User login
Retrograde Reamer/Irrigator/Aspirator Technique for Autologous Bone Graft Harvesting With the Patient in the Prone Position
The Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania) has become a powerful tool for harvesting autologous bone graft from the intramedullary canal of the long bones of the lower extremity for the treatment of osseous defects, nonunions, and joint fusions.1,2 The RIA system provides satisfactory quality and quantity of bone graft (range, 40-90 mL)3-5 with osteogenic properties that rival those harvested from the iliac crest.6,7 Minimal donor-site morbidity and mortality have been reported in association with the RIA technique compared with iliac crest bone graft harvest.8
The RIA technique for the femur—with the antegrade approach and the supine position,8 with the antegrade approach and the prone position,9 and with the retrograde approach and the supine position4—has been described in the literature. To our knowledge, however, the RIA technique for the femur with the retrograde approach and the prone position has not been described. Antegrade harvesting uses the trochanteric entry point, and retrograde harvesting uses an entry at the intercondylar notch just anterior to the posterior cruciate ligament. In this article, we detail the technique for RIA harvesting of the femur with the patient in the prone position. Patient positioning is based on the diagnosis and the proposed procedure.
Advantages of a retrograde starting point include a more concentric trajectory (vs that of an antegrade starting point) and more efficient canal pressure reduction, which might decrease the risk of intraoperative fat embolization.10 This technique offers a more efficient solution to any procedure that requires the prone position, and it avoids the need to reposition, reprepare, or redrape the extremity. It is also very useful in treating obese patients.
After obtaining institutional review board (IRB) approval, we retrospectively reviewed patient files. Because the study was retrospective, the IRB waived the requirement for informed consent. The patients described here provided written informed consent for print and electronic publication of these case reports.
Surgical Technique
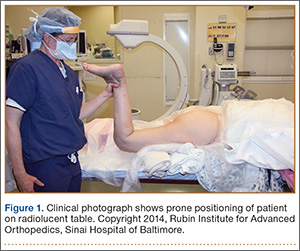
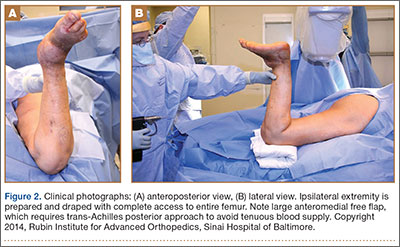
The patient is placed in a prone position on a radiolucent table with a bump under the thigh to allow access to the knee joint with full extension of the hip (Figures 1, 2A, 2B). The knee is then flexed to gain access to the intercondylar notch.
The anatomical axis of the femur is identified in the coronal and sagittal planes with the help of an image intensifier. Frequent intraoperative fluoroscopic imaging is required to prevent eccentric reaming and guide-wire movement from causing iatrogenic fractures and perforations, respectively.8 A 2-mm Steinmann pin is used to identify the point of entry into the femoral canal, which is located just above the posterior cruciate ligament insertion in the intercondylar notch, and care is taken not to ream this structure. A minimally invasive incision of about 15 mm is centered on this pin using a patellar tendon–splitting approach.
An 8-mm cannulated anterior cruciate ligament reamer is passed over the pin to enlarge the opening at the entry point, and a 2.5-mm ball-tipped guide wire is positioned in the femur. The image intensifier is used to confirm positioning of the guide in the trochanteric region and centered in the intramedullary canal. A radiolucent diving board facilitates fluoroscopic imaging.
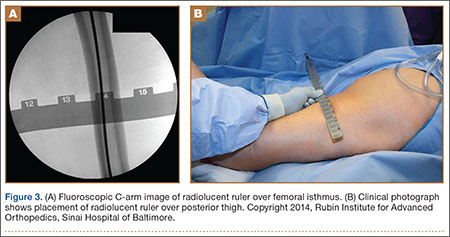
The diameter (12.5 or 16.5 mm) of the reaming head is selected after the intramedullary guide is placed in the femoral canal. The isthmus of the femur is then identified radiographically, and a radiopaque ruler with increments in millimeters is used to measure the canal diameter (Figures 3A, 3B). Because the femoral canal is an ellipsoid, the canal diameter usually is much larger anteroposteriorly than laterally.8 We prefer to use a reaming head that overlaps the inner cortical diameter by 1 mm on each side. An alternative method includes measuring the outer diameter of the narrowest portion of the bone and using a reamer head no more than 45% of the outer diameter at the isthmus.8
The RIA system is prepared on the back table by attaching the reaming head to the irrigation and suction systems. As the reamer head enters the intramedullary canal, an approach–withdraw–pause technique is used to slowly advance the reamer through the femur. It is crucial to use the image intensifier to guide reaming in order to avoid overdrilling the anterior cortex and prevent eccentric reaming of the canal, which more commonly occurs in patients with large anterior femoral bows.11 When the collection filter becomes full, reaming is stopped. The bone graft in the filter is emptied into a specimen cup for measurement and storage until subsequent use (Figure 4). Suctioning is suspended when reaming is stopped because substantial blood loss can occur with prolonged suction and aspiration.12 When repeat reaming is required, care is taken not to overream the cortices, thereby avoiding the risk of iatrogenic fracture.10,12

The knee joint is irrigated to remove any intramedullary debris. Typically there is no debris, as it is captured by the RIA. The wound is closed in 2 layers. Dressing with Ace bandage (3M, St. Paul, Minnesota) is placed around the knee for comfort. Weight-bearing status is determined by the index procedure.
Case Reports
Case 1
A 68-year-old female smoker presented to our facility with right ankle pain after recent ankle arthrodesis for pilon fracture nonunion. Almost 3 years earlier, the patient sustained a Gustilo-Anderson type II open pilon fracture in a motorcycle accident. She underwent antibiotic therapy, irrigation and débridement of the fracture site, and external fixation before definitive treatment with repeat irrigation and débridement and open reduction and internal fixation of the tibial plafond. About 6 months after surgery, she presented to her surgeon with a draining abscess over the anteromedial surgical incision. Multiple débridement procedures were performed, the implant was removed, the ankle was stabilized with a bridging external fixator, and culture-specific antibiotic therapy was administered. Intraoperative cultures confirmed methicillin-resistant Staphylococcus aureus. Vancomycin was administered intravenously for 6 weeks. Once C-reactive protein level and erythrocyte sedimentation rate returned to normal, repeat débridement with a rectus abdominis free flap and ankle fusion were performed.
When the patient presented to our clinic, we saw atrophic nonunion of the ankle fusion on radiographs. Smoking cessation was encouraged but not required before surgery. The patient returned to the operating suite for tibiotalocalcaneal fusion with a retrograde intramedullary nail. With the patient in the prone position, retrograde femoral RIA reaming was performed to harvest 30 mL of autologous bone. After resection of the nonunion site using a trans-Achilles approach and insertion of the intramedullary nail, the autologous bone graft was mixed with recombinant human bone morphogenetic protein 2 (BMP-2), and the mixture was introduced into the fusion site. At final follow-up, 18 months after surgery, the patient was clinically asymptomatic and radiographically healed—without further intervention and despite continued smoking. She did not report any knee pain from the harvest site.
Case 2
A 59-year-old noncompliant woman with diabetes and Charcot neuropathy sustained a trimalleolar ankle fracture-dislocation that was initially treated with ankle and hindfoot arthrodesis. The postoperative course was uneventful, and she was discharged home. Less than a week later, she presented to the emergency department with a midshaft tibial fracture just proximal to the ankle and hindfoot fusion nail. She subsequently had the device removed and a long arthrodesis rod inserted to span the fracture site up to the proximal tibial metadiaphysis. About 9 months later, she returned to our office complaining of ankle pain. No signs of infection were clinically evident. Radiographs showed nonunion of the ankle and subtalar joint. Findings of the initial bone biopsy and pathologic examination were negative for infection. The patient returned to the operating room 4 weeks later for revision ankle fusion. With the patient in the prone position, autologous bone (~30 mL) was harvested using retrograde femoral RIA reaming. The nonunion site was resected, and a mixture of autologous bone graft and BMP-2 was applied. Through a posterior approach, an anterior ankle arthrodesis locking plate was applied to the posterior aspect of the calcaneus and tibia. The patient was kept non-weight-bearing for 3 months and progressed in weight-bearing for another 4 to 6 weeks. Ambulatory status was restored about 4 months after surgery. No harvest-site knee pain was reported.
Discussion
Given its osteogenic, osteoconductive, and osteoinductive properties, autologous cancellous bone graft is the gold standard for reconstruction and fusion procedures in foot and ankle surgery.13 Bone graft can be obtained from many potential donor sites, but the most common is the iliac crest.2 However, many comorbidities, such as residual donor-site pain, neurovascular injuries, infection, and increased surgical time, have been reported in the literature.14,15 The RIA system was initially developed for simultaneous reaming and aspiration to reduce intramedullary pressure, heat generation, operating time, and the systemic effects of reaming, such as the embolic phenomenon.16-22 The single-pass reamer has provided a minimally invasive strategy for procuring voluminous amounts of autologous cancellous bone from the intramedullary canal of lower extremity long bones. Schmidmaier and colleagues3 recently quantified the measurements of several growth factors, such as insulinlike growth factor 1, transforming growth factor β 1, and BMP-2—proving that RIA-derived aspirates have amounts comparable to if not larger than those of iliac crest autologous bone graft. Pratt and colleagues23 provided insight into the possibility of induction of mesenchymal stem cells using the previously unwanted supernatant reamings after filtration. Recently, the RIA technique of autologous tibial and hindfoot bone graft harvest was described for use in ankle or tibiotalocalcaneal arthrodesis.2 Although this technique is a useful surgical option, tibia size remains a limiting factor. Kovar and Wozasek24 reported harvesting significantly more bone graft in the femur than in the tibia. A tibia that cannot accommodate the 12-mm (smallest) reamer head in the RIA system would be a contraindication. In addition, concerns about the association between tibial stress fractures and reaming of the entire tibial canal and concerns about the overall donor-site morbidity of the tibial shaft remain.
Conclusion
With its retrograde approach and prone positioning, this RIA technique is an effective and efficient solution for harvesting autologous femoral bone graft. Although we have described its use in ankle and hindfoot arthrodesis, this technique can be applied to any prone-position surgical procedure, including spine surgery.
1. Kobbe P, Tarkin IS, Frink M, Pape HC. Voluminous bone graft harvesting of the femoral marrow cavity for autologous transplantation. An indication for the “reamer-irrigator-aspirator-” (RIA-)technique [in German]. Unfallchirurg. 2008;111(6):469-472.
2. Herscovici D Jr, Scaduto JM. Use of the reamer-irrigator-aspirator technique to obtain autograft for ankle and hindfoot arthrodesis. J Bone Joint Surg Br. 2012;94(1):75-79.
3. Schmidmaier G, Herrmann S, Green J, et al. Quantitative assessment of growth factors in reaming aspirate, iliac crest, and platelet preparation. Bone. 2006;39(5):1156-1163.
4. Qvick LM, Ritter CA, Mutty CE, Rohrbacher BJ, Buyea CM, Anders MJ. Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series. Injury. 2013;44(10):1263-1269.
5. Lehman AA, Irgit KS, Cush GJ. Harvest of autogenous bone graft using reamer-irrigator-aspirator in tibiotalocalcaneal arthrodesis: surgical technique and case series. Foot Ankle Int. 2012;33(12):1133-1138.
6. Wildemann B, Kadow-Romacker A, Haas NP, Schmidmaier G. Quantification of various growth factors in different demineralized bone matrix preparations. J Biomed Mater Res A. 2007;81(2):437-442.
7. Sagi HC, Young ML, Gerstenfeld L, Einhorn TA, Tornetta P. Qualitative and quantitative differences between bone graft obtained from the medullary canal (with a reamer/irrigator/aspirator) and the iliac crest of the same patient. J Bone Joint Surg Am. 2012;94(23):2128-2135.
8. Belthur MV, Conway JD, Jindal G, Ranade A, Herzenberg JE. Bone graft harvest using a new intramedullary system. Clin Orthop. 2008;466(12):2973-2980.
9. Nichols TA, Sagi HC, Weber TG, Guiot BH. An alternative source of autograft bone for spinal fusion: the femur: technical case report. Neurosurgery. 2008;62(3 suppl 1):E179.
10. Van Gorp CC, Falk JV, Kmiec SJ Jr, Siston RA. The reamer/irrigator/aspirator reduces femoral canal pressure in simulated TKA. Clin Orthop. 2009;467(3):805-809.
11. Quintero AJ, Tarkin IS, Pape HC. Technical tricks when using the reamer irrigator aspirator technique for autologous bone graft harvesting. J Orthop Trauma. 2010;24(1):42-45.
12. Stafford PR, Norris B. Reamer-irrigator-aspirator as a bone graft harvester. Tech Foot Ankle Surg. 2007;6(2):100-107.
13. Whitehouse MR, Lankester BJ, Winson IG, Hepple S. Bone graft harvest from the proximal tibia in foot and ankle arthrodesis surgery. Foot Ankle Int. 2006;27(11):913-916.
14. Scharfenberger A, Weber T. RIA for bone graft harvest: applications for grafting large segmental defects in the tibia and femur. Presented at: 21st Annual Meeting of the Orthopaedic Trauma Association; 2005; Ottawa, Canada.
15. Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Orthop. 1996;(329):300-309.
16. Bedi A, Karunakar MA. Physiologic effects of intramedullary reaming. Instr Course Lect. 2006;55:359-366.
17. Higgins TF, Casey V, Bachus K. Cortical heat generation using an irrigating/aspirating single-pass reaming vs conventional stepwise reaming. J Orthop Trauma. 2007;21(3):192-197.
18. Husebye EE, Lyberg T, Madsen JE, Eriksen M, Røise O. The influence of a one-step reamer-irrigator-aspirator technique on the intramedullary pressure in the pig femur. Injury. 2006;37(10):935-940.
19. Müller CA, Green J, Südkamp NP. Physical and technical aspects of intramedullary reaming. Injury. 2006;37(suppl 4):S39-S49.
20. Pape HC, Dwenger A, Grotz M, et al. Does the reamer type influence the degree of lung dysfunction after femoral nailing following severe trauma? An animal study. J Orthop Trauma. 1994;8(4):300-309.
21. Pape HC, Zelle BA, Hildebrand F, Giannoudis PV, Krettek C, van Griensven M. Reamed femoral nailing in sheep: does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am. 2005;87(11):2515-2522.
22. Schult M, Küchle R, Hofmann A, et al. Pathophysiological advantages of rinsing-suction-reaming (RSR) in a pig model for intramedullary nailing. J Orthop Res. 2006;24(6):1186-1192.
23. Pratt DJ, Papagiannopoulos G, Rees PH, Quinnell R. The effects of medullary reaming on the torsional strength of the femur. Injury. 1987;18(3):177-179.
24. Kovar FM, Wozasek GE. Bone graft harvesting using the RIA (reamer irrigation aspirator) system—a quantitative assessment. Wien Klin Wochenschr. 2011;123(9-10):285-290.
The Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania) has become a powerful tool for harvesting autologous bone graft from the intramedullary canal of the long bones of the lower extremity for the treatment of osseous defects, nonunions, and joint fusions.1,2 The RIA system provides satisfactory quality and quantity of bone graft (range, 40-90 mL)3-5 with osteogenic properties that rival those harvested from the iliac crest.6,7 Minimal donor-site morbidity and mortality have been reported in association with the RIA technique compared with iliac crest bone graft harvest.8
The RIA technique for the femur—with the antegrade approach and the supine position,8 with the antegrade approach and the prone position,9 and with the retrograde approach and the supine position4—has been described in the literature. To our knowledge, however, the RIA technique for the femur with the retrograde approach and the prone position has not been described. Antegrade harvesting uses the trochanteric entry point, and retrograde harvesting uses an entry at the intercondylar notch just anterior to the posterior cruciate ligament. In this article, we detail the technique for RIA harvesting of the femur with the patient in the prone position. Patient positioning is based on the diagnosis and the proposed procedure.
Advantages of a retrograde starting point include a more concentric trajectory (vs that of an antegrade starting point) and more efficient canal pressure reduction, which might decrease the risk of intraoperative fat embolization.10 This technique offers a more efficient solution to any procedure that requires the prone position, and it avoids the need to reposition, reprepare, or redrape the extremity. It is also very useful in treating obese patients.
After obtaining institutional review board (IRB) approval, we retrospectively reviewed patient files. Because the study was retrospective, the IRB waived the requirement for informed consent. The patients described here provided written informed consent for print and electronic publication of these case reports.
Surgical Technique
The patient is placed in a prone position on a radiolucent table with a bump under the thigh to allow access to the knee joint with full extension of the hip (Figures 1, 2A, 2B). The knee is then flexed to gain access to the intercondylar notch.
The anatomical axis of the femur is identified in the coronal and sagittal planes with the help of an image intensifier. Frequent intraoperative fluoroscopic imaging is required to prevent eccentric reaming and guide-wire movement from causing iatrogenic fractures and perforations, respectively.8 A 2-mm Steinmann pin is used to identify the point of entry into the femoral canal, which is located just above the posterior cruciate ligament insertion in the intercondylar notch, and care is taken not to ream this structure. A minimally invasive incision of about 15 mm is centered on this pin using a patellar tendon–splitting approach.
An 8-mm cannulated anterior cruciate ligament reamer is passed over the pin to enlarge the opening at the entry point, and a 2.5-mm ball-tipped guide wire is positioned in the femur. The image intensifier is used to confirm positioning of the guide in the trochanteric region and centered in the intramedullary canal. A radiolucent diving board facilitates fluoroscopic imaging.
The diameter (12.5 or 16.5 mm) of the reaming head is selected after the intramedullary guide is placed in the femoral canal. The isthmus of the femur is then identified radiographically, and a radiopaque ruler with increments in millimeters is used to measure the canal diameter (Figures 3A, 3B). Because the femoral canal is an ellipsoid, the canal diameter usually is much larger anteroposteriorly than laterally.8 We prefer to use a reaming head that overlaps the inner cortical diameter by 1 mm on each side. An alternative method includes measuring the outer diameter of the narrowest portion of the bone and using a reamer head no more than 45% of the outer diameter at the isthmus.8
The RIA system is prepared on the back table by attaching the reaming head to the irrigation and suction systems. As the reamer head enters the intramedullary canal, an approach–withdraw–pause technique is used to slowly advance the reamer through the femur. It is crucial to use the image intensifier to guide reaming in order to avoid overdrilling the anterior cortex and prevent eccentric reaming of the canal, which more commonly occurs in patients with large anterior femoral bows.11 When the collection filter becomes full, reaming is stopped. The bone graft in the filter is emptied into a specimen cup for measurement and storage until subsequent use (Figure 4). Suctioning is suspended when reaming is stopped because substantial blood loss can occur with prolonged suction and aspiration.12 When repeat reaming is required, care is taken not to overream the cortices, thereby avoiding the risk of iatrogenic fracture.10,12
The knee joint is irrigated to remove any intramedullary debris. Typically there is no debris, as it is captured by the RIA. The wound is closed in 2 layers. Dressing with Ace bandage (3M, St. Paul, Minnesota) is placed around the knee for comfort. Weight-bearing status is determined by the index procedure.
Case Reports
Case 1
A 68-year-old female smoker presented to our facility with right ankle pain after recent ankle arthrodesis for pilon fracture nonunion. Almost 3 years earlier, the patient sustained a Gustilo-Anderson type II open pilon fracture in a motorcycle accident. She underwent antibiotic therapy, irrigation and débridement of the fracture site, and external fixation before definitive treatment with repeat irrigation and débridement and open reduction and internal fixation of the tibial plafond. About 6 months after surgery, she presented to her surgeon with a draining abscess over the anteromedial surgical incision. Multiple débridement procedures were performed, the implant was removed, the ankle was stabilized with a bridging external fixator, and culture-specific antibiotic therapy was administered. Intraoperative cultures confirmed methicillin-resistant Staphylococcus aureus. Vancomycin was administered intravenously for 6 weeks. Once C-reactive protein level and erythrocyte sedimentation rate returned to normal, repeat débridement with a rectus abdominis free flap and ankle fusion were performed.
When the patient presented to our clinic, we saw atrophic nonunion of the ankle fusion on radiographs. Smoking cessation was encouraged but not required before surgery. The patient returned to the operating suite for tibiotalocalcaneal fusion with a retrograde intramedullary nail. With the patient in the prone position, retrograde femoral RIA reaming was performed to harvest 30 mL of autologous bone. After resection of the nonunion site using a trans-Achilles approach and insertion of the intramedullary nail, the autologous bone graft was mixed with recombinant human bone morphogenetic protein 2 (BMP-2), and the mixture was introduced into the fusion site. At final follow-up, 18 months after surgery, the patient was clinically asymptomatic and radiographically healed—without further intervention and despite continued smoking. She did not report any knee pain from the harvest site.
Case 2
A 59-year-old noncompliant woman with diabetes and Charcot neuropathy sustained a trimalleolar ankle fracture-dislocation that was initially treated with ankle and hindfoot arthrodesis. The postoperative course was uneventful, and she was discharged home. Less than a week later, she presented to the emergency department with a midshaft tibial fracture just proximal to the ankle and hindfoot fusion nail. She subsequently had the device removed and a long arthrodesis rod inserted to span the fracture site up to the proximal tibial metadiaphysis. About 9 months later, she returned to our office complaining of ankle pain. No signs of infection were clinically evident. Radiographs showed nonunion of the ankle and subtalar joint. Findings of the initial bone biopsy and pathologic examination were negative for infection. The patient returned to the operating room 4 weeks later for revision ankle fusion. With the patient in the prone position, autologous bone (~30 mL) was harvested using retrograde femoral RIA reaming. The nonunion site was resected, and a mixture of autologous bone graft and BMP-2 was applied. Through a posterior approach, an anterior ankle arthrodesis locking plate was applied to the posterior aspect of the calcaneus and tibia. The patient was kept non-weight-bearing for 3 months and progressed in weight-bearing for another 4 to 6 weeks. Ambulatory status was restored about 4 months after surgery. No harvest-site knee pain was reported.
Discussion
Given its osteogenic, osteoconductive, and osteoinductive properties, autologous cancellous bone graft is the gold standard for reconstruction and fusion procedures in foot and ankle surgery.13 Bone graft can be obtained from many potential donor sites, but the most common is the iliac crest.2 However, many comorbidities, such as residual donor-site pain, neurovascular injuries, infection, and increased surgical time, have been reported in the literature.14,15 The RIA system was initially developed for simultaneous reaming and aspiration to reduce intramedullary pressure, heat generation, operating time, and the systemic effects of reaming, such as the embolic phenomenon.16-22 The single-pass reamer has provided a minimally invasive strategy for procuring voluminous amounts of autologous cancellous bone from the intramedullary canal of lower extremity long bones. Schmidmaier and colleagues3 recently quantified the measurements of several growth factors, such as insulinlike growth factor 1, transforming growth factor β 1, and BMP-2—proving that RIA-derived aspirates have amounts comparable to if not larger than those of iliac crest autologous bone graft. Pratt and colleagues23 provided insight into the possibility of induction of mesenchymal stem cells using the previously unwanted supernatant reamings after filtration. Recently, the RIA technique of autologous tibial and hindfoot bone graft harvest was described for use in ankle or tibiotalocalcaneal arthrodesis.2 Although this technique is a useful surgical option, tibia size remains a limiting factor. Kovar and Wozasek24 reported harvesting significantly more bone graft in the femur than in the tibia. A tibia that cannot accommodate the 12-mm (smallest) reamer head in the RIA system would be a contraindication. In addition, concerns about the association between tibial stress fractures and reaming of the entire tibial canal and concerns about the overall donor-site morbidity of the tibial shaft remain.
Conclusion
With its retrograde approach and prone positioning, this RIA technique is an effective and efficient solution for harvesting autologous femoral bone graft. Although we have described its use in ankle and hindfoot arthrodesis, this technique can be applied to any prone-position surgical procedure, including spine surgery.
The Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania) has become a powerful tool for harvesting autologous bone graft from the intramedullary canal of the long bones of the lower extremity for the treatment of osseous defects, nonunions, and joint fusions.1,2 The RIA system provides satisfactory quality and quantity of bone graft (range, 40-90 mL)3-5 with osteogenic properties that rival those harvested from the iliac crest.6,7 Minimal donor-site morbidity and mortality have been reported in association with the RIA technique compared with iliac crest bone graft harvest.8
The RIA technique for the femur—with the antegrade approach and the supine position,8 with the antegrade approach and the prone position,9 and with the retrograde approach and the supine position4—has been described in the literature. To our knowledge, however, the RIA technique for the femur with the retrograde approach and the prone position has not been described. Antegrade harvesting uses the trochanteric entry point, and retrograde harvesting uses an entry at the intercondylar notch just anterior to the posterior cruciate ligament. In this article, we detail the technique for RIA harvesting of the femur with the patient in the prone position. Patient positioning is based on the diagnosis and the proposed procedure.
Advantages of a retrograde starting point include a more concentric trajectory (vs that of an antegrade starting point) and more efficient canal pressure reduction, which might decrease the risk of intraoperative fat embolization.10 This technique offers a more efficient solution to any procedure that requires the prone position, and it avoids the need to reposition, reprepare, or redrape the extremity. It is also very useful in treating obese patients.
After obtaining institutional review board (IRB) approval, we retrospectively reviewed patient files. Because the study was retrospective, the IRB waived the requirement for informed consent. The patients described here provided written informed consent for print and electronic publication of these case reports.
Surgical Technique
The patient is placed in a prone position on a radiolucent table with a bump under the thigh to allow access to the knee joint with full extension of the hip (Figures 1, 2A, 2B). The knee is then flexed to gain access to the intercondylar notch.
The anatomical axis of the femur is identified in the coronal and sagittal planes with the help of an image intensifier. Frequent intraoperative fluoroscopic imaging is required to prevent eccentric reaming and guide-wire movement from causing iatrogenic fractures and perforations, respectively.8 A 2-mm Steinmann pin is used to identify the point of entry into the femoral canal, which is located just above the posterior cruciate ligament insertion in the intercondylar notch, and care is taken not to ream this structure. A minimally invasive incision of about 15 mm is centered on this pin using a patellar tendon–splitting approach.
An 8-mm cannulated anterior cruciate ligament reamer is passed over the pin to enlarge the opening at the entry point, and a 2.5-mm ball-tipped guide wire is positioned in the femur. The image intensifier is used to confirm positioning of the guide in the trochanteric region and centered in the intramedullary canal. A radiolucent diving board facilitates fluoroscopic imaging.
The diameter (12.5 or 16.5 mm) of the reaming head is selected after the intramedullary guide is placed in the femoral canal. The isthmus of the femur is then identified radiographically, and a radiopaque ruler with increments in millimeters is used to measure the canal diameter (Figures 3A, 3B). Because the femoral canal is an ellipsoid, the canal diameter usually is much larger anteroposteriorly than laterally.8 We prefer to use a reaming head that overlaps the inner cortical diameter by 1 mm on each side. An alternative method includes measuring the outer diameter of the narrowest portion of the bone and using a reamer head no more than 45% of the outer diameter at the isthmus.8
The RIA system is prepared on the back table by attaching the reaming head to the irrigation and suction systems. As the reamer head enters the intramedullary canal, an approach–withdraw–pause technique is used to slowly advance the reamer through the femur. It is crucial to use the image intensifier to guide reaming in order to avoid overdrilling the anterior cortex and prevent eccentric reaming of the canal, which more commonly occurs in patients with large anterior femoral bows.11 When the collection filter becomes full, reaming is stopped. The bone graft in the filter is emptied into a specimen cup for measurement and storage until subsequent use (Figure 4). Suctioning is suspended when reaming is stopped because substantial blood loss can occur with prolonged suction and aspiration.12 When repeat reaming is required, care is taken not to overream the cortices, thereby avoiding the risk of iatrogenic fracture.10,12
The knee joint is irrigated to remove any intramedullary debris. Typically there is no debris, as it is captured by the RIA. The wound is closed in 2 layers. Dressing with Ace bandage (3M, St. Paul, Minnesota) is placed around the knee for comfort. Weight-bearing status is determined by the index procedure.
Case Reports
Case 1
A 68-year-old female smoker presented to our facility with right ankle pain after recent ankle arthrodesis for pilon fracture nonunion. Almost 3 years earlier, the patient sustained a Gustilo-Anderson type II open pilon fracture in a motorcycle accident. She underwent antibiotic therapy, irrigation and débridement of the fracture site, and external fixation before definitive treatment with repeat irrigation and débridement and open reduction and internal fixation of the tibial plafond. About 6 months after surgery, she presented to her surgeon with a draining abscess over the anteromedial surgical incision. Multiple débridement procedures were performed, the implant was removed, the ankle was stabilized with a bridging external fixator, and culture-specific antibiotic therapy was administered. Intraoperative cultures confirmed methicillin-resistant Staphylococcus aureus. Vancomycin was administered intravenously for 6 weeks. Once C-reactive protein level and erythrocyte sedimentation rate returned to normal, repeat débridement with a rectus abdominis free flap and ankle fusion were performed.
When the patient presented to our clinic, we saw atrophic nonunion of the ankle fusion on radiographs. Smoking cessation was encouraged but not required before surgery. The patient returned to the operating suite for tibiotalocalcaneal fusion with a retrograde intramedullary nail. With the patient in the prone position, retrograde femoral RIA reaming was performed to harvest 30 mL of autologous bone. After resection of the nonunion site using a trans-Achilles approach and insertion of the intramedullary nail, the autologous bone graft was mixed with recombinant human bone morphogenetic protein 2 (BMP-2), and the mixture was introduced into the fusion site. At final follow-up, 18 months after surgery, the patient was clinically asymptomatic and radiographically healed—without further intervention and despite continued smoking. She did not report any knee pain from the harvest site.
Case 2
A 59-year-old noncompliant woman with diabetes and Charcot neuropathy sustained a trimalleolar ankle fracture-dislocation that was initially treated with ankle and hindfoot arthrodesis. The postoperative course was uneventful, and she was discharged home. Less than a week later, she presented to the emergency department with a midshaft tibial fracture just proximal to the ankle and hindfoot fusion nail. She subsequently had the device removed and a long arthrodesis rod inserted to span the fracture site up to the proximal tibial metadiaphysis. About 9 months later, she returned to our office complaining of ankle pain. No signs of infection were clinically evident. Radiographs showed nonunion of the ankle and subtalar joint. Findings of the initial bone biopsy and pathologic examination were negative for infection. The patient returned to the operating room 4 weeks later for revision ankle fusion. With the patient in the prone position, autologous bone (~30 mL) was harvested using retrograde femoral RIA reaming. The nonunion site was resected, and a mixture of autologous bone graft and BMP-2 was applied. Through a posterior approach, an anterior ankle arthrodesis locking plate was applied to the posterior aspect of the calcaneus and tibia. The patient was kept non-weight-bearing for 3 months and progressed in weight-bearing for another 4 to 6 weeks. Ambulatory status was restored about 4 months after surgery. No harvest-site knee pain was reported.
Discussion
Given its osteogenic, osteoconductive, and osteoinductive properties, autologous cancellous bone graft is the gold standard for reconstruction and fusion procedures in foot and ankle surgery.13 Bone graft can be obtained from many potential donor sites, but the most common is the iliac crest.2 However, many comorbidities, such as residual donor-site pain, neurovascular injuries, infection, and increased surgical time, have been reported in the literature.14,15 The RIA system was initially developed for simultaneous reaming and aspiration to reduce intramedullary pressure, heat generation, operating time, and the systemic effects of reaming, such as the embolic phenomenon.16-22 The single-pass reamer has provided a minimally invasive strategy for procuring voluminous amounts of autologous cancellous bone from the intramedullary canal of lower extremity long bones. Schmidmaier and colleagues3 recently quantified the measurements of several growth factors, such as insulinlike growth factor 1, transforming growth factor β 1, and BMP-2—proving that RIA-derived aspirates have amounts comparable to if not larger than those of iliac crest autologous bone graft. Pratt and colleagues23 provided insight into the possibility of induction of mesenchymal stem cells using the previously unwanted supernatant reamings after filtration. Recently, the RIA technique of autologous tibial and hindfoot bone graft harvest was described for use in ankle or tibiotalocalcaneal arthrodesis.2 Although this technique is a useful surgical option, tibia size remains a limiting factor. Kovar and Wozasek24 reported harvesting significantly more bone graft in the femur than in the tibia. A tibia that cannot accommodate the 12-mm (smallest) reamer head in the RIA system would be a contraindication. In addition, concerns about the association between tibial stress fractures and reaming of the entire tibial canal and concerns about the overall donor-site morbidity of the tibial shaft remain.
Conclusion
With its retrograde approach and prone positioning, this RIA technique is an effective and efficient solution for harvesting autologous femoral bone graft. Although we have described its use in ankle and hindfoot arthrodesis, this technique can be applied to any prone-position surgical procedure, including spine surgery.
1. Kobbe P, Tarkin IS, Frink M, Pape HC. Voluminous bone graft harvesting of the femoral marrow cavity for autologous transplantation. An indication for the “reamer-irrigator-aspirator-” (RIA-)technique [in German]. Unfallchirurg. 2008;111(6):469-472.
2. Herscovici D Jr, Scaduto JM. Use of the reamer-irrigator-aspirator technique to obtain autograft for ankle and hindfoot arthrodesis. J Bone Joint Surg Br. 2012;94(1):75-79.
3. Schmidmaier G, Herrmann S, Green J, et al. Quantitative assessment of growth factors in reaming aspirate, iliac crest, and platelet preparation. Bone. 2006;39(5):1156-1163.
4. Qvick LM, Ritter CA, Mutty CE, Rohrbacher BJ, Buyea CM, Anders MJ. Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series. Injury. 2013;44(10):1263-1269.
5. Lehman AA, Irgit KS, Cush GJ. Harvest of autogenous bone graft using reamer-irrigator-aspirator in tibiotalocalcaneal arthrodesis: surgical technique and case series. Foot Ankle Int. 2012;33(12):1133-1138.
6. Wildemann B, Kadow-Romacker A, Haas NP, Schmidmaier G. Quantification of various growth factors in different demineralized bone matrix preparations. J Biomed Mater Res A. 2007;81(2):437-442.
7. Sagi HC, Young ML, Gerstenfeld L, Einhorn TA, Tornetta P. Qualitative and quantitative differences between bone graft obtained from the medullary canal (with a reamer/irrigator/aspirator) and the iliac crest of the same patient. J Bone Joint Surg Am. 2012;94(23):2128-2135.
8. Belthur MV, Conway JD, Jindal G, Ranade A, Herzenberg JE. Bone graft harvest using a new intramedullary system. Clin Orthop. 2008;466(12):2973-2980.
9. Nichols TA, Sagi HC, Weber TG, Guiot BH. An alternative source of autograft bone for spinal fusion: the femur: technical case report. Neurosurgery. 2008;62(3 suppl 1):E179.
10. Van Gorp CC, Falk JV, Kmiec SJ Jr, Siston RA. The reamer/irrigator/aspirator reduces femoral canal pressure in simulated TKA. Clin Orthop. 2009;467(3):805-809.
11. Quintero AJ, Tarkin IS, Pape HC. Technical tricks when using the reamer irrigator aspirator technique for autologous bone graft harvesting. J Orthop Trauma. 2010;24(1):42-45.
12. Stafford PR, Norris B. Reamer-irrigator-aspirator as a bone graft harvester. Tech Foot Ankle Surg. 2007;6(2):100-107.
13. Whitehouse MR, Lankester BJ, Winson IG, Hepple S. Bone graft harvest from the proximal tibia in foot and ankle arthrodesis surgery. Foot Ankle Int. 2006;27(11):913-916.
14. Scharfenberger A, Weber T. RIA for bone graft harvest: applications for grafting large segmental defects in the tibia and femur. Presented at: 21st Annual Meeting of the Orthopaedic Trauma Association; 2005; Ottawa, Canada.
15. Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Orthop. 1996;(329):300-309.
16. Bedi A, Karunakar MA. Physiologic effects of intramedullary reaming. Instr Course Lect. 2006;55:359-366.
17. Higgins TF, Casey V, Bachus K. Cortical heat generation using an irrigating/aspirating single-pass reaming vs conventional stepwise reaming. J Orthop Trauma. 2007;21(3):192-197.
18. Husebye EE, Lyberg T, Madsen JE, Eriksen M, Røise O. The influence of a one-step reamer-irrigator-aspirator technique on the intramedullary pressure in the pig femur. Injury. 2006;37(10):935-940.
19. Müller CA, Green J, Südkamp NP. Physical and technical aspects of intramedullary reaming. Injury. 2006;37(suppl 4):S39-S49.
20. Pape HC, Dwenger A, Grotz M, et al. Does the reamer type influence the degree of lung dysfunction after femoral nailing following severe trauma? An animal study. J Orthop Trauma. 1994;8(4):300-309.
21. Pape HC, Zelle BA, Hildebrand F, Giannoudis PV, Krettek C, van Griensven M. Reamed femoral nailing in sheep: does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am. 2005;87(11):2515-2522.
22. Schult M, Küchle R, Hofmann A, et al. Pathophysiological advantages of rinsing-suction-reaming (RSR) in a pig model for intramedullary nailing. J Orthop Res. 2006;24(6):1186-1192.
23. Pratt DJ, Papagiannopoulos G, Rees PH, Quinnell R. The effects of medullary reaming on the torsional strength of the femur. Injury. 1987;18(3):177-179.
24. Kovar FM, Wozasek GE. Bone graft harvesting using the RIA (reamer irrigation aspirator) system—a quantitative assessment. Wien Klin Wochenschr. 2011;123(9-10):285-290.
1. Kobbe P, Tarkin IS, Frink M, Pape HC. Voluminous bone graft harvesting of the femoral marrow cavity for autologous transplantation. An indication for the “reamer-irrigator-aspirator-” (RIA-)technique [in German]. Unfallchirurg. 2008;111(6):469-472.
2. Herscovici D Jr, Scaduto JM. Use of the reamer-irrigator-aspirator technique to obtain autograft for ankle and hindfoot arthrodesis. J Bone Joint Surg Br. 2012;94(1):75-79.
3. Schmidmaier G, Herrmann S, Green J, et al. Quantitative assessment of growth factors in reaming aspirate, iliac crest, and platelet preparation. Bone. 2006;39(5):1156-1163.
4. Qvick LM, Ritter CA, Mutty CE, Rohrbacher BJ, Buyea CM, Anders MJ. Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series. Injury. 2013;44(10):1263-1269.
5. Lehman AA, Irgit KS, Cush GJ. Harvest of autogenous bone graft using reamer-irrigator-aspirator in tibiotalocalcaneal arthrodesis: surgical technique and case series. Foot Ankle Int. 2012;33(12):1133-1138.
6. Wildemann B, Kadow-Romacker A, Haas NP, Schmidmaier G. Quantification of various growth factors in different demineralized bone matrix preparations. J Biomed Mater Res A. 2007;81(2):437-442.
7. Sagi HC, Young ML, Gerstenfeld L, Einhorn TA, Tornetta P. Qualitative and quantitative differences between bone graft obtained from the medullary canal (with a reamer/irrigator/aspirator) and the iliac crest of the same patient. J Bone Joint Surg Am. 2012;94(23):2128-2135.
8. Belthur MV, Conway JD, Jindal G, Ranade A, Herzenberg JE. Bone graft harvest using a new intramedullary system. Clin Orthop. 2008;466(12):2973-2980.
9. Nichols TA, Sagi HC, Weber TG, Guiot BH. An alternative source of autograft bone for spinal fusion: the femur: technical case report. Neurosurgery. 2008;62(3 suppl 1):E179.
10. Van Gorp CC, Falk JV, Kmiec SJ Jr, Siston RA. The reamer/irrigator/aspirator reduces femoral canal pressure in simulated TKA. Clin Orthop. 2009;467(3):805-809.
11. Quintero AJ, Tarkin IS, Pape HC. Technical tricks when using the reamer irrigator aspirator technique for autologous bone graft harvesting. J Orthop Trauma. 2010;24(1):42-45.
12. Stafford PR, Norris B. Reamer-irrigator-aspirator as a bone graft harvester. Tech Foot Ankle Surg. 2007;6(2):100-107.
13. Whitehouse MR, Lankester BJ, Winson IG, Hepple S. Bone graft harvest from the proximal tibia in foot and ankle arthrodesis surgery. Foot Ankle Int. 2006;27(11):913-916.
14. Scharfenberger A, Weber T. RIA for bone graft harvest: applications for grafting large segmental defects in the tibia and femur. Presented at: 21st Annual Meeting of the Orthopaedic Trauma Association; 2005; Ottawa, Canada.
15. Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Orthop. 1996;(329):300-309.
16. Bedi A, Karunakar MA. Physiologic effects of intramedullary reaming. Instr Course Lect. 2006;55:359-366.
17. Higgins TF, Casey V, Bachus K. Cortical heat generation using an irrigating/aspirating single-pass reaming vs conventional stepwise reaming. J Orthop Trauma. 2007;21(3):192-197.
18. Husebye EE, Lyberg T, Madsen JE, Eriksen M, Røise O. The influence of a one-step reamer-irrigator-aspirator technique on the intramedullary pressure in the pig femur. Injury. 2006;37(10):935-940.
19. Müller CA, Green J, Südkamp NP. Physical and technical aspects of intramedullary reaming. Injury. 2006;37(suppl 4):S39-S49.
20. Pape HC, Dwenger A, Grotz M, et al. Does the reamer type influence the degree of lung dysfunction after femoral nailing following severe trauma? An animal study. J Orthop Trauma. 1994;8(4):300-309.
21. Pape HC, Zelle BA, Hildebrand F, Giannoudis PV, Krettek C, van Griensven M. Reamed femoral nailing in sheep: does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am. 2005;87(11):2515-2522.
22. Schult M, Küchle R, Hofmann A, et al. Pathophysiological advantages of rinsing-suction-reaming (RSR) in a pig model for intramedullary nailing. J Orthop Res. 2006;24(6):1186-1192.
23. Pratt DJ, Papagiannopoulos G, Rees PH, Quinnell R. The effects of medullary reaming on the torsional strength of the femur. Injury. 1987;18(3):177-179.
24. Kovar FM, Wozasek GE. Bone graft harvesting using the RIA (reamer irrigation aspirator) system—a quantitative assessment. Wien Klin Wochenschr. 2011;123(9-10):285-290.

Emerging Biologics in Orthopedics
The discipline of orthopedic medicine and surgery has dramatically advanced over the last several decades. Improved understanding of biomechanics, tissue healing, and the pathogenesis of musculoskeletal diseases has allowed us to make significant progress in the diagnosis, treatment, and rehabilitation of our patients. Despite these advancements, there is still much to be learned, especially in the field of orthobiologics and regenerative medicine. As our understanding of existing technologies, such as bone marrow aspirate, platelet-rich plasma, and adult stem cells, continues to evolve, even newer biologic treatment options are being developed. This issue of The American Journal of Orthopedics focuses on emerging biologics across the spectrum of orthopedic care.
In this issue, on pages 202-205, Mansour and Conway describe a new prone retrograde technique for obtaining bone graft using the Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania). While iliac crest bone graft has been the gold standard for many years, use of the RIA system to obtain bone graft has been studied and has been shown to have decreased morbidity when compared with iliac crest harvest.1 Additionally, intramedullary bone graft from the femur appears to be just as concentrated with biologically active bone marrow as iliac crest harvest.2 This new technique allows increased efficiency, especially for surgeries that are done in the prone position.
Melamed and colleagues examine a new biologic to augment repair of rotator cuff tears (see pages 212-216). Chitosan, a linear polysaccharide, has been shown to help with soft-tissue healing. Although in the past its use has been limited secondary to problems with the compound precipitating at physiologic pH, new formulations mitigate that problem. In the authors’ animal model of acute supraspinatus repair, the use of chitosan gel increased the number of fibroblasts and the amount of repair tissue when compared with untreated controls. Additionally, the experimental group showed a decreased inflammatory response when compared with the control group. This is very exciting research as the biologic enhancement of rotator cuff tendon healing could potentially help decrease the rate of rotator cuff repair failure.
Lenehan and colleagues analyze the long-term outcomes of anterior cruciate ligament reconstruction in a cohort of patients studied over an 8-year period (see pages 217-222). During this period, 99 patients were reconstructed with allograft tissue and 24 with autograft. Their analysis, like other recently published work, shows that the rates of revision were much higher for patients under 25 years of age who were reconstructed using allograft tissue. The rate of revision for NCAA (National Collegiate Athletic Association) Division I athletes reconstructed with allograft tissue was found to be 62%, while the revision rate for all patients under the age of 25 years who received an allograft was found to be 20.5%. Clearly, there is still a great deal to learn about the biology of graft incorporation and healing, especially as it relates to allograft tissue.
These 3 articles exemplify the breadth of orthopedic biologics and their potential role in orthopedic surgery. Through efforts of investigators highlighted in this journal and in others, biologics will become better understood and more widely used when appropriate, leading to improved patient outcomes.
1. Calori GM, Colombo M, Mazza EL, Mazzola S, Malagoli E, Mineo GV. Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury. 2014;45 Suppl 6:S116-S120.
2. van der Bel R, Blokhuis TJ. Increased osteogenic capacity of Reamer/Irrigator/Aspirator derived mesenchymal stem cells. Injury. 2014;45(12):2060-2064.
The discipline of orthopedic medicine and surgery has dramatically advanced over the last several decades. Improved understanding of biomechanics, tissue healing, and the pathogenesis of musculoskeletal diseases has allowed us to make significant progress in the diagnosis, treatment, and rehabilitation of our patients. Despite these advancements, there is still much to be learned, especially in the field of orthobiologics and regenerative medicine. As our understanding of existing technologies, such as bone marrow aspirate, platelet-rich plasma, and adult stem cells, continues to evolve, even newer biologic treatment options are being developed. This issue of The American Journal of Orthopedics focuses on emerging biologics across the spectrum of orthopedic care.
In this issue, on pages 202-205, Mansour and Conway describe a new prone retrograde technique for obtaining bone graft using the Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania). While iliac crest bone graft has been the gold standard for many years, use of the RIA system to obtain bone graft has been studied and has been shown to have decreased morbidity when compared with iliac crest harvest.1 Additionally, intramedullary bone graft from the femur appears to be just as concentrated with biologically active bone marrow as iliac crest harvest.2 This new technique allows increased efficiency, especially for surgeries that are done in the prone position.
Melamed and colleagues examine a new biologic to augment repair of rotator cuff tears (see pages 212-216). Chitosan, a linear polysaccharide, has been shown to help with soft-tissue healing. Although in the past its use has been limited secondary to problems with the compound precipitating at physiologic pH, new formulations mitigate that problem. In the authors’ animal model of acute supraspinatus repair, the use of chitosan gel increased the number of fibroblasts and the amount of repair tissue when compared with untreated controls. Additionally, the experimental group showed a decreased inflammatory response when compared with the control group. This is very exciting research as the biologic enhancement of rotator cuff tendon healing could potentially help decrease the rate of rotator cuff repair failure.
Lenehan and colleagues analyze the long-term outcomes of anterior cruciate ligament reconstruction in a cohort of patients studied over an 8-year period (see pages 217-222). During this period, 99 patients were reconstructed with allograft tissue and 24 with autograft. Their analysis, like other recently published work, shows that the rates of revision were much higher for patients under 25 years of age who were reconstructed using allograft tissue. The rate of revision for NCAA (National Collegiate Athletic Association) Division I athletes reconstructed with allograft tissue was found to be 62%, while the revision rate for all patients under the age of 25 years who received an allograft was found to be 20.5%. Clearly, there is still a great deal to learn about the biology of graft incorporation and healing, especially as it relates to allograft tissue.
These 3 articles exemplify the breadth of orthopedic biologics and their potential role in orthopedic surgery. Through efforts of investigators highlighted in this journal and in others, biologics will become better understood and more widely used when appropriate, leading to improved patient outcomes.
The discipline of orthopedic medicine and surgery has dramatically advanced over the last several decades. Improved understanding of biomechanics, tissue healing, and the pathogenesis of musculoskeletal diseases has allowed us to make significant progress in the diagnosis, treatment, and rehabilitation of our patients. Despite these advancements, there is still much to be learned, especially in the field of orthobiologics and regenerative medicine. As our understanding of existing technologies, such as bone marrow aspirate, platelet-rich plasma, and adult stem cells, continues to evolve, even newer biologic treatment options are being developed. This issue of The American Journal of Orthopedics focuses on emerging biologics across the spectrum of orthopedic care.
In this issue, on pages 202-205, Mansour and Conway describe a new prone retrograde technique for obtaining bone graft using the Reamer/Irrigator/Aspirator (RIA) system (Synthes, West Chester, Pennsylvania). While iliac crest bone graft has been the gold standard for many years, use of the RIA system to obtain bone graft has been studied and has been shown to have decreased morbidity when compared with iliac crest harvest.1 Additionally, intramedullary bone graft from the femur appears to be just as concentrated with biologically active bone marrow as iliac crest harvest.2 This new technique allows increased efficiency, especially for surgeries that are done in the prone position.
Melamed and colleagues examine a new biologic to augment repair of rotator cuff tears (see pages 212-216). Chitosan, a linear polysaccharide, has been shown to help with soft-tissue healing. Although in the past its use has been limited secondary to problems with the compound precipitating at physiologic pH, new formulations mitigate that problem. In the authors’ animal model of acute supraspinatus repair, the use of chitosan gel increased the number of fibroblasts and the amount of repair tissue when compared with untreated controls. Additionally, the experimental group showed a decreased inflammatory response when compared with the control group. This is very exciting research as the biologic enhancement of rotator cuff tendon healing could potentially help decrease the rate of rotator cuff repair failure.
Lenehan and colleagues analyze the long-term outcomes of anterior cruciate ligament reconstruction in a cohort of patients studied over an 8-year period (see pages 217-222). During this period, 99 patients were reconstructed with allograft tissue and 24 with autograft. Their analysis, like other recently published work, shows that the rates of revision were much higher for patients under 25 years of age who were reconstructed using allograft tissue. The rate of revision for NCAA (National Collegiate Athletic Association) Division I athletes reconstructed with allograft tissue was found to be 62%, while the revision rate for all patients under the age of 25 years who received an allograft was found to be 20.5%. Clearly, there is still a great deal to learn about the biology of graft incorporation and healing, especially as it relates to allograft tissue.
These 3 articles exemplify the breadth of orthopedic biologics and their potential role in orthopedic surgery. Through efforts of investigators highlighted in this journal and in others, biologics will become better understood and more widely used when appropriate, leading to improved patient outcomes.
1. Calori GM, Colombo M, Mazza EL, Mazzola S, Malagoli E, Mineo GV. Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury. 2014;45 Suppl 6:S116-S120.
2. van der Bel R, Blokhuis TJ. Increased osteogenic capacity of Reamer/Irrigator/Aspirator derived mesenchymal stem cells. Injury. 2014;45(12):2060-2064.
1. Calori GM, Colombo M, Mazza EL, Mazzola S, Malagoli E, Mineo GV. Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury. 2014;45 Suppl 6:S116-S120.
2. van der Bel R, Blokhuis TJ. Increased osteogenic capacity of Reamer/Irrigator/Aspirator derived mesenchymal stem cells. Injury. 2014;45(12):2060-2064.

Epigenomic findings may help predict relapse in DLBCL

Photo by Rhoda Baer
Epigenomic heterogeneity at diagnosis may predict relapse in diffuse large B-cell lymphoma (DLBCL), according to research published in Nature Communications.
Investigators made this connection by reviewing biopsies taken from DLBCL patients before and after treatment.
The epigenome in these patients’ cancer cells changed greatly after treatment, and the global epigenome of pretreatment biopsies was substantially different in patients who relapsed and those who did not. There was more cell-to-cell heterogeneity in patients who relapsed.
“This is the first study I know of in cancer that looks at changes in the epigenome before and after treatment, and what we found could ultimately make traditional treatments much more effective,” said study author Olivier Elemento, PhD, of Weill Cornell Medical College in New York, New York.
To uncover the role of epigenetic involvement in DLBCL, Dr Elemento and his colleagues analyzed banked biopsies from patients. In each sample set, the investigators looked at sites in the epigenome where a methyl group was added or removed after DLBCL recurred.
They found a change in methylation that occurred between 39,808 and 1,035,960 specific methylation sites, depending on the sample. In addition, they identified between 78 and 13,162 differently methylated regions in the epigenome in relapsed disease.
“These are massive changes, given that the epigenome has 20 million methylation sites,” Dr Elemento said. “Our study shows that, in some cases, up to one-twentieth of the entire epigenome is changed after treatment. There are many more epigenetic changes than there are altered genes in DLBCL.”
“Once you have changes in methylation, the end result is an imbalanced expression of proteins,” added Giorgio Inghirami, MD, also of Weill Cornell.
“The tumor after chemotherapy is not the same as the tumor before treatment. This why it is so critical to have biopsies before any treatment of [primary or relapsed] lesions.”
The investigators hope this work will ultimately allow clinicians and researchers to predict treatment resistance in individual patients. ![]()
Photo by Rhoda Baer
Epigenomic heterogeneity at diagnosis may predict relapse in diffuse large B-cell lymphoma (DLBCL), according to research published in Nature Communications.
Investigators made this connection by reviewing biopsies taken from DLBCL patients before and after treatment.
The epigenome in these patients’ cancer cells changed greatly after treatment, and the global epigenome of pretreatment biopsies was substantially different in patients who relapsed and those who did not. There was more cell-to-cell heterogeneity in patients who relapsed.
“This is the first study I know of in cancer that looks at changes in the epigenome before and after treatment, and what we found could ultimately make traditional treatments much more effective,” said study author Olivier Elemento, PhD, of Weill Cornell Medical College in New York, New York.
To uncover the role of epigenetic involvement in DLBCL, Dr Elemento and his colleagues analyzed banked biopsies from patients. In each sample set, the investigators looked at sites in the epigenome where a methyl group was added or removed after DLBCL recurred.
They found a change in methylation that occurred between 39,808 and 1,035,960 specific methylation sites, depending on the sample. In addition, they identified between 78 and 13,162 differently methylated regions in the epigenome in relapsed disease.
“These are massive changes, given that the epigenome has 20 million methylation sites,” Dr Elemento said. “Our study shows that, in some cases, up to one-twentieth of the entire epigenome is changed after treatment. There are many more epigenetic changes than there are altered genes in DLBCL.”
“Once you have changes in methylation, the end result is an imbalanced expression of proteins,” added Giorgio Inghirami, MD, also of Weill Cornell.
“The tumor after chemotherapy is not the same as the tumor before treatment. This why it is so critical to have biopsies before any treatment of [primary or relapsed] lesions.”
The investigators hope this work will ultimately allow clinicians and researchers to predict treatment resistance in individual patients. ![]()
Photo by Rhoda Baer
Epigenomic heterogeneity at diagnosis may predict relapse in diffuse large B-cell lymphoma (DLBCL), according to research published in Nature Communications.
Investigators made this connection by reviewing biopsies taken from DLBCL patients before and after treatment.
The epigenome in these patients’ cancer cells changed greatly after treatment, and the global epigenome of pretreatment biopsies was substantially different in patients who relapsed and those who did not. There was more cell-to-cell heterogeneity in patients who relapsed.
“This is the first study I know of in cancer that looks at changes in the epigenome before and after treatment, and what we found could ultimately make traditional treatments much more effective,” said study author Olivier Elemento, PhD, of Weill Cornell Medical College in New York, New York.
To uncover the role of epigenetic involvement in DLBCL, Dr Elemento and his colleagues analyzed banked biopsies from patients. In each sample set, the investigators looked at sites in the epigenome where a methyl group was added or removed after DLBCL recurred.
They found a change in methylation that occurred between 39,808 and 1,035,960 specific methylation sites, depending on the sample. In addition, they identified between 78 and 13,162 differently methylated regions in the epigenome in relapsed disease.
“These are massive changes, given that the epigenome has 20 million methylation sites,” Dr Elemento said. “Our study shows that, in some cases, up to one-twentieth of the entire epigenome is changed after treatment. There are many more epigenetic changes than there are altered genes in DLBCL.”
“Once you have changes in methylation, the end result is an imbalanced expression of proteins,” added Giorgio Inghirami, MD, also of Weill Cornell.
“The tumor after chemotherapy is not the same as the tumor before treatment. This why it is so critical to have biopsies before any treatment of [primary or relapsed] lesions.”
The investigators hope this work will ultimately allow clinicians and researchers to predict treatment resistance in individual patients. ![]()
Measures improve use of VTE prophylaxis

Photo courtesy of CDC
Programs that give physicians real-time feedback and financial incentives may lead to improvements in hospital safety, according to a study published in the Journal of Hospital Medicine.
The study showed that hospitalists significantly improved their compliance with practice guidelines for preventing venous thromboembolism (VTE)
when they could get feedback on their compliance rates and a direct financial incentive for improving their performance.
“Our study confirms there is a real return on investment in such programs, not only for patient safety but also for hospitals,” said study author Henry Michtalik, MD, of Johns Hopkins Hospital in Baltimore, Maryland.
“Metrics such as the use of preventive drugs for [VTE] are already being monitored but only really improve a hospital’s quality of care when programs get data back to the people who are treating patients to directly improve care.”
Dr Michtalik and his team found that, by providing such information to physicians through web-based, real-time displays, monthly VTE prophylaxis compliance rates improved from 86% to 90% in 6 months.
Adding pay-for-performance to the real-time feedback for the following 18 months boosted compliance rates to 94%.
Dr Michtalik pointed out that “no one got wealthy off of the pay-for-performance program. Instead, we believe the money served more as a method to engage the providers.”
Payments ranged from $53 to $1244, with all but 2 of the incentive payments totaling under $1000. And it was during the 6-month feedback-only period that compliance rose the fastest.
The study involved 38 part-time and full-time academic hospitalists and the analysis of 3144 inpatients with a median stay of 3 days. The most common diagnoses were heart failure, acute kidney failure, temporary loss of consciousness (syncope), pneumonia, and chest pain.
Following the evidence-based guidelines of the American College of Chest Physicians for VTE prevention, physicians in the study were required to complete a VTE-risk assessment for each patient by using the hospital’s computerized provider order entry system.
“It sort of walks you through the thinking process” for making the VTE-risk assessment, Dr Michtalik said.
The system then prompted physicians with a risk-appropriate recommendation, but it was up to physicians to order the treatment itself. That allowed for physician discretion among types of prevention, as well as for patient and physician preference.
Before implementing the feedback system, the researchers established a 2-year baseline and found that physicians in the study prescribed inappropriate prophylaxis 7.9% of the time and did not prescribe prophylaxis when indicated 6.1% of the time.
Overall, the choice of inappropriate preventive treatment dropped to 6.2% with real-time feedback and to 2.6% with the addition of pay-for-performance. Lack of prophylaxis when indicated fell to 3.2% with feedback and to 3.1% with pay-for-performance.
Dr Michtalik noted that continuous improvements depend not only on the right kind of feedback but also on efforts to avoid “information overload,” especially now that an increasing amount of health and medical records are electronic.
“So you specifically target a few things that need to be improved,” he said, “and really incorporate them into the hospital’s culture.” ![]()
Photo courtesy of CDC
Programs that give physicians real-time feedback and financial incentives may lead to improvements in hospital safety, according to a study published in the Journal of Hospital Medicine.
The study showed that hospitalists significantly improved their compliance with practice guidelines for preventing venous thromboembolism (VTE)
when they could get feedback on their compliance rates and a direct financial incentive for improving their performance.
“Our study confirms there is a real return on investment in such programs, not only for patient safety but also for hospitals,” said study author Henry Michtalik, MD, of Johns Hopkins Hospital in Baltimore, Maryland.
“Metrics such as the use of preventive drugs for [VTE] are already being monitored but only really improve a hospital’s quality of care when programs get data back to the people who are treating patients to directly improve care.”
Dr Michtalik and his team found that, by providing such information to physicians through web-based, real-time displays, monthly VTE prophylaxis compliance rates improved from 86% to 90% in 6 months.
Adding pay-for-performance to the real-time feedback for the following 18 months boosted compliance rates to 94%.
Dr Michtalik pointed out that “no one got wealthy off of the pay-for-performance program. Instead, we believe the money served more as a method to engage the providers.”
Payments ranged from $53 to $1244, with all but 2 of the incentive payments totaling under $1000. And it was during the 6-month feedback-only period that compliance rose the fastest.
The study involved 38 part-time and full-time academic hospitalists and the analysis of 3144 inpatients with a median stay of 3 days. The most common diagnoses were heart failure, acute kidney failure, temporary loss of consciousness (syncope), pneumonia, and chest pain.
Following the evidence-based guidelines of the American College of Chest Physicians for VTE prevention, physicians in the study were required to complete a VTE-risk assessment for each patient by using the hospital’s computerized provider order entry system.
“It sort of walks you through the thinking process” for making the VTE-risk assessment, Dr Michtalik said.
The system then prompted physicians with a risk-appropriate recommendation, but it was up to physicians to order the treatment itself. That allowed for physician discretion among types of prevention, as well as for patient and physician preference.
Before implementing the feedback system, the researchers established a 2-year baseline and found that physicians in the study prescribed inappropriate prophylaxis 7.9% of the time and did not prescribe prophylaxis when indicated 6.1% of the time.
Overall, the choice of inappropriate preventive treatment dropped to 6.2% with real-time feedback and to 2.6% with the addition of pay-for-performance. Lack of prophylaxis when indicated fell to 3.2% with feedback and to 3.1% with pay-for-performance.
Dr Michtalik noted that continuous improvements depend not only on the right kind of feedback but also on efforts to avoid “information overload,” especially now that an increasing amount of health and medical records are electronic.
“So you specifically target a few things that need to be improved,” he said, “and really incorporate them into the hospital’s culture.” ![]()
Photo courtesy of CDC
Programs that give physicians real-time feedback and financial incentives may lead to improvements in hospital safety, according to a study published in the Journal of Hospital Medicine.
The study showed that hospitalists significantly improved their compliance with practice guidelines for preventing venous thromboembolism (VTE)
when they could get feedback on their compliance rates and a direct financial incentive for improving their performance.
“Our study confirms there is a real return on investment in such programs, not only for patient safety but also for hospitals,” said study author Henry Michtalik, MD, of Johns Hopkins Hospital in Baltimore, Maryland.
“Metrics such as the use of preventive drugs for [VTE] are already being monitored but only really improve a hospital’s quality of care when programs get data back to the people who are treating patients to directly improve care.”
Dr Michtalik and his team found that, by providing such information to physicians through web-based, real-time displays, monthly VTE prophylaxis compliance rates improved from 86% to 90% in 6 months.
Adding pay-for-performance to the real-time feedback for the following 18 months boosted compliance rates to 94%.
Dr Michtalik pointed out that “no one got wealthy off of the pay-for-performance program. Instead, we believe the money served more as a method to engage the providers.”
Payments ranged from $53 to $1244, with all but 2 of the incentive payments totaling under $1000. And it was during the 6-month feedback-only period that compliance rose the fastest.
The study involved 38 part-time and full-time academic hospitalists and the analysis of 3144 inpatients with a median stay of 3 days. The most common diagnoses were heart failure, acute kidney failure, temporary loss of consciousness (syncope), pneumonia, and chest pain.
Following the evidence-based guidelines of the American College of Chest Physicians for VTE prevention, physicians in the study were required to complete a VTE-risk assessment for each patient by using the hospital’s computerized provider order entry system.
“It sort of walks you through the thinking process” for making the VTE-risk assessment, Dr Michtalik said.
The system then prompted physicians with a risk-appropriate recommendation, but it was up to physicians to order the treatment itself. That allowed for physician discretion among types of prevention, as well as for patient and physician preference.
Before implementing the feedback system, the researchers established a 2-year baseline and found that physicians in the study prescribed inappropriate prophylaxis 7.9% of the time and did not prescribe prophylaxis when indicated 6.1% of the time.
Overall, the choice of inappropriate preventive treatment dropped to 6.2% with real-time feedback and to 2.6% with the addition of pay-for-performance. Lack of prophylaxis when indicated fell to 3.2% with feedback and to 3.1% with pay-for-performance.
Dr Michtalik noted that continuous improvements depend not only on the right kind of feedback but also on efforts to avoid “information overload,” especially now that an increasing amount of health and medical records are electronic.
“So you specifically target a few things that need to be improved,” he said, “and really incorporate them into the hospital’s culture.” ![]()
Analyses reveal higher-than-expected pediatric cancer rates in Florida

Photo by Bill Branson
Several statistical analyses have revealed higher-than-expected rates of pediatric cancers in 2 regions of Florida—the Miami metro area and an area west of the Everglades.
The anomalous rates were detected by 5 different research teams—each using different epidemiological and statistical methodology—on a data set spanning the period from 2000 to 2010 that was provided by the Florida Association of Pediatric Tumor Programs (FAPTP).
Lance A. Waller, PhD, of Emory University in Atlanta, Georgia, reviewed the different analyses and described his findings in Statistics and Public Policy.
The research groups applied different analytical approaches to achieve the same goal: detect spatio-temporal pediatric cancer clusters. The analyses used familiar methods—scan statistics, classification, and hierarchical Bayesian modeling—as well as some ideas new to disease clustering: wombling and machine learning.
During their respective analyses of the FAPTP data, the research groups found several suggestive results. For instance, each approach identified local areas in which the observed pediatric cancer rate is significantly higher than the rate expected, given the number of people at risk.
While the precise areas of high reported risk differ between methods, the groups identified a few common results that overlap but are not identical.
For example, all 5 teams identified significantly elevated rates of pediatric cancers in an urban area within collections of ZIP code tabulation areas (ZCTAs) in the Miami metro area and in an area just west of the Everglades. (ZCTAs are geographic areas defined by the US Census Bureau to provide a link between census geography—blocks, block groups, and tracts—and US Postal Service ZIP code areas.)
One analysis suggested the local increase west of the Everglades is based on 2 cases, both classified as “other” race, while another analysis indicated that this cluster is limited to the year 2000.
The observed elevated rates near Miami involved a much larger population size and many more cases, factors that complicate the identification of any shared characteristics common to cases in the cluster.
The analyses also revealed other patterns in the data. Dr Waller said an analysis that revealed a statewide increase in the baseline pediatric cancer incidence rate occurring between 2005 and 2006 merits a closer look to see whether this result represents an overall increase in risk or a change in reporting, because the statistical analysis does not reveal potential reasons for the change.
There also are subtle differences between the specific clusters identified by the various analytical approaches. Comparisons across analyses revealed characteristics of the detected patterns, including the number of cases (2), types of cancer (leukemia or brain/central nervous system cancer), and the racial composition and timing of the cluster west of the Everglades.
As the methods the researchers used don’t completely agree on the precise location, boundaries, and make-up of the detected clusters, the findings suggest a single method may not prove sufficient for such analyses, Dr Waller said.
He added that the identified clusters are geographically quite large and therefore unlikely to provide clear links between particular environmental exposures to local risks.
“While the results do not identify a ‘smoking gun’ in the form of a shared environmental exposure in high-incidence areas, the results do provide epidemiologic insight into the local demographics of the incidence of pediatric cancer cases and suggest more detailed assessment of migration patterns in the Miami area,” Dr Waller said.
“Policy-wise, the results point to responsibly responsive next steps of detailed description of the cases and the at-risk population in the detected areas to summarize local features in the data, particularly the race of cases west of the Everglades and demographic descriptors of any shifts in the at-risk population in the Miami area during the study period.”
Policy responses by local and state health officials may involve more detailed follow-up, including additional data collection, exposure surveys, or in-depth investigation of case histories within a reported cluster.
Dr Waller added that estimated cancer rates consist of the local number of cases (reported by the FAPTP) and the local number of children at risk (reported by the decennial census). Higher-than-expected rates can result from unusually high numbers of reported cases or low numbers of reported local residents.
Since Miami, like many urban areas, often experiences rapid changes in population size and composition between decennial censuses, it is important to assess the accuracy of both data components. Dr Waller suggested, as a first step, assessing the accuracy of the case counts and the inter-census population projections defining the local rates.
“State and local health departments and public health agencies regularly respond to cluster reports from the public,” he said. “Typically, a responsive and effective response is not based on a detailed new epidemiologic study but, rather, is based on education, assessments of local concentrations of demographic risk factors associated with the reported cluster, and an assessment of the distribution of numbers of cases expected given the local demographics.” ![]()
Photo by Bill Branson
Several statistical analyses have revealed higher-than-expected rates of pediatric cancers in 2 regions of Florida—the Miami metro area and an area west of the Everglades.
The anomalous rates were detected by 5 different research teams—each using different epidemiological and statistical methodology—on a data set spanning the period from 2000 to 2010 that was provided by the Florida Association of Pediatric Tumor Programs (FAPTP).
Lance A. Waller, PhD, of Emory University in Atlanta, Georgia, reviewed the different analyses and described his findings in Statistics and Public Policy.
The research groups applied different analytical approaches to achieve the same goal: detect spatio-temporal pediatric cancer clusters. The analyses used familiar methods—scan statistics, classification, and hierarchical Bayesian modeling—as well as some ideas new to disease clustering: wombling and machine learning.
During their respective analyses of the FAPTP data, the research groups found several suggestive results. For instance, each approach identified local areas in which the observed pediatric cancer rate is significantly higher than the rate expected, given the number of people at risk.
While the precise areas of high reported risk differ between methods, the groups identified a few common results that overlap but are not identical.
For example, all 5 teams identified significantly elevated rates of pediatric cancers in an urban area within collections of ZIP code tabulation areas (ZCTAs) in the Miami metro area and in an area just west of the Everglades. (ZCTAs are geographic areas defined by the US Census Bureau to provide a link between census geography—blocks, block groups, and tracts—and US Postal Service ZIP code areas.)
One analysis suggested the local increase west of the Everglades is based on 2 cases, both classified as “other” race, while another analysis indicated that this cluster is limited to the year 2000.
The observed elevated rates near Miami involved a much larger population size and many more cases, factors that complicate the identification of any shared characteristics common to cases in the cluster.
The analyses also revealed other patterns in the data. Dr Waller said an analysis that revealed a statewide increase in the baseline pediatric cancer incidence rate occurring between 2005 and 2006 merits a closer look to see whether this result represents an overall increase in risk or a change in reporting, because the statistical analysis does not reveal potential reasons for the change.
There also are subtle differences between the specific clusters identified by the various analytical approaches. Comparisons across analyses revealed characteristics of the detected patterns, including the number of cases (2), types of cancer (leukemia or brain/central nervous system cancer), and the racial composition and timing of the cluster west of the Everglades.
As the methods the researchers used don’t completely agree on the precise location, boundaries, and make-up of the detected clusters, the findings suggest a single method may not prove sufficient for such analyses, Dr Waller said.
He added that the identified clusters are geographically quite large and therefore unlikely to provide clear links between particular environmental exposures to local risks.
“While the results do not identify a ‘smoking gun’ in the form of a shared environmental exposure in high-incidence areas, the results do provide epidemiologic insight into the local demographics of the incidence of pediatric cancer cases and suggest more detailed assessment of migration patterns in the Miami area,” Dr Waller said.
“Policy-wise, the results point to responsibly responsive next steps of detailed description of the cases and the at-risk population in the detected areas to summarize local features in the data, particularly the race of cases west of the Everglades and demographic descriptors of any shifts in the at-risk population in the Miami area during the study period.”
Policy responses by local and state health officials may involve more detailed follow-up, including additional data collection, exposure surveys, or in-depth investigation of case histories within a reported cluster.
Dr Waller added that estimated cancer rates consist of the local number of cases (reported by the FAPTP) and the local number of children at risk (reported by the decennial census). Higher-than-expected rates can result from unusually high numbers of reported cases or low numbers of reported local residents.
Since Miami, like many urban areas, often experiences rapid changes in population size and composition between decennial censuses, it is important to assess the accuracy of both data components. Dr Waller suggested, as a first step, assessing the accuracy of the case counts and the inter-census population projections defining the local rates.
“State and local health departments and public health agencies regularly respond to cluster reports from the public,” he said. “Typically, a responsive and effective response is not based on a detailed new epidemiologic study but, rather, is based on education, assessments of local concentrations of demographic risk factors associated with the reported cluster, and an assessment of the distribution of numbers of cases expected given the local demographics.” ![]()
Photo by Bill Branson
Several statistical analyses have revealed higher-than-expected rates of pediatric cancers in 2 regions of Florida—the Miami metro area and an area west of the Everglades.
The anomalous rates were detected by 5 different research teams—each using different epidemiological and statistical methodology—on a data set spanning the period from 2000 to 2010 that was provided by the Florida Association of Pediatric Tumor Programs (FAPTP).
Lance A. Waller, PhD, of Emory University in Atlanta, Georgia, reviewed the different analyses and described his findings in Statistics and Public Policy.
The research groups applied different analytical approaches to achieve the same goal: detect spatio-temporal pediatric cancer clusters. The analyses used familiar methods—scan statistics, classification, and hierarchical Bayesian modeling—as well as some ideas new to disease clustering: wombling and machine learning.
During their respective analyses of the FAPTP data, the research groups found several suggestive results. For instance, each approach identified local areas in which the observed pediatric cancer rate is significantly higher than the rate expected, given the number of people at risk.
While the precise areas of high reported risk differ between methods, the groups identified a few common results that overlap but are not identical.
For example, all 5 teams identified significantly elevated rates of pediatric cancers in an urban area within collections of ZIP code tabulation areas (ZCTAs) in the Miami metro area and in an area just west of the Everglades. (ZCTAs are geographic areas defined by the US Census Bureau to provide a link between census geography—blocks, block groups, and tracts—and US Postal Service ZIP code areas.)
One analysis suggested the local increase west of the Everglades is based on 2 cases, both classified as “other” race, while another analysis indicated that this cluster is limited to the year 2000.
The observed elevated rates near Miami involved a much larger population size and many more cases, factors that complicate the identification of any shared characteristics common to cases in the cluster.
The analyses also revealed other patterns in the data. Dr Waller said an analysis that revealed a statewide increase in the baseline pediatric cancer incidence rate occurring between 2005 and 2006 merits a closer look to see whether this result represents an overall increase in risk or a change in reporting, because the statistical analysis does not reveal potential reasons for the change.
There also are subtle differences between the specific clusters identified by the various analytical approaches. Comparisons across analyses revealed characteristics of the detected patterns, including the number of cases (2), types of cancer (leukemia or brain/central nervous system cancer), and the racial composition and timing of the cluster west of the Everglades.
As the methods the researchers used don’t completely agree on the precise location, boundaries, and make-up of the detected clusters, the findings suggest a single method may not prove sufficient for such analyses, Dr Waller said.
He added that the identified clusters are geographically quite large and therefore unlikely to provide clear links between particular environmental exposures to local risks.
“While the results do not identify a ‘smoking gun’ in the form of a shared environmental exposure in high-incidence areas, the results do provide epidemiologic insight into the local demographics of the incidence of pediatric cancer cases and suggest more detailed assessment of migration patterns in the Miami area,” Dr Waller said.
“Policy-wise, the results point to responsibly responsive next steps of detailed description of the cases and the at-risk population in the detected areas to summarize local features in the data, particularly the race of cases west of the Everglades and demographic descriptors of any shifts in the at-risk population in the Miami area during the study period.”
Policy responses by local and state health officials may involve more detailed follow-up, including additional data collection, exposure surveys, or in-depth investigation of case histories within a reported cluster.
Dr Waller added that estimated cancer rates consist of the local number of cases (reported by the FAPTP) and the local number of children at risk (reported by the decennial census). Higher-than-expected rates can result from unusually high numbers of reported cases or low numbers of reported local residents.
Since Miami, like many urban areas, often experiences rapid changes in population size and composition between decennial censuses, it is important to assess the accuracy of both data components. Dr Waller suggested, as a first step, assessing the accuracy of the case counts and the inter-census population projections defining the local rates.
“State and local health departments and public health agencies regularly respond to cluster reports from the public,” he said. “Typically, a responsive and effective response is not based on a detailed new epidemiologic study but, rather, is based on education, assessments of local concentrations of demographic risk factors associated with the reported cluster, and an assessment of the distribution of numbers of cases expected given the local demographics.” ![]()
Fake malaria drugs may be less common than we thought

Photo courtesy of the
London School of Hygiene
& Tropical Medicine
Investigations into antimalarial drug quality conducted in Cambodia and Tanzania uncovered no evidence of fake medicines.
Previous reports had suggested that up to a third of antimalarials might be falsified, or do not contain the stated active pharmaceutical ingredient.
The new research revealed no falsified drugs in either country, but it did unearth substandard antimalarial drugs, or genuine medicines that do not have the correct amount of the active ingredient.
These findings were published in 2 articles in the American Journal of Tropical Medicine and Hygiene.
“Although there have been alarming reports about the prevalence of fake antimalarials, our study provides ample data showing that the quality of drugs is not so bad based on comprehensive sampling and analysis presented here,” said Harparkash Kaur, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“The lack of falsified medicines in Cambodia and Tanzania are reassuring, but the presence of substandard medicines is definitely a concern.”
The researchers analyzed 2028 antimalarials from Tanzania and Cambodia at 3 independent laboratories in the UK and US. They classified drugs as acceptable, falsified, or substandard.
In Tanzania, the researchers used an “overt sampling” system, telling vendors they were going to analyze the quality of their medicines.
In Cambodia, the researchers used overt sampling as well as a “mystery client” approach, where actors pretended to be patients with malaria, or their relatives, and bought the medicines offered to them.
Both studies used a randomized approach to sampling of drug outlets, which differs from previous studies that mostly used non-representative methods for selecting drugs for analysis.
Neither study unearthed falsified drugs, but substandard drugs were found in 31% of samples in Cambodia and 12% of samples in Tanzania.
“Falsified medicines have received much attention globally, but substandard drugs are far more prevalent and of great concern,” said Shunmay Yeung, MBBS, PhD, also of the London School of Hygiene & Tropical Medicine.
“Not only do they leave patients with malaria undertreated, which could be fatal, but they may also contribute to the development of resistance to [artemisinin-based combination therapies], the most effective drugs for malaria. Generally, the fact that no falsified antimalarials were identified reflects the positive impact of the [countries’ efforts] to control drug quality.” ![]()
Photo courtesy of the
London School of Hygiene
& Tropical Medicine
Investigations into antimalarial drug quality conducted in Cambodia and Tanzania uncovered no evidence of fake medicines.
Previous reports had suggested that up to a third of antimalarials might be falsified, or do not contain the stated active pharmaceutical ingredient.
The new research revealed no falsified drugs in either country, but it did unearth substandard antimalarial drugs, or genuine medicines that do not have the correct amount of the active ingredient.
These findings were published in 2 articles in the American Journal of Tropical Medicine and Hygiene.
“Although there have been alarming reports about the prevalence of fake antimalarials, our study provides ample data showing that the quality of drugs is not so bad based on comprehensive sampling and analysis presented here,” said Harparkash Kaur, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“The lack of falsified medicines in Cambodia and Tanzania are reassuring, but the presence of substandard medicines is definitely a concern.”
The researchers analyzed 2028 antimalarials from Tanzania and Cambodia at 3 independent laboratories in the UK and US. They classified drugs as acceptable, falsified, or substandard.
In Tanzania, the researchers used an “overt sampling” system, telling vendors they were going to analyze the quality of their medicines.
In Cambodia, the researchers used overt sampling as well as a “mystery client” approach, where actors pretended to be patients with malaria, or their relatives, and bought the medicines offered to them.
Both studies used a randomized approach to sampling of drug outlets, which differs from previous studies that mostly used non-representative methods for selecting drugs for analysis.
Neither study unearthed falsified drugs, but substandard drugs were found in 31% of samples in Cambodia and 12% of samples in Tanzania.
“Falsified medicines have received much attention globally, but substandard drugs are far more prevalent and of great concern,” said Shunmay Yeung, MBBS, PhD, also of the London School of Hygiene & Tropical Medicine.
“Not only do they leave patients with malaria undertreated, which could be fatal, but they may also contribute to the development of resistance to [artemisinin-based combination therapies], the most effective drugs for malaria. Generally, the fact that no falsified antimalarials were identified reflects the positive impact of the [countries’ efforts] to control drug quality.” ![]()
Photo courtesy of the
London School of Hygiene
& Tropical Medicine
Investigations into antimalarial drug quality conducted in Cambodia and Tanzania uncovered no evidence of fake medicines.
Previous reports had suggested that up to a third of antimalarials might be falsified, or do not contain the stated active pharmaceutical ingredient.
The new research revealed no falsified drugs in either country, but it did unearth substandard antimalarial drugs, or genuine medicines that do not have the correct amount of the active ingredient.
These findings were published in 2 articles in the American Journal of Tropical Medicine and Hygiene.
“Although there have been alarming reports about the prevalence of fake antimalarials, our study provides ample data showing that the quality of drugs is not so bad based on comprehensive sampling and analysis presented here,” said Harparkash Kaur, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“The lack of falsified medicines in Cambodia and Tanzania are reassuring, but the presence of substandard medicines is definitely a concern.”
The researchers analyzed 2028 antimalarials from Tanzania and Cambodia at 3 independent laboratories in the UK and US. They classified drugs as acceptable, falsified, or substandard.
In Tanzania, the researchers used an “overt sampling” system, telling vendors they were going to analyze the quality of their medicines.
In Cambodia, the researchers used overt sampling as well as a “mystery client” approach, where actors pretended to be patients with malaria, or their relatives, and bought the medicines offered to them.
Both studies used a randomized approach to sampling of drug outlets, which differs from previous studies that mostly used non-representative methods for selecting drugs for analysis.
Neither study unearthed falsified drugs, but substandard drugs were found in 31% of samples in Cambodia and 12% of samples in Tanzania.
“Falsified medicines have received much attention globally, but substandard drugs are far more prevalent and of great concern,” said Shunmay Yeung, MBBS, PhD, also of the London School of Hygiene & Tropical Medicine.
“Not only do they leave patients with malaria undertreated, which could be fatal, but they may also contribute to the development of resistance to [artemisinin-based combination therapies], the most effective drugs for malaria. Generally, the fact that no falsified antimalarials were identified reflects the positive impact of the [countries’ efforts] to control drug quality.” ![]()
Alzheimer’s drug improves cognitive function after RT for brain tumors
Adult brain tumor survivors taking donepezil, a drug approved for the treatment of Alzheimer’s disease, showed significant improvements in the cognitive functions of memory, motor speed, and dexterity, compared with those taking a placebo. However, improvements in the primary outcome of composite cognitive function were similar for the two arms, investigators reported.
The study results were published online April 20 in the Journal of Clinical Oncology.
Patients with greater pretreatment deficits saw greater improvements in cognitive functioning with donepezil treatment, reported Stephen Rapp, Ph.D., professor of psychiatry and behavioral medicine at Wake Forest School of Medicine, Winston-Salem, N.C., and associates.
“This suggests that treatment with a daily dose of donepezil can provide benefit to some adult long-term brain tumor survivors after PBI or WBI [partial- or whole-brain irradiation], particularly those with greater pretreatment cognitive impairment,” they wrote (J. Clin. Oncol. 2015 Apr. 20 [doi: 10.1200/JCO.2014.58.4508]).
The phase III trial enrolled 198 primary or metastatic brain tumor survivors who underwent fractionated PBI or WBI at least 6 months previously. Patients received either donepezil at 5 mg daily for 6 weeks, followed by 10 mg daily for 18 weeks if well tolerated, or placebo for 24 weeks. Composite cognitive scores improved for both arms and did not differ significantly. Donepezil treatment resulted in significantly greater improvements in memory (recognition, P = .027; discrimination, P = .007) and motor speed and dexterity (P = .016).
Donepezil was generally well tolerated, except for diarrhea in 25% of the active arm vs. 9% in the placebo arm (P = .005). The study retention rate was 74% at 24 weeks for both groups.
Although enrolled patients had a high level of cognitive impairment relative to noncancer controls, with 91% having at least one test score at least 1.5 standard deviations below the normal comparison group, scores across most measures varied widely from significantly lower to higher than the comparison group. This heterogeneity may underlie the less than significant improvement observed with the study treatment. Patients with greater cognitive deficits saw greater benefits.
“This indicates that brain tumors and their treatments, including cranial irradiation, are associated with clinically significant cognitive impairment among some but not all patients. In future studies, demonstrable cognitive impairment should be an inclusion criterion for enrollment,” Dr. Rapp and associates wrote.
The study by Rapp et al. suggests that for brain tumor survivors experiencing cognitive difficulties, intervention with donepezil, a drug approved for use in Alzheimer’s disease (AD), may be helpful. Although average improvements were small, the trial indicates clear benefit for some patients, especially those most impaired. The study followed patients taking the drug for 6 months, but patients who responded to treatment likely will continue with lifelong therapy, based on experience with donepezil in AD. After cessation of the agent, neurocognitive function of treated AD patients declined to the level of untreated patients.
The results of the current study justify administering the drug to affected patients and monitoring for effects. In the absence of evidence of clinical benefit, the data do not support continuing treatment. Donepezil use in AD is continued for some patients even without signs of improvement, on the basis of slowing expected decline. However, cognitive declines due to tumor and treatment injury do not progress over time, and donepezil use in this population is supported only with evidence of benefit.
Optimal dosing for cancer patients requires further study, but studies with AD patients showed no clear benefit of dose escalation that outweighed GI adverse effects.
Maintaining maximal cognitive functioning in patients who often begin treatment with brain injury due to the tumor and unrelated illnesses, requires first the prevention of further damage. Strategies include functional image-guided surgery, limiting daily radiation fraction size, improved image-guided radiotherapy target definition, highly conformal radiotherapy administration techniques, and highly focused stereotactic radiosurgery in place of whole-brain radiotherapy for many patients with brain metastasis. Research on improvements in imaging of tumor and functional brain to better guide surgery and radiation is worthwhile.
Neurocognitive rehabilitation is recommended for patients with cognitive deficits that persist after therapy had ended. A recent randomized study showed clear benefit of rehabilitation for attention, verbal memory, and mental fatigue.
By taking steps to prevent injury, rehabilitate patients with deficits, and administer drug therapies while monitoring for benefit, improvements to cognitive function in brain tumor survivors may begin to increase. To best employ these strategies, a validated, easy-to-use instrument that measures mild to moderate impairment is needed for routine oncology practice.
Dr. Lawrence Kleinberg is associate professor of radiation oncology and molecular radiation sciences at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore. These comments were excerpted from the editorial accompanying the report by Dr. Rapp et al. (J. Clin. Oncol. 2015 April 20 [doi: 10.1200/JCO.2014.60.2805]).
The study by Rapp et al. suggests that for brain tumor survivors experiencing cognitive difficulties, intervention with donepezil, a drug approved for use in Alzheimer’s disease (AD), may be helpful. Although average improvements were small, the trial indicates clear benefit for some patients, especially those most impaired. The study followed patients taking the drug for 6 months, but patients who responded to treatment likely will continue with lifelong therapy, based on experience with donepezil in AD. After cessation of the agent, neurocognitive function of treated AD patients declined to the level of untreated patients.
The results of the current study justify administering the drug to affected patients and monitoring for effects. In the absence of evidence of clinical benefit, the data do not support continuing treatment. Donepezil use in AD is continued for some patients even without signs of improvement, on the basis of slowing expected decline. However, cognitive declines due to tumor and treatment injury do not progress over time, and donepezil use in this population is supported only with evidence of benefit.
Optimal dosing for cancer patients requires further study, but studies with AD patients showed no clear benefit of dose escalation that outweighed GI adverse effects.
Maintaining maximal cognitive functioning in patients who often begin treatment with brain injury due to the tumor and unrelated illnesses, requires first the prevention of further damage. Strategies include functional image-guided surgery, limiting daily radiation fraction size, improved image-guided radiotherapy target definition, highly conformal radiotherapy administration techniques, and highly focused stereotactic radiosurgery in place of whole-brain radiotherapy for many patients with brain metastasis. Research on improvements in imaging of tumor and functional brain to better guide surgery and radiation is worthwhile.
Neurocognitive rehabilitation is recommended for patients with cognitive deficits that persist after therapy had ended. A recent randomized study showed clear benefit of rehabilitation for attention, verbal memory, and mental fatigue.
By taking steps to prevent injury, rehabilitate patients with deficits, and administer drug therapies while monitoring for benefit, improvements to cognitive function in brain tumor survivors may begin to increase. To best employ these strategies, a validated, easy-to-use instrument that measures mild to moderate impairment is needed for routine oncology practice.
Dr. Lawrence Kleinberg is associate professor of radiation oncology and molecular radiation sciences at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore. These comments were excerpted from the editorial accompanying the report by Dr. Rapp et al. (J. Clin. Oncol. 2015 April 20 [doi: 10.1200/JCO.2014.60.2805]).
The study by Rapp et al. suggests that for brain tumor survivors experiencing cognitive difficulties, intervention with donepezil, a drug approved for use in Alzheimer’s disease (AD), may be helpful. Although average improvements were small, the trial indicates clear benefit for some patients, especially those most impaired. The study followed patients taking the drug for 6 months, but patients who responded to treatment likely will continue with lifelong therapy, based on experience with donepezil in AD. After cessation of the agent, neurocognitive function of treated AD patients declined to the level of untreated patients.
The results of the current study justify administering the drug to affected patients and monitoring for effects. In the absence of evidence of clinical benefit, the data do not support continuing treatment. Donepezil use in AD is continued for some patients even without signs of improvement, on the basis of slowing expected decline. However, cognitive declines due to tumor and treatment injury do not progress over time, and donepezil use in this population is supported only with evidence of benefit.
Optimal dosing for cancer patients requires further study, but studies with AD patients showed no clear benefit of dose escalation that outweighed GI adverse effects.
Maintaining maximal cognitive functioning in patients who often begin treatment with brain injury due to the tumor and unrelated illnesses, requires first the prevention of further damage. Strategies include functional image-guided surgery, limiting daily radiation fraction size, improved image-guided radiotherapy target definition, highly conformal radiotherapy administration techniques, and highly focused stereotactic radiosurgery in place of whole-brain radiotherapy for many patients with brain metastasis. Research on improvements in imaging of tumor and functional brain to better guide surgery and radiation is worthwhile.
Neurocognitive rehabilitation is recommended for patients with cognitive deficits that persist after therapy had ended. A recent randomized study showed clear benefit of rehabilitation for attention, verbal memory, and mental fatigue.
By taking steps to prevent injury, rehabilitate patients with deficits, and administer drug therapies while monitoring for benefit, improvements to cognitive function in brain tumor survivors may begin to increase. To best employ these strategies, a validated, easy-to-use instrument that measures mild to moderate impairment is needed for routine oncology practice.
Dr. Lawrence Kleinberg is associate professor of radiation oncology and molecular radiation sciences at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore. These comments were excerpted from the editorial accompanying the report by Dr. Rapp et al. (J. Clin. Oncol. 2015 April 20 [doi: 10.1200/JCO.2014.60.2805]).
Adult brain tumor survivors taking donepezil, a drug approved for the treatment of Alzheimer’s disease, showed significant improvements in the cognitive functions of memory, motor speed, and dexterity, compared with those taking a placebo. However, improvements in the primary outcome of composite cognitive function were similar for the two arms, investigators reported.
The study results were published online April 20 in the Journal of Clinical Oncology.
Patients with greater pretreatment deficits saw greater improvements in cognitive functioning with donepezil treatment, reported Stephen Rapp, Ph.D., professor of psychiatry and behavioral medicine at Wake Forest School of Medicine, Winston-Salem, N.C., and associates.
“This suggests that treatment with a daily dose of donepezil can provide benefit to some adult long-term brain tumor survivors after PBI or WBI [partial- or whole-brain irradiation], particularly those with greater pretreatment cognitive impairment,” they wrote (J. Clin. Oncol. 2015 Apr. 20 [doi: 10.1200/JCO.2014.58.4508]).
The phase III trial enrolled 198 primary or metastatic brain tumor survivors who underwent fractionated PBI or WBI at least 6 months previously. Patients received either donepezil at 5 mg daily for 6 weeks, followed by 10 mg daily for 18 weeks if well tolerated, or placebo for 24 weeks. Composite cognitive scores improved for both arms and did not differ significantly. Donepezil treatment resulted in significantly greater improvements in memory (recognition, P = .027; discrimination, P = .007) and motor speed and dexterity (P = .016).
Donepezil was generally well tolerated, except for diarrhea in 25% of the active arm vs. 9% in the placebo arm (P = .005). The study retention rate was 74% at 24 weeks for both groups.
Although enrolled patients had a high level of cognitive impairment relative to noncancer controls, with 91% having at least one test score at least 1.5 standard deviations below the normal comparison group, scores across most measures varied widely from significantly lower to higher than the comparison group. This heterogeneity may underlie the less than significant improvement observed with the study treatment. Patients with greater cognitive deficits saw greater benefits.
“This indicates that brain tumors and their treatments, including cranial irradiation, are associated with clinically significant cognitive impairment among some but not all patients. In future studies, demonstrable cognitive impairment should be an inclusion criterion for enrollment,” Dr. Rapp and associates wrote.
Adult brain tumor survivors taking donepezil, a drug approved for the treatment of Alzheimer’s disease, showed significant improvements in the cognitive functions of memory, motor speed, and dexterity, compared with those taking a placebo. However, improvements in the primary outcome of composite cognitive function were similar for the two arms, investigators reported.
The study results were published online April 20 in the Journal of Clinical Oncology.
Patients with greater pretreatment deficits saw greater improvements in cognitive functioning with donepezil treatment, reported Stephen Rapp, Ph.D., professor of psychiatry and behavioral medicine at Wake Forest School of Medicine, Winston-Salem, N.C., and associates.
“This suggests that treatment with a daily dose of donepezil can provide benefit to some adult long-term brain tumor survivors after PBI or WBI [partial- or whole-brain irradiation], particularly those with greater pretreatment cognitive impairment,” they wrote (J. Clin. Oncol. 2015 Apr. 20 [doi: 10.1200/JCO.2014.58.4508]).
The phase III trial enrolled 198 primary or metastatic brain tumor survivors who underwent fractionated PBI or WBI at least 6 months previously. Patients received either donepezil at 5 mg daily for 6 weeks, followed by 10 mg daily for 18 weeks if well tolerated, or placebo for 24 weeks. Composite cognitive scores improved for both arms and did not differ significantly. Donepezil treatment resulted in significantly greater improvements in memory (recognition, P = .027; discrimination, P = .007) and motor speed and dexterity (P = .016).
Donepezil was generally well tolerated, except for diarrhea in 25% of the active arm vs. 9% in the placebo arm (P = .005). The study retention rate was 74% at 24 weeks for both groups.
Although enrolled patients had a high level of cognitive impairment relative to noncancer controls, with 91% having at least one test score at least 1.5 standard deviations below the normal comparison group, scores across most measures varied widely from significantly lower to higher than the comparison group. This heterogeneity may underlie the less than significant improvement observed with the study treatment. Patients with greater cognitive deficits saw greater benefits.
“This indicates that brain tumors and their treatments, including cranial irradiation, are associated with clinically significant cognitive impairment among some but not all patients. In future studies, demonstrable cognitive impairment should be an inclusion criterion for enrollment,” Dr. Rapp and associates wrote.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Among adult brain tumor survivors who underwent partial- or whole-brain irradiation, treatment with donepezil compared with placebo was associated with significant improvements in memory and motor speed and dexterity, but composite cognitive scores were similar.
Major finding: After 24 weeks of treatment, patients taking donepezil (vs. placebo) had significantly more improvement in memory (recognition, P = .027; discrimination, P = .007) and motor speed and dexterity (P = .016).
Data source: A double-blind phase III trial that randomized 198 patients who had undergone irradiation at least 6 months previously to receive donepezil (5 mg for 6 weeks followed by 10 mg for 18 weeks) or placebo (24 weeks).
Disclosures: Dr. Rapp reported having no financial disclosures.
ABVD and Stanford V similar for bulky mediastinal Hodgkin’s lymphoma
Failure-free survival and overall survival were similar between two combined modality therapies in patients with stage I or II bulky mediastinal Hodgkin’s lymphoma, investigators reported.
The results were published online April 20 in the Journal of Clinical Oncology.
The phase III trial evaluated outcomes following treatment with either doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) or mechlorethamine, doxorubicin, vincristine, bleomycin, vinblastine, etoposide, and prednisone (Stanford V).
Median failure-free survival (FFS) and overall survival (OS) were not reached in either arm. The 5-year FFS and OS were 85% and 96% for ABVD, respectively, and 79% and 92% for Stanford V, reported Dr. Ranjana H. Advani, professor of oncology at Stanford (Calif.) University, and associates.
At a median follow up of 6.54 years, 19 treatment failures occurred in the ABVD arm and 23 in the Stanford V arm. In total, 14 deaths occurred, 5 in the ABVD group and 9 in the Stanford V group.
Approximately 20%-25% of patients with stage I or II Hodgkin’s lymphoma (HL) have bulky mediastinal involvement, and this was the first contemporary prospective trial to evaluate this patient subgroup, the investigators wrote (J. Clin. Oncol. 2015 April 20 [doi:10.1200/JCO.2014.57.8138]).
“This is important because ongoing trials in North America use mediastinal bulk as an eligibility criterion, and contemporary guidelines use it to define treatment algorithms,” Dr. Advani and associates said, noting that both regimens are acceptable treatment options.
“In addition, these results provide an important contemporary benchmark for comparison of ongoing and future studies,” they wrote.
Out of 854 patients with HL enrolled in the trial, 264 with bulky disease were eligible for the subgroup analysis; 135 received ABVD and 129 received Stanford V. After completion of chemotherapy, all patients received 36 Gy of modified involved field radiotherapy (IFRT). Patterns of relapse were similar between treatment arms, and less than 10% of patients had in-field recurrences, a finding that indicated effective local control with IFRT.
Both treatment arms had similar rates of grade 3-4 neutropenia, and the Stanford V arm had more grade 3 lymphopenia (83% vs. 46%, P < .001) and grade 3 and 4 sensory neuropathy. At 5 years, both groups had similar risks of second cancers: two in the ABVD group and six in the Stanford group. The assessment of risks associated with higher doses of anthracycline and bleomycin in ABVD and larger radiation fields in Stanford V requires longer follow-up, the researchers wrote.
Failure-free survival and overall survival were similar between two combined modality therapies in patients with stage I or II bulky mediastinal Hodgkin’s lymphoma, investigators reported.
The results were published online April 20 in the Journal of Clinical Oncology.
The phase III trial evaluated outcomes following treatment with either doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) or mechlorethamine, doxorubicin, vincristine, bleomycin, vinblastine, etoposide, and prednisone (Stanford V).
Median failure-free survival (FFS) and overall survival (OS) were not reached in either arm. The 5-year FFS and OS were 85% and 96% for ABVD, respectively, and 79% and 92% for Stanford V, reported Dr. Ranjana H. Advani, professor of oncology at Stanford (Calif.) University, and associates.
At a median follow up of 6.54 years, 19 treatment failures occurred in the ABVD arm and 23 in the Stanford V arm. In total, 14 deaths occurred, 5 in the ABVD group and 9 in the Stanford V group.
Approximately 20%-25% of patients with stage I or II Hodgkin’s lymphoma (HL) have bulky mediastinal involvement, and this was the first contemporary prospective trial to evaluate this patient subgroup, the investigators wrote (J. Clin. Oncol. 2015 April 20 [doi:10.1200/JCO.2014.57.8138]).
“This is important because ongoing trials in North America use mediastinal bulk as an eligibility criterion, and contemporary guidelines use it to define treatment algorithms,” Dr. Advani and associates said, noting that both regimens are acceptable treatment options.
“In addition, these results provide an important contemporary benchmark for comparison of ongoing and future studies,” they wrote.
Out of 854 patients with HL enrolled in the trial, 264 with bulky disease were eligible for the subgroup analysis; 135 received ABVD and 129 received Stanford V. After completion of chemotherapy, all patients received 36 Gy of modified involved field radiotherapy (IFRT). Patterns of relapse were similar between treatment arms, and less than 10% of patients had in-field recurrences, a finding that indicated effective local control with IFRT.
Both treatment arms had similar rates of grade 3-4 neutropenia, and the Stanford V arm had more grade 3 lymphopenia (83% vs. 46%, P < .001) and grade 3 and 4 sensory neuropathy. At 5 years, both groups had similar risks of second cancers: two in the ABVD group and six in the Stanford group. The assessment of risks associated with higher doses of anthracycline and bleomycin in ABVD and larger radiation fields in Stanford V requires longer follow-up, the researchers wrote.
Failure-free survival and overall survival were similar between two combined modality therapies in patients with stage I or II bulky mediastinal Hodgkin’s lymphoma, investigators reported.
The results were published online April 20 in the Journal of Clinical Oncology.
The phase III trial evaluated outcomes following treatment with either doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) or mechlorethamine, doxorubicin, vincristine, bleomycin, vinblastine, etoposide, and prednisone (Stanford V).
Median failure-free survival (FFS) and overall survival (OS) were not reached in either arm. The 5-year FFS and OS were 85% and 96% for ABVD, respectively, and 79% and 92% for Stanford V, reported Dr. Ranjana H. Advani, professor of oncology at Stanford (Calif.) University, and associates.
At a median follow up of 6.54 years, 19 treatment failures occurred in the ABVD arm and 23 in the Stanford V arm. In total, 14 deaths occurred, 5 in the ABVD group and 9 in the Stanford V group.
Approximately 20%-25% of patients with stage I or II Hodgkin’s lymphoma (HL) have bulky mediastinal involvement, and this was the first contemporary prospective trial to evaluate this patient subgroup, the investigators wrote (J. Clin. Oncol. 2015 April 20 [doi:10.1200/JCO.2014.57.8138]).
“This is important because ongoing trials in North America use mediastinal bulk as an eligibility criterion, and contemporary guidelines use it to define treatment algorithms,” Dr. Advani and associates said, noting that both regimens are acceptable treatment options.
“In addition, these results provide an important contemporary benchmark for comparison of ongoing and future studies,” they wrote.
Out of 854 patients with HL enrolled in the trial, 264 with bulky disease were eligible for the subgroup analysis; 135 received ABVD and 129 received Stanford V. After completion of chemotherapy, all patients received 36 Gy of modified involved field radiotherapy (IFRT). Patterns of relapse were similar between treatment arms, and less than 10% of patients had in-field recurrences, a finding that indicated effective local control with IFRT.
Both treatment arms had similar rates of grade 3-4 neutropenia, and the Stanford V arm had more grade 3 lymphopenia (83% vs. 46%, P < .001) and grade 3 and 4 sensory neuropathy. At 5 years, both groups had similar risks of second cancers: two in the ABVD group and six in the Stanford group. The assessment of risks associated with higher doses of anthracycline and bleomycin in ABVD and larger radiation fields in Stanford V requires longer follow-up, the researchers wrote.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: No significant differences in outcomes were observed after treatment with ABVD vs. Stanford V in patients with stage I or II bulky mediastinal Hodgkin’s lymphoma.
Major finding: At a median follow-up of 6.5 years, ABVD and Stanford V resulted in similar numbers of treatment failures (19 vs. 23), complete remission rate (75% vs. 81%), and overall response rate (83% vs. 88%), respectively.
Data source: A subgroup analysis of a phase III trial of patients with stage I or II bulky disease, in which 135 were assigned ABVD and 129 received Stanford V.
Disclosures: Dr. Advani reported receiving research funds from Millennium, Takeda Oncology, Seattle Genetics, Genentech/Roche, Allos Therapeutics, Pharmacyclics, Janssen Pharmaceuticals, Celgene, and Idera Pharmaceuticals. Many of his coauthors reported ties to several industry sources.
NSAIDs for depression
At the risk of stating the obvious, our patients are becoming increasingly complex. Life is prolonged and comorbidities accumulate, creating dizzying laundry lists of medical problems.
Within the context of clinical or, increasingly, nonreimbursed telephonic or electronic visits, we attack the medical problem with the worst severity in an attempt to tamp it down to the level of its comorbid brethren.

Almost without exception, depression rears its ugly head in our sickest patients. Antidepressants will be started and added to the three pages (double-spaced, with 1-inch margins) of medications.
But in all of these patients, are we treating the disease or just the symptom? What if inflammation is causing the depression? Will reduction of inflammation treat the depression?
Dr. Ole Köhler of Aarhus University Hospital, Denmark, and his colleagues conducted a systematic review on the antidepressant effects of anti-inflammatory medications (JAMA Psychiatry 2014;71:1381-91). Fourteen trials informed the meta-analysis, 10 that evaluated NSAID drugs (for example, celecoxib, naproxen, ibuprofen), and 4 that investigated cytokine inhibitors (for example, etanercept, infliximab). Six of the 10 NSAID studies evaluated NSAIDs as monotherapy. All four of the cytokine-inhibitor trials evaluated them as monotherapy. Length of treatment was between 6 and 12 weeks.
The pooled effect suggests that anti-inflammatory treatment reduced depressive symptoms. Celecoxib seemed to have the strongest effect on remission and clinical response. No increase in adverse events was reported.
We know that proinflammatory drugs can induce depression. So the opposite is quite possibly true, and these data suggest it to be so. Findings suggest that reducing the inflammatory state among our patients with depression may be a useful adjunct to antidepressant therapy, at least in the initial period.
Whatever we can do to facilitate depressive symptom relief seems a worthy goal. So, here again, we could tell our patients presenting with depression to take two (with an SSRI, perhaps) and call us in the morning. But how best to do this and in what patients remains uncertain.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified, practicing clinician.
At the risk of stating the obvious, our patients are becoming increasingly complex. Life is prolonged and comorbidities accumulate, creating dizzying laundry lists of medical problems.
Within the context of clinical or, increasingly, nonreimbursed telephonic or electronic visits, we attack the medical problem with the worst severity in an attempt to tamp it down to the level of its comorbid brethren.
Almost without exception, depression rears its ugly head in our sickest patients. Antidepressants will be started and added to the three pages (double-spaced, with 1-inch margins) of medications.
But in all of these patients, are we treating the disease or just the symptom? What if inflammation is causing the depression? Will reduction of inflammation treat the depression?
Dr. Ole Köhler of Aarhus University Hospital, Denmark, and his colleagues conducted a systematic review on the antidepressant effects of anti-inflammatory medications (JAMA Psychiatry 2014;71:1381-91). Fourteen trials informed the meta-analysis, 10 that evaluated NSAID drugs (for example, celecoxib, naproxen, ibuprofen), and 4 that investigated cytokine inhibitors (for example, etanercept, infliximab). Six of the 10 NSAID studies evaluated NSAIDs as monotherapy. All four of the cytokine-inhibitor trials evaluated them as monotherapy. Length of treatment was between 6 and 12 weeks.
The pooled effect suggests that anti-inflammatory treatment reduced depressive symptoms. Celecoxib seemed to have the strongest effect on remission and clinical response. No increase in adverse events was reported.
We know that proinflammatory drugs can induce depression. So the opposite is quite possibly true, and these data suggest it to be so. Findings suggest that reducing the inflammatory state among our patients with depression may be a useful adjunct to antidepressant therapy, at least in the initial period.
Whatever we can do to facilitate depressive symptom relief seems a worthy goal. So, here again, we could tell our patients presenting with depression to take two (with an SSRI, perhaps) and call us in the morning. But how best to do this and in what patients remains uncertain.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified, practicing clinician.
At the risk of stating the obvious, our patients are becoming increasingly complex. Life is prolonged and comorbidities accumulate, creating dizzying laundry lists of medical problems.
Within the context of clinical or, increasingly, nonreimbursed telephonic or electronic visits, we attack the medical problem with the worst severity in an attempt to tamp it down to the level of its comorbid brethren.
Almost without exception, depression rears its ugly head in our sickest patients. Antidepressants will be started and added to the three pages (double-spaced, with 1-inch margins) of medications.
But in all of these patients, are we treating the disease or just the symptom? What if inflammation is causing the depression? Will reduction of inflammation treat the depression?
Dr. Ole Köhler of Aarhus University Hospital, Denmark, and his colleagues conducted a systematic review on the antidepressant effects of anti-inflammatory medications (JAMA Psychiatry 2014;71:1381-91). Fourteen trials informed the meta-analysis, 10 that evaluated NSAID drugs (for example, celecoxib, naproxen, ibuprofen), and 4 that investigated cytokine inhibitors (for example, etanercept, infliximab). Six of the 10 NSAID studies evaluated NSAIDs as monotherapy. All four of the cytokine-inhibitor trials evaluated them as monotherapy. Length of treatment was between 6 and 12 weeks.
The pooled effect suggests that anti-inflammatory treatment reduced depressive symptoms. Celecoxib seemed to have the strongest effect on remission and clinical response. No increase in adverse events was reported.
We know that proinflammatory drugs can induce depression. So the opposite is quite possibly true, and these data suggest it to be so. Findings suggest that reducing the inflammatory state among our patients with depression may be a useful adjunct to antidepressant therapy, at least in the initial period.
Whatever we can do to facilitate depressive symptom relief seems a worthy goal. So, here again, we could tell our patients presenting with depression to take two (with an SSRI, perhaps) and call us in the morning. But how best to do this and in what patients remains uncertain.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified, practicing clinician.

Low-risk PE patients can be treated as outpatients
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).