User login
Should we be concerned about thyroid cancer in patients taking glucagon-like peptide 1 receptor agonists?
The question is complicated, as there are different types of thyroid cancer, and a causal relationship is hard to prove.
Glucagon-like peptide 1 (GLP-1) receptor agonists can be safely used in all patients with thyroid cancers that are derived from the thyroid follicular epithelium (papillary and follicular thyroid cancer). However, they are currently contraindicated in patients with medullary thyroid cancer and in patients with multiple endocrine neoplasia 2 (MEN-2), which is not a form of thyroid cancer but is relevant to our discussion. We probably should be cautious about using them in patients with familial thyroid cancer and those with a genetic predisposition for papillary or follicular thyroid cancer.
GLP-1 DRUGS ARE WIDELY USED
The glucagon-like peptide 1 (GLP-1) receptor agonists are widely used to treat type 2 diabetes mellitus. The currently available drugs of this class—exenatide (Byetta), liraglutide (Victoza), albiglutide (Tanzeum), dulaglutide (Trulicity), and extended-release exenatide (Bydureon)—are popular because they lower glucose levels, pose a low risk of hypoglycemia, can induce weight loss,1 and, in the case of extended-release exenatide and albiglutide, are given once weekly. They are currently recommended as add-on therapy to metformin. These drugs mimic the action of GLP-1, an endogenous hormone released by the intestine in response to food. They bind to receptors on beta cells, stimulating insulin production.1
FOUR TYPES OF THYROID CANCER
There are four types of thyroid cancer: medullary (a contraindication to GLP-1 agonists), papillary, follicular, and anaplastic.
Medullary thyroid cancer is extremely rare in humans, with 976 cases diagnosed from 1992 to 2006 in the United States, compared with 36,583 cases of papillary and 4,560 cases of follicular cancer. Anaplastic cancer is also rare (556 cases).2 The highest incidence rates of medullary thyroid cancer are in people of Hispanic descent (0.21 per 100,000 woman-years and 0.18 per 100,000 man-years).2
EXPERIMENTAL EVIDENCE
Pancreatic beta cells are not the only cells in the body that can express GLP-1 receptors. Notably, the parafollicular cells (also called C cells) of the thyroid, which secrete calcitonin and which are the cells involved in medullary thyroid cancer, also sometimes express these receptors if cancer develops.
In experiments in mice and rats, the incidence of thyroid C-cell tumors was higher in animals given GLP-1 analogues. Liraglutide, exenatide, taspoglutide, and lixisenatide potently activated GLP-1 receptors in thyroid C cells, increasing calcitonin gene expression and stimulating calcitonin release in a dose-dependent manner.3 Moreover, sustained activation of these receptors caused C-cell hyperplasia and resulted in medullary thyroid cancer. However medullary thyroid cancer also occurred in rodents receiving placebo.
C cells in monkeys and humans express fewer GLP-1 receptors than those in rodents; in fact, healthy human C cells do not express them at all.3,4 In rats with C-cell hyperplasia or medullary thyroid cancer, GLP-1 receptors are present in 100% of cases (and in increased density), compared with 27% of human medullary thyroid cancers.4
In addition to medullary thyroid cancer, various other human tumors have been shown to express GLP-1 receptors.5 Based on limited data, KÖrner et al5 found that these receptors are also present in various other human tumors, eg:
- Pheochromocytoma (60%)
- Paraganglioma (28%)
- Meningioma (35%)
- Astrocytoma (25%)
- Glioblastoma (9%)
- Ependymoma (16%)
- Medulloblastoma (25%)
- Nephroblastoma (22%)
- Neuroblastoma (18%)
- Ovarian adenocarcinoma (16%)
- Prostate carcinoma (5%).
Madsen et al6 reported that liraglutide binding to the GLP-1 receptor on murine thyroid C cells led to C-cell hyperplasia. However, prolonged administration of liraglutide at very high doses did not produce C-cell proliferation in monkeys.3
Gier et al7 looked at GLP-1 receptor expression in normal human C cells, hyperplastic C cells, and medullary thyroid cancer cells, as well as in papillary thyroid cancer cells, which do not arise from C cells. They demonstrated concurrent calcitonin and GLP-1 receptor immunostaining, not only in those with C-cell hyperplasia (9 of 9 cases) and medullary thyroid cancer (11 of 12 cases), but also in 3 (18%) of 17 patients with papillary thyroid cancer and 5 (33%) of 15 with normal thyroid follicular cells. However, the choice of polyclonal antibodies and radioligands used and concerns about methodology have led investigators to interpret these results cautiously.8–10
STUDIES OF GLP-1 AGONISTS IN HUMANS
Several prospective clinical studies showed no increase in calcitonin levels during therapy with GLP-1 receptor agonists in patients with type 2 diabetes.3,11 Long-term use of liraglutide in high doses (up to 3 mg per day) did not lead to elevations in serum calcitonin levels.11
In a retrospective Adverse Event Reporting System database review, the incidence rate of thyroid cancer in patients treated with exenatide was higher—with an odds ratio of 4.7 (30 events)—than with a panel of control drugs (3 events).12 However, this study did not differentiate between types of thyroid cancer, and the inherent limitations of retrospective databases complicate its interpretation. Such a high odds ratio would imply a significant increase in the incidence of medullary thyroid cancer, but this does not seem to be true.
Alves et al13 performed a meta-analysis of randomized controlled trials and long-term observational studies. None of the studies evaluating exenatide reported cases of thyroid cancer, whereas five of the studies evaluating liraglutide did. In total, nine patients treated with liraglutide were diagnosed with thyroid cancer, compared with one patient on glimepiride. The odds ratio for thyroid cancer occurrence associated with liraglutide treatment was 1.54, but that was not statistically significant (95% confidence interval 0.40–6.02, P = .53, I2 = 0%).
These studies are hypothesis-generating and do not prove that GLP-1 receptor agonists cause medullary thyroid cancer. Given the extremely low incidence of medullary thyroid cancer, to prove or disprove a causal relationship would require an enormous number of patients, who would need to be followed for several years.
OFFICIAL RECOMMENDATIONS
Considerable differences in the biology of the rodent vs human thyroid GLP-1 receptor systems have led regulatory authorities to conclude that the risk for development of medullary thyroid cancer with GLP-1 therapy in humans is difficult to quantify, but low.14 Consequently, the US Food and Drug Administration recommends neither monitoring of calcitonin levels nor ultrasound imaging as a screening tool in patients taking GLP-1 agonists.14
BENEFITS OUTWEIGH RISKS
At present, the benefits of using GLP-1 receptor agonists to treat type 2 diabetes mellitus outweigh the risks, and there seems to be little reason to withhold this effective therapy except in patients who have a personal or family history of medullary thyroid cancer or MEN-2. Until the effects of GLP-1 agonists are systematically studied in follicular-cell-derived thyroid cancer, we also recommend caution when considering their use in patients with familial thyroid cancer and those with a genetic predisposition for papillary and follicular thyroid cancer—eg, patients with familial adenomatous polyposis, phosphate and tensin homolog hamartoma tumor syndrome, Carney complex type 1, Werner syndrome, or familial papillary thyroid cancer.
Methodologically superior studies and careful long-term monitoring of patients treated with GLP-1 agonists are required to clarify the risk vs benefit of these therapies.
- Samson SL, Garber A. GLP-1R agonist therapy for diabetes: benefits and potential risks. Curr Opin Endocrinol Diabetes Obes 2013; 20:87–97.
- Aschebrook-Kilfoy B, Ward MH, Sabra MM, Devesa SS. Thyroid cancer incidence patterns in the United States by histologic type, 1992–2006. Thyroid 2011; 21:125–134.
- Bjerre Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
- Waser B, Beetschen K, Pellegata NS, Reubi JC. Incretin receptors in non-neoplastic and neoplastic thyroid C cells in rodents and humans: relevance for incretin-based diabetes therapy. Neuroendocrinology 2011; 94:291–301.
- Körner M, Stöckli M, Waser B, Reubi JC. GLP-1 receptor expression in human tumors and human normal tissues: potential for in vivo targeting. J Nucl Med 2007; 48:736–743.
- Madsen LW, Knauf JA, Gotfredsen C, et al. GLP-1 receptor agonists and the thyroid: C-cell effects in mice are mediated via the GLP-1 receptor and not associated with RET activation. Endocrinology 2012; 153:1538–1547.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
- Drucker DJ, Sherman SI, Bergenstal RM, Buse JB. The safety of incretin-based therapies—review of the scientific evidence. J Clin Endocrinol Metab 2011; 96:2027–2031.
- Gagel RF. Activation of G-protein-coupled receptors and thyroid malignant tumors: the jury is still out. Endocr Pract 2011; 17:957–959.
- Nauck MA. A critical analysis of the clinical use of incretin-based therapies: the benefits by far outweigh the potential risks. Diabetes Care 2013; 36:2126–2132.
- Hegedüs L, Moses AC, Zdravkovic M, Le Thi T, Daniels GH. GLP-1 and calcitonin concentration in humans: lack of evidence of calcitonin release from sequential screening in over 5000 subjects with type 2 diabetes or nondiabetic obese subjects treated with the human GLP-1 analog, liraglutide. J Clin Endocrinol Metab 2011; 96:853–860.
- Elashoff M, Matveyenko AV, Gier B, Elashoff R, Butler PC. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 2011; 141:150–156.
- Alves C, Batel-Marques F, Macedo AF. A meta-analysis of serious adverse events reported with exenatide and liraglutide: acute pancreatitis and cancer. Diabetes Res Clin Pract 2012; 98:271–284.
- Parks M, Rosebraugh C. Weighing risks and benefits of liraglutide—the FDA’s review of a new antidiabetic therapy. N Engl J Med 2010; 362:774–777.
The question is complicated, as there are different types of thyroid cancer, and a causal relationship is hard to prove.
Glucagon-like peptide 1 (GLP-1) receptor agonists can be safely used in all patients with thyroid cancers that are derived from the thyroid follicular epithelium (papillary and follicular thyroid cancer). However, they are currently contraindicated in patients with medullary thyroid cancer and in patients with multiple endocrine neoplasia 2 (MEN-2), which is not a form of thyroid cancer but is relevant to our discussion. We probably should be cautious about using them in patients with familial thyroid cancer and those with a genetic predisposition for papillary or follicular thyroid cancer.
GLP-1 DRUGS ARE WIDELY USED
The glucagon-like peptide 1 (GLP-1) receptor agonists are widely used to treat type 2 diabetes mellitus. The currently available drugs of this class—exenatide (Byetta), liraglutide (Victoza), albiglutide (Tanzeum), dulaglutide (Trulicity), and extended-release exenatide (Bydureon)—are popular because they lower glucose levels, pose a low risk of hypoglycemia, can induce weight loss,1 and, in the case of extended-release exenatide and albiglutide, are given once weekly. They are currently recommended as add-on therapy to metformin. These drugs mimic the action of GLP-1, an endogenous hormone released by the intestine in response to food. They bind to receptors on beta cells, stimulating insulin production.1
FOUR TYPES OF THYROID CANCER
There are four types of thyroid cancer: medullary (a contraindication to GLP-1 agonists), papillary, follicular, and anaplastic.
Medullary thyroid cancer is extremely rare in humans, with 976 cases diagnosed from 1992 to 2006 in the United States, compared with 36,583 cases of papillary and 4,560 cases of follicular cancer. Anaplastic cancer is also rare (556 cases).2 The highest incidence rates of medullary thyroid cancer are in people of Hispanic descent (0.21 per 100,000 woman-years and 0.18 per 100,000 man-years).2
EXPERIMENTAL EVIDENCE
Pancreatic beta cells are not the only cells in the body that can express GLP-1 receptors. Notably, the parafollicular cells (also called C cells) of the thyroid, which secrete calcitonin and which are the cells involved in medullary thyroid cancer, also sometimes express these receptors if cancer develops.
In experiments in mice and rats, the incidence of thyroid C-cell tumors was higher in animals given GLP-1 analogues. Liraglutide, exenatide, taspoglutide, and lixisenatide potently activated GLP-1 receptors in thyroid C cells, increasing calcitonin gene expression and stimulating calcitonin release in a dose-dependent manner.3 Moreover, sustained activation of these receptors caused C-cell hyperplasia and resulted in medullary thyroid cancer. However medullary thyroid cancer also occurred in rodents receiving placebo.
C cells in monkeys and humans express fewer GLP-1 receptors than those in rodents; in fact, healthy human C cells do not express them at all.3,4 In rats with C-cell hyperplasia or medullary thyroid cancer, GLP-1 receptors are present in 100% of cases (and in increased density), compared with 27% of human medullary thyroid cancers.4
In addition to medullary thyroid cancer, various other human tumors have been shown to express GLP-1 receptors.5 Based on limited data, KÖrner et al5 found that these receptors are also present in various other human tumors, eg:
- Pheochromocytoma (60%)
- Paraganglioma (28%)
- Meningioma (35%)
- Astrocytoma (25%)
- Glioblastoma (9%)
- Ependymoma (16%)
- Medulloblastoma (25%)
- Nephroblastoma (22%)
- Neuroblastoma (18%)
- Ovarian adenocarcinoma (16%)
- Prostate carcinoma (5%).
Madsen et al6 reported that liraglutide binding to the GLP-1 receptor on murine thyroid C cells led to C-cell hyperplasia. However, prolonged administration of liraglutide at very high doses did not produce C-cell proliferation in monkeys.3
Gier et al7 looked at GLP-1 receptor expression in normal human C cells, hyperplastic C cells, and medullary thyroid cancer cells, as well as in papillary thyroid cancer cells, which do not arise from C cells. They demonstrated concurrent calcitonin and GLP-1 receptor immunostaining, not only in those with C-cell hyperplasia (9 of 9 cases) and medullary thyroid cancer (11 of 12 cases), but also in 3 (18%) of 17 patients with papillary thyroid cancer and 5 (33%) of 15 with normal thyroid follicular cells. However, the choice of polyclonal antibodies and radioligands used and concerns about methodology have led investigators to interpret these results cautiously.8–10
STUDIES OF GLP-1 AGONISTS IN HUMANS
Several prospective clinical studies showed no increase in calcitonin levels during therapy with GLP-1 receptor agonists in patients with type 2 diabetes.3,11 Long-term use of liraglutide in high doses (up to 3 mg per day) did not lead to elevations in serum calcitonin levels.11
In a retrospective Adverse Event Reporting System database review, the incidence rate of thyroid cancer in patients treated with exenatide was higher—with an odds ratio of 4.7 (30 events)—than with a panel of control drugs (3 events).12 However, this study did not differentiate between types of thyroid cancer, and the inherent limitations of retrospective databases complicate its interpretation. Such a high odds ratio would imply a significant increase in the incidence of medullary thyroid cancer, but this does not seem to be true.
Alves et al13 performed a meta-analysis of randomized controlled trials and long-term observational studies. None of the studies evaluating exenatide reported cases of thyroid cancer, whereas five of the studies evaluating liraglutide did. In total, nine patients treated with liraglutide were diagnosed with thyroid cancer, compared with one patient on glimepiride. The odds ratio for thyroid cancer occurrence associated with liraglutide treatment was 1.54, but that was not statistically significant (95% confidence interval 0.40–6.02, P = .53, I2 = 0%).
These studies are hypothesis-generating and do not prove that GLP-1 receptor agonists cause medullary thyroid cancer. Given the extremely low incidence of medullary thyroid cancer, to prove or disprove a causal relationship would require an enormous number of patients, who would need to be followed for several years.
OFFICIAL RECOMMENDATIONS
Considerable differences in the biology of the rodent vs human thyroid GLP-1 receptor systems have led regulatory authorities to conclude that the risk for development of medullary thyroid cancer with GLP-1 therapy in humans is difficult to quantify, but low.14 Consequently, the US Food and Drug Administration recommends neither monitoring of calcitonin levels nor ultrasound imaging as a screening tool in patients taking GLP-1 agonists.14
BENEFITS OUTWEIGH RISKS
At present, the benefits of using GLP-1 receptor agonists to treat type 2 diabetes mellitus outweigh the risks, and there seems to be little reason to withhold this effective therapy except in patients who have a personal or family history of medullary thyroid cancer or MEN-2. Until the effects of GLP-1 agonists are systematically studied in follicular-cell-derived thyroid cancer, we also recommend caution when considering their use in patients with familial thyroid cancer and those with a genetic predisposition for papillary and follicular thyroid cancer—eg, patients with familial adenomatous polyposis, phosphate and tensin homolog hamartoma tumor syndrome, Carney complex type 1, Werner syndrome, or familial papillary thyroid cancer.
Methodologically superior studies and careful long-term monitoring of patients treated with GLP-1 agonists are required to clarify the risk vs benefit of these therapies.
The question is complicated, as there are different types of thyroid cancer, and a causal relationship is hard to prove.
Glucagon-like peptide 1 (GLP-1) receptor agonists can be safely used in all patients with thyroid cancers that are derived from the thyroid follicular epithelium (papillary and follicular thyroid cancer). However, they are currently contraindicated in patients with medullary thyroid cancer and in patients with multiple endocrine neoplasia 2 (MEN-2), which is not a form of thyroid cancer but is relevant to our discussion. We probably should be cautious about using them in patients with familial thyroid cancer and those with a genetic predisposition for papillary or follicular thyroid cancer.
GLP-1 DRUGS ARE WIDELY USED
The glucagon-like peptide 1 (GLP-1) receptor agonists are widely used to treat type 2 diabetes mellitus. The currently available drugs of this class—exenatide (Byetta), liraglutide (Victoza), albiglutide (Tanzeum), dulaglutide (Trulicity), and extended-release exenatide (Bydureon)—are popular because they lower glucose levels, pose a low risk of hypoglycemia, can induce weight loss,1 and, in the case of extended-release exenatide and albiglutide, are given once weekly. They are currently recommended as add-on therapy to metformin. These drugs mimic the action of GLP-1, an endogenous hormone released by the intestine in response to food. They bind to receptors on beta cells, stimulating insulin production.1
FOUR TYPES OF THYROID CANCER
There are four types of thyroid cancer: medullary (a contraindication to GLP-1 agonists), papillary, follicular, and anaplastic.
Medullary thyroid cancer is extremely rare in humans, with 976 cases diagnosed from 1992 to 2006 in the United States, compared with 36,583 cases of papillary and 4,560 cases of follicular cancer. Anaplastic cancer is also rare (556 cases).2 The highest incidence rates of medullary thyroid cancer are in people of Hispanic descent (0.21 per 100,000 woman-years and 0.18 per 100,000 man-years).2
EXPERIMENTAL EVIDENCE
Pancreatic beta cells are not the only cells in the body that can express GLP-1 receptors. Notably, the parafollicular cells (also called C cells) of the thyroid, which secrete calcitonin and which are the cells involved in medullary thyroid cancer, also sometimes express these receptors if cancer develops.
In experiments in mice and rats, the incidence of thyroid C-cell tumors was higher in animals given GLP-1 analogues. Liraglutide, exenatide, taspoglutide, and lixisenatide potently activated GLP-1 receptors in thyroid C cells, increasing calcitonin gene expression and stimulating calcitonin release in a dose-dependent manner.3 Moreover, sustained activation of these receptors caused C-cell hyperplasia and resulted in medullary thyroid cancer. However medullary thyroid cancer also occurred in rodents receiving placebo.
C cells in monkeys and humans express fewer GLP-1 receptors than those in rodents; in fact, healthy human C cells do not express them at all.3,4 In rats with C-cell hyperplasia or medullary thyroid cancer, GLP-1 receptors are present in 100% of cases (and in increased density), compared with 27% of human medullary thyroid cancers.4
In addition to medullary thyroid cancer, various other human tumors have been shown to express GLP-1 receptors.5 Based on limited data, KÖrner et al5 found that these receptors are also present in various other human tumors, eg:
- Pheochromocytoma (60%)
- Paraganglioma (28%)
- Meningioma (35%)
- Astrocytoma (25%)
- Glioblastoma (9%)
- Ependymoma (16%)
- Medulloblastoma (25%)
- Nephroblastoma (22%)
- Neuroblastoma (18%)
- Ovarian adenocarcinoma (16%)
- Prostate carcinoma (5%).
Madsen et al6 reported that liraglutide binding to the GLP-1 receptor on murine thyroid C cells led to C-cell hyperplasia. However, prolonged administration of liraglutide at very high doses did not produce C-cell proliferation in monkeys.3
Gier et al7 looked at GLP-1 receptor expression in normal human C cells, hyperplastic C cells, and medullary thyroid cancer cells, as well as in papillary thyroid cancer cells, which do not arise from C cells. They demonstrated concurrent calcitonin and GLP-1 receptor immunostaining, not only in those with C-cell hyperplasia (9 of 9 cases) and medullary thyroid cancer (11 of 12 cases), but also in 3 (18%) of 17 patients with papillary thyroid cancer and 5 (33%) of 15 with normal thyroid follicular cells. However, the choice of polyclonal antibodies and radioligands used and concerns about methodology have led investigators to interpret these results cautiously.8–10
STUDIES OF GLP-1 AGONISTS IN HUMANS
Several prospective clinical studies showed no increase in calcitonin levels during therapy with GLP-1 receptor agonists in patients with type 2 diabetes.3,11 Long-term use of liraglutide in high doses (up to 3 mg per day) did not lead to elevations in serum calcitonin levels.11
In a retrospective Adverse Event Reporting System database review, the incidence rate of thyroid cancer in patients treated with exenatide was higher—with an odds ratio of 4.7 (30 events)—than with a panel of control drugs (3 events).12 However, this study did not differentiate between types of thyroid cancer, and the inherent limitations of retrospective databases complicate its interpretation. Such a high odds ratio would imply a significant increase in the incidence of medullary thyroid cancer, but this does not seem to be true.
Alves et al13 performed a meta-analysis of randomized controlled trials and long-term observational studies. None of the studies evaluating exenatide reported cases of thyroid cancer, whereas five of the studies evaluating liraglutide did. In total, nine patients treated with liraglutide were diagnosed with thyroid cancer, compared with one patient on glimepiride. The odds ratio for thyroid cancer occurrence associated with liraglutide treatment was 1.54, but that was not statistically significant (95% confidence interval 0.40–6.02, P = .53, I2 = 0%).
These studies are hypothesis-generating and do not prove that GLP-1 receptor agonists cause medullary thyroid cancer. Given the extremely low incidence of medullary thyroid cancer, to prove or disprove a causal relationship would require an enormous number of patients, who would need to be followed for several years.
OFFICIAL RECOMMENDATIONS
Considerable differences in the biology of the rodent vs human thyroid GLP-1 receptor systems have led regulatory authorities to conclude that the risk for development of medullary thyroid cancer with GLP-1 therapy in humans is difficult to quantify, but low.14 Consequently, the US Food and Drug Administration recommends neither monitoring of calcitonin levels nor ultrasound imaging as a screening tool in patients taking GLP-1 agonists.14
BENEFITS OUTWEIGH RISKS
At present, the benefits of using GLP-1 receptor agonists to treat type 2 diabetes mellitus outweigh the risks, and there seems to be little reason to withhold this effective therapy except in patients who have a personal or family history of medullary thyroid cancer or MEN-2. Until the effects of GLP-1 agonists are systematically studied in follicular-cell-derived thyroid cancer, we also recommend caution when considering their use in patients with familial thyroid cancer and those with a genetic predisposition for papillary and follicular thyroid cancer—eg, patients with familial adenomatous polyposis, phosphate and tensin homolog hamartoma tumor syndrome, Carney complex type 1, Werner syndrome, or familial papillary thyroid cancer.
Methodologically superior studies and careful long-term monitoring of patients treated with GLP-1 agonists are required to clarify the risk vs benefit of these therapies.
- Samson SL, Garber A. GLP-1R agonist therapy for diabetes: benefits and potential risks. Curr Opin Endocrinol Diabetes Obes 2013; 20:87–97.
- Aschebrook-Kilfoy B, Ward MH, Sabra MM, Devesa SS. Thyroid cancer incidence patterns in the United States by histologic type, 1992–2006. Thyroid 2011; 21:125–134.
- Bjerre Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
- Waser B, Beetschen K, Pellegata NS, Reubi JC. Incretin receptors in non-neoplastic and neoplastic thyroid C cells in rodents and humans: relevance for incretin-based diabetes therapy. Neuroendocrinology 2011; 94:291–301.
- Körner M, Stöckli M, Waser B, Reubi JC. GLP-1 receptor expression in human tumors and human normal tissues: potential for in vivo targeting. J Nucl Med 2007; 48:736–743.
- Madsen LW, Knauf JA, Gotfredsen C, et al. GLP-1 receptor agonists and the thyroid: C-cell effects in mice are mediated via the GLP-1 receptor and not associated with RET activation. Endocrinology 2012; 153:1538–1547.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
- Drucker DJ, Sherman SI, Bergenstal RM, Buse JB. The safety of incretin-based therapies—review of the scientific evidence. J Clin Endocrinol Metab 2011; 96:2027–2031.
- Gagel RF. Activation of G-protein-coupled receptors and thyroid malignant tumors: the jury is still out. Endocr Pract 2011; 17:957–959.
- Nauck MA. A critical analysis of the clinical use of incretin-based therapies: the benefits by far outweigh the potential risks. Diabetes Care 2013; 36:2126–2132.
- Hegedüs L, Moses AC, Zdravkovic M, Le Thi T, Daniels GH. GLP-1 and calcitonin concentration in humans: lack of evidence of calcitonin release from sequential screening in over 5000 subjects with type 2 diabetes or nondiabetic obese subjects treated with the human GLP-1 analog, liraglutide. J Clin Endocrinol Metab 2011; 96:853–860.
- Elashoff M, Matveyenko AV, Gier B, Elashoff R, Butler PC. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 2011; 141:150–156.
- Alves C, Batel-Marques F, Macedo AF. A meta-analysis of serious adverse events reported with exenatide and liraglutide: acute pancreatitis and cancer. Diabetes Res Clin Pract 2012; 98:271–284.
- Parks M, Rosebraugh C. Weighing risks and benefits of liraglutide—the FDA’s review of a new antidiabetic therapy. N Engl J Med 2010; 362:774–777.
- Samson SL, Garber A. GLP-1R agonist therapy for diabetes: benefits and potential risks. Curr Opin Endocrinol Diabetes Obes 2013; 20:87–97.
- Aschebrook-Kilfoy B, Ward MH, Sabra MM, Devesa SS. Thyroid cancer incidence patterns in the United States by histologic type, 1992–2006. Thyroid 2011; 21:125–134.
- Bjerre Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
- Waser B, Beetschen K, Pellegata NS, Reubi JC. Incretin receptors in non-neoplastic and neoplastic thyroid C cells in rodents and humans: relevance for incretin-based diabetes therapy. Neuroendocrinology 2011; 94:291–301.
- Körner M, Stöckli M, Waser B, Reubi JC. GLP-1 receptor expression in human tumors and human normal tissues: potential for in vivo targeting. J Nucl Med 2007; 48:736–743.
- Madsen LW, Knauf JA, Gotfredsen C, et al. GLP-1 receptor agonists and the thyroid: C-cell effects in mice are mediated via the GLP-1 receptor and not associated with RET activation. Endocrinology 2012; 153:1538–1547.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
- Drucker DJ, Sherman SI, Bergenstal RM, Buse JB. The safety of incretin-based therapies—review of the scientific evidence. J Clin Endocrinol Metab 2011; 96:2027–2031.
- Gagel RF. Activation of G-protein-coupled receptors and thyroid malignant tumors: the jury is still out. Endocr Pract 2011; 17:957–959.
- Nauck MA. A critical analysis of the clinical use of incretin-based therapies: the benefits by far outweigh the potential risks. Diabetes Care 2013; 36:2126–2132.
- Hegedüs L, Moses AC, Zdravkovic M, Le Thi T, Daniels GH. GLP-1 and calcitonin concentration in humans: lack of evidence of calcitonin release from sequential screening in over 5000 subjects with type 2 diabetes or nondiabetic obese subjects treated with the human GLP-1 analog, liraglutide. J Clin Endocrinol Metab 2011; 96:853–860.
- Elashoff M, Matveyenko AV, Gier B, Elashoff R, Butler PC. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 2011; 141:150–156.
- Alves C, Batel-Marques F, Macedo AF. A meta-analysis of serious adverse events reported with exenatide and liraglutide: acute pancreatitis and cancer. Diabetes Res Clin Pract 2012; 98:271–284.
- Parks M, Rosebraugh C. Weighing risks and benefits of liraglutide—the FDA’s review of a new antidiabetic therapy. N Engl J Med 2010; 362:774–777.
Outcome measures need context

Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
Dr. Vinay Prasad, in his commentary in this issue of CCJM, argues that, to best inform clinical decision-making, interventional and observational studies should measure multiple outcomes whenever possible, including all-cause mortality. He cites examples, such as calcium supplementation for bone health and aspirin for primary cardiovascular prevention, where favorable effects on focused clinical outcomes were not paralleled by favorable effects on overall morbidity. The study was a success, but the patient died.
Reading his commentary got me thinking about the many ways that the results of interventional studies and population data increasingly affect how we practice and teach medicine. Measuring an outcome in the population of interest (study volunteers, patient panels, trainees) is all the rage and is almost always more useful than only tracking interim metrics. True outcome measures are clearly useful when comparing groups and, hopefully, help assess the core reason the study was done.
Yet at the same time that group outcome measures are emphasized for many useful reasons, personalized medicine has a growing appeal: don’t let the individual get lost in the group, and pay attention to the outliers as well as the mean.
Positive results from a well-designed, prospective, controlled trial provide confidence that a drug or procedure has efficacy compared with placebo or a known effective comparator. But before recommending a therapy to a specific patient, we need to carefully evaluate whether the likely benefit in an individual patient is worth the clinical and financial cost. The information to make that evaluation doesn’t come easily from simply looking at a P value in a clinical study. Not only do we need to look at the size of the effect of an efficacious treatment and ask whether our specific patient is comparable to the study participants, but, as Dr. Prasad emphasizes, we must also look closely at the actual outcome measures of the study to see if they match our patient’s short- and long-term goals.
How significant is a statistically significant finding if the measured outcome is not the one the patient cares the most about? For example, a recent extremely well-done study that led to US Food and Drug Administration (FDA) approval of branded colchicine for acute gout used the efficacy measure of 50% reduction in pain at 24 hours.1 But what our patients really want is attack resolution (which usually requires medication in addition to what was used in the trial, increasing the risk of side effects). Proof of concept (a rational dose of colchicine has benefit) was very well demonstrated; that this dosing regimen should be standard of care, I think, remains unsupported.
We must also try to assess the long-term relevance (clinical outcome) of results based initially on surrogate markers. For example, not all drugs that increase bone density reduce the long-term fracture rate, and not all drugs that lower the blood glucose level reduce cardiovascular complications of diabetes. This has seemingly become a linchpin concept in the FDA’s approach to drug approval, with attendant increases in the cost and time to get drug approval.
We teach that the tools of evidence-based medicine should be routinely and appropriately employed in clinical practice. The premises of evidence-based medicine are deeply rooted in clinical studies. But our patients’ genetic background, individual preferences, and specific concerns regarding management of their disease and the side effects of medications should also be seriously discussed. We can then jointly define individualized outcome goals in the examination room. These may not exactly match the outcomes chosen by clinical investigators in designing their studies, and the plan may not match the policy of an insurance plan or a “pay-for-performance” metric. I hope that the opportunity for reconciliation of these differences will always be available.
The increasing demand for physicians and health systems to meet specific outcome and performance measures brings up the same concerns that arise when applying the results of a clinical study to a specific patient: will striving to match a group-based outcome be beneficial to the patient in front of us? My major goal as a physician is to care for the individual patient. My patient may not exactly match the population studied to prove that an intervention worked (or didn’t), so the data from that study may not fully apply. In the same way, care for all of our patients with the same diagnosis may not fit into the same performance rubric. The same attention that goes into determining appropriately relevant outcome measures for clinical studies needs to go into dictating performance outcome metrics by which physicians and health care systems are measured. They should be patient-centered and, to maintain face validity, somewhat flexible. On any given night, what keeps me awake is not population-based outcomes, but concern over the outcome of the individual patients I saw in clinic that day.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, dou-ble-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62:1060–1068.
But how many people died? Health outcomes in perspective
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
Before we dispense advice about staying healthy, we should know the effect of whatever we are recommending—be it diet, supplements, chemoprevention, or screening—on all meaningful outcomes, including overall mortality, quality of life, harms, inconveniences, and cost. Even though looking at all these outcomes may seem self-evidently wise, many research studies do not do it, and health care providers do not do it enough.
How would looking at all the outcomes change our opinion of health practices?
COMPARING GRAPEFRUIT AND PEACHES
A 2013 study linked eating berries with lower rates of myocardial infarction in women,1 another found that people who ate some fruits (blackberries and grapefruit) but not others (peaches and oranges) had a lower rate of incident diabetes,2 and a third linked a healthy diet to a lower incidence of pancreatic cancer.3 However, none of these studies examined all-cause mortality rates. A fourth study found that drinking green tea was associated with a lower risk of death from pneumonia in Japanese women, but not men.4
For the sake of argument, let us put aside concern about whether observational studies can reliably inform recommendations for clinical practice5 and concede that they can. The point is that studies such as those above look at some but not all meaningful outcomes, undermining the utility of their findings. If healthy people conclude that they should eat grapefruit instead of peaches, they may miss out on benefits of peaches that the study did not examine. Eating a healthy diet remains prudent, but the study linking it to a lower rate of pancreatic cancer is no tipping point, as pancreatic cancer is just one way to die. And advocating green tea to Japanese women but not men, to avoid pneumonia, would be a questionable public health strategy. Pneumonia is the sixth leading cause of death and accounts for 3.9% of disability-adjusted life-years lost,6 but what about the first five causes, which account for 96.1%?
These and many other studies of dietary habits of people who are well fail to consider end points that healthy people care about. Suppose that drinking more coffee would prevent all deaths from pancreatic cancer but would modestly increase cardiovascular deaths—say, by 5%. On a population level, recommending more coffee would be wrong, because it would result in far more deaths. Suppose that drinking tea decreased deaths from pneumonia—we should still not advise patients to drink tea, as we do not know whether tea’s net effect is beneficial.
Some may argue that these epidemiologic studies are merely hypothesis-generating, but my colleagues and I analyzed all the nonrandomized studies published in several leading medical journals in 1 year and found that 59% made specific practice recommendations.5 Other studies may be misused in this fashion, even though the authors refrained from doing so.
CALCIUM PROTECTS BONES, BUT WHAT ABOUT THE HEART?
Narrow end points are not limited to dietary studies. Calcium supplementation with or without vitamin D has been vigorously promoted for decades7 to treat and prevent osteoporosis in pre- and postmenopausal women, and data confirm that these agents decrease the risk of fracture.8
But bone health is only one end point important to women, and long-term supplementation of a mineral or vitamin with the goal of strengthening bones may have unforeseen adverse effects.
In 2010, calcium supplementation without vitamin D was linked to higher rates of myocardial infarction (with some suggestion of increased rates of all-cause death) in pooled analyses of 15 trials.9 In 2011, a higher risk of cardiovascular events (stroke and myocardial infarction) was found in recipients of calcium with vitamin D in a reanalysis of the Women’s Health Initiative Calcium/Vitamin D Supplementation Study,10 adjusting for the widespread use of these supplements at baseline, and this was corroborated by a meta-analysis of eight other studies.10 A more recent study confirmed that supplemental calcium increases cardiovascular risk in men.11
Although the increase in cardiovascular risk seems to be modest, millions of people take calcium supplements; thus, many people may be harmed. Our exuberance for bone health suggests that, at times, a single outcome can distract.
DOES SCREENING IMPROVE SURVIVAL?
On the whole, the evidence for screening continues to focus only on certain outcomes. With the exception of the National Lung Cancer Screening Trial,12 to date, no cancer screening trial has shown an improvement in the overall survival rate.
In fact, a 2013 Cochrane review13 found that mammographic screening failed to lower the rate of death from all cancers, including breast cancer, after 10 years (relative risk [RR] 1.02, 95% confidence interval [CI] 0.95–1.10) and the rate of death from all causes after 13 years (RR 0.99, 95% CI 0.95–1.03). Although screening lowered the breast cancer mortality rate, the authors argued that we should not look at only some outcomes and concluded that “breast cancer mortality was an unreliable outcome” that was biased in favor of screening, mainly because of “differential misclassification of cause of death.”13
Black et al14 found that of 12 major cancer screening trials examining both disease-specific mortality and all-cause mortality, 5 had differences in mortality rates that went in opposite directions (eg, the rate of disease-specific mortality improved while overall survival was harmed, or vice-versa), suggesting paradoxical effects. In another 2 studies, differences in all-cause mortality exceeded gains in disease-specific mortality. Thus, in 7 (58%) of the 12 trials, inconsistencies existed between rates of disease-specific mortality and all-cause mortality, prompting doubt about the conclusions of the studies.14
For some cancers, data suggest that screening increases deaths from other causes, and these extra deaths are not included in the data on disease-specific mortality. For instance, men who are screened for prostate cancer have higher rates of death from cardiovascular disease and suicide,15 which might negate the tenuous benefits of screening in terms of deaths from prostate cancer.
Studies of screening for diseases other than cancer have also focused on only some outcomes. For example, the United States Preventive Services Task Force supports screening for abdominal aortic aneurysm once with ultrasonography in men ages 65 to 75 who have ever smoked,16 but the recommendation is based on improvements in the death rate from abdominal aortic aneurysm, not in all-cause mortality.17 This, along with a declining incidence of this disease and changes in how it is treated (with endovascular repair on the rise and open surgical repair declining), has led some to question if we should continue to screen for it.18
CHEMOPREVENTION: NO FREE LUNCH
Finasteride
In 2013, an analysis19 that looked at all of the outcomes laid to rest 10 years of debate over the Prostate Cancer Prevention Trial, which had randomized more than 18,000 healthy men over age 55 with no signs or symptoms of prostate cancer to receive finasteride or placebo, with the end point of prostate cancer incidence. The initial results, published in 2003,20 had found that the drug decreased the rate of incident prostate cancer but paradoxically increased the rate of high-grade (Gleason score ≥ 7) tumors. Whether these results were real or an artifact of ascertainment was debated, as was whether the adverse effects—decreases in sexual potency, libido, and ejaculation—were worth the 25% reduction in prostate cancer incidence.
Much of the debate ended with the 2013 publication, which showed that regardless of finasteride’s effect on prostate cancer, overall mortality curves at 18-year follow-up were absolutely indistinguishable.19 Healthy patients hoping that finasteride will help them live longer or better can be safely told that it does neither.
Statins as primary prevention
As for statin therapy as primary prevention, the best meta-analysis to date (which meticulously excluded secondary-prevention patients after analyzing individual patient-level data) found no improvement in overall mortality despite more than 240,000 patient-years of follow-up.21 Because of this, and because the harms of statin therapy are being increasingly (but still poorly) documented, widespread use of statins has been questioned.22
Proponents point to the ability of statins to reduce end points such as revascularization, stroke, and nonfatal myocardial infarction.23 But the main question facing healthy users is whether improvement in these end points translates to longer life or better quality of life. These questions remain unresolved.
Aspirin as primary prevention
Another example of the importance of considering all the outcomes is the issue of aspirin as primary prevention.
Enthusiasm for aspirin as primary prevention has been recently reinvigorated, with data showing it can prevent colorectal cancers that overexpress cyclooxygenase-2.24 But a meta-analysis of nine randomized trials of aspirin25 with more than 1,000 participants found that, although aspirin decreases the rate of nonfatal myocardial infarction (odds ratio [OR] 0.80, 95% CI 0.67–0.96), it does not significantly reduce cancer mortality (OR 0.93, 95% CI 0.84–1.03), and it increases the risk of nontrivial bleeding (OR 1.31; 95% CI 1.14–1.50). Its effects on overall mortality were not statistically significant but were possibly favorable (OR 0.94, 95% CI 0.88–1.00), so this requires further study.
After broad consideration of the risks and benefits of aspirin, the US Food and Drug Administration has issued a statement that aspirin is not recommended as primary prevention.26
WHY STUDIES LOOK ONLY AT SOME OUTCOMES
There are many reasons why researchers favor examining some outcomes over others, but there is no clear justification for ignoring overall mortality. Overall mortality should routinely be examined in large population studies of diet and supplements and in trials of medications27 and cancer screening.
With regard to large observational studies, it is hard to understand why some would not include survival analyses, unless the results would fail to support the study’s hypothesis. In fact, some studies do report overall survival results,28 but others do not. The omission of overall survival in large data-set research should raise concerns of multiple hypothesis testing and selective reporting. Eating peaches as opposed to grapefruit may not be associated with differences in rates of all-cause mortality, myocardial infarction, pneumonia, or lung cancer, but if you look at 20 different variables, chances are that one will have a P value less than .05, and an investigator might be tempted to report it as statistically significant and even meaningful.
Empirical studies support this claim. One group found that for 80% of ingredients randomly selected from a cookbook, there existed Medline-indexed articles assessing cancer risk, with 65% of studies finding nominally significant differences in the risk of some type of cancer.29
An excess of significant findings such as this argues that significance-chasing and selective reporting are common in this field and has led to calls for methodologic improvements, including routine falsification testing30 and up-front registration of observational studies.31
WHY ALL OUTCOMES MATTER
Healthy people do not care about some outcomes; they care about all outcomes. Some patients may truly have unique priorities (quality of life vs quantity of life), but others may overestimate their risk of death from some causes and underestimate their risk from others, and practitioners have the obligation to counsel them appropriately.
For instance, a patient who watches a brother pass away from pancreatic adenocarcinoma may wish to do everything possible to avoid that illness. But often, as in this case, fear may surpass risk. The patient’s risk of pancreatic cancer is no different than that in the general population: the best data show32 an odds ratio of 1.8, with a confidence interval spanning 1. As such, pancreatic cancer is still not among his five most likely causes of death.
Some patients may care about their bone mineral density or cholesterol level. But again, physicians have an obligation to direct patients’ attention to all of the outcomes that should be of interest to them.
OBJECTIONS TO INCLUDING ALL OUTCOMES
There are important objections to the argument I am presenting here.
First, including all outcomes is expensive. For studies involving retrospective analysis of existing data, looking at overall mortality would not incur additional costs, only an additional analysis. But for prospective trials to have statistical power to detect a difference in overall mortality, larger sample sizes or longer follow-up might be needed—either of which would add to the cost.
In chemoprevention trials, the rate of incident cancer has been called the gold standard end point.33 To design a thrifty chemoprevention study, investigators can either target a broad population and aim for incident malignancy, or target a restricted, high-risk population and aim for overall mortality. The latter is preferable because although it can inform the decisions of only some people, the former cannot inform any people, as was seen with difficulties in interpreting the Prostate Cancer Prevention Trial and trials showing reduced breast cancer incidence from tamoxifen, raloxifene, and exemestane.
In large cancer screening trials, the cost of powering the trial for overall mortality would be greater, and though a carefully selected, high-risk population can be enrolled, historically this has not been popular. In cancer screening, it is a mistake to contrast the costs of trials powered for overall mortality with those of lesser studies examining disease-specific death. Instead, we must consider the larger societal costs incurred by cancer screening that does not truly improve quantity or quality of life.34
The recent reversal of recommendations for prostate-specific antigen testing by the United States Preventive Services Task Force35 suggests that erroneous recommendations, practiced for decades, can cost society hundreds of billions of dollars but fail to improve meaningful outcomes.
The history of medicine is replete with examples of widely recommended practices and interventions that not only failed to improve the outcomes they claimed to improve, but at times increased the rate of all-cause mortality or carried harms that far outweighed benefits.36,37 The costs of conducting research to fully understand all outcomes are only a fraction of the costs of a practice that is widely disseminated.38
A second objection to my analysis is that there is more to life than survival, and outcomes besides overall mortality are important. This is a self-evident truth. That an intervention improves the rate of overall mortality is neither necessary nor sufficient for its recommendation. Practices may improve survival but worsen quality of life to such a degree that they should not be recommended. Conversely, practices that improve quality of life should be endorsed even if they fail to prolong life.
Thus, overall mortality and quality of life must be considered together, but the end points that are favored currently (disease-specific death, incident cancer, diabetes mellitus, myocardial infarction) do not do a good job of capturing either. Disease-specific death is not meaningful to any patient if deaths from other causes are increased so that overall mortality is unchanged. Furthermore, preventing a diagnosis of cancer or diabetes may offer some psychological comfort, but well-crafted quality-of-life instruments are best suited to capture just how great that benefit is and whether it justifies the cost of such interventions, particularly if the rate of survival is unchanged.
Preventing stroke or myocardial infarction is important, but we should be cautious of interpreting data when decreasing the rate of these morbid events does not lead to commensurate improvements in survival. Alternatively, if morbid events are truly avoided but survival analyses are underpowered, quality-of-life measurements should demonstrate the benefit. But the end points currently used capture neither survival nor quality of life in a meaningful way.
WHEN ADVISING HEALTHY PEOPLE
Looking at all outcomes is important when caring for patients who are sick, but even more so for patients who are well. We need to know an intervention has a net benefit before we recommend it to a healthy person. Overall mortality should be reported routinely in this population, particularly in settings where the cost to do so is trivial (ie, in observational studies). Designers of thrifty trials should try to include people at high risk and power the trial for definite end points, rather than being broadly inclusive and reaching disputed conclusions. Research and decision-making should look at all outcomes. Healthy people deserve no less.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.
- Cassidy A, Mukamal KJ, Liu L, Franz M, Eliassen AH, Rimm EB. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013; 127:188–196.
- Muraki I, Imamura F, Manson JE, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ 2013; 347:f5001.
- Arem H, Reedy J, Sampson J, et al. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J Natl Cancer Inst 2013; 105:1298–1305.
- Watanabe I, Kuriyama S, Kakizaki M, et al. Green tea and death from pneumonia in Japan: the Ohsaki cohort study. Am J Clin Nutr 2009; 90:672–679.
- Prasad V, Jorgenson J, Ioannidis JP, Cifu A. Observational studies often make clinical practice recommendations: an empirical evaluation of authors’ attitudes. J Clin Epidemiol 2013; 66:361–366.e4.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380:2197–2223.
- Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med 1998; 338:736–746.
- Looker AC. Interaction of science, consumer practices and policy: calcium and bone health as a case study. J Nutr 2003; 133:1987S–1991S.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010; 341:c3691
- Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011; 342:d2040.
- Xiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA Intern Med 2013; 173:639–646.
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365:395–409.
- Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2013 Jun 4;6:CD001877.
- Black WC, Haggstrom DA, Welch HG. All-cause mortality in randomized trials of cancer screening. J Natl Cancer Inst 2002; 94:167–173.
- Fall K, Fang F, Mucci LA, et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: prospective cohort study. PLoS Med 2009; 6:e1000197.
- Prasad V. An unmeasured harm of screening. Arch Intern Med 2012; 172:1442–1443.
- Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a sytematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321–329.
- Harris R, Sheridan S, Kinsinger L. Time to rethink screening for abdominal aortic aneurysm? Arch Intern Med 2012; 172:1462–1463.
- Thompson IM Jr, Goodman PJ, Tangen CM, et al. Long-term survival of participants in the prostate cancer prevention trial. N Engl J Med 2013; 369:603–610.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:216–224.
- Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010; 170:1024–1031.
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA 2012; 307:1491–1492.
- McEvoy JW, Blumenthal RS, Blaha MJ. Statin therapy for hyperlipidemia. JAMA 2013; 310:1184–1185.
- Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med 2007; 356:2131–2142.
- Seshasai SR, Wijesuriya S, Sivakumaran R, et al. Effect of aspirin on vascular and nonvascular outcomes: meta-analysis of randomized controlled trials. Arch Intern Med 2012; 172:209–216.
- US Food and Drug Administration. Use of aspirin for primary prevention of heart attack and stroke. www.fda.gov/Drugs/ResourcesForYou/Consumers/ucm390574.htm. Accessed February 5, 2015.
- Ioannidis JP. Mega-trials for blockbusters. JAMA 2013; 309:239–240.
- Dunkler D, Dehghan M, Teo KK, et al; ONTARGET Investigators. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern Med 2013; 173:1682–1692.
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr 2013; 97:127–134.
- Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 2013; 309:241–242.
- Ioannidis JPA. The importance of potential studies that have not existed and registration of observational data sets. JAMA 2012; 308:575–576.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res 2004; 64:2634–2638.
- William WN Jr, Papadimitrakopoulou VA. Optimizing biomarkers and endpoints in oral cancer chemoprevention trials. Cancer Prev Res (Phila) 2013; 6:375–378.
- Prasad V. Powering cancer screening for overall mortality. Ecancermedicalscience 2013 Oct 9; 7:ed27.
- US Preventive Services Task Force. Final recommendation statement. Prostate cancer: screening. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/prostate-cancer-screening. Accessed February 5, 2015.
- Prasad V, Cifu A, Ioannidis JP. Reversals of established medical practices: evidence to abandon ship. JAMA 2012; 307:37–38.
- Prasad V, Vandross A, Toomey C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790–798.
- Elshaug AG, Garber AM. How CER could pay for itself—insights from vertebral fracture treatments. N Engl J Med 2011; 364:1390–1393.

Headway being made in developing biomarkers for PTSD
HUNTINGTON BEACH, CALIF. – Researchers are making significant headway in developing objective, reliable, and valid biomarkers to discriminate individuals with warzone post traumatic stress disorder from healthy controls, according to Dr. Charles R. Marmar.
“It’s clear that over the next four or five years we will identify very clear biological, psychological, and other behavioral risk and resilience profiles,” Dr. Marmar told attendees at the annual meeting of the American College of Psychiatrists.
Currently, clinicians largely rely on patient self-reports and clinical observations to diagnose PTSD in military personnel, said Dr. Marmar, professor and chair of the department of psychiatry at NYU Langone Medical Center and director of NYU’s Steven and Alexandra Cohen Veterans Center.

“The problem from the military and law enforcement perspective is that the majority of war fighters experience tremendous stigma in acknowledging their symptoms, particularly active duty military personnel,” he said. “A minority will exaggerate to avoid service or for compensation. Given that we’ve had nearly three million men and women serve in Iraq and Afghanistan, and the fact that we have no objective way yet of determining which ones continue to be fit for redeployment, which ones are in urgent need of help, and which ones deserve compensation, we need to develop better ways to determine if treatments are effective, to inform new treatment selection, and to define new targets for treatment.”
The scope of the problem is underscored in an analysis of data from 289,328 veterans entering VA Healthcare for the first time beginning on April 1, 2002 through March 31, 2006 (Am J. Pub. Health 2009;99[9]:1651-8). Prior to the invasion of Iraq, the distribution of mental health problems was very similar among veterans as in the general population: depression being most common, and low rates of PTSD and alcohol and drug abuse. However, “with each quarter since the invasion of Iraq, there’s been an incubative growth in the prevalence of PTSD, which has now eclipsed depression,” Dr. Marmar said. “We have a toll, a generational effect which looks similar in magnitude with the Vietnam War, both in the number of men and women who serve and in the prevalence of PTSD, depression and alcohol- and drug-related disorders.”
In the general population, risk factors include female sex, child abuse, genetics, which in twin studies account for 30-40% of the risk, lower IQ and lower educational attainment, stressful life events in the prior and following year, and panic reaction at the time of event, such as racing heart, shaking, and sweating.
According to findings from the National Vietnam Veterans Readjustment Study, risk factors for chronic warzone PTSD include high school dropout rate, history of child abuse, high warzone exposure, serious warzone injury, killing combatants, prisoners, and civilians, peritraumatic dissociation, hostile homecoming, post-discharge trauma, and genetics. “These are the risk profiles, and they should give us some clues about where to look for biological factors,” Dr. Marmar said.
The risks of service are not limited to stress, anxiety, depression, alcohol and drug abuse, or traumatic brain injury (TBI). “If you compare men and women returning from Iraq and Afghanistan with no mental health issues to those who have a diagnosis of either PTSD, depression, or the combination, the [diagnosed] cases have 2.5 times the risk of tobacco use, hypertension, dyslipidemia, obesity, and type 2 diabetes,” he said. “These are people in their late 20s and early 30s. So the costs of warzone-related stress and depression are enormous on general health.”
Dr. Marmar presented preliminary findings from the ongoing PTSD Systems Biology Consortium, an effort by researchers at seven universities to establish biomarkers for PTSD. Funded by the Department of Defense, the National Institutes of Health, and other sources, the consortium is comprised of integrated cores including neurocognition, genetics, structural and functional brain imaging, endocrinology, metabolism, genomics, proteomics, metabolomics, and bioinformatics.
To date, the researchers have screened 2,215 veterans from service in Iraq and Afghanistan, all of whom have been deployed to war at least once. Cases were PTSD positive and had a CAPS (Clinician-Administered PTSD scale) score of 20 or greater. Controls were PTSD negative and had a CAPS score of less than 20. They excluded subjects with lifetime psychosis, bipolar disorder, or OCD, as well as alcohol dependence in the past eight months, and drug abuse in the past year. They also excluded veterans with TBI “because we’re trying to be very careful to see if we can get a biological signal comparing combat PTSD cases with controls,” Dr. Marmar noted.
Dr. Marmar presented preliminary findings from 52 PTSD cases and 52 controls that were matched for sex, ethnicity, and age. The sample was entirely men, their mean age was 34 years, and they had a mean of 14.8 years of education. The researchers covaried for depression and other known confounders. “It’s very difficult to disentangle the effects of PTSD and depression because 50% of the cases of warzone PTSD also meet criteria for current major depression, and over 80% meet criteria for lifetime depression,” he said.
In results from the clinical diagnostic evaluation, PTSD cases, compared with controls, were significantly more likely to have current anxiety (7% vs. 0%, respectively; P = .041); lifetime anxiety (9.6% vs. 0%; P = .022); current major depressive disorder (51.5% vs. 1.9%; P<.001); lifetime MDD (84.6% vs. 23.1%; P<.001); and lifetime alcohol abuse dependence (63.5% vs. 25%; P = .001). There was also a non-signficant trend toward lifetime substance abuse/dependence (13.5% vs. 3.9%; P = .081).
Results from the neurocognitive assessments revealed that PTSD positive men had a significantly lower estimated IQ, compared with their PTSD negative counterparts (a mean of 99.3 vs. 107.9, respectively; P = .031). Other significant differences between the two groups were observed in tests of auditory and working memory, specifically digit span (8.67 vs. 10.04; P = .02), and the visual memory sum (9.1 vs. 10.67; P = .01).
One of the consortium collaborators developed a test to compare reward and punishment learning. For the test, “the subject is required to understand what the meaning of a symbol is in a task, and they have no prior knowledge [of the meaning],” Dr. Marmar explained. “They’re either rewarded for guessing correctly or punished for guessing incorrectly.” So far, the healthy controls “are performing much better in identifying the symbols when they’re rewarded, compared with the PTSD cases, and there’s no difference in punishment,” he said. “So there’s impaired reward learning and intact punishment learning in PTSD cases compared to controls, which likely reflects underlying disturbances in dopamine reward circuitry.”
Investigators in the neurogenetics core hypothesized that DNA variants in stress-response genes identified from previous medical studies will be associated with PTSD. These included FKBP5, COMT, APOE, BDNF, PACAP/PAC1R, and OPRL1. Initial analysis revealed that there were a greater number of BDNF allele frequencies among cases, compared with controls (P = .008). “It would appear that BDNF variants confer resilience for combat-related PTSD,” Dr. Marmar said.
The researchers also found a single nucleotide polymorphism never previously described on Chromosome 4. “It’s in a region between genes, probably a micro-RNA regulatory gene on the 4th chromosome,” he said. “That gene in our sample was associated with higher levels of PTSD. In addition, fMRI studies found that carrying this allele was associated with weaker activation of prefrontal cortical areas in the brain to empirical faces tasks.”
The endocrine core found that PTSD cases had lower ambient cortisol levels, compared with controls (P = .051). They also had significantly greater cortisol suppression following dexamethasone administration, compared with controls (P = .013). “This is evidence that there is increased glucocorticoid receptor sensitivity in PTSD expressing as elevated cortisol suppression,” Dr. Marmar said.
Investigators from the structural imaging core found no significant differences in overall hippocampal volume or in the five major hippocampal subfields between PTSD cases and controls, nor in difference in the volume of other brain structures previously implicated in PTSD, such as the amygdala and the thalamus. However, the researchers are finding some differences between cases and controls on functional imaging, including increased spontaneous activity in the amygdala and the insula, and decreased spontaneous activity in the precuneus. “The overall findings on fMRI are that there’s increased activity in the regions [of the brain] associated with fear and decreased connectivity between the frontal cortex and the amygdala,” he said. “This is consistent with the model of dysregulated fear activity in PTSD.”
Researchers have also observed that many markers of metabolic syndrome are significantly elevated between PTSD cases and controls, including fasting glucose (P = .001), weight (P = .03), and resting pulse (P = .003). “When you covary for depression, these findings remain,” Dr. Marmar said. “It’s important to note that these are men mostly in their early 30s recently returned from war and recently in military training, physically fit to be deployed to war.”
He closed his presentation by noting that mounting evidence from animal and human studies suggests evidence of mitochondrial dysfunction in PTSD. In the current analysis, researchers observed a reduced abundance of citrate and other mitochondrial metabolites in PTSD cases compared with controls, as well as an increased abundance of “premitochondrial” metabolites such as pyruvate and lactate. “These findings stand when you covary for depression and for metabolic syndrome,” Dr. Marmar said.
“We believe that these may be very important potential future candidate biomarkers to differentiate PTSD cases from controls.”
The next step in this effort, he added, is to replicate the consortium’s overall findings in a cross-validation sample of 50 male cases and 50 male controls. “We also have a sample of 40 female cases and 40 controls to see if the markers are the same or different,” he said. The researchers are also conducting a prospective study of 1,200 active duty military personnel, who will be evaluated before and after deployment.
For now, some clinicians wonder what should be done for men and women who carry the PTSD risk alleles, or carry the endocrine or metabolism vulnerability to develop complications from combat exposure. “That’s a very sensitive national question,” Dr. Marmar said. “People want to serve their country. The answer may be to allow service but to have a more nuanced approach to what people’s roles should be within the military, to match individuals’ stress resilience with the responsibilities they have.”
Dr. Marmar reported that he had no relevant financial conflicts.
On Twitter @dougbrunk
HUNTINGTON BEACH, CALIF. – Researchers are making significant headway in developing objective, reliable, and valid biomarkers to discriminate individuals with warzone post traumatic stress disorder from healthy controls, according to Dr. Charles R. Marmar.
“It’s clear that over the next four or five years we will identify very clear biological, psychological, and other behavioral risk and resilience profiles,” Dr. Marmar told attendees at the annual meeting of the American College of Psychiatrists.
Currently, clinicians largely rely on patient self-reports and clinical observations to diagnose PTSD in military personnel, said Dr. Marmar, professor and chair of the department of psychiatry at NYU Langone Medical Center and director of NYU’s Steven and Alexandra Cohen Veterans Center.
“The problem from the military and law enforcement perspective is that the majority of war fighters experience tremendous stigma in acknowledging their symptoms, particularly active duty military personnel,” he said. “A minority will exaggerate to avoid service or for compensation. Given that we’ve had nearly three million men and women serve in Iraq and Afghanistan, and the fact that we have no objective way yet of determining which ones continue to be fit for redeployment, which ones are in urgent need of help, and which ones deserve compensation, we need to develop better ways to determine if treatments are effective, to inform new treatment selection, and to define new targets for treatment.”
The scope of the problem is underscored in an analysis of data from 289,328 veterans entering VA Healthcare for the first time beginning on April 1, 2002 through March 31, 2006 (Am J. Pub. Health 2009;99[9]:1651-8). Prior to the invasion of Iraq, the distribution of mental health problems was very similar among veterans as in the general population: depression being most common, and low rates of PTSD and alcohol and drug abuse. However, “with each quarter since the invasion of Iraq, there’s been an incubative growth in the prevalence of PTSD, which has now eclipsed depression,” Dr. Marmar said. “We have a toll, a generational effect which looks similar in magnitude with the Vietnam War, both in the number of men and women who serve and in the prevalence of PTSD, depression and alcohol- and drug-related disorders.”
In the general population, risk factors include female sex, child abuse, genetics, which in twin studies account for 30-40% of the risk, lower IQ and lower educational attainment, stressful life events in the prior and following year, and panic reaction at the time of event, such as racing heart, shaking, and sweating.
According to findings from the National Vietnam Veterans Readjustment Study, risk factors for chronic warzone PTSD include high school dropout rate, history of child abuse, high warzone exposure, serious warzone injury, killing combatants, prisoners, and civilians, peritraumatic dissociation, hostile homecoming, post-discharge trauma, and genetics. “These are the risk profiles, and they should give us some clues about where to look for biological factors,” Dr. Marmar said.
The risks of service are not limited to stress, anxiety, depression, alcohol and drug abuse, or traumatic brain injury (TBI). “If you compare men and women returning from Iraq and Afghanistan with no mental health issues to those who have a diagnosis of either PTSD, depression, or the combination, the [diagnosed] cases have 2.5 times the risk of tobacco use, hypertension, dyslipidemia, obesity, and type 2 diabetes,” he said. “These are people in their late 20s and early 30s. So the costs of warzone-related stress and depression are enormous on general health.”
Dr. Marmar presented preliminary findings from the ongoing PTSD Systems Biology Consortium, an effort by researchers at seven universities to establish biomarkers for PTSD. Funded by the Department of Defense, the National Institutes of Health, and other sources, the consortium is comprised of integrated cores including neurocognition, genetics, structural and functional brain imaging, endocrinology, metabolism, genomics, proteomics, metabolomics, and bioinformatics.
To date, the researchers have screened 2,215 veterans from service in Iraq and Afghanistan, all of whom have been deployed to war at least once. Cases were PTSD positive and had a CAPS (Clinician-Administered PTSD scale) score of 20 or greater. Controls were PTSD negative and had a CAPS score of less than 20. They excluded subjects with lifetime psychosis, bipolar disorder, or OCD, as well as alcohol dependence in the past eight months, and drug abuse in the past year. They also excluded veterans with TBI “because we’re trying to be very careful to see if we can get a biological signal comparing combat PTSD cases with controls,” Dr. Marmar noted.
Dr. Marmar presented preliminary findings from 52 PTSD cases and 52 controls that were matched for sex, ethnicity, and age. The sample was entirely men, their mean age was 34 years, and they had a mean of 14.8 years of education. The researchers covaried for depression and other known confounders. “It’s very difficult to disentangle the effects of PTSD and depression because 50% of the cases of warzone PTSD also meet criteria for current major depression, and over 80% meet criteria for lifetime depression,” he said.
In results from the clinical diagnostic evaluation, PTSD cases, compared with controls, were significantly more likely to have current anxiety (7% vs. 0%, respectively; P = .041); lifetime anxiety (9.6% vs. 0%; P = .022); current major depressive disorder (51.5% vs. 1.9%; P<.001); lifetime MDD (84.6% vs. 23.1%; P<.001); and lifetime alcohol abuse dependence (63.5% vs. 25%; P = .001). There was also a non-signficant trend toward lifetime substance abuse/dependence (13.5% vs. 3.9%; P = .081).
Results from the neurocognitive assessments revealed that PTSD positive men had a significantly lower estimated IQ, compared with their PTSD negative counterparts (a mean of 99.3 vs. 107.9, respectively; P = .031). Other significant differences between the two groups were observed in tests of auditory and working memory, specifically digit span (8.67 vs. 10.04; P = .02), and the visual memory sum (9.1 vs. 10.67; P = .01).
One of the consortium collaborators developed a test to compare reward and punishment learning. For the test, “the subject is required to understand what the meaning of a symbol is in a task, and they have no prior knowledge [of the meaning],” Dr. Marmar explained. “They’re either rewarded for guessing correctly or punished for guessing incorrectly.” So far, the healthy controls “are performing much better in identifying the symbols when they’re rewarded, compared with the PTSD cases, and there’s no difference in punishment,” he said. “So there’s impaired reward learning and intact punishment learning in PTSD cases compared to controls, which likely reflects underlying disturbances in dopamine reward circuitry.”
Investigators in the neurogenetics core hypothesized that DNA variants in stress-response genes identified from previous medical studies will be associated with PTSD. These included FKBP5, COMT, APOE, BDNF, PACAP/PAC1R, and OPRL1. Initial analysis revealed that there were a greater number of BDNF allele frequencies among cases, compared with controls (P = .008). “It would appear that BDNF variants confer resilience for combat-related PTSD,” Dr. Marmar said.
The researchers also found a single nucleotide polymorphism never previously described on Chromosome 4. “It’s in a region between genes, probably a micro-RNA regulatory gene on the 4th chromosome,” he said. “That gene in our sample was associated with higher levels of PTSD. In addition, fMRI studies found that carrying this allele was associated with weaker activation of prefrontal cortical areas in the brain to empirical faces tasks.”
The endocrine core found that PTSD cases had lower ambient cortisol levels, compared with controls (P = .051). They also had significantly greater cortisol suppression following dexamethasone administration, compared with controls (P = .013). “This is evidence that there is increased glucocorticoid receptor sensitivity in PTSD expressing as elevated cortisol suppression,” Dr. Marmar said.
Investigators from the structural imaging core found no significant differences in overall hippocampal volume or in the five major hippocampal subfields between PTSD cases and controls, nor in difference in the volume of other brain structures previously implicated in PTSD, such as the amygdala and the thalamus. However, the researchers are finding some differences between cases and controls on functional imaging, including increased spontaneous activity in the amygdala and the insula, and decreased spontaneous activity in the precuneus. “The overall findings on fMRI are that there’s increased activity in the regions [of the brain] associated with fear and decreased connectivity between the frontal cortex and the amygdala,” he said. “This is consistent with the model of dysregulated fear activity in PTSD.”
Researchers have also observed that many markers of metabolic syndrome are significantly elevated between PTSD cases and controls, including fasting glucose (P = .001), weight (P = .03), and resting pulse (P = .003). “When you covary for depression, these findings remain,” Dr. Marmar said. “It’s important to note that these are men mostly in their early 30s recently returned from war and recently in military training, physically fit to be deployed to war.”
He closed his presentation by noting that mounting evidence from animal and human studies suggests evidence of mitochondrial dysfunction in PTSD. In the current analysis, researchers observed a reduced abundance of citrate and other mitochondrial metabolites in PTSD cases compared with controls, as well as an increased abundance of “premitochondrial” metabolites such as pyruvate and lactate. “These findings stand when you covary for depression and for metabolic syndrome,” Dr. Marmar said.
“We believe that these may be very important potential future candidate biomarkers to differentiate PTSD cases from controls.”
The next step in this effort, he added, is to replicate the consortium’s overall findings in a cross-validation sample of 50 male cases and 50 male controls. “We also have a sample of 40 female cases and 40 controls to see if the markers are the same or different,” he said. The researchers are also conducting a prospective study of 1,200 active duty military personnel, who will be evaluated before and after deployment.
For now, some clinicians wonder what should be done for men and women who carry the PTSD risk alleles, or carry the endocrine or metabolism vulnerability to develop complications from combat exposure. “That’s a very sensitive national question,” Dr. Marmar said. “People want to serve their country. The answer may be to allow service but to have a more nuanced approach to what people’s roles should be within the military, to match individuals’ stress resilience with the responsibilities they have.”
Dr. Marmar reported that he had no relevant financial conflicts.
On Twitter @dougbrunk
HUNTINGTON BEACH, CALIF. – Researchers are making significant headway in developing objective, reliable, and valid biomarkers to discriminate individuals with warzone post traumatic stress disorder from healthy controls, according to Dr. Charles R. Marmar.
“It’s clear that over the next four or five years we will identify very clear biological, psychological, and other behavioral risk and resilience profiles,” Dr. Marmar told attendees at the annual meeting of the American College of Psychiatrists.
Currently, clinicians largely rely on patient self-reports and clinical observations to diagnose PTSD in military personnel, said Dr. Marmar, professor and chair of the department of psychiatry at NYU Langone Medical Center and director of NYU’s Steven and Alexandra Cohen Veterans Center.
“The problem from the military and law enforcement perspective is that the majority of war fighters experience tremendous stigma in acknowledging their symptoms, particularly active duty military personnel,” he said. “A minority will exaggerate to avoid service or for compensation. Given that we’ve had nearly three million men and women serve in Iraq and Afghanistan, and the fact that we have no objective way yet of determining which ones continue to be fit for redeployment, which ones are in urgent need of help, and which ones deserve compensation, we need to develop better ways to determine if treatments are effective, to inform new treatment selection, and to define new targets for treatment.”
The scope of the problem is underscored in an analysis of data from 289,328 veterans entering VA Healthcare for the first time beginning on April 1, 2002 through March 31, 2006 (Am J. Pub. Health 2009;99[9]:1651-8). Prior to the invasion of Iraq, the distribution of mental health problems was very similar among veterans as in the general population: depression being most common, and low rates of PTSD and alcohol and drug abuse. However, “with each quarter since the invasion of Iraq, there’s been an incubative growth in the prevalence of PTSD, which has now eclipsed depression,” Dr. Marmar said. “We have a toll, a generational effect which looks similar in magnitude with the Vietnam War, both in the number of men and women who serve and in the prevalence of PTSD, depression and alcohol- and drug-related disorders.”
In the general population, risk factors include female sex, child abuse, genetics, which in twin studies account for 30-40% of the risk, lower IQ and lower educational attainment, stressful life events in the prior and following year, and panic reaction at the time of event, such as racing heart, shaking, and sweating.
According to findings from the National Vietnam Veterans Readjustment Study, risk factors for chronic warzone PTSD include high school dropout rate, history of child abuse, high warzone exposure, serious warzone injury, killing combatants, prisoners, and civilians, peritraumatic dissociation, hostile homecoming, post-discharge trauma, and genetics. “These are the risk profiles, and they should give us some clues about where to look for biological factors,” Dr. Marmar said.
The risks of service are not limited to stress, anxiety, depression, alcohol and drug abuse, or traumatic brain injury (TBI). “If you compare men and women returning from Iraq and Afghanistan with no mental health issues to those who have a diagnosis of either PTSD, depression, or the combination, the [diagnosed] cases have 2.5 times the risk of tobacco use, hypertension, dyslipidemia, obesity, and type 2 diabetes,” he said. “These are people in their late 20s and early 30s. So the costs of warzone-related stress and depression are enormous on general health.”
Dr. Marmar presented preliminary findings from the ongoing PTSD Systems Biology Consortium, an effort by researchers at seven universities to establish biomarkers for PTSD. Funded by the Department of Defense, the National Institutes of Health, and other sources, the consortium is comprised of integrated cores including neurocognition, genetics, structural and functional brain imaging, endocrinology, metabolism, genomics, proteomics, metabolomics, and bioinformatics.
To date, the researchers have screened 2,215 veterans from service in Iraq and Afghanistan, all of whom have been deployed to war at least once. Cases were PTSD positive and had a CAPS (Clinician-Administered PTSD scale) score of 20 or greater. Controls were PTSD negative and had a CAPS score of less than 20. They excluded subjects with lifetime psychosis, bipolar disorder, or OCD, as well as alcohol dependence in the past eight months, and drug abuse in the past year. They also excluded veterans with TBI “because we’re trying to be very careful to see if we can get a biological signal comparing combat PTSD cases with controls,” Dr. Marmar noted.
Dr. Marmar presented preliminary findings from 52 PTSD cases and 52 controls that were matched for sex, ethnicity, and age. The sample was entirely men, their mean age was 34 years, and they had a mean of 14.8 years of education. The researchers covaried for depression and other known confounders. “It’s very difficult to disentangle the effects of PTSD and depression because 50% of the cases of warzone PTSD also meet criteria for current major depression, and over 80% meet criteria for lifetime depression,” he said.
In results from the clinical diagnostic evaluation, PTSD cases, compared with controls, were significantly more likely to have current anxiety (7% vs. 0%, respectively; P = .041); lifetime anxiety (9.6% vs. 0%; P = .022); current major depressive disorder (51.5% vs. 1.9%; P<.001); lifetime MDD (84.6% vs. 23.1%; P<.001); and lifetime alcohol abuse dependence (63.5% vs. 25%; P = .001). There was also a non-signficant trend toward lifetime substance abuse/dependence (13.5% vs. 3.9%; P = .081).
Results from the neurocognitive assessments revealed that PTSD positive men had a significantly lower estimated IQ, compared with their PTSD negative counterparts (a mean of 99.3 vs. 107.9, respectively; P = .031). Other significant differences between the two groups were observed in tests of auditory and working memory, specifically digit span (8.67 vs. 10.04; P = .02), and the visual memory sum (9.1 vs. 10.67; P = .01).
One of the consortium collaborators developed a test to compare reward and punishment learning. For the test, “the subject is required to understand what the meaning of a symbol is in a task, and they have no prior knowledge [of the meaning],” Dr. Marmar explained. “They’re either rewarded for guessing correctly or punished for guessing incorrectly.” So far, the healthy controls “are performing much better in identifying the symbols when they’re rewarded, compared with the PTSD cases, and there’s no difference in punishment,” he said. “So there’s impaired reward learning and intact punishment learning in PTSD cases compared to controls, which likely reflects underlying disturbances in dopamine reward circuitry.”
Investigators in the neurogenetics core hypothesized that DNA variants in stress-response genes identified from previous medical studies will be associated with PTSD. These included FKBP5, COMT, APOE, BDNF, PACAP/PAC1R, and OPRL1. Initial analysis revealed that there were a greater number of BDNF allele frequencies among cases, compared with controls (P = .008). “It would appear that BDNF variants confer resilience for combat-related PTSD,” Dr. Marmar said.
The researchers also found a single nucleotide polymorphism never previously described on Chromosome 4. “It’s in a region between genes, probably a micro-RNA regulatory gene on the 4th chromosome,” he said. “That gene in our sample was associated with higher levels of PTSD. In addition, fMRI studies found that carrying this allele was associated with weaker activation of prefrontal cortical areas in the brain to empirical faces tasks.”
The endocrine core found that PTSD cases had lower ambient cortisol levels, compared with controls (P = .051). They also had significantly greater cortisol suppression following dexamethasone administration, compared with controls (P = .013). “This is evidence that there is increased glucocorticoid receptor sensitivity in PTSD expressing as elevated cortisol suppression,” Dr. Marmar said.
Investigators from the structural imaging core found no significant differences in overall hippocampal volume or in the five major hippocampal subfields between PTSD cases and controls, nor in difference in the volume of other brain structures previously implicated in PTSD, such as the amygdala and the thalamus. However, the researchers are finding some differences between cases and controls on functional imaging, including increased spontaneous activity in the amygdala and the insula, and decreased spontaneous activity in the precuneus. “The overall findings on fMRI are that there’s increased activity in the regions [of the brain] associated with fear and decreased connectivity between the frontal cortex and the amygdala,” he said. “This is consistent with the model of dysregulated fear activity in PTSD.”
Researchers have also observed that many markers of metabolic syndrome are significantly elevated between PTSD cases and controls, including fasting glucose (P = .001), weight (P = .03), and resting pulse (P = .003). “When you covary for depression, these findings remain,” Dr. Marmar said. “It’s important to note that these are men mostly in their early 30s recently returned from war and recently in military training, physically fit to be deployed to war.”
He closed his presentation by noting that mounting evidence from animal and human studies suggests evidence of mitochondrial dysfunction in PTSD. In the current analysis, researchers observed a reduced abundance of citrate and other mitochondrial metabolites in PTSD cases compared with controls, as well as an increased abundance of “premitochondrial” metabolites such as pyruvate and lactate. “These findings stand when you covary for depression and for metabolic syndrome,” Dr. Marmar said.
“We believe that these may be very important potential future candidate biomarkers to differentiate PTSD cases from controls.”
The next step in this effort, he added, is to replicate the consortium’s overall findings in a cross-validation sample of 50 male cases and 50 male controls. “We also have a sample of 40 female cases and 40 controls to see if the markers are the same or different,” he said. The researchers are also conducting a prospective study of 1,200 active duty military personnel, who will be evaluated before and after deployment.
For now, some clinicians wonder what should be done for men and women who carry the PTSD risk alleles, or carry the endocrine or metabolism vulnerability to develop complications from combat exposure. “That’s a very sensitive national question,” Dr. Marmar said. “People want to serve their country. The answer may be to allow service but to have a more nuanced approach to what people’s roles should be within the military, to match individuals’ stress resilience with the responsibilities they have.”
Dr. Marmar reported that he had no relevant financial conflicts.
On Twitter @dougbrunk
EXPERT ANALYSIS AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF PSYCHIATRISTS

Telltale sonographic features of simple and hemorrhagic cysts
Pelvic ultrasonography remains the preferred imaging method to evaluate most adnexal cysts, given its ability to accurately characterize their various aspects:
- Simple cysts are uniformly hypoechoic, with thin walls and no blood flow on color Doppler (FIGURE 1).
- Hemorrhagic cysts produce lacy/reticular echoes and clot with concave margins
(FIGURE 2). - Mature cystic teratomas produce hyperechoic lines and dots, sometimes known as “dermoid mesh,” acoustic shadowing, and a hyperechoic nodule (FIGURE 3).
- Endometriomas produce diffuse, low-level internal echoes and a “ground glass” appearance (FIGURE 4).
In the first of this 4-part series on the sonographic features of cystic adnexal pathology, we focus on simple and hemorrhagic cysts. In the following parts we will highlight:
- mature cystic teratomas and endometriomas (Part 2)
- hydrosalpinx and pelvic inclusion cysts (Part 3)
- cystadenoma and ovarian neoplasia (Part 4).
An earlier installment of this series entitled “Hemorrhagic ovarian cysts: one entity with many appearances” (May 2014) also focused on cystic pathology.
Figure 1: Simple cyst
A simple cyst in a 32-year-old patient. Figure 2: Hemorrhagic cyst
Note the lacy/reticular internal echoes and lack of internal blood flow on color Doppler. Figure 3: Cystic teratoma
This cyst exhibits the “dermoid mesh” and hyperechoic lines that correspond with hair. Figure 4: Endometrioma
Note diffuse low-level internal echoes (“ground glass”) and no “ring of fire” on color Doppler. |
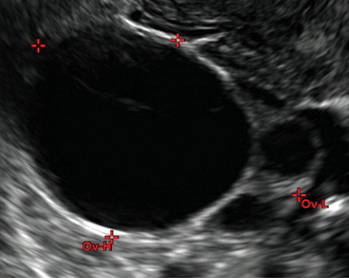
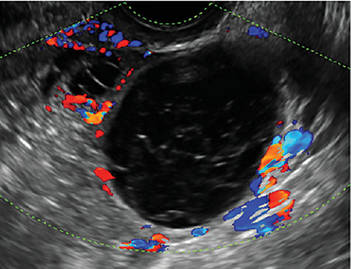

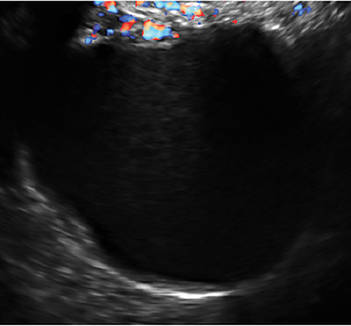
Characteristics of simple cysts
A simple cyst typically is round or oval, anechoic, and has smooth, thin walls. It contains no solid component or septation (with rare exceptions), and no internal flow is visible on color Doppler imaging.
Levine and colleagues observed that simple adnexal cysts as large as 10 cm carry a risk of malignancy of less than 1%, regardless of the age of the patient. In its 2010 Consensus Conference Statement,1 the Society of Radiologists in Ultrasound recommended the following management strategies for women with simple cysts:
Reproductive-aged women
- Cyst <3 cm: No action necessary; the cyst is a normal physiologic finding and should be referred to as a follicle.
- 3–5 cm: No follow-up necessary; the cyst is almost certainly benign.
- 5–7 cm: Yearly imaging; the cyst is highly likely to be benign.
- >7 cm: Additional imaging is recommended.
Postmenopausal women
- <1 cm: No follow-up necessary; the cyst is almost certainly benign.
- 1–7 cm: Yearly imaging; the cyst is likely to be benign.
- >7 cm: Additional imaging is recommended.
Characteristics of hemorrhagic cysts
These cysts can be quite variable in appearance. Among their sonographic features:
- reticular (lacy, cobweb, or fishnet) internal echoes, due to fibrin strands
- solid-appearing areas with concave margins
- on color Doppler, there may be circumferential peripheral flow (“ring of fire”) and no internal flow.
In its 2010 Consensus Conference Statement, the Society of Radiologists in Ultrasound recommended the following management strategies1:
Premenopausal women
- ≤5 cm: No follow-up imaging unless the diagnosis is uncertain.
- >5 cm: Short-interval follow-up ultrasound (6–12 weeks).
Recently menopausal women
- Any size: Follow-up ultrasound in 6–12 weeks to ensure resolution.
Later postmenopausal women
- Any size: Consider surgical removal, as the cyst may be neoplastic.
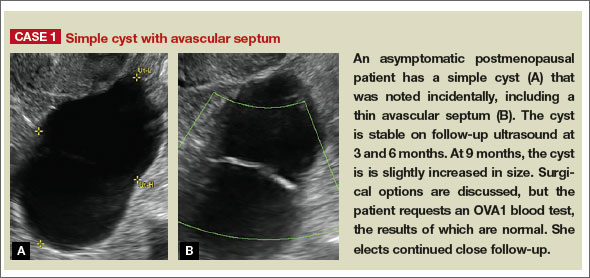
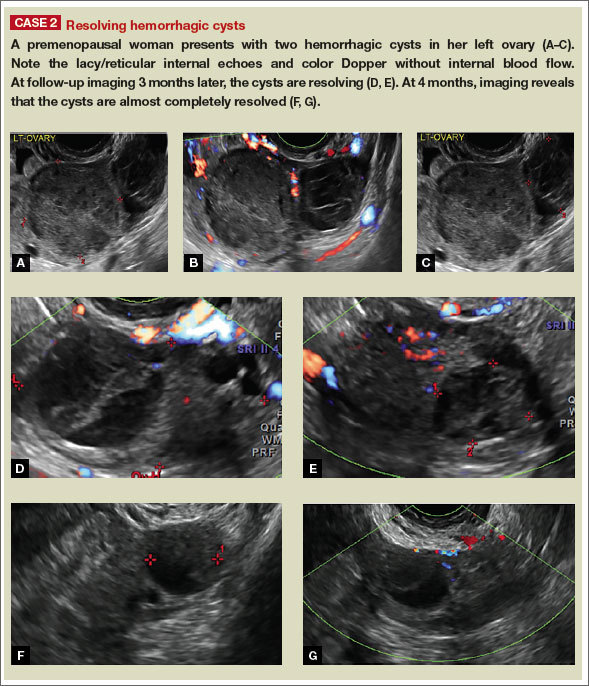
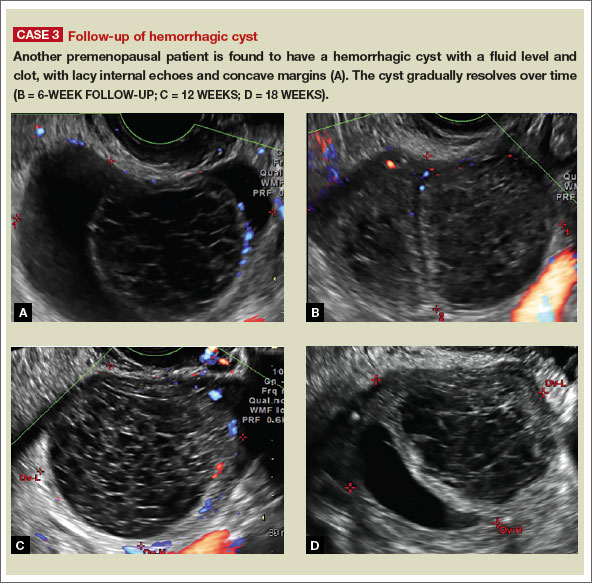
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Reference
1. Levine D, Brown DL, Andreotti RF, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010;256(3):943–954.
Michelle Stalnaker Ozcan, MD, and Andrew M. Kaunitz, MD

Dr. Ozcan is Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville.

Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
Michelle Stalnaker Ozcan, MD, and Andrew M. Kaunitz, MD
Dr. Ozcan is Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
Michelle Stalnaker Ozcan, MD, and Andrew M. Kaunitz, MD
Dr. Ozcan is Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
Pelvic ultrasonography remains the preferred imaging method to evaluate most adnexal cysts, given its ability to accurately characterize their various aspects:
- Simple cysts are uniformly hypoechoic, with thin walls and no blood flow on color Doppler (FIGURE 1).
- Hemorrhagic cysts produce lacy/reticular echoes and clot with concave margins
(FIGURE 2). - Mature cystic teratomas produce hyperechoic lines and dots, sometimes known as “dermoid mesh,” acoustic shadowing, and a hyperechoic nodule (FIGURE 3).
- Endometriomas produce diffuse, low-level internal echoes and a “ground glass” appearance (FIGURE 4).
In the first of this 4-part series on the sonographic features of cystic adnexal pathology, we focus on simple and hemorrhagic cysts. In the following parts we will highlight:
- mature cystic teratomas and endometriomas (Part 2)
- hydrosalpinx and pelvic inclusion cysts (Part 3)
- cystadenoma and ovarian neoplasia (Part 4).
An earlier installment of this series entitled “Hemorrhagic ovarian cysts: one entity with many appearances” (May 2014) also focused on cystic pathology.
Figure 1: Simple cyst
A simple cyst in a 32-year-old patient. Figure 2: Hemorrhagic cyst
Note the lacy/reticular internal echoes and lack of internal blood flow on color Doppler. Figure 3: Cystic teratoma
This cyst exhibits the “dermoid mesh” and hyperechoic lines that correspond with hair. Figure 4: Endometrioma
Note diffuse low-level internal echoes (“ground glass”) and no “ring of fire” on color Doppler. |
Characteristics of simple cysts
A simple cyst typically is round or oval, anechoic, and has smooth, thin walls. It contains no solid component or septation (with rare exceptions), and no internal flow is visible on color Doppler imaging.
Levine and colleagues observed that simple adnexal cysts as large as 10 cm carry a risk of malignancy of less than 1%, regardless of the age of the patient. In its 2010 Consensus Conference Statement,1 the Society of Radiologists in Ultrasound recommended the following management strategies for women with simple cysts:
Reproductive-aged women
- Cyst <3 cm: No action necessary; the cyst is a normal physiologic finding and should be referred to as a follicle.
- 3–5 cm: No follow-up necessary; the cyst is almost certainly benign.
- 5–7 cm: Yearly imaging; the cyst is highly likely to be benign.
- >7 cm: Additional imaging is recommended.
Postmenopausal women
- <1 cm: No follow-up necessary; the cyst is almost certainly benign.
- 1–7 cm: Yearly imaging; the cyst is likely to be benign.
- >7 cm: Additional imaging is recommended.
Characteristics of hemorrhagic cysts
These cysts can be quite variable in appearance. Among their sonographic features:
- reticular (lacy, cobweb, or fishnet) internal echoes, due to fibrin strands
- solid-appearing areas with concave margins
- on color Doppler, there may be circumferential peripheral flow (“ring of fire”) and no internal flow.
In its 2010 Consensus Conference Statement, the Society of Radiologists in Ultrasound recommended the following management strategies1:
Premenopausal women
- ≤5 cm: No follow-up imaging unless the diagnosis is uncertain.
- >5 cm: Short-interval follow-up ultrasound (6–12 weeks).
Recently menopausal women
- Any size: Follow-up ultrasound in 6–12 weeks to ensure resolution.
Later postmenopausal women
- Any size: Consider surgical removal, as the cyst may be neoplastic.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Pelvic ultrasonography remains the preferred imaging method to evaluate most adnexal cysts, given its ability to accurately characterize their various aspects:
- Simple cysts are uniformly hypoechoic, with thin walls and no blood flow on color Doppler (FIGURE 1).
- Hemorrhagic cysts produce lacy/reticular echoes and clot with concave margins
(FIGURE 2). - Mature cystic teratomas produce hyperechoic lines and dots, sometimes known as “dermoid mesh,” acoustic shadowing, and a hyperechoic nodule (FIGURE 3).
- Endometriomas produce diffuse, low-level internal echoes and a “ground glass” appearance (FIGURE 4).
In the first of this 4-part series on the sonographic features of cystic adnexal pathology, we focus on simple and hemorrhagic cysts. In the following parts we will highlight:
- mature cystic teratomas and endometriomas (Part 2)
- hydrosalpinx and pelvic inclusion cysts (Part 3)
- cystadenoma and ovarian neoplasia (Part 4).
An earlier installment of this series entitled “Hemorrhagic ovarian cysts: one entity with many appearances” (May 2014) also focused on cystic pathology.
Figure 1: Simple cyst
A simple cyst in a 32-year-old patient. Figure 2: Hemorrhagic cyst
Note the lacy/reticular internal echoes and lack of internal blood flow on color Doppler. Figure 3: Cystic teratoma
This cyst exhibits the “dermoid mesh” and hyperechoic lines that correspond with hair. Figure 4: Endometrioma
Note diffuse low-level internal echoes (“ground glass”) and no “ring of fire” on color Doppler. |
Characteristics of simple cysts
A simple cyst typically is round or oval, anechoic, and has smooth, thin walls. It contains no solid component or septation (with rare exceptions), and no internal flow is visible on color Doppler imaging.
Levine and colleagues observed that simple adnexal cysts as large as 10 cm carry a risk of malignancy of less than 1%, regardless of the age of the patient. In its 2010 Consensus Conference Statement,1 the Society of Radiologists in Ultrasound recommended the following management strategies for women with simple cysts:
Reproductive-aged women
- Cyst <3 cm: No action necessary; the cyst is a normal physiologic finding and should be referred to as a follicle.
- 3–5 cm: No follow-up necessary; the cyst is almost certainly benign.
- 5–7 cm: Yearly imaging; the cyst is highly likely to be benign.
- >7 cm: Additional imaging is recommended.
Postmenopausal women
- <1 cm: No follow-up necessary; the cyst is almost certainly benign.
- 1–7 cm: Yearly imaging; the cyst is likely to be benign.
- >7 cm: Additional imaging is recommended.
Characteristics of hemorrhagic cysts
These cysts can be quite variable in appearance. Among their sonographic features:
- reticular (lacy, cobweb, or fishnet) internal echoes, due to fibrin strands
- solid-appearing areas with concave margins
- on color Doppler, there may be circumferential peripheral flow (“ring of fire”) and no internal flow.
In its 2010 Consensus Conference Statement, the Society of Radiologists in Ultrasound recommended the following management strategies1:
Premenopausal women
- ≤5 cm: No follow-up imaging unless the diagnosis is uncertain.
- >5 cm: Short-interval follow-up ultrasound (6–12 weeks).
Recently menopausal women
- Any size: Follow-up ultrasound in 6–12 weeks to ensure resolution.
Later postmenopausal women
- Any size: Consider surgical removal, as the cyst may be neoplastic.
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Reference
1. Levine D, Brown DL, Andreotti RF, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010;256(3):943–954.
Reference
1. Levine D, Brown DL, Andreotti RF, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010;256(3):943–954.
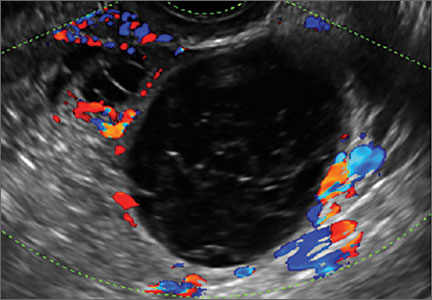
Product Update: InTone, E-Sacs, traxi, Saliva Fertility Monitor
FEMALE URINARY INCONTINENCE DEVICE

The InTone® system from InControl Medical™ is a noninvasive home-based pelvic-floor rehabilitation program to treat female urinary incontinence. InControl offers two customizable probes. Apex, for women with mild to moderate stress urinary incontinence, delivers electro-stimulation to strengthen pelvic floor muscles and eliminate leakage associated with coughing, laughing, or exercise. ApexM, for women with urgency and mixed urinary incontinence, provides alternating-frequency stimulation to strengthen the pelvic floor muscles and calm detrusor muscle spasms.
The InTone system for moderate to severe incontinence combines muscle stimulation with pelvic-floor exercises. A hand-held control unit allows the patient to listen to prerecorded exercises at home. The control unit also offers visual biofeedback to ensure that the exercises are being completed properly. The patient can present the data from her workouts, stored by the handheld control unit, to her physician, who can then individualize the exercise plan. InTone is indicated for use in 12-minute sessions, six times a week, for 90 days to treat stress urinary incontinence, and for 180 days for urgency or mixed incontinence.
FOR MORE INFORMATION, VISIT www.incontrolmedical.com
TISSUE RETRIEVAL SACS

Espiner Medical offers E-Sacs, a variety of tissue retrieval sacs for minimally invasive surgery. E-Sacs are manufactured from Superamine66™ fabric, a lightweight, ripstop nylon coated with polyurethane designed to make them strong, rupture proof, leak resistant, easy to deploy, and x-ray opaque. Standard E-Sacs, made of one-piece construction with an integral tail that can be deployed using 5-mm instruments, do not require claw forceps to extract. Super E-Sacs are ideal for larger specimens and have colored tabs to facilitate placement. Master E-Sacs open automatically, have stronger arms to reinforce the mouth opening, a drawstring closure, and can accept tissue sizes up to a large spleen, ovary, or kidney. EcoSacs, for bottom-first abdominal entry, have a large open mouth to facilitate tissue capture with a drawstring closure.
FOR MORE INFORMATION, VISIT www.espinermedical.com
PANNICULUS RETRACTOR

traxi can be applied and used as a sterile or nonsterile product in conjunction with both external and internal retractors. The manufacturer explains that traxi works by anchoring at the xiphoid and distributing the patient’s weight rather than applying it fully on the sternum, which can make it difficult for the patient to breathe. traxi should not be left on the patient for longer than 24 hours. traxi is labeled with HOLD and PULL HERE tabs, as well as A, B, and C tabs to guide the clinician through the retractor application process.
FOR MORE INFORMATION, VISIT www.clinicalinnovations.com
SALIVA FERTILITY MONITOR

The KNOWHEN® Saliva Fertility Monitor is a handheld mini-microscope that monitors a woman’s ovulation using just a single drop of saliva. A woman’s daily test results can be tracked on an ovulation mobile app provided with the product, allowing her to better plan her sexual activity to achieve fertility goals.
First thing each morning, before eating, drinking, smoking, or brushing teeth, a woman applies a thick drop of saliva to the glass surface and waits for it to dry (5–15 minutes). Then she compares the image she sees through the lens to the chart supplied with the kit and inputs her results on the KNOWHEN app. If she is not ovulating, dots and circles may appear. When she sees a few fernlike crystals, it means she is starting to ovulate, or has just finished ovulating. Consistent fern-like crystals in the viewer indicate that she is ovulating. During ovulation, high estrogen levels raise the percentage of salt in a woman’s body. In saliva, these salts take the shape of ferns under the 60X magnification of the KNOWHEN microscope. The kit includes the app and educational material, including an instructional video.
FOR MORE INFORMATION, VISIT www.knowhen.com
FEMALE URINARY INCONTINENCE DEVICE
The InTone® system from InControl Medical™ is a noninvasive home-based pelvic-floor rehabilitation program to treat female urinary incontinence. InControl offers two customizable probes. Apex, for women with mild to moderate stress urinary incontinence, delivers electro-stimulation to strengthen pelvic floor muscles and eliminate leakage associated with coughing, laughing, or exercise. ApexM, for women with urgency and mixed urinary incontinence, provides alternating-frequency stimulation to strengthen the pelvic floor muscles and calm detrusor muscle spasms.
The InTone system for moderate to severe incontinence combines muscle stimulation with pelvic-floor exercises. A hand-held control unit allows the patient to listen to prerecorded exercises at home. The control unit also offers visual biofeedback to ensure that the exercises are being completed properly. The patient can present the data from her workouts, stored by the handheld control unit, to her physician, who can then individualize the exercise plan. InTone is indicated for use in 12-minute sessions, six times a week, for 90 days to treat stress urinary incontinence, and for 180 days for urgency or mixed incontinence.
FOR MORE INFORMATION, VISIT www.incontrolmedical.com
TISSUE RETRIEVAL SACS
Espiner Medical offers E-Sacs, a variety of tissue retrieval sacs for minimally invasive surgery. E-Sacs are manufactured from Superamine66™ fabric, a lightweight, ripstop nylon coated with polyurethane designed to make them strong, rupture proof, leak resistant, easy to deploy, and x-ray opaque. Standard E-Sacs, made of one-piece construction with an integral tail that can be deployed using 5-mm instruments, do not require claw forceps to extract. Super E-Sacs are ideal for larger specimens and have colored tabs to facilitate placement. Master E-Sacs open automatically, have stronger arms to reinforce the mouth opening, a drawstring closure, and can accept tissue sizes up to a large spleen, ovary, or kidney. EcoSacs, for bottom-first abdominal entry, have a large open mouth to facilitate tissue capture with a drawstring closure.
FOR MORE INFORMATION, VISIT www.espinermedical.com
PANNICULUS RETRACTOR
traxi can be applied and used as a sterile or nonsterile product in conjunction with both external and internal retractors. The manufacturer explains that traxi works by anchoring at the xiphoid and distributing the patient’s weight rather than applying it fully on the sternum, which can make it difficult for the patient to breathe. traxi should not be left on the patient for longer than 24 hours. traxi is labeled with HOLD and PULL HERE tabs, as well as A, B, and C tabs to guide the clinician through the retractor application process.
FOR MORE INFORMATION, VISIT www.clinicalinnovations.com
SALIVA FERTILITY MONITOR
The KNOWHEN® Saliva Fertility Monitor is a handheld mini-microscope that monitors a woman’s ovulation using just a single drop of saliva. A woman’s daily test results can be tracked on an ovulation mobile app provided with the product, allowing her to better plan her sexual activity to achieve fertility goals.
First thing each morning, before eating, drinking, smoking, or brushing teeth, a woman applies a thick drop of saliva to the glass surface and waits for it to dry (5–15 minutes). Then she compares the image she sees through the lens to the chart supplied with the kit and inputs her results on the KNOWHEN app. If she is not ovulating, dots and circles may appear. When she sees a few fernlike crystals, it means she is starting to ovulate, or has just finished ovulating. Consistent fern-like crystals in the viewer indicate that she is ovulating. During ovulation, high estrogen levels raise the percentage of salt in a woman’s body. In saliva, these salts take the shape of ferns under the 60X magnification of the KNOWHEN microscope. The kit includes the app and educational material, including an instructional video.
FOR MORE INFORMATION, VISIT www.knowhen.com
FEMALE URINARY INCONTINENCE DEVICE
The InTone® system from InControl Medical™ is a noninvasive home-based pelvic-floor rehabilitation program to treat female urinary incontinence. InControl offers two customizable probes. Apex, for women with mild to moderate stress urinary incontinence, delivers electro-stimulation to strengthen pelvic floor muscles and eliminate leakage associated with coughing, laughing, or exercise. ApexM, for women with urgency and mixed urinary incontinence, provides alternating-frequency stimulation to strengthen the pelvic floor muscles and calm detrusor muscle spasms.
The InTone system for moderate to severe incontinence combines muscle stimulation with pelvic-floor exercises. A hand-held control unit allows the patient to listen to prerecorded exercises at home. The control unit also offers visual biofeedback to ensure that the exercises are being completed properly. The patient can present the data from her workouts, stored by the handheld control unit, to her physician, who can then individualize the exercise plan. InTone is indicated for use in 12-minute sessions, six times a week, for 90 days to treat stress urinary incontinence, and for 180 days for urgency or mixed incontinence.
FOR MORE INFORMATION, VISIT www.incontrolmedical.com
TISSUE RETRIEVAL SACS
Espiner Medical offers E-Sacs, a variety of tissue retrieval sacs for minimally invasive surgery. E-Sacs are manufactured from Superamine66™ fabric, a lightweight, ripstop nylon coated with polyurethane designed to make them strong, rupture proof, leak resistant, easy to deploy, and x-ray opaque. Standard E-Sacs, made of one-piece construction with an integral tail that can be deployed using 5-mm instruments, do not require claw forceps to extract. Super E-Sacs are ideal for larger specimens and have colored tabs to facilitate placement. Master E-Sacs open automatically, have stronger arms to reinforce the mouth opening, a drawstring closure, and can accept tissue sizes up to a large spleen, ovary, or kidney. EcoSacs, for bottom-first abdominal entry, have a large open mouth to facilitate tissue capture with a drawstring closure.
FOR MORE INFORMATION, VISIT www.espinermedical.com
PANNICULUS RETRACTOR
traxi can be applied and used as a sterile or nonsterile product in conjunction with both external and internal retractors. The manufacturer explains that traxi works by anchoring at the xiphoid and distributing the patient’s weight rather than applying it fully on the sternum, which can make it difficult for the patient to breathe. traxi should not be left on the patient for longer than 24 hours. traxi is labeled with HOLD and PULL HERE tabs, as well as A, B, and C tabs to guide the clinician through the retractor application process.
FOR MORE INFORMATION, VISIT www.clinicalinnovations.com
SALIVA FERTILITY MONITOR
The KNOWHEN® Saliva Fertility Monitor is a handheld mini-microscope that monitors a woman’s ovulation using just a single drop of saliva. A woman’s daily test results can be tracked on an ovulation mobile app provided with the product, allowing her to better plan her sexual activity to achieve fertility goals.
First thing each morning, before eating, drinking, smoking, or brushing teeth, a woman applies a thick drop of saliva to the glass surface and waits for it to dry (5–15 minutes). Then she compares the image she sees through the lens to the chart supplied with the kit and inputs her results on the KNOWHEN app. If she is not ovulating, dots and circles may appear. When she sees a few fernlike crystals, it means she is starting to ovulate, or has just finished ovulating. Consistent fern-like crystals in the viewer indicate that she is ovulating. During ovulation, high estrogen levels raise the percentage of salt in a woman’s body. In saliva, these salts take the shape of ferns under the 60X magnification of the KNOWHEN microscope. The kit includes the app and educational material, including an instructional video.
FOR MORE INFORMATION, VISIT www.knowhen.com
David Henry's JCSO podcast, February 2015
The line-up for David Henry’s monthly podcast for The Journal of Community and Supportive Oncology includes an Original Report in which investigators report complete response rates (no emesis, no rescue medication) APF530, a sustained-release granisetron, during the acute and delayed phases of chemotherapy-induced nausea and vomiting over multiple cycles of the therapy. He also discusses the findings from a study on joint breast and colorectal cancer screenings in medically underserved women, and another in women with self-reported lower limb lymphedema after treatment for gynecological cancers and their use of services. A fourth Original Report examines perceptions about participation in cancer clinical trials in New York state and how increased outreach and a team approach to educating and enrolling patients in trials are important to increase participation and ensure a diverse sample of participants. Finally, a feature article on new therapies looks at the significant challenges – and recent advances – in the treatment of head and neck cancers.
The line-up for David Henry’s monthly podcast for The Journal of Community and Supportive Oncology includes an Original Report in which investigators report complete response rates (no emesis, no rescue medication) APF530, a sustained-release granisetron, during the acute and delayed phases of chemotherapy-induced nausea and vomiting over multiple cycles of the therapy. He also discusses the findings from a study on joint breast and colorectal cancer screenings in medically underserved women, and another in women with self-reported lower limb lymphedema after treatment for gynecological cancers and their use of services. A fourth Original Report examines perceptions about participation in cancer clinical trials in New York state and how increased outreach and a team approach to educating and enrolling patients in trials are important to increase participation and ensure a diverse sample of participants. Finally, a feature article on new therapies looks at the significant challenges – and recent advances – in the treatment of head and neck cancers.
The line-up for David Henry’s monthly podcast for The Journal of Community and Supportive Oncology includes an Original Report in which investigators report complete response rates (no emesis, no rescue medication) APF530, a sustained-release granisetron, during the acute and delayed phases of chemotherapy-induced nausea and vomiting over multiple cycles of the therapy. He also discusses the findings from a study on joint breast and colorectal cancer screenings in medically underserved women, and another in women with self-reported lower limb lymphedema after treatment for gynecological cancers and their use of services. A fourth Original Report examines perceptions about participation in cancer clinical trials in New York state and how increased outreach and a team approach to educating and enrolling patients in trials are important to increase participation and ensure a diverse sample of participants. Finally, a feature article on new therapies looks at the significant challenges – and recent advances – in the treatment of head and neck cancers.
Factor Xa antidote gets orphan designation

Photo by Piotr Bodzek
The US Food and Drug Administration (FDA) has granted orphan designation to andexanet alfa for reversing the anticoagulant effect of factor Xa inhibitors in patients experiencing a serious, uncontrolled bleeding event and those who require urgent or emergent surgery.
At present, there is no approved antidote for these patients.
Andexanet alfa is the only compound being studied as a reversal agent for factor Xa inhibitors that directly and specifically corrects anti-factor Xa activity.
The drug is a modified human factor Xa molecule that acts as a decoy to target and sequester both oral and injectable factor Xa inhibitors in the blood. Once bound, the inhibitors are unable to bind to and inhibit native factor Xa, thus allowing for the restoration of normal hemostatic processes.
Andexanet alfa has the potential to address several clinical scenarios where a factor Xa antidote is needed by allowing for flexible and controlled reversal. This can be short-acting, through the administration of an intravenous (IV) bolus, or longer-acting with the addition of an extended infusion.
The FDA previously granted andexanet alfa breakthrough therapy designation, which is intended to expedite the development and review of a drug candidate intended to treat a serious or life-threatening condition.
“Orphan drug designation for andexanet alfa recognizes its potential to address a significant unmet medical need and to advance the field by helping patients who currently have no treatment options,” said Bill Lis, chief executive officer of Portola Pharmaceuticals, the company developing andexanet alfa.
The FDA’s orphan drug designation program provides orphan status to drugs and biologics that are intended for the treatment, diagnosis, or prevention of rare diseases/disorders that currently affect fewer than 200,000 people in the US.
Orphan designation qualifies a company for certain benefits, including an accelerated approval process, 7 years of market exclusivity following the drug’s approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Clinical development of andexanet alfa
Researchers are currently evaluating andexanet alfa in 2 randomized, placebo-controlled, phase 3 trials—ANNEXA-A and ANNEXA-R.
They previously reported promising results from the first part of the ANNEXA-A study, a test of andexanet alfa’s ability to reverse the effects of apixaban in healthy subjects when the antidote was given as a single IV bolus.
Researchers also reported favorable results from the first part of the ANNEXA-R study, in which they evaluated andexanet alfa’s ability to reverse the effects of rivaroxaban in healthy subjects when the antidote was given as a single IV bolus.
The second parts of the ANNEXA-A and ANNEXA-R studies are ongoing. The researchers are evaluating the use of andexanet alfa given as a bolus and a continuous infusion.
ANNEXA-4, a phase 4, single-arm, confirmatory study is also ongoing. Researchers are evaluating the drug in patients receiving apixaban, rivaroxaban, edoxaban, or enoxaparin who present with an acute major bleed. ![]()
Photo by Piotr Bodzek
The US Food and Drug Administration (FDA) has granted orphan designation to andexanet alfa for reversing the anticoagulant effect of factor Xa inhibitors in patients experiencing a serious, uncontrolled bleeding event and those who require urgent or emergent surgery.
At present, there is no approved antidote for these patients.
Andexanet alfa is the only compound being studied as a reversal agent for factor Xa inhibitors that directly and specifically corrects anti-factor Xa activity.
The drug is a modified human factor Xa molecule that acts as a decoy to target and sequester both oral and injectable factor Xa inhibitors in the blood. Once bound, the inhibitors are unable to bind to and inhibit native factor Xa, thus allowing for the restoration of normal hemostatic processes.
Andexanet alfa has the potential to address several clinical scenarios where a factor Xa antidote is needed by allowing for flexible and controlled reversal. This can be short-acting, through the administration of an intravenous (IV) bolus, or longer-acting with the addition of an extended infusion.
The FDA previously granted andexanet alfa breakthrough therapy designation, which is intended to expedite the development and review of a drug candidate intended to treat a serious or life-threatening condition.
“Orphan drug designation for andexanet alfa recognizes its potential to address a significant unmet medical need and to advance the field by helping patients who currently have no treatment options,” said Bill Lis, chief executive officer of Portola Pharmaceuticals, the company developing andexanet alfa.
The FDA’s orphan drug designation program provides orphan status to drugs and biologics that are intended for the treatment, diagnosis, or prevention of rare diseases/disorders that currently affect fewer than 200,000 people in the US.
Orphan designation qualifies a company for certain benefits, including an accelerated approval process, 7 years of market exclusivity following the drug’s approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Clinical development of andexanet alfa
Researchers are currently evaluating andexanet alfa in 2 randomized, placebo-controlled, phase 3 trials—ANNEXA-A and ANNEXA-R.
They previously reported promising results from the first part of the ANNEXA-A study, a test of andexanet alfa’s ability to reverse the effects of apixaban in healthy subjects when the antidote was given as a single IV bolus.
Researchers also reported favorable results from the first part of the ANNEXA-R study, in which they evaluated andexanet alfa’s ability to reverse the effects of rivaroxaban in healthy subjects when the antidote was given as a single IV bolus.
The second parts of the ANNEXA-A and ANNEXA-R studies are ongoing. The researchers are evaluating the use of andexanet alfa given as a bolus and a continuous infusion.
ANNEXA-4, a phase 4, single-arm, confirmatory study is also ongoing. Researchers are evaluating the drug in patients receiving apixaban, rivaroxaban, edoxaban, or enoxaparin who present with an acute major bleed. ![]()
Photo by Piotr Bodzek
The US Food and Drug Administration (FDA) has granted orphan designation to andexanet alfa for reversing the anticoagulant effect of factor Xa inhibitors in patients experiencing a serious, uncontrolled bleeding event and those who require urgent or emergent surgery.
At present, there is no approved antidote for these patients.
Andexanet alfa is the only compound being studied as a reversal agent for factor Xa inhibitors that directly and specifically corrects anti-factor Xa activity.
The drug is a modified human factor Xa molecule that acts as a decoy to target and sequester both oral and injectable factor Xa inhibitors in the blood. Once bound, the inhibitors are unable to bind to and inhibit native factor Xa, thus allowing for the restoration of normal hemostatic processes.
Andexanet alfa has the potential to address several clinical scenarios where a factor Xa antidote is needed by allowing for flexible and controlled reversal. This can be short-acting, through the administration of an intravenous (IV) bolus, or longer-acting with the addition of an extended infusion.
The FDA previously granted andexanet alfa breakthrough therapy designation, which is intended to expedite the development and review of a drug candidate intended to treat a serious or life-threatening condition.
“Orphan drug designation for andexanet alfa recognizes its potential to address a significant unmet medical need and to advance the field by helping patients who currently have no treatment options,” said Bill Lis, chief executive officer of Portola Pharmaceuticals, the company developing andexanet alfa.
The FDA’s orphan drug designation program provides orphan status to drugs and biologics that are intended for the treatment, diagnosis, or prevention of rare diseases/disorders that currently affect fewer than 200,000 people in the US.
Orphan designation qualifies a company for certain benefits, including an accelerated approval process, 7 years of market exclusivity following the drug’s approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Clinical development of andexanet alfa
Researchers are currently evaluating andexanet alfa in 2 randomized, placebo-controlled, phase 3 trials—ANNEXA-A and ANNEXA-R.
They previously reported promising results from the first part of the ANNEXA-A study, a test of andexanet alfa’s ability to reverse the effects of apixaban in healthy subjects when the antidote was given as a single IV bolus.
Researchers also reported favorable results from the first part of the ANNEXA-R study, in which they evaluated andexanet alfa’s ability to reverse the effects of rivaroxaban in healthy subjects when the antidote was given as a single IV bolus.
The second parts of the ANNEXA-A and ANNEXA-R studies are ongoing. The researchers are evaluating the use of andexanet alfa given as a bolus and a continuous infusion.
ANNEXA-4, a phase 4, single-arm, confirmatory study is also ongoing. Researchers are evaluating the drug in patients receiving apixaban, rivaroxaban, edoxaban, or enoxaparin who present with an acute major bleed. ![]()
Nanotechnology: Why Should We Care?
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
The orthopedic community is increasingly deluged with advancements in the basic sciences. With each step, we must evaluate the necessity of new information and the relevance of these topics for clinical practice. Since the late 1990s, the promise of nanotechnology to effect significant changes in the medical field has been heralded. However, in this coming decade, we as a profession will see unprecedented advances in the movement of this technology “from the bench to the bedside.” Not unlike many other basic science advancements in our field, nanotechnology is poorly understood among clinicians and residents. As the use of biologics and drug delivery systems expands in orthopedics, nanoparticle-based devices will become more prevalent and have a momentous impact on the way we treat and diagnose orthopedic patients.
A nanoparticle is generally defined as a particle in which at least 1 dimension is between 1 to 100 nanometers and has material properties consistent with quantum mechanics.1 Nanomaterials can be composed of organic and inorganic chemical elements that enable basic chemical processes to create more complex systems. Individual nanoparticle units can be synthesized to form nanostructures, including nanotubes, nanoscaffolds, nanofibers, and even nanodiamonds.2-4 Nanoparticles at this scale display unique optical, chemical, and physical properties that can be manipulated to create specific end-use applications. Such uses may include glass fabrication, optical probes, television screens, drug delivery, gene delivery, and multiplex diagnostic assays.5-7 By crossing disciplines of physics, engineering, and medical sciences, we can create novel technology that includes nanomanufacturing, targeted drug delivery, nanorobotics in conjunction with artificial intelligence, and point-of-care diagnostics.7-9
The field of orthopedics has benefited from nanotechnologic advances, such as new therapeutics and implant-related technology. Nanotubes are hollow nanosized cylinders that are commonly created from titania, silica, or carbon-based substrates. They have garnered significant interest for their high tensile and shear strength, favorable microstructure for bony ingrowth, and their capacity to hold antibiotics or growth factors, such as bone morphogenic proteins (BMPs).10 The current local delivery limitations of BMPs via a collagen sponge have the potential to be maximized and better controlled with a nanotechnology-based approach. The size, internal structure, and shape of the nanoparticle can be manipulated to control the release of these growth factors, and certain nanoparticles can be dual-layered, allowing for release of multiple growth factors at once or in succession.11,12 A more powerful and targeted delivery system of these types of growth factors may result in improved or more robust outcomes, and further research is warranted.
It is possible that carbon-based nanotubes can be categorized as a biomedical implant secondary to their mechanical properties.13 Their strength and ability to be augmented with osteogenic materials has made them an attractive area of research as alternative implant surfaces and stand-alone implants. Nanotubes are capable of acting as a scaffold for antibiotic-loaded, carbon-based nanodiamonds for localized treatment of periprosthetic infection, and research has been directed toward controlled release of the nanodiamond-antibiotic construct from these scaffolds or hydrogels.4,14 Technologies like this may allow the clinician to treat periprosthetic infections locally and minimize the use of systemic antibiotics. The perfection of this type of delivery system may augment the role of antibiotic-laden cement and improve our treatment success rates, even in traditionally hard-to-treat organisms.
Nanoscaffolds and nanofibers are created from nanosized polymers and rendered into a 3-dimensional structure that can be loaded with biologic particles or acting as a scaffold/template for tissue or bone ingrowth. Nanofibers created using biodegradable substrates such as poly(lactic-co-glycolic acid) (PLGA) and chitosan have been extensively studied for their delayed-release properties and biocompatibility.15 These scaffolds are often soaked or loaded with chondrogenic, osteogenic, or antibacterial agents, and have been evaluated in both in vitro and in vivo studies with promising results.15,16 They have been an exciting area of research in tissue engineering, and have been accepted as an adjunct in tendon-repair treatments and local bone regeneration.3,17 As this technology is perfected, the potential to treat more effectively massive rotator cuff tears or tears with poor tissue integrity will dramatically improve and expand the indications for rotator cuff repair.
Augmentation of implant surfaces with nanomaterials that improve osseointegration, or that act as antimicrobial agents have also been a focus of research in hopes of decreasing the rates of aseptic failure and periprosthetic infection in arthroplasty procedures. Nanocrystalline surfaces made of hydroxyapatite and cobalt chromium have been evaluated for their enhanced osteoconductive properties, and may replace standard surfaces.18-20 Recent work evaluating nanoparticle-antibiotic constructs that have been covalently bound to implant surfaces for delayed release of antibiotics during the perioperative period has shown promise, and may allow a more targeted and localized treatment strategy for periprosthetic infection.21,22
Major limitations regarding successful clinical implementation of nanotechnology include both cost and regulatory processes. Currently, pharmaceutical companies estimate that, on average, successful clinical trials from phase 1 to completion for new drugs can cost hundreds of millions of dollars.23 Such high costs result partially from the laborious and capital-intensive process of conducting clinical trials that meet US Food and Drug Administration (FDA) requirements. These regulations would apply to both surface-coated implants and nanoparticle-based drug delivery systems. These types of implants would not be expedited into the market secondary to their drug delivery component and would likely require lengthy clinical studies. Implant companies may be reluctant to invest millions of dollars in multiple FDA trials when they have lucrative implants on the market.
Other limitations include the particles’ complex 3-dimensional structure, which can present challenges for mass production. Producing large quantities of nanoparticles at a consistent quality may be a major limitation to the more unique and target-based nanotherapies. Recent concerns with the toxicity profile of nanotechnology-based medicines have resulted in more intense scrutiny of the nanotechnology safety profile.24,25 Currently, nanoparticle technology is evaluated case by case with each technology requiring its own toxicology and safety profile testing if it is intended for human use. These tests can be cost-prohibitive and require extensive private and government capital for successful market entry. Despite these limitations, nanotechnology will impact the next generation of orthopedic surgeons. Current estimates project the nanomedicine market to be worth $177.6 billion by 2019.26
Advances in nanobased orthopedic technologies have expanded dramatically in the past decade, and we, as the treating physicians, must make educated decisions on how and when to use nanoparticle-based therapies and treatment options. Nanotechnology’s basic science is confusing and often burdensome, but contemporary review articles may be helpful in keeping the orthopedic resident and clinician current with advancements.10,27,28 The more we educate ourselves about evolving nanotechnologies, the less reluctance we will have when evaluating new diagnostic and therapeutic treatment modalities.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
1. Hewakuruppu YL, Dombrovsky LA, Chen C, et al. Plasmonic “pump-probe” method to study semi-transparent nanofluids. Appl Opt. 2013;52(24):6041-6050.
2. Balasundaram G, Webster TJ. An overview of nano-polymers for orthopedic applications. Macromol Biosci. 2007;7(5):635-642.
3. Zhang Z, Hu J, Ma PX. Nanofiber-based delivery of bioactive agents and stem cells to bone sites. Adv Drug Deliv Rev. 2012;64(12):1129-1141.
4. Mochalin VN, Shenderova O, Ho D, Gogotsi Y. The properties and applications of nanodiamonds. Nat Nanotechnol. 2012;7(1):11-23.
5. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological applications based on surface-enhanced Raman scattering from indocyanine green on gold nanoparticles. Anal Chem. 2005;77(8):2381-2385.
6. Wang L, O’Donoghue MB, Tan W. Nanoparticles for multiplex diagnostics and imaging. Nanomedicine (Lond). 2006;1(4):413-426.
7. Krebs MD, Salter E, Chen E, Sutter KA, Alsberg E. Calcium phosphate-DNA nanoparticle gene delivery from alginate hydrogels induces in vivo osteogenesis. J Biomed Mater Res A. 2010;92(3):1131-1138.
8. Myers FB, Lee LP. Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip. 2008;8(12):2015-2031.
9. Sacha GM, Varona P. Artificial intelligence in nanotechnology. Nanotechnology. 2013;24(45):452002.
10. Ganguly DY, Shahbazian R, Shokuhfar T. Recent advances in nanotubes for orthopedic implants. J Nanotech Smart Mater. 2014;1:1-10.
11. Srivastava S, Kotov NA. Composite Layer-by-Layer (LBL) assembly with inorganic nanoparticles and nanowires. Acc Chem Res. 2008;41(12):1831-1841.
12. Panda HS, Srivastava R, Bahadur D. Shape and size control of nano dispersed Mg/Al layered double hydroxide. J Nanosci Nanotechnol. 2008;8(8):4218-4223.
13. Wang X, Li Q, Xie J, et al. Fabrication of ultralong and electrically uniform single-walled carbon nanotubes on clean substrates. Nano Lett. 2009;9(9):3137-3141.
14. Zhu Y, Li J, Li W, et al. The biocompatibility of nanodiamonds and their application in drug delivery systems. Theranostics. 2012;2(3):302-312.
15. Wu L, Ding J. In vitro degradation of three-dimensional porous poly(D,L-lactide-co-glycolide) scaffolds for tissue engineering. Biomaterials. 2004;25(2):5821-5830.
16. Wu X, Rabkin-Aikawa E, Guleserian KJ, et al. Tissue-engineered microvessels on three-dimensional biodegradable scaffolds using human endothelial progenitor cells. Am J Physiol Heart Circ Physiol. 2004;287(2):H480-H487.
17. Xia W, Liu W, Cui L, et al. Tissue engineering of cartilage with the use of chitosan-gelatin complex scaffolds. J Biomed Mater Res B Appl Biomater. 2004;71(2):373-380.
18. Laurencin CT, Kumbar SG, Nukavarapu SP. Nanotechnology and orthopedics: a personal perspective. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2009;1(1):6-10.
19. Webster TJ, Ejiofor JU. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials. 2004;25(19):4731-4739.
20. Webster TJ, Ergun C, Doremus RH, Siegel RW, Bizios R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials. 2000;21(17):1803-1810.
21. Stewart S, Barr S, Engiles J, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: a proof-of-concept study. J Bone Joint Surg Am. 2012;94(15):1406-1415.
22. Hickok NJ, Shapiro IM. Immobilized antibiotics to prevent orthopaedic implant infections. Adv Drug Deliv Rev. 2012;64(12):1165-1176.
23. DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ. 2003;22(2):151-185.
24. Vines T, Faunce T. Assessing the safety and cost-effectiveness of early nanodrugs. J Law Med. 2009;16(5):822-845.
25. Nel A, Xia T, Mädler L, Li N. Toxic potential of materials at the nanolevel. Science. 2006;311(5761):622-627.
26. Nanomedicine Market (Neurology, Cardiovascular, Anti-Inflammatory, Anti-Infective, and Oncology Applications): Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013-2019. Transparency Market Research website. http://www.transparencymarketresearch.com/nanomedicine-market.html. Published August 1, 2014. Accessed January 20, 2015.
27. Sullivan MP, McHale KJ, Parvizi J, Mehta S. Nanotechnology: current concepts in orthopaedic surgery and future directions. Bone Joint J. 2014;96-B(5):569-573.
28. Pleshko N, Grande DA, Myers KR. Nanotechnology in orthopaedics. J Am Acad Orthop Surg. 2012;20(1):60-62.
Intragrade Intramedullary Nailing of an Open Tibial Shaft Fracture in a Patient With Concomitant Ipsilateral Total Knee Arthroplasty
Fracture of the tibial shaft below an ipsilateral total knee arthroplasty (TKA) is an infrequently occurring injury pattern that presents a unique treatment scenario. The high predilection for open wounds associated with these diaphyseal fractures further complicates the treatment algorithm.1,2 The standard principles of treatment for open tibial shaft fractures entail open fracture débridement followed by adequate fracture reduction and stable skeletal fixation in a manner that limits adverse complications of this injury, which include nonunion, malunion, infection, soft-tissue compromise, and reoperation.3,4
Antegrade intramedullary (IM) tibial nailing has become standard treatment for tibial shaft fractures.5-7 This minimally invasive method of fixation limits damage to the soft-tissue envelope, provides superior neutralization of the mechanical forces to provide a template for biologic fracture healing, and allows the best options for revision procedures in the event of inadequate healing. This case report examines treatment options for an open tibial shaft fracture of an ipsilateral TKA, complicating the standard treatment of antegrade tibial nailing. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old woman became light-headed and fell down a flight of stairs at her home. She was taken to the local emergency room where she presented with left leg pain, deformity, and a skin wound. The wound was dressed with sterile gauze and the extremity immobilized in a temporary plaster splint after which the patient was transferred to our level I trauma center. The accident occurred shortly after dawn, and she received definitive evaluation at the level I trauma center before noon the same day, making the time from injury to evaluation less than 6 hours.
The patient’s medical history was significant for depressive and anxiety disorders, fibromyalgia, hypertension, peripheral vascular disease, and lymphedema. Her surgical history was significant for a remote left TKA and remote open reduction with internal fixation of a left lateral malleolus fracture. She was prescribed antidepressant and anti-anxiolytic medications, narcotic medication, and antihypertensive therapy. She smoked 1 pack of cigarettes per day for approximately 20 years and denied alcohol consumption or illicit drug use. Her body mass index was 37.5, and she ambulated independently in the community.
Upon presentation at our hospital, the patient was hemodynamically stable with no discernable systemic compromise from the extremity injury. An examination of the left lower extremity showed a large longitudinal skin wound over the anteromedial surface of the lower leg measuring roughly 10 cm in length with obvious periosteal stripping and protrusion of the proximal fracture segment. Neurologic motor and sensory function was intact in the lower extremities and pulses were strong. Lower leg compartments were soft. Radiographic imaging confirmed a short oblique fracture of the distal third of the tibial diaphysis. The left TKA was intact with no signs of component loosening or periprosthetic fracture (Figures 1A, 1B).
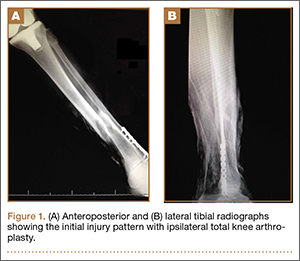
The patient urgently received broad-spectrum antibiotics with intravenous (IV) cefazolin and IV gentamicin as well as tetanus vaccination. Her fracture was temporarily stabilized in a long-leg splint before she was transported to the operating room. Based upon the characteristics of the patient and the open fracture, we had an extensive discussion with the patient regarding the severity of her injury and treatment options, including nonoperative treatment, operative irrigation and débridement with skeletal stabilization, or below-knee amputation. The patient was adamant that limb salvage be attempted despite adequate understanding that she was exposing herself to risk of multiple reoperations from potential complications, as well as systemic medical compromise. Thus, we considered possible techniques for internal fixation of the tibial shaft fracture and treatment of the open wound.
Two primary technical concerns were addressed in the preoperative planning phase: the first was the need for primary closure of the open wound. This patient had a large wound over the anteromedial surface of the distal third of the tibia with scant soft-tissue coverage. Consequently, skin graft alone would not be adequate. While a muscle flap is another option, it would be prone to failure because of the patient’s age and comorbidities, including hypertension, peripheral vascular disease, lymphedema, and tobacco use. Therefore, we hoped to achieve primary closure. Our second major concern was that the method of fixation must be biomechanically sound without impeding our first goal of primary wound closure. In the setting of an ipsilateral TKA, standard antegrade IM nail fixation would not be possible. While we considered plate fixation, it is biomechanically less stable than an IM nail, and we had great concerns about wound complications. External fixation—uniplanar and mutliplanar (eg, Ilizarov)—was limited by issues of long-term fracture stability and risk of pin-site infection. Both methods appeared less desirable compared with IM nail fixation. Thus, we devised an innovative technique to implant an IM nail into the tibial canal.
The operative procedure first entailed standard open fracture care comprising débridement of nonviable soft tissue from the traumatic anteromedial tibial wound, curettage of the fractured bone ends, and irrigation with pulse-jet lavage. Then, we turned to reduction and internal fixation of the bony injury. The large traumatic wound was not extended and was used as the primary surgical approach to permit introduction of the IM nail into the canal. Through the traumatic wound, we performed limited reaming of the proximal and distal fracture segments. Using a cannulated technique over guide wires, we reamed to 11 mm (Figure 2). The tourniquet was not used during the IM reaming. We determined the maximum nail length (approximately 22 cm) by measuring the distance from the fracture to the bone interface with the tibial component. We used a 10×200-mm femoral retrograde Synthes nail (Synthes, Inc, West Chester, Pennsylvania) for the procedure, although we considered an IM humerus nail. Through the traumatic wound, the nail was advanced in its entirety into the proximal tibial segment (Figure 3). The fracture was reduced anatomically and held with a bone tenaculum (Figures 4A, 4B). A medial cortical window proximal to the proximal extent of the IM nail was created through which the Synthes IM reduction tool (aluminum femoral finger) was advanced to impact the IM nail antegrade through the fracture site into the distal segment (Figure 5). After placement of the nail was complete, the excised fragment of bone was reinserted into the cortical window. The Synthes IM reduction tool was chosen for its diameter, length, and, most important, its relative flexibility. While maintaining reduction of the fracture, cross-locking of the nail was performed at the distal and proximal ends with perfect circle technique through stab incisions. Length, alignment, and rotation of the affected tibia were deemed symmetric to the contralateral side based on preoperative clinical measurements. Final fluoroscopic images showed appropriate alignment and proper implant placement.


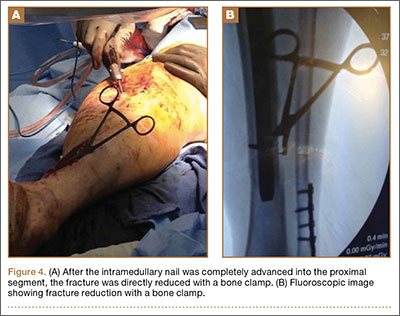
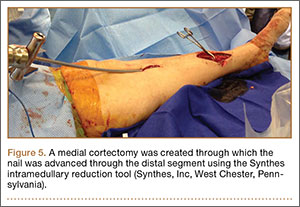
Following open reduction and internal fixation of the fracture, the traumatic and surgical wounds were closed in a layered fashion. A subcutaneous drain and an incisional vacuum-assisted closure (VAC) device were applied to the closed traumatic wound, and a second subcutaneous drain was placed at the site of the cortical window. The patient tolerated the procedure well without perioperative complications.
In the acute period after surgery, the patient’s neurologic and vascular status remained stable. Her muscular compartments remained soft and compressible on physical examination, and her pain was well controlled. The incisional VAC and the 2 Hemovac drains were removed within a few days of the operation. Intravenous cefazolin was continued through her hospital stay and she was transitioned to oral cephalexin at discharge as recommended by our infectious disease colleagues to complete a 10-day course of antibiotic therapy.
At the time of discharge—within 1 week of her initial injury—the patient’s wounds were dry and she was ambulatory with a walker. She was instructed to remain non-weight-bearing and to keep her wounds clean and dry with follow-up in 2 weeks. Over 6 to 8 weeks after surgery, the patient’s weight-bearing status was gradually advanced to full weight-bearing, and she achieved union of the fracture and uneventful healing of the traumatic wound (Figures 6A, 6B, 7).
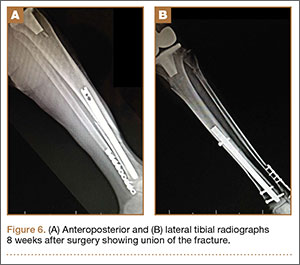

Discussion
We have presented a case of an open distal-third tibial shaft fracture in a 66-year-old obese woman with an ipsilateral TKA. Open fracture of the tibial shaft is potentially limb-threatening because of the challenging management of the bone and soft-tissue injury. The presence of an ipsilateral TKA adds a degree of complexity. From a biomechanical standpoint, the lower interdigitation of cortical bone, coupled with weight-bearing of the lower extremity, subjects the tibia diaphysis to issues of rotation, length, and angular control.8 Due to the diaphyseal nature of the fracture, consisting of cortical bone with comparably lower vascularity and a small soft-tissue envelope, these fractures heal very slowly and often take as many as 6 to 9 months to achieve union.9,10 Furthermore, as was the case here, short oblique fractures of the tibial shaft often occur under bending stresses that also cause significant damage to the tibial soft-tissue envelope and periosteum, as indicated by the open wound. This disruption deprives the fracture and soft tissues of important vascular supply that is critical to healing and to avoiding infection and soft-tissue necrosis.11-13 The effects of treatment may magnify these biomechanical and biologic consequences. Ideal fixation serves to minimize potential complications by neutralizing the biomechanical forces to permit fracture healing while also limiting the amount of soft-tissue trauma and tension. Because the challenges associated with treatment of open tibial shaft fractures make it a limb-threatening injury in a patient with poor peripheral circulation, it is appropriate to consider primary amputation.14
If circumstances warrant an attempt at limb salvage, IM nailing with static interlocking screws would typically be the standard of care for treatment of an open fracture of the tibia shaft. This provides stable internal fixation that controls tibial alignment in 6° of freedom and neutralizes bending forces with less strain on the implant because of the IM position.15,16 In addition to superior neutralization of the biomechanical forces, IM nailing is also a minimally invasive approach that limits further trauma to the periosteum and soft-tissue envelope surrounding the fracture site. This optimizes biologic fracture healing and minimizes complications of malunion, infection, and nonunion.17-19 Moreover, by limiting further damage to the surrounding soft tissue, there is a diminished need for a plastic surgery procedure to reestablish soft-tissue integrity overlying the fracture site. This is particularly advantageous in patients with medical comorbidities that make skin grafts and muscle flaps less likely to succeed. For these reasons, IM nailing was our preferred method of fixation in our patient; however, the presence of an ipsilateral TKA made this standard treatment through an antegrade approach impossible.
Consequently, we considered other methods of fixation, including internal fixation with plate application or external fixation with a multiplanar construct, such as an Ilizarov frame. Some orthopedists consider plate application a superior technique for achieving fracture union because it results in interfragmentary compression, which promotes primary healing. Interestingly, some would argue that the absolute stability provided by the plate may be too rigid a construct to enable optimal fracture healing biology if compression is not achieved.20 However, to allow primary healing to complete fracture union, absolute stability with rigid and strong fixation must be provided. In the tibial shaft, with large bending forces and rotational moments, this is difficult to achieve with plate fixation alone.8 Furthermore, plate application often requires relatively extensive soft-tissue dissection and may impede biologic factors in healing of the bone and soft tissue, increasing the likelihood of infection.21 Finally, adequate plate fixation would significantly increase the soft-tissue volume at this location, further compromising the soft tissues and impeding our goal of primary wound closure.
A uniplanar or mutliplanar external fixator would be an appealing option for definitive fixation because of minimal additional soft-tissue damage that is created during its application. However, it is difficult to achieve adequate stability to encourage either primary, or more commonly, secondary healing in the adult or elderly population.22 An Ilizarov frame is a multiplanar external construct, which allows reconstructive applications because of multiple points of fixation in bone.23 However, the multiple fixation points result in burdensome size of the implant for the patient and requires patient compliance to minimize risk of pin-site infection, which is magnified in a patient with multiple medical comorbid conditions. Furthermore, when comparing treatment options that aim to minimize additional soft-tissue trauma at the site of injury, there is little evidence to show a lower risk of infection at the open fracture site compared with IM nailing.24,25 Thus, in our patient, customary treatment of an open tibial shaft fracture using antegrade IM nailing was not possible, while plate application and external fixation, though potential treatment options, would be relatively contraindicated due to a higher likelihood of failure.
Consequently, primary amputation may be the most appropriate treatment option in a patient with multiple comorbid medical conditions, including peripheral vascular disease. Primary amputation prevents morbidity and mortality associated with complications related to the aforementioned treatment options, as well as limiting risks associated with multiple reoperations.14,25 Studies illustrate that patient functional outcomes after primary amputation are equal to and, in some cases, superior to those patients undergoing limb salvage procedures for open tibial shaft fractures.26-28
Despite the appropriateness of primary amputation in this case, the patient requested limb salvage. Therefore, other innovative treatment options were explored to achieve our goals of primary wound closure and stable internal fixation. Previous case reports have examined retrograde IM nailing as a means of rigidly fixing tibial shaft fractures in the setting of poor soft tissues or ipsilateral knee arthroplasty.29-31 However, the retrograde approach to IM nailing requires passage of reamers through the subtalar and ankle joints, leading to associated arthritis in these joints or, more commonly, rigidity because the final nail position often crosses these joints in addition to the fracture site. Therefore, a novel approach for IM nailing was performed using the large open-fracture wound. Through the traumatic wound, open-fracture débridement was first performed, followed by placement of a nail into the medullary canal with little additional disruption of the surrounding periosteum or soft tissue.
Possible complications of this novel method for IM nail passage warrant discussion. First, potentially unfavorable aspects associated with IM reaming include impairment of endosteal blood circulation in the subacute postoperative period.32-34 If the patient develops complications, such as deep infection, nonunion, hardware failure, or periprosthetic fracture, treatment options that require removal of the nail would be very difficult to execute because this nail was passed “intragrade,” or through the fracture site, not from the knee or the calcaneus. However, unique to this case of intragrade nailing, complications associated with the proximal cortical window may occur. In particular, unintended cortical fracture may happen during impaction of the nail into the distal segment of the fracture after reduction. However, this complication may be avoided with the use of a 1-cm wide and 2-cm long window and the use of the malleable aluminum femoral finger (Synthes). Furthermore, use of a femoral nail is recommended because the Herzog curve of a tibial nail cannot be inserted in the proximal tibial segment using an “intragrade” nailing technique. However, fracture may occur intraoperatively or during rehabilitation after surgery because the cortical window creates a region of high stress distal to the tibial arthroplasty component. Likewise, the area of bone between the proximal extent of the IM nail and tibial component of the TKA represents an area of high stress susceptible to periprosthetic fracture.
Conclusion
We have presented a case of a high-energy open distal tibial diaphyseal fracture in a 66-year-old woman with medical comorbidities and treatment complicated by the presence of an ipsilateral TKA. Intramedullary nailing has become the standard of care for open fractures of the tibial diaphysis because of the high rate of union with little additional soft-tissue damage at the fracture site. Despite these advantages, the ipsilateral TKA complicated the placement of an antegrade tibial nail. An alternative treatment, such as an external fixation using an Ilizarov frame, would present equally challenging treatment aspects, including patient compliance, with little proven benefit over an IM nail. Application of a plate would be less desirable because of increased risk of infection at the fracture site, soft-tissue and periosteum disruption, and muscle necrosis compared with other treatment options. Primary amputation was an appropriate consideration for this patient given her comorbid medical circumstances, but the patient refused this treatment option. Therefore, we created a novel approach to place an IM nail, using the traumatic wound to achieve access to the medullary canal proximally and distally.
1. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop. 1989;243:36-40.
2. Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br. 1995;77(3):417-421.
3. Puno RM, Teynor JT, Nagano J, Gustilo RB. Critical analysis of results of treatment of 201 tibial shaft fractures. Clin Orthop. 1986;212:113-121.
4. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhal JL, Mehta S. Open tibial shaft fractures: I. Evaluation and initial wound management. J Am Acad Orthop Surg. 2010;18(1):10-19.
5. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
6. SPRINT Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): study rationale and design. BMC Musculoskelet Disord. 2008;9:91.
7. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008;90(12):2567-2578.
8. Burr DB, Milgrom C, Fyhrie D, et al. In vivo measurement of human tibial strains during vigorous activity. Bone. 1996;18(5):405-410.
9. Edwards P. Fracture of the shaft of the tibia: 492 consecutive cases in adults: Importance of soft tissue injury. Acta Orthop Scand (Suppl). 1965;76(suppl 76):1-82.
10. Papakostidis C, Kanakaris NK, Pretel J, Faour O, Morell DJ, Giannoudis PV. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo–Anderson classification. Injury. 2011;42(12):1408-1415.
11. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742-746.
12. DeLong WG Jr, Born CT, Wei SY, Petrik ME, Ponzio R, Schwab CW. Aggressive treatment of 119 open fracture wounds. J Trauma. 1999;46(6):1049-1054.
13. Tielinen L, Lindahl JE, Tukiainen EJ. Acute unreamed intramedullary nailing and soft tissue reconstruction with muscle flaps for the treatment of severe open tibial shaft fractures. Injury. 2007;38(8):906-912.
14. Georgiadis GM, Behrens FF, Joyce MJ, Earle AS, Simmons AL. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. J Bone Joint Surg Am. 1993;75(10):1431-1441.
15. Hansen M, Mehler D, Hessmann MH, Blum J, Rommens PM. Intramedullary stabilization of extraarticular proximal tibial fractures: a biomechanical comparison of intramedullary and extramedullary implants including a new proximal tibia nail (PTN). J Orthop Trauma. 2007;21(10):701-709.
16. Hoegel FW, Hoffmann S, Weninger P, Bühren V, Augat P. Biomechanical comparison of locked plate osteosynthesis, reamed and unreamed nailing in conventional interlocking technique, and unreamed angle stable nailing in distal tibia fractures. J Trauma Acute Care Surg. 2012;73(4):933-938.
17. Brumback RJ, Reilly JP, Poka A, Lakatos RP, Bathon GH, Burgess AR. Intramedullary nailing of femoral shaft fractures. Part 1: Decision-making errors with interlocking fixation. J Bone Joint Surg Am. 1988;70(10):1441-1452.
18. Hooper GJ, Keddell RG, Penny ID. Conservative management or closed nailing for tibial shaft fractures. A randomised prospective trial. J Bone Joint Surg Br. 1991;73(1):83-85.
19. Karladani AH, Granhed H, Edshage B, Jerre R, Styf J. Displaced tibial shaft fractures: a prospective randomized study of closed intramedullary nailing versus cast treatment in 53 patients. Acta Orthop Scand. 2000;71(12):160-167.
20. Kenwright J, Richardson JB, Goodship AE, et al. Effect of controlled axial micromovement on healing of tibial fractures. Lancet. 1986;22(8517):1185-1187.
21. Im GI, Tae SK. Distal metaphyseal fractures of tibia: a prospective randomized trial of closed reduction and intramedullary nail versus open reduction and plate and screws fixation. J Trauma. 2005;59(5):1219-1223.
22. Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998;12(1):1-7.
23. Ramos T, Ekholm C, Eriksson BI, Karlsson J, Nistor L. The Ilizarov external fixator - a useful alternative for the treatment of proximal tibial fractures. A prospective observational study of 30 consecutive patients. BMC Musculoskelet Disord. 2013;14:11.
24. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
25. Webb LX, Bosse MJ, Castillo RC, MacKenzie EJ; LEAP Study Group. Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am. 2007;89(5):923-928.
26. Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P, Browner BD. The medical and economic impact of severely injured lower extremities. J Trauma. 1988;28(8):1270-1273.
27. Bosse MJ, MacKenzie EJ, Kellam JF, et al. An analysis of outcomes of reconstruction or amputation of leg-threatening injuries. N Engl J Med. 2002;347(24):1924-1931.
28. MacKenzie EJ, Bosse MJ, Pollak AN, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg Am. 2005;87(8):1801-1809.
29. Doulens KM, Joshi AB, Wagner RA. Tibial fracture after total knee arthroplasty treated with retrograde intramedullary fixation. Am J Orthop. 2007;36(7):E111-E113.
30. Zafra-Jiménez JA, Pretell-Mazzini J, Resines-Erasun C. Distal tibial fracture below a total knee arthroplasty: retrograde intramedullary nailing as an alternative method of treatment: a case report. J Orthop Trauma. 2011;25(7):e74-e76.
31. Loosen S, Preuss S, Zelle BA, Pape HC, Tarken IS. Multimorbid patients with poor soft tissue conditions: Treatment of distal tibia fractures with retrograde intramedullary nailing. Unfallchirurg. 2012;116(6):553-558.
32. Kessler SB, Hallfeldt KJ, Perren SM, Schweiberer L. The effects of reaming and intramedullary nailing on fracture healing. Clin Orthop. 1986;212:18-25.
33. Klein MP, Rahn BA, Frigg R, Kessler S, Perren SM. Reaming versus non-reaming in medullary nailing: interference with cortical circulation of the canine tibia. Arch Orthop Trauma Surg. 1990;109(6):314-316.
34. Reichert IL, McCarthy ID, Hughes SP. The acute vascular response to intramedullary reaming. Microsphere estimation of blood flow in the intact ovine tibia. J Bone Joint Surg Br. 1995;77(3):490-493.
Fracture of the tibial shaft below an ipsilateral total knee arthroplasty (TKA) is an infrequently occurring injury pattern that presents a unique treatment scenario. The high predilection for open wounds associated with these diaphyseal fractures further complicates the treatment algorithm.1,2 The standard principles of treatment for open tibial shaft fractures entail open fracture débridement followed by adequate fracture reduction and stable skeletal fixation in a manner that limits adverse complications of this injury, which include nonunion, malunion, infection, soft-tissue compromise, and reoperation.3,4
Antegrade intramedullary (IM) tibial nailing has become standard treatment for tibial shaft fractures.5-7 This minimally invasive method of fixation limits damage to the soft-tissue envelope, provides superior neutralization of the mechanical forces to provide a template for biologic fracture healing, and allows the best options for revision procedures in the event of inadequate healing. This case report examines treatment options for an open tibial shaft fracture of an ipsilateral TKA, complicating the standard treatment of antegrade tibial nailing. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old woman became light-headed and fell down a flight of stairs at her home. She was taken to the local emergency room where she presented with left leg pain, deformity, and a skin wound. The wound was dressed with sterile gauze and the extremity immobilized in a temporary plaster splint after which the patient was transferred to our level I trauma center. The accident occurred shortly after dawn, and she received definitive evaluation at the level I trauma center before noon the same day, making the time from injury to evaluation less than 6 hours.
The patient’s medical history was significant for depressive and anxiety disorders, fibromyalgia, hypertension, peripheral vascular disease, and lymphedema. Her surgical history was significant for a remote left TKA and remote open reduction with internal fixation of a left lateral malleolus fracture. She was prescribed antidepressant and anti-anxiolytic medications, narcotic medication, and antihypertensive therapy. She smoked 1 pack of cigarettes per day for approximately 20 years and denied alcohol consumption or illicit drug use. Her body mass index was 37.5, and she ambulated independently in the community.
Upon presentation at our hospital, the patient was hemodynamically stable with no discernable systemic compromise from the extremity injury. An examination of the left lower extremity showed a large longitudinal skin wound over the anteromedial surface of the lower leg measuring roughly 10 cm in length with obvious periosteal stripping and protrusion of the proximal fracture segment. Neurologic motor and sensory function was intact in the lower extremities and pulses were strong. Lower leg compartments were soft. Radiographic imaging confirmed a short oblique fracture of the distal third of the tibial diaphysis. The left TKA was intact with no signs of component loosening or periprosthetic fracture (Figures 1A, 1B).
The patient urgently received broad-spectrum antibiotics with intravenous (IV) cefazolin and IV gentamicin as well as tetanus vaccination. Her fracture was temporarily stabilized in a long-leg splint before she was transported to the operating room. Based upon the characteristics of the patient and the open fracture, we had an extensive discussion with the patient regarding the severity of her injury and treatment options, including nonoperative treatment, operative irrigation and débridement with skeletal stabilization, or below-knee amputation. The patient was adamant that limb salvage be attempted despite adequate understanding that she was exposing herself to risk of multiple reoperations from potential complications, as well as systemic medical compromise. Thus, we considered possible techniques for internal fixation of the tibial shaft fracture and treatment of the open wound.
Two primary technical concerns were addressed in the preoperative planning phase: the first was the need for primary closure of the open wound. This patient had a large wound over the anteromedial surface of the distal third of the tibia with scant soft-tissue coverage. Consequently, skin graft alone would not be adequate. While a muscle flap is another option, it would be prone to failure because of the patient’s age and comorbidities, including hypertension, peripheral vascular disease, lymphedema, and tobacco use. Therefore, we hoped to achieve primary closure. Our second major concern was that the method of fixation must be biomechanically sound without impeding our first goal of primary wound closure. In the setting of an ipsilateral TKA, standard antegrade IM nail fixation would not be possible. While we considered plate fixation, it is biomechanically less stable than an IM nail, and we had great concerns about wound complications. External fixation—uniplanar and mutliplanar (eg, Ilizarov)—was limited by issues of long-term fracture stability and risk of pin-site infection. Both methods appeared less desirable compared with IM nail fixation. Thus, we devised an innovative technique to implant an IM nail into the tibial canal.
The operative procedure first entailed standard open fracture care comprising débridement of nonviable soft tissue from the traumatic anteromedial tibial wound, curettage of the fractured bone ends, and irrigation with pulse-jet lavage. Then, we turned to reduction and internal fixation of the bony injury. The large traumatic wound was not extended and was used as the primary surgical approach to permit introduction of the IM nail into the canal. Through the traumatic wound, we performed limited reaming of the proximal and distal fracture segments. Using a cannulated technique over guide wires, we reamed to 11 mm (Figure 2). The tourniquet was not used during the IM reaming. We determined the maximum nail length (approximately 22 cm) by measuring the distance from the fracture to the bone interface with the tibial component. We used a 10×200-mm femoral retrograde Synthes nail (Synthes, Inc, West Chester, Pennsylvania) for the procedure, although we considered an IM humerus nail. Through the traumatic wound, the nail was advanced in its entirety into the proximal tibial segment (Figure 3). The fracture was reduced anatomically and held with a bone tenaculum (Figures 4A, 4B). A medial cortical window proximal to the proximal extent of the IM nail was created through which the Synthes IM reduction tool (aluminum femoral finger) was advanced to impact the IM nail antegrade through the fracture site into the distal segment (Figure 5). After placement of the nail was complete, the excised fragment of bone was reinserted into the cortical window. The Synthes IM reduction tool was chosen for its diameter, length, and, most important, its relative flexibility. While maintaining reduction of the fracture, cross-locking of the nail was performed at the distal and proximal ends with perfect circle technique through stab incisions. Length, alignment, and rotation of the affected tibia were deemed symmetric to the contralateral side based on preoperative clinical measurements. Final fluoroscopic images showed appropriate alignment and proper implant placement.
Following open reduction and internal fixation of the fracture, the traumatic and surgical wounds were closed in a layered fashion. A subcutaneous drain and an incisional vacuum-assisted closure (VAC) device were applied to the closed traumatic wound, and a second subcutaneous drain was placed at the site of the cortical window. The patient tolerated the procedure well without perioperative complications.
In the acute period after surgery, the patient’s neurologic and vascular status remained stable. Her muscular compartments remained soft and compressible on physical examination, and her pain was well controlled. The incisional VAC and the 2 Hemovac drains were removed within a few days of the operation. Intravenous cefazolin was continued through her hospital stay and she was transitioned to oral cephalexin at discharge as recommended by our infectious disease colleagues to complete a 10-day course of antibiotic therapy.
At the time of discharge—within 1 week of her initial injury—the patient’s wounds were dry and she was ambulatory with a walker. She was instructed to remain non-weight-bearing and to keep her wounds clean and dry with follow-up in 2 weeks. Over 6 to 8 weeks after surgery, the patient’s weight-bearing status was gradually advanced to full weight-bearing, and she achieved union of the fracture and uneventful healing of the traumatic wound (Figures 6A, 6B, 7).
Discussion
We have presented a case of an open distal-third tibial shaft fracture in a 66-year-old obese woman with an ipsilateral TKA. Open fracture of the tibial shaft is potentially limb-threatening because of the challenging management of the bone and soft-tissue injury. The presence of an ipsilateral TKA adds a degree of complexity. From a biomechanical standpoint, the lower interdigitation of cortical bone, coupled with weight-bearing of the lower extremity, subjects the tibia diaphysis to issues of rotation, length, and angular control.8 Due to the diaphyseal nature of the fracture, consisting of cortical bone with comparably lower vascularity and a small soft-tissue envelope, these fractures heal very slowly and often take as many as 6 to 9 months to achieve union.9,10 Furthermore, as was the case here, short oblique fractures of the tibial shaft often occur under bending stresses that also cause significant damage to the tibial soft-tissue envelope and periosteum, as indicated by the open wound. This disruption deprives the fracture and soft tissues of important vascular supply that is critical to healing and to avoiding infection and soft-tissue necrosis.11-13 The effects of treatment may magnify these biomechanical and biologic consequences. Ideal fixation serves to minimize potential complications by neutralizing the biomechanical forces to permit fracture healing while also limiting the amount of soft-tissue trauma and tension. Because the challenges associated with treatment of open tibial shaft fractures make it a limb-threatening injury in a patient with poor peripheral circulation, it is appropriate to consider primary amputation.14
If circumstances warrant an attempt at limb salvage, IM nailing with static interlocking screws would typically be the standard of care for treatment of an open fracture of the tibia shaft. This provides stable internal fixation that controls tibial alignment in 6° of freedom and neutralizes bending forces with less strain on the implant because of the IM position.15,16 In addition to superior neutralization of the biomechanical forces, IM nailing is also a minimally invasive approach that limits further trauma to the periosteum and soft-tissue envelope surrounding the fracture site. This optimizes biologic fracture healing and minimizes complications of malunion, infection, and nonunion.17-19 Moreover, by limiting further damage to the surrounding soft tissue, there is a diminished need for a plastic surgery procedure to reestablish soft-tissue integrity overlying the fracture site. This is particularly advantageous in patients with medical comorbidities that make skin grafts and muscle flaps less likely to succeed. For these reasons, IM nailing was our preferred method of fixation in our patient; however, the presence of an ipsilateral TKA made this standard treatment through an antegrade approach impossible.
Consequently, we considered other methods of fixation, including internal fixation with plate application or external fixation with a multiplanar construct, such as an Ilizarov frame. Some orthopedists consider plate application a superior technique for achieving fracture union because it results in interfragmentary compression, which promotes primary healing. Interestingly, some would argue that the absolute stability provided by the plate may be too rigid a construct to enable optimal fracture healing biology if compression is not achieved.20 However, to allow primary healing to complete fracture union, absolute stability with rigid and strong fixation must be provided. In the tibial shaft, with large bending forces and rotational moments, this is difficult to achieve with plate fixation alone.8 Furthermore, plate application often requires relatively extensive soft-tissue dissection and may impede biologic factors in healing of the bone and soft tissue, increasing the likelihood of infection.21 Finally, adequate plate fixation would significantly increase the soft-tissue volume at this location, further compromising the soft tissues and impeding our goal of primary wound closure.
A uniplanar or mutliplanar external fixator would be an appealing option for definitive fixation because of minimal additional soft-tissue damage that is created during its application. However, it is difficult to achieve adequate stability to encourage either primary, or more commonly, secondary healing in the adult or elderly population.22 An Ilizarov frame is a multiplanar external construct, which allows reconstructive applications because of multiple points of fixation in bone.23 However, the multiple fixation points result in burdensome size of the implant for the patient and requires patient compliance to minimize risk of pin-site infection, which is magnified in a patient with multiple medical comorbid conditions. Furthermore, when comparing treatment options that aim to minimize additional soft-tissue trauma at the site of injury, there is little evidence to show a lower risk of infection at the open fracture site compared with IM nailing.24,25 Thus, in our patient, customary treatment of an open tibial shaft fracture using antegrade IM nailing was not possible, while plate application and external fixation, though potential treatment options, would be relatively contraindicated due to a higher likelihood of failure.
Consequently, primary amputation may be the most appropriate treatment option in a patient with multiple comorbid medical conditions, including peripheral vascular disease. Primary amputation prevents morbidity and mortality associated with complications related to the aforementioned treatment options, as well as limiting risks associated with multiple reoperations.14,25 Studies illustrate that patient functional outcomes after primary amputation are equal to and, in some cases, superior to those patients undergoing limb salvage procedures for open tibial shaft fractures.26-28
Despite the appropriateness of primary amputation in this case, the patient requested limb salvage. Therefore, other innovative treatment options were explored to achieve our goals of primary wound closure and stable internal fixation. Previous case reports have examined retrograde IM nailing as a means of rigidly fixing tibial shaft fractures in the setting of poor soft tissues or ipsilateral knee arthroplasty.29-31 However, the retrograde approach to IM nailing requires passage of reamers through the subtalar and ankle joints, leading to associated arthritis in these joints or, more commonly, rigidity because the final nail position often crosses these joints in addition to the fracture site. Therefore, a novel approach for IM nailing was performed using the large open-fracture wound. Through the traumatic wound, open-fracture débridement was first performed, followed by placement of a nail into the medullary canal with little additional disruption of the surrounding periosteum or soft tissue.
Possible complications of this novel method for IM nail passage warrant discussion. First, potentially unfavorable aspects associated with IM reaming include impairment of endosteal blood circulation in the subacute postoperative period.32-34 If the patient develops complications, such as deep infection, nonunion, hardware failure, or periprosthetic fracture, treatment options that require removal of the nail would be very difficult to execute because this nail was passed “intragrade,” or through the fracture site, not from the knee or the calcaneus. However, unique to this case of intragrade nailing, complications associated with the proximal cortical window may occur. In particular, unintended cortical fracture may happen during impaction of the nail into the distal segment of the fracture after reduction. However, this complication may be avoided with the use of a 1-cm wide and 2-cm long window and the use of the malleable aluminum femoral finger (Synthes). Furthermore, use of a femoral nail is recommended because the Herzog curve of a tibial nail cannot be inserted in the proximal tibial segment using an “intragrade” nailing technique. However, fracture may occur intraoperatively or during rehabilitation after surgery because the cortical window creates a region of high stress distal to the tibial arthroplasty component. Likewise, the area of bone between the proximal extent of the IM nail and tibial component of the TKA represents an area of high stress susceptible to periprosthetic fracture.
Conclusion
We have presented a case of a high-energy open distal tibial diaphyseal fracture in a 66-year-old woman with medical comorbidities and treatment complicated by the presence of an ipsilateral TKA. Intramedullary nailing has become the standard of care for open fractures of the tibial diaphysis because of the high rate of union with little additional soft-tissue damage at the fracture site. Despite these advantages, the ipsilateral TKA complicated the placement of an antegrade tibial nail. An alternative treatment, such as an external fixation using an Ilizarov frame, would present equally challenging treatment aspects, including patient compliance, with little proven benefit over an IM nail. Application of a plate would be less desirable because of increased risk of infection at the fracture site, soft-tissue and periosteum disruption, and muscle necrosis compared with other treatment options. Primary amputation was an appropriate consideration for this patient given her comorbid medical circumstances, but the patient refused this treatment option. Therefore, we created a novel approach to place an IM nail, using the traumatic wound to achieve access to the medullary canal proximally and distally.
Fracture of the tibial shaft below an ipsilateral total knee arthroplasty (TKA) is an infrequently occurring injury pattern that presents a unique treatment scenario. The high predilection for open wounds associated with these diaphyseal fractures further complicates the treatment algorithm.1,2 The standard principles of treatment for open tibial shaft fractures entail open fracture débridement followed by adequate fracture reduction and stable skeletal fixation in a manner that limits adverse complications of this injury, which include nonunion, malunion, infection, soft-tissue compromise, and reoperation.3,4
Antegrade intramedullary (IM) tibial nailing has become standard treatment for tibial shaft fractures.5-7 This minimally invasive method of fixation limits damage to the soft-tissue envelope, provides superior neutralization of the mechanical forces to provide a template for biologic fracture healing, and allows the best options for revision procedures in the event of inadequate healing. This case report examines treatment options for an open tibial shaft fracture of an ipsilateral TKA, complicating the standard treatment of antegrade tibial nailing. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old woman became light-headed and fell down a flight of stairs at her home. She was taken to the local emergency room where she presented with left leg pain, deformity, and a skin wound. The wound was dressed with sterile gauze and the extremity immobilized in a temporary plaster splint after which the patient was transferred to our level I trauma center. The accident occurred shortly after dawn, and she received definitive evaluation at the level I trauma center before noon the same day, making the time from injury to evaluation less than 6 hours.
The patient’s medical history was significant for depressive and anxiety disorders, fibromyalgia, hypertension, peripheral vascular disease, and lymphedema. Her surgical history was significant for a remote left TKA and remote open reduction with internal fixation of a left lateral malleolus fracture. She was prescribed antidepressant and anti-anxiolytic medications, narcotic medication, and antihypertensive therapy. She smoked 1 pack of cigarettes per day for approximately 20 years and denied alcohol consumption or illicit drug use. Her body mass index was 37.5, and she ambulated independently in the community.
Upon presentation at our hospital, the patient was hemodynamically stable with no discernable systemic compromise from the extremity injury. An examination of the left lower extremity showed a large longitudinal skin wound over the anteromedial surface of the lower leg measuring roughly 10 cm in length with obvious periosteal stripping and protrusion of the proximal fracture segment. Neurologic motor and sensory function was intact in the lower extremities and pulses were strong. Lower leg compartments were soft. Radiographic imaging confirmed a short oblique fracture of the distal third of the tibial diaphysis. The left TKA was intact with no signs of component loosening or periprosthetic fracture (Figures 1A, 1B).
The patient urgently received broad-spectrum antibiotics with intravenous (IV) cefazolin and IV gentamicin as well as tetanus vaccination. Her fracture was temporarily stabilized in a long-leg splint before she was transported to the operating room. Based upon the characteristics of the patient and the open fracture, we had an extensive discussion with the patient regarding the severity of her injury and treatment options, including nonoperative treatment, operative irrigation and débridement with skeletal stabilization, or below-knee amputation. The patient was adamant that limb salvage be attempted despite adequate understanding that she was exposing herself to risk of multiple reoperations from potential complications, as well as systemic medical compromise. Thus, we considered possible techniques for internal fixation of the tibial shaft fracture and treatment of the open wound.
Two primary technical concerns were addressed in the preoperative planning phase: the first was the need for primary closure of the open wound. This patient had a large wound over the anteromedial surface of the distal third of the tibia with scant soft-tissue coverage. Consequently, skin graft alone would not be adequate. While a muscle flap is another option, it would be prone to failure because of the patient’s age and comorbidities, including hypertension, peripheral vascular disease, lymphedema, and tobacco use. Therefore, we hoped to achieve primary closure. Our second major concern was that the method of fixation must be biomechanically sound without impeding our first goal of primary wound closure. In the setting of an ipsilateral TKA, standard antegrade IM nail fixation would not be possible. While we considered plate fixation, it is biomechanically less stable than an IM nail, and we had great concerns about wound complications. External fixation—uniplanar and mutliplanar (eg, Ilizarov)—was limited by issues of long-term fracture stability and risk of pin-site infection. Both methods appeared less desirable compared with IM nail fixation. Thus, we devised an innovative technique to implant an IM nail into the tibial canal.
The operative procedure first entailed standard open fracture care comprising débridement of nonviable soft tissue from the traumatic anteromedial tibial wound, curettage of the fractured bone ends, and irrigation with pulse-jet lavage. Then, we turned to reduction and internal fixation of the bony injury. The large traumatic wound was not extended and was used as the primary surgical approach to permit introduction of the IM nail into the canal. Through the traumatic wound, we performed limited reaming of the proximal and distal fracture segments. Using a cannulated technique over guide wires, we reamed to 11 mm (Figure 2). The tourniquet was not used during the IM reaming. We determined the maximum nail length (approximately 22 cm) by measuring the distance from the fracture to the bone interface with the tibial component. We used a 10×200-mm femoral retrograde Synthes nail (Synthes, Inc, West Chester, Pennsylvania) for the procedure, although we considered an IM humerus nail. Through the traumatic wound, the nail was advanced in its entirety into the proximal tibial segment (Figure 3). The fracture was reduced anatomically and held with a bone tenaculum (Figures 4A, 4B). A medial cortical window proximal to the proximal extent of the IM nail was created through which the Synthes IM reduction tool (aluminum femoral finger) was advanced to impact the IM nail antegrade through the fracture site into the distal segment (Figure 5). After placement of the nail was complete, the excised fragment of bone was reinserted into the cortical window. The Synthes IM reduction tool was chosen for its diameter, length, and, most important, its relative flexibility. While maintaining reduction of the fracture, cross-locking of the nail was performed at the distal and proximal ends with perfect circle technique through stab incisions. Length, alignment, and rotation of the affected tibia were deemed symmetric to the contralateral side based on preoperative clinical measurements. Final fluoroscopic images showed appropriate alignment and proper implant placement.
Following open reduction and internal fixation of the fracture, the traumatic and surgical wounds were closed in a layered fashion. A subcutaneous drain and an incisional vacuum-assisted closure (VAC) device were applied to the closed traumatic wound, and a second subcutaneous drain was placed at the site of the cortical window. The patient tolerated the procedure well without perioperative complications.
In the acute period after surgery, the patient’s neurologic and vascular status remained stable. Her muscular compartments remained soft and compressible on physical examination, and her pain was well controlled. The incisional VAC and the 2 Hemovac drains were removed within a few days of the operation. Intravenous cefazolin was continued through her hospital stay and she was transitioned to oral cephalexin at discharge as recommended by our infectious disease colleagues to complete a 10-day course of antibiotic therapy.
At the time of discharge—within 1 week of her initial injury—the patient’s wounds were dry and she was ambulatory with a walker. She was instructed to remain non-weight-bearing and to keep her wounds clean and dry with follow-up in 2 weeks. Over 6 to 8 weeks after surgery, the patient’s weight-bearing status was gradually advanced to full weight-bearing, and she achieved union of the fracture and uneventful healing of the traumatic wound (Figures 6A, 6B, 7).
Discussion
We have presented a case of an open distal-third tibial shaft fracture in a 66-year-old obese woman with an ipsilateral TKA. Open fracture of the tibial shaft is potentially limb-threatening because of the challenging management of the bone and soft-tissue injury. The presence of an ipsilateral TKA adds a degree of complexity. From a biomechanical standpoint, the lower interdigitation of cortical bone, coupled with weight-bearing of the lower extremity, subjects the tibia diaphysis to issues of rotation, length, and angular control.8 Due to the diaphyseal nature of the fracture, consisting of cortical bone with comparably lower vascularity and a small soft-tissue envelope, these fractures heal very slowly and often take as many as 6 to 9 months to achieve union.9,10 Furthermore, as was the case here, short oblique fractures of the tibial shaft often occur under bending stresses that also cause significant damage to the tibial soft-tissue envelope and periosteum, as indicated by the open wound. This disruption deprives the fracture and soft tissues of important vascular supply that is critical to healing and to avoiding infection and soft-tissue necrosis.11-13 The effects of treatment may magnify these biomechanical and biologic consequences. Ideal fixation serves to minimize potential complications by neutralizing the biomechanical forces to permit fracture healing while also limiting the amount of soft-tissue trauma and tension. Because the challenges associated with treatment of open tibial shaft fractures make it a limb-threatening injury in a patient with poor peripheral circulation, it is appropriate to consider primary amputation.14
If circumstances warrant an attempt at limb salvage, IM nailing with static interlocking screws would typically be the standard of care for treatment of an open fracture of the tibia shaft. This provides stable internal fixation that controls tibial alignment in 6° of freedom and neutralizes bending forces with less strain on the implant because of the IM position.15,16 In addition to superior neutralization of the biomechanical forces, IM nailing is also a minimally invasive approach that limits further trauma to the periosteum and soft-tissue envelope surrounding the fracture site. This optimizes biologic fracture healing and minimizes complications of malunion, infection, and nonunion.17-19 Moreover, by limiting further damage to the surrounding soft tissue, there is a diminished need for a plastic surgery procedure to reestablish soft-tissue integrity overlying the fracture site. This is particularly advantageous in patients with medical comorbidities that make skin grafts and muscle flaps less likely to succeed. For these reasons, IM nailing was our preferred method of fixation in our patient; however, the presence of an ipsilateral TKA made this standard treatment through an antegrade approach impossible.
Consequently, we considered other methods of fixation, including internal fixation with plate application or external fixation with a multiplanar construct, such as an Ilizarov frame. Some orthopedists consider plate application a superior technique for achieving fracture union because it results in interfragmentary compression, which promotes primary healing. Interestingly, some would argue that the absolute stability provided by the plate may be too rigid a construct to enable optimal fracture healing biology if compression is not achieved.20 However, to allow primary healing to complete fracture union, absolute stability with rigid and strong fixation must be provided. In the tibial shaft, with large bending forces and rotational moments, this is difficult to achieve with plate fixation alone.8 Furthermore, plate application often requires relatively extensive soft-tissue dissection and may impede biologic factors in healing of the bone and soft tissue, increasing the likelihood of infection.21 Finally, adequate plate fixation would significantly increase the soft-tissue volume at this location, further compromising the soft tissues and impeding our goal of primary wound closure.
A uniplanar or mutliplanar external fixator would be an appealing option for definitive fixation because of minimal additional soft-tissue damage that is created during its application. However, it is difficult to achieve adequate stability to encourage either primary, or more commonly, secondary healing in the adult or elderly population.22 An Ilizarov frame is a multiplanar external construct, which allows reconstructive applications because of multiple points of fixation in bone.23 However, the multiple fixation points result in burdensome size of the implant for the patient and requires patient compliance to minimize risk of pin-site infection, which is magnified in a patient with multiple medical comorbid conditions. Furthermore, when comparing treatment options that aim to minimize additional soft-tissue trauma at the site of injury, there is little evidence to show a lower risk of infection at the open fracture site compared with IM nailing.24,25 Thus, in our patient, customary treatment of an open tibial shaft fracture using antegrade IM nailing was not possible, while plate application and external fixation, though potential treatment options, would be relatively contraindicated due to a higher likelihood of failure.
Consequently, primary amputation may be the most appropriate treatment option in a patient with multiple comorbid medical conditions, including peripheral vascular disease. Primary amputation prevents morbidity and mortality associated with complications related to the aforementioned treatment options, as well as limiting risks associated with multiple reoperations.14,25 Studies illustrate that patient functional outcomes after primary amputation are equal to and, in some cases, superior to those patients undergoing limb salvage procedures for open tibial shaft fractures.26-28
Despite the appropriateness of primary amputation in this case, the patient requested limb salvage. Therefore, other innovative treatment options were explored to achieve our goals of primary wound closure and stable internal fixation. Previous case reports have examined retrograde IM nailing as a means of rigidly fixing tibial shaft fractures in the setting of poor soft tissues or ipsilateral knee arthroplasty.29-31 However, the retrograde approach to IM nailing requires passage of reamers through the subtalar and ankle joints, leading to associated arthritis in these joints or, more commonly, rigidity because the final nail position often crosses these joints in addition to the fracture site. Therefore, a novel approach for IM nailing was performed using the large open-fracture wound. Through the traumatic wound, open-fracture débridement was first performed, followed by placement of a nail into the medullary canal with little additional disruption of the surrounding periosteum or soft tissue.
Possible complications of this novel method for IM nail passage warrant discussion. First, potentially unfavorable aspects associated with IM reaming include impairment of endosteal blood circulation in the subacute postoperative period.32-34 If the patient develops complications, such as deep infection, nonunion, hardware failure, or periprosthetic fracture, treatment options that require removal of the nail would be very difficult to execute because this nail was passed “intragrade,” or through the fracture site, not from the knee or the calcaneus. However, unique to this case of intragrade nailing, complications associated with the proximal cortical window may occur. In particular, unintended cortical fracture may happen during impaction of the nail into the distal segment of the fracture after reduction. However, this complication may be avoided with the use of a 1-cm wide and 2-cm long window and the use of the malleable aluminum femoral finger (Synthes). Furthermore, use of a femoral nail is recommended because the Herzog curve of a tibial nail cannot be inserted in the proximal tibial segment using an “intragrade” nailing technique. However, fracture may occur intraoperatively or during rehabilitation after surgery because the cortical window creates a region of high stress distal to the tibial arthroplasty component. Likewise, the area of bone between the proximal extent of the IM nail and tibial component of the TKA represents an area of high stress susceptible to periprosthetic fracture.
Conclusion
We have presented a case of a high-energy open distal tibial diaphyseal fracture in a 66-year-old woman with medical comorbidities and treatment complicated by the presence of an ipsilateral TKA. Intramedullary nailing has become the standard of care for open fractures of the tibial diaphysis because of the high rate of union with little additional soft-tissue damage at the fracture site. Despite these advantages, the ipsilateral TKA complicated the placement of an antegrade tibial nail. An alternative treatment, such as an external fixation using an Ilizarov frame, would present equally challenging treatment aspects, including patient compliance, with little proven benefit over an IM nail. Application of a plate would be less desirable because of increased risk of infection at the fracture site, soft-tissue and periosteum disruption, and muscle necrosis compared with other treatment options. Primary amputation was an appropriate consideration for this patient given her comorbid medical circumstances, but the patient refused this treatment option. Therefore, we created a novel approach to place an IM nail, using the traumatic wound to achieve access to the medullary canal proximally and distally.
1. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop. 1989;243:36-40.
2. Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br. 1995;77(3):417-421.
3. Puno RM, Teynor JT, Nagano J, Gustilo RB. Critical analysis of results of treatment of 201 tibial shaft fractures. Clin Orthop. 1986;212:113-121.
4. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhal JL, Mehta S. Open tibial shaft fractures: I. Evaluation and initial wound management. J Am Acad Orthop Surg. 2010;18(1):10-19.
5. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
6. SPRINT Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): study rationale and design. BMC Musculoskelet Disord. 2008;9:91.
7. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008;90(12):2567-2578.
8. Burr DB, Milgrom C, Fyhrie D, et al. In vivo measurement of human tibial strains during vigorous activity. Bone. 1996;18(5):405-410.
9. Edwards P. Fracture of the shaft of the tibia: 492 consecutive cases in adults: Importance of soft tissue injury. Acta Orthop Scand (Suppl). 1965;76(suppl 76):1-82.
10. Papakostidis C, Kanakaris NK, Pretel J, Faour O, Morell DJ, Giannoudis PV. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo–Anderson classification. Injury. 2011;42(12):1408-1415.
11. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742-746.
12. DeLong WG Jr, Born CT, Wei SY, Petrik ME, Ponzio R, Schwab CW. Aggressive treatment of 119 open fracture wounds. J Trauma. 1999;46(6):1049-1054.
13. Tielinen L, Lindahl JE, Tukiainen EJ. Acute unreamed intramedullary nailing and soft tissue reconstruction with muscle flaps for the treatment of severe open tibial shaft fractures. Injury. 2007;38(8):906-912.
14. Georgiadis GM, Behrens FF, Joyce MJ, Earle AS, Simmons AL. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. J Bone Joint Surg Am. 1993;75(10):1431-1441.
15. Hansen M, Mehler D, Hessmann MH, Blum J, Rommens PM. Intramedullary stabilization of extraarticular proximal tibial fractures: a biomechanical comparison of intramedullary and extramedullary implants including a new proximal tibia nail (PTN). J Orthop Trauma. 2007;21(10):701-709.
16. Hoegel FW, Hoffmann S, Weninger P, Bühren V, Augat P. Biomechanical comparison of locked plate osteosynthesis, reamed and unreamed nailing in conventional interlocking technique, and unreamed angle stable nailing in distal tibia fractures. J Trauma Acute Care Surg. 2012;73(4):933-938.
17. Brumback RJ, Reilly JP, Poka A, Lakatos RP, Bathon GH, Burgess AR. Intramedullary nailing of femoral shaft fractures. Part 1: Decision-making errors with interlocking fixation. J Bone Joint Surg Am. 1988;70(10):1441-1452.
18. Hooper GJ, Keddell RG, Penny ID. Conservative management or closed nailing for tibial shaft fractures. A randomised prospective trial. J Bone Joint Surg Br. 1991;73(1):83-85.
19. Karladani AH, Granhed H, Edshage B, Jerre R, Styf J. Displaced tibial shaft fractures: a prospective randomized study of closed intramedullary nailing versus cast treatment in 53 patients. Acta Orthop Scand. 2000;71(12):160-167.
20. Kenwright J, Richardson JB, Goodship AE, et al. Effect of controlled axial micromovement on healing of tibial fractures. Lancet. 1986;22(8517):1185-1187.
21. Im GI, Tae SK. Distal metaphyseal fractures of tibia: a prospective randomized trial of closed reduction and intramedullary nail versus open reduction and plate and screws fixation. J Trauma. 2005;59(5):1219-1223.
22. Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998;12(1):1-7.
23. Ramos T, Ekholm C, Eriksson BI, Karlsson J, Nistor L. The Ilizarov external fixator - a useful alternative for the treatment of proximal tibial fractures. A prospective observational study of 30 consecutive patients. BMC Musculoskelet Disord. 2013;14:11.
24. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
25. Webb LX, Bosse MJ, Castillo RC, MacKenzie EJ; LEAP Study Group. Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am. 2007;89(5):923-928.
26. Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P, Browner BD. The medical and economic impact of severely injured lower extremities. J Trauma. 1988;28(8):1270-1273.
27. Bosse MJ, MacKenzie EJ, Kellam JF, et al. An analysis of outcomes of reconstruction or amputation of leg-threatening injuries. N Engl J Med. 2002;347(24):1924-1931.
28. MacKenzie EJ, Bosse MJ, Pollak AN, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg Am. 2005;87(8):1801-1809.
29. Doulens KM, Joshi AB, Wagner RA. Tibial fracture after total knee arthroplasty treated with retrograde intramedullary fixation. Am J Orthop. 2007;36(7):E111-E113.
30. Zafra-Jiménez JA, Pretell-Mazzini J, Resines-Erasun C. Distal tibial fracture below a total knee arthroplasty: retrograde intramedullary nailing as an alternative method of treatment: a case report. J Orthop Trauma. 2011;25(7):e74-e76.
31. Loosen S, Preuss S, Zelle BA, Pape HC, Tarken IS. Multimorbid patients with poor soft tissue conditions: Treatment of distal tibia fractures with retrograde intramedullary nailing. Unfallchirurg. 2012;116(6):553-558.
32. Kessler SB, Hallfeldt KJ, Perren SM, Schweiberer L. The effects of reaming and intramedullary nailing on fracture healing. Clin Orthop. 1986;212:18-25.
33. Klein MP, Rahn BA, Frigg R, Kessler S, Perren SM. Reaming versus non-reaming in medullary nailing: interference with cortical circulation of the canine tibia. Arch Orthop Trauma Surg. 1990;109(6):314-316.
34. Reichert IL, McCarthy ID, Hughes SP. The acute vascular response to intramedullary reaming. Microsphere estimation of blood flow in the intact ovine tibia. J Bone Joint Surg Br. 1995;77(3):490-493.
1. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop. 1989;243:36-40.
2. Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br. 1995;77(3):417-421.
3. Puno RM, Teynor JT, Nagano J, Gustilo RB. Critical analysis of results of treatment of 201 tibial shaft fractures. Clin Orthop. 1986;212:113-121.
4. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhal JL, Mehta S. Open tibial shaft fractures: I. Evaluation and initial wound management. J Am Acad Orthop Surg. 2010;18(1):10-19.
5. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
6. SPRINT Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): study rationale and design. BMC Musculoskelet Disord. 2008;9:91.
7. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008;90(12):2567-2578.
8. Burr DB, Milgrom C, Fyhrie D, et al. In vivo measurement of human tibial strains during vigorous activity. Bone. 1996;18(5):405-410.
9. Edwards P. Fracture of the shaft of the tibia: 492 consecutive cases in adults: Importance of soft tissue injury. Acta Orthop Scand (Suppl). 1965;76(suppl 76):1-82.
10. Papakostidis C, Kanakaris NK, Pretel J, Faour O, Morell DJ, Giannoudis PV. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo–Anderson classification. Injury. 2011;42(12):1408-1415.
11. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742-746.
12. DeLong WG Jr, Born CT, Wei SY, Petrik ME, Ponzio R, Schwab CW. Aggressive treatment of 119 open fracture wounds. J Trauma. 1999;46(6):1049-1054.
13. Tielinen L, Lindahl JE, Tukiainen EJ. Acute unreamed intramedullary nailing and soft tissue reconstruction with muscle flaps for the treatment of severe open tibial shaft fractures. Injury. 2007;38(8):906-912.
14. Georgiadis GM, Behrens FF, Joyce MJ, Earle AS, Simmons AL. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. J Bone Joint Surg Am. 1993;75(10):1431-1441.
15. Hansen M, Mehler D, Hessmann MH, Blum J, Rommens PM. Intramedullary stabilization of extraarticular proximal tibial fractures: a biomechanical comparison of intramedullary and extramedullary implants including a new proximal tibia nail (PTN). J Orthop Trauma. 2007;21(10):701-709.
16. Hoegel FW, Hoffmann S, Weninger P, Bühren V, Augat P. Biomechanical comparison of locked plate osteosynthesis, reamed and unreamed nailing in conventional interlocking technique, and unreamed angle stable nailing in distal tibia fractures. J Trauma Acute Care Surg. 2012;73(4):933-938.
17. Brumback RJ, Reilly JP, Poka A, Lakatos RP, Bathon GH, Burgess AR. Intramedullary nailing of femoral shaft fractures. Part 1: Decision-making errors with interlocking fixation. J Bone Joint Surg Am. 1988;70(10):1441-1452.
18. Hooper GJ, Keddell RG, Penny ID. Conservative management or closed nailing for tibial shaft fractures. A randomised prospective trial. J Bone Joint Surg Br. 1991;73(1):83-85.
19. Karladani AH, Granhed H, Edshage B, Jerre R, Styf J. Displaced tibial shaft fractures: a prospective randomized study of closed intramedullary nailing versus cast treatment in 53 patients. Acta Orthop Scand. 2000;71(12):160-167.
20. Kenwright J, Richardson JB, Goodship AE, et al. Effect of controlled axial micromovement on healing of tibial fractures. Lancet. 1986;22(8517):1185-1187.
21. Im GI, Tae SK. Distal metaphyseal fractures of tibia: a prospective randomized trial of closed reduction and intramedullary nail versus open reduction and plate and screws fixation. J Trauma. 2005;59(5):1219-1223.
22. Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998;12(1):1-7.
23. Ramos T, Ekholm C, Eriksson BI, Karlsson J, Nistor L. The Ilizarov external fixator - a useful alternative for the treatment of proximal tibial fractures. A prospective observational study of 30 consecutive patients. BMC Musculoskelet Disord. 2013;14:11.
24. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68.
25. Webb LX, Bosse MJ, Castillo RC, MacKenzie EJ; LEAP Study Group. Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am. 2007;89(5):923-928.
26. Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P, Browner BD. The medical and economic impact of severely injured lower extremities. J Trauma. 1988;28(8):1270-1273.
27. Bosse MJ, MacKenzie EJ, Kellam JF, et al. An analysis of outcomes of reconstruction or amputation of leg-threatening injuries. N Engl J Med. 2002;347(24):1924-1931.
28. MacKenzie EJ, Bosse MJ, Pollak AN, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg Am. 2005;87(8):1801-1809.
29. Doulens KM, Joshi AB, Wagner RA. Tibial fracture after total knee arthroplasty treated with retrograde intramedullary fixation. Am J Orthop. 2007;36(7):E111-E113.
30. Zafra-Jiménez JA, Pretell-Mazzini J, Resines-Erasun C. Distal tibial fracture below a total knee arthroplasty: retrograde intramedullary nailing as an alternative method of treatment: a case report. J Orthop Trauma. 2011;25(7):e74-e76.
31. Loosen S, Preuss S, Zelle BA, Pape HC, Tarken IS. Multimorbid patients with poor soft tissue conditions: Treatment of distal tibia fractures with retrograde intramedullary nailing. Unfallchirurg. 2012;116(6):553-558.
32. Kessler SB, Hallfeldt KJ, Perren SM, Schweiberer L. The effects of reaming and intramedullary nailing on fracture healing. Clin Orthop. 1986;212:18-25.
33. Klein MP, Rahn BA, Frigg R, Kessler S, Perren SM. Reaming versus non-reaming in medullary nailing: interference with cortical circulation of the canine tibia. Arch Orthop Trauma Surg. 1990;109(6):314-316.
34. Reichert IL, McCarthy ID, Hughes SP. The acute vascular response to intramedullary reaming. Microsphere estimation of blood flow in the intact ovine tibia. J Bone Joint Surg Br. 1995;77(3):490-493.
