grossly evident), or clinically important (overt with compromised hemodynamics or requiring transfusion).3
The majority of clinically significant GI bleeding events occur in critically ill patients. Although more than 75% of patients have endoscopic evidence of SRMD within 24 hours of ICU admission, lesions often resolve spontaneously as patients stabilize, and the average frequency of significant bleeding is only 6%. However, when present, SRMB in ICU patients increases the length of hospitalization, cost, and mortality rates.1,3 By contrast, significant GI bleeding occurs in less than 1% of inpatients without critical illness.4
While preventing clinically important bleeding in hospitalized patients is a crucial objective, current practice reflects significant stress ulcer phophylaxis (SUP) overutilization, with substantial economic impact and potential for harm. One in three patients takes antisecretory therapy (AST) upon admission.5 Additionally, SUP is prescribed in 32% to 54% of general medical inpatients, despite the low risk for SRMB. Importantly, these prophylactic agents are continued on discharge in more than half of these patients.6-9 Clinician prescribing practices potentially can set an unfounded standard of care for obligatory prophylaxis among inpatients.
Data for Clinical Decision-Making
Several studies report the risks for gastrointestinal hemorrhage related to acute illness. In a prospective study of 2,252 ICU patients, two independent predictors of clinically important, new-onset SRMB were identified: mechanical ventilation for more than 48 hours and coagulopathy (see Table 1). Of these risk factors, respiratory failure was present in virtually all patients with GI hemorrhage; only one patient had coagulopathy alone. Mechanical ventilation or coagulopathy was associated with a 4% risk of clinically important GI bleeding, whereas patients with neither symptom had a 0.1% risk.
Though GI bleeding was uncommon, mortality associated with bleeding was 49%, compared with 9% in the nonbleeding group. In the absence of one of these two risk factors, 900 ICU patients would need to be treated to prevent one clinically important GI bleeding event.3 Other studies identify an increased risk of GI bleeding in subsets of patients with trauma, thermal injury, and organ transplantation. Additional possible risk factors might include septic shock, glucocorticoid or NSAID use, renal or hepatic failure, and prior GI bleeding or ulcer.10 The likelihood of GI bleeding increases proportionate to the number of risk factors present.
Limited data for non-ICU patients demonstrate an increased bleeding risk in the presence of ischemic heart disease, chronic renal failure, mechanical ventilation, or prior ICU stay.11 One study of 17,707 general medical patients found a low overall incidence (0.4%) of overt or clinically important GI bleeding, mainly in patients treated with anticoagulants without a mortality difference related to bleeding events.4
The 1999 American Society of Health System Pharmacists (ASHP) Therapeutic Guidelines on Stress Ulcer Prophylaxis reviewed extensive data by level of evidence to identify clinical indicators of patients at higher risk (see Table 2, p. 31).10 The bottom line is that stress-related bleeding depends on the type and severity of illness. Independent risk factors for critically ill patients include mechanical ventilation or coagulopathy. Stable general medical inpatients are at very low risk of clinically significant GI bleeding.

Clinical predictors help define patients at the greatest risk of SRMB. However, to be meaningful, SUP must improve clinical outcomes. Despite extensive studies on the efficacy of pharmacologic agents in the prevention of significant bleeding, several trials do not show a benefit of SUP over placebo, even in patients with major risk factors.4,12,13 Other independent studies and meta-analyses demonstrate that H2-receptor antagonists (H2RAs) prevent ICU bleeding, reducing events by approximately 50%.10 Of all the available prophylactic agents, H2RAs are FDA-approved for this use, proton pump inhibitors (PPIs) are likely as effective, and both are well-tolerated. However, data suggest that the use of AST is associated with C. difficile-associated disease, hip fracture, and pneumonia.
Outside of the ICU, there is no difference in de novo GI bleeding among general medical patients prescribed SUP. The ASHP guidelines thus conclude there is no indication for SUP in stable, general medical inpatients.10
Prevention Strategies

A subset of seriously ill patients has an increased risk for significant SRMB, but ideal prevention is not well-defined. As noted in the ASHP guidelines, “prophylaxis does not necessarily prevent bleeding in patients with documented risk factors, and the efficacy of prophylaxis varies in different patient populations.”
Given the effect of SRMB, it is reasonable to provide preventive agents to subgroups of critically ill patients with significant risk factors of mechanical ventilation for more than 48 hours and underlying coagulopathy. Studies report that judicious SUP prescription when these risks are present reduces cost without increasing morbidity or mortality in the ICU.14
Back to the Case
Our case addresses a patient in both an ICU and general medical setting. Based on his lack of risk factors for significant GI bleeding, SUP was not indicated. In this case, the patient improved. Had he developed ventilatory failure requiring intubation, the risk of clinically important GI bleeding would have approached 4%, and H2RA prophylaxis would have been recommended. Although the optimal length of prophylaxis is unknown, SUP likely can be discontinued on transfer out of the ICU, as clinical stability is associated with a substantially lower risk of clinically important bleeding.
Bottom Line
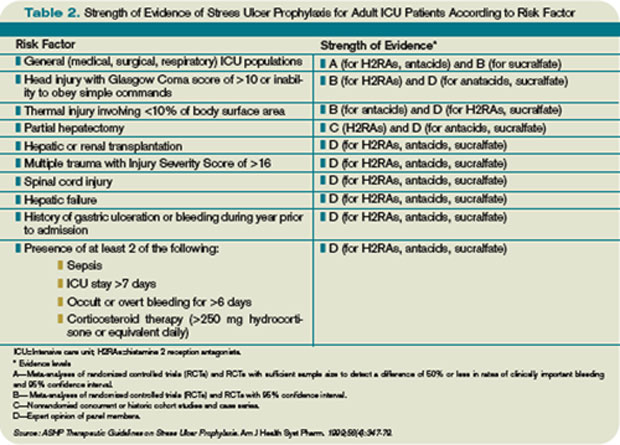
Literature supports the limited use of SUP in hospitalized medical inpatients. SUP can be reserved for critically-ill patients with major risk factors, including prolonged mechanical ventilation or coagulopathy. TH
Dr. Wright is associate professor and head of the section of hospital medicine of the Department of Medicine at the University of Wisconsin School of Medicine and Public Health.
References
1. Stollman N, Metz D. Pathophysiology and prophylaxis of stress ulcer in intensive care unit patients. J Crit Care. 2005;20:35-45.
2. Fennerty M. Pathophysiology of the upper gastrointestinal tract in the critically ill patient: rationale for the therapeutic benefits of acid suppression. Crit Care Med. 2002;30(6 Suppl):S351-S355.
3. Cook D, Fuller H, Guyatt G, et al. Risk factors for gastrointestinal bleeding in critically ill patients. New Engl J Med. 1994;330:377-381.
4. Qadeer M, Richter J, Brotman D. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1:13-20.
5. Heidelbaugh J, Inadomi J. Magnitude and economic impact of inappropriate use of stress ulcer prophylaxis in non-ICU hospitalized patients. Am J Gastroenterol. 2006;101:2200-2205.
6. Nardino R, Vender R, Herbert P. Overuse of acid-suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95:3118-3122.
7. Pham C, Regal R, Bostwick T, Knauf K. Acid suppressive therapy use on an inpatient internal medicine service. Ann Pharmacother. 2006;40:1261-1266.
8. Hwang K, Kolarov S, Cheng L, Griffith R. Stress ulcer prophylaxis for non-critically ill patients on a teaching service. J Eval Clin Pract. 2007;13:716-721.
9. Wohlt P, Hansen L, Fish J. Inappropriate continuation of stress ulcer prophylactic therapy after discharge. Ann Pharmachother. 2007;41:1611-1616.
10. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm. 1999;56:347-379.
11. Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2:86-92.
12. Faisy C, Guerot E, Diehl J, Iftimovici E, Fagon J. Clinically significant gastrointestinal bleeding in critically ill patients with and without stress-ulcer prophylaxis. Intensive Care Med. 2003;29:1306-1313.
13. Kantorova I, Svoboda P, Scheer P, et al. Stress ulcer prophylaxis in critically ill patients: a randomized controlled trial. Hepatogastroenterology. 2004;51:757-761.
14. Coursol C, Sanzari S. Impact of stress ulcer prophylaxis algorithm study. Ann Pharmacother. 2005;39:810-816.
Case
A 69-year-old man with Type 2 diabetes mellitus and chronic obstructive pulmonary disease is admitted to the ICU with respiratory compromise related to community-acquired pneumonia (CAP), accompanied by delirium, hyperglycemia, and hypovolemia. He responds well to supportive, noninvasive ventilatory therapy, but develops positive stool occult blood testing during the second day in the ICU. Upon clinical improvement, you transfer him to the general medical floor. What is the best strategy for preventing clinically significant gastrointestinal (GI) bleeding during his hospitalization?
Background
Stress-related mucosal disease (SRMD) refers to superficial erosions or focal ulceration of the proximal gastrointestinal mucosa resulting from physiologic demand in acute illness. Multiple factors contribute to its development, including disruption of the protective mucosal barrier, splanchnic vasculature hypoperfusion, and release of inflammatory mediators.1,2 Increasing severity and number of lesions are associated with the propensity for stress-related mucosal bleeding (SRMB). Based on severity, GI hemorrhage can be defined as occult (detected on chemical testing), overt (grossly evident), or clinically important (overt with compromised hemodynamics or requiring transfusion).3
The majority of clinically significant GI bleeding events occur in critically ill patients. Although more than 75% of patients have endoscopic evidence of SRMD within 24 hours of ICU admission, lesions often resolve spontaneously as patients stabilize, and the average frequency of significant bleeding is only 6%. However, when present, SRMB in ICU patients increases the length of hospitalization, cost, and mortality rates.1,3 By contrast, significant GI bleeding occurs in less than 1% of inpatients without critical illness.4
While preventing clinically important bleeding in hospitalized patients is a crucial objective, current practice reflects significant stress ulcer phophylaxis (SUP) overutilization, with substantial economic impact and potential for harm. One in three patients takes antisecretory therapy (AST) upon admission.5 Additionally, SUP is prescribed in 32% to 54% of general medical inpatients, despite the low risk for SRMB. Importantly, these prophylactic agents are continued on discharge in more than half of these patients.6-9 Clinician prescribing practices potentially can set an unfounded standard of care for obligatory prophylaxis among inpatients.
Data for Clinical Decision-Making
Several studies report the risks for gastrointestinal hemorrhage related to acute illness. In a prospective study of 2,252 ICU patients, two independent predictors of clinically important, new-onset SRMB were identified: mechanical ventilation for more than 48 hours and coagulopathy (see Table 1). Of these risk factors, respiratory failure was present in virtually all patients with GI hemorrhage; only one patient had coagulopathy alone. Mechanical ventilation or coagulopathy was associated with a 4% risk of clinically important GI bleeding, whereas patients with neither symptom had a 0.1% risk.
Though GI bleeding was uncommon, mortality associated with bleeding was 49%, compared with 9% in the nonbleeding group. In the absence of one of these two risk factors, 900 ICU patients would need to be treated to prevent one clinically important GI bleeding event.3 Other studies identify an increased risk of GI bleeding in subsets of patients with trauma, thermal injury, and organ transplantation. Additional possible risk factors might include septic shock, glucocorticoid or NSAID use, renal or hepatic failure, and prior GI bleeding or ulcer.10 The likelihood of GI bleeding increases proportionate to the number of risk factors present.
Limited data for non-ICU patients demonstrate an increased bleeding risk in the presence of ischemic heart disease, chronic renal failure, mechanical ventilation, or prior ICU stay.11 One study of 17,707 general medical patients found a low overall incidence (0.4%) of overt or clinically important GI bleeding, mainly in patients treated with anticoagulants without a mortality difference related to bleeding events.4
The 1999 American Society of Health System Pharmacists (ASHP) Therapeutic Guidelines on Stress Ulcer Prophylaxis reviewed extensive data by level of evidence to identify clinical indicators of patients at higher risk (see Table 2, p. 31).10 The bottom line is that stress-related bleeding depends on the type and severity of illness. Independent risk factors for critically ill patients include mechanical ventilation or coagulopathy. Stable general medical inpatients are at very low risk of clinically significant GI bleeding.
Clinical predictors help define patients at the greatest risk of SRMB. However, to be meaningful, SUP must improve clinical outcomes. Despite extensive studies on the efficacy of pharmacologic agents in the prevention of significant bleeding, several trials do not show a benefit of SUP over placebo, even in patients with major risk factors.4,12,13 Other independent studies and meta-analyses demonstrate that H2-receptor antagonists (H2RAs) prevent ICU bleeding, reducing events by approximately 50%.10 Of all the available prophylactic agents, H2RAs are FDA-approved for this use, proton pump inhibitors (PPIs) are likely as effective, and both are well-tolerated. However, data suggest that the use of AST is associated with C. difficile-associated disease, hip fracture, and pneumonia.
Outside of the ICU, there is no difference in de novo GI bleeding among general medical patients prescribed SUP. The ASHP guidelines thus conclude there is no indication for SUP in stable, general medical inpatients.10
Prevention Strategies
A subset of seriously ill patients has an increased risk for significant SRMB, but ideal prevention is not well-defined. As noted in the ASHP guidelines, “prophylaxis does not necessarily prevent bleeding in patients with documented risk factors, and the efficacy of prophylaxis varies in different patient populations.”
Given the effect of SRMB, it is reasonable to provide preventive agents to subgroups of critically ill patients with significant risk factors of mechanical ventilation for more than 48 hours and underlying coagulopathy. Studies report that judicious SUP prescription when these risks are present reduces cost without increasing morbidity or mortality in the ICU.14
Back to the Case
Our case addresses a patient in both an ICU and general medical setting. Based on his lack of risk factors for significant GI bleeding, SUP was not indicated. In this case, the patient improved. Had he developed ventilatory failure requiring intubation, the risk of clinically important GI bleeding would have approached 4%, and H2RA prophylaxis would have been recommended. Although the optimal length of prophylaxis is unknown, SUP likely can be discontinued on transfer out of the ICU, as clinical stability is associated with a substantially lower risk of clinically important bleeding.
Bottom Line
Literature supports the limited use of SUP in hospitalized medical inpatients. SUP can be reserved for critically-ill patients with major risk factors, including prolonged mechanical ventilation or coagulopathy. TH
Dr. Wright is associate professor and head of the section of hospital medicine of the Department of Medicine at the University of Wisconsin School of Medicine and Public Health.
References
1. Stollman N, Metz D. Pathophysiology and prophylaxis of stress ulcer in intensive care unit patients. J Crit Care. 2005;20:35-45.
2. Fennerty M. Pathophysiology of the upper gastrointestinal tract in the critically ill patient: rationale for the therapeutic benefits of acid suppression. Crit Care Med. 2002;30(6 Suppl):S351-S355.
3. Cook D, Fuller H, Guyatt G, et al. Risk factors for gastrointestinal bleeding in critically ill patients. New Engl J Med. 1994;330:377-381.
4. Qadeer M, Richter J, Brotman D. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1:13-20.
5. Heidelbaugh J, Inadomi J. Magnitude and economic impact of inappropriate use of stress ulcer prophylaxis in non-ICU hospitalized patients. Am J Gastroenterol. 2006;101:2200-2205.
6. Nardino R, Vender R, Herbert P. Overuse of acid-suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95:3118-3122.
7. Pham C, Regal R, Bostwick T, Knauf K. Acid suppressive therapy use on an inpatient internal medicine service. Ann Pharmacother. 2006;40:1261-1266.
8. Hwang K, Kolarov S, Cheng L, Griffith R. Stress ulcer prophylaxis for non-critically ill patients on a teaching service. J Eval Clin Pract. 2007;13:716-721.
9. Wohlt P, Hansen L, Fish J. Inappropriate continuation of stress ulcer prophylactic therapy after discharge. Ann Pharmachother. 2007;41:1611-1616.
10. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm. 1999;56:347-379.
11. Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2:86-92.
12. Faisy C, Guerot E, Diehl J, Iftimovici E, Fagon J. Clinically significant gastrointestinal bleeding in critically ill patients with and without stress-ulcer prophylaxis. Intensive Care Med. 2003;29:1306-1313.
13. Kantorova I, Svoboda P, Scheer P, et al. Stress ulcer prophylaxis in critically ill patients: a randomized controlled trial. Hepatogastroenterology. 2004;51:757-761.
14. Coursol C, Sanzari S. Impact of stress ulcer prophylaxis algorithm study. Ann Pharmacother. 2005;39:810-816.
Case
A 69-year-old man with Type 2 diabetes mellitus and chronic obstructive pulmonary disease is admitted to the ICU with respiratory compromise related to community-acquired pneumonia (CAP), accompanied by delirium, hyperglycemia, and hypovolemia. He responds well to supportive, noninvasive ventilatory therapy, but develops positive stool occult blood testing during the second day in the ICU. Upon clinical improvement, you transfer him to the general medical floor. What is the best strategy for preventing clinically significant gastrointestinal (GI) bleeding during his hospitalization?
Background
Stress-related mucosal disease (SRMD) refers to superficial erosions or focal ulceration of the proximal gastrointestinal mucosa resulting from physiologic demand in acute illness. Multiple factors contribute to its development, including disruption of the protective mucosal barrier, splanchnic vasculature hypoperfusion, and release of inflammatory mediators.1,2 Increasing severity and number of lesions are associated with the propensity for stress-related mucosal bleeding (SRMB). Based on severity, GI hemorrhage can be defined as occult (detected on chemical testing), overt (grossly evident), or clinically important (overt with compromised hemodynamics or requiring transfusion).3
The majority of clinically significant GI bleeding events occur in critically ill patients. Although more than 75% of patients have endoscopic evidence of SRMD within 24 hours of ICU admission, lesions often resolve spontaneously as patients stabilize, and the average frequency of significant bleeding is only 6%. However, when present, SRMB in ICU patients increases the length of hospitalization, cost, and mortality rates.1,3 By contrast, significant GI bleeding occurs in less than 1% of inpatients without critical illness.4
While preventing clinically important bleeding in hospitalized patients is a crucial objective, current practice reflects significant stress ulcer phophylaxis (SUP) overutilization, with substantial economic impact and potential for harm. One in three patients takes antisecretory therapy (AST) upon admission.5 Additionally, SUP is prescribed in 32% to 54% of general medical inpatients, despite the low risk for SRMB. Importantly, these prophylactic agents are continued on discharge in more than half of these patients.6-9 Clinician prescribing practices potentially can set an unfounded standard of care for obligatory prophylaxis among inpatients.
Data for Clinical Decision-Making
Several studies report the risks for gastrointestinal hemorrhage related to acute illness. In a prospective study of 2,252 ICU patients, two independent predictors of clinically important, new-onset SRMB were identified: mechanical ventilation for more than 48 hours and coagulopathy (see Table 1). Of these risk factors, respiratory failure was present in virtually all patients with GI hemorrhage; only one patient had coagulopathy alone. Mechanical ventilation or coagulopathy was associated with a 4% risk of clinically important GI bleeding, whereas patients with neither symptom had a 0.1% risk.
Though GI bleeding was uncommon, mortality associated with bleeding was 49%, compared with 9% in the nonbleeding group. In the absence of one of these two risk factors, 900 ICU patients would need to be treated to prevent one clinically important GI bleeding event.3 Other studies identify an increased risk of GI bleeding in subsets of patients with trauma, thermal injury, and organ transplantation. Additional possible risk factors might include septic shock, glucocorticoid or NSAID use, renal or hepatic failure, and prior GI bleeding or ulcer.10 The likelihood of GI bleeding increases proportionate to the number of risk factors present.
Limited data for non-ICU patients demonstrate an increased bleeding risk in the presence of ischemic heart disease, chronic renal failure, mechanical ventilation, or prior ICU stay.11 One study of 17,707 general medical patients found a low overall incidence (0.4%) of overt or clinically important GI bleeding, mainly in patients treated with anticoagulants without a mortality difference related to bleeding events.4
The 1999 American Society of Health System Pharmacists (ASHP) Therapeutic Guidelines on Stress Ulcer Prophylaxis reviewed extensive data by level of evidence to identify clinical indicators of patients at higher risk (see Table 2, p. 31).10 The bottom line is that stress-related bleeding depends on the type and severity of illness. Independent risk factors for critically ill patients include mechanical ventilation or coagulopathy. Stable general medical inpatients are at very low risk of clinically significant GI bleeding.
Clinical predictors help define patients at the greatest risk of SRMB. However, to be meaningful, SUP must improve clinical outcomes. Despite extensive studies on the efficacy of pharmacologic agents in the prevention of significant bleeding, several trials do not show a benefit of SUP over placebo, even in patients with major risk factors.4,12,13 Other independent studies and meta-analyses demonstrate that H2-receptor antagonists (H2RAs) prevent ICU bleeding, reducing events by approximately 50%.10 Of all the available prophylactic agents, H2RAs are FDA-approved for this use, proton pump inhibitors (PPIs) are likely as effective, and both are well-tolerated. However, data suggest that the use of AST is associated with C. difficile-associated disease, hip fracture, and pneumonia.
Outside of the ICU, there is no difference in de novo GI bleeding among general medical patients prescribed SUP. The ASHP guidelines thus conclude there is no indication for SUP in stable, general medical inpatients.10
Prevention Strategies
A subset of seriously ill patients has an increased risk for significant SRMB, but ideal prevention is not well-defined. As noted in the ASHP guidelines, “prophylaxis does not necessarily prevent bleeding in patients with documented risk factors, and the efficacy of prophylaxis varies in different patient populations.”
Given the effect of SRMB, it is reasonable to provide preventive agents to subgroups of critically ill patients with significant risk factors of mechanical ventilation for more than 48 hours and underlying coagulopathy. Studies report that judicious SUP prescription when these risks are present reduces cost without increasing morbidity or mortality in the ICU.14
Back to the Case
Our case addresses a patient in both an ICU and general medical setting. Based on his lack of risk factors for significant GI bleeding, SUP was not indicated. In this case, the patient improved. Had he developed ventilatory failure requiring intubation, the risk of clinically important GI bleeding would have approached 4%, and H2RA prophylaxis would have been recommended. Although the optimal length of prophylaxis is unknown, SUP likely can be discontinued on transfer out of the ICU, as clinical stability is associated with a substantially lower risk of clinically important bleeding.
Bottom Line
Literature supports the limited use of SUP in hospitalized medical inpatients. SUP can be reserved for critically-ill patients with major risk factors, including prolonged mechanical ventilation or coagulopathy. TH
Dr. Wright is associate professor and head of the section of hospital medicine of the Department of Medicine at the University of Wisconsin School of Medicine and Public Health.
References
1. Stollman N, Metz D. Pathophysiology and prophylaxis of stress ulcer in intensive care unit patients. J Crit Care. 2005;20:35-45.
2. Fennerty M. Pathophysiology of the upper gastrointestinal tract in the critically ill patient: rationale for the therapeutic benefits of acid suppression. Crit Care Med. 2002;30(6 Suppl):S351-S355.
3. Cook D, Fuller H, Guyatt G, et al. Risk factors for gastrointestinal bleeding in critically ill patients. New Engl J Med. 1994;330:377-381.
4. Qadeer M, Richter J, Brotman D. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1:13-20.
5. Heidelbaugh J, Inadomi J. Magnitude and economic impact of inappropriate use of stress ulcer prophylaxis in non-ICU hospitalized patients. Am J Gastroenterol. 2006;101:2200-2205.
6. Nardino R, Vender R, Herbert P. Overuse of acid-suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95:3118-3122.
7. Pham C, Regal R, Bostwick T, Knauf K. Acid suppressive therapy use on an inpatient internal medicine service. Ann Pharmacother. 2006;40:1261-1266.
8. Hwang K, Kolarov S, Cheng L, Griffith R. Stress ulcer prophylaxis for non-critically ill patients on a teaching service. J Eval Clin Pract. 2007;13:716-721.
9. Wohlt P, Hansen L, Fish J. Inappropriate continuation of stress ulcer prophylactic therapy after discharge. Ann Pharmachother. 2007;41:1611-1616.
10. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm. 1999;56:347-379.
11. Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2:86-92.
12. Faisy C, Guerot E, Diehl J, Iftimovici E, Fagon J. Clinically significant gastrointestinal bleeding in critically ill patients with and without stress-ulcer prophylaxis. Intensive Care Med. 2003;29:1306-1313.
13. Kantorova I, Svoboda P, Scheer P, et al. Stress ulcer prophylaxis in critically ill patients: a randomized controlled trial. Hepatogastroenterology. 2004;51:757-761.
14. Coursol C, Sanzari S. Impact of stress ulcer prophylaxis algorithm study. Ann Pharmacother. 2005;39:810-816.
Misunderstood Modifiers
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Armed with HM Knowledge
Many physicians use traditional practice as their stepping stone to a hospitalist career. David M. Grace, MD, took a far more unconventional path.
He served as a combat medic in the Army National Guard, joined a disaster medical assistance team at the Federal Emergency Management Agency (FEMA), and volunteered to help the American Red Cross in times of crisis—all before entering medical school.
Dr. Grace became a hospitalist in 2002, and now serves as hospitalist division area medical officer for The Schumacher Group, a staffing and consulting firm in Lafayette, La., that hires physicians as independent contractors to work in hospitals across the country.
But 21 years into his healthcare career, he continues to seek opportunities that offer the same two rewards: “I want to be filled with Adrenalin,” he says, “but I still want to use my brains.”
—David M. Grace, MD, The Schumacher Group, Lafayette, La.
Question: Given your varied background, how did you wind up becoming a hospitalist?
Answer: My predoctoring resume reads like a fast track of becoming an emergency physician. In residency, I had heard the term “hospitalist.” I knew I liked dealing with sick patients. Emergency departments act as a fairly good filter, and anyone who gets through and upstairs truly is a sick patient. I figured if I were a hospitalist, all my patients would be sick, as opposed to just some. That really drove me to hospital medicine.
Q: You founded your own hospitalist company in 2005, but within two years, you joined The Schumacher Group. Why did you make the switch?
A: With the speed with which hospital medicine is growing, I thought if I could tap into their resources and infrastructure … I’d be able to do things I couldn’t do in my own group for years, if not decades. I really thought I would be able to impact a far larger portion of patient lives with them than I could in my own smaller, somewhat homemade group.
Q: When The Schumacher Group formed, it focused on emergency departments. In 2007, it launched a hospitalist service. What’s the benefit?
A: If you put good hospitalist systems under the same umbrella as good emergency department systems, you can do things to boost the synergy between the two disciplines and improve patient care. In the facilities where we’re managing both the ED and the hospitalists, we can effect patient care from the moment the patient swings through the ambulance bay doors until the moment they are discharged.
Q: How successful has the HM effort been?
A: The hospitalist side, by the end of the year, will have about 20 to 25 practices up and running, with growth in the neighborhood of 10 to 15 practices a year expected to come on line.
Q: What are the advantages to a private corporation setup?
A: At the end of the day, doctors need to be patient-care advocates. But if you are employed by a hospital, they sign your check. When push comes to shove on a quality issue, I think there’s a tendency not to shove as hard when the person you’re shoving is the person employing you.
Q: Could this approach be the wave of the future?
A: I think so. It goes back to the idea of focusing all of your resources into one small area, such as hospital medicine or inpatient medicine, so there’s far fewer distractions than for a hospital that runs its own hospitalist program. We saw that in the 1970s, when hospitals were buying primary-care practices left and right. They realized they didn’t have the skills or the resources to make that effective, and they rapidly divested.
Q: Most doctors at the executive level of The Schumacher Group—including yourself—still practice medicine. Why is that so integral to the mission?
A: When I served in the military, the best officers I served under were officers who had been enlisted men earlier in their career. The same follows suit in hospital medicine. When I make an administrative decision, it can affect thousands of patient lives tomorrow. I can mentally track the effects of my decision all the way back to how it will affect the patient laying in the bed. If you’re not having that constantly reinforced by seeing patients, it’s very easy to lose track of it, and that has such a profound effect on patient care.
Q: SHM recently designated you one of the inaugural “Fellows in Hospital Medicine.” What is the biggest reward of a HM career?
A: For me, there are two. One is the ability to see the fruits of your labor much more rapidly than in the outpatient world. I can have a patient in bed in front of me actively dying and watch them a week later walk out of hospital in good condition. That’s a very different timetable than the outpatient world, when you may put a patient on all the right medicines to reduce the risk of a heart attack and, over 60 years, watch them not have a heart attack. The other thing I find very rewarding is the amount of measurements and data collected on what we do. We get feedback ranging from patient satisfaction scores to referring physician scores to readmission rates to data that shows if we are able to get patients better outcomes at lower costs. You just don’t get that type of feedback in many other fields.
Q: What is the greatest challenge facing the profession?
A: One of the biggest is the supply and demand mismatch. Right now, one of the hardest jobs is a hospitalist recruiter. With every physician having five to 10 open job offers …recruiting is difficult, and recruiting the right physician is extremely difficult.
Q: How can that be addressed?
A: One way is to be efficient. Can we see more patients in the same amount of time with no decrease in quality? For us, it involves the use of what we call a practice coordinator. It’s an employee of The Schumacher Group who is located in the individual hospital who does everything from assisting with managing the practice to answering telephone calls. This really allows us to help us organize our time better, so we don’t get bogged down in nonclinical work. Every minute spent on the phone with an insurance company or home health agency is a minute not spent at the bedside. Another way is expanding the use of midlevel providers. The key is not to use them as a replacement for a physician, but as an assistant to the physician—again, to boost capacity.
Q: How did your background with the military, FEMA, and the Red Cross prepare you for what you’re doing now?
A: Business as usual is very difficult to do in a chaotic environment, so I began to appreciate the importance of systems. If you’re relying on an individual and that individual leaves, your entity is in trouble. If you put good systems into place, you’re not so reliant on any one individual. Systems can function long after any individual doctor has come and gone. In the world of hospitalists—where there’s still fairly high turnover, being a young field and there are many opportunities—it’s imperative the systems approach is taken. TH
Mark Leiser is a freelance writer in New Jersey.
Many physicians use traditional practice as their stepping stone to a hospitalist career. David M. Grace, MD, took a far more unconventional path.
He served as a combat medic in the Army National Guard, joined a disaster medical assistance team at the Federal Emergency Management Agency (FEMA), and volunteered to help the American Red Cross in times of crisis—all before entering medical school.
Dr. Grace became a hospitalist in 2002, and now serves as hospitalist division area medical officer for The Schumacher Group, a staffing and consulting firm in Lafayette, La., that hires physicians as independent contractors to work in hospitals across the country.
But 21 years into his healthcare career, he continues to seek opportunities that offer the same two rewards: “I want to be filled with Adrenalin,” he says, “but I still want to use my brains.”
—David M. Grace, MD, The Schumacher Group, Lafayette, La.
Question: Given your varied background, how did you wind up becoming a hospitalist?
Answer: My predoctoring resume reads like a fast track of becoming an emergency physician. In residency, I had heard the term “hospitalist.” I knew I liked dealing with sick patients. Emergency departments act as a fairly good filter, and anyone who gets through and upstairs truly is a sick patient. I figured if I were a hospitalist, all my patients would be sick, as opposed to just some. That really drove me to hospital medicine.
Q: You founded your own hospitalist company in 2005, but within two years, you joined The Schumacher Group. Why did you make the switch?
A: With the speed with which hospital medicine is growing, I thought if I could tap into their resources and infrastructure … I’d be able to do things I couldn’t do in my own group for years, if not decades. I really thought I would be able to impact a far larger portion of patient lives with them than I could in my own smaller, somewhat homemade group.
Q: When The Schumacher Group formed, it focused on emergency departments. In 2007, it launched a hospitalist service. What’s the benefit?
A: If you put good hospitalist systems under the same umbrella as good emergency department systems, you can do things to boost the synergy between the two disciplines and improve patient care. In the facilities where we’re managing both the ED and the hospitalists, we can effect patient care from the moment the patient swings through the ambulance bay doors until the moment they are discharged.
Q: How successful has the HM effort been?
A: The hospitalist side, by the end of the year, will have about 20 to 25 practices up and running, with growth in the neighborhood of 10 to 15 practices a year expected to come on line.
Q: What are the advantages to a private corporation setup?
A: At the end of the day, doctors need to be patient-care advocates. But if you are employed by a hospital, they sign your check. When push comes to shove on a quality issue, I think there’s a tendency not to shove as hard when the person you’re shoving is the person employing you.
Q: Could this approach be the wave of the future?
A: I think so. It goes back to the idea of focusing all of your resources into one small area, such as hospital medicine or inpatient medicine, so there’s far fewer distractions than for a hospital that runs its own hospitalist program. We saw that in the 1970s, when hospitals were buying primary-care practices left and right. They realized they didn’t have the skills or the resources to make that effective, and they rapidly divested.
Q: Most doctors at the executive level of The Schumacher Group—including yourself—still practice medicine. Why is that so integral to the mission?
A: When I served in the military, the best officers I served under were officers who had been enlisted men earlier in their career. The same follows suit in hospital medicine. When I make an administrative decision, it can affect thousands of patient lives tomorrow. I can mentally track the effects of my decision all the way back to how it will affect the patient laying in the bed. If you’re not having that constantly reinforced by seeing patients, it’s very easy to lose track of it, and that has such a profound effect on patient care.
Q: SHM recently designated you one of the inaugural “Fellows in Hospital Medicine.” What is the biggest reward of a HM career?
A: For me, there are two. One is the ability to see the fruits of your labor much more rapidly than in the outpatient world. I can have a patient in bed in front of me actively dying and watch them a week later walk out of hospital in good condition. That’s a very different timetable than the outpatient world, when you may put a patient on all the right medicines to reduce the risk of a heart attack and, over 60 years, watch them not have a heart attack. The other thing I find very rewarding is the amount of measurements and data collected on what we do. We get feedback ranging from patient satisfaction scores to referring physician scores to readmission rates to data that shows if we are able to get patients better outcomes at lower costs. You just don’t get that type of feedback in many other fields.
Q: What is the greatest challenge facing the profession?
A: One of the biggest is the supply and demand mismatch. Right now, one of the hardest jobs is a hospitalist recruiter. With every physician having five to 10 open job offers …recruiting is difficult, and recruiting the right physician is extremely difficult.
Q: How can that be addressed?
A: One way is to be efficient. Can we see more patients in the same amount of time with no decrease in quality? For us, it involves the use of what we call a practice coordinator. It’s an employee of The Schumacher Group who is located in the individual hospital who does everything from assisting with managing the practice to answering telephone calls. This really allows us to help us organize our time better, so we don’t get bogged down in nonclinical work. Every minute spent on the phone with an insurance company or home health agency is a minute not spent at the bedside. Another way is expanding the use of midlevel providers. The key is not to use them as a replacement for a physician, but as an assistant to the physician—again, to boost capacity.
Q: How did your background with the military, FEMA, and the Red Cross prepare you for what you’re doing now?
A: Business as usual is very difficult to do in a chaotic environment, so I began to appreciate the importance of systems. If you’re relying on an individual and that individual leaves, your entity is in trouble. If you put good systems into place, you’re not so reliant on any one individual. Systems can function long after any individual doctor has come and gone. In the world of hospitalists—where there’s still fairly high turnover, being a young field and there are many opportunities—it’s imperative the systems approach is taken. TH
Mark Leiser is a freelance writer in New Jersey.
Many physicians use traditional practice as their stepping stone to a hospitalist career. David M. Grace, MD, took a far more unconventional path.
He served as a combat medic in the Army National Guard, joined a disaster medical assistance team at the Federal Emergency Management Agency (FEMA), and volunteered to help the American Red Cross in times of crisis—all before entering medical school.
Dr. Grace became a hospitalist in 2002, and now serves as hospitalist division area medical officer for The Schumacher Group, a staffing and consulting firm in Lafayette, La., that hires physicians as independent contractors to work in hospitals across the country.
But 21 years into his healthcare career, he continues to seek opportunities that offer the same two rewards: “I want to be filled with Adrenalin,” he says, “but I still want to use my brains.”
—David M. Grace, MD, The Schumacher Group, Lafayette, La.
Question: Given your varied background, how did you wind up becoming a hospitalist?
Answer: My predoctoring resume reads like a fast track of becoming an emergency physician. In residency, I had heard the term “hospitalist.” I knew I liked dealing with sick patients. Emergency departments act as a fairly good filter, and anyone who gets through and upstairs truly is a sick patient. I figured if I were a hospitalist, all my patients would be sick, as opposed to just some. That really drove me to hospital medicine.
Q: You founded your own hospitalist company in 2005, but within two years, you joined The Schumacher Group. Why did you make the switch?
A: With the speed with which hospital medicine is growing, I thought if I could tap into their resources and infrastructure … I’d be able to do things I couldn’t do in my own group for years, if not decades. I really thought I would be able to impact a far larger portion of patient lives with them than I could in my own smaller, somewhat homemade group.
Q: When The Schumacher Group formed, it focused on emergency departments. In 2007, it launched a hospitalist service. What’s the benefit?
A: If you put good hospitalist systems under the same umbrella as good emergency department systems, you can do things to boost the synergy between the two disciplines and improve patient care. In the facilities where we’re managing both the ED and the hospitalists, we can effect patient care from the moment the patient swings through the ambulance bay doors until the moment they are discharged.
Q: How successful has the HM effort been?
A: The hospitalist side, by the end of the year, will have about 20 to 25 practices up and running, with growth in the neighborhood of 10 to 15 practices a year expected to come on line.
Q: What are the advantages to a private corporation setup?
A: At the end of the day, doctors need to be patient-care advocates. But if you are employed by a hospital, they sign your check. When push comes to shove on a quality issue, I think there’s a tendency not to shove as hard when the person you’re shoving is the person employing you.
Q: Could this approach be the wave of the future?
A: I think so. It goes back to the idea of focusing all of your resources into one small area, such as hospital medicine or inpatient medicine, so there’s far fewer distractions than for a hospital that runs its own hospitalist program. We saw that in the 1970s, when hospitals were buying primary-care practices left and right. They realized they didn’t have the skills or the resources to make that effective, and they rapidly divested.
Q: Most doctors at the executive level of The Schumacher Group—including yourself—still practice medicine. Why is that so integral to the mission?
A: When I served in the military, the best officers I served under were officers who had been enlisted men earlier in their career. The same follows suit in hospital medicine. When I make an administrative decision, it can affect thousands of patient lives tomorrow. I can mentally track the effects of my decision all the way back to how it will affect the patient laying in the bed. If you’re not having that constantly reinforced by seeing patients, it’s very easy to lose track of it, and that has such a profound effect on patient care.
Q: SHM recently designated you one of the inaugural “Fellows in Hospital Medicine.” What is the biggest reward of a HM career?
A: For me, there are two. One is the ability to see the fruits of your labor much more rapidly than in the outpatient world. I can have a patient in bed in front of me actively dying and watch them a week later walk out of hospital in good condition. That’s a very different timetable than the outpatient world, when you may put a patient on all the right medicines to reduce the risk of a heart attack and, over 60 years, watch them not have a heart attack. The other thing I find very rewarding is the amount of measurements and data collected on what we do. We get feedback ranging from patient satisfaction scores to referring physician scores to readmission rates to data that shows if we are able to get patients better outcomes at lower costs. You just don’t get that type of feedback in many other fields.
Q: What is the greatest challenge facing the profession?
A: One of the biggest is the supply and demand mismatch. Right now, one of the hardest jobs is a hospitalist recruiter. With every physician having five to 10 open job offers …recruiting is difficult, and recruiting the right physician is extremely difficult.
Q: How can that be addressed?
A: One way is to be efficient. Can we see more patients in the same amount of time with no decrease in quality? For us, it involves the use of what we call a practice coordinator. It’s an employee of The Schumacher Group who is located in the individual hospital who does everything from assisting with managing the practice to answering telephone calls. This really allows us to help us organize our time better, so we don’t get bogged down in nonclinical work. Every minute spent on the phone with an insurance company or home health agency is a minute not spent at the bedside. Another way is expanding the use of midlevel providers. The key is not to use them as a replacement for a physician, but as an assistant to the physician—again, to boost capacity.
Q: How did your background with the military, FEMA, and the Red Cross prepare you for what you’re doing now?
A: Business as usual is very difficult to do in a chaotic environment, so I began to appreciate the importance of systems. If you’re relying on an individual and that individual leaves, your entity is in trouble. If you put good systems into place, you’re not so reliant on any one individual. Systems can function long after any individual doctor has come and gone. In the world of hospitalists—where there’s still fairly high turnover, being a young field and there are many opportunities—it’s imperative the systems approach is taken. TH
Mark Leiser is a freelance writer in New Jersey.