User login
Number of Zika-infected pregnancies jumps in states/D.C.
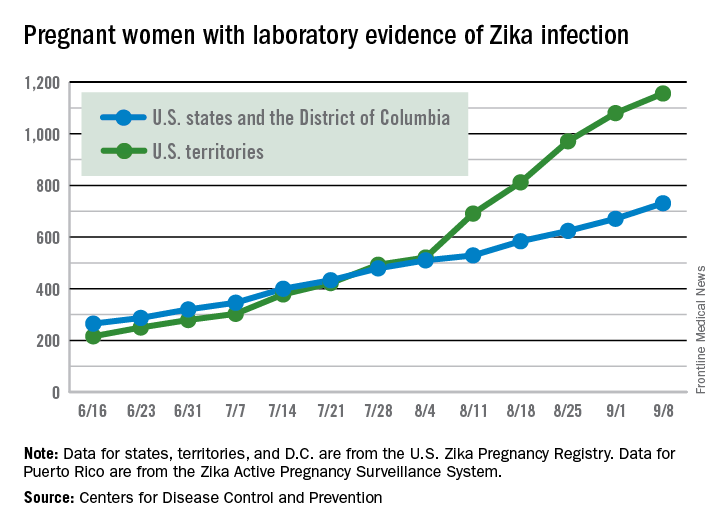
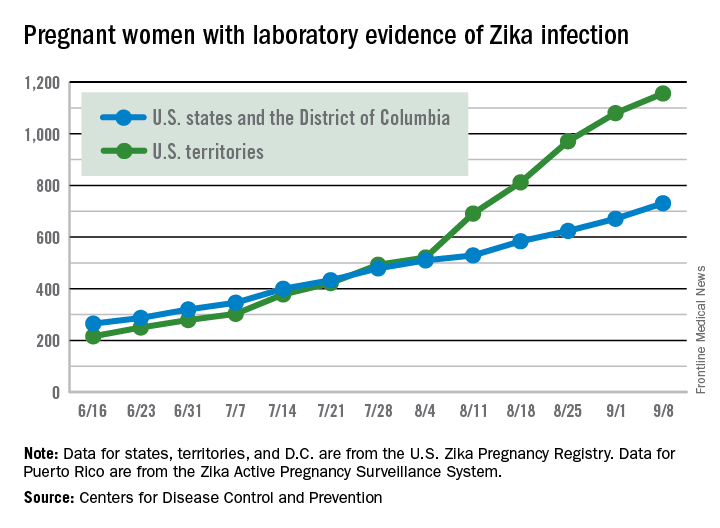
There were 60 more pregnant women in the 50 states and the District of Columbia with laboratory evidence of Zika infection for the week ending Sept. 8, according to the Centers for Disease Control and Prevention.
That is the largest weekly increase yet among that population, and it brings the total number of Zika-infected pregnant women to 731 in the 50 states and D.C. so far in 2016. The U.S. territories reported 76 new cases for the week ending Sept. 8, for a territorial total of 1,156 and a combined U.S. total of 1,887 pregnant women with Zika virus, the CDC reported Sept. 15.
For the second week in a row, a liveborn infant with Zika-related birth defects was born in the 50 states/D.C. The total is now 19 for the year: 18 in the states/D.C. and 1 in the territories. There were no new pregnancy losses with Zika-related birth defects, so the number holds at six for the year: five in the states/D.C. and one in the territories, the CDC said.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 60 more pregnant women in the 50 states and the District of Columbia with laboratory evidence of Zika infection for the week ending Sept. 8, according to the Centers for Disease Control and Prevention.
That is the largest weekly increase yet among that population, and it brings the total number of Zika-infected pregnant women to 731 in the 50 states and D.C. so far in 2016. The U.S. territories reported 76 new cases for the week ending Sept. 8, for a territorial total of 1,156 and a combined U.S. total of 1,887 pregnant women with Zika virus, the CDC reported Sept. 15.
For the second week in a row, a liveborn infant with Zika-related birth defects was born in the 50 states/D.C. The total is now 19 for the year: 18 in the states/D.C. and 1 in the territories. There were no new pregnancy losses with Zika-related birth defects, so the number holds at six for the year: five in the states/D.C. and one in the territories, the CDC said.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 60 more pregnant women in the 50 states and the District of Columbia with laboratory evidence of Zika infection for the week ending Sept. 8, according to the Centers for Disease Control and Prevention.
That is the largest weekly increase yet among that population, and it brings the total number of Zika-infected pregnant women to 731 in the 50 states and D.C. so far in 2016. The U.S. territories reported 76 new cases for the week ending Sept. 8, for a territorial total of 1,156 and a combined U.S. total of 1,887 pregnant women with Zika virus, the CDC reported Sept. 15.
For the second week in a row, a liveborn infant with Zika-related birth defects was born in the 50 states/D.C. The total is now 19 for the year: 18 in the states/D.C. and 1 in the territories. There were no new pregnancy losses with Zika-related birth defects, so the number holds at six for the year: five in the states/D.C. and one in the territories, the CDC said.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Pain starting in knee later arises in other joints
People who develop knee pain associated with osteoarthritis often subsequently develop pain in other joints, according to a study of two observational, community-based cohorts that could not discern any pattern of new pain sites.
In the “first investigation of the association of knee pain with pain in multiple other sites,” David T. Felson, MD, of Boston University and his colleagues reported that the regions where pain developed after first appearing in the knee varied from person to person and occurred in both upper and lower extremities, which goes against the hypothesis that adjacent joints are most often affected by knee pain.

The study involved patients from the MOST (Multicenter Osteoarthritis Study) trial, including 281 with knee pain at the index visit (168 unilaterally) and 852 without, as well as patients from OAI (the Osteoarthritis Initiative), including 412 with knee pain at the index visit (241 unilaterally), and 1,941 without. The investigators assessed the patients’ data for 14 total joints outside of the knees: 2 each of feet, ankles, hips, hands, wrists, elbows, and shoulders (Arthritis Rheumatol. 2016 Sep 2. doi: 10.1002/art.39848).
Patients with new-onset knee pain at the index visit reported a mean of 2.3 painful joints outside the knee, compared with a significantly lower number of 1.3 reported by those without knee pain. The mean number of nonknee joints with pain was higher among patients with bilateral knee pain, compared with unilateral knee pain. The percentage of patients who reported pain outside the knee rose with the number of painful knees: 80% for two, 64% for one, and 50% for none.
The patients who developed new unilateral knee pain at the index visit also experienced an increase in prevalent joint pain in multiple joints in upper- and lower-extremity sites. In particular, the investigators noted that ipsilateral prevalent hip joint pain, which they characterized as pain in the groin or front of the thigh, was more than twice as likely to occur among those with new unilateral knee pain at the index visit, but the odds for contralateral hip joint pain did not reach statistical significance. The comparisons were adjusted for age, sex, body mass index, depression at the index visit, study (MOST or OAI), and count of painful upper and lower limb joints at the index visit (excluding knees).
When examining only patients with new-onset joint pain outside of the knee, the odds of patients with new knee pain to later develop new-onset joint pain outside the knee were 30% higher than for those without knee pain. Patients with new knee pain had a mean 2.6 new painful joints out of 12.1 eligible joints, compared with 2.0 new painful joints in those without knee pain out of 12.7 eligible joints. (Joint regions with prevalent symptoms at the index visit were excluded as incident painful sites.) Patients with knee pain also had a consistently higher rate of new-onset pain in nonknee joints when compared with patients without knee pain in at least half of the follow-up visits over the course of the MOST and OAI studies. Sensitivity analyses indicated that the association between knee pain and subsequent pain in other joints was not driven by the inclusion of patients with widespread pain.
“There was no clear-cut predilection for pain in any specific lower-extremity joint region,” the investigators wrote.
The investigators noted that other researchers have suggested that patients with knee pain may be at higher risk for lower-extremity joint pain because of changes to their gait that gradually cause damage to other joints, but evidence in this study doesn’t “necessarily support the argument that in persons with knee pain, aberrant loading by altered movement patterns induces pain in only nearby joints. Our findings suggest that the sites affected are more than just hip and ankle and that there is no special predilection for pain in these locations.”
While the investigators cannot differentiate underlying mechanisms for their study’s finding of multiple co-occurring sites of joint pain in people with new-onset knee pain, they suggested that it “supports either a predilection for osteoarthritic changes at multiple joint sites and/or raises the possibility that nervous system–driven pain sensitization increases the risk not only of widespread pain but even of regional pain. Since symptomatic OA is unusual in some of these painful sites (e.g., elbow, shoulder, ankle), pain sensitization would seem a more likely explanation.”
Some of the study’s limitations described by the investigators included the uncertainty surrounding whether new-onset knee pain was truly new onset or whether it was a reoccurrence, and also the fact that most of the people in the two cohorts had multiple sites of joint pain at both the baseline and the index visit and there were too few people with no sites of pain outside the knee to carry out subanalyses in that group, which “speaks to the high prevalence of multiple joint pains in older adult cohorts.”
The research was supported by grants from the National Institutes of Health. The authors had no disclosures to report.
People who develop knee pain associated with osteoarthritis often subsequently develop pain in other joints, according to a study of two observational, community-based cohorts that could not discern any pattern of new pain sites.
In the “first investigation of the association of knee pain with pain in multiple other sites,” David T. Felson, MD, of Boston University and his colleagues reported that the regions where pain developed after first appearing in the knee varied from person to person and occurred in both upper and lower extremities, which goes against the hypothesis that adjacent joints are most often affected by knee pain.
The study involved patients from the MOST (Multicenter Osteoarthritis Study) trial, including 281 with knee pain at the index visit (168 unilaterally) and 852 without, as well as patients from OAI (the Osteoarthritis Initiative), including 412 with knee pain at the index visit (241 unilaterally), and 1,941 without. The investigators assessed the patients’ data for 14 total joints outside of the knees: 2 each of feet, ankles, hips, hands, wrists, elbows, and shoulders (Arthritis Rheumatol. 2016 Sep 2. doi: 10.1002/art.39848).
Patients with new-onset knee pain at the index visit reported a mean of 2.3 painful joints outside the knee, compared with a significantly lower number of 1.3 reported by those without knee pain. The mean number of nonknee joints with pain was higher among patients with bilateral knee pain, compared with unilateral knee pain. The percentage of patients who reported pain outside the knee rose with the number of painful knees: 80% for two, 64% for one, and 50% for none.
The patients who developed new unilateral knee pain at the index visit also experienced an increase in prevalent joint pain in multiple joints in upper- and lower-extremity sites. In particular, the investigators noted that ipsilateral prevalent hip joint pain, which they characterized as pain in the groin or front of the thigh, was more than twice as likely to occur among those with new unilateral knee pain at the index visit, but the odds for contralateral hip joint pain did not reach statistical significance. The comparisons were adjusted for age, sex, body mass index, depression at the index visit, study (MOST or OAI), and count of painful upper and lower limb joints at the index visit (excluding knees).
When examining only patients with new-onset joint pain outside of the knee, the odds of patients with new knee pain to later develop new-onset joint pain outside the knee were 30% higher than for those without knee pain. Patients with new knee pain had a mean 2.6 new painful joints out of 12.1 eligible joints, compared with 2.0 new painful joints in those without knee pain out of 12.7 eligible joints. (Joint regions with prevalent symptoms at the index visit were excluded as incident painful sites.) Patients with knee pain also had a consistently higher rate of new-onset pain in nonknee joints when compared with patients without knee pain in at least half of the follow-up visits over the course of the MOST and OAI studies. Sensitivity analyses indicated that the association between knee pain and subsequent pain in other joints was not driven by the inclusion of patients with widespread pain.
“There was no clear-cut predilection for pain in any specific lower-extremity joint region,” the investigators wrote.
The investigators noted that other researchers have suggested that patients with knee pain may be at higher risk for lower-extremity joint pain because of changes to their gait that gradually cause damage to other joints, but evidence in this study doesn’t “necessarily support the argument that in persons with knee pain, aberrant loading by altered movement patterns induces pain in only nearby joints. Our findings suggest that the sites affected are more than just hip and ankle and that there is no special predilection for pain in these locations.”
While the investigators cannot differentiate underlying mechanisms for their study’s finding of multiple co-occurring sites of joint pain in people with new-onset knee pain, they suggested that it “supports either a predilection for osteoarthritic changes at multiple joint sites and/or raises the possibility that nervous system–driven pain sensitization increases the risk not only of widespread pain but even of regional pain. Since symptomatic OA is unusual in some of these painful sites (e.g., elbow, shoulder, ankle), pain sensitization would seem a more likely explanation.”
Some of the study’s limitations described by the investigators included the uncertainty surrounding whether new-onset knee pain was truly new onset or whether it was a reoccurrence, and also the fact that most of the people in the two cohorts had multiple sites of joint pain at both the baseline and the index visit and there were too few people with no sites of pain outside the knee to carry out subanalyses in that group, which “speaks to the high prevalence of multiple joint pains in older adult cohorts.”
The research was supported by grants from the National Institutes of Health. The authors had no disclosures to report.
People who develop knee pain associated with osteoarthritis often subsequently develop pain in other joints, according to a study of two observational, community-based cohorts that could not discern any pattern of new pain sites.
In the “first investigation of the association of knee pain with pain in multiple other sites,” David T. Felson, MD, of Boston University and his colleagues reported that the regions where pain developed after first appearing in the knee varied from person to person and occurred in both upper and lower extremities, which goes against the hypothesis that adjacent joints are most often affected by knee pain.
The study involved patients from the MOST (Multicenter Osteoarthritis Study) trial, including 281 with knee pain at the index visit (168 unilaterally) and 852 without, as well as patients from OAI (the Osteoarthritis Initiative), including 412 with knee pain at the index visit (241 unilaterally), and 1,941 without. The investigators assessed the patients’ data for 14 total joints outside of the knees: 2 each of feet, ankles, hips, hands, wrists, elbows, and shoulders (Arthritis Rheumatol. 2016 Sep 2. doi: 10.1002/art.39848).
Patients with new-onset knee pain at the index visit reported a mean of 2.3 painful joints outside the knee, compared with a significantly lower number of 1.3 reported by those without knee pain. The mean number of nonknee joints with pain was higher among patients with bilateral knee pain, compared with unilateral knee pain. The percentage of patients who reported pain outside the knee rose with the number of painful knees: 80% for two, 64% for one, and 50% for none.
The patients who developed new unilateral knee pain at the index visit also experienced an increase in prevalent joint pain in multiple joints in upper- and lower-extremity sites. In particular, the investigators noted that ipsilateral prevalent hip joint pain, which they characterized as pain in the groin or front of the thigh, was more than twice as likely to occur among those with new unilateral knee pain at the index visit, but the odds for contralateral hip joint pain did not reach statistical significance. The comparisons were adjusted for age, sex, body mass index, depression at the index visit, study (MOST or OAI), and count of painful upper and lower limb joints at the index visit (excluding knees).
When examining only patients with new-onset joint pain outside of the knee, the odds of patients with new knee pain to later develop new-onset joint pain outside the knee were 30% higher than for those without knee pain. Patients with new knee pain had a mean 2.6 new painful joints out of 12.1 eligible joints, compared with 2.0 new painful joints in those without knee pain out of 12.7 eligible joints. (Joint regions with prevalent symptoms at the index visit were excluded as incident painful sites.) Patients with knee pain also had a consistently higher rate of new-onset pain in nonknee joints when compared with patients without knee pain in at least half of the follow-up visits over the course of the MOST and OAI studies. Sensitivity analyses indicated that the association between knee pain and subsequent pain in other joints was not driven by the inclusion of patients with widespread pain.
“There was no clear-cut predilection for pain in any specific lower-extremity joint region,” the investigators wrote.
The investigators noted that other researchers have suggested that patients with knee pain may be at higher risk for lower-extremity joint pain because of changes to their gait that gradually cause damage to other joints, but evidence in this study doesn’t “necessarily support the argument that in persons with knee pain, aberrant loading by altered movement patterns induces pain in only nearby joints. Our findings suggest that the sites affected are more than just hip and ankle and that there is no special predilection for pain in these locations.”
While the investigators cannot differentiate underlying mechanisms for their study’s finding of multiple co-occurring sites of joint pain in people with new-onset knee pain, they suggested that it “supports either a predilection for osteoarthritic changes at multiple joint sites and/or raises the possibility that nervous system–driven pain sensitization increases the risk not only of widespread pain but even of regional pain. Since symptomatic OA is unusual in some of these painful sites (e.g., elbow, shoulder, ankle), pain sensitization would seem a more likely explanation.”
Some of the study’s limitations described by the investigators included the uncertainty surrounding whether new-onset knee pain was truly new onset or whether it was a reoccurrence, and also the fact that most of the people in the two cohorts had multiple sites of joint pain at both the baseline and the index visit and there were too few people with no sites of pain outside the knee to carry out subanalyses in that group, which “speaks to the high prevalence of multiple joint pains in older adult cohorts.”
The research was supported by grants from the National Institutes of Health. The authors had no disclosures to report.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:People with frequently painful knees often develop pain in joints outside the knee, and the sites vary from person to person.
Major finding: The odds of patients with new knee pain to later develop joint pain outside the knee were 30% higher than for those without knee pain.
Data source: A study of 693 persons with index visit knee pain and 2,793 without it from two community-based cohorts.
Disclosures: The research was supported by grants from the National Institutes of Health. The authors had no disclosures to report.

Telerehabilitation May Be As Effective As In-Person Rehabilitation in MS
LONDON—In patients with multiple sclerosis (MS), telerehabilitation is a convenient and practical method of performing physical therapy with efficacy comparable to that of conventional in-person physical therapy, as measured by objective outcomes of gait and balance. Telerehabilitation should be investigated further and used more extensively as a means of improving function and quality of life in MS, according to researchers who spoke at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS).
MS often results in physical and cognitive disability. Rehabilitation methods that include physical therapy can achieve functional improvement of established physical deficits. Factors such as availability, geographical distance, mobility, transportation, and cost, however, limit access to specialized rehabilitation services. Telecommunication technology opens the possibility of supervising and directing a physical therapy program remotely through audio and visual communication in real time.
Gabriel Pardo, MD, Director of the Oklahoma Medical Research Foundation MS Center of Excellence in Oklahoma City, and colleagues sought to demonstrate the feasibility of a tele-health rehabilitation program in individuals with ambulatory deficits secondary to MS. The researchers also intended to evaluate the efficacy of the tele-health rehabilitation program and compare it with that of conventional physical therapy.

Dr. Pardo and colleagues included 30 individuals in a single-center, prospective, randomized, three-arm, evaluator-blinded study that lasted for eight weeks. About 69% of participants were female, and the population’s mean age was 54.7. Approximately 60% of participants had relapsing-remitting MS, 23% had secondary progressive MS, and 17% had primary progressive MS. The population’s mean Expanded Disability Status Scale (EDSS) score was 4.3.
All participants performed a home-based exercise program (HEP) unsupervised on five days per week for eight weeks. Participants were randomized to three intervention groups. Group 1 underwent HEP alone. Group 2 underwent HEP plus remote physical therapy supervised via audio and visual real-time telecommunication two to three times per week. Group 3 underwent HEP plus in-person physical therapy at the medical facility two to three times per week. The study outcomes were multiple measurements of gait and balance, as well as patient-reported outcomes. Selected outcomes were performed with a computerized system (ie, Neurocom SmartBalance).
Functional gait assessment improved from baseline in all groups. Improvements were no different between the telerehabilitation and the conventional PT groups, but this finding was not statistically significant. Other outcomes that were similar for Groups 2 and 3 were the Timed 25-Foot Walk, stride length, the Berg balance scale, step width, tandem sway, tandem width, limits of stability, and the sensory organization test. One participant dropped out of the study because of an MS relapse.
The researchers observed no problems with adherence in any of the groups. “If we are to demonstrate a more significant intergroup difference, we need [larger] cohorts, and consequently, further research is needed,” Dr. Pardo concluded.
LONDON—In patients with multiple sclerosis (MS), telerehabilitation is a convenient and practical method of performing physical therapy with efficacy comparable to that of conventional in-person physical therapy, as measured by objective outcomes of gait and balance. Telerehabilitation should be investigated further and used more extensively as a means of improving function and quality of life in MS, according to researchers who spoke at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS).
MS often results in physical and cognitive disability. Rehabilitation methods that include physical therapy can achieve functional improvement of established physical deficits. Factors such as availability, geographical distance, mobility, transportation, and cost, however, limit access to specialized rehabilitation services. Telecommunication technology opens the possibility of supervising and directing a physical therapy program remotely through audio and visual communication in real time.
Gabriel Pardo, MD, Director of the Oklahoma Medical Research Foundation MS Center of Excellence in Oklahoma City, and colleagues sought to demonstrate the feasibility of a tele-health rehabilitation program in individuals with ambulatory deficits secondary to MS. The researchers also intended to evaluate the efficacy of the tele-health rehabilitation program and compare it with that of conventional physical therapy.
Dr. Pardo and colleagues included 30 individuals in a single-center, prospective, randomized, three-arm, evaluator-blinded study that lasted for eight weeks. About 69% of participants were female, and the population’s mean age was 54.7. Approximately 60% of participants had relapsing-remitting MS, 23% had secondary progressive MS, and 17% had primary progressive MS. The population’s mean Expanded Disability Status Scale (EDSS) score was 4.3.
All participants performed a home-based exercise program (HEP) unsupervised on five days per week for eight weeks. Participants were randomized to three intervention groups. Group 1 underwent HEP alone. Group 2 underwent HEP plus remote physical therapy supervised via audio and visual real-time telecommunication two to three times per week. Group 3 underwent HEP plus in-person physical therapy at the medical facility two to three times per week. The study outcomes were multiple measurements of gait and balance, as well as patient-reported outcomes. Selected outcomes were performed with a computerized system (ie, Neurocom SmartBalance).
Functional gait assessment improved from baseline in all groups. Improvements were no different between the telerehabilitation and the conventional PT groups, but this finding was not statistically significant. Other outcomes that were similar for Groups 2 and 3 were the Timed 25-Foot Walk, stride length, the Berg balance scale, step width, tandem sway, tandem width, limits of stability, and the sensory organization test. One participant dropped out of the study because of an MS relapse.
The researchers observed no problems with adherence in any of the groups. “If we are to demonstrate a more significant intergroup difference, we need [larger] cohorts, and consequently, further research is needed,” Dr. Pardo concluded.
LONDON—In patients with multiple sclerosis (MS), telerehabilitation is a convenient and practical method of performing physical therapy with efficacy comparable to that of conventional in-person physical therapy, as measured by objective outcomes of gait and balance. Telerehabilitation should be investigated further and used more extensively as a means of improving function and quality of life in MS, according to researchers who spoke at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS).
MS often results in physical and cognitive disability. Rehabilitation methods that include physical therapy can achieve functional improvement of established physical deficits. Factors such as availability, geographical distance, mobility, transportation, and cost, however, limit access to specialized rehabilitation services. Telecommunication technology opens the possibility of supervising and directing a physical therapy program remotely through audio and visual communication in real time.
Gabriel Pardo, MD, Director of the Oklahoma Medical Research Foundation MS Center of Excellence in Oklahoma City, and colleagues sought to demonstrate the feasibility of a tele-health rehabilitation program in individuals with ambulatory deficits secondary to MS. The researchers also intended to evaluate the efficacy of the tele-health rehabilitation program and compare it with that of conventional physical therapy.
Dr. Pardo and colleagues included 30 individuals in a single-center, prospective, randomized, three-arm, evaluator-blinded study that lasted for eight weeks. About 69% of participants were female, and the population’s mean age was 54.7. Approximately 60% of participants had relapsing-remitting MS, 23% had secondary progressive MS, and 17% had primary progressive MS. The population’s mean Expanded Disability Status Scale (EDSS) score was 4.3.
All participants performed a home-based exercise program (HEP) unsupervised on five days per week for eight weeks. Participants were randomized to three intervention groups. Group 1 underwent HEP alone. Group 2 underwent HEP plus remote physical therapy supervised via audio and visual real-time telecommunication two to three times per week. Group 3 underwent HEP plus in-person physical therapy at the medical facility two to three times per week. The study outcomes were multiple measurements of gait and balance, as well as patient-reported outcomes. Selected outcomes were performed with a computerized system (ie, Neurocom SmartBalance).
Functional gait assessment improved from baseline in all groups. Improvements were no different between the telerehabilitation and the conventional PT groups, but this finding was not statistically significant. Other outcomes that were similar for Groups 2 and 3 were the Timed 25-Foot Walk, stride length, the Berg balance scale, step width, tandem sway, tandem width, limits of stability, and the sensory organization test. One participant dropped out of the study because of an MS relapse.
The researchers observed no problems with adherence in any of the groups. “If we are to demonstrate a more significant intergroup difference, we need [larger] cohorts, and consequently, further research is needed,” Dr. Pardo concluded.
Retinal Measurements Predict 10-Year Disability in MS
LONDON—As has been previously shown with brain atrophy and lesion volume, retinal measures can have predictive value for medium-term disability in multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). “Our preliminary findings support the utility of optical coherence tomography (OCT) as a tool to predict neurodegeneration and disease progression over time in patients with MS,” said Alissa M. Rothman, MD, a post-doctoral research coordinator at the Johns Hopkins MS Center in Baltimore.
Measures of retinal layer thicknesses obtained with OCT have been shown to correlate with visual function, grey matter volume, and Expanded Disability Status Scale (EDSS) scores in MS. However, the prognostic value of retinal measurements for predicting long-term disability in patients with MS is still being evaluated. In the present study, Dr. Rothman and colleagues sought to determine whether retinal thicknesses as assessed by OCT predicts disability in MS 10 years later.
A total of 89 patients with MS were scanned on Stratus OCT between 2006 and 2007. During 2015 and 2016, these patients underwent formal, blinded EDSS determination. Average peripapillary retinal nerve fiber layer (RNFL) thickness and total macular volume (TMV) were assessed by calculating the mean value of these measures for both eyes in each subject. Patients were categorized by baseline diagnosis as relapsing remitting (RRMS), secondary progressive (SPMS), or primary progressive MS (PPMS). Mixed effects linear regression models were used to investigate whether average TMV and RNFL thicknesses at baseline predict EDSS scores after 10 years.
The final analysis included 75 patients with RRMS, nine patients with SPMS, and five patients with PPMS. Fourteen of the 75 patients with a baseline diagnosis of RRMS transitioned to SPMS during the follow-up period. Baseline analyses revealed that the RRMS cohort was significantly younger than the SPMS and PPMS cohorts (mean differences = 21.5 years and 11.7 years, respectively) and that patients with SPMS patients had a longer disease duration than patients with RRMS and PPMS (mean differences = 14.2 years and 13.2 years, respectively). A history of optic neuritis (ON) was observed in the RRMS and SPMS cohorts (41% and 44%, respectively), but not in the PPMS cohorts (0%). Adjusting for age, sex, and a history of ON, the mean TMV values at baseline predicted EDSS scores after a median follow-up of 9.3 years. On average, a 1 mm3 lower TMV value at baseline predicted a mean decrease of 2 in EDSS at follow-up. Mean baseline RNFL values did not significantly predict EDSS scores.
—Glenn S. Williams
LONDON—As has been previously shown with brain atrophy and lesion volume, retinal measures can have predictive value for medium-term disability in multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). “Our preliminary findings support the utility of optical coherence tomography (OCT) as a tool to predict neurodegeneration and disease progression over time in patients with MS,” said Alissa M. Rothman, MD, a post-doctoral research coordinator at the Johns Hopkins MS Center in Baltimore.
Measures of retinal layer thicknesses obtained with OCT have been shown to correlate with visual function, grey matter volume, and Expanded Disability Status Scale (EDSS) scores in MS. However, the prognostic value of retinal measurements for predicting long-term disability in patients with MS is still being evaluated. In the present study, Dr. Rothman and colleagues sought to determine whether retinal thicknesses as assessed by OCT predicts disability in MS 10 years later.
A total of 89 patients with MS were scanned on Stratus OCT between 2006 and 2007. During 2015 and 2016, these patients underwent formal, blinded EDSS determination. Average peripapillary retinal nerve fiber layer (RNFL) thickness and total macular volume (TMV) were assessed by calculating the mean value of these measures for both eyes in each subject. Patients were categorized by baseline diagnosis as relapsing remitting (RRMS), secondary progressive (SPMS), or primary progressive MS (PPMS). Mixed effects linear regression models were used to investigate whether average TMV and RNFL thicknesses at baseline predict EDSS scores after 10 years.
The final analysis included 75 patients with RRMS, nine patients with SPMS, and five patients with PPMS. Fourteen of the 75 patients with a baseline diagnosis of RRMS transitioned to SPMS during the follow-up period. Baseline analyses revealed that the RRMS cohort was significantly younger than the SPMS and PPMS cohorts (mean differences = 21.5 years and 11.7 years, respectively) and that patients with SPMS patients had a longer disease duration than patients with RRMS and PPMS (mean differences = 14.2 years and 13.2 years, respectively). A history of optic neuritis (ON) was observed in the RRMS and SPMS cohorts (41% and 44%, respectively), but not in the PPMS cohorts (0%). Adjusting for age, sex, and a history of ON, the mean TMV values at baseline predicted EDSS scores after a median follow-up of 9.3 years. On average, a 1 mm3 lower TMV value at baseline predicted a mean decrease of 2 in EDSS at follow-up. Mean baseline RNFL values did not significantly predict EDSS scores.
—Glenn S. Williams
LONDON—As has been previously shown with brain atrophy and lesion volume, retinal measures can have predictive value for medium-term disability in multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). “Our preliminary findings support the utility of optical coherence tomography (OCT) as a tool to predict neurodegeneration and disease progression over time in patients with MS,” said Alissa M. Rothman, MD, a post-doctoral research coordinator at the Johns Hopkins MS Center in Baltimore.
Measures of retinal layer thicknesses obtained with OCT have been shown to correlate with visual function, grey matter volume, and Expanded Disability Status Scale (EDSS) scores in MS. However, the prognostic value of retinal measurements for predicting long-term disability in patients with MS is still being evaluated. In the present study, Dr. Rothman and colleagues sought to determine whether retinal thicknesses as assessed by OCT predicts disability in MS 10 years later.
A total of 89 patients with MS were scanned on Stratus OCT between 2006 and 2007. During 2015 and 2016, these patients underwent formal, blinded EDSS determination. Average peripapillary retinal nerve fiber layer (RNFL) thickness and total macular volume (TMV) were assessed by calculating the mean value of these measures for both eyes in each subject. Patients were categorized by baseline diagnosis as relapsing remitting (RRMS), secondary progressive (SPMS), or primary progressive MS (PPMS). Mixed effects linear regression models were used to investigate whether average TMV and RNFL thicknesses at baseline predict EDSS scores after 10 years.
The final analysis included 75 patients with RRMS, nine patients with SPMS, and five patients with PPMS. Fourteen of the 75 patients with a baseline diagnosis of RRMS transitioned to SPMS during the follow-up period. Baseline analyses revealed that the RRMS cohort was significantly younger than the SPMS and PPMS cohorts (mean differences = 21.5 years and 11.7 years, respectively) and that patients with SPMS patients had a longer disease duration than patients with RRMS and PPMS (mean differences = 14.2 years and 13.2 years, respectively). A history of optic neuritis (ON) was observed in the RRMS and SPMS cohorts (41% and 44%, respectively), but not in the PPMS cohorts (0%). Adjusting for age, sex, and a history of ON, the mean TMV values at baseline predicted EDSS scores after a median follow-up of 9.3 years. On average, a 1 mm3 lower TMV value at baseline predicted a mean decrease of 2 in EDSS at follow-up. Mean baseline RNFL values did not significantly predict EDSS scores.
—Glenn S. Williams
VIVA: Assessing aortic repair and more in the latest trials
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.

United States an expensive place for knee, hip replacement
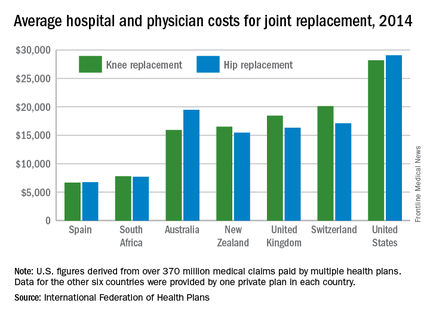
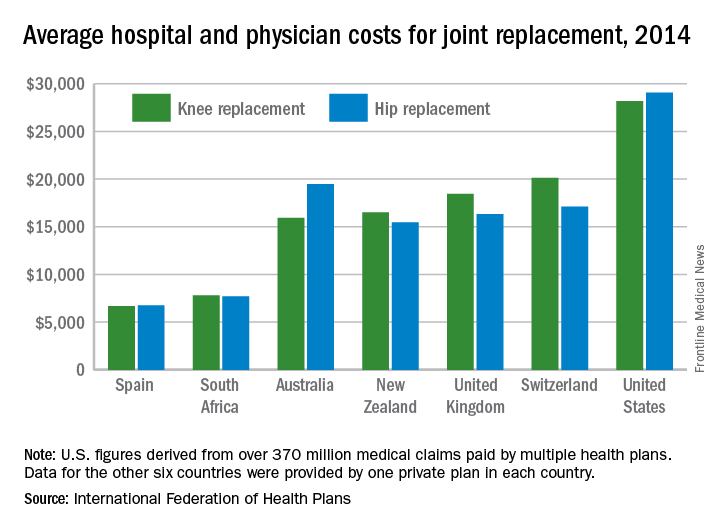
Knee and hip replacement surgeries were more expensive in the United States than in a group of six other industrialized countries in 2014, according to a report from the International Federation of Health Plans.
The U.S. average for total hospital and physician costs was $28,184 for knee replacement and $29,067 for hip replacement. Switzerland was the next most expensive country for knee replacements at $20,132, and Australia was second for hip replacements at $19,484. Spain had the lowest average cost for both surgeries: $6,687 for knee replacement and $6,757 for hip replacement, the IFHP reported.
“We look at these numbers every year and it’s always a shocking demonstration of how much procedures and prescription drugs actually cost,” IFHP Chief Executive Tom Sackville said in a written statement. “There is no reason why identical procedures and products should vary in price so much across countries: it illustrates the damaging effects of an inadequately regulated health care market.”
The IFHP consists of 80 member companies in 25 countries. For the survey, costs for each country were submitted by participating member plans. Costs for the United States are derived from over 370 million employer-sponsored medical claims incurred from Jan. 1, 2014, to Dec. 31, 2014, and paid by multiple health plans. Cost data for the other six countries were provided by one private plan in each country.
Knee and hip replacement surgeries were more expensive in the United States than in a group of six other industrialized countries in 2014, according to a report from the International Federation of Health Plans.
The U.S. average for total hospital and physician costs was $28,184 for knee replacement and $29,067 for hip replacement. Switzerland was the next most expensive country for knee replacements at $20,132, and Australia was second for hip replacements at $19,484. Spain had the lowest average cost for both surgeries: $6,687 for knee replacement and $6,757 for hip replacement, the IFHP reported.
“We look at these numbers every year and it’s always a shocking demonstration of how much procedures and prescription drugs actually cost,” IFHP Chief Executive Tom Sackville said in a written statement. “There is no reason why identical procedures and products should vary in price so much across countries: it illustrates the damaging effects of an inadequately regulated health care market.”
The IFHP consists of 80 member companies in 25 countries. For the survey, costs for each country were submitted by participating member plans. Costs for the United States are derived from over 370 million employer-sponsored medical claims incurred from Jan. 1, 2014, to Dec. 31, 2014, and paid by multiple health plans. Cost data for the other six countries were provided by one private plan in each country.
Knee and hip replacement surgeries were more expensive in the United States than in a group of six other industrialized countries in 2014, according to a report from the International Federation of Health Plans.
The U.S. average for total hospital and physician costs was $28,184 for knee replacement and $29,067 for hip replacement. Switzerland was the next most expensive country for knee replacements at $20,132, and Australia was second for hip replacements at $19,484. Spain had the lowest average cost for both surgeries: $6,687 for knee replacement and $6,757 for hip replacement, the IFHP reported.
“We look at these numbers every year and it’s always a shocking demonstration of how much procedures and prescription drugs actually cost,” IFHP Chief Executive Tom Sackville said in a written statement. “There is no reason why identical procedures and products should vary in price so much across countries: it illustrates the damaging effects of an inadequately regulated health care market.”
The IFHP consists of 80 member companies in 25 countries. For the survey, costs for each country were submitted by participating member plans. Costs for the United States are derived from over 370 million employer-sponsored medical claims incurred from Jan. 1, 2014, to Dec. 31, 2014, and paid by multiple health plans. Cost data for the other six countries were provided by one private plan in each country.
‘Toe and flow’ approach to CLI management lowers amputation risk
Amputation in diabetes is less likely when critical limb ischemia is approached in a multidisciplinary way, according to the coauthor of clinical recommendations issued earlier this year. But to ensure optimal patient outcomes, just who should be on the interdisciplinary care team, how should it be coordinated, and what algorithms are best?
To help navigate these concerns, Joseph L. Mills, MD, professor and chief of vascular surgery and endovascular therapy at Baylor College of Medicine in Houston, will discuss “the toe and flow” model of care on Sunday morning, Sept. 18, as part of the presymposium Addressing Core Questions in Critical Limb Ischemia session.
“This model of care combines podiatrists and orthopedists with vascular specialists who provide advanced open surgery and endovascular therapy, to provide best treatment for patients,” said Dr. Mills, who coauthored the Society for Vascular Surgery Threatened Limb Classification (Wound, Ischemia, and foot Infection), or “WIfI,” as well as a clinical guideline on management of the diabetic foot, released earlier this year by the SVS in collaboration with the American Podiatric Medical Association, and the Society for Vascular Medicine.
Every 20 seconds, somewhere in the world a person with diabetes undergoes leg amputation as a result of the disease, according to Dr. Mills. Not only are the resulting costs of care unmanageable, fragmented diabetic foot care compromises a patient’s quality and longevity of life, he said.
The unfortunate path to amputation in diabetes most commonly begins with a simple neuropathic foot ulcer, often made worse by peripheral artery disease. The wound eventually moves through acute and chronic stages of neuropathy, vasculopathy, and infection, until amputation is necessary. Offering appropriate intervention at any point in this trajectory, or avoiding it altogether, means the ideal care team should include specialists with expertise in these disciplines. Beyond the core team members of a vascular surgeon, podiatrist, and orthopedic specialist, Dr. Mills said that other interdisciplinary team configurations might include a diabetologist, orthopedist, plastic surgeon, infectious disease specialist, general surgeon, and pedorthist/prosthetist.
“Learning how to build ‘toe and flow’ teams into your local environment can help improve outcomes in this challenging patient population,” Dr. Mills said. “Methods and flow diagrams concerning how this can be done will be a major focus of the talk.”
Dr. Mills will cover how patient responsibilities should be divided between team members across varying levels of clinical care, ranging from basic clinics to centers of excellence. The talk will also address aftercare, as well as how to facilitate effective communication between team members and patients.
“Enthusiasm for this model is the key ingredient to helping reduce the number of amputations in your patients,” he said.
On Twitter @whitneymcknight
Amputation in diabetes is less likely when critical limb ischemia is approached in a multidisciplinary way, according to the coauthor of clinical recommendations issued earlier this year. But to ensure optimal patient outcomes, just who should be on the interdisciplinary care team, how should it be coordinated, and what algorithms are best?
To help navigate these concerns, Joseph L. Mills, MD, professor and chief of vascular surgery and endovascular therapy at Baylor College of Medicine in Houston, will discuss “the toe and flow” model of care on Sunday morning, Sept. 18, as part of the presymposium Addressing Core Questions in Critical Limb Ischemia session.
“This model of care combines podiatrists and orthopedists with vascular specialists who provide advanced open surgery and endovascular therapy, to provide best treatment for patients,” said Dr. Mills, who coauthored the Society for Vascular Surgery Threatened Limb Classification (Wound, Ischemia, and foot Infection), or “WIfI,” as well as a clinical guideline on management of the diabetic foot, released earlier this year by the SVS in collaboration with the American Podiatric Medical Association, and the Society for Vascular Medicine.
Every 20 seconds, somewhere in the world a person with diabetes undergoes leg amputation as a result of the disease, according to Dr. Mills. Not only are the resulting costs of care unmanageable, fragmented diabetic foot care compromises a patient’s quality and longevity of life, he said.
The unfortunate path to amputation in diabetes most commonly begins with a simple neuropathic foot ulcer, often made worse by peripheral artery disease. The wound eventually moves through acute and chronic stages of neuropathy, vasculopathy, and infection, until amputation is necessary. Offering appropriate intervention at any point in this trajectory, or avoiding it altogether, means the ideal care team should include specialists with expertise in these disciplines. Beyond the core team members of a vascular surgeon, podiatrist, and orthopedic specialist, Dr. Mills said that other interdisciplinary team configurations might include a diabetologist, orthopedist, plastic surgeon, infectious disease specialist, general surgeon, and pedorthist/prosthetist.
“Learning how to build ‘toe and flow’ teams into your local environment can help improve outcomes in this challenging patient population,” Dr. Mills said. “Methods and flow diagrams concerning how this can be done will be a major focus of the talk.”
Dr. Mills will cover how patient responsibilities should be divided between team members across varying levels of clinical care, ranging from basic clinics to centers of excellence. The talk will also address aftercare, as well as how to facilitate effective communication between team members and patients.
“Enthusiasm for this model is the key ingredient to helping reduce the number of amputations in your patients,” he said.
On Twitter @whitneymcknight
Amputation in diabetes is less likely when critical limb ischemia is approached in a multidisciplinary way, according to the coauthor of clinical recommendations issued earlier this year. But to ensure optimal patient outcomes, just who should be on the interdisciplinary care team, how should it be coordinated, and what algorithms are best?
To help navigate these concerns, Joseph L. Mills, MD, professor and chief of vascular surgery and endovascular therapy at Baylor College of Medicine in Houston, will discuss “the toe and flow” model of care on Sunday morning, Sept. 18, as part of the presymposium Addressing Core Questions in Critical Limb Ischemia session.
“This model of care combines podiatrists and orthopedists with vascular specialists who provide advanced open surgery and endovascular therapy, to provide best treatment for patients,” said Dr. Mills, who coauthored the Society for Vascular Surgery Threatened Limb Classification (Wound, Ischemia, and foot Infection), or “WIfI,” as well as a clinical guideline on management of the diabetic foot, released earlier this year by the SVS in collaboration with the American Podiatric Medical Association, and the Society for Vascular Medicine.
Every 20 seconds, somewhere in the world a person with diabetes undergoes leg amputation as a result of the disease, according to Dr. Mills. Not only are the resulting costs of care unmanageable, fragmented diabetic foot care compromises a patient’s quality and longevity of life, he said.
The unfortunate path to amputation in diabetes most commonly begins with a simple neuropathic foot ulcer, often made worse by peripheral artery disease. The wound eventually moves through acute and chronic stages of neuropathy, vasculopathy, and infection, until amputation is necessary. Offering appropriate intervention at any point in this trajectory, or avoiding it altogether, means the ideal care team should include specialists with expertise in these disciplines. Beyond the core team members of a vascular surgeon, podiatrist, and orthopedic specialist, Dr. Mills said that other interdisciplinary team configurations might include a diabetologist, orthopedist, plastic surgeon, infectious disease specialist, general surgeon, and pedorthist/prosthetist.
“Learning how to build ‘toe and flow’ teams into your local environment can help improve outcomes in this challenging patient population,” Dr. Mills said. “Methods and flow diagrams concerning how this can be done will be a major focus of the talk.”
Dr. Mills will cover how patient responsibilities should be divided between team members across varying levels of clinical care, ranging from basic clinics to centers of excellence. The talk will also address aftercare, as well as how to facilitate effective communication between team members and patients.
“Enthusiasm for this model is the key ingredient to helping reduce the number of amputations in your patients,” he said.
On Twitter @whitneymcknight
Cortical thinning may not be tied to executive dysfunction in late-life depression
SAN FRANCISCO – Frontal cortical thinning was common in late-life depression but generally did not predict executive dysfunction, according to magnetic resonance imaging studies of 157 adults.
The only exception was the left middle fronto-orbital gyrus. Thinning there predicted significantly worse performance on tests of executive function and processing speed, said Krista Farley of the late-life depression program at the University of California, San Francisco. Based on this limited finding, “further investigation of the etiology of executive dysfunction in late-life depression is warranted,” Ms. Farley said in a poster presented at the 2016 congress of the International Psychogeriatric Association.

About 5%-10% of community-dwelling older adults meet criteria for major depressive disorder, which is even more common in acute care and long-term care settings, and is often refractory to pharmacotherapy. Although late-life depression has been linked to cortical atrophy and executive dysfunction, it was unknown whether those two aspects of the disorder were related, Ms. Farley said.
The study by Ms. Farley and her associates of adults aged 65 years and older included 65 normal controls and 92 patients who met DSM-IV criteria for major depressive disorder, scored at least 19 on the Hamilton Depression Rating Scale, and had no evidence of dementia, having scored at least 25 on the Mini–Mental State Examination. Using T1– and T2–weighted structural MRI scans, the researchers measured the cortical thickness of six individual regions of the frontal lobe as well as the anterior cingulate gyrus. The patient and control groups resembled one another in terms of education, IQ, and age, but 71% of patients with late-life depression were female, compared with only 50% of controls.
Patients with late-life depression had significantly more thinning of the middle frontal gyrus, the inferior frontal gyrus, and the middle fronto-orbital gyrus, compared with controls, even after the investigators adjusted for age and sex (P less than .05 for all comparisons). Analyzing the left and right brain hemispheres separately localized the differences to the left hemisphere and additionally implicated the left lateral frontal orbital gyrus (mean thickness in patients, 3.2 mm; standard deviation, 0.2; versus 3.4 mm [SD = 0.31] in controls; P = .03).
Patients with late-life depression also scored significantly lower than controls on the Symbol Digit Modalities Test for information processing speed (P = .001) and the Stroop test of executive function (P = .002). The thickness of the left middle fronto-orbital gyrus was significantly inversely correlated with performance on both tests, with P values of .01 and .03, respectively. “The negative association with focal frontal regions was unexpected and deserves further investigation,” Ms. Farley said. But because cortical thinning in other locations did not predict cognitive performance, “cortical abnormalities may have a limited role in the manifestation of cognitive dysfunction in this vulnerable patient population,” Ms. Farley concluded.
The National Institutes of Health and the Leon J. Epstein Psychiatry Fund at the University of California, San Francisco, supported the work. Ms. Farley had no relevant financial disclosures.
SAN FRANCISCO – Frontal cortical thinning was common in late-life depression but generally did not predict executive dysfunction, according to magnetic resonance imaging studies of 157 adults.
The only exception was the left middle fronto-orbital gyrus. Thinning there predicted significantly worse performance on tests of executive function and processing speed, said Krista Farley of the late-life depression program at the University of California, San Francisco. Based on this limited finding, “further investigation of the etiology of executive dysfunction in late-life depression is warranted,” Ms. Farley said in a poster presented at the 2016 congress of the International Psychogeriatric Association.
About 5%-10% of community-dwelling older adults meet criteria for major depressive disorder, which is even more common in acute care and long-term care settings, and is often refractory to pharmacotherapy. Although late-life depression has been linked to cortical atrophy and executive dysfunction, it was unknown whether those two aspects of the disorder were related, Ms. Farley said.
The study by Ms. Farley and her associates of adults aged 65 years and older included 65 normal controls and 92 patients who met DSM-IV criteria for major depressive disorder, scored at least 19 on the Hamilton Depression Rating Scale, and had no evidence of dementia, having scored at least 25 on the Mini–Mental State Examination. Using T1– and T2–weighted structural MRI scans, the researchers measured the cortical thickness of six individual regions of the frontal lobe as well as the anterior cingulate gyrus. The patient and control groups resembled one another in terms of education, IQ, and age, but 71% of patients with late-life depression were female, compared with only 50% of controls.
Patients with late-life depression had significantly more thinning of the middle frontal gyrus, the inferior frontal gyrus, and the middle fronto-orbital gyrus, compared with controls, even after the investigators adjusted for age and sex (P less than .05 for all comparisons). Analyzing the left and right brain hemispheres separately localized the differences to the left hemisphere and additionally implicated the left lateral frontal orbital gyrus (mean thickness in patients, 3.2 mm; standard deviation, 0.2; versus 3.4 mm [SD = 0.31] in controls; P = .03).
Patients with late-life depression also scored significantly lower than controls on the Symbol Digit Modalities Test for information processing speed (P = .001) and the Stroop test of executive function (P = .002). The thickness of the left middle fronto-orbital gyrus was significantly inversely correlated with performance on both tests, with P values of .01 and .03, respectively. “The negative association with focal frontal regions was unexpected and deserves further investigation,” Ms. Farley said. But because cortical thinning in other locations did not predict cognitive performance, “cortical abnormalities may have a limited role in the manifestation of cognitive dysfunction in this vulnerable patient population,” Ms. Farley concluded.
The National Institutes of Health and the Leon J. Epstein Psychiatry Fund at the University of California, San Francisco, supported the work. Ms. Farley had no relevant financial disclosures.
SAN FRANCISCO – Frontal cortical thinning was common in late-life depression but generally did not predict executive dysfunction, according to magnetic resonance imaging studies of 157 adults.
The only exception was the left middle fronto-orbital gyrus. Thinning there predicted significantly worse performance on tests of executive function and processing speed, said Krista Farley of the late-life depression program at the University of California, San Francisco. Based on this limited finding, “further investigation of the etiology of executive dysfunction in late-life depression is warranted,” Ms. Farley said in a poster presented at the 2016 congress of the International Psychogeriatric Association.
About 5%-10% of community-dwelling older adults meet criteria for major depressive disorder, which is even more common in acute care and long-term care settings, and is often refractory to pharmacotherapy. Although late-life depression has been linked to cortical atrophy and executive dysfunction, it was unknown whether those two aspects of the disorder were related, Ms. Farley said.
The study by Ms. Farley and her associates of adults aged 65 years and older included 65 normal controls and 92 patients who met DSM-IV criteria for major depressive disorder, scored at least 19 on the Hamilton Depression Rating Scale, and had no evidence of dementia, having scored at least 25 on the Mini–Mental State Examination. Using T1– and T2–weighted structural MRI scans, the researchers measured the cortical thickness of six individual regions of the frontal lobe as well as the anterior cingulate gyrus. The patient and control groups resembled one another in terms of education, IQ, and age, but 71% of patients with late-life depression were female, compared with only 50% of controls.
Patients with late-life depression had significantly more thinning of the middle frontal gyrus, the inferior frontal gyrus, and the middle fronto-orbital gyrus, compared with controls, even after the investigators adjusted for age and sex (P less than .05 for all comparisons). Analyzing the left and right brain hemispheres separately localized the differences to the left hemisphere and additionally implicated the left lateral frontal orbital gyrus (mean thickness in patients, 3.2 mm; standard deviation, 0.2; versus 3.4 mm [SD = 0.31] in controls; P = .03).
Patients with late-life depression also scored significantly lower than controls on the Symbol Digit Modalities Test for information processing speed (P = .001) and the Stroop test of executive function (P = .002). The thickness of the left middle fronto-orbital gyrus was significantly inversely correlated with performance on both tests, with P values of .01 and .03, respectively. “The negative association with focal frontal regions was unexpected and deserves further investigation,” Ms. Farley said. But because cortical thinning in other locations did not predict cognitive performance, “cortical abnormalities may have a limited role in the manifestation of cognitive dysfunction in this vulnerable patient population,” Ms. Farley concluded.
The National Institutes of Health and the Leon J. Epstein Psychiatry Fund at the University of California, San Francisco, supported the work. Ms. Farley had no relevant financial disclosures.
AT IPA 2016
Key clinical point: Cortical thinning may not be the major reason for executive dysfunction among patients with late-life depression.
Major finding: Among all brain regions studied, only thinning in the middle frontal orbital gyrus predicted significantly worse performance on the Symbol Digit Modalities and Stroop tests.
Data source: Magnetic resonance imaging scans and cognitive tests of 92 patients with late-life depression and 65 controls.
Disclosures: The National Institutes of Health and the Leon J. Epstein Geriatric Psychiatry Fund at the University of California, San Francisco, supported the work. Ms. Farley had no relevant financial disclosures.

Dulaglutide plus insulin glargine drops HbA1c in poorly controlled type 2
MUNICH – Once-weekly dulaglutide paired with insulin glargine plus metformin allowed 69% of patients with poorly controlled type 2 diabetes to achieve a hemoglobin A1c of 7% or lower.
Over the 28-week study, 51% of the group reached an HbA1c of 6.5% or lower – significantly better than the 17% who achieved this goal on insulin glargine with or without metformin, Paolo Pozzilli, MD, reported at the annual meeting of the European Association for the Study of Diabetes.

The combination was safe, with just one incident of severe hypoglycemia, and well tolerated, said Dr. Pozzilli of the University Campus Bio-Medico, Rome. Nausea – the most troublesome side effect of any glucagonlike peptide receptor agonist occurred in 12% of those taking the drug. Diarrhea occurred in 11% and vomiting in 6%. All of the gastrointestinal side effects were significantly more common than they were in the placebo group.
“I would say that the combination treatment of dulaglutide and insulin glargine – with or without metformin – is a reasonable, well-tolerated, and effective option for patients with type 2 diabetes who are not hitting their treatment goals,” he said.
Dr. Pozzilli reported results of Lily’s AWARD-9 trial. The placebo-controlled trial comprised 300 patients with poorly controlled type 2 diabetes (HbA1c, 7%-10.5%), despite being on insulin glargine and metformin. They were randomized to weekly subcutaneous placebo or 1.5 mg dulaglutide injections, in addition to their usual medications. There was no up titration on the study drug – patients started out with the full dose immediately. The study’s completion rate was high, with 92% of the investigational group and 87% of the control group finishing the 28-week treatment.
The group was typical for poorly controlled type 2 patients. Their mean age was 60 years; about 60% were men; and almost all were white. The mean body mass index was 32 kg/m2. The mean disease duration was 13 years, and the mean HbA1c was 8.4%. Their mean fasting plasma glucose was 8.7 mmol/L.
The effect of dual therapy was quickly evident, with HbA1c levels beginning to drop within 2 weeks. By 12 weeks, the separation between groups was statistically significant (dulaglutide HbA1c about 7%, placebo about 8%). By 28 weeks, the combination group had reached a mean HbA1c of 6.92%, compared with 7.69% in the placebo group. The response curve of the combination group appeared to be on a continuing decline when the study ended. The final measure represented an HbA1c decrease of 1.44% for the combination group and 0.67% for the placebo group.
By 28 weeks, 69% of the dulaglutide group and 35% of the placebo group had achieved an HbA1c of 7% or lower – a significant difference. Half of the dulaglutide group (51%) achieved a measure of 6.5% or lower, compared with 17% of the placebo group – also a significant difference.
The addition of dulaglutide moderated the need to increase the insulin that occurred over the study period. By 28 weeks, those taking dulaglutide had increased their insulin by a mean of 0.14 U/kg, compared with an increase of 0.27 U/kg in the placebo group. This difference was also statistically significant.
Patients in the combination group lost significantly more weight as well (mean 1.91 kg vs. a gain of 0.5 kg in the placebo group). Weight loss was quickly evident; by 4 weeks, patients had lost more than 1 kg. This “encouraging sign might help boost patient compliance,” Dr. Pozzilli said.
The side-effect profile was acceptable, compared with placebo. Hypoglycemia occurred in about 55% of those taking dulaglutide and 51% of those taking the placebo; it was symptomatic in 35% and 30%, respectively. Nocturnal hypoglycemia occurred in 28% and 29%, respectively. There was one case of severe hypoglycemia, which occurred in the dulaglutide group.
In addition to the GI side effects, there was one injection site reaction in the dulaglutide group. There were no cases of pancreatitis or pancreatic cancer.
The study was sponsored by Eli Lilly. Dr. Pozzilli is on the company’s speakers’ bureau and receives research grant money from it.
MUNICH – Once-weekly dulaglutide paired with insulin glargine plus metformin allowed 69% of patients with poorly controlled type 2 diabetes to achieve a hemoglobin A1c of 7% or lower.
Over the 28-week study, 51% of the group reached an HbA1c of 6.5% or lower – significantly better than the 17% who achieved this goal on insulin glargine with or without metformin, Paolo Pozzilli, MD, reported at the annual meeting of the European Association for the Study of Diabetes.
The combination was safe, with just one incident of severe hypoglycemia, and well tolerated, said Dr. Pozzilli of the University Campus Bio-Medico, Rome. Nausea – the most troublesome side effect of any glucagonlike peptide receptor agonist occurred in 12% of those taking the drug. Diarrhea occurred in 11% and vomiting in 6%. All of the gastrointestinal side effects were significantly more common than they were in the placebo group.
“I would say that the combination treatment of dulaglutide and insulin glargine – with or without metformin – is a reasonable, well-tolerated, and effective option for patients with type 2 diabetes who are not hitting their treatment goals,” he said.
Dr. Pozzilli reported results of Lily’s AWARD-9 trial. The placebo-controlled trial comprised 300 patients with poorly controlled type 2 diabetes (HbA1c, 7%-10.5%), despite being on insulin glargine and metformin. They were randomized to weekly subcutaneous placebo or 1.5 mg dulaglutide injections, in addition to their usual medications. There was no up titration on the study drug – patients started out with the full dose immediately. The study’s completion rate was high, with 92% of the investigational group and 87% of the control group finishing the 28-week treatment.
The group was typical for poorly controlled type 2 patients. Their mean age was 60 years; about 60% were men; and almost all were white. The mean body mass index was 32 kg/m2. The mean disease duration was 13 years, and the mean HbA1c was 8.4%. Their mean fasting plasma glucose was 8.7 mmol/L.
The effect of dual therapy was quickly evident, with HbA1c levels beginning to drop within 2 weeks. By 12 weeks, the separation between groups was statistically significant (dulaglutide HbA1c about 7%, placebo about 8%). By 28 weeks, the combination group had reached a mean HbA1c of 6.92%, compared with 7.69% in the placebo group. The response curve of the combination group appeared to be on a continuing decline when the study ended. The final measure represented an HbA1c decrease of 1.44% for the combination group and 0.67% for the placebo group.
By 28 weeks, 69% of the dulaglutide group and 35% of the placebo group had achieved an HbA1c of 7% or lower – a significant difference. Half of the dulaglutide group (51%) achieved a measure of 6.5% or lower, compared with 17% of the placebo group – also a significant difference.
The addition of dulaglutide moderated the need to increase the insulin that occurred over the study period. By 28 weeks, those taking dulaglutide had increased their insulin by a mean of 0.14 U/kg, compared with an increase of 0.27 U/kg in the placebo group. This difference was also statistically significant.
Patients in the combination group lost significantly more weight as well (mean 1.91 kg vs. a gain of 0.5 kg in the placebo group). Weight loss was quickly evident; by 4 weeks, patients had lost more than 1 kg. This “encouraging sign might help boost patient compliance,” Dr. Pozzilli said.
The side-effect profile was acceptable, compared with placebo. Hypoglycemia occurred in about 55% of those taking dulaglutide and 51% of those taking the placebo; it was symptomatic in 35% and 30%, respectively. Nocturnal hypoglycemia occurred in 28% and 29%, respectively. There was one case of severe hypoglycemia, which occurred in the dulaglutide group.
In addition to the GI side effects, there was one injection site reaction in the dulaglutide group. There were no cases of pancreatitis or pancreatic cancer.
The study was sponsored by Eli Lilly. Dr. Pozzilli is on the company’s speakers’ bureau and receives research grant money from it.
MUNICH – Once-weekly dulaglutide paired with insulin glargine plus metformin allowed 69% of patients with poorly controlled type 2 diabetes to achieve a hemoglobin A1c of 7% or lower.
Over the 28-week study, 51% of the group reached an HbA1c of 6.5% or lower – significantly better than the 17% who achieved this goal on insulin glargine with or without metformin, Paolo Pozzilli, MD, reported at the annual meeting of the European Association for the Study of Diabetes.
The combination was safe, with just one incident of severe hypoglycemia, and well tolerated, said Dr. Pozzilli of the University Campus Bio-Medico, Rome. Nausea – the most troublesome side effect of any glucagonlike peptide receptor agonist occurred in 12% of those taking the drug. Diarrhea occurred in 11% and vomiting in 6%. All of the gastrointestinal side effects were significantly more common than they were in the placebo group.
“I would say that the combination treatment of dulaglutide and insulin glargine – with or without metformin – is a reasonable, well-tolerated, and effective option for patients with type 2 diabetes who are not hitting their treatment goals,” he said.
Dr. Pozzilli reported results of Lily’s AWARD-9 trial. The placebo-controlled trial comprised 300 patients with poorly controlled type 2 diabetes (HbA1c, 7%-10.5%), despite being on insulin glargine and metformin. They were randomized to weekly subcutaneous placebo or 1.5 mg dulaglutide injections, in addition to their usual medications. There was no up titration on the study drug – patients started out with the full dose immediately. The study’s completion rate was high, with 92% of the investigational group and 87% of the control group finishing the 28-week treatment.
The group was typical for poorly controlled type 2 patients. Their mean age was 60 years; about 60% were men; and almost all were white. The mean body mass index was 32 kg/m2. The mean disease duration was 13 years, and the mean HbA1c was 8.4%. Their mean fasting plasma glucose was 8.7 mmol/L.
The effect of dual therapy was quickly evident, with HbA1c levels beginning to drop within 2 weeks. By 12 weeks, the separation between groups was statistically significant (dulaglutide HbA1c about 7%, placebo about 8%). By 28 weeks, the combination group had reached a mean HbA1c of 6.92%, compared with 7.69% in the placebo group. The response curve of the combination group appeared to be on a continuing decline when the study ended. The final measure represented an HbA1c decrease of 1.44% for the combination group and 0.67% for the placebo group.
By 28 weeks, 69% of the dulaglutide group and 35% of the placebo group had achieved an HbA1c of 7% or lower – a significant difference. Half of the dulaglutide group (51%) achieved a measure of 6.5% or lower, compared with 17% of the placebo group – also a significant difference.
The addition of dulaglutide moderated the need to increase the insulin that occurred over the study period. By 28 weeks, those taking dulaglutide had increased their insulin by a mean of 0.14 U/kg, compared with an increase of 0.27 U/kg in the placebo group. This difference was also statistically significant.
Patients in the combination group lost significantly more weight as well (mean 1.91 kg vs. a gain of 0.5 kg in the placebo group). Weight loss was quickly evident; by 4 weeks, patients had lost more than 1 kg. This “encouraging sign might help boost patient compliance,” Dr. Pozzilli said.
The side-effect profile was acceptable, compared with placebo. Hypoglycemia occurred in about 55% of those taking dulaglutide and 51% of those taking the placebo; it was symptomatic in 35% and 30%, respectively. Nocturnal hypoglycemia occurred in 28% and 29%, respectively. There was one case of severe hypoglycemia, which occurred in the dulaglutide group.
In addition to the GI side effects, there was one injection site reaction in the dulaglutide group. There were no cases of pancreatitis or pancreatic cancer.
The study was sponsored by Eli Lilly. Dr. Pozzilli is on the company’s speakers’ bureau and receives research grant money from it.
AT EASD 2016
Key clinical point: Adding dulaglutide to insulin glargine and metformin significantly improved long-term blood glucose levels.
Major finding: The combination of dulaglutide plus insulin glargine and metformin took 69% of patients to an HbA1c of 7% or lower.
Data source: The randomized, placebo-controlled AWARD-9 study comprised 300 patients with poorly controlled type 2 diabetes.
Disclosures: Eli Lilly sponsored the trials. Dr. Pozzilli is on the company’s speaker’s bureau and receives research funding from it.

Checklist may prompt cuts in unneeded antibiotic prescriptions
Primary care practitioners’ use of a seven-item checklist may reduce the number of pediatric patients with respiratory tract infections who are prescribed unnecessary antibiotics, a prognostic cohort study suggests.
The study revealed short illness (a duration of illness of 3 days or less), temperature (a body temperature of 37.8°C or greater at presentation), age (being under 2 years), intercostal or subcostal recession, wheeze on auscultation, asthma, and vomiting (moderate or severe in the previous 24 hours) were each independently associated with hospital admission (P less than .01 for all associations).

The checklist includes these seven characteristics or risk variables (short illness, temperature, age, recession, wheeze, asthma, and vomiting [mnemonic STARWAVe]). To use the checklist, a primary care practitioner would assign one point for the presence of each item in a patient then add up all of the points to determine that patient’s risk level for future hospital admission for respiratory tract infection. A score of 1 point or less, observed in 5,593 (67%) cases would be considered indicative of a very low rate of risk for hospitalization (0.3%, 0.2%-0.4%). A score of 2 or 3 points, found for 2,520 (30%) children, would be considered as a normal level of risk (1.5%, 1.0%-1.9%), and a score of 4 or more points, seen in 204 (3%) children, would signify a high risk level (11.8%, 7.3%-16.2%).
Of the 8,394 children assessed, 78 (0.9%; 95% confidence interval, 0.7%-1.2%) were admitted to a hospital. Most were admitted on days 2-7 (33, 42%) and on days 8-30 (30, 39%) following recruitment. Only 15 (19%) were admitted on the day of recruitment (day 1).
“Many clinicians report that they prescribe antibiotics just in case, to mitigate perceived risk of future hospital admission and complications, and that failing to provide a prescription for a child who subsequently becomes seriously unwell is professionally unacceptable. If primary care clinicians could identify children at low (or very low) risk of such future complications, the reduced clinical uncertainty could lead to a reduced use of antibiotics in these groups of patients,” wrote first author Alastair Hay, MD, from the Centre for Academic Primary Care in the School of Social and Community Medicine at the University of Bristol (England), and his colleagues.
These researchers conducted the study based on a structured, blinded review of the medical records from children aged between 3 months and 16 years presenting with acute cough (less than or equal to 28 days) and respiratory tract infection treated by 519 general practitioners in 247 practices in England between July 2011 and June 2013. The primary study outcome was hospital admission for respiratory tract infection within 30 days.
Additionally, a multivariable model was employed to detect factors associated with increased risk of hospital admission. As measured by receiver operating characteristic curve analysis, the accuracy of the STARWAVe score checklist in predicting risk groups and associated risk of hospitalization was found to be high (0.81; 95% CI, 0.77-0.86). The suggested probability of hospital admission for children who did not have any of the seven characteristics included in the checklist was found to be exceptionally low (0.14%).
Significantly associated parent-reported variables included both moderate or severe vomiting and severe fever, each in the previous 24 hours. Significant clinician-reported variables included intercostal or subcostal recession and wheeze on auscultation.
“The main value of our results is to reduce clinical uncertainty and antibiotic use in children least likely to benefit from them, namely those at very low risk of future hospital admission,” Dr. Hay and his associates noted in The Lancet Respiratory Medicine (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30223-5).
Funding for this study was provided by the National Institute for Health Research and sponsored by the University of Bristol. Only one of the study’s authors, Dr. Peter Muir, reported ties to industry sources.
There are few efficacious interventions for respiratory tract infection available to primary care clinicians beyond offering reassurance and self-management advice, so the modest benefit offered by antibiotics can persuade general practitioners to prescribe them.
To derive (and validate) a clinical prediction rule to improve targeted antibiotic prescribing in children with respiratory tract infections, Hay et al determined the seven characteristics independently associated (P less than .01 for all associations) with hospital admission for children presenting to primary care physicians with cough and respiratory tract infection (STARWAVe). Using this seven-item checklist to help structure point-of-care assessment for this patient population should predict the risk of hospital admission with remarkable accuracy (area under the received operating characteristic curve, 0.81; 95% CI, 0.76-0.85).
STARWAVe offers primary care clinicians an evidence-based practical tool to help guide antibiotic prescription decisions and, through shared decision-making, has the potential to reduce antibiotic prescription based on prognostic uncertainty or on nonmedical grounds.
If STARWAVe leads to an increase in antibiotic prescription (to 90%) in high-risk children and a parallel halving of prescription to those at low risk of hospital admission, it could achieve a 10% overall reduction in primary care antibiotic prescriptions for respiratory tract infections.
These comments are excerpted from a commentary by Dr. Christopher C. Winchester from Oxford PharmaGenesis and Durham University (England), Alison Chisholm, MSc, from the Respiratory Effectiveness Group in Cambridge (England), and Dr. David Price from the University of Aberdeen (Scotland) and the Observational and Pragmatic Research Institute in Singapore. Dr. Winchester and Dr. Price disclosed financial relationships with numerous industry sources; Ms. Chisholm indicated no financial relationships relevant to this article. Funded information was not provided. (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30272-7).
There are few efficacious interventions for respiratory tract infection available to primary care clinicians beyond offering reassurance and self-management advice, so the modest benefit offered by antibiotics can persuade general practitioners to prescribe them.
To derive (and validate) a clinical prediction rule to improve targeted antibiotic prescribing in children with respiratory tract infections, Hay et al determined the seven characteristics independently associated (P less than .01 for all associations) with hospital admission for children presenting to primary care physicians with cough and respiratory tract infection (STARWAVe). Using this seven-item checklist to help structure point-of-care assessment for this patient population should predict the risk of hospital admission with remarkable accuracy (area under the received operating characteristic curve, 0.81; 95% CI, 0.76-0.85).
STARWAVe offers primary care clinicians an evidence-based practical tool to help guide antibiotic prescription decisions and, through shared decision-making, has the potential to reduce antibiotic prescription based on prognostic uncertainty or on nonmedical grounds.
If STARWAVe leads to an increase in antibiotic prescription (to 90%) in high-risk children and a parallel halving of prescription to those at low risk of hospital admission, it could achieve a 10% overall reduction in primary care antibiotic prescriptions for respiratory tract infections.
These comments are excerpted from a commentary by Dr. Christopher C. Winchester from Oxford PharmaGenesis and Durham University (England), Alison Chisholm, MSc, from the Respiratory Effectiveness Group in Cambridge (England), and Dr. David Price from the University of Aberdeen (Scotland) and the Observational and Pragmatic Research Institute in Singapore. Dr. Winchester and Dr. Price disclosed financial relationships with numerous industry sources; Ms. Chisholm indicated no financial relationships relevant to this article. Funded information was not provided. (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30272-7).
There are few efficacious interventions for respiratory tract infection available to primary care clinicians beyond offering reassurance and self-management advice, so the modest benefit offered by antibiotics can persuade general practitioners to prescribe them.
To derive (and validate) a clinical prediction rule to improve targeted antibiotic prescribing in children with respiratory tract infections, Hay et al determined the seven characteristics independently associated (P less than .01 for all associations) with hospital admission for children presenting to primary care physicians with cough and respiratory tract infection (STARWAVe). Using this seven-item checklist to help structure point-of-care assessment for this patient population should predict the risk of hospital admission with remarkable accuracy (area under the received operating characteristic curve, 0.81; 95% CI, 0.76-0.85).
STARWAVe offers primary care clinicians an evidence-based practical tool to help guide antibiotic prescription decisions and, through shared decision-making, has the potential to reduce antibiotic prescription based on prognostic uncertainty or on nonmedical grounds.
If STARWAVe leads to an increase in antibiotic prescription (to 90%) in high-risk children and a parallel halving of prescription to those at low risk of hospital admission, it could achieve a 10% overall reduction in primary care antibiotic prescriptions for respiratory tract infections.
These comments are excerpted from a commentary by Dr. Christopher C. Winchester from Oxford PharmaGenesis and Durham University (England), Alison Chisholm, MSc, from the Respiratory Effectiveness Group in Cambridge (England), and Dr. David Price from the University of Aberdeen (Scotland) and the Observational and Pragmatic Research Institute in Singapore. Dr. Winchester and Dr. Price disclosed financial relationships with numerous industry sources; Ms. Chisholm indicated no financial relationships relevant to this article. Funded information was not provided. (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30272-7).
Primary care practitioners’ use of a seven-item checklist may reduce the number of pediatric patients with respiratory tract infections who are prescribed unnecessary antibiotics, a prognostic cohort study suggests.
The study revealed short illness (a duration of illness of 3 days or less), temperature (a body temperature of 37.8°C or greater at presentation), age (being under 2 years), intercostal or subcostal recession, wheeze on auscultation, asthma, and vomiting (moderate or severe in the previous 24 hours) were each independently associated with hospital admission (P less than .01 for all associations).
The checklist includes these seven characteristics or risk variables (short illness, temperature, age, recession, wheeze, asthma, and vomiting [mnemonic STARWAVe]). To use the checklist, a primary care practitioner would assign one point for the presence of each item in a patient then add up all of the points to determine that patient’s risk level for future hospital admission for respiratory tract infection. A score of 1 point or less, observed in 5,593 (67%) cases would be considered indicative of a very low rate of risk for hospitalization (0.3%, 0.2%-0.4%). A score of 2 or 3 points, found for 2,520 (30%) children, would be considered as a normal level of risk (1.5%, 1.0%-1.9%), and a score of 4 or more points, seen in 204 (3%) children, would signify a high risk level (11.8%, 7.3%-16.2%).
Of the 8,394 children assessed, 78 (0.9%; 95% confidence interval, 0.7%-1.2%) were admitted to a hospital. Most were admitted on days 2-7 (33, 42%) and on days 8-30 (30, 39%) following recruitment. Only 15 (19%) were admitted on the day of recruitment (day 1).
“Many clinicians report that they prescribe antibiotics just in case, to mitigate perceived risk of future hospital admission and complications, and that failing to provide a prescription for a child who subsequently becomes seriously unwell is professionally unacceptable. If primary care clinicians could identify children at low (or very low) risk of such future complications, the reduced clinical uncertainty could lead to a reduced use of antibiotics in these groups of patients,” wrote first author Alastair Hay, MD, from the Centre for Academic Primary Care in the School of Social and Community Medicine at the University of Bristol (England), and his colleagues.
These researchers conducted the study based on a structured, blinded review of the medical records from children aged between 3 months and 16 years presenting with acute cough (less than or equal to 28 days) and respiratory tract infection treated by 519 general practitioners in 247 practices in England between July 2011 and June 2013. The primary study outcome was hospital admission for respiratory tract infection within 30 days.
Additionally, a multivariable model was employed to detect factors associated with increased risk of hospital admission. As measured by receiver operating characteristic curve analysis, the accuracy of the STARWAVe score checklist in predicting risk groups and associated risk of hospitalization was found to be high (0.81; 95% CI, 0.77-0.86). The suggested probability of hospital admission for children who did not have any of the seven characteristics included in the checklist was found to be exceptionally low (0.14%).
Significantly associated parent-reported variables included both moderate or severe vomiting and severe fever, each in the previous 24 hours. Significant clinician-reported variables included intercostal or subcostal recession and wheeze on auscultation.
“The main value of our results is to reduce clinical uncertainty and antibiotic use in children least likely to benefit from them, namely those at very low risk of future hospital admission,” Dr. Hay and his associates noted in The Lancet Respiratory Medicine (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30223-5).
Funding for this study was provided by the National Institute for Health Research and sponsored by the University of Bristol. Only one of the study’s authors, Dr. Peter Muir, reported ties to industry sources.
Primary care practitioners’ use of a seven-item checklist may reduce the number of pediatric patients with respiratory tract infections who are prescribed unnecessary antibiotics, a prognostic cohort study suggests.
The study revealed short illness (a duration of illness of 3 days or less), temperature (a body temperature of 37.8°C or greater at presentation), age (being under 2 years), intercostal or subcostal recession, wheeze on auscultation, asthma, and vomiting (moderate or severe in the previous 24 hours) were each independently associated with hospital admission (P less than .01 for all associations).
The checklist includes these seven characteristics or risk variables (short illness, temperature, age, recession, wheeze, asthma, and vomiting [mnemonic STARWAVe]). To use the checklist, a primary care practitioner would assign one point for the presence of each item in a patient then add up all of the points to determine that patient’s risk level for future hospital admission for respiratory tract infection. A score of 1 point or less, observed in 5,593 (67%) cases would be considered indicative of a very low rate of risk for hospitalization (0.3%, 0.2%-0.4%). A score of 2 or 3 points, found for 2,520 (30%) children, would be considered as a normal level of risk (1.5%, 1.0%-1.9%), and a score of 4 or more points, seen in 204 (3%) children, would signify a high risk level (11.8%, 7.3%-16.2%).
Of the 8,394 children assessed, 78 (0.9%; 95% confidence interval, 0.7%-1.2%) were admitted to a hospital. Most were admitted on days 2-7 (33, 42%) and on days 8-30 (30, 39%) following recruitment. Only 15 (19%) were admitted on the day of recruitment (day 1).
“Many clinicians report that they prescribe antibiotics just in case, to mitigate perceived risk of future hospital admission and complications, and that failing to provide a prescription for a child who subsequently becomes seriously unwell is professionally unacceptable. If primary care clinicians could identify children at low (or very low) risk of such future complications, the reduced clinical uncertainty could lead to a reduced use of antibiotics in these groups of patients,” wrote first author Alastair Hay, MD, from the Centre for Academic Primary Care in the School of Social and Community Medicine at the University of Bristol (England), and his colleagues.
These researchers conducted the study based on a structured, blinded review of the medical records from children aged between 3 months and 16 years presenting with acute cough (less than or equal to 28 days) and respiratory tract infection treated by 519 general practitioners in 247 practices in England between July 2011 and June 2013. The primary study outcome was hospital admission for respiratory tract infection within 30 days.
Additionally, a multivariable model was employed to detect factors associated with increased risk of hospital admission. As measured by receiver operating characteristic curve analysis, the accuracy of the STARWAVe score checklist in predicting risk groups and associated risk of hospitalization was found to be high (0.81; 95% CI, 0.77-0.86). The suggested probability of hospital admission for children who did not have any of the seven characteristics included in the checklist was found to be exceptionally low (0.14%).
Significantly associated parent-reported variables included both moderate or severe vomiting and severe fever, each in the previous 24 hours. Significant clinician-reported variables included intercostal or subcostal recession and wheeze on auscultation.
“The main value of our results is to reduce clinical uncertainty and antibiotic use in children least likely to benefit from them, namely those at very low risk of future hospital admission,” Dr. Hay and his associates noted in The Lancet Respiratory Medicine (Lancet Respir Med. 2016 Sep 1. doi: 10.1016/S2213-2600(16)30223-5).
Funding for this study was provided by the National Institute for Health Research and sponsored by the University of Bristol. Only one of the study’s authors, Dr. Peter Muir, reported ties to industry sources.
FROM THE LANCET RESPIRATORY MEDICINE
Key clinical point: Use of a checklist of seven characteristics independently associated with hospital admission for children presenting to primary care physicians with cough and respiratory tract infection may lead to more appropriate prescribing of antibiotics in this patient population.
Major finding: Only 0.9% of 8,394 pediatric patients presenting to primary care with acute cough and respiratory tract infections were admitted to hospitals. A checklist based on seven characteristics observed in study participants (short illness, temperature, age, recession, wheeze, asthma, and vomiting [mnemonic STARWAVe]) that were independently associated with hospital admission (P less than .01 for all associations) was developed to define three risk categories for future hospital admission for respiratory tract infection.
Data sources: A prognostic cohort study of children aged between 3 months and 16 years presenting with acute cough (28 days or fewer) and respiratory tract infection treated by 519 general practitioners in 247 practices in England between July 2011 and June 2013.
Disclosures: Funding for this study was provided by the National Institute for Health Research and sponsored by the University of Bristol. Only Dr. Peter Muir reported ties to industry sources.
